As soon as I began writing about COVID in the spring of 2020, I made the case that SARS-CoV-2 hadn’t been proved to exist.
I then met Tom Cowan, Andrew Kaufman, and Christine Massey. I became aware of the work of Stefan Lanka. They were making a wide challenge about viruses in general:
No actual isolation; no proof of existence; instead, a parade of false claims and obfuscations from official sources.
A few years later…and the number of serious researchers who are coming to the same conclusion has expanded significantly. (You can find links to some of these researchers at Christine Massey’s Substack page )
The new work isn’t just a repetition of the original challenge to official authority. It attacks fake viruses from a number of angles. The shocks keep coming.
This story isn’t going away. It’s building.
It reminds me of the vaccine story. When I first started writing about dangerous and ineffective vaccines, in 1987, there were dozens of writers, present and past, who had covered similar ground—going back many decades. But that was nothing compared with…
The strength of that story now, in 2023, after the catastrophe of the COVID vaccines.
This is what I believe is going to happen to the fake virus story—against even longer odds. I say “longer,” because the proofs that viruses aren’t real by any scientific standard will undermine and detonate the very center of the medical cartel, which is all about germ theory.
Germ theory is marketing. The marketing of (toxic) drugs and vaccines for thousands of so-called distinct diseases, each supposedly caused by a unique germ.
When that fiction falls, the whole house collapses.
Going back as far as the beginning of the 20th century (and farther), another paradigm about disease emerged. It came to be called “holistic.” Probably not the best label. But the idea was: look at the whole body, the whole person. Look at body processes as connected and inter-related. Understand disease and health in those larger terms. Include environmental effects—basic sanitation, pollution, toxic chemicals, nutrition, the rise of the middle class out of poverty.
Something needs to be pointed out here. The holistic paradigm is a very difficult approach, in terms of making it pay off in real cures. It always has been difficult. Thousands of methods have been suggested. Many of these tend to mirror the medical strategy: find magic bullet solutions, take short cuts. Market them. Claim temporary fixes are permanent.
Treating the body and the person as a whole, taking in the mind-body connection—this is by no means a walk in the park.
Therefore, sooner or later, many people, discouraged, fall back on medical answers and germ theory.
The work of the no-virus pioneers provides an absolutely essential antidote to that surrender.
Because what are people surrendering to? The convenient fiction that viruses are everywhere, causing separate diseases. Convenient fiction was how viruses were willed into existence in the first place:
Doctors couldn’t cure their patients. So they looked for “something that was missing.” A hole in their hypotheses. And they claimed they found it.
Tiny particles no one had ever seen. No one had ever isolated. “This is the key. This is the great discovery.” It was a self-serving fairy tale. An excuse for treatment failure.
It kicked off millions of efforts to assure one and all that viruses were real. Marketing, parading as science.
Where were these viruses being discovered? In proprietary labs. No civilians permitted. Doors locked. Only the experts could understand the details of their own isolation of the tiny particles.
The particles which had been fantasized into existence.
We’re actually looking at a magic-myth story. Explorer-knights (doctors, researchers) are searching for an invisible dragon object which is crippling the population. These heroes finally corner it and isolate it and go to work decimating it and all its variants.
But the real ending to that story is now being provided by the multiplying number of independent researchers, who are proving the invisible dragon object was never cornered or identified or isolated.
Instead, the so-called explorer-knights made up, invented, fabricated the idea of the object to begin with.
That’s the magic. Sleight of hand. That’s the myth. Secret lab procedures that, when exposed, turn out to assume what they’re trying to prove. Also known as circular reasoning.
The whole story has come unglued.
For now, I’ll conclude with this analogy. A group of elite researchers claim that, 49 trillion light years from Earth, there is a flaming star the size of the Milky Way. At the center of that star, buried within a supernatural vault, there is a tiny, tiny purple man with green toes and orange hair who is causing all trouble and all destruction circulating throughout the universe. He’s there. He’s been “isolated.”
Given that incredible tale, would you expect, would you really expect there can be ANY sort of test which would prove the existence of that tiny man?
Could ANY test be produced that would be authentic?
So, in the case of the wild virus fairy tale, are we looking at proofs of existence and isolation that need to be improved, in order for us to accept them?
Or are we, instead, looking at the tiny purple man, about whose existence there are no possible proofs at all?
Because the story is so absurdly outrageous.
I’m thinking we’re dealing with the tiny purple man. And this may be the next chapter in the no-virus revelation:
The original concoction of viruses was so crazy, every so-called proof is going to be circular, mindless, and futile.
Drs. Tom Cowan and Mark Bailey challenge an article posted on October 4, 2023 by HART (a group of scientists in the UK) titled “Why HART uses the virus model — Arguments against ‘the virus doesn’t exist’ “.
Tom and Mark go over all key points made in the article.
It’s clear that the HART group has no idea what has been revealed in the research done by those who been exposing the false foundation of virology.
HART has somehow missed a foundational point of the “no virus” research — that no infectious “virus” has ever been isolated in the entire history of virology and that the “no virus” research shines a light on the fraud of all so-called infectious viruses.
Here is how HART group describes themselves at their website:
“HART is a group of highly qualified UK doctors, scientists, economists, psychologists and other academic experts. We came together over shared concerns about policy and guidance recommendations relating to the COVID-19 pandemic.
We continue to be concerned about the lack of open scientific debate in mainstream media and the worrying trend of censorship and harassment of those who question the narrative. Science without question is dogma.”
Instead of focusing on the DNA-contaminated mRNA vaccines, the central question should be: Has the basic assumption about “pathogenic particles (viruses)” ever been scientifically proven/confirmed? The answer is NO , and therefore every vaccination is inherently illegal and dangerous.
It is ironic that if the assumptions of genetic theory were correct, critics would be right. This irony shows that pharmaceuticals are paradoxically finding themselves caught in the crossfire due to theses held by both critics and the mainstream.
What does that mean?
The idea that DNA is the unchanging blueprint of life has been promoted for over 40 years. But in 2006, leading researchers confirmed: This idea was naive. DNA is dynamic and constantly changing.
The human genome
Complete decoding of the human genome (in reality just reading rows of letters that are not understood) is impossible. No two people are “genetically” alike, not even one cell is another. When you consider that the individual genomes of less than 0.0003% of the 8 billion people have been sequenced (and incompletely), one thing becomes clear: assignments of genetic letter orders for cancer, eye color, height, etc. are impossible.
An example: the color of the eyes
It was believed that it was simply genetically determined. This idea turned out to be a forced interpretation of the current data, which was refuted by more recent data. So parents with blue eyes can have a child with brown eyes. This makes it clear that the idea of a fixed genetic section has been scientifically refuted.
Plain language: If every genome is unique, we only know a tiny fraction of all genomes (0.0003%) and they are constantly changing themselves, then the attempt to define fixed gene sections for certain characteristics such as eye color or cancer is worth it , like trying to catch a river with a sieve – it’s not only inaccurate, it’s simply unattainable.
The madness of genetics
When even simple examples such as eye color cannot be assigned, it seems bizarre when parties claim that foreign “specific” DNA can precisely change human genetics and cause cancer. Dr. Kary Mullis summed it up well: With PCR you can find everything in every person if you do it right. This means that every DNA or RNA sequence can be found in every person, whether healthy, sick, vaccinated or unvaccinated.
The strategy of fighting like with like may seem promising at first glance. But on closer inspection it turns out to be a theoretical trap. Instead of focusing on the DNA-contaminated mRNA vaccines, the central question should be: Has the basic assumption about “pathogenic particles (viruses)” ever been scientifically proven/confirmed? The answer is NO , and therefore every vaccination is inherently illegal and dangerous.
The current approach offers the pharmaceutical apparatus a back door: they could argue that there are better, uncontaminated vaccines or present other methods that would then have to be accepted within the long-refuted genetics thesis.
The technical implementation of the laboratory in Magdeburg is vulnerable even within the narrative
The detection is based on non-exact methods such as Qubit Flex Fluorometer and qPCR that have been performed. Neither the plasmids were directly isolated and detected nor were they properly sequenced.
First, we lack detailed information about the exact conditions and protocols under which these experiments were conducted.
Secondly, we know nothing about the negative and positive controls carried out.
Third, no sequencing or isolation of the plasmids was performed. This means that we do not know exactly which DNA sequences were present in the samples. Sequencing would have been necessary to determine the “theoretically” accurate nature of the DNA detected and to ensure that it was in fact plasmid DNA and not other forms of DNA.
What do burkas, tichels, yarmulkes, hijabs, kapps, fezzes, dukus, and surgical masks all have in common? Religious cultures mandate or strongly encourage these head coverings to comply with dogma. Although most of these are rooted in ethnic and religious traditions of any denomination to reflect humility before G-d and modesty before man, surgical masks have become the morality trend of the Western world for those who fear The Science before they fear any god.
As absurd as that last sentence may sound, the People of the United States are under siege–a war that is targeting our greatest claim to fame, our pride and joy: our freedom. Our Forefathers determined at the inception of this nation that all men have the inviolate right to life and liberty. Recognizing some freedoms that are indelible to the identity of a human are especially at risk of infringement, the Founders drafted the Bill of Rights to expressly protect freedom of religion, freedom of speech, freedom of the press, freedom to peaceably assemble, and freedom to petition the government among other activities.
Yet over the last three years, our government has encroached on these unalienable freedoms in the name of public health and following The Science. The few government officials and bureaucrats sitting in D.C. and Georgia imposed their beliefs on what makes the public healthy on the masses, without regard for dissenting opinions or contrary beliefs. Such factional tyranny is exactly the breach of social contract the Framers aimed to prevent.
After initially telling the country that masks would not work against this virus, Anthony Fauci fell in step, ordering persons be masked and directing both government and non-government actors alike to hold their fellow citizens accountable for failing to mask. A futile exercise in the name of “public health” given research predating the pandemic had already put to bed the idea that masking could prevent respiratory infections. Even following the Cochrane Review’s pandemic masking study showing little-to-no efficacy at masks preventing infection, the Biden administration still tells the People we should be masking.
Beyond inefficacy, recent studies are also researching possible adverse consequences from constant mask-wearing, now termed “Mask-Induced Exhaustion Syndrome.” The illness bears many of the same symptoms as “long covid,” begging the question: are the health risks of long-term masking worth the miniscule efficacy? I digress. Masking mandates began to die down when the CDC lost a legal battle where the court only addressed the agency’s statutory authority to impose such a mandate. The question of whether such mandates are constitutional at all was never reached. Despite the open question in the courts, I firmly believe mask mandates do not pass constitutional muster.
Recalling my extreme parallel of religious head coverings to surgical masks, compare this scenario: one day, the bureaucrats in Washington decide that for public health and decency, everyone must wear a burka. The land would cry, “Foul!” Non-muslim citizens would lose their minds that Sharia law was being imposed on them in violation of their First Amendment right to be free from the establishment of religion! Only the worshippers of the public health fascists would gladly adorn the dress as a testament to their true belief that the burka would save them from illness. I ask you, how is our current masking guidelines any different? Because masking is not a teaching from an institutionalized religion? Is trusting The Science not a form of having faith?
In truth, our courts have held time and time again that government actors cannot infringe on our clothing under both freedom-tenants of religion and speech. Our Constitution contracts our appointed government to respect and defend our human right to liberty, which includes our ability to express ourselves and beliefs through our clothing and appearances. After all, our appearance is all a part of our individual identities. Covering one’s face, one’s physical identity, must be a choice and not a requirement.
Moreover, our individual identities are not just linked to our physical attributes. Nay, our speech is also core to our humanity and identities. Speech is the expression of one’s soul, subjective based upon the speaker’s own perceptions and experiences. How I speak and what I say is part of how others (and I) recognize me as who I am!
Like any painting serves as a window into the artist’s being, so is speech into a person’s mind, heart, and soul. It is as complex as the human body that produces such words and sounds: the speaker’s larynx, vocal chords, pharynx, palate, tongue, teeth, cheeks, lips, and nose are all coordinating in harmony to make what we think in our minds come out of our mouths. Speech is as unique to each individual as a person’s fingerprints or DNA. Muffling a person’s voice, covering the delicate facets producing speech, hiding non-verbal facial cues, and restricting air flow via masks is not natural.
Masking inhibits self-expression. Even prior to physical masking, virtue-signalers touted policing one’s own speech as being “politically correct.” Policing and masking speech is toxic to both individuals and humankind. It evokes the same hesitancy as does domestic abuse–the feeling of “walking on eggshells” for fear your words will trigger and bring you harm. It further causes an identity crisis–a dissociation within oneself, wherein the mind is policing the heart and soul for fear of offending any listener (or observer). Both perpetuate the victimhood complex where one believes she cannot live without fear because others will not do “what they are supposed to do.”
It is true that internal perceptions expressed outwardly are not always correct or palatable. Such is the beauty of allowing one to convey his opinions and beliefs in his own words: the listener can understand the person with whom she is speaking and take the opportunity to debate and educate, correct her own misunderstanding, or completely discredit the speaker of value within her own mind. Speech is not just about speaking, but about hearing and deciding what one believes to be true. Speech of our own and listening to others’ speech helps us understand and develop our own identities.
It is not that constant expletives and hyperboles should become the norm of self-expression through speech. No, language itself is so vastly malleable that it can be morphed to rise to any situation–to connect with one’s listeners. For instance, there are different ages of communication. You would not use the same words with a child as you would with adults, unless your intention is to be misunderstood or completely unintelligible like the unseen adult characters of Charlie Brown. To be understood by your listeners, you must change your speech to be appropriate for the venue and target audience.
How is any of this relevant to the topic of mask mandates eroding freedom? Requiring people to cover the face and bodily member responsible for speaking and being heard and understood is inhumane. It strips children of their ability to learn how to speak, how to use their body to produce sounds and words and sentences, and how to connect those words to facial expressions to add context for listeners. It socially distances people from each other, deteriorating the human connection that allows us to communicate and understand each other.
There is no replacement for that connection. As I discussed in a prior article, humans are a social species. Although we are capable as individuals, we fail to thrive when deprived of interacting with others. During lockdowns, people yearned to visit family, go out to restaurants, to resume “normalcy.” Zoom meetings, video calls, and text messages were not enough to curb the cravings for human connection.
Masking is just another degree of separation from one another. Although it is less obvious than the isolation of quarantines, it is just another lonely reminder that we are not free. Not free to be ourselves, not free to connect, not free from fear, not free to breathe, not free to decide for ourselves what is in our own best interest. Even President Biden joked during a recent press conference that, “they keep telling me… I got to keep wearing [a mask], but don’t tell them I didn’t have it on when I walked in,” defiantly waving his surgical mask away from his face.
Who are “they” to decide what is in any individual’s best interest? Are we children and “they” our parents? Do we lack the mental capacity to think for ourselves? Are we not developed and educated enough to decide what is healthy and what is not? Are our God-given immune systems so defective that we can no longer survive colds? I find it a hard blue pill to swallow that humanity has survived on this planet for hundreds of thousands of years for a coronavirus variant to suddenly confound our natural biological defenses.
Who are “they” at all? “They” are not our duly-elected legislators who oathed to uphold and defend our Constitution and who are the only branch of government who the People gave authority to create laws. In fact, Senator JD Vance (R-OH) is now fighting this usurpation of legislative authority by “them.” On September 7, 2023, he brought to the Senate floor the “Freedom to Breathe” Act, which would prohibit mask mandates. Senator Ed Markey (D-MA) objected to the call for unanimous consent, arguing that this legislation would infringe on the health powers of the states.
An interesting and seemingly Constitution-based argument by Senator Markey, but it presupposes masking mandates on the public are a health-related decision at all, which is not supported by scientific evidence, and that such mandates are not otherwise constitutionally prohibited.
Though the People granted health powers to the states, those powers are still limited by the People’s ultimate right to life and liberty, including the free exercise of religion without a state-sanctioned religion (The Science) and free speech without intrusions on the speech-producing orifice or physical identity of the speaker.
Masking restrictions are not a “health power” the state governments are permitted to enforce. Masking mandates are not a public health measure the federal government is permitted to sanction. Both impede life and liberty guaranteed to the People by being human and safeguarded by the People through enforcing our Constitution. As such, the People will not comply.
The parents of 62-day-old Sawyer learned their baby’s blood contained 95 micrograms per liter of aluminum, a level that would be toxic for adults. The toxicologist who read Sawyer’s report said the aluminum and antigen levels in the blood were due to the vaccines.
A Maine couple last week finally got the answers they’d been seeking for nearly a year, ever since their 62-day-old son, Sawyer, died Oct. 28, 2022 — 34 hours after receiving his scheduled childhood vaccines.
According to a toxicology report, Sawyer’s blood contained 95 micrograms per liter of aluminum, a level that would be toxic for adults.
A toxicologist told the couple the aluminum and antigen levels in the blood were due to the vaccines. She also said a viral infection Sawyer was being treated for could have been a contributing factor.
Sawyer’s parents, Melissa — a registered nurse — and her fiancé Nick shared their story last week with journalist Jennifer Margulis.
In an interview this week with The Defender, the couple detailed their search for truth, beginning with how Maine’s medical examiner refused repeated requests to perform lab tests that might have shown the culpability of the vaccines — and instead initially ruled Sawyer’s death “asphyxiation due to inappropriate sleep position and environment.”
The story of baby Sawyer
On Oct. 20, 2022, Melissa took Sawyer to a doctor for a persistent rash around his torso. The doctor diagnosed a viral infection, gave Melissa some medicinal cream and told her to monitor Sawyer’s temperature for possible fever.
Exactly one week later, Melissa went to the same pediatrician for a baby wellness checkup, where the doctor insisted Sawyer, despite Melissa’s reservations and the baby still having a rash, receive the scheduled childhood vaccines.
These included: RotaTeq (for rotavirus), Hib (for Haemophilus influenzae b), Prevnar 13 (for 13 types of pneumococcal bacteria) and Pediarix (for diphtheria, tetanus, pertussis, hepatitis B and polio).
Dr. Lawrence Palevsky, a pediatrician, told The Defender, “I don’t know of any official warnings against vaccinating sick children,” but “there are no upsides to vaccinating a sick child. There are only downsides.” He added, “And, there are no upsides to vaccinating any child.”
Melissa told The Defender that, despite her medical training, she became skeptical of vaccines just two days prior when she watched a video of a toxicologist talking about the dangers of vaccines for children. She discussed the upcoming vaccinations with her fiancé, and they decided to go ahead with them.
“We were afraid that the medical system was going to judge him and judge us and not let him into school,” Nick said. “We just hadn’t done any research on it.”
Nick has two daughters from a previous marriage, ages 11 and 19, who received all of their childhood vaccines “and nothing ever happened,” he said.
After the doctor’s visit, Sawyer arrived home screaming and Melissa gave him the baby Tylenol recommended by the doctor.
By the next day, the baby had calmed somewhat but was still acting “fussy and uncomfortable,” so Melissa gave him more Tylenol and some expressed breastmilk.
When Nick got home from work that day, they put Sawyer into his bassinet for a nap around 5:30. By 6:15 the baby was fussing, and with some help was able to get back to sleep. He slept off and on for another four hours, while his parents kept tabs on him via his baby monitor and visits to his room.
The last time Melissa checked on Sawyer, he wasn’t moving or breathing. She picked up his limp and lifeless body and started screaming. Nick rushed in to help but it was already too late.
Emergency medical technicians arrived after the couple called 911. They tried but were unable to revive Sawyer.
The county and state police also responded and, because it was an infant death, opened a formal investigation and ordered an autopsy.
Chief Medical Examiner Mark Flomenbaum performed the autopsy the next day. Although he found Sawyer to be “well developed” and without signs of injury or bruising, Flomenbaum filed a death certificate citing asphyxiation due to a “sub-optimal sleeping environment” — essentially blaming the parents.
“It was near Christmas when we got the autopsy results,” Melissa told The Defender. “We read them on Christmas Eve. … We did nothing for the entire weekend.”
Asked if they ever learned what the medical examiner saw to make his determination, they said no. “The only thing in his basket was the blanket he was laying on.”
The police looked for evidence of child abuse or alcoholism, but quickly concluded it was an accidental death.
Melissa, grief-stricken, told everyone she could to investigate the possible role of vaccines in Sawyer’s death.
She first called the medical examiner to see if he would do testing to determine if sudden infant death syndrome (SIDS) was responsible, but was told there was no need “because it wouldn’t show the cause of his passing,” she recalled being told.
The hunt for answers
That’s when the couple’s hunt for answers began. “I was looking up people on the internet, on social media. I was calling any number I could find,” Melisssa said.
Finally, she discovered a suite of pathology tests that could determine whether vaccines played a role in Sawyer’s death.
The tests measure C-reactive protein (indicating brain inflammation), liver enzymes, aluminum and mercury in brain and blood tissue, formaldehyde and formalin (another name for formaldehyde). A cytokine panel would also identify various blood factors and vaccine titer levels.
Melissa mailed and emailed Flomenbaum’s office to formally request the full battery of tests. The doctor refused, dismissing her concerns and telling her that heavy metals do not cause SIDS.
“They gave me a reason why each test didn’t need to be done,” she said.
Further emails to the state medical examiner’s office, from both parents, have been bouncing back as “undeliverable” since.
A friend of Melissa’s told her about Health Choice Maine, a statewide nonprofit working to protect health freedom and parental rights. There she met Tiffany Kreck, Health Choice Maine’s executive director, who helped Melissa organize her own investigation.
“Families being bullied by a doctor or threatened with CPS [child protective services] or whatever, can reach out, and we will, to the best of our ability, help them navigate it,” Kreck told The Defender.
Melissa said Tiffany gave her a list of things they had to do, “like getting reports and billing information, people to contact, and that’s what I did.”
Their primary goal was to find a competent pathologist to perform the lab tests Melissa had requested. They searched the entire country — even enlisting the help of Laura Bono, vice president of Children’s Health Defense, Kreck told The Defender — but came up empty.
Kreck told Melissa they would not be mentioning anything about vaccines to the prospective pathologists, so they would be less likely to reject the request.
The biggest obstacle was finding a doctor who was willing to order the tests.
Her ob-gyn told her that it was “out of his scope of practice.”
She called her primary care physician and told him she thought the vaccines had played a role in her son’s death “and he denied it,” she said. Her pediatrician also said no.
The toxicology report and next steps
Finally, they found someone in-state who, responding to Melissa’s grief, agreed to perform the tests on June 21. Although some of Sawyer’s tissue samples had degraded, the pathologist was able to perform enough tests to issue a definitive report last month.
The report was technical and was not accompanied by any guidance or recommendations.
Melissa said, “They never called me and said, ‘Oh, listen, this is high. This could be due to his vaccines. We will do a VAERS [Vaccine Adverse Event Reporting System] report, you know, and advocate for other infants that pass away.’ No, we didn’t get anything from them.”
So they had to hire a private toxicologist who could interpret the report. That second report arrived last week.
“And she was the one that called us the other day and told us that his aluminum levels were very high,” Melissa said, “and that we needed to seek some legal services.”
The report showed baby Sawyer had 95 micrograms of aluminum per liter of blood, a level that would be toxic for adults. The toxicologist told the couple the aluminum and antigen levels in the blood were due to the vaccines. She also said the baby’s illness could have been a contributing factor.
Kreck told Margulis, “This additional pathology report shows how much are medical examiners don’t know because they won’t look.”
The report also showed high levels of lead, which would not be due to vaccines, the toxicologist said, and asked about lead levels in their house or water. But given that the baby had only consumed breastmilk and was not yet old enough to crawl around on the floor, the question remains open.
After receiving the confirmation about the aluminum, the couple felt “exonerated” from the implication they were responsible for Sawyer dying from asphyxiation, “but we also still feel like we failed our baby,” Melissa told The Defender.
“Me being a nurse,” she said, “I felt like I failed him both as a nurse and a mother.”
Nick added, “From the father’s standpoint, you’re supposed to protect your family, and I failed at that. It weighs on me every second of the day.”
Melissa and Nick are planning to file a claim with the National Vaccine Injury Compensation Program (VICP). She said she still feels skeptical “because I know how the government and the medical system are.”
Kreck is helping the couple prepare for the VICP meeting. “We are doing every test that we can possibly do and trying to cross all of our t’s and dot all of our i’s before we go into the VICP,” Kreck said, “which is historically difficult and harsh on what they perceive to be SIDS cases.”
A couple told The Defender they got help reporting the case to VAERS last November, but have never received any follow-up. They did, however, confirm that Sawyer’s case was in the database.
Health Choice Maine is also exploring options for a lawsuit challenging the finding on the state medical examiner’s death certificate.
Dealing with the grief
Just three months after the ordeal, a therapist told Melissa, who was still grieving for her child and searching for answers, that she had an “adjustment disorder.”
“She was pretty much telling me that I was not adjusting to losing my son quick enough, and recommended trauma therapy,” Melissa said.
She left the office crying, wondering if something was wrong with her or not being able to let go of her grief. “I haven’t had good luck with therapists,” she told The Defender.
“I’ve been going through this all on my own, trying to go through reports and all the information about my baby’s life and his medical records. And I’m doing all this while trying to grieve the loss of him and it is horrifically painful,” she said. “It’s something no parent should ever have to go through.”
One therapist told Melissa to take mood stabilizers and anti-depressants. “The mental health care system has not been very helpful in this at all,” Nicked added.
Nick found that going back to work and keeping busy was the most therapeutic approach for him. “Just keeping my mind focused on other stuff, you know, while carrying all that around,” he said.
Nick has joined Melissa in several of her therapy sessions, which he found very helpful.
The couple found a grief support group called Empty Arms for parents who have lost a child, which has been “amazing,” Melissa said. The group does a butterfly release for the deceased on Memorial Day and an annual remembrance walk.
They have found support from family members as well, although Melissa said it has been hard to talk to her family about the vaccine connection.
The couple said the loss has brought them closer together. “I couldn’t keep going, fighting the fight we’re fighting right now, without her,” Nick said. “And you don’t realize how much you love someone and just how precious life is and what you have in front of you is.”
“Cherish it and love it, don’t let it go,” he said.
“We lost the biggest and best part of us both and if we didn’t stay together, I’d feel like I was losing another piece,” Melissa said.
The couple’s journey to warn others
“I just want to make other people aware and I want to put a stop to this,” Melissa said.
Melissa said she warns mothers of sick children to cancel their appointments for vaccines at least until the child has recovered. She added:
“Children do not need vaccines. And if they were to get them, they don’t need them until they’re at least two years old. The problem is, is they have a blood-brain barrier that has not closed up until they’re two years old or later.
“And if you get vaccinated before two years old, the aluminum can cross that blood-brain barrier. That’s why levels are so high and it stops respiration and causes cardiac arrest.”
Nick said, “I wouldn’t tell anybody ‘Don’t vaccinate your children.’ But I would definitely say ‘Do your research. Go to the end of the internet, make sure what you’re doing is right, that you know all the possible outcomes.’”
“Be more educated and be a strong advocate for your baby,” he added. “Because it’s your baby, not the doctor’s.”
Asked why more medical professionals don’t speak out, Melissa simply said “Career suicide.”
“I don’t even wanna be a nurse anymore,” she said. “Why would I want to be? But I have to pay my bills.”
“Doctors don’t have any better education on vaccines than most 10th graders,” she said. “Even as a nurse, we don’t get the education. We just got the schedule.”
She also said that medical examiners should have the right to test for vaccine injuries during the autopsy and identify them as a cause on the death certificate. “The vaccines are killing people and babies and they’re trying to cover it up,” she said.
While the couple said they found it helpful to share their story, they also admitted to wanting to keep a low profile. “It’s kind of a quiet subject for us because we’ve got to protect ourselves now,” Melissa said.
The couple is looking for a good support system. “We’re looking for people to stand behind us and support us as we go through this journey, for the next questionable amount of years, to get justice for our baby. It might drag on for a while,” Melissa said.
When asked about what gives them the strength to stand up and share their story, despite the backlash that such activism could invite, Melissa said:
“This is the only way that I feel like I can mother my baby anymore. And my baby deserves justice. And we deserve to know the truth.
“He is our reason for living right now. And he is our motivation.”
Questions about the state medical examiner
Kreck told The Defender that state medical examiner Flomenbaum came from Massachusetts where he had been fired as the state medical examiner. “It looks like he tried to sue them for wrongful termination and lost,” Kreck said.
Flomenbaum earned a national reputation as a top medical examiner through his work identifying bodies in New York City after the 9/11 attack in 2001, according to an article in the Portland Press Herald.
He was fired from his Massachusetts position for losing a body and having a backlog of bodies waiting to be examined.
In 2019, the Maine attorney general’s office investigated and later cleared Flomenbaum over criticism that he was running a side business as a consultant in out-of-state death cases.
The Press Herald article details more of Flomenbaum’s controversial history, which included a Connecticut prosecutor’s letter to then-Attorney General Jane Mills telling her that a judge had determined his testimony in a child manslaughter case was “not credible.”
Flomenbaum was reprimanded in 2021 by Maine Governor Mills for inappropriate and unprofessional behavior in the workplace, after which he announced he would not be seeking reassignment to the position.
“He was only supposed to have a month or so left of his term back then and he’s still in office now. That all sounds very odd and fishy,” Kreck said.
Melissa told The Defender that Flomenbaum had recently left the medical examiner’s office, putting the disposition of Sawyer’s remains in question.
The couple, with the aid of Health Choice Maine, is seeking to remove Sawyer’s blood and tissue samples from the medical examiner’s office.
Anyone with information about where a new location might be found to accommodate Sawyer’s remains is encouraged to email Tiffany Kreck at tiffany@healthchoicemaine.org.
Dr. Rima Laibow, M.D. is a graduate of Albert Einstein College of Medicine (1970) who believes passionately in the right of Americans to choose their own health paths. She has practiced drug-free, natural medicine for 50 years by seeking the underlying cause of every illness and ailment and treating that root cause.
In 2002 one of her patients from a very rich family told her about detailed plans from her circles for a new world order (NWO). This also included the reduction of the world population by 90%, because they would be “useless eaters”. Based on these stories, Dr. Laibow began to do research on these topics.
In 2004 she founded the “Natural Solutions Foundation” together with her late husband, an organization dedicated to health through food and freedom.
In this episode of ICIC, Dr. Reiner Fuellmich and co-host Attorney Dagmar Schön talk with Dr. Rima Laibow, a psychiatrist and specialist in child & adolescent psychiatry in the US, about the untrustworthy and demonstrably long-planned agenda of a psychopathic minority of self-proclaimed elites who stop at no crime to achieve their inhuman goals.
In their dangerous megalomania to decimate humanity by 95% and to keep the rest under their totalitarian control like cattle and to abuse them as they see fit, they do not even stop at the cruelest violence against the weakest members of our society, the children.
If it’s possible to indoctrinate all children worldwide using mind control and MK-Ultra programs with early sexualization, uprooting and identity confusion, which they incorporate into all areas of our daily lives, and to poison them by means of so-called vaccinations and in the worst case by gene-altering, experimental injections to damage their DNA, it will be easy in the future to manipulate and control humanity and to eradicate the qualities that make up being human, such as love, compassion, friendship, social connectedness.
Thus, the “useless eaters” who, in their view, burden the planet to which they have issued a sole claim, should disappear. Useful slaves, without human characteristics, created in laboratories in the best case, shall be available for them, without feelings and without polluting the planet unnecessarily and wasting resources.
Dr. Laibow speaks clearly using plain words to expose it all, and bring into the light of day this terrible plan which the power-hungry and their henchmen, who she calls “monsters”, have subtly forged under the guise of private organizations like the WHO, EU, UN, Unicef and Unesco etc., which were founded especially for this purpose. It does not gloss over anything, and points out the impending dangers to our existence and that of our children and our children’s children.
We as sentient beings, as people with strength, creativity, courage and a sense of justice must no longer remain silent in the hope that ‘it’ will eventually pass and we will be able to live a normal life again, because it was not normal before either, only that it could not be perceived due to the brainwashing and drug treatments. But now that we have seen it clearly, what has been done to us just in the last three years and they are waiting in the wings again with panic and torture, we have to stand up and protectively put ourselves in front of our children.
Dr. Laibow advises everyone to declare loud and clear, “Don’t you dare lay a hand on our children, and don’t you dare try to control our lives!”
This is the language that they understand and it is the power of community and cohesion that we need to hunt down these ‘monsters’ and hold them accountable.
About Dr. Sam Bailey: After training and practicing within the medical system for two decades, she commenced a new phase of understanding and promoting health as a wider concept.
In 2019, Sam launched her YouTube channel exposing the hidden scientific truths about health.
A few years later and after taking the red pill, Bailey’s channel has become a runaway hit with 20+ million views and 300,000+ subscribers to help people understand the simple ways they can take control of their health.
She is the co-author of Virus Mania, which examines how the medical industry continually invents epidemics to make billion-dollar profits at our expense.
About Dr. Mark Bailey: Mark is the husband of Dr Sam Bailey and when you see one of them, you are really seeing both of them. They started working together when they first met in 2007 and have been a close team ever since. Mark and Sam are based in New Zealand and have three children together.
Since early 2020 he has been the duo’s chief researcher with a focus on microbiology, the existence of viruses, as well as historical and epistemological issues within medical science.
Is There Anything Floating in the Air – Trying to Infect Us?
“CONCOCTED science is the modern version of spiritual revelation. The Roman Church—while it was carrying out witch hunts and inquisitions replete with confessions obtained through torture and capped off with death by burning at the stake—was claiming Jesus Himself had passed the keys of the Kingdom to the Church…and He tacitly approved its policies.
“These days, debilitating, brain damaging, and life-destroying vaccines are the scientific revelations the Church of Federal Medicine stands for.
I continue to write about this subject because it’s vital.
NIH, the US National Institutes of Health, is the largest medical research facility in the world. It has 18,000 employees and runs on an annual budget of $45 billion.
I once suggested to Jim Warner, a White House policy analyst under Ronald Reagan, that somebody should do an audit of NIH and determine exactly what medical advancements the agency had actually made during its long history. He thought that was a terrific idea. But nothing came of it.
I assure you, an audit would reveal much less than meets the eye. Much less in the way of useful discoveries and technology. Along with mountains of useless and fraudulent science.
BUT NIH stands as a center of knowledge and a symbol, a reference point, a proof positive that medical science is marching forward.
It’s a very expensive public relations tool.
How could we not accept and signal our obedience to medicine, when we have such an awesome modern cathedral for its research?
Ditto for the CDC and the FDA. Both infernally corrupt agencies.
CONCOCTED science is the modern version of spiritual revelation. The Roman Church—while it was carrying out witch hunts and inquisitions replete with confessions obtained through torture and capped off with death by burning at the stake—was claiming Jesus Himself had passed the keys of the Kingdom to the Church…and He tacitly approved its policies.
These days, debilitating, brain damaging, and life-destroying vaccines are the scientific revelations the Church of Federal Medicine stands for.
Concocted science.
People accept science as fact, based on the IMPRESSION that actual knowledge is being discovered.
PR people make sure this impression is delivered.
Just as the Roman Church never confesses to fraud in its doctrine, the centers of modern medical knowledge never confess fraud.
Last week it was reported that the Australian state of Victoria may be considering “permanent” facemask mandates to achieve “zero-Covid”.
Now, we don’t need to get into the personal liberty implications of such a law, or the near-infinite supply of evidence that masks don’t work to prevent the transmission of respiratory disease.
They don’t work, they never worked. Mandating them was a political move designed to make the fake Covid “pandemic” appear real, and their continued use is a symptom of brainwashing or a by-product of chronic virtue signaling.
The mask debate, such as it was, is over.
No, the only aspect of this development worth talking about is the “evidence” used to support the position – and trust me, the quotes are entirely justified.
“Simulation modelling study” is very much the key phrase there. For those who don’t know, “simulation modelling studies” involve feeding data into a computer programme, then asking it to form conclusions.
Clearly, they are only as reliable and useful as the data you use. In fact, you can very easily make them produce any result you want by feeding in the “right” (bad) data.
In this particular modelling study they started out by telling the computer that cloth masks reduce transmission by 53% and respirators reduced it by 80%:
Odds ratios for the relative risk of infection for people exposed to an infected person (wearing a mask v not wearing a mask) were set at 0.47 for cloth and surgical masks and 0.20 for respirators
Essentially, they told their computer that masks prevent disease…and then said “ok, computer, since you now know masks prevent disease – what would happen if everybody wore them all the time?”
The computer then told them – obviously – that nobody would get sick.
Because they made it logically impossible for it to say anything else.
But there’s a bit more to it.
The next layer of interest is where they got their input data from.
After all there have been dozens of studies done on masks over the years, 98% of which say masks don’t work.
So, did our guys they choose a peer-reviewed real-time control trial relying on lab-tested double-blind results?
Perhaps one of the dozen or so such trials listed in our40 facts article?
Did they maybe average the results of multiple studies?
In this *ahem* “scientific study”, they had people randomly call up those who had recently been tested for “Covid”, ask them “did you wear a mask?” and then published the conclusion – “masks reduce transmission by 53%” – as if they meant something.
Interestingly, if you scroll down to the “affiliations” section you can see that one of the authors is a Pfizer grant recipient.
What we have here is not “science” it’s a computer model based on the results of a subjective phone survey conducted by a government agency with a vested interest. It is entirely meaningless, and yet is published in journals and cited by “experts”, perhaps even used as the basis of introducing new laws.
This is how “The ScienceTM” works. And, although Covid has maybe opened many people’s eyes to this issue, it is far from unique to “Covid”. You are just as likely to find this kind of “research” published on any topic – especially those that serve a political purpose – and have been for years if not decades.
This has nothing to do with the “pandemic”, and everything to do with the difference between science and “The Science”. So let’s examine that distinction.
“Science” is an approach to the world. A rational method for gathering information, testing new ideas and forming evidence-based conclusions.
“The Science” is a self-sustaining industry of academics who need jobs and owe favours.
An ongoing quid pro quo relationship between the researchers – who want honors and knighthoods and tenure and book deals and research grants and to be the popular talking head explaining complex ideas to the multitudes on television – and the corporations, governments and “charitable foundations” who have all of those things in their gift.
This system doesn’t produce research intended to be read, it creates headlines for celebrities to tweet, links for “journalists” to embed, sources for other researchers to cite.
An illusion of solid substantiation that comes apart the moment you actually read the words, examine the methodology or analyse the data.
Self-reporting surveys, manipulated data, “modelling studies” that spit-out pre-ordained results. Affiliated-authors paid by the state or corporate interests to provide “evidence” that supports highly profitable or politically convenient assumptions.
This mask study is the perfect example of that.
Interlacing layers of nothing designed to create the impression of something.
That’s why they want you to trust it, rather than read it.
In this episode of ICIC, Dr Reiner Fuellmich talks to Dr Gerd Reuther, medical doctor and radiologist, about the historical background of medicine and the genesis of diseases and epidemics over the centuries, from the pre-Christian era to the present day.
He points out numerous connections and parallels to so-called pandemics of antiquity and current events, i.e. the “Corona pandemic”. The criers of these “pandemics” have always used the same methods earlier and to this day: the creation of fear and panic.
It sheds light on the role of the Church and its representatives and how far their powerful arm has reached in science, research as well as medicine at all times. These areas were entirely under the control of the Church, and even today these exercises of power continue.
One could call this behaviour opportunistic, since throughout history the Church has always turned to those who were in power. It is currently showing this pattern again, namely when it unhesitatingly fired up the Covid vaccination propaganda. Compared to then, not much has changed:
It was and is about trivial monetary claims to power and ownership, manipulating people for their own benefit, keeping them in dependencies, e.g. on the pharmaceutical industry, and exerting control over life itself.
Historical events such as outbreaks of plague and cholera are analysed and examined for their truthfulness. The history of the origin of “vaccination” and what the belief in its effectiveness is based on are also discussed in detail.
Since when have disease patterns and symptoms been defined and documented, and why were there no “civilisation diseases” in the past? How can it be that not all people fall ill with one and the same “pathogen” and what role do the improper handling of toxins and the natural immune system play?
Dr Gerd Reuther and his wife Dr phil. Renate Reuther, historian and English specialist, have summarised all these medical-historical findings and events compactly on 150 pages in a book entitled “Hauptsache Panik” (Panic is the main thing), which, despite its historical focus, is more up-to-date than ever. For only those who know the past can shape the present and change the future.
via ANTIJANTEPODDEN: Investigative journalist James Corbett has investigated how psychology is being weaponized to target dissidents.
In this episode he explains the absurdity of the old diagnoses of anarchia, which was too much love for freedom, and drapetomania, which was the mental illness of slaves running away from their masters.
Over the last three years, we have seen a medical doctor being diagnosed and force medicated for corona insanity. This was because of his resistance to the government narrative in Switzerland. We have also seen an increased willingness to pathologize conspiracy theorists, and to label people as domestic terrorists for using their right to share their opinions.
Even though the methods used against us are ugly, and the majority just go along uncritically, James Corbett shows examples of how modeling disobedience can dramatically turn the situation around.
The Bravo channel’s TV show I Am Jazz followed the adventures of Jazz Jennings, a spunky little boy who wanted to be a girl. The GLAAD crowd got a front man (well, boy) to push its trans movement upon boys and girls. Barbara Walters got an exclusive interview with him for Disney’s ABC. Bravo made money. He got attention. Everybody was happy.
His story was the LGBTQ version of Pinocchio but without a Jiminy Cricket to steer him clear of those who would exploit him — such as Barbara Walters and the producers of the I Am Jazz TV show. On June 20, 2018, doctors sliced and diced the 17-year-old in transsexual surgery — which is now called gender-affirming health care because everyone is too ashamed to call it a sex change.
The TV show went on a hiatus because Jazz was not too pleased with the result. He gained 100 pounds. He should have been more careful of what he wished for because he did not become a glamorous girl but a fat chick whose emotional problems grew worse.
When the show resumed, he returned to a public spotlight he had first entered at 7; Jazz now was fat and unhappy. The TV show recorded his first post-op date with a man. It was awkward and awful. Much like Kim Kardashian’s cosmetic doctoring, Jazz could change how he looked but not who he really is — a boy who never grew to be a man.
He has a trump card. He can sue. He was a minor when doctors began feeding him pills and under age when they performed this ultimate cosmetic surgery in him.
While he denies having regrets, Jazz’s behavior shows he is having second thoughts. I am pretty sure GLAAD and Bravo are sweating this one out. The stakes are so high that people are getting nosebleeds as they try to keep him away from personal injury lawyers.
My hope is that every ambulance chaser in the nation enters the detransitioning lawsuit business because it will be bigger than that Camp Lejeune water case they are advertising for plaintiffs. If suspected carcinogens — not proven, but suspected — can yield millions in legal fees, just think of the billions that could be there for the raking for a medication known to be toxic. The money is there. For example, Boston Children’s Hospital has an endowment of $7 billion.
That hospital’s Center for Gender Surgery said, “As the first pediatric center in the country dedicated to the surgical care of transgender patients, we take an interdisciplinary approach from the start to ensure exceptional patient care.”
But the children’s hospital also claims not to perform sex-change surgery on minors.
However, it is not just the surgery that is the problem. It is the pills. Puberty blockers expand the targets of litigation to include not just doctors and hospitals, but drug companies as well. It also expands the universe of plaintiffs.
The American College of Pediatricians warns, “There is not a single long-term study to demonstrate the safety or efficacy of puberty blockers, cross-sex hormones and surgeries for transgender-believing youth. This means that youth transition is experimental, and therefore, parents cannot provide informed consent, nor can minors provide assent for these interventions. Moreover, the best long-term evidence we have among adults shows that medical intervention fails to reduce suicide.
“Puberty blockers may actually cause depression and other emotional disturbances related to suicide. In fact, the package insert for Lupron, the number one prescribed puberty blocker in America, lists ‘emotional instability’ as a side effect and warns prescribers to ‘Monitor for development or worsening of psychiatric symptoms during treatment.’
“Similarly, discussing an experimental trial of puberty blockers in the U.K., Oxford University Professor Michael Biggs wrote, ‘There was no statistically significant difference in psychosocial functioning between the group given blockers and the group given only psychological support. In addition, there is unpublished evidence that after a year on [puberty blockers] children reported greater self-harm, and the girls also experienced more behavioral and emotional problems and expressed greater dissatisfaction with their body—so puberty blockers exacerbated gender dysphoria.’
“Puberty blockers may cause permanent physical harm.
“Temporary use of Lupron has also been associated with and may be the cause of many serious permanent side effects including osteoporosis, mood disorders, seizures, cognitive impairment and, when combined with cross-sex hormones, sterility.”
Right now, there is big money in transing kids. Obama approved having Medicaid and Medicare pay for transsexual operations and the like. He also forced insurers to cover transing, and the transing industry took off — and best of all for these ghouls is the poisonous side effects make the transed kids customers for life.
Fox reported, “A young male, who formerly identified as a trans woman, who was castrated and became a patient for life as part of gender-affirming care, wants to warn others not to follow in his footsteps. He discussed his story of resilience and learning to accept himself for who he is, for the first time, with Fox News Digital.”
He appears in a video.
The story said, “Kobe, whose name is being withheld for privacy reasons, had ‘checked every box for what they call a trans adolescent.’ He was always effeminate and loved pink and playing with Barbies. If he had never been exposed to gender ideology, he says he probably ‘would have just stayed a feminine boy. And there’s nothing wrong with that.’”
He said, “I felt unlovable as an effeminate man in society and everything. A feminine boy, actually. I was never a man, I’m trying to reclaim my manhood now and everything. It’s hard. I have breasts, I have the hip development of a woman, because I started the estrogen young. I have no gonads. You know, it’s hard. My skull never really masculinized.”
We won’t let kids smoke at 10, why do we allow them to take experimental drugs that will cause such damage?
Litigation will stop this quicker than the politicians will. Heck, the pols are still arguing over which bathroom drag queens use.
In February, Fox reported, “A prominent detransitioner sued a nationwide medical group and its doctors Thursday who she said ‘decided to perform a mutilating, mimicry sex change experiment’ on her, according to the lawsuit.
“The Center for American Liberty sued Kaiser Hospitals on behalf of detransitioner Chloe Cole ‘for pushing her into medical mutilation instead of properly treating her,’ according to Cole’s lawyer Harmeet K. Dhillon. Between the ages 13–17 years, Cole underwent a transgender transition, including the off-label use of puberty blockers, cross-sex hormones and a double mastectomy.”
Dhillon tweeted, “What Kaiser did, for profit, to Chloe in the name of woke ideology instead of sound medical practice, should not happen to any child in America!”
Win the case and it won’t.
The left knows these lawsuits are a bigger threat to LGBT than Ron DeSantis. In May, NYT tried to play down the kids who want their old bodies back — which will never happen. NYT objected to using detransitioners to push bans on transsexual operations for kids.
NYT said, “As more American teenagers have identified as transgender, it is difficult to say how many will transition medically — many transgender people do not — and precisely how many will later change course. Methodology, demographics and even the definition of detransition vary widely from study to study, which typically show that between 2% and 13% of people detransition, and not always because of regret.”
Only 2% to 13%?
We shut down the world’s economy because of a virus that killed less than 1% of those infected.
The story said, “Elisa Rae Shupe was well known in the transgender rights movement: first as an outspoken transgender woman, and then as the first American to change her legal sex to nonbinary.
“So when she published an essay in 2019 saying that her transition ‘was all a sham’ and that she wanted ‘to live again as the man that I am,’ conservatives took immediate notice.”
And lefties dropped her like a hot brick.
But the radioactive brick is litigation, not legislation.
The Economist reported in March, “Legal action may change transgender care in America. Some detransitioners are starting to take their doctors to court.”
The story said, “Most Americans favour protecting trans people from discrimination, but they sharply disagree on medically transitioning children. Whereas 72% of Republicans believe it should be illegal to provide a minor with medical care for gender transition, just 26% of Democrats agree, according to the Pew Research Centre, a think-tank. Activists who believe such care saves lives have tried to discredit Ms Cole, by focusing on the support she receives from firebrands on the right. But the facts of this case—if they are as claimed—could give at least some of them pause for thought.”
A Jazz Jennings lawsuit would stop hospitals from preying on kids.
“Covid” Vaccines Were Deployed by the US Department of Defense as “Countermeasure Prototypes” With No Safety Testing Required, Using the General Public as Guinea Pigs
“As if that news were not troubling enough, Katherine and Sasha learned that anyone who examines the contents of the vaccines vials can be legally punished for doing so. Pharmacists and doctors warned that the vials are property of the US government, so having the vials tested would expose them to criminal charges.”
I found Sasha Latypova through a colleague in Europe. The day I met Sasha at her villa in California, the skies were overcast, which correlated with the subject matter of the interview. Now retired, Sasha had had a very successful career as an independent contractor designing clinical trials for the largest pharmaceutical companies in the world.
During our interview, I was stunned by some of the conclusions Sasha had reached regarding which government agencies actually authorized the vaccines. Through the COVID crisis, Sasha teamed up with a paralegal in Pennsylvania named Katherine Watt who conducted very thorough research that unearthed the legal framework through which the vaccines were approved and deployed. You can find her work here.
Katherine Watt discovered that the covid vaccines were authorized not by the FDA but by the US Department of Defense as countermeasure prototype demonstrations. This revelation ties in with a prior BIG PICTURE interview with Brook Jackson, who managed a piece of the Pfizer clinical trials for a Pfizer contractor, found fraud, and was fired for bringing the irregularities to the attention of her superiors. When Brook later sued the government for purchasing vaccines that were not properly FDA approved, the government’s response was that they were not FDA approved but approved instead by the DOD.
Coincidentally, Katherine Watt uncovered the existence of a joint Health and Human Services and Department of Defense program to combat bioterrorism or natural outbreaks through the rapid deployment of “countermeasure prototype demonstrations.” This is a shockingly broad term that basically means “anything whipped up by the military that they think may be of use.” In other words, they are rapidly whipped-up secret recipe military vaccines that require no approval other than the say so of the HHS secretary and his belief they may be of benefit. No testing needed, no clinical trials required.
The general public is now the unwitting guinea pig. This means all the COVID vaccines everyone has been receiving were actually produced by the military under a martial law legal structure and the public is being unwittingly injected with not just experimental vaccines, but with military prototypes that were never intended to receive any FDA approval.
This strange scenario explains why the regulators (FDA) behaved so strangely and why no one was ever punished for the rushed and fraudulently conducted clinical trials.
Operation Warp Speed was a military operation complete with sophisticated propaganda strategies. These psychological propaganda programs targeted films like my Planet Lockdown film. The public was encouraged to take the vaccines by psychological warfare units of the military. Yet it is illegal under the 1878 Posse Comitatus Act for the military to operate on US soil.
As if that news were not troubling enough, Katherine and Sasha learned that anyone who examines the contents of the vaccines vials can be legally punished for doing so. Pharmacists and doctors warned that the vials are property of the US government, so having the vials tested would expose them to criminal charges.
I must ask: If these are simply experimental vaccinations for a novel flu, why on god’s green earth are all these unusual measures needed? This is quite suspicious, and, in my experience, suspicious people tend to act suspiciously . . . and are up to something they don’t want you to know . . .
Please join me and learn just how Sasha discovered what she did, the logic she followed, and where it led her. I think you will understand why the truth disturbed her enough to come forward and share it with the world. She is committed to getting this information so that we cannot be fooled the next time a “pandemic” is announced.
Video available at PlanetLockdown Odysee & Rumble channels.
“The truth is, no one can get to health through vaccinations. If a person is sickly, vaccines won’t help. If he’s healthy, he doesn’t need vaccines.
“The bad news is, vaccines destroy. Whether it’s the so-called adjuvants they put in the shots, the goop they think are pieces of viruses (that don’t exist), the preservatives, the lipid nanoparticles, the coatings on the particles, the little segments of RNA—the injections attack the body. In all sorts of ways. In all sorts of places.”
When I think about what piece to write next, or when for the moment my tank is empty, I come up with VACCINES. That’s the subject.
It’s been that way for a long time.
I could be accused of having a grand obsession, but this isn’t the case. I’m responding to the civilizational obsession with vaccination.
At the same time, it IS personal. Because of the outrage I feel, watching medical storm troopers who have been on the march for more than a hundred years.
Watching their arrogance, their blunt stupidity, their “rational” madness. As they keep marching and invading.
If we were living in an absolute monarchy and I were King, there would be hell to pay. The troopers would pay, dearly.
Over the past 35 years, I’ve written countless articles on vaccination. I’ve run down the evidence from all the angles. Now I’m left with the feeling when all the data detailing crimes have been exhausted. I’m at the end of that trail.
It’s not THE end, though. Not by a long shot.
The troopers and their allies represent, for me, everything that’s insane about our society—especially the bland acceptance by the willing victims. The silent majority.
Including, of course, the educated classes, who proudly wear their badges of science, the ultimate virtue signal. They live in a harsh bombed out desert and think it’s a pretty garden.
Some of them watch their children go crazy from the shots, suffering massive brain damage—and still these parents won’t admit what happened.
They refuse to see what they saw.
—It might have been after a talk I gave. I had mentioned the fact that improved sanitation and nutrition in the West accounted for the decline in all sorts of illness—not the widespread introduction of vaccines.
The person said, “But for children who still can’t get nutritious food, vaccines protect them.”
It was a mindless “save the children” remark.
Of course, when the body’s defense is chronically deficient, a vaccine isn’t going to pump it up. Because there isn’t anything THERE to pump up. That’s a ridiculous fairy tale. And a vaccine isn’t food.
Bill Gates tried to pull off the same sort of nonsense, when he announced with great personal fanfare, that he’d just read a book about contaminated water supplies in the Third World—as if he’d just discovered what everyone else had known for 50 years.
So he said something like this: I saw that bad water accounted for horrific chronic diarrhea, a killer. We have to clean up the water. But meanwhile, my anti-diarrheal vaccine will help.
No it won’t. The sick child, who is wasting away, has no immune system left. The vaccine won’t build up what isn’t there.
—Belief across a population is a powerful thing. It can operate like a bulldozer, flattening all obstacles and objections. And at the end of the day, it stands naked, amid the ruins. When the belief is demanding a solution that won’t work. Vaccines.
I come from an era when vaccinations were few and far between. A poke here, a stab there. There was no CDC shouting about schedules. The big Pharma money wasn’t rolling in yet. The predators knew the public wouldn’t go for 30 or 40 shots during childhood.
But now it’s a lifeline. Oh, the kids will die if you don’t shoot them up.
Bleeding heart liberals, clueless rubes, and Big Pharma. A jackpot sales team.
And a bland Howdy Doody monster like Bill Gates in the background, pouring billions of dollars into MORE vaccines.
As I predicted early on during Warp Speed, the introduction of RNA technology was going to create a bonanza for Pharma. They’d redo every vaccine in the book with the new tech. They’re working in that direction now.
Because vaccines injure and kill, this civilization is on wartime footing. We’re under attack. Half the effort to censor us is devoted to the vaccine issue. The enemy knows what’s at stake.
If we take their prime weapon away from them—by walking away from it in huge numbers—they fall.
After the COVID fiasco, when millions of people DID walk away from the injection…the public is primed to take a look at the whole range of vaccines.
I’ve watched some of the new pundits who appeared during COVID to expose that shot. Some of them are close. They’re close to seeing that the whole arsenal of vaccines is nothing less than a doomsday weapon. They haven’t crossed that line yet. But they’re on the verge.
I crossed the line in 1988, when I wrote AIDS INC. Because I realized “the virus” wasn’t causing anything, I was looking for real causes of immune suppression—since that was what so-called AIDS was.
And that’s when I saw The Big One looming up on the horizon. Vaccines.
I started talking to Health Freedom advocates who’d been in the trenches for decades. I started reading hard to find books that investigated vaccines. And then, there it was.
I saw it.
I couldn’t look away from it.
