David Icke w/ Former FEMA Operative Celeste Solum: Barcoding You Via PCR Tests, Vaccines, Mass Depopulation, Terraforming & Transforming All Life on Earth
“My breaking news is, anyone, anyone who has taken a covid test — they have placed a magnetic beacon. You have been tagged. You have been barcoded. And I am going to provide you the evidence of that today…”
“I also want to draw people’s attention to the word ‘illuminate’…I don’t know if you’ve recognized it, but as an organic farmer, I have. It’s like things looked like a different color. The colors were not the same as before. .. I tripped on, in my research, that these forces and powers that are retooling and restructuring our planet, have restructured light.”
David Icke:
“A lot of people are now seeing about changing humans and barcoding humans — changing the nature of humans — but they want to change the nature of all life on earth, no matter what it is…”
###
Celeste Solum:
“Right now, your doctor can get paid for your execution…”
David Icke:
“It’s a difficulty that people have… to grasp just the scale of psychopathic, frikking evil that we’re dealing with.”
###
Celeste Solum:
You can imagine my horror when, in January, I went to the World Economic Forum and I saw all those plans and they had been operationalized. So, no longer were they on the shelf. No longer were they sitting in computers. All the public leaders around the world were declaring that they were operationalized, which means that they were activated…
This covid situation is the first deployment of a construct, a new lifeform, if you will It is not a virus. It is a nano, synthetic, biological life…– and what I mean by that is they have learned how, through evil technology, to fuse biological life and robotics. And the purpose of that is for extermination — because they don’t want anything of the old world. They want a new world…
I can show you military documents that talk about the old humans and the new humans. And they want, by 2025, to have the old humans eradicated. And any human from now on basically has to be engineered in a laboratory and enhanced and augmented and part of the matrix…”
###
David Icke:
“It makes perfect sense to me because, where I’m coming from… is that behind all this is a force that isn’t human. And it’s working through this network of, I think, largely hybrids — running this web that I call the global cult. And this non-human force is basically assimilating and transforming humans and human life — and, indeed, all life on earth, to fit its own design. And it’s been operating in the background. You can see it mentioned in all the ancient cultures, the Bible, everywhere… And it then makes sense that they would see us, as humans, in the way some humans see animals.”
Celeste Solum:
“Yeah. Basically, they believe that they are the custodians of the animals or the stock, the chattel. We’re nothing to them. And now is the time. They tolerated us for a time… But now is the time that they want to eradicate all life that is not made in a laboratory…”
###
David Icke:
“…It seems, as I’ve observed their mentality through the years, that they are obsessed with order… They are very ill-at-ease with states of flux that they don’t control…”
###
Celeste Solum:
“They are retooling and rewiring our bodies. Each one of us right now has 20,000 to 30,000 nanoparticles… They’re not active… Right now, they are in a sensory capacity…”
David Icke:
“It’s clear — the whole agenda of transforming the human body. How is this going to be impacted by the covid vaccine? Because when you’ve got these psychopaths insistent, not least through mandatory, that every man, woman and child on the planet is vaccinated with this thing. It’s obviously not about a virus. It’s about the transformation of everyone’s body….”
Celeste Solum:
“So many years ago, like over decades ago, DARPA wanted to put chips into…”
David Icke:
“For people who don’t know, DARPA is the technological development arm of the Pentagon and gives evil a bad name.”
Celeste Solum:
” Well, they do black ops…
So they wanted to put chips and RFIDs… in people’s brains but they didn’t want to have to do surgery. So after many, many years they came up with a gel that would do the same thing… This gel is called hydrogel or Quantum Dot…
So what will happen with the vaccine is, you’ll get it injected into you and then it assembles — it self assembles. And then it swarms through your body. There are 33 different classifications… of robots — each with a different mission and a payload deployed into your body…”
###
David Icke:
“What’s the relevance to all of this… of the whole tecno-electromagnetic-5G web that’s being built all around us?… Does it have an effect of activating this to another level?”
Celeste Solum:
“So basically, how it works is they deployed all these…nano synbios into our body that… Their bellies are hollow. They can carry a poison… It can carry a virus, a bacteria, a fungus. It can carry… it has explosive capabilities — more explosive capability (one nanoparticle) than TNT… It gets its marching orders from the frequency that is being aimed at it. “
###
Celeste Solum:
“Back at the parting of the Red Sea in the Bible, it says the seas split. In the Hebrew… it talked about the sea coagulated like curds… And so, another breaking news story that I’m going to be sharing this week is — between an enzyme and these nanoparticles they are coagulating our body like cheese curds.
…what the doctor’s perceived as pneumonia was not pneumonia but a swarming of the nanoparticles into the lungs, making a… primitive coagulation– but they intend to do this to the whole bloodstream. So, if they’re not going to get you one way, they’re going to get you another way.”
###
David Icke:
“What’s the significance then of … sticking this probe up people’s noses — just fo this test — right up to the brain?”
Celeste Solum:
“A couple of different things. One, if you pierce the blood-brain barrier… But they really don’t need that because they’ve already figured out how to get this — these nanoparticles — to cross the blood-brain barrier. But you are then getting, in many instances, the hydrogel straight into the brain. It doesn’t even have to travel through the body…”
###
David Icke:
“The bottom line is, take your mind back. And stop just doing or believing what authority tells you…
Whatever happens, we keep going. Because not keeping going is just not an option.”
[As a service to protect truth from censorship & to share widely, mirrored copies of this video will be available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Free content for Celeste will be coming soon on YouTube. Previously her free content was shared at diamondisc channel but will be moving to a new channel. Check back with diamondisc for details: https://www.youtube.com/user/diamondisc/videos
Connect with David Icke at DavidIcke.com & Ickonic.com
See videos related to The Story of Adam and Eve unclassified CIA document:
The court stated, the test’s reliability depends on the number of cycles used and the viral load present. Citing Jaafar et al. 2020, the court concludes that
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the rule in most laboratories in Europe and the US), the probability that said person is infected is less than 3%, and the probability that said result is a false positive is 97%.”
The court further notes that the cycle threshold used for the PCR tests currently being made in Portugal is unknown.
The threshold cycles used in PCR tests in India is between 37 and 40, which makes the reliability of the PCR test less than 3% and the false positive rate as high as 97%.
This case concerned the fact that four people had been quarantined by the Regional Health Authority. Of these, one had tested positive for COVID using a PCR test; the other three were deemed to have undergone a high risk of exposure. Consequently, the Regional Health Authority decided that all four were infectious and a health hazard, which required that they go into isolation.
Dr. Tom Cowan: The PCR Test is NOT a Valid Diagnostic Tool
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Del Bigtree asked ICAN’s attorneys to explain when someone can claim a medical exemption and whether a business can ask for proof of the medical exemption.
ICAN’s attorneys, led by Aaron Siri, provided this letter. In short, ICAN has been advised that, upon asserting a medical exemption to wearing a mask, the business cannot ask for proof of the medical exemption.
If you want to complete a self-assessment to determine if you have a medical exemption to wearing a mask, here are self-assessment forms for residents in New York, California, and Texas. If you would like a self-assessment form for another state, please let us know!
With so little information public, and the information we do have is not genuinely encouraging, a cynical person might suggest the only thing breathless media coverage of Covid vaccine news has done is create pump-and-dump stock opportunities for investors.
As Bloomberg wrote: There’s ‘a wave of euphoria’ surging through global finance markets. Hooray? Pfizer’s latest stock surge was supported by press release hopium rooted in Science™. Like corporate media’s reporting on vaccine Science™, inconvenient truths are misrepresented, glossed over or outright ignored.
Just as Pfizer’s recent press release hyped its first interim analysis from its phase 3 study, the company’s CEO Albert Bourla sold 61% of his stock, netting him a cool $5.6M.
The sale was part of a pre-scheduled 10b5-1 trading plan. So were Moderna’s Chief Medical Officer Tal Zaks and their CEO Stephan Bancel, who made $63,069,210 and $58,591,783 respectively over the last six months with the world’s eyes on their vaccine development milestones. Optics be damned, as the companies simultaneously gobble up taxpayer money while their leadership unload stocks at record pace.
Science™ by press releases get dissected almost immediately nowadays, laying bare their shortcomings. Covid vaccine makers and their front men are throwing out big numbers to grab headlines across corporate media. Operation Warp Speed head contractor Dr. Moncef Slaoui said Friday, speaking from the White House Rose Garden (through a mask), that 20 million Americans could receive the shot by December. Followed up with 25-30 million each month after that.
Two narratives are running parallel throughout media to direct two different types of consumers. While the ‘pump and dump’ headlines target investors, the ‘vaccine will save us all’ reporting aims at the eventual mandatory consumers.
Reading between the lines, Reuters might be telling investors to be on the lookout for the next Science™ by press release before making any financial moves, while commoners in Europe under second lockdown, “must grit [your] teeth.” Or perhaps another translation: Don’t mistake our media hype aimed at investors to think you’ll get out of your [second] unscientific lockdown anytime soon, Europe!
Similarly, Yahoo News ran the headline, Pfizer vaccine could be key to conquering COVID-19 — but don’t throw away your mask yet. One statement message for investors, another for people under authoritarian edicts.
A recent BMJ analysis by Peter Doshi reviewed Covid vaccine frontrunners. Current trials, hyped at every turn, aren’t designed to save lives. Doshi writes, “None of the trials currently underway are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.”
He continues, “In all the ongoing phase III trials for which details have been released, laboratory confirmed infections even with only mild symptoms qualify as meeting the primary endpoint definition. In Pfizer and Moderna’s trials, for example, people with only a cough and positive laboratory test would bring those trials one event closer to their completion.”
So why are we waiting for a vaccine to save us when its basic metrics aren’t designed to do so? In the early days of the coronavirus response, all measures were predicated on things going back to normal once the vaccine arrived. Now headlines have drastically changed. Lockdowns are here and increasing and your masks aren’t coming off when the vaccine savior arrives.
Yet that’s not stopping Ticketmaster or the airlines. Both are now considering digital vaccine verification to attend concerts or travel. A billboard.com exclusive reports, “After purchasing a ticket for a concert, fans would need to verify that they have already been vaccinated (which would provide approximately one year of COVID-19 protection)” Where the claim ‘approximately one year of COVID-10 protection’ comes from is anyone’s guess.
Meanwhile, the World Economic Forum’s CommonPass [for the commoners] is being tested for international flight travel. The CommonPass takes traveler’s vaccine status or Covid test and prints out a scannable QR code used by airlines or border officials.
Then there’s Microsoft founder and not a doctor Bill Gates who previously claimed countries could be back to normal by “late 2021” if a vaccine is found. The Sun reports that Gates will meet with UK Prime Minister Boris Johnson to “plan a national vaccine rollout plan with the pharma giants.”
Johnson has taken criticism for announcing a second lockdown, a move he deemed a ‘nuclear deterrent’ not to be embarked upon again after the collateral damage and life-years-lost recorded from the first round of UK lockdowns.
Even the notorious Dr. Fauci’s flip flops are now openly abusive as he ratchets up the rhetoric. Fauci recently stated the UK and US are countries that “have that independent spirit.” But now is the time to “do what you’re told” continued Fauci with an uncomfortable laugh.
Upon Pfizer’s latest press release, The Lancet’s editor-in-chief Richard Horton tweeted:
On the Pfizer COVID-19 vaccine: publishing interim results through a press release is neither good scientific practice nor does it help to build public trust in vaccines. An announcement should come with full publication of a peer-reviewed research paper in a scientific journal.
Unfortunately for many like Horton, the realization should be arriving that public trust may have never been a primary goal of vaccine-makers. Science™ regularly takes a backseat to profits and ethics [see Pfizer hit with $2.3B largest criminal fraud fine in history by Justice Department]. And even when proper science should be followed, it is often sidestepped. Regularly failing to use inert placebos during vaccine trials, using trial designs with obscenely short observation windows to monitor serious adverse events, refusing to conduct vaccinated vs unvaccinated trials to compare total health outcomes and deep conflicts of interest are all in a day’s work for vaccine makers.
It should be noted that one ofthe biggest retractions in modern history by a journal, The Lancet, happened on Horton’s watch. The investigation leading to the retraction wasn’t prompted by some internal watchdogs or misinformation czars, it was driven from public pressure by independent scientists and researchers.
Second waves of lockdowns are upon us. Many who thought the vaccine would return us to normalcy have had a rude awakening. Since we are given no clear exit plan by ‘officials,’ perhaps it’s time to make our own.
Patrick Bet-David and Dr. Reiner Fuellmich discuss revelations around the covid narrative, including a breakdown of what’s really been going on and how we are going to hold the people who orchestrated all of this accountable.
Patrick Bet-David has a virtual sit down with consumer protection trial lawyer Reiner Fuellmich to talk about the Coronavirus and his work on the German Corona investigation committee.
Panic Paper (in German) https://bit.ly/3f3IZRF
About the guest: Dr Reiner Fuellmich is one of four members of the German Corona Investigative Committee, which since July 10, 2020, has been listening to large number of international scientists’ and experts’ testimonies, to find answers to questions about the pandemic, being asked by people worldwide.
Connect with the Corona Investigative Committee at Corona Ausschuss
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Medical Doctor/Manager for Wyoming’s State Public Health Department/Preparedness Unit Warns About Unfolding Medical Tyranny & Dark, Deadly History of Covid Vaccine Development
Dr. Igor Shepherd: Covid Vaccinations Are “Global Genetic Genocide” and “Biological Weapons of Mass Destruction”
Truth Comes to Light editor’s note: The article below is sourced from garydbarnett.com. The video is from Julie Formsby YouTube channel. As is heard in the introduction to Dr. Igor Shepherd’s talk and further detailed in Gary Barnett’s article, Dr. Igor Shepherd’s scientific background, life experience and areas of study are extensive, beginning in communist Soviet Union. In the video, Dr. Shepherd shares his background and offers his perspective on current events — tying in his knowledge of totalitarian government agenda, biological weapons and vaccines as tools for the tyrannical takeover and destruction of humanity.
Dr. Igor Shepherd is a medical doctor/manager for Wyoming’s State Public Health Department/Preparedness Unit, and is on the Covid response team.
I was able to have a conversation with Dr. Shepherd after he did a talk for “Keep Colorado Free and Open” this past Tuesday. Dr. Shepherd wrote to me, and I was able to get a copy of his important talk. He has taken great risk to do this talk about the horrors of this new ‘Covid-19’ vaccine, so I recommend that all watch and listen. It is a fairly long talk and questions are answered at the end, but it is worth every minute of your time. He calls them “Biological Weapons of Mass Destruction.”
Dr. Shepherd was born and raised in the Soviet Union, and became a Military Doctor in St. Petersburg, Russia, and studied under the Strategic Rocket Force. He is an expert today on bio-weapons, Chemical, Biological, Radiological, Nuclear, and high yield Explosives,(CBRNE) and Pandemic preparedness. His view is that these vaccines are very similar technology to the bio-weapon RND used to develop viral weapons. He fully understands that the plan of depopulation and mandatory vaccinations will be at our doorstep very soon, and is shocked that the American people are so passive concerning this enemy takeover. He believes that this fake pandemic is the means by which a communist global government will be ushered into existence; one that cannot be voted out. I agree with this thinking, as this technocratic takeover and economic destruction will be communistic in nature.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
A new report from the state of New Hampshire has concluded that the safety of 5G technology is a concern for the health of the people, the animals, and the environment.
On November 1, a 111-page report describing the health concerns associated with 5G technology was released by the New Hampshire Commission to Study the Environmental and Health Effects of evolving 5G technology. The report was released to New Hampshire Governor Christopher T. Sununu, Speaker of the House Stephen J. Shurtleff, and President of the Senate Donna Soucy.
The recommendations include:
– state agencies include information on their websites regarding the dangers of radiofrequency (RF) microwave radiation from all sources;
– calling on state agencies to add warnings concerning newborns, young children and pregnant women;
– ensuring any new wireless antennae installation located on private property to be placed away from residences, businesses, and schools;
– encourage the deployment of fiber optic cables and wired connections;
– recommend that state agencies work with scientific experts to develop RF radiation safety limits to protect trees, plants, birds, insects, and pollinators
5G — or 5th generation cellular technology — is the name for the latest telecom technology upgrade. The new technology is expected to herald the beginning of Smart Cities, where driverless cars, pollution sensors, cell phones, traffic lights, and thousands of other devices interact in what is known as “The Internet of Things.” However, there have been a number of health and privacy concerns raised by opponents of the rapidly advancing 5G expansion.
These concerns led the New Hampshire house to pass HB 522 in 2019, a bill which created the commission, tasking it to “study the environmental and health effects of evolving 5G technology.” The Commission was made up of several legislators who are also medical doctors and engineers, a scientist with expertise in electromagnetic radiation, a New Hampshire Town Councilperson and representatives from the New Hampshire Attorney General’s Office, Department of Health & Human Services and the Department of Business and Economic Affairs.
The Commission also featured members of the wireless industry, including the CTIA, the largest wireless industry lobby which has been instrumental in promoting 5G. The members of the industry signed onto the “minority report” that stated “the scientific consensus” is that wireless technology is safe. However, the “majority report” documents substantial scientific evidence finding harmful health and environmental impacts.
In early November, the commission concluded that the safety of 5G has “come into question because of the thousands of peer-reviewed studies documenting deleterious health effects associated with cellphone radiation exposure.” The majority of the commission voted in favor of sending 15 recommendations to the Governor.
The report also recommends US federal agencies coordinate “to protect people, wildlife, and the environment from harmful levels of radiation” and states that “until there is Federal action, New Hampshire should take the initiative to protect its environment.” The strongest call to action was a recommendation that a resolution be introduced to the House of the U.S. Congress to require the Federal Communication Commission (FCC) to commission an independent review of the current radiofrequency (RF)
standards of the electromagnetic radiation in the 300MHz to 300GHz microwave spectrum.
The 5G Commission’s goal was to answer several questions regarding the safety of 5G. The commission asked the following:
– “Why are the FCC radiofrequency exposure limits set for the United States 100 times higher than countries like Russia, China, Italy, Switzerland, and most of Eastern Europe?”
– “Why have more than 220 of the world’s leading scientists signed an appeal to the WHO and the United Nations to protect public health from wireless radiation and nothing has been done?”
– “Why have the cumulative biological damaging effects of ever-growing numbers of pulse signals riding on the electromagnetic sine waves not been explored, especially as the world embraces the Internet of Things, meaning all devices being connected by electromagnetic waves, and the exploration of the number of such pulse signals that will be created by implementation of 5G technology?”
Devra Davis PhD, MPH, President of Environmental Health Trust, commended the state of New Hampshire for “taking the time to generate such an important and historic document.” Davis also called for reducing wireless exposure in light of the growing body of evidence. Davis has previously published research documenting the scientific evidence which indicates that radiofrequency radiation from mobile phones and other wireless devices is a possible human carcinogen and recently published a paper on cell phone radiation and colon cancer.
Davis and the Environmental Health Trust have also partnered with the Children’s Health Defense in a join lawsuit against the FCC. The suit, filed in July, accuses the FCC of failing to protect human health and the environment by dismissing scientific evidence of harm from wireless radiation. The suit alleges that the FCC violated numerous laws and ignored scientific evidence when it decided on December 4, 2019 that FCC radiofrequency-exposure limits and regulations provide adequate protection and thus, should not be updated.
New Hampshire is not the first state to call for independent study of 5G technology. Back in May 2019, the Louisiana House unanimously voted to have the Louisiana Department of Environmental Quality and the Department of Health study the effects of 5G technology on the environment and public health.
Corruption Written Into Law
According to the FCC’s regulations, local governing bodies are not allowed to consider health risks when making their decisions. This is because the federal law known as the Wireless Communications Act of 1996 prohibits local jurisdictions from considering perceived health effects when taking an action on a proposed facility. Instead, cities and towns can only regulate cell sites based on the aesthetics and placement of the devices.
This problem was only made worse in September 2018, when the FCC passed a new rule putting the federal government in complete control of the 5G rollout. In April 2019, President Trump issued an executive order stating that local and state bodies must now approve new 5G infrastructure within 90 days. The Trump administration also initiated a cap on the fees local governments can charge telecom companies wanting to install 5G technology.
Additionally, in early February 2019, the Senate Commerce, Science, and Transportation Committee held a hearing on the future of 5G wireless technology and its impact on the American people and economy. At the hearing, U.S. Senator Richard Blumenthal (D-CT) raised concerns about the lack of scientific research and data on the technology’s potential health risks. In early December 2018, Senator Blumenthal and California Representative Anna Eshoo held a press conference asking the FCC to provide evidence that 5G technology is safe.
New York Congressman Thomas Suozzi also sent a letter to the FCC seeking answers about the technology. “Small cell towers are being installed in residential neighborhoods in close proximity to houses throughout my district,” said Rep. Suozzi in his letter. “I have heard instances of these antennae being installed on light poles directly outside the window of a young child’s bedroom. Rightly so, my constituents are worried that should this technology be proven hazardous in the future, the health of their families and value of their properties would be at serious risk.”
New Jersey Congressman Andy Kim sent a letter as well, noting that, “Current regulations governing radiofrequency (RF) safety were put in place in 1996 and have not yet been reassessed for newer generation technologies. Despite the close proximity to sensitive areas where these high-band cells will be installed, little research has been conducted to examine 5G safety.” Oregon Representative Peter A. DeFazio, House Transportation and Infrastructure Committee Chairman, wrote a letter to FCC Chairman Ajit Pai and acting FDA Commissioner Sharpless regarding the status of the government’s research into the potential health effects of RF radiation and its relation to the FCC’s guidelines for safe human RF exposure levels.
Despite the growing concern from state representatives, scientists, health professionals and journalists, the FCC has wholeheartedly endorsed the rollout of 5G, claiming that there are no public health concerns. Additionally, many cities and localities are raising alarm bells due to the federal government and their partners in Big Wireless usurping local control of 5G expansion. The Mayor of Danville, California went so far as to admit that the city council had “lost control” of the 5G rollout to the federal government and Big Wireless.
It is this revolving-door relationship between Big Wireless and the U.S. government regulatory agencies that has corrupted the research around the dangers of radiofrequency radiation and placed the American people directly in harm’s way.
Aided by British military, Liverpool have initiated a mass covid testing program on its population, in an attempt “to control #Covid19”. No matter how often tests prove to be inaccurate, it doesn’t seem to be stopping governing authorities in Europe, and parts of the US, from tightening their grip on the people. But there is hope. True to the spirit and tradition of Liverpool lore, the people, and elements of the science and academia, are challenging the draconian measures.
What is a #Vaxhole? A person who quotes vaccine safety science that does not exist. What compelled Del to resurrect this HighWire tradition? British reporter Piers Morgan posted a tweet about the #Covid19 Vaccine you have to see to believe.
Vaccine certificates and immunity passports were just “conspiracy theories” 6 months ago and now they’re conspiracy fact as IBM, the CDC and the WHO are conspiring together to mass inoculate as much of the population as possible with a COVID-19(84) vaccine. In this video Dan Dicks of Press For Truth explains why IBM is a terrible choice for third party data handling while proving that so called “conspiracy theories” are slowly becoming conspiracy facts as the powers that ought not to be incrementally crank up the heat in a boiling frog scenario that is starting to get extremely hot!
I’ve described how the major clinical trials of the COVID vaccine are designed to prevent nothing more than a cough, or chills and fever [1] [2].
The whole plan to gain FDA approval of the vaccine is a stark fraud.
Now let’s move on to the next con: how to make it seem the vaccine is a roaring success.
Brief background: My readers know I’ve presented a complete case to show the SARS-CoV-2 virus was never proved to exist in the first place [3] [4] [5] [6] [7] [8] [9] [10]. So the whole idea of a vaccine is a non-sequitur, an absurdity. Likewise, the PCR test for “the virus” is a fraud on several levels [11]:
For example, the number of “cycles” for which the test is set is a key factor. Each cycle is a huge amplification of the tissue sample taken from the patient.
When you blow up that tissue sample above 34 cycles, you get gigantic numbers of false-positive results, even by the standards of the test. Fauci has admitted it. I’ve pointed out that FDA guidelines nevertheless recommend doing the test at up to 40 cycles. This alone explains reports of “rising COVID case numbers.”
