As the FDA looks into the known data from #Covid19 trials, we take a look at the ten biggest unknowns, including the duration of protection, effectiveness against mortality, and the vaccine’s effectiveness against transmission of the virus.
Our vaccination programs are not based on complete science of the ingredients or long term health impacts. Our children have been suffering as a consequence. CDC and other agencies are now pushing for increased adult vaccination schedules. Their goal is pre-cradle to grave vaccination for all.
And none of it is has a foundation in science. All of it ignores the concerning independent studies about risks, and all of it ignores the current understanding of human immunity and the symbiotic relationships that support it.
Recently, a landmark study was conducted by Dr. James Lyons-Weiler and Dr. Paul Thomas. The study compared vaccinated children and unvaccinated children and was published in the International Journal of Environmental Research and Public Health on November 22, 2020 after being peer reviewed.
Dr. Weiler, a research scientist and co-author of the study, was recently interviewed by Activist Post Contributor Spiro Skouras. In the interview, Weiler breaks down the data from the study which indicates children who were vaccinated showed a higher rate of medical office visits and experienced an elevated rate of medical symptoms ranging from Asthma and behavioral issues, to ADHD and Anemia.
In this report, Spiro interviews Dr. Paul Thomas, a prominent pediatrician in Portland, Oregon who also co-authored the study and used 10+ years of data from his medical practice to conduct the study.
Shortly after the vaccinated versus unvaccinated study was published, five days in fact, the Oregon State Medical Board held an emergency meeting declaring that Dr. Paul was an immediate threat to his patients and the public and suspended his medical license.
In this must-see interview, Dr. Paul addresses the accusations leveled against himself and his practice, in addition to breaking down in detail the study’s findings. Dr. Paul also weighs in on the CDC recommended vaccine schedule and the experimental Covid vaccine.
Video available at Spiro Skouras YouTube and BitChute channels.
The only way to deal with an unfree world is to become so absolutely free that your very existence is an act of rebellion.” ~ Albert Camus
While loyalty to self and truth is not slavery, allegiance to any country, government, or ruling class is slavery. Inherent in this thinking is the fact that believing or trusting any ruling individual or entity without absolute verification at every level, is the basis for societal destruction at the hands of the few due to blind obedience to falsely claimed authority. Lies and deceit are the tools of tyrants, and come in the forms of outright deception to manipulative propaganda. These traits are always evident, but today they are completely overt, as lies and truth are both used in devious ways in order to gain compliance and control.
This can be seen in that a non-existent virus pandemic has been used to instill great fear in the unsuspecting minds of the masses to such an extent, that most have been willing to give up all normalcy and sanity in their lives and the lives of their families. They have due to false trust been duped into behavior that can only be described as psychotic in nature. This has led to voluntary self-imprisonment, isolation, business and job destruction, mask wearing, travel immobilization, and total lockdowns. It has led to greater sickness, death, and economic devastation as well, all in the name of ‘health security’ and obedience to power at the expense of all freedom. This should serve as the final valuable lesson learned by even the most common of men, because it should be obvious that relying on the state in any capacity whatsoever can only lead to an enslaved society dependent on a master class for its very existence and survival. This of course is what is sought; a communistic based technocratic ‘civilization’ controlled by the few.
Everything that happens with governments and the entire state apparatus is planned in advance. Nothing concerning the ruling class is organic or natural in any way. All action and reaction to any event by the government and its controllers is by design. Most everything that happens has been foretold or predicted by the state oligarchic perpetrators. This is usually done by very deceptive means meant either to create a false crisis, or to use indoctrination methods in order to plant in the minds of the people what to expect from some imagined future adversary or terrifying event that has already been devised or created. These tactics of course are psychological in nature, but if the psyche of the majority can be captured to such an extent as to cause the proper desired reaction, then they can be easily controlled. In a world of logic and reason, this current situation should serve as definitive proof of this hypothesis, but sadly, I doubt that any such mass revelation by the people at large will be forthcoming. I base this on Einstein’s statement that doing the same thing over and over again while expecting a different outcome is insanity. This seems to sum up the mentality of the American herd.
This analysis can be supported easily by history, and that may be part of the reason that our real history is being hidden and destroyed every single day at this juncture. This is happening through censorship of course, but also through the physical destruction of historical records including books, the closing off of access to original sources, and elimination of important factual information in every form imaginable.
This current hoax is nothing new, as similar events have happened before, and have been played out over and over again in real life and in staged table top exercises meant to condition the public for future planned actual incidents. This was a way to set up, to promote, and to prepare the public for events that could be used to alter society and change the common mindset from one of individual liberty to one of collective compliance. Of course, this change began very long ago, but it has escalated beyond imagination over the past two decades, and in this past year alone, the idea of a society based on total voluntary servitude has seemingly come to fruition. It is all a set up!
In 2001, an exercise called “Dark Winter,” a favored term of Joe Biden about our current situation, was set up by Johns Hopkins and others to simulate a covert smallpox attack on the U.S., and to see what a government response might look like under those circumstances.
In 2005, “Atlantic Storm,” was organized by the Center for Biosecurity at the University of Pittsburgh Medical Center. This was a simulation about an international smallpox outbreak that turned into a pandemic.
In 2010, a Rockefeller Foundation paper called Lock Step, analyzed a scenario as to how governments would respond with authoritarian measures to react to a worldwide flu pandemic. This is very similar to what is happening today. “During the pandemic, national leaders around the world flexed their authority and imposed airtight rules and restrictions, from the mandatory wearing of face masks to body-temperature checks at the entries to communal spaces like train stations and supermarkets.”
In 2017, a novel coronavirus outbreak was simulated in Minnesota. This exercise was called “The SPARS Pandemic 2025-2028,” and comprised a futuristic scenario that illustrated communication dilemmas concerning medical countermeasures (MCMs) that could plausibly emerge in the not-so-distant future.
The next exercise in August of 2019 was a Trump administration and Health and Human Services major exercise called Crimson Contagion. This simulation was almost identical to the Covid-19 plot today. “It tried to model what would happen if an influenza pandemic that started in China spread through the U.S. with no treatment, leaving 7.7 million Americans hospitalized and 586,000 dead.”
The last exercise that took place was the evil Gates Foundation Event 201 in October of 2019. This was nearly an exact replica of what has happened this past year concerning the response to this fraudulent virus pandemic. The fact that the Gates foundation along with Johns Hopkins were involved in this set-up to prepare the sheep, is damning at every level, and exposes that all government tyranny is planned in advance, and telegraphed in order to condition the public.
What all these simulations, and many others, have in common is that the promoters and preparers of these events all claim to have no foreknowledge of any real future like situations, and allege that these are only done so as to be prepared to help the lowly proletariat in case of some biowarfare or health emergency. This is an outright lie. They are never prepared to stop any risk, but are always prepared to use it in order to gain power and control over humanity. The government and its partners in crime create and publically announce these simulations for the specific purpose of psychological preparedness training of the common people. It is no different than any propaganda campaign that is based on implanting ideas in the minds of its victims through projection and repetition.
It cannot be overstated that every act of government, its controllers, and its partners, is never accidental, or caused by unknown factors; it is always plotted and planned in order to benefit the ruling class. Every claimed emergency, whether national or state, is known about beforehand, and any response will be specifically generated to first benefit the oligarchy. This is true even in the case of natural disasters, as all preparedness first helps those insider entities that stand to gain from disaster.
This specific and purposely-manufactured virus ‘pandemic’ has been in the works for almost twenty years, and situations like this have been discussed for decades by the controlling ‘elites’ and their pawns in government. Because of this, all should understand that this is not over, and will never end without a large and sustained uprising by the citizenry. The escalation of extreme tyrannical measures is only going to dramatically increase in the coming year. Once this ludicrous presidential selection process ends in January, the political class will be completely free to pursue its globalist agendas without restriction. Those agendas, if allowed to go forward, will be the most devastating and draconian that we have ever faced.
The chosen masters that you have voluntarily allowed to rule over you have intentionally created this crisis, and are fully prepared to use it to destroy your life and family. You have suffered for almost a year, and this is only the beginning. The state’s agenda is crystal clear; propaganda is their weapon of choice, and total submission is their goal. Are you prepared to stop them by whatever means necessary, or will you comply and become slaves. Those are the only choices left!
First of all, very high praise goes to Christine Massey, for her work in exposing the coronavirus fraud. In a half-sane world, she would have received many awards by now.
Her latest communication reads: “Freedom of Information reveals Public Health Agency of Canada has no record of ‘SARS-COV-2’ isolation performed by anyone, anywhere, ever” [1]
I urge readers to visit Massey’s site and read her new article and follow all the links. Her findings are stunning. She and her team have made about 40 FOI requests to public health agencies in various countries, requesting proof that SARS-CoV-2 has been isolated. You’ll see from the responses that not one agency has records demonstrating isolation.
This means exactly what it seems to mean: the virus has not been proven to exist.
As for the people who keep chanting that the virus has been isolated, I can keep explaining why this is not so. I can do this forever. [2] [3]
Whether it’s a scientist, a gaggle of scientists, a government official, a person waving a study around like a newspaper with a hot headline from an old movie, my response is the same, and I make it knowing that some people will intentionally refuse to understand it:
ONE: SAYING the virus has been isolated is not the same thing as proving it’s been isolated.
TWO: Researchers routinely twist the meaning of the word “isolated” to mean its very opposite.
Isolation is absurdly taken to mean: “We have the virus in a soup in a dish in the lab. It is not separated out (isolated) from the soup. The soup contains various cells—human, monkey—and an array of (toxic) chemicals and drugs. We know the virus is there, because it is infecting and killing some of the cells.”
A reasonably bright junior high school student would immediately realize this is not a description of isolation.
A reasonably bright high school student would point out that there is no proof the virus is infecting and killing cells, because the toxic chemicals and drugs in the soup are sufficient to do the cell-killing. He might also mention the cells in the soup are being starved of nutrients, and this alone could cause their death.
Therefore, there is no evidence that “the virus” is actually in the soup.
Therefore, there is no evidence in this situation for claiming the virus exists at all.
On to the next factor: the ever-present claims of having “sequenced the genetic structure of the virus.” Again, SAYING the sequencing has been achieved is not the same thing as proving it.
And proving it is impossible, if you don’t already have the virus in a purified and isolated state. Instead of proof, you have shady inference and assumption and guesswork and deception.
How can you sequence something you don’t have? You can’t.
I’ve used several analogies to explain this nonsense. Here is another one:
An art restorer, conservationist, and historian is called to the home of a well-known mob enforcer.
The enforcer tells him he has something to show him in the attic. On the way, they pass through the living room, where several open suitcases are sitting on the floor. They’re spilling over with stacks of cash. Automatic weapons and boxes of ammo are laid out on a long table. In an open closet, the art expert sees a row of jackets with designations indicating: FBI, BATF, Federal Marshal, sheriff, local police.
In the attic, the mob enforcer points to a small pile of tiny chips on the floor.
“These are from a lost Rembrandt self-portrait,” he says. “Collect them, go to work on them, give me a favorable report. Or else.”
Back in his lab, the obedient art expert quickly divides the chips into three groups. The first group is water-color chips from a child’s toy set. The second group is mid-20th-century acrylic chips. The third group is lead white chips, used for a hundred years on either side of the rough date when Rembrandt could have painted the lost self-portrait.
The art expert finds that Rembrandt (and hundreds of other painters) used this general type of lead white.
The expert constructs, from other scholars’ work, an essay claiming there was and is a lost Rembrandt self-portrait. He excludes commentary that denies the existence of this painting.
He “sequences” all this information and conjecture and guesswork (and con) into a convincing report, which points to the small pile of chips in the mob enforcer’s attic.
(It turns out the enforcer intends to accuse a rival mob boss of stealing the “lost Rembrandt self-portrait.”)
The existence of the self-portrait is thus “established,” which is to say, it is put together, cobbled from various sources, concocted, smoothed out by ignoring counter-information—employing a vast generality about lead white paint.
Of course, in all this ridiculous invention, the self-portrait itself is not there, it is not in hand, its existence has not been demonstrated, it is a story, THERE IS NO ISOLATION OF IT from surrounding assumption and gimcrackery.
So it is with SARS-CoV-2. Pieces of data that reference prior supposed RNA sequences in libraries are all strung together, to resemble what is claimed to be a new and unique coronavirus—without having the actual virus, without having shown it exists at all.
In past articles, I’ve quoted two key documents, one from the CDC, and one from “the Drosten group.” These documents were describing how to perform the PCR test for the new virus—and in both documents, the authors state they don’t have the virus.
So…a test for what? The virus you don’t have.
All claims that these authors eventually DID obtain the virus are based on the crooked definition of “isolated” I’ve explained above.
Yes, they got hold of “isolated virus,” meaning the soup in the dish in the lab—and we’re back where we began. Isolation meaning non-isolation.
I’ve explained all this several times, in detail, in past articles, and of course people here and there continue to send me studies claiming isolation.
I can do this forever.
People can say, “Well, we know from photos of Martian soil samples that on the second Tuesday in March, 1843, there was a picnic on Mars attended by three virologists from the Martian Institute of Epidemiology, and they ate baloney sandwiches on rye toast and drank Miller Lite.”
I enjoy these fictional tales in a vacuum. I would leave them alone, except that the failure to prove the existence of SARS-Cov-2 is at the bottom of all the lies that have been used to steal the freedom and assets and livelihoods from at least a billion people.
I won’t leave that alone.
Neither should you.
“…but wait, Mr. Rappoport, here is a study from Outer Mongolia that states the virus has been isolated. This seems to settle the science on this issue, once and for all.”
Sure. Sure it does. And the sun sets every day at noon in Cincinnati.
The Pfizer Covid vaccine is already being administered to the public in the UK, and the first doses have been given in the US ahead of a mass vaccination campaign on a global scale.
It is important to recognize that the Pfizer Covid vaccine has not been approved by the FDA. It has only received Emergency Use Authorization (EUA), meaning the vaccine has not gone through the standard process to get official approval from the regulatory agency.
Now Moderna’s experimental Covid vaccine is set to get the same Emergency Use Authorization, allowing the shot to be distributed to millions of people.
We have already witnessed short-term adverse events (side effects) from the Pfizer vaccine. Truth is, nobody knows what the long-term effects could be and it appears the public is being subjected to an experiment on a global scale.
In this report, we examine discrepancies in the FDA Moderna report that was voted on by an advisory panel. The panel voted 20-0 recommending EUA.
Some of the discrepancies include cherry picked trial participants to achieve the desired results to gain EUA, as well as 13 total deaths in the trials – 6 in the vaccinated group and 7 in the placebo. Something the media refuses to address.
Brandy Vaughan founded a non-profit organization called “Learn the Risk” in 2015 in order to expose the great risk of vaccination. She became one of the premier spokesmen against dangerous vaccines, and compromised her very life to do so. She worked for Merck, an evil pharmaceutical company, but resigned in 2003 due to the horrible consequences and death that was due to a Merck drug called Vioxx. She could not stomach the fact that this company had full knowledge of the danger of this drug, and the deaths that it caused, but sold it anyway for huge profit.
Her desire was to attempt to create a healthier world by becoming an advocate against harmful pharmaceutical drugs and poisonous vaccines. Her mission began due to a mandatory vaccination law in her home state of California.
Due to her courage, she wanted to spread truth to help others, but she became a target of the pharmaceutical industry, and therefore the state. Her house was broken into on multiple occasions, and this was made obvious so as to relay to her that she was being threatened. These were no normal break ins according to private investigation, and were done by professionals with much information and skill.
She knew her life was in mortal danger, and in December of 2019, she made a public statement indicating that she was in perfect health, was taking no drugs or medication of any kind, lived for her young son, and would never under any circumstances commit suicide. A few days before her death, she was visiting close friends, laughing, having great dinners, and playing games into the night. In addition, she stated that if anything happened to her, it would indicate foul play. She was only 47 years old, and extremely healthy according to her own assessment and that of her friends, so her death should be heavily scrutinized.
It is very disturbing to me that after eleven days since her death, nothing definitive has been announced, and a so-called investigation was not considered until this past Monday, just three days ago. This is with the knowledge that she had been threatened, her house broken into several times, and was certain she was a target by evil forces. One unfounded report attempted to claim without one shred of evidence that she had a bladder condition. This is interesting given that she had recently stated that she was in perfect health.
It is my deepest suspicion that Brandy was murdered. Her enemies were in the pharmaceutical business and the government that protected these companies, and allowed them to profit at the expense of American citizens by exempting them from liability. She was a problem for them because she was honest and well spoken in her attempts to expose murderous corruption. In addition, she was gaining a larger audience, and understood the inner workings of these heinous companies.
This has cover-up written all over it. A late investigation was only begun due to pressure, with the stated comment that nothing could be done for 4 to 6 weeks due to waiting for toxicology screening. I firmly believe that the hope of all those involved in this investigation and probable coverup is that this will be forgotten by then, and can be swept under the rug. If and when a cause of death is announced by the state, it should be totally disregarded unless it can be verified by multiple trusted outside sources. But that would not be allowed, so who is going to come forward with vital information to expose this travesty meant to hide the murder of this young vibrant woman who wanted only to raise her son and alert others to the dangers of the evil among us?
We should never forget, and not let this go forward until we know the absolute truth.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
For those of you who have been following my work concerning COVID-19, you know that the entire foundation of the story of the virus rests on whether the novel “corona virus” has been properly isolated and its entire genome characterized. Many of you have sent papers to me that have been published in prestigious peer-reviewed journals that claim to have isolated and characterized this new virus. They are all incorrect.
In fact, the original Corman-Drosten et al paper on which this edifice of viral causation is based states that they used an “in silico” genome of an “in silico” virus. “In silico” is Latin for “theoretical.” In common English, synonyms for theoretical are “imaginary” or “make-believe.”
The CDC in its July 2020 monograph states “no quantified isolated of the 2019-nCov are available.” Again, in simple English, this means they have no examples of an isolated virus in their possession. In Freedom of Information requests, the Canadian health ministry, the Australian health ministry and the governments of many Commonwealth countries admit that they do not possess any studies that show the isolation of this purported virus.
In this interview, and hopefully for the final time, Jon Rappaport and I describe in common language and precise detail the steps that are needed to properly isolate and characterize a virus. We did this so we could empower our readers and listeners to know for themselves how to read and identify fraudulent science. Among the many challenges we face, one is the rampant scientific illiteracy. In some ages this may not have been relevant, but if we are going to live in an era in which “science” is the new religion and its tenets control our lives, we had better understand what its unquestioned “priests” are saying.
I can tell you, the more I look into what passes for “science,” the more I see how rotten it is to the core. If we are to have a new “religion,” let’s have one of truth, freedom, justice and the sense of wonder and awe at the phenomena of life. Let us celebrate what it means to be a human being endowed with a free spirit in a loving relationship with the mystery that is our world. Please join me in this interview.
I keep hammering on the test because it is the main piece of public fakery that holds this whole pandemic illusion in place.
If it falls, the illusion disappears.
In numerous past articles, I’ve shown the PCR test is useless and deceptive, from several angles.
Recently, I wrote about a Florida directive, issued by the governor and his department of public health: it forces labs to reveal the number of cycles at which each PCR test is run. [1]
A cycle is a quantum leap in amplification of the original sample taken from the patient.
Anthony Fauci himself has asserted that 35 cycles or higher makes the test result useless. Yet the FDA and the CDC recommend running the test at up to 40 cycles. This has opened the door to millions of false positives. [2] [3]
The cherry on the cake? Test labs never tell doctors or their patients how many cycles are deployed in the test. [4]
My first point today is this: if other states wake up and follow Florida’s lead, the whole false edifice of the test would collapse.
My second point: at labs all over the country (and the world), thousands and thousands of PCR tech employees understand the con, the hustle, and the crime—because they are participating in it EVERY DAY.
They are all silent.
If 20 of them stepped forward and told the truth, we would see the PCR test wobble and the fakery called “case numbers” and “pandemic” and “lockdowns” start to crumble.
These PCR techs would confess that they’re running the test at 40 cycles and therefore the results are MEANINGLESS.
So we need pressure on these PCR techs. Lots and lots of pressure. From us. From court cases. From every source we can muster.
The PCR techs are good Germans. They’re complicit and silent. THIS HAS TO END.
In 1992, strategist James Carville helped Bill Clinton win the presidency by suggesting that, coming out of a recession, the campaign should use the slogan, “It’s the economy, stupid!” It worked like a charm.
Now, the slogans/memes should be: IT’S THE CYCLES, STUPID! and IT’S THE TEST, STUPID!
The test spits out false positives like a fire hose, creating the impression of escalating COVID case numbers, which are used as the rationale for the lockdowns and the economic devastation.
Without those fake numbers, the authorities have NOTHING.
So get busy. Get the message about the tests out to one and all. Be relentless. Don’t curl up into a ball when people reject what you’re communicating. Keep going. Expose the fraudulent test cycles. Point to the PCR techs at labs as complicit enablers in the ongoing crime.
Here is my article from several weeks ago about Fauci and the test:
Smoking gun: Fauci states COVID test has fatal flaw; confession from the “beloved” expert of experts [5]
The COVID delusion is finished, blown apart
by Jon Rappoport
December 17, 2020
OK, here we go. Smoking gun. Jackpot.
Right from the horse’s mouth. Right from the man we’re told is the number-one COVID expert in the nation. What Fauci says is golden truth.
Well, how about THIS?
July 16, 2020, podcast, “This Week in Virology”: Tony Fauci makes a point of saying the PCR COVID test is useless and misleading when the test is run at “35 cycles or higher.” A positive result, indicating infection, cannot be accepted or believed.
“…If you get [perform the test at] a cycle threshold of 35 or more…the chances of it being replication-confident [aka accurate] are miniscule…you almost never can culture virus [detect a true positive result] from a 37 threshold cycle…even 36…”
Each “cycle” of the test is a quantum leap in amplification and magnification of the test specimen taken from the patient.
Too many cycles, and the test will turn up all sorts of irrelevant material that will be wrongly interpreted as relevant.
That’s called a false positive.
What Fauci failed to say on the video is: the FDA, which authorizes the test for public use, recommends the test should be run up to 40 cycles. Not 35.
Therefore, all labs in the US that follow the FDA guideline are knowingly or unknowingly participating in fraud. Fraud on a monstrous level, because…
Millions of Americans are being told they are infected with the virus on the basis of a false positive result, and…
The total number of COVID cases in America—which is based on the test—is a gross falsity.
The lockdowns and other restraining measures are based on these fraudulent case numbers.
Let me back up and run that by you again. Fauci says the test is useless when it’s run at 35 cycles or higher. The FDA says run the test up to 40 cycles, in order to determine whether the virus is there. This is the crime in a nutshell.
If anyone in the White House has a few brain cells to rub together, pick up a giant bullhorn and start revealing the truth to the American people.
“Hello, America, you’ve been tricked, lied to, conned, and taken for a devastating ride. On the basis of fake science, the country was locked down.”
If anyone in the Congress has a few brain cells operating, pull Fauci into a televised hearing and, in ten minutes, make mincemeat out of the fake science that has driven this whole foul, stench-ridden assault on the US economy and its citizens.
All right, here are two chunks of evidence for what I’ve written above. First, we have a CDC quote on the FDA website, in a document titled [6]: “CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel For Emergency Use Only.” See pdf page 38 (doc page 37). This document is marked, “Effective: 12/01/2020.” That means, even though the virus is being referred to by its older name, the document is still relevant as of Dec 2020. “For Emergency Use Only” refers to the fact that the FDA has certified the PCR test under a traditional category called “Emergency Use Authorization.”
FDA: “…a specimen is considered positive for 2019-nCoV [virus] if all 2019-nCoV marker (N1, N2) cycle threshold growth curves cross the threshold line within 40.00 cycles ([less than] 40.00 Ct).”
Naturally, MANY testing labs reading this guideline would conclude, “Well, to see if the virus is there in a patient, we should run the test all the way to 40 cycles. That’s the official advice.”
“Most tests set the limit at 40 [cycles]. A few at 37.”
“Set the limit” would usually mean, “We’re going to look all the way to 40 cycles, to see if the virus is there.”
The Times: “This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients…”
Boom. That’s the capper, the grand finale. Labs don’t or won’t reveal their collusion in this crime.
Get the picture?
I hope so.
If a lawyer won’t go to court with all this, or if a judge won’t pay attention and see the light, they should be stripped of their jobs and sent to the Arctic to sell snow.
I start with Public Health officials making a startling admission, then I move to 4 more examples of persecution of people who are questioning the government’s Big Pharma response to COVID, and then I go through who “they” are.
Who is it behind the persecution, censorship & vaccine narrative???
CNN has the story. And it’s quite a story: “Why vaccinate our most frail? Odd vote out shows the dilemma”, December 4. [1]
“The vote to recommend long-term care residents be among the first to receive Covid-19 vaccinations was not unanimous.”
“Out of a panel of 14 CDC vaccine advisers, a lone doctor said no.”
“’Odd woman out, I guess,’ Dr. Helen ‘Keipp’ Talbot, of Vanderbilt University, told her colleagues. ‘I still struggle with this. This was not an easy vote’.”
“Talbot was worried about whether the vaccine would even work in such frail, vulnerable patients. Even more, she worried about how it might look if the vaccine failed in that group, or how it would affect public perception if residents died soon after getting the vaccine.”
“The Covid-19 vaccines have not been tested in the frail elderly, many of whom are residents of long-term care facilities.”
Let’s stop here for a moment. First, we learn that the clinical trials of the COVID vaccine have not used the frail and elderly as volunteers. Therefore, there is NO evidence that the vaccine is safe or effective in that very large group. If this doesn’t give the frail and elderly and their families pause for thought, nothing will.
Second, Dr. Talbot is worried about “public perception,” when the elderly die right after getting the vaccination.
Well, what would YOU think if your mother died the day after she received the COVID shot?
The CNN article gets worse. Read on. Next up is a comment from Dr. Kelly Moore, “associate director of the Immunization Action Coalition, which is supporting frontline workers who will administer Covid-19 vaccinations.”
“’Since they [the COVID vaccines] haven’t been studied in people in those [elderly] populations, we don’t know how well the vaccine will work for them. We know that most vaccines don’t work nearly as well in a frail elderly person as they would in someone who is fit and vigorous, even if they happen to be the same age,’ Moore said.”
Again—zero evidence the COVID vaccines work in elderly and frail populations. Most vaccines don’t “work nearly as well.”
CNN: “When shots begin to go into arms of [nursing home and long-term care facility] residents, Moore said Americans need to understand that deaths may occur that won’t necessarily have anything to do with the vaccine.”
“’We would not at all be surprised to see, coincidentally, vaccination happening and then having someone pass away a short time after they receive a vaccine, not because it has anything to do with the vaccination but just because that’s the place where people at the end of their lives reside,’ Moore said.”
“’One of the things we want to make sure people understand is that they should not be unnecessarily alarmed if there are reports, once we start vaccinating, of someone or multiple people dying within a day or two of their vaccination who are residents of a long-term care facility. That would be something we would expect, as a normal occurrence, because people die frequently in nursing homes’.”
Right. Don’t be alarmed.
Don’t worry if people who are doing reasonably well suddenly die right after getting the COVID shot. It’s just a coincidence.
Their long-term health conditions just happened to kick in a day or two after vaccination. Nothing to wonder about.
Don’t kick up a fuss if it’s YOUR father or mother who died. Stay calm. You can be sure the doctors will let you know if your mother died from the vaccine. Of course they will.
Even though the vaccine has never been tested on the elderly and frail, the doctors know whether a death occurred from the vaccination or from other causes. And they’ll tell the truth. They always do.
The doctors quoted in this CNN article are obviously worried about people dying as a result of the vaccine. They know it’s going to happen. They’re thinking out loud about what they can do to stem the tide of public outrage—particularly from the families of those who die.
The best idea they can come up with is: “these people die anyway.”
I remind readers that, for months, I’ve been reporting on the huge percentage of all so-called COVID deaths that have been occurring among the elderly in nursing homes, in long-term care facilities, in hospitals, in their homes. [2]
These people were already suffering from multiple long-term serious health conditions. On top of that, they had been treated for years with an array of toxic medical drugs.
And then, they’re absolutely terrified when they receive a diagnosis of COVID. Then they’re isolated, cut off from family and friends.
And they give up and die.
NO VIRUS IS REQUIRED TO EXPLAIN THESE DEATHS.
This is forced premature killing of old people. It’s murder by COVID diagnosis and isolation. [2]
And now, these people will receive an experimental RNA vaccine, whose effects include auto-immune reactions; the body basically attacks itself. [3]
More killing.
And doctors advising the CDC are telling us not to be alarmed.
The deaths are just routine.
Lots and lots of doctors who know what’s going on are thinking, “What if all this comes back on ME?”
Well, it IS coming back on you, Doctors.
You’re killers in white coats who are supposed to be saving lives.
The #Covid19 vaccine rollout is underway in the US, yet legitimate claims and fears of serious adverse reactions persist.
From the alarming number of test subjects developing facial paralysis, to the NHS in England warning of serious allergic reactions, the Covid vaccine injury ‘elephant in the room’ is looming ever larger.
An Austrian parliamentary member exposed the defectiveness of the government’s COVID-19 tests by demonstrating in the parliament how a glass of Coca Cola tested positive for COVID-19.
In footage from the meeting in Vienna Friday, FPO General Secretary Michael Schnedlitz brings a glass of Coca Cola to the podium, from which he proceeds to collect drops to use on an antigen rapid test being used on a mass scale.
After going to the lectern and starting his speech, the politician sprinkled few drops of cola on corona rapid test. Three minutes later the test showed a result: Coca Cola was COVID-19 positive.
After demonstrating a positive result, Schnedlitz goes on to slam the tests as a waste of taxpayer resources.
“Mr. President, we are likely to have a problem now, we have a positive corona test in parliament, namely this cola triggered a positive corona test. I don’t know how to deal with it now!
With things like this you are throwing tens of millions of euros in tax money out of the window instead of providing real protection for old people’s and nursing homes, instead of investing money in our hospitals.
The corona mass tests are worthless! This was also shown by a simple experiment in parliament, in which a cola had a positive result! But this black-green government spends tens of millions in tax money on precisely these tests.”
Robert F. Kennedy, Jr. interviews Dr. Zach Bush about alternative routes to achieving optimal health, including how improving the gut microbiome can strengthen the immune system.
In the latest episode of our second season of “TRUTH” with Robert F. Kennedy, Jr., Kennedy interviewed Dr. Zach Bush who specializes in internal medicine, endocrinology and hospice care with a focus on the microbiome as it relates to health, disease and food systems.
Kennedy and Bush covered a wide range of topics, including:
the widely misunderstood history of the polio virus
Pharma’s takeover of the federal regulatory health system
All “Truth” episodes can be found on Children’s Health Defense’s social media, and on Children’s Health Defense’s channel found on Peeps TV, a network on Roku. Roku is accessible from any Smart TV and can be purchased separately for older TVs.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
More Than 50% of NY Firefighters Say No to Covid19 Vaccine
For the past 30 years, I’ve written about the dangers and ineffectiveness of vaccines, including the new COVID vaccine.
I’ve written about cutting edge nanotechnology research and its use, in vaccines, as implanted sensors, which would surveil body and brain processes in real time, and also send instructions to the body and brain.
I’ve written about the absurdity of basic vaccine theory; the unproven notion that the body needs a “rehearsal,” in order to prepare for the “real disease.”
I’ve written about how vaccines, in suppressing the immune system and its full inflammatory response, also suppress the outward signs of diseases, thus presenting a false picture of conquest of those diseases—when in fact the overall health and vitality of the body are reduced.
I’ve written about how criminal word games are played. For example, vaccines causing brain damage in children are shunted into a category called “autism”; and then, researchers claim autism is a separate disease with a genetic cause.
I’ve written about the destructive effects of a hundred years of wall-to-wall promotion of the one-disease-one-germ lie.
I’ve written about DNA vaccines permanently altering the genetic makeup of the recipients.
I’ve written about vaccines used to cause miscarriages in women when they later become pregnant.
But this article is about something else.
It’s about the dawn of a new pharmaceutical era, which was born the moment the Pfizer/BioNTech COVID vaccine was approved.
This marks the first time RNA technology deployed in a drug or vaccine has been dragged across the finish line and conditionally certified as safe and effective—which it is not.
But no matter. Bill Gates and other elite planners and money titans have won what for them is a great victory.
Because RNA vaccines are much faster, easier, and cheaper to produce than traditional vaccines.
Instead of years in the making, they can be developed in months.
And this means…bonanza.
Whole lists of so-called diseases—West Nile, Bird Flu, Zika, Swine Flu, SARS—can now be brought to soaring profits by making RNA vaccines to “prevent them.”
And not only that, a whole parade of older vaccines—hepatitis, measles, seasonal flu, diphtheria, whooping cough, tetanus, etc., can be recast with brand new updated RNA versions.
Researchers can pretend to discover a whole slew of “new viruses” that require RNA vaccines jammed into the marketplace in record time.
Don’t forget the domesticated animal market; RNA vaccines for every conceivable invented purpose sold to big corporations that operate cattle, pig, chicken, and fish “factories.”
We’re talking about trillions and trillions of dollars. More dollars than Amazon dreams of.
This is why the Pfizer RNA COVID vaccine is first in line, and why the Moderna RNA vaccine is next.
Quick, easy, and cheap RNA technology will mean endless numbers of new vaccines. And therefore, a day will come when every person routinely takes a DNA test to establish a profile, and every profile will be fitted to customized sets of vaccines.
In the same way that cosmetics are designed for every shade of skin tone, vaccines will be designed for every DNA profile.
The whole apparatus will be a highly dangerous and ineffective hoax, but what else is new? Vaccines have been a hoax since the beginning. We’re talking about MONEY.
So much money, pharmaceutical companies will be bankrolled directly by governments, after a currency reset makes new money invented out of thin air replace the old “thin air money.” Patients will receive all these vaccines “for free.” Governments will pay the vaccines companies.
UNLESS THESE LUNATICS ARE STOPPED.
Unless the people rebel and refuse the vaccines—no matter what.
If you think the futuristic vaccine-world I’m describing could only be a fantasy, what would masks, distancing, lockdowns, and planetary destruction of national economies have been called 15 years ago?
Think of past vaccines as giant clunky IBM computers sitting in empty rooms…and future vaccines as cell phones carried by billions of people.
Because RNA technology opened the door to faster, easier, and cheaper production.
What remains the same—past, present, and future—is FREEDOM.
The natural right to say NO. And mean it, come hell or high water.
CODA: What could be more awkward and foolish than the Pfizer regimen for their COVID vaccine? A first shot followed by a later booster.
I don’t care how many apps and reminders are built into this system. The fall-off from the first shot to the second will be enormous. People will opt out, after they experience severe adverse effects from the initial injection. They’ll forget to show up according to the prescribed schedule.
As I’ve detailed, the Pfizer and Moderna clinical trials of their vaccines were only designed to prevent mild illness—a cough, or chills and fever. Not serious illness. Not hospitalization. Not death. And cough, chills, and fever cure themselves. No need for a vaccine.
But none of this makes any difference to the vaccine kings. They and their public health colleagues can easily rig COVID case numbers in a downward direction—and then claim the success of the vaccine is the reason and the cause.
No, commercially speaking, the point of gaining approval of the vaccine was planting the flag of RNA technology in the marketplace.
This is the equivalent of building the first railroad tracks, digging the first big canals, flying the first air freight carriers.
New markets, new products, new customers, new money.
Marry these with a vast weakening of human vitality and a strengthening of control over populations, through vaccination, and you have the fascist Holy Grail.
Under section 564 of the Federal Food, Drug, and Cosmetic Act (FD&C Act), the FDA commissioner has the authority to allow unapproved medical products to be used in an “emergency” when there are no approved alternatives.
Before rushing into The Final Frontier traveling faster than the speed of light, why not heed the wisdom of Jean Luc Picard, Captain of the Enterprise, when he warned, “No being is so important that he can usurp the rights of another.”
Focus on the Headlines
CNN mainstream newswarns,“Don’t be alarmed if people start dying after taking the vaccine.”
Huh?
If ever there was a blatant warning that does not require reading between the headlines, it is this: Beware of the new, untested, genetically modified COVID vaccine. Don’t say we didn’t warn you. Collateral damage happens.
Whenever the government has rushed an experimental vaccine to market, the outcomes have been disastrous. The story has been told many times before through the media headlines.
Nothing ever needs to be rushed when it comes to ensuring safety because alternatives do exist, from the drug, Hydroxychloroquine, to mineral supplementation and medicinal herbs. Survivors of the Spanish Flu pandemic used homeopathy, a proven holistic alternative, with great success, even though there is no mention in the headlines.
