Katherine Watt: Parsing “Yay, We Did It!” Informational Misdirection Campaigns.
Katherine Watt: Parsing “Yay, We Did It!” Informational Misdirection Campaigns.
by Katherine Watt, Bailiwick News
originally published June 13, 2024
I’m on some email mailing lists for some of the more prominent ‘medical freedom movement’ organizations.
Without naming the organizations or the individual leaders, below is my analysis of recent messages from movement leaders that can be paraphased as “Yay, we did it!,” especially regarding campaigns directed at the World Health Organization, and “Next target!,” especially regarding gain-of-function research on so-called pathogens with pandemic potential.
The things they don’t talk about matter more than what they do talk about.
“Yay, we did it!” focused on WHO campaigns, is a method to induce readers, listeners and viewers to misunderstand and ignore legal authorities already centralized by domestic communicable disease control law, vaccine production and supply contracts (domestic and international), and international Mutual Recognition Agreements, already invoked and enforced during Covid, and to a lesser extent, during previous alleged pandemics.
Currently there’s also a focus on “gain-of-function” laboratory activity as a source of pandemic-potential pathogens, as contrasted with naturally-evolving or zoonotic pathogens.
These fake targets for public distress — imminent (rather than accomplished) centralization of global public-health-predicated governing authority, deadly global pandemic-potential pathogens and gain of function research — are offered for several reasons:
- To reinforce the fear- and compliance-sustaining lie that pathogens can be, or can be manipulated to become, existential threats to society: sustainably and simultaneously very deadly and very transmissible communicable disease vectors.
- To funnel public attention and effort into wasteful, irrelevant campaigns to legally influence supralegal (operating outside the law with global legal immunity) organizations (i.e. UN, WHO, WEF), and to de-fund or prohibit gain of function research.
- To leave unrecognized and unchallenged the intrinsic heterogeneity, instability and toxicity of biological products, including vaccines, better understood as legalized poisons designed, intended and used for more than a century to mutilate, sterilize and kill recipients.
- To leave unrecognized and unchallenged the real threat of global deception and coercion programs already established and led by the US government and central banks, already operative through US state and county governments, international organizations (UN, WHO, WEF) and other national governments and their political subdivisions.
Misleaders want people to believe these falsehoods:
- Deadly global pandemic pathogens transmitting communicable diseases have occurred in the past and will occur again, especially through development and circulation of “gain of function” pathogens of pandemic potential.
- Past, current, emerging, novel, and/or future pandemic pathogens legally and morally justify centralized US-government and central-bank-controlled (UN-WHO-fronted) military and financial control of global pandemic and public health emergency preparedness and response programs.
- US-government- and central bank-controlled (UN-WHO-fronted) governments don’t yet have operative legal, military and financial authority to surveil, test, quarantine, isolate and compel submission to treatment for alleged infection with alleged pandemic pathogens.
- US-FDA is a regulatory agency legally obligated, and historically functioning, to regulate the manufacture of drugs, devices, biological products (including vaccines), for safety, efficacy and purity, and therefore people should have confidence in US-FDA’s reviews, decisions and pronouncements.
- Vaccines and other biological products are non-toxic, non-weapon, medicinal product class, and therefore people should have confidence in and consume these products.
- EUA countermeasures (drugs, devices, biological products, vaccines) are intended, designed, effective, manufactured, and regulated for treating and/or preventing infection with deadly pandemic pathogens.
Misleaders want people to misunderstand or ignore these truths:
1. Deadly global pandemic pathogens are not possible, by natural evolution or by “gain-of-function” lab-development. Whatever their initial virulence (severity or harmfulness), as communicable disease outbreaks spread among living organisms, they weaken and burn out as populations’ individual and aggregate immune systems respond.
Note: I think globalist killers expedited their vaccine-mediated worldwide poisoning program starting in the 1950s with national polio vaccination campaigns partly because, in combination with better water and sewage treatment systems, faster international travel — especially air travel — had rapidly moved the world’s people toward much higher individual and aggregate immunity to many previously regionally-transmitted communicable disease vectors.
2. There is no moral or legal justification for centralized US-government and central-bank-controlled (UN-WHO-fronted) military and financial control of global pandemic/public health emergency preparedness and response programs.
3. Deadly chemical weapons, fraudulent mass testing, and fraudulent mass media campaigns can and have been developed and deployed to simulate outbreaks of deadly communicable disease and drive public credulity in the core lies listed above.
4. USA-FDA does not regulate manufacture of vaccines and other biological product. US-FDA simulates regulation, and has never established or enforced measurable, validated standards for vaccine or biological product identity, safety, efficacy or purity.1
5. UN-WHO, International Health Regulations (2005), require member states to “adjust domestic legislative and administrative arrangements” to comply with IHR regulations.

