Norway upped the number of deaths under investigation, from 23 last week to 33, while in Germany, health officials said they are investigating 10 deaths that occurred among elderly patients who received the COVID vaccine.
Norway health officials said last week they were investigating the deaths of 23 elderly people who died shortly after receiving the vaccine, and had confirmed 13 of those were directly related to the vaccine.
Today, Bloomberg reported that the number of deaths under investigation in Norway had risen to 33 and that all had occurred in people ranging from age 75 to 80. According to Bloomberg, Camilla Stoltenberg, head of the Norwegian Institute of Public Health, said at a press conference today:
“It is important to remember that about 45 people die every day in nursing homes in Norway, so it is not a given that this represents any excess mortality or that there is a causal connection.”
The Norwegian Medicines Agency previously told Bloomberg that all of the deaths occurred in people who received the Pfizer-BioNTech vaccine, which until Friday was the only COVID vaccine approved for use in Norway.
The Norwegian Institute of Public Health, which had originally prioritized the elderly for the vaccine, has since revised its advice to urge more caution when vaccinating the elderly, especially those with underlying conditions.
The institute told Bloomberg that “for those with the most severe frailty, even relatively mild vaccine side effects can have serious consequences. For those who have a very short remaining life span anyway, the benefit of the vaccine may be marginal or irrelevant.”
The Institute also admitted to Global Times that the clinical trials that resulted in emergency approval of the vaccine included “very few people over the age of 85,” but added “we assume that the side effects will largely be the same in the elderly as in those over 65 years of age.”
According to the Global Times, a Beijing-based immunologist who requested anonymity said the mRNA vaccines had not proven safe for large-scale use or for preventing infectious diseases. Noting that people over 80 have weaker immune systems, he said they should not receive the vaccine, but instead should take medicines to improve their immune systems.
Meanwhile, The BMJ and other news outlets reported last week that in Germany, the Paul Ehrlich Institute is investigating 10 deaths in people ranging in age from 79 to 93 who died shortly after receiving the COVID vaccine.
U.S. health officials continue to push COVID vaccinations in nursing homes, despite growing resistance among nursing home employees to take the vaccine.
So far, there’s no word of any investigation into the deaths of 29 elderly people at a nursing home in New York. According to a Jan. 9 news report from Syracuse.com, a single nursing home in upstate New York vaccinated 193 residents beginning on Dec. 22 and subsequently reported 24 deaths within the span of a couple of weeks.
The facility attributed the deaths to a COVID-19 “outbreak,” even though there had been no COVID-19 deaths in any nursing homes in the entire county “until the first three deaths … were reported Dec. 29.”
Florida health officials and the U.S. Centers for Disease Control and Prevention are investigating the death of a 56-year-old doctor who died of a rare autoimmune disease 15 days after getting the Pfizer vaccine. A Johns Hopkins scientist told the New York Times it was a “medical certainty” that the death was related to Pfizer’s vaccine.
The U.S. Food and Drug Administration is investigating numerous severe allergic reactions, including anaphylaxis, in healthcare workers who received the vaccine.
Sunday night, California health officials called for a pause on the use of a huge batch of Moderna’s COVID vaccine due to its ”higher-than-usual number of possible allergic reactions.” As The Defender reported this morning, California’s top epidemiologist Dr. Erica S. Pan is recommending providers pause the administration of lot ‘041L20A’ of the Moderna COVID vaccine.
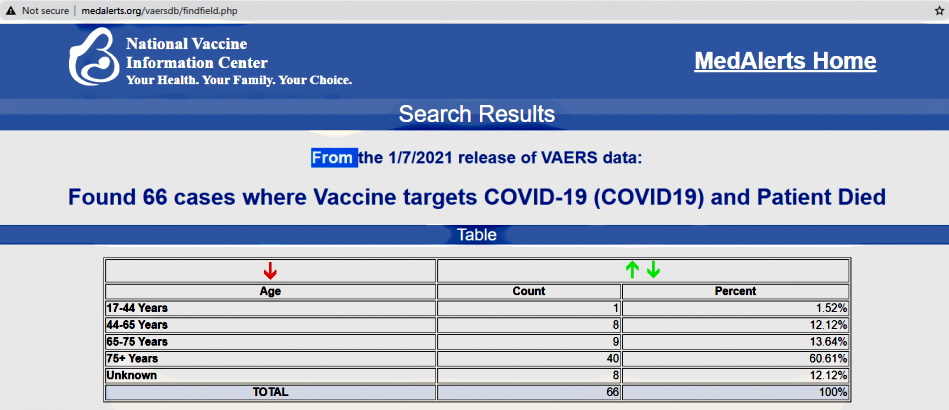
According to the latest figures, updated Jan. 7, from the Vaccine Adverse Event Reporting System (VAERS), 66 deaths have been reported in the U.S. as being possibly related to a COVID vaccine. It’s estimated that only 1% of vaccine injuries are reported to VAERS.
Anyone who suspects an injury or death related to the COVID vaccine, or any vaccine, can go to the VAERS website and file a report.
Coffey County, Kansas, Health Department Nurses Refuse to Give COVID-19 Vaccines
Coffee County in Kansas has roughly 8,500 residents, but they won’t be getting their COVID-19 shots from the county health department’s four nurses.
Department chief Lindsay Payer and her staffers have opted out of giving the injections because they have doubts about the safety of the Moderna vaccine, which the county is offering, local TV station WIBW reported.
Payer told WIBW that her employees made up their own minds and “not without considerable thought.” The county will hire at least one outside nurse, who will be paid with COVID-19 funds.
“I will tell you we will have to contract staff…because my staff is not comfortable with that. It’s a new technology. We’ve never seen it before. It was only studied in 45 people before it was approved…,” Payer said.
“It’s somewhat discomforting to a nurse who has to put that in people’s bodies.”
In December, 3,916 COVID vaccine-related adverse events, including 13 deaths, were reported to VAERS. As more adverse events — ranging from life-threatening anaphylaxis to death — occur, it will be tougher to “sell” the experimental injections.
By Jan. 11, counting China and Russia, 43 countries had administered at least 26 million doses of vaccine — especially Pfizer’s — with far more ambitious plans for the coming year. The companies’ global delivery targets for 2021 include two billion Pfizer/BioNTech doses and at least 600 million Moderna shots.
Drawing on the tried-and-true marketing technique of drumming up the “illusion of scarcity” to “accelerate demand,” U.S. officials have been attempting to direct the public’s attention to the concocted drama of vaccine supply shortages and a slower-than-expected rollout.
However, as the early warning signs already apparent during clinical trials begin to translate into serious adverse reactions on a wider scale, officials now face a new public relations challenge — that of “managing expectations” to ensure population willingness to take the vaccine.
As more people hear about adverse events, and more adverse events occur — ranging from life-threatening anaphylaxis and emergency room visits to brain inflammation and death — “selling” the experimental injections may become an increasingly uphill battle.
Deaths … so far
In the U.S., the primary mechanism for reporting adverse reactions is the Vaccine Adverse Event Reporting System (VAERS), a flawed passive surveillance system that relies on the willingness and ability of parents and professionals to submit reports voluntarily.
As Children’s Health Defense Chairman Robert F. Kennedy, Jr. wrote on Dec. 18, 2020 to the co-chair of the new COVID-19 Advisory Board, VAERS has been an abject failure, with fewer than 1% of adverse events ever reported, according to a 2010 federal study.
Given the abysmal track record of VAERS in capturing serious adverse events, it is noteworthy that 13 deaths — a subset of 3,916 total adverse events reported following COVID-19 vaccination — had already been recorded by the system by the end of December (as per the MedAlerts search engine).
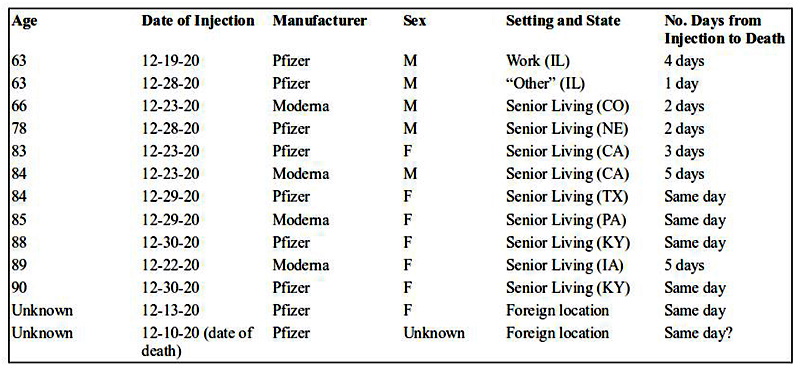
Nine of the deaths followed the Pfizer vaccine and four followed the Moderna shot (see table below). Nearly all of the deceased were institutionalized (primarily in nursing homes), although one 63-year-old male received the injection at work.
Five (and possibly six) of the deaths occurred on the same day as vaccination, all in women and sometimes within 60 to 90 minutes of the injection — and without any “immediate adverse reaction” having been observed.
The reports describe outcomes ranging from “foaming at the mouth” to “massive heart attacks.” Three of the deceased were in their early to mid-60s.
The write-ups that accompany VAERS reports furnish details about these sad fatalities, including the astonishing fact that some of the deceased had actually experienced and recovered from COVID-19 (raising questions about why they were vaccinated).
The write-ups also illustrate the subtle pressure to attribute the cause of death to something other than COVID-19 vaccination. For example, a grandchild who submitted a report wrote, “My grandmother [age 85] died a few hours after receiving the moderna covid vaccine booster 1. While I don’t expect that the events are related, the treating hospital did not acknowledge this and I wanted to be sure a report was made.”
A nursing home submitting a report on behalf of an 89-year-old who died five days after receiving the Moderna injection likewise wrote, “Due to proximity of vaccination we felt we should report the death, even though it is not believed to be related.”
And when a 78-year-old died two days after the Pfizer shot, the report simply stated, “no adverse events and no issues yesterday; Death today … (unknown if related – Administrator marked as natural causes).”
The 13 deaths communicated to VAERS do not include any deaths in the state of New York. However, a disturbing news report from Syracuse.com suggests that COVID-19 vaccines could be linked to a shocking number of additional deaths in the elderly in that state.
According to the news account, a single nursing home in upstate New York vaccinated 193 residents beginning on Dec. 22 and subsequently reported 24 deaths within the span of a couple of weeks. Although the facility has attributed the deaths to a COVID-19 “outbreak,” there had been no COVID-19 deaths in any nursing homes in the entire county “until the first three deaths … were reported Dec. 29.”
Pointing out that 24 deaths among 193 vaccinated residents equates to a 12.4% mortality rate, one observer notes that this reflects a “124-fold increase in mortality over and above the COVID-19 death rate for the population at large.”
Another compelling source of data about deaths following receipt of the experimental Pfizer/BioNTech shot comes from a growing number of incidents being reported from Israel and Europe:
Israel: Four individuals die “shortly after receiving the vaccination,” including two elderly men, aged 75 and 88, who experience apparent heart attacks two to three hours post-Pfizer-vaccine.
Norway: Two nursing home residents die within “a few days” of Pfizer COVID-19 vaccination.
Portugal: Health worker Sonia Acevedo, 41-year-old mother of two, dies suddenly two days after receiving the Pfizer injection.
Sweden: An elderly man, age 85, dies of a heart attack one day after receiving the Pfizer vaccine.
Switzerland: An elderly man, age 91, dies not long after getting the Pfizer shot.
Finally, in early January, news outlets, including The Defender, also described the tragic U.S. case involving Miami obstetrician-gynecologist Gregory Michael, who at age 56 died within two weeks of receiving the Pfizer vaccine — with the cause of death attributed to a “highly unusual clinical case of severe [immune] thrombocytopenia” (ITP).
ITP is considered a Type II “hypersensitivity reaction” (“immune responses that are exaggerated or inappropriate against an antigen or allergen”). Because Michael did not start experiencing symptoms until three days post-vaccination, his case was not captured in a Jan. 6 Centers for Disease and Control (CDC) report on serious allergic reactions following COVID-19 vaccination that limited the analysis to reactions occurring within the first 24 hours.
Serious allergic reactions
Critics familiar with VAERS’ shortcomings — and the ways in which officials can manipulate its data — bluntly condemn VAERS as “nothing more than window dressing, and a part of U.S. authorities’ systematic effort to reassure/deceive us about vaccine safety.”
As an example of the “effort to reassure,” one need look no further than the Jan. 6 CDC news release about post-vaccination anaphylaxis and non-anaphylaxis allergic reactions. In this report, the CDC’s tally of the hundreds of VAERS reports received per day during the first 10 days of the Pfizer vaccine rollout totaled 4,393 adverse events from December 14 to 23 — including 175 incidents flagged by CDC “for further review as possible cases of severe allergic reactions, including anaphylaxis, based on descriptions of signs and symptoms.”
Following its review, the CDC chose to include only 21 cases, excluding 154 cases either because they did not meet narrow criteria defined by the Brighton Collaboration (a global group that publishes “standardized case definitions” for countable adverse events); or because symptom onset occurred “later than the day after vaccination”; or because CDC judged the events to be “nonallergic” despite signs and symptoms to the contrary.
Based on the 21 cases, the public health agency then produced an estimate of 11.1 cases of anaphylaxis per million vaccine doses, whereas including all 175 events reported as severe allergic reactions would have yielded a rate of 92.4 cases per million doses.
Even so, the CDC’s conservative estimate of the anaphylaxis rate for experimental COVID-19 mRNA vaccines is roughly 10 times greater than for flu shots, including in individuals with no prior history of allergic reactions.
News reports have added to the frightening picture of post-COVID-19 allergic reactions that is emerging. These include the “hundreds” of Israelis describing “severe anaphylactic shock,” other allergic symptoms such as tongue and throat swelling, tingling sensations, dizziness and weakness; the two health workers in the UK who suffered “anaphylactoid reactions” on the first day of the Pfizer vaccine rollout; the two hospital workers in Alaska who experienced allergic symptoms — a serious anaphylactic reaction in one case and “eye puffiness, light headedness and scratchy throat” in the second case — within 10 minutes of getting the Pfizer jab; and the “mild to moderate” side effects from the Pfizer injection, including pain and dizziness, reported by four Bulgarians.
Reactions have not been confined to allergic symptoms, however. Additional descriptions of adverse events include:
A “rare, multisystem inflammatory syndrome,” including heart damage, developed by a 23-year-old male social worker in Israel 24 hours after receiving the Pfizer injection.
The seizures and encephalomyelitis (brain and spinal cord inflammation) experienced by 32-year-old Mexican internist Karla Cecilia Perez hours after getting the Pfizer shot.
The Bell’s palsy developed by a U.S. nurse within three days of her injection. On YouTube, she warns Americans, “Do not take this vaccination,” saying “I would not wish this on my worst enemy.”
Adverse mRNA vaccine reactions — no picnic
Setting the stage to “manage expectations,” The Atlantic told readers in mid-December that while COVID-19 injections have “a kick” and involve “more than the usual unpleasantness of getting a shot,” they are still “nowhere near as bad as COVID-19 itself.”
Some of the individuals described above and others submitting reports to VAERS might beg to differ.
For example, in a write-up accompanying one VAERS report (available through MedAlerts), a 36-year-old female who received the Pfizer vaccine on Dec. 17 was described as experiencing “disabling” light-headedness and dizziness 15 to 20 minutes post-vaccination, followed by an elevated heart rate and “really high” blood pressure.
After several hours in a monitoring station, where health workers gave her Benadryl and “lots of water” along with measuring her blood pressure “every five minutes,” she spent another four hours undergoing “continual monitoring” in the emergency room, followed by “a few more hours” in the ER the following day and a recommendation to start taking blood pressure medication. By Dec. 20, her blood pressure still had not normalized, and she had developed a bad headache. The health provider who submitted the report to VAERS on the woman’s behalf concluded that a causal association between Pfizer’s vaccine and the event could not be ruled out “based on a compatible temporal relation.”
Among Pfizer vaccine recipients with reactions categorized in VAERS as “life-threatening,” there are many other disquieting write-ups, often concerning young women in their 30s:
Female, age 31: “40 min after injection my throat and tongue started to feel weird and tight, pharmacy…gave me [Benadryl and Tylenol]. At about 1 hr 45 min after injection my throat got to the point of so swollen and itchy I couldn’t swallow. I went to nearest emergency room….”
Female, age 35: “5 minutes after getting the vaccine began itching that quickly developed into rash/hives to face, neck, chest, abdomen. At 20 minutes post vaccine developed severe leg weakness with lightheadedness, chest tightness, and [shortness of breath]. 22 minutes out collapsed to the floor unable to bear weight…and had severe cramping and tingling in legs, still unable to move them. Was rushed to the ER….”
Female, age 30: “Approximately 2 minutes after injection, felt flushed and tingly. This subsided, but developed a cough. Felt fine enough to leave the vaccination area after being monitored for 15 minutes. Cough continued, and developed a scratchy throat that eventually led to swelling of the throat at approximately 30-35 mins post administration. Sought care in the ED, where I was tachycardic and hypertensive…. Discharged home, but symptoms returned around 2pm. Sought care in a different ED, where I remained hypertensive and tachycardic.”
What’s next?
An objective analysis of the COVID-19 vaccine rollout necessarily raises serious questions about product safety and the assessment of risks versus benefits.
The VAERS reports submitted through December indicate that over half (53%) of those affected by mRNA vaccine reactions are 17-44 year-olds in the prime of life.
More than one in five (n=877) adverse events resulted in an emergency visit, 140 were rated “serious,” 100 led to hospitalization, 41 were “life-threatening” and 5 produced permanent disability.
Supplementing VAERS, the CDC has been encouraging COVID-19 vaccine recipients to use a smartphone app called v-safe to “quickly tell CDC” about mRNA vaccine side effects. On Dec. 19, v-safe tallies for the first five days of COVID-19 vaccination showed that among 215,362 vaccine recipients registered with v-safe, 5,052 individuals self-reported serious “health impact events” following their first dose of vaccine — events requiring care from a fellow health professional and rendering the person unable to work or perform normal daily activities. This, too, is concerning, translating into a one-in-43 injury rate (2.3%) for the v-safe group.
This has prompted concerns among allergists, in particular, who question whether drive-thru sites and under-trained personnel will be able to recognize and handle the sudden adverse reactions that the two mRNA vaccines seem capable of eliciting — especially since both contain the notorious allergenic ingredient polyethylene glycol (PEG).
In the U.S., some allergists are recommending that consumers with known allergies be “proactive” and ask prospective vaccination venues “pointed questions” about their emergency training, equipment and ability “to respond swiftly if something goes wrong.”
A growing number of healthcare experts are going even further, with one Wyoming public health official describing the injections as “biological weapons of mass destruction,” and many others urging the public to “just say no” to experimental injections that health officials and the vaccine makers admit aren’t proven to prevent COVID or stop transmissibility, but could do long-lasting harm.
“I Am Open”: 50,000 Italian Restaurant Owners Plan to Ignore Lockdown
Today – Friday 15th January – over 50,000 restaurants are planning to open, an act of mass civil disobedience against “anti-Covid” lockdown measures which have massively hurt the restaurant business, especially small family-owned businesses.
Spreading through social media under the hashtag #IoOpro (“I am opening”), the movement is largest country-wide act of civil disobedience since lockdowns began.
Italain opposition MP Vittorio Sgarbi has backed the movement, saying in an interview:
Open up, & don’t worry, in the end we will make them eat their fines”.
A similar movement already started in Mexico on January 12th, when hundreds of restaurant owners gathered to protest the lockdowns:
Mexico ?? Epic scenes, Over 500 restaurants have joined forces, agreeing to open up together, defying LOCKDOWN. Forced closed since Dec 18, they’ve stated it’s either ‘WE OPEN UP OR WE DIE’. Long Live the People ?? pic.twitter.com/PeSQpaGtqb
The “I am Open” protest is spreading across Europe as well, with variants already taking hold in German-speaking Switzerland (#Wirmachenauf) and Poland (#OtwieraMY).
It’s good to be reminded that, no matter how much it looks like the new normal is spreading unopposed, it’s not. People all over the world are resisting where they can. That’s what “Covid Positive” is all about.
To follow the progress of this movement we recommended following Robin Monotti and the It’s Time to Rise accounts on twitter and other platforms.
“…the WHO protocols Pfizer used to produce the mRNA [for the vaccine] do not appear to identify any nucleotide sequences that are unique to the SARS-CoV-2 virus. When investigator Fran Leader questioned Pfizer they confirmed: ‘The DNA template does not come directly from an isolated virus from an infected person’.”
And there we are, right back where I started, some time ago. If you don’t have the isolated virus, how can you claim you’ve sequenced it?
And if you’ve sequenced it by ASSUMPTION and GUESS, how can you claim the sequence—or the virus—is real?
Answer: You SAY the sequence and the virus are real, but you have zero proof. Because you’re a “scientific authority,” people automatically believe what you SAY.
A man visits a vast auto junkyard looking for parts. Over the office door, he sees a sign: “1972 Ferrari 365 GTB/4 Daytona Spider. Inquire within.”
The owner of the junkyard tells him, “We’re offering shares in the Ferrari. Three thousand a share. When we eventually sell it, you’ll make at least double your investment.”
The man says, “Where is the car? I’d like to see it.”
“Well,” the junkyard owner says, “look around you. We’ve got several square miles of cars and parts. The Ferrari is out there somewhere. We recently ran a test on exhaust fumes with a special instrument. It concluded that the ’72 Ferrari had recently been driven through the yard here…”
This is the sort of thing that happens in virology.
Of course, no mainstream virologist would admit it. He would talk about analogues and gene banks and PCR and representative samples and in silico (computer modeling).
But the stark reality is clear.
Assumption and guess and slippery inference do not carry the day.
You either have the isolated virus or you don’t. If you don’t, anything you say about “it” is useless. You can’t validly claim it exists.
As I’ve written and said dozens of times now, the virological meaning of the word “isolate” is quite different from the ordinary meaning.
In the technical world of the con and the hustle, “isolated virus” means: “We have the virus in a soup in a dish in the lab. The soup contains human and monkey cells, toxic drugs and chemicals, and other genetic material. Some of the cells are dying. This means the virus is killing them.”
That assertion is false. The drugs and chemicals can be killing the cells. And the cells are being starved of vital nutrients. That alone could explain the cell-death.
Furthermore, a supposed virus mixed in a soup in a dish in a lab is definitely not “isolated.”
Bottom line: there is no persuasive evidence that a virus is in the soup.
What’s in the COVID vaccine? Among other material, a supposed fragment from a supposed virus that hasn’t been proven to exist.
Consider the PCR test. Several levels of valid criticism have been aimed at the test.
First, different labs will come up with different contradictory test results. This is true.
Drilling down a little deeper, the test, when it amplifies the tissue sample taken from a patient, is useless and dangerous when more than 34 cycles or steps of amplification are deployed. Why? Because then, huge numbers of false-positives occur.
Down yet another level, we discover that the PCR doesn’t detect a virus at all. It identifies a piece of RNA presumed to come from a virus.
And finally, the test identifies a piece of RNA from a virus that hasn’t been proven to exist.
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Declarations by health officials and vaccine makers that deaths and injuries following COVID vaccinations are unrelated coincidences are becoming a pattern. They’re also depriving people of the information they need to make informed decisions.
The official handling last week of the deaths of two Danes and a Miami doctor following their COVID jabs highlights the gaping holes in the government’s surveillance system for detecting post-marketing vaccine reactions.
These incidents suggest that health officials will be unlikely to give the public authentic risk profiles for the emergency use COVID vaccines.
Accurate risk profiles allow regulators to determine if a medical intervention is causing more harm than good and consumers to make rational choices about their own use of a product.
Regulators usually develop risk assessments during preclinical trials by comparing health outcomes in individuals receiving the intervention against a placebo group. Such studies must be large enough to detect rare injuries and of sufficient duration to reveal ailments with long diagnosis horizons.
The existence of the placebo group makes it difficult to conceal or misattribute injuries. Conversely, the absence of a placebo group in post-vaccination surveillance systems makes it easy for self-interested pharmaceutical and regulatory officials to undercount injuries by attributing them to coincidence.
Coincidence is turning out to be quite lethal to COVID vaccine recipients.
Death by coincidence
Shortly after reporting the Danish deaths and prior to any autopsies, Tanja Eriksen, acting head of Denmark’s Pharmacovigilance Unit, told the Danish newspaper, EkstaBladet, that the Danish Medicines Agency had determined that coincidence probably killed the two Danish citizens whose deaths followed their vaccinations.
One of the deaths was a citizen who had “severe lung disease.” The existence of the comorbidity suggested that the death was therefore coincidental. The second citizen received the vaccine at a “very old age,” and therefore also expired from coincidence.
“When vaccinated in fragile groups, one would expect there to be deaths,” explained Eriksen, using logic seldom applied by health officials to deaths from the COVID-19 virus. “This will happen regardless of whether they are vaccinated or not.”
These simple declarations — that deaths and injuries following vaccination are unrelated coincidences — are becoming a pattern.
On Dec. 20, 2020, World Today News reported the death of an 85-year-old man in Kalmar, Sweden, one day after he received the vaccine. Dr. Mattias Alvunger of the Kalmar Hospital dismissed concerns about the death being related to the vaccine, calling the fact that it was reported to the Swedish Medical Products Agency as “routine.”
On January 1, Sonia Acevedo, a 41-year-old Portugese nurse and mother of two, died two days after receiving the Pfizer/BioNtech vaccine. Her father told the Daily Mail that she never drank alcohol and was in perfect health. Nevertheless, Portugal’s Health Authority dismissed her death as a sad coincidence.
Israel also reported two deaths from the coincidence pandemic: one in a 75-year-old man in Beit She’an, and the other an 88-year-old man. Both died two hours after vaccination. Israeli health officials warned the public not to attribute the deaths to the vaccine.
In Lucerne, Switzerland, a 91-year-old man died five days after getting Pfizer/BioNtech’s vaccine. Swiss authorities called any connection “highly unlikely.”
On January 3, Dr. Gregory Michael, a beloved Miami obstetrician and enthusiastic COVID-19 vaccine booster, died of a hemorrhagic stroke after receiving Pfizer/BioNtech’s vaccine. Dr. Michael developed acute idiopathic thrombocytopenia purpura (ITP) — a known vaccine side effect — immediately after receiving the jab. His platelet count dropped from 150,000 to zero and never rebounded.
An army of experts from around the world, involved in the vaccine program, consulted in doomed efforts to restore Dr. Michael’s platelet count. The inevitable brain hemorrhage killed him two weeks later. Michael’s wife said that her husband’s death was “100% linked to the vaccine. She added that he was physically healthy, exercised often, rarely drank alcohol, never smoked cigarettes and had no known comorbidities.
Nevertheless, Pfizer dismissed Michael’s injuries as another sad coincidence: “We do not believe at this time that there is any direct connection to the vaccine.” Pfizer pointed out that ITP is also caused by excess drinking and reasoned that “there have been no recorded safety signals identified in trials from vaccinations so far.”
On Tuesday, the New York Times quoted Dr. Jerry Spivak, a blood disorder expert at Johns Hopkins University, saying “I think it’s a medical certainty that the vaccine was related.”
An injury that occurs at that frequency would not likely be seen in Pfizer/BioNtech’s Phase II clinical trial because only 22,000 people received the vaccine. However, an injury of this severity occurring once in every 25,000 shots could debilitate or kill 12,000 of the 300 million Americans to whom the company hopes to give the jab.