The headlines love software developer and appointed COVID spokesperson, Bill Gates, who disclosed that 700,000 people could die from this vaccine. This figure is suspiciously close to the figure seen on the Georgia Guidestones, whose message is to maintain humanity under 500,000,000 (from 7 billion).
If you scan the news, you will find the high-risk groups for COVID deaths. The headlines read: “40% of Central Florida COVID deaths from nursing homes,” and “more than 6,000 coronavirus deaths are tied to Massachusetts long-term care facilities.” Nursing homes and long-term care facilities are the same groups targeted for the first round of vaccines.
Don’t be alarmed if people start dying after taking the vaccine. – CNN
Is CNN warning that the first to be jabbed will be the first to die? Are they disclosing a pattern for past epidemics and mass vaccination campaigns? Is truth being disclosed in the headlines? Do the headlines provide informed consent for the masses?
Vaccine makers, who are not liable for vaccine injuries and deaths, claim that they have a limited number of vaccines to deploy in the first phase. For instance, Moderna, says most people in the US will have to wait several months before they might have access to a coronavirus vaccine. And it could be years before everyone in the world can get vaccinated against COVID-19. Pfizer, which says its vaccine is 95% effective at preventing coronavirus infections, is expected to produce the first COVID-19 vaccine to receive FDA authorization in the coming weeks.
Before you consider if you belong to any of the priority groups, ponder this: What good is a 95% effective vaccine to prevent an infection that could make you a death statistic in the process?
If those most likely to die are the same people taking the vaccine first, then …“Don’t be alarmed if people start dying after taking the vaccine.”
Past Vaccine Disasters
If hindsight is 20/20, then people should be able to track past vaccine disasters for Polio, Swine flu, and H1N1, to name a few. However, people also have short attention spans.
Polio
In 1955, the government announced the first vaccine to protect kids against polio. More than 200,000 children got the polio vaccine, but within days the government had to abandon the program. The Cutter Incident resulted in 40,000 kids getting polio, including 10 deaths, from the polio vaccine. Later, from 1955 to 1963, it was found that between 10% and 30% of polio vaccines were contaminated with simian virus 40, which later resulted in an increased incidence of certain cancers among the 98 million people exposed to contaminated polio vaccine. About 90% of children and 60% of adults in the U.S. were inoculated for polio and possibly exposed to SV40.
Swine flu
In 1976, forty-five years ago, scientists predicted a pandemic of a new dangerous strain of influenza dubbed, Swine Flu. The federal government planned to buy 200 million doses of vaccines developed by drug companies and distribute them for free to state health agencies. President Ford misled people into believing that Swine Flu could be as bad as the Spanish Flu. The prediction that 50 million Americans would be sickened by swine flu never came to fruition.
Of the 46 million people who obediently took the shot, 4,000 Americans claimed damages from Uncle Sam amounting to three and a half billion dollars due to vaccine damage. Many developed Guillain-Barré syndrome — a disorder attributed to vaccines that can cause muscle weakness, paralysis, and even death. The program ended when 25% of the populated got the jab. See Mike Wallace of 60 Minutes expose the 1976 Swine Flu Pandemic Vaccine Injuries. During the fall of the following year, people feared getting the flu shot.
“I am terrified about getting a flu shot after all the troubles it caused last year,”wrote Martha W. on Sept. 26, 1977.
H1N1
In June 2009, the World Health Organization declared an H1N1 pandemic, marking the first global pandemic since the 1968 Hong Kong flu. The H1N1 strain of flu was the result of a reassortment of human influenza and swine influenza viruses. This suggests that viruses can jump the species barrier [more on that later]. In October, 2009, president Obama declared a National Emergency. The declaration gave DHHS Secretary extraordinary powers during a crisis. Health experts called it a false pandemic, insisting it was “just a normal kind of flu.” Ten years later, history repeats itself…
…the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%). – Anthony Fauci, March 26, 2020, New England Journal of Medicine editorial
Question the Narrative
Has vaccine science evolved since 1955, or 1976, or 2009 if the same pattern keeps repeating? Question the research:
When politics and science form a consensus, integrity and truth are lost.
Perhaps the greatest deception in repeat pandemics is that “the virus” has never been isolated. There is no true viral pandemic in human history since humans make viruses (exosomes) within their own cells.
The only person you’re truly competing against is yourself. – Jean Luc Picard, Captain, Starship Enterprise
As all students of biology know, viruses are not alive. They depend on the components of a cell for survival. Therefore, a virus is not contagious. The Coronavirus deception will never be reported in the headlines because a protein sequence is not a Bestseller. The CDC states:
Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA.
If viruses do not live outside cells, then how do they cross a species barrier to become a chimera, part pig and part human? The same way SARS and CoV2 meet and mingle. In a petri dish of a laboratory. The virus is nothing more than an elaborate distraction to reset society under global mandates to coerce compliance in illegal dictates because people have allowed themselves to be easily misled.
There can be no justice so long as laws are absolute. – Jean Luc Picard, Captain, Starship Enterprise
Next up
After January 2021, the simulation continues. The next president would lock down the U.S. for 4-6 weeks to “contain the spread of the virus” that did not respond to the first lockdown. Viruses do not respond to lockdowns, face masks, social distancing, or vaccine mandates because they are not alive. They are not a threat. However, the politicians and scientists who promote the virus deception are.
As people buy into Operation Warp Speed, politicians and scientists are hopeful that people will also buy into the latest, December 2020 headline declaring that a new annual, “universal flu vaccine shows promise.” However….
“Don’t be alarmed if people start dying after taking the vaccine.” – CNN News Headline
With the UK being the first western country to greenlight the #Covid19 vaccine to healthcare workers and the elderly, the media lauded the first recipient this week, a 90 year old woman, with their usual fanfare and excitement despite extensive safety concerns.
#UKVaccineApproval #UKVaccineRollout
CHD Article on Big-Picture Look at Current Pandemic Beneficiaries Accepted by Peer-Reviewed Journal
An article by Children’s Health Defense on how the pandemic facilitated a financial, tech, biopharmaceutical and military-intelligence push for centralized, technocratic control has been accepted by the International Journal of Vaccine Theory, Practice and Research.
“Planned Surveillance and Control by Global Technocrats: A Big-Picture Look at the Current Pandemic Beneficiaries,” a peer-reviewed article by Children’s Health Defense, has been accepted for publication in the journal, International Journal of Vaccine Theory, Practice and Research. The journal was launched in 2020 by John W. Oller, Jr., Ph.D. (editor-in-chief) and Christopher A. Shaw, Ph.D. (senior editor) “to make independent research, free from constraints of monetary, political, or any other undisclosed influence, about vaccine theory and practice freely accessible.”
The Children’s Health Defense article, which will appear in the journal by year’s end, assesses how the pandemic has facilitated a financial, tech, biopharmaceutical and military-intelligence push for centralized, technocratic control.
Here’s the article:
Abstract
Global financial patterns and pronouncements point to a seismic overhaul of governance and financial systems that is playing out beneath the surface of the Covid-19 pandemic, reaching far beyond the health domain. Increased centralized control has the potential to create an unbridgeable chasm between a tiny handful of winners and a majority of losers. To foster an integrated analysis of the technocratic and financial forces and agendas at play, this rapid review identifies some of the pandemic’s principal beneficiaries across the interwoven financial, tech, biopharmaceutical, and military-intelligence sectors, assessing developments in the context of the accelerating global push for technocratic consolidation and control. The evidence suggests that Trojan horse coronavirus vaccines may challenge bodily integrity and informed consent in entirely new ways, transporting invasive technologies into people’s brains and bodies. Technologies such as brain-machine interfaces, digital identity tracking devices, and cryptocurrency-compatible chips would contribute to the central banking goal of replacing currencies with digital transaction and identification systems and creating a global control grid that connects the world population to the military-pharma-intelligence cloud of the global technocrats. Moreover, using vaccines as a delivery vehicle for surveillance technologies cancels any legal liability.
Keywords: Biopharmaceuticals; central banks; Covid-19 pandemic; digital identity; Operation Warp Speed; technocracy; vaccines
Introduction
On March 11, 2020, the World Health Organization (WHO) upgraded a reportedly novel coronavirus from a global health emergency (as of January 30) to a global pandemic, having given the name “Covid-19” to the newly minted disease associated with the virus (Forster, 2020; World Health Organization, 2020a). If one examines actions taken both before and since the WHO’s March decree, it seems evident that many highly placed individuals and sectors were able to strategically position themselves to benefit from the declared crisis (Children’s Health Defense, 2020b). At the same time, with a “new form of economic shock” being imposed worldwide under cover of Covid-19 (Lagarde, 2020), it has become apparent that old-fashioned corporate profiteering is far from the whole story.
In fact, global financial patterns and pronouncements point to a seismic overhaul of governance and financial systems that is playing out beneath the surface of the pandemic, reaching far beyond the health domain. These developments highlight a disturbing push for global technocracy — a form of centralized, expert-led control over resource production and consumption that the Wall Street Journal has characterized as “anti-democratic rule by elites who think they know better” (Wood, 2018, 2020; Fitts, 2020a; Schinder, 2020; Schumacher, 2020; White, 2020). In the U.S., many of the actions unfolding behind the scenes are also benefiting from a climate of institutionalized secrecy enabled by the October 2018 adoption of a game-changing policy statement (FASAB Statement 56), which turned financial disclosure rules upside-down to allow the U.S. government and its contractors to maintain secret books (Federal Accounting Standards Advisory Board, 2018; Ferri & Lurie, 2018).
As 2020’s rapid-fire events suggest, substantially increased centralized control and secrecy have the potential to create an unbridgeable chasm between a tiny handful of elite winners and a majority of upper and lower middle class losers. In early June, CNBC’s Wall Street analyst Jim Cramer heatedly pointed out the fact that the pandemic had already produced “one of the greatest wealth transfers in history” (Clifford, 2020). Others have echoed these observations, describing the “monumental transfer of wealth from the bottom of the economic ladder to the top” (Barnett, 2020; Kampf-Lassin, 2020). In comparison to the benefits flowing to large corporations and billionaires, Cramer bluntly observed that pandemic-related restrictions have had a “horrible effect” on America’s small-business economy, with a similar pattern on display outside the U.S. (Clifford, 2020). Even the World Economic Forum — which has promoted many of the structural changes now underway at its annual Davos meetings — acknowledges the “asymmetric nature” of Covid-19-related hardships and the “greater ferocity and velocity” of the pandemic’s impact on populations already under stress before 2020 (World Economic Forum, 2020).
By early fall, fifty million Americans (many with already high burdens of debt) had lost jobs; financial forecasters were issuing warnings about further layoffs; and millions of the still-employed were earning less than pre-pandemic (Andriotis, 2020). In addition, the bulk of the trillions in federal stimulus (which by early May exceeded the gross domestic product of all but six nations worldwide) had made its way to large corporations; Forbes reported that roughly 70 percent of the initial $350 billion intended for struggling small businesses went to large companies (Simon, 2020). Observers suggest that by channeling taxpayer bailouts to the companies that already had the greatest ability to withstand the shutdowns, the largest players have been able to gain even more of a “stranglehold” over the economy (Kampf-Lassin, 2020).
As U.S. billionaires’ wealth increased by almost a trillion dollars (a weekly average of $42 billion), weekly jobless claims, requests for food bank assistance, and reports of addiction, overdoses, depression, and suicide began “shatter[ing] all historical records” (Feeding America, n.d.; Alcorn, 2020; Americans for Tax Fairness, 2020; Baldor & Burns, 2020; Community FoodBank of New Jersey, 2020; Dubey et al., 2020; Ettman et al., 2020; Hollyfield, 2020; Lerma, 2020; Prestigiacomo, 2020; Schwarz, 2020; Sergent et al., 2020; Thorbecke, 2020; Wan & Long, 2020). Outside the U.S., the situation is similar (Bueno-Notivol et al., 2020). As a marker of the global surge in hunger, the Nobel Committee awarded its 2020 Peace Prize to the World Food Programme, prompting the agency’s head to warn that the world is “on the brink of a hunger pandemic” that could result in “famines of biblical proportions” in the coming year (Lederer, 2020).
In November, the Centers for Disease Control and Prevention (CDC) released data identifying over 100,000 excess U.S. deaths “indirectly” associated with the pandemic (Rossen et al., 2020), including a “stunning 26.5% jump” in excess deaths in young adults in their mid-twenties through mid-forties (Prestigiacomo, 2020). Commenting on these mortality data — which reflect “a death count well beyond what [researchers] would normally expect” (Preidt, 2020) — the former U.S. Food and Drug Administration (FDA) Commissioner Scott Gottlieb voiced his suspicion that “a good portion of the deaths in that younger cohort were deaths due to despair,” including drug overdoses (Squawk Box, 2020). University researchers writing about mortality in JAMA concurred that “Excess deaths attributed to causes other than COVID-19 could reflect deaths . . . resulting from disruptions produced by the pandemic” (Woolf et al., 2020), including “spillover effects . . . such as delayed medical care, economic hardship or emotional distress” (Preidt, 2020). Multilateral entities like the Organisation for Economic Co-operation and Development (OECD) emphasize that it will be essential to assess the long-term impact of “confinement and deteriorating financial conditions” on mortality and warn that the social and economic fallout is likely to be “significant” (Morgan et al., 2020).
As an ideology, technocracy is recognized for exalting knowledge and expertise as the principal sources of legitimate power and authority and for asserting that there is “one best way” that only “the experts” (e.g., engineers, scientists, and doctors) can determine (Burris, 1989). However, critics of technocracy have long pointed out that, particularly in crisis situations, the know-how, “discretionary interventions” and seemingly “elastic” power claimed by technocrats can end up blurring the line between useful expertise and “arbitrary rule” (White, 2020). Moreover, technocrats typically resist attempts to make explicit “the non-rational attributes of technocratic decision-making” (Burris, 1989).
With the noticeable absence of any cost-benefit analysis and the increasingly “non-rational” justifications being put forth for Covid-19 restrictions (Handley, 2020; Kristen, 2020; Kulldorff et al., 2020; The Reaction Team, 2020) — as well as the economic, political, social, and cultural changes rolling out at dizzying speed — it is important to try to understand the technocratic and financial agendas at play. Three increasingly interwoven sectors (Big Finance, Big Tech, and Big Pharma) are reaping rewards from Covid-19, benefiting from close relationships with the military-intelligence apparatus (Glaser, 2020; Usdin, 2020). This rapid review seeks to (1) identify some of the pandemic’s principal beneficiaries (financial and otherwise) across these sectors, and (2) assess these parties’ actions in the context of the accelerating global push for technocratic consolidation and control through invasive surveillance.
Methods
Rapid reviews are used to synthesize evidence in a streamlined manner, abbreviating the timeline and requirements of more involved systematic reviews (Ganann et al., 2010). A rapid review is particularly well suited to emerging current event sequences, and the dynamic Covid-19-related situation certainly qualifies. Though not exhaustive, rapid reviews make it possible to quickly summarize available evidence across multiple disciplines, whether for the purpose of informing policy-making and decision-making or to identify patterns and take stock of the bigger picture.
For the purposes of this broad overview of current events, we relied primarily on the so-called grey literature as well as media accounts (from both the legacy media and independent journalists) and various online sources. We also consulted relevant peer-reviewed literature. Notably, while the peer-review process is ordinarily slow-moving, Covid-19-related studies have been making their way through the pipeline at breakneck speed (Packer, 2020).
Examples of sources consulted for this review include conventional and alternative financial commentary; webpages and communications from public health agencies, international organizations, and universities; individual blogs and commentary; and peer-reviewed studies cataloguing the impact of Covid-19 restrictions.
Big Finance
Assisted by the media, commentators have had an easy time framing the events of 2020 principally as a health crisis. With each passing month, however, those claims wear thinner (Barnett, 2020). In a comprehensive analysis titled The State of Our Currencies, former U.S. Assistant Secretary of Housing Catherine Austin Fitts (2020a) offers a broader and more instructive interpretation. Informed by close attention to financial patterns, Fitts asserts that the “shock doctrine” measures being imposed under cover of Covid-19 are helping lay the train tracks for a new global central banking machine and a technocratic “regulatory and economic model that permits far greater central control.”
Fitts calls attention to G7 central bankers’ August 2019 approval in Jackson Hole, Wyoming of a plan called “Going Direct” (Bartsch et al., 2019) that makes the case for a novel “blurring [of] the lines between government fiscal policy and central bank monetary policy” (Martens & Martens, 2020). Drafted months before Covid-19, the plan — co-branded by the World Economic Forum (n.d.) as “the Great Reset” — evokes the prospect of a serious economic downturn and “unusual circumstances” that could be used to justify “unprecedented” global measures (Bartsch et al., 2019).
Fitts (2020a) postulates that central bankers have both a short-term aim (to extend the existing dollar-based reserve currency system) and an ambitious longer-term goal: to implement a “new global governance and financial transaction system, and gather the power necessary to herd all parties into the new system”. Characterizing these aspirations as nothing short of ending currency as we know it, Fitts suggests that the top-down digital-currency-based model being promoted as a replacement could end up sidelining traditional intermediaries and instead directly furnish populations with something akin to a “credit at the company store”. Spelling out the implications of such a model, Fitts notes that with the help of digital surveillance and a social credit system, the central-bank-controlled “credit” could easily be “adjusted or turned off on an individual basis”. General Manager Agustín Carstens of the Bank for International Settlements (BIS) — the central bank of central banks — recently acknowledged as much, stating that in stark contrast to cash, a Central Bank Digital Currency (CBDC) would give central banks “absolute control” over CBDC use “and the technology to enforce” CBDC rules and regulations (International Monetary Fund, 2020). With a vaccine-injected digital surveillance program in individuals, the CBDC would have dictatorial power at the level of individual buying and selling.
Fitts’ analysis suggests that central bankers began laying the groundwork for the desired global transition well in advance of the coronavirus mayhem. In 2019 alone, G7 finance ministers endorsed a cryptocurrency action plan in July; in August, the G7 central bankers approved “Going Direct”; in September, the U.S. Federal Reserve (“the Fed”) started making hundreds of billions of dollars in loans “direct” to Wall Street trading houses; and in October, the BIS issued a major report on global cryptocurrencies (Bank for International Settlements, 2019; Helms, 2019; Fitts, 2020a; Martens & Martens, 2020). In the middle of the frenzy of central bank activity in October, the Bill & Melinda Gates Foundation (along with the World Economic Forum and Johns Hopkins Center for Health Security) held the well-publicized “pandemic tabletop exercise” called Event 201, which played out a global coronavirus outbreak scenario strikingly similar to 2020’s actual events (Center for Health Security, n.d.).
In January 2020, U.S. corporations witnessed a record number of CEO departures (Ausick, 2020; Marinova, 2020) — a mass exodus that strategically allowed over 200 departing executives to sell their stock at or near the market high (see Table 1). Other wealthy and influential insiders also engaged in surprisingly well-timed stock market transactions. For example, following a late-January, behind-closed-doors briefing about the virus (which had yet to affect a single American), certain U.S. senators sold hundreds of thousands of dollars of stock, “unloading shares that plummeted in value a month later” (Lane, 2020). The world’s wealthiest person, Amazon CEO Jeff Bezos, sold nearly $4.1 billion over an 11-day period in early February after having also sold $2.8 billion in shares in August 2019 (Palmer, 2020).
Table 1. U.S. CEO Departures in January 2020
Sources: Ausick, 2020; ChallengerGray, 2020
As the U.S. government turned on the stimulus spigot in March, the Fed sustained its irregular intervention in the U.S. economy. By the summer of 2020, the Fed had expanded its balance sheet by $2.9 trillion — much of it unaccounted for, according to Fed-watcher John Titus (2020) — and financial observers were warning that “the market is no longer the biggest factor in selecting [economic] winners and losers” (Whalen, 2020). Titus (2020) concurs with this assessment, baldly characterizing 2020’s events as a Fed-led “coup d’état”. Titus (2014) has been chronicling major financial forces and legal changes since the 2008 financial crisis, describing how central banks are not only able to “loot” the American people “in broad daylight” but can do so without fear of prosecution — probably because, as Titus and Fitts (2020a) both point out, the Department of Justice depends on Fed member banks for its financial operations.
The coronavirus stimulus has provided abundant financial opportunities advantageous to Fed member banks. Over a two-week period in April, for example, large banks earned $10 billion in fees (ranging from 1 to 5 percent) simply for processing the government’s loans to businesses (Sullivan et al., 2020). Class-action lawsuits subsequently alleged that the banks prioritized larger loans (and larger companies) in order to garner the largest fees, while shutting out “tens of thousands” of eligible but smaller businesses (Sullivan et al., 2020). Serving as lender to the parent company of a national restaurant chain, Fed member bank JPMorgan Chase (the largest and most profitable bank in the U.S.) earned a $100,000 fee for a single “one-time transaction for which it assumed no risk and could pass through with fewer requirements than for a regular loan” (Sullivan et al., 2020).
In September, Senator Marco Rubio (Chairman of the Senate Committee on Small Business and Entrepreneurship) wrote to the JPMorgan Chase CEO expressing “alarm” about allegations that JPMorgan employees “may have been involved in potentially illegal conduct” in the distribution of Paycheck Protection Program and Economic Injury Disaster Loan funds (Rubio, 2020). Bloomberg later confirmed the possibility of Covid-19-related banking abuse on a wide scale (David, 2020). Importantly, this is not a new pattern of behavior for the U.S. banking behemoth. Since 2002 (and primarily since the 2008 financial crisis), JPMorgan Chase has paid out at least $42 billion in settlements for questionable, unethical, or illegal behavior (Fitts, 2019); its public-facing Wikipedia page lists involvement in 22 different “controversies,” including the economically shattering Enron and Madoff scandals (“JPMorgan Chase”, n.d.). Nevertheless, JPMorgan continues to earn glowing accolades from the financial community. In June 2020, Forbes urged investors to “bank on the best” in the uncertain Covid-19 environment (Trainer, 2020), citing JPMorgan’s post-2009 “industry-leading profitability” and asserting that the bank is exceptionally well positioned to expand its market share both during and post-pandemic. In October, JPMorgan rolled out a new smartphone credit card reader designed to compete with Square and PayPal (Son, 2020).
Big Tech
By July 2020, global billionaires’ wealth had surged to an all-time high of $10.2 trillion — an increase of 27.5 percent since April, and a 41.3 percent increase for tech billionaires (Phillipps, 2020). U.S. billionaires accrued a significant share of this pandemic wealth bonus, increasing their worth by $845 billion from mid-March to mid-September and prompting the observation that “for American billionaires specifically, things have never looked better” (Lerma, 2020). As a whole, U.S. billionaires’ wealth reached the equivalent of almost one-fifth of the U.S. gross domestic product, with four tech billionaires (Jeff Bezos, Bill Gates, Elon Musk, and Mark Zuckerberg) plus Warren Buffett seeing their total wealth climb by 59 percent (da Costa, 2020). Calling attention to Bezos, in particular, the Institute for Policy Studies described his surge in wealth as “unprecedented in modern financial history”, requiring “a real-time hour-by-hour tracker” to keep up (Collins et al., 2020).
The companies with which top-tier billionaires are affiliated include Amazon and Amazon Web Services (Bezos), Apple (Tim Cook), Facebook (Zuckerberg), Google/Alphabet (Larry Page and Sergey Brin), Microsoft (Steve Ballmer and Gates), Oracle (Larry Ellison), Zoom (Eric Yuan), and the variety of companies (including Neuralink, SpaceX, and Tesla) spearheaded by Musk (Alcorn, 2020; Collins et al., 2020; Toh, 2020). In July, as Bloomberg described these companies’ “outsized influence on U.S. markets”, it noted that they are as well-situated to profit from the U.S. shutdown as they are to take advantage of a recovering Europe and Asia — a “one-two punch” that has already increased FAANG companies’ market (Facebook, Amazon, Apple, Netflix, and Google, plus Microsoft) by 62 percent (Ritholtz, 2020). Suggesting that Silicon Valley will go down in history as “the standout sector” (Divine, 2020a), a U.S. News analyst unabashedly recommended Facebook as a 2020 “best buy” because “it’s gobbling up the world, and reasonable people could argue that if privacy is dying, individual investors may as well profit alongside Silicon Valley” (Divine, 2020b).
Covid-19 has provided Big Tech (and Big Telecom) with an opportunity to bring a range of controversial technologies further out into the open, despite many unresolved concerns about safety and ethics (Boteler, 2017; Gohd, 2017; Ross, 2018; Boyle, 2019; Feiner, 2019; Markman, 2019; Plautz, 2019; Zhang et al., 2019; Bajpai, 2020; Goodwin, 2020; Gyarmathy, 2020; McGovern, 2020; Novet, 2020; Reuters, 2020; Tucker, 2020; U.S. Department of Defense, 2020). Singly and in combination, the technologies (some of which are listed in Table 2) have the potential to usher in unprecedented societal changes, strengthening technocrats’ ability to control many facets of daily life. Artificial intelligence (AI), 5G, “smart” utility meters, and the Internet of Things (IoT), for example, are rapidly and fundamentally changing the nature of cities, businesses, and homes — what Fitts (2020a) calls the “final mile” — forming an essential part of the strategy to convert the economic model to a technocratic model that uses AI and software to achieve centrally controlled resource allocation.
Table 2. Covid-19 and the Rollout of Control Technologies
In October 2020, the World Economic Forum — the Great Reset’s front-row marketer — released a report on the future of jobs, describing the significant displacement of workers resulting from the pandemic and the related global restructuring that the organization has been taking the opportunity to promote (Petzinger, 2020). With automation and Covid-19 causing a “double-disruption” that is not only accelerating job destruction in the short term but “shrinking opportunities” in the longer term, the report solemnly pronounced a “new division of labour between humans, machines and algorithms” (World Economic Forum, 2020). Well before the pandemic, Amazon had established a robot-centric system at its fulfillment centers, with a process focused on “limit[ing] movement of people [and] let[ting] robots move everything” (Masud, 2019). This downsizing of humans has apparently served Amazon well; by May 2020, Amazon’s e-commerce business had shot up by 93 percent compared to the previous May (Klebnikov, 2020).
A September 2020 survey showed that many other companies plan to substantially boost their spending on AI and machine learning, citing Covid-19 as their rationale for prioritizing “the adoption of new technologies that enhance and enable automation” (Shein, 2020). Observers also predict, however, that the AI gold rush will lead to even more market consolidation and control by Amazon and three other big Covid-19 winners — Alphabet, Facebook, and Microsoft. These four companies, according to Forbes, have the “scale to push the envelope”, the “talent and the technology to perfect [AI]”, and the computing power to dominate the field (Markman, 2019). Amazon already controls nearly 46 percent of the worldwide public cloud-computing infrastructure that is a key backstop for AI functions such as parallel processing and the digestion of Big Data (Atlantic.Net, 2018; Nix, 2019).
Before Covid-19, consumer rejection of 5G wireless technology had been growing (Castor, 2020). However, the imposition of social distancing measures, remote learning, and online work requirements has provided the telecommunications industry with a ready-made pretext to fast-forward 5G’s deployment while attempting to burnish the industry’s unfavorable public image. Taking advantage of virus fears, Big Tech and Big Telecom are claiming that 5G can help enable “a future in which business, health care and human interaction must be at more than an arm’s length” (Wasserman, 2020). Forbes has praised communication service providers for responding to the coronavirus lockdowns “with a sense of urgency, purpose and empathy” (Wilson, 2020). Describing areas requiring more “advanced connectivity”, a technology expert at Deloitte Consulting cited the example of “cameralytics” (video surveillance) “to help worker safety and social distancing” (Howell, 2020). Whatever the rationale, the reality on the ground has been a massive increase in U.S. telecom companies’ capital spending on 5G and a “full steam ahead” rollout of spectrum and infrastructure that has placed the U.S. “ahead of schedule” (Knight, 2020; Ludlum, 2020). The European Commission is now attempting to follow the U.S.’s lead by pushing for the removal of “regulatory hurdles” and making the case that 5G will aid the region’s post-coronavirus economic recovery (McCaskill, 2020).
Covid-19 has also brought another of Big Tech’s interests into sharper focus: food. Billionaires such as Bill Gates and Peter Thiel have, for some time, been investing in biotech start-ups that aim to produce, in a lab, stem-cell-based “meat”, “fish”, “dairy”, and “breastmilk” (Kerr, 2016; Kosoff, 2017; Beres, 2020; Wuench, 2020). These start-ups and their investors have been only too happy to position the burgeoning industry as a partial solution to pandemic-related food insecurity and supply chain interruptions (Galanakis, 2020; Pereira & Oliveira, 2020; Yeung, 2020), welcoming Covid-19 as an “accelerator” as well as an opportunity to overcome consumer skepticism (Siegner, 2019; Morrison, 2020). In addition, as the coronavirus breathes new life into the term “sustainability” — long used by technocrats as a cover term for more centralized control (Wood, 2018) — global partners like the United Nations and the World Economic Forum are making the improbable claim that the complex, high-dollar, lab-created food substitutes (which require genetically stable cell lines, bioreactors, “edible scaffolds”, and cell culture media) are a “sustainable” option (Whiting, 2020). The biopharma giant Merck is also getting in on the “cultured meat” action, offering to make its “extensive knowledge of the relevant science and biotechnology” available to companies seeking to overcome “critical technological challenges” (Whiting, 2020). Merck frequently collaborates with the Gates Foundation, including in the development of Covid-19 vaccines (Lardieri, 2020).
Big Pharma
In September 2019, an annual Gallup poll reported that the restaurant industry was America’s top-ranked and most-liked among the 25 industries regularly assessed by the polling group (McCarthy, 2019). Sadly, less than a year later the Independent Restaurant Coalition predicted the permanent demise of up to 85 percent of independent restaurants (Jiang, 2020). In contrast, the pharmaceutical industry came in “dead last” in the 2019 poll, despite $9.6 billion spent annually on direct-to-consumer advertising and another $20 billion on marketing to health professionals (McCarthy, 2019; Schwartz & Woloshin, 2019). The U.S. is one of only two countries in the world that allows drug companies to market directly to consumers and, in non-election years, roughly 70 percent of news outlets’ advertising revenues come from pharma (Solis, 2019).
The pharmaceutical industry’s history of “fraud, bribery, lawsuits and scandals” is well known (Compton, n.d.), and no less a figure than Bill Gates has suggested that the public perceives Big Pharma as “kind of selfish and uncooperative”; however, Mr. Gates and Fortune magazine propose that Covid-19 may offer the industry an opportunity for “redemption” (Leaf, 2020). The stage may have been set for Big Pharma’s year of opportunity in January, when JPMorgan Chase held its 38th annual invitation-only health care conference. The business press describes the yearly conference as “one of the biggest biotech dealmaking events, often setting the tone for funding rounds, partnerships and mergers and acquisitions” (Leuty, 2020). Thus, just when the coronavirus ball was getting rolling, the conference brought an estimated 20,000 venture capitalists, investment bankers, and drug development executives and entrepreneurs to San Francisco to hear keynote addresses by JPMorgan’s and GlaxoSmithKline’s CEOs and to stoke expectations of a strong year for the biotech-plus-pharma chimera known as “biopharma” (JPMorgan, n.d.; Leuty, 2020; Lipschultz, 2020). In 2014, McKinsey & Company described the investment opportunities in biopharmaceuticals as “big and growing too rapidly to ignore”, with an annual growth rate more than double that of conventional pharma and a 20 percent share of global pharmaceutical revenues (Otto et al., 2014).
A few weeks after the JPMorgan conference — and well before any Covid-19 deaths in the U.S. — the Department of Health and Human Services (HHS) helped ensure that significant pandemic benefits would flow into the biopharma and medical space. HHS did so by issuing a declaration (on February 4) making vaccines and all Covid-19-related medical countermeasures immune from legal liability (HHS, 2020a). On March 6, roughly a week after the first reported coronavirus death, President Trump sweetened the pot by signing into law the first in a series of emergency stimulus packages, earmarking 40 percent of the $8.3-billion bill for vaccines and drugs under terms the pharmaceutical industry openly dictated (Karlin-Smith, 2020).
Following the February 4 HHS declaration eliminating legal liability, Bill and Melinda Gates instantly pledged $100 million in funding for coronavirus vaccine research and treatments, followed by another $150 million in mid-April (Bill & Melinda Gates Foundation, 2020; Voytko, 2020). When Operation Warp Speed followed, making untold billions available for research and development of therapeutics and vaccines at taxpayer expense (see Table 3), dozens of biopharma companies jumped into the fray (HHS, n.d.). Catherine Austin Fitts notes that a system that exempts from liability anything labeled as a “vaccine” amounts to “an open invitation to make billions . . . particularly where government regulations and laws can be used to create a guaranteed market through mandates” (Fitts, 2020b). Moreover, each time the CDC’s Advisory Committee on Immunization Practices (ACIP) adds a given vaccine to the CDC schedule, it is not only the equivalent of a “golden ticket” for the vaccine manufacturer but also directly benefits the CDC, which owns dozens of vaccine-related patents and routinely shares licensing agreements with manufacturers (Taylor, 2017; Children’s Health Defense, 2019).
Currently, there is one injury for every 39 vaccinations administered (2.6%), often resulting in a “disastrous outcome of life-altering iatrogenic illnesses” (Harvard Pilgrim Health Care, n.d.; Kennedy Jr., 2019; Kristen, 2019). A CDC study published in JAMA in 2016 reported that one in five young children (19.5%) under age five who were admitted to emergency rooms for drug reactions were suffering from vaccine injuries (Shehab et al., 2016). Early clinical trial results and Covid-19 vaccines’ use of an array of experimental, never-before-approved technologies suggest that comparable (or worse) levels of injury could follow the rollout of coronavirus vaccines (Children’s Health Defense, 2020a, 2020c, 2020d, 2020e). The Moderna and Pfizer vaccines, for example, feature mRNA molecules that are known to be “intrinsically unstable and prone to degradation”, with an inflammatory component that risks dangerous immune reactions (Feuerstein, Garde, & Joseph, 2020; Jackson et al., 2020; Wadhwa et al., 2020). Assuming the same vaccine injury rate of 2.6 percent, Operation Warp Speed’s projected vaccination of roughly 25 million Americans per month (Owermohle, 2020b) could conceivably result in 3.9 million injuries over just the first six months. (Given that the leading vaccines will require two initial doses and probable boosters thereafter, this figure could even be an underestimate.) If Bill Gates and other technocrats succeed in their declared aspiration to manufacture billions of doses of coronavirus vaccine and “get them out to every part of the world” (Gates, 2020), the scale of injury would not only be unprecedented but could open a lucrative, long-term gateway to the wider drug market to manage the injuries (Kristen, 2019).
*HHS note on Operation Warp Speed funding: “Congress has directed almost $10 billion to this effort through supplemental funding, including the CARES Act. Congress has also appropriated other flexible funding. The almost $10 billion specifically directed includes more than $6.5 billion designated for countermeasure development through BARDA and $3 billion for NIH research.”
By mid-October, 44 candidate vaccines were in clinical evaluation worldwide, with another two hundred or so in the pipeline (Agrawal et al., 2020; World Health Organization, 2020b). Furnishing predictably uncritical coverage ensured by the pharmaceutical industry’s strategic entanglements with the media, scientists, and medical journals, the press has been telling the public that the vaccines will play “an important role in most response scenarios”, including “‘sav[ing] the world’ in worse scenarios” and serving as an “insurance policy against continued health and economic shocks” (Agrawal et al., 2020). Only a handful of journalists have called attention to Big Pharma’s pandemic profiteering, pointing out that “insiders at companies developing experimental vaccines and treatments . . . aren’t waiting until they finish the job to collect their reward” (Wallack, 2020).
An October piece in the Boston Globe cited the example of Moderna (Wallack, 2020). It took Moderna a mere three weeks after Bill Gates’ initial funding installment to send its first batch of experimental vaccine to research and patent partner, the National Institute of Allergy and Infectious Diseases (NIAID), leading to an immediate surge in share price of 28 percent (Lee, 2020; Loftus, 2020). By early April, Moderna’s CEO had become an overnight billionaire; by October, he had sold nearly $58 million in stock, followed by another $2 million in mid-November, just ahead of the company’s intended filing for vaccine Emergency Use Authorization (Nagarajan, 2020; Tognini, 2020; Wallack, 2020). Meanwhile, Moderna’s chief medical officer has been “systematically liquidating all of his company stock” — about $70 million — “in a series of pre-planned trades that have made him roughly $1 million richer each week” (Wallack, 2020). Thus far this year, company insiders have sold $309 million in stock versus under $2 million in 2019, fueling suspicion that they may be “downplaying possible obstacles to goose stock prices — and increase their personal profits” (Wallack, 2020). Also among those selling Moderna stock options is Moncef Slaoui, the former Moderna board member and former GlaxoSmithKline executive who now heads up Operation Warp Speed (Rozsa & Spencer, 2020).
