In the middle of the 19th century, starting in Germany, a misleading and dangerous worldview was imposed on all of humanity – by means of fraud. It was disguised as science. The function: to rule by creating fear, after the nobility and churches, which previously carried out this task, were disempowered by money. Life no longer has any meaning or value, since everything came about by chance. Deriving from the erroneous atomic theory, it was claimed that cells existed as the smallest indivisible units of life.
All illnesses are caused by pathogenic substances in the cells. The body can no longer be trusted, as pathogenic substances such as metastases and viruses constantly pose a fatal threat to people from the outside and inside. Only state medicine and its measures can save people. The cell theory, which has never been scientifically proven and has only ever been refuted, forces those involved to believe in genetic material as a book of life, because since the introduction of the atomic theory in “science” there has been no spirit, no consciousness and no information field to produce life from the all-connecting substance, the ether, Akasha in Indian, rediscovered as the primordial substance of life by Dr. Augustin.
By the year 2000, all geneticists knew that all their ideas had been refuted by their own findings, partly because the so-called genetic material DNA is constantly changing in every nucleus . So the claim of a functioning mRNA is just as much scientific fraud as the claim of pathogenic viruses or metastases. Until the second largest mass murder after AIDS , Corona , no one claimed that mRNA could work . Suddenly, with the invention of SARS-Cov2 in the PC, a compulsive logic became a billion-dollar product, the danger of which, however, does not result from the harmless mRNA, but from the dangerous nanoparticles it contains and the psychosomatics when people are thrown into a terrorist panic.
After Ernst Wolff revealed that when President Trump left the WHO in 2020, he transferred the funds to the GAVI vaccination alliance, which was founded in 2001 at the WEF and financed by the Bill and Melinda Gates Foundation , here is a collage of Trump’s statements on vaccinations and here is the bombshell. Trump is investing $500 billion in mRNA vaccinations against cancer ! In the upcoming part 2, we will explain why mRNA vaccinations are helpful in voodoo cancer diagnoses for completely different reasons and in addition to the nanoparticle effects. And in the coming episodes, we will explain that we have all, in many aspects, been in this mechanistic thought trap since 1858, which, when we leave it together, rewards us with a sustaining and wonderful feeling of cosmic involvement and connection with things and beings.
Since ‘hindsight is 20/20,’ what happened in 2020?
In 2020, the new, experimental mRNA injections rolled out as a premeditated response to Coronavirus. What was on the package inserts of the products?
Nothing.
The inserts were blank. This way, companies could not be held liable for any ill effects following injection. It’s called indemnity, an exemption from penalties.
Fast forward to 2024. Eureka! Suddenly scientists know what was in those Emergency Use Authorized (EUA), FDA-unapproved COVID injections!
Among the undeclared chemical elements were detected 11 of the 15 cytotoxic lanthanides used in electronic devices and optogenetics. In addition, among the undeclared elements were all 11 of the heavy metals: chromium was found in 100% of the samples; arsenic 82%; nickel 59%; cobalt and copper 47%; tin 35%; cadmium, lead and manganese in 18%; and mercury in 6%. A total of 55 undeclared chemical elements were found and quantified…
James Lyons-Weiler, Ph.D., a member of the journal’s editorial board said, “Individually, these chemicals are known to cause neurological, cardiovascular and immunological damage.”
No matter where the information is found in the media, whether in an article, social media, cinema,documentary, or hidden in a medical journal study, the architects who create toxic products must disclose the information somewhere, whether perceived positively or negatively. Of course how you perceive the information is up to you.
As long as the deed is visible, it has been exposed, even if it is after the fact. This is called implied consent.
No response is considered to be silent acquiescence. This means that by your non response, you have agreed to the methods used.
When hindsight is 20/20, it means “too little, too late.” The deed is done.
Biodigital Convergence
There is another purpose to the disclosing information after the fact; that is to misdirect an investigation. Four years later, mRNA is old information since, in the Information Age, old news happens yesterday, not four years ago.
For at least two decades, scientists and governments have been paving the way toward Transhumanism, the merging of humans and machines. The way to Transhumanism is through Biodigital Convergence. Read more here.
In the coming years, biodigital technologies could be woven into our lives in the way that digital technologies are now. Biological and digital systems are converging, and could change the way we work, live, and even evolve as a species. More than a technological change, this biodigital convergence may transform the way we understand ourselves and cause us to redefine what we consider human or natural.
The positive side of Hindsight is Foresight. Instead of looking to the past, we can focus on what is unfolding now, and into the near future.
Biodigital Convergence leads to Smart cities, Cognitive(C40) cities, Blockchain, Reverse engineering, Digital Twin, Self-assembly nanotechnologies, the Internet of Bodies, and more… in the connected future of the Metaverse.
If Biodigital Convergence sound like a Virtual Reality, then you are one step closer to your Avatar. Will you become an Avatar in the Metaverse? Watch the feature film, Avatar for disclosure.
The architects of converging technologies want everyone to live a Metaverse of their construction.
The NNI recently celebrated its 20th birthday. This proves that mRNA nanotechnology is old news. It does not discriminate against gender, sex, race, or religion. This global initiative seeks to incorporate everyone, everywhere. They have our consent through silent acquiescence.
The concept of ‘vaccine status,’ along with related vaccine science and laws are mere propaganda and distraction. These are symptoms of past strategies that lead to future ‘connectivity.’ Unfortunately, focus on vaccines is exactly where architects want people to be.
Foresight might be fuzzy, but without it, we are left scrambling in the past.
Conclusions of this observational study in ~800K children and adolescents in the UK: covid vaccines had no efficacy and were associated with ALL cases of myocarditis and pericarditis! Anyone injecting kids with this garbage is simply poisoning them for no reason at all. You can read for yourself:
OpenSAFELY: Effectiveness of COVID-19 vaccination in children and adolescents
Colm D Andrews[1] , Edward P K Parker[2] , Elsie Horne[4] , Venexia Walker[4] , Tom Palmer[4] , Andrea L Schaffer[1] , Amelia CA Green[1] , Helen J Curtis[1] , Alex J Walker[1] , Lucy Bridges[1] , Christopher Wood[1] , Victoria Speed[1] , Christopher Bates[3] , Jonathan Cockburn[3] , John Parry[3] , Amir Mehrkar[1] , Brian MacKenna[1], Sebastian CJ Bacon[1] , Ben Goldacre[1] , Miguel A Hernan[5] , Jonathan AC Sterne[4] , The OpenSAFELY Collaborative, and William J Hulme[1] .
[1]Bennett Institute for Applied Data Science, Nuffield Department of Primary Care Health Sciences, University of Oxford, OX2 6GG, UK
[2] London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, UK
[4] Population Health Sciences, University of Bristol, Oakfield House, Oakfield Grove, Bristol, BS8 2BN, UK
[5] Departments of Epidemiology and Biostatistics, Harvard T.H. Chan School of Public Health, Boston, MA 02115
Abstract:
Background Children and adolescents in England were offered BNT162b2 as part of the national COVID-19 vaccine roll out from September 2021. We assessed the safety and effectiveness of first and second dose BNT162b2 COVID-19 vaccination in children and adolescents in England.
Methods:
With the approval of NHS England, we conducted an observational study in the OpenSAFELY-TPP database, including a) adolescents aged 12-15 years, and b) children aged 5-11 years and comparing individuals receiving i) first vaccination with unvaccinated controls and ii) second vaccination to single-vaccinated controls. We matched vaccinated individuals with controls on age, sex, region, and other important characteristics. Outcomes were positive SARS-CoV-2 test (adolescents only); COVID-19 A&E attendance; COVID-19 hospitalisation; COVID-19 critical care admission; COVID-19 death, with non-COVID-19 death and fractures as negative control outcomes and A&E attendance, unplanned hospitalisation, pericarditis, and myocarditis as safety outcomes.
Results:
Amongst 820,926 previously unvaccinated adolescents, the incidence rate ratio (IRR) for positive SARS-CoV-2 test comparing vaccination with no vaccination was 0.74 (95% CI 0.72-0.75), although the 20-week risks were similar. The IRRs were 0.60 (0.37-0.97) for COVID-19 A&E attendance, 0.58 (0.38-0.89) for COVID-19 hospitalisation, 0.99 (0.93-1.06) for fractures, 0.89 (0.87- 0.91) for A&E attendances and 0.88 (0.81-0.95) for unplanned hospitalisation. Amongst 441,858 adolescents who had received first vaccination IRRs comparing second dose with first dose only were 0.67 (0.65-0.69) for positive SARS-CoV-2 test, 1.00 (0.20-4.96) for COVID-19 A&E attendance, 0.60 (0.26-1.37) for COVID-19 hospitalisation, 0.94 (0.84-1.05) for fractures, 0.93 (0.89-0.98) for A&E attendance and 0.99 (0.86-1.13) for unplanned hospitalisation. Amongst 283,422 previously unvaccinated children and 132,462 children who had received a first vaccine dose, COVID-19-related outcomes were too rare to allow IRRs to be estimated precisely. A&E attendance and unplanned hospitalisation were slightly higher after first vaccination (IRRs versus no vaccination 1.05 (1.01- 1.10) and 1.10 (0.95-1.26) respectively) but slightly lower after second vaccination (IRRs versus first dose 0.95 (0.86-1.05) and 0.78 (0.56-1.08) respectively). There were no COVID-19-related deaths in any group. Fewer than seven (exact number redacted) COVID-19-related critical care admissions occurred in the adolescent first dose vs unvaccinated cohort.
Among both adolescents and children, myocarditis and pericarditis were documented only in the vaccinated groups, with rates of 27 and 10 cases/million after first and second doses respectively. Conclusion BNT162b2 vaccination in adolescents reduced COVID-19 A&E attendance and hospitalisation, although these outcomes were rare. Protection against positive SARS-CoV-2 tests was transient.
A federal judge rejected the EPA’s argument that the exact level at which fluoride is hazardous is too unclear to determine if the chemical presents an unreasonable risk, and ruled the agency must take regulatory action.
In a decision that could end the practice of water fluoridation in the U.S., a federal judge late Tuesday ruled that water fluoridation at current U.S. levels poses an “unreasonable risk” of reduced IQ in children.
The U.S. Environmental Protection Agency (EPA) can no longer ignore that risk, and must take regulatory action, Judge Edward Chen of the U.S. District Court of the Northern District of California wrote in the long-awaited landmark decision.
More than 200 million Americans drink water treated with fluoride at the “optimal” level of 0.7 milligrams per liter (mg/L). However, Chen ruled that a preponderance of scientific evidence shows this level of fluoride exposure may damage human health, particularly that of pregnant mothers and young children.
The verdict delivers a major blow to the EPA, public health agencies like the Centers for Disease Control and Prevention (CDC) and professional lobbying groups like the American Dental Association (ADA), which have staked their reputations on the claim that water fluoridation is one of the greatest public health achievements of the 20th century and an unqualified public good.
Rick North, board member of Fluoride Action Network, one of the plaintiffs in the lawsuit, told The Defender, “What’s false is the CDC claiming that fluoridation is one of the 10 greatest health achievements of the 20th century. What’s true is that ending fluoridation will be one of the 10 greatest health achievements of the 21st century.”
“The judge did what EPA has long refused to do, and that is to apply the EPA standard risk assessment framework to fluoride,” said Michael Connett, attorney for the plaintiffs. “In so doing, the court has shown that the widespread exposure to fluoride that we now have in the United States is unreasonably and precariously close to the levels that we know cause harm.”
The EPA can appeal Tuesday’s decision. The agency told The Defender it is reviewing the decision and has no comment at this time. The U.S. Department of Justice, which represents the EPA in the lawsuit, also said it has no comment.
It is the first lawsuit to go to a federal trial under the Toxic Substances Control Act (TSCA), as amended by Congress in 2016. The TSCA allows U.S. citizens to petition the EPA to evaluate whether a chemical presents an unreasonable risk to public health and should be regulated.
If the EPA denies a TSCA citizen petition — which the agency did when the plaintiffs asked it to reexamine water fluoridation in 2016 — the petitioners are entitled to a “de novo” judicial review of the science without the deference to the agency typically afforded it in legal cases.
Chen’s 80-page ruling, issued six months after closing arguments in February, offers a careful and detailed articulation of the EPA’s review process for chemicals that pose a hazard to human health and evaluates and summarizes the extensive scientific data presented at trial.
Chen wrote, “EPA’s own expert agrees that fluoride is hazardous at some level.” He cited a key report issued by the U.S. Department of Health and Human Services (HHS) National Toxicology Program (NTP), which undertook a systematic review of all available scientific research at the time of publication.
The report “concluded that fluoride is indeed associated with reduced IQ in children, at least at exposure levels at or above 1.5 mg/L,” Chen wrote.
The NTP also reported that although there are technical challenges to measuring fluoride’s toxic effects at low levels, “scientists have observed a statistically significant association between fluoride and adverse effects in children even at such ‘lower’ exposure levels,” Chen wrote.
He said that despite recognizing that fluoride is hazardous, the EPA’s defense rested largely on the fact that the exact level at which it is hazardous is too unclear for the agency to determine whether the chemical presents an unreasonable risk.
This argument is “not persuasive,” Chen wrote.
Pregnant women exposed to fluoride in water at levels exceeding the hazard level
The EPA requires a margin of error by a factor of at least 10 to exist between the hazard level for a toxin and the acceptable human exposure level. “Put differently, only an exposure that is below 1/10th of the hazard level would be deemed safe under Amended TSCA, given the margin of error required,” Chen wrote.
That means that even if the hazard level were 4 mg/L — well above the 1.5 mg/L identified by the NTP — the safe level of fluoride exposure would be 0.4 mg/L, well below the current “optimal” fluoride level in the U.S., Chen wrote.
The much lower probable hazard level established by high-quality studies indicates that many pregnant women in the U.S. are already exposed to fluoride in water at levels exceeding the hazard level.
“Under even the most conservative estimates of this level, there is not enough of a margin between the accepted hazard level and the actual human exposure levels to find that fluoride is safe,” Chen concluded.
“Simply put, the risk to health at exposure levels in United States drinking water is sufficiently high to trigger regulatory response by the EPA under Amended TSCA.”
The law dictates that the EPA must take regulatory action, but it does not specify what that action has to be. EPA regulatory actions can range from notifying the public of risks to banning chemicals.
Philippe Grandjean, M.D., Ph.D., adjunct professor in environmental health at Harvard and chair of environmental medicine at the University of Southern Denmark, top researcher on fluoride’s neurotoxicity and expert witness for plaintiffs in the case told The Defender he thought the court’s decision was “well-justified.”
He said the ruling made it incumbent on the EPA to go beyond simply ending water fluoridation.
“EPA will have to consider what to do in the southwestern parts of the country where the fluoride content of groundwater is too high due to minerals in the soil containing fluoride,” he said. “And then there is the question about ingestion of toothpaste.”
The CDC and the ADA did not immediately respond to The Defender’s request for comment.
More than 70 years of controversy
For more than seven decades, U.S. public health officials have steadfastly supported water fluoridation, claiming the practice is a key strategy for maintaining and improving dental health.
The EPA in 1975 recommended adding fluoride to water at an optimal level of 1.2 mg/L for its dental benefits, but recommended a maximum level of 4 mg/L, the ruling said.
As more evidence has emerged about fluoride’s adverse health effects, including skeletal fluorosis, recommended levels were revised.
Surgeon General Vivek Murthy, officially lowered the recommended dosage for water fluoridation in 2015 from 0.7-1.2 mg/L to 0.7 mg/L after considering “adverse health effects” along with alleged benefits.
However, evidence that fluoride poses a neurotoxic risk has existed for decades.
A seven-day trial took place in federal court in San Francisco in June 2020, but Chen put the proceedings on hold pending the release of the NTP’s systematic review of research available on the neurotoxic effects of fluoride.
The NTP sought to publish its report — which consisted of a “state of the science” monograph and a meta-analysis — in May 2022, but dental officials at the CDC and the National Institutes of Health National Institute of Dental and Craniofacial Research pressured HHS Assistant Secretary for Health Rachel Levine to prevent the review from being published.
Levine told the NTP to not publish the report but to put it on hold and allow for further review.
Plaintiffs submitted documents obtained via the Freedom of Information Act exposing this intervention to the court. The revelation prompted Chen to rule that the trial should go forward using the draft report from the NTP.
The trial resumed in January in San Francisco, with arguments presented over the course of two weeks.
Connett said that Congress created the citizen petition provision in TSCA as a counterweight to bureaucratic lethargy and as a check on the EPA.
The statute, he said, is a powerful tool for overcoming politicized science.
“When science becomes fossilized in political inertia, the citizen petition provision of TSCA is a very powerful tool for citizens,” Connett said. “Through this case, we have been able to effectuate what Congress had envisioned with this part of the statute.”
The difference between conspiracy realists and conspiracy deniers is, of course, that the latter never question anything, never think for themselves, never do their own research.
They simply lap up every last drop of drivel and delusion presented to them, including the laughable conceit that in so doing they are proving themselves somehow more “advanced”, more “adult”, more “astute” than those tin-foil-hat-wearing idiots who dare challenge official top-down truth.
As they remain rooted to their theatre seats, stuffing their faces with propaganda popcorn and fizzy fakery, their scientifically-sealed minds cannot even grasp the possibility that others might have taken the initiative to have a peek backstage and work out what The Spectacle is all about.
I don’t suppose there are many conspiracy deniers reading this, but just in case one or two have wandered in by mistake, here are some more stones to look under, if you can find the courage to face the reality of the seething maggot-infested corruption that lies beneath the surface of our society.
First of all, have a read of Hedley Rees’ Inside Pharma blog and in particular his reporting on what he describes as “the latest Big Pharma feeding frenzy”.
He points us to the existence of an annual J.P. Morgan Healthcare Conference, which will next be held in San Francisco in January 2025.
Its site states: “This premier conference is the largest and most informative healthcare investment symposium in the industry which connects global industry leaders, emerging fast-growth companies, innovative technology creators and members of the investment community”.
Hmmm…
J.P. Morgan is, as I set out in Enemies of the People, a longstanding front for the Rothschilds, those leading members of “the investment community” who have long been involved in profiting from bio-tech and the grotesquely-misnamed “healthcare” industry.
As I report in my booklet, International Biotechnology Trust (IBT), a division of Rothschilds, says on its website that it “offers investors access to the fast-growing biotechnology sector”.
Predictably, in view of the Rothschilds’ intimacy with UK governments, their biotech wing was involved in the country’s “response” to Covid.
IBT proudly relates that its investment manager Kate Bingham was in May 2020 appointed chair of the UK Vaccine Taskforce “reporting to the Prime Minster to lead UK efforts to find and manufacture a COVID-19 vaccine, on a six-month engagement”.
It says: “On December 8th 2020 the UK started COVID-19 vaccinations – the first Western country to do so. She [Bingham] was awarded a DBE in the Queen’s Birthday Honours in June 2021 for services to the procurement, manufacture and distribution of COVID-19 vaccines”.
One of the most prominent UK enthusiasts for the Covid jabs, vaccine passports and the digital ID to which they were designed to lead is former Prime Minister Tony Blair.
Last November I wrote about the research by the UK Column’s Ben Rubin which revealed that in June 2022 Blair was the main speaker at a conference on the “Future of Britain” hosted, with the organisation My Life My Say, by the Institute of Global Health Innovation at Imperial College, London.
In investigating My Life My Say, Rubin discovered that trustee Glen Manning was a senior banker with Rothschild & Co.
Blair himself, after resigning from British politics, in January 2008 joined the Rothschilds’ JPMorgan Chase in a “senior advisory capacity”, on a modest salary of £2.52m per year.
A thank-you, perhaps, for having led the UK into the invasion of Iraq in 2003, among many other invaluable services to the money power?
Blair is very keen on the “modernisation” of public services in the UK, including, of course, the National Health Service.
This would involve our data being held centrally in a “new NHS cloud infrastructure” and “used as a collective national asset to help our life-science sector to be world-leading”.
Marvellous.
In the light of all that, it is hardly surprising to read, back on the Inside Pharma blog, that the key speaker at the 2024 JP Morgan Healthcare Conference was none other than “The Rt. Hon. Tony Blair: Executive Chairman of the Institute for Global Change”.
I would once again echo Rubin’s warning that “Tony Blair is coordinating with the Rothschild family to fundamentally reshape British society and implement a global, digital slave state”.
Of course, for my (probably imaginary) conspiracy-denying readers this will all no doubt be seen as a meaningless series of complete coincidences.
So I would suggest they also take a peek at this article from Australian researcher Warren Ross about the climate scam.
Rightly describing this as “a whole new area of investment and opportunity” for the billionaire class, he notes that “BlackRock are eager to fill as much of this space as they can and have proved their commitment to this by purchasing infrastructure investment fund Global Infrastructure Partners”.
He adds: “ESG compliance is used by companies like BlackRock to direct investment away from companies that choose not to comply or don’t comply with sufficient zealotry”.
In addition, as I note in Enemies of the People, Edmund de Rothschild was the key player behind the World Conservation Bank, later renamed Global Environment Facility (GEF).
The Corbett Report has explained that the idea for an international “conservation” bank had been around for some time before France put forward a formal proposal at a joint ministerial meeting of the IMF in 1989.
“The project was put under the umbrella of the World Bank and by 1991 the World Conservation Bank was formally established”.
The article adds that the GEF has made and co-financed tens of billions of dollars worth of grants and “is the funding mechanism for five different UN conventions, including the United Nations Framework Convention on Climate Change”.
As well as establishing so-called “protected areas”, it has funded Chinese companies producing solar cells and wind farm technology…
The reality that conspiracy deniers cannot bear to see, and that those in power want to keep hidden, is that our society is dominated by one single giant global organisation.
This mega-organisation is not one that aims to do good for us or for our world, which is why it has to take such pains to conceal its existence and its activities.
It is an unimaginably vast, ruthless, greedy, destructive crime syndicate which has grabbed global control by means of lies and usury, blackmail and bribery, manipulation and murder.
The sooner we all wake up to this nauseating reality, and get together to do something about it, the better.
Recently published research from Korea and Japan confirm previous reports we’ve heard of nanotech in the COVID-19 injectables.
Contents of the COVID-19 injectables produced by Pfizer and Moderna were examined under a stereo-microscope at four-hundred-times magnification. Specimens were cultured in different media to observe the effect they had on living cells.
The study concluded that the anomalous injuries that have occurred worldwide since the injectables were “pressed upon billions of individuals,” were caused by the nanotechnology contents of the COVID-19 injectables.
The research found cellular toxicity, and over the course of a few weeks, simple one dimensional structures grew into complex three dimensional structures. Numerous artificial self-assembling nano-sized objects of many different shapes. Including animated worm-like entities, discs, chains, spirals, tubes, and right-angle structures containing other artificial structures within them. Some structures even “seemed to appear and then disappear over time.” All of this was found to be well “beyond any expected and acceptable levels of contamination.”
This was first reported on nearly three years ago by Ricardo Delgado and La Quinta Columna, out of Spain. Who found a relationship between the nano-tech and 5G
“The Fifth Column recently published their findings and conclusions on the strange self-assembling nano tech they discovered in the Pfizer mRNA vaccines via Optical Microscopy Analysis.”
The objects they found in the vaccine correspond with known items in the scientific record. And the conclusion they come to seems quite clear, that the well documented scientific goal to use nanotechnology in living human beings to form networks capable of controlling several nanomachines, is currently being deployed in the COV-19 vaccines”
~ Greg Reese “5G Powered Graphene Based Nano-Tech in the Pfizer Vaccine” (2022)
5G towers were fired up for the first time in Wuhan the same time they were reportedly experiencing a COVID-19 outbreak. David Icke said there was a relationship between COVID-19 and 5G back in 2020. And it got him banned.
Using Dark-field microscopy, Doctor Ana Maria Mihalcea has found these same artificial nano-structures in the blood of both those who got the COVID-19 injectables, and those who did not.
Decades ago, Silicon Valley guru Ray Kurzweil, said that by 2045, most of human civilization will be non-biological machines thanks to the advancements of nano-robots which could cure aging and death.
While talk of mRNA is making it easily into the mainstream, the nano-tech is being ignored.
Hopefully this nicotine study will be repeated by other independent scientists, because the mass infection of humanity with experimental nano-tech has now been ignored for at least three years. And all sides of political leadership are steering us towards a brave new world of A.I. and the internet of things. Where being an organic human being seems to not be an option.
A FOIA request was filed with the U.S. Centers for Disease Control and Prevention (CDC)and the Agency for Toxic Substances and Disease Registry (ATSDR) (see pages 1 & 2) for all studies/reports in the possession, custody or control of the institutions:
that scientifically prove/provide evidence of the existence of any alleged “hantavirus” (showing that the alleged particles exist and cause the illness/symptoms they are alleged to cause), or
that even describe purification of particles alleged to be “hantavirus” directly from bodily fluid/tissue/excrement of “hosts”, with purification confirmed via EM imaging, or
wherein the purported genome of the alleged “hantavirus” was found intact (as opposed to fabricated in silico aka computer modeled), or
that scientifically demonstrate contagion of the illness / symptoms that are allegedly caused by said purported “virus”.
As usual I asked that if records matching my request were held but were already publicly available, I be given citations so that I may identify and access each one. I also clarified that my request was not limited to records authored by the CDC or ATSDR but included records authored by anyone, anywhere, ever.
May 10, 2024, #24-00976-FOIA:
Roger Andoh acting as CDC/ATSDR FOIA Officer in the Office of the Chief Operating Officer responded, citing only the first section of my request where I asked for studies providing scientific evidence of the existence of the alleged virus.
Before looking at Roger’s response, please review the exact wording of that section of my request. I hadn’t even asked for evidence of particles infecting cells, hijacking them and making copies of themselves, which according to “virus” dogma “viruses” do. I have never asked for such evidence in any of my requests. My requests have been much simpler than that.
And yet, despite the simplicity of my request, not only did Roger confess that “we do not have any documents pertaining to your request” (written by anyone, anywhere, ever)…
… he also disclosed that the “experts” in the Division of High-Consequence Pathogens and Pathology have never obtained scientific evidence of purported “viruses” existing in “hosts” and causing the illness/symptoms that they are claimed to cause. Because virology was never a science.
“The Division of High-Consequence Pathogens and Pathology has stated that the procedure asked about in this FOIA request is not a methodology or procedure that the branch utilizes or has ever implemented. DHCPP routinely, per protocol, places samples on cell culture post sample receipt or conduct RT-PCR.” (emphasis added)
(The various problems with PCR “tests” and the use of cell cultures in virology have already been discussedby many at great length.)
I followed up with Roger (pg 9) asking about the remaining sections of the request: records of the alleged “virus” simply being found and purified from bodily fluid/tissue/excrement of “hosts” (required for valid analysis and experiments), records of the alleged “viral genome” having been found intact anywhere, and studies providing scientific evidence of illness contagion.
Roger never responded. Based on my knowledge of the virology literature and the 100% failure rate of 224 institutions in 40 countries responding to requests for foundational “virus” evidence I am confident that such studies do not exist, anywhere.
Here is the CDC’s web page on imaginary “hantaviruses”. Hmm, where have we seen those “signs and symptoms” before?
(Note: this information has been sent to ~200 people who work for “the state”, lamestream media, etc. at Canada, Isle of Man, England and the U.S., so that they can’t claim later that they didn’t know.)
More Official Confessions/Evidence Showing that Virology is Pseudoscience
3000+ pages of “virus” FOIs in 8 compilation pdfs, and my notarized declarations re the anti-scientific nature of virology: https://tinyurl.com/IsolationFOIs
Because “they” (HIV, influenza virus, HPV, measles virus, etc., etc., etc.) have never been shown to exist, clearlydon’t exist and virology isn’t a science.
Twenty-six U.S. governors — over half of the nation’s state leaders — have stated publicly that they will not comply with a World Health Organization (WHO)-led global attempt at controlling U.S. Americans’ health.
In their Aug. 29 statement, the 26 governors — all Republicans — and the Republican Governors Association accused the WHO of “attempting one world control over health policy” by promoting a “pandemic agreement” or “pandemic treaty.”
“Put simply,” they wrote, “Republican Governors will not comply.”
Since 2021, the WHO has been drafting proposals for a pandemic agreement and amendments to its International Health Regulations.
During the organization’s most recent World Health Assembly session, which ended on June 1, WHO negotiators did not agree on a final draft of a pandemic agreement. However, they did make “concrete commitments to completing negotiations on a global pandemic agreement within a year, at the latest, and possibly in 2024,” the WHO stated.
Health freedom activist Dr. Meryl Nass, an internist and founder of Door to Freedom, an organization that lobbied against the WHO pandemic treaty proposals, told The Defender the governors’ statement is “very necessary at this time” because the United Nations (U.N.) — which runs the WHO — “seeks to gain world control over emergencies such as cyber emergencies, supply chain emergencies or outer space emergencies.”
“The jig is up,” Nass said. “It has become widely understood that the U.N. system is being used in an attempt to centralize its control and usurp national sovereignty.”
The governors said they refuse to comply with a WHO pandemic agreement because it would consolidate power in the hands of the WHO, thereby threatening nationa
Nass said:
“This was every Republican governor in the United States with the single exception of Vermont Republican governor [Phil Scott]. He governs a state that is strongly Democrat and may have felt he could not expend the political capital required to go along and make this statement unanimous.”
The 26 governors pointed to a May 22 letter to President Joe Biden in which 24 Republican governors voiced their concerns about the WHO’s proposal.
According to the letter, the WHO’s proposed treaty would “empower the WHO, particularly its uncontrollable Director-General, with the authority to restrict the rights of U.S. citizens, including freedoms such as speech, privacy, travel, choice of medical care, and informed consent, thus violating our Constitution’s core principles.”
WHO fails to pass pandemic treaty but says it’s still committed to it
In December 2021, the agency’s World Health Assembly established an “intergovernmental negotiating body” to draft an international agreement under the WHO’s constitution to strengthen the agency’s pandemic prevention, preparedness and response. The U.S. federal government supported the initiative.
Although WHO negotiators disagreed on a final draft of the agreement during the most recent World Health Assembly session, they did approve a set of revisions to the WHO’s International Health Regulations.
However, the approved revisions did not include many of the most restrictive proposals that worried health freedom advocates, The Defender reported.
Nass wrote on her Substack that the World Health Assembly “had to adopt something to save face, and it had become apparent to the globalists that they would not do any better if they delayed a decision.”
U.S. states’ actions ‘central’ to defeating WHO pandemic plan
Action by U.S. states was “central” to defeating the WHO plan to centralize control of public health during declared emergencies, Nass told The Defender.
“Children’s Health Defense and Door to Freedom were central in devising this strategy,” she said, adding:
“The Constitution’s 10th Amendment reserves for the states all powers that were not specifically granted to the central government. Healthcare was never a federal authority.
“Therefore, we urged citizens to contact their attorneys general, governors, legislators — and federal officials — to demand they not turn over authority for health to the WHO.”
Additionally, 22 attorneys general told Biden they would “resist any attempt to enable the WHO to directly or indirectly set public policy for our citizens.”
Numerous states — including Utah, Florida, Louisiana and Oklahoma — wrote legislation to prevent the WHO from overriding states’ authority on matters of public health policy.
“I am certain,” Nass added, “that these efforts reverberated around the world and helped lead to rejection” of the WHO’s proposals.
Truth Comes to Light editor’s note: Below you will find a video released today by La Quinta Columna wherein Ricardo Delgado shares the work of one of their associates, Rafa Calvin, who demonstrates the destruction of (apparent) nanotechnology as found in dental anesthetics (used locally via injection) by applying drops of a distilled water/tobacco mixture. As readers here will know, La Quinta Columna has done great work in researching the graphene and nanoparticles found in the so-called covid vaccines. They have also revealed similar toxins in dental anesthetics.
The video speaks for itself. As the video was produced in Spanish, I have included their transcript (as found in the video) along with a few additional translated notes that were displayed in Spanish without English translation. You will need to watch the video to understand context of Richardo’s words. At approximately 5:05 minutes into the video, the demonstration begins.
This has inspired me to begin researching the medicinal uses of tobacco throughout history and spanning many cultures. As with most natural healing options gifted to us by nature, the strange humans who seek to control by any means have buried the truth and offer us endless toxins in their place — all requiring “money”, thus not only poisoning us, but harvesting our energy by making us work within their system to supply them with “payment”.
La Quinta Columna would like to inform you that we are working on further studies in the light of the recent findings.
Today, Friday 23rd August, we will begin to carry out more tests directly on the Pfizer “vaccine”.
We do not want with this discovery to encourage smoking in the population, only to show the evidence that nicotine, as we already suspected, apparently interacts negatively with what has been introduced to millions of people around the world.
We are continuing our research and will show more results in the near future.
Yours sincerely;
La Quinta Columna,.Ricardo Delgado
Transcript:
Let’s remember some news. Some articles that were published at the time and recently as well.
For example, Turkish doctor:
‘Smoking and drinking alcohol make COVID-19 vaccines less effective.’
And someone will say, from now on… Well, if precisely what they call vaccines, we now know that it is a neuronal implant that precisely amplifies and catalyzes microwave electromagnetic radiation because it contains graphene.
In this sense. Smoking and drinking, as they say here, and we’re not going to encourage that here, eh?
But smoking, which is what we are focusing on, does make them less effective, since it would cause fewer deaths. Right?
That’s the first logic that comes to mind.
The following study tells us:
Vaccines COVID [covid vaccines] and tobacco. Here we are focusing precisely on nicotine.
‘Can smoking affect the effectiveness of Pfizer doses?’ he says.
A study that has yet to be reviewed claims that people who smoke develop fewer antibodies.
Another example. The Infobae newspaper published: ‘Are COVID vaccines less effective in smokers?’
This is to say, do they do less harm? This is the question we have to ask ourselves?
A recent review of studies showed that antibody levels are lower in this group compared to non-smokers.
What is the cause? Well, we are going to read it here because these are his arguments — his lies, in short.
The study here or the news, February 2022, okay?
And we must remember the emphasis that the Minister of Health, Monica Garcia, places on the issue of tobacco. Listen.
[Monica Garcia] ‘Today is a great day for quality of life. Today, the plan for tobacco control that had not been updated for 14 years was approved and I insist that it puts our country back on track…’
And after 14 years it had not been updated and now they are making it more restrictive for the health of the Spanish people above all, right?
[Monica Garcia] ‘The vanguard of the world in the fight of tobacco, which is the main cause of preventable mortality. As I said, it is the cause of 30% of cancers in our country and is also the cause of more than 16 types of cancer. Today we do it…’
We don’t talk about graphene, the cancers it causes and so on. No, we don’t say that. It far exceeds those of tobacco, almost certainly. And in record time, too, eh?
[Monica Garcia] ‘We are going with ambition, we are doing it with pride, we are doing it with coherence, and we are also doing it without fear. Dusting off this plan will give more years of life to our citizens and that will give a better quality of life in those years.’
Clear!…
[Monica Garcia] ‘It is others who will have to explain why they do not want to adhere to this plan. It is others who will have to explain why they turn their back on scientific evidence, why they turn their back on health, why they turn their back on their own technicians, and they will have to explain why they are not in favour of a consensus that I believe is a fairly broad social consensus. Regardless of this refusal, the origin of which we do not know exactly, they will have to explain it to us. I don’t know if they have given in to the pressure. We don’t know if they have already embarked on this established denialism.’
Wow!
[Monica Garcia] ‘that some people in this country have, we don’t know if..’
So, denialism has to do with tobacco?
Do you see how this woman’s subconscious instinctively betrays her?
What does denialism have to do with a proposal to restrict, after all — the sale or prohibition of tobacco in this regard? See?
Because they’re not very smart, huh?
And when she’s reading, it all seems somewhat coherent since they write the speech for her, but when she interprets, she completely screws up.
[Monica Garcia] ‘As if it were already the result of the obsessive attack on the central government. But this attitude will not tarnish the splendid and wonderful news we have today. And I insist that in our country we will once again be at the forefront of the fight against smoking and at the forefront of the fight for the health of our citizens.’
Denialism, smoking!
But this all stinks pretty bad, huh? In the sense of making you see that now, precisely now. This incisive fight against tobacco and which reduces the effectiveness of the COVID vaccine and the effectiveness of what they call a vaccine, which is not a vaccine — will not in any case reduce the effectiveness of this intracorporeal technology introduced?
Indeed, La Quinta Columna has carried out some kind of tests on the part of that follower Rafa Calvin. And he has mixed. Let’s watch the video.
[Video begins.]
