Moral Courage and Our Common Future—A Foreword to “Plague of Corruption”
Moral Courage and Our Common Future—A Foreword to Plague of Corruption
by Robert F. Kennedy, Jr., Chairman, Children’s Health Defense
May 12, 2020
“And yet, it moves!” Galileo whispered those defiant words in 1615 as he left the Roman Inquisition tribunal before which he repudiated his theory that the Earth—the immovable center of the Universe according to contemporary orthodoxy—revolves around the sun. Had he not recanted, his life would be forfeit. We like to think of Galileo’s struggles as the quaint artifact of a dark, ignorant, and tyrannical era where individuals challenged government-anointed superstitions only at grave personal risk. Dr. Judy Mikovits’ story shows that stubborn orthodoxies anointed by pharmaceutical companies and corrupt government regulators to protect power and profits remain a dominant force in science and politics.
A pioneer in the field of human retrovirology
By any standard, Dr. Judy Mikovits was among the most skilled scientists of her generation. She entered professional science from the University of Virginia with a BA degree in chemistry on June 10, 1980, as a protein chemist for the National Cancer Institute (NCI) working on a life-saving project to purify interferon. The quality of her work and her reliable flashes of genius soon propelled her to the apex of the male-dominated world of scientific research. At NCI, Mikovits began what would become a twenty-year collaboration with Dr. Frank Ruscetti, a pioneer in the field of human retrovirology. While heading up the lab of Robert Gallo in 1977, Ruscetti made scientific history by co-discovering with Bernie Poiesz the first human retrovirus, HTLV-1 (human T-cell leukemia virus). A retrovirus is a “stealth virus” that, like HIV, enters the host without alerting the immune systems.
It may then lie dormant for years without causing harm. Before killing a person, a retrovirus will usually destroy their immune system. As a result, many retroviruses cause cancer. With an escalating understanding of retrovirus behavior, the Ruscetti/ Mikovits collaboration and Mikovits’s award-winning PhD thesis from George Washington University in 1991 changed the paradigm of HIV-AIDS treatment, turning the disease from a death sentence into a manageable condition.
Integrity before personal ambition
From the outset, the most daunting obstacle to Mikovits’ career advancement was her scientific integrity. She always placed it ahead of personal ambition. Judy Mikovits never meant to wade into a public health brawl. She never considered herself a renegade or revolutionary. Judy’s relatives mainly worked in government or law enforcement. They believed in the bedrock American principles of hard work, respect for authority, and, above all, telling the truth. That backdrop made it impossible for her to abandon her high natal standards of honesty and integrity even when they became a hindrance.
After leaving NIH, she worked a stint for Upjohn—leading a project to prove the safety of the company’s blockbuster Bovine Growth Hormone. When Mikovits discovered the company’s formula could cause precancerous changes in human cell cultures, she refused direct orders from her boss to hide her discoveries. Mikovits’ revelation suggested that the ubiquitous presence of the hormone in milk could lead to breast cancer in women who drank it. Her refusal to back down precipitated her departure from Upjohn and her return to NIH and graduate school. Judy’s war on BGH eventually led to Upjohn abandoning the product.
A new retrovirus—a ticking timebomb
In 2009, now in academia, Mikovits and Ruscetti, who was still at NCI, led a team that discovered a strong association between a previously unknown retrovirus and myalgic encephalomyelitis, commonly known as chronic fatigue syndrome (ME/CFS). Predictably, the retrovirus was also linked to certain blood cancers. Collaborators had named it Xenotropic Murine Leukemia Related Virus (XMRV), when they first detected in DNA sequences in prostate cancer a few years earlier.
The medical community had dealt with Chronic Fatigue Syndrome, which strikes mostly women, in bad faith since its appearance in the mid- 1980s. The medical establishment derided ME/CFS as “yuppie flu” and attributed it to the inherent psychological fragility of career women pursuing professions in high-pressure corporate ecosystems. Mikovits found evidence for the retrovirus in approximately 67 percent of women afflicted with ME/CFS, and in a little less than 4 percent of the healthy population.
On October 8, 2009, Mikovits and Ruscetti published their explosive findings in the journal Science, describing the first-ever isolation of the recently discovered retrovirus XMRV, and its association to ME/CFS. Her revelation about ME/CFS immediately triggered angry reactions from jealous cancer power centers, stubbornly resistant to science that attributed cancer and neuroimmune diseases to viruses.
The blowback grew even grimmer when Mikovits’ subsequent research suggested that the new retrovirus, originally found in mice, had somehow jumped into humans via contaminated vaccines.
Even more troubling to the medical establishment, Dr. Mikovits’ research revealed that many of the female patients afflicted with XMRV had children with autism. Suspecting XMRV might be passed from mother to child, as with HIV, Mikovits tested seventeen of the children. Fourteen showed evidence of the virus. Those findings dovetailed with parental reports of autistic regression following vaccination. Subsequent studies linked XMRV to epidemics in leukemia, prostate cancer, autoimmune disease, and the explosion of Alzheimer’s disease.
Mikovits’ data suggest that more than ten million Americans are harboring this virus like a ticking time bomb—a potential threat far greater than the HIV-AIDS epidemic.
Worse yet, research also found widespread XMRV contamination in the blood supply and blood products. Based on her research and the findings of others, it seemed that anywhere from 3 to 8 percent of the population now carry the virus—XMRV has become part of human ecology, passed from mother to child in vitro or through breast milk. Mikovits’ data suggest that more than ten million Americans are harboring this virus like a ticking time bomb—a potential threat far greater than the HIV- AIDS epidemic.