From Moderna’s perspective, the Covid-19 vaccine represents a lifeline, rescuing the company from a shaky bottom line due to its prior inability to bring any products to market (Garde, 2017; Nathan-Kazis, 2020). Other biopharma companies formerly on the skids are likewise poised to make record profits from the coronavirus (Webb & Diego, 2020). Characterizing the business model for Covid-19 (and other) vaccines as a “great scheme” — particularly given the HHS-guaranteed, risk-free environment — a watchdog group spokesman told the Boston Globe, “Taxpayers cover the upfront investment costs and shoulder any downside, while their [biopharma’s] executives and shareholders can capture the upside if their drugs pan out and are shoveling obscene amounts of money into their pockets throughout the process” (Wallack, 2020). In the words of a business school professor, “You announce a sliver of positive hope about a product and your stock price goes up,” even though “the chances of that product panning out might be relatively low” (Wallack, 2020). In 2020, the company Vaxart saw its per-share stock price rise from 27 cents to a high of $17.49 (Wallack, 2020).
Rolling Stone journalist Matt Taibbi (2020) describes Covid-19 as “the ultimate cash cow,” a “subsidy-laden scam,” and a legal opportunity for “giant-scale gouging”, quoting a legislator who admits that while the public is paying for the research and manufacturing, “the profits will be privatized”. Writing in August about how the government-subsidized business model played out for Gilead’s drug remdesivir, Taibbi (2020) recounted: “Gilead, a company with a market capitalization of more than $90 billion, making it bigger than Goldman Sachs, develops an antiviral drug with the help of $99 million in American government grant money. Though the drug may cost as little as $10 per dose to make, and is being produced generically in Bangladesh at about a fifth of the list price, and costs about a third less in Europe than it does in the U.S., Gilead ended up selling hundreds of thousands of doses at the maximum conceivable level, i.e., the American private-insurance price — which, incidentally, might be about 10 times what it’s worth, given its actual medical impact.”
Always a major lobbying presence on Capitol Hill, the pharmaceutical industry has been more lavish than usual with its political spending in 2020, donating over $11 million to individual candidates involved with health care policy and related political action committees (Facher, 2020a). Although the overall amounts represent a pittance for companies earning tens of billions a year, pharma and its lobbying groups recognize that “small chunks of corporate change”, when strategically allocated, “can have a significant impact” (Facher, 2020b). Coronavirus vaccine frontrunner Pfizer, the second-largest drug and biotech company in the world and the fourth-highest earner of vaccine revenues (Statista, n.d.; Hansen, 2020), has been the top political spender, likely laying the groundwork for its November 20 filing for Emergency Use Authorization for its coronavirus vaccine (Chander, 2020; Children’s Health Defense, 2020d). Pfizer has also benefited from repeated endorsements from the financial community and self-proclaimed spokesmen like Bill Gates (Speights, 2020a, 2020b).
The Military-Intelligence Complex
Traditional vaccines have their fair share of safety problems, but coronavirus and other 21st-century vaccines promise to challenge bodily integrity and informed consent in entirely new ways, particularly given their strong reliance on various forms of nanotechnology (Health and Environment Alliance, 2008; Li et al., 2009; Chauhan et al., 2020; Children’s Health Defense, 2020a). Many of the technologies being rolled into Covid-19 vaccines and their delivery systems originated in the military sphere or benefited from Defense Advanced Research Projects Agency (DARPA) funding. DARPA has had a Biological Technologies Office since 2014 and, since the emergence of Covid-19, has specifically directed many of its pandemic-related efforts toward coronavirus therapeutics and vaccines (Gallo, 2020). Far from being suspect, the military’s role has been celebrated. A BioCentury report optimistically suggested in March that as an agency “that specializes in turning science fantasies into realities”, DARPA might offer the “best hopes” for Covid-19 biotech solutions due to its willingness to pursue “high-risk, high-reward technologies”, set goals “that defy conventional wisdom”, and go after its goals with a “laser” focus (Usdin, 2020).
One of the principal DARPA-incubated vaccine technologies to gain prominence in the Covid-19 era are the nucleic acid (mRNA and DNA) vaccines that turn the human body into its own “bioreactor” (Ghose, 2015; Usdin, 2020). Vaccines using mRNA (such as Moderna’s and Pfizer’s) — which developers compare to “software” (Garde, 2017) and praise for their “programmability” (Al-Wassiti, 2019) — target the cell’s cytoplasm and rely on delivery technologies such as lipid nanoparticles to “ensure stabilization of mRNA under physiological conditions” (Wadhwa et al., 2020). DNA vaccines (such as Inovio’s) are intended to penetrate all the way into a cell’s nucleus and come with the risk of “integration of exogenous DNA into the host genome, which may cause severe mutagenesis and induced new diseases” (Zhang, Maruggi, Shan, & Li, 2019). Describing the scientific community’s early doubts about nucleic acid vaccines — arising from the potential for “many things” to go wrong — a DARPA program manager recently noted, “It was something that was much too risky for groups like the NIH to fund” (Usdin, 2020).
Risks aside, DARPA and vaccine manufacturers are attracted to one chief benefit of nucleic acid vaccines: They can be developed much more quickly and cheaply. Other military-initiated technologies are also coming into view with Covid-19 vaccines. These include electroporation, which applies a high-voltage electrical pulse to make cell membranes permeable to a vaccine’s foreign DNA (Inovio Pharmaceuticals, 2020); syringe-injected biosensors that enable continuous wireless monitoring of vital signs and body chemistry (Peer, n.d.; Profusa, n.d.; Diego, 2020b; Tucker, 2020); and the quantum-dot-based infrared detectors that are under discussion as a tool for tracking vaccination status (Johnson, 2011; Trafton, 2019). DARPA has also played a leading role in developing and funding technologies that “blur the lines between computers and biology”, including brain-machine interfaces and neuromonitoring and mind-reading devices (CB Insights, 2019; Gent, 2019; Tullis, 2019).
Some of Moderna’s earliest funding came from DARPA, which awarded the company $25 million in 2013 to develop the mRNA platform that has become a key feature of its coronavirus vaccine (Usdin, 2020). Other DARPA beneficiaries now involved in efforts to develop Covid-19 vaccines or therapeutics include AbCellera Biologics, CureVac, Inovio Pharmaceuticals, Regeneron Pharmaceuticals, and Vir Biotechnology; some of AbCellera’s partners include major players like Pfizer and Gilead (Usdin, 2020).
The Pentagon’s involvement in coronavirus-related efforts goes well beyond DARPA-funded research. Four-star General Gustave Perna is serving as chief operating officer of Operation Warp Speed alongside chief advisor Moncef Slaoui. General Perna, in charge of U.S. Army Materiel Command, oversees the global supply chain for over 190,000 U.S. Army employees (HHS, 2020b). For the first time ever, the distribution of the eventual coronavirus vaccines is being planned as a “joint venture” between the CDC and the Pentagon, with the latter overseeing “all the logistics of getting the vaccines to the right place, at the right time, in the right condition” (Owermohle, 2020a). In a CBS “60 Minutes” appearance in early November, General Perna indicated that Operation Warp Speed already had doses of (currently unapproved) vaccine and syringes stockpiled and protected by armed guards, and intends to get them out the door “within 24 hours” of vaccine approval and delivered “to every zip code in this country” (Martin, 2020).
The Pentagon has indicated that private-sector involvement could be a key feature of the distribution strategy, and the private sector is positioning itself to participate. Merck, for example, is testing drone delivery of vaccines in partnership with Volansi, Inc., a company that provides “on-demand” drone services for the military (Landi, 2020; Simmie, 2020). In July, Merck’s CEO set the stage for its logistics involvement by describing vaccine distribution as “even a harder problem” than the “scientific conundrum of coming forward with a vaccine that works” (Murray & Griffin, 2020).
Outside the pharmaceutical arena, technological transformations that are speeding the world toward more centralized control also reveal the influence of the military-intelligence sector. For example, Amazon Web Services has held cloud-computing contracts with the CIA since 2013, with the original $600 million contract extending to all 17 intelligence agencies (Konkel, 2014). In October of 2019, the Department of Defense awarded the $10 billion JEDI cloud computing contract to Microsoft, a decision that Amazon has unsuccessfully disputed in court (Sandler, 2020). In early 2020, the U.S. Navy awarded a cloud computing contract to Leidos (Leidos, 2020).
5G, too, relies in part on the high-range millimeter-wave spectrum previously used almost entirely by the military for “non-lethal” crowd dispersal weapons (Joint Intermediate Force Capabilities Office, n.d.). In October, the Department of Defense announced it would spend $600 million to test “dual-use” applications of 5G to enhance the U.S. military’s “leap-ahead capabilities”, including applications such as 5G-enabled augmented/virtual reality, 5G-enabled “smart” warehouses, and 5G technologies “to aid in Air, Space, and Cyberspace lethality” (U.S. Department of Defense, 2020).
Both 5G and cloud computing are critical components of the Big Data and IoT build-out that is enabling the conversion of individual data into the “new oil” (Fitts, 2020a), and both have exploded in 2020 (Howell, 2020; Klebnikov, 2020). The technologies are essential to the “centrally controlled digital financial transaction systems” envisioned by central bankers, who plan to rely on seamless data flows to and from “every smartphone, community, and home without exception” (Fitts, 2020a).
Discussion
As more individuals and organizations connect the technocratic dots and look beneath the coronavirus pandemic’s seductively simple surface, it should become increasingly apparent that the pandemic profiteers do not have people’s best interests at heart. In The State of Our Currencies and other pandemic-related writings, Catherine Austin Fitts (2020a, 2020b) strongly emphasizes the importance of accepting that what is transpiring in the financial, tech, biopharmaceutical, and military-intelligence sectors is interconnected. Part of this involves recognizing that the coronavirus vaccines currently dominating the headlines represent something likely to go far beyond the simple health intervention being held out by scientists and officials as a panacea. Instead, the evidence suggests that Covid-19 vaccines are intended to serve as a Trojan horse to transport invasive technologies into people’s brains and bodies. These technologies could include brain-machine interface nanotechnology, digital identity tracking devices, technology that can be turned on and off remotely, and cryptocurrency-compatible chips (Fitts, 2020b).
In Fitts’ (2020a, 2020b) view, this type of intimate access — achieved “without notice, disclosure, or compensation” — represents the “final inch” of interest to technocrats. Together with external technologies to control behavior (Max, 2020), such access could permit the achievement of several goals: (1) replacing currencies with a digital transaction system, digital identification, and tracking (an “embedded credit card system”); (2) creating a global control grid that connects the population to the military-intelligence clouds; and (3) obtaining continuous access to valuable individual data on a 24/7 basis (Fitts, 2020b). Countries in West Africa are already piloting a venture by the Gates Foundation, the Gates-funded GAVI vaccine alliance, and Mastercard that “marks a novel approach towards linking a biometric digital identity system, vaccination records, and a payment system into a single cohesive platform” (Diego, 2020a). As Fitts (2020b) summarizes, “Just as Gates installed an operating system in our computers, now the vision is to install an operating system in our bodies and use ‘viruses’ to mandate an initial installation followed by regular updates”. The “neat trick”, as Fitts sees it, is that the use of vaccines as the delivery vehicle cancels out legal liability.
It is noteworthy that Bill Gates announced that he was stepping down from the Microsoft board of directors on March 13 — the same day that President Trump declared the pandemic a national emergency (Haselton & Novet, 2020). That same month, the Pentagon reaffirmed its intention for the JEDI cloud-computing contract to go to Microsoft (Rash, 2020; Sun, 2020). By distancing himself from the appearance of conflicts of interest with Microsoft’s Defense Department commitments and the Pentagon’s subsequent role in Operation Warp Speed, Mr. Gates had more freedom to make the rounds and begin promoting worldwide vaccination and digital certificates (Haggith, 2020). Gates has been less successful in distracting attention from other potential conflicts of interest. An exposé by The Nation (ironically also published in March) showed that the Gates Foundation gives billions to corporations in which the foundation holds stocks and bonds — including all of the major pharmaceutical companies — creating a “welter of conflicts of interest” (Schwab, 2020). A dozen years ago, around the time of the 2007-2008 financial crisis, the Los Angeles Times outlined the Gates Foundation’s numerous holdings in a number of notoriously “destructive or unethical” companies (Piller et al., 2007).
Mr. Gates is not the only party strenuously promoting digital IDs and “no-escape” financial tracking (marketed under the benevolent guise of “financial inclusion”). In October, Kristalina Georgieva, the International Monetary Fund’s (IMF’s) Managing Director, evoked “a world in which digital is the way in which financial transactions take place” and made it clear that she views universal digital IDs as a non-negotiable requirement for moving in the “right direction” (International Monetary Fund, 2020). Georgieva has, not unhappily, described Covid-19 as a “once in a lifetime pandemic” (Bello, 2020).
Georgieva’s remarks should be examined in the context of a proposal by the U.S. House of Representatives to bestow the IMF with $3 trillion “no-strings-attached” U.S. dollars as “coronavirus relief aid” (Huessy, 2020; Roberts, 2020). A U.S. taxpayer-funded gift of this magnitude would be unprecedented and would increase the IMF’s lending resources (called Special Drawing Rights or SDRs) by as much as 10-fold (Roberts, 2020). 2020’s events (including global debt entrapment and actual or potential food shortages) and the IMF’s bullying track record (Bello, 2020) suggest that the IMF could then wield the $3 trillion as a weapon, strong-arming countries into accepting an array of unwanted measures such as digital identities, forced vaccination, and eventually (as the World Economic Forum predicts), the relinquishment of private property (World Economic Forum, 2016). As a step in this general direction, the IMF has strongly praised India’s leadership in biometric identification systems. It celebrates the “delivery of social benefits through direct electronic payments to eligible bank account holders”, but glosses over the systems’ vulnerability to “unauthorized access” and the data breaches that are already rampant (Jha, 2018).
While current prospects for ordinary citizens certainly appear challenging, nothing is a foregone conclusion. Large-scale protests against the curtailment of civil rights have occurred and continue to occur in many countries, most notably in Germany (Depuydt, 2020). The Great Barrington Declaration — a statement crafted by public health scientists from Harvard, Stanford, and Oxford — has garnered signatures from over 12,000 scientists, over 35,000 medical practitioners, and nearly 639,000 citizens from around the world, all concerned about “the damaging physical and mental health impacts of the prevailing COVID-19 policies” (Kulldorff et al., 2020). Similarly, an Appeal authored in May by Archbishop Carlo Maria Viganò, former Apostolic Nuncio to the United States, gathered 40,000 signatures within a few days, with the signatories (religious leaders, doctors, journalists, lawyers, and other professionals) all seeking to draw attention to the threats to sovereignty and freedom that pandemic-related mandates have unleashed (Tosatti, 2020). Archbishop Viganò has also penned severe critiques of the Great Reset, describing its architects as “a global elite that wants to subdue all of humanity, imposing coercive measures [and a health dictatorship] with which to drastically limit individual freedoms and those of entire populations” (Viganò, 2020).
One of the signatories of Archbishop Viganò’s Appeal is attorney Robert F. Kennedy, Jr., founder and chief legal counsel of Children’s Health Defense, an organization dedicated to ending childhood epidemics by working to eliminate harmful exposures, holding those responsible accountable, and establishing stronger safeguards. In late October, Kennedy recorded a 19-minute video message to people around the world, describing the “coup d’état by big data, by big telecom, by big tech, by the big oil and chemical companies and by the global public health cartel” (Kennedy Jr., 2020). In his closing remarks, Kennedy also indicated that citizens who wish to maintain their freedoms cannot afford to remain complacent: “You are on the front lines of the most important battle in history, and it is the battle to save democracy, and freedom, and human liberty, and human dignity from this totalitarian cartel that is trying to rob us simultaneously, in every nation in the world, of the rights that every human being is born with.”
Andriotis, A. (2020, September 20). No job, loads of debt: Covid upends middle-class family finances. The Wall Street Journal. https://archive.is/mZAme
Bank for International Settlements. (2019, October 18). Investigating the impact of global stablecoins. G7 Working Group on Stablecoins. https://www.bis.org/cpmi/publ/d187.pdf
Bueno-Notivol, J., Gracia-García, P., Olaya, B., Lasheras, I., López-Antón, R., & Santabárbara, J. (2020). Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. International Journal of Clinical and Health Psychology, 2020 Aug 31. doi: 10.1016/j.ijchp.2020.07.007
Chauhan, G., Madou, M. J., Kalra, S., Chopra, V., Ghosh, D., & Martinez-Chapa, S. O. (2020). Nanotechnology for COVID-19: Therapeutics and vaccine research. ACS Nano. doi: 10.1021/acsnano.0c04006
Community FoodBank of New Jersey. (2020, September 30). COVID-19’s Impact on Food Insecurity in New Jersey. Hillside, NJ: CFBNJ. https://cfbnj.org/covidimpact/
Dubey, M. J., Ghosh, R., Chatterjee, S., Biswas, P., Chatterjee, S., & Dubey, S. (2020). COVID-19 and addiction. Diabetes & Metabolic Syndrome, 14(5), 817-823. doi: 10.1016/j.dsx.2020.06.008
Ettman, C. K., Abdalla, S. M., Cohen, G. H., Sampson, L., Vivier, P. M., & Galea, S. (2020). Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Network Open, 3(9), e2019686. doi: 10.1001/jamanetworkopen.2020.19686
Federal Accounting Standards Advisory Board. (2020, October 4). Statement of Federal Financial Accounting Standards 56: Classified Activities. FASAB Handbook, Version 18 (06/19). Retrieved September 26, 2020, from http://files.fasab.gov/pdffiles/handbook_sffas_56.pdf
Ganann, R., Ciliska, D., & Thomas, H. (2010). Expediting systematic reviews: methods and implications of rapid reviews. Implementation Science, 5, 56. doi: 10.1186/1748-5908-5-56
HHS. (2020a, February 4). Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID-19. U.S. Department of Health and Human Services. Federal Register, 85(52), 15198–15203. https://www.law360.com/articles/1253029/attachments/0
Jackson, N. A. C., Kester, K. E., Casimiro, D., Gurunathan, S., & DeRosa, F. (2020). The promise of mRNA vaccines: a biotech and industrial perspective. NPJ Vaccines, 5, 11. doi: 10.1038/s41541-020-0159-8
Pereira, M., & Oliveira, A. M. (2020). Poverty and food insecurity may increase as the threat of COVID-19 spreads. Public Health Nutrition, 1-5. doi: 10.1017/S1368980020003493
Profusa. (n.d.). Profusa is pioneering tissue-integrating biosensors for continuous monitoring of body chemistries. Retrieved October 26, 2020 from https://profusa.com/
Rossen, L. M., Branum, A. M., Ahmad, F. B., Sutton, P., & Anderson, R. N. (2020, October 23). Excess deaths associated with COVID-19, by age and race and ethnicity — United States, January 26–October 3, 2020. Morbidity and Mortality Weekly Report, 69(42), 1522-1527. doi: 10.15585/mmwr.mm6942e2
Shehab, N., Lovegrove, M. C., Geller, A. I., Rose, K. O., Weidle, N. J., Budnitz, D. S. (2016). US emergency department visits for outpatient adverse drug events, 2013-2014. JAMA, 316(20, 2115-2125. doi: 10.1001/jama.2016.16201
Wadhwa, A., Aljabbari, A., Lokras, A., Foged C., & Thakur, A. (2020). Opportunities and challenges in the delivery of mRNA-based vaccines. Pharmaceutics, 12(2), 102. doi: 10.3390/pharmaceutics12020102
Woolf, S. H., Chapman, D. A., Sabo, R. T., Weinberger, D.M., Hill, L., & Taylor, D. D. H. (2020). JAMA, 324(15), 1562-1564. doi: 10.1001/jama.2020.19545
Zhang, C., Maruggi, G., Shan, H., & Li, J. (2019). Advances in mRNA vaccines for infectious diseases. Frontiers in Immunology, 10, 594. doi: 10.3389/fimmu.2019.00594
Zhang, J., Xu, K., Zhang, S., Wang, Y., Zheng, N., Pan, G. et al. (2019). Brain-machine interface-based rat-robot behavior control. Advances in Experimental Medicine and Biology, 1101: 123-147. doi: 10.1007/978-981-13-2050-7_5
From the UK, The Guardian has the story: “People with a history of significant allergic reactions should not receive the Covid vaccine, the medicines regulator has said, after two NHS workers experienced symptoms on Wednesday.”
They just figured this out? Now?
The Guardian is referring to the Pfizer/BioNTech vaccine, which has just been approved in the US.
Two people experiencing significant adverse effects may not sound important, particularly since they already a history of allergic reactions, but the following quote in the Guardian article raises major red flags a mile high:
“The MHRA [UK Medicines and Healthcare products Regulatory Agency] advice states: ‘Any person with a history of a significant allergic reaction to a vaccine, medicine or food (such as previous history of anaphylactoid reaction or those who have been advised to carry an adrenaline autoinjector) should not receive the Pfizer/BioNtech vaccine. Resuscitation facilities should be available at all times for all vaccinations. Vaccination should only be carried out in facilities where resuscitation measures are available’.”
First of all, a very large number of people have a history of allergic reactions to a vaccine or medicine or food. Automatically, these people should not take the vaccine. But how many people in the general public are aware of this restriction?
Second, with the operation to vaccinate hundreds of millions of people running at top speed, who actually believes that many locations where shots are given will have the necessary resuscitation equipment on hand? Sheer insanity.
Then, on top of all this, we have a bombshell statement from the Denver Post: “Documents published by the two [vaccine] companies [Pfizer and BioNTech] showed that people with a history of severe allergic reactions were excluded from the [clinical vaccine] trials, and doctors were advised to look out for such reactions in trial participants who weren’t previously known to have severe allergies.”
In other words, the clinical trials were already biased, because they excluded people with a history of allergic reactions. Therefore, the performance of the vaccine looked safer. Therefore, no one would find out that allergic reactions to the vaccine are a MAJOR danger.
And NOW, as if it’s nothing more than an afterthought, we get—“Oh, by the way, if people have allergies, they shouldn’t take the vaccine.”
Why don’t regulators simply admit, “This vaccine is as disastrous as possible, but we can’t let that cat out of the bag.”
I have written about the inherent dangers of the new experimental RNA technology deployed with this COVOD vaccine. The world population is a vast group of guinea pigs. Past efforts to introduce RNA tech have failed because serious autoimmune reactions have occurred. The body basically attacks itself.
What rational person would line up to take this shot?
You have to ask yourself why some Pittsburgh and Chicago medical centers aren’t making the new COVID vaccine mandatory for their own healthcare workers.
They’ve issued that announcement on the basis of wait-and-see. They know the vaccine carries major risks, and the clinical trials were far from convincing.
According to WebMD, “more than 50 million Americans suffer from allergies each year.” 200,000 people come to the ER with food allergies. 4-5% of the population have food allergies. Who can say, with certainty, how many Americans would experience, say, life- threatening anaphylactic shock from the COVID vaccine?
And when it comes to medicines, consider just one type of allergic reaction—to penicillin or antibiotics. Is the outbreak of a rash serious enough to warrant automatic exemption from the COVID vaccine? Should shortness of breath be the standard? No one knows.
Finally, as I’ve reported in these pages several times, the 3 major clinical trials of COVID vaccines (Pfizer, Moderna, AstraZeneca) were designed to prevent nothing more than a “mild case of COVID-19.” That means a cough, or chills and fever.
Serious cases of illness? Hospitalization? Death? These were not on the radar of the clinical trials.
Cough, or chills and fever, cure themselves naturally. No need for a vaccine.
So again, what rational person would line up to take the COVID shot?
What rational person would imagine the celebratory media coverage of the vaccine rollout, or the carnival barking of Trump, amounts to more than a typical sales job and a hustle and a con?
Of course, you’re not supposed to know about the information in this article, even though it’s readily available in open source literature and in mainstream news. Social media censor the ANALYSIS OF THE MEANING OF THIS INFORMATION.
That’s called a clue.
That’s called medical tyranny.
A dictatorship wants you to take the COVID shot.
That’s another clue.
Spiro Skouras w/ Dr. James Lyons-Weiler: Vaccinated vs Unvaccinated — The Study the CDC Refused to Do
COVID-19 has reignited the vaccine debate worldwide as significant portions of the population express their unwillingness or hesitancy to take the experimental vaccine. A vaccine that was developed in record time with rolled back regulations, limited oversight, as well as a limited scope in the safety trials.
The vaccine manufacturers conducting the trials carefully screened potential volunteers, and carefully selected candidates to help them ensure a passing grade for government regulators and then mass distribution.
In this interview, Spiro is joined by Dr. James Lyons-Weiler who recently co-authored a study comparing vaccinated and unvaccinated children. A study the CDC has refused to perform despite four different congressional bills which would have obligated them to conduct. All four bills failed.
The fact that all four bills failed may not come as a surprise, considering Big Pharma is the largest lobby in DC. But the key findings of the study, may indeed surprise you.
The study was independently conducted, peer reviewed and publicly funded.
The UK and Russia have begun their mass COVID vaccination campaigns and it won’t be long from now until the experimental shot is deployed in your town.
Meanwhile, Canada, the US and Mexico are among a growing list of countries who have approved the Pfizer vaccine.
In this report, we examine some of the possible adverse events the CDC and FDA will be looking for, according to the agencies’ own virtual meeting on surveillance and vaccine safety held in October 2020.
We will also take a look at some of the adverse events experienced by the volunteers who participated in the trials according to an FDA review of the trial, as well as those who experienced adverse events outside of the trials.
Gates and his minions insist the billionaire never said we’d need digital vaccine passports. But in a June 2020 TED Talk, Gates said exactly that. Someone edited out the statement, but CHD tracked down the original.
Some chiseler altered Bill Gates’ June 2020 TED Talk to edit out his revealing prediction that we will all soon need digital vaccine passports (slide 1). But after considerable effort, we tracked down the original video (slide 2).
Gates’ minions on cable and network news, his public broadcasting, social media and fact-checker toadies all now insist that Gates never said such things. They say he never intended to track and trace us with subdermal chips or injected tattoos.
Gates’ company, Microsoft, has patented a sinister technology that uses implanted chips with sensors that will monitor body and brain activity. It promises to reward compliant humans with crypto currency payments when they perform assigned activities.
Gates also invested approximately $20 million in MicroCHIPS, a company that makes chip-based devices, including birth-control implant chips with wireless on/off switches for remote-controlled drug-delivery by medical authorities.
In July 2019, months before the COVID pandemic, Gates bought 3.7M shares of Serco, a military contractor with U.S. and UK government contracts to track and trace pandemic infections and vaccine compliance.
To facilitate our transition to his surveillance society, Gates invested $1 billion in EarthNow, which promises to blanket the globe in 5G video surveillance satellites. EarthNow will launch 500 satellites allowing governments and large enterprises to live-stream monitor almost every “corner” of the Earth, providing instantaneous video feedback with one-second delay.
The Bill and Melinda Gates Foundation also acquired 5.3 million shares of Crown Castle, which owns 5G spy antennas including more than 40,000 cell towers and 65,000 small cells.
Please make your own copy of these clips — as Gates’ power to disappear inconvenient facts is expanding every digital day.
###
[Truth Comes to Light editor’s note: The link in this article to the missing Gates’ clip sends you to Instagram. If, like me, you don’t use that platform, you won’t be able to view it. It can also be viewed HERE on BitChute at SansVimeo channel. – Kathleen]
Now that governments are going to roll out “a vaccine to save the world” (see here and here), people should become aware of a history they don’t know exists.
The article below was a small section of my book, AIDS INC., which I wrote in 1987-8. At the time, I decided to take a look at vaccines and see what I could find out about them.
My ensuing research led me into all sorts of surprising areas.
Since the period of 1987-8, much more has come to light about vaccine safety and efficacy. Here is what I discovered way back when—
“The combined death rate from scarlet fever, diphtheria, whooping cough and measles among children up to fifteen shows that nearly 90 percent of the total decline in mortality between 1860 and 1965 had occurred before the introduction of antibiotics and widespread immunization. In part, this recession may be attributed to improved housing and to a decrease in the virulence of micro-organisms, but by far the most important factor was a higher host-resistance due to better nutrition.” Ivan Illich, Medical Nemesis, Bantam Books, 1977
“In a recent British outbreak of whooping cough, for example, even fully immunized children contracted the disease in fairly large numbers; and the rates of serious complications and death were reduced only slightly. In another recent outbreak of pertussis, 46 of the 85 fully immunized children studied eventually contracted the disease.
“In 1977, 34 new cases of measles were reported on the campus of UCLA, in a population that was supposedly 91% immune, according to careful serological testing. Another 20 cases of measles were reported in the Pecos, New Mexico, area within a period of a few months in 1981, and 75% of them had been fully immunized, some of them quite recently. A survey of sixth-graders in a well-immunized urban community revealed that about 15% of this age group are still susceptible to rubella, a figure essentially identical with that of the pre-vaccine era.” Richard Moskowitz, MD, The Case Against Immunizations, 1983, American Institute of Homeopathy.
“Of all reported whooping cough cases between 1979 and 1984 in children over 7 months of age – that is, old enough to have received the primary course of the DPT shots (diphtheria, pertussis, tetanus) – 41% occurred in children who had received three or more shots and 22% in children who had one or two immunizations.
“Among children under 7 months of age who had whooping cough, 34% had been immunized between one and three times…
“… Based on the only U.S. findings on adverse DPT reactions, an FDA-financed study at the University of California, Los Angeles, one out of every 350 children will have a convulsion; one in 180 children will experience high-pitched screaming; and one in 66 will have a fever of 105 degrees or more.” Jennifer Hyman, Democrat and Chronicle, Rochester, New York, special supplement on DPT, dated April, 1987.
“A study undertaken in 1979 at the University of California, Los Angeles, under the sponsorship of the Food and Drug Administration, and which has been confirmed by other studies, indicates that in the U.S.A. approximately 1,000 infants die annually as a direct result of DPT vaccinations, and these are classified as SIDS (Sudden Infant Death Syndrome) deaths. These represent about 10 to 15% of the total number of SIDS deaths occurring annually in the U.S.A. (between 8,000 and 10,000 depending on which statistics are used).” Leon Chaitow, Vaccination and Immunization, CW Daniel Company Limited, Saffron Walden, Essex, England, 1987.
“Assistant Secretary of Health Edward Brandt, Jr., MD, testifying before the U.S. Senate Committee on Labor and Human Resources, rounded… figures off to 9,000 cases of convulsions, 9,000 cases of collapse, and 17,000 cases of high-pitched screaming for a total of 35,000 acute neurological reactions occurring within forty-eight hours of a DPT shot among America’s children every year.” DPT: A Shot in the Dark, by Harris L. Coulter and Barbara Loe Fischer, Harcourt Brace Jovanovich.
“While 70-80% of British children were immunized against pertussis in 1970-71, the rate is now 39%. The committee predicts that the next pertussis epidemic will probably turn out to be more severe than the one in 1974/75. However, they do not explain why, in 1970/71, there were more than 33,000 cases of pertussis with 41 fatal cases among the very well immunized British child population; whereas in 1974/75, with a declining rate of vaccination, a pertussis epidemic caused only 25,000 cases with 25 fatalities.” Wolfgang Ehrengut, Lancet, Feb. 18, 1978, p. 370.
“… Barker and Pichichero, in a prospective study of 1232 children in Denver, Colorado, found after DTP that only 7% of those vaccinated were free from untoward reactions, which included pyrexia (53%), acute behavioral changes (82%), prolonged screaming (13%), and listlessness, anorexia and vomiting. 71% of those receiving second injections of DTP experienced two or more of the reactions monitored.” Lancet, May 28, 1983, p. 1217
“Publications by the World Health Organization show that diphtheria is steadily declining in most European countries, including those in which there has been no immunization. The decline began long before vaccination was developed. There is certainly no guarantee that vaccination will protect a child against the disease; in fact, over 30,000 cases of diphtheria have been recorded in the United Kingdom in fully immunized children.” Leon Chaitow, Vaccination and Immunization, p. 58.
“Pertussis (whooping cough) immunization is controversial, as the side effects have received a great deal of publicity. The counter claim is that the effectiveness and protection offered by the procedure far outweigh the possible ill effects… annual deaths, per million children, from this disease over the period from 1900 to the mid-nineteen seventies, shows that from a high point of just under 900 deaths per million children (under age 15) in 1905, the decline has been consistent and dramatic. There had been a lowering of mortality rates of approximately 80% by the time immunization was introduced on a mass scale, in the mid-nineteen fifties. The decline has continued, albeit at a slower rate, ever since. No credit can be given to vaccination for the major part of the decline since it was not in use.” Chaitow, Vaccination and Immunization, p. 63.
“… the swine-flu vaccination program was one of its (CDC) greatest blunders. It all began in 1976 when CDC scientists saw that a virus involved in a flu attack outbreak at Fort Dix, N.J., was similar to the swine-flu virus that killed 500,000 Americans in 1918. Health officials immediately launched a 100-million dollar program to immunize every American. But the expected epidemic never materialized, and the vaccine led to partial paralysis in 532 people. There were 32 deaths.” U.S. News and World Report, Joseph Carey, October 14, 1985, p. 70, “How Medical Sleuths Track Killer Diseases.”
“Despite (cases) in which (smallpox) vaccination plainly failed to protect the population, and despite the rampant side-effects of the methods, the proponents of vaccination continued their attempts to justify the methods by claims that the disease had declined in Europe as a whole during the period of its compulsory use. If the decline could be correlated with the use of the vaccination, then all else could be set aside, and the advantage between its current low incidence could be shown to outweigh the periodic failures of the method, and to favour the continued use of vaccination. However, the credit for the decline in the incidence of smallpox could not be given to vaccination. The fact is that its incidence declined in all parts of Europe, whether or not vaccination was employed.” Chaitow, Vaccination and Immunization, pp. 6-7.
“Smallpox, like typhus, has been dying out (in England) since 1780. Vaccination in this country has largely fallen into disuse since people began to realize how its value was discredited by the great smallpox epidemic of 1871-2 (which occurred after extensive vaccination).” W. Scott Webb, A Century of Vaccination, Swan Sonnenschein, 1898.
“In this incident (Kyoto, Japan, 1948) – the most serious of its kind – a toxic (vaccine) batch of alum-precipitated toxoid (APT) was responsible for illness in over 600 infants and for no fewer than 68 deaths.
“On 20 and 22 October, 1948, a large number of babies and children in the city of Kyoto received their first injection of APT. On the 4th and 5th of November, 15,561 babies and children aged some months to 13 years received their second dose. One to two days later, 606 of those who had been injected fell ill. Of these, 9 died of acute diphtheritic paralysis in seven to fourteen days, and 59 of late paralysis mainly in four to seven weeks.” Sir Graham Wilson, Hazards of Immunization, Athone Press, University of London, 1967.
“Accidents may, however, follow the use of this so-called killed (rabies) vaccine owing to inadequate processing. A very serious occurrence of this sort occurred at Fortaleza, Ceara, Brazil, in 1960. No fewer than 18 out of 66 persons vaccinated with Fermi’s carbolized (rabies) vaccine suffered from encephalomyelitis and every one of the eighteen died.” Sir Graham Wilson, Hazards of Immunization.
“At a press conference in Washington on 24 July, 1942, the Secretary of War reported that 28,585 cases of jaundice had been observed in the (American) Army between 1 January and 4 July after yellow fever vaccination, and of these 62 proved fatal.” Sir Graham Wilson, Hazards of Immunization.
“The world’s biggest trial (conducted in south India) to assess the value of BCG tuberculosis vaccine has made the startling revelation that the vaccine ‘does not give any protection against bacillary forms of tuberculosis.’ The study said to be ‘most exhaustive and meticulous,’ was launched in 1968 by the Indian Council of Medical Research (ICMR) with assistance from the World Health Organization (WHO) and the U.S. Centers for Disease Control in Atlanta, Georgia.
“The incidence of new cases among the BCG vaccinated group was slightly (but statistically insignificantly) higher than in the control group, a finding that led to the conclusion that BCG’s protective effect ‘was zero.’” New Scientist, November 15, 1979, as quoted by Hans Ruesch in Naked Empress, Civis Publishers, Switzerland, 1982.