The public can expect to see more of this strategic chicanery: When a healthy 32-year-old Mexican doctor was hospitalized with encephalitis — inflammation of his brain and spinal cord — after receiving the Pfizer/BioNtech vaccine, Mexican doctors dismissed the injury as unrelated to the vaccination, reasoning that the condition had not been detected in Pfizer/ BioNtech’s clinical trials.
This week an Auburn, New York nursing home reported, without any apparent irony, that 32 of 193 residents have died since the facility began administering the Pfizer vaccine on Dec. 21. The company claims that its clients are dying of COVID-19 infections, not the vaccine.
Equally disturbing, additional deaths may have gone altogether unreported.
Among Dr. Michael’s many grateful patients was Tessa Levy, who had a scheduled appointment with him for the Tuesday after his death on Jan. 3. Michaels delivered all four of Tessa’s children, saving one of them with an ingenious split-second diagnosis of a rare heart condition that would have otherwise killed the boy.
Tessa is the daughter of my close friend, the famous Beverly Hills surgeon, Dr. George Boris. “He was a healthy, strong, vigorous guy,” Tessa told me about Michaels. “He never showed any health problems.”
On New Year’s Eve, Dr. Boris’s brother-in-law, Murray Brazner, also died suddenly, one week after receiving the Pfizer vaccine. Neither the vaccine company nor any health agency took notice of his sudden unexpected death. “No autopsy was performed, and his death isn’t recorded as a vaccine injury. It makes you wonder,” Dr. Boris told me.
Mr. Brazner’s death illustrates an even graver problem: Many injuries may be escaping notice by the surveillance system and the media. Unreported stories similar to Dr. Brazner’s tragedy are already common complaints on social media.
On Jan. 2, Janice Hisle lamented on Facebook that her friend’s mom, an Ohio woman, died after receiving the vaccine. According to Hisle, the woman developed a high fever hours after the jab and died a “couple days” later. “I am so angry for my friend,” she commented, “who is crying because relatives were not allowed to see her before she was vaccinated. They thought the vaccine would ‘open the door.’”
We could find no mention of the Ohio woman’s death in media records or official COVID-vaccine death tallies.
One might assume that if deaths following COVID-19 vaccine can be so easily dismissed or ignored, lesser injuries will also escape notice.
The all-too-familiar vaccine propaganda playbook
The routine of reflexively dismissing suspicious deaths and injuries as unrelated to vaccination not only calls into doubt the official data tallies on vaccine injuries, it also contrasts markedly with the habit among public health officials of authoritatively attributing every death to COVID-19 so long as the deceased tested positive for COVID within 60 days of death using a PCR test notorious for producing false positives.
In fact, the $48 billion COVID vaccine enterprise shares three defining features with every new vaccine introduced since 1986:
1. Systematic exaggeration of risk from the target disease. (Pharma calls this project “Disease Branding.”)
2. Systematic exaggeration of vaccine efficacy.
3. Systematically downplaying vaccine risks.
1. Exaggerating disease risk:
Regulatory agencies count every death as a COVID death, so long as the deceased tested positive for COVID within 60 days of death — no matter that he may have died in a motorcycle crash.
In September, the Centers for Disease Control and Prevention (CDC) admitted that 94% of individuals whose deaths the CDC officially attributed to COVID had other illnesses that may have actually killed them. The average deceased had 2.8 comorbidities. Yet in CDC’s official tabulations, CDC always presumes that COVID-19 did the killing.
But as we see from the examples above, when it comes to COVID vaccine injuries, the opposite presumption governs: the comorbidity is always the cause of death — even when, as with Dr. Michaels, there are no known comorbidities.
2. Systematic exaggeration of vaccine efficacy:
Pfizer touts a 95% efficacy rate in its clinical trials, but this is a meaningless measure of “relative efficacy” based on a tiny cohort of 94 people in the placebo group who got mild cases of COVID during the clinical trials.
The true risk of vaccine injury will continue to be obscured by the habit among public health officials of routinely dismissing reported injuries as unrelated to vaccination.
The practices of systematically overestimating vaccine safety, underestimating vaccine deaths, and exaggerating risks of COVID-19 effectively deprive the public of their right to informed consent.
And so what do we really know about the true risk of COVID-19 vaccines?
Public health officials and industry spokespeople like to say that the risks of serious injury from vaccination are “one in one million.. However, in the first week of distribution, Americans took 200,000COVID vaccines and reported 5,000 “serious” (meaning missed workdays or medical intervention required) injuries.
This is an injury rate of 1 in every 40 jabs. This means that the 150 shots necessary to avert one mild case of COVID will cause serious injury to at least three people.
If the clinical trials are good predictors, that rate is likely to increase dramatically after the second shot (the clinical trials suggested that almost all the benefits of COVID vaccination and vast majority of injuries were associated with the second dose).
We don’t know the true risk of death from the vaccine since regulators have rendered virtually every death invisible by attributing them all to coincidence.
The 1-in-40 risk of “serious injury” from Pfizer’s COVID vaccine is consistent with what we know about other vaccines.
Nevertheless, it is only by clinging to this “designed to fail” system that regulators and industry have maintained their pretense that current vaccine risk profiles are acceptable.
A 2010 study funded by HHS concluded that VAERS captured “fewer than 1% of injuries.” In other words, the actual injury rates from mandated vaccines are more than 100x what HHS has been telling the public!
The 2010 HHS study found that the true risk for serious adverse events was 26/1,000, or one in 37.
Similarly, Merck’s clinical trials for Gardasil found that an astonishing half of all vaccine recipients suffered from adverse events, which Merck euphemistically called “new medical conditions,” and that 2.3% of vaccine recipients (1 in 43) suffered from autoimmune disease within six months of vaccination.
Similarly, a recent Italian study found that 41% of vaccine recipients (412 adverse events per 1,000 doses) suffered adverse events, with 11% of these rated “serious,” meaning 38 serious adverse events per 1,000 vaccinated individuals. These include grave gastrointestinal and “serious neurological disorders.” This amounts to a “serious” injury rate of 1/26.
Holocaust survivor Vera Sharav of the Alliance for Human Research Protection has observed that, “Everyone who gets any of these vaccines is participating in a vast medical experiment.”
Health officials generally concur that the granting of “emergency use authorization” to the rollout of experimental vaccine technologies with only a few weeks of safety testing, two years before the scheduled completion of Phase 2 testing, is a great human experiment, involving millions of subjects.
But researchers are unlikely to see all of the safety signals if a badly designed surveillance system allows local health officials and company employees the discretion to dismiss any serious injury as unrelated.
This is an injury rate of 1 in every 40 jabs. This means that the 150 shots necessary to avert one mild case of COVID will cause serious injury to at least three people.
If the clinical trials are good predictors, that rate is likely to increase dramatically after the second shot (the clinical trials suggested that almost all the benefits of COVID vaccination and vast majority of injuries were associated with the second dose).
We don’t know the true risk of death from the vaccine since regulators have rendered virtually every death invisible by attributing them all to coincidence.
The 1-in-40 risk of “serious injury” from Pfizer’s COVID vaccine is consistent with what we know about other vaccines.
Nevertheless, it is only by clinging to this “designed to fail” system that regulators and industry have maintained their pretense that current vaccine risk profiles are acceptable.
A 2010 study funded by HHS concluded that VAERS captured “fewer than 1% of injuries.” In other words, the actual injury rates from mandated vaccines are more than 100x what HHS has been telling the public!
The 2010 HHS study found that the true risk for serious adverse events was 26/1,000, or one in 37.
Similarly, Merck’s clinical trials for Gardasil found that an astonishing half of all vaccine recipients suffered from adverse events, which Merck euphemistically called “new medical conditions,” and that 2.3% of vaccine recipients (1 in 43) suffered from autoimmune disease within six months of vaccination.
Similarly, a recent Italian study found that 41% of vaccine recipients (412 adverse events per 1,000 doses) suffered adverse events, with 11% of these rated “serious,” meaning 38 serious adverse events per 1,000 vaccinated individuals. These include grave gastrointestinal and “serious neurological disorders.” This amounts to a “serious” injury rate of 1/26.
Holocaust survivor Vera Sharav of the Alliance for Human Research Protection has observed that, “Everyone who gets any of these vaccines is participating in a vast medical experiment.”
Health officials generally concur that the granting of “emergency use authorization” to the rollout of experimental vaccine technologies with only a few weeks of safety testing, two years before the scheduled completion of Phase 2 testing, is a great human experiment, involving millions of subjects.
But researchers are unlikely to see all of the safety signals if a badly designed surveillance system allows local health officials and company employees the discretion to dismiss any serious injury as unrelated.
Alert: The Operation to Squash Protests in America
The Department of Justice has announced it’s mounting a full-scale operation to arrest and charge people who broke into the Capitol on January 6.
There will be a wide-ranging menu of charges, starting with criminal trespass, and moving all the way to weapons possession, theft of National Security data, assault, and sedition.
The DOJ list of charges is meant to impress the American people.
Of course, an impressive DOJ list could have been leveled against thousands of people who participated in Antifa/BLM-led burning, looting, theft, and assault across the US over the past six months.
But that didn’t happen.
Those violent riots were a form of “insurrection,” but the label was never applied.
And Big Tech never considered banning social media users who planned and supported the riots.
From here on out, people will need to announce quite specifically what they’re protesting against. I’m talking, of course, about protests against the brutal COVID lockdowns.
Because you can be sure the government/media complex will paint such people with the “Capitol-break-in” brush. That’s part of this operation to squash dissent.
On a related note, social media are censoring users, and news media are censoring their own talent, if the issue of the stolen election continues to be raised. However, there is no expiration date on accusations of vote fraud.
Remember, after Trump won the 2016 election, Democrats spent the next three years claiming he didn’t win, but instead was part of a Russian conspiracy that handed him the presidency. Who was censored for saying THAT?
Back to the protests: As I’ve mentioned in prior articles, equating distinct events, and thus turning them into “the same event,” is part and parcel of mind control.
A hundred bereft business owners, who have been driven into bankruptcy by the COVID lockdowns, gathering near a governor’s office to protest, will be equated with “crazy dangerous Trumpers who believe the election was stolen.”
This is no accident. It’s standard operating procedure in the world of intelligence-agency campaigns.
If the CIA wants to maintain a foreign dictator in office, because he makes favorable deals with mega-corporations to loot and plunder his country, they’ll spread vast disinformation about the rebels who want free elections:
“The rebel force threatening to unseat the president is led by the cult of child-killers who have been ravaging families in the countryside…”
Closer to home, imagine something like this: “The group called Citizens for a Free Nation, who showed up at the governors’ mansion last week to protest COVID safety measures, is largely composed of unhinged anti-vaxxers and Trump supporters, some of whom may have attended the January 6 rally at the Capitol, which resulted in an act of insurrection. Police and FBI are investigating…”
Behind it all? A determination to suppress resistance to the COVID lockdowns, aka mass imprisonments.
The Police State knows the months of lockdowns and economic destruction have driven more and more people to the wall. The US population is a dry tinder forest in a season of high heat and no rain.
Controlling the population is a major problem. So those who stand up and visibly break out of jail have to be made into despicable illustrations of Something Else.
What label is at hand? By mere coincidence: INSURRECTIONISTS, “who broke into the Capitol on January 6, the day that will live in infamy.”
That label can now be applied anywhere. It’s a major item on the game board of intelligence-agency operations. When dissenting heads pop up, paint them with it.
Nevertheless, protests are still legal and legitimate. People who run them need to articulate what they’re about, over and over, in very clear fashion.
Americans, who’ve lived with more freedom and security than people in other parts of the world, tend to think their government, when it muscles in, signifies The End and Total Defeat.
Nothing could be further from the truth.
Freedom never dies.
It is an eternal quality.
PART TWO
You see, it wasn’t just Trump waving six loaded machine guns and a Stinger missile in the air and ordering his million troops to march on the Capitol and break in. It wasn’t just the Trumpers inside the Capitol looking for legislators to kidnap and ransom. It wasn’t just that.
No, it was/is Trumpers planning and carrying out assaults on all 50 state Capitols.
INSURRECTION against the very foundations of our democracy and way of life.
Domestic terrorism (unless somehow the Russians could also be dragged into the story).
It’s NATIONAL SECURITY.
And…we’re clear. That’s tonight’s news broadcast. Thanks, everybody. Get some sleep. We start this same train moving again tomorrow morning. Same story. New made-up details.
What’s going on?
Here’s one thing: stop the COVID protests.
Conflate people breaking out of COVID lockdowns because they’re desperate…with evil plots to blow up Capitol buildings because of Trump.
Mix and match. Merge. Melt one into the other.
Broadcast the impression that “it’s all one thing.”
This is a rerun of the old playbook strategy from the 1960s. Conflate marches against the Vietnam War with kids dropping LSD and trying to fly off buildings, with Black Panther members committing murder, with the Weather Underground planting bombs, with the Yippie-led street riots at the 1968 Democratic National Convention in Chicago.
Outcome? Nixon won the election and kept the War going. FBI agents were infiltrating Leftist groups and urging “violent solutions.”
Don’t you think we could be seeing some of that FBI COINTELPRO action now?
In the 1960s, roughly speaking, the playbook was used against the Left. Now it’s being used against the Right.
It’s the same op, different players.
In both cases, “Democracy is hanging by a thread…” That’s the message. “Insurrection must be stopped.”
Then, the short-term goal was to keep the Vietnam War humming. Now, it’s destroy resistance to the brutal lockdowns.
Paid propaganda pros don’t care which messages they’re hired to spread. They only care about technique.
In the 1960s, the political Right was the Establishment. Now it’s the political Left. They’re both controlled by Money.
Big Money. New World Order money. Call it Fascism, Socialism, Communism, Globalism, Technocracy, it doesn’t matter. All these names mean: top-down control.
The elite players are bent on destroying the essence of the Constitution and individual freedom.
Here is a backgrounder I wrote on this whole subject:
Socialism: triumph for corporate criminals
In several recent articles, I’ve exposed the myth that socialism is a revolution of and for the people.
I’ve presented evidence that socialism is actually a movement owned, operated, and funded by ultra-wealthy elites.
Dupes, foot soldiers, blind idealists, indoctrinated students, and low-level thugs are recruited through cutouts to serve the agenda of Rockefeller Globalists, for example, who are determined to bring about worldwide socialism.
Socialism, in a nutshell, equals ultra-rich elites (represented by the Council on Foreign Relations, Trilateral Commission, Bilderberg, etc.) owning the free market, cutting out competition, and creating more powerful, overarching, central governments.
Hidden in the plan is the granting of greater dominion to mega-corporations. This is a key fact.
The US Constitution was a document that established extremely limited central government. Regardless of the motives of the authors and the state legislatures that ratified it, the ideas contained in the Constitution were, and are, extremely oppressive toward large centralized structures controlling the people.
But there was another factor present at the beginning of the American Republic.
At the dawn of the United States, corporations were chartered and thus allowed to operate by the individual states. If a corporation, in the eyes of a state legislature, violated a basic trust by harming the people, committing offenses against the citizenry, the legislature could summarily cancel their charter and literally exile them from the state.
This power followed, in part, from the fact that corporations were not and are not individuals. They do not have the rights and freedoms of individuals. Corporations were not granted the rights of citizens in the Constitution.
Richard Grossman, an activist and scholar of US corporate history, unearthed and made lucid these facts.
At the birth of the American Republic, therefore, there was a double limitation on power. Central government and corporations were both strapped and shackled.
Of course, just as the federal government has been allowed to expand like an unchecked fungus, so has corporate power.
Under socialism (aka Globalism), mega-corporate power is the prow of a ship that sails on and on and conquers the economies of the world.
Corporate crimes go unpunished.
Contrary to popular belief, the real agenda of socialism has nothing to do with prosecuting those crimes.
The idea, for example, that greater socialism in America would defeat Monsanto [now Bayer] is ludicrous in the extreme.
Monsanto [Bayer] is one of the components of actual socialism—the real, not the fake, version.
Again, socialism is by, for, and of the ultra-wealthy elites. It is not a movement on behalf of the downtrodden.
As Gary Allen puts it in his 1971 classic, None Dare call It Conspiracy: “…pressure from above and pressure from below… The pressure from above comes from secret, ostensibly respectable Comrades in the government and [elite Globalist] Establishment, forming, with the radicalized mobs in the streets below, a giant pincer around middle-class society. The street rioters are pawns, shills, puppets, and dupes for an oligarchy of elitist conspirators working above to turn America’s limited government into an unlimited government with total control over our lives and property.”
“The American middle class is being squeezed to death by a vise. In the streets we have avowed revolutionary groups… Virtually all members of these groups sincerely believe that they are fighting the Establishment. In reality they are an indispensable ally of the Establishment in fastening Socialism on all of us. The naive radicals think that under Socialism the ‘people’ will run everything. Actually, it will be a clique of Insiders in total control, consolidating and controlling all wealth. That is why these schoolboy Lenins and teenage Trotskys are allowed to roam free and are practically never arrested or prosecuted. They are protected. If the Establishment wanted the revolutionaries stopped, how long do you think they would be tolerated?”
Gary Allen wrote that passage in 1971. Does it ring a familiar bell now?
As philosopher George Santayana famously wrote in 1905, “Those who cannot remember the past are condemned to repeat it.”
Equally famous is the prescription for all advertising: repeat the same message over and over, so it sinks into the mind and forms a false impression of truth.
Thus it has been with the basic message of socialism. “This is a form of government that finally serves the people. It is the people rising up to take the reins of power.”
Once that notion is rigidly fixed in consciousness, it is impossible to believe socialism is actually emanating from the elite of the elite.
Fortunately, more and more people are waking up to the basic con of fake news, which doesn’t only broadcast distorted current events spooling out through screens, day by day.
Basic themes of fake news also span decades and even centuries.
What will happen when enough young people, who want to tear down the structures of the monopolists, realize those same men are bankrolling them in the streets?
What will happen when these young people realize their teachers and mentors and handlers and professors have been feeding them the precise reverse of the truth?
As long as independent media continue to proliferate, that day is coming.
‘The New Normal’ Documentary: What the 1% Has to Gain and the Rest of Us Are About to Lose
Original video is available at happen.network. It has already been banned and deleted from YouTube.
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
It’s January 2021, the world is in lockdown and our economy is on the brink of collapse.
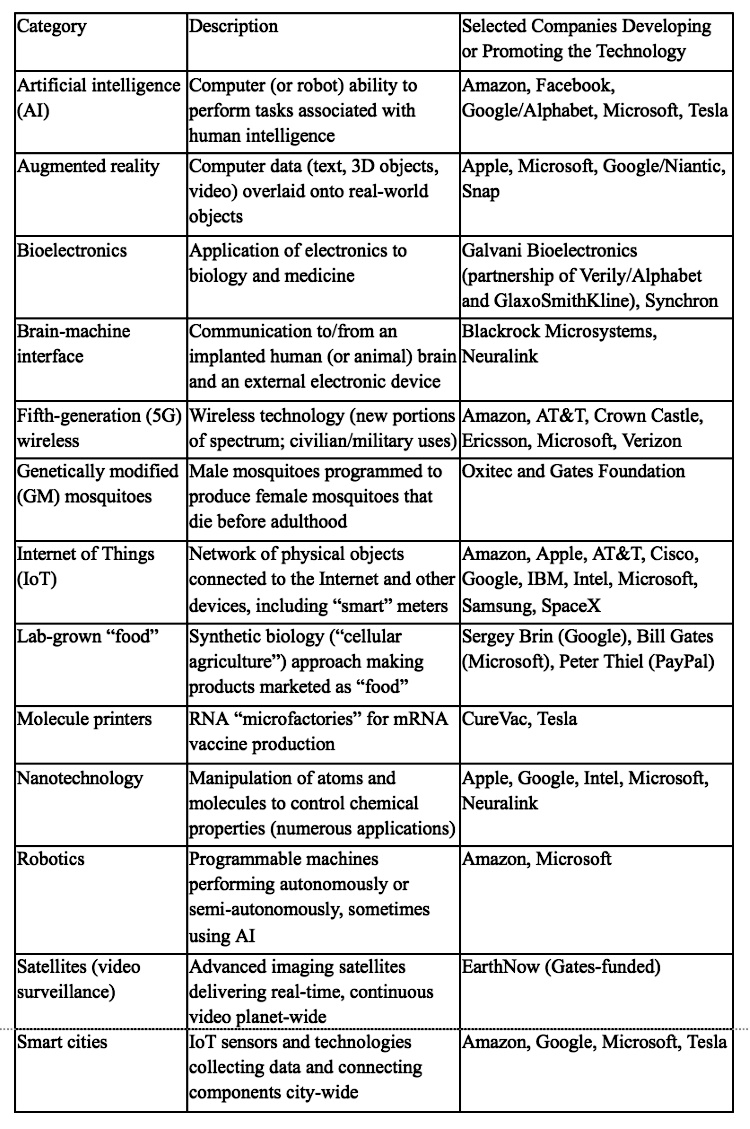
Will the new vaccine enable our lives to return back to normal or does it mark a pivotal point in the evolution of humanity (one that is driven by artificial intelligence, will reimagine capitalism and be governed by extreme tyrannical laws that are dictated by global elites)?
The New Normal, a factual, 50-minute documentary, investigates The Fourth Industrial Revolution, what the 1% has to gain and the rest of us are about to lose.
happen.network is a forward-thinking digital media and social platform that values integrity, curating independent current-affairs content for a free-thinking community.
Johns Hopkins Scientist: ‘A Medical Certainty’ Pfizer Vaccine Caused Death of Florida Doctor
Dr. Jerry L. Spivak, an expert on blood disorders at Johns Hopkins University, told the New York Times Tuesday that he believes “it is a medical certainty” that Pfizer’s COVID vaccine caused the death of Dr. Gregory Michael.
The Florida Health Department and the Centers for Disease Control and Prevention are investigating the death of a Florida doctor who died Jan. 3 from a rare autoimmune disorder he developed on Dec. 21, three days after receiving Pfizer’s COVID vaccine.
As The Defender reported last week, Heidi Neckelmann, the wife of Dr. Gregory Michael, said that in her mind, her 56-year-old husband’s death was “100% linked” to the vaccine.
Now, at least one doctor has come forward publicly to say he also believes the vaccine caused Michael to develop acute idiopathic thrombocytopenic purpura (ITP), the disorder that killed him.
“Dr. Jerry L. Spivak, an expert on blood disorders at Johns Hopkins University, who was not involved in Dr. Michael’s care, said that based on Ms. Neckelmann’s description, ‘I think it is a medical certainty that the vaccine was related.’
“‘This is going to be very rare,’ said Dr. Spivak, an emeritus professor of medicine. But he added, ‘It happened and it could happen again.’”
Spivak told the Times he based his reasoning on the fact that Michael’s disorder came on quickly after the shot, and “was so severe that it made his platelet count ‘rocket’ down.”
Spivak also offered two other reasons to back up his theory. One, the fact that Michael was healthier and younger than most people who develop chronic forms of ITP. And two, the fact that about 70% of people who develop ITP are women.
As Spivak told the Times: “A sudden case in a man, especially a relatively young, healthy one, suggests a recent trigger.”
Pfizer said it is also investigating Michael’s death, though the drugmaker told multiple news outlets it doesn’t “believe at this time that there is any direct connection to the vaccine.”
Shortly after the first reports surfaced of Michael’s death, Pfizer told USA Today:
“There is no indication — either from large clinical trials or among people who have received the vaccine since the government authorized its use last month — that it could be connected to thrombocytopenia.”
The vaccine most often implicated in ITP is the measles-mumps-rubella (MMR) vaccine, where the disease occurs in approximately 1 in every 25,000 to 40,000 doses of the vaccine, Redwood said.
According to Redwood, a study comparing adverse effects following influenza vaccination found that ITP was the third most common autoimmune condition (after Guillain Barre and rheumatoid arthritis).
An official with the Miami Dade medical examiner’s office on Jan. 11 told the media that the cause of Michael’s death is “pending the completion of studies” by the medical examiner and the Centers for Disease Control and Prevention.
Dr. Tom Cowan: Overview of the Real Science Related to the COVID Narrative; How Science is Being Weaponized Against Us
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Topics covered:
How science is being weaponized against us and why we must understand real science.
What do virologists actually do?
Where do they get the genome?
The creation of an imaginary genome of a make-believe virus.
Looking into the science of the so-called COVID vaccine — an injectable product that is nothing like any vaccine ever made.
Genetic engineering.
The theory of vaccines.
mRNA drug development meant to act as an operating system in our bodies.
Dr. Tom Cowen’s strategies for keeping himself and his family well.
Excerpts — Unofficial Partial Transcript
…There’s nothing unique about this. They’re simply testing for pieces of genetic material, having no idea the origin of this genetic material.
So, as far as I know, and I know this, I think, as well as anybody could know it. There is not one study out there — there has never been with this virus or many other viruses — that has properly isolated the virus, properly sequenced the virus. And if you can’t properly isolate it, you cannot say that a sequence of it comes only from that virus.
And, if you’ve never isolated it… you could never prove that the virus is the cause of this disease.
Isolation is the key. And no matter how many people say they’ve isolated, no matter how many people criticize me and us for saying it, I still contend that there is simply no evidence that this kind of isolation has ever happened with this or many other of the viruses that we are told cause disease.”
___
“Let’s move on a little bit to talk about… the so-called COVID vaccine… We need to understand thoroughly that this injectable product is nothing like any vaccine that has ever been made, and actually, in no way should be called a vaccine…
The first thing we have to know is that in genetics… there is something called a central dogma.
The central dogma of genetics — meaning the foundational principle of genetics — is that the genetic material in all animals, including humans, is found in the nucleus it’s found in this substance called DNA, which we’re told is the house of the genes. In other words, each strand of DNA contains many different genes which are composed of so-called nucleotides, which are composed of base pairs, which are either A, T, C or G.
So a gene is a long string, like word, made of say AATTCGAT, etc. So it’s got a certain number of length. And the sequence of those nucleotides is what constitutes a gene. And there’s many genes in sequence, not necessarily one after the other, laying on this piece of DNA.
Now, the central dogma is, this DNA, which is formed sort of like a zipper, right? So there’s a strand here and this is A. And every A matches up with T. And then the next one is C and every C matches up with G, and then so on down the line.
[Dr. Cowan is demonstrating with his hands during this explanation — near the 21 minute mark in the video.]
So they’re like this and then you separate them. And then two strands will form if it’s mitosis, so that A always matches up again with T and the C always matches up again with G. And so then you make two exact copies of it. And that’s how a cell reproduces itself.
Now, sometimes the DNA — let’s just use the word “wants” — to make protein. So the way that works is, you get this separation, And so, here’s the A — and it makes T, C…whatever the complimentary nucleotide. And that new structure is called m (or messenger) RNA. And that process of turning the DNA into a homologous copy of RNA, messenger RNA, is called transcription.
Now, that process, we think, happens in the nucleus. Then the mRNA goes out of the nucleus into the cytoplasm. And now we have a homologous copy. And then through a process called translation, this RNA is converted into a protein, which obviously has the same sequence as the DNA did in the first place…
And that sequence of nucleotides creates the amino acids, which is essentially the backbone or the material out of which a protein is made. And then the protein does all the functions that are happening in a living organism.
So, again, the central dogma is, quite simply — this is a one-directional process. DNA makes messenger RNA, called transcription. Messenger RNA makes protein, which is called translation.
The central dogma tells us that protein never makes RNA, RNA never makes DNA, and DNA never makes protein directly.