Nicotine extracted directly from a gram of tobacco with distilled water and added it to a sample of a dental anesthetic, local, for dental use, where that micro tech appears.
First part 5cc of distilled water, 1 gram of tobacco. Place the mixture in the centre of the object holder.
[Image] Dental anesthetic 30 days drying.
[Hundreds of micro tech bits can be observed at 100x magnification.]
Well, I’m going to make a little clarification for people who are asking what this is. Surely there is still a lot of research time left, even from the year 2021-2022 until now of La Quinta Columna. What we are seeing is an intracorporeal network of biosensors introduced in local anesthetics. OK?
[I put a small amount of the water/tobacco mixture.]
Well, good for Rafa Calvin. Let’s watch another video. I think they show more results here. There it goes.
Let us also remember what we said about nicotine having a neuroprotective action, and that there were some studies that seemed to determine that it could be an effective treatment for diseases such as Alzheimer’s, Parkinson’s and other types of neuropathies.
However, it does not necessarily have to be inhaled and smoked. There are many ways to administer nicotine, including chewing gum. This substance passes in certain doses into the blood, which we now know is contaminated with you know what.
It is an indication that should be tested and more tests must obviously be done.
Starting tomorrow, I’m going to get pure liquid nicotine, which they also sell, and we’re going to test the Pfizer vaccine in different doses and quantities. We will show the results as soon as we have it.
Remember, the original Monkeypox story from 2022? If not, read The Monkeypox Story:
Do you have a desire to swing from trees, pick breakfast bugs off your mate, to screech, yell, and generally monkey around? But seriously….
Back in 2022, the CDC called Monkeypox a “rare” disease, but spreading. The World Health Organization (WHO) declared it a public health emergency of international concern. Amidst many contradictions, suddenly, the story ended. Nothing more was reported. Of course, at the time. another event had taken center stage.
But we all know how stories become epic sagas.
What is once considered rare soon becomes ripe (as a banana) for an epidemic then a pandemic. Give it two years and one outbreak of rash goes global. Today’s Monkeypox story claims that back in 2023 there were warnings similar to HIV-AIDS in how the disease was targeted:
Some of these cases are being found in communities of gay, bisexual and other men who have sex with men. Transgender people and gender-diverse people may also be more vulnerable in the context of the current outbreak.
However, in 2024, Monkeypox has been renamed Mpox, perhaps because we all have shorter attention spans. All reference to HIV-AIDS has all but disappeared. Early reviews of this feature story include the following:
Mpox is an infectious disease closely related to but much less severe than smallpox, and is suspected to originate in African rodents and non-human primates. Mpox spreads through close contact with an infected person, including from sexual and skin-to-skin-contact. Pregnant people can also pass the virus to their child during pregnancy and after birth. The most common symptom of mpox is a blister-like rash that typically lasts for two to four weeks. Other symptoms include fever, fatigue, muscle aches, cough, and sore throat.
New Classification System
This time, Mpox is divided into two clades. A clade indicates a grouping of animals or plants (or in this case, a strain of virus) from a shared ancestor.
There are two main strains of mpox: clade I, which causes more severe illness and has historically been confined to central Africa, and clade II, which has historically caused infections in west Africa.
Why call it a clade when we all know a group of monkeys is a troop?
while the virus was first discovered in monkeys, it’s thought that the natural reservoir of the virus may be a rodent, leading to complaints that monkeypox is a misnomer.
Why shorten the name from Monkeypox to Mpox? Why not just make the “k” silent?
According to a situational WHO report, published in August 2024, as ofJune 2024, there were 175 cases (of Monkeypox) reported across North, Central, and South America; 100 cases were reported in Europe, and 11 cases were reported in Southeast Asian countries.
Looking closer, any image labelled “Monkeypox” could double as an image labelled as Shingles.
Any skin rash often traces back to a congested liver. The liver needs to be cleansed for the skin to clear. According to Traditional Chinese Medicine, there is a blood imbalance, which involves the health of the liver. Even the 2007 Journal of Hepatologystates:
Chronic liver disease of any origin can cause typical skin findings.
What the WHO and CDC have not disclosed is that vaccine ingredients are widely known to cause rashes, often a full body rash.
A vaccine-associated rash is a consequence of an influx of toxins to the body that results in a suppressed immune system. Frequent Strep Throat infections are another indication of a suppressed immune system. A.S.I.A is not a continent when it comes to vaccine damage. A.S.I.A is Autoimmune/Inflammatory Syndrome Induced by Adjuvants, (ie, induced by toxins), where adjuvants are vaccine ingredients (eg. aluminum sulphate).
Dermatological reactions have been reported following Shingrix vaccine administration.
Will Chickenpox become Cpox? Will Horsepox become Hpox?
It is recommended to do your own research. Reflect before you inject.
Spoilers to Endings
Beware of the spoilers! We may know how the story ends! The question is, do we share it and spoil the ending for everyone else?
Recent news reports fail to disclose that in February of 2021, patent application #20210260182 was filed for RECOMBINANT POXVIRUS BASED VACCINE AGAINST SARS-CoV-2 VIRUS. This is a combination pox/COVID vaccine patent filed over a year ago. After all, where there is a will, there is a vaccine patent!
The terms “chimeric” or “engineered” or “modified” (e.g., chimeric poxvirus, engineered polypeptide, modified polypeptide, engineered nucleic acid, modified nucleic acid) or grammatical variations thereof are used interchangeably herein to refer to a non-native sequence that has been manipulated to have one or more changes relative a native sequence.
In some embodiments, the SARS-CoV-2 protein is inserted into the Thymidine Kinase (TK) locus (Gene ID HPXV095; positions 992077-92610; SEQ ID NO: 1) of the horsepox virus or the synthetic horsepox virus.
There are more than 292 COVID-19 candidates’ vaccines being developed as of July 2021 of which 184 are in human preclinical trials.
Problem-Reaction-Solution
In the movie business, sequels are made to increase profit not gained by the first movie. The directors do not always expect people to remember the first version, especially if it was a flop. But now, the virus has mutated! It’s spreading!
But the era of Reverse Genetics is here. That is: engineering viruses from deadly Smallpox, which they admit could lead to the reemergence of Smallpox, as well as to future pandemics.
It’s an aluminosilicate mineral by definition. Silico-aluminate. Powdered aluminum.
Toxic.
Ironically, in the natural health world, zeolite is advertised and promoted as a metal detoxifier; something that binds to and removes metal toxins from the body. Zeolites are promoted in industry to minimize environmental issues linked to landfill disposal leakage.
Zeolites constituent [SiO4]4 −and [AlO4]5 . According to this 2005 article, they share all corners to create a three-dimensional framework structure carrying a negative charge.
Nearly 100 different frameworks have been crystallographically defined for zeolites, and related structures, each one having a unique molecular architecture. The internal dimensions of their channels and cavities are close to molecular dimensions and this has led to their employment as ‘molecular sieves’ and catalysts.
Some zeolite structures, high in aluminum, cannot be used in living systems (in vivo) because they are not stable in acids. But how do zeolite manufacturers assure the right form is used in human health applications?
Normally, waste is incinerated and sent to landfills for disposal. However, with the problems of available landfill space decreasing, hazardous substances leaching out of landfills, not to mention the cost of solidification, or burial of hazardous waste, what can be done?
The ash or residue materials containing rich silica and alumina are dissolved in the alkaline solution to form the aluminosilicate as the precursors of zeolite, after aging for a period of time, the aluminosilicate solution is put into an autoclave to conduct hydrothermal reactions at a specific temperature and pressure and the crystalline zeolite is formed gradually.
The recycling of hazardous waste to become a “healthy” additive is nothing new.
The CDC and U.S. Environmental Protection Agency (U.S. EPA) allow HSFA to be added as “fluoride” to municipal drinking water. For more than 80 years, HFSA has been deemed by “experts” as “safe” in preventing tooth decay. Even though there is plenty of proof that HFSA causes dental fluorosis.
The studies show a lowered I.Q. in any population that drinks fluoridated water. Within phosphate fertilizer waste (HFSA) is arsenic and lead, among other toxins. This leads to numerous forms of cancer in any population that drinks municipal fluoridated, water.
Nanotechnology can be defined as “the art and science of manipulating matter at the nanoscale (down to 1/100,000 the width of a human hair) to create new and unique materials and products…seemingly ordinary materials may behave completely differently than in their larger bulk or macro form.
Due to their small size, nanoparticles can cross biological membranes, cells, tissues and organs more readily than larger particles. Once in the blood stream, nanomaterials can circulate throughout the body and can lodge in organs and tissues including the brain, liver, heart, kidneys, spleen, bone marrow and nervous system. Once inside cells, they may interfere with normal cellular function, cause oxidative damage and even cell death.
Ironically, calcium nano-fertilizer is being used to counter the effects of oxidative stress from fluoride uptake in rice!
More broadly, zeolites are important to the industries of Artificial Intelligence, A.I. Their nano-crystalline structure is useful to biomedical applications, not only as biosensors, but also as: Vaccine adjuvants, Antimicrobial agents, Drug and Gen delivery, Hemodyalisis, external applications, Diabetes Mellitus, Detoxicants, Bone formation, Anti-diarrheal agents, Anti-tumor adjuvants, and Enzyme mimetics.
Before applying zeolite to your routine, or listening to “experts” who promote it for their own profit, do your own research. Even with a lowered I.Q. from drinking fluoridated water, anyone can protect themselves by asking questions and checking the source.
These days, toxins are not only in the water, but also in fast foods, and in the air we breathe. People, who turn to supplements for help, need to ask if any new-and-improved product is safe or shaky?
“Vaxxed III: Authorized To Kill,” launching in over 200 theaters on Sept. 18, chronicles the stories of people injured or killed by the COVID-19 vaccines or hospital protocols. Children’s Health Defense gathered the testimonials during a nine-month, 50,000-mile bus tour across America.
“Vaxxed III: Authorized To Kill” sheds light on the devastating risks of severe injury and death associated with COVID-19 vaccines.
The documentary, which also highlights the tragic fatalities that resulted from COVID-19 hospital protocols, will be released nationwide on Wednesday, Sept. 18.
Children’s Health Defense (CHD) gathered the powerful testimonies that will be featured in the documentary during its 2023-2024 bus tour across America — “The People’s Study.”
According to CHD.TV Program Director Polly Tommey, even before the film’s release, Facebook is reportedly removing posts about “Vaxxed III,” claiming it has been discredited by people around the world.
Tommey described the painful stories she witnessed during the CHD bus tour:
“We were horrified by the COVID hospital protocol deaths, which just kept coming and still are. The injuries from the COVID shots were beyond belief. We thought we had seen it all with the babies’ deaths following routine vaccinations and the Gardasil HPV vaccine injuries and deaths. This time around, we were not prepared for so much death — it was everywhere.”
“Vaxxed III” will launch via a “People’s Premiere,” showing simultaneously in over 200 theaters across the country. Tommey said the film aims to create a powerful grassroots movement, bringing communities around the nation together and empowering more people to share their stories.
The film’s creators are asking people to find a screening near you and buy tickets before Aug. 18, to ensure each theater meets its minimum target — at least 50% of seats must be sold for the showing to proceed, or tickets will be refunded.
Whether a parent, healthcare professional or concerned citizen, “Vaxxed III” offers an opportunity to engage with these critical issues and join a movement dedicated to transparency, accountability and informed choice.
“This film is powerful. It’s the result of 50,000 miles on a bus across the country, hundreds of interviews with doctors, scientists, nurses and parents who will no longer be silenced about the vaccine injuries and hospital protocol deaths they have witnessed.
“‘Vaxxed III’ is more than a movie — it’s a call to action. We encourage everyone to find their nearest showing, invite friends and family and engage in discussion with your local community.”
Be part of the conversation, share your story and help shape the future of public health reform in America. Together, we can prevent this catastrophe from ever happening again.
A multistate outbreak of HPAI A(H5N1) bird flu in dairy cows was first reported on March 25, 2024. This is the first time that these bird flu viruses had been found in cows.
Highly pathogenic avian influenza (HPAI) H5N1 in the hemagglutinin clade 2.3.4.4b,” the virus associated with the dairy cow outbreak, was first detected in a Texas dairy cow on March 25, 2024. Since then, there have been 172 confirmed cases of infected dairy milking cows in 13 states.
The CDC states that today’s suspicious strain of “Bird Flu” is known to cross the species barrier in poultry, dairy cows, as well as in dairy workers! That’s three different species!
Why lump humans into animal categories, unless the government considers humans part of the herd?
The species barrier still exists, even if the definition has been scrubbed from the Internet! Read more here. The UK Dictionary once defined it as:
The natural mechanisms that prevent a virus or disease from spreading from one species to another.
The ‘species barrier’ explains why certain species of animals are not affected by a given infectious agent or parasite. It also describes the phenomenon of natural genetic resistance to pathogens. In general, a pathogen may encounter three successive lines of defense in attempts to infect or parasitize a potential host:
first, the pathogen has to encounter the host animal;
next, the pathogen has to penetrate the body, overcoming mechanisms of nonspecific, natural, constitutional or innate resistance;
the pathogen may also face specific, adaptive or acquired resistance.
In other words, the species barrier makes animals, including humans, capable of resisting major infections. Such a concept explains the strength and power of an individual immune system. However, this would not apply when a substance breaks through the protective skin barrier, say, through an injection.
We don’t catch diseases, we create them by breaking down the natural defenses according to the way we eat, drink, think and live. – Dr. Constantine Hering, Father of American Homeopathy, Hering’s Law of Cure
Culling of Livestock is Common Practice
Whether designated “beef,” “poultry” or “dairy,” if an animal is deemed to be infected with bird flu, what follows is a mass extinction event of the herd and the subsequent elimination of the food supply.
According to Farm Policy News, today, states known for diary and beef herds are reporting higher death rates among cattle. And yet, the USDA insists the meat supply is safe.
Why suggest the flu results in immediate death by culling?
Why? Because every few years, the government justifies livestock depopulation. During the 2020 human pandemic, animal culling promoted vaccination as a viable option for animals [and for humans, as well].
Official 2019 Guidelines for the euthanasia of animals was established in “response to natural or human-made disasters”… “in as humane a manner as possible.”
Is the meat supply safe from Bird flu, but not mRNA, unless you know your farmer?
Fear Dismantles Food Supply Chains
Fear is commonly observed in the face of a pandemic. However, fear and panic should not be the drivers because they lead to irrational reactions. Culling millions of animals with no evidence of actual danger but simply on the basis of fear is setting up a dangerous precedent. – Journal New Microbes New Infect. 2020 Nov
In 2023, ranchers said the killing of 19 feral cattle by helicopter in a New Mexico wilderness area was inhumane. [Note: Feral refers to freely roaming animals]. Yet, ground-based and aerial removal efforts, since October 2021, have substantially reduced the feral cattle population, even without blaming Bird Flu.
Does Bird Flu sound like a bunch of bull?
Long before culling Guidelines, in 2014, under the Obama presidency, the Dept. of Agriculture had killed 2,713,570 animals, of 319 different species. A 2015 article in Mother Jones stated:
much like the actual kill list—the USDA’s operations are shrouded in secrecy, prone to collateral damage…The contradictions can be glaring.
To wit, the USDA killed cats (730) to save rats, but if you’re scoring at home, it also killed 1,327 black rats, 353 Norway rats, 74 Hutia rats, 7 Polynesian rats, 4 bushy-tailed woodrats, and 3 kangaroo rats. It slaughtered more than 16,500 double-breasted cormorants to save salmon. It’s shooting white-tailed deer (5,321) to save various plant species and the small fauna, like rabbits, that eat them. But the woods aren’t safe for Thumper either—the agency bagged 7,113 cottontail rabbits, plus assorted varieties of jackrabbits, swamp rabbits, and feral pet rabbits. The USDA killed 322 wolves and 61,702 coyotes to save livestock, perhaps in an attempt to atone for the 16 unspecified livestock it killed by accident.
If any excuse can result in the official culling of livestock, or freely roaming animals, and flying creatures, then does government-sponsored euthanasia of animals also include the human species?
This essay was written to address the fallacy that technological advances in the 21st century have provided evidence for the virus model. In essence, the technology-driven approach cannot change the fact that the concept of ‘virus’ remains as it was in the 1800s: a mental construct that attempts to explain why organisms become diseased.
The paper also examines the misinterpretations concerning bacteriophages and giant “viruses” and how these entities have been inappropriately placed in the virological realm. As former virologist Dr Stefan Lanka has explained, these entities can be found in nature, isolated and characterised, but they are not pathogenic. The linguistic legerdemain employed by the virologists cannot change biological reality.
Here comes the rain again
Raining in my head like a tragedy
– The Eurythmics, “Here Comes the Rain Again”
The pandemic pandemonium machine appears to be revving up its engines for yet another campaign as Bird Flu Mania Redux is being unleashed across the airwaves, onto every screen and into every cranium still naive enough to believe the masters of microbial terror are on the up and up.
The pandemia industry is rolling out its version of stale, exaggerated plot lines and ham-fisted Hollywood sequels that make Grade ‘B’ movies seem avant-garde.
Hysterical headlines fill the airwaves screeching end-times tales of the coming avian apocalypse:
Running counter to the unsubstantiated caterwauling of the pharma influenced media parrots Mexican Health Secretary Jorge Alcocer countered the WHO’s claim that a 59 year old Mexican man had died from this latest presumed bird flu strain.
In unequivocal terms Alcocer rebuffed the WHO’s latest round of fear mongering stating, “I can point out that the statement made by the World Health Organization is pretty bad, since it speaks of a fatal case (of bird flu), which was not the case.” Noting that the man had numerous underlying medical conditions and had been bedridden for three weeks Alcocer added that the man had, “died from other causes, mainly kidney and respiratory failure.”
Lead role in this latest bird-brained episode of the Avian Flu H5N1 sequel seems to have been handed over to lifelong bureaucrat Rick Bright, former director of the Biomedical Advanced Research and Development Authority (BARDA) and self described Pandemic Nemesis.
Pandemia Theater
All the world’s a stage, And all the men and women merely players; They have their exits and their entrances; And one man in his time plays many parts
– William Shakespeare, from “As You Like It”, spoken by Jaques
No stranger to the bright lights of pandemic theatrics, Rick Bright was recently showcased at a Council on Foreign Relations (CFR) webinar, “Avian Flu Outbreak and Preventing the Next Pandemic,” that was broadcast to 300 state and local officials from 47 states.
Bright kicked off the hifalutin CFR symposium with an oblique reference to this latest viral hobgoblin, menacingly pronouncing it to be a “shapeshifter.”
With nary a piece of evidence in sight, Bright commenced to “educate” the audience on this potential plague with a performance reminiscent of the Mad Hatter:
“We know it can rapidly change. We know it can jump to different hosts and different species rapidly, and change, and evolve.
“And those mutations can help it be more lethal, or adapt, or spread to humans and other hosts. Sometimes because the genetic makeup of the virus is fragmented, there’s all these segments inside that virus, you can have two viruses infect a person, or an animal, or a seasonal virus and the H5N1 virus. And they’ll recombine and reassort. And you’ll have this virus that comes out with some of the best or worst of all worlds. And so we know the tricks of this virus.”
Bright’s breathless rambling of ifs,ands, ors and mights, coming on the heels of the most massive medical money grab in history might cause one to pause and consider the reliability, if not integrity, of such pronouncements.
These doomsday warnings come from the same pandemic fanatic “man-in-the-know” who in October of 2019 bizarrely foreshadowed the coming covid storm, “But it is not too crazy to think that an outbreak of a novel avian virus could occur in China somewhere.”
Lessons From the Past: Avian Flu 2005
“I don’t know of any biotech company that’s so politically well-connected”
– Andrew McDonald, analyst at Think Equity Partners referring to Gilead Sciences Inc.
For those who still do history it’s worth noting that the original H5N1 fright flick was shown across TV screens back in 2005.
In the original screenplay then President Bush primed the panic button by declaring that a minimum of 200,000 people would die from the avian flu, with as many as 2 million dying in the US alone.
President Bush called for $7.1 billion in spending to “stop the spread” of this fearful, feathered contagion and prompted Congress’ enactment of the infamous Public Readiness and Emergency Preparedness Act (PREP Act).
This key Act, invoked during the covid crisis, protects pharmaceutical manufacturers from financial risk during a declared public health emergency. The act specifically provides immunity, from Federal and State liability, to drug makers involved in the manufacture, testing, distribution, administration and use of countermeasures, arising from public health emergencies.
While it’s not clear if even a single soul in the US perished from this predicted plague, what is clear is that certain companies and well-connected individuals made a killing off these dire prophecies.
Before taking a position in the Bush administration, as US Secretary of Defense, Donald H. Rumsfeld, served as Chairman of the Board of Gilead Sciences Inc., a biopharmaceutical company that focuses on developing antiviral drugs. In 1996 Gilead would patent the drug Tamiflu which was marketed as salvation for the pending avian armageddon of 2005. Gilead Inc., is also the developer of the controversial drug remdesivir that was used in covid protocols.
The avian flu scare of 2005, promoted by the Bush administration, would ultimately be used to justify the purchase of $2 billion worth of Tamiflu and as luck would have it Donald Rumsfeld would make more than $5 million in capital gains from selling his shares in Gilead.
Back to the Future: Follow the Money
Birds have been on this planet, Miss Daniels, since Archaeopteryx, a hundred and forty million years ago. Doesn’t it seem odd that they’d wait all that time to start a…a war against humanity.
In Hitchock’s classic, while trapped in a house that is being pecked into oblivion by an inexplicable mass bird attack, Cathy desperately asks a beleaguered Mitch, “Why are they doing this, the birds, why are they trying to kill people?” Mitch responds, “We don’t know, honey. I wish I could say.”
In this latest Pharma production there’s no need to look to the heavens for a supernatural explanation. Bereft of new ideas the pandemic profiteers pull from their predictable playbook, complete with tired lines delivered by some of the same seedy CDC actors, Reciting the sweet syrupy notes straight from the BioPharma hymn book, the all too human actors and their mendacious mouthpieces give away the hustle.
Shortly after his performance at the influential CFR, Rick Bright made an appearance on the Biocentury Show and spoke to the supposed need for better surveillance, speedy mRNA vaccines, better therapeutics and the need to stockpile all of the above to be better prepared for alleged bird germ emergencies.
In that interview Bright went through the entire pandemic preparedness inventory, a wish list every Pharma executive dreams about. In a single sentence the not-so-subtle Pharma lifer gave away the not-so-hidden secret as to how this racket would be financed, “Industry will respond if the government makes the money available.”
When translated, Bright’s coy confessional is an unambiguous lesson in how to siphon off public monies for private interests.
They will invent the problem.
Problem-Reaction-Solution
One day, a leaf landed on Chicken Little’s tail. Chicken Little feels the leaf and jumps in surprise. He ran to Henny Penny and cried, “The sky is falling!” “Oh, I must tell everyone!” cried Henny Penny. Chicken Little jumps up and down in panic! Henny Penny looks worried. Soon, Henny Penny met Ducky Lucky. “The sky is falling!” cried Henny Penny. Ducky Lucky asked, “How do you know that?” “Chicken Little told me,” said Henny Penny. “We must tell everyone!” cried Ducky Lucky. … Soon, they met Foxy Loxy. “The sky is falling!” cried Turkey Lurkey. Foxy Loxy asked, “How do you know that?” “Goosey Loosey told me,” cried Turkey Lurkey. “Ducky Lucky told me,” cried Goosey Loosey. “Henny Penny told me,” cried Ducky Lucky. “Chicken Little told me,” cried Henny Penny. The birds point back at each other. Chicken Little covers his eyes.
“Look!” said Foxy Loxy. “Do you see the sky falling?” “No, we don’t see it falling,” they said. “Listen!” said Foxy Loxy. “Do you hear the sky falling?” “No, we don’t hear it falling,” they said. “Feel!” said Foxy Loxy. “Do you feel the sky falling?” “No, we don’t feel it falling,” they said. “Silly birds!” said Foxy Loxy. “Next time, see, hear, and feel for yourselves before you tell everyone else!”.
– “Chicken Little: The Sky is Falling” – An English Folk Tale.
The pattern of problem-reaction-solution embedded in The Hegelian Dialectic is a repeating pattern that plays out in reality.
This analytical lens is “frequently used to scrutinize major global events and policies [and] suggests that powerful groups or entities engineer a problem, anticipating a public reaction that allows them to offer a pre-planned solution. While ostensibly solving the issue, these solutions often serve hidden interests, whether they be financial gains, increased power, or expanded control.”
In the universe of the Pharmaceutical Industry this is a seasoned and time honored strategy.
In the theatrical production of Avian Flu 2024, the media-manufactured fowl-based fear factor was founded on a mere four “confirmed” cases “discovered” in dairy workers. The primary symptom that sounded the alarms for the Pharma friendly bureaucrats at CDC Inc. was conjunctivitis (pink eye), a catch-all term for inflammation of the eye.
Eliminated from consideration were more reasonable explanations for why farm workers might have eye irritations such as, ever-present dust and dander found on farms, the boatload of chemical residues (from Roundup e.g.) that circulate throughout factory farms, or the ubiquitous dairy farm mountains of manure which release toxic ammonia.
To kick start the next pandemic bonanza the virus hunters, who dutifully serve the pharmaceutical syndicate, call upon the tried and true PCR shell game to hornswoggle the public into believing that another sinister, free-floating microbe is on-the-move.
Known for its ability to be manipulated in order to obtain the desired results, the decidedly non-diagnostic PCR process has proven to be the perfect tool for the art of medical deception and for casting a spell on an ill-informed public. No matter the well-documented history of PCR being used to invent non-existent epidemics and to “identify” non-existent diseases the PCR voodoo is being rolled out yet again as proof positive that this bird flu baddie represents reality.
Truth to be told, identifying The Virus™ is nearly superfluous, as all they need to do is create the perception of a pandemic, manufacture mass panic with staged Hollywood productions, and doomsday models and use the fraudulent PCR tests to manufacture the perception of an incoming alien invasion.
The CDC then starts squawking about another “deadly virus” in order to justify a multi million dollar government handout to a Pharma darling, like the recent $176 million government giveaway to Moderna to develop an “mRNA bird flu pandemic vaccine.”
Voila! Another boondoggle to funnel tax dollars to Pharma executives and shareholders.
You’d think by now it would be glaringly obvious the emperor’s wearing no clothes and that the only pandemic to be feared is not coming from barnyard animals but one of snake oil salesmen.
Whatever their motives, be it the sadistic inclinations of Nurse Ratched dying to jab everyone again; or Billy Bug Gates and Co. looking to decimate the food supply by culling millions of birds and cattle in order to crank up his failing bug and chemical fake meat factories; or central bankers looking to give payouts of fake currency to farmers for their “losses” in order to further exacerbate hyperinflation in order roll out their CBDCs, one thing is for sure, despite all advertisements none of this is being done for public health.
So the next time you hear the carnival barkers of the Medical Mafia and their media parrots whistling dixie about some deadly bird bug ignore their self-serving hype and whistle your own tune:
Take these disasters: pesticides that disrupt hormone levels; plastics everywhere; chemicals in dead processed foods; infant formula replacing breast milk; vaccines that disrupt and shred the immune system.
THEN researchers come along.
They take the symptoms these disasters create and cluster them in groups and put medical labels on them.
ADHD, depression, Bipolar, gender dysphoria…
When it comes to disruption of the immune system from pesticides, plastics, no breast milk, dead processed food, etc., look at this boggling list of “immune system diseases” the medical system has invented:
Other Conditions:
Inflammatory Bowel Disease (IBD), including Crohn’s Disease and Ulcerative Colitis
Guillain-Barre Syndrome
Dermatomyositis
Scleroderma
These guys really know how to label.
They’re experts.
They can cluster and carve up symptoms and come up with medical names from here to the horizon.
They can resist any attempt to see how pesticides or infant formula or processed foods are the actual realities.
You can see why.
For every disease label, there are medical treatments. Drugs.
Treatments and drugs=$$$.
Plus control over the lives of patients.
There’s a much longer list than the one I just published above. It’s the total of diseases based on…
Viruses that don’t exist.
Brought to you by The Label Kings.
If I were a greedy young psychopath starting out in the world today, I would major in Communications at a prestigious college and write a thesis titled:
“100 ways to recycle death and label it with many disease names.”
With that thesis in hand, I would land a very nice starting position with one of the largest pharmaceutical companies in the world.
They would see my value immediately.
Now consider a doctor’s point of view. A patient comes in with complaints. The doctor can listen, run a few tests, slap on a disease label, and prescribe a drug, or he can say:
“Looks to me like you have pesticide poisoning. I don’t know what to do about that. I don’t have a remedy that takes the poison out of your body.”
He wouldn’t say THAT if you had him in chains and were beating him with a club.
If he had that degree of honesty, he’d be out of business pretty quick. And eventually he’d find himself in front of a state medical board trying (and failing) to keep his license.
The board idiots and sold out quacks would rake him over the coals.
Why not take easy road instead? He closes his eyes, throws an imaginary dart at an imaginary dart board and comes up with a disease name the patient never heard of.
“This is what you’ve got,” he says to the patient. “We have a course of treatment for it. Let’s begin.”
And so they do.
On the long march to nowhere.
CODA: To explore the fake science that led to the fake pandemic that led to the COVID “vaccines,” read Dr. Mark Bailey’s and Dr Sam Bailey’s book, The Final Pandemic. This dynamic duo has their hands on real science. It’s a powerful antidote to mainstream nonsense.
by Andrew Kaufman, MD sourced from Andrew Kaufman MD newsletter May 31, 2024
When it comes to diet and nutrition, the last place you want to go for advice is the medical establishment. Their definition of a “healthy” diet will likely put you on the stretcher…
That means that you’re going to have to do your own homework, and that’s no small feat considering all the conflicting views on what a “healthy” human diet actually is, especially when it comes to men’s health…
Knowing full-well that grocery shelves are filled with synthetic, hormone-disrupting garbage—slowly turning strong, defiant men into docile yellow-bellies—the ability to recognize which foods will optimally strengthen you both physically and mentally becomes critical in these times…
I’ve been tumbling down this neverending nutritional rabbit hole for a long time now, and I’ve encountered many invaluable voices. But there’s one individual who stood out like nobody else… the illustrious Dr. Paul Saladino.
Paul has been at the forefront of the carnivore community for a long time, so much so that he has even worn the title of “Carnivore MD”…. And he’s an archnemesis of Big Pharma and its evil twin-brother, Big Food…
Occasionally dropping by places like McDonald’s and Chipotle to reveal the harmful ingredients contained in their infamous “Happy” meals and Mexican burritos made him extremely popular on Youtube…
(It’s useful to know when your son’s Chicken McNuggets are fried in seed oils and contain a whopping 30 ingredients you couldn’t pronounce if you tried.)
After 2 years of doing the carnivore diet, Paul eventually decided to add organic fruit and honey into his diet. And since those foods don’t exactly typify a carnivorous diet, he morphed it into the rubric of ‘animal-based,’ with the addition of various organ meats and raw dairy products.
Being a broad-minded thinker, and no stranger to controversy, like myself; Paul was bound to be a guest on my Healthy Living Interviews series, and today we finally made it happen!
During our remarkable discussion, Paul reflects on his long-distance journey of becoming a psychiatrist, and how he eventually parted ways with the allopathic priesthood and adopted a natural approach to healing…
“On the first day of medical school, they told me: ’50% of what you’ll learn is going to be wrong.’ I found it very ironic when a physician questions anything dogmatic in medicine and then gets thrown out of the kingdom.”
We also touched on the difference between beneficial and unhealthy carbohydrates, the xenoestrogen deluge and its effects on men’s hormones, and the perils of seed oil consumption.
I have much appreciation for Paul and his inspiring work. It’s rare to find avid contrarians like himself who continue to point our collective understanding of health in the right direction.
The World Health Organization (WHO) is set to convene the 77th World Health Assembly (WHA) meeting for May 27 – June 1, 2024 at the plush InterContinental Hotel in Geneva, Switzerland.
This in-person meeting of the WHA, the decision-making body of WHO, will bring together senior representatives from governments, multilateral organizations, and the private sector to discuss two international legal instruments intended to increase WHO’s authority in identifying and managing health emergencies.
The two documents, (1) Amendments to the 2005 International Health Regulations (IHR), and (2) A Pandemic Treaty, termed ‘ÇA+’ by the WHO, when viewed together in the context of the globalist pandemic preparedness agenda represent an ambitious attempt towards monopoly power in global health governance.
These two instruments, the Pandemic Treaty and the IHR Amendments, are designed to operate in concert and consolidate the influence of the WHO as the world’s “global health authority.” If adopted and approved by member states these proposals would bring about significant changes in how the WHO operates.
The draft IHR amendments would lay out new powers for the WHO during health emergencies, and broaden the context within which they can be used. The draft CA+ (‘treaty’) if implemented would support the bureaucracy, financing and governance that underpins the expanded IHR amendments.
Under the guise of a “One Health” approach these proposals and amendments would grant the WHO sweeping powers, under its Director General, in the arena of health management and broaden the WHO’s reach into areas of governance on food economies, the environment and issues surrounding allocation of national resources.
If implemented, the IHR Amendments and the Pandemic Treaty working in tandem would grant administrative authority to unelected and unaccountable bureaucrats at the WHO.
These unilateral, wide-ranging decisions would assuredly benefit those who work for the various public-private partnerships that control the financial and political machinery of the WHO.
While there are countless reasons this latest hijacking of power by the WHO must be opposed, the list below highlights some of the primary concerns and consequences entailed in the IHR amendments and Pandemic Treaty:
Changes the existing IHR provisions from non-binding “advice” to legally binding regulations;
Allows the WHO to declare a Public Health Emergency of International Concern (PHEIC) which can oblige national governments to “undertake” border closures, lockdown of individuals, mandated medical examinations and vaccination;
Expands the WHO Director General’s (DG) authority to unilaterally declare a Public Health Emergency of International Concern (PHEIC);
Empowers Regional Directors to declare regional public health emergencies;
Expands the definitions of what constitutes pandemics and health emergencies;
Maintain a perpetually operative pandemic preparedness bureaucracy through the development of a “framework convention” that would establish a new $30 billion per year international health authority. This new global health bureaucracy would choreograph the WHO’s role in developing global “allocation plans for health products” (including vaccines);
Require member States to support censorship and suppression of information that diverges or dissents from WHO opinions and directives;
Sets up wide-ranging health surveillance systems in all member States, which WHO will monitor regularly through administrative mechanisms;
Gives WHO control over some measure of country resources, including requirements for financial contributions to fund “capacity building and “technical assistance” structures by requiring a percentage of national health budgets be devoted to health emergencies as defined by the WHO;
Removal of a clause that required regulations must be in accordance “with full respect for the dignity, human rights and fundamental freedoms of persons”, and replacing it with a new clause that reads regulations shall be “based on the principles of equity, inclusivity, coherence and in accordance with their common but differentiated responsibilities of the States Parties, taking into consideration their social and economic development”;
Expands WHO’s scope by emphasizing a ‘One Health’ agenda which includes a broad range of health, economic, social and political life which impact health, and therefore fall under the dictates of a declared international health emergency.
In addition to creating a multi-billion dollar self-perpetuating pandemic-preparedness industry, which will fund itself by looting the world’s taxpayers, this latest power grab by the WHO and its globalist sponsors represents a fundamental threat to national, medical and bodily autonomy and is a clear and present danger to the citizens of the world.
This entire process under which unelected delegates negotiate terms and conditions which would place people at the mercy of medical officers, public health bureaucrats and health enforcement gendarmes, who will be immune to any penalty for any acts carried out in the name of “public good,” stands in direct opposition to, and are in direct violation of informed consent and stands in direct opposition to multiple long-standing national and international principles of medical ethics such as:
The Nuremberg Code of 1947: ′′The consent of the human subject is absolutely essential. The International Covenant on Civil and Political Rights resumed this ban against unintentional experimentation, in its 1966 text, which states: no one may be subjected without his consent to medical or scientific experiment.”
The Geneva statement for doctors from 1948: “I will respect the autonomy and dignity of my patient. I will not use my medical knowledge to infringe human rights and civil liberties, even under force. I will keep absolute respect for human life, from conception. I will consider my patient’s health as my first concern.”
The Declaration of Geneva of the World Medical Association that binds the physician with the words, “The health of my patient will be my first consideration,” and the International Code of Medical Ethics declares that, “A physician shall act only in the patient’s interest when providing medical care which might have the effect of weakening the physical and mental condition of the patient.”