In January of 2011, HIV-AIDS expert Ben Berkhout published these explosive revelations in the journal Frontiers in Microbiology. He included Mikovits’ evidence that mouse tissue used in vaccine production was the likely vector for human contamination. Unbeknownst to Judy, her co-author on this book, Kent Heckenlively, had already independently discovered published medical research showing that the first recorded outbreak of ME/CFS was among 198 doctors and nurses at the Los Angeles County Hospital in 1934–1935, following their injection with an experimental polio vaccine grown in mouse brain tissue.
Big pharma fights back
Mikovits’ evidence threatened financial catastrophe for the world’s pharmaceutical companies because of their negligent use of animal cell cultures to produce vaccines and other pharmaceutical products. Her findings put at risk billions of dollars of revenues from an entire branch of medicine called “biologics,” which depends on animal tissue and products.
Pharmaceutical companies and their captive regulators unleashed a furious broadside against Mikovits and Ruscetti, besieging them from every stronghold.
The journal Science feverishly pressed Mikovits to retract her October 2009 article. In September of 2011, the Whittemore Peterson Institute at the University of Nevada, Reno, fired Judy from her faculty job. Judy and her family noticed menacing-looking men following her in pickup trucks and other incidents indicating she was under surveillance. In one incident, burley thugs surrounded her home and forced her to flee in a boat. After she escaped, they barged into her home, claiming to work for the government. In November, Ventura Police arrested Judy without a warrant and held her in jail for five days without bail. The police searched her house from top to bottom, strewing her papers everywhere. That same day, cops raided the home of her friend, Lilly, and forced her to sit in a chair for several hours while they ransacked the building. NIH officials told Nevada police that Dr. Mikovits had illegally taken her research notebooks from their lab. This was a fabricated charge. As the principle investigator on two government grants, it was Dr. Mikovits’ obligation to retain all of her research papers. Furthermore, Judy had left all of the notebooks in her university office on September 29. That same day, someone illegally burglarized Judy’s office, removed her notebooks, and then somehow planted them in a closet of her home, apparently to incriminate her. Weeks later, as Judy languished in a cell, her husband, David, found the journals neatly packed in a linen beach bag in an obscure closet in her Southern California home. David frantically took them to the jail after midnight and then handed them over to Ventura Police.
… the pharmaceutical cartel and its captive scientific journals launched a campaign of vilification against her.
While she was in jail, Judy’s former boss told her husband and Dr. Ruscetti that if she just signed an apology admitting her paper was wrong, the police would release her from confinement and she could salvage her science career. Judy refused. No prosecutor has ever filed charges against her, but the pharmaceutical cartel and its captive scientific journals launched a campaign of vilification against her. Less than two years earlier, the journal Science had celebrated her. Now, the same journal published her mug shot and retracted her paper.
Judy lost federal grants for which she was the principle investigator. She has gone bankrupt trying to find work and restore her good name. The scientific journals, admittedly all now controlled by Big Pharma, have refused to publish her papers. The NIH medical libraries have locked her out. Despite spending hundreds of thousands of dollars in legal fees, she has not been able to get her day in court. The US Attorney in Nevada has kept the case “under seal” for years. Fraudulent acts of public health officials at the highest levels of Health and Human Services (HHS) have effectively rendered her unemployable.
Challenging contemporary orthodoxies is an occupational hazard
The persecution of scientists and doctors who dare to challenge contemporary orthodoxies did not take a rest after Galileo: it has always been, and remains today, an occupational hazard. Henrik Ibsen’s 1882 play An Enemy of the People is a parable for the pitfall of scientific integrity. Ibsen tells the story of a doctor in southern Norway who discovers that his town’s popular and lucrative public baths were actually sickening the visitors who flocked to them for rejuvenation. Discharges from local tanneries had infected the spas with lethal bacteria. When the doctor goes public with the information, local merchants, joined by government officials, their allies in the “liberal-minded independent press,” and other financially interested parties move to muzzle him. The medical establishment pulls his medical license, the townsfolk vilify and brand him “an enemy of the people.”
Ibsen’s fictional doctor experienced what social scientists call the “Semmelweis reflex.” This term describes the knee-jerk revulsion with which the press, the medical and scientific community, and allied financial interests greet new scientific evidence that contradicts an established scientific paradigm. The reflex can be particularly fierce in cases where new scientific information suggests that established medical practices are actually harming public health.
The real-life plight of Ignaz Semmelweis, a Hungarian physician, inspired the term and Ibsen’s play. In 1847, Dr. Semmelweis was an assistant professor at Vienna’s General Hospital maternity clinic, where around 10 percent of women died from puerperal “birth bed” fever. Based on his pet theory that cleanliness could mitigate transmission of disease-causing “particles,” Semmelweis introduced the practice of mandatory hand washing for interns between performing autopsies and delivering babies. The rate of fatal puerperal fever immediately dropped to around 1 percent. Semmelweis published these findings.
Rather than building a statue to Semmelweis, the medical community, unwilling to admit culpability in the injury of so many patients, expelled the doctor from the medical profession. His former colleagues tricked Dr. Semmelweis into visiting a mental institution in 1865, then committed him against his will. Semmelweis died mysteriously two weeks later. A decade afterward, Louis Pasteur’s germ theory and Joseph Lister’s work on hospital sanitation vindicated Semmelweis’s ideas.
