(OMNS Oct 20, 2020) In treating the sick, Hippocrates, the Father of Medicine counselled, “First, do no harm.” Unfortunately, this cherished principle has not been followed in caring for patients with coronavirus infection. Losing a loved one due to cancer and other diseases is always tragic. But losing one due to the coronavirus pandemic when it could be prevented is an unforgivable act resulting in the mass murder of innocent lives. It has happened due to ignorance about history, hypocrisy, a lack of training of doctors about alternative medicine, and closed minds about the life-saving medical benefits of high doses of intravenous vitamin C.
I would not have the knowledge to write this article if one event in my life had not happened. At 74 years of age I nearly died of a serious heart attack. Doctors said I’d be dead in a few years without the help of cholesterol-lowering drugs. Luckily, several years earlier I had interviewed Dr. Linus Pauling, two-time winner of the Nobel Prize. He advised me of the important role of vitamin C in decreasing the risk of coronary disease. This is when I made one of the most vital decisions of my life. I decided to take 10,000 milligrams (mg) of vitamin C daily, rather than believe Big Pharma. But I also worried because Pauling, although a brilliant chemist, was not a doctor. Was he right about vitamin C? It was only years later when Dr. Sidney Bush, a English researcher proved that vitamin C could reverse atherosclerosis (hardening of arteries) that I knew I had made the right decision. [1]
Now, 22 years later, the doctors who told me I’d be dead in a few years without cholesterol-lowering drugs are dead, and I’m in my 97th year, still alive. It’s this experience with the cardiovascular effects of vitamin C that’s triggered my interest in the anti-infective and other medical benefits of vitamin C, especially how it can decrease deaths from viral and bacterial diseases.
Klenner went on to show that large doses of vitamin C could also cure other viral diseases such as meningitis, hepatitis, measles, mumps, pneumonia, shingles and even the poisonous bite of a rattlesnake. [2-4] Since that time other researchers have reported that there is no viral disease that high-dose IVC cannot successfully treat.
But Klenner did not win a popularity contest with his colleagues. He wrote in frustration that “Some physicians would stand by and see their patient die rather than use ascorbic acid because in their finite minds it exists only as a vitamin.”
Since that time closed medical minds have resulted in thousands of deaths from coronavirus and other diseases in Canada and worldwide. Because of a misconception that vitamin C is just another vitamin. But there is proof that vitamin C is a potent anti-infective nutrient that attacks both viral and bacterial diseases.
Infection triggers a severe inflammatory cellular reaction in the body which results in a decrease in vitamin C. It’s like being caught in a snow storm on a lonely road and running out of gas. But in this case white blood cells need C to fight the infection. And if you have not been taking C on a regular basis, your white blood cells without C are like a gun without bullets.
Many people do not realize that nearly all animals make their own vitamin C. Humans lost this ability eons ago due to a genetic mutation. For instance, dogs produce 5,000 milligrams (mgs) daily. Health Canada maintains humans need only 90 mgs. But if a dog gets an infection, it will automatically produce up to 20,000 mgs daily!
During the coronavirus pandemic I’ve listened to Medical Officers of Health, TV anchors, politicians and medical experts all discuss the importance of distancing and frequent hand washing. But I have only heard one discuss the advantages of vitamin C and D in building up the body’s immunity. [5] And I have not heard any explain how the use of high doses of IVC could save lives.
Dr. Lendon H. Smith outlined the clinical experiences of Frederick Klenner in “Clinical Guide to the Use of Vitamin C”. It contains a wealth of information on how vitamin C treats many diverse diseases. And how prescribing insufficient amounts of vitamin C can lead to failure in therapy. This medical information is available for all to read. [6]
I’ve have written before that if a family member died due to coronavirus infection and doctors and hospital refused to use IVC, I would contest this situation in a court of law. I believe I would win because historical evidence is so overwhelming that large doses of C save lives.
The hypocrisy surrounding vitamin C is mind boggling. Dr, Linus Pauling complained, “The medical community requires rigorous evidence supporting vitamin C, but accepts flimsy evidence against it.” Little has changed since I interviewed Pauling. This deficit is evidently caused by the minds of medical professionals refusing to accept scientific fact. And we will never know the number of needless deaths this has caused during the pandemic.
A year ago, as a journalist, I was invited to be a member of the Orthomolecular Medical News Service. It’s international editorial board is composed of distinguished physicians, professors, and researchers. Several months ago I asked all members how they would treat several viral infections. The overwhelming response was “high dose intravenous vitamin C.” OMNS has published twenty-two physician case reports of success with IVC. [7]
Since February, researchers in China have been conducting double-blind studies on IVC. This means one group will receive IVC and a control group will get a placebo. Some studies have already been completed, and the results show that IVC saves more lives than placebo. [8]
“Dr. Enqiang Mao, chief of emergency medicine
at Ruijin Hospital, Shanghai, stated that his group
treated ~50 moderate to severe cases of COVID-19
infection with high dose intravenous vitamin C.
“The IVC dosing was for 7-10 days, with 10,000 mg
for moderate cases and 20,000 mg for more severe cases.
“All patients who received intravenous vitamin C
improved, and there was no mortality.”
“There were no side effects reported from any of
the cases treated with high dose IVC.”
But even in one of these recent laudable studies, there was a flaw. According to the report, all patients received a certain dose for moderate infection while others a higher dose for a more severe one. But patients who died had not received the higher dose. [9]
This reflects everything that Dr. Linus Pauling and Dr. Frederick Klenner stressed. As Pauling told his critics, “It’s the dosage!” Or, as Klenner claimed, “Some infections require a much larger dose.” As we all know, half an aspirin will not cure a migraine headache.
But there is more disturbing news. Chinese researchers are experiencing trouble getting their findings published. Contacts also tell me that doctors who use IVC in North America are being harassed by authorities. In some case, being told that if they persist they will lose their license to practice medicine.
To get an update on what was happening in some parts of Canada and the U.S I contacted several infectious disease specialists, Medical Officers of Health (MOH), and university hospitals, asking a simple question. “Do you prescribe intravenous vitamin C or know of anyone who does to treat coronavirus infection? And if terminal patients are not receiving IVC, why is this the case”?
It proved to be a time-consuming assignment. Many replied they would get back to me but failed to do so. I could only conclude they were not using IVC and did not want anyone to know about it.
Or they responded, “We have checked with our infectious disease specialist and confirm that high dose C is not being used to treat coronavirus infection.”
What was shocking is that not a single Medical Officer of Health replied that IVC was being prescribed to those dying from coronavirus infection.
Another surprise was the reaction of Johns Hopkins one of the great hospitals of the world. Its distinguished professors were the first to introduce the value of bedside teaching for students. During this pandemic they were considered the authority in reporting the number of coronavirus deaths. So, I was shocked to receive this response, “We are not conducting clinical trials or administering C as a treatment for COVID 19.” And even Harvard Medical School where I spent so many years as a student and later training as a surgeon, never replied to me.
What is going to happen? It’s that the Chinese study will likely fail to end the controversy and patients will continue to die needlessly of this virus. I was hoping that one infectious expert, or Medical Officer of Health, would possess the intellectual curiosity to ask, “I wonder if high does IVC could save lives?” It’s tragic this has not occurred. Some would label this as medical ignorance, others as malpractice, or if a loved one has died as murder, and finally a court of law looking all the facts decide it’s been mass murder.
So, we have a unique situation. It’s been said that war is far too important to be left to generals. Due to the economic chaos caused by coronavirus this disaster may be much too important to be left to medical experts when so many North Americans have suffered.
It’s time for the government to demand that our medical schools conduct a study of IVC. There is no shortage of patients. We have the scientific talent in our universities. Vitamin C is inexpensive and will virtually never cause complications. Vitamin C has never killed anyone. Besides, this study could be done in a short time and not require thousands of patients.
Who will grasp the moment and save countless lives?
(Syndicated columnist W. Gifford-Jones, MD, (also known as Kenneth Walker, MD) graduated from Harvard Medical School in 1950. He did surgical residencies at McGill University, the University of Rochester, and Harvard Medical School. Still an activist, his website is http://www.docgiff.com.)
1. Bush SJ (2010) 700 Vitamin C Secrets. Northampton, England: Direct Print on Demand Ltd. ISBN-13: 978-0956651990; ISBN-10: 0956651992 978-0956651990.
6. Smith, LH. Clinical guide to the use of vitamin C: The clinical experiences of Frederick R. Klenner, M.D.. Portland, OR: Life Sciences Press, 1988. Originally titled: Vitamin C as a fundamental medicine: Abstracts of Dr. Frederick R. Klenner, MD’s published and unpublished work. ISBN 0-943685-01-X. Reprinted 1991, ISBN 0-943685-13-3. http://www.whale.to/a/smith1988.html or https://www.seanet.com/~alexs/ascorbate/198x/smith-lh-clinical_guide_1988.htm
(The views expressed in this article are the author’s and not necessarily that of all members of the Orthomolecular Medicine News Service Editorial Review Board. OMNS welcomes discussion on a variety of subjects. Readers may submit their own article drafts to the Editor at the contact email below.)
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Ron Erlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Felix I. D. Konotey-Ahulu, MD, FRCP, DTMH (Ghana)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, M.D. (USA)
Ken Walker, M.D. (Canada)
Raymond Yuen, MBBS, MMed (Singapore)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, French Edition: Vladimir Arianoff, M.D. (Belgium)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Assistant Editor: Helen Saul Case, M.S. (USA)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
We were told initially that the premise for lockdown was to ‘flatten the curve’ and therefore protect the NHS from being overwhelmed.
It is clear that at no point was the National Health Service (NHS) in any danger of being overwhelmed, and since May 2020 covid wards have been largely empty; and crucially the death toll from covid has remained extremely low.
We now have hundreds of thousands of so-called ‘cases’, ‘infections’ and ‘positive tests’ but hardly any sick people. Recall that four fifths (80%) of ‘infections’ are asymptomatic (1) Covid wards have been by and large empty throughout June, July, August and September 2020. Most importantly covid deaths are at an all-time low. It is clear that these ‘cases’ are in fact not ‘cases’ but rather they are normal healthy people.
So-called asymptomatic cases have never in the history of respiratory disease been the driver for spread of infection. Rather it is symptomatic people who spread respiratory infections – not asymptomatic people.(2)
It is also abundantly clear that the ‘pandemic’ is basically over and has been since June 2020. (3)
We have very highly likely reached herd immunity and therefore have no need for a vaccine.
We have safe and very effective treatments and preventative treatments for covid, we therefore call for an immediate end to all lockdown measures, social distancing, mask wearing, testing of healthy individuals, track and trace, immunity passports, the vaccination program and so on.
There has been a catalogue of unscientific, non-sensical policies enacted which infringe our inalienable rights, such as – freedom of movement, freedom of speech and freedom of assembly. These draconian totalitarian measures must never be repeated.
LOCKDOWN
Covid has proved less deadly than previous influenza seasons – There were 50,100 flu deaths from December 2017 to March 2018 in England and Wales. There were 80,000 flu deaths in 1969. To date we have circa 42,000 covid related deaths in the UK.
We have never locked down society for a respiratory virus before.
The basis for lockdown was a mathematical model by Professor Neil Ferguson. His modelling which predicted half a million deaths in the UK has been roundly condemned as being not fit for purpose. His estimated death figures were clearly wrong by a factor of 10 or 12 times. (1)
Professor Ferguson’s modelling was not even peer reviewed before being acted upon by several nations. Eminent epidemiologists such as Professor Gupta from Oxford University were ignored, they estimated the death count would be far lower in the UK.
Professor Ferguson has a long track record of woeful modelling he was entirely wrong about sars, mers, mad cow’s disease (CJD), and swine flu. Why did the world listen to him again? (2)
Countries which did not lock down Sweden, Japan, Taiwan, South Korea and Belarus have all done significantly better than us in terms of percentage of population deaths. They also have herd immunity and intact economies.
Lockdown did not save lives, and this has been published in the Lancet ‘….in our analysis, full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.’ (3)
The vast majority of deaths occurred in elderly and very elderly people
The vast majority of deaths occurred in people with pre-existing serious health issues such as cancer, cardiovascular disease, Alzheimer’s, diabetes etc
Covid poses virtually zero risk to the under 45’s who have more chance of being struck by lightning than dying from covid.
Covid poses a very small risk for healthy under 60 year olds who have a greater chance of accidental drowning than dying from covid.
The entire nation was essentially placed under house arrest. We have never isolated the healthy before.
Isolating the sick and those who are immunocompromised makes sense. Isolating the healthy has hampered the establishment of herd immunity and makes no sense.
To put it into perspective we had 115,000 smoking related deaths in the UK in 2015 compared to the 42,000 deaths from covid.
We usually have around 600,000 deaths every year in the UK, roughly 1600 deaths per day.
COLLATERAL DAMAGE THE CURE IS WORSE THAN THE VIRUS
Placing the public under virtual house arrest has caused untold damage to both physical and mental health.(1)
Ventilating patients instead of oxygenating patients proved to be a deadly policy and an unwarranted failure. Ventilation resulted in many unnecessary deaths. (2)
Sending infected people from hospitals to care homes placed the elderly and frail under unnecessary risk and resulted in many unnecessary deaths. (3)
Blanket Do Not Resuscitate (DNR) orders were imposed on thousands of people without their consent nor the consent of their families – this is both unlawful and immoral and lead to unnecessary deaths in care homes. (4)
Hospitals became essentially ‘covid only’ centres vast numbers of patients were wilfully neglected, resulting in many thousands of unnecessary deaths. (5)
The government’s own report estimates that some two hundred thousand (200,000) people will die as a direct result of lockdown – not the virus. Hospitals being closed, suicide and poverty will result in more deaths than the virus. (6)
The cure is worse than the disease!
DEATH CERTIFICATES (1)
The majority of people who died had significant comorbidities, such as Alzheimer’s, cancer, cardiovascular disease and diabetes.
Counting death certificates with a ‘mention’ of covid as being a death caused by covid is a gross misrepresentation of the facts and has vastly over exaggerated the death toll.
The rules for the signing of death certificates have been changed solely for covid by the Coronavirus 2020 Act.
Doctors do not even need to have physically seen the patient in order to sign death certificates.
The Act has removed the need for a confirmatory medical certificate for cremations.
Autopsies have virtually been banned, no doubt leading to misdiagnosis of the true cause of deaths; and also reducing our understanding of the disease itself.
Worse still, care home staff who largely have no medical training are able to give a statement as to the cause of death.
Covid was put on death certificates merely on the ‘suspicion’ of people having covid. This may well be unlawful, since it is a crime to falsify death certificates.
People who die within 28 days of a positive pcr test are deemed to have died from covid, even if they die in a car crash or from a heart attack; clearly over inflating the death toll (2)
ECONOMIC RUIN
Reports now estimate that as many as six and a half million (6,500,000) people in the UK will lose their jobs as a result of lockdown. (1)
It is well known that poverty directly adversely affects health, we can expect to see many people suffering with poor health and resulting in many premature deaths, as a direct result of lockdown.
CENSORSHIP
Government have acted maliciously in censoring doctors, nurses and NHS staff. The people have the perfect right to hear what is going on in hospitals, and the medical profession have a duty to look after the public and to reassure them. (1)
The medical profession have not been allowed to let the public know that covid wards have been empty for months, nor that covid deaths have reached an all-time low for months, and this has unnecessarily added to the public’s distress and anxiety.
Doctors and scientists with views that differ from the government narrative have had their videos and articles removed from the internet
TESTING – FALSE POSITIVES
PCR tests cannot be verified for accuracy as there is no ‘gold standard’ against which to check them. The virus has not been purified. (1)
PCR tests cannot detect viral loads and are prone to false positives. (2)
A positive PCR test does not mean that an individual is infected nor infective. (3)
In fact approximately 90% of the PCR positive ‘cases’ are false positives. We therefore have no second wave and no pandemic. (4 , 5)
The government’s report estimates a false positive rate of between 0.8 to 4.0 % using data from other viral infections – not from covid (6)
Viral fragments may remain in people’s bodies for several weeks following recovery from infection. (7)
The crisis will never end if we are waiting for zero positive tests. Everyone has probably had a cold caused by a coronavirus and will likely have a few viral fragments matching those of the cousin SARS-CoV-2 virus (8)
Testing healthy asymptomatic individuals is non-sensical, unscientific and a colossal waste of money. The governments moon shot daily testing program will cost £100 Billion roughly two thirds of the annual NHS budget.
Antibody testing is not the gold standard as many people have T-cell immunity, and antibodies may not circulate following recovery from infection.
HYDROXYCHLOROQUINE
The controversial drug Hydroxychloroquine (HCQ) has been unfairly smeared, by the WHO, CDC, NIH and the media.
However HCQ has very firm support from, amongst others: Professor Harvey Risch epidemiologist from Yale, The American Association of Physicians and Surgeons (AAPS), American Frontline Doctors, the Henry Ford Health System and Professor Didier Raoult microbiologist and infectious disease specialist – to name but a few. (1)
The Lancet was even forced to retract a study on HCQ after it was revealed by the Guardian newspaper that they had been completely fabricated and written by a sci-fi writer and a porn star. Even following this astounding revelation HCQ was still banned in most countries. (2)
HCQ according to AAPS has a ninety per cent (90%) cure rate when given early and alongside zinc (3)
HCQ is safer than many over the counter drugs such as aspirin, Benadryl and Tylenol.
The AAPS also point out that there has never been a vaccine as safe as HCQ. (4)
HCQ has been licensed for over sixty years and has been safely used by billions of people worldwide. There is a very small risk of arrythmia which is easily monitored.
Why was HCQ banned then? Could it be that there are no huge profits to be made from this out-of-patent drug?
HCQ was used to great effect in the Sars1 outbreak of 2005 (5)
In short had HCQ been available then there would not have been a pandemic !
PREVENTION
Preventative measures such as hydroxychloroquine or vitamins D, C and zinc should have been recommended for the public. (1)
Early calcifediol (25-hydroxyvitamin D) treatment to hospitalized COVID-19 patients significantly reduced intensive care unit admissions (2)
Vit D reduces the severity of covid. (2,3)
Voluntary isolation of the frail – should they so choose; in combination with preventative measures would have been a far better strategy. The rest of society could and should have continued as normal.
VACCINE
A rushed vaccine is clearly not in the public’s best interest
Indemnifying vaccine manufacturers against all liability is also clearly not in the public’s best interest
CONFLICTS OF INTEREST
Chief Scientific Officer Sir Patrick Vallance has £600,000 worth of shares in GSK Glaxo Smith Klein. He has in recent years sold £5 million of shares in GSK which he ‘earned’ whilst chief of GSK (1)
Sir Chris Whitty, Chief Medical Officer UK, accepted over £30 million in funding from the Bill and Melinda Gates foundation to study malaria vaccines. (2)
It has become clear that members of SAGE, Public Health England (PHE), World Health Organisation (WHO), Centre for Disease Control (CDC), National institute for Health (NIH) etc have many conflicts of interests. They all accept very large ‘donations’ from the pharmaceutical and vaccine industry. These conflicts of interests may well have effectively corrupted their integrity. (3)
It is also clear that governments are heavily lobbied by the pharmaceutical industry and the vaccine industry, again this may have compromised their integrity. (4)
CUI BONO? WHO BENEFITS?
Vaccine manufacturers will make trillions from this, as will track and trace manufacturers, and the pharmaceutical industry stand to make trillions from covid testing.
Prime minister Boris Johnson announced the new ‘moon shot’ testing will cost £100 Billion, approximately two thirds of the annual NHS budget.
Surely these vast sums would be far better spent on treating all of the neglected patients who have been wilfully neglected during lockdown and who now face huge waiting lists.
CONCLUSIONS
We have effective and safe treatments and preventative medications for covid, therefore there is no need for any lockdown restrictions and associated measures. The pandemic is essentially over as can be seen by the consistent low death rate and hospital admissions over the past four months.
We demand the immediate and permanent ceasing of all lockdown measures.
Lockdowns do not save lives, that is why they have never been used before. Civil liberties and fundamental freedoms have been unnecessarily removed from the public and this must never happen again.
Preventative measures such as Hydroxychloroquine, vitamin C, Vitamin D and zinc must be made readily available to the public.
Isolation must be voluntary. People are perfectly capable of making their own assessment of the risks and must be free to go about their lives as they so choose. People must have the right to choose whether to isolate or not.
Likewise, businesses must have the right to remain open if they so choose.
We demand that doctors, nurses, scientists and healthcare professionals must be permitted free speech and never be censored again.
Professor Mark Woolhouse epidemiologist and specialist in infectious diseases, Edinburgh University Member of the Scientific Pandemic Influenza Group on Behaviours, that advises the Government stated that –
‘…Lockdown was a monumental disaster on a global scale. The cure was worse than the disease.’
‘I never want to see national lockdown again. It was always a temporary measure that simply delayed the stage of the epidemic we see now. It was never going to change anything fundamentally, however low we drove down the number of cases,’
‘We absolutely should never return to a position where children cannot play or go to school.’
I believe the harm lockdown is doing to our education, health care access, and broader aspects of our economy and society will turn out to be at least as great as the harm done by Covid-19.’(1)
The World Doctors Alliance agree fully with Prof Woolhouse’s assertions, he is right! We must never lockdown again!
NB the term ‘covid’ has been used to represent Sars-CoV-2 and Covid-19
The fight for America’s soul escalates by the day.
Much of the planet appears on the verge of a new set of restrictions and lockdowns. Spain, the U.K., and some American states are already clamping back down, an unwelcome sequel to the blockbuster bomb from last spring.
Like Hollywood, which seems to refuse to learn any lessons about insulting its audience, the medical/political establishment seems hell-bent upon ignoring any lessons learned from the first lockdown- faltering economies, explosive nursing home mortality rates, mass childhood anxiety and depression, increasing deaths of despair. All of it again unaccounted for and unacknowledged by ‘experts’ and ‘officials’ planning round two.
Fortunately, Team Science and Team Humanity now have a seat at the table in this debate as it plays out on the global stage. Record protests are now happening regularly in several European countries, with little sign of respite.
While CNN is busy “reporting” to its bleating acolytes that things will never go back to normal and we’ve all just got to shrug and accept it, the science is far far far from settled. It’s clear to nearly everyone that lockdowns caused undue harm. That must be why outlets like CNN have switched to pure pro-new normal psychological operations, reminiscent of Tokyo Rose during World War II.
As the controversial camps spar over science and professional recommendations, ABC News reports that the CDC is slowing its pace for releasing new coronavirus health guidance. The agency hasn’t updated its position since September 24th.
Meanwhile, CDC director Robert Redfield and White House coronavirus Task Force member Dr. Scott Atlas keeps appearing in competing public Q&As to transmit the truest, most up-to-date science surrounding the coronavirus. For readers keeping score, Dr. Atlas is in the lead.
Perhaps the biggest news in the world was the announcement that President Trump and the First Lady both tested positive for COVID late Thursday. Though the public has been told the President’s symptoms are mild (so far), questions remain about the upcoming presidential debates with Joe Biden. The President tested positive, presumably on October 1st. The debate is scheduled for October 15th. His self-imposed White House quarantine will be over on debate day.
‘Out of an abundance of caution’ the President was taken to Walter Reed Medical Center on Friday night, according to a memo issued to reporters that same day. The President’s physician, Navy Cmdr. Dr. Sean Conley wrote:
“Following PCR-confirmation of the President’s diagnosis, as a precautionary measure, he received a single 8-gram dose of Regeneron’s polyclonal antibody cocktail…In addition to the polyclonal antibodies, the President has been taking zinc, vitamin D, famotidine, melatonin and a daily aspirin.”
The President then made a short video appearance from Walter Reed Hospital to update the nation yet showing some signs of illness. On Saturday, Dr. Conley released a memo stating the President had made ‘substantial progress’ and was ‘fever free and off supplemental oxygen.’He also completed his second does of Remdesivir yet Dr. Conley warned the President was ‘not out of the woods yet.’