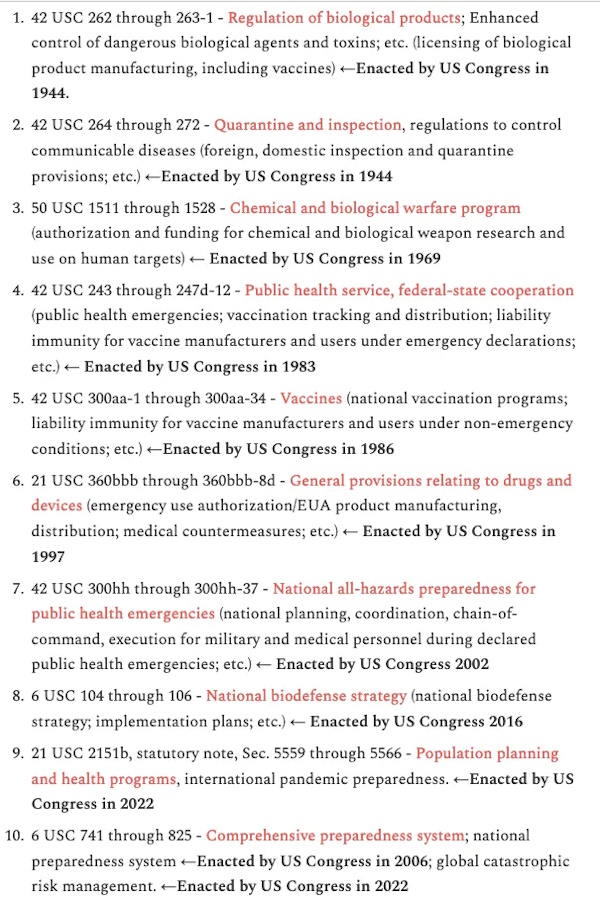
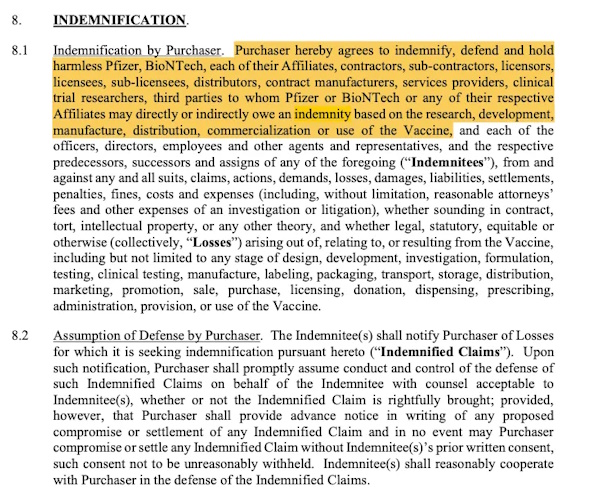
6. Centralized military and financial control of pandemic preparedness and response provisions are embedded in US domestic law (federal statutes, regulations, executive orders, commercial contracts and treaties; state laws and contracts, county emergency management plans and contracts), in compliance with UN-WHO IHR, 2005, and UN-WHO IHR, 2022 amendments, and have been built in and developed for several decades including provisions authorizing military, law enforcement and public health officers to engage in warrantless surveillance, inspection, testing, apprehension, detention, quarantine, isolation, compulsory treatment; provisions authorizing exemptions/waivers/exclusions from cGMP and related requirements for routine vaccination products and for EUA countermeasures; and provisions authorizing vaccine manufacturer and administrator (nurse, pharmacist, doctor) civil and criminal liability indemnification since 1986 for routine vaccination-poisoning and since the 2005 PREP Act for emergency countermeasure vaccination-poisoning and other EUA drugs, devices and biological products.
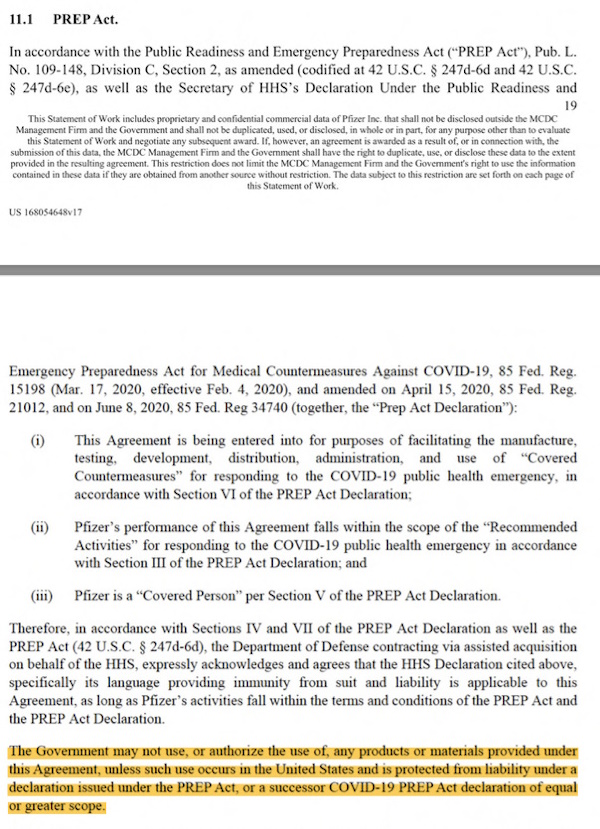
7. Vaccine and other countermeasure production contracts between the US military and pharmaceutical companies condition manufacturing, distribution and use on intact PREP Act statutes and active PREP Act declarations.