“Between 10 December 1929 and 30 April 1930, 251 of 412 infants born in Lubeck received three doses of BCG vaccine by the mouth during the first ten days of life. Of these 251, 72 died of tuberculosis, most of them in two to five months and all but one before the end of the first year. In addition, 135 suffered from clinical tuberculosis but eventually recovered; and 44 became tuberculin-positive but remained well. None of the 161 unvaccinated infants born at the time was affected in this way and none of these died of tuberculosis within the following three years.” Hazards of Immunization, Wilson.
“We conducted a randomized double-blind placebo-controlled trial to test the efficacy of the 14-valent pneumococcal capsular polysaccharide vaccine in 2295 high-risk patients… Seventy-one episodes of proved or probable pneumococcal pneumonia or bronchitis occurred among 63 of the patients (27 placebo recipients and 36 vaccine recipients)… We were unable to demonstrate any efficacy of the pneumococcal vaccine in preventing pneumonia or bronchitis in this population.” New England Journal of Medicine, November 20, 1986, p. 1318, Michael Simberkoff et al.
“But already before Salk developed his vaccine, polio had been constantly regressing; the 39 cases out of every 100,000 inhabitants registered in 1942 had gradually diminished from year to year until they were reduced to only 15 cases in 1952… according to M. Beddow Baylay, the English surgeon and medical historian.” Slaughter of the Innocent, Hans Reusch, Civitas Publishers, Switzerland, and Swain, New York, 1983.
“Many published stories and reports have stated, implied and otherwise led professional people and the public to believe that the sharp reduction of cases (and of deaths) from poliomyelitis in 1955 as compared to 1954 is attributable to the Salk vaccine… That it is a misconception follows from these considerations. The number of children inoculated has been too small to account for the decrease. The sharp decrease was apparent before the inoculations began or could take effect and was of the same order as the decrease following the immediate post-inoculation period.” Dr. Herbert Ratner, Child and Family, vol. 20, no. 1, 1987.
“So far it is hardly possible to gain insight into the extent of the immunization catastrophe of 1955 in the United States. It may be considered certain that the officially ascertained 200 cases (of polio) which were caused directly or indirectly by the (polio) vaccination constitute minimum figures… It can hardly be estimated how many of the 1359 (polio) cases among vaccinated persons must be regarded as failures of the vaccine and how many of them were infected by the vaccine. A careful study of the epidemiologic course of polio in the United States yields indications of grave significance. In numerous states of the U.S.A., typical early epidemics developed with the immunizations in the spring of 1955… The vaccination incidents of the year 1955 cannot be exclusively traced back to the failure of one manufacturing firm.” Dr. Herbert Ratner, Child and Family, 1980, vol. 19, no. 4, “Story of the Salk Vaccine (Part 2).”
“Suffice it to say that most of the large (polio) epidemics that have occurred in this country since the introduction of the Salk vaccine have followed the wide-scale use of the vaccine and have been characterized by an uncommon early seasonal onset. To name a few, there is the Massachusetts epidemic of 1955; the Chicago epidemic of 1956; and the Des Moines epidemic of 1959.” Dr. Herbert Ratner, Child and Family, 1980 vol. 19, no. 4.
“The live (Sabin) poliovirus vaccine has been the predominant cause of domestically arising cases of paralytic poliomyelitis in the United States since 1972. To avoid the occurrence of such cases, it would be necessary to discontinue the routine use of live poliovirus vaccine.” Jonas Salk, Science, March 4, 1977, p. 845.
“By the (U.S.) government’s own admission, there has been a 41% failure rate in persons who were previously vaccinated against the (measles) virus.” Dr. Anthony Morris, John Chriss, BG Young, “Occurrence of Measles in Previously Vaccinated Individuals,” 1979; presented at a meeting of the American Society for Microbiology at Fort Detrick, Maryland, April 27, 1979.
“Prior to the time doctors began giving rubella (German measles) vaccinations, an estimated 85% of adults were naturally immune to the disease (for life). Because of immunization, the vast majority of women never acquire natural immunity (or lifetime protection).” Dr. Robert Mendelsohn, Let’s Live, December 1983, as quoted by Carolyn Reuben in the LA WEEKLY, June 28, 1985.
“Adminstration of KMV (killed measles vaccine) apparently set in motion an aberrant immunologic response that not only failed to protect children against natural measles, but resulted in heightened susceptibility.” JAMA Aug. 22, 1980, vol. 244, p. 804, Vincent Fulginiti and Ray Helfer. The authors indicate that such falsely protected children can come down with “an often severe, atypical form of measles. Atypical measles is characterized by fever, headache… and a diverse rash (which)… may consist of a mixture of macules, papules, vesicles, and pustules… ”
The above quotes reflect only a mere fraction of an available literature which shows there is a need for an extensive review of vaccination. It is certain that undisclosed, unlooked for illness occurs as a result of vaccines, or as a result of infection after protective immunity should have been conferred but wasn’t. A certain amount of this sort of illness is immunosuppressive in the widest sense, and some in a narrower sense (depression of T-cell numbers, etc.). When looking for unusual illness and immune depression, vaccines are one of those areas which remain partially hidden from investigation. That is a mistake. It is not adequate to say, “Vaccines are simple; they stimulate the immune system and confer immunity against specific germ agents.” That is the glossy presentation. What vaccines often do is something else. They engage some aspect of the body’s immune-response, but to what effect over the long term? Why, for example, do children who have measles vaccine develop a susceptibility to another more severe, atypical measles? Is that virulent form of the disease the result of reactivation of the virus in the vaccine?
Official reports on vaccine reactions are often at odds with unofficial estimates because of the method of analysis used. If vaccine-reaction is defined as a small set of possible effects experienced within 72 hours of an inoculation, then figures will be smaller. But doctors like G.T. Stewart, of the University of Glasgow, have found through meticulous investigation, including visits to hospitals and interviews with parents of vaccinated children, that reactions as severe as brain-damage (e.g., from the DPT vaccine) can be overlooked, go unreported and can be assumed mistakenly to have come from other causes.
Oregon Pediatrician Dr. Paul Thomas, MD has come under fire by the Oregon Medical Board for providing informed consent to his patients.
After publishing a study using the data from his more than 13000 patients, the Oregon Medical, in an attempt to silence the highly controversial study results, suspended his license.
In an article on the COVID vaccine rollout, CNN says that Americans shouldn’t be alarmed if people start dying after taking the vaccine because “deaths may occur that won’t necessarily have anything to do with the vaccine.”
The advisory appeared in an article titled ‘Why vaccinate our most frail? Odd vote out shows the dilemma’ in which Dr. Kelly Moore, associate director of the Immunization Action Coalition, cautions that vaccines don’t work as well on the frail and elderly compared to healthy people.
“When shots begin to go into arms of residents, Moore said Americans need to understand that deaths may occur that won’t necessarily have anything to do with the vaccine,” states the report.
“We would not at all be surprised to see, coincidentally, vaccination happening and then having someone pass away a short time after they receive a vaccine, not because it has anything to do with the vaccination but just because that’s the place where people at the end of their lives reside,” Moore said.
She then said Americans shouldn’t be alarmed to see people dying a day or two after receiving the COVID vaccination.
“One of the things we want to make sure people understand is that they should not be unnecessarily alarmed if there are reports, once we start vaccinating, of someone or multiple people dying within a day or two of their vaccination who are residents of a long-term care facility. That would be something we would expect, as a normal occurrence, because people die frequently in nursing homes.”
While deaths in care homes of people who take the vaccine are described as normal and nothing to do with the vaccine, some would suggest that you could make the exact same argument about deaths of those with multiple comorbidities in care homes that were put down to COVID.
Many have and have been shouted down for doing so.
In a 2012 meeting, the FDA voted to allow the use of human fetal cells and adult human tumor cells in vaccines, despite acknowledging the many risks, including that vaccine recipients might later develop cancer.
“If the American people knew some of the things that went on at the FDA, they’d never take anything but Bayer aspirin.” — Len Lutwalk, FDA scientist
“The FDA, by spinelessly knuckling under to every whim of the drug companies, has thrown away its high reputation, and in doing so, forfeited our trust.” — Drummond Rennie, deputy editor of JAMA
“[The] honest employee fears the dishonest employee. There is also irrefutable evidence that managers at CDER (Center for Drug Evaluation and Research of the FDA) have placed the nation at risk by corrupting the evaluation of drugs and by interfering with our ability to ensure the safety and efficacy of drugs. While I was at FDA, drug reviewers were clearly told not to question drug companies and that our job was to approve drugs … If we asked questions that could delay or prevent a drug’s approval — which of course was our job as drug reviewers — management would reprimand us, reassign us, hold secret meetings about us or worse … When you are able to dig in, if you found issues that would make you turn down a drug, you could be pressured to reverse your decision, or the review would then be handed off to someone who would simply copy and paste whatever claims the company made in the summary document … I believe I also have documentation of falsification of documents, fraud, perjury and widespread racketeering, including witnesses tampering and witness retaliation.” — Ronald Kavanagh, Ph.D., pharmacist who reviewed medications for the FDA from 1998 to 2008
Vaccines and related biological products advisory committee today
Today — Thursday, Dec. 10 — the Vaccines and Related Biological Products Advisory Committee (VRBPAC), which is the U.S. Food and Drug Administration’s (FDA) internal panel that licenses new vaccines as “safe and effective,” will meet to consider Pfizer’s COVID vaccine. VRBAC will meet in one week, Dec. 17, to consider approval of the Moderna vaccine.
The damning safety studies in Pfizer’s late release clinical trial data dump, and the severe (life-threatening) allergic reactions that bedeviled the vaccine’s UK rollout, have raised red flags and public anxiety about the safety of the companies’ mRNA vaccines. Anthony Fauci has addressed growing skepticism about COVID vaccines and the Operation Warp Speed program, by reassuring the public that “VRBPAC” is an “independent panel of leading experts” whom the public can absolutely trust to assure vaccine safety.
In order to help you make your own conclusion about how reliably VRBPAC will protect your health, I excerpt below the transcripts from the cavalier, ignorant and astonishingly unethical deliberations during the 2012 VRBPAC meeting where panelists voted unanimously to allow use of human tumor cells in vaccines. I urge you to read and make up your own mind whether you want to place your health — and perhaps your life — in the hands of these reckless charlatans and irresponsible clowns.
How FDA originally approved use of fetal cells in vaccines
FDA allows both human fetal cells and adult human tumor cells in vaccines. Both types have cancer risks. While both Pfizer and Moderna tested their mRNA vaccine using fetal cells, there are no fetal cells, cell debris or DNA in their final products.
However, according to company documents, Johnson and Johnson (Janssen) and Altimmune’s COVID vaccines are manufactured in the human fetal cell line PER-C6, and thus the final vaccine products will contain cellular debris and DNA fragments from these cells. Researchers harvested these cell lines from the eyeball of an 18-week-old human fetus aborted in 1985, and then rendered them immortal by making them cancerous.
The AstraZeneca, Cansino, Gamayela, Vaxart, LongComm and Upitt vaccines are manufactured in the human fetal cell line HEK293, and thus the final vaccine products will contain cellular debris and DNA fragments from the fetal HEK-293 cell line. Scientists harvested this cell line from the kidney of a female Dutch fetus legally aborted in 1973 and then immortalized the cells by rendering them cancerous.
Normal primary cells, which are unable to replicate indefinitely, ultimately die. Immortalized cell lines are derived from known malignant cancer cells such as those obtained from Henrietta Lacks (HeLa) or created in the laboratory by introducing viral oncogenes or chemical exposures capable of mutating normal primary cells into immortal tumor cells.
According to FDA’s “The Pink Sheet” dated Nov. 29, 1999, for two decades the agency has been acutely aware of the inherent risks of using immortalized cell lines for vaccine development. The FDA CBER Director Dr. Peter Patriarca, M.D. explained that continuous cell lines are used for their ability to self-propagate, making them an ideal substrate on which to grow viruses, “the worst thing we are concerned about is … malignancy, because some of these continuous cells have the potential for growing tumors in laboratory animals.”
Patriarca further conceded that “the technology to make these vaccines actually exceeds the science and technology to understand how these vaccines work and to predict how they will work.” This dire “black box” conundrum that Patriarca described in 1999 is even more acute today with the urgent pressure to develop COVID vaccines before manufacturers have tested them in animals or subjected them to long-term safety studies.
We call vaccines “biologics” because vaccinologists have traditionally grown their antigens on biological substrates — usually animal tissue. Competing companies culture COVID vaccines on a variety of animal strata. The Merck and IAVA COVID vaccines are manufactured in vero monkey cells, and thus contain cellular debris and DNA fragments from vero monkeys in the final product. The Sanofi, GSK, and Novavax COVID jabs are manufactured in insect cells and thus contain insect cellular debris and DNA fragments in the final products.
Public health advocates criticize the use of animal tissues in vaccines due to risks that they carry endogenous viruses, microbes, parasites and lack safety testing. (Plague of Corruption, Mikovits 2020).The first use of human fetal cells in vaccines occurred around 60 years ago, but the practice is increasingly popular. It was always controversial. Immunologists long considered using cells from aborted human fetuses in vaccines to be a high-risk gambit; human DNA debris is much more likely to infiltrate cells in vaccinated individuals than insect or monkey DNA.
Researchers and regulatory agencies have worried for more than 50 years about the potential for injected DNA to cause cancer. According to Dr. Theresa Deisher, a research scientist, primitive (unmethylated) DNA chains from human fetuses have the ability to 1) activate immune receptors that could lead to autoimmune attacks in susceptible individuals who have genetic predispositions that cause their own DNA to be under-methylated, or 2) insert into cells where they could combine with host DNA and cause mutations.
Regulators have in the past predicted that the odds of that happening were less than 1 in a trillion. However, in early gene therapy trials this event did indeed occur in 4 of 9 boys, 1 of whom died from the leukemia the insertions caused.
“Researchers have long observed that when introduced DNA enters a cell, it chooses a region of the cell that gives it a survival advantage. These could be the regions that are most likely to produce long-living cancer cells,” Dr. Deisher told me. FDA has never made any effort to test the safety of this practice or to determine whether the epidemic of soft-tissue cancers is “vaccine-generation” children is related to the use of cancerous fetal cells in vaccines. Even worse, in 2002, FDA green-lighted vaccine companies to use cancerous tumor cells from adults in vaccines.
FDA as an arm of Big Pharma
Before reviewing the shocking transcript of the FDA meeting that approved this dubious practice, we need to understand the conflicts and corruption that pervade this rogue agency. If we are to ever develop safe, effective COVID vaccines, we need first to stop thinking of the FDA as a regulatory agency; it is an arm of the notoriously corrupt pharmaceutical industry.
According to a 2017 Emory University study entitled “Thick as Thieves? Big Pharma Wields Its Power with the Help of Government Regulation,” FDA bureaucrats act as “enablers, or perhaps worse still, [they are] complicit in questionable or ethically unsound activity as a result of being driven by self-serving motives ….” A 1992 law that allows drugmakers to buy fast-track approvals for new products from FDA has poured concrete on a regulatory dynamic already corrupted by all the ubiquitous mechanisms of “agency capture.”
No one at FDA wins kudos for slowing down those money flows. To the contrary, according to FDA’s own employees, drug company payments bias regulators, with “an inclination toward approval.”
According to Dr. Michael Carome, a former Health and Human Services (HHS) official and a director of the advocacy group Public Citizen, “Instead of a regulator and a regulated industry, we now have a partnership … That relationship has tilted [the FDA] away from a public health perspective to an industry friendly perspective.”
Corrupt vaccine approval panels
But as corrupt as FDA is, the internal panels — VRBAC — that approve new vaccines make the rest of the agency look like a Sunday church picnic.
When Dr. Fauci, Paul Offit, Peter Hotez and Bill Gates tell you that you needn’t worry because FDA is the “gold standard” for vaccine safety and that the ultimate licensing decision will be made by an “independent panel of experts,” they are talking about VRBPAC. But VRBPAC is far from “independent.” It is not even comprised exclusively of public officials. Instead, it is populated by outside “experts” who are almost all pharmaceutical industry insiders.
In 2003, following a 3-year investigation, the United States Congress’s House Oversight Committee found VRBAC was completely dominated by the vaccine industry.
According to findings of the congressional investigation, VRBAC’s “independent” vaccine panel members often share vaccine patents with the pharmaceutical companies whose products they are evaluating. They “own stock in those vaccine companies, receive payment from those companies for research and paid speeches. They occupy consulting lofty and powerful sinecures and accept payments to monitor vaccine trials and funding for their academic departments.”
The 2000-2003 U.S. House Government Reform Committee’s investigation of VRBPAC found that: (1) “The overwhelming majority of members, both voting members and consultants, have substantial ties to the pharmaceutical industry.” (2) “Conflict of interest rules employed by the FDA … have been weak, enforcement has been lax and committee members with substantial ties to pharmaceutical companies have been given waivers to participate in committee proceedings … In many cases, significant conflicts of interest are not deemed to be conflicts at all.”
Congressional investigators offered a typical example of the sort of financial entanglements that put VRBPAC under Pharma’s slavish control. That example was the December 12, 1997, VRBPAC meeting that approved Wyeth’s (now Pfizer’s) rotavirus vaccine, Rotashield.
The Congressional investigators detailed the committee’s cozy nepotism with vaccine makers.
“Examples of Conflicts of Interest:
“For instance, 3 out of 5 FDA advisory committee (VRBPAC) members who voted to approve the rotavirus vaccine in December 1997 had financial ties to pharmaceutical companies that were developing different versions of the vaccine.
“One out of five voting members’ employer had a $9,586,000 contract for a rotavirus vaccine.
“One out of five voting members was the principal investigator for a Merck grant to develop a rotavirus vaccine.
“One out of five voting members received approximately $1 million from vaccine manufacturers toward vaccine development.”
Congressional investigators concluded that, “Altogether, four out of the five committee members had conflicts of interest that required waivers, and their recommendation for approval of the vaccine was unanimous.”
Here’s what happened at the 2012 FDA meeting on fetal cells
HHS acknowledges that the FDA and Centers for Disease Control committees that contract and review new vaccines have historically not used “evidence-based medicine.” To illustrate what this means, one only need read (below) the astonishing transcript of the 2012 panel that first approved the use of adult cancer tumor cells in vaccines.
This transcript shows what the public is never supposed to see: the behind-the-scenes sausage-making of federal vaccine approvals. Here, you will read for yourself how the “independent,” “gold standard” panelists entrusted with protecting your children made monumentally consequential decisions, not on evidence-based science, but by rolling the dice and taking what they knew was a horrendously risky bet on public health
In any other realm, this transcript would be proof of negligent homicide. The sickening side-view of VRBAC’s deliberations reveals FDA’s “trusted experts” for what they are; sadistic boys in lab coats giddily discussing the removal of wings from flies. We are all lab rats in their high-risk population-wide experiment. At FDA’s vaccine division, that sort of reckless decision-making is routine.
In 2012, most live virus vaccines were from animal tissue and the idea of putting potentially cancerous tumor cells from adult “donors” in vaccines was still a daring and audacious gamble. That September, the FDA VRBPAC committee met to discuss this risky innovation. The transcript of that meeting — showing captive FDA officials considering a proposal by the pharma cabal to allow the use of human cancer cells (HeLa) to replace animal tissue in the manufacture of vaccines — is proof of reckless criminal conduct.
The HeLa cells are well known to cause cancer in animals, but Big Pharma wanted to lower production costs of vaccines and this method is cheaper and faster than using animal tissue for the cultivated media. The obvious question of whether such vaccines might induce cancer in recipients was on the top of the VRBPAC agenda. Health authorities and vaccine manufacturers blatantly acknowledged their uncertainty regarding the safety of vaccines made from HeLa cancer tumors as they voted to make a dangerous high-stakes gamble that would lower costs for vaccine makers
Unbelievably, FDA voted to allow pharmaceutical companies to produce vaccines using human cells without reviewing a single scientific study to determine if the outcome would be safe.
Before, I quoted some of the criminally reckless statements from the meeting directly. A more detailed account appears in this article.
This was a full meeting of FDA’s VRBPAC in 2012 to decide on the use of human tumor cell lines for the production of vaccines. I list these speakers and their titles at that time:
Dr. Philip Krause, Acting Deputy Director of OVRR (Office of Vaccine Research and Review) and FDA’s CBER (Center for Biologics Evaluation and Research). Also, Principal Investigator for Vaccine Safety: Virus Detection and Latency.
Dr. Doug Lowy, Director of the National Cancer Institute of the NIH.
Dr. Robert Daum, Chair of the VRBPAC.
Donald W. Jehn M.S., Designated Federal Officer for VRBPAC.
Keith Peden, PhD, Chief of LDNAV, DVP/OVRR/CBER.
Dr. Marion Gruber, Director of the FDA’s Office of Vaccines.
Dr. Nathanial Brady, a self-described clinician.
Dr. Pamela McInnes, a vaccine development expert and the Director of the Division of Extramural Research at the NIH’s National Institute of Dental and Craniofacial Research, and previously a Deputy Director under Anthony Fauci at the National Institute of Allergy and Infectious Diseases.
Pharma knew that their tumorigenic vaccines might cause tumors in recipients.
Dr. Philip Krause acknowledged the risks when he said: “We have really identified three major factors that could potentially convey risk from tumor-derived cells. And these include the cells themselves … and if they were tumor-derived cells then maybe they themselves could form tumors in a vaccine recipient.”
Government regulators acknowledged that tumor cell lines can cause tumors.
Dr. Doug Lowy acknowledged this when he said: “What I think is qualitatively different about the tumor cell lines is the fact that they can cause tumors.”
FDA officials knew that tumors might occur decades after vaccination.
Dr. James Cook acknowledged this when he commented: “But certainly, if you are going to address this question about tumor risk from vaccines made in tumor cell lines, it’s going to have to be a decade’s question.”
FDA openly acknowledged that its primary objective was not to assure public safety but to help vaccine manufacturers.
Dr. Robert Daum, the leader of the meeting, commented: “ …but we are here to consider the issues that we would like to advise the agency to consider in helping the company continue the manufacturing process, what should they be concerned about, what should they be watching for.”
FDA officials knew that they could not prove vaccine safety using test animals to assess oncogenicity.
Dr. Keith Peden acknowledged this fact when he said: “I’m not optimistic that we’re going to find animal models to assess oncogenicity of DNA. That’s why I’m feeling that maybe it’s the clearance aspect that we have to deal with, with respect to DNA.”
FDA officials deliberately terminated animal safety tests too early in order to conceal consequences.
Dr. Robert Daum acknowledged this fact when he said: “Are they watching these animals long enough? Should it be longer?”
Dr. Keith Peden acknowledged this fact when he said: “Is it relevant to safety that a cell forms a tumor after a year, a year-and-a-half?”
FDA decided to keep the tumor cell lines secret, because doctors and the public may be alarmed and say “Oh, my God!” if they knew the truth.
Dr. Nathanael Brady acknowledged this when he said: “How is this group (of vaccines) going to be able to be accepted by the consumers … As soon as you hear “a tumor-derived cell line,” how do you explain that, put the public at ease?”
Dr. Robert Daum further acknowledged these facts: “ …the practicing medical community and also the lay public. They are going to hear that we are recommending, or that the manufacturers are making, vaccines with tumorigenic cell lines and say, ‘Oh, my God,’ even if there’s no scientific basis to say, ‘Oh, my God.’”
FDA decided to use deceptive language to convince doctors and the public that the vaccines were safe even when they, themselves, were unconvinced of safety.
Dr. Philip Krause acknowledged this when he said: “… because it’s a discussion of how one communicates these issues and how the public will perceive them. But I’m not completely sure that we have a complete answer on the fundamental scientific question. So how can you communicate a scientific consensus that the product is safe unless we’re sure that you, the experts we are asking to advise us, are convinced that it’s safe?”
FDA decided to hide information about their use of tumor cells and omit it from package inserts.
Dr. Marion Gruber proposed this deception when he said: “The minute you describe something in the package insert in terms of potential clinical safety concerns, I think that really precludes using these cell substrates.”
Dr. James Cook agreed to the deception when he said: “When it gets right down to what’s in the vial and what the patient is going to ask me about, whether it’s safe, I’m not going to say, well, you know, HeLa cells kill nude mice.”
Dr. Robert Daum acknowledged the deception when he said: “I don’t know that our charge is to micromanage the package insert today. I think that’s a new discussion, with lots of issues that we haven’t really aired completely.”
Health authorities were skeptical about safety of the tumor lines, but they decided to subject the public to the risk, so that they could perform a global population-wide live human experiment.
Dr. Robert Daum agreed to conduct the mass human experiment with the following statement: “So I’m not sure that we can give a certainty there’s no risk — don’t worry about this … It’s sort of a brave new world. We’re all doing it together. But I think that you are doing a beautiful job.”
FDA officials opted to toss the dice, perform the population-wide human experiment, and learn about the risks as time goes by.
FDA officials even cast this experiment as a noble venture in the quest for scientific knowledge. Dr. Pamela McInnes made this stunning appeal to her colleagues: “… even though there are challenges [risks to humans] to using the new technologies, they have to be embraced and we have to continue to try to learn from them and struggle through that learning curve.”
In the end, FDA decided to take the risks. The leader of the committee says, “I’m a vaccine guy,” then urged his cronies to approve.
Dr. Robert Daum said: “I’m a vaccine guy. They are wonderful to prevent infectious diseases … I hope that I’m speaking for everybody when I say that’s the answer to your question. If not, please chime in now.”
The committee formally approves the method of making vaccines from human cancer tumors.
Dr. Robert Daum said: “To come back to the agency’s question of whether this committee believes it’s correct scientifically to go forward with the development of these vaccines, our answer is yes.”
Prior to voting to go forward, the committee made the following conclusions:
Making vaccines with cells that are directly derived from human cancer tumors is faster and cheaper than breeding animals for the culture media.
Millions of potentially cancer-causing vaccines will be produced.
The vaccines may possibly cause genetic mutations.
Millions of dollars will be made by vaccine promoters.
The health of millions of consumers may be jeopardized.
Information about how vaccines are made will be hidden from doctors and consumers.
This 2012 VRBPAC meeting perfectly illustrates the reckless, malevolent and murderous zeitgeist underlying the Pharma/HHS partnership. VRBPAC’s “devil-may-care” decision-making allowed pharmaceutical companies to use potentially cancerous fetal cells to make millions of vaccines.
Since that meeting, vaccines containing cancerous cells and DNA strands from aborted fetuses have become pervasive among the 72 doses of vaccines that FDA has approved, and CDC “recommends” for American children. Today, the vaccines for chickenpox, MMR, hepatitis A and shingles contain fetal DNA.
There is little chance of consequence to vaccine makers from making this reckless choice, and much potential benefit. The 1986 National Vaccine Injury Act makes pharmaceutical companies immune from negligence claims and from product defect lawsuits by injured plaintiffs. Since cancer takes years to develop, causation is virtually impossible for injured petitioners to prove in the Federal Vaccine Court where HHS is the defendant.
Furthermore, by the time a tumor develops, the three-year statute of limitations for the vaccine injury has long expired. Pharma is therefore recklessly and pathologically bold about putting carcinogens in vaccines.
Finally, it’s worth considering that cancer treatment drugs like Keytruda are among pharmaceutical companies’ largest profit makers. Precipitating a cancer epidemic in human populations only benefits vaccine makers’ bottom line.
Remember, these are the same companies and the same FDA regulators that brought us the opioid epidemic.
A new experimental, genetically engineered, recombinant mRNA COVID vaccine is being released ‘at warp speed’. China biotech companies are promising millions of doses of COVID vaccines. The United States paid billions to six other companies, including Pfizer pharmaceutical, which are ready to deploy their versions of the not-yet-FDA-approved shot.
Pfizer Warning Disclosed
In a December 2020 article in LifeNews.com, Pfizer pharmaceutical WARNED pregnant women not to use the COVID-19 mRNA vaccine due to fertility and breastfeeding risks. While this is important news for millions of women, Pfizer has not warned anyone that their study excluded two other groups: 1) those who had a previous diagnosis of COVID-19 disease, and those who are immunocompromised. Immunocompromised people fail to adequately to clear infections. Those with an autoimmune disease create autoantibodies that attack their own tissues. They also fail to clear infections adequately. According to medical doctors, “both groups can create potentially life-threatening conditions.”
On December 1, 2020, the ex-Pfizer head of respiratory research Dr. Michael Yeadon requested the European Union to halt the COVID vaccine, calling it female sterilization:
The vaccinations are expected to produce antibodies against spike proteins of SARS-CoV-2. However, spike proteins also contain syncytin-homologous proteins, which are essential for the formation of the placenta in mammals such as humans. It must be absolutely ruled out that a vaccine against SARS-CoV-2 could trigger an immune reaction against syncytin-1, as otherwise infertility of indefinite duration could result in vaccinated women.
The COVID vaccine follows in the wake of the last recombinant vaccine for the human papilloma virus (HPV).
In 2007, the HPV4, quadravalent, GARDASIL triple-shot series was introduced to girls ages 9-26, to prevent infertility. Then came HPV9 given as two or three shots. No one reported that Gardasil-9 contains more than double the toxic aluminum content of the original vaccine and has no fewer reported side effects.
After more than a decade of reviews, GARDASIL has proved to do exactly the opposite of what it claimed. For more, see my 2014 article Guard Against GARDASIL and a 2018 article by the Weston A. Price Foundation.
The deployment of the HPV GARDASIL vaccine worldwide resulted thousands of young women in the E.U. who suffered. In the U.S., over fifty-eight thousand adverse reactions—including four hundred twenty-seven deaths—have been reported after HPV vaccine injections. The primary adverse effect experienced by recipients was listed as Primary Ovarian Insufficiency (POI) resulting in premature menopause.
An adolescent infertility shot that increases the risk of infertility and autoimmunity?
Imposter DNA
According to pathologist, Dr. Sin Hang Lee, well-known for using cutting-edge DNA sequencing for molecular diagnoses:
Once a segment of recombinant DNA is inserted into a human cell, the consequences are hard to predict. It may be in the cell temporarily or stay there forever, with or without causing a mutation. Now the host cell contains human DNA as well as genetically engineered viral DNA.
Under the Trojan Horse of a vaccine, imposter DNA can be injected and incorporated into your own DNA that manufacture proteins, aka autoantibodies, that attack your cells. Not only do autoantibodies lead to autoimmune diseases, but also to ADHD, seizures, autism, Alzheimer’s and Sudden Infant Death Syndrome (SIDS). All fall under the heading of Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Adjuvants are aluminum-based neurotoxins of vaccines.
In 2016, Dr. Lee sent an open letter of complaint to the World Health Organization’s Global Advisory Committee on Vaccine Safety citing lack of safety data on the vaccine and lack of credibility. But global authorities pay no attention to deaths and injuries caused by vaccine products since vaccine makers are not held accountable for any damages from their products under Bubble Indemnity.
The medical narrative uses fear and contradiction to confuse. They suggest that a virus called HPV “makes it more difficult for a woman to conceive and remain pregnant.” Yet in the next sentence they disclose “However, it is important to remember that most cases of HPV clear up without any need for treatment.” In the fine print, scientists also disclose that no study suggests that HPV contributes to infertility.
The media promoted the experimental HPV jab, not only as a prevention to infertility, but also as a “cure-all” for cervical cancer and genital warts.
Scientists admit that the immune system clear up infections on its own, without treatment. If you consider that clue, you might say goodbye to the germ theory. Under The Terrain Theory, viruses are called exosomes, like enzymes, created within your own cells to cleanse the cells of toxins, a self-cleaning service by your cells. So, while the Germ Theory of disease paints a virus as an enemy, the Terrain Theory of disease welcomes a virus as a friend. The deception of virology and vaccines says that viruses are alive and contagious when they are not:
The entirety of virology and vaccine science is predicated on one thing—that viruses are infectious agents that cause disease. Without this theory, vaccines would not be ‘effective’ or ‘work’ in the minds of the people. Without the virus theory, vaccines would crumble like a house of cards.
The Mandate Strategy
The HPV recombinant vaccine mandate was part of a strategy to coerce compliance with vaccines that genetically modify human DNA. In 2007, both Merck Pharmaceutical and Texas Governor Rick Perry, pushed an HPV vaccine mandate for young girls, ages 9-14. Parents had to consent. However, the editor of JAMA opposed mandating vaccinating girls against the virus.
Note: there will always be two opposing scientific narratives to keep people confused about their inherent right to refuse. Science is a distraction in the health freedom equation.
The HPV vaccine mandate failed. Then, in 2018, scientists pushed the vaccine on boys, suggesting that the presence of HPV in contaminated sperm negatively affects pregnancy outcomes. The CDC claimed that it provides long-lasting protection against penile and anal cancer. But what happens after the vaccine efficacy wanes after 3-5 years?
When women face only a 0.6 percent risk of cervical cancer and men face a 0.2 percent risk of rare anal and penile cancers, is it logical to continue to use a vaccine with so many complications?
We detected disproportionate reports of premature ovarian insufficiency (POI) and related events, including amenorrhea, menstruation irregular, FSH increased, and premature menopause, following human papillomavirus (HPV) vaccine from FDA Vaccine Adverse Event Reporting System (VAERS).
An anti-cancer shot that increases the risk of cancer?
Ironically, HPV vaccines have injured and killed far more children than ever would have gone on to develop HPV-associated cancers without the vaccine. Before the ‘warp speed’ deployment of the next experimental, recombinant shot, it might be wise to assess the damage from the consequences of the last one.
HPV Vaccine Damage Report
A May 2007 editorial in the New England Journal of Medicine questioned the vaccine’s “overall vaccine effectiveness, duration of protection, and adverse effects that may emerge over time,” as the clinical trials did not provide these answers.
VAERS, continues to receive reports of young girls experiencing serious reactions to GARDASIL Adverse reactions include unconsciousness, seizures and facial paralysis, Bells Palsy, Guillain Barre syndrome, speech and vision problems, arthritis, and lupus, and death, after being injected.
Public Interest Group, Judicial Watch, reported in May 11, 2007, that the VAERS data base showed 1,637 adverse reaction reports. Of 42 women who were vaccinated with GARDASIL while pregnant, 18 experienced complications, ranging from miscarriages to fetal abnormalities. As of Dec. 13, 2013, there were a total of 29,918 vaccine reaction reports made to the VAERS associated with GARDASIL vaccinations, including 140 deaths.
In 2011, the Institute of Medicine (IOM) produced a report, Adverse Effects of Vaccines: Evidence and Causality, concluding that “evidence convincingly supports a causal relationship between HPV vaccine and syncope (fainting), and anaphylaxis.”
In a December 2012 study in the journal Advances in Bioscience and Biotechnology, Dr. Lee confirmed the presence of vaccine DNA fragments (HPV-16 L1) in the postmortem blood of a girl who had died shortly after receiving the GARDASIL vaccine, noting the vaccine has the ability to provoke an exaggerated immune response. He also pointed out that the rate of anaphylaxis in girls receiving GARDASIL is five to 20 times higher than any other school-based vaccination program.
In a 2014 study from Keele University in England, Dr. Christopher Exley, examined sixty-two semen samples and found “unequivocal evidence” of high concentrations of aluminum, especially in the semen of men with low sperm counts.
Along with the introduction of the HPV vaccines, several cases of onset or exacerbations of autoimmune diseases following the vaccine shot have been reported in the literature and pharmacovigilance databases, triggering concerns about its safety.
A 2015 study at the University of Texas showed that young women, ages 20-26, who received the four-strain GARDASIL vaccine were more likely than non-HPV-vaccinated women to be infected with high-risk nonvaccine strains of HPV ten years later. In other words, there is a greater risk of infection in those who take the vaccine.
In the 2018 Journal Pediatrics, a Vaccine Safety Datalink study titled, “Primary Ovarian Insufficiency and Adolescent Vaccination,” correlated ovarian failure with vaccinations, including HPV vaccines.
The March 24, 2020 British Medical Journaltitled “Ongoing inadequacy of quadrivalent HPV vaccine safety studies” concluded, “Cochrane could not exclude an increased risk of HPV vaccine mortality “and “medical journals are at risk of becoming arms of the pharmaceutical industry highlights an increased scientific need for alert and active critique of industry-funded trials. [BMJ Evidence-Based Medicine 2020;25:44-45].
A June 2018 study (retracted) in the Journal of Toxicology and Environmental Health analyzed a database of more than eight million American women and found a 25 percent lowered probability of pregnancy associated with HPV vaccination.
As of December 2019, data from the CDC shows that more than one in eight American women—12 percent—have trouble conceiving and bearing a child.
Based on this review, will the COVID19 shot increase the risk for respiratory distress, infertility, autoimmunity and cancer all in one?
Trust Your Innate Immune System
If you are a woman of child-bearing age, do you want the choice to be a mother?