Questions still remain about the President’s PCR test. Independent journalist Jon Rappoport asked on Twitter “How many cycles was your PCR test set to?”
Meanwhile, a Summit News article published Friday titled, ‘Could Trump’s Coronavirus Test Be a False Positive?’ points out that even the New York Times has cast widespread doubt on the testing accuracy.
“In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus,” the NYT reported.
Widespread testing has led to impacts at the population level, driving everything from reopenings to lockdowns depending on how state and local governments interpret the results, it’s the vaccine that everyone is watching.
WIth the world’s eyes on the coronavirus vaccine development, more people have come forward, admitting adverse reactions in the experimental COVID vaccine group.
AstraZeneca’s vaccine has been the focus since neurological issues were flagged in its September Phase 3 trials. European regulators are set to announce a review of AstraZeneca’s vaccine as soon as this week, according to Bloomberg. The U.S. trials, however, are still on hold as the FDA has announced a broadened investigation into the suspected adverse reaction of a participant in AstraZeneca’s vaccine trial.
It is now widely reported that Moderna and Pfizer’s coronavirus vaccine trial participants are experiencing high fever, body aches, headaches and exhaustion, among other symptoms, after receiving the shots. In interviews, five participants — three in Moderna’s study and two in Pfizer’s late-stage trials — said they experienced discomfort.
Closely mirroring the coordinated American vaccine push during the measles panic of 2019, medical journals are now pre-positioning talking points and strategies to mandate the still-experimental and questionable COVID vaccine. One coronavirus vaccine trial participant, testing Pfizer’s candidate, woke up with chills, shaking so hard he cracked a tooth after taking the second dose, reports CNBC.
An unwelcome development for many this past week has been the discredited New England Medical Journal (NEJM) beginning to bang the drum of mandatory COVID vaccination.
The NEJM makes the case that the mandate may only need to cover the “elderly, health professionals working in high-risk situations or working with high-risk patients (e.g., nursing home residents and patients with severe respiratory symptoms), and persons with certain underlying medical conditions may be high-priority groups.”
Yet the slippery slope of vaccine mandates already has a distasteful history in the U.S. with 2019’s measles outbreak. During that time, health officials’ used the increased measles cases as a trojan horse to mandate the MMR in some states. However, that operation quickly gave way to bills removing religious exemptions, parental consent and attempts to eliminate a host of other barriers to full vaccine schedules.
Draconian developments on the medical freedom front are quickly threatening to change the shape of the USA. If they take a turn for the worse (the President’s health diminishes, vaccine mandates are pushed and implemented, a second lockdown), each has the ability to plunge this nation into a chaotic spiral that may result in unknown upheaval.
Like rapt moviegoers, the world is on the edge of its seat as we enter October. Expect surprises. Hopefully, a few good ones.
Is President Trump’s “Illness” Really a Commercial for Regeneron’s New COVID Drug?
The same day it was announced that President Trump was tested positive for COVID, it was immediately announced that the President was being administered a new experimental COVID drug, Regeneron’s REGN-COV2.
Business journals apparently already had press releases ready about the drug, and the company’s stock immediately went up on Friday.
FiercePharma, one the Pharmaceutical companies’ main marketing trade publications, was one of the first to publish the story:
In a bombshell development Thursday, President Donald J. Trump tested positive for COVID-19, sending shockwaves through the country with just weeks until Election Day. One unanswered question was how the president’s physicians would navigate an uncertain treatment course—and an unproven antibody cocktail from Regeneron is now in the spotlight.
Trump’s personal doctor confirmed Friday that the president was treated with an 8-gram dose of Regeneron’s investigational antibody cocktail for COVID-19, dubbed REGN-COV2, along with aspirin and famotidine, better known as branded Pepcid. He’s also taking zinc and vitamin D, two typical immune-boosting supplements.
Trump’s early treatment with Regeneron’s cocktail was an immediate boon for investors with the drugmaker’s stock trading up around $20—or 3%—in after-market hours Friday.
Regeneron does not even have emergency use approval yet. FiercePharma also reports that Regeneron’s CEO Len Schleifer has been a guest at the White House during the pandemic.
Kyle Blankenship reports:
Unlike another highly touted COVID-19 hopeful, Gilead Sciences’s Veklury (remdesivir), REGN-COV2 has no emergency use approvals anywhere in the world—a fact that could underscore Trump’s relationship with New York-based Regeneron and CEO Len Schleifer, who has been a guest at the White House during the pandemic.
The company said late Friday that Trump’s doctors had requested the therapy under its compassionate use program.
An eventual clean bill of health for Trump could go a long way to boosting confidence in Regeneron’s therapy, which is already raising hopes of $6 billion in sales per year—assuming it can secure the FDA’s approval.
Compared with vaccines, which are being supplied to the U.S. government at $24 on average for a two-dose regimen, antibody drugs could be far more expensive, as they are typically priced well into the thousands, Morningstar analyst Karen Andersen told clients last month. But antibodies could be particularly useful for older adults, whose immune systems may not respond as well to vaccination. (Full article.) (Emphasis Added)
President Trump has transferred more wealth to Big Pharma during the COVID Plandemic than probably all the previous administrations put together, with his Operation Warp Speed and other emergency measures that have given hundreds of BILLIONS of dollars to Big Pharma.
With the Rockefellers controlling the pharmaceutical industry in the U.S. and around the world, this might have been President Trump’s ticket stamped to assure his second term.
T-cells Are the Superstars in Fighting COVID-19 — But Why Are Some People So Poor at Making Them?
by Eshani M King, Evidence Based Research in Immunology and Health sourced from the Children’s Health Defense September 24, 2020
Thank you to Eshani M King for allowing Children’s Health Defense to run her letter in response to Dr. Peter Doshi’s article — Covid-19: Do many people have pre-existing immunity? — that was featured in The BMJ last week.
Dear Editor,
Thank you to Dr. Doshi for raising the profile of T-cells. Incidentally, German researchers found that a staggering 81% of individuals had pre-existing T-cells that cross-react with SARS-CoV-2 epitopes. This fits with modelling in May by Imperial College’s Professor Friston, a world authority in mathematical modelling of complex dynamic biological systems, indicating that around 80% and 50% of the German and UK populations, respectively, are resistant to COVID-19.
Antibodies can only latch onto and help destroy pathogens outside cells and may also occasionally, paradoxically, enhance a pathogen’s ability to infect cell instead by antibody dependent “enhancement” or ADE. It is only the T-cell that can cleverly sense and destroy pathogens inside infected cells using “sensors” which detect foreign protein fragments.
In the late 60’s, the Lancet described a case of a child with agammaglobulinemia, a condition in which absence of B cells prevent them from producing antibodies, who overcame a measles infection quite normally and did not become re-infected thereafter. We now know that, although this condition can compromise immunity, in that particular case the rest of the immune functions, including T-cells, must have been perfectly up to the job of clearing infection and establishing immune memory without help from antibodies. The importance of T-cells in fighting SARS-CoV-1 and establishing immune memory has also been well documented and discussed in a number of pre-COVID papers from 2017 and earlier.
Then, early in April, it was reported that two patients with agammaglobulinemia overcame COVID-19 infections without requiring ventilation, prompting the Italian authors to write: “This observation suggests that T‐cell response is probably important for immune protection against the virus, while B‐cell response might be unessential.”
All this should have shifted the focus of efforts towards T-cells at an early stage — the real question is why mainstream media and others continued to focus efforts and narrative on antibodies. Is it because vaccines are good at provoking antibody responses but not so great at generating T-cells? Some of the vaccines presently under trial do elicit some T-cells but it seems that neither the quantity nor variety are hugely impressive.
Does this matter? Apparently so: Research establishments including Yale found that in mild or asymptomatic cases, many T-cells are produced. These were highly varied, responding not just to parts of the Spike, S protein or Receptor Binding Domain but to many other parts of the virus. Notably, in these mild cases there were few or no detectable antibodies. Conversely, the severely ill produced few T-cells with less variety but had plenty of antibodies. What is also of interest is that men produced fewer T-cells than women, and unlike women, their T-cell response reduced with age.
So why are some people unable to mount a good protective T-cell response? The key to this question might be a 10-year-old Danish study led by Carsten Geisler, head of the Department of International Health, Immunology and Microbiology at the University of Copenhagen. Geisler noted that “When a T cell is exposed to a foreign pathogen, it extends a signalling device or ‘antenna’ known as a vitamin D receptor, with which it searches for vitamin D,” and if there is an inadequate vitamin D level, “they won’t even begin to mobilize.” In other words, adequate vitamin D is critically important for the activation of T-cells from their inactive naïve state. The question of whether T-cells might also need a continuing supply of vitamin D to prevent the T-cell exhaustion and apoptosis observed in some serious COVID-19 cases deserves further research.
High levels of vitamin D are also critical for first line immune defences including physical mucosal defences, human antiviral production, modulating cytokines, reducing blood clotting and a whole host of other important immune system functions. The obese, diabetics and people of BAME origin are far more deficient in vitamin D and men have lower levels than women.
Another intriguing clue is that Japan has the highest proportion of elderly on the planet but despite lack of lockdowns, little mask wearing and high population densities in cities, it escaped with few COVID deaths. Could this, at least in part, be because of extraordinarily high vitamin D levels of over 30 ng/ml in 95% of the active elderly? By comparison, UK average levels are below 20ng/ml. Vitamin D is made in the skin from the action of UV sunlight, food usually being a poor source, but the Japanese diet includes unusually high levels. Sunny countries near the equator (e.g. Nigeria, Singapore, Sri Lanka) also have very low COVID related deaths.
The results of the first vitamin D intervention double blind RCT for COVID was published on 29 August by researchers in Córdoba, Spain. This very well conducted study produced spectacular outcomes for the vitamin D group (n=50), virtually eliminating the need for ICU (reducing it by 96%) and eliminating deaths (8% in the n=26 control group). Although this was a small trial, the ICU results are so dramatic that they are statistically highly significant.
Substantially more vitamin D is required for optimal immune function than for bone health. It seems Dr Fauci is not ignorant of this, having apparently confirmed on TV and by email that he takes 6,000 IU daily! (see Dr John Campbell on YouTube Vitamin D and pandemic science, 16 September 2020). Meanwhile the US’s health body continues to recommend only 600-800 IU and the UK’s, only 400 IU.
It is high time for joined up solid scientific rationale to overthrow mainstream narratives based on an alternative “science” controlled by industry interests/politics. Beda M Stadler, the former Director of the Institute for Immunology at the University of Bern, a biologist and Professor Emeritus, certainly appears to think so (see Ivor Cummins Ep91 Emeritus Professor of Immunology…Reveals Crucial Viral Immunity Reality on YouTube, 28 July 2020).
In the same way that prior infections protect us against future infections by means of cross-reacting T-cells, overcoming COVID-19 naturally offers potential for greater protection against future coronaviruses. Vaccines have their place but so do our amazingly complex, sophisticated, highly effective immune systems which have evolved over millennia to protect us from a world teeming with trillions of pathogens.
Dr. Tom Cowan & Sally Fallon Morrell: Why Viruses (including “Coronavirus”) Are Not the Cause of Disease | Highly Protective Foods in This Toxic World
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light BitChute, LBRY & Brighteon channels. All credit goes to the original source of this video.]
This well-researched, thought-provoking guide to traditional foods contains a startling message: animal fats and cholesterol are not villains but vital factors in the diet, necessary for normal growth, proper function of the brain and nervous system, protection from disease and optimum energy levels.
The culinary ideas introduced in Nourishing Traditions® have stimulated the growth of a variety of small businesses providing traditional nutrient-dense foods including lacto-fermented condiments, kombucha and other lacto-fermented soft drinks, bone broth and genuine sourdough bread.
Raw milk production is flourishing as are direct farm-to-consumer buying arrangements. Sally is frequent contributors to holistic health publications.
Her work is widely respected for providing accurate and understandable explanations of complicated subjects in the field of nutrition and health. Several articles on the dangers of modern soy products have generated intense controversy in the health food industry.
Her presentations on Nourishing Traditions Diets and The Oiling of America have earned highly complimentary reviews throughout the US and overseas.
For readers of Plague of Corruption, Thomas S. Cowan, MD, and Sally Fallon Morell ask the question: are there really such things as “viruses”? Or are electro smog, toxic living conditions, and 5G actually to blame for COVID-19?
The official explanation for today’s COVID-19 pandemic is a “dangerous, infectious virus.” This is the rationale for isolating a large portion of the world’s population in their homes so as to curb its spread. From face masks to social distancing, from antivirals to vaccines, these measures are predicated on the assumption that tiny viruses can cause serious illness and that such illness is transmissible person-to-person.
It was Louis Pasteur who convinced a skeptical medical community that contagious germs cause disease; his “germ theory” now serves as the official explanation for most illness. However, in his private diaries he states unequivocally that in his entire career he was not once able to transfer disease with a pure culture of bacteria (he obviously wasn’t able to purify viruses at that time). He admitted that the whole effort to prove contagion was a failure, leading to his famous death bed confession that “the germ is nothing, the terrain is everything.”
While the incidence and death statistics for COVID-19 may not be reliable, there is no question that many people have taken sick with a strange new disease—with odd symptoms like gasping for air and “fizzing” feelings—and hundreds of thousands have died. Many suspect that the cause is not viral but a kind of pollution unique to the modern age—electromagnetic pollution. Today we are surrounded by a jangle of overlapping and jarring frequencies—from power lines to the fridge to the cell phone. It started with the telegraph and progressed to worldwide electricity, then radar, then satellites that disrupt the ionosphere, then ubiquitous Wi-Fi. The most recent addition to this disturbing racket is fifth generation wireless—5G. In The Contagion Myth: Why Viruses (including Coronavirus) are Not the Cause of Disease, bestselling authors Thomas S. Cowan, MD, and Sally Fallon Morell tackle the true causes of COVID-19.
On September 26, 2019, 5G wireless was turned on in Wuhan, China (and officially launched November 1) with a grid of about ten thousand antennas—more antennas than exist in the whole United States, all concentrated in one city. A spike in cases occurred on February 13, the same week that Wuhan turned on its 5G network for monitoring traffic. Illness has subsequently followed 5G installation in all the major cities in America.
Since the dawn of the human race, medicine men and physicians have wondered about the cause of disease, especially what we call “contagions,” numerous people ill with similar symptoms, all at the same time. Does humankind suffer these outbreaks at the hands of an angry god or evil spirit? A disturbance in the atmosphere, a miasma? Do we catch the illness from others or from some outside influence?
As the restriction of our freedoms continues, more and more people are wondering whether this is true. Could a packet of RNA fragments, which cannot even be defined as a living organism, cause such havoc? Perhaps something else is involved—something that has upset the balance of nature and made us more susceptible to disease? Perhaps there is no “coronavirus” at all; perhaps, as Pasteur said, “the germ is nothing, the terrain is everything.”
This well-researched, thought-provoking guide to traditional foods contains a startling message: Animal fats and cholesterol are not villains but vital factors in the diet, necessary for normal growth, proper function of the brain and nervous system, protection from disease and optimum energy levels. Sally Fallon dispels the myths of the current low-fat fad in this practical, entertaining guide to a can-do diet that is both nutritious and delicious.
Nourishing Traditions will tell you:
Why your body needs old fashioned animal fats
Why butter is a health food
How high-cholesterol diets promote good health
How saturated fats protect the heart
How rich sauces help you digest and assimilate your food
Why grains and legumes need special preparation to provide optimum benefits
About enzyme-enhanced food and beverages that can provide increased energy and vitality
Why high-fiber, lowfat diets can cause vitamin and mineral deficiencies
Topics include the health benefits of traditional fats and oils (including butter and coconut oil); dangers of vegetarianism; problems with modern soy foods; health benefits of sauces and gravies; proper preparation of whole grain products; pros and cons of milk consumption; easy-to-prepare enzyme enriched condiments and beverages; and appropriate diets for babies and children.
Dr. Anthony Fauci has served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984, but has yet to come out with the “Big One” — a vaccine or infectious disease treatment that will allow him to retire with a victory under his belt
Fauci has flip-flopped on the use of masks, first mocking people for wearing them, and then insisting they should. In mid-July, he suddenly urged governments to “be as forceful as possible” on mask rules
While Fauci still claims there’s only anecdotal evidence supporting the use of hydroxychloroquine, and that the drug doesn’t work for COVID-19, the scientific support for it goes as far back as 2005
In April, Fauci praised the NIAID-sponsored drug Remdesivir, saying it “has a clear-cut and significant positive effect in diminishing the time to recovery.” Overall, the improvement rate for the drug was 31%
Research now shows hydroxychloroquine reduced mortality by 50% when given early, and many doctors anecdotally claim survival rates close to 100%. Despite such excellent results, Fauci continues to disparage and cast doubt on hydroxychloroquine
At 79 years old, Dr. Anthony Fauci — who has served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984 — has yet to come out with the “Big One” — a vaccine or infectious disease treatment that will allow him to retire with a victory under his belt.
He failed to create a successful vaccine for AIDS, SARS, MERS and Ebola. A COVID-19 vaccine is essentially his last chance to go out in a blaze of glory. As evidenced by his history, he will stop at nothing to protect Moderna’s COVID-19 vaccine and Gilead’s antiviral Remdesivir.
He even threw tried and true pandemic protocols out the window when COVID-19 hit, turning into an unquestioning spokesman for draconian liberty-stripping measures instead. To echo a question asked by Dr. Sal Martingano in his article,1 “Dr. Fauci: ‘Expert’ or Co-Conspirator,” why are we not questioning this so-called expert?
Fauci ‘Has Been Wrong About Everything’
The risk we take when listening to Fauci is that, so far, he’s been wrong about most things. In a July 14, 2020, “Opposing View” editorial in USA Today, White House adviser Peter Navarro, director of the Office of Trade and Manufacturing Policy, stated that Fauci “has been wrong about everything that I have interacted with him on.”2 According to Navarro, Fauci’s errors in judgment include:3
•Opposing the ban on incoming flights from China in late January 2020.
•Telling the American people the novel virus outbreak was nothing to worry about well into February.
•Flip-flopping on the use of masks — first mocking people for wearing them, and then insisting they should. In fact, mid-July, he suddenly urged governments to “be as forceful as possible” on mask rules.4
•Claiming there was only anecdotal evidence supporting the use of hydroxychloroquine, when the scientific grounds for it go as far back as 2005, when the study,5 “Chloroquine Is a Potent Inhibitor of SARS Coronavirus Infection and Spread,” was published in the Virology Journal.
Fauci should have been well aware of this publication. According to that study,6 “Chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage,” the study authors said. In other words, the drug worked both for prevention and treatment.
As noted by Navarro, more recent research found hydroxychloroquine reduced the mortality rate among COVID-19 patients by 50% when used early.
Interestingly, in a March 24, 2020, interview7 with Chris Stigall, Fauci did say that — were he to speak strictly as a doctor treating patients — he would certainly prescribe chloroquine to COVID-19 patients, particularly if there were no other options.
Then, in August, he flipped back to insisting hydroxychloroquine doesn’t work,8 even though by that time, there were several studies demonstrating its effectiveness against COVID-19 specifically.
So, it appears Fauci has had a hard time making up his mind on this issue as well, on the one hand dismissing the drug as either untested or ineffective against COVID-19, and on the other admitting it would be wise to use, seeing how the options are so limited.
Navarro continues:9
“Now Fauci says a falling mortality rate doesn’t matter when it is the single most important statistic to help guide the pace of our economic reopening. The lower the mortality rate, the faster and more we can open. So when you ask me whether I listen to Dr. Fauci’s advice, my answer is: only with skepticism and caution.”
Fauci Has Done Nothing to Help Unite the Country
While Fauci claims to be exasperated by how political the pandemic has become,10 Robert F. Kennedy Jr. pointed out in an August 2, 2020, Instagram post11 that Fauci himself is, at least in part, part of the problem, as his double standards on hydroxychloroquine have done much to polarize and divide the nation:
“Fauci insists he will not approve HCQ for COVID until its efficacy is proven in ‘randomized, double blind placebo studies.’ To date, Dr. Fauci has never advocated such studies for any of the 72 vaccine doses added to the mandatory childhood schedule since he took over NIAID in 1984. Nor is he requiring them for the COVID vaccines currently racing for approval.
Why should chloroquine be the only remedy required to cross this high hurdle? HCQ is less in need of randomized placebo studies than any of these vaccines since its safety is well established after 60 years of use and decades on WHO’s listed of ‘essential medicines.’
Fauci’s peculiar hostility towards HCQ is consistent with his half century bias favoring vaccines and patent medicines. Dr. Fauci’s double standards create confusion, mistrust and polarization.”
In a June 10, 2020, article,12 Global Research also questioned Fauci’s many attempts to disparage the drug for no apparently valid reason; even promoting the fake (and ultimately retracted) Lancet study that claimed to show hydroxychloroquine was dangerous. At the end of the day, who benefits? Well, certainly it benefits the drug and vaccine industries, which seems to be where Fauci’s loyalties lie.
Fauci’s Bias Is Hard to Miss
While Fauci is not named on the patents of either Moderna’s vaccine or Remdesivir, the NIH does have a 50% stake in Moderna’s vaccine,13 and the recognition that would come with a successful vaccine launch would certainly include Fauci.
He also has lots to lose — if nothing else, his pride — if Remdesivir doesn’t become a blockbuster, as his NIAID is sponsoring the clinical trials.14 The NIAID also supported the original research into Remdesivir, when it was aimed at treating Ebola.15
His bias here is clear for anyone to see. April 29, 2020, he stated16 Remdesivir “has a clear-cut and significant positive effect in diminishing the time to recovery.” How good is that? Patients on the drug recovered in 11 days, on average, compared to 15 days among those receiving a placebo. Overall, the improvement rate for the drug was 31%.
Meanwhile, research17 now shows hydroxychloroquine reduced mortality by 50% when given early, and many doctors anecdotally claim survival rates close to 100%. This still isn’t good enough for Fauci, who continues insisting hydroxychloroquine is a bust.18
His stance on these two drugs certainly doesn’t make sense based on the data alone. But it does make sense if he wants (or has been instructed) to protect the profits of Remdesivir.
As director of NIAID, which has been part of Remdesivir’s development from the start, why wouldn’t he want to see it become a moneymaker for the agency he dedicated his career to? It also makes sense when you consider his primary job is to raise funds for biodefense research, primarily vaccines but also diagnostics and drug therapies.19,20
Fauci Doubts Safety of Russian Vaccine
Early in August 2020, Russia announced they would begin vaccinating citizens with its own COVID-19 vaccine, despite not finishing large-scale human trials.21 The announcement drew skepticism from American infectious disease specialists, including Fauci, who said he has “serious doubts” that Russia’s COVID-19 vaccine is actually safe and effective.22
He’s probably right on that point. It’s hard to imagine you can prove safety and effectiveness in a mere two months of trials. But the fast-tracked vaccine efforts of the U.S. and EU are hardly bound to be significantly better, considering the many shortcuts that are being taken.
Fauci Ignores Two Decades of Failed Coronavirus Vaccines
Despite being in a position to know better, Fauci conveniently ignores the many failed attempts to create other coronavirus vaccines over the past two decades, including vaccines against SARS and MERS. A paper23 by Eriko Padron-Regalado, “Vaccines for SARS-CoV-2: Lessons From Other Coronavirus Strains” reviews some of these past experiences. As noted in the Conservative Review:24
“Since their emergence in 2003 and 2012 respectively, no safe and efficacious human vaccines for either SARS-Cov1 or MERS have been developed.
