
Lethal Injection; Frontline E.R. Doctor Gives Chilling Account of Unusual Vaccine-Induced Illness
by Mike Whitney, The Unz Review
November 20, 2021
“Americans are scared to death…. People are walking off the job, not because they want to lose their jobs, but they don’t want to die from the vaccine! … They say, ‘Listen, I don’t want to die. That’s the reason I’m not taking the vaccine.’ It’s that clear.” Dr. Peter McCullough
A report in the U.K. Telegraph explains how the Covid-19 vaccine has led to a sharp rise in excess deaths. Here’s an excerpt from the article:
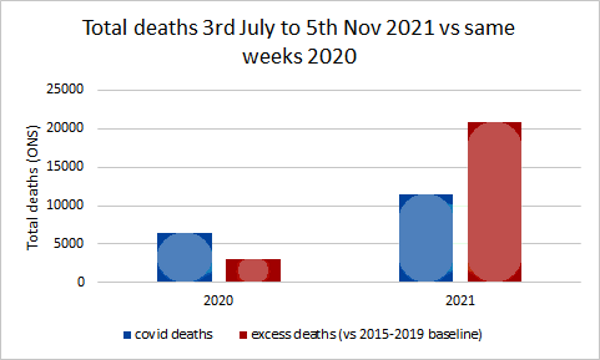
“Nearly 10,000 more people than usual have died in the past four months from non-Covid reasons, as experts called for an urgent government inquiry into whether the deaths were preventable….
Latest figures from the Office for National Statistics showed that England and Wales registered 20,823 more deaths than the five-year average in the past 18 weeks. Only 11,531 deaths involved Covid.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
Mortality is rising because more people are dying. And more people are dying because more people have been vaccinated. There’s a link between rising mortality and the Covid-19 vaccine. Naturally, the media wants to shift responsibility for the fatalities to “delayed treatments” and “the lack of preventable care”. But this is just a diversion. The primary cause of death is the injection of a toxic pathogen into the bloodstreams of roughly 70% of the population. That’s what’s causing the clotting, the bleeding, the pulmonary embolisms, the heart attacks, the strokes, and the premature deaths. It’s the vaccine. Here’s more
“Weekly figures for the week ending November 5 showed that there were 1,659 more deaths than would normally be expected at this time of year. Of those, 700 were not caused by Covid.
The excess is likely to grow as more deaths are registered in the coming weeks.
Data from the UK Health Security Agency show there have been thousands more deaths than the five-year average in heart failure, heart disease, circulatory conditions and diabetes since the summer.
The number of deaths in private homes is also 40.9 per cent above the five-year average, with 964 excess deaths recorded in the most recent week, which runs up to November 5.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
The sudden surge in mortality is not a meaningless blip on the radar. It’s a red flag indicating a significant break in the five-year trend. Something has gone terribly wrong. Mass vaccination was supposed to reduce the number of cases, hospitalizations and deaths. Instead, the fatalities continue to rise.
Why?
The answer to that question can be found in the data itself. As the author admits, there has been a sharp uptick in heart failure, heart disease, circulatory conditions and strokes. (Diabetes is the outlier) These are precisely the ailments one would expect to see if one had just injected millions of people with a clot-generating biologic that triggers a violent immune response that attacks the inner lining of the blood vessels inflicting severe damage to the body’s critical infrastructure. So, yes, all-cause mortality is up, and it is certain to climb even higher as more people are vaccinated and gradually succumb to the (frequently) delayed effects of a hybrid concoction that is the cornerstone of a malign plan to dramatically reduce global population. Check out this chart followed by a brief comment by diagnostic pathologist, Dr Claire Craig:
So, not only are more people dying, but the demographic has shifted downwards as younger and younger people are drawn into the vaccine vortex. Simply put, the number of young people dying from vaccine-inflicted cardiac arrest and myocarditis continues to increase with no end in sight.
Not surprisingly, all-cause mortality is higher among the vaccinated than the unvaccinated which, again, makes it easier to trace the problem back to its root, a cytotoxic “poison-death shot” that suppresses the innate immune system, damages vital organs and shaves years off the lives of normal, healthy people.
Perhaps, you’ve seen one of the many short videos of fit, young athletes who suddenly have dropped dead on the field of play or been rushed to hospital shortly after getting injected. If not, here’s a link to two of them. (Athletes collapse following vaccination: See here and here)
According to Israeli Real-Time News, there has been a “500% increase in deaths of players in 2021… Since December, 183 professional athletes and coaches have suddenly collapsed! 108 of them died!”