If you are pregnant or nursing, congratulations. Avoid the the two-shot COVID-19 mRNA Vaccine if you want to have more children. According to a UK government document for medical professionals states that there is little data about the risks of the vaccine thus far, and animal reproductive toxicity studies are not finished. Therefore, the Pfizer vaccine, BNT162b2, “is not recommended during pregnancy.”
Pregnant or not, know you always have a choice. You can choose to trust a vaccine maker who is not liable, or reliable, because they do not stand behind their products. Or you can trust your gut, the center of your innate immune system, the defense system you were born with.
Your immune system is designed to work in balance with nature, under the laws of nature, or Holism. This innate system is balanced between two poles: 1) cellular or T cell-mediated immunity, and 2) humoral or B cell-mediated immunity, and they have a reciprocal relationship. When one is artificially stimulated, the other is suppressed.
When viruses are injected into the body, an imbalance occurs—only B cells are activated to create antibodies. Killer T cells are subsequently inhibited, and an engineered virus can temporarily inactivate killer T cells. Dr. Rebecca Carley, M.D. writes, “The ‘prevention’ of a disease via vaccination is, in reality, an inability to expel organisms due to the suppression of the cell-mediated response. Thus, rather than preventing disease, the disease is actually prevented from ever being resolved.”
Holism explains that when people are exposed to a virus, not everyone gets sick. Researchers at the University of Michigan (U of M) showed that when injected with infectious viral agents, a strong immune system and infectious disease could not co-exist. That’s because the cells of your immune system determines whether a virus manifests or not.
When it comes to COVID or any condition, why inject a virus which medical experts claim causes disease? If it is well established that autoimmunity is induced by aluminum adjuvants, then is this shot safe for anyone?
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Transcript:
Imagine this. A man and a woman get into a car. The woman sits in the driving seat. The man in the passenger seat. The woman is taking her driving test and the man beside her is the examiner. The woman is a terrible driver and no one thinks she will pass the test.
Before she starts the car the woman unfastens her handbag, removes her purse and takes out £1,000 in nice new banknotes. She then turns to the driving examiner.
`I know you and your wife both need a nice holiday,’ she says, handing over the money. `This has nothing to do with the driving test I’m about to take but I’d like you have this.’
`Well, thank you, very much,’ says the driving examiner. `Now, let’s see how you get on with your driving test, shall we?’
You might think a trifle unlikely.
But listen to this.
The Bill and Melinda Gates Foundation has a chunky sized investment in the drug company Pfizer which is making the new vaccine which has just been approved for covid-19 in the UK.
The MHRA in the UK is the first regulator in the world to approve the vaccine. It’s fair to say that other countries are possibly a bit puzzled. I don’t think anyone envies Britain for having the fastest regulator in the world. In the US, Dr Fauci, originally said the UK regulators had rushed their approval. But, predictably, he later apologised for saying that. What a surprise that was to us all.
But in 2017 the Bill and Melinda Gates Foundation entered into what I can only call a financial arrangement with the MHRA – the bit of the UK government which regulates medicines and makes sure that they are safe. (MHRA stands for the Medicines and Healthcare Products Regulatory Agency).
Bill and Melinda’s Foundation handed over £980,000 to the MHRA.
So bear with me if I go over this again.
First, the Bill and Melinda Gates Foundation makes a big investment in Pfizer.
Second, the Bill and Melinda Gates Foundation hands over £980,000 and the MHRA smiles sweetly and says thank you very much.
Third, the MHRA is the first agency in the world to approve the new Pfizer vaccine. It is, I suspect, the fastest ever approval of a vaccine.
Even if this tripartite relationship is entirely innocent it should never have happened. What is yet another Government agency doing accepting money from Gates? It was Gates who said that if they were very good at vaccinating people they could reduce the population considerably.
And Pifzer?
Well, to be honest with you, Pfizer’s record isn’t anything you would want to boast about. If you worked there you’d keep quiet about it I think and say you worked for the tax people or robbed banks for living.
So, for example, in the UK, Pfizer was fined £84.2 million for overcharging the NHS by 2,600% and in the US Pfizer was hit with a $2.3 billion fine for mis-promoting medicines and paying kickbacks to doctors. At the time I think the $2.3 billion fine was one of the biggest fines for fraud in American history. It might still be for all I know.
The MHRA should be closed down immediately.
And how did my imaginary driving test student get on?
Oh, to everyone’s surprise she passed her test. She hit a bus, ran over two old ladies and collided with a lamppost when she tried to park. But she passed.
And so this is Britain today.
I have been writing about doctors and drug companies for half a century. My first book on drugs and drug companies was called `The Medicine Men’ and it was published in 1975. I can honestly say I have never come across anything quite so disgraceful, so blatant as the MHRA, Bill Gates and Pfizer link.
And no one cares.
Have you heard about this on the BBC?
Have MPs been shouting about it?
Have the papers run this story on their front pages?
I despair. I really do.
Meanwhile, the confusion goes on and on.
Matt Hancock’s chum and co-author, who is now in charge of vaccinations in the UK or is it just England or maybe just Stratford-upon-Avon, suggested that people who don’t have the covid-19 vaccination might not be allowed to enter cinemas or watch football matches.
I wasn’t surprised. They were always going to say that.
And then senior ministers seemed to change their mind and overrule him. But I rather bet that people who have the vaccine will be given some sort of certificate. After all the EU has been planning a vaccination passport since 2018.
The American government has a clinical trial under way which is testing messages to see which ones are most likely to persuade people that they should have the vaccination.
If you want to get your freedom back,’ then accept the vaccine.’
`If you want to keep your job,’ then accept the vaccine.’
That sort of thing. All devised by psychologists to manipulate, blackmail and coerce. And all for a vaccine which experts around the world agree is for an infection which is no more lethal than the ordinary, annual flu. You can see why the trickery is necessary.
Almost every survey I have seen suggests that most people don’t want the vaccine. Even many health professionals don’t want it. My friend Dr Colin Barron reported that even a great chunk of GPs said they wouldn’t have the vaccine – and they’re making over £12 a jab for giving it.
Of course, if governments everywhere wanted to persuade people to have the vaccine they could be a little more open about the advantages and disadvantages: the benefits and the risks.
It is normal in medicine for doctors to tell patients about all the side effects which may be associated with the treatment they are having.
Indeed, it isn’t just normal, it’s compulsory.
If you go into hospital to have an operation they’ll list all the possible things that can go wrong.
If you are given medication then they’ll tell you about the hazards. Or they should. It’s called informed consent.
There is only one exception: vaccines.
There is no such thing as `informed consent’ about vaccines because doctors aren’t allowed to question vaccines and vaccination in public.
Since anyone who questions the safety or efficacy of vaccines is automatically defined as an anti-vaxxer they can hardly expect doctors to tell patients about the risks. If they did then every doctor would automatically be an anti-vaxxer and be demonised.
You don’t have to be spreading rumours about vaccines to be classified as a dangerous anti-vaxxer.
Some are asking if the first dose of the vaccine will be merely a placebo – to encourage everyone to believe the vaccine is safe. I’m not surprised people are asking that.
After all, lots of dirty things happen in the world of vaccines. Back in 2009, Time magazine reported that Germany had been accused of offering a flu vaccine made by one company, and believed to have fewer side effects, to politicians, civil servants and soldiers and another, potentially riskier vaccine to everyone else.
The riskier vaccine was called Pandemrix. And I dealt with that in my book `Covid 19: The Greatest Hoax of the Century’ – which was banned almost everywhere but which is now available free as a pdf on my website www.vernoncoleman.com and is also free on the Light Paper website – thelightpaper.co.uk
Any doctor who questions the efficacy of a vaccine is officially an anti-vaxxer. If the alleged virus has never been isolated and identified how have they managed to make a vaccine? Why is the vaccine said to be better than natural immunity? Why will people need more than one dose? Why will they need it every year? It’s illegal to ask the questions so there are no answers.
The social media channels such as ScrewYouTube don’t differentiate between loonies suggesting that vaccines will make your hands drop off and turn you bright blue and experienced physicians asking for more information about vaccines.
Everyone asking for information about vaccines is officially an anti-vaxxer – and will be silenced.
The British Army is now concentrating on removing material from the internet if it questions vaccines and vaccination.
I doubt if the soldiers doing this work are qualified doctors – they aren’t expected to judge between serious, professional questions and wild accusations.
They just take down everything.
ScrewYouTube does the same, of course.
Any video which questions vaccine safety, reports acknowledged vaccine problems or criticises drug companies which make vaccines will be deleted.
No questions asked. No chance to defend.
Simple, rapid execution.
The authorities seem to me to have created a problem, the alleged covid-19 epidemic, and they have created a solution – a vaccine.
And yet the list of questions which need to be asked grows longer every day.
I predicted some time ago that there could be infertility problems with the vaccine, and on 3rd December Richie Allen broadcast details of government guidelines which suggested a huge – but not entirely unexpected – cover up.
Richie revealed that although health care professions are warned that it is unknown whether the vaccine has an impact on infertility this warning was not included in the information for those having the vaccine. Maybe there will be an infertility problem and it won’t be apparent for another five or ten years when a few thousand nurses and doctors find they can’t get pregnant. Bill Gates has a certain amount of history in this area.
Medical journal articles have suggested that there are a lot of questions still unanswered.
It’s difficult to know precisely what has been tested, of course, because there is a great deal of secrecy about the trials.
A vaccine should stop serious illness developing and it should interfere with the transmission of a disease and it should be safe.
Do any of the covid-19 vaccines do all or any of these?
The mysteries seem endless.
Will the vaccine really be safe for 80-year-olds? Has it been tested on 80-year-olds? Back in March 2020 I warned that one of the aims of this whole hoax was to get rid of old people. Is this what is going to happen now? Back in March I also warned that another aim was to introduce mandatory vaccinations.
It is said that 100% of those who had two doses of Moderna’s mRNA vaccine had what are called systemic adverse events. Not nice.
And 50% of those who had the Pfizer vaccine were said to be ill.
The Astra Zeneca trial was similar.
And The Lancet reported that there was a possibility that people who had one of the vaccines might have an increased risk of developing an HIV infection.
When testing new drugs, companies usually test against a placebo. Half the patients in a trial get the new drug and half get a sugar pill.
But in their trial it seems that Astra Zeneca tested their new covid-19 vaccine against a meningitis vaccine which is known to produce significant adverse effects.
Why would they do this?
Well, at the risks of upsetting the 77th Brigade, could it be because this would enable them to argue that their vaccine was safer than the placebo?
Is that entirely fair? I doubt if I am the only doctor to think it isn’t.
Even the Financial Times seemed upset by Astra Zeneca. In an article headlined, `Doubts raised over Astra Zeneca Oxford Vaccine Data’ the FT reported that there had been a mistake in the dosage given and that all the people testing the vaccine had been under 55 years of age.
By questioning the vaccine has the FT has become an anti-vaxxer newspaper? Will their website will now be taken down?
The questions keep on coming I’m afraid.
The head of `Operation Warp Speed’ in the USA, who is helping to get vaccines ready for use, is apparently a former GSK executive which seems to me to be a tad incestuous. Mind you, the Chief Scientific Officer in the UK is a former GSK executive.
What else can’t I tell you?
Well, it seems that a little quiet scepticism might not be entirely unfair. At least 66 fully tested and approved vaccines in the US have, over the years, been discontinued – largely for safety reasons. And billions of dollars have been paid in compensation to patients injured by vaccines – or paid to their relatives when patients died or were very severely injured. The UK Government has its standard, miserly £120,000 fee for vaccine damaged patients. And that is paid by taxpayers not drug companies.
What steps is the MHRA taking to ensure that any side effects are properly and speedily recorded?
Why did the drug companies insist on being given indemnity if their vaccines cause no problems? No other companies are indemnified if they produce dangerous products. Well, Bill Gates insisted on indemnity being given. The UK Government has, I think, finally agreed to give its standard £120,000 vaccine damage fee to anyone with severe side effects. But try living on £120,000 if you’re paralysed for life.
Still, there is one bright thought I can share with you.
The vaccine companies want their products to be given emergency approval. This will enable the vaccines to be brought out quickly – by accepting a lower standard of effectiveness and safety.
But when a vaccine is brought out using Emergency Use Authorisation the States in America are banned I believe from mandating the vaccine. They can’t force people to take it.
And a full licence, which would allow mandatory vaccines, will or should take years to acquire.
So here’s a thought: will it be legal for individual companies, schools and so on to insist that people have the vaccination?
And although the drug companies and doctors have been given legal immunity – they can’t be sued if their product is dangerous – does that immunity stretch to company bosses and teachers demanding that you have a vaccine?
One thing is for certain: if someone tries to force you to have a vaccine then it would be wise to insist that the boss signs and dates a letter confirming that he or she is forcing you to be vaccinated and that he or she takes responsibility for any health problems which ensue.
I wonder how many bosses would risk that.
Finally, don’t try bribing your driving instructor.
You could probably go to prison for that.
Only governments and billionaires can get away with that sort of behaviour scot free.
“We slow the progress of science today for all sorts of ethical reasons. Biomedicine could advance much faster if we abolished our rules on human experimentation in clinical trials, as Nazi researchers did.” ~ Paul Nitze
The idea of brutal experimentation on animals has always been justified by claiming that it is necessary in order to benefit the health or mental well being of humans. This propagandist thinking could and would lead to a public acceptance of experimenting and torture of living things in the false name of human progress. But it was also meant to condition man to accept harm to one species in order to better his own. It stands to reason that once this mindset was in place, it could be argued that human experimentation could enhance that ‘progress’ much further, thereby becoming a necessary evil that could be seen as beneficial, especially if it began with psychological experimentation, and not physical. Now that the psyche and body are in many cases being seen as one and the same, why not use medical testing of some humans so as to benefit the collective? In this scenario, the individual would be destroyed in favor of the group, and this could easily lead to sacrificing some for the good of all. The result of this progression would be that we are all lab animals now.
In this era of the fraudulent coronavirus ‘pandemic,’ most are well on their way to becoming a nation of mindless drones that will be accepting of human experimentation. This is in fact already happening, but it seems that it will get much worse very soon. Fear can breed aggression, but considering the herd mentality of the human species, it is much more likely to breed passivity and compliance, both very detrimental to survival in what could be considered any normal way of life. It is not that this government and its controllers have not used its citizens and others for these purposes in the past, but today it is becoming rampant, and is even out in the open concerning current policies in place.
Most all that is now being mandated by the political class is based on experimentation. That experimentation is predicated on compliance testing, this regardless of the gross harm caused. You see, when experimenting with the human animal, it is first necessary to gauge the psyche of the average person in order to know how far the experiment can advance. Because of this, it is crucial to perform psychological experimentation prior to physical experimentation. This of course is not necessary with animals, but is vital with ‘reasoning’ humans. With mass compliance, it becomes evident to the ruling sector of society that the people are prepared to become guinea pigs, and therefore are ripe for abuse. These lockdowns, distancing rules, mask wearing, voluntary business closings, virus testing, and restrictions to liberty at every level, are simply tests to see if the people are willing to follow ludicrous and dangerous instructions in order to gain some sort of false safety due only to pre-planned government propaganda. It has been obvious that Americans in large part have been willing to do absolutely anything they were told to do, including allowing their older family members to be psychologically tortured, and effectively murdered, due to forced isolation by the state.
The ultimate goal of the state here is to first destroy the human spirit, leaving an empty mind and a blank slate so that the people at large are ready and willing to become the test subjects for their claimed masters. The day of the first significant physical experiment on this population is fast approaching, and at this time seems imminent. That experiment will rival many of the heinous and torturous ‘scientific’ persecutions of the past, but will be unique in that it will be made to seem voluntary instead of being done through incarceration and brute force. But there is a sinister aspect of this feigned voluntarism that exposes a heinous psychological manipulation.
I am speaking here of course of the coming poisonous ‘Covid-19’ vaccination. The contradiction and foretelling of doom is obvious, so why are so many already willing to be used as lab animals? The first sign of great danger lies in the fact that the state has exempted the pharmaceutical companies developing these experimental toxins from all liability. The state with your money is also paying for the development of these virulent injections, while allowing unlimited profit to its partners in crime. In addition, the government is claiming to be liable, but that is a lie, as government has nothing, and produces nothing; it only steals from those that do. So each and every citizen guinea pig taking this deadly and experimental vaccine is personally liable for any and all harm. What this means is that vaccine manufacturers, deliverers, and the government have zero risk, while the people retain all the physical, mental, medical, and financial liability. This is a true government coup d’état, in that the human lab animals take all the risk, contract all the sickness, disease and even face death, and also pay for all the damages.
While the political class will crow loudly about this not being mandatory, they will at the same time threaten every single individual that does not bow down to the state and take this vaccine. Those threats will be brutal, and meant to destroy any that do not comply. So this vaccine will really be mandated in that those that disobey will be abused, and attempts by the government to force consent will be completely inhumane. The ability to get daily necessities including food will be eliminated, as will most all travel, working and supporting family without an immunization pass, gaining medical care, access to any service, all public entertainment and activities, and most anything vital to life. Does this sound voluntary to you?
But this experimentation will not end here, but will also continue as long as the people allow it to continue. There will be new experimental vaccines, new updated injections, injectable nanoparticles, chips, property confiscation and redistribution, RNA and DNA experimentation, universal basic income, governmental digital money, tracking devices, and many other intrusions said to be necessary for any citizen wanting to be able to move about or function in any ‘new normal’ manner. So long as the people comply with these orders, the list of demands by the state will be innumerable.
We are all facing one giant experiment where the powerful controlling ‘elites’ and their pawns in government are the mad scientists, and the common masses are the lab animal test subjects.
There is only one answer to this madness: Disobey every government order and be prepared to defend at all costs your life, your family, your property, and your freedom!
“The enrichment center would like to announce a new employee initiative of forced voluntary participation.
If any Aperture Science employee would like to opt out of this new voluntary testing program, please remember; science rhymes with compliance.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Call to Action: Join RFK, Jr. and Children’s Health Defense in Urging the FDA to Slow Down the COVID-19 Vaccine Approval Process
On December 4, Robert F. Kennedy, Jr. sent a letter to Peter Marks, Director of the Center for Biologics Evaluation and Research’s (CBER), on behalf of Children’s Health Defense (CHD) asking the Food and Drug Administration (FDA) to take a cautious approach in approving COVID-19 vaccines that have been developed at “warp speed.” Considering that almost $4.5 billion has been paid out to vaccine injured individuals from vaccines developed in traditional timelines, caution, and concern for human safety should be the FDA’s top priority in the approval process.
This coming Thursday, December 10, CBER’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) will meet in open session to discuss Emergency Use Authorization (EUA) of the Pfizer-BioNTech COVID-19 vaccine for the prevention of COVID-19 in individuals 16 years of age and older. CHD asks that you take the following steps to urge VRBPAC to make safety the chief concern in its considerations:
Send the letter below to your representatives in the House and Senate letting them know that you support Mr. Kennedy’s call for caution in making decisions regarding emergency use authorization of Pfizer’s COVID vaccine as well as any other COVID vaccine in development.
With the VRBPAC meeting coming up so quickly, the time to act is now.
As I’ve reported, COVID testing labs never tell doctors or patients how the PCR test is run. [1]
This means the number of cycles is a secret.
A cycle is a step up in amplification of the tissue sample taken from the patient.
As even Tony Fauci has asserted, tests run at 35 cycles or above are useless. [1] [2] They’re also misleading. The results tend to be positive, meaning the patient is “infected with the virus.” But this is false.
However, as I’ve also reported, the CDC and the FDA recommend that the test should be run at up to 40 cycles. [1] [3] This is a direct hustle. It ensures false positives and higher COVID case numbers—used as justification for lockdowns.
Now, the state of Florida is doing something unheard of. It’s demanding that labs report the “cycle threshold” for every test they run.
Here is the relevant wording in a release from the Florida governor, Ron DeSantis, and the state Department of Health, dated December 3, 2020 [4]:
“Cycle threshold (CT) values and their reference ranges, as applicable, must be reported by laboratories to FDOH via electronic laboratory reporting or by fax immediately.”
“If your laboratory is not currently reporting CT values and their reference ranges, the lab should begin reporting this information to FDOH within seven days of the date of this memorandum.”
We can assume there is only one reason for this order. The Florida governor and the Department of Health are aware that tests run at 35 cycles or higher are useless and misleading, and they want to stop this crime.
Imagine what happens if the trend of “new COVID cases” in Florida soon takes a sudden dip and keeps on falling—because labs are finally telling the truth. Because their deceptive test results are being rejected. The con will be exposed.
And imagine other states following Florida’s example.
I have a few concerns. The term “cycle threshold” is taken to be more or less synonymous with “number of cycles.” But I would prefer Florida simply say: “All labs must report the number of cycles for each PCR test they run.” For me, that would be clearer.
And then, down in the Florida memo, we have this: “If your laboratory is unable to report CT values and their reference ranges, please fill out the brief questionnaire attached to this memorandum and submit by facsimile to the FDOH’s Bureau of Epidemiology confidential fax line…” [the link to the questionnaire is in [4]]
Unable to report? Why would any lab be unable?
The questionnaire offers two bizarre possibilities. The first: “Although the qualitative result is generated based on a CT value, the assay/instrument does not provide the user [the lab] with the actual CT value—it only provides the qualitative result.”
What?? This indicates the lab’s PCR equipment is internally pre-programmed to run the test at a certain number of cycles, and the lab doesn’t know what that number is, can’t find out, and can’t demand the equipment manufacturer disclose that vital piece of information. ABSURD. We’re dealing with a state secret?
The second item in the questionnaire for labs: “The laboratory does not have a separate mechanism to report the CT value to FDOH [Florida Dept. of Health] since the CT value does not get reported to the submitting provider.”
No mechanism for reporting? SET ONE UP. Email, fax, pencil and paper, carrier pigeon. Also ABSURD.
As always, the devil is in the details. I’m sure many labs will try to avoid reporting. They don’t want to be exposed as the charlatans they are.
Memo to Florida Governor DeSantis: Don’t let the labs weasel out of this one. Don’t let them give you excuses. Don’t let them off the hook. Failure to report true facts during a public health crisis is felony. Charge a few labs, drag them into court. Put fear of prosecution into state labs. You’re on the right track. You’ve made a major breakthrough. You see the con at work. You don’t want your state to be pressured into lockdowns based on fake case numbers derived from deceptive tests. Now make sure your enforcement personnel crack down on reluctant labs. Go the distance. If labs have equipment pre-set for the number of cycles, and they don’t know how to get inside the equipment to find that number, bring in pros who will do the job for them. I believe you’ll uncover a major scandal. Much of that equipment will be pre-set for 40 cycles. Keep updating the public on what you discover. Blow this crime wide open. Keep a very close eye on your public health officials. Among them, you’ll find agents who don’t want the truth to emerge. They’ll try to sabotage your good efforts every which way they can.
New details have emerged about the test used for #COVID19, highlighting serious inaccuracies in results and past comments by the tests’ creator doubting the accuracy of PCR testing.
German virologist Christian Drosten’s guidelines on detection of the novel coronavirus for the PCR tests was accepted after only 24 hours of surveillance before becoming the standard. His paper is now being contested and peer reviewed for the first time allowing for some shocking discoveries of error that would potentially render the PCR test completely useless.
Last week, the United Kingdom jumped in front of all other Western nations when it was the first to give emergency approval to Pfizer’s experimental Covid vaccine.
As Pfizer’s novel injectable product got the green light from Britain’s Medicines & Healthcare products Regulatory Agency (MHRA), The New York Times wrote:
“European regulators on Wednesday cast doubt on the rigor of Britain’s review and said that the authorization was limited to specific batches of the vaccine, a claim that Pfizer denied and British officials did not address.”
Echoing the doubt in part was Switzerland’s medical regulator Swissmedic publicly declared necessary information was lacking, and it would not sign off on three different coronavirus vaccines [Pfizer, Moderna and AstraZeneca’s] ordered by the Swiss government.
Swissinfo.ch noted: “The regulator said important data on safety, efficacy and quality are still missing. It has reached out to the manufacturers, who provided data from their studies.”
At a press briefing last Tuesday organized by the Federal Office of Public Health., Swissmedic’s Claus Bolte threw down the gauntlet: “We lack data on the effectiveness of the clinical trials and on the important subgroups that participated in these large studies,” Bolte, head of the authorization division, explained as Swissmedic demurred from endorsing the unproven jabs.
Nevertheless the UK marched forward with their strategy, echoed by most nations around the world, to target frontline health workers and everyone who lives or works in long term care facilities, for the first round of experimental vaccines.
Swaths of the medical community are increasingly hesitant at being… steamrolled? Socially pressured? Coerced? Given an offer they can’t refuse?…into becoming Phase 4 Post-Marketing data points for Pfizer’s experimental vaccine – and for good reason!
Until recently, the bulk of scientific data known publicly about Pfizer’s shot came via the company’s carefully worded press releases. This inconvenient truth has dawned on the medical community who are first in line for the shot.
Doctors and nurses are not convinced about the vaccine data. To those ends, large health systems, medical societies and the federal government are launching an effort to persuade front-line health-care providers to take experimental shots.
A rushed propaganda arm is kicking into gear behind the scenes in an attempt to quell widespread vaccine hesitancy erupting within the medical community. Unanswered questions, lack of transparency, questionable safety profiles, absent liability and the limited trial endpoints of the experimental vaccines deserve further public debate before premature assumptions of widespread uptake are made by health officials and national leaders.
In the US, vaccine-makers are given legal protection from any injuries or death caused by their injectable products. Outside America, this concept is foreign and scoffed at (as it should be!), by citizens of other countries. After the rushed approval of Pfizer’s shot, the UK population received a sobering lesson in Big Pharma’s modus operandi.
Mere days after the UK gave Pfizer’s Covid vaccine the green light, Pfizer’s Department of Health and Social Care confirmed the company had also been given indemnity protecting it from legal action as a result of any problems with the vaccine.
Simultaneously, in the true spirit of transparency, Pfizer’s UK management spoke to journalists at a press conference but refused to explain why the company needed an indemnity, according to The Independent: “We’re not actually disclosing any of the details around any of the aspects of that agreement and specifically around the liability clauses.”
Ministers have also changed the law in recent weeks to give new protections to companies such as Pfizer, giving them immunity from being sued by patients in the event of any complications, according to reports.
The UK government has published information regarding Pfizer’s COVID-19 mRNA Vaccine BNT162b2 for UK health professionals. Comprised of the latest, most up-to-date data and science, from the company itself, the information leaflet notes the following points:
“It is unknown whether COVID-19 mRNA Vaccine BNT162b2 has an impact on fertility.”
“Animal studies into potential toxicity to reproduction and development have not been completed.”
“The most frequent adverse reactions in participants 16 years of age and older were pain at the injection site (> 80%), fatigue (> 60%), headache (> 50%), myalgia (> 30%), chills (> 30%), arthralgia (> 20%) and pyrexia (> 10%) and were usually mild or moderate in intensity and resolved within a few days after vaccination.”
“In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products.”
Major bombshell’s were delivered last week. The first one was from doctors Wolfgang Wodarg and Michael Yeadon, in the form of a legal petition to the European Medicines Agency. They have demanded a “stay,” or halt, to Phase III trials of Pfizer’s BNT162 in Germany, and in all other EU protocol countries until study design is amended.
The doctors deemed the current study designs for the Phase II/III trials of Pfizer/BioNTech to be inadequate for several reasons.
One such reason are that the clinical trials for new experimental Covid vaccines candidates, which use polymerase chain reaction (PCR) tests as the primary evidence of infection, are inadequate to accurately assess efficacy, say the doctors.
Along the lines of understanding safety, or a lack thereof, the doctors also raised the very real issue of Antibody Dependent Enhancement (ADE). This is a common problem with the family of coronaviruses and a major, well-documented reason why many previous vaccine trials for other coronaviruses failed.
The doctors write: “Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place.”
Once thought to be a baseless theory, the admittedly untested effects on fertility from Pfizer’s shot has scientific standing to be questioned. The petition reads:
Syncytin-1…is derived from human endogenous retroviruses (HERV) and is responsible for the development of a placenta in mammals and humans and is therefore an essential prerequisite for a successful pregnancy, is also found in homologous form in the spike proteins of SARS viruses. There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile. To my knowledge, Pfizer/BioNTech has yet to release any samples of written materials provided to patients, so it is unclear what, if any, information regarding (potential) fertility-specific risks caused by antibodies is included.
Here’s EMA co-petitioner Dr. Wolfgang Wodarg speaking about his action in a recent interview with Del Bigtree on The HighWire:
Threaded throughout the paper was information discovered from the second major bombshell: The paper purporting to validate the primary RT-PCR test to detect SARS-CoV-2 used since January for the detection of coronavirus has been deemed “useless” by an external peer-review.
This is the same test used to determine if the new Covid vaccines are effective! Starting to see the house of cards yet? Listen to this guy:
Dr. Michael Yeadon, co-petitioner on the EMA legal document and one of the 22 medical professionals who has signed onto the external peer-review of the PCR test. This interview is with talkRADIO’s Julia Hartley-Brewer:
Do You Trust A Pharm Tech to Administer the Most Complex Vaccine In Human History?
I am not belittling the career choice of pharma tech. But you should know that a person with a high school diploma or GED who makes $21,000 will be injecting you with this brand new vaccine. A Pharmacy Intern is a pharmacy school student. The vaccine needs to be stored, thawed, mixed, spoken to in a soft voice and told that it is the prettiest vaccine ever according to documentation. UK Pfizer Covid Doc – Read it
Salary for a Pharm Teach ranges from high $20Ks to low $30Ks. Source Zip recruiter
From the CVS hiring site:
Education: High School diploma or equivalent (preferred).
Bill Gates is actively financing and promoting new untested vaccines supposed to keep us at least somewhat safe from a ‘ghastly” death from the novel coronavirus and supposedly allow us to resume somewhat “normal” lives. The Pharma giant Pfizer has now announced what they claim were spectacular results in initial human tests. They use an experimental technology known as gene editing, specifically mRNA gene-editing, something never before used in vaccines. Before we rush to get jabbed in hopes of some immunity, we should know more about the radical experimental technology and its lack of precision.
The financial world went ballistic on November 9 when the pharma giant Pfizer and its German partner, BioNTech, announced in a company press release that it had developed a vaccine for Covid19 that was “90%” effective.
The controversial US head of NIAID, Tony Fauci (right) rushed to greet the news and the EU announced it had purchased 300 million doses of the costly new vaccine. If you believe financial markets, the pandemic is all but past history.
Suspicious events
However it seems Albert Bourla, the CEO of Pfizer, doesn’t share the confidence of his own claims. On the day his company issued its press release on the proposed vaccine trials, he sold 62% of his stock in Pfizer, making millions profit in the deal. He made the sell order in a special option in August so it would not appear as “insider selling”, however he also timed it just after the US elections and the mainstream media illegitimately declared Joe Biden President-elect. It seems from appearances that Bourla had a pretty clear conflict of interest in the timing of his press release on the same day.
Bourla lied and denied to the Press that his company had received any funds from the Trump Administration to develop the vaccine when it came out they contracted in summer to deliver 100 million doses to the US Government. Further adding to the suspect actions of Pfizer was the fact the company first informed the team of Joe biden rather than the relevant US government agencies.
But this is far from the only thing alarming about the much-hyped Pfizer announcement.
The German Partner
Pfizer, famous for its Viagra and other drugs, has partnered with a small Mainz, Germany company, BioNTech, which has developed the radical mRNA technique used to produce the new corona vaccine. BioNTech was only founded in 2008. BioNTech signed an agreement with the Bill & Melinda Gates Foundation in September, 2019, just before announcement in Wuhan China of the Novel Coronavirus and just before BioNTech made its stock market debut. The agreement involved cooperation on developing new mRNA techniques to treat cancer and HIV. Curiously that press release, “The Gates Foundation sees BioNTech potential to ‘dramatically reduce global HIV and tuberculosis’” 05. September 2019, has now been deleted.
BioNTech also has an agreement with one of the largest drug producers in China, Shanghai Fosun Pharmaceutical Co., Ltd (“Fosun Pharma”) to develop a version of its mRNA vaccine for novel coronavirus for the Chinese market. Ai-Min Hui, President of Global R&D of Fosun Pharma said in an August statement, “Dosing the first Chinese subject with BNT162b1 marks a milestone of the global co-development program in China. We are closely working with BioNTech and regulatory authorities to evaluate the safety and efficacy of BNT162b1 and other mRNA vaccine candidates…”
This means that the same German biotech company is behind the covid vaccines being rushed out in China as well as the USA and EU. The vaccine is being rushed through to eventual approval in an alarmingly short time.
Both US and EU authorities and presumably also Chinese, waived the standard animal tests using ferrets or mice and have gone straight to human “guinea pigs.” Human tests began in late July and early August. Three months is unheard of for testing a new vaccine. Several years is the norm. Because of the degree of global panic engendered by WHO over the coronavirus, caution is thrown to the wind. Vaccine makers all have legal indemnity, meaning they can’t be sued if people die or are maimed from the new vaccine. But the most alarming fact about the new Pfizer-BioNTech gene edited vaccine is that the gene edited mRNA for human vaccine application has never before been approved. Notably, two year peer reviewed tests with mice fed genetically modified corn sprayed with Monsanto glyphosate-rich Roundup first showed cancer tumors after nine months as well as liver and other organ damage. Earlier Monsanto company tests ended at three months and claimed no harm. A similar situation exists with the gene edited mRNA vaccines that are being rushed out after less than 90 days human tests.
“Explicitly experimental”
Dr. Michael Yeadon replied in a recent public social media comment to a colleague in the UK; “All vaccines against the SARS-COV-2 virus are by definition novel. No candidate vaccine has been… in development for more than a few months.” Yeadon then went on to declare,
“If any such vaccine is approved for use under any circumstances that are not EXPLICITLY experimental, I believe that recipients are being misled to a criminal extent. This is because there are precisely zero human volunteers for…whom there could possibly be more than a few months past-dose safety information.”
Yeadon is well qualified to make the critique. As he notes in the comment, “I have a degree in Biochemistry & Toxicology & a research based PhD in pharmacology. I have spent 32 years working in pharmaceutical R&D, mostly in new medicines for disorders of lung & skin. I was a VP at Pfizer & CEO…. of a biotech I founded (Ziarco – acquired by Novartis). I’m knowledgeable about new medicine R&D.” He was formerly with Pfizer at a very senior level.
Human guinea pigs?
The Pfizer-BioNTech vaccine is experimental and far from guaranteed safe, despite the fact that Pfizer, the EU and the notorious Dr Tony Fauci seem ready to roll it out even before year end to hundreds of millions of humans.
The experimental technology is based on a rather new gene manipulation known as gene editing. In a major article in the 2018 New York Council on Foreign Relations magazine, Foreign Affairs, Bill Gates effusively promoted the novel gene editing CRISPR technology as being able to “transform global development.” He noted that his Gates Foundation had been financing gene editing developments for vaccines and other applications for a decade.
But is the technology for breaking and splicing of human genes so absolutely safe that it is worth risking on a novel experimental vaccine never before used on humans? Contrary to what Bill Gates claims, the scientific answer is no, it is not proven so safe.
In a peer reviewed article in the October, 2020 journal Trends in Genetics, the authors conclude that “the range of possible molecular events resulting from genome editing has been underestimated and the technology remains unpredictable on, and away from, the target locus.”
Dr. Romeo Quijano, retired professor of Pharmacology and Toxicology at the College of Medicine, University of the Philippines Manila, noted some of the dangers of the experimental gene editing when applied to human vaccines. Quijano warns of,
“the danger that the vaccine might actually “enhance” the pathogenicity of the virus, or make it more aggressive possibly due to antibody-dependent enhancement (ADE), as what happened with previous studies on test vaccines in animals. If that should happen in a major human trial the outcome could be disastrous. This serious adverse effect may not even be detected by a clinical trial especially in highly biased clinical trials laden with conflicts of interest involving vaccine companies. Even when a serious adverse event is detected, this is usually swept under the rug.”
He cites the case of another Gates mRNA vaccine candidate, Moderna, where “three of the 15 human experimental subjects in the high dose group suffered serious and medically significant symptoms. Moderna, however, concluded that the vaccine was “generally safe and well tolerated, which the corporate-dominated media dutifully reported, covering-up the real danger…”
He notes,
“Exogenous mRNA is inherently immune-stimulatory, and this feature of mRNA could be beneficial or detrimental. It may provide adjuvant activity and it may inhibit antigen expression and negatively affect the immune response. The paradoxical effects of innate immune sensing on different formats of mRNA vaccines are incompletely understood.” Quijano adds, “A mRNA-based vaccine could also induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity… and may promote blood coagulation and pathological thrombus formation.”