It’s always in that very specific sequence: DNA, messenger RNA, protein. Transcription, translation, action. The action molecule is the protein. The blueprint is the DNA.
Now, here’s the interesting thing, all those facts that I just said — and, I’m sure some of you this won’t come as a surprise to — are actually incorrect. One of the things I’m going to do in this next year is dissect that whole process and show very clearly how many of the things that I just said, which are reported as fact, are actually not fact at all.
And one of the things that’s not fact is, starting with the discovery of what are called retroviruses (or in other words RNA viruses)…
So again, a virus is a piece of genetic material, either DNA or RNA, in a protein coating. So that’s what a virus is.
Then a bunch of people — Gallo, Montagnier and others — came up with the theory that this disease called AIDS is caused by a virus called HIV. Human Immunodeficiency Virus. But the trouble was, this virus, which also was never isolated or proven to cause anything (but that’s another story) was an RNA virus. And the question then for them was, how does this RNA virus insert itself into the DNA of the tissues and the cells to make copies of itself.
Since there is no — or at that time, there was no idea that RNA could reverse this central dogma and make DNA. So, they discovered in researching this that there’s something called reverse transcriptase (which is abbreviated RT — which is what the RT-PCR test means) that can convert RNA, messenger RNA, into DNA , that can then get itself inserted into the animal or human DNA. And this process is basically based on an enzyme called reverse transcriptase. And, at the time, the theory was this reverse transcriptase, this enzyme that could do this process of reversing the central dogma, was only found in so-called retroviruses. There was no normally, naturally-occurring reverse transcriptase in any animal or any human…
___
What we didn’t know is that this process of converting RNA into DNA is actually a normal repair process, and any tissue in any system, any mammalian living system, actually has it’s own reverse transcriptase. And that there is a continual interplay between RNA and DNA…
So, you may be asking why is this something I need to know about? The reason is, for the first time humans are injecting other humans with messenger RNA…
…The expectation of the injection of messenger RNA into an animal is to make that messenger RNA insert itself into the human DNA, the human genome, which is basically the definition of genetic engineering…”
Once more, dear reader, I venture into the insane world where experts falsely claim they’ve proved SARS-CoV-2 exists. Within that world, they contradict themselves. They just can’t keep their story straight.
So let’s begin with Tony Fauci. We have him on video making the following statement: “…In all the history of respiratory borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks…Even if there’s a rare asymptomatic person that might transmit [the virus], an epidemic is not driven by an asymptomatic carrier.” [1]
Fauci is emphatic. People with no symptoms who are carrying a virus? Not a problem. They don’t spread the virus to other people. They don’t cause or maintain an epidemic.
Now let’s turn to the CDC. Jay Butler, CDC deputy director for infectious diseases just told the Washington Post, “The bottom line is controlling the COVID-19 pandemic really is going to require controlling the silent pandemic of transmission from persons without symptoms.” [2] [3]
Just the opposite of what Fauci said.
So now we have this:
ONE: People who carry the virus but have no symptoms don’t cause or maintain an epidemic.
TWO: Those very people ARE a major problem, and the epidemic can’t be controlled without controlling them—with masks, distancing, and lockdowns.
Follow the science? What science?
On the back of this gibberish, nations all over the world are seeing their economies destroyed, and hundreds of millions of lives ruined.
It’s a freak show, and the freaks are running it.
Of course, the experts can lie their way out of this. They can say, “Well, this is the FIRST TIME in human history that people with no symptoms are driving an epidemic. We’ve never seen it before…”
Right. This is a special case. Astounding.
If you believe that, I have condos for sale on the far side of the moon.
The truth is, the experts are starting backwards from an unexpressed premise, which is: WE WANT TO LOCK DOWN THE PLANET AND WRECK ITS ECONOMY, AS THE FIRST STEP TO CREATING A BRAND NEW WORLD OF TECHNOCRATIC CONTROL. NOW, WHAT DO WE HAVE TO SAY IN ORDER TO MAKE THAT HAPPEN?
This is how official science operates. It’s political and totalitarian, and it pretends to be objective.
So Jay Butler, the CDC deputy director, rounds off his statement to the Washington Post with this: “The community mitigation tools that we have [masks, distancing, lockdowns] need to be utilized broadly to be able to slow the spread of SARS-CoV-2 from all infected persons, at least until we have those vaccines widely available.”
Translation: We have to keep lying, to keep the global population under lock and key. Putting the Chinese model of control in place, in Western countries, takes time. Buy the con for another few years and we’ll have an iron grip on the population.
Things seem to be working backwards at The Commons on St. Anthony nursing home in Auburn, New York. Vaccinating people is supposed to reduce or end coronavirus deaths. Right? But, at The Commons, such deaths are reported to have occurred only after residents began receiving coronavirus vaccinations.
James T. Mulder wrote Saturday at syracuse.com that until December 29 there had been no coronavirus deaths at The Commons. December 29, when deaths of residents with coronavirus began occurring at The Commons, is also, Mulder’s article discloses, seven days days after the nursing home began giving coronavirus vaccinations to residents, with 80 percent of residents so far having been vaccinated.
Over a period of less than two weeks since December 29, Mulder relates that 24 coronavirus-infected residents at the 300-bed nursing home have died.
This is the penultimate paragraph of Mulder’s article, where vaccinations at The Commons is mentioned:
The nursing home began vaccinating residents Dec. 22. So far 193 residents, or 80%, and 113 employees, or less than half the staff, have been vaccinated. The nursing home plans to do more vaccinations Jan. 12.
You see them everywhere. Men and women walking down the street, all of them with masks on their faces and cell phones in their hands. People jogging, with masks covering their faces and cell phones in their hands. Mothers wheeling their babies with one hand, holding a cell phone in the other hand, with a mask covering their face.
The world has gone insane.
Back in May, the President of Tanzania announced that a goat, a quail, and a papaya had tested positive for COVID-19. People did not stop eating papayas. But when farmed minks began testing positive, the response has been to kill them all.
After a few minks in the Netherlands tested positive in April, 570,000 minks were slaughtered. Minks started testing positive and being killed in Denmark in June, and on November 4, Denmark announced it would destroy the rest of its 17 million minks. Sanity finally broke out in that country, and the eradication campaign stopped after only 2.5 million minks were slaughtered. But minks have also been killed in Spain, Sweden, Greece, France, and the United States.
Lions, tigers and leopards in zoos have tested positive.
This is what you are supposed to do: “Isolate the pet from everyone else, including other pets.” “Keep your pet at least 6 feet away from other pets and people.”
“If you have a private backyard where your dog can go to the bathroom, do not take them for walks.” But, the CDC warns, “Do not wipe or bathe your pet with… hand sanitizer,” and “Do not try to put a mask on your pet.”
It is becoming obvious that no matter what you test — minks, lions, dogs, papayas, people, or anything else — you will get positive results, and that the results mean nothing. Just wait until someone tests a cow. Kill all the cows, and no more meat or dairy products! Vaccinate every pet and farm animal in the world! Do contact tracing for every pet that comes in contact with an infected pet!
We have a pandemic, all right, but it is a pandemic of insanity, not COVID-19. The world — the entire world, not just a few people or a few countries or a few cultures — has forgotten what life is. Life is community. It is social contact, touching, breathing, sharing. It is oxygen. People are dying because their masks are making them hypoxic. Cancer cells thrive in the absence of oxygen.
If you have cancer, and you wear a mask, you are making your cancer grow. And life is bacteria and viruses. Ninety-nine percent of all bacteria and viruses are beneficial and necessary — necessary for life, and necessary for evolution. If you disinfect the surface of the earth, you will put an end to life. We did not disinfect the world for smallpox, influenza, measles, or tuberculosis. But we are doing it for “COVID-19.”
And we are blaming every symptom known to man on “COVID-19.” COVID-19 is a respiratory virus, closely related to the common cold. But we have made a caricature of it. Suddenly a coronavirus is a magical piece of RNA, created by Dracula, that will damage your kidneys or your heart or give you a stroke.
There is another, very real pandemic that is out of control: a pandemic of radiation. A pandemic that does cause kidney and heart damage and strokes, in addition to pneumonia. The radiation is produced by cell phones. The cell phones with which mothers are irradiating their babies, and joggers are irradiating their hearts. The cell phones with which 7 billion people are irradiating the birds, insects and flowers around them. The radiation that will kill all 7 billion of us, unless we put an end to it.
Take Back Your Health Conference, January 23-24, 2021
I will be speaking about these issues at the 2021 Take Back Your Health (TBYH) Conference. This year’s conference, featuring doctors, immunologists, environmental experts, and others, is titled Our Global Microbiome: Understanding Our Relationship with the Viruses, Bacteria and Molds Around Us.
The conference will be held online January 23 and 24. Details and registration information are here: https://conference.tbyhguide.com/.
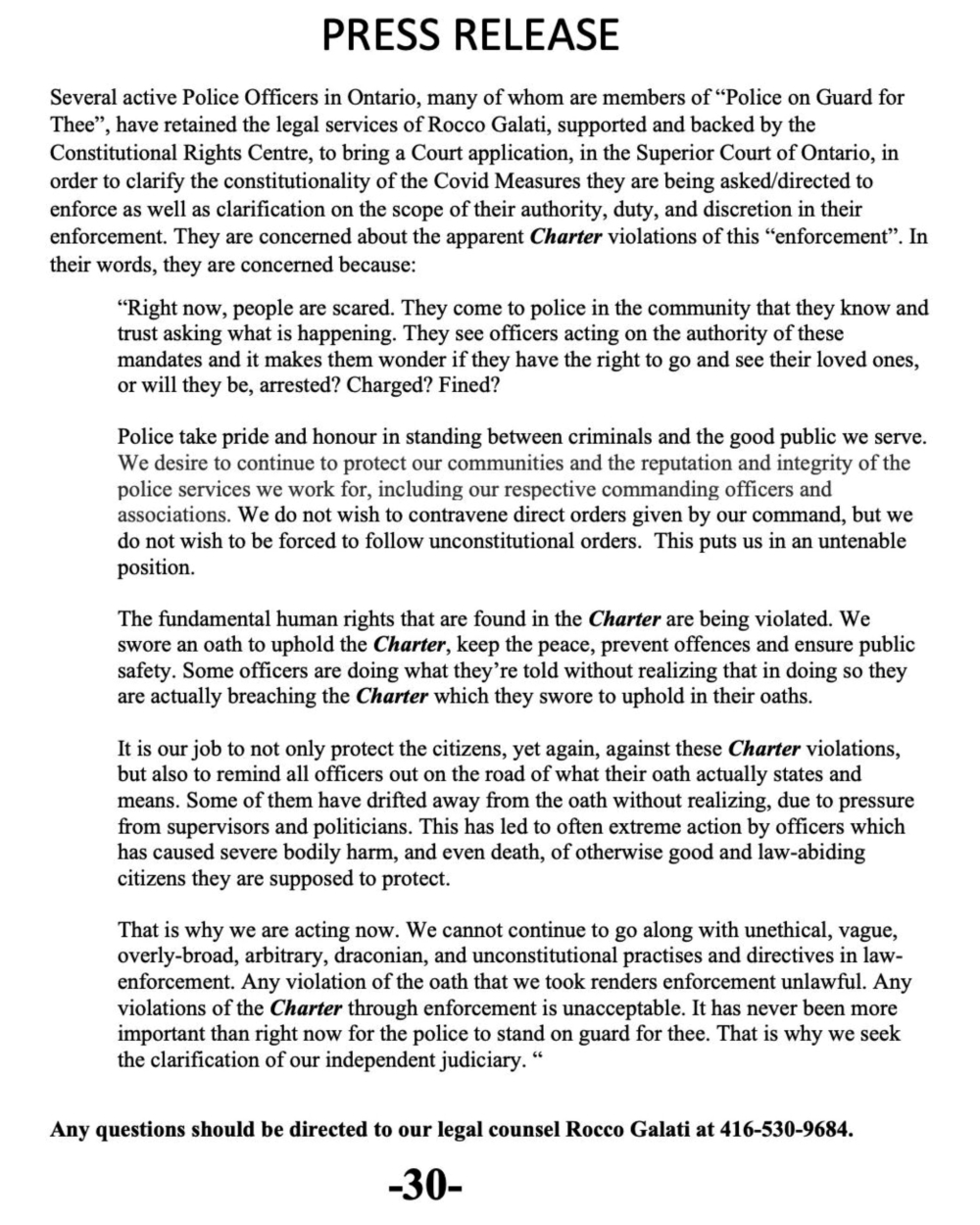
Dear Police, First Responders and Healthcare Workers
Re: COVID-19 Vaccine Concerns
I am writing on behalf of Vaccine Choice Canada to express our deep concern for you and your colleagues.
We understand that first responders and frontline healthcare workers are being targeted to receive the initial deployment of the COVID-19 vaccine. After a thorough review of the available scientific literature, it is our contention that the Pfizer and Moderna products authorized for use in Canada carry substantial risks.
We recognize the importance of first responders and frontline workers and feel a sense of urgency to share this information with those we rely on most during times of emergency. The attached document addresses the following concerns:
Human experimentation: The Pfizer and Moderna vaccines granted ‘interim approval’ by Health Canada have not been adequately tested for either safety or efficacy. This means that the use of the COVID-19 vaccine is human experimentation.
The Vaccine May Not Prevent Infection or Transmission: COVID-19 vaccine makers are not required to demonstrate that their product prevents either infection or transmission of the virus.
COVID-19 – A Low Lethality Illness: The coronavirus is statistically shown to be far less deadly than portrayed by mainstream media and health officials.
Health Canada Oversight Insufficient: The safety testing of the COVID-19 vaccine products is incomplete and less rigorous than that for other vaccines.
No Individualized Risk-Benefit Analysis: A proper risk-benefit analysis has not been conducted. Implementing a “one-size-fits-all” policy fails to recognize that the risk of infection varies greatly depending upon several variables including age and pre-existing conditions.
Informed Consent: Those advocating for mandates and coercive measures that remove the right to consent are undermining essential individual rights and freedoms. This is a clear violation of the Canadian Charter and also medical ethics.
Our intention in writing this letter is to bring to your awareness the experimental nature of this vaccine. It is our hope that this information will help to protect your right to voluntary informed consent, free of any coercion or constraint. Thank you for your service to Canadians.
Sincerely,
Vaccine Choice Canada
1. The COVID Vaccine Is Human Experimentation
The Pfizer and Moderna vaccines were granted ‘interim approval’ by Health Canada but have not been adequately tested for either safety or efficacy. This means that the use of the COVID-19 vaccine is technically considered to be human experimentation. [i]
The normal development timeline of a vaccine product is 5 – 10 years. It is impossible to identify the effects of a vaccine in the few months the product has existed. The most significant concern with the Pfizer and Moderna vaccines is the introduction of ‘messenger RNA/DNA technology’. This technology has never before been injected into humans on such a mass scale. The consequences of injecting genetic altering technology into a human body is unknown.
The potential exists for catastrophic consequences, not only for the person receiving the vaccine, but for all future generations as it is highly likely that the mRNA/DNA in the vaccine will combine with the recipient’s own DNA and be transmitted to their offspring.
The use of this novel technology is especially disconcerting given COVID-19 vaccine manufacturers have been granted total immunity from liability for any harm or injury caused by their products. Federal procurement minister Anita Anand justified the indemnity in the following statement – “All countries, generally speaking, are faced with the issue of indemnification of companies, especially in cases of novel technologies like this.”[ii] Ordinarily, a ‘novel technology’ would demand a higher level of oversight and accountability, not less.
Normal protocols to test the safety of vaccines include testing in animals prior to testing in human subjects. This protocol is even more essential for a coronavirus vaccine. All previous efforts to develop a coronavirus vaccine over the last 60 years have failed because the vaccine caused an exaggerated immune response upon re-exposure to the virus. [iii] This ‘pathological priming’ resulted in severe injury and death to the test animals. An earlier attempt to create a similar RSV vaccine resulted in an 80% hospitalization rate and the death of two of the 35 children in the trial. In the rush to develop a COVID vaccine, Health Canada has permitted vaccine makers to bypass animal testing and move directly to testing on humans.
Health Canada has also granted Pfizer and Moderna permission to deploy their vaccines in the general population without completing Phase III trials. This is unprecedented in vaccine development. Health authorities admit that long-term safety data does not exist for the vaccine. [iv] There is no data that defines the vaccine’s interaction with other vaccines or prescription medications. [v] COVID-19 vaccines have not been tested for their ability to cause cancer, induce organ damage, change genetic information, impact the fetus of a pregnant woman or to impair fertility. William Haseltine, a former Harvard Medical School professor states that, “These protocols seem designed to get a drug on the market on a timeline arguably based more on politics than public health.” [vi]
2. The Vaccine May Not Prevent Infection or Transmission
Many individuals eager to receive a COVID-19 vaccine are under the notion that the vaccine will protect them from the SARS-CoV-2 virus. The reality is that COVID-19 vaccine makers are not required to demonstrate that their product prevents either infection or transmission of the virus. Vaccine manufacturers are also not required to demonstrate that the vaccine will result in a reduction in severe illness, hospitalization, or death.[vii][viii][ix]
According to a report in the British Medical Journal, “Hospital admissions and deaths from COVID-19 are simply too uncommon in the population being studied for an effective vaccine to demonstrate statistically significant differences in a trial of 30,000 people. The same is true of its ability to save lives or prevent transmission: the trials are not designed to find out.” [x]
This begs the question – what benefit will the COVID-19 vaccine actually confer?
Public health authorities have stated that vaccine recipients will still be required to wear a face covering, maintain physical distance, and avoid crowds. CDC’s own data confirms that over 80% of individuals who test positive for COVID-19 are asymptomatic. For these individuals a risk-benefit analysis could only conclude that a COVID-19 vaccine will result in substantially more risk than benefit.
3. COVID-19 Is A Low Lethality Illness
Many individuals who intend to be at the front of the line for a COVID-19 vaccine will do so because they believe COVID-19 is an illness with a high rate of mortality. This fear creates a sense of panic that compels people to accept a medical product with an unknown safety profile.
Our federal and provincial governments and the mainstream media persist in describing COVID-19 as a “deadly” condition. This is simply not true for the vast majority of the population. The risk of mortality is primarily to those over 80 years of age in poor health, residing in extended care facilities. [xi] The median age of death attributed to COVID-19 is 82 years. Almost all were frail with several co-morbidities. According to the CDC, the case survival rate of COVID-19 in patients ages 0 – 19 is 99.997%, 99.98% in patients 20 – 49 years, and 99.5% in patients 50 – 69 years. [xii][xiii]
What is also rarely acknowledged by our government, public health officers, and the corporate media is that safe and effective drugs for the prevention and treatment of COVID-19 have been identified.[xiv][xv][xvi] Such treatments negate the need for an ‘emergency use’ vaccine. Unfortunately, these treatments are rarely discussed, much less encouraged.
4. Health Canada Oversight Insufficient
Many Canadians assume Health Canada provides rigorous oversight and would never permit a vaccine to be introduced to the Canadian public without robust testing to ensure both safety and effectiveness. The fact is that Health Canada does not conduct its own clinical trials to determine the safety and efficacy of a vaccine. Instead, Health Canada relies on the data provided by the vaccine manufacturers. Health Canada also holds the perspective that it is not necessary for vaccine makers to test their products against a neutral placebo, the gold standard for safety testing.
Canadians may not be aware that vaccine producers such as Pfizer, Merck and GlaxoSmithKline have paid billions in criminal penalties and settlements for research fraud, faking drug safety studies, failing to report safety problems, bribery, kickbacks, and false advertising. [xvii][xviii] In 2009, Pfizer paid $2.3 billion to resolve criminal and civil allegations in what was then the largest health care fraud settlement in history. [xix] Canadians may also not be aware that the Vaccine Injury Compensation Program in the United States has paid out more than $4.4 B in compensation for vaccine injury and death since 1989, and that Canada is one of only two G20 Nations without a national vaccine injury compensation program. While a vaccine injury compensation program has been promised, the details have yet to be announced.
Vaccines are not benign medical products. Vaccination is an invasive medical procedure that delivers by injection complex biochemical drugs and now genetic modifying technology. Because of this complexity and uncertainty, the level of safety testing ought to be even more rigorous. But this is not the case. The safety testing of the COVID-19 vaccine is less rigorous and more incomplete as compared with other pharmaceutical drugs.
The consequences of rushing a novel and inadequately tested product can be serious, permanent, and even deadly. Data following the administration of the Pfizer vaccine reveals that 3.6% of test subjects experienced a ‘health impact’ significant enough such that they were “unable to perform normal daily activities, unable to work, and required care from a health professional.” [xx]
5. No Individualized Risk-Benefit Analysis
The arguments used to legitimize, legalize and implement COVID-19 vaccination are political and ideological rather than evidence-based. In the rush to approve a COVID-19 vaccine an analysis of the risks vs benefits has not been conducted. Indeed, how does one conduct a risk-benefit analysis when both the risks and the benefits are unknown? Some researchers have described the use of a COVID-19 vaccine in the general population as the most reckless and brazen experiment in the history of humanity.
Further, implementing a “one-size-fits-all” policy assumes the risk-benefit is the same for everyone. This fails to take into consideration the established fact that the risk of COVID-19 infection varies greatly depending upon several known variables, most especially age and pre-existing conditions. These variables must be considered when assessing the risk and benefit of this medical device.
6. Informed Consent Is Essential
The mandate of Vaccine Choice Canada has been and continues to be protecting the health sovereignty of Canadians, which inherently includes the right to informed consent. Informed consent is the most fundamental aspect of health sovereignty, an ethical medical system, and a free and democratic society.
It is imperative that any individual contemplating getting a COVID-19 vaccine be fully aware that the vaccine has not undergone the most basic testing to demonstrate either safety or efficacy and that they are participating in human experimentation. In a letter dated October 3, 2020, Dr. Michael Yeadon, a former Vice President of Pfizer stated – “All vaccines against the SARS-CoV-2 virus are by definition novel. If any such vaccine is approved for use under any circumstances that are not EXPLICITLY experimental, I believe that recipients are being misled to a criminal extent.”
Secondly, we hold that any medical intervention requires voluntary consent. Canada is a signatory to The Universal Declaration of Bioethics and Human Rights which describes consent as follows: “Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information. The consent should, where appropriate, be expressed and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice.”
According to the Nuremberg Code, developed in response to the medical abuses of the Nazi regime, informed voluntary consent means that “the person involved… should be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion.”
Those advocating for mandates and other coercive measures that remove the right to voluntary consent are undermining essential individual rights and freedoms. This is a clear violation of the Canadian Charter and also medical ethics. It is important to understand that we have the legal right to refuse any unwanted medical intervention.
We would be glad to provide you with further documentation should you wish.
Welcome to 2021, the theatrical performance for which 2020 was merely a dress rehearsal. If you haven’t been deplatformed yet, don’t worry, you will be. That is, unless we can get our shit together as a species and work together to pry the boot off our faces. The sooner we do that, the better.
Spiro was recently booted off Twitter for wrongthink. There’s a lot of that going around these days, no matter how meticulously-researched one’s content is. We are an information war – don’t bring a plastic fork to a drone strike.
‘Like,’ share, & subscribe if you got something out of this content, because it probably won’t be around much longer. Download this (& the other videos on both of our channels) & repost it to your own channel or platform.
It started with the rapid emergency use authorizations (EUA) of experimental Covid vaccines from Pfizer and Moderna (and now AstraZeneca in some countries).
It’s concerning. Nearly zero caution was observed as Big Pharma rolled out a product with so many unknowns upon the entire public worldwide. But it’s okay! Just believe!
The primary endpoints for the Covid vaccine trials were a positive SARS-CoV-2 PCR test and mild symptoms. There was just one problem: The PCR test protocol to identify SARS-CoV-2 had, and still has, known and concerning errors, as well as inherent fallacies that render it useless. Yet that didn’t stop Pfizer and Moderna from leaning hard on them to validate their experimental Covid shots’ efficacy.
Others in the scientific community who saw through the issues and errors sounded the alarm in the form of a legal motion to stop the clinical studies until the protocol could be amended. Again, Science™ ignored the warnings, data and facts to recklessly roll out their experimental shot on the world…Just believe!
Now the lines are further blurred and the waters are even more murky. Unhinged health officials are creating their own reality as the corporate media gleefully ramps up its medical gas-lighting of the public to support their delusions. We are entering cult-like territory…Just believe!
Pregnant women and children are considered more sensitive and vulnerable biologically. The far-reaching effects from adverse events have the potential to yield a greater impact upon these groups. Therefore, batteries of studies and experimental data usually proceed recommendations for them to take risks on new products.
As it stands, both Moderna and Pfizer’s experimental Covid vaccine trials lack the data to give guidance to pregnant women. In fact, they specifically state:
“8.4 Unknown Risks/Data Gaps Safety in certain subpopulations
There are currently insufficient data to make conclusions about the safety of the vaccine in subpopulations such as children…pregnant and lactating individuals, and immunocompromised individuals.”
That did not stop the U.S. Centers For Disease Control and Prevention (CDC) from making a potentially catastrophic and unscientific appeal to faith and belief. The agency took to Twitter shortly after the EUA vaccine approvals to specifically target pregnant women.
Pregnant? You may discuss #COVID19 vaccines with your doctor, but it’s not required before vaccination. While studies have not yet been done, experts believe mRNA vaccines like COVID-19 vaccines are unlikely to pose a risk for #pregnant people. More: https://t.co/pBVlI6STf8. pic.twitter.com/N2o76U4L4T
We’ve seen this scam before from the U.S. Food and Drug Administration (FDA), when they approved and then solicited both flu shots and TdaP vaccines to pregnant women without the proper studies.
After failing to produce the clinical trials and safety studies that were allegedly used to license both sets of shots for use in pregnant women when presented with a FOIA request, the FDA was taken to court in 2019.
At the time, Scott Gottlieb’s FDA conceded, “Clinical studies for TdaP and inactivated influenza vaccines did not specifically enroll pregnant women.” The FDA legal response went on to admit they “have no records responsive to your [plaintiff’s] request.”
In short, the agency that licensed both flu and TdaP shots for use in pregnant women did so without the required scientific studies to ensure safety.
In addition to the FDA licensing the flu and TdaP vaccines outside of law and their own policy, the agency also actively promoted and marketed the flu shot to pregnant women – much like the CDC is doing presently with the experimental Covid shots.
Ringing in 2021 were sudden, predictable stories of up to half of health care workers saying they would avoid the vaccine alongside headlines claiming thousands of reported vaccine reactions.
The ‘wobbly’ frontline healthcare appeared to be growing weary. Amidst the chaos, chief medical officers for England, Scotland, Wales and Northern Ireland announced a delay in giving the second dose of shots to recipients.
There was just one problem. All the Covid vaccine trials were tested using two doses, not one, to achieve their endpoint results in which an EUA was based upon. Put another way, trials weren’t designed to test the safety and efficacy of one dose. Just believe!
The lockstep vaccine operation was thrown into upheaval. Pfizer broke rank and publicly refuted UK health officials in a rare distancing from their previously cozy relationship:
“Pfizer and BioNTech’s Phase 3 study for the Covid-19 vaccine was designed to evaluate the vaccine’s safety and efficacy following a 2-dose schedule, separated by 21 days,” Pfizer said in a statement on Thursday. “There are no data to demonstrate that protection after the first dose is sustained after 21 days.“
Even Time magazine’s Person of the Year and In Style fashion icon and cover star Dr. Anthony Fauci rebuked UK’s chief medical officers, telling CNN the U.S. would not adapt such an unscientific position by delaying the second dose.
