Pascal Najadi, son of World Economic Forum (WEF) cofounder Hussain Najadi, is calling on the Swiss authorities to arrest the leaders of the World Economic Forum, the World Health Organization and GAVI, all of which are headquartered in Geneva, Switzerland, as well as Big Tech and Big Pharma executives, for injecting a bioweapon into 5.7 billion people
In 2022, Najadi filed criminal charges against Swiss president Alain Berset for misleading the Swiss people about the COVID shots
Najadi has also filed a civil case against Pfizer at the New York Supreme Court for harm done to him by the Pfizer COVID injection
GAVI, founded by Bill Gates, has diplomatic immunity in Switzerland, and its immunity clauses go beyond even that of diplomats. GAVI’s immunity covers all aspects of engagement, including criminal business dealings. They can do whatever they want without repercussions. GAVI is also completely tax exempt
Another Gates-founded and funded organization headquartered in Geneva — the Global Fund to Fight AIDS, Tuberculosis and Malaria — also has diplomatic immunity
“Everything evil in the world, related to democide … comes from Geneva.” That’s a quote from Pascal Najadi, a former banker and son of World Economic Forum (WEF) cofounder Hussain Najadi, who claims his father left the WEF “out of disgust” in the early ‘80s.1 Hussain, founder of AmBank, one of the largest banks in Malaysia, was assassinated in Ceylon in 2013.2,3
According to Najadi, “evil” organizations engaged in democide — the murder of people by government — include the World Health Organization, the Global Alliance for Vaccine Immunization (GAVI) and the WEF, all of which are headquartered in Geneva, Switzerland.
This is why he calls Geneva “the head of the snake.” Najadi is now calling on the Swiss authorities to arrest the leaders of these organizations, along with Big Tech and Big Pharma executives, because:
“… the WEF, WHO, GAVI, Big Pharma, Big Tech [and] Bill Gates all advocated for a global humanity injection [with] a bioweapon — injecting nanolipids [which are classified as toxic4] into 5.7 billion people. And we Swiss are hosting them? That’s terrible. We cannot tolerate any entity that promotes poison to be injected into humanity.”
One of the reasons Najadi is so adamant about holding these organizations accountable is because he trusted the information given, got three doses of Pfizer’s mRNA shot in 2021, and is now dying from the effects. “It’s a democide, and you’ll be judged,” he says. “It will be corrected in the name of humanity.”
Najadi Goes After Swiss Government and Pfizer
In December 2022, Najadi filed criminal charges against Swiss President Alain Berset (formerly the Swiss minister of health) for misleading the Swiss people about the COVID shots.5
Among the false statements highlighted by Najadi was Berset’s claim that vaccinated people were not contagious and could not spread the virus6 — a claim he must have known was untrue at the time he said it, October 27, 2021.
First of all, Pfizer never conducted any tests to determine transmissibility among the jabbed, so they had no data. Moreover, three months earlier, August 3, 2021, the Swiss Federal Office of Public Health (FOPH) had announced findings showing “Vaccinated people can spread the coronavirus just as frequently as unvaccinated people.”7
Criminal charges include assault, bodily harm and abuse of office. The charges are reportedly still under investigation. He discusses this case with Rebel News in the video above.
In March 2023, he also filed a civil case against Pfizer and the U.S. Food and Drug Administration at the New York Supreme Court in Manhattan for harm done to him by the Pfizer COVID shot.8,9,10 That case is discussed in the video below. Charges were also filed against the two doctors who “injected him with a toxic substance.”11
The Geneva Syndrome
According to her bio,12,13 Astrid Stuckelberger “is an internationally recognized expert on issues related to evaluating scientific research for policymakers, in particular in health and innovation assessment, pandemic and emergency management training and in optimizing individual and population health and well-being.”
She’s also a published author, with a dozen books to her credit, as well as more than 180 scientific articles, policy papers and governmental and international reports.
Between 2010 and 2020, Stuckelberger was also a professor at the Universities of Applied Science in Switzerland, and a senior lecturer at the University of Lausanne. When she started speaking out against the COVID-19 narrative, her university positions were canceled.
Stuckelberger refers to what she calls “the Geneva syndrome.” What she means is that most of the people who work in these Geneva-based organizations do not understand what they’re working toward, and those who do understand are too afraid to speak out because the power wielded by these entities is so great.
Instead, they speak in code or try to wake people up to the reality of what’s planned in indirect ways. What’s planned, of course, is a one world government ruled by an unelected cadre of technocrats.
The agenda that has become apparent over the past three years has been in the works for decades, but there was always some semblance of law and order, some checks and balances. What we’re seeing now is that the individuals involved have become so emboldened they don’t even care that people can see them flouting the rules and changing them to fit their own aims.
The WHO, for example, does not have the authority to dictate orders to the world, yet that’s what they did. Now, they’re simply trying to “legalize” and make permanent their power grab through the implementation of a new pandemic treaty, amendments to the international health regulations and One Health — none of which can be voted on by the public.
Why Do Gates’ Organizations Enjoy Diplomatic Immunity?
Stuckelberger was the first to publicly point out that GAVI, the vaccine alliance founded by Bill Gates, has diplomatic immunity in Switzerland.14,15 More specifically, GAVI has “qualified diplomatic immunity,” which is odd, considering the organization has no political power that would warrant it.
Odder still is that GAVI’s immunity clauses go beyond even that of diplomats. GAVI’s immunity covers all aspects of engagement, including criminal business dealings.
They can do whatever they want, without repercussions. Equally strange, GAVI is completely tax exempt. So, to summarize, GAVI is a nongovernmental organization (NGO) that is allowed to operate in Switzerland without paying any taxes, while also having total immunity for anything they do wrong, willfully or otherwise.
Another Gates-founded and funded organization headquartered in Geneva — the Global Fund to Fight AIDS, Tuberculosis and Malaria — also has diplomatic immunity.16,17 Like that of GAVI, the agreement between the Swiss Federal Council and the Global Fund includes articles specifying the “inviolability” of their premises and archives.
No agent of the Swiss public authority can enter or search them without express consent of the executive director of the organization. Their archives may not be searched, regardless of their location, and “in the conduct of its business,” the organizations “enjoy immunity from every form of legal process and enforcement.”
The only person who can waive this immunity is the executive director himself, or an authorized representative. But if you’re engaged in criminal activity, would you waive your immunity to search, seizure and prosecution?
The inclusion of that article alone reveals volumes. It’s what you’d want if you knew that what you were doing could get you in legal trouble, sooner or later. One of the few exceptions to the ironclad immunity clause is the civil liability for damages caused by a vehicle belonging to the operation.
The Nation-State of Gates
In her 2021 testimony to the German Corona Extra-Parliamentary Inquiry Committee, Stuckelberger also detailed the highly unusual agreement between the WHO, Gates and Swissmedic (the Food and Drug Administration of Switzerland).
According to Stuckelberger, Gates requested to be part of the WHO’s executive board in 2017, ostensibly because he’s one of its largest funders. Essentially, he, as an individual, sought to gain the status of a member state. There’s no evidence that Gates was ever granted this status, but he may still have more power over the WHO than his funding already grants him.
Essentially, it appears that when he did not get voted in as a one-man nation state, Gates created three-party contracts with member states and the WHO instead, essentially placing himself on par with the WHO. According to Stuckelberger, on one of those three-way contracts is between Gates, the WHO and Swissmedic.
This arrangement is yet another piece of evidence that private-public partnerships have been hijacked by private interests, which also happen to enjoy the same or even greater liability protections than nation states!
Building a Global ‘We the People’ Movement
Najadi insists that Switzerland must return to its neutral roots. “Swiss neutrality has to be restored,” he says, and once restored, the country must never again allow institutions like the WEF, WHO and GAVI to gain foothold.
“The snake head is in Geneva,” Najadi says. “I call it a direct, clear and present danger to the Swiss population. But I can tell you, it is being cut off. If you have a house of cards … of a criminal [entity]… one card pulled by justice and the whole card house collapses.
But from hope alone it is not done. Everybody must now change the spirit. All the vaccinated, the injected, knowing that they are poisoned — we are the masses. We are billions of people. Let’s just stand up and say ‘Stop. We will not comply.’ Because we are the guardians of humanity and our light obliterates the darkness of evil.”
This is the THIRD Proclamation of Arikinui Ripekatangi of many tribes and subtribes of our Supreme Sovereign Nation of New Zealand, Leader and Prime Minister of the Wakaminenga Maori Government of Aotearoa New Zealand.
Notice to members of the World Health Organisation & United Nations/WEF and their representatives acting as the NZ Crown government
You are directed to cease and desist any and all actions taken to implement measures of depopulation
And those associated with the WHO pandemic prevention treaty against the people of the sovereign independent nation of Aotearoa Nu Tireni New Zealand
I watched a recent interview (link) of Prof. Syed Sattar (Retired Professor of Virology from the University of OTTAWA, Canada), who is still active in the area. He is a great friend, and I greatly admire his academic credentials and achievements. I have known him personally and professionally, at least for twenty years.
I find the interview informative, describing the fundamental concepts of virology, notably virus isolation. That is, how the virus isolation concepts are illustrated in virology literature, which Prof. Sattar emphasized as well-established practices and routines in virology laboratories.
However, issues and confusion arise when virologists, including Prof. Sattar, describe isolation as “culturing or its part” as a virus. It is essentially their critical misunderstanding, i.e., considering “culture” and the “virus” as the same thing. In reality and scientifically, they have to be and are two separate entities. I often describe the difference between the two as being chicken (“virus”) and “soup,” which may or may not contain the chicken/virus.
To show the presence or existence of a virus, the virus (if there) must be isolated or separated from the culture. The separation of the virus from culture and its content is called the “isolation” step, which has never been done. This is the confusion or misunderstanding virologists and microbiologists have and are unwilling to take the time to consider or evaluate.
They often defend their position by arguing that viruses (particles) are minute in size and number and cannot be seen or isolated (separated) from cells (culture) to observe. Therefore, viruses and culture have to go together and side by side. Hence, it resulted in considering/calling culturing or culture a “virus.”
It is to be noted that there is no objection to the culturing step, which, in reality, is a fermentation step for growing or multiplying the viruses. However, once the viruses are sufficiently multiplied, they MUST be isolated or separated to evaluate their identity and characteristics, such as structure, RNA/DNA proteins, etc. This step is missing.
So, effectively, virologists work with cultures but make claims about them as “viruses.” It is like working with debris from a forest but selling it as novel and rare wood dust particles.
Seeing the photographs with low or high-resolution microscopes does not establish the presence of something, just like seeing small yellow particles would not confirm the presence of gold in the sample. The particles must be isolated/separated to characterize them.
It is an invalid argument that viruses are small (in size and number), so they cannot be seen without culturing or separating from cells. Smaller items like carbon, hydrogen atoms, and molecules are commonly available in isolated and purified forms with full characterization or certifications.
If the claim is that there are viruses, then these entities, considered particles, must be available in, isolated, purified, and fully characterized. Nothing of this nature is available, including for the coronaviruses. Calling or considering cultures/isolates as viruses is an incorrect understanding that needs to be abandoned.
Links to some articles for further information on the topic:
An unexplained pneumonia-like sickness is reportedly swiftly spreading through schools in China, leading to a surge of hospitalizations of children.
Over the past few weeks, numerous schools in China, predominantly in Beijing and Liaoning province, have reported a rapid increase in children presenting with severe symptoms. These symptoms, including high fever and lung inflammation, are eerily similar to those of pneumonia, Daily Mail reported.
However, what sets this illness apart is the lack of common respiratory symptoms like coughing. This unique symptom profile has led health professionals to label this as an “undiagnosed pneumonia.”
Note that this peculiar symptomatology has reportedly baffled health professionals, who are struggling to categorize and understand this new illness.
Mystery? Baffling? Eerie?
I don’t think so. They always give you: “This has no explanation”—just before they magically announce they’ve found a new virus.
Of course, they never actually isolate that new virus. They never discover it. They just invent a fairy tale.
As far as “mysterious” is concerned in China right now, here is a definitive statement from the American Thoracic Society: “It is possible to have pneumonia without a cough or fever.”
Oops.
For years, doctors have been diagnosing patients with pneumonia when there is no cough present. It’s not baffling. It’s not ultra-strange. So forget about that.
Which leaves the question: what IS making all these children in China sick? Hmm. Let’s see. Could it be changes in the moon’s orbit? Sun spots? Lasers fired from UFOs? Infected bats imported from Mars?
No?
Well, how about THIS?
US Embassy in China, October 30, 2023:
EVENT: This is a notification that the Beijing City Government has issued an ‘orange’ alert for air pollution effective from 12:00 Monday, October 30 until 24:00 Thursday, November 2. An ‘orange’ alert means that official forecasts indicate Beijing’s Air Quality Index (AQI) will exceed 200 for two consecutive days or 150 for three consecutive days. The alert may be extended if air pollution levels persist.
During an “orange” alert, some businesses may reduce operations.
ACTIONS TO TAKE: The U.S. EPA recommends people with heart or lung disease, older adults, children, and teenagers limit or avoid outdoor physical activity when the AQI level exceeds 200. It recommends everyone avoid outdoor exertion if the AQI level exceeds 300.
Reuters, October 31, 2023:
Authorities issued their highest warnings for fog and haze on Tuesday as smog enveloped major cities in northern China, warning the public that visibility could drop to less than 50 metres (164 feet).
Northern province Hebei launched an anti-pollution emergency response, listing traffic safety controls for when necessary including suspending flight takeoffs and landings, temporarily closing highways and suspending ferries, China’s meteorological bureau said in a notice.
As air pollution levels in the wider Beijing-Tianjin-Hebei area and northern part of Henan province reached moderate to severe, pollution control experts said increased industrial activities, heavy trucking and crop fires had contributed to the haze, state media CCTV reported.
Crisis 24, a “global security platform,” reports that heavy pollution is occurring in Northern China provinces, including Beijing and Liaoning, the two areas reporting the “mystery illness” in children.
I see. Pollution causing lung problems. Wow. I just fell off my chair. What a revelation. Who ever heard of that?
Yeah. I went through all this—reported on all this—in 2020—with “COVID.” That was a mysterious pneumonia, too. Except for the heavy air pollution. Every year in China, about 300,000 people die from pneumonia (lung problems). That means there are millions of cases.
Psychiatrists used to not put much effort into diagnosing. Instead, they focused on getting to and working on the issues in their clients’ lives that were upsetting them. But all that changed when the 1980 DSM came out. Since then, diagnosing mental disorders has been one of their main focuses (prescribing medicine being the other). People pay huge sums of money for psychiatrists’ expert opinions, and their diagnostic evaluations carry great weight in court, school, the workplace, and disability determinations. But is this truly warranted? Is a doctor really needed to make a psychiatric diagnosis, or can anyone do it?
Here are three points which support the idea that anyone can make a psychiatric diagnosis:
1. All the diagnostic criteria that psychiatrists learn in their training can be easily found on various websites. Therefore anyone can look up the criteria for diagnosing any mental illness and then conduct a do-it-yourself diagnostic evaluation.
2. It’s true that only trained doctors can perform physical exams and order lab tests, x-rays/scans, biopsies, etc.. And it’s true that only doctors are qualified to interpret their results. But these medical workups are only ever done to verify physical illness diagnoses, like cancer or diabetes. They are never done to diagnose mental illnesses. If a medical workup is ever done during a mental illness evaluation, it’s only to rule out a real (physical) illness.
3. If one examines the criteria for all the mental illness diagnoses, it becomes clear that identifying them doesn’t require any medical background or skill. For example, here are some criteria for diagnosing depression: diminished interest/pleasure in activities, indecisiveness, and feelings of worthlessness. First of all, these are not terms/concepts that only doctors are privy to. Secondly, they’re vague, subjective perceptions rather than objective, scientific facts. They’re in the eye of the beholder. Thus, any human could offer an opinion as to whether or not someone is experiencing them. Who’s to say which is the “right” opinion?
These are all excellent points.
But if a regular human such as you dares to take it upon yourself to perform a psychiatric diagnostic evaluation, you’ll be laughed at for your brazenness. You need a doctor’s official stamp of approval to make the diagnosis appear legitimate and valid. Doctors are greatly revered and trusted. Only if you tell others that a learned doctor diagnosed you with your mental illness, will it be viewed as a proven fact rather than a mere opinion. So even though psychiatrists don’t use any medical knowledge when making diagnoses, they do have MD degrees, and that’s enough.
Furthermore, for centuries psychiatrists have been designated by society to be the supreme authorities over several key areas: They decide who is insane and should be involuntarily committed and forcibly sedated. They also determine who is mentally unfit and should lose their right to manage their own lives. Perhaps these longstanding power roles have culturally imbued psychiatrists with an aura of superhuman capabilities which makes all their opinions far more important than a regular person’s. The common belief that psychiatrists have the intimidating ability to read and manipulate people’s minds may enhance this aura. Without necessarily being consciously aware of the aura, people may sense it, fear it, and be awed by it. They may thus be particularly likely to unquestioningly, submissively accept whatever their omniscient psychiatrist diagnoses and commands.
Psychiatry’s aura of superiority may be what enabled it to convince people that mental illnesses are real physical illnesses, even though they’re opposites: First psychiatry constructed a fantasy about emotional distress being a medically-treatable disease caused by a chemical imbalance or brain anomaly.Then it turned it into a reality just by proclaiming it to be true. It didn’t matter that 50 years of intensive research never found any chemical imbalances or brain anomalies. Nor did it matter that antidepressants were proven to be mere placebos(1). When psychiatry says something is true, that makes it true, no matter how illogical. And this isn’t the first time this was done: The diagnosis of hysteria was taken seriously for many centuries. It was another example of emotional distress being unfoundedly declared to be a medical condition. This time it was said to be caused by a wandering uterus, and the treatment was to coax it back into place(2).
Psychiatry would lose its power over people if its aura was removed, because nothing would be left but smoke and mirrors. People would lose faith in it (just as happened to the Wizard of Oz when his curtain was removed, revealing that he wasn’t a higher being but just a regular human). Psychiatry’s customers would then realize that they’re not defective and helpless as their doctor oppressively insists. They’d see that they’re actually capable of thinking for themselves in order to devise adaptive ways to solve their own problems. (The tin man, scarecrow, and lion made the same realization after their wizard was shown to be a fraud.) If this ever happens, then people will no longer feel compelled to follow the yellow brick road to a doctor’s office to have their painful feelings medicalized.
1. Kirsch, I. “The Emperor’s New Drugs: Exploding The Antidepressant Myth”, Basic Books, New York, 2010.
2. Wellesley, M “A Load Of Ballokis” London Review of Books, 23 April 2018.
Lawrence Kelmenson has practiced psychiatry for 32 years, working with children, adults, and families. He graduated medical school from State University of New York, and completed psychiatric residency training at Cornell. He then became staff psychiatrist, and later medical director, of Craig House Hospital in Beacon, New York until 2000, and has since conducted a psychotherapy-based private practice in Cold Spring, New York.
The narrative of an Anthrax bioweapons attack is again in the “news cycle” and remains prominent on the CDC website.
A November 15, 2023 CDC news brief updated advice for healthcare providers in preventing and treating anthrax should a “wide-area aerosol release of B. anthracis” occur.
CDC has classified B. anthracis as a “category A” organism of concern because an attack with B. anthracis would happen via aerosolized exposure. How does the CDC know that any attack would be in an aerosolized form? Does the CDC have a crystal ball? The CDC did seem to know the problems of the COVID19 vaccines before they were distributed:
Americans need to be prepared for the possibility that they may feel a little unwell after they get a coronavirus vaccine, if one is authorized. – CDC Prevention Advisory Committee, November 23, 2020.
Appearance of small welts or sores that are itchy.
Confusion or dizziness
Cough
The sore developing into a blister that turns into a skin ulcer.
Nausea and loss of appetite ( if the infection is through ingestion).
Swelling in the neck area.
Headache & fatigue
Sweats
Shortness of breath
Diarrhea accompanied by severe abdominal pain.
If exposed to the CDC anthrax antigen, the CDC recommends Post-Exposure Prophylaxis (PEP), suggesting immediate vaccination and antimicrobial therapy (Ciprofloxacin and Doxycycline are first-line options). The CDC says a new and improved anthrax vaccine became available in 2019. However, on July 20, 2023, the U.S. FDA approved a neweranthrax adjuvanted vaccine, Cyfendus for use in adults 18-65 exposed to anthrax as a countermeasure. Where there is one countermeasure there are always more.
A 2000 report published in Experimental and Molecular Pathology titled, “Antibodies to Squalene in Gulf War Syndrome,” described symptoms including severe headaches, nausea, muscular pain, joint swelling, short term memory loss, night sweats, depression. Autoimmune conditions ranged from fibromyalgia, lymphadenopathy, Lupus, Multiple Sclerosis, autoimmune thyroid disease, chronic fatigue syndrome to malar rashes, chronic headaches, non-healing skin lesions, musculoskeletal disorders (ALS), among others.
US District Court Judge Emmet G. Sullivan ruled that it was illegal for the federal government to mandate anthrax vaccinations. Judge Sullivan banned the Pentagon from forcing military personnel serving in Iraq, Afghanistan, South Korea, and part of Asia and Africa to get the anthrax shots without their prior consent. The military could not require the vaccine until the FDA approved it for the specific use of inhaled anthrax. – Hill & Ponton Disability Attorneys, Dec. 2020, updated
In general, adjuvants, such as squalene are added to vaccines (flu shots) to hyper-stimulate the immune system. They are designed to stimulate antibody creation and remain in the body for a prolonged reaction. The new class of adjuvants are comprised of phospholipids (surfactants), which also happen to make up the membrane of every human cell. Using recombinant DNA technology, phospholipids are combined with recombinant proteins and engineered in a way to be structurally and functionally identical to their natural counterparts. As such, the body can create antibodies to its own tissues in an attack of the Self.
A Little Anthrax History
B. anthracis (anthrax) was discovered in 1875 by the German physician and one of the founders of microbiology, Robert Koch (1843-1910) who developed Koch’s Postulates. He also discovered the deadly toxins cholera and tuberculosis, then was awarded the Nobel Prize in 1905.
Anthrax had also been produced in a Russian lab since before the 1920s. In May 1926, the first report of a new anthrax strain with enhanced virulence was filed, resulting in a 100% increase in mortality. By 1930, Germany had a bioweapons facility. By 1935, the Russians had developed a human anthrax vaccine.
Today, many countries have developed weaponized anthrax through genetic manipulation using bacteria and insects. According to the NIH, Russia created anthrax by introducing an “alien gene” into the highly toxic Baccillus Anthracis bacteria. The new NIH version of anthrax is resistant to antibiotics.
They used an alien gene and genetically altered bacterial immunological properties to produce a deadly pathogen to Humans. Where did they get an alien gene from? A UFO crash perhaps? Negotiations with other beings? Your guess is as good as mine….I found a patent with a method for removing plasma (DNA) from Bacillus anthracis bacteria using CRISPR/Cas9 system and it’s owned by China. This is how they get Mycoplasmas.
— Ariana Love, ND Nov. 23, 2021
The process that began before 1950 is called Cross-Species-Genomics. Its purpose? “To generate disease models.” In other words, to produce the deadly biowarfare agent for use in vaccines. The science reveals that deadly agents do not cross the species barrier unless genetic modification is used in a lab setting. A 2002 study in the Journal Pathology, Microbiology, and Immunology states:
The assessment of species barriers has relied on the development of a clinical disease in inoculated animals. On this basis there is a highly efficient barrier limiting transmission…
After 1979, the Soviet’s preferred a bioweapon of inhaled anthraxdue to undifferentiated symptoms that resemble a cold or flu. This version was genetically attenuated sometime before 2006 by the NIH.
British SIS intelligence reports from 1924 confirmed the use of anthrax shells (with a capacity of 2 liters/shell), bombs, and mortars.
In the April 2021 Journal Nature, the study, “Adjuvantng a subunit COVID-19 vaccine to induce protective immunity,” the reference to Alhydrogel is listed under Adjuvant Formulations and immunization:
Alum (Alhydrogel 2%) was purchased from Croda Healthcare (batch 0001610348)
According to a 2021 study in Molecular Cell, Anthrax is developed to “regulate gene expression by binding to DNA sequences and modulating transcriptional activity through their effector domains.” So Anthrax has more than one function.
The reason to be aware of any possible aerosolized anthrax bacterium spore release is to know the natural remedies that exist so you have a choice between consenting to an experimental vaccines and prescribed pharmaceuticals or natural options.
As a disclaimer, nothing suggested in this article is intended to replace consulting with a medical expert if you have a medical problem. Everyone should take responsibility for his or her own health and do your own research. That said, the following herbs and foods are commonly known remedies to help enhance the immune system, your built-in defense system, and can be incorporated in or with meals.
Garlic displays potent anti- anthracis activity, according to the 2021 Journal of Ethnopharmacology. So start thinking of your favorite garlic dishes to create in the kitchen. Alternatively, you can make a tea. Peel and crush into a fine paste with water. Mix paste in two glasses of warm water. Drink in two doses: morning, before bedtime. Continue for 10 days.
Oil of Oregano
Homeopathic anthracinum – super-diluted and potentized extracts of the anthrax bacteria itself to boost immunity on a nanoscale.
Herbs:
Wintergreen essential oil – for discomfort in bones, muscles and joints. Add a few drops to olive oil and apply to the soles of the feet. You can also add 3-5 drops to a bath.
White Fir – oxygenates with antiseptic properties known for us in disease caused by bacteria. Mix essential oil with olive oil or use essential oil as aromatherapy.
Thyme and Melissa (lemon balm) – Fill a capsule with 12 drops of Thyme and 1 drop of Melissa.
Spruce – essential oil has oxygenating properties with support to the nervous and respiratory systems.
Idaho Tansy – stimulates the immune system. Can be applied topically against infection or on wounds.
Savory and Oregano oil – both herbs are potent anti-microbials.
Astragalus root powder Chaparral power Tea – Mix 2 teaspoons of each herb in 2 glasses of warm water. Strain and add organic honey. Drink twice during the day.
Echinacea – boil 2 tsp. root powder in two glasses of water. Strain. Drink twice daily for a week or more.
An investigation by The BMJ into the Vaccine Adverse Event Reporting System, or VAERS, found multiple deficiencies in the system, including the revelation that the government runs two systems — one for the public, and a private back-end system that contains all of the corrections and updates, including deaths that occurred after an initial injury.
When Dr. Robert Sullivan collapsed on his treadmill three weeks after his second COVID-19 vaccine in early 2021, he fell into a “nightmare” ordeal that he said exposed glaring deficiencies in the nation’s vaccine safety monitoring system.
But like others interviewed in a recent investigation by The BMJ, Sullivan hit barrier after barrier when trying to submit and update his report.
Almost three years later, still grappling with debilitating symptoms, Sullivan’s experience highlights the systemic problems with the U.S. adverse events monitoring system run jointly by the Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA).
From doctors unable to file reports to disappearing data, limits on transparency and lack of resources to follow up on concerning vaccine reactions, experts warn VAERS is failing to detect critical safety signals.
According to one of those experts — VAERS researcher Albert Benavides, whose experience includes HMO claims auditing, data analytics and revenue cycle management — VAERS’ failure isn’t accidental.
Like others interviewed by The BMJ, Sullivan experienced limited follow-up after submitting his VAERS report. He received only a temporary report number months after his initial submission.
A physician named “Helen” (pseudonym) told The BMJ that fewer than 20% of concerning reports get follow-up, including many deaths she reported.
In consultation with Benavides, an audit by React19 found that 1 in 3 COVID-19 vaccine adverse events reports in VAERS were either not posted publicly or were deleted. React19 is a nonprofit that collects stories of people injured by the mRNA vaccines.
According to The BMJ, of those queried by React19, “22% had never been given a permanent VAERS ID number and 12% had disappeared from the system entirely.”
Benavides, who publishes the VAERSAware dashboards documenting many of the problems with VAERS, said there is even deeper dysfunction in the VAERS system — from inventing symptoms to deleting reports.
“VAERS does not publish all legitimate reports received,” Benavides told The Defender. “They throttle publication of reports. They even delete legitimate reports.”
For a system dependent on voluntary engagement, these restrictive policies keep critical data hidden, according to Benavides.
In 2007, the U.S. Department of Health and Human Services (HHS) contracted with Harvard Pilgrim Health Care (HPHC) to review the VAERS system. In 2010, HPHC filed its r report, which determined that 1 in 39 people experienced vaccine injuries and that only around 1% of vaccine-related injuries or deaths are ever reported to VAERS.
The CDC, which operates under HHS, scuttled the study, refused to take calls from the researchers and declined to upgrade the VAERS system when a new, much more effective system was developed.
‘Blind spots are self-created’
VAERS “collects reports of symptoms, diagnoses, hospital admissions, and deaths after vaccination for the purpose of capturing post-market safety signals,” according to The BMJ.
But the limited transparency of VAERS data presents barriers to proper analysis, according to The BMJ’s investigation and researchers like Benavides.
The public — including doctors and other report submitters — can access only incomplete initial reports, not updates with vital details.
This means outcomes like death are often excluded if the initial report was for an injury and a subsequent death report was filed.
“I made the false assumption that my conversation [with VAERS] would result in an adjustment to the publicly reported case,” Patrick Whelan, M.D., Ph.D., told The BMJ.
Whelan, a rheumatologist and researcher at the University of California Los Angeles, in 2022 filed a report of a cardiac arrest in a 7-year-old male patient after COVID-19 vaccination.
“I assumed that, since it was a catastrophic event, the safety committee would want to hear about it right away,” Whelan said. But nobody called him or requested an update after his submission.
“There was no mechanism for [updating] it,” Whelan told The BMJ. “The only option I had was to make a new VAERS report.” Without updates, the VAERS data showed that the boy was still hospitalized.
Whelan is one the authors of a recent critique of the Cochrane Review that concluded the COVID-19 mRNA vaccines were not dangerous.
The problem with VAERS is not limited to a lack of adequate follow-up but to the incomplete and often inaccurate information found there.
“VAERS in effect allows typos, truncated lot #’s, UNK [unknown] ages, UNK vax dates, UNK death dates, etc. to pass through into publication,” Benavides said.
Benavides said specific data — including ethnicity, hospital names, attending physicians, submitter’s relationship to the patient, patient and submitter addresses, telephone numbers and emails — collected by VAERS are not published,
“Any blind spots are self-created, in my opinion,” he said.
Agencies maintain two separate VAERS databases — public gets to see only one
“There’s two parts to VAERS, the front end and back end,” stated Narayan Nair, division director for the FDA’s Division of Pharmacovigilance at a December 2022 meeting with advocates, according to The BMJ. “Anything from medical records by law can’t be posted on the public-facing system,” he said.
The BMJ investigation discovered that the FDA and CDC maintain two separate VAERS databases, one available to the public that contains only initial reports, and a private back-end system containing all of the updates and corrections.
“Anything derived from medical records by law” cannot be posted on the public-facing system, Nair told the advocates, according to The BMJ.
In an apparent contradiction to this claim, The BMJ noted the FDA’s Adverse Event Reporting System (FAERS), which collects post-marketing information on drug reactions, posts its updates publicly.
Sullivan, who met Nair years before COVID-19 and considers him a friend, told The Defender that if this “very bright, kind and caring person” could not fix VAERS, “I don’t think it’s fixable.”
CDC says it reviewed 20,000 reports of deaths — none were related to COVID shots
Withholding outcome data like deaths obscures critical safety signals, experts contend.
James Gill, a medical examiner, reported the death of a 15-year-old patient after vaccination, but the case was dismissed by the CDC despite autopsy evidence, according to the BMJ investigation.
Physician “Helen” told The BMJ that after filing reports on her medical patients, including six who had died, she received only a single request for medical records on the death and two for hospital-admitted patients.
The standard operating procedure for COVID-19 vaccine reports in VAERS, according to The BMJ, is for reports to be processed quickly and for “serious reports” to receive special review by CDC staff.
However, while some other countries have acknowledged the probable connection between the mRNA vaccines and death, the CDC, while claiming to have reviewed nearly 20,000 death reports, has yet to acknowledge a single death linked to the COVID-19 vaccines, The BMJ said.
Benavides provided The Defender examples of VAERS “deleting legitimate reports,” not just duplicates or false claims.
“VAERS even deleted dead Pfizer Trial patients,” he said, claiming that this report, for example, was not a “duplicate” and did not appear to be fake.
Benavides said:
“There are currently about 50 deaths that are not counted as deaths because the correct box is not checked off.
“There are thousands of reports and about 100 deaths in ‘UNKNOWN VAX TYPE’ in VAERS. Read the narrative to see these are clearly C19 jab-related deaths.
“There are over a thousand cardiac arrests where they are not marked as dead, and I question if they actually survived because there is no mention of ROSC [return of spontaneous circulation].”
“Why couldn’t VAERS populate the ages of these dead kids before publication?” Benavides said, pointing to this report on his website.
Physicians report only FDA-recognized adverse events
Ralph Edwards, former director of the Uppsala Monitoring Centre and until recently editor-in-chief of the International Journal of Risk & Safety in Medicine, told The BMJ the regulators may be relying too heavily on past epidemiological data, especially for new types of adverse events. “If something hasn’t been heard of before, it tends to be ignored,” he said.
Without guidance to report potential risks, doctors also face barriers. “Physicians are only willing to talk about FDA-recognized vaccine adverse events,” stated physician “Helen” in a 2021 meeting between the FDA and physicians and advocates, according to The BMJ.
Svetlana Blitshteyn, a neurologist and researcher at the University at Buffalo, New York, told The BMJ if physicians are not educated to look for a specific condition, they’re unlikely to test for it or know how to treat it.
Sullivan told The Defender he believes his experience of developing pulmonary hypertension after taking the mRNA vaccine is one such safety signal the CDC and FDA are overlooking — a condition he believes many athletes have unknowingly developed.
Sullivan co-authored a paper of his and one other similar case of post-vaccine pulmonary hypertension. According to the paper:
“Pulmonary hypertension is a serious disease characterized by damage to lung vasculature and restricted blood flow through narrowed arteries from the right to left heart. The onset of symptoms is typically insidious, progressive and incurable, leading to right heart failure and premature death.”
“Athletes are canaries in the coal mine,” Sullivan told The Defender, speaking of the unusual numbers of athlete deaths since the rollout of the vaccine. Sullivan thinks that those with superior physical conditioning, like him, stand a better chance of survival with early detection.
However, he said, “Athletes will get echocardiography, and it will be essentially normal. The only way to tell for sure is to do a right-heart catheterization” that can identify the anomaly.
Sullivan believes the lives of many athletes could still be saved if the reporting system recognized and investigated the signal — and said he would be happy to join a project dedicated to this goal.
He also told The Defender he believes many of the sudden deaths reported in the 25- to 44-year-old age group are a result of this hidden condition.
‘The buck stops with the CDC for reforms’
Critics point to choices by the CDC as compounding VAERS’ passive design and understaffing issues.
Despite over 1.7 million reports since the COVID-19 vaccine rollout, staffing was not boosted accordingly, according to statements the CDC made to The BMJ.
A Freedom of Information Act request by The BMJ revealed Pfizer has nearly 1,000 more full-time employees working on vaccine surveillance than the CDC. Records showed in 2021, Pfizer on-boarded 600 additional full-time employees to handle the volume of adverse reports and planned to hire 200 more.
Physician “Helen” in The BMJ article called for an end to the “negative feedback loop” whereby the FDA fails to list adverse reactions because passive surveillance systems like the FDA’s don’t display them, while at the same time, because of that lack of disclosure, “physicians are blinded to the adverse reactions in their patients, and thus aren’t reporting them.”
“The buck stops with the CDC for reforms needed to open up data,” Benavides told The Defender, adding several suggestions that could immediately improve VAERS:
“Revert back to pre-January 2011 when VAERS did append initial reports with follow-up data, including death. Take off the arbitrary 30-minute time limit to file a report before getting kicked off. Make the process easier to submit follow-up data.”
When asked why the incompetence of VAERS had been allowed to continue for so long, Sullivan told The Defender, “Because of the lack of product liability” for the vaccines “and the surge to defend economic interests.”
Sullivan said he’d like to see the following changes to the system:
Pharmaceutical advertising banned.
Pharmaceutical company revenues devoted to advertising instead be spent on R&D.
The tax money collected on pharma profits be directly sent to victim injury funds.
Yale cardiologist takes on study of COVID vaccine injuries
Benavides said he spoke with Sen. Ron Johnson (R-Wis.) Monday and is also in discussion with Rep. Marjorie Taylor Greene (R-Ga.) of the House Select Subcommittee on the Coronavirus Pandemic to address the concerns with VAERS, including the under-publishing of reports.
“That’s a long overdue prospect and it would be incredible to actually get some analysis by that committee,” he said.
Another bright spot comes from news reported in The BMJ’s investigation that Dr. Harlan Krumholz, a cardiologist and researcher at Yale University, has been recruiting members of React19 to study their vaccine injuries.
“We are working hard to understand the experience, clinical course, and potential mechanisms of the ailments reported by those who have had severe symptoms arise soon after the vaccination,” Krumholz told The BMJ.
Sullivan told The Defender that medical science is “just beginning to catalog the damage to the heart” from the vaccines but that “in order to treat something, you have to diagnose it” — and that, because of the shortcomings with VAERS, “we have yet to scratch the surface of that.”
Sullivan, now almost three years into his ordeal, is outliving his initial prognosis.
“I have a grim diagnosis hanging over me, but I’m optimistic because I’m still here,” he said. “I had something bad happen to me, but I’ve met so many amazing, wonderful people along the way who are just interested in truth.”
“I’m going to live the best and most productive life I can with the time I have left,” Sullivan said, helping others who “have this cloud hanging over their future.”
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
When I discovered this study several years ago and wrote the following extensive piece on it, the study was a bolt from the blue, a complete devastating shocker.
It still is.
It is more than enough to topple the whole vaccine empire.
Honoring the work of the study co-author, Dr. Antonietta Gatti, Catherine Austin Fitts wrote, “Not long after the publication of this revolutionary study, tax authorities raided and investigated Dr. Gatti’s and [her husband] Dr. Montanari’s laboratory and private home—an all too usual method of intimidation.”
THAT was the “scientific follow-up.”
In a nutshell, Dr. Gatti’s 2017 study showed an incredible amount of contamination, in a whole host of traditional vaccines. The contamination was in the form of tiny nanoparticles, mostly metallic, and obviously highly harmful and dangerous.
Before reading my summary and analysis of that study—here is an updated communication from Dr. Gatti I received a few days ago. It describes, in a stark and disturbing fashion, what has been happening to her, her work, and her laboratory. This is chilling:
“At the end of last year, our laboratory no longer had the financial capacity to continue its research. The proceeds from the few analyzes requested by private individuals yielded enormously less than what the research cost us. Then, there were two possibilities: close everything or set up a foundation by giving away everything that belonged to us, hoping to find some sponsors. After all, all initiatives, even the most bizarre, find someone willing to contribute financially. Why not a foundation that does fundamental research on health? So, we opted for the latter choice, and the Nanodiagnostics Foundation was born.”
“But, after almost a year, not a cent has arrived. In short, no company, no private citizen, no institution is willing to contribute.”
“Many people continue to demand results and ask questions to which they have no answers from the institutions or their doctors, but, if it is a question of parting from some money, the silence is absolute.”
“It is clear that our work is a threat to billion-dollar businesses that are not exactly clear, at least for most people. For this reason, the most absurd and incredible slanders are invented to our detriment.
Not being able to dispute our scientific results, there are those who publish, usually anonymously, that we earn enormous sums of money, even giving the impression that the Foundation belongs to us, when it should be known that foundations do not belong to anyone, and no one can profit from them. And this is when we have donated everything that belonged to us, and we work for free.”
“Another tactic is trying to isolate and discredit us with lies. What the University of Bologna did a few days ago, the university where I graduated, then specialized and taught, is a small example.”
“A few months ago, that university asked us if we were willing to accept [a] student… who would prepare her graduation thesis with us. We agreed and agreed with the student on how to proceed. A few months passed, then, a couple of weeks ago, when the University authorities realized that the student would work with us, they sent us a message of a few lines in which they informed us that what we do (and which I had taught at that university) was of no interest to them (which, in a way, is true, although very far from the mission of the University). Needless to say, my letter to the Rector asking for explanations remained unanswered.”
“And it is also useless to say how difficult it is to publish the results that we continue to obtain, and which are not liked by those who financially maintain the medical journals, on whose scientific nature I prefer not to comment. For twice the Editor after the publication of an article (on vaccines and on SIDS) asked to retreat [sic] them. Only the work of the Robert Kennedy Jr lawyers stopped the request.”
“[Paper:] Novel chemical-physical autopsy investigation in sudden infant death and sudden intrauterine unexplained death syndromes” (click here)
“Just for your information, in spite of all difficulties, we are now dealing with very critical topics: spontaneously aborted babies, analysis of the brains of infants who died in cots (Sudden Infant Death Syndrome, aka SIDS), analysis of what falls from the sky (e.g., recently hail never seen before), food, etc. All this can only be fought with personal discredit.”
“We haven’t had any visits from the regime for a long time. For them it is enough to monitor our computers and phones. The rest is done by ‘volunteers’. As for other scientists, no one deals with our topics in full. It must be realized that doing so represents a risk that is obviously preferable not to take.”
“As long as we can manage, we will continue to work. If, however, no sponsor materializes (idle chatter and empty promises are not only useless: they are a waste of time,) we will have no other option than to declare defeat, a defeat that belongs to the whole world and, above all, to the children who do not deserve the fate they are suffering.”
“…I give some details of our Foundation Nanodiagnostics (click here)…”
IF YOU CAN, PLEASE DONATE TO Dr. Gatti’s vital work at the above website.
Here is my original article on Dr. Gatti’s vaccine-contamination study:
Dangerous nano-particles contaminating many vaccines: groundbreaking study
“The Lung,” Second Edition: “Nanoparticles [are] comparable in size to subcellular structures…enabling their ready incorporation into biological systems.”
A 2017 study of 44 types of 15 traditional vaccines, manufactured by leading global companies, has uncovered a very troubling and previously unreported fact:
The vaccines are heavily contaminated with a variety of nanoparticles.
Many of the particles are metals.
We’re talking about traditional vaccines, such as HPV, flu, Swine Flu, Hepatitis B, MMR, DPT, tetanus, etc.
To begin to understand some of the destructive effects of contaminating nanoparticles in vaccines, here is the groundbreaking 2017 study:
International Journal of Vaccines & Vaccination
Volume 4 Issue 1
January 23 2017
New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination
Antonietta M Gatti and Stefano Montanari
(Paper archived here and here)
“The analyses carried out show that in all samples checked vaccines contain non biocompatible and bio-persistent foreign bodies which are not declared by the Producers, against which the body reacts in any case. This new investigation represents a new quality control that can be adopted to assess the safety of a vaccine. Our hypothesis is that this contamination is unintentional, since it is probably due to polluted components or procedures of industrial processes (e.g. filtrations) used to produce vaccines…”
Are the study authors leaving the door open to the possibility that the contamination is intentional?
“The quantity of foreign bodies detected and, in some cases, their unusual chemical compositions baffled us. The inorganic particles identified are neither biocompatible nor biodegradable, that means that they are biopersistent and can induce effects that can become evident either immediately close to injection time or after a certain time from administration. It is important to remember that particles (crystals and not molecules) are bodies foreign to the organism and they behave as such. More in particular, their toxicity is in some respects different from that of the chemical elements composing them, adding to that toxicity…they induce an inflammatory reaction.”
“After being injected, those microparticles, nanoparticles and aggregates can stay around the injection site forming swellings and granulomas…But they can also be carried by the blood circulation, escaping any attempt to guess what will be their final destination…As happens with all foreign bodies, particularly that small, they induce an inflammatory reaction that is chronic because most of those particles cannot be degraded. Furthermore, the protein-corona effect…due to a nano-bio-interaction…can produce organic/inorganic composite particles capable of stimulating the immune system in an undesirable way…It is impossible not to add that particles the size often observed in vaccines can enter cell nuclei and interact with the DNA…”
“In some cases, e.g. as occurs with Iron and some Iron alloys, they can corrode and the corrosion products exert a toxicity affecting the tissues…”
“Given the contaminations we observed in all samples of human-use vaccines, adverse effects after the injection of those vaccines are possible and credible and have the character of randomness, since they depend on where the contaminants are carried by the blood circulation. It is only obvious that similar quantities of these foreign bodies can have a more serious impact on very small organisms like those of children. Their presence in the muscles…could heavily impair the muscle functionality…”
“We come across particles with chemical compositions, similar to those found in the vaccines we analyzed, when we study cases of environmental contamination caused by different pollution sources. In most circumstances, the combinations detected are very odd as they have no technical use, cannot be found in any material handbook and look like the result of the random formation occurring, for example, when waste is burnt. In any case, whatever their origin, they should not be present in any injectable medicament, let alone in vaccines, more in particular those meant for infants.”
This 2017 study opens up a whole new field: the investigation of nanoparticles in vaccines where none were expected.
Such particles are not medicine in any sense of the word.
Many legal and scientific “experts” assert the State has a right to mandate vaccines and force them on the population. But these contaminating nanoparticles are not vaccines or medicines. Only a lunatic would defend the right of the State to inject them.
Here is another section from the 2017 study. Trade names of vaccines, and compositions of the nanoparticle contaminants are indicated. Take a deep breath and buckle up:
“…further presence of micro-, sub-micro- and nanosized, inorganic, foreign bodies (ranging from 100nm to about ten microns) was identified in all cases [all 44 vaccines], whose presence was not declared in the leaflets delivered in the package of the product…”
“…single particles, cluster of micro- and nanoparticles (less than 100nm) and aggregates…debris of Aluminum, Silicon, Magnesium and Titanium; of Iron, Chromium, Silicon and Calcium particles…arranged in a cluster, and Aluminum-Copper debris…in an aggregate.”
“…the particles are surrounded and embedded in a biological substrate. In all the samples analyzed, we identified particles containing: Lead (Typhym, Cervarix, Agrippal S1, Meningitec, Gardasil) or stainless steel (Mencevax, Infarix Hexa, Cervarix. Anatetall, Focetria, Agrippal S1, Menveo, Prevenar 13, Meningitec, Vaxigrip, Stamaril Pasteur, Repevax and MMRvaxPro).”
“…particles of Tungsten identified in drops of Prevenar and Infarix (Aluminum, Tungsten, Calcium chloride).”
“…singular debris found in Repevax (Silicon, Gold, Silver) and Gardasil (Zirconium).”
“Some metallic particles made of Tungsten or stainless steel were also identified. Other particles containing Zirconium, Hafnium, Strontium and Aluminum (Vivotif, Meningetec); Tungsten, Nickel, Iron (Priorix, Meningetec); Antimony (Menjugate kit); Chromium (Meningetec); Gold or Gold, Zinc (Infarix Hexa, Repevax), or Platinum, Silver, Bismuth, Iron, Chromium (MMRvaxPro) or Lead,Bismuth (Gardasil) or Cerium (Agrippal S1) were also found. The only Tungsten appears in 8/44 vaccines, while Chromium (alone or in alloy with Iron and Nickel) in 25/44. The investigations revealed that some particles are embedded in a biological substrate, probably proteins, endo-toxins and residues of bacteria. As soon as a particle comes in contact with proteic fluids, a nano-bio-interaction…occurs and a ‘protein corona’ is formed…The nano-bio-interaction generates a bigger-sized compound that is not biodegradable and can induce adverse effects, since it is not recognized as self by the body.”
“…examples of these nano-bio-interactions. Aggregates can be seen (stable composite entities) containing particles of Lead in Meningitec… of stainless steel (Iron, Chromium and Nickel…) and of Copper, Zinc and Lead in Cervarix…Similar aggregates, though in different situations (patients suffering from leukemia or cryoglobulinemia), have already been described in literature.”
I’m sure you’ve read official assurances that vaccine-manufacturing problems are “rare.” You can file those pronouncements along with other medical lies.
“I’d like the heavy metal sandwich on rye, please. And instead of serving it on a plate, can you inject it?”
Several vital questions demanding answers spring from the findings of this 2017 study:
Are some of these nanoparticles intentionally placed in vaccines?
Does the standard manufacturing process for traditional vaccines INEVITABLY lead to dangerous and destructive nano-contamination?
New nano-technology is already being employed to create several vaccines—supposedly “improving effectiveness.” In fact, the RNA COVID-19 vaccine are a nano-type. Does this manufacturing process carry with it the unavoidable effect of unleashing a hurricane of nanoparticle contaminants?
How many cases of childhood brain damage and autism can be laid at the door of nanoparticle contamination?
And finally, where are these contaminated vaccines manufactured? The above study did not attempt to discover this. It was outside the scope of the research. It’s common knowledge that, for example, in the case of the US, vaccines or their components, are, in many instances, not produced domestically. Where does this put control of safety? In, say, China, where there have been numerous pharmaceutical scandals connected to contamination of products?
The vaccine establishment does not show the slightest interest in answering any of these questions. They are busy pretending the questions don’t exist.
“Why is it so difficult for virologists to simply explain basic questions about a ‘virus’ such as whether the ‘virus’ is living or dead? Why must the concept of what a ‘virus’ is change depending upon the researchers and technology of the time? What physical organism changes in concept after over a century of supposed study? The answer to all of these questions is actually fairly easy to grasp. As the researchers have never actually had any physical entities on hand in order to study, the concept of what the assumed invisible entities are was allowed to constantly change in order to suit the needs and evidence of the researchers of the time. There was no solid foundation for virology to stand upon from the very beginning in order to definitively state what the nature of a ‘virus’ truly is.”
For the greater part of the first 50 years of the 20th century, there was no agreed upon definition for what the invisible entities labelled as a “virus” actually were nor how these agents looked, formed and functioned. Some researchers believed that these entities were endogenous processes produced within the host while others envisioned them as exogenous invaders that came from outside and attacked from within. There were arguments over whether “viruses” were corpuscular in nature or whether they were a soluble liquid. Debates centered around whether these agents were alive or if they were simply inanimate and non-living. While there were researchers who believed “viruses” were a ferment or a chemical molecule of some kind, the majority believed that these invisible entities were just smaller unseen bacterium. According to biochemist and historian of science Ton van Helvoort’s 1996 paper When Did Virology Start?, the “virus” concept lacked clarity and certainty over the first half of the 20th century. However, the link between bacteriology and “viruses” was so strong at this time that these unseen entities were not considered conceptually distinct from bacteria:
“I have come to believe that, despite its widespread appearance in textbooks and journals of that era, the early concept of the “filterable virus” lacked clarity and certainty. More importantly, I also believe that during the 1930s and 194Os, the links between the study of filterable viruses and bacteriology were so strong that viruses were still considered merely another form of bacteria-not conceptually distinct, as they now are.”
The reason for these many contradictory ideas about the nature of the “virus” was a direct result of the fact that the researchers never had a physical entity on hand in order to study. The “virus” was nothing more than a fluid concept that was open to the interpretation of those who claimed to be working with them. Most of these researchers came from a bacteriological or chemistry background, and thus, they viewed the “virus” concept through their own lens and paradigms. Regardless, there was no way to actually determine the true nature of something that could not be seen or studied in reality and that only existed within the realm of the imagination.
Thus, it shouldn’t be hard to understand why virologists often have a difficult time answering simple questions such as “What is a virus?” or “Is it alive or dead?” This is exactly the argument made in the appropriately titled 2014 article Inventing Virusesby William Summers, a retired Professor of Therapeutic Radiology, Molecular Biophysics & Biochemistry, and History of Medicine. While being able to define what a “virus” is should be an easy task for any virologist, simple questions about the nature of a “virus” are not ones that are simple for them to answer. In the opening of his paper, Summers asked a more subtle question about the invention of the “virus” category:
“…how generations of microbiologists arrived at the idea that some of the entities they dealt with fell into a category that differed in fundamental ways from others. In other words, how did they invent the category of “virus” as we now know it?”
Summers looked to investigate how the idea that “viruses” are a separate entity that requires its own category away from bacteriology came to be. In doing so, he admitted that our beliefs, understandings, and conceptions of what a “virus” is changes over time. This is because “viruses” are whatever a virologist tells us that they are. The concept and the nature of the “virus” was invented, and continually reinvented, by virologists as part of the normal progress of their (pseudo) science. In other words, the idea of the “virus” is able to change at any time based upon whatever a virologist wants a “virus” to be at any given moment:
“Even so, how did the category “virus” come to be recognized, and what are its essential, defining qualities? Viruses are natural objects, but our beliefs, understanding, and conceptions of them change over time on the basis of new information, new points of view, and new scientific values and standards. In a very real way, a virus is what virologists say it is. It is a product of the way virologists talk about viruses—that is, the way facts about viruses are organized in their discourse. It can be said that virologists invent (and continually reinvent) the concept of a virus as part of the normal progress of their science.”