“500% increase in the deaths” of athletes?!? What are we to make of this?
For starters; the Covid-19 vaccine is not a medication. It is the essential component in the elitist plan for industrial-scale extermination. It is designed to inflict severe physical injury on the people who take it. It’s shocking that people are so deep in denial that can’t see what’s going on right before their eyes. (Please, watch the video clips of the athletes. These are the fittest people on the planet and, yet, they are being struck down by the mystery substance in the vaccine.) Here’s how South African doctor Shankara Chetty summed it up in a recent video posted on Bitchute:
“The pathogen that is causing all the deaths from the illness is the spike protein. And the spike protein is what the vaccine is supposed to make in your body. …Spike protein is one of the most contrived poisons that man has ever made. And, the aim of this toxin, is to kill billions of people without anyone noticing it. So it is a poison with an agenda.” (“South African Physician Dr. Shankara Chetty Talks about “The Bigger Plan”, Bitchute)
There it is in a nutshell. And Chetty is not alone in linking the vaccine to the agenda of the globalist elites who plan to use the cover of a pandemic to implement their “population management” scheme. Former Pfizer vice president, Mike Yeadon, offered a similar view just days ago on his website. He said:
“We are in the midst of the biggest depopulation program the world has ever seen, where most of humanity are acting as useful idiots to it and to their own demise.”
Indeed, and we have tried to provide as much information as possible on the biologic agent that is being used to pursue this malign agenda, the spike protein. In early reports we passed along the research of Dr. Patrick Whelan who grasped the danger of the spike protein before anyone else. Here’s a brief recap of his analysis from a letter he submitted to the FDA on December 8, 2020:
“I am concerned about the possibility that the new vaccines aimed at creating immunity against the SARS-CoV-2 spike protein have the potential to cause microvascular injury to the brain, heart, liver, and kidneys in a way that does not currently appear to be assessed in safety trials of these potential drugs.
… Meinhardt et al…. show that the spike protein in brain endothelial cells is associated with formation of microthrombi (clots)… In other words, viral proteins appear to cause tissue damage without actively replicating virus…. The Pfizer/BioNTech vaccine (BNT162b2) is composed of an mRNA that produces a membrane-anchored full-length spike protein. The mouse studies suggest that an untruncated form of the S1 protein like this may cause a microvasculopathy in tissues that express much ACE2 receptor.
…it appears that the viral spike protein… is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung, and kidney. Before any of these vaccines are approved for widespread use in humans, it is important to assess in vaccinated subjects the effects of vaccination on the heart…. As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs. (“FDA shrugs off dire warning about lethal spike protein“, Truth in the Age of Covid)
From the very beginning, government regulators and their allies in public health establishment have ignored (or censored) the warnings of capable physicians and researchers. They also waved-off career immunologist and vaccinologist, Dr Byram Bridle who was the first in his profession to identify the spike protein as “a specific causative agent of disease”; aka–“a pathogen”. Here’s Bridle:
“‘We have known for a long time that the spike protein is pathogenic…. It is a toxin. It can cause damage in our body if it’s in circulation. Now, we have clear-cut evidence that . . . the vaccine itself, plus the protein, gets into blood circulation.’”
Once that happens, the spike protein can combine with receptors on blood platelets and with cells that line our blood vessels. This is why, paradoxically, it can cause both blood clotting and bleeding. ‘And of course the heart is involved, as part of the cardiovascular system… That’s why we’re seeing heart problems. The protein can also cross the blood-brain barrier and cause neurological damage.…
‘In short,… we made a big mistake. We didn’t realize it until now. We didn’t realize that by vaccinating people we are inadvertently inoculating them with a toxin.”… (“Vaccine scientist: ‘We’ve made a big mistake’“, Conservative Woman)
Here again, we have a highly-regarded immunologist, with more than 3 decades of experience under his belt, who offered his informed and evidence-based research on an issue that should have been of great interest to the regulators that were making decisions about the long-term safety of the experimental drug they were foisting on millions of people across the country. But there was no interest at all. Despite the fact that the science supported his conclusions, Bridle was viciously attacked, censored, dragged through the mud, and forced to leave his place of employment.
Why?
Because he drew the same conclusions as Dr. Patrick Whelan. There’s really no substantive difference between the two except that Bridle’s comments attracted more attention in the media which made him a greater threat to the “universal vaccination” strategy. That was his real crime; he discovered the truth and made his findings available to the public, basically alerting them to the dangers of the “poison-death shot”. For that he was crushed.