Whatever I thought a career in journalism was, could be, should be, that career took a sharp turn.
I had no idea how much passivity I would encounter.
Pure, dumb, conformist passivity.
But with Warp Speed, and everything that followed, I saw the apathy in the public begin to dissolve.
I saw foundational pillars begin to crack.
The truth is, no one can get to health through vaccinations. If a person is sickly, vaccines won’t help. If he’s healthy, he doesn’t need vaccines.
The bad news is, vaccines destroy. Whether it’s the so-called adjuvants they put in the shots, the goop they think are pieces of viruses (that don’t exist), the preservatives, the lipid nanoparticles, the coatings on the particles, the little segments of RNA—the injections attack the body. In all sorts of ways. In all sorts of places.
In England, right at the start, when THE one shot was for smallpox, there were whole cities with high vaccination rates where people were dropping like flies. And cities where the vaccination rate was low, people came through all right.
When the authorities finally began cleaning off the raw sewage running down the city streets, when they installed public sanitation systems, disease took a very sharp downturn.
These things aren’t hard to understand.
But they’ve been hidden from the public.
We’re looking at a revolution of simple truth. Which can be spoken and delivered simply.
And widely.
By us all.
In this war.
During which we’re under attack.
Many foot soldiers happen to be doctors, who have the advantage of seeming neutral. They wave no flags. They salute no dictator. They’re calm and rational. Nevertheless, they wield the weapon, and they use it.
We can’t let that oddity deter us.
If you need a push, talk to the mother of a severely autistic child. That is, a child whose brain was assaulted by a vaccine. Have her tell you what she goes through every day of her life, with that child.
It seems difficult to believe a modern civilization could have gone so far off the track as this one has.
The difficulty in facing that fact is what drives people back into their huts and their television screens and online games.
But you know, believing something that happens to be true and then acting on it is more powerful than any civilization.
In my last interview with Del Bigtree on The Highwire I sounded the alarm regarding the future of aluminium adjuvants in vaccines. I urged against complacency and warned that next generation vaccines would continue to rely upon aluminium adjuvants. Well, we now know this to be true direct from the horse’s mouth.
The latest vaccine industry funded paper entitled ‘Aluminium Adjuvants – Back to the Future’ leaves no doubt that the vaccine industry is not contemplating a future without aluminium adjuvants. The paper is published in a special issue of the journal Pharmaceutics called Designing and Developing the Next Generation of Vaccine Adjuvants. The vaccine industry will continue to use aluminium adjuvants well into the future. They will continue to promote the injection of aluminium into our body, from new born infants to vulnerable individuals and the elderly.
Their rationale for continuing the use of aluminium adjuvants? Well, first and foremost, though not mentioned in this latest review, is cost. As I have written about in previous substacks and in my book, aluminium adjuvants are dirt cheap, they add absolutely nothing to the cost of a vaccine. Why would industry invest in new adjuvants when aluminium adjuvants are effective and cheap. The bottom line is always the deciding factor for profit-led industry.
However, their cost effectiveness is not worthy of a mention in this latest industry review. The major selling point for aluminium adjuvants in this paper is ‘their excellent safety profile, which has been established through the use of hundreds of millions of doses in humans over many years’. This stomach churning statement, taken from the abstract of the published paper, is pure aluminium industry speak. It reminds me of their often used defence of the safety of aluminium, wheeled out at many scientific meetings, that the fact that aluminium is present throughout the body must prove that it is good for you.
The fact that such a statement is in the abstract of this paper demonstrates that it went unchallenged by the so-called peer review process. Indeed there is no evidence that this paper was peer reviewed. The Guest Editor of the Special Issue where the paper is published is the lead author of the paper. The Editor of Pharmaceutics is a vaccine industry stooge. This journal, published by MDPI (see my criticism of this publisher in my book), is simply a vehicle for the vaccine industry to legitimise their messages regarding the safety and efficacy of vaccines.
It is, of course, common knowledge and scientific fact that the safety of aluminium adjuvants in humans has NEVER been tested for any vaccine in use today. To my knowledge the only vaccine ‘safety trial’ where a saline control was used was carried out by Merck on Gardasil. The results of this trial, available through clinicaltrials.gov, showed an incidence of serious adverse events of 2.4% both for the whole vaccine and for the aluminium adjuvant alone while the incidence was 0% for a saline control. Make of this what you will but my interpretation is that an unacceptably high incidence of serious adverse events in recipients of Gardasil was due to the aluminium adjuvant.
Further indirect evidence of the toxicity of aluminium adjuvants comes from the work of vaccine advocate Peter Aaby working in Guinea-Bissau, Africa. He has shown in multiple studies that mortality in children receiving aluminium-adjuvanted vaccines is significantly higher than unvaccinated children. He does not find a similar effect in live attenuated vaccines that do not use an aluminium adjuvant.
Any form of true peer review of this paper in Pharmaceutics would have prevented such lies from being published. The true safety profile of the use of hundreds of millions of doses of aluminium adjuvants in humans is all about us for anyone willing to look and see. True epidemics of industry sponsored human disease including Alzheimer’s disease and autism. Shame on those in scientific publishing who turn a blind eye to the truth and worse promote lies that can only result in further human suffering and death.
The extensive history of the pharmaceutical industry is filled with stories and deeds of adventures, misadventures, profit-making, profit-taking, fraud, bribery, false claims, messianic promises, and criminal conduct.
Few companies in the history of medicine have received as much attention as Pfizer Inc. has received these last three years of the Corona Crisis.
Through the course of relentless media coverage and amidst all the sound and fury, Pfizer has managed to avoid scrutiny of its previous criminal conduct and is universally portrayed in the mainstream media as a benevolent enterprise whose mission is to nobly service humanity.
In an effort to set the record straight we embark upon a comprehensive historical examination of this company which sprouted from humble beginnings into one of the most influential corporate behemoths walking the earth today.
History
The story of Pfizer begins in New York City in 1849, when a pair of German immigrants, cousins Charles Pfizer and Charles F. Erhart, received a $2,500 loan from Charles Pfizer’s father to purchase a commercial building in Williamsburg, Brooklyn where they would embark upon a joint business venture in the nascent chemical manufacturing industry.
Charles Pfizer had been a pharmacist’s apprentice in Germany and possessed commercial training as a chemist. Charles Erhart was a confectioner.
Originally named Charles Pfizer and Company the business would initially focus on the production of chemical compounds. Their first product was a pharmaceutical called Santonin which was used to treat parasitic worms.
Combining their talents the cousins housed their product within tasty confections such as candy lozenges and toffee-flavored sugar cream cones. This strategy proved to be a success, setting the stage for the company’s future development.
The drug Santonin would be used as an anthelmintic up until the 1950’s, when it fell out of favor due to noted toxic effects which posed serious risks to patients.
Pfizer would quickly expand into the realm of fine chemicals for commercial sale to wholesalers and retailers.
In 1862, Pfizer would become the first U.S. company to domestically produce tartaric acid and cream of tartar.
With the outbreak of the American Civil War a massive need for painkillers and antiseptics erupted, creating an “opportunity” for the pharmaceutical industry.
Pfizer quickly expanded its production of both, as well as of iodine, morphine, chloroform, camphor, and mercurials. By 1868, Pfizer revenues had doubled and its product line had increased substantially.
The big boon for the company would come in the 1880’s with its production of industrial grade citric acid, widely used in soft drinks like Coca-Cola and Dr. Pepper. This would become the company’s centerpiece and drive their growth for decades.
Another fortuitous change for the “small New York firm” would arrive in 1919, when its scientists would pioneer and develop a deep tank fermentation process, the principles of which would later be applied to the production of penicillin.
This prowess in fermentation and large-scale pharmaceutical production would put Pfizer in a lead position in WW2, when the US government appealed to the pharma industry for support in producing penicillin for the war effort.
Working with government scientists, Pfizer began pursuing mass production of penicillin utilizing its deep-tank fermentation technology and in 1944 became the first company to mass produce penicillin.
As penicillin prices and usage declined post-WW2, Pfizer began searching for more profitable antibiotics. The move into commercial production of antibiotics signaled a pivot in Pfizer’s business model.
The company’s operations shifted from the manufacture of fine chemicals to research-based pharmaceuticals, giving birth to Pfizer’s new drug discovery program, which focused on vitro synthesis.
In 1950 Pfizer would develop its first proprietary pharmaceutical product, Terramycin, a broad-spectrum antibiotic.
By 1951, Pfizer had established offices in Belgium, Brazil, Canada, Cuba, England, Mexico, Panama, and Puerto Rico. As its power and profits mushroomed, Pfizer would augment its portfolio through various acquisitions and entries into multiple areas of research and development, including an animal health division.
As the Pfizer pharmaceutical kingdom expanded, however, questions about salacious business practices began to surface.
Violations
Despite portraying itself as a righteous corporate citizen, Pfizer is no stranger to controversies and scandals. As early as 1958 it was one of six drug companies accused of price fixing by the Federal Trade Commission.
In 1961 the Justice Department filed criminal antitrust charges against Pfizer, American Cyanamid, and Bristol-Myers, accusing top executives at each company of charging egregiously high prices and monopolizing the production and distribution of drugs dating back to 1953.
In 1963 the FTC ruled that the accused companies in its 1958 complaint did in fact rig antibiotic prices. The FTC also noted that “unclean hands and bad faith played a major role”in Pfizer being granted the tetracycline patent.
By the 1960s, Pfizer was at its most diversified point in history, with interests ranging from pills to perfume to petrochemicals to pet products.
The company’s shift toward bringing out new products culminated with the establishment of the Central Research Division in the early 1970s. A full 15% of Pfizer’s revenue was directed to this research department.
This focus on innovation brought about Pfizer’s development of blockbuster drugs, which are described as “drugs that generate at least $1 billion in revenue a year for the pharmaceutical companies that produce them.”
While these drugs can be extremely profitable for pharmaceutical companies, the blockbuster drug business model presents certain long-term problems. Beyond the time and money that goes into their development, there are the exigencies of patent issues. Pharma companies see the “patent window” of 20 years as a severe limitation, since it often takes them a full decade to bring a new drug to market, thus shortening both the time allowed to reclaim profits from development costs and the time allotted to reap maximum profits from their new product.
Due to patent laws, the success of blockbuster drugs is often short-lived. Also, reliance on blockbusters means that if a product fails, the consequences for the manufacturer can be catastrophic.
Using this business model, the need for pharmaceutical companies to constantly produce blockbuster drugs is difficult to overstate. Naturally, they go to great lengths to protect their golden goose.
Accompanying Pfizer’s string of blockbusters was a massive surge in the company’s fortunes in tandem with a procession of controversial products, felony offenses and multiple fines—including the largest criminal fine in US history.
Take, for example, Pfizer’s first blockbuster drug, the anti-inflammatory Feldene, which would also become one of its initial contentious products.
Pfizer submitted a new-drug application for Feldene to the FDA in March 1978 and again in May 1980. The applications were rejected due to poor testing protocols. In September 1981, Pfizer resubmitted an application to the FDA, using old data.
Multiple questions surrounding Feldene, including the route taken toward its ultimate approval, would make it one of Project Censored’s top “Censored” news stories in 2015.
In that story, Project Censored noted:
”Then, while the FDA was still considering the application, Pfizer sponsored a reception at the meeting of the American Rheumatism Association in Boston and showed a film promoting Feldene which the FDA said was illegal. Nevertheless, on April 6, 1982, the FDA approved Feldene for use in the U.S.”
Even though Feldene would go on to become Pfizer’s most lucrative product, questions about the drug quickly surfaced. By 1986 the FDA was being petitioned to relabel the drug due to serious concerns about its long half-life and its tendency to accumulate in the blood.
The watchdog organization Public Citizen Health Research Group (PCHRG) would later charge that this widely prescribed arthritis drug created risks of gastrointestinal bleeding among the elderly.
Citing reports of 2,621 adverse events and as many as 182 deaths among patients taking the drug, PCHRG requested that the FDA ban Feldene for patients 60 and over, “as an imminent hazard to the public health.”
Dr. Sidney Wolfe, director of the PCHRG stated, “At least 1.75 million elderly American people now receiving this drug are at risk of developing life-threatening gastrointestinal reactions.”
PCHRG’s Wolfe would later cite internal documents from Pfizer that voiced concerns about the drug. By 1995 he called for a complete ban on the drug for all ages.
This was just the beginning of a series of high-profile scandals and legal problems that would come to define Pfizer’s business-as-usual practices.
For instance, reports of serious issues surrounding a heart valve produced by Pfizer’s Shiley division began to plague the company. This problem would result in the cessation of production of all models of the faulty valves by 1986.
A 1991 FDA task force charged that Shiley withheld information about safety problems from regulators in order to get initial approval for its valves. A November 7, 1991, investigation in The Wall Street Journal asserted that Shiley had deliberately falsified manufacturing records relating to valve fractures.
These fractures resulted in catastrophic consequences for numerous patients. By 2012 it was reported that 663 individuals had died as a result of the defective valves.
It also agreed to pay $10.75 million to settle US Justice Department charges that it lied to regulators in seeking approval for the valves.
The parade of corrupt practices and legal problems that has come to define this pharmaceutical Leviathan was just getting underway. From then on, Pfizer was cited and prosecuted for a litany of illegal acts ranging from price fixing, product safety, bribery, advertising and marketing scandals all the way to environmental and human rights violations.
In 1999 Pfizer pled guilty to criminal antitrust charges and agreed to pay fines totaling $20 million. In that case, Pfizer was charged with “participating in a conspiracy to raise and fix prices and allocate market shares in the U.S. for a food preservative called sodium erythorbate, and to allocate customers and territories for a flavoring agent called maltol.”
In 2000 The Washington Post published a six-part exposé accusing Pfizer of testing a dangerous experimental antibiotic Trovafloxacin (trade name Trovan) on children in Nigeria without receiving proper consent from their parents.
Trovan was slated to become Pfizer’s next blockbuster drug, according to Wall Street analysts, one of whom claimed, “Pfizer might reap $1 billion a year if Trovan could gain approval for all its potential uses.” But when the company was unable to find enough patients in the United States, its researchers went in search of new patients in Kano, Nigeria.
This unapproved clinical trial on 200 Nigerian children resulted in the death of 11 children. It is alleged that many more children later suffered “serious side-effects ranging from organ failure to brain damage.”
In 2001 Pfizer was sued by 30 Nigerian families, who accused the company of using their children as “human guinea pigs.” The families contended that “Pfizer violated the Nuremberg Code as well as UN human rights standards and other ethical guidelines” and alleged that Pfizer exposed the children to “cruel, inhuman and degrading treatment.”
After years of legal battles, Pfizer agreed in 2009 to pay $75 million to settle some of the lawsuits that had been brought in Nigerian courts.
Trovan never became the blockbuster Pfizer had envisioned. The company admitted to stockholders it had “suffered a disappointment” with this experimental meningitis drug. Trovan was never approved for use by children in the United States, so production was halted. The European Union banned it in 1999.
Below is a chronology of still more Pfizer misadventures.
— In 2002 Pfizer agreed to pay $49 million to settle charges that one of its subsidiaries defrauded the federal Medicaid program by overcharging for its cholesterol-lowering drug Lipitor.
— In 2003 Pfizer paid $6 million to settle with 19 states that accused it of using misleading ads to promote the antibiotic Zithromax (also called Z-Pak), used for children’s ear infections. The claim alleged that Pfizer “overstated the benefits and efficiency of Zithromax when compared to other comparable antibiotics.”
— In 2004 Pfizer agreed to a $60 million settlement in a class-action suit brought by users of a diabetic medication developed by Warner-Lambert, which Pfizer acquired in 2000. The drug Rezulin had been withdrawn from the market after numerous patients died from acute liver failure said to be caused by the drug.
— In 2004 Pfizer agreed to halt ads for its painkiller Celebrex, and the following year it admitted that 1999 clinical trials found that elderly patients taking the drug were far more likely to incur risks of heart problems.
— 2004 also saw Pfizer plead guilty to two felonies and pay $430 million in penalties for fraudulently promoting the epilepsy blockbuster drug Neurontin for unapproved uses. Pfizer claimed it could also be used for “bipolar disorder, pain, migraine headaches, and drug and alcohol withdrawal.”
Pfizer’s underhanded tactics involving Neurontin also included bribing doctors with luxury trips and monies to promote the drug and planting operatives at medical education events.
Documents later came to light suggesting that Pfizer arranged for delays in the publication of scientific studies that undermined its claim for the other uses of Neurontin. In one of these documents, it was found that a Neurontin team leader at Pfizer said, “I think we can limit the potential downside of the 224 study by delaying publication for as long as possible.”
Finally, in 2010, a federal jury found that Pfizer committed racketeering fraud in its marketing of Neurontin; the judge in the case subsequently ordered the company to pay $142 million in damages.
— In 2005 Pfizer withdrew its painkiller Bextra from the market after the FDA cited “inadequate information on possible heart risks from long-term use of the drug as well as ‘life-threatening’ skin reactions, including deaths.”
— That same year the FDA approved a black box warning on Pfizer’s other blockbuster painkiller, Celebrex, citing elevated risks of “cardiovascular events and life-threatening gastrointestinal bleeding.”
— In 2007 Pfizer agreed to pay $34.7 million to settle federal charges relating to the marketing of its Genotropin human growth hormone. Pharmacia & Upjohn Co., a Pfizer subsidiary, agreed to pay $19.7 million for “offering a kickback to a pharmacy benefit manager to sell more of the drug,” while Pfizer agreed to pay another $15 million for “promotion of Genotropin for uses not approved by the Food and Drug Administration.”
— In 2008 Pfizer paid out a whopping $894 million fine to settle lawsuits “alleging that its withdrawn Bextra painkiller and widely used Celebrex arthritis drug harmed U.S. patients and defrauded consumers.” Of the total fine, $745 million was set aside to “resolve personal injury claims.”
— The very next year, 2009, Pfizer was fined $2.3 billion gaining the dubious distinction of being tagged with the largest health care settlement in history. GlaxoSmithKline would up the ante with a $3 billion settlement in 2012.
The fine was a combination of civil and criminal settlements relating to Pfizer’s “allegedly illegal promotion of certain drugs, most notably Bextra.” Pfizer pled guilty to “misbranding the painkiller Bextra with the intent to defraud or mislead, promoting the drug to treat acute pain at dosages the FDA had previously deemed dangerously high.”
The Justice Department also noted Pfizer had “allegedly paid kickbacks to compliant doctors and promoted three other drugs illegally: the antipsychotic Geodon, an antibiotic Zyvox, and the antiepileptic drug Lyrica.”
When interviewed by The New York Times, former Pfizer sales representative John Kopchinski, who helped initiate the federal investigation, stated, “The whole culture of Pfizer is driven by sales, and if you didn’t sell drugs illegally, you were not seen as a team player.”
The criminal fine of $1.195 billion in that settlement still represents the largest criminal fine ever imposed in the United States for any matter.
Even after entering an expansive corporate integrity agreement with the Office of Inspector General of the Department of Health and Human Services as part of the 2009 settlement, Pfizer’s unprincipled and injurious behavior continued. The band played on.
In 2010 The New York Timesreported on Pfizer’s admission that it had paid around “$20 million to 4,500 doctors and other medical professionals for consulting and speaking on its behalf in the last six months of 2009.”
The Times also mentioned that Pfizer had paid “$15.3 million to 250 academic medical centers and other research groups for clinical trials in the same period.”
In reference to the amounts disclosed by Pfizer, Dr. Marcia Angell, former editor of The New England Journal of Medicine and author of The Truth About the Drug Companies: How They Deceive Us and What to Do About It, admitted that while she had no specific knowledge of the matter, she believed the publicly revealed amounts Pfizer disclosed “seemed low.” She added: “I can’t help but think something has escaped.”
In 2011 Pfizer agreed to pay $14.5 million to resolve False Claims Act accusations that it illegally marketed its bladder drug Detrol.
The SEC alleged that “employees and agents of Pfizer’s subsidiaries in Bulgaria, China, Croatia, Czech Republic, Italy, Kazakhstan, Russia, and Serbia made improper payments to foreign officials to obtain regulatory and formulary approvals, sales, and increased prescriptions for the company’s pharmaceutical products.”
According to Kara Brockmeyer, Chief of the SEC Enforcement Division’s Foreign Corrupt Practices Act Unit, “Pfizer subsidiaries in several countries had bribery so entwined in their sales culture that they offered points and bonus programs to improperly reward foreign officials who proved to be their best customers.”
In 2012, Pfizer was hit with another massive fine—this time to settle claims that the side effects of its Hormone Replacement Therapy (HRT) drug Prempro cause breast cancer. Around 10,000 women filed a lawsuit against the company, alleging that the drug maker withheld information about the potential risks of breast cancer from HRTs. The $1.2 billion settlement came after six years of trials.
The FDA had placed a black box warning on Chantix, the highest safety-related warning assigned by the FDA, “to alert patients and doctors to the risk of psychiatric side effects” and had noted that the drug is “probably associated with a higher risk of a heart attack.”
Pharmaceutical companies make every effort to circumvent black box warnings. They generate bad publicity and negatively impact the marketability of the drug in question, which leads to adverse financial consequences for the company.
In 2016, after years of lobbying, Pfizer managed to get the FDA to lift the black box designation from Chantrix in a 10-9 vote, giving the controversial blockbuster drug a “new lease on life.”
In 2013 Pfizer reached a $35 million settlement relating to the alleged improper marketing and promotion of the immunosuppressive drug Rapamune. When New York Attorney General Eric T. Schneiderman announced that he and 40 other state attorneys general had arrived at the settlement, he remarked, “There has to be one set of rules for everyone, no matter how rich or powerful, and that includes big pharmaceutical companies that make unapproved and unsubstantiated claims about products in order to boost profits.”
While this article’s list of Pfizer’s corporate crimes is prodigious by any measure of shady business practices, it is far from exhaustive. In total, since 2000 Pfizer has accumulated $10,945,838,549 in penalties and incurred 96 violations covering a wide range of offenses.
A Company You Can Trust?
Pfizer’s portfolio of corporate crimes rivals that of the most corrupt companies in history. But that did not stop Pfizer from becoming a corporate celebrity with its COVID-19 vaccine. Indeed, the company has benefited handsomely from that product, whose $36.8 billion in 2021 sales made it the highest-selling pharmaceutical product in history.
When the pharma company’s 2022 revenues reached an all-time, single-year high of $100.3 billion, COVID-19 vaccine sales accounted for nearly 38 percent of those revenues.
Yet, while Pfizer was basking in the glow of mainstream media cheerleading and record-setting profits, honest inquiries into its unremitting record of corruption were kept from public view.
We were told we must “Trust in Pfizer” to vaccinate the world and save humanity from the so-called COVID crisis.
Given Pfizer’s documented record of misdeeds, any reasonable person would ask:
“Is this a company that belongs behind the wheel of the most widespread mass vaccination campaign in history?”
“Is this a company we should trust with experimental medical technology?”
“Is this a company we want to be in control of the most radical mass medical experiment in human history?”
“How is it that a company that habitually engaged in such illegal practices was able to reinvent itself as the savior of humanity?”
At that commemoration, then-president of Pfizer Global Manufacturing Natale Ricciardi told attendees, “We have always had a very noble mission.” Despite cryptically lamenting, “A lot of things have changed at Pfizer, and unfortunately, we had to make certain decisions,” Ricciardi went on to assert, “But the nobility of what we do, the nobility of what has been done and continues to be done has never changed and will never change.”
All these years later—and despite Mr. Ricciardi’s insistence on Pfizer’s magnanimity—a thinking person might look through the company’s checkered catalog of crimes and fines and recognize that noble experiments are hardly the realm of “alleged” serial felons like Pfizer.
June 15, 2023, podcast host Joe Rogan interviewed Robert F. Kennedy Jr., who is currently running as a Democratic presidential candidate
In 2005, Kennedy started suing coal-burning powerplants and cement kilns for releasing mercury into waterways. He also pushed legislation to protect children against mercury and gave lectures on its dangers
During those lectures, mothers started approaching him saying they suspected their children had been injured by mercury-containing vaccines. They told him that if he was really interested in protecting children against mercury, he had to investigate vaccines
The mother of a vaccine-injured child brought him a thick stack of published research, and after looking through it, Kennedy realized that what health officials told us was very different from what the science showed
Kennedy is now also legally representing people who claim they’ve been injured by cellphone radiation, which science shows can cause cancer, degrade mitochondria and make your blood-brain barrier more permeable, allowing toxins in your system to flood into your brain
Still, if anything in that book was false, Kennedy would have been sued to high heaven by now, Rogan reasoned. Reading that book opened Rogan’s eyes to the fact that what we’re told by public officials and the media isn’t necessarily the truth. He also realized just how easy it is to fall for a false narrative — especially when it’s all you’re ever allowed to really hear.
For the first several minutes of the interview, Kennedy reviewed his background and how he got to where he is today. He started his legal career as an environmental lawyer in the mid-1960s, suing 500 polluters who had turned the Hudson River into a sewer, on behalf of commercial fishermen whose livelihoods were threatened.
As a result of those lawsuits, the Hudson River was cleaned up and restored. These successes led Kennedy to found Riverkeeper,2 which patrols waterways in 46 countries, holds polluters accountable and defends clean drinking water.
How Kennedy Got Involved With Vaccine Safety
I would strongly encourage you to listen to this interview as around the 10-minute mark Rogan asks Kennedy how he got into the vaccine controversy. Although Kennedy had presented some of his comments in the media previously, this is the first time he was ever allowed to give his uninterrupted one-hour fascinating story on major media.
In 2005, Kennedy started suing coal-burning powerplants and cement kilns for releasing mercury into waterways. He launched these lawsuits on behalf of local Riverkeeper chapters after learning that mercury was being found in the flesh of most freshwater fish. Pregnant women were also found to have levels that might put their children at risk of developmental problems.
Kennedy also pushed legislation to protect children against mercury and gave lectures on its dangers. During those lectures, mothers started approaching him saying they suspected that mercury (thimerosal) in the childhood vaccines had injured their children. They told him that if he was really interested in protecting children against mercury, he had to investigate vaccines.
He resisted, as his focus was on environmental pollution and he didn’t want to get involved in public health. However, mothers of developmentally challenged children kept coming to his speeches, wanting to talk to him about vaccines.
Their continued pressure eventually changed his mind, and he decided to listen to their concerns. The true turning point came when a psychologist named Sarah Bridges found his home address and delivered an 18-inch thick stack of scientific papers, saying she would not leave until he’d read them.
Bridges was one of the few people who had been awarded $20 million by the vaccine court, which had concluded that her son’s autism had been caused by a vaccine. She just didn’t want other parents to go through the same heartache.
Huge Gap Between Public Narrative and Published Science
Kennedy began reading, and by the time he’d gone through a third of the pile, he came to the realization that there was a huge gap between what the public health agencies were saying about vaccine safety and what the published science showed.
Kennedy then started calling high-level public health officials and regulators, asking them about these studies and, to his surprise, he realized none of them had read them. They were all just repeating what they had been told about the science. Stranger still, they told him to take his questions to people in the vaccine industry.
Kennedy did contact Dr. Paul Offit, as suggested, and caught Offit in a blatant lie. He asked Offit, how come pregnant women are told not to eat tuna fish to avoid mercury, but are then told to get flu shots that contain a huge bolus of mercury? Offit told him “there are two kinds of mercury, a good mercury and a bad mercury.” According to Offit, fish contain the bad kind, whereas the mercury in vaccines is harmless.
The problem was, Kennedy is an expert on mercury, having spent years suing mercury polluters. He has a deep understanding of the two types of mercury (ethylmercury in vaccines and methylmercury in fish), and there’s no such thing as a “good” or harmless mercury.
Kennedy, an excellent storyteller, goes on to review the history of vaccine science and why toxic elements like mercury are used at all. This interview is without doubt one of the most educational “lectures” on vaccines available right now, so I encourage you to listen to at least the first hour, if you don’t have time for the whole thing.
Ethylmercury Lodges in the Brain
Importantly, he reviews crucial research that firmly debunks the claim that ethylmercury is excreted from the body within a week. Studies on monkeys, where the animals were sacrificed after vaccination (which you cannot do with children), showed that the reason there was no ethylmercury in the blood after several days was because it had traveled into the brain, where it stayed, causing inflammation.
When Kennedy challenged Offit on this point, Offit insisted that, while this research did show that ethylmercury lodged in the brain, “the mosaic of studies” proved it was harmless and left the body.
Kennedy asked him to share those studies, which Offit promised to do but never did. Kennedy never heard from him again. At that point, Kennedy realized that something was terribly wrong, and he couldn’t walk away.
Kennedy also challenged Dr. Anthony Fauci — who is a close friend of the Kennedy family — to show him a single placebo-controlled trial of a vaccine listed on the childhood vaccination schedule. Fauci said he would send him the studies, but, like Offit, never did.
The reality is, none of the mandated vaccines has ever been tested against a true placebo, such as saline. Most are tested against other vaccines, and if you’re testing two products that contain a similar toxin, of course, the outcomes will be similar. That doesn’t mean you’ve proven safety. Not even close.
Kennedy eventually sued the Health and Human Services Department to obtain the evidence Fauci claimed to have, and after a year the HHS finally returned a letter saying there were no such safety studies. “So, nobody knows what the risk profiles of these products are,” Kennedy says.
The sheer lack of data also means that anyone who claims vaccines have saved more lives by preventing disease than they’ve destroyed through side effects is simply guessing and making assumptions. There’s no scientific data to back that up.
Also, Kennedy points out that while many vaccines are now mercury-free, they’re loaded with aluminum adjuvant instead, which is just as bad. So they’ve just exchanged one neurotoxin for another.
Intentional Suppression of the Autism Signal
Kennedy goes on to tell the story of a secret meeting3 organized by the U.S. Centers for Disease Control and Prevention in 1999 after they conducted an internal study of their database, which contains the medical records, including the vaccination records, of 10 million children from the 10 biggest HMOs.
Specifically, they wanted to know whether mercury-containing vaccines might be causing autism. One of the first comparisons of health outcomes was done on the hepatitis B vaccine.
The data showed that infants who had received the hepatitis B vaccine within 30 days of birth had a 1,135% higher risk of autism compared to infants who either did not get the hepatitis B vaccine at all or received it after 30 days of age. “At that point, they knew what caused the autism epidemic,” Kennedy told Rogan, because “that’s a relative risk of 11.35, and a relative risk of 2 is proof of causation.”
As panic spread through the industry, the CDC put together this secret meeting at a retreat center in Georgia. It was intentionally held outside the CDC campus to circumvent FOIA laws. The meeting included representatives from all the major vaccine companies, regulatory agencies that administer vaccines, the U.S. Food and Drug Administration, the National Institutes of Health, the Health and Human Services Department and leading academic institutions that conduct clinical trials.
The first day was spent discussing the reality of the problem, and the second day was spent discussing how to hide it. While the meeting was held in secret, someone did record it and, in 2005, Kennedy obtained a copy of it. You can read the transcript on the Children’s Health Defense website.
Early on in that 286-page transcript, we find the following admission by Walter Orenstein, then-director of the National Immunization Program at the CDC:4
“Initial concerns were raised last summer that mercury, as methylmercury in vaccines, might exceed safe levels … Analysis to date raise some concerns of a possible dose-response effect of increasing levels of methylmercury in vaccines and certain neurologic diagnoses.”
What happened to this safety signal? As explained by Kennedy, it was intentionally “vanished” by reworking the study four times, using statistical tricks.5 After the fourth iteration, the signal linking thimerosal with autism and a half dozen other neurodevelopmental disorders were no longer detectable.
The CDC published that final version and announced thimerosal had been investigated and found to be safe. And when investigators asked to see the raw data, the CDC claimed the data had been “lost,” so no one was ever able to verify the results. The fabrication stuck and has been peddled ever since.
We Live in a Toxic Soup
Kennedy stresses that vaccines are not the only factor in the epidemics of chronic disease and autism in children. There are many other factors as well. Children are exposed to an enormous amount of toxins from many different sources, including electromagnetic fields (EMF) and wireless radiation.
Kennedy is currently representing people who blame their brain tumors on cellphone radiation, and “we have the science,” he says. “Tens of thousands of studies show the dangers of Wi-Fi radiation.”
Aside from cancer, cellphone radiation degrades your mitochondria and makes your blood-brain barrier more permeable, Kennedy says, allowing all the other toxins in your system to flood in. So, this too, could play a significant role in the neurological dysfunction we now see in so many children. Kennedy also discusses the history behind and toxic influence of glyphosate, especially on your gut. (Incidentally, gut dysfunction is also a hallmark in autism.)
This is an interesting part of the interview as when Kennedy first mentions EMF, Rogan doubts it is true and doesn’t believe him. After Kennedy’s explanation you see Rogan morph in real time to a believer in EMF dangers and even ask his assistant Jamie to look into getting rid of the Wi-Fi.
Rogan Invites Dr. Hotez to Debate RFK
Yesterday, I published an article reviewing the online debate that erupted after this interview, when Dr. Peter Hotez took to Twitter, slamming Spotify for not clamping down on Rogan’s “vaccine misinformation.”6 Never mind the fact that Hotez, in April 2020, was allowed to argue his own irrational vaccine stance on Rogan’s show.7
Rogan replied to Hotez’s tweet, saying, “Peter, if you claim what RFK Jr. is saying is ‘misinformation,’ I am offering you $100,000.00 to the charity of your choice if you’re willing to debate him on my show with no time limit.” Others further sweetened Rogan’s offer by adding their own donations and, by 9 a.m. EST on June 18, the pot had reached $1.52 million.
Hotez refused, albeit indirectly. Instead of giving Rogan a direct answer, he went on the MSNBC show “Rising Reacts” and said he wasn’t willing to participate in an event that would get turned into “The Jerry Springer Show” by having Kennedy there.
Once you’ve listened to this interview, you can probably understand why no one is willing to engage in a public debate with Kennedy on this issue, particularly if you also heard Rogan’s interview8 with Hotez and compare the two. Kennedy has the data to back his claims and they have none.
On a side note, I find it curious that after Rogan took a beating in the press for discussing how he used ivermectin to treat a bout of COVID-19, he really hasn’t had any hard-hitting health-related truthtellers on his show — until Kennedy.
In my view, Spotify is hardly a free speech platform, so maybe that shouldn’t be that surprising. Spotify killed our account due to a discussion about EMF, and they didn’t just take that episode down. They removed all of my content.
Rogan has an exclusive contract with Spotify that grants him more freedom than most others, but I doubt he has completely free reign. That said, I’m glad he brought Kennedy on, and allowed him to talk uninterrupted.
I am an accomplished interdisciplinary scientist and physicist, and a former tenured Full Professor of physics and lead scientist, originally at the University of Ottawa.
I have written over 30 scientific reports relevant to COVID, starting April 18, 2020 for the Ontario Civil Liberties Association (ocla.ca/covid), and recently for a new non-profit corporation (correlation‑canada.org/research). Presently, all my work and interviews about COVID are documented on my website created to circumvent the barrage of censorship (denisrancourt.ca).
In addition to critical reviews of published science, the main data that my collaborators and I analyse is all‑cause mortality.
All-cause mortality by time (day, week, month, year, period), by jurisdiction (country, state, province, county), and by individual characteristics of the deceased (age, sex, race, living accomodations) is the most reliable data for detecting and epidemiologically characterizing events causing death, and for gauging the population-level impact of any surge or collapse in deaths from any cause.
Such data is not susceptible to reporting bias or to any bias in attributing causes of death. We have used it to detect and characterize seasonality, heat waves, earthquakes, economic collapses, wars, population aging, long-term societal development, and societal assaults such as those occurring in the COVID period, in many countries around the world, and over recent history, 1900-present.
Interestingly, none of the post-second-world-war Centers-for-Disease-Control-and-Prevention-promoted (CDC‑promoted) viral respiratory disease pandemics (1957-58, “H2N2”; 1968, “H3N2”; 2009, “H1N1 again”) can be detected in the all‑cause mortality of any country. Unlike all the other causes of death that are known to affect mortality, these so‑called pandemics did not cause any detectable increase in mortality, anywhere.
The large 1918 mortality event, which was recruited to be a textbook viral respiratory disease pandemic (“H1N1”), occurred prior to the inventions of antibiotics and the electron microscope, under horrific post-war public-sanitation and economic-stress conditions. The 1918 deaths have been proven by histopathology of preserved lung tissue to have been caused by bacterial pneumonia. This is shown in several independent and non-contested published studies.
My first report analysing all-cause mortality was published on June 2, 2020, at censorship-prone Research Gate, and was entitled “All-cause mortality during COVID-19 – No plague and a likely signature of mass homicide by government response”. It showed that hot spots of sudden surges in all‑cause mortality occurred only in specific locations in the Northern-hemisphere Western World, which were synchronous with the March 11, 2020 declaration of a pandemic. Such synchronicity is impossible within the presumed framework of a spreading viral respiratory disease, with or without airplanes, because the calculated time from seeding to mortality surge is highly dependent on local societal circumstances, by several months to years. I attributed the excess deaths to aggressive measures and hospital treatment protocols known to have been applied suddenly at that time in those localities.
The work was pursued in greater depth with collaborators for several years and continues. We have shown repeatedly that excess mortality most often refused to cross national borders and inter-state lines. The invisible virus targets the poor and disabled and carries a passport. It also never kills until governments impose socio-economic and care-structure transformations on vulnerable groups within the domestic population.
Here are my conclusions, from our detailed studies of all-cause mortality in the COVID period, in combination with socio-economic and vaccine-rollout data:
If there had been no pandemic propaganda or coercion, and governments and the medical establishment had simply gone on with business as usual, then there would not have been any excess mortality
There was no pandemic causing excess mortality
Measures caused excess mortality
COVID-19 vaccination caused excess mortality
Regarding the vaccines, we quantified many instances in which a rapid rollout of a dose in the imposed vaccine schedule was synchronous with an otherwise unexpected peak in all-cause mortality, at times in the seasonal cycle and of magnitudes that have not previously been seen in the historic record of mortality.
In this way, we showed that the vaccination campaign in India caused the deaths of 3.7 million fragile residents. In Western countries, we quantified the average all-ages rate of death to be 1 death for every 2000 injections, to increase exponentially with age (doubling every additional 5 years of age), and to be as large as 1 death for every 100 injections for those 80 years and older. We estimated that the vaccines had killed 13 million worldwide.
If one accepts my above-numbered conclusions, and the analyses that we have performed, then there are several implications about how one perceives reality regarding what actually did and did not occur.
First, whereas epidemics of fatal infections are very real in care homes, in hospitals, and with degenerate living conditions, the viral respiratory pandemic risk promoted by the USA‑led “pandemic response” industry is not a thing. It is most likely fabricated and maintained for ulterior motives, other than saving humanity.
Second, in addition to natural events (heat waves, earthquakes, extended large-scale droughts), significant events that negatively affect mortality are large assaults against domestic populations, affecting vulnerable residents, such as:
sudden devastating economic deterioration (the Great Depression, the dust bowl, the dissolution of the Soviet Union),
war (including social-class restructuring),
imperial or economic occupation and exploitation (including large-scale exploitative land use), and
the well-documented measures and destruction applied during the COVID period.
Otherwise, in a stable society, mortality is extremely robust and is not subject to large rapid changes. There is no empirical evidence that large changes in mortality can be induced by sudden appearances of new pathogens. In the contemporary era of the dominant human species, humanity is its worst enemy, not nature.
Third, coercive measures imposed to reduce the risk of transmission (such as distancing, direction arrows, lockdown, isolation, quarantine, Plexiglas barriers, face shields and face masks, elbow bumps, etc.) are palpably unscientific; and the underlying concern itself regarding “spread” was not ever warranted and is irrational, since there is no evidence in reliable mortality data that there ever was a particularly virulent pathogen.
In fact, the very notion of “spread” during the COVID period is rigorously disproved by the temporal and spatial variations of excess all-cause mortality, everywhere that it is sufficiently quantified, worldwide. For example, the presumed virus that killed 1.3 million poor and disabled residents of the USA did not cross the more-than-thousand-kilometer land border with Canada, despite continuous and intense economic exchanges. Likewise, the presumed virus that caused synchronous mortality hotspots in March-April-May 2020 (such as in New York, Madrid region, London, Stockholm, and northern Italy) did not spread beyond those hotspots.
Interestingly, in this regard, the historical seasonal variations (12 month period) in all-cause mortality, known for more than 100 years, are inverted in the northern and southern global hemispheres, and show no evidence of “spread” whatsoever. Instead, these patterns, in a given hemisphere, show synchronous increases and decreases of mortality across the entire hemisphere. Would the “spreading” causal agent(s) always take exactly 6 months to cross into the other hemisphere, where it again causes mortality changes that are synchronous across the hemisphere? Many epidemiologists have long-ago concluded that person-to-person “contact” spreading of respiratory diseases cannot explain and is disproved by the seasonal patterns of all-cause mortality. Why the CDC et al. are not systematically ridiculed in this regard is beyond this scientist’s comprehension.
Instead, outside of extremely poor living conditions, we should look to the body of work produced by Professor Sheldon Cohen and co‑authors (USA) who established that two dominant factors control whether intentionally challenged college students become infected and the severity of the respiratory illness when they are infected:
degree of experienced psychological stress
degree of social isolation
The negative impact of experienced psychological stress on the immune system is a large current and established area of scientific study, dutifully ignored by vaccine interests, and we now know that the said impact is dramatically larger in elderly individuals, where nutrition (gut biome ecology) is an important co-factor.
Of course, I do not mean that causal agents do not exist, such as bacteria, which can cause pneumonia; nor that there are not dangerous environmental concentrations of such causal agents in proximity to fragile individuals, such as in hospitals and on clinicians’ hands, notoriously.
Fourth, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, the debate about gain-of-function research and an escaped bioweapon is irrelevant.
I do not mean that the Department of Defence (DoD) does not fund gain-of-function and bioweapon research (abroad, in particular), I do not mean that there are not many US patents for genetically modified microbial organisms having potential military applications, and I do not mean that there have not previously been impactful escapes or releases of bioweapon vectors and pathogens. For example, the Lyme disease controversy in the USA may be an example of a bioweapon leak (see Kris Newby’s 2019 book “Bitten: The Secret History of Lyme Disease and Biological Weapons”).
Generally, for obvious reasons, any pathogen that is extremely virulent will not also be extremely contagious. There are billions of years of cumulative evolutionary pressures against the existence of any such pathogen, and that result will be deeply encoded into all lifeforms.
Furthermore, it would be suicidal for any regime to vehemently seek to create such a pathogen. Bioweapons are intended to be delivered to specific target areas, except in the science fiction wherein immunity from a bioweapon that is both extremely virulent and extremely contagious can be reliably delivered to one’s own population and soldiers.
In my view, if anything COVID is close to being a bioweapon, it is the military capacity to massively, and repeatedly, rollout individual injections, which are physical vectors for whichever substances the regime wishes to selectively inject into chosen populations, while imposing complete compliance down to one’s own body, under the cover of protecting public health.
This is the same regime that practices wars of complete nation destruction and societal annihilation, under the cover of spreading democracy and women’s rights. And I do not mean China.
Fifth, again, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, there was no need for any special treatment protocols, beyond the usual thoughtful, case-by-case, diagnostics followed by the clinician’s chosen best approach.
Instead, vicious new protocols killed patients in hotspots that applied those protocols in the first months of the declared pandemic.
This was followed in many states by imposed coercive societal measures, which were contrary to individual health: fear, panic, paranoia, induced psychological stress, social isolation, self-victimization, loss of work and volunteer activity, loss of social status, loss of employment, business bankruptcy, loss of usefulness, loss of caretakers, loss of venues and mobility, suppression of freedom of expression, etc.
Only the professional class did better, comfortably working from home, close to family, while being catered to by an army of specialised home-delivery services.
Unfortunately, the medical establishment did not limit itself to assaulting and isolating vulnerable patients in hospitals and care facilities. It also systematically withdrew normal care, and attacked physicians who refused to do so.
In virtually the entire Western World, antibiotic prescriptions were cut and maintained low by approximately 50% of the pre-COVID rates. This would have had devastating effects in the USA, in particular, where:
the CDC’s own statistics, based on death certificates, has approximately 50% of the million or so deaths associated with COVID having bacterial pneumonia as a listed comorbidity (there was a massive epidemic of bacterial pneumonia in the USA, which no one talked about)
the Southern poor states historically have much higher antibiotic prescription rates (this implies high susceptibility to bacterial pneumonia)
excess mortality during the COVID period is very strongly correlated (r = +0.86) — in fact proportional to — state-wise poverty
Sixth, since our conclusion is that there is no evidence that there was any particularly virulent pathogen causing excess mortality, there was no public-health reason to develop and deploy vaccines; not even if one accepted the tenuous proposition that any vaccine has ever been effective against a presumed viral respiratory disease.
Add to this that all vaccines are intrinsically dangerous and our above-described vaccine-dose fatality rate quantifications, and we must recognize that the vaccines contributed significantly to excess mortality everywhere that they were imposed.
In conclusion, the excess mortality was not caused by any particularly virulent new pathogen. COVID so-called response in-effect was a massive multi-pronged state and iatrogenic attack against populations, and against societal support structures, which caused all the excess mortality, in every jurisdiction.
It is only natural now to ask “what drove this?”, “who benefited?” and “which groups sustained permanent structural disadvantages?”
In my view, the COVID assault can only be understood in the symbiotic contexts of geopolitics and large-scale social-class transformations. Dominance and exploitation are the drivers. The failing USA-centered global hegemony and its machinations create dangerous conditions for virtually everyone.
“Gates’ actual goal in reaching the poor is to use them as guinea pigs in his experiments in culling the human race. It is also a virtue signal — a means of getting away with his brand of predatory philanthropy…”
…
“The lack of access to c-19 injections was not a tragedy, it was a fantastically lucky break for the world’s poor. Thank heaven the world’s poor were not served equitably with the toxic jabs.
“In the rich countries whose people did get them, millions have been injured and killed. It is hard to imagine that an on-the-ground practicing doctor could miss the non-evidence of a pandemic, and the dangers of giving totally new medical products from felony-convicted drug companies to everyone in the world, without delay.”
Until we have vaccines & medicines, mask wearing is one of the best tools we have to stop the spread of COVID-19. #WearAMask and upload a photo to social media, then ask your friends to do the same 😷 🤳 #WorldMaskWeekpic.twitter.com/ypA07gNI7J
A good job, wealth, honors, and prestige are hard to come by if you’re outside the establishment.
At the time of his death almost a year and a half ago, Dr. Paul Farmer had all the honors —co-founder of Partners In Health, University Professor at Harvard, a department chief at Boston’s Brigham and Women’s Hospital, UN envoy, recipient of prestigious awards, subject of the New York Times bestseller Mountains Beyond Mountains — but his reputation was built on not being part of the establishment. Perhaps his biggest honor was that he was allowed to have it both ways.
He was praised for setting up clinics and living among the poor in Haiti and Rwanda, yet he was well connected with a very corrupt global health establishment — the WHO, the UN, the Bill and Melinda Gates Foundation, USAID, and the Clinton Global Initiative — and no one mentioned a conflict.
In August 2021 Farmer co-signed a letter to President Biden saying,
“The time is now for ambitious leadership to vaccinate the world. The need to be on a “wartime footing” to secure the world against this pandemic viral threat is paramount. Any global COVID vaccination program must be structured to address multiple interlinked priorities. First, the manufacturing capacity of mRNA vaccines in the US must be rapidly scaled up to reach approximately 4 billion people by the end of 2021 . . . . “
This is the same message Bill Gates had for us at about the same time when he informed us that “we need to vaccinate everyone on the planet.”
When it came to covid, Farmer’s message was not that untested mRNA vaccines might possibly be unsafe but that a special effort should be made to get them to the poor right away.
“By massively boosting vaccine production and removing barriers to an equitable rollout,” he said, “we can help vaccinate the world to the benefit of all.” ‘Equity’ was also the message put out by Bill Gates almost every time he gave an interview. “The lack of equitable access to COVID-19 vaccines is a public health tragedy,” Gates said.
Gates’ actual goal in reaching the poor is to use them as guinea pigs in his experiments in culling the human race. It is also a virtue signal — a means of getting away with his brand of predatory philanthropy. And, no matter if a country is poor, Gates looks to make a profit on his investments — something the devil apparently allows.
The Clinton Foundation used the poor in a similar way in Haiti, using the plight of Haiti’s devastating 2010 earthquake to raise $9 billion in charitable donations, only 10% of which actually went to Haitian organizations. Bill Clinton was envoy to the UN in this scam and Paul Farmer was directly involved as UN special envoy under Clinton.
So, Farmer was a front man for Clinton and accepted money (and pandemic talking points) from Gates. One wonders why.
One might now also question if Dr. Farmer’s bringing Anthony Fauci-underwritten HIV/AIDS drugs to Haiti in the 1990s was more of a benefit to Haitians or to the pharmaceutical companies who sold them for up to $16,000 per patient. If it hadn’t been for the gross malfeasance revealed in the covid era, we might never have asked.
The lack of access to c-19 injections was not a tragedy, it was a fantastically lucky break for the world’s poor. Thank heaven the world’s poor were not served equitably with the toxic jabs.
In the rich countries whose people did get them, millions have been injured and killed. It is hard to imagine that an on-the-ground practicing doctor could miss the non-evidence of a pandemic, and the dangers of giving totally new medical products from felony-convicted drug companies to everyone in the world, without delay.
Farmer rightly gained his reputation showing the connections between poverty and disease, but he made a terrible mistake getting caught up in the designs of predatory pharmaceutical companies and profit-making philanthropists.
Considering the small number of wealthy psychopaths who planned and conducted the covid operation, the war on the poor includes just about everyone — not just people in remote villages in Haiti — and doctors of medicine were its main lieutenants.
This great humanitarian seems to have missed the fact that the fake pandemic was a broad-daylight attack in an overall war on humanity.
In February 2022, Partners in Health announced that Paul Farmer died of “an acute cardiac event while he was sleeping.” He was 62. He is thus among the thousands who “died suddenly” — the meme for healthy people who quite likely died from covid “vaccination,” though we’re never told.
The kindest interpretation is that, unlike Gates, Paul Farmer was not among the cognoscenti, and that he unwittingly took the same poison he was pushing for all.
The moral of the story: you may gain fame and fortune, but end up being just a dupe. What a terrific waste for a man who apparently spent his life caring for the poor.
Let the well-off and well-connected take note: no matter the fame and status the establishment gives you, you can be used and discarded just like everybody else. There are other goals more worth achieving.
“The point is, separately, in different venues, the Breggins and Jane Ruby are individuals who rose to the challenge to try to inform a brutalized public about what turns out to have been a war: a war of fear, fraud and bioweaponry waged against us by own government. Their contributions were, are and will continue to be vitally important to the flow of essential and also life-saving information.
Ask yourself: Why would anyone want to deflect these valuable contributors from their important vocations?…”
Do you remember how hard it was to get good information, especially in 2020, back at the Beginning of the End? It is hard still, but it was much worse before so many of us had delved into the sciences with a doggedness we never mustered in high school; before we had learned to see into the geysers of government and media disinformation about the “plandemic,” the “scamdemic,” the garbage-demic, to take apart and stomp on all of the Big Lies we were and are still beset by. And that was even before the government’s biochemical attack on the world via “mRNA vaccine” had begun.
The totalitarian-style censorship and disinformation which government, media and social media imposed upon us were (are) catastrophic and also fatal in all too many cases. That’s why when we learn, through arduous court-ordered FOIA research or congressional hearings or secret interviews or confessions … or autopsies that we were right to doubt and disbelieve and not comply, there are dead bodies, broken homes, ruined lives and a shattered future to embitter our vindication. To intensify our rage. That’s why Dr. Robert Malone’s openly stated goal in 2023 to use the courts to have a “chilling effect’ on debate in the public square, which he’s trying to rebrand as “defamation,” is so disturbing, bizarre and fraught with peril.
Malone’s interlocuters-turned-“defendants” are Dr. Peter Breggin, Ginger R. Breggin and Dr. Jane Ruby — outlandish words to write about such worthies. I don’t recall exactly when in the dark of lockdown I first came upon them. I do remember Dr. Jane’s exciting reports on the then-new Stew Peters Show, her tenacity, her blinking neon commitment to finding the truth, were an immediate godsend. At some point, too, I matched with the Breggins, Dr. Peter Breggin, “Conscience of Psychiatry,” and his wife and co-author Ginger Breggin, benefiting enormously from their warm and civilized discourse, which included (bonus) two interviews with me about American Betrayal. I was delighted to learn my book had inspired the Breggins to dig into the research that became their 2021 success, COVID 19 and the Global Predators: We Are the Prey.
The point is, separately, in different venues, the Breggins and Jane Ruby are individuals who rose to the challenge to try to inform a brutalized public about what turns out to have been a war: a war of fear, fraud and bioweaponry waged against us by own government. Their contributions were, are and will continue to be vitally important to the flow of essential and also life-saving information.
Ask yourself: Why would anyone want to deflect these valuable contributors from their important vocations? So what if they said something, many things, with which you disagree, even violently disagree? So what if they reject and even rebut your theories? So what if they engage you in a veritable “war of words”? To quote vintage Michelle Malkin, “Boo-the-heck-hoo.” Argue. Gnash your teeth. Write a rebuttal. Quote Voltaire. Exult in the First Amendment. But this — resorting to the punitive enforcement mechanism of a defamation lawsuit — is not right. Asking for $25 million in damages is an outrage. Such aggressive lawfare is akin to dropping a cluster bomb. The landscape that was is no more.
As many know, I am referring to the tantrum-esque defamation lawsuit D. Robert Malone has brought against the Breggins and Jane Ruby. I wrote a book about 15 years ago called The Death of the Grown-Up, which employs the metaphor to explore chaos and decline in our time. However, the absence of bona fide adults is not just a metaphorical problem. We could really use some grown-ups here. To wit:
If there happens to be an adult in the vicinity of Dr. Malone’s circle, please, could you instruct the “inventor of the mRNA vaccine” to pack his marbles and come home from the playground? Given the catastrophic impact of his precious invention as deployed by the governments of the world, he’s surely the last man on earth who should be trying to exert a “chilling effect” on anything — and especially not on the speech of doctors and scientists. People are dying from these shots all around. We need help. Debate. Breakthroughs. Not silence, not fear of being dragged to court for speaking up. Sticks and stones, anyone? Like Rick said in Casablanca, the problems of three (or four) little people don’t amount to a hill of beans in this crazy world; however, if Malone were to win this lawsuit, American jurisprudence would feature a jihad-style trip-wire on public debate by public figures on public issues. Then again, if the First Amendment and American tradition count for anything at all anymore, the court will rule decisively against Malone. One man’s “defamation” will be everyone else’s free speech.
But at what cost? Stories of case-related censorship and acrimony buzz around the erstwhile medical freedom movement. Wouldn’t it be a better use of everyone’s time to try to figure out how to heal mRNA-injected humanity?
It was about half-way through 2021 when Dr. Malone showed his face in public discourse. Remember the weird thrill that rippled through the battered band of shot-resisters? Look: the mRNA inventor was throwing shade, some, anyway, on the mass injection program at that time in full-throttle- enforcement. Yes, to be sure, Xyklon B isn’t for everybody….How exciting? I’m not sure what psychological buttons Malone’s arrival on the scene pushed; as I think back on it now, such enthusiasm doesn’t make a lot of sense. After all, he didn’t come forward expressing remorse, as lots of great inventors have done before him, rueing their sometimes literally earth-shaking inventions, from the atom bomb and the Kalashnikov, to the office cubicle and the labradoodle. Notably, “The History of mRNA Vaccines” still unfolds under a spray of lovely pink blossoms here on Malone’s website.