The deliberate ever-changing concept of the “virus” shifted away from its original invention as an agent of disease transmission to its modern day concept as a genetic assembly that sometimes causes disease when it integrates into its host in order to survive. This reinvention of the concept happened in 1957 when French microbiologist Andre Lwoff took many competing and contradictory ideas and mashed them together into the modern definition of a “virus” based upon work done with bacteriophages. Prior to his reinvention of the concept, in 1953, Lwoff actually questioned whether a bacteriophage was a “virus” and wanted to know exactly what a “virus” was. He even noted that “viruses” are defined to be exogenous (coming from outside of the body) while bacteriophages are “always formed inside its host” and “could therefore be described as endogenous,” i.e. originating from within the host. In fact, Lwoff stated that “if prophage is phylogenetically endogenous, the temperate phage produced by a lysogenic bacterium must be described as endogenous,” meaning that the phage is from within the host, thus negating it as an exogenous entity in line with the definition of a “virus.” Ironically, after redefining the “virus” as a genetic code in 1957, Lwoff would ultimately warn in 1991 that virology was “in danger of losing its soul, since viruses now show a strong tendency to become sequences.” He also argued that the abundance of discoveries was causing “the very concept of virus” to waver “on its foundations,” noting that the “problem today and in future is to keep abreast of its whereabouts.”
Regardless, Summers stated that his paper was not about the “triumphant accumulation of knowledge by the heroic scientists” of the past. Rather, it was an examination of the “continual struggle to understand and organize observations.” This struggle was showcased by Lwoff’s own attempts to rationalize and combine contradictory evidence in order to create the modern genetic concept of the “virus” from an entity that did not meet the necessary requirements:
“Nobelist Andre Lwoff, perhaps in a Gertrude Stein frame of mind, famously answered “viruses are viruses” (9), but the question “What is virus?” has been notoriously fraught since the role of virus in late nineteenth-century germ theories became central to medicine, and later, in the midtwentieth-century, to biology in general. The evolution, or perhaps deliberate and continuous reformulation, of the meaning of “virus” from an agent of disease transmission in the nineteenth century to a molecular assembly with remarkable properties by the end of the twentieth century is the subject of this article. This is not a story of the triumphant accumulation of knowledge by the heroic scientists of the past so much as it is an examination of the continual struggle to understand and organize observations that challenged and made obsolete the comfortable certainties of the often recent past. This examination requires consideration of past science on its own terms, without judgment in light of present-day understanding, and it requires consideration of the context and extent of background knowledge of the particular period considered.”
This struggle to answer the question “What is a virus?” was ongoing, even in the so-called “modern age” of virology. There was no consensus as to the true nature of a “virus.” Summers shared a quote by Joseph Beard that stated that the “virus” was a fabric of concepts that had been “woven of a plethora of woof and a paucity of warp.” In weaving terms, this makes for an unstable foundation upon which to weave. Another example was of plant virologist N.W. Pirie who was considered “agnostic” (impossible to know one way or the other) on whether a “virus” was a molecule or a microbe. However, he seemed to argue that the variability in the chemical composition of the same “virus” went against the modern molecular hypothesis. Thus, we can see that there was no agreement on the nature of the “virus:”
“The construction of the virus as a living molecule in the middle decades of the twentieth century generated wide debate as to the correct answer to the question, “What is a virus?” Having rejected filterability, negative growth properties, and size as defining characteristics, microbiologists searched for new ways to think about viruses. Even at the beginning of what might be called the modern era, there was remarkably little consensus on this subject. Joseph Beard, in 1945, famously remarked, “Viruses are said to be living molecules and autocatalytic enzymes and are likened to genes and mitochondria—in short, a fabric of concepts has been woven of a plethora of woof with a paucity of warp” (quoted in 47, p. 332). N.W. Pirie, one of the pioneers in the study of plant viruses, even in 1949 was agnostic as to whether viruses were microbes or molecules. In a long review of the problem in the British Medical Bulletin (47), he argued that the variation in chemical composition reported for the same virus suggested a level of heterogeneity not compatible with the molecular hypothesis. He noted that “all the viruses purified so far have contained nucleoprotein, but this generalization may lack significance because the viruses that have been studied are a group selected to some extent on a chemical basis.”
Summers ultimately concluded that each generation of virologists will look at “viruses” in their own way and will alter the concept of the “virus” based upon the “science” of the time. Thus, the “virus” is left to be a concept that is allowed to be continually reinvented at the whims of the researchers:
“Although “viruses are viruses,” each generation of scientists looks anew at these fascinating entities in its own way, endowing them with properties, relationships, and capacities that reflect the science of the time. Truly, they are microbes being continually reinvented by their most ardent admirers.”
In his summary, Summers laid out 5 very revealing points to end his paper on. Sharing similar sentiments as van Helvoort, he stated that the “virus” concept is an unstable one that “evolved,” not due to an accumulation of facts, but rather due to an ongoing reformulation of the “virus” concept on the basis of “scientific” focus at a given time. This reinvention was determined by technological advances rather than scientific understanding. Thus, the answer as to what a “virus” is will depend upon the discourse at the time more so than the “known” characteristics of “viruses:”
The concept of a virus has not been stable and has evolved since its introduction in the latter half of the nineteenth century.
This evolution has been not a linear accumulation of facts but rather an ongoing reformulation of the virus concept on the basis of scientific focus at a given time, e.g., growth, metabolism, chemical composition, genetics, or physical structure.
The concept of a virus has particularly been determined by technological advances ratherthan scientific understanding.
The answer to the question “What is a virus?” is one that depends on the particular scientific discourse at a given time.
The discourse with respect to the physical object “virus” is based on the particular concerns and problems of interest at a given time more than on any one set of intrinsic characteristics known about viruses.
Why is it so difficult for virologists to simply explain basic questions about a “virus” such as whether the “virus” is living or dead? Why must the concept of what a “virus” is change depending upon the researchers and technology of the time? What physical organism changes in concept after over a century of supposed study? The answer to all of these questions is actually fairly easy to grasp. As the researchers have never actually had any physical entities on hand in order to study, the concept of what the assumed invisible entities are was allowed to constantly change in order to suit the needs and evidence of the researchers of the time. There was no solid foundation for virology to stand upon from the very beginning in order to definitively state what the nature of a “virus” truly is.
While Summers paper on the invention of the “virus” offers some great modern insight into the problems related to defining the nature of the invisible beast, there is a much earlier paper by prominent virologist Thomas Rivers from 1932 that details the many issues with trying to give life to the imaginary shortly after its conception. You may know Rivers due to his 1937 proclamation that “It is obvious that Koch’s postulates have not been satisfied in viral diseases.” This shockingly honest admittance that the essential logical criteria considered necessary in order to prove a microbe causes disease remains unfulfilled for “viruses” and continues to haunt virology to this day. As it is a rather long 18 pages that I have reproduced here, I will try to keep my commentary throughout brief. However, what Rivers highlighted as key problems in 1932 during the formative years of virology compliments Summers 2014 paper on why virologists needed to invent, and then continually reinvent, the concept of the “virus” that was dreamt up in the late 1800s.
Thomas Rivers immediately began his 1932 paper on the nature of “viruses” by admitting that, up to 1932, “viruses” were defined solely based upon their absence as well as for what they were not. “Viruses” were defined in negative terms as they were:
Invisible to ordinary microscopic methods.
Unable to be obtained via filtration.
Unable to propagate in the absence of susceptible cells.
Interestingly, things did not progress away from defining “viruses” in negative terms even with Andre Lwoff’s 1957 modern reinvention of the concept as noted by Professor Milton W. Taylor, teacher of virology and world-renowned historian from Indiana University. In a 2014 paper examining what a “virus” is, Taylor explained that Lwoff’s reinvention of the “virus” concept was also a “negative definition” that “stresses the non-cellular nature of viruses.” By Lwoff’s own words from his 1971 paper From Protozoa to Bacteria and Viruses. Fifty Years with Microbes, he defined “viruses” by the “inability to grow and to divide, absence of metabolism, absence of the information for the enzymes of energy metabolism…the absence of transfer RNA and of ribosomes and also of the corresponding information.” In other words, even by the modern definition, “viruses” were still defined by what they were not.
While Rivers attempted to define “viruses” in what he felt were positive terms of what was “definitely known” about these invisible agents, he admitted that the biological nature was still a moot question, i.e. one open to debate and challenges with no foreseeable solution or answer. Perhaps this was due to his feelings that, while there was plenty of data concerning the nature of “viruses,” the accumulated data was “distinctly lacking in quality,” and that “enough reliable data have not been acquired to establish the nature of the viruses.”
The Nature of Viruses
Thomas M. Rivers
The Rockefeller Institute for Medical Research, New York
Viruses are usually characterized by three negative properties, namely, invisibility by ordinary microscopic methods, failure to be retained by filters impervious to well-known bacteria, and inability to propagate themselves in the absence of susceptible cells. I prefer a positive characterization of the viruses, one emphasizing the intimate relation that exists between them and their host cells. The multiplication of viruses only in the presence of susceptible cells, their regeneration and production of disease in many instances in only one species of host, the marked stimulation and destruction of cells induced by their activity which on the one hand gives rise to tumors, such as Rous’ sarcoma, and on the other to vesicular lesions, as fever blisters, the intracellular pathology frequently evidenced in virus diseases by inclusion bodies, and, finally, the lasting immunity that follows the majority of virus maladies, are essential phenomena that serve to stress the intimate type of parasitism encountered in working with these active agents. Such a characterization of viruses implies much, not only as concerns their biological nature which is still a moot question, but as regards their activities about which something is definitely known.
Data concerning the nature of viruses are sufficiently adequate in quantity but distinctly lacking in quality. According to reports, some of which have come from eminent investigators, most of these active agents have been seen and have been cultivated on lifeless media. If such statements are correct, viruses are autonomous living agents, and further discussion of their biological nature should deal with their place in the scale of living entities and their relation to other forms of life. Reports of work in this field are confusing, however, particularly to the uninitiated, and critical investigators are of the opinion that enough reliable data have not been acquired to establish the nature of the viruses. Inasmuch as this is a subject of fundamental biological importance, I shall review some of the recently accumulated data regarding the size, electrical charge, purification, spontaneous generation, adaptations, elementary bodies, metabolism, immunological phenomena and cultivation of viruses that might be of assistance in the elucidation of the origin and constitution of these peculiar incitants of disease.
One of the only indirect means which early virologists could use to conclude that a “virus” was “present” in a sample was by claiming that the invisible entities passed through filters of a certain size that retained all known bacteria, thus allowing them to guess as to the size of the unseen particles. Rivers noted that a “virus” was generally accepted as “an object less than 0.2 p or 200 ppl in diameter” and that it was not capable of being seen under light microscopy. In other words, “viruses” were too small to be seen and were defined by their absence. He noted that figures regarding the size of “viruses” derived from stained preparations were apt to be inaccurate and misleading. This lines up with his 1927 statement on filtration in his paper Filterable Viruses: A Critical Review, claiming that the methods were “crude and inaccurate.”
Rivers then presented evidence for the size of eight “viruses,” which were contradictory depending upon the researchers cited. He utilized hemoglobin as a comparison and stated that if the figure for hemoglobin is incorrect (which had contradictory estimates as to its size as well), many statements concerning the size of “viruses” were also inaccurate. Rivers was dismayed that certain researchers did not account for the possibility that they might have been estimating the size of particles of degraded cells to which the “viruses” were attached. He noted that other researchers took this into consideration and that they were unable to be assured that they had been successful in obtaining the correct figures for the size of the different “viruses.” Rivers concluded that none of the figures could be accepted without reservations and that the exact size of any “virus” was unknown. The numerous contradictory results stemmed from “inadequate experimentation, careless thinking, prejudice, imperfect experimental methods, and the difficult nature of the problems.”
SIZE. The size of minute particles may be determined in several ways, namely, by direct mensuration provided the objects are capable of resolution under the microscope; by filtration and ultrafiltration if the factors that influence the passage of the particles through pores of graded diameters are known and controlled; by diffusion, and, finally, by centrifugation. All of these methods have been employed in the study of the magnitude of viruses and the results obtained will be discussed.
It is generally accepted that an object less than 0.2 p or 200 ppl in diameter is not capable of resolution under the microscope when ordinary light is used. Furthermore, it is understood that mordants and stains usually increase the magnitude of small particles. Some of the “larger” viruses, e.g., those of fowl-pox (log), smallpox, vaccinia (122, 123), and rabies, are said to be just visible after treatment with certain mordants and dyes. Consequently, one is justified in concluding that most of the viruses have a diameter of less than 200 pp and in an unstained state are not mensurable by means of ordinary light. Moreover, figures regarding their size derived from stained preparations are apt to be inaccurate and misleading. The use of light of short wave lengths makes possible the mensuration of particles smaller than 0.2 p in diameter. So far, however, this method of investigation has yielded no convincing evidence concerning the magnitude of viruses. It appears, therefore, that direct methods of mensuration only indicate that the active agents are considerably smaller than ordinary bacteria.
The sizes of at least eight viruses have been estimated by means of ultrafiltration, diffusion, or centrifugation. The results obtained for these active agents together with figures for the diameter of the hemoglobin molecule for comparison are given below.
Hemoglobin. For a number of years the molecule of hemoglobin was thought to be 30 uu in diameter. Recently, however, figures (34) derived from the results of Svedberg and Nichol’s (33) centrifugation experiments and Northrop and Anson’s (30) diffusion experiments with hemoglobin indicate that its diameter is approximately 5.5 uu. Many estimations regarding the magnitude of viruses have been based on the former figure for the diameter of the hemoglobin molecule, 30 uu. If this figure is incorrect, many statements concerning the size of viruses are also inaccurateMosaic virus. Duggar and Karrer (17) by means of ultrafiltration found the infectious particles of mosaic virus to be of the same order of magnitude as hemoglobin molecules, namely, 30 uu in diameter. Vinson (34), however, says that Duggar’s experiments interpreted in the light of recent work regarding the size of hemoglobin molecules indicates that the diameter of mosaic virus is about 5.5 uu.
Herpetic virus. Zinsser and Tang (38) by means of ultrafiltration estimated the diameter of herpetic virus to be 20-100 uu. Levaditi and Nicolau (27) in the same way found that the virus passed through membranes which retained toxins, hemolysins, complement, and serum globulins. Bedson (13), however, unable to confirm Levaditi and Nicolau’s (27) results, obtained evidence by centrifugation that herpetic virus is probably of sufficient size to be visible.
Foot-and-mouth disease virus. Olitsky and Boez (31), using ultrafiltration, found that the virus of foot-and-mouth disease is 20-100 uu in diameter. Elford by means of his special membranes estimated it to be 8-12 uu.
Poliomyelitic virus. By means of ultrafiltration, Krueger and Schultz (25), in 1929, found that the virus of poliomyelitis possesses a magnitude not greater than 300 uu. In 1931, by the same means, Clifton, Schultz, and Gebhardt (16) obtained results indicating that the diameter of the virus lies below 50 uu.
Fowl plague virus. By means of ultrafiltration Andriewsky (8) secured a figure of 2.5 uu for the diameter of fowl plaguevirus, while Bechhold and Schlesinger (11) by centrifugation found it to be 120-130 uu.
Bacteriophage. According to d’Herelle (22) and Elford (19), both of whom used ultrafiltration, the diameter of the bacteriophage is approximately 30 uu. Kruger and Tamada (26) by means of purified bacteriophage preparations and ultrafiltration found it to be 5 uu, and Hetler and Bronfenbrenner (24) by means of a diffusion method estimated it to be 1.2-22.8 uu.
Rous virus. According to Zinsser and Tang (38), the Rous virus is 20-100 uu; according to Mendelsohn, Clifton and Lewis (29), 50 uu; according to Frankel (20), 10 uu. All these workers obtained their figures by means of ultrafiltration.
Vaccine virus. Levaditi and Nicolau (27) reported that vaccine virus passes through membranes impervious to toxins, hemolysins, complement, and serum globulins. Bland (15), however, from the results of his centrifugation experiments not only concluded that Levaditi and Nicolau’s findings are incorrect but that vaccine virus is probably large enough to be seen. Bechhold and Schlesinger (11) by means of centrifugation estimated that the active agent is 210-230 uu in diameter, while Yaoi and Kasai (37) working with “purified” virus found that it diffused at the rate of fuchsin particles and is, therefore, not capable of being seen.
One cannot consider the results cited above without being amused and dismayed. Many of the workers seemed in no way concerned about the possibility that they might have been estimating not the magnitude of viruses, but the size of particles of degraded cells to which the viruses were attached. Other investigators, cognizant of the difficulties of the problem! attempted to remove the viruses from such carriers. They were unable, however, to be assured that they had been successful and that they had obtained the correct figures for the size of the different viruses.
From the results of indirect methods of mensuration it is safe to conclude that viruses are small and that some of them may be exceedingly minute. If the figure of 210 uu for the diameter of vaccine virus is accurate, there is no reason as far as size is concerned to suppose that the virus is not a living organism. On the other hand, if the figures of 1.2 uu, 5.5 uu, and 8 uu for the bacteriophage, mosaic virus, and foot-and-mouth disease virus, respectively, are correct, it is obvious that these agents cannot be highly organised, because it is impossible that with such a magnitude they can consist of more than one, or at most several, molecules of protein. Unfortunately, none of the figures can be accepted without reservations. At present the exact size of
The numerous discordant results encountered in the literature dealing with the filterability, size, and visibility of viruses are probably due to inadequate experimentation, careless thinking, prejudice, imperfect experimental methods, and the difficult nature of the problems. One of the great needs at present is improvement in methods of microscopy, filtration, and purification of viruses in order that results obtained will approximate the true size of viruses and not the size of particles of other sorts on which the agents are adsorbed. It must be remembered, however, that the determination of the size of one virus will not establish the magnitude of another, because no more uniformity of dimensions should be expected among these agents than is found among bacteria and protozoa. Furthermore, it is not possible to derive proof of the animate or inanimate nature of viruses even from a correct estimation of their diameters, for, within limits as yet undetermined, life and death are not functions of size.
In this next section on electrical charges, take note once again of the range in estimates and contradictory conclusions made by the researchers. Rivers pointed out that “virus” preparations consisted principally of proteins and bits of degraded cells from the host. This meant that the electrical charge results might not be those of the “virus” particles themselves but of the other materials present within the sample. This inability to distinguish the assumed “virus” from the remaining host and foreign constituents present in the sample is the reason why complete purification and isolation of the assumed “viral” particles from the host components, which has never been achieved, is absolutely necessary. Rivers admitted that there were few experiments that were performed with “protein-free” preparations of “viruses,” and that the methods of purification did not convince him that such purified “viruses” had ever been completely separated from their carriers (i.e. host materials). Even with the modern advances in technology, this inability to completely separate “viruses” from host components was noted in a May 2020 article that stated that “to date, a reliable method that can actually guarantee a complete separation does not exist.” Rivers concluded that the lack of purity meant that it was impossible to state definitely what electrical charge is carried by the “viruses.”
ELECTRICAL CHARGE. Most bacteria and proteins under ordinary biological conditions of hydrogen ion concentration carry a negative electrical charge. When the nature of the viruses became a question of interest, attempts were made to ascertain their behavior in an electrical field in order that it might be compared with the action of proteins and bacteria under similar circumstances.
Bacteriophage. Kligler and his co-workers (41) using a so-called “protein-free” bacteriophage found that the active agent was amphoteric in acid and decidedly alkaline solutions and chiefly negatively charged in neutral and mildly alkaline solutions. Krueger and his associates (42) stated that the bacteriophage is negatively charged between the hydrogen ion concentrations of 9.0-3.4, and positively charged at pH 3.35. Todd (48) found that the active agent carried a negative charge between the hydrogen ion concentrations of 3.36-7.6. The results of Natarajan and Hyde’s (43) experiments indicate (1) that bacteriophages for typhoid bacilli and Flexner’s dysentery bacilli are only electronegative between pH 4.9-9.3 and 5.4-9.3 respectively, (2) that small plaque coliphage is electronegative below pH 8.3, but with greater alkalinity moves to both poles, and (3) that large plaque coliphage is electronegative over a range of pH 5.4-6.1, while at a higher alkalinity it wanders to both poles.
Rabic virus. According to Glusman (40) and his associates fixed rabic virus is negatively charged over a range of pH 6.0-9.3.
Vaccine virus. Douglas and Smith (39) found that vaccine virus carried a negative charge between the hydrogen ion concentrations of 5.5-8.4. The experiments of Yaoi and Kasai (49) revealed that between pH 6-7 more virus collected at the positive than at the negative pole, and between pH 8-9 the active agent was demonstrable only at the anode.
Fowl-pox virus. Kligler and his co-workers (41) found fowl-pox virus in “protein-free” preparations to be positively charged on the acid side, amphoteric in neutral solutions, and negatively charged in alkaline solutions. According to Natarajan and Hyde (43), the active agent is amphoteric over a range of pH 6.4-9.3.
Foot-and-mouth disease virus. Olitsky and Bo& (44) believe that the virus of foot-and-mouth disease is positively charged, while Sichert-Modrow (47) is of the opinion that the active agent carries a negative charge over a range of pH 7.0-8.1.
Pcliomyelitic virus. According to Olitsky, Rhoads, and Long (45) poliomyelitic virus wanders to the anode.
Rous virus. Pulcher (46) found that the Rous virus was adsorbed on electropositive and not on electronegative hemoglobins and concluded that the active agent is negatively charged.
Virus of infectious myxomatosis of rabbits. According to Natarajan and Hyde (43), the virus of infectious myxomatosis of rabbits is electronegative over a range of pH 4.9-9.3.
Herpetic virus. Natarajan and Hyde (43) found herpetic virus to be electronegatively charged only between the hydrogen ion concentrations of 7.0-8.9.
From the results of the work cited above it is obvious that most workers have found that under ordinary biological conditions of hydrogen ion concentration certain viruses in an electrical field wander to the anode. Moreover, many investigators have stated that the viruses under these conditions are negatively charged and in this respect are similar to bacteria, cells, and numerous proteins. Others, however, aware of the fact that virus preparations usually consist principally of proteins and bits of degraded cells from the host, realize that the electrical charges determined might not be those of the virus particles themselves but of their carriers, i.e., material on which the virus particles are adsorbed. It is true that a few experiments have been performed with “protein-free” preparations of viruses. But an examination of the methods of purification fails to convince one that such purified viruses had been completely separated from their carriers. Therefore, at present it is impossible to state definitely what electrical charge is carried by the viruses.
This next section is probably my favorite of the entire paper as Rivers sums up the purification problem perfectly. He started off by admitting that “virus-containing” emulsions consisted chiefly of substances unrelated to the “virus.” Thus, he stated that researchers needed to attempt to obtain the “viruses” either in a pure or in a relatively pure state as it was realized that purified “viruses” are essential for the proper study of problems in the field. These problems related to the aforementioned estimation of the size of “viruses” and the determination of the electrical charge, as well as any investigation into the “immunological” responses attributed to “viruses.” He shared a quote by Murphy who, in working to purify the Rous sarcoma “virus” through various manipulative purification processes, stated that it was “hardly conceivable that the active fraction” obtained after these processes could “carry with it through all these manipulations any living organism or virus.” Murphy felt that he was dealing with an enzyme rather than a “virus.” Rivers then backed up his own assertion from five years earlier in 1927 that “No virus had been obtained in an absoutely pure state” by reiterating that it was unlikely that a “virus” had ever been obtained in a state of absolute purity.
PURIFICATION. Inasmuch as virus-containing emulsions consist chiefly of substances unrelated to the active agents themselves, it is natural that workers should attempt to obtain the viruses either in a pure or in a relatively pure state. Moreover, it is being realized that purified viruses are essential for the proper study of problems in this field, such as the estimatlion of the size of viruses, the determination of their electrical charge, and the investigation of immunological responses excited by them. In addition to the fact that purified viruses are of practical value, it is obvious that such preparations will also be of value to investigators interested in the theoretical problem of the nature of viruses. Indeed, Murphy (52, 55) has already concluded from the results of his experiments on the purification of the Rous agent that this disease-incitant is neither a virus nor a living organism. He states, “It is hardly conceivable that the active fraction which I have thus succeeded in obtaining, a substance purified by repeated precipitations, could carry with it through all these manipulations any living organism or virus. To me the enzyme-like nature of the principle seems to have been conclusively established. . . . .” However, most workers do not believe that Murphy is justified in concluding from the results of such experiments that the Rous agent is not a virus, because at least eight other viruses, e.g., the incitants of infectious myxomatosis of rabbits (58), foot-and-mouth disease (64)) bacteriophagy (50, 56, 57), fowl-pox (56), vaccinia (66, 68)) rabies (66), poliomyelitis (65), and mosaic disease (67) have been subjected to manipulations similar to those used by Murphy and have been obtained, still active, in various states of purity.
Most methods of purification of viruses are based on the principles of precipitation by a variety of chemicals and selective adsorption and elution as used extensively in enzyme work. As yet, it is unlikely that a virus has been obtained in a state of absolute purity. Nevertheless, the results already secured are encouraging and should excite further investigations. It may be possible in this way to attain eventually a more accurate concept of the nature of some viruses. For instance, it may be shown that in certain purified virus preparations the number of nitrogen atoms for each infectious unit or particle is insufficient to warrant the supposition that the agents are living, organized structures. Krueger and Tamada (57) have already suggested this viewpoint.
While it is now stated that “viruses” require a host cell and must be cultured in order to be observed and studied, in the past, claims were made that “viruses” could be grown without cells. Rivers stated that these claims of successful cultivation on lifeless media were not uncommon, and he noted a few cases:
Frosch and Dahmen stated that they were able to cultivate the “virus” of foot-and-mouth disease on ordinary media.
Olitsky reported the cultivation of mosaic “virus” in a cell-free medium.
Eagles and McClean reported that vaccine “virus” is capable of regeneration in a cell-free medium.
Rivers ultimately decided that none of these were true examples of “viruses” being grown in cell-free media, and thus, it was chalked up to contradictory evidence that was brushed aside in favor of the prevailing belief that “viruses” are invisible and incapable of regeneration in the absence of living susceptible host cells. Rivers did note that such a state of affairs would prevent a complete definition of the nature of “viruses.” However, he believed that it was not absolutely essential to see and to cultivate the “viruses” on simple media.
CULTIVATING. In the literature of twenty years ago it is not uncommon to encounter reports in which it was claimed that viruses had been successfully cultivated on lifeless media. These reports have not been confirmed and at present such claims are rarely made. A few, however, have been made in recent years. Frosch and Dahmen (78) stated that they were able to cultivate the virus of foot-and-mouth disease on ordinary media. But the German, English, and American Foot-and-Mouth Disease Commissions were unable to confirm their work. Olitsky (91) reported the cultivation of mosaic virus in a cell-free medium. Nevertheless, upon repeating his work he (92) has been forced to conclude that true multiplication of the virus was not obtained. Recently, Eagles and McClean (75, 76) reported that vaccine virus is capable of regeneration in a cell-free medium. A careful examination of their papers, however, leaves one in doubt as to whether some of their media were cell-free, and as to whether multiplication of the virus occurred in the nutrient materials that undoubtedly contained no cells. In my laboratory (86, 90, 93) during the last four years, Haagen, Muckenfuss, Li, and I have made numerous attempts to cultivate vaccine virus in cell-free media, many of which were similar to if not identical with those employed by Eagles and McClean. None of our efforts was successful. On the other hand, the cultivation of vaccine virus in the presence of cells surviving in vitro has been more consistently successful in our hands and in Maitland’s (88) than it has been in Eagles and McClean’s.
Although the cultivation of viruses in lifeless media has not been accomplished, it is generally conceded that these agents are capable of pullulation in the presence of susceptible cells either surviving or growing in vitro. The viruses of Rous sarcoma (72), Virus III infection of rabbits (69), herpes febrilis (70), fowl-pox (77), vaccinia (79, 80, 86, 88)) rabies (94), foot-and-mouth disease (83,84,85? 89), vesicular stomatitis (73), infectious myxomatosis of rabbits (71, Sl), fowl plague (82), and probably the agents causing common colds (74) and poliomyelitis (87), have been cultivated in the presence of tissues surviving in vitro.
Moreover, the characteristic of species specificity possessed by many viruses is frequently reflected in their in vitro cultivation. For instance, fowl-pox virus (77), innocuous for mice and rats, does not regenerate in cultures of their tissues. Foot-and-mouth disease does not attack chickens and the virus (89) does not grow in cultures consisting of minced chick embryo and plasma. In addition to a species specificity, some viruses exhibit in cultivation experiments a predilection for certain kinds of cells. Fowl plague virus (82) multiplies in the presence of chick embryo skin and brain, but does not regenerate in pure cultures of fibroblasts. Foot-and-mouth disease virus (85) increases in amount when the culture medium contains minced guinea-pig embryo, but does not grow when fibroblasts or bits of heart muscle alone are present. Thus it appears that many viruses are capable of multiplication in tissue cultures and frequently retain under such conditions their species and cellular specificity. Nevertheless, it will be interesting to observe the results of further attempts to circumvent this species and cellular specificity of viruses by in vitro methods of cultivation.
A crucial experiment, if there be one, to decide the question of the autonomy of the viruses is their undisputed cultivation on lifeless media. It may be impossible, however, to accomplish such an experiment with all of the viruses, because some of them may be obligate parasites, as is the malarial organism. Thus in the quest for proof of the nature of viruses, we may find that many of them are invisible and incapable of regeneration in the absence of living susceptible host cells. Such a state of affairs will prevent, for a time at least, a complete definition of the nature of these peculiar incitants of disease. Nevertheless, we should obtain all the facts and make the most of them in the study of biological phenomena and in the better understanding and control of disease. For this purpose it is not absolutely essential to see and to cultivate the viruses on simple media any more than it is imperative to see and to know what electricity is in order to study the phenomena produced by it and to control its activity for our daily needs.
Regarding whether “viruses” are alive or not due to having their own metabolism, Rivers stated that the evidence was that they did not have any such metabolic capabilities. However, he felt that conclusions could not be drawn that “viruses” do not have a metabolism and that they are inanimate because the methods used may not have been adequate.
Adaptation of the “virus” to different hosts was used by researchers in order to state whether or not “viruses” were alive. This essentially meant drawing conclusions from using different materials and different methods in different animals while generating different results. One set of researchers viewed the contradicting outcomes as the result of a “living virus” while another set of researchers saw it as a result of the hosts response. Neither seemed to recognize the fact that it was the different experimental procedures generating different responses and results rather than the act of any “virus” adapting.
METABOLISM. Much of the discussion conc.erning the nature of viruses has centered around the question as to whether they are animate or inanimate. In this relation, one would like to know what the evidence is regarding independent metabolic activities of these active agents. Technical difficulties have hindered this type of experimentation with viruses. Nevertheless, a few investigations (95-99) have been made, the result,s of which were negative. One must not conclude from such negative results, however, that viruses do not possess an independent metabolism and are, therefore, inanimate substances, because the methods used for the detection of the metabolic activities may not have been sufficiently delicate.
ADAPTATION. Certain viruses inoculated into new hosts apparently undergo changes in some of theircharacteristics. Smallpox virus (100, 101) passed through monkeys to rabbits and calves and then back to man is no longer smallpox virus but vaccine virus, a.nd the disease, vaccinia, caused by it is not contagious as is smallpox. The incitant of yellow fever (106, 107) passed through a large number of mice by means of intracerebral inoculations loses much of its pathogenicity for monkeys when inoculated intravenously or intraperitoneally, but gains the power of producing a transmissible encephalitis in monkeys receiving the inoculum in the brain. Such phenomena are spoken of as adaptations of viruses to new hosts, and, inasmuch as adaptation is considered a characteristic of living rather than lifeless material, they have been cited by some investigators (103) as proof of the animate nature of the viruses. On the other hand, workers, who believe that viruses are products of cellular perversion, state that the changes observed in the characteristics of the active agents when they are inoculated into alien hosts are to be expected, inasmuch as mouse, rabbit, monkey, and human cells, because of intrinsic differences, may not always manufacture identical substances as the result of similar stimuli. Therefore, they contend that the changes and adaptations are not accomplished by the agents themselves but by their hosts and, consequently, are not admissible as proof of the living nature of the viruses.
As ”viruses” were incapable of being observed and studied directly, various forms of indirect evidence were utilized in order to infer the presence of these entities. One of the earliest ways to do so was by claiming that a phenomenon known as inclusion bodies was a sign that a “virus” was present. These “bodies” are aggregates of proteins seen in various tissues under microscopy that were taken as an indicator by the researchers that they were dealing with a “virus.” However, it is well-known that inclusion bodies are not specific to “viral” cases and can be found in those without a “viral” disease. They are also not found in all cases of a particular disease, can be found in those without the disease, and are even found in uninoculated cell cultures, as seen with RSV. A 1941 paper by Alfred M. Lucas stated that the “existence of an object which appears to be an inclusion body is not proof of the presence of a virus but merely an indication that a virus should be considered if no bacterial agent can be found.” What this means is that inclusion bodies are nothing more than non-specific indirect evidence used to infer an assumed “virus” if other “causes” are ruled out. This means that finding inclusion bodies is essentially meaningless as a specific sign for the presence of any “virus.” Rivers appeared to understand this as well. After presenting various contradictory interpretations and presentations of inclusion bodies by different researchers, he noted that “inclusions may arise in a number of ways and that they may or may not contain virus.” He felt that making conclusions about what these “peculiar structures” represented was “hazardous at present.”
INCLUSIONS. Within the nucleus and cytoplasm of cells injured by viruses, certain peculiar structures, inclusion bodies, are frequently observed. Although many of these bodies are of importance in diagnostic and experimental work, numerous opinions exist concerning their nature. Lipschtitz believes that the inclusions in many diseases (119) consist of compact masses of virus particles, yet he is of the opinion that such structures in measles (120) are nothing more than altered central bodies. Goodpasture (113) thinks that Negri bodies in rabies are composed of degenerated mitochondria and neurofibrils, while Levaditi (118) and Manouelian (121) consider them protozoa and designate them, respectively, Glugea lyssae and Encephalitoxoon rabiei. Goodpasture and his associates (124, 125) have demonstrated that the incitant of fowl-pox is intimately associated with the Bollinger bodies which are made up of a lipoid capsule within which numerous small coccoid bodies are embedded in a protein matrix. On the other hand, Glaser (112) has presented evidence that the polyhedral bodies, the characteristic inclusions in wilt diseases of caterpillars, consist of non-infectious crystalline protein. Thus, it appears that inclusions may arise in a number of ways and that they may or may not contain virus. Consequently, generalizations regarding these peculiar structures are hazardous at present.
The small coccoid bodies found in fowl-pox by Borrel (109) and in vaccinia by Paschen (122,123) appear to be extremely minute organisms. In fact, one is justified in asking why these bodies are not convincing evidence of the organismal nature of certain viruses. The first reason is that one cannot by morphological and tinctorial data alone determine whether autonomous life exists in such small objects. Another reason is the fact that Goodpasture, while holding the belief that the small coccoid bodies in fowl-pox (124, 125) represent the virus, stated that similar structures, seen in rabic brains (113) and considered of etiological importance by Babes (108) and Koch (114-116), are probably degenerated mitochondria. Moreover, Borrel (110) has described similar bodies in other virus diseases the etiological agents of which have been shown by ultrafiltration to be incapable of resolution by microscopic methods. Furthermore, Craciun and Oppenheimer (111)) who cultivated the small bodies of vaccinia and showed that they are closely associated with the virus, made the following statement, “We have from these studies no morphological proof of an increase in the number of granules, since they cannot readily be distinguished from other granules normally seen in tissue cultures.” Finally, mitochondria in some respects resemble bacteria. They may decrease or increase numerically within cells, and their size and shape may be altered by appropriate stimuli. At times, they actually divide. Nevertheless, mitochondria are not considered autonomous living agents. Consequently, so far as I am aware, there is no convincing evidence-the specific agglutination of virus elementary bodies (184) by antiviral sera will be discussed later-to invalidate the conception that cells under the stimulus of viruses may react by the formation of numerous small coccoid bodies uniform in size and intimately associated with the stimulating agents. One would not consider such bodies microorganisms or hold that they consist of virus alone. Therefore, in spite of definite proof that viruses are present in certain types of inclusions, doubt still exists regarding the organismal nature of the small coccoid bodies found within them.
Other features observed in pathological processes induced by viruses, e.g., hyperplasia and necrosis, are fully as important as are the inclusion bodies. The excessive stimulation of cells seen in some virus diseases, e.g., fowl-pox and warts, leads one by analogy to think of mdignant neoplasms. Undoubtedly a number of fowl tumors are caused by agents separable from cells, and, although there is no proof that mammalian tumors arise in this way, the possibility is worthy of consideration and offers an attractive field for work. The fact, however, that some tumors are produced by filterable agents is by no means conclusive evidence that all neoplasms (217) arise through the activity of such incitants.
In this next section, Rivers admitted that there was an increasing chorus of researchers who believed that “viruses” were nothing more than “merely filterable, invisible, and noncultivable elements of ordinary bacteria.” He presented many scenarios, such as:
The bacteriophage is a form in the life cycle of lysogenic bacteria.
The “viruses” of yellow fever and hog cholera are invisible forms of Leptospira icteroides and B. suipestifer respectively.
The etiological agent of scarlet fever is a filterable form of hemolytic streptococci.
The incitants of poliomyelitis, epidemic encephalitis, fox encephalitis, common colds, measles, and influenza represent certain stages in the life cycle of green streptococci.
Apparently, Rivers was unfamiliar with the fact that this bacterial life cycle process, known as pleomorphism, was observed by many researchers such as Antoine Bechamp, Günther Enderlein, Royal Raymond Rife, and later by many others with the use of dark field microscopy. That bacteria are pleomorphic entities, i.e. having the ability to assume different forms, is an established fact.
VIRUSES AS FILTERABLE FORMS OF BACTERIA. For a long time a few investigators have held that certain virus diseases are induced by ordinary bacteria. Now that attention is being focused on filterable forms of bacteria, workers in increasing numbers (128, 131, 132, 134, 135) are adopting the belief that viruses are merely filterable, invisible, and noncultivable elements of ordinary bacteria. It has been claimed, and evidence of a kind has been offered to substantiate the assertions, that the bacteriophage (165, 166) is a form in the life cycle of lysogenic bacteria, that the viruses of yellow fever (131, 134, 135) and hog cholera (134, 135) are invisible forms of Leptospira icteroides and B. suipestifer respectively, that the etiological agent of scarlet fever (134, 135) is a filterable form of hemolytic streptococci, and that the incitants of poliomyelitis, epidemic encephalitis, fox encephalitis, common colds, measles, and influenza represent certain stages in the life cycle of green streptococci (131). Without going into details of the available knowledge of bacterial life cycles and their invisible and noncultivable forms, one can say that proof of many of the claims regarding them is lacking. In fact, if certain reports are correct, some of the filterable forms of bacteria are much smaller than are many of the viruses. Kendall (131) recently stated that “egg white, filtered through Berkefeld W filters (after dilution with sterile physiological saline solution) is rarely sterile.” Such a statement raises embarrassing questions for workers in the virus field because many viruses will not pass through W filters. Since the existence of bacterial life cycles is doubtful, it seems unwarrantable to offer the presumptive filterable forms of them as evidence upon another unsolved problem, the nature of the viruses.
The thing to notice in this next section on physical and chemical agents is, once again, the often contradictory nature of the evidence presented by different researchers. One researcher would find a certain chemical that had an effect on the “virus,” while another researcher would state otherwise. Some viewed that chemical tests proved “viruses” were protozoa. Others felt that their tests proved the “virus” was an enzyme. Sanderson showed that bacteriophages were not killed by successive freezing and thawings and believed that they were unliving. However, Rivers showed that bacteriophages can be killed by repeated freezing and thawing, thus contradicting Sanderson’s interpretation. Ultimately, Rivers concluded that, regardless of the number of tests with chemical and physical agents that had been devised as criteria for the presence of life or to define the nature of “viruses,” not a single one of them was found to be satisfactory.
EFFECT OF PHYSICAL AND CHEMICAL AGENTS ON VIRUSES. Many years ago it was discovered that bile and saponin are injurious to protozoa but with a few exceptions are innocuous for bacteria. Consequently, when the question of the nature of viruses began to attract attention, tests were made to determine what effect bile and saponin have on these incitants of disease. Many viruses, e.g., rabic virus (141, 144), were found to be inactivated and because of this fact certain workers concluded that they are protozoa. Sufficient exceptions, however, have been encountered to invalidate the test as a means either of separating bacteria from protozoa or of defining the nature of viruses. The agent causing Rous’ sarcoma (140) is more resistant to ultraviolet light than are bacteria, and Murphy (220) considers this fact as evidence in favor of his hypothesis of the enzyme-like nature of the virus. On the other hand, bacteriophage (139), the living nature of which many doubt, is just as sensitive to ultraviolet light as are bacteria. Sanderson (153), using a temperature of -78°C., found no diminution in the titer of two strains of bacteriophage subjected to 20 successive freezings and thawings. Since bacteria and cells are killed by repeated freezing and thawing, he concluded that bacteriophage must be something other than a living organism. Rivers (151) showed, however, that colon bacilli, Virus III, vaccine virus, herpetic virus, bacteriophage, complement, and trypsin are all either killed or inactivated by repeated freezing (-185°C.) and thawing and that, as might be expected, some of the agents are more resistant than are others. Hence it is obvious that destruction or inactivation of an active agent by repeated freezing and thawing is not evidence that it possesses life. The observations on heat, desiccation, oxidation, and the effect of dyes have likewise yielded no convincing evidence concerning the nature of viruses. Thus it appears that a number of tests with chemical and physical agents have been devised as criteria for the presence of life or to define the nature of viruses, but no one of them has been found satisfactory.
The spontaneous generation of “viruses” by the host is a concept that defeats the idea that these entities are exogenous outside invaders. If something like a bacteriophage can be produced by a normal bacterium without any external phage present, it shows that these entities arise from a process initiated from within the organism. Rivers noted that Hadley and his co-workers stated that it was possible to obtain bacteriophage from normal bacterial cultures by means of enforced dissociation. Thus, no external source of phage was necessary. Nobel Prize-winning immunologist Jules Bordet was able to do the same, as did other researchers. Rivers presented a few scenarios where “viral” diseases could be induced by injecting toxic substances such as tar and arsenic into chickens, as well as an instance where a tumor-producing extract could be obtained from healthy chickens. While Rivers thought that the interpretation of the evidence was potentially fundamental to biology, he excused it as being due to contamination by the researchers working in labs with similar materials as well as the possibility that “latent viruses” were hiding within the healthy hosts.
SPONTANEOUS GENERATION OF VIRUSES. The origin as well as the nature of viruses constitutes a question of interest. The intimate relation between these active agents and their host cells has induced more than one investigator to view the host cell as the source or origin of viruses. Indeed, reports of experimental work have appeared leading to claims that normal cells have been induced to manufacture certain viruses. According to Carrel (156, 157), minced chick embryo mixed with tar, indol, or arsenic and injected into normal chickens in a small percentage of instances gives rise to tumors resembling Rous’ sarcoma no. 1 and transmissible by cell-free filtrates. Fischer (163) by treating cultures of normal cells with arsenic obtained on one occasion a filterable agent capable of causing tumors. Carrel was unable to confirm Fischer’s work. Murphy (52, 167), by means of a method the details of which have not been described, reported that he was able to extract a filterable tumor-producing agent from the gonads of normal-appearing Plymouth Rock roosters.Recently, Hadley and his co-workers (166) stated that it is possible to obtain bacteriophage from normal bacterial cultures by means of enforced dissociation. Although no worker in this field has claimed to have generated living organisms from inanimate matter, it appears that a few believe that they have by certain manipulations induced cells to yield substances which possess some of the attributes of life, notably that of increasing without limit.
The observations described above are suggestive, and, if confirmed and found to warrant the interpretation given them by Carrel, Murphy, Fischer, and Hadley, will prove to be of fundamental biological importance. Unfortunately, however, all of the experiments yielding the observations were actively referred to were conducted in laboratories where workers engaged in the study of agents similar to those supposedly brought into existence. In such laboratories and with such materials it is always difficult for one to rule out the possibility of contaminating normal animals, tissues, bacteria, emulsions, and filtrates. This fact has long been appreciated by workers in vaccine virus laboratories and it delayed the acceptance of the experimental transformation of smallpox virus into vaccine virus. Therefore, experiments of the nature described should never be conducted in rooms used for the study of agents similar to those for which a search is being made. The workers who believe that they have induced viruses to come into existence have not excluded the possibility of the preexistence of latent viruses or of small amounts of virus in the supposedly normal embryos, gonads, chickens, and bacterial cultures utilized in the experiments. This possibility is emphasized by Flexner’s (164) work on poliomyelitis, for he was able to demonstrate the presence of virus in the nasal washings from normal contacts. The possibility outlined is further emphasized by Andrewes and Miller’s (155) experience with Virus III in rabbits, by Cole and Kuttner’s (158) work with the salivary-gland virus in guinea pigs, and by the work upon virus carriers in general among animals, plants (168) and bacteria.
CGI (Computer-Generated Imagery): The only way you will ever see “antibodies” attacking “viruses.”
Rivers next discussed “immunity” in relation to establishing the nature of “viruses.” It is important to note that, regarding antibodies and “immunity,” researchers are utilizing one hypothetical entity in order to define another. While Rivers spoke as if the antibody and antigen concepts are established facts, he remarked that if the concept of the nature of antigens is correct, “viruses” are proteins or are closely linked to proteins. Thus, the interpretation of the nature of the “virus” rests upon the correctness of the nature of the antigen concept. He felt that the rise of these (hypothetical) antibodies that differed between host cell and antigen adduced (led one to believe) the exogenous rather than the endogenous origin of the “viruses.” Regardless, Rivers admitted that the mode of action of neutralizing antibodies was not clearly understood, and when speaking of antibodies causing flocculation (clumping together), he shared that various researchers noted the “immunological” phenomena in “virus” maladies are comparable to those induced by toxins. While Rivers felt that “immunological” observations were important, he admitted that this method of approach had not brought about a definite solution to the problem of the nature of “viruses.”
IMMUNITY. Most virus diseases lead to a marked and lasting immunity in recovered hosts. Not only are the but in their sera antibodies capable of hosts refractory to reinfection neutralizing the viruses are demonstrable. What bearing have these facts upon the nature of viruses? In the first place, it is certain that viruses are highly antigenic. Furthermore, if our concept of the nature of antigens is correct, the viruses are proteins or are closely linked to proteins. Moreover, the agents are not only antigenic, but they give rise to antibodies different from those excited by proteins of the host cells. This is true even of the bacteriophage (188). These facts have been adduced as evidence of the exogenous rather than the endogenous origin of the viruses. Thus, the antigenic nature of viruses appears to be prejudicial to the idea that they are products of cellular activity. The notion, however, that a lifeless agent may be injurious to the cell creating it and that it may induce immunological responses independent of those excited by the cell, loses some of its fantastic qualities when one considers the well-known facts that lens protein is not species specific but organ specific and that sympathetic uveitis in the uninjured eye is caused not by microorganisms but by the reaction of the body to substances derived from injured cells of the other uveal tract.
In addition to the neutralizing antibodies, whose mode of action is not clearly understood, complement-fixing antibodies and antibodies causing flocculation in virus emulsions have been described. Schultz and his associates (191-195) contend that the latter types of antibodies are not excited by viruses and that the immunological phenomena in virus maladies are comparable to those induced by toxins. In spite of their contentions, sufficient evidence has been adduced by different workers to make it more than likely that certain virus diseases lead to the production (176, 177, 180, 199) of the antibodies mentioned. Furthermore, Ledingham (184) has recently demonstrated that Borrel bodies in fowl-pox and Paschen bodies in vaccinia are specifically agglutinated by antifowl-pox and antivaccinal sera respectively. The results of these experiments indicate to Ledingham that the elementary bodies are living organisms and represent the virus. There is no reason to doubt that specific agglutinations of the bodies occurred in the manner described by Ledingham, and one cannot deny that such a phenomenon is presumptive evidence of the organismal nature of the bodies. Yet one dare not say categorically that his experiments are unequivocal evidence that the elementary bodies represent virus alone, because it has been shown by Jones (182, 183) that collodion particles treated with a variety of proteins and then thoroughly washed are specifically agglutinated by the proper antisera. Thus, the Borrel and Paschen bodies without being organisms yet having virus adsorbed on them might nevertheless be specifically agglutinated by appropriate antiviral sera.
Gye (181) states that Rous virus repeatedly injected into alien hosts excites two groups of antibodies, one of which acts on the virus itself, while the other operates on the “specific factor” derived from the host cell. According to him, either set of antibodies inactivates the virus. This fact is offered by him as further evidence of the dual nature of the causative agent of fowl tumors. Murphy (189) and Sittenfield (196-198) have reported the presence in Rous sarcoma of a substance that inhibits the action of the etiological agent, and the first mentioned worker is of the opinion that the “inhibitor” differs from ordinary virus antibodies. The presence of this “inhibitor” together with other phenomena has induced Murphy (220) to believe that immunity to the Rous agent is unlike that observed in virus maladies and lends evidence to his view that the Rous agent is not a virus. Inhibiting substances, however, have been obtained from tissues infected with viruses, for example, a substance restraining the action of rabic virus has been demonstrated by Marie (186) in the brains of rabid animals. Furthermore, Andrewes’ (172, 173) work appears to indicate that the immune responses excited by the filterable agents of fowl tumors may not be unique and may possess much in common with those encountered in other virus diseases.
From what has been said, it is obvious that immunological phenomena are playing an important role in discussions concerning the nature of viruses. As yet this method of approach has not brought us to a definite solution of the problem.
Rivers finished up his review on the nature of “viruses” by presenting the various differing interpretations on the concept of the “virus.” These invisible entities were regarded as either:
Living contagious fluids
Oxidizing enzymes
Protozoan parasites
Inanimate chemical substances
Minute living organisms (related to bacteria)
Rivers noted that depending on the researchers, the rabies “virus” was either an enzyme, a parasite, a protozoon, or an unknown living organism. He stated that researchers were divided over whether bacteriophages were an inanimate agent or a living organism. The fowl-pox “virus” was thought of as either a protozoan parasite, a nucleoprotein poison manufactured by “infected” cells, or a minute coccoid organism capable of regeneration in parasitized cells. The agent associated with Rous sarcoma was either animate, a living organism mixed with an inanimate substance, an enzyme-like substance, or a transmissible mutagen.
Rivers highlighted these numerous competing concepts in order to show how radically different the ideas concerning the nature of “viruses” are from one another. He then proceeded to explain the main conceptions of “viruses,” with the first two scenarios explaining how a stimulus induces a normal cell to create a substance X, which may either remain free or become closely bound to a part of the cell. In Rivers’ third example, which he considered the most popular, X is a minute living organism that enters cells, multiplies, and produces disease. Thus, there is a distinct difference where X is considered an inanimate substance that results from cellular perversion in the first two scenarios, while X is viewed as an autonomous organism in the last scenario. Regardless of the scenarios that Rivers provided attempting to explain “viral” formation, he admitted that there was no unequivocal evidence of the validity of any of these concepts.
CONCEPTS OF THE NATURE OF VIRUSES. A review of the data by means of which one arrives at a concept of the nature of viruses has been presented. Now it will be interesting to see what notions certain workers have concerning some of them.
Beijerinck (202) considers the virus of mosaic disease to be a living contagious fluid; Woods (228), an oxidizing enzyme; Goldstein (212), a protozoan parasite; Vinson (67), an inanimate chemical substance. Most workers, however, believe that it is a minute living organism.
Hijgyes (216) is of the opinion that the incitant of rabies is an enzyme or “alternatively, that the tissues themselves might spontaneously become virulent as the result of changes in their chemical composition.” At one time Remlinger said, “The rabies virus, which is at once filterable, diffusible and capable of reproducing the disease from case to case, appears to occupy a place midway between the microbes and the diastases.” Recently, however, he (221) has published an article on the evolution of the parasite of rabies. Levaditi (118) and others (121, 225) have presented evidence in favor of the idea that the causal agent is a protozoon. The majority of investigators hold the concept that the incitant is a living organism whose nature is not definitely known.
Numerous workers believe that the bacteriophage is an inanimate agent, while others are convinced that it is a living organism. Ideas, however, concerning the nature of the inanimate transmissible substance or the animate organism vary. For details of the different concepts one is referred to papers by Twort (226, 227), d’Herelle (103), Bordet (203), Bronfenbrenner (95), Burnet (206), and Hadley (165, 166).
The incitant of fowl-pox has been described by certain investigators as a protozoan parasite. Sanfelice (222, 223) suggested that it is a nucleoproteid poison manufactured by infected cells. Borrel (log), Goodpasture (124, 125), and Ledingham (184) hold that it is a minute coccoid organism capable of regeneration in parasitized cells.
Rous and others are prepared to entertain the idea that the causal agent of Chicken Tumor No. I is animate. Gye (215) believes that it consists of two factors, one of which is a living exogenous organism, the other an inanimate specific factor derived from infected cells. Murphy (52, 55), at one time, spoke of the Rous agent as an enzyme-like substance. Recently, however, he (220) has compared it to filterable substances capable of transforming melitensis (204,205) into paramelitensis organisms and of converting one type specific pneumococcus (201) into another type specific form. In regard to the matter he says (22O), “Thus we have a group of agents, products of specialized cells capable of conferring the peculiar type quality to undifferentiated cells of the same species which, in turn, may produce the active factor and transmit this to their descendants.” For this type of agent he proposes the name transmissible mutagens.
Sufficient ideas concerning the nature of viruses have been cited to illustrate how radically some differ from others. Many of them, particularly the ones dealing with the origin and reproduction of inanimate substances that behave in a manner similar to that of living organisms, lack precision. In a general way, however, the different concepts can be arranged in groups and it seems advisable to state and to portray diagrammatically several of the popular ones.