The Belmont Report on voluntariness which asserts, “[the] element of informed consent requires conditions free of coercion and undue influence. Coercion occurs when an overt threat of harm is intentionally presented by one person to another in order to obtain compliance. Undue influence, by contrast, occurs through an offer of an excessive, unwarranted, inappropriate or improper reward or other overture in order to obtain compliance.
Unjustifiable pressures usually occur when persons in positions of authority or commanding influence — especially where possible sanctions are involved — urge a course of action for a subject.”
UNESCO’s Universal Declaration on Bioethics and Human Rights in 2005: “to provide a universal framework of principles and procedures to guide States in the formulation of their legislation, policies or other instruments in the field of bioethics [and to] promote respect for human dignity and protect human rights, by ensuring respect for the life of human beings, and fundamental freedoms, consistent with international human rights law.”
The World Health Organization, a UN agency with no national legal oversight and no legal accountability at all, seeks to establish itself as global health dictator by demanding member States respond to perceived threats through autocratic decrees formulated and given by the WHO which are certain to accrue profits and power to its corporate sponsors.
Make no mistake, whatever bylines and selling points the WHO offers, be it called “treaty,” “agreement” or “accord,”the practical intent and desired effect of this latest autocratic assault on our rights is to create the legal and financial basis for an internationally coordinated bio-surveillance regime that will significantly strengthen the authority of the World Health Organisation.
The historical precedence of coercive and oppressive actions seen throughout the Covid-19 crisis provides a clear warning to all and demonstrates that the WHO will assuredly attempt to leverage the Pandemic Treaty and IHR Amendments to gain monopoly power through a global health governance pact that will inevitably result in global health despotism.
The WHO Pandemic Treaty which creates a world of “declared pandemics” and rolling “perpetual lockdowns” that will take away people’s inalienable human rights and bodily autonomy must be rebuked by all citizens of the world and formally rejected by all local, state, regional and national governments of the world.
“The degree to which the psychiatric community is complicit with abusive parents in drugging non-compliant children is a war crime across the generations, and there will be a Nuremberg at some point in the future”
~ Stefan Molyneux
I will step away from my normal correspondence in order to address a purposely-generated problem that has reached heights of abuse so extreme as to have grossly compromised one in nine children in this country. This intentionally manufactured problem is insanely egregious, and has caused irreparable harm due to the administration of psycho-stimulation drugs prescribed to mostly children, and in many (most) cases, has destroyed their ability to think, function normally, live active and fulfilling lives, and to exist without devastation of their health, mind, body, and soul. I am speaking of what is dishonestly labeled as ‘ADHD,’ or Attention Deficit/Hyperactivity ‘Disorder,’ a bogus scam meant only to achieve wealth, power, and control of a large segment of the young in society, without any physiological evidence whatsoever.
I was first introduced to this State-supported atrocity 25 years ago, when the government (‘public) school system attempted to erroneously ‘diagnose’ and drug my granddaughter with what is the equivalent of cocaine on steroids for a non-existent ‘disorder.’ She was only 6 years old at the time, but I was able to get her out of the heinous ‘public’ school system and into a private school that did not promote (force) the drugging of children. This began my research efforts into this collaborative and criminal government’s fascist partnership with pharmaceutical companies targeting kids.
This was (and is) in essence, a domestic false flag operation targeting the young, with a multi-dimensional agenda that could at the same time disturb the mental capabilities of a large swath of the youngest generations. This of course, would lead to a compounding effect over time, breeding a more obedient and a less intellectual population. It could cause additional health-related problems for life, serve as a control mechanism based on the compromising of brain and motor functions of the young through central nervous system damage, and could easily lead to a much more compliant society so as to enhance the ability to manage and regulate large numbers. This is all based on the greatly enhanced wealth of the few, gaining governing power, and a higher level of control over the collective herd of the dumbed-down masses.
There is no such thing as ADHD! Period. No brain condition, no brain damage, ‘mental’ or physical, no physiological evidence whatsoever exists, or has ever been demonstrated to prove that any cause dishonestly referred to as ADHD is valid. None.
What has been proven and is obvious, is the horrible damage done due to the administration of harmful drugs, especially to the bodies and minds of the not fully developed, and immature young. The so-called (illegitimate) ‘treatment’ for the fake ‘disorder’ called ADHD is Ritalin, a most devastating and mind-altering drug to be certain. The properties of Ritalin as opposed to cocaine are staggeringly similar, and in fact, are two sides of the same coin, except that Ritalin has longer lasting adverse effects. Cocaine is said to be plant based, while Ritalin is said to be chemically based. In simple terms, and from a comparative analysis, the differences are few. Ritalin is the immediate-release form of methylphenidate, and is classified as a central nervous system stimulant or psychostimulant. in fact, it has been classified as a Schedule II drug, which is in the same class as cocaine, Vicodin, methamphetamine, methadone, hydromorphone, Demerol, OxyContin, fentanyl, Dexedrine, Adderall, and Ritalin.
Ritalin’s side effects, and many are not even listed here, are astounding. They include allergies, hives, swelling, extreme heart problems, psychosis, circulation problems, increased blood pressure, mood changes, anxiety, nervousness, irritability, inability to sleep, fast heart rate, heart arrhythmia, no appetite, extreme weight loss, nausea, vomiting, pain, headache, dizziness, disorientation, aggression, hostility, paranoia, and loss of coordination. This is in addition to possible permanent brain damage. All of these side effects can also be enhanced to even more dangerous levels when other drugs, anti-depressants, and even over-the-counter ‘medications.’ are co-mingled. Given the massive prescribing and administration of drugs for everything and everybody today, the risks are astronomical. Also, the risk of dependency (addiction) is great as well.
The incidence of diagnosis of this bogus ‘disorder’ has increased steadily year after year. Since 1997, and just up to 2017, the increase in stated cases rose by approximately 145%. The rate of diagnosed cases by that time were over 11% of children under 12 years of age. In addition, more cases are said to be dramatically increasing in older children and adults, opening up much larger markets for higher profits for the murderous pharmaceutical companies.
This is an abomination, as it is the literal destruction of a large percentage of children. Much of this criminal medical scam is based on fear of one’s child being ‘different,’ which should be applauded, instead of suppressed. Today’s parents are much at fault (or most) for allowing the State and its partners in crime, to dictate how their children should be raised and drugged to suit the perverted mores of the ruling class’s idea of societal collective mediocrity. There is another degrading aspect to this dilemma, as parents today, many who have been ‘forced,’ (due to voluntary support of the State) both married couples and single parents, to work outside the home, leaving their children to be raised by the evil governing and schooling systems. This in my mind is the abandonment of family for the sake of material survival, which would never have been prevalent if government instead of family had been abandoned.
Every child, every human in fact, is different from every other. We are unique as individuals, and that uniqueness should be cherished. Wants, needs, intelligence, interests, personality, desire, energy levels, talents, hopes, and dreams, are destroyed when all attempt to stifle individual excellence in favor of conformity. When the individual is sacrificed for the so-called ‘good’ of the collective crowd, an inferior society will be the result, and independence, strength, self-ownership, and self-responsibility, will be discarded in favor of sameness, universal attitudes of victimization, boredom, and depression.
This is why the drugging of society, especially the current and future generations of the impressionable young, are targeted by this fascist and criminal State. The older generations still exist in large numbers, but their lives are not long for this world. In two generations only, all will dramatically change. If the young are fully controlled due to indoctrination, AI, technocratic design, drugs, and propagandized from birth, the controlling element of this world will have an easy time eliminating all dissent, while creating an entire society of drone-like mannequins accepting of their own dependency and enslavement.
There is a reason that the young are being dumbed down and targeted from every angle, manipulated to never question false ‘authority,’ to forget and eliminate tradition, to abandon family, and to hate everything and everybody. The State and its criminal partners fully understand the path they are taking in order to achieve its goal of creating a kept and indifferent society of slaves. The medical fraud, including the toxic and fatal poisoning by lethal injection of bioweapons called ‘vaccines,’, and the extreme drugging of youth, including the ADHD and Ritalin crime, is just one aspect of this terror being inflicted on society.
To stop this deadly assault, parents have to once again become parents, instead of worthless, pathetic, dolts worried more about their phone, games, and constant personal desires that run completely counter to the well-being of their own children.
In an April 16th interview with Polly Tommey, Dr. Paul Thomas, explained how the American medical establishment incentivizes pediatricians to fully vaccinate their young patients, and fines them if they don’t. Vaccinations that have been proven to cause more death and harm than the diseases they are said to be preventing.
“Well, as other practices started kicking people out of their practices if they weren’t following the CDC schedule, I was getting more and more families who didn’t want to do any vaccines. Which was fine with me. So we took an entire month of every single billing sheet. And on every visit, on the back of that, our providers would mark off what vaccines we recommend according to the CDC schedule. Families could decline them. And then our billing department, insurance company by insurance company, vaccine by vaccine, we looked at how much money was being lost for vaccines that were refused, just the admin fee.
So there’s three main ways you make money off of vaccines in pediatrics. The number one is the admin fee. And you get about, it depends on the insurance company, every contract’s different, but I would average it out to say about $40 for the first antigen and $20 for each subsequent antigen. So let’s just say a two month well baby visit. There’s a DPT. That’s three shots, three antigens. Hib, Prevnar, HepB, Polio, Rotavirus, six shots, eight antigens, about $240. Thank you for giving those shots. Multiply that by the fact that I was getting 30 to 40 newborns per month. They’re coming in repeatedly at two months, four months, six months, nine months, twelve months, fifteen, eighteen months, and age two. So we looked at the admin fee loss and from my practice that was billing at that time, about 3 million gross, we were losing a million dollars, over a million dollars, in vaccines that were refused. So you cannot stay in business if you’re not giving, pretty close to the CDC schedule. It just doesn’t pencil out economically at all.
But let me tell you about the other two ways we make money from vaccines. One is the markup. That’s,that’s small. They don’t allow a lot of profit on vaccines as far as markups. But they do this thing called incentives or bonuses. And it’s called a “Quality Bonus.” Well in pediatrics, one of the main quality measures is how well you vaccinate. Isn’t that interesting? It has nothing to do with how healthy your kids are. Like when I studied my vaxed vs unvaxed patients, the unvaxed were so incredibly healthy. They rarely got sick. They rarely would end up in an emergency room or in a hospital or with any chronic condition. So being unvaxed results in very healthy kids who don’t use a lot of medical dollars. Every health system should want that. But it’s reversed, it’s all flipped, It’s bizarre.
You’re supposed to have had your kids up to date about 80% of them by age two. Guess what percentage of my population was at fully vaccinated at age two? 1%. The goal is 80%. So Doctor Paul gets an F minus. Basically what that means is not only do I not get paid the normal amount for everything else we do in the office, I get dinged maybe 10 or 15% off of those RVUs, relative value units, that are ascribed. To everything you do in medicine is given a value. If you do very well on your quality measures, you’re a really good vaccinator, you may get an additional 10% on everything you do in your office. That’s huge.
SIDs is sudden infant death syndrome. When you hear the word syndrome, it means we don’t know what it is. We don’t know what causes it. Well, we actually have a pretty good clue because there are six data sets. Studies that looked at SIDs when that infant died, relative to when they got a vaccine. In one data set, 97% were in the first ten days after the vaccine. For the six other studies, a couple of them showed that 50% of the deaths happened in the first week. But 75 to about 90% of those deaths are happening in the first week after vaccines in all these studies. We’ve known this for decades. The countries that have the most infant vaccines have the highest infant mortality. Guess where the US stands? We are number one in infant vaccines. We are number one in industrial countries for infant mortality.
There’s a document, 450 page legal document, that has tables showing for every single disease for which we have a vaccine, there are more deaths from the vaccine than there are from the disease for which we have that vaccine.”
I’ve been told the CDC expects every child to receive 70 shots in the arm between birth and 18 years of age.
I recently took a look at the CDC childhood vaccine schedule. I found the tables confusing.
But I did note the two lists of vaccines they want kids to take between birth and 15 months, and then between 18 months and 18 years old.
This isn’t the number of injections; it’s the number of vaccines.
Between birth and 15 months: 20 vaccines.
Between 18 months and 18 years old: 20 vaccines.
40 vaccines. FORTY.
20 during the most vulnerable period possible—birth to 15 months. And that doesn’t include vaccines the mother took during pregnancy.
So the CDC is Murder Incorporated.
Show me the hundred well done studies that prove 20 plus 20 vaccines are safe.
Also—show me one well done study against another large study of children who were never vaccinated. Compare overall health in the 2 groups.
No? You can’t?
There is no science going on.
Imagine this. A sales person approaches a parent. He says, “I have a very low-cost offer. Here are dozens and dozens of chemicals and random biological materials I can inject into your child between birth and 18 years of age. How about it? It’s a great deal.”
Did you know that the CDC has an adult vaccination schedule?1 It’s been around for 22 years, growing and changing.2 Promotion of routine adult immunization started around 1990 but wasn’t formalized into a schedule until 2002.
The federal government has embraced vaccination as “a lifespan approach, covering vaccination from before birth into old age,”3 basically, from womb to tomb. This is laid out in its National Vaccination Plans, which were mandated by U.S. Congress in 1987.
The Adult Immunization Schedule has been a bit of a sleeper, but in recent years, when listening to the CDC’s Advisory Council on Immunization Practices (ACIP) meetings, we hear about it more and more. What changed? Let’s start at the beginning.
What Is the Adult Schedule?
In 1991, the CDC acknowledged in its weekly public health report that vaccination in adults wasn’t typical.4
The very first time the CDC pulled all their immunization recommendations into one place was in their weekly publication “Morbidity and Mortality Weekly Report” (MMWR) in 1969.5 Those recommendations laid the foundation for what we now recognize as the “schedule.” This first publication included dosage recommendations for adults, but those dosages generally were for shots missed in childhood or special circumstances like travel. It was not until many years later that the idea of an adult schedule was independently promoted. Other than influenza, the shots were targeted toward common childhood illnesses, and there wasn’t much to promote for adults.
The face of public health, and thus immunization, changed in 1979 when the federal Department of Health, Education, and Welfare (the predecessor to Health and Human Services) released a report titled “Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention.”6 That publication marked the beginning of a new era of emphasis on population health. It was unique in its structured, data-driven approach to setting and surveilling health policy goals for our nation.7 This approach gave it longevity and flexibility and created the foundation for a new, decades-long infrastructure of setting health policy goals through identification of specific objectives with measurable targets, starting with “Healthy People 1990,” (launched in 1980) that continues to the latest “Healthy People 2030.”
The 1980s were tumultuous for vaccine policy. The expose “Vaccine Roulette” aired in 1982, helping parents across the country (and the globe) connect the dots on symptoms their children suddenly acquired after routine vaccination with DPT. The awareness congealed into a movement of parents who ignited a fire under U.S. Congress about the injustice of following the federally recommended childhood schedule only to find it was not safe for their babies. This outcry culminated in the National Childhood Vaccine Injury Act, known by many as the “1986 Act,” which removed liability from manufacturers. (You can do a deep dive on DPT in our article, “Shining a light on Pertussis & DPT: the vaccine that shut the courthouse doors.”)
While the 1986 Act was being debated, 1985 saw two measles outbreaks on college campuses.8 With vaccines in mind, a joint resolution was adopted by Congress that was signed by Ronald Reagan into law, acknowledging the last week in October as “National Adult Immunization Awareness Week.”9 The intent behind the resolution was to prevent deaths from influenza and pneumonia in older adults, but the college measles outbreaks were mentioned as justification for needing to raise awareness of vaccination among adults.10 Baked into federal adult immunization policy was the intent that the awareness week was “only the beginning.”
Source: Congressional Record, Aug. 13, 1986; remarks by Sen. Orrin Hatch, sponsor of the joint resolution.
A National Coalition for Adult Immunization (NCAI) was formed shortly after, in 1988, to align “public and private resources to achieve Healthy People national goals.”
The 1979 report that inspired “Healthy People” only mentioned adult immunization in passing.
And the follow up report in 1980, “Promoting Health, Preventing Disease,” which came to be known as “Healthy People 1990,” provided 226 health policy goals with targets to be reached by 1990, but did not dive into adult vaccination.11
Regardless, the CDC fell in line with NCAI and started calling on doctors to include adult immunization as “a routine part of their practice.” In the 1991 publication where the CDC changed its tune on adult immunization, they reasoned that we couldn’t eliminate all illnesses because some adults were still “at risk” of getting sick from diseases on the childhood schedule if they were never vaccinated or weren’t sick in childhood. That said, there weren’t many action items because there weren’t many vaccines licensed to be marketed to adults.
After the 1986 Act, many vaccines were added to the childhood schedule. When the pneumococcal vaccine was added in 2001, it was licensed both for adolescents and adults. The promotion of adult vaccines picked up again for that moment in time. In 2002, the CDC unveiled its first official adult schedule. In short, healthy adults who had already been following the CDC’s childhood schedule were recommended annual flu shots, tetanus boosters every 10 years (generally at the time given in tandem with diphtheria as a TD shot), and the newly added pneumococcal recommendation for people who were 65 and over.
Note that right now COVID is recommended as “one or more doses,” which basically means there’s a blank check for how many shots will be recommended. The FDA and the CDC, along with their advisory committees (ACIP and VRBPAC respectively), have contemplated annual doses, but there’s also discussion of targeting strains. In other words, what will be recommended is yet to be seen.
One thing we can say for certain is that back in 2002 when the adult schedule table was first unveiled, the dose counts recommended were a lot lower.
Barriers to Success for the Adult Schedule
Simplification: The American Family Physician group says of the adult schedule, “The success of the childhood immunization program is partly because of the annual publication of the Recommended Childhood Immunization Schedule that summarizes the current recommendations and that it can be posted in the office for quick reference. We suggest that physicians post the Recommended Adult Immunization Schedule in the office as a quick reference tool and that it be used as part of a larger office-based program to improve adult immunization rates.”
Access: A study published on February 4, 2014, in the Annals of Internal Medicinerecommended that physicians refer patients to get the vaccines they did not stock to a pharmacy or public health department to get vaccinated.12 The reason for referring patients outside their clinic was either “lack of insurance coverage for the vaccine (55% for general internists and 62% for family physicians) or inadequate reimbursement (36% for general internists and 41% for family physicians).” Dr. Laura Hurley, one of the authors of the paper,13 that improving the delivery of recommended vaccines to adults will require a concerted effort to resolve financial barriers, especially for smaller practices and for general internists who see more patients with Medicare Part D.
In short, access comes down to whether a doctor is going to be paid enough to go to the trouble of stocking a shot.
The current White House has been promoting increased uptake of immunizing agents in adults. And the CDC, the agency in charge of getting “shots in arms,” has increased both propaganda and financial incentives. The 2023 Inflation Reduction Act (IRA), for example, was14
Conveniently, any American with Medicare or Medicaid can get any shot on the schedule at no cost to them. But some states did not require payment through their Medicaid for certain vaccines, and this federal law overrode their autonomy to decide how to spend taxpayer money. The new policy addresses that.
Biden’s policy follows the footsteps laid by Obama’s Affordable Care Act in 2010, which expanded access to vaccines with cost-sharing. The Healthy People plan was mentioned in the Affordable Care Act four times.15
The IRA law also highlights the importance of the schedule itself — insurance payments hinge on whether the vaccine is on the schedule, not simply whether it has been recommended. Not surprisingly, for the first time in history, the ACIP chose to update its annual schedule to a rolling schedule to keep up with all the anticipated changes and additional recommendations. For the first time in the history of the schedule, the ACIP left the last page blank so new recommendations could be quickly added through the year, rather than waiting for the annual update. This was done in the name of access.
You may have also been hearing of calls for financing called Vaccines for Adults. This will have to be legislated through the budget.
Why the Sudden Push for Vaccines for Adults?
A review of 100 vaccines in development by “Vaccines Today,” found a staggering 80% percent are aimed at adults.16 A survey of the vaccines and immunizing agents approved for use by the FDA over the past five years shows 11 of 15 can be marketed to adults, nine of which are only approved for those over 18 years of age.17 This is a shift from around the 1960s where we saw an explosion in new vaccines aimed at children, especially after the 1986 Act removed liability for injury from manufacturers and providers for shots on the childhoodschedule.
One of the goals of the plan is to simply increase demand. In other words, the federal government wants you to want these products. The plan was launched in 2015, a year after the CDC announced it was collaborating with Pfizer and a company called CECity to increase adult immunization rates.19 We know Pfizer makes vaccines (and “immunizing agents”); CECity is a company that specializes in electronic health records and was brought on board to implement a cloud-based “Adult Immunization Registry.” The initiative was released during the World Health Organization’s “Decade of Vaccines,” where their “Global Immunization Vision and Strategy 2006-2015” expanded the target group for routine immunizations to include adults.
The plan integrates health data transfer goals with calls for “interoperability” and “bidirectional exchange” of personal data between electronic health records (EHRs) and Immunization Information Systems (IIS’s).
Can adults injured by vaccines sue the manufacturer? It depends.
The 1986 Act and subsequent court cases removed liability from manufacturers and providers of vaccines if a person is injured or killed from vaccines. Does that apply to all vaccines? No, it only applies to shots that are on the childhood schedule. So if an adult takes a vaccine that is on the childhood schedule, like HPV or tetanus, they are bound by law to lose their right to a day in court and instead go through an administrative process many call “Vaccine Court,” which removes the right to a trial by jury. But if an adult takes the vaccine for shingles, which is not on the childhood schedule and therefore not under the umbrella of the VICP, an injured person can sue in court. It makes one wonder if those legal rights could be taken away and swept up into an amendment to the 1986 Act with a normalized Adult Immunization Schedule.
References:
“Recommended Adult Immunization Schedule.” CDC. February 28, 2024. https://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf.
“2020 National Vaccine Plan Development: Recommendations from the National Vaccine Advisory Committee.” Public Health Reports, 135(2):181–188. https://pubmed.ncbi.nlm.nih.gov/12418546/.
MMWR Morb Mortal Wkly Rep., (1991): 40(RR-12). v “ACIP Recommendations 1969: Collected Recommendations of the Public Health Service Advisory Committee on Immunization Practices.” National Communicable Disease Center 18, no. 43. https://stacks.cdc.gov/view/cdc/818.
“Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention.” Public Health Service 79-55071, U.S. Department of Health and Welfare (1979). https://files.eric.ed.gov/fulltext/ED186357.pdf.
“The Evolution of the Healthy People Initiative: A Look Through the Decades.” J Public Health Manag Pract, (2021): 27(6):S225–S234. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8478310/. ↩︎
“Current Trends Measles on College Campuses.” Morbidity and Mortality Weekly Report, (1985): 34(29);445-9. https://www.cdc.gov/mmwr/preview/mmwrhtml/00000581.htm.
“Public Law 99-528.” Congressional Record, 99th Congress 132, (1986). https://www.govinfo.gov/content/pkg/STATUTE-100/pdf/STATUTE-100-Pg3009.pdf.
Congressional Record, 99th Congress 132, part 15 (1986): 21399. https://www.congress.gov/bound-congressional-record/1986/08/13/senate-section?p=1.
“Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention.” Public Health Service 79-55071, U.S. Department of Health and Welfare (1979). https://files.eric.ed.gov/fulltext/ED186357.pdf.
“Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention.” Public Health Service 79-55071, U.S. Department of Health and Welfare (1979). https://files.eric.ed.gov/fulltext/ED186357.pdf.
”US Physicians’ Perspective of Adult Vaccine Delivery. Annals of Internal Medicine. Volume 160. No. 3. https://www.acpjournals.org/doi/10.7326/M13-2332?articleid=1819120
“National Adult Immunization Plan.” U.S. Department of Health and Human Services. https://www.hhs.gov/sites/default/files/nvpo/national-adult-immunization-plan/naip.pdf.
“Several Changes to Adult Vaccine Access Enacted Through IRA.” Avalere, (2022). https://avalere.com/insights/several-changes-to-adult-vaccine-access-enacted-through-ira.
“Compilation of Patient Protection and Affordable Care Act.” U.S. House of Representatives, (2010). https://housedocs.house.gov/energycommerce/ppacacon.pdf.
Future of Immunisation: 100 Vaccines in the Pipeline.” Vaccines Today, Gary Finnegan (2023). https://www.vaccinestoday.eu/stories/future-of-immunisation-100-vaccines-in-the-pipeline/.
“Biological Approvals by Year.” The Center for Biologics Evaluation and Research, U.S.FDA (2024). https://www.fda.gov/vaccines-blood-biologics/development-approval-process-cber/biological-approvals-year.
“Adult Immunization Plans.” U.S. Department of Health and Human Services, (2019). https://www.hhs.gov/vaccines/national-adult-immunization-plan/index.html.
“American College of Physicians, CECity, and Pfizer Collaborate to Increase Adult Immunization Rates.” Pfizer, (2014). https://www.pfizer.com/news/press-release/press-release-detail/american_college_of_physicians_cecity_and_pfizer_collaborate_to_increase_adult_immunization_rates
There are children who get all sorts of ideas in their heads. They change their minds every day.
In the current culture, on a given Tuesday, a boy might decide he wants to be a girl, and vice versa.
But then comes Wednesday, and the world is completely different.
Except we have the psycho meddlers. Parents, teachers, counselors, government-backed groups, pedophiles…
They enter the scene and they’re committed to making that random Tuesday last forever.
I put most of this on the parents. The mind-controlled parents who believe in total permissiveness and “the new cultural imperatives” at the same time.
They weren’t fit to have the children in the first place.
When I was a kid, I entertained all sorts of crazy ideas. It was fun. I went to my father with a plan to buy a pet rattlesnake and bring it in the house. I told him I could tame the snake.
He came down on me like a ton of bricks. NO took ten seconds.
He wasn’t pleasant and kind and understanding and supportive of my claim that I was a wild animal tamer and a healer.
If it were possible (it isn’t), I’d like to see one of these oh so permissive parents put on trial, with a sane jury behind the rail. And a sentence of 30 years in prison for the parent’s encouragement—which led to his child taking toxic meds, ruinous hormones, and going into an operating room for life-destroying surgery.
Few of us were born when the forces for milk pasteurization launched the first major attack on Nature’s perfect food. In 1945, a magazine called Coronet published an article, “Raw Milk Can Kill You,” blaming raw milk for an outbreak of brucellosis in a town called Crossroads, U.S.A., killing one-third of the inhabitants. The Reader’s Digest picked up the story and ran it a year later.
Just one problem with this piece of “reporting.” There was no town called Crossroads and no outbreak of brucellosis. The whole story was a fabrication—otherwise known as a lie. And lies about raw milk have continued ever since.
Unfortunately, the fictitious Crossroads story paved the way for laws against selling raw milk, starting with Michigan in 1948.
Here’s another example of lies against raw milk (which I referenced in an earlier post,[i] but it is worth repeating). In 2007, John F. Sheehan, BSc (Dy), JD, US Food & Drug Administration, Center for Food Safety & Applied Nutrition (USFDA/CFSAN), Division of Dairy and Egg Safety, prepared a Powerpoint maligning raw milk; it was presented to the 2005 National Conference on Interstate Milk Shipments (NCIMS) by Cindy Leonard, MS.[ii]
As shown in the table below, all of the fifteen reports associating outbreaks of foodborne illness with raw milk that Sheehan cites are seriously flawed. For example, in two of the fifteen, the study authors presented no evidence that anyone consumed raw milk products and in one of them, the outbreak did not even exist. Not one of the studies showed that pasteurization would have prevented the outbreak.
No Valid Positive Milk Sample
12/15
80%
No Valid Statistical Association with Raw Milk
10/15
67%
Findings Misrepresented by FDA
7/15
47%
Alternatives Discovered, Not Pursued
5/15
33%
No Evidence Anyone Consumed Raw Milk Products
2/15
13%
Outbreak Did Not Even Exist
1/15
13%
Did Not Show that Pasteurization Would Have Prevented Outbreak
15/15
100%
Fast forward to the present and the ruckus about bird flu in dairy cows—more lies, very clever lies, but lies nevertheless.
In a press release dated March 25, 2024 ,[iii] the U.S. Department of Agriculture (USDA), Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC), as well as state veterinary and public health officials, announced investigation of “an illness among primarily older dairy cows in Texas, Kansas, and New Mexico that is causing decreased lactation, low appetite, and other symptoms.”
The agencies claim that samples of unpasteurized milk from sick cattle in Kansas and Texas have tested positive for “highly pathogenic avian influenza (HPAI).” Officials blame the outbreak on contact with “wild migratory birds” and possibly from transmission between cattle. The press release specifically warns against consumption of raw milk, a warning repeated in numerous publications and Internet postings.
According to the press release, national laboratories have confirmed the presence of HPAI (Highly Pathogenic Avian Influenza) through testing, but it does not reveal the type of test used to detect this so-called viral illness.
THE FIRST LIE: Researchers have found HPAI virus in the milk of sick cows.
Officials have NOT found any viruses in the milk or any other secretions of the sick cows. The CDC has yet to reply to repeated requests for proof of finding the isolated HPAI virus in any fluid of any sick chicken or other animal.[iv] Nor have health and agriculture agencies in Canada,[v] Japan[vi], the UK[vii] and Europe[viii] provided any proof of an isolated avian influenza virus.
As for all the studies you can find in a PubMed search claiming “isolation” of a virus, not one of them shows the true isolation of a virus, any virus, from the fluids (phlegm, blood, urine, lung fluids, etc) of any animal, bird or human.[ix]
The truth is that “viruses” serve as the whipping boy for environmental toxins, and in the confinement animal system, there are lots of them–hydrogen sulfide, carbon dioxide, methane and ammonia from excrement, for example.[x] Then there are toxins in the feed, such as arsenic added to chicken feed, and mycotoxins, tropane and β-carboline alkaloids in soybean meal.[xi] By blaming nonexistent viruses, agriculture officials can avoid stepping on any big industry toes nor add to the increasing public disgust with the confinement animal system.
Way back in 2006, researchers Crowe and Englebrecht published an article entitled, “Avian flu virus H5N1: No proof for existence, pathogenicity, or pandemic potential; non-‘H5N1’z causation omitted.”[xii]Nothing has changed since then.
Here’s your homework assignment: Contact USDA at Aphispress@usda.gov and ask them to provide proof of the isolation of the HPAI virus or any virus in the milk of the sick cattle.
SECOND LIE: National laboratories have confirmed the presence of HPAI (Highly Pathogenic Avian Influenza) through testing.
They don’t say anything about the kind of test they used, but it almost certainly the PCR (polymerase chain reaction) test. The PCR test detects genetic material from a pathogen or abnormal cell sample and allows researchers to make many copies of a small section of DNA or RNA. The test was not designed to determine or diagnose disease, it was designed to amplify or increase a certain piece of genetic material.
Each “amplification” is a doubling of the material. If you amplify thirty times you will get a negative; amplify 36 times or more, and you will get a positive. At 60 amplifications, everyone will “test positive” for whatever bit of genetic material you believe can cause disease.[xiii] If you want to show that you have a pandemic brewing, just amplify, amplify, amplify. Folks, this is not a valid test, not good science by any stretch of the imagination—especially as there was no virus to begin with.
How many times did our health officials amplify the samples they obtained from the milk of the sick cows? Be sure to ask them when you email Aphispress@usda.gov for proof of the virus.
THIRD LIE: The “virus” is highly pathogenic.
According to the Wall Street Journal, one—just one–person working in the dairies got sick and tested positive for avian influenza after exposure to dairy cattle presumed to be infected with the H5N1 bird flu.[xiv] The person reported eye redness, or conjunctivitis, as his only symptom—a symptom that can be explained by exposure to any of the many airborne toxins in confinement dairies. (How are they treating the illness? With vitamin A and herbal eyedrops? No, the poor sod is getting treatment with a toxic antiviral drug.)
According to the CDC, the disease in humans ranges from mild infections, which include upper-respiratory and eye-related symptoms, to severe pneumonia. If the “virus” is so highly pathogenic, we’d expect a lot of workers working around these sick cows to end up in the hospital. . . but we’ve heard of none so far.
FOURTH LIE: You can get avian fly from drinking raw milk, but pasteurized milk is safe
According to medical biologist Peg Coleman,[xv] “Recent risk communications from CDC, FDA, and USDA regarding transmission of highly pathogenic avian influenza virus or HPAI (subtype H5N1) to humans via raw milk include no supporting evidenceof viral transmission from raw milk to humans in the peer-reviewed literature. . . An extensive body of scientific evidence from the peer-reviewed literature . . . does not support the assumption by these US government agencies that [non-existent] HPAI transmits to humans via milkborne or foodborne routes and causes disease. Nor does the scientific evidence support the recommendation that consumers should avoid raw milk and raw milk products [emphasis in the original].”[xvi]
Coleman notes the suite of bioactive components in raw milk, including bovine milk, that destroy pathogens and strengthen the gut wall. “Many of these bioactive components of raw milk are . . . sensitive to heat and may be absent, inactive, or present in lower concentrations in pasteurized milks. . . Cross-disciplinary evidence demonstrates that raw milk from healthy cows is not inherently dangerous, consistent with the CDC evidence of trends for 2005-2020 and evidence of benefits and risks. There is no scientific evidence that HPAI in raw milk causes human disease.”
And while USDA, FDA and CDC assure the public that pasteurization will make milk safe, they note that “Milk from infected animals is being diverted or destroyed,” implying that pasteurization alone does not guarantee safety. In any event, sales of industrial pasteurized milk continue their relentless decline.
Fortunately, raw milk drinkers are already skeptical of government pronouncements and are skilled at seeing through lies. Both large and small raw milk dairy farms report that sales are booming. The current bird flu fracas is just another Crossroads, U.S.A., a bunch of lies fostered by a dishonest dairy industry taking aim at the competition.
In the Covidian Era, science has moved on to a digital upgrade of itself called Scientism, the religion of science, where science is god, and part of a new global Technocracy.
Social engineering used to mean molding the minds of people to conform to new norms. This goes back to 1928, Ed Bernays, and his book Propaganda. However, in a Technocracy, not only minds, but bodies, too, can be molded. If you did not get the memo, Technocracy has brought humanity from Human to Posthuman and Transhuman.
In the 2022 Journal Global Trends, Russian scientists describe the difference between Posthuman and Transhuman:
The fundamental idea of posthumanism is the rejection of biological, ethical, and ontological anthropocentrism. Transhumanism focuses on changing and improving natural human characteristics through biological, technological, and cognitive modifications…Transhumanism has the potential to preserve man as an effective economic and cognizing agent.
In other words, man as an “economic agent” refers to the cybernetic human as a commodity in a modern world. This means the laws of the nations need to change to catch up.
The new law amends the Federal Food, Drug, and Cosmetic Act by authorizing sponsors of novel drugs to make use of “certain alternatives to animal testing, including cell-based assays and computer models, to obtain an exemption from the Food and Drug Administration to investigate the safety and effectiveness of a drug.
After decades of extrapolating animal studies to humans, suddenly animals are no longer scientifically valid. Does this transition make obsolete more than a century of animal-based research? In one sense, such a transition is long-awaited and frees innocent animals from needless torture. In another sense, it moves the mark to a new target.
Scientists now claim humans are diverse, and therefore require different models. They propose, “human cell-based models that more accurately reflect the diversity of human genetics may guide the development of treatments that are more reliable and successful in real-world applications.”
In Scientism, humans are considered commodities. Some Transhumanists propose transferring consciousness to a machine to create a brain-machine interface. The Russian Posthuman authors propose that consciousness may be a feature exclusive to humans. They appear not to know for sure. They state:
Accordingly, it is still possible that there is a fundamental difference between man and other objects of the world.
Digital IDs reflect a digital avatar in Precision Healthcare. “Precision Healthcare” refers to a remote medical model of healthcare. According to a 2021 study in the Journal of Personalized Medicine:
A digital twin is a virtual model of a physical entity, with dynamic, bi-directional links between the physical entity and its corresponding twin in the digital domain.
In March 2024, Dept. of Defense (DoD) officials testified on its own priorities before the House Armed Services Subcommittee. The digital ID is a natural progression from the trend toward non-binary humans who do not identify with a specific gender. This makes the transition, from human to digital Posthuman, effortless. All humans with a digital ID belong to an A.I., industrial (not biological) system—Transhumanism.
The rapid development of technology—in particular, artificial intelligence—accelerates the processes of industrial automation. This, in turn, raises the question of the role of man in the economy of the future: if artificial systems can more effectively perform the functions of man, then what place will man, as a potentially inefficient economic agent, take in the economy?