Modern analogs abound
Modern analogs abound. Herbert Needleman of the University of Pittsburgh endured the Semmelweis reflex when he revealed the brain-killing toxicity of lead in the 1980s. Needleman published a groundbreaking study in 1979 in the New England Journal of Medicine showing that children with high levels of lead in their teeth scored significantly lower than their peers on intelligence tests, on auditory and speech processing, and on attention measurements. Beginning in the early 1980s, the lead and oil industries (leaded gasoline was a lucrative petroleum product) mobilized public relations firms and scientific and medical consultants to lambast Needleman’s research and his credibility. Industry pressured the Environmental Protection Agency, the Office of Scientific Integrity at the National Institutes of Health, and the University of Pittsburgh to launch investigations against Needleman. Ultimately the federal government and the University vindicated Needleman. But the impact of the industry’s scathing assault ruined Needleman’s academic career and stagnated the field of lead research. The episode offered an enduring demonstration of industry power to disrupt the lives of researchers who dare to question their products’ safety.
Trade journals and the popular media disparaged [Rachel Carson] as a ‘hysterical woman.’
Rachel Carson ran the same gauntlet in the early 1960s when she exposed the dangers of Monsanto’s DDT pesticide, which the medical community then promoted as prophylactic against body lice and malaria. Government officials and medical professionals led by the American Medical Association joined Monsanto and other chemical manufacturers, attacking Carson viciously. Trade journals and the popular media disparaged her as a “hysterical woman.” Industry talking points derided Carson as a “spinster,” the contemporary euphemism for lesbian, and for being unscientific. Vicious criticisms of her book appeared in editorial pages in Time, Life, Newsweek, the Saturday Evening Post, US News and World Report, and even Sports Illustrated. I am immensely proud that my uncle, President John F. Kennedy, played a critical role in vindicating Carson. In 1962, he defied his own USDA, a captive agency in league with Monsanto, and appointed a panel of independent scientists who validated every material assertion in Carson’s book Silent Spring.
The experience of British physician and epidemiologist Alice Stewart offers a near-perfect analogy to the Medical cartel’s lynching of Judy Mikovits. In the 1940s, Stewart was one of the rare women in her profession and the youngest fellow ever elected at the time to the Royal College of Physicians. She began investigating the high occurrences of childhood cancers in well-to-do families, a puzzling phenomenon given that disease often correlated with poverty, and seldom with affluence. Stewart published a paper in The Lancet in 1956 offering strong evidence that the common practice of giving X-rays to pregnant women was the culprit in carcinomas that would later afflict their children. According to Margaret Heffernan, author of Willful Blindness, Stewart’s finding “flew in the face of conventional wisdom”—the medical profession’s enthusiasm for the new technology of X-rays—as well as “doctors’ idea of themselves, which was as people who helped patients.” A coalition of government regulators, nuclear promoters, and the nuclear industry joined the US and British medical establishments in launching a brutal attack on Stewart. Stewart, who died in 2002 at the age of ninety-five, never again received another major research grant in England. It took twenty-five years after the publication of Stewart’s paper for the medical establishment to finally acknowledge her findings and abandon the practice of X-raying expectant mothers.
Punished, exiled, and ruined
Judy Mikovits is heir to these martyrs and, more directly, to a long line of scientists, whom public health officials have punished, exiled, and ruined specifically for committing heresy against reigning vaccine orthodoxies.
Dr. Bernice Eddy was an award-winning virologist, and one of the highest-ranking female scientists in NIH history. She and her research partner Elizabeth Stewart were the first researchers to isolate the Polyomavirus—the first virus proven to cause cancer. In 1954, NIH asked Eddy to direct testing of the Salk polio vaccine. She discovered, while testing eighteen macaques, that Salk’s vaccine contained residual live polio virus that was paralyzing the monkeys. Dr. Eddy warned her NIH bosses that the vaccine was virulent, but they dismissed her concerns. The distribution of that vaccine by Cutter Labs in California caused the worst polio outbreak in history. Health officials infected 200,000 people with live polio; 70,000 became sick, leaving 200 children paralyzed and ten dead.
 In 1961, Eddy discovered that a cancer-causing monkey virus, SV40, had contaminated ninety-eight million Salk polio vaccines. When she injected the SV40 virus into newborn hamsters, the rodents sprouted tumors. Eddy’s discovery proved an embarrassment to many scientists working on the vaccine. Instead of rewarding her for her visionary work, NIH officials banned her from polio research and assigned her to other duties. The NIH buried the alarming information and continued using the vaccines.
In 1961, Eddy discovered that a cancer-causing monkey virus, SV40, had contaminated ninety-eight million Salk polio vaccines. When she injected the SV40 virus into newborn hamsters, the rodents sprouted tumors. Eddy’s discovery proved an embarrassment to many scientists working on the vaccine. Instead of rewarding her for her visionary work, NIH officials banned her from polio research and assigned her to other duties. The NIH buried the alarming information and continued using the vaccines.
In the autumn of 1960, the New York Cancer Society invited Eddy to address its annual conference. Eddy chose the subject of tumors induced by the polyoma virus. However, she also described tumors induced by the SV40 viral agent in monkey kidney cells. Her NIH supervisor angrily reprimanded Eddy for mentioning the discovery publicly and banned her from public health crisis statements. Eddy argued for publication of her work on the virus, casting the contaminated vaccine supply on an urgent public health crisis. Agency bigwigs stonewalled publication, allowing Merck and Parke-Davis to continue marketing the oncogenic vaccine to millions of American adults and children.
On July 26, 1961, the New York Times reported that Merck and Parke-Davis were withdrawing their Salk vaccines. The article said nothing about cancer. The Times ran the story next to an account about overdue library fines on page 33.
While two drug companies, Merck and Parke-Davis, recalled their polio vaccine in 1961, NIH officials refused to pursue a total recall of the rest of the supply, fearing reputational injury to the vaccine program if Americans learned that PHS had infected them with a cancer-producing virus. As a result, millions of unsuspecting Americans received carcinogenic vaccines between 1961 and 1963. The Public Health Service then concealed that “secret” for forty years.