Moreover, experimental non-human (animal model) evaluations of four SARS-Cov1 candidate vaccine types, revealed that despite conferring some protection against infection with SARS-Cov1, each also caused serious lung injury, caused by an overreaction of the immune system, upon viral challenge.25
Identical ‘hypersensitive-type’ lung injury occurred26 when mice were administered a candidate MERS-Cov vaccine, then challenged with infectious virus, negating the ostensible benefit achieved by their development of promising … ‘antibodies’ … which might have provided immunity to MERS-Cov.
These disappointing experimental observations must serve as a cautionary tale for SARS-Cov2 vaccination programs to control epidemic COVID-19 disease.”
NIAID Safety Controversies and Ethics Violations
When recently asked for a rebuttal to criticism of his leadership during the pandemic, Fauci replied, “I think you can trust me,” citing his long record of service in government medicine. However, that long service record is fraught with ethics and safety lapses.
For example, in 2005, NPR reported27 the NIH tested novel AIDS drugs on hundreds of HIV-positive children in state foster care during the late 1980s and90s without assigning patient advocates to monitor the children’s health, as is required by law in most states.
Fauci was appointed director of the NIAID in 1984. The AIDS research was part of his research portfolio, and the AIDS research division reported directly to him, so these violations occurred on his watch.28 In 2008, two NIH biomedical ethicists published a paper on the controversial practice of using wards of the state as guinea pigs, noting:29
“Enrolling wards of the state in research raises two major concerns: the possibility that an unfair share of the burdens of research might fall on wards, and the need to ensure interests of individual wards are accounted for … Having special protections only for some categories is misguided. Furthermore, some of the existing protections ought to be strengthened.”
Under Fauci, the NIAID became the largest funder of HIV/AIDS in the world.30 Despite that, numerous articles over the years have discussed how AIDS activists have been less than satisfied with Fauci and the NIAID.31,32,33 A 1986 article stated:34
“If Fauci were less intent on amassing power within the federal health bureaucracy … he would have left AIDS treatment research with the NCI, where it began, relying on that institute’s proven expertise in organizing large, multisite clinical trials for cancer therapies.”
A July 23, 2020, article in Just the News lists several other safety and ethics problems that Fauci has been involved in through the years, including conflict of interest violations in vaccine research.35
Just the News also interviewed NIAID chief of ethics and regulatory compliance Dr. Jonathan Fishbein, whom the NIAID was forced to reinstate in 2005 after it was determined that Fishbein had been wrongly fired in retaliation for raising concerns about lack of safety in some of the agency’s research:36
“Fishbein said … Fauci failed to take responsibility for the managers and researchers working below him when signs of trouble emerged, allowing problems to persist until others intervened. ‘Fauci is all about Fauci,’ Fishbein said. ‘He loves being the headline. It’s his ego.’”
Fauci’s Connections to Wuhan Lab
By now, you probably also know that the NIAID funded gain-of-function research on coronaviruses at the Wuhan Institute of Virology. As reported by Newsweek:37
“In 2019, with the backing of NIAID, the National Institutes of Health committed $3.7 million over six years for research that included some gain-of-function work. The program followed another $3.7 million, 5-year project for collecting and studying bat coronaviruses, which ended in 2019, bringing the total to $7.4 million.”
This money was not given directly, but rather funneled to the Wuhan lab via the EcoHealth Alliance. According to a recent report by The Wall Street Journal,38 the NIH is now insisting EcoHealth Alliance submit all information and materials from the Wuhan lab before it’s allowed to resume funding.
Fauci is a longtime proponent of dangerous gain-of-function research. In 2003, he wrote an article39 published in the journal Nature on how “the world needs new and creative ways to counter bioterrorism.”
“We will pursue innovative approaches for modulating innate immunity to induce and enhance protection against many biological pathogens, as well as simple and rapid molecularly based diagnostics to detect, characterize and quantify infectious threats,” Fauci wrote.
“These are lofty goals that may take many years to accomplish — but we must aspire to them. Third, we must enormously strengthen our interactions with the private sector, including biotechnology companies and large pharmaceutical corporations.
Many biodefence-related products that we are pursuing do not provide sufficient incentives for industry — the potential profit margin for companies is tenuous, and there is no guarantee that products would be used.
Therefore, we will seek non-traditional collaborations with industry, for example guaranteeing that products will be purchased if companies sign up … so that we can quickly make available effective vaccines and treatments …”
With that, there can be little question about which team Fauci is on. He’s on the side of drug and vaccine makers, and has been for decades. There’s no money to be made by either the agency or its private collaborators from natural products such as vitamin D, vitamin C, quercetin or its drug equivalent, hydroxychloroquine. All of these are dirt-cheap and off patent.
Prediction Track Record = Null
Fauci’s predictions for COVID-19 mortality have also turned out to be as inaccurate as all of his previous predictions. In 1987, he predicted heterosexual infection of HIV/AIDS would rise to 10% by 1991. It never rose above 4%.
He predicted the bird flu would result in 2 million to 7 million deaths. In the end, the avian H5N1 flu killed 440 worldwide. He sought billions of dollars to combat the threat of Zika, a virus that fizzled without making much of an impact anywhere.40
When you look at his track record, you realize he’s predicted “nightmare” scenarios for decades, none of which have materialized. Last but not least, Dr. Fauci serves on Bill Gates leadership council.
Attack of the Tomato Killers: The Police State’s War on Weed and Backyard Gardens
“They came again this morning at about 8:00 o’clock. A large cargo-type helicopter flew low over the cabin, shaking it on its very foundations. It shook all of us inside, too. I feel frightened … I see how helpless and tormented I am becoming with disgust and disillusionment with the government which has turned this beautiful country into a police state … I feel like I am in the middle of a war zone.”—Journal entry from a California resident describing the government’s aerial searches for marijuana plants
Backyard gardeners, beware: tomato plants have become collateral damage in the government’s war on drugs, especially marijuana.
In fact, merely growing a vegetable garden on your own property, or in a greenhouse on your property, or shopping at a gardening store for gardening supplies—incredibly enough—could set you up for a drug raid sanctioned by the courts.
It’s happened before.
After shopping for hydroponic tomatoes at their local gardening store, a Kansas family found themselves subjected to a SWAT team raid as part of a multi-state, annual campaign dubbed “Operation Constant Gardener,” in which police collected the license plates of hundreds of customers at the gardening store and then investigated them for possible marijuana possession.
By “investigated,” I mean that police searched through the family’s trash. (You can thank the Supreme Court and their 1978 ruling in California v. Greenwood for allowing police to invade your trash can.) Finding “wet glob vegetation” in the garbage, the cops somehow managed to convince themselves—and a judge—that it was marijuana.
In fact, it was loose-leaf tea, but those pesky details don’t usually bother the cops when they’re conducting field tests.
There’s a long list of innocent ingredients that could be mistaken for drugs and get you subjected to a raid, because that’s all it takes—just the barest whiff of a suspicion by police that you might be engaged in criminal activity—to start the ball rolling.
From there, these so-called “investigations” follow the usual script: judge issues a warrant for a SWAT raid based on botched data, cops raid the home and terrorize the family at gunpoint, cops find no drugs, family sues over a violation of their Fourth Amendment rights, and then the courts protect the cops and their botched raid on the basis of qualified immunity.
Surely, you might think, the government has enough on its hands right now—policing a novel coronavirus pandemic, instituting nationwide lockdowns, quelling civil unrests over police brutality—that it doesn’t need to waste time and resources ferreting out pot farmers.
You’d be wrong.
This is a government that excels at make-work projects in which it assigns at-times unnecessary jobs to government agents to keep them busy or employed.
Back in 2013, an aerial surveillance mission spotted what police thought might be marijuana plants. Two days later, dozens of city officials, SWAT team, police officers and code compliance employees, and numerous official vehicles including dozens of police cars and several specialized vehicular equipment, including helicopters and unmanned flying drones, descended on The Garden of Eden, a 3.5-acre farm in Arlington, Texas, for a 10-hour raid in search of marijuana that turned up nothing more than tomato, blackberry and okra plants.
These aerial and ground sweeps have become regular occurrences across the country, part of the government’s multi-million dollar Domestic Cannabis Eradication Program. Local cops refer to the annual military maneuvers as “Eradication Day.”
Writing for The Washington Post, Radley Balko describes how these raids started off, with the National Guard, spy planes and helicopters:
The project was called the Campaign Against Marijuana Production, or CAMP… In all, thirteen California counties were invaded by choppers, some of them blaring Wagner’s “Ride of the Valkyries” as they dropped Guardsmen and law enforcement officers armed with automatic weapons, sandviks, and machetes into the fields of California … In CAMP’s first year, the program conducted 524 raids, arrested 128 people, and seized about 65,000 marijuana plants. Operating costs ran at a little over $1.5 million. The next year, 24 more sheriffs signed up for the program, for a total of 37. CAMP conducted 398 raids, seized nearly 160,000 plants, and made 218 arrests at a cost to taxpayers of $2.3 million.
The area’s larger growers had been put out of business (or, probably more accurately, had set up shop somewhere else), so by the start of the second campaign in 1984, CAMP officials were already targeting increasingly smaller growers. By the end of that 1984 campaign, the helicopters had to fly at lower and lower altitudes to spot smaller batches of plants. The noise, wind, and vibration from the choppers could knock out windows, kick up dust clouds, and scare livestock. The officials running the operation made no bones about the paramilitary tactics they were using. They considered the areas they were raiding to be war zones. In the interest of “officer safety,” they gave themselves permission to search any structures relatively close to a marijuana supply, without a warrant. Anyone coming anywhere near a raid operation was subject to detainment, usually at gunpoint.
But how do you go from a “war on drugs” to SWAT-style raids on vegetable gardens?
Connect the dots, starting with the government’s war on marijuana, the emergence of SWAT teams, the militarization of local police forces through the federal 1033 Program, which allows the Pentagon to transfer “vast amounts of military equipment—machine guns and ammunition, helicopters, night-vision gear, armored cars—to local police departments,” and the transformation of American communities into battlefields: as always, it comes back to the make work principle, which starts with local police finding ways to justify the use of military equipment and federal funding.
Mark my words: the use of police drones will make these kinds of aerial missions even more common.
For the most part, aerial surveillance is legal. As Arthur Holland Michel writes for The Atlantic: “When it comes to law enforcement, police are likewise free to use aerial surveillance without a warrant or special permission. Under current privacy law, these operations are just as legal as policing practices whereby an officer spots unlawful activity while walking or driving through a neighborhood.”
In Philip Cobbs’ case, helicopter spotters claimed to have seen two lone marijuana plants growing in the wreckage of a fallen oak tree on the Virginia native’s 39-acre family farm.
What the cops were really after was an excuse to search Cobbs’ little greenhouse, which he had used that spring to start tomato plants, cantaloupes, and watermelons, as well as asters and hollyhocks, which he planned to sell at a roadside stand near his home. The search of the greenhouse turned up nothing more than used tomato seedling containers.
Nevertheless, police charged Cobbs with misdemeanor possession of marijuana for the two plants they claimed to have found. Eventually, the charges were dismissed but not before The Rutherford Institute took up Cobbs’ case, which revealed that police hadn’t even bothered to secure a warrant before embarking on their raid of Cobbs’ property—a raid that had to cost taxpayers upwards of $25,000, at the very least—part of their routine sweep of the countryside in search of pot-growing operations.
Two plants or two hundred or no plants at all: it doesn’t matter.
A SWAT team targeted one South Carolina man for selling $50 worth of pot on two different occasions. The Washington Postreports: The SWAT team “broke down Betton’s door with a battering ram, then fired at least 57 bullets at him, hitting him nine times. He lost portions of his gallbladder, colon, bowel and rectum, and is paralyzed from the waist down. He also suffered damage to his liver, lung, small intestine and pancreas. Two of his vertebrae were damaged, and another was partially destroyed. Another bullet shattered his leg.” After security footage showed that most of what police said about the raid was a lie, the cops settled the case for $2.75 million.
Monetary awards like that are the exception, however.
Most of the time, the cops get away with murder and mayhem. Literally.
Bottom line: no amount of marijuana is too insignificant if it allows police to qualify for federal grants and equipment and lay claim to seized assets (there’s the profit motive) under the guise of fighting the War on Drugs.
Although growing numbers of states continue to decriminalize marijuana use and 9 out of 10 Americans favor the legalization of either medical or recreational/adult-use marijuana, the government’s profit-driven “War on Drugs”—waged with state and local police officers dressed in SWAT gear, armed to the hilt, and trained to act like soldiers on a battlefield, all thanks to funding provided by the U.S. government, particularly the Pentagon and Department of Homeland Security (DHS)—has not abated.
Since the formation of the DHS post-9/11, hundreds of billions of dollars in grants have flowed to local police departments for SWAT teams, giving rise to a “police industrial complex” that routinely devastates communities, terrorizes families, and destroys innocent lives.
No longer reserved exclusively for deadly situations, SWAT teams are now increasingly being deployed for relatively routine police matters, with some SWAT teams being sent out as much as five times a day. Nationwide, SWAT teams have been employed to address an astonishingly trivial array of criminal activity or mere community nuisances: angry dogs, domestic disputes, improper paperwork filed by an orchid farmer, and misdemeanor marijuana possession, to give a brief sampling.
Unfortunately, general incompetence, collateral damage (fatalities, property damage, etc.) and botched raids tend to go hand in hand with an overuse of paramilitary forces.
In some cases, officers misread the address on the warrant. In others, they simply barge into the wrong house or even the wrong building. In another subset of cases, police conduct a search of a building where the suspect no longer resides.
SWAT teams have even on occasion conducted multiple, sequential raids on wrong addresses or executed search warrants despite the fact that the suspect is already in police custody. Police have also raided homes on the basis of mistaking the presence or scent of legal substances for drugs. Incredibly, these substances have included tomatoes, sunflowers, fish, elderberry bushes, kenaf plants, hibiscus, and ragweed.
All too often, the shock-and-awe tactics utilized by many SWAT teams only increases the likelihood that someone will get hurt with little consequences for law enforcement, even when the raids are botched.
Botched SWAT team raids have resulted in the loss of countless lives, including children and the elderly. Usually, however, the first to be shot are the family dogs.
SWAT raids are usually carried out late at night or shortly before dawn. Unfortunately, to the unsuspecting homeowner—especially in cases involving mistaken identities or wrong addresses—a raid can appear to be nothing less than a violent home invasion, with armed intruders crashing through their door.
That’s exactly what happened to Jose Guerena, the young ex-Marine who was killed after a SWAT team kicked open the door of his Arizona home during a drug raid and opened fire. According to news reports, Guerena, 26 years old and the father of two young children, grabbed a gun in response to the forced invasion but never fired. In fact, the safety was still on his gun when he was killed. Police officers were not as restrained. The young Iraqi war veteran was allegedly fired upon 71 times. Guerena had no prior criminal record, and the police found nothing illegal in his home.
The problems inherent in these situations are further compounded by the fact that SWAT teams are granted “no-knock” warrants at high rates such that the warrants themselves are rendered practically meaningless.
This sorry state of affairs is made even worse by U.S. Supreme Court rulings that have essentially done away with the need for a “no-knock” warrant altogether, giving the police authority to disregard the protections afforded American citizens by the Fourth Amendment.
When the war on drugs—a.k.a. the war on the American people—becomes little more than a thinly veiled attempt to keep SWAT teams employed and special interests appeased, it’s time to revisit our drug policies and laws.
“You take the Constitution, the Bill of Rights, all the rights you expect to have—when they come in like that, the only right you have is not to get shot if you cooperate. They open that door, your life is on the line,” concluded Bob Harte, whose home was raided by a SWAT team simply because the family was seen shopping at a garden store, cops found loose tea in the family’s trash and mistook it for marijuana.
“Our family will never be the same,” said Addie Harte, recalling the two-hour raid that had police invading their suburban home with a battering ram and AR-15 rifles. As The Washington Post reports:
Bob found himself flat on floor, hands behind his head, his eyes locked on the boots of the officer standing over him with an AR-15 assault rifle. “Are there kids?” the officers were yelling. “Where are the kids?” “And I’m laying there staring at this guy’s boots fearing for my kids’ lives, trying to tell them where my children are,” Harte recalled later in a deposition on July 9, 2015. “They are sending these guys with their guns drawn running upstairs to bust into my children’s house, bedroom, wake them out of bed.”
It didn’t matter that no drugs were found—nothing but a hydroponic tomato garden and loose tea leaves. The search and SWAT raid were reasonable, according to the courts.
A collaborative film by Spacebusters and Dr. Andrew Kaufman about how authentic medicine was hijacked by the power elite and turned into a deadly, sickness for profit industry.
Written by : Dr. Andrew Kaufman and Steven S. Busters Produced by: Spacebusters Technical advisor: Rosco S. Busters
[Truth Comes to Light Editor’s note: This transcript is provided by Truth Comes to Light as a service to sharing truth. It has not been verified by the authors, so 100% accuracy is not guaranteed.]
TRANSCRIPT
This tale of two snakes is the story of how medicine in the United States, and eventually the world, was subverted into a commerce business enterprise with the central goal of creating and maintaining illness throughout the population for profit.
We have been kept from fully developing our potential to reason, our intuition, to become enlightened and to be the godlike beings that is our true nature.
Animal man can be domesticated and controlled. Enlightened man cannot.
The unholy trinity of corporate allopathic medicine, which is our mainstream medical system today — utilizing synthetic Big Pharma drugs, surgery and radiation — drains the body’s corpuscles through medical treatment strategies based on suppressing symptoms through synthetic drugs instead of targeting the cause of disease and removing it.
What causes disease or cellular dis-ease?
Toxic industrial environments. Toxic foods. Over-acidic diets. Polluted air and water. Prolonged states of mental stress and emotional distress. Lack of sleep. Drugs. Alcohol. Cigarettes. Electrosmog. Heavy-metal poisoning. Vaccines. And even prescription drugs.
The Rod of Asclepius has been the exoteric symbol for medical healing since as far back as 1400 to 1200 BC.
He was the son of Apollo, the god of healing, immortalized forever in the stars as Ophiuchus, the serpent holder standing on the male genital phallus and corpuscle destroyer, Scorpio, which we’ll cover in the plot twist at the end of this film.
It is the staff with the single snake, completely misunderstood exotericly, to be a symbol of the snakes possession of anti-venom against its own poisons and its ability to shed its skin and renew — an exoteric symbol of longevity and immortality.
But in 1902 a captain in the US Army Medical Corps mistook the caduceus for the Rod of Asclepius and he proposed the adoption of the caduceus as the Medical Corps official symbol.
The two-snake caduceus is the symbol of the Roman god Mercury, whereas the one-snake rod is the symbol of Asclepius.
Natural Healing
Before 1902, the caduceus was used as a symbol for commerce and companies in printing, as Mercury or Hermes was the messenger of the gods.
It was used in mining, chemistry and metallurgy, as alchemy was a hermetic science.
Exotericly Mercury is the god of commerce, trade, merchants, outlaws, thieves and tricksters and is represented by two serpents to show the opposing meanings of polarization.
One snake is the healing — remediating and curative — the upward flow of living corpuscles from the spleen to the cerebral crown chakra, supporting positive energy, inner development and enlightenment.
The other serpent is the poisonous, debilitating, drainage of the living corpuscles away from the higher-self, body and mind.
It is this second serpent that has infiltrated medicine.
It has convinced us that paying for poison is the cure for cellular poisoning.
It is no accident that this symbol was first adopted by the army. The bogus germ theory, driving allopathic medicine, states that microorganisms invade our bodies and require military defense.
This model of disease, the warfare model, where illness comes from an uncontrollable enemy outside of us, necessitates a drug from the medical machine as our only chance of survival. We fight this imagined enemy with chemical weapons and machines, just as any warfare.
Allopathic medicine blames these enemy diseases on bad genes or evil germs, mysterious and deadly cancers, unexplained autoimmune and neurodegenerative diseases, and many more — always outside of our control with causes unknown and no ability to address or reverse ourselves.
Thus, we are dependent on the medical system to rescue us.
How did this happen?
In 1847 the American Medical Association was founded. The largest association of medical students and physicians — both doctors of medicine and doctors of osteopathy, which is a type of alternative medicine — much of which is now said to have no therapeutic value and is labeled pseudoscience by the medical cartel.
From the very beginning, the AMA urged all state governments to adopt measures to register all births, marriages and deaths, which is a form of commerce itself — the way shipments are registered to port authorities as property of the receiving country’s government.
In 1897 the AMA incorporated into a private corporation and by 1899 they were already pushing for mandatory, untested smallpox vaccinations.
Then, in 1901, the AMA started a committee on national legislation, starting the trend of non-elected NGOs directing elected lawmakers policy decisions.
In 1905 they created the Council on Pharmacy and Chemistry to set standards for drug manufacturing and advertising, asking drug companies to show proof of effectiveness of their drugs or pay corrupt bribes to “Doc” Simmons in order to advertise those drugs in the Journal of the American Medical Association.
They basically became the first drug catalog sales reps. Obviously, drug manufacturers had great incentive to get in good favors with “Doc” Simmons and the AMA, later known as the Big Pharma revolving door.
But the real horror started in 1904 when the AMA founded the Council on Medical Education to regulate medical schools and what type of medicine could be taught in them.
As osteopathic and homeopathic medicine had no commercial profit incentive to these snakes, they had to go.
From its earliest inception, the American Medical Association has had one principal objective: attaining and defending a total monopoly of the practice of medicine in the United States.
From its outset, the AMA made the unholy trinity of allopathy the basis of its practice.
Allopathy set up an intense rivalry with the prevalent 19th century School of Medicine, the practice of homeopathy.
The AMA is one of the biggest frauds in history, involved in medical bribery, racketeering, corruption, coercion, and deception.
The former quack heads of the organization — like the failed journalist “Doc” Simmons, who never attended a medical school or worked for an actual hospital, and his protege Dr. Morris Fishbein, an aspiring circus trapeze artist and part-time opera singer who never worked a day as a physician in his life, but somehow headed the American Medical Association — were to set the standard for the disgraceful fraud still going on to this day.
You can find the shocking details of this in the first two chapters of the book Murder by Injection.
In 1907 the American Medical Association involved the Carnegie Foundation in elaborating a book-length study of medical education in the United States and Canada, also known as the Carnegie Foundation Bulletin, Number Four.
Its author, Abraham Flexner, was an ambitious educator, neither a physician nor a medical scientist, but the brother of Simon Flexner, employed by the Rockefeller Institute for medical research. Later on, Flexner became the first director of the Rockefeller philanthropy programs in medical education.
Andrew Carnegie was regarded as the second richest man in history after John D. Rockefeller. While Carnegie played a leading role in the American steel industry and education, Rockefeller was interested in the oil industry and medical research.
Flexner’s report was published in 1910 and the purpose was to improve the quality of medical service by establishing professional medical education based on mainstream scientific principles.
But what was accepted as science in the early 20th century?
The theory of materialism — rising in the 17th century — holds that the only existing thing is matter, everything is composed of material and all phenomena (including consciousness, human soul and spirit) are the result of material interactions.
In other words, matter is the only substance.
Scientific materialism or physicalism became the philosophical position of the early 20th century. The main statement of physicalism is that there are no kinds of things other than physical things.
Before the Flexner Report was released, twice as many physicians practiced alternative medicine than conventional allopathic medicine, and medical knowledge was taught in small private schools all over the United States.
The report changed everything. And backed by the police power of each American state, medical schools were obliged to follow the trends set by the Carnegie Foundation.
The Flexner Report stated that the human body belongs to the animal world. It is put together of tissues and organs. It grows, reproduces itself, decays, according to general laws. It is liable to attack by hostile physical and biological agencies.
Herbs, homeopathy, chiropractic & massage were demoted as quackery.
Small medical schools were either closed or merged into universities financially supported by large industrial companies.
In less than 10 years the number of medical schools dropped from 650 to just 50. The number of medical students decreased from 7500 to 2500 and they were unable to afford the high education fees.
The report included a detailed regulation of medical education and pharmacology as the only solution against dreadful diseases.