Let’s say Pfizer and then Moderna win FDA approval to release their vaccines in the US. With the military doing the logistics of shipping, millions of doses move out, and soon, an extraordinary number of Americans are lining up to take the shot.
After a suitable period of time, the elite medical planners will change the way the PCR test is done. The number of cycles will be drastically reduced. That order will go out to labs in the US.
What does this mean? It means that far fewer positive test results will occur.
Therefore, the trend of “new COVID cases” will stop rising. It will level off, and then it will fall.
This rigging will be heralded as proof that that vaccine is producing a victory over the virus.
There is another strategy: change the definition of “a case of COVID.” Make the new definition, in terms of clinical symptoms, more restrictive. Something like this would do the trick: “The patient must exhibit a body temperature of at least 100 for 48 consecutive hours.”
That will automatically cause a significant drop in the number of cases. The drop will be attributed to the salutary effect of the vaccine.
For purposes of lockdowns and general clampdowns [12], to promote more fear and punish areas where the economy is “too open,” a reverse-technique can be applied:
Make PCR tests adjust their cycles UPWARD, thus producing huge numbers of positive results and “new cases.”
“Well, in South Dakota, we have to mandate at least 100,000 more vaccinations in each of the following ‘hot spots,’ where case numbers have suddenly escalated. And we must lock down those areas immediately…”
Needless to say, any and all serious harm and death caused by the vaccine anywhere will be attributed to “the pandemic disease.”
And there you have it. Simple, brutal, criminal, and controlled from the federal level. A strategy for making it seem the COVID vaccine is effective, and saved the day.
Here is a backgrounder I wrote on the subject of COVID vaccine fraud:
Making a vaccine look like it’s a champion isn’t difficult for public health agencies. There are a number of strategies.
Of course, these fraudulent strategies would be serious crimes. But when has that stopped the CDC or the World Health Organization?
In no particular order—-
ONE: Rework the definition of a “COVID case.” Presently, the CDC absurdly allows doctors to diagnose a person with COVID who has a cough, or chills and fever, and lives in an area where cases are being claimed. No test necessary.
So change this practice, once the vaccine is approved. Demand testing for a diagnosis. State that cough alone is not enough. Chills and fever must also be present. Require fever to be above 100.
These and other changes would automatically shrink the number of cases. The drop in numbers would be attributed to the vaccine.
This “definitional shrinking” was, in fact, deployed in the 1950s, after the introduction of the polio vaccine.
TWO: Order a change in the way the PCR diagnostic test is done. The practice of amplifying the original test sample from the patient occurs in cycles, or jumps. The greater the number of cycles, the more likely the test will result in a COVID diagnosis. Therefore, order a reduced number of cycles for all testing labs.
Outcome? Fewer COVID diagnoses. Fewer case numbers. “The vaccine is working.”
THREE: Quietly restrict the present hospital practice of arbitrarily writing “COVID” on patient case and death files.
FOUR: Cook up and publish false studies showing more and more people are developing immunity to the virus. Attribute this to the vaccine.
FIVE: Another type of false study—“the transmission of the virus from person to person is slowing, thanks to the vaccine.”
SIX: Pump up the success of issuing Immunity certificates after vaccination. “People are feeling safer now. More businesses are reopening…”
SEVEN: Using the compliant press, simply issue bald declarations that the vaccine is a success.
EIGHT: Hide the many instances of injury and death from the vaccine. When necessary, claim COVID was the cause.
NINE: Warn that the wonderful vaccine-derived immunity is not permanent, and frequent booster shots are necessary.
TEN: Rework the definition of “vaccine-acquired immunity.” Even a very weak antibody response from the shot would qualify as “protective immunity.”
ELEVEN: Huge numbers of people with ordinary flu-like illness, pneumonia, and other traditional lung infections are being called “COVID.” Change this practice. Go back to calling many of these people “flu,” “pneumonia,” etc. COVID case numbers will drop. Claim the drop is the effect of the vaccine.
TWELVE: Presently, millions of so-called COVID cases have “co-morbidities.” These are prior serious health conditions which are, in fact, the true causes of illnesses and death. Of course, this is denied. But after the vaccine is introduced… scale back the practice of counting all these ill and deceased co-morbid patients as “COVID.” Case and death numbers will drop. Claim the vaccine is the reason.
THIRTEEN: After the vaccine is introduced, slow down testing for a brief period. This will automatically reduce the rate of new cases. Attribute the decline to the vaccine.
Committing these crimes are a walk in the park for public health agencies.
And appointing official mouthpieces to carry lies to the public is as easy as training little Faucis to sit up and bark.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Our book, The Contagion Myth, is now available (banned on Amazon but sold on other outlets) and has already generated dozens of comments, many of them challenging our contention that the corona “virus” does not exist and that the illness attributed to this virus is not contagious—one referred to our book as a fairy tale!
However, unlike most coronavirus skeptics, we are not arguing that the illness is just a bad case of the flu, with deaths due solely to pre-existing conditions or inappropriate hospital care; rather we postulate that the illness can be very serious and that the likely cause is radiation poisoning, probably from the worldwide deployment of 5G, starting in Wuhan, China and followed by major cities throughout the world.
Comments we have received include the following:
Okinawa does not have 5G but people are getting infected there;
Some friends went to a wedding in Kirkland, Washington and got Covid, so it must be infectious;
There’s 5G in New Zealand but very few cases of illness;
A school in our neighborhood has opened for in-person classes and there has been an outbreak—two people have tested positive;
A lot of people “got the virus” after a big no-mask motorcycle rally in Sturgis, South Dakota;
What about rabbits getting myxomatosis, a known viral disease.
With the exception of the rabbit comment (a subject to be explored in a future blog), these observations are just that—epidemiological observations, which are certainly interesting and deserve further exploration, but these in no way disprove our main contention that this virus does not exist and the illness attributed to it is not contagious.
Why take our word for the shocking claim that no scientist has found the so-called coronavirus? Of course, you shouldn’t take our word for it, you should listen to what the experts are saying. In July 2020, the FDA posted a CDC document entitled “CDC 2019-Novel Coronavirus (2019-nCoV), Real-Time RT-PCR diagnostic Panel. For Emergency Use Only. Instructions for Use.” Buried in the text, on page 39, is the following statement: “. . . no quantified virus isolates of the 2019-nCoV are currently available.”
In other words, our government is telling us that there are no purified isolated samples of this “novel coronavirus,” which means that the virus has never been isolated and purified. What they are finding in the RT-PCR tests are fragments of genetic material, which actually come from human chromosome #8. This means that the results of all RT-PCR tests are invalid—the only thing they can tell us is that we are human beings.
Here is an analogy to describe what is going on. Let’s say you are a paid Lego specialist and someone offers to reward you if you can construct an exact replica of King Beauregard’s Medieval castle. The referees put all the known Lego pieces out on a table and promise to pay you well to do the reconstruction. Naturally, you ask to see a picture of what the castle looked like or at least some sort of architectural plan so you know what to build. But the referees say that you must reconstruct the castle without having access to any information about the original castle. You think this is downright bizarre, but since a job is a job, you start looking. You find pieces for a moat; you know that castles have moats and think that this must be part of the castle. Then you find windows, turrets, soldiers, etc.–with each new finding you are given a castle-building Lego award and an increase in salary. You write some software that fills in the rest of the castle from the fragments you have. Then you publish a peer reviewed paper on the “completed” castle for all the world to see.
Unfortunately, a child appears who looks like he has time traveled from the Middle Ages. You show him the castle. “Everybody knows that Beauregard didn’t have a castle.” He says. “Beauregard was an impoverished aristocrat who was afraid of moats; he lived in a garret in London.” But the show must go on, so his remarks are never published, while the Lego expert (who knows the child is right) keeps quiet and enjoys his hefty salary.
A number of readers have sent us studies “proving” the existence of pathogenic viruses. In fact, one virologist claimed that “thousands of papers” show that isolated bacteria or viruses cause disease. (He also tried to convince us that one could sterilize one’s hands, cover them and they would remain sterile “indefinitely.”)
One was a link to a study with the promising title “Koch’s postulates fulfilled for SARS virus”, published 2003 in the prestigious journal Nature. We discuss this study in The Contagion Myth. The researchers claim that Severe Acute Respiratory Syndrome (SARS) is also caused by a coronavirus. The title itself is misleading, not to say fraudulent, because the researchers did not satisfy Koch’s postulates—which is the common-sense way of proving that a microbe causes disease. They did not satisfy River’s postulates either—River’s postulates are for proving that a virus causes a disease. These methods involve isolating and purifying a specific microbial organism from a number of individuals suffering from a specific disease and injecting the isolated, purified bacteria or virus into healthy organisms (animal or human). If every sick person has the organism and every test subject becomes ill, then you know that the specific microbe causes the specific disease.
Let’s focus on the process of isolating and purifying a virus—it’s hard to do but not impossible. In 1973, the Pasteur Institute published guidelines for doing this. First the virologist takes mucus or secretions from a person with the disease. The secretions are diluted and then put into a kind of blender. The resultant liquid is then passed through a very fine filter—fine enough to keep out bacteria and fungi but let the viruses through; the resulting liquid is called a supernatant. It contains the virus but also lots of other stuff as well. The supernatant must then be centrifuged in such a way that you get bands of particles of the same size and weight. The scientist can determine which band is the virus using the known size and weight of viruses. This band is removed from the supernatant with a pipette. This is the properly isolated and purified virus. The virus is then transferred to some tissue to grow and multiply.
An important point is that when the virologist has finished the purification process of macerating, filtering and ultracentrifugation, he must then take an electron micrograph of the final, purified virus to show his colleagues that he has in fact successfully purified and isolated the virus. Virologists have done this many times and for many different viruses. Without an electron micrograph picture showing purification, no reputable journal would publish this work. The reason is simple: scientists are essentially told not to believe each other because someone says so. If you say you isolated a virus you must show the picture to prove it, period. Absent the picture it could be a total fabrication. The way science is supposed to work, after you have isolated and photographed the virus, other scientists in other labs follow the exact steps that you outlined in your paper and show pictures of the same isolated virus. Once a number of labs have done this, you have real proof that the virus exists.
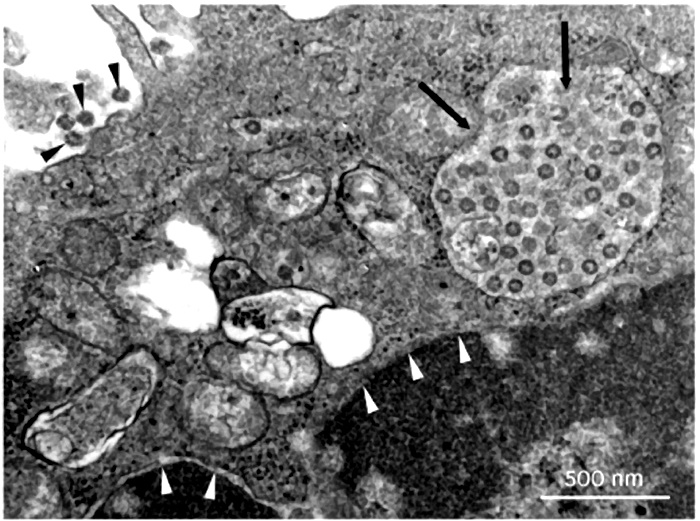
In the case of the novel corona virus, every single published photograph we have seen showing the “isolated” virus shows no such thing. Instead, it shows tissue with a number of dots, usually with an arrow pointing to the so-called coronavirus. If you see tissue in the photograph, by definition, it’s not isolated. An example of such a photograph comes from “Virus Isolation from the First Patient with SARS-CoV-2 in Korea,” published February 24, 2020 in the Journal of Korean Medical Science. Although the authors claim to have isolated the virus, the photographs they publish show “virus” structures inside and outside a cell (indicated by arrows), not isolated.
You can see a properly isolated “virus” in the electron microscopy image of the chicken pox “virus,” below. (By the way, although health officials claim that chicken pox is “highly contagious,” no studies have shown that exposing people to isolated chicken pox virus makes them sick.)
What virologists do today is use the liquid—called the supernatant–after either filtration or centrifuging to get rid of the bacteria, fungi and other larger material. This is what they refer to as “purification.” This is like filtering the grounds out of coffee to get caffeine so you can study its effects. But there are hundreds or thousands of other compounds in the coffee, so you still need to isolate the caffeine. What the researchers should then do is put the supernatant in what’s called a sucrose density centrifuge column, which spins out the various compounds into bands. One of these bands will contain the pure virus, which can then be photographed and analyzed.
Instead of working with pure virus, researchers use the supernatant, which contains all kinds of molecules and particles. Instead of doing a genetic analysis of the isolated virus, they do genetic analysis on the mess of compounds in the supernatant.
Now to get enough “virus” to use experimentally, virologists must grow it in a biological medium such as an animal or at least cells from an animal. Unlike bacteria, which can be grown in petri dishes, viruses are not alive and can only “grow” in other living cells.
So they transfer the supernatant not to healthy tissue, but to tissue that has been starved of nutrients and poisoned with strong antibiotics—to make sure that what is left is only viruses and not bacteria and fungi. The main type of tissue they use is kidney cells from various species, often monkey kidney cells (called Vero cells), and lung cancer cells. The “viruses” seem to multiply. The resultant mess of “viruses,” particles, poisons, dead tissue and cellular debris—called “cultured” virus– is then sold to researchers as samples of “purified virus” for them to use in studies.
By the way, the CDC has published guidelines on “transport medium” for viruses. This is what they use to inoculate the starved tissue which then grows the “virus.” The three main ingredients are fetal bovine serum (extracted from still-living fetal calves and preserved with anti-fungals, among other poisons) along with two highly toxic antibiotics, amphotericin (affectionately called ampho-terrible) and gentamicin. This ungodly mixture is then grown on monkey or fetal kidney cells. Interestingly, all doctors know that the main organ affected by gentamicin and ampho-terrible is the kidneys. So you poison the kidney, the kidney breaks down and then the virologist claims that the virus killed the kidney—without performing any controls. Don’t look behind the curtain, folks!
This practice is fraught with obvious problems for proving it is the virus and not the cancer cells or poisoned kidney cells that are causing disease when these viruses get injected into healthy test animals.
Remember that to prove that a specific virus is making humans or animals sick, they need to find the identical virus in many subjects who are sick with the same symptoms—and then make healthy humans or animals sick by exposing them to this virus. But when researchers try to grow the purified virus on healthy cells, they don’t get a lot of viruses; and when they subject healthy tissue, healthy animals or healthy people to these “viruses,” illness does not result—and this is the wily virus that is going to kill us all!
Why do “viruses” multiply in the starved and poisoned kidney or cancer cells? Because when cells are starved or poisoned, they produce exosomes, which are identical in appearance and characteristics to what are called “viruses.” These tiny particles are helpful, not toxic. They do not attack the cells and then multiply; rather, they are produced inside the cell, often in large amounts, when the cells are stressed by poison and starvation.
Viruses and exosomes are indistinguishable, as we learn from a study entitled “The Role of Extracellular Vesicles as Allies of HIV, HCV and SARS viruses,” published in the journal Viruses, May 2020. To quote from the paper, “The remarkable resemblance between EVs [extracellular vesicles, that is, exosomes] and viruses has caused quite a few problems in the studies focused on the analysis of EVs released during viral infection. Nowadays it is an almost impossible mission to separate EVs and viruses by means of canonical vesicle isolation methods, such as differential ultracentrifugation, because they are frequently co-pelleted due to their similar dimensions. To overcome this problem, different studies have proposed the separation of EVs from virus particles by exploiting their different migration velocity in a density gradient or using the presence of specific markers that distinguish viruses from EVs. However, to date, a reliable method that can actually guarantee a complete separation does not exist [emphasis added]. “
In other words, researchers can’t distinguish viruses from exosomes—that’s because they are the same thing and in reality, all viruses are exosomes. Scientists are discovering that all of these “viruses” originate in our own tissues—they don’t attack us from the outside.
With this background, let’s then look at the study, “Koch’s Postulates fulfilled for SARS Virus.” The researchers took unpurified sediment from the snot of sick people, grew that in lung cancer cells until they got a sufficient quantity of cellular material to work with. Then they centrifuged this mess again, not even attempting to purify any virus from the mixture. Finally, they took this unholy mixture of snot sediment, lung cancer cells and who-knows-what-else and injected that into two unfortunate monkeys. They didn’t do a control group by injecting saline into other monkeys or injecting lung cancer cells into monkeys or even injecting the liquid from the centrifuged material into monkeys. They just injected the cellular-debris-laden goop. One of the monkeys got pneumonia, the other got a rash. That, claim the researchers, is the proof that a “coronavirus” can cause disease and that Koch’s postulates have been satisfied.
“The Coronavirus Unveiled,” appearing in the New York Times, gives the impression that researchers are working with a genuine isolated coronavirus. Nevertheless, the article tells us that “In February, as the new coronavirus swept across China and shut down entire cities, . . . the best pictures anyone had managed to take were low-resolution images, in which the virus looked like a barely discernible smudge.”
How did the researchers isolate the virus? They “doused the viruses with chemicals to render them harmless. . .” In other words, they poisoned them. Then they somehow “concentrated the virus-laden fluid from a quart down to a single drop” after which they flash froze the drop. Then in the microscope they saw structures they called viruses.
This is not the proper way to isolate and characterize a virus, either. Proper isolation involves ultrafiltration and centrifuging–not dousing with chemicals and flash freezing–and then performing various physical, biochemical and immunological analyses.
After seeing these particles—most likely helpful exosomes responding to the poisonous chemicals–the researchers state that “its intimately twisted genes commandeer our biochemistry [and] wrenches into our cellular factories, while others build nurseries for making new viruses.” This is highly imaginative horror-movie speculation, not science.
Virologist have three “hosts” they can use in their attempts to prove that viruses cause illness. After “isolating” the virus, they can expose humans to the virus; they can expose animals to the virus; or they can use tissue cultures taken from various animal or human sources and expose the tissue culture to the virus. Leaving aside the fact that they never actually isolate and purify the virus, which they openly admit, let’s assume that the unpurified fluid they are using does contain the relevant virus and therefore should be able to transmit infection. I
In the history of virology, most virologists have decided not to do their experiments on human subjects as this is considered unethical. In the case of the SARS-CoV-2 virus, we know of no published study that used humans as the test subjects.
Virologists also admit that in the case of most viral infections, there are no studies available proving infection in animals. How a virus can infect and kill humans but not animals is left unexplained. Researchers get around this obvious biological conundrum by saying, “there are no animal models on which to test such-and-such a virus.” In other words, “We know that the virus infects and kills humans even though we’ve never tested the virus on humans because that would be unethical. Therefore, we do our tests on animals, even though when we test animals. they don’t get sick, because they are not proper “hosts” for the virus. So, you’ll just have to trust us.”
In the case of SARS CoV-2, we know of two studies that used unpurified “virus” on animal models, one with hamsters and one with mice. In the hamster study, researchers took the unpurified, lung-cancer-grown, centrifuged animal secretions and squirted it down the throats and into the lungs of a group of unfortunate hamsters. Some but not all of the hamsters got pneumonia and some even died. We have no idea what would have happened if they had squirted plain lung cancer cells into the lungs of these hamsters, probably not anything good. Even more perplexing, some of the hamsters didn’t even get sick at all, which certainly doesn’t square with the deadly contagious virus theory.
In the mouse study, researchers infected both transgenic mice and wild (normal) mice with unpurified virus. None of the wild mice exposed to the “virus” got sick. Of the mice genetically programmed to get sick, a statistically insignificant number either lost some fur luster or had an insignificant weight loss. Thus, scientists have not been able to show that the Covid-19 “virus” causes harm to animals.
The purpose of the study was for a group of about twenty virologists to describe the state of the science dealing with the isolation and purification, and the biological characteristics of the new SARS-CoV-2 virus, and to share this information with other scientists for their own research. A thorough and careful reading of this important paper reveals some shocking findings.
First, in the section titled “Whole Genome Sequencing,” we find that rather than having isolated the virus and sequencing the genome from end to end, they “designed 37 pairs of nested PCRs spanning the genome on the basis of the coronavirus reference sequence. . . “ This means they actually looked at a mere thirty-seven primers out of the approximately thirty thousand base pairs claimed to be the genome of an intact virus. They then took these thirty-seven segments and put them into a computer program, which filled in the rest of the genome.
This computer-generation step—called “whole genome sequencing”–constitutes scientific fraud of the highest order. Here is an equivalency: a group of researchers claim to have found a unicorn because they found a piece of a hoof, a hair from a tail, and a sliver of a horn. They then put that information into a computer and program it to re-create the unicorn, claiming that this computer re-creation is the real unicorn. Of course, they have never actually seen a unicorn so could not possibly have examined its genetic makeup to compare their samples with the actual unicorn’s hair, hooves and horn.
The researchers claim they decided which is the real genome of SARS-CoV-2 by “consensus,” sort of like a vote. As different computer programs will come up with different versions of the imaginary “unicorn,” they come together as a group and decide which is the real imaginary unicorn. (By the way, this is how scientists characterized the measles “virus”—by consensus!)
But the real blockbuster finding in this study comes later, a finding so shocking that it’s hard to believe what we are reading. “Therefore, we examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549), human liver cells (HUH 7.0), and human embryonic kidney cells (HEK-293T). In addition to Vero E6 and Vero CCL81 cells . . . Each cell line was inoculated at high multiplicity of infection and examined 24h post-infection.”
This is the third method virologists use to prove infection and pathogenicity — the method they usually rely on—namely, the inoculation of solutions they say contain the virus onto a variety of tissue cultures. As we have pointed out, such inoculation has never been shown to kill (lyse) the tissue, unless the tissue is first poisoned and starved (grown in a “minimal-nutrient medium.”)
In the Results section, the authors state: “Therefore, we examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549), human liver cells (HUH7.0), and human embryonic kidney cells (HEK-293T) . . . Each cell line was inoculated at high multiplicity of infection and examined 24h post infection. No CPE was observed in any of the cell lines except in Vero cells.”
Note, CPE means “cytopathic effect,” which refers to structural changes in host cells that are caused by “viral invasion.” The infecting virus is said to cause lysis (breaking up) of the host cell or, when the cell dies without lysis, an inability to reproduce. Both of these effects are said to occur due to CPEs.
So did this viral material with its “intimately twisted genes commandeer the cellular biochemistry [and] wrench into the cellular factories, while others build nurseries for making new viruses?” Nothing of the sort!
The shocking thing about the findings is that using their own methods, the virologists found that solutions claimed to contain SARS-CoV-2 (as well as poisons)—even in high amounts –were not infective to any of the three human tissue cultures they tested. In plain English, this means they proved, on their terms, that this “new coronavirus” is not infectious to human beings. It is only infective to monkey kidney cells, and only when you add two potent drugs (gentamicin and amphotericin), known to be toxic to kidneys, to the mix.
Interestingly, in their conclusion the authors don’t mention this important fact. Only virologists reading the whole paper will find out that if you want to grow the virus, don’t bother to use human cell lines.
Meanwhile we have worldwide lockdown predicated on the idea that something called coronavirus causes disease. As you can read, in all three of the human cell lines no CPE (no cell death, no infection) was observed. Only Vero cells (monkey kidney cells) were adversely affected—and remember, the material injected into these cells contained kidney toxins. So basically, they proved that the SARS-CoV-2 virus does not infect human tissue.
The researchers used “The wild type chimpanzee adenovirus isolate Y25 [which] was originally obtained from William Hillis, John Hopkins University of Medicine. The virus was passaged in HEK293A cells (Invitrogen, Cat. R705-07) and purified by CsCl gradient . . . Viral DNA was phenol extracted for genomic sequencing and cloning.”
The researchers purchased some material (not properly isolated even though it is called an “isolate”) which they then “passaged” through human embryonic kidney cells (called HEK293A), and then they “purified” it by CsCl gradient. You can read about this technique here. It separates DNA molecules (not viruses) after mixing them with cesium chloride (a heavy metal salt) and ethidium bromide (a mutagen that can affect DNA biological processes, like DNA replication and transcription.)