Quijano writes in the extensively documented article,
“among other dangers, the virus-vectored vaccines could undergo recombination with naturally occurring viruses and produce hybrid viruses that could have undesirable properties affecting transmission or virulence. The…possible outcomes of recombination are practically impossible to quantify accurately given existing tools and knowledge. The risks, however, are real, as exemplified by the emergence of mutant types of viruses, enhanced pathogenicity and unexpected serious adverse events (including death) following haphazard mass vaccination campaigns and previous failed attempts to develop chimeric vaccines using genetic engineering technology.”
Bill Gates, the mRNA vaccine makers including Pfizer/BioNTech and Moderna, and their close allies such as Dr. Tony Fauci of the NIAID are clearly playing fast and loose with human lives in their rush to get these experimental vaccines into our bodies. Notably, the same Dr. Fauci and his NIAID owns the patent on a vaccine for dengue fever known as Dengvaxia, marketed by Sanofi-Pasteur and promoted as an “essential” vaccine by Tedros’ WHO since 2016. Robert F. Kennedy Jr. (right) noted that Fauci and NIAID “knew from the clinical trials that there was a problem with paradoxical immune response,” but they gave it to several hundred thousand Filipino kids anyway. It was estimated that as many as 600 vaccinated children died before the government stopped the vaccinations.
Clearly the well-established Precautionary Principle–if in serious doubt, don’t– is being ignored by Fauci, Pfizer/BioNTech and others in rushing to approve the new mRNA vaccine for coronavirus. Messenger RNA technology has yet to produce an approved medicine, let alone a vaccine.
Bill Gates on How the New Vaccine Is Designed to Change Our DNA Forever
Bill Gates on How the New Vaccine Is Designed to Change Our DNA Forever
This past week, vaccine safety advocates put up informative banners across major highways throughout all 50 states and in 3 countries.
Del chats with organizers Joshua Coleman and Olivia Mikos from V is for Vaccine who used the biggest traffic day of the year to their advantage to draw attention to #Covid19 vaccine safety.
To track COVID vaccine recipients, Operation Warp Speed has resurrected a program devised after the September 11 attacks that was quickly defunded following public backlash over privacy concerns.
Operation Warp Speed (OWS), a joint operation between U.S. Health and Human Services and the Department of Defense, continues to be shrouded in secrecy.
OWS is a public-private partnership tasked with producing therapeutics and a fast-tracked COVID-19 vaccine — 300 million doses’ worth that are intended to be made available starting in January 2021.
OWS has plans to engage an “active pharmacovigilance surveillance system” to track Americans for 24 months following vaccination.
One of OWS’ four key tenets is “traceability,” which includes confirming which of the approved vaccines were administered regardless of location (public or private), reminding recipients to return for a second dose and ensuring that the correct second dose is administered.
Google and Oracle, multinational computer technology corporations headquartered in California, in the heart of Silicon Valley, have been contracted to “collect and track vaccine data” as part of OWS’ surveillance systems.
OWS, rather than being directed by public health officials, is heavily dominated by military, technology companies and U.S. intelligence agencies, likening it to a successor for Total Information Awareness (TIA), a program that sprang up after the September 11 attacks but was quickly defunded following public backlash over privacy concerns.
Operation Warp Speed, a joint operation between U.S. Health and Human Services (HHS) and the Department of Defense (DOD), continues to be shrouded in secrecy, but little by little information is emerging that long-term monitoring of the U.S. public is part of the plan.
At face value, OWS is a public-private partnership tasked with producing therapeutics and a fast-tracked COVID-19 vaccine — 300 million doses’ worth that are intended to be made available starting in January 2021.
But it appears the involvement doesn’t end there. Rather than just ensuring a vaccine is produced and made available for those who want it, Moncef Slaoui, the chief scientific adviser for Operation Warp Speed, dubbed the coronavirus vaccine czar, said in an interview with The Wall Street Journal that the rollout will include “incredibly precise … tracking systems.”
Their purpose? “To ensure that patients each get two doses of the same vaccine and to monitor them for adverse health effects.” In an interview with The New York Times, Slaoui described it as a “very active pharmacovigilance surveillance system.”
What will the vaccine monitoring system entail?
This is the number one question, and one that hasn’t been answered, at least not officially. “While Slaoui himself was short on specifics regarding this ‘pharmacovigilance surveillance system,’” news outlet Humans Are Free reported, “the few official documents from OWS that have been publicly released offer some details about what this system may look like and how long it is expected to ‘track’ the vital signs and whereabouts of Americans who receive a Warp Speed vaccine.”
One of the documents, “From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine,” was released by HHS. It also mentions the use of pharmacovigilance surveillance along with Phase 4 (post-licensure) clinical trials in order to assess the vaccines’ long-term safety, since “some technologies have limited previous data on safety in humans.”
The report, which lays out a strategy for distributing a COVID-19 vaccine, from allocation and distribution to administration and more, continues:
“The key objective of pharmacovigilance is to determine each vaccine’s performance in real-life scenarios, to study efficacy, and to discover any infrequent and rare side effects not identified in clinical trials. OWS will also use pharmacovigilance analytics, which serves as one of the instruments for the continuous monitoring of pharmacovigilance data.
“Robust analytical tools will be used to leverage large amounts of data and the benefits of using such data across the value chain, including regulatory obligations. Pharmacovigilance provides timely information about the safety of each vaccine to patients, healthcare professionals, and the public, contributing to the protection of patients and the promotion of public health.”
Similar language was reiterated in an October 2020 perspective article published in The New England Journal of Medicine (NEJM), written by Slaoui and Dr. Matthew Hepburn.
Hepburn is a former program manager for the U.S. Defense Advanced Research Projects Agency (DARPA), where he oversaw the development of Profusa an implantable biosensor that allows a person’s physiology to be examined at a distance via smartphone connectivity. Profusa is also backed by Google, the largest data mining company in the world.
In NEJM, the duo writes, “Because some technologies have limited previous data on safety in humans, the long-term safety of these vaccines will be carefully assessed using pharmacovigilance surveillance strategies.”
‘Traceability’ a key tenet of operation warp speed
Humans Are Free also references an OWS infographic, which details the COVID-19 vaccine distribution and administration process. One of the four key tenets is “traceability,” which includes confirming which of the approved vaccines were administered regardless of location (public or private), reminding recipients to return for a second dose and ensuring that the correct second dose is administered.
That word — pharmacovigilance — is used again, this time as a heading inferring that the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention will be involved in “24-month post trial monitoring for adverse effects/additional safety feature.” Pharmacovigilance, also known as drug safety, generally refers to the collection, analysis, monitoring and prevention of adverse effects from medications and other therapies.
Passive reporting systems for adverse events, like the Vaccines Adverse Event Reporting System, already exist and are managed by the FDA and CDC.
However, a report released by Johns Hopkins Bloomberg School of Public Health, Center for Health Security suggests that passive systems that rely on people to send in their experiences should be made into an “active safety surveillance system directed by the CDC that monitors all vaccine recipients — perhaps by short message service or other electronic mechanisms — with criteria based on the World Health Organization Global Vaccine Safety Initiative.”
What’s more, according to Humans Are Free, “Despite the claims in these documents that the ‘pharmacovigilance surveillance system’ would intimately involve the FDA, top FDA officials stated in September that they were barred from attending OWS meetings and told reporters they could not explain the operation’s organization or when or with what frequency its leadership meets.” STAT News further reported:
“The Food and Drug Administration, which is playing a critical role in the response to the pandemic, has virtually no visibility into OWS — but that’s by design … The FDA has set up a firewall between the vast majority of staff and the initiative to separate any regulatory decisions from policy or budgetary decisions.
“FDA officials are still allowed to interact with companies developing products for OWS, but they’re barred from sitting in on discussions regarding other focuses of OWS, like procurement, investment or distribution.”
Johns Hopkins Bloomberg School of Public Health, Center for Health Security, by the way, has ties to Event 201, a pandemic preparedness simulation for a “novel coronavirus” that took place in October 2019, along with Dark Winter, another simulation that took place in June 2001, which predicted major aspects of the subsequent 2001 anthrax attacks.
Hepburn also reportedly “ruffled feathers” during a June 2020 presentation to the CDC’s Advisory Committee on Immunization Practices because he offered no data-rich slides, which are typically part of such presentations, and, STAT News reported, “Several members asked Hepburn pointed questions he pointedly did not answer.”
Google and Oracle contracted to collect vaccine data
Google and Oracle, multinational computer technology corporations headquartered in California, in the heart of Silicon Valley, have been contracted to “collect and track vaccine data” as part of OWS’ surveillance systems, a partnership Slaoui reportedly revealed in his Wall Street Journal interview. According to Humans Are Free:
“If the Warp Speed contracts that have been awarded to Google and Oracle are anything like the Warp Speed contracts awarded to most of its participating vaccine companies, then those contracts grant those companies diminished federal oversight and exemptions from federal laws and regulations designed to protect taxpayer interests in the pursuit of the work stipulated in the contract.
“It also makes them essentially immune to Freedom of Information Act requests. Yet, in contrast to the unacknowledged Google and Oracle contracts, vaccine companies have publicly disclosed that they received OWS contracts, just not the terms or details of those contracts. This suggests that the Google and Oracle contracts are even more secretive.”
In an interview with investigative journalist Whitney Webb, it’s also revealed that Slaoui, a long-time head of GlaxoSmithKline’s vaccine division, is a leading proponent of bioelectronic medicine, which is the use of injectable or implantable technology for the purpose of treating nerve conditions.
The MIT Technology review has referred to it as hacking the nervous system. But it also allows monitoring of the physiology of the human body from the inside.
Slaoui is also invested in a company called Galvani Bioelectronics, which was cofounded by a Google subsidiary. “So, you have Google being contracted to monitor this pharmacovigilance surveillance system that aims to monitor the physiology and the human body for two years,” Webb says.
“And then you have the ties to the Profusa project,” she adds, “which oddly enough is supposed to work inside the human body for 24 months — the exact window they’ve said will be used to monitor people after the first [vaccine] dose.”
The conflict of interest is massive, in part because Google owns YouTube, which has been banning our videos, a majority of which are interviews with health experts sharing their medical or scientific expertise and viewpoints on COVID-19, since June 2020. As noted by Humans Are Free:
“With Google now formally part of OWS, it seems likely that any concerns about OWS’s extreme secrecy and the conflicts of interest of many of its members (particularly Moncef Slaoui and Matt Hepburn) as well as any concerns about Warp Speed vaccine safety, allocation and/or distribution may be labeled ‘COVID-19 vaccine misinformation’ and removed from YouTube.”
Is total surveillance set to become the new normal?
OWS, rather than being directed by public health officials, is heavily dominated by military, technology companies and U.S. intelligence agencies, likening it to a successor for TIA, a program managed by DARPA that sprang up after the September 11 attacks.
At the time, TIA was seeking to collect Americans’ medical records, fingerprints and other biometric data, along with DNA and records relating to personal finances, travel and media consumption. According to Webb:
“We now know, for example, that the NSA and the Department of Homeland Security are directly involved in Operation Warp Speed, But there are some indications as to what they could be involved with.
“And the fact that Silicon Valley companies that have been known to collaborate with intelligence [agencies] for the purpose of spying on innocent Americans — Google and Oracle, for example — are going to be involved in this surveillance system … for everyone that gets the vaccine.
“It’s certainly alarming, and it seems to point to the fulfillment of an agenda that was attempted to be pushed through or foisted on the American public after September 11, called Total Information Awareness, which was managed, originally, by DARPA.
“It was about using medical data and non-medical data — essentially all data about you — to prevent terror attacks before they could happen, and also to prevent bioterror attacks and even prevent naturally occurring disease outbreaks.
“A lot of the same initiatives proposed under that original program after September 11 have essentially been resurrected, with updated technology, under the guise of combating COVID-19.”
A key difference is that TIA was quickly defunded by Congress after significant public backlash, including concerns that TIA would undermine personal privacy. In the case of OWS, there’s little negative press and media outlets are overwhelmingly supportive of the operation as a way to resolve the COVID-19 crisis.
But what if it’s not actually about COVID-19 at all, but represents something bigger, something that’s been in the works for decades? As Humans Are Free puts it:
“The total-surveillance agenda that began with TIA and that has been resurrected through Warp Speed predated COVID-19 by decades.
“Its architects and proponents have worked to justify these extreme and invasive surveillance programs by marketing this agenda as the ‘solution’ to whatever Americans are most afraid of at any given time. It has very little to do with ‘public health’ and everything to do with total control.”
Bill Clinton, George W. Bush, and Barack Obama all say they will be getting the new Coronavirus vaccine. As if we didn’t trust the ruling class already, this should seal the deal. This is an obvious bit of propaganda.
The three former presidents from both sides of the aisle (political parasites and members of the ruling class) have all pledged to take a COVID-19 vaccine on camera when it’s available to them, hoping to assuage fears at a time when recent polls have shown that just under half of Americans said they would not take a vaccine, according to a report by Today.
As Brian with High Impact TVsays, “anytime a world leader takes a V-A-double-X on TV, it might behoove the general public to take a closer look.”
We know these three former presidents have all lied to us and deceived us, so the very idea of them taking the vaccine on video is laughable. Even if they do get a shot, does anyone honestly believe it’s anything more than a simple saline solution? Wake up, folks. It’s 2020 and people are still falling for this.
Obama said on “The Joe Madison Show” on SiriusXM Wednesday that he was committed to taking a vaccine. “I promise you that when it’s then made for people who are less at risk, I will be taking it, and I may end up taking it on TV or having it filmed just so that people know that I trust this science, and what I don’t trust is getting COVID,” he said.
A statement by Bush aide Freddy Ford provided to NBC News and first reported by CNN indicated that the 43rd president (who lied extensively about weapons of mass destruction and 9/11 to send the troops into endless wars) would also be publicly taking the vaccine when it becomes available. “A few weeks ago President Bush asked me to let Dr. Fauci and Dr. Birx know that, when the time is right, he wants to do what he can to help encourage his fellow citizens to get vaccinated,” Ford said. “First, the vaccines need to be deemed safe and administered to the priority populations. Then, President Bush will get in line for his, and will gladly do so on camera.”
So that’s it! Roll up your sleeve and submit, slaves. The presidents are going to. And there’s no way they’d ever lie and fake these videos of them getting the vaccine. Of course, they’ll be getting the same shot they want us to take… (sarcasm again)
The CEO of Australian airline Qantas triggered a frenzy by being the first major airline to announce their intention to require #Covid19 vaccines for their passengers. The HighWire reports.
Operation VECTOR Exposed — This Is Why the Coming Vaccine Rollout Must Be Rejected!
The Canadian Armed Forces have engaged operation VECTOR, its vaccine rollout plan to immunize the entire population of Canada.
The plan is being rushed through under the guise that COVID-19(84) is the biggest threat to humanity and therefore the military (who have recently been caught engaging in propaganda campaigns to scare the Canadian people) is now tasked with ensuring a nationwide rollout as early as Spring of 2021.
In this video Dan Dicks of Press For Truth exposes operation vector as a plan that must be avoided at all costs!
DO NOT get the shot because the shot IS the pandemic!
“When wearing a mask, most of us breathe with our upper chest muscles and with our mouth open,” states Children’s Minnesota on their website. While the hospital admits this can cause “increased stress and anxiety” there are other more long-lasting concerns.
According to a paper, in the peer-reviewed journal General Dentistry, “children’s whose mouth breathing is untreated” may develop the following deformities:
long, narrow faces
narrow mouths
high palatal vaults
misalignment between the teeth of the two dental arches
gummy smiles
As well as “many other unattractive facial features.”
Yet, how many children are being taught how to breathe while wearing a mask? Instead, many (if not most) are sucking in air through their mouth, as an instinctual reaction to the rise in carbon dioxide. This lowers the position of their tongue, which is key factor in normal facial development.
As the author of the paper, Dr. Yosh Jefferson, DMD, states: “If mouth breathing is treated early, its negative effect on facial and dental development and the medical and social problems associated with it can be reduced or averted.”
Instead, face masks may very well exacerbate the problem leading to a generation of deformed children. Because, it’s not just the mouth breathing. How will a growing face and two developing ears respond to a muzzle stretched around it for hours each day?
John C. A. Manley has spent over a decade ghostwriting for medical doctors, as well as naturopaths, chiropractors and Ayurvedic physicians. He publishes the COVID-19(84) Red Pill Posts – an email-based newsletter dedicated to preventing the governments of the world from using an exaggerated pandemic as an excuse to violate our freedom, health, privacy, livelihood and humanity. You can visit his website at: MuchAdoAboutCorona.ca
Under Guise of ‘Racial Justice,’ Johns Hopkins Lays Out Plan to Vaccinate Ethnic Minorities and Mentally Challenged First
Claims made by Johns Hopkins Center for Health Security about its strategy for vaccinating ethnic minorities and the mentally challenged first, “as a matter of justice,” suggest ulterior motives.
With the first COVID-19 vaccine candidate set to receive an Emergency Use Authorization from the U.S. government in a matter of days, its distribution and allocation is set to begin “within 24 hours” of that vaccine’s imminent approval.
The allocation strategy of COVID-19 vaccines within the U.S. is set to dramatically differ from previous national vaccination programs. One key difference is that the vaccine effort itself, known as Operation Warp Speed, is being almost completely managed by the U.S. military, along with the Department of Homeland Security and the National Security Agency, as opposed to civilian health agencies, which are significantly less involved than previous national vaccination efforts and have even been barred from attending some Warp Speed meetings. In addition, for the first time since 2001, law enforcement officers and Department of Homeland Security officials are set to not be prioritized for early vaccination.
Another key difference is the plan to utilize a phased approach that targets “populations of focus” identified in advance by different government organizations, including the CDC’s Advisory Committee on Immunization Practices (ACIP). Characteristics of those “populations of focus,” also referred to as “critical populations” in official documentation, will then be identified by the secretive, Palantir-developed software tool known as “Tiberius” to guide Operation Warp Speed’s vaccine distribution efforts. Tiberius will provide Palantir access to sensitive health and demographic data of Americans, which the company will use to “help identify high-priority populations at highest risk of infection.”
This report is the first of a three-part series unmasking the racist components of the Pentagon-run project to both develop and distribute a COVID-19 vaccine. It explores the COVID-19 vaccine allocation strategy first outlined by the Johns Hopkins Center for Health Security and subsequent government allocation strategies that were informed by Johns Hopkins.
The main focus of this allocation strategy is to deliver vaccines first to racial minorities but in such a way as to make those minorities feel “at ease” and not like “guinea pigs” when receiving an experimental vaccine that those documents admit is likely to cause “certain adverse effects … more frequently in certain population subgroups.” Research has shown that those “subgroups” most at risk for adverse effects are these same minorities.
The documents also acknowledge that information warfare and economic coercion will likely be necessary to combat “vaccine hesitancy” among these minority groups. It even frames this clearly disproportionate focus on racial minorities as related to national concerns over “police brutality,” claiming that giving minorities the experimental vaccine first is necessary to combat “structural racism” and ensure “fairness and justice” in the healthcare system and society at large.
Part 2 of this series will discuss how Palantir, a company currently helping Department of Homeland Security and law enforcement violently target African Americans and Latinos, will be in charge of allocating “tailored” COVID-19 vaccines to those same minorities as well as Palantir’s origins and its executives’ views on race. Part 3 will explore the direct ties between a COVID-19 vaccine front-runner and the Eugenics Society, which was re-named the Galton Institute in 1989.
The planners
The Trump administration has been criticized for its rush to develop and deploy a COVID-19 vaccine and particularly for installing Monclef Slaoui, a former pharmaceutical executive with ongoing conflicts of interest, as chief scientific adviser for Operation Warp Speed, the Pentagon-run program to produce and distribute the vaccine. Yet, if and when a Biden administration takes power, Operation Warp Speed is set to proceed with little, if any, modification.
The Johns Hopkins Center for Health Security (CHS) director Tom Inglesby, who will serve on the Biden Health and Human Services (HHS) transition team, has praised Slaoui, telling Stat News that the longer someone like him can remain in charge of the nation’s COVID-19 vaccine effort, “the better it is for the country.”
Inglesby, who led discussions at the CHS’s Event 201 exercise in October 2019 and who was one of the primary authors of the controversial Johns Hopkins Dark Winter exercise in 2001, is emblematic of the U.S. government’s and the mainstream media’s general reliance on the Johns Hopkins Bloomberg School of Public Health (of which CHS is part) for pandemic-related matters. Slaoui regularlyappearsonnetworkTV as a COVID-19 oracle and has been called “one of the nation’s go-to experts on the spread of the coronavirus.” Readers may note that the Johns Hopkins “coronavirus tracker” has been used by virtually everymainstreamnews source since the beginning of COVID-19 reporting. This relationship is expected to continue, if not intensify, in a Biden administration.
Both Kathleen Hicks, the lead on Biden’s Department of Defense (DOD) transition team, and Alexander Bick, on Biden’s National Security Council transition team, are scholars at Johns Hopkins Kissinger Center for Global Affairs, reflecting the university’s broader influence on a future Biden administration. Yet, the most significant way the Biden transition intersects with Johns Hopkins is through the CHS.
Originally called the Center for Civilian Biodefense Strategies, the CHS is a think tank within Johns Hopkins that regularly gives recommendations to both the U.S. government and the World Health Organization (WHO) and, like the Bill and Melinda Gates Foundation, has emerged as a voiceof authority on all matters COVID-19 in the U.S. The center’s founding director was D. A. Henderson, best known for his role in the WHO-sponsored smallpox vaccination campaign. Henderson also held several government positions, including serving as associate director of the Office of Science and Technology Policy under George H. W. Bush. He was also the longtime dean of the Johns Hopkins School of Public Health.
Another member of the Biden transition team is Luciana Borio, a current member of the CHS steering committee. As both a former FDA scientist and former National Security Council member, Borio signifies the relationship between the national security state and the biosecurity state. She’s currently a vice president of In-Q-Tel, the venture-capital arm of the CIA.
In-Q-Tel’s current executive vice president, Tara O’Toole, who at the onset of the COVID-19 outbreak declared that “the best way ever to protect those who are well is with vaccines,” is Inglesby’s mentor and predecessor as director of the CHS. She was also a key player and the lead author of the CHS’s Dark Winter and CladeX bioterror simulations. The Engineering Contagion series published by The Last American Vagabond earlier this year explored the Dark Winter simulation in depth, including how the simulation eerily predicted the 2001 anthrax attacks that followed soon after September 11, 2001, with several participants demonstrating apparent foreknowledge of those attacks.
Ending racism with vaccines?
The Centers for Disease Control and Prevention (CDC) has consistently referenced materials developed by the CHS in its recent COVID-19 vaccine allocation literature. These CDC-issued materials form the backbone of the various vaccine allocation strategies issued by many state governments. Chief among these is the COVID-19 Vaccination Program Interim Playbook, published at the end of October. A key aspect of that program is the determination of “critical populations for COVID-19 vaccination, including those groups identified to receive the first available doses of COVID-19 vaccine when supply is expected to be limited.”
In August, the CHS published its Inglesby cowritten Interim Framework for COVID-19 Vaccine Allocation and Distribution, which is cited by the CDC as a key reference for its nationwide COVID-19 vaccine-allocation strategy. This report will examine this document, in particular, as well as other related documents that reveal that ethnic and racial minorities, specifically those over sixty-five and those who make up part of the “essential” workforce, are set to be the first to receive experimental COVID-19 vaccines.
The Interim Framework argues there is a need to prioritize ethnic minorities, particularly African Americans and Latino Americans, in order to reflect “fairness and justice.” It states that “a critical difference” between COVID-19 vaccine allocation and the “context envisioned in the 2018 guidance for pandemic influenza vaccine allocation” is the fact that the U.S. is “currently in the midst of a national reckoning on racial injustice, prompted by cases of police brutality and murder.” It goes on to state that “although structural racism was as present in the 2018 and previous influenza epidemics as it is today, the general public acknowledgment of racial injustice was not.”
It goes without saying that police brutality is decidedly unrelated to vaccine allocation as is increased national awareness of racial injustice as it relates to police brutality. This is further compounded by the police, in this document, being removed as a priority group for COVID-19 vaccine allocation, despite having been designated a priority group in all other government vaccine-allocation guidance since the 2001 anthrax attacks. Also odd is that it is only increased access of minorities to the COVID-19 vaccine that is cited as a way to address “structural racism in health systems,” not other policies that would be more likely to address the problem such as Medicare for All.
In addition, the Interim Framework admits that “communities of color, particularly Black populations, may be more wary of officials responsible for vaccine-related decisions due to past medical injustices committed by authorities on Black communities.” There is a long list of these “medical injustices” committed against minority communities by the U.S. government, including the infamous Tuskegee syphilis experiments, which are discussed in detail later.
Another odd passage on “justice” and “equity” as it relates to vaccinating ethnic minorities first states:
“In the context of vaccine allocation, treating individuals fairly has sometimes been defined as treating everyone the same or equally, for example, by distributing vaccines on a first-come, first-served basis or by giving everyone an equal chance at getting a vaccine via a lottery. Because the impact of the vaccine is different for different people (i.e., some people are at greater risk of death), the straightforward ways of treating people equally are often rejected as unfair or as an inefficient use of vaccine …
“In the context of vaccine allocation, promoting equity and social justice requires addressing higher rates of COVID-19–related severe illness and mortality among systematically disadvantaged or marginalized groups …
“As a matter of justice, these disparities in COVID-19 risk and adverse outcomes across racial and ethnic groups should be addressed in our overall COVID-19 response.”
This extreme emphasis on the “fairness and justice” of prioritizing minorities for the vaccine is contradicted by other claims made in the same document. For example, the document also states:
“The ultimate safety of an approved vaccine is not completely knowable until it has been administered to millions of people. During clinical trials, tens of thousands of individuals will receive the vaccine but that may fail to show safety concerns that occur with less frequency, such as 1 in a million. This can be a concern for particularly severe adverse effects.”
It also notes: “It is also possible that certain adverse effects may occur more frequently in certain population subgroups, which may not be apparent until millions are vaccinated.”
Notably, African Americans are understood to be at a higher risk for adverse reactions to vaccines. According to a study by the University of Pennsylvania, African Americans exhibit a disproportionately higher immune response to certain flu shots. And in 2014, the Mayo Clinic found that African Americans have almost double the immune response to the rubella vaccine as Caucasian Americans. Immune reactions that are too strong can result in more adverse events and inflammatory responses such as transverse myelitis, a debilitating inflammation and paralysis of the spinal cord. A 2010 study in the Journal of Toxicology and Environmental Health showed that African American boys were at significantly greater risk of suffering severe neurological injury from the hepatitis B shot as compared to Caucasians.
This raises the question as to whether African Americans should be prioritized for a poorly tested vaccine when the available science shows that this demographic may be at a higher risk for adverse reactions to vaccines. Previous coronavirus vaccine projects triggered immune responses so strong that the test animals died, and the vaccine projects got scrapped. The Johns Hopkins CHS Interim Framework claiming that vaccinating African Americans and other ethnic minorities first represents “fairness and justice” and would address “structural racism” does not square with its admission that the safety of the COVID-19 vaccine is “not completely knowable” until millions have received it and that “certain adverse effects may occur more frequently in certain population subgroups.”
Who is really to blame for ‘vaccine hesitancy’?
For a successful rollout of a COVID-19 vaccine, the federal government will need to reckon with “vaccine hesitancy,” which the WHO named as one of the top ten threats to global health in 2019 and which is a major concern discussed at length in the August Interim Framework on COVID-19 vaccination strategies.
According to recentpolls, such hesitancy is, understandably, most prevalent among African Americans, the group that has most commonly been used as human guinea pigs by the U.S. government and associated scientific and medical institutions. For instance, there are the infamous Tuskegee University experiments, devised by the U.S. Public Health Service (now a division of HHS) and the CDC. The unwitting participants in the study, all of whom were African American, were told that they were receiving free health-care services from the federal government, while actually they were being intentionally untreated for syphilis so government scientists could study the devastating progression of the disease. Deception was critical to the experiment, as the participants did not know they were part of an experiment at all and were also kept unaware of their true diagnosis. While Tuskegee may be the most well-known example of racist medical experimentation in the U.S., it’s far from the only one.
For example, during the Manhattan Project, the undertaking that produced the atom bomb, the U.S. government contracted dozens of physicians to inject unknowing hospital patients with up to 4.7 micrograms of radioactive plutonium, forty-one times normal lifetime exposure. The goal of this experiment was to pinpoint the dosage at which radioactive elements such as plutonium would cause illnesses like leukemia, and to measure the amount of radioactivity that lingers in the blood, tissues, bones, and urine. Between 1944 and 1994 the Atomic Energy Commission supported thousands of experimental projects sanctioning such radiation on human subjects, most of whom were African Americans.
From 1954 to 1962, the Sloan-Kettering Institute, which receives hundreds of millions of dollars of NIH funds annually, injected over four hundred African American inmates at Ohio State Prison with live cancer cells to observe how the body might destroy them. The primary sponsor for this research was the National Institutes of Health, which also partially sponsored the Tuskegee experiments.
From 1987 through 1991, U.S. researchers administered as much as five hundred times the approved dosage of the Edmonton-Zagreb (EZ) measles vaccine to African American and Latino babies in low-income Los Angeles neighborhoods as part of a vaccine experiment. Consent forms did not inform parents of the increased dosage or of the fact that the vaccine was experimental. Parents were also not informed that the vaccine had already been given to 2,000 children in Haiti, Senegal, and Guinea-Bissau with disastrous results. For example, in Senegal, children who received the jab died at a rate 80% higher than children who did not receive it. The CDC would later characterize the U.S. trials as “clearly a mistake.”
Between 1992 and 1997, Columbia University’s Lowenstein Center for the Study and Prevention of Childhood Disruptive Behavior Disorders conducted studies that sought to establish a link between genetics and violence, focusing on minority children in New York City. These experiments targeted 126 boys between the ages of six and ten, 100% of whom were either African American, Latino, or biracial. In exchange for $100 and a $25 Toys “R” Us gift card, the children, selected because their older brothers had come into contact with the juvenile probation system, were taken from their homes, denied food and water, and given a drug called fenfluramine. Prior to these experiments, fenfluramine had never been administered to people under the age of twelve, and it was already known that the drug was associated with heart-valve damage, brain damage, and death.
Such historical facts raise obvious questions about the reasons for “vaccine hesitancy” and how they are currently being approached by the U.S. government and related institutions. While it would make the most sense to combat this problem by holding to account the people responsible for past abuses, such as those described above, the opposite has been the case. Instead, the CHS and other institutions, particularly regarding the coming COVID-19 vaccination campaign, have proposed several other means of combatting “vaccine hesitancy,” ranging from deception to information warfare to economic coercion.
A dark legacy poised to continue
Given the long-standing exploitive relationship between U.S. medicine and ethnic minorities, the August Interim Framework addresses the situation that communities of color, and in particular black populations, “may be more wary of officials responsible for vaccine-related decisions due to past medical injustices.” It states: “Anticipate hesitancy among marginalized populations who may be fearful or wary of seeking vaccination at sites that have historically caused mistrust.”
Another CHS paper, published in July, “The Public’s Role in COVID-19 Vaccination,” which is cited heavily in the August framework, acknowledged the U.S. “legacy of experimentation on Black men and women.”
However, the CHS document also notes that more than one COVID-19 vaccine candidate “may be available at the same time” and they “may have different safety and efficacy profiles across different population groups and may have different logistical requirements.” It adds that “it is also possible that certain adverse effects may occur more frequently in certain population subgroups, which may not be apparent until millions are vaccinated.”
It is notable that Palantir, the CIA-linked government technology contractor, has been put in charge of creating the software that will “decide” which “population subgroups” are given what vaccine. Palantir is perhaps best known for its controversial role in targeting undocumented immigrants through its contracts with ICE and its role in predictive-policing efforts that disproportionately targeted African Americans. It is certainly unsettling that those same ethnic groups that Palantir is most controversial for targeting on behalf of the national-security state and law enforcement are the same “critical populations” that the company will initially identify for the U.S. military–led COVID-19 vaccination program, Operation Warp Speed.
In addition, in a move that can only aggravate minority community “vaccine hesitancy,” the August CHS Interim Framework recommends that the CDC transform the current “vaccines adverse-event reporting system” from a voluntary system that relies on individuals sending in reports to the government to “an active surveillance system” that “monitors all vaccine recipients,” possibly via unspecified “electronic mechanisms.”
The Last American Vagabond reported last month that Operation Warp Speed, seemingly having taken a cue from the Interim Framework, plans to utilize “incredibly precise … tracking systems” that will “ensure that patients each get two doses of the same vaccine and to monitor them for adverse health effects.” Those systems will be managed, in part, by the intelligence-linked tech giants Google and Oracle.
The main stated purpose of these “tracking systems,” referred to in other Warp Speed documents as “pharmacovigilance systems,” is to monitor the longer-term effects of new, unlicensed vaccine-production methods that are being used in the production of every Warp Speed COVID-19 vaccine candidate. Per Warp Speed’s own documents, these methods “have limited previous data on safety in humans … the long-term safety of these vaccines will be carefully assessed using pharmacovigilance surveillance and Phase 4 (post-licensure) clinical trials,” following the administration of the COVID-19 vaccines to the prioritized “critical populations.”
A strategy takes shape
Given the above, the unprecedented facets of the Warp Speed COVID-19 vaccination plan — that is, its focus on ethnic minorities as the first to receive the experimental COVID-19 vaccine, its interest in giving different vaccine candidates to “different population groups,” and studying the largely unknown effects through “tracking systems” and unspecified “electronic mechanisms”— are all things that would obviously further fuel mistrust by those ethnic groups that have historically been targets of medical experimentation by the U.S. government.
Furthermore, that COVID-19 vaccine development and distribution efforts are being spearheaded by the military and national-security apparatus, as well as having the intimate involvement of controversial contractors such as Palantir, will likely exacerbate minority distrust as Operation Warp Speed advances, given that these same groups are those most often found to be on the receiving end of militarized state violence.
Also concerning is that law enforcement, military, and Department of Homeland Security officials will no longer be priority vaccine-allocation targets, for the first time since the 2001 anthrax attacks, while no convincing reason for their exclusion is offered.
Yet, instead of honestly addressing these unprecedented recommendations, the effort to get around the “vaccine hesitancy” issue as it relates to minorities plans to rely on tactics that avoid addressing any of these issues directly. In one example, although the August Interim Framework recommends “directly prioritizing” ethnic minorities, it recognizes that doing so “could further threaten the fragile trust that some have in the medical and public health system, particularly if there is the perception that there has been a lack of testing to assess vaccine safety and that they are the ‘guinea pigs.’” The document also states that “the implementation of directly prioritizing communities of color could also be challenging and divisive, as determining how to access specific populations and how to determine eligibility based on race or ethnicity includes many sensitive challenges.”
As a workaround for such concerns, the CHS suggests that “prioritizing other cohorts of the population, such as essential workers or those with underlying health conditions associated with poorer COVID-19 outcomes, could also indirectly help address the disproportionate burden of this pandemic on communities of color” due to the high representation of those minorities in the essential workforce.
The document continues: “While this approach might avoid some of the challenges outlined above, it would also need to be implemented in a way that ensures vaccines are equitably distributed across subcategories of these categories.” Thus, it suggests prioritizing “those individuals and groups who face both severe health and severe economic risks, specifically essential workers at higher risk of severe illness — or whose household members are at higher risk — who will suffer severe economic harm if they stop working.” Those groups at “higher risk of severe illness,” the document later notes, are incidentally ethnic minorities.
In other words, the strategy proposed by the CHS is to specifically prioritize cohorts of the U.S. population that contain high proportions of ethnic minorities without directly prioritizing those minorities in order to, somewhat deceptively, avoid exacerbating “vaccine hesitancy” concerns among those groups by directly singling them out.
The Interim Framework acknowledges the high prevalence of ethnic minorities in the essential workforce and cites a paper published in April 2020 by the Center for Economic and Policy Research that notes “people of color are overrepresented in many occupations with frontline industries.”
In addition to prioritizing essential workforce cohorts, which have a high percentage of ethnic minorities, the CHS document also suggests that prisoners, another group where ethnic minorities are heavily overrepresented, and “undocumented immigrant communities of color” should also be prioritized. Like the essential workforce strategy, this would ensure increased vaccine uptake by ethnic minorities without prioritizing them directly.
It is also worth noting that, in addition to the focus on ethnic minorities, the Interim Framework also recommends that “differently abled and mentally challenged populations, who can experience difficulties in accessing healthcare and could be in higher-risk living settings, such as assisted living facilities,” be included as a “target population” along with ethnic minorities.