According to the present day consequences of this report, no medical school can be created without the permission of government and medical research adheres fully to the protocols of scientific research of the 1910s — materialism, medication and vaccination.
Supply of physicians were restricted, incomes of the remaining practitioners raised, and conventional medical schools began to be centralized.
in 1997 the WHO obtained full control over medicine, as the validity of the Flexner report extended worldwide.
And what was the long-term result of reforming medical education and practice?
Hardly any news on the media.
According to the 2003 medical report Death by Medicine, 784,000 people in the United States die every year from conventional medicine mistakes.
This is 16,400% of the victims of September 11th, 2001 — the equivalent of six jumbo jet crashes a day for an entire year. A hundred and six thousand of these deaths each year are from prescription drugs.
The United States spends 282billiondollars annually on deaths due to medical mistakes or iatrogenic deaths. According to a 1995 US iatrogenic report, the annual automobile accident mortality rate is 45,000 people. On the other hand, annually over a million patients get injured in hospitals and 280,000 of these cases result in death.
In 2004 the US spent 1.4 trillion dollars, 15,5% of the GDP, on health care. More than one third was paid to the pharmaceutical industry.
In 2010 alone, the top 20 pharmaceutical companies profited the equivalent of $97 per person times six billion people.
Back in 2001 Pfizer was the number-one most profitable company — with 7.8 billion dollar profit — of all the Fortune 500 companies.
In 2002 the combined profits of the top 10 drug companies of the Fortune 500 were nearly 36 billion dollars. That is more than the profits of the other 490 businesses put together.
After a hundred years, we must raise the question: what went wrong?
Despite the huge amount of money accumulated by the pharma industry, there are more dreadful diseases and sick people today than ever. You will find the answers in the Flexner Report — a document that created and enabled the terms of a centralized medical system and the pharma industry to take over the control of healthcare for profit.
“When we interfere with the processes of nature, and breed efficient plants and efficient animals, there’s always some way in which we have to pay for it. We do not really know how to interfere with the way the world is…
The way the world actually is, is an enormously complex, interrelated organism. The same problem arises in medicine because the body is a very complex, interrelated organism.
And if you look at the body in a superficial way, you may see there’s something wrong with it.
Here’s chicken pox.
And there’s spots that itch that come out all over the place. Well, you might say ‘Well, spots are there. Cut ’em off,’ So you kill the bug. Well, then you find you got real problems.
Well, then you think ‘Well now, wait a minute, it wasn’t the bugs in the blood. There are bugs all over the place.
What was wrong with this person?
His resistance wasn’t out there.
For what you should have given him was not an antibiotic but vitamins…
See, we always look at the human being medically, in bits and pieces, because we have heart specialists, lung specialists, bone specialists, nerve specialists and so on.
And they each see the human being from their point of view. There are a few generalists, but they realize the human body is so complicated that no one mind can understand it.”
~ Alan Watts
And that’s the problem with compartmentalized allopathic medicine.
Imagine your car doesn’t work because it’s out of gas and has a dead battery.
The allopathic, Big Pharma approach is to charge you big money to send five people to push your car. And then they say ‘See, it’s moving. We’ve fixed it.’
Sure it’s moving, but not very fast. Nothing inside works without power and you won’t make it more than a few miles before those people are too tired to push, no matter how much you pay them.
A mechanic wouldn’t fix a blown engine valve or gasket leaking oil by telling you to just add more oil every day. That would be stupid. You have to fix the cause.
But this logic is perfectly normal in modern medicine. We end up with specialists and general practitioners trained in which symptoms hint at which specific part of the physical anatomy may be in dis-ease — but have zero non-specialized education in nutrition, biochemistry, plant medicines, molecular biology, naturopathy, homeopathy, exercise, psychology or any other sciences that can tell them how to diagnose and eliminate the cause of cellular dis-ease.
So out of ignorance and frustration, they are left with three unholy options.
Synthetic Drugs
Most synthetic drugs circulate through the entire body and have a chemical effect on every biological system in the body, not just the specific area of cellular dis-ease they are meant to help.
While they may sometimes help the problem area, they simultaneously disrupt perfectly working functions in other parts of our body.
Have you ever noticed the dozens of side effects listed on drug inserts or at the end of commercial disclaimers?
“Kurt quit smoking with Chantix and support. Talk to your doctor about Chantix and a support plan that’s right for you. Some people have had changes in behavior, hostility, agitation, depressed mood and suicidal thoughts or actions while taking or after stopping Chantix. If you notice agitation, hostility, depression or changes in behavior, thinking or mood that are not typical for you, or if you develop suicidal thoughts or actions, stop taking Chantix and call your doctor right away. Talk to your doctor about any history of depression or other mental health problems which can get worse while taking Chantix. Some people can have allergic or serious skin reactions to Chantix, some of which can be life-threatening. If you notice swelling of face, mouth, throat or a rash, stop taking Chantix and see your doctor right away. Tell your doctor which medicines you’re taking as they may work differently when you quit smoking. Chantix dosing may be different if you have kidney problems. The most common side effect is nausea. Patients also reported trouble sleeping and vivid, unusual or strange dreams. Until you know how Chantix may affect you, use caution when driving or operating machinery. Chantix should not be taken with other quit-smoking products.
‘The urges weren’t like they used to be and that helped me quit.’
Talk to your doctor to find out if prescription Chantix is right for you.”
Talk to your doctor to see if a drug twenty times more dangerous than smoking is right for you?
Then these “side effects” require more drugs to balance the new problems caused by the first drug. And on and on this vicious circle goes.
Because these drugs relieve symptoms, but don’t eliminate the cause of the cellular dis-ease, many people are on their meds for life — raking in huge repeat customer profits for the big pharma snakes.
Surgery
After enough neglect — cells, tissues and organs eventually die, putrefy and go into sepsis — inducing internal bacteria to eat you alive.
Rather than addressing and reversing the reasons why, the allopathic strategy is to just remove parts or all of various organs, or even hack off the limbs — not stop the cause.
And when the dis-ease expresses itself again, they’ll just cut out more of you, until there’s nothing left of you to cut out anymore.
But don’t worry, your insurance will pay for it. And, if not, they’ll take your house and life savings in return for the “favor”.
Surgery has been around since ancient times. And there are brilliant trauma, heart and transplant surgeons — and others — saving millions of lives when absolutely no other option is left.
This is in no way meant to attack them.
But allopathic medicine is the reason we now need so many of them so often.
Radiation
You already know about the effects of acute radiation syndrome on cellular biology.
To even discuss the absurdity of this allopathic form of medical treatment, as some sort of cure for cellular dis-ease, is an insult to human intelligence — sheer lunacy. So we won’t even bother going there.
If your doctor even suggests this — run very far and fast.
“A better thing to talk about, however, is the relationship between profits and cancer. In the United States, there was a study that was published — I believe it was in 1994 — it was a 12 year program, 12-year study.
They looked at adults who had developed cancer as an adult — not childhood cancer, but adult cancer. Right? This is the main type of cancer that we get here in the United States. They did a meta-analysis of these people, all around the world, who developed cancer as adults for 12 years and were treated with chemo.
They looked at the results and they published the results in the Journal of Clinical Oncology. And the results? Ninety-seven percentof the time chemotherapy does not work. Ninety-seven percent of the time it doesn’t work.
So why is it still used? It’s one reason and one reason only. Money.
If you go to a medical doctor, an MD, with a sinus infection and that doctor prescribes an antibiotic, he gets no financial kickback. Now if he prescribes 5000, you know, of that antibiotic in one month, the drug company that makes it might send him to Cancun for a conference. Right? But he gets no direct remuneration.
It’s not… with chemotherapeutic drugs it’s different. Chemotherapeutic drugs are the only classification of drugs that the prescribing doctor gets direct cut of.
So, if your doctor prescribes chemotherapy for you, here’s how it goes, more or less:
The doctor buys it from the pharmaceutical company for five thousand dollars, sells it to the patient for $12,000. Insurance pays nine thousand dollars and the doctor pockets the four thousand dollar difference. And there ought to be a law.
The only reason chemotherapy is used is because doctors make money from it. Period.
It doesn’t work! Ninety-seven percent of the time!
If Ford Motor Company made an automobile that exploded 97% of the time, would they still be in business? No.
This is the tip of the iceberg of the control that the pharmaceutical industry has on us.
We — most people — have no idea of this at all now.
In my book, I have a bulleted list of 10 questions that every cancer patient could ask their doctor. Ten questions.
I’ve had patients checked out, literally kicked out of the oncologists office, because the doctor was p-o’d that thepatient was asking them these questions. And these are just common sense questions.
Cancer treatment in the United States — we have lost the war on cancer. We have lost the war on cancer.
Why?
Because cancer is not a reductionistic phenomenon. Cancer is a holistic phenomenon.
When you try to bring a reductionistic methodology, like drugs and surgery, to bear on a holistic phenomenon, you will completely miss the boat each and every time.
Medical doctors are like colorblind art critics. They can see that that’s a boat — they can see the black and white outline — but they’re completely blind to all of colors and textures that make up the substance of the thing.
It’s no difference with cancer. The reason that people get cancer in the United States, and the reason that we have completely lousy outcomes, is because medical doctors are driving the research bus.
When women get together and do a 5k run for breast cancer, all of that money — do you think any of that money goes to nutritional research?
Do you think any of that money goes to homeopathic research? Or acupuncture? Or traditional Chinese medicine? Or naturopathic research? No.
All of it goes to drugs and surgery — which do not work.
Now, why aren’t those women running for selenium? If every girl in this country took 200 micrograms of selenium, in one generation we’d eliminate breast cancer by 82%.
That’s a big number.
Why aren’t we doing that? Because medicine in the United States is a for-profit industry and most people are completely unaware of this. And most people bow down to the altar of MD-directed high-tech medicine.”
Chemotherapy is in fact nitrogen mustard, the cell killing compound used to make chemical warfare mustard gas n World War I and II,
Why does it have a 97% failure rate?
It doesn’t just kill cancer cells. it kills all cells.
It’s poison.
The exoteric correlation between the caduceus and our double helix DNA cannot be ignored — as DNA alteration is the target of Bill Gates and the current Big Pharma vaccine cartel — set to become the world’s first medical mafia trillionaires.
“They’re using a new technology for this vaccine, which they say allows them to develop it more rapidly.
But, you know, they’ve developed it in record time. I mean, obviously they have developed this before– before the plandemic actually came to fruition. But what these vaccines are is, they have DNA.
And they — using this technology called microporation, where they apply an electric current through two additional needles. And it causes little holes to open up in your cells, so that this foreign DNA can go into your cells and basically turn you into a genetically modified organism
Now they say that the gene is the gene of a virus, so we’re gonna have our own cells making virus proteins and somehow that’s gonna trigger an immune response.
You know, I don’t buy that at all.
S,o what these genes are I don’t know.
You know, I have some guesses because I know one of the goals of the vaccine is for infertility. Right? Because it’s all about population reduction.”
~ Dr. Andrew Kaufman
By either coincidence or conspiracy, at the very same time the WHO and NGOs were giving out hundreds of millions of free poisonous smallpox vaccinesall over Africa.
The continent erupted with the biggest autoimmune disorder epidemic in known history.
What wasn’t free, and ended up indebting several African governments, were the hundreds of millions of PCR tests already manufactured to test for the new unheard of autoimmune disorder called HIV/AIDS.
And the bogus-treatment-drug AZT — called one of the most toxic, expensive and controversial drugs in the history of medicine — this disease may result in the deaths of 90 million African people by the year 2025.
We saw the same trend in India when a polio epidemic and hundreds of thousands of paralyzed children coincided with a mass polio vaccination campaign there.
And today, we can now recognize the same alarming pattern happening with the blatant fudging of statistics and the orchestrated villainization of the common cold and flu — to force a worldwide multi-trillion-dollar profit vaccination agenda.
“There’s no paper that shows, based on its experiment, that this virus causes anything. So there’s not one paper and the conclusion that said ‘as a result of this study, we’ve determined that this virus is the cause of this disease’.
So that’s not even stated in the literature as a conclusion.
But if, in fact, if you look at the methods that they use to supposedly isolate viruses, they’re doing no such thing whatsoever.
And this was really something that I learned about only in studying this illness, because I had looked into germ theory, and I knew germ theory had lots of experiments that disproved it. And that it was, you know, something that was pervasive in medicine.
But what I’ve ultimately come to learn is that they discovered a technique that essentially has these culture cells decay. And they say that that’s proof that a virus is causing the decay of those cells.
But, in actuality, they’ve never run a control experiment. And what they’re doing is taking those cells and giving them inadequate nutrition, and exposing them to toxic chemicals. And so, that’s the reason the cells are decaying.
And that’s the only thing that they say that proves a virus.
So they’ve not actually isolated any virus whatsoever. They have shown that they can do this isolation technique in bacterial viruses. They call them bacteriophages. And they’ve shown that they can use this technique to isolate exosomes. And the technique is fairly simple.
You just filter out these small particles and then you put them through a centrifuge to have them segregate together based on their density. And then you hold a syringe or a pipette and you can look at them under the microscope.
You can characterize them chemically. You can take out the genetic material and sequence it.
And they’ve done these experiments for exosomes and bacteriophages. But they’ve never done it for a virus. And the simple reason is because there must not be any virus, that exists, that causes disease.
So they have this other procedure that just shows damage to cells in a culture and they say that that’s evidence of a virus. And it’s really quite astounding when I uncovered this. Because it’s not just in the studies for the SARS-CoV-2 virus that, you know, they say is associated with COVID-19, but it’s true for every single virus paper that I’ve looked at for any type of virus.
So really, there’s really no evidence that any virus that is alleged to cause a disease has ever been isolated, or proven to cause any disease whatsoever.”
~ Dr. Andrew Kaufman
___
“Yeah and here we see this response, which is unprecedented.
And the interesting thing, like you mentioned exosomes. And in one of the first discussions that I heard you talk about this, you mentioned the fact that, well actually, when you look at an exosome, you look at its makeup, you look at the way it reacts and its characteristics, and then you look at COVID-19. Well, you go, well hey, it’s actually exactly the same thing.
So they’ve basically taken this normal part of our immune system, which is just a response to toxicity in the cells, and categorize it as this terrible pandemic. And it’s going to appear in basically anybody who’s stressed or got toxicity in the cell.
So it’s a total win-win situation for them. But there appears that there is no virus at all. They’re simply, you know, re-diagnosed or re-labeled, part of our immune system. And the response has been like, you know, it’s been over-the-top. Absolutely over-the-top.
And even when you look at the death figures for this year, it’s less deaths this year than it has been for the last five years. And no one seems to be dying of anything else anymore.”
~ Max Igan
___
“Well, essentially — see what what they’re seeing under the microscope — it could very well be exosomes because they’ve they pretty much created a recipe to make exosomes. Because they’re usually using monkey kidney cells for this purpose and they’re mixing it with antibiotics. And it’s well known that antibiotics induce exosomes. But the thing is that these cells are basically dying cells and they’re putting out all kinds of debris.
And early on, in the study of virology, they actually really wrestled with this problem and pretty much gave up on trying to find a virus — until this new technique that I described was invented. So we could very well be seeing pictures of exosomes when we see those pictures But they could also be other kinds of cellular debris particles.
The thing i, we just don’t know because they’ve never taken those particles and then purified them and characterized exactly what they are. So that’s really never been done. And what you’re talking about with the test — the test is a little bit different because the PCR test, which is the main test, it doesn’t test for a virus at all. What that tests for is a sequence of RNA, which is genetic material.
And the way they obtain that is also — they take the impure sample basicall, like the lung fluidn ithis case, from some people who are sick or possibly a throat swab. And they amplify short little sequences. And sequences that they’re specifically looking for mostly because they have this library of gene sequences of viruses.
But the thing is, if you go back, they’ve always characterized them this way. So they’ve never once had a intact virus particle and then sliced it open and taken the RNA out and done a sequence from end to end.
That’s never been done. What they do instead is, they take this impure sample and they look for specific sequence that they’ve pre-identified as being viral in nature from this database. And then what they’re doing is amplifying these short little sequences — maybe 150 to 250 base pairs — and they’re splicing them together into this one long strand of 30,000 which they say is the viral genome. But it’s actually just this Frankenstein-type of assembly of all these little pieces that we don’t even have any proof they’re related. They could even come from different types of cells or different creatures.
And when there’s gaps, they’re basically using sequences that they get from that database of other viruses that are also put together in this Frankenstein-type way. And they sew all those together, you know, and say that this is the sequence, the genome sequence of this virus.
And that’s the procedure. And that’s — they’re testing for something from that. But we don’t really know what it is. Except it’s most likely our own sequences.
So that’s why there’s so many positive results, because they’re essentially testing our own genetic sequences.”
~ Dr. Andrew Kaufman
In other words, more medical fraud for profit and control by keeping people in fear and ignorance of the truth — the promised plot twist.
Which is the actual, secret, hidden and misunderstood esoteric meaning of Mercury — the metaphoric symbol representing the higher mind, spirit and belief. In the Cerebrum and his caduceus are actual two hemisphere cerebrum, spinal cord, cerebrospinal fluid and two snakes representing the two sensory and motor nervous systems of our body, through which we experience everything.
The science of epigenetics states that what you are thinking is translated by the brain into body chemistry that will determine what you physically become.
As Dr. Bruce Lipton explains, the function of Mercury or mind is to create coherence between what we believe and the physical reality that we experience.
If you believe there’s a threat, signals of threat released into the blood will prepare the cells to engage in a protection area response. But if the perceived threat is imaginary stress, emotion or worry from an imbalanced mind, our cells don’t know if a threat is real or not — because cells only respond to the chemicals. They do not see the real external environment.
If we believe we are under threat or stress, we manifest stress in our cellular physiology, even though the environment in which we live is not really promoting that. Our thoughts, Mercury, whether they are right or wrong are actually changing our cellular biology through his caduceus.
What we think we become. Signal plus protein equals behavior.
So when our behavior is not supporting health or us, we can say we are expressing dis-ease.
So it’s either defective proteins or the signal causing disease. Defective proteins lead to defective functions creating disharmonious behavior in your cells which can cause disease.
Which is why a COVID-19 vaccine, using electroporation to fuse foreign bat or pig DNA into your cells, to create new protein instruction codes, is most certainly going to lead to both disease and your demise.
Luckily for those wise enough to reject the new RNA/DNA recombinant COVID-19 vaccines, flawed protein expression genes caused less than 1% of all natural disease. The signal causes up to 90% of all dis-ease.
How can it interfere with health? Trauma — physical damage to the brain, spine or parts of the body related to the nervous system — can interfere with the flow of information from the nervous system to the cells, altering communication and leading to a misunderstanding by the responding cells — because the signals are altered.
Toxins cause disease by interfering with the propagation of the signals from the brain to the cells. If we put toxic elements into our body, including vaccine adjuvants and even toxins from eating industrial farmed food, these toxic chemicals can engage in the signal pathway.
But if they do, they don’t promote a normal signal propagation. Toxic chemistry can distort the signal.
If the brain is sending a signal to control the cells and there’s toxic chemistry in the pathway, then the signal that reaches the cell is altered, and then the behavior of the altered cell can lead to disease.
But the real secret of Mercury mind, is that our thoughts become translated into chemistry that can either cure or create disease.
A dis-ease caused by thought is not because the body is defective, it’s because the signal is inappropriate.
Because this esoteric science is hidden — consciousness, emotion, worry and stress are the primary problems contributing to issues regarding health on this planet. Too many people are sending inappropriate signals at inappropriate times, leading to inappropriate behavior which we call disease or dis-ease.
The truth is that these are two sides to the same coin.
Metaphysically, mercury is mind.
Physiologically, Mercury is the nerves and the cerebrospinal system. The cerebrospinal system is the generator and carrier of physicochemical electricity, which is simply energy or life.
Our mind and the sensory nerves utilize the electrical energy of thought and the subtle nerve fluids in the cerebral spinal fluid.
Depending on our thoughts and actions, Mercury may do this beneficially and positively, or negatively and destructively.
Chemically, Mercury is quicksilver which, is an oily fatty substance. the “argentum vivum” or “living philosophical silver” that rises back up from our sacrum to our cerebrum to be converted back to electricity infinitely if not wasted
The real interpretation of “quick” means living.
And as oil is the physical manifestation of energy, mercury or quicksilver, means the oil of life.
We are told by the AMA that a quack is a medical charlatan. Takes one to know one.
But actually quack is short for the 1570s Dutch term quacksalver or the German quacksalber, and the Danish quakzalver, meaning “hawker of salve” or oil or to rub with ointment.
Quakzalver sounds remarkably close to quicksilver. Wouldn’t you say
As usual, the snakes have inverted the true meaning of healing — for profit.
And that is the real reason Mercury is the father of merchants and thieves.
Mind, which is the father of thought, can actually rob the physical body by wasting living electricity through thought, emotion, action and physical merchandise — through riotous and gluttonous thought and living habits.
The “brain esse”[esence] and thought power or electricity constitute the true merchandise of every human body.
And thus, the job of the great physician Mercury, your mind, is to electrochemically heal all dis-eases.
Not just through pure thought and action, but through pure food sustenance and plant medicine on the physical plane. The cerebrospinal fluid around our brain, spinal cord, and nerves, cushions those organs.
It picks up supplies from the blood and gets rid of toxic waste products. It is a colorless, transparent alkaline fluid — 99% water, 1% monoatomic potassium — which creates healing and toxic-dissolving oils, glucose, protein amino acid molecules, enzymes, hormones, antibodies, etc.
It is how the brain talks to cells.
In esoteric biblical biochemistry, the healing Rod of Asclepius is the staff of Moses.
The electrical seed germination that creates the healing corpuscles of the cells (created in our spleen) that make up our blood, lymph and nerve endings, brought down to the spleen from the cerebrum (or Aries the lamb or Ram of God), also known as Brahma or Abraham, by Mercury, the messenger of the Godhead.
That is why Moses, or the electric seed of the corpuscles, is the descendant of Abraham, our cerebrum.
The winged caduceus of Mercury is the Tree of Life.
While the serpents represent the tree of knowledge of good and evil, or cellular ease and dis-ease, one is the sensory system, the other the motor system, doing work pertaining to motion. But perverted it becomes e-motion, meaning energy wasted, substance lost, death and dis-ease.
All around us today, we see its effect.
Humanity as a whole, floundering in chaos instead of harmony, lost in a sea of emotion — energy wasted, substance lost.
The blood corpuscles carry not only nutriment to every cell, but air as well. Our cerebral cells, as well as all other cells, must be supplied with the proper mineral foods and salts, and kept free from acid accumulation and toxic poison.
Each individual has his own Tree of Life. No one but himself can destroy that tree and no one but himself can cultivate it or supply it with nutriment.
There are links to details on this beautiful esoteric science in the description.
But know that oils neutralize and dissolve body toxins and poisons.
Water keeps fibers fluid and in motion.
Spirit (electricity) moves the body and the 12 mineral salts that manifest electricity to biology are the physical body.
Physician heal thyself. This is not medicine.
And this is not the cause of disease.
At a glance, on the surface symbols, are just pictures that represent an idea in the consciousness of those who look at them. But while we may think symbols are just pictures, they do act on our subconscious mind to bring about the desired influence of the sigil creator.
The actual intent of the symbol may be unknown to the viewer or even be inverted in its true meaning. For example the peace symbol, or inverted Algiz, is actually a Proto-Germanic death ruin that was inscribed on tombstones. Death is peace.
The swastika had a positive meaning in ancient times. Its Sanskrit name was svasktika, literally meaning “it is”, well being, good existence, and good luck. For the Hindus it was a symbol for Vishnu and the Sun or, when inverted, Kali and magic.
Thus we can invert the meaning of the caduceus to serve our health, rather than drain our corpuscles.
In our current reality, war is peace, freedom is slavery, ignorance is strength, and poison is medicine. But it does not have to be that way, if we do not want it to.