In total, ninety-eight million Americans received shots potentially containing the cancer-producing virus, which is now part of the human genome. In 1996, government researchers identified SV-40 in 23 percent of the blood specimens and 45 percent of the sperm specimens collected from healthy adults. Six percent of the children born between 1980 and 1995 are infected. Public health officials gave millions of people the vaccine for years after they knew it was infected. They contaminated humanity with a monkey virus and refused to admit what they’d done.
Today, scientists find SV-40 in a wide range of deadly tumors, including between 33 percent and 90 percent of brain tumors, eight of eight ependymomas, and nearly half of the bone tumors tested.
Today, SV-40 is used in research laboratories throughout the world because it is so reliably carcinogenic. Researchers use it to produce a wide variety of bone and soft-tissue cancers including mesothelioma and brain tumors in animals. These cancers have exploded in the baby boom generation, which received the Salk and Sabin polio vaccines between 1955 and 1963. Skin cancers are up by 70 percent, lymphoma and prostate by 66 percent, and brain cancer by 34 percent. Prior to 1950, mesothelioma was rare in humans. Today, doctors diagnose nearly 3,000 Americans with mesotheliomas every year; 60 percent of the tumors that were tested contained SV-40. Today, scientists find SV-40 in a wide range of deadly tumors, including between 33 percent and 90 percent of brain tumors, eight of eight ependymomas, and nearly half of the bone tumors tested.
In successive measures, NIH forbade Bernice Eddy from speaking publicly or attending scholarly conferences, held up her papers, removed her from vaccine research altogether, and eventually destroyed her animals and took away access to her labs. Her treatment continues to mark an enduring scandal with the scientific community, yet NIH’s Bernice Eddy playbook has become a standardized template for Federal vaccine regulators in their treatment of dissident vaccine scientists who seek to tell the truth about vaccines.
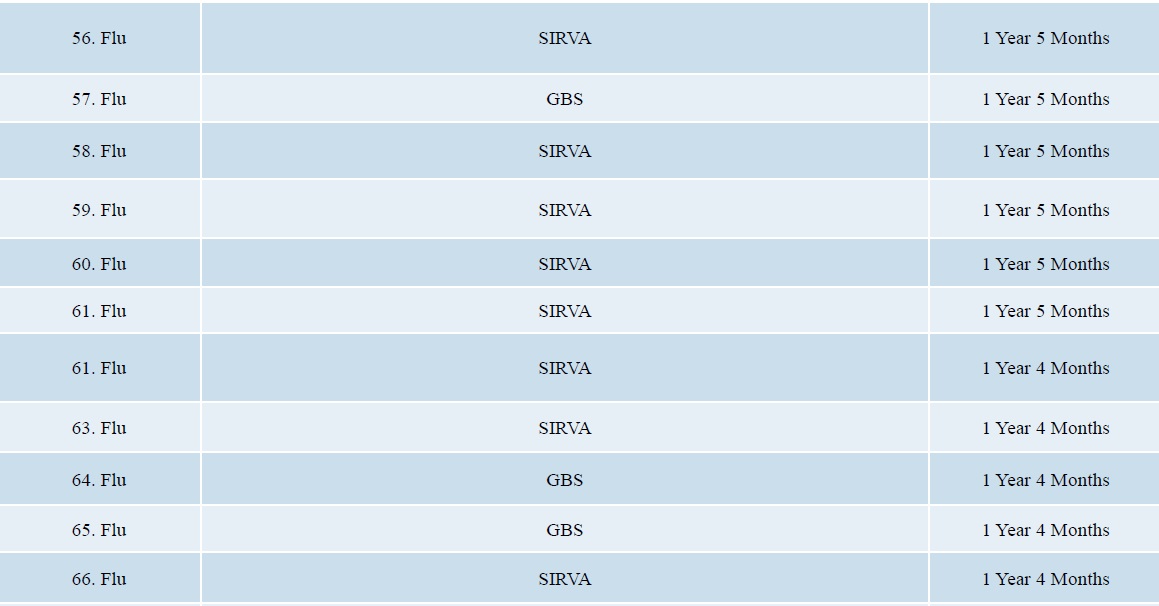