Studying humans in large-scale experiments has already happened. The deployment of COVID EUA medical countermeasures (MCMs), sometimes referred to as vaccines, was tested during the COVID pandemic. However, unlike vaccines, which are FDA-approved, MCMs are not. According to the CDC, MCMs include: biological products, drugs, and devices.
Testing humans in Real Time, as a digital Avatar, puts the Tele in Telehealth. It is a strategy of “emergent technology,” even though emergent technology, such as TeleMedicine, is already 10 years old. Further, this technology prevents the need for long-term genotoxicological and carcino-toxicological vaccine studies. Any adverse events (AEs) can be released later. Or not.
Without defining, ‘modernization 2.o,’ in human terms, science and government have paved the way for a new religion in a Posthuman synthetic, digital world. To maintain the inner human is to be aware of Technocracy, and turn toward the Natural world, and the heart center.
Along with our allies we have spent the last four years dismantling every aspect of the virus model whether it concerns “isolation”, antibodies, genomics, PCR, proteomics, electron microscopy, or animal and human studies. In 2022, I published A Farewell to Virology, to date one of the only treatises that outlines a formal refutation of the entire virus model. This was inspired The Perth Group’s 2017 epic HIV – a virus like no other, the most comprehensive document refuting the existence of ‘HIV’ specifically.
In my recent webinars with Dr Tom Cowan we have been discussing the scientific method, along with the concepts of independent variables and controlled experiments. Clearly the virologists have resorted to anti-scientific practices to make their various claims including the foundational claim of virus existence.
It motivated me to write an essay specifically addressing the apical logical fallacy in the cell culture technique – something that has been noticed previously but perhaps not formally expressed. The virologists have claimed they perform control experiments and sometimes describe these as ‘mock-infected’ cultures. In recent months we have also been contacted by people in the ‘no virus’ community asking whether John Enders inadvertently performed a control experiment in his 1954 measles paper. Dr Stefan Lanka exposed the lack of a control experiment in this paper in the Stuttgart Higher Regional Court in 2016 and I make some further comments expanding on this in note 20.
The pivotal issue is that the virologists do not have an independent variable and their experiments cannot make a hypothetical particle real. The ‘gold standard’ technique for “isolation” cannot possibly determine the presence (or existence) of viruses no matter how they attempt to control it. The paradigm that was created in the 1940s to keep virology alive was dead on arrival because the technique relies on a reification fallacy and logical errors that disqualify the entire process from being scientific.
We have had some feedback that although fairly brief, this paper is difficult to follow in some parts. (It helps to read all the endnotes.) If you have not already seen it, I would recommend watching Kate Sugak’s excellent presentation at the XXII Russian Scientific Conference: “The scientific vacuum: The scientific method and its absence in virology“. Kate covers the crucial scientific considerations articulated in my paper in an easy to follow format and shows that the virologists have nowhere left to hide.
How safe is our drinking water? Do you even know what is in it? What would you say if you were told you were being medicated with a very dangerous chemical, without consent, through your drinking water? No doubt the majority of us would be up in arms, but in 2024 this is exactly what the UK Government is planning on doing. Already in the UK, six million people drink fluoridated water, but the addition of fluoride at source is about to be expanded throughout the whole of England.
Debi Evans is joined by Joy Warren, National Coordinator of Fluoride Free Alliance UK. She has been active against water fluoridation since soon after gaining a BSc (Hons) in Environmental Science in 2002. Her catalyst for action was attending a Friends of the Earth meeting in early 2003 at which a medical doctor gave an account of her long struggle against hypothyroidism after moving to fluoridated Coventry. After researching the issue of fluoride’s negative effect on the endocrine system and much else, Joy became convinced that the practice of adding a medicine to drinking water was a thoroughly unethical medical practice. Part of her journey has involved excluding fluoride from her environment—which was no mean feat, living as she does in a fluoridated city.
Joy joined the National Pure Water Association in 2005 and soon became an Executive Director. In 2010, she left NPWA to start West Midlands Against Fluoridation and ran a very successful website and fluoride analysis service. During this time, she gained a Certificate in Health and Nutrition. In 2018, encouraged by friends, she set up the Fluoride Free Alliance UK (FFAUK), which became the national organisation campaigning on the issue, NPWA having been wound up a few years earlier.
There have been several attempts to add fluoride to English drinking water since 2003 and Joy Warren has been actively involved in ensuring that each attempt failed. The current climate is more challenging, with the Conservative government and advisors since 2022 trying to get England and Wales fluoridated, and this has meant Joy exercising her coordination and IT skills to the full.She has been involved against all attempts since 2004 to fluoridate a population and has a 100% success record.
This interview covers what fluoride is and how dangerous it is. What is a neurotoxin? Can you stop your area from being fluoridated? Joy Warren reveals the extent of the Government’s plan to medicate us with fluoride through our drinking water, without our consent. Why has the Government taken this potentially disastrous decision, and how will it affect you and future generations?
Fluoride is also present in many medicines and foods; are you aware of how much fluoride your body is ingesting? Do you know the dangers to children and babies? Dental vans will be visiting primary schools to paint children’s teeth with fluoride varnish. Do you consent?
Joy Warren discusses what the public can do to object to the fluoridation of water. Fluoride is invisible, and the Government would like it remain that way. It is up to every one of us to inform others of the dangers of fluoride.
Contact Details:
Joy Warren, National Coordinator, Fluoride Free Alliance UK
Public health and regulatory systems have consistently hidden those truths behind false claims about the effects of vaccines, and behind legalized non-regulation of biological product manufacturing.
The US Food and Drug Administration and other drug manufacturing regulators claim that drug manufacturing regulation is about assessing product purity, sterility, potency, safety and efficacy to protect humans and animals from impure, adulterated, contaminated, impotent, harmful, and/or ineffective products.
Biological products can be defined as a subset of the larger category of drugs. Biological products are drugs manufactured through biological processes that take place within living organisms. Drugs that aren’t biological products are manufactured through chemical processes. Vaccines are included in the biological products class of drugs.
A defining characteristic of biological products, in legal terms, is their rule-governed exemption from regulatory oversight that applies to and is enforceable for drugs manufactured using chemical processes.
One of several defining characteristics of biological products as murder weapons, is their ability to biologically incorporate into the target’s body, such that weapons become indistinguishable from victims. Empty vials, syringes and other residual evidence disappears into garbage dumps and medical waste incinerators.
Eleanor McBean published a book in 1957 called Poisoned Needle.
She carefully documented the history of vaccination lies prior to and since Edward Jenner’s cow-pox and smallpox lies. She collected dozens of doctors’ observations throughout the 1700s, 1800s and early 1900s, supporting the conclusion that vaccines have always been nothing more than toxic slurries introduced into healthy people and animals for the purpose of making them weaker and sicker and dead, while enabling the poisoners to lie to themselves and to their victims about what they’re doing, how and why.
One example from Poisoned Needle:
Dr. J. W. Hodge had considerable experience with vaccination before he denounced it and wrote a book on his collected data. In his [1902] book The Vaccination Superstition (p. 41) he states:
“After a thorough investigation of the most authentic records and facts in harmony with the physician’s daily observations and experiences, the conclusion is drawn that instead of protecting its subjects from contagion of smallpox, vaccination actually renders them more susceptible to it.
“Vaccination is the implantation of disease — that is its admitted purpose. Health is the ideal state to be sought, not disease . . . Every pathogenic disturbance in the infected organism wastes and lowers the vital powers, and thus diminishes its natural resisting capacity.
“This fact is well known and so universally conceded that it seems superfluous to cite authorities. Nevertheless, I shall mention one. The International Textbook of Surgery – Vol. 1. p. 263, is authority for the following statement: ‘Persons weakened by disease or worn out by excessive labor yield more readily to infection than healthy individuals.’
“If this is true, it explains why, in various epidemics, smallpox always attacks the vaccinated first, and why these diseases continue to infest the civilized world while its allied (unvaccinated) ‘filth diseases’ have disappeared before the advance of civilization, through the good offices of sanitation, hygiene and improved nutrition.”
For the last few years, I’ve been documenting the development of American public health emergency anti-law as a distinct layer of statutes, regulations, executive orders and court cases that overrides and suspends good laws criminalizing (among other crimes) intentional use of poisons, including vaccines, to injure and kill people.
Public health emergency law as a tool to enable deniable, spatially-distant, time-shifted homicide became more visible because public health emergency law was used to start the Covid-19 killing programs and is still being used to maintain the Covid-19 killing programs.
Public health emergency statutes, regulations, executive orders and court cases govern, among other things, non-regulation of poisons (i.e. emergency use authorization/EUA countermeasures) during declared emergencies.
In December 2023, I located a Federal Register Notice of Final Rule through which then-FDA Commissioner Scott Gottlieb shut the doors of all biological product manufacturing facilities to FDA inspections, effective May 2, 2019, eight months before public announcement of Covid-19, and more than a year and a half before the Covid-19 mass vaccination campaign got underway in December 2020.
This fact helps to answer the question: How could hundreds of millions of doses be manufactured, shipped and ready for use a few weeks after the FDA’s December 2020 “emergency use authorization” decisions? Manufacturing began well before Covid was announced, inside factories not subject to inspection. That’s how.
Reading Gottlieb’s rule-change a few months ago, I realized that non-regulation of biological product manufacturing under routine, non-emergency conditions, had been in effect — or, rather, non-effect — since long before Covid, and will still be in effect/non-effect even if emergency declarations about Covid and other fake communicable disease and public health threats are revoked someday.
So for the last couple of months, I’ve been thinking about and collecting more legal evidence that biological product anti-law under non-emergency conditions also suspends or overrides good laws criminalizing (among other crimes) intentional use of poisons to injure and kill people, just as effectively as public health emergency anti-laws do.
The legal history of routine non-regulation of all biological products can be assembled in the same way the legal history of emergency-predicated non-regulation of EUA countermeasures has been assembled.
Such a collection would document how, over time, built-in exemptions from otherwise applicable, enforceable manufacturing rules, along with rule changes, and explicit notices from FDA to manufacturers (called Guidance for Industry) that FDA would not, will not and does not enforce rules, have rendered biological product non-regulation more non-regulatory as each year has passed.
However, sifting through hundreds of rule changes to track each rule as it’s become increasingly inapplicable and unenforceable, is an exercise in grasping at smoke. So I’m not planning to pursue it further, unless an attorney contacts me with a credible proposal for a case that would be strengthened by detailed accounts of FDA Federal Register rule-making activities over the past half-century or so.
At 21 CFR 610.11, the 1973 FDA rules established that the only “general safety” test (GST) required to claim a biological product was safe, was to inject a sample into two mice and two guinea pigs. If the two mice and two guinea pigs didn’t get “significant symptoms” or die within seven days, “the product meets the requirements for general safety.”
FDA authorized “exceptions to this test…when more than one lot is processed each day” and “variations of this test…whenever required.” Manufacturers were directed to apply to the Bureau of Biologics (now the Center for Biologics Evaluation and Research) for exemptions.
After a series of revisions, FDA eliminated general safety test requirements for biological products, effective Aug. 3, 2015 (80 FR 37971).
FDA has made dozens of similar rule changes, weakening and eliminating rules about samples, protocols and lot-by-lot release; establishment and product licensing applications; post-approval manufacturing process changes; mixing, diluting and repackaging and more, including the elimination of facility inspections Gottlieb put in place effective May 2, 2019.
It’s important to understand that the acts FDA officials have committed, to eliminate applicability and enforceability of drug manufacturing regulations for biological product manufacturing, have not been acts to eliminate actual regulation of medicines.
They have been acts to eliminate what has, from the start, been pretend-regulation to enable unimpeded manufacture, distribution and use of intentional poisons, so that their true character as poisons could be hidden from and invisible to the public.
A few weeks ago, I located Mutual Recognition Agreements. MRAs are international trade treaties. When signed and ratified by national governments, MRAs authorize national regulators — including drug regulators — to be “relieved of” their regulatory obligations and instead, recognize and rely on the regulatory decisions of other countries’ regulators, especially the US Food and Drug Administration.
The two systems interlock.
Under the legal terms of MRA treaties, US-FDA can be legally construed as the sole regulator for worldwide drug manufacturing and distribution systems.
Under the legal terms of the US-FDA drug regulation system, all biological product manufacturing can be legally conducted with no substantive disclosure, monitoring or enforcement of rules controlling purity, sterility, safety, potency, efficacy, raw materials, manufacturing processes, or chemical and biological composition of finished, packaged, distributed products.
Also note, the legal structure of Mutual Recognition Agreements plus FDA-non-regulation-of-biological-products, operates separate from and in addition to the UN-World Health Organization, International Health Regulations system.
National governments interested in shielding their populations from intentional poisoning must withdraw from the United Nations and WHO treaties; must withdraw from the IHR treaty; and also must withdraw from each Mutual Recognition Agreement treaty that subordinates their own federal drug regulation to other countries’ regulators, including the US-FDA non-regulation, poison-facilitation system.
It’s plausible that some simpler biological products (insulin, for example) may have historically been manufactured, and may still today be manufactured, to meet measurable, achievable standards of safety and batch-to-batch consistency, because doing that would help US-FDA and pharmaceutical companies maintain public confidence and reduce the likelihood that the public would begin to see and understand the biological-product-based intentional poisoning program.
It’s also plausible that biological products labeled as vaccines have had, for many decades and still today, a high degree of batch-to-batch variation ranging from low to high toxicity, because that also would be a sensible way for US-FDA and pharmaceutical companies to maintain high levels of public ignorance, complacency and compliance with vaccination programs.
March 5, 2024 – Four questions and four responses “…Due to changes in US law, acts that are crimes in other legal contexts, such as poisoning, battery, torture and homicide, if carried out by vaccines (and many other drugs, devices and biological products) are legal. Perpetrators cannot be held liable under civil tort law and cannot be prosecuted under criminal law. This intentional poisoning is much more visible to the public because of the Covid-19 events since 2020, so there are more possibilities for stopping the programs. One of the main methods to carry out the mass deception is false attribution of cause and effect…”
Isolation means the separation of one thing from everything else. This is the only way to scientifically identify a thing. This is done with everything from large organic material to the smallest nano-particles. It is done with Gold and Silver. And it is done in basic chemistry, but it has never been done with a virus. Several have claimed to have done so, but have since been exposed as frauds. And today, virologists claim that isolation is not possible because of the obligate intracellular nature of a virus. This means that they cannot exist outside of a living cell. But if this were true, then it would also be true that they can not spread from one person to another. The pseudo-science of virology is full of logical fallacies that any inquisitive person can recognize.
Scientific studies require a control group. Meaning that two samples are needed where every factor is the same except for the presence of the thing being studied. But this can not be done in virology because a virus has never been isolated. When virologists claim they are isolating it, they are lying. This is evident today with the latest so-called proofs that SARS-CoV-2 has been isolated.
In both the “Isolation and rapid sharing of the 2019 novel coronavirus” published by the Medical Journal of Australia. And in the “Viral isolation analysis of SARS-CoV-2” from Japan’s Journal of Infection and Chemotherapy, the titles suggest that they isolated a virus. But they clearly did not.
They took material from the most contaminated source possible, the nose, which acts as a filter by capturing particulates inhaled from the environment. And at no point did they isolate a virus from this sample. What they did was run the entire mix of unknown material through a PCR test, and claimed that it tested positive for SARS-CoV-2. But we know that the PCR test is not capable of isolating a virus, and we know it’s been deliberately adjusted to give false positive results. So this is not science, it is fraud. They then inoculated a culture of cells with the entire mix of nose material, added in unspecified material, and the cells died. At no point in these experiments was a virus ever isolated. They in fact did the opposite of isolation by adding foreign material to a mix of unknown material from a person’s nose. So even if the cells died as a result, there is no way of knowing what killed them.
There is an alternative theory that does not have massive funding from spurious foundations and Nobel Peace prizes to convince the public of it’s validity.
Terrain theory tells us that most of what we are told is a disease, is nothing more than the symptoms of a natural bodily process of healing and repairing tissues damaged from stress and external toxins. Cells naturally die and break down in a way that is identical to how virologists claim a virus behaves. And the very same foundations pushing the theory of the virus, have been simultaneously creating a more toxic world with petrochemical drugs that earn billions in profits. There are far more so-called diseases today than existed before this pseudo science was unleashed on society.
In 1859 Florence Nightingale published, Notes on Nursing, where in she wrote that “all disease… is more or less a reparative process… an effort of nature to remedy a process of poisoning or of decay, which has taken place… sometimes years beforehand.” She is saying that what we are told today are symptoms of a disease, are actually natural processes of the body healing itself from damage.
Manly P Hall, known best for his 1928 publication, The Secret Teachings of All Ages, gave a lecture in 1989 called, Magnetic Fields of the Human Body. In this lecture he described this same sentiment.
He said that each human body is surrounded by its own magnetic field which provides tremendous protection. And as long as the individual takes proper care of this magnetic field, it will heal all wounds and recover all bodily functions and organs. He said that the law of the energy field is also the law of integrity. When we break the laws of nature, we damage this flow, which in turn damages the individual’s vitality. This magnetic field can be damaged by negative attitudes such as fear, and destructive attitudes towards others. It can be damaged by drugs and alcohol, toxic substances, and any action contrary to the common good.
He went on to say that in ancient times looking upon objects perfect and complete in structure was therapeutic because looking upon them inspired an acceptance of perfect symmetry that positively effects our energy field. And conversely, when we accept discord as inevitable, our energy field is damaged.
For the past hundred years the same families and foundations have created a world of chaos and discord. And perhaps Terrain theory is correct, and the ancients were right, and we have been given a perfect divine vessel that will protect us so long as we look after it and live in accordance with the common good.
Since the onset of the Covidan Era in 2019, the “alternative media” and its alternative media celebrities, have occupied a greater percentage of center stage. They didn’t have to push their way into the spotlight since they own part of it, a section further upstage.
The “alternative media” has upstaged the mainstream media in the promotion, and selling, of “alternative remedies ” for COVID-19. Among the many options is Ivermectin.
In 2020, I wrote an article on the dangers of Ivermectin in the article, The Rise of Ivermectin, found here. Additional information was published by Vaccine Impact here. Why bring up yesterday’s news?
Old news is new again when new information becomes available. What the many “alternative” faces did not reveal about their “alternative” products is that they were not alternative at all. They contain the same materials as the standard issue EUA injectables and pills. They only come packaged with a less inflammatory script.
But what about the stories of people Ivermectin has helped?
Pharmaceuticals may help the body, before they hurt it. Ivermectin is a known anti-parasitic. If it helps people, then they have parasites. And these days, who doesn’t have parasites? Especially when there are parasites among us, parasites in high places. However, Ivermectin studied in randomized, controlled trials showed no clinical benefit in the prevention or treatment of Covid-19.Toxic effects include: severe confusion, ataxia, seizures, and hypotension.
How much help “alternative” products offer depends upon the individual ingredients, and whether they are injected (vaccine), ingested (pill), or inhaled (airborne). The most immediate and potentially dangerous delivery system is by injection, since the materials bypass the body’s innate immune system to be delivered directly into the bloodstream. From the blood, electromagnetic nanomaterials (lipdnanoparticles, graphene, and hydrogels), are carried to organs, tissues and cells, where they take up residence and become embedded into tissue.
Nanobots are self-assembling and self-replicating. They have artificial intelligence (A.I.). They take orders and commands, military-style. The National Nanotechnology Initiative (NNI) has been around for 25 years. NNI is the new supplement to the president’s 2024 budget called for under the provisions of the 21st Century Nanotechnology Research and Development Act (15 USC §7501). If the president is supplementing with A.I. as a budget item, then Americans should be aware of the updated national diet.
The “Alternative” Pharma Products
Ivermectin is not only an off-label, anti-parasitic medication, but a novel drug delivery system with nanostructured lipid carriers.
Oral Antibodies marketed as “natural food antibodies,” these are the new oral vaccines. Same ingredients, different form. “Guaranteed Titre Levels” means synthetic.
Monoclonal antibody vaccines (mAB) are chimeric injections made of mice and men- “a combination of part mouse and part human.” In 2022, an Emergency Task Force warned that monoclonal antibodies are not effective. Then again, the meaning of “effective” may depend upon one’s point of view.
Ascorbic acid (GMO product) with graphene nanocomposites.
Choosing an “alternative” medication is still a medication. Thus, it is important to read the labels and do the research.
The REAL McCoy
With definitions ever-changing under a NanoNarrative, we need to return to “REAL.” “Real” is eating clean with organic, grass fed meat and milk, pastured eggs, locally-grown vegetables and fruits, eating with the seasons. “Real” is connecting to Nature and the world of plants and herbs as medicine. “Real” does not require a label.
Food is the main fuel of the body. Still, in today’s world, food as fuel is not enough due to our many toxic exposures.
It is important to supplement with “real” ingredients, not “alternatives.” Supplementing foods should be food-based, such as fruit freshly harvested, nutrient-rich broths, and herbal preparations, such as teas and tinctures. For example, when sourcing vitamin C, choose food-based C over ascorbic acid.
Real foods resemble body parts. Citrus fruits have a similar appearance to female mammals’ mammary glands. These fruits support breast health and lymphatic flow into and out of the breasts.
In a world of nanotech, it takes an effort to be natural. Get to know your local ‘small farmer’ as someone not small in stature, but small in commercial operation. The Weston A. Price Foundation connects people to local small farmers to source real foods. Find a local chapter here.
The farther from nature, the closer to synthetic A.I., the door to Cyborgs, and the realm of Transhumanism.
A new class of “encrypted RNA” vaccines are being developed where the RNA would piggyback onto an existing wild virus and spread from person to person without any person’s knowledge or consent.
This so-called “therapy” uses a technology called TIPs (Therapeutic Interfering Particles), which are described as “engineered molecular parasites” that piggyback on a wild virus. If you get the virus, you also get these parasites. Once inside an infected person, the TIPs are supposed to rapidly multiply, hijacking the resources the wild virus needs to multiply and therefore stopping the virus.
Supporters of this technology claim it will “solve” several problems with traditional vaccine delivery, including “behavior barriers” like noncompliance. Meaning everyone gets vaccinated—whether they like it or not.
Let me try to disentangle this.
Some naturally circulating virus (which doesn’t exist) will be captured and outfitted with lab-created molecular parasites.
The virus (which doesn’t exist) plus its attached parasites will enter the body, where the parasites will “hijack the resources” the virus (which doesn’t exist) needs to survive and multiply.
What resources would these be? The bloodstream? The nervous system? The brain? The anus?
And what does “hijack” mean? Destroy? Disable? Wall off from the rest of the body?
The virus (which doesn’t exist) stops multiplying and dies. Then that person is immune from further infection by that type of virus (which doesn’t exist).
I assume, when the wild virus plus the parasites enter the body, even though the virus doesn’t exist it’s a tiny blob of SOMETHING, rather than just an idea.
What would that something be? No idea.
Whatever the parasites are actually doing in the body, we know they’re not aiding in destroying the virus, because the virus doesn’t exist.
SSRIs (Selective Serotonin Re-Uptake Inhibitors) are a common class of antidepressants used to treat depression, anxiety and other mental health problems. Popular SSRIs include Fluoxetine (Prozac), Escitalopram (Lexapro), and Sertraline (Zoloft). Something well established about these drugs is that they have sexual side-effects. In fact, between 40 and 65% of people who take an SSRI are thought to experience some form of sexual dysfunction. What few people know, though, is these side effects can persist even after coming off of the drugs—a condition called Post-SSRI Sexual Dysfunction (PSSD).
This is more than just low libido. It can be a total loss of libido, genital numbness, erectile dysfunction, an inability to orgasm and complete lack of sexual attraction. Emotional blunting is also common, with sufferers describing a numbing of positive emotions, no romantic feelings, and difficulty connecting with others…
In the UK, 1 in 3 teenagers aged 12 to 18 has been prescribed antidepressants. In 2022 alone, the number of children aged 13 to 19 taking antidepressants rose by 6,000 to 173,000…
And increasingly before puberty! In the UK, antidepressant prescriptions for children aged five to 12 years increased by more than 40% between 2015 and 2021. Aged five! Before they’ve even had the chance to develop normally! Online forums are already full of people sharing their experiences of puberty on SSRIs and now dealing with sexual dysfunction as adults. Stories of starting Zoloft at age 11 and never developing normal sexual sensation. Of being prescribed Prozac at 14 and not knowing what it’s like to have a libido. Of taking Lexapro for less than a month and still having genital numbness six years on.
Loss of sexual feeling, desire, interest.
And on top of that, tons of assurances from the Woke mob that having no sexuality is just fine. It’s a gender identity.
As opposed to a CHEMICAL DISASTER.
I went to Google and typed in “SSRIs loss of sexual feeling.” Here are the entries that sprang up:
NIH: “Sexual dysfunction in [SSRIs].”
Harvard Health: “Some people taking SSRIs aren’t able to have an orgasm at all. These symptoms tend to become more common with age…”
Mayo Clinic: “Effects on sexual function can include: A change in your desire for sex; Erectile problems; Orgasm problems; Problems with arousal, comfort and satisfaction.”
New York Times: “Doctors and patients have long known that antidepressants can cause sexual problems. No libido. Pleasureless orgasms. Numb genitals…”
So it’s no secret.
Except—how many doctors who are about to prescribe antidepressants to children tell their parents, “The drug can have serious sexual side effects”?
So there’s that. Widespread ignorance, because doctors keep their mouths shut about what they know.
And when all sexual feeling shuts down, a child is told, “Non-binary…asexual…gender…trans…it’s all fine…no problem…”
The kid thinks he’s on the cutting edge of a new society, a new culture, a new way of seeing male and female, a revolution.
One new study, supporting the “millions” assertion, claims the most common long COVID symptom people report is tiredness after light physical or mental exercise.
Aha.
As we all know, feeling tired can only be caused by THE VIRUS.
“Doctor, six months ago, I was fine. But since then, I’ve been fatigued.”
“Right, Ms. Jones. You have long COVID.”
“Say what?”
“I diagnosed you with COVID six months ago. The disease is persisting.”
“Oh. Come to think of it, I started feeling tired right after you diagnosed me.”
“A coincidence.”
“I don’t think so. I left your office. I was depressed by the diagnosis, and when I got home I couldn’t run my usual nine miles for the day.”
“Are you saying I made you tired?”
“Yes, I believe I am.”
“I’ll write a note to Homeland Security. Expect a visit to your house. Open the door carefully and assure the agents you have no weapons and no dogs.”
Long COVID is long money. For doctors.
And of course, the virus doesn’t exist. So there’s that.
I’ve felt tired since 1952. I’ve successfully fought it off by limiting my conversations with long idiots.
If I were the predatory CEO of a pharmaceutical company, I’d establish studies proving every disease under the sun can have a long component, which must be treated with drugs and prevented by vaccines. For years.
Long flu, long colds, long eyestrain, long ass ache, etc.
Doctors received special training in medical school so they could make absurd diagnoses with a straight face.
Otherwise, this would happen:
“Doctor, when you just told me I have long COVID, you smiled. Why?”
“Sorry, I was keeping myself from laughing.”
“What?”
“Sometimes it gets to be too much.”
“You lost me.”
“Have you ever said something so stupid you busted out laughing?”
“I’m not sure.”
“Ha-ha. Sorry. I’m trying to be serious, but long COVID? I mean, come on. When I first read about it, I cracked up. I had to go home from the office. Everything started to seem funny. I couldn’t control myself.”
Someday, somebody will come up with Long Pregnancy. Women can remain pregnant for up to three years. But at the end, they don’t give birth. The baby they’ve been carrying is only a few cells. However, this is a serious condition and must be treated for the full duration of the pregnancy. Treated with very expensive drugs. Otherwise the patient could develop Chronic Fatigue, Mononucleosis, Rocky Mountain Spotted Fever, etc.
Some of these women, when untreated, also develop Tourette’s, even speak in tongues—which can be quite embarrassing in social situations. Like Thanksgiving dinner.
There is also a condition known as Long Sermons. People are exposed to it during church services. Some houses of worship may have to be closed down, in order to curb contagion out in the community. Psychiatrists can treat the disorder, with anti-psychotic drugs.
All of these long illnesses can be avoided if we start diagnosing doctors. You don’t need a license to participate. Invent your own disease and disorder labels. Offer the doctors help—at a price. No insurance, no Medicare or Medicaid. Straight cash for your services.
For every diagnosis you make, be sure to attach the word “long.”
You’ll be correct. What these doctors are suffering from, they’ve had for a long time. Possibly since college. Maybe even earlier.
Hell, tell them it’s genetic. Doing that lets you get away with anything.
Remind them of the story about Jesus and the Money Changers. Tell them they’re suffering from Long Money Changing. That’ll hit them where they live.
When it’s Children’s Mental Health Week, it’s ironic that attention isn’t actually focused on children’s mental health. Instead the focus is on mental illness and the host of psychiatric ‘disorders’ being used to label various aspects of childhood.
It would be more accurate to call it children’s mental illness week. Rather than label children mentally healthy, psychiatrists have for decades been unscientifically labelling them as mentally ill.
Through the redefinition of difficulties associated with the early years, psychiatrists have been editing childhood and adolescence out of existence. Challenging behaviour has gone under the psychiatric microscope, redefined, before being categorised as criteria for so-called mental ‘disorders.’
It’s an obsessive habit resulting in the regular use of meaningless and stigmatising psychiatric labels that can create even more difficulties for young people. Nothing appears to be off limits for editing psychiatrists.
Reading, writing and maths have been included in diagnostic manuals. They have been unscientifically classified as “impairment in reading,” “impairment in written expression” and “impairment in mathematics.”
The habit, which includes the use of labels like “ADHD” and “conduct disorder,” lead a young person down the road of mind-altering prescribed drugs. It demonstrates a focus on mental illness, not on mental health.
Children and adolescents are being chemically restrained, some for lengthy periods of time. Consequently, they experience the debilitating effects that go hand-in-hand with the drugs. The saddest and most tragic aspect of it all is some children don’t make it. They take their own lives after taking antidepressants known to cause suicidal thoughts and suicidal behaviour.
If psychiatric solutions worked, we wouldn’t keep hearing the psychiatric mantra that more and more children are suffering with mental illness. They fall into the category of having mental difficulties on the basis that boisterous or argumentative childhood behaviour has been redefined.
Parents who have lost their children have said they would never have let their children take the psychiatric drugs if they had been fully informed and knew the truth. It’s therefore vital we keep on beating the drum to expose damaging psychiatric habits.
In Children’s Mental Health Week, we must be reminded that children are not experimental animals. They are human beings who have every youthful right to expect protection, care, love and the chance to reach their full potential in life.
The bright new dawn of genetic engineering of life has a few problems. My, my.
Of course, the engineering companies pitching investors for money downplay the problems, and so do governments. Remember when Biden issued a release glorifying “overwriting cells of the body” (*) to achieve new breakthroughs in…something or other?
From Gene Watch UK, here are documented cases of genetic editing screw-ups. The language is technical, but you can grasp the essentials. Scientists are playing with fire.
“Petri et al. (2022) reported unintended genetic insertions and deletions in zebrafish following prime editing…Prime editing does not induce double stranded breaks and thus is often proposed to be safer than standard CRISPR/Cas systems. Nonetheless, integration of guide RNA derived DNA sequences was detected, showing that even using a technique without introducing foreign DNA, or double-stranded breaks, the technique does not rule out the potential for unintended insertion of exogenous DNA.”
“Tao et al. (2022) reported insertions of transposable elements in human cells in vitro following both standard CRISPR/Cas9 and prime editing systems, though these unintended changes were more common with CRISPR/Cas9 systems. Moreover, hundreds of integrated copies of vector plasmid DNA used to deliver the prime editing machinery were also detected…Moreover, insertions occurred at induced DNA breaks where CRISPR/Cas9 has been applied for controversial therapeutic editing…”
“Weiss et al. (2022) reported that in Arabidopsis plants, the DNA repair pathway chosen by the plant cells to repair the CRISPR-induced DNA breaks was influenced by the epigenetic status of the genome, including DNA methylation status… This in turn, influences the final mutational outcomes. This paper highlights limitations in relying on predictive tools that only take into consideration sequence information when trying to predict efficiency, specificity and mutational outcomes of genome editing. Bigger complexities beyond the level of the genome are also involved.”
“Höijer et al. (2022) reported large structural unintended on-target changes, including 4.8kb deletions to 1.4kn insertions, in zebrafish. This study showed the passing down of these mutations to the next generation.”
“Huang et al. (2022) reported that following CRISPR/Cas12 editing in fungal species, doublestranded breaks are repaired with multiple DNA repair pathways, each with different mutational profiles. This study highlights the lack of current understanding around the various DNA pathways that exist in various species, and how they may impact editing outcomes. Rather than being able to predict or even control CRISPR mutations outcomes as is often presented by GMO proponents, this study instead shows how CRISPR is being used in research to try to understand the basic mechanisms and complexities of DNA repair. Without a full understanding of the underlying science, assertions of precision and thus safety are unfounded.”
“Park et al. (2022) reported high levels of on-target unintended changes, when assessed using a new analytical tool that can sequence larger segments of the target site. Long range sequencing was able to detect a variety of changes including large deletions, highlighting the need for detailed analytical tools to assess on-target impacts.”
“Geng et al. (2022) report on-target unintended changes including genomic inversions, duplications, rearrangements and integration of exogenous DNA at the target-site in human cells, resulting in alterations in cell proliferation. This study highlights the potential impacts of unintended changes on target cell function, with implications for both edited plants and animals.”
But don’t worry, be happy. These genetic engineers all over the world may be bulls charging through shops shattering objects…but I’m sure they’ll eventually fix all their mistakes. Right?
For a final note—I’m not confident these genetic madmen even know what they’re playing with in the first place. When they see their errors, what are they really looking at? They make so many basic assumptions and guesses about DNA and genes, they could be operating in the dark, clueless and lost.
“Here’s a break in DNA where the repair after the cut failed.”
“Really? Are you sure that’s DNA?”
“It has to be.”
“Why?”
“Because if it isn’t, we have no idea what we’re doing.”
You know, THAT kind of thing.
The same kind of thing that happens when biologists trying to alter a virus fail to realize there isn’t any virus there…
These awesome problems can only be ignored in one way: by deciding that the 8 billion people on planet Earth are merely subjects in a vast ongoing experiment. And therefore have no reason to complain.
— Jon Rappoport
(*) FURTHER READING:
The Biden White House Executive Order: “Executive Order on Advancing Biotechnology and Biomanufacturing Innovation for a Sustainable, Safe, and Secure American Bioeconomy” (September 12, 2022). The link to this EO is here. My comments on this EOare here—as a “breaking news” update—at the very beginning of this podcast.
See also this podcast: “DARPA/Pentagon research projects to create future humans,”here.
And so here we are again with yet another ‘health scare’ story hitting the headlines. This time it’s measles.
Although this is a UK storyline, I would point out that the WHO published a News Release dated 16 November 2023 entitled Global measles threat continues to grow as another year passes with millions of children unvaccinated.
So I suppose it shouldn’t be at all surprising to see reports about an upsurge in measles cases in the UK, such as the BBC article entitled Measles: Why are cases rising and what are the symptoms?
The article gets straight to the point in the opening sentence,
“Measles cases are likely to spread rapidly unless more people are vaccinated, the UK Health Security Agency has warned.”
The next sentence states,
“Pop-up clinics are being opened to get more children vaccinated.”
Another BBC article, entitled Get measles vaccine to avoid rapid spread, says UK health boss, refers to Helen Bedford, professor of children’s health at University College London, and states, under the heading What is causing the drop in vaccinations?
“The pandemic also had an impact, with “some parents afraid to attend clinics for fear of catching Covid or because they were not clear that vaccination services were continuing”, Prof Bedford adds.”
Could it also be that some parents have actually started to earnestly research the real nature of vaccines and have decided not to subject their precious babies to that procedure?
Both BBC articles describe measles as ‘highly contagious’ and state that,
“It normally clears up after seven to 10 days.”
This raises the obvious question of why the alleged increase in cases is of such concern if it is a condition that is self-limiting and only lasts about a week or so?
The first cited article professes to address this issue by claiming that,
“…it can lead to serious problems if it infects other parts of the body, such as the lungs or brain.”
This is followed by the claim that,
“Complications can include pneumonia, meningitis, blindness and seizures.”
Although the article claims that ‘measles can be fatal’, it recognises that ‘this is rare’.
So why is this being reported as a serious problem when the number of deaths from ‘measles or related infections’ between 2000 and 2022 was 23? I am not denying that children and adults experience illness, and I would add that a single death is one too many. What I am contending is that claims that any death is caused by an ‘infection’, whether measles or something else, is grossly misleading, which is putting it mildly, because there is no evidence for the existence of any ‘infectious virus’.
