Lies passed around like conjured pieces of gold. Medical liars speaking their messages with straight faces, from their pulpits of influence.
We’ve watched them work. We’ve experienced the inner sensation of blood boiling; outrage.
Who are these people? Where did they come from? How did they attain their positions of power? Are they a different species?
And like you, I have watched the passive faces of audiences as they take in these lies, as they know something is wrong, as they refuse to act.
If you control the meaning of words like “evidence,” “cause,” “relationship between,” you own the playing field. You can manipulate outcomes and conclusions, and you can define science itself.
Your power derives from ownership of those simple words.
Suppose a healthy baby with all his faculties intact receives a barrage of vaccines at 15 months. Then, three days later, his temperature soars to 105, he has seizures, he screams, and then he goes silent. He withdraws from the world, from his parents. In the ensuing months, he doesn’t speak. He doesn’t laugh. He shows no interest in life around him. He doesn’t recover from this. He doesn’t regain his former health.
In what sense can it be said that the vaccines caused his condition? That may seem like an absurd question to be asking, but scientists claim it is important. So do judges and government officials. So do drug companies who make and sell vaccines.
They claim it’s very important, because they want to maintain control over the concept of “cause.” It’s their protection in the racket they are running.
Can we track the path, step by step, of these vaccine ingredients as they are injected into a baby and make their way through his system? Can we observe every reaction they produce, in sequence, all the way into and through the recesses of the nervous system and the brain?
Of course not.
By such an impossible standard, everyone falls short.
If perverse officials and scientists suddenly invoke that standard, can anyone fulfill it? No.
But make sure you understand that scientists and bureaucrats judge their own work by far looser principles.
They assert, for example, with psychotic arrogance that the underlying cause of autism is in the genes, although their research has only given them the foggiest of reasons for even beginning to crawl out on that limb—where they crow and lie and ask for more research money.
They say ADHD is created by certain brain abnormalities, even though their scans produce on-again off-again evidence—which, finally, is no evidence at all.
In fact, for every one of the 297 so-called mental disorders that are named and defined and described in the official bible of psychiatric literature, there is not one, not one lucid diagnostic test to back up, biologically, their disease labels and descriptions and definitions.
It’s a game. “We may hold you to an impossible standard. We hold ourselves to no standard at all.”
So you should be aware that, if you choose to enter this game, for whatever reasons, you are playing against a monumentally stacked deck.
The powers-that-be will do everything they can to subvert, deny, and destroy THE STORY OF ONE PARENT ABOUT ONE CHILD.
Why? Because the story is too convincing. It’s too obvious. It’s too real. It’s too DEVASTATING. It’s too dangerous.
“My child was healthy. He was vaccinated. Then he collapsed. He never recovered.”
With that, you are setting dynamite on the rails of the medical princes.
And you are also waking up other parents whose stories are essentially the same. You are igniting a fire in their heads.
Can you imagine what would happen if you said, “Look, my child was hit by a cluster of vaccines delivered when he was fifteen months old, and he was never the same after that, and THAT is what I’m seeking compensation for, and that is ALL I’m seeking compensation for. I don’t care what you call it, what name you give to it.”
And the government said, “Well, all right.”
The ensuing flood would drown them. And would drown the vaccine manufacturers, too.
You must be stopped.
And the way they will stop you is by manipulating the word “cause.” That’s all. That’s their entire policy and program. They execute it on an arcane and pseudo-technical level, employing models and constructs and numbers in their private little universe, while they polish their credentials.
They don’t want YOUR STORY to stand naked in front of the public.
Of course it is obvious that, when health turns to tragedy, the vaccines were at fault, just as when a blow to the head causes memory loss. Of course everyone concerned knows the truth.
But they say: science is not done this way. We must have “evidence of causation.” They occasionally throw a few crumbs to parents whose child was brain-damaged by a vaccine. But in the main, they conjure up a version of pseudo-science and use it to obfuscate the otherwise unpardonable reality of what the vaccine has done.
And how does this conjured and manufactured science work?
It starts with the owned and operated definition of a disease or disorder. In the case of autism, the old behavioral criteria are dragged out. Here they are. I’m sorry for loading the full display on you, but I want you to see it in print:
The following is from Diagnostic and Statistical Manual of Mental Disorders: DSM IV
(I) A total of six (or more) items from (A), (B), and (C), with at least two from (A), and one each from (B) and (C)
(A) qualitative impairment in social interaction, as manifested by at least two of the following:
1. marked impairments in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body posture, and gestures to regulate social interaction
2. failure to develop peer relationships appropriate to developmental level
3. a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people, (e.g., by a lack of showing, bringing, or pointing out objects of interest to other people)
4. lack of social or emotional reciprocity ( note: in the description, it gives the following as examples: not actively participating in simple social play or games, preferring solitary activities, or involving others in activities only as tools or “mechanical” aids )
(B) qualitative impairments in communication as manifested by at least one of the following:
1. delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime)
2. in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others
3. stereotyped and repetitive use of language or idiosyncratic language
4. lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level
(C) restricted repetitive and stereotyped patterns of behavior, interests and activities, as manifested by at least two of the following:
1. encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
2. apparently inflexible adherence to specific, nonfunctional routines or rituals
3. stereotyped and repetitive motor mannerisms (e.g hand or finger flapping or twisting, or complex whole-body movements)
4. persistent preoccupation with parts of objects
(II) Delays or abnormal functioning in at least one of the following areas, with onset prior to age 3 years:
(A) social interaction
(B) language as used in social communication
(C) symbolic or imaginative play
(III) The disturbance is not better accounted for by Rett’s Disorder or Childhood Disintegrative Disorder
And now you have the full and complete definition of autism from the official manual. There is no other definition. There are no physical tests or blood tests or brain scans. There is only this menu of behaviors.