>Bridle has since made other claims that should concern anyone whose cancer might be in remission. Here’s what he said in a recent interview:
“What I’ve seen way too much of is people who had cancers that were in remission, or that were being well controlled; their cancers have gone completely out of control after getting this vaccine. And we know the vaccine causes a drop in T-cell numbers, and those T-cells are part of our immune system and they are part of the critical weapons our immune system has to fight off cancer cells; so there’s a potential mechanism there. All I can say, is I’ve had way too many people contact me with these reports for me to feel comfortable. I would say that is my newest major safety concern, and it’s also the one that’s going to be the most under-reported in the adverse data base, because if someone has had cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine.” (“Dr Byram Bridle speaks”, Bitchute, :55 second-mark)
So, the vaccine suppresses the immune system?
Yes, it does, and author Alex Berenson provided evidence of this just recently in an article he posted on Substack. Here’s an excerpt:
“… the British government…. admitted today, in its newest vaccine surveillance report, that:
“N antibody levels appear to be lower in people who acquire infection following two doses of vaccination.” (Page 23)
What’s this mean?…
What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus….
This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE…
… it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.” (“URGENT: Covid vaccines will keep you from acquiring full immunity EVEN IF YOU ARE INFECTED AND RECOVER”, Alex Berenson, Substack)
Berenson’s observations square with research that was compiled earlier in the year by scientists in The Netherlands and Germany who:
“….warned that the … (COVID-19) vaccine induces complex reprogramming of innate immune responses that should be considered in the development and use of mRNA-based vaccines… the research team from Radboud University Medical Center and Erasmus MC in the Netherlands… showed that the vaccine altered the production of inflammatory cytokines by innate immune cells following stimulation with both specific (SARS-CoV-2) and non-specific stimuli.
Following vaccination, innate immune cells had a reduced response to toll-like receptor 4 (TLR4), TLR7 and TLR8 – all ligands that play an important role in the immune response to viral infection…. an unexplored area is whether BNT162b2 vaccination has long-term effects on innate immune responses …
This could be very relevant in COVID-19, in which dysregulated inflammation plays an important role in the pathogenesis and severity of the disease,” writes the team. “Multiple studies have shown that long-term innate immune responses can be either increased (trained immunity) or down-regulated (innate immune tolerance) after certain vaccines or infections.” (Research suggests Pfizer-BioNTech COVID-19 vaccine reprograms innate immune responses, new-medical-net)
Berenson’s finding also align with with cutting-edge research showing that the spike protein greatly “impedes adaptive immunity” by preventing DNA from repairing damaged cells. The paper suggests that the spike protein does in fact “impact on the nucleus of the cell, where we store our DNA, our core genetic material.” Here’s more from Berenson’s breakdown of the paper:
“…. our cells have mechanisms to repair their own DNA.
But – at least in the experiments these two scientists ran – the spike protein appeared to interfere with our own DNA repair proteins: “Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site.”
To be clear, the scientists did NOT prove the spike protein was causing these problems in people, or even animals… Nonetheless, at a time when advanced countries that have high mRNA (and DNA/AAV) vaccination rates are seeing unusually full hospitals and higher-than-normal death rates, they are yet more cause for concern. As the authors explained:
“Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.” (“URGENT: Worrisome paper about the spike protein’s impact on DNA and DNA repair”, Alex Berenson, Substack)
Bottom line: If the vaccine does in fact inhibit the body’s innate immune response, then people are going to get alot sicker from seasonal infections that routinely spread through the population. Their path to recovery will also be alot more difficult.
But rather that belabor the immunity angle, let’s move on to the research of Dr Charles Hoffe who was the first physician to provide hard evidence that the vaccines generate blood clots by triggering an immune response in which the body attacks the thin layer of cells lining the walls of the blood vessels. Hoffe found that 62% of his patients that had been vaccinated tested positive for blood clots on a D-dimer test. Naturally, he was alarmed by what he found, particularly since the vaccine “was causing serious neurological events, and even death. When he raised his concerns with the BC College of Physicians, they immediately implemented a gag order, and reprimanded him in an attempt to intimidate, and silence him.”