I would point out that, by comparison, almost nothing is reported about the very real information relating to the much greater numbers of adults and children who have died as the result of the Covid-19 injections.
Nevertheless, the following claim is found under the heading Why are measles cases rising and where are outbreaks?
“Some 85% of children in 2022-23 had received two MMR doses by the time they were five years old, the lowest level since 2010-11. The goal is 95%.”
The idea of a required ‘target’ percentage of vaccination coverage is based on the concept of ‘herd immunity’. In order for ‘herd immunity’ to be valid, there needs to be evidence that the disease in question fulfils certain criteria, which are: that it is caused by a virus; that it can be prevented by a vaccine; and that one person’s ‘immunity’ – which really means their health status – affects another person’s health status.
These criteria have never been proven in reality. Herd immunity is a fallacy.
The advice, under the heading What should you do if you get measles? includes,
“rest and drink plenty of fluids.”
This is actually sound advice – although I must add that I am not providing anything that should be construed as ‘medical advice’.
The symptoms that are labelled ‘measles’ are part of the body’s normal processes of self-healing.
Unfortunately, the core message of both articles is to promote the MMR vaccine using propaganda rather than actual evidence of its efficacy, because there is none. No vaccine has ever been proven to prevent any ‘disease’ and all vaccines produce side effects, which the article claims to address under the healing What are the side effects of the MMR jab? with the comment that,
“Most side effects are mild and do not last long.”
The propaganda continues within the statement that Andrew Wakefield ‘wrongly’ claimed that the MMR vaccine was associated with autism. Although he was struck off the register as the result of his work, which was the discovery of a link between autism and gut issues, Andrew Wakefield was never against the use of vaccines, he merely questioned the use of multiple vaccines, like MMR, instead of single ones.
What IS conspicuous by its absence in either of these articles, is any reference to the Stefan Lanka court case in 2016, the result of which was a clear demonstration that the study papers that are used as ‘proof’ that measles is caused by a virus, do not actually provide that proof. In other words, it has never been proven that measles is caused by a virus.
It is obvious that this is another case of fear-mongering aimed mainly at parents of young children with the objective of increasing vaccine uptake and thereby boosting the profits of Big Pharma.
The question is: How many will comply?
I would also ask: Have enough people seen through the lies regarding the claims of safety and effectiveness of vaccines? Is that why the vaccination uptake has reduced?
I suppose only time will tell.
I am ever hopeful that there is an increasing number of people who are awakening to the truth about the so-called ‘healthcare system’ we are supposed to follow; and learning how they really can take back control of their own health and the health of their family, especially their babies.
The CDC withheld an “alert on myocarditis and mRNA vaccines” warning of the connection between heart inflammation and Covid-19 shots in May 2021, the Epoch Times has revealed.
The agency never published the alert; instead, its authors pushed vaccines on all age groups across the country.
Dr. Demetre Daskalakis was the author of the draft. He gained minor celebrity status during the response to Covid and Monkeypox, appearing on magazine covers dressed in bondage and posting shirtless photos demanding Americans wear masks.
The proposed alert came in response to two fatal post-Pfizer vaccination myocarditis deaths in Israel and repeated warnings from the Department of Defense.
Despite voicing private concern, Daskalakis publicly promoted the products. In the same month he sent the warning, he wrote, “Data over dogma. Vaccines Work,” in response to a CDC tweet allowing “fully vaccinated” Americans to “resume activities without wearing a mask or staying 6 feet apart.” He then posted, “Highly effective prevention means fewer barriers, physical or social. #Covidvaccine.”
At the time, the overwhelming majority of American teenagers had not received Covid shots. No state had a vaccination rate above 20% for 12- to 17-year-olds. In California, 90% of that age cohort remained unvaccinated. Indeed, the age gradient of risk was so steep – medically significant outcomes from the virus centered on the age and infirm – there was never a reason to push them on the general population.
Over the following two years, Dr. Daskalakis and his colleagues pushed the shots on every age group and deliberately withheld publishing its alert on myocarditis. Instead, the CDC sent repeated alerts encouraging Covid-19 vaccination for everyone.
Two months after the unpublished warning, the CDC sent an alert to doctors to “remind patients that vaccination is recommended for all persons aged 12 years of age and older, even for those with prior SARS-CoV-2 infection.”
The propaganda efforts, in conjunction with President Biden’s mandates, succeeded. By May 2023, a large majority of American teenagers had received at least one dose of a Covid vaccine. The vaccination rate for 12 to 17-year-olds in California skyrocketed from 10% to 84%, with one in five receiving an additional booster, according to CDC data.
The rate of vaccination for 12 to 17-year-olds went from 3% to 47% in Mississippi, 15% to 87% in Virginia, and 19% to 94% in Vermont from May 2021 to May 2023.
During that time period, Dr. Daskalakis repeatedly avoided voicing concerns over the risk of myocarditis. “I am so excited for my #Covid19 booster on Monday! I love vaccines!” he posted on Twitter in September 2022. In October 2023, he posted a photo of him receiving another Covid shot.
Daskalakis sent the draft alert to Henry Walke and John Brooks, both senior officials at the CDC. Their social media accounts do not share the same penchant for nudity and mRNA shots as Dr. Demetre’s, but, like Daskalakis, they continued to promote the shots without mentioning the discarded myocarditis alert.
In January 2022, Walke joined Dr. Rochelle Walensky in a CDC telebriefing that recommended a “safe and effective vaccine” for “all children five and older.” Brooks blamed “people who are not vaccinated” as “the source of new emerging [Covid] variants” in March 2022.
To this day, the CDC recommends children begin receiving Covid vaccines once they are six months old. It is not possible for immigrants to obtain legal permission to work in the US without one.
Fifty years ago, the most incisive questions from the Watergate hearings came from Senator Howard Baker: “What did the President know, and when did he know it?” The inquiry, ostensibly simple, encompassed the entire scandal.
The corruption of our public health apparati demands a similar probe. What did they know, and when did they know it? As the Covid regime demands “a pandemic amnesty,” the report from the Epoch Times adds to the plethora of evidence that their misdeeds were not mere mistakes; they were deliberate acts of fraud and deceit.
They knew of the risks, and they withheld the information from the American people. Stripped of informed consent, millions of citizens took the shots while doctors like Demetre Daskalakis denied them the right to know the risks of the product.
In spite of the mention of “spike protein” which seems to have a mythology all of its own within medical freedom groups, Greg Reese’s latest work is worth watching.
Here Reese shares the important work of Denis Rancourt wherein Rancourt analyzes death data during “covid” and demonstrates clearly how the cures for this made-up disease, along with cruel external force and mind control, were the actual cause of increased deaths.
Humanity historically has been bewitched and held spellbound by political and religious leaders, faux science and fear-based beliefs into cooperating with its own enslavement, self-harm and death.
As so many great researchers continue to look at what the so-called mRNA vaccines are about, what the actual contents are, and how they affect our biology, we do know that ALL vaccines have always been toxic and that NO virus has ever been isolated. All vaccines are forced upon us via lies and are all part of an incredibly ignorant (and nefarious) agenda.
Greg Reese has a unique way of writing and producing short impactful videos as he continues expanding his own awareness. This one is worth sharing.
~ Kathleen]
17 Million Murdered by COVID Vaccines and Voodoo Death
Denis Rancourt has a PhD in Physics, he is a former tenured Full Professor, and has published over one hundred articles in leading science journals. Rancourt and his team have used all-cause-mortality data to prove there have been about seventeen million deaths as a result of official COVID-19 measures, but not from Covid, which was a lie.
As far as I can tell, from the all cause mortality data that we’ve been studying extensively for a long time, there’s no such thing as a viral respiratory pandemic. (Denis Rancourt)
There was no pandemic in the sense that there was not a particularly virulent new pathogen that was spreading and causing death. That is not what happened. What happened was huge assaults against vulnerable people by many different methods. And every time you did that, you caused excess mortality. In all the countries where they were not doing that, there was absolutely no excess mortality, even if it was a jurisdiction that was right beside the one that was doing this. (Denis Rancourt)
Rancourt explains a science of psychological murder that has been officially studied and documented for well over a century. It wasn’t just the spike protein that killed us, it was the whole damn thing.
Psychological stress and social isolation are dominant determinants of an individual’s health that causes a suppression of your immune system. And you’re going to get some kind of infection, cancer, heart disease. And very often the lungs are very exposed to the environments and they’re subjected to all the bacteria that you live with all the time. You get bacterial pneumonia and it’s a huge killer when a society is stressed, meaning all of its individuals are stressed. The kind of psychological stress that kills you is when you’re entire world is turned upside down. Your whole life you thought you had a place in the world and it’s gone. That will kill you within a very short time.
We always occupy a dominance hierarchy, a social dominance hierarchy. That is how we organize our societies because we are social animals. It is a fundamental truth of how we organize societies. The stress that is intended to keep you in your place within that dominance hierarchy is an everyday chronic stress, and the stressors have to keep changing how they’re going to stress you because you get habituated to the stress. So they have to randomly hit you with hard things every once in a while to really make sure you understand what your place is. That stress is one of the biggest determinants of health.
But we have to admit that medicine itself is a massive killer. It’s a massive cause of premature death of individuals. (Denis Rancourt)
Modern Western medicine is officially recognized as the third highest cause of death. It was designed to be a way of controlling the population.
It was designed to be a way of controlling the population. The role of medicine as an institution in our society is to maintain the dominance hierarchy, is to keep people sick and to put them in their place. It’s just part of that institutionally. (Denis Rancourt)
Financed by the Carnegie Foundation and published in 1910, the Flexner report was used to outlaw natural medicine practices in America. The Rockefeller foundation then funded a new kind of medicine. An inverted form of heath care that utilized petrochemical drugs and experimental surgery to keep people sick, and in many cases, kill the patient. As Denis Rancourt has pointed out, this is how societies have been run for centuries.
A de-classified document entitled, “Geomagnetic Factors In Spontaneous Subjective Telepathic, Precognitive And Postmortem Experiences”, as well as decades of Trauma Based Mind Control research, shows us that the CIA and our governments are well aware of the deadly effects that traumatizing a population can induce. They are killing us with fear and trauma.
This is known as psychogenic death or psychosomatic death, It is the phenomenon of sudden death brought about by strong emotional shock. Chairman of the Department of Physiology at Harvard Medical School, Walter Cannon, called it Voodoo death because mind control is the main method used in Voodoo rituals. Which is well understood by our world leaders. Bill and Hillary Clinton spent their honeymoon in Haiti at a Voodoo ritual which Bill claims inspired him to run for political office.
I was particularly intrigued by the Voodoo religion.
Voodoo’s central ritual is a dance during which spirits possessed believers. On the most interesting day of the trip, I got the chance to observe voodoo in practice. After several minutes of rhythmic dancing to pounding drums, the spirits arrived, seizing a woman and a man. The man proceeded to rub a burning torch all over his body and walk on hot coals without being burned. The woman in a frenzy, screamed repeatedly, then grabbed a live chicken and bit its head off.
By the time we got back from Haiti, I had determined to run for attorney general.
On January 7, 2024, my research uncovered an official Department of Defense publication (DoD) from May 15, 2020, describing the masterplan for Operation WARP Speed, confirming DoD’s unprecedented role in running Warp Speed as a military operation:(1)
U.S. Department of Defense
IMMEDIATE RELEASE
Trump Administration Announces Framework
and Leadership for ‘Operation Warp Speed’
May 15, 2020 |The opening paragraph of the release places the U.S. military at the center of developing and controlling WARP Speed:(2)
On Friday, the Trump Administration announced the appointment of Moncef Slaoui as chief advisor and General Gustave F. Perna as chief operating officer of Operation Warp Speed (OWS), the administration’s national program to accelerate the development, manufacturing, and distribution of COVID-19 vaccines, therapeutics, and diagnostics (medical countermeasures).
Dr. Slaoui is a venture capitalist and, formerly, Chairman of Global Research and Development and Chairman of Global Vaccines at GlaxoSmithKline, where he led the development of five major novel vaccines. As the four-star general in charge of the U.S. Army Materiel Command, General Perna oversees the global supply chain and installation and materiel readiness for the U.S. Army, including more than 190,000 military, civilian, and contract employees.
From the start, Warp Speed was a Great Reset operation with the chief advisor, a “venture capitalist,” and the man in charge was a four-star general in the U.S. Army. This is an extraordinary example of the military-industrial complex at work, this time directing and organizing the greatest assault ever made on the lives of Americans and the U.S. Constitution. It is the U.S. Army acting as the assault troops for the global predators.
The DoD release describes how the heart of the defense establishment is fully geared up for Warp Speed:
“In addition to deploying 62,000 military service members in direct support of fighting COVID-19 on frontlines across the globe, the Department of Defense is racing towards a vaccine,” said Defense Secretary Mark T. Esper. “Through our research and development labs, such as DARPA and the Defense Health Agency, and our massive logistical knowledge and capacity, we are committed to achieving the goal of Operation Warp Speed for the American people.”
DoD Controls the Entire “Approval” Process for Safety and Effectiveness
The DoD press release makes clear that the FDA, which supervises and evaluates pharmaceutical industry studies for safety and effectiveness, is no longer in charge of vaccine development. The entire process is in the hands of the “government,” meaning the military:
The protocols for the trials will be overseen and set by the federal government, as opposed to traditional public-private partnerships, in which pharmaceutical companies decide on their own protocols.
The “protocols” for the trials are the entire basis of how and by what standards the clinical trials will be performed if they are performed at all. The “government,” in this case, is the DoD with some advisory input from HHS, neither of which has the legal right or the capacity to take this role.
Meanwhile, when discussing the organization of WARP Speed in 2020, Paul Mango, HHS deputy chief of staff for policy, disavowed any government role for testing the vaccines, stating, “Quite honestly, we are not conducting any science whatsoever inside the government to support Operation Warp Speed, none.”(3,4)
So, from the start, the government was completely in charge of the protocols for drug company research, removing the drug approval process from the hands of the FDA and the drug companies; but the “government” itself was doing none of the scientific work. That made a catastrophe inevitable because no one was authorized to conduct a scientific evaluation of the safety and efficacy of the mRNA platform injections that are causing so much death and destruction—and none has ever been done!
As we demonstrated in our book, COVID-19 and the Global Predators: We Are the Prey, and elsewhere,(5) it was well-known in the scientific community by 2020 that efforts to make vaccines for SARS-CoVs in animal experiments had such deadly results they were too lethal to the animals to ever attempt to test on human beings.
Proving the lethality of the mRNA platform and the “vaccines,” the death toll has been climbing since the opening day of the jabs, now with 20,000 reports to the VAERS reporting system monitored by both the CDC and FDA, with most of the deaths occurring in the first three days of the injection. For reasons I’ve already analyzed, based on scientific research and my forensic research experience, fewer than 1 in 100 serious adverse vaccine reactions are reported. Thus, 20,000 reports of death to VAERS indicate a real death toll of 2,000,000 or more.(6) Not only did they fail to do the preliminary scientific evaluation on humans, but they then also ignored and denied the death toll that continues to grow in the U.S. and around the world.
The Military Masterplan Chart Gets Leaked
In September 2020, the journal STAT published an article by Nicholas Florko, which displayed a leaked organization in July 2020 elaborate schematic for Operation Warp Speed, further documenting the vast military involvement. The chart divides responsibility for Warp Speed between “HHS” and “Defense.” The print is too small for a legible reproduction in this column but can be easily found at this link.(7) STAT reported:
The labyrinthine chart, dated July 30, shows that roughly 60 military officials — including at least four generals — are involved in the leadership of Operation Warp Speed, many of whom have never worked in health care or vaccine development. Just 29 of the roughly 90 leaders on the chart aren’t employed by the Department of Defense; most of them work for the Department of Health and Human Services and its subagencies.
Confirming the Groundbreaking Work of Sasha Latypova and Katherine Watt
Although we just located this May 2020 DOD Press Release, the role of the DoD in Operation Warp Speed has been under diligent examination for some time by brilliant researchers in the health freedom movement, including Sasha Latypova and Katherine Watt.
Sasha Latypova has recently published her “Summary of Everything and Quick Links, Updated –Year End 2023,” which covers research on the militarization of Warp Speed, including her work as well as Katherine Watt’s.(8)
Katherine Watt recently cut to the heart of the matter in regard to the sham role played by the drug companies:
All FDA activity that appeared to be license-related, pertaining to all biological products manufactured since May 2019, has been fraudulent, performative, charade, pretextual, and any other word or phrase that means not real, not substantive, not legally relevant.(9)
Implications for Robert Malone’s Role
Among the Deep State organizations described in the DoD press release as collaborators was “NIH’s ACTIV partnership for vaccine and therapeutic development.” ACTIV is essentially a Great Reset Center in the federal government for these collaborations between government and outside sources of wealth of power. Representatives on NIH ACTIV include The Gates Foundation, many top drug companies, and key government agencies.
In a sworn statement for a legal case dated October 21, 2021, Robert Malone, MD declared himself an “active member of NIH ACTIV” (p. 4 ) and further listed his participation in “Accelerated COVID-19 Therapeutic Interventions and Vaccines: ACTIV Therapeutics Clinical Working Group, NIH. Invited Participant. June, 2020-present” (p. 16).(10)
We were the first to make public Dr. Malone’s participation in NIH ACTIV, and more recently Dr. Malone has declared he is no longer a member. It seems probable that his role on ACTIV made him aware from early on that Operation Warp Speed was, in fact, a DoD operation and the drug companies had a sham role, but we are not aware of his bringing that information to the health freedom movement when he arrived.
As documented in his same sworn statement dated October 21, 2021, Malone also has a long and very active business and professional involvement with the Department of Defense, including managing large contracts and sitting on important committees at DoD and DTRA, The Defense Threat Reduction Agency, a defense and a combat support agency within DoD. Malone also denies any more recent or current involvements with DoD and DTRA.
Our earlier disclosures about Malone’s background were among his reasons for bringing a $25 million defamation lawsuit against us and against Dr. Jane Ruby, on whose show I discussed related issues. The judge has recently dismissed Malone’s defamation suit against all of us. The judge has also warned Malone that he might declare his lawsuit “frivolous,” and he has ordered Malone to explain why he should not be forced to pay the legal expenses of the Breggins and Dr. Ruby.(11)
Overall Implications of DoD Running WARP Speed
The implications of the DoD’s role in Operation WARP Speed are complex and require continuing unraveling. But these investigations may not substantially change the big picture because the ultimate villains are higher up the totalitarian totem pole and remain the same: the international governance being imposed upon the world by the global predators, including many multi-billionaires and the institutions they have captured from the UN and the World Health Organization (WHO) to the global banking system and the military-industrial complex—all of which we thoroughly document in our book, COVID-19 and the Global Predators: We Are the Prey.
4 There is a fascinating Government Accounting Office (GAO) memo from January 2022, stating that HHS took over control from the defense department in early 2022 and that GAO found that HHS itself did not have the ability to manage Operation WARP speed. https://www.gao.gov/products/gao-22-104453
When people, including “experts,” describe science, they usually mean “medical science,” which is a nonexistent or imaginary thing like viruses, but imply they are referring to actual science (chemistry, physics, and mathematics, mainly chemistry). Generally, they cannot talk directly about the actual science because they have not studied or practiced it significantly. In most cases, they lack understanding, even at the basic level.
So, when reading articles and comments about science from such “expert” or their “research,” make sure to know which science is referred to, the fake one (like medicine, virology, etc) or the actual one.
There is hardly any critique from knowledgeable people about the well-established and well-understood principles and practices of the actual science.
Viruses, variants, PCR testing, sequencing, RNA, mRNA, spike protein, vaccines, gain of function research, etc., are all fake science inventions. They can ONLY be resolved, and quickly, by applying the well-understood and well-established principles and techniques of actual science.
Fake science and its promoters are confusing and hindering resolving the issues – be cautious and seek help from actual science experts or scientists (link).
If someone has not studied and practiced chemistry, physics and/or mathematics in exhaustive detail and does not have hands-on experience but claims to be a science expert or scientist, in that case, they are fake and must be ignored. (link)
Viruses and their existence and isolation, RNA, spike protein, sequencing, PCR testing, and developing vaccines resulted from fake science/scientists. The science (chemistry) does not support any of these claims. There should not be any debate or argumentation about it.
Furthermore, whenever you see the word “study” or “research,” including those published in peer-reviewed “scientific” journals concerning the virus and its RNA, spike protein, mRNA and/or vaccine, consider that you are presented with false and fraudulent information.
Nobody can do such studies or research as none of the above items are available. No study has ever been done or can be done until they are available in physical form and pure from somewhere. It is not an opinion but a scientific fact.
You are not a fool, but fake scientists have fooled and tricked you with scientific-sounding jargon.
Medical experts, particularly physicians, are often presented as science experts or scientists, which is categorically a false and invalid claim. It is not just my claim or observation; anyone can form this opinion by studying the curriculum of any medical/medicine (M.D.) degree program. (link, link)
You will quickly observe an absence of science teaching and training. The medical degree emphasizes memorizing some physiological and chemical terms to associate with the patient’s symptoms to prescribe well-established allopathic medicines (mostly pure chemicals and non-physiological). There is no actual science or its research anywhere.
Therefore, it is not difficult to understand that medical experts can not follow the concepts and practices of isolation, purification, and characterization of viruses, RNA, spike protein, and vaccines. These are chemistry-based substances or molecules. Furthermore, it is unfortunate that they do not even try to understand the shortcomings (link) but demean the others, the genuine and actual scientists. The real tragedy!
Unfortunately, the public suffers from fake and false science propaganda, and so do the countries. The tragic mindset needs to be addressed – and quickly.
Information on my training, expertise, and experience is provided here.
Each of these supposed (fake) viruses traveled. In each case, they traveled from a foreign country to the US.
Name several viruses that, during the past 65 years, traveled from the US to foreign nations caused epidemics there.
No?
Can’t?
Why not?
Purported viruses can originate anywhere. They can travel anywhere. What’s the problem?
On top of all this, we have the “Hot Zone” theory/prediction of emerging deadly viruses:
They come from jungles and rainforests far away, and because modern travel is so frequent, they come to America, and…
Because our immune systems have no previous history of encountering these viruses, the germs sweep through our population and create pandemics.
Given that description, why haven’t the proponents of the theory cited viruses that originate in the US and travel to jungles and rainforests in other nations and cause deadly epidemics there? The people in those remote places have no experience with OUR viruses.
What’s the problem?
What’s going on is really quite simple. STORIES are being told about supposed viruses. The stories inevitably feature origins in foreign lands, and the germs travel to the US.
By any measure, we should have heard press reports, over the past 65 years, of the Chicago or New York or Miami or San Francisco or Des Moines Flu showing up in Germany, France, Brazil, West Africa, China, India…
But we haven’t.
And the reason is, those aren’t the STORIES. That’s all. This has nothing to do with science.
Nothing at all.
Therefore, all the stories of foreign viruses landing here are on the level of man in the moon and Cinderella and Snow White.
If these US outbreaks of illness in the US were caused by foreign viruses, we would have witnessed similar viral outbreaks in other countries that originated here.
Last night, as an unpaid subscriber, I received an email from Dr. Meryl Nass Substack titled “The “No Viruses exist” cult has been out in force lately.” (link)
After reading it, I am confused about whether to cry with the absurd logic presented or laugh at the arguments (hilarious science). I could not decide, so in my frustration, I am leaving it to you to decide – my thoughts or questions are highlighted in bold.
@ “I told Christine Massey over and over that her FOIAs were answered by all countries in the same manner because a) the countries lie about everything related to COVID, …”
So, why is it difficult to accept that they lied about the virus existence as well?
@ “These people want everything to be isolated the way they decide it should be isolated.”
No, the question is where this (the virus) has been isolated as claimed. The result of an isolation step is an isolated item, in this case, the virus – where is it?
@ “Some things require indirect measurements.”
True, but those things have to exist first. Where is that thing (the virus)? Please provide (scientific) evidence of its existence. Moreover, the measuring instrument must be calibrated/validated independently to show that it can measure lengths or distances. Where is the (“indirect”) test/method independently calibrated/validated to measure the viruses? There is none, and it is a fact.
@ “But here is the kicker. Have none of these pseudo-scientists ever had a cold? Have they never had flu? No cold sores? No genital herpes? No warts? All these are due to viruses.”
That is the question. How have these observations been linked to the viruses? Where are these viruses? Who has them (samples or specimens of the isolated viruses)?
Please bring these questions/thoughts to Dr. Meryl Nass’s attention.
Former Italian Health Minister Roberto Speranza is under investigation for homicide after emails reveal that, from the very start of the vaccinations, he knew the shots were killing people and gave orders to local health authorities to conceal deaths and serious side effects in order to reassure Italian citizens of their safety and to not jeopardize the vaccination campaign.
The story has been reported on both German and Italian news networks.
I will now provide an English translation.
The Rome Public Prosecutor’s Office is investigating Roberto Speranza, the Italian government’s health minister, during the time of COVID measures. He was responsible for the vaccination campaign.
The investigations are the result of complaints related to the so-called AIFA emails from the Italian Medicines Agency. The former director of AIFA, Nicola Magrini, is also under investigation.
The publication of these internal emails revealed that they had been aware of the dangers of the COVID vaccination from the start.
The accusation is that the responsible minister and the head of the drug authority knowingly and deliberately exposed the unsuspecting Italian population to this risk. Yes, they encouraged Italians to get vaccinated.
Vaccination was even made mandatory for certain professional groups. Consequently, many side effects, including fatal ones, came to light.
The investigations are for murder, serious bodily harm, and more, because Speranza and Magrini evidently gave instructions to the local health authorities to conceal the deaths and serious side effects that occurred immediately after the vaccinations began, in order not to jeopardize the vaccination campaign and to reassure the citizens about their safety.
The responsible minister and the head of AIFA are now expected to answer for these actions.
According to the complaints from the police unions and the financial police, as well as from the private organization Listen to Me, which represents 4,200 people damaged by vaccines.
In Italy, police officers and teachers were subjected to mandatory COVID vaccination.
Here is the former health minister, Roberto Speranza, proudly announcing vaccination statistics in Italy.
“We have now reached a massively significant percentage of vaccinated people in Italy, 89.41%. Therefore, currently in Italy, just over 10% of the population remains unvaccinated.”
Well, today Roberto Speranza is under investigation for lies he allegedly told about vaccines.
Among the crimes he is accused of are ideological falsehood and murder.
“Look, this is the document we are showing you tonight exclusively. It states the former minister Roberto Speranza, along with Nicola Magrini, the former general manager of AIFA, are both registered in the investigative records of the Rome Prosecutor’s Office.”
Last week, the House of Representatives of the Philippines passed a resolution to investigate over 260,000 unexplained excess deaths in 2021 and 67,000 unexplained excess deaths in 2022.
The next day, they were hit by a 7.6 magnitude earthquake.
“Oh, you can’t come in here, are you kidding? This is a high-security lab. Only certified professionals can enter. We’re dealing with viruses. Off limits to you and all civilians. WE tell you what we discover. YOU accept our findings. Now shut up and get lost…”
That’s the attitude of elite researchers who claim to be discovering and isolating new viruses…
When, in fact, as many of us have detailed…
They’re doing no such thing.
They’re faking it, in multiple ways.
They’re in charge of faking it.
A reader, in a comment, mentioned that WE should be able to go into those labs WITH VIDEO CAMERAS and record everything going on in there.
BANG.
BOOM.
Exactly.
We should be able to get in there with a pro video crew and cameras that record every single action these bozo researchers perform.
Many cameras catching the action from every possible angle. Up very close, medium range, ceiling angles, angles from the floor.
With sound. And send a few people in there who have previously detailed how the virus fakery is accomplished. They stand close to the researchers and stop them at any moment and ask questions.
“Why did you just do that?” “What’s in that dish?” “You claim you just proved WHAT? Explain how you proved it.” And so on.
Every single step of the so-called isolation of new viruses is questioned and criticized—and recorded on video, with sound—until there are no more secrets, no more proprietary information, no more missing pieces in the process. To OUR satisfaction.
Otherwise, there is no reason under the sun to accept what these weasels are telling us.
“Doctor, you just SAID you separated the virus from the solution in this dish of soup. You SAID it but you didn’t show it. We all know that. When are you going to SHOW the isolation?”
“Why did you just dip that instrument in the soup? What are you doing? You’re measuring something? Prove it. What are you measuring?”
“You SAY you just removed a virus from this soup you created, and you’re purifying it, and then you’re going to put a sample under an electron microscope, and then you’re going to say the particles that show up are viruses. So we’ll have to go over all these steps very carefully and slowly, because we’ll have many questions. Many pointed questions you’ll need to answer.”
All this is happening live, on camera, with sound.
In the moment.
Then we’ll see what these elite researchers know and don’t know.
It is important to note that physicians are taught and trained to write prescriptions for well-established pharmaceuticals (aka potent chemicals and mostly physiologically irrelevant) – no more, no less.
For this purpose, they must memorize some physiology, biology, and chemistry words during the training/education.
Furthermore, they do not study or get training to invent or identify new diseases or develop new treatments (pharmaceuticals/chemicals) – scientifically.
It is unclear how they consider and promote themselves to be scientists and practitioners of science. It is hard to find the basis for their claims. There is practically none. Wrong? Prove it!
Using the vocabulary from the subjects mentioned above, without relevant laboratory work and with the help of computer drawing software, they declared the existence of the viruses, their RNAs, and spike proteins. It is purely a fictional story without any scientific evidence. No physical specimens of these things are available anywhere. Everything is illusionary or mythical. Wrong? Prove it!
On top of that, mysterious vaccines have been developed for the imaginary virus or illness. Sketchy details describing the vial’s content have been provided. There is a strong possibility that these vials may contain some unknown content, potentially harmful (microbial) gunk, without usual and standard scientific characterization. Wrong? Prove it!
Every claim is based on peer/buddy-reviewed articles/”research” from journals labeled “scientific” without accreditation by any independent third party, but primarily by self or news media-proclaimed experts.
In short, the claims about the virus, RNA, spike protein, vaccines, and so-called medical science, in general, are textbook cases of quackery and science fraud. Wrong? Prove it!
It should not, then, be surprising to note that medical/pharmaceutical experts sell/promote vaccines through authorities’ sponsorship and mandates and with the highest levels of immunity. It indicates that they may be aware of the uselessness and harmfulness of the products; otherwise, they would sell directly to consumers/patients like other safe and effective products. Use caution in accepting these experts’ claims. In most cases, they are factually false or not science-based.
The above views are based on my working experience (30 years) as a research scientist at Health Canada for the assessment and evaluation of pharmaceutical products. Further information about related work may be found here: Helpful Notes and the Book by (Dr. Qureshi, co-author), who has extensive experience in substance isolation, characterization, and analytical testing, among other specialties.
I watched a recent interview (link) of Prof. Syed Sattar (Retired Professor of Virology from the University of OTTAWA, Canada), who is still active in the area. He is a great friend, and I greatly admire his academic credentials and achievements. I have known him personally and professionally, at least for twenty years.
I find the interview informative, describing the fundamental concepts of virology, notably virus isolation. That is, how the virus isolation concepts are illustrated in virology literature, which Prof. Sattar emphasized as well-established practices and routines in virology laboratories.
However, issues and confusion arise when virologists, including Prof. Sattar, describe isolation as “culturing or its part” as a virus. It is essentially their critical misunderstanding, i.e., considering “culture” and the “virus” as the same thing. In reality and scientifically, they have to be and are two separate entities. I often describe the difference between the two as being chicken (“virus”) and “soup,” which may or may not contain the chicken/virus.
To show the presence or existence of a virus, the virus (if there) must be isolated or separated from the culture. The separation of the virus from culture and its content is called the “isolation” step, which has never been done. This is the confusion or misunderstanding virologists and microbiologists have and are unwilling to take the time to consider or evaluate.
They often defend their position by arguing that viruses (particles) are minute in size and number and cannot be seen or isolated (separated) from cells (culture) to observe. Therefore, viruses and culture have to go together and side by side. Hence, it resulted in considering/calling culturing or culture a “virus.”
It is to be noted that there is no objection to the culturing step, which, in reality, is a fermentation step for growing or multiplying the viruses. However, once the viruses are sufficiently multiplied, they MUST be isolated or separated to evaluate their identity and characteristics, such as structure, RNA/DNA proteins, etc. This step is missing.
So, effectively, virologists work with cultures but make claims about them as “viruses.” It is like working with debris from a forest but selling it as novel and rare wood dust particles.
Seeing the photographs with low or high-resolution microscopes does not establish the presence of something, just like seeing small yellow particles would not confirm the presence of gold in the sample. The particles must be isolated/separated to characterize them.
It is an invalid argument that viruses are small (in size and number), so they cannot be seen without culturing or separating from cells. Smaller items like carbon, hydrogen atoms, and molecules are commonly available in isolated and purified forms with full characterization or certifications.
If the claim is that there are viruses, then these entities, considered particles, must be available in, isolated, purified, and fully characterized. Nothing of this nature is available, including for the coronaviruses. Calling or considering cultures/isolates as viruses is an incorrect understanding that needs to be abandoned.
Links to some articles for further information on the topic:
An unexplained pneumonia-like sickness is reportedly swiftly spreading through schools in China, leading to a surge of hospitalizations of children.
Over the past few weeks, numerous schools in China, predominantly in Beijing and Liaoning province, have reported a rapid increase in children presenting with severe symptoms. These symptoms, including high fever and lung inflammation, are eerily similar to those of pneumonia, Daily Mail reported.
However, what sets this illness apart is the lack of common respiratory symptoms like coughing. This unique symptom profile has led health professionals to label this as an “undiagnosed pneumonia.”
Note that this peculiar symptomatology has reportedly baffled health professionals, who are struggling to categorize and understand this new illness.
Mystery? Baffling? Eerie?
I don’t think so. They always give you: “This has no explanation”—just before they magically announce they’ve found a new virus.
Of course, they never actually isolate that new virus. They never discover it. They just invent a fairy tale.
As far as “mysterious” is concerned in China right now, here is a definitive statement from the American Thoracic Society: “It is possible to have pneumonia without a cough or fever.”
Oops.
For years, doctors have been diagnosing patients with pneumonia when there is no cough present. It’s not baffling. It’s not ultra-strange. So forget about that.
Which leaves the question: what IS making all these children in China sick? Hmm. Let’s see. Could it be changes in the moon’s orbit? Sun spots? Lasers fired from UFOs? Infected bats imported from Mars?
No?
Well, how about THIS?
US Embassy in China, October 30, 2023:
EVENT: This is a notification that the Beijing City Government has issued an ‘orange’ alert for air pollution effective from 12:00 Monday, October 30 until 24:00 Thursday, November 2. An ‘orange’ alert means that official forecasts indicate Beijing’s Air Quality Index (AQI) will exceed 200 for two consecutive days or 150 for three consecutive days. The alert may be extended if air pollution levels persist.
During an “orange” alert, some businesses may reduce operations.
ACTIONS TO TAKE: The U.S. EPA recommends people with heart or lung disease, older adults, children, and teenagers limit or avoid outdoor physical activity when the AQI level exceeds 200. It recommends everyone avoid outdoor exertion if the AQI level exceeds 300.
Reuters, October 31, 2023:
Authorities issued their highest warnings for fog and haze on Tuesday as smog enveloped major cities in northern China, warning the public that visibility could drop to less than 50 metres (164 feet).
Northern province Hebei launched an anti-pollution emergency response, listing traffic safety controls for when necessary including suspending flight takeoffs and landings, temporarily closing highways and suspending ferries, China’s meteorological bureau said in a notice.
As air pollution levels in the wider Beijing-Tianjin-Hebei area and northern part of Henan province reached moderate to severe, pollution control experts said increased industrial activities, heavy trucking and crop fires had contributed to the haze, state media CCTV reported.
Crisis 24, a “global security platform,” reports that heavy pollution is occurring in Northern China provinces, including Beijing and Liaoning, the two areas reporting the “mystery illness” in children.
I see. Pollution causing lung problems. Wow. I just fell off my chair. What a revelation. Who ever heard of that?
Yeah. I went through all this—reported on all this—in 2020—with “COVID.” That was a mysterious pneumonia, too. Except for the heavy air pollution. Every year in China, about 300,000 people die from pneumonia (lung problems). That means there are millions of cases.