Nor did he arrive on the medical freedom scene waving an antidote to mRNA technology, which, they say, has now been “delivered” into 70 percent of humanity and linked to a scale of death and injury that is unimaginable.
Kristen Napolillo asked Malone on Twitter: “What are you doing to find a way to blunt the effects of your invention?”
One thing about quoting Dr. Robert Malone: There is no need to underscore or add anything.
On June 8, 2023, Dr. Malone set forth his legal thinking on Substack:
My criteria for taking legal action has been whether or not someone seems to be doing significant reputational damage, while also factoring in the quirky nature of various clauses in defamation law.
It’s almost touching, isn’t it, to see someone who “invented the mRNA vaccine” fretting about “reputational damage”?
In some cases I have proceeded to delivering a cease and desist and that was enough. Dr. Richard Fleming was one such case. I sent him a letter, and he stopped. Seems rational enough. Thank you, Richard (and I seriously mean that).
Again, no comment necessary — but I do want to write that again: Thank you, Richard (and I seriously mean that).
He continues:
Turns out that response is the exception rather than the rule. Others double down, go public, get even nastier and more personally vindictive.
No! Can you beat that? Malone sends out a “cease and desist” and some people … refuse?
So then you have the same dilemma. Act on it or not. Fish or cut bait. First stop is to ask a mutual colleague to intervene. In almost all cases they refused. So you then pay the lawyer to prepare and file the suit. And in some cases the accused gets even nastier, and seeks to cause yet more pain.
It’s a marvel but he soldiers on:
There are all of the armchair quarterbacks, some of who are employers, friends or associates with the ones doing the harassment and defamation. “Why are you suing the ____ (fill in the blank)!!??!!” “You just want to destroy the medical freedom movement!” (whatever that is). “You are just doing it for money!” (what a horrible business plan that would be, given the paltry odds of winning a defamation lawsuit).
“Fill in the blank”? Somehow, I feel bidden to provide photos of the people, the experts, including an eminent doctor, the writers and commentators, the human beings whom Dr. Malone has just turned into a blank.
Now, let him rip.
No, I am suing because I am having something taken from me, and it is both wrong and illegal. My reputation, my peace of mind, and that of those close to me. Cyberstalking, cyberbullying, malicious defamation. These things are wrong. They are not what civilized, mentally healthy people do to each other. And they often seem to involve some odd perverse obsession.
But it is also true that hate and defamation is a very good business model and a great way to build up a follower base. People are building their audiences by employing this strategy based on tall tales, lies, name calling and hate. But maybe, just maybe, if I win a case, this will become a disincentive for those prone to this sort of behavior in the future, directed towards me or to others.
And then there are the ones that are shunning me because I am (legally) fighting back against those that are doing this to Jill and I [sic]. That part is a real mind-bender for me. Somehow fighting back against those who are aggressively cyberstalking and defaming me on a daily basis makes me the bad guy. Now if that is not pretzel logic, I do not know what is.
I suppose, in an intellectual sense, it is a fascinating question to ponder – what makes these people behave in this way? Why do haters hate? Why do others support them? I do not have an answer, only informed speculation. Personally, I think it somehow relates to the mental state of other types of stalkers, such as the ones that shot President Regan [sic] and John Lennon. And it clearly relates to envy, jealousy, and greed. Spreading hate can be quite lucrative in the age of the internet, where attention seeking behavior can be monetized. So there is that. (Emphasis added.)
I have no quip to make when the rhetoric is so troubling. Consider seriously that Dr. Malone has first blanked the names of the Breggins and Jane Ruby, and then created an escalating series of fantastical enemies, from imaginary cyberstalkers, cyberbullies, malicious defamers, to not civilized, not mentally healthy people, to haters with a mentality “somehow related” to that of notorious violent criminals: John Hinkley and Mark David Chapman, the former, the attempted-assassin who wounded Ronald Reagan and paralyzed James Brady; the latter, the assassin of John Lennon.
Still, no one around him has put a hand on his shoulder and said, Enough.
—
Let’s pick up on p. 13 of a recent Motion to Dismiss by Dr. Peter Breggin and Ginger R. Breggin.
The Breggin Motion is discussing the thirteenth bulleted item in Malone’s Complaint. This Item 13 contains four separate allegations of defamation purported to be found in an online interview of Dr. Breggin by Pete Santilli.
From the Breggins’ Motion to Dismiss:
Malone alleges that Breggins stated: Dr. Malone is part of the “Deep State” oppressors. Dr. Malone’s concept of mass formation psychosis is calculated to protect the “mass murderers of COVID-19.” Dr. Malone is a Hitler apologist and “excuser.” “Malone wake up to history.”
The Breggins:
When examining the entire interview of Dr. Breggin on this show, nowhere in the show can it be found that Dr. Breggin made the statement that Malone atrributes to him that he is a part of the “Deep State oppressors.”
Malone’s allegations that Breggin stated that “Dr. Malone’s concept of mass formation psychosis is calculated to protect the `mass murderers of COVID-19′ is actually Breggin talking about Dr. Desmet,not Dr. Malone.
And lastly, nowhere in this recorded interview (or anywhere else for that matter) can it be found where Dr. Breggin ever stated that Dr. Malone is “a Hitler apologist and excuser.”
First of all, may I say (shout): Who cares! Say what you will! These are public commentators debating the onset of totalitarianism in our time. Hitler, Stalin, Mao are the totalitarian all-stars, at least up to now, and are gonna come up. Boo-the-heck-hoo. Still, there is a crucially important legal (and moral) point here: The Breggins’ brief states that certain of these quotations are not to be found on video, or anywhere else. If this is true — and I cannot find them, either — the Malone Complaint includes false allegations. Put that in your syringe and shoot it. What will the judge say about that?
And now this:
Moreover, the only quote that can be found to be semi-accurate, “Desmet, Malone, wake up to history,” is a pejorative at best, and an admonition even, but it is not defamatory.
No, it is not. But ponder the legal mind that sees fit to include such an innocuous comment, with its pleasantly archaic rhetorical flourish, into a defamation brief. Ponder the scientific mind that hopes for a “chilling effect.” Frankly, if Dr. Robert Malone is so darn worried about reputational damage, he should drop this stupid lawsuit ASAP and wake up. Wake up to free speech.
According to the science we learn in our indoctrination center called the educational system, leukemia or blood cancer is a disease in which an overproduction of white blood cells is created. Many of those cells are damaged or not developed enough, and this is caused by the damaged bone marrow which produces them.
We are educated/indoctrinated to believe that white blood cells are our immune system, created to protect us from the pathogen that has attacked our body. So, when the pathogen occurs, the white blood cell blood count increases. As the pathogen gets gobbled up by the white blood cells/macrophage, (the process science has named autophagy), the threat no longer exists, and the number of white blood cells reduces to the ”normal” levels.
When the blood count of white blood cells is high and no pathogen is detected, and the situation persists without the white blood cell count dropping to the normal level, this is when the body is declared by our experts to be diseased with leukemia.
Is this what really happens?
We are “educated” to recognize leukemia through the symptoms that accompany it. Those symptoms are; fever or chills, persistent fatigue, frequent infections, losing weight, swollen lymph nodes, easy bleeding or bruising, tiny red spots in the skin, excessive sweating, and bone pain and tenderness.
In which way an increased white blood cell count causes such symptoms? This makes no sense.
When we look at those symptoms, everyone who is familiar with my work immediately comes to the conclusion that those are symptoms of toxic blood and a toxic body in general.
Since white blood cells are not what we are told, a defense mechanism created to attack the intruder/pathogen, instead, they are a garbage disposal system, as the level of the garbage increases in the blood, the body increases the production of white blood cells to dispose of this garbage.
This means that the body is functioning correctly in the given circumstance. Since doctors cannot identify any pathogen and the blood level of white blood cells remains high, they blame the bone, thymus, and lymph nodes for overproducing white blood cells for no apparent reason, and through the implementation of toxic chemicals, they attack those organs to suppress white blood cell production.
Through their action, doctors increase the blood´s toxicity which stimulates the body to further increase the white blood cell count, and the battle with the “disease” becomes eventually lost because the overly toxic patient dies.
Doctors proudly declare that they have extended the patient’s life/suffering for as long as they could and without their intervention, the patient would have died sooner.
Well, it is obvious that doctors are incompetent and they are the reason why their patient has died.
What is the cause of increased white blood cell count and why it remains high?
The symptoms reveal that the blood is toxic. Since the white blood cell count has increased, this means that the body senses a toxin that can be eliminated by disposing of it through white blood cells (most likely an organic compound).
The bone marrow thymus and lymph nodes start to produce white blood cells, but they cannot recognize the “garbage” because it is not labeled. Since the toxic level is not dropping, the body continues producing white blood cells and at the same time, some of them are expiring and undergo autophagy and appear damaged or undeveloped.
The reason why the poison is not labeled is the lack of GcMAF because of the incorrect genetic expression caused by eating starches/glucose. The cells are forced to produce nagalase to be able to hydrolyze glucose and use it as fuel. This prevents them to produce GcMAF since the same pair of genes is responsible for the signaling to the cell what the cell should manufacture in this given environment.
This is another example of how eating starches contributes to a diseased state of our body.
Since those people that follow the SHP are forbidden to consume starches, their cells start to produce GcMAF marker, the toxins become marked and eliminated through macrophage, and as the blood toxic level drops, the production of the white blood cells stops and leukemia miraculously disappears.
I have noticed that green tea has toxins that stimulate white cell production, and preservatives of meat in canned food and sausages do the same. This is why we see leukemia often in people that consume large quantities of green tea and children that eat colorful cereals, frankfurters or ham, or other types of salami.
Also, cats fed with can foods and dry food loaded with carbohydrates will develop leukemia.
They all heal when their food is corrected.
It was brought to my attention that by July people will be able to start scheduling their med bed appointments. They will be free so if someone wants to sell you an appointment, this is a fraudster, do not fall for it.
What makes us sick and what doesn’t make us sick? To answer that question, our first step is to understand how we as human beings come to know something. There are two basic ways. First, we can have a sensory experience of something that tells us that this thing is real. We might study a particular tree in its habitat and see whether it produces fruit or observe what type of birds it attracts. Or we could study frogs and learn about where they live, what they eat and their interaction with the wider ecosystem.
But there are also things for which no sensory experience is possible, perhaps because they’re too small to see. That doesn’t mean they don’t exist, but in this situation, we have to do something called “science”— meaning looking for and establishing the existence of things that we don’t experience directly through our senses.
When we do science—and this is important—we have to make sure, during every single step of the process, that we haven’t altered the nature of the thing we’re studying, or even brought that thing into existence through our intervention. Analytical chemists understand this; they tell me that in their line of work (which amounts to finding things they cannot experience through their senses), they have to validate that their procedures—taking something out of its habitat and shining a light on it or adding chemicals—didn’t in fact actually create what they ended up with. Otherwise, they can’t know whether or not the thing actually exists. Stated another way, when researchers test cause and effect by changing an independent variable to see whether it has an effect on a dependent variable, they have to make sure, every step of the way, that they are measuring just the relationship between those two variables. This is the essence of the “scientific method.” When we don’t follow the true scientific method, we can end up in a world of illusions, delusions and make-believe.
What if there is no possible way to do an experiment? In that case, you are relying on something that is more like faith, and you should acknowledge that. You should state, “This is what I believe to be true and I’m going to dedicate myself to figuring out whether I can validate that it actually is true.” In other words, the goal is to go from “I believe” to “I know.”
How Do Viruses Make You Ill
AWOL Viruses
What is the agreed-on definition of a virus? A virus is described as a disease-causing microbe with a piece of either DNA or RNA in the middle surrounded by a protein coat, and is said to be self-replicating in a host. It gets into the host’s cells, makes more of itself and then causes disease by bursting open the cells.
According to the definition, the expected natural habitat of this organism is the lungs, the blood, the lymph nodes, the urine, the cerebrospinal fluid and so on. However—and there is no scientific disagreement on this important point whatsoever—there is not a single study in the published medical literature for the past one hundred years that reports finding such a particle in any biological fluid of any plant, animal or human being. This is true whether you’re talking about the fluid from someone’s “herpes” lesion, or the lungs of someone with “Covid-19,” or the snot from a person with “measles,” or the blood of someone with “Ebola” or the lymph nodes of a person with “AIDS.” There is not one published study in the scientific/medical literature showing that someone found such a particle in any one of those bodily fluids—and nobody disagrees with that! This should make you suspicious. As Mark Twain once stated, “It ain’t what you don’t know that gets you into trouble. It’s what you know for sure that just ain’t so.”
WC Fields said, “If you can’t dazzle them with brilliance, baffle them with bullshit,” and I think he was talking about virology. Consider this: we now have over two hundred ten responses from various health departments around the world to the question, “Do you have any published study that shows that you directly isolated SARS-CoV-2 from any human being on the planet?”1 (SARS-CoV-2 is the alleged virus, and Covid-19 is the disease alleged to be caused by the virus.) They all say the same thing: “We have no record of SARS-CoV-2 having been purified.” They’ve never found it, nor have they found any of the other pathogenic viruses. (We also have around forty or fifty similar responses pertaining to Ebola, Zika, HIV, measles and the like.)
Colleagues of mine have asked the authors of four of the most important papers written about SARS-CoV-2, some of which bafflingly have the word “isolation” in the title, “Did you isolate this virus in your study?” Their answer was not only “No” but also, “We didn’t even try to find it in any biological fluid of any person who was sick.” In the early days of virology, scientists did look, but they were never able to find such a particle using the very tool—the electron microscope—that should have allowed them to find it. After twenty years, they abandoned ship and said, “There’s nothing to this theory.” But then later, it got resurrected.
What Are You Sick With
A Belief System
Note that virology has methods and techniques to truly isolate a virus.2 Using ultracentrifugation and something called a “sucrose density gradient,” virologists can separate a fluid sample into bands by molecular weight. Ultracentrifugation will spin viruses out into their own band, which virologists can then extract with a pipette and check for purity.
But they don’t use these techniques! Instead, I’ll give an example of what a virologist says if you ask, “Why do you think this virus exists? If you can’t find it, why do you think it’s in the lungs?” A virologist told me that someone would have to be “incredibly ill and shedding extremely large amounts of virus, and the fluid from their lungs would have to have a large amount of virus—and even then, it wouldn’t be possible.” In other words, “There’s not enough virus to find.”
Think about this. Your lungs are said to be the perfect culture medium—at the ideal temperature (thirty-seven degrees Celsius) for viruses to reproduce—and the lung environment is, therefore, supposedly teeming with viruses. After they reproduce, viruses reportedly kill millions and billions of cells, and that, we are told, is how they cause disease. Supposedly, there are twenty million copies of a virus in a single sneeze. But the virologist’s answer is, “There’s not enough to see.”
Remember, a virus is described as incredibly tiny—something like one-thousandth of a pinhead or less—which means that when viruses explode, they are exploding perhaps one hundredth of a pinhead of your lungs. Yet you could take out even a baseball-sized piece of your lungs, and while that might be called “having a bad day,” you won’t die. The body also isn’t crazy enough to make an abnormal and excessive immune response to losing less than a pinhead size of the lungs. So, it is logical to ask, “If the virus is exploding the cells in a portion of your lungs that is the equivalent of less than a pinhead, how is it causing disease?”
There is a second reason virologists give for not using the tools at their disposal to isolate a virus. They say that the virus is an intracellular parasite organism, meaning it is only inside the cell and doesn’t go outside the cell. But if that is the case, how does it get to the next person? This starts to strain credulity. Here’s how that nutty conversation might go:
Q: “Why can’t you catch the virus when it goes from one person to another person?”
A: “Well, it’s not there for more than about six hours. We don’t have enough money to pay someone to look every six hours to find the organism in the snot.”
We asked one eminent virologist, “If you put ten thousand people together and collected all their sputum, would that be enough to find the virus?” His answer: “No, that’s not enough.”
Poisoning, Not Purification
There are something like ten thousand published papers that refer to the “isolation” of such-and-such a virus. Virologists will show you the title of these papers and say, “See, how can you say this isn’t true?” But since they aren’t using the proper steps, you have to know what they did instead. And you have to ask, did they rigorously validate every step of their process?
In 1954, a researcher named John Franklin Enders established the procedures that rejuvenated the then-languishing field of virology.3 Here are Enders’ basic steps:
Virologists take snot from somebody alleged to have a certain disease (such as measles or Covid-19).
Sometimes they centrifuge (not ultracentrifuge) or filter the mixture to get rid of cells, fungi and debris. That has become a sticking point because some people call this “purification.” However, purifying the snot a little is not equivalent to purifying out a virus.
Next, they put the snot in a cell culture of green monkey kidney cells—cells that happen to be highly inbred and tend to break down easily.
Then they mix in antibiotics—and specifically antibiotics that are kidney-toxic (gentamicin and amphotericin)—and they take away the cell culture medium’s nutrients. (This is the equivalent of being forced onto a standard American diet after thriving on a Wise Traditions diet.)
Next, they mix in fetal bovine serum, a product sucked out of the heart of a newborn calf.
Maintaining the cell culture at a steady temperature, they then watch what happens. In about five days, the cells break down— which is called a cytopathic effect (CPE)—and they call the CPE the “proof” that the virus exists and causes damage.
Understand that virologists consider this process—which inevitably generates cell breakdown—not “a” proof but “the” proof for the existence of all pathogenic viruses. You might reasonably ask, “How do you know the CPE is not due to starving the cells, or poisoning them with gentamicin and amphotericin, or using fetal bovine serum, or because of some other toxin in the sick person’s snot?” Virologists’ answer is that they do a “mock infection” as a control. However, if you go to the hundreds of papers I and my colleagues have read over the past two years, you will not find even one actual mock infection. In fact, it can’t be done because the independent variable would necessarily need to be the very virus that they have not isolated. Often, the study authors don’t even provide details, and if you try to obtain more information, you invariably learn that they did not conduct a properly controlled experiment.
Interestingly, Enders’ procedures are also how pharmaceutical companies make viral vaccines.4 For example, they take someone with measles and put their unpurified snot into a monkey kidney cell culture, add fetal bovine serum, gentamicin, and amphotericin, and then when the cells break down, they call that “isolation” of the measles virus. They put that goop into a vial—and that is called a “live” virus vaccine. They can also cycle the goop over and over in huge vats, removing some of the proteins, and that is an “attenuated” viral vaccine. But at no point did they ever demonstrate there is a virus in there. With mRNA and newer technologies, they are just putting different stuff—known and unknown—in their vaccines. In short, vaccines are biotoxins, and they make people sick. How could biotoxins possibly prevent people from getting sick?
The Lanka Experiments
There is one scientist, Stefan Lanka, who contracted with an independent professional lab to try to answer the question of whether the culturing process itself, rather than a pathogenic virus, might be causing the CPE.
The lab conducted four experiments. In the first, they cultured normal cells with a normal nutrient medium, adding only a small amount of antibiotics—and no snot from a sick person. Five days later, the cell growth was perfectly normal. The second experiment was the same as the first, but with the addition of 10 percent fetal bovine serum. Again, five days later there was no cell breakdown.
The third experiment replicated Enders’ procedures, lowering the percentage of fetal bovine serum from 10 percent to 1 percent (that is, starving the cells) and tripling the amount of antibiotics. On day five, the characteristic CPE that “proves” the existence and pathogenicity of a virus was evident—except that Lanka had not added any fluid from a sick person or anything else that could have had a virus in it.
The fourth experiment repeated the third but with the addition of RNA from yeast. It so happens that monkey kidney cells don’t like yeast any more than they like kidney-toxic antibiotics. Unsurprisingly, the fourth experiment produced the same CPE result—clearly showing that the CPE is the result of the culturing technique rather than any virus.
After they “prove” the existence of a virus using their cell culturing process, virologists “find” the genome of the virus using fragments of the RNA in the broken-down cell culture to create the assembled genome of the alleged virus. This is called “sequencing.” What is important to understand is that this process generates a genome that is purely theoretical (“in silico”). As I explain in my booklet Breaking the Spell:
“This genome never exists in any person, and it never exists intact even in the culture results; it exists only inside the computer, based on an alignment process that arranges these short pieces [of RNA] into an entire ‘genome.’”5
In the case of SARS-CoV-2, sequencing software generated anywhere from three hundred forty-two thousand to one million different possibilities of how to arrange the fragments. A small group of scientists then decided which arrangement they liked—by “consensus”—and then, for every subsequent analysis, they put that first consensus-derived genome in and told the computer to make another one along the same lines. When they turn out a sequence that is a bit different from the original consensus-derived “genome,” that’s called a “variant.”
Note that all of this applies both to so-called “natural” viruses and to so-called lab-engineered “gain-of-function” viruses—which no more exist than any “natural” virus exists. So, here you have biologists in their hazmat suits, protecting themselves against a genome from a virus that exists only in a computer.
As for the PCR test, the whole premise of the test is also nonsense. You cannot say that a PCR sequence came from a thing you have not isolated. It makes no sense to even talk about “false-positives,” because the results are just plain false.
Identical Pictures, Delusional Thoughts
At some point, people say to me, “But Tom, we’ve seen electron microscope pictures of SARS-CoV-2,” complete with “spikes” and something that looks like a “corona”! However, I have a picture from a kidney biopsy produced before the year 2000 (when there was no possibility that it was SARS-CoV-2) that looks just the same. In fact, I have eleven electron microscope pictures—labeled as kidney biopsies, lung biopsies or SARS-CoV-2—and there is no way to tell the difference between them. They are morphologically indistinguishable—they all look the same. In fact, the CDC has known since the 1970s that electron microscopy cannot tell the difference between a kidney biopsy, lung cancer, cellular debris, SARS-CoV-2 or any so-called pathogenic virus; it simply is not possible.
The cellular debris, by the way, comes from poisoning—whether from putting yeast, antibiotics or fetal bovine serum on a culture, or from EMFs, or from not eating a Wise Traditions diet. It can even be from “wonky” or delusional thinking. For example, I knew an anthroposophical doctor who spent his career giving AIDS drugs to so-called “HIV-positive” people because he believed in the delusional germ theory, and then, because of this belief, he took four Covid shots. Five days after the fourth one, he was dead. You could say he died from the shots, but I say he died because he spent his entire life believing in something that is completely make-believe.
An Even Bigger Delusion
It turns out that the delusion is even bigger than viruses—we didn’t just make up viruses, we made up diseases. Consider what happens if you get a splinter in your finger. In medical school, I was taught that pus is a sign of infection, but actually, the pus is the body’s therapeutic response to the splinter; if you suppress the pus, you will never get the splinter out. We need to stop thinking of the body’s responses as “diseases”; they are the wisdom of the body coming through.
We can look at many other conditions—and the body’s wise therapies—in the same way. For example, if you put toxic junk in your lungs, the body will cough it up because it wants to get rid of dead, dying and poisoned tissue. In Wuhan, which has some of the worst air pollution in the world, bronchitis is the therapy for breathing air. It’s not a disease.
Or consider chickenpox, which might have something to do with malnutrition or a collagen deficiency or a toxic environment—but is also a normal maturation and cleansing process. If you come along and poison a child with a chickenpox vaccine so they cannot go through that cleansing process, they will instead have a life of asthma, allergies, eczema and all these other made-up terms that really mean you stopped the process of healing. It may look like you lessened the incidence of “chickenpox,” but by interfering with the cleansing process you have increased lots of chronic things, which never go away.
There are no vaccines that are exceptions to that rule—they all poison you, and you end up worse. When you cannot go through the normal maturation and healing steps, you eventually may end up with cancer. You’re depositing one poison after another throughout your life, and now you’ve got a garbage can of poisons otherwise known as a “tumor.” What would you do if you kept being poisoned over and over, and someone prevented you from getting the poisons out? It’s very simple: you would buy a garbage can and put the poison in there. But what happens if you keep putting in garbage, and it starts piling up in your basement, garage, kitchen and bedroom until you can’t live? That’s called “metastasis,” and then you die.
What Are We Made Of?
To examine more deeply the question of what makes us sick, let’s consider what we’re made of. To start on safe ground, let’s accept that we’re made of a head, ears, eyes, mouth, chest, arms, fingers, legs, toes and a bunch of other things. Inside, we also have things like a heart, bones, blood vessels, nerves, a liver, kidneys and other things. As far as I can tell, older healing traditions like Chinese and Ayurvedic medicine also believe there is a heart and liver and spleen and all the rest of it. In fact, not only do they believe it, they put huge stock in the energy flow through those organs.
Now remember, there are two ways of knowing. In the first instance, you can observe, but if you can’t observe, you have to do science—and you have to be sure that any science you do isn’t affecting what you’re seeing. And if it is, you have to control for that.
We’re told that hepatocytes are the main functional cells of the liver, but we might ask, “How do we know that?” How many of us have actually seen hepatocytes in the liver of an intact living organism? Nobody. That may not mean they’re not there, but it means we’ve got a question that requires further experimentation. We can take someone and anesthetize them (or at least some part of them), and stick a needle in, and suck out a piece of the liver, and stain it with toxic chemicals, and shine a high-powered light on it, and then say that what we see are the hepatocytes.
But how do we know that the process of anesthetizing (that is, poisoning) the person, removing the sample from a living organism and putting chemical stains on it didn’t create the structures we’re seeing?
For example, we know that bacteria, when stressed, will create a storage form called bacteriophages, and the same is true for other organisms like fungus spores. How do we know that stressing the liver by removing it from the living organism that nourishes it didn’t create the appearance of the liver cells? I’m not necessarily saying that this proves there are no liver cells, but I’m saying you need to ask the question if you want to do real science.
My thinking on these matters owes a lot to thinkers like the British biologist Harold Hillman, who spent fifty years and thousands of pages asking these kinds of questions.6 If you really want to understand biology, read Hillman. Another influence is Gilbert Ling, a brilliant Chinese-born American scientist who challenged the accepted view of the cell.7
Let’s remember that in addition to sensory observations and science, you may get to a point where you simply can’t know something. Going back to virology, if you can’t take the virus out of the sample that you inoculate, the best you might be able to say is, “We have no actual evidence that the virus exists. It doesn’t mean it doesn’t, but we have no evidence.” How different would the world be if, in March 2020, they had announced: “We did some experiments, and we have some idea there might be a virus, but we can’t really prove it, and all the experiments have shown it’s not really there—but we think we should lock you down and make you wear a mask and starve you anyway.” Of course, they don’t say it like that. My point is that it may not be possible to prove the existence of those liver cells—or any cells.
What is also interesting is that of the approximately one hundred eighty-four different tissue types, we know that forty-four don’t have any cells. Examples are the crystalline lens of the eye, and the bursae—sacs of fluid (colorfully described as “miniature water balloons”) that facilitate the frictionless movement of the joints.8 The absence of cells makes sense because this organized water tissue is much stronger and more coherent than if it were broken up into little cells.
Historically, what did Chinese and Ayurvedic medicine have to say about cells? Nothing. There is no mention of cells in either of those traditions. By the way, they never mentioned contagion or germ theory either. It was the German physician Rudolf Virchow who popularized the idea that we are made of cells. In the 1850s, Virchow wrote a book about cellular physiology essentially based on his dissection of an onion; he saw that it had compartments and from there he asserted that all living things were made of cells and that “all cells come from cells.” Although many people initially thought he was nuts, somehow that became the cellular theory of biology and medicine, despite the theory never having been “proven” in any meaningful sense of the word.
Ribosome Fairy Tales?
For the time being, let’s assume that cells do exist in those one hundred forty or so human tissues. Then we can ask, what is a cell made of? In addition to a cell membrane, standard textbooks show pictures with structures called organelles that include a nucleus, an endoplasmic reticulum, ribosomes, mitochondria, lysosomes, the Golgi apparatus and others (see Figure 1). This definition of a cell is the basis of all medicine and biology.
Now, let’s consider the ribosomes. Cell biology tells us that ribosomes are the place where mRNA is translated into proteins, describing ribosomes as the cells’ protein-making “factories” or “machinery.” Ribosomes also happen to be an important part of the Covid story— remember, the official rationale for putting mRNA in the injections was so it could instruct the ribosomes to produce the SARS-CoV-2 spike protein.9
As an aside, if you say, “I’m going to make tires out of rubber,” it would not be unusual to be asked, “How do you know that works?” Then you could describe the process, including the quantity of rubber needed to produce a set number of tires, and they could repeat the process to see whether they end up with the same number of tires from the same amount of rubber. Along these lines, you would expect there to be hundreds of studies showing that if you put “X” amount of mRNA into a human being, you get “Y” amount of spike protein. But do you know how many studies there are like that? Zero. Instead, we just heard, “We had to move at the speed of science,”10 which really means “We made it up.”
There is an interesting thing going on with the ribosomes, because we’re talking about the place in a cell where the essence of you, biologically, is made. We are made of proteins. The creation of you, we’re told, is in the ribosomes. The question is, is there such a thing as a ribosome, or did they make it up?
FIGURE 1. A standard (make-believe) cell diagram.
One clue that there is something fishy going on is that no one can tell you how many ribosomes a cell contains, other than a vague “millions.” However, we can do some basic arithmetic (which will be an approximation because we’re mixing volume and linear measurement). We’re told that a ribosome measures about twenty-five nanometers (0.025 micrometers)—and if we conservatively estimate that a mammalian cell has about four million ribosomes, then that would equal one hundred thousand micrometers. However, a typical mammalian cell is something like one hundred micrometers, and the cytoplasm (which contains the ribosomes) is only 70 percent of the cell, meaning that its volume is seventy micrometers. Not only that, but the mitochondria—which are hundreds or thousands of times bigger than the putative ribosomes—are also in there. So, how does something that is one hundred thousand micrometers fit into a space that is seventy micrometers and also houses millions of mitochondria? Doesn’t anybody study arithmetic?
A second clue that ribosomes are imaginary comes from electron microscope pictures, which always show the ribosome as a perfect circle. If it is a perfect circle on a two-dimensional picture, that means it had to have been a sphere in real life. Now think about how biologists obtain these pictures: they take some tissue, put it in a blender, grind and macerate it, freeze it to minus one hundred twenty degrees centigrade, stain it with heavy metals and shoot a high-energy electron beam at it to evaporate all the water from the tissue. How does a sphere that has been ground up in a blender, frozen, poisoned and had all its water evaporated end up—every single time—as a perfect circle? It is not possible for those circles to be real cellular structures. (This is a good time to remember WC Fields’ quote about “baffling them with bullshit.”)
Fortunately, Harold Hillman had the genius to take something that could not possibly have ribosomes in it and put it through the same process (staining and so forth), and he got the exact same pictures. It turns out that those are just typical images of dead and dying tissue (remember that pictures of “viruses” also come from stained tissue that is dead and dying), and those perfect circles are gas bubbles—in which case, there are no ribosomes. And if there are no ribosomes, there is no place for the translation of RNA into protein to occur. And if that is the case, what the heck is going on, and how do we actually make the stuff that we’re made of?
More Cell Make-Believe
For another example, let’s look at the cell component called the endoplasmic reticulum (ER). Textbooks describe the ER as “a netlike labyrinth of branching tubules and flattened sacs”11 that serve as the cell’s “transportation system.” The millions of ribosomes in a cell are said to line the surface of the “rough” part of the ER.
Why does the ER even have to be there? Before I answer that question, let’s consider that the cytoplasm of a cell (which is the gel-like liquid inside a cell membrane but external to the nucleus) has a different pH level than the pH inside the cell nucleus—and that is a verifiable, measurable phenomenon. You can measure the two pH values one hundred times and they will never be the same. Why is the pH different? The reason can only be due to the cytoplasm and nucleus having different concentrations of hydrogen ions—because that is where pH comes from. And for the pH values to be different, there has to be an impenetrable barrier between the cytoplasm and nucleus, or some other mechanism that keeps the hydrogen ions from equilibrating across the two. If there were no mechanism, they would equilibrate and their pH would be the same—but it never is.
Now, we run into the conceptual problem of the mRNA. They say DNA makes mRNA in the nucleus; then, the mRNA exits the nucleus through pores in the nuclear membrane and heads to the imaginary ribosomes, where it is translated into protein. So, how does the mRNA get out without letting any hydrogen ions in to equilibrate? An mRNA molecule is at least thousands and maybe millions of times bigger than a hydrogen ion. Picture the problem this way: Something the size of an elephant can go out, but something the size of a mosquito can’t get in.
Believe it or not, we’re expected to believe that there is something like a whirligig that attaches to the mRNA (the “elephant”) and spins around like a conveyor belt and takes the mRNA to the other side of the cell. Meanwhile, no one has ever seen the whirligig. (“But it must be a whirligig, because how else did the elephant get out?”) But then you have to ask, how does it go round and round and not tangle up the “branching” components of the ER? If you picture them like ropes, wouldn’t you have to untangle the ropes? (Didn’t any scientist ever go on a merry-go-round?) Once again, Hillman provided a common-sense answer. He showed that when you take tissue and quickly freeze it, it makes fracture lines—and that’s what we call the endoplasmic reticulum. The ER doesn’t exist.
In short, using basic principles of geometry, mathematics and logic, you can go through the same process with every component of the cell. Nothing on a standard cell diagram—with the exception of the nucleus, the mitochondria and a thin cell wall—has ever been proven to exist. It’s all make-believe.
Other Things That Just Ain’t So
In addition to the imaginary cell components, there are a lot of other things in science that, as Mark Twain put it, “we believe in but just ain’t so.” Consider “Neurology 101.” A neurologist’s explanation of how nerves work goes like this: We have nerves made up of nerve cells called “neurons”; they transmit electrical and chemical signals via “axons” that end in “synapses.” Something called the “presynaptic junction” releases chemical messengers called “neurotransmitters” (such as serotonin and dopamine), which swim across the junction and attach to “postsynaptic receptors,” where they “depolarize” the next neuron and start the next impulse—and so on, until the nerve ends at its destination and “fires.” But the process can’t work like that; it’s nonsense. This becomes immediately obvious if you ask someone to wiggle the tip of their right or left index finger as soon as they hear the word “right” or “left”; they do it virtually instantaneously, with no lag time for this hypothesized neurotransmitter journey.12
In addition, if you dissect a nerve, you never see a synapse. Now, you could have the problem of “maybe it’s just too small to see,” but most things aren’t too small to see with an electron microscope. If you hunt down a picture of what an anatomical synapse is supposed to look like, what you’ll find are pictures of stained nerves. That’s not a synapse—because there are no synapses. The nerve is continuous.
Think about how much in medicine is based on neurotransmitters and receptors (such as the famed “ACE2 receptors,” “opiate receptors,” “dopamine receptors,” or “serotonin receptors”). They even tell us that it is oxytocin, a hormone that “acts as a neurotransmitter,” that makes us love someone. It couldn’t be because they’re a nice person or they give you a backrub—no, it’s the “love hormone” oxytocin.
Here is another example. How many of you have heard of the “blood-brain barrier” or believe there is such a barrier? We often hear about it from people opposed to vaccination, who say that vaccines make your blood-brain barrier “leaky.” The implication is that we’re talking about an actual anatomical structure—a physical barrier that stretches out like a piece of cellophane along the border between the blood vessels and your brain tissue so that nothing gets in or out—except vaccines. . . and except anesthetics because drug-makers “know how to get anesthetics through the blood-brain barrier.” Nonetheless, no one has ever proven the existence of such a barrier.
Just to be clear, I am not saying that there aren’t substances that get into the brain in a different way than they get into the liver. The liver and the brain each have a different composition of water and lipids, so logically, some things will dissolve and get into the liver differently from how they get into the brain. But just because things get in the brain differently does not mean there is an anatomical barrier.
Finally, we can scrutinize the notion that DNA is the mechanism of heredity. The premise of genetics is that you have a stable fixed code that is the same in every cell of your body. That fixed, stable DNA makes proteins, and the proteins make you. But there are probably two hundred thousand different types of protein, and only twenty thousand genes or units that code for these proteins. We’re told that one gene makes one protein, so how does that work? Where did the other one hundred eighty thousand proteins come from? The central dogma that one gene makes one protein cannot be true. So, how we are made can’t have anything to do with DNA and, therefore, DNA cannot be the code for biological systems. In fact, DNA changes from minute to minute—Barbara McClintock proved this decades ago13—so there is no stable DNA. We do not have the same DNA in all the tissues and cells of our body. These things have been 100 percent disproven.
It’s the Structured Water
The ribosomes, endoplasmic reticulum, synapses, neurotransmitters and blood-brain barrier represent just a partial list—and I do mean partial—of things of which I either doubt the existence or suspect their function is different from what we have been told. If you are still wondering what we are made up of, the reality is more beautiful, simpler, easier to understand and more logical and rational. The real answer to what we’re made of is structured water. Structured water, which creates free electrons, is the only possible explanation for how we’re able to instantaneously wiggle our index finger when we hear the word “right” or left.”
FIGURE 2. Dark-field microscope image of cells showing cell membrane, nucleus, mitochondria and structured water.
Figure 2 is an image of a cell produced with dark-field microscopy, which is the most reliable technique for viewing live, unstained biological samples. In the image, you see a thin membrane (the outer coating); you see organized water (also called structured water, coherent water, EZ water, the fourth phase of water or liquid crystalline water); you see little black dots in the structured water (the mitochondria) and you see a nucleus that is always circular or dome-shaped—and that’s it.
Note that the mitochondria help structure our water by making ATP—which is not “energy” as we’ve been told. Think of structured water like jello. If you add water to gelatin proteins, nothing happens, but if you heat the mixture, the heat unfolds the proteins and you get water that gels. As for us, we have all these proteins, and the mitochondria make the ATP that unfolds them so that the proteins can interact with water and form gels. All gels create a negative charge and an electromagnetic field around them, which is the voltage—the energy—of life. To put it simply, we are living liquid crystals.
The dome in the middle (the nucleus) also has something sticking out that collects energy from the world. It may be DNA, but it is not a double helix—it’s a spiral sticking out of the nucleus. The way it works is similar to a radio antenna. It “downloads” information coming in through “radio waves” that get picked up by the “antenna,” and out of that emerge proteins and life (or sound and song in the case of a radio). And this dynamic, tunable, responsive, liquid crystalline medium pervades the whole body—from the organs and tissues to the interior of every cell.
Note that in Genesis, before God created the Earth, plants or people, he created water and light energy. No one can enter the kingdom of God unless they are born of the water and the Spirit. The Spirit is the information field that comes in through our antenna. Every scriptural tradition says that all living things and the universe itself are made of water.
What Does Make Us Sick?
If we now circle back to “what doesn’t make us sick,” we could summarize the answer in one word: “viruses.” And if we ask, “What does make us sick?”, the answer is also straightforward. We get sick when we mess up our structured water. If we disturb the gels by putting “schmutz” in them—which could be aluminum, mercury, glyphosate, bad food, EMFs, or even negative emotions like anger, fear, shame or guilt—that will distort or dissolve the gels. If we do that in our eye, we get a distorted gel that has a film on it, and we call that a “cataract.” If we distort the bursa in our knee, so that the gels that are supposed to protect both sides of the knee start sticking together, then we have bone on bone and we call that “arthritis.” Public health officials create epidemics by pulling different manifestations of distorted water into a single diagnosis—such as AIDS or Covid-19—and when they are ready to make the epidemic go away, they separate them back out into twenty different diagnoses. It’s very clever—and it’s nothing new.
Without describing it as such, medicine does sometimes assess the coherence of your water to see if you are sick. For example, doctors use MRIs to diagnose cancer. What is the MRI measuring? It’s measuring the coherence of your water. When your water goes from a gel-like jello to a puddle-like liquid, it sends a different signal to the MRI.
Imagine you have a poison grape in your “jello.” Your body heats up the gel and you get a fever—that’s hyperthermia. The heat dissolves the gel and makes it runny, creating mucus that you can spit out or cough up, or creating something you can push out through your skin. That’s what we call “being sick.” It makes perfect sense. If you want to flush out the poison grape, all you have to do is clean your gels—which is what detoxification approaches like the Gerson diet and water fasting are all about—and clean up the field and you will heal. If you want to know why you are sick, think about how you are structuring your water, what you’re putting into your water, the quality of the water and the quality or composition of the field that you’re exposed to.
I’m not the first person to say that water creates life. Mae Wan-Ho, a past speaker at Weston A. Price Foundation conferences, wrote books about “the role of biological water in organising living processes.”14 Marcel Vogel,15 who knew more about crystals than any human being ever alive and who invented liquid crystal screens, discovered that he could use the energetic fields of quartz crystals to structure water.16
We are made of a living, evolving, changing crystal, which is why we are not made of quartz. One way of viewing Covid-related events is that people like Bill Gates are trying to make us be made of quartz, not water. In some ways, that is what this is all about. As a fixed, perfect quartz crystal, they tell us, nothing will ever change and we can live forever. But that is not what I want. I want to change, grow, evolve and be a human being who has to be watered.
We’re swimming along with misconceptions in a make-believe world—and we have to get rid of this garbage. We can find a much better way once we explore and learn what we’re really made of and how it all works. Every reason we get sick has to do with a distortion of the field coming in.
Continuing with the radio analogy, you need to find the good signal instead of the distorted signal. The good signal is the sun, moon and the earth; good friends; your dog; community; clean, nutrient-dense food, clean water and clean air; good music; and love, safety and freedom. That is the field that you “download” into the gel to give it information to organize progressively into the more and more perfect crystal that is you.
Sidebar
No Deathbed Confession
How have virology’s luminaries been able to claim they found a virus when we know they have never found one in any biological fluid? Let’s consider Luc Montagnier, the prestigious virologist who won a Nobel Prize for discovering HIV. He died in 2022. Montagnier acknowledged that purification was a necessary step to prove the existence of a virus (or, in the case of HIV, a retrovirus) but admitted, “We did not purify.”17 The technician who performed his electron microscopy for twenty years even said, “It turns out we never saw a virus. All we saw was junk.” But to his dying day, Montagnier never “fessed up” or acknowledged, “We don’t have a real virus.”
On what did Montagnier base his claim that he had found HIV? It’s very simple:
• He took lymphocytes from the lymph nodes of a person said to have AIDS.
• He stimulated them to grow with a chemical called PHA (phytohaemagglutinin).
• When the lymphocytes grew, he assayed them for an enzyme called reverse transcriptase.
• When he found reverse transcriptase, he said that it proved the existence of a new retrovirus eventually called HIV.
• To “prove” that HIV was transmissible to other people, Montagnier took his PHA-stimulated lymphocyte culture and put it in a lymphocyte culture from a healthy person. When he found reverse transcriptase in that culture as well, that was the “proof” that HIV is a transmissible disease.
There was only one problem. Ten years previously, Robert Gallo had written a paper reporting reverse transcriptase in every single culture from anybody with lymphocytes stimulated with PHA. Both Gallo and Montagnier knew that his experiment had nothing to do with proving that there was a retrovirus or any kind of virus at all. Later, the scientist credited with discovering the reverse transcriptase enzyme, David Baltimore, also admitted as much.18
Water Pictures
Veda Austin, a “water researcher,” has dedicated many years to observing the life of water, which she describes as “fluid intelligence.”19
Veda has developed techniques for photographing water in its “state of creation.” This work explores whether, if she asks water a question, the water can take in and download the information and, given the right circumstances, make structures that essentially answer that question. And what she has found is that if she puts the water in a dish and freezes it, the water organizes its crystals and makes pictures.
For example, when she showed the dish of water a wedding invitation and said, “Water, show me the wedding invitation,” the frozen water created an amazing artistic depiction of a wedding ring. But my favorite example is when she said, “Water, what is falling down?” The water did not create anything as straightforward as an image of rain; instead, the water produced an image of “London Bridge is falling down.”
“Safe and Free” by Jude Roberts20
In the last two years, I’ve learned important things from my cat Pumpkin. One stormy evening, with coyotes howling in the distance, I walked with Pumpkin toward the greenhouse where he sleeps, but Pumpkin started heading for the woods instead. When I called him, he gave me a look that seemed to say, “There’s no point in being safe if I can’t be free.” My friend Jude Roberts understands this, too. His song “Safe and Free” reminds us what this is all about.
I got up to go to work today,
there was no work for me.
Governor closed my shop, he say
to keep me safe and free
I’ve had my shop for twenty years,
It feeds my family,
And now we have to stay inside,
To keep us safe and free
To keep us safe and free
Called my dear old mother,
My mother said to me
“Son, I miss you dearly,
But you cannot come to tea”
“The children miss you, Mamma,
They’re healthy as can be.”
“A hug could kill their Grandma,
Keep them away from me.
Keep me safe and free.”
Giant tech and billionaires
And pharmacology
Spinning like a top to move
The wheels of industry
Amazon and Walmart,
The consumer pedigree,
They can do their business,
Because anyone can see
They keep us safe and free
Technocrats and robot gods
And blind authority,
Sell your soul and pray to them,
They’ll keep you safe and free
Biotech behemoths say
They have a shot for me.
I trust them with my body,
And forgive them for their greed
If it keeps me safe and free
Keep us safe from terrorists,
Keep us free from germs,
Keep us from the danger
Of the wisdom we have learned
Until the books are burned
Governor says to wear a mask
I cannot disagree
I cannot breathe or speak my mind,
But at least I’m safe and free
I’ll wear my mask for you my friend,
You wear your mask for me.
Worried eyes and faceless fear
Is all that we can see.
Sure feel safe and free
Keep us free from choices,
Keep us stuck in blame,
Keep us in a toxic state,
Of poverty and shame
While they run their game
I’ll open up my shop today
Even if they come for me.
If I can’t feed my family,
We’re neither safe nor free.
I may not be a scientist,
And I’m damn sure not a priest
Ain’t a fool on God’s green Earth
Can keep life safe for me.
So better I live free.
Alberts B. et al. “The endoplasmic reticulum.” In Molecular Biology of the Cell, 4th edition. New York: Garland Science; 2002.
Cowan T. Human Heart, Cosmic Heart: A Doctor’s Quest to Understand, Treat, and Prevent Cardiovascular Disease. White River Junction, VT: Chelsea Green Publishing; 2016, pp. 102- 105.
Halpern ME. Barbara McClintock on defining the unstable genome. Genetics. 2016;204:3-4.
Dr. Tom Cowan has been one of the leading voices speaking out against the mainstream medical narrative and coordinated agenda of masking, social distancing and forced vaccinations. His messages of health freedom and personal autonomy have resonated with millions of people around the world. Dr. Cowan challenges conventional medicine to explore health and wellness in holistic terms, seeking to provide a collaborative forum for the exchange of knowledge, products and practices that enable us to forge a new world together, governed by truth.
“Therefore, one of the answers I would provide to the question of why the ‘no virus’ issue is so important is: that fear of ‘germs’ makes people believe that ‘disease’ can be transmitted between people, which means that we have to continue being afraid of each other.
“In fact, one of the fundamental problems with all of this is that it keeps people in a state of unjustified fear, which is disempowering. Releasing unjustified fear is empowering.”
It seems that many people wonder why the ‘no virus’ issue remains important now that the ‘pandemic’ is over.
To add to that, there are some people in the ‘freedom movement’ who have recently asserted that there are many aspects of the globalists’ agenda that are not related to health and are far more dangerous to humanity, such as technocracy, transhumanism, digital currencies, smart cities etc.
Yes, these are important issues – really important issues, I totally agree – but so is the idea that ‘pathogenic agents’ exist because it has tentacles that reach into many aspects of our lives, so it cannot be brushed aside as if irrelevant, especially in view of the complete lack of evidence to support this idea.
I would therefore recommend that people who believe in ‘pathogenic agents’ become aware of the various reports that claim there will be ‘future pandemics’. For just one example, a 22nd May 2023 ‘News’ item on the UN website states,
“Although COVID-19 may no longer be a global public health emergency, countries must still strengthen response to the disease and prepare for future pandemics and other threats, the Director-General of the World Health Organization (WHO) said on Monday in Geneva.”
There has never been a ‘pandemic’ due to an infectious agent and there never could be. But, whilst people believe that pathogenic infectious agents exist, they will believe in the possibility of other ‘pandemics’.
Therefore, one of the answers I would provide to the question of why the ‘no virus’ issue is so important is: that fear of ‘germs’ makes people believe that ‘disease’ can be transmitted between people, which means that we have to continue being afraid of each other.
In fact, one of the fundamental problems with all of this is that it keeps people in a state of unjustified fear, which is disempowering. Releasing unjustified fear is empowering.
Furthermore, fear of ‘germs’ makes people acquiesce to measures that are claimed to be for their benefit but are far more likely to be harmful, and in many cases potentially or even actually fatal.
For example, the maintenance of a belief in pathogens permits the maintenance of a belief in the idea that STIs are real, as demonstrated by a recent BBC article Gonorrhoea and syphilis sex infections reach record levels in England,
“England is seeing record high levels of gonorrhoea and syphilis sexually transmitted infections, following a dip during Covid years, new figures reveal.”
Is the claim that these STIs ‘dipped’ during the Covid years intended to suggest that people maintaining their distance from one another was beneficial? This point is not elaborated upon, so maybe it was not intended to imply that. Still, the point was stated, so maybe it was intended to be drawn into the sub-conscious mind.
One of the key messages in the BBC article is that people should ‘practise safe sex’ – whatever that means. In order to be ‘safe’, people are encouraged to ‘get themselves tested’ – does this sound familiar?
In addition, the article states that,
“The age group most likely to be diagnosed with a sexually transmitted infection (STI) is people who are 15-24.”
The reason for STIs to mainly affect young people is not explained, although it is possibly because this age group is more likely to be tested, as the article indicates,
“Some of the rise will be due to increased testing, but the scale of the surge strongly suggests that there are more of the infections around, says the UKHSA.”
A particularly significant comment made by the spokesperson for the UKHSA, and reported in the article, is that,
“Testing is important because you may not have any symptoms of an STI.”
Yet, according to the CDC,
“An infection occurs when germs enter the body, increase in number, and cause a reaction of the body.”
In other words, an infection causes a reaction or ‘symptoms’, but infected people may not have symptoms. A contradiction in terms, surely!
Just to be clear, the definition of ‘symptom’ according to the online Merriam-Webster dictionary is,
“…subjective evidence of disease or physical disturbance.”
So, to summarise: according to the medical establishment, a symptom is evidence of disease and ‘germs’ are pathogens, which means they cause disease, which is defined by the presence of symptoms. Yet ‘germs’ are said to be able to cause an infection even in the complete absence of symptoms.
Confused? You should be, because this is all nonsense!
But it is nonsense that people are not only expected to believe without question, but are not allowed to question.
Maybe it is because this is all so confusing that people are likely to just switch off their thinking, because they don’t understand it, and instead defer to the so-called ‘experts’. I am not being disrespectful. I do wonder, however, whether this approach may be intentional and that those in control of the narrative intentionally promote contradictory information to ensure that people are confused.
Deferring to ‘experts’ is however, a serious error of judgement, because it means people will believe the experts’ reports about ‘germs’ and become trapped in a false narrative that they may have been ‘infected’. This in turn will make them believe that they need to take certain drugs and act in a certain way to ‘protect’ themselves from other people or protect other people from them, especially people with whom they are in a loving relationship. They are made to believe the idea that they could cause harm to their partner or vice versa, and they therefore live in fear.
This fear is fuelled by a variety of statements, such as the claim in the BBC article that,
“An untreated infection can lead to infertility, pelvic inflammatory disease and can be passed on to a child during pregnancy.”
There is no evidence for this claim. Yet, this is exactly the kind of message that will encourage people to want to be tested to make sure they are ‘safe’. Again, does this sound familiar?
An even deeper problem is highlighted by the comment from the Chief Executive of the Terrence Higgins who is reported to have said that,
“Sexual health services and public health budgets have been cut to the bone.”
This comment was followed by his statement that,
“This was exacerbated and laid bare by last year’s mpox outbreak, which left sexual health clinics in the most affected areas unable to provide HIV and STI testing, HIV prevention and access to contraception due to the displacement of these core and vital services. Until sexual health is properly resourced – with an appointment easier to access than a (sic) – we won’t see the number of STIs heading in the right direction.”
Where do I start with this?
OK, so the Terrence Higgins Trust web page About our charity states,
“We’re the UK’s leading HIV and sexual health charity. We support people living with HIV and amplify their voices, and help the people using our services to achieve good sexual health.”
I realise that I don’t have a Substack article specifically about HIV, but this is one I wrote about STDs,
HIV is a huge topic, but the fundamental point to convey here is that there is no evidence, and there never was, that there is such a thing as a ‘virus’ called HIV that is the cause of a health problem called AIDS – or any other health problem for that matter.
It is abundantly clear that there is a lot at stake here. It is also crystal clear that belief in the existence of any kind of pathogenic agent is absolutely essential for organisations such as the Terrence Higgins Trust (THT), as well as ‘health’ institutions, such as the WHO, CDC, NHS, and all the other alphabet agencies.
I have no idea of the motives of those who are in charge of the THT, nor do I intend to speculate on them. However, whether they know it or not, what they are promoting on their website is fully supportive of Agenda 2030 and the ‘Global Goals’, as the message at the foot of their website claims,
“Time is running out. Donate now and together we can end new cases of HIV in the UK by 2030.”
To those in the ‘truther’ community who claim that the 2030 Agenda has nothing to do with the ‘virus’ issue I would strongly suggest that they read SDG3, especially target 3.3.
And target 3b
The ‘no virus’ issue – and the associated understanding that there is no proof that any ‘diseases’ are caused by any ‘microorganism’, whether bacteria, fungi or parasites (‘viruses’ aren’t relevant in this context) – is and remains an extremely important issue; especially in view of the intended 2030 Agenda rollout of vaccines, because vaccines rely on the existence of pathogenic infectious agents.
Another reason to understand its importance is because the idea that ‘germs’ cause illness that only the medical establishment can address supports the idea that we need a ‘health service’ to look after us when we become ill, which is not the case. To this, I would add a caveat that accident and emergency services ARE important and should remain in place, although those who work in that sector should receive further training to teach them how the body actually works, and how it can and does heal itself; this knowledge will certainly improve patient recovery times and outcomes.
We may not reach everyone, but the importance of the ‘no virus’ issue cannot be underestimated. When people lose their fear of ‘germs’ of all descriptions, they will be able to concentrate their efforts on all the other aspects of their lives.
People can only make informed decisions when they are in possession of all the relevant information.
Technology expert Michael Rectenwald, Ph.D., told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The World Health Organization (WHO) and the European Commission — the executive branch of the European Union (EU) — on Monday launched a “landmark digital health partnership” marking the beginning of the WHO Global Digital Health Certification Network (GDHCN) to promote a global interoperable digital vaccine passport.
Beginning this month, the WHO will adopt the EU’s system of digital COVID-19 certification “to establish a global system that will help facilitate global mobility and protect citizens across the world from on-going and future health threats, including pandemics,” according to Monday’s announcements by the WHO and the European Commission.
WHO & @EU_Commission launch landmark digital health initiative to help protect people across the world from on-going & future health threats
This is the first building block of the WHO Global Digital Health Certification Network that will develop a wide range of digital products… pic.twitter.com/IPlxn8wAXv
— World Health Organization (WHO) (@WHO) June 5, 2023
The WHO and European Commission claim the GDHCN initiative, which has been in the works since 2021, “will develop a wide range of digital products to deliver better health for all.”
The organizations said the WHO will not collect individuals’ personal data via these digital passports — stating that such data collection “would continue to be the exclusive domain of governments.”
WHO Director-General Tedros Adhanom Ghebreyesus lauded the new agreement:
“Building on the EU’s highly successful digital certification network, WHO aims to offer all WHO Member States access to an open-source digital health tool, which is based on the principles of equity, innovation, transparency and data protection and privacy.
“New digital health products in development aim to help people everywhere receive quality health services quickly and more effectively.”
However, experts who spoke with The Defender said the ramifications of such a system for human liberty and freedom of movement raised concerns.