Fauci quickly changed his tune to get back on script telling NBC news that spreading out doses is now “under consideration.”
The Washington Post began banging the drums for the delay writing:
Is there any potential downside to a delay? “Yes. The strategy hasn’t been studied, so we don’t know if and when the immunity from the first shot begins to wane. But data from Moderna, for example, is reassuring. It shows robust immune response four weeks after the first shot, and most experts believe it is extremely unlikely immunity would somehow plummet by week eight or even week 12 following a single shot.”
Just believe! Yet not all experts do.
The Times of Israel writes, “It’s an act of desperation. It also contravenes the scientific protocols,” said Israeli epidemiologist Ron Balicer on Saturday, in an interview with Channel 12. He underlined the unknown risks, as well as the questions about how effective a single dose will be in shielding elderly and high-risk people from the virus.
That made it an all ‘round embarrassing day for the Science™ crowd. In the past, there was at least a public relations effort, a united front feigning thorough science in order to back health policies and recommendations when such data was insufficient or just plain missing. The public has been asked often during the Covid response to believe [and comply] with unscientific policies yielding well-known detrimental ends.
Universal lockdowns, across-the-board school closures for children, a heavy reliance on highly erroneous PCR tests and packing nursing homes with Covid-positive patients have extended out deaths and despair while grinding down societal health and well-being to a nearly unrecognizable state.
Experts and policy-makers, among others, are to blame. But now something has changed. A worn facade of proclaiming to be following the science only to act contrary to it has given way to a religious-like fervor. A strange, uncomfortable, cult-like brainwashing and intimidation scheme is attempting to mesmerize, bully or otherwise lure the public into compliance.
Society is being led further away from sound science by ‘officials’ and ‘experts’ who ask for our trust based upon magical thinking. Why have we allowed such a degree of medical and health charlatanism, often favoring corporate bottom lines and the vertical integration of power, to be wielded by those who have not earned the trust of The People?
What will you do in 2021 to avoid this continued sliding away from truth, reality and common sense?
Study Finds 68% of Children Report Side Effects from Wearing Masks (Germany)
The results the first German study on children and teenagers wearing mouth and nose coverings reveal 68% complain of wearing a mask. Researchers at the university of Witten Herdecke had set up the first registry to report effects of wearing a mask in children. 363 doctors were invited to report their findings and ask parents and teachers to register side effects of masks. They were surprised by the elevated number of reports, as they found complaints affecting 25,930 children were entered in less than 6 days
Most common issues were
Irritability (60%)
Headaches (53%)
Difficulties concentrating (50%)
Sadness (49%)
Reluctance to attend school (44%)
Malaise (42%)
Impaired learning (38%)
Fatigue and drowsiness (37%)
Other physical symptoms included rashes and allergies around the mouth, syncope (20%)nausea (16, 6%), hyperventilation (12%) fainting spells (2,2%)
In addition 25% of the children had developed anxieties. Asked what they were thinking about the measures, 41% of the parents estimated they should be milder and 31,6% estimated they were inappropriate.
The investigation concludes that high frequency and type of symptoms reported ask for a broader investigation into specific risks for children and to reevaluate measures imposing mouth and nose covering for young people.
The “adults need to collectively reflect the circumstances under which they would be willing to take a residual risk upon themselves in favour of enabling children to have a higher quality of life without having to wear a mask”.
New York Senate Bill 416 authorizes quarantine of individuals or groups who “potentially pose a threat to public health,” including forced testing and vaccinations. This must stop now. This Ice Age Farmer broadcast is NOT available on youtube due to the subject matter.
We welcome Reiner Fuellmich. After a general presentation and his analysis on the pandemic, he tells us about the actions he is leading, the legal and judicial situation in Germany where the system is locally under the influence of certain companies, international cooperation and “loaded dice” by the PCR tests of the much criticized Dr. Drosten.
Truth Comes to Light editor’s note: This video made use of YouTube’s transcript option and, unedited, it naturally contains a lot of errors. Below, we are providing some excerpts where you will find corrected names, etc.
[Original video available at FranceSoir YouTube channel. As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Topics of discussion include:
Background of Dr. Reiner Fuellmich’s involvement with the lawsuits
Key lies that are the basis for the fraudulent pandemic
Class action in the United States, Canada and Australia
Malpractice lawsuits internationally
Various lawsuits for individual situations
Excerpts:
I did remember, however, that there was a similar thing that happened years ago but I couldn’t quite remember the details of this. And that’s why I called my friend Wolfgang Wodarg who was a medical doctor. And I asked him about what he thought about it. He explained to me that I was remembering the right thing — it was the swine flu, which was 12 years ago. And he said it looks very much like the swine flu all over again — because it’s the same people playing the same roles. Panic. Making people panic. The same professor Drosten of Charity University, the same Neil Ferguson of the Imperial College in London. Same people.
And he told me to take a closer look at what some of the other experts said, because we knew very quickly that the only person who the German government relied on was this infamous, now infamous, professor Drosten. So he pointed out to me that there’s Ioannidis of Stanford University and Michael Levitt of Stanford University. Plus a number of German scientists who have a entirely different view of the situation.
___
…it’s quite clear that this is like World War III, and probably worse. A lot of people are committing suicide.
___
So the final question was, ‘what about the PCR tests?’. And when we looked at this, it turns out that there’s one major player who’s — now it’s called the Drosten paper which was published on, I think January 23rd. This major player is professor Drosten — who as it turns out is neither a professor nor is he a doctor. Because the dissertation, that finally was found by the people… who had been looking for it for months and months and months, turns out to be a piece that was probably produced in June of this year, but not in 2003 or 2002 as he as he claims it was.
So that got us really interested in this, because if somebody lies about his academic background then the next question is — is he telling the truth as far as what he’s saying in this now infamous Drosten paper, in this paper he claims that he had invented a new PCR test which was capable of detecting infections.
In another paper, that was published a little later, he claims that there are asymptomatic infections. Now you have to read this together because — what does that mean? If there really are asymptomatic infections, that means that people out there who have no infections whatsoever are dangerous because they may be infectious. If it’s not true then we don’t have to worry about that.
Up until then it was quite clear that anybody who didn’t have any any symptoms is not infectious — is a healthy person. I mean, who goes to see a doctor when they don’t have any symptoms? But all of a sudden this brand new claim stated there are asymptomatic infections. And this is, I think, really important to know because, if there were asymptomatic infections, then it would make sense to be afraid of everyone. If not, then the whole thing collapses like a house of cards.
The other thing is, what about the PCR tests? And it turns out that PCR tests — even though a PCR test is a great thing to amplify things that the human eye normally cannot see — it doesn’t and cannot tell you anything about infections. The inventor of the PCR test Kary Mullis said this over and over and over again. I listened to all of his videos. Great guy. Intelligent. Witty. Smart.
___
So we listened to, I think in the meantime, over a hundred experts from all over the world — scientists, doctors, economists, lawyers — and as far as the scientists are concerned — the immunologists, the biologists, all of them said ‘No way can a PCR test tell you anything about infections’.
Because the one major problem it has — first of all it isn’t designed and it isn’t admitted for diagnostic purposes.
___
So what do we have here? We have two blatant lies. These are false statements. And we know that this man made them knowingly because he’s supposedly an expert on PCR tests. And we know that he lied on purpose because there’s an interview with him from six years ago, I think that was during the MERS flu, which is also a corona virus, a different one, but still. And that’s when he said that the PCR tests are so sensitive that they test positive to almost anything — and that, in many cases, it tests positive on healthy people. So he knew what was going on. And, even then, he also knew that the mainstream media played a big role in this. Because in this interview, he said ‘and you also have to take into consideration’, he pointed out that the mainstream media are causing quite a ruckus, quite an uproar.
___
If there are no asymptomatic infections, what’s going on? So we arrive at the conclusion — that is our current conclusion — that there’s some other agenda being pushed, which has nothing to do with health, and everything to do with control and power and money.
___
A class action is something that you can use when you have a huge, or a large number, of people who suffered damages because of one single damaging action. In this case it’s the lockdowns. The Drosten-PCR-test-induced lockdowns. And that’ll be a problem for Mr. Drosten and the people who he cooperates with — W.H.O. and others who are behind this — because they sold these PCR tests, these Drosten PCR tests, throughout the world.
___
…it looks as though the mistakes were made on purpose in order to drive up the numbers of infections which are really only false positives.
___
…The first complaint that we filed is — we’re representing our friend Wolfgang Wodarg because he was accused by a group of what is now called “fact checkers” (which is nothing else but people who are bought and paid for by youtube, twitter, facebook in order to defame people who express an opinion that is not in agreement with the government’s opinion, in particular when it comes to covid and PCR). So these people called him a liar because he explained that PCR tests cannot tell you anything about infections. Now if they call him a liar, they have to prove that he’s the liar. So we’re suing them for defamation… Today we’re sending out another brief to Drosten himself, explaining to him that he has to retract his ideas, but that, even at this point, he is civilly liable for the damages that he caused.
___
The most important thing is, of course, to get these class actions started, both in the United States and in Canada, and if possible, also in Australia. How this works is as follows: A person who suffered damages in the United States, or in Canada, or in Australia, because of these Drosten-PCR-test-induced lockdowns can file a complaint against Drosten, against the W.H.O. — or anyone else who, in the United States, Canada or in Australia claims that the PCR test that they’re selling tells you something about infections.
Now, if then, they explain to the judge that they’re not the only ones who are suffering harm, but that there’s thousands and thousands of more people who suffer the same kind of damage, they can ask the court to let this case go forward as a class action. Meaning, if the judge decides, yes, this makes sense to be tried as a class action, then anybody who suffered the same kinds of damages can join this class. What the judge will then do is publish this. And, if it’s going to be an international case, then he’s going to publish this worldwide in all the mainstream media — so that anyone who suffered damages because of this same illegal action can join the class. They don’t have to, but they can. They can still file their own complaints but the power of this class action is that you have — in the end, you have probably hundreds of thousands, I think even millions, of plaintiffs who are all in this one case together. But only one case, for the so-called representative plaintiff — someone who suffered typical damages — one case is tried. If this case is won then everybody else wins too.
___
We’re cooperating with all of our colleagues in Italy and France, in Spain, Austria, Switzerland — all of the countries from which lawyers have approached us. And they all get everything they need from us.
___
There are other actions that are going to be filed for malpractice. Yes. Because we know that, in particular when it comes to New York and Bergamo, Italy… The pictures of these places were shown all over the world in order to scare people, in order to tell them ‘this is what’s going to happen if you don’t do as we are telling you’. Because they needed these pictures in order to make people panic — put them in panic modes — so that they won’t ask any questions but do as they’re told. Wear masks, for example. Social distancing, for example. You have to have a lockdown, for example.
We know now from talking to the doctors from New York and from the United States, and from talking to a network of doctors in Italy and in other places that these pictures were staged.
___
…We’re waiting for a trial date to be set by the court here in Berlin. I know that, very soon, there’s going to be a similar complaint to be filed someplace in the United States — within the next couple of days I think. And I know that within the next couple of weeks a real PCR class action case will be filed in Canada.
___
I wish we had acted sooner, but it took us a while to understand what was going on. And you can’t go to court unless you have the full picture. Now we have the full picture, we believe. In our opinion, this is a staged pandemic — staged for completely other purposes than health care.
As I said, this is about money, power, and control over the people. And so this is actually the last step. Collecting damages should be the last step.
What we’re all working on right now — because we have to get our priorities straight — is to… we’re filing criminal complaints and administrative law complaints in order to stop the EMA [European Medicines Agency] — the European commission that decides on whether or not to admit these vaccines — in order to stop them from admitting these vaccines, because as we know now they’re extremely dangerous.
They’re not vaccines. This is genetic engineering.
___
[speaking about situation in Germany] I think there are about thirty percent of the population who are completely in line with the government, and who, if they had a choice but probably would wear three or four or five masks on top of each other. But then, there’s 20 percent who are of the opinion that there’s something seriously wrong and this should be stopped very soon. But 50 percent of the people — that’s what we estimate — are beginning to ask more and more questions. And, if I read my sister correctly, and other nurses and doctors who I spoke with, at least 90 percent of the people do not want vaccinations.
Tomorrow we’re meeting with a large group of lawyers and we’re going to decide who’s going to do what. Some of us are going to go to administrative law courts, some of us are going to work with the tort law cases — which is my specialty– and others are going to do criminal law.
___
More and more doctors are coming out of hiding and are approaching us, the Corona Committee, through our whistleblower tool. So things are beginning to boil…
The Italian citizens’ organization Corvelva has finally forced an inquiry into the quality of vaccine lots after having financed independent analyzes of different vaccines that showed many samples are not compliant with quality standards and health product regulations.
Corvelva just issued a press release of the decision made by the Public Prosecutor’s Office in Rome on December 28th. They proudly announced that « our analyzes, which had led to a complaint to the Public Prosecutor’s Office of Rome, after a request for dismissal made by the Public Minister and with our subsequent opposition last year, were today considered worthy of further study. The judge in charge issued AN ORDER in which he indicates to the Public Prosecutor the need to proceed with investigations.
Particularly interesting is a quote of this decision that emphasizes the need to provide real scientific answers and not get away with administrative or legal arguments.“It is believed that a merely formal response to the complaint is not sufficient to overcome the technical and scientific arguments of the exponent”. This sentence was written as a response to the Public Ministry who had motivated his request to dismiss, by arguing that the effectiveness of the controls of the Italian and European health agencies “cannot be questioned by the results of the analyzes carried out by private individuals”.
The order finds that arguments of the complaint are “detailed” and that it is therefore considered necessary to investigate what was reported.
Therefore there is an indication to proceed with independent analyzes by the health security police department to see if the findings can be reproduced.
Mattia Marchi a member of the Corvelva team summarizes the whole story:
On July 31, 2017 the Italian government decided to impose 10 mandatory vaccines for children. In our opinion this law made no sense, was contrary to science and logic and to our fundamental rights.So from that moment on our organization Corvelva decided to oppose it in every way. One of the strategies chosen was to go verify the compliance of vaccines marketed in Italy and Europe. Initially we had identified 7 vaccines (1) of which 5 vaccines had shown major discrepancies compared to the data sheets. From here we decided to study in depth both the efficacy and safety of 4 vaccines, analyzing them both under the chemical and metagenomics (biological) aspects. We found issues so serious that we were obliged to proceed with the investigation, always making everything public. (2)
While we proceeded with the study and analysis of these 4 vaccines, Priorix Tetra, Gardasil9, Hexyon and Infanrix Hexa, we deposited the results to all Italian and European control bodies, also opening a complaint to the criminal court of Rome. For almost 2 years we have received summary and delayed responses, focused more on the fact that we are considered antivaccine rather than on the merits of the data presented, but today we are proud and happy to share the big news: our complaint is validated and the judge has instructed an investigation”.
This decision is truly unprecedented worldwide and signs a first victory against the lack of accountability of vaccine makers and health institutions.The issue of vaccine quality is of extreme importance as the public needs to be certain that vaccine products contain what they claim, nothing less and nothing more. It goes beyond the pro- or anti-vaccine debate and it can open new legal avenues.
Children’s Health Defense has been following Corvelva’s work closely and had published some of their findings relevant for the American public on their website. Read here the articles reporting about the quality issues (for example the presence of amphetamine residues and retroviruses) in theGardasil vaccine and about the DNA from fetal cell lines contained in vaccines last year.
You can read all details on their website in the series ‘Vaccinegate’ with specific analysis for each vaccine. For the European people, the reports on the MMRV Priorix Tetra vaccine (GSK), Hexyon (Sanofi) and Infanrix Hexa (GSK) are a must read as these are major pediatric vaccines marketed in Europe.
We will not review their findings here, but some of the results are very concerning, for example the fact that in some cases (Priorix and Infanrix) the required quantity of antigen could not be detected. No antigen means it can’t work and it should normally be withdrawn from the market with immediate effect.Will the Italian investigators do their job?How far can we trust our health institutions in their mission to protect the public? This time we need answers.
The latest example of hypocrisy is Dr. Deborah Birx, White House coronavirus advisor. It turns out she traveled to meet her family for Thanksgiving after telling Americans not to travel, not to gather with family outside their immediate households.
Gavin Newsom, the governor of California, told the public they should celebrate Thanksgiving outdoors. Then he was caught having dinner, indoors, at a restaurant, unmasked, with 12 people.
There are other examples.
The usual explanation: these officials are arrogant and believe they’re above the law. They want to thumb their noses at the little people.
Yes, no doubt. But a more direct reason is staring us in the face.
The hypocritical officials know the whole COVID pandemic is a fraud.
They know there is no danger.
They know the lockdowns are unnecessary.
That’s why these officials break their own rules.
Why would they expose themselves to “the virus,” unless they knew they were safe?
Some of them believe they’re trapped in a political apparatus that offers no exit. They must go along with the show. They must participate in the fraud because, for example, federal dollars flow into their states, and those dollars are contingent on “playing the COVID game.”
Other officials have been bribed, blackmailed, threatened.
Regardless, they know they can flout their own rules because there is no health risk, no danger.
The risk is on the level of betting on a boxing match, when the bout is fixed, and you know who will win.
People will say, “These officials aren’t smart enough to figure out COVID is a fraud.”
You don’t have to be smart, you don’t have to understand all the intricate details of the fake test, the fake case and death numbers based on the test. You just need to understand enough.
You just need to be clued in.
This would suggest the COVID fraud is an open secret, shared by many in power. I believe that is exactly the case.
For purposes of comparison, consider a level of “secret understanding” slightly above that of politicians. Government scientists.
These scientists are fully aware that the PCR test for COVID is a complete hoax—for reasons I’ve detailed over the past nine months. Therefore, the scientists also know the case numbers based on those tests are fraudulent. And they know the case numbers are used as the rationale for the lockdowns.
That’s a lot of knowing. That’s a lot of “open secret.”
Here’s another comparison. PCR techs in labs all over the world, who are running the test, are fully cognizant of the crimes they’re committing every day—by utilizing “too many cycles” and therefore destroying any shred of validity when diagnosing ANYTHING.
Sharing this open secret among themselves, they otherwise remain silent.
Getting the picture?
The open secret of the COVID fraud isn’t confined to a dozen people in a sealed room. It’s high and wide. It’s understood by many in positions of power and responsibility, all over the world.
You can add your own lists of “secret sharers.” Mainstream physicians, for example. Physicians who are in charge of administering the COVID vaccines they know are unnecessary and dangerous. They also remain silent. So do certain news media people.
And since there are so many people who know the real score, we can begin to see the degree and extent of complicity that is driving the whole pandemic hoax.
This isn’t only a small conspiracy of movers and shakers who planned it and launched it.
This is a very wide-ranging conspiracy of silence.
“Don’t blame me. I’m just following orders.”
“But you know COVID is a total fraud.”
“Of course I know.”
“And you know others who know.”
“Many others.”
“Case closed.”
Which is to say, case WIDE OPEN.
The COVID situation is directly analogous to the Nazi, USSR, and Chinese bureaucracies; faceless workers passing on and obeying orders.
Many of the workers know those orders, no matter how they are dressed up, are arbitrary and evil.
The orders are initiated to destroy lives and freedom, and are transferred through the human machinery of The Complicit Silent Ones.
In early 2020, the WHO accepted a PCR test for “SARS-CoV-2” that was designed without having possession of the virus. Yet the test is meant to detect…the missing virus. This is evidence of deep criminal intent. [1]
But as of December 14, 2020, WHO has made a correction [2]. Thereby blowing its own cover. Why?
Two reasons. Huge numbers of people have caught on to the PCR test scam. And by their correction, WHO paves the way for “declining COVID case numbers”—thereby making it appear the new vaccine is a roaring success. I predicted this development. [3] [4]
A brief review. The PCR test (a complete fraud for several reasons) is run in “cycles.” Each cycle is a giant magnification of a tiny portion of the swab sample taken from the patient.
As I’ve reported, even Tony Fauci readily asserts that if the PCR is run at 35 cycles or higher, it’s meaningless. [5] [6]
Every positive result—indicating “infection with the virus”—occurring at 35 cycles or higher is meaningless.
BUT, as I’ve also pointed out, public health agencies recommend running the PCR test at up to 40 cycles. Therefore, labs comply.
Therefore, millions upon millions of PCR tests results, over the last nine months, which indicate “infection,” are a vast lie.
Therefore, the COVID case numbers are a vast lie, and the lockdowns, which are based on those numbers, are absurd, insane, criminal, and predatory.
NOW, the WHO is walking back their stance on how the PCR should be run, for the reasons I mentioned above.
The WHO document is titled, “WHO Information Notice for IVD Users/Nucleic acid testing (NAT) technologies that use real-time polymerase chain reaction (RT-PCR) for detection of SARS-CoV-2.” [2]
Here are the money quotes. The language is mealy-mouthed, intentionally confusing, cautious, and sterile. Nevertheless, we can see the intent to lower the number of test cycles.
“Users of RT-PCR reagents should read the IFU [Information for Use] carefully to determine if manual adjustment of the PCR positivity threshold is necessary to account for any background noise which may lead to a specimen with a high cycle threshold (Ct) value result being interpreted as a positive result.”
Translation: Using too many test cycles—aka “high cycle threshold (Ct) value”—has resulted in patients being told they’re infected, which is a lie.
“In some cases, the IFU will state that the cut-off should be manually adjusted to ensure that specimens with high Ct values are not incorrectly assigned SARS-CoV-2 detected due to background noise.”
Translation: Running the test with a high number of cycles yields “background noise”—aka a false positive result. The patient is told he’s infected but he’s not.
“The design principle of RT-PCR means that for patients with high levels of circulating virus (viral load), relatively few cycles will be needed to detect virus and so the Ct value will be low. Conversely, when specimens return a high Ct value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain.”
Translation: When the test is run with a high number of cycles, we can’t tell the difference between “irrelevant” and “meaningful.”
A frank and honest translation of the WHO message: “We’re changing the way we’re doing PCR tests. We were running them with a high number of cycles and getting millions of false positives, and those numbers were deployed to justify the lockdowns—but NOW we’re moving to a lower number of cycles. This change, all on its own, will result in fewer positive results, fewer case numbers, making the vaccine look VERY GOOD.”
The WHO is still crazy, still criminal, but not entirely stupid. They know what they’re doing and why.
Trial Lawyer Dr. Reiner Fuellmich: International Lawsuits Take on the Fraudulent Pandemic, Based on the Big Lies Around PCR Tests & Asymptomatic Infections
Dr. Reiner Fuellmich is a German American lawyer with experience going after large companies like Deutsche Bank.
He is a member of the German Corona Investigative Committee. He discusses the current situation and his efforts to bring justice to the situation.
This interview was done as apart of the full length documentary. We are releasing the full interview for the betterment of public understanding of the situation.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Excerpts:
“Our focus is on the PCR test because if we manage to convince a court of law that this is a fraudulent enterprise — the PCR test being marketed with the assertion that it can detect infections. If we can convince a court of law that this is a false statement, then the whole house of cards is going to come crashing down because there’s nothing else.
That is the tool that they’re that they’re using in order to keep people in panic mode. And there’s no basis for this panic because, as I just pointed out, even according to the WHO which couldn’t quite escape the conclusions of John Ioannidis, the mortality is, or lethality is, roughly the same as that of the common flu.”
___
“And also there’s already herd immunity. That’s another thing that has been overlooked. So there’s absolutely no reason for vaccines except for the pharmaceutical industry to make money and probably cause a lot of damage as far as health. And even there’s probably going to be a lot of fatalities too because these vaccines haven’t really been tested properly.”
___
“This is not gonna be one single lawsuit. It’s gonna be a number of different lawsuits that are going to be filed both on here in Germany on this side of the Atlantic and in the United States.”
___
“The intent is, or the intention that we think is important here, is to uncover the whole thing– to use what we’ve learned through the corona committee — to use these pieces of evidence and the experts that we’ve heard in order to convince a court of law that this is a staged pandemic and that there’s other goals, other people who are behind this, and trying to push completely different goals. This has nothing to do with the world’s health.”
___
“We know that there’s something in the background but it’s not important for our lawsuit. For a lawsuit, we can concentrate on one thing only. These people lied when they’re telling the general public that PCR tests can tell us something about infections. “
___
“…but trying to use fear so that people will believe everyone, even their closest neighbors and relatives is a danger to them could be a super spreader, even if they’re completely healthy and show no symptoms. That’s why I’m saying. It’s not just a lie about ‘PCR tests can tell us something about infections’. In addition, they needed to lie about ‘people can be infectious even if they don’t show any symptoms’.”
___
“One of the law professors who advises us in the background pointed out to me, in this tort case there are two really important lies that have to be put front and center: One is PCR tests can tell us something about infections. The truth is it cannot. In particular, not the way these PCR tests, the Drosten tests are set up…”
___
“Lie number one, you cannot tell anything about infections by using these PCR tests because what they do is they test positive to almost everything, including, for example the debris, the fragments, of a common cold, of of your immune system’s fight against the common cold.
Lie number two, even more important I think, is — he says that there are asymptomatic infections. Which basically means anyone who is surrounding us, our relatives, our friends, and who shows no symptoms, who’s perfectly healthy or appears perfectly healthy, could be a threat. That’s what this induces. That’s what this fraud — there are asymptomatic infections — induces. It tells us, ‘oh my god, everybody could be potentially dangerous’. That is not true.”
___
“We have had not just lawyers who are trying to help, more and more lawyers who are coming out of hiding more or less, but we’ve also — The Corona Committee, that is — we’ve also had judges calling us, getting in touch with us, and asking us how they can help. “
___
“From what I’ve read and the people who we talked to here on this committee, historians and journalists, this is the so-called Great Reset that some very rich players of the corporate world, including Bill Gates, but also including Klaus Schwab. He’s using his World Economic Forum as a meeting forum for the corporate elite, self-appointed corporate elite, and the self-appointed political elite — to influence them, to manipulate them, to basically lobby them. What the goal is probably — probably population reduction is one of the goals, so that the resources of the world will last longer for those who will survive this. That, in my opinion, is one of the goals, maybe the basic goal.”
Every Scary Thing You’re Being Told Depends on the Unreliable PCR Test
Since the COVID-19 crisis began, all of the WHO and Government so-called ‘mitigation’ policies – lockdowns, social distancing, masks, shutting schools etc, have all been based on data of coronavirus “cases” gathered from the increasingly dubious PCR Test. Despite its many fundamental flaws – and even an warning by its inventor, Nobel Prize winner Kerry Mullis, who explicitly said not to use his test as a diagnostic for any virus – governments, the medical establishment, and even Dr Anthony Fauci himself, have chosen to base their entire COVID ‘pandemic’ narrative on this highly inaccurate testing regime.
The following video presentation is a summary of the pitfalls of the PCR Test and why no responsible medical professional or public health official should be treating it as a legitimate medical diagnostic tool, but rather only, as Mullis himself instructed, as an auxiliary ‘research aid’. Research links for this video have been provided below.
Carl Heneghan Giving Evidence to House of Commons Committee:
https://www.parliamentlive.tv/Event/Index/52ee1eec-a2bf-403d-a27d-7bba077ebfcc
RELATED INFORMATION:
An essential problem that many PCR tests have is called the “cycle quantification” (Cq), also know as the “cycle threshold” (Ct), these two different terms are explained here:
https://archive.is/R0QgM
The Cq/Ct value specifies how many cycles of DNA replication are required to detect a real signal from biological samples. As it says in the MIQE guidelines (https://bit.ly/2T5Wpm2) “Cq values higher than 40 are suspect because of the implied low efficiency and generally should not be reported.”