Psychiatrists used to not put much effort into diagnosing. Instead, they focused on getting to and working on the issues in their clients’ lives that were upsetting them. But all that changed when the 1980 DSM came out. Since then, diagnosing mental disorders has been one of their main focuses (prescribing medicine being the other). People pay huge sums of money for psychiatrists’ expert opinions, and their diagnostic evaluations carry great weight in court, school, the workplace, and disability determinations. But is this truly warranted? Is a doctor really needed to make a psychiatric diagnosis, or can anyone do it?
Here are three points which support the idea that anyone can make a psychiatric diagnosis:
1. All the diagnostic criteria that psychiatrists learn in their training can be easily found on various websites. Therefore anyone can look up the criteria for diagnosing any mental illness and then conduct a do-it-yourself diagnostic evaluation.
2. It’s true that only trained doctors can perform physical exams and order lab tests, x-rays/scans, biopsies, etc.. And it’s true that only doctors are qualified to interpret their results. But these medical workups are only ever done to verify physical illness diagnoses, like cancer or diabetes. They are never done to diagnose mental illnesses. If a medical workup is ever done during a mental illness evaluation, it’s only to rule out a real (physical) illness.
3. If one examines the criteria for all the mental illness diagnoses, it becomes clear that identifying them doesn’t require any medical background or skill. For example, here are some criteria for diagnosing depression: diminished interest/pleasure in activities, indecisiveness, and feelings of worthlessness. First of all, these are not terms/concepts that only doctors are privy to. Secondly, they’re vague, subjective perceptions rather than objective, scientific facts. They’re in the eye of the beholder. Thus, any human could offer an opinion as to whether or not someone is experiencing them. Who’s to say which is the “right” opinion?
These are all excellent points.
But if a regular human such as you dares to take it upon yourself to perform a psychiatric diagnostic evaluation, you’ll be laughed at for your brazenness. You need a doctor’s official stamp of approval to make the diagnosis appear legitimate and valid. Doctors are greatly revered and trusted. Only if you tell others that a learned doctor diagnosed you with your mental illness, will it be viewed as a proven fact rather than a mere opinion. So even though psychiatrists don’t use any medical knowledge when making diagnoses, they do have MD degrees, and that’s enough.
Furthermore, for centuries psychiatrists have been designated by society to be the supreme authorities over several key areas: They decide who is insane and should be involuntarily committed and forcibly sedated. They also determine who is mentally unfit and should lose their right to manage their own lives. Perhaps these longstanding power roles have culturally imbued psychiatrists with an aura of superhuman capabilities which makes all their opinions far more important than a regular person’s. The common belief that psychiatrists have the intimidating ability to read and manipulate people’s minds may enhance this aura. Without necessarily being consciously aware of the aura, people may sense it, fear it, and be awed by it. They may thus be particularly likely to unquestioningly, submissively accept whatever their omniscient psychiatrist diagnoses and commands.
Psychiatry’s aura of superiority may be what enabled it to convince people that mental illnesses are real physical illnesses, even though they’re opposites: First psychiatry constructed a fantasy about emotional distress being a medically-treatable disease caused by a chemical imbalance or brain anomaly.Then it turned it into a reality just by proclaiming it to be true. It didn’t matter that 50 years of intensive research never found any chemical imbalances or brain anomalies. Nor did it matter that antidepressants were proven to be mere placebos(1). When psychiatry says something is true, that makes it true, no matter how illogical. And this isn’t the first time this was done: The diagnosis of hysteria was taken seriously for many centuries. It was another example of emotional distress being unfoundedly declared to be a medical condition. This time it was said to be caused by a wandering uterus, and the treatment was to coax it back into place(2).
Psychiatry would lose its power over people if its aura was removed, because nothing would be left but smoke and mirrors. People would lose faith in it (just as happened to the Wizard of Oz when his curtain was removed, revealing that he wasn’t a higher being but just a regular human). Psychiatry’s customers would then realize that they’re not defective and helpless as their doctor oppressively insists. They’d see that they’re actually capable of thinking for themselves in order to devise adaptive ways to solve their own problems. (The tin man, scarecrow, and lion made the same realization after their wizard was shown to be a fraud.) If this ever happens, then people will no longer feel compelled to follow the yellow brick road to a doctor’s office to have their painful feelings medicalized.
1. Kirsch, I. “The Emperor’s New Drugs: Exploding The Antidepressant Myth”, Basic Books, New York, 2010.
2. Wellesley, M “A Load Of Ballokis” London Review of Books, 23 April 2018.
Lawrence Kelmenson has practiced psychiatry for 32 years, working with children, adults, and families. He graduated medical school from State University of New York, and completed psychiatric residency training at Cornell. He then became staff psychiatrist, and later medical director, of Craig House Hospital in Beacon, New York until 2000, and has since conducted a psychotherapy-based private practice in Cold Spring, New York.
The narrative of an Anthrax bioweapons attack is again in the “news cycle” and remains prominent on the CDC website.
A November 15, 2023 CDC news brief updated advice for healthcare providers in preventing and treating anthrax should a “wide-area aerosol release of B. anthracis” occur.
CDC has classified B. anthracis as a “category A” organism of concern because an attack with B. anthracis would happen via aerosolized exposure. How does the CDC know that any attack would be in an aerosolized form? Does the CDC have a crystal ball? The CDC did seem to know the problems of the COVID19 vaccines before they were distributed:
Americans need to be prepared for the possibility that they may feel a little unwell after they get a coronavirus vaccine, if one is authorized. – CDC Prevention Advisory Committee, November 23, 2020.
Appearance of small welts or sores that are itchy.
Confusion or dizziness
Cough
The sore developing into a blister that turns into a skin ulcer.
Nausea and loss of appetite ( if the infection is through ingestion).
Swelling in the neck area.
Headache & fatigue
Sweats
Shortness of breath
Diarrhea accompanied by severe abdominal pain.
If exposed to the CDC anthrax antigen, the CDC recommends Post-Exposure Prophylaxis (PEP), suggesting immediate vaccination and antimicrobial therapy (Ciprofloxacin and Doxycycline are first-line options). The CDC says a new and improved anthrax vaccine became available in 2019. However, on July 20, 2023, the U.S. FDA approved a neweranthrax adjuvanted vaccine, Cyfendus for use in adults 18-65 exposed to anthrax as a countermeasure. Where there is one countermeasure there are always more.
A 2000 report published in Experimental and Molecular Pathology titled, “Antibodies to Squalene in Gulf War Syndrome,” described symptoms including severe headaches, nausea, muscular pain, joint swelling, short term memory loss, night sweats, depression. Autoimmune conditions ranged from fibromyalgia, lymphadenopathy, Lupus, Multiple Sclerosis, autoimmune thyroid disease, chronic fatigue syndrome to malar rashes, chronic headaches, non-healing skin lesions, musculoskeletal disorders (ALS), among others.
US District Court Judge Emmet G. Sullivan ruled that it was illegal for the federal government to mandate anthrax vaccinations. Judge Sullivan banned the Pentagon from forcing military personnel serving in Iraq, Afghanistan, South Korea, and part of Asia and Africa to get the anthrax shots without their prior consent. The military could not require the vaccine until the FDA approved it for the specific use of inhaled anthrax. – Hill & Ponton Disability Attorneys, Dec. 2020, updated
In general, adjuvants, such as squalene are added to vaccines (flu shots) to hyper-stimulate the immune system. They are designed to stimulate antibody creation and remain in the body for a prolonged reaction. The new class of adjuvants are comprised of phospholipids (surfactants), which also happen to make up the membrane of every human cell. Using recombinant DNA technology, phospholipids are combined with recombinant proteins and engineered in a way to be structurally and functionally identical to their natural counterparts. As such, the body can create antibodies to its own tissues in an attack of the Self.
A Little Anthrax History
B. anthracis (anthrax) was discovered in 1875 by the German physician and one of the founders of microbiology, Robert Koch (1843-1910) who developed Koch’s Postulates. He also discovered the deadly toxins cholera and tuberculosis, then was awarded the Nobel Prize in 1905.
Anthrax had also been produced in a Russian lab since before the 1920s. In May 1926, the first report of a new anthrax strain with enhanced virulence was filed, resulting in a 100% increase in mortality. By 1930, Germany had a bioweapons facility. By 1935, the Russians had developed a human anthrax vaccine.
Today, many countries have developed weaponized anthrax through genetic manipulation using bacteria and insects. According to the NIH, Russia created anthrax by introducing an “alien gene” into the highly toxic Baccillus Anthracis bacteria. The new NIH version of anthrax is resistant to antibiotics.
They used an alien gene and genetically altered bacterial immunological properties to produce a deadly pathogen to Humans. Where did they get an alien gene from? A UFO crash perhaps? Negotiations with other beings? Your guess is as good as mine….I found a patent with a method for removing plasma (DNA) from Bacillus anthracis bacteria using CRISPR/Cas9 system and it’s owned by China. This is how they get Mycoplasmas.
— Ariana Love, ND Nov. 23, 2021
The process that began before 1950 is called Cross-Species-Genomics. Its purpose? “To generate disease models.” In other words, to produce the deadly biowarfare agent for use in vaccines. The science reveals that deadly agents do not cross the species barrier unless genetic modification is used in a lab setting. A 2002 study in the Journal Pathology, Microbiology, and Immunology states:
The assessment of species barriers has relied on the development of a clinical disease in inoculated animals. On this basis there is a highly efficient barrier limiting transmission…
After 1979, the Soviet’s preferred a bioweapon of inhaled anthraxdue to undifferentiated symptoms that resemble a cold or flu. This version was genetically attenuated sometime before 2006 by the NIH.
British SIS intelligence reports from 1924 confirmed the use of anthrax shells (with a capacity of 2 liters/shell), bombs, and mortars.
In the April 2021 Journal Nature, the study, “Adjuvantng a subunit COVID-19 vaccine to induce protective immunity,” the reference to Alhydrogel is listed under Adjuvant Formulations and immunization:
Alum (Alhydrogel 2%) was purchased from Croda Healthcare (batch 0001610348)
According to a 2021 study in Molecular Cell, Anthrax is developed to “regulate gene expression by binding to DNA sequences and modulating transcriptional activity through their effector domains.” So Anthrax has more than one function.
The reason to be aware of any possible aerosolized anthrax bacterium spore release is to know the natural remedies that exist so you have a choice between consenting to an experimental vaccines and prescribed pharmaceuticals or natural options.
As a disclaimer, nothing suggested in this article is intended to replace consulting with a medical expert if you have a medical problem. Everyone should take responsibility for his or her own health and do your own research. That said, the following herbs and foods are commonly known remedies to help enhance the immune system, your built-in defense system, and can be incorporated in or with meals.
Garlic displays potent anti- anthracis activity, according to the 2021 Journal of Ethnopharmacology. So start thinking of your favorite garlic dishes to create in the kitchen. Alternatively, you can make a tea. Peel and crush into a fine paste with water. Mix paste in two glasses of warm water. Drink in two doses: morning, before bedtime. Continue for 10 days.
Oil of Oregano
Homeopathic anthracinum – super-diluted and potentized extracts of the anthrax bacteria itself to boost immunity on a nanoscale.
Herbs:
Wintergreen essential oil – for discomfort in bones, muscles and joints. Add a few drops to olive oil and apply to the soles of the feet. You can also add 3-5 drops to a bath.
White Fir – oxygenates with antiseptic properties known for us in disease caused by bacteria. Mix essential oil with olive oil or use essential oil as aromatherapy.
Thyme and Melissa (lemon balm) – Fill a capsule with 12 drops of Thyme and 1 drop of Melissa.
Spruce – essential oil has oxygenating properties with support to the nervous and respiratory systems.
Idaho Tansy – stimulates the immune system. Can be applied topically against infection or on wounds.
Savory and Oregano oil – both herbs are potent anti-microbials.
Astragalus root powder Chaparral power Tea – Mix 2 teaspoons of each herb in 2 glasses of warm water. Strain and add organic honey. Drink twice during the day.
Echinacea – boil 2 tsp. root powder in two glasses of water. Strain. Drink twice daily for a week or more.
An investigation by The BMJ into the Vaccine Adverse Event Reporting System, or VAERS, found multiple deficiencies in the system, including the revelation that the government runs two systems — one for the public, and a private back-end system that contains all of the corrections and updates, including deaths that occurred after an initial injury.
When Dr. Robert Sullivan collapsed on his treadmill three weeks after his second COVID-19 vaccine in early 2021, he fell into a “nightmare” ordeal that he said exposed glaring deficiencies in the nation’s vaccine safety monitoring system.
But like others interviewed in a recent investigation by The BMJ, Sullivan hit barrier after barrier when trying to submit and update his report.
Almost three years later, still grappling with debilitating symptoms, Sullivan’s experience highlights the systemic problems with the U.S. adverse events monitoring system run jointly by the Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA).
From doctors unable to file reports to disappearing data, limits on transparency and lack of resources to follow up on concerning vaccine reactions, experts warn VAERS is failing to detect critical safety signals.
According to one of those experts — VAERS researcher Albert Benavides, whose experience includes HMO claims auditing, data analytics and revenue cycle management — VAERS’ failure isn’t accidental.
Like others interviewed by The BMJ, Sullivan experienced limited follow-up after submitting his VAERS report. He received only a temporary report number months after his initial submission.
A physician named “Helen” (pseudonym) told The BMJ that fewer than 20% of concerning reports get follow-up, including many deaths she reported.
In consultation with Benavides, an audit by React19 found that 1 in 3 COVID-19 vaccine adverse events reports in VAERS were either not posted publicly or were deleted. React19 is a nonprofit that collects stories of people injured by the mRNA vaccines.
According to The BMJ, of those queried by React19, “22% had never been given a permanent VAERS ID number and 12% had disappeared from the system entirely.”
Benavides, who publishes the VAERSAware dashboards documenting many of the problems with VAERS, said there is even deeper dysfunction in the VAERS system — from inventing symptoms to deleting reports.
“VAERS does not publish all legitimate reports received,” Benavides told The Defender. “They throttle publication of reports. They even delete legitimate reports.”
For a system dependent on voluntary engagement, these restrictive policies keep critical data hidden, according to Benavides.
In 2007, the U.S. Department of Health and Human Services (HHS) contracted with Harvard Pilgrim Health Care (HPHC) to review the VAERS system. In 2010, HPHC filed its r report, which determined that 1 in 39 people experienced vaccine injuries and that only around 1% of vaccine-related injuries or deaths are ever reported to VAERS.
The CDC, which operates under HHS, scuttled the study, refused to take calls from the researchers and declined to upgrade the VAERS system when a new, much more effective system was developed.
‘Blind spots are self-created’
VAERS “collects reports of symptoms, diagnoses, hospital admissions, and deaths after vaccination for the purpose of capturing post-market safety signals,” according to The BMJ.
But the limited transparency of VAERS data presents barriers to proper analysis, according to The BMJ’s investigation and researchers like Benavides.
The public — including doctors and other report submitters — can access only incomplete initial reports, not updates with vital details.
This means outcomes like death are often excluded if the initial report was for an injury and a subsequent death report was filed.
“I made the false assumption that my conversation [with VAERS] would result in an adjustment to the publicly reported case,” Patrick Whelan, M.D., Ph.D., told The BMJ.
Whelan, a rheumatologist and researcher at the University of California Los Angeles, in 2022 filed a report of a cardiac arrest in a 7-year-old male patient after COVID-19 vaccination.
“I assumed that, since it was a catastrophic event, the safety committee would want to hear about it right away,” Whelan said. But nobody called him or requested an update after his submission.
“There was no mechanism for [updating] it,” Whelan told The BMJ. “The only option I had was to make a new VAERS report.” Without updates, the VAERS data showed that the boy was still hospitalized.
Whelan is one the authors of a recent critique of the Cochrane Review that concluded the COVID-19 mRNA vaccines were not dangerous.
The problem with VAERS is not limited to a lack of adequate follow-up but to the incomplete and often inaccurate information found there.
“VAERS in effect allows typos, truncated lot #’s, UNK [unknown] ages, UNK vax dates, UNK death dates, etc. to pass through into publication,” Benavides said.
Benavides said specific data — including ethnicity, hospital names, attending physicians, submitter’s relationship to the patient, patient and submitter addresses, telephone numbers and emails — collected by VAERS are not published,
“Any blind spots are self-created, in my opinion,” he said.
Agencies maintain two separate VAERS databases — public gets to see only one
“There’s two parts to VAERS, the front end and back end,” stated Narayan Nair, division director for the FDA’s Division of Pharmacovigilance at a December 2022 meeting with advocates, according to The BMJ. “Anything from medical records by law can’t be posted on the public-facing system,” he said.
The BMJ investigation discovered that the FDA and CDC maintain two separate VAERS databases, one available to the public that contains only initial reports, and a private back-end system containing all of the updates and corrections.
“Anything derived from medical records by law” cannot be posted on the public-facing system, Nair told the advocates, according to The BMJ.
In an apparent contradiction to this claim, The BMJ noted the FDA’s Adverse Event Reporting System (FAERS), which collects post-marketing information on drug reactions, posts its updates publicly.
Sullivan, who met Nair years before COVID-19 and considers him a friend, told The Defender that if this “very bright, kind and caring person” could not fix VAERS, “I don’t think it’s fixable.”
CDC says it reviewed 20,000 reports of deaths — none were related to COVID shots
Withholding outcome data like deaths obscures critical safety signals, experts contend.
James Gill, a medical examiner, reported the death of a 15-year-old patient after vaccination, but the case was dismissed by the CDC despite autopsy evidence, according to the BMJ investigation.
Physician “Helen” told The BMJ that after filing reports on her medical patients, including six who had died, she received only a single request for medical records on the death and two for hospital-admitted patients.
The standard operating procedure for COVID-19 vaccine reports in VAERS, according to The BMJ, is for reports to be processed quickly and for “serious reports” to receive special review by CDC staff.
However, while some other countries have acknowledged the probable connection between the mRNA vaccines and death, the CDC, while claiming to have reviewed nearly 20,000 death reports, has yet to acknowledge a single death linked to the COVID-19 vaccines, The BMJ said.
Benavides provided The Defender examples of VAERS “deleting legitimate reports,” not just duplicates or false claims.
“VAERS even deleted dead Pfizer Trial patients,” he said, claiming that this report, for example, was not a “duplicate” and did not appear to be fake.
Benavides said:
“There are currently about 50 deaths that are not counted as deaths because the correct box is not checked off.
“There are thousands of reports and about 100 deaths in ‘UNKNOWN VAX TYPE’ in VAERS. Read the narrative to see these are clearly C19 jab-related deaths.
“There are over a thousand cardiac arrests where they are not marked as dead, and I question if they actually survived because there is no mention of ROSC [return of spontaneous circulation].”
“Why couldn’t VAERS populate the ages of these dead kids before publication?” Benavides said, pointing to this report on his website.
Physicians report only FDA-recognized adverse events
Ralph Edwards, former director of the Uppsala Monitoring Centre and until recently editor-in-chief of the International Journal of Risk & Safety in Medicine, told The BMJ the regulators may be relying too heavily on past epidemiological data, especially for new types of adverse events. “If something hasn’t been heard of before, it tends to be ignored,” he said.
Without guidance to report potential risks, doctors also face barriers. “Physicians are only willing to talk about FDA-recognized vaccine adverse events,” stated physician “Helen” in a 2021 meeting between the FDA and physicians and advocates, according to The BMJ.
Svetlana Blitshteyn, a neurologist and researcher at the University at Buffalo, New York, told The BMJ if physicians are not educated to look for a specific condition, they’re unlikely to test for it or know how to treat it.
Sullivan told The Defender he believes his experience of developing pulmonary hypertension after taking the mRNA vaccine is one such safety signal the CDC and FDA are overlooking — a condition he believes many athletes have unknowingly developed.
Sullivan co-authored a paper of his and one other similar case of post-vaccine pulmonary hypertension. According to the paper:
“Pulmonary hypertension is a serious disease characterized by damage to lung vasculature and restricted blood flow through narrowed arteries from the right to left heart. The onset of symptoms is typically insidious, progressive and incurable, leading to right heart failure and premature death.”
“Athletes are canaries in the coal mine,” Sullivan told The Defender, speaking of the unusual numbers of athlete deaths since the rollout of the vaccine. Sullivan thinks that those with superior physical conditioning, like him, stand a better chance of survival with early detection.
However, he said, “Athletes will get echocardiography, and it will be essentially normal. The only way to tell for sure is to do a right-heart catheterization” that can identify the anomaly.
Sullivan believes the lives of many athletes could still be saved if the reporting system recognized and investigated the signal — and said he would be happy to join a project dedicated to this goal.
He also told The Defender he believes many of the sudden deaths reported in the 25- to 44-year-old age group are a result of this hidden condition.
‘The buck stops with the CDC for reforms’
Critics point to choices by the CDC as compounding VAERS’ passive design and understaffing issues.
Despite over 1.7 million reports since the COVID-19 vaccine rollout, staffing was not boosted accordingly, according to statements the CDC made to The BMJ.
A Freedom of Information Act request by The BMJ revealed Pfizer has nearly 1,000 more full-time employees working on vaccine surveillance than the CDC. Records showed in 2021, Pfizer on-boarded 600 additional full-time employees to handle the volume of adverse reports and planned to hire 200 more.
Physician “Helen” in The BMJ article called for an end to the “negative feedback loop” whereby the FDA fails to list adverse reactions because passive surveillance systems like the FDA’s don’t display them, while at the same time, because of that lack of disclosure, “physicians are blinded to the adverse reactions in their patients, and thus aren’t reporting them.”
“The buck stops with the CDC for reforms needed to open up data,” Benavides told The Defender, adding several suggestions that could immediately improve VAERS:
“Revert back to pre-January 2011 when VAERS did append initial reports with follow-up data, including death. Take off the arbitrary 30-minute time limit to file a report before getting kicked off. Make the process easier to submit follow-up data.”
When asked why the incompetence of VAERS had been allowed to continue for so long, Sullivan told The Defender, “Because of the lack of product liability” for the vaccines “and the surge to defend economic interests.”
Sullivan said he’d like to see the following changes to the system:
Pharmaceutical advertising banned.
Pharmaceutical company revenues devoted to advertising instead be spent on R&D.
The tax money collected on pharma profits be directly sent to victim injury funds.
Yale cardiologist takes on study of COVID vaccine injuries
Benavides said he spoke with Sen. Ron Johnson (R-Wis.) Monday and is also in discussion with Rep. Marjorie Taylor Greene (R-Ga.) of the House Select Subcommittee on the Coronavirus Pandemic to address the concerns with VAERS, including the under-publishing of reports.
“That’s a long overdue prospect and it would be incredible to actually get some analysis by that committee,” he said.
Another bright spot comes from news reported in The BMJ’s investigation that Dr. Harlan Krumholz, a cardiologist and researcher at Yale University, has been recruiting members of React19 to study their vaccine injuries.
“We are working hard to understand the experience, clinical course, and potential mechanisms of the ailments reported by those who have had severe symptoms arise soon after the vaccination,” Krumholz told The BMJ.
Sullivan told The Defender that medical science is “just beginning to catalog the damage to the heart” from the vaccines but that “in order to treat something, you have to diagnose it” — and that, because of the shortcomings with VAERS, “we have yet to scratch the surface of that.”
Sullivan, now almost three years into his ordeal, is outliving his initial prognosis.
“I have a grim diagnosis hanging over me, but I’m optimistic because I’m still here,” he said. “I had something bad happen to me, but I’ve met so many amazing, wonderful people along the way who are just interested in truth.”
“I’m going to live the best and most productive life I can with the time I have left,” Sullivan said, helping others who “have this cloud hanging over their future.”
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
When I discovered this study several years ago and wrote the following extensive piece on it, the study was a bolt from the blue, a complete devastating shocker.
It still is.
It is more than enough to topple the whole vaccine empire.
Honoring the work of the study co-author, Dr. Antonietta Gatti, Catherine Austin Fitts wrote, “Not long after the publication of this revolutionary study, tax authorities raided and investigated Dr. Gatti’s and [her husband] Dr. Montanari’s laboratory and private home—an all too usual method of intimidation.”
THAT was the “scientific follow-up.”
In a nutshell, Dr. Gatti’s 2017 study showed an incredible amount of contamination, in a whole host of traditional vaccines. The contamination was in the form of tiny nanoparticles, mostly metallic, and obviously highly harmful and dangerous.
Before reading my summary and analysis of that study—here is an updated communication from Dr. Gatti I received a few days ago. It describes, in a stark and disturbing fashion, what has been happening to her, her work, and her laboratory. This is chilling:
“At the end of last year, our laboratory no longer had the financial capacity to continue its research. The proceeds from the few analyzes requested by private individuals yielded enormously less than what the research cost us. Then, there were two possibilities: close everything or set up a foundation by giving away everything that belonged to us, hoping to find some sponsors. After all, all initiatives, even the most bizarre, find someone willing to contribute financially. Why not a foundation that does fundamental research on health? So, we opted for the latter choice, and the Nanodiagnostics Foundation was born.”
“But, after almost a year, not a cent has arrived. In short, no company, no private citizen, no institution is willing to contribute.”
“Many people continue to demand results and ask questions to which they have no answers from the institutions or their doctors, but, if it is a question of parting from some money, the silence is absolute.”
“It is clear that our work is a threat to billion-dollar businesses that are not exactly clear, at least for most people. For this reason, the most absurd and incredible slanders are invented to our detriment.
Not being able to dispute our scientific results, there are those who publish, usually anonymously, that we earn enormous sums of money, even giving the impression that the Foundation belongs to us, when it should be known that foundations do not belong to anyone, and no one can profit from them. And this is when we have donated everything that belonged to us, and we work for free.”
“Another tactic is trying to isolate and discredit us with lies. What the University of Bologna did a few days ago, the university where I graduated, then specialized and taught, is a small example.”
“A few months ago, that university asked us if we were willing to accept [a] student… who would prepare her graduation thesis with us. We agreed and agreed with the student on how to proceed. A few months passed, then, a couple of weeks ago, when the University authorities realized that the student would work with us, they sent us a message of a few lines in which they informed us that what we do (and which I had taught at that university) was of no interest to them (which, in a way, is true, although very far from the mission of the University). Needless to say, my letter to the Rector asking for explanations remained unanswered.”
“And it is also useless to say how difficult it is to publish the results that we continue to obtain, and which are not liked by those who financially maintain the medical journals, on whose scientific nature I prefer not to comment. For twice the Editor after the publication of an article (on vaccines and on SIDS) asked to retreat [sic] them. Only the work of the Robert Kennedy Jr lawyers stopped the request.”
“[Paper:] Novel chemical-physical autopsy investigation in sudden infant death and sudden intrauterine unexplained death syndromes” (click here)
“Just for your information, in spite of all difficulties, we are now dealing with very critical topics: spontaneously aborted babies, analysis of the brains of infants who died in cots (Sudden Infant Death Syndrome, aka SIDS), analysis of what falls from the sky (e.g., recently hail never seen before), food, etc. All this can only be fought with personal discredit.”
“We haven’t had any visits from the regime for a long time. For them it is enough to monitor our computers and phones. The rest is done by ‘volunteers’. As for other scientists, no one deals with our topics in full. It must be realized that doing so represents a risk that is obviously preferable not to take.”
“As long as we can manage, we will continue to work. If, however, no sponsor materializes (idle chatter and empty promises are not only useless: they are a waste of time,) we will have no other option than to declare defeat, a defeat that belongs to the whole world and, above all, to the children who do not deserve the fate they are suffering.”
“…I give some details of our Foundation Nanodiagnostics (click here)…”
IF YOU CAN, PLEASE DONATE TO Dr. Gatti’s vital work at the above website.
Here is my original article on Dr. Gatti’s vaccine-contamination study:
Dangerous nano-particles contaminating many vaccines: groundbreaking study
“The Lung,” Second Edition: “Nanoparticles [are] comparable in size to subcellular structures…enabling their ready incorporation into biological systems.”
A 2017 study of 44 types of 15 traditional vaccines, manufactured by leading global companies, has uncovered a very troubling and previously unreported fact:
The vaccines are heavily contaminated with a variety of nanoparticles.
Many of the particles are metals.
We’re talking about traditional vaccines, such as HPV, flu, Swine Flu, Hepatitis B, MMR, DPT, tetanus, etc.
To begin to understand some of the destructive effects of contaminating nanoparticles in vaccines, here is the groundbreaking 2017 study:
International Journal of Vaccines & Vaccination
Volume 4 Issue 1
January 23 2017
New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination
Antonietta M Gatti and Stefano Montanari
(Paper archived here and here)
“The analyses carried out show that in all samples checked vaccines contain non biocompatible and bio-persistent foreign bodies which are not declared by the Producers, against which the body reacts in any case. This new investigation represents a new quality control that can be adopted to assess the safety of a vaccine. Our hypothesis is that this contamination is unintentional, since it is probably due to polluted components or procedures of industrial processes (e.g. filtrations) used to produce vaccines…”
Are the study authors leaving the door open to the possibility that the contamination is intentional?
“The quantity of foreign bodies detected and, in some cases, their unusual chemical compositions baffled us. The inorganic particles identified are neither biocompatible nor biodegradable, that means that they are biopersistent and can induce effects that can become evident either immediately close to injection time or after a certain time from administration. It is important to remember that particles (crystals and not molecules) are bodies foreign to the organism and they behave as such. More in particular, their toxicity is in some respects different from that of the chemical elements composing them, adding to that toxicity…they induce an inflammatory reaction.”
“After being injected, those microparticles, nanoparticles and aggregates can stay around the injection site forming swellings and granulomas…But they can also be carried by the blood circulation, escaping any attempt to guess what will be their final destination…As happens with all foreign bodies, particularly that small, they induce an inflammatory reaction that is chronic because most of those particles cannot be degraded. Furthermore, the protein-corona effect…due to a nano-bio-interaction…can produce organic/inorganic composite particles capable of stimulating the immune system in an undesirable way…It is impossible not to add that particles the size often observed in vaccines can enter cell nuclei and interact with the DNA…”
“In some cases, e.g. as occurs with Iron and some Iron alloys, they can corrode and the corrosion products exert a toxicity affecting the tissues…”
“Given the contaminations we observed in all samples of human-use vaccines, adverse effects after the injection of those vaccines are possible and credible and have the character of randomness, since they depend on where the contaminants are carried by the blood circulation. It is only obvious that similar quantities of these foreign bodies can have a more serious impact on very small organisms like those of children. Their presence in the muscles…could heavily impair the muscle functionality…”
“We come across particles with chemical compositions, similar to those found in the vaccines we analyzed, when we study cases of environmental contamination caused by different pollution sources. In most circumstances, the combinations detected are very odd as they have no technical use, cannot be found in any material handbook and look like the result of the random formation occurring, for example, when waste is burnt. In any case, whatever their origin, they should not be present in any injectable medicament, let alone in vaccines, more in particular those meant for infants.”
This 2017 study opens up a whole new field: the investigation of nanoparticles in vaccines where none were expected.
Such particles are not medicine in any sense of the word.
Many legal and scientific “experts” assert the State has a right to mandate vaccines and force them on the population. But these contaminating nanoparticles are not vaccines or medicines. Only a lunatic would defend the right of the State to inject them.
Here is another section from the 2017 study. Trade names of vaccines, and compositions of the nanoparticle contaminants are indicated. Take a deep breath and buckle up:
“…further presence of micro-, sub-micro- and nanosized, inorganic, foreign bodies (ranging from 100nm to about ten microns) was identified in all cases [all 44 vaccines], whose presence was not declared in the leaflets delivered in the package of the product…”
“…single particles, cluster of micro- and nanoparticles (less than 100nm) and aggregates…debris of Aluminum, Silicon, Magnesium and Titanium; of Iron, Chromium, Silicon and Calcium particles…arranged in a cluster, and Aluminum-Copper debris…in an aggregate.”
“…the particles are surrounded and embedded in a biological substrate. In all the samples analyzed, we identified particles containing: Lead (Typhym, Cervarix, Agrippal S1, Meningitec, Gardasil) or stainless steel (Mencevax, Infarix Hexa, Cervarix. Anatetall, Focetria, Agrippal S1, Menveo, Prevenar 13, Meningitec, Vaxigrip, Stamaril Pasteur, Repevax and MMRvaxPro).”
“…particles of Tungsten identified in drops of Prevenar and Infarix (Aluminum, Tungsten, Calcium chloride).”
“…singular debris found in Repevax (Silicon, Gold, Silver) and Gardasil (Zirconium).”
“Some metallic particles made of Tungsten or stainless steel were also identified. Other particles containing Zirconium, Hafnium, Strontium and Aluminum (Vivotif, Meningetec); Tungsten, Nickel, Iron (Priorix, Meningetec); Antimony (Menjugate kit); Chromium (Meningetec); Gold or Gold, Zinc (Infarix Hexa, Repevax), or Platinum, Silver, Bismuth, Iron, Chromium (MMRvaxPro) or Lead,Bismuth (Gardasil) or Cerium (Agrippal S1) were also found. The only Tungsten appears in 8/44 vaccines, while Chromium (alone or in alloy with Iron and Nickel) in 25/44. The investigations revealed that some particles are embedded in a biological substrate, probably proteins, endo-toxins and residues of bacteria. As soon as a particle comes in contact with proteic fluids, a nano-bio-interaction…occurs and a ‘protein corona’ is formed…The nano-bio-interaction generates a bigger-sized compound that is not biodegradable and can induce adverse effects, since it is not recognized as self by the body.”
“…examples of these nano-bio-interactions. Aggregates can be seen (stable composite entities) containing particles of Lead in Meningitec… of stainless steel (Iron, Chromium and Nickel…) and of Copper, Zinc and Lead in Cervarix…Similar aggregates, though in different situations (patients suffering from leukemia or cryoglobulinemia), have already been described in literature.”
I’m sure you’ve read official assurances that vaccine-manufacturing problems are “rare.” You can file those pronouncements along with other medical lies.
“I’d like the heavy metal sandwich on rye, please. And instead of serving it on a plate, can you inject it?”
Several vital questions demanding answers spring from the findings of this 2017 study:
Are some of these nanoparticles intentionally placed in vaccines?
Does the standard manufacturing process for traditional vaccines INEVITABLY lead to dangerous and destructive nano-contamination?
New nano-technology is already being employed to create several vaccines—supposedly “improving effectiveness.” In fact, the RNA COVID-19 vaccine are a nano-type. Does this manufacturing process carry with it the unavoidable effect of unleashing a hurricane of nanoparticle contaminants?
How many cases of childhood brain damage and autism can be laid at the door of nanoparticle contamination?
And finally, where are these contaminated vaccines manufactured? The above study did not attempt to discover this. It was outside the scope of the research. It’s common knowledge that, for example, in the case of the US, vaccines or their components, are, in many instances, not produced domestically. Where does this put control of safety? In, say, China, where there have been numerous pharmaceutical scandals connected to contamination of products?
The vaccine establishment does not show the slightest interest in answering any of these questions. They are busy pretending the questions don’t exist.
“Why is it so difficult for virologists to simply explain basic questions about a ‘virus’ such as whether the ‘virus’ is living or dead? Why must the concept of what a ‘virus’ is change depending upon the researchers and technology of the time? What physical organism changes in concept after over a century of supposed study? The answer to all of these questions is actually fairly easy to grasp. As the researchers have never actually had any physical entities on hand in order to study, the concept of what the assumed invisible entities are was allowed to constantly change in order to suit the needs and evidence of the researchers of the time. There was no solid foundation for virology to stand upon from the very beginning in order to definitively state what the nature of a ‘virus’ truly is.”
For the greater part of the first 50 years of the 20th century, there was no agreed upon definition for what the invisible entities labelled as a “virus” actually were nor how these agents looked, formed and functioned. Some researchers believed that these entities were endogenous processes produced within the host while others envisioned them as exogenous invaders that came from outside and attacked from within. There were arguments over whether “viruses” were corpuscular in nature or whether they were a soluble liquid. Debates centered around whether these agents were alive or if they were simply inanimate and non-living. While there were researchers who believed “viruses” were a ferment or a chemical molecule of some kind, the majority believed that these invisible entities were just smaller unseen bacterium. According to biochemist and historian of science Ton van Helvoort’s 1996 paper When Did Virology Start?, the “virus” concept lacked clarity and certainty over the first half of the 20th century. However, the link between bacteriology and “viruses” was so strong at this time that these unseen entities were not considered conceptually distinct from bacteria:
“I have come to believe that, despite its widespread appearance in textbooks and journals of that era, the early concept of the “filterable virus” lacked clarity and certainty. More importantly, I also believe that during the 1930s and 194Os, the links between the study of filterable viruses and bacteriology were so strong that viruses were still considered merely another form of bacteria-not conceptually distinct, as they now are.”