Independent journalist James Roguski told The Defender the WHO is not waiting for a successful conclusion of these negotiations in order to implement initiatives such as a global digital vaccine passport. He said:
“The announcement by the WHO and the European Commission regarding the launch of their digital health partnership was hardly a surprise. Over a month ago, the WHO quietly published that they were working on ‘operationalizing’ the very things that were being ‘negotiated.’
“This is just one example that clearly shows that the super-secret ‘negotiations’ regarding the International Health Regulations (IHR) are a charade.”
Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom,” told The Defender that, under the guise of preserving freedom, a digital passport system “means restraints on movement and living for the unvaccinated and forced vaccination to participate in life.”
The announcement of the WHO-European Commission collaboration came just days after the conclusion of the WHO’s annual World Health Assembly (WHA).
While the pandemic treaty and IHR amendments were not finalized at this year’s meeting, high-level WHO officials warned of the risk of a future pandemic and spread of a deadly “Disease X,” and expressed the need to “restrict personal liberties” during a future health emergency.
The EU has been a strong proponent of digital vaccine passports, first launched for its member states in late 2020 — concurrent with the introduction of the COVID-19 vaccines — under the name “Green Pass.” The EU’s experience with the digital passes is noted in Monday’s announcement, which states:
“One of the key elements in the European Union’s work against the COVID-19 pandemic has been digital COVID-19 certificates. To facilitate free movement within its borders, the EU swiftly established interoperable COVID-19 certificates.
“Based on open-source technologies and standards it allowed also for the connection of non-EU countries that issue certificates … becoming the most widely used solution around the world.”
Roguski told The Defender the EU also was among the strongest proponents of vaccine passports during ongoing negotiations for the WHO’s “pandemic treaty” and amendments to the IHR.
“They really want the global digital health certificate,” Roguski told The Defender in March. “Primarily, that’s coming from the European Union.”
‘Pandemic passports a death sentence for millions’
According to Roguski, the EU, during negotiations for the IHR amendments, put forth proposals that seek to “‘normalize’ the implementation of a global digital health certificate.”
The Czech Republic called for Passenger Locator Forms “containing information concerning traveller’s destination,” preferably in digital form, for the purpose of contact tracing.
They also proposed that the WHO’s Health Assembly “may adopt, in cooperation with the International Civil Aviation Organization [ICAO] … and other relevant organisations, the requirements that documents in digital or paper form shall fulfill with regard to interoperability of information technology platforms, technical requirements of health documents, as well as safeguards to reduce the risk of abuse and falsification.”
The Czech Republic and the EU proposed documentation not just for vaccination, but “test certificates and recovery certificates” in cases “where a vaccine or prophylaxis has not yet been made available for a disease in respect of which a public health emergency of international concern has been declared.”
Plans for the WHO’s GDHCN have been in the works since at least August 2021, when the WHO released a document titled “Digital documentation of COVID-19 certificates: vaccination status: technical specifications and implementation guidance, 27 August 2021.”
“The Secretariat has developed SMART (Standards-based, Machine-readable, Adaptive, Requirements-based, and Testable) Guidelines on the digital documentation of COVID-19 certificates, comprising recommendations on the data, digital functionality, ethics, and trust architecture needed to ensure the interoperability of immunization and health records globally.”
The WHO also announced the successful completion of a “technical feasibility study for establishing a federated global trust network, which tested the ability to interoperate the health content and trust networks across existing regional efforts.”
EU officials have frequently praised themselves over the launch of the bloc’s “Green Pass,” touting how individuals’ privacy would be protected on the app. The introduction of the “Green Pass” was accompanied by statements by European Commission President Ursula von der Leyen calling for a “discussion” on mandatory vaccinations in the EU.
One of the EU’s stated priorities as part of its 2019-2024 five-year plan is to create a “Digital Identity for all Europeans.” Namely, each EU citizen and resident would have access to a “personal digital wallet,” which would include national ID cards, birth and medical certificates, and drivers’ licenses.
These proposals and initiatives appear to be closely aligned with the United Nations’ Sustainable Development Goals (SDGs), and in particular, Target 16.9, which calls for the provision of a digital legal identity for all, including newborns, by 2030.
Tedros said the SDGs are “our north star,” while addressing this year’s WHA.
Rectenwald called “pandemic passports” a “death sentence for millions.” He told The Defender:
“Despite the studies demonstrating that vaccines to curb pandemics have been deadly and useless, the WHO is doubling down on vaccine mandates.
“Pandemic passports equal a death sentence for millions and the abrogation of rights for the non-compliant. The WHO should be stopped before it completes the construction of a global totalitarian system.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
Video available at La Quinta Columna Odysee & Rumble channels. Follow at La Quinta Columna telegram channel: https://t.me/laquintacolumnainternational
They are introducing nanotechnology into all sorts of injectable products, especially in what they call vaccines for Covid.
Self-assembled nanotechnologies, based on graphene, are advanced non-human technologies, but implemented by humans.
The parasitization of our species ordered by “them” will lead to the extinction of human beings as we know them, who will become transhuman, monitored, with non-human thoughts that can in turn be read remotely via electromagnetic waves. Managed by AI, we will become what they call enhanced humans. Augmented humans.
Helpful list from FDA, found while doing research and organizing my files on:
Public Health Emergency (PHE), Emergency Use Authorization (EUA) and PREP Act notices, declarations, determinations and authorizations issued by HHS Secretaries and their delegees from Jan. 2020 to the present;
Legal advisory opinions about PREP Act liability immunity, issued by the HHS Office of General Counsel from Jan. 2020 to the present; and
Guidance to pharmacists about PREP Act liability immunity, issued by the Office of the Assistant Secretary of Health, from Jan. 2020 to the present; and
May biochemical weapon uptake rates approach zero in coming months and years, as rational popular response to the truth rendered much more visible since January 2020, and in firm opposition to all “recommendations” of the CDC Advisory Committee on Immunization Practices (ACIP).
Biochemical weapons deployed by injection have been intrinsically injurious from the start of government campaigns promoting their use more than a century ago.
The “Covid-19” weapons have been the most deadly to date, with some lots deadlier than others, and contents of many lots still unidentified.
A poultry farm in Yaroslavl has been ordered to cull 800,000 chickens, as regions introduce arbitrary “public health” measures to stop the spread of “bird flu”
On May 12, Russian media reported that an “infected” gull had been discovered near a pond in a village in Moscow Oblast.
What happened next was practically preordained.
Moscow Mayor Sergey Sobyanin—the poster boy for New Normal Russia—issued a decree on May 18 imposing “quarantine” measures on 11 districts in the capital.
The order placed restrictions on public events where birds might be congregating, and also banned the transportation of feathered creatures in the aforementioned districts.
Of course, birds could always just, you know, fly into one of these “quarantined” districts, and spread their devilish flu, but that’s neither here nor there.
Moscow is the trend-setter when it comes to enterprising public health policy in Russia, so of course other regions have been eager to follow suit with their own arbitrary bird flu edicts.
Just hours after Sobyanin’s decree was published, Kaliningrad imposed its own “quarantine” on a 10km perimeter around another bird flu Ground Zero.
The restrictions, which will remain in place until August 1, included a ban on the “import and export of birds and hatching eggs, the relocation of birds, procurement and export of bird feed, as well as holding agricultural fairs, exhibitions, auctions and other events.”
A week later, the discovery of dead, flu-riddled gulls in Nizhny Novgorod prompted officials to introduce a 30-day quarantine in one of the region’s districts.
Health authorities “seized poultry within a radius of five kilometers [from where the dead gulls were found], and poultry farms in the region were transferred to enhanced security protocols.”
Locals were also advised to only buy poultry from “verified” sources—the good, factory-farmed corporate stuff; don’t even think about buying poultry from your unverified neighbor!
But confiscating all chickens in a 5km radius is amateur hour compared to the health-boosting measures adopted in Yaroslavl.
The Romanovskaya poultry farm in Yaroslavl has been instructed to cull its livestock, and destroy all animal products on its premises, following an alleged bird flu outbreak:
All birds, more than 800 thousand in total, will be killed … The destruction of the carcasses, along with poultry products (eggs), will be carried out via incineration at a specially designated site. […]
The poultry farm has not disclosed any details about the order. When a 76.RU correspondent tried to contact company representatives, they declined to comment.
“We are in quarantine. That’s all,” a receptionist said, before hanging up.
The region is a major agricultural hub, so there’s no reason to believe that this bird-liquidation will cause a shortage of poultry or eggs. But…it’s also 800,000 chickens?
Finally, like a bad omen, Tatarstan (which was arguably the most Virus Crazy region in Russia after Moscow/St. Petersburg) is already bracing for the bird flu apocalypse:
It was clear that the COVID grift was rapidly losing its potency when Virus Nanny Anna Popova announced an imminent wave of “Arcturus”.
How many waves of severe-sounding Greek letters and words are possible, before people stop paying attention? Or worse, starting asking questions?
Well, now Russia is sacrificing 800,000 chickens to the Global Health Gods.
By the way: Where did this scary outbreak of bird flu begin? Hard to say for sure, but China recorded the world’s first human death from the new and improved “H3N8 avian influenza strain” in mid-April.
The bird flu scam actually predates COVID by many years. In fact, many of the trusted experts who demanded large-scale chicken slaughter (for public health) later went on to become celebrated “coronavirus experts” who championed worldwide house arrest for the proles—resulting in another mass culling.
Have you ever heard of a psychopath named David Nabarro?
source / source (to be fair to Nabarro, he later described lockdown as a “last resort”, which makes him slightly less disgusting than the typical WHO-certified Neanderthal.)
Let’s not deceive ourselves, friends. Global Biosecurity Theater is forever.
“…This is a pseudoscientific concept that is also an oxymoron as two entirely contradictory terms were put together in order to create this illogical state. Asymptomatic is characterized by a lack of signs and symptoms of illness, whereas disease is characterized by signs and symptoms of illness…
Asymptomatic carriers are nothing but healthy people who have been labelled with disease minus signs of any disease who are then told that they can infect others. They are treated as a sick individual based upon results generated using fraudulent tests.
[…]
The “viral” theory is a load of BS, and there is no such thing as a healthy sick person capable of transmitting disease. We have no reason to fear the walking healthy.”
“In areas where there are limited number of new cases, State or local public health officials may request to test a small number of asymptomatic ‘healthy people,’ particularly from vulnerable populations”
In the not so distant past, when we walked around feeling healthy without any symptoms of disease, most of us would consider that we were, in fact, free of any disease. There would be no thoughts about going to the doctor for a PCR test in order to determine whether or not we were unknowingly a walking talking “virus” spewing host harboring billions of “infectious” particles capable of transmitting disease to our loved ones. We would not subject ourselves to quarantines and daily testing due to the remote possibility of being around someone who tested positive with symptoms, let alone for anyone testing positive without any signs of disease. We did not go around covering our faces with masks out of fear that those around us may be silent spreaders. We didn’t bust out our rulers in order to measure 6 feet of distance between us and another living soul. None of these irrational actions were ever even a glimmer of a thought until the well-orchestrated fear propaganda campaign promoted the pseudoscientific concept of the asymptomatic carrier of disease and catapulted it into the public consciousness.
Even though this idea has been effectively weaponized against us over the last few years, it is not a new one. In fact, as will be shown later, the notion of the asymptomatic carrier began at the same time germ theory was born. The idea is that one can be silently harboring and able to transmit a pathogen without displaying any symptoms of disease whatsoever. This has resulted in the highly illogical creation of asymptomatic disease:
What Does it Mean to Have an Asymptomatic Disease?
“Asymptomatic disease is where a person is infected with a disease (or develops a disease; diagnosed) but fails to display any noticeable symptoms.”
Asymptomatic until symptomatic – silent diseases
“Many diseases and infections can be asymptomatic, including those that may be potentially fatal in some people. These include (but are not limited to): tuberculosis, breast cancer, endometriosis, HIV/AIDS, herpes, hepatitis, chlamydia, hypertension, common colds/flu, and type-2 diabetes mellitus. Many of these conditions remain largely asymptomatic until very advanced disease stages when they suddenly become symptomatic. Others can remain more or less asymptomatic throughout their disease course.”
“Infectious diseases can also be completely asymptomatic (with no symptoms ever manifesting), particularly in younger and healthier individuals. For example, hepatitis (hepatitis C) infections can take up to 6 months to develop, and even then, approximately 80% of infected individuals may not experience any symptoms. Other examples include cholera, herpes, measles, and rubella which can be completely asymptomatic.”
“In summary, asymptomatic disease refers to diseases and infections which do not lead to any symptoms in patients (subclinical) for the whole disease course or until they develop symptoms in which the asymptomatic phase is referred to as pre-symptomatic.
In many respiratory infections including COVID-19, asymptomatic disease is common and may be a source of transmission within the community, though more research is needed to establish the exact contribution asymptomatic transmission has on the community rates of infection.”
As can be seen, many so-called “infectious diseases” are said to be asymptomatic. If one is labelled as asymptomatic, one never develops the disease at any point in time even though they are diagnosed with asymptomatic disease. This is a pseudoscientific concept that is also an oxymoron as two entirely contradictory terms were put together in order to create this illogical state. Asymptomatic is characterized by a lack of signs and symptoms of illness, whereas disease is characterized by signs and symptoms of illness. One can not have disease if one is not displaying signs of disease:
Asymptomatic carriers are nothing but healthy people who have been labelled with disease minus signs of any disease who are then told that they can infect others. They are treated as a sick individual based upon results generated using fraudulent tests. In the past, most would have scoffed at this idea and never willingly subjected themselves to quarantines and further testing. In fact, they would have never tested to begin with. However, in the face of a “pandemic” with a “novel virus,” many lined up for the mass testing agenda in order to ensure that they were amongst the “uninfected.” This willingness to subject to testing despite a clear lack of symptoms was primarily driven by fear. This old concept was thrust onto a frightened population and then ramped up in a way that had never been done so before.
In order to understand why there was never any reason to ever participate in this irrational belief of such a ridiculous concept, let’s examine how the asymptomatic carrier first came about at the dawn of germ theory. We will then examine how this idea was weaponized against the public during the “pandemic” despite a complete lack of any scientific evidence in support of the asymptomatic disease carrier.
When German bacteriologist Robert Koch was looking for the causative agents of certain diseases in the late 1800’s, he formulated a series of four logical requirements that needed to be met in order for anyone to claim that a certain microbe caused a specific disease. These were as follows:
The microorganism must be found in abundance in all hosts suffering from the disease but should not be found in healthy hosts.
The microorganism must be isolated from a diseased host and grown in pure culture.
The cultured microorganism should cause the same symptoms of disease when introduced into a healthy host.
The microorganism must be re-isolated from the inoculated, diseased experimental host and shown to be identical to the original causative agent.
While these logic-based postulates were accepted by and large within the scientific community, Koch quickly discovered a problem with his very first criterion. Whether it was tuberculosis, typhoid, malaria, or cholera, the microbe that he was claiming as causative agents were regularly found in healthy individuals. Thus, Koch was unable to satisfy his very own first Postulate. However, rather than realize that his criteria had worked as he had envisioned and had actually ruled out bacteria and other microbes as a causative agent of disease, Koch allowed for himself and others to bend not only his first postulate, but the others as well. Allowing for the bacteria and other microbes claimed to be causative agents of disease to be found in those without disease lead to the creation of the illogical concept that became known as the asymptomatic carrier of disease. Koch’s entire claim to fame rested entirely on the perception that he was a microbe-hunter. Bending his own rules saved Koch from giving up his prestige, kept his findings intact, and helped to establish the germ theory on unfalsifiable pseudoscientific grounds.
Koch’s idea of asymptomatic “infection” received a big push shortly afterwards when the media released propaganda promoting the idea of an asymptomatic carrier in 1907 by targeting an Irish immigrant by the name of Mary Mollen. Mary was a cook for wealthy families and ended up employed by banker Charles Henry Warren when he rented a summer home for himself and his family. When 6 of the 11 family members came down with the symptoms of typhoid fever over the last week of August, the property owners feared that no one would rent the house again if they believed that the property was the source of the outbreak. A man named George Roper was hired to investigate the situation and he came to the conclusion that it was Mary who had passed on the bacteria to the family through her cooking. This led to a modern day witch-hunt for Mary who refused to believe that she was the source of illness. Sadly, Mary was eventually involuntarily quarantined for the majority of the rest of her life. This ordeal led to Mary being notoriously and unfairly known by the moniker Typhoid Mary, even though many of her stool samples came back negative for the bacterium:
Typhoid Mary: the Tragedy of Mary Mallon
“On 11 November 1938, a 69 year old Irishwoman died on North Brother Island, New York. She had been held in isolation for 23 years, yet she had not been charged or convicted with any criminal offence.
Mary Mallon was born in Cookstown, Ireland in 1869. She immigrated to America when she was a teenager and found employment in domestic service. She developed an aptitude for cooking, and as this paid more than basic service, Mary accepted several jobs as a cook for the wealthy. In 1906, Charles Henry Warren, a New York banker, rented a summer home for himself and his family on Long Island. Mary Mallon was engaged as a cook for the duration of their stay. From the end of August, one by one people began to fall ill with typhoid fever, in all, six of the eleven occupants of the house developed typhoid fever.
The owners of the property feared that they would be unable to secure further tenants if the public believed that the source of the outbreak was their property and so hired Dr George Soper to investigate the cause. Soper came to the conclusion that Mary Mallon was to blame for the spread of disease. Hindering his efforts, Mary had left their employment three weeks after the outbreak. Soper started to investigate the previous situations held by Mary Mallon. From 1900 to 1907 there had been seven jobs where, it was reported, somewhere between twenty-three and thirty-eight people became ill and one person, a child, died. Soper believed that Mary was the source of typhoid fever that had followed her employment history, but he needed biological samples to affirm his hypothesis.”
“The Greater New York Charter allowed for ‘all reasonable means for ascertaining the existence and cause of disease’. It essentially gave health officials the authority to remove Mary Mallon and quarantine her against her will. After two years of isolation, with only a dog for company, Mary sued the health department. They had tested her stools approximately weekly and 120 out of 163 samples proved positive. Yet Mary countered with her own private analysis, sampled over the preceding year, all coming back negative. Mary’s laboratory results proved for her, her healthy status and she failed to understand that she was diagnosed a healthy typhoid carrier. She was arguably the first person identified as such, and having not been charged with a criminal offence she felt it was barbaric to be treated like a criminal (and a ‘leper’) when she was innocent of any crime.”
Mary was falsely quarantined against her will due to one man’s suspicion and hypothesis that rested solely on correlation equaling causation. No scientific experiments were ever carried out proving that Mary was spreading disease to her patrons. As with all claims of asymptomatic transmission, it was a circumstantial case built upon faulty epidemiological data. George Roper is the man who ultimately condemned Mary by labeling her as the cause without any scientific evidence proving his hypothesis. Based upon his own words presented below, he assumed certain premises, such as the bacterium should be in the urine (which it was not) and in the feces. He claimed that stool examinations only failed twice over the course of two weeks to find the bacterium. However, he later recounted several instances of failure to detect the bacterium over the course of several months. In the summer months, few bacterial colonies were found and in the month of July, there were five consecutive negative tests. During the month of August, no typhoid was ever found in Mary’s stools. In September, they began to appear again. However, from September 11 to October 14, 1907, the stools failed to yield any typhoid bacilli. From October 16, 1907, to February 5, 1908, weekly examinations of the stools showed anywhere from 25 to 50 percent “typhoid-like” colonies on the culture plates. There were two instances within that period where no bacilli were found. Taking into account that Mary’s own independent lab results showed that no bacilli were found within her stools, Soper’s consistently contradictory evidence should have been questioned.
After recounting these failures, Soper shared his thoughts on how Mary transmitted the bacterium through having not washed her hands properly while preparing the food. He based his conclusion upon his interviews where he stated that no housekeeper ever told him that Mary was a clean cook. He did not say whether he asked them or not or rather just assumed that their lack of addressing it was proof that Mary was unsanitary. Soper then stated that, in the most thorough “investigation,” he believed that the bacterium was carried from Mary’s hands to the people who ate ice cream containing cut-up peaches that she had prepared. Again, no evidence was provided beyond his belief. Soper was amazed that no one had ever discovered an asymptomatic carrier in America before him. Interestingly, Soper revealed that he was long interested in the transmission of typhoid fever and knew of Robert Koch’s work. He stated that his interest in this area was longstanding and that Koch’s work was the basis for his own investigation. He admitted that he had read several papers on the probable role of healthy carriers in producing typhoid. Soper was made aware by Dr. Simon Flexner, of the infamous Flexner report, to some of these references after he had concluded his work on the Mary Mallon case. It is very clear that Soper went looking for evidence to fit his preconceived conclusions as to what the cause was. He was also potentially guided along the way:
The Military Surgeon Vol. XLV July, 1919 Number 1 Original Articles Typhoid Mary
By Major GEORGE A. SOPER
“It was expected by me that the germs might be found in the urine, but more probably in the stools. None was found in the urine. The stools contained the germs in great numbers. Daily examinations made for over two weeks failed only twice to reveal the presence of the Bacillus typhoid and on these occasions the sample taken was perhaps too small to reveal them. The blood gave a positive Widal reaction. The cook appeared to be in perfect health.
The feces were examined on an average of three times a week from March 20 to November 16, 1907, and in only a comparatively few instances did the investigators fail to find the bacilli. During the summer months the culture plates contained only a few typhoid-like colonies. In July there were five consecutive negative tests followed by a positive one.
During August the stool showed no typhoid; in September they began to appear again; from September 11 to October 14, 1907, the feces failed to yield typhoid bacilli. During this time the patient’s diet was carefully regulated and she was receiving mild laxatives. On October 16, 1907, a very thorough test showed that the germs were again present. From October 16, 1907, to February 5, 1908, weekly examinations of the stools gave, with only two exceptions, from 25 to 50 per cent typhoid-like colonies on the culture plates. These exceptions were on November 13 and December 4, when no typhoid was found. The implication was plain. The cook was virtually a living culture tube in which the germs of typhoid multiplied and from which they escaped in the movements from her bowels. When at toilet her hands became soiled, perhaps unconsciously and invisibly so. When she pre-pared a meal, the germs were washed and rubbed from her fingers into the food. No housekeeper ever gave me to understand that Mary was a particularly clean cook. In the Oyster Bay outbreak, which was studied with more particularity than the others, the infectious matter is believed to have been carried from the cook’s hands to the people who were later taken sick by means of ice cream containing cut-up peaches. Mary prepared this herself. In this instance no heat sterilized the washings from her hands. Mary Mallon was kept virtually a prisoner by the Department of Health for three years. At first she was held at the hospital for contagious diseases at the foot of East 16th Street, Manhattan; later she was removed to Riverside Hospital on North Brother’s Island in the East River, between Hell Gate and Long Island Sound.”
“The case is least remarkable for the reason that it was the first of its kind to be worked out in America. It is surprising that nobody bad discovered a carrier before. They are now known to be rather common.
Somewhat similar investigations bad been made in Germany) and I make no claim of originality or for any other credit in her discovery. My interest and experience in the epidemiology of typhoid had been of long standing. I had read the address which Koch had delivered before the Kaiser Wilhelm’s Akademie, November 28, 1902, and his investigation into the prevalence of typhoid at Trier 3 and thought it was one of the most illuminating of documents.In fact it had been the basis of much of tile epidemic work with which I had been connected.
Koch’s address was not the only one printed about this time to show that healthy carriers might exist and give rise to typhoid. Conradi and Drigalski4 had anticipated Koch and it was probably on the suggestion contained in their paper to the effect that with their new culture medium they had found typhoid bacilli in the stools of several well persons that Koch’s flying laboratory was sent to Trier and the ground prepared for his Kaiser Wilhelm’s Akademic address.
In the Festschrift Zum SeclizigstenGeburstag von Robert Koch, which appeared in 1903, there are several papers on the probable role of healthy carriers in producing typhoid. About this time Kayser, Klinger and others were publishing in Arbeiten aus dem Kaiserlichen Gesundheit-smate reports of cases which they found to be due to persons whose condition was much like Typhoid Mary’s. Dr. Simon Flexner kindly called my attention to some of these references after I had concluded my work on the Mary Mallon case.”
After the highly publicized Typhoid Mary case, this idea of asymptomatic carriers simmered in the background over the next century. While there were claims of such a state in certain diseases, this has never been scientifically proven. However, that did not stop Koch’s escape clause from taking a prominent role in the “Covid crisis,” primarily due to a mass testing campaign that was bound to identify positive cases in healthy people using fraudulent tests never calibrated and validated to purified and isolated “virus.” Although all PCR results are false-positives, we can see that even the CDC noted that testing people without symptoms generates false-positive cases. They stated as much under their PCR guidelines for pertussis when recommending not to test those without symptoms:
Diagnosis PCR Best Practices
“However, only patients with signs and symptoms consistent with pertussis should be tested by PCR to confirm the diagnosis. Testing asymptomatic persons should be avoided as it increases the likelihood of obtaining falsely-positive results. Asymptomatic close contacts of confirmed cases should not be tested and testing of contacts should not be used for post-exposure prophylaxis decisions.”
Thus, we can see that the CDC were well aware that testing people without symptoms will lead to an influx of cases labelled as asymptomatic “infections” when they are, in fact, not “infected” or diseased at all. This massive amount of asymptomatic cases of “SARS-COV-2” based upon fraudulent test results has cemented the illogical concept of the asymptomatic carrier into the minds of the populace. A timely December 2020 review, while reiterating the history of the asymptomatic carrier described above, pointed out the fact that even though asymptomatic infection and transmission has always been a concept waiting it the wings, it has only recently been thrust into the limelight with this “pandemic:”
Invisible epidemics: ethics and asymptomatic infection
History
“Dr Robert Koch was one of the founders of modern microbiology, and his work is particularly well known for a set of postulates (first published in 1890) linking microbes with the causation of infectious disease (Gradmann 2010). Though variously expressed, one of Koch’s initial postulates was that the microbe putatively responsible for a disease should be found in all people suffering from the disease, but not in healthy individuals (Gradmann 2010). Koch soon realised that this did not hold true in all cases, since many potentially pathogenic organisms are frequently found in healthy people. For example, Koch observed that asymptomatic carriers of cholera, typhoid, and malaria could spread these diseases to others, and he is credited for inventing the concept of the carrier state (i.e., in which healthy people asymptomatically carry an infection) (Gradmann 2010).
Public awareness of asymptomatic carriage of infection increased, especially in English-speaking countries, with media reporting of the case of Mary Mallon (known as “Typhoid Mary”) beginning in 1907. Mallon was a cook working in New York who, although showing no signs of typhoid disease herself, spread typhoid bacteria to many other people, resulting in several deaths (Brooks 1996; Soper 1939). For the general population, this revealed an important truth: that “persons, rather than things” (Soper 1939) were the source of many infectious diseases. Despite this Copernican revolution in public health (an epidemiological parallel of the microbiological revolution of germ theory), Mary Mallon and many others found it difficult to believe that healthy people could spread disease. Mallon repeatedly resisted public health restrictions and refused to believe she was infected or posed risks to others. She spent the latter years of her life living in public health confinement on North Brother Island, working as an assistant in the local infectious disease laboratory (Soper 1939).”
Implications for outbreaks, epidemics, and pandemics
“Asymptomatic infection was recognised to be a significant factor in the 2015–2016 Zika virus epidemic, particularly because many of those who were infected—including some women who acquired infection during pregnancy and gave birth to children severely affected by congenital Zika syndrome—showed few or no symptoms (Jamrozik and Selgelid 2018). Although less well recognised, transmission of asymptomatic Middle Eastern Respiratory Syndrome (MERS) coronavirus infection (perhaps both camel-human and human–human transmission) may play an important role in the epidemiology of MERS—which is all the more remarkable because people who develop symptomatic MERS infection have a high fatality risk of around 35% (Grant et al. 2019). Asymptomatic infection has also been reported for viruses closely related to the coronavirus that caused the earlier severe acute respiratory syndrome (SARS) epidemic. In one study from 2003, around 40% of Chinese wild animal traders had serological evidence of having been exposed to coronaviruses that closely resembled SARS-coronavirus, raising questions about whether people in high risk occupations should be screened for asymptomatic infection to detect potential “spillover” events of pathogens with epidemic potential (Guan et al. 2003). We initiated the November 2018 Brocher Foundation workshop upon which this Special Issue is based partly in light of the growing awareness of such cases of asymptomatic infection—and their ethical implications for policy and practice.
Since that time general awareness of asymptomatic infection has skyrocketed in light of its role in the coronavirus disease 2019 (Covid19) pandemic, in virtue of which the term ‘asymptomatic infection’ has become highly familiar to ordinary members of the general public. Early data, which were later widely confirmed, suggested that asymptomatic transmission of Covid19 occurs both in cases where the individual transmitting the virus goes on to develop symptoms later (i.e., they were “pre-symptomatic” at the time of transmission) and in cases where they never develop symptoms (Hu et al. 2020). Asymptomatic individuals can, under certain conditions, transmit to large numbers of other people (e.g., one person was shown to infect 71 others) (Liu et al. 2020). The overall degree to which asymptomatic transmission contributes to local Covid19 epidemics likely varies in different contexts and has not always been well-characterised (in part because of the difficulties of identifying all asymptomatic infections during an epidemic). In any case, asymptomatic transmission of Covid19 raises a number of ethical issues similar to those discussed above, including those related to the justification of public health interventions such as screening and isolation for asymptomatic cases.”
While the asymptomatic carrier was made a star of the “Covid” show in order to generate fear and drive compliance towards quarantines, lockdowns, social-distancing, and masking, the message has been entirely inconsistent throughout, and the lack of any valid scientific evidence proving such a carrier state was on full display from the very beginning. At a White House press briefing on January 28th 2020, the idea of asymptomatically transmitting the “novel coronavirus” was floated out there as a possibility. The CDC claimed to have heard reports about asymptomatic cases but had not seen any of the data. At the time, poster boy Anthony Fauci stated that, based upon past evidence from respiratory “viruses” of any type, asymptomatic transmission was never a driver behind any outbreaks or spread of disease:
Asymptomatic transmission
“There’s a difference between someone who has the virus and is about to show symptoms and someone who gets it and never has any noticeable sign. The second type is purely asymptomatic and there was a lot of uncertainty on this point at a Jan. 28 White House briefing. The CDC said there were reports of it, but they hadn’t seen the data.
Fauci put the question into the context of past coronaviruses.
“We would really like to see the data because, if there is asymptomatic transmission, it impacts certain policies that you do regarding screening, etc. But the one thing historically people need to realize is that, even if there is some asymptomatic transmission, in all the history of respiratory-born viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there’s a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.”
However, a few days later on February 3rd, 2020, Anthony Fauci had changed his tune and stated that, based upon a single paper, he had no doubt that asymptomatic transmission was occurring and that the study he had read had laid the case to rest. Unfortunately for Fauci, the conclusive evidence that asymptomatic transmission occurred was based upon false information. The study in question claimed that a woman, who had been in a meeting in Germany with four people who later became ill, was an asymptomatic carrier as she had no symptoms at the time of the meeting and became ill upon her flight home to China. For some reason, the authors of the paper failed to actually speak to the woman and wrote the paper solely based upon what the four patients told them. Ironically, the Robert Koch Institute actually spoke to the woman and confirmed that she was symptomatic at the time of the meeting, thus giving Fauci a nice serving of egg on his face:
“Chinese researchers had previously suggested asymptomatic people might transmit the virus but had not presented clear-cut evidence. “There’s no doubt after reading [the NEJM] paper that asymptomatic transmission is occurring,” Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases, told journalists. “This study lays the question to rest.”
But now, it turns out that information was wrong.
The letter in NEJM described a cluster of infections that began after a businesswoman from Shanghai visited a company near Munich on 20 and 21 January, where she had a meeting with the first of four people who later fell ill. Crucially, she wasn’t sick at the time: “During her stay, she had been well with no sign or symptoms of infection but had become ill on her flight back to China,” the authors wrote. “The fact that asymptomatic persons are potential sources of 2019-nCoV infection may warrant a reassessment of transmission dynamics of the current outbreak.
But the researchers didn’t actually speak to the woman before they published the paper. The last author, Michael Hoelscher of the Ludwig Maximilian University of Munich Medical Center, says the paper relied on information from the four other patients: “They told us that the patient from China did not appear to have any symptoms.” Afterward, however, officials at the Robert Koch Institute (RKI), Germany’s federal public health agency, and the Health and Food Safety Authority of the state of Bavaria did talk to the Shanghai patient on the phone, and it turned out she did have symptoms while in Germany. According to people familiar with the call, she felt tired, suffered from muscle pain, and took paracetamol, a fever-lowering medication. (An RKI spokesperson would only confirm to Science that the woman had symptoms.)”
In March 2020, a top Chinese health official completely contradicted Fauci by stating that there was no evidence that asymptomatic carriers could spread illness to others:
‘No evidence’ asymptomatic carriers spread coronavirus, Chinese health official claims
“A top Chinese health official sought to allay growing fears over asymptomatic coronavirus carriers on Monday, saying there was “no evidence” they could spread the illness but medical workers should remain alert to the risk.”
Not one to be made the fool, in April 2020, Fauci suggested that there were millions of silent spreaders in the US. In fact, he claimed that asymptomatic infections made up anywhere from 25 to 50% of the infections. He backed his figures up by confidently stating that they were just guessing as they had no scientific data to support these guesstimates. Fauci stated that he wouldn’t have any “scientific” data until mass antibody testing was carried out. He said that it was impossible to know who is infected without symptoms until you test everyone who has no symptoms. This lends credence to the fact that testing people without symptoms will, as the CDC stated with pertussis, create nothing but false-positives:
Fauci once dismissed concerns about ‘silent carriers’ of coronavirus. Not anymore.
At Sunday’s White House briefing, Dr. Anthony Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases, suggested that hundreds of thousands — or even millions — of “silent carriers” may be unwittingly spreading the coronavirus across the United States because they don’t realize they’re infected.
The idea that at least some coronavirus carriers don’t feel sick isn’t new. But the scale of Fauci’s estimate was.”
“It’s somewhere between 25 and 50 percent” of the total, Fauci said. But “right now,” he went on, “we’re just guessing.”
“The first thing to note is that Fauci himself expressed a high degree of uncertainty about his own numbers. “I don’t have any scientific data to say that,” he admitted Sunday. “You know when we’ll get the scientific data? When we get those antibody tests out there and we really know what the penetrance is. Then we can answer the questions in a scientifically sound way.”
“Fauci was right to be cautious. As he noted, it’s impossible to say how many carriers never showed symptoms until you’ve tested a bunch of people who never showed symptoms — something that will only happen after the worst of the pandemic is over and scientists start trying to determine, en masse, who does and doesn’t have immunity. (More on that later.)”
“Last week Centers for Disease Control and Prevention Director Robert Redfield told NPR that “one of the [pieces of] information that we have pretty much confirmed now is that a significant number of individuals that are infected actually remain a asymptomatic.”
In June 2020, the WHO’s Maria Van Kerkhove disagreed with Fauci’s assessment of asymptomatic transmission by claiming that it appears to be rare based upon the data that was seen. In fact, she claimed that investigators were not finding any cases of secondary transmission from an asymptomatic carrier to anyone else:
Coronavirus spread by asymptomatic people ‘appears to be rare,’ WHO official says
“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,” Van Kerkhove said on Monday.
“We have a number of reports from countries who are doing very detailed contact tracing. They’re following asymptomatic cases, they’re following contacts and they’re not finding secondary transmission onward. It is very rare — and much of that is not published in the literature,” she said. “We are constantly looking at this data and we’re trying to get more information from countries to truly answer this question. It still appears to be rare that an asymptomatic individual actually transmits onward.”
However, by November 2020, Fauci was defiant against the WHO’s admittance that no secondary transmissions were occurring and stated that he was certain that 40-45% of the transmission was due to asymptomatic carriers. Fauci hammered home the point as to why masks, which he had claimed offered no protection in March 2020, were now essential in November 2020:
Anthony Fauci’s Thoughts on Covid-19 Transmission, Treatments, and Vaccines
“Speaking of asymptomatic spread, Fauci says that 40–45% of transmission is due to asymptomatic people unwittingly infecting others. This is why masks are so essential — by wearing one, you protect other people even if you don’t know that you’re infected.”
In December 2021, Fauci was defeated yet again when the “discoverer” of Omicron, Dr. Angelique Coetzee, questioned whether such a thing as an asymptomatic carrier even existed at all. She stated that they had seen no asymptomatic cases of Omicron and then recommended that those without symptoms need not test:
‘There’s no reason to test if you have no symptoms,’ and 2 other findings from the woman instrumental in first identifying omicron
“Notably, Coetzee suggested that asymptomatic cases of the omicron variant are rare, if such a condition exists at all.
Asked during a Christmas Eve interview on MSNBC if “there was not such a thing as an asymptomatic case of omicron,” Coetzee responded: “We haven’t seen it.”
Secondly, the chairwoman of the South African Medical Association also told MSNBC on Friday that she doesn’t recommend testing by individuals until, and if, symptoms arise from the variant. “There’s no reason to test if you don’t have symptoms,” she said.”
In another blow to the ego of “Science,” an April 2021 study published by the CDC saw Fauci’s statements contradicted yet again when the researchers found no asymptomatic transmission. In fact, they stated that their findings were in line with other studies and that asymptomatic transmission was unlikely to contribute to the spread of “Covid,” which torpedoed Fauci’s claims of 40-45% of transmission being due to those without symptoms:
Analysis of Asymptomatic and Presymptomatic Transmission in SARS-CoV-2 Outbreak, Germany, 2020
“We determined secondary attack rates (SAR) among close contacts of 59 asymptomatic and symptomatic coronavirus disease case-patients by presymptomatic and symptomatic exposure. We observed no transmission from asymptomatic case-patients and highest SAR through presymptomatic exposure. Rapid quarantine of close contacts with or without symptoms is needed to prevent presymptomatic transmission.”
Conclusions
“In this cluster of COVID-19 cases, little to no transmission occurred from asymptomatic case-patients. Presymptomatic transmission was more frequent than symptomatic transmission. The serial interval was short; very short intervals occurred.
The fact that we did not detect any laboratory-confirmed SARS-CoV-2 transmission from asymptomatic case-patients is in line with multiple studies (9–11).”
“In conclusion, our study suggests that asymptomatic cases are unlikely to contribute substantially to the spread of SARS-CoV-2. COVID-19 cases should be detected and managed early to quarantine close contacts immediately and prevent presymptomatic transmissions.”
While Fauci’s claims of asymptomatic transmission were obviously unfounded, there were many asymptomatic cases being generated due to the fraudulent testing, as predicted by the CDC with pertussis. Thus, the perception that asymptomatic people were spreading a “virus” was easily conveyed to the public based upon unscientific data. We can see evidence of the massive amounts of healthy people testing positive for a “virus” by way of the mandatory mass testing data that came out of China throughout the “pandemic.” For instance, in March of 2022, Shanghai reported that over 70% of their cases were asymptomatic.
Why is Shanghai seeing so many asymptomatic Covid-19 infections?
“China is in the grip of an Omicron wave, but about 70 percent of cases reported in March have not had any symptoms.”
“Of the 103,965 locally acquired cases reported in March, only 3,046 had symptoms, according to National Health Commission data. And most of the asymptomatic infections were reported in Shanghai.”
By November of 2022, China was seeing upwards of 90% of their reported cases described as asymptomatic.
China Reports Third Consecutive Daily Record for New COVID Cases
“China reported 35,183 new COVID-19 infections on Friday, of which 3,474 were symptomatic and 31,709 were asymptomatic, the National Health Commission said on Saturday, setting a new high for the third consecutive day.
That compared with 32,943 new cases a day earlier — 3,103 symptomatic and 29,840 asymptomatic infections, which China counts separately.
Excluding imported cases, China reported 34,909 new local cases on Friday, of which 3,405 were symptomatic and 31,504 were asymptomatic, up from 32,695 a day earlier.”
By December 2022, China had given up on reporting their overwhelming amount of asymptomatic cases in their daily Covid counts:
China stops publishing asymptomatic COVID cases, reports no deaths
“China’s National Health Commission (NHC) will as of Wednesday stop reporting new asymptomatic COVID-19 infections, as many people without symptoms no longer participate in testing, making it hard to accurately tally the total count, it said.”
There were many reasons provided for why China had so many asymptomatic cases but it easily boiled down to their untargeted mass surveillance testing of the entire population. It is clear that if one goes looking for cases, one will find them whether symptomatic or not. In China, it was very much the latter as they were seeing over 98% asymptomatic rates in Shanghai based upon their testing data. This goes against the idea that mass testing would find more symptomatic cases. As more healthy people were subjected to a fraudulent test, the more “healthy sick” people that could be added to the overall totals:
Explainer-Why are Shanghai’s COVID infections nearly all asymptomatic?
“The number of new confirmed community transmitted cases in the major financial hub of Shanghai reached 4,477 on Tuesday, a record high, but only 2.1% showed symptoms. The share of symptomatic cases over the previous seven days was around 1.6%.”
“Following are some explanations for why the rate of asymptomatic cases is so high.
Surveillance Testing
China is also the only major country to do mass, untargeted surveillance testing, which is bound to uncover more asymptomatic cases, although it could also be expected to reveal more symptomatic cases.
“Surely, high levels of testing will pick up more rather than less asymptomatic cases,” said Adrian Esterman, an expert in biostatistics at the University of South Australia.”
Mass testing with fraudulent tests led to a surge in healthy people being fraudulently labelled as asymptomatic carriers. It doesn’t matter that this very act of mass testing, as the CDC stated, increases the likelihood of false-positives (even though they are all false-positives). This perception of a massive number of “infections” of a “virus” regardless of any disease being present only helped to further solidify this illogical concept into the minds of a fearful public as if it were a scientifically proven fact when it is anything but. Ironically, despite their “test, test, test” mantra, the WHO actually claimed that its guidelines never recommended mass testing of asymptomatic people as was being done in China due to high costs involved and the lack of data of its effectiveness:
Analysis: Test, test, test? Scientists question costly mass COVID checks
“WHO guidelines have never recommended mass screening of asymptomatic individuals – as is currently happening in China – because of the costs involved and the lack of data on its effectiveness.”
Thus, we can see that there truly is nothing behind the claim of an asymptomatic carrier of disease other than the fraudulent label provided by technology never meant for diagnostic use, especially on such a massive scale as we witnessed during this “pandemic.” PCR can find anything in anyone and the result is utterly meaningless, as stated by inventor Kary Mullis:
“Anyone can test positive for practically anything with a PCR test, if you run it long enough with PCR if you do it well, you can find almost anything in anybody.”
“[PCR is] just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick, it doesn’t tell you that the thing you’ve ended up with really was going to hurt you or anything like that.”
The asymptomatic excuse was created in face of conflicting evidence by a man who wanted nothing more than to protect his prestige and his findings. Robert Koch was under pressure from a growing field of researchers who were either contradicting his own findings or making new discoveries of their own. Koch needed a way to ensure that his own research would stand up to scrutiny. Bending his own logical postulates in order to allow for the asymptomatic carrier to exist allowed for his contradictory findings, as well as those put forward by later researchers, to persevere in the face of any further challenges by opponents:
“Whatever I undertake these days, there will be a bunch of the envious and jealous at hand. They will try to challenge me and if they don’t succeed, try to make me turn away from my work in disgust.”
“Those happy days are gone when the number of bacteriologists was small and each of them could research wide areas in an undisturbed manner…So now in making the most modest and most careful delineation of a research area you will step on the first colleagues’ toes or bump into a second one unintentionally, or come too close to the third’s field of work. Before you even realise it, you are surrounded by opponents.”
It is clear to anyone looking at the idea of an asymptomatic carrier of disease logically that this very notion does not stand up under scrutiny. This nonsense was summed up brilliantly by the late great Canadian researcher David Crowe:
“Someone who believes in the virus can explain this conundrum to me.
“It has been strongly stated that asymptomatic people can be infectious for quite a long time (I can provide references if you don’t believe me, but this has been widely stated). This means that for quite a long time their body has a large quantity of virus particles, otherwise infection wouldn’t be possible. But their body doesn’t react to these particles, an immune reaction would at least result in a fever. But without an immune reaction they can never get rid of the virus particles. And how is it that virus particles running around the body of some people don’t do anything, whereas other people get seriously ill and die? How do all the virus particles in one person know that they shouldn’t mess with the cells to cause symptoms, whereas in another person they all go crazy and cause devastation?
“So we can conclude that (1) Asymptomatic people never get rid of the virus and therefore must be quarantined forever; (2) It’s the virus that’s deficient, not the person, which must mean there are multiple dramatically different strains; or (3) the viral theory is a load of BS.
“Please help me.”
-David Crowe March 31st, 2020
It is obviously number 3. The “viral” theory is a load of BS, and there is no such thing as a healthy sick person capable of transmitting disease. We have no reason to fear the walking healthy.
“…And he described it as a kill box and then I looked that up and it turned out it’s a military term for establishing a geographic space or three-dimensional area for a military attack by air and by surface to kill the people who are in it and then dismantle the kind of framework and move on to the next campaign.
And what the DoD and the World Health Organization intend to do and have gotten quite far in doing, but not completely reached their goals, is to set up the entire world as their geographic terrain, their target population as all the people in the world, the duration of their campaign as permanent…”
Transcript: Jan. 24, 2023 Legal Walls of the Covid-19 Kill Box Presentation
…And the basic idea is that public health has been militarized and the military has been sort of turned into a public health front or Potemkin Village such that they are using public health language and public health laws to actually carry out a military campaign.
And I would not call them DoD vaccines.
I would call them DoD weapons.
So, I call it the kill box because the first sort of lead that I had was Todd Callender’s January 30th 2022 interview on Elizabeth Lee Vliet’s podcast called Truth for Health.
And he described it as a kill box and then I looked that up and it turned out it’s a military term for establishing a geographic space or three-dimensional area for a military attack by air and by surface to kill the people who are in it and then dismantle the kind of framework and move on to the next campaign.
And what the DoD and the World Health Organization intend to do and have gotten quite far in doing, but not completely reached their goals, is to set up the entire world as their geographic terrain, their target population as all the people in the world, the duration of their campaign as permanent.
And the weapons that they’re using are, number one, informational. That’s the propaganda piece and the censorship piece.
Number two, psychological. That’s the fear and terrorism piece of telling people they need to be afraid all the time and they need to listen to the government.
And then the third piece is the chemical, biological, radiological, and nuclear [CBRN] weapons, which are called in their campaign pharmaceuticals, vaccines but are actually toxins and pathogens.
So I started, after I heard that interview — I had already been wondering what was going on but I started trying to track down some of the things Todd Callender talked about in his interview and figure out what the legal frameworks were and how they were set up and what the financial coercion mechanisms were.
My finding, which many other people have found in various, from various other angles, was that this project has been going on for centuries.
It’s basically globalist central bankers and lots of related organizations trying to get complete control of human beings through banking programs and through military programs.
And they kicked it into higher gear in 1913 with the Federal Reserve Act, and then they kicked the public health aspect of it into higher gear starting in the 1930s and 40s.
Before the 1960s, they mostly did it through orchestrated armed conflicts and financial depressions and wars, which are very loud and messy and destructive to infrastructure.
And it makes it difficult for them to have plausible deniability and legal impunity for what they’re doing.
So in the mid-60s they got much better at inducing suicide and homicide by fraudulently labeling poisons as medicines or as vaccines or as prophylactics and telling people that submitting to that poisoning process was their civic duty. And that’s — we saw that in Covid with the shorthand for “Do this or you’re going to kill your grandma.”
And the way that the pharmaceutical method is primarily useful to them is that plausible deniability is much easier and legal impunity is a lot easier.
They can achieve the same goal of killing lots of people without their fingerprints being all over it.
I looked into the coercion cascades, mostly financial. I’m not going to go into a lot of detail with that but it starts at the top with the Bank for International Settlements and they can use their control of other federal central banks, access to financial systems, and then all the way down through state governments, national governments, local, municipal, school districts, hospitals. Everything.
If you comply with what they’re telling you to do as far as masking and testing, isolating yourself, taking injections, then you will get the financial access that you need to run your business or to have a job. And if you don’t comply, they can cut you off from those services. And so that is one of the main mechanisms through which the whole thing was carried out.
The U.S. Congress passed the law to set up the Chemical and Biological Warfare program. And in that law, which is 50 USC Chapter 32, there are very important key terms including “protective,” “prophylactic” and “defensive,” which is how they justified doing it.
They were using those words because the international community of ordinary non-insane people were concerned about biological and chemical weapons and they were working on international treaties to prohibit them.
And so they needed to build in loopholes and the loopholes they built in were that, “We’re not going to do biological and chemical research and weapons development except for protective or prophylactic or defensive purposes.”
And that’s a false characterization because all biologically active products are intrinsically aggressive and toxic and lethal. And that’s where we get disciplines or, that’s the thing that disciplines like toxicology, pharmacokinetics, genotoxicity, drug-drug interactions, are all related to that fact: that everything that goes into the human body or any living body has some effects which can be toxic. So that was the way they tried to get around that.
And then the foundational Public Health Emergencies platform came out in 1983 when Congress passed the Public Health Service Act Amendment and that set up the Public Health Emergencies program under the 1944 law that had originally set up the Public Health Service. Which is a branch of the military.
And it also, in 1983, Congress and Reagan set up a 30 million dollar slush fund and that has continued. It’s got a different name now than it did then, [Public Health and Social Services Emergency Fund] but it’s still being funded as recently as the NDAA and the Consolidated Appropriations Act in December of 2022.
The other thing they did in the 80s was set up the 1986 National Vaccine Program and National Childhood Vaccine Injury Act.
And that’s the one that set up the liability exemption for manufacturers and funneled anyone who was injured by a vaccine into this different compensation program. And that’s been used as a model since Covid started, for the Countermeasures Injury Compensation Program.
So the international piece, the cornerstone, is the World Health Organization, which is not a health organization. It’s a military organization, because of this merger that I’m talking about. It’s sort of the military arm of the one-world government that they’re trying to set up.
And they did a set of amendments to the International Health Regulations in 2005 that entered into force in June 2007. But basically the IHR, which are currently going through another round of amendments to make them worse, called on national governments to strengthen their own domestic laws and fund more programs for surveillance, testing, detention and quarantine — physical control and forced treatment — during international outbreaks of communicable diseases.
And the pretext that they used, because it was bankers who were doing this, was that they needed to protect international trade from disruptions caused by disease outbreaks. But the real intent was to set up these legal systems that transferred sovereign government from the nation-state to the World Health Organization and the BIS automatically when a “public health emergency of international concern” [PHEIC] has been declared.
And Congress and U.S presidents and the cabinet complied with that demand from the World Health Organization.
So two of the key years were 1997 and 1998. That was when the beginnings of the emergency use authorization program was set up and when they transferred the CBRN [chemical, biological, radiological, nuclear] weapons stockpile from DOD, classification I guess, to HHS or CDC classification and control.
It was the same products, as far as I can tell. It was just a relabeling and a re-homing of them.
The EUA [Emergency Use Authorization], that was kind of a two-step thing. At the time the public was really upset about the use of unapproved vaccines for anthrax on military troops and the horrible adverse effects they were having.
So Congress passed a law in November [1997] to kind of revoke authorization for testing or using unapproved products on military troops. But three days later in a different law, made it so that the same programs could be done but the target population would be expanded from just military troops to the entire American population.
Then around 2000 to 2002, using the momentum from 9/11 and the anthrax attacks on Congress, they set up, through the statutes again, program management sort of structures. They did that through the 2000 Public Health Threats and Emergencies Act, [and] through the 2001 Authorization for Use of Military Force.
And people talked about this at the time. It was construed as putting the country into a permanent state of war — the Global War on Terror — with every other country in the world. So there was no geographic limitation. There was no time limitation. There was no identified enemy other than “terror” and through that — I think other people figured this out at the time and then it sort of got suppressed — but it made everyone in the world into a presumptive combatant or enemy target.
So it was essentially a de facto covert global martial law act by the US government.
And then in those early 2000s we also got the PATRIOT Act, the Public Health Security and Bioterrorism Preparedness and Response Act and the Homeland Security Act.
And those were just more of the merging of the DHS [Department of Homeland Security], the DOJ [Department of Justice], the HHS [Health and Human Services], the Department of Defense: all of the cabinet agencies.
So since then, 2003 to [2019] there have been lots and lots of executive orders on these things. Lots more statutes and appropriations. Lots of agency regulations, guidance reports that were circulated to state, local and tribal authorities and law enforcement so that they would know that under a public health emergency, they are subordinated to the federal military.
FDA [Food and Drug Administration] issued a lot of Guidance for Industry documents and sent
those out to the pharmaceuticals and to the academic organizations and NGOs [non-governmental organizations] to let them know about how FDA was going to handle experimental products like “vaccines,” “gene therapies,” “biologics.”
And they did more test runs like 2003 SARS, 2006 MERS and 2009 H1N1.
That brings us up to the Other Transactions Authority [OTA]. And this was revealed through Pfizer’s April 2022 motion to dismiss whistleblower Brook Jackson’s False Claims Act case.
They said, “This was not a vaccine. It was a DoD prototype and we were never obligated to do valid clinical trials. We were never obligated to prove safety or efficacy to anyone. We never had to get FDA authorization through any of the normal guidance for industry channels, because it was a prototype.”
On October 4th, 2022, the US government endorsed that view and filed a statement of interest and support for the motion to dismiss, basically saying that clinical trials were never material or necessary for DOD to pay the contractors for producing and distributing the bioweapons known as Covid-19 vaccines.
And so all of this became visible from 2020 to the present when the World Health Organization Secretary-General issued the “public health emergency of international concern” [PHEIC] at the end of January 2020 and the HHS secretary immediately triggered the domestic frameworks through the “determination that a public health emergency exists” followed by PREP Act declarations for “medical countermeasures,” which are the weapons.
And then Congress and the presidents — Trump and Biden — passed several additional Congressional acts funding and reinforcing the structure of the kill box and issued more executive orders under the Defense Production Act, under the Stafford Act, under the National Emergencies Act, to sort of build out the program.
Basically what it built is a huge public and private funding stream for military-led bioweapons research and use; eliminated informed consent by reclassifying people who could potentially be carrying a disease as presumptive national security threats, so that you could do anything you want to them because you’re on a war footing.
And to shield the products and weapons from product liability, to shield all the people involved from criminal liability and civil liability, and to shield the government funders, developers and regulators from criminal prosecution under the other laws — which are in place but are sort-of superseded by this framework — for use of bioweapons [18 USC 175] use of chemical weapons [18 USC 229], terrorism [18 USC 2331] things like that.
…I see it as a joint project between the U.S Department of Defense — a coordinating committee of that, the Federal Reserve, and the World Health Organization, and the Bank for International Settlements and the United Nations. But the World Health Organization is like a subsidiary of the U.N.
And there are things that the globalists do not like. They don’t like constitutions and charters. They don’t like the conflicting statutory frameworks around bioterrorism, war crimes, genocide, torture. They don’t like any of that stuff.
They don’t like when states and provinces and counties and towns pass their own laws protecting informed consent, protecting people from, for consumer safety. They actually put out a report in October 2022, State Laws Limiting Public Health Protections: Hazardous for Our Health. And there’s a whole bunch of things in there that states have started doing that the globalists do not like.
So doing more of those things, more bringing control back to the state, more using Article 10 of the Constitution, to reclaim state authority, those are all extremely useful.
And I do think it’s going to break. I think there’s going to be a tipping point and the criminal prosecutions are going to start.
And we have all the evidence. And every time they try to answer what we’re talking about by saying national security, they reinforce that this is the right way to go.
This is what they’re doing.
They’re doing war crimes.