This strategy as laid out by the CHS appears to have been embraced by the CDC’s ACIP, which is the official government body that will designate the “target populations” of the COVID-19 vaccination strategy.
Also in August, Kathleen Dooling, a CDC epidemiologist writing on behalf of ACIP’s COVID-19 Vaccines Work Group, stated that “groups for early phase vaccination” should be those that “overlap” the most with, first, those with “high risk” medical conditions, second, essential workers, and, third, adults over sixty-five. As previously noted, the essential workforce is predominantly composed of ethnic minorities.
Notably, the “high risk” medical conditions listed in this same document are conditions that are all significantly more prevalent among ethnic minorities, such as type 2 diabetes, obesity, chronic kidney disease, serious heart conditions, and sickle cell disease. Cancer is also listed and, while prevalent across the U.S. population at large, the incidence of cancer is highest among African Americans.
Particularly notable is the inclusion of sickle cell disease, as African Americans in the U.S. have a much higher probability of having that condition than any other group. According to 2010 data analyzed by the CDC, the sickle cell gene, which is necessary in both parents for a child to inherit sickle cell disease, is present in 73 per 1,000 African American newborns, compared to three per 1,000 Caucasian newborns.
The “overlap” strategy fits with current CDC ACIP guidelines for vaccine recommendations, which hold that, if vaccination supply is limited, the CDC should “reduce the extra burden the disease is having on people already facing disparities.” The “overlap” strategy as laid out in the recent ACIP COVID-19 Vaccines Work Group document, however, has the inevitable end result of ensuring that the vast majority of those who will first receive the experimental COVID-19 vaccine will be ethnic minorities over the age of sixty-five and ethnic minorities in the essential workforce.
Also noteworthy in relation to the prioritization of ethnic minorities is that in March the government interpreted federal regulations to grant liability immunity to any entity producing, distributing, manufacturing, or administering COVID-19 countermeasures, including vaccines. According to HHS, this move may also “provide immunity from certain liability under civil rights laws,” meaning that those involved with the COVID-19 vaccination campaign may not be liable if found to violate the rights of groups protected under civil rights law, that is, ethnic minorities.
Controlling the narrative
Another tactic promoted by the CHS, as well as the CDC and Warp Speed, to combat “vaccine hesitancy” is aggressive communication strategies that include “saturating” the media landscape with provaccine content while greatly reducing content deemed to promote “vaccine hesitancy.” The national-security state, which is managing Operation Warp Speed, has become increasingly involved in this media effort, particularly by censoring content that is considered to be anti-vaccine (including, in their view, news outlets critical of the pharmaceutical industry and vaccine manufacturers) by using counterterror tools that have previously been used to disrupt online terrorist propaganda.
After the October 2019 coronavirus pandemic simulation, Event 201, the CHS issued a statement that media companies have a responsibility to ensure that “authoritative messages are prioritized.” The CHS had co-sponsored Event 201 alongside the World Economic Forum and the Bill and Melinda Gates Foundation.
There is much more to this information war than just the rapidly accelerating online censorship effort. For instance, the official Operation Warp Speed document “From the Factory to the Frontlines” notes that “strategic communications and public messaging are critical to ensure maximum acceptance of vaccines, requiring a saturation of messaging across the national media.” It also states that “working with established partners — especially those that are trusted sources for target audiences — is critical to advancing public understanding of, access to, and acceptance of eventual vaccines” and that “identifying the right messages to promote vaccine confidence, countering misinformation, and targeting outreach to vulnerable and at-risk populations will be necessary to achieve high coverage.”
The document also notes that Warp Speed will employ the CDC’s three-pronged strategic framework known as “Vaccinate with Confidence” for its communications thrust. The third pillar of that strategy is called “Stop Myths” and has as a main focus “establish[ing] partnerships to contain the spread of misinformation” as well as “work[ing] with local partners and trusted messengers to improve confidence in vaccines.”
Like the official Warp Speed guidance, the CDC Interim Framework also sees “community outreach” as an essential element for a successful vaccine campaign and suggests funding and training community health workers to promote vaccination specifically to “underserved, disproportionately affected groups.” It details how the U.S. government might engage African Americans, Latino Americans, and lower-income populations to build trust in connection with vaccine recommendations and get around “concerns that they are ‘testing subjects’ for a novel vaccine.”
The CHS document notes, for example, the importance of cultural competence when promoting vaccines, advising that vaccinating at “churches, schools, culturally specific community centers or senior centers” might sit better with marginalized populations and make them feel more at ease. Such considerations were further elaborated on by Luciana Borio in September. That month, the vice president of In-Q-Tel and member of Biden’s transition team, wrote that while it may be appropriate to use U.S. military resources for vaccination efforts, “any such federal engagement must be done in a collaborative manner sensitive to public perceptions that may be engendered by having a public health function fulfilled by individuals in uniform.”
A July CHS paper, “The Public’s Role in COVID-19 Vaccination,” a document Luciana Borio also helped write, argued, “Vaccination sites should not be heavily policed or send any signals that the site may be unsafe for Black or other minority communities.” This CHS paper further states that “trusted community spokespersons” should be utilized for a “communication campaign,” amplifying “vaccine-affirming, personally relevant messages.” Like similar WHO materials, it advocates tailoring the campaign to specific audiences and identifying a network of spokespeople to deliver a “salient and specific message repeatedly, delivered by multiple trusted messengers and via diverse media channels.”
The CDC also recommends vaccine administration at places such as university parking lots, soup kitchens, public libraries, and faith-based organizations. An October CDC report reads: “For people living in institutions, consider vaccination at intake; for people attending colleges/universities, vaccinate at enrollment.” It also proposes that U.S. states and territories utilize nontraditional vaccination sites such as homeless shelters and food pantries.
The prospect of red-carpet celebrities, influencers, and “trusted messengers” endorsing public-health policy is not unthinkable. According to NBC New York, New York and New Jersey have already recruited celebrities to urge residents to follow CDC guidelines. Actors including Julia Roberts, Penelope Cruz, Sarah Jessica Parker, Robin Wright, and Hugh Jackman earlier this year joined a coordinated campaign to “pass the mic to COVID-19 experts.”
In addition, this summer the WHO paid PR firm Hill & Knowlton Strategies $135,000 to identify micro-influencers, macro-influencers, and what it calls “hidden heroes” who “shape and guide conversations” to promote WHO messaging on social media and promote the organization’s image as a COVID-19 authority. Hill & Knowlton are controversial for having previously manufactured the false “incubator baby” testimony delivered in front of Congress that propelled the U.S. into the first Gulf War in the early 1990s.
“The Public’s Role in COVID-19 Vaccination” also urges using groups such as faith-based organizations, schools, homeowners’ associations, and unions trusted by “hard-to-reach audiences” to convey positive vaccine messages and to “modulate public perceptions of vaccination.” Accordingly, the July CHS paper notes “the importance of using outside groups who have relationships with the community, instead of direct government involvement.” It should be noted that during the Tuskegee experiments, the U.S. Public Health Service hired Eunice Rivers, a black nurse with a close relationship to the local minority community, to maintain contact with those who were part of the experiment to ensure they continued to participate.
This outsourcing framework as laid out by the CHS is reproduced in the federal government’s own literature. An October CDC report, Interim Playbook for Jurisdiction Operations, describes the importance of engaging what minority populations would consider “trusted sources” such as union representatives, college presidents, athletic coaches, state licensure boards, homeless shelter staff, soup kitchen managers, and faith leaders to “address hesitancy” in relation to the COVID-19 vaccine.
Operation Warp Speed’s document “From the Factory to the Frontlines,” released the same day as the CDC Interim Playbook, gives more specific examples of the government’s ongoing work with organizations “representing minority populations,” stating that faith-based organizations can be critical. “HHS’s Center for Faith and Opportunity Initiatives is working with minority-serving faith and community groups … and encouraging participation in the vaccination program,” the document reads. It also states that an “information campaign” led by HHS’s public affairs department is already working to “target key populations and communities to ensure maximum vaccine acceptance.”
Of note is that a member of Biden’s Office of Management and Budget (OMB) transition team is Bridget Dooling. The OMB houses the Office of Information and Regulatory Affairs, which reviews all regulations across the federal government. Dooling previously worked at OIRA, and from 2009 until 2011 worked under the direction of then-OIRA administrator Cass Sunstein. On Twitter, Dooling regularly interacts with Sunstein. She has frequently promoted Sunstein’s work on Twitter, especially this past month.
Notably, in 2008, Sunstein authored a paper encouraging the U.S. government to employ covert agents to “cognitively infiltrate” online dissident groups that promote antigovernment “conspiracy theories” and to maintain a vigorous “counter misinformation establishment.”
Elements of his strategy for tackling anti-government “conspiracy theories” are analogous to the aforementioned CHS theme of using “outside groups who have relationships with the community” instead of the government directly. “Governments can supply these independent bodies with information and perhaps prod them into action from behind the scenes,” he contended in his paper.
Sunstein was recently made chair of the World Health Organization’s Technical Advisory Group on Behavioral Insights and Sciences for Health to ensure “vaccine acceptance and uptake in the context of COVID-19.”
In September he also wrote an opinion piece for Bloomberg, “How to Fight Back against Coronavirus Vaccine Phobia,” suggesting that “high-profile people who are respected and admired by those who lack confidence in vaccines” will help sell the public on the safety of vaccines. “Trusted politicians, athletes or actors — thought to be ‘one of us’ rather than ‘one of them’ — might explicitly endorse vaccination,” he writes.
When all else fails, coerce
In addition to this information warfare approach to combating “vaccine hesitancy,” the government also intends to stave off possible hesitancy through economic coercion, that is, by using economic incentives, even linking vaccination to entrance into the workforce, housing assistance, food, travel, and education.
Sunstein’s Bloomberg piece, for example, states that when a vaccine is available, “an economic incentive, such as a small gift certificate, can help” make it easy for “people who are at particular risk. Such gift cards will inevitably be more effective at swaying decisions of the poor.”
Former 2020 Presidential Candidate and U.S. Representative for Maryland’s 6th congressional district John Delaney recently penned an article in the Washington Post, “Pay Americans to Take a Coronavirus Vaccine,” in which he argues a way to overcome the “historical level of distrust” in the vaccine development process is to take advantage of the current economic crisis and “pay people to take a COVID vaccine.” Delaney writes, “Such an incentive might be the most effective way to persuade people to overcome suspicion or even fear …”
CHS’s “The Public’s Role in COVID-19 Vaccination,” paper also details how bundling services like “food security, rent assistance, [and] free clinic services” with vaccination can increase vaccine intake. “Local and state public health agencies should explore opportunities to bundle COVID-19 vaccination with other safety net services,” it suggests. One way of doing this is to simply provide “food aid, employment aid, or other preventative health services” that “may be urgently needed” at vaccination sites. “[And] in some cases,” says the CHS, “it also may be acceptable and feasible to deliver vaccination via home visits by community health nurses when vaccination is bundled with delivery of other services.”
This strategy for increasing vaccine intake parallels what the CHS proposes in order to make digital contact tracing technology (DCTT) widespread in the population without mandating it outright. “Instead of making use fully voluntary and initiated by users, there are ways that DCTT could be put into use without users’ voluntary choice,” a recent CHS paper “Digital Contact Tracing for Pandemic Response” reads. It continues: “For example, use of an app could be mandated as a precondition for returning to work or school, or even further, to control entry into a facility or transportation (such as airplanes) through scanning of a QR code.”
Palantir and priority populations
Aside from the troubling aspects of the COVID-19 vaccination strategy as outlined above, there is the separate issue of the way in which these “populations of focus” will be chosen and identified. Palantir, the big data firm with deep and persisting ties to the CIA, has created a new software tool expressly for Warp Speed called Tiberius. Not only will Tiberius use Palantir’s Gotham software and its artificial intelligence components to “help identify high-priority populations,” it will produce delivery timetables and map out the locations for vaccine distribution based on the masses of data it has collected through various contracts with HHS and data-sharing alliances with In-Q-Tel, Amazon, Google and Microsoft, among others.
These data include extremely sensitive information about American citizens and the lack of privacy safeguards governing Palantir’s growing access to American healthcare data has even gotten the attention of Congress, with several senators and representatives warning in July that Palantir’s massive stores of data “could be used by other federal agencies in unexpected, unregulated, and potentially harmful ways, such as in the law and immigration enforcement context.”
Given that Palantir, at present, is best known for targeting the same minorities that are slated to be “priority populations” for early receipt of the experimental COVID-19 vaccine, Tiberius and the company behind it, including the obsessive “race war” fears of its top executive, will be explored in Part 2 of this series.
Don’t blink. Johns Hopkins may delete or retract their analysis at any moment. Their author’s study is devastating. Too hot to handle.
UPDATE: Yes, I wrote that opener a few hours before Johns Hopkins stepped in and DID retract the article. Boom. [1] [2] [3] [4]
Hopkins claims the article has been used to spread misinformation about the pandemic, and contains factual errors. CDC is cited as one correct source of facts. Hmm.
Regardless, here is my article, finished before the Johns Hopkins retraction. Since then, I’ve only polished it a bit in several places, for clarity:
Months ago, I told you this, in a number of articles: The overwhelming percentage of people who are “dying from the virus” are actually dying from traditional diseases.
These people have been relabeled and repackaged as “COVID-19.”
It has nothing to do with “the virus.”
A new analysis from Johns Hopkins confirms this in spades.
The Johns Hopkins News-Letter article, in a student publication, is headlined, “A closer look at US deaths due to COVID-19.” It lays out the case made by “Genevieve Briand, assistant program director of the Applied Economics master’s degree program at Hopkins.”
As you keep reading, keep this in mind: If the so-called increase in mortality from COVID is offset, almost exactly, by a decrease in deaths from all other major diseases…
Indicating that the so-called COVID deaths are nothing more than an exercise in re-labeling, then…
You can say there is a new coronavirus, but it’s even less harmful than flu, because virtually everybody recovers…
Or you can say the whole story of a new coronavirus is a fake narrative. There is no new virus.
My readers know I’ve been offering much evidence for the latter conclusion.
Here are key quotes from the Johns Hopkins News-Letter article:
“These data analyses suggest that in contrast to most people’s assumptions, the number of deaths by COVID-19 is not alarming. In fact, it has relatively no effect on deaths in the United States.”
“This comes as a shock to many people. How is it that the data lie so far from our perception?”
“When Briand looked at the 2020 data during that seasonal period, COVID-19-related deaths exceeded deaths from heart diseases. This was highly unusual since heart disease has always prevailed as the leading cause of deaths. However, when taking a closer look at the death numbers, she noted something strange. As Briand compared the number of deaths per cause during that period in 2020 to [deaths per cause in] 2018, she noticed that instead of the expected drastic increase across all causes, there was a significant decrease in deaths due to heart disease. Even more surprising, as seen in the graph below, this sudden decline in deaths is observed for all other causes.”
“This trend is completely contrary to the pattern observed in all previous years. Interestingly, as depicted in the table below, the total decrease in deaths by other causes almost exactly equals the increase in deaths by COVID-19. This suggests, according to Briand, that the COVID-19 death toll is misleading. Briand believes that deaths due to heart diseases, respiratory diseases, influenza and pneumonia may instead be [may have been] recategorized as being due to COVID-19.”
“The CDC classified all deaths that are related to COVID-19 simply as COVID-19 deaths. Even patients dying from other underlying diseases but are infected with COVID-19 count as COVID-19 deaths. This is likely the main explanation as to why COVID-19 deaths drastically increased while deaths by all other diseases experienced a significant decrease.”
“’All of this points to no evidence that COVID-19 created any excess deaths. Total death numbers are not above normal death numbers. We found no evidence to the contrary,’ Briand concluded.”
“’If [the COVID-19 death toll] was not misleading at all, what we should have observed is an increased number of heart attacks and increased COVID-19 numbers. But a decreased number of heart attacks and all the other death causes doesn’t give us a choice but to point to some misclassification [re-labeling],’ Briand replied.”
“In other words, the effect of COVID-19 on deaths in the U.S. is considered problematic only when it increases the total number of deaths or the true death burden by a significant amount in addition to the expected deaths by other causes. Since the crude number of total deaths by all causes before and after COVID-19 [was first announced] has stayed the same, one can hardly say, in Briand’s view, that COVID-19 deaths are concerning.”
Of course, there is some mealy-mouthed backtracking in the article. The virus is deadly and the pandemic is real, etc. But the data are the data.
The whole COVID operation is a hoax.
If I thought other honest researchers would investigate and re-calculate the Hopkins analysis, I would say, let’s see what they come up with. But based on my experience, there will be, at best, a brief flurry of articles in the press about this extraordinary finding, and then the scientific and press denizens will move on, as if nothing happened. That is their way. They briefly expose a scandal and then they slither off to cover up the scandal.
The other possibility is: Hopkins will retract the analysis, claiming it was flawed. That is the other strategy the low-crawling creatures sometimes deploy.
So there you have it.
Hoax. Con. Fake.
As I keep reporting, the virus (never proven to exist) is the cover story for the true phase-one goal: destruction of the economy.
If the virus were real, if it were attacking people left and right, the all-cause mortality numbers would be through the roof.
But they aren’t.
“I have a great idea, Bill. Let’s declare a fake pandemic. We’ll report all sorts of high death numbers. But really, we’ll just be subtracting numbers from other traditional diseases that cause deaths, and we’ll add those numbers to our fake pandemic.”
“Sounds great, Tony. Can you pull it off? I mean, it’s pretty obvious.”
“Sure, we can pull it off. And if some journalist with a mainstream reputation or an institution suddenly develops a brief infection of ETHICS, we’ll call their work a mistake or a lapse in judgment.”
“You mean an institution like the World Health Organization or Johns Hopkins?”
“Right. We’ll say the institution didn’t issue the study, it was just one of their people, a lone researcher. And if necessary, the institution, under pressure, will back off. But that’s assuming anyone noticed the study in the first place. Normally, these ‘revelations’ surface for a moment and then sink like a stone. No one cares. A pandemic is a money waterfall. The beneficiaries won’t sacrifice their bottom lines, or their reputations…”
Of course, people can rise up and raise holy hell.
I remember vividly the day, at the tail end of March, when facemasks suddenly became synonymous with morality: either one cared about the lives of others and donned a mask, or one was selfish and refused to do so. The shift occurred virtually overnight.
Only a day or two before, I had associated this attire solely with surgeons and people living in heavily polluted regions. Now, my friends’ favorite pastime during our weekly Zoom sessions was excoriating people for running or socializing without masks in Prospect Park. I was mystified by their certitude that bits of cloth were the only thing standing between us and mass death, particularly when mere weeks prior, the message from medical experts contradicted this new doctrine.
On February 29, the U.S. surgeon general infamously tweeted: “Seriously people – STOP BUYING MASKS. . . They are NOT effective in preventing general public from catching #Coronavirus.” Anthony Fauci, the best-known member of the coronavirus task force, advised Americans not to wear masks around this time. Similarly, in the earliest weeks of the pandemic, the CDC maintained that masks should be worn only by individuals who were symptomatic or caring for a sick person, a position that the WHO stood by even longer.
As rapidly as mask use became a matter of ethics, the issue transformed into a political one, exemplified by an article printed on March 27 in the New York Times, entitled “More Americans Should Probably Wear Masks for Protection.” The piece was heavy on fear-mongering and light on evidence. While acknowledging that “[t]here is very little data showing that flat surgical masks, in particular, have a protective effect for the general public,” the author went on to argue that they “may be better than nothing,” and cited a couple of studies in which surgical masks ostensibly reduced influenza transmission rates.
One report reached its conclusion based on observations of a “dummy head attached to a breathing simulator.” Another analyzed use of surgical masks on people experiencing at least two symptoms of acute respiratory illness. Incidentally, not one of these studies involved cloth masks or accounted for real-world mask usage (or misusage) among lay people, and none established efficacy of widespread mask-wearing by people not exhibiting symptoms. There was simply no evidence whatsoever that healthy people ought to wear masks when going about their lives, especially outdoors. Yet by April, to walk the streets of Brooklyn with one’s nose and mouth exposed evoked the sort of reaction that in February would have been reserved for the appearance of a machine gun.
In short order, the politicization intensified. President Trump refused to wear a mask relatively early on, so resistance to them was equated with support for him. By the same token, Democratic politicians across the board eagerly adopted the garb; accordingly, all good liberals were wearing masks religiously by the beginning of April. Likewise, left-leaning newspapers such as theNew York Times and theWashington Post unequivocally promoted mask-wearing after that March 27 article, with no real analysis or consideration of opposing views and evidence.
The speed with which mask-wearing among the general public transitioned from unheard of to a moral necessity struck me as suspicious. After all, if the science was as airtight as those around me claimed, surely masks would have been recommended by January or February, not to mention during prior infectious disease outbreaks such as the 2009 swine flu. It seemed unlikely that the scientific proof became incontrovertible sometime between late February and late March, particularly in the absence of any new evidence surfacing during that time period.
Perhaps none of this is particularly surprising in this hyper-political era. What is shocking is the scientific community’s participation in subverting evidence that does not comport with the consensus. A prime example is the Institute of Health Metrics Evaluation’s (“IHME”) rather astounding claim, published in the journal Nature-Medicine and echoed in countless articles afterward, that the lives of 130,000 people could be saved with a nationwide mask mandate.
As my colleague Phil Magness pointed out in an op-ed in the Wall Street Journal, the IHME model was predicated upon faulty data: it assumed that 49% of Americans were wearing masks based on a survey conducted between April and June, while claiming that statistic represented the number of Americans wearing masks as of September 21. In fact, by the summer, around 80% of Americans were regularly wearing them. (Ironically, had Dr. Fauci and the Surgeon General not bungled the message in March, mask use probably would have reached much higher rates much earlier on).
This called into question the accuracy of the 130,000 figure, since many more people habitually used masks than the study presumed.
Although Magness contacted Nature-Medicine to point out the problem, after stalling for nearly two weeks, the journal declined to address it. Needless to say, the damage had been done: newspapers such as the New York Times undoubtedly would fail to correct the error and any retractions certainly would be placed far from the front page, where the initial article touting the IHME figure appeared. Thus, as expected, the unfounded claim that 130,000 lives could be saved with a nationwide mask-mandate continues to be repeated, including by president-elect Joe Biden and National Institutes of Health Director Francis Collins.
That the science behind mask-wearing is questionable at best is further exemplified by a letter to the editor written in response to Magness’s article. Dr. Christopher Murray acknowledged that rates of mask-wearing have steadily increased, but then concluded that masks should be used because they are “our first line of defense against the pandemic” and current IHME modeling indicates that “if 95% of U.S. residents were to wear masks when leaving home, we could prevent the deaths of tens of thousands of Americans” because “masks work,” and “much deeper pain is ahead if we refuse to wear them.”
None of this accounts for the failure of either Nature-Medicine or the IHME modelers to recognize and correct the error. Moreover, neither the IHME modelers nor Dr. Murray provide any evidence that masks work. They assume masks are extremely effective at preventing spread of the coronavirus, and then claim that the model is correct for that reason. This sort of circular reasoning is all-too typical of those who so vociferously insist that masks are effective without going to the trouble of substantiating that contention – or differentiating what is likely a modest benefit from mask-wearing in specific indoor locations and around high-risk individuals from the media-driven tendency to depict masks as a silver bullet for stopping the virus in all circumstances.
Coverage of a recent mask study conducted in Denmark likewise epitomizes the failure of the scientific community to rigorously engage with results that do not fit the prevailing masks-as-a-panacea narrative. The first randomized and controlled study of its kind (another appeared in May but it pertained to flu and had similar results), it found an absence of empirical evidence that masks provide protection to people wearing them, although it apparently did not assess whether they prevent infection of those who encounter the wearer. The report was covered in a New York Times article bearing the patronizing headline, “A New Study Questions Whether Masks Protect Wearers. You Need to Wear Them Anyway.”
Noting that the results “conflict with those from a number of other studies,” primarily “laboratory examinations of the particles blocked by materials of various types,” the author remarked that, therefore, this research “is not likely to alter public health recommendations in the United States.” Notably, laboratory examinations, as opposed to the Danish study, do not account for the realities of everyday mask usage by non-medical professionals.
The author then quotes Susan Ellenberg, a biostatistician at the University of Pennsylvania, who claims that the study indicates a trend: “‘in the direction of benefit’ even if the results were not statistically significant. ‘Nothing in this study suggests . . . that it is useless to wear a mask,’” according to Dr. Ellenberg.
Nor does anything in this study suggest that it is useful to wear a mask, a fact that Dr. Ellenberg (and the headline) conveniently ignores. Furthermore, if a result is statistically insignificant, it should not be used to make the case for any proposition — as even I, a layperson, know.
Scientists ought to dispassionately analyze data that contradicts their biases and assumptions, and be open to changing their beliefs accordingly. That the results of the only randomized, controlled study were and continue to be automatically discounted demonstrates that, when it comes to the subject of masks, anything approximating the scientific method has gone out the window. That is all the more evident given the lack of interest that mask proponents have shown in conducting a randomized, controlled study themselves.
An article in the Los Angeles Times went even further: it twisted the findings of the Danish study to argue, incomprehensibly, that the research demonstrated more mask-wearing is warranted. The author cited, as supposedly compelling evidence that masks work, the low Covid-19 death rates in Singapore, Vietnam, and Taiwan. Indeed, according to the latest YouGov poll, administered in mid-November, 83% of Americans now wear masks in public, higher rates than Vietnam (77%) and Taiwan (82%).
Furthermore, there are other explanations, apart from widespread mask usage, for the remarkably low death rates in these countries. Some scientists believe that previous exposure to other coronaviruses in these regions may confer partial or total immunity to SARS-CoV-2. Others have speculated that obesity, environment or genetics could be the reason that Europe and the United States have substantially higher death rates than many Asian and African countries; after all, obesity is one of the most significant risk factors for severe illness.
To conclude on the basis of low death rates in several countries that masks prevent coronavirus transmission is patently absurd, illogical, and unscientific. A casual observer might also note that coronavirus cases (albeit not necessarily deaths) are rising in many parts of the world, regardless of mask mandates or rates of implementation. While not a controlled experiment, this fact at least ought to be addressed when making such sweeping claims.
Ultimately, I do not have the credentials to determine whether or not –or to what extent — masks work. But it is obvious that the issue has become so politicized that mainstream media outlets, politicians, and even scientists seize upon the slightest bit of favorable evidence, dismiss out of hand anything that conflicts with their theory, and most egregiously of all misrepresent the data, to support the conclusion that masks worn by asymptomatic people prevent coronavirus transmission.
And masks are only one part of this story: school closures, lockdowns, and social distancing all have been dogmatically embraced as a means of controlling infection. The substantial evidence that these mechanisms are not effective, particularly beyond their duration, has been automatically rejected for too long. This is not science: it is politics, and those within the profession who have refused to examine their confirmation biases, or manipulated the evidence to score political points, are utterly unqualified for the job.
Jenin Younes is a public defender in New York City. She enjoys running, restaurants, and reading in her free time.
Attorney Dr. Reiner Fuellmich: 1st of Many Lawsuits Has Been Filed to Attack Use of PCR Tests Which Are the Cornerstone of “Crimes Against Humanity” Crisis
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Throughout the coronavirus response, those within ‘official’ positions around the world have chimed in on the idea of a mandatory Covid shot. Their hopes and potential future plans have been all over the board causing apprehension and confusion within the public. Whether you want the eventual shot, being rushed through emergency use authorization, or not, answers have not been clear.
In what has been a growing trend in political, and now health reporting, shadowy anonymous sources have driven headlines and news cycles. Always framed as ‘for their protection,’ yet ignoring accuracy or ability to verify their prognostications, the vaccine narrative hasn’t escaped it.
CNBC is now reporting that “The Food and Drug Administration has asked a group of advisors to set aside three days in early December for potential meetings to discuss Covid-19 vaccines…according to two people familiar with the plans. The advisory group may be asked to weigh in on Pfizer and Moderna’s vaccines, said the people, who asked not to be named because the plans aren’t yet public.”
Biden gave his answers in October during an ABC News Town Hall saying “we should be thinking about making it mandatory.” When asked how he would enforce that, Biden appeared to describe a scenario where he would ask Governors and mayors to execute the mandates.
Anyone paying attention to the last few years of American legislation sweeping across states [originally justified due to a measles outbreak] will easily see how such mandates will roll out. They will take the form of coercion by law, threatening to take away anything from access to school [for children] and daycare all the way to unemployment benefits for adults. Meanwhile, grocery stores, travel, and concert venues have already signaled they are open to denying access unless proof of vaccination is shown.
Frontline workers are being targeted for the first round of the Covid shots. It will be no surprise if hospitals treat their previously celebrated frontline heroes like subhuman rule-violators if they refuse the experimental shot.
Tests cases have already proven themselves in thorough court settings when it came to mandatory flu shots for healthcare workers. The “vaccinate or mask” policy was ruled unreasonable and called “a coercive tool” instead of a protective health policy in a case brought against the Sault Area Hospital in Sault Ste. Marie.
Nevertheless, the medical community, whose aggressively protected dictum of lauding the safety and efficacy of vaccination when doling them out to kids, are now suddenly questioning the coming shots they’ll be coerced into taking. Or through the lens of the mainstream media’s open discriminatory stance, the medical community has turned into ‘anti-vaxxers.’
A Facebook group titled NHS Workers for Choice, No Restrictions for Declining a Vaccine insist they are not an anti-vaccine – but that didn’t stop the media from calling them names. The group was made up of “hundreds of NHS staff” including “a GP, several A&E nurses, healthcare assistants, lab workers, and care home staff” according to the Daily Star hit piece.
Meanwhile, here in the U.S. the Washington Post spins their coverage a little gentler with its piece titled Doctors and nurses want more data before championing vaccines to end the pandemic. WaPo writes of a propaganda push when describing “Large health systems, medical societies and the federal government are launching an effort to persuade front-line health-care providers to take novel vaccines.”
The endless hype surrounding the endpoint data from Pfizer, Moderna and AstraZeneca’s shot is not thorough at this stage, published in peer-reviewed journals or even transparent for the public to access. It’s from simple science by press release public relations statements. In addition, the data being submitted for Emergency Use Authorization to the FDA is often resting on a small number of the total participants involved in the trials.
Speaking to the matter, vaccine safety scientist and infectious diseases physician Rebecca Chandler wrote:
“Perhaps watching a scientific community praise and promote vaccines based on press releases rather than review of data may actually promote vaccine skepticism.”
The hesitancy among doctors and nurses is not the same as the anti-vaccine movement, writes the WaPo who appear to be correct. Traditionally, what the media labels ‘anti-vaxxers’ were parents who were ‘pro-vax’ until experiencing an injury in their child after following recommended schedules put forth by officials. In juxtaposition, the WaPo writes of New Jersey State doctors “Among professionals contacted by the state, “some did not want to be in the first round, so they could wait and see if there are potential side effects,” New Jersey Health Commissioner Judith M. Persichilli said at a Nov. 9 news briefing. Of those who said they would not take the vaccine, many said they would be more than willing to get the vaccine at a later date, when more data is available,” she said.” It appears those doctors are going to wait around and see if the people they inject will show adverse reactions before deciding to take the shot themselves.
A survey of 609 healthcare workers in Los Angeles found respondents reported unwillingness to participate in a coronavirus vaccine trial, with 66.5% intending to delay vaccination.
Over the last month, headlines abound intending to shape the public narrative around the coming Covid shot. Global News Canada asksA coronavirus vaccine is almost ready. But will you take it? Forbes tells youWhat The Public Thinks About Mandatory Covid-19 Vaccinations.
Some within government are already taking counter-actions.Florida state Rep. Anthony Sabatini took to Twitter writing:
I will be filing a Bill next week to eliminate the State’s power to mandate and force vaccines upon citizens during a state of emergency. Government should not be able to forcibly vaccinate—it should be an individual choice.
Florida Gov. DeSantis stated regarding the hyped press releases from Covid vaccine-makers hype, “I do believe that these breakthroughs represent probably the greatest rays of hope that we have seen since the pandemic began,”
Gov. DeSantis stated that Florida residents will not be mandated to take either vaccine.
While states are also now chiming in about how they will handle getting the shot into the arms of their residents. Law.com writes, “The New York State Bar Association on Saturday passed a resolution urging the state to consider making it mandatory for all New Yorkers to undergo COVID-19 vaccination when a vaccine becomes available, even if people object to it for “religious, philosophical or personal reasons.
Regarding the kids, government contractor Dr. Moncef Slaoui said in a recent interview, “the plan is to run trials at an expedited pace over the coming months, first with younger adolescents, then toddlers, and, finally, infants. If that goes well, Slaoui, expects most kids will be able to get vaccinated by the middle of next year.” writes Yahoo news.
The final word is that of Dr. Michael Yeadon, who holds a degree in Biochemistry & Toxicology & a research-based PhD in pharmacology. Dr. Yeadon spent 32 years working in pharmaceutical R&D and was a VP at Pfizer. He posted this letter to Twitter,
“Whatever one’s views are about political management of the pandemic in [the] U.K., we believe strongly that mandated or coerced use in the wider population of part-developed vaccines should play no role whatsoever in recovering from it.
Those at distinctly elevated risk of severe illness & death, of course should be offered it, using fully informed consent. But absolutely not mandated or coerced vaccination. We so argue this, because it’s illegal and unethical. It might be countered that this letter is superfluous because no one is suggesting it. Sadly, that isn’t true. On the contrary, senior figures from governments across the world are proposing exactly this. Leading U.K. politicians have worryingly even said that “our national policy now is to suppress the virus as much as possible until a vaccine becomes available.”
Despite any promises of a non-coercive Covid shot, the government’s apparatus for ramming through all sorts of legislation to eliminate any barrier hindering injectable pharmaceutical product lines making their way into your body is well-established over the last few years. Starting with a measles outbreak in 2019, nearly 200 bills suddenly appeared, as if waiting for the right moment. It was clear it wasn’t about measles then, and perhaps in a short time, we may discover there may be more to this new vaccine push than simply attempting to stop a cold virus or save lives – a primary endpoint that the Covid trials weren’t even designed for in the first place.
COVID 19, and the subsequent governmental responses, appear to be part of an international conspiracy to commit fraud. It seems there is no evidence that a virus called SARS-CoV-2 causes a disease called COVID 19.
Sometimes you have to go with your gut. I am not an expert in genetics and, as ever, stand to be corrected. However my attention was drawn to some research published by the Spanish medical journal D-Salud-Discovery. Their advisory board of eminently qualified physicians and scientists lends further credibility to their research. Their claim is astounding.
The genetic primers and probes used in RT-PCR tests to identify SARS-CoV-2 do not target anything specific. I followed the search techniques outlined in this English translation of their report and can corroborate the accuracy of their claims about the nucleotide sequences listed in the World Health Organisations protocols. You can do the same.
D-Salud-Discovery state there are no tests capable of identifying SARS-CoV-2. Consequently all claims about the alleged impact of COVID 19 on population health are groundless.
The entire official COVID 19 narrative is a deception. Ostensibly, there is no scientific foundation for any part of it.
If these claims are accurate we can state that there is no evidence of a pandemic, merely the illusion of one. We have suffered incalculable loss for no evident reason, other than the ambitions of unscrupulous despots who wish to transform the global economy and our society to suit their purposes.
In doing so this “parasite class” have potentially committed countless crimes. These crimes can and should be investigated and prosecuted in a court of law.
Identification of What Exactly?
The World Health Organisation (WHO) classified COVID-19 (COronaVIrus Disease 2019). They declared a global COVID 19 pandemic on March 11th 2020.
“The etiologic agent [causation for the disease] responsible for the cluster of pneumonia cases in Wuhan has been identified as a novel betacoronavirus, (in the same family as SARS-CoV and MERS-CoV) via next generation sequencing (NGS) from cultured virus or directly from samples received from several pneumonia patients.”
The WHO’s claim is that the SARS-CoV-2 virus causes the disease COVID-19. They also allege this virus has been clearly identified by researchers in Wuhan.
“The Chinese authorities identified a new type of coronavirus, which was isolated on 7 January 2020……On 12 January 2020, China shared the genetic sequence of the novel coronavirus for countries to use in developing specific diagnostic kits.”
These two statements from the WHO clearly suggest the SARS-CoV-2 virus was isolated (meaning purified for study) and then genetic sequences were identified from the isolated sample. From this, diagnostic kits were developed and distributed globally to test for the virus in towns, cities and communities around the world. According to the WHO and Chinese researchers, these tests will find the virus that causes COVID 19.
Yet the WHO also state:
“Working directly from sequence information, the team developed a series of genetic amplification (PCR) assays used by laboratories.”