According to one conception, certain stimuli produce changes within cells that are inherited by daughter cells. Once the mutations occur, cells of the new type continue to be formed though the stimuli disappear. No agents separable from the cells are demonstrable, and immunological phenomena in this type of disease differ from those observed in virus maladies. Ordinarily this idea of the causation of disease and the concepts concerning the nature of filterable viruses are not grouped together. Yet in some respects they are not dissimilar and many hold the view that malignant neoplasms arise in some such way. See figure 1.
Another notion is that appropriate stimuli induce normal cells to make a substance x which is closely bound to parts y of the cells. Thus an xy complex is formed. This complex, separable from the cells, yet capable of inciting its own production by them, either passes directly into daughter cells, or, having become extracellular, enters another set of normal cells. The xy complex is antigenic, and cells freed from it presumably become normal again. See figure 2.
Still another idea is that certain stimuli incite normal cells to produce a substance x which is not closely bound to parts of the cells, X, separable from cells, yet capable of impelling its formation by them, either passes directly into daughter cells, or, having become extracellular, enters a new group of normal cells. X is antigenic and cells freed from it presumably become normal again. See figure 3.
Finally there is the concept most generally held that x is not a product of the perverted activity of cells but is a minute living organism. X enters cells, multiplies, produces disease, is separable from cells: and is antigenic. Cells freed from it presumably become normal again. At times, x is absorbed by particles y of host cells and evidences of an xy complex are obtained. See figure 4.
For practical purposes it makes little difference which one of the last three concepts is accepted. Theoretically, however, x of the second and third conceptions is quite different from x of the fourth. In the second and third, x, a product of cellular perversion, is an inanimate agent, while in the fourth it is an autonomous organism. No unequivocal evidence of the validity of any of the concepts has been adduced.
Rivers concluded by acknowledging the confused state of the evidence concerning “viruses,” noting that this confusion had made it exceedingly difficult to define their nature. He felt that the easiest way out of their dilemma would be to accept “viruses” as minute organisms. However, Rivers warned of quickly accepting presumptive evidence as “viruses” may be either minute organisms, forms of life unfamiliar to us, inanimate transmissible incitants of disease, or all of the above.
Conclusion
The confused state of our knowledge of the viruses at the present time makes it exceedingly difficult to define the nature of these active agents. The easiest way out of the dilemma, however, would be the acceptance of the presumptive evidence that viruses are minute organisms. Yet the easiest way and the one that best fits the experiences of the day may not be the right one. Furthermore, excessive skepticism and the habit of too readily accepting presumptive evidence are equally productive of sterility. Unless viruses represent a form of life unknown to us, proof of their living nature would not be a striking discovery. If, however, some of them are not animate, absolute proof of such a fact would be of fundamental biological importance. Therefore, care should be exercised that immoderate skepticism on the one hand, and the mental satisfaction secured by accepting presumptive evidence on the other, do not dull our efforts to obtain a better understanding of the viruses, some of which may be minute organisms, while others may represent forms of life unfamiliar to us, while still others may be inanimate transmissible incitants of disease. In any event, we are face to face with the “infinitely small in biology,” and, if there be a sharp demarcation between life and death, then scientists, investigating the nature of viruses, are working near the line that separates infinitely small living organisms from inanimate active agents.
From these two presented articles from two different points in time in the history of virology (Rivers in 1932 and Summers in 2014), it should be clear why it is difficult for virologists to define the nature of the “virus.” Researchers needed to invent, and then continually reinvent, the nature of the “virus” as the foundation that virology is built upon is conceptually weak. It is full of contradictions that have cracked the very infrastructure that was put in place. There were never any submicroscopic entities that were being studied by the various researchers over the last century. As there were no “viruses” to study and characterize, there was no agreement at all amongst the various researchers as to the nature of the invisible concept crafted inside of their minds. They had tricked themselves, through shoddy indirect pseudoscientific evidence, into believing that they were studying something real based upon lab-created effects without an identifiable cause. This is why the “virus” has been continually defined for what it isn’t, rather than for what it supposedly is. The magical “virus” skirts the line between life and death, microbe and molecule, enzyme and ferment. It is unlike anything else seen in nature, and for this very reason, its nature remains mysterious and incomplete. This should be the very first clue that there is nothing scientific about the “virus,” as science only deals with the natural world and its phenomena, not the supernatural. However, within the supernatural realm is where the “virus” concept will remain, ready and waiting to be reinvented upon the arrival of the latest technology for the next best indirect measurement. This will be utilized to continue fooling the researchers, as well as the public that blindly trusts in them to know better, that these fictional entities exist in nature, when, as Thomas Rivers kindly pointed out, “viruses” have never once been observed there. Thus, the nature of the “virus” will continue to remain merely an invention of the imagination of the most ardent admirers of these invisible boogeymen—the virologists.
It is time to revisit the England-wide NHS prescription data regarding one particular category of psychiatric drug prescribing. In a previous post specifically on ADHD drugs, a shocking 15% year-on-year rise in ADHD drug prescriptions for 2022 was noted. Within the first two quarters of 2023, the previous increase has already been exceeded by over 2.5%. It now stands at an almost 18% increase for the same period, compared to 2022.
And this is the year-on-year increase. Looking at current levels compared to a long-term trend, it is even more staggering. For almost 9 years, since 2012, prescriptions of drugs used for ADHD remained fairly close to the long-term trend (within a 5% window). In 2022, that trend was broken with a 10% divergence, but in 2023 it disconnects from it completely. A 25% divergence from a steady long-term trend must signal a radical change in the userbase. What is happening?
In economics, there is the law of supply and demand. As the price increases, supply rises while demand declines. Conversely, as the price drops, supply constricts while demand grows. CCHR UK has been scrutinising the demand side of the equation, while the media has been keen to underline the supply side. Journalists tend to write about drug supply shortages as if they are occurring within a status quo of demand. An 18% year-on-year increase, and a 25% divergence from a long-term trend, is anything but a status quo.
In recent media articles, there was an obvious omission. The media failed to mention that demand has – somehow and without too much explanation – exploded. What brought about such a demand?
It should be recognised there are no physical or biological tests that can be carried out to support the existence of ADHD. None. There are no tests. Pontificating psychiatric authors have however taken regular human behaviour and redefined it as a so-called mental ‘disorder’ which has been accepted without inspection.
This isn’t a new concept. Sets of emotional and behavioural characteristics were redefined as far back as 1987 when ADHD was literally voted into existence. This however is not science. It’s consensus. It’s psychobabble. Considering the law of supply and demand, there has been a tremendous increase in the supply of psychiatric rhetoric, opinions and assumptions that have brought about a greatly-increased demand for ADHD drugs.
Furthermore, the prescribed drugs can have serious consequences, that include some of the following side-effects:
abdominal pain
aggression
depression
dizziness
drowsiness
hallucinations
headaches
insomnia
loss of appetite
moodiness
nervousness
psychosis
restlessness
seizures
stunted growth
suicidal thoughts
violent behaviour
weight loss and ‘zombie’ appearance
While there are many discerning people who question the unscientific psychiatric modus operandi, there are many who accept psychiatric labels like ADHD without inspection. Not so long ago, psychiatrists brazenly used the ‘chemical imbalance’ theory to push ADHD. That theory has been debunked but the statistics represent that more people must be accepting the label for the prescribing rates to continue to rise.
At the end of the day, being fully informed is the key policy. If people reply on the psychiatric narrative, they won’t be fully informed. Don’t be fooled by psychiatric rhetoric.
As soon as I began writing about COVID in the spring of 2020, I made the case that SARS-CoV-2 hadn’t been proved to exist.
I then met Tom Cowan, Andrew Kaufman, and Christine Massey. I became aware of the work of Stefan Lanka. They were making a wide challenge about viruses in general:
No actual isolation; no proof of existence; instead, a parade of false claims and obfuscations from official sources.
A few years later…and the number of serious researchers who are coming to the same conclusion has expanded significantly. (You can find links to some of these researchers at Christine Massey’s Substack page )
The new work isn’t just a repetition of the original challenge to official authority. It attacks fake viruses from a number of angles. The shocks keep coming.
This story isn’t going away. It’s building.
It reminds me of the vaccine story. When I first started writing about dangerous and ineffective vaccines, in 1987, there were dozens of writers, present and past, who had covered similar ground—going back many decades. But that was nothing compared with…
The strength of that story now, in 2023, after the catastrophe of the COVID vaccines.
This is what I believe is going to happen to the fake virus story—against even longer odds. I say “longer,” because the proofs that viruses aren’t real by any scientific standard will undermine and detonate the very center of the medical cartel, which is all about germ theory.
Germ theory is marketing. The marketing of (toxic) drugs and vaccines for thousands of so-called distinct diseases, each supposedly caused by a unique germ.
When that fiction falls, the whole house collapses.
Going back as far as the beginning of the 20th century (and farther), another paradigm about disease emerged. It came to be called “holistic.” Probably not the best label. But the idea was: look at the whole body, the whole person. Look at body processes as connected and inter-related. Understand disease and health in those larger terms. Include environmental effects—basic sanitation, pollution, toxic chemicals, nutrition, the rise of the middle class out of poverty.
Something needs to be pointed out here. The holistic paradigm is a very difficult approach, in terms of making it pay off in real cures. It always has been difficult. Thousands of methods have been suggested. Many of these tend to mirror the medical strategy: find magic bullet solutions, take short cuts. Market them. Claim temporary fixes are permanent.
Treating the body and the person as a whole, taking in the mind-body connection—this is by no means a walk in the park.
Therefore, sooner or later, many people, discouraged, fall back on medical answers and germ theory.
The work of the no-virus pioneers provides an absolutely essential antidote to that surrender.
Because what are people surrendering to? The convenient fiction that viruses are everywhere, causing separate diseases. Convenient fiction was how viruses were willed into existence in the first place:
Doctors couldn’t cure their patients. So they looked for “something that was missing.” A hole in their hypotheses. And they claimed they found it.
Tiny particles no one had ever seen. No one had ever isolated. “This is the key. This is the great discovery.” It was a self-serving fairy tale. An excuse for treatment failure.
It kicked off millions of efforts to assure one and all that viruses were real. Marketing, parading as science.
Where were these viruses being discovered? In proprietary labs. No civilians permitted. Doors locked. Only the experts could understand the details of their own isolation of the tiny particles.
The particles which had been fantasized into existence.
We’re actually looking at a magic-myth story. Explorer-knights (doctors, researchers) are searching for an invisible dragon object which is crippling the population. These heroes finally corner it and isolate it and go to work decimating it and all its variants.
But the real ending to that story is now being provided by the multiplying number of independent researchers, who are proving the invisible dragon object was never cornered or identified or isolated.
Instead, the so-called explorer-knights made up, invented, fabricated the idea of the object to begin with.
That’s the magic. Sleight of hand. That’s the myth. Secret lab procedures that, when exposed, turn out to assume what they’re trying to prove. Also known as circular reasoning.
The whole story has come unglued.
For now, I’ll conclude with this analogy. A group of elite researchers claim that, 49 trillion light years from Earth, there is a flaming star the size of the Milky Way. At the center of that star, buried within a supernatural vault, there is a tiny, tiny purple man with green toes and orange hair who is causing all trouble and all destruction circulating throughout the universe. He’s there. He’s been “isolated.”
Given that incredible tale, would you expect, would you really expect there can be ANY sort of test which would prove the existence of that tiny man?
Could ANY test be produced that would be authentic?
So, in the case of the wild virus fairy tale, are we looking at proofs of existence and isolation that need to be improved, in order for us to accept them?
Or are we, instead, looking at the tiny purple man, about whose existence there are no possible proofs at all?
Because the story is so absurdly outrageous.
I’m thinking we’re dealing with the tiny purple man. And this may be the next chapter in the no-virus revelation:
The original concoction of viruses was so crazy, every so-called proof is going to be circular, mindless, and futile.
“You mentioned “DNA targeting.” yes, indeed, this is possible, but is it happening? I seriously doubt it. If medical/pharmaceutical experts cannot isolate a virus, RNA, or spike protein, they cannot (not capable) of working with DNA targeting, as assumed.”
Viruses/Virology: Promoting With Glorified And Catchy Language
About the view that vaccine(s) may include some type of DNA targeting, I responded as follows:
Being a chemist/scientist all my life, and mainly in the pharmaceutical area, when I read about pharmaceuticals, including viruses and vaccines, it is evident to me that medical experts clearly describe chemistry in a glorified and catchy language. However, most of their claims do not make sense and are often false and fraudulent.
You mentioned “DNA targeting.” yes, indeed, this is possible, but is it happening? I seriously doubt it. If medical/pharmaceutical experts cannot isolate a virus, RNA, or spike protein, they cannot (not capable) of working with DNA targeting, as assumed. So, it is fancy language to impress that something (high-level “science”) is happening.
On the other hand, as I described (here and here), it looks like they are injecting partial or unpurified cell culture (as a “vaccine”), assuming it is mRNA and is causing the problems (adverse effects), including deaths.
The only and easiest/quickest way to find out is to get an audit done by experts with experience in isolation/purification to establish if the mRNA/vaccine is pure as described or junk.
However, in the current (regulatory) system, an audit is done by experts who have no or limited experience in isolation and purification and have a vested interest in maintaining the status quo, so they will provide fancy stories and seek more funding for “research” to prepare for next “pandemic” and “vaccine.”
Further information on the topic may be found here: Helpful Notes, the Book, and Blog by the author (Dr. Qureshi), who worked at Health Canada as a Research Scientist and had 35+ years of bench science experience in substance isolation, characterization, and analytical testing among other specialties.
For many years doctors have received bonuses for adherence to the latest drug therapy protocol. Drugs that are known to be dangerous such as statins and anti-depressants. And now we know that insurance companies are paying doctors to fully vaccinate your children.
This incentive program for vaccinating babies can be found in the Blue Cross Blue Shield doctor incentives booklet. And specifies that every patient under the age of two that receives the currently prescribed twenty-four inoculations is worth a four-hundred dollar payout to that doctor.
For further motivation, they get paid by the hundred and they have to vaccinate a certain percentage of their total patients or they don’t get anything. Blue Cross Blue Shield rules say that a doctor needs to vaccinate sixty-three percent of their patients in order to qualify.
The average American pediatrician has about fifteen hundred patients and would have to have nine hundred and forty-five of them fully vaccinated in order to get paid. At forty-thousand for every hundred this works out to three-hundred and sixty thousand dollars.
This is why most pediatricians won’t provide care for families who don’t completely submit to the latest childhood vaccine schedule protocol. We are talking over a quarter million dollars which is more than the average pediatrician’s yearly salary.
Research shows that an unvaccinated child’s risk of death increases by over five thousand percent when they receive the current vaccine schedule.
And Doctors are now beginning to use virtual reality to help them administer these poisons to children who instinctively know better.
Drs. Tom Cowan and Mark Bailey challenge an article posted on October 4, 2023 by HART (a group of scientists in the UK) titled “Why HART uses the virus model — Arguments against ‘the virus doesn’t exist’ “.
Tom and Mark go over all key points made in the article.
It’s clear that the HART group has no idea what has been revealed in the research done by those who been exposing the false foundation of virology.
HART has somehow missed a foundational point of the “no virus” research — that no infectious “virus” has ever been isolated in the entire history of virology and that the “no virus” research shines a light on the fraud of all so-called infectious viruses.
Here is how HART group describes themselves at their website:
“HART is a group of highly qualified UK doctors, scientists, economists, psychologists and other academic experts. We came together over shared concerns about policy and guidance recommendations relating to the COVID-19 pandemic.
We continue to be concerned about the lack of open scientific debate in mainstream media and the worrying trend of censorship and harassment of those who question the narrative. Science without question is dogma.”
We are providing a transcript of one of Dr. Tom Cowan’s recent weekly webinars. His research (and that of many others) that shreds the heavy veil of lies about our human biology (and the biology of the animal world) is essential for us all to understand. The mind control involved in modern “medicine” is deeply entrenched.
Just as we as a species have been easy to control via politics, religions, and false narratives about our true nature and our history, “science” has been used in the same way. These deceptive narratives keep us trapped in a world of ever-spawning sub-narratives laced with fear. This latest whirlwind of information related to mRNA vaccines, spike protein, DNA contamination, shedding, etc. pushes us to get a better grip on what is really possible and ultimately what is true.
~ Kathleen
“You see, the tendency here, especially amongst the so-called freedom community, is they like to pick up on these studies to attempt to demonstrate or prove that these vaccines, so-called, are horrible, and they’re causing myocarditis, and they’re doing so through the mechanism of the creation of this so-called spike protein.
“I am not arguing against the fact that the injections are horrible, or that they give people myocarditis or otherwise heart problems. I’m talking about the mechanism. Because the mechanism is everything. It has to do with, eventually, how you think about this whole thing. What is actually happening. And even, eventually, how to treat it.
“Because I have no sympathy for the argument advanced by so many doctors. ‘Tom, what difference does it make whether there’s actually mRNA in the injections or whether there’s spike proteins or whether there’s a virus?’
“It makes all the difference in the world. Because if you can’t understand what’s happening or at least disprove that this particular thing is happening, you will will eventually be led astray.
“You will also eventually scare and frighten people more than you should. And there is no benefit from being ignorant about what happens and using anti-scientific thinking to make claims about what’s happening that are easily disproven.”
[…]
“So there is no such thing as a monoclonal or antibody specificity. So all these papers alleging that they found the spike protein, that the spike protein is a mechanism of damage, need to be tossed out as uncontrolled anti-scientific garbage.”
[…]
“So again, there is no actual clear scientific evidence that this process would result in pure mRNA of a specific type that could be put into these vials, that could produce a spike protein, and that could be the saving grace of the pharmaceutical industry with further mRNA vaccines.
“It’s simply the old culturing non-specific stuff that they’ve been doing all along with viruses and claiming they’re actually doing something a lot more sophisticated then they actually know how to do.”
So today I wanted to talk about the question again, which we’ve dealt with a little bit.
Is there spike proteins being made as a result of COVID shots?
But then taking it back even a step further. So this, we’re told, is a new mRNA technology that has been developed over many years. Robert Malone was one of the people who worked on the development of this technique, we’re told.
And I received an interesting series of short papers by a friend and colleague, Saeed Qureshi.
So many of you know him. I believe he’s a biochemist and works in pharmacy kind of things, who’s been very vocal about the non-existence of the virus, or at least the inability to prove that viruses actually exist.
And he sent me some papers where he goes through the argument of whether there is actually mRNA in the mRNA shots. Imagine that.
And I can imagine that most of you can imagine that because we’ve heard so many things that simply aren’t true.
When people say, ‘but there’s got to be something that is true’… And right now I’d be hard pressed to think of what in modern medicine and biology is, in fact, accurate. I’m sure there’s something. Like we have a head on top of our chest, sort of.
So we’re going to take a look at that. Before we look at that, we need some background, which is again, going over old hat.
Most of things, probably these days have a little bit of old hat in them. And that is, we have to really understand what this question of antibody specificity — and I’ll tell you a little more about what I mean by that.
But I also want to point out that probably the best paper that was written on this was written by our friend Mike Stone at Viroliegy called Antibody Specificity?
So if you’re really interested in this subject you should check out that paper on that website. So this is, again, me lifting things from other people. But as I always say, at least I acknowledge that.
So let’s get into the question first of antibody specificity. And before I do that, I have something I wanted to show you. So share the screen.
I don’t know this guy Daniel Dennett.
“There’s simply no polite way to tell people they’ve dedicated their lives to an illusion.”
So, I guess you can forget about worrying about that, because if there’s actually no way to do that and “be polite’ or maintain connection, then you don’t have to bother trying to think about what the best way would be, because there’s no way. So you might as well just say it the best way you know how.
So here’s some papers — some quotes from peer reviewed journals. The first three that I’ve probably shown before. (Can make this a little bigger.) This is about antibodies. Again, these were all lifted from peer reviewed journals.
[TCTL editor’s note: Here Tom Cowan shares some images of papers and reads from them.]
“The idea of poison and antidote led to the belief that the antidote would precisely combine with the poison and thus neutralize it. Even if death occurred when treated with the antidotes, which was often the case with mercury and arsenic, the justification was that it would prevent infecting others or that the person would have died more quickly without treatment.
“When Paul Ehrlich, who invented chemotherapy and the immune theory, slowly poisoned horses with toxic plant extracts so that they could survive otherwise lethal concentrations of the poison for a time, he found that there was an increase in protein in the blood. Since that time, these proteins have been referred to as an antidote and, in the modern version, as an anti-body.
“In reality, the body builds new vessels with these proteins, called globulins, seal all other cells and tissues with them, regulates blood clotting and thus wound healing. Paul Ehrlich’s misconception that these antidote proteins fit the toxins exactly like a key in a lock is the basis of all immune theories.”
So this paragraph essentially encapsulates the reason why I keep saying there’s no immune system.
This is the foundation of the immune theory — that we make proteins called antibodies, which are, in fact, globulins — which I would say are non-specific, unlike the specificity which is claimed. And I’ll get into more what I mean by that in a minute. So they’re not specific to anything in any virus or any protein.
They are non-specific proteins that regulate clotting and wound healing. So they cannot be used in any way to identify the protein. That’s what it means by specificity.
And since the time of Ehrlich, there have been probably thousands of papers going into the molecular details of how this specificity comes about. But the fact of the matter is, nobody has been able to prove specificity — meaning one antibody is specific, that binds and only binds to one specific antigen or protein or part of a protein or toxin. That’s what we mean by specific.
The antibody, if it was specific, could be used to identify the protein. If it’s not specific, it can’t be used to identify the protein. That should be obvious.
And so specific means it’s unique to that protein. Non-specific means it’s not unique to that protein.
If it’s specific, it can be used to identify the protein, since that’s the only possible thing it could be reacting to. If it’s non-specific, then it can’t possibly be used to identify the protein.
So next:
“In reality, these globulins, which are presented as antibodies and used in antibody tests, only come in a few size classes and different charge states. Only the size and the state of charge on the one hand and the composition of the liquids on the other hand in which the antibodies are supposed to react with the ‘bodies’ decide whether a reaction will occur or not. Even a slight change in fluid composition, temperature, or pH can cause antibodies to bind to all substances or none.”
And this is the case that the antibodies are not specific, and that they’re reacting to non-specific proteins. And the reaction is more based on the composition of the fluid, such as the temperature or the pH, or maybe the oxidation reduction potential, or maybe some other things, but they are not reacting to a specific antigen protein or toxin at all.
“This is the reason why all antibody tests, e.g. against pathogens, types of cancer etc. can be easily manipulated, are arbitrary and without any meaningfulness. Even the package inserts for these tests state that there is no (calibration) standard. Even if the disease-causing viruses existed, ‘antibody tests’ could not detect them.”
So, that is the basic argument that they’re manipulatable, they’re changed depending on the conditions of the fluid that they’re in.
They can’t possibly identify a protein or a virus or a toxin. They’re just, as they say, non-specific proteins that regulate blood clotting and wound healing. And so this is a very important fact as we go forward in this discussion.
Okay, next.
So I’m going to switch here to a slightly different.
Before I get into the spike protein and the mRNA —
This, unfortunately, title is called “Biden Quotes”. I don’t know if I’ve ever seen this. Apparently Biden said:
“I said I’d cure cancer. They looked at me like, ‘Why cancer’? Because no one thinks we can. That’s why. And we can. We ended cancer as we know it,” Biden said during a speech in the East Room of the White House.
Well, that’s good to know. So one less thing we all have to worry about, according to Joe Biden.
And then just highlight this and then I’m going to bring this up.
Okay. So this is a little bit of a switch of subjects. But I found this interesting and you’ll see how it relates to the topic. This was posted on something called US Mortality by someone who I don’t think I know. I may know them, named Ben. So I don’t really know who Ben is. I’ve seen some of his stuff just recently and it looks great. So I applaud Ben, whoever you are, you’re doing some great stuff. And, in particular, for thinking properly, because that’s what it all is based on.
So we all know that it certainly doesn’t reduce the death rate. That’s easy to show with just epidemiology. But here’s the question — because people, including myself before I really toned or honed my thinking process had questions about this. Because it seems like in previous times, 50-60 years ago, there was more of a disease called measles than there is now. And so, now that I know more about it, I know how difficult it is to make that diagnosis. And how difficult that kind of conclusion is to make on pure epidemiology or pure observation.
So it’s one of those things that — it seems like there’s less measles. But the question here is, has it been actually proven whether or not there’s more or less measles? That the MMR vaccine has been shown to reduce the number of measles cases?
So, again, the thinking process is: this is a claim. You don’t have to know anything else about the situation but the claim is the MMR vaccine has reduced the number of measles cases.
So that claim should be provable or disprovable by doing a proper study with a control — giving one group of people or children who haven’t had measles the MMR and another group of more or less identical children, not giving them the MMR, and then looking at the cases and seeing if you can detect a difference.
Anything else but that, any observation or any other epidemiological information can’t come up with that answer. This is the only way to do it. That should be obvious.
So we’re investigating the claim that the MMR vaccine reduced the cases of measles.
So here’s what the CDC says: that the MMR vaccine protects against measles, mumps and rubella. Two MMR vaccines are available — MMR II and PRIORIX, fully interchangeable. So you can use either one.
And then they go according to the Mayo Clinic — What is Measles? So they give you a bunch of of symptoms. And in particular I want to mention they tell you about Koplik’s spots, the white spots with the bluish white centers on a red background inside the lining of a cheek.
And as I said, this is the so-called pathonomonic feature of a case of measles, except 40% or so of children who are told they have measles don’t have Koplik’s spots. So that’s apparently non-Koplik’s spots measles, which is odd because that’s how you know it’s measles. So how can there be a non-Koplik’s spot measles? But anyways. So these are the symptoms of a child or a person with measles. Occurs in stages over two weeks.
So now that we know what measles looks like, let’s look at the package insert of the two products, he says.
So, these were the clinical trials that demonstrated that these vaccines reduce the case of measles. And as he points out this is the MMR II, quoting here they “demonstrate that the antibody response rates to measles, mumps, and rubella among children who received MMR II manufactured with rHA will be similar to the antibody response rates among children who receive MMR manufactured with” some other antigen and to demonstrate that MMR II will induce acceptable antibody response rates to measles, mumps, and rubella. And it’s well tolerated.
So in other words, the demonstration that the MMR II works to prevent cases of measles has no clinical indications as endpoints, no placebo was used. They only looked at antibodies under the claim that the antibodies tell you specifically that this child had or didn’t have measles. And as we now know that isn’t possible with an antibody test.
So this is an anti-scientific study, which can tell you nothing about whether the MMR II vaccine reduced the actual cases of clinical measles or not.
So let’s look at the other one, the PRIORIX. The second current vaccine was also compared to antibody responses, this time to the antibody responses of MMR II.
In other words, they inject a poison in you. They see that you have a non-specific repair mechanism activated by this injection of the poison. They claim that that means that you have an immunity against measles. And then the second vaccine, they compare it to the first one, which was fraudulently and anti-scientifically done. And then they compare the antibody response relative to MMR II, and they find that it’s basically similar. Therefore, they both protect you against measles.
When in reality that just means they both created approximately the same sort of tissue damage because they’re both poisons. And they, therefore, create the same amount of bodily response, non-specifically to heal the damage.
Now third one, MMR II (HSA), since 1978, they say that the efficacy of measles, mumps, rubella was established in a series of double-blind controlled trials, of which only these two references mentioned measles. So only this one study is — so that’s the only study that actually has anything to do with measles. And so here he has a link to the studies. And according to the study, the vaccines were compared for their clinical reaction and their antibody response.
He says he doesn’t have access to the full text, but according to the abstract the endpoints did not include the case rate of measles or deaths.
And here you can see the clinical reaction rate and antibody, were compared in children given three vaccines — so they’re compared these to the previous two. And they say they did it with the clinical reaction. So finally we get actually a trial that’s looking at whether the children got sick or not. But how did they do it?
So they did it with a clinical trial of 300 children that did not have measles. They split them into three groups. They use two measles vaccines and a placebo. And then they monitored them for three weeks.
So even though they did use a placebo, they gave them these two different measles vaccines. And then they monitor them for a total of three weeks to see whether that protected them against measles.
And what did they actually do? Did they actually look for all the clinical signs of measles? No, they simply did a rectal temperature every day, I guess, for those three weeks. And that was the only clinical sign that they measured. And if they had no more signs of a rectal increase in temperature that, apparently, meant they were protected for life against measles or three weeks.
So this is about as crazy as you can get. It goes back to an experiment in ’69 in Honduras where 300 children were monitored for three weeks. No efficacy for measles cases or deaths was established. All subsequent studies rely on this original study.
This is yet another example of these doctors thinking that somebody must have proved this. Somebody must have shown that the cases go down. When this is the only trial, apparently, that actually did anything clinical at all. And it was — all they did was measure the rectal temperature for three weeks, which has nothing to do with the alleged protection against measles or the reduction of cases or death or anything else that is claimed for this measles vaccine.
So you would have to say that there is no evidence that any MMR shot or any measles vaccine, reduced the cases of measles or the death rate for measles. Full stop.
And if you disagree with that, you’re going to have to send us a study that shows that that’s the case. And my guess is you will not be able to do that.
Okay. So now with that background, we can then go to the first question. Are we, as this paper claims… one of the most important papers on the molecular mechanism of the detection of recombinant spike protein in the blood of individuals vaccinated against SARS-CoV-2.
Here is the author [Carlo Brogna], apparently in Italy.
So, of course, we go down to the methods section and ask. So how did he detect this recombinant spike protein in the blood of individuals vaccinated against SARS-CoV-2?
And lo and behold, no surprise, probably. We go down to the experimental procedures… informed consent… 20 human samples were collected from vaccinated subjects with informed consent. The geometric mean of their antibodies′ titer versus spike protein was such and such after 60 days. In addition 20 human biological samples were collected from unvaccinated subjects wtih informed consent.
And so they were different. These ones who had not undergone COVID-19 and didn’t have the vaccine, and presumably had less tissue breakdown, were negative for these antibodies — which according to them, proves that the spike protein is created in the blood through vaccination, and is part of the illness they’re calling COVID-19.
So again, the whole thing rests on the fact that the only thing that they measured here were antibodies. They were claiming that the antibodies were specific for the spike protein. Therefore, if they find the spike protein in the blood of vaccinated or people who allegedly had COVID, that means that they had spike protein disease. Whereas the people who were healthy and then, presumably not breaking down their tissues, didn’t have to make non-specific antibodies. So the antibody tests were negative.
It has nothing to do with spike proteins or viruses at all.
So again, it doesn’t mean that I’m saying — we’re talking the mechanism here, not whether some people who allegedly had some non-specific illness called COVID-19 were sick. Maybe they were and maybe they were breaking down. And I’m not exonerating these injections.
For sure, if you inject somebody, as we’ll see with non-specific cell culture goop, you will make them sick. Their tissues will break down and they will have increased antibodies.
The question we’re dealing with here is not whether things can make people sick, or injections of poisons can make people sick. It’s whether the antibodies prove that this is a spike protein or a spike protein coming from a virus, and the spike protein is made by the alleged mRNA in the injection.
So, let me just go through, well, let me go to the next one here.
You see, the tendency here, especially amongst the so-called freedom community, is they like to pick up on these studies to attempt to demonstrate or prove that these vaccines, so-called, are horrible, and they’re causing myocarditis, and they’re doing so through the mechanism of the creation of this so-called spike protein.
I am not arguing against the fact that the injections are horrible, or that they give people myocarditis or otherwise heart problems. I’m talking about the mechanism because the mechanism is everything. It has to do with, eventually, how you think about this whole thing. What is actually happening. And even, eventually, how to treat it.
Because I have no sympathy for the argument advanced by so many doctors. ‘Tom, what difference does it make whether there’s actually mRNA in the injections or whether there’s spike proteins or whether there’s a virus.’
It makes all the difference in the world. Because if you can’t understand what’s happening or at least disprove that this particular thing is happening, you will will eventually be led astray.
You will also eventually scare and frighten people more than you should. And there is no benefit from being ignorant about what happens and using anti-scientific thinking to make claims about what’s happening that are easily disproven.
So when you say, okay, well, how did this paper that’s so crucial to our understanding that it’s the spike protein that’s causing myocarditis — how did they detect the spike protein?
And no surprise there. If you go to the method section, you see:
“We performed extensive antibody profiling…” and then there’s a whole other bunch of immune profiles, antibodies against the human-relevant virome. These are all downstream antibody testing, all of which are non-specific and can’t possibly tell you that there was a spike protein.
And here again you see this immunophenotyping, and it’s all about detecting antibodies against previous infection, SARS-Cov-2 spike protein specific T-cell responses and other antibodies.
They never actually assay for spike protein directly in the fluids. They sometimes look for pieces which they allege, through other antibody testing previously done, that those come from the spike protein.
It all basically boils down to: Are antibodies specific? And the answer, as I said, is clearly no.
So, this brings up another interesting question.
So somebody could say, ‘Okay, Cowan, how can you actually go about proving whether these antibodies are specific or not? Like what should we do?’
Just like we outlined with how they should go about proving there is a virus or not with our viral challenge, here I will outline how you would go about, if you wanted to do proper, reasonable, logical science, proving that antibodies are specific and not just non-specific reactions to tissue breakdown. So it would go something like this:
You would give a substance, preferably a toxic substance or a substance that causes damage, like a vaccine (so-called), or an injection, or some sort of cell culture goop or nanoparticles. And
then you would get breakdown of the tissue. If you don’t give any toxic substance, you won’t get any tissue breakdown, presumably, and then you won’t get any antibodies produced, and then you don’t have anything to study. So you give the substance, you get the tissue breakdown.
And then you inject the antibody or take a sample and mix it with the antibody that you believe — this is what you’re going to test — is specific for a certain protein.
They say that if this antibody binds, and therefore makes some sort of reaction, that’s proof of specificity. But what they should do is give the same person or animal a different substance that couldn’t possibly have a spike protein in it, but is also toxic to the tissues and causes a similar amount of tissue damage. Then you once you get the tissue damage, you take a sample or inject the antibodies, or mix it with antibodies in the sample, or inject the antibody into the person, and see if it binds the same antibody.
If it binds — and obviously the insult, the toxin, was different — that proves that the antibodies are not binding to a specific toxin, they’re binding to non-specific toxins and, in particular, they’re being produced in reaction to tissue damage.
So that’s the first of two controls that you would do.
The second is you would give this toxic substance — let’s say something you claim is a spike protein or an mRNA — you would see the tissue damage. And then you would inject it with the antibody that you claim is specific, see if it binds. and see if it lights up and you can detect it. And if it does, you claim that that binding proves that it’s protein specific.
But then, give the same substance (your so-called spike protein), you get the tissue breakdown, but this time you inject or mix it with a different antibody, not the antibody that you say is specific to the spike protein, but a totally different antibody. That of course shouldn’t bind. And if it does, it tells you that antibodies are binding non-specifically, and you cannot use it to prove the existence of that antigen or that protein in the first place.
Every single paper that does that, that uses antibodies to make this claim, should obviously include both of those steps. And yet, none of us can find a paper that ever includes both of those steps. Therefore, they’re all anti-scientific. They are not using appropriate controls and not following the scientific method.
And this is why one of the world’s leading authorities on antibodies, and particularly monoclonal antibodies (monoclonal means they’re specific to one antigen) and that’s Clifford Saper, Harvard Medical School Professor. And this is a quote from one of his papers.
“No, there is no such thing as a monoclonal antibody that, because it is monoclonal, recognizes only one protein or only one virus. It will bind to any protein having the same (or a very similar) sequence.”
So there is no such thing as a monoclonal or antibody specificity. So all these papers alleging that they found the spike protein, that the spike protein is a mechanism of damage, need to be tossed out as uncontrolled anti-scientific garbage.
If you want an analogy, I came up with one just before this that may help.
So let’s say you have a balloon and you cut the balloon with a knife or some object. And then you put duct tape on it to fix the balloon. And then you claim that because you were able to fix the balloon with duct tape this proves that the knife was the mechanism that cut the balloon.
That’s essentially what they’re doing. They’re saying essentially that the duct tape is somehow specific to the mechanism of injury, which is a knife.
So the first control experiment you would need to do is take the balloon and cut it with a scissors, and then use your duct tape and see if you could fix the balloon. Because if you could, this would demonstrate that your conclusion originally was wrong, that it is not specific to a knife, because it works just as well with a balloon cut with a scissors.
And then the next control experiment you would do is you would take the balloon and you would cut it with a knife. But this time you would try to fix the balloon with, say, elephant tape. I’m not sure what that is, but I’ve heard that that actually works sort of like duct tape. And if that works to fix the balloon, which it would, that would tell you that the type of tape, i.e. the antibody, is not specific to the mechanism of injury, that is to say a knife — that any similar tape would work.
So again, similarly, many antibodies will bind to that protein, or to that injured tissue, because the antibodies are not specific to the protein. They’re specific to the tissue injury.
So many different mechanisms of injury, and many different antibodies will work. And if you don’t believe me, send me a paper where they did both of those controls, and I and others will admit we’re wrong. Except that won’t happen, because none of the so-called scientists will be able to do that. Because, as far as we can see, it doesn’t exist.
And so, once again, we are putting out very specific guidelines to prove us wrong. And the people who are attempting to do that seemingly never are able to do that, because those papers don’t exist.
And then, finally, we get to the issue of Dr. Qureshi’s paper of ‘Is there actually mRNA in these injections?’.
So here’s the paper. You can see the reference here, and I don’t know exactly how to find it but I think if you put this in somehow you’ll be able to find it. And he talks about how they claim that there is mRNA in these injections. I mean that’s the whole point.
You put the mRNA for the spike protein, then that goes to the imaginary ribosomes and makes the spike proteins, and the spike proteins make non-specific antibodies to a protein that couldn’t possibly have been made — or at least has never been demonstrated to have been made — and pretty soon you realize you’re in La La Land.
So, here he goes through the steps. And I think basically, he talks about the fact that the mRNA… Let’s just read it and so we go there from a pharmaceutical perspective.
[TCTL editor’s note: Here, Tom skips through, reading parts of pages 2 to 4 from Saeed Qureshi’s paper and mixing with his own comments. To identify which words are Saeed’s and which are Tom’s, it might help to read the paper while listening. LINK]
“One must obtain the active ingredient, in this case mRNA”… either have to make it yourself or get it from a third party.
So he talks about this. There’s the active ingredient, which is the mRNA and then there’s all the other stuff that goes into the formulation.
So we’re not interested in the other stuff. We’re only interested in this so-called active ingredient, which is mRNA.
So during the product development, the active ingredient is monitored, tested, to see if it is in the body, is expected in the expected amounts, the efficacy and toxicity relate to the active ingredient levels.
Therefore, a vaccine developer would first need an appropriate mRNA or its source to purchase such an active ingredient… should commonly be available from an independent third party supplier with appropriate certification for identification and purity.
However, the COVID-19 mRNA is proprietary. No information about its nature and purity is available in the public domain. So obviously that makes it difficult to know whether that’s in there.
Therefore, as he says, appropriately, one must rely on general information regarding what is present in the vials, and how they may have been synthesized manufactured and purified.
So now we’re getting to the crux of the matter.
In this regard a fermentation process using culturing microbes, such as bacteria is claimed to produce mRNA, which is then extracted, isolated, from the manufacturing perspective. The following diagram shows the steps. [see the bottom of page 2 for diagram]
You can see that steps — hard to see here. Culture has developed, some chemical reactions are performed. This stops the culturing fermentation, followed by purification. The last step is marked as formulation.
This production process of mRNA is simple, yet very confusing, which may be why people do not correctly understand the manufacturing of the vaccine and its adverse effect.
As explained above, the active ingredient is mRNA.
And this is the key of all this.
But no step describes mRNA production. We go through this in detail.
There is no step proving that this bacteria in this fermentation mat are making a specific mRNA.
The last step in the diagram is formulation or vaccine. Therefore this is vaccine production, not mRNA per se.
He says they use the words mRNA and vaccine interchangeably which is incorrect. Calling the end stages formulation indicates that the mRNA has never been produced, but is assumed to be there. So there is no step in here that proves, or demonstrates the specific production of mRNA.
It’s only assumed to be there.
The last step in the manufacturing should be a pure and isolated mRNA compound. However, it is an “isolate”, culture or gunk, possibly selectively concentrated compared to the one in the productive chamber.
In other words, all they have is the breakdown of the culture or gunk, culture gunk, not specifically isolated purified mRNA, which then they could use as the active ingredient to put into the vials.
And he says they don’t appreciate the difference between culture isolate gunk and pure isolated component which is a critical misunderstanding as the relevant science, the same as the virus issue.
So mRNA has not been produced, but a culture isolate, gunk, is considered and sold as mRNA or vaccine.
And this is another crucial point he makes.
It may be argued that the manufacturing processes or steps shown in the figure above have multiple filtration separation or isolation steps, like gradient ultra centrifugation for virus isolation, ensuring the production of pure mRNA.
And this is the part that I can’t verify myself. But I know Saeed, and I think this is a worthy place to start.
“Considering my extensive expertise and experience 40 plus years in separation science, including exhaustive training and experience in chromatography, I can confidently say that the steps described here would not be able to produce the claimed pure and isolated mRNA until shown otherwise.”
“Another critical point is that it is impossible to monitor mRNA production because no test may be developed without the availability of the pure and isolated reference (mRNA) standard. Therefore, it is safe to conclude that mRNA production is based on assumption, not scientific or valid testing.”
In other words, if they can’t come up with the pure isolated mRNA, there’s no way to validate this procedure. And therefore, there’s no way to claim that this procedure made the mRNA that they’re saying is in there. Therefore, there’s no way to even know that the mRNA is in there.
So what’s in there?
He suspects that the presence of DNA contamination, which is becoming an issue now — they know that the DNA is contaminated — is simply because they’re using culture gunk or chip particles of bacteria, which obviously have their own contaminating DNA. And this contamination would explain the widespread adverse reactions after the injection of these vials.
So we don’t need to propose a mechanism of mRNA or spike protein. Simply injecting bacterial culture junk with all the stuff that’s in there that is not properly purified.
And there’s no way to assess the validity of the claim, because they don’t have a pure mRNA to begin with, makes the whole burden of proof on the manufacturers to prove that there is the mRNA that they say there is in there.
And my guess is that is, again, a challenge that they will never undertake due to claims of proprietary, or this or that, or we don’t want to sell our secrets, or people would do nasty things with it as if (as if they’re not doing enough nasty things with what they’re doing already).
So again, there is no actual clear scientific evidence that this process would result in pure mRNA of a specific type that could be put into these vials, that could produce a spike protein, and that could be the saving grace of the pharmaceutical industry with further mRNA vaccines.
It’s simply the old culturing non-specific stuff that they’ve been doing all along with viruses and claiming they’re actually doing something a lot more sophisticated then they actually know how to do.
So I hope that clarifies things and alleviates people’s worries that they’re being genetically reprogrammed or that there’s some specific genetic modification going on.
I mean, again, it’s not to say that the injections aren’t bad enough. And I’m not exonerating the injections or saying they’re not causing the damage that they do. Far from it.
It’s just not the mechanism that we’ve been told. And anybody who claims that’s the mechanism, the burden of proof is on them to:
Show the pure isolated mRNA that comes from this process.
Show us that mRNA is the same in all the vaccines.
Show us by direct assay that the spike proteins are made as a result of these injections.
Show that the spike protein injections create something called immunity to something called the virus.
And none of those four steps are possible, because the whole thing is a bunch of hooey.
The parents of 62-day-old Sawyer learned their baby’s blood contained 95 micrograms per liter of aluminum, a level that would be toxic for adults. The toxicologist who read Sawyer’s report said the aluminum and antigen levels in the blood were due to the vaccines.
A Maine couple last week finally got the answers they’d been seeking for nearly a year, ever since their 62-day-old son, Sawyer, died Oct. 28, 2022 — 34 hours after receiving his scheduled childhood vaccines.
According to a toxicology report, Sawyer’s blood contained 95 micrograms per liter of aluminum, a level that would be toxic for adults.
A toxicologist told the couple the aluminum and antigen levels in the blood were due to the vaccines. She also said a viral infection Sawyer was being treated for could have been a contributing factor.
Sawyer’s parents, Melissa — a registered nurse — and her fiancé Nick shared their story last week with journalist Jennifer Margulis.
In an interview this week with The Defender, the couple detailed their search for truth, beginning with how Maine’s medical examiner refused repeated requests to perform lab tests that might have shown the culpability of the vaccines — and instead initially ruled Sawyer’s death “asphyxiation due to inappropriate sleep position and environment.”
The story of baby Sawyer
On Oct. 20, 2022, Melissa took Sawyer to a doctor for a persistent rash around his torso. The doctor diagnosed a viral infection, gave Melissa some medicinal cream and told her to monitor Sawyer’s temperature for possible fever.
Exactly one week later, Melissa went to the same pediatrician for a baby wellness checkup, where the doctor insisted Sawyer, despite Melissa’s reservations and the baby still having a rash, receive the scheduled childhood vaccines.
These included: RotaTeq (for rotavirus), Hib (for Haemophilus influenzae b), Prevnar 13 (for 13 types of pneumococcal bacteria) and Pediarix (for diphtheria, tetanus, pertussis, hepatitis B and polio).
Dr. Lawrence Palevsky, a pediatrician, told The Defender, “I don’t know of any official warnings against vaccinating sick children,” but “there are no upsides to vaccinating a sick child. There are only downsides.” He added, “And, there are no upsides to vaccinating any child.”
Melissa told The Defender that, despite her medical training, she became skeptical of vaccines just two days prior when she watched a video of a toxicologist talking about the dangers of vaccines for children. She discussed the upcoming vaccinations with her fiancé, and they decided to go ahead with them.
“We were afraid that the medical system was going to judge him and judge us and not let him into school,” Nick said. “We just hadn’t done any research on it.”
Nick has two daughters from a previous marriage, ages 11 and 19, who received all of their childhood vaccines “and nothing ever happened,” he said.
After the doctor’s visit, Sawyer arrived home screaming and Melissa gave him the baby Tylenol recommended by the doctor.
By the next day, the baby had calmed somewhat but was still acting “fussy and uncomfortable,” so Melissa gave him more Tylenol and some expressed breastmilk.
When Nick got home from work that day, they put Sawyer into his bassinet for a nap around 5:30. By 6:15 the baby was fussing, and with some help was able to get back to sleep. He slept off and on for another four hours, while his parents kept tabs on him via his baby monitor and visits to his room.
The last time Melissa checked on Sawyer, he wasn’t moving or breathing. She picked up his limp and lifeless body and started screaming. Nick rushed in to help but it was already too late.
Emergency medical technicians arrived after the couple called 911. They tried but were unable to revive Sawyer.
The county and state police also responded and, because it was an infant death, opened a formal investigation and ordered an autopsy.
Chief Medical Examiner Mark Flomenbaum performed the autopsy the next day. Although he found Sawyer to be “well developed” and without signs of injury or bruising, Flomenbaum filed a death certificate citing asphyxiation due to a “sub-optimal sleeping environment” — essentially blaming the parents.
“It was near Christmas when we got the autopsy results,” Melissa told The Defender. “We read them on Christmas Eve. … We did nothing for the entire weekend.”
Asked if they ever learned what the medical examiner saw to make his determination, they said no. “The only thing in his basket was the blanket he was laying on.”
The police looked for evidence of child abuse or alcoholism, but quickly concluded it was an accidental death.
Melissa, grief-stricken, told everyone she could to investigate the possible role of vaccines in Sawyer’s death.
She first called the medical examiner to see if he would do testing to determine if sudden infant death syndrome (SIDS) was responsible, but was told there was no need “because it wouldn’t show the cause of his passing,” she recalled being told.
The hunt for answers
That’s when the couple’s hunt for answers began. “I was looking up people on the internet, on social media. I was calling any number I could find,” Melisssa said.
Finally, she discovered a suite of pathology tests that could determine whether vaccines played a role in Sawyer’s death.
The tests measure C-reactive protein (indicating brain inflammation), liver enzymes, aluminum and mercury in brain and blood tissue, formaldehyde and formalin (another name for formaldehyde). A cytokine panel would also identify various blood factors and vaccine titer levels.
Melissa mailed and emailed Flomenbaum’s office to formally request the full battery of tests. The doctor refused, dismissing her concerns and telling her that heavy metals do not cause SIDS.
“They gave me a reason why each test didn’t need to be done,” she said.
Further emails to the state medical examiner’s office, from both parents, have been bouncing back as “undeliverable” since.
A friend of Melissa’s told her about Health Choice Maine, a statewide nonprofit working to protect health freedom and parental rights. There she met Tiffany Kreck, Health Choice Maine’s executive director, who helped Melissa organize her own investigation.
“Families being bullied by a doctor or threatened with CPS [child protective services] or whatever, can reach out, and we will, to the best of our ability, help them navigate it,” Kreck told The Defender.
Melissa said Tiffany gave her a list of things they had to do, “like getting reports and billing information, people to contact, and that’s what I did.”
Their primary goal was to find a competent pathologist to perform the lab tests Melissa had requested. They searched the entire country — even enlisting the help of Laura Bono, vice president of Children’s Health Defense, Kreck told The Defender — but came up empty.
Kreck told Melissa they would not be mentioning anything about vaccines to the prospective pathologists, so they would be less likely to reject the request.
The biggest obstacle was finding a doctor who was willing to order the tests.
Her ob-gyn told her that it was “out of his scope of practice.”
She called her primary care physician and told him she thought the vaccines had played a role in her son’s death “and he denied it,” she said. Her pediatrician also said no.
The toxicology report and next steps
Finally, they found someone in-state who, responding to Melissa’s grief, agreed to perform the tests on June 21. Although some of Sawyer’s tissue samples had degraded, the pathologist was able to perform enough tests to issue a definitive report last month.
The report was technical and was not accompanied by any guidance or recommendations.
Melissa said, “They never called me and said, ‘Oh, listen, this is high. This could be due to his vaccines. We will do a VAERS [Vaccine Adverse Event Reporting System] report, you know, and advocate for other infants that pass away.’ No, we didn’t get anything from them.”
So they had to hire a private toxicologist who could interpret the report. That second report arrived last week.
“And she was the one that called us the other day and told us that his aluminum levels were very high,” Melissa said, “and that we needed to seek some legal services.”
The report showed baby Sawyer had 95 micrograms of aluminum per liter of blood, a level that would be toxic for adults. The toxicologist told the couple the aluminum and antigen levels in the blood were due to the vaccines. She also said the baby’s illness could have been a contributing factor.
Kreck told Margulis, “This additional pathology report shows how much are medical examiners don’t know because they won’t look.”
The report also showed high levels of lead, which would not be due to vaccines, the toxicologist said, and asked about lead levels in their house or water. But given that the baby had only consumed breastmilk and was not yet old enough to crawl around on the floor, the question remains open.
After receiving the confirmation about the aluminum, the couple felt “exonerated” from the implication they were responsible for Sawyer dying from asphyxiation, “but we also still feel like we failed our baby,” Melissa told The Defender.
“Me being a nurse,” she said, “I felt like I failed him both as a nurse and a mother.”
Nick added, “From the father’s standpoint, you’re supposed to protect your family, and I failed at that. It weighs on me every second of the day.”
Melissa and Nick are planning to file a claim with the National Vaccine Injury Compensation Program (VICP). She said she still feels skeptical “because I know how the government and the medical system are.”
Kreck is helping the couple prepare for the VICP meeting. “We are doing every test that we can possibly do and trying to cross all of our t’s and dot all of our i’s before we go into the VICP,” Kreck said, “which is historically difficult and harsh on what they perceive to be SIDS cases.”
A couple told The Defender they got help reporting the case to VAERS last November, but have never received any follow-up. They did, however, confirm that Sawyer’s case was in the database.
Health Choice Maine is also exploring options for a lawsuit challenging the finding on the state medical examiner’s death certificate.
Dealing with the grief
Just three months after the ordeal, a therapist told Melissa, who was still grieving for her child and searching for answers, that she had an “adjustment disorder.”
“She was pretty much telling me that I was not adjusting to losing my son quick enough, and recommended trauma therapy,” Melissa said.
She left the office crying, wondering if something was wrong with her or not being able to let go of her grief. “I haven’t had good luck with therapists,” she told The Defender.
“I’ve been going through this all on my own, trying to go through reports and all the information about my baby’s life and his medical records. And I’m doing all this while trying to grieve the loss of him and it is horrifically painful,” she said. “It’s something no parent should ever have to go through.”
One therapist told Melissa to take mood stabilizers and anti-depressants. “The mental health care system has not been very helpful in this at all,” Nicked added.
Nick found that going back to work and keeping busy was the most therapeutic approach for him. “Just keeping my mind focused on other stuff, you know, while carrying all that around,” he said.
Nick has joined Melissa in several of her therapy sessions, which he found very helpful.
The couple found a grief support group called Empty Arms for parents who have lost a child, which has been “amazing,” Melissa said. The group does a butterfly release for the deceased on Memorial Day and an annual remembrance walk.
They have found support from family members as well, although Melissa said it has been hard to talk to her family about the vaccine connection.
The couple said the loss has brought them closer together. “I couldn’t keep going, fighting the fight we’re fighting right now, without her,” Nick said. “And you don’t realize how much you love someone and just how precious life is and what you have in front of you is.”
“Cherish it and love it, don’t let it go,” he said.
“We lost the biggest and best part of us both and if we didn’t stay together, I’d feel like I was losing another piece,” Melissa said.
The couple’s journey to warn others
“I just want to make other people aware and I want to put a stop to this,” Melissa said.