MIQE stands for “Minimum Information for Publication of Quantitative Real-Time PCR Experiments”, a set of guidelines that describe the minimum information necessary for evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
The inventor of the PCR test himself, Kary Banks Mullis, agreed, when he stated: “If you have to go more than 40 cycles to amplify a single-copy gene, there is something seriously wrong with your PCR.” Source for the above quote: https://bit.ly/346XeRY
The MIQE guidelines have been developed under the guidance of Stephen A. Bustin, Professor of Molecular Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of Quantitative PCR which has been called “the bible of qPCR (https://en.wikipedia.org/wiki/Stephen_Bustin). According to Bustin, a Cq in the 20s to 30s should be aimed at and there is concern regarding the reliability of the results for any Cq over 35. If the Cq value gets too high, it becomes difficult to distinguish real signal from background, for example due to reactions of primers and fluorescent probes, and hence there is a higher probability of false positives.
PCR Test unable to distinguish between signals from dead or live viruses: “Molecular techniques based on real-time polymerase chain reaction (qPCR) allow the detection and quantification of DNA but are unable to distinguish between signals from dead or live cells.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4889745/ (archive: https://archive.is/x5gak)
Covid19 PCR Tests are scientifically meaningless:
https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/ (archive: https://archive.is/R4gPW)
The Trouble With PCR Tests:
https://swprs.org/the-trouble-with-pcr-tests/ (archive: https://archive.is/g1PKx)
PCR as “Useless Testing”:
http://eu-chronicle.eu/2020/08/useless-testing/ (archive: https://archive.is/IF4yS)
Was the Covid-19 test meant to detect a virus?
https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/ (archive: https://archive.is)
Corona: creating the illusion of a pandemic through diagnostic tests:
https://blog.nomorefakenews.com/2020/04/08/corona-creating-illusion-of-pandemic-through-diagnostic-test/ (archive: https://archive.is/noPQz)
Are you infectious if you have a positive PCR test result for COVID-19?
https://www.cebm.net/covid-19/infectious-positive-pcr-test-result-covid-19/ (archive: https://archive.is/sv06K)
BBC: Coronavirus: Tests ‘could be picking up dead virus’:
https://www.bbc.com/news/health-54000629
(archive: https://archive.vn/vx6JG)
[Truth Comes to Light editor’s note: The PCR tests are being completely misused when looking for cause of infectious disease. In the case of Covid19, they are looking for a virus that has never been isolated — meaning they are looking for something not known to exist outside of a computer model. To say that a certain number of cycles, as stated by several in this video, will help in determining who is infectious, makes no sense at all. Exactly what are they looking for when the virus itself has never been isolated? Kary Mullis, inventor of the PCR test, tried to make it very clear that this test could not be used for determining infectious disease. Add that to the questions about the role of viruses in infectious disease and the entire convoluted narrative falls apart. The Covid19 narrative is fraud to the bone. To understand the unfolding truth revelations, see the work of Jon Rappoport, Dr. Andrew Kaufman, Dr. Tom Cowan, Dr. Zach Bush, and many others whose work we share here. ~ Kathleen]
Catherine Austin Fitts: The “Pandemic” as Cover for a Coup D’Etat Aimed at Taking Over the Planet — Converting Democratic Process to Technocracy, Imposing Complete Economic & Political Control
“If you look at what needs to be done, the problem — we don’t have the power to stop the central bankers from doing what they’re doing, but my prediction is they will fail. It’s too hard. It’s too complicated. And it’s too outside the laws of nature or the laws of divine intelligence.” ~ Catherine Austin Fitts
This sit down interview with Catherine covers the spectrum of the current situation we find ourselves in.
It was conducted as apart of the full length documentary. We are releasing the full interview for the betterment of public understanding of the situation.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Transcript:
“I used to say — I used to have a pastor who would say “If we can face it, God can fix it”. And I believe that many things are possible if we can face it.
So again, transparency is very important.
If you look at what needs to be done, the problem — we don’t have the power to stop the central bankers from doing what they’re doing, but my prediction is they will fail.
It’s too hard. It’s too complicated. And it’s too outside the laws of nature or the laws of divine intelligence. And the issue then becomes, how do we as a people, pick up and build a human civilization? So, you know, they decided they couldn’t do a human civilization. They’re doing something I think will fail. And the question for all of us is, how can we make sure we can take things right if, and when, they fail.
So everybody knows my favorite bible story is the story of Gideon. And that’s my prediction for what’s going to happen…”
___
“The story of Gideon is a long story. I won’t tell the whole thing. But, essentially an angel of the Lord comes and asks Gideon to throw the Midianites out of Israel and Gideon insists he’s too unimportant, and too helpless to do it. And the angel of the Lord says, ‘Well, that’s okay we’re gonna do it. You’re perfect because everybody will know it was us, not you.’
So, in fact, Gideon calls for an army and the angel of the Lord… makes him go through very many tests to make him realize that he doesn’t need a big army, he just needs people who are faithful and competent. And, in fact, in this environment my advice to everybody after they come clean is strip your life down to the people who are, you know, faithful and competent. And then, so Gideon comes down the side of the mountains. The Midianites are sleeping in the valley below. And he comes down with Gideon’s army, banging pitchers and lanterns. And the Midianites are so hateful and suspicious of each other, they jump up at the dark and kill each other.
And, in fact, every time I’ve seen someone bring tremendous transparency to what’s happening, that’s what happens. The Midianites — fight breaks out and the Midianites start killing each other. And if you look at what these guys are trying to do, it’s so hard and complicated, I think the Midianite thing is going to happen par excellence.
And the question for all of us is, okay, what’s our plan, if and when that happens…”
___
“My plan is to build a human civilization. And, again, first you bring transparency, then you rebuild the economy, bottom up…
We are now integrating very powerful technology and that means we have to be — we have to grow spiritually. You can’t have this kind of advanced technology managed by cavemen. And, to a certain extent, that’s what we’re watching. We’re giving very powerful weaponry and very powerful surveillance technology to people who are using it, behaving like cavemen.”
___
“…I think, first and foremost, what we’re dealing with is spiritual. You know, this is part of a ten thousand year old war and the outcome depends on our our ability to spiritually evolve and grow up.
So, you know, I tell everybody death is not the worst thing that can happen… What can happen is, you can lose your immortal soul. That’s your danger. So stop worrying about death and start worrying about, you know, whether you’re going to be free or not.”
Truth Comes to Light editor’s note: This documentary appears to be linked with the Plandemic — Indoctornation project. It was created with the invitation “please share” at the close of the video. Our original source was davidicke.com but it is found on many platforms and websites. None of the sources that we found share creator/producer information. ~ Kathleen
Available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels.
[Satire] UK Bans Certain Spoken Sounds That Are Believed to Spread Covid-19
[Truth Comes to Light editor’s note: Satire by retired PR consultant and freelance translator, Peter Prowse. Peter announces the new UK policy wherein sounds produced by the letters P, T and C will be phased out and replaced with the sounds produced by N, F and L. The video went viral and is now found all over the internet.]
Ever since the world became aware of Covid-19 in early 2020, we have warned of the possibility that the government response may turn out to be worse than the condition itself.
Many have described this response as a form of medical tyranny, sold to us as a temporary measure for the greater good. Two weeks to flatten the curve they said.
Four months into the lockdowns, some of us half jokingly said things like, “I hope they lift the lockdowns before the 4th of July, so we can celebrate our freedoms.”
Now we find ourselves eight months into a two-week lockdown with no end in sight, despite the fact that a federal judge in Pennsylvania ruled the shut downs were unconstitutional. The Michigan Supreme Court also ruled that the Governor’s emergency orders had violated the Constitution. So why hasn’t anything changed?
In this interview, Spiro’s guest Dr. Pamela Popper discusses two new lawsuits that she believes could end Covid-1984. The two lawsuits, one in Ohio and one in New Mexico, challenge the root of the problem: the emergency itself.
In a CDC document titled, “Coronavirus Disease 2019 (COVID-19) 2020 Interim Case Definition, Approved April 5, 2020,” under the section, “Laboratory Criteria,” we have this: [1]
“Detection of severe acute respiratory syndrome coronavirus 2 ribonucleic acid (SARS-CoV-2 RNA) in a clinical specimen using a molecular amplification detection test.”
The test referred to is the PCR. And as you can plainly see, it is detecting, not the virus itself, but a piece of RNA.
A piece of RNA ASSUMED to come from the virus, SARS-CoV-2.
I say ASSUMED because, where is the actual virus? Where is the virus isolated from all surrounding material?
If you don’t have the virus, you can’t say, with any degree of certainty at all, that you have a piece of it (the RNA).
As I’ve described many times, “isolated” is a term that is tortured by researchers and public health officials, so that it means just the opposite of what it is supposed to mean. [2]
Numerous studies that claim the virus has been isolated actually turn out to mean: “We have the virus in a soup in a dish in the lab. The soup contains various types of animal and humans cells, toxic chemicals and drugs, and other genetic material. The virus is completely surrounded, but it is there. We know this, because some of the cells are dying, and this dying must be the result of infection with the virus…”
This argument not only turns the definition of “isolation” on its head, it reveals, upon a moment’s consideration, that the dying of the cells could come from the action of the toxic chemicals and drugs; and on top of that, the cells are being starved of nutrients, so they could be dying as a result of that deprivation.
Therefore, to say “the virus must be in the soup in the dish in the lab” because is killing cells…well, that’s completely unproven, and therefore…
There is no reason under the sun to claim that the virus is there in the soup at all.
Hence, the claim that the PCR test is detecting a piece of RNA from the virus is unwarranted. Because, again…where is the virus? Where is the truly isolated virus?
Nowhere.
And on that basis alone, the PCR test is irrelevant, useless, and deceptive.
It is set up to look for and detect a piece of RNA material that has never been proved to come from this un-isolated phantom ASSUMPTION, called “SARS-CoV-2.”
A few more moments of clear thought, and you realize the whole string of “science” that leads to the lockdowns and the economic devastation is not science at all.
It is what is called, in the intelligence community, a cover story. A story launched to justify crimes.
As we approach the final days of 2020, Spiro is joined by author, journalist and recently retired registered nurse, James Perloff, to reflect on what is widely considered to be the wildest and worst year perhaps in our lifetimes.
The media and the governments around the world would like us to believe this is all by chance and we must blindly follow their mandates and restrictions in order to mitigate this crisis.
Spiro and Perloff delve beyond the surface of this crisis to explore potential motives behind what appears to be a pre-planned agenda attached to the current crisis in order to facilitate the most significant transition in human history.
James Perloff shares information from his new book titled COVID-19 and the Agendas to Come, Red-Pilled which reveals what the social engineers have in store for the future of humanity.
So the gov’s latest wheeze in an effort to breathe more life into its dying terror campaign has been to respond to “advice” from “experts” that it should be “worried” and “concerned” the COVID9 bug has developed a mysterious “variant” that has caused it to accelerate the rate at which it is spreading.
Having received their stimuli, Boris and Co have duly reacted in the manner of Pavlov’s dogs, turned up the dictatorship another notch and launched WEDs (Weapons of Economic Destruction) against London, ably assisted by its Mayor, Genghis Khan.
This is all being done according to the scientific methodology known as MSU (Making Sh*t Up) so favoured by oppressive regimes the length and breadth of the United Kingdom.
In line with MSU’s compulsory voluntary guidelines there’s no actual scientific evidence produced unless you count “advice” from faceless subversives, and “concern” or “worry” or Barmy Boris looking mental on TV (or Hatt Mancock looking shifty) as scientific evidence.
The government of course feels that telling everybody repeatedly that it is “following the science” is enough science, especially as science can be inconvenient and time-consuming if you have to spend days or weeks rigging the results or faking the stats – the time after all can be better spent panicking or grinding down small businesses and other government programs.
So what we apparently have is a government “concerned” about an accelerated spread of the bug because of “advice”it has received from somebody or other whose identities must remain secret for reasons of state secrecy.
That’s evidence is it?
Apparently it is at least enough evidence to justify bypassing Parliament (yet again) attacking London and turning various screws (social, economic, Yuletide, patience etc) on the populace.
And who are these freakin’ experts on whose puppet strings Barmy Boris and the rest of his intellectually challenged crew of nation wreckers are so happy to dance?
We are going to leave aside the fact that, by the way, the statistical evidence for the spread of the disease is derived from the ruddy PCR test.
The PCR test has more things wrong with it than Boris’ haircut. One of these is the minor technical point that it does not establish and never hasestablished the existence in anyone who tests positive (even in the minuscule percentage of cases where the positive is not false) of a live infectious virus.
Because of this (along with a host of other reasons) relying on the PCR test to “prove” the spread of the virus is about as sound as referring to the movie “Independence Day” to prove there’s a threat of alien invasion.
You can find out more on why the PCR test is a total fraud here
So who are those very wise but anonymous people with brains the size of a planet?
Well, professor Neil Ferguson for one, as the following article from the Spectator explains.
Leaving aside the fact that he is still advising the government when the government (in YET ANOTHER lie) said he would not be, why the hell does the government insist on using this bloke whose mathematical predictions (not to mention his personal ethics) were utterly, abysmally, horribly, blatantly, glaringly indisputably and undeniably wrong?
With the resources of the entire scientific community at its disposal, virologists, epidemiologists, mathematicians, statisticians and so forth, the gov is still taking advice from Ferguson? Is this indicative of the standards it will accept when the well being of the country is at stake?
Another, deeper, mystery in back of all this of course is this:
Why are we letting ourselves be governed to destruction by people so bereft of common sense, competence, sanity, honesty or even an interest in the survival of our country?
The Spectator at least has sided with the People and its article is well worth a read. Find it here.
Between Dec. 11 and 18, 2020, the U.S. Food and Drug Administration (FDA) granted Pfizer/BioNTech and Moderna pharmaceutical companies an Emergency Use Authorization (EUA)1 to distribute COVID-19 vaccines using messenger RNA (mRNA) technology that to date has not been licensed for use in humans.2345 Although the Advisory Committee on Immunization Practices (ACIP) of the U.S. Centers for Disease Control and Prevention (CDC) held two special Saturday meetings to create national vaccine use recommendations for the two vaccines,67 legally both vaccines remain experimental until they have been formally licensed by the FDA.8 As initial supplies of the vaccines roll out into the states and health care workers treating COVID-19 patients in hospitals and medical facilities are the first to be vaccinated, reports of vaccine reactions are emerging.9
On Dec. 19, 2020, at a special meeting of the ACIP,10 the CDC presented information released by the ACIP COVID-19 Vaccines Work Group “Anaphylaxis Following mRNA COVID-19 Vaccine Receipt.”11 According to the CDC, by Dec. 18 there had been six case reports of anaphylaxis following Pfizer/BioNTech vaccinations that met the Brighton Collaboration criteria for anaphylaxis, which is a potentially life threatening reaction that occurs when immune cells overreact to a substance that has entered the body and a hyper-inflammatory response is triggered involving sudden release of histamine and other chemicals that may cause:1213
skin redness, hives, and itching;
swelling of the eyes, lips, tongue, throat, hands, feet;
trouble swallowing and breathing, wheezing;
diarrhea or vomiting;
abdominal or chest pain;
fast or irregular heartbeat;
dizziness, sudden drop in blood pressure;
headache;
confusion, vision and speech problems;
shock/loss of consciousness;
cardiac arrest;
death
Foods are the most common triggers for anaphylactic reactions, followed by drugs/biologicals, insect stings, and idiopathic anaphylaxis (anaphylaxis of unknown cause). A shot of epinephrine is the first-line immediate treatment for anaphylaxis.14
Vaccines are known to cause allergic and anaphylactic reactions within minutes to four hours of vaccination, but CDC officials have long considered vaccine-associated anaphylaxis to be rare, stating in a 2018 study that:
Vaccine-associated hypersensitivity reactions are not infrequent; however, serious acute-onset, presumably IgE–mediated or IgG and complement-mediated anaphylactic or serious delayed-onset T cell–mediated systemic reactions are considered extremely rare.
The CDC confirmed that one person, who had an anaphylactic reaction following administration of the Pfizer/BioNTech COVID-19 vaccine, had a previous history of anaphylaxis after a rabies vaccination. The CDC said the reported cases of anaphylaxis are being reviewed by federal health officials.15
CDC Reports More Than 3,000 “Health Impact Events” After COVID-19 Shots
At the Dec. 19 ACIP meeting, a chart entitled “V-safe Active Surveillance for COVID-19 Vaccines” was presented indicating that between Dec. 14 and Dec. 18, there were 272,001 doses of the Pfizer/BioNTech vaccine administered and 3,150 “Health Impact Events” recorded, including 514 events in pregnant women after receipt of the Pfizer/BioNTech vaccine. The chart gave no further details about the nature of the more than 3,000 Health Impact Events recorded by the CDC.16
The CDC’s definition of Health Impact Events is “unable to perform normal daily activities, unable to work, required care from doctor or health care professional.”
Great Britain First Reported Anaphylaxis Cases After COVID-19 Shots
Britain was the first country to vaccinate frontline health workers and the elderly with the Pfizer/BioNTech COVID-19 vaccine beginning on Dec. 8. Within 24 hours, Reuters reported that there had been two cases anaphylaxis and one possible allergic reaction in health care workers receiving the first doses of the vaccine. Reportedly, both health care workers had a history of allergic reactions and carried an epi-pen. On Dec. 9, the chief executive of Britain’s Medicines and Healthcare Products Regulatory Agency (MHRA) stated that, “any person with a history of anaphylaxis to a vaccine, medicine or food should not receive the Pfizer/BioNTech vaccine.”17
Alaska Health Care Workers Had Allergic Reactions to Covid-19 Vaccine
On Dec. 16, The New York Times reported that two health care workers in Alaska who got the Pfizer/BioNTech vaccine suffered allergic reactions. One worker had a reaction serious enough to require hospitalization.18
A middle aged woman with no history of allergies experienced shortness of breath, elevated heart rate and a rash covering her face and torso within 10 minutes of receiving the vaccine. She was immediately treated with epinephrine and her reaction subsided but then re-emerged and she was given IV epinephrine and steroids, hospitalized in the intensive care unit for one night and spent a second night in the hospital further recovering. According to CNN, the allergic reactions experienced by the two Alaska health care workers after the Pfizer/BioNTech COVID-19 vaccinations were reported to the federal Vaccine Adverse Events Reporting System (VAERS).19
History of Anaphylactic Reaction to Previous Dose of COVID-19 Vaccine Only Contraindication
The CDC states there is one contraindication to the Pfizer/BioNTech COVID-19 vaccine: “Severe allergic reaction (e.g. anaphylaxis) to any component of the Pfizer-BioNTech COVID-19 vaccine listed in the prescribing information is a contraindication to vaccination.” However, there is one precaution:20
CDC considers a history of severe allergic reaction such as anaphylaxis to any vaccine or to any injectable therapy (e.g., intramuscular, intravenous or subcutaneous) as a precaution, but not a contraindication.
Currently, the government does not consider a history of severe allergic reactions, including anaphylaxis, to foods, drugs, other vaccines or environmental substances to be a reason to not receive mRNA COVID-19 vaccines.
Dermal Fillers May Be Associated with Facial, Lip Swelling After Moderna COVID-19 Shots
On Dec. 17, there was a report published in Drug Discovery and Development, that “temporary facial swelling might be another mild side effect for [Moderna Covid-19] vaccine recipients who have had prior dermal fillers,” such as injectable hyaluronic acid (HA) used in certain plastic surgery procedures.
Reportedly, in Moderna’s Phase 3 trials, three people developed facial or lip swelling after receiving the vaccine and two of the patients had prior dermal fillers in their cheeks within six months before vaccination. The third patient had received dermal filler in the lip two days after receiving the vaccine and had reported similar swelling in the past after receiving a flu vaccine. Antihistamines and steroids were used to treat the patients.
FDA Recommends Watching for Bell’s Palsy After COVID-19 Vaccinations
On Dec. 15, CNBC reported that the FDA staff recommends monitoring people who get COVID-19 vaccines manufactured by Pfizer/BioNTech and Moderna for symptoms of Bell’s palsy, which involves inflammation and paralysis of the nerve that controls facial muscles.21 The recommendation came after clinical trial data for both vaccines was analyzed by FDA staff.
In trials of the Moderna vaccine involving about 30,000 participants, there were four reported cases of Bell’s palsy and three had received the mRNA COVID-19 vaccine, while one received a placebo. In clinical trials of the Pfizer/BioNTech vaccine involving about 42,000 participants, there were four reported cases of Bell’s palsy and all had received the experimental vaccine while no cases of Bell’s palsy occurred in the placebo arm of the trial.
FDA staff said there wasn’t enough data from the trials to determine causation, but that there should be increased monitoring for cases of Bell’s palsy as the mRNA vaccines are given to millions of people.
Bell’s palsy can cause facial paralysis (usually one side of face) and drooling, pain around jaw and ear, increased sensitivity to sound, headache, loss of taste and changes in production of tears and saliva.22 It can develop after a viral infection and has been reported following influenza vaccination.2324
According to Mayo Clinic, “For most people, Bell’s palsy is temporary. Symptoms usually start to improve within a few weeks, with complete recovery in about six months. A small number of people continue to have some Bell’s palsy symptoms for life. Rarely, Bell’s palsy can recur.”25
Both the Pfizer/BioNTech and Moderna COVID-19 vaccines require two doses given three to four weeks apart. The CDC states that most common side effects of mRNA COVID-19 vaccines are injection site redness and pain, fever, chills, fatigue (tiredness) and headache.
The CDC warns that, “these side effects may feel like the flu and may even affect your ability to do daily activities, but they should go away in a few days,” and instructs people to “get the second shot even if you have side effects after the first one, unless a vaccination provider or your doctor tells you not to get a second shot.”26
Vaccine Companies, Providers Shielded from Liability for COVID-19 Vaccine Injuries and Deaths
The vaccine manufacturers, doctors and all COVID-19 vaccine providers are completely shielded from civil liability for vaccine injuries and deaths that occur in the U.S. after COVID-19 vaccinations under the Public Readiness and Emergency Preparedness (PREP) Act passed by Congress in 2005.27 The Act gives a liability shield to the manufacturer of any vaccine or drug developed in response to a health emergency like a pandemic causes when a vaccine or drug causes the death or permanent injury of an individual who receives it during pre-licensure clinical trials or after it is released for public use.
Individuals who die or suffer serious harm directly caused by the administration of covered countermeasures, such as vaccines, may be eligible to receive compensation through the Countermeasures Injury Compensation Program operated by the U.S. Department of Health and Human Services,28 whether or not the harm was a result of willful misconduct on the part of the vaccine manufacturer or person administering the vaccine.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Report from CDC, in PDF format, mentioned in Dr. Vernon Coleman’s video:
“My father told me when I was a child: people in authority lie.
If we are going to continue to live in a democracy we need to understand that people in authority lie.
People in authority will abuse every power that we relinquish to them and right now we are giving them the power to micro-manage every bit of our lives, 24 hours a day. They’re going to know where we are, they’re going to know the money that we spend, they’re going to have access to our children.
They’re going to have the right to compel unwanted medical interventions on us. You know, the NAZIs did that in the camps, in World War 2—they tested the vaccines on Gypsies and Jews.
And the world was so horrified after the war that we signed the Nuremburg Charter and we all pledged when we do that, we would never again impose unwanted medical interventions on human beings without informed consent.
And yet in two years all of that conviction has suddenly disappeared, and people are walking around in masks where the science has not been explained to them—they are doing what they’re told.
These government agencies are orchestrating obedience and it is not democratic—it’s not the product of democracy. It’s the product of a pharmaceutical-driven, bio-security agenda that will enslave the entire human race and plunge us into a dystopian nightmare where the apocalyptical forces of ignorance and greed will be running our lives and ruining our children and destroying all the dreams and dignity that we hope to give to our children.”
Robert F. Kennedy Jr.
Top Catholic Cardinal Warns COVID-19 Being Used to Usher in “Evil” Great Reset
A top ranking Catholic Cardinal has warned that the COVID-19 pandemic is being exploited by proponents of “The Great Reset” to “advance their evil agenda.”
Cardinal Raymond Burke, one of the most powerful Catholics in the United States, gave a homily in which he savaged “secular forces” who want to “make us slaves to their godless and murderous agenda.”
“Then there is the mysterious Wuhan virus about whose nature and prevention the mass media daily give us conflicting information,” said Burke. “What is clear, however, is that it has been used by certain forces, inimical to families and to the freedom of nations, to advance their evil agenda. These forces tell us that we are now the subjects of the so-called ‘Great Reset,’ the ‘new normal,’ which is dictated to us by their manipulation of citizens and nations through ignorance and fear.”
The Cardinal also slammed the United States’ fealty to China as a dangerous threat to Christian identity in America.
“To attain economic gains, we as a nation have permitted ourselves to become dependent upon the Chinese Communist Party, an ideology totally opposed to the Christian foundations upon which families and our nation remain safe and prosper,” he said.
Burke, who sits on the Church’s Supreme Tribunal of the Apostolic Signatura, the highest judicial authority in the Catholic Church, is not the first prominent figure in the Catholic Church to warn about the dark objectives behind the Great Reset.
As we highlighted back in November, Archbishop Carlo Maria Viganò wrote an open letter to President Trump claiming that the COVID-19 pandemic is part of a plot to impose a “health dictatorship.”
“We see heads of nations and religious leaders pandering to this suicide of Western culture and its Christian soul, while the fundamental rights of citizens and believers are denied in the name of a health emergency that is revealing itself more and more fully as instrumental to the establishment of an inhuman faceless tyranny,” wrote Viganò.
He added that The Great Reset sought to inflict “the imposition of liberticidal measures, hidden behind tempting promises of ensuring a universal income and cancelling individual debt.”
Doctor Who Warned Americans Not to Travel for Thanksgiving Traveled for Thanksgiving
White House coronavirus response Dr. Deborah Birx traveled to meet family during Thanksgiving after warning Americans to avoid doing the same in yet another example of rampant COVID hypocrisy.
According to an Associated Press report, Birx traveled to her vacation home on Fenwick Island in Delaware the day after Thanksgiving to gather with her daughter, son-in-law and grandchildren.
Birx claimed the family members were all part of her “immediate household,” but all of those family members do not live in the same home.
The doctor had previously urged Americans to “take it upon yourself to be restrictive” when it came to Thanksgiving travel and not meet with people from outside one household.
Dr. Deborah Birx: Keep Thanksgiving to your immediate household
“I don’t like it to be any number… if you say it can be 10, and it’s eight people from four different families, then that probably is not the same degree of safe as 10 people from your immediate household.” pic.twitter.com/lumNHf3H75
Birx’s own relative Kathleen Flynn told the AP that her behavior had caused tension within the family.
“She cavalierly violated her own guidance,” Flynn said.
The scandal may harm Birx’s effort to secure a public health role within the Biden administration.
“To me this disqualifies her from any future government health position,” said Dr. Angela Rasmussen, a virologist at the Georgetown Center for Global Health Science and Security. “It’s a terrible message for someone in public health to be sending to the American people.”
Birx’s behavior is par for the course given similar instances of public officials repeatedly violating coronavirus rules while insisting other Americans abide by them.
California Governor Gavin Newsom’s rampant hypocrisy was exposed when he was caught on camera unmasked eating indoors at a Michelin star restaurant with a group of 12 people while telling Californians they could only celebrate Thanksgiving outside.