This is the same smoke and mirrors—not true separation and isolation but “surrogate” techniques that use various poisons.
Another study sent to us is entitled, “SARS-CoV-2 structure and replication characterized by in situ cryo-electron tomography,” published June 23, 2020. The authors begin with the creed of the faithful: “β-coronaviruses, including SARS-CoV-1 and Middle Eastern Respiratory Virus (MERS-CoV) are highly contagious pathogens that can cause severe lower respiratory infections. At the end of 2019, SARS-CoV-2 emerged in the city of Wuhan, China, likely through zoonotic transmission via a bat reservoir and a still unidentified intermediate host that subsequently led to a pandemic, accumulating to date to over 8 million cases and close to 500,000 deaths worldwide.”
The article provides no references for the statement that the SARS virus is “highly contagious” but does contain a lot of fuzzy electron-microscope photographs of tissues and cells whose genetic material they determined using PCR tests—the equivalent of finding moats and turrets in a bunch of Lego pieces.
The researchers did not isolate and purify the virus but instead used “monkey kidney derived VeroE6 cells” and “human pulmonary cell lines.” In other words, they used cell lines grown in starved and poisoned cultures.
Later in the paper the authors state that they get different “morphologies” of the virus depending on which cell line they use. In other words when grown on monkey kidney cells the virus looks one way, grown on lung cancer the same virus looks different. That is like saying that if you plant some seeds in one garden you will get tomatoes but if you plant them in another garden you will get turnips. What this observation tells us is that what they find comes from the tissue not the source “virus,” that is why they are different.
According to the authors, “Our report provides the first in situ cryo-ET analysis of coronaviruses at high preservation levels.” Wait a minute—this study was published on June 23, 2020. You mean they had no analyses of this virus before health officials called for universal lockdown?
Says Scoglio, “At the center of the pandemic project stands the Covid swab test, which is based on the RT-PCR (Reverse Transcriptase- Polymerase Chain reaction): a sample of organic material is taken from the throat, or more rarely from the broncho-alveolar fluid, of the individual, and then the presence of the SARS-Cov-2 virus in the sample is tested. This is done by using the same RT-PCR methodology used to originally “isolate” the virus from patient zero. Thus, the Covid test depends essentially on the original isolation, or lack thereof, of the SARS-Cov2 virus, the original PCR isolation of the virus constituting the golden standard necessary to validate any subsequent Covid test. The problems with the original virus isolation, and thus with the ensuing swab test, are many, and they all point to the truth that the SARS-Cov2 virus has never been isolated and never tested for its pathogenicity.”
One argument we hear is that Koch’s postulates are irrelevant, out of date, useless or even “wrong.” If so, why do researchers claim to have satisfied Koch’s postulates, not only for Covid-19 but for other diseases like HIV/AIDS and Lyme’s disease.
For example, in 1997, scientists announced that human immunodeficiency virus (HIV) does fulfill Koch’ postulates and hence is the proven cause of AIDS. The study involved taking the blood from an HIV-positive person and injecting it into one chimpanzee. They didn’t purify or isolate anything, just injected the blood into one chimpanzee. They kept the chimp for ten years–who knows what they fed it or anything about its conditions of confinement. After ten years the chimp developed an “opportunistic infection” (which could even be a yeast infection) and tested HIV-positive (a test result that occurs in at least thirty-three other conditions). The study had no controls–like injecting the chimp with blood from someone with cancer or with blood from a healthy person. This was the proof that HIV causes AIDS! This is not science, but it keeps the grant money flowing.
With Lyme’s disease the “proof” that Koch’s postulates were fulfilled comes from a paper published in 1983, which reported detection of spirochete [spiral-shaped bacteria] in the blood of two patients with Lyme. The researchers then examined some ticks in the neighborhood and found the same spirochete. That’s it, that was the “proof” of Koch’s postulates.
As we have explained, finding bacteria at the site of an injury or in a person with a disease in no way constitutes proof of causation any more than finding firemen at the site of a fire means they caused the fire. Among other roles, bacteria act as scavengers in nature, they “eat” dead or diseased tissue. Maggots play the same role; if you see a dead dog crawling with maggots, it would be crazy conclude that the maggots killed the dog. So why do scientists assume that the presence of “viruses” in a cell means that the cell has been attacked from the outside and taken over by hostile compounds?
If anyone can show us a properly done study in which the “coronavirus” from many sick people was isolated, purified, photographed and characterized according to the consensus agreement of the 1973 Pasteur Institute guidelines, and then shown to cause disease in healthy organisms (animals or humans), we will gladly withdraw the book. Meanwhile, we contend that the idea of a contagious coronavirus is a fairy tale.
The Contagion Myth is banned on Amazon but available at:
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Description of video from Children’s Health Defense YouTube channel:
In the latest episode of our second season of “TRUTH” with Robert F. Kennedy, Jr., Kennedy interviews Dr. David Martin.
The two primarily discussed medical patents and the involvement from Dr. Anthony Fauci. Highlights of their conversation include:
– Breaking down Dr. David Martin’s company ‘M·CAM’ and how he found a way to put up intangible assets as collateral security.
– The Bayn – Dole Act that led to Fauci profiting from royalties off University patents.
– Fauci working for the NIAID but failing to study infectious diseases and allergies.
– Fauci involved in dodgy deals and price-fixing medicine in the USA.
– SARS vaccine patented in March 2019, 8 months before the COVID-19 outbreak.
Dr. Andrew Kaufman w/ Jason Liosatos: Manipulation of Humanity Via Nonsense PCR Test Results & Fear [Operation Moonshot]
Dr. Andrew Kaufman w/ Jason Liosatos: Manipulation of Humanity Via Nonsense PCR Test Results & Fear [Operation Moonshot]
“The test…it doesn’t measure a virus and it doesn’t actually anything that they know what it is… It’s simply a test that’s easy to manipulate to get a certain percent positive…
…In the UK, I think we have an interesting story because the plans from the government leaked and published in a British medical journal… I’m talking about Operation Moonshot which is this plan to basically create a testing industrial complex.” ~ Dr. Andrew Kaufman
Dr Andrew Kaufman PCR Testing False Positives – COVID-19 Interview with Jason Liosatos
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry & Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
The horseshoe crab is thought to be 300 million years old; that’s 200 million years older than dinosaurs. They don’t sting, don’t bite and don’t harm us in any way. The annual spring congregation of egg-laden horseshoe crabs on the east coast provides a vital food source for annual migrations of millions of shorebirds.
But even this harmless sea creature may be annihilated by pharma’s insatiable drive to make a universal coronavirus vaccine. In 1990, biologists estimated 1.24 million crabs spawned in Delaware Bay, a main egg-laying nursery grounds and prime collection point for the companies. By 2019, that number had dropped to 335,211. Conservation groups feel that the planned harvest by vaccine manufacturers may lead to the species’ extinction.
Horseshoe crabs are known for their unique blue blood. But it’s not the blood’s color that is the attraction. A unique chemical found in its blood, called coagulogen, is used by the drug companies to detect as little as a few parts per billion of dangerous endotoxin bacterial contamination in any medication, medical devise or vaccine. According to Associates of Cape Cod, Inc, one of a handful of horseshoe crab blood processors, that’s like “finding a grain of sand in an Olympic swimming pool.”
First licensed in the 1970’s, coagulogen has become the gold standard of pharmaceutical purity testing. This simple test, referred to as a limulus amebocyte lysate test, or LAL for short, is named after the white blood cells (amebocytes) from which the chemical is harvested. The extract is so powerful that if even a trace of endotoxin is present, coagulogen will neutralize it into a gel. If no gel is formed, the product is considered to be free of bacteria. The FDA mandates that all injectable or indwelling materials to be certified as endotoxin-free using the LAL test before a product can be manufactured and sold into the market.
Harvesting the Crab: Big Business
The American LAL industry has been around a long time. The first commercial LAL production facility was established in Chincoteague, VA in 1971. Currently, several production facilities are located from Massachusetts to South Carolina. After the FDA granted approval for the commercial use of the LAL test in 1987, demand for testing reagents soared through the 1990s. Currently, drug companies require at least 80 million test units each year for drug and device testing. With the specter of using the LAL test to certify more than 15 billion COVID vaccines – two shots for every human on planet – the demand for horseshoe crab blood and LAL testing reagents may soom be stratospheric.
The crabs are harvested by local fisherman and taken to collection facilities which then return them to water within 24 to 72 hours of harvesting their blood. The crabs are returned to the ocean a great distance from where they were initially picked up to avoid recurrent rebleeding from the same crab. The process is rather straight forward: the animals are strapped into collection devices and a catheter is inserted into the sinuses where their blood is removed. Pharma claims it is a harmless procedure, similar to a human giving blood.
But how harmless is exsanguinating 30 percent of the animals’ blood?
Nearly 500,000 sea creatures are caught and then bled each year. This number is about to explode. The value of the commercial harvest of horseshoe crabs grew from about $400,000 in 2004 to more than $1.8 million in 2014. In 2018, a teaspoon of LAL was worth about $75 and the market value had ballooned to $112 million.
“The problem is that the companies need a large supply of the blood from live crabs,” a 2014 article in The Atlantic noted. “Horseshoe crabs live on the seafloor, near the shore. When they want to mate, they swim into very shallow water, and horseshoe crab collectors wade along, snatching the crabs out of their habitat.
Synthetic Alternatives
Because the demand for the LAL agent is about to explode as global vaccine demand is ramped up, alternatives for coagulogen are being explored. It appears a replacement for the blood harvesting may have been found.
Numerous articles have been published about the development of a recombinant Factor C (rFC) test, a recombinate, synthetic alternative to the LAL test. Comparative testing of samples tested with both the LAL and recombinant rFC suggests that the new test may even be superior for identifying bacterial endotoxins.
The results of a six-year study was published in the journal, Microorganisms, in March 2020. The study, which compared endotoxin sensitivity of LAL assay and two different rFC-based assays, demonstrated that both rFC-based assays were comparable to LAL. In fact, the rFC-based methods generated even better endotoxin recovery rates than traditional LAL testing. The researchers concluded:
“The rFC-based tests were found to represent reliable methods, as equivalent or even superior to LAL assays and suitable for routine bacterial endotoxin testing.”
A similar study, released in July 2020, concluded:
“rFC assays offer a number of benefits, including compliance with the principles of the 3Rs, i.e., replacement, reduction, and refinement of animal testing by safeguarding animal welfare and promoting more ethical and sustainable use of animals for testing… In summary, we demonstrated that both LAL and rFC assays are adequate for testing and releasing four vaccine products.”
Conservationists fear that the demand for horseshoe crab blood for COVID-19 vaccines may exterminate the crabs and greatly impact the shorebird population that depends on them. A synthetic substitution would be good news for the horseshoe crab population and for the entire environmental and marine ecosystem. And better for humans too.
If it becomes impossible for people to refuse the hydrogel-contaminated COVID19 vaccine, at least the vaccine will not decimate the horseshoe crab population for its manufacturing process.
Are you ok with your 11-year-old consenting to a medical procedure at school without your parental consent?
The new “Minor Consent for Vaccinations Amendment Act” Bill would give children the authority to get a vaccine at school without permission from their parents or legal guardians.
Dawn Richardson, director of Advocacy at NVIC, speaks with Del about this potentially dangerous overreach and how to stop it.
As I keep making the case that the SARS-CoV-2 virus has not been proven to exist, I’m also making this point:
There is no honest and prolonged mainstream debate on this issue, and there has to be. Reputable journals should be opening up their pages to such a debate from all comers, and they aren’t. They’re ignoring, side-stepping, and suppressing a debate. This is not science. It’s not even a shadow of science.
And the COVID virus is not the first time the issue of existence has arisen. If more people understood that, they wouldn’t be so shocked.
Here are several cases from recent history:
In the early part of the 20th century, a very nasty skin disease called pellagra took hold in the American South, affecting several million people.
The elite medical view, of course: a germ was the cause. But no one could find it in the ensuing decades. Finally, a small group of independent researchers, relentlessly pursuing a different course, convinced the establishment that the true cause was a niacin deficiency.
In the 1960s and 70s, Japan experienced a strange nervous-system affliction labeled SMON. Again the clarion call was: find the virus, it must be a virus. But no, in a landmark court case, the cause was shown to be a gastrointestinal drug, clioquinol, manufactured by Ciba-Geigy. The company apologized and paid out damages. Since then, some research has suggested that clioquinol fails to explain all the SMON cases.
SARS, 2003. During the height of hysteria in Canada about this flu-like illness, famous WHO researcher, Frank Plummer, wandered off the reservation and told the press that fewer and fewer SARS patients showed any sign of having the virus—in fact, the percentage was shrinking to zero. Therefore: what virus?
Swine Flu, 2009. As I detailed in a recent article, CBS investigative reporter Sharyl Attkisson uncovered the fact that the CDC had secretly stopped counting cases, because the overwhelming percentage of patients’ samples coming back from testing labs showed no sign of the Swine Flu virus or any other flu virus.
HIV, first announced as the cause of AIDS in 1984, has been challenged by a number of independent researchers. I have published Christine Johnson’s explosive and detailed interview with Eleni Papadopulos, “a biophysicist and leader of a group of HIV/AIDS scientists from Perth in Western Australia.” The subject? Does HIV exist? I’m reprinting my article and the Papadopulos interview below.
There are other illnesses in which the existence of the virus has been challenged: for example, polio and the Swine Flu of the 1970s.
Mainstream and independent investigators should also be aware there are analogous “missing causes” within the medical framework. The most egregious example is certainly psychiatry.
Following the breakthrough work of psychiatrist Peter Breggin, I’ve written extensively on this subject. In a nutshell, there are NO defining lab tests for ANY of the 300 so-called mental disorders. Every one of these disorders is arbitrarily assembled by committees of psychiatrists, from menus of behaviors. This is about as far from science as you can get.
Is there an open and honest prolonged debate about this stunning situation in the psychiatric literature? Absolutely not.
Here is my article, Does HIV Exist? Buckle up:
Before we get to Christine Johnson’s interview, a bit of background.
My first book, AIDS INC., was published in 1988. The research I engaged in then formed a foundation for my recent work in exposing the vast fraud called COVID-19.
In 1987-88, my main question eventually became: does HIV cause AIDS? For months, I had blithely assumed the obvious answer was yes. This created havoc in my investigation, because I was facing contradictions I couldn’t solve.
For example, in parts of Africa, people who were chronically ill and dying obviously needed no push from a new virus. All their “AIDS” conditions and symptoms could be explained by their environment: contaminated water supplies; sewage pumped directly into the drinking water; protein-calorie malnutrition; hunger, starvation; medical treatment with immunosuppressive vaccines and drugs; toxic pesticides; fertile farm land stolen by corporations and governments; wars; extreme poverty. The virus cover story actually obscured all these ongoing crimes.
Finally, in the summer of 1987, I found several researchers who were rejecting the notion that HIV caused AIDS. Their reports were persuasive.
I’m shortcutting a great deal of my 1987-8 investigation here, but once HIV was out of the picture for me, many pieces fell into place. I discovered that, in EVERY group supposedly at “high-risk” for AIDS, their conditions and symptoms could be entirely explained by factors that had nothing to do with a new virus.
AIDS was not one condition. It was an umbrella label, used to re-package a number of immunosuppressive conditions and create the illusion of a new and unique and single “pandemic.”
Several years after the publication of AIDS INC, I became aware of a quite different emerging debate going on under the surface of research: DOES HIV EXIST?
Was the purported virus ever truly discovered?
And THAT question led to: what is the correct procedure for discovering a new virus?
The following 1997 interview, conducted by brilliant freelance journalist, Christine Johnson, delves into these questions:
How should researchers prove that a particular virus exists? How should they isolate it? What are the correct steps?
These questions, and their answers, reside at the heart of most disease research—and yet, overwhelmingly, doctors never explore them or even consider them.
Johnson interviews Dr. Eleni Papadopulos, “a biophysicist and leader of a group of HIV/AIDS scientists from Perth in Western Australia. Over the past decade and more she and her colleagues have published many scientific papers questioning the HIV/AIDS hypothesis…”
Here I’m publishing and highlighting excerpts from the interview. Technical issues are discussed. Grasping them is not the easiest exercise you’ve ever done, but I believe the serious reader can comprehend the vital essentials.
Christine Johnson: Does HIV cause AIDS?
Eleni Papadopulos: There is no proof that HIV causes AIDS.
CJ: Why not?
EP: For many reasons, but most importantly, because there is no proof that HIV exists.
… CJ: Didn’t Luc Montagnier and Robert Gallo [purportedly the co-discoverers of HIV] isolate HIV back in the early eighties?
EP: No. In the papers published in Science by those two research groups, there is no proof of the isolation of a retrovirus from AIDS patients. [HIV is said to be a retrovirus.]
CJ: They say they did isolate a virus.
EP: Our interpretation of the data differs. To prove the existence of a virus you need to do three things. First, culture cells and find a particle you think might be a virus. Obviously, at the very least, that particle should look like a virus. Second, you have to devise a method to get that particle on its own so you can take it to pieces and analyze precisely what makes it up. Then you need to prove the particle can make faithful copies of itself. In other words, that it can replicate.
CJ: Can’t you just look down a microscope and say there’s a virus in the cultures?
EP: No, you can’t. Not all particles that look like viruses are viruses.
… CJ: My understanding is that high-speed centrifugation is used to produce samples consisting exclusively of objects having the same density, a so-called “density-purified sample.” Electron microscopy is used to see if these density-purified samples consist of objects which all have the same appearance — in which case the sample is an isolate — and if this appearance matches that of a retrovirus, in terms of size, shape, and so forth. If all this is true, then you are three steps into the procedure for obtaining a retroviral isolate. (1) You have an isolate, and the isolate consists of objects with the same (2) density and (3) appearance of a retrovirus. Then you have to examine this isolate further, to see if the objects in it contain reverse transcriptase [an enzyme] and will replicate when placed in new cultures. Only then can you rightfully declare that you have obtained a retroviral isolate.
EP: Exactly. It was discovered that retroviral particles have a physical property which enables them to be separated from other material in cell cultures. That property is their buoyancy, or density, and this was utilized to purify the particles by a process called density gradient centrifugation.
The technology is complicated, but the concept is extremely simple. You prepare a test tube containing a solution of sucrose, ordinary table sugar, made so the solution is light at the top but gradually becomes heavier, or more dense, towards the bottom. Meanwhile, you grow whatever cells you think may contain your retrovirus. If you’re right, retroviral particles will be released from the cells and pass into the culture fluids. When you think everything is ready, you decant a specimen of culture fluids and gently place a drop on top of the sugar solution. Then you spin the test tube at extremely high speeds. This generates tremendous forces, and particles present in that drop of fluid are forced through the sugar solution until they reach a point where their buoyancy prevents them from penetrating any further. In other words, they drift down the density gradient until they reach a spot where their own density is the same as that region of the sugar solution. When they get there they stop, all together. To use virological jargon, that’s where they band. Retroviruses band at a characteristic point. In sucrose solutions they band at a point where the density is 1.16 gm/ml.
That band can then be selectively extracted and photographed with an electron microscope. The picture is called an electron micrograph, or EM. The electron microscope enables particles the size of retroviruses to be seen, and to be characterized by their appearance.
CJ: So, examination with the electron microscope tells you what fish you’ve caught?
EP: Not only that. It’s the only way to know if you’ve caught a fish. Or anything at all.
CJ: Did Montagnier and Gallo do this?
EP: This is one of the many problems. Montagnier and Gallo did use density gradient banding, but for some unknown reason they did not publish any Ems [photos] of the material at 1.16 gm/ml…this is quite puzzling because in 1973 the Pasteur Institute hosted a meeting attended by scientists, some of whom are now amongst the leading HIV experts. At that meeting the method of retroviral isolation was thoroughly discussed, and photographing the 1.16 band of the density gradient was considered absolutely essential.
CJ: But Montagnier and Gallo did publish photographs of virus particles.
EP: No. Montagnier and Gallo published electron micrographs of culture fluids that had not been centrifuged, or even separated from the culture cells, for that matter. These EMs contained, in addition to many other things, including the culture cells and other things that clearly are not retroviruses, a few particles which Montagnier and Gallo claimed are retroviruses, and which all belonged to the same retroviral species, now called HIV. But photographs of unpurified particles don’t prove that those particles are viruses. The existence of HIV was not established by Montagnier and Gallo — or anyone since — using the method presented at the 1973 meeting.
CJ: And what was that method?
EP: All the steps I have just told you. The only scientific method that exists. Culture cells, find a particle, isolate the particle, take it to pieces, find out what’s inside, and then prove those particles are able to make more of the same with the same constituents when they’re added to a culture of uninfected cells.
CJ: So before AIDS came along there was a well-tried method for proving the existence of a retrovirus, but Montagnier and Gallo did not follow this method?
EP: They used some of the techniques, but they did not undertake every step including proving what particles, if any, are in the 1.16 gm/ml band of the density gradient, the density that defines retroviral particles.
CJ: But what about their pictures?
EP: Montagnier’s and Gallo’s electron micrographs…are of entire cell cultures, or of unpurified fluids from cultures…”
—end of interview excerpt—
If you grasp the essentials of this discussion, you’ll see there is every reason to doubt the existence of HIV, because the methods for proving its existence were not followed.
And so…as I’ve reported these past few months, there is every reason to doubt and reject the existence of the COVID virus, since correct large-scale electron microscope studies have never been done.
I kept the Christine Johnson interview, and other similar information, in mind when, for example, I explored the dud epidemics called SARS and 2009 Swine Flu.
How many viruses have been named as causes of disease, when in fact those viruses have never been isolated or proved to exist?
Of course, conventional-consensus researchers and doctors will scoff at any attempt to raise these issues. For them, “the science is settled.” Meaning: they don’t want to think. They don’t want to stir the waters.
After 30 years working as a reporter in the area of deep medical-research fraud, I’ve seen that false science occurs in levels.
The deeper you go, the stranger it gets. To put it another way: the deeper you go, the worse it gets.
“In the minds of those abused in the behavioral/ psychiatric system, they’ve suffered child abuse, punishment and torture. Many of them are silenced, however, out of fear, or because of damage—too scared to speak out. This is exacerbated by the lack of oversight and accountability.”
Diagnosing (pathologizing) troubled children as mentally disordered is a huge industry—whether incarcerating them in behavioral or psychiatric facilities, wilderness camps or subjecting them to psychological behavior modification programs. In the minds of those abused in this system, they’ve suffered child abuse, punishment and torture. Many of them are silenced, however, out of fear, or because of damage—too scared to speak out.
This is exacerbated by the lack of oversight and accountability in the behavioral/psychiatric industry—putting children’s welfare at risk, traumatizing them, then labeling that normal reaction to an abusive abnormal situation as “Post-Traumatic Stress Disorder.” Approximately one-third of UHS’s Behavioral Division’s revenues are derived from taxpayer dollars, such as Medicare, TRICARE, and Medicaid, with the remaining two-thirds from commercial payers.[1]
In July 2020, Modern Healthcare reported that 19 individual complaints were made public after being kept under seal throughout Federal Department of Justice fraud case that alleged Universal Health Services’ psychiatric hospitals had a range of techniques to “Maximize payment by admitting as many patients as possible and keeping them as long as possible.” “Each describes a methodical scheme whereby administrators pressured staff to admit patients even when it wasn’t necessary and hold them for as long as their insurance paid out. From there, the allegations detail a hodge-podge of contrasting methods and effects on patients and government programs.”[2]
When such practices involve children, it is even more egregious. The following is but a small example of abuses documented from Universal Health Services (UHS), with similar abuses found in other chains of behavioral facilities. It shows patient sexual abuse, suicides and restraint assault, even death. Some of the facilities were shut down, but too many still remain open.