Hoffe has been interviewed a number of times and always provides a detailed and riveting account of his findings. In a recent interview, he predicted that some vaccinees suffering from clot-related issues would likely die in just three years. Here’s what he said:
“… once you block off a significant number of blood vessels to your lungs, your heart must pump at a much greater resistance to get the blood through your lungs. That causes a condition called pulmonary artery hypertension, which is high blood pressure in your lungs because so many of the blood vessels in your lungs are blocked. And the terrifying thing about this is tha t people with pulmonary artery hypertension usually die of right-sided heart failure in three years… And not only is the long-term outlook very grim, but with each successive shot, the damage will add and add and add. It’s going to be cumulative because you are getting more and more damaged capillaries.” (“Shock: Doctor Warns That Majority Of Vaccinated Patients Could HavePermanent Heart Damage, Some May Die Within Three Years”Permanent Heart Damage, Some May Die Within Three Years”, Infowars; Minute 6:10)
Once again, there is no discrepancy between the analysis of Whelan, Bridle and Hoffe. And while the focus of their attention might vary slightly, their conclusions are the same. These experimental injections pose serious risks for anyone who allows himself to be inoculated.
Now check out how similar Hoffe’s analysis is to Dr. Rochagne Kilian who was an Emergency Room physician at the GBHS hospital until she resigned in protest. This is a particularly important video as it describes the “oddball” symptoms and exceedingly rare conditions that are now presenting in emergency rooms everywhere following the mass vaccination of millions of people with the “poison-death shot”. (I transcribed the video myself, so there could be errors.)
Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels
“What I was seeing in my ER department especially in the last 8 to 9 months is related to the D-Dimer levels. We use D-Dimers specifically related to pulmonary embolisms as well as Deep Vein Thrombosis. D-Dimer detects any thrombosis (clots) in the body but it doesn’t give you a diagnosis it gives you a basis for going further and doing an ultrasound and CT scan to either confirm or deny the presence of a pulmonary embolism or Deep Vein Thrombosis.
The first part of 2020 was probably the slowest ever in the emergency department, but when we went into 2021 and the vaccination rollout started, we ended up seeing an increase in stroke, transient ischemic attacks and stroke like presentations. (There were) definitely significant larger numbers of those people coming in. I ended up doing D-dimer tests on these people and never before in my clinical experience had I seen D-dimers and the amount of people with positive D-dimers higher than 2,000, higher than 3,000 and higher than 5,000. My clinical experience told me a needed to go look for a large clot either in their legs or their lungs. And I ended up doing a CT scan on these people. Most of them, and I will say almost all of them, had negative scans which started making me think that if there was not a significant clot in their lungs, but my D-dimer was so much higher than what I was usually seeing, it might not be concentrated in one clot. But that it is multiple micro-thrombi extended throughout the body, and that is so easy to miss because the CT scan is not going to pick it up.
“These people coming into the ER were all people anywhere from about a week to four months after receiving their 2nd injections. There are certain factors that can influence a D-dimer test that can give you a sense of a higher level than would be expected in the body. That said, the patients I was doing D-Dimer tests on did not have a level of maybe a positive 500 or 400 reading. It was more than 3500, more than 5000 ng/ml. So those are significantly positive without any proof of having a pulmonary embolism. If I was seeing high levels of D-dimer without a definite diagnosis, I needed to ask more questions.
One study said, never ignore extremely elevated D-dimer levels. They are specific for serious illness, including venous thrombosis, sepsis, and/or cancer. Even if sharply elevated D-dimer are a seemingly solitary finding, clinical suspicion of severe underlying disease should be maintained.
There were two conditions that stood out and the first one was disseminated intravascular coagulation also known as DIC. The second one is antiphosphlipid syndrome. Both of these conditions are related to an abnormality in either the initiation or the feedback of the coagulation pathway as well as thrombosis or the thrombosis cycle where clots are being broken down. DIC is a serious sometimes life threatening situation in which the proteins in the blood involved in blood clotting become overactive. It’s a cascade that’s difficult to stop once it’s reached a certain level. There are certain conditions that trigger DIC; significant sepsis, underlying viruses, trauma, major surgery, pregnancy and childbirth. And less common causes toxic drug reaction, blood transfusion reaction, and organ transplants. So there was a connection with intravascular products and a possible DIC.