And there are many so-called related disorders, and each one has its similar complex behavioral definition. These depictions overlap. But no matter. As far as the psychiatrists and pediatricians and medical bureaucrats are concerned, autism is defined. Engraved on tablets.
Does, in the judgment of a doctor, your child fit the definition or doesn’t he? The word is given from on high. The decision is rendered. And we are then one step removed from the reality of the simple and brutal destroying effects of the vaccines. This is good for them. They are now in familiar territory. Protected land.
Now they can say, “Your child, who at fifteen months collapsed, has autism.”
This is the bridge to the next giant step. Which is:
“We have determined that vaccines are not the cause of autism.”
“We know this.”
“We have proved this.”
Therefore, you’re trapped. Your child has been painted with the label “autism”–and perhaps you were actually hoping for that, because you knew something was terribly wrong, and the designation confirms you were correct. But as far as making a link to the vaccines, you’re suddenly at their mercy.
If they decide to compensate you through the federal vaccine compensation system, they will say, “Well, your child actually is suffering from encephalopathy and has autism-like symptoms.” But far more frequently, they will fall back on their pronouncement that vaccines and autism are unconnected, and you will get nothing.
How did these medical experts and their bureaucratic partners determine that vaccines are not the cause of autism?
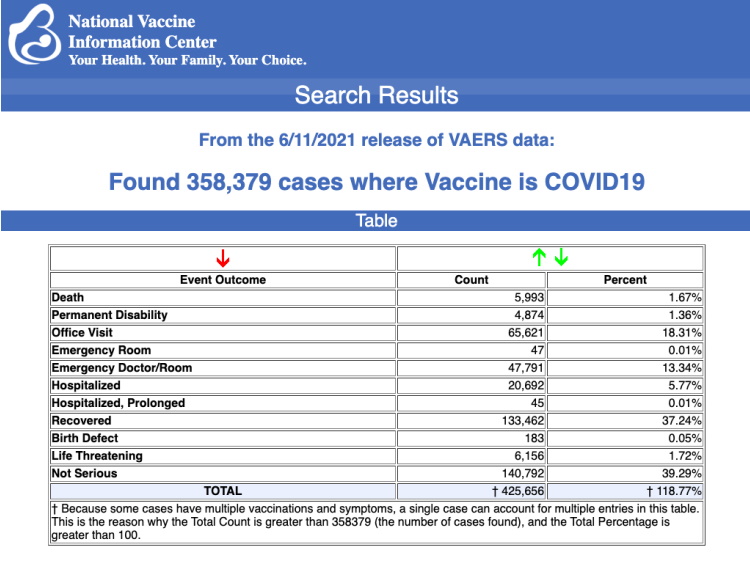
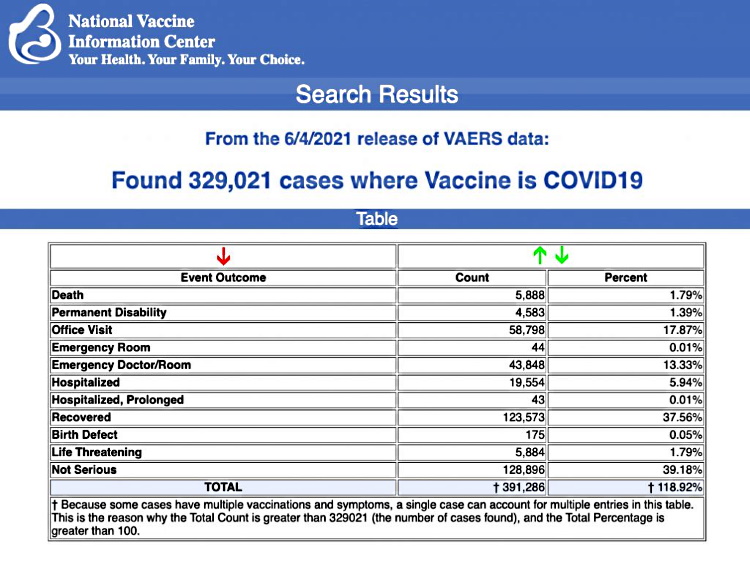
They examined studies. And the studies “found no link.” In particular, there is the key Verstraeten study, published in two phases. Three HMOs’ records of babies were considered by Verstraeten and his colleagues.