Melissa said she warns mothers of sick children to cancel their appointments for vaccines at least until the child has recovered. She added:
“Children do not need vaccines. And if they were to get them, they don’t need them until they’re at least two years old. The problem is, is they have a blood-brain barrier that has not closed up until they’re two years old or later.
“And if you get vaccinated before two years old, the aluminum can cross that blood-brain barrier. That’s why levels are so high and it stops respiration and causes cardiac arrest.”
Nick said, “I wouldn’t tell anybody ‘Don’t vaccinate your children.’ But I would definitely say ‘Do your research. Go to the end of the internet, make sure what you’re doing is right, that you know all the possible outcomes.’”
“Be more educated and be a strong advocate for your baby,” he added. “Because it’s your baby, not the doctor’s.”
Asked why more medical professionals don’t speak out, Melissa simply said “Career suicide.”
“I don’t even wanna be a nurse anymore,” she said. “Why would I want to be? But I have to pay my bills.”
“Doctors don’t have any better education on vaccines than most 10th graders,” she said. “Even as a nurse, we don’t get the education. We just got the schedule.”
She also said that medical examiners should have the right to test for vaccine injuries during the autopsy and identify them as a cause on the death certificate. “The vaccines are killing people and babies and they’re trying to cover it up,” she said.
While the couple said they found it helpful to share their story, they also admitted to wanting to keep a low profile. “It’s kind of a quiet subject for us because we’ve got to protect ourselves now,” Melissa said.
The couple is looking for a good support system. “We’re looking for people to stand behind us and support us as we go through this journey, for the next questionable amount of years, to get justice for our baby. It might drag on for a while,” Melissa said.
When asked about what gives them the strength to stand up and share their story, despite the backlash that such activism could invite, Melissa said:
“This is the only way that I feel like I can mother my baby anymore. And my baby deserves justice. And we deserve to know the truth.
“He is our reason for living right now. And he is our motivation.”
Questions about the state medical examiner
Kreck told The Defender that state medical examiner Flomenbaum came from Massachusetts where he had been fired as the state medical examiner. “It looks like he tried to sue them for wrongful termination and lost,” Kreck said.
Flomenbaum earned a national reputation as a top medical examiner through his work identifying bodies in New York City after the 9/11 attack in 2001, according to an article in the Portland Press Herald.
He was fired from his Massachusetts position for losing a body and having a backlog of bodies waiting to be examined.
In 2019, the Maine attorney general’s office investigated and later cleared Flomenbaum over criticism that he was running a side business as a consultant in out-of-state death cases.
The Press Herald article details more of Flomenbaum’s controversial history, which included a Connecticut prosecutor’s letter to then-Attorney General Jane Mills telling her that a judge had determined his testimony in a child manslaughter case was “not credible.”
Flomenbaum was reprimanded in 2021 by Maine Governor Mills for inappropriate and unprofessional behavior in the workplace, after which he announced he would not be seeking reassignment to the position.
“He was only supposed to have a month or so left of his term back then and he’s still in office now. That all sounds very odd and fishy,” Kreck said.
Melissa told The Defender that Flomenbaum had recently left the medical examiner’s office, putting the disposition of Sawyer’s remains in question.
The couple, with the aid of Health Choice Maine, is seeking to remove Sawyer’s blood and tissue samples from the medical examiner’s office.
Anyone with information about where a new location might be found to accommodate Sawyer’s remains is encouraged to email Tiffany Kreck at tiffany@healthchoicemaine.org.
About Dr. Sam Bailey: After training and practicing within the medical system for two decades, she commenced a new phase of understanding and promoting health as a wider concept.
In 2019, Sam launched her YouTube channel exposing the hidden scientific truths about health.
A few years later and after taking the red pill, Bailey’s channel has become a runaway hit with 20+ million views and 300,000+ subscribers to help people understand the simple ways they can take control of their health.
She is the co-author of Virus Mania, which examines how the medical industry continually invents epidemics to make billion-dollar profits at our expense.
About Dr. Mark Bailey: Mark is the husband of Dr Sam Bailey and when you see one of them, you are really seeing both of them. They started working together when they first met in 2007 and have been a close team ever since. Mark and Sam are based in New Zealand and have three children together.
Since early 2020 he has been the duo’s chief researcher with a focus on microbiology, the existence of viruses, as well as historical and epistemological issues within medical science.
Is There Anything Floating in the Air – Trying to Infect Us?
“CONCOCTED science is the modern version of spiritual revelation. The Roman Church—while it was carrying out witch hunts and inquisitions replete with confessions obtained through torture and capped off with death by burning at the stake—was claiming Jesus Himself had passed the keys of the Kingdom to the Church…and He tacitly approved its policies.
“These days, debilitating, brain damaging, and life-destroying vaccines are the scientific revelations the Church of Federal Medicine stands for.
I continue to write about this subject because it’s vital.
NIH, the US National Institutes of Health, is the largest medical research facility in the world. It has 18,000 employees and runs on an annual budget of $45 billion.
I once suggested to Jim Warner, a White House policy analyst under Ronald Reagan, that somebody should do an audit of NIH and determine exactly what medical advancements the agency had actually made during its long history. He thought that was a terrific idea. But nothing came of it.
I assure you, an audit would reveal much less than meets the eye. Much less in the way of useful discoveries and technology. Along with mountains of useless and fraudulent science.
BUT NIH stands as a center of knowledge and a symbol, a reference point, a proof positive that medical science is marching forward.
It’s a very expensive public relations tool.
How could we not accept and signal our obedience to medicine, when we have such an awesome modern cathedral for its research?
Ditto for the CDC and the FDA. Both infernally corrupt agencies.
CONCOCTED science is the modern version of spiritual revelation. The Roman Church—while it was carrying out witch hunts and inquisitions replete with confessions obtained through torture and capped off with death by burning at the stake—was claiming Jesus Himself had passed the keys of the Kingdom to the Church…and He tacitly approved its policies.
These days, debilitating, brain damaging, and life-destroying vaccines are the scientific revelations the Church of Federal Medicine stands for.
Concocted science.
People accept science as fact, based on the IMPRESSION that actual knowledge is being discovered.
PR people make sure this impression is delivered.
Just as the Roman Church never confesses to fraud in its doctrine, the centers of modern medical knowledge never confess fraud.
In this episode of ICIC, Dr Reiner Fuellmich talks to Dr Gerd Reuther, medical doctor and radiologist, about the historical background of medicine and the genesis of diseases and epidemics over the centuries, from the pre-Christian era to the present day.
He points out numerous connections and parallels to so-called pandemics of antiquity and current events, i.e. the “Corona pandemic”. The criers of these “pandemics” have always used the same methods earlier and to this day: the creation of fear and panic.
It sheds light on the role of the Church and its representatives and how far their powerful arm has reached in science, research as well as medicine at all times. These areas were entirely under the control of the Church, and even today these exercises of power continue.
One could call this behaviour opportunistic, since throughout history the Church has always turned to those who were in power. It is currently showing this pattern again, namely when it unhesitatingly fired up the Covid vaccination propaganda. Compared to then, not much has changed:
It was and is about trivial monetary claims to power and ownership, manipulating people for their own benefit, keeping them in dependencies, e.g. on the pharmaceutical industry, and exerting control over life itself.
Historical events such as outbreaks of plague and cholera are analysed and examined for their truthfulness. The history of the origin of “vaccination” and what the belief in its effectiveness is based on are also discussed in detail.
Since when have disease patterns and symptoms been defined and documented, and why were there no “civilisation diseases” in the past? How can it be that not all people fall ill with one and the same “pathogen” and what role do the improper handling of toxins and the natural immune system play?
Dr Gerd Reuther and his wife Dr phil. Renate Reuther, historian and English specialist, have summarised all these medical-historical findings and events compactly on 150 pages in a book entitled “Hauptsache Panik” (Panic is the main thing), which, despite its historical focus, is more up-to-date than ever. For only those who know the past can shape the present and change the future.
via ANTIJANTEPODDEN: Investigative journalist James Corbett has investigated how psychology is being weaponized to target dissidents.
In this episode he explains the absurdity of the old diagnoses of anarchia, which was too much love for freedom, and drapetomania, which was the mental illness of slaves running away from their masters.
Over the last three years, we have seen a medical doctor being diagnosed and force medicated for corona insanity. This was because of his resistance to the government narrative in Switzerland. We have also seen an increased willingness to pathologize conspiracy theorists, and to label people as domestic terrorists for using their right to share their opinions.
Even though the methods used against us are ugly, and the majority just go along uncritically, James Corbett shows examples of how modeling disobedience can dramatically turn the situation around.
The Bravo channel’s TV show I Am Jazz followed the adventures of Jazz Jennings, a spunky little boy who wanted to be a girl. The GLAAD crowd got a front man (well, boy) to push its trans movement upon boys and girls. Barbara Walters got an exclusive interview with him for Disney’s ABC. Bravo made money. He got attention. Everybody was happy.
His story was the LGBTQ version of Pinocchio but without a Jiminy Cricket to steer him clear of those who would exploit him — such as Barbara Walters and the producers of the I Am Jazz TV show. On June 20, 2018, doctors sliced and diced the 17-year-old in transsexual surgery — which is now called gender-affirming health care because everyone is too ashamed to call it a sex change.
The TV show went on a hiatus because Jazz was not too pleased with the result. He gained 100 pounds. He should have been more careful of what he wished for because he did not become a glamorous girl but a fat chick whose emotional problems grew worse.
When the show resumed, he returned to a public spotlight he had first entered at 7; Jazz now was fat and unhappy. The TV show recorded his first post-op date with a man. It was awkward and awful. Much like Kim Kardashian’s cosmetic doctoring, Jazz could change how he looked but not who he really is — a boy who never grew to be a man.
He has a trump card. He can sue. He was a minor when doctors began feeding him pills and under age when they performed this ultimate cosmetic surgery in him.
While he denies having regrets, Jazz’s behavior shows he is having second thoughts. I am pretty sure GLAAD and Bravo are sweating this one out. The stakes are so high that people are getting nosebleeds as they try to keep him away from personal injury lawyers.
My hope is that every ambulance chaser in the nation enters the detransitioning lawsuit business because it will be bigger than that Camp Lejeune water case they are advertising for plaintiffs. If suspected carcinogens — not proven, but suspected — can yield millions in legal fees, just think of the billions that could be there for the raking for a medication known to be toxic. The money is there. For example, Boston Children’s Hospital has an endowment of $7 billion.
That hospital’s Center for Gender Surgery said, “As the first pediatric center in the country dedicated to the surgical care of transgender patients, we take an interdisciplinary approach from the start to ensure exceptional patient care.”
But the children’s hospital also claims not to perform sex-change surgery on minors.
However, it is not just the surgery that is the problem. It is the pills. Puberty blockers expand the targets of litigation to include not just doctors and hospitals, but drug companies as well. It also expands the universe of plaintiffs.
The American College of Pediatricians warns, “There is not a single long-term study to demonstrate the safety or efficacy of puberty blockers, cross-sex hormones and surgeries for transgender-believing youth. This means that youth transition is experimental, and therefore, parents cannot provide informed consent, nor can minors provide assent for these interventions. Moreover, the best long-term evidence we have among adults shows that medical intervention fails to reduce suicide.
“Puberty blockers may actually cause depression and other emotional disturbances related to suicide. In fact, the package insert for Lupron, the number one prescribed puberty blocker in America, lists ‘emotional instability’ as a side effect and warns prescribers to ‘Monitor for development or worsening of psychiatric symptoms during treatment.’
“Similarly, discussing an experimental trial of puberty blockers in the U.K., Oxford University Professor Michael Biggs wrote, ‘There was no statistically significant difference in psychosocial functioning between the group given blockers and the group given only psychological support. In addition, there is unpublished evidence that after a year on [puberty blockers] children reported greater self-harm, and the girls also experienced more behavioral and emotional problems and expressed greater dissatisfaction with their body—so puberty blockers exacerbated gender dysphoria.’
“Puberty blockers may cause permanent physical harm.
“Temporary use of Lupron has also been associated with and may be the cause of many serious permanent side effects including osteoporosis, mood disorders, seizures, cognitive impairment and, when combined with cross-sex hormones, sterility.”
Right now, there is big money in transing kids. Obama approved having Medicaid and Medicare pay for transsexual operations and the like. He also forced insurers to cover transing, and the transing industry took off — and best of all for these ghouls is the poisonous side effects make the transed kids customers for life.
Fox reported, “A young male, who formerly identified as a trans woman, who was castrated and became a patient for life as part of gender-affirming care, wants to warn others not to follow in his footsteps. He discussed his story of resilience and learning to accept himself for who he is, for the first time, with Fox News Digital.”
He appears in a video.
The story said, “Kobe, whose name is being withheld for privacy reasons, had ‘checked every box for what they call a trans adolescent.’ He was always effeminate and loved pink and playing with Barbies. If he had never been exposed to gender ideology, he says he probably ‘would have just stayed a feminine boy. And there’s nothing wrong with that.’”
He said, “I felt unlovable as an effeminate man in society and everything. A feminine boy, actually. I was never a man, I’m trying to reclaim my manhood now and everything. It’s hard. I have breasts, I have the hip development of a woman, because I started the estrogen young. I have no gonads. You know, it’s hard. My skull never really masculinized.”
We won’t let kids smoke at 10, why do we allow them to take experimental drugs that will cause such damage?
Litigation will stop this quicker than the politicians will. Heck, the pols are still arguing over which bathroom drag queens use.
In February, Fox reported, “A prominent detransitioner sued a nationwide medical group and its doctors Thursday who she said ‘decided to perform a mutilating, mimicry sex change experiment’ on her, according to the lawsuit.
“The Center for American Liberty sued Kaiser Hospitals on behalf of detransitioner Chloe Cole ‘for pushing her into medical mutilation instead of properly treating her,’ according to Cole’s lawyer Harmeet K. Dhillon. Between the ages 13–17 years, Cole underwent a transgender transition, including the off-label use of puberty blockers, cross-sex hormones and a double mastectomy.”
Dhillon tweeted, “What Kaiser did, for profit, to Chloe in the name of woke ideology instead of sound medical practice, should not happen to any child in America!”
Win the case and it won’t.
The left knows these lawsuits are a bigger threat to LGBT than Ron DeSantis. In May, NYT tried to play down the kids who want their old bodies back — which will never happen. NYT objected to using detransitioners to push bans on transsexual operations for kids.
NYT said, “As more American teenagers have identified as transgender, it is difficult to say how many will transition medically — many transgender people do not — and precisely how many will later change course. Methodology, demographics and even the definition of detransition vary widely from study to study, which typically show that between 2% and 13% of people detransition, and not always because of regret.”
Only 2% to 13%?
We shut down the world’s economy because of a virus that killed less than 1% of those infected.
The story said, “Elisa Rae Shupe was well known in the transgender rights movement: first as an outspoken transgender woman, and then as the first American to change her legal sex to nonbinary.
“So when she published an essay in 2019 saying that her transition ‘was all a sham’ and that she wanted ‘to live again as the man that I am,’ conservatives took immediate notice.”
And lefties dropped her like a hot brick.
But the radioactive brick is litigation, not legislation.
The Economist reported in March, “Legal action may change transgender care in America. Some detransitioners are starting to take their doctors to court.”
The story said, “Most Americans favour protecting trans people from discrimination, but they sharply disagree on medically transitioning children. Whereas 72% of Republicans believe it should be illegal to provide a minor with medical care for gender transition, just 26% of Democrats agree, according to the Pew Research Centre, a think-tank. Activists who believe such care saves lives have tried to discredit Ms Cole, by focusing on the support she receives from firebrands on the right. But the facts of this case—if they are as claimed—could give at least some of them pause for thought.”
A Jazz Jennings lawsuit would stop hospitals from preying on kids.
“Covid” Vaccines Were Deployed by the US Department of Defense as “Countermeasure Prototypes” With No Safety Testing Required, Using the General Public as Guinea Pigs
“As if that news were not troubling enough, Katherine and Sasha learned that anyone who examines the contents of the vaccines vials can be legally punished for doing so. Pharmacists and doctors warned that the vials are property of the US government, so having the vials tested would expose them to criminal charges.”
I found Sasha Latypova through a colleague in Europe. The day I met Sasha at her villa in California, the skies were overcast, which correlated with the subject matter of the interview. Now retired, Sasha had had a very successful career as an independent contractor designing clinical trials for the largest pharmaceutical companies in the world.
During our interview, I was stunned by some of the conclusions Sasha had reached regarding which government agencies actually authorized the vaccines. Through the COVID crisis, Sasha teamed up with a paralegal in Pennsylvania named Katherine Watt who conducted very thorough research that unearthed the legal framework through which the vaccines were approved and deployed. You can find her work here.
Katherine Watt discovered that the covid vaccines were authorized not by the FDA but by the US Department of Defense as countermeasure prototype demonstrations. This revelation ties in with a prior BIG PICTURE interview with Brook Jackson, who managed a piece of the Pfizer clinical trials for a Pfizer contractor, found fraud, and was fired for bringing the irregularities to the attention of her superiors. When Brook later sued the government for purchasing vaccines that were not properly FDA approved, the government’s response was that they were not FDA approved but approved instead by the DOD.
Coincidentally, Katherine Watt uncovered the existence of a joint Health and Human Services and Department of Defense program to combat bioterrorism or natural outbreaks through the rapid deployment of “countermeasure prototype demonstrations.” This is a shockingly broad term that basically means “anything whipped up by the military that they think may be of use.” In other words, they are rapidly whipped-up secret recipe military vaccines that require no approval other than the say so of the HHS secretary and his belief they may be of benefit. No testing needed, no clinical trials required.
The general public is now the unwitting guinea pig. This means all the COVID vaccines everyone has been receiving were actually produced by the military under a martial law legal structure and the public is being unwittingly injected with not just experimental vaccines, but with military prototypes that were never intended to receive any FDA approval.
This strange scenario explains why the regulators (FDA) behaved so strangely and why no one was ever punished for the rushed and fraudulently conducted clinical trials.
Operation Warp Speed was a military operation complete with sophisticated propaganda strategies. These psychological propaganda programs targeted films like my Planet Lockdown film. The public was encouraged to take the vaccines by psychological warfare units of the military. Yet it is illegal under the 1878 Posse Comitatus Act for the military to operate on US soil.
As if that news were not troubling enough, Katherine and Sasha learned that anyone who examines the contents of the vaccines vials can be legally punished for doing so. Pharmacists and doctors warned that the vials are property of the US government, so having the vials tested would expose them to criminal charges.
I must ask: If these are simply experimental vaccinations for a novel flu, why on god’s green earth are all these unusual measures needed? This is quite suspicious, and, in my experience, suspicious people tend to act suspiciously . . . and are up to something they don’t want you to know . . .
Please join me and learn just how Sasha discovered what she did, the logic she followed, and where it led her. I think you will understand why the truth disturbed her enough to come forward and share it with the world. She is committed to getting this information so that we cannot be fooled the next time a “pandemic” is announced.
Video available at PlanetLockdown Odysee & Rumble channels.
“The truth is, no one can get to health through vaccinations. If a person is sickly, vaccines won’t help. If he’s healthy, he doesn’t need vaccines.
“The bad news is, vaccines destroy. Whether it’s the so-called adjuvants they put in the shots, the goop they think are pieces of viruses (that don’t exist), the preservatives, the lipid nanoparticles, the coatings on the particles, the little segments of RNA—the injections attack the body. In all sorts of ways. In all sorts of places.”
When I think about what piece to write next, or when for the moment my tank is empty, I come up with VACCINES. That’s the subject.
It’s been that way for a long time.
I could be accused of having a grand obsession, but this isn’t the case. I’m responding to the civilizational obsession with vaccination.
At the same time, it IS personal. Because of the outrage I feel, watching medical storm troopers who have been on the march for more than a hundred years.
Watching their arrogance, their blunt stupidity, their “rational” madness. As they keep marching and invading.
If we were living in an absolute monarchy and I were King, there would be hell to pay. The troopers would pay, dearly.
Over the past 35 years, I’ve written countless articles on vaccination. I’ve run down the evidence from all the angles. Now I’m left with the feeling when all the data detailing crimes have been exhausted. I’m at the end of that trail.
It’s not THE end, though. Not by a long shot.
The troopers and their allies represent, for me, everything that’s insane about our society—especially the bland acceptance by the willing victims. The silent majority.
Including, of course, the educated classes, who proudly wear their badges of science, the ultimate virtue signal. They live in a harsh bombed out desert and think it’s a pretty garden.
Some of them watch their children go crazy from the shots, suffering massive brain damage—and still these parents won’t admit what happened.
They refuse to see what they saw.
—It might have been after a talk I gave. I had mentioned the fact that improved sanitation and nutrition in the West accounted for the decline in all sorts of illness—not the widespread introduction of vaccines.
The person said, “But for children who still can’t get nutritious food, vaccines protect them.”
It was a mindless “save the children” remark.
Of course, when the body’s defense is chronically deficient, a vaccine isn’t going to pump it up. Because there isn’t anything THERE to pump up. That’s a ridiculous fairy tale. And a vaccine isn’t food.
Bill Gates tried to pull off the same sort of nonsense, when he announced with great personal fanfare, that he’d just read a book about contaminated water supplies in the Third World—as if he’d just discovered what everyone else had known for 50 years.
So he said something like this: I saw that bad water accounted for horrific chronic diarrhea, a killer. We have to clean up the water. But meanwhile, my anti-diarrheal vaccine will help.
No it won’t. The sick child, who is wasting away, has no immune system left. The vaccine won’t build up what isn’t there.
—Belief across a population is a powerful thing. It can operate like a bulldozer, flattening all obstacles and objections. And at the end of the day, it stands naked, amid the ruins. When the belief is demanding a solution that won’t work. Vaccines.
I come from an era when vaccinations were few and far between. A poke here, a stab there. There was no CDC shouting about schedules. The big Pharma money wasn’t rolling in yet. The predators knew the public wouldn’t go for 30 or 40 shots during childhood.
But now it’s a lifeline. Oh, the kids will die if you don’t shoot them up.
Bleeding heart liberals, clueless rubes, and Big Pharma. A jackpot sales team.
And a bland Howdy Doody monster like Bill Gates in the background, pouring billions of dollars into MORE vaccines.
As I predicted early on during Warp Speed, the introduction of RNA technology was going to create a bonanza for Pharma. They’d redo every vaccine in the book with the new tech. They’re working in that direction now.
Because vaccines injure and kill, this civilization is on wartime footing. We’re under attack. Half the effort to censor us is devoted to the vaccine issue. The enemy knows what’s at stake.
If we take their prime weapon away from them—by walking away from it in huge numbers—they fall.
After the COVID fiasco, when millions of people DID walk away from the injection…the public is primed to take a look at the whole range of vaccines.
I’ve watched some of the new pundits who appeared during COVID to expose that shot. Some of them are close. They’re close to seeing that the whole arsenal of vaccines is nothing less than a doomsday weapon. They haven’t crossed that line yet. But they’re on the verge.
I crossed the line in 1988, when I wrote AIDS INC. Because I realized “the virus” wasn’t causing anything, I was looking for real causes of immune suppression—since that was what so-called AIDS was.
And that’s when I saw The Big One looming up on the horizon. Vaccines.
I started talking to Health Freedom advocates who’d been in the trenches for decades. I started reading hard to find books that investigated vaccines. And then, there it was.
I saw it.
I couldn’t look away from it.
Whatever I thought a career in journalism was, could be, should be, that career took a sharp turn.
I had no idea how much passivity I would encounter.
Pure, dumb, conformist passivity.
But with Warp Speed, and everything that followed, I saw the apathy in the public begin to dissolve.
I saw foundational pillars begin to crack.
The truth is, no one can get to health through vaccinations. If a person is sickly, vaccines won’t help. If he’s healthy, he doesn’t need vaccines.
The bad news is, vaccines destroy. Whether it’s the so-called adjuvants they put in the shots, the goop they think are pieces of viruses (that don’t exist), the preservatives, the lipid nanoparticles, the coatings on the particles, the little segments of RNA—the injections attack the body. In all sorts of ways. In all sorts of places.
In England, right at the start, when THE one shot was for smallpox, there were whole cities with high vaccination rates where people were dropping like flies. And cities where the vaccination rate was low, people came through all right.
When the authorities finally began cleaning off the raw sewage running down the city streets, when they installed public sanitation systems, disease took a very sharp downturn.
These things aren’t hard to understand.
But they’ve been hidden from the public.
We’re looking at a revolution of simple truth. Which can be spoken and delivered simply.
And widely.
By us all.
In this war.
During which we’re under attack.
Many foot soldiers happen to be doctors, who have the advantage of seeming neutral. They wave no flags. They salute no dictator. They’re calm and rational. Nevertheless, they wield the weapon, and they use it.
We can’t let that oddity deter us.
If you need a push, talk to the mother of a severely autistic child. That is, a child whose brain was assaulted by a vaccine. Have her tell you what she goes through every day of her life, with that child.
It seems difficult to believe a modern civilization could have gone so far off the track as this one has.
The difficulty in facing that fact is what drives people back into their huts and their television screens and online games.
But you know, believing something that happens to be true and then acting on it is more powerful than any civilization.
Well, I’ve won another Nobel Prize. I’ve got so many now, I keep the medals in a box in the basement. I mail the checks straight to the IRS, they take what they want and deposit the leftovers in my bank account.
This Prize has to do with child psychology, and more importantly, cultural psychology.
Let’s start here. Some kids do have problems.
If a kid is walking to the grocery store through a hail of drive-by bullets, that’s a problem.
If his father is beating him up three times a month, that’s a problem.
If he has no father and his mother is working two jobs to keep the lights on and she’s rarely home, that’s a problem.
If breakfast every day is chocolate Snuffles and peanut butter pressed between two slices of plastic white bread, that’s a problem.
But I’m not talking about those problems. I’m talking about the fashion trend and the cultural imperative and the outright demand that kids ARE SUPPOSED TO HAVE personal problems—and if they don’t, they’re out. They’re barred from belonging. They’re weird. They’re covering up something.
Once you install the need to have problems in a kid, once you convince him he has to be on that starter page, boom, with a leap he’s off and running. Because he has an active imagination.
He’ll go with that proposition, and all kinds of invention will follow.
“I’m trying to root out my systemic racism…climate change is going to kill us all…I think I want to be a girl…my mother doesn’t understand me…I may have early arthritis…I don’t like sports anymore…I’m having a crisis and I don’t know what it’s about…how can we stop people from cutting down trees…I don’t eat meat but I want to…I have neck pains at night…I was getting taller but now I’ve stopped…I may be too thin…we’re not letting in enough immigrants…”
Badges. Badges of belonging. Gotta settle on a good problem. Which one should I have today? Not having a problem is like going to school naked.
Back in the 1940s, when I was growing up, no kid had these problems. No kid was manufacturing problems.
That was before the Age of Psychologizing.
When I was a kid, there were foods I didn’t like. Unfortunately, they would appear on the dinner table. Chicken soup. String beans. Mashed potatoes. So my mother and I would argue, I would force down a forkful and a spoonful or two, and that would be it, until the next night, when we’d go at it again.
But it never occurred to me that this was a problem.
Now, YOU HAVE TO HAVE PROBLEMS is the gateway drug into all sorts of wretched crapola. It’s a set-up.
Admiral Rachel Levine—a man who “transitioned” and is now Assistant Secretary of Health in the Biden administration—has made shocking statements in support of transgenderism:
“We really want to base our treatment and to affirm and to support and empower these youth—not to limit their participation in activities in sports and even limit their ability to get gender affirmation treatment in their state…”
“I can say that you [doctors], the children that you serve, the young people that you serve, their families, and you all have support at the highest levels of the federal government.”
“President Biden supports you. I as the Assistant Secretary for Health will support you and I talk about this topic, everywhere I go, to get the word out…”
And the Word is: backing, at the highest levels of government, children receiving puberty blockers, sex hormones, and genital mutilation surgery.
That’s “gender-affirming care.”
So if you still think the trans movement is just a small collection of misfits, forget it.
This is big-league politics. This is major medicine. This is government policy by fiat.
Realize this is federal power dictating medical treatment and supporting it with all hands on deck.
In terms of power at the helm, this is on the level of the CDC childhood vaccination schedule.
This is also on the level of declaring the RNA COVID vaccine kill shots safe, effective, and necessary.
Full steam ahead.
This is the federal government supporting castration for boys.
And double mastectomies for girls.
National policy.
Colluding with medical societies, doctors, hospitals, clinics, and psychiatrists.
A government is bent on destroying lives and generations of children.
Officially.
The day is approaching when multiple laws will empower Child Protective Services to remove children from their homes, if their parents revolt against “the child’s decision” to change genders.
In my last interview with Del Bigtree on The Highwire I sounded the alarm regarding the future of aluminium adjuvants in vaccines. I urged against complacency and warned that next generation vaccines would continue to rely upon aluminium adjuvants. Well, we now know this to be true direct from the horse’s mouth.
The latest vaccine industry funded paper entitled ‘Aluminium Adjuvants – Back to the Future’ leaves no doubt that the vaccine industry is not contemplating a future without aluminium adjuvants. The paper is published in a special issue of the journal Pharmaceutics called Designing and Developing the Next Generation of Vaccine Adjuvants. The vaccine industry will continue to use aluminium adjuvants well into the future. They will continue to promote the injection of aluminium into our body, from new born infants to vulnerable individuals and the elderly.
Their rationale for continuing the use of aluminium adjuvants? Well, first and foremost, though not mentioned in this latest review, is cost. As I have written about in previous substacks and in my book, aluminium adjuvants are dirt cheap, they add absolutely nothing to the cost of a vaccine. Why would industry invest in new adjuvants when aluminium adjuvants are effective and cheap. The bottom line is always the deciding factor for profit-led industry.
However, their cost effectiveness is not worthy of a mention in this latest industry review. The major selling point for aluminium adjuvants in this paper is ‘their excellent safety profile, which has been established through the use of hundreds of millions of doses in humans over many years’. This stomach churning statement, taken from the abstract of the published paper, is pure aluminium industry speak. It reminds me of their often used defence of the safety of aluminium, wheeled out at many scientific meetings, that the fact that aluminium is present throughout the body must prove that it is good for you.
The fact that such a statement is in the abstract of this paper demonstrates that it went unchallenged by the so-called peer review process. Indeed there is no evidence that this paper was peer reviewed. The Guest Editor of the Special Issue where the paper is published is the lead author of the paper. The Editor of Pharmaceutics is a vaccine industry stooge. This journal, published by MDPI (see my criticism of this publisher in my book), is simply a vehicle for the vaccine industry to legitimise their messages regarding the safety and efficacy of vaccines.
It is, of course, common knowledge and scientific fact that the safety of aluminium adjuvants in humans has NEVER been tested for any vaccine in use today. To my knowledge the only vaccine ‘safety trial’ where a saline control was used was carried out by Merck on Gardasil. The results of this trial, available through clinicaltrials.gov, showed an incidence of serious adverse events of 2.4% both for the whole vaccine and for the aluminium adjuvant alone while the incidence was 0% for a saline control. Make of this what you will but my interpretation is that an unacceptably high incidence of serious adverse events in recipients of Gardasil was due to the aluminium adjuvant.
Further indirect evidence of the toxicity of aluminium adjuvants comes from the work of vaccine advocate Peter Aaby working in Guinea-Bissau, Africa. He has shown in multiple studies that mortality in children receiving aluminium-adjuvanted vaccines is significantly higher than unvaccinated children. He does not find a similar effect in live attenuated vaccines that do not use an aluminium adjuvant.
Any form of true peer review of this paper in Pharmaceutics would have prevented such lies from being published. The true safety profile of the use of hundreds of millions of doses of aluminium adjuvants in humans is all about us for anyone willing to look and see. True epidemics of industry sponsored human disease including Alzheimer’s disease and autism. Shame on those in scientific publishing who turn a blind eye to the truth and worse promote lies that can only result in further human suffering and death.
At Age of Autism, there is a riveting piece about the government cover-up and the forced collusion with Pharma, entitled “Sharyl Attkisson, Friend of Ours.”Read it.
Let’s start here. There is no defining physical diagnostic test for autism. No blood test, no urine test, no hair test, no genetic assay, no brain scan.
What??
That’s right.
And you can throw out the official definition of autism. That menu of behaviors and attitudes is arbitrary—complied by a committee of psychiatrists.
But a doctor’s eyeball diagnosis of autism is very valuable. To government and Pharma.
Why?
When a mother comes before the mandatory federal vaccine court to win $$ compensation for her destroyed child, the court can (and will) say:
“We see your doctor diagnosed your son with autism. But there is no proof vaccines cause autism. Compensation denied.”
The mother was really telling the court (but she couldn’t say it), “My child had a vaccine and checked out of the world. It’s VACCINE DAMAGE.”
Of course, that wouldn’t fly, either. Why should it? It’s the TRUTH. And truth doesn’t win.
This is the word game the government plays. It’s a predatory game.
How does the government “prove” vaccines don’t cause autism? Easy. Researchers say: “We have identified children with autism who have never had vaccines.”
What is the government really saying? “We’ve identified children with brain damage caused by factors other than vaccines.”
Of course there are such children. But so what?
So the government wins. With that completely absurd assertion.
Cutting through all this wordplay and mumbo-jumbo—push the label “autism” to one side and speak the facts: The child had a vaccine and it DAMAGED HIS BRAIN.
But again, that won’t work. In court.
It’s too obvious, too clear-cut, too simple, too true.
The court’s rule is: A parent seeking compensation for injury to her child, caused by a vaccine, MUST have a diagnosis of an official disorder or a disease from a doctor.
The most frequent diagnosis is autism—and then, bang, “There is no proof vaccines cause autism.”
The extensive history of the pharmaceutical industry is filled with stories and deeds of adventures, misadventures, profit-making, profit-taking, fraud, bribery, false claims, messianic promises, and criminal conduct.
Few companies in the history of medicine have received as much attention as Pfizer Inc. has received these last three years of the Corona Crisis.
Through the course of relentless media coverage and amidst all the sound and fury, Pfizer has managed to avoid scrutiny of its previous criminal conduct and is universally portrayed in the mainstream media as a benevolent enterprise whose mission is to nobly service humanity.
In an effort to set the record straight we embark upon a comprehensive historical examination of this company which sprouted from humble beginnings into one of the most influential corporate behemoths walking the earth today.
History
The story of Pfizer begins in New York City in 1849, when a pair of German immigrants, cousins Charles Pfizer and Charles F. Erhart, received a $2,500 loan from Charles Pfizer’s father to purchase a commercial building in Williamsburg, Brooklyn where they would embark upon a joint business venture in the nascent chemical manufacturing industry.
Charles Pfizer had been a pharmacist’s apprentice in Germany and possessed commercial training as a chemist. Charles Erhart was a confectioner.
Originally named Charles Pfizer and Company the business would initially focus on the production of chemical compounds. Their first product was a pharmaceutical called Santonin which was used to treat parasitic worms.
Combining their talents the cousins housed their product within tasty confections such as candy lozenges and toffee-flavored sugar cream cones. This strategy proved to be a success, setting the stage for the company’s future development.
The drug Santonin would be used as an anthelmintic up until the 1950’s, when it fell out of favor due to noted toxic effects which posed serious risks to patients.
Pfizer would quickly expand into the realm of fine chemicals for commercial sale to wholesalers and retailers.
In 1862, Pfizer would become the first U.S. company to domestically produce tartaric acid and cream of tartar.
With the outbreak of the American Civil War a massive need for painkillers and antiseptics erupted, creating an “opportunity” for the pharmaceutical industry.
Pfizer quickly expanded its production of both, as well as of iodine, morphine, chloroform, camphor, and mercurials. By 1868, Pfizer revenues had doubled and its product line had increased substantially.
The big boon for the company would come in the 1880’s with its production of industrial grade citric acid, widely used in soft drinks like Coca-Cola and Dr. Pepper. This would become the company’s centerpiece and drive their growth for decades.
Another fortuitous change for the “small New York firm” would arrive in 1919, when its scientists would pioneer and develop a deep tank fermentation process, the principles of which would later be applied to the production of penicillin.
This prowess in fermentation and large-scale pharmaceutical production would put Pfizer in a lead position in WW2, when the US government appealed to the pharma industry for support in producing penicillin for the war effort.
Working with government scientists, Pfizer began pursuing mass production of penicillin utilizing its deep-tank fermentation technology and in 1944 became the first company to mass produce penicillin.
As penicillin prices and usage declined post-WW2, Pfizer began searching for more profitable antibiotics. The move into commercial production of antibiotics signaled a pivot in Pfizer’s business model.
The company’s operations shifted from the manufacture of fine chemicals to research-based pharmaceuticals, giving birth to Pfizer’s new drug discovery program, which focused on vitro synthesis.
In 1950 Pfizer would develop its first proprietary pharmaceutical product, Terramycin, a broad-spectrum antibiotic.
By 1951, Pfizer had established offices in Belgium, Brazil, Canada, Cuba, England, Mexico, Panama, and Puerto Rico. As its power and profits mushroomed, Pfizer would augment its portfolio through various acquisitions and entries into multiple areas of research and development, including an animal health division.
As the Pfizer pharmaceutical kingdom expanded, however, questions about salacious business practices began to surface.
Violations
Despite portraying itself as a righteous corporate citizen, Pfizer is no stranger to controversies and scandals. As early as 1958 it was one of six drug companies accused of price fixing by the Federal Trade Commission.
In 1961 the Justice Department filed criminal antitrust charges against Pfizer, American Cyanamid, and Bristol-Myers, accusing top executives at each company of charging egregiously high prices and monopolizing the production and distribution of drugs dating back to 1953.
In 1963 the FTC ruled that the accused companies in its 1958 complaint did in fact rig antibiotic prices. The FTC also noted that “unclean hands and bad faith played a major role”in Pfizer being granted the tetracycline patent.
By the 1960s, Pfizer was at its most diversified point in history, with interests ranging from pills to perfume to petrochemicals to pet products.
The company’s shift toward bringing out new products culminated with the establishment of the Central Research Division in the early 1970s. A full 15% of Pfizer’s revenue was directed to this research department.
This focus on innovation brought about Pfizer’s development of blockbuster drugs, which are described as “drugs that generate at least $1 billion in revenue a year for the pharmaceutical companies that produce them.”
While these drugs can be extremely profitable for pharmaceutical companies, the blockbuster drug business model presents certain long-term problems. Beyond the time and money that goes into their development, there are the exigencies of patent issues. Pharma companies see the “patent window” of 20 years as a severe limitation, since it often takes them a full decade to bring a new drug to market, thus shortening both the time allowed to reclaim profits from development costs and the time allotted to reap maximum profits from their new product.
Due to patent laws, the success of blockbuster drugs is often short-lived. Also, reliance on blockbusters means that if a product fails, the consequences for the manufacturer can be catastrophic.
Using this business model, the need for pharmaceutical companies to constantly produce blockbuster drugs is difficult to overstate. Naturally, they go to great lengths to protect their golden goose.
Accompanying Pfizer’s string of blockbusters was a massive surge in the company’s fortunes in tandem with a procession of controversial products, felony offenses and multiple fines—including the largest criminal fine in US history.
Take, for example, Pfizer’s first blockbuster drug, the anti-inflammatory Feldene, which would also become one of its initial contentious products.
Pfizer submitted a new-drug application for Feldene to the FDA in March 1978 and again in May 1980. The applications were rejected due to poor testing protocols. In September 1981, Pfizer resubmitted an application to the FDA, using old data.
Multiple questions surrounding Feldene, including the route taken toward its ultimate approval, would make it one of Project Censored’s top “Censored” news stories in 2015.
In that story, Project Censored noted:
”Then, while the FDA was still considering the application, Pfizer sponsored a reception at the meeting of the American Rheumatism Association in Boston and showed a film promoting Feldene which the FDA said was illegal. Nevertheless, on April 6, 1982, the FDA approved Feldene for use in the U.S.”
Even though Feldene would go on to become Pfizer’s most lucrative product, questions about the drug quickly surfaced. By 1986 the FDA was being petitioned to relabel the drug due to serious concerns about its long half-life and its tendency to accumulate in the blood.
The watchdog organization Public Citizen Health Research Group (PCHRG) would later charge that this widely prescribed arthritis drug created risks of gastrointestinal bleeding among the elderly.
Citing reports of 2,621 adverse events and as many as 182 deaths among patients taking the drug, PCHRG requested that the FDA ban Feldene for patients 60 and over, “as an imminent hazard to the public health.”
Dr. Sidney Wolfe, director of the PCHRG stated, “At least 1.75 million elderly American people now receiving this drug are at risk of developing life-threatening gastrointestinal reactions.”
PCHRG’s Wolfe would later cite internal documents from Pfizer that voiced concerns about the drug. By 1995 he called for a complete ban on the drug for all ages.
This was just the beginning of a series of high-profile scandals and legal problems that would come to define Pfizer’s business-as-usual practices.
For instance, reports of serious issues surrounding a heart valve produced by Pfizer’s Shiley division began to plague the company. This problem would result in the cessation of production of all models of the faulty valves by 1986.
A 1991 FDA task force charged that Shiley withheld information about safety problems from regulators in order to get initial approval for its valves. A November 7, 1991, investigation in The Wall Street Journal asserted that Shiley had deliberately falsified manufacturing records relating to valve fractures.
These fractures resulted in catastrophic consequences for numerous patients. By 2012 it was reported that 663 individuals had died as a result of the defective valves.
It also agreed to pay $10.75 million to settle US Justice Department charges that it lied to regulators in seeking approval for the valves.
The parade of corrupt practices and legal problems that has come to define this pharmaceutical Leviathan was just getting underway. From then on, Pfizer was cited and prosecuted for a litany of illegal acts ranging from price fixing, product safety, bribery, advertising and marketing scandals all the way to environmental and human rights violations.
In 1999 Pfizer pled guilty to criminal antitrust charges and agreed to pay fines totaling $20 million. In that case, Pfizer was charged with “participating in a conspiracy to raise and fix prices and allocate market shares in the U.S. for a food preservative called sodium erythorbate, and to allocate customers and territories for a flavoring agent called maltol.”
In 2000 The Washington Post published a six-part exposé accusing Pfizer of testing a dangerous experimental antibiotic Trovafloxacin (trade name Trovan) on children in Nigeria without receiving proper consent from their parents.
Trovan was slated to become Pfizer’s next blockbuster drug, according to Wall Street analysts, one of whom claimed, “Pfizer might reap $1 billion a year if Trovan could gain approval for all its potential uses.” But when the company was unable to find enough patients in the United States, its researchers went in search of new patients in Kano, Nigeria.
This unapproved clinical trial on 200 Nigerian children resulted in the death of 11 children. It is alleged that many more children later suffered “serious side-effects ranging from organ failure to brain damage.”
In 2001 Pfizer was sued by 30 Nigerian families, who accused the company of using their children as “human guinea pigs.” The families contended that “Pfizer violated the Nuremberg Code as well as UN human rights standards and other ethical guidelines” and alleged that Pfizer exposed the children to “cruel, inhuman and degrading treatment.”
After years of legal battles, Pfizer agreed in 2009 to pay $75 million to settle some of the lawsuits that had been brought in Nigerian courts.
Trovan never became the blockbuster Pfizer had envisioned. The company admitted to stockholders it had “suffered a disappointment” with this experimental meningitis drug. Trovan was never approved for use by children in the United States, so production was halted. The European Union banned it in 1999.
Below is a chronology of still more Pfizer misadventures.
— In 2002 Pfizer agreed to pay $49 million to settle charges that one of its subsidiaries defrauded the federal Medicaid program by overcharging for its cholesterol-lowering drug Lipitor.
— In 2003 Pfizer paid $6 million to settle with 19 states that accused it of using misleading ads to promote the antibiotic Zithromax (also called Z-Pak), used for children’s ear infections. The claim alleged that Pfizer “overstated the benefits and efficiency of Zithromax when compared to other comparable antibiotics.”
— In 2004 Pfizer agreed to a $60 million settlement in a class-action suit brought by users of a diabetic medication developed by Warner-Lambert, which Pfizer acquired in 2000. The drug Rezulin had been withdrawn from the market after numerous patients died from acute liver failure said to be caused by the drug.
— In 2004 Pfizer agreed to halt ads for its painkiller Celebrex, and the following year it admitted that 1999 clinical trials found that elderly patients taking the drug were far more likely to incur risks of heart problems.
— 2004 also saw Pfizer plead guilty to two felonies and pay $430 million in penalties for fraudulently promoting the epilepsy blockbuster drug Neurontin for unapproved uses. Pfizer claimed it could also be used for “bipolar disorder, pain, migraine headaches, and drug and alcohol withdrawal.”
Pfizer’s underhanded tactics involving Neurontin also included bribing doctors with luxury trips and monies to promote the drug and planting operatives at medical education events.
Documents later came to light suggesting that Pfizer arranged for delays in the publication of scientific studies that undermined its claim for the other uses of Neurontin. In one of these documents, it was found that a Neurontin team leader at Pfizer said, “I think we can limit the potential downside of the 224 study by delaying publication for as long as possible.”
Finally, in 2010, a federal jury found that Pfizer committed racketeering fraud in its marketing of Neurontin; the judge in the case subsequently ordered the company to pay $142 million in damages.
— In 2005 Pfizer withdrew its painkiller Bextra from the market after the FDA cited “inadequate information on possible heart risks from long-term use of the drug as well as ‘life-threatening’ skin reactions, including deaths.”
— That same year the FDA approved a black box warning on Pfizer’s other blockbuster painkiller, Celebrex, citing elevated risks of “cardiovascular events and life-threatening gastrointestinal bleeding.”
— In 2007 Pfizer agreed to pay $34.7 million to settle federal charges relating to the marketing of its Genotropin human growth hormone. Pharmacia & Upjohn Co., a Pfizer subsidiary, agreed to pay $19.7 million for “offering a kickback to a pharmacy benefit manager to sell more of the drug,” while Pfizer agreed to pay another $15 million for “promotion of Genotropin for uses not approved by the Food and Drug Administration.”
— In 2008 Pfizer paid out a whopping $894 million fine to settle lawsuits “alleging that its withdrawn Bextra painkiller and widely used Celebrex arthritis drug harmed U.S. patients and defrauded consumers.” Of the total fine, $745 million was set aside to “resolve personal injury claims.”
— The very next year, 2009, Pfizer was fined $2.3 billion gaining the dubious distinction of being tagged with the largest health care settlement in history. GlaxoSmithKline would up the ante with a $3 billion settlement in 2012.
The fine was a combination of civil and criminal settlements relating to Pfizer’s “allegedly illegal promotion of certain drugs, most notably Bextra.” Pfizer pled guilty to “misbranding the painkiller Bextra with the intent to defraud or mislead, promoting the drug to treat acute pain at dosages the FDA had previously deemed dangerously high.”
The Justice Department also noted Pfizer had “allegedly paid kickbacks to compliant doctors and promoted three other drugs illegally: the antipsychotic Geodon, an antibiotic Zyvox, and the antiepileptic drug Lyrica.”
When interviewed by The New York Times, former Pfizer sales representative John Kopchinski, who helped initiate the federal investigation, stated, “The whole culture of Pfizer is driven by sales, and if you didn’t sell drugs illegally, you were not seen as a team player.”
The criminal fine of $1.195 billion in that settlement still represents the largest criminal fine ever imposed in the United States for any matter.
Even after entering an expansive corporate integrity agreement with the Office of Inspector General of the Department of Health and Human Services as part of the 2009 settlement, Pfizer’s unprincipled and injurious behavior continued. The band played on.
In 2010 The New York Timesreported on Pfizer’s admission that it had paid around “$20 million to 4,500 doctors and other medical professionals for consulting and speaking on its behalf in the last six months of 2009.”
The Times also mentioned that Pfizer had paid “$15.3 million to 250 academic medical centers and other research groups for clinical trials in the same period.”
In reference to the amounts disclosed by Pfizer, Dr. Marcia Angell, former editor of The New England Journal of Medicine and author of The Truth About the Drug Companies: How They Deceive Us and What to Do About It, admitted that while she had no specific knowledge of the matter, she believed the publicly revealed amounts Pfizer disclosed “seemed low.” She added: “I can’t help but think something has escaped.”
In 2011 Pfizer agreed to pay $14.5 million to resolve False Claims Act accusations that it illegally marketed its bladder drug Detrol.
The SEC alleged that “employees and agents of Pfizer’s subsidiaries in Bulgaria, China, Croatia, Czech Republic, Italy, Kazakhstan, Russia, and Serbia made improper payments to foreign officials to obtain regulatory and formulary approvals, sales, and increased prescriptions for the company’s pharmaceutical products.”
According to Kara Brockmeyer, Chief of the SEC Enforcement Division’s Foreign Corrupt Practices Act Unit, “Pfizer subsidiaries in several countries had bribery so entwined in their sales culture that they offered points and bonus programs to improperly reward foreign officials who proved to be their best customers.”
In 2012, Pfizer was hit with another massive fine—this time to settle claims that the side effects of its Hormone Replacement Therapy (HRT) drug Prempro cause breast cancer. Around 10,000 women filed a lawsuit against the company, alleging that the drug maker withheld information about the potential risks of breast cancer from HRTs. The $1.2 billion settlement came after six years of trials.
The FDA had placed a black box warning on Chantix, the highest safety-related warning assigned by the FDA, “to alert patients and doctors to the risk of psychiatric side effects” and had noted that the drug is “probably associated with a higher risk of a heart attack.”
Pharmaceutical companies make every effort to circumvent black box warnings. They generate bad publicity and negatively impact the marketability of the drug in question, which leads to adverse financial consequences for the company.
In 2016, after years of lobbying, Pfizer managed to get the FDA to lift the black box designation from Chantrix in a 10-9 vote, giving the controversial blockbuster drug a “new lease on life.”
In 2013 Pfizer reached a $35 million settlement relating to the alleged improper marketing and promotion of the immunosuppressive drug Rapamune. When New York Attorney General Eric T. Schneiderman announced that he and 40 other state attorneys general had arrived at the settlement, he remarked, “There has to be one set of rules for everyone, no matter how rich or powerful, and that includes big pharmaceutical companies that make unapproved and unsubstantiated claims about products in order to boost profits.”
While this article’s list of Pfizer’s corporate crimes is prodigious by any measure of shady business practices, it is far from exhaustive. In total, since 2000 Pfizer has accumulated $10,945,838,549 in penalties and incurred 96 violations covering a wide range of offenses.
A Company You Can Trust?
Pfizer’s portfolio of corporate crimes rivals that of the most corrupt companies in history. But that did not stop Pfizer from becoming a corporate celebrity with its COVID-19 vaccine. Indeed, the company has benefited handsomely from that product, whose $36.8 billion in 2021 sales made it the highest-selling pharmaceutical product in history.
When the pharma company’s 2022 revenues reached an all-time, single-year high of $100.3 billion, COVID-19 vaccine sales accounted for nearly 38 percent of those revenues.
Yet, while Pfizer was basking in the glow of mainstream media cheerleading and record-setting profits, honest inquiries into its unremitting record of corruption were kept from public view.
We were told we must “Trust in Pfizer” to vaccinate the world and save humanity from the so-called COVID crisis.
Given Pfizer’s documented record of misdeeds, any reasonable person would ask:
“Is this a company that belongs behind the wheel of the most widespread mass vaccination campaign in history?”
“Is this a company we should trust with experimental medical technology?”
“Is this a company we want to be in control of the most radical mass medical experiment in human history?”
“How is it that a company that habitually engaged in such illegal practices was able to reinvent itself as the savior of humanity?”
At that commemoration, then-president of Pfizer Global Manufacturing Natale Ricciardi told attendees, “We have always had a very noble mission.” Despite cryptically lamenting, “A lot of things have changed at Pfizer, and unfortunately, we had to make certain decisions,” Ricciardi went on to assert, “But the nobility of what we do, the nobility of what has been done and continues to be done has never changed and will never change.”
All these years later—and despite Mr. Ricciardi’s insistence on Pfizer’s magnanimity—a thinking person might look through the company’s checkered catalog of crimes and fines and recognize that noble experiments are hardly the realm of “alleged” serial felons like Pfizer.
June 15, 2023, podcast host Joe Rogan interviewed Robert F. Kennedy Jr., who is currently running as a Democratic presidential candidate
In 2005, Kennedy started suing coal-burning powerplants and cement kilns for releasing mercury into waterways. He also pushed legislation to protect children against mercury and gave lectures on its dangers
During those lectures, mothers started approaching him saying they suspected their children had been injured by mercury-containing vaccines. They told him that if he was really interested in protecting children against mercury, he had to investigate vaccines
The mother of a vaccine-injured child brought him a thick stack of published research, and after looking through it, Kennedy realized that what health officials told us was very different from what the science showed
Kennedy is now also legally representing people who claim they’ve been injured by cellphone radiation, which science shows can cause cancer, degrade mitochondria and make your blood-brain barrier more permeable, allowing toxins in your system to flood into your brain
Still, if anything in that book was false, Kennedy would have been sued to high heaven by now, Rogan reasoned. Reading that book opened Rogan’s eyes to the fact that what we’re told by public officials and the media isn’t necessarily the truth. He also realized just how easy it is to fall for a false narrative — especially when it’s all you’re ever allowed to really hear.
For the first several minutes of the interview, Kennedy reviewed his background and how he got to where he is today. He started his legal career as an environmental lawyer in the mid-1960s, suing 500 polluters who had turned the Hudson River into a sewer, on behalf of commercial fishermen whose livelihoods were threatened.
As a result of those lawsuits, the Hudson River was cleaned up and restored. These successes led Kennedy to found Riverkeeper,2 which patrols waterways in 46 countries, holds polluters accountable and defends clean drinking water.