The reason for these many contradictory ideas about the nature of the “virus” was a direct result of the fact that the researchers never had a physical entity on hand in order to study. The “virus” was nothing more than a fluid concept that was open to the interpretation of those who claimed to be working with them. Most of these researchers came from a bacteriological or chemistry background, and thus, they viewed the “virus” concept through their own lens and paradigms. Regardless, there was no way to actually determine the true nature of something that could not be seen or studied in reality and that only existed within the realm of the imagination.
Thus, it shouldn’t be hard to understand why virologists often have a difficult time answering simple questions such as “What is a virus?” or “Is it alive or dead?” This is exactly the argument made in the appropriately titled 2014 article Inventing Virusesby William Summers, a retired Professor of Therapeutic Radiology, Molecular Biophysics & Biochemistry, and History of Medicine. While being able to define what a “virus” is should be an easy task for any virologist, simple questions about the nature of a “virus” are not ones that are simple for them to answer. In the opening of his paper, Summers asked a more subtle question about the invention of the “virus” category:
“…how generations of microbiologists arrived at the idea that some of the entities they dealt with fell into a category that differed in fundamental ways from others. In other words, how did they invent the category of “virus” as we now know it?”
Summers looked to investigate how the idea that “viruses” are a separate entity that requires its own category away from bacteriology came to be. In doing so, he admitted that our beliefs, understandings, and conceptions of what a “virus” is changes over time. This is because “viruses” are whatever a virologist tells us that they are. The concept and the nature of the “virus” was invented, and continually reinvented, by virologists as part of the normal progress of their (pseudo) science. In other words, the idea of the “virus” is able to change at any time based upon whatever a virologist wants a “virus” to be at any given moment:
“Even so, how did the category “virus” come to be recognized, and what are its essential, defining qualities? Viruses are natural objects, but our beliefs, understanding, and conceptions of them change over time on the basis of new information, new points of view, and new scientific values and standards. In a very real way, a virus is what virologists say it is. It is a product of the way virologists talk about viruses—that is, the way facts about viruses are organized in their discourse. It can be said that virologists invent (and continually reinvent) the concept of a virus as part of the normal progress of their science.”
The deliberate ever-changing concept of the “virus” shifted away from its original invention as an agent of disease transmission to its modern day concept as a genetic assembly that sometimes causes disease when it integrates into its host in order to survive. This reinvention of the concept happened in 1957 when French microbiologist Andre Lwoff took many competing and contradictory ideas and mashed them together into the modern definition of a “virus” based upon work done with bacteriophages. Prior to his reinvention of the concept, in 1953, Lwoff actually questioned whether a bacteriophage was a “virus” and wanted to know exactly what a “virus” was. He even noted that “viruses” are defined to be exogenous (coming from outside of the body) while bacteriophages are “always formed inside its host” and “could therefore be described as endogenous,” i.e. originating from within the host. In fact, Lwoff stated that “if prophage is phylogenetically endogenous, the temperate phage produced by a lysogenic bacterium must be described as endogenous,” meaning that the phage is from within the host, thus negating it as an exogenous entity in line with the definition of a “virus.” Ironically, after redefining the “virus” as a genetic code in 1957, Lwoff would ultimately warn in 1991 that virology was “in danger of losing its soul, since viruses now show a strong tendency to become sequences.” He also argued that the abundance of discoveries was causing “the very concept of virus” to waver “on its foundations,” noting that the “problem today and in future is to keep abreast of its whereabouts.”
Regardless, Summers stated that his paper was not about the “triumphant accumulation of knowledge by the heroic scientists” of the past. Rather, it was an examination of the “continual struggle to understand and organize observations.” This struggle was showcased by Lwoff’s own attempts to rationalize and combine contradictory evidence in order to create the modern genetic concept of the “virus” from an entity that did not meet the necessary requirements:
“Nobelist Andre Lwoff, perhaps in a Gertrude Stein frame of mind, famously answered “viruses are viruses” (9), but the question “What is virus?” has been notoriously fraught since the role of virus in late nineteenth-century germ theories became central to medicine, and later, in the midtwentieth-century, to biology in general. The evolution, or perhaps deliberate and continuous reformulation, of the meaning of “virus” from an agent of disease transmission in the nineteenth century to a molecular assembly with remarkable properties by the end of the twentieth century is the subject of this article. This is not a story of the triumphant accumulation of knowledge by the heroic scientists of the past so much as it is an examination of the continual struggle to understand and organize observations that challenged and made obsolete the comfortable certainties of the often recent past. This examination requires consideration of past science on its own terms, without judgment in light of present-day understanding, and it requires consideration of the context and extent of background knowledge of the particular period considered.”
This struggle to answer the question “What is a virus?” was ongoing, even in the so-called “modern age” of virology. There was no consensus as to the true nature of a “virus.” Summers shared a quote by Joseph Beard that stated that the “virus” was a fabric of concepts that had been “woven of a plethora of woof and a paucity of warp.” In weaving terms, this makes for an unstable foundation upon which to weave. Another example was of plant virologist N.W. Pirie who was considered “agnostic” (impossible to know one way or the other) on whether a “virus” was a molecule or a microbe. However, he seemed to argue that the variability in the chemical composition of the same “virus” went against the modern molecular hypothesis. Thus, we can see that there was no agreement on the nature of the “virus:”
“The construction of the virus as a living molecule in the middle decades of the twentieth century generated wide debate as to the correct answer to the question, “What is a virus?” Having rejected filterability, negative growth properties, and size as defining characteristics, microbiologists searched for new ways to think about viruses. Even at the beginning of what might be called the modern era, there was remarkably little consensus on this subject. Joseph Beard, in 1945, famously remarked, “Viruses are said to be living molecules and autocatalytic enzymes and are likened to genes and mitochondria—in short, a fabric of concepts has been woven of a plethora of woof with a paucity of warp” (quoted in 47, p. 332). N.W. Pirie, one of the pioneers in the study of plant viruses, even in 1949 was agnostic as to whether viruses were microbes or molecules. In a long review of the problem in the British Medical Bulletin (47), he argued that the variation in chemical composition reported for the same virus suggested a level of heterogeneity not compatible with the molecular hypothesis. He noted that “all the viruses purified so far have contained nucleoprotein, but this generalization may lack significance because the viruses that have been studied are a group selected to some extent on a chemical basis.”
Summers ultimately concluded that each generation of virologists will look at “viruses” in their own way and will alter the concept of the “virus” based upon the “science” of the time. Thus, the “virus” is left to be a concept that is allowed to be continually reinvented at the whims of the researchers:
“Although “viruses are viruses,” each generation of scientists looks anew at these fascinating entities in its own way, endowing them with properties, relationships, and capacities that reflect the science of the time. Truly, they are microbes being continually reinvented by their most ardent admirers.”
In his summary, Summers laid out 5 very revealing points to end his paper on. Sharing similar sentiments as van Helvoort, he stated that the “virus” concept is an unstable one that “evolved,” not due to an accumulation of facts, but rather due to an ongoing reformulation of the “virus” concept on the basis of “scientific” focus at a given time. This reinvention was determined by technological advances rather than scientific understanding. Thus, the answer as to what a “virus” is will depend upon the discourse at the time more so than the “known” characteristics of “viruses:”
The concept of a virus has not been stable and has evolved since its introduction in the latter half of the nineteenth century.
This evolution has been not a linear accumulation of facts but rather an ongoing reformulation of the virus concept on the basis of scientific focus at a given time, e.g., growth, metabolism, chemical composition, genetics, or physical structure.
The concept of a virus has particularly been determined by technological advances ratherthan scientific understanding.
The answer to the question “What is a virus?” is one that depends on the particular scientific discourse at a given time.
The discourse with respect to the physical object “virus” is based on the particular concerns and problems of interest at a given time more than on any one set of intrinsic characteristics known about viruses.
Why is it so difficult for virologists to simply explain basic questions about a “virus” such as whether the “virus” is living or dead? Why must the concept of what a “virus” is change depending upon the researchers and technology of the time? What physical organism changes in concept after over a century of supposed study? The answer to all of these questions is actually fairly easy to grasp. As the researchers have never actually had any physical entities on hand in order to study, the concept of what the assumed invisible entities are was allowed to constantly change in order to suit the needs and evidence of the researchers of the time. There was no solid foundation for virology to stand upon from the very beginning in order to definitively state what the nature of a “virus” truly is.
While Summers paper on the invention of the “virus” offers some great modern insight into the problems related to defining the nature of the invisible beast, there is a much earlier paper by prominent virologist Thomas Rivers from 1932 that details the many issues with trying to give life to the imaginary shortly after its conception. You may know Rivers due to his 1937 proclamation that “It is obvious that Koch’s postulates have not been satisfied in viral diseases.” This shockingly honest admittance that the essential logical criteria considered necessary in order to prove a microbe causes disease remains unfulfilled for “viruses” and continues to haunt virology to this day. As it is a rather long 18 pages that I have reproduced here, I will try to keep my commentary throughout brief. However, what Rivers highlighted as key problems in 1932 during the formative years of virology compliments Summers 2014 paper on why virologists needed to invent, and then continually reinvent, the concept of the “virus” that was dreamt up in the late 1800s.
Thomas Rivers immediately began his 1932 paper on the nature of “viruses” by admitting that, up to 1932, “viruses” were defined solely based upon their absence as well as for what they were not. “Viruses” were defined in negative terms as they were:
Invisible to ordinary microscopic methods.
Unable to be obtained via filtration.
Unable to propagate in the absence of susceptible cells.
Interestingly, things did not progress away from defining “viruses” in negative terms even with Andre Lwoff’s 1957 modern reinvention of the concept as noted by Professor Milton W. Taylor, teacher of virology and world-renowned historian from Indiana University. In a 2014 paper examining what a “virus” is, Taylor explained that Lwoff’s reinvention of the “virus” concept was also a “negative definition” that “stresses the non-cellular nature of viruses.” By Lwoff’s own words from his 1971 paper From Protozoa to Bacteria and Viruses. Fifty Years with Microbes, he defined “viruses” by the “inability to grow and to divide, absence of metabolism, absence of the information for the enzymes of energy metabolism…the absence of transfer RNA and of ribosomes and also of the corresponding information.” In other words, even by the modern definition, “viruses” were still defined by what they were not.
While Rivers attempted to define “viruses” in what he felt were positive terms of what was “definitely known” about these invisible agents, he admitted that the biological nature was still a moot question, i.e. one open to debate and challenges with no foreseeable solution or answer. Perhaps this was due to his feelings that, while there was plenty of data concerning the nature of “viruses,” the accumulated data was “distinctly lacking in quality,” and that “enough reliable data have not been acquired to establish the nature of the viruses.”
The Nature of Viruses
Thomas M. Rivers
The Rockefeller Institute for Medical Research, New York
Viruses are usually characterized by three negative properties, namely, invisibility by ordinary microscopic methods, failure to be retained by filters impervious to well-known bacteria, and inability to propagate themselves in the absence of susceptible cells. I prefer a positive characterization of the viruses, one emphasizing the intimate relation that exists between them and their host cells. The multiplication of viruses only in the presence of susceptible cells, their regeneration and production of disease in many instances in only one species of host, the marked stimulation and destruction of cells induced by their activity which on the one hand gives rise to tumors, such as Rous’ sarcoma, and on the other to vesicular lesions, as fever blisters, the intracellular pathology frequently evidenced in virus diseases by inclusion bodies, and, finally, the lasting immunity that follows the majority of virus maladies, are essential phenomena that serve to stress the intimate type of parasitism encountered in working with these active agents. Such a characterization of viruses implies much, not only as concerns their biological nature which is still a moot question, but as regards their activities about which something is definitely known.
Data concerning the nature of viruses are sufficiently adequate in quantity but distinctly lacking in quality. According to reports, some of which have come from eminent investigators, most of these active agents have been seen and have been cultivated on lifeless media. If such statements are correct, viruses are autonomous living agents, and further discussion of their biological nature should deal with their place in the scale of living entities and their relation to other forms of life. Reports of work in this field are confusing, however, particularly to the uninitiated, and critical investigators are of the opinion that enough reliable data have not been acquired to establish the nature of the viruses. Inasmuch as this is a subject of fundamental biological importance, I shall review some of the recently accumulated data regarding the size, electrical charge, purification, spontaneous generation, adaptations, elementary bodies, metabolism, immunological phenomena and cultivation of viruses that might be of assistance in the elucidation of the origin and constitution of these peculiar incitants of disease.
One of the only indirect means which early virologists could use to conclude that a “virus” was “present” in a sample was by claiming that the invisible entities passed through filters of a certain size that retained all known bacteria, thus allowing them to guess as to the size of the unseen particles. Rivers noted that a “virus” was generally accepted as “an object less than 0.2 p or 200 ppl in diameter” and that it was not capable of being seen under light microscopy. In other words, “viruses” were too small to be seen and were defined by their absence. He noted that figures regarding the size of “viruses” derived from stained preparations were apt to be inaccurate and misleading. This lines up with his 1927 statement on filtration in his paper Filterable Viruses: A Critical Review, claiming that the methods were “crude and inaccurate.”
Rivers then presented evidence for the size of eight “viruses,” which were contradictory depending upon the researchers cited. He utilized hemoglobin as a comparison and stated that if the figure for hemoglobin is incorrect (which had contradictory estimates as to its size as well), many statements concerning the size of “viruses” were also inaccurate. Rivers was dismayed that certain researchers did not account for the possibility that they might have been estimating the size of particles of degraded cells to which the “viruses” were attached. He noted that other researchers took this into consideration and that they were unable to be assured that they had been successful in obtaining the correct figures for the size of the different “viruses.” Rivers concluded that none of the figures could be accepted without reservations and that the exact size of any “virus” was unknown. The numerous contradictory results stemmed from “inadequate experimentation, careless thinking, prejudice, imperfect experimental methods, and the difficult nature of the problems.”
SIZE. The size of minute particles may be determined in several ways, namely, by direct mensuration provided the objects are capable of resolution under the microscope; by filtration and ultrafiltration if the factors that influence the passage of the particles through pores of graded diameters are known and controlled; by diffusion, and, finally, by centrifugation. All of these methods have been employed in the study of the magnitude of viruses and the results obtained will be discussed.
It is generally accepted that an object less than 0.2 p or 200 ppl in diameter is not capable of resolution under the microscope when ordinary light is used. Furthermore, it is understood that mordants and stains usually increase the magnitude of small particles. Some of the “larger” viruses, e.g., those of fowl-pox (log), smallpox, vaccinia (122, 123), and rabies, are said to be just visible after treatment with certain mordants and dyes. Consequently, one is justified in concluding that most of the viruses have a diameter of less than 200 pp and in an unstained state are not mensurable by means of ordinary light. Moreover, figures regarding their size derived from stained preparations are apt to be inaccurate and misleading. The use of light of short wave lengths makes possible the mensuration of particles smaller than 0.2 p in diameter. So far, however, this method of investigation has yielded no convincing evidence concerning the magnitude of viruses. It appears, therefore, that direct methods of mensuration only indicate that the active agents are considerably smaller than ordinary bacteria.
The sizes of at least eight viruses have been estimated by means of ultrafiltration, diffusion, or centrifugation. The results obtained for these active agents together with figures for the diameter of the hemoglobin molecule for comparison are given below.
Hemoglobin. For a number of years the molecule of hemoglobin was thought to be 30 uu in diameter. Recently, however, figures (34) derived from the results of Svedberg and Nichol’s (33) centrifugation experiments and Northrop and Anson’s (30) diffusion experiments with hemoglobin indicate that its diameter is approximately 5.5 uu. Many estimations regarding the magnitude of viruses have been based on the former figure for the diameter of the hemoglobin molecule, 30 uu. If this figure is incorrect, many statements concerning the size of viruses are also inaccurateMosaic virus. Duggar and Karrer (17) by means of ultrafiltration found the infectious particles of mosaic virus to be of the same order of magnitude as hemoglobin molecules, namely, 30 uu in diameter. Vinson (34), however, says that Duggar’s experiments interpreted in the light of recent work regarding the size of hemoglobin molecules indicates that the diameter of mosaic virus is about 5.5 uu.
Herpetic virus. Zinsser and Tang (38) by means of ultrafiltration estimated the diameter of herpetic virus to be 20-100 uu. Levaditi and Nicolau (27) in the same way found that the virus passed through membranes which retained toxins, hemolysins, complement, and serum globulins. Bedson (13), however, unable to confirm Levaditi and Nicolau’s (27) results, obtained evidence by centrifugation that herpetic virus is probably of sufficient size to be visible.
Foot-and-mouth disease virus. Olitsky and Boez (31), using ultrafiltration, found that the virus of foot-and-mouth disease is 20-100 uu in diameter. Elford by means of his special membranes estimated it to be 8-12 uu.
Poliomyelitic virus. By means of ultrafiltration, Krueger and Schultz (25), in 1929, found that the virus of poliomyelitis possesses a magnitude not greater than 300 uu. In 1931, by the same means, Clifton, Schultz, and Gebhardt (16) obtained results indicating that the diameter of the virus lies below 50 uu.
Fowl plague virus. By means of ultrafiltration Andriewsky (8) secured a figure of 2.5 uu for the diameter of fowl plaguevirus, while Bechhold and Schlesinger (11) by centrifugation found it to be 120-130 uu.
Bacteriophage. According to d’Herelle (22) and Elford (19), both of whom used ultrafiltration, the diameter of the bacteriophage is approximately 30 uu. Kruger and Tamada (26) by means of purified bacteriophage preparations and ultrafiltration found it to be 5 uu, and Hetler and Bronfenbrenner (24) by means of a diffusion method estimated it to be 1.2-22.8 uu.
Rous virus. According to Zinsser and Tang (38), the Rous virus is 20-100 uu; according to Mendelsohn, Clifton and Lewis (29), 50 uu; according to Frankel (20), 10 uu. All these workers obtained their figures by means of ultrafiltration.
Vaccine virus. Levaditi and Nicolau (27) reported that vaccine virus passes through membranes impervious to toxins, hemolysins, complement, and serum globulins. Bland (15), however, from the results of his centrifugation experiments not only concluded that Levaditi and Nicolau’s findings are incorrect but that vaccine virus is probably large enough to be seen. Bechhold and Schlesinger (11) by means of centrifugation estimated that the active agent is 210-230 uu in diameter, while Yaoi and Kasai (37) working with “purified” virus found that it diffused at the rate of fuchsin particles and is, therefore, not capable of being seen.
One cannot consider the results cited above without being amused and dismayed. Many of the workers seemed in no way concerned about the possibility that they might have been estimating not the magnitude of viruses, but the size of particles of degraded cells to which the viruses were attached. Other investigators, cognizant of the difficulties of the problem! attempted to remove the viruses from such carriers. They were unable, however, to be assured that they had been successful and that they had obtained the correct figures for the size of the different viruses.
From the results of indirect methods of mensuration it is safe to conclude that viruses are small and that some of them may be exceedingly minute. If the figure of 210 uu for the diameter of vaccine virus is accurate, there is no reason as far as size is concerned to suppose that the virus is not a living organism. On the other hand, if the figures of 1.2 uu, 5.5 uu, and 8 uu for the bacteriophage, mosaic virus, and foot-and-mouth disease virus, respectively, are correct, it is obvious that these agents cannot be highly organised, because it is impossible that with such a magnitude they can consist of more than one, or at most several, molecules of protein. Unfortunately, none of the figures can be accepted without reservations. At present the exact size of
The numerous discordant results encountered in the literature dealing with the filterability, size, and visibility of viruses are probably due to inadequate experimentation, careless thinking, prejudice, imperfect experimental methods, and the difficult nature of the problems. One of the great needs at present is improvement in methods of microscopy, filtration, and purification of viruses in order that results obtained will approximate the true size of viruses and not the size of particles of other sorts on which the agents are adsorbed. It must be remembered, however, that the determination of the size of one virus will not establish the magnitude of another, because no more uniformity of dimensions should be expected among these agents than is found among bacteria and protozoa. Furthermore, it is not possible to derive proof of the animate or inanimate nature of viruses even from a correct estimation of their diameters, for, within limits as yet undetermined, life and death are not functions of size.
In this next section on electrical charges, take note once again of the range in estimates and contradictory conclusions made by the researchers. Rivers pointed out that “virus” preparations consisted principally of proteins and bits of degraded cells from the host. This meant that the electrical charge results might not be those of the “virus” particles themselves but of the other materials present within the sample. This inability to distinguish the assumed “virus” from the remaining host and foreign constituents present in the sample is the reason why complete purification and isolation of the assumed “viral” particles from the host components, which has never been achieved, is absolutely necessary. Rivers admitted that there were few experiments that were performed with “protein-free” preparations of “viruses,” and that the methods of purification did not convince him that such purified “viruses” had ever been completely separated from their carriers (i.e. host materials). Even with the modern advances in technology, this inability to completely separate “viruses” from host components was noted in a May 2020 article that stated that “to date, a reliable method that can actually guarantee a complete separation does not exist.” Rivers concluded that the lack of purity meant that it was impossible to state definitely what electrical charge is carried by the “viruses.”
ELECTRICAL CHARGE. Most bacteria and proteins under ordinary biological conditions of hydrogen ion concentration carry a negative electrical charge. When the nature of the viruses became a question of interest, attempts were made to ascertain their behavior in an electrical field in order that it might be compared with the action of proteins and bacteria under similar circumstances.
Bacteriophage. Kligler and his co-workers (41) using a so-called “protein-free” bacteriophage found that the active agent was amphoteric in acid and decidedly alkaline solutions and chiefly negatively charged in neutral and mildly alkaline solutions. Krueger and his associates (42) stated that the bacteriophage is negatively charged between the hydrogen ion concentrations of 9.0-3.4, and positively charged at pH 3.35. Todd (48) found that the active agent carried a negative charge between the hydrogen ion concentrations of 3.36-7.6. The results of Natarajan and Hyde’s (43) experiments indicate (1) that bacteriophages for typhoid bacilli and Flexner’s dysentery bacilli are only electronegative between pH 4.9-9.3 and 5.4-9.3 respectively, (2) that small plaque coliphage is electronegative below pH 8.3, but with greater alkalinity moves to both poles, and (3) that large plaque coliphage is electronegative over a range of pH 5.4-6.1, while at a higher alkalinity it wanders to both poles.
Rabic virus. According to Glusman (40) and his associates fixed rabic virus is negatively charged over a range of pH 6.0-9.3.
Vaccine virus. Douglas and Smith (39) found that vaccine virus carried a negative charge between the hydrogen ion concentrations of 5.5-8.4. The experiments of Yaoi and Kasai (49) revealed that between pH 6-7 more virus collected at the positive than at the negative pole, and between pH 8-9 the active agent was demonstrable only at the anode.
Fowl-pox virus. Kligler and his co-workers (41) found fowl-pox virus in “protein-free” preparations to be positively charged on the acid side, amphoteric in neutral solutions, and negatively charged in alkaline solutions. According to Natarajan and Hyde (43), the active agent is amphoteric over a range of pH 6.4-9.3.
Foot-and-mouth disease virus. Olitsky and Bo& (44) believe that the virus of foot-and-mouth disease is positively charged, while Sichert-Modrow (47) is of the opinion that the active agent carries a negative charge over a range of pH 7.0-8.1.
Pcliomyelitic virus. According to Olitsky, Rhoads, and Long (45) poliomyelitic virus wanders to the anode.
Rous virus. Pulcher (46) found that the Rous virus was adsorbed on electropositive and not on electronegative hemoglobins and concluded that the active agent is negatively charged.
Virus of infectious myxomatosis of rabbits. According to Natarajan and Hyde (43), the virus of infectious myxomatosis of rabbits is electronegative over a range of pH 4.9-9.3.
Herpetic virus. Natarajan and Hyde (43) found herpetic virus to be electronegatively charged only between the hydrogen ion concentrations of 7.0-8.9.
From the results of the work cited above it is obvious that most workers have found that under ordinary biological conditions of hydrogen ion concentration certain viruses in an electrical field wander to the anode. Moreover, many investigators have stated that the viruses under these conditions are negatively charged and in this respect are similar to bacteria, cells, and numerous proteins. Others, however, aware of the fact that virus preparations usually consist principally of proteins and bits of degraded cells from the host, realize that the electrical charges determined might not be those of the virus particles themselves but of their carriers, i.e., material on which the virus particles are adsorbed. It is true that a few experiments have been performed with “protein-free” preparations of viruses. But an examination of the methods of purification fails to convince one that such purified viruses had been completely separated from their carriers. Therefore, at present it is impossible to state definitely what electrical charge is carried by the viruses.
This next section is probably my favorite of the entire paper as Rivers sums up the purification problem perfectly. He started off by admitting that “virus-containing” emulsions consisted chiefly of substances unrelated to the “virus.” Thus, he stated that researchers needed to attempt to obtain the “viruses” either in a pure or in a relatively pure state as it was realized that purified “viruses” are essential for the proper study of problems in the field. These problems related to the aforementioned estimation of the size of “viruses” and the determination of the electrical charge, as well as any investigation into the “immunological” responses attributed to “viruses.” He shared a quote by Murphy who, in working to purify the Rous sarcoma “virus” through various manipulative purification processes, stated that it was “hardly conceivable that the active fraction” obtained after these processes could “carry with it through all these manipulations any living organism or virus.” Murphy felt that he was dealing with an enzyme rather than a “virus.” Rivers then backed up his own assertion from five years earlier in 1927 that “No virus had been obtained in an absoutely pure state” by reiterating that it was unlikely that a “virus” had ever been obtained in a state of absolute purity.
PURIFICATION. Inasmuch as virus-containing emulsions consist chiefly of substances unrelated to the active agents themselves, it is natural that workers should attempt to obtain the viruses either in a pure or in a relatively pure state. Moreover, it is being realized that purified viruses are essential for the proper study of problems in this field, such as the estimatlion of the size of viruses, the determination of their electrical charge, and the investigation of immunological responses excited by them. In addition to the fact that purified viruses are of practical value, it is obvious that such preparations will also be of value to investigators interested in the theoretical problem of the nature of viruses. Indeed, Murphy (52, 55) has already concluded from the results of his experiments on the purification of the Rous agent that this disease-incitant is neither a virus nor a living organism. He states, “It is hardly conceivable that the active fraction which I have thus succeeded in obtaining, a substance purified by repeated precipitations, could carry with it through all these manipulations any living organism or virus. To me the enzyme-like nature of the principle seems to have been conclusively established. . . . .” However, most workers do not believe that Murphy is justified in concluding from the results of such experiments that the Rous agent is not a virus, because at least eight other viruses, e.g., the incitants of infectious myxomatosis of rabbits (58), foot-and-mouth disease (64)) bacteriophagy (50, 56, 57), fowl-pox (56), vaccinia (66, 68)) rabies (66), poliomyelitis (65), and mosaic disease (67) have been subjected to manipulations similar to those used by Murphy and have been obtained, still active, in various states of purity.
Most methods of purification of viruses are based on the principles of precipitation by a variety of chemicals and selective adsorption and elution as used extensively in enzyme work. As yet, it is unlikely that a virus has been obtained in a state of absolute purity. Nevertheless, the results already secured are encouraging and should excite further investigations. It may be possible in this way to attain eventually a more accurate concept of the nature of some viruses. For instance, it may be shown that in certain purified virus preparations the number of nitrogen atoms for each infectious unit or particle is insufficient to warrant the supposition that the agents are living, organized structures. Krueger and Tamada (57) have already suggested this viewpoint.
While it is now stated that “viruses” require a host cell and must be cultured in order to be observed and studied, in the past, claims were made that “viruses” could be grown without cells. Rivers stated that these claims of successful cultivation on lifeless media were not uncommon, and he noted a few cases:
Frosch and Dahmen stated that they were able to cultivate the “virus” of foot-and-mouth disease on ordinary media.
Olitsky reported the cultivation of mosaic “virus” in a cell-free medium.
Eagles and McClean reported that vaccine “virus” is capable of regeneration in a cell-free medium.
Rivers ultimately decided that none of these were true examples of “viruses” being grown in cell-free media, and thus, it was chalked up to contradictory evidence that was brushed aside in favor of the prevailing belief that “viruses” are invisible and incapable of regeneration in the absence of living susceptible host cells. Rivers did note that such a state of affairs would prevent a complete definition of the nature of “viruses.” However, he believed that it was not absolutely essential to see and to cultivate the “viruses” on simple media.
CULTIVATING. In the literature of twenty years ago it is not uncommon to encounter reports in which it was claimed that viruses had been successfully cultivated on lifeless media. These reports have not been confirmed and at present such claims are rarely made. A few, however, have been made in recent years. Frosch and Dahmen (78) stated that they were able to cultivate the virus of foot-and-mouth disease on ordinary media. But the German, English, and American Foot-and-Mouth Disease Commissions were unable to confirm their work. Olitsky (91) reported the cultivation of mosaic virus in a cell-free medium. Nevertheless, upon repeating his work he (92) has been forced to conclude that true multiplication of the virus was not obtained. Recently, Eagles and McClean (75, 76) reported that vaccine virus is capable of regeneration in a cell-free medium. A careful examination of their papers, however, leaves one in doubt as to whether some of their media were cell-free, and as to whether multiplication of the virus occurred in the nutrient materials that undoubtedly contained no cells. In my laboratory (86, 90, 93) during the last four years, Haagen, Muckenfuss, Li, and I have made numerous attempts to cultivate vaccine virus in cell-free media, many of which were similar to if not identical with those employed by Eagles and McClean. None of our efforts was successful. On the other hand, the cultivation of vaccine virus in the presence of cells surviving in vitro has been more consistently successful in our hands and in Maitland’s (88) than it has been in Eagles and McClean’s.
Although the cultivation of viruses in lifeless media has not been accomplished, it is generally conceded that these agents are capable of pullulation in the presence of susceptible cells either surviving or growing in vitro. The viruses of Rous sarcoma (72), Virus III infection of rabbits (69), herpes febrilis (70), fowl-pox (77), vaccinia (79, 80, 86, 88)) rabies (94), foot-and-mouth disease (83,84,85? 89), vesicular stomatitis (73), infectious myxomatosis of rabbits (71, Sl), fowl plague (82), and probably the agents causing common colds (74) and poliomyelitis (87), have been cultivated in the presence of tissues surviving in vitro.
Moreover, the characteristic of species specificity possessed by many viruses is frequently reflected in their in vitro cultivation. For instance, fowl-pox virus (77), innocuous for mice and rats, does not regenerate in cultures of their tissues. Foot-and-mouth disease does not attack chickens and the virus (89) does not grow in cultures consisting of minced chick embryo and plasma. In addition to a species specificity, some viruses exhibit in cultivation experiments a predilection for certain kinds of cells. Fowl plague virus (82) multiplies in the presence of chick embryo skin and brain, but does not regenerate in pure cultures of fibroblasts. Foot-and-mouth disease virus (85) increases in amount when the culture medium contains minced guinea-pig embryo, but does not grow when fibroblasts or bits of heart muscle alone are present. Thus it appears that many viruses are capable of multiplication in tissue cultures and frequently retain under such conditions their species and cellular specificity. Nevertheless, it will be interesting to observe the results of further attempts to circumvent this species and cellular specificity of viruses by in vitro methods of cultivation.
A crucial experiment, if there be one, to decide the question of the autonomy of the viruses is their undisputed cultivation on lifeless media. It may be impossible, however, to accomplish such an experiment with all of the viruses, because some of them may be obligate parasites, as is the malarial organism. Thus in the quest for proof of the nature of viruses, we may find that many of them are invisible and incapable of regeneration in the absence of living susceptible host cells. Such a state of affairs will prevent, for a time at least, a complete definition of the nature of these peculiar incitants of disease. Nevertheless, we should obtain all the facts and make the most of them in the study of biological phenomena and in the better understanding and control of disease. For this purpose it is not absolutely essential to see and to cultivate the viruses on simple media any more than it is imperative to see and to know what electricity is in order to study the phenomena produced by it and to control its activity for our daily needs.
Regarding whether “viruses” are alive or not due to having their own metabolism, Rivers stated that the evidence was that they did not have any such metabolic capabilities. However, he felt that conclusions could not be drawn that “viruses” do not have a metabolism and that they are inanimate because the methods used may not have been adequate.
Adaptation of the “virus” to different hosts was used by researchers in order to state whether or not “viruses” were alive. This essentially meant drawing conclusions from using different materials and different methods in different animals while generating different results. One set of researchers viewed the contradicting outcomes as the result of a “living virus” while another set of researchers saw it as a result of the hosts response. Neither seemed to recognize the fact that it was the different experimental procedures generating different responses and results rather than the act of any “virus” adapting.
METABOLISM. Much of the discussion conc.erning the nature of viruses has centered around the question as to whether they are animate or inanimate. In this relation, one would like to know what the evidence is regarding independent metabolic activities of these active agents. Technical difficulties have hindered this type of experimentation with viruses. Nevertheless, a few investigations (95-99) have been made, the result,s of which were negative. One must not conclude from such negative results, however, that viruses do not possess an independent metabolism and are, therefore, inanimate substances, because the methods used for the detection of the metabolic activities may not have been sufficiently delicate.
ADAPTATION. Certain viruses inoculated into new hosts apparently undergo changes in some of theircharacteristics. Smallpox virus (100, 101) passed through monkeys to rabbits and calves and then back to man is no longer smallpox virus but vaccine virus, a.nd the disease, vaccinia, caused by it is not contagious as is smallpox. The incitant of yellow fever (106, 107) passed through a large number of mice by means of intracerebral inoculations loses much of its pathogenicity for monkeys when inoculated intravenously or intraperitoneally, but gains the power of producing a transmissible encephalitis in monkeys receiving the inoculum in the brain. Such phenomena are spoken of as adaptations of viruses to new hosts, and, inasmuch as adaptation is considered a characteristic of living rather than lifeless material, they have been cited by some investigators (103) as proof of the animate nature of the viruses. On the other hand, workers, who believe that viruses are products of cellular perversion, state that the changes observed in the characteristics of the active agents when they are inoculated into alien hosts are to be expected, inasmuch as mouse, rabbit, monkey, and human cells, because of intrinsic differences, may not always manufacture identical substances as the result of similar stimuli. Therefore, they contend that the changes and adaptations are not accomplished by the agents themselves but by their hosts and, consequently, are not admissible as proof of the living nature of the viruses.
As ”viruses” were incapable of being observed and studied directly, various forms of indirect evidence were utilized in order to infer the presence of these entities. One of the earliest ways to do so was by claiming that a phenomenon known as inclusion bodies was a sign that a “virus” was present. These “bodies” are aggregates of proteins seen in various tissues under microscopy that were taken as an indicator by the researchers that they were dealing with a “virus.” However, it is well-known that inclusion bodies are not specific to “viral” cases and can be found in those without a “viral” disease. They are also not found in all cases of a particular disease, can be found in those without the disease, and are even found in uninoculated cell cultures, as seen with RSV. A 1941 paper by Alfred M. Lucas stated that the “existence of an object which appears to be an inclusion body is not proof of the presence of a virus but merely an indication that a virus should be considered if no bacterial agent can be found.” What this means is that inclusion bodies are nothing more than non-specific indirect evidence used to infer an assumed “virus” if other “causes” are ruled out. This means that finding inclusion bodies is essentially meaningless as a specific sign for the presence of any “virus.” Rivers appeared to understand this as well. After presenting various contradictory interpretations and presentations of inclusion bodies by different researchers, he noted that “inclusions may arise in a number of ways and that they may or may not contain virus.” He felt that making conclusions about what these “peculiar structures” represented was “hazardous at present.”
INCLUSIONS. Within the nucleus and cytoplasm of cells injured by viruses, certain peculiar structures, inclusion bodies, are frequently observed. Although many of these bodies are of importance in diagnostic and experimental work, numerous opinions exist concerning their nature. Lipschtitz believes that the inclusions in many diseases (119) consist of compact masses of virus particles, yet he is of the opinion that such structures in measles (120) are nothing more than altered central bodies. Goodpasture (113) thinks that Negri bodies in rabies are composed of degenerated mitochondria and neurofibrils, while Levaditi (118) and Manouelian (121) consider them protozoa and designate them, respectively, Glugea lyssae and Encephalitoxoon rabiei. Goodpasture and his associates (124, 125) have demonstrated that the incitant of fowl-pox is intimately associated with the Bollinger bodies which are made up of a lipoid capsule within which numerous small coccoid bodies are embedded in a protein matrix. On the other hand, Glaser (112) has presented evidence that the polyhedral bodies, the characteristic inclusions in wilt diseases of caterpillars, consist of non-infectious crystalline protein. Thus, it appears that inclusions may arise in a number of ways and that they may or may not contain virus. Consequently, generalizations regarding these peculiar structures are hazardous at present.