You can decide yourself, right now, that poison is poison, but plants, clean nutrient-filled food and positive mind is medicine.
Our bodies have amazing capabilities to heal if we simply provide the right environment, free of toxins, full of nutrition, purity of mind and spirit.
There is no form of cellular disease we cannot heal from.
International best-selling author, Dr Vernon Coleman MB ChB DSc FRSA, explains that the people planning to rule the world want to reduce the global population to 500 million. And he then explains how’ll they’ll kill the six billion of us they want to eliminate. For more unbiased information, please visit http://www.vernoncoleman.com
The transcripts of the videos that YouTube banned are also on the website.
In the event that the original video is censored and deleted by the source social media platform,
link here to a mirrored copy on TCTL Bitchute & Lbry channels.
TRANSCRIPT:
There are people around who believe that if we all wear masks, obey the social distancing laws and become true slaves to the system, then everything will be back to normal by Christmas at the latest.
In the last 24 hours I have read, and been dismayed by, three articles by writers who believe that if we all behave properly, and do exactly as we are told to do, the coronavirus will slink off and all will be well with everyone back at work, the economy beginning to boom and the world well on its way to a recovery. There are even some who were shocked at the suggestion that taxes will rise dramatically in the next 12 months or so. Where do these people think the money came from – the money that an ex Goldman Sachs, currently the UK Chancellor, was throwing around with such gay abandon.
Of course, they add as a rider, we won’t be able to forget about social distancing, and we may have to keep on our masks until the vaccine is ready, but everything will be normal apart from that.
I wonder what these people have inside their skulls. Porridge? Those little white polystyrene balls that are used for packaging? Bubble wrap?
They certainly don’t have brains.
The people now planning to rule the world, a group of billionaires and would-be billionaires who I will, for ease, refer to as the enemy, have decided that there are too many people in the world and that the earth would be more comfortable for them if the total were reduced to around 500,000,000.
Since the current population is around 7 billion that means that at least 6 billion of us are surplus to requirements, unnecessary, not wanted on voyage. Since their ambition has a convincingly eugenic flavour they will presumably want to get rid of the weak and the poor and the elderly and the frail.
So how are they going to do that?
Well, the ignorant, scare mongering climate change nutters have done some of their work for those who want us dead. The brainwashed children and idiots who believe in man-made global warming are helping the enemy enormously. Cutting back on our use of oil and gas will kill hundreds of millions who will die of hunger and cold.
And I have no doubt that the enemy will manage another plandemic.
The abominable Gates and his wife have already said that people will pay attention when the next pandemic arrives. And I thought they both smirked very knowingly when Bill made this prediction.
It wouldn’t be difficult.
They could just say that the coronavirus which caused Covid-19 had mutated. Or they could blame a pig virus or a cuckoo virus or maybe a virus from the Gates family – something unpleasant.
It wouldn’t really need to be something too nasty. After all, a really bad virus might kill off some of the billionaires.
I rather suspect that we are going to have more alleged virus health calamities coming up. If it isn’t the coronavirus in a pre-ordained second wave it will be something else. If they can make up one crisis then they can, and will, make up many more.
All it needs is good marketing, and organisations like the BBC will provide all the myths and fake news that the enemy will need.
The BBC, The Guardian and the Daily Mail could turn tapioca into a deadly threat.
Of course, the plan to reduce the global population is already doing well.
The enemy has got everyone social distancing. And that is known to cause illness and to kill people. The CIA reckon that social distancing is one of the most powerful weapons there is for controlling large numbers of people.
They managed to murder huge numbers in the care homes and they have killed vast numbers of the sick by closing down hospitals for absolutely no good reason.
They put everyone under house arrest – and isolation damages the immune system. Prisoners of War have confirmed that isolation does more damage than physical torture. Stress and anxiety affect the immune system too.
The masks will kill quite a few people too. It’s well known that they reduce blood oxygen levels, and those with respiratory and cardiac disorders will die. It’s true that surgeons wear masks but the circumstances are entirely different. Women’s movement enthusiasts used to burn their bras. Perhaps, we should burn our masks – in an environmentally acceptable way, of course.
Even the sanitising gel they insist we use a dozen times a day will kill some people. (If you haven’t seen it, watch my video on hand sanitisers. Or read the script on this website.)
And then there is the cold in the winter months. They are stopping us using gas and there are going to be electricity outages. Many will freeze to death in the winter months.
But I think their biggest weapon is food.
That’s how they are going to bring the population crashing right down.
Food shortages are coming and the cost of food is going to rise even faster than it has been doing. And it isn’t because of global warming or whatever other lies they tell you – it is, however, a side effect of the coronavirus hoax.
All around the world food is in short supply. The price of the world’s most important staple food – rice – has risen by 70%. Food prices in the US have recently seen a historic jump and are, I believe, destined to stay high and go higher. Countries which have good food production are halting their exports. Vietnam, for example, has stopped exporting because they need their food supplies at home. And you cannot blame them. Some authorities condemn it as nationalism but all countries, all villages, all homes would do much the same.
And it is the managed over-reaction to a virus known to be no more dangerous than the flu that is causing the problem – and that will result in millions of deaths to add to the millions who are going to die as a result of the lockdowns.
The global death rate because of the food shortage is going to be measured in hundreds of millions – and eventually in billions. Africa and Asia are going to see the worst levels of starvation ever seen. I fear that those countries which have some grain will flog it to America – despite massive starvation. Black lives matter protestors, who have been manipulated by professionals, would be wise to forget about Cecil Rhodes’s statue, and where they’d like to see it placed, and concentrate instead on helping Africans who are going to be subjected to the worst genocide in history.
So, how is the coronavirus scandal responsible for the food shortages that are coming?
That’s easy to explain.
Processing plants and distribution centres all around the world have been deliberately severely disrupted by the massive over-reaction to this fairly ordinary virus.
Around the world more and more testing is being done. And although the tests are about as trustworthy as Gates, Clinton and Soros – your local purveyors of fear and death – they are treated with undeserved reverence. Curiously, it seems to me that farms and food distribution centres are being tested more than, say, civil servants or tax officials. This is odd because the chances of the virus being carried on food are roughly the same as the chance that the moon is made of cheese.
And so if one worker on a farm or in a warehouse falls ill with flu like symptoms then the authorities will close down that farm or the warehouse. Delivery systems have been massively affected as drivers are sent home for two weeks and all their colleagues sent home for two weeks too.
As a result, huge crops of vegetables and fruit are being ploughed into the ground. Millions of animals are being slaughtered and then buried or burnt because the supply chains have been shut down. America, almost unbelievably, has been importing beef because of the shortages.
The world lockdown, and the mass house arrests that were engineered to keep us all subservient, mean that thousands of farmers cannot get their crops picked. Fruit in particular is likely to rot in the fields, and tankers full of milk are being poured away. Controls on transport have meant that it has been difficult to move food from where there is a glut to where there is a dearth. It would have been easy for governments to insist that furloughed workers should help pick the crops but they didn’t do so. And why would they? The plan is to eradicate the poor and the weak.
And the unsurprising consequence of all this is that there are going to be massive shortages of fruit and vegetables, and prices are going to rocket.
In the UK, the most toxic of the Remainers, the fascist EU loving lunatics, bigoted, soaked in their own prejudices and consumed by ignorance, will blame Brexit for the shortages. But then, if they develop a bald spot or lose their keys they blame Brexit.
In the US, the media will doubtless blame Trump for the food shortages.
Sadly for them all, the shortages will be global.
All around the world there will be a shortage of almost all foods.
This isn’t the sort of fear-porn favoured by irresponsible main stream media giants such as the EU and Gates supported BBC.
This is real.
Other factors are going to ensure that the shortage just gets worse.
If and when the economy is allowed to stutter into action again, the price of oil will doubtless eventually rise because the existing supplies are diminishing rapidly and most oil companies have pretty well given up exploration.
The rising price of oil will mean that farming and transportation costs will rise and that will push up the price of food still further.
I tell you this not to scare you but because when you know something is happening you can do something about it.
You may think it is worthwhile building up your stocks of long-dated food staples such as rice and pasta. Dried and tinned foods which have long dates are good. As you eat your stocks, replace them with more.
Governments tell us not to store stuff but the military don’t buy bullets the day they need them, do they? If you have a garden and can grow your favourite vegetables or fruit that’s probably a good idea but watch that no one climbs over your fence and steals them. I don’t recommend having an allotment – the chances of you being able to harvest your own crops are too remote because they will be stolen. It might also be a good idea to stock up on vitamin and mineral supplements if you usually take them.
I’ve always been a bit of contrarian, though I don’t suppose anyone would notice, and I’m convinced that the time to panic buy is when there is no panic.
I hope the advice here will help you and your family to have a better chance to be strong and healthy. Countries look after themselves and we all need to do so. It isn’t selfish. It’s survival. If you buy food you will eat anyway, and you store it carefully, what have you got to lose? If I’m wrong and there is no enemy and there are no food shortages then you can always eat what you’re stored.
If and when your government finally warns you of this problem it will be far too late.
Remember: you should stockpile food now – don’t wait for the panic
Copyright Vernon Coleman July 2020
Vernon Coleman’s book Coming Apocalypse explains how the hoax developed and what our future will be. Coming Apocalypse is available on Amazon as a paperback and an eBook.
Vitamin D Deficiency Is Associated with COVID-19 Severity and Mortality
On April 7th, we proposed that Vitamin D might be important in COVID-19 infections based on the timing of the pandemic and the “at risk” populations. We cited literature showing that Vitamin D sufficiency reduced the risk of acute respiratory infections and the severity of infection by other viruses. We found several studies using high-dose Vitamin D in patients on ventilators that showed improved outcomes including decreased mortality. A month ago, we called for more research.
Now, new studies in COVID-19 patients suggest Vitamin D sufficiency might reduce disease severity and death.
The Associations are Strong
On April 9th, initial data from the Philippines on 212 confirmed COVID-19 patients showed that Vitamin D status was strongly associated with severity of COVID-19. The study sorted patients into 4 categories of severity based on criteria established in Wuhan. The levels were:
Mild – Mild clinical features without pneumonia
Ordinary – Confirmed pneumonia by CT with fever and other respiratory symptoms
Severe – Hypoxia (low oxygen) and respiratory distress
Critical – Respiratory failure requiring intensive care monitoring.
In the analysis, 85.5% of patients with sufficient (>30ng/ml) Vitamin D had mild cases while 72.8% of patients who were deficient in Vitamin D (<20ng/ml) had severe or critical cases.
On April 26th, a second retrospective study came out of Indonesia. This larger study investigated Vitamin D status in 780 confirmed COVID-19 cases. The researchers collected data on Vitamin D status, age, sex and the presence of comorbidities along with mortality data. The study confirmed what we know—that male patients, those over age 50, and those with pre-existing conditions were all significantly more likely to die of COVID-19. However, the most dramatic finding was that patients with Vitamin D insufficiency (between 20 and 30 ng/ml) were 12.55 times more likely to die and patients with Vitamin D deficiency (<20ng/ml) were 19.12 times more likely to die from the disease than patients with sufficient Vitamin D.
Since age, sex and comorbidities can also be associated with Vitamin D deficiency, the researchers then did an adjusted analysis. The key finding is that, even after controlling for age, sex and having a comorbidity, “When compared to cases with normal Vitamin D status, death was approximately 10.12 times more likely for Vitamin D deficient cases.”
Strikingly, 100% of ICU patients less than 75 years old had Vitamin D insufficiency.
A third small study out of Louisiana State University Health Sciences Center dated April 24th, examined Vitamin D insufficiency (VDI) in severe COVID-19 patients and discussed possible Vitamin D-related mechanisms for the coagulopathy and immune responses that are being seen. It stated that, “Among ICU subjects, 11 (84.6%) had VDI, vs. 4 (57.1%) of floor subjects. Strikingly, 100% of ICU patients less than 75 years old had VDI.” The study is limited by its small sample size but is consistent with the above studies.
In an excellent 2018 review paper on Vitamin D in critical care, the authors stated, “Vitamin D deficiency is common in critical illness with prevalence between 40 and 70%.” They continue, “Vitamin D deficiency has been shown to be associated with sepsis, acute respiratory distress syndrome and acute kidney injury and three different meta-analyses confirm that patients with low Vitamin D status have a longer ICU stay and increased morbidity and mortality.”
More recently, in another review paper (2020) investigating the potential links between Vitamin D status and risk of Influenza and COVID-19, the authors point out that, “Through several mechanisms, Vitamin D can reduce the risk of infections. Those mechanisms include inducing cathelicidins and defensins that can lower viral replication rates and reducing concentrations of pro-inflammatory cytokines that produce the inflammation that injures the lining of the lungs, leading to pneumonia.” Cathelicidins and defensins are molecules your body produces to protect you against bacteria, viruses and fungi and modulate your immune system.
If Vitamin D can reduce severity of COVID-19, it is a potential game-changer.
Why Vitamin D Should Be Studied in Large Clinical Trials
Currently, only Remdesivir has been FDA approved for severe cases of COVID-19. It is an IV pro-drug (the drug is a precursor; the body creates the active compound) that is both expensive at a potential price of $4500 per patient and challenging to scale up quickly. The NIAID/NIH Remdesivir trial was double-blinded and placebo-controlled. Participants had to test positive for the virus and have evidence of lung problems. Remdesivir improved time to recovery (discharge from the hospital or ability to return to normal activity) by 4 days, from 15 days to 11 days. However, the overall survival difference in the trial did not reach statistical significance (8% mortality in the treatment group, 11.6% in the placebo group). So, Remdesivir is unlikely to be a significant factor in the U.S. or the solution on a global scale.
By contrast, Vitamin D is free from the sun and widely available. It is inexpensive in typical supplements and costs about $100 for a typical IV formulation which may be needed for patients with kidney disease. It is manufactured around the globe and is not subject to patent restrictions. Its safety is well-established and understood. If Vitamin D can reduce severity of COVID-19, it is a potential game-changer. Taking the pressure off of hospitals and health care workers, protecting our elderly, veterans and prisoners, and preventing a resurgence of hospitalizations and deaths are all on the table.
An April 28th press release from the Medical University of South Carolina is encouraging. Long-time Vitamin D researchers, Bruce Hollis, PhD, and Dr. Carol Wagner, are starting to study COVID-19. Hollis and Wagner have recently been studying the impact of Vitamin D in pregnancy and during breast-feeding on infant outcomes. They have over 60 years of combined experience with Vitamin D research.
There are currently 10 clinical trials including Vitamin D for COVID-19, some in addition to standard therapies and some in specific combinations with other drugs and supplements. Unfortunately, several of these trials are not well-designed to show significant outcomes because the doses proposed are fairly low.
The Bottom Line
Vitamin D might be a game changer, reducing deaths and disease severity. Vitamin D from sunshine is free and regular exposure for 20 minutes a day this time of year will provide about 1000 IU for people living in mid-latitudes who expose about 30% of their body surface. Vitamin D is available to almost everyone, even the poorest and recently unemployed. Populations that can’t get outside easily (the elderly, prison populations, indoor workers) may need Vitamin D supplements to achieve sufficient blood levels. We should work towards testing Vitamin D levels in those populations to ensure that they are sufficient.
Please share this information; it might save a life.
COVID-19 and Vitamin D: Could We Be Missing Something Simple?
[CHD note: With the United States largely shut down and the deaths from COVID-19 rising, we wanted to share the following information and questions with our readers. Please share this widely on social media, particularly with health professionals on the front lines, government officials and anyone who might be interested in studying Vitamin D and coronaviruses.]
Introduction
Briefly, the literature on Vitamin D’s role in immune health has exploded in the past 10 years, particularly in relation to viral infections and autoimmune disorders. Approximately 80% of the literature is new in the past decade and much of it has been published overseas. There are studies showing that Vitamin D sufficiency is important to reduce mortality in ventilated patients. There is a large and growing literature on Vitamin D’s role in preventing viral infections and reducing their severity.
A 2018 study based on NHANES data from 2001-2010 found that 28.9% of American adults were Vitamin D deficient (serum 25(OH)D<20ng/ml) and an additional 41.4% of American adults were Vitamin D insufficient (serum 25(OH)D between 20ng/ml and 30ng/ml). Americans who were black, less-educated, poor, obese, current smokers, physically inactive or infrequently consumed milk had higher prevalence of Vitamin D deficiency. Those with intestinal disorders (Crohn’s or celiac) that reduce dietary uptake of Vitamin D and those with liver or kidney diseases that may reduce the body’s conversion of Vitamin D to its active form may also be at increased risk of deficiency regardless of age. Vitamin D is a fat-soluble steroid hormone that regulates over 200 genes in the human body.
Questions that need answers
Based on the breadth of the research on Vitamin D in acute respiratory disorders and the many viral infections in which Vitamin D status plays a role, the following questions need to be answered:
Are hospitalized COVID-19 patients Vitamin D deficient (serum 25(OH)D levels < 20ng/ml) or insufficient (levels between 20ng/ml and 30ng/ml)?
Are hospitalized COVID-19 patients more Vitamin D deficient than would be expected in matched controls?
Are hospitalized COVID-19 patients who need intensive care more Vitamin D deficient?
Does giving high-dose Vitamin D to COVID-19 patients reduce their need for mechanical ventilation and/or reduce the amount of time that they require mechanical ventilation?
Does giving high-dose Vitamin D to health-care workers reduce their risk of COVID-19?
If Vitamin D deficiency is found in severe COVID-19 patients, what recommendation should be made to the general public, particularly those who are quarantined and/or fighting infections at home?
While only time and studies will give us definitive answers to these questions, Vitamin D testing is widely available, supplements are inexpensive and in a COVID-19 critical care setting we should consider anything that might reduce the number of cases, hospitalizations and deaths. Even a 10% reduction in one of these metrics would have a major impact.
The literature supports the importance of Vitamin D sufficiency
There are studies suggesting that sufficient Vitamin D reduces the risk of acute respiratory infections. Also, the literature supports the importance of Vitamin D sufficiency in reducing morbidity and mortality in critical care settings. This is a sample of the literature.
A 2017 article in the BMJ states the following: “25 eligible randomized controlled trials (total 11 321 participants, aged 0 to 95 years) were identified… Vitamin D supplementation reduced the risk of acute respiratory tract infection among all participants (adjusted odds ratio 0.88, 95% confidence interval 0.81 to 0.96; P for heterogeneity <0.001).” The protective effects were greatest in those who were deficient (serum levels <25 nmol/L = 10ng/ml) and in those who took Vitamin D regularly (on a daily or weekly basis) compared to large bolus doses.
Another 2018 review of the literature specifically in intensive care settings suggests that the non-significant results in some large trials of Vitamin D supplementation are likely the result of including subjects who are Vitamin D sufficient in the trials and not excluding Vitamin D supplements in the control groups. The authors are clear that “three different meta-analyses confirm that patients with low vitamin D status have a longer ICU stay and increased morbidity and mortality” and that “this hormone plays an important pleiotropic (having more than one effect) role in the setting of critical illness and may support recovery from severe acute illness.”
A small 2019 Iranian study recommended larger follow-up studies after randomizing 44 mechanically ventilated adult patients to 300,000 IU of Vitamin D vs. placebo. The study found a significant reduction in mortality (61.1% vs. 36.3%) and a non-significant 10-day reduction in time on the ventilator.
In a 2018 follow-up pilot study they found that in critically ill, ventilated patients, with Vitamin D deficiency and anemia, high-dose Vitamin D increased hemoglobin.
Additionally, a research group at Emory published a 2016 pilot study showing that high-dose Vitamin D decreased hospital length of stay in ventilated ICU patients. In a 2018 follow-up pilot study they found that in critically ill, ventilated patients, with Vitamin D deficiency and anemia, high-dose Vitamin D increased hemoglobin.
A 2017 study found that “Monthly high-dose vitamin D3 supplementation reduced the incidence of ARI (acute respiratory infections) in older long-term care residents but was associated with a higher rate of falls without an increase in fractures.”
A 2015 study in Thorax found that Vitamin D deficiency was common in patients who developed acute respiratory distress syndrome after esophagectomy.
A 2018 study in the Indian Journal of Anesthesia reported no significant results in mechanically respirated patients based on Vitamin D deficiency vs. sufficiency at admission, but this was likely due to small sample size. The trends for days in the ICU, days on mechanical ventilation, days to spontaneous breathing trial and 30-day mortality were all more favorable in the group with sufficient Vitamin D.
In another 2018 Iranian study of 46 patients with Vitamin D deficiency and Ventilator-Associated Pneumonia, a single dose of 300,000 IU of Vitamin D compared to placebo significantly reduced serum levels of IL-6 and significantly reduced mortality. IL-6 is a cytokine that is typically elevated in acute respiratory distress syndrome.
Unlike the above studies, a large 2014 Austrian study of 492 critically ill patients with Vitamin D deficiency did not find significant results with Vitamin D supplementation for most of its outcome measures. The only significant result was decreased hospital mortality in the severely Vitamin D deficient subgroup. However, this study population included surgical, neurological and medical patients and it is possible that Vitamin D is only relevant for respiratory infections. Also, this study reported no serious adverse events using very high doses of Vitamin D in a critically ill population.
A 2017 rat study showed that pretreatment with calcitriol (the active form of Vitamin D) reduced lipopolysaccharide-induced acute lung injury by modulating the renin-angiotensin system. ACE and ACE2 are part of this system and ACE2 is the binding site of SARS-CoV2 on cells. There is an unresolved ongoing debate on whether angiotensin converting enzyme inhibitors (ACE inhibitors) used to treat blood pressure and heart conditions increase or decrease the risk of SARS-CoV2 infection. How Vitamin D deficiency might fit into this discussion is an open question.
Interestingly, a 2018 case-control study of 532 Japanese workers found that in a subgroup of participants without vaccination, vitamin D sufficiency was associated with a significantly lower risk of influenza.
Research on Vitamin D in other viral infections
Vitamin D deficiency has been studied in many viruses and, generally, sufficient Vitamin D levels lead to lower rates of infection and less severe cases. This research is a combination of in vitro and in vivo studies. There is no specific literature on coronaviruses so we looked for research on Vitamin D in other viral infections including Influenza, HIV, Dengue, Epstein Barr, Hepatitis B and Hepatitis C. Some examples follow:
A 2018 Chinese trial of two different doses of Vitamin D in 400 infants showed significantly lower risk of influenza A, reduced viral load and reduced duration of symptoms in the group on the higher dose. A similar 2010 study in Japanese school children found that 1200 IU/day of Vitamin D reduced Influenza A infections from 18.6% in the placebo group to 10.8% in the supplemented group. The supplemented children with asthma also had a reduced risk of asthma attacks. Interestingly, a 2018 case-control study of 532 Japanese workers found that “In a subgroup of participants without vaccination, vitamin D sufficiency (≥30 ng/mL) was associated with a significantly lower risk of influenza (odds ratio 0.14; 95% confidence interval 0.03-0.74)”.
A 2018 study of youth with HIV showed that high-dose Vitamin D attenuated immune activation and exhaustion from anti-retroviral therapy. A 2016 study of 466 South African infants (half HIV-infected) found that low Vitamin D and SNPs on certain genes increased the risk of tuberculosis and death. A 2018 review of Vitamin D in HIV infection states, “High levels of VitD and VDR expression are also associated with natural resistance to HIV-1 infection. Conversely, VitD deficiency is linked to more inflammation and immune activation, low peripheral blood CD4+ T-cells, faster progression of HIV disease, and shorter survival time in HIV-infected patients.”
A small 2020 study of healthy patients showed that higher dose Vitamin D supplementation reduced susceptibility to DENV-2 (dengue) infection in blood cells. A 2017 study of human monocyte-derived macrophages found that “DENV bound less efficiently to vitamin D3-differentiated macrophages, leading to lower infection”.