An October 2020 lawsuit against UHS’s Cumberland Child and Adolescent behavioral hospital in Virginia exemplifies such risks: Twenty former patients from the hospital alleged sexual abuse, physical assaults and attempts to deceive public and state health officials. Seeking $127 million in damages, attorneys for the plaintiffs alleged that Dr. Daniel N. Davidow, the former medical director of Cumberland since 1996 inappropriately touched young female patients during routine medical exams and that employees and fellow patients physically struck or sexually abused other residents.[3] Twelve female patients alleged sexual abuse, including some as young as nine.[4] It was reported that Davidow was under police investigation.[5] Herschel C. Harden III, a former psychotherapist at Cumberland was also indicted on two counts of object sexual penetration by force of a former patient in 2018 and 2019 while Harden worked at the hospital.[6] [See entry October 2020]
Playing through the greenery and litter of a mini forest’s undergrowth for just one month may be enough to change a child’s immune system, according to a small new experiment.
When daycare workers in Finland rolled out a lawn, planted forest undergrowth such as dwarf heather and blueberries, and allowed children to care for crops in planter boxes, the diversity of microbes in the guts and on the skin of young kids appeared healthier in a very short space of time.
Compared to other city kids who play in standard urban daycares with yards of pavement, tile and gravel, 3-, 4-, and 5-year-olds at these greened-up daycare centres in Finland showed increased T-cells and other important immune markers in their blood within 28 days.
“We also found that the intestinal microbiota of children who received greenery was similar to the intestinal microbiota of children visiting the forest every day,” says environmental scientist Marja Roslund from the University of Helsinki.
One daycare before (left) and after introducing grass and planters (right). (University of Helsinki)
Prior research has shown early exposure to green space is somehow linked to a well-functioning immune system, but it’s still not clear whether that relationship is causal or not.
The experiment in Finland is the first to explicitly manipulate a child’s urban environment and then test for changes in their micriobiome and, in turn, a child’s immune system.
While the findings don’t hold all the answers, they do support a leading idea – namely that a change in environmental microbes can relatively easily affect a well-established microbiome in children, giving their immune system a helping hand in the process.
The notion that an environment rich in living things impacts on our immunity is known as the ‘biodiversity hypothesis’. Based on that hypothesis, a loss of biodiversity in urban areas could be at least partially responsible for the recent rise in immune-related illnesses.
“The results of this study support the biodiversity hypothesis and the concept that low biodiversity in the modern living environment may lead to an un-educated immune system and consequently increase the prevalence of immune-mediated diseases,” the authors write.
The study compared the environmental microbes found in the yards of 10 different urban daycares looking after a total of 75 kids between the ages of 3 and 5.
Some of these daycares contained standard urban yards with concrete and gravel, others took kids out for daily nature time, and four had their yards updated with grass and forest undergrowth.
Over the proceeding 28 days, kids in these last four daycares were given time to play in their new backyard five times a week.
When researchers tested the microbiota of their skin and gut before and after the trial, they found improved results compared to the first group of kids that played in daycares with less greenery for the same amount of time.
Even in that short duration of the study, researchers found microbes on the skin and guts of children who regularly played in green spaces had increased in diversity – a feature which is tied to an overall healthier immune system.
Their results largely matched the second group of kids at daycares who had outings for daily nature time.
Among kids who got outside, playing in the dirt, the grass and among the trees, an increase in a microbe called gammaproteobacteria appeared to boost the skin’s immune defence, as well as increase helpful immune secretions in the blood and reduce the content of interleukin-17A, which is connected to immune-transmitted diseases.
“This supports the assumption that contact with nature prevents disorders in the immune system, such as autoimmune diseases and allergies,” says Sinkkonen.
In the world of science, beliefs typically die a long, slow death. Such is the case with the germ theory, which really took off in the late 1800s.
At that time, the main proponents of the germ theory, including the Frenchman Louis Pasteur and the German Robert Koch, ardently believed that all the bacteria in living organisms, including human beings, were invaders from the outside. In other words, from our skin inward, we were sterile, except if we had been invaded by a pathogen. Today, 150 years later, this idea seems laughably incorrect and naïve.
Almost everyone now knows that trillions of bacteria live in and on every surface of our bodies. Some people have even attempted to demonstrate that most of our genetic material is bacterial rather than human in origin. We now have conclusive evidence that these trillions of bacteria living in us help digest our food, synthesize crucial nutrients, participate in detoxification functions, help regulate and control our emotions and, in some ways, participate in every normal human function. The early proponents of the germ theory were not only completely inaccurate in their conclusions about the role of bacteria in the human organism, but, more important, they established a framework that postulated that human beings were somehow separate from nature. This insidious and unscientific conclusion, which continues to the present time, has caused grave harm to all living systems.
In the case of viruses, a similar shift is just beginning to happen in the scientific community. The old paradigm about viruses is that we are essentially “virus-free” in our healthy, natural state, and the only viruses that are inside us must be pathogens that came from the outside. This belief was, of course, never proven; it was just stated as dogma, and it dovetailed nicely with the narrative of “nature is out to get us.”
If we fast forward to modern virology, we now know that these particles called viruses can be exosomes, also called extracellular vesicles (EVs), which are generated from the tissues as a way of detoxification and communication. The way it works is that when a tissue is exposed to a certain toxin, especially one that breaks down the genetic material (i.e., EMF poisoning), the tissue packages this broken-down genetic material into vesicles so they can be excreted from the body. This is what I mean when I say a virus is the body’s way of “pooping out poisons.”
This excreted package of poisons is not only a vital detoxification strategy, but it also serves as a communication vehicle that can be sent out to the world. Through a kind of resonance, exosomes communicate from one part of the body to another, or from one organism to its community of friends, that a poison has been encountered, so prepare to make a defensive response. The conclusion, then, is that these internally generated exosomes (EVs) are the agent of adaption for living beings. They are not pathogens. Unfortunately, the medical/scientific community has mistaken these detoxification-communication messengers for pathogenic viruses. But that narrative is starting to crumble. Consider this quote from a recent paper published in the journal Viruses 2020 May; 12(5). 571. The paper was written by Gianessi, F et al and is titled: “The Role of Extracellular Vesicles as Allies of HIV, HCV and SARS Viruses.” Here is a quote from Section 3 of the paper:
The remarkable resemblance between EVs and viruses has caused quite a few problems in the studies on the analysis of EVs released during viral infections. Nowadays, it is an almost impossiblemission to separate EVs and viruses by means of canonical vesicle isolation methods, such as differential ultracentrifugation, because they are frequently co-pelleted due to their similar dimension. To overcome this problem, different studies have proposed the separation of EVs from virus particles by exploiting their different migration velocity in a density gradient or using the presence of specific markers that distinguish viruses from EVs. However, to date, a reliable method that can actually guarantee a complete separation does not exist.
Read the final line again: A way to distinguish external “pathogenic” viruses from particles generated from our own tissues to help us adapt to a novel toxin does NOT exist, period. Perhaps the reason virologists can’t find any method to distinguish these particles from each other, in spite of the fact that they can pull a single molecule out of virtually any complex solution, can only be because there is nothing to distinguish. I submit that all viruses are exosomes/EVs. They are all generated from our tissues. None are pathogens. See you later, close up shop, it’s time to get honest work.
This change in how we view viruses (exosomes) will happen, but possibly only when the old guard dies out. Paradigms are hard to change. This one, however, is threatening to destroy the world, and we don’t have time for the virologists to fade away. We must understand this shift ourselves. It’s not that complicated once you remove the veil. It’s obvious: We humans are part of the joyous dance of life, viruses and bacteria are our dance partners, and without them we will trip on our own two feet and fall flat on our collective faces.
In 2016, MSNBC host Melissa Harris Perry made a concerning statement. Discussing public education, Harris Perry said, “We have to break through our kind of private idea that kids belong to their parents or kids belong to their families.”
In the four years since, concepts like “kids belong to the community” have been insidiously melded into “greater good” public health vaccination talking points from politicians deciding policy.
This move is now supercharged with the coronavirus response. We’re being told, ‘we’re all in this together,’ a mantra-like chant droned into society’s consciousness.
This debate is reaching critical mass because corporate media has long refused to provide public balance to the issue. Big Media has neutralized parents’ concerns via limited, unscientific Big Pharma talking points. The division between facts and propaganda has been percolating.
Religious, medical and philosophical barriers protecting children from historically criminal, unethical corporations have been systematically removed. It was inevitable that the final battle would be to remove the ‘parent barrier.’ That’s where we are now.
Directly before the world experienced the coronavirus, the vaccine debate had devolved to whether parents should be removed from the picture entirely when it comes to vaccine decisions. The health community and government representatives deemed parents and the need for parental consent ‘a barrier to obtaining vaccination.’
The world’s people are staring down a possible future reality in which they remain confined to their homes without an experimental COVID shot rushed to market. Meanwhile, Big Pharma is working through governmental officials and still targeting children.
Washington D.C.’s B23-0171 is a big carny in the coal mine to make the medical-industrial complex the parents of future generations of American children. Put forth in 2019, the bill had no activity for over a year. During a public hearing in June 2019, pediatrician Dr. Helene Felman, representing Washington D.C.’s chapter of the American Academy of Pediatrics (AAP), stated:
“As a pediatrician, I like the legislation as it stands because it offers the opportunity to capture those young adults who can make informed decisions at technically any age.”
Several other proponents of the bill who testified similarly danced around committing to an age they believed would be appropriate for a child to make their own medical decisions.
Fast forward. Present-day. The bill was just passed by a voice vote in a virtual meeting of D.C.’s Health Committee and, as the DCPost.com put it in their headline, D.C. Paves Way for Permitting Vaccination of Kids Without Parental Consent.
They decided that 11 years of age was the magic number for kids to okay vaccination behind closed doors with a provider who is protected from liability and has no accountability for what happens to the child after vaccination.
Don’t worry, the child still ‘has to meet the gatekeeper’ as described in hearing comments. “The physical still has to meet the judgment that the minor is capable of informed consent,” said Councilmember Mary Cheh.
What if the parents find out? Don’t worry, they probably won’t, it’ll be our little secret. The bill contains “many protections so that the confidentiality and privacy of the minor’s actions are maintained.”
The chair of the Health Committee who passed the bill, Vincent C. Gray (D-Ward 7), was quoted in the Washington Post saying, “the hope of an imminent coronavirus vaccine gave the bill new urgency.” This seems to imply that the Covid shot, sans parental consent, will be given to all children. Children are of the lowest risk of the coronavirus. Children are minimally if at all, represented in the current Covid vaccine trials.
Acknowledging that The Tuskegee Experiment was still in the minds of many people, Gray didn’t see that the legislation committee members were engaged in “would ever possibly have that kind of situation once again.”
The bill now goes to a second reading on October 10th. If the bill passes the second reading, it goes to the Mayor, who has up to 10 days to sign the bill, let it go into effect without a signature, or veto it. If the Mayor vetoes the bill, the Council can override the veto by a two-thirds vote.
There is no justification to override a parent’s legal right to make an informed benefit and risk decision about vaccination on behalf of their minor children, ignore their religious rights to decline vaccination, and then hand that responsibility to vaccine providers who are protected from liability and have no accountability for what happens to the child after vaccination.
A child is less likely than their parent to understand personal and family medical history, including vaccine reactions, allergies, and autoimmune or neurological disorders.
Kids do not have the same kind of critical thinking skills or emotional maturity required to make a vaccine benefit-risk decision compared to an adult. Vaccines can cause injury and death, as evidenced by the National Vaccine Injury Compensation Program, which has paid out over $4.4 billion dollars to vaccine victims.
Children and adolescents are vulnerable to peer and authority-figure persuasion.
If a child consents to vaccination without their parent knowing and has a reaction, the parent may not recognize the reason for their child’s decline in health, and this lack of knowledge could be life-threatening for the child.
This puts minor children at risk of being pressured and coerced into getting a COVID-19 vaccine behind their parents’ back once it is available and added to the ACIP recommended schedule for children.“
A new page has been turned. The medical community, with the help of the government, has created a beachhead in the nation’s capital, supporting the effort to remove parental consent.
Robert F. Kennedy, Jr.: International Message for Freedom and Hope, October 24, 2020 | “You Are on the Front Lines of the Most Important Battle in History”
Today, October 24, 2020, there are many rallies around the world. Activists in these countries are joining in a common voice: Argentina; Bolivia; Peru; Uruguay; Italy; Germany; Poland; Belgium; Netherlands; United Kingdom; Ireland; Sweden; Denmark; France; and Austria.
Citizens of all countries are paying an enormous price for the epidemic.
They have not only lost their loved ones, but their freedoms, their livelihood, their joy. Children and youth are suffering due to this crisis too.
Without their friends and social activities, mental health problems in our young is at an all-time high.
People around the world are demanding to be spared from the devastating consequences of the epidemic.
Robert F. Kennedy, Jr., Chairman of Children’s Health Defense, provides an inspirational message for freedom and hope to activists around the world.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry & Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Transcript:
Hey everybody.
It’s Robert F. Kennedy, Jr. here and I cannot tell you how happy I am to be able to have this opportunity to talk to thousands of citizens, in 15 countries on all the continents in the world, who have come together today to protest this coup d’etat — by Big Data, by Big Telecom, by Big Tech, by the big oil and chemical companies, and by this global public health cartel led by Bill Gates and the W.H.O — and now amounts to two trillion dollars and wants to magnify and amplify its wealth and its power over our lives, over our liberties — that wants to subvert our democracies and want to destroy our sovereignty and our control over our lives and our children’s health.
And I want to remind you, those of you who are not Americans, of something that every American child learns when we’re growing up in this country about our history. During the Great Depression, Franklin Roosevelt, who was one of the greatest presidents in American history, said to the American people: the only thing that we have to fear is fear itself. And we grow up hearing that but people don’t really understand what it means.
But it was a very, very profound warning by Roosevelt because he saw what the Great Depression was doing in Eastern Europe and Italy, in Germany and Spain, where that crisis was turning people towards fascism — in the eastern countries, where the same crisis was turning citizens and governments towards communism and also causing the collapse of governments all over the world.
And in our country, in the United States, it’s hard for people to remember today that that almost a third of the people in our country were completely disillusioned with capitalism and wanted to turn to communism. And another third wanted to turn to fascism. And Franklin Roosevelt wanted to preserve our country for democracy, for free market capitalism, for civil rights and to preserve our constitution.
And he recognized that the weapon of authoritarian control was going to be feared.
And when I spoke a few weeks ago in Berlin, I reminded the people of Germany of a very famous story that happened during the Nuremberg trials after World War II, when Hitler’s closest lieutenant, the head of the Luftwaffe, Hermann Goring, was asked by one of the prosecutors: how did you get the German people (the German people, the most educated people in the world that were some of the most tolerant people in the world — the Weimar Republic was one of the strongest democracies in the world) — how did you take — these people were so well educated and so awakened and so tolerant — and turn them into obedient slaves who committed some of the worst atrocities in human history. And Goring said: Oh, that’s a simple thing. (And any of you can look up his quote and I urge you to do so). And he said that it works not just in a fascist government but it works in a democracy, in a monarchy, in a communist government, in any government that you want.
The job of the government is to put the people in fear. And if you can keep them in fear, you can get them to do anything that you want them to do — that they will turn into sheep.
And there’s a famous book by Naomi Klein that all of us should read called Disaster Capitalism. And that book shows — it’s a historical chronology of all of the times during American History and the history of the world. During the Great Depression, and during the financial collapse in 2008, during the financial collapse in Chile for example in 1973, during the time of the World Trade Center bombing — that authoritarian elements in a society, and large corporations, and wealthy plutocrats and oligarchs, wealthy families and individuals use crises to shift wealth upward, to obliterate the middle classes of those countries and to clamp down totalitarian controls.
And, of course, it’s an obvious thing that people who are used to voting for their governments are not going to vote for policies that make the rich people richer, that give corporations even more power over their lives, that reduce democracy and reduce civil rights. These are not good vessels for populism.
In order to transform the government so that it will reward the rich with even more wealth, the people who want to do that in the large corporations — who want to orchestrate that kind of change — have to get rid of civil rights. And the first civil right that they begin with is freedom of speech.
They need to clamp down censorship because censorship is the most important right. In our country, we put it number one — the first amendment, the constitution. Because all the other rights depend on it.
If a government can hide what it’s doing, it can get away with anything it wants. If a corporation can lie to you and conceal information, if there’s no transparency in a democracy, you do not have a democracy.
Oh, if you want to get rid of all the other rights like freedom of assembly, which you are exercising today.
Some of you are exercising at great threats. Some of you will suffer. Some of you will be jailed. Some of you will suffer injuries. But that is a basic right.
The right to freedom of expression.
The right to to jury trial.
The right to freedom of religion.
The right to privacy.
The right to have governments that don’t spy on you and keep your information.
All of those other rights can only be subverted if they begin by imposing censorship, by being able to silence people who want to speak.
So, the coup d’etat that we are all fighting today is a coup d’etat that starts with a conspiracy between the government agencies and the big technology companies — the Silicon Valley billionaires.
People like Zuckerberg and Bill Gates.
And the people who run Google and Facebook and Pinterest and all of these other Silicon Valley corporations who are now in this conspiracy — to make sure that we cannot talk about our grievances.
We cannot say bad things about pharmaceutical products.
We cannot question government policies that make no sense to us.
And I’m going to say a few things about some of those government policies.
Number one: I am not a conspiracy theorist. I follow the facts. I don’t know that the COVID illness was laboratory generated in Wuhan. There is plenty of evidence that it was, but not enough evidence for me to say that it’s a fact.
But my question is:
Why don’t we know the answer to that?
Why is Tony Fauci not being asked that question?
Why is President Trump not launching an investigation?
Or President Xi?
Or the president of any of these countries saying: Where did this come from? Because we need to know that!
The global citizens — This is the worst calamity in history! And nobody seems curious about where this actually comes from.
We know it didn’t come from a bat in the wet market in Wuhan.
And that story was a fable, that it now has no basis in fact.
And we have Nobel laureates, and we have large institutions, and investigative agencies. And prosecutorial agencies are saying: we think it came from Wuhan lab and we think that it may have come from studies that were funded by Bill Gates and Tony Fauci.
I don’t know if this is true, but why are our government officials not asking that as the number one question?
Why, instead of sending their police to suppress dissent, are they not sending the police to question people who may know the answer to that question?
There are many other questions that I’d like to know the answer.
Questions about masks.
I’m very willing to accept if the masks work then I want to wear them. If they’re going to protect other people from transmissibility then I want to wear them. But the studies that I’ve seen indicate that they do not work against viral transmission for the most part. There are some that say they may work under limited circumstances.
What I don’t want to be told is: they work, and you’re going to wear them, and you better not ask questions about it.
Most Americans and most of the people on this planet — we want leadership but we don’t want bullying. And we know the difference between bullying and leadership.
We want to know the truth about hydroxychloroquine.
We want to know why are we spending 18 billion dollars on vaccines and only 1.4 billion on therapeutic drugs. What is the sense of that?
There are many, many other questions that we, in a democracy, have a right to have answered — without being called conspiracy theorists, without being vilified as being inconsiderate, or being bad citizens.
Everybody who’s part of these demonstrations are people who are striving with their lives to become good citizens.
Now, let me tell you what we need to do to win this battle.
The only way we can win it is with democracy. We need to fight to get our democracy back, to reclaim our democracy from these villains who are stealing it from us.
And you notice the people who are getting riches from this quarantine are the same people who are censoring criticism of the quarantine.
Who is becoming the richest?
Jeffrey Bezos. Eighty-three billion dollars he’s made. And he owns Amazon. And he is censoring books that criticize the quarantine.
Zuckerberg — who owns Facebook ,who’s made tens of billions of dollars by this quarantine. And he is censoring information that is critical of the quarantine. He censors my Instagram. He censors my Facebook. My Twitter page is also censored.
And all of these people are the people who are making billions of dollars on the quarantine.
And what I want to know is a simple question.
Is the quarantine actually effective?
You know, we’ve had plenty of pandemics in the past. In 1969 we had a Hong Kong flu pandemic that killed 100,000 people in the United States. It’s the equivalent of 200 000 people today.
That’s the same number of people were being killed by coronavirus.
Did we go on to lock down? No. Did we wear masks? No.
We went to Woodstock. We went to the Democratic convention in Chicago and had huge crowds of people.
Nobody was told to lock down. And don’t see your girlfriend. And wear a mask. And don’t go out of your house. And shut down your business. And bankrupt every business in the country.
Last year there were 1.6 million people in the world who died from tuberculosis. We have 1.6 million people die every year from tuberculosis.
We’re not wearing masks. We’re not on lock down.
What’s the difference between tuberculosis and coronavirus? Tuberculosis has a vaccine. And the vaccine costs about three dollars. And that’s why we’re not on lock down — because nobody is making thirty-nine dollars a vaccine or three hundred dollars a vaccine — the way that Moderna and Astrazeneca and Johnson & Johnson are making from this catastrophe. And that is the only reason that I can think of.
And I’m happy if somebody tells me there’s another reason. But, let’s hear it.
Don’t just shut me up.
Don’t just tell me that I can’t debate.
Here’s what we need to do. We need to do exactly what you’re doing today. We need to come out on the street and we need to stick together.
What the big tech villains and scoundrels and Mark Zuckerberg and Jeffrey Bezos and Bill Gates and Tony Fauci want you to do is — they want us fighting with each other.
They want blacks fighting against whites.
They want Republicans fighting against Democrats.
They want everybody polarized.
They want everybody fragmented.
Because they know that if we all get together we’re going to start asking questions.
And those are questions that they can’t answer.
Why are you getting rich?
And why are we all getting poor?
And what’s the difference between tuberculosis and coronavirus?
And why are we not wearing masks for the tuberculosis, but we are for the coronavirus?
And where did it all come from?
And all of those questions that we deserve an answer to and we’re not getting answers.
We need to stick together.
If you’re a Republican or Democrat, stop talking about that.
Stop identifying yourself.
The enemy is Big Tech, Big Data, Big Oil, Big Pharma, the medical cartel, the government totalitarian elements that are trying to oppress us — that are trying to rob us of our liberties, of our democracy, of our freedom of thought, of our freedom of expression, of our freedom of assembly, and all of the freedoms that give dignity to humanity.
And the last thing that all of us need to do is we need to stay educated and informed.
And one of the things that I want to announce to you today is that Children’s Health Defense, my organization, with the help of many of you who are on these crowds, is launching a journal — a daily journal.
And we are going to weaponize information for you.
We’re going to tell you what the newest science is. We’re going to take all the information that is censored everywhere else and we’re going to reprint it in our publication.
And you can get that every day.
So if you see something that is censored, we want to hear about it. Because we want to put it up.
We are going to be the enemies of censorship. We are going to be the refuge. And we’re going to allow debate.
We’re going to make sure it’s civil debate. We’re going to encourage people to be non-partisan.
We’re gonna allow people to come and have different opinions than us. We are not scared of debate the way pharmaceutical company and Bill Gates and Mark Zuckerberg and Jeffrey Bezos and Tony Fauci are terrified of debate. We welcome debate.
We want to hear if you’ve got a different opinion than me — I want to hear about it. And I want to see your science. And I want the public to hear us talking about it and debating about it, because the free flow of information, the cauldron of debate, is the only thing that allows governments to develop rational policies in which self-governance will actually work and triumph.
You are on the front lines of the most important battle in history and it is the battle to save democracy, and freedom, and human liberty, and human dignity from this totalitarian cartel that is trying to rob us –simultaneously in every nation in the world — of the rights that every human being is born with.
So, thank you for your courage.
Thank you for your commitment.
And thank you for your brotherhood.
And I can pledge to you — and I will go down dying with my boots on, fighting side by side with all of you — to make sure that we return these rights and preserve them for our children.
And I will see all of you on the barricades.
Thank you.
36 Deaths Isn’t Enough to Stop Flu Vax Program in S. Korea
Note: This is becoming almost a joke. Except people are dying, which is a tragedy. How many people must die before a vaccine program is halted? Meanwhile, how many people must be shunted into social isolation with devastating result while we (not us, that’s the royal we…(Wait. it’s not really royal, I don’t think the Queen of England is holding her breath for a vaccine either) “We” wait for a vaccine like refugees on the Titanic waiting for lifeboats. Spoiler alert – the lifeboats are made of rotten Swiss cheese.