I’m going to quote from the study and then comment:
“Results. In phase I at HMO A, cumulative exposure at 3 months resulted in a significant positive association with tics (relative risk [RR]: 1.89; 95% confidence interval [CI]: 1.05–3.38). At HMO B, increased risks of language delay were found for cumulative exposure at 3 months (RR: 1.13; 95% CI: 1.01–1.27) and 7 months (RR: 1.07; 95% CI: 1.01–1.13). In phase II at HMO C, no significant associations were found. In no analyses were significant increased risks found for autism or attention-deficit disorder.”
“Conclusions. No consistent significant associations were found between TCVs and neurodevelopmental outcomes. Conflicting results were found at different HMOs for certain outcomes. For resolving the conflicting findings, studies with uniform neurodevelopmental assessments of children with a range of cumulative thimerosal exposures are needed.”
First of all, notice how far away we are from that basic fact that vaccines were delivered to your child and your child collapsed and never recovered. We are miles from that. We’re now discussing correlations between vaccines containing mercury (thimerosal) and various indicators and labels: tics, language delay, autism, attention-deficit disorder, neurodevelopmental outcomes.
We now have a complex situation. First of all, in order to conclude that mercury-containing vaccines are correlated with autism or attention-deficit disorder, the researchers would have to have observed, in these children’s medical records, reports detailing all the behavioral criteria THE RESEARCHERS ASSUME add up to a positive diagnosis of these two INVENTED disorders—neither of which even exists on the basis of actual biological or chemical tests of any kind.
So essentially, if we make the translation from psychiatric-speak to basic English, we have this: “There is no convincing correlation between mercury-containing vaccines and those disorders we invented by slicing and dicing human behavior into compartments and giving them disease-labels.”
This is staggering when you think about it.
Continuing: In the first HMO records, Verstraeten and his colleages found a significant correlation between the vaccines and tics. As in facial tics. Why is that important? Because tics can be a sign of motor brain damage. They have a name for that: tardive dyskinesia. But it means brain damage.
However, if you look at the concocted definitions of the concocted disorders called autism and ADD, you’ll find no mention of tics or tardive dyskinesia. Therefore, an increased risk of tics doesn’t bring the researchers any closer to connecting vaccines and autism—simply because autism wasn’t defined that way. It wasn’t invented that way.
Perusing the records at the second HMO, Verstraeten found an increased risk of language delay. The babies didn’t start speaking when normally expected to. This is one of the listed criteria for a diagnosis of autism, but of course it is not enough, by the concocted rules of the game, to rate a placing of the invented label, autism, on any of those children.
At the third HMO, which was investigated as a separate phase 2 of the study, researchers found no significant associations—meaning no tics, no language delay…nothing that would rate a diagnosis of autism or suggest the presence of any of the invented symptoms of autism.
All in all, Verstraeten and his colleagues found no reason to conclude that mercury-containing vaccines were correlated with autism or other signals of neurological problems.
He played off one HMO against another: “In this one, we found X. But in the other one, we didn’t. We found Y instead. And in the third one, we found neither X nor Y.” Why didn’t he simply use all three HMOs as one reservoir? Possibly because he was trying to guard against the possibility of biased records at one HMO. Who knows?
And why didn’t he conclude, “All in all, we discovered some evidence of harm from the vaccines.”
Again, notice how far we are from the actual event of vaccines causing brain damage in a child.
The study decides that there is no increased risk, from vaccines, for autism or ADD. And that’s that. “Further research” is needed.
A child harmed by vaccines could have a tiny brain lesion or severe immune deficiency or a rewired connection somewhere deep in the recesses of the brain—undetected—but none of this matches up to the invented criteria for a diagnosis of autism.
But millions of people actually believe that autism is a distinct entity which was “discovered,” like a pre-set embedded pattern of errant pathways in the brain. And when those people are told, by experts, that vaccines don’t cause it, the PR value is enormous. For doctors who give the vaccines, for drug companies, for public-health agencies.
This is all a ruse. It’s a fabrication, and the studies that follow from it serve to mask the facts of vaccine damage.
They invent define the disorder, they have no definitive diagnostic tests for it, they conclude that vaccines don’t cause it. It’s one fantasy after another.
It’s as if you drew a map of a gold mine that doesn’t exist, and then you passed a law forbidding people from searching for it.
There are various degrees and events of tragic and lasting impact-damage that are laid upon children. The causes are multiple. One significant cause is vaccines. There is no such thing as autism. It is a construct ultimately designed to get certain people off the hook. And to make profit. And to engender money for research.
They will never find a cure for autism, because it doesn’t exist, except as a menu of behaviors wrapped inside their fantasy. Of course, if they were in the world, the world you live in, they would acknowledge that vaccines do cause brain and neurological damage, and they would compensate for that. They would act in a straightforward and honest fashion.
I spoke to one psychiatrist off the record, who said, “A genetic cause for autism? Are you serious? Autism is an artifact to begin with. So how do you find a gene that causes a fairy tale?”