Recently, a landmark study was conducted by Dr. James Lyons-Weiler and Dr. Paul Thomas. The study compared vaccinated children and unvaccinated children and was published in the International Journal of Environmental Research and Public Health on November 22, 2020 after being peer reviewed.
Dr. Weiler, a research scientist and co-author of the study, was recently interviewed by Activist Post Contributor Spiro Skouras. In the interview, Weiler breaks down the data from the study which indicates children who were vaccinated showed a higher rate of medical office visits and experienced an elevated rate of medical symptoms ranging from Asthma and behavioral issues, to ADHD and Anemia.
In this report, Spiro interviews Dr. Paul Thomas, a prominent pediatrician in Portland, Oregon who also co-authored the study and used 10+ years of data from his medical practice to conduct the study.
Shortly after the vaccinated versus unvaccinated study was published, five days in fact, the Oregon State Medical Board held an emergency meeting declaring that Dr. Paul was an immediate threat to his patients and the public and suspended his medical license.
In this must-see interview, Dr. Paul addresses the accusations leveled against himself and his practice, in addition to breaking down in detail the study’s findings. Dr. Paul also weighs in on the CDC recommended vaccine schedule and the experimental Covid vaccine.
Video available at Spiro Skouras YouTube and BitChute channels.
The only way to deal with an unfree world is to become so absolutely free that your very existence is an act of rebellion.” ~ Albert Camus
While loyalty to self and truth is not slavery, allegiance to any country, government, or ruling class is slavery. Inherent in this thinking is the fact that believing or trusting any ruling individual or entity without absolute verification at every level, is the basis for societal destruction at the hands of the few due to blind obedience to falsely claimed authority. Lies and deceit are the tools of tyrants, and come in the forms of outright deception to manipulative propaganda. These traits are always evident, but today they are completely overt, as lies and truth are both used in devious ways in order to gain compliance and control.
This can be seen in that a non-existent virus pandemic has been used to instill great fear in the unsuspecting minds of the masses to such an extent, that most have been willing to give up all normalcy and sanity in their lives and the lives of their families. They have due to false trust been duped into behavior that can only be described as psychotic in nature. This has led to voluntary self-imprisonment, isolation, business and job destruction, mask wearing, travel immobilization, and total lockdowns. It has led to greater sickness, death, and economic devastation as well, all in the name of ‘health security’ and obedience to power at the expense of all freedom. This should serve as the final valuable lesson learned by even the most common of men, because it should be obvious that relying on the state in any capacity whatsoever can only lead to an enslaved society dependent on a master class for its very existence and survival. This of course is what is sought; a communistic based technocratic ‘civilization’ controlled by the few.
Everything that happens with governments and the entire state apparatus is planned in advance. Nothing concerning the ruling class is organic or natural in any way. All action and reaction to any event by the government and its controllers is by design. Most everything that happens has been foretold or predicted by the state oligarchic perpetrators. This is usually done by very deceptive means meant either to create a false crisis, or to use indoctrination methods in order to plant in the minds of the people what to expect from some imagined future adversary or terrifying event that has already been devised or created. These tactics of course are psychological in nature, but if the psyche of the majority can be captured to such an extent as to cause the proper desired reaction, then they can be easily controlled. In a world of logic and reason, this current situation should serve as definitive proof of this hypothesis, but sadly, I doubt that any such mass revelation by the people at large will be forthcoming. I base this on Einstein’s statement that doing the same thing over and over again while expecting a different outcome is insanity. This seems to sum up the mentality of the American herd.
This analysis can be supported easily by history, and that may be part of the reason that our real history is being hidden and destroyed every single day at this juncture. This is happening through censorship of course, but also through the physical destruction of historical records including books, the closing off of access to original sources, and elimination of important factual information in every form imaginable.
This current hoax is nothing new, as similar events have happened before, and have been played out over and over again in real life and in staged table top exercises meant to condition the public for future planned actual incidents. This was a way to set up, to promote, and to prepare the public for events that could be used to alter society and change the common mindset from one of individual liberty to one of collective compliance. Of course, this change began very long ago, but it has escalated beyond imagination over the past two decades, and in this past year alone, the idea of a society based on total voluntary servitude has seemingly come to fruition. It is all a set up!
In 2001, an exercise called “Dark Winter,” a favored term of Joe Biden about our current situation, was set up by Johns Hopkins and others to simulate a covert smallpox attack on the U.S., and to see what a government response might look like under those circumstances.
In 2005, “Atlantic Storm,” was organized by the Center for Biosecurity at the University of Pittsburgh Medical Center. This was a simulation about an international smallpox outbreak that turned into a pandemic.
In 2010, a Rockefeller Foundation paper called Lock Step, analyzed a scenario as to how governments would respond with authoritarian measures to react to a worldwide flu pandemic. This is very similar to what is happening today. “During the pandemic, national leaders around the world flexed their authority and imposed airtight rules and restrictions, from the mandatory wearing of face masks to body-temperature checks at the entries to communal spaces like train stations and supermarkets.”
In 2017, a novel coronavirus outbreak was simulated in Minnesota. This exercise was called “The SPARS Pandemic 2025-2028,” and comprised a futuristic scenario that illustrated communication dilemmas concerning medical countermeasures (MCMs) that could plausibly emerge in the not-so-distant future.
The next exercise in August of 2019 was a Trump administration and Health and Human Services major exercise called Crimson Contagion. This simulation was almost identical to the Covid-19 plot today. “It tried to model what would happen if an influenza pandemic that started in China spread through the U.S. with no treatment, leaving 7.7 million Americans hospitalized and 586,000 dead.”
The last exercise that took place was the evil Gates Foundation Event 201 in October of 2019. This was nearly an exact replica of what has happened this past year concerning the response to this fraudulent virus pandemic. The fact that the Gates foundation along with Johns Hopkins were involved in this set-up to prepare the sheep, is damning at every level, and exposes that all government tyranny is planned in advance, and telegraphed in order to condition the public.
What all these simulations, and many others, have in common is that the promoters and preparers of these events all claim to have no foreknowledge of any real future like situations, and allege that these are only done so as to be prepared to help the lowly proletariat in case of some biowarfare or health emergency. This is an outright lie. They are never prepared to stop any risk, but are always prepared to use it in order to gain power and control over humanity. The government and its partners in crime create and publically announce these simulations for the specific purpose of psychological preparedness training of the common people. It is no different than any propaganda campaign that is based on implanting ideas in the minds of its victims through projection and repetition.
It cannot be overstated that every act of government, its controllers, and its partners, is never accidental, or caused by unknown factors; it is always plotted and planned in order to benefit the ruling class. Every claimed emergency, whether national or state, is known about beforehand, and any response will be specifically generated to first benefit the oligarchy. This is true even in the case of natural disasters, as all preparedness first helps those insider entities that stand to gain from disaster.
This specific and purposely-manufactured virus ‘pandemic’ has been in the works for almost twenty years, and situations like this have been discussed for decades by the controlling ‘elites’ and their pawns in government. Because of this, all should understand that this is not over, and will never end without a large and sustained uprising by the citizenry. The escalation of extreme tyrannical measures is only going to dramatically increase in the coming year. Once this ludicrous presidential selection process ends in January, the political class will be completely free to pursue its globalist agendas without restriction. Those agendas, if allowed to go forward, will be the most devastating and draconian that we have ever faced.
The chosen masters that you have voluntarily allowed to rule over you have intentionally created this crisis, and are fully prepared to use it to destroy your life and family. You have suffered for almost a year, and this is only the beginning. The state’s agenda is crystal clear; propaganda is their weapon of choice, and total submission is their goal. Are you prepared to stop them by whatever means necessary, or will you comply and become slaves. Those are the only choices left!
First of all, very high praise goes to Christine Massey, for her work in exposing the coronavirus fraud. In a half-sane world, she would have received many awards by now.
Her latest communication reads: “Freedom of Information reveals Public Health Agency of Canada has no record of ‘SARS-COV-2’ isolation performed by anyone, anywhere, ever” [1]
I urge readers to visit Massey’s site and read her new article and follow all the links. Her findings are stunning. She and her team have made about 40 FOI requests to public health agencies in various countries, requesting proof that SARS-CoV-2 has been isolated. You’ll see from the responses that not one agency has records demonstrating isolation.
This means exactly what it seems to mean: the virus has not been proven to exist.
As for the people who keep chanting that the virus has been isolated, I can keep explaining why this is not so. I can do this forever. [2] [3]
Whether it’s a scientist, a gaggle of scientists, a government official, a person waving a study around like a newspaper with a hot headline from an old movie, my response is the same, and I make it knowing that some people will intentionally refuse to understand it:
ONE: SAYING the virus has been isolated is not the same thing as proving it’s been isolated.
TWO: Researchers routinely twist the meaning of the word “isolated” to mean its very opposite.
Isolation is absurdly taken to mean: “We have the virus in a soup in a dish in the lab. It is not separated out (isolated) from the soup. The soup contains various cells—human, monkey—and an array of (toxic) chemicals and drugs. We know the virus is there, because it is infecting and killing some of the cells.”
A reasonably bright junior high school student would immediately realize this is not a description of isolation.
A reasonably bright high school student would point out that there is no proof the virus is infecting and killing cells, because the toxic chemicals and drugs in the soup are sufficient to do the cell-killing. He might also mention the cells in the soup are being starved of nutrients, and this alone could cause their death.
Therefore, there is no evidence that “the virus” is actually in the soup.
Therefore, there is no evidence in this situation for claiming the virus exists at all.
On to the next factor: the ever-present claims of having “sequenced the genetic structure of the virus.” Again, SAYING the sequencing has been achieved is not the same thing as proving it.
And proving it is impossible, if you don’t already have the virus in a purified and isolated state. Instead of proof, you have shady inference and assumption and guesswork and deception.
How can you sequence something you don’t have? You can’t.
I’ve used several analogies to explain this nonsense. Here is another one:
An art restorer, conservationist, and historian is called to the home of a well-known mob enforcer.
The enforcer tells him he has something to show him in the attic. On the way, they pass through the living room, where several open suitcases are sitting on the floor. They’re spilling over with stacks of cash. Automatic weapons and boxes of ammo are laid out on a long table. In an open closet, the art expert sees a row of jackets with designations indicating: FBI, BATF, Federal Marshal, sheriff, local police.
In the attic, the mob enforcer points to a small pile of tiny chips on the floor.
“These are from a lost Rembrandt self-portrait,” he says. “Collect them, go to work on them, give me a favorable report. Or else.”
Back in his lab, the obedient art expert quickly divides the chips into three groups. The first group is water-color chips from a child’s toy set. The second group is mid-20th-century acrylic chips. The third group is lead white chips, used for a hundred years on either side of the rough date when Rembrandt could have painted the lost self-portrait.
The art expert finds that Rembrandt (and hundreds of other painters) used this general type of lead white.
The expert constructs, from other scholars’ work, an essay claiming there was and is a lost Rembrandt self-portrait. He excludes commentary that denies the existence of this painting.
He “sequences” all this information and conjecture and guesswork (and con) into a convincing report, which points to the small pile of chips in the mob enforcer’s attic.
(It turns out the enforcer intends to accuse a rival mob boss of stealing the “lost Rembrandt self-portrait.”)
The existence of the self-portrait is thus “established,” which is to say, it is put together, cobbled from various sources, concocted, smoothed out by ignoring counter-information—employing a vast generality about lead white paint.
Of course, in all this ridiculous invention, the self-portrait itself is not there, it is not in hand, its existence has not been demonstrated, it is a story, THERE IS NO ISOLATION OF IT from surrounding assumption and gimcrackery.
So it is with SARS-CoV-2. Pieces of data that reference prior supposed RNA sequences in libraries are all strung together, to resemble what is claimed to be a new and unique coronavirus—without having the actual virus, without having shown it exists at all.
In past articles, I’ve quoted two key documents, one from the CDC, and one from “the Drosten group.” These documents were describing how to perform the PCR test for the new virus—and in both documents, the authors state they don’t have the virus.
So…a test for what? The virus you don’t have.
All claims that these authors eventually DID obtain the virus are based on the crooked definition of “isolated” I’ve explained above.
Yes, they got hold of “isolated virus,” meaning the soup in the dish in the lab—and we’re back where we began. Isolation meaning non-isolation.
I’ve explained all this several times, in detail, in past articles, and of course people here and there continue to send me studies claiming isolation.
I can do this forever.
People can say, “Well, we know from photos of Martian soil samples that on the second Tuesday in March, 1843, there was a picnic on Mars attended by three virologists from the Martian Institute of Epidemiology, and they ate baloney sandwiches on rye toast and drank Miller Lite.”
I enjoy these fictional tales in a vacuum. I would leave them alone, except that the failure to prove the existence of SARS-Cov-2 is at the bottom of all the lies that have been used to steal the freedom and assets and livelihoods from at least a billion people.
I won’t leave that alone.
Neither should you.
“…but wait, Mr. Rappoport, here is a study from Outer Mongolia that states the virus has been isolated. This seems to settle the science on this issue, once and for all.”
Sure. Sure it does. And the sun sets every day at noon in Cincinnati.
The Pfizer Covid vaccine is already being administered to the public in the UK, and the first doses have been given in the US ahead of a mass vaccination campaign on a global scale.
It is important to recognize that the Pfizer Covid vaccine has not been approved by the FDA. It has only received Emergency Use Authorization (EUA), meaning the vaccine has not gone through the standard process to get official approval from the regulatory agency.
Now Moderna’s experimental Covid vaccine is set to get the same Emergency Use Authorization, allowing the shot to be distributed to millions of people.
We have already witnessed short-term adverse events (side effects) from the Pfizer vaccine. Truth is, nobody knows what the long-term effects could be and it appears the public is being subjected to an experiment on a global scale.
In this report, we examine discrepancies in the FDA Moderna report that was voted on by an advisory panel. The panel voted 20-0 recommending EUA.
Some of the discrepancies include cherry picked trial participants to achieve the desired results to gain EUA, as well as 13 total deaths in the trials – 6 in the vaccinated group and 7 in the placebo. Something the media refuses to address.
Video available at Spiro Skouras BitChute and YouTube channels.
America’s frontline workers are now receiving the Covid vaccine. It was reported that two health care workers who received the experimental Covid shot in Alaska experienced severe adverse events minutes after taking it.
Both were admitted to the ER and one was transferred to the ICU after experiencing severe adverse events, both are expected to survive. One of the health care workers had not history of allergies.
This is similar to two health care workers who also experienced adverse events in the UK after receiving the experimental shot, prompting the government to issue a warning that pregnant women, children and people who have clergies to medicine, vaccines or food avoid the shot for now.
Today, health care workers in Chicago received the vaccine; and about 10 minutes later, a nurse who reviewed the vaccine passed out on TV.
The local media reported that the nurse did regain consciousness and appeared to be OK, which is a good thing.
But remember, this is an experimental vaccine that has not received official approval from government regulators. The Pfizer vaccine has only received EUA (Emergency Use Authorization) and the trials are still ongoing. So, that makes this an experimental vaccine in my book and the public appear to be the guinea pigs.
We know that the PCR tests being used are not “fit for purpose”, that they are for Research Use Only. They are not meant to be used as diagnostic tools, and the late inventor of the RT-PCR instruments was very clear about this. According to the late Dr. Kary Mullis,
“PCR detects a very small segment of the nucleic acid which is part of a virus itself. The specific fragment detected is determined by the somewhat arbitrary choice of DNA primers used which become the ends of the amplified fragment. “ (1)
We also know that Coding changes to Death Certificates have fabricated false perceptions about COVID lethality. CDC coding changes blurred the important distinction between dying OF COVID and dying WITH COVID. Consequently co-morbidities such as heart disease, cancer, etc. have been largely negated and COVID has been relegated an artificially high importance in terms of Cause of Death reporting.
Dr. Ngozi Ezike explained the “death count” in a May 2020 press conference with these words:
“I just want to be clear in terms of the definition of ‘people dying of COVID’.
So, the case definition is very simplistic. It means, at the time of death, it was a COVID positive diagnosis.
So, that means that if you were in hospice and had already been given, you know, a few weeks to live, and then you were also to have found to have COVID, that would have counted as a COVID death.
It means that if technically even if you died of a clear alternate cause, but you had COVID at the same time, it’s still listed as a COVID death.
So, everyone who is listed as a COVID death, doesn’t mean that that was the cause of death, but they had COVID at the time of death.
I hope that’s helpful.” (2)
According to H. Ealy, M. McEvoy et al in “Covid-19: Questionable Policies, Manipulated Rules of Data Collection and Reporting. Is It Safe for Students to Return to School?”:
“The 2003 guidelines for establishing death certificates had been cancelled. “Had the CDC used its industry standard, Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting Revision 2003, as it has for all other causes of death for the last 17 years, the COVID-19 fatality count would be approximately 90.2% lower than it currently is.” (3)
To summarize then, the tests that are widely used to test for COVID are not fit for diagnostic purposes. Additionally, prior to the announced pandemic, coding changes made to Death Certificates falsely and very significantly increase COVID Death Statistics.
These two factors alone create substantial misperceptions about the danger and lethality of COVID-19.
CNN has the story. And it’s quite a story: “Why vaccinate our most frail? Odd vote out shows the dilemma”, December 4. [1]
“The vote to recommend long-term care residents be among the first to receive Covid-19 vaccinations was not unanimous.”
“Out of a panel of 14 CDC vaccine advisers, a lone doctor said no.”
“’Odd woman out, I guess,’ Dr. Helen ‘Keipp’ Talbot, of Vanderbilt University, told her colleagues. ‘I still struggle with this. This was not an easy vote’.”
“Talbot was worried about whether the vaccine would even work in such frail, vulnerable patients. Even more, she worried about how it might look if the vaccine failed in that group, or how it would affect public perception if residents died soon after getting the vaccine.”
“The Covid-19 vaccines have not been tested in the frail elderly, many of whom are residents of long-term care facilities.”
Let’s stop here for a moment. First, we learn that the clinical trials of the COVID vaccine have not used the frail and elderly as volunteers. Therefore, there is NO evidence that the vaccine is safe or effective in that very large group. If this doesn’t give the frail and elderly and their families pause for thought, nothing will.
Second, Dr. Talbot is worried about “public perception,” when the elderly die right after getting the vaccination.
Well, what would YOU think if your mother died the day after she received the COVID shot?
The CNN article gets worse. Read on. Next up is a comment from Dr. Kelly Moore, “associate director of the Immunization Action Coalition, which is supporting frontline workers who will administer Covid-19 vaccinations.”
“’Since they [the COVID vaccines] haven’t been studied in people in those [elderly] populations, we don’t know how well the vaccine will work for them. We know that most vaccines don’t work nearly as well in a frail elderly person as they would in someone who is fit and vigorous, even if they happen to be the same age,’ Moore said.”
Again—zero evidence the COVID vaccines work in elderly and frail populations. Most vaccines don’t “work nearly as well.”
CNN: “When shots begin to go into arms of [nursing home and long-term care facility] residents, Moore said Americans need to understand that deaths may occur that won’t necessarily have anything to do with the vaccine.”
“’We would not at all be surprised to see, coincidentally, vaccination happening and then having someone pass away a short time after they receive a vaccine, not because it has anything to do with the vaccination but just because that’s the place where people at the end of their lives reside,’ Moore said.”
“’One of the things we want to make sure people understand is that they should not be unnecessarily alarmed if there are reports, once we start vaccinating, of someone or multiple people dying within a day or two of their vaccination who are residents of a long-term care facility. That would be something we would expect, as a normal occurrence, because people die frequently in nursing homes’.”
Right. Don’t be alarmed.
Don’t worry if people who are doing reasonably well suddenly die right after getting the COVID shot. It’s just a coincidence.
Their long-term health conditions just happened to kick in a day or two after vaccination. Nothing to wonder about.
Don’t kick up a fuss if it’s YOUR father or mother who died. Stay calm. You can be sure the doctors will let you know if your mother died from the vaccine. Of course they will.
Even though the vaccine has never been tested on the elderly and frail, the doctors know whether a death occurred from the vaccination or from other causes. And they’ll tell the truth. They always do.
The doctors quoted in this CNN article are obviously worried about people dying as a result of the vaccine. They know it’s going to happen. They’re thinking out loud about what they can do to stem the tide of public outrage—particularly from the families of those who die.
The best idea they can come up with is: “these people die anyway.”
I remind readers that, for months, I’ve been reporting on the huge percentage of all so-called COVID deaths that have been occurring among the elderly in nursing homes, in long-term care facilities, in hospitals, in their homes. [2]
These people were already suffering from multiple long-term serious health conditions. On top of that, they had been treated for years with an array of toxic medical drugs.
And then, they’re absolutely terrified when they receive a diagnosis of COVID. Then they’re isolated, cut off from family and friends.
And they give up and die.
NO VIRUS IS REQUIRED TO EXPLAIN THESE DEATHS.
This is forced premature killing of old people. It’s murder by COVID diagnosis and isolation. [2]
And now, these people will receive an experimental RNA vaccine, whose effects include auto-immune reactions; the body basically attacks itself. [3]
More killing.
And doctors advising the CDC are telling us not to be alarmed.
The deaths are just routine.
Lots and lots of doctors who know what’s going on are thinking, “What if all this comes back on ME?”
Well, it IS coming back on you, Doctors.
You’re killers in white coats who are supposed to be saving lives.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
RFK, Jr. w/ Dr. Zach Bush: On What Is Really Making Us Sick | Shifting Away From Big Pharma Health Paradigm
Robert F. Kennedy, Jr. interviews Dr. Zach Bush about alternative routes to achieving optimal health, including how improving the gut microbiome can strengthen the immune system.
In the latest episode of our second season of “TRUTH” with Robert F. Kennedy, Jr., Kennedy interviewed Dr. Zach Bush who specializes in internal medicine, endocrinology and hospice care with a focus on the microbiome as it relates to health, disease and food systems.
Kennedy and Bush covered a wide range of topics, including:
the widely misunderstood history of the polio virus
Pharma’s takeover of the federal regulatory health system
All “Truth” episodes can be found on Children’s Health Defense’s social media, and on Children’s Health Defense’s channel found on Peeps TV, a network on Roku. Roku is accessible from any Smart TV and can be purchased separately for older TVs.
[As a service to protect truth from censorship & to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, Lbry/Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
‘YOU CAN’T SHUT US DOWN’ – New York City Bar Owners Defy Lockdown Orders
STATEN ISLAND, NY – This week New York bar owners held a press conference to reaffirm their commitment to defy the city and state’s unlawful lockdown orders.
Danny Presti and Keith McAlarney, the co-owners of Mac’s Public House, recently gained national headlines by breaking COVID curfew, and for serving patrons indoors, and by lampooning the radical left and Antifa by declaring their bar to be an ‘Autonomous Zone’.
Despite harassment from police, they have continued to defy New York Gov. Andrew Cuomo’s ‘pandemic’ restrictions, and have been arrested twice in the last two weeks.
The struggling owners, along with their customers, were made fun of by the elite cast of Saturday Night Live (SNL) for daring to protest Cuomo’s draconian lockdown orders. The swipe by SNL appears to have backfired though, as working class New Yorkers have voiced their dismay at the mainstream media’s attack on the city’s small businesses being devastated by lockdowns.
In their sidewalk presser event, Presti and McAlarney were joined by community activists, and also by their lawyer Lou Gelormino, who remarked, “Maybe Saturday Night Live should be mocking the people that looted and rioted our great city of Manhattan and the rest of the great cities of this country.” Watch:
“Informed Consent” a New Documentary by Jaymie Icke About the Dangers of the Vaccine Rollout
Available at Press for Truth Lbry and BitChute channels.
Informed Consent is the newest film by Jamie Icke that exposes the dangers associated with taking a vaccine.
A global inoculation rollout is currently underway with a rushed Pfizer vaccine that has already proven to be dangerous yet scores of people are willingly lining up to take the experimental jab simply because they are watching far too much mainstream news on the television.
In this video Dan Dicks of Press For Truth speaks with Jaymie Icke about his newest film “Informed Consent” and the balance he hopes to bring to the minds of the masses so that they can truly make an informed decision when it comes to accepting the Covid-19(84) vaccine.
Under section 564 of the Federal Food, Drug, and Cosmetic Act (FD&C Act), the FDA commissioner has the authority to allow unapproved medical products to be used in an “emergency” when there are no approved alternatives.
Before rushing into The Final Frontier traveling faster than the speed of light, why not heed the wisdom of Jean Luc Picard, Captain of the Enterprise, when he warned, “No being is so important that he can usurp the rights of another.”
Focus on the Headlines
CNN mainstream newswarns,“Don’t be alarmed if people start dying after taking the vaccine.”
Huh?
If ever there was a blatant warning that does not require reading between the headlines, it is this: Beware of the new, untested, genetically modified COVID vaccine. Don’t say we didn’t warn you. Collateral damage happens.
Whenever the government has rushed an experimental vaccine to market, the outcomes have been disastrous. The story has been told many times before through the media headlines.
Nothing ever needs to be rushed when it comes to ensuring safety because alternatives do exist, from the drug, Hydroxychloroquine, to mineral supplementation and medicinal herbs. Survivors of the Spanish Flu pandemic used homeopathy, a proven holistic alternative, with great success, even though there is no mention in the headlines.
The headlines love software developer and appointed COVID spokesperson, Bill Gates, who disclosed that 700,000 people could die from this vaccine. This figure is suspiciously close to the figure seen on the Georgia Guidestones, whose message is to maintain humanity under 500,000,000 (from 7 billion).
If you scan the news, you will find the high-risk groups for COVID deaths. The headlines read: “40% of Central Florida COVID deaths from nursing homes,” and “more than 6,000 coronavirus deaths are tied to Massachusetts long-term care facilities.” Nursing homes and long-term care facilities are the same groups targeted for the first round of vaccines.
Don’t be alarmed if people start dying after taking the vaccine. – CNN
Is CNN warning that the first to be jabbed will be the first to die? Are they disclosing a pattern for past epidemics and mass vaccination campaigns? Is truth being disclosed in the headlines? Do the headlines provide informed consent for the masses?
Vaccine makers, who are not liable for vaccine injuries and deaths, claim that they have a limited number of vaccines to deploy in the first phase. For instance, Moderna, says most people in the US will have to wait several months before they might have access to a coronavirus vaccine. And it could be years before everyone in the world can get vaccinated against COVID-19. Pfizer, which says its vaccine is 95% effective at preventing coronavirus infections, is expected to produce the first COVID-19 vaccine to receive FDA authorization in the coming weeks.
Before you consider if you belong to any of the priority groups, ponder this: What good is a 95% effective vaccine to prevent an infection that could make you a death statistic in the process?
If those most likely to die are the same people taking the vaccine first, then …“Don’t be alarmed if people start dying after taking the vaccine.”
Past Vaccine Disasters
If hindsight is 20/20, then people should be able to track past vaccine disasters for Polio, Swine flu, and H1N1, to name a few. However, people also have short attention spans.
Polio
In 1955, the government announced the first vaccine to protect kids against polio. More than 200,000 children got the polio vaccine, but within days the government had to abandon the program. The Cutter Incident resulted in 40,000 kids getting polio, including 10 deaths, from the polio vaccine. Later, from 1955 to 1963, it was found that between 10% and 30% of polio vaccines were contaminated with simian virus 40, which later resulted in an increased incidence of certain cancers among the 98 million people exposed to contaminated polio vaccine. About 90% of children and 60% of adults in the U.S. were inoculated for polio and possibly exposed to SV40.