Links:
Jan. 24, 2023 – DoD ‘Vaccines’ Press Conference. (L4Atv1, 2 hrs — 0:00:30 Sam Dube – Host Open; 0:03:04 Glen Macko – Overview of DoD Vaccines; 0:05:28 Katherine Watt – Legal: Laws, Contracts, FOIA, SEC; 0:24:39 Sasha Latypova – Manufacturing, Safety, Quality, Intent; 0:33:32 Phillip Altman – Conformation of Skills/Knowledge of Katherine & Sasha; 0:38:08 LTC (Ret) Pete Chambers – Vaccine observations in Military; 0:46:13 Dr Sam Dube – Guidance on “Going Local” for personal protection; 0:56:47 Q&A)
It’s worth asking why now, because by any objective measure, there has been no virus activity worthy of the words ‘pandemic’ or ‘emergency’ for a very long time. The answer seems to be the failure of Corona to return in the winter, as long-absent influenza succeeded in suppressing Corona infections (in accordance with my prediction), and the increasing disinterest of the public in obtaining official test results has put all virus statistics in the toilet. They’re ending it now, in other words, not because anything on the ground has changed, but because they no longer have any hope of the scary headlines necessary to keep the machine up and running.
As in the beginning, so in the end: The pandemicists will give you always and forever the maximum virus suppression and the maximum vaccination that is politically possible. Not what is prudent, or what has any hope of achieving anything, or what has evidence in its favour, but simply the maximum that they can give you, for as long as they can give it to you. That is a reason in itself, never to let the pandemicists anywhere near the levers of power ever again.
With the Covid vaccination campaigns concluded, the European Union is sitting on an enormous vaccine surplus – and hundreds of millions more doses are expected to arrive this year and next… Because they are not needed, EU member states have been trying for months to retroactively adjust the contracts, without much success.
One country has now lost patience in the face of the tough negotiations, and is venting its anger. The Polish Health Minister Adam Niedzielski on Tuesday sent a letter to the “shareholders of Pfizer” [which] says that the delivery of hundreds of millions of doses planned by Pfizer despite a “stable epidemic situation” is “completely pointless.”
The excess doses can no longer even be given away; there is no government “interested” in Covid vaccines, said the minister …
Niedzielski also breaks prior agreements on the confidentiality of talks between governments, pharmaceutical companies and the mediating EU Commission … [and] reveals what Pfizer is offering the states: They’ll reduce the total quantity of the outstanding orders, in exchange for half the price of each dose that is not produced: “That’s a charge for literally non-existent doses that were never produced and will never be produced and that don’t cost Pfizer a penny.”
No wonder there has been such urgency to keep these negotiations secret.
Niedzielski writes that he is “extremely” sorry, but he is forced to conclude that the company is not prepared to show “a satisfactory level of flexibility and make any realistic proposals.” … The health minister called on Pfizer to “live up to its responsibility towards EU citizens and member states and work in good faith towards a solution that is fair for everyone.” Poland wants to continue to believe that the pharmaceutical industry is not only about money.
Some guests have argued why there is no such thing as an immune system.
Some guests have thought about alternative causes of illness.
The point is that there are good reasons to question the conventional model of “Rockefeller medicine”. Much of it doesn’t make sense and desperately requires critique.
Blindly believing what the pharmaceutical industry, governments and media preach from their pulpits, after observing the Covid™ scam, is utterly ludicrous. I have become an allopathic atheist. An apostate.
Climate science is drowning in pseudoscience and so is virology.
Andrew Kaufman, who has been on my show a few times before, joined me for the following conversation of conversations.
A beginner’s guide to Germ Theory.
He approached important concepts, including
virus definitions, isolation and fake existence claims;
understanding contagion and “catching” something from somebody;
bacteria and germs in general;
why all vaccines are toxic;
what is disease, actually;
shifting paradigms about health and wellbeing and
the significance of bringing down this house of germs cards.
Dr. Melissa McCann raised more than $110,000 to crowdfund the case, which accuses the Australian government of negligence related to the approval and monitoring of COVID-19 vaccines.
At least 500 Australians have already joined a “landmark” COVID-19 vaccine injury class action lawsuit filed this week against the Australian government and the medicines regulator seeks redress for those allegedly injured or left bereaved by the COVID-19 vaccines.
The action was filed in the Federal Court of Australia, New South Wales Registry.
According to the lawsuit, the respondents approved the vaccines “with no proper or reasonable evidentiary or logical basis to reasonably determine the Vaccines to be safe, effective and possessing a positive risk-benefit profile.”
“The action will argue that the Therapeutic Goods Administration did not fulfil their duty to properly regulate the Covid-19 vaccines, resulting in considerable harm and damage to Australians.”
The suit alleges the government “acted negligently in approving the vaccines and also by failing to withdraw them” based upon the “known evidence” of risk.
“Australians who have experienced a serious adverse event following Covid-19 vaccination are invited to step forward and register for this class action,” Strijland said.
A spokesperson for the Department of Health and Aged Care said that the department “is aware” of the lawsuit and that “as the matter is before the court it is not appropriate to comment further.
Class actions provide “a path to justice” for people who may not have the resources to file a court claim on their own, said Alison Bevege, a journalist who has written for Reuters and Daily Mail, in an April 26 Substack post.
Those injured by COVID-19 vaccines have been “ignored, denied, belittled and marginalised,” Bevege added.
Australian doctor crowdsourced $110,000 to bring class action suit
Thank you for sharing this news @RefugeOfSinner5 These injured and bereaved have suffered immense loss, pain and grief. Just as heartbreaking has been the gaslighting and silence, which has left them feeling abandoned. We cannot simply 'move on' from covid and leave them behind. https://t.co/TSxqYaqtOf
According to McCann, the class action suit was necessary because Australia’s federal vaccine injury compensation program — the COVID-19 Vaccine Claims Scheme — was “not fit for purpose” and had left many vaccine-injured Australians “abandoned with no support” after being promised “fair and accessible” compensation.
Services Australia as of April 12 had received 3,501 applications and paid 137 claims totaling more than $7.3 million, with 2,263 claims still in progress and 696 deemed not payable, news.com.au reported.
By comparison, the U.S. government, as of April 1, approved its first three payments to people injured by COVID-19 vaccines — amounting to a total of $4,634.89. Since the start of the pandemic, Americans claiming injuries related to COVID-19 vaccines and other countermeasures submitted 11,425 requests for compensation.
“TGA had determined that several young previously healthy children died of COVID-19 vaccine-induced myocarditis. Redacted letters from the TGA to McCann indicated these facts and an admission of willful concealment,” McCullough said.
‘I’d never known what a heart attack would feel like’
Among those represented in the lawsuit is Melbourne teacher Gareth O’Gradie, a previously healthy father of two who before he got his first Pfizer shot in July 2021, was into running, footy, cricket and tennis.
“Six days after [the vaccination] I had sudden-onset chest pain, shortness of breath, fever, chills, sweats,” he told World Freedom Alliance. “I’d never known what a heart attack would feel like, but that’s the type of thing I expected.”
O’Gradie, 41, was rushed to the hospital, where he was diagnosed with vaccine-induced pericarditis. He said:
“In the end I had open heart surgery to remove the pericardium, which had become inflamed and stuck to my heart. It’s extreme.
“All the heads of different departments, cardiology, rheumatology, cardiothoracic, all had conferences to say, ‘We’ve tried this, what is the next step for this recurrent pericarditis we can’t control the pain for?’ It wasn’t an easy decision.
“They said, ‘Nothing’s working — this is what we can offer.’”
“There was a lot of, you know, ‘We need to not scare the public as part of the vaccine rollout, so let’s not publicise these things,” he told news.com.au. “There was a large, intentional withholding of information — that doesn’t give people informed consent.”
TCTL editor’s note: As shared here yesterday, Marvin Haberland went to court in Hamburg, Germany, early today with the intention of challenging the entire basis of virology. See yesterday’s article for understanding the case and the strategy.
Below you will find the announcement following the trial that appeared in German at Next Level telegram channel. You will also find an interview of Marvin immediately following the trial.
At this point, all information sources are in German. I have used various software tools to create rough transcriptions and translations, which were then edited. Please understand that I do not speak German, so consider these rough translations.
From the gist of it, it seems that the case against Marvin was dismissed and that the state must bear all costs of the trial. Marvin was not allowed to present any information to the court. Yet, this is one of four dismissals that Marvin has witnessed, all using this same strategy. Clearly, the courts are avoiding admitting the evidence that reveals the fraud of virology into public record.
The video includes interviews with a few of the attendees who shared their observations and perspectives. ~ Kathleen
In short: Our press spokesman Marvin Haberland won the trial as expected, in which the court dropped the case and paid the costs.
The subtleties in this are the big win:
(a) We went into this trial without a lawyer.
No lawyer wanted to defend us by supporting our strategy. Thus, we had no legal fees either. So it can be done without.
b) Our strategy is direct and clear
It aims to clarify the lack of science in virology in court, since Paragraph 1 of the Infection Protection Act requires it.
c) We have thus shown that the measures based on an imaginary virus are not justifiable and not tenable.
d) As has been shown, there is no need for complicated strategies, 400-page justifications or briefs. The only thing that needs to be attacked is the basis.
e) The possible avalanche effect
If many people would follow our argumentation, probably either all fines would be stopped, or someone would go to the next instance, where then the scientificity has to be clarified.
f) Our strategy and our expertise, as well as the evidence requests that could not be refuted, were known to all involved, both to the court apparatus and to the many employees whom we contacted throughout to make it clear that we were looking forward to the trial. Perhaps this was also one of the reasons why our trial was constantly postponed and unclear statements were made by staff.
Especially Important:
If the court, the state and others had known of something that they could have used to make a legal example of us regarding our requests for evidence, they certainly would have done so.
Thus, they obviously used the easiest “escape option” and simply discontinued the proceedings.
Notice:
We will get our chance, we will not let go. Virology will get mighty problems, we are sure.
Marvin is interviewed by Jen of Grosse Freiheit TV (found at Odysee & YouTube.)
Jen: [00:00:00]
Hello. Hello and welcome to a new episode of Grosse Freiheit TV. We are in Hamburg at the district court. Here was just the trial of Marvin. You probably know Marvin from my video. We made a video about how he wants to bring down the whole virology in court about five five months ago. And now here was just finally the trial. Marvin, what was it like for you?
Marvin: [00:00:21]
Yeah, so I wasn’t expecting that much of an audience at first. The room was super full. Very thankful for everyone who came. Yes, it was unfortunately only a partial victory, you can say.
As expected, the proceedings were discontinued. So the court costs etc. are borne by the state treasury. One does not have to pay anything, no misdemeanor. But of course, this is not the result one would have wished for now.
I would have liked either to be sentenced or to get an acquittal, so that somehow you have something in writing in your hand. That way, when it’s stopped…
I mean, the judges are also clever, of course. They want to stop it so that they don’t get into trouble, and so that they don’t open up a big can of worms, of course. But that’s not the desired result.
But well, in the end, the judge summoned a witness, a police officer. She couldn’t remember anything and then he stopped the proceedings immediately.
So I had no chance at all to say anything. He then said yes, you have submitted numerous motions for evidence here, but I don’t want to keep you in suspense any longer. I will stop this today, he said, but then I wanted to declare him biased, because this does not meet his responsibility, so to speak. And he didn’t allow that anymore, because he said that the proceedings are over.
So it was obvious to them, to the spectators, of course, that this was just embarrassing. But well, he got quite red in the face, the judge But that’s how it is.
Jen: [00:01:55]
He then also immediately threatened the audience. Then it got a little bit louder, so the people. Yeah, I did too. I thought ‘so, now it’s about to start, now he’s going to be insulted by everybody’. But fortunately the people held back. And then he also said something like, yes, hold back, otherwise I’ll have to have the hall cleared and you’ll be reported to the police. He impressed the people with his authority, so to speak.
Marvin: [00:02:20]
Yes, right, exactly, yes, hides there just a bit behind the barricades, behind this legal facade. But he was visibly uncomfortable. Did you, did you notice? But he probably just has too big problems when he gets involved.
So in my opinion, there were also a lot of people there today. You can then spread this, carry it out, Look here, if you go this way or if you get fines or also with other topics, with vaccinations, if you address the scientificity, so to speak, the virus existence question, which is always played down or ignored by everyone or by many.
That is the only way to lead these things to success, because an attitude is also a success in itself.You just don’t have to pay the money.
If everyone knew that, every citizen would no longer have to abide by these rules, no one would have to follow the vaccinations or other things and would just not have to be afraid of anything, because that only works on this fear basis. Exactly.
Jen: [00:03:25]
Can you report back. You’ve seen other trials in Hamburg. Have they all been stopped?
Marvin: [00:03:30]
Yes, all the trials that used the argumentation with paragraph one, that the scientific nature of virology is not given and therefore the penalty notices are all illegal, they were all dropped.
That was a total of four that I accompanied, including my own proceedings. And they were all simply discontinued, even two of them by the same judge without justification, simply ‘I will discontinue it now. Done.’
Jen: [00:03:56]
And what was your impression here on site?
So you wrote me yesterday evening, you wrote me only then, so about yes, here are security checks and then I have, when I came in here, I have just seen how at the airport you become. You have to leave cell phones there. I had to leave my camera in the car and now someone from the audience, you’re about to see the whole player again. He also said that it seemed to him a bit like sabotage, that the people were left outside, that they didn’t deliberately create a queue, that they deliberately chose a small hall. I also said, I don’t know what it’s like here otherwise, I’m never here otherwise. What is your impression? Do you think it was deliberately done that way, because of course they got it? It gets big media noticed that it gets a big media attention. What is your impression? You have also been standing here in front of the lock.
Marvin: [00:04:49]
Exactly. So I’ve been here a couple of times. So I can’t agree with that. I don’t think that there was blocking, I haven’t been able to determine that now. It was a long queue, because many people were there. But they got in quite quickly. I think the hall is actually the largest one they have here. Well, or there is a bigger one. Okay, but it was definitely big, I think.
Of course, not everybody got in. I didn’t see exactly how many didn’t get in, but I think there were about 40 people sitting in the back of the hall.
Yes, basically you can say that the judge knows from the beginning that he wants to stop it.
It doesn’t matter what I said. It doesn’t matter what the witnesses said or didn’t say, in the case that it is to be stopped. That’s programmed from the beginning. And yes, that is already valuable to know, if you have this strategy, then you are just so strongly right that the legal system cannot help itself any more than to just stop it. That’s their only chance to even cover this thing.
Jen: [00:05:58]
Yes, I say the judge, then his hands were more or less tied. If he had actually said, I’ll invite an expert and that would have come out accordingly, that the whole virology, that this is simply not scientific, then it would probably have been the same for him as for the judge in Weimar. Or what would you say to that?
Marvin: [00:06:15]
Yes, that’s exactly how I see it! So of course the judge is under extreme pressure. I mean, if he had done that, then it would certainly have been similar to the judge in Weimar or it would have had other consequences. He also happened to be ill two weeks earlier in October, when the actual hearing was scheduled. I don’t know whether that was for strategic reasons.
In any case, I can say that ‘I saw you here’ in the building during this time shortly afterwards. He had other OWI proceedings that I was in the room for at the time. So he was, in any case, healthy again shortly afterwards and then it still took half a year until I got the invitation here again.
So you can think about it, was that just to annoy him or to put him on the rack? Well, I mean, in the end it doesn’t matter. I just want to show the public that this kind of thing is simply stopped. Everybody can follow that and that’s good.
Jen: [00:07:14]
So what’s the way forward now? Are you going to pursue further litigation or what is your next course of action now to bring down this viral lie?
Marvin: [00:07:25]
Yes, so I’ve talked to some audience members today who actually still have cases pending, some of them even now in the second instance. So we can certainly support there.
And yes, I will simply continue to get involved in the area and of course by making this so public, that was also my goal, people also see from this. Hey, this will simply be stopped.
These arguments are not discussed at all in court, they are not even taken up, they are simply dropped.
So there’s probably something really hot cooking. So it can’t be completely wrong.
And of course also with friends and family, etc., who have all understood that in the meantime, even those who were super-pro, so to speak, on the subject of vaccination or corona have apologized to me in the meantime and also understood that, so to speak.
And that is actually the only thing that we also want to achieve, which is simply to provide clarification and in what way it is now done, whether with attitudes or with a verdict, it is actually the same for us, because we make it public anyway.
And yes, with the attitude is the thing actually, so to speak. Silence can also be something — can also be a statement in that case.
Jen: [00:08:37]
All right? Yeah, thank you so much for putting yourself out there. And now here are a few more impressions from the hearing here.
Trial Attendee#1: [00:08:43]
Our jurisprudence is totally screwed up, so screwed up. The judge already had his verdict. It was so obvious, because yeah well, there was another policewoman called as a witness, but she couldn’t remember. A subject, that was a joke. So that was to make it appear it was a really good trial. No, it wasn’t. He then also outed himself, after all, by saying, ‘Yes, I don’t want to keep them in suspense for long. I’m going to stop the proceedings.’
Trial Attendee #2: [00:09:11]
And they weren’t up for the expertise thing and that’s why they said okay, let’s shut this thing down before we do any more damage to our already placed ship. That was actually my impression.
And it was also interesting that the judge, when asked why he had made this decision, only referred to his judicial sovereignty. So one cannot say more to it… Now that the fairy tale, the narrative, so to speak, little by little disintegrates, one simply does not want to let in still such long discussions, which could still increase the damage…
Trial Attendee #3: [00:09:45] That happened very quickly. The policewoman couldn’t remember. Right. But when the judge asked again if there was anything with an affidavit or something. then all of a sudden she could remember, but not really. So it seemed to me like it was a little comedy that was being performed. The policewoman then also went out again and then then the judge then stated ‘yes, I’ll put that then’.
Jen: [00:10:10]
On, Have you been in the room?
Trial Attendee #4: [00:10:12]
[This clearly did not translate well.] No, So we were actually, let’s say in a relatively strange way ultra-slow dispatched here I as extra because of the process traveled to and did not know that here somehow so a kind of combination control, courtroom and airport takes place. Was there but male female separated, there it went already. Then was yes the process begins.
Jen: [00:10:33]
Let’s see, it was missing.
Trial Attendee #4: [00:10:35]
Exactly and 10:30 only up. So there was already the smell of sabotage somehow in the air, I say. We were then still upstairs and then Mr. Marvin already came out and announced, the process was stopped. So all in all, half hour wait and one minute information.
Trial Attendee #5: [00:11:02]
I’m not a lawyer. Maybe they have their formal legal reasons, but it makes you wonder if it’s our court and our state.
Trial Attendee#1: [00:11:12]
It is. I would have quite liked to see 100 years of virology just go down the drain. But that’s not going to happen because they’re just too powerful.
Dear friends, here is the recording of my very interesting conversation with Marvin Haberland. Marvin is an engineer and he comes from Germany. As a result of a tragedy in his family, he decided to investigate the subject of medicine. This investigation led him to virology, and he eventually discovered that the foundations of virology were based on anti-scientific misconceptions. After realizing this, Marvin decided to act.
Our conversation today will focus on his upcoming trial in Germany on April 26, 2023, in Hamburg. This trial will be the second trial in history designed to disprove virology and demonstrate the lack of real science behind it.
References cited in the interview with Marvin Haberland.
Marvin’s letter to the court and his Freedom of Information request:
Transcript of first 25 mins. prepared by TCTL editor:
Katie:
Hello everyone. My name is Katie and today my very special guest is Marvin Haberland.
Marvin is an engineer and he comes from Germany.
As a result of a health tragedy in his family, he decided to take a deep look at medicine. That exploration led him eventually to virology and, as a consequence, he discovered that the foundations of virology are based on anti-scientific misconceptions.
Marvin decided to do something about this realization.
Our today’s conversation will revolve around his upcoming court case in Germany, which as far as I am aware, will be the 2nd court case in history that aims to disprove virology and demonstrate the lack of real science behind it.
So, Marvin, I think it would be great to talk about your story.
What got you interested in the subject of virology and how did you start noticing there is something wrong with it?
Marvin:
Yes, thank you for the invitation.
Katie:
You’re welcome. Thank you for coming.
Marvin:
So, like you said, basically due to a tragedy in my family. So my grandmother, she died when I was studying in the US.
And that got me quite interested in the topic; as she, before she was diagnosed with the cancer, she always asked me, ‘Marvin, you’re always so smart. You’re always researching things. Can you help me?’.
And I was always saying, which I now regret, ‘Grandmother, look, I don’t know. I have no knowledge on this topic. Please go consult the doctors.’ And so on.
I was kind of ignorant, which from today’s perspective, of course, I regret. But this is the way it is.
So when she died, this triggered something in me and I started to then really research the topic of chemotherapy. And I found out that basically it’s not really based on evidence. There are very, very low-quality studies without any control groups. There is always comparing chemotherapy to another chemotherapy, or chemotherapy to chemotherapy plus a new drug. But there is never the zero control group, without any therapy, or very rare to find that.
And actually if you research the real figures, the efficiency of the five-year survival rate is about 2.3% only, which is basically zero because the statistical fluctuations.
So when I found this out it was very surprising to me. And then from that point, I also looked right and left of this topic to nutritionist sciences where I found very, very similar results. And also infectious disease and germ theory. And that got me interested in the field.
Katie:
From when you started your research, what was the first thing that you started to research the virology topic?
Marvin:
Yeah. So first was basically chemotherapy/ cancer, then nutritional sciences. And from that I moved on to virology and I found out about Stefan Lanka’s work.
So basically, first was the measles virus and the early scientific practices, or unscientific practices, of Enders and Peebles in 1954. And then I also researched, of course, Pasteur and Robert Koch, from the really early beginnings of germ theory and vaccinations.
And then from there I moved on to HIV.
I bought the book — I have it here — the ‘Virus Mania’ book from Engelbrecht… and other authors, which got me very interested in HIV also.
And then I discovered there is a pattern in virology. It’s always the same.
So, measles, HIV, SARS-CoV-1… These are repeating patterns which I found very interesting.
And then when covid or corona came up, I immediately did the research.
I remember in January 2020 when this came up, I went to GISAID [China National GeneBank] and other platforms where they upload the genomes. And I tried to figure out — OK, maybe this time they did the correct isolation, the correct scientific procedures.
And I figured out, OK, this is the same like with the swine flu, with the bird flu, with the SARS-1.
So from very early on, I was interested again.
I decided to start to be more active in speaking out and do work in this field to spread the misconceptions and the scientific fraud, basically.
I thought this was important because many people don’t know about this and I felt responsible to share.
Katie:
Let’s talk about the court case and what motivated you to go there, to do it. And what did you do?
This is important. What did you do to get there? And why are you doing it? And what is your goal?
Marvin:
First of all, I got motivated to do it, basically, also by Stefan Lanka who had a court case in 2015 about measles virus.
So little different strategy than mine, but pretty similar.
And he was saying in the beginning of covid, ‘OK, people of Germany, if you get these fines because you’re not wearing the mask or because you are meeting with other people during the lockdown, and so on, just…’. He laid out the basic strategy how to go to court.
And what I did is I just didn’t wear the mask. I had a mask zone directly in front of my house, so I couldn’t even exit my door without wearing a mask, which I didn’t want to do.
And after receiving the fine, I just objected it and I sent the court specific abstract from the law, which is basically the first paragraph, in Germany, of the infectious disease law, which says that every virologist, every institutional authority, has to work according to the status quo of science, scientific practice.
And I am basically saying that in virology this is not at all the case. And they are not following the scientific method. And not any sort of scientific method that is required.
And I sent proof to the court from several different Freedom of Information acts…
I sent one to the University of Melbourne in Australia and several others.
So my argumentation is basically the law is is not fulfilled, and these are my proofs. And this is why I am not willing to pay the fine.
Basically this is just the strategy. And we will see how this goes.
It will be on the 26th of April.
After my first invitation got cancelled. It was originally scheduled the 19th of October last year, but then I received a cancellation letter because the judge apparently got sick.
And now I have the second invitation. So we will see.
And there are many others that do this in Germany, so I have already consulted three other people with the same strategy and all three of these cases got closed.
So basically the people didn’t have to pay anything. But the court did not really issue a official statement. They just closed the case.
So what I want to achieve is official statement by the court. Because if they close my case, basically I cannot do anything about it. I have to accept it. But it has not the effect that I would like to have — basically to have an official statement ‘Yes, indeed, paragraph one of the infectious law of diseases is broken. Virologists are not working according to the scientific method.’ This would be my goal.
Or something else they could say, which is also possible, they could say that the law states that they should work according to the scientific method, but they don’t have to, right?
If the court says something like this and I have to pay the fine, it’s OK for me.
But then I have the official statement ‘Virologists are not obliged to work scientifically’. Which would be fine. This is just about our goal to to share the the situation — how it is.
Katie:
So let’s talk a little bit more about the main problem of virology, so people who are completely new to this, they can understand better the lack of scientific method behind it.
Let’s talk about all of this — about controls and about your Freedom of Information requests.
Marvin:
Sure. So basically, in science how it works is, you observe something in nature and then you come up with a hypothesis on how this could work. And then you try to come up with an experiment to test this hypothesis. And if the experiments support the hypothesis, then the hypothesis turns into a theory, and the theory gets tested over and over and over again. And all experiments support it. OK?
But if the experiment, the outcome, is against the hypothesis, then you falsify the hypothesis. This is basically how it works.
And in virology the hypothesis is fair. OK?
You say that you get sick from some viruses infecting you, coming from the outside. Infectious disease are being spread and so on.
And the experiments should be that you bring together sick and healthy animals or people and you show that you can really transmit this.
Or you try to extract these particles, these viruses, and then you take them and put them in the food or you spread them in the air of the animals or of the humans. And you show, by doing that, that you can replicate the symptoms.
That has never been done in virology.
What they are doing instead of doing it in the way I just stated, is they try to come up with some sort of excuse. They say that they cannot really do it in the correct way because the viruses are too small. Or too little in quantity. Or they only can live inside the cell and so on.
So they try to find excuses why they cannot extract the particle. And then they do some experiments in the lab.
So they never do it in a real ‘in vivo’. They only do it ‘in vitro’ in the lab. They take cell cultures and then they mix a lot of different chemicals, antibiotics and other substances together with fetal bovine serum, cell cultures from monkey kidney cells and so on.
They have a big brew of different components and then they observe that this cell culture basically disintegrates or dies. And they say, ‘OK, this is the proof for a virus’.
But this is impossible scientifically because there are so many variables. There are the toxic antibiotics, the fetal bovine serum.
Then they take off the fetal bovine serum so they remove the nutrition.
Then there is different other chemicals involved — trypsin sometimes and several different steps along the way.
So it’s impossible to say that the result is caused by a virus.
And what is on top of that unscientific — and everyone can understand this: They don’t have the control experiment.
So they are just running all these steps and they are doing what is called circular reasoning. And they don’t have any control.
They are trying to find causative results, cause and effect, but it’s impossible to do it. This is just a correlation. They observe that something happens, but they are not really using the scientific method to come up with the cause/effect relation.
The control experiment would be — for the viewers. You do the exact same experiment. You do the cell culture experiment with the chemicals, same antibiotics, same steps, everything the same. But you don’t add the so-called virus. This would be the only variable that should be different from the other experiment.
And the outcome then should be different.
If the virus would exist, and would be the cause of this cell culture disintegration, thy so-called cytopathic effect, then, only then you would prove that this is the determining variable.
But, of course, as they never have isolated the virus in the first place, they cannot even do this control experiment. It’s impossible.
And this is the big scientific problem.
I am willing to say that on some levels this is also fraud because they know. Because we asked them.
The virologists. Most of them know that the control experiments are missing and are important. They are trying to find excuses why they are not doing them, so they know exactly they should do them.
It’s not that they are unconscious. So I can say that this is basically fraud. Maybe not for everyone, but certainly for many virologists. They know exactly about this this issue.
Katie:
So in the court, you are going to point at this exactly — the lack of controls.
Marvin:
The center of the argumentation is the lack of control. And this is the reason why the first paragraph which states that everything should be done according to the scientific method, the recent scientific techniques and so on. And we have the German Association of Science which says that in order to work according to the scientific method, everything has to be controlled, right? Every experimental step has to be controlled and so on.
So this is very easy to then demonstrate to the judge that it has not been done in virology ever.
And I have many proof. Not not only me, many people have done that.
But for my case I have asked the University of Melbourne, in the Doherty Institute, which is their virology institute, basically, and they have published one of the first SARS-Cov-2 isolation publications. And it was the first publication outside of China.
And I asked them very early on if they did the control experiments for every step, including the genome sequencing. And they clearly answered that they did not do it. Very clearly. No excuse. Very, very straightforward. They said no, we didn’t do it for any of the steps.
And then I asked them why did you not perform the controls. And they told me very, very straightforward again. ‘We didn’t have the resources to do it. We were just focusing on the positive culture. And we had to work quickly. And we had no time.’ Basically, this was their answer.
So everyone can see that this is extremely unscientific. And the German Association of Science even clearly states quoting — I’m quoting them basically that they say that nobody should issue any sort of scientific paper, unless they have followed all the scientific steps, even if economic factors, monetary factors or the economic pressure is high. So you should not publish anything before following all the scientific steps.
And I think everyone would agree. So this is, as a proof, is a very good proof. Because usually if you ask virologists around the world, if you ask the official institutions — CDC, RKI, Pasteur Institute and so on — it is very unlikely to to get a straightforward answer like this. It’s very rare to get it. I was very lucky to get this straightforward answer. And this is what I’m using as a main proof. But then I use other proofs as well.
Katie:
Yes. Another question that I had is that there is this group you are working with that is called The Next Level and they help you.
Could you talk a little bit about them, who they are?
Marvin:
So, basically, next level is like a joint venture. We are basically coming out of two different telegram groups or channels that have evolved during covid and we are now working together with different scientists, doctors, engineers (like I am), mathematicians, computer scientists, and so on.
So we are quite a diverse team and what our main focus is basically health topics. So we try to dig deep into virology, germ theory, medications, disease in general, biology and so on. And our focus is the scientific area.
So we try to be very scientific in our articles and our work. And we try to read through papers and explain to the audience why a certain paper, or why a certain scientific document, is methodically not good, or what is the problem with it, why is it not scientific. Or we try to also educate on other health topics. This is what we are doing.
Katie:
This sounds amazing. And I also noticed that Germany specifically, and German-speaking countries are extremely active in this area.
Like there are so many knowledgeable people, a lot of activists, a lot of channels and people talking about it.
I really noticed in Germany, I even had one of my videos, that was translated in German… I think, around 1,000,000 people watched it in German.
I noticed how this topic is really popular and a lot of people are working towards solutions. So we really need to also take example from them.
Marvin:
I’m not really sure why that is in Germany. As in every other country, in Germany you have a lot of people that are just following the western medicine blindly. But you have a lot of people also that are very critical and trying to dig deep into the topics, and educate themselves, and doing the research.
So I think we have just had a history. Many, many scientists — so-called scientists of the past — of these areas came from Germany. Or from Europe basically.
And, we had — with Doctor Stefan Lanka we had a very prominent biologist/virologist who came out to the public and tried to educate and spread the truth basically about the practices, scientific practices, in virology. So that gave the whole movement a boost, I would say, in Germany.
And also he was working together with the Perth Group in Australia, which in the 80s, 90s, were very, very clearly doing a lot of good work in HIV research. So I think this is also part of the reason why, specifically in German-speaking countries, many people are already aware of these topics.
Katie:
So how people can support you and what you are doing this court case and everything that you require to do?
Marvin:
So one support would, of course, to be there at the day. So for everyone maybe who is around Hamburg could come there and just — at the 26th of April — think it’s at 10:45 am. I can share the address later, but that would be great for sure.
And then, of course, you can support our Next Level, so our work what we are doing. We have a website and we also have a magazine that comes out regularly. So you can do any sort of donation.
You can buy the magazine and you can also interact with other critical thinkers in the online forums — telegram — and just support this community. That would be also very great because we are doing a lot of work.
Basically all of us do this in our free time. So we have all our main jobs, and apart from that, we do this in our free time because we are very passionate about this.
We don’t want a future for our families and friends and children and so on that is continuing with this craziness basically. And with these pandemics over and over again, with vaccinations and medical drugs and so on.
It is all going against, basically, our health and is not based on science.
This people really should understand that this is not really scientific.
If you take your time, some hours, weeks, and you really try to figure it out, you will quickly understand that this is not based on science.
This is based on fraud. Sometimes on misinterpretation. OK? Misinterpretation. Very often, due to lacking control experiments, they misinterpreted the results they get. They don’t know what exactly is cause and effect because they don’t have any controls. So they just take it for granted; and this is also unscientific.
Part 1: The New Body Soul Biology (English voice over) Dr Stefan Lanka
In 2021 Interview, RFK Jr. Reveals How Former Pres. Trump, Who Was Very Aware of the Serious Injuries Caused by Vaccines, Asked RFK Jr. to Lead a Commission on Vaccine Safety. Trump Changed His Mind Following Pfizer’s Million Dollar Contribution to His Inauguration
TCTL editor’s note: In 2021, Theo Von interviewed Robert F. Kennedy, Jr. Clips from this interview are found mirrored around the internet. In this interview, RFK Jr. talked about his meetings with Donald Trump wherein Trump asked RFK Jr. to head a vaccine safety commission. Trump was well aware of the serious dangers and great harm caused by vaccines as he personally knew people whose children developed serious health issues following vaccination. However, Trump changed his mind about the vaccine safety commission following a million dollar contribution from Pfizer to Trump’s inauguration. RFK Jr. was pushed aside and Scott Gottlieb, who was a Pfizer consultant, was selected by Trump to run the FDA. ~ Kathleen
Partial transcript:
Theo Von:
…Trump almost gave you a position… Wasn’t there talk of that? And then it kind of went away…
RFK, Jr.
Well, what happened was he … over the Christmas vacation… 2016, he’s elected right? And obviously the election is in November.
So I was skiing and with my kids in Colorado over Christmas vacation and I got a call from his chief of staff saying the president-elect wants to meet and he wants to talk about vaccines.
So, you know, I’ve been an activist on trying to get safer vaccines for a long time. And, of course, I agreed to meet with him.
So…immediately after getting home, I went … to New York and met with him at Trump Tower. It was about a two hour meeting.
Theo Von:
Had you ever met with him before?
RFK Jr.
I had sued him twice before successfully. And I had met him. And, you know, the lawsuit was not something that had hurt our relationship. I stopped him from building two golf courses in the New York City watershed. And those lawsuits were about two or three years apart.
And he knew me, and he knew my family… When my sister ran for governor of Maryland, he made a big contribution to that.
He contributed to my brother, who was then in Congress. And I had a cousin who was a congressman from Rhode Island, and he made a contribution. He was a big democratic donor at that point.
He called me. He asked me to come in. I had, as I said, about a two hour meeting with him. At that meeting, people were coming in and out of that meeting.
So Steve Bannon was there. Reince Priebus. You remember him? Hope Hill was there. Kellyanne Conway. And Jared Kushner. And both the president’s sons at various times were in that meeting.
Theo Von:
A lot of people.
RFK Jr.:
I had a lot of time alone with President Trump too.
He said that he believed that vaccines were making people sick. Specifically, he had three women friends who were mothers, one who was in the building that day, who had perfectly healthy kids who had gotten … their wellness visits. And they were around two years old.
And the children never were the same after those visits. And they all had been subsequently diagnosed with autism. And he believed that it was linked to vaccines.
And… because he had been open about that during the campaign, hundreds of women had — the same thing that happened to me, that got me into this, you know, this career killing advocacy, vaccine safety advocacy…
People start coming up to you and saying… “This happened to me. This happened to my son.”
“I had a perfectly healthy child who exceeded all his milestones. And I took him in at 16 months and he, you know, he was speaking, he was toilet trained, he had social interactions. And I took him in and he had a shot or a series of shots usually — could be up to nine — and that night, he’s like fever 103.”
I mean the stories were usually all identical. They had a seizure. And then over the next three months, they lose all of their capacity to… their social interactions, their eye contact…
I go in there and he tells me these stories. He wants to do something about it.
Theo Von:
And does he seem serious when he’s saying that?…
RFK Jr.:
Yeah, he was dead serious. And he asked… whether I would run a vaccine safety commission. And then he asked what I would do.
And I said, listen, I don’t think you have to do a big political lift. All I think you need to do is open up the databases and allow independent scientists in there to actually look at the science. Because the HMOs have all the vaccine data down to batch for every child in America. And they also have the medical records.
So all you have to do — in fact… AI can do machine counting and you can do cluster analysis.
And you can figure out very, very quickly whether all of these epidemics — not just of neurodevelopmental diseases like all the ADD, the ADHD… Tourette’s syndrome, narcolepsy… Autism. The allergic diseases, food allergies, peanut allergies… Asthma and then all the autoimmune diseases…
And they’re all listed, by the way, on the vaccine inserts, as vaccine side effects.
Because the only way that you can sue — you know, they passed this law in 1986 and made it illegal to sue a vaccine company for injury.
You still can sue them if they know of an injury that’s caused by their vaccine and they don’t list it on the side effects.
So they list 400 injuries…
But they’re not allowed to list it unless there is significant evidence that it is actually being caused by the vaccine.
FDA is not allowed to allow them to list it unless FDA believes it’s being caused by the vaccine.
Theo Von:
So you have this meeting with Trump, just to get back to that… Did you leave out of the meeting kind of hopeful about it?
RFK Jr.:
Well, I said to him, what do you want me to do? And he said we want you to announce it. Jared Kushner escorted me to the press scrum…
So then I went down and announced it. Talked to the press.
And then a week later, Pfizer made a million dollar contribution to Trump’s inaugural.
And then Trump comes in. And we continue to have some meetings with Fauci — that he had set up, were part of this process and we’re rolling, to get this thing started.
Theo Von:
Did Fauci seem legit when you talked to him?…
RFK Jr.:
Oh, he’s very, very charming…
Listen, Fauci — I’m about to publish a book on Fauci [see “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health”, published by Children’s Health Defense in November 2021]… He’s been there for 50 years, so he’s like J. Edgar Hoover.
And the only way that you last at that agency for 50 years is by carrying water for the pharmaceutical industry.
And under his watch, he’s supposed to prevent autoimmune and allergic diseases. Under his watch, chronic disease has gone from affecting 12% of the American population to 54%. And we take more pharmaceutical drugs than anybody in the world. We pay the highest prices.
He’s made this country Pharmaceutical Nation.
Theo Von:
My brother is allergic to sesame seeds.
RFK Jr.:
…And the way that you get allergies is from the aluminum adjuvant in the vaccine, which is meant — is put in that vaccine to initiate an allergic response.
So if you have sesame seed oil as an excipient in the vaccine, or if you’re eating sesame seeds when you have that aluminum adjuvant in you, it can provoke a permanent allergy…
So anybody who was born after 89 — I think it’s one in 12 now. Autism went from one in 10,000, in my generation, to one in every 34 kids. And it’s the same with all these chronic diseases that are all listed as side effects.
Theo Von:
So the proof seems to be right there.
RFK Jr.:
Well, that’s correlation, which isn’t actually proof. But if you actually go into the scientific literature, the proof is there.
Theo Von:
… So whenever you talked to Trump, you said, okay, let’s open up this database, right, this information…
RFK Jr.:
Yeah… I said you don’t have to do any heavy lifting. You don’t have to go to Congress. You don’t have to change regulations. All you have to do is open up the vaccine safety data link, which is the medical records for the top nine HMOs, and allow independent scientists to go in there. And just open it up so they can start publishing.
Theo Von:
And did he do it?
RFK Jr.:
No, he didn’t. It’s still… locked down.
Tony Fauci makes sure nobody can get in there.
And you know, even when Congress ordered these two scientists … to go in there, and they let them into the place, they gave them one study room. They would not allow them near a copy machine. They allowed them pencils and they had to write down the data. And they cranked the heat in the room up to 105…
So anyway, so Big Pharma stepped in and Trump appoints Pfizer’s lobbyist to run FDA (Scott Gottlieb) and Eli Lilly’s lobbyist is Alex Azar to run HHS. And as soon as they came and they shut us down.
“With hundreds of billions of “viruses” at peak infection, there is absolutely no reason that virologists should not be able to purify and isolate the assumed “viral” particles directly from the fluids of a sick human or animal.”
Last week, I took a look at the very illogical excuse that virologists make in regard to why they are unable to purify and isolate the particles that are claimed to be “viruses” directly from the fluids of a sick human or animal. As a reminder, below is the response I received from biologist Thomas Baldwin, who studies “pathogenic” plant “viruses” and goes by the Twitter handle Sense_Strand:
It is claimed that there are just not enough of these “viral” particles within the fluids and thus, the purification procedures will result in too little of the “virus” remaining after these steps are performed. Due to this lack of particles, it is claimed that the “viruses” can not be found in electron microscopy images, and it is for this very reason that the “virus” particles must be grown in cell culture so that the “virus” can replicate to a large enough number in order to be visualized and studied. While I won’t rehash my counterargument here, I will allow Debunked to help me demonstrate why this is a ridiculous excuse:
When virologists claim incredible numbers like that, it is pretty reasonable to conclude that there should be plenty of “viral” particles within the fluids of a sick animal or human in order to purify, isolate, visualize, characterize, and study. Alas, virologists defiantly cling to their laughable excuse in order to cover up for the fact that they just cannot find the assumed “viral” particles anywhere directly within the fluids. While this statement clearly defies logic, the lack of “virus” is only one aspect of the excuse. There is another component that is used to explain why, even if they could purify and isolate the particles, it wouldn’t ultimately matter. Beyond the lack of enough “viral” particles within the fluids, virologists claim that there are not enough “infectious” particles present after purification in order to be able to “infect” an animal or human on order to prove pathogenicity. It is stated that this purification process damages the “virus” and causes it to lose “infectivity.” This excuse was illustrated in a response interviewer Djamel Tahi received from HIV “discoverer” Luc Montagnier:
“I believe we published in Science (May 1983) a gradient which showed that the RT had exactly the density of 1.16. So one had a ‘peak’ which was RT. So one has fulfilled this criterion for purification. But to pass it on serially is difficult because when you put the material in purification, into a gradient, retroviruses are very fragile, so they break each other and greatly lose their infectivity.”
“I repeat we did not purify. We purified to characterise the density of the RT, which was soundly that of a retrovirus. But we didn’t take the “peak”…or it didn’t work…because if you purify, you damage.So for infectious particles it is better to not touch them too much.”
As can be seen, if the particles are purified, it is assumed that they lose their “infectivity.” Thus, virologists must not touch their fragile little “virus” particles too much or they will be damaged and will not work properly. With statements like this, it makes the story about how these non-living entities somehow survive the harsh environmental conditions of the great outdoors in order to invade a body, bypass the hosts “immune system,” and hijack the cells so that it can create more copies of itself, seem rather ridiculous. According to virologists, in order to retain “infectivity,” the “virus” particles must remain unpurified and proceed to be mixed into a foreign animal or cancer cell with toxic antibiotics, antifungaks, fetal calf blood, chemicals and “nutrients,” etc. and incubated for days. However, this is normally not enough to create the necessary “infective” particles, so virologists will remove the top layer of one culture and then add it to another culture with a fresh round of toxic compounds mixed in. This new culture is then incubated further until signs of cell death are observed. Only then can there be enough “infectious viral” particles to visualize and establish pathogenicity.
To the outside observer who looks at this critically and logically, it is clear that all virologists are doing is creating a toxic soup of many foreign and chemical elements in which they get to claim a “virus” resides within. This sludge is then forcefully and unnaturally inoculated into animals in many disgusting ways, either through the nose, the skin, the muscles, the eyes, the throat, the stomach, the brain, or even the testicles. Virologist then determine what is an “infectious” dose based upon how much of this toxic soup is used as an injection into the animal at the time any symptoms appear. Virologists will determine how much “virus” is present in the soup by utilizing either one of two methods: the tissue culture infectious dose (TCID50) and the plaque assay. Let’s examine these methods briefly and then see, according to virology’s own theoretical narrative, how many “viral” particles it takes to cause infection and disease. We can then determine whether or not it is reasonable to believe that there are not enough “infectious” particles present after purification and isolation in order to determine pathogenicity.
Tissue Culture Infectious Dose (TCID50)
This first method for estimating how many “virus” particles are necessary for “infection” relies on the observation of the cytopathogenic effect (CPE) that is created during the cell culture experiment. CPE is an effect that is observed when the cells start to die and break apart during the cell culture process after the cell has been starved and poisoned. To calculate how many “viruses” they believe are present and “infectious,” virologists will use varying “virus” dilutions that are added as an endpoint dilution to host cell populations in a 96 well plate format. They will then incubate these mixtures until a cytopathic effect can be observed. The wells are either inspected by visually counting the CPE in the affected wells or by using assay readouts. Once 3 of the same CPE readings in separate cells for the same dilution are observed, the dose is calculated using one of various mathematical equations. The dilution at which 50% of the cell cultures are “infected” is determined and used to mathematically calculate a TCID50 result:
Tissue Culture Infectious Dose (TCID50) Assays: How to determine virus infectivity?
TCID50 assays: How do they work?
“50% Tissue Culture Infectious Dose (TCID50) assays are virus titration experiments which can be used to quantify virus titers by investigating the cytopathic effects of a virus on an inoculated host cell culture4. Compared to the widely used plaque assays, which are also used in virus quantification, TCID50 assays offer the advantage that even viruses that do not form plaques or infect cell monolayers can be quantified.
In TCID50 assays, varying virus dilutions are added as an endpoint dilution to host cell populations with the same number of cells and incubated until a cytopathic effect can be seen. Here, the TCID50 value represents the amount of virus dilution required to induce cytopathic effects in 50% of wells containing the inoculated cell culture after a defined period of time.
TCID50 assays assess this threshold either by visually counting the number of affected wells or by using cell viability assays as readout. The TCID50value is determined when the cytopathic effect or cell viability assay read-out appear the same for a dilution in 3 separate readings. An example of the application of cell viability/toxicity assays for the evaluation of viral cytopathic effects can be found in the AN 363: Viral cytopathic effects measured in a drug discovery screen.
TCID50 calculation
The results of 50% Tissue Culture Infectious Dose (TCID50) assays can be analysed by different calculations 5. Several mathematical approaches have been developed for this purpose, including the Reed-Muench 4, Spearman-Kärber or Weil method. The formula after Reed-Muench is depicted as an example below.
Where I is the interpolated value of the 50% endpoint and h is the dilution factor.
Since most often, the exact 50% endpoint is not observed in TCID50 assays, an approximate value can be obtained factoring in the dilutions closest below and above the 50% threshold. Independent of the method, the dilution at which 50% of the cell cultures are infected is determined and used to mathematically calculate a TCID50 result which is expressed as 50% infectious dose (ID50) per millilitre (ID50/mL) after a defined period of time. For example, if 0.2 mL of a 1:10,000 virus dilution infects 50% of the cells in 2 days the titer is expressed as 104 TCID50/0.2 mL in 2 days.”
As can be seen, this method relies on the observation of CPE as evidence of a “virus” and then attempts to calculate how many of these invisible entities reside within the fluids. However, as should be expected when dealing with attempts to count something that can not be seen, this method has its drawbacks. For one, the Poisson distribution that is utilized, which takes the TCID50 value and multiplies it by 0.7, is admittedly only an approximation and is said to not always be true. The serial dilution method itself is also a source of error by its very nature. If any fluid remains at the end of the pipette used to suction out the “virus,” it is said that this can greatly influence the quantification results. Another issue is attempting to keep all of the variables exactly the same across all cultures, which is admitted to not always be the case. Thus, there is a lot of guesswork and assumption involved in calculating the infectious dose of the unseen entity:
Timeless TCID50: One solution to many viruses
From dilutions to titres
“TCID50 values give an indication of how many viruses is needed to have CPE in 50% of the cells. But how to go from this to the actual amount of virus per ml? The formula is quite simple, and it consists in multiplying the TCID50 value by 0.7. This comes from the Poisson distribution applied to viral infection which states that, in a fully permissive cell line, the probability of reaching 50% infection is achieved by a multiplicity of infection of approximately 0.7. This is not always true, but it’s a good approximation for most applications.
The troubles of counting viruses
As accurate as one can be, counting viruses is never easy. First, serial dilutions are -by their own nature- a source of error. Second -and this is particularly relevant for high titres of virus- even the tiniest volume that remains attached to the very end of a pipette tip can carry enough viral particles to make a substantial difference in the quantification. Third, the biological variation of the system is high. Plate the same amount of cells, add the same amount of virus, stop the infection at the same time, and the percentage of infection may be close, but never exactly the same.
Finally, when assessing a treatment that (as you would hope!) decreases virus titres, the amount of virus may fall below the assay detection threshold.”
However, if relying on an indirect effect and spotty mathematical equations to calculate how many “viruses” it takes to “infect” a cell is not to your liking, you may appreciate this next method even less. Plaque assays also rely on the observation of CPE in cultured cells. As the cells break apart and die, the “viral” particles are assumed to travel to neighboring cells, infecting them and creating plaques, or holes, in the dish. The cells are then fixed and stained, killing everything in order to be observed. It is said that the cells that remain adhered to the surface are assumed to be uninfected, and any observed plaques are assumed to arise from cell death caused by “viral infection.” Virologists will look for the dilution that led to the optimal observed plaques; too little dilution leads to too many plaques while too much dilution yields none. The titre is then calculated using arithmetic based on the volume of the aliquot added to the cells and the sample dilution the aliquot was drawn from. The assay is designed so that each plaque represents infection by only a single “viral” particle:
Measuring infectious virus: the plaque assay
Infection and plaque formation
Plaque assays require cultured cells susceptible to infection by the virus of interest. The cells are first seeded onto a surface they can adhere to and grow on, then left overnight to form a confluent monolayer (a cohesive sheet of cells covering the entire growth surface). A virus sample is then diluted several times, and an aliquot of each dilution is added to a dish or well of cells. An incubation period allows the virus to attach to target cells before removing the inoculum. The culture is then covered with a medium containing nutrients and a substance, such as agarose or methylcellulose, forming a gel or semisolid overlay. Infectious virus particles that enter cells and replicate can then trigger the release of progeny virions. The gel restricts particle movement so that newly produced viruses can only infect neighbouring cells. If the virus kills infected cells, the dead (or dying) cells detach and create a hole in the monolayer through lysis or other means. This space – now devoid of cells –is called a plaque and appears as circular spots on the growth surface.
The plaques are allowed to grow until visible to the naked eye. The cells are then fixed with formaldehyde to lock cellular structures while killing the cells and virus. Dyes that stain cells are added for contrast, making plaques easier to see. Purple violet stains the cells purple, while plaques, lacking cells, remain clear. Cells that remain adhered to the surface are assumed to be uninfected, and apparent plaques are assumed to arise from cell death caused by infection. That is why the virus dilutions must be added to confluent monolayers with no gaps that might later be mistaken for plaques.
Viral titre: PFU/ml
Multiple dilutions of the stock sample are analysed to identify one or more dilutions that give rise to a countable number of plaques. At the lowest dilutions, too many infectious particles will destroy large swaths of the cell monolayer or create plaques too numerous and overlapping to distinguish. At the highest dilutions, there may be no plaques at all. At the optimal dilutions, plaques are counted to determine the titre of the original stock sample, typically reported as the number of plaque-forming units per millilitre (PFU/ml).
For a given plaque count, the stock titre can be calculated by simple arithmetic based on the volume of the aliquot added to the cells and the sample dilution the aliquot was drawn from. As a basic example, if 35 plaques were counted when a 0.1 ml aliquot of the 10-5 dilution was added to the cells, the titre of the undiluted stock is 3.5×107 PFU/ml. For reliable titres, each sample dilution should be plated multiple times, at least in duplicate and preferably in triplicate. Furthermore, multiple dilutions may result in countable plaques. More elaborate formulas incorporating all relevant plaque counts are typically used to calculate titres.
PFU/ml vs IU/ml
The assay is designed so that each plaque results from infection by multiplying a single infectious virus particle. As such, PFU/ml is considered a measure of the number of infectious units per millilitre (IU/ml), with the caveat that one cannot be certain of a one-to-one ratio of plaques to infectious particles in the applied aliquot. Also, be aware that the titre of a sample is specific to the assay conditions used to determine it, as infectivity is influenced by many factors, such as the type of host cell, pH, and culture medium. Titres can differ by several orders of magnitude by changing key assay parameters.”
As with the TCID50, there are some definite drawbacks when trying to “accurately” estimate how much of an invisible entity can cause infection and disease using the plaque assay. For starters, as noted above, the “infectivity” is said to be influenced by many factors within the culture itself. This includes the type of host cell, the pH level, as well as the culture medium used. Thus, the calculated titres can vary wildly by several orders of magnitude just by changing the assay parameters. The determination of what exactly constitutes a plaque is very subjective as well, which can mislead the results. In other words, plaque counting is prone to human error.
Beyond these issues, as noted before, both TCID50 and plaque assays rely on the observation of a cytopathogenic effect in order to claim the presence and infectivity of any “virus.” However, CPE is not specific to “viruses” as there are many known factors that can result in this effect being observed that do not require the presence of a fictional entity in order to explain, such as:
Bacteria
Parasites
Amoebas
Chemical Contaminants
Age of the Cell
Incubation Temperature
Length of Incubation
Antibiotics/Antifungals
It is entirely unscientific to rely on an effect in order to presume a cause. However, this pseudoscientific concept is central to the cell culture method as well as to the processes utilized to guesstimate how many “infectious viruses” are present. In other words, there is no direct evidence any “viruses” are present in any sample used to determine an “infectious” dose. All of these results claiming how much “virus” is present and can ultimately cause an infection are entirely hypothetical and calculated based on the presence of cell death. It is nothing but guesswork.
However, if it wasn’t clear that these numbers are pseudoscientific fraud, a 2003 OSHA White Paper looking at the determination of the infectious dose (ID) may help to sell the fact that virologists honestly have no clue what an infectious dose is. While this refers to calculating ID using animals, the same criticisms can apply to utilizing lab-created cell cultures as a surrogate. The White Paper concluded that there is no clear definition of what an infectious dose is and that there is no single standardized method for determining ID. The extrapolation of data to humans is unreliable and is a poor surrogate for human responses. There are various secondary interactions that can impact the estimates. The “pathogens” vary wildly in “virulence” and data on the ID via route of exposure is unavailable. In other words, virologists just make things up as they go along:
“In summary, the studies described above support ABSA’s position that attempts to develop quantitative values for human infectious dose are not currently feasible. Infectious dose values developed using past studies would not accurately characterize the relative hazard of pathogenic organisms in humans. The reasons for this conclusion are:
• Lack of a clear and universally acceptable definition of the term “infectious dose.”
• There is no single standardized protocol for testing infectious dose in animals, making legitimate controlled comparisons ofstudy results very difficult.
• Extrapolation of infection and toxicity data among animal species and from animals to humans has proven to be unreliable for most biological (and chemical) agents.
• Inbred animal strains are a poor surrogate for predicting human response, as humans are a highly variable outbred population.
• Infectious dose is affected by numerous, complex secondary interactions to include condition of the host, its genetics, and previous exposure to the biological agent or vaccine. Risk estimates must take these and many other factors into consideration.
• Bacteria of a single species can vary widely in virulence and infectious dose. It is not possible to make a broad or generalized statement about the infectious dose of a species of bacteria.
• Infectious dose in part depends on the route of exposure. A complete picture of a single pathogen’s infectious dose profile requires inhalation, percutaneous, oral, im, ip, iv, etc. data. These data are currently unavailable.”