South Korea is preparing to fight two infectious diseases this winter: the novel coronavirus and the flu. But reports of deaths after flu shot vaccination may jeopardize the second effort.
As of Friday afternoon local time, 36 people have died in Korea after getting flu shots, including a 17-year-old high schooler, Korea Biomedical Review reported. Some district and municipal governments have put out requests to hospitals to suspend influenza vaccination, but the Korea Disease Control and Prevention Agency (KDCA) still wants the national program to move ahead, refuting a link between the vaccines and the deaths.
“The number of deaths has increased, but our team sees the low possibility that the deaths resulted from the shots,” KDCA Commissioner Jeong Eun-kyeong told lawmakers at a hearing on Thursday, according to Reuters. Health Minister Park Neung-hoo, for his part, promised to “thoroughly examine the entire process in which various government agencies are involved, from production to distribution.”
Fake Placebo Meningitis Vaccine May Have Killed Healthy 28-Year-Old Brazilian Covid Vaccine Volunteer
If you ask anyone with middle school grasp of science what is a “placebo,” they will likely say, “a sugar pill.” A placebo has always meant an inert, benign substitute for the drug being tested. How many Earthlings understand that with this Covid vaccine, the placebo is another vaccine? And in this case, it may well have killed a healthy, altruistic 28 year young man. Our sincere condolences to his grieving family. He volunteered to help others. And what of every parent whose child needs a meningitis vaccine for school? Are they to feel comforted?
noun
noun: placebo; plural noun: placebos
a harmless pill, medicine, or procedure prescribed more for the psychological benefit to the patient than for any physiological effect.
“his Aunt Beatrice had been kept alive on sympathy and placebos for thirty years”
a substance that has no therapeutic effect, used as a control in testing new drugs.
a measure designed merely to calm or please someone.
“pacified by the placebos of the previous year, they claimed a moral victory”
###
SAO PAULO/FRANKFURT (Reuters) – Brazilian health authority Anvisa said on Wednesday that a volunteer in a clinical trial of the COVID-19 vaccine developed by AstraZeneca and Oxford University had died but added that the trial would continue.Oxford confirmed the plan to keep testing, saying in a statement that after careful assessment “there have been no concerns about safety of the clinical trial.”
AstraZeneca declined to comment immediately.
A source familiar with the matter told Reuters the trial would have been suspended if the volunteer who died had received the COVID-19 vaccine, suggesting the person was part of the control group that was given a meningitis jab. Read more here.
[Truth Comes to Light Editor’s note: See related video by Del Bigtree & Jefferey Jaxen at The HighWire.]
DEATH DURING COVID VACCINE TRIAL
Dr. Peter Breggin: Fauci’s Pandemic — How He Caused It and Uses It
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry & Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Based on the in-depth scientific and historical report, “Fauci’s COVID-19 Treachery with Chilling Ties to the Chinese Military” on Breggin.com in the Coronavirus Resource Center.
We’ve seen how the EU produced the dumbest propaganda video ever, but did you know they also produced the dumbest propaganda comic book ever? Well, they did! Join James for today’s edition of #PropagandaWatch and read along as we thrill and chill to an exciting story of time traveling pandemic survivors and learn how the EU (and big pharma) teamed up to save the world from a deadly (fictional) virus.
(OMNS Oct 20, 2020) In treating the sick, Hippocrates, the Father of Medicine counselled, “First, do no harm.” Unfortunately, this cherished principle has not been followed in caring for patients with coronavirus infection. Losing a loved one due to cancer and other diseases is always tragic. But losing one due to the coronavirus pandemic when it could be prevented is an unforgivable act resulting in the mass murder of innocent lives. It has happened due to ignorance about history, hypocrisy, a lack of training of doctors about alternative medicine, and closed minds about the life-saving medical benefits of high doses of intravenous vitamin C.
I would not have the knowledge to write this article if one event in my life had not happened. At 74 years of age I nearly died of a serious heart attack. Doctors said I’d be dead in a few years without the help of cholesterol-lowering drugs. Luckily, several years earlier I had interviewed Dr. Linus Pauling, two-time winner of the Nobel Prize. He advised me of the important role of vitamin C in decreasing the risk of coronary disease. This is when I made one of the most vital decisions of my life. I decided to take 10,000 milligrams (mg) of vitamin C daily, rather than believe Big Pharma. But I also worried because Pauling, although a brilliant chemist, was not a doctor. Was he right about vitamin C? It was only years later when Dr. Sidney Bush, a English researcher proved that vitamin C could reverse atherosclerosis (hardening of arteries) that I knew I had made the right decision. [1]
Now, 22 years later, the doctors who told me I’d be dead in a few years without cholesterol-lowering drugs are dead, and I’m in my 97th year, still alive. It’s this experience with the cardiovascular effects of vitamin C that’s triggered my interest in the anti-infective and other medical benefits of vitamin C, especially how it can decrease deaths from viral and bacterial diseases.
Klenner went on to show that large doses of vitamin C could also cure other viral diseases such as meningitis, hepatitis, measles, mumps, pneumonia, shingles and even the poisonous bite of a rattlesnake. [2-4] Since that time other researchers have reported that there is no viral disease that high-dose IVC cannot successfully treat.
But Klenner did not win a popularity contest with his colleagues. He wrote in frustration that “Some physicians would stand by and see their patient die rather than use ascorbic acid because in their finite minds it exists only as a vitamin.”
Since that time closed medical minds have resulted in thousands of deaths from coronavirus and other diseases in Canada and worldwide. Because of a misconception that vitamin C is just another vitamin. But there is proof that vitamin C is a potent anti-infective nutrient that attacks both viral and bacterial diseases.
Infection triggers a severe inflammatory cellular reaction in the body which results in a decrease in vitamin C. It’s like being caught in a snow storm on a lonely road and running out of gas. But in this case white blood cells need C to fight the infection. And if you have not been taking C on a regular basis, your white blood cells without C are like a gun without bullets.
Many people do not realize that nearly all animals make their own vitamin C. Humans lost this ability eons ago due to a genetic mutation. For instance, dogs produce 5,000 milligrams (mgs) daily. Health Canada maintains humans need only 90 mgs. But if a dog gets an infection, it will automatically produce up to 20,000 mgs daily!
During the coronavirus pandemic I’ve listened to Medical Officers of Health, TV anchors, politicians and medical experts all discuss the importance of distancing and frequent hand washing. But I have only heard one discuss the advantages of vitamin C and D in building up the body’s immunity. [5] And I have not heard any explain how the use of high doses of IVC could save lives.
Dr. Lendon H. Smith outlined the clinical experiences of Frederick Klenner in “Clinical Guide to the Use of Vitamin C”. It contains a wealth of information on how vitamin C treats many diverse diseases. And how prescribing insufficient amounts of vitamin C can lead to failure in therapy. This medical information is available for all to read. [6]
I’ve have written before that if a family member died due to coronavirus infection and doctors and hospital refused to use IVC, I would contest this situation in a court of law. I believe I would win because historical evidence is so overwhelming that large doses of C save lives.
The hypocrisy surrounding vitamin C is mind boggling. Dr, Linus Pauling complained, “The medical community requires rigorous evidence supporting vitamin C, but accepts flimsy evidence against it.” Little has changed since I interviewed Pauling. This deficit is evidently caused by the minds of medical professionals refusing to accept scientific fact. And we will never know the number of needless deaths this has caused during the pandemic.
A year ago, as a journalist, I was invited to be a member of the Orthomolecular Medical News Service. It’s international editorial board is composed of distinguished physicians, professors, and researchers. Several months ago I asked all members how they would treat several viral infections. The overwhelming response was “high dose intravenous vitamin C.” OMNS has published twenty-two physician case reports of success with IVC. [7]
Since February, researchers in China have been conducting double-blind studies on IVC. This means one group will receive IVC and a control group will get a placebo. Some studies have already been completed, and the results show that IVC saves more lives than placebo. [8]
“Dr. Enqiang Mao, chief of emergency medicine
at Ruijin Hospital, Shanghai, stated that his group
treated ~50 moderate to severe cases of COVID-19
infection with high dose intravenous vitamin C.
“The IVC dosing was for 7-10 days, with 10,000 mg
for moderate cases and 20,000 mg for more severe cases.
“All patients who received intravenous vitamin C
improved, and there was no mortality.”
“There were no side effects reported from any of
the cases treated with high dose IVC.”
But even in one of these recent laudable studies, there was a flaw. According to the report, all patients received a certain dose for moderate infection while others a higher dose for a more severe one. But patients who died had not received the higher dose. [9]
This reflects everything that Dr. Linus Pauling and Dr. Frederick Klenner stressed. As Pauling told his critics, “It’s the dosage!” Or, as Klenner claimed, “Some infections require a much larger dose.” As we all know, half an aspirin will not cure a migraine headache.
But there is more disturbing news. Chinese researchers are experiencing trouble getting their findings published. Contacts also tell me that doctors who use IVC in North America are being harassed by authorities. In some case, being told that if they persist they will lose their license to practice medicine.
To get an update on what was happening in some parts of Canada and the U.S I contacted several infectious disease specialists, Medical Officers of Health (MOH), and university hospitals, asking a simple question. “Do you prescribe intravenous vitamin C or know of anyone who does to treat coronavirus infection? And if terminal patients are not receiving IVC, why is this the case”?
It proved to be a time-consuming assignment. Many replied they would get back to me but failed to do so. I could only conclude they were not using IVC and did not want anyone to know about it.
Or they responded, “We have checked with our infectious disease specialist and confirm that high dose C is not being used to treat coronavirus infection.”
What was shocking is that not a single Medical Officer of Health replied that IVC was being prescribed to those dying from coronavirus infection.
Another surprise was the reaction of Johns Hopkins one of the great hospitals of the world. Its distinguished professors were the first to introduce the value of bedside teaching for students. During this pandemic they were considered the authority in reporting the number of coronavirus deaths. So, I was shocked to receive this response, “We are not conducting clinical trials or administering C as a treatment for COVID 19.” And even Harvard Medical School where I spent so many years as a student and later training as a surgeon, never replied to me.
What is going to happen? It’s that the Chinese study will likely fail to end the controversy and patients will continue to die needlessly of this virus. I was hoping that one infectious expert, or Medical Officer of Health, would possess the intellectual curiosity to ask, “I wonder if high does IVC could save lives?” It’s tragic this has not occurred. Some would label this as medical ignorance, others as malpractice, or if a loved one has died as murder, and finally a court of law looking all the facts decide it’s been mass murder.
So, we have a unique situation. It’s been said that war is far too important to be left to generals. Due to the economic chaos caused by coronavirus this disaster may be much too important to be left to medical experts when so many North Americans have suffered.
It’s time for the government to demand that our medical schools conduct a study of IVC. There is no shortage of patients. We have the scientific talent in our universities. Vitamin C is inexpensive and will virtually never cause complications. Vitamin C has never killed anyone. Besides, this study could be done in a short time and not require thousands of patients.
Who will grasp the moment and save countless lives?
(Syndicated columnist W. Gifford-Jones, MD, (also known as Kenneth Walker, MD) graduated from Harvard Medical School in 1950. He did surgical residencies at McGill University, the University of Rochester, and Harvard Medical School. Still an activist, his website is http://www.docgiff.com.)
1. Bush SJ (2010) 700 Vitamin C Secrets. Northampton, England: Direct Print on Demand Ltd. ISBN-13: 978-0956651990; ISBN-10: 0956651992 978-0956651990.
6. Smith, LH. Clinical guide to the use of vitamin C: The clinical experiences of Frederick R. Klenner, M.D.. Portland, OR: Life Sciences Press, 1988. Originally titled: Vitamin C as a fundamental medicine: Abstracts of Dr. Frederick R. Klenner, MD’s published and unpublished work. ISBN 0-943685-01-X. Reprinted 1991, ISBN 0-943685-13-3. http://www.whale.to/a/smith1988.html or https://www.seanet.com/~alexs/ascorbate/198x/smith-lh-clinical_guide_1988.htm
(The views expressed in this article are the author’s and not necessarily that of all members of the Orthomolecular Medicine News Service Editorial Review Board. OMNS welcomes discussion on a variety of subjects. Readers may submit their own article drafts to the Editor at the contact email below.)
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Ron Erlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Tonya S. Heyman, M.D. (USA)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Robert E. Jenkins, D.C. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Felix I. D. Konotey-Ahulu, MD, FRCP, DTMH (Ghana)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Thomas Levy, M.D., J.D. (USA)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Charles C. Mary, Jr., M.D. (USA)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, M.D. (USA)
Ken Walker, M.D. (Canada)
Raymond Yuen, MBBS, MMed (Singapore)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, French Edition: Vladimir Arianoff, M.D. (Belgium)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Assistant Editor: Helen Saul Case, M.S. (USA)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
With “Operation Warp Speed” being one of the biggest (over $1 billion) government funded vaccine projects in history, a major conflict of interest has come to light with Moncef Slaoui, the White House Scientific Head of Operations.
Not only has he been the CEO to two of the largest drug companies in the world, both contenders in this race, but he also refuses to give up his $10 million in GlaxoSmithKline stock.
This week, my colleague and friend Sally Fallon Morell brought to my attention an amazing article put out by the CDC. The link to the article is here, and it was published in June 2020. The purpose of the article was for a group of about 20 virologists to describe the state of the science of the isolation, purification and biological characteristics of the new SARS-CoV-2 virus, and to share this information with other scientists for their own research. A thorough and careful reading of this important paper reveals some shocking findings.
First, in the section titled “Whole Genome Sequencing,” we find that rather than having isolated the virus and sequencing the genome from end to end, they found 37 base pairs from unpurified samples using PCR probes This means they actually looked at 37 out of the approximately 30,000 of the base pairs that are claimed to be the genome of the intact virus. They then took these 37 segments and put them into a computer program, which filled in the rest of the base pairs.
To me, this computer-generation step constitutes scientific fraud. Here is an equivalency: A group of researchers claim to have found a unicorn because they found a piece of a hoof, a hair from a tail, and a snippet of a horn. They then add that information into a computer and program it to re-create the unicorn, and they then claim this computer re-creation is the real unicorn. Of course, they had never actually seen a unicorn so could not possibly have examined its genetic makeup to compare their samples with the actual unicorn’s hair, hooves and horn.
The researchers claim they decided which is the real genome of SARS-CoV-2 by “consensus,” sort of like a vote. Again, different computer programs will come up with different versions of the imaginary “unicorn,” so they come together as a group and decide which is the real imaginary unicorn.
The real blockbuster finding in this study comes later, a finding so shocking that I had to read it many times before I could believe what I was reading. Let me quote the passage intact:
“Therefore, we examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549), human liver cells (HUH 7.0), and human embryonic kidney cells (HEK-293T). In addition to Vero E6 and Vero CCL81 cells. … Each cell line was inoculated at high multiplicity of infection and examined 24h post-infection. No CPE was observed in any of the cell lines except in Vero cells, which grew to greater than 10 to the 7th power at 24 h post-infection. In contrast, HUH 7.0 and 293T showed only modest viral replication, and A549 cells were incompatible with SARS CoV-2 infection.”
What does this language actually mean, and why is it the most shocking statement of all from the virology community? When virologists attempt to prove infection, they have three possible “hosts” or models on which they can test. The first is humans. Exposure to humans is generally not done for ethical reasons and has never been done with SARS-CoV-2 or any coronavirus. The second possible host is animals. Forgetting for a moment that they never actually use purified virus when exposing animals, they do use solutions that they claim contain the virus. Exposure to animals has been done once with SARS-CoV-2, in an experiment that used mice. The researchers found that none of the wild (normal) mice got sick. In a group of genetically modified mice, a statistically insignificant number lost some fur. They experienced nothing like the illness called Covid 19.
The third method virologists use to prove infection and pathogenicity — the method they most rely on — is inoculation of solutions they say contain the virus onto a variety of tissue cultures. As I have pointed out many times, such inoculation has never been shown to kill (lyse) the tissue, unless the tissue is first starved and poisoned.
The shocking thing about the above quote is that using their own methods, the virologists found that solutions containing SARS-CoV-2 — even in high amounts — were NOT, I repeat NOT, infective to any of the three human tissue cultures they tested. In plain English, this means they proved, on their terms, that this “new coronavirus” is not infectious to human beings. It is ONLY infective to monkey kidney cells, and only then when you add two potent drugs (gentamicin and amphotericin), known to be toxic to kidneys, to the mix.
My friends, read this again and again. These virologists, published by the CDC, performed a clear proof, on their terms, showing that the SARS-CoV- 2 virus is harmless to human beings. That is the only possible conclusion, but, unfortunately, this result is not even mentioned in their conclusion. They simply say they can provide virus stocks cultured only on monkey Vero cells, thanks for coming.
If people really understood how this “science” was done, I would hope they would storm the gates and demand honesty, transparency and truth.
In a frenzy brought on by this pandemic, we find ourselves in a web of Big Tech censorship. Facebook and Twitter now openly censor posts and stories by public figures and reputable media outlets with no reason, sometimes apologizing, but leaving a dangerous precedent in their wake. Not even White House coronavirus task force member Dr. Scott Atlas is immune to Big Tech’s hammer as they removed his tweet stating:
“Masks work? NO” followed by a series of misrepresentations about the science behind the effectiveness of masks in combating the pandemic.”
The media-fueled coronavirus response has kept fear stoked among much of the world’s population. And yet…numbers from both the U.S. Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) signal, as many said from the beginning of this pandemic, the virus to be no more than a bad flu season.
Nevertheless, the world needs a savior. Media has conditioned us for a one-shot hero to save us and lead us into a Hollywood-honed ‘new normal’—or so we are led to believe.
What about…Aggressively shielding those who we now have the data to prove—beyond doubt—are the most vulnerable? At least cautiously allowing the economy to reengage and avoid the mounting ‘deaths of despair’? Opening schools, since children are the least vulnerable physically but most damaged psychologically?
Nope.
Goldman Sachs analysts, in their infinite wisdom, have come out to proclaim that “The vaccine represents a more important factor than the election result for the path of equities…” No mention of the initial, unscientific lockdowns that throttled the economy. They then went on to warn, the biggest challenge is “convincing the population to get vaccinated…” Really?
In 2018, those same minds at Goldman Sachs asked ‘Is curing patients a sustainable business model?’….and they were serious.
In a report titled “Genome Revolution,” their analysts wrote, “The potential to deliver ‘one shot cures’ is one of the most attractive aspects of gene therapy, genetically-engineered cell therapy and gene editing. However, such treatments offer a very different outlook with regard to recurring revenue versus chronic therapies.”
Two years later, Goldman now has the best of both worlds, a so-called ‘one shot vaccine cure’ that is also tinkering with what vaccine-maker, Moderna, calls ‘the software of life,’ a quasi gene therapy and germ line reprogramming by an experimental mechanism of action in cancer patients.
Another Wall Street power player JP Morgan recently pegged its prediction for a deployable vaccine by mid-2021: “Let’s put it this way: Life can’t fully return to normal until a vaccine exists and is distributed to the masses…Consensus feels like there is a speed limit on the recovery—it can only go so far and so fast without a vaccine.”
Another company toying with the ‘software of life’ is America’s most loved corporate criminal, Johnson & Johnson (J&J) and their Covid vaccine-maker subsidiary, Janssen.
Recently forced to pause their trial due to ‘an unexplained illness’ in a study participant, it’s been nearly a week and still no updates. By comparison, AstraZeneca’s UK vaccine trial went from stop to restart in four days – the FDA still has it paused here in the U.S.
Over the past few years, reporting on J&J has read like a fictional crime novel. Labeled a ‘kingpin’ and blamed for causing the opioid crisis in Oklahoma in 2019, J&J’s opioid-making subsidiary Janssen was ordered to pay $572M, later reduced to $107M. As a side note, in July, HHS’s Biomedical Advanced Research and Development Authority awarded Janssen with $456M taxpayer dollars for ‘clinical trials and other vaccine development activities.’ One month later, Janssen secured over a billion dollars from HHS to manufacture 100 million doses of its COVID-19 vaccine for use in clinical trials, or to vaccinate Americans if authorized by the Food and Drug Administration.
A day after J&J’s vaccine safety trial pause, additional news broke regarding their potential master settlement against litigation alleging its involvement fueling the U.S. opioid epidemic. Last week J&J felt the need to pile on another billion to its already $4B settlement framework negotiated with a group of state attorneys general.
All under the veil of J&J’s public promise to be more ethical with its newfound vaccine contract.
As the popular maxim goes ‘the best predictor of future behavior is…past behavior.’
J&J also recently discontinued its century-plus legacy talc baby powder product. They claimed it was because of misinformation about the product’s safety. Yet internal emails, memos and documents showed the company knew it was harmful and sought to suppress the science and those who spoke out against it…for decades.
The company also recently paid over $100M to settle more than 1000 talc lawsuits. J&J still faces more than 19,000 lawsuits from consumers and their survivors, claiming its talc products caused cancer due to contamination with asbestos, a known carcinogen.
Over $2 billion to the Department of Justice to resolve criminal and civil investigation including off-label marketing and kickbacks to doctors and pharmacists for their prescription drugs. A billion to settle their mounting medical device hip implant lawsuits in 2019. Ordered to lay $8 billion (later reduced to $1.2B) in damages in a Risperdal lawsuit also in 2019. It just doesn’t end.
But they’ll act differently this time with their Covid vaccine. This time you can trust them to be ethical and transparent about any safety issues. Right?
And if they aren’t? Well at least those harmed in the future by Janssen’s products can sue J&J and have their day in court like so many victims before them for against J&J’s talc, Risperdal, opioid and medical device products. Right?
In conclusion, here’s a quote from October 11, 2020 by J&J’s Chief Scientific Officer Paul Stoffels speaking with the Wall Street Journal:
“It’s important for people, if there would be side effects, that they get compensated,” Johnson & Johnson’s chief scientific officer, Paul Stoffels, told the Journal. “But for the industry to make multiple billion vaccines available, you also have to have” liability protection, he said.
You’ll recall that back in April of this year I examined the question of whether or not there was foreknowledge of the plandemic. Specifically, that episode of Questions For Corbett looked at:
and several other signs that those in positions of power knew that 2020 was going to be the year of COVID.
But April seems like an eternity ago and many more pieces of suspiciously predictive activities been dug up in the meantime.
So, in the interest of continuing this exploration, let’s examine 10 more signs of plandemic foreknowledge.
1) Crimson Contagion
In 2019 the US Department of Health and Human Services (HHS) held a pandemic exercise called Crimson Contagion, which, the mainstream press notes, was “eerily similar” to the current scamdemic. The exercise scenario envisioned a novel strain of pandemic influenza originating in China and being brought back to the US by international tourists.
So why did the exercise make it into the mainstream press at all? Because Orange Man Bad, of course. More specifically, because it provides the “Bin Ladin Determined to Strike in US” cover story for this neo-9/11, subtly reinforcing the narrative by suggesting that COVID-19 is a real and existential threat to the US and that the valiant leadership of the HHS tried to warn the White House about PPE shortages and other preparedness shortcomings.
2) Canada’s Pandemic Warning System Shut Down Right Before COVID-19
Canada’s international alert system for disease outbreaks—the Global Public Health Intelligence Network, or GPHIN, which, The Globe and Mail helpfully informs us, is “highly regarded”—was “silenced” by the Canadian government in early 2019. And we all know what happened at the end of 2019.
This story once again serves to bolster the mainstream narrative by portraying the novel coronavirus as a real and existential threat that could have been prevented if only the government had plowed more money into its public health department and paid more attention to the epidemiologists (who, as we have seen this year, never get anything wrong).
3) “Simulation” of the Deliberate Release of a Lethal Respiratory Pathogen Planned for 2020
The Global Preparedness Monitoring Board is a body convened by the World Bank and the World Health Organization (WHO) that seeks to “ensure preparedness for global health crises.” In their 2019 “Annual report on global preparedness for health emergencies” they warned, a propos of absolutely nothing, of the “very real threat of a rapidly moving, highly lethal pandemic of a respiratory pathogen killing 50 to 80 million people and wiping out nearly 5% of the world’s economy.”
They also set a number of goals for 2020, including:
The United Nations (including WHO) conducts at least two system-wide training and simulation exercises, including one for covering the deliberate release of a lethal respiratory pathogen.