Swine flu
In 1976, forty-five years ago, scientists predicted a pandemic of a new dangerous strain of influenza dubbed, Swine Flu. The federal government planned to buy 200 million doses of vaccines developed by drug companies and distribute them for free to state health agencies. President Ford misled people into believing that Swine Flu could be as bad as the Spanish Flu. The prediction that 50 million Americans would be sickened by swine flu never came to fruition.
Of the 46 million people who obediently took the shot, 4,000 Americans claimed damages from Uncle Sam amounting to three and a half billion dollars due to vaccine damage. Many developed Guillain-Barré syndrome — a disorder attributed to vaccines that can cause muscle weakness, paralysis, and even death. The program ended when 25% of the populated got the jab. See Mike Wallace of 60 Minutes expose the 1976 Swine Flu Pandemic Vaccine Injuries. During the fall of the following year, people feared getting the flu shot.
“I am terrified about getting a flu shot after all the troubles it caused last year,”wrote Martha W. on Sept. 26, 1977.
H1N1
In June 2009, the World Health Organization declared an H1N1 pandemic, marking the first global pandemic since the 1968 Hong Kong flu. The H1N1 strain of flu was the result of a reassortment of human influenza and swine influenza viruses. This suggests that viruses can jump the species barrier [more on that later]. In October, 2009, president Obama declared a National Emergency. The declaration gave DHHS Secretary extraordinary powers during a crisis. Health experts called it a false pandemic, insisting it was “just a normal kind of flu.” Ten years later, history repeats itself…
…the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%). – Anthony Fauci, March 26, 2020, New England Journal of Medicine editorial
Question the Narrative
Has vaccine science evolved since 1955, or 1976, or 2009 if the same pattern keeps repeating? Question the research:
When politics and science form a consensus, integrity and truth are lost.
Perhaps the greatest deception in repeat pandemics is that “the virus” has never been isolated. There is no true viral pandemic in human history since humans make viruses (exosomes) within their own cells.
The only person you’re truly competing against is yourself. – Jean Luc Picard, Captain, Starship Enterprise
As all students of biology know, viruses are not alive. They depend on the components of a cell for survival. Therefore, a virus is not contagious. The Coronavirus deception will never be reported in the headlines because a protein sequence is not a Bestseller. The CDC states:
Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA.
If viruses do not live outside cells, then how do they cross a species barrier to become a chimera, part pig and part human? The same way SARS and CoV2 meet and mingle. In a petri dish of a laboratory. The virus is nothing more than an elaborate distraction to reset society under global mandates to coerce compliance in illegal dictates because people have allowed themselves to be easily misled.
There can be no justice so long as laws are absolute. – Jean Luc Picard, Captain, Starship Enterprise
Next up
After January 2021, the simulation continues. The next president would lock down the U.S. for 4-6 weeks to “contain the spread of the virus” that did not respond to the first lockdown. Viruses do not respond to lockdowns, face masks, social distancing, or vaccine mandates because they are not alive. They are not a threat. However, the politicians and scientists who promote the virus deception are.
As people buy into Operation Warp Speed, politicians and scientists are hopeful that people will also buy into the latest, December 2020 headline declaring that a new annual, “universal flu vaccine shows promise.” However….
“Don’t be alarmed if people start dying after taking the vaccine.” – CNN News Headline
With the UK being the first western country to greenlight the #Covid19 vaccine to healthcare workers and the elderly, the media lauded the first recipient this week, a 90 year old woman, with their usual fanfare and excitement despite extensive safety concerns.
#UKVaccineApproval #UKVaccineRollout
CHD Article on Big-Picture Look at Current Pandemic Beneficiaries Accepted by Peer-Reviewed Journal
An article by Children’s Health Defense on how the pandemic facilitated a financial, tech, biopharmaceutical and military-intelligence push for centralized, technocratic control has been accepted by the International Journal of Vaccine Theory, Practice and Research.
“Planned Surveillance and Control by Global Technocrats: A Big-Picture Look at the Current Pandemic Beneficiaries,” a peer-reviewed article by Children’s Health Defense, has been accepted for publication in the journal, International Journal of Vaccine Theory, Practice and Research. The journal was launched in 2020 by John W. Oller, Jr., Ph.D. (editor-in-chief) and Christopher A. Shaw, Ph.D. (senior editor) “to make independent research, free from constraints of monetary, political, or any other undisclosed influence, about vaccine theory and practice freely accessible.”
The Children’s Health Defense article, which will appear in the journal by year’s end, assesses how the pandemic has facilitated a financial, tech, biopharmaceutical and military-intelligence push for centralized, technocratic control.
Here’s the article:
Abstract
Global financial patterns and pronouncements point to a seismic overhaul of governance and financial systems that is playing out beneath the surface of the Covid-19 pandemic, reaching far beyond the health domain. Increased centralized control has the potential to create an unbridgeable chasm between a tiny handful of winners and a majority of losers. To foster an integrated analysis of the technocratic and financial forces and agendas at play, this rapid review identifies some of the pandemic’s principal beneficiaries across the interwoven financial, tech, biopharmaceutical, and military-intelligence sectors, assessing developments in the context of the accelerating global push for technocratic consolidation and control. The evidence suggests that Trojan horse coronavirus vaccines may challenge bodily integrity and informed consent in entirely new ways, transporting invasive technologies into people’s brains and bodies. Technologies such as brain-machine interfaces, digital identity tracking devices, and cryptocurrency-compatible chips would contribute to the central banking goal of replacing currencies with digital transaction and identification systems and creating a global control grid that connects the world population to the military-pharma-intelligence cloud of the global technocrats. Moreover, using vaccines as a delivery vehicle for surveillance technologies cancels any legal liability.
Keywords: Biopharmaceuticals; central banks; Covid-19 pandemic; digital identity; Operation Warp Speed; technocracy; vaccines
Introduction
On March 11, 2020, the World Health Organization (WHO) upgraded a reportedly novel coronavirus from a global health emergency (as of January 30) to a global pandemic, having given the name “Covid-19” to the newly minted disease associated with the virus (Forster, 2020; World Health Organization, 2020a). If one examines actions taken both before and since the WHO’s March decree, it seems evident that many highly placed individuals and sectors were able to strategically position themselves to benefit from the declared crisis (Children’s Health Defense, 2020b). At the same time, with a “new form of economic shock” being imposed worldwide under cover of Covid-19 (Lagarde, 2020), it has become apparent that old-fashioned corporate profiteering is far from the whole story.
In fact, global financial patterns and pronouncements point to a seismic overhaul of governance and financial systems that is playing out beneath the surface of the pandemic, reaching far beyond the health domain. These developments highlight a disturbing push for global technocracy — a form of centralized, expert-led control over resource production and consumption that the Wall Street Journal has characterized as “anti-democratic rule by elites who think they know better” (Wood, 2018, 2020; Fitts, 2020a; Schinder, 2020; Schumacher, 2020; White, 2020). In the U.S., many of the actions unfolding behind the scenes are also benefiting from a climate of institutionalized secrecy enabled by the October 2018 adoption of a game-changing policy statement (FASAB Statement 56), which turned financial disclosure rules upside-down to allow the U.S. government and its contractors to maintain secret books (Federal Accounting Standards Advisory Board, 2018; Ferri & Lurie, 2018).
As 2020’s rapid-fire events suggest, substantially increased centralized control and secrecy have the potential to create an unbridgeable chasm between a tiny handful of elite winners and a majority of upper and lower middle class losers. In early June, CNBC’s Wall Street analyst Jim Cramer heatedly pointed out the fact that the pandemic had already produced “one of the greatest wealth transfers in history” (Clifford, 2020). Others have echoed these observations, describing the “monumental transfer of wealth from the bottom of the economic ladder to the top” (Barnett, 2020; Kampf-Lassin, 2020). In comparison to the benefits flowing to large corporations and billionaires, Cramer bluntly observed that pandemic-related restrictions have had a “horrible effect” on America’s small-business economy, with a similar pattern on display outside the U.S. (Clifford, 2020). Even the World Economic Forum — which has promoted many of the structural changes now underway at its annual Davos meetings — acknowledges the “asymmetric nature” of Covid-19-related hardships and the “greater ferocity and velocity” of the pandemic’s impact on populations already under stress before 2020 (World Economic Forum, 2020).
By early fall, fifty million Americans (many with already high burdens of debt) had lost jobs; financial forecasters were issuing warnings about further layoffs; and millions of the still-employed were earning less than pre-pandemic (Andriotis, 2020). In addition, the bulk of the trillions in federal stimulus (which by early May exceeded the gross domestic product of all but six nations worldwide) had made its way to large corporations; Forbes reported that roughly 70 percent of the initial $350 billion intended for struggling small businesses went to large companies (Simon, 2020). Observers suggest that by channeling taxpayer bailouts to the companies that already had the greatest ability to withstand the shutdowns, the largest players have been able to gain even more of a “stranglehold” over the economy (Kampf-Lassin, 2020).
As U.S. billionaires’ wealth increased by almost a trillion dollars (a weekly average of $42 billion), weekly jobless claims, requests for food bank assistance, and reports of addiction, overdoses, depression, and suicide began “shatter[ing] all historical records” (Feeding America, n.d.; Alcorn, 2020; Americans for Tax Fairness, 2020; Baldor & Burns, 2020; Community FoodBank of New Jersey, 2020; Dubey et al., 2020; Ettman et al., 2020; Hollyfield, 2020; Lerma, 2020; Prestigiacomo, 2020; Schwarz, 2020; Sergent et al., 2020; Thorbecke, 2020; Wan & Long, 2020). Outside the U.S., the situation is similar (Bueno-Notivol et al., 2020). As a marker of the global surge in hunger, the Nobel Committee awarded its 2020 Peace Prize to the World Food Programme, prompting the agency’s head to warn that the world is “on the brink of a hunger pandemic” that could result in “famines of biblical proportions” in the coming year (Lederer, 2020).
In November, the Centers for Disease Control and Prevention (CDC) released data identifying over 100,000 excess U.S. deaths “indirectly” associated with the pandemic (Rossen et al., 2020), including a “stunning 26.5% jump” in excess deaths in young adults in their mid-twenties through mid-forties (Prestigiacomo, 2020). Commenting on these mortality data — which reflect “a death count well beyond what [researchers] would normally expect” (Preidt, 2020) — the former U.S. Food and Drug Administration (FDA) Commissioner Scott Gottlieb voiced his suspicion that “a good portion of the deaths in that younger cohort were deaths due to despair,” including drug overdoses (Squawk Box, 2020). University researchers writing about mortality in JAMA concurred that “Excess deaths attributed to causes other than COVID-19 could reflect deaths . . . resulting from disruptions produced by the pandemic” (Woolf et al., 2020), including “spillover effects . . . such as delayed medical care, economic hardship or emotional distress” (Preidt, 2020). Multilateral entities like the Organisation for Economic Co-operation and Development (OECD) emphasize that it will be essential to assess the long-term impact of “confinement and deteriorating financial conditions” on mortality and warn that the social and economic fallout is likely to be “significant” (Morgan et al., 2020).
As an ideology, technocracy is recognized for exalting knowledge and expertise as the principal sources of legitimate power and authority and for asserting that there is “one best way” that only “the experts” (e.g., engineers, scientists, and doctors) can determine (Burris, 1989). However, critics of technocracy have long pointed out that, particularly in crisis situations, the know-how, “discretionary interventions” and seemingly “elastic” power claimed by technocrats can end up blurring the line between useful expertise and “arbitrary rule” (White, 2020). Moreover, technocrats typically resist attempts to make explicit “the non-rational attributes of technocratic decision-making” (Burris, 1989).
With the noticeable absence of any cost-benefit analysis and the increasingly “non-rational” justifications being put forth for Covid-19 restrictions (Handley, 2020; Kristen, 2020; Kulldorff et al., 2020; The Reaction Team, 2020) — as well as the economic, political, social, and cultural changes rolling out at dizzying speed — it is important to try to understand the technocratic and financial agendas at play. Three increasingly interwoven sectors (Big Finance, Big Tech, and Big Pharma) are reaping rewards from Covid-19, benefiting from close relationships with the military-intelligence apparatus (Glaser, 2020; Usdin, 2020). This rapid review seeks to (1) identify some of the pandemic’s principal beneficiaries (financial and otherwise) across these sectors, and (2) assess these parties’ actions in the context of the accelerating global push for technocratic consolidation and control through invasive surveillance.
Methods
Rapid reviews are used to synthesize evidence in a streamlined manner, abbreviating the timeline and requirements of more involved systematic reviews (Ganann et al., 2010). A rapid review is particularly well suited to emerging current event sequences, and the dynamic Covid-19-related situation certainly qualifies. Though not exhaustive, rapid reviews make it possible to quickly summarize available evidence across multiple disciplines, whether for the purpose of informing policy-making and decision-making or to identify patterns and take stock of the bigger picture.
For the purposes of this broad overview of current events, we relied primarily on the so-called grey literature as well as media accounts (from both the legacy media and independent journalists) and various online sources. We also consulted relevant peer-reviewed literature. Notably, while the peer-review process is ordinarily slow-moving, Covid-19-related studies have been making their way through the pipeline at breakneck speed (Packer, 2020).
Examples of sources consulted for this review include conventional and alternative financial commentary; webpages and communications from public health agencies, international organizations, and universities; individual blogs and commentary; and peer-reviewed studies cataloguing the impact of Covid-19 restrictions.
Big Finance
Assisted by the media, commentators have had an easy time framing the events of 2020 principally as a health crisis. With each passing month, however, those claims wear thinner (Barnett, 2020). In a comprehensive analysis titled The State of Our Currencies, former U.S. Assistant Secretary of Housing Catherine Austin Fitts (2020a) offers a broader and more instructive interpretation. Informed by close attention to financial patterns, Fitts asserts that the “shock doctrine” measures being imposed under cover of Covid-19 are helping lay the train tracks for a new global central banking machine and a technocratic “regulatory and economic model that permits far greater central control.”
Fitts calls attention to G7 central bankers’ August 2019 approval in Jackson Hole, Wyoming of a plan called “Going Direct” (Bartsch et al., 2019) that makes the case for a novel “blurring [of] the lines between government fiscal policy and central bank monetary policy” (Martens & Martens, 2020). Drafted months before Covid-19, the plan — co-branded by the World Economic Forum (n.d.) as “the Great Reset” — evokes the prospect of a serious economic downturn and “unusual circumstances” that could be used to justify “unprecedented” global measures (Bartsch et al., 2019).
Fitts (2020a) postulates that central bankers have both a short-term aim (to extend the existing dollar-based reserve currency system) and an ambitious longer-term goal: to implement a “new global governance and financial transaction system, and gather the power necessary to herd all parties into the new system”. Characterizing these aspirations as nothing short of ending currency as we know it, Fitts suggests that the top-down digital-currency-based model being promoted as a replacement could end up sidelining traditional intermediaries and instead directly furnish populations with something akin to a “credit at the company store”. Spelling out the implications of such a model, Fitts notes that with the help of digital surveillance and a social credit system, the central-bank-controlled “credit” could easily be “adjusted or turned off on an individual basis”. General Manager Agustín Carstens of the Bank for International Settlements (BIS) — the central bank of central banks — recently acknowledged as much, stating that in stark contrast to cash, a Central Bank Digital Currency (CBDC) would give central banks “absolute control” over CBDC use “and the technology to enforce” CBDC rules and regulations (International Monetary Fund, 2020). With a vaccine-injected digital surveillance program in individuals, the CBDC would have dictatorial power at the level of individual buying and selling.
Fitts’ analysis suggests that central bankers began laying the groundwork for the desired global transition well in advance of the coronavirus mayhem. In 2019 alone, G7 finance ministers endorsed a cryptocurrency action plan in July; in August, the G7 central bankers approved “Going Direct”; in September, the U.S. Federal Reserve (“the Fed”) started making hundreds of billions of dollars in loans “direct” to Wall Street trading houses; and in October, the BIS issued a major report on global cryptocurrencies (Bank for International Settlements, 2019; Helms, 2019; Fitts, 2020a; Martens & Martens, 2020). In the middle of the frenzy of central bank activity in October, the Bill & Melinda Gates Foundation (along with the World Economic Forum and Johns Hopkins Center for Health Security) held the well-publicized “pandemic tabletop exercise” called Event 201, which played out a global coronavirus outbreak scenario strikingly similar to 2020’s actual events (Center for Health Security, n.d.).
In January 2020, U.S. corporations witnessed a record number of CEO departures (Ausick, 2020; Marinova, 2020) — a mass exodus that strategically allowed over 200 departing executives to sell their stock at or near the market high (see Table 1). Other wealthy and influential insiders also engaged in surprisingly well-timed stock market transactions. For example, following a late-January, behind-closed-doors briefing about the virus (which had yet to affect a single American), certain U.S. senators sold hundreds of thousands of dollars of stock, “unloading shares that plummeted in value a month later” (Lane, 2020). The world’s wealthiest person, Amazon CEO Jeff Bezos, sold nearly $4.1 billion over an 11-day period in early February after having also sold $2.8 billion in shares in August 2019 (Palmer, 2020).
Table 1. U.S. CEO Departures in January 2020
Sources: Ausick, 2020; ChallengerGray, 2020
As the U.S. government turned on the stimulus spigot in March, the Fed sustained its irregular intervention in the U.S. economy. By the summer of 2020, the Fed had expanded its balance sheet by $2.9 trillion — much of it unaccounted for, according to Fed-watcher John Titus (2020) — and financial observers were warning that “the market is no longer the biggest factor in selecting [economic] winners and losers” (Whalen, 2020). Titus (2020) concurs with this assessment, baldly characterizing 2020’s events as a Fed-led “coup d’état”. Titus (2014) has been chronicling major financial forces and legal changes since the 2008 financial crisis, describing how central banks are not only able to “loot” the American people “in broad daylight” but can do so without fear of prosecution — probably because, as Titus and Fitts (2020a) both point out, the Department of Justice depends on Fed member banks for its financial operations.
The coronavirus stimulus has provided abundant financial opportunities advantageous to Fed member banks. Over a two-week period in April, for example, large banks earned $10 billion in fees (ranging from 1 to 5 percent) simply for processing the government’s loans to businesses (Sullivan et al., 2020). Class-action lawsuits subsequently alleged that the banks prioritized larger loans (and larger companies) in order to garner the largest fees, while shutting out “tens of thousands” of eligible but smaller businesses (Sullivan et al., 2020). Serving as lender to the parent company of a national restaurant chain, Fed member bank JPMorgan Chase (the largest and most profitable bank in the U.S.) earned a $100,000 fee for a single “one-time transaction for which it assumed no risk and could pass through with fewer requirements than for a regular loan” (Sullivan et al., 2020).
In September, Senator Marco Rubio (Chairman of the Senate Committee on Small Business and Entrepreneurship) wrote to the JPMorgan Chase CEO expressing “alarm” about allegations that JPMorgan employees “may have been involved in potentially illegal conduct” in the distribution of Paycheck Protection Program and Economic Injury Disaster Loan funds (Rubio, 2020). Bloomberg later confirmed the possibility of Covid-19-related banking abuse on a wide scale (David, 2020). Importantly, this is not a new pattern of behavior for the U.S. banking behemoth. Since 2002 (and primarily since the 2008 financial crisis), JPMorgan Chase has paid out at least $42 billion in settlements for questionable, unethical, or illegal behavior (Fitts, 2019); its public-facing Wikipedia page lists involvement in 22 different “controversies,” including the economically shattering Enron and Madoff scandals (“JPMorgan Chase”, n.d.). Nevertheless, JPMorgan continues to earn glowing accolades from the financial community. In June 2020, Forbes urged investors to “bank on the best” in the uncertain Covid-19 environment (Trainer, 2020), citing JPMorgan’s post-2009 “industry-leading profitability” and asserting that the bank is exceptionally well positioned to expand its market share both during and post-pandemic. In October, JPMorgan rolled out a new smartphone credit card reader designed to compete with Square and PayPal (Son, 2020).
Big Tech
By July 2020, global billionaires’ wealth had surged to an all-time high of $10.2 trillion — an increase of 27.5 percent since April, and a 41.3 percent increase for tech billionaires (Phillipps, 2020). U.S. billionaires accrued a significant share of this pandemic wealth bonus, increasing their worth by $845 billion from mid-March to mid-September and prompting the observation that “for American billionaires specifically, things have never looked better” (Lerma, 2020). As a whole, U.S. billionaires’ wealth reached the equivalent of almost one-fifth of the U.S. gross domestic product, with four tech billionaires (Jeff Bezos, Bill Gates, Elon Musk, and Mark Zuckerberg) plus Warren Buffett seeing their total wealth climb by 59 percent (da Costa, 2020). Calling attention to Bezos, in particular, the Institute for Policy Studies described his surge in wealth as “unprecedented in modern financial history”, requiring “a real-time hour-by-hour tracker” to keep up (Collins et al., 2020).
The companies with which top-tier billionaires are affiliated include Amazon and Amazon Web Services (Bezos), Apple (Tim Cook), Facebook (Zuckerberg), Google/Alphabet (Larry Page and Sergey Brin), Microsoft (Steve Ballmer and Gates), Oracle (Larry Ellison), Zoom (Eric Yuan), and the variety of companies (including Neuralink, SpaceX, and Tesla) spearheaded by Musk (Alcorn, 2020; Collins et al., 2020; Toh, 2020). In July, as Bloomberg described these companies’ “outsized influence on U.S. markets”, it noted that they are as well-situated to profit from the U.S. shutdown as they are to take advantage of a recovering Europe and Asia — a “one-two punch” that has already increased FAANG companies’ market (Facebook, Amazon, Apple, Netflix, and Google, plus Microsoft) by 62 percent (Ritholtz, 2020). Suggesting that Silicon Valley will go down in history as “the standout sector” (Divine, 2020a), a U.S. News analyst unabashedly recommended Facebook as a 2020 “best buy” because “it’s gobbling up the world, and reasonable people could argue that if privacy is dying, individual investors may as well profit alongside Silicon Valley” (Divine, 2020b).
Covid-19 has provided Big Tech (and Big Telecom) with an opportunity to bring a range of controversial technologies further out into the open, despite many unresolved concerns about safety and ethics (Boteler, 2017; Gohd, 2017; Ross, 2018; Boyle, 2019; Feiner, 2019; Markman, 2019; Plautz, 2019; Zhang et al., 2019; Bajpai, 2020; Goodwin, 2020; Gyarmathy, 2020; McGovern, 2020; Novet, 2020; Reuters, 2020; Tucker, 2020; U.S. Department of Defense, 2020). Singly and in combination, the technologies (some of which are listed in Table 2) have the potential to usher in unprecedented societal changes, strengthening technocrats’ ability to control many facets of daily life. Artificial intelligence (AI), 5G, “smart” utility meters, and the Internet of Things (IoT), for example, are rapidly and fundamentally changing the nature of cities, businesses, and homes — what Fitts (2020a) calls the “final mile” — forming an essential part of the strategy to convert the economic model to a technocratic model that uses AI and software to achieve centrally controlled resource allocation.
Table 2. Covid-19 and the Rollout of Control Technologies
In October 2020, the World Economic Forum — the Great Reset’s front-row marketer — released a report on the future of jobs, describing the significant displacement of workers resulting from the pandemic and the related global restructuring that the organization has been taking the opportunity to promote (Petzinger, 2020). With automation and Covid-19 causing a “double-disruption” that is not only accelerating job destruction in the short term but “shrinking opportunities” in the longer term, the report solemnly pronounced a “new division of labour between humans, machines and algorithms” (World Economic Forum, 2020). Well before the pandemic, Amazon had established a robot-centric system at its fulfillment centers, with a process focused on “limit[ing] movement of people [and] let[ting] robots move everything” (Masud, 2019). This downsizing of humans has apparently served Amazon well; by May 2020, Amazon’s e-commerce business had shot up by 93 percent compared to the previous May (Klebnikov, 2020).
A September 2020 survey showed that many other companies plan to substantially boost their spending on AI and machine learning, citing Covid-19 as their rationale for prioritizing “the adoption of new technologies that enhance and enable automation” (Shein, 2020). Observers also predict, however, that the AI gold rush will lead to even more market consolidation and control by Amazon and three other big Covid-19 winners — Alphabet, Facebook, and Microsoft. These four companies, according to Forbes, have the “scale to push the envelope”, the “talent and the technology to perfect [AI]”, and the computing power to dominate the field (Markman, 2019). Amazon already controls nearly 46 percent of the worldwide public cloud-computing infrastructure that is a key backstop for AI functions such as parallel processing and the digestion of Big Data (Atlantic.Net, 2018; Nix, 2019).
Before Covid-19, consumer rejection of 5G wireless technology had been growing (Castor, 2020). However, the imposition of social distancing measures, remote learning, and online work requirements has provided the telecommunications industry with a ready-made pretext to fast-forward 5G’s deployment while attempting to burnish the industry’s unfavorable public image. Taking advantage of virus fears, Big Tech and Big Telecom are claiming that 5G can help enable “a future in which business, health care and human interaction must be at more than an arm’s length” (Wasserman, 2020). Forbes has praised communication service providers for responding to the coronavirus lockdowns “with a sense of urgency, purpose and empathy” (Wilson, 2020). Describing areas requiring more “advanced connectivity”, a technology expert at Deloitte Consulting cited the example of “cameralytics” (video surveillance) “to help worker safety and social distancing” (Howell, 2020). Whatever the rationale, the reality on the ground has been a massive increase in U.S. telecom companies’ capital spending on 5G and a “full steam ahead” rollout of spectrum and infrastructure that has placed the U.S. “ahead of schedule” (Knight, 2020; Ludlum, 2020). The European Commission is now attempting to follow the U.S.’s lead by pushing for the removal of “regulatory hurdles” and making the case that 5G will aid the region’s post-coronavirus economic recovery (McCaskill, 2020).
Covid-19 has also brought another of Big Tech’s interests into sharper focus: food. Billionaires such as Bill Gates and Peter Thiel have, for some time, been investing in biotech start-ups that aim to produce, in a lab, stem-cell-based “meat”, “fish”, “dairy”, and “breastmilk” (Kerr, 2016; Kosoff, 2017; Beres, 2020; Wuench, 2020). These start-ups and their investors have been only too happy to position the burgeoning industry as a partial solution to pandemic-related food insecurity and supply chain interruptions (Galanakis, 2020; Pereira & Oliveira, 2020; Yeung, 2020), welcoming Covid-19 as an “accelerator” as well as an opportunity to overcome consumer skepticism (Siegner, 2019; Morrison, 2020). In addition, as the coronavirus breathes new life into the term “sustainability” — long used by technocrats as a cover term for more centralized control (Wood, 2018) — global partners like the United Nations and the World Economic Forum are making the improbable claim that the complex, high-dollar, lab-created food substitutes (which require genetically stable cell lines, bioreactors, “edible scaffolds”, and cell culture media) are a “sustainable” option (Whiting, 2020). The biopharma giant Merck is also getting in on the “cultured meat” action, offering to make its “extensive knowledge of the relevant science and biotechnology” available to companies seeking to overcome “critical technological challenges” (Whiting, 2020). Merck frequently collaborates with the Gates Foundation, including in the development of Covid-19 vaccines (Lardieri, 2020).