Now that we know that this process for counting the invisible “viruses” is fraught with drawbacks that leave the “accuracy” of these results extremely questionable, let’s take a look at some of these wildly varying estimates in order to see how many particles are necessary to cause an infection according to virology’s fictional narrative. As “SARS-COV-2” is the soup du jour at the moment, here are a few key highlights from a systematic review of many studies attempting to find the minimal ID for the “novel coronavirus.” What you will see from the August 2022 review is that there is absolutely no experimental data for humans, with one study admittedly presenting a hypothetical estimate (technically, they are all hypothetical). The minimal ID for “SARS-COV-2” is extrapolated from animal studies with estimates that vary wildly between the papers:
Minimum infective dose of severe acute respiratory syndrome coronavirus 2 based on the current evidence: A systematic review
“The main methods for reporting the infective dose were through tissue culture infectious dose (TCID50) and by counting plaque-forming units (PFU).33
In TCID50, the viral dose in 5% of inoculated tissue culture made pathological changes or cell death. PFU is estimated of viral concentration in plaque-forming units by measuring the number of particles that form a plaque.34 The minimum infective doses have been summarized in Table 2.
Human studies on infective dose of SARS-CoV-2
“We found no experimental studies that assess the infective dose in human, so we included observational human studies.”
“Finding the minimum infective dose of the virus can be extremely useful in determining the transmission pattern. This represents itself in inconsistent results across the included studies; similar viral load did not cause the same outcome. This indicates that despite having a similar minimum infective dose, the infection rate could differ so this minimum is not the same across the same population. On the other hand, there are some human studies which have shown some hypothetical infective viral dosages.”
Conclusion
“The results of this review suggest that one of the key factors to control the pandemic could be the study of virus transmission. The minimum infective dose is one of the main components of virus transmission. In this study, we have presented a range of minimum infective doses in humans and various animal species, yet such numbers can possibly vary between the individuals based on numerous factors. Measuring the minimum infective dose can provide a clearer overall understanding of the disease and its transmissibility and help better halt its spreading.”
While it is fun to see how much their guesstimates can range between studies, the above paper doesn’t give us a great idea as to what this minimal ID is for “SARS-COV-2” in terms of an actual number of particles it may take in order to cause infection. Let’s see if we can put a number to it based upon what the “experts” are saying:
SARS-CoV-2 Infectious Dose
“Some experts estimate that exposure to as few as 1000 SARS-CoV-2 viral particles can cause an infection. This dose of virus could occur by inhaling 1000 infectious viral particles in a single breath, 100 viral particles in 10 breaths, or 10 viral particles in 100 breaths.”
According to the “experts,” as little as 1000 “SARS-COV-2” particles are enough to cause infection. Where did they get this magical number from? Who knows? However, a separate study gave an even smaller estimate of just 100 “viral” particles:
Review of infective dose, routes of transmission and outcome of COVID-19 caused by the SARS-COV-2: comparison with other respiratory viruses
“An accurate quantitative estimate of the infective dose of SARS-CoV-2 in humans is not currently feasible and needs further research. Our review suggests that it is small, perhaps about 100 particles.”
It appears that virologists have the ability to just pull any ID number that they want out of thin air. When we factor in their other imaginary numbers, such as those who are at “peak viral infection” harboring 10 to 100 billion “viral” particles while breathing out 10 million “viruses” per breath, it seems rather illogical to claim that there would not be enough “infectious virus” after purification in order to prove pathogenicity.
Examining the issue a bit further, let’s look at a few other sources and see just how little “virus” is said to actually be necessary in order to cause an infection. According to virology’s pseudoscientific narrative, would you believe that just one airborne particle can cause you to become infected? That is exactly what we are told by this next source which dealt a fatal blow to mask supporters everywhere. The researchers based their claim upon theoretical modeling (aren’t they all), and concluded that only one airborne particle is enough to cause infection and disease:
What if just one airborne particle was enough to infect you?
“For some diseases, exposure to just a single airborne particle containing virus, bacteria or fungi can be infectious. When this happens, understanding and predicting airborne disease spread can be a whole lot easier.
That’s the result of a new study by a Lawrence Livermore National Laboratory (LLNL) scientist who developed a new theory of airborne infectious disease spread. This research, which appears in the journal Applied and Environmental Microbiology, demonstrated good agreement with data from Q fever, Legionnaire’s disease and Valley fever outbreaks. The authors hope to use it to understand and mitigate COVID-19 spread.”
Unfortunately, the authors did not give us any idea as to how many “viral” particles would be in one airborne particle. Hypothetically, it could be one “virion” or it could be quite a few more. Let’s see if we can get some concrete guesstimates as to how many of the “viral” particles it may take to cause infection and disease. According to the CDC, “norovirus” only requires a few particles in order to cause infection and disease:
About Norovirus
“People with norovirus illness can shed billions of norovirus particles. And only a few virus particles can make other people sick.”
When looking to insect “viruses,” researchers set up an experiment with two “marked virus variants.” They exposed a population of caterpillars to both variants, and based upon these results, established a probability model to determine that it is theoretically possible for just one “virus” particle to cause infection and disease:
One Virus Particle Is Enough To Cause Infectious Disease
“Can exposure to a single virus particle lead to infection or disease? Until now, solid proof has been lacking. Experimental research with insect larvae has shown that one virus particle is theoretically enough to cause infection and subsequent disease.”
“Based on the assumption that every virus particle operates independently from all other virus particles,the researchers set up a probability model. This model predicts how many virus particles have caused an infection and how many different virus genotypes are present in infected hosts, such as plants, insects or people. The results of the infection experiment with the susceptible insects are in agreement with the model predictions. From this it can be derived that the virus particles have an independent effect, and that a single virus particle can indeed cause infection and/or disease.”
We have now officially gone from 1000 “viral” particles to just one particle. Let’s see if any other sources make such a bold claim. In a CDC study that looked to establish a quantifiable estimation of how many “variola” (a.k.a. smallpox) particles are necessary to cause infection, the researchers concured that only one “virus” particle was sufficient to cause infection and disease:
The infectious dose of variola (smallpox) virus.
“Quantitative estimation of an individual’s risk of infection due to airborne pathogens requires knowledge of the pathogen’s infectious dose, in addition to estimates of the pathogen’s airborne concentration and the person’s exposure duration. Based on our review of the published literature on poxvirus infection, we conclude that the infectious dose of variola (smallpox) virus is likely one virus particle and that infection can be initiated in either the upper respiratory tract or pulmonary region. Studies of airborne transmission of poxvirus in monkeys and rabbits show that primary infection can occur in both regions of the respiratory tract. A quantitative study of poxvirus inhalation transmission in rabbits indicates that the deposition of one pock-forming unit (PFU) carried on respirable particles can cause infection. Findings in both in vitro and in vivo studies of the number of virus particles comprising a PFU are consistent with a “one-hit” phenomenon–namely, the cellular uptake of just one virus particle can lead to infection of a cell or an area of cell growth, creating a pock (an infected area of cells). Variability in virulence among different virus strains may involve differences in the probability of infection per virus particle, where a highly virulent strain has a probability close to one of successful infection for each virus particle.”
“On balance, we believe there is adequate in vitro and in vivo evidence that infection can be produced by a single particle of variola virus. Across different experimental systems the number of poxvirus per infectious unit has been found to vary, but it appears that favorable conditions enable all virus particles to infect (Overman & Tamm, 1956; Parker, Bronson, & Green, 1941; Sprunt & McDearman, 1940).”
The CDC has also stated that only one “viral” particle from rabies is enough to cause infection and disease:
Rabies
“During clinical disease, millions of viral particles may be found intermittently in the saliva. In theory, only a single rabies particle or virion is required to result in a productive infection.”
This one “viral” particle is supported as well by OSHA in regard to the Ebola “virus:”
Ebola
“In areas of Africa where Ebola viruses are common, suspected reservoirs include primate and bat populations. While there are no known animal reservoirs of the disease in the U.S., there is concern related to possible spread of EVD among human populations due to the availability and reach of global travel. Under certain conditions, exposure to just one viral particle can result in development of EVD. Depending on the strain and the individual infected with the disease, EVD may be fatal in 50-90 percent of cases.1”
It is clear that, according to virology’s own pseudoscientific narrative, only one “viral” particle is theoretically necessary in order to cause infection and disease. Therefore, there is absolutely no reason to assume that there are not enough infectious “viral” particles remaining after purification and isolation directly from the fluids to be used in order to prove pathogenicity. The reason this excuse is presented is because virologists are unable to recreate disease using just the fluids from a sick host. In order to even attempt to show pathogenicity, they claim that the unpurifued fluids must be added to a foreign animal or cancer cell along with antibiotics, antifungals, fetal calf blood, chemicals, “nutrients,” etc. and then injected unnaturally into an animal either through the nose, the blood, the throat, the skin, the brain, the stomach, the eyes, the feet, and/or the testicles. There is nothing natural or scientific about this process.
However, as virology is pseudoscience, it falls back on unfalsifiable concepts in order to excuse away the lack of scientific evidence. Instead of being able to find the “virus” particles directly in the fluids, they get to claim that there is not enough “virus” there despite their own numbers making this an impossibility. As virologists know that they can not prove pathogenicity using nothing but the assumed “viral” particles, they get to claim that the purification process creates a yield loss and that the “viruses” lose infectivity. Therefore, virologists get to excuse away that they can not show that the particles created after the cell culture experiment ever existed within the fluids of a sick host to begin with. They get to explain away that they can not prove pathogenicity using nothing but the assumed “viral” particles without culturing. Yet, despite their excuses, the numbers supplied by virologys own pseudoscientific narrative fail them. With hundreds of billions of “viruses” at peak infection, there is absolutely no reason that virologists should not be able to purify and isolate the assumed “viral” particles directly from the fluids of a sick human or animal. If only one “viral” particle is necessary theoretically in order to cause infection and disease, there is no reason virologists cannot use a purified sample to prove pathogenicity naturally via the scientific method. By their own admission, all it takes is just one particle to cause infection and disease. One particle from a sea of billions.
“It is also clear that the dramatic events of the past three years, events that have devastated the lives of many people all over the world, are based on this very misconception that so-called pathogenic viruses exist. This misconception has been around for a very long time, and it has led to damaging public health measures, the most notorious being vaccines, which have themselves harmed and killed millions of animals and people during their long and sordid history.
—This carnage needs to stop.”
~~~
TCTL editor’s note:
In the video below, Samantha Bailey reads the written statement “Why Are We Doing This?” which was signed by Tom Cowan, Andrew Kaufman, Mark and Samantha Bailey.
Following that reading, each of the four makes a brief personal statement about why they continue to speak out about lies at the foundation of virology.
Sadly, the level of rancor between those in the “freedom” community taking the “no-virus” position and those taking the “pro-virus” position has reached higher and higher levels.
Videos, Instagram posts and tweets are put out by both sides claiming to “debunk’ the other side or sometimes to just call names.
Mikki Willis, the producer and director of the documentary series Plandemic, has created a new video urging unity among those who claim to be on the side of freedom, along with a subtle accusation that dissenters against this unity are classic disinformation agents.
Given this background, we, as some of the recognized leaders of the “no-virus team,” thought it would be a good opportunity to reconnect and even restate why we are doing this.
Why we will not just be good team players and participate in the growing worldwide movement fighting for the universal principles of freedom, bodily autonomy and the ability to guide one’s life based on one’s own beliefs and decisions? Why keep speaking out?
It seems obvious to us and, in fact, has been a guiding principle throughout our entire lives that a life based in freedom and integrity must have a solid, factual foundation. In other words, if the foundation is not based on the truth, as best we can see it, our entire lives are based on mistruths and are in danger of collapse at any moment.
Imagine building a relationship, a family, a homestead based on love between two people when the reality is that, rather than love, there is distrust, suspicion and even ill will. Sooner or later, that life will collapse into ruins.
This is the same with a financial system based on fiat currency, an agricultural system based on inattention to the health of the soil, or a medical system based on anti-scientific medical hypotheses.
After careers of examining medical research and theories and three years of intensive investigation into the question of whether particles or, perhaps better said, entities known as viruses actually exist, it is our clear conclusion that no such particle has ever been shown to exist, let alone cause any disease in plants, animals or people. For us, this conclusion stands as a clear fact.
It is also clear that the dramatic events of the past three years, events that have devastated the lives of many people all over the world, are based on this very misconception that so-called pathogenic viruses exist. This misconception has been around for a very long time, and it has led to damaging public health measures, the most notorious being vaccines, which have themselves harmed and killed millions of animals and people during their long and sordid history.
—This carnage needs to stop.
People need to experience the world with new eyes and with a new concept of life, biology and health. This new conception can begin only when we realize, once and for all, that the idea of contagious, pathogenic viruses, or viral-like entities of any sort — natural, lab created, clones or otherwise —is simply a scientific misconception, or possibly a fraud.
Why we are doing this is straightforward: It’s so that no woman, man, child or animal ever has to be subjected again to abuse based on a long, bankrupt theory of biology and medicine.
We have nothing personally to gain from this quest. No prestigious awards are coming our way, and we likely will get nothing but further scorn and derision from colleagues, public institutions, and the general media.
Yet, when we think of our children, grandchildren, our friends, our families, our beloved animals, and animals in labs who are tortured and killed in this clearly futile effort to demonstrate the “reality” of viruses, everything in our being cries out, “this must stop.”
Therefore, we ask all people of good will to accept the following challenge. Please send us any genuine scientific information that demonstrates that viruses exist and cause disease.
We are not interested in any comments about our motivations or the consequences of our quests for us personally. Absent that evidence, we and our good friends will keep going. We believe that the future for all of us depends on it.
Dr. Thomas Cowan
Dr. Andrew Kaufman
Drs. Samantha & Mark Bailey
Time marker 5:03 — Dr. Tom Cowan:
So we’ve been talking a fair amount about why we’re doing this. The this being talking about the fact that there’s no virus, never had a virus that’s been shown to exist or cause any disease.
So what difference does it make?
So there’s obviously a whole lot of reasons including all the social distancing and the masks and the viral vaccines and the devastation of the adults and the lives of children.
But one thing that we haven’t, unfortunately, talked about much is its effect on the animals and the widespread frank torture and mutilation of millions of animals in labs and so-called science experiments all over the world.
And for whatever reason, I hadn’t appreciated this so much until I actually have animals of my own. And I think you could see our three cats and six chickens and we’re getting three goats this week.
When you realize all the mutilated animals, the ferrets with the cell culture stuffed down their throats, the 15,000 monkeys that were allegedly killed by Sabin to make an ineffective and dangerous polio vaccine.
When you realize all the mutilated dogs that have been left in dumpsters, which I’ve heard from many people who actually witnessed this themselves, the mice who’ve been injected with debris into their brain.
And you realize that all these experiments have no possible benefit. They’re just basically sadistic, torturing of innocent animals.
And at some point in your life, everything cries out to say this has to stop.
Time marker 7:04 — Dr. Andrew Kaufman:
Hello, I’m Dr. Andrew Kaufman. And today I’m here to answer the question why is it important to me to tell the whole truth about viruses? Meaning that they don’t actually exist or cause disease.
When faced with a lot of opposition and resistance to this message, you know, why am I communicating this over and over and sticking to this position.
And my answer is simple and I can answer in one word which is justice. But let me explain.
So if we look up the definition of justice, it means the maintenance or establishment of that which is just.
And I have here the definition of the word just from Merriam Webster: “Having a basis in or conforming to fact or reason.” Fact or reason.
So those are the two principal aspects that need to be established and known in order to bring about justice. Fact and Reason.
Now justice, for me, is a guiding factor in my life’s work or my mission.
What I would want to achieve and leave as my legacy on earth at the end of my life is related to bringing about justice.
So earlier in my career, this led me to the specialty of forensic psychiatry because I had learned that there was a great injustice perpetrated on the mentally ill individuals of the world. And this was so-called the deinstitutionalization movement which took people out of mental institutions — which at least were established with some purpose of helping and supporting and bettering those individuals — into the homeless crisis as well as jails and prisons.
So I was specifically going to try and help those mentally ill individuals who were essentially warehoused in jails and prisons, even without perpetrating any immoral crimes.
So many of them are there for things, because they were homeless, for example. So when it was really cold out, they went inside a storage facility to stay warm and escape frostbite. But that was trespassing so they ended up incarcerated, for example. And I’ve seen individuals in that scenario.
So this principle of justice has been a guiding force for me in my life. And it’s no different in the era of covid, where as I wanted to use fact and reason to make an opinion and see what is just with relationship to the announcement of this pandemic which occurred in 2020. And so, of course, I used my reasoning abilities to establish what are the facts.
And that led me to look at the initial fact, which was the establishment of this so-called virus that was causing this pandemic. Everything downstream of that was based upon this assumption.
And what I found out was that this assumption did not have a factual basis. And I simply applied logic and reason, and application of the scientific method to see that the experiments used to establish this basis of a new disease were simply unscientific and false.
And this helped me, of course, have a unique understanding of everything that occurred over the past several years. And I could easily look through the lens of judgment and see what was just and what was unjust in terms of people’s reactions, especially the government and various industries.
And this leads ultimately to holding the perpetrators of this tyranny accountable.
And one of the criticisms that has come from some of the health freedom leaders have been that if we look at the truth that there was no virus, that somehow that lets people like Anthony Fauci off the hook. But it’s actually the opposite because until we establish a factual basis of the crimes that were committed — and namely, in my opinion, they were the complete fabrication of an imaginary new disease that allowed justification of tyrannical policies that reduce freedom and inhibited commerce and allowed all types of manipulation to occur.
And we, to this day, don’t really know who are the main leaders behind this psychological operation that established this false disease, not based on fact. But perhaps if we hold people like Anthony Fauci accountable for participating in this charade that we can extract information and find out who the originators are. And that would be the only way to establish a true justice and accountability for what we’ve experienced.
And I know that going forward it continues to be the utmost important element in our analysis is to establish the facts and to use reasoning to understand what’s going on.
And of course this is true, especially with respect to our health.
So I hope this provides some inspiration to see how important it is to really get to the bottom of this issue.
Time marker 13:10 — Dr. Mark Bailey:
For more than three years I have researched the virus hypothesis, digesting virology textbooks and thousands of publications — from Ivanovsky’s claimed tobacco mosaic virus in 1903 through to Fan Wu’s claimed novel coronavirus in early 2020.
Virology’s world is arcane and most people have barely scratched the surface, content to believe viruses exist and often outraged that we would question such a thing.
However, we did question and haven’t stopped after we broke away from our conventional training and examined this issue for ourselves.
When I completed A Farewell to Virology, even I was surprised at the patent lack of evidence for these alleged infectious particles. It wasn’t just a few areas where the virologist evidence was lacking. It was in every area.
The techniques have shifted over the past century as their own experiments have consistently refuted themselves.
Now their remaining “evidence” lies in inadequate methodologies, uncontrolled studies and media releases.
Some time ago, we witnessed a move away from genuine experimental studies and into what I suspect is their final resort — genomics and proteomics.
But as I wrote in A Farewell to Virology, this approach is built on bankrupt foundations and will only delay the wider realization that the virus model is done for.
In the meantime, the carnage will continue for those still inside the viral paradigm. Experiencing disease, detecting genetic sequences, looking at electron microscopy images or obtaining test results — whether they be through the PCR or alleged antibodies — do not require the existence of viruses, as we and others have repeatedly exposed.
Mankind can make up stories to explain these various phenomena, but cannot change the underlying principles, no matter how sophisticated the technology.
I don’t know how much of the virus fallacy is a misconception, and how much is outright fraud.
It probably doesn’t matter because what is important is that more people are waking up to the fallacy and rejecting the virus and germ theory models outright.
Like our family, they have worked out that none of the touted solutions, whether they be public health measures, vaccines or drugs, offer any benefit to our well-being.
They can see the destruction to humanity, the animals and the environment based on this fraudulent war against imaginary infectious particles.
The real enemy is fear and ignorance, something each of us must overcome. Our world does not need to be feared, with the insight that nature does not make mistakes. And this divine biology is always pro-life and for our benefit.
We may still be in the minority, but we are already victorious as we share this new freedom, wisdom and prosperity with the next generation.
Time marker 16:10 — Dr. Samantha Bailey
In 2020, I first started questioning the covid-19 fraud because I could see that people were fearing for their lives.
The public were being told to stay indoors, to obtain food only from corporate outlets, to avoid relatives and neighbours, all while staying close to their phones and TVs to keep up to date with government announcements.
The fear of the supposed virus was clearly out of proportion with reality. My gut feeling was that I had to try to reduce people’s fear by researching the science honestly and presenting my findings to anyone that would listen.
Our research into SARS-CoV-2 quickly morphed into searching for evidence for the existence of any virus. By mid 2020, it was apparent to us that the key scientific evidence was absent and the level of the fraud was massive.
The powers that shouldn’t be had been building up to the staging of a huge pandemic like covid-19 for decades. Finally, they had their formula correct and almost everyone was complying with the new totalitarian rule under the mistaken belief of contagion.
The key to unravelling the fraud lay with explaining the viral delusion as well as the lies of germ theory to allay the public’s fear.
I investigate the science and follow the trails wherever they may lead. I then release my findings to the public so that I can sleep at night.
I want my children to have a life where they do not live in fear of nature, where they can understand the true causes of disease and how to be healthy through right thinking and right living.
It is a joy to watch them grow to their full potential and I hope that many more people will share the benefits of ignoring the virus model and its associated carnage.
On March 15, 2003 the World Health Organization (WHO) issued a global alert warning of a new virus spreading through Asia and causing Severe Acute Respiratory Syndrome (SARS), a potentially fatal disease, similar to pneumonia. Photos from China depicting ballet dancers and bridal parties wearing white masks appeared in western newspapers while health departments across the country issued notices to hospitals detailing the symptoms of the new virus and asking for immediate notification of suspect cases. Until the global alert, reports referred to an “unknown virus” first striking in Guangdong Province, China, although some reports place the origin in the Philippines. With the March 15 WHO report, the SARS virus became official and reports of new cases came flooding in.
By late May, officials had reported over 8,000 cases worldwide, with almost 700 deaths.1 Of the 65 suspected SARS victims in the US, all but a few had traveled by airplane to areas where the outbreak has been most severe, including mainland China, Hong Kong, Singapore, Hanoi and Toronto. The Chinese economy has taken a hit and some Chinese airline routes were virtually empty due to SARS fear.2
Serious Drama
The SARS outbreak has revived discussion of forced quarantine. According to a study by the American Public Health Laboratory Association and quoted by Senator Edward M. Kennedy, Democrat of Massachusetts, few cities have enough hospital space to quarantine patients in the event of a large-scale outbreak of an infectious disease like SARS. According to Lawrence O. Gostin, director of the Center for Law and the Public’s Health at Georgetown University’s Law Center, public health laws date back to the 19th century and are “wholly inadequate to deal with an emergency.”
“The need for public health law reform is urgent,” said Mr. Gostin. “It should have provisions for surveillance, vaccination, treatment, isolation and quarantine in a way that gives decisive powers to health authorities while respecting the Constitution.” So far, all but one of the SARS victims has submitted to voluntary isolation. The one exception, a New York man, was involuntarily contained until his symptoms passed. Federal quarantine law now includes SARS among its disease guidelines.
Mr. Gostin was the author of the draconian Emergency State Health Powers Act, which has been adopted (fortunately in softened form) by 22 states. According to Gostin, “The need for effective state compulsory power is beyond doubt. But that’s not a given in our country, which is now so tied to the rhetoric of individual rights. It seems we’ve lost the tradition of the common good.”3
Kill the Carrier
In China, a country where the “rhetoric of individual rights” is lacking, the government has announced it would kill SARS carriers who refused quarantine.4 Malaysian officials threatened imprisonment.5 In Hong Kong, officials motivated by the “tradition of common good” have suggested that “families of SARS patients be rounded up, and sent to quarantine camps.”6 In Nanjing, China, 10,000 have been quarantined, and in Beijing 16,000 as of May 6, 2003.7
Official Disease Definition
SARS means “Severe Acute Respiratory Syndrome.” This wide-open definition encompasses many diseases common in the affected regions. Symptoms range from flu-like to pneumonia.8 Dr. Frank Plummer, director of the National Microbiology Laboratory in Canada stated, “Of course, the case definition of SARS is a little loose.”9
The World Health Organization (WHO) has defined SARS in the following way: a) a person presenting after 1 November 2002 with history of high fever (greater than 100.4° F) and cough or breathing difficulty; or b) a person who was not autopsied but with acute respiratory disease and who has been in close contact within 10 days of someone who had SARS.10
This definition alone should give thoughtful readers cause to question the SARS phenomenon. Firstly, is a temperature of 1.8 degrees F over normal really a “high fever”? The CDC used “mild fever” in their case definition. Secondly, should WHO install a historical bias before the history of SARS is even written? WHO has made it impossible to place the discovery of SARS before November 2002, or even think of it as preceding that date, thus guaranteeing its status as an “emerging epidemic.”
In the US, the Centers for Disease Control (CDC) defines SARS differently: a) Illness of unknown aetiology [cause not already ascertained] and onset after February 1, 2003, AND, b) Temperature over 100.5 degrees F, AND, c) respiratory illness, AND, d) Recent contact with a SARS patient or travel to epidemic region.
This defines the new epidemic as an arrival from southeast Asia, China or Toronto. This definition obviates any need to test for the SARS virus in patients who contracted pneumonia before February 2003, AND, who had not traveled to the Orient or met such a traveler. With this definition, the diagnosis of any SARS-like case, determined previously to be of non-viral origin, would be secured from contradictions. The usual one-disease, one-cause theme for epidemics is thereby maintained.
SARS Virology
Due to the wide-ranging definition, the only unique quality of SARS is the associated virus. But association is not enough and a single association is not a rigorous, convincing proof.
On April 16, 2003, WHO announced that SARS virus, a member of the coronavirus family, was definitely causative for the disease. The report referred to a study carried out by a team led by Dr. Albert Osterhaus, the director of virology at Erasmus Medical Centre in Rotterdam. Media reports used the terms “unequivocal,” “definite,” and “beyond a doubt” to describe the work at Erasmus.
Osterhaus reported that his team infected one group of monkeys with SARS virus, a second group with the metapneumonvirus (also found in some SARS patients), and a third group with SARS virus and then the metapneumovirus. The monkeys infected with the metapneumonvirus alone developed mild symptoms, compared to the “full-blown disease” seen in the first group. The third group “did not develop a more serious version of SARS.” From this Osterhaus concluded, “the coronavirus alone is capable of causing the typical symptoms…”11
Virology in Doubt
Press releases about the “definitive” Erasmus study, distributed by AP, WHO, Nature Magazine and others, cannot be taken seriously without further details. Here are a few unanswered questions:
a) Since laboratory virus stocks are poisoned with antibiotics, or are derived by a process that utilizes poisons, then which poisons were present in Erasmus University virus stocks?
b) Were the toxicities of virus stocks included in the assessment of the study results?
c) How was the virus stock obtained?
d) Was a comprehensive test for other viruses performed on the experimental stock?
e) Are the laboratory-produced viruses chimeric viruses, that is, synthetic viruses?
f) What quantity of virus medium was applied to each monkey; that is, what multiple of real-world conditions?
g) What concentration of viruses were applied; that is, what multiple of real-world conditions?
h) How was the medium applied; would the application method be possible in real-world conditions?
i) Which chemicals were added to the medium in addition to antibiotics? Do these interact or promote the toxicity of other chemicals in the virus stock?
j) How many monkeys were in each group? Were there enough for a valid assessment?
k) What was the condition of each monkey prior, during and at the conclusion of the experiment? Monkeys have been regarded as poor experimental subjects because of their intelligent sensitivity, and maltreatment received from handlers and distributors. Stress alone, incurred by the monkeys due to cruelty, cage conditions and poor nutrition, can cause illness or susceptibility.
l) Was the virus used in the experiment actually “isolated”? The word, when used by virologists, means something entirely different from the meaning assumed by non-virologists (including doctors), and this word serves as the basis for misinformation regarding virus proof. The details of “isolation of the virus” need to be explained.
m) Were any of the experimental animals, or tests, rerun after unexpected results occurred? What were the circumstances?
At this writing, one further detail of the Erasmus study has been obtained, “Osterhaus and colleagues completed the final ones [Koch Postulates] when they infected two macaque monkeys with the virus from a SARS patient and isolated it from the animals.”12
So, the “definite” proof is based on two monkeys injected with the supposed SARS virus. What happened to independent confirmation, randomized controls, and probability analysis that determine the possibility that a test on two monkeys is valid? The hyped language, the major institutions and funding sources involved, juxtaposed against the meager number of monkeys in the experiment, point to extreme bias in the search for a microbial demon. I look forward to more details of the Erasmus study.
As of late May, tests for the virus in Toronto “failed to spot a targeted virus in 30% to 50% of infected patients.”13 This was attributed to inaccurate testing methods, not the absence of the virus. Nevertheless, no matter how often SARS virus is found, the virus is present only in trace amounts and not in quantities large enough to cause disease, leaving infection and pathology in doubt.14
Convenient Scapegoats
In spite of the nagging inconsistencies in the viral theory for SARS, scientists and the press have gone one step further with reports that SARS originated in a live meat market in China’s Guangdong province in November, 2002. Researchers in Hong Kong and Shenzhen, China found a virus that is “almost identical” to the human SARS coronavirus in six masked palm civets (cat-sized animals) and a raccoon dog sold in these open air markets,15 a convenient discovery that will bring official pressure on China’s traditional farmers and food-sellers, now in competition with new, “sanitary” western-style supermarkets.
Viral demons are fair game for the media. Dramatic realities merge with scenes from class B sci-fi movies, as doctors and nurses scream through hospital wards, airports are closed and police round up infected carriers. In China, such dreadful acts are all too real. In addition to the proposed human executions, millions of cats, dogs, farm animals and wildlife may be slaughtered to stop the deadly viral plague. Precedent is found in Britain’s Mad Cow and Hoof and Mouth epidemics, and supposed viral epidemics in Malaysia and Taiwan during 1997-1998. In this scenario, medical workers come to the rescue like soldiers, heroically primed to save lives with deadly force.
The pharmaceutical companies, of course, are playing a leading role. Roche, “the global leader in the $22-billion-a-year clinical-diagnostics market” is developing a test that should be able to “flag SARS in the first days of an infection, possibly even when the virus isn’t causing symptoms.” This will allow officials “to identify superspreaders (patients whose SARS infections are highly transmissible) before they become superspreaders,” says a Roche executive.16 As all diagnostic tests generate false positives, anyone suffering from a fever and a cough risks being branded as a modern Typhoid Mary should he or she submit to such a procedure.
SARS Critics
In spite of the fearful headlines, the SARS paradigm has met widespread criticism.
An insider, Dr. Frank Plummer, spilled the beans: “The director… told The Scientist yesterday (April 10) that the new coronavirus implicated as the cause of the disease is certainly around in the environment but is unlikely to be the causative agent. Frank Plummer is director of Canada’s National Microbiology Laboratory in Winnipeg.”17
Plummer stated, “we are finding some of the best-characterized [SARS disease] cases are negative [for the SARS virus]. So it’s puzzling. As is the fact the amounts of virus we are finding, when we find it, are very small–only detectable by very sensitive PCR.
“That’s what the majority of labs [nasopharyngeal swabs] around the world are testing, it’s where you find most respiratory viruses. It’s strange [that there’s so little virus there] because it seems to be transmitted by close contact.”
After the announcement of the Erasmus study, Plummer stated, “Once you conclude that this coronavirus is the sole cause of SARS then you move into a different phase and you move to test only for it. . . to the exclusion of other things. And I think. . . at least based on what we’re seeing in Canada. . . it’s a little early to do that. We are in many ways behaving as if this is the cause.”18
According to a CBC news report, “No classic respiratory or bacterial respiratory pathogen was consistently identified. Scientists have not definitively shown the new coronavirus causes SARS. To do that, they need to see the virus in infected lung samples from all patients and show the virus causes SARS in an animal model.”19 Implicit in this statement is the fact that SARS symptoms are not unique to the disease, or that tests were finding other (non-SARS) pathogens in the victims, or tests were not consistently performed for other pathogens.
Jon Rappoport, an independent journalist who has written for CBS Healthwatch, writes, “This [SARS] insanity is multiplied beyond all sense when you consider that, in Canada, they are now finding the [SARS] coronavirus in ZERO PERCENT of diagnosed SARS cases.”20
Nicholas Regush, veteran journalist of ABC News, admits no contact with Rappoport, yet writes, “We’re in very deep trouble… the COMING OF SARS. Having been a member of the reporting classes for many years, I can’t say that I’m surprised. More like disappointed. Disgusted. Outraged.”21
Fintan Dunne, who edits a website entitled www.SickOfDoctors.com, is also critical: “More of the hype machine and further global economic damage, over a spurious syndrome which is a drop in the disease ocean.”22
Dr. Donald Low, one of Canada’s leading infectious disease experts and a key member of the SARS containment team, described WHO’s policies for Toronto as “a bunch of bullshit” and “inappropriate.”23
According to Peter Duesberg, the well-known microbiologist at the University of California at Berkeley, the list of badly diagnosed, yet strongly hyped epidemics is lengthy: Ebola, Hepatitis C, AIDS, SMON, and others.24 According to the German virologist Stefan Lanka, the list of pseudo-epidemics is nearly endless.25
Toxicology
The orthodox SARS paradigm completely omits and avoids toxicology for good reason: SARS disease symptoms are identical to pesticide and air pollution disease symptoms. And these poisons correlate in time and place with SARS epidemics.
Only virology holds SARS together, and by including toxicology, the virus theory of SARS can be entirely rebutted.
Airline Pesticides
As the SARS syndrome “appears to be spreading via air travel, the CDC advised travelers to postpone any non-essential travel to affected areas, which include China, Hong Kong, the Philippines, Singapore, Thailand, and Vietnam, according to WHO.”26
What most travelers don’t realize is that airlines routinely apply pesticides to airplanes, especially those on Asian routes. Airlines call their pesticide application “disinsection.” A US Department of Transportation memo describes two methods of application: “Either spray the aircraft cabin, with an aerosolized insecticide, while passengers are on board or treat the aircraft’s interior surfaces with a residual insecticide.” 27
On August 2, 2001, CNN reported on a lawsuit filed by United Airlines stewardesses for damages caused by pesticides sprayed in United Airlines planes on Australian and New Zealand routes.28 No further mention of the lawsuit has appeared in the press.
However, on March 17, 2003, Pesticide Action Network Updates Service (PANUPS) announced: “An airline flight to the tropics may involve greater health risks. . . pesticides are routinely sprayed in aircraft cabins by US airlines, sometimes over the heads of passengers during flight.”29
Details on airline pesticide protocols for southeast Asian airline flights emerge from the US Department of Transportation memo: “Guam requires disinsection, but permits the residual method, of all flights from the Commonwealth of the Northern Mariana Islands, Thailand, Philippines, Korea, Indonesia, Malaysia, the Federated States of Micronesia, Papua New Guinea, Solomon Islands, and the Republic of the Marshall Islands and, during certain months, of flights from Taiwan, Korea and Japan.”30
The pesticides used in airlines are synthetic pyrethrin pesticides (pyrethroids), which in some countries have been banned from agricultural use.31 SARS symptoms are nearly identical to those of pyrethrin pesticides, as shown in the table on Page 19.
There are other chemical risks found in aircraft. Diana Fairechild, who worked decades for the airline industry and spent years litigating against that industry over issues related to pesticide protocols, describes the liabilities of airline travel on her website.46
Airport Pollution
Airports are notoriously air polluted. A single airliner at take-off emits tremendous volumes of pollutants.47 JFK airport in New York City, has its own oil refinery on the airport grounds, nearly two football fields in area. How common is that practice? Oil refinery emissions correlate exceedingly well with recent so-called viral disease epidemics. The West Nile virus epidemic was first noticed in the neighborhoods beneath one of the busiest take-off lanes in the US, La Guardia Airport, New York City.48
Industrial Emissions
The greatest SARS epidemic region in the world is the Guangdong province of China. That heavily populated province also vies for position as the most highly polluted region on earth, due to the presence of oil refineries, metal smelters and other chemical industries in a country with lower environmental standards.
Writing for The Atlantic Monthly, Mark Hertsgaard describes Guangdong province as “A fiendish laboratory experiment that was mushrooming beyond control. . . . Shanxi, a day’s journey west of Beijing. . . the land. . . scalped, the water poisoned, the air made toxic and dark. . . . At least five of the cities with the worst air pollution in the world are in China. Sixty to 90 percent of the rainfall in Guangdong. . . is acid rain. . . people’s lungs and nervous systems are bombarded by an extraordinary volume and variety of deadly poisons. One of every four deaths in China is caused by lung disease.”49 Hertsgaard found that total suspended particulates (an air pollution index) can be, in some cities in China, 12 times higher than in New York City. Obviously, non-viral forms of SARS exist in Guangdong. SARS is far from atypical.
Deforestation by fire can also cause the respiratory problems associated with SARS. Huge fires are set or occur accidentally in Singapore, Malaysia and China. Major fires ravaged southeast Asia in September 2002, just two months before officials announced the SARS epidemic.50
Tan Ee Lyn (Reuters) describes the air environment in Hong Kong and southern China, the major SARS epicenters: “[Title:] CHINA: September 9, 2002, Thick smog shrouds Hong Kong, health warning issued. [Text:]Hong Kong–Thick smog blanketed Hong Kong last week, a clear sign that the territory and southern China are still a long way from cleaning up their bad air. The government urged people with respiratory problems to avoid heavily congested traffic areas and cut back on outdoor physical activity.”
Toxicology = Virology
Even if a perfect (according to the rules of virology) laboratory proof for virus causation existed, such proofs still involve high use of artifice, far from the reality of everyday life. Even if SARS virology could have isolated and properly identified a real virus, questions still remain. A SARS virus may be a natural endogenous virus (from within) serving a normal adaptive function. It might not be the infectious, exogenous virus (from without) as described by media hype.
Not well known, but well established, is the fact that virus-like genetic material (RNA) is often expressed from poisoned cellular tissue as an adaptive and defensive response to poisoning.51 Expressing virus-like genes is part of the cellular “SOS response” of cells engaged in accelerated genetic recombination.52 The so-called SARS virus can be interpreted as such a genetic expression occurring in humans, as well as the exotic animals, palm civet cats and raccoon dogs sold in Guangdong live animal markets and recently found positive for SARS.
Virus Is Us
The cutting-edge biochemist, Howard Urnovitz, views SARS virus as human genes rearranged by pollution stress: “I do not see a virus. I see a unique and complete rearrangement of genomic elements. For example, when I look at what is believed to be the gene sequence coding for the spike protein of this coronavirus, I see a complicated gene rearrangement of a region of human chromosome. As I did in our studies of Gulf War Syndrome, when I see gene rearrangements like this, I immediately search for an associated catastrophic environmental event that could have caused such genomic rearrangement.”53 (Emphasis added.)
SARS epidemics correspond strongly with such “catastrophic environmental events.”
SARS Redefined
SARS is not a unique disease, since its symptoms coincide with pyrethrin poisoning and air pollution diseases.
Orthodox science damns itself by beginning with a virus hypothesis when toxicological evidence is plentiful. Orthodox journalism promotes the discovery of the “SARS virus” with little criticism of the virology and a deafening silence regarding toxicology.
Apparently the virus paradigm is a necessary cover for industrial pollution. WHO’s promotion of the virus disease paradigm is a tremendous boon for industry, which requires free disposal of industrial wastes into the lungs. . . correction. . . the atmosphere.
The preponderance of evidence indicates that SARS is the direct result of regional industrial pollution, airport pollution, with an optional coup de grace from pyrethroid pesticides applied directly upon the passengers or as a residue vapor. Essentially, airlines are enclosed, fabric-filled containers where air is circulated several times before it is vented to the outside. They are not the kind of chamber that environmentalists would prefer to enter following “disinsection.” SARS, like St. Louis virus (SLE), West Nile Virus (WNV) and non-toxicological asthma definitions guarantee spin control for emerging epidemics.
Neenyah Ostrom discusses the general relationship between pollution in China and the SARS virus– and the relation between poisoning and cellular RNA: “But Guangdong and Hong Kong share another distinction: They are in perhaps the most polluted area on the planet. Should we be asking questions like, what new types of pollutants have been introduced into this gene-swapping microenvironment? So, the question becomes: Is pollution a causative agent in SARS?”
If SARS disease is another semantic flag for industrial pollution, then SARS functions by punishing the economy of polluting regions without specifically placing blame on powerful industries. Military groups have long employed such a method–where the group is punished to correct individual behavior. Within industry, SARS will bring about a reassessment of economic priorities (industrial need versus human worth) without the complications of public blame games.
Sidebars
West Nile Virus
West Nile Virus (WNV) arrived in New York City in 1999 and soon grew into an “epidemic” characterized by a sea of contradictions.54 Medical press agencies proclaimed the “first arrival of the West Nile virus to the Western Hemisphere”55 but a more accurate description of the situation would be the “first testing of the West Nile virus in the Western Hemisphere.”
Mayor Giuliani personally announced the epidemic. He also announced the immediate commencement of a six-week pesticide spray campaign over the city, dispensed by helicopters. Meanwhile, the TV and newspaper headlines chanted, “The Deadly Virus.” The disease was at first attributed to the St. Louis encephalitis virus (SLE) but a few weeks later blame shifted to West Nile virus.
The United States Geological Survey (“USGS”) issued a press release one year later “confirming” the pathological effect of WNV on crows. This was hyped and widely distributed. Having read many other virological studies, I found the USGS results incredibly odd. The crows were injected intramuscularly with a virus extract and a few days later all met death. The filter used to separate the virus from tissue extract was nearly six times the diameter of the virus.56 Nearly all non-injected crows in the same cage also died. The success of the experiment was too convincing to be true, especially for a study that did not employ the common, harsh, intracranial injection method. The study outcome was also odd because WNV had been considered a mild virus and not especially dangerous to birds. The USGS laboratory ignored my repeated inquiries for the published details. After going through another scientist, who contacted the USGS, I received an emailed response from the USGS indicating low confidence for their study. The agency indicated their study would not be published or discussed and they expressed an intention to perform a better experiment in the future. I doubt they would want to take a chance on another such experiment.
SLE and WNV epidemics occur annually in air-polluted petrochemical regions (such as eastern New Jersey and St. Louis) during the warm spring and summer months, with an apex in July and August. The incidence correlates daily with air pollution brought to ground level by warm air and loss of convection efficiency for exhaust sources. SLE epidemics have a long history in the US (in petrochemical regions) and these epidemics don’t spread infectiously to other regions. The two great epicenters for WNV/SLE disease are the two great petrochemical industrial regions in the US–southern Louisiana and New Jersey.
During the summers of 1999 and 2000, air pollution levels reached record levels, correlating with the incidence of “West Nile virus” cases, both human and avian. The gasoline additive MTBE represents perhaps the greatest production volume for any industrial poison in the US, yet it has received little publicity. The public became aware of its dangers only when the EPA suggested that MTBE be phased out on July 27,1999. That date also represents the apex of the West Nile virus avian epidemic for 1999.63
Like so many widely dispensed industrial poisons, the physiological effects of MTBE have only become known through usage on the public. However, Dr. Peter Joseph correlated MTBE with neurological disease in his 1997 study, “Changes in Disease Rates Following the Introduction of Oxygenated Fuels.” Neurological symptoms also characterize West Nile virus disease. Avian mortality further distinguishes this “viral” disease. Yet, avian mortality is an early warning system for human air pollution disease, as evidenced by the traditional air assay test, the “miners’ canary.”
Legionnaires’ Disease
Another acute respiratory disease is Legionnaires’ disease, also characterized by sloppy science. The disease was claimed causative for 182 casualties and 29 deaths within a few days in 1976 at the bicentennial celebration of the American Legion at the Bellevue Stratford Hotel in Philadelphia.
After several months of study, CDC scientists announced the discovery of Legionella bacteriumas as the cause for Legionnaires’ disease. Virologists Peter Duesberg and Brian Ellison relate the story.57 “One month before the CDC isolated the bacterium, a US House of Representatives Investigative Committee held hearings excoriating the CDC for not having looked for toxic chemicals as a possible cause of the 1976 epidemic. Chairman John Murphy of New York sharply attacked the investigation because ‘The CDC, for example, did not have a toxicologist present in their initial team of investigators sent to deal with the epidemic. No apparent precautions were taken to deal with the possibility, however remote at the time, that something else might have been the cause.’”
According to Duesberg, “The evidence indicates Legionella is actually quite harmless. Since 1976, CDC and public health investigators have found the bacteria all over the country, in water cooling towers, condensers, shower heads, faucets, humidifiers, whirlpools, swimming pools and even hot-water tanks, assorted plumbing, mud, and lakes. The bacterium is so universal that between 20 percent and 30 percent of the American population has already been infected, yet virtually no one ever develops Legionnaires’ disease symptoms.” Calling the organism Aguanella–indicating it is simply water-borne–wouldn’t serve the CDC’s purpose. Quite by chance, the CDC’s interpretation happens to protect the chemical industry, which sells poisonous deodorants, pesticides, antibiotics, carpets, paints, pharmaceuticals, cosmetics and beverages to hotels–and airlines.
Two SARS Disease Paradigms: Comparison of Symptoms
Symptom
As SARS Virus32-35
As Airline Pesticide Poisoning
(mostly Pyrethrin formulations)36-45
Coughing
Yes
Yes
Malaise
Yes
Yes
Fever
Yes
Yes
Headaches
Yes
Yes
Nausea
Yes
Yes
Vomiting
Yes
Yes
Rash
Yes
Yes
Respiratory distress
Yes
Yes
Respiratory failure
Yes
Yes
Neurological dysfunction
Yes
Yes
Cardiac dysfunction
Yes
Yes
Irritability
Yes
Yes
Diarrhea
Yes
Yes
Pneumonia
Yes
Yes
Lung damage (as measles symptoms, see below)
Yes
Yes
Dyspnoea (breathing difficulty related to hypoxemia)
Yes
Yes
Hypoxemia (low oxygen level)
Yes
Yes
Proteinaceous pulmonary edema
Yes
Yes
Leukocyte inhibition
Yes
Yes
Increases sodium ion permeability in tissue
Not Listed
Yes
Affects nasal, windpipe and lung surfaces
Yes
Yes
Shock
Not Listed
Yes
Seizures
Not listed
Yes
Salivation
Yes
Yes
Neurological damage
Yes
Yes
Muscular stiffness
Yes
Not listed
Like measles (Syncytial lung)
Yes
Yes*
Like flu
Yes
Yes
Like common cold
Yes
Yes
Like mumps
Yes
Yes*
*In terms of listed symptoms
SARS – Other Theories
Len Horowitz, PhD, author of Emerging Viruses: SARS is simply the flu, which kills 36,000 people annually in the US. Death comes to those whose immunity has been compromised by drugs and vaccines.58 The media has created great fear among the public by grossly overstating mortality rates and exaggerating the danger to healthy individuals.
Mae-Wan Ho, PhD, president of the London-based Institute of Science in Society: SARS is a highly infectious disease caused by a new bacterium of the Chlamydia family that was created accidentally through genetic engineering. Disease-causing viruses and bacteria and their genetic material are the predominant materials and tools of genetic engineering. The artificial constructs created by genetic engineering are designed to cross species barriers and to jump into genomes, creating the possibility of new, highly virulent micro-organisms.59
Marshall Smith, Editor, BroJon Gazette: The SARS virus, like all flu viruses, is a variant caused by the rural Chinese custom of raising flocks of geese side-by-side with herds of swine. If a pig is ill with a porcine flu and then eats droppings from an avian-virus-infected goose, the result is a new cross-species flu virus with the outer lining of a pig and the inner viral core of a goose. Whether or not this theory is correct, Smith’s advice is sound: Do not suppress a fever. Fever is the body’s way of preventing the invading virus from reproducing and spreading massively throughout the body. Unfortunately, most cold and flu medications reduce fever, setting the stage for massive viral proliferation. Unfortunately, the current definition of SARS may cause many people to take drugs to suppress fever, in order to avoid quarantine.
Linda Saif, professor of food animal health at Ohio State University: Coronavirus causes cough and pneumonia, so-called shipping fever, in animals packed together in cattle cars. The stresses of air travel–large numbers of people together in small spaces, being away from home, being close to other strangers, moving across time zones, rushing to catch flights–are conditions that make the coronavirus dangerous to humans as well.60 (Saif does not explain why airline travel, which has been a fact of life for millions of people for the last 40 years, has not caused SARS until recently.)
Richard Fisher, senior fellow at the Jamestown Foundation, a Washington-based think tank: “. . . there are compelling reasons. . . to at least ask whether there might be any linkage between SARS and China’s biological-warfare efforts.”61
Chandra Wickramasinghe, professor of applied mathematics and astronomy at Cardiff University: The SARS virus comes from outer space, hitched a ride on a comet and then drifted down to earth.62
References:
Washington Post, May 24, 2003
AP, May 15, 2003. “SARS has caused more damage to the global airline industry than the Sept. 11 attacks and the war in Iraq combined, the world’s airline association said Thursday.”
NY Times 5/5/03
“China has threatened to execute or jail for life anyone who breaks SARS quarantine orders and spreads the deadly virus intentionally.” Beijing (Reuters), May 15, 2003
“Malaysia ordered a quarantine for 203 citizens, mostly low waged earners, who had visited a SARS-infected produce market in Singapore and warned that it would imprison those who would break the orders.” www.rediff.com/news/2003/apr/24sars1.htm
“Rotterdam-led scientists confirm virus as cause of SARS”, Bio Aspects Newsletter, Vol 6, April 24, 2003, www.geneyous.nl/docs/BioASPects20030424.html#article-marktontwikkeling1
“Tests Confirm Coronavirus Is Sars Source”, Patricia Reaney, May 15, 2003, NIH/Reuters, MedlinePlus
Fortune Magazine, 5/26/03
www.biomedcentral.com/news/20030411/04
Washington Times, February 24, 2003
Fortune Magazine, May 25, 2003
Walgate 4/11/03, Ibid
“Containment Controversy”, Global Sunday, 4/25/03, an interview by Troy Reeb with Dr. Frank Plummer, Global Sunday, www.canada.com/national/globalsunday
“Scientists make small steps in identifying cause of SARS”, CBC NEWS, April 10, 2003, www.cbc.ca/stories/2003/04/10/sars_sci030410
Neenyah Ostrom, “Why is SARS Such a Mystery? Virus, Bacteria, Fungus, Parasite – Why Can’t Researchers ID the Bug?”, March 20, 2003, www.chronicillnet.org
Aviation Policy, U.S. Dept. of Trans., http://ostpxweb.dot.gov/policy/safety/disin.htm
“United Sued Over Pesticide In Planes”, August 2, 2001, CHICAGO, Illinois (AP) — Flight attendants are being sickened by exposure to pesticides that are sprayed on airplanes serving Australia and New Zealand, a lawsuit filed against United Airlines claims,” www.cnn.com/2001/TRAVEL/NEWS/08/02/unitedairlines.pesticides.ap/index.html
“Airline Passengers Are Sprayed for Bugs”, March 17, 2003: “An airline flight to the tropics may involve greater health risks… pesticides are routinely sprayed in aircraft cabins by U.S. airlines sometimes over the heads of passengers during flight.” PANNA mentions Asian routes as specifically at risk for this procedure.
“Aviation Policy”, U.S. Dept. of Trans., http://ostpxweb.dot.gov/policy/safety/
Cynthia Olsen, “A Safe Alternative Treatment for Head Lice”, Alive Magazine, October 2000, “Pyrethrins have been banned from agricultural use as a pesticide.”
CDC Case Definition for SARS (March 22, 2003): Measured temperature > 100.5F; cough; hypoxia; shortness of breath; pneumonia; acute respiratory distress.
Gavin Joynt and Charles Gomersall, “Severe acute respiratory syndrome (SARS)”,
Tamer Fouad, M.D., SARS Symptoms: “headache, muscular stiffness, loss of appetite, malaise, confusion, rash, and diarrhea. Early laboratory findings include low platelet and white blood cell counts. In some cases, those symptoms are followed by pneumonia in both lungs, sometimes requiring use of a respirator.” The Doctor’s Lounge.NET. http://thedoctorslounge.net/medlounge/articles/sars
Maggie Fox, April 10, 2003 (Ibid). Early SARS symptoms: like flu, measles, mumps.
Olsen, 2000, Ibid. Symptoms listed for permethrin (a type of synthetic pyrethrin used on airlines): “Side effects include vomiting, respiratory failure, pneumonia and asthma.”
Becky Riley, “Flyers Beware: Pesticide Use on International and U.S. Domestic Aircraft and Flights”, Northwest Coaltion Against Pesticides (NCAMP), 1998, “… “in-flight spraying, Airosol Aircraft Insecticide, says that acute health hazards of exposure to the product include dizziness, skin irritation, and frostbite, and that overexposure due to inhalation may cause temporary central nervous system effects: dizziness, headache, confusion, stupor with the exclusion of oxygen and with grossly excessive overexposure. Additional warnings state that individuals with preexisting diseases of the cardiovascular system may have increased susceptibility to the toxicity of excessive exposures, and to heart irregularities (Airosol Company, 1992).”
Ibid, “Two other U.S.-registered permethrin-containing products with labeled aircraft uses, but theoretically not for use in passenger cabins (though this is far from clear from reading the product labels), are Dragnet FT Termiticide/Insecticide and Flea Insecticide. According to information provided by the FMC Corporation, manufacturer of the above products, symptoms of overexposure to both of the products include hypersensitivity to touch and sound, tremors, and convulsions. Overexposure of animals via inhalation has also produced symptoms such as squinting eyes, irregular and rattling breathing, and ataxia (loss of muscular coordination). Inhalation of stoddard solvent vapors [present in both of the above products] may cause dizziness, disturbances in vision, drowsiness, respiratory irritation, and eye and skin and mucous membrane irritation (FMC, 1998; FMC, 1993).
Ibid. Airline pesticides: “Organophosphates are efficiently absorbed by inhalation, ingestion, and skin penetration. Symptoms of acute exposure to organophosphates include: headache, nausea, dizziness and anxiety, followed by muscle twitching, weakness, tremor, incoordination, vomiting, abdominal cramps, diarrhea, tightness in the chest, and coughing. Severe organophosphate poisonings can lead to incontinence, paralysis, unconsciousness, convulsions, and life-threatening respiratory failure (US EPA, 1989).”
Ibid. “Bendicarb: Highly toxic carbamate nerve poison (US EPA, 1989). Causes eye irritation. Exposure (poisoning) symptoms include tightness in chest, sweating, stomach pains, vomiting, and diarrhea (US EPA, 1979).”
Ibid. Piperonyl butoxide (used on aircraft): “Classified by EPA as a possible human carcinogen (US EPA, 1998-3). In animal tests, causes liver tumors and lung damage, hemorrhages, and anemia (Takahashi, 1994).”
“MSDS: Permethrin,” Universal Crop Protection Alliance LLC, “…moderate eye and skin irritation… Eye: There may be moderate stinging, tearing and redness… mild skin irritation… Disturbances in vision, drowsiness, respiratory irritation… High oral doses can result in damage to the liver and kidneys… Long term feeding studies in animals resulted in increased liver and kidney weights, induction of the liver microsomal drug metabolizing enzyme system, and histopathological changes in the lungs and liver.”