The situation with Vitamin D deficiency and Epstein-Barr virus infection in Relapsing/Remitting Multiple Sclerosis (RRMS) is more nuanced. While each is an independent risk factor for RRMS, recent studies have found that high-dose Vitamin D supplementation resulted in significantly lower antibody levels to EBNA-1. In this case the lower antibody levels lead to lower risk of relapse and lower risk of new lesions on MRI.
A 2019 meta-analysis of studies of Vitamin D status in chronic Hepatitis B infections found that “Vitamin D levels were lower in CHB patients and inversely correlated with viral load”. A 2018 Israeli study found that Hepatitis B transfected liver cancer cells actually downregulate Vitamin D receptors to allow the virus to replicate.
In a 2012 Israeli study, the addition of Vitamin D to standard anti-viral therapy in patients with chronic Hepatitis C infections improved viral response. A 2015 study of Egyptian children with Hepatitis C found that cases treated with Vitamin D along with antivirals showed significantly higher “early and sustained virological response” compared to controls.
One additional factor should be considered. Single nucleotide polymorphisms that affect Vitamin D Receptor function and metabolism of Vitamin D to its active form affect sufficiency, so identifying patients with those polymorphisms will help identify those at greater risk for Vitamin D deficiency. There is a growing literature on these genetic factors as well.
Last week, former CDC Director, Dr. Tom Frieden, suggested that Vitamin D might decrease coronavirus infections. We hope this article will convince doctors and researchers to take a closer look at Vitamin D as a potential preventative and therapeutic option. As we stated in our recent video, we think that scarce resources should be focused on treatment versus a vaccine that may never materialize.
Last, a caveat
This is not medical advice and you should not take high doses of Vitamin D without checking with your doctor, particularly if you have any underlying health conditions. Vitamin D does have potential toxicity at high levels including hypercalcemia and kidney stones. A daily dose of 800 IU – 2000 IU of Vitamin D is generally regarded as safe and will produce sufficiency in most people, but more is not necessarily better. NIH’s information on Vitamin D dosing and drug interactions can be found here.
Please share this information.
China Cures Coronavirus with Vitamin C; Research Suggests Selenium
I live in China. This year, like every other, people with severely compromised immune systems were and are suffering from pneumonia. In early January 2020, in Wuhan, China – a place with dreadful air quality—hospitals started receiving patients.
In fact, for most of November, all of December, and most of January, the air quality index (AQI) was so bad that local governments regularly issued standard health warnings due to high levels of particulate matter. (At my school in Shanghai, if the AQI is over 150, children are cannot play outside. This is based on government advisories.)
And please be aware, far from hiding the problem, government officials in China at the regional and national level, readily provide daily and historical reports of the air quality index, noting particulate matter (PM2.5) and more. Thus we can track data for Wuhan — and most other large cities and urban areas — for the past six years.
Unsurprisingly, those diagnosed with severe forms of COVID-19 are the elderly and the immunocompromised. Additionally, people who have a host of pre-existing conditions are at higher risk. (NEJM March 30th, 2020). The Boston-based non-profit, Health Effects Institute, says anywhere from 500,000 to 1,250,000 Chinese die due to air pollution alone each year. (see pages 11-13). But the question discussed in this report is, “When people have pneumonia or other respiratory difficulties, what are the best treatment protocols?”
Ceep it Cimple Ctupid: Intravenous Vitamin C … Again?
All across China, not just in Wuhan, but also in other cities that saw pneumonia cases (and note, Chinese medical teams discuss COVID-19 as pneumonia), people are being cured with vitamin C.
I am including the details from a public report written in Chinese and published by a medical team Xibei Hospital, affiliated with Jiao Tong University, in the city of Xi’an, Shaanxi province. (To complete the translation I used a combination of programs and resources: Google Translate, Pleco, and Baidu Fanyi).
Given what the doctors in Xi’an knew of reports from Wuhan (which is 500 miles away from Xi’an, in the neighboring province of Hubei), and from seeing pneumonia patients in early February 2020, a team at the Xibei Hospital, devised a protocol centered on the use of intravenous (IV) vitamin C against the Coronavirus. They first treated patients on February 10th. Critically ill patients received 200 mg of soluble vitamin C per kg body weight, once every 12 hours. After the first two treatments, the patient would get 100 mg/kg, every 24 hours, for the next four days. (Those presenting with moderate symptoms were given 100 mg/kg on day one).
Arguably, these doses are too low. Practitioners and researchers like Dr. Suzanne Humphries (2014) and Thomas Levy, J.D., Ph.D. (2017), posit that intravenous infusions of vitamin C should be from 50-100g per day, and can be repeated every 3-7 days.
Even with their relatively low doses, patients in Xi’an were released after four to eight days of vitamin C. Thus, the protocol, emphasizing the antioxidant, ascorbic acid, has been a clear success.
Nevertheless, my question is, Why don’t we hear of anything about intravenous vitamin C as a routine practice in the United States, or even in other developed countries with reported COVID19 cases like Italy, Spain, Germany, France, or Iran?
What Does the Research Say about Vitamin C?
The teams in China did not choose to administer vitamin C due to mere guesswork. To make the decision, they cited the medical literature and used their knowledge about respiratory diseases and oxidative stress.
Dr. Zhi Yong Peng, at the Zhongnan Hospital, at Wuhan University, justified his decision to use vitamin C, noting:
For most viral infections, there is a lack of effective antiviral drugs … Vitamin C, ascorbic acid, has antioxidant properties. Clinical studies have shown that vitamin C can effectively prevent [sepsis and related cytokine storms]. In addition, vitamin C can [protect the lungs].
Vitamin C can effectively shorten the duration of (or even prevent) the common cold. In a controlled … trial, 85% of 252 students experienced a reduction in [cold] symptoms, [after receiving] high-dose vitamin C group (1g per hour for 6 hours, followed by 1g every 8 hours).
Xibei Report on Vitamin C
According to the Xibei Hospital (2020) report:
For patients with severe neonatal pneumonia and critically ill patients, vitamin C treatments should be initiated as soon as possible after admission. This is because whether the illness was similiar to infections seen in the past like Keshan disease, SARS, Middle East respiratory syndrome (MERS), or the current new [COVID19] pneumonia, the main cause of death of patients is cardiopulmonary failure caused by increased acute oxidative stress. When the virus causes increased oxidative stress in the body and increased capillary permeability, early application of large doses of vitamin C can have a strong antioxidant effect, reduce inflammatory responses, and improve endothelial (heart tissue) function.
They add:
Numerous studies have shown that treatment with doses of vitamin C promote excellent results. Our past experience in successfully rescuing acute Keshan disease and current studies at home and abroad show that high-dose vitamin C can not only improve viral resistance, but more importantly, can prevent and treat acute lung injury and acute respiratory distress (ARDS).
Why not nutrition?
Dr. Thomas Levy has written many books and has given many lectures on the benefits of vitamin C for curing disease and body detoxification. Of course, Levy attributes this information great pioneer Frederick Klenner, MD. Klenner used ascorbic acid and developed protocols with intravenous and intramuscular applications of high dose vitamin C. He is published as early as 1949—reporting cures of polio, measles, mumps, chickenpox and more.
Because I knew of the benefits of high dose vitamin C in early February, I encouraged four ex-pat doctors, working in Wenzhou, China, to give it to their patients. Wenzhou, a city of over 10 million, was the second Chinese city placed under a complete quarantine. These doctors ridiculed me and scoffed at the idea that nutrition could provide any relief to coronavirus patients. One actually said: “A vaccine is the only solution, as a virus has no effective treatment.” I voiced my objection to that idea, and had plans to use the antiviral drugs — then being touted by the WHO.
Again, I insisted that antioxidants could save the sick. To this, the M.D. added: “Nutrition is important, but if nutrition is enough, why do governments make hospitals and medical colleges?”
Why, indeed.
What about Selenium?
When I read the press release and protocol from Jiao Tong University Hospital, I wanted to learn more about Keshan disease. That rabbit hole only introduced me to more evidence that confirmed how nutrition can cure. Below are some excerpts from the Wikipedia entry on Keshan disease:
Keshan disease, named after Keshan County of Heilongjiang province in Northeast China, is a congestive cardiomyopathy caused by a combination of dietary deficiency of selenium and the presence of a mutated [sic] strain of Coxsackievirus [sic] … Often fatal, the disease afflicts children and women of child-bearing age. It is characterized by heart failure and pulmonary edema.
After reading all the references cited by the Wiki page, I concluded the following about Keshan disease and the state of scientific knowledge:
(a) Symptoms of respiratory difficulty and congestive heart disease were found to be prevalent in a wide belt of territory extending from northeast to southwest China (including parts of Shaanxi province. (See Ge and Yang 1979); those areas which are replete with selenium-deficient soils.
(c) Intentional dietary supplementation with selenium reduced the incidence and harm of Keshan disease in China. (See Ge and Yang 1979).
Keshan Disease
Beck et al. (2003) cited a 1979 report from China. The report declared, unequivocally: “Populations living in areas of China with selenium-rich soils did not develop Keshan disease.”
Given their interest, Beck et al. (2003) conducted research into the role of selenium and Keshan disease. They concluded:
“[Experiments with mice] suggest that together with the deficiency in selenium, an infection with coxsackievirus was required for the development of Keshan disease.”
Please appreciate the idea that viruses cause disease is not universally accepted—and arguably wrong for Keshan disease in particular. Ge and Yang (1979) claimed that Keshan disease was and is not related to any virus. Instead, they note it as seasonal – coming in the winter. Ge and Yang (1979) explored the question of a viral cause for Keshan disease but rejected that hypothesis due to a lack of evidence. Though most medical practitioners insist that viruses cause disease, recall that in 2005, Peter Doshi discovered that despite claims that influenza virus kills thousands of Americans every year, for 2001, America had only 18 confirmed flu deaths.
The lack of evidence for a viral infection causing Keshan disease and the failure to find a flu virus in fatalities attributed to a virus should guide our thinking about COVID-19 today. Remember, the Chinese doctors in Xi’an treat pneumonia as pneumonia. And they lump together different viruses (SARS, MERS, etc.), saying that each causes oxidative stress.
If disease—all disease—is really about oxidative stress, as Dr. Thomas Levy holds, maybe the type of virus is irrelevant. Keep in mind, even though virologists categorize many types of viruses, there are no true species of viruses (Racaniello 2019, Lecture #1, minutes 56-57).
To determine whether selenium deficiency was a specific link to the coxsackievirus, Beck et al. (2003) injected the influenza virus into selenium-deficient mice and mice fed with adequate amounts of selenium. As we should expect, the selenium-deficient mice had more severe pathology, more inflammatory distress, and produced more T-cells, antibodies, and hormones when they developed the respiratory infection.
Consider that the viruses associated with pneumonia and other types of respiratory distress are different. In human populations, we generally see respiratory ailments with flu-like symptoms, and/or pneumonia, during the winter months. Additionally, we see respiratory illness in persons depleted of an essential antioxidant, selenium. That is, they are suffering from oxidative stress when exposed to the pathogen.
Deficiency in Cuba
Going back to Beck et al. (2003), because their investigation into Keshan disease attributed the ailment to both selenium deficiency and a virus [sic], the team wanted to bolster their thesis with a case study. They provided some discussion about the relationship between said virus and selenium, in another part of the world—Cuba.
During a period of severe nutritional deficit in Cuba (1989-1993), doctors found a rash of patients developing optic and peripheral neuropathy (Beck et al. 2003). The Cuban doctors discovered that their sick patients had oxidative stress due to selenium deficiency, and 84% had some mutated form of coxsackievirus. And the outbreaks occurred in the winter months when vitamin D3 blood-levels would be lowest (Beck et al. 2003).
Just putting these few sources together, we know that:
people get sick in winter
a virus is not essential to the formation of an illness or disease.
More significantly, neither specific viruses nor any distinct diseases have a link to selenium deficiency. Selenium is an antioxidant. And when we raise our antioxidant levels and reduce oxidative stress, we can stay infection-free. Ergo, the key to beating or avoiding pneumonia, a cold, the flu, or any respiratory ailment, is to consume adequate amounts of selenium and vitamin C.
Other important nutrients to take as supplements are vitamins A, E, and K, B-complex, magnesium, and zinc.
Conquer COVID Craziness—and Encourage Others Too
The last time I took a class at a university was spring 2001. Since that time, I’ve been enjoying the benefits of my virtual university—the Internet. Over the last 20 years, I have heard lectures from professors and researchers on radio, podcasts, and YouTube. We now have access to millions of peer-reviewed articles, books, and historical accounts. I studied the best that our information age can offer. I learn from Drs. Viera Scheibner, Gary Null, Sherri Tenpenny, Thomas Levy, Rashid Buttar, Sherry Rogers, Nick Gonzales, Leonard Coldwell, Linus Pauling, Fred Klenner, Toni Bark, William Kelley, and many more.
But I have not just absorbed their information, I have used their work as a jumping-off point to do further research … and you can too.
The allopaths either do not know or do not care about nutrition (just ask Allan Smith). There is a general awareness of the intellectual laziness of American physicians. I have observed this after interactions with Western-trained doctors from South Africa, India, and the Middle East, the arrogance of their ignorance is endemic.
From my survey of the current news, if you are in America or Europe, all you hear is that the best doctors can offer is hydroxychloroquine, antivirals or a future vaccine. But from the research, we can see that, instead of their pharmaceutical drugs (which can mask symptoms, but does not cure), what we all need is selenium-rich food (or whole food supplements) and high doses of vitamin C.
Can We Get Back To Normalcy?
There will always be people with viruses and respiratory difficulties. They will be suffering from oxidative stress—and that is NOT contagious. The numbers will rise in the winter when there is less sun. Less sun lowers vitamin D3 levels and reduces the absorption of phosphorous. Additionally, people are more likely to eat more starchy foods and get less vitamin C in their diet.
This is why we hear of members of Congress, professional athletes in NBA, NHL, and world-class soccer players testing positive for COVID. These people were not in China, not eating bat soup, and not sharing ventilators with older people in Italian ICU wards. They did not contract an exogenous virus—their bodies made the virus due to oxidative stress. In fact, spontaneous endogenous generation of viruses, referred to by some as exosomes, would explain why Beck et al. (2003) discovered mutated and more virulent strains of the coxsackievirus in their selenium-depleted mice. They also discovered these strains in human subjects with low selenium. This also notes why researchers are forever finding new and mutated versions of viruses.
Regardless, as Del Bigtree (2020) showed from the European data (minutes 80-90), in the winter of 2018, death rates across Europe were far higher than today—but there was no declaration of an epidemic or pandemic, and there was no global shut down.
No Fear of the Unknown
This is not a time to accept economic stagnation and the social dislocation that will accompany it. It is not a time to fear that which you cannot see (a virus)—especially given that no medical doctor has ever proven that said viruses cause illness. (I will present more on the virus theory in future articles).
Get your Vitamin C, selenium, and zinc, wash your hands to prevent bacterial infection and tell your friends to do the same.
Vitamin B1 Is Vital to Protect Against Infectious Disease
Thiamine (vitamin B1) deficiency syndrome (beriberi) has many similarities to sepsis — a primary cause of COVID-19 mortality — and thiamine deficiency is relatively common in critically ill patients in general
Thiamine deficiency is prevalent in pulmonary tuberculosis, and the more severe the case, the more severe the thiamine deficiency. Thiamine has been shown to limit Mycobacterium tuberculosis by regulating your innate immunity
Thiamine deficiency is also associated with the development of high fever, and some researchers have suggested that serious infections may in fact be a presenting manifestation of thiamine deficiency
Clinical case reports have shown thiamine injections reversed a number of acute illnesses in which high fever was a factor, including one case where the patient presented with high fever, headache and asphyxia, and another where the patient had high fever and severe pneumonia
Thiamine is required for metabolism of some of the metabolites of vitamin C. Vitamin C also works synergistically with corticosteroids, which helps explain why the Marik Sepsis Protocol is so effective. Magnesium may also be important, as it is required for the activation of thiamine
While a limited number of drugs have been enlisted in the treatment of severe coronavirus (SARS-CoV-2) infection, a number of nutritional supplements have risen to the forefront for their apparent usefulness. In addition to quercetin, zinc and vitamins C and D, vitamin B1 (thiamine) may be vital to protect against infectious respiratory illness.
Thiamine is also part of Dr. Paul Marik’s sepsis treatment, which calls for 1,500 milligrams (mg) of intravenous ascorbic acid every six hours, 200 mg of thiamine every 12 hours and 50 mg of hydrocortisone every six hours.1
Sepsis, as you may have heard, is a major contributor in influenza deaths in general, and a primary cause for COVID-19 deaths specifically. In one clinical trial,2,3 Marik, a critical care doctor at Sentara Norfolk General Hospital in East Virginia, showed his treatment reduced sepsis-related mortality nearly fivefold.
More recent research,4,5 published online January 9, 2020, found Marik’s sepsis protocol lowered mortality in pediatric patients as well. At the 30-day mark, controls and the hydrocortisone-only groups had a mortality rate of 28% while the treatment group had a mortality rate of just 9%.
Vitamin C, Thiamine and Steroids Have Synergistic Effects
All three ingredients in Marik’s sepsis protocol have synergistic effects, which seems to be why it’s so effective. Vitamin C is well-known for its ability to prevent and treat infectious diseases on its own.
Influenza,6 encephalitis and measles7 have all been successfully treated with high-dose vitamin C, and previous research has shown it effectively lowers proinflammatory cytokines and C-reactive protein.8,9,10
Vitamin C and corticosteroids, however, have been shown to work synergistically. This was demonstrated in a study11 by Marik in collaboration with John Catravas, Ph.D., a pharmacology researcher at Old Dominion University, and others, in which endothelial cells from lung tissue were exposed to lipopolysaccharide — a type of endotoxin found in patients with sepsis — in the absence or presence of ascorbic acid and hydrocortisone.
Interestingly, when either vitamin C or the steroid was administered in isolation, very little improvement in endothelial barrier function occurred. When administered together, however, the infection was successfully eradicated and the cells were restored to normal.
The addition of thiamine (vitamin B1) is also important. Not only is thiamine required for metabolism of some of the metabolites of vitamin C, thiamine deficiency syndrome (beriberi) has many similarities to sepsis, and thiamine deficiency is relatively common in critically ill patients.12
As noted in a 1955 study,13 thiamine deficiency is also prevalent in pulmonary tuberculosis, and the more severe the case, the more severe the thiamine deficiency.
Studies have also shown thiamine can be helpful for a long list of diseases and disorders, including mitochondrial disorders,14 heart failure,15 delirium,16 thyroid fatigue and Hashimoto’s (a thyroid autoimmune disorder).17 These and other health effects may help explain why thiamine works so well in conjunction with vitamin C and hydrocortisone for sepsis.
Thiamine Deficiency Implicated in Severe Infections
Thiamine deficiency has also been implicated in severe infections specifically. A 2016 study18 in the journal Psychosomatics sought to investigate this by looking at 68 patients with Korsakoff syndrome, a memory disorder caused by severe thiamine deficiency.
While thiamine deficiency is often the result of alcohol misuse, it’s also associated with chronic infections, poor nutrition and/or malabsorption. As explained by the Alzheimer’s Association, “Thiamine helps brain cells produce energy from sugar. When levels fall too low, brain cells cannot generate enough energy to function properly.”19
In the Psychosomatics study, they found that 35 of 68 Korsakoff patients suffered severe infections during the acute phase of the illness, including meningitis, pneumonia and sepsis. According to the authors, “Infections may be the presenting manifestation of thiamine deficiency.”
Thiamine Helps Regulate Your Immune Function
Another study20 published in 2018 found thiamine helps limit Mycobacterium tuberculosis (MTB) by regulating your innate immunity. According to this paper:
“… vitamin B1 promotes the protective immune response to limit the survival of MTB within macrophages and in vivo through regulation of peroxisome proliferator-activated receptor γ (PPAR-γ).
Vitamin B1 promotes macrophage polarization into classically activated phenotypes with strong microbicidal activity and enhanced tumor necrosis factor-α and interleukin-6 expression at least in part by promoting nuclear factor-κB signaling.
In addition, vitamin B1 increases mitochondrial respiration and lipid metabolism and PPAR-γ integrates the metabolic and inflammatory signals regulated by vitamin B1 … We demonstrate that vitamin B1 enhances anti-MTB activities in macrophages and in vivo by down-regulating PPAR-γ activity.
Our data demonstrate important functions of thiamine VB1 in regulating innate immune responses against MTB and reveal novel mechanisms by which vitamin B1 exerts its function in macrophages.”
The Link Between Thiamine Deficiency and Fever
Thiamine deficiency is also associated with the development of high fever, and according to a letter to the editor,21 “Is Parenteral Thiamin a Super Antibiotic?” published in the Annals of Nutrition & Metabolism in 2018, thiamine injections are “likely to eradicate microbial infections” causing the fever.
The authors cite some clinical case reports in which thiamine injections were able to reverse a number of acute illnesses in which high fever was a factor, including one case where the patient presented with high fever, headache and asphyxia (feelings of suffocation), and another where a comatose patient had high fever and severe pneumonia.
“… another laborer with much milder pneumonia, 38°C fever with few rales in the left lung died within 24 h, although a full dose of penicillin G was used, but no thiamin was given,” the authors note.
“This sharp contrast between the two cases made such a deep impression that it was strongly remembered. Fifty-six years later, it became a life-saving suggestion for a critical case with fatal viral pneumonia.”
The authors go on to detail an even more remarkable case involving a 38-year-old Chinese woman who was brought to the hospital with high fever (39 to 40 degrees C), pain, swollen legs and bloody sputum. Laboratory testing showed she was anemic and had low platelets, severe pneumonia, femoral thromboses and heart failure. She also tested positive for hepatitis C.
“An exhaustive identification study revealed that the pathogen of her pneumonia was diagnosed to be an unknown kind of virus,” the authors note. “Pulmonary lesions were extremely severe, strange, and rare with multiple small perforations in the left lung …
After 12 days of immunoglobulin, anti-viral, antithrombotic, and antipyretic medication, she was about to die when her family promptly carried her home … At home, thiamin 200 mg and VB complex 1 ampule (containg thiamin 10 mg, riboflavin 2 mg, niacinamide 30 mg, pyridoxin 2 mg, pantothenic acid 1 mg) were injected thrice daily.
Temperature returned to normal after 2 days and leg edema disappeared in 5 days … After 58 days, she was checked in the Beichen Hospital … The results revealed a normal heart; hepatitis C negative … less effusion in the left thoracic cavity; pleural thickness especially on the left side but no adhesion. Lung perforation was absent … She thereafter enjoyed excellent health without any sign of embolism or pneumonia recurrence.”
About 10 months after her initial hospitalization, she underwent a second follow-up, which revealed normal blood counts and electrocardiography. Her lungs also looked completely normal on X-rays, “with no thickening or adhesion of pleura except for a few texture thickenings in the lungs.”
According to the authors, this case made them wonder whether thiamine might be “a super antibiotic.” “It seemed to be surely so and was emerging to be a powerful alternative in the event of antibiotics failing,” they said.
Thiamine Deficiency Might Impact Pandemics
The World Health Organization has also published information about the importance of thiamine and how to prevent deficiency during major emergencies.22 According to WHO:
“Thiamine deficiency occurs where the diet consists mainly of milled white cereals, including polished rice, and wheat flour, all very poor sources of thiamine. Thiamine deficiency can develop within 2-3 months of a deficient intake and can cause disability and death.”
Other evidence suggests thiamine insufficiency or deficiency can develop even faster than that, perhaps as quickly as two weeks, as its half-life in your system is only nine to 18 days.23
The WHO report also points out that “Thiamine deficiency occurs sporadically in people who are socially isolated, suffer loss of appetite and self-neglect” — a point that is particularly pertinent in current circumstances of global “shelter in place” requirements. What’s more:
“The requirement of thiamine is increased when carbohydrates are taken in large amounts and is raised during periods of increased metabolism, for example, fever, muscular activity, hyperthyroidism and also during pregnancy and lactation. A diet based on polished rice is high in carbohydrates which augments the thiamine requirement and is compounded by a low thiamine content.”