How Kennedy Got Involved With Vaccine Safety
I would strongly encourage you to listen to this interview as around the 10-minute mark Rogan asks Kennedy how he got into the vaccine controversy. Although Kennedy had presented some of his comments in the media previously, this is the first time he was ever allowed to give his uninterrupted one-hour fascinating story on major media.
In 2005, Kennedy started suing coal-burning powerplants and cement kilns for releasing mercury into waterways. He launched these lawsuits on behalf of local Riverkeeper chapters after learning that mercury was being found in the flesh of most freshwater fish. Pregnant women were also found to have levels that might put their children at risk of developmental problems.
Kennedy also pushed legislation to protect children against mercury and gave lectures on its dangers. During those lectures, mothers started approaching him saying they suspected that mercury (thimerosal) in the childhood vaccines had injured their children. They told him that if he was really interested in protecting children against mercury, he had to investigate vaccines.
He resisted, as his focus was on environmental pollution and he didn’t want to get involved in public health. However, mothers of developmentally challenged children kept coming to his speeches, wanting to talk to him about vaccines.
Their continued pressure eventually changed his mind, and he decided to listen to their concerns. The true turning point came when a psychologist named Sarah Bridges found his home address and delivered an 18-inch thick stack of scientific papers, saying she would not leave until he’d read them.
Bridges was one of the few people who had been awarded $20 million by the vaccine court, which had concluded that her son’s autism had been caused by a vaccine. She just didn’t want other parents to go through the same heartache.
Huge Gap Between Public Narrative and Published Science
Kennedy began reading, and by the time he’d gone through a third of the pile, he came to the realization that there was a huge gap between what the public health agencies were saying about vaccine safety and what the published science showed.
Kennedy then started calling high-level public health officials and regulators, asking them about these studies and, to his surprise, he realized none of them had read them. They were all just repeating what they had been told about the science. Stranger still, they told him to take his questions to people in the vaccine industry.
Kennedy did contact Dr. Paul Offit, as suggested, and caught Offit in a blatant lie. He asked Offit, how come pregnant women are told not to eat tuna fish to avoid mercury, but are then told to get flu shots that contain a huge bolus of mercury? Offit told him “there are two kinds of mercury, a good mercury and a bad mercury.” According to Offit, fish contain the bad kind, whereas the mercury in vaccines is harmless.
The problem was, Kennedy is an expert on mercury, having spent years suing mercury polluters. He has a deep understanding of the two types of mercury (ethylmercury in vaccines and methylmercury in fish), and there’s no such thing as a “good” or harmless mercury.
Kennedy, an excellent storyteller, goes on to review the history of vaccine science and why toxic elements like mercury are used at all. This interview is without doubt one of the most educational “lectures” on vaccines available right now, so I encourage you to listen to at least the first hour, if you don’t have time for the whole thing.
Ethylmercury Lodges in the Brain
Importantly, he reviews crucial research that firmly debunks the claim that ethylmercury is excreted from the body within a week. Studies on monkeys, where the animals were sacrificed after vaccination (which you cannot do with children), showed that the reason there was no ethylmercury in the blood after several days was because it had traveled into the brain, where it stayed, causing inflammation.
When Kennedy challenged Offit on this point, Offit insisted that, while this research did show that ethylmercury lodged in the brain, “the mosaic of studies” proved it was harmless and left the body.
Kennedy asked him to share those studies, which Offit promised to do but never did. Kennedy never heard from him again. At that point, Kennedy realized that something was terribly wrong, and he couldn’t walk away.
Kennedy also challenged Dr. Anthony Fauci — who is a close friend of the Kennedy family — to show him a single placebo-controlled trial of a vaccine listed on the childhood vaccination schedule. Fauci said he would send him the studies, but, like Offit, never did.
The reality is, none of the mandated vaccines has ever been tested against a true placebo, such as saline. Most are tested against other vaccines, and if you’re testing two products that contain a similar toxin, of course, the outcomes will be similar. That doesn’t mean you’ve proven safety. Not even close.
Kennedy eventually sued the Health and Human Services Department to obtain the evidence Fauci claimed to have, and after a year the HHS finally returned a letter saying there were no such safety studies. “So, nobody knows what the risk profiles of these products are,” Kennedy says.
The sheer lack of data also means that anyone who claims vaccines have saved more lives by preventing disease than they’ve destroyed through side effects is simply guessing and making assumptions. There’s no scientific data to back that up.
Also, Kennedy points out that while many vaccines are now mercury-free, they’re loaded with aluminum adjuvant instead, which is just as bad. So they’ve just exchanged one neurotoxin for another.
Intentional Suppression of the Autism Signal
Kennedy goes on to tell the story of a secret meeting3 organized by the U.S. Centers for Disease Control and Prevention in 1999 after they conducted an internal study of their database, which contains the medical records, including the vaccination records, of 10 million children from the 10 biggest HMOs.
Specifically, they wanted to know whether mercury-containing vaccines might be causing autism. One of the first comparisons of health outcomes was done on the hepatitis B vaccine.
The data showed that infants who had received the hepatitis B vaccine within 30 days of birth had a 1,135% higher risk of autism compared to infants who either did not get the hepatitis B vaccine at all or received it after 30 days of age. “At that point, they knew what caused the autism epidemic,” Kennedy told Rogan, because “that’s a relative risk of 11.35, and a relative risk of 2 is proof of causation.”
As panic spread through the industry, the CDC put together this secret meeting at a retreat center in Georgia. It was intentionally held outside the CDC campus to circumvent FOIA laws. The meeting included representatives from all the major vaccine companies, regulatory agencies that administer vaccines, the U.S. Food and Drug Administration, the National Institutes of Health, the Health and Human Services Department and leading academic institutions that conduct clinical trials.
The first day was spent discussing the reality of the problem, and the second day was spent discussing how to hide it. While the meeting was held in secret, someone did record it and, in 2005, Kennedy obtained a copy of it. You can read the transcript on the Children’s Health Defense website.
Early on in that 286-page transcript, we find the following admission by Walter Orenstein, then-director of the National Immunization Program at the CDC:4
“Initial concerns were raised last summer that mercury, as methylmercury in vaccines, might exceed safe levels … Analysis to date raise some concerns of a possible dose-response effect of increasing levels of methylmercury in vaccines and certain neurologic diagnoses.”
What happened to this safety signal? As explained by Kennedy, it was intentionally “vanished” by reworking the study four times, using statistical tricks.5 After the fourth iteration, the signal linking thimerosal with autism and a half dozen other neurodevelopmental disorders were no longer detectable.
The CDC published that final version and announced thimerosal had been investigated and found to be safe. And when investigators asked to see the raw data, the CDC claimed the data had been “lost,” so no one was ever able to verify the results. The fabrication stuck and has been peddled ever since.
We Live in a Toxic Soup
Kennedy stresses that vaccines are not the only factor in the epidemics of chronic disease and autism in children. There are many other factors as well. Children are exposed to an enormous amount of toxins from many different sources, including electromagnetic fields (EMF) and wireless radiation.
Kennedy is currently representing people who blame their brain tumors on cellphone radiation, and “we have the science,” he says. “Tens of thousands of studies show the dangers of Wi-Fi radiation.”
Aside from cancer, cellphone radiation degrades your mitochondria and makes your blood-brain barrier more permeable, Kennedy says, allowing all the other toxins in your system to flood in. So, this too, could play a significant role in the neurological dysfunction we now see in so many children. Kennedy also discusses the history behind and toxic influence of glyphosate, especially on your gut. (Incidentally, gut dysfunction is also a hallmark in autism.)
This is an interesting part of the interview as when Kennedy first mentions EMF, Rogan doubts it is true and doesn’t believe him. After Kennedy’s explanation you see Rogan morph in real time to a believer in EMF dangers and even ask his assistant Jamie to look into getting rid of the Wi-Fi.
Rogan Invites Dr. Hotez to Debate RFK
Yesterday, I published an article reviewing the online debate that erupted after this interview, when Dr. Peter Hotez took to Twitter, slamming Spotify for not clamping down on Rogan’s “vaccine misinformation.”6 Never mind the fact that Hotez, in April 2020, was allowed to argue his own irrational vaccine stance on Rogan’s show.7
Rogan replied to Hotez’s tweet, saying, “Peter, if you claim what RFK Jr. is saying is ‘misinformation,’ I am offering you $100,000.00 to the charity of your choice if you’re willing to debate him on my show with no time limit.” Others further sweetened Rogan’s offer by adding their own donations and, by 9 a.m. EST on June 18, the pot had reached $1.52 million.
Hotez refused, albeit indirectly. Instead of giving Rogan a direct answer, he went on the MSNBC show “Rising Reacts” and said he wasn’t willing to participate in an event that would get turned into “The Jerry Springer Show” by having Kennedy there.
Once you’ve listened to this interview, you can probably understand why no one is willing to engage in a public debate with Kennedy on this issue, particularly if you also heard Rogan’s interview8 with Hotez and compare the two. Kennedy has the data to back his claims and they have none.
On a side note, I find it curious that after Rogan took a beating in the press for discussing how he used ivermectin to treat a bout of COVID-19, he really hasn’t had any hard-hitting health-related truthtellers on his show — until Kennedy.
In my view, Spotify is hardly a free speech platform, so maybe that shouldn’t be that surprising. Spotify killed our account due to a discussion about EMF, and they didn’t just take that episode down. They removed all of my content.
Rogan has an exclusive contract with Spotify that grants him more freedom than most others, but I doubt he has completely free reign. That said, I’m glad he brought Kennedy on, and allowed him to talk uninterrupted.
I am an accomplished interdisciplinary scientist and physicist, and a former tenured Full Professor of physics and lead scientist, originally at the University of Ottawa.
I have written over 30 scientific reports relevant to COVID, starting April 18, 2020 for the Ontario Civil Liberties Association (ocla.ca/covid), and recently for a new non-profit corporation (correlation‑canada.org/research). Presently, all my work and interviews about COVID are documented on my website created to circumvent the barrage of censorship (denisrancourt.ca).
In addition to critical reviews of published science, the main data that my collaborators and I analyse is all‑cause mortality.
All-cause mortality by time (day, week, month, year, period), by jurisdiction (country, state, province, county), and by individual characteristics of the deceased (age, sex, race, living accomodations) is the most reliable data for detecting and epidemiologically characterizing events causing death, and for gauging the population-level impact of any surge or collapse in deaths from any cause.
Such data is not susceptible to reporting bias or to any bias in attributing causes of death. We have used it to detect and characterize seasonality, heat waves, earthquakes, economic collapses, wars, population aging, long-term societal development, and societal assaults such as those occurring in the COVID period, in many countries around the world, and over recent history, 1900-present.
Interestingly, none of the post-second-world-war Centers-for-Disease-Control-and-Prevention-promoted (CDC‑promoted) viral respiratory disease pandemics (1957-58, “H2N2”; 1968, “H3N2”; 2009, “H1N1 again”) can be detected in the all‑cause mortality of any country. Unlike all the other causes of death that are known to affect mortality, these so‑called pandemics did not cause any detectable increase in mortality, anywhere.
The large 1918 mortality event, which was recruited to be a textbook viral respiratory disease pandemic (“H1N1”), occurred prior to the inventions of antibiotics and the electron microscope, under horrific post-war public-sanitation and economic-stress conditions. The 1918 deaths have been proven by histopathology of preserved lung tissue to have been caused by bacterial pneumonia. This is shown in several independent and non-contested published studies.
My first report analysing all-cause mortality was published on June 2, 2020, at censorship-prone Research Gate, and was entitled “All-cause mortality during COVID-19 – No plague and a likely signature of mass homicide by government response”. It showed that hot spots of sudden surges in all‑cause mortality occurred only in specific locations in the Northern-hemisphere Western World, which were synchronous with the March 11, 2020 declaration of a pandemic. Such synchronicity is impossible within the presumed framework of a spreading viral respiratory disease, with or without airplanes, because the calculated time from seeding to mortality surge is highly dependent on local societal circumstances, by several months to years. I attributed the excess deaths to aggressive measures and hospital treatment protocols known to have been applied suddenly at that time in those localities.
The work was pursued in greater depth with collaborators for several years and continues. We have shown repeatedly that excess mortality most often refused to cross national borders and inter-state lines. The invisible virus targets the poor and disabled and carries a passport. It also never kills until governments impose socio-economic and care-structure transformations on vulnerable groups within the domestic population.
Here are my conclusions, from our detailed studies of all-cause mortality in the COVID period, in combination with socio-economic and vaccine-rollout data:
If there had been no pandemic propaganda or coercion, and governments and the medical establishment had simply gone on with business as usual, then there would not have been any excess mortality
There was no pandemic causing excess mortality
Measures caused excess mortality
COVID-19 vaccination caused excess mortality
Regarding the vaccines, we quantified many instances in which a rapid rollout of a dose in the imposed vaccine schedule was synchronous with an otherwise unexpected peak in all-cause mortality, at times in the seasonal cycle and of magnitudes that have not previously been seen in the historic record of mortality.
In this way, we showed that the vaccination campaign in India caused the deaths of 3.7 million fragile residents. In Western countries, we quantified the average all-ages rate of death to be 1 death for every 2000 injections, to increase exponentially with age (doubling every additional 5 years of age), and to be as large as 1 death for every 100 injections for those 80 years and older. We estimated that the vaccines had killed 13 million worldwide.
If one accepts my above-numbered conclusions, and the analyses that we have performed, then there are several implications about how one perceives reality regarding what actually did and did not occur.
First, whereas epidemics of fatal infections are very real in care homes, in hospitals, and with degenerate living conditions, the viral respiratory pandemic risk promoted by the USA‑led “pandemic response” industry is not a thing. It is most likely fabricated and maintained for ulterior motives, other than saving humanity.
Second, in addition to natural events (heat waves, earthquakes, extended large-scale droughts), significant events that negatively affect mortality are large assaults against domestic populations, affecting vulnerable residents, such as:
sudden devastating economic deterioration (the Great Depression, the dust bowl, the dissolution of the Soviet Union),
war (including social-class restructuring),
imperial or economic occupation and exploitation (including large-scale exploitative land use), and
the well-documented measures and destruction applied during the COVID period.
Otherwise, in a stable society, mortality is extremely robust and is not subject to large rapid changes. There is no empirical evidence that large changes in mortality can be induced by sudden appearances of new pathogens. In the contemporary era of the dominant human species, humanity is its worst enemy, not nature.
Third, coercive measures imposed to reduce the risk of transmission (such as distancing, direction arrows, lockdown, isolation, quarantine, Plexiglas barriers, face shields and face masks, elbow bumps, etc.) are palpably unscientific; and the underlying concern itself regarding “spread” was not ever warranted and is irrational, since there is no evidence in reliable mortality data that there ever was a particularly virulent pathogen.
In fact, the very notion of “spread” during the COVID period is rigorously disproved by the temporal and spatial variations of excess all-cause mortality, everywhere that it is sufficiently quantified, worldwide. For example, the presumed virus that killed 1.3 million poor and disabled residents of the USA did not cross the more-than-thousand-kilometer land border with Canada, despite continuous and intense economic exchanges. Likewise, the presumed virus that caused synchronous mortality hotspots in March-April-May 2020 (such as in New York, Madrid region, London, Stockholm, and northern Italy) did not spread beyond those hotspots.
Interestingly, in this regard, the historical seasonal variations (12 month period) in all-cause mortality, known for more than 100 years, are inverted in the northern and southern global hemispheres, and show no evidence of “spread” whatsoever. Instead, these patterns, in a given hemisphere, show synchronous increases and decreases of mortality across the entire hemisphere. Would the “spreading” causal agent(s) always take exactly 6 months to cross into the other hemisphere, where it again causes mortality changes that are synchronous across the hemisphere? Many epidemiologists have long-ago concluded that person-to-person “contact” spreading of respiratory diseases cannot explain and is disproved by the seasonal patterns of all-cause mortality. Why the CDC et al. are not systematically ridiculed in this regard is beyond this scientist’s comprehension.
Instead, outside of extremely poor living conditions, we should look to the body of work produced by Professor Sheldon Cohen and co‑authors (USA) who established that two dominant factors control whether intentionally challenged college students become infected and the severity of the respiratory illness when they are infected:
degree of experienced psychological stress
degree of social isolation
The negative impact of experienced psychological stress on the immune system is a large current and established area of scientific study, dutifully ignored by vaccine interests, and we now know that the said impact is dramatically larger in elderly individuals, where nutrition (gut biome ecology) is an important co-factor.
Of course, I do not mean that causal agents do not exist, such as bacteria, which can cause pneumonia; nor that there are not dangerous environmental concentrations of such causal agents in proximity to fragile individuals, such as in hospitals and on clinicians’ hands, notoriously.
Fourth, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, the debate about gain-of-function research and an escaped bioweapon is irrelevant.
I do not mean that the Department of Defence (DoD) does not fund gain-of-function and bioweapon research (abroad, in particular), I do not mean that there are not many US patents for genetically modified microbial organisms having potential military applications, and I do not mean that there have not previously been impactful escapes or releases of bioweapon vectors and pathogens. For example, the Lyme disease controversy in the USA may be an example of a bioweapon leak (see Kris Newby’s 2019 book “Bitten: The Secret History of Lyme Disease and Biological Weapons”).
Generally, for obvious reasons, any pathogen that is extremely virulent will not also be extremely contagious. There are billions of years of cumulative evolutionary pressures against the existence of any such pathogen, and that result will be deeply encoded into all lifeforms.
Furthermore, it would be suicidal for any regime to vehemently seek to create such a pathogen. Bioweapons are intended to be delivered to specific target areas, except in the science fiction wherein immunity from a bioweapon that is both extremely virulent and extremely contagious can be reliably delivered to one’s own population and soldiers.
In my view, if anything COVID is close to being a bioweapon, it is the military capacity to massively, and repeatedly, rollout individual injections, which are physical vectors for whichever substances the regime wishes to selectively inject into chosen populations, while imposing complete compliance down to one’s own body, under the cover of protecting public health.
This is the same regime that practices wars of complete nation destruction and societal annihilation, under the cover of spreading democracy and women’s rights. And I do not mean China.
Fifth, again, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, there was no need for any special treatment protocols, beyond the usual thoughtful, case-by-case, diagnostics followed by the clinician’s chosen best approach.
Instead, vicious new protocols killed patients in hotspots that applied those protocols in the first months of the declared pandemic.
This was followed in many states by imposed coercive societal measures, which were contrary to individual health: fear, panic, paranoia, induced psychological stress, social isolation, self-victimization, loss of work and volunteer activity, loss of social status, loss of employment, business bankruptcy, loss of usefulness, loss of caretakers, loss of venues and mobility, suppression of freedom of expression, etc.
Only the professional class did better, comfortably working from home, close to family, while being catered to by an army of specialised home-delivery services.
Unfortunately, the medical establishment did not limit itself to assaulting and isolating vulnerable patients in hospitals and care facilities. It also systematically withdrew normal care, and attacked physicians who refused to do so.
In virtually the entire Western World, antibiotic prescriptions were cut and maintained low by approximately 50% of the pre-COVID rates. This would have had devastating effects in the USA, in particular, where:
the CDC’s own statistics, based on death certificates, has approximately 50% of the million or so deaths associated with COVID having bacterial pneumonia as a listed comorbidity (there was a massive epidemic of bacterial pneumonia in the USA, which no one talked about)
the Southern poor states historically have much higher antibiotic prescription rates (this implies high susceptibility to bacterial pneumonia)
excess mortality during the COVID period is very strongly correlated (r = +0.86) — in fact proportional to — state-wise poverty
Sixth, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, there was no public-health reason to develop and deploy vaccines; not even if one accepted the tenuous proposition that any vaccine has ever been effective against a presumed viral respiratory disease.
Add to this that all vaccines are intrinsically dangerous and our above-described vaccine-dose fatality rate quantifications, and we must recognize that the vaccines contributed significantly to excess mortality everywhere that they were imposed.
In conclusion, the excess mortality was not caused by any particularly virulent new pathogen. COVID so-called response in-effect was a massive multi-pronged state and iatrogenic attack against populations, and against societal support structures, which caused all the excess mortality, in every jurisdiction.
It is only natural now to ask “what drove this?”, “who benefited?” and “which groups sustained permanent structural disadvantages?”
In my view, the COVID assault can only be understood in the symbiotic contexts of geopolitics and large-scale social-class transformations. Dominance and exploitation are the drivers. The failing USA-centered global hegemony and its machinations create dangerous conditions for virtually everyone.
“Gates’ actual goal in reaching the poor is to use them as guinea pigs in his experiments in culling the human race. It is also a virtue signal — a means of getting away with his brand of predatory philanthropy…”
…
“The lack of access to c-19 injections was not a tragedy, it was a fantastically lucky break for the world’s poor. Thank heaven the world’s poor were not served equitably with the toxic jabs.
“In the rich countries whose people did get them, millions have been injured and killed. It is hard to imagine that an on-the-ground practicing doctor could miss the non-evidence of a pandemic, and the dangers of giving totally new medical products from felony-convicted drug companies to everyone in the world, without delay.”
Until we have vaccines & medicines, mask wearing is one of the best tools we have to stop the spread of COVID-19. #WearAMask and upload a photo to social media, then ask your friends to do the same 😷 🤳 #WorldMaskWeekpic.twitter.com/ypA07gNI7J
A good job, wealth, honors, and prestige are hard to come by if you’re outside the establishment.
At the time of his death almost a year and a half ago, Dr. Paul Farmer had all the honors —co-founder of Partners In Health, University Professor at Harvard, a department chief at Boston’s Brigham and Women’s Hospital, UN envoy, recipient of prestigious awards, subject of the New York Times bestseller Mountains Beyond Mountains — but his reputation was built on not being part of the establishment. Perhaps his biggest honor was that he was allowed to have it both ways.
He was praised for setting up clinics and living among the poor in Haiti and Rwanda, yet he was well connected with a very corrupt global health establishment — the WHO, the UN, the Bill and Melinda Gates Foundation, USAID, and the Clinton Global Initiative — and no one mentioned a conflict.
In August 2021 Farmer co-signed a letter to President Biden saying,
“The time is now for ambitious leadership to vaccinate the world. The need to be on a “wartime footing” to secure the world against this pandemic viral threat is paramount. Any global COVID vaccination program must be structured to address multiple interlinked priorities. First, the manufacturing capacity of mRNA vaccines in the US must be rapidly scaled up to reach approximately 4 billion people by the end of 2021 . . . . “
This is the same message Bill Gates had for us at about the same time when he informed us that “we need to vaccinate everyone on the planet.”
When it came to covid, Farmer’s message was not that untested mRNA vaccines might possibly be unsafe but that a special effort should be made to get them to the poor right away.
“By massively boosting vaccine production and removing barriers to an equitable rollout,” he said, “we can help vaccinate the world to the benefit of all.” ‘Equity’ was also the message put out by Bill Gates almost every time he gave an interview. “The lack of equitable access to COVID-19 vaccines is a public health tragedy,” Gates said.
Gates’ actual goal in reaching the poor is to use them as guinea pigs in his experiments in culling the human race. It is also a virtue signal — a means of getting away with his brand of predatory philanthropy. And, no matter if a country is poor, Gates looks to make a profit on his investments — something the devil apparently allows.
The Clinton Foundation used the poor in a similar way in Haiti, using the plight of Haiti’s devastating 2010 earthquake to raise $9 billion in charitable donations, only 10% of which actually went to Haitian organizations. Bill Clinton was envoy to the UN in this scam and Paul Farmer was directly involved as UN special envoy under Clinton.
So, Farmer was a front man for Clinton and accepted money (and pandemic talking points) from Gates. One wonders why.
One might now also question if Dr. Farmer’s bringing Anthony Fauci-underwritten HIV/AIDS drugs to Haiti in the 1990s was more of a benefit to Haitians or to the pharmaceutical companies who sold them for up to $16,000 per patient. If it hadn’t been for the gross malfeasance revealed in the covid era, we might never have asked.
The lack of access to c-19 injections was not a tragedy, it was a fantastically lucky break for the world’s poor. Thank heaven the world’s poor were not served equitably with the toxic jabs.
In the rich countries whose people did get them, millions have been injured and killed. It is hard to imagine that an on-the-ground practicing doctor could miss the non-evidence of a pandemic, and the dangers of giving totally new medical products from felony-convicted drug companies to everyone in the world, without delay.
Farmer rightly gained his reputation showing the connections between poverty and disease, but he made a terrible mistake getting caught up in the designs of predatory pharmaceutical companies and profit-making philanthropists.
Considering the small number of wealthy psychopaths who planned and conducted the covid operation, the war on the poor includes just about everyone — not just people in remote villages in Haiti — and doctors of medicine were its main lieutenants.
This great humanitarian seems to have missed the fact that the fake pandemic was a broad-daylight attack in an overall war on humanity.
In February 2022, Partners in Health announced that Paul Farmer died of “an acute cardiac event while he was sleeping.” He was 62. He is thus among the thousands who “died suddenly” — the meme for healthy people who quite likely died from covid “vaccination,” though we’re never told.
The kindest interpretation is that, unlike Gates, Paul Farmer was not among the cognoscenti, and that he unwittingly took the same poison he was pushing for all.
The moral of the story: you may gain fame and fortune, but end up being just a dupe. What a terrific waste for a man who apparently spent his life caring for the poor.
Let the well-off and well-connected take note: no matter the fame and status the establishment gives you, you can be used and discarded just like everybody else. There are other goals more worth achieving.
“The point is, separately, in different venues, the Breggins and Jane Ruby are individuals who rose to the challenge to try to inform a brutalized public about what turns out to have been a war: a war of fear, fraud and bioweaponry waged against us by own government. Their contributions were, are and will continue to be vitally important to the flow of essential and also life-saving information.
Ask yourself: Why would anyone want to deflect these valuable contributors from their important vocations?…”
Do you remember how hard it was to get good information, especially in 2020, back at the Beginning of the End? It is hard still, but it was much worse before so many of us had delved into the sciences with a doggedness we never mustered in high school; before we had learned to see into the geysers of government and media disinformation about the “plandemic,” the “scamdemic,” the garbage-demic, to take apart and stomp on all of the Big Lies we were and are still beset by. And that was even before the government’s biochemical attack on the world via “mRNA vaccine” had begun.
The totalitarian-style censorship and disinformation which government, media and social media imposed upon us were (are) catastrophic and also fatal in all too many cases. That’s why when we learn, through arduous court-ordered FOIA research or congressional hearings or secret interviews or confessions … or autopsies that we were right to doubt and disbelieve and not comply, there are dead bodies, broken homes, ruined lives and a shattered future to embitter our vindication. To intensify our rage. That’s why Dr. Robert Malone’s openly stated goal in 2023 to use the courts to have a “chilling effect’ on debate in the public square, which he’s trying to rebrand as “defamation,” is so disturbing, bizarre and fraught with peril.
Malone’s interlocuters-turned-“defendants” are Dr. Peter Breggin, Ginger R. Breggin and Dr. Jane Ruby — outlandish words to write about such worthies. I don’t recall exactly when in the dark of lockdown I first came upon them. I do remember Dr. Jane’s exciting reports on the then-new Stew Peters Show, her tenacity, her blinking neon commitment to finding the truth, were an immediate godsend. At some point, too, I matched with the Breggins, Dr. Peter Breggin, “Conscience of Psychiatry,” and his wife and co-author Ginger Breggin, benefiting enormously from their warm and civilized discourse, which included (bonus) two interviews with me about American Betrayal. I was delighted to learn my book had inspired the Breggins to dig into the research that became their 2021 success, COVID 19 and the Global Predators: We Are the Prey.
The point is, separately, in different venues, the Breggins and Jane Ruby are individuals who rose to the challenge to try to inform a brutalized public about what turns out to have been a war: a war of fear, fraud and bioweaponry waged against us by own government. Their contributions were, are and will continue to be vitally important to the flow of essential and also life-saving information.
Ask yourself: Why would anyone want to deflect these valuable contributors from their important vocations? So what if they said something, many things, with which you disagree, even violently disagree? So what if they reject and even rebut your theories? So what if they engage you in a veritable “war of words”? To quote vintage Michelle Malkin, “Boo-the-heck-hoo.” Argue. Gnash your teeth. Write a rebuttal. Quote Voltaire. Exult in the First Amendment. But this — resorting to the punitive enforcement mechanism of a defamation lawsuit — is not right. Asking for $25 million in damages is an outrage. Such aggressive lawfare is akin to dropping a cluster bomb. The landscape that was is no more.
As many know, I am referring to the tantrum-esque defamation lawsuit D. Robert Malone has brought against the Breggins and Jane Ruby. I wrote a book about 15 years ago called The Death of the Grown-Up, which employs the metaphor to explore chaos and decline in our time. However, the absence of bona fide adults is not just a metaphorical problem. We could really use some grown-ups here. To wit:
If there happens to be an adult in the vicinity of Dr. Malone’s circle, please, could you instruct the “inventor of the mRNA vaccine” to pack his marbles and come home from the playground? Given the catastrophic impact of his precious invention as deployed by the governments of the world, he’s surely the last man on earth who should be trying to exert a “chilling effect” on anything — and especially not on the speech of doctors and scientists. People are dying from these shots all around. We need help. Debate. Breakthroughs. Not silence, not fear of being dragged to court for speaking up. Sticks and stones, anyone? Like Rick said in Casablanca, the problems of three (or four) little people don’t amount to a hill of beans in this crazy world; however, if Malone were to win this lawsuit, American jurisprudence would feature a jihad-style trip-wire on public debate by public figures on public issues. Then again, if the First Amendment and American tradition count for anything at all anymore, the court will rule decisively against Malone. One man’s “defamation” will be everyone else’s free speech.
But at what cost? Stories of case-related censorship and acrimony buzz around the erstwhile medical freedom movement. Wouldn’t it be a better use of everyone’s time to try to figure out how to heal mRNA-injected humanity?
It was about half-way through 2021 when Dr. Malone showed his face in public discourse. Remember the weird thrill that rippled through the battered band of shot-resisters? Look: the mRNA inventor was throwing shade, some, anyway, on the mass injection program at that time in full-throttle- enforcement. Yes, to be sure, Xyklon B isn’t for everybody….How exciting? I’m not sure what psychological buttons Malone’s arrival on the scene pushed; as I think back on it now, such enthusiasm doesn’t make a lot of sense. After all, he didn’t come forward expressing remorse, as lots of great inventors have done before him, rueing their sometimes literally earth-shaking inventions, from the atom bomb and the Kalashnikov, to the office cubicle and the labradoodle. Notably, “The History of mRNA Vaccines” still unfolds under a spray of lovely pink blossoms here on Malone’s website.
Nor did he arrive on the medical freedom scene waving an antidote to mRNA technology, which, they say, has now been “delivered” into 70 percent of humanity and linked to a scale of death and injury that is unimaginable.
Kristen Napolillo asked Malone on Twitter: “What are you doing to find a way to blunt the effects of your invention?”
One thing about quoting Dr. Robert Malone: There is no need to underscore or add anything.
On June 8, 2023, Dr. Malone set forth his legal thinking on Substack:
My criteria for taking legal action has been whether or not someone seems to be doing significant reputational damage, while also factoring in the quirky nature of various clauses in defamation law.
It’s almost touching, isn’t it, to see someone who “invented the mRNA vaccine” fretting about “reputational damage”?
In some cases I have proceeded to delivering a cease and desist and that was enough. Dr. Richard Fleming was one such case. I sent him a letter, and he stopped. Seems rational enough. Thank you, Richard (and I seriously mean that).
Again, no comment necessary — but I do want to write that again: Thank you, Richard (and I seriously mean that).
He continues:
Turns out that response is the exception rather than the rule. Others double down, go public, get even nastier and more personally vindictive.
No! Can you beat that? Malone sends out a “cease and desist” and some people … refuse?
So then you have the same dilemma. Act on it or not. Fish or cut bait. First stop is to ask a mutual colleague to intervene. In almost all cases they refused. So you then pay the lawyer to prepare and file the suit. And in some cases the accused gets even nastier, and seeks to cause yet more pain.
It’s a marvel but he soldiers on:
There are all of the armchair quarterbacks, some of who are employers, friends or associates with the ones doing the harassment and defamation. “Why are you suing the ____ (fill in the blank)!!??!!” “You just want to destroy the medical freedom movement!” (whatever that is). “You are just doing it for money!” (what a horrible business plan that would be, given the paltry odds of winning a defamation lawsuit).
“Fill in the blank”? Somehow, I feel bidden to provide photos of the people, the experts, including an eminent doctor, the writers and commentators, the human beings whom Dr. Malone has just turned into a blank.
Now, let him rip.
No, I am suing because I am having something taken from me, and it is both wrong and illegal. My reputation, my peace of mind, and that of those close to me. Cyberstalking, cyberbullying, malicious defamation. These things are wrong. They are not what civilized, mentally healthy people do to each other. And they often seem to involve some odd perverse obsession.
But it is also true that hate and defamation is a very good business model and a great way to build up a follower base. People are building their audiences by employing this strategy based on tall tales, lies, name calling and hate. But maybe, just maybe, if I win a case, this will become a disincentive for those prone to this sort of behavior in the future, directed towards me or to others.
And then there are the ones that are shunning me because I am (legally) fighting back against those that are doing this to Jill and I [sic]. That part is a real mind-bender for me. Somehow fighting back against those who are aggressively cyberstalking and defaming me on a daily basis makes me the bad guy. Now if that is not pretzel logic, I do not know what is.
I suppose, in an intellectual sense, it is a fascinating question to ponder – what makes these people behave in this way? Why do haters hate? Why do others support them? I do not have an answer, only informed speculation. Personally, I think it somehow relates to the mental state of other types of stalkers, such as the ones that shot President Regan [sic] and John Lennon. And it clearly relates to envy, jealousy, and greed. Spreading hate can be quite lucrative in the age of the internet, where attention seeking behavior can be monetized. So there is that. (Emphasis added.)
I have no quip to make when the rhetoric is so troubling. Consider seriously that Dr. Malone has first blanked the names of the Breggins and Jane Ruby, and then created an escalating series of fantastical enemies, from imaginary cyberstalkers, cyberbullies, malicious defamers, to not civilized, not mentally healthy people, to haters with a mentality “somehow related” to that of notorious violent criminals: John Hinkley and Mark David Chapman, the former, the attempted-assassin who wounded Ronald Reagan and paralyzed James Brady; the latter, the assassin of John Lennon.
Still, no one around him has put a hand on his shoulder and said, Enough.
—
Let’s pick up on p. 13 of a recent Motion to Dismiss by Dr. Peter Breggin and Ginger R. Breggin.
The Breggin Motion is discussing the thirteenth bulleted item in Malone’s Complaint. This Item 13 contains four separate allegations of defamation purported to be found in an online interview of Dr. Breggin by Pete Santilli.
From the Breggins’ Motion to Dismiss:
Malone alleges that Breggins stated: Dr. Malone is part of the “Deep State” oppressors. Dr. Malone’s concept of mass formation psychosis is calculated to protect the “mass murderers of COVID-19.” Dr. Malone is a Hitler apologist and “excuser.” “Malone wake up to history.”
The Breggins:
When examining the entire interview of Dr. Breggin on this show, nowhere in the show can it be found that Dr. Breggin made the statement that Malone atrributes to him that he is a part of the “Deep State oppressors.”
Malone’s allegations that Breggin stated that “Dr. Malone’s concept of mass formation psychosis is calculated to protect the `mass murderers of COVID-19′ is actually Breggin talking about Dr. Desmet,not Dr. Malone.
And lastly, nowhere in this recorded interview (or anywhere else for that matter) can it be found where Dr. Breggin ever stated that Dr. Malone is “a Hitler apologist and excuser.”
First of all, may I say (shout): Who cares! Say what you will! These are public commentators debating the onset of totalitarianism in our time. Hitler, Stalin, Mao are the totalitarian all-stars, at least up to now, and are gonna come up. Boo-the-heck-hoo. Still, there is a crucially important legal (and moral) point here: The Breggins’ brief states that certain of these quotations are not to be found on video, or anywhere else. If this is true — and I cannot find them, either — the Malone Complaint includes false allegations. Put that in your syringe and shoot it. What will the judge say about that?
And now this:
Moreover, the only quote that can be found to be semi-accurate, “Desmet, Malone, wake up to history,” is a pejorative at best, and an admonition even, but it is not defamatory.
No, it is not. But ponder the legal mind that sees fit to include such an innocuous comment, with its pleasantly archaic rhetorical flourish, into a defamation brief. Ponder the scientific mind that hopes for a “chilling effect.” Frankly, if Dr. Robert Malone is so darn worried about reputational damage, he should drop this stupid lawsuit ASAP and wake up. Wake up to free speech.
In the glorious aftermath of Robert Kennedy Jr. red-pilling Joe Rogan about vaccines; other toxic but government approved products like glyphosate, atrazine, and PFOAs; and the malfeasance of government agencies, vaccine developer Dr. Peter Hotez seriously miscalculated or suffered an unfortunate lapse of judgement when he accused Kennedy of spreading misinformation. He thus unleashed a storm of criticism he surely never expected. Rogan publicly offered Hotez $100,000 donated to the charity of his choice if he would come on the show to debate Kennedy. Other onlookers chipped in and the donation promise mounted. Last I looked, the offer stood at $2.6 million but Hotez is not taking it!
Never before has the refusal of vaccine apologists to debate vaccine critics spoken louder of their ties to big pharma, big media, big government, and big academia.
Observing the last few years, millions have not just awoken to the reality of conflicts of interest and captured media, industry, and government, but also to true authoritarian censorship. Unfortunately, while millions may be forgiven for believing this is a recent development, the reality is far different.
I’ve been smeared by media outlets like the New York Times and CBS. Congressman Adam Schiff wrote to big tech and had my movie The Greater Good and the movies and books of many others removed from big tech platforms. Those of us working on vaccine safety awareness and health freedom issues know this is nothing new and has, instead, been standard practice for decades.
And Peter Hotez has acted as a loyal foot soldier to the big pharma lobby in their condemnable battle against honest citizens who’ve witnessed vaccine injury close up. His dishonesty is now on full display for all to see – but again, it’s not new.
In 2021, Hotez tweeted false claims about investigative reporter Sharyl Attkisson alleging she had endorsed an article comparing him to Joseph Mengele, placed him in harm’s way through “dangerous and hurtful” conduct, and called for his doxing. He even suggested she was connected to white nationalists and was sending him images of Nuremberg. To call Hotez a liar is an understatement. Hotez exhibits a particularity dangerous and pathological behavior in that he is not merely dishonest but a fabricator of falsehoods intended to destroy those with different opinions.
Unfortunately, I have had my own experience with Hotez.
On October 2, 2019, a pediatrician, the Idaho State Health and Welfare epidemiologist, Hotez, and I, were guests on the NPR/Boise Public Radio show Idaho Matters. Some might argue 2019 was a prelude to what was to come in 2020 as the relatively small increase in measles cases was being hyped worldwide and weaponized against those demanding bodily autonomy and truth in science. Hotez’ conduct on the show illustrates perfectly the kind of person we’re now seeing unmasked – and it’s not a very flattering image.
Hotez employs slurs, ad hominem attacks, and falsehoods to smear his challengers from the vaccine safety awareness community. Again, this kind of treatment is not new. During the radio show, Hotez made the following statements:
1) that there is an “aggressive anti-vaccine lobby”
2) that I repeated “anti-vaccine tropes”
3) that I compared the measles cases in NY to the national population to “deliberately mislead”
4) that the concept of health and medical freedom is a “phony concept”
5) that I and other parents “download vaccine misinformation” from the internet
6) that the “anti-vaccine lobby is a media empire” with over 480 “misinformation websites”
7) that parents can’t put children in harm’s way because of “misinformation”
8) that I stated 89,000 vaccine “injuries” have been reported to VAERS after MMR
9) that Hotez is going to “correct the misinformation” I gave and give the “real information”
Additionally, Hotez insinuated I was lying when I stated that a local woman developed MS from a vaccine by saying there is no evidence of that. The young woman in question had to leave our community with her three children as she was no longer able to care for her family. She spent time on a neurological ward at a hospital in Salt Lake City, UT and there were many others suffering neurological complications from flu vaccines.
So, let’s address his claims:
1) There is a genuine grassroots effort of vaccine injured families raising awareness about the lack of quality science on vaccines. Specific problems with vaccine safety studies are the lack of genuine placebos (mercury, aluminum or another vaccine is used), short duration (studies can last as few as 3 days), lack of comparison to completely unvaccinated populations, lack of studies evaluating all the combinations in which vaccines are given, lack of studies evaluating health outcomes of the vaccination schedule. There are a couple of studies comparing health outcomes of vaccinated versus unvaccinated children and they overwhelmingly show the health of unvaccinated children is superior. The truth is that big pharma, which includes the vaccine industry, is the largest lobby group in the US shelling out $250 million each year, spends $35 billion on ads annually thereby “owning” the media, pays more than half the drug approvers’ salaries at FDA, and controls the medical journals through the purchase of glossy reprints.
2) Everything I stated was based on official data from US agencies or data from peer-reviewed published studies. It’s there for anyone to see – you just have to dig a little deeper than the mainstream media. In fact, these days, you may have to employ an independent search engine because google rigs its results to downplay anything that challenges officialdom. I don’t repeat tropes, I know the science and would gladly debate Hotez or any other vaccine pusher about the true science of vaccines, including all we don’t know.
3) I did not compare measles cases in NY to the national population. I compared the total amount of measles cases according to CDC to the total US population. To understand how the public has been misled about the dangers of measles, the cases, and the role of vaccines, check out these articles at Children’s Health Defense.
4) Health and medical freedom are not a “phony” concept. Children have been kidnapped by hospitals and CPS for refusing the Hep B shot at birth or deciding a fever has passed and there’s no need for medical attention. There is nothing phony about parents having their children stolen from them because they’ve done what they think is best for their children. Millions have been injured by vaccines and there is a mountain of science documenting the risks and shortcomings of vaccines. To suggest otherwise is not only dishonest, it’s immoral.
5) All the information I give in all forums is, to the best of my knowledge, accurate and derived from published peer-reviewed research or US government data. It is not misinformation in any way, shape or form, no matter how often or loudly Hotez or other vaccine industry stakeholders shout about it. (Notice, Hotez and his ilk were calling us misinformation spreaders years ago – it’s not a new derision.) Rather, parents like me have advanced degrees and are highly educated. We can read science and discern when we’re being misled. We understand when an issue is being whitewashed. We understand experts can be bought and we’re smart enough, strong enough, and well-educated enough to call them out – we’re just not usually given the chance.
6) The vaccine awareness safety movement is largely not “anti-vaccine”. Rather, it is comprised primarily of ex-vaccinators who’ve witnessed the dangers of vaccines first hand. Would you call them anti-car seat for wanting safe car seats for their children? If someone chooses to only eat organic food, does that make them anti-food? If someone chooses filtered water based on the science related to a specific filter does that make them anti-water? If someone chooses to live in the countryside does that make them anti-city? This slur has been weaponized to smear and dehumanize individuals and their choices rather than address the damage sustained by them or their children from government approved products. It’s a ridiculous leap that has been normalized and is the go-to rhetoric for dismissing well-educated, well-researched individuals as loony dissenters. Many parents who once enthusiastically embraced vaccinations have now adjusted their posture choosing not to vaccinate and challenging the official narrative, but that results from personal negative experience, not some words they read on the internet.
7) Parents are protecting their children and themselves from the injection of known toxins that can damage the neurological system, the immune system, the gastrointestinal system, and more. Vaccines contain myriad toxins which have never been tested singly or in combination for toxicity, yet they are readily injected into our tiny, newborn babies as though no possible downside exists. This is prima facie not just wrong, but indisputably unethical.
8) I stated correctly that there have been 89,000 reports of adverse reactions to measles vaccines. Hotez’ number of 221 is the number who actually received compensation from the impossibly corrupted Vaccine Compensation Program.
“While the current vaccine is acknowledged as a good vaccine, we and others have demonstrated that the immune response to measles vaccine varies substantially in actual field use. Multiple studies demonstrate that 2–10% of those immunized with two doses of measles vaccine fail to develop protective antibody levels, and that immunity can wane over time and result in infection (so-called secondary vaccine failure) when the individual is exposed to measles. For example, during the 1989–1991 U.S. measles outbreaks 20–40% of the individuals affected had been previously immunized with one to two doses of vaccine. In an October 2011 outbreak in Canada, over 50% of the 98 individuals had received two doses of measles vaccine. The Table shows that this phenomenon continues to play a role in measles outbreaks. Thus, measles outbreaks also occur even among highly vaccinated populations because of primary and secondary vaccine failure, which results in gradually larger pools of susceptible persons and outbreaks once measles is introduced [8]. This leads to a paradoxical situation whereby measles in highly immunized societies occurs primarily among those previously immunized [8].”
Call me a lay person, but it does not take a scientist to understand words like “primary and secondary vaccine failure” or the “paradoxical situation of highly vaccinated groups being more susceptible.” Hmmm. When have I heard about vaccines undermining the immune system and rendering vaccinees more susceptible to illness?
While it wasn’t Hotez who made the absurd claim that vaccines are one of the best tested medicines available, I feel I’d be remiss by not correcting that whopper. The truth is vaccine safety studies do not use genuine placebos, they instead utilize another vaccine or solution containing mercury or aluminum as the placebo. Absent placebo-controlled studies, it is preposterous to claim that vaccines are well tested and one cannot make any claims about safety or efficacy without a proper placebo-controlled study. NONE. Not to mention that vaccine safety studies evaluate one vaccine but vaccines are administered in groups of as many as 8 doses of vaccines in a day. Nor are the health outcomes of vaccinated compared to those of the unvaccinated. To argue this is robust science is laughable. To understand the shortcomings of vaccine science, watch my movie, The Greater Good.
Hotez has deep ties to the pharmaceutical industry, spent his career developing vaccines and holds patents on vaccines, rendering him a seriously conflicted participant in any debate about vaccines. One would never ask someone from the coal industry about the safety of coal-fired power plants but when it comes to vaccine-connected physicians and scientists, we somehow give them a free pass. Perhaps worse still is the glaring lack of disclosure made by media when media presents these so-called experts with vested interests. Nary a word was mentioned about Hotez’ background in his introduction on the show.
In addition, Hotez makes disparaging remarks about those who deviate from the official orthodoxy of vaccines dispensed by the pharmaceutical industry and the health agencies that receive vast sums from that industry without any consequence or challenge from the compliant media.
As I wrap things up, let me share one last tidbit which illustrates the type of sick individual Hotez is; I did not have time to mention this during the show, but he has stated that the parents of vaccine injured children “hate their children and are a hate group.” Seriously.
It beggars belief that Hotez has any credibility as an expert but the pharma-influenced media doesn’t bat an eye at such outrageous comments.
Robert F. Kennedy Jr. would do the world a service by debating Hotez but my experience speaks volumes about Hotez’ true colors – he’s not interested in an exchange of different views, respectable debate, or an examination of the body of science. You can hear it yourself in the show, all he does is disparage me and those who have concerns about the safety of vaccines likely in the hopes that others will dismiss our concerns without further investigation.
Hopefully, his latest antics will undermine any vestigial credibility he may have had.
[TCTL editor’s note: To keep up with growing amount of money being offered to Peter Hotez (for his favorite charity) for a debate with RFK Jr., see Joe Rogan’s twitter feed. TCTL is still suspended from twitter (that happened years ago) but you can view JRE’s feed whether you have an account or not.]
According to the science we learn in our indoctrination center called the educational system, leukemia or blood cancer is a disease in which an overproduction of white blood cells is created. Many of those cells are damaged or not developed enough, and this is caused by the damaged bone marrow which produces them.
We are educated/indoctrinated to believe that white blood cells are our immune system, created to protect us from the pathogen that has attacked our body. So, when the pathogen occurs, the white blood cell blood count increases. As the pathogen gets gobbled up by the white blood cells/macrophage, (the process science has named autophagy), the threat no longer exists, and the number of white blood cells reduces to the ”normal” levels.
When the blood count of white blood cells is high and no pathogen is detected, and the situation persists without the white blood cell count dropping to the normal level, this is when the body is declared by our experts to be diseased with leukemia.
Is this what really happens?
We are “educated” to recognize leukemia through the symptoms that accompany it. Those symptoms are; fever or chills, persistent fatigue, frequent infections, losing weight, swollen lymph nodes, easy bleeding or bruising, tiny red spots in the skin, excessive sweating, and bone pain and tenderness.
In which way an increased white blood cell count causes such symptoms? This makes no sense.
When we look at those symptoms, everyone who is familiar with my work immediately comes to the conclusion that those are symptoms of toxic blood and a toxic body in general.
Since white blood cells are not what we are told, a defense mechanism created to attack the intruder/pathogen, instead, they are a garbage disposal system, as the level of the garbage increases in the blood, the body increases the production of white blood cells to dispose of this garbage.
This means that the body is functioning correctly in the given circumstance. Since doctors cannot identify any pathogen and the blood level of white blood cells remains high, they blame the bone, thymus, and lymph nodes for overproducing white blood cells for no apparent reason, and through the implementation of toxic chemicals, they attack those organs to suppress white blood cell production.
Through their action, doctors increase the blood´s toxicity which stimulates the body to further increase the white blood cell count, and the battle with the “disease” becomes eventually lost because the overly toxic patient dies.
Doctors proudly declare that they have extended the patient’s life/suffering for as long as they could and without their intervention, the patient would have died sooner.
Well, it is obvious that doctors are incompetent and they are the reason why their patient has died.
What is the cause of increased white blood cell count and why it remains high?
The symptoms reveal that the blood is toxic. Since the white blood cell count has increased, this means that the body senses a toxin that can be eliminated by disposing of it through white blood cells (most likely an organic compound).
The bone marrow thymus and lymph nodes start to produce white blood cells, but they cannot recognize the “garbage” because it is not labeled. Since the toxic level is not dropping, the body continues producing white blood cells and at the same time, some of them are expiring and undergo autophagy and appear damaged or undeveloped.
The reason why the poison is not labeled is the lack of GcMAF because of the incorrect genetic expression caused by eating starches/glucose. The cells are forced to produce nagalase to be able to hydrolyze glucose and use it as fuel. This prevents them to produce GcMAF since the same pair of genes is responsible for the signaling to the cell what the cell should manufacture in this given environment.
This is another example of how eating starches contributes to a diseased state of our body.
Since those people that follow the SHP are forbidden to consume starches, their cells start to produce GcMAF marker, the toxins become marked and eliminated through macrophage, and as the blood toxic level drops, the production of the white blood cells stops and leukemia miraculously disappears.
I have noticed that green tea has toxins that stimulate white cell production, and preservatives of meat in canned food and sausages do the same. This is why we see leukemia often in people that consume large quantities of green tea and children that eat colorful cereals, frankfurters or ham, or other types of salami.
Also, cats fed with can foods and dry food loaded with carbohydrates will develop leukemia.
They all heal when their food is corrected.
It was brought to my attention that by July people will be able to start scheduling their med bed appointments. They will be free so if someone wants to sell you an appointment, this is a fraudster, do not fall for it.
“Is this intentional? Are we subjected to this slow genocide as part of the global eugenic effort to rid the world of useless eaters?—or even more horrifying, to rid the world of all humans who are made in the image of God along with nature herself? An agenda chillingly made clear in C.S. Lewis’ tome That Hideous Strength seen as well in the works of numerous others such as George Orwell and Aldous Huxley.
“Probably not everything I have mentioned here has come about as part of this nefarious evil intention. But I would be willing to bet a lot of it has (see the work of David Icke). It may just have become the nature of the beast to create a culture in its atheistic hubris that ignores the subtleties of life and living.”
We have, for quite some time, been exposed to a myriad of silent killers. These are the subtle murderers of both the physical body as well as the spirit.
I used to think most of these killers were unintentional and merely the result of ignorance or a non-existent understanding of the non-material world of spirit. I also felt that science was rather inept in detecting subtle shifts of emotion, such as depression or “just not feeling well.” All such “measurements” were simply too nuanced to show up in their metrics.
Now I believe a lot of what I am speaking of is intentional. We are intentionally being eliminated or, at the very least, intentionally being made ill. Humanity is purposefully being murdered.
That’s a rather radical assumption, eh? Well, let’s just put it aside for the moment if this bothers you. I can make a good argument even if you are unwilling to accept that extreme notion. And, as the eminent Swiss psychiatrist Carl Jung used to often say to his patients, “Well, I could be wrong.”
There are many obvious things out in the world that are killing us softly…and not all of them so softly. Pollution is a big one; the air we breathe and the water we drink are toxic—probably more toxic than we are led to believe (that’s the “softly” part). Then on the toxic list we’ve got most of what we eat, the obvious being fast food, the not so obvious being processed food, and the really soft culprit being GMO. There are more “obvious killers” out there as well, I just don’t have the space to include all of them.
Some of the more “not so obvious” things, which some of you may have issue with, are things like 5G, and really any EMF pollution, which even includes radio waves. Most medicine is toxic, doctors themselves can be quite toxic and guilty of killing us softly, although I still would bet most of them do this unintentionally (how many times have you read statistics that “deaths due to doctors, hospitals, and pharmaceuticals” rank in the top five of global killers?) There are so many things on this list it would take volumes to present them all.
Actually, I would not be surprised if every single thing we encounter every day is chemically toxic in some way (meaning it is responsible for destroying the tissue of our physical body). Fun stuff.