Shirley A. Briggs and Rachel Carson Council, Inc., “Excerpts From Basic Guide To Pesticides”, Pyrethroid symptoms: “tremors; exaggerated startle response; hyperthermia [fever]”
Lance C. Villers, MA, NREMTP, “Managing organophosphate exposures”, Texas Dept. of Health, EMS Management, OP Symptoms: “respiratory depression, bronchospasm, bronchial secretions, pulmonary edema, muscular weakness, resulting in hypoxemia.” www.tdh.state.tx.us/hcqs/ems/MJCEPesticideExp.htm
INCHEM, “Pyrethrin”, Symptoms: “cough, wheeze, dyspnoea, bronchospasm or pulmonary oedema.”, Chemical Safety Information From Intergovernmental Organizations. www.inchem.org
“Airports create smog; a single 747 arriving and departing… produces as much smog as a car driven more that 5,600 miles, and as much NOx as a car driven almost 26,500 miles (source: Natural Resources Defense Council).” Queens College School of Earth and Environmental Science www.qc.edu/EES/ENSCI111/Air/air.html
Jim West, “The Dangers of MTBE-Gasoline Additive: Its Connection to the West Nile Virus”, Townsend Letter For Doctors And Patients, July 2002, v228, p64-76.
Mark Hertzgaard, “Our Real China Problem”, The Atlantic Monthly, November 1997.
Ralph Scobey, M.D., “Is Human Poliomyelitis Caused By An Exogenous
Virus?”, Archive Of Pediatrics (April/May,1954) v71, p111. From Jim West’s
analysis of Scobey, www.geocities.com/harpub/scobexog.htm
Mark Ptashne, A Genetic Switch (1992), p62. Cell Press and Blackwell Scientific Publications, 50 Church St., Cambridge, MA 02138
“Dr. Urnovitz rejects the theory of a coronavirus as being the cause of SARS”, May 14, 2003. www.chronixbiomedical.com/Research/press_release3.html
Eric Ammerman , Senior Public Health Sanitarian, Monroe County Department of Health. “Experts agree that WNV most likely arrived in the Western Hemisphere as some ‘accidental tourist’ aboard a ship or in an airplane.”
“A panel appointed by the EPA is set to report on Tuesday that use of the much-debated ingredient M.T.B.E. . . should be ‘reduced substantially’. .. ” The New York Times, July 27, 1999.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly magazine of the Weston A. Price Foundation, Summer 2003.
The release of the National Toxicology Program’s (NTP) systematic review of fluoride’s neurotoxicity was blocked by government officials and concealed from the public since May 2022
Fluoride Action Network’s lawsuit against the U.S. Environmental Protection Agency (EPA) to ban the deliberate addition of fluoridating chemicals to U.S. drinking water has been on hold waiting for the release of the NTP report
Prior to the NTP report’s scheduled release in May 2022, it was shared with members of dental groups like the American Dental Association, which urged officials to alter the report
After a court order, the NTP report was released, showing that out of 55 studies included, 52 found that increased fluoride exposure was associated with decreases in child IQ
The meta-analysis noted that no safe exposure level could be confirmed, including exposure to fluoride levels found in artificially fluoridated water
In 2015, the U.S. Centers for Disease Control and Prevention labeled community water fluoridation as one of the 10 greatest public health achievements of the 20th century.1 To this day, relatively few consumers are aware of water fluoridation’s sordid history or the battle that’s been going on behind the scenes to get this toxin out of U.S. drinking water.
I’ve been warning of the risks for well over a decade and have been ridiculed as a result. In one example from 2013, an article published by mainstream media outlet Slate scoffed at the idea of fluoride as a neurotoxin, insulting me directly in the process.2
Vindication is upon us, however, following the court-ordered release of the National Toxicology Program’s (NTP) systematic review of fluoride’s neurotoxicity — a release that was blocked by government officials and concealed from the public since May 2022.3
Fluoride Lawsuit Delayed for Years, Waiting on NTP Report
Paul Connett, Ph.D., executive director of the Fluoride Action Network (FAN), has been instrumental in catalyzing the movement to remove fluoride from water supplies in the U.S. as well as internationally. FAN filed a historic lawsuit against the U.S. Environmental Protection Agency (EPA) in federal court.
In 2016, FAN and coalition partners filed a petition asking the EPA to ban the deliberate addition of fluoridating chemicals to U.S. drinking water under Section 21 of the Toxic Substances Control Act (TSCA).
The EPA dismissed FAN’s petition, prompting the lawsuit challenging the EPA’s denial. Although the EPA filed a motion to dismiss the case, the motion was denied by the court in 2017.4 The trial was held in June 2020, but the judge was unable to make a final ruling.5
At the time, he requested more information, including the NTP’s systematic review of fluoride’s neurotoxicity, as well as the benchmark dose analysis of fluoride’s neurotoxicity.6 Status hearings for the case have been delayed since. In December 2021, an update from FAN explained:7
“The document the Court wanted was the systematic review of fluoride’s neurotoxicity from the National Toxicology Program’s (NTP). The NTP spent 4-5 years and at least a million dollars to produce two draft systematic reviews8 on fluoride’s neurotoxicity. Both draft reviews stated, ‘NTP concludes that fluoride is presumed to be a cognitive neurodevelopmental hazard to humans.’
However, on February 9, 2021, seven months after the trial ended, the NTP wrote a private statement, not released to the press or to the public, that it would not complete its systematic review.
Instead, NTP wrote that it would do a ‘state of the science’ report on fluoride’s neurotoxicity. The public learned of NTP’s private statement after lawyers representing the U.S. EPA in the TSCA trial submitted it into the record on February 22, 2021 …
The National Toxicology Program is well aware that the Court is waiting for its document. The presumption is that powerful forces within the National Institutes of Health were behind the ending of the NTP’s systematic review and that they may be involved in the ‘state of the science’ report as well.”
Multiple delays, including cancelations and rescheduling, followed, with the EPA continuing to ask that the trial be delayed indefinitely until NTP published the report.
Finally, at a January 2023 hearing, FAN reported, “the judge acknowledged that “justice delayed is justice denied,” ultimately ruling against them. The court directed the plaintiffs and defendants to start the process of adjudicating whether the final NTP report and accompanying agency comments ought to be made public in preparation for the final phase of the trial.”9
Dental Groups Urged Officials to Alter NTP Fluoride Report
Reports suggest that prior to the NTP report’s scheduled release in May 2022, it was shared with members of dental groups like the American Dental Association. Linda Birnbaum, who was NTP director until 2019, said the report was set to be released until, “They were blocked.” Capital & Main reported a clear conflict, as dental groups got ahold of the NTP report and worried its findings would threaten the future of water fluoridation:10
“Leading up to the report’s intended release, individuals from dental organizations including the American Dental Association (ADA) scrutinized the report’s scientific credibility in communications with staff from other dental groups and health agencies including the National Institutes of Health and the NTP, divisions of HHS, records show.
This January, Birnbaum issued a scathing legal declaration as part of the lawsuit, writing, ‘The decision to set aside the results of an external peer review process based on concerns expressed by agencies with strong policy interests on fluoride suggests the presence of political interference in what should be a strictly scientific endeavor.’
… If federal health agencies shared the report with outside organizations, ‘That was completely inappropriate,’ said Birnbaum. ‘It’s either everybody gets a chance to look at it, or only very restricted government entities,’ Birnbaum added. ‘That trust, I would say, was broken.’
In a February 2022 email to various senior health officials including HHS Assistant Secretary for Health Rachel Levine, ADA senior manager for strategic advocacy and public policy Robert Burns asked the NTP to ‘exclude — or carefully consider how to characterize — any lingering neurotoxin claims’ from the upcoming report.
He wrote that ‘such claims are often taken out of context,’ and might ‘undermine national, state, and local efforts to expand community water fluoridation’ at the CDC’s recommended levels.”
NTP Report — 52 of 55 Studies Link Fluoride to Lower IQ
So, what did the NTP report11 reveal about fluoride’s neurotoxicity? Out of 55 studies included in the review, 52 found that increased fluoride exposure was associated with decreases in child IQ.
“Our meta-analysis confirms results of previous meta-analyses and extends them by including newer, more precise studies … The data support a consistent inverse association between fluoride exposure and children’s IQ,” the report found.12 While some have stated that the data only apply to water fluoride concentrations above those commonly found in U.S. drinking water, NTP didn’t agree, stating:13
“We do not agree with this comment … our assessment considers fluoride exposures from all sources, not just water … because fluoride is also found in certain foods, dental products, some pharmaceuticals, and other sources … Even in the optimally fluoridated cities … individual exposure levels … suggest widely varying total exposures from water combined with fluoride from other sources.
… We have no basis on which to state that our findings are not relevant to some children or pregnant people in the United States … Several of the highest quality studies showing lower IQs in children were done in optimally fluoridated (0.7 mg/L) areas…many urinary fluoride measurements exceed those that would be expected from consuming water that contains fluoride at 1.5 mg/L.”
No Safe Level of Fluoride in Water
The report also identified a drop of about seven IQ points over a fluoride range of 0.2 to 1.5 mg/L, which a peer reviewer described as “substantial … That’s a big deal.”14 The meta-analysis noted that no safe exposure level could be confirmed, including exposure to fluoride levels found in artificially fluoridated water.15 The next hearing for FAN’s lawsuit against the EPA is set for April 11, 2023.16
FAN obtained documents via the Freedom of Information Act that further showed dental groups’ attempts to “water down the report.” FAN explained:17
“When the NTP held firm, these agencies got HHS Assistant Administrator Rachel Levine to block its release. Only one historical example exists of an NTP report being blocked from release, a report on the carcinogenicity of asbestos-contaminated talc.
Talc industry groups conducted an aggressive lobbying campaign, enlisting friendly congresspeople to intervene. FAN was able to force today’s release of the NTP report by using leverage from the ongoing lawsuit against the EPA.
Fluoridation defenders have falsely claimed draft versions of the report had been ‘rejected’ by a National Academies committee. In fact, the committee recommended that NTP clarify their methods and reasoning for reaching their conclusions because the issue was considered so contentious. The NTP has done that in the report …
There is now little question that a large body of scientific evidence supports a conclusion that fluoride can lower child’s IQ, including at exposure levels from fluoridated water … With the release of this report, dental interests may have to rethink their denial of the evidence that fluoridation can reduce children’s IQ.”
97% of Western Europe Has Rejected Water Fluoridation
If the U.S. got it wrong about water fluoridation after declaring it a top public health achievement, it makes you wonder what else they’re wrong about. And it’s important to understand that water fluoridation is not the norm worldwide. In fact, 97% of people living in western Europe drink nonfluoridated water, including those in: Austria
Belgium, Denmark, Finland, France, Germany, Greece, Iceland, Italy, Luxembourg, Netherlands, Northern Ireland, Norway, Portugal, Scotland, Sweden, Switzerland
Fluoride in drinking water is an industrial waste product from the phosphate fertilizer industry.19 More than 300 studies have shown fluoride’s toxic effects on the brain,20 including 2006 National Research Council review that suggested fluoride exposure may be associated with brain damage, endocrine system disruption and bone cancer.21
In 2012, Harvard researchers also revealed that children living in high-fluoride areas had significantly lower IQ scores than those who lived in low-fluoride areas22 and suggested high fluoride exposure may have an adverse effect on children’s neurodevelopment.
A study of Mexican women and children also raised concern, showing that higher exposure to fluoride while in utero is associated with lower scores on tests of cognitive function in childhood, both at the age of 4 and 6 to 12 years.23
Each 0.5 milligram per liter increase in pregnant women’s fluoride levels was associated with a reduction of 3.15 and 2.5 points on the children’s scores on the General Cognitive Index (GCI) of the McCarthy Scales of Children’s Abilities and the Wechsler Abbreviated Scale of Intelligence (WASI), respectively.
Fluorosilicic acid, which is the fluoride chemical added to drinking water, may also be contaminated with additional harmful compounds, including lead and arsenic. Children, in particular, are at risk from ingesting fluoride, but they are exposed to the same levels in drinking water as adults. According to Steven Gilbert, Ph.D., founder and director of the Institute of Neurotoxicology and Neurological Disorders:24
“From the 1950s the PHS [Public Health Service] recommendation for the concentration of fluoridated water has been 1.0 mg/L (milligrams per liter or ppm) for most of the U.S., with a range of 0.7 to 1.2 mg/L. In 2015, this recommendation was lowered to 0.7 mg/L to reduce the toxic side effects of fluoride ingestion while attempting to maintain its beneficial effects.
For toxicological assessment, ingested doses are typically adjusted by body weight. Kids eat more, breathe more, and drink more than adults on a body weight basis so they will have higher fluoride doses than adults. Moreover, child organ systems such as the brain and bones are still developing, making them more vulnerable to the toxic effects of fluoride.”
Hopefully, now that the NTP review has been released, the truth about water fluoridation’s toxicity will come out, and the archaic practice can be ended in the U.S. and worldwide.
Help End the Practice of Fluoridation
There’s no doubt about it: Fluoride should not be ingested. Even scientists from the EPA’s National Health and Environmental Effects Research Laboratory have classified fluoride as a “chemical having substantial evidence of developmental neurotoxicity.”
Furthermore, according to screenings conducted for the Centers for Disease Control and Prevention (CDC), 65% of American adolescents now have dental fluorosis — unattractive discoloration and mottling of the teeth that indicate overexposure to fluoride — up from 41% a decade ago. Clearly, children are continuing to be overexposed, and their health and development put in jeopardy. Why?
The only real solution is to stop the archaic practice of artificial water fluoridation in the first place. Fortunately, the Fluoride Action Network (FAN), has a game plan to END fluoridation worldwide.
Clean pure water is a prerequisite to optimal health. Industrial chemicals, drugs and other toxic additives really have no place in our water supplies. So please, protect your drinking water and support the fluoride-free movement by making a tax-deductible donation to the Fluoride Action Network today.
Internet Resources Where You Can Learn More
I encourage you to visit the website of the Fluoride Action Network and visit the links below:
10 Facts About Fluoride — Attorney Michael Connett summarizes 10 basic facts about fluoride that should be considered in any discussion about whether to fluoridate water. Also see 10 Facts Handout (PDF).
Moms2B Avoid Fluoride — Help spread the word to expecting parents to avoid fluoride during pregnancy due to potential harm to the fetus.
Health Effects Database — FAN’s database sets forth the scientific basis for concerns regarding the safety and effectiveness of ingesting fluorides. They also have a Study Tracker with the most up-to-date and comprehensive source for studies on fluoride’s effects on human health.
“It is abundantly clear that the incessant reporting about so-called ‘pathogens’ that can ‘infect’ us, continues to promulgate the idea that ‘viruses’ are not only real, but they are also pathogenic and therefore pose a risk to our health. This serves to keep many people confused and fearful – which is of course part of the intention of such reporting.”
An article posted on the BBC website on 5th April caught my eye because it provides yet another example of why it is so important to not only expose the lies about ‘viruses’ being pathogens, but to also refute the claims by many voices in the ‘alternative health movement’ that the ‘no virus’ position is divisive and of no real importance.
I strongly disagree that it is divisive and of no importance.
In fact, I would say that it is absolutely central to our ability to live in freedom that we understand that there is no evidence for the existence of a pathogenic ‘virus’ – or any other so-called ‘germ’ for that matter – because it enables us to live without fear and to take responsibility for our own health.
The aforementioned BBC article, entitled Rare tick disease found in England, health officials say, begins with the following claim,
“A virus carried by ticks, which is common in many parts of the world, is now present in the UK and health officials are reminding the public how to avoid bites from the tiny bugs.”
The idea that it is ‘now’ present in the UK would seem to be contradicted by a later statement in the article,
“But the tick species which carries the virus is widespread in the UK.”
There are similarities with the claims about this tick and those about the mosquitoes that are claimed to cause malaria, because they are also said to be widespread in the UK; a situation that raises the obvious question: Why are there no cases of malaria in the UK? Maybe they have not yet added malaria to their list of ‘diseases’ to scare us with!! But if they do, rest assured I am ready with my rebuttal!
The problem with ticks is claimed to be that they could cause tick-borne encephalitis (TBE), although the BBC article states that the risk is ‘low’. Which raises the question of what is the purpose of this article if the risk of health problems is low? I would suggest it is merely another fear-mongering exercise!
There are other similarities with these ticks and mosquitoes, one of which is that they are not born with ‘viruses’, but, according to a page entitled The Lifecycle of a Blacklegged (Deer) Tick on the TickTalk website,
“Ticks do not hatch with any diseases or infections, however the smaller animals that they typically feed on at this stage of their life can carry disease-causing pathogens.”
Note the use of the word ‘can’ with respect to the ability of the animals they feed on to carry pathogens.
The web page also makes the statement that,
“If a larva feeds on an infected animal, the pathogen can be transmitted to the tick and they become a carrier.”
It is interesting that a so-called ‘infection’ can happen in both directions because, according to the BBC article,
“While feeding, they can transmit viruses and infections that cause disease, with the most common being Lyme disease – a bacterial infection which can be treated with antibiotics.”
The vital question that needs to be asked is: Where is the evidence that animals carry the ‘pathogens’ in the first place and that these ‘pathogens’ are passed to ticks during a blood meal?
I won’t hold my breath waiting for the answer.
However, it should be noted that there is to be increased ‘testing’, as the BBC article states,
“The UK Health Security Agency has recommended changes to testing in hospital so that any new cases can be picked up quickly.
Enhanced surveillance for the virus is now being carried out in England and Scotland, where there is one probable case of tick-borne encephalitis.”
Unsurprisingly, the types of ‘test’ used seem to be either PCR or antigen tests, neither of which have been proven to be able to detect the existence of a pathogen or to show that a pathogen was the cause of a person’s health problem.
Another really interesting question that does not seem to be asked – or answered – is: How can the tick transmit a virus that is said to cause serious health problems to a human but not be adversely affected itself? To simply state that the tick is a ‘carrier’ is woefully inadequate and parallels the nonsense of ‘asymptomatic carriers’, which I have discussed in earlier articles.
Furthermore, there is no explanation for the claim that the tick is able to receive a ‘virus’ from the few drops of blood it draws from an ‘infected’ animal. Surely the odds of that happening are minuscule – unless the animal is riddled with ‘viruses’, in which case the animal would be extremely ill, according to the mainstream view of ‘infections’. This clearly makes no sense.
Nor is there proof for the claim about the process by which the ‘virus’ passes to a human host when the tick is drawing blood, because this would involve the virus travelling to the human body from the tick’s body, which is in the opposite direction to the flow of blood.
There is an attempt at an explanation of this process in a 2013 study article entitled Tick salivary compounds: their role in modulation of host defences and pathogen transmission, which states that,
“Pathogens exploit tick salivary molecules for their survival and multiplication in the vector and transmission to and establishment in the hosts.”
The answer to the question about transmission is that no ‘virus’ does this; because, as I have repeatedly shown, there is no evidence for the existence of ‘pathogenic viruses’.
I am not denying that tick bites cause reactions and can make some people feel unwell and experience various symptoms.
Although I cannot possibly speculate on what does cause these problems, I can share some information I have found.
The first piece of information involves the use of ‘insect repellants’, such as DEET, which is recommended by the NHS. Interestingly, it is claimed that scientists do not know how DEET works to repel insects. Although DEET has not been found to be particularly toxic, it has been found to be an irritant, which may explain why some people react to this substance.
I would strongly suggest, therefore, that people research the ingredients of insect repellants before using them, as it is possible that these chemicals enter the body through the open wound of the tick bite and thereby cause a reaction.
It is also reported, such as in the 2013 study article mentioned above, that ticks inject ‘salivary molecules’ into the host to ‘modulate’ the response. Maybe some people react strongly to these ‘molecules’ for various reasons, which may depend on the overall health of their body.
There is, however, another aspect to this fear-mongering about ticks, which is an alleged connection to ‘climate change’, as can be seen in this comment in the BBC article,
“They speculate that infected ticks may have been brought into the UK by migratory birds because of climate change.”
This is nonsense!
I am NOT denying that the climate changes. What I am denying is the claim that human activities are driving changes in the climate as the result of increased levels of atmospheric carbon dioxide. There is no evidence to support such a claim.
What I would also like to emphasise is that the environment has been and is still being damaged; but a substantial proportion of that damage is due to pollutants, none of it is caused by increased levels of carbon dioxide. In fact, carbon dioxide is essential for life – without it, plants would die; and so would we.
Do people who are making every effort to reduce their ‘carbon footprint’ not understand this?
I will return to the topic of ‘climate change’ at some stage because again we are being made to fear the wrong ‘enemy’.
Back to the ‘ticks’. The most important point to make is that they are not ‘infected’ with any virus or bacterium that can be transmitted to humans or animals and make them ill.
Bacteria, which are claimed to be the cause of Lyme disease, another ‘tick-borne disease’, have similarly never been proven to be the cause of any disease. This is important because the NHS website advises people, if bitten, to,
“…clean the bite area with antibacterial wash/soap and water, and monitor it for several weeks for any changes.”
Antibacterial products are, by their very nature, toxic and therefore harmful. The application of antibacterial substances is another likely cause of health problems after a bite.
It is abundantly clear that the incessant reporting about so-called ‘pathogens’ that can ‘infect’ us, continues to promulgate the idea that ‘viruses’ are not only real, but they are also pathogenic and therefore pose a risk to our health. This serves to keep many people confused and fearful – which is of course part of the intention of such reporting.
And it is for this reason that people need to recognise that they are being made to fear ‘germs’ – an invisible ‘enemy’. But, in the case of a ‘virus’, this enemy has never been proven to exist in the way it is described.
I would dearly love to write about other topics, but the ‘germ theory’ lie needs to be dismantled – once and for all – a task that I do not accept is unimportant or ‘divisive’.
Cover image credit: Nel_Botha-NZ
(Photo of oxpeckers, native to sub-Saharan Africa. They feed on ticks, larvae
and other parasites that infest large mammals such as the giraffe shown in the image.)
Can Atmospheric Electricity Contribute to Pilots Collapsing From Blood Clots? How Does Electrically Responsive Hydrogel React Under Increasing Voltage of Electrostatic Fields at High Altitude?
We know that the C19 shots contain lipid nanoparticles with are the components of hydrogel like Polyethylene Glycol in Pfizer and SM 102 in Moderna. Hydrogel is a self assembly polymer that grows under the exposure of electrical and electromagnetic fields. I have shown the work of Clifford Carnicom, that low level electrical fields can change the blood to an unrecognizable filament network within an extremely short amount of time. I have discussed our Infrared Spectroscopy, patents and historical work on CDB aka Morgellons – indicate the presence of hydrogel. I have written about this here:
It has been known for over a century and been described by Georges Lakhovsky in 1939, that the electric potential of the terrestrial atmosphere increases with height at the rate of 1 volt per cm. The more modern values are described here:
The electrostatic field and the difference of potential of the earth field according to investigations, is in summer about 60 to 100 volts and in winter 300 to 500 volts per meter of difference in height, a simple calculation gives the result that when such a collector is arranged for example on the ground, and a second one is mounted vertically over it at a distance of 2000 meters and both are connected by a conducting cable, there is a difference in potential in summer of about 2,000,000 volts and in winter even of 6,000,000 volts and more.[11]
Many explain electricity in a wire with the analogy of a water pipe. The pressure in the pipe is the voltage (V) and the flow velocity of the current is measured in amperes (A). Power, which is measured in watts (W), is the energy unit per time. Their mathematical relationship is: V x A = W
Imagine our experiment done by Clifford Carnicom even on unvaccinated blood applying 10 micro amps of current for two hours.
Now remember the analysis of Mike Adams on the cadaver blood clots, taken from vaccinated individuals. It contained conductive metals and self assembly carbon rich polymer.
I have discussed my concerns about hydrogel being the culprit of these rubbery blood clots after the documentary “Died suddenly” came out:
How much electricity is in the human body? Scientists agree that the human body, at rest, can produce around 100 watts of power on average. This is enough electricity to power up a light bulb. Some humans have the ability to output over 2,000 watts of power, for instance if sprinting.
Summary:
I have been sounding the alarm that the rubbery clots seen in deceased vaccinated individuals are made from hydrogel, which is what Mike Adams confirmed. We have shown how blood changes under low level electrical current, clearly growing a filament network, aka rubbery clot like structures. High altitudes voltage increased to anywhere between 2-6 million ( or more) volts at high altitude, could increase the electrical power in the body significantly and contribute to sudden growth of hydrogel filaments. The same can happen with exercise, as the body can increase its power output from 100 to 2000 watts. We must consider that hydrogel self assembly is not only enhanced via electromagnetic fields like 5G but also via electricity. We are a body electric. Could it be that the hydrogel is harnessing our own electric field, as well as that of the environment to produce a “kill switch?”
The evidence so far certainly suggests this and I urge scientists and doctors worldwide to explore this causal relationship. Aviation safety should explore these causalities and their obvious emerging scientific questions. Once again, I ask doctors to use the diagnostic tool of live blood analysis to see if pilots and athletes have these structures. Voltammetry testing on blood of high risk individuals may be an unconsidered valuable diagnostic tool to prevent catastrophic events like airplanes falling out of the sky or people dying suddenly.
All pilots and athletes especially, aside from every human being on the face of the earth, should have live blood analysis BEFORE flights or engaging in exercise. If the hydrogel structures are visible, the blood needs to be cleared and these contributing activities avoided. As you know, I recommend EDTA Chelation with other extensive protocols that I have mentioned in prior substacks and interviews. Most of all, the conversation about this concerning association needs to be taking place worldwide.
“It is high time that We, the People, around the world gain consciousness and become aware of the dictatorial measures waiting just a short stretch down road to be implemented. Then, the bulk of The Great Reset / Agenda 2030 would have been achieved. Once that happens, it will be difficult to escape.”
Two kinds of absolute controls are being prepared to implement The Great Reset, alias UN Agenda 2030. A potentially straitjacket and total control by programmable Central Bank Digital Currency (CBDC), and an all-oppressive health tyranny by WHO, overriding national Constitutional rights and national sovereignty as far as health measures are concerned.
The former will be “managed”, coordinated and supervised for faultless implementation, by the so-called Central Bank of Central Banks, the Bank for International Settlement (BIS); the latter by the 1948 Rockefeller-created, falsely called UN-agency WHO. The emerging tyrant’s budget is to 80% pharma, Gates and otherwise privately funded. Both are criminal organizations.
These are plans, not yet implemented. But the world better be aware, so We, the People, may stop this terrifying assault on humanity in its tracks.
CBDC may be upon us, humanity, rather sooner than later. Programmable CBDC is a weapon of mass destruction. The weapon has been in the planning for decades – and it fits right into the Bigger Picture of the Great Reset / Agenda 2030.
Programmable – means the money can be programmed on how it is to be spent by an individual, or blocked, or made to expire, or made to be used for certain goods or services – or it can be totally withheld, wiped out, depending on how well you behave, according to the standards of the all-commandeering death cult elite.
CBDC is a master control element, a stranglehold on the population.
Simultaneously, an all controlling health tyranny is being prepared by WHO. The plan is that the new totalitarian rules – Biden Administration initiated revised International Health Regulations (IHR), including a new Pandemic Treaty – are to be ratified by the World Health Assembly, presumably by the end of May 2023. If approved, by a two-thirds majority, the new rules will become effective in 2024.
Health Tyranny and Control by WHO
The elite who pretends to rule over humanity acts most silently from the shadows. It includes the financial giants, the largest funders of the World Economic Forum (WEF), the Davos Boys. The financial elite calls the shots on integrated and willing Klaus Schwab, WEF’s CEO.
In turn, Mr. Schwab passes on instructions to the World Health Organization (WHO), for example, to redesign and implement the revision of the IHR which now also includes a Pandemic Treaty.
First, Bill Gates, also one of the key sponsors of WHO, puts a shady Ethiopian politician, Tedros Adhanom Ghebreyesus, at the helm of WHO. Tedros, a buddy of Bill Gates, is former DG of the GAVI Vaxx-Alliance, also created and funded by the Gates Foundation. – So much for WHO being a UN Agency.
If these new IHR / Pandemic Treaty are approved by the World Health Assembly at the end of May 2023, the world (currently 194 WHO members) will be living under a “health tyranny”.
WHO would have overreaching powers over otherwise autonomous countries, being able to overrule national Constitutions and decide whether a disease must be treated as a pandemic, i.e., with massive vaccination.
For example, WHO could decide that henceforth the common flue must be treated as a pandemic. Since “covid”, any “vaccination” will be the gene-modifying mRNA type. The same viral-technology that has, with covid inoculations, caused already tens of millions of deaths around the world. Of course, not openly recognized, but over-mortality statistics, especially in the western world, alias, Global North, speak for themselves. They are congruent with the countries’ vaxx-injection rates.
People have no clue that when they next take their kid for a polio, or measles vaccination, their child will be injected with a potentially deadly mRNA-type toxic solution, producing immune-averse spike proteins. See this by Dr. Mike Yeadon, former VP and Chief Science Officer of Pfizer.
Total Obedience
To assure utmost obedience of countries, Klaus Schwab has on several occasions boasted that the WEF was infiltrating scholars of the WEF “Academy” for Young Global Leaders (YGL) into governments around the world. They often are placed in Prime Minister’s or President’s positions. To name just a few of the more prominent ones – Justin Trudeau, Canada; Emmanuel Macron, France; Mark Rutte, Netherlands; former German Chancellor Angela Merkel; as well as Olaf Scholz, current Chancellor of Germany.
Central Bank Digital Currency (CBDC) – Welcome to the New Money Prison
The decision to introduce CBDC so-to-speak at warp speed was made at a Jackson Hole, WY, meeting in August 2019 by the Central Bankers of the G7 nations. They voted on a financial coup which was “Going Direct Reset”.
This was planned way ahead for at least the last 20 years, and now needed to be consolidated for the final stage of total and absolute financial control – the end game of the coming world tyranny. First applied by the Global North, where the impact will be greatest. See brief 1 min. video by Katherine Austin Fitts, it says it all.
It is weaponizing money into programmable and controllable CBDC – a Weapon of Mass Destruction.
The rest of the world will follow suit. That’s what they think. Destruction of the industrialized world is first. Germany is supposed to lead deindustrialization of Europe, prompted by artificially caused energy shortages. Then comes the absolute control of the world’s natural resources – so that reconstruction of the system, with a drastically reduced world population, may progress rather fast.
The US / NATO Ukraine proxy-war against Russia is a forerunner aiming at dominating Russia and her wealth of natural resources.
Governments and banksters are the people’s biggest, most nefarious, but least recognized enemies. How much longer does it take until a majority of people will wake up and stop this crime on humanity?
According to Katherine Austin Fitts, the introduction of CBDC, may put half a billion people out of work. That is just one part of the warfare. It is intimately connected to the plandemic. People did not die of covid, most perished from toxic vaxxes and from “covid” caused misery.
Dr. Michael Yeadon, former VP and Chief Scientist of Pfizer repeatedly said in his interviews and special addresses, the real, potentially massive dying, of the coerced vaxx-campaign – will take place after three and up to about ten years from the beginning of the vaxx-drive. Injections of mRNA material into people’s bodies began in December 2020. We are now entering year three. And hundreds of thousands, if not millions, around the world have already died due to the “vaxxes”, NOT covid.
Today, truth-seeking scientists and medical doctors warn – “don’t get vaxxed, it is dangerous for your health, the jabs may kill you.” If not, they may maim you for life, or reduce massively women’s and men’s fertility. The latter shows already up in statistics – in Europe from 20% to 40% reduced fertility in 2022. Yet, worldwide vaxx-drives go on – a bulldozer stopping from nothing.
How to weaponize money?
A threesome tyranny – a “trinity”, is at it. The WEF and it’s behind the scene giant financiers; the Governments, and the banksters, through a network of national central banks, all controlled by the Bank for International Settlement (BIS), in Basel, Switzerland. The “health industry” – Big Pharma, health- and hospital facilities and insurances are following the line with digitized health records and digitized health services.
The 2019 G7 Jackson Hole decision on massive bank failures to bring about CBDC, started in early March 2023 on a relatively light note in the United States. The opening was the apparent collapse of California’s Silicon Valley Bank (SVB), California’s Silvergate Capital and NYC’s Signature Bank. None of them really needed to go into bankruptcy. They were “bailed out” by the Biden Administration, put in control of the “Regulator”, before rumors of failure could trigger a run on the bank.
We know how “rumors” can be fabricated or enhanced and how they may mobilize people.
On the other side of the Atlantic, Credit Suisse, second largest Swiss bank, had been plagued for the last two decades by scandals and “financial irregularities” one after the other, including drug money laundering, and helping Russian oligarch escape western sanctions by “disappearing “ documents linking them to their luxury yachts which were supposed to be confiscated.
Since earlier this year, the bank’s share value plummeted, first by the week, then by the day. For a complete list of financial scandals and more, see this.
Much of the loss of confidence was, again, based on rumors – and rumors can be spread – true or false.
There was never a need to put CS into receivership. The bank, according to many analysts, also FINMA (the Swiss banking “regulator”) was solvent, especially after CS supposedly received on Friday, 17 March, a 50 billion franc “bail-out” loan from the Swiss Central Bank.
According to insiders (CS analysts)- and outsiders, this amount of cash would have been enough to restructure the bank, including quietly getting rid of undesirable skeletons – regaining trust of people and shareholders – and be functional again within less than a year.
However, there may be another agenda for the sudden change in direction, during the weekend, 18/19 March. Janet Yellen, US Secretary of Treasury, UK and German senior Ministry of Finance officials were in “consultation” with the Swiss Minister of Finance.
Outside pressure again cut into Swiss sovereignty politically and in terms of Swiss reputed private banking services.
What happened then, is the complete opposite to what the 50 billion “bail-out” should have achieved. One may ask, was the CHF 50 billion government “bail-out” just a disguise?
In an apparent sudden change of direction, the Swiss Government, without any consultation of shareholders and holders of some CHF 16 billion worth of bonds, forced UBS, the largest Swiss bank, to take over its slightly smaller sister, CS. Even stranger, this happened by applying a shady emergency decree. CS was never in an emergency of insolvency.
CS shareholders had to accept a take-over price of CHF 3 billion, about CHF 0.76 / share, less than half its last quoted share value. The bank’s infrastructure alone is worth a multiple of the take-over price.
On Sunday, March 19, the Swiss regulator FINMA announced that the so-called additional tier-one bonds (AT1) of about CHF 16 billion will be written to zero as part of the deal. Neither the shareholders or the bondholders were warned.
This precipitous coerced deal has not gone down well in Europe. A famous law Professor at the Swiss Fribourg law-specialized university, called Switzerland a “Banana Republic”.
The conservative Swiss newspaper NZZ reported on 19 March 2023 that a few months ago nobody would have believed the downfall of CS was possible. In 2007, CS had a stock value of over CHF 100 billion. It was gradually reduced to CHF 7 billion, less than a week before the decreed take-over. The paper concludes that Switzerland got rid of a Zombie-bank, but acquired instead a Monster-bank. After the merger, UBS will have about 5 trillion worth of managed assets. Compare this with about 10 trillion of BlackRock.
Instead of a 50 billion bailout credit – which would have been paid back, the new deal costs Switzerland about 230 billion – a 200 billion Central Bank line of credit, of which hundred billion are fully guaranteed by the Swiss Government (taxpayers), plus a 9 billion guarantee (taxpayer) for UBS losses, plus other guarantees in case of defaults.
As a sideline, the Swiss Central Bank, on 5 March declared one of the biggest losses in its recent history, of CHF132.5 billion. You add to this a potential loss position of another some CHF 100 to 200 billion – that makes you think – what else is planned to wipe out this debt?
The major CS shareholders may launch a massive law suit against the Swiss Government. Saudi National Bank (10%), Saudi Olayan Group (5%), plus Qatar Holding (5%), hold together about 20%. For these oil-producing countries legal fees may not be an issue, but creating a precedent will be important. BlackRock with about 4.1% CS shares stays for now on the sidelines.
Looks and smells like all of this has been planned by a long hand. Remember the G7 Central Bankers meeting at Jackson Hole, Wy in 2019?
Financial Times and Forbes report that there are about 200 small-to medium size US banks “at the brink” of collapse. The Credit Suisse collapse, one of the world’s 30 systemically most important banks, also one of the “Too Big to Fail” banks, rescued by the Swiss Government, may just set the beginning of a massive domino of bank failures in the US and Europe. See this.
BlackRock’s Vice Chairman, responsible for Investments, Philipp Hildebrand, is the former President of the Swiss National Bank (forced out in 2016, because of a personal scandal), then joined BlackRock. He knows how the wheels turn in Switzerland.
The Biden Administration’s rule of order, ignores the 2010 Dodd-Frank Act that eliminates government bail-outs and opened the door for bail-ins, allowing banks to confiscating creditors’ money and converting it into equity. If this government bail-out policy continues, a never-seen before government debt will accrue. The same may apply in Europe, amassing potentially hundreds of trillions of national debts, on both sides of the Atlantic.
This would be the ideal moment to introduce at once in the western world – US, UK, Canada, Europe, but also Japan and Australia – programmable Central Bank Digital Currency (CBDC).
These countries’ combined 2022 GDP amounts to about US$ 50 trillion equivalent, almost half of the 2022 world GDP (US$ 103.86 trillion). See this (World Bank data).
*
Within the shortest period of time, the western US-dollar-based economy’s debt could be wiped out with one stroke – with a new kind of money, the CBDC. With another stroke, the entire ignorant western population could be doubly straitjacketed – by WHO’s Health Tyranny, as well as by programmable CBDC.
It is high time that We, the People, around the world gain consciousness and become aware of the dictatorial measures waiting just a short stretch down road to be implemented. Then, the bulk of The Great Reset / Agenda 2030 would have been achieved. Once that happens, it will be difficult to escape.
It is time that We the People, request our governments to exit WHO – in Switzerland a referendum to this effect has already been initiated – and that we are prepared for setting up parallel governments with local money, totally delinked from existing banking and central banks.
Peter Koenig is a geopolitical analyst and a former Senior Economist at the World Bank and the World Health Organization (WHO), where he worked for over 30 years around the world. He lectures at universities in the US, Europe and South America. He writes regularly for online journals and is the author of Implosion – An Economic Thriller about War, Environmental Destruction and Corporate Greed; and co-author of Cynthia McKinney’s book “When China Sneezes: From the Coronavirus Lockdown to the Global Politico-Economic Crisis” (Clarity Press – November 1, 2020).
Peter is a Research Associate of the Centre for Research on Globalization (CRG). He is also a non-resident Senior Fellow of the Chongyang Institute of Renmin University, Beijing.
A new report estimates that 26.6 million people were injured, 1.36 million disabled, and 300,000 excess deaths can be attributed to COVID-19 vaccine damages in 2022 alone, which cost the economy nearly $150 billion.
Research firm Phinance Technologies, founded and operated by former Blackrock portfolio manager Ed Dowd, Yuri Nunes (PhD Physics, MSc Mathematics) and Carlos Alegria (PhD Physics, Finance), split the impact of the vaccines into four broad categories to estimate the human costs associated with the Covid-19 vaccine; no effect or asymptomatic, those who sustained injuries (mild-to-moderate outcome), those who became disabled (severe outcome), and death (extreme outcome). Data on vaccine disabilities and injuries comes directly from the Bureau of Labor Statistics (BLS), while the excess death figures are derived from official figures on deaths in the US via two different methods (methodology here).
It’s important to note that people in one category (injured, for example) can move into latter categories of severity – which this analysis does not take into consideration.
“We need to remember that not only are these groupings an attempt to characterize different levels of damage from the inoculations, they are not static and could interact with each other,” reads the report. “For instance, there might be individuals who had no visible effects after vaccination but nonetheless could still be impacted.”
“Individuals with mild injuries from the inoculations could, over time, develop severe injuries to the extent of being disabled, or an extreme outcome such as death.”
🚨🚨Estimated 2022 US Vaccine Damage Report:
Estimated Human Cost: ✅26.6 million Injuries ✅1.36 million Disabilities ✅300k excess deaths
In analyzing each of the above categories, Phinance used absolute excess lost worktime (see previous report) to determine that the direct economic cost of vaccine injuries was $79.5 billion in 2022, and $52.2 billion for those with severe disabilities.
For deaths, Phinace used the average yearly absolute rise in excess deaths since 2021, which was 0.05% for the 25-64 year-old demographic, which amounted to $5.6 billion in lost productivity.
In total, they found a total “economic cost” of $147.8 billion in 2022 due to the Covid-19 vaccines.
As Dowd notes, these figures are just what can be currently measured, as things like “The knock effects such as lost productivity due to a worker being present but working at say 50%-75% of capacity is missed plus burn out from those picking up slack.”
I’ve grown increasingly frustrated about the way debate is controlled around the topic of origins of the alleged novel virus, SARS-CoV-2, and I have come to disbelieve it’s ever been in circulation, causing massive scale illness and death. Concerningly, almost no one will entertain this possibility, despite the fact that molecular biology is the easiest discipline in which to cheat. That’s because you really cannot do it without computers, and sequencing requires complex algorithms and, importantly, assumptions. Tweaking algorithms and assumptions, you can hugely alter the conclusions.
This raises the question of why there is such an emphasis on the media storm around Fauci, Wuhan and a possible lab escape. After all, the ‘perpetrators’ have significant control over the media. There’s no independent journalism at present. It is not as though they need to embarrass the establishment. I put it to readers that they’ve chosen to do so.
So who do I mean by ‘they’ and ‘the perpetrators? There are a number of candidates competing for this position, with their drug company accomplices, several of whom are named in Paula Jardine’s excellent five-part series for TCW, Anatomy of the sinister Covid project. High on the list is the ‘enabling’ World Economic Forum and their many political acolytes including Justin Trudeau and Jacinda Ardern.
But that doesn’t answer the question why are they focusing on the genesis of the virus. In my view, they are doing their darnedest to make sure you regard this event exactly as they want you to. Specifically, that there was a novel virus.
I’m not alone in believing that myself at the beginning of the ‘pandemic’, but over time I’ve seen sufficient evidence to cast strong doubt on that idea. Additionally, when considered as part of a global coup d’état, I have put myself in the position of the most senior, hidden perpetrators. In a Q&A, they would learn that the effect of a released novel pathogen couldn’t be predicted accurately. It might burn out rapidly. Or it might turn out to be quite a lot more lethal than they’d expected, demolishing advanced civilisations. Those top decision-makers would, I submit, conclude that this natural risk is intolerable to them. They crave total control, and the wide range of possible outcomes from a deliberate release militates against this plan of action: ‘No, we’re not going to do this. Come back with a plan with very much reduced uncertainty on outcomes.’
The alternative I think they’ve used is to add one more lie to the tall stack of lies which has surrounded this entire affair. This lie is that there has ever been in circulation a novel respiratory virus which, crucially, caused massive-scale illness and deaths. In fact, there hasn’t.
Instead, we have been told there was this frightening, novel pathogen and ramped up the stress-inducing fear porn to 11, and held it there. This fits with cheating about genetic sequences, PCR test protocols (probes, primers, amplification and annealing conditions, cycles), ignoring contaminating genetic materials from not only human and claimed viral sources, but also bacterial and fungal sources. Why for example did they need to insert the sampling sticks right into our sinuses? Was it to maximise non-human genetic sequences?
Notice the soft evidence that our political and cultural leaders, including the late Queen, were happy to meet and greet one another without testing, masking or social distancing. They had no fear. In the scenario above, a few people would have known there was no new hazard in their environment. If there really was a lethal pathogen stalking the land, I don’t believe they’d have had the courage or the need to act nonchalantly and risk exposure to the virus.
Most convincingly for me is the US all-cause mortality (ACM) data by state, sex, age and date of occurrence, as analysed by Denis Rancourt and colleagues. The pattern of increased ACM is inconsistent with the presence of a novel respiratory virus as the main cause.
If I’m correct that there was no novel virus, what a genius move it was to pretend there was! Now they want you only to consider how this ‘killer virus’ got into the human population. Was it a natural emergence (you know, a wild bat bit a pangolin and this ended up being sold at a wet market in Wuhan) or was it hubristically created by a Chinese researcher, enabled along the way by a researcher at the University of North Carolina funded by Fauci, together making an end run around a presidential pause on such work? Then there’s the question as to whether the arrival of the virus in the general public was down to carelessness and a lab leak, or did someone deliberately spread it?
I also need to point out that the perpetrators have hermetic control of the mass media via a Big Tech and government stranglehold documented in part here, here and here. That’s why they’ve found it so easy to censor people like me. If a story appears on multiple TV networks, it’s because they’re either OK with it or it has been actively planted. It won’t be genuine. They never tell the truth. I don’t think they’ve told the truth since this coup began and probably much earlier. Most so-called journalists have lost sight of what truth ever was.
I believe that the perpetrators (who could be all or any of Gates, Fauci, Farrar, Vallance, CEPI, EcoHealth Alliance, DARPA and numerous others) planted the controversy about the origins of SARS-CoV-2 because a little embarrassment of the establishment was a small price to persuade most of us that there surely must be a novel virus when there isn’t. (And they have got away with it to date.)
I have colleagues who do not believe what we’ve been told (i.e. that a virus has been experimentally constructed) is even possible technologically. I don’t have the background to assess that idea. But the rest hangs together for me in a way that no other explanation does.
To this point, an ex-pharmaceutical industry executive Sasha Latypova, speaking with Robert F Kennedy Jr on his podcast of last Thursday, March 16, describes the extensive evidence of the contracts and relationships that were in place before the Covid era. Contracts were signed for billions of dollars in February 2020. Not only would the required production never happen (from a standing start, to sign such a large commitment is ridiculous) but it cannot be done. She estimated that approximately one kilogram of DNA was required. There isn’t that much medicinal grade DNA on the planet at any one time. That’s because it’s hard to do, very expensive, wholly bespoke and difficult to store for long periods. Also, the amounts of any specific DNA sequence required and held in store by commercial suppliers would be milligrams or perhaps grams at a stretch. So it was always completely unfeasible, regardless of how much money was thrown at the problem, to have accomplished what they claim to have done in a short time.
Consequently, no other conclusion is supported by the facts than that it’s a huge crime, extensively planned. In itself, that rules out a natural emergence of a pathogen, unless divine providence occurred. Logically we’re left with a leak or, as I argue, a lie plus a PsyOp. The former may or may not be possible, but what isn’t arguable is that something like this could be done and would be likely to run smoothly, with a real pathogen. Almost any outcome but the one presumably wanted is likely if a pathogen is released. I can reach no other conclusion than that it’s fake.
In closing, I’m not saying people weren’t sick or that they didn’t die in huge numbers. I’m arguing only about the causes of illnesses and deaths. People were made sick and some killed by all the pre-existing causes, amplified by fear, resulting in immunosuppression and then a host of revolting actions. Note even the official overlap of signs and symptoms of ‘Covid-19’ and existing illnesses. Notably, they chopped antibiotic prescriptions in the US by 50 per cent during 2020. They ensured large numbers of frail elderly people were mechanically ventilated, a procedure which, in such subjects, is close to contraindicated. Some were administered remdesivir, which is a poison for the kidneys. In care homes, they were given midazolam and morphine, respiratory depressant drugs which in combination are all but contraindicated in patients with breathing difficulties. If used, close monitoring is required, most usually automated alarm systems attached to vital cardiorespiratory monitoring, including fingertip monitoring for blood gases. That didn’t happen in care homes.
I believe the main reason for the lies about the novel virus is a desire for total predictability and control, with the clearly articulated intention of transforming society; beginning by dismantling the financial system through lockdowns and furlough, while the immediate practical goal of lockdown was to provide the causus belli for injecting as many people as possible with materials designed not to induce immunity, but to demand repeat inoculation, to cause injury and death, and to control freedom of movement. I’m sure they’re pretty content with getting at least one needle into 6,000,000,000 people.
Note that though an estimated 10-15million have been killed with poisonous ‘vaccines’, these are the but first of many mRNA injections to come. The indications are that ways to force you to accept ten more have been anticipated, because that’s the number of doses your government has agreed to purchase. Purchasing what? Well, it’s already been mooted that all existing vaccines are to be reformatted as mRNA types. If this happens, I don’t believe anyone injected ten more times is likely to escape death or severe, life-limiting illnesses. Inducing your body to manufacture non-self proteins will axiomatically induce an autoimmune attack by your own body. Your disease will be related to where the injected dose goes and of course the consistency of that injected product. They’ve been horribly erratic so far. It’s not certain they ever could have been made and launched if they had been subject to the usual quality requirements and not granted ’emergency use’ authorisations. Of course, as we now know, the regulators played an important role beyond lying for the US military, the organisation which made the original orders for ‘vaccines’, and set all the contractual conditions for companies such as Moderna and Pfizer.
The chickens are coming home to roost right now in the banking system.
As I always say, I cannot know much for sure. I don’t have a copy of the script of this, the greatest crime in history. But, whatever Covid actually is, I don’t believe that what was called influenza disappeared conveniently in early 2020. It’s another lie. It’s what they do. It’s all they do.
To those who sense that all is not well but are unwilling to make the psychological leap to the diabolical world I believe we’re now living in, I point out the asymmetry of risk. If you follow the official narrative and I’m right, you and your children will lose all your freedoms and probably your lives. If you believe what I’m saying and I’m wrong, you’ll be laughed at. These options aren’t faintly balanced. A rational actor should cease believing what we’re being told. It’s not a safe position, keeping your counsel and your head down. It’s the most dangerous thing you could do.
“The cabal of pandemic fraudsters must be laughing. As cartoonist Bob Moran quipped, gain of function is really gain of fiction. To date, there is no actual evidence that viruses can be made more lethal, despite the huge amounts of research grant money awarded and theoretical reports.”
Why Wuhan? For the most deadly pandemic since the Spanish influenza of 1918-1919, an enormous but hardly known metropolis from the Chinese interior was the source. The official story was zoonotic transmission of a bat coronavirus, blamed on poor hygiene at the city’s wet market.
While I saw from the outset the malevolent plot of Covid-19 to erect an authoritarian regime through an exaggerated threat to lives, I was temporarily drawn to the alternative explanation. The Wuhan Institute of Virology, funded by the US government for ‘gain of function’ viral research, seemed an obvious origin. While the lab leak was dismissed as conspiracy theory by political leaders and most mainstream media, investigative journalism by Ian Birrell in the Mail on Sundayreported lax practices and broken seals in the Wuhan laboratory, despite its intended operation at the highest level of biosecurity.
I suggested a laboratory accident in my report Year of the Bat, written for Civitas think-tank during the first lockdown. But months later I changed my mind, having listened to the likes of Patrick Henningsen of 21st Century Wire, doctors Sam Bailey and Tom Cowan, Jeff Berwick of Dollar Vigilante, and seasoned conspiracy theorist David Icke. In his Perceptions of a Renegade Mind, Icke argued that it was easier to enact a technocratic coup with a fake rather than real virus. A released pathogen would be unpredictable, likely to lose lethality, and scientific analysis would soon diverge from an initially contrived consensus.
Why didn’t medics and scientists see the scam? Covid-19 was, in my view, a carefully planned emergency, in which normal standards of science and ethics would be overridden. As the new virus began to spread in January 2020, Christian Drosten and colleagues in Germany provided the concrete foundation for the entire edifice, by identifying a genetic sequence through PCR testing, enabling screening for the disease. Incredibly, this paper was approved by peer review in 24 hours. Testing kits were already available in bulk supply across the world – one of many curious instances of readiness for a nasty viral surprise.
Doctors and health authorities uncritically accepted the existence of Covid-19 and its testing standard. Kary Mullis, inventor of the PCR test, emphasised that this tool should not be used for diagnostic purpose, and that with high level of amplification of samples, almost anything in the atmosphere could be found by the test. Perhaps too conveniently, Mullis died in August 2019.
Instead of the widely depicted CGI rendering of a sphere with spikes (like a naval mine, but typically coloured in a sinister deep purple), the reality of SARSCOV2 is a code for a genetic sequence generated with ‘next generation’ genomic sequencing software found in human beings here, there and everywhere. It may be merely dead cellular material, possibly more prevalent with seasonal respiratory infection. This code, rather than any viral sample, was all that Pfizer and Moderna used to produce their ‘vaccines’.
The origins of Covid-19 has become a major talking point recently, after the Department of Energy suggested that, after years of denial by the US government, that a lab leak was ‘possible’. The hypothesis was then elevated to ‘probable’ by FBI chief Christopher Wray. Cue a deluge of ‘told you so’ from the sceptical margins.
As lamented by Patrick Henningsen on UK Column News (3 March 2023), some of the most respected and influential dissidents are riding on the crest of this wave of sudden Covid-19 revisionism. Robert Malone, mRNA vaccine inventor, tweeted on the ‘narrative collapsing’, asserting that ‘the lab leak killed millions of people’. Stanford University professor of medicine Jay Bhattacharya, initiator of the Great Barrington Declaration, saw a belated shift ‘from putative conspiracy to legitimate science’. Fox News and Republican politicians such as Rand Paul renewed their calls for prosecution of Dr. Anthony Fauci and demand for reparations from China.
According to Henningsen, the lab leak is nothing but an official conspiracy theory. The narrative, far from collapsing, is unwittingly reinforced by halfway house sceptics. Everything reported on mainstream media is for a purpose, serving the ‘progressive’ agenda. What may appear as mea culpa is a staged performance involving well-remunerated fall guys such as Fauci, and British health secretary Matt Hancock.
Not only does the lab leak cause obfuscation and futile debate, it fools unwary sceptics into perpetrating the big lie. If you fall for this tale, you fall for everything founded on the fundamental falsehood of a ‘novel’ (and possibly manmade) virus. It diverts attention from the iatrogenic scandal of the vaccines, while also preparing the ground for a global pandemic treaty. Instead of fumbling politicians with their petty squabbles and egos, the unelected and unaccountable World Health Organisation will assume control of every nation’s public health response to any future threat of a contagion. This will be justified by the many ‘mistakes’ governments made with Covid-19, as now being highlighted in mass media. By the same token, it also serves to excuse any ‘mistakes’ by governments and the pharmaceutical firms, as they can simply say they were trying to react quickly to a potentially engineered pathogen from an unregulated lab in Wuhan.
The cabal of pandemic fraudsters must be laughing. As cartoonist Bob Moran quipped, gain of function is really gain of fiction. To date, there is no actual evidence that viruses can be made more lethal, despite the huge amounts of research grant money awarded and theoretical reports.
As the dust settles on Covid-19, even the sceptical community has much to learn. They are not always as ‘awake’ as they believe.
The stunning confluence of events and coincidences suggests that the Covid-19 global pandemic took years of planning. If so, it was the work of misanthropic geniuses who saw the potential for a power grab through a global campaign of fear and control, leading to a ‘new normal’ of digital surveillance and constraints on population and resources. The true sequence of events was in reverse. Rather than a virus leading to a vaccine leading to digital identity, the end point was achieved by mass vaccination, for which a virus was invented. Covid-19 arose not from a laboratory, but from a laptop.
Under the 1984 Bayh-Dole Act, government scientists can collect royalties from drug companies for discoveries they make while working on the public’s dime
Taxpayers fund government research, while Big Pharma, the National Institutes of Health and NIH scientists keep all the profits
As a patent holder who profits from royalties, the NIH has a significant stake in regulations that impact patents and vaccine mandates, and may use its influence to benefit itself rather than the public
The NIH distributes $32 billion of taxpayer funds as research grants each year. As the largest federal grant-maker, the NIH has a monopoly on what research gets done and what doesn’t
Scientists vying for grants also recognize that in order to get funding, they have to play by the rules, and that means doing work that supports establishment narratives on public health policy
In late February 2023, Moderna agreed to pay $400 million to the National Institute of Allergy and Infectious Diseases (NIAID) for the patent it holds on Moderna’s mRNA shot.1
The patent process is a part of the COVID mRNA shots that the media haven’t really addressed and people in general don’t know anything about — probably because it’s a total racket. Based on internal documents and correspondence, it appears the NIAID funded the creation of SARS-CoV-2. At the same time, it patented and receives royalty payments for the “vaccine” against said virus.
The National Institutes of Health (NIH) is supposed to be the primary government agency responsible for public health research, but by the looks of it, it appears instead to be in the business of creating public health threats in order to profit from them.