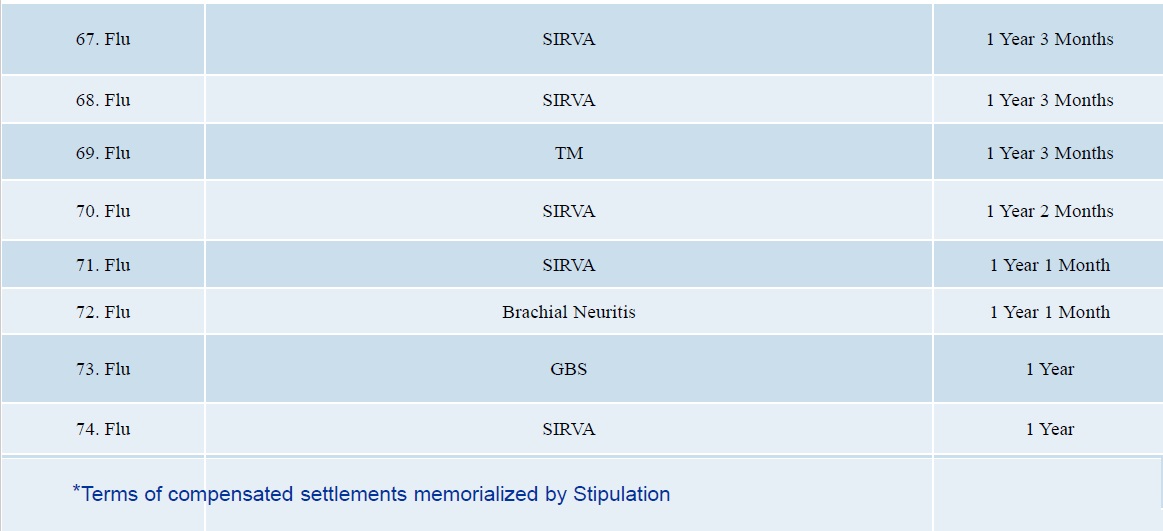
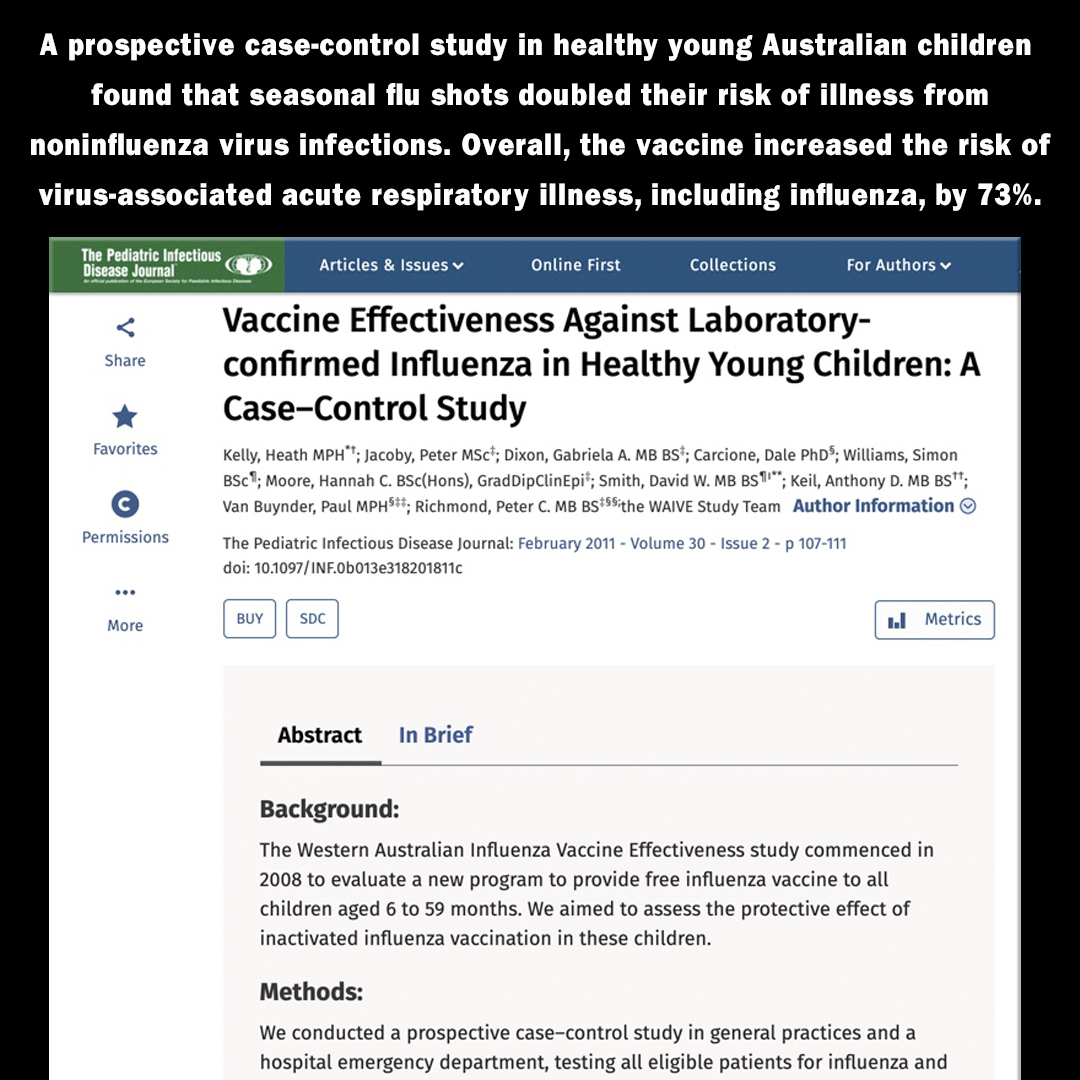
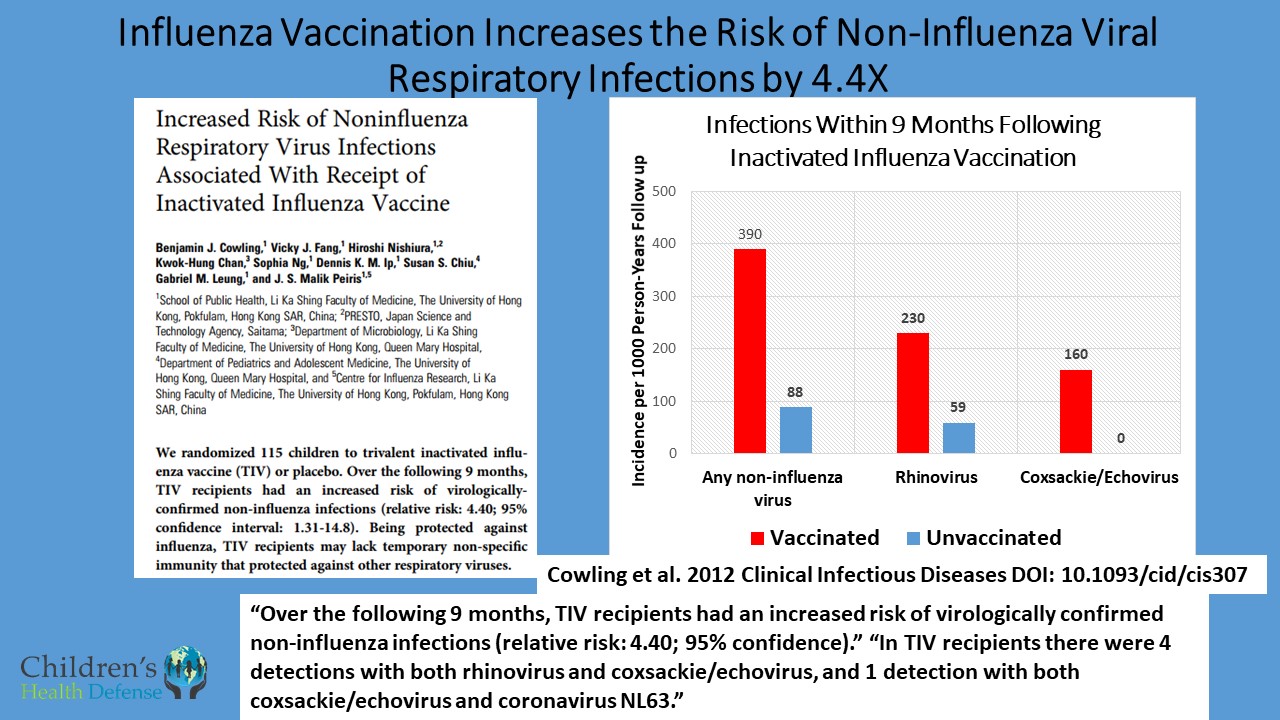
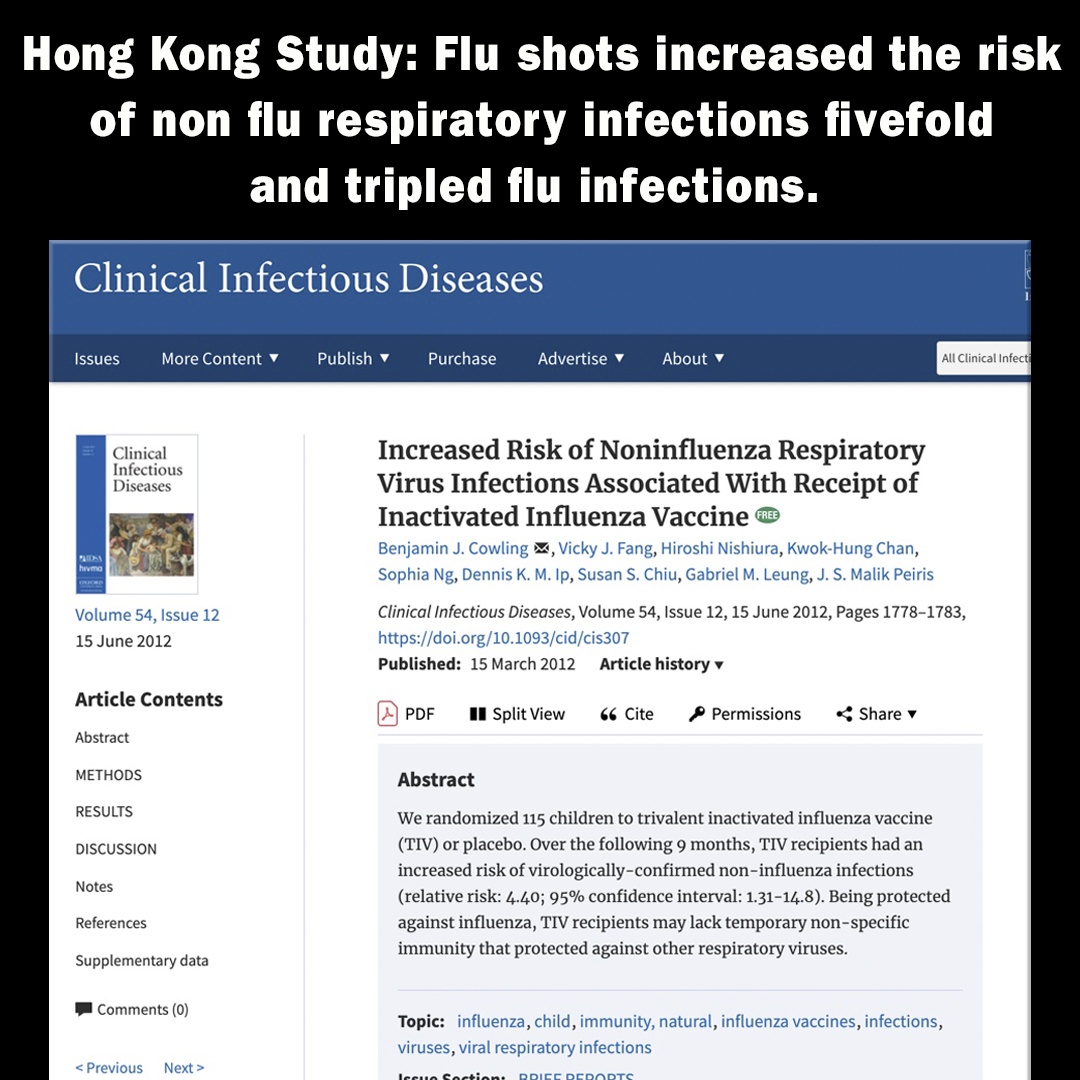
 Dr. John Anthony Morris was a bacteriologist and virologist who worked for thirty-six years at NIH and the Food and Drug Administration (FDA), beginning in 1940. Morris served as the chief vaccine officer for the Bureau of Biological Standards (BBS) at the National Institute of Health and later with the FDA when the BBS transferred to that agency in the 1970s. Dr. Morris irked his superiors by arguing that the research carried out by his unit demonstrated there was no reliable proof that flu vaccines were effective in preventing influenza; in particular, he accused his supervisor of basing HHS’s mass vaccination program for the swine flu primarily on a scientifically baseless fear campaign and on false claims made by pharmaceutical manufacturers. He warned that the vaccine was dangerous and could induce neurological injuries. His CDC superior warned Dr. Morris, “I would advise you not to talk about this.”