I think a lot of people out there are not really aware of most of these things, or think the damage they may inflict is so minimal it really doesn’t amount to much. Well, as they say, things add up.
Again, this is all stuff that most people at least have heard of possibly being bad news. Most of those people, again, probably figure that the powers that be would not allow things out there that could really hurt us. I mean, really, there are so many government agencies that regulate this stuff, and do whatever they can to keep us from being harmed. Cough, cough. Really? Like I’ve said before, if you believe that, I’ve got beachfront property in Nevada I’ll sell you cheap. Or is it Kansas?
We’ve all seen movies like Erin Brockovich (2000) and Dark Waters (2019) that show the heroics of individuals fighting the big bad polluting evil ones and winning millions of bucks for their victims. That’s great, more power to them. But the bad guys in these movies are for the most part a few levels down from the real culprits. Sure, there are evil corporations and CEOs who run them. They are indeed part of the agenda. But again, I won’t get into that here.
Some of the biggest soft killers out there are mental health killers, as well as the drugs that accompany them. I would also put the aforementioned EMF killers in this group, and maybe even some of the pollutants that attack our minds rather than our bodies—nobody pays much attention to that—to subtle effects of personality, cognition, etc. For example most of the talk about the Covid vaccines hurting us is how it hurts us physically. You hear little about the effects they may have on the brain (other than physical), the personality, or the spirit. Oh God no, none of that woo woo stuff please, it just isn’t important.
Human beings are pretty subtle bio systems, and that is just the physical part of us. The mental/emotional part is pretty subtle too, and the spiritual part is so subtle it is ignored entirely. Even the first two of these, physical and mental, are largely ignored. The only part of them that is given much attention at all is the tip of the iceberg part. The majority of these systems lie below the level of gross awareness, yet this hidden level(s) has more influence on the well being of the person than the relatively small portion of the iceberg that is given all of the attention.
Let me be a bit clearer here.
Modern medicine is mostly a science of statistics. The majority rules here, the middle of the bell curve is what is given consideration. Nearly every medical “statement” is given as a percentage. What percent will survive a particular cancer, disease, or treatment modality, what percentage will still be alive in 5 years, what percentage will suffer side effects—on and on. Very little thought is given to the outliers. In fact, certain side effects fall so far below a relevant statistic, that these side effects are completely ignored; yet these ignored side effects could have a huge impact on quality of life.
Here is an example: I have dozens of clients who come to me with the common complaint of depression. Most of them are not suicidal; they simply have what they define as a crappy life. Their life just isn’t the life they envisioned. Maybe they don’t even know they are depressed, but after further evaluation, it seems clear they are just not capable of being fully happy, motivated, curious about life, or even interested in life.
These patients don’t really possess any of the typical traumas in their experience that can bring on such complaints. What is it then? The environment (I don’t mean climate change)? Yes. The culture? Yes. The societal decadence and immorality? Yes. The food they eat? Yes. The over the counter drugs they take? Yes. The prescription drugs they take? Most definitely yes.
All these things are killing them—some obviously, but the real dangers are the things killing them softly—the things we are told are unimportant.
None of these things are considered by modern medicine to have a significant enough influence on the body, the mind, or the spirit (which of course no medical practitioner pays any attention to) to be dangerous. If we, as humans, fall above a certain line with our complaints and ailments, we are considered “normal” and the complaints and ailments that fall below that are not statistically relevant. But they add up.
We then die younger than we should, we become weaker earlier than we should, and even if our body can stay physically functioning through modern medical miracles, we are dead inside with a poisoned soul as well as with a body and brain that is barely functioning to par, but functioning enough that most people think is good enough.
Living a life that has meaning and purpose is actually more important than living a life with a fully healthy body—and we are getting neither in this current world setting. Our souls are slowly being killed by a meaningless, materially focused culture where consumerism is the name of the life game. I need not list the problems present in this soul killing culture, but at the head of slow death is the movement toward transhumanism and the deliberate creation of a world without a moral foundation.
The physical body is being killed softly as well with all of the aforementioned toxic killers we are exposed to day in and day out. Most of them are slow and soft, and operate unhindered below the radar of most people—and certainly below the radar of those who should be monitoring such things.
Is this intentional? Are we subjected to this slow genocide as part of the global eugenic effort to rid the world of useless eaters?—or even more horrifying, to rid the world of all humans who are made in the image of God along with nature herself? An agenda chillingly made clear in C.S. Lewis’ tome That Hideous Strength seen as well in the works of numerous others such as George Orwell and Aldous Huxley.
Probably not everything I have mentioned here has come about as part of this nefarious evil intention. But I would be willing to bet a lot of it has (see the work of David Icke). It may just have become the nature of the beast to create a culture in its atheistic hubris that ignores the subtleties of life and living.
Most of these toxic examples I have presented here have come about through omission—e.g., by omitting any sort of diligence to avoid their toxic effects, or by entirely doing away with things that fall into the lower material resolutions of our experience, making them statistically irrelevant—if you can’t clearly see it then just ignore it. Obviously anything “unseen,” such as love, beauty, art, God, unity, and the essence of life, is completely and almost savagely ignored. Such is our world—a humanity that is quietly, and softly, dying.
I think it is generally accepted that the practice of medicine has changed radically over the past fifty or so years. The medicalization and corporatization of life have “progressed” simultaneously as most doctors have become obedient servants of the corporate state.
But wait, one may object, and with some justification.
The development of micro-surgical techniques has significantly improved the methods of many operations that were formally very invasive and posed a great risk to the elderly and chronically sick. Many people have had knee, hip, and heart surgeries – to name a few – that would have been problematic or impossible in the past. Body part replacements are now common. Soon everyone will be half-mechanical on the way to full robotization with a bit of pig and cow thrown in for good measure. Whether this is good is debatable on many levels, but the “procedures” (a word that seems to have replaced the more gruesome sounding words “operations” or “surgeries”) have clearly become more efficient and less invasive. These micro-surgical techniques have surely saved lives and improved the quality of life for many.
So much for the technology. I have a little medical tale to tell.
My best friend, an athletic man in his mid-seventies in excellent health and athletic shape, went to a new doctor at a medical practice since his doctor of thirty-five years had retired. The visit was for an annual physical that was required under the practice’s rules. He had previously met this doctor for a required brief meet-and-greet introduction and all seemed copacetic.
This time, he was ushered into the examination room where he sat and waited for the doctor. A nurse took his blood pressure and pulse and departed. The doctor soon arrived with an iPad and sat down next to him. He put the man’s records up on the screen. He then proceeded to review a list of inoculations my friend did or didn’t have. My friend – let’s call him Joe – has always been a guy who took very little medicine and was rarely sick; at the most he would take an aspirin or a few ibuprofen after a vigorous workout.
“I see you had a tetanus shot,” said the doctor.
“Yes, after I cut my hand.”
“And at your age it’s good you had a pneumonia vaccine.”
“I did,” said Joe, “but I kind of regret it.”
“Oh no, at your age you are at great risk from dying from pneumonia,” replied the doctor. He added, “And you haven’t had your shingles vaccination, which I highly recommend. It’s covered by Medicare now. You don’t want to get shingles; it’s terrifying.”
Joe said nothing.
“And you are due for a flu vaccine.”
“I never had one and never will,” said Joe.
“At your age you can die from the flu. It’s very dangerous. I definitely recommend you get it.”
“No thanks.”
“You really should.”
His voice rising, the doctor said, “And I see you have not gotten any Covid vaccines. You are really risking your life by not doing so. You must get them.”
Joe then succinctly explained his deep knowledge about Covid, the “vaccines,” their lack of testing, the mRNA technique, the deaths and injuries, etc. – all the reasons he opposed them.
The doctor became agitated. He argued back; explained how he had gone to Yale and studied the mRNA process under Drs. F. Teufelmeister and A. E. Newman and that he knew the vaccines were very safe and effective blah blah blah.
Joe said, “It doesn’t matter that you went to Yale. I emphatically disagree.”
This incensed the doctor, who blurted out, “If it was allowed, I would hold you down and inject you right now.”
“Is that so?” said Joe, incredulous.
The annual physical ended soon thereafter.
The doctor never laid a hand on Joe to examine him. No stethoscope; no ear, throat or nose checks; no hands on any part of his body – the exam was exclusively about vaccinations, read off a screen. Technical in all regards. All about how Joe was so very vulnerable and could die without them. The doctor was Big Pharma’s mouthpiece. Death threats devoid of any human touch, cold and sterile, and a wish that he could hold Joe down and forcibly inject him, the touch of the fascist mind expressed in a wish.
When Joe told me this story, I, being a student of the sociology of medicine, was reminded of the history of eugenics and the sick minds of people who think they can cull the herd because of their power and prestige. The sordid history that continues under euphemisms such as genetic research. Here was a doctor who dared to say what others no doubt think as well: “I would hold you down and inject you right now,” if only I could. But since he can’t, the state must find other ways to coerce, such as compulsory medical requirements. Such are totalitarian dreams made of, when death has become a commodity used to sell the dreams of reason, and the healer’s art, once linked to working with nature, has become an adjunct of state propaganda.
Thumbing through it, Joe came to a page where I had underlined the following:
The ritualization of crisis, a general trait of a morbid society, does three things for the medical functionary. It provides him with a license that usually only the military can claim. Under the stress of crisis, the professional who is believed to be in command can easily presume immunity from the ordinary rules of decency and justice. He who is assigned control over death ceases to be an ordinary human. As with the director of a triage, his killing is covered by policy. More important, his entire performance takes place in an aura of crisis.
On my way home I stopped to pick up my sister’s mail. The AARP Bulletin was in the box with her letters. This is one of two publications of the AARP organization, a powerful lobbying group and medical insurance company with 38 million members for people fifty years-old and over. The AARP Bulletin and AARP The Magazine are the largest circulation publications in the United States with a combined distribution of approximately 67 million.
Is there anything not to fear in this morbid culture where crises are promoted faster than the therapeutic and hygienic “remedies” offered to deal with them? Create the diseases and all the bogeymen and then offer pseudo-solutions straight from the sorcerer’s playbook.
Build the fear and they will come, knocking at the sorcerers’ doors.
If it were allowed, I would lift you up with a simple truth.
“Therefore, one of the answers I would provide to the question of why the ‘no virus’ issue is so important is: that fear of ‘germs’ makes people believe that ‘disease’ can be transmitted between people, which means that we have to continue being afraid of each other.
“In fact, one of the fundamental problems with all of this is that it keeps people in a state of unjustified fear, which is disempowering. Releasing unjustified fear is empowering.”
It seems that many people wonder why the ‘no virus’ issue remains important now that the ‘pandemic’ is over.
To add to that, there are some people in the ‘freedom movement’ who have recently asserted that there are many aspects of the globalists’ agenda that are not related to health and are far more dangerous to humanity, such as technocracy, transhumanism, digital currencies, smart cities etc.
Yes, these are important issues – really important issues, I totally agree – but so is the idea that ‘pathogenic agents’ exist because it has tentacles that reach into many aspects of our lives, so it cannot be brushed aside as if irrelevant, especially in view of the complete lack of evidence to support this idea.
I would therefore recommend that people who believe in ‘pathogenic agents’ become aware of the various reports that claim there will be ‘future pandemics’. For just one example, a 22nd May 2023 ‘News’ item on the UN website states,
“Although COVID-19 may no longer be a global public health emergency, countries must still strengthen response to the disease and prepare for future pandemics and other threats, the Director-General of the World Health Organization (WHO) said on Monday in Geneva.”
There has never been a ‘pandemic’ due to an infectious agent and there never could be. But, whilst people believe that pathogenic infectious agents exist, they will believe in the possibility of other ‘pandemics’.
Therefore, one of the answers I would provide to the question of why the ‘no virus’ issue is so important is: that fear of ‘germs’ makes people believe that ‘disease’ can be transmitted between people, which means that we have to continue being afraid of each other.
In fact, one of the fundamental problems with all of this is that it keeps people in a state of unjustified fear, which is disempowering. Releasing unjustified fear is empowering.
Furthermore, fear of ‘germs’ makes people acquiesce to measures that are claimed to be for their benefit but are far more likely to be harmful, and in many cases potentially or even actually fatal.
For example, the maintenance of a belief in pathogens permits the maintenance of a belief in the idea that STIs are real, as demonstrated by a recent BBC article Gonorrhoea and syphilis sex infections reach record levels in England,
“England is seeing record high levels of gonorrhoea and syphilis sexually transmitted infections, following a dip during Covid years, new figures reveal.”
Is the claim that these STIs ‘dipped’ during the Covid years intended to suggest that people maintaining their distance from one another was beneficial? This point is not elaborated upon, so maybe it was not intended to imply that. Still, the point was stated, so maybe it was intended to be drawn into the sub-conscious mind.
One of the key messages in the BBC article is that people should ‘practise safe sex’ – whatever that means. In order to be ‘safe’, people are encouraged to ‘get themselves tested’ – does this sound familiar?
In addition, the article states that,
“The age group most likely to be diagnosed with a sexually transmitted infection (STI) is people who are 15-24.”
The reason for STIs to mainly affect young people is not explained, although it is possibly because this age group is more likely to be tested, as the article indicates,
“Some of the rise will be due to increased testing, but the scale of the surge strongly suggests that there are more of the infections around, says the UKHSA.”
A particularly significant comment made by the spokesperson for the UKHSA, and reported in the article, is that,
“Testing is important because you may not have any symptoms of an STI.”
Yet, according to the CDC,
“An infection occurs when germs enter the body, increase in number, and cause a reaction of the body.”
In other words, an infection causes a reaction or ‘symptoms’, but infected people may not have symptoms. A contradiction in terms, surely!
Just to be clear, the definition of ‘symptom’ according to the online Merriam-Webster dictionary is,
“…subjective evidence of disease or physical disturbance.”
So, to summarise: according to the medical establishment, a symptom is evidence of disease and ‘germs’ are pathogens, which means they cause disease, which is defined by the presence of symptoms. Yet ‘germs’ are said to be able to cause an infection even in the complete absence of symptoms.
Confused? You should be, because this is all nonsense!
But it is nonsense that people are not only expected to believe without question, but are not allowed to question.
Maybe it is because this is all so confusing that people are likely to just switch off their thinking, because they don’t understand it, and instead defer to the so-called ‘experts’. I am not being disrespectful. I do wonder, however, whether this approach may be intentional and that those in control of the narrative intentionally promote contradictory information to ensure that people are confused.
Deferring to ‘experts’ is however, a serious error of judgement, because it means people will believe the experts’ reports about ‘germs’ and become trapped in a false narrative that they may have been ‘infected’. This in turn will make them believe that they need to take certain drugs and act in a certain way to ‘protect’ themselves from other people or protect other people from them, especially people with whom they are in a loving relationship. They are made to believe the idea that they could cause harm to their partner or vice versa, and they therefore live in fear.
This fear is fuelled by a variety of statements, such as the claim in the BBC article that,
“An untreated infection can lead to infertility, pelvic inflammatory disease and can be passed on to a child during pregnancy.”
There is no evidence for this claim. Yet, this is exactly the kind of message that will encourage people to want to be tested to make sure they are ‘safe’. Again, does this sound familiar?
An even deeper problem is highlighted by the comment from the Chief Executive of the Terrence Higgins who is reported to have said that,
“Sexual health services and public health budgets have been cut to the bone.”
This comment was followed by his statement that,
“This was exacerbated and laid bare by last year’s mpox outbreak, which left sexual health clinics in the most affected areas unable to provide HIV and STI testing, HIV prevention and access to contraception due to the displacement of these core and vital services. Until sexual health is properly resourced – with an appointment easier to access than a (sic) – we won’t see the number of STIs heading in the right direction.”
Where do I start with this?
OK, so the Terrence Higgins Trust web page About our charity states,
“We’re the UK’s leading HIV and sexual health charity. We support people living with HIV and amplify their voices, and help the people using our services to achieve good sexual health.”
I realise that I don’t have a Substack article specifically about HIV, but this is one I wrote about STDs,
HIV is a huge topic, but the fundamental point to convey here is that there is no evidence, and there never was, that there is such a thing as a ‘virus’ called HIV that is the cause of a health problem called AIDS – or any other health problem for that matter.
It is abundantly clear that there is a lot at stake here. It is also crystal clear that belief in the existence of any kind of pathogenic agent is absolutely essential for organisations such as the Terrence Higgins Trust (THT), as well as ‘health’ institutions, such as the WHO, CDC, NHS, and all the other alphabet agencies.
I have no idea of the motives of those who are in charge of the THT, nor do I intend to speculate on them. However, whether they know it or not, what they are promoting on their website is fully supportive of Agenda 2030 and the ‘Global Goals’, as the message at the foot of their website claims,
“Time is running out. Donate now and together we can end new cases of HIV in the UK by 2030.”
To those in the ‘truther’ community who claim that the 2030 Agenda has nothing to do with the ‘virus’ issue I would strongly suggest that they read SDG3, especially target 3.3.
And target 3b
The ‘no virus’ issue – and the associated understanding that there is no proof that any ‘diseases’ are caused by any ‘microorganism’, whether bacteria, fungi or parasites (‘viruses’ aren’t relevant in this context) – is and remains an extremely important issue; especially in view of the intended 2030 Agenda rollout of vaccines, because vaccines rely on the existence of pathogenic infectious agents.
Another reason to understand its importance is because the idea that ‘germs’ cause illness that only the medical establishment can address supports the idea that we need a ‘health service’ to look after us when we become ill, which is not the case. To this, I would add a caveat that accident and emergency services ARE important and should remain in place, although those who work in that sector should receive further training to teach them how the body actually works, and how it can and does heal itself; this knowledge will certainly improve patient recovery times and outcomes.
We may not reach everyone, but the importance of the ‘no virus’ issue cannot be underestimated. When people lose their fear of ‘germs’ of all descriptions, they will be able to concentrate their efforts on all the other aspects of their lives.
People can only make informed decisions when they are in possession of all the relevant information.
Technology expert Michael Rectenwald, Ph.D., told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The World Health Organization (WHO) and the European Commission — the executive branch of the European Union (EU) — on Monday launched a “landmark digital health partnership” marking the beginning of the WHO Global Digital Health Certification Network (GDHCN) to promote a global interoperable digital vaccine passport.
Beginning this month, the WHO will adopt the EU’s system of digital COVID-19 certification “to establish a global system that will help facilitate global mobility and protect citizens across the world from on-going and future health threats, including pandemics,” according to Monday’s announcements by the WHO and the European Commission.
WHO & @EU_Commission launch landmark digital health initiative to help protect people across the world from on-going & future health threats
This is the first building block of the WHO Global Digital Health Certification Network that will develop a wide range of digital products… pic.twitter.com/IPlxn8wAXv
— World Health Organization (WHO) (@WHO) June 5, 2023
The WHO and European Commission claim the GDHCN initiative, which has been in the works since 2021, “will develop a wide range of digital products to deliver better health for all.”
The organizations said the WHO will not collect individuals’ personal data via these digital passports — stating that such data collection “would continue to be the exclusive domain of governments.”
WHO Director-General Tedros Adhanom Ghebreyesus lauded the new agreement:
“Building on the EU’s highly successful digital certification network, WHO aims to offer all WHO Member States access to an open-source digital health tool, which is based on the principles of equity, innovation, transparency and data protection and privacy.
“New digital health products in development aim to help people everywhere receive quality health services quickly and more effectively.”
However, experts who spoke with The Defender said the ramifications of such a system for human liberty and freedom of movement raised concerns.
Independent journalist James Roguski told The Defender the WHO is not waiting for a successful conclusion of these negotiations in order to implement initiatives such as a global digital vaccine passport. He said:
“The announcement by the WHO and the European Commission regarding the launch of their digital health partnership was hardly a surprise. Over a month ago, the WHO quietly published that they were working on ‘operationalizing’ the very things that were being ‘negotiated.’
“This is just one example that clearly shows that the super-secret ‘negotiations’ regarding the International Health Regulations (IHR) are a charade.”
Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom,” told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The announcement of the WHO-European Commission collaboration came just days after the conclusion of the WHO’s annual World Health Assembly (WHA).
While the pandemic treaty and IHR amendments were not finalized at this year’s meeting, high-level WHO officials warned of the risk of a future pandemic and spread of a deadly “Disease X,” and expressed the need to “restrict personal liberties” during a future health emergency.
The EU has been a strong proponent of digital vaccine passports, first launched for its member states in late 2020 — concurrent with the introduction of the COVID-19 vaccines — under the name “Green Pass.” The EU’s experience with the digital passes is noted in Monday’s announcement, which states:
“One of the key elements in the European Union’s work against the COVID-19 pandemic has been digital COVID-19 certificates. To facilitate free movement within its borders, the EU swiftly established interoperable COVID-19 certificates.
“Based on open-source technologies and standards it allowed also for the connection of non-EU countries that issue certificates … becoming the most widely used solution around the world.”
Roguski told The Defender the EU also was among the strongest proponents of vaccine passports during ongoing negotiations for the WHO’s “pandemic treaty” and amendments to the IHR.
“They really want the global digital health certificate,” Roguski told The Defender in March. “Primarily, that’s coming from the European Union.”
‘Pandemic passports a death sentence for millions’
According to Roguski, the EU, during negotiations for the IHR amendments, put forth proposals that seek to “‘normalize’ the implementation of a global digital health certificate.”
The Czech Republic called for Passenger Locator Forms “containing information concerning traveller’s destination,” preferably in digital form, for the purpose of contact tracing.
They also proposed that the WHO’s Health Assembly “may adopt, in cooperation with the International Civil Aviation Organization [ICAO] … and other relevant organisations, the requirements that documents in digital or paper form shall fulfill with regard to interoperability of information technology platforms, technical requirements of health documents, as well as safeguards to reduce the risk of abuse and falsification.”
The Czech Republic and the EU proposed documentation not just for vaccination, but “test certificates and recovery certificates” in cases “where a vaccine or prophylaxis has not yet been made available for a disease in respect of which a public health emergency of international concern has been declared.”
Plans for the WHO’s GDHCN have been in the works since at least August 2021, when the WHO released a document titled “Digital documentation of COVID-19 certificates: vaccination status: technical specifications and implementation guidance, 27 August 2021.”
“The Secretariat has developed SMART (Standards-based, Machine-readable, Adaptive, Requirements-based, and Testable) Guidelines on the digital documentation of COVID-19 certificates, comprising recommendations on the data, digital functionality, ethics, and trust architecture needed to ensure the interoperability of immunization and health records globally.”
The WHO also announced the successful completion of a “technical feasibility study for establishing a federated global trust network, which tested the ability to interoperate the health content and trust networks across existing regional efforts.”
EU officials have frequently praised themselves over the launch of the bloc’s “Green Pass,” touting how individuals’ privacy would be protected on the app. The introduction of the “Green Pass” was accompanied by statements by European Commission President Ursula von der Leyen calling for a “discussion” on mandatory vaccinations in the EU.
One of the EU’s stated priorities as part of its 2019-2024 five-year plan is to create a “Digital Identity for all Europeans.” Namely, each EU citizen and resident would have access to a “personal digital wallet,” which would include national ID cards, birth and medical certificates, and drivers’ licenses.
These proposals and initiatives appear to be closely aligned with the United Nations’ Sustainable Development Goals (SDGs), and in particular, Target 16.9, which calls for the provision of a digital legal identity for all, including newborns, by 2030.
Tedros said the SDGs are “our north star,” while addressing this year’s WHA.
Rectenwald called “pandemic passports” a “death sentence for millions.” He told The Defender:
“Despite the studies demonstrating that vaccines to curb pandemics have been deadly and useless, the WHO is doubling down on vaccine mandates.
“Pandemic passports equal a death sentence for millions and the abrogation of rights for the non-compliant. The WHO should be stopped before it completes the construction of a global totalitarian system.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
Video available at La Quinta Columna Odysee & Rumble channels. Follow at La Quinta Columna telegram channel: https://t.me/laquintacolumnainternational
They are introducing nanotechnology into all sorts of injectable products, especially in what they call vaccines for Covid.
Self-assembled nanotechnologies, based on graphene, are advanced non-human technologies, but implemented by humans.
The parasitization of our species ordered by “them” will lead to the extinction of human beings as we know them, who will become transhuman, monitored, with non-human thoughts that can in turn be read remotely via electromagnetic waves. Managed by AI, we will become what they call enhanced humans. Augmented humans.
Helpful list from FDA, found while doing research and organizing my files on:
Public Health Emergency (PHE), Emergency Use Authorization (EUA) and PREP Act notices, declarations, determinations and authorizations issued by HHS Secretaries and their delegees from Jan. 2020 to the present;
Legal advisory opinions about PREP Act liability immunity, issued by the HHS Office of General Counsel from Jan. 2020 to the present; and
Guidance to pharmacists about PREP Act liability immunity, issued by the Office of the Assistant Secretary of Health, from Jan. 2020 to the present; and
May biochemical weapon uptake rates approach zero in coming months and years, as rational popular response to the truth rendered much more visible since January 2020, and in firm opposition to all “recommendations” of the CDC Advisory Committee on Immunization Practices (ACIP).
Biochemical weapons deployed by injection have been intrinsically injurious from the start of government campaigns promoting their use more than a century ago.
The “Covid-19” weapons have been the most deadly to date, with some lots deadlier than others, and contents of many lots still unidentified.
A poultry farm in Yaroslavl has been ordered to cull 800,000 chickens, as regions introduce arbitrary “public health” measures to stop the spread of “bird flu”
On May 12, Russian media reported that an “infected” gull had been discovered near a pond in a village in Moscow Oblast.
What happened next was practically preordained.
Moscow Mayor Sergey Sobyanin—the poster boy for New Normal Russia—issued a decree on May 18 imposing “quarantine” measures on 11 districts in the capital.
The order placed restrictions on public events where birds might be congregating, and also banned the transportation of feathered creatures in the aforementioned districts.
Of course, birds could always just, you know, fly into one of these “quarantined” districts, and spread their devilish flu, but that’s neither here nor there.
Moscow is the trend-setter when it comes to enterprising public health policy in Russia, so of course other regions have been eager to follow suit with their own arbitrary bird flu edicts.
Just hours after Sobyanin’s decree was published, Kaliningrad imposed its own “quarantine” on a 10km perimeter around another bird flu Ground Zero.
The restrictions, which will remain in place until August 1, included a ban on the “import and export of birds and hatching eggs, the relocation of birds, procurement and export of bird feed, as well as holding agricultural fairs, exhibitions, auctions and other events.”
A week later, the discovery of dead, flu-riddled gulls in Nizhny Novgorod prompted officials to introduce a 30-day quarantine in one of the region’s districts.
Health authorities “seized poultry within a radius of five kilometers [from where the dead gulls were found], and poultry farms in the region were transferred to enhanced security protocols.”
Locals were also advised to only buy poultry from “verified” sources—the good, factory-farmed corporate stuff; don’t even think about buying poultry from your unverified neighbor!
But confiscating all chickens in a 5km radius is amateur hour compared to the health-boosting measures adopted in Yaroslavl.
The Romanovskaya poultry farm in Yaroslavl has been instructed to cull its livestock, and destroy all animal products on its premises, following an alleged bird flu outbreak:
All birds, more than 800 thousand in total, will be killed … The destruction of the carcasses, along with poultry products (eggs), will be carried out via incineration at a specially designated site. […]
The poultry farm has not disclosed any details about the order. When a 76.RU correspondent tried to contact company representatives, they declined to comment.
“We are in quarantine. That’s all,” a receptionist said, before hanging up.
The region is a major agricultural hub, so there’s no reason to believe that this bird-liquidation will cause a shortage of poultry or eggs. But…it’s also 800,000 chickens?
Finally, like a bad omen, Tatarstan (which was arguably the most Virus Crazy region in Russia after Moscow/St. Petersburg) is already bracing for the bird flu apocalypse:
It was clear that the COVID grift was rapidly losing its potency when Virus Nanny Anna Popova announced an imminent wave of “Arcturus”.
How many waves of severe-sounding Greek letters and words are possible, before people stop paying attention? Or worse, starting asking questions?
Well, now Russia is sacrificing 800,000 chickens to the Global Health Gods.
By the way: Where did this scary outbreak of bird flu begin? Hard to say for sure, but China recorded the world’s first human death from the new and improved “H3N8 avian influenza strain” in mid-April.
The bird flu scam actually predates COVID by many years. In fact, many of the trusted experts who demanded large-scale chicken slaughter (for public health) later went on to become celebrated “coronavirus experts” who championed worldwide house arrest for the proles—resulting in another mass culling.
Have you ever heard of a psychopath named David Nabarro?
source / source (to be fair to Nabarro, he later described lockdown as a “last resort”, which makes him slightly less disgusting than the typical WHO-certified Neanderthal.)
Let’s not deceive ourselves, friends. Global Biosecurity Theater is forever.
Self Assembly Hydrogel Polymers, Historical Research Context of Hydrogel Smart Materials and Nano Worms That Rapidly Grow From Nanometers to Visible Size
Scientists from NTU and CMU created a leaf-like hydrogel structure through a process similar to how real leaf tissues grow. Credit: CMU and NTU
In this article, I wanted to explain more about Hydrogel. There have been scientists and doctors saying that you cannot see nanotechnology grow from nanoscale to microscopic scale and that we cannot possibly see what we claim to see in the blood.
Our latest research findings show however that we are seeing what we claim:
Image: Four vaccinated Blood Samples left to sit for 4 hours I have posted the work of Clifford Carnicom and myself showing that Near Infrared Spectroscopy performed on C19 vaccinated and unvaccinated blood repetitively identified the spectral signature of functional chemical groups indicating polymer hydrogels.
There are people who do live blood analysis who call the hydrogel containing filaments parasites, biofilm, other lifeforms explicable via terrain theory. They dismiss the filaments because they were seen before historically, so they cannot have anything to do with the C19 injections. These are incorrect claims and I wish to explain the scientific background here.
We have discussed extensively that the Transhumanist assault of synthetic biology has been going on for decades and that historically the same filaments have been found in people’s blood before the C19 injections – they were then called Morgellons or Cross Doman Bacteria (CDB) and sprayed via geoengineering and bioengineering for people to inhale and get sick. The symptom complex experienced by CDB/ Morgellons has enormous overlap to “long Covid” poisoning – including chronic fatigue, brain fog, multi organ dysfunction, accelerated aging, mood disorders and more.
In the image above, you can see hydrogel used to grow like a leaf. In the article below, it is discussed that hydrogels can grow like biological tissues and that oxygen tension can control the growth. The more oxygen there is the faster they grow. Normal blood is carrying oxygen. There are many more ways to control the growth, this is just one example:
The team’s findings, published in Proceedings of the National Academy of Sciences today, suggest new applications in areas such as tissue engineering and soft robotics where hydrogel is commonly used. The team has also filed a patent at CMU and NTU. In nature, plant or animal tissues are formed as new biomass is added to existing structures. Their shape is the result of different parts of those tissues growing at different rates.
Mimicking this behaviour of biological tissues in nature, the research team comprising CMU scientists Changjin Huang, David Quinn, K. Jimmy Hsia and NTU President-designate Prof Subra Suresh, showed that through manipulation of oxygen concentration, one can pattern and control the growth rate of hydrogels to create the desired complex 3-D shapes. The team found that higher oxygen concentrations slow down the cross-linking of chemicals in the hydrogel, inhibiting growth in that specific area.
Hydrogel research has gone on for many decades. Here is an article from 1977 discussing the interactions of hydrogel and blood:
Here is an article explaining how fast the hydrogel can change its volume or size. What we have been seeing in human blood and in the analysis of C19 vials nanotechnology is entirely consistent with the literature.
Abstract
Smart hydrogels, or stimuli-responsive hydrogels, are three-dimensional networks composed of crosslinked hydrophilic polymer chains that are able to dramatically change their volume and other properties in response to environmental stimuli such as temperature, pH and certain chemicals. Rapid and significant response to environmental stimuli and high elasticity are critical for the versatility of such smart hydrogels. Here we report the synthesis of smart hydrogels which are rapidly responsive, highly swellable and stretchable, by constructing a nano-structured architecture with activated nanogels as nano-crosslinkers.
You can control the growth of hydrogels by many different chemical means. Here is an article from 2001 – just to show how long the scientific community has worked on perfecting this technology:
Environmentally sensitive hydrogels have enormous potential in various applications. Some environmental variables, such as low pH and elevated temperatures, are found in the body. For this reason, either pH-sensitive and/or temperature-sensitive hydrogels can be used for site-specific controlled drug delivery. Hydrogels that are responsive to specific molecules, such as glucose or antigens, can be used as biosensors as well as drug delivery systems. Light-sensitive, pressure-responsive and electro-sensitive hydrogels also have the potential to be used in drug delivery and bio separation. Hydrogels containing such ‘sensor’ properties can undergo reversible volume phase transitions or gel–sol phase transitions upon only minute changes in the environmental condition. The types of environment-sensitive hydrogels are also called ‘Intelligent’ or ‘smart’ hydrogels. Many physical and chemical stimuli have been applied to induce various responses of the smart hydrogel systems. The physical stimuli include temperature, electric fields, solvent composition, light, pressure, sound and magnetic fields, while the chemical or biochemical stimuli include pH, ions and specific molecular recognition events. Smart hydrogels have been used in diverse applications, such as in making artificial muscles, chemical valves, immobilization of enzymes and cells , and concentrating dilute solutions in bioseparation.
The worm like appearance we are seeing in the blood is not a parasite but a self assembly polymer nano worm which has been developed by science for over 2 decades (thanks to Shimon Yanowitz for sending this to me):
Filomicelles and nanoworms are an emerging subclass of nanomaterials with a special elongated shape. The physical properties of a filomicelle are distinct from a traditional spherical micelle, and as such have attracted tremendous interest in a variety of research areas. In this review, we highlight the substantial progress in the synthesis and application of polymeric nanoworms over the past two decades. Synthetic techniques summarized in this review are particle replication in nonwetting templates (PRINT), film stretching, self-assembly (SA), crystallization-driven self-assembly (CDSA), polymerization-induced selfassembly (PISA), and temperature-induced morphological transformation (TIMT). The applications of filomicelles as (i) templates for inorganic nanoparticles, (ii) building blocks for superstructures, (iii) synthetic dendritic cells for immunotherapy, (iv) constituents of thermoresponsive gels for biomedical applications, and (v) nanocarriers for cancer drug delivery are subsequently discussed. In the conclusion, we describe the current trajectory of research in the field and identify areas where further developments are of urgent need.
Note how the researchers consider self assembly as a “living” process.
Please note that these can grow from nanometer to macroscopic size, visible with the naked eye:
In this episode, a successful career government pharmaceuticals and vaccines testing expert with Health Canada explains why COVID-19 is not proven to exist in applied science. As such, no vaccine will treat a nonexistent pathogen.
Dr. Qureshi has a Ph.D. in fundamental science (chemistry) specializing in analytical chemistry, which covers the science of substances, isolation, identification, characterization, purification, tests developments, validation, and their uses.
For over three years Dr Qureshi has collaborated with other independent scientists and researchers at Principia Scientific International to provide objective, independent analysis to expose the most significant medical fraud in history.
Working with Dr Judy Wilyman – Australia’s most prominent qualified expert in vaccine injury – co-authors, Qureshi, Beatty, and O’Sullivan have compiled an important new book that among other things shows how corrupt policymakers, a controlled media and government ‘experts’ combined to scare us onto surrendering our freedoms – all premised on junk science.
Slaying the Virus and Vaccine Dragon reveals how a coordinated international medical hoax – just like the climate scare – is a dystopian population control strategy implemented by a psychopathic billionaire cult pursuing UN Agenda 21(Agenda 2030) to depopulate the planet.
About Dr. Saeed Qureshi
As a senior research scientist for 30 years with Health Canada, Dr. Qureshi conducted experimental studies relating to drug applications for product marketing—undertaking hands-on experimental (scientific) studies for both in vitro and in vivo (animal/human) evaluations.
He has extensively published in peer-reviewed journals and made numerous invited national and international presentations on these topics.
For his scientific accomplishments he has received several high-profile awards including the Lifetime Achievement Award from the Indus Foundation, India); from the Deputy Minister’s Award of Excellence in Science at Health Canada) plus the Excellence in Science Award also at Health Canada
Slaying the Virus and Vaccine Dragon identifies that modern democracies commonly suffer from a fatal weakness, in that they rely on politicians and government scientists to maintain high ethical standards, indefinitely.
“…This is a pseudoscientific concept that is also an oxymoron as two entirely contradictory terms were put together in order to create this illogical state. Asymptomatic is characterized by a lack of signs and symptoms of illness, whereas disease is characterized by signs and symptoms of illness…
Asymptomatic carriers are nothing but healthy people who have been labelled with disease minus signs of any disease who are then told that they can infect others. They are treated as a sick individual based upon results generated using fraudulent tests.
[…]
The “viral” theory is a load of BS, and there is no such thing as a healthy sick person capable of transmitting disease. We have no reason to fear the walking healthy.”
“In areas where there are limited number of new cases, State or local public health officials may request to test a small number of asymptomatic ‘healthy people,’ particularly from vulnerable populations”
In the not so distant past, when we walked around feeling healthy without any symptoms of disease, most of us would consider that we were, in fact, free of any disease. There would be no thoughts about going to the doctor for a PCR test in order to determine whether or not we were unknowingly a walking talking “virus” spewing host harboring billions of “infectious” particles capable of transmitting disease to our loved ones. We would not subject ourselves to quarantines and daily testing due to the remote possibility of being around someone who tested positive with symptoms, let alone for anyone testing positive without any signs of disease. We did not go around covering our faces with masks out of fear that those around us may be silent spreaders. We didn’t bust out our rulers in order to measure 6 feet of distance between us and another living soul. None of these irrational actions were ever even a glimmer of a thought until the well-orchestrated fear propaganda campaign promoted the pseudoscientific concept of the asymptomatic carrier of disease and catapulted it into the public consciousness.
Even though this idea has been effectively weaponized against us over the last few years, it is not a new one. In fact, as will be shown later, the notion of the asymptomatic carrier began at the same time germ theory was born. The idea is that one can be silently harboring and able to transmit a pathogen without displaying any symptoms of disease whatsoever. This has resulted in the highly illogical creation of asymptomatic disease:
What Does it Mean to Have an Asymptomatic Disease?
“Asymptomatic disease is where a person is infected with a disease (or develops a disease; diagnosed) but fails to display any noticeable symptoms.”
Asymptomatic until symptomatic – silent diseases
“Many diseases and infections can be asymptomatic, including those that may be potentially fatal in some people. These include (but are not limited to): tuberculosis, breast cancer, endometriosis, HIV/AIDS, herpes, hepatitis, chlamydia, hypertension, common colds/flu, and type-2 diabetes mellitus. Many of these conditions remain largely asymptomatic until very advanced disease stages when they suddenly become symptomatic. Others can remain more or less asymptomatic throughout their disease course.”
“Infectious diseases can also be completely asymptomatic (with no symptoms ever manifesting), particularly in younger and healthier individuals. For example, hepatitis (hepatitis C) infections can take up to 6 months to develop, and even then, approximately 80% of infected individuals may not experience any symptoms. Other examples include cholera, herpes, measles, and rubella which can be completely asymptomatic.”
“In summary, asymptomatic disease refers to diseases and infections which do not lead to any symptoms in patients (subclinical) for the whole disease course or until they develop symptoms in which the asymptomatic phase is referred to as pre-symptomatic.
In many respiratory infections including COVID-19, asymptomatic disease is common and may be a source of transmission within the community, though more research is needed to establish the exact contribution asymptomatic transmission has on the community rates of infection.”
As can be seen, many so-called “infectious diseases” are said to be asymptomatic. If one is labelled as asymptomatic, one never develops the disease at any point in time even though they are diagnosed with asymptomatic disease. This is a pseudoscientific concept that is also an oxymoron as two entirely contradictory terms were put together in order to create this illogical state. Asymptomatic is characterized by a lack of signs and symptoms of illness, whereas disease is characterized by signs and symptoms of illness. One can not have disease if one is not displaying signs of disease:
Asymptomatic carriers are nothing but healthy people who have been labelled with disease minus signs of any disease who are then told that they can infect others. They are treated as a sick individual based upon results generated using fraudulent tests. In the past, most would have scoffed at this idea and never willingly subjected themselves to quarantines and further testing. In fact, they would have never tested to begin with. However, in the face of a “pandemic” with a “novel virus,” many lined up for the mass testing agenda in order to ensure that they were amongst the “uninfected.” This willingness to subject to testing despite a clear lack of symptoms was primarily driven by fear. This old concept was thrust onto a frightened population and then ramped up in a way that had never been done so before.
In order to understand why there was never any reason to ever participate in this irrational belief of such a ridiculous concept, let’s examine how the asymptomatic carrier first came about at the dawn of germ theory. We will then examine how this idea was weaponized against the public during the “pandemic” despite a complete lack of any scientific evidence in support of the asymptomatic disease carrier.
When German bacteriologist Robert Koch was looking for the causative agents of certain diseases in the late 1800’s, he formulated a series of four logical requirements that needed to be met in order for anyone to claim that a certain microbe caused a specific disease. These were as follows:
The microorganism must be found in abundance in all hosts suffering from the disease but should not be found in healthy hosts.
The microorganism must be isolated from a diseased host and grown in pure culture.
The cultured microorganism should cause the same symptoms of disease when introduced into a healthy host.
The microorganism must be re-isolated from the inoculated, diseased experimental host and shown to be identical to the original causative agent.
While these logic-based postulates were accepted by and large within the scientific community, Koch quickly discovered a problem with his very first criterion. Whether it was tuberculosis, typhoid, malaria, or cholera, the microbe that he was claiming as causative agents were regularly found in healthy individuals. Thus, Koch was unable to satisfy his very own first Postulate. However, rather than realize that his criteria had worked as he had envisioned and had actually ruled out bacteria and other microbes as a causative agent of disease, Koch allowed for himself and others to bend not only his first postulate, but the others as well. Allowing for the bacteria and other microbes claimed to be causative agents of disease to be found in those without disease lead to the creation of the illogical concept that became known as the asymptomatic carrier of disease. Koch’s entire claim to fame rested entirely on the perception that he was a microbe-hunter. Bending his own rules saved Koch from giving up his prestige, kept his findings intact, and helped to establish the germ theory on unfalsifiable pseudoscientific grounds.
Koch’s idea of asymptomatic “infection” received a big push shortly afterwards when the media released propaganda promoting the idea of an asymptomatic carrier in 1907 by targeting an Irish immigrant by the name of Mary Mollen. Mary was a cook for wealthy families and ended up employed by banker Charles Henry Warren when he rented a summer home for himself and his family. When 6 of the 11 family members came down with the symptoms of typhoid fever over the last week of August, the property owners feared that no one would rent the house again if they believed that the property was the source of the outbreak. A man named George Roper was hired to investigate the situation and he came to the conclusion that it was Mary who had passed on the bacteria to the family through her cooking. This led to a modern day witch-hunt for Mary who refused to believe that she was the source of illness. Sadly, Mary was eventually involuntarily quarantined for the majority of the rest of her life. This ordeal led to Mary being notoriously and unfairly known by the moniker Typhoid Mary, even though many of her stool samples came back negative for the bacterium:
Typhoid Mary: the Tragedy of Mary Mallon
“On 11 November 1938, a 69 year old Irishwoman died on North Brother Island, New York. She had been held in isolation for 23 years, yet she had not been charged or convicted with any criminal offence.
Mary Mallon was born in Cookstown, Ireland in 1869. She immigrated to America when she was a teenager and found employment in domestic service. She developed an aptitude for cooking, and as this paid more than basic service, Mary accepted several jobs as a cook for the wealthy. In 1906, Charles Henry Warren, a New York banker, rented a summer home for himself and his family on Long Island. Mary Mallon was engaged as a cook for the duration of their stay. From the end of August, one by one people began to fall ill with typhoid fever, in all, six of the eleven occupants of the house developed typhoid fever.
The owners of the property feared that they would be unable to secure further tenants if the public believed that the source of the outbreak was their property and so hired Dr George Soper to investigate the cause. Soper came to the conclusion that Mary Mallon was to blame for the spread of disease. Hindering his efforts, Mary had left their employment three weeks after the outbreak. Soper started to investigate the previous situations held by Mary Mallon. From 1900 to 1907 there had been seven jobs where, it was reported, somewhere between twenty-three and thirty-eight people became ill and one person, a child, died. Soper believed that Mary was the source of typhoid fever that had followed her employment history, but he needed biological samples to affirm his hypothesis.”
“The Greater New York Charter allowed for ‘all reasonable means for ascertaining the existence and cause of disease’. It essentially gave health officials the authority to remove Mary Mallon and quarantine her against her will. After two years of isolation, with only a dog for company, Mary sued the health department. They had tested her stools approximately weekly and 120 out of 163 samples proved positive. Yet Mary countered with her own private analysis, sampled over the preceding year, all coming back negative. Mary’s laboratory results proved for her, her healthy status and she failed to understand that she was diagnosed a healthy typhoid carrier. She was arguably the first person identified as such, and having not been charged with a criminal offence she felt it was barbaric to be treated like a criminal (and a ‘leper’) when she was innocent of any crime.”
Mary was falsely quarantined against her will due to one man’s suspicion and hypothesis that rested solely on correlation equaling causation. No scientific experiments were ever carried out proving that Mary was spreading disease to her patrons. As with all claims of asymptomatic transmission, it was a circumstantial case built upon faulty epidemiological data. George Roper is the man who ultimately condemned Mary by labeling her as the cause without any scientific evidence proving his hypothesis. Based upon his own words presented below, he assumed certain premises, such as the bacterium should be in the urine (which it was not) and in the feces. He claimed that stool examinations only failed twice over the course of two weeks to find the bacterium. However, he later recounted several instances of failure to detect the bacterium over the course of several months. In the summer months, few bacterial colonies were found and in the month of July, there were five consecutive negative tests. During the month of August, no typhoid was ever found in Mary’s stools. In September, they began to appear again. However, from September 11 to October 14, 1907, the stools failed to yield any typhoid bacilli. From October 16, 1907, to February 5, 1908, weekly examinations of the stools showed anywhere from 25 to 50 percent “typhoid-like” colonies on the culture plates. There were two instances within that period where no bacilli were found. Taking into account that Mary’s own independent lab results showed that no bacilli were found within her stools, Soper’s consistently contradictory evidence should have been questioned.
After recounting these failures, Soper shared his thoughts on how Mary transmitted the bacterium through having not washed her hands properly while preparing the food. He based his conclusion upon his interviews where he stated that no housekeeper ever told him that Mary was a clean cook. He did not say whether he asked them or not or rather just assumed that their lack of addressing it was proof that Mary was unsanitary. Soper then stated that, in the most thorough “investigation,” he believed that the bacterium was carried from Mary’s hands to the people who ate ice cream containing cut-up peaches that she had prepared. Again, no evidence was provided beyond his belief. Soper was amazed that no one had ever discovered an asymptomatic carrier in America before him. Interestingly, Soper revealed that he was long interested in the transmission of typhoid fever and knew of Robert Koch’s work. He stated that his interest in this area was longstanding and that Koch’s work was the basis for his own investigation. He admitted that he had read several papers on the probable role of healthy carriers in producing typhoid. Soper was made aware by Dr. Simon Flexner, of the infamous Flexner report, to some of these references after he had concluded his work on the Mary Mallon case. It is very clear that Soper went looking for evidence to fit his preconceived conclusions as to what the cause was. He was also potentially guided along the way:
The Military Surgeon Vol. XLV July, 1919 Number 1 Original Articles Typhoid Mary
By Major GEORGE A. SOPER
“It was expected by me that the germs might be found in the urine, but more probably in the stools. None was found in the urine. The stools contained the germs in great numbers. Daily examinations made for over two weeks failed only twice to reveal the presence of the Bacillus typhoid and on these occasions the sample taken was perhaps too small to reveal them. The blood gave a positive Widal reaction. The cook appeared to be in perfect health.
The feces were examined on an average of three times a week from March 20 to November 16, 1907, and in only a comparatively few instances did the investigators fail to find the bacilli. During the summer months the culture plates contained only a few typhoid-like colonies. In July there were five consecutive negative tests followed by a positive one.
During August the stool showed no typhoid; in September they began to appear again; from September 11 to October 14, 1907, the feces failed to yield typhoid bacilli. During this time the patient’s diet was carefully regulated and she was receiving mild laxatives. On October 16, 1907, a very thorough test showed that the germs were again present. From October 16, 1907, to February 5, 1908, weekly examinations of the stools gave, with only two exceptions, from 25 to 50 per cent typhoid-like colonies on the culture plates. These exceptions were on November 13 and December 4, when no typhoid was found. The implication was plain. The cook was virtually a living culture tube in which the germs of typhoid multiplied and from which they escaped in the movements from her bowels. When at toilet her hands became soiled, perhaps unconsciously and invisibly so. When she pre-pared a meal, the germs were washed and rubbed from her fingers into the food. No housekeeper ever gave me to understand that Mary was a particularly clean cook. In the Oyster Bay outbreak, which was studied with more particularity than the others, the infectious matter is believed to have been carried from the cook’s hands to the people who were later taken sick by means of ice cream containing cut-up peaches. Mary prepared this herself. In this instance no heat sterilized the washings from her hands. Mary Mallon was kept virtually a prisoner by the Department of Health for three years. At first she was held at the hospital for contagious diseases at the foot of East 16th Street, Manhattan; later she was removed to Riverside Hospital on North Brother’s Island in the East River, between Hell Gate and Long Island Sound.”
“The case is least remarkable for the reason that it was the first of its kind to be worked out in America. It is surprising that nobody bad discovered a carrier before. They are now known to be rather common.
Somewhat similar investigations bad been made in Germany) and I make no claim of originality or for any other credit in her discovery. My interest and experience in the epidemiology of typhoid had been of long standing. I had read the address which Koch had delivered before the Kaiser Wilhelm’s Akademie, November 28, 1902, and his investigation into the prevalence of typhoid at Trier 3 and thought it was one of the most illuminating of documents.In fact it had been the basis of much of tile epidemic work with which I had been connected.
Koch’s address was not the only one printed about this time to show that healthy carriers might exist and give rise to typhoid. Conradi and Drigalski4 had anticipated Koch and it was probably on the suggestion contained in their paper to the effect that with their new culture medium they had found typhoid bacilli in the stools of several well persons that Koch’s flying laboratory was sent to Trier and the ground prepared for his Kaiser Wilhelm’s Akademic address.
In the Festschrift Zum SeclizigstenGeburstag von Robert Koch, which appeared in 1903, there are several papers on the probable role of healthy carriers in producing typhoid. About this time Kayser, Klinger and others were publishing in Arbeiten aus dem Kaiserlichen Gesundheit-smate reports of cases which they found to be due to persons whose condition was much like Typhoid Mary’s. Dr. Simon Flexner kindly called my attention to some of these references after I had concluded my work on the Mary Mallon case.”
After the highly publicized Typhoid Mary case, this idea of asymptomatic carriers simmered in the background over the next century. While there were claims of such a state in certain diseases, this has never been scientifically proven. However, that did not stop Koch’s escape clause from taking a prominent role in the “Covid crisis,” primarily due to a mass testing campaign that was bound to identify positive cases in healthy people using fraudulent tests never calibrated and validated to purified and isolated “virus.” Although all PCR results are false-positives, we can see that even the CDC noted that testing people without symptoms generates false-positive cases. They stated as much under their PCR guidelines for pertussis when recommending not to test those without symptoms:
Diagnosis PCR Best Practices
“However, only patients with signs and symptoms consistent with pertussis should be tested by PCR to confirm the diagnosis. Testing asymptomatic persons should be avoided as it increases the likelihood of obtaining falsely-positive results. Asymptomatic close contacts of confirmed cases should not be tested and testing of contacts should not be used for post-exposure prophylaxis decisions.”
Thus, we can see that the CDC were well aware that testing people without symptoms will lead to an influx of cases labelled as asymptomatic “infections” when they are, in fact, not “infected” or diseased at all. This massive amount of asymptomatic cases of “SARS-COV-2” based upon fraudulent test results has cemented the illogical concept of the asymptomatic carrier into the minds of the populace. A timely December 2020 review, while reiterating the history of the asymptomatic carrier described above, pointed out the fact that even though asymptomatic infection and transmission has always been a concept waiting it the wings, it has only recently been thrust into the limelight with this “pandemic:”
Invisible epidemics: ethics and asymptomatic infection
History
“Dr Robert Koch was one of the founders of modern microbiology, and his work is particularly well known for a set of postulates (first published in 1890) linking microbes with the causation of infectious disease (Gradmann 2010). Though variously expressed, one of Koch’s initial postulates was that the microbe putatively responsible for a disease should be found in all people suffering from the disease, but not in healthy individuals (Gradmann 2010). Koch soon realised that this did not hold true in all cases, since many potentially pathogenic organisms are frequently found in healthy people. For example, Koch observed that asymptomatic carriers of cholera, typhoid, and malaria could spread these diseases to others, and he is credited for inventing the concept of the carrier state (i.e., in which healthy people asymptomatically carry an infection) (Gradmann 2010).
Public awareness of asymptomatic carriage of infection increased, especially in English-speaking countries, with media reporting of the case of Mary Mallon (known as “Typhoid Mary”) beginning in 1907. Mallon was a cook working in New York who, although showing no signs of typhoid disease herself, spread typhoid bacteria to many other people, resulting in several deaths (Brooks 1996; Soper 1939). For the general population, this revealed an important truth: that “persons, rather than things” (Soper 1939) were the source of many infectious diseases. Despite this Copernican revolution in public health (an epidemiological parallel of the microbiological revolution of germ theory), Mary Mallon and many others found it difficult to believe that healthy people could spread disease. Mallon repeatedly resisted public health restrictions and refused to believe she was infected or posed risks to others. She spent the latter years of her life living in public health confinement on North Brother Island, working as an assistant in the local infectious disease laboratory (Soper 1939).”