The Wuhan scientists developed their genetic amplification assays from “sequence information” because there was no isolated, purified sample of the so called SARS-CoV-2 virus. They also showed electron microscope images of the newly discovered virions (the spiky protein ball containing the viral RNA.)
However, such protein structures are not unique. They look just like other round vesicles, such as endocytic vesicles and exosomes.
Virologists claim that it is not possible to “isolate” a virus because they only replicate inside host cells. They add that Koch’s postulates do not apply because they relate to bacteria (which are living organisms). Instead, virologists observe the virus’ cytopathogenic effects (CPE), causing cell mutation and degradation, in cell cultures.
When Chinese researchers first sequenced the full SARS-CoV-2 genome they observed CPE in Vero E6 and Huh7 cells. Vero E6 are an immortalised monkey cell line and Huh7 are immortalised cancer (tumorigenic) cells. Meaning they have been maintained in vitro (in petri dish cultures) for many years.
Central to the official SARS-CoV-2 story is the idea that it is a zoonotic virus, capable of bridging the species gap from animals to humans. When scientists from the U.S. CDC“infected” various cells with the novel virus they noted the following:
“We examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549) [lung celles], human liver cells (HUH7.0), and human embryonic kidney cells (HEK-293T), in addition to Vero E6 and Vero CCL81 [monkey cells]……No cytopathic effect was observed in any of the cell lines except in Vero cells [monkey cells]…….HUH7.0 and 293T cells showed only modest viral replication and A549 cells [human lung tissue cells] were incompatible with SARS-CoV-2 infection.”
The CDC did not observe any CPE in human cells. They saw no evidence that this alleged virus caused any human illness. Nor did this supposed human virus show any notable replication in human cells, suggesting human to human infection would be impossible.
Noting this problem, a team of Polish scientists introduced this sequenced “virus” to human epithethelium (airway) cells. They observed the effects on these HAE cultures for 5 days. They noted much greater replication than the CDC scientists but ultimately stated:
“We did not observe any release of the virus from the basolateral side of the HAE culture.”
Meaning they did not see any evidence of the supposed virions breaching the cell wall membrane. Again suggesting this so called virus isn’t infectious in human beings.
It is not clear that SARS-CoV-2 is a human virus capable of causing illness. It may not even physically exist. Is it nothing more than a concept based upon predictive genetic sequences?
Voyage Of Discovery
The Wuhan Center for Disease Control and Prevention and the Shanghai Public Health Clinical Centre published the first full SARS-CoV-2 genome (MN908947.1 ). This has been updated many times. However, MN908947.1 was the first genetic sequence describing the alleged COVID 19 etiologic agent (SARS-CoV-2).
All subsequent claims, tests, treatments, statistics, vaccine development and resultant policies are based upon this sequence. If the tests for this novel virus don’t identify anything capable of causing illness in human beings, the whole COVID 19 narrative is nothing but a charade.
The WUHAN researchers stated that they had effectively pieced the SARS-CoV-2 genetic sequence together by matching fragments found in samples with other, previously discovered, genetic sequences. From the gathered material they found an 87.1% match with SARS coronavirus (SARS-Cov). They used de novo assembly and targeted PCR and found 29,891-base-pair which shared a 79.6% sequence match to SARS-CoV.
They had to use de novo assembly because they had no priori knowledge of the correct sequence or order of those fragments. Quite simply, the WHO’s statement that Chinese researchers isolated the virus on the 7th January is false.
The Wuhan team used 40 rounds of RT-qPCR amplification to match fragments of cDNA (complimentary DNA constructed from sampled RNA fragments) with the published SARS coronavirus genome (SARS-CoV). Unfortunately it isn’t clear how accurate the original SARS-CoV genome is either.
In 2003 a team of researchers from from Hong Kong studied 50 patients with severe acute respiratory syndrome (SARS). They took samples from 2 of these patients and developed a culture in fetal monkey liver cells.
They created 30 clones of the genetic material they found. Unable to find evidence of any other known virus, in just one of these cloned samples they found genetic sequences of “unkown origin.”
CHART: E Gene target sequence
Examining these unknown RNA sequences they found 57% match to bovine coronavirus and murine hepatitis virus and deduced it was of the family Coronaviridae. Considering these sequences to suggest a newly discovered SARS-CoV virus (new discoveries being ambrosia for scientists), they designed RT-PCR primers to test for this novel virus. The researchers stated:
“Primers for detecting the new virus were designed for RT-PCR detection of this human pneumonia-associated coronavirus genome in clinical samples. Of the 44 nasopharyngeal samples available from the 50 SARS patients, 22 had evidence of human pneumonia-associated coronavirus RNA.”
Half of the tested patients, who all had the same symptoms, tested positive for this new alleged virus. No one knows why the other half tested negative for this novel SARS-CoV virus. The question wasn’t asked.
This supposed virus had just a 57% sequence match to allegedly known coronavirus. The other 43% was just “there.” Sequenced data was produced and recorded as a new genome as GenBank Accession No. AY274119.
The Wuhan researchers subsequently found an 79.6% sequence match to AY274119 and therefore called it a novel strain of SARS-CoV (2019-nCoV – eventually renamed SARS-CoV-2). No one, at any stage of this process, had produced any isolated, purified sample of any virus. All they had were percentage sequence matches to other percentage sequence matches.
Isolate Nothing
Scientists are very annoyed because they keep saying the virus has been isolated but no one believes them. This is because, as yet, no one has provided a single purified sample of the SARS-CoV-2 virus. What we have instead is a completed genome and, as we are about to discover, it isn’t particularly convincing.
Investigative journalists Torsten Engelbrecht and Konstantin Demeter asked some of the scientists who said they had images of SARS-C0V-2 virions to confirm these were images of an isolated, purified, virus. None of them could.
“The reliability of COVID-19 tests is uncertain due to the limited evidence base…There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.”
In The UK, in July, a group of concerned academics wrote a letter to the UK Prime Minister Boris Johnson in which they asked him to:
“Produce independently peer reviewed scientific evidence proving that the Covid-19 virus has been isolated.”
To date they have not received a reply.
Similarly, UK researcher Andrew Johnson made a Freedom of Information Request to Public Health England (PHE). He asked them to provide him with their records describing the isolation of a SARS-COV-2 virus. To which they responded:
“PHE can confirm it does not hold information in the way suggested by your request.”
Canadian researcher Christine Massey made a similar freedom of information request, asking the Canadian government the same. To which the Canadian government replied:
“Having completed a thorough search, we regret to inform you that we were unable to locate any records responsive to your request.”
“…No quantified virus isolates of the 2019-nCoV are currently available……..Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.”
Last updated on 13th July 2020, the CDC are yet to obtain any pure viral sample from any patient said to have the disease of COVID-19. They openly admit their tests don’t necessarily show if SARS-CoV-2 is either present or causes COVID 19.
We are told that none of this matters. That we are ignorant and just don’t understand virology. Therefore, we must except pictures of things we know could be something else and genetic sequences (which could be anything else) as conclusive proof that this virus, and the disease it is supposed to cause, are real.
Testing For Nothing
The WHO, and every government, think tank, policy steering committee, government scientific advisor, supranational institutions and others who promote the official COVID 19 narrative, assert that SARS-CoV-2 causes COVID 19. While no one has ever produced a sample of this supposed virus, the alleged SARS-CoV-2 genome has been published. It is in the public domain.
Key genetic sequences, in the SARS-CoV-2 genome, are said to have specific functions. These are the target proteins that scientists test for to identify the presence of the “virus”. These include:
RNA-polymerase (Rd-Rp) gene – This enables the SARS-CoV-2 RNA to replicate inside the cytoplasm of COVID 19 diseased epithelial cells.
S gene (Orf2) – this glycoprotein forms the spike on the SARS-CoV-2 virion surface which supposedly facilitates SARS-CoV-2 binding to the ACE2 receptors on cells, allowing the RNA inside the virion protein shell (capsid) to pass into the now infected cell.
E gene (Orf1ab) – small membrane protein used in viral assembly
N gene (Orf9a) – the nucleocapsid gene which binds the RNA in capsid formation
The WHO maintain a publicly available record of the RT-PCR primers and probes used to test for SARS-CoV-2. The primers are specific nucleotide sequences that bind (anneal) to the antisense and sense strands of the synthesised cDNA (called forward and reverse primers respectively.)
The cDNA strands separate when heated and reform when cooled. Prior to cooling, nucleotide sequences called probes are introduced to anneal to specific target regions of the suspected viral genome. During amplification, as the regions between primers elongate, when a primer strikes a probe, the probe decays releasing a fluorescent or dye which can then be read by researchers.
It is the identification of these markers which scientists claim to prove the presence of SARS-CoV-2 in a sample.
Something else which is publicly available is the Basic Local Alignment Search Tool (BLAST). This allows anyone to compare published nucleotide sequences with all those stored by the U.S. National Institutes of Health (NIH) genetic database called GenBank. Therefore we can BLAST the claimed SARS-CoV-2 primers, probes and target gene sequences.
The WHO’s forward, reverse primers and probe protocols, for the alleged SARS-CoV-2 viral genome, are based upon RdRp, Orf1, N and E gene profiles. Anyone can run them through BLAST to see what we find.
The vital RdRP nucleotide sequence, used as a forward primer is – ATGAGCTTAGTCCTGTTG. If we run a nucleotide BLAST this is recorded as a complete SARS-CoV-2 isolate with a 100% matched sequence identity. Similarly the reverse E gene primer sequence – ATATTGCAGCAGTACGCACACA – reveals the presence of the Orf1ab sequence which also identifies SARS-CoV-2.
However, BLAST also enables us to search the nucleotide sequences of the microbial and human genomes. If we search for the RdRp SARS-CoV-2 sequence it reveals 99 human chromosome with a 100% sequence identity match. The Orf1ab (E gene) returns 90 with a 100% sequence identity match to human chromosomes.
Doing the same for these sequences with a microbial search finds 92 microbes with a 100% match to the SARS-CoV-2 E gene and 100 matched microbes, with a 100% sequence identity, to the vital SARS-CoV-2 RdRp gene.
Whenever we check the so called unique genetic markers for SARS-CoV-2, recorded in the WHO protocols, we find complete or high percentage matches with various fragments of the human genome. This suggests that the genetic sequences, which are supposed to identify SARS-CoV-2, are not unique. They could be anything from microbial sequences to fragments of human chromosomes.
So called fact checkers, like Reuters’ Health Feedback project, have been quick to dismiss the claims of those who have noticed the apparent lack of specificity in the supposed SARS-CoV-2 genome. Using a slew of strawman arguments like, “this claim suggests every test should be positive,” (which it doesn’t) their debunking attempt runs something like this:
Primers are designed to bind to specific nucleotide sequences that are unique to the virus. The forward primer may bind to a particular chromosome but the reverse primer doesn’t bind to the same chromosome and so the chromosome is not present in the SARS-CoV-2 virus. Moreover because the forward and perverse primers envelop the sequence to be amplified the cDMA sequence between primers is unique to the virus.
This seems to deliberately misrepresent the significance of these findings by forwarding an argument that no one, other than the fact checkers themselves, are making. BLAST searches show that these target sequences are not unique to SARS-CoV-2. Nor do all targets need to be found for a result to be deemed positive.
Moroccan researchers investigated the epidemiology of Moroccan alleged cases of SARS-CoV-2. Nine percent were positive for three genes, eighteen percent were positive for two genes and seventy three percent for just one. As we have just discussed, many may have been positive for none.
“An optimal diagnosis consists of a NAAT [nucleic acid amplification test] with at least two genome-independent targets of the SARS-CoV-2; however, in areas where transmission is widespread, a simple single-target algorithm can be used……One or more negative results do not necessarily rule out the SARS-CoV-2 infection.”
Regardless of the spurious arguments of well funded fact checkers, if the forward and reverse primers identify junk, perhaps one being the fragment of a chromosome and the other a microbial sequence, then the amplified region between them is probably junk too.
The argument that RT-PCR only finds RNA is specious. Natural transcription (the separation of DNA strands) occurs during gene expression. No one is saying whole chromosomes or microbes are sequenced in the alleged SARS-CoV-2 genome. Though they may, for all we know. They are saying the alleged markers, used to test for this supposed virus, are not fit for purpose.
RT-PCR tests do not sequence the entire genome. They look for incidents of specific probe florescence to indicate the presence of sequences said to exist. These sequences are defined by MN908947.1 and the subsequent updates. These primers and probes could reveal nothing but RNA matches extracted from non-coding, sometimes called “junk,” DNA (cDNA.)
For example the SARS-CoV-2 S gene is meant to be highly specific to the SARS-CoV-2 virus genome. The target sequence is – TTGGCAAAATTCAAGACTCACTTTC. A microbial BLAST search returns 97 microbial matches with 100% identity sequence match. The lowest identity percentage match, within the top 100, is 95%. A human genome BLAST also finds a 100% sequence match to 86 human chromosome fragments.
No matter where you look in the supposed genome of SARS-CoV-2, there is nothing in the WHO’s test protocols that clearly identifies what it is. The whole genome could be false. The tests do not prove the existence of SARS-CoV-2. All they reveal is a soup of unspecified genetic material.
If so, as there are no isolates or purified samples of the virus, without a viable test, there is no evidence that SARS-CoV-2 exists. Therefore, nor is there any evidence that a disease called COVID 19 exists.
This infers that there is no scientific basis for any claims about COVID 19 case numbers, hospital admissions or mortality figures. All measures taken to combat this deadly virus are quite possibly founded upon nothing.
“Some deceitful practice or willful device, resorted to with intent to deprive another of his right, or in some manner to do him an injury.”
The Legal definition of a conspiracy is:
“A combination or confederacy between two or more persons formed for the purpose of committing, by their joint efforts, some unlawful or criminal act”
It seems, those who claim we face a pandemic have not provided any evidence to show that a virus called SARS-CoV-2 causes a disease called COVID 19. All of the information strongly suggesting this possibility is readily available in the public domain. Anyone can read it.
For there to be a fraud the deceit must be wilful. The intention must be to deliberately deprive others of their rights or injure them in some other way. If there is evidence of collusion between individuals ad/or organisations to commit fraud, then this is a conspiracy (in Common Law jurisdictions) or a Joint Criminal Enterprise (JCE) under International Law.
It seems COVID 19 has been deliberately used as a casus belli to wage war on humanity. We have been imprisoned in our own homes, our freedom to roam restricted, freedom of speech and expression eroded, rights to protest curtailed, separated from loved ones, our businesses destroyed, psychologically bombarded, muzzled and terrorised.
Worse still, while there is no evidence of unprecedented all cause mortality, there were unseasonable spikes in deaths. These correlate precisely with Lockdown measures which saw the withdrawal of the health services we pay for and a reorientation of public health services to treat one alleged disease at the exclusion of all others.
Further, it is proposed by those who have forwarded the COVID 19 story, that this alleged disease provides justification for the complete restructuring of the global economy, our political systems, societies, cultures and humanity itself.
To be allowed to participate in their so called “new normal,” which is the wholesale transformation of our entire society without our consent, they insist we submit to their conditions.
These include, but aren’t limited to, bio-metric surveillance of everyone, the centralised control and monitoring of all of our transactions, oppressive business and social restrictions and an effective demand that we have no right to sovereignty over our own bodies. This constitutes the condition of slavery.
There is no doubt that we have been deprived of our rights and injured. In Common Law jurisdictions innocence is presumed, but the evidence that harm has been deliberately caused by an international conspiracy is overwhelming. Destructive policies, enacted by governments across the world, clearly originated among globalist think tanks and supranational institutions long before the emergence of this non existent pandemic.
In Napoleonic Code jurisdictions, guilt is presumed. In order for the accused conspirators to prove their innocent they must show that, despite their immeasurable resources, they have collectively been unable to access or understand any of the freely available evidence suggesting COVID 19 is a myth.
Those responsible for the crime of conspiracy to commit global fraud should be tried. If found guilty they should be imprisoned while the rest of us get on with trying to repair the damage they have already inflicted.
Author Iain Davis is an independent researcher and short filmmaker and the author of the new book, A Dangerous Ideology. See more of Iain’s work at his blog site In This Together and follow him at Twitter & Steemit & MINDS.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
(OMNS Nov 20, 2020) On an orthomolecular farm, one that uses no agricultural chemicals, and no pharmaceutical products with animals or farmers, we have a different perspective on viruses, and thus our response to the COVID19 situation may be counter to what is generally propagating in the mainstream.
For those who are unfamiliar with this topic, just a warning. This might be uncomfortable to read, but healing is not necessarily comfortable. It would be good to start with some history.
Vitamin C Mutants
In 1979, Irwin Stone published a paper, a medical hypothesis, entitled Homo Sapiens Ascorbicus, a Biochemically Corrected Robust Human Mutant. [1] Stone had been researching vitamin C and publishing papers on it for decades, and personally was taking lots of vitamin C in an attempt to match the levels he knew that animals make in their bodies continuously.
He and his wife had been in a head-on collision years earlier where he had broken most of his bones. Both had been taking many grams of vitamin C daily, and, to the surprise of medics that arrived on the scene, neither were in shock when the ambulance arrived. He was told that he would never walk again, but he was fully recovered and walking in 3 months, and he attributed that to his taking 50-60 grams of vitamin C a day while in the hospital. Stone and his wife had both experienced being the robust human mutants that he described in his paper.
What Irwin Stone knew was that a goat our size, when under stress, can produce up to 100 grams per day of vitamin C, converting glucose, blood sugar, to ascorbate. [2] Humans produce none, but we have the same mammalian cells as a goat and the same need for ascorbate, according to Stone. Stone called ascorbate “the healing factor” and he and other vitamin C researchers felt that calling ascorbate a “vitamin” did not adequately describe its necessity in helping humans prevent and heal from disease and injury.
Orthomolecular vs Pharma
Double Nobel Laureate, Linus Pauling, coined the term “orthomolecular” in 1968 in an article he published in the journal Science which was titled “Orthomolecular Psychiatry.” [3] In 1970, he wrote the bestselling book Vitamin C and the Common Cold. [4] In it is a chapter where he criticizes the pharmaceutical industry of the time for selling toxic chemicals as cold remedies when all humanity needed to know was to take high levels of ascorbate to neutralize viral infections.
Also in the 1970s, Pauling’s colleague at Stanford, Dr. Robert Cathcart treated thousands of people for various diseases in his private practice using only oral ascorbic acid. His research showed us that any viral infection could be addressed by raising the ascorbate level in the body high enough. [5] So viruses, even viral pneumonia, handled by people who are “skilled at taking vitamin C” as Cathcart put it, were a non-issue. Essentially Cathcart showed that, to the robust human mutant called Homo Sapiens Ascorbicus, viruses are a non-issue. [6]
Also by the 1970’s, the pharmaceutical industry apparently had been granted controlling influence by the mass media and governments of the world, and had a huge influence on the information distributed through our educational systems. They had essentially programmed humanity into building a dependency on their industry and products. They took control of both sides of every argument, arguing that vitamin C was important for every human, and that everyone needed to take vitamin C daily only in MILLIGRAM quantities, and they propagated rumors about the dangers of overdosing vitamin C. Mainstream medicine marginalized the information that Pauling was trying to get out, shoved his message off into a hidden corner, and those of us who grew up in the 60’s and 70’s simply weren’t trained to understand vitamin C and our human need for vitamin C. Today, the mainstream is still trapped in a model that was essentially obsoleted by Pauling and his orthomolecular colleagues in the 1970s. This industrial medicine model leads us astray from optimal health for ourselves and our children, even though it claims to offer “advanced” solutions.
Fortunately, Pauling’s Orthomolecular medicine continued to develop over the decades, in the background, and it continues to evolve today, healing people using only proper doses of nutrients. [7,8] Today, orthomolecular medicine, with only nutrients in its tool chest, is a serious competitor to the dominant pharmaceutical medicine model. Many of orthomolecular treatments are effective at relieving disease in a few hours or even a few minutes, as in the case of using vitamin C in a nebulizer for lung issues like asthma. [9] And it’s very easy for any human to prove that taking a few grams of vitamin C every 15 or 30 minutes during a day can shut down a virus, any virus, even a “novel” virus. [10,11]
Orthomolecular Farming
Somewhat battered by the dominant “health care” paradigm, my wife, Kira, and I started livestock farming with a commitment to living in a new paradigm: being pharmaceutical free and chemical free in all of our living and farming methods. We had knowledge and experience using vitamin C when we started this 160-acre farm. We had already used it for things like shutting down viral pneumonia and eliminating Kira’s dependency on epi-pens when she got stung by a wasp, and we used it to help a horse heal a broken hip bone. I had personally shut down many colds and other viruses in a day or two and was discovering how I could prevent sunburn and other radiation damage using Vitamin C and E [12, 13]. We kept my handicapped son Cameron going for years beyond his life expectancy by high dosing him with vitamin C when he had respiratory issues. We already had one grandchild, Helios, who was a vitamin C baby, and since then, we’ve welcomed more vitamin C baby grandchildren.
Each of these cascading experiences are powerful revelations on our journey to a new paradigm based on truth. Through our personal experiences, and by contrasting our gullibility earlier in life with the dramatic health benefits we realized and observed by high dosing vitamin C, we are becoming . . .
A New Farmer Species
One cause of “circling disease” in cattle is listeriosis, an infection that inflames the covering of the cow brain, similar to meningitis in humans. [14] In the mainstream veterinary model, this is a fatal disease in cows. A circling cow is about to die without massive antibiotic treatment, and even with that expensive treatment, it’s most likely to die. But with an understanding of the biochemistry of ascorbate in animals, this is a simple disease to treat, completely resolvable within hours. [15].
As orthomolecular practitioners with extensive experience dealing with all kinds of animal and human health issues using only high dose nutrients, we are simply not impressed by the mainstream COVID19 misinformation. Since we started this farm, we have been telling people that we are immersed in misinformation: lies about raw milk being dangerous, lies about food additives being safe, lies and obfuscation about nutrients, lies about vaccines being safe and useful, and, by omission, about the importance and power of a balanced microbiome in the soil, plants, animals, and humans.
When you have proven for yourself the truth, the lies have no traction. We have become, in essence, immune to the lies.
Mask-free, Gloves-free, Disinfectant-free
I titled this article “COVID19 vs Homo Sapiens Ascorbicus” because I think one of the main things we’ve proven in the years on this farm, and continue to prove daily, is Irwin Stone’s hypothesis. On this farm, we strive to match the levels of vitamin C in our bodies that animals produce. In doing so, we have become the robust human mutants that Irwin Stone predicted was possible all the way back in 1979. The reason we don’t worry about viruses, even novel viruses, is because they don’t affect the animals here and they don’t affect the homo sapiens ascorbicus farmers that we have become.
To the robust mutant, I have to say that the world has looked very strange for a long time, way before the COVID19 craze.
Out in the world, back when we were “original-recipe” homo sapiens, we were ignorantly downing food additives like polysorbate-80 (an emulsifier) in processed foods assuming it was safe, when in actuality it was damaging our gut microbiome, and we were injecting the same additive in vaccines to “boost the immunity of our children,” when in actuality it was opening up their blood brain barriers to the flow of more toxins.
Now, as transformed mutants, we no longer buy into the logic behind these practices. Homo sapiens ascorbicus aren’t affected by, and certainly don’t fear, viruses. So using pharmaceutical products to treat disease or alter our immune systems or the immune systems of our animals doesn’t make any sense.
As homo sapiens ascorbicus, we choose not to comply with unconstitutional dictates like masks, gloves, and Purell to avoid a disease that will never affect us. To our subspecies, those dictates look positively tyrannical. We know how to prevent viral infection using vitamin C, and, fortunately, we also know that high dosing vitamin C will protect us from the carcinogenic “sanitation” products being sprayed and spread freely now from shopping cart to shopping cart, on plexiglass and pin pads, and airborne in the stores that we must frequent in our quest to recruit and transform new homo sapiens ascorbicus. If you happen to see a maskless farmer in the crowd, you may be looking at one of the new, robust homo sapiens ascorbicus “mutants” that Irwin Stone predicted back in 1979. We are that new orthomolecular “species.”
A New Model
One of the founding quotes of our farm is from Buckminster Fuller, who was a brilliant contemporary of Linus Pauling. Fuller said, “You never change things by fighting against the existing reality. To change something, build a new model that makes the old model obsolete.”
For the last decade, we have been busy building a new reality, a farm community that homo-sapiens ascorbicus prefer to live in, one that better fits our robust mutant transformation. In observing the happenings of 2020, it seems that the existing reality, which is currently dominated by homo sapiens (original version), is failing and fading away into fear and overdue obsolescence. The new model is ours for the building, and the new model will be occupied by fearless mutants of the species homo sapiens ascorbicus and many others who, in their own way, have transcended the hysteria of the mainstream narrative.
So that’s an orthomolecular farmer’s response to COVID19. If you haven’t already figured out your relationship to ascorbic acid, ascorbate, the healing factor, vitamin C, you might want to. It will change your life. However, be aware that you may become a robust human mutant as well and you may find yourself with a naked face in a crowd of masked homo-sapiens who live in an obsolete reality.
(Theo Farmer administers the Facebook and MeWe groups titled “Vitamin C and Animals.” He is also the author of the children’s book Buttercup, Me and Vitamin C, a free pdf download at https://www.hfpma.online/shop )
Editor’s note: The views expressed in this article are the author’s and not necessarily that of all members of the Orthomolecular Medicine News Service Editorial Review Board. OMNS welcomes divergent opinions and discussion on a variety of subjects. Readers may submit their own article drafts to the Editor at the contact email below.
References
1. Stone, I. (1979) Homo Sapiens Ascorbicus, A Biochemically Corrected Robust Human Mutant. Med Hypotheses, 5:711-721. https://pubmed.ncbi.nlm.nih.gov/491997
3. Pauling L. (1968) Orthomolecular psychiatry. Varying the concentrations of substances normally present in the human body may control mental disease. Science. 160:265-271. https://pubmed.ncbi.nlm.nih.gov/5641253
4. Pauling L. (1970) Vitamin C and the Common Cold. W.H.Freeman & Co. ISBN-13:978-0425048535
5. Cathcart RF (1981) Vitamin C, titrating to bowel tolerance, anascorbemia, and acute induced scurvy. Med Hypotheses, 7:1359-1376. http://doctoryourself.com/titration.html
11. AscorbateWeb. An historical compendium of 20th-Century medical & scientific literature attesting to the efficacy of ascorbate (a.k.a. “Vitamin C”) in the treatment and prevention of human and animal illnesses and diseases. https://www.seanet.com/~alexs/ascorbate
13. Hickey S, Yanagisawa A, Saul AW, Schuitemaker GE, Downing D. (2012) Fukushima Radiation Release is Worse than You Have Been Told: What You Can Do to Protect Yourself. Orthomolecular Medicine News Service http://orthomolecular.org/resources/omns/v08n17.shtml
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Ron Erlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Felix I. D. Konotey-Ahulu, MD, FRCP, DTMH (Ghana)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, M.D. (USA)
Ken Walker, M.D. (Canada)
Raymond Yuen, MBBS, MMed (Singapore)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, French Edition: Vladimir Arianoff, M.D. (Belgium)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Assistant Editor: Helen Saul Case, M.S. (USA)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
Comments and media contact: drsaul@doctoryourself.com OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication.
Truth Comes to Light editor’s note: I recommend the work of Dr. Andrew Kaufman and Dr. Tom Cowan to understand the research showing that viruses are not at all what we have been taught. ~ Kathleen
Available at Dr. Andrew Kaufman’s LBRY or YouTube channels.
After being denied publication by three major journals, the Danish group has finally been published in the Annals of Internal Medicine. You won’t be surprised by what they found if you are part of this community. We now have some high quality evidence on our side. Check out the paper here:
The court stated, the test’s reliability depends on the number of cycles used and the viral load present. Citing Jaafar et al. 2020, the court concludes that
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the rule in most laboratories in Europe and the US), the probability that said person is infected is less than 3%, and the probability that said result is a false positive is 97%.”
The court further notes that the cycle threshold used for the PCR tests currently being made in Portugal is unknown.
The threshold cycles used in PCR tests in India is between 37 and 40, which makes the reliability of the PCR test less than 3% and the false positive rate as high as 97%.
This case concerned the fact that four people had been quarantined by the Regional Health Authority. Of these, one had tested positive for COVID using a PCR test; the other three were deemed to have undergone a high risk of exposure. Consequently, the Regional Health Authority decided that all four were infectious and a health hazard, which required that they go into isolation.

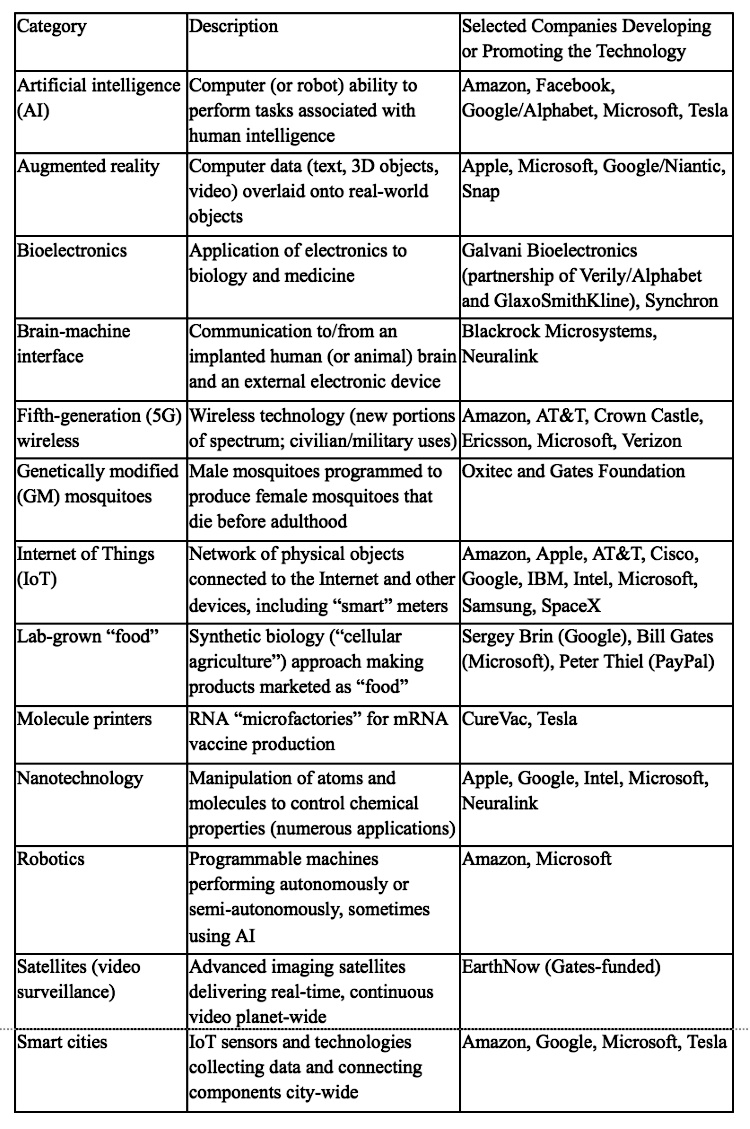
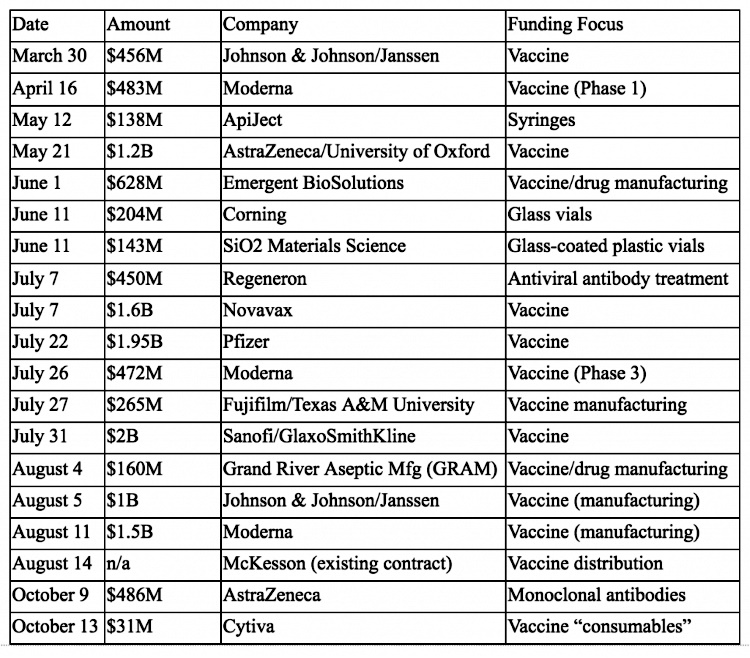
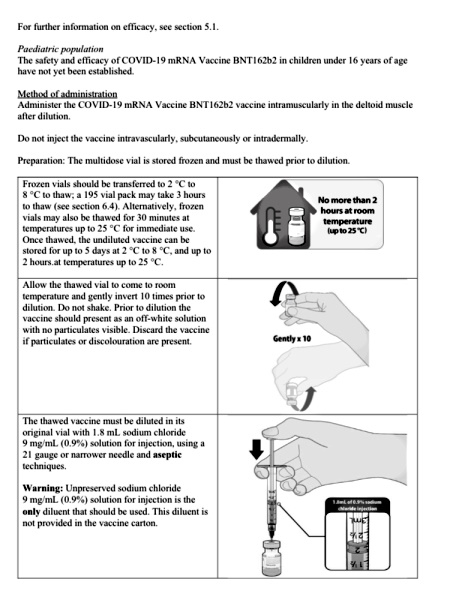
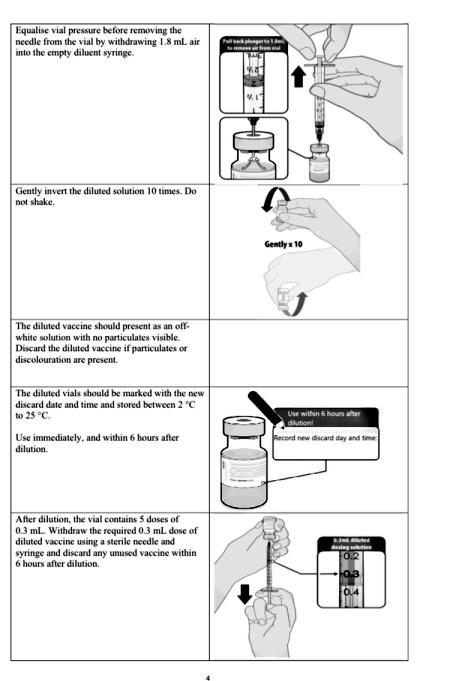
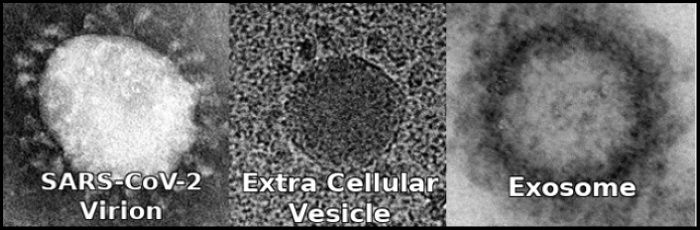
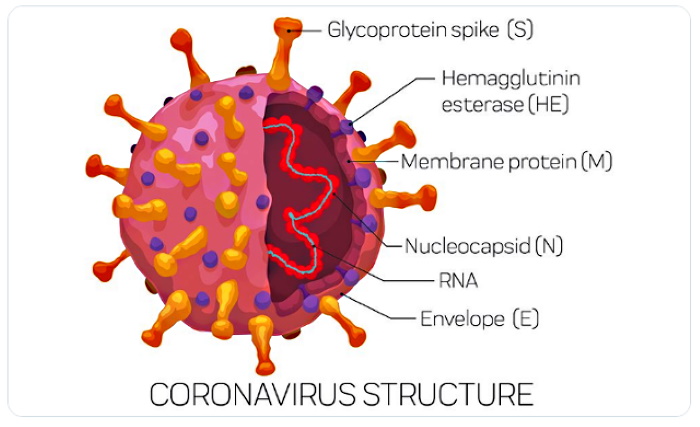
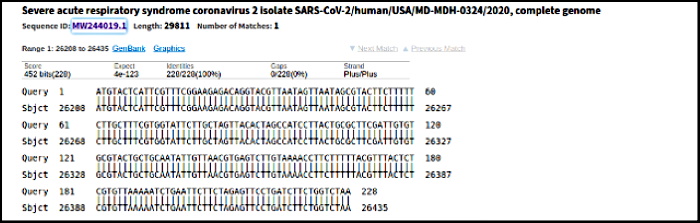 CHART: E Gene target sequence
CHART: E Gene target sequence