Aside from rice, junk food of all kinds tends to be loaded with carbohydrates as well, which could necessitate a higher-than normal thiamine intake to prevent side effects of thiamine deficiency. In adults, thiamine deficiency is divided into two primary types:24,25
Dry beriberi (thiamine deficiency with peripheral neuropathy) — Polyneuropathy with paraesthesia of the extremities (especially the legs), reduced knee jerk and other tendon reflexes, progressive severe weakness and wasting of muscles, and greatly increased susceptibility to infections.
Web beriberi (thiamine deficiency with cardiomyopathy) — Edema (especially of the legs, but also the trunk and face), high cardiac output, ventricular failure, sinus rhythm, dilatation of arterioles, depressed erythrocyte and leukocyte transketolase, elevated serum lactate and pyruvate, and pulmonary congestion with pleural effusions; death from congestive heart failure may occur abruptly.
By dramatically increasing susceptibility to infections, thiamine deficiency could potentially have the ability to impact the spread of just about any pandemic infectious disease.
The Importance of Thiamine in Septic Shock
With regard to sepsis — which is a primary reason why people die from COVID-19 — thiamine may be of vital importance. In a Journal of Thoracic Disease article with the evocative title, “Do Not Forget to Give Thiamine to Your Septic Shock Patient!” the authors stress that:26
“[Thiamine] is a water-soluble vitamin that is an indispensable constituent of cellular metabolism. A lack of this vitamin can, therefore, be potentially life-threatening … Thiamine diphosphate, also known as thiamine pyrophosphate (TPP) … is the most important and active form of this vitamin …
Thiamine pyrophosphate … acts in concomitance with magnesium to expedite various mitochondrial oxidative decarboxylation reactions.
Thiamine pyrophosphate is necessary as a cofactor for branched-chain ketoacid dehydrogenase complex essential for the metabolism of the branched-chain amino acids and for two critical complexes required for the mitochondrial synthesis of adenosine triphosphate (ATP): pyruvate and 2-oxoglutarate dehydrogenase (α-ketoglutarate) complexes …
Also, TPP serves as a coenzyme for transketolase, a cytosolic enzyme implicated in the pentose phosphate pathway that functions in maintaining cell redox status through the production of NADPH (reduced nicotinamide adenine dinucleotide phosphate) and glutathione …
Lack of thiamine leads to alterations in intermediate metabolism that end-up in lactic acidosis …
Thiamine deficiency is also prevalent in septic shock patients, with rates ranging from 20% to 70% depending on the cutoff value used to define the presence of thiamine deficiency. Lack of thiamine reduces the flux of pyruvate to the Krebs cycle, thus increasing lactate production by altering the aerobic metabolism.
In a prospective, observational study, Donnino et al. investigated the relationship between thiamine levels and lactic acidosis in 30 septic shock patients …
After excluding patients with abnormal liver function tests, the authors observed a significant negative correlation between thiamine concentrations and lactic acidosis, implying a potential association between thiamine levels and lactic acidosis in septic shock patients with normal liver function.
Thus, the possibility that by decreasing the activity of pyruvate dehydrogenase complex, thiamine deficiency can contribute to increased production of lactic acid in critically ill septic patients exists.”
The authors cite additional research strongly suggesting “the administration of thiamine is advantageous in septic shock patients with severe thiamine deficiency (thiamine level ≤7 nmol/L).” Considering the safety of thiamine, even at high doses, the authors stress that “septic shock patients should be given thiamine … without waiting for the results of thiamine level.”
The European Society for Clinical Nutrition and Metabolism guidelines for patients in intensive care situations are 100 to 300 mg of thiamine per day “during the first three days in the ICU for all patients with suspected thiamine deficiency.”27
In cases of septic shock, however, dosages of 500 mg may be required. According to “Do Not Forget to Give Thiamine to Your Septic Shock Patient!”:28
“Because anaphylaxis has been reported in rare instances, guidelines in the United Kingdom have recommended that thiamine should be administered over 15- to 30-minute interval in a mixture of saline solution or dextrose, with the intention of averting potential adverse reactions.”
Vitamins C, D, Thiamine and Magnesium for Critical Illness
A 2018 report29 in Intensive Care Medicine also focuses on thiamine — here in conjunction with vitamins C and D. It cites research showing septic shock patients with thiamine deficiency who were given thiamine had far lower mortality (13%) than those who did not receive it (46%).30 They were also far less likely to suffer kidney failure.
Like thiamine, acute vitamin C deficiency is very common during critical illness yet tends to go unnoticed. As noted in this report, “Acute vitamin C deficiency may contribute to hypotension, exaggerated inflammation, capillary leakage, microcirculatory compromise, oxidative organ injury, and impaired immune defense and wound healing.”
Vitamin D deficiency is also common, and can worsen illness and increase the risk of death from acute illness. According to the authors of this report:
“Preliminary data using novel methods suggest that glutathione and glutamate pathway metabolism, which are important for redox regulation and immunomodulation, are affected by vitamin D status …
The VITdAL-ICU study (n = 475) did not find a difference in the length of hospital stay between groups, but there was a significant reduction in mortality in the predefined subgroup of patients with severe vitamin D deficiency. The most recent meta-analysis concludes that vitamin D in the ICU may be associated with mortality reduction.”
Surprisingly, magnesium has not been given much, if any, attention in all this. It may be just as important for the prevention and treatment of infection, however, seeing how magnesium is required for the activation of both thiamine31 and vitamin D.32,33,34
Published Research and Articles on Vitamin C as a Consideration for Pneumonia, Lung Infections, and the Novel Coronavirus (SARS-CoV-2/COVID-19)
by Graham Player, PhD, Andrew W. Saul, Damien Downing, MBBS, MRSB and Gert Schuitemaker, PhD
(OMNS Mar 22, 2020) In 1936 Gander and Niederberger found that vitamin C lowered fever and reduced pain in pneumonia patients. Also in 1936, Hochwald independently reported similar results. In 1946 Slotkin further reported that “Vitamin C has been used routinely by the general surgeons in the Millard Fillmore Hospital, Buffalo, as a prophylactic against pneumonia, with complete disappearance of this complication.”
It is one thing to be sick from a virus and another thing entirely to die from a viral-instigated disease. A 1994 randomised double-blind trial involving vitamin C/placebo supplementation was conducted on 57 elderly patients admitted to hospital with acute respiratory infections (bronchitis and bronchopneumonia). Using a clinical scoring system based on major symptoms of the respiratory condition, patients supplemented with the vitamin fared significantly better than those on placebo. This was particularly the case for those commencing the trial most severely ill, many of whom had very low plasma and white cell vitamin C concentrations on admission.
Vitamin C supports your immune system. Vitamin C helps to kill viruses and reduces the symptoms of infection. It’s not a COVID-19 “cure,” but nothing is. It might just save your life, though, and will definitely reduce the severity of the infection. If someone tells you it’s not proven, consider two things:
Nothing is proven to work against COVID-19, because it is a new virus
Vitamin C has worked against every single virus including influenzas, pneumonia, and even poliomyelitis.
In the medical literature, there are more than 64,000 published articles and studies on Vitamin C available at The U.S. National Library of Medicine National Center for Biotechnology Information. Vitamin C is arguably one of the most researched substances in existence. Much of the research is very positive. Ignorance of the research, benefits and use of Vitamin C is not a valid excuse for it not to be used as a therapy, particularly when there are no other known medications available, and it is not likely to cause damage, and the published research is readily accessible for everybody.
Following is a brief selection of articles and research from the medical literature that are educational and helpful in considering the use of Vitamin C.
(Graham Player, PhD, is a member of the Royal Society of Medicine, UK and member of the American Academy of Anti-Aging Medicine. He currently resides in Hong Kong. Andrew W. Saul is Editor-in-Chief of the Orthomolecular Medicine News Service. He co-founded it in 2005 with Drs. Abram Hoffer and Hugh D. Riordan. Drs. Damien Downing and Gert Schuitemaker are both long-time members of the Orthomolecular Medicine News Service Editorial Review Board.)
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness.
For more information: http://www.orthomolecular.org
(OMNS February 10, 2020) Most deaths from coronavirus are caused by pneumonia. Vitamin C has been known, for over 80 years, to greatly benefit pneumonia patients.
In 1936 Gander and Niederberger found that vitamin C lowered fever and reduced pain in pneumonia patients. [1]
Also in 1936, Hochwald independently reported similar results. He gave 500 mg of vitamin C every ninety minutes. [2]
McCormick gave 1000 mg vitamin C intravenously, followed by 500 mg orally every hour. He repeated the injection at least once. On the fourth day, his patient felt so well that he voluntarily resumed work, with no adverse effects. [3]
In 1944 Slotkin and Fletcher reported on the prophylactic and therapeutic value of vitamin C in bronchopneumonia, lung abscess, and purulent bronchitis. “Vitamin C has greatly alleviated this condition and promptly restored normal pulmonary function.” [4]
Slotkin further reported that “Vitamin C has been used routinely by the general surgeons in the Millard Fillmore Hospital, Buffalo, as a prophylactic against pneumonia, with complete disappearance of this complication.” [5]
According to the US Centers for Disease Control, there are about 80,000 dead from annual influenzas, escalating to pneumonia, in the USA. Coronavirus is a very serious contagious disease. But contagion to a virus largely depends on the susceptibility of the host. It is well established that low vitamin C levels increase susceptibility to viruses. [6]
Vitamin C lowers mortality
It is one thing to be sick from a virus and another thing entirely to die from a viral-instigated disease. It must be emphasized that a mere 200 mg of vitamin C/day resulted in an 80% decrease in deaths among severely ill, hospitalized respiratory disease patients. [7]
“Vitamin C is effective in reducing duration of severe pneumonia in children less than five years of age. Oxygen saturation was improved in less than one day.”[10]
A single, cheap, big-box discount store vitamin C tablet will provide more than twice the amount used in the study above.
And yes, with vitamin C, more is better.
Frederick R. Klenner and Robert F. Cathcart successfully treated influenza and pneumonia with very high doses of vitamin C. Klenner published on his results beginning in the 1940s; [8] Cathcart beginning in the 1960s. [9] They used both oral and intravenous administration.
A recent placebo controlled study concluded that “vitamin C should be included in treatment protocol of children with pneumonia so that mortality and morbidity can be reduced.” In this study, the majority of the children were infants under one year of age. By body weight, the modest 200 mg dose given, to tiny babies, would actually be the equivalent of 2,000-3,000 mg/day for an adult. [10]
Although many will rightly maintain that the dose should be high, even a low supplemental amount of vitamin C saves lives. This is very important for those with low incomes and few treatment options.
We’re talking about twenty cents’ worth of vitamin C a day to save lives now.
References:
1. Gander and Niederberger. Vitamin C in the handling of pneumonia.” Munch. Med. Wchnschr., 31: 2074, 1956.
2. Hochwald A. Beobachtunger fiber Ascorbinsaure Wirkung bei der Krupposen Pneumonia.” Wien. Arch. f. inn. Med., 353, 1936.
4. Slotkin & Fletcher. Ascorbic acid in pulmonary complications following prostatic surgery.” Jour. Urol., 52: Nov. 6, 1944.
5. Slotkin GE. Personal communication with WJ McCormick. December 2, 1946.
6. Saul AW. Nutritional treatment of coronavirus. Orthomolecular Medicine News Service, 16:6, Jan 30, 2020. http://orthomolecular.org/resources/omns/v16n06.shtml (22 references and 50 recommended papers for further reading)
7. Hunt C et al. The clinical effects of Vitamin C supplementation in elderly hospitalised patients with acute respiratory infections. Int J Vitam Nutr Res 1994;64:212-19. https://www.ncbi.nlm.nih.gov/pubmed/7814237
8. Klenner FR. Observations on the dose and administration of ascorbic acid when employed beyond the range of a vitamin in human pathology. J Applied Nutrition 1971, 23:3&4. http://www.doctoryourself.com/klennerpaper.html
Klenner, FR. (1951) Massive doses of vitamin C and the virus diseases. J South Med and Surg, 113:101-107.
Klenner, FR. (1971) Observations on the dose and administration of ascorbic acid when employed beyond the range of a vitamin in human pathology. J. App. Nutr., 23:61-88.
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, M.D. (Australia)
Richard Cheng, M.D., Ph.D. (USA)
Prof. Gilbert Henri Crussol (Spain)
Carolyn Dean, M.D., N.D. (USA)
Damien Downing, M.D. (United Kingdom)
Michael Ellis, M.D. (Australia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Michael Janson, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Dave McCarthy, M.D. (USA)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Dag Viljen Poleszynski, Ph.D. (Norway)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, MD (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Robert G. Smith, Ph.D. (USA), Associate Editor
Helen Saul Case, M.S. (USA), Assistant Editor
Michael S. Stewart, B.Sc.C.S. (USA), Technology Editor
Jason M. Saul, JD (USA), Legal Consultant
Hospital-based Intravenous Vitamin C Treatment for Coronavirus and Related Illnesses
When you go to the hospital, bring along a big red pen, and cross out anything that you don’t like in the hospital’s permission form. And before you sign it, add anything you want. Write out “I want intravenous vitamin C, 25 grams per day, until I state otherwise.” And should they say, “We’re not going to admit you,” you reply, “Please put it in writing that you refuse to admit me.” What do you think their lawyers are going to do with that? They have to admit you. It’s a game, and you can win it. But you can’t win it if you don’t know the rules. And basically, they don’t tell you the rules.
(OMNS February 2, 2020) No matter which hospital a coronavirus patient may seek help from, the question is, Will they be able to leave walking out the front door, or end up being wheeled out the basement backdoor? Prompt administration of intravenous vitamin C, in high doses, can make the difference.
Abundant clinical evidence confirms vitamin C’s effectiveness when used in sufficient quantity. [1]
Physicians have demonstrated the powerful antiviral action of vitamin C for decades. [2]
Specific instructions for intravenous vitamin C
The Japanese College of Intravenous Therapy (JCIT) recommends intravenous vitamin C (IVC) 12.5/25g (12,500 – 25,000 mg) for acute viral infections (influenza, herpes zoster, common cold, rubella, mumps, etc.) and virus mimetic infections (idiopathic sudden hearing loss, Bell’s palsy). In adults, IVC 12.5g is given for early stage illness with mild symptoms, and IVC 25g for moderate to severe symptoms. IVC is usually administered once or twice a day for 2-5 continuous days, along with or without general treatments for viral infections.
IVC 12.5g cocktail
Sterile water
125 mL
50% Vitamin C
25 mL (12. 5g)
0.5M Magnesium sulfate
10 mL
Add Vitamin B complex
Drip for 30-40 min
IVC 25g cocktail
Sterile water
250 mL
50% Vitamin C
50 mL (25g)
0.5M Magnesium sulfate
20 mL
Add Vitamin B complex
Drip for 40-60 min
Patients with acute viral infections show a depletion of vitamin C and increasing free radicals and cellular dysfunction. Such patients should be treated with vitamin C, oral or IV, for neutralizing free radicals throughout the body and inside cells, maintaining physiological functions, and enhancing natural healing. If patients progress to sepsis, vitamin C should be added intravenously as soon as possible along with conventional therapy for sepsis.
Toronto Star, 30 May 2003: “Fred Hui, MD believes that administering vitamin C intravenously is a treatment worth trying. And he’d like to see people admitted to hospital for the pneumonia-like virus treated with the vitamin intravenously while also receiving the usual drugs for SARS. ‘I appeal to hospitals to try this for people who already have SARS,’ says Hui. Members of the public would also do well to build up their levels of vitamin C, he says, adding that there is nothing to lose in trying it. ‘This is one of the most harmless substances there is,’ Hui states. ‘There used to be concern about kidney stones, but that was theoretical. It was never borne out in an actual case.’ Hui says he has found intravenous vitamin C effective in his medical practice with patients who have viral illnesses.”[3]
Additional administration details are readily obtained from a free download of the complete Riordan Clinic Intravenous Vitamin C Protocol. [4] Although initially prepared for cancer patients, the protocol has found widespread application for many other diseases, particularly viral illnesses.
“Research and experience has shown that a therapeutic goal of reaching a peak-plasma concentration of ~20 mM (350- 400 mg/dL) is most efficacious. (No increased toxicity for posoxidant IVC plasma vitamin C levels up to 780 mg/dL has been observed.) . . . [T]he administering physician begins with a series of three consecutive IVC infusions at the 15, 25, and 50 gram dosages followed by post IVC plasma vitamin C levels in order to determine the oxidative burden for that patient so that subsequent IVCs can be optimally dosed.”
Pages 16-18 of the Riordan protocol present IVC administration instructions.
“Given the rapid rate of success of intravenous vitamin C in viral diseases, I strongly believe it would be my first recommendation in the management of corona virus infections.”
(Victor A. Marcial-Vega, MD)
Puerto Rico
“It is of great importance for all doctors to be informed about intravenous vitamin C. When a patient is already in hospital severely ill, this would be the best solution to help save her or his life.”
(Karin Munsterhjelm, MD)
Finland
Winning the hospital game
When faced with hospitalization, the most powerful person in the most entire hospital system is the patient. However, in most cases, the system works on the assumption that the patient will not claim that power. If on your way in you signed the hospital’s legal consent form, you can unsign it. You can revoke your permission. Just because somebody has permission to do one thing doesn’t mean that they have the permission to do everything. There’s no such thing as a situation that you cannot reverse. You can change your mind about your own personal healthcare. It concerns your very life. The rights of the patient override the rules of any institution.
If the patient doesn’t know that, or if they’re not conscious, or if they just don’t have the moxie to do it, the next most powerful person is the spouse. The spouse has enormous influence and can do almost as much as the patient. If the patient is incapacitated, the spouse can, and must, do all the more. If there is no spouse present, the next most powerful people in the system are the children of the patient.
When you go to the hospital, bring along a big red pen, and cross out anything that you don’t like in the hospital’s permission form. And before you sign it, add anything you want. Write out “I want intravenous vitamin C, 25 grams per day, until I state otherwise.” And should they say, “We’re not going to admit you,” you reply, “Please put it in writing that you refuse to admit me.” What do you think their lawyers are going to do with that? They have to admit you. It’s a game, and you can win it. But you can’t win it if you don’t know the rules. And basically, they don’t tell you the rules.
This is deadly serious. Medical mistakes are now the third leading cause of death in the US. Yes, medical errors kill over 400,000 Americans every year. That’s 1,100 each day, every day. [5]
There are mistakes of commission and mistakes of omission. Failure to provide intravenous vitamin C is, literally, a grave omission. Do not allow yourself or your loved ones to be deprived of a simple, easy to prepare and administer IV of vitamin C.
“If a family member of mine died due to coronavirus infection, after a doctor refused to use intravenous vitamin C, I would challenge his or her treatment in a court of law. I would win.” (Kenneth Walker, MD, surgeon)
It can be done
Vitamin IVs can be arranged in virtually any hospital, anywhere in the world. Attorney and cardiologist Thomas E. Levy’s very relevant presentation is free access.
Both the letter and the intent of new USA legislation now make this easier for you.
“The new federal Right to Try Act provides patients suffering from life-threatening diseases or conditions the right to use investigational drugs… It amends the Food, Drug, and Cosmetic Act to exempt investigational drugs provided to patients who have exhausted approved treatment options and are unable to participate in a clinical trial involving the drug. Advocates of right to try laws have sought to accelerate access to new drugs for terminally ill patients who are running out of options. Arguably, the law does not represent a radical change in this and several other states, however, because in 2016, California had already joined the majority of other states in adopting a law enabling physicians to help terminally ill patients pursue investigational therapies, without fear of Medical Board or state civil or criminal liability. . . The new Right to Try law should give physicians, as well as drug manufacturers, some added comfort about FDA enforcement in these cases.”[8]
Therefore, in regards to intravenous vitamin C, do not accept stories that “the hospital can’t” or “the doctor can’t” or that “the state won’t allow it.” If you hear any of this malarkey, please send the Orthomolecular Medicine News Service the text of the policy or the law that says so. In the meantime, take the reins and get vitamin C in the veins.
Mikirova N, Hunninghake R. (2014) Effect of high dose vitamin C on Epstein-Barr viral infection. Med Sci Monit. 20:725-732. https://www.ncbi.nlm.nih.gov/pubmed/24793092. “The clinical study of ascorbic acid and EBV infection showed the reduction in EBV EA IgG and EBV VCA IgM antibody levels over time during IVC therapy that is consistent with observations from the literature that millimolar levels of ascorbate hinder viral infection and replication in vitro.”
Gonzalez MJ, Berdiel MJ, Duconge J, Levy TE, Alfaro IM, Morales-Borges R, Marcial-Vega, V, Olalde J. (2018) High Dose Vitamin C and Influenza: A Case Report. J Orthomol Med. 33(3) https://isom.ca/article/high-dose-vitamin-c-influenza-case-report/ “Based on the positive outcome in this case, we propose that Intravenous Vitamin C should be studied as a vital component of the treatment protocol for acute viral infections.”
Murata A. (1975) Virucidal activity of vitamin C: Vitamin C for the prevention and treatment of viral diseases. Proceedings of the First Intersectional Congress of Microbiological societies, Science Council of Japan, 3:432-42.
Note: The Japanese College of Intravenous Therapy (JCIT) was founded in 2007. JCIT has organized educational seminar on intravenous nutrient therapy and integrative medicine for 13 years. JCIT now consists of 850 active members of physician and dentists. Every year, the College organizes 10 or more educational seminars with protocols for intravenous vitamin C therapy, mainly along with the Riordan Protocol, for patients with acute and chronic diseases. More than 2500 physicians in Japan have learned these protocols, and patients can easily find member’s clinics all over Japan. In addition, JCIT recommends that physicians stock extra vitamin C vials in case of a pandemic. The JCIT website (Japanese language only): https://www.iv-therapy.org
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, M.D. (Australia)
Prof. Gilbert Henri Crussol (Spain)
Carolyn Dean, M.D., N.D. (USA)
Damien Downing, M.D. (United Kingdom)
Michael Ellis, M.D. (Australia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Michael Janson, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Dave McCarthy, M.D. (USA)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Dag Viljen Poleszynski, Ph.D. (Norway)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, MD (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Robert G. Smith, Ph.D. (USA), Associate Editor
Helen Saul Case, M.S. (USA), Assistant Editor
Michael S. Stewart, B.Sc.C.S. (USA), Technology Editor
Jason M. Saul, JD (USA), Legal Consultant
(OMNS January 29, 2020) The ability of properly-dosed vitamin C before and after a vaccination to block any potential short- and long-term toxic side effects while enhancing the antibody-forming aim of the injection was covered in an earlier OMNS article. [1] The points made in that article, along with their validation in the scientific literature, remain pertinent 8 years later. As emphasized in that article, the purpose of this article is not to praise or condemn the administration of vaccinations. Most who know me know my stance on this issue, coming from what I consider to be a purely scientific perspective. But that is not the purpose of this article.
Even the most ardent of vaccine supporters should be able to admit that vaccinations, however infrequently, sometimes result in an undesired outcome on the health status of the recipient. The “argument” then shifts as to whether the chance of such an outcome is so rare as to be reasonably and permissibly ignored. The pro-vaccine community maintains that population-wide vaccinations confer a high degree of protection against even more morbidity and mortality that would otherwise be inflicted by the diseases or conditions for which the vaccines are being given. However, here I emphasize the need for mitigation of the side effects of vaccination.