Most cases of DIC are diagnosed rapidly and suddenly which is the acute presentation. But there are cases where it develops gradually, occurring over a longer period of time. This is known as a chronic form of DIC and I would go as far to say a subacute form of DIC that is very easy to miss. Simultaneous clotting and bleeding can occur with chronic DIC. The bleeding part comes in blood in the urine, headaches and other symptoms associated with brain bleeds, bruising, inflammation of red, small dots on the limbs, bleeding at sites of wounds and mucosal bleeding. which means bleeding out of the gums and nose. I definitely saw an increase in nose bleeds and bleeding from previous wound sites. ulcers, as well as rashes that couldn’t be explained. Blood clotting symptoms and signs were symptoms like chest pains, heart attacks, strokes, TIAs, and headaches either related to bleeding or not. As well as symptoms related to kidney failure, because of the clotting of those smaller blood vessels that go to the kidneys. Antiphosphlipid syndrome is a very similar type of condition. But the basis of the antiphosphlipid syndrome is an autoimmune disorder meaning that the body’s immune system makes proteins–known as antibodies–that mistakenly attacks its own body or tissues. That gives the skin the cascading effect of clotting disorder but it is linked to an autoimmune trigger. Basically, it presented in exactly the same way; high blood pressure which I was seeing alot of; first diagnosis of high blood pressure, heart attacks, strokes, TIAs, heart valve problems, repeated headaches or migraines, vision loss, balance and mobility problems, difficulty concentrating or thinking clearly,
The astute listener would start forming a picture of what we’ve been told about Covid-19, and there are research papers connecting Covid 19 with an underlying vascular disease. One of these was a study called “Covid 19; unraveling the clinical progression of Nature’s Virtually perfect Biological weapon.”
“SARS-Cov-2, presenting as Covid-19 syndrome, was not a respiratory basis, but an underlying vascular basis. which had certain phases of incubation, pulmonary phase, pro inflammatory phase, (which once again comes into a cytotoxic inflammation process) then moves into a protothrombic phase . Covid-19 is a thrombotic disease. implications for prevention, antithrombotic therapy and follow up…..
This picture shows us certain risk factors, Homeostatic Abnormalities, as well as clinical outcomes. It indicates increased D-dimer levels. It also mentions Venous Thromboembolism, Myocardial Infarction, and Disseminated Intravascular Coagulation that is connected to postulated mechanisms of coagulathopy as well as parthenogenesis of thrombosis in Covid-19…
I started asking the question, if we are able to detect certain connections between vascular abnormalities and Covid-19, and we based our proposed treatment on the spike protein, which includes the Pfizer and Moderna injections, shouldn’t we be looking for similar side effects or complications from that same injection?
If we are mandating certain treatments, we do need to do the due diligence to make sure what the side effects and complications especially in a time where there has not been long term studies.”And that’s what led me to focusing on D-dimers.” (“Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels“, Bitchute)
Kilian’s statement should be read over and over again. It is the most detailed description we have of the mysterious and deeply sinister machinations of a laboratory-engineered bioweapon that, in effect, turns the vascular and immune systems against the person who was vaccinated. Disseminated intravascular coagulation and antiphosphlipid syndrome are names that are entirely unknown to the American people, and yet, these freakish conditions are now responsible for a growing number of patients that are experiencing bleeding, clotting, headaches, rashes, bruising, high blood pressure, and inflammation . And– in more extreme cases– chest pains, heart attacks, strokes, heart-valve problems, and brain bleeds. One can only guess how the media will try to cover-up these extraordinarily-rare and potentially life-threatening conditions??
When Kilian asks:
“If we are able to detect certain connections between vascular abnormalities and Covid-19… shouldn’t we be looking for similar side effects or complications from that same injection?”
>Bingo! If the spike protein produced by the vaccines, inflicts the same internal damage as Covid-19, then shouldn’t doctors expect to see the same symptoms?
Yes, they should. And if the symptoms are the same, then there’s a good chance that vaccine-induced injuries are being misdiagnosed as Covid-19.
Think about that for a minute. That would be the perfect scenario for the pandemic managers and their billionaire backers who’d love to see the impending mountain of carnage blamed on the waning virus instead of on their own poison-death shot.
And that is the evil-genius of the globalist strategy; to remove the fingerprints from the smoking gun before the investigators even arrive at the scene of the crime.
The amount of planning that must have gone into this scam, is simply breathtaking.
Read more by Mike Whitney at The Unz Review
cover image credit: paulbr75 / pixabay


Truth Comes to Light highlights writers and video creators who ask the difficult questions while sharing their unique insights and visions.
Everything posted on this site is done in the spirit of conversation. Please do your own research and trust yourself when reading and giving consideration to anything that appears here or anywhere else.