But don’t worry, guys! That’s just a “simulation,” and we all know that drills never go live.
4) The WHO Warns of “New Normal” of Pandemic Outbreaks . . . in 2019
Last June, Dr. Michael Ryan—the executive director of the WHO’s health emergencies programme—told BBC News that “We are entering a very new phase of high impact epidemics and this isn’t just Ebola.” In case you didn’t get the warning, he added: “This is a new normal, I don’t expect the frequency of these events to reduce.”
Look out, folks, we’ve got a regular Nostradamus here.
Dr. Ryan, it should be noted, is the same WHO official who announced that the “new normal” of the COVID-19 era involves governments forcibly removing those suspected of infection from their homes and separating them from their families. Oddly, he forgot to mention that part when speaking to the BBC last year.
5) A Comic Book Published by the EU Envisioned A Global Pandemic Stopped by the EU
This one has to be seen to be believed:
What you are looking at is a page from Infected, a comic book published by the EU Publications Office in 2012.
No, you read that right. A comic book published by the EU Publications Office.
And what’s the story of this comic book adventure?
During a tour of a P4 biosecurity lab in China, a time traveler from the year 2111 arrives to warn the assembled scientists that, in the future, a pandemic will ravage the planet. In order to prevent the calamity, the time traveler provides the scientists with a some vials of biological material that he says will be necessary to “nip any pandemic in the bud.”
Terrorists try to steal the material *blah blah blah* man scratched by a monkey *yadda yadda* global infectious outbreak *etc., etc.* and then . . . (you guessed it!) . . . the EU saves the day through an unprecedented global health campaign dubbed “The Way Forward.”
Yes, luckily for humanity, the EU-led “one health” approach saved us all from this “new era” of zoonotic pandemic outbreaks that we have just entered.
Personally, if I were a citizen of the EU I’d be upset that some portion of my taxes go toward paying for the production of propaganda schlock like this. After all, these are the same people who produced the dumbest propaganda video ever.
Oh, and just for the record, although the imaginary P4 lab in the comic is said to be in “Beijing,” China’s first (and only) P4 lab is in fact in Wuhan.
6) COVID-19 Test Kits Being Sold in 2017?
The World Bank runs a website called the World Integrated Trade Solution (WITS) that tracks global trade data by product using their “Harmonized System” (HS) tracking codes. On September 4, 2020, they posted data on COVID-19 test kits that raised some eyebrows. You see, the website indicated that these COVID-19 test kits were being sold as far back as 2017!
Proof positive that the whole thing was planned years in advance, right?
Sigh.
A cursory glance at the data would give even the most credulous truther pause for thought about the significance of this “find.” If we were to take this posting at face value, then we have to believe that not only were 58 separate countries producing and exporting these COVID-19 test kits (meaning that tens of thousands of people would have been involved in their production, sale, shipping and storage), but that countries like Switzerland were producing over 2,000,000 kg worth of these kits (valued at a cool $23 billion) without a single person anywhere in this supply chain asking, “What’s COVID-19, anyway?” and not a single person coming out afterward to say, “You know, I thought it was odd that we were exporting billions of dollars worth of these COVID-19 test kits, but it was even weirder when COVID-19 was identified and named three years later.”
Or, you know, the test kits were general medical test kits that were relabeled for COVID-19 use in April of this year and retroactively relabeled in the WITS system. Because that’s exactly what the fact checkers are saying.
And you know what? I believe them. (“Oooooooh, I just knew James was a globalist shill!” jeers the crowd.)
This is another example of how poorly researched information gets passed around online so that the fact checkers can arrive on their white horses and save the day by dispelling the obvious misinformation (Gates and the God gene vaccine at the CIA, anyone?).
So I don’t consider this one plandemic foreknowledge at all, but thought I would throw it in to put the debunking on record.
7) A White House Advisory Group Published a Report on How a Pandemic Would Ravage the Economy . . . Last September
In September 2019 the White House’s Council of Ecnomic Advisors published a report on “Mitigating the Impact of Pandemic Influenza through Vaccine Innovation.” The report warned of “the potentially large health and economic losses in the United States associated with influenza pandemics,” estimating that such a pandemic would cause “from $413 billion to $3.79 trillion” worth of damage to the economy. And, as the title suggests, it argues that “[n]ewer technologies, like cell-based or recombinant vaccines” could help drastically mitigate that damage.
Unsurprisingly, the usual MSM presstitutes used the story to reinforce the narrative that pandemic diseases are the new normal, that the US is woefully unprepared to fight the war on the invisible enemy, and that investment in novel vaccine technologies can help save the country from economic ruination.
8) Central Bank Gold Repatriation
You might remember back in 2013 when Germany’s Bundesbank issue a remarkable statement announcing that they would repatriate 674 tons of their gold holding from the New York Fed. You may even remember that they specifically set a 2020 deadline for that repatriation.
But did you know that Austria’s central bank followed suit in 2015 with an announcement that they, too, would repatriate the country’s gold by 2020? And did you know that the Polish central bank repatriated 100 tonnes of its gold from the Bank of England’s vaults in a series of secret airlifts ending in November 2019?
All of these pieces of evidence led analysts like Ronan Manly to predict that 2020 would be the year of the great “system reset,” a transformation of the world financial system that would ultimately be used to usher in a new international monetary order.
This has nothing to do with a pandemic, of course, but then again, neither does the financial crisis we’re living through. The truth is that the current financial meltdown has been gathering steam for years and was well underway for at least a year prior to any of this COVID-19 hysteria. “Following the money” to track down the real perpetrators of this crime seems as good advice for would-be scamdemic investigators as it is for 9/11 investigators.
Conclusion
As you can see, there were many different warnings that a pandemic emergency was set to take place this year. As you can also see, there is no “smoking gun” that proves anything specific about COVID-19. Even worse, many of these “warnings” actually serve to bolster the narrative that this scamdemic really is an emergency—one that we could have prevented if only we’d thrown more money at big pharma and given more power to the public health technocrats.
But such is the nature of these large-scale events. Amateur sleuthers get caught up searching for the single, undeniable “smoking gun” and lose sight of the bigger picture.
The bigger picture here is that—exactly as I have demonstrated in my work on Medical Martial Law and Medical Martial Law 2020 and COVID-911—the groundwork for the emergence of the biosecurity state has been carefully laid over the course of the past two decades (at least). From the passage of emergency health legislation to the creation of new pandemic preparedness offices to the signing of international health treaties, this medical martial law infrastructure has ensured that—regardless of whether it is real or fake, planned or unplanned—any public health crisis could be used as the trigger for the beginning of the biosecurity era.
By all means, keep looking for that smoking gun (and, if you happen to find it, let me know in the comments below). But unless we discuss What No One Is Saying About the Corona Crisis and address the root of this new biosecurity paradigm, the bioterrorists will get away with their scam.
We were told initially that the premise for lockdown was to ‘flatten the curve’ and therefore protect the NHS from being overwhelmed.
It is clear that at no point was the National Health Service (NHS) in any danger of being overwhelmed, and since May 2020 covid wards have been largely empty; and crucially the death toll from covid has remained extremely low.
We now have hundreds of thousands of so-called ‘cases’, ‘infections’ and ‘positive tests’ but hardly any sick people. Recall that four fifths (80%) of ‘infections’ are asymptomatic (1) Covid wards have been by and large empty throughout June, July, August and September 2020. Most importantly covid deaths are at an all-time low. It is clear that these ‘cases’ are in fact not ‘cases’ but rather they are normal healthy people.
So-called asymptomatic cases have never in the history of respiratory disease been the driver for spread of infection. Rather it is symptomatic people who spread respiratory infections – not asymptomatic people.(2)
It is also abundantly clear that the ‘pandemic’ is basically over and has been since June 2020. (3)
We have very highly likely reached herd immunity and therefore have no need for a vaccine.
We have safe and very effective treatments and preventative treatments for covid, we therefore call for an immediate end to all lockdown measures, social distancing, mask wearing, testing of healthy individuals, track and trace, immunity passports, the vaccination program and so on.
There has been a catalogue of unscientific, non-sensical policies enacted which infringe our inalienable rights, such as – freedom of movement, freedom of speech and freedom of assembly. These draconian totalitarian measures must never be repeated.
LOCKDOWN
Covid has proved less deadly than previous influenza seasons – There were 50,100 flu deaths from December 2017 to March 2018 in England and Wales. There were 80,000 flu deaths in 1969. To date we have circa 42,000 covid related deaths in the UK.
We have never locked down society for a respiratory virus before.
The basis for lockdown was a mathematical model by Professor Neil Ferguson. His modelling which predicted half a million deaths in the UK has been roundly condemned as being not fit for purpose. His estimated death figures were clearly wrong by a factor of 10 or 12 times. (1)
Professor Ferguson’s modelling was not even peer reviewed before being acted upon by several nations. Eminent epidemiologists such as Professor Gupta from Oxford University were ignored, they estimated the death count would be far lower in the UK.
Professor Ferguson has a long track record of woeful modelling he was entirely wrong about sars, mers, mad cow’s disease (CJD), and swine flu. Why did the world listen to him again? (2)
Countries which did not lock down Sweden, Japan, Taiwan, South Korea and Belarus have all done significantly better than us in terms of percentage of population deaths. They also have herd immunity and intact economies.
Lockdown did not save lives, and this has been published in the Lancet ‘….in our analysis, full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.’ (3)
The vast majority of deaths occurred in elderly and very elderly people
The vast majority of deaths occurred in people with pre-existing serious health issues such as cancer, cardiovascular disease, Alzheimer’s, diabetes etc
Covid poses virtually zero risk to the under 45’s who have more chance of being struck by lightning than dying from covid.
Covid poses a very small risk for healthy under 60 year olds who have a greater chance of accidental drowning than dying from covid.
The entire nation was essentially placed under house arrest. We have never isolated the healthy before.
Isolating the sick and those who are immunocompromised makes sense. Isolating the healthy has hampered the establishment of herd immunity and makes no sense.
To put it into perspective we had 115,000 smoking related deaths in the UK in 2015 compared to the 42,000 deaths from covid.
We usually have around 600,000 deaths every year in the UK, roughly 1600 deaths per day.
COLLATERAL DAMAGE THE CURE IS WORSE THAN THE VIRUS
Placing the public under virtual house arrest has caused untold damage to both physical and mental health.(1)
Ventilating patients instead of oxygenating patients proved to be a deadly policy and an unwarranted failure. Ventilation resulted in many unnecessary deaths. (2)
Sending infected people from hospitals to care homes placed the elderly and frail under unnecessary risk and resulted in many unnecessary deaths. (3)
Blanket Do Not Resuscitate (DNR) orders were imposed on thousands of people without their consent nor the consent of their families – this is both unlawful and immoral and lead to unnecessary deaths in care homes. (4)
Hospitals became essentially ‘covid only’ centres vast numbers of patients were wilfully neglected, resulting in many thousands of unnecessary deaths. (5)
The government’s own report estimates that some two hundred thousand (200,000) people will die as a direct result of lockdown – not the virus. Hospitals being closed, suicide and poverty will result in more deaths than the virus. (6)
The cure is worse than the disease!
DEATH CERTIFICATES (1)
The majority of people who died had significant comorbidities, such as Alzheimer’s, cancer, cardiovascular disease and diabetes.
Counting death certificates with a ‘mention’ of covid as being a death caused by covid is a gross misrepresentation of the facts and has vastly over exaggerated the death toll.
The rules for the signing of death certificates have been changed solely for covid by the Coronavirus 2020 Act.
Doctors do not even need to have physically seen the patient in order to sign death certificates.
The Act has removed the need for a confirmatory medical certificate for cremations.
Autopsies have virtually been banned, no doubt leading to misdiagnosis of the true cause of deaths; and also reducing our understanding of the disease itself.
Worse still, care home staff who largely have no medical training are able to give a statement as to the cause of death.
Covid was put on death certificates merely on the ‘suspicion’ of people having covid. This may well be unlawful, since it is a crime to falsify death certificates.
People who die within 28 days of a positive pcr test are deemed to have died from covid, even if they die in a car crash or from a heart attack; clearly over inflating the death toll (2)
ECONOMIC RUIN
Reports now estimate that as many as six and a half million (6,500,000) people in the UK will lose their jobs as a result of lockdown. (1)
It is well known that poverty directly adversely affects health, we can expect to see many people suffering with poor health and resulting in many premature deaths, as a direct result of lockdown.
CENSORSHIP
Government have acted maliciously in censoring doctors, nurses and NHS staff. The people have the perfect right to hear what is going on in hospitals, and the medical profession have a duty to look after the public and to reassure them. (1)
The medical profession have not been allowed to let the public know that covid wards have been empty for months, nor that covid deaths have reached an all-time low for months, and this has unnecessarily added to the public’s distress and anxiety.
Doctors and scientists with views that differ from the government narrative have had their videos and articles removed from the internet
TESTING – FALSE POSITIVES
PCR tests cannot be verified for accuracy as there is no ‘gold standard’ against which to check them. The virus has not been purified. (1)
PCR tests cannot detect viral loads and are prone to false positives. (2)
A positive PCR test does not mean that an individual is infected nor infective. (3)
In fact approximately 90% of the PCR positive ‘cases’ are false positives. We therefore have no second wave and no pandemic. (4 , 5)
The government’s report estimates a false positive rate of between 0.8 to 4.0 % using data from other viral infections – not from covid (6)
Viral fragments may remain in people’s bodies for several weeks following recovery from infection. (7)
The crisis will never end if we are waiting for zero positive tests. Everyone has probably had a cold caused by a coronavirus and will likely have a few viral fragments matching those of the cousin SARS-CoV-2 virus (8)
Testing healthy asymptomatic individuals is non-sensical, unscientific and a colossal waste of money. The governments moon shot daily testing program will cost £100 Billion roughly two thirds of the annual NHS budget.
Antibody testing is not the gold standard as many people have T-cell immunity, and antibodies may not circulate following recovery from infection.
HYDROXYCHLOROQUINE
The controversial drug Hydroxychloroquine (HCQ) has been unfairly smeared, by the WHO, CDC, NIH and the media.
However HCQ has very firm support from, amongst others: Professor Harvey Risch epidemiologist from Yale, The American Association of Physicians and Surgeons (AAPS), American Frontline Doctors, the Henry Ford Health System and Professor Didier Raoult microbiologist and infectious disease specialist – to name but a few. (1)
The Lancet was even forced to retract a study on HCQ after it was revealed by the Guardian newspaper that they had been completely fabricated and written by a sci-fi writer and a porn star. Even following this astounding revelation HCQ was still banned in most countries. (2)
HCQ according to AAPS has a ninety per cent (90%) cure rate when given early and alongside zinc (3)
HCQ is safer than many over the counter drugs such as aspirin, Benadryl and Tylenol.
The AAPS also point out that there has never been a vaccine as safe as HCQ. (4)
HCQ has been licensed for over sixty years and has been safely used by billions of people worldwide. There is a very small risk of arrythmia which is easily monitored.
Why was HCQ banned then? Could it be that there are no huge profits to be made from this out-of-patent drug?
HCQ was used to great effect in the Sars1 outbreak of 2005 (5)
In short had HCQ been available then there would not have been a pandemic !
PREVENTION
Preventative measures such as hydroxychloroquine or vitamins D, C and zinc should have been recommended for the public. (1)
Early calcifediol (25-hydroxyvitamin D) treatment to hospitalized COVID-19 patients significantly reduced intensive care unit admissions (2)
Vit D reduces the severity of covid. (2,3)
Voluntary isolation of the frail – should they so choose; in combination with preventative measures would have been a far better strategy. The rest of society could and should have continued as normal.
VACCINE
A rushed vaccine is clearly not in the public’s best interest
Indemnifying vaccine manufacturers against all liability is also clearly not in the public’s best interest
CONFLICTS OF INTEREST
Chief Scientific Officer Sir Patrick Vallance has £600,000 worth of shares in GSK Glaxo Smith Klein. He has in recent years sold £5 million of shares in GSK which he ‘earned’ whilst chief of GSK (1)
Sir Chris Whitty, Chief Medical Officer UK, accepted over £30 million in funding from the Bill and Melinda Gates foundation to study malaria vaccines. (2)
It has become clear that members of SAGE, Public Health England (PHE), World Health Organisation (WHO), Centre for Disease Control (CDC), National institute for Health (NIH) etc have many conflicts of interests. They all accept very large ‘donations’ from the pharmaceutical and vaccine industry. These conflicts of interests may well have effectively corrupted their integrity. (3)
It is also clear that governments are heavily lobbied by the pharmaceutical industry and the vaccine industry, again this may have compromised their integrity. (4)
CUI BONO? WHO BENEFITS?
Vaccine manufacturers will make trillions from this, as will track and trace manufacturers, and the pharmaceutical industry stand to make trillions from covid testing.
Prime minister Boris Johnson announced the new ‘moon shot’ testing will cost £100 Billion, approximately two thirds of the annual NHS budget.
Surely these vast sums would be far better spent on treating all of the neglected patients who have been wilfully neglected during lockdown and who now face huge waiting lists.
CONCLUSIONS
We have effective and safe treatments and preventative medications for covid, therefore there is no need for any lockdown restrictions and associated measures. The pandemic is essentially over as can be seen by the consistent low death rate and hospital admissions over the past four months.
We demand the immediate and permanent ceasing of all lockdown measures.
Lockdowns do not save lives, that is why they have never been used before. Civil liberties and fundamental freedoms have been unnecessarily removed from the public and this must never happen again.
Preventative measures such as Hydroxychloroquine, vitamin C, Vitamin D and zinc must be made readily available to the public.
Isolation must be voluntary. People are perfectly capable of making their own assessment of the risks and must be free to go about their lives as they so choose. People must have the right to choose whether to isolate or not.
Likewise, businesses must have the right to remain open if they so choose.
We demand that doctors, nurses, scientists and healthcare professionals must be permitted free speech and never be censored again.
Professor Mark Woolhouse epidemiologist and specialist in infectious diseases, Edinburgh University Member of the Scientific Pandemic Influenza Group on Behaviours, that advises the Government stated that –
‘…Lockdown was a monumental disaster on a global scale. The cure was worse than the disease.’
‘I never want to see national lockdown again. It was always a temporary measure that simply delayed the stage of the epidemic we see now. It was never going to change anything fundamentally, however low we drove down the number of cases,’
‘We absolutely should never return to a position where children cannot play or go to school.’
I believe the harm lockdown is doing to our education, health care access, and broader aspects of our economy and society will turn out to be at least as great as the harm done by Covid-19.’(1)
The World Doctors Alliance agree fully with Prof Woolhouse’s assertions, he is right! We must never lockdown again!
NB the term ‘covid’ has been used to represent Sars-CoV-2 and Covid-19
In this interview, social justice and anti-GMO advocate Vandana Shiva, Ph.D., discusses her book, “Oneness Vs. the 1%: Shattering Illusions, Seeding Freedom,” which she co-wrote with her son, in which she argues that the ultra-wealthy elite are responsible for a majority of the environmental, financial and health crises currently facing us.
• In “Oneness Vs. the 1%: Shattering Illusions, Seeding Freedom,” Vandana Shiva, Ph.D., argues that the ultra-wealthy elite are responsible for a majority of the environmental, financial and health crises currently facing us
• Bill Gates’ wealth and “philanthropic” efforts, for example, have allowed him to gain unprecedented influence over agriculture and global health policies that threaten food security and human health
• The COVID-19 pandemic has catalyzed a massive transfer of wealth to the rich
• While global lockdowns have decimated small businesses and left many to struggle financially, wealthy globalists have amassed immense profits, and lockdowns have prevented public mobilization against tech and retail giants
• To facilitate the transfer of wealth, the elite lobby for the elimination of labor and environmental laws, as well as human and farmer’s rights
With a new epilogue about Bill Gates’s global agenda and how we can resist the billionaires’ war on life
Widespread poverty and malnutrition, an alarming refugee crisis, social unrest, and economic polarization have become our lived reality as the top 1% of the world’s seven-billion-plus population pushes the planet―and all its people―to the social and ecological brink.
In Oneness vs. the 1%, Vandana Shiva takes on the Billionaires Club of Gates, Buffet, and Zuckerberg, as well as other modern empires whose blindness to the rights of people, and to the destructive impact of their construct of linear progress, have wrought havoc across the world. Their single-minded pursuit of profit has undemocratically enforced uniformity and monocultures, division and separation, monopolies and external control―over finance, food, energy, information, healthcare, and even relationships.
Basing her analysis on explosive, little-known facts, Shiva exposes the 1%’s model of philanthrocapitalism, which is about deploying unaccountable money to bypass democratic structures, derail diversity, and impose totalitarian ideas based on One Science, One Agriculture, and One History. She calls for the “resurgence of real knowledge, real intelligence, real wealth, real work, real well-being,” so that people can reclaim their right to: Live Free. Think Free. Breathe Free. Eat Free.
The annual spring congregation of egg-laden horseshoe crabs on the east coast provide a vital food source for annual migrations of millions of shore birds.
The $18 billion gold rush for liability free COVID vaccines now threatens that ancient Atlantic coast ritual. COVID vaccine makers plot to harvest tens of thousands of these primitive and beloved sea creatures. The horseshoe crab’s blue blood is the only known natural source of limulus amebocyte lysate, a substance that detects and eliminates a potentially deadly vaccine contaminant called endotoxin.
In 1990, biologists estimated 1.24 million crabs spawned in Delaware Bay, a main egg-laying nursery grounds and prime collection point for the companies. By 2019, that number had dropped to 335,211. Conservation groups feel that the planned harvest by vaccine manufacturers may lead to the species’ extinction.
Starting in July, Swiss-based Lonza will begin manufacturing a COVID-19 vaccine for human clinical trials. The company will use lysate in the vaccine it plans to sell it in the U.S.
The horseshoe crab is already on the brink of extinction. Conservationists fear that the demand for horseshoe crab blood for COVID-19 vaccines may exterminate the crabs and destroy the shore birds and the marine ecosystem that depend on them.
Conservationists observe that the harvesting of wild animals like sharks and horseshoe crabs for exploding vaccine manufacturing is unsustainable.
David Icke Shares Work of German Neurologist: Masks Are Destroying Children’s Brains
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light BitChute, Lbry, Odysee & Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video.]
Philanthrocapitalism — epitomized by the Bill & Melinda Gates Foundation — has emerged over the last 30 years as a major force with the potential to “push the future of our planet towards extinction and ecological collapse,” according to a report launched Wednesday by Navdanya International.
“Gates to a Global Empire” sheds light on how philanthrocapitalism accelerates the corporate takeover of our seed, agriculture, food, knowledge and global health systems, and how it manipulates information and erodes democracies — all in the name of corporate profits.
The report explores how the Gates Foundation, powered by an “unholy alliance” between big capital, science and technology institutions and states, has established a global empire over life, through monocultures, patents and monopolies designed to destroy the natural world of diversity, self-organization and freedom.
In her introduction to the report, Navdanya International’s founder, Vandana Shiva, said:
“The European Court of Justice has ruled that gene-edited organisms are GMOs. However, Gates is hastily pushing for deregulation with no regard for caution or potentially dangerous consequences. His ‘Gates AgOne’ … initiative is a clear declaration of his intent to create an Empire over life and biodiversity, over food and farming, and over our daily bread.”
With a net worth of nearly $117 billion, Gates is now the most powerful philanthropist in modern history, according to a synthesis of the report. After making technology available to the masses through his popularization of the at-home personal computer, the founder of Microsoft has “taken to reinventing himself as a benevolent philanthropist who uses his technologic influence and private market savvy to solve the world’s most pressing problems through his and his wife’s foundation: The Bill & Melinda Gates Foundation.”
Through its various initiatives, sub-organizations, development schemes and funding mechanisms, Gates weaves, according to the report, “an intricate web of wide-ranging power and influence.”
“Gates to a Global Empire” Report Launch and Online Conferenceby Seed Freedom
Original video available at Seed Freedom YouTube channel.
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light BitChute, Lbry, Odysee & Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video.]