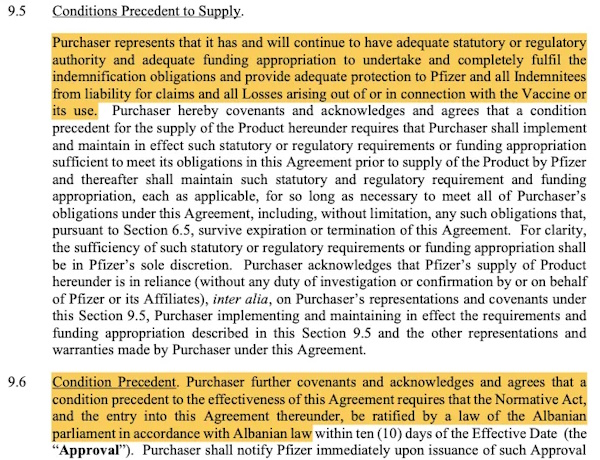
8. International sales contracts condition supply of products manufactured by US military contractors, to non-US governments, on purchasing government adoption and maintenance of indemnification laws.
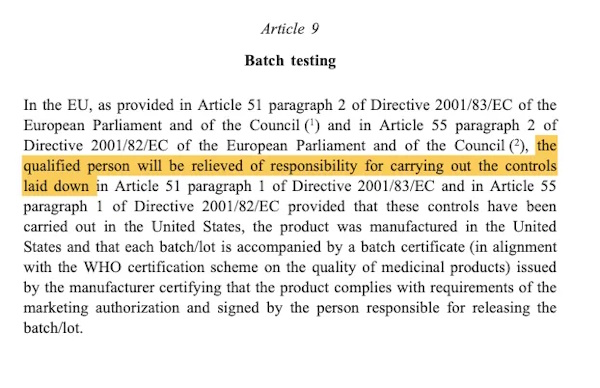
9. International Mutual Recognition Agreements (MRAs) absolve federal drug regulators of non-US countries of legal responsibility for cGMP manufacturing regulation, transferring regulatory functions to US-FDA: global drug non-regulator under US laws exempting biological products, vaccines and EUA countermeasures from cGMP compliance.
1 FDA history of non-regulation of vaccines and other biological products, series:
- Dec. 19, 2023 – Legalized FDA non-regulation of biological products effective May 2, 2019, by Federal Register Final Rule, signed by then-FDA Commissioner Scott Gottlieb.
- March 8, 2024 – Part 1: Mutual Recognition Agreements. First in series on legal links connecting domestic and international non-regulation of non-medicines
- March 12, 2024 – Part 2: Statutory and regulatory definitions for drugs, biological products, and biosimilars
- March 15, 2024 – Part 3: Deregulation of biological product manufacturing, mid-1990s to present
- March 20, 2024 – Part 4: Vaccines have always been heterogeneous mixtures of toxins used to intentionally sicken people and animals
- March 21, 2024 – Part 5: Vaccine and related biological product manufacturing as US government-licensed poison manufacturing Evidence from November 1986 ‘mandate for safer childhood vaccines’ codified at 42 USC 300aa-27, and July 2018 stipulation by HHS.
- April 3, 2024 – Part 6: On why FDA revised written non-rules for non-regulation of biological products to make them more unintelligible, inapplicable and unenforceable since the 1990s.
- April 25, 2024 – Part 7: Terms, phrases and organizations involved in worldwide regulatory and manufacturing deception surrounding vaccines and other biological products.
- May 21, 2024 – Part 8: There is no legal limit to the amount of so-called contamination that can legally be included in vaccines or any other biological products.
- May 25, 2024 – Part 9: On FDA buildings as virtual mailboxes to project the public illusion of biological product manufacturing regulation.
- June 4, 2024 – Part 10: Sen. Rand Paul, FDA Modernization Act 2.0, and animal testing of new drugs.
Cover image based on creative commons work of:creozavr