Dr. John Anthony Morris was a bacteriologist and virologist who worked for thirty-six years at NIH and the Food and Drug Administration (FDA), beginning in 1940. Morris served as the chief vaccine officer for the Bureau of Biological Standards (BBS) at the National Institute of Health and later with the FDA when the BBS transferred to that agency in the 1970s. Dr. Morris irked his superiors by arguing that the research carried out by his unit demonstrated there was no reliable proof that flu vaccines were effective in preventing influenza; in particular, he accused his supervisor of basing HHS’s mass vaccination program for the swine flu primarily on a scientifically baseless fear campaign and on false claims made by pharmaceutical manufacturers. He warned that the vaccine was dangerous and could induce neurological injuries. His CDC superior warned Dr. Morris, “I would advise you not to talk about this.”
When vaccine recipients began reporting adverse reactions, including Guillain-Barré, Dr. Morris disobeyed that order and went public. He declared that the flu vaccine was ineffective and potentially dangerous and said that he could find no evidence that this swine flu was dangerous or that it would spread from human to human.
In retaliation, FDA officials confiscated his research materials, changed the locks on his laboratory, reassigned his laboratory staff, and blocked his efforts to publish his findings. The FDA assigned Dr. Morris to a small room with no telephone. Anyone who wished to see him had to secure permission from the chief of the lab. In 1976, HHS fired Dr. Morris on the pretext that he failed to return library books on time.
Among the vaccine’s victims were 500 cases of Guillain-Barré, including 200 people paralyzed and thirty-three dead.
Subsequent events supported Dr. Morris’s skepticism about the swine flu shot. The 1976 swine flu vaccination program was so fraught with problems that the government discontinued inoculations after forty-nine million people had received the vaccine. Among the vaccine’s victims were 500 cases of Guillain-Barré, including 200 people paralyzed and thirty-three dead. Furthermore, the incidence of swine flu among vaccinated was seven times greater than among those who were unvaccinated, according to news reports.
According to his New York Times obituary, Dr. Morris said, “The producers of these (influenza) vaccines know they are worthless, but they go on selling them anyway.” He told the Washington Post in 1979, “It’s a medical ripoff I believe the public should have truthful information on the basis of which they can determine whether or not to take the vaccine,” adding, “I believe that given full information, they won’t take the vaccine.”
 FDA used the same playbook in 2002 to isolate, silence, and drive from government service its star epidemiologist, Dr. Bart Classen, when his massive epidemiologic studies, the largest ever performed, linked Hib vaccines to the juvenile diabetes epidemic. FDA ordered Dr. Classen to refrain from publishing the government-funded studies, forbade him from talking publicly about the alarming outbreak, and eventually forced him out of government service.
FDA used the same playbook in 2002 to isolate, silence, and drive from government service its star epidemiologist, Dr. Bart Classen, when his massive epidemiologic studies, the largest ever performed, linked Hib vaccines to the juvenile diabetes epidemic. FDA ordered Dr. Classen to refrain from publishing the government-funded studies, forbade him from talking publicly about the alarming outbreak, and eventually forced him out of government service.
In 1995, the CDC hired a PhD computer analytics expert, Dr. Gary Goldman, to perform the largest-ever CDC-funded study of the chickenpox vaccine. Goldman’s results on an isolated population of 300,000 residents of Antelope Valley, California, showed that the vaccine waned, leading to dangerous outbreaks of chickenpox in adults and that ten-year-old children who received the vaccine were getting shingles at over three times the rate of unvaccinated children. Shingles has twenty times the death rate of chickenpox and causes blindness. CDC ordered Goldman to hide his findings and forbade him from publishing his data. In 2002, Goldman resigned in protest. He sent a letter to his bosses saying that he was resigning because “I refuse to participate in research fraud.”
Our corrupt medical officials have systematically disgraced and silenced them.
Recent medical history overflows with other examples of the brutal suppression of any science that exposes vaccines’ risks; its casualties include brilliant and compassionate doctors and scientists like Dr. Waney Squier, the railroaded British gastroenterologist Andy Wakefield, the steadfast father/ son research team David and Dr. Mark Geier, Italian biochemist Antionetta Gatti, and Danish epidimiologist Peter Goetzsche. Any just society would have built statues to these visionaries and honored them with laurels and leadership. Our corrupt medical officials have systematically disgraced and silenced them.
In England a neuropathologist, Dr. Waney Squier of the Radcliffe Hospital in Oxford, testified in a series of cases on behalf of defendants accused of inflicting shaken baby syndrome. Squier believed that, in these cases, vaccines and not physical trauma had caused the infants’ brain injuries. In March 2016, the Medical Practitioner’s Tribunal Service (MPTS) charged her with falsifying evidence and lying and struck her from the medical register. Squier appealed the tribunal’s decision in November 2016. The High Court of England reversed the MPTS’s decision, concluding, “The determination of the MPTS is in many significant ways flawed.”