Implications for outbreaks, epidemics, and pandemics
“Asymptomatic infection was recognised to be a significant factor in the 2015–2016 Zika virus epidemic, particularly because many of those who were infected—including some women who acquired infection during pregnancy and gave birth to children severely affected by congenital Zika syndrome—showed few or no symptoms (Jamrozik and Selgelid 2018). Although less well recognised, transmission of asymptomatic Middle Eastern Respiratory Syndrome (MERS) coronavirus infection (perhaps both camel-human and human–human transmission) may play an important role in the epidemiology of MERS—which is all the more remarkable because people who develop symptomatic MERS infection have a high fatality risk of around 35% (Grant et al. 2019). Asymptomatic infection has also been reported for viruses closely related to the coronavirus that caused the earlier severe acute respiratory syndrome (SARS) epidemic. In one study from 2003, around 40% of Chinese wild animal traders had serological evidence of having been exposed to coronaviruses that closely resembled SARS-coronavirus, raising questions about whether people in high risk occupations should be screened for asymptomatic infection to detect potential “spillover” events of pathogens with epidemic potential (Guan et al. 2003). We initiated the November 2018 Brocher Foundation workshop upon which this Special Issue is based partly in light of the growing awareness of such cases of asymptomatic infection—and their ethical implications for policy and practice.
Since that time general awareness of asymptomatic infection has skyrocketed in light of its role in the coronavirus disease 2019 (Covid19) pandemic, in virtue of which the term ‘asymptomatic infection’ has become highly familiar to ordinary members of the general public. Early data, which were later widely confirmed, suggested that asymptomatic transmission of Covid19 occurs both in cases where the individual transmitting the virus goes on to develop symptoms later (i.e., they were “pre-symptomatic” at the time of transmission) and in cases where they never develop symptoms (Hu et al. 2020). Asymptomatic individuals can, under certain conditions, transmit to large numbers of other people (e.g., one person was shown to infect 71 others) (Liu et al. 2020). The overall degree to which asymptomatic transmission contributes to local Covid19 epidemics likely varies in different contexts and has not always been well-characterised (in part because of the difficulties of identifying all asymptomatic infections during an epidemic). In any case, asymptomatic transmission of Covid19 raises a number of ethical issues similar to those discussed above, including those related to the justification of public health interventions such as screening and isolation for asymptomatic cases.”
While the asymptomatic carrier was made a star of the “Covid” show in order to generate fear and drive compliance towards quarantines, lockdowns, social-distancing, and masking, the message has been entirely inconsistent throughout, and the lack of any valid scientific evidence proving such a carrier state was on full display from the very beginning. At a White House press briefing on January 28th 2020, the idea of asymptomatically transmitting the “novel coronavirus” was floated out there as a possibility. The CDC claimed to have heard reports about asymptomatic cases but had not seen any of the data. At the time, poster boy Anthony Fauci stated that, based upon past evidence from respiratory “viruses” of any type, asymptomatic transmission was never a driver behind any outbreaks or spread of disease:
Asymptomatic transmission
“There’s a difference between someone who has the virus and is about to show symptoms and someone who gets it and never has any noticeable sign. The second type is purely asymptomatic and there was a lot of uncertainty on this point at a Jan. 28 White House briefing. The CDC said there were reports of it, but they hadn’t seen the data.
Fauci put the question into the context of past coronaviruses.
“We would really like to see the data because, if there is asymptomatic transmission, it impacts certain policies that you do regarding screening, etc. But the one thing historically people need to realize is that, even if there is some asymptomatic transmission, in all the history of respiratory-born viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there’s a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.”
However, a few days later on February 3rd, 2020, Anthony Fauci had changed his tune and stated that, based upon a single paper, he had no doubt that asymptomatic transmission was occurring and that the study he had read had laid the case to rest. Unfortunately for Fauci, the conclusive evidence that asymptomatic transmission occurred was based upon false information. The study in question claimed that a woman, who had been in a meeting in Germany with four people who later became ill, was an asymptomatic carrier as she had no symptoms at the time of the meeting and became ill upon her flight home to China. For some reason, the authors of the paper failed to actually speak to the woman and wrote the paper solely based upon what the four patients told them. Ironically, the Robert Koch Institute actually spoke to the woman and confirmed that she was symptomatic at the time of the meeting, thus giving Fauci a nice serving of egg on his face:
“Chinese researchers had previously suggested asymptomatic people might transmit the virus but had not presented clear-cut evidence. “There’s no doubt after reading [the NEJM] paper that asymptomatic transmission is occurring,” Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases, told journalists. “This study lays the question to rest.”
But now, it turns out that information was wrong.
The letter in NEJM described a cluster of infections that began after a businesswoman from Shanghai visited a company near Munich on 20 and 21 January, where she had a meeting with the first of four people who later fell ill. Crucially, she wasn’t sick at the time: “During her stay, she had been well with no sign or symptoms of infection but had become ill on her flight back to China,” the authors wrote. “The fact that asymptomatic persons are potential sources of 2019-nCoV infection may warrant a reassessment of transmission dynamics of the current outbreak.
But the researchers didn’t actually speak to the woman before they published the paper. The last author, Michael Hoelscher of the Ludwig Maximilian University of Munich Medical Center, says the paper relied on information from the four other patients: “They told us that the patient from China did not appear to have any symptoms.” Afterward, however, officials at the Robert Koch Institute (RKI), Germany’s federal public health agency, and the Health and Food Safety Authority of the state of Bavaria did talk to the Shanghai patient on the phone, and it turned out she did have symptoms while in Germany. According to people familiar with the call, she felt tired, suffered from muscle pain, and took paracetamol, a fever-lowering medication. (An RKI spokesperson would only confirm to Science that the woman had symptoms.)”
In March 2020, a top Chinese health official completely contradicted Fauci by stating that there was no evidence that asymptomatic carriers could spread illness to others:
‘No evidence’ asymptomatic carriers spread coronavirus, Chinese health official claims
“A top Chinese health official sought to allay growing fears over asymptomatic coronavirus carriers on Monday, saying there was “no evidence” they could spread the illness but medical workers should remain alert to the risk.”
Not one to be made the fool, in April 2020, Fauci suggested that there were millions of silent spreaders in the US. In fact, he claimed that asymptomatic infections made up anywhere from 25 to 50% of the infections. He backed his figures up by confidently stating that they were just guessing as they had no scientific data to support these guesstimates. Fauci stated that he wouldn’t have any “scientific” data until mass antibody testing was carried out. He said that it was impossible to know who is infected without symptoms until you test everyone who has no symptoms. This lends credence to the fact that testing people without symptoms will, as the CDC stated with pertussis, create nothing but false-positives:
Fauci once dismissed concerns about ‘silent carriers’ of coronavirus. Not anymore.
At Sunday’s White House briefing, Dr. Anthony Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases, suggested that hundreds of thousands — or even millions — of “silent carriers” may be unwittingly spreading the coronavirus across the United States because they don’t realize they’re infected.
The idea that at least some coronavirus carriers don’t feel sick isn’t new. But the scale of Fauci’s estimate was.”
“It’s somewhere between 25 and 50 percent” of the total, Fauci said. But “right now,” he went on, “we’re just guessing.”
“The first thing to note is that Fauci himself expressed a high degree of uncertainty about his own numbers. “I don’t have any scientific data to say that,” he admitted Sunday. “You know when we’ll get the scientific data? When we get those antibody tests out there and we really know what the penetrance is. Then we can answer the questions in a scientifically sound way.”
“Fauci was right to be cautious. As he noted, it’s impossible to say how many carriers never showed symptoms until you’ve tested a bunch of people who never showed symptoms — something that will only happen after the worst of the pandemic is over and scientists start trying to determine, en masse, who does and doesn’t have immunity. (More on that later.)”
“Last week Centers for Disease Control and Prevention Director Robert Redfield told NPR that “one of the [pieces of] information that we have pretty much confirmed now is that a significant number of individuals that are infected actually remain a asymptomatic.”
In June 2020, the WHO’s Maria Van Kerkhove disagreed with Fauci’s assessment of asymptomatic transmission by claiming that it appears to be rare based upon the data that was seen. In fact, she claimed that investigators were not finding any cases of secondary transmission from an asymptomatic carrier to anyone else:
Coronavirus spread by asymptomatic people ‘appears to be rare,’ WHO official says
“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,” Van Kerkhove said on Monday.
“We have a number of reports from countries who are doing very detailed contact tracing. They’re following asymptomatic cases, they’re following contacts and they’re not finding secondary transmission onward. It is very rare — and much of that is not published in the literature,” she said. “We are constantly looking at this data and we’re trying to get more information from countries to truly answer this question. It still appears to be rare that an asymptomatic individual actually transmits onward.”
However, by November 2020, Fauci was defiant against the WHO’s admittance that no secondary transmissions were occurring and stated that he was certain that 40-45% of the transmission was due to asymptomatic carriers. Fauci hammered home the point as to why masks, which he had claimed offered no protection in March 2020, were now essential in November 2020:
Anthony Fauci’s Thoughts on Covid-19 Transmission, Treatments, and Vaccines
“Speaking of asymptomatic spread, Fauci says that 40–45% of transmission is due to asymptomatic people unwittingly infecting others. This is why masks are so essential — by wearing one, you protect other people even if you don’t know that you’re infected.”
In December 2021, Fauci was defeated yet again when the “discoverer” of Omicron, Dr. Angelique Coetzee, questioned whether such a thing as an asymptomatic carrier even existed at all. She stated that they had seen no asymptomatic cases of Omicron and then recommended that those without symptoms need not test:
‘There’s no reason to test if you have no symptoms,’ and 2 other findings from the woman instrumental in first identifying omicron
“Notably, Coetzee suggested that asymptomatic cases of the omicron variant are rare, if such a condition exists at all.
Asked during a Christmas Eve interview on MSNBC if “there was not such a thing as an asymptomatic case of omicron,” Coetzee responded: “We haven’t seen it.”
Secondly, the chairwoman of the South African Medical Association also told MSNBC on Friday that she doesn’t recommend testing by individuals until, and if, symptoms arise from the variant. “There’s no reason to test if you don’t have symptoms,” she said.”
In another blow to the ego of “Science,” an April 2021 study published by the CDC saw Fauci’s statements contradicted yet again when the researchers found no asymptomatic transmission. In fact, they stated that their findings were in line with other studies and that asymptomatic transmission was unlikely to contribute to the spread of “Covid,” which torpedoed Fauci’s claims of 40-45% of transmission being due to those without symptoms:
Analysis of Asymptomatic and Presymptomatic Transmission in SARS-CoV-2 Outbreak, Germany, 2020
“We determined secondary attack rates (SAR) among close contacts of 59 asymptomatic and symptomatic coronavirus disease case-patients by presymptomatic and symptomatic exposure. We observed no transmission from asymptomatic case-patients and highest SAR through presymptomatic exposure. Rapid quarantine of close contacts with or without symptoms is needed to prevent presymptomatic transmission.”
Conclusions
“In this cluster of COVID-19 cases, little to no transmission occurred from asymptomatic case-patients. Presymptomatic transmission was more frequent than symptomatic transmission. The serial interval was short; very short intervals occurred.
The fact that we did not detect any laboratory-confirmed SARS-CoV-2 transmission from asymptomatic case-patients is in line with multiple studies (9–11).”
“In conclusion, our study suggests that asymptomatic cases are unlikely to contribute substantially to the spread of SARS-CoV-2. COVID-19 cases should be detected and managed early to quarantine close contacts immediately and prevent presymptomatic transmissions.”
While Fauci’s claims of asymptomatic transmission were obviously unfounded, there were many asymptomatic cases being generated due to the fraudulent testing, as predicted by the CDC with pertussis. Thus, the perception that asymptomatic people were spreading a “virus” was easily conveyed to the public based upon unscientific data. We can see evidence of the massive amounts of healthy people testing positive for a “virus” by way of the mandatory mass testing data that came out of China throughout the “pandemic.” For instance, in March of 2022, Shanghai reported that over 70% of their cases were asymptomatic.
Why is Shanghai seeing so many asymptomatic Covid-19 infections?
“China is in the grip of an Omicron wave, but about 70 percent of cases reported in March have not had any symptoms.”
“Of the 103,965 locally acquired cases reported in March, only 3,046 had symptoms, according to National Health Commission data. And most of the asymptomatic infections were reported in Shanghai.”
By November of 2022, China was seeing upwards of 90% of their reported cases described as asymptomatic.
China Reports Third Consecutive Daily Record for New COVID Cases
“China reported 35,183 new COVID-19 infections on Friday, of which 3,474 were symptomatic and 31,709 were asymptomatic, the National Health Commission said on Saturday, setting a new high for the third consecutive day.
That compared with 32,943 new cases a day earlier — 3,103 symptomatic and 29,840 asymptomatic infections, which China counts separately.
Excluding imported cases, China reported 34,909 new local cases on Friday, of which 3,405 were symptomatic and 31,504 were asymptomatic, up from 32,695 a day earlier.”
By December 2022, China had given up on reporting their overwhelming amount of asymptomatic cases in their daily Covid counts:
China stops publishing asymptomatic COVID cases, reports no deaths
“China’s National Health Commission (NHC) will as of Wednesday stop reporting new asymptomatic COVID-19 infections, as many people without symptoms no longer participate in testing, making it hard to accurately tally the total count, it said.”
There were many reasons provided for why China had so many asymptomatic cases but it easily boiled down to their untargeted mass surveillance testing of the entire population. It is clear that if one goes looking for cases, one will find them whether symptomatic or not. In China, it was very much the latter as they were seeing over 98% asymptomatic rates in Shanghai based upon their testing data. This goes against the idea that mass testing would find more symptomatic cases. As more healthy people were subjected to a fraudulent test, the more “healthy sick” people that could be added to the overall totals:
Explainer-Why are Shanghai’s COVID infections nearly all asymptomatic?
“The number of new confirmed community transmitted cases in the major financial hub of Shanghai reached 4,477 on Tuesday, a record high, but only 2.1% showed symptoms. The share of symptomatic cases over the previous seven days was around 1.6%.”
“Following are some explanations for why the rate of asymptomatic cases is so high.
Surveillance Testing
China is also the only major country to do mass, untargeted surveillance testing, which is bound to uncover more asymptomatic cases, although it could also be expected to reveal more symptomatic cases.
“Surely, high levels of testing will pick up more rather than less asymptomatic cases,” said Adrian Esterman, an expert in biostatistics at the University of South Australia.”
Mass testing with fraudulent tests led to a surge in healthy people being fraudulently labelled as asymptomatic carriers. It doesn’t matter that this very act of mass testing, as the CDC stated, increases the likelihood of false-positives (even though they are all false-positives). This perception of a massive number of “infections” of a “virus” regardless of any disease being present only helped to further solidify this illogical concept into the minds of a fearful public as if it were a scientifically proven fact when it is anything but. Ironically, despite their “test, test, test” mantra, the WHO actually claimed that its guidelines never recommended mass testing of asymptomatic people as was being done in China due to high costs involved and the lack of data of its effectiveness:
Analysis: Test, test, test? Scientists question costly mass COVID checks
“WHO guidelines have never recommended mass screening of asymptomatic individuals – as is currently happening in China – because of the costs involved and the lack of data on its effectiveness.”
Thus, we can see that there truly is nothing behind the claim of an asymptomatic carrier of disease other than the fraudulent label provided by technology never meant for diagnostic use, especially on such a massive scale as we witnessed during this “pandemic.” PCR can find anything in anyone and the result is utterly meaningless, as stated by inventor Kary Mullis:
“Anyone can test positive for practically anything with a PCR test, if you run it long enough with PCR if you do it well, you can find almost anything in anybody.”
“[PCR is] just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick, it doesn’t tell you that the thing you’ve ended up with really was going to hurt you or anything like that.”
The asymptomatic excuse was created in face of conflicting evidence by a man who wanted nothing more than to protect his prestige and his findings. Robert Koch was under pressure from a growing field of researchers who were either contradicting his own findings or making new discoveries of their own. Koch needed a way to ensure that his own research would stand up to scrutiny. Bending his own logical postulates in order to allow for the asymptomatic carrier to exist allowed for his contradictory findings, as well as those put forward by later researchers, to persevere in the face of any further challenges by opponents:
“Whatever I undertake these days, there will be a bunch of the envious and jealous at hand. They will try to challenge me and if they don’t succeed, try to make me turn away from my work in disgust.”
“Those happy days are gone when the number of bacteriologists was small and each of them could research wide areas in an undisturbed manner…So now in making the most modest and most careful delineation of a research area you will step on the first colleagues’ toes or bump into a second one unintentionally, or come too close to the third’s field of work. Before you even realise it, you are surrounded by opponents.”
It is clear to anyone looking at the idea of an asymptomatic carrier of disease logically that this very notion does not stand up under scrutiny. This nonsense was summed up brilliantly by the late great Canadian researcher David Crowe:
“Someone who believes in the virus can explain this conundrum to me.
“It has been strongly stated that asymptomatic people can be infectious for quite a long time (I can provide references if you don’t believe me, but this has been widely stated). This means that for quite a long time their body has a large quantity of virus particles, otherwise infection wouldn’t be possible. But their body doesn’t react to these particles, an immune reaction would at least result in a fever. But without an immune reaction they can never get rid of the virus particles. And how is it that virus particles running around the body of some people don’t do anything, whereas other people get seriously ill and die? How do all the virus particles in one person know that they shouldn’t mess with the cells to cause symptoms, whereas in another person they all go crazy and cause devastation?
“So we can conclude that (1) Asymptomatic people never get rid of the virus and therefore must be quarantined forever; (2) It’s the virus that’s deficient, not the person, which must mean there are multiple dramatically different strains; or (3) the viral theory is a load of BS.
“Please help me.”
-David Crowe March 31st, 2020
It is obviously number 3. The “viral” theory is a load of BS, and there is no such thing as a healthy sick person capable of transmitting disease. We have no reason to fear the walking healthy.
“…And he described it as a kill box and then I looked that up and it turned out it’s a military term for establishing a geographic space or three-dimensional area for a military attack by air and by surface to kill the people who are in it and then dismantle the kind of framework and move on to the next campaign.
And what the DoD and the World Health Organization intend to do and have gotten quite far in doing, but not completely reached their goals, is to set up the entire world as their geographic terrain, their target population as all the people in the world, the duration of their campaign as permanent…”
Transcript: Jan. 24, 2023 Legal Walls of the Covid-19 Kill Box Presentation
…And the basic idea is that public health has been militarized and the military has been sort of turned into a public health front or Potemkin Village such that they are using public health language and public health laws to actually carry out a military campaign.
And I would not call them DoD vaccines.
I would call them DoD weapons.
So, I call it the kill box because the first sort of lead that I had was Todd Callender’s January 30th 2022 interview on Elizabeth Lee Vliet’s podcast called Truth for Health.
And he described it as a kill box and then I looked that up and it turned out it’s a military term for establishing a geographic space or three-dimensional area for a military attack by air and by surface to kill the people who are in it and then dismantle the kind of framework and move on to the next campaign.
And what the DoD and the World Health Organization intend to do and have gotten quite far in doing, but not completely reached their goals, is to set up the entire world as their geographic terrain, their target population as all the people in the world, the duration of their campaign as permanent.
And the weapons that they’re using are, number one, informational. That’s the propaganda piece and the censorship piece.
Number two, psychological. That’s the fear and terrorism piece of telling people they need to be afraid all the time and they need to listen to the government.
And then the third piece is the chemical, biological, radiological, and nuclear [CBRN] weapons, which are called in their campaign pharmaceuticals, vaccines but are actually toxins and pathogens.
So I started, after I heard that interview — I had already been wondering what was going on but I started trying to track down some of the things Todd Callender talked about in his interview and figure out what the legal frameworks were and how they were set up and what the financial coercion mechanisms were.
My finding, which many other people have found in various, from various other angles, was that this project has been going on for centuries.
It’s basically globalist central bankers and lots of related organizations trying to get complete control of human beings through banking programs and through military programs.
And they kicked it into higher gear in 1913 with the Federal Reserve Act, and then they kicked the public health aspect of it into higher gear starting in the 1930s and 40s.
Before the 1960s, they mostly did it through orchestrated armed conflicts and financial depressions and wars, which are very loud and messy and destructive to infrastructure.
And it makes it difficult for them to have plausible deniability and legal impunity for what they’re doing.
So in the mid-60s they got much better at inducing suicide and homicide by fraudulently labeling poisons as medicines or as vaccines or as prophylactics and telling people that submitting to that poisoning process was their civic duty. And that’s — we saw that in Covid with the shorthand for “Do this or you’re going to kill your grandma.”
And the way that the pharmaceutical method is primarily useful to them is that plausible deniability is much easier and legal impunity is a lot easier.
They can achieve the same goal of killing lots of people without their fingerprints being all over it.
I looked into the coercion cascades, mostly financial. I’m not going to go into a lot of detail with that but it starts at the top with the Bank for International Settlements and they can use their control of other federal central banks, access to financial systems, and then all the way down through state governments, national governments, local, municipal, school districts, hospitals. Everything.
If you comply with what they’re telling you to do as far as masking and testing, isolating yourself, taking injections, then you will get the financial access that you need to run your business or to have a job. And if you don’t comply, they can cut you off from those services. And so that is one of the main mechanisms through which the whole thing was carried out.
The U.S. Congress passed the law to set up the Chemical and Biological Warfare program. And in that law, which is 50 USC Chapter 32, there are very important key terms including “protective,” “prophylactic” and “defensive,” which is how they justified doing it.
They were using those words because the international community of ordinary non-insane people were concerned about biological and chemical weapons and they were working on international treaties to prohibit them.
And so they needed to build in loopholes and the loopholes they built in were that, “We’re not going to do biological and chemical research and weapons development except for protective or prophylactic or defensive purposes.”
And that’s a false characterization because all biologically active products are intrinsically aggressive and toxic and lethal. And that’s where we get disciplines or, that’s the thing that disciplines like toxicology, pharmacokinetics, genotoxicity, drug-drug interactions, are all related to that fact: that everything that goes into the human body or any living body has some effects which can be toxic. So that was the way they tried to get around that.
And then the foundational Public Health Emergencies platform came out in 1983 when Congress passed the Public Health Service Act Amendment and that set up the Public Health Emergencies program under the 1944 law that had originally set up the Public Health Service. Which is a branch of the military.
And it also, in 1983, Congress and Reagan set up a 30 million dollar slush fund and that has continued. It’s got a different name now than it did then, [Public Health and Social Services Emergency Fund] but it’s still being funded as recently as the NDAA and the Consolidated Appropriations Act in December of 2022.
The other thing they did in the 80s was set up the 1986 National Vaccine Program and National Childhood Vaccine Injury Act.
And that’s the one that set up the liability exemption for manufacturers and funneled anyone who was injured by a vaccine into this different compensation program. And that’s been used as a model since Covid started, for the Countermeasures Injury Compensation Program.
So the international piece, the cornerstone, is the World Health Organization, which is not a health organization. It’s a military organization, because of this merger that I’m talking about. It’s sort of the military arm of the one-world government that they’re trying to set up.
And they did a set of amendments to the International Health Regulations in 2005 that entered into force in June 2007. But basically the IHR, which are currently going through another round of amendments to make them worse, called on national governments to strengthen their own domestic laws and fund more programs for surveillance, testing, detention and quarantine — physical control and forced treatment — during international outbreaks of communicable diseases.
And the pretext that they used, because it was bankers who were doing this, was that they needed to protect international trade from disruptions caused by disease outbreaks. But the real intent was to set up these legal systems that transferred sovereign government from the nation-state to the World Health Organization and the BIS automatically when a “public health emergency of international concern” [PHEIC] has been declared.
And Congress and U.S presidents and the cabinet complied with that demand from the World Health Organization.
So two of the key years were 1997 and 1998. That was when the beginnings of the emergency use authorization program was set up and when they transferred the CBRN [chemical, biological, radiological, nuclear] weapons stockpile from DOD, classification I guess, to HHS or CDC classification and control.
It was the same products, as far as I can tell. It was just a relabeling and a re-homing of them.
The EUA [Emergency Use Authorization], that was kind of a two-step thing. At the time the public was really upset about the use of unapproved vaccines for anthrax on military troops and the horrible adverse effects they were having.
So Congress passed a law in November [1997] to kind of revoke authorization for testing or using unapproved products on military troops. But three days later in a different law, made it so that the same programs could be done but the target population would be expanded from just military troops to the entire American population.
Then around 2000 to 2002, using the momentum from 9/11 and the anthrax attacks on Congress, they set up, through the statutes again, program management sort of structures. They did that through the 2000 Public Health Threats and Emergencies Act, [and] through the 2001 Authorization for Use of Military Force.
And people talked about this at the time. It was construed as putting the country into a permanent state of war — the Global War on Terror — with every other country in the world. So there was no geographic limitation. There was no time limitation. There was no identified enemy other than “terror” and through that — I think other people figured this out at the time and then it sort of got suppressed — but it made everyone in the world into a presumptive combatant or enemy target.
So it was essentially a de facto covert global martial law act by the US government.
And then in those early 2000s we also got the PATRIOT Act, the Public Health Security and Bioterrorism Preparedness and Response Act and the Homeland Security Act.
And those were just more of the merging of the DHS [Department of Homeland Security], the DOJ [Department of Justice], the HHS [Health and Human Services], the Department of Defense: all of the cabinet agencies.
So since then, 2003 to [2019] there have been lots and lots of executive orders on these things. Lots more statutes and appropriations. Lots of agency regulations, guidance reports that were circulated to state, local and tribal authorities and law enforcement so that they would know that under a public health emergency, they are subordinated to the federal military.
FDA [Food and Drug Administration] issued a lot of Guidance for Industry documents and sent
those out to the pharmaceuticals and to the academic organizations and NGOs [non-governmental organizations] to let them know about how FDA was going to handle experimental products like “vaccines,” “gene therapies,” “biologics.”
And they did more test runs like 2003 SARS, 2006 MERS and 2009 H1N1.
That brings us up to the Other Transactions Authority [OTA]. And this was revealed through Pfizer’s April 2022 motion to dismiss whistleblower Brook Jackson’s False Claims Act case.
They said, “This was not a vaccine. It was a DoD prototype and we were never obligated to do valid clinical trials. We were never obligated to prove safety or efficacy to anyone. We never had to get FDA authorization through any of the normal guidance for industry channels, because it was a prototype.”
On October 4th, 2022, the US government endorsed that view and filed a statement of interest and support for the motion to dismiss, basically saying that clinical trials were never material or necessary for DOD to pay the contractors for producing and distributing the bioweapons known as Covid-19 vaccines.
And so all of this became visible from 2020 to the present when the World Health Organization Secretary-General issued the “public health emergency of international concern” [PHEIC] at the end of January 2020 and the HHS secretary immediately triggered the domestic frameworks through the “determination that a public health emergency exists” followed by PREP Act declarations for “medical countermeasures,” which are the weapons.
And then Congress and the presidents — Trump and Biden — passed several additional Congressional acts funding and reinforcing the structure of the kill box and issued more executive orders under the Defense Production Act, under the Stafford Act, under the National Emergencies Act, to sort of build out the program.
Basically what it built is a huge public and private funding stream for military-led bioweapons research and use; eliminated informed consent by reclassifying people who could potentially be carrying a disease as presumptive national security threats, so that you could do anything you want to them because you’re on a war footing.
And to shield the products and weapons from product liability, to shield all the people involved from criminal liability and civil liability, and to shield the government funders, developers and regulators from criminal prosecution under the other laws — which are in place but are sort-of superseded by this framework — for use of bioweapons [18 USC 175] use of chemical weapons [18 USC 229], terrorism [18 USC 2331] things like that.
…I see it as a joint project between the U.S Department of Defense — a coordinating committee of that, the Federal Reserve, and the World Health Organization, and the Bank for International Settlements and the United Nations. But the World Health Organization is like a subsidiary of the U.N.
And there are things that the globalists do not like. They don’t like constitutions and charters. They don’t like the conflicting statutory frameworks around bioterrorism, war crimes, genocide, torture. They don’t like any of that stuff.
They don’t like when states and provinces and counties and towns pass their own laws protecting informed consent, protecting people from, for consumer safety. They actually put out a report in October 2022, State Laws Limiting Public Health Protections: Hazardous for Our Health. And there’s a whole bunch of things in there that states have started doing that the globalists do not like.
So doing more of those things, more bringing control back to the state, more using Article 10 of the Constitution, to reclaim state authority, those are all extremely useful.
And I do think it’s going to break. I think there’s going to be a tipping point and the criminal prosecutions are going to start.
And we have all the evidence. And every time they try to answer what we’re talking about by saying national security, they reinforce that this is the right way to go.
This is what they’re doing.
They’re doing war crimes.
Links:
Jan. 24, 2023 – DoD ‘Vaccines’ Press Conference. (L4Atv1, 2 hrs — 0:00:30 Sam Dube – Host Open; 0:03:04 Glen Macko – Overview of DoD Vaccines; 0:05:28 Katherine Watt – Legal: Laws, Contracts, FOIA, SEC; 0:24:39 Sasha Latypova – Manufacturing, Safety, Quality, Intent; 0:33:32 Phillip Altman – Conformation of Skills/Knowledge of Katherine & Sasha; 0:38:08 LTC (Ret) Pete Chambers – Vaccine observations in Military; 0:46:13 Dr Sam Dube – Guidance on “Going Local” for personal protection; 0:56:47 Q&A)
Laura Bartlett and Greta Crawford have founded an organization to address the forced treatments patients receive when they’re hospitalized for COVID-19, but the same strategy can be used to protect yourself against other medical hazards as well
The Caregivers and Consent document they created is an “advance decision” document. So, the moment you enter the hospital, the hospital staff know what they can and cannot do to you; they are legally required to respect your current care decisions. And unlike an Advance Directive (which only kicks in when you are incapacitated) the Caregivers and Consent document goes into effect immediately
It’s important to complete and notarize your Caregivers and Consent document BEFORE you ever need to go to the hospital
Make sure you send the completed, signed and notarized document to the CEO of the hospital in two ways: (1) via a professional courier (one that specializes in delivering legal documents); and (2) via the Postal system with certified mail, return receipt requested. The CEO is responsible for all legal business relating to the hospital, including the medical records, so the CEO, not your attending physician, is the one whose responsibility it is to get your consent document entered into your electronic medical record
Make at least 10 copies of the signed, notarized document and keep one copy on your person, in case you ever have an accident or acute illness requiring hospitalization. Also provide copies to the attending physician and nurse once hospitalized
Also, should you become hospitalized (and therefore unable to personally send the document to the CEO), designate a family member or friend to send your Caregivers and Consent document on your behalf. Additional recommendations to ensure your safety are included
In this interview, Laura Bartlett and Greta Crawford detail how you can protect yourself from one of the top contributors to premature death, namely conventional hospital care. The key here is to understand what the dangers are and take proactive measures to guard yourself and your family from them.
Nearly 10 years ago, I interviewed Dr. Andrew Saul, author of “Hospitals and Health: Your Orthomolecular Guide to a Shorter, Safer Hospital Stay,” in which he details how to minimize your risk of being a victim of a medical error.
First and foremost, Saul recommended making sure you have a patient advocate, someone who can speak on your behalf if you’re incapacitated and make sure you’re receiving the correct medication and treatment. During COVID, however, family or friends were not allowed into the hospital, and patients were routinely bullied into treatments they did not want or consent to.
The good news is, Bartlett and Crawford have developed a legal document that, when served to the hospital in the proper way, can ensure that your medical wishes are honored. By eliminating any confusion about your consent (or denial of consent), this document can literally save your life.
Why ProtocolKills.com Was Created
Bartlett and Crawford have founded an organization to address the lethal and, in many cases, forced treatments patients receive when they’re hospitalized for COVID-19, but the same strategy can be used to protect yourself against other medical hazards as well. Crawford explains:
“I created a website called ProtocolKills.com. This came after I was in the hospital with COVID. In the process of going to the hospital, I was denied informed consent and was completely unaware of some of the things they were doing to me. I was given five rounds of remdesivir, which nearly took my life, and I did not even know that I was being poisoned at the time …
During that time in the hospital, I went from thinking I was going to go home after I got oxygen to actually feeling like that I was going to die. I was almost certain I was going to die after being given just the first dose of remdesivir …
[And then there was] the constant push for the vaccine in the hospital, the harassment for not getting vaxxed, and the fact that I was given medication without my knowledge at all, which led me to start the website to not only inform people about what was going on, but [as] a platform to allow other victims who were not as fortunate as me.
Many of them, the majority of them, did not make it out alive. So, it’s a platform for them to share their story. We have over 250 stories on there about what they faced in the hospital. We really wanted to get this information out there to the public, but we also wanted to give a solution, not just to scare people. And that’s where I ended up meeting Laura.”
National Hospital Hostage Hotline to the Rescue
Bartlett continues:
“Before I met Greta at the beginning of COVID, in early 2020, I started helping my brother, Dr. Richard Bartlett, who had a protocol utilizing inhaled budesonide steroid as part of his protocol to treat COVID early. We also found it very effective once people were in the hospital to help reverse [the infectious process] and also the scarring and the inflammation of the lungs.
There are instances where it even helped people who were on ventilators as long as 30 days come off the ventilator and go home. So, I was helping him get that message out in early 2020. I’m not a doctor. I’m not a nurse. I’m just somebody who could help get that known around the world. My background is in media PR …
In the process, people who knew my brother, knew me, started reaching out to both of us with stories that they were in the hospital and they were having a hard time getting the doctor to respect their right to informed consent. It was an overwhelming number of instances where people just felt like they were being bullied or coerced, that their right to try budesonide, for instance, was just dismissed.
And it was almost as if informed consent didn’t exist. But in fact, it never went away. Even during the COVID shielding for hospitals, informed consent between the doctor and the patient never went away. You always had the right to informed consent.
So that’s where my work started. In the process, since there were so many people reaching out for help, I thought, ‘Well, why doesn’t somebody come up with a way for people to quickly access some information of what their rights are and their patient rights?’
So, I started a nationwide hotline, called the Hospital Hostage Hotline [call or text 888-c19-emergency, or 888-219-3637]. It’s still in effect. I still get calls from all over the country. And I’ve been able to help people who went in even for non-COVID reasons like a urinary tract infection that was [also] diagnosed as COVID, and they were being pushed towards a protocol and told they couldn’t leave the hospital.
They needed to know they could, that they always had the right to leave AMA — Against Medical Advice — if that’s what they chose. They also have the right to either consent or not consent to things and it should be respected. I realized that one of the biggest tools for getting that informed consent notice to the doctor was not to just verbally say it, but to have it in writing. These aren’t my original ideas.
I actually had a hospital insider reach out … somebody who had been in the system and knew how to navigate the system at a high level in administration, give me some tips and tools on how to navigate the hospital system to make sure that informed consent was not only documented and delivered effectively to get into the electronic medical record, but also, what their basic patient rights were and how to advocate for them.”
You Have the Right to Leave
One drawback of signing an AMA is that insurance won’t pay for your treatment. That threat will often keep patients in the hospital because they’ll have to pay out of pocket. So, it can be used against you.
“Profit has been a big factor in a lot of suffering,” Bartlett says. “Patients were afraid to leave because they were told, like in the instance of a gentleman that I was helping in New Jersey who went in for a urinary tract infection.
He was an elderly man. This was early 2020. They quickly tested him for COVID and started him on that road towards a ventilator. And they told him flat out, ‘If you leave, none of this will be covered by insurance.’ So that was a big factor.”
Hospitals may also misinform you about your AMA rights, as we’ve seen repeatedly during COVID. More often than not, the hospital’s reluctance to release a patient has to do with protecting its revenues. Bartlett offers the following story to illustrate:
“Somebody that I was helping advocate for said the doctor actually said to them, ‘You cannot leave.’ This person was 15 or 16 days into their COVID diagnosis and they were feeling better. They were likely not COVID positive …
That’s where the name of the hotline came from. They actually felt like hostages. That’s what they were reporting to me. ‘I feel like I’m held prisoner.’ But in fact, they always had the right to leave a hospital whenever they chose to. It’s not up to the doctor when they can leave. They have to make that medical choice for themselves, whether or not they feel like they can leave.”
A Novel Consent Document That Can Save Your Life
Patients clearly need a way to put themselves back in the driver’s seat, and the novel medical consent document Bartlett and Crawford created, available on OurPatientRights.com, is the most powerful way I’ve seen so far to do that. As explained by Bartlett:
“What we learned from this whole ordeal over the last couple of years is that there was a need for a novel document that did not exist, to our knowledge, that covers your written consent. A document that documents your current consent, not an advance directive that kicks in after you’re incapacitated.
Before you go into the hospital, write down your consent wishes so that everybody involved in your care within the hospital will have eyes on it because it’s put into your electronic medical record. It’s notarized. It’s signed before you go in. That’s the key. So do it while you have full capacity.
It’s a novel strategy. I’m so grateful to the hospital insider who saw the problem and helped us navigate the system, so that we have an insider’s perspective on how to do this to keep people safe.”
As noted by Crawford, while COVID-19 may seem like a distant memory, people are still being hospitalized and diagnosed with COVID, and are being held hostage by a hostile medical system seemingly intent on milking them for all their worth, until death, if need be.
This is where filing a written medical consent form can help save your life. No doctor can override your written decision (consent) declining certain medications or treatments. Verbal communication is not enough. It must be in writing, notarized and delivered in a manner that formally serves the hospital and puts their physicians on notice.
General Consent Vs. Specific Consent
As explained by Bartlett, when you enter a hospital, you must sign a general consent authorization form. This is basically a contract between you and the hospital. Since you have bodily autonomy, they need your consent before they can do anything to you.
Typically, the general consent form authorizes hospital staff to test, treat and care for you in whatever way they see fit — and when a patient signs the general consent authorization, physicians feel justified that they can implement a hospital protocol without further explaining the risks, benefits or alternatives of that protocol to the patient.
Now, if you’re well enough to read the entire document, and see something in there that you don’t agree with, you can strike the sentence or paragraph and initial it, to indicate that you do not consent to that specific detail. However, that still doesn’t offer you much protection.
What you need is a much more specific document where you detail the types of treatments you consent to and the ones you don’t. You need to carve out a niche from the general consent form that specifies exactly what you do (and do not) consent to. And you need to be clear. Fortunately, the Caregivers and Consent document carves out that niche to communicate clearly to all physicians your exact consent wishes.
“You need a written consent document that, in addition to just the general consent, is a contract between you and the doctor, so he knows, he’s put on notice, what it is that you absolutely do not consent to. For instance, a COVID injection, if that’s your wishes,” Bartlett explains.
“They have a code of ethics, the American Medical Association guidance to physicians, per the ethics opinion 2.1.1, that when the patient surrogate has provided specific written consent, the consent form should be included in the record. This is key. Write it down. You don’t need an attorney. You don’t need any fancy training. You don’t need to be a doctor, don’t need to be a nurse.
You can write it down, and then, when you deliver it in our specific way — and it’s very important how you deliver it — it gets put into the electronic medical record for everybody to see. Now you’ve got receipts, that if you do something against consent, it’s intentional. OK?
So, here’s the website you can find a template for that.
What you’ll see there are two PDF documents. [On one of the PDFs there are two pages.] One is the actual template, the other one is instructions on how to deliver it. And you can edit the document by the way. You can write your own. It’s just a template. But there’s also very specific instructions on how you are going to deliver this so it’s not disregarded.
Here’s what you’re going to see in the document. ‘I [your name] advise all physicians, nurses, and other caregivers that this Caregivers and Consent document reflects my current wishes for my care and are carefully planned and intentional wishes.’ That’s very important because it’s current. It’s not going to kick in when I’m incapacitated.”
Your Written Consent Must Be Respected
Advance medical directives don’t kick in until or unless you’re incapacitated, so that’s another completely different kind of document reflecting current consent wishes. What Bartlett and Crawford have created is an “advance decision” document. So, the moment you enter the hospital, they know what they can and cannot do to you. And, they are legally required to respect your written directives. The following section of the document reads:
“Receipt of this Caregivers and Consent document by the hospital serves as notice that I will report to the Medical Board any physician who violates my carefully planned and intentional wishes that are based upon my deeply held religious and spiritual beliefs and are delineated within this Caregivers and Consent document.”
This puts the doctor on notice. This isn’t a threat. It’s merely a factual statement that if anyone goes against your wishes, they’re intentionally disregarding your consent. Once it’s in your electronic medical record, they can’t say they didn’t know that you did not consent to a specific test, drug, vaccine or procedure. So, ignoring your written consent is then actually a criminal offense akin to assault and battery. It’s also medical malpractice.
“Let me tell you, there are good physicians and they are clamoring for something like this,” Bartlett says. “They are thankful there is something they can use to push back against administration and say, ‘I’m not going to violate this person’s written consent. I’m not going to do this to this person …’
With these documents, if you are blatantly refusing to honor a patient’s wishes and religious beliefs, and you’re doing it against these documented legal forms, then you risk losing your license altogether as a physician and never working in medicine again …
But you need it in writing … and it needs to be served in a very specific way. You need to do this before you ever go to the hospital. Have it handy in case you get yourself into a predicament, like a multi-car pileup on the highway and an ambulance transports you to the hospital. The time to have this done is before there’s a problem.”
The document also specifies that “All items in this Caregivers and Consent document shall remain in effect unless I choose to revoke in writing; no one else may alter or amend this Caregivers and Consent document.” So there can be no misunderstanding. Your doctor or nurse cannot claim you gave implied consent because you mumbled something incoherent in your sleep. In other words, if you didn’t change your consent wishes in writing, you didn’t change your consent wishes. Period.
What’s in the Caregivers and Consent Document Template
As mentioned, you can customize your Caregivers and Consent document any way you like. But to give people a starting point, the template, available on OurPatientRights.com, includes things like:
“I do not consent to the use of medications without my being informed of each medication’s risks, benefits and alternatives before they are ordered. Only after that information is communicated shall I choose to either grant consent or to not grant consent for each and every medication that is ordered.”
“I do not consent to receiving any vaccine or booster for COVID-19 or COVID-19 variant.”
“I do not consent to receiving the seasonal flu vaccine.”
“I request and consent to the use of 1 mg of budesonide via nebulizer every 4 to 6 hours for COVID-19 or COVID-19 variant diagnosis with respiratory issues.”
If you want to, you could change the verbiage to state that you do not consent to ANY vaccine. If you have allergies, add that to the list. Personally, I would recommend adding the following dietary notice:
“I do not consent to receiving ANY processed food, such as high-fructose corn syrup or seed oils. The only acceptable oil for me is butter, ghee, beef tallow or coconut oil. Acceptable forms of protein would be eggs, lamb, bison, beef or non-farmed seafood; but they must not be prepared with seed oils. If the hospital is unable to provide this food for me, my family or friends will bring it for me.
Additionally, I do not consent to not being able to take my normal supplements while in the hospital.”
I would strongly recommend that you integrate this additional clause because it’s a stealth form of abuse. These kinds of foods can only impair your effort to get well, no matter what your problem is. You may also want to add a notice saying you do not consent to receive blood donations from COVID-19 vaccinated donors, and that all blood donations must be from donors confirmed to have not received any COVID-19 vaccines.
Important: Follow Proper Procedure!
As mentioned multiple times in this interview, it’s crucial to follow the proper procedure. Here’s a summary of the necessary steps:
1.Complete your customized and personalized Caregivers and Consent form BEFORE you ever need to go to the hospital.
2.Get the form notarized. Make sure you sign the form in front of the notary.
3.Send the completed, signed, notarized form to the CEO of the hospital in two ways: (1) via a professional courier (one that specializes in delivering legal documents); and (2) via the Postal system with certified mail, return receipt requested.
The CEO is responsible for all legal business relating to the hospital, including the medical records, so the CEO, not your attending physician, is the one whose responsibility it is to get your consent forms entered into your electronic medical record.
4.Make at least 10 copies of the signed, notarized form and keep one copy on your person or in your wallet or purse, and another in the glove compartment of your car, in case you ever have an accident. Also provide copies to family or friends. If you happen to be hospitalized before you’ve had the chance to send the documents, have one of them follow the delivery procedure outlined on the General Instructions form.
5.Once you’re hospitalized, you or one of your contacts will give one copy to your attending physician and another to your nurse, and inform them that this document is already in your electronic medical record, or that the hospital will be served the documents shortly. Distribute additional copies to other care providers as needed.
6.Also, upon hospitalization, request to see your electronic medical record to make sure your Caregivers and Consent form has been entered. It is your right to see your electronic medical record, and it’s available through an online portal, so don’t let anyone tell you otherwise.
Also routinely check your medical record (or have your patient advocate do it for you) to make sure your wishes are being followed and that you’re not being given something you’ve denied consent for.
Crawford notes:
“What we’ve experienced using these documents is a complete change in the attending physician, from being aggressive and maybe trying to push you, to being very helpful and efficient. Once they receive these documents, they just do a 180. As a matter of fact, one patient’s brother told me he’s getting treated better than he’s ever been treated at a hospital before.”
Again, having this document in your medical record virtually guarantees that they cannot harm you by doing something you don’t agree with. Of course, some psychopath might ignore your directives, but they’ll have to pay a hefty price, as they’re guaranteed to lose a malpractice suit and be stripped of their medical license. The legal consequences are so severe that the person doing it would have to be beyond irrational.
Keep in mind that while you can request and consent to certain treatments, such as ivermectin, for example, this document CANNOT force your doctor or hospital to use that treatment. They can still refuse to administer something you’ve consented to.
They cannot, however, administer something that you’ve declined consent for. The ace up your sleeve at that point is that you can still sign out AMA (against medical advice), get out alive, and seek desired treatment elsewhere. Getting out alive is the key goal.
More Information
Again, here are the three resources created by Bartlett and Crawford:
ProtocolKills.com — Here you can find a hospital protocol for COVID, information about remdesivir, patient rights information, alternative health care options and patient testimonies
OurPatientRights.com — Here you can download the template for the Caregivers and Consent document and general instructions
In closing, please share this information with everyone you know. Bring it to your church, synagogue and local community groups. Everyone needs to know they can secure their patient right to informed consent and how to do it so that their wishes cannot be ignored. This is the most effective way to empower yourself when it comes to your medical care. So please, help spread the word.
It’s worth asking why now, because by any objective measure, there has been no virus activity worthy of the words ‘pandemic’ or ‘emergency’ for a very long time. The answer seems to be the failure of Corona to return in the winter, as long-absent influenza succeeded in suppressing Corona infections (in accordance with my prediction), and the increasing disinterest of the public in obtaining official test results has put all virus statistics in the toilet. They’re ending it now, in other words, not because anything on the ground has changed, but because they no longer have any hope of the scary headlines necessary to keep the machine up and running.
As in the beginning, so in the end: The pandemicists will give you always and forever the maximum virus suppression and the maximum vaccination that is politically possible. Not what is prudent, or what has any hope of achieving anything, or what has evidence in its favour, but simply the maximum that they can give you, for as long as they can give it to you. That is a reason in itself, never to let the pandemicists anywhere near the levers of power ever again.
With the Covid vaccination campaigns concluded, the European Union is sitting on an enormous vaccine surplus – and hundreds of millions more doses are expected to arrive this year and next… Because they are not needed, EU member states have been trying for months to retroactively adjust the contracts, without much success.
One country has now lost patience in the face of the tough negotiations, and is venting its anger. The Polish Health Minister Adam Niedzielski on Tuesday sent a letter to the “shareholders of Pfizer” [which] says that the delivery of hundreds of millions of doses planned by Pfizer despite a “stable epidemic situation” is “completely pointless.”
The excess doses can no longer even be given away; there is no government “interested” in Covid vaccines, said the minister …
Niedzielski also breaks prior agreements on the confidentiality of talks between governments, pharmaceutical companies and the mediating EU Commission … [and] reveals what Pfizer is offering the states: They’ll reduce the total quantity of the outstanding orders, in exchange for half the price of each dose that is not produced: “That’s a charge for literally non-existent doses that were never produced and will never be produced and that don’t cost Pfizer a penny.”
No wonder there has been such urgency to keep these negotiations secret.
Niedzielski writes that he is “extremely” sorry, but he is forced to conclude that the company is not prepared to show “a satisfactory level of flexibility and make any realistic proposals.” … The health minister called on Pfizer to “live up to its responsibility towards EU citizens and member states and work in good faith towards a solution that is fair for everyone.” Poland wants to continue to believe that the pharmaceutical industry is not only about money.
Some guests have argued why there is no such thing as an immune system.
Some guests have thought about alternative causes of illness.
The point is that there are good reasons to question the conventional model of “Rockefeller medicine”. Much of it doesn’t make sense and desperately requires critique.
Blindly believing what the pharmaceutical industry, governments and media preach from their pulpits, after observing the Covid™ scam, is utterly ludicrous. I have become an allopathic atheist. An apostate.
Climate science is drowning in pseudoscience and so is virology.
Andrew Kaufman, who has been on my show a few times before, joined me for the following conversation of conversations.
A beginner’s guide to Germ Theory.
He approached important concepts, including
virus definitions, isolation and fake existence claims;
understanding contagion and “catching” something from somebody;
bacteria and germs in general;
why all vaccines are toxic;
what is disease, actually;
shifting paradigms about health and wellbeing and
the significance of bringing down this house of germs cards.
Dr. Melissa McCann raised more than $110,000 to crowdfund the case, which accuses the Australian government of negligence related to the approval and monitoring of COVID-19 vaccines.
At least 500 Australians have already joined a “landmark” COVID-19 vaccine injury class action lawsuit filed this week against the Australian government and the medicines regulator seeks redress for those allegedly injured or left bereaved by the COVID-19 vaccines.
The action was filed in the Federal Court of Australia, New South Wales Registry.
According to the lawsuit, the respondents approved the vaccines “with no proper or reasonable evidentiary or logical basis to reasonably determine the Vaccines to be safe, effective and possessing a positive risk-benefit profile.”
“The action will argue that the Therapeutic Goods Administration did not fulfil their duty to properly regulate the Covid-19 vaccines, resulting in considerable harm and damage to Australians.”
The suit alleges the government “acted negligently in approving the vaccines and also by failing to withdraw them” based upon the “known evidence” of risk.
“Australians who have experienced a serious adverse event following Covid-19 vaccination are invited to step forward and register for this class action,” Strijland said.
A spokesperson for the Department of Health and Aged Care said that the department “is aware” of the lawsuit and that “as the matter is before the court it is not appropriate to comment further.
Class actions provide “a path to justice” for people who may not have the resources to file a court claim on their own, said Alison Bevege, a journalist who has written for Reuters and Daily Mail, in an April 26 Substack post.
Those injured by COVID-19 vaccines have been “ignored, denied, belittled and marginalised,” Bevege added.
Australian doctor crowdsourced $110,000 to bring class action suit
Thank you for sharing this news @RefugeOfSinner5 These injured and bereaved have suffered immense loss, pain and grief. Just as heartbreaking has been the gaslighting and silence, which has left them feeling abandoned. We cannot simply 'move on' from covid and leave them behind. https://t.co/TSxqYaqtOf
According to McCann, the class action suit was necessary because Australia’s federal vaccine injury compensation program — the COVID-19 Vaccine Claims Scheme — was “not fit for purpose” and had left many vaccine-injured Australians “abandoned with no support” after being promised “fair and accessible” compensation.
Services Australia as of April 12 had received 3,501 applications and paid 137 claims totaling more than $7.3 million, with 2,263 claims still in progress and 696 deemed not payable, news.com.au reported.
By comparison, the U.S. government, as of April 1, approved its first three payments to people injured by COVID-19 vaccines — amounting to a total of $4,634.89. Since the start of the pandemic, Americans claiming injuries related to COVID-19 vaccines and other countermeasures submitted 11,425 requests for compensation.
“TGA had determined that several young previously healthy children died of COVID-19 vaccine-induced myocarditis. Redacted letters from the TGA to McCann indicated these facts and an admission of willful concealment,” McCullough said.
‘I’d never known what a heart attack would feel like’
Among those represented in the lawsuit is Melbourne teacher Gareth O’Gradie, a previously healthy father of two who before he got his first Pfizer shot in July 2021, was into running, footy, cricket and tennis.
“Six days after [the vaccination] I had sudden-onset chest pain, shortness of breath, fever, chills, sweats,” he told World Freedom Alliance. “I’d never known what a heart attack would feel like, but that’s the type of thing I expected.”
O’Gradie, 41, was rushed to the hospital, where he was diagnosed with vaccine-induced pericarditis. He said:
“In the end I had open heart surgery to remove the pericardium, which had become inflamed and stuck to my heart. It’s extreme.
“All the heads of different departments, cardiology, rheumatology, cardiothoracic, all had conferences to say, ‘We’ve tried this, what is the next step for this recurrent pericarditis we can’t control the pain for?’ It wasn’t an easy decision.
“They said, ‘Nothing’s working — this is what we can offer.’”
“There was a lot of, you know, ‘We need to not scare the public as part of the vaccine rollout, so let’s not publicise these things,” he told news.com.au. “There was a large, intentional withholding of information — that doesn’t give people informed consent.”