Big Pharma
In September 2019, an annual Gallup poll reported that the restaurant industry was America’s top-ranked and most-liked among the 25 industries regularly assessed by the polling group (McCarthy, 2019). Sadly, less than a year later the Independent Restaurant Coalition predicted the permanent demise of up to 85 percent of independent restaurants (Jiang, 2020). In contrast, the pharmaceutical industry came in “dead last” in the 2019 poll, despite $9.6 billion spent annually on direct-to-consumer advertising and another $20 billion on marketing to health professionals (McCarthy, 2019; Schwartz & Woloshin, 2019). The U.S. is one of only two countries in the world that allows drug companies to market directly to consumers and, in non-election years, roughly 70 percent of news outlets’ advertising revenues come from pharma (Solis, 2019).
The pharmaceutical industry’s history of “fraud, bribery, lawsuits and scandals” is well known (Compton, n.d.), and no less a figure than Bill Gates has suggested that the public perceives Big Pharma as “kind of selfish and uncooperative”; however, Mr. Gates and Fortune magazine propose that Covid-19 may offer the industry an opportunity for “redemption” (Leaf, 2020). The stage may have been set for Big Pharma’s year of opportunity in January, when JPMorgan Chase held its 38th annual invitation-only health care conference. The business press describes the yearly conference as “one of the biggest biotech dealmaking events, often setting the tone for funding rounds, partnerships and mergers and acquisitions” (Leuty, 2020). Thus, just when the coronavirus ball was getting rolling, the conference brought an estimated 20,000 venture capitalists, investment bankers, and drug development executives and entrepreneurs to San Francisco to hear keynote addresses by JPMorgan’s and GlaxoSmithKline’s CEOs and to stoke expectations of a strong year for the biotech-plus-pharma chimera known as “biopharma” (JPMorgan, n.d.; Leuty, 2020; Lipschultz, 2020). In 2014, McKinsey & Company described the investment opportunities in biopharmaceuticals as “big and growing too rapidly to ignore”, with an annual growth rate more than double that of conventional pharma and a 20 percent share of global pharmaceutical revenues (Otto et al., 2014).
A few weeks after the JPMorgan conference — and well before any Covid-19 deaths in the U.S. — the Department of Health and Human Services (HHS) helped ensure that significant pandemic benefits would flow into the biopharma and medical space. HHS did so by issuing a declaration (on February 4) making vaccines and all Covid-19-related medical countermeasures immune from legal liability (HHS, 2020a). On March 6, roughly a week after the first reported coronavirus death, President Trump sweetened the pot by signing into law the first in a series of emergency stimulus packages, earmarking 40 percent of the $8.3-billion bill for vaccines and drugs under terms the pharmaceutical industry openly dictated (Karlin-Smith, 2020).
Following the February 4 HHS declaration eliminating legal liability, Bill and Melinda Gates instantly pledged $100 million in funding for coronavirus vaccine research and treatments, followed by another $150 million in mid-April (Bill & Melinda Gates Foundation, 2020; Voytko, 2020). When Operation Warp Speed followed, making untold billions available for research and development of therapeutics and vaccines at taxpayer expense (see Table 3), dozens of biopharma companies jumped into the fray (HHS, n.d.). Catherine Austin Fitts notes that a system that exempts from liability anything labeled as a “vaccine” amounts to “an open invitation to make billions . . . particularly where government regulations and laws can be used to create a guaranteed market through mandates” (Fitts, 2020b). Moreover, each time the CDC’s Advisory Committee on Immunization Practices (ACIP) adds a given vaccine to the CDC schedule, it is not only the equivalent of a “golden ticket” for the vaccine manufacturer but also directly benefits the CDC, which owns dozens of vaccine-related patents and routinely shares licensing agreements with manufacturers (Taylor, 2017; Children’s Health Defense, 2019).
Currently, there is one injury for every 39 vaccinations administered (2.6%), often resulting in a “disastrous outcome of life-altering iatrogenic illnesses” (Harvard Pilgrim Health Care, n.d.; Kennedy Jr., 2019; Kristen, 2019). A CDC study published in JAMA in 2016 reported that one in five young children (19.5%) under age five who were admitted to emergency rooms for drug reactions were suffering from vaccine injuries (Shehab et al., 2016). Early clinical trial results and Covid-19 vaccines’ use of an array of experimental, never-before-approved technologies suggest that comparable (or worse) levels of injury could follow the rollout of coronavirus vaccines (Children’s Health Defense, 2020a, 2020c, 2020d, 2020e). The Moderna and Pfizer vaccines, for example, feature mRNA molecules that are known to be “intrinsically unstable and prone to degradation”, with an inflammatory component that risks dangerous immune reactions (Feuerstein, Garde, & Joseph, 2020; Jackson et al., 2020; Wadhwa et al., 2020). Assuming the same vaccine injury rate of 2.6 percent, Operation Warp Speed’s projected vaccination of roughly 25 million Americans per month (Owermohle, 2020b) could conceivably result in 3.9 million injuries over just the first six months. (Given that the leading vaccines will require two initial doses and probable boosters thereafter, this figure could even be an underestimate.) If Bill Gates and other technocrats succeed in their declared aspiration to manufacture billions of doses of coronavirus vaccine and “get them out to every part of the world” (Gates, 2020), the scale of injury would not only be unprecedented but could open a lucrative, long-term gateway to the wider drug market to manage the injuries (Kristen, 2019).
*HHS note on Operation Warp Speed funding: “Congress has directed almost $10 billion to this effort through supplemental funding, including the CARES Act. Congress has also appropriated other flexible funding. The almost $10 billion specifically directed includes more than $6.5 billion designated for countermeasure development through BARDA and $3 billion for NIH research.”
By mid-October, 44 candidate vaccines were in clinical evaluation worldwide, with another two hundred or so in the pipeline (Agrawal et al., 2020; World Health Organization, 2020b). Furnishing predictably uncritical coverage ensured by the pharmaceutical industry’s strategic entanglements with the media, scientists, and medical journals, the press has been telling the public that the vaccines will play “an important role in most response scenarios”, including “‘sav[ing] the world’ in worse scenarios” and serving as an “insurance policy against continued health and economic shocks” (Agrawal et al., 2020). Only a handful of journalists have called attention to Big Pharma’s pandemic profiteering, pointing out that “insiders at companies developing experimental vaccines and treatments . . . aren’t waiting until they finish the job to collect their reward” (Wallack, 2020).
An October piece in the Boston Globe cited the example of Moderna (Wallack, 2020). It took Moderna a mere three weeks after Bill Gates’ initial funding installment to send its first batch of experimental vaccine to research and patent partner, the National Institute of Allergy and Infectious Diseases (NIAID), leading to an immediate surge in share price of 28 percent (Lee, 2020; Loftus, 2020). By early April, Moderna’s CEO had become an overnight billionaire; by October, he had sold nearly $58 million in stock, followed by another $2 million in mid-November, just ahead of the company’s intended filing for vaccine Emergency Use Authorization (Nagarajan, 2020; Tognini, 2020; Wallack, 2020). Meanwhile, Moderna’s chief medical officer has been “systematically liquidating all of his company stock” — about $70 million — “in a series of pre-planned trades that have made him roughly $1 million richer each week” (Wallack, 2020). Thus far this year, company insiders have sold $309 million in stock versus under $2 million in 2019, fueling suspicion that they may be “downplaying possible obstacles to goose stock prices — and increase their personal profits” (Wallack, 2020). Also among those selling Moderna stock options is Moncef Slaoui, the former Moderna board member and former GlaxoSmithKline executive who now heads up Operation Warp Speed (Rozsa & Spencer, 2020).
From Moderna’s perspective, the Covid-19 vaccine represents a lifeline, rescuing the company from a shaky bottom line due to its prior inability to bring any products to market (Garde, 2017; Nathan-Kazis, 2020). Other biopharma companies formerly on the skids are likewise poised to make record profits from the coronavirus (Webb & Diego, 2020). Characterizing the business model for Covid-19 (and other) vaccines as a “great scheme” — particularly given the HHS-guaranteed, risk-free environment — a watchdog group spokesman told the Boston Globe, “Taxpayers cover the upfront investment costs and shoulder any downside, while their [biopharma’s] executives and shareholders can capture the upside if their drugs pan out and are shoveling obscene amounts of money into their pockets throughout the process” (Wallack, 2020). In the words of a business school professor, “You announce a sliver of positive hope about a product and your stock price goes up,” even though “the chances of that product panning out might be relatively low” (Wallack, 2020). In 2020, the company Vaxart saw its per-share stock price rise from 27 cents to a high of $17.49 (Wallack, 2020).
Rolling Stone journalist Matt Taibbi (2020) describes Covid-19 as “the ultimate cash cow,” a “subsidy-laden scam,” and a legal opportunity for “giant-scale gouging”, quoting a legislator who admits that while the public is paying for the research and manufacturing, “the profits will be privatized”. Writing in August about how the government-subsidized business model played out for Gilead’s drug remdesivir, Taibbi (2020) recounted: “Gilead, a company with a market capitalization of more than $90 billion, making it bigger than Goldman Sachs, develops an antiviral drug with the help of $99 million in American government grant money. Though the drug may cost as little as $10 per dose to make, and is being produced generically in Bangladesh at about a fifth of the list price, and costs about a third less in Europe than it does in the U.S., Gilead ended up selling hundreds of thousands of doses at the maximum conceivable level, i.e., the American private-insurance price — which, incidentally, might be about 10 times what it’s worth, given its actual medical impact.”
Always a major lobbying presence on Capitol Hill, the pharmaceutical industry has been more lavish than usual with its political spending in 2020, donating over $11 million to individual candidates involved with health care policy and related political action committees (Facher, 2020a). Although the overall amounts represent a pittance for companies earning tens of billions a year, pharma and its lobbying groups recognize that “small chunks of corporate change”, when strategically allocated, “can have a significant impact” (Facher, 2020b). Coronavirus vaccine frontrunner Pfizer, the second-largest drug and biotech company in the world and the fourth-highest earner of vaccine revenues (Statista, n.d.; Hansen, 2020), has been the top political spender, likely laying the groundwork for its November 20 filing for Emergency Use Authorization for its coronavirus vaccine (Chander, 2020; Children’s Health Defense, 2020d). Pfizer has also benefited from repeated endorsements from the financial community and self-proclaimed spokesmen like Bill Gates (Speights, 2020a, 2020b).
The Military-Intelligence Complex
Traditional vaccines have their fair share of safety problems, but coronavirus and other 21st-century vaccines promise to challenge bodily integrity and informed consent in entirely new ways, particularly given their strong reliance on various forms of nanotechnology (Health and Environment Alliance, 2008; Li et al., 2009; Chauhan et al., 2020; Children’s Health Defense, 2020a). Many of the technologies being rolled into Covid-19 vaccines and their delivery systems originated in the military sphere or benefited from Defense Advanced Research Projects Agency (DARPA) funding. DARPA has had a Biological Technologies Office since 2014 and, since the emergence of Covid-19, has specifically directed many of its pandemic-related efforts toward coronavirus therapeutics and vaccines (Gallo, 2020). Far from being suspect, the military’s role has been celebrated. A BioCentury report optimistically suggested in March that as an agency “that specializes in turning science fantasies into realities”, DARPA might offer the “best hopes” for Covid-19 biotech solutions due to its willingness to pursue “high-risk, high-reward technologies”, set goals “that defy conventional wisdom”, and go after its goals with a “laser” focus (Usdin, 2020).
One of the principal DARPA-incubated vaccine technologies to gain prominence in the Covid-19 era are the nucleic acid (mRNA and DNA) vaccines that turn the human body into its own “bioreactor” (Ghose, 2015; Usdin, 2020). Vaccines using mRNA (such as Moderna’s and Pfizer’s) — which developers compare to “software” (Garde, 2017) and praise for their “programmability” (Al-Wassiti, 2019) — target the cell’s cytoplasm and rely on delivery technologies such as lipid nanoparticles to “ensure stabilization of mRNA under physiological conditions” (Wadhwa et al., 2020). DNA vaccines (such as Inovio’s) are intended to penetrate all the way into a cell’s nucleus and come with the risk of “integration of exogenous DNA into the host genome, which may cause severe mutagenesis and induced new diseases” (Zhang, Maruggi, Shan, & Li, 2019). Describing the scientific community’s early doubts about nucleic acid vaccines — arising from the potential for “many things” to go wrong — a DARPA program manager recently noted, “It was something that was much too risky for groups like the NIH to fund” (Usdin, 2020).
Risks aside, DARPA and vaccine manufacturers are attracted to one chief benefit of nucleic acid vaccines: They can be developed much more quickly and cheaply. Other military-initiated technologies are also coming into view with Covid-19 vaccines. These include electroporation, which applies a high-voltage electrical pulse to make cell membranes permeable to a vaccine’s foreign DNA (Inovio Pharmaceuticals, 2020); syringe-injected biosensors that enable continuous wireless monitoring of vital signs and body chemistry (Peer, n.d.; Profusa, n.d.; Diego, 2020b; Tucker, 2020); and the quantum-dot-based infrared detectors that are under discussion as a tool for tracking vaccination status (Johnson, 2011; Trafton, 2019). DARPA has also played a leading role in developing and funding technologies that “blur the lines between computers and biology”, including brain-machine interfaces and neuromonitoring and mind-reading devices (CB Insights, 2019; Gent, 2019; Tullis, 2019).
Some of Moderna’s earliest funding came from DARPA, which awarded the company $25 million in 2013 to develop the mRNA platform that has become a key feature of its coronavirus vaccine (Usdin, 2020). Other DARPA beneficiaries now involved in efforts to develop Covid-19 vaccines or therapeutics include AbCellera Biologics, CureVac, Inovio Pharmaceuticals, Regeneron Pharmaceuticals, and Vir Biotechnology; some of AbCellera’s partners include major players like Pfizer and Gilead (Usdin, 2020).
The Pentagon’s involvement in coronavirus-related efforts goes well beyond DARPA-funded research. Four-star General Gustave Perna is serving as chief operating officer of Operation Warp Speed alongside chief advisor Moncef Slaoui. General Perna, in charge of U.S. Army Materiel Command, oversees the global supply chain for over 190,000 U.S. Army employees (HHS, 2020b). For the first time ever, the distribution of the eventual coronavirus vaccines is being planned as a “joint venture” between the CDC and the Pentagon, with the latter overseeing “all the logistics of getting the vaccines to the right place, at the right time, in the right condition” (Owermohle, 2020a). In a CBS “60 Minutes” appearance in early November, General Perna indicated that Operation Warp Speed already had doses of (currently unapproved) vaccine and syringes stockpiled and protected by armed guards, and intends to get them out the door “within 24 hours” of vaccine approval and delivered “to every zip code in this country” (Martin, 2020).
The Pentagon has indicated that private-sector involvement could be a key feature of the distribution strategy, and the private sector is positioning itself to participate. Merck, for example, is testing drone delivery of vaccines in partnership with Volansi, Inc., a company that provides “on-demand” drone services for the military (Landi, 2020; Simmie, 2020). In July, Merck’s CEO set the stage for its logistics involvement by describing vaccine distribution as “even a harder problem” than the “scientific conundrum of coming forward with a vaccine that works” (Murray & Griffin, 2020).
Outside the pharmaceutical arena, technological transformations that are speeding the world toward more centralized control also reveal the influence of the military-intelligence sector. For example, Amazon Web Services has held cloud-computing contracts with the CIA since 2013, with the original $600 million contract extending to all 17 intelligence agencies (Konkel, 2014). In October of 2019, the Department of Defense awarded the $10 billion JEDI cloud computing contract to Microsoft, a decision that Amazon has unsuccessfully disputed in court (Sandler, 2020). In early 2020, the U.S. Navy awarded a cloud computing contract to Leidos (Leidos, 2020).
5G, too, relies in part on the high-range millimeter-wave spectrum previously used almost entirely by the military for “non-lethal” crowd dispersal weapons (Joint Intermediate Force Capabilities Office, n.d.). In October, the Department of Defense announced it would spend $600 million to test “dual-use” applications of 5G to enhance the U.S. military’s “leap-ahead capabilities”, including applications such as 5G-enabled augmented/virtual reality, 5G-enabled “smart” warehouses, and 5G technologies “to aid in Air, Space, and Cyberspace lethality” (U.S. Department of Defense, 2020).
Both 5G and cloud computing are critical components of the Big Data and IoT build-out that is enabling the conversion of individual data into the “new oil” (Fitts, 2020a), and both have exploded in 2020 (Howell, 2020; Klebnikov, 2020). The technologies are essential to the “centrally controlled digital financial transaction systems” envisioned by central bankers, who plan to rely on seamless data flows to and from “every smartphone, community, and home without exception” (Fitts, 2020a).
Discussion
As more individuals and organizations connect the technocratic dots and look beneath the coronavirus pandemic’s seductively simple surface, it should become increasingly apparent that the pandemic profiteers do not have people’s best interests at heart. In The State of Our Currencies and other pandemic-related writings, Catherine Austin Fitts (2020a, 2020b) strongly emphasizes the importance of accepting that what is transpiring in the financial, tech, biopharmaceutical, and military-intelligence sectors is interconnected. Part of this involves recognizing that the coronavirus vaccines currently dominating the headlines represent something likely to go far beyond the simple health intervention being held out by scientists and officials as a panacea. Instead, the evidence suggests that Covid-19 vaccines are intended to serve as a Trojan horse to transport invasive technologies into people’s brains and bodies. These technologies could include brain-machine interface nanotechnology, digital identity tracking devices, technology that can be turned on and off remotely, and cryptocurrency-compatible chips (Fitts, 2020b).
In Fitts’ (2020a, 2020b) view, this type of intimate access — achieved “without notice, disclosure, or compensation” — represents the “final inch” of interest to technocrats. Together with external technologies to control behavior (Max, 2020), such access could permit the achievement of several goals: (1) replacing currencies with a digital transaction system, digital identification, and tracking (an “embedded credit card system”); (2) creating a global control grid that connects the population to the military-intelligence clouds; and (3) obtaining continuous access to valuable individual data on a 24/7 basis (Fitts, 2020b). Countries in West Africa are already piloting a venture by the Gates Foundation, the Gates-funded GAVI vaccine alliance, and Mastercard that “marks a novel approach towards linking a biometric digital identity system, vaccination records, and a payment system into a single cohesive platform” (Diego, 2020a). As Fitts (2020b) summarizes, “Just as Gates installed an operating system in our computers, now the vision is to install an operating system in our bodies and use ‘viruses’ to mandate an initial installation followed by regular updates”. The “neat trick”, as Fitts sees it, is that the use of vaccines as the delivery vehicle cancels out legal liability.
It is noteworthy that Bill Gates announced that he was stepping down from the Microsoft board of directors on March 13 — the same day that President Trump declared the pandemic a national emergency (Haselton & Novet, 2020). That same month, the Pentagon reaffirmed its intention for the JEDI cloud-computing contract to go to Microsoft (Rash, 2020; Sun, 2020). By distancing himself from the appearance of conflicts of interest with Microsoft’s Defense Department commitments and the Pentagon’s subsequent role in Operation Warp Speed, Mr. Gates had more freedom to make the rounds and begin promoting worldwide vaccination and digital certificates (Haggith, 2020). Gates has been less successful in distracting attention from other potential conflicts of interest. An exposé by The Nation (ironically also published in March) showed that the Gates Foundation gives billions to corporations in which the foundation holds stocks and bonds — including all of the major pharmaceutical companies — creating a “welter of conflicts of interest” (Schwab, 2020). A dozen years ago, around the time of the 2007-2008 financial crisis, the Los Angeles Times outlined the Gates Foundation’s numerous holdings in a number of notoriously “destructive or unethical” companies (Piller et al., 2007).
Mr. Gates is not the only party strenuously promoting digital IDs and “no-escape” financial tracking (marketed under the benevolent guise of “financial inclusion”). In October, Kristalina Georgieva, the International Monetary Fund’s (IMF’s) Managing Director, evoked “a world in which digital is the way in which financial transactions take place” and made it clear that she views universal digital IDs as a non-negotiable requirement for moving in the “right direction” (International Monetary Fund, 2020). Georgieva has, not unhappily, described Covid-19 as a “once in a lifetime pandemic” (Bello, 2020).
Georgieva’s remarks should be examined in the context of a proposal by the U.S. House of Representatives to bestow the IMF with $3 trillion “no-strings-attached” U.S. dollars as “coronavirus relief aid” (Huessy, 2020; Roberts, 2020). A U.S. taxpayer-funded gift of this magnitude would be unprecedented and would increase the IMF’s lending resources (called Special Drawing Rights or SDRs) by as much as 10-fold (Roberts, 2020). 2020’s events (including global debt entrapment and actual or potential food shortages) and the IMF’s bullying track record (Bello, 2020) suggest that the IMF could then wield the $3 trillion as a weapon, strong-arming countries into accepting an array of unwanted measures such as digital identities, forced vaccination, and eventually (as the World Economic Forum predicts), the relinquishment of private property (World Economic Forum, 2016). As a step in this general direction, the IMF has strongly praised India’s leadership in biometric identification systems. It celebrates the “delivery of social benefits through direct electronic payments to eligible bank account holders”, but glosses over the systems’ vulnerability to “unauthorized access” and the data breaches that are already rampant (Jha, 2018).
While current prospects for ordinary citizens certainly appear challenging, nothing is a foregone conclusion. Large-scale protests against the curtailment of civil rights have occurred and continue to occur in many countries, most notably in Germany (Depuydt, 2020). The Great Barrington Declaration — a statement crafted by public health scientists from Harvard, Stanford, and Oxford — has garnered signatures from over 12,000 scientists, over 35,000 medical practitioners, and nearly 639,000 citizens from around the world, all concerned about “the damaging physical and mental health impacts of the prevailing COVID-19 policies” (Kulldorff et al., 2020). Similarly, an Appeal authored in May by Archbishop Carlo Maria Viganò, former Apostolic Nuncio to the United States, gathered 40,000 signatures within a few days, with the signatories (religious leaders, doctors, journalists, lawyers, and other professionals) all seeking to draw attention to the threats to sovereignty and freedom that pandemic-related mandates have unleashed (Tosatti, 2020). Archbishop Viganò has also penned severe critiques of the Great Reset, describing its architects as “a global elite that wants to subdue all of humanity, imposing coercive measures [and a health dictatorship] with which to drastically limit individual freedoms and those of entire populations” (Viganò, 2020).
One of the signatories of Archbishop Viganò’s Appeal is attorney Robert F. Kennedy, Jr., founder and chief legal counsel of Children’s Health Defense, an organization dedicated to ending childhood epidemics by working to eliminate harmful exposures, holding those responsible accountable, and establishing stronger safeguards. In late October, Kennedy recorded a 19-minute video message to people around the world, describing the “coup d’état by big data, by big telecom, by big tech, by the big oil and chemical companies and by the global public health cartel” (Kennedy Jr., 2020). In his closing remarks, Kennedy also indicated that citizens who wish to maintain their freedoms cannot afford to remain complacent: “You are on the front lines of the most important battle in history, and it is the battle to save democracy, and freedom, and human liberty, and human dignity from this totalitarian cartel that is trying to rob us simultaneously, in every nation in the world, of the rights that every human being is born with.”
Andriotis, A. (2020, September 20). No job, loads of debt: Covid upends middle-class family finances. The Wall Street Journal. https://archive.is/mZAme
Bank for International Settlements. (2019, October 18). Investigating the impact of global stablecoins. G7 Working Group on Stablecoins. https://www.bis.org/cpmi/publ/d187.pdf
Bueno-Notivol, J., Gracia-García, P., Olaya, B., Lasheras, I., López-Antón, R., & Santabárbara, J. (2020). Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. International Journal of Clinical and Health Psychology, 2020 Aug 31. doi: 10.1016/j.ijchp.2020.07.007
Chauhan, G., Madou, M. J., Kalra, S., Chopra, V., Ghosh, D., & Martinez-Chapa, S. O. (2020). Nanotechnology for COVID-19: Therapeutics and vaccine research. ACS Nano. doi: 10.1021/acsnano.0c04006
Community FoodBank of New Jersey. (2020, September 30). COVID-19’s Impact on Food Insecurity in New Jersey. Hillside, NJ: CFBNJ. https://cfbnj.org/covidimpact/
Dubey, M. J., Ghosh, R., Chatterjee, S., Biswas, P., Chatterjee, S., & Dubey, S. (2020). COVID-19 and addiction. Diabetes & Metabolic Syndrome, 14(5), 817-823. doi: 10.1016/j.dsx.2020.06.008
Ettman, C. K., Abdalla, S. M., Cohen, G. H., Sampson, L., Vivier, P. M., & Galea, S. (2020). Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Network Open, 3(9), e2019686. doi: 10.1001/jamanetworkopen.2020.19686
Federal Accounting Standards Advisory Board. (2020, October 4). Statement of Federal Financial Accounting Standards 56: Classified Activities. FASAB Handbook, Version 18 (06/19). Retrieved September 26, 2020, from http://files.fasab.gov/pdffiles/handbook_sffas_56.pdf
Ganann, R., Ciliska, D., & Thomas, H. (2010). Expediting systematic reviews: methods and implications of rapid reviews. Implementation Science, 5, 56. doi: 10.1186/1748-5908-5-56
HHS. (2020a, February 4). Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID-19. U.S. Department of Health and Human Services. Federal Register, 85(52), 15198–15203. https://www.law360.com/articles/1253029/attachments/0
Jackson, N. A. C., Kester, K. E., Casimiro, D., Gurunathan, S., & DeRosa, F. (2020). The promise of mRNA vaccines: a biotech and industrial perspective. NPJ Vaccines, 5, 11. doi: 10.1038/s41541-020-0159-8
Pereira, M., & Oliveira, A. M. (2020). Poverty and food insecurity may increase as the threat of COVID-19 spreads. Public Health Nutrition, 1-5. doi: 10.1017/S1368980020003493
Profusa. (n.d.). Profusa is pioneering tissue-integrating biosensors for continuous monitoring of body chemistries. Retrieved October 26, 2020 from https://profusa.com/
Rossen, L. M., Branum, A. M., Ahmad, F. B., Sutton, P., & Anderson, R. N. (2020, October 23). Excess deaths associated with COVID-19, by age and race and ethnicity — United States, January 26–October 3, 2020. Morbidity and Mortality Weekly Report, 69(42), 1522-1527. doi: 10.15585/mmwr.mm6942e2
Shehab, N., Lovegrove, M. C., Geller, A. I., Rose, K. O., Weidle, N. J., Budnitz, D. S. (2016). US emergency department visits for outpatient adverse drug events, 2013-2014. JAMA, 316(20, 2115-2125. doi: 10.1001/jama.2016.16201
Wadhwa, A., Aljabbari, A., Lokras, A., Foged C., & Thakur, A. (2020). Opportunities and challenges in the delivery of mRNA-based vaccines. Pharmaceutics, 12(2), 102. doi: 10.3390/pharmaceutics12020102
Woolf, S. H., Chapman, D. A., Sabo, R. T., Weinberger, D.M., Hill, L., & Taylor, D. D. H. (2020). JAMA, 324(15), 1562-1564. doi: 10.1001/jama.2020.19545
Zhang, C., Maruggi, G., Shan, H., & Li, J. (2019). Advances in mRNA vaccines for infectious diseases. Frontiers in Immunology, 10, 594. doi: 10.3389/fimmu.2019.00594
Zhang, J., Xu, K., Zhang, S., Wang, Y., Zheng, N., Pan, G. et al. (2019). Brain-machine interface-based rat-robot behavior control. Advances in Experimental Medicine and Biology, 1101: 123-147. doi: 10.1007/978-981-13-2050-7_5