I have written several recent articles documenting the fact that the COVID virus is missing in action. [1] [2] [3] [4]
And when I say missing, I’m talking about two MAJOR confessions, from both the CDC and a group of study-authors in Europe…and in each case, these people were in the process of assembling instructions on how to perform the diagnostic PCR test for that very virus. The virus they said they didn’t have.
They didn’t have it because they couldn’t get it.
They couldn’t get it because no one had it.
In other words, the existence of the COVID virus is unproven.
Now, I want to point out three factors that produce a hypnotic effect. Even in the absence of the virus, these factors seem to indicate the virus “must exist.” I’m not talking about government or media pronouncements, which are obvious.
ONE: Scientists and public health agencies claim they’ve ISOLATED the virus.
There is no reason to believe them. The term “isolation” is thrown around like a politician throws around the term, “the people.”
Isolation of a virus SHOULD mean it is separated out from all the genetic, cellular, microbial, and waste material that surrounds it. But don’t assume, when professionals are talking or writing, that this is what they DO mean. Do not assume that.
For example, they often mean: “We have the virus in a dish in the lab. The soup in the dish contains human cells, chemicals, drugs, and other material. However, we know the virus is there and growing, because it is killing the human cells…”
Wrong. There is more than sufficient non-viral substance in the soup that could be doing the cell-killing. And obviously, “the virus” in the dish is surrounded by this mix of material. It is far from isolated.
And, as I’ve documented in a previous article, if the CDC, one of the biggest public health agencies in the world, couldn’t get the virus, as of July of this year, and admitted it in writing…“the virus” isn’t isolated.
TWO: This hypnotic effect ropes in some of the brightest medical and scientific professionals, who otherwise challenge all sorts of medical dogma. It is: “The genetic sequence of the virus is well established. Many studies confirm this.”
Well, sure. If experts have mapped out the genetic structure of the virus, the virus must exist. Right?
Wrong. The sequence is INFERRED. It is ASSUMED.
Inferred from what? The genetic sequence could be cobbled together from several sources: the unseparated material “in the dish in the lab”; a piece or pieces of RNA that have been arbitrarily chosen as “relevant clues”; a piece or pieces of synthetic RNA that, again, have been arbitrarily selected according to a bias in favor of a certain type of virus.
Bias? What does that mean? I’ll explain. When a few dozen people in Wuhan fell ill, back in 2019, there were a million ways researchers could have gone, in trying to figure out the cause.
Of course, as I’ve written, they could have looked out their windows and observed the horrific air pollution hanging over the city, and realized these “unexplained cases” of pneumonia had a ridiculously simple origin. [5] But no.
The researchers opted, as they always do, for a “new virus.” And, they chose, without a shred of evidence, to “look for” a germ from the coronavirus family. That was the pre-planned story. That was the bias.
From that point on, the die was cast. The “genetic sequencing” involved cobbling together, by assumption and inference, a collage of INFORMATION, into code, which would satisfy the pre-ordained scenario.
They ASSEMBLED a genetic sequence that matched what they were going for: a coronavirus.
Don’t imagine genetic sequencing is performed by people looking directly at a virus through a cosmic microscope and jotting down the names of rows of genes sitting side by side like cars in a supermarket parking lot.
THREE: The other hypnotic factor is the PCR test. “If the test exists to detect the virus, the virus must exist.”
Wrong. The test—which has irreparable and fatal flaws, as I’ve documented—is working, at best, from a fragment of RNA which is ASSUMED to come from the virus. If the test appears to identify that fragment as “relevant,” the test result clams the person is “infected.”
People believe the test must mean something. And the only thing it could mean is: it finds the virus in a person, or the virus isn’t in that person’s body. But either way, the virus is real.
Wrong.
The deck is stacked. The game is rigged. Welcome to the Deep Medical State.
As in any truly deep operation, only a small number of elite professionals understand the basic con. The rest are blind, and accepting. Some are willfully blind. They see the truth in a flash of insight, and then they shut up.
However, in this mad “COVID landscape,” minds and doors are opening. The hypnotic haze is receding. The truth is coming out. Doctors, scientists, reporters, and members of the public are discovering and rejecting the Big Con.
“Liberty, then, is the sovereignty of the individual, and never shall man know liberty until each and every individual is acknowledged to be the only legitimate sovereign of his or her person, time, and property, each living and acting at his own cost.”
~ Josiah Warren, “Equitable Commerce”. Book by Josiah Warren, 1848.
The essence of freedom is based on individual sovereignty, while the essence of servitude is based on compliance and obedience to false authority. Any claimed authority is illegitimate if it is not voluntary, and therefore administered by force. That means that all government authority is improper unless each and every individual agrees with that governance, and also has the ability to throw it aside, and leave at any time of his choosing. We have never lived under a system that allowed real freedom in this country.
In order for freedom to exist, it is up to the people at large to ensure that no government has enough power to infringe on the liberty of any individual citizen. Obviously, the people have failed miserably in any effort to secure individual independence, as every aspect of life in the United States is now surveilled, regulated, monitored, and controlled by a government claiming to be sovereign over the individual, and all of this is enforced by brutal and violent means. In order for people to wake up to their own servitude, and care enough to take risk to change, they have to have enough individual incentive to seek that on their own. That is not evident yet, and because people still clamor to be led instead of ruling self, the situation is worsening at every juncture.
The most telling aspect of this phenomenon is the near total compliance by the general population of mandated mask wearing and social distancing. By acquiescing to these orders handed down by the political class, it is apparent that the masses are nothing more than slaves, and are either totally indifferent or ignorant of any reality concerning their own well-being or any natural desire for freedom. When people en masse are willing to take orders from a controlling force called government, then they become the greatest threat to the whole, which means they are the greatest threat to the individual sovereignty of all.
Thinking of this in logical terms should scare the living daylights out of any sane person. How can a country that claims to be the most free on earth, a country of well over 300 million people, give up everything they have worked for and gained in life, everything they hold dear, and cower and hide in the shadows hoping that they will be granted by their masters a partial return to normalcy if they do as they are told? They do this because they have been fooled into believing that a common flu will attack and kill them all. Never mind that there are no additional deaths, there is no pandemic, and that no so-called virus has ever been found to exist. It has never been isolated or separated, never been identified, and never satisfied Koch’s Postulates to prove that it is even real. How could so many be fooled by a lie so obvious? Is this simply because of what the master propagandists claim when they say the bigger the lie, the more that will believe it? Or is it just that so many have become dependent on others telling them what to do and how to live for so long that they no longer have any desire or ability to question false authority?
Mask wearing and social distancing are nothing more than compliance tests used by the controlling ‘elite’ to see how weak and pathetic this population has become. This was necessary in order to find out if this country was ready to be taken over by the few oligarchs in power. All indications are that the America of the past has come and gone, and all that is left is a once dynamic and strong land now filled with mindless and obtuse citizens with robotic personalities waiting for their next order. As I wrote recently:
“Forced mask wearing due to political control over people is a major aspect of the tyrannical response to this fraudulent virus ‘pandemic.’ Social distancing, forced testing, quarantines, mandated business closings, temperature checks, mass surveillance, and any number of other atrocious invasions of privacy are all demeaning and oppressive, but the state and local orders supported by the national political and ‘health’ organizations to wear masks, is especially instructive of the real agenda sought. That agenda is as clear as day, and is being implemented not only as a test of mass societal compliance, but also to force people apart and to remove closeness, expression, and emotion from the human psyche. This is a purposeful state exercise with the intent of destroying the spirit of the American public, leaving only a society of unfeeling and obedient drones awaiting the next order handed down from on high”.
People that live in constant fear have no ability to think or reason. Their primary goal is to seek safety regardless of the consequences. Their ability to love and care for others is diminished, and their compassion for friends and family disappears in an effort to attain what they falsely believe to be self-preservation. By becoming completely indifferent to their surroundings and personal relationships, they become dangerous to themselves and others. The ruling class fully understands this dynamic, and has used it to gain an advantageous position of power over the entire country. We are in the midst of a coup that is turning one against another, and all against all. The people themselves are being used to destroy each other, and all those that comply with the state’s directives to hide their faces with a mask, to eliminate expression, and to isolate themselves from friends and family, are not only destroying their own lives, but are a great risk to all others. There is no excuse for this behavior.
Masks and distancing will lead to vaccination, and once a majority receives any fraudulent Covid vaccination, physical and mental problems will escalate, and sickness will become prevalent. Every aspect of the state’s plan for population control, takeover, and global reset is dependent on compliance by the herd at every stage of tyranny. So long as the crowd continues to submit to these draconian mandates, the plan will be able to be advanced. The biggest push to further this nefarious agenda is coming soon, and continuous compliance by the people will guarantee a state of totalitarian rule.
“Sovereignty is not given, it is taken.” ~ Mustafa Kemal Ataturk (Unsourced)
Yet Another Case of the Missing Virus; They Lied and Locked Down the World
I’ve been exposing the fact that the CDC, in July of this year, admitted, in a document, that…
They didn’t have the SARS-CoV-2 virus. It wasn’t “available.”
This means they couldn’t obtain an isolated specimen of the virus. There is only one reason why.
The virus hasn’t been isolated. And THAT means no one has proved it exists.
And now, I’ve discovered ANOTHER key document. This one apparently formed the basis for the first PCR test aimed at detecting the COVID virus all over the world.
READ WHAT THIS STUDY SAYS. These quotes should be engraved in stone above the entrance to a museum dedicated to the history of medical fraud.
“We aimed to develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus material available.”
TRANSLATION: We want to develop a test to detect the new COVID virus without having the virus.
“Here we present a validated diagnostic workflow for 2019-nCoV, its design relying on close genetic relatedness of 2019-nCoV with SARS coronavirus, making use of synthetic nucleic acid technology.”
TRANSLATION: We HAVE developed a diagnostic test to detect the new COVID virus. We ASSUME this new virus is closely related to an older coronavirus. We ASSUME we know HOW it is related. We ASSUME, because we don’t have the new COVID virus. Therefore, all our assumptions are made out of nothing. Actually, we have no proof there is a new coronavirus.
“The workflow reliably detects 2019-nCoV, and further discriminates 2019-nCoV from SARS-CoV.”
TRANSLATION: Our new test to detect the new virus? We don’t have the new virus. We’ve never observed it. We can’t study it directly. There is no proof it exists. But we will use the test to detect it.
Those quotes from the study are astounding. A diagnostic test for the virus, but there is no virus. No standard against which to compare the reliability of the test.
The authors blithely assume they can somehow infer that the virus exists in the first place, without having an isolated specimen.
Then they assume they can understand the structure of the virus that isn’t there.
The virus isn’t there. It has NOT been isolated. It has NOT been separated out from other material. Therefore, it has not been observed and its existence has not been proved.
And yet, the test which these authors have developed is launched, all over the world, to detect that virus; to promote the unproven notion that there is a pandemic; to form the basis for counting COVID case numbers; and ultimately to justify all the lockdowns which have crashed the global economy and destroyed millions upon millions of lives.
A great deal of confusion has been created, because scientists are now talking about the “new virus” as if they understand its structure and sequence. No. They’ve INTERPRETED that genetic structure. And once they’ve made their interpretations, they gibber about what it means.
It’s like this. A man has a very thick steel vault. He clams there is a pile of treasure inside. But no one can open the door to the vault. People show up with all sorts of fancy instruments, and they make indirect measurements. They then issue very authoritative-sounding statements about what is inside the vault.
But no one can get in there. This is a magic vault, you see. You can’t drill into it. You can’t blow it up. But in its vicinity, all sorts of hustlers are gathered. And they PONTIFICATE. They BLOVIATE. They wave their credentials. Reporters interview them. Governments follow their recommendations.
And that’s all it is. It’s that kind of party.
There is also confusion about what the word “isolate” means, when it comes to viruses. SAYING you have isolated a virus doesn’t mean you have.
It may mean you THINK you have the virus inside a mess of material which contains many different genetic sequences and all manner of cellular debris and who knows what.
Some scientists will claim “a lesser amount of mess” entitles them to state they’ve “isolated” the virus.
Other scientists will claim that because they can grow, in a dish, what they BELIEVE to be the virus, this is “proof” that the virus exists.
They’re wrong.
Still other scientists will say that, in a dish in a lab, they “have the virus growing”, and they know it, because the virus is destroying certain cells in the soup in the dish. But in this soup, there are various added chemicals, and those chemicals could easily be doing the cell-killing.
So they are wrong, too.
As the late independent researcher David Crowe has written: “And the word ‘isolation’ has been so debased by virologists it means nothing (e.g. adding impure materials to a cell culture and seeing cell death is [as] ‘isolation’).”
This is why something called real-world experiments were introduced into science. Experiments that were forced out of the lab into the arena where actual humans live.
In my last article, I described exactly the kind of experiment that should have been initiated five minutes after scientists claimed there was an “outbreak in China.” It’s a large scale study involving humans who were diagnosed with the “epidemic illness.” Tissue samples would be taken from 500 of these patients and correctly analyzed via electron microscope photography.
But studies of that dimension and precision don’t interest scientists who live in the lab. Such studies are too dangerous. There is every chance that, in the harsh glare of sunlight, all their warnings about a vast pandemic will be shown to be false. False and ridiculous. Absurd. And insane.
These “experts” don’t want to take that chance.
So they fiddle and diddle in their labs, and they make wild claims based on nothing, on NO VIRUS.
For them, there is no such thing as NO VIRUS. There must always be a virus. They will build strings of thought that circle around and meet up and shake hands and justify themselves, BY DEFINITION.
When all is said and done, that is what they are playing at. “We make all the definitions, and therefore we can conclude anything we want to conclude. And call it science.”
That’s what’s going on.
I see the con and I’m pointing out the con.
I’m telling scientists who are honest to call it a con, too.
Empty out the house of modern virology; open the windows and let the fresh air in; and then we’ll be living in a far better world.
And, oh yes, prosecute these researchers who devised a test for the virus they never found. Prosecute them for crimes against humanity, and send them to prison.
Original video available at The HighWire BitChute & Brighteon channels.
As we mask our kids all day at school, keep them from interacting with others, and attempt to block them from every virus & bacteria, Del questions the physical toll lockdown restrictions have on our children’s immune system.
Johnson & Johnson Latest to Halt COVID-19 Vaccine Trial Over Unspecified Illness
Yet another high-profile Phase 3 vaccine trial has been temporarily halted after one of the participants developed a suspicious illness.
According to a report published Monday night by STAT News, Johnson & Johnson has informed participants and researchers that its 60,000-person trial would be temporarily paused as the company and the Data and Safety Monitoring Board, the organization overseeing all the US COVID-19 trials.
JNJ confirmed the pause when contacted by STAT, though it offered no details about the illness or the patient.
Contacted by STAT, J&J confirmed the study pause, saying it was due to “an unexplained illness in a study participant.”
The company declined to provide further details. “We must respect this participant’s privacy. We’re also learning more about this participant’s illness, and it’s important to have all the facts before we share additional information,” the company said in a statement.
According to STAT, the DSMB was convened late Monday evening to start looking into the case. J&J said that in cases like this, “it is not always immediately apparent” whether the participant who experienced an adverse event received the experimental vaccine, or a placebo.
Pauses like these aren’t uncommon in vaccine trials.
“If we do a study of 60,000 people, that is a small village,” the source said. “In a small village there are a lot of medical events that happen.”
But these trials are drawing more scrutiny ever since the AstraZeneca-Oxford trial was put on hold by regulators in the UK after a participant was sickened with symptoms of what was believed to be transverse myelitis, a serious spinal issue. Trials resumed in the UK, India and elsewhere days later, but in the US, an AZ trial remains on hold due to an unspecified issue. Both AZ and US regulators have been suspiciously tight-lipped.
Already, public health officials in the US, Europe and around the world are worried about waning confidence in the vaccine, with some surveys showing that roughly half the public would rather not take it.
In a research note published earlier, analysts at Goldman Sachs wrote that trust in the vaccine could be a serious barrier to its ultimate eradication. “We think that the biggest challenge to ultimately lowering the disease burden and virus circulation to very low levels will be convincing the broad population to take the vaccine. Our base case assumes such broad uptake but this will likely require a safe and very effective vaccine, trust in the approval and rollout process, no out-of -pocket costs, and effective public and community campaigns.”
JNJ is using an adenovirus vector, like several other top vaccine projects.
Original video available at The HighWire BitChute & Brighteon channels.
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light Lbry & Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video.]
As AstraZeneca’s vaccine trial adverse reactions are being investigated by the FDA, Moderna and Pfizer are now grabbing mainstream headlines for their vaccine side effects.
Bed-ridden trial participants, some with chills so bad they cracked a tooth, are openly speaking about second-dose warnings, informing the public that they’ll need to “toughen up” if they plan on taking the shot.
Jon Rappoport: The Virus That Isn’t There and the Vaccine That Doesn’t Work
Catherine Austin Fitts: The Fight For the Future | “Leveraged Buyout of the Planet” During This Orchestrated Global Disaster, Transhumanist Depopulation, Humanity as Livestock, Space Surveillance
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light BitChute, Lbry, Odysee & Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video.]
CATHERINE AUSTIN FITTS REVEALS SPACE SURVEILLANCE!
In this explosive Part 2 of a 3 part interview series, Dark Journalist Daniel Liszt welcomes back Former Assistant Secretary of HUD Catherine Austin Fitts.
Catherine has spent two decades tracking Missing Trillions from Government agencies including HUD and the Department of Defense.
TRANSHUMANIST AGENDA
Catherine goes deep on the Transhumanist Agenda promoted by the World Economic Forum and Big Tech, which she compares to “Livestock Management”.
She shows how their goal is to convert the world’s population into mind-controlled technology slaves and sheds light on a hidden system of economic and political control dominated by a parasitical group that is attempting to depopulate humanity.
Catherine reveals the covert agenda behind the massive surveillance infrastructure and the Secret Space Program that is being developed with public money.
Imagine! – Tomorrow, or one of these days, a gigantic earth or seaquake would shake the Atlantic Ocean or the Pacific, or god-forbid, a meteorite would hit one of these Great Seas – triggering a monster tsunami that would devastate most of the US East Coast – New York, Washington, all the way up to Boston and all the way down to Miami; as well as the Western European Coastline, including the UK; London under water, the Bretagne (Britany) flooded – and flood waters would reach all the way to Paris.
Or, imagine a similar scenario at the US Pacific Coast: San Francisco, Los Angeles, devastated and Baja California outright disappeared under gigantic tidal waves. No global warming. Just Mother Nature. The cosmic forces.
Or, in yet another scenario, imagine, one of Washington’s presumptuous warmongers would through a preemptive act of arrogant stupidity trigger a nuclear war… the worst of all situations.
What would happen?
Covid would be gone at once.
From one moment to the next. The, oh-so deadly “pandemic”- that never was – but we were made believe – the so heavily touted contagion that just devastated during the months past the entire world economy, caused unfathomable suffering, misery, death by desperation, death by famine – death by suicide and mass human auto-destruction, death by associated causes by the millions, hundreds of millions, billions perhaps – that worst of all viral diseases humanity has ever known and suffered from – would suddenly come to a shrieking halt.
A genius virus – so genius, must be man-made – that hits the entire world, summer or winter – 193 UN member countries – at once – coincidentally beginning with the tolling of the bells into the Decade of the 2020s, triggering a global lockdown of 193 nations exactly at the same time – mid-March 2020. That genius non-visible enemy induces all 193 UN member governments to impose the same measures to save humanity – face masks that deprive you from properly breathing your life-supporting oxygen, social distancing – that prevents sharing and socializing with friends, lockdown of everything, shops, workplaces, entertainment, even a walk in the park is forbidden – all at once.
Every one of the 193 UN members experiences simultaneously the same predicament – a humongous danger to humanity. An invisible enemy that hits at once all corners of the globe indiscriminately, the South, North, East and West. Nowhere to escape. Only the moon, but the moon is already controlled and monopolized by one of our planet’s richest billionaires.
The corrupt politicians and so-called leaders of all the 193 UN member countries, sadly, they are all puppets of a Higher Power, all of them had let themselves be bought or coerced into the diabolical game plan of total digital control of body and mind, using this dubious invisible enemy – a virus – with a monstrous fear-propaganda, with falsified and manufactured statistics, leading 7 billion people into believing that they are at risk of death, and that only a total lockdown, in other words, annihilation of the global economy, can save them. Never mind your life-support activity and livelihood.
A catastrophic event, hypothetical, for sure, as described before, and Covid is gone. As if it never was.
All coopted and/or coerced – or generously remunerated politicians of the 193 UN member nations, would now scramble to get into their readily prepared bunkers and other safety holes. Suddenly, they couldn’t care less about the deadly virus that threatens the rest of the world. They were never threatened themselves; they were always safe.
Occasionally to strengthen their covid propaganda the one or the other announced with big-big brouhaha how suddenly covid-sick he or she became. Ambulance- and airlifting them into emergency rooms, with hourly media reporting, is part of the game. The public is in sympathy and believing that if they are not obedient… this nasty virus may hit them too.
A few days later, the “cured-again” politician emerges from his or her emergency situation – a brilliant PR stint. And very successful. It helped the bought and betraying government officials increasing their handle on the necks of people, their repression, and heightening their tyranny a notch or two. Their egocentric selves would seek the highest points to save themselves from the tidal waves, or the deepest bunkers to protect themselves from the nuclear dust and radioactive fallout, from the all-burning and obliterating mushroom cloud.
And then there are leaders (sic-sic leaders), who this very moment boldly, non-apologetically and without any scruples and empathy for their frightened-to-death co-citizens, declare, “Many of us are pondering when things will return to normal. The short response is never.”
And Boris Johnson, the self-styled czar of the United Kingdom, continues, “We have been through too much frustration and hardship just to settle for the status quo ante – to think that life can go on as it was before the plague; and it will not… We are resolving not to go back to 2019.”
Mr. BoJo shamelessly quotes from the infamous and diabolical book, ‘Covid-19: The Great Reset’, by Klaus Schwab, founder and President of the WEF – World Economic Forum, as reported today, 8 October by RT. The Great Reset is a disaster foretold – see this and this.
The 8th of October 2020, may be just a short time away from the hypothetical Blast of Nature, that would make Covid go away for good and forever – and would obliterate the UK czar’s and WEF’s dreams.
All those mediocre and outright immoral politicians have known all the time and know today, that the luciferian game they are playing is against the very people of their countries they were elected by. Can you even call this worthless lot ‘criminal’? Doubtful. Criminal requires some kind of value. These abject individuals have none. They know they are betraying the people, their co-citizens, their compatriots, with the masquerades, with the social distancing, with the segregation into solidary confinement. They know they are killing “their people” with fear and constant, everyday fear.
They know that all of what they are propagating and lying about to make you scared, is but a miserable farce, a scam. They know the fear they impose day after day, hour after hour, makes you vulnerable to diseases, all kind of diseases, because fear kills your immune system. These masters of evil do it anyway – and coopt their aids, doctors, scientists, by threatening them, directly or indirectly with job loss, with loss of reputation — and yes, they have families and many oblige for the sake of their families.
Not all. Thanks-god for the brave who come forward in Germany, Belgium, Austria, the Netherlands, Italy, Spain, the United States – and from ever more countries, to speak the truth. Speaking Truth to Power can never be defeated.
All these high-ranking government officials, the sold-and bought ones, those without conscience, those that have sold you, who would also sell their mothers for the sake of being rewarded with positive recognition by the little dirty, devoid-of-any-ethics elite; an elite, who just want to control the world, its resources. And, not to forget – an elite who assume for themselves the right to dispose of how many people they deem worthy to live on this Blue Marvelous Planet. The masters of eugenics.
Before the hypothetical catastrophe hit, this little elite was able to buy the entire United Nations system, so as to have all 193 members, and countless UN agencies, with the World Health Organization (WHO) as their forerunner. They adopt the same cruel and unbelievable measures against a virus, that may not be more than a flu-virus, called Covid-19, a derivation of the SARS-Cov-2 virus – a virus that is no threat at all, and least a pandemic. But with the power of WHO and her billion-dollar-profit interest groups, a pandemic was declared on 11 March 2020. No justification, and no questions asked.