The small coccoid bodies found in fowl-pox by Borrel (109) and in vaccinia by Paschen (122,123) appear to be extremely minute organisms. In fact, one is justified in asking why these bodies are not convincing evidence of the organismal nature of certain viruses. The first reason is that one cannot by morphological and tinctorial data alone determine whether autonomous life exists in such small objects. Another reason is the fact that Goodpasture, while holding the belief that the small coccoid bodies in fowl-pox (124, 125) represent the virus, stated that similar structures, seen in rabic brains (113) and considered of etiological importance by Babes (108) and Koch (114-116), are probably degenerated mitochondria. Moreover, Borrel (110) has described similar bodies in other virus diseases the etiological agents of which have been shown by ultrafiltration to be incapable of resolution by microscopic methods. Furthermore, Craciun and Oppenheimer (111)) who cultivated the small bodies of vaccinia and showed that they are closely associated with the virus, made the following statement, “We have from these studies no morphological proof of an increase in the number of granules, since they cannot readily be distinguished from other granules normally seen in tissue cultures.” Finally, mitochondria in some respects resemble bacteria. They may decrease or increase numerically within cells, and their size and shape may be altered by appropriate stimuli. At times, they actually divide. Nevertheless, mitochondria are not considered autonomous living agents. Consequently, so far as I am aware, there is no convincing evidence-the specific agglutination of virus elementary bodies (184) by antiviral sera will be discussed later-to invalidate the conception that cells under the stimulus of viruses may react by the formation of numerous small coccoid bodies uniform in size and intimately associated with the stimulating agents. One would not consider such bodies microorganisms or hold that they consist of virus alone. Therefore, in spite of definite proof that viruses are present in certain types of inclusions, doubt still exists regarding the organismal nature of the small coccoid bodies found within them.
Other features observed in pathological processes induced by viruses, e.g., hyperplasia and necrosis, are fully as important as are the inclusion bodies. The excessive stimulation of cells seen in some virus diseases, e.g., fowl-pox and warts, leads one by analogy to think of mdignant neoplasms. Undoubtedly a number of fowl tumors are caused by agents separable from cells, and, although there is no proof that mammalian tumors arise in this way, the possibility is worthy of consideration and offers an attractive field for work. The fact, however, that some tumors are produced by filterable agents is by no means conclusive evidence that all neoplasms (217) arise through the activity of such incitants.
In this next section, Rivers admitted that there was an increasing chorus of researchers who believed that “viruses” were nothing more than “merely filterable, invisible, and noncultivable elements of ordinary bacteria.” He presented many scenarios, such as:
The bacteriophage is a form in the life cycle of lysogenic bacteria.
The “viruses” of yellow fever and hog cholera are invisible forms of Leptospira icteroides and B. suipestifer respectively.
The etiological agent of scarlet fever is a filterable form of hemolytic streptococci.
The incitants of poliomyelitis, epidemic encephalitis, fox encephalitis, common colds, measles, and influenza represent certain stages in the life cycle of green streptococci.
Apparently, Rivers was unfamiliar with the fact that this bacterial life cycle process, known as pleomorphism, was observed by many researchers such as Antoine Bechamp, Günther Enderlein, Royal Raymond Rife, and later by many others with the use of dark field microscopy. That bacteria are pleomorphic entities, i.e. having the ability to assume different forms, is an established fact.
VIRUSES AS FILTERABLE FORMS OF BACTERIA. For a long time a few investigators have held that certain virus diseases are induced by ordinary bacteria. Now that attention is being focused on filterable forms of bacteria, workers in increasing numbers (128, 131, 132, 134, 135) are adopting the belief that viruses are merely filterable, invisible, and noncultivable elements of ordinary bacteria. It has been claimed, and evidence of a kind has been offered to substantiate the assertions, that the bacteriophage (165, 166) is a form in the life cycle of lysogenic bacteria, that the viruses of yellow fever (131, 134, 135) and hog cholera (134, 135) are invisible forms of Leptospira icteroides and B. suipestifer respectively, that the etiological agent of scarlet fever (134, 135) is a filterable form of hemolytic streptococci, and that the incitants of poliomyelitis, epidemic encephalitis, fox encephalitis, common colds, measles, and influenza represent certain stages in the life cycle of green streptococci (131). Without going into details of the available knowledge of bacterial life cycles and their invisible and noncultivable forms, one can say that proof of many of the claims regarding them is lacking. In fact, if certain reports are correct, some of the filterable forms of bacteria are much smaller than are many of the viruses. Kendall (131) recently stated that “egg white, filtered through Berkefeld W filters (after dilution with sterile physiological saline solution) is rarely sterile.” Such a statement raises embarrassing questions for workers in the virus field because many viruses will not pass through W filters. Since the existence of bacterial life cycles is doubtful, it seems unwarrantable to offer the presumptive filterable forms of them as evidence upon another unsolved problem, the nature of the viruses.
The thing to notice in this next section on physical and chemical agents is, once again, the often contradictory nature of the evidence presented by different researchers. One researcher would find a certain chemical that had an effect on the “virus,” while another researcher would state otherwise. Some viewed that chemical tests proved “viruses” were protozoa. Others felt that their tests proved the “virus” was an enzyme. Sanderson showed that bacteriophages were not killed by successive freezing and thawings and believed that they were unliving. However, Rivers showed that bacteriophages can be killed by repeated freezing and thawing, thus contradicting Sanderson’s interpretation. Ultimately, Rivers concluded that, regardless of the number of tests with chemical and physical agents that had been devised as criteria for the presence of life or to define the nature of “viruses,” not a single one of them was found to be satisfactory.
EFFECT OF PHYSICAL AND CHEMICAL AGENTS ON VIRUSES. Many years ago it was discovered that bile and saponin are injurious to protozoa but with a few exceptions are innocuous for bacteria. Consequently, when the question of the nature of viruses began to attract attention, tests were made to determine what effect bile and saponin have on these incitants of disease. Many viruses, e.g., rabic virus (141, 144), were found to be inactivated and because of this fact certain workers concluded that they are protozoa. Sufficient exceptions, however, have been encountered to invalidate the test as a means either of separating bacteria from protozoa or of defining the nature of viruses. The agent causing Rous’ sarcoma (140) is more resistant to ultraviolet light than are bacteria, and Murphy (220) considers this fact as evidence in favor of his hypothesis of the enzyme-like nature of the virus. On the other hand, bacteriophage (139), the living nature of which many doubt, is just as sensitive to ultraviolet light as are bacteria. Sanderson (153), using a temperature of -78°C., found no diminution in the titer of two strains of bacteriophage subjected to 20 successive freezings and thawings. Since bacteria and cells are killed by repeated freezing and thawing, he concluded that bacteriophage must be something other than a living organism. Rivers (151) showed, however, that colon bacilli, Virus III, vaccine virus, herpetic virus, bacteriophage, complement, and trypsin are all either killed or inactivated by repeated freezing (-185°C.) and thawing and that, as might be expected, some of the agents are more resistant than are others. Hence it is obvious that destruction or inactivation of an active agent by repeated freezing and thawing is not evidence that it possesses life. The observations on heat, desiccation, oxidation, and the effect of dyes have likewise yielded no convincing evidence concerning the nature of viruses. Thus it appears that a number of tests with chemical and physical agents have been devised as criteria for the presence of life or to define the nature of viruses, but no one of them has been found satisfactory.
The spontaneous generation of “viruses” by the host is a concept that defeats the idea that these entities are exogenous outside invaders. If something like a bacteriophage can be produced by a normal bacterium without any external phage present, it shows that these entities arise from a process initiated from within the organism. Rivers noted that Hadley and his co-workers stated that it was possible to obtain bacteriophage from normal bacterial cultures by means of enforced dissociation. Thus, no external source of phage was necessary. Nobel Prize-winning immunologist Jules Bordet was able to do the same, as did other researchers. Rivers presented a few scenarios where “viral” diseases could be induced by injecting toxic substances such as tar and arsenic into chickens, as well as an instance where a tumor-producing extract could be obtained from healthy chickens. While Rivers thought that the interpretation of the evidence was potentially fundamental to biology, he excused it as being due to contamination by the researchers working in labs with similar materials as well as the possibility that “latent viruses” were hiding within the healthy hosts.
SPONTANEOUS GENERATION OF VIRUSES. The origin as well as the nature of viruses constitutes a question of interest. The intimate relation between these active agents and their host cells has induced more than one investigator to view the host cell as the source or origin of viruses. Indeed, reports of experimental work have appeared leading to claims that normal cells have been induced to manufacture certain viruses. According to Carrel (156, 157), minced chick embryo mixed with tar, indol, or arsenic and injected into normal chickens in a small percentage of instances gives rise to tumors resembling Rous’ sarcoma no. 1 and transmissible by cell-free filtrates. Fischer (163) by treating cultures of normal cells with arsenic obtained on one occasion a filterable agent capable of causing tumors. Carrel was unable to confirm Fischer’s work. Murphy (52, 167), by means of a method the details of which have not been described, reported that he was able to extract a filterable tumor-producing agent from the gonads of normal-appearing Plymouth Rock roosters.Recently, Hadley and his co-workers (166) stated that it is possible to obtain bacteriophage from normal bacterial cultures by means of enforced dissociation. Although no worker in this field has claimed to have generated living organisms from inanimate matter, it appears that a few believe that they have by certain manipulations induced cells to yield substances which possess some of the attributes of life, notably that of increasing without limit.
The observations described above are suggestive, and, if confirmed and found to warrant the interpretation given them by Carrel, Murphy, Fischer, and Hadley, will prove to be of fundamental biological importance. Unfortunately, however, all of the experiments yielding the observations were actively referred to were conducted in laboratories where workers engaged in the study of agents similar to those supposedly brought into existence. In such laboratories and with such materials it is always difficult for one to rule out the possibility of contaminating normal animals, tissues, bacteria, emulsions, and filtrates. This fact has long been appreciated by workers in vaccine virus laboratories and it delayed the acceptance of the experimental transformation of smallpox virus into vaccine virus. Therefore, experiments of the nature described should never be conducted in rooms used for the study of agents similar to those for which a search is being made. The workers who believe that they have induced viruses to come into existence have not excluded the possibility of the preexistence of latent viruses or of small amounts of virus in the supposedly normal embryos, gonads, chickens, and bacterial cultures utilized in the experiments. This possibility is emphasized by Flexner’s (164) work on poliomyelitis, for he was able to demonstrate the presence of virus in the nasal washings from normal contacts. The possibility outlined is further emphasized by Andrewes and Miller’s (155) experience with Virus III in rabbits, by Cole and Kuttner’s (158) work with the salivary-gland virus in guinea pigs, and by the work upon virus carriers in general among animals, plants (168) and bacteria.
CGI (Computer-Generated Imagery): The only way you will ever see “antibodies” attacking “viruses.”
Rivers next discussed “immunity” in relation to establishing the nature of “viruses.” It is important to note that, regarding antibodies and “immunity,” researchers are utilizing one hypothetical entity in order to define another. While Rivers spoke as if the antibody and antigen concepts are established facts, he remarked that if the concept of the nature of antigens is correct, “viruses” are proteins or are closely linked to proteins. Thus, the interpretation of the nature of the “virus” rests upon the correctness of the nature of the antigen concept. He felt that the rise of these (hypothetical) antibodies that differed between host cell and antigen adduced (led one to believe) the exogenous rather than the endogenous origin of the “viruses.” Regardless, Rivers admitted that the mode of action of neutralizing antibodies was not clearly understood, and when speaking of antibodies causing flocculation (clumping together), he shared that various researchers noted the “immunological” phenomena in “virus” maladies are comparable to those induced by toxins. While Rivers felt that “immunological” observations were important, he admitted that this method of approach had not brought about a definite solution to the problem of the nature of “viruses.”
IMMUNITY. Most virus diseases lead to a marked and lasting immunity in recovered hosts. Not only are the but in their sera antibodies capable of hosts refractory to reinfection neutralizing the viruses are demonstrable. What bearing have these facts upon the nature of viruses? In the first place, it is certain that viruses are highly antigenic. Furthermore, if our concept of the nature of antigens is correct, the viruses are proteins or are closely linked to proteins. Moreover, the agents are not only antigenic, but they give rise to antibodies different from those excited by proteins of the host cells. This is true even of the bacteriophage (188). These facts have been adduced as evidence of the exogenous rather than the endogenous origin of the viruses. Thus, the antigenic nature of viruses appears to be prejudicial to the idea that they are products of cellular activity. The notion, however, that a lifeless agent may be injurious to the cell creating it and that it may induce immunological responses independent of those excited by the cell, loses some of its fantastic qualities when one considers the well-known facts that lens protein is not species specific but organ specific and that sympathetic uveitis in the uninjured eye is caused not by microorganisms but by the reaction of the body to substances derived from injured cells of the other uveal tract.
In addition to the neutralizing antibodies, whose mode of action is not clearly understood, complement-fixing antibodies and antibodies causing flocculation in virus emulsions have been described. Schultz and his associates (191-195) contend that the latter types of antibodies are not excited by viruses and that the immunological phenomena in virus maladies are comparable to those induced by toxins. In spite of their contentions, sufficient evidence has been adduced by different workers to make it more than likely that certain virus diseases lead to the production (176, 177, 180, 199) of the antibodies mentioned. Furthermore, Ledingham (184) has recently demonstrated that Borrel bodies in fowl-pox and Paschen bodies in vaccinia are specifically agglutinated by antifowl-pox and antivaccinal sera respectively. The results of these experiments indicate to Ledingham that the elementary bodies are living organisms and represent the virus. There is no reason to doubt that specific agglutinations of the bodies occurred in the manner described by Ledingham, and one cannot deny that such a phenomenon is presumptive evidence of the organismal nature of the bodies. Yet one dare not say categorically that his experiments are unequivocal evidence that the elementary bodies represent virus alone, because it has been shown by Jones (182, 183) that collodion particles treated with a variety of proteins and then thoroughly washed are specifically agglutinated by the proper antisera. Thus, the Borrel and Paschen bodies without being organisms yet having virus adsorbed on them might nevertheless be specifically agglutinated by appropriate antiviral sera.
Gye (181) states that Rous virus repeatedly injected into alien hosts excites two groups of antibodies, one of which acts on the virus itself, while the other operates on the “specific factor” derived from the host cell. According to him, either set of antibodies inactivates the virus. This fact is offered by him as further evidence of the dual nature of the causative agent of fowl tumors. Murphy (189) and Sittenfield (196-198) have reported the presence in Rous sarcoma of a substance that inhibits the action of the etiological agent, and the first mentioned worker is of the opinion that the “inhibitor” differs from ordinary virus antibodies. The presence of this “inhibitor” together with other phenomena has induced Murphy (220) to believe that immunity to the Rous agent is unlike that observed in virus maladies and lends evidence to his view that the Rous agent is not a virus. Inhibiting substances, however, have been obtained from tissues infected with viruses, for example, a substance restraining the action of rabic virus has been demonstrated by Marie (186) in the brains of rabid animals. Furthermore, Andrewes’ (172, 173) work appears to indicate that the immune responses excited by the filterable agents of fowl tumors may not be unique and may possess much in common with those encountered in other virus diseases.
From what has been said, it is obvious that immunological phenomena are playing an important role in discussions concerning the nature of viruses. As yet this method of approach has not brought us to a definite solution of the problem.
Rivers finished up his review on the nature of “viruses” by presenting the various differing interpretations on the concept of the “virus.” These invisible entities were regarded as either:
Living contagious fluids
Oxidizing enzymes
Protozoan parasites
Inanimate chemical substances
Minute living organisms (related to bacteria)
Rivers noted that depending on the researchers, the rabies “virus” was either an enzyme, a parasite, a protozoon, or an unknown living organism. He stated that researchers were divided over whether bacteriophages were an inanimate agent or a living organism. The fowl-pox “virus” was thought of as either a protozoan parasite, a nucleoprotein poison manufactured by “infected” cells, or a minute coccoid organism capable of regeneration in parasitized cells. The agent associated with Rous sarcoma was either animate, a living organism mixed with an inanimate substance, an enzyme-like substance, or a transmissible mutagen.
Rivers highlighted these numerous competing concepts in order to show how radically different the ideas concerning the nature of “viruses” are from one another. He then proceeded to explain the main conceptions of “viruses,” with the first two scenarios explaining how a stimulus induces a normal cell to create a substance X, which may either remain free or become closely bound to a part of the cell. In Rivers’ third example, which he considered the most popular, X is a minute living organism that enters cells, multiplies, and produces disease. Thus, there is a distinct difference where X is considered an inanimate substance that results from cellular perversion in the first two scenarios, while X is viewed as an autonomous organism in the last scenario. Regardless of the scenarios that Rivers provided attempting to explain “viral” formation, he admitted that there was no unequivocal evidence of the validity of any of these concepts.
CONCEPTS OF THE NATURE OF VIRUSES. A review of the data by means of which one arrives at a concept of the nature of viruses has been presented. Now it will be interesting to see what notions certain workers have concerning some of them.
Beijerinck (202) considers the virus of mosaic disease to be a living contagious fluid; Woods (228), an oxidizing enzyme; Goldstein (212), a protozoan parasite; Vinson (67), an inanimate chemical substance. Most workers, however, believe that it is a minute living organism.
Hijgyes (216) is of the opinion that the incitant of rabies is an enzyme or “alternatively, that the tissues themselves might spontaneously become virulent as the result of changes in their chemical composition.” At one time Remlinger said, “The rabies virus, which is at once filterable, diffusible and capable of reproducing the disease from case to case, appears to occupy a place midway between the microbes and the diastases.” Recently, however, he (221) has published an article on the evolution of the parasite of rabies. Levaditi (118) and others (121, 225) have presented evidence in favor of the idea that the causal agent is a protozoon. The majority of investigators hold the concept that the incitant is a living organism whose nature is not definitely known.
Numerous workers believe that the bacteriophage is an inanimate agent, while others are convinced that it is a living organism. Ideas, however, concerning the nature of the inanimate transmissible substance or the animate organism vary. For details of the different concepts one is referred to papers by Twort (226, 227), d’Herelle (103), Bordet (203), Bronfenbrenner (95), Burnet (206), and Hadley (165, 166).
The incitant of fowl-pox has been described by certain investigators as a protozoan parasite. Sanfelice (222, 223) suggested that it is a nucleoproteid poison manufactured by infected cells. Borrel (log), Goodpasture (124, 125), and Ledingham (184) hold that it is a minute coccoid organism capable of regeneration in parasitized cells.
Rous and others are prepared to entertain the idea that the causal agent of Chicken Tumor No. I is animate. Gye (215) believes that it consists of two factors, one of which is a living exogenous organism, the other an inanimate specific factor derived from infected cells. Murphy (52, 55), at one time, spoke of the Rous agent as an enzyme-like substance. Recently, however, he (220) has compared it to filterable substances capable of transforming melitensis (204,205) into paramelitensis organisms and of converting one type specific pneumococcus (201) into another type specific form. In regard to the matter he says (22O), “Thus we have a group of agents, products of specialized cells capable of conferring the peculiar type quality to undifferentiated cells of the same species which, in turn, may produce the active factor and transmit this to their descendants.” For this type of agent he proposes the name transmissible mutagens.
Sufficient ideas concerning the nature of viruses have been cited to illustrate how radically some differ from others. Many of them, particularly the ones dealing with the origin and reproduction of inanimate substances that behave in a manner similar to that of living organisms, lack precision. In a general way, however, the different concepts can be arranged in groups and it seems advisable to state and to portray diagrammatically several of the popular ones.
According to one conception, certain stimuli produce changes within cells that are inherited by daughter cells. Once the mutations occur, cells of the new type continue to be formed though the stimuli disappear. No agents separable from the cells are demonstrable, and immunological phenomena in this type of disease differ from those observed in virus maladies. Ordinarily this idea of the causation of disease and the concepts concerning the nature of filterable viruses are not grouped together. Yet in some respects they are not dissimilar and many hold the view that malignant neoplasms arise in some such way. See figure 1.
Another notion is that appropriate stimuli induce normal cells to make a substance x which is closely bound to parts y of the cells. Thus an xy complex is formed. This complex, separable from the cells, yet capable of inciting its own production by them, either passes directly into daughter cells, or, having become extracellular, enters another set of normal cells. The xy complex is antigenic, and cells freed from it presumably become normal again. See figure 2.
Still another idea is that certain stimuli incite normal cells to produce a substance x which is not closely bound to parts of the cells, X, separable from cells, yet capable of impelling its formation by them, either passes directly into daughter cells, or, having become extracellular, enters a new group of normal cells. X is antigenic and cells freed from it presumably become normal again. See figure 3.
Finally there is the concept most generally held that x is not a product of the perverted activity of cells but is a minute living organism. X enters cells, multiplies, produces disease, is separable from cells: and is antigenic. Cells freed from it presumably become normal again. At times, x is absorbed by particles y of host cells and evidences of an xy complex are obtained. See figure 4.
For practical purposes it makes little difference which one of the last three concepts is accepted. Theoretically, however, x of the second and third conceptions is quite different from x of the fourth. In the second and third, x, a product of cellular perversion, is an inanimate agent, while in the fourth it is an autonomous organism. No unequivocal evidence of the validity of any of the concepts has been adduced.
Rivers concluded by acknowledging the confused state of the evidence concerning “viruses,” noting that this confusion had made it exceedingly difficult to define their nature. He felt that the easiest way out of their dilemma would be to accept “viruses” as minute organisms. However, Rivers warned of quickly accepting presumptive evidence as “viruses” may be either minute organisms, forms of life unfamiliar to us, inanimate transmissible incitants of disease, or all of the above.
Conclusion
The confused state of our knowledge of the viruses at the present time makes it exceedingly difficult to define the nature of these active agents. The easiest way out of the dilemma, however, would be the acceptance of the presumptive evidence that viruses are minute organisms. Yet the easiest way and the one that best fits the experiences of the day may not be the right one. Furthermore, excessive skepticism and the habit of too readily accepting presumptive evidence are equally productive of sterility. Unless viruses represent a form of life unknown to us, proof of their living nature would not be a striking discovery. If, however, some of them are not animate, absolute proof of such a fact would be of fundamental biological importance. Therefore, care should be exercised that immoderate skepticism on the one hand, and the mental satisfaction secured by accepting presumptive evidence on the other, do not dull our efforts to obtain a better understanding of the viruses, some of which may be minute organisms, while others may represent forms of life unfamiliar to us, while still others may be inanimate transmissible incitants of disease. In any event, we are face to face with the “infinitely small in biology,” and, if there be a sharp demarcation between life and death, then scientists, investigating the nature of viruses, are working near the line that separates infinitely small living organisms from inanimate active agents.
From these two presented articles from two different points in time in the history of virology (Rivers in 1932 and Summers in 2014), it should be clear why it is difficult for virologists to define the nature of the “virus.” Researchers needed to invent, and then continually reinvent, the nature of the “virus” as the foundation that virology is built upon is conceptually weak. It is full of contradictions that have cracked the very infrastructure that was put in place. There were never any submicroscopic entities that were being studied by the various researchers over the last century. As there were no “viruses” to study and characterize, there was no agreement at all amongst the various researchers as to the nature of the invisible concept crafted inside of their minds. They had tricked themselves, through shoddy indirect pseudoscientific evidence, into believing that they were studying something real based upon lab-created effects without an identifiable cause. This is why the “virus” has been continually defined for what it isn’t, rather than for what it supposedly is. The magical “virus” skirts the line between life and death, microbe and molecule, enzyme and ferment. It is unlike anything else seen in nature, and for this very reason, its nature remains mysterious and incomplete. This should be the very first clue that there is nothing scientific about the “virus,” as science only deals with the natural world and its phenomena, not the supernatural. However, within the supernatural realm is where the “virus” concept will remain, ready and waiting to be reinvented upon the arrival of the latest technology for the next best indirect measurement. This will be utilized to continue fooling the researchers, as well as the public that blindly trusts in them to know better, that these fictional entities exist in nature, when, as Thomas Rivers kindly pointed out, “viruses” have never once been observed there. Thus, the nature of the “virus” will continue to remain merely an invention of the imagination of the most ardent admirers of these invisible boogeymen—the virologists.
It is time to revisit the England-wide NHS prescription data regarding one particular category of psychiatric drug prescribing. In a previous post specifically on ADHD drugs, a shocking 15% year-on-year rise in ADHD drug prescriptions for 2022 was noted. Within the first two quarters of 2023, the previous increase has already been exceeded by over 2.5%. It now stands at an almost 18% increase for the same period, compared to 2022.
And this is the year-on-year increase. Looking at current levels compared to a long-term trend, it is even more staggering. For almost 9 years, since 2012, prescriptions of drugs used for ADHD remained fairly close to the long-term trend (within a 5% window). In 2022, that trend was broken with a 10% divergence, but in 2023 it disconnects from it completely. A 25% divergence from a steady long-term trend must signal a radical change in the userbase. What is happening?
In economics, there is the law of supply and demand. As the price increases, supply rises while demand declines. Conversely, as the price drops, supply constricts while demand grows. CCHR UK has been scrutinising the demand side of the equation, while the media has been keen to underline the supply side. Journalists tend to write about drug supply shortages as if they are occurring within a status quo of demand. An 18% year-on-year increase, and a 25% divergence from a long-term trend, is anything but a status quo.
In recent media articles, there was an obvious omission. The media failed to mention that demand has – somehow and without too much explanation – exploded. What brought about such a demand?
It should be recognised there are no physical or biological tests that can be carried out to support the existence of ADHD. None. There are no tests. Pontificating psychiatric authors have however taken regular human behaviour and redefined it as a so-called mental ‘disorder’ which has been accepted without inspection.
This isn’t a new concept. Sets of emotional and behavioural characteristics were redefined as far back as 1987 when ADHD was literally voted into existence. This however is not science. It’s consensus. It’s psychobabble. Considering the law of supply and demand, there has been a tremendous increase in the supply of psychiatric rhetoric, opinions and assumptions that have brought about a greatly-increased demand for ADHD drugs.
Furthermore, the prescribed drugs can have serious consequences, that include some of the following side-effects:
abdominal pain
aggression
depression
dizziness
drowsiness
hallucinations
headaches
insomnia
loss of appetite
moodiness
nervousness
psychosis
restlessness
seizures
stunted growth
suicidal thoughts
violent behaviour
weight loss and ‘zombie’ appearance
While there are many discerning people who question the unscientific psychiatric modus operandi, there are many who accept psychiatric labels like ADHD without inspection. Not so long ago, psychiatrists brazenly used the ‘chemical imbalance’ theory to push ADHD. That theory has been debunked but the statistics represent that more people must be accepting the label for the prescribing rates to continue to rise.
At the end of the day, being fully informed is the key policy. If people reply on the psychiatric narrative, they won’t be fully informed. Don’t be fooled by psychiatric rhetoric.
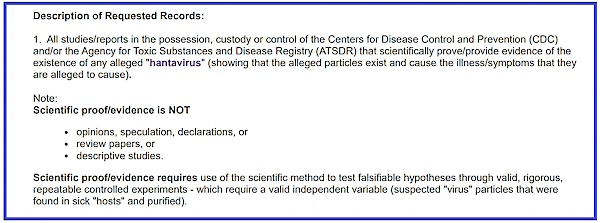
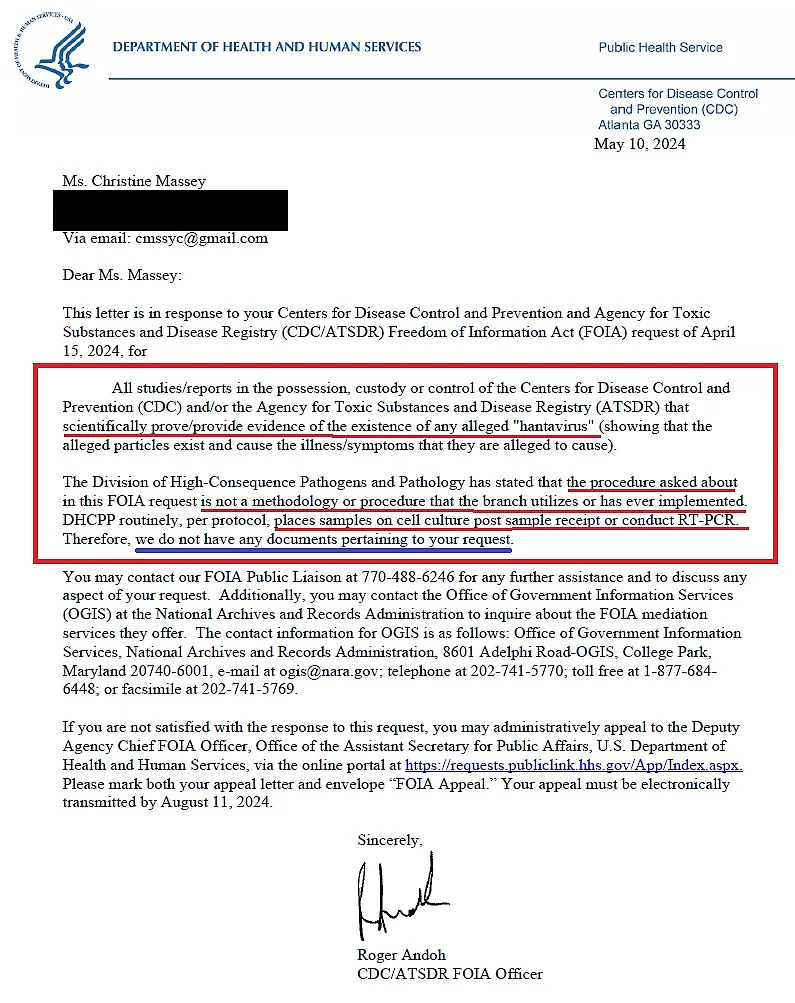




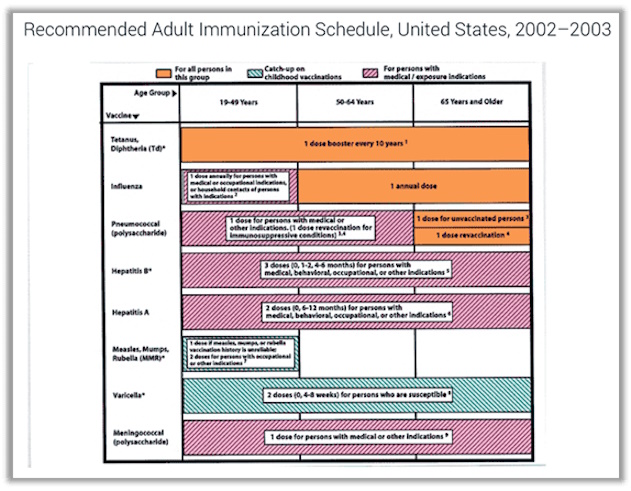
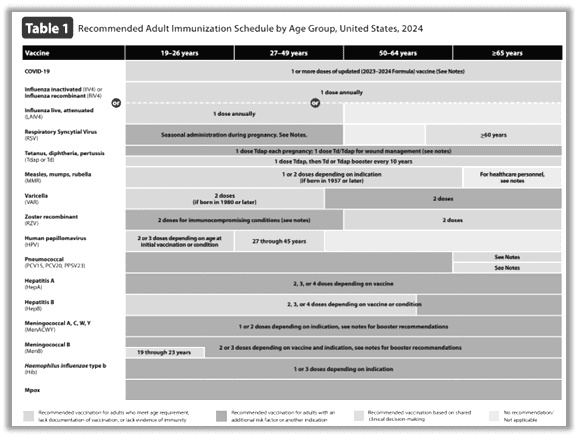
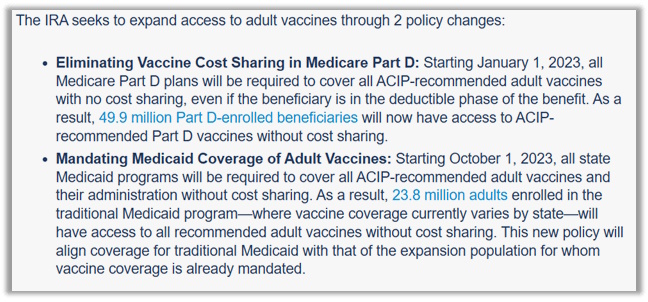
 Few of us were born when the forces for milk pasteurization launched the first major attack on Nature’s perfect food. In 1945, a magazine called Coronet published an article, “Raw Milk Can Kill You,” blaming raw milk for an outbreak of brucellosis in a town called Crossroads, U.S.A., killing one-third of the inhabitants. The Reader’s Digest picked up the story and ran it a year later.
Few of us were born when the forces for milk pasteurization launched the first major attack on Nature’s perfect food. In 1945, a magazine called Coronet published an article, “Raw Milk Can Kill You,” blaming raw milk for an outbreak of brucellosis in a town called Crossroads, U.S.A., killing one-third of the inhabitants. The Reader’s Digest picked up the story and ran it a year later.

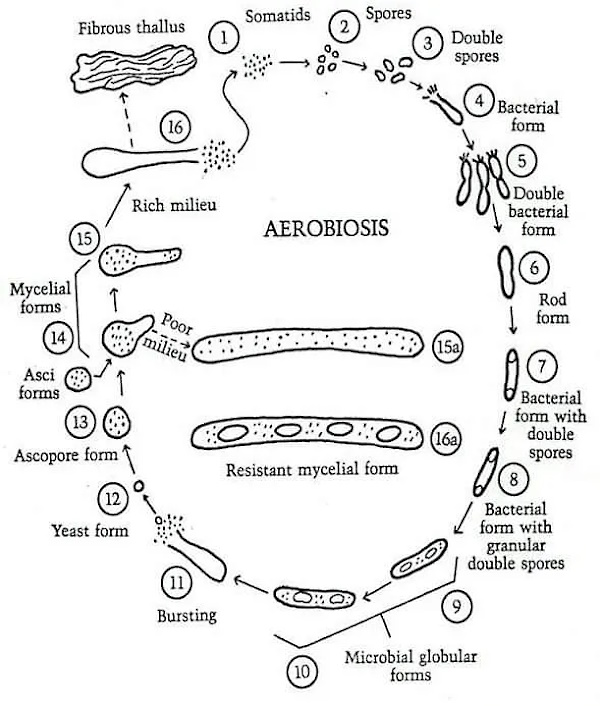
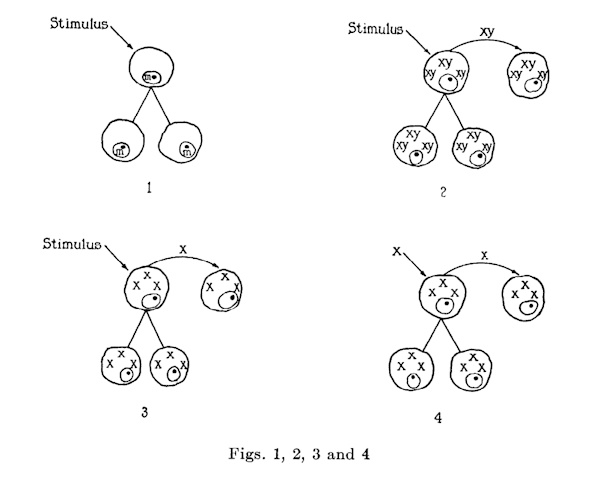
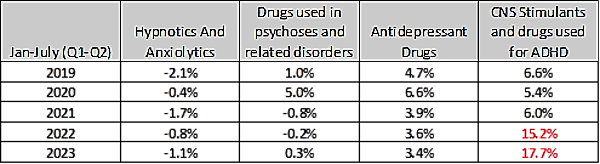
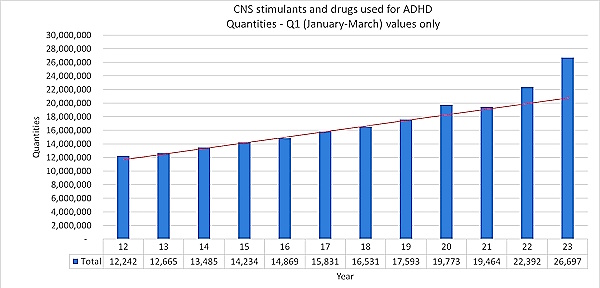
{kind=link}