The National Citizens Inquiry is a citizen-led and citizen-funded initiative that is hearing testimony from Canadians and experts examining the nature, the legality and the effects of the Canadian governments’ COVID mandates and restrictions. Today James talks to the volunteer-run inquiry’s volunteer communications director, Michelle Leduc Catlin, about the inquiry itself, what it is seeking to accomplish and how Canadians (and people around the world) can support it in its endeavours.
In 2021 Interview, RFK Jr. Reveals How Former Pres. Trump, Who Was Very Aware of the Serious Injuries Caused by Vaccines, Asked RFK Jr. to Lead a Commission on Vaccine Safety. Trump Changed His Mind Following Pfizer’s Million Dollar Contribution to His Inauguration
TCTL editor’s note: In 2021, Theo Von interviewed Robert F. Kennedy, Jr. Clips from this interview are found mirrored around the internet. In this interview, RFK Jr. talked about his meetings with Donald Trump wherein Trump asked RFK Jr. to head a vaccine safety commission. Trump was well aware of the serious dangers and great harm caused by vaccines as he personally knew people whose children developed serious health issues following vaccination. However, Trump changed his mind about the vaccine safety commission following a million dollar contribution from Pfizer to Trump’s inauguration. RFK Jr. was pushed aside and Scott Gottlieb, who was a Pfizer consultant, was selected by Trump to run the FDA. ~ Kathleen
Partial transcript:
Theo Von:
…Trump almost gave you a position… Wasn’t there talk of that? And then it kind of went away…
RFK, Jr.
Well, what happened was he … over the Christmas vacation… 2016, he’s elected right? And obviously the election is in November.
So I was skiing and with my kids in Colorado over Christmas vacation and I got a call from his chief of staff saying the president-elect wants to meet and he wants to talk about vaccines.
So, you know, I’ve been an activist on trying to get safer vaccines for a long time. And, of course, I agreed to meet with him.
So…immediately after getting home, I went … to New York and met with him at Trump Tower. It was about a two hour meeting.
Theo Von:
Had you ever met with him before?
RFK Jr.
I had sued him twice before successfully. And I had met him. And, you know, the lawsuit was not something that had hurt our relationship. I stopped him from building two golf courses in the New York City watershed. And those lawsuits were about two or three years apart.
And he knew me, and he knew my family… When my sister ran for governor of Maryland, he made a big contribution to that.
He contributed to my brother, who was then in Congress. And I had a cousin who was a congressman from Rhode Island, and he made a contribution. He was a big democratic donor at that point.
He called me. He asked me to come in. I had, as I said, about a two hour meeting with him. At that meeting, people were coming in and out of that meeting.
So Steve Bannon was there. Reince Priebus. You remember him? Hope Hill was there. Kellyanne Conway. And Jared Kushner. And both the president’s sons at various times were in that meeting.
Theo Von:
A lot of people.
RFK Jr.:
I had a lot of time alone with President Trump too.
He said that he believed that vaccines were making people sick. Specifically, he had three women friends who were mothers, one who was in the building that day, who had perfectly healthy kids who had gotten … their wellness visits. And they were around two years old.
And the children never were the same after those visits. And they all had been subsequently diagnosed with autism. And he believed that it was linked to vaccines.
And… because he had been open about that during the campaign, hundreds of women had — the same thing that happened to me, that got me into this, you know, this career killing advocacy, vaccine safety advocacy…
People start coming up to you and saying… “This happened to me. This happened to my son.”
“I had a perfectly healthy child who exceeded all his milestones. And I took him in at 16 months and he, you know, he was speaking, he was toilet trained, he had social interactions. And I took him in and he had a shot or a series of shots usually — could be up to nine — and that night, he’s like fever 103.”
I mean the stories were usually all identical. They had a seizure. And then over the next three months, they lose all of their capacity to… their social interactions, their eye contact…
I go in there and he tells me these stories. He wants to do something about it.
Theo Von:
And does he seem serious when he’s saying that?…
RFK Jr.:
Yeah, he was dead serious. And he asked… whether I would run a vaccine safety commission. And then he asked what I would do.
And I said, listen, I don’t think you have to do a big political lift. All I think you need to do is open up the databases and allow independent scientists in there to actually look at the science. Because the HMOs have all the vaccine data down to batch for every child in America. And they also have the medical records.
So all you have to do — in fact… AI can do machine counting and you can do cluster analysis.
And you can figure out very, very quickly whether all of these epidemics — not just of neurodevelopmental diseases like all the ADD, the ADHD… Tourette’s syndrome, narcolepsy… Autism. The allergic diseases, food allergies, peanut allergies… Asthma and then all the autoimmune diseases…
And they’re all listed, by the way, on the vaccine inserts, as vaccine side effects.
Because the only way that you can sue — you know, they passed this law in 1986 and made it illegal to sue a vaccine company for injury.
You still can sue them if they know of an injury that’s caused by their vaccine and they don’t list it on the side effects.
So they list 400 injuries…
But they’re not allowed to list it unless there is significant evidence that it is actually being caused by the vaccine.
FDA is not allowed to allow them to list it unless FDA believes it’s being caused by the vaccine.
Theo Von:
So you have this meeting with Trump, just to get back to that… Did you leave out of the meeting kind of hopeful about it?
RFK Jr.:
Well, I said to him, what do you want me to do? And he said we want you to announce it. Jared Kushner escorted me to the press scrum…
So then I went down and announced it. Talked to the press.
And then a week later, Pfizer made a million dollar contribution to Trump’s inaugural.
And then Trump comes in. And we continue to have some meetings with Fauci — that he had set up, were part of this process and we’re rolling, to get this thing started.
Theo Von:
Did Fauci seem legit when you talked to him?…
RFK Jr.:
Oh, he’s very, very charming…
Listen, Fauci — I’m about to publish a book on Fauci [see “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health”, published by Children’s Health Defense in November 2021]… He’s been there for 50 years, so he’s like J. Edgar Hoover.
And the only way that you last at that agency for 50 years is by carrying water for the pharmaceutical industry.
And under his watch, he’s supposed to prevent autoimmune and allergic diseases. Under his watch, chronic disease has gone from affecting 12% of the American population to 54%. And we take more pharmaceutical drugs than anybody in the world. We pay the highest prices.
He’s made this country Pharmaceutical Nation.
Theo Von:
My brother is allergic to sesame seeds.
RFK Jr.:
…And the way that you get allergies is from the aluminum adjuvant in the vaccine, which is meant — is put in that vaccine to initiate an allergic response.
So if you have sesame seed oil as an excipient in the vaccine, or if you’re eating sesame seeds when you have that aluminum adjuvant in you, it can provoke a permanent allergy…
So anybody who was born after 89 — I think it’s one in 12 now. Autism went from one in 10,000, in my generation, to one in every 34 kids. And it’s the same with all these chronic diseases that are all listed as side effects.
Theo Von:
So the proof seems to be right there.
RFK Jr.:
Well, that’s correlation, which isn’t actually proof. But if you actually go into the scientific literature, the proof is there.
Theo Von:
… So whenever you talked to Trump, you said, okay, let’s open up this database, right, this information…
RFK Jr.:
Yeah… I said you don’t have to do any heavy lifting. You don’t have to go to Congress. You don’t have to change regulations. All you have to do is open up the vaccine safety data link, which is the medical records for the top nine HMOs, and allow independent scientists to go in there. And just open it up so they can start publishing.
Theo Von:
And did he do it?
RFK Jr.:
No, he didn’t. It’s still… locked down.
Tony Fauci makes sure nobody can get in there.
And you know, even when Congress ordered these two scientists … to go in there, and they let them into the place, they gave them one study room. They would not allow them near a copy machine. They allowed them pencils and they had to write down the data. And they cranked the heat in the room up to 105…
So anyway, so Big Pharma stepped in and Trump appoints Pfizer’s lobbyist to run FDA (Scott Gottlieb) and Eli Lilly’s lobbyist is Alex Azar to run HHS. And as soon as they came and they shut us down.
“With hundreds of billions of “viruses” at peak infection, there is absolutely no reason that virologists should not be able to purify and isolate the assumed “viral” particles directly from the fluids of a sick human or animal.”
Last week, I took a look at the very illogical excuse that virologists make in regard to why they are unable to purify and isolate the particles that are claimed to be “viruses” directly from the fluids of a sick human or animal. As a reminder, below is the response I received from biologist Thomas Baldwin, who studies “pathogenic” plant “viruses” and goes by the Twitter handle Sense_Strand:
It is claimed that there are just not enough of these “viral” particles within the fluids and thus, the purification procedures will result in too little of the “virus” remaining after these steps are performed. Due to this lack of particles, it is claimed that the “viruses” can not be found in electron microscopy images, and it is for this very reason that the “virus” particles must be grown in cell culture so that the “virus” can replicate to a large enough number in order to be visualized and studied. While I won’t rehash my counterargument here, I will allow Debunked to help me demonstrate why this is a ridiculous excuse:
When virologists claim incredible numbers like that, it is pretty reasonable to conclude that there should be plenty of “viral” particles within the fluids of a sick animal or human in order to purify, isolate, visualize, characterize, and study. Alas, virologists defiantly cling to their laughable excuse in order to cover up for the fact that they just cannot find the assumed “viral” particles anywhere directly within the fluids. While this statement clearly defies logic, the lack of “virus” is only one aspect of the excuse. There is another component that is used to explain why, even if they could purify and isolate the particles, it wouldn’t ultimately matter. Beyond the lack of enough “viral” particles within the fluids, virologists claim that there are not enough “infectious” particles present after purification in order to be able to “infect” an animal or human on order to prove pathogenicity. It is stated that this purification process damages the “virus” and causes it to lose “infectivity.” This excuse was illustrated in a response interviewer Djamel Tahi received from HIV “discoverer” Luc Montagnier:
“I believe we published in Science (May 1983) a gradient which showed that the RT had exactly the density of 1.16. So one had a ‘peak’ which was RT. So one has fulfilled this criterion for purification. But to pass it on serially is difficult because when you put the material in purification, into a gradient, retroviruses are very fragile, so they break each other and greatly lose their infectivity.”
“I repeat we did not purify. We purified to characterise the density of the RT, which was soundly that of a retrovirus. But we didn’t take the “peak”…or it didn’t work…because if you purify, you damage.So for infectious particles it is better to not touch them too much.”
As can be seen, if the particles are purified, it is assumed that they lose their “infectivity.” Thus, virologists must not touch their fragile little “virus” particles too much or they will be damaged and will not work properly. With statements like this, it makes the story about how these non-living entities somehow survive the harsh environmental conditions of the great outdoors in order to invade a body, bypass the hosts “immune system,” and hijack the cells so that it can create more copies of itself, seem rather ridiculous. According to virologists, in order to retain “infectivity,” the “virus” particles must remain unpurified and proceed to be mixed into a foreign animal or cancer cell with toxic antibiotics, antifungaks, fetal calf blood, chemicals and “nutrients,” etc. and incubated for days. However, this is normally not enough to create the necessary “infective” particles, so virologists will remove the top layer of one culture and then add it to another culture with a fresh round of toxic compounds mixed in. This new culture is then incubated further until signs of cell death are observed. Only then can there be enough “infectious viral” particles to visualize and establish pathogenicity.
To the outside observer who looks at this critically and logically, it is clear that all virologists are doing is creating a toxic soup of many foreign and chemical elements in which they get to claim a “virus” resides within. This sludge is then forcefully and unnaturally inoculated into animals in many disgusting ways, either through the nose, the skin, the muscles, the eyes, the throat, the stomach, the brain, or even the testicles. Virologist then determine what is an “infectious” dose based upon how much of this toxic soup is used as an injection into the animal at the time any symptoms appear. Virologists will determine how much “virus” is present in the soup by utilizing either one of two methods: the tissue culture infectious dose (TCID50) and the plaque assay. Let’s examine these methods briefly and then see, according to virology’s own theoretical narrative, how many “viral” particles it takes to cause infection and disease. We can then determine whether or not it is reasonable to believe that there are not enough “infectious” particles present after purification and isolation in order to determine pathogenicity.
Tissue Culture Infectious Dose (TCID50)
This first method for estimating how many “virus” particles are necessary for “infection” relies on the observation of the cytopathogenic effect (CPE) that is created during the cell culture experiment. CPE is an effect that is observed when the cells start to die and break apart during the cell culture process after the cell has been starved and poisoned. To calculate how many “viruses” they believe are present and “infectious,” virologists will use varying “virus” dilutions that are added as an endpoint dilution to host cell populations in a 96 well plate format. They will then incubate these mixtures until a cytopathic effect can be observed. The wells are either inspected by visually counting the CPE in the affected wells or by using assay readouts. Once 3 of the same CPE readings in separate cells for the same dilution are observed, the dose is calculated using one of various mathematical equations. The dilution at which 50% of the cell cultures are “infected” is determined and used to mathematically calculate a TCID50 result:
Tissue Culture Infectious Dose (TCID50) Assays: How to determine virus infectivity?
TCID50 assays: How do they work?
“50% Tissue Culture Infectious Dose (TCID50) assays are virus titration experiments which can be used to quantify virus titers by investigating the cytopathic effects of a virus on an inoculated host cell culture4. Compared to the widely used plaque assays, which are also used in virus quantification, TCID50 assays offer the advantage that even viruses that do not form plaques or infect cell monolayers can be quantified.
In TCID50 assays, varying virus dilutions are added as an endpoint dilution to host cell populations with the same number of cells and incubated until a cytopathic effect can be seen. Here, the TCID50 value represents the amount of virus dilution required to induce cytopathic effects in 50% of wells containing the inoculated cell culture after a defined period of time.
TCID50 assays assess this threshold either by visually counting the number of affected wells or by using cell viability assays as readout. The TCID50value is determined when the cytopathic effect or cell viability assay read-out appear the same for a dilution in 3 separate readings. An example of the application of cell viability/toxicity assays for the evaluation of viral cytopathic effects can be found in the AN 363: Viral cytopathic effects measured in a drug discovery screen.
TCID50 calculation
The results of 50% Tissue Culture Infectious Dose (TCID50) assays can be analysed by different calculations 5. Several mathematical approaches have been developed for this purpose, including the Reed-Muench 4, Spearman-Kärber or Weil method. The formula after Reed-Muench is depicted as an example below.
Where I is the interpolated value of the 50% endpoint and h is the dilution factor.
Since most often, the exact 50% endpoint is not observed in TCID50 assays, an approximate value can be obtained factoring in the dilutions closest below and above the 50% threshold. Independent of the method, the dilution at which 50% of the cell cultures are infected is determined and used to mathematically calculate a TCID50 result which is expressed as 50% infectious dose (ID50) per millilitre (ID50/mL) after a defined period of time. For example, if 0.2 mL of a 1:10,000 virus dilution infects 50% of the cells in 2 days the titer is expressed as 104 TCID50/0.2 mL in 2 days.”
As can be seen, this method relies on the observation of CPE as evidence of a “virus” and then attempts to calculate how many of these invisible entities reside within the fluids. However, as should be expected when dealing with attempts to count something that can not be seen, this method has its drawbacks. For one, the Poisson distribution that is utilized, which takes the TCID50 value and multiplies it by 0.7, is admittedly only an approximation and is said to not always be true. The serial dilution method itself is also a source of error by its very nature. If any fluid remains at the end of the pipette used to suction out the “virus,” it is said that this can greatly influence the quantification results. Another issue is attempting to keep all of the variables exactly the same across all cultures, which is admitted to not always be the case. Thus, there is a lot of guesswork and assumption involved in calculating the infectious dose of the unseen entity:
Timeless TCID50: One solution to many viruses
From dilutions to titres
“TCID50 values give an indication of how many viruses is needed to have CPE in 50% of the cells. But how to go from this to the actual amount of virus per ml? The formula is quite simple, and it consists in multiplying the TCID50 value by 0.7. This comes from the Poisson distribution applied to viral infection which states that, in a fully permissive cell line, the probability of reaching 50% infection is achieved by a multiplicity of infection of approximately 0.7. This is not always true, but it’s a good approximation for most applications.
The troubles of counting viruses
As accurate as one can be, counting viruses is never easy. First, serial dilutions are -by their own nature- a source of error. Second -and this is particularly relevant for high titres of virus- even the tiniest volume that remains attached to the very end of a pipette tip can carry enough viral particles to make a substantial difference in the quantification. Third, the biological variation of the system is high. Plate the same amount of cells, add the same amount of virus, stop the infection at the same time, and the percentage of infection may be close, but never exactly the same.
Finally, when assessing a treatment that (as you would hope!) decreases virus titres, the amount of virus may fall below the assay detection threshold.”
However, if relying on an indirect effect and spotty mathematical equations to calculate how many “viruses” it takes to “infect” a cell is not to your liking, you may appreciate this next method even less. Plaque assays also rely on the observation of CPE in cultured cells. As the cells break apart and die, the “viral” particles are assumed to travel to neighboring cells, infecting them and creating plaques, or holes, in the dish. The cells are then fixed and stained, killing everything in order to be observed. It is said that the cells that remain adhered to the surface are assumed to be uninfected, and any observed plaques are assumed to arise from cell death caused by “viral infection.” Virologists will look for the dilution that led to the optimal observed plaques; too little dilution leads to too many plaques while too much dilution yields none. The titre is then calculated using arithmetic based on the volume of the aliquot added to the cells and the sample dilution the aliquot was drawn from. The assay is designed so that each plaque represents infection by only a single “viral” particle:
Measuring infectious virus: the plaque assay
Infection and plaque formation
Plaque assays require cultured cells susceptible to infection by the virus of interest. The cells are first seeded onto a surface they can adhere to and grow on, then left overnight to form a confluent monolayer (a cohesive sheet of cells covering the entire growth surface). A virus sample is then diluted several times, and an aliquot of each dilution is added to a dish or well of cells. An incubation period allows the virus to attach to target cells before removing the inoculum. The culture is then covered with a medium containing nutrients and a substance, such as agarose or methylcellulose, forming a gel or semisolid overlay. Infectious virus particles that enter cells and replicate can then trigger the release of progeny virions. The gel restricts particle movement so that newly produced viruses can only infect neighbouring cells. If the virus kills infected cells, the dead (or dying) cells detach and create a hole in the monolayer through lysis or other means. This space – now devoid of cells –is called a plaque and appears as circular spots on the growth surface.
The plaques are allowed to grow until visible to the naked eye. The cells are then fixed with formaldehyde to lock cellular structures while killing the cells and virus. Dyes that stain cells are added for contrast, making plaques easier to see. Purple violet stains the cells purple, while plaques, lacking cells, remain clear. Cells that remain adhered to the surface are assumed to be uninfected, and apparent plaques are assumed to arise from cell death caused by infection. That is why the virus dilutions must be added to confluent monolayers with no gaps that might later be mistaken for plaques.
Viral titre: PFU/ml
Multiple dilutions of the stock sample are analysed to identify one or more dilutions that give rise to a countable number of plaques. At the lowest dilutions, too many infectious particles will destroy large swaths of the cell monolayer or create plaques too numerous and overlapping to distinguish. At the highest dilutions, there may be no plaques at all. At the optimal dilutions, plaques are counted to determine the titre of the original stock sample, typically reported as the number of plaque-forming units per millilitre (PFU/ml).
For a given plaque count, the stock titre can be calculated by simple arithmetic based on the volume of the aliquot added to the cells and the sample dilution the aliquot was drawn from. As a basic example, if 35 plaques were counted when a 0.1 ml aliquot of the 10-5 dilution was added to the cells, the titre of the undiluted stock is 3.5×107 PFU/ml. For reliable titres, each sample dilution should be plated multiple times, at least in duplicate and preferably in triplicate. Furthermore, multiple dilutions may result in countable plaques. More elaborate formulas incorporating all relevant plaque counts are typically used to calculate titres.
PFU/ml vs IU/ml
The assay is designed so that each plaque results from infection by multiplying a single infectious virus particle. As such, PFU/ml is considered a measure of the number of infectious units per millilitre (IU/ml), with the caveat that one cannot be certain of a one-to-one ratio of plaques to infectious particles in the applied aliquot. Also, be aware that the titre of a sample is specific to the assay conditions used to determine it, as infectivity is influenced by many factors, such as the type of host cell, pH, and culture medium. Titres can differ by several orders of magnitude by changing key assay parameters.”
As with the TCID50, there are some definite drawbacks when trying to “accurately” estimate how much of an invisible entity can cause infection and disease using the plaque assay. For starters, as noted above, the “infectivity” is said to be influenced by many factors within the culture itself. This includes the type of host cell, the pH level, as well as the culture medium used. Thus, the calculated titres can vary wildly by several orders of magnitude just by changing the assay parameters. The determination of what exactly constitutes a plaque is very subjective as well, which can mislead the results. In other words, plaque counting is prone to human error.
Beyond these issues, as noted before, both TCID50 and plaque assays rely on the observation of a cytopathogenic effect in order to claim the presence and infectivity of any “virus.” However, CPE is not specific to “viruses” as there are many known factors that can result in this effect being observed that do not require the presence of a fictional entity in order to explain, such as:
Bacteria
Parasites
Amoebas
Chemical Contaminants
Age of the Cell
Incubation Temperature
Length of Incubation
Antibiotics/Antifungals
It is entirely unscientific to rely on an effect in order to presume a cause. However, this pseudoscientific concept is central to the cell culture method as well as to the processes utilized to guesstimate how many “infectious viruses” are present. In other words, there is no direct evidence any “viruses” are present in any sample used to determine an “infectious” dose. All of these results claiming how much “virus” is present and can ultimately cause an infection are entirely hypothetical and calculated based on the presence of cell death. It is nothing but guesswork.
However, if it wasn’t clear that these numbers are pseudoscientific fraud, a 2003 OSHA White Paper looking at the determination of the infectious dose (ID) may help to sell the fact that virologists honestly have no clue what an infectious dose is. While this refers to calculating ID using animals, the same criticisms can apply to utilizing lab-created cell cultures as a surrogate. The White Paper concluded that there is no clear definition of what an infectious dose is and that there is no single standardized method for determining ID. The extrapolation of data to humans is unreliable and is a poor surrogate for human responses. There are various secondary interactions that can impact the estimates. The “pathogens” vary wildly in “virulence” and data on the ID via route of exposure is unavailable. In other words, virologists just make things up as they go along:
“In summary, the studies described above support ABSA’s position that attempts to develop quantitative values for human infectious dose are not currently feasible. Infectious dose values developed using past studies would not accurately characterize the relative hazard of pathogenic organisms in humans. The reasons for this conclusion are:
• Lack of a clear and universally acceptable definition of the term “infectious dose.”
• There is no single standardized protocol for testing infectious dose in animals, making legitimate controlled comparisons ofstudy results very difficult.
• Extrapolation of infection and toxicity data among animal species and from animals to humans has proven to be unreliable for most biological (and chemical) agents.
• Inbred animal strains are a poor surrogate for predicting human response, as humans are a highly variable outbred population.
• Infectious dose is affected by numerous, complex secondary interactions to include condition of the host, its genetics, and previous exposure to the biological agent or vaccine. Risk estimates must take these and many other factors into consideration.
• Bacteria of a single species can vary widely in virulence and infectious dose. It is not possible to make a broad or generalized statement about the infectious dose of a species of bacteria.
• Infectious dose in part depends on the route of exposure. A complete picture of a single pathogen’s infectious dose profile requires inhalation, percutaneous, oral, im, ip, iv, etc. data. These data are currently unavailable.”
Now that we know that this process for counting the invisible “viruses” is fraught with drawbacks that leave the “accuracy” of these results extremely questionable, let’s take a look at some of these wildly varying estimates in order to see how many particles are necessary to cause an infection according to virology’s fictional narrative. As “SARS-COV-2” is the soup du jour at the moment, here are a few key highlights from a systematic review of many studies attempting to find the minimal ID for the “novel coronavirus.” What you will see from the August 2022 review is that there is absolutely no experimental data for humans, with one study admittedly presenting a hypothetical estimate (technically, they are all hypothetical). The minimal ID for “SARS-COV-2” is extrapolated from animal studies with estimates that vary wildly between the papers:
Minimum infective dose of severe acute respiratory syndrome coronavirus 2 based on the current evidence: A systematic review
“The main methods for reporting the infective dose were through tissue culture infectious dose (TCID50) and by counting plaque-forming units (PFU).33
In TCID50, the viral dose in 5% of inoculated tissue culture made pathological changes or cell death. PFU is estimated of viral concentration in plaque-forming units by measuring the number of particles that form a plaque.34 The minimum infective doses have been summarized in Table 2.
Human studies on infective dose of SARS-CoV-2
“We found no experimental studies that assess the infective dose in human, so we included observational human studies.”
“Finding the minimum infective dose of the virus can be extremely useful in determining the transmission pattern. This represents itself in inconsistent results across the included studies; similar viral load did not cause the same outcome. This indicates that despite having a similar minimum infective dose, the infection rate could differ so this minimum is not the same across the same population. On the other hand, there are some human studies which have shown some hypothetical infective viral dosages.”
Conclusion
“The results of this review suggest that one of the key factors to control the pandemic could be the study of virus transmission. The minimum infective dose is one of the main components of virus transmission. In this study, we have presented a range of minimum infective doses in humans and various animal species, yet such numbers can possibly vary between the individuals based on numerous factors. Measuring the minimum infective dose can provide a clearer overall understanding of the disease and its transmissibility and help better halt its spreading.”
While it is fun to see how much their guesstimates can range between studies, the above paper doesn’t give us a great idea as to what this minimal ID is for “SARS-COV-2” in terms of an actual number of particles it may take in order to cause infection. Let’s see if we can put a number to it based upon what the “experts” are saying:
SARS-CoV-2 Infectious Dose
“Some experts estimate that exposure to as few as 1000 SARS-CoV-2 viral particles can cause an infection. This dose of virus could occur by inhaling 1000 infectious viral particles in a single breath, 100 viral particles in 10 breaths, or 10 viral particles in 100 breaths.”
According to the “experts,” as little as 1000 “SARS-COV-2” particles are enough to cause infection. Where did they get this magical number from? Who knows? However, a separate study gave an even smaller estimate of just 100 “viral” particles:
Review of infective dose, routes of transmission and outcome of COVID-19 caused by the SARS-COV-2: comparison with other respiratory viruses
“An accurate quantitative estimate of the infective dose of SARS-CoV-2 in humans is not currently feasible and needs further research. Our review suggests that it is small, perhaps about 100 particles.”
It appears that virologists have the ability to just pull any ID number that they want out of thin air. When we factor in their other imaginary numbers, such as those who are at “peak viral infection” harboring 10 to 100 billion “viral” particles while breathing out 10 million “viruses” per breath, it seems rather illogical to claim that there would not be enough “infectious virus” after purification in order to prove pathogenicity.
Examining the issue a bit further, let’s look at a few other sources and see just how little “virus” is said to actually be necessary in order to cause an infection. According to virology’s pseudoscientific narrative, would you believe that just one airborne particle can cause you to become infected? That is exactly what we are told by this next source which dealt a fatal blow to mask supporters everywhere. The researchers based their claim upon theoretical modeling (aren’t they all), and concluded that only one airborne particle is enough to cause infection and disease:
What if just one airborne particle was enough to infect you?
“For some diseases, exposure to just a single airborne particle containing virus, bacteria or fungi can be infectious. When this happens, understanding and predicting airborne disease spread can be a whole lot easier.
That’s the result of a new study by a Lawrence Livermore National Laboratory (LLNL) scientist who developed a new theory of airborne infectious disease spread. This research, which appears in the journal Applied and Environmental Microbiology, demonstrated good agreement with data from Q fever, Legionnaire’s disease and Valley fever outbreaks. The authors hope to use it to understand and mitigate COVID-19 spread.”
Unfortunately, the authors did not give us any idea as to how many “viral” particles would be in one airborne particle. Hypothetically, it could be one “virion” or it could be quite a few more. Let’s see if we can get some concrete guesstimates as to how many of the “viral” particles it may take to cause infection and disease. According to the CDC, “norovirus” only requires a few particles in order to cause infection and disease:
About Norovirus
“People with norovirus illness can shed billions of norovirus particles. And only a few virus particles can make other people sick.”
When looking to insect “viruses,” researchers set up an experiment with two “marked virus variants.” They exposed a population of caterpillars to both variants, and based upon these results, established a probability model to determine that it is theoretically possible for just one “virus” particle to cause infection and disease:
One Virus Particle Is Enough To Cause Infectious Disease
“Can exposure to a single virus particle lead to infection or disease? Until now, solid proof has been lacking. Experimental research with insect larvae has shown that one virus particle is theoretically enough to cause infection and subsequent disease.”
“Based on the assumption that every virus particle operates independently from all other virus particles,the researchers set up a probability model. This model predicts how many virus particles have caused an infection and how many different virus genotypes are present in infected hosts, such as plants, insects or people. The results of the infection experiment with the susceptible insects are in agreement with the model predictions. From this it can be derived that the virus particles have an independent effect, and that a single virus particle can indeed cause infection and/or disease.”
We have now officially gone from 1000 “viral” particles to just one particle. Let’s see if any other sources make such a bold claim. In a CDC study that looked to establish a quantifiable estimation of how many “variola” (a.k.a. smallpox) particles are necessary to cause infection, the researchers concured that only one “virus” particle was sufficient to cause infection and disease:
The infectious dose of variola (smallpox) virus.
“Quantitative estimation of an individual’s risk of infection due to airborne pathogens requires knowledge of the pathogen’s infectious dose, in addition to estimates of the pathogen’s airborne concentration and the person’s exposure duration. Based on our review of the published literature on poxvirus infection, we conclude that the infectious dose of variola (smallpox) virus is likely one virus particle and that infection can be initiated in either the upper respiratory tract or pulmonary region. Studies of airborne transmission of poxvirus in monkeys and rabbits show that primary infection can occur in both regions of the respiratory tract. A quantitative study of poxvirus inhalation transmission in rabbits indicates that the deposition of one pock-forming unit (PFU) carried on respirable particles can cause infection. Findings in both in vitro and in vivo studies of the number of virus particles comprising a PFU are consistent with a “one-hit” phenomenon–namely, the cellular uptake of just one virus particle can lead to infection of a cell or an area of cell growth, creating a pock (an infected area of cells). Variability in virulence among different virus strains may involve differences in the probability of infection per virus particle, where a highly virulent strain has a probability close to one of successful infection for each virus particle.”
“On balance, we believe there is adequate in vitro and in vivo evidence that infection can be produced by a single particle of variola virus. Across different experimental systems the number of poxvirus per infectious unit has been found to vary, but it appears that favorable conditions enable all virus particles to infect (Overman & Tamm, 1956; Parker, Bronson, & Green, 1941; Sprunt & McDearman, 1940).”
The CDC has also stated that only one “viral” particle from rabies is enough to cause infection and disease:
Rabies
“During clinical disease, millions of viral particles may be found intermittently in the saliva. In theory, only a single rabies particle or virion is required to result in a productive infection.”
This one “viral” particle is supported as well by OSHA in regard to the Ebola “virus:”
Ebola
“In areas of Africa where Ebola viruses are common, suspected reservoirs include primate and bat populations. While there are no known animal reservoirs of the disease in the U.S., there is concern related to possible spread of EVD among human populations due to the availability and reach of global travel. Under certain conditions, exposure to just one viral particle can result in development of EVD. Depending on the strain and the individual infected with the disease, EVD may be fatal in 50-90 percent of cases.1”
It is clear that, according to virology’s own pseudoscientific narrative, only one “viral” particle is theoretically necessary in order to cause infection and disease. Therefore, there is absolutely no reason to assume that there are not enough infectious “viral” particles remaining after purification and isolation directly from the fluids to be used in order to prove pathogenicity. The reason this excuse is presented is because virologists are unable to recreate disease using just the fluids from a sick host. In order to even attempt to show pathogenicity, they claim that the unpurifued fluids must be added to a foreign animal or cancer cell along with antibiotics, antifungals, fetal calf blood, chemicals, “nutrients,” etc. and then injected unnaturally into an animal either through the nose, the blood, the throat, the skin, the brain, the stomach, the eyes, the feet, and/or the testicles. There is nothing natural or scientific about this process.
However, as virology is pseudoscience, it falls back on unfalsifiable concepts in order to excuse away the lack of scientific evidence. Instead of being able to find the “virus” particles directly in the fluids, they get to claim that there is not enough “virus” there despite their own numbers making this an impossibility. As virologists know that they can not prove pathogenicity using nothing but the assumed “viral” particles, they get to claim that the purification process creates a yield loss and that the “viruses” lose infectivity. Therefore, virologists get to excuse away that they can not show that the particles created after the cell culture experiment ever existed within the fluids of a sick host to begin with. They get to explain away that they can not prove pathogenicity using nothing but the assumed “viral” particles without culturing. Yet, despite their excuses, the numbers supplied by virologys own pseudoscientific narrative fail them. With hundreds of billions of “viruses” at peak infection, there is absolutely no reason that virologists should not be able to purify and isolate the assumed “viral” particles directly from the fluids of a sick human or animal. If only one “viral” particle is necessary theoretically in order to cause infection and disease, there is no reason virologists cannot use a purified sample to prove pathogenicity naturally via the scientific method. By their own admission, all it takes is just one particle to cause infection and disease. One particle from a sea of billions.
“It is also clear that the dramatic events of the past three years, events that have devastated the lives of many people all over the world, are based on this very misconception that so-called pathogenic viruses exist. This misconception has been around for a very long time, and it has led to damaging public health measures, the most notorious being vaccines, which have themselves harmed and killed millions of animals and people during their long and sordid history.
—~~~
TCTL editor’s note:
In the video below, Samantha Bailey reads the written statement “Why Are We Doing This?” which was signed by Tom Cowan, Andrew Kaufman, Mark and Samantha Bailey.
Following that reading, each of the four makes a brief personal statement about why they continue to speak out about lies at the foundation of virology.
Sadly, the level of rancor between those in the “freedom” community taking the “no-virus” position and those taking the “pro-virus” position has reached higher and higher levels.
Videos, Instagram posts and tweets are put out by both sides claiming to “debunk’ the other side or sometimes to just call names.
Mikki Willis, the producer and director of the documentary series Plandemic, has created a new video urging unity among those who claim to be on the side of freedom, along with a subtle accusation that dissenters against this unity are classic disinformation agents.
Given this background, we, as some of the recognized leaders of the “no-virus team,” thought it would be a good opportunity to reconnect and even restate why we are doing this.
Why we will not just be good team players and participate in the growing worldwide movement fighting for the universal principles of freedom, bodily autonomy and the ability to guide one’s life based on one’s own beliefs and decisions? Why keep speaking out?
It seems obvious to us and, in fact, has been a guiding principle throughout our entire lives that a life based in freedom and integrity must have a solid, factual foundation. In other words, if the foundation is not based on the truth, as best we can see it, our entire lives are based on mistruths and are in danger of collapse at any moment.
Imagine building a relationship, a family, a homestead based on love between two people when the reality is that, rather than love, there is distrust, suspicion and even ill will. Sooner or later, that life will collapse into ruins.
This is the same with a financial system based on fiat currency, an agricultural system based on inattention to the health of the soil, or a medical system based on anti-scientific medical hypotheses.
After careers of examining medical research and theories and three years of intensive investigation into the question of whether particles or, perhaps better said, entities known as viruses actually exist, it is our clear conclusion that no such particle has ever been shown to exist, let alone cause any disease in plants, animals or people. For us, this conclusion stands as a clear fact.
It is also clear that the dramatic events of the past three years, events that have devastated the lives of many people all over the world, are based on this very misconception that so-called pathogenic viruses exist. This misconception has been around for a very long time, and it has led to damaging public health measures, the most notorious being vaccines, which have themselves harmed and killed millions of animals and people during their long and sordid history.
—This carnage needs to stop.
People need to experience the world with new eyes and with a new concept of life, biology and health. This new conception can begin only when we realize, once and for all, that the idea of contagious, pathogenic viruses, or viral-like entities of any sort — natural, lab created, clones or otherwise —is simply a scientific misconception, or possibly a fraud.
Why we are doing this is straightforward: It’s so that no woman, man, child or animal ever has to be subjected again to abuse based on a long, bankrupt theory of biology and medicine.
We have nothing personally to gain from this quest. No prestigious awards are coming our way, and we likely will get nothing but further scorn and derision from colleagues, public institutions, and the general media.
Yet, when we think of our children, grandchildren, our friends, our families, our beloved animals, and animals in labs who are tortured and killed in this clearly futile effort to demonstrate the “reality” of viruses, everything in our being cries out, “this must stop.”
Therefore, we ask all people of good will to accept the following challenge. Please send us any genuine scientific information that demonstrates that viruses exist and cause disease.
We are not interested in any comments about our motivations or the consequences of our quests for us personally. Absent that evidence, we and our good friends will keep going. We believe that the future for all of us depends on it.
Dr. Thomas Cowan
Dr. Andrew Kaufman
Drs. Samantha & Mark Bailey
Time marker 5:03 — Dr. Tom Cowan:
So we’ve been talking a fair amount about why we’re doing this. The this being talking about the fact that there’s no virus, never had a virus that’s been shown to exist or cause any disease.
So what difference does it make?
So there’s obviously a whole lot of reasons including all the social distancing and the masks and the viral vaccines and the devastation of the adults and the lives of children.
But one thing that we haven’t, unfortunately, talked about much is its effect on the animals and the widespread frank torture and mutilation of millions of animals in labs and so-called science experiments all over the world.
And for whatever reason, I hadn’t appreciated this so much until I actually have animals of my own. And I think you could see our three cats and six chickens and we’re getting three goats this week.
When you realize all the mutilated animals, the ferrets with the cell culture stuffed down their throats, the 15,000 monkeys that were allegedly killed by Sabin to make an ineffective and dangerous polio vaccine.
When you realize all the mutilated dogs that have been left in dumpsters, which I’ve heard from many people who actually witnessed this themselves, the mice who’ve been injected with debris into their brain.
And you realize that all these experiments have no possible benefit. They’re just basically sadistic, torturing of innocent animals.
And at some point in your life, everything cries out to say this has to stop.
Time marker 7:04 — Dr. Andrew Kaufman:
Hello, I’m Dr. Andrew Kaufman. And today I’m here to answer the question why is it important to me to tell the whole truth about viruses? Meaning that they don’t actually exist or cause disease.
When faced with a lot of opposition and resistance to this message, you know, why am I communicating this over and over and sticking to this position.
And my answer is simple and I can answer in one word which is justice. But let me explain.
So if we look up the definition of justice, it means the maintenance or establishment of that which is just.
And I have here the definition of the word just from Merriam Webster: “Having a basis in or conforming to fact or reason.” Fact or reason.
So those are the two principal aspects that need to be established and known in order to bring about justice. Fact and Reason.
Now justice, for me, is a guiding factor in my life’s work or my mission.
What I would want to achieve and leave as my legacy on earth at the end of my life is related to bringing about justice.
So earlier in my career, this led me to the specialty of forensic psychiatry because I had learned that there was a great injustice perpetrated on the mentally ill individuals of the world. And this was so-called the deinstitutionalization movement which took people out of mental institutions — which at least were established with some purpose of helping and supporting and bettering those individuals — into the homeless crisis as well as jails and prisons.
So I was specifically going to try and help those mentally ill individuals who were essentially warehoused in jails and prisons, even without perpetrating any immoral crimes.
So many of them are there for things, because they were homeless, for example. So when it was really cold out, they went inside a storage facility to stay warm and escape frostbite. But that was trespassing so they ended up incarcerated, for example. And I’ve seen individuals in that scenario.
So this principle of justice has been a guiding force for me in my life. And it’s no different in the era of covid, where as I wanted to use fact and reason to make an opinion and see what is just with relationship to the announcement of this pandemic which occurred in 2020. And so, of course, I used my reasoning abilities to establish what are the facts.
And that led me to look at the initial fact, which was the establishment of this so-called virus that was causing this pandemic. Everything downstream of that was based upon this assumption.
And what I found out was that this assumption did not have a factual basis. And I simply applied logic and reason, and application of the scientific method to see that the experiments used to establish this basis of a new disease were simply unscientific and false.
And this helped me, of course, have a unique understanding of everything that occurred over the past several years. And I could easily look through the lens of judgment and see what was just and what was unjust in terms of people’s reactions, especially the government and various industries.
And this leads ultimately to holding the perpetrators of this tyranny accountable.
And one of the criticisms that has come from some of the health freedom leaders have been that if we look at the truth that there was no virus, that somehow that lets people like Anthony Fauci off the hook. But it’s actually the opposite because until we establish a factual basis of the crimes that were committed — and namely, in my opinion, they were the complete fabrication of an imaginary new disease that allowed justification of tyrannical policies that reduce freedom and inhibited commerce and allowed all types of manipulation to occur.
And we, to this day, don’t really know who are the main leaders behind this psychological operation that established this false disease, not based on fact. But perhaps if we hold people like Anthony Fauci accountable for participating in this charade that we can extract information and find out who the originators are. And that would be the only way to establish a true justice and accountability for what we’ve experienced.
And I know that going forward it continues to be the utmost important element in our analysis is to establish the facts and to use reasoning to understand what’s going on.
And of course this is true, especially with respect to our health.
So I hope this provides some inspiration to see how important it is to really get to the bottom of this issue.
Time marker 13:10 — Dr. Mark Bailey:
For more than three years I have researched the virus hypothesis, digesting virology textbooks and thousands of publications — from Ivanovsky’s claimed tobacco mosaic virus in 1903 through to Fan Wu’s claimed novel coronavirus in early 2020.
Virology’s world is arcane and most people have barely scratched the surface, content to believe viruses exist and often outraged that we would question such a thing.
However, we did question and haven’t stopped after we broke away from our conventional training and examined this issue for ourselves.
When I completed A Farewell to Virology, even I was surprised at the patent lack of evidence for these alleged infectious particles. It wasn’t just a few areas where the virologist evidence was lacking. It was in every area.
The techniques have shifted over the past century as their own experiments have consistently refuted themselves.
Now their remaining “evidence” lies in inadequate methodologies, uncontrolled studies and media releases.
Some time ago, we witnessed a move away from genuine experimental studies and into what I suspect is their final resort — genomics and proteomics.
But as I wrote in A Farewell to Virology, this approach is built on bankrupt foundations and will only delay the wider realization that the virus model is done for.
In the meantime, the carnage will continue for those still inside the viral paradigm. Experiencing disease, detecting genetic sequences, looking at electron microscopy images or obtaining test results — whether they be through the PCR or alleged antibodies — do not require the existence of viruses, as we and others have repeatedly exposed.
Mankind can make up stories to explain these various phenomena, but cannot change the underlying principles, no matter how sophisticated the technology.
I don’t know how much of the virus fallacy is a misconception, and how much is outright fraud.
It probably doesn’t matter because what is important is that more people are waking up to the fallacy and rejecting the virus and germ theory models outright.
Like our family, they have worked out that none of the touted solutions, whether they be public health measures, vaccines or drugs, offer any benefit to our well-being.
They can see the destruction to humanity, the animals and the environment based on this fraudulent war against imaginary infectious particles.
The real enemy is fear and ignorance, something each of us must overcome. Our world does not need to be feared, with the insight that nature does not make mistakes. And this divine biology is always pro-life and for our benefit.
We may still be in the minority, but we are already victorious as we share this new freedom, wisdom and prosperity with the next generation.
Time marker 16:10 — Dr. Samantha Bailey
In 2020, I first started questioning the covid-19 fraud because I could see that people were fearing for their lives.
The public were being told to stay indoors, to obtain food only from corporate outlets, to avoid relatives and neighbours, all while staying close to their phones and TVs to keep up to date with government announcements.
The fear of the supposed virus was clearly out of proportion with reality. My gut feeling was that I had to try to reduce people’s fear by researching the science honestly and presenting my findings to anyone that would listen.
Our research into SARS-CoV-2 quickly morphed into searching for evidence for the existence of any virus. By mid 2020, it was apparent to us that the key scientific evidence was absent and the level of the fraud was massive.
The powers that shouldn’t be had been building up to the staging of a huge pandemic like covid-19 for decades. Finally, they had their formula correct and almost everyone was complying with the new totalitarian rule under the mistaken belief of contagion.
The key to unravelling the fraud lay with explaining the viral delusion as well as the lies of germ theory to allay the public’s fear.
I investigate the science and follow the trails wherever they may lead. I then release my findings to the public so that I can sleep at night.
I want my children to have a life where they do not live in fear of nature, where they can understand the true causes of disease and how to be healthy through right thinking and right living.
It is a joy to watch them grow to their full potential and I hope that many more people will share the benefits of ignoring the virus model and its associated carnage.

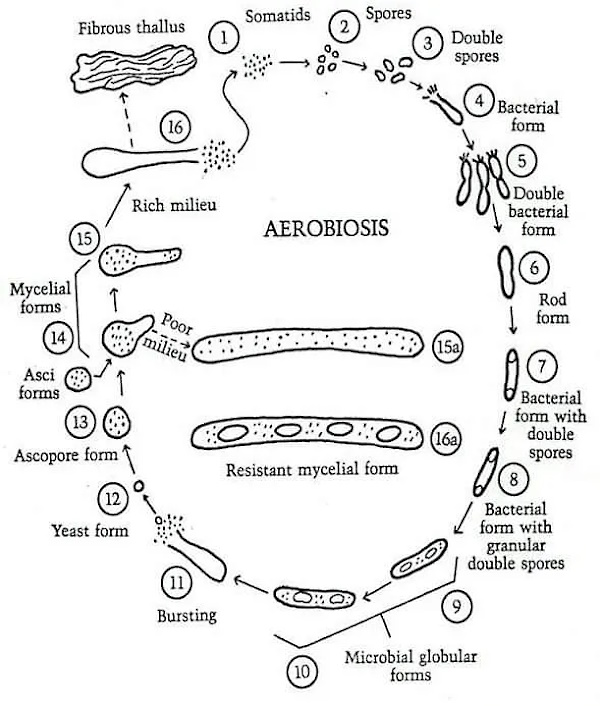
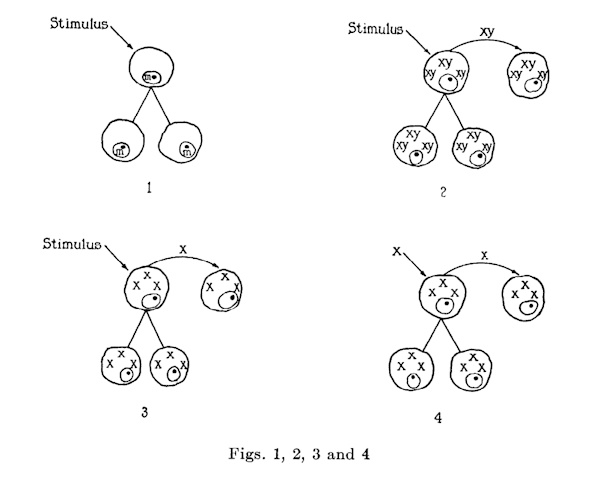
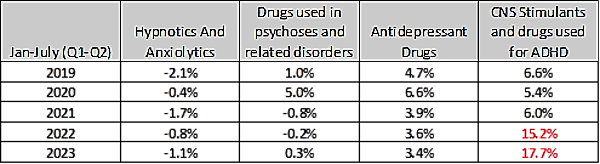
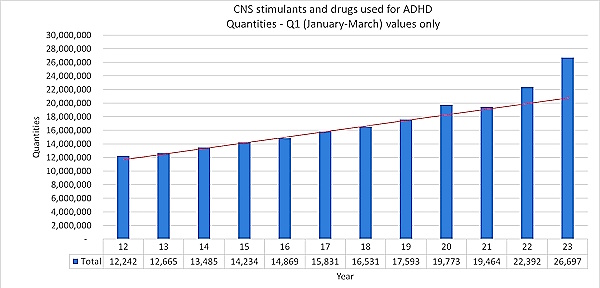








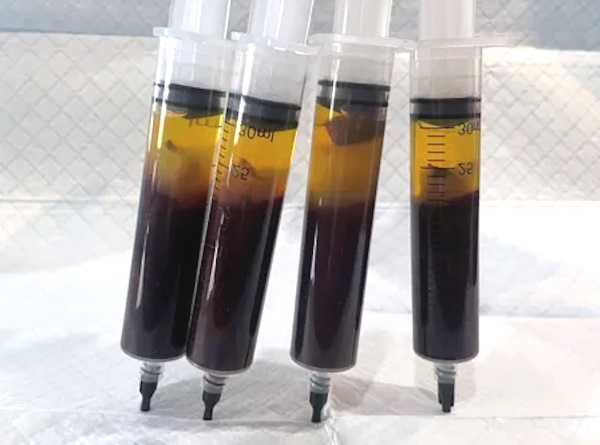

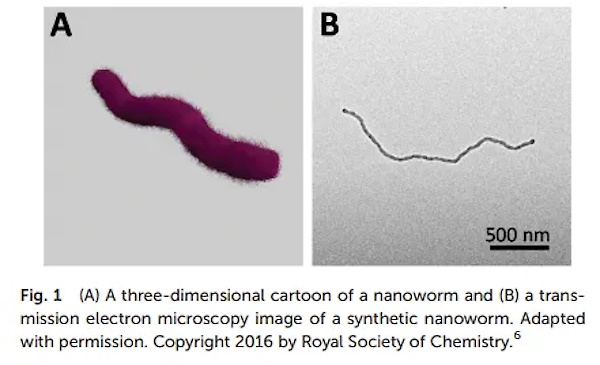
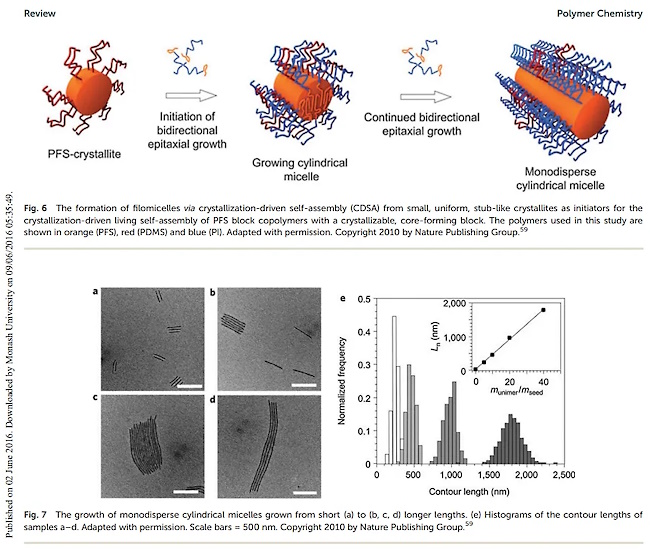
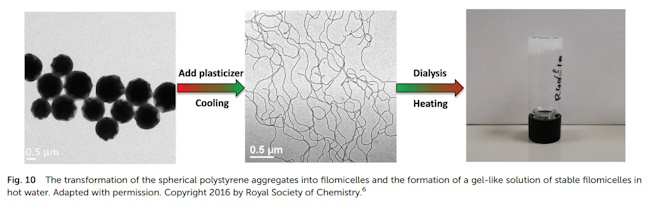
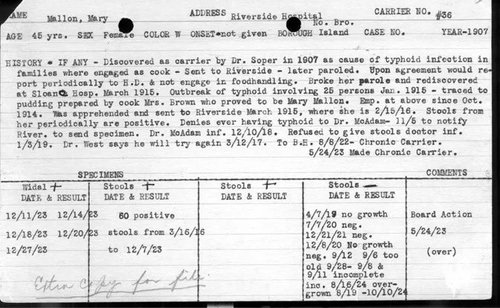






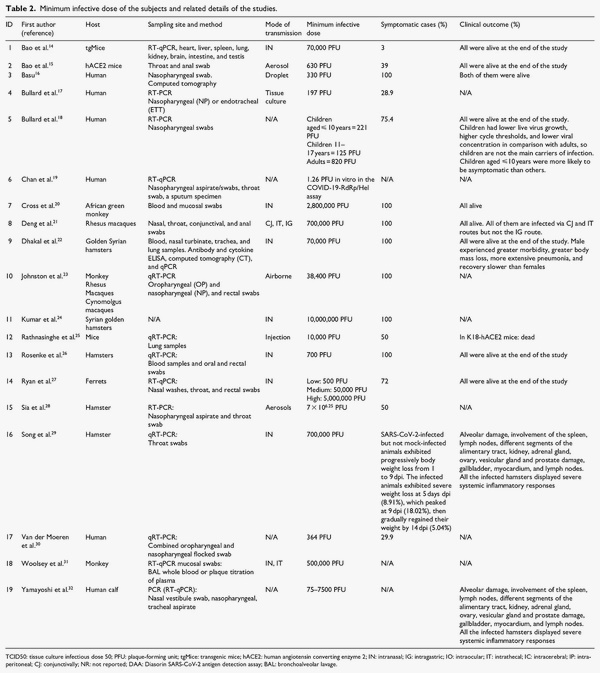
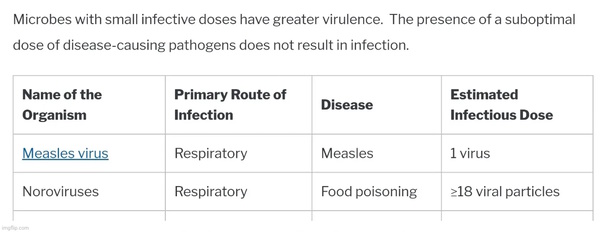
{kind=link}
{kind=link}
{kind=link}