To fully appreciate the toxic origins of all disease, it is very important to understand the critical roles played by vitamin C and other major antioxidants in counteracting and minimizing the impact of new toxin exposures and old toxin damage. All toxins, whether originating from an infection, food or water intake, or environmental source, or even as an unintended consequence of a vaccination, inflict their damage on the body by directly or indirectly causing the oxidation of critical biomolecules in the body. When biomolecules are oxidized (depleted of electrons), they lose some or all of their natural chemical roles throughout the body and inside the cells. Essentially, oxidation inactivates the natural physiological role of a biomolecule.
Biomolecules include proteins, sugars, fats, enzymes, nucleic acid, or structural molecules. Depending on the chemical nature of a given toxin, it will oxidize a unique array of biomolecules, varying in location, concentration, and degree. These are the primary factors that determine the resulting clinical medical condition. And the presence of sufficient antioxidants can either prevent this oxidation from taking place by directly donating electrons to the electron-seeking toxins, or it can repair the toxin-oxidized biomolecules by contributing electrons back to them (reduction). However, it essential to realize that the oxidized state of the biomolecules is the disease, or toxicity. There is no additional ill-defined “disease” that is impacting the cells and tissues with the increased numbers of oxidized biomolecules. Once enough biomolecules are restored to the reduced state, “disease” no longer exists. [2]
With this concept of the etiology of all diseases in mind, it can then be appreciated that any potential toxic side effect of a vaccination (or any other toxin exposure) can literally always be blocked or rapidly repaired by counterbalancing it with sufficient levels of antioxidants (primarily vitamin C). When this is combined with the established concept that vitamin C is essential for a fully competent immune system capable of producing an optimal antibody response to an antigen presented by a vaccination, it is only logical that optimizing the vitamin C status of a baby, child, or adult (as with influenza vaccinations) should always be an essential clinical goal.
Numerous articles in the mainstream medical literature clearly indicate that the infectious diseases for which vaccinations are given are effectively prevented by vitamin C. [1-3] Furthermore, when vitamin C levels are low in the body, infectious diseases are effectively eradicated by vitamin C-centered protocols (that can include other anti-pathogen interventions). [1-5]
The pharmaceutical industry makes billions of dollars on selling vaccinations and continuing to develop new vaccines for different conditions in an ongoing basis. However, in the current environment of politics, big business, and the law, such billion-dollar businesses will arguably never lose. They also will never be minimized and their profits will never be substantially decreased. Such businesses have many congressmen and senators owing them for campaign contributions, along with many judges as well. Furthermore, most of those politicians and members of the judicial system actually believe that opposing vaccinations is tantamount to opposing the most significant intervention available supporting optimal public health. Many of us understand how much this enrages those who are convinced that vaccinations are doing a great deal of harm.
With all of these issues in mind, the overriding concern is how to protect as many babies, children, and adults from any possibility of a negative vaccine side effect. Even if, say, 10 years from now the scientific community finds that some vaccines are doing more harm than good and largely eliminates them, how many more lives (and families) will have been devastated in the meantime? Whether autism ever results from vaccination is actually not the primary issue. The issue is how to protect the infants that will be vaccinated today. All old and new evidence of any vaccination-induced toxicity should continue to be revisited and given its due publicity. But protection needs to take place now.
Also, while it will likely displease most of the anti-vaccination community, a successful vitamin C-centered vaccine-protection protocol will make the vaccine manufacturers look like the good guys. Very few individuals will sustain side effects, and the vaccine companies will ultimately be given credit for making “better and safer” vaccines, and they will ultimately make more money rather than less. However, and this cannot be overemphasized, the vaccine damage will drop, and even largely disappear. The immediate protection of everyone’s health has to be the top priority.
My personal recommendations for an effective program of toxin protection with optimization of a vaccine antibody response are as follows:
Start the supplementation at least 7 days before a planned vaccination (the longer, the better since everyone at any age should regularly supplement vitamin C). This regimen should be followed as well on the day of vaccination and continued for at least one week following the vaccination. However, it will be best to continue the recommended vitamin C dosing for life. [1-5]
For infants and very young children, 1,000 mg of liposome-encapsulated vitamin C. This can readily be mixed in a flavored yogurt or other favorite baby food. This higher dose is possible relative to the sodium ascorbate powder below since liposomes only rarely cause the loose bowel effect seen with higher doses of vitamin C. Liposomes also allow a much better intracellular uptake of vitamin C to occur.
When liposome-encapsulated vitamin C is not available, proceed with sodium ascorbate powder (this can also be done in addition to the liposome form for even better protection). Infants under 10 pounds can be given 500 mg daily in a favorite juice (just a salty taste). For infants between 10 and 20 pounds, this can be increased to as much as 1,000 mg daily, in divided doses. Very roughly, the daily amount of non-liposome-encapsulated vitamin C can be increased by 1,000 mg per year of life.
Magnesium chloride can significantly augment the anti-toxin and pro-immune effect of vitamin C. [6,7] Mix 25 grams in a quart of water. Depending on body size, give 1 TBSP to 1/2 cup (15 to 125 ml) of this solution at least once and preferably twice daily in the days leading up to vaccination. As with vitamin C, the solution is salty (and a little bitter) and to be palatable is best diluted further in juice.
Vitamin D3 and zinc supplementation can also afford additional benefits. Again, depending on body size, 1,000 to 25,000 units of D3 can be given daily. These doses should not be continued in small children beyond a week after the vaccination. However, D3 is a valuable supplement, and it is of value for everyone. Long-term dosing requires validation that the regularly administered dose is raising the blood level to the range of 50 to 100 ng/ml. 10 to 50 mg of zinc (as zinc gluconate or other well-absorbed form) daily can be given by pill or drops for the week before and the week after vaccination. Long-term supplementation with zinc (and D3) should be done in concert with the advice of your integrative physician.
Finally, if a vaccination simply can’t wait, taking the recommended doses of vitamin C, magnesium chloride, vitamin D3, and zinc the same day or just following the vaccination, and continuing for several weeks can also offer enormous protection. The above regimen simply aims to help optimize the protection being provided.
An addendum regarding a practical treatment approach to coronavirus, currently at epidemic levels in China:
If the virus is actually as contagious as is being currently asserted, modern air travel and the purported time of incubation and asymptomatic status (about 2 weeks) means it can spread anywhere on the planet. As with nearly all other contagious viruses, spread is most commonly due to airborne virus in microdroplets from sneezing, coughing, and the exhalation of infected individuals. Similarly, when the virus gets on the hands in a sufficient amount, touching the nose, eyes, and mouth can initiate the process of transmission as well.
The measures that most readily inhibit transmission include regular hand washing or sanitizing, containment of the microdroplets with high virus concentration (protective masks), and avoidance of areas with multiple infected individuals. And even when these measures do not completely block the transmission of virus, they massively decrease the amount of viral exposure, and a strong immune system will often do the rest.
A strong immune system is really the only significant protection an individual has, unless, of course, an individual can completely eliminate the possibility of virus exposure, which is virtually impossible.
A great deal of immune system strength, possibly most of it, comes from the vitamin C content in the immune cells. When the levels of vitamin C in the body are low, the immune system can never function at full capacity. There are many measures that can strengthen and support the immune system, but regular supplementation of vitamin C with multi-gram doses (2,000 mg daily or more) is probably the single most important preventive measure. Much larger doses can be given if it is determined that the virus has already been contracted. If IV vitamin C is available, this is optimal. But always take as much as can be afforded and tolerated, in both liposome-encapsulated form and sodium ascorbate powder and by intravenous administration.
Follow the magnesium chloride regimen discussed above, but take the recommended doses four times daily during a time of active infection.
The virus grows rapidly in the mucosa of the naso- and oropharynx. It is this quickly-growing “reservoir” of virus that continues to feed the viral presence throughout the body and sustain the infected state. Nebulization with 3% hydrogen peroxide quickly destroys all or most of this source of virus, and the body, with the help of vitamin C and magnesium, can then “mop up” the rest of the virus and rapidly accelerate clinical resolution. This is arguably the MOST IMPORTANT intervention to rapidly eradicate any systemic viral infection. Also, if available, ozone treatments of the blood can further accelerate the clinical resolution of infections such as the coronavirus.
Note:
By way of disclosure, I am a paid consultant to LivOn Labs. I am only comfortable recommending their liposome-encapsulated products, including vitamin C. Although “liposome” products are available from a variety of other vendors, many contain no liposomes at all. Also, contrary to popular belief, there are no liposomes in many homemade versions of “liposome” vitamin C. (See my article https://www.peakenergy.com/articles/nh20140411/Exposing-the-truth-about-liposomal-nutrients)
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, M.D. (Australia)
Prof. Gilbert Henri Crussol (Spain)
Carolyn Dean, M.D., N.D. (USA)
Damien Downing, M.D. (United Kingdom)
Michael Ellis, M.D. (Australia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Michael Janson, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Dave McCarthy, M.D. (USA)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Dag Viljen Poleszynski, Ph.D. (Norway)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, MD (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Robert G. Smith, Ph.D. (USA), Associate Editor
Helen Saul Case, M.S. (USA), Assistant Editor
Michael S. Stewart, B.Sc.C.S. (USA), Technology Editor
Jason M. Saul, JD (USA), Legal Consultant
Vitamin C Protects Against Coronavirus
Vitamin C Protects Against Coronavirus
by Andrew W. Saul, Editor
Orthomolecular Medicine News Service, Jan 26, 2020
(OMNS January 26, 2020) The coronavirus pandemic can be dramatically slowed, or stopped, with the immediate widespread use of high doses of vitamin C. Physicians have demonstrated the powerful antiviral action of vitamin C for decades. There has been a lack of media coverage of this effective and successful approach against viruses in general, and coronavirus in particular.
It is very important to maximize the body’s anti-oxidative capacity and natural immunity to prevent and minimize symptoms when a virus attacks the human body. The host environment is crucial. Preventing is obviously easier than treating severe illness. But treat serious illness seriously. Do not hesitate to seek medical attention. It is not an either-or choice. Vitamin C can be used right along with medicines when they are indicated.
“I have not seen any flu yet that was not cured or markedly ameliorated by massive doses of vitamin C.”
(Robert F. Cathcart, MD)
The physicians of the Orthomolecular Medicine News Service and the International Society for Orthomolecular Medicine urge a nutrient-based method to prevent or minimize symptoms for future viral infection. The following inexpensive supplemental levels are recommended for adults; for children reduce these in proportion to body weight:
Vitamin C: 3,000 milligrams (or more) daily, in divided doses.
Vitamin D3: 2,000 International Units daily. (Start with 5,000 IU/day for two weeks, then reduce to 2,000)
Magnesium: 400 mg daily (in citrate, malate, chelate, or chloride form)
Zinc: 20 mg daily
Selenium: 100 mcg (micrograms) daily
Vitamin C [1], Vitamin D [2], magnesium [3], zinc [4], and selenium [5] have been shown to strengthen the immune system against viruses.
The basis for using high doses of vitamin C to prevent and combat virus-caused illness may be traced back to vitamin C’s early success against polio, first reported in the late 1940s.[6] Many people are unaware, even surprised, to learn this. Further clinical evidence built up over the decades, leading to an anti-virus protocol published in 1980.[7]
It is important to remember that preventing and treating respiratory infections with large amounts of vitamin C is well established. Those who believe that vitamin C generally has merit, but massive doses are ineffective or somehow harmful, will do well to read the original papers for themselves. To dismiss the work of these doctors simply because they had success so long ago sidesteps a more important question: Why has the benefit of their clinical experience not been presented to the public by responsible governmental authorities, especially in the face of a viral pandemic?
Gorton HC, Jarvis K (1999) The effectiveness of vitamin C in preventing and relieving the symptoms of virus-induced respiratory infections. J Manip Physiol Ther, 22:8, 530-533. https://www.ncbi.nlm.nih.gov/pubmed/10543583
Yejin Kim, Hyemin Kim, Seyeon Bae et al. (2013) Vitamin C is an essential factor on the anti-viral immune responses through the production of interferon-α/β at the initial stage of influenza A virus (H3N2) infection. Immune Netw. 13:70-74. https://www.ncbi.nlm.nih.gov/pubmed/23700397.
Ginde AA, Mansbach JM, Camargo CA Jr. (2009) Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med. 169:384-390. https://www.ncbi.nlm.nih.gov/pubmed/19237723.
Martineau AR, Jolliffe DA, Hooper RL et al. (2017) Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 356:i6583. https://www.ncbi.nlm.nih.gov/pubmed/28202713.
Urashima M, Segawa T, Okazaki M et al. (2010) Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr. 91:1255-60. https://www.ncbi.nlm.nih.gov/pubmed/20219962.
von Essen MR, Kongsbak M, Schjerling P et al. (2010) Vitamin D controls T cell antigen receptor signaling and activation of human T cells. Nat Immunol. 11:344-349. https://www.ncbi.nlm.nih.gov/pubmed/20208539.
Dean C. (2017) The Magnesium Miracle. 2nd Ed., Ballantine Books. ISBN-13: 978-0399594441.
Levy TE (2019) Magnesium: Reversing Disease. Medfox Pub. ISBN-13: 978-0998312408
4. Zinc:
Fraker PJ, King LE, Laakko T, Vollmer TL. (2000) The dynamic link between the integrity of the immune system and zinc status. J Nutr. 130:1399S-406S. https://www.ncbi.nlm.nih.gov/pubmed/10801951.
Liu MJ, Bao S, Gálvez-Peralta M, et al. (2013) ZIP8 regulates host defense through zinc-mediated inhibition of NF-кB. Cell Rep. 3:386-400. https://www.ncbi.nlm.nih.gov/pubmed/23403290.
Mocchegiani E, Muzzioli M. (2000) Therapeutic application of zinc in human immunodeficiency virus against opportunistic infections. J Nutr. 130:1424S-1431S. https://www.ncbi.nlm.nih.gov/pubmed/10801955.
Shankar AH, Prasad AS. (1998) Zinc and immune function: the biological basis of altered resistance to infection. Am J Clin Nutr. 68:447S-463S. https://www.ncbi.nlm.nih.gov/pubmed/9701160.
Steinbrenner H, Al-Quraishy S, Dkhil MA et al. (2015) Dietary selenium in adjuvant therapy of viral and bacterial infections. Adv Nutr. 6:73-82. https://www.ncbi.nlm.nih.gov/pubmed/25593145.
7. Cathcart RF. The method of determining proper doses of vitamin C for treatment of diseases by titrating to bowel tolerance. Australian Nurses J 1980, 9(4):9-13. http://www.doctoryourself.com/titration.html
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, M.D. (Australia)
Prof. Gilbert Henri Crussol (Spain)
Carolyn Dean, M.D., N.D. (USA)
Damien Downing, M.D. (United Kingdom)
Michael Ellis, M.D. (Australia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Michael Janson, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Dave McCarthy, M.D. (USA)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Dag Viljen Poleszynski, Ph.D. (Norway)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, MD (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Robert G. Smith, Ph.D. (USA), Associate Editor
Helen Saul Case, M.S. (USA), Assistant Editor
Michael S. Stewart, B.Sc.C.S. (USA), Technology Editor
Jason M. Saul, JD (USA), Legal Consultant
Here is what modern medicine did to quash the compelling though preliminary data showing vitamin C saves lives of sepsis patients.
The biggest study yet published, in the Journal of the American Medical Association no less, utilized 46 “end points” (measures) to assess whether vitamin C is effective in the treatment of sepsis. The study involved 167 vitamin C-treated sepsis patients from seven intensive care units in the U.S.
The study concluded, based upon the un-weighted measures, that vitamin C is ineffective. In their own words, study evaluators concluded “there was no significant difference between vitamin C and placebo-treated patients.”
Markers of organ failure, inflammation, blood clotting, number of days in the intensive care unit and hospital readmissions, were not improved. But the most important measure, mortality, plummeted (from 46.3% in the placebo group to 29.8% in the vitamin C-treated group)! The researchers didn’t rank mortality over less consequential markers of disease.
An analytical article written at NPR.org said doctors “were interested in blood test results while patients are concerned whether they live or die.” What reviewers won’t say is that the study was designed to fail, designed to overlook the importance of mortality over all other measured factors of sepsis. In spite of the fact none of the many clinical measurements associated with better outcomes explain why vitamin C-treated patients are more likely to survive suggests the important of vitamin C as a life saver. Vitamin C vanquished the mortal consequences of sepsis despite insignificant changes in other markers.
When a man has fallen overboard on a ship into icy waters, if physicians pull him out of the water and measure his blood pressure, heart rate, body temperature, level of inflammation, and level of stress hormones, they will likely be abnormal, but the simple fact is, throwing a life preserver to save the drowning man would be a life-saving intervention regardless of any of those other numbers. The same is true for vitamin C.
Sepsis is the major cause of death in hospitals by far
Sepsis is the number one reason why patients die in hospitals today. Sepsis accounts for ~52% of hospital deaths, above cancer (16%) and heart failure (7%). Sepsis is a bloodstream infection, involving any bacterium or virus, which often occurs among patients who have a weakened immune system and is accompanied by other diseases such as cancer, heart or lung disease, among patients that are in the intensive care unit of the hospital because of their life-threatening condition.
Their blood pressure is low. Their kidneys aren’t functioning normally. Urine flow is nil. Breathing is difficult. Body temperature falls. Blood doesn’t clot effectively. The sepsis patient is often in a state of mental delirium (confusion). In other words, patients in septic shock are helpless to even help themselves. Multiple organ failure is common.
The stand-out statistic from Dr. Marik’s study is that none (zero) of the vitamin C-treated sepsis patients died of sepsis in the intensive care unit, they were transferred to general nursing units where some succumbed to their lung, heart or malignant diseases! The positive published result is overwhelming.
While modern medicine drags its feet, a pooled analysis of the three small studies that employed vitamin C in the treatment of sepsis concluded “the evidence is stronger than first thought” that vitamin C results in a marked reduction in mortality.
Yet, there is no question that sepsis patients are, as a group, severely deficient in vitamin C, a shortage that is in need of correction. Intravenous vitamin C therapy has been safely used since the 1970s.
In an editorial published in Critical Care journal, Mr. Marik’s title is pointed: “Doctor – your septic patients have scurvy!” It’s not just the sepsis patients who have scurvy in the intensive care unit, 50% of the non-sepsis patients have vitamin C levels that are so low as to be classified as scurvy too!
Dr. Marik writes that clinicians “would undoubtedly be shocked to learn that about 40% of the patients in their intensive care unit with septic shock have serum levels of vitamin C supporting a diagnosis of scurvy.” So scurvy is the true definition of sepsis, induced by increased demand rather than a shortage of intake of vitamin C.
Dr. Marik writes: “These astonishing revelations are not new. It has been known for over two decades that acute illness results in an acute deficiency of vitamin C.” An unwelcome development is that in acute disease, a key vitamin C transporter is reduced, which limits delivery of vitamin C when given orally. Oral absorption of vitamin C is hindered too. Therefore, intravenous vitamin C is required.
Dr. Tom Levy MD, author of Curing The Incurable, says “sepsis is when you have two or three molecules of vitamin C left in your body in the presence of any infection. In the final stage of almost any disease you die of scurvy because disease increases demand for this essential vitamin.”
How many lives could be saved with vitamin C therapy?
Let’s do some guesstimating. Some 19 million people worldwide which includes 1.7 million Americans, are diagnosed with sepsis annually. The mortality rate for hospital-treated sepsis cases is 34.7%. Dr. Marik’s small study brought the overall mortality rate down to 8.5%.
About 6,593,000 sepsis patients worldwide and 589,900 sepsis patients in the U.S. die annually due to this bloodstream infection. It appears a regimen of vitamin C + vitamin B1 and cortisone (steroid) would reduce those numbers to 1,615,000 worldwide and 114,500 in the U.S. annually. By extrapolation of Dr. Marik’s data, close to 5 million (4,978,000) lives worldwide and close to a half-million (475,400) lives in the U.S. could be saved annually by intravenous +B1 + cortisone therapy.
The 19 million worldwide sepsis figure is lacking data from lower income countries. By extrapolation of data from high-income countries, global incidence and death from sepsis may be much higher (31.5 million and 5.3 million deaths).
Modern medicine has done a good job of throwing vitamin C therapy under the rug. Its use threatens the modern model of developing patentable synthetic drugs to conquer disease.
The demand for double-blind placebo-controlled studies is unethical when it comes to sepsis. Patients receiving placebo would essentially be left to die. Historically, it should be noted that penicillin, insulin, digoxin, aspirin, acetaminophen, nitroglycerin all came into common use without controlled studies.
Intravenous vitamin C reduces absolute, not relative risk, from 40 in 100 to zero in 100. The number of sepsis patients that need to be treated to save one life is 1. With vitamin C therapy deaths occur after discharge from the intensive care unit and are due to other causes. Yet medical skeptics argue over the safety and effectiveness of vitamin C (??). Potentially the lives of all 1.7 million hospitalized cases of sepsis can be saved (100% survival from sepsis), but some (~8.5%) will die of other diseases (overall survival).
The clock is ticking. Every hour another 57 Americans die of sepsis in the hospital. The remaining question is not whether vitamin C will be proven to save lives of sepsis patients but whether our overseers will allow this to happen.

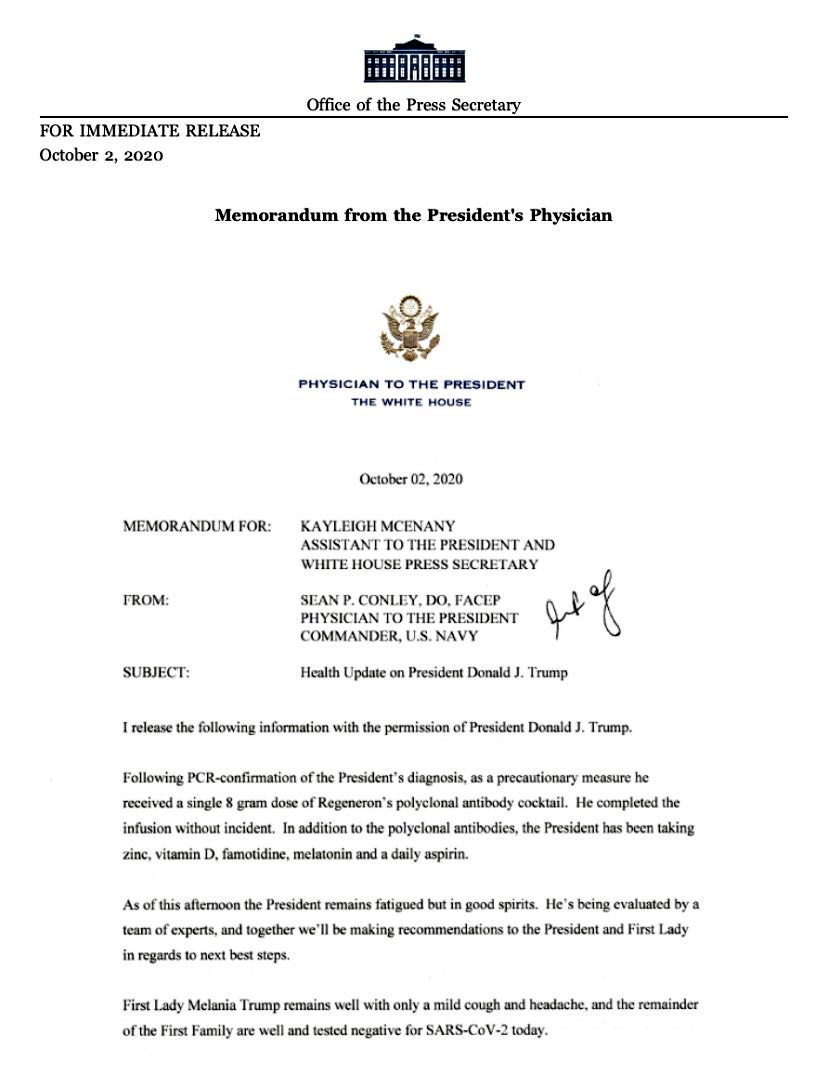



 His resistance wasn’t out there.
His resistance wasn’t out there.