 Professor Peter Gøtzsche co-founded the Cochrane Collaboration in 1993 to remedy the overwhelming corruption of published science and scientists by pharmaceutical companies. Over 30,000 of the world’s leading scientists joined Cochrane as volunteer reviewers hoping to restore independence and integrity to published science. Gøtzsche was responsible for making Cochrane the world’s leading independent research institute. He also founded the Nordic Cochrane Center in 2003. On October 29, 2018, pharmaceutical interests, led by Bill Gates, finally succeeded in ousting Professor Gøtzsche. A stacked board controlled by Gates fired Gøtzsche from the Cochrane Collaboration after he published a well-founded criticism of the HPV vaccine. In 2018, the Danish government, under pressure from pharma, fired Peter Gøtzsche from Rigshospitalet in Copenhagen. His findings about the HPV vaccine threatened the pharmaceutical industry’s earnings.
Professor Peter Gøtzsche co-founded the Cochrane Collaboration in 1993 to remedy the overwhelming corruption of published science and scientists by pharmaceutical companies. Over 30,000 of the world’s leading scientists joined Cochrane as volunteer reviewers hoping to restore independence and integrity to published science. Gøtzsche was responsible for making Cochrane the world’s leading independent research institute. He also founded the Nordic Cochrane Center in 2003. On October 29, 2018, pharmaceutical interests, led by Bill Gates, finally succeeded in ousting Professor Gøtzsche. A stacked board controlled by Gates fired Gøtzsche from the Cochrane Collaboration after he published a well-founded criticism of the HPV vaccine. In 2018, the Danish government, under pressure from pharma, fired Peter Gøtzsche from Rigshospitalet in Copenhagen. His findings about the HPV vaccine threatened the pharmaceutical industry’s earnings.
A search for existential truth
Science, at its best, is a search for existential truth. Sometimes, however, those truths threaten powerful economic paradigms. Both science and democracy rely on the free flow of accurate information. Greedy corporations and captive government regulators have consistently shown themselves willing to twist, distort, falsify, and corrupt science, hide information, and censor open debate to protect personal power and corporate profits. Censorship is the fatal enemy of both democracy and public health. Dr. Frank Ruscetti often quotes Valery Legasov, the courageous Russian physicist who braved censor, torture, and threats on his life by the KGB to reveal to the world the true cause of the Chernobyl disaster. “To be a scientist is to be naïve. We are so focused on our search for the truth, we fail to consider how few actually want us to find it. But it is always there, whether we can see it or not, whether we choose to or not. The truth doesn’t care about our needs or our wants. It doesn’t care about our governments, our ideologies, our religions. It will lie in wait for all time.”
This account by Judy Mikovits and Kent Heckenlively is vitally important both to the health of our children and the vitality of our democracy. My father believed moral courage to be the rarest species of bravery. Rarer even than the physical courage of soldiers in battle or great intelligence. He thought it the one vital quality required to salvage the world.
If we are to continue to enjoy democracy and protect our children from the forces that seek to commoditize humanity, then we need courageous scientists like Judy Mikovits who are willing to speak truth to power, even at terrible personal cost.

 The Patent
The Patent Maintaining and analyzing the data
Maintaining and analyzing the data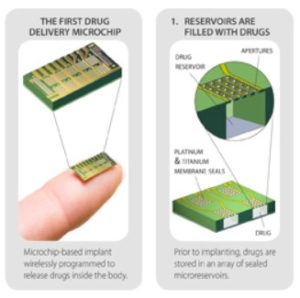 Gates will
Gates will 
 Robert Cinque
Robert Cinque


 Instead of holding officials accountable for their negligence , doctors on the front lines are being fired for speaking up! It happened to a medical whistleblower in China and it happens to
Instead of holding officials accountable for their negligence , doctors on the front lines are being fired for speaking up! It happened to a medical whistleblower in China and it happens to 





 Doctors, Nurses, Cops, Firefighters, Lawyers, and anyone with a tie. You will kill more by following orders. Do your homework. Stop pretending there’s such a thing as experts. Compliance will lead to millions of lives lost as a result of mass economic collapse. The Great Depression killed 7 million people. All of our food comes from the same trucks. The situation will be nineteen times worse by Winter and history will claim it was the fault of the unvaccinated and the result of Covid-19, the humanity virus. Your doctor is the military now.
Doctors, Nurses, Cops, Firefighters, Lawyers, and anyone with a tie. You will kill more by following orders. Do your homework. Stop pretending there’s such a thing as experts. Compliance will lead to millions of lives lost as a result of mass economic collapse. The Great Depression killed 7 million people. All of our food comes from the same trucks. The situation will be nineteen times worse by Winter and history will claim it was the fault of the unvaccinated and the result of Covid-19, the humanity virus. Your doctor is the military now.

 SOURCE:
SOURCE:  This is not necessary, nor smart. SOURCE: sciencemag.org
This is not necessary, nor smart. SOURCE: sciencemag.org SOURCE: Pesticide Action Network
SOURCE: Pesticide Action Network Did someone mention that the virus was “airborne”?
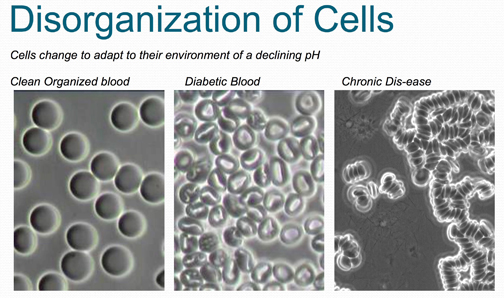
Did someone mention that the virus was “airborne”? Low electrical charge, proton dominant blood. Dehydrated cells are collapsed.
Low electrical charge, proton dominant blood. Dehydrated cells are collapsed. Electron-sufficient environment, hydrated cells, functional Krebs Cycle.
Electron-sufficient environment, hydrated cells, functional Krebs Cycle.