Covid is a man-made virus, part of a bio-war arsenal, that can at will be mutated to become fiercer. Indeed, it may most likely already exist in such mutated strings and invade different parts of the world in various forms of severity.
Now, with Covid gone – hypothetically, that is – these un-people, at the helm of the 193 UN members, as they are not deserving being called people, these 193 heads of states and their obeying lackeys, they are now fighting for themselves. The vaccines that they so cruelly were coercing you to accept – or else; or fearing you into wanting – these meekly beings, are now at the mercy of nature. And so, would be the arrogant little politician, who unwittingly triggered the hypothetical nuclear blast, that, in turn triggered other blasts of worldwide dimension, catastrophe no end. – But, but honestly – who is to blame? Of course, Russia and China.
These covid-king politicians couldn’t care less about you. These now angst-ridden politicians, once seemingly preoccupied for your health, who insistently told you to get covid-inoculated to save your skin, they so easily abandon you to safe their own skin.
They are now so adamant to seek refuge — from nature. They let covid go.
Nature may know no mercy.
Not with them, not with the rest of us, Global Northerners, who have been sleepwalking like zombies in pre-lockstep conditions, despite the numerous warnings: Decades, if not more, of preparation, the 2010 Rockefeller Report, numerous WHO commissioned preparatory reports, then Event 201, that struck on 18 October 2019 in NYC, in full sight, just a few weeks before the well-planned worldwide “outbreak of the fierce covid disease”.
We were and are being clouded by cognitive dissonance – to remain voicelessly in our comfort zones. Yes, I’m talking about us in the Global North, or we, westerners, who are so much superior to those poor people in the Global South, those that we in the Global North have exploited and ransacked for centuries, have stolen their resources and deprived them of education and of a decent livelihood.
We of the Global North, we who have obeyed the 193 crooked and dishonest heads of states and their obedient servants, their bought medical crews, we too, are now exposed without mercy to this – hypothetical – natural catastrophe – or nuclear blast – whatever fate may hypothetically have in store for us. We too deserve it.
For the grace of being recognized by our immoral leaders, puppets to a higher force, a deep state, a dark state or a non-state monster, for that recognition, for that egocentric flaw of being accepted by the powerful, we have closed our eyes and let the devil walk right over us – and into us.
Covid is gone. For good. Never came back.
Hypothetically, the world as we knew it, is gone. By Nature. Mother Earth’s cleansing. Reset, yes, but not WEF-style. So easy. Universal Reset, caused by the real forces of Mother Universe – not by our lousy, man-made, bribe-prone fiat money.
Covid is gone – from one instant to the next. That shows once more how ignorant, selfish, and unconscious we are; unconscious of our fellow human beings, those from the Global South, whom we deprived of their wealth and education, and whom, to this day, we colonize with debt and by using them as guinea pigs, for example, to test all kinds of dangerous and controversial medication, including vaccines. In their wisdom as victims they may understand sooner than we do, what the 193 tyrannical governments are up to.
Hail to Covid. It may bring us the Light by suddenly disappearing – compliments of Nature’s Wrath.
Peter Koenig is an economist and geopolitical analyst. He is also a water resources and environmental specialist. He worked for over 30 years with the World Bank and the World Health Organization around the world in the fields of environment and water. He lectures at universities in the US, Europe and South America. He writes regularly for online journals such as Global Research; ICH; New Eastern Outlook (NEO) and more. He is the author of Implosion – An Economic Thriller about War, Environmental Destruction and Corporate Greed – fiction based on facts and on 30 years of World Bank experience around the globe. He is also a co-author of The World Order and Revolution! – Essays from the Resistance. He is a Research Associate of the Centre for Research on Globalization.
Electroconvulsive Therapy on Autistic Youth Unjustified and Dangerous
The 1975 film, “One Flew Over the Cuckoo’s Nest,” directed the public’s attention to a 1930s-era procedure termed lobotomy: a brain-altering intervention described by one of its leading proponents, Dr. Walter Freeman, as “soul surgery.” Lobotomies were performed on thousands of American adults, and some children, well into the 1980s before being somewhat (but not entirely) retired.
The procedure acquired the nickname “ice pick lobotomy” in the 1940s and 1950s because practitioners used a “pick-like instrument” to reach through the eye sockets to sever nerve connections in the brain, after first “subduing” patients with electroshock treatments. “One Flew Over the Cuckoo’s Nest” portrayed the lobotomy as a crude tool to “stabilize” personality and eliminate “excess emotion” — with often drastic and sometimes fatal results.
The late 1930s were a heyday for experimenting on the brains of those pronounced schizophrenic, bipolar or severely depressed — or as psychiatrist and psychiatric whistleblower Dr. Peter Breggin puts it, for seeking out “new ways to inflict controlled damage on [a] patient’s brain without completely destroying its function.” Shortly after the birth of lobotomy, Italian psychiatrists focused on the procedure’s electroshock component, and began promoting electrically induced seizures as a psychiatric intervention.
Eighty years later, the use of electroconvulsive therapy (ECT) is not only commonly used to treat psychosis and other illnesses, but is a disturbingly acceptable “off-label” option for expanded indications like severe autism. Governed by the hypothesis that intense seizures can have therapeutic effects (a strange proposition for the many individuals with autism who already suffer from intractable seizures), the aim of ECT is to pass electricity through the brain to induce a generalized epileptic-like seizure.
Proponents of ECT for autistic youth and depressed adults argue that “modern-day ECT is a far cry from the old methods that earned ECT its sinister reputation.” Those “old methods” produced violent seizures which caused the body “to thrash with a force great enough to break bones.” But modern ECT’s elicitation of a temporary coma and a flatlining of brain waves hardly sounds more reassuring.
A 2006 review in Advances in Psychiatric Treatment stated that “Newer methods of ECT have not resulted in an appreciable decrease in adverse effects.” Moreover, while ECT fans tout 21st century-ECT as being highly “controlled” and “refined,” they also admit “the optimal seizure duration remains unclear” and that they do not really understand how ECT works.
‘Side effects’ — matter of perspective?
Neurosurgeons admit that psychiatric brain interventions represent an “ethical quagmire.” Yet undergirding the practice of ECT is the persistent conviction that “psychiatric diseases can be treated by the selective destruction of healthy brain tissue.” For this reason — and because they are institutionally and professionally invested in ECT’s promulgation — proponents casually dismiss known ECT outcomes, such as confusion and memory loss, as mere “side effects.”
Not everyone agrees. Dr. Peter Breggin, a Harvard-trained psychiatrist, explains that because ECT works by intentionally damaging the brain, its effects are comparable to a traumatic brain injury. After as few as one to three ECT sessions, the damage can not only provoke physical symptoms such as headaches and nausea, but can also permanently impair memory and concentration, and “demolish” the sense of self. Breggin summarizes:
“After several routine ECTs, the damaged person becomes increasingly apathetic, indifferent, unable to feel genuine emotions, and even robotic. Memory loss and confusion worsen. This helpless individual becomes unable to voice distress or complaints, and becomes docile and manageable. ECT doctors mistakenly call this an improvement but it indicates severe and disabling brain injury.”
According to other critics, “Any claim that ECT does not cause brain damage ignores basic electrical science.” A bioengineering expert points out that ECT is capable of prompting brain cell effects including dysfunction, temporary injury, permanent damage cell death and, as a result of the pulsing nature of the voltage, “a jackhammer effect that can tear holes in cell walls … leading to the alteration or destruction of cell membranes.”
Echoing the comparison of lobotomy to “soul surgery,” Breggin states that the targeting of vital regions of the brain has far-reaching implications:
“The electricity not only travels through the frontal lobes — that’s the seat of intelligence and thoughtfulness and creativity and judgment — it also goes through the temporal lobes — the seat of memory. You are damaging the very expression of the personality, the character, the individuality and even, if you believe in it, the expression of the soul.”
Autism — addressing underlying medical conditions yields better outcomes than ECT
Labeling autism as a psychiatric illness may be one of the most tragic wrong turns ever taken in modern medicine. For at least two decades, parents, clinicians and researchers have pushed back against this diagnostic pigeon-holing, showing how “autism” is an umbrella term for a “highly diverse set of abnormalities affecting multiple systems of the body.”
Moreover, critics say these systems, which manage metabolic, mitochondrial, immunological, gastrointestinal and neurological functions,“interact in complex and highly interdependent ways.”
In July 2013, Harvard physician Dr. Timothy Buie presented case studies (timestamp 1:08) to the Interagency Autism Coordinating Committee (IACC), a federal advisory committee on autism.The studies illustrate how autism behaviors often labeled as psychological have a medical underpinning. Sharing video footage of two young people experiencing acute gastrointestinal distress and pain, Buie emphasized that “inflammation anywhere in the body could be a trigger for brain effects.” Even more crucially, according to Buie, when the underlying medical problems are appropriately addressed, problem behaviors such as self-injury can resolve “completely.”
In short, recognizing that the brain and nervous system are interconnected with other body systems opens up the possibility for tackling some of autism’s core symptoms, thus vastly improving quality of life.
Sadly, the IACC presentation that immediately followed Buie’s talk reflected a different approach, one that didn’t address the underlying medical factors (such as chronic pain or sensory onslaught) that might provoke self-injury. Dr. Lee Wachtel, a leading ECT proponent at the Johns Hopkins School of Medicine, instead presented ECT as a means of halting the challenging behaviors without addressing any of the underlying issues.
Wachtel continues to promote ECT. In a 2018 article in Psychiatric Times, Wachtel advocated for ECT specifically for adolescents with autism and self-injurious behavior. Comparing ECT to renal dialysis, Wachtel spelled out the aggressive treatment protocol, which involves not just electrode stimulation, but also general anesthesia, muscle relaxants (to avoid damaging convulsions) and continuous oxygenation — administered as often as several times a week initially and every five to ten days for “maintenance,” amounting to hundreds of sessions over time.
Other physicians using ECT with younger patients agree on the need for ongoing maintenance sessions to retain “clinical stability.” One ECT promoter at Johns Hopkins has acknowledged that when ECT is used in autistic patients to curtail self-injurious behaviors, the patients “can’t be tapered well off of ECT” and require ongoing treatments. He adds, “nobody really knows the long-term effects of ECT at that frequency and started at such a young age.”
Time to ban, not promote, ECT for children and teenagers
When doctors use ECT with autistic children and teenagers they are administering the procedure off-label. That’s because ECT devices are not FDA-approved for autism. The insurer Aetna considers ECT “experimental and investigational” for the treatment of autism spectrum disorders.
In the 1970s, the FDA classified ECT devices as high-risk Class III devices. But beginning in 2009, the regulatory agency launched a process to reclassify them as lower-risk Class II devices. Despite a majority (79%) of public and expert comments being strongly opposed, the FDA went ahead with a Class II classification in late 2018, including for teenagers with catatonia (a frequent feature of autism), bipolar disorder and major depression.
Breggin has, since 1979, heroically advocated for a total ban on ECT, a practice he characterizes as both dangerous and abusive. Breggin strongly favors abolishing the practice in minors, noting that long-term follow-up studies of ECT patients now definitively document “massive harm to the brain and mind.”
Unfortunately, as the FDA reclassification illustrates, the U.S. is moving in the wrong direction. Even though the World Health Organization stated in a 2005 resource book on mental health that there are “no indications for the use of ECT on minors, and hence this should be prohibited through legislation” (p. 64), the American Academy of Child and Adolescent Psychiatry, around the same time, published parameters for ECT’s use in adolescents. Unfortunately, these guidelines are often used to justify the increasing use of ECT in younger populations.
Wachtel and colleagues dismiss objections to ECT’s use in children as being the result of uninformed “resistance and stigma.” But those who have studied the procedure’s long-term risks, like Breggin and other critics, view ECT as barbaric. As one UK professor stated, “Common sense says you don’t put a high voltage of electricity through children’s brains.” A mental health professional in Australia, critical of the “dumbing down” of psychiatry as a profession, said:
“[W]hen [today’s psychiatrists] get a complicated patient, they don’t actually know what to do. […] Thus, they very quickly reach the limit of their skill set and have no option but to reach for the electrodes. A psychiatrist who says, ‘You need ECT’ is really only saying, ‘I don’t know what else to do.’”
This article is the first in a series about electroconvulsive therapy.
COVID: The Virus That Isn’t There: The Root Fraud Exposed
This is a follow-up to yesterday’s article, in which I exposed the fact that the CDC does not have the COVID coronavirus in its possession, because it is “unavailable.” Their word, not mine.
The CDC is admitting the virus hasn’t been isolated. In other words, its existence is unproven.
You need to realize the CDC, during its own published confession (see below), is discussing this explosive situation in the context of instructing the world how to perform the PCR test.
The test to detect a virus that isn’t there.
This would be on the order of NASA issuing a guide for navigating a fleet of ships to a planet whose existence has not been established—and the population of the whole world is going to board those ships for the voyage.
The CDC is saying: here is how you detect the virus in a human, here is the test on which we’re going to rely, here is the test on the basis of which we’re going to identify all case numbers and demand all lockdowns—except we don’t have the virus.
Why don’t they have it?
Because they can’t isolate it. That’s obvious.
If they could isolate it, they would.
Let’s not tap dance around this central fact. Let’s not make excuses for the CDC. They have a problem the size of Jupiter. It’s their problem, not ours. But they’re foisting their problem on us, in the form of a STORY ABOUT A PANDEMIC. AND ALL THE LOCKDOWNS THAT FLOW FROM THE STORY.
To say this is unacceptable is a vast understatement. The CDC is committing a crime that has no bounds.
For months, I’ve been writing about the “missing virus” and the studies that should be done to prove it exists—real-world studies that have never been done and will never be done. Now, here is the smoking gun.
I’m aware that many scientists and doctors, who are otherwise exposing the pandemic as a fraud on legitimate grounds, don’t want to touch what I’m revealing here. I would remind them that, months ago, when some of us were already exposing the PCR test as unreliable and useless and deceptive, THAT ISSUE was too hot to touch. But now it isn’t.
The issue of the existence of the SARS-CoV-2 virus may seem as if it’s too hot, but it isn’t. It’s time to launch a full-on attack. Immediately.
The truth is only bitter for those who are hiding it.
I’m also aware there are people who have been building scenarios about how the virus is “activated.” Certain frequencies wake it up, and so on. Well, the question is: WHAT VIRUS? THE ONE THAT ISN’T THERE?
Still other people would say, “Then what are all these scientists sequencing in their labs, if it’s not the virus?” Again, not our problem. They might start with a piece of RNA, and then claim, without proof, it’s part of SARS-CoV-2; and they go to work on it. They claim anything they want to. It’s not science.
If a mechanic says he has a piece of a fender from a car that has never been seen before; if he claims he knows the car exists; but he can’t show you the car; are you going to buy his story? Are you going to invest your life-savings and life-savings of your family and friends in this car he admits is “unavailable?” Are you going to invest and go broke and sit in your home and wear a mask and keep your distance from other people and close your business and declare bankruptcy? Are you going to consent to that?
Another question that arises: if the virus is missing and has never been isolated, has never been proved to exist, what are they putting in the COVID vaccine? That’s a question that should be answered by law-enforcement agencies raiding many facilities and seizing materials and finding honest scientists who will discover what is really in the COVID vaccine brews. Waiting for that to happen…the sun could go dark first. In the meantime, do you want to take the shot in the arm?
Some people have claimed there are “animal models” which prove the coronavirus exists and is harmful, because the animals become sick, when they are “injected with the virus.” This is incorrect on two counts.
First, the animal models are supposed to progress through various species, until they arrive at animals that most closely resemble humans; chimps. The animal models being cited are mice or hamsters, which are very, very low on the totem pole.
Second, what are these mice being injected with? It’s supposed to be pure virus. But instead, it’s a soup which contains all sorts of material, including chemicals. The chemicals could be causing the animals to become ill.
Here is my breaking story about the virus that isn’t there, from yesterday:
Buried deep in the document, on page 39, in a section titled, “Performance Characteristics,” we have this: “Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
The key phrase there is: “Since no quantified virus isolates of the 2019-nCoV are currently available…”
Every object that exists can be quantified, which is to say, measured. The use of the term “quantified” in that phrase means: the CDC has no measurable amount of the virus, because it is unavailable. THE CDC HAS NO VIRUS.
A further tip-off is the use of the word ‘isolates.” This means NO ISOLATED VIRUS IS AVAILABLE.
Another way to put it: NO ONE HAS AN ISOLATED SPECIMEN OF THE COVID-19 VIRUS.
NO ONE HAS ISOLATED THE COVID-19 VIRUS.
THEREFORE, NO ONE HAS PROVED THAT IT EXISTS.
As if this were not enough of a revelation to shock the world, the CDC goes on to say they are presenting a diagnostic PCR test to detect the virus-that-hasn’t-been-isolated…and the test is looking for RNA which is PRESUMED to come from the virus that hasn’t been proved to exist.
And using this test, the CDC and every other public health agency in the world are counting COVID cases and deaths…and governments have instituted lockdowns and economic devastation using those case and death numbers as justification.
If people believe “you have the virus but it is not available,” and you have the virus except it is buried within other material and hasn’t been extracted and purified and isolated, these people believe the moon is made of green cheese.
This is like saying. “We have the 20 trillion dollars, they are contained somewhere in our myriad accounts, we just don’t know where.” If you don’t know where, you don’t know you have the money.
“The car keys are somewhere in the house. We just don’t where.” Really? If you don’t know where, you don’t know the keys are in the house.
“The missing cruise missile is somewhere in the arsenal, we just don’t where.” No. If you don’t know where, you don’t know the missile is in the arsenal.
“The COVID-19 virus is somewhere in the material we have—we just haven’t removed it from that material. But we know what it is and we’ve identified it and we know its structure.” NO YOU DON’T. YOU ASSUME THAT.
Science is not assumptions.
“But…but…there is a study which says a few researchers in a lab isolated the virus…”
They say they did. But in July, the CDC is saying no virus is available. I guess that means trucks were not available to bring the virus from that lab to the CDC. The trucks were out of gas. It was raining. The bridge was washed out. The trucks were in the shop. Joe, the driver, couldn’t find his mask, and he didn’t want to leave home without it…
Science is not assumptions.
The pandemic is a fraud, down to the root of the poisonous tree.
Medical Nanobots Designed to Track & “Save” You During Times of Epidemic
From a research paper titled “Nanorobot Hardware Architecture for Medical Defense”
ISSN 1424-8220
www.mdpi.org/sensors
Sensors 2008, 8, 2932-2958; DOI: 10.3390/s8052932
Published May 6, 2008
[As a service to protect truth from censorship, mirrored copies of this video are available at Truth Comes to Light BitChute, Lbry, Odysee & Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video.]
Bill Gates on Track to Grow His Fortune Through Foundation’s Ties to Vaccine Makers
A telling piece in The Nation this week reports some of the conflicts of interest the Bill & Melinda Gates Foundation holds in the world’s quest for a COVID-19 vaccine. According to the article, the foundation’s investments in companies working to develop COVID-19 vaccines put Gates “in a position to potentially reap considerable financial gains from the COVID-19 pandemic.”
The Nation cites the example of the foundation’s $40 million stake in CureVac, a German pharmaceutical company whose stock soared 400% after going public in August. A similar Nation article from earlier this year reported the Gates Foundation also holds corporate stocks and bonds in drug companies Merck, GlaxoSmithKline, Novartis and Sanofi, and the foundation gives these same companies charitable grants for projects like developing new drugs.
AstraZeneca, the British pharmaceutical company that gained an exclusive license to control the COVID-19 vaccine produced by Oxford University research, is considered a frontrunner in the vaccine race. According to The Nation: “Gates himself described his foundation as intimately involved in the partnership between AstraZeneca and the University of Oxford.” Gates had the leverage to push the university … because the foundation is one of the founders and largest funders of the Coalition for Epidemic Preparedness Innovations, which in turn funds the University of Oxford’s vaccine development (to the tune of some $384 million).”
AstraZeneca also received $750 million from the Global Alliance for Vaccines and Immunization, an organization the Gates Foundation helped set up and continues to fund to this day. Despite questions on the safety of the AstraZeneca vaccine, governments worldwide have already bought it, on the taxpayers dime.
Also notable is the Gates Foundation’s grants, totaling $20 million, to Moderna, whose vaccine has also been described as a COVID-19 frontrunner. The foundation has a “global health project framework agreement” with the company, agreeing to give it up to $100 million to develop its mRNA technology, in exchange for receiving “certain non-exclusive licenses,” which have yet to be publicly specified.
Even with all this, Gates doesn’t publicly disclose his conflicts of interest when appearing on TV as an expert on COVID-19. And, as The Nation reports, when Gates wrote an article in the New England Journal of Medicine, he simply listed his conflicts of interest as “numerous.” According to Forbes, Gates has seen his personal net worth increase by more than $10 billion since the onset of the pandemic.
Despite the Gates Foundation’s candid declaration to pursue “mutually beneficial opportunities” with vaccine manufacturers, it is rare to find reporting in mainstream media on the foundation’s conflicts of interest. This may be because the foundation funds a number of major media outlets, including NPR, BBC, ABC and Al Jazeera, as well as publications like The Daily Telegraph and the Financial Times. The Guardian’s entire “Global Development” section is made possible through a partnership with the Gates Foundation.
The foundation also invests in journalism training programs. According to the Seattle Times, “experts coached in Gates-funded programs write columns that appear in media outlets from The New York Times to the Huffington Post, while digital portals blur the line between journalism and spin.”
According to Robert F. Kennedy, Jr., chairman of Children’s Health Defense, The Nation’s exposé “is a refreshing change for those searching for critical reporting on the self-declared ‘biggest funder of vaccines in the world.’”
Jeremy Loffredo is a reporter for Children’s Health Defense.
The Smoking Gun: Where Is the Coronavirus? The CDC Says It Isn’t Available.
Buried deep in the document, on page 39, in a section titled, “Performance Characteristics,” we have this: “Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
The key phrase there is: “Since no quantified virus isolates of the 2019-nCoV are currently available…”
Every object that exists can be quantified, which is to say, measured. The use of the term “quantified” in that phrase means: the CDC has no measurable amount of the virus, because it is unavailable. THE CDC HAS NO VIRUS.
A further tip-off is the use of the word ‘isolates.” This means NO ISOLATED VIRUS IS AVAILABLE.
Another way to put it: NO ONE HAS AN ISOLATED SPECIMEN OF THE COVID-19 VIRUS.
NO ONE HAS ISOLATED THE COVID-19 VIRUS.
THEREFORE, NO ONE HAS PROVED THAT IT EXISTS.
As if this were not enough of a revelation to shock the world, the CDC goes on to say they are presenting a diagnostic PCR test to detect the virus-that-hasn’t-been-isolated…and the test is looking for RNA which is PRESUMED to come from the virus that hasn’t been proved to exist.
And using this test, the CDC and every other public health agency in the world are counting COVID cases and deaths…and governments have instituted lockdowns and economic devastation using those case and death numbers as justification.
If people believe “you have the virus but it is not available,” and you have the virus except it is buried within other material and hasn’t been extracted and purified and isolated, these people believe the moon is made of green cheese.
This is like saying. “We have the 20 trillion dollars, they are contained somewhere in our myriad accounts, we just don’t know where.” If you don’t know where, you don’t know you have the money.
“The car keys are somewhere in the house. We just don’t where.” Really? If you don’t know where, you don’t know the keys are in the house.
“The missing cruise missile is somewhere in the arsenal, we just don’t where.” No. If you don’t know where, you don’t know the missile is in the arsenal.
“The COVID-19 virus is somewhere in the material we have—we just haven’t removed it from that material. But we know what it is and we’ve identified it and we know its structure.” NO YOU DON’T. YOU ASSUME THAT.
Science is not assumptions.
“But…but…there is a study which says a few researchers in a lab isolated the virus…”
They say they did. But in July, the CDC is saying no virus is available. I guess that means trucks were not available to bring the virus from that lab to the CDC. The trucks were out of gas. It was raining. The bridge was washed out. The trucks were in the shop. Joe, the driver, couldn’t find his mask, and he didn’t want to leave home without it…
Science is not assumptions.
The pandemic is a fraud, down to the root of the poisonous tree.