And the agency itself isn’t the only one raking in profits. Many patents are held by individuals working at the NIH/NIAID. So, taxpayers fund research that may or may not work out, while Big Pharma, the NIH and individuals at the NIH profit from products that end up on the market. This is a clear conflict of interest that can hurt public health in any number of ways.
For starters, it incentivizes the NIH to support and promote potentially dangerous drugs, as we’ve clearly seen during the COVID pandemic. The NIH also has a significant stake in regulations that impact patents and vaccine mandates, and may use its influence to benefit itself rather than the public.
Conflicts of Interest Influence Public Health Policy
In the Full Measure video above, investigative journalist Sharyl Attkisson reports the findings of watchdog group Open The Books, which recently took a deep dive into “the issue of government scientists collecting royalty payments from pharmaceutical companies for discoveries made while working on your dime.”
According to OpenTheBooks.com founder and CEO Adam Andrzejewski, the NIH distributes $32 billion of taxpayer funds as research grants each year to an estimated 56,000 different entities. “That basically buys you the entire American health care space,” he says.
As the largest federal grant-maker, the NIH has a monopoly on what research gets done and what doesn’t, as it decides which scientists and projects get that money. Scientists vying for grants also recognize that in order to get a piece of that pie, they have to play by the rules, and that means doing work that supports establishment narratives on public health policy.
But that’s not all. The NIH is also gobbling up patents, which further weakens its incentive to protect and promote what’s truly in the public’s best interest due to the financial conflicts of interest that come into play.
How the Third-Party Royalty Complex Works
As explained by Andrzejewski, under the 1984 Bayh-Dole Act, government scientists can collect royalties from drug companies for discoveries they make while working on the public’s dime:
“Here’s how the third-party royalty complex works. You have a government scientist funded by taxpayers, and they work in a government lab that’s also funded by taxpayers. And when they have an invention [a drug, device or therapeutic] … the NIH … then licenses that invention … to the private sector.
And the private sector then pays royalties back to NIH. NIH then distributes those royalties on a royalty split schedule, back to the scientist. Details of those royalty payments to government scientists are kept as strictly held secrets.”
In fact, these royalty payments are kept under such closed wraps, scientists who receive them aren’t even required to divulge them on their financial statements, let alone to the public. Congress can’t even access those data.
In mid-June 2022, Sen. Rand Paul questioned then-NIAID chief Dr. Anthony Fauci about whether he’d ever received royalty payments from an entity to which he had given a research grant, and whether he or anyone else on the vaccine committee had ever received payments from vaccine makers.2 Fauci suffered one of his now-famous lapses of memory and wouldn’t answer.
NIH Fights to Shield Conflicted Parties
Paul’s questioning of Fauci came on the heels of a lawsuit filed against the NIH to obtain these payment disclosures. The lawsuit was filed by Open The Books in October 2021. But while the NIH eventually did release them, many of the most crucial pieces of information were redacted, and Paul’s attempt to get answers led nowhere. As noted by Andrzejewski:
“That lawsuit unearthed 3,000 pages of royalty payments to NIH scientists from 2010 to 2021. During that time, 2,407 government scientists received $325 million in secretive royalty payments, averaging out to more than $135,000 each.
But much is left unknown. NIH redacted or blacked out key details. We don’t know who paid it. We don’t know how much each individual scientist received. We can only see their names and count the number of times that each scientist received a payment.
And they also redacted the invention, the license number or the patent number … So, every single one of those individual, third-party royalty payments has the appearance of a conflict of interest …
We need to be able to follow the money. Unelected bureaucrats are running the entire American health care complex without any scrutiny. They’re basically telling the American people, ‘Sit down, shut up, pay up. We’ll run things.’ And that’s not how the federal government is supposed to operate.”
COVID Jabs Are Rife With Conflicts of Interest
Conflicts of interest also appear to have played a role in the U.S. government’s preferential treatment of Pfizer and Moderna during the pandemic. Pfizer was the first to receive government authorization for its COVID jab, and it just so happens to be part of an NIH royalty-sharing agreement.
Moderna also has such an agreement. What this all means is that the NIH helped invent certain technologies that went into these shots, and then licensed those technologies to Pfizer and Moderna in return for royalty payments.
So, the NIH has been making tens of millions of dollars from the COVID shots. Could that financial incentive influence the NIH’s stance on vaccine mandates? What do you think?
As you may recall, Johnson & Johnson’s COVID jab was vilified for causing blood clots, and the U.S. Food and Drug Administration even limited the authorized use of the Janssen shot to people over the age of 18 who have no access to Moderna’s or Pfizer’s jabs, and/or those who voluntarily opt for the Janssen shot, understanding the risks.3
Meanwhile, Pfizer’s and Moderna’s shots also cause blood clots, but neither of them was placed under restrictions. Instead, both were added to the U.S. childhood and adult vaccination schedules. Janssen wasn’t.
The NIH Royalty Cash Cow
The NIH’s secret royalties and the conflicts of interest these payments create were also addressed by “Rising” hosts Robby Soave and Briahna Joy Gray in a recent episode (video above). Alexander Zaitchik, author of “Owning the Sun: A People’s History of Monopoly Medicine from Aspirin to COVID-19 Vaccines,” also joined them on the program.
In Zaitchik’s view, the biggest scandal is not that government scientists are receiving royalty payments from drug companies but, rather, the intimate relationship that exists between government and “an industry that is using the monopoly system to price gouge the American people.”
“The NIH has basically abandoned its role to serve the public,” Zaitchik says, “and instead has become much too aligned with the industry and is an enabler, an accomplice and a protector of these monopolies. The vaccines are a point in case.
Government science was basically given, along with these massive research subsidies, through Warp Speed, to Moderna, for example. And there were no public interest provisions attached.
There were no pricing promises, there were no requests that technology be transferred [shared] with other parts of the world. It was basically a conveyor belt for private industry … So, for me, the real problem is NIH [being] fully aligned with industry on the monopoly question when public science is involved …”
Public Gets Fleeced Coming and Going
When public monies are being used for research, any scientific discoveries ought to be used for the public’s benefit, and the patents should remain public property with broad licensing rights.
This used to be the default position, but not anymore. In the 1970s, Big Pharma convinced Congress that this policy was slowing down innovation, and that if companies were allowed to claim exclusive rights to the patents, they’d be more apt to innovate. The Bayh-Dole Act was an outgrowth of this.
But we can now see why and how that doesn’t work. Public health is literally being sacrificed for profit, and since government agencies are in on it, there’s no one left to look out for the public’s interests.
Additionally, the public ends up getting fleeced twice. First, our tax dollars are being used to fund the research that private companies then lay claim to, and then we end up paying top dollar for the products we funded the development of, as there’s no price competition.
As noted by Zaitchik, while the Bayh-Dole Act is a bad law, it does have a rider that says generic production of drugs created with government funding can be mandated. However, every time patient groups have approached the NIH and asked for this provision to be enforced, as the monopoly is hurting patients who cannot afford the exorbitant prices, the NIH has rejected those requests.
For example, the U.S. Army invented a breakthrough prostate cancer drug, and Americans are paying six times the price for this drug compared to other parts of the world. But even though the government has the power to lower the price by mandating generic production, it refuses to do so.
“The whole system, up and down, has been completely corrupted by the amount of money and power the industry has been allowed to amass, because of the corruption in the patent system in general,” Zaitchik says.
Big Pharma Endangers Public Health
In closing, I’d like to draw attention to a paper published in Surgical Neurology International in October 2022, titled “The Pharmaceutical Industry Is Dangerous To Health. Further Proof With COVID-19.”4
“The COVID-19 period highlights a huge problem that has been developing for decades, the control of science by industry,” the author, Fabien Deruelle, an independent researcher in France, writes.
“In the 1950s, the tobacco industry set the example, which the pharmaceutical industry followed. Since then, the latter has been regularly condemned for illegal marketing, misrepresentation of experimental results, dissimulation of information about the dangers of drugs, and considered as criminal.
Therefore, this study was conducted to show that knowledge is powerfully manipulated by harmful corporations, whose goals are: 1) financial; 2) to suppress our ability to make choices to acquire global control of public health.”
Deruelle’s paper reviews a long list of techniques that drug companies use to shape and control the science, including the following:
Falsification of clinical trials and making data inaccessible
Faked studies
Conflict-of-interest studies
Concealment of the jab’s short-term side effects
Concealment of the fact there is no knowledge of the long-term effects of the COVID-19 jab
Dubious composition of the COVID shots, with many ingredients remaining unlisted
Inadequate testing methods
Conflicts of interest within governments and international organizations
Bribing of physicians
Denigration of renowned scientists who express differing views
The banning of alternative effective treatments
Unscientific countermeasures that eviscerate liberties and freedoms
Government use of behavior modification and social engineering techniques to impose isolation, masks wearing and vaccine acceptance
Scientific censorship by the media
White Collar Crooks Are Running the Show
Deruelle points out that all but one of the primary drug companies producing COVID “vaccines” — Pfizer, Moderna, AstraZeneca, Merck and Johnson & Johnson — have long criminal histories, having been busted and fined huge sums for illegal marketing, recommending drugs for off-label use, misrepresenting trial results and concealing information about known dangers of their drugs. Moderna is the only exception, as it’s only been around since 2010. Deruelle writes:5
“In 2007, Merck paid $670 million, in 2009, Pfizer paid $2.3 billion, in 2010, AstraZeneca paid $520 million, and in 2012, Johnson and Johnson paid a fine of $1.1 billion …
Since 1995, Pfizer has been assessed more than $6.5 billion in penalties for 42 instances of misconduct; 36 instances of misconduct since 1995, resulting in over $11.5 billion in penalties for Johnson and Johnson; 35 instances of misconduct since 1995 and $8.8 billion in penalties for Merck.
Pfizer is singled out as having persistent criminal behavior and casual disregard for the health and well-being of patients. Pfizer is no different from other pharmaceutical companies, but it is larger and more egregious. Pfizer is a habitual offender, persistently engaging in illegal business practices, bribing physicians, and suppressing unfavorable trial results.”
Will Pfizer Stand Trial?
True to form, Pfizer is also accused of scientific fraud in its COVID-19 jab trial. Brook Jackson, who worked at one of Pfizer’s trial sites, sued Pfizer in 2021 for violating the False Claims Act.6 U.S. District Judge Michael Truncale heard oral arguments on the motions to dismiss, March 1, 2023.
As reported by The Epoch Times March 2, 2023,7 defense attorneys for Pfizer argued that “whether protocol violations occurred was ultimately irrelevant because the federal government was made aware of them but still granted emergency authorization to Pfizer’s vaccine.”
Jackson’s lawyers countered by saying the FDA authorized the vaccine before reviewing Jackson’s complaint. Judge Truncale has not issued a ruling as of this writing, and Jackson’s attorney suspects it may be weeks or even months before the judge issues his opinion.8
Conflicts of Interest Shaped COVID Responses
Deruelle also specifically delves into the conflicts of interest and relationships between the drug companies involved during COVID-19 and governments, international organizations and media — and how they worked the COVID “emergency” for their own benefit. Here are some select excerpts:9
“In 2009, the H1N1 episode should already have been enough to reveal that governments and the WHO are not autonomous. Work has shown that the 2009 H1N1 pandemic seems (based on case fatality rates [CFRs]) to have been the mildest influenza pandemic on record. Following investigations by the BMJ, it appears that this event declared by the WHO is significantly tainted by conflicts of interest.
A report by the Parliamentary Assembly of the Council of Europe has heavily criticized the WHO, national governments, and EU agencies for their handling of the swine flu pandemic: distortion of priorities of public health services all over Europe, waste of huge sums of public money, provocation of unjustified fear among Europeans, and creation of health risks through vaccines and medications which might not have been sufficiently tested before being authorized in fast-track procedures.
According to former head of health at the Council of Europe, W. Wodarg, the swine flu outbreak was a false pandemic driven by drug companies that influenced scientists and official agencies …
During the COVID-19 period, France hired private consulting firms, mainly McKinsey and Company, which is known for working with pharmaceutical companies. The Senate Inquiry Commission reports that McKinsey contributed on all aspects of the health crisis, notably for social engineering strategies on the vaccination campaign and the extension of the health pass …
The suppression of good science and scientists is not new, but COVID-19 unleashed state corruption on a grand scale, suppressing science for political and financial reasons … Since the beginning of COVID-19, much scientific data and expert opinion have been censored or labeled as false or misleading by many internet platforms …
In June 2019, the World Economic Forum (WEF) and the United Nations signed a partnership (2030 agenda). In the field of health, this alliance is designed to combat key emerging global health threats and achieve universal health coverage. In October 2019, in New York City, the Johns Hopkins Center for Health Security and its partners the WEF and the Gates Foundation, hosted Event 201, a fictional coronavirus pandemic …
Among the partners of the WEF, there are: Pfizer, AstraZeneka, Johnson and Johnson, Moderna, McKinsey, and Facebook et Google. A few months later, a coronavirus pandemic is declared, accompanied by its highly mediatized universal solution, the vaccine …
In addition to Event 201, other pandemic simulations, civil (MARS and SPARS in 2017) and military (Dark Winter in 2001, Atlantic Storm in 2003 and 2005, Global mercury in 2003, and Crimson Contagion in 2019), have taken place over the past 20 years. All these simulations correspond to fear programs induced by false media.
For the general welfare of the population, all these scenarios lead to the same methods (identical to those used during COVID-19): Isolation, control of movements and liberties, censorship, propaganda, and coercive vaccination of the population …
[T]here is no doubt that this is an event manipulated by governments, international agencies, pharmaceutical industries, and the media. In addition to the huge profits obtained by the pharmaceutical groups involved, the primary goal of this ‘pandemic’ seems to be compulsory vaccination, because the introduction of a European vaccine passport had already been planned since 2019 …
The objective of the WHO is to impose the Chinese model to become the norm. That is to say, a system with centralization of each person’s health data and restriction of freedoms for the unvaccinated … A period such as COVID-19 represents a powerful lever for increasing the effectiveness of global governance.”
Conflicts of Interest Threaten Our Freedom
In the final analysis, conflicts of interest and the collusion between government and industry does more than rob us of our hard-earned money. It now threatens our very freedom, as these monopolies are being used to further a totalitarian takeover of global proportions.
As such, we can no longer turn a blind eye or accept excuses such as “these relationships don’t influence our decision-making.” They absolutely influence the decisions being made, and the public is consistently on the losing end. Congress needs to start taking this seriously, and revisit laws such as the Bayh-Dole Act, which is currently allowing private monopolies to profit while no one is looking out for our interests.
The medical system in the UK, known as the NHS, is currently in crisis and I wholeheartedly agree!
But the real nature of the crisis is not how it is portrayed by the mainstream media, which is demonstrated by a January 2023 BBC article entitled The NHS crisis – decades in the making that states,
“The NHS is in the middle of its worst winter in a generation, with senior doctors warning that hospitals are facing intolerable pressures that are costing lives.”
The article adds that,
“The health service was already under pressure – the result of long-standing problems – but Covid, flu and now strike action by staff have all added to the sense of crisis this winter.”
Strike action by staff was not restricted to the early winter months, further strikes have occurred very recently. On 12th March, the BBC reported the then impending 3-day strike by junior doctors in an article entitled Why are doctors demanding the biggest pay rise?
“On Monday, thousands of junior doctors in England will start a 72-hour strike. They want a 35% pay rise. Yet doctors are among the highest paid in the public sector. So why do they have the biggest pay claim?”
A key concern will be that these strikes will cost lives.
A 13th March BBC article entitled I’ve never seen the NHS this bad – junior doctor refers to the conditions suffered by junior doctors that include workplace pressures and financial difficulties.
These conditions are not exclusive to junior doctors!
The point of these reports would seem to be to foster public sympathy and support for the junior doctors and deepen people’s concern for the future of the NHS.
The ‘official’ view of the pressures on the NHS is endorsed by a June 2022 opinion article entitled The steady crisis across the NHS published in the BMJ, which claims that the main issue is ‘chronic workforce shortages’ and states,
“The NHS has shown in the past that it can deliver rapid improvements to patient care when it has enough staff to tackle these challenges. If we want to break the cycle of consistently poor performance, the government needs a fully funded workforce plan for the whole health and social care system.”
The emphasis in these articles is clearly on the idea that doctors save lives and that they need better pay and working conditions, without which they would be unable to provide the proper level of care for their patients, as the 13th March article indicates,
“More pay and better working conditions would allow doctors to retain a work-life balance and would allow them to deliver the care they wanted to deliver, he said, adding taking industrial action was a “last resort” for doctors.”
The problem is that this is not an accurate view of the real problems and the inability of the NHS to provide adequate ‘healthcare’ to patients and enable them to be restored to health.
One of the alleged ‘problems’ that face the NHS, and every other ‘health service’ based on the practices of ‘modern medicine’, is expressed by the January BBC article, which states that,
“Advances in medicine over recent decades have meant people are living longer.
That is a success story. But it means the NHS, like every health service in the developed world, is having to cope with an ageing population.”
This is a misleading perspective – to put it mildly!
I must make it absolutely clear that I am not denying that there are some situations in which doctors absolutely do save lives – these situations mainly occur at the scene of accidents or emergencies or within the A&E (accident & emergency) department of hospitals. This is where the NHS provides an invaluable service.
However, can it really be claimed that the NHS and all other medical systems based on ‘modern medicine’ actually save lives in situations other than accidents and emergencies?
The evidence strongly suggests that this is not the case.
In response to a June 2000 article in the BMJ entitled Doctors’ strike in Israel may be good for health is a comment dated March 2001 with the intriguing title Doctor strikes, lowered mortality – Happens every time which includes the following,
“The 1960’s saw physicians in Canada go on strike and the mortality rate dropped.
Los Angeles physicians associated with a USC hospital went on strike in the 1970’s and the mortality rate dropped.
Physicians went on strike in South America (Columbia?) later that same decade and the mortality rate dropped.
Physicians have now gone on strike on 3 different occasions in Israel –in the 1950’s, again in the 1970’s or 80’s and now in the the year 2000. In all 3 occasions the mortality rate has dropped, on one or two occasions by 50%.”
In a December 2008 study article published on PubMed and entitled Doctors’ strikes and mortality: a review, the authors report their review of strikes around the world between 1976 and 2003 and state, with respect to the 7 studies they found that matched their criteria,
“All reported that mortality either stayed the same or decreased during, and in some cases, after the strike. None found that mortality increased during the weeks of the strikes compared to other time periods.”
One of the ‘reasons’ given is that elective surgeries were halted during the strikes. But this does not explain why mortality reduced – surely a lack of doctors ought to result in higher mortality!
For an explanation of why mortality decreases when doctors strike, I would remind readers of the phenomenon known as ‘iatrogenesis’ and recommend the July 2000 JAMA article by Dr Barbara Starfield MD entitled Is US Health Really the Best in the World? In her article, Dr Starfield shows that Americans are by no means the healthiest in the world, despite the huge costs of healthcare in that country. (The links to all articles can be found in the References at the foot of this article.)
I would also recommend people read the Death by Medicine study by Gary Null et al. that includes the chart in the image below.
The conclusion, which may be unpalatable to many people – although that does not make it untrue – is succinctly stated by the author of the March 2001 BMJ article,
“Conclusion? I’m sorry to say, but conventional, allopathic, (drug and surgery happy) physicians remain very, very dangerous to our health…”
The sad truth is that ‘modern medicine’ is not a ‘healthcare system’. Instead, as more people are discovering for themselves, it is a ‘sick-care’ system that merely manages symptoms but never truly allows people’s bodies to heal. The reason for this is because ‘modern medicine’ is based on a faulty paradigm and relies on our continuing ignorance of this fact to perpetuate that flawed system.
The empowering truth, by contrast, is that the human body is an amazing living organism that has the ability to self-heal – but implementing this understanding within our lives requires us to reclaim responsibility for our health and not outsource our healthcare to flawed systems that have no understanding of the body’s innate self-healing abilities.
The National Toxicology Program on Wednesday Released a Draft Report Linking Prenatal and Childhood Fluoride Exposure to Reduced IQ in Children, After Public Health Officials Tried for Almost a Year to Block Its Publication.
The National Toxicology Program (NTP) on Wednesday released a draft report linking prenatal and childhood fluoride exposure to reduced IQ in children, after public health officials tried for almost a year to block its publication.
The U.S. Department of Health and Human Services (HHS) and the Centers for Disease Control and Prevention (CDC) initially blocked the NTP from releasing the report, according to emails obtained via a Freedom of Information Act (FOIA) request.
But a court order stemming from a lawsuit filed by Food and Water Watch against the U.S. Environmental Protection Agency (EPA) forced the report’s release this week.
The NTP, an interagency program run by HHS that researches and reports on environmental toxins, conducted a six-year systematic review to assess scientific studies on fluoride exposure and potential neurodevelopmental and cognitive health effects in humans.
The report, containing a monograph and a meta-analysis, went through two rounds of peer review by the National Academies of Sciences, Engineering, and Medicine. Comments from reviewers and HHS and NTP’s responses also were included in the report released Wednesday.
According to its website, the NTP “removed the hazardous classification of fluoride” in response to comments in the peer-review process. Yet, the report states:
“Our meta-analysis confirms results of previous meta-analyses and extends them by including newer, more precise studies with individual-level exposure measures.
“The data support a consistent inverse association between fluoride exposure and children’s IQ …
“The results were robust to stratifications by risk of bias, gender, age group, outcome assessment, study location, exposure timing, and exposure type (including both drinking water and urinary fluoride).”
“These findings fly in the face of the empty, unscientific claims U.S. health officials have propagated for years, namely that water fluoridation is safe and beneficial,” said Robert F. Kennedy, Jr., Children’s Health Defense chairman and chief litigation counsel. “It’s past time to eliminate this neurotoxin from our water supply.”
The controversial report will play a key role in determining the outcome of a lawsuit brought in 2017 by several nonprofits against the EPA to end fluoridation of drinking water, plaintiffs’ attorney Michael Connett told The Defender.
“We had to fight hard to have this report even made public,” Connett said. “They [CDC and HHS] buried this. If they had gotten their way, this report would have never even seen the light of day,” Connett said.
Since the trial began in 2020, U.S. District Judge Edward Chen has been waiting for the NTP to complete a systematic review of fluoride’s neurotoxicity before ruling on the case.
Groups like the American Dental Association publicly pressured the NTP to “exclude any neurotoxin claims” from the reports.
Connett said during the trial, the EPA repeatedly claimed that the plaintiffs’ allegations about toxicity could not be verified because there was no “systematic review.”
The documents released Wednesday fill that gap.
Connett said:
“So now what do we have? We have a systematic review by one of the pioneering, leading, most authoritative research groups on toxicology in the world.
“They just completed a systematic review that took them six years to complete, so if that’s not enough to demonstrate a hazard under the toxic substances control act, then how would any citizen group ever be able to meet the standard?”
The findings: fluoride and lowered IQ in children
According to the NTP report:
“The current bodies of experimental animal studies and human mechanistic evidence do not provide clarity on the association between fluoride exposure and cognitive or neurodevelopmental human health effects.”
Yet, the report’s summary contradicts this statement by summarizing the evidence informing this conclusion, stating that nearly all studies examined for this literature review found evidence of cognitive or developmental issues associated with fluoride.
According to the report, 8 of the 9 “high-quality studies examining cognitive or neurodevelopmental outcomes reported associations with fluoride exposure.”
Of the 19 high-quality studies assessing the association between fluoride and IQ in children, 18 reported an association between higher fluoride exposure and lower IQ in children. Forty-six of the 53 low-quality studies also found evidence of that association.
The meta-analysis also states:
“The body of evidence from studies on adults is also limited and provides low confidence that fluoride exposure is associated with adverse effects on adult cognition. There is, however, a large body of evidence on IQ effects in children.”
The monograph and meta-analysis found that fluoride exposure at levels equivalent to 1.5 mg/L is associated with lower IQ in children. The abstract concludes:
“This review finds, with moderate confidence, that higher fluoride exposure (e.g., represented by populations whose total fluoride exposure approximates or exceeds the World Health Organization Guidelines for Drinking-water Quality of 1.5 mg/L of fluoride) is consistently associated with lower IQ in children.”
Levels of fluoride found in drinking water in the U.S. are typically 0.7 mg/L, which is lower than the 1.5 mg/L levels found to be neurotoxic by the reports.
On that basis, HHS’ review of the reports recommended the NTP revise its assessment such that, “all conclusory statements in this document should be explicit that any findings from the included studies only apply to water fluoride concentrations above 1.5 mg/L.”
The NTP responded:
“We do not agree with this comment. Our assessment considers fluoride exposures from all sources, not just water.
As discussed in the pre-publication 2022 NTP Monograph, because fluoride is also found in certain foods, dental products, some pharmaceuticals, and other sources, individual behaviors are likely an important determinant of actual exposures.”
Rick North, former CEO of the American Cancer Society’s Oregon division and Fluoride Action Network board member told The Defender that “people consume large amounts of fluoride through tea and other drinks and processed foods made with fluoridated water, not to mention pesticide ingestion and fluoride from air pollution.”
He also said that people’s fluoride exposure can depend on how much water they drink.
“Think about it,” North said. “Your level of risk depends upon, incredibly, how thirsty you are. That’s how absurd the entire premise of water fluoridation is,” he said.
The NTP confirmed that people exposed to levels of fluoride lower than 1.5 mg/L in the water system could have high levels of fluoride in their systems. It stated:
“Even in the optimally fluoridated cities [fluoridated at 0.7 mg/L] in Canada studied by Green et al. (2019), individual exposure levels, as documented by repeated urinary measurements, suggest widely varying total exposures from water combined with fluoride from other sources.”
It added, “our moderate confidence conclusion is primarily based on studies with total fluoride exposure that approximates or exceeds what is generally associated with consumption of optimally fluoridated water [0.7 mg/L] in the United States.”
“We have stressed in our monograph that our conclusions apply to total fluoride exposures rather than to exposures exclusively through drinking water.”
“What the NTP is pointing to here is that in some communities, where the dose of fluoride in the water is 0.7 mg/L, the NTP has found levels of fluoride found to be associated with lower IQ,” Connett told The Defender.
Also, different people have different risk levels, he said. Pregnant women and bottle-fed babies, for example, are some of the populations at highest risk.
On this point, the NTP responded to a different HHS critique, writing, “We have no basis on which to state that our findings are not relevant to some children or pregnant people in the United States.”
“The margin of safety here just doesn’t exist — it is precariously small,” Connett said. He added that the lawsuit is “basically a risk assessment of fluoride.”
To do a risk assessment, the EPA first identifies a hazard and determines at what dose — what level of human exposure — that hazard harms human health.
Then the agency determines in a given case whether the margin between the existing hazard levels and the human exposure levels is unacceptably close, which would make a toxin pose a risk to human health.
Connett said that in EPA’s previous risk assessments for other chemicals, such as methylene chloride or bromopropane, evaluated according to the 2020 risk evaluation method that guides this case, the agency found the hazard level exceeds the human exposure level by much higher margins — “usually in a range of ten to 20 times higher,” yet it has deemed those chemicals to present an unreasonable risk to human health.
In other words, the substances were found to be toxic to humans at levels significantly lower than what people may be exposed to in regular use, yet the EPA determined them to be risks.
When it makes that determination, the EPA must then take steps to mitigate the risk.
That can also be the finding in this case. According to a pre-trial document, both sides in the case agreed to the “undisputed fact” that the “EPA does not require that human exposure levels exceed a known adverse effect level to make an unreasonable risk determination under TSCA.”
The NTP documents also raised flags about the implications of seemingly small neurotoxic effects:
“Research on other neurotoxicants has shown that subtle shifts in IQ at the population level can have a profound impact on the number of people who fall within the high and low ranges of the population’s IQ distribution.
“For example, a 5-point decrease in a population’s IQ would nearly double the number of people classified as intellectually disabled.”
Top HHS and CDC officials tried to ‘water down’ and block the report
In 2016, a group of six nonprofit organizations and several individuals petitioned the EPA to end fluoridation of drinking water in the U.S. based on evidence of health risks associated with fluoride, namely neurotoxicity.
The EPA rejected the petition.
In response, Food and Water Watch, Fluoride Action Network and others sued the EPA in 2017, seeking an end to water fluoridation.
They based their initial claims on dozens of studies and reviews demonstrating fluoride’s neurotoxicity. Studies have also linked fluoride to a variety of other health risks in both children and adults, and evidence shows it to be an endocrine disruptor.
The EPA denied water fluoridation causes harm.
A seven-day trial took place in federal court in San Francisco in June 2020, but Judge Chen put the proceedings on hold pending the release of NTP’s systematic review of research available on the neurotoxic effects of fluoride.
The report, slated for release in May 2022, was delayed several times and sent for several rounds of peer review.
“The people on the [NTP] committee were experts in their fields who put years into this study, going back and forth with one external review after another,” North said. “You couldn’t ask for more peer review than what it already had. There were constant attempts to delay it, to water it down.”
In late October 2022, Judge Chen ended the stay on the NTP review, ruling that the parties involved could view the NTP review in its unpublished form to better inform his final decision.
However, due to concerns from the EPA, he also ruled the report could not be made public unless the NTP released it.
In December 2022, the plaintiffs filed several exhibits with Judge Chen, including a redacted version of the NTP’s assessment of fluoride’s neurotoxicity and internal emails between the CDC and the NTP obtained through FOIA demonstrating that HHS blocked the release of the long-delayed review, the plaintiffs argued.
The documents showed that on May 11, NTP notified the agencies that it was going to release the report on May 18, but the CDC opposed the release.
Emails also indicated that HHS Assistant Secretary for Health Rachel Levine was going to “get involved,” and, “the May 18 release date for [the monograph] is almost certainly not going to happen,” the Defender reported.
Connett said:
“It was only because we were tipped off by someone with knowledge on the inside that something was amiss that we went and did extensive FOIA requests and we were able to get documents showing that the NTP scientists considered this report to be complete and ready for publication last May, May of 2022.”
North said it was clear the agencies were blocking the release of the report, which was ready for publication.
“This was a clear case of stonewalling,” North said. “The National Toxicology Program, after over six years of research and numerous outside peer reviews, had completed its state-of-the-science report.”
Connett added:
“We have emails showing that Levine is the one who put it on hold. Rachel Levine said not to publish this report at this time. Then we got the FOIA emails showing that and NTP said they may not publish this [the report] at all. They may not publish it in final form but we did get them to agree to at least post a draft report. They will consider it a draft report.”
On January 20, Judge Chen denied the EPA’s request to add another six-month period to the stay he lifted in his October ruling.
The monograph and meta-analysis released yesterday on the NTP’s website are both labeled “draft.”
“Unfortunately, fluoridation promoters and high-level government officials have continued to label it a draft,” North said. “It wasn’t.”
Experts associated with the lawsuit against the EPA will now analyze and interpret the report in future hearings and then Judge Chen will rule.
The next hearing date is scheduled for April 11, 2023. At that time, the judge will set a date for the next phase of the trial.
The bill in question, Washington State Legislature House Bill 1333, “Establishing the domestic violent extremism commission,” would, according to its critics, “criminalize thought and expression under an invented category of offences called ‘domestic violent extremism'” and allow the state’s attorney general to “prosecute some people for words and speech, rather than violent acts.”
Although there is nothing in the bill itself declaring that “political enemies” of the state will be sent to “psych wards,” the idea that psychologists and psychiatrists might be employed on such a “domestic violent extremism commission” to diagnose political dissidents with some form of mental disorder is not a misplaced one.
In fact, as it turns out, there is a long and worrying history of psychiatry being used as a weapon to silence those declared to be enemies of the state. And, more worrying still, recent events have demonstrated that—far from being a relic of the past—the pathologization of political dissent is becoming even more widespread than ever before.
The Bad Old Days
The history of psychology is, to a large extent, the history of cruel and unusual punishments meted out by rulers on political dissidents.
That psychology has always been a convenient tool for the ruling class to wield against dissenters may seem like a controversial observation at first glance. But this is precisely what the most mainstream of establishment sources tell us . . . when they’re talking about the establishment’s enemies.
In 1983, for example, Dr. Walter Reich was afforded prime journalistic real estate in America’s newspaper of record, The New York Times, for a lengthy report on “The World of Soviet Psychiatry.” After reporting that the 1977 congress of the World Psychiatric Association in Hawaii had voted to condemn “the systematic abuse of psychiatry for political purposes in the U.S.S.R.,” Reich notes that “Western concern over pyschiatric abuse in the Soviet Union had only grown” since the congress’ vote and that “the Russians were in danger of being suspended or even expelled from the international psychiatric organization.”
Reich then spends the majority of the rest of his 6,000-word article contrasting the American approach to mental health—in which “psychiatric treatment has become acceptable enough during the last few decades for people in emotional distress to seek it out”—with the Soviet approach—in which “the need for psychiatric care is more likely to be seen as a cause for shame.”
The Soviets, we are told, had taken the honourable study of the human mind and weaponized it, turning it into an instrument of political oppression.
For years, Soviet psychiatrists had been accused in the West of diagnosing as mentally ill political dissidents they knew to be mentally well. According to both Western critics and Soviet dissidents, the K.G.B.—especially after it was taken over in 1967 by Yuri V. Andropov, now the top Soviet leader—had regularly referred dissidents to psychiatrists for such diagnoses in order to avoid embarrassing public trials and to discredit dissent as the product of sick minds. Once in psychiatric hospitals, usually special institutions for the criminally insane, the dissidents were said to be treated with particular cruelty—for example, given injections that caused abscesses, convulsions and torpor, or wrapped in wet canvas that shrank tightly upon drying.
Lest the reader be left in any doubt as to his message, Reich states it clearly later on in the piece: “[T]he experience of Soviet psychiatry had a lot to teach,” he tells us, “about the vulnerabilities of psychiatry to misuse wherever it is practiced.”
To be sure, Reich isn’t wrong. The horrors of the Soviet psychiatric system—in which political dissidents were routinely diagnosed with “sluggish schizophrenia,” psychiatric hospitals were used as temporary prisons during periods of protest, and troublesome rebels were kept in medically induced comas or drug-induced catatonic states for extended periods of time—has been well documented in numerous mainstream sources, both popular and academic. But these horrors were given their most poignant expression in the words of Alexander Solzhenitsyn:
The incarceration of free thinking healthy people in madhouses is spiritual murder, it is a variation of the gas chamber, even more cruel; the torture of the people being killed is more malicious and more prolonged. Like the gas chambers, these crimes will never be forgotten and those involved in them will be condemned for all time during their life and after their death.
As Reich correctly observes in his report, the Soviet pathologization of dissent does indeed serve as a warning that psychiatry is vulnerable to being misused “wherever it is practiced.” But, by a funny coincidence, these concerns only ever seem to come up when psychiatry is being “misused” in countries that are on the US State Department’s enemies list.
Thus, there are no shortage of sources that will tell you about:
the abuses that Japanese psychiatrists inflicted on their patients during and immediately after WWII, resulting in an abnormally large number of patient deaths;
the Cuban revolutionary government’s use of psychotropic drugs and electroconvulsive therapy in order to obtain information from, punish, demoralize, coerce, subdue, terrorize, and cause psychological damage to those deemed a threat to state security;
. . . and any number of similar examples of psychiatric abuse by governments at war with or in the crosshairs of the US government.
Often excluded from this analysis, however, are the horrific abuses that psychiatrists in the West have inflicted on their patients in the name of state security.
For example, while the history books will rightly condemn the horrors of the Nazi eugenic sterilization program, they seldom explore the roots of that program. As it turns out, those roots were in the Kaiser Wilhelm Institute of Anthropology, Human Heredity, and Eugenics, which was funded by the Rockefeller Foundation. What’s more, Ernst Rüdin—the director of the also-Rockefeller-funded Kaiser Wilhelm Institute for Psychiatry and one of the key architects of Germany’s eugenics program—modeled the Nazi eugenics legislation on America’s own “Model Eugenical Sterilization Law.”
In fact, America’s first professor of psychology, James McKeen Cattell, helped bring the eugenics pseudoscience to the shores of America in the first place. Having befriended Francis Galton, the progenitor of eugenics, during a trip to England in 1887, Cattell returned to the US with an enthusiasm for the idea. He later wrote a letter to Galton bragging, “We are following in America your advice and example.”
Still further back in history, Benjamin Rush—one of the founding fathers of the United States and the man officially recognized by the American Psychiatric Association as the “father of American psychiatry”—made early contributions to the weaponization of psychiatry by inventing a number of mental disorders to pathologize dissent. The most notable of these made-up disorders was “anarchia,” a type of madness Rush defined as “an excess of the passion for liberty,” which “could not be removed by reason, nor restrained by government” and “threatened to render abortive the goodness of heaven to the United States.”
And what did this “father of American psychiatry” prescribe for those he deemed to be suffering from mental illness? Well, for starters, he “treated his patients with darkness, solitary confinement, and a special technique of forcing the patient to stand erect for two to three days at a time, poking them with sharp pointed nails to keep them from sleeping—a technique borrowed from a British procedure for taming horses.” He also invented two mechanical devices for the treatment of the insane: a “tranquilizing chair,” in which the patient’s “body is immobilized by straps at the shoulders, arms, waist, and feet [and] a box-like apparatus is used to confine the head,” and a “gyrator,” “which was a horizontal board on which torpid patients were strapped and spun to stimulate blood circulation.”
The cause in the most of cases, that induces the negro to run away from service, is as much a disease of the mind as any other species of mental alienation, and much more curable, as a general rule. With the advantages of proper medical advice, strictly followed, this troublesome practice that many negroes have of running away, can be almost entirely prevented, although the slaves be located on the borders of a free state, within a stone’s throw of the abolitionists.
Yes, the history of psychiatry is replete with examples of political dissidents, unruly populations or other “social undesirables” being labeled as insane and sent to the madhouse . . . or worse.
But that was then, many would be inclined to argue. This is now. Surely psychiatry isn’t used to suppress dissent any more, is it? . . .
The Bad New Days
. . . It sure is! And I’m not just talking about psychiatric repression in some backward, evil dictatorship like Russia. (Although, to be sure, there is that, too.)
No, once again, it is the “liberal,” “enlightened,” “free and democratic” West that is leading the way in weaponizing psychiatry against the masses. And, incredibly, the wielders of this psychiatric weapon don’t try to hide the fact, but have instead actively sought to codify it in their “bible.”
Since 1952, the American Psychiatric Association has published the Diagnostic and Statistical Manual of Mental Disorders, or the DSM, as a guideline for the classification and diagnoses of mental health issues. Commonly referred to as the psychiatric diagnostic bible, the DSM, according to the APA itself, “is the standard classification of mental disorders used by mental health professionals in the United States and contains a listing of diagnostic criteria for every psychiatric disorder recognized by the U.S. healthcare system.”
Critics have long questioned the influence that Big Pharma has had in pressuring the APA to diagnose more and more behaviour as “abnormal” in order to prescribe pharmaceutical interventions to a greater and greater percentage of the public.
Concerns over Big Pharma’s influence on the creation of DSM are not trivial. In 2012, a study led by University of Massachusetts-Boston researcher Lisa Cosgrove noted that 69% of the DSM-5 task force members had ties to the pharmaceutical industry, including paid work as consultants and spokespersons for drug manufacturers. On certain panels, the conflict of interest was even more profound: 83% of the members of the panel working on mood disorders had pharamaceutical industry ties, and 100%—every single member—of the sleep disorder panel had “ties to the pharmaceutical companies that manufacture the medications used to treat these disorders or to companies that service the pharmaceutical industry.”
If these task force members’ goal is to make sure that more and more pharmaceuticals are sold, then by every measure they’ve been remarkably successful. Recent surveys indicate one in six American adults report taking a psychiatric drug, such as an antidepressant or a sedative. Worryingly, the number of children being prescribed antipsychotic medications like Adderall and Ritalin has continued to increase decade after decade.
But more worrying still is the way that this increase in antipsychotic prescriptions has been justified—by the invention of a new “mental disorder” called Oppositional Defiance Disorder.
Clinical psychologist Bruce Levine, who has spent decades ringing the alarm bell about the ways in which his profession is being used to repress legitimate political dissent, explains in his 2018 book, Resisting Illegitimate Authority:
Beginning in 1980, for noncompliant children who are not engaged in any illegal practices, the APA (in its DSM-III diagnostic manual) created the disruptive disorder diagnosis “oppositional defiant disorder” (ODD). For an ODD diagnosis, a youngster needs only four of the following eight symptoms for six months: often loses temper; often touchy or easily annoyed; often angry and resentful; often argues with authority figures; often actively defies or refuses to comply with requests from authority figures or with rules; often deliberately annoys others; often blames others for his or her mistakes or misbehavior; spitefulness or vindictiveness at least twice within the past six months.
Levine goes on to point out that the front line of this assault on the human psyche are the children who are diagnosed with a mental disorder for demonstrating previously normal childhood behaviour:
In 2012, the Archives of General Psychiatry reported that between 1993 through 2009, there was a sevenfold increase of children 13 years and younger being prescribed antipsychotic drugs, and that disruptive behavior disorders such as ODD and CD were the most common diagnoses in children medicated with antipsychotics, accounting for 63% of those medicated.
But the pathologization of those who show signs of “oppositional defiance” is not confined to children. Levine also observes, citing his own clinical experience:
Among the people I have talked with who have been previously diagnosed with psychiatric illnesses, I am struck by how many of them, compared to the general population, are essentially anti-authoritarians. Unluckily for them, the professionals who have diagnosed them are not.
As we shall see next week, the weaponization of psychology against those independent, free-thinkers who tend to question authority is not some vague, amorphous concern about a Big Pharma boondoggle that is hurting people in the pocketbook. Rather, this weapon is now being used against critics of the biosecurity agenda and others who dare point out that the globalist, transhuman emperor is wearing no clothes.
But if it is true that the study of the mind has been weaponized and that that weapon is being deployed against conspiracy realists, the obvious question then becomes . . .
Published in 1946 as “The Reestablishment of Peacetime Psychiatry,” the lecture includes a proclamation that psychiatrists should take it upon themselves to rid the population of the concept of good and evil entirely: “If the race is to be freed from its crippling burden of good and evil it must be psychiatrists who take the original responsibility. This is a challenge which must be met.”
Perhaps unsurprisingly, Chisholm’s call to action was taken up by the British military. The “challenge” of “freeing the race” from the “crippling burden of good and evil” was taken up by British military psychiatrist Colonel John Rawlings Rees, the first president of Chisholm’s World Federation of Mental Health and chair of the infamous Tavistock Institute from 1933 to 1947.
In 1940, Rees gave an address to the annual meeting of the UK’s National Council for Mental Hygiene in which he laid out in predictably militaristic terms how this ambitious plan for reforming the public psyche was to be achieved. In “Strategic Planning for Mental Health,” Rees—after claiming that the psychiatrists of the council “can justifiably stress our particular point of view with regard to the proper development of the human psyche, even though our knowledge be incomplete”—asserts that they must aim to make that point of view “permeate every educational activity in our national life.”
He then launches into a startling confession:
[W]e have made a useful attack upon a number of professions. The two easiest of them naturally are the teaching profession and the Church; the two most difficult are law and medicine.” [. . .] “If we are to infiltrate the professional and social activities of other people I think we must imitate the Totalitarians and organize some kind of fifth column activity!”
Then Rees brazenly proclaims that “Parliament, the Press and other publications are the most obvious ways by which our propaganda can be got across” before reminding his audience once again of the need for secrecy if this plan to influence the development of the public psyche is to succeed: “Many people don’t like to be ‘saved’, ‘changed’ or made healthy,” he remarks.
So what were Rees and his fellow travelers really aiming at in their “fifth column” campaign to “attack” the professions and propagandize the public? His true intentions are revealed through his work for the British military—including his alleged drugging, poisoning and mesmerizing of Rudolf Hess, the Deputy Führer of the Nazi party who was captured and held by the British for decades after making a still-unexplained solo flight to Scotland in 1941—and through his work at the Tavistock Institute, where he attempted to mould public opinion in the UK to his liking.
As The Campaigner magazine explained in a Tavistock exposé published in 1978: “The theme of all of Rees’s known work is the development of the uses of psychiatry as a weapon of the ruling class.” That work, the article elaborates, included advising Rees’ superiors how they “can succeed in structuring a stressed individual’s or group’s situation appropriately, the victim(s) can be induced to develop for himself a special sort of ‘reaction formation’ through which he ‘democratically’ arrives precisely at the attitudes and decisions which the dictators would wish to force upon him.”
In other words, Rees’ work centered on the Problem-Reaction-Solution method of mass social control that Corbett Reporteers will be very familiar with by now. It should be no surprise, then, to learn that Rees’ research heavily influenced the operations of a budding young intelligence service that was then forming in the United States: the Central Intelligence Agency.
Indeed, the CIA has always been interested in weaponizing psychiatry as a way of achieving success in their covert operations. In fact, the CIA even openly advertises job opportunities for psychiatrists to “help the CIA mission where it intersects with psychiatric and broader behavioral issues.”
But when most people think of the CIA and weaponized psychiatry, they think of MKUltra and mind control.
As even the Wikipedia article on the subject admits, the CIA’s “Project MKUltra” was “an illegal human experimentation program designed and undertaken by the U.S. Central Intelligence Agency (CIA), intended to develop procedures and identify drugs that could be used in interrogations to weaken individuals and force confessions through brainwashing and psychological torture.”
There is much that the public still does not know about this project, its forerunner programs, Project Bluebird and Project ARTICHOKE, and the depths to which agents of the US government sank to discover ways of manipulating, melding, erasing or reprogramming individuals’ psyches. But what we do know about the program is chilling enough.
One series of experiments, presided over by Sidney Gottlieb, involved administering LSD to unwitting Americans, including mental patients, prisoners, drug addicts and prostitutes. This included “Operation Midnight Climax,” in which unsuspecting men were drugged and lured to CIA safe houses by prostitutes on the CIA payroll. Their sexual activity was monitored behind one-way mirrors and was used to study the effect of sexual blackmail and the use of mind-altering substances in field operations.
Another experiment, dubbed MKULTRA Subproject 68, was overseen by the esteemed psychiatrist Dr. Ewen Cameron. This subproject involved Dr. Cameron using LSD, paralytic drugs, electroshock therapy and drug-induced comas to attempt to wipe patients’ memories and reprogram their psyche. When brought to light, the program was identified as an attempt to refine methods of medical torture for the purpose of extracting information from unwilling sources and was condemned. Lawsuits regarding the blatantly illegal experimentation conducted by Cameron continue into the current era.
Although MKUltra “officially ended” after its exposure in the 1970s, the CIA has not stopped employing psychiatrists to find new and innovative ways to psychologically torment their opponents.
In May 2002, Martin Seligman, an influential American professor of psychology and a former president of the American Psychological Association, delivered a lecture at the San Diego Naval Base explaining how his research could help American personnel to—in his own words—”resist torture and evade successful interrogation by their captors.”
Among the hundred or so people in attendance at that lecture was one particularly enthused fan of Selgiman’s work: Dr. Jim Mitchell, a military retiree and psychologist who had contracted to provide training services to the CIA. Although Seligman had no idea of it at the time, Mitchell was—as we now know—one of the key architects of the CIA’s illegal torture program.
Naturally, Mitchell’s interest in Seligman’s talk was not in how it could be applied to help American personnel overcome learned helplessness and resist torture but rather how it could be used to induce learned helplessness in a CIA target and enhance torture. As it turns out, Mitchell’s theory (that “producing learned helplessness in a Qaeda interrogation subject might ensure that he would comply with his captor’s demands”) was bogus. More experienced interrogators objected at the time, noting that torture would only induce a prisoner to say what his captor wants, not what he knows.
What those interrogators didn’t understand was that extracting false confessions from prisoners was actually the point of the CIA torture program. It was “confessions” extracted under torture, after all, that went on to form the backbone of the 9/11 Commission Report, with a full quarter of all of the report’s footnotes deriving from torture testimony.
The Worst is Yet to Come . . .
Yes, from mind control experiments to torture programs to brainwashing and lobotomization, there can be no doubt that the governments, militaries and intelligence agencies of every major nation have devoted considerable resources to the weaponization of psychiatry over the course of the past century.
But, as it turns out, one of the simplest and easiest techniques for controlling dissent is simply to pathologize it. As we are beginning to see, simply declaring resistance to the status quo to be a form of mental disorder can be an exceptionally powerful tool for silencing opposition.
Next week, we will examine the ways this technique is now being employed against the conspiracy realists who seek to point out the obvious truths about the homeland security state and the biosecurity state.
Three years ago the Western World came to a standstill. The official Covid-19 narrative depicted a strange suddenly-super-spreading, deadlier-than-flu virus hailing from China that landed in Northern Italy.
On February 20, 2020 the first alleged case of Covid-19 was discovered in the West in the Lombardy town of Codogno, Italy. Later that day the Italian government reported their first “Covid-19 death.”
Dramatic media reports emerging from Northern Italy were hammered into and onto the Western psyche giving the impression there was a mysterious “super spreading” and “super lethal” novel virus galloping across the region infecting and killing scores of people.
Harrowing reports out of Bergamo, a city in the alpine Lombardy region of Northern Italy, spoke of coffins stacked high, “covid-related deaths growing relentlessly” and the alarming need for military assistance to remove the grim volume of dead bodies piling up.
Using the entire machinery of the state, Italian Prime Minister Giuseppe Conte began issuing a rolling set of government decrees culminating in Italy becoming the first country in the world to implement a national lockdown. These mandates would set the stage for lockdowns throughout the Western world.
Three years later a comprehensive evaluation of the story about the alleged Italian medical emergency in Spring 2020, reveals a tale of the disturbing epidemiological history of Northern Italy, mass media manipulation and deceptive reporting utilized to create the illusion of a new epidemic.
A multitude of questions and inconsistencies surrounding the Italian story soon surfaced. Ascribing this strange set of convergent circumstances to a viral event strained credulity.
Were these overcrowded conditions in Italian hospitals genuinely the result of a unique viral pathogen or were there other causal factors?
Were these anomalous spikes in excess deaths in Northern Italy verifiably caused by the arrival and spread of a novel deadly virus?
How was it that this virus spread across thousands of kilometers within days and peaked synchronously in selected locations?
How was it that this virus was able to spread so fast across thousands of kilometers, peaking at the same time in those selected locations, yet wasn’t contagious enough to spread to nearby locations?
How was it that this virus waited for a government decree and only then began to create excess death?
How was it possible that all countries in the West and beyond adopted similar “health” measures as carried out in Italy, virtually “overnight”, measures that resembled a de facto police state rather than medical initiatives?
Why Italy?
A brief timeline of the series of events as they unfolded in Northern Italy in Spring 2020:
January 31, 2020 – The Italian Council of Ministers declares a 6-month national emergency handing the coordination of the COVID-19 emergency responses to the Head the Civil Protection Department, following the detection of the first two COVID-19 positive people in Rome – two Chinese tourists traveling from Wuhan;
February 20, 2020 – First Covid-19 case of Italian citizen diagnosed in Codogno.
78-year-old Adriano Trevisan, a retired bricklayer from the village of Vo’ Euganeo near Padua in the Veneto region became the first Covid death of a European recorded. The deceased tested positive for the virus and died in the hospital while being treated for pneumonia.
February 27, 2020 – A National Surveillance system, coordinated by the ISS (National Institute of Health) is set up to oversee the collection and collation of daily data.
March 9, 2020 – The government of Italy under Prime Minister Giuseppe Conte extends the lockdown to the whole of Italy restricting the movement of the population except for necessity, work, and health circumstances.
March 11, 2020 – The World Health Organization declares the novel coronavirus (COVID-19) outbreak a global pandemic. Italy declares closure of all restaurants, pubs, theaters and social activities.
April 9, 2020 – ‘Liquidità’ Decree goes into full effect, including temporary measures to facilitate access to loans, support business continuity and corporate liquidity and measures to support export, internationalization and business investment.
May 4, 2020 – Reopening of most factories and various wholesale businesses, within pre-set health safety protocols.
While such a chronology can serve to refresh our memory and provide a coherent understanding of the sequence of events, it is not a substitute for real history.
As they say– the devil is in the details.
The details in Northern Italy start with massive pollution problems and the accompanying long-standing chronic health conditions which have afflicted the region for years.
Pollution and Chronic Illness
Everyday life in the Lombardy region is bedeviled with dangerous living conditions and health challenges– numerous acute health problems facing an aging population have been documented for a long period of time.
The Po River Valley in Northern Italy is cited as having the worst air quality in all of Europe. The air quality in the region has been deteriorating for many years. The cities in the Po River Valley are cited as having the highest mortality burdens associated with air pollution in all of Europe.
Along with the sheer volume of pollutants, the Po River Valley is known for its unique characteristics of low winds and prolonged episodes of climatic inversions turning it into a holding tank for atmospheric pollution.
The Lancet Planetary Health report from January 2021 estimated death rates associated with fine particulate matter and nitrogen dioxide pollution in 1000 European cities. Brescia and Bergamo in the Lombardy region held the morbid distinction of having the highest death rate from fine particulate matter in Europe. Two other Northern Italian cities, Vicenza and Saronno placed fourth and eighth respectively, in the list of top ten cities in this category. These locations correspond precisely with the highest incidents of upper respiratory infections occurring in Northern Italy as reported in the official pandemic narrative.
In the Lombardy region there is also an ongoing asbestos problem from occupational asbestos exposure in the 1960s and 1970s. A 2016 study, “Incidence of mesothelioma in Lombardy, Italy: exposure to asbestos, time patterns and future projections, predicted a rise of malignant mesothelioma (MM), an aggressive and deadly form of cancer primarily impacting the linings of the chest and abdomen. “This study documented a high burden of MM in both genders in the Lombardy Region, reflecting extensive occupational (mainly in men) and non-occupational (mainly in women) exposure to asbestos in the past. Incidence rates are still increasing; a downturn in occurrence of MM is expected to occur after 2019.”
A further study, “Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14–2016/17 seasons)”, reveals that rates of death due to the common flu have increased markedly over the past decade. This study described a nearly fourfold increase in flu mortality during the covered time period. By the 2016/17 season the totals skyrocketed to 24,981 excess deaths attributable to flu epidemics.
Adding to the ongoing problems of air pollution, residents in the Po River Valley are plagued by high levels of industrial livestock runoff in rivers and tributaries.
Dioxin is a known cancer-causing agent and many people who were living in and around Seveso at the time would be at increased risk of cancers later in life. Someone who turned 20 years of age in 1976 would now be in their 60’s during the Covid Era.
This is consistent with what has been widely reported among Nembro men, with cancer being the leading cause of death in this demographic and lung cancer being the most common type of cancer.
Austerity Measures and Health Infrastructure
Compounding the abysmal environmental conditions facing the people of Northern Italy are austerity measures of the past two decades which have decimated Italian public services, severely decreasing health care resources.
Examining the state of the hospitals in northern Italy, long before the “pandemic”, a pattern starts to emerge.
A 2019 review on the current state of Italian hospitals, “Health & Hospitals in Italy. 17th Annual Report”, noted a “significant increase in 2019 of people on waiting lists and for longer times, compared to the already problematic situation in 2018,” and a, “pronounced deterioration, over the last 5 years, of the “connection” systems between general medicine and hospitals and between these and post-hospitalization services (rehabilitation, long-term care, assisted living homes and home care service).”
The charged atmosphere and resulting firestorm created by a trumpeted “viral invasion” brutally exposed the effects of 20 years of cuts to the national health care system.
The report noted that in 2000, Italy was 2nd in the world for health coverage. The reports cited that by 2011, due to yearly declines in health spending, “more than nine million people declared that they could not access some health services for economic reasons.”
Further cuts magnified an already volatile situation. Over the period 2010–19, the Italian National Healthcare Service suffered financial cuts of more than €37 billion as it experienced a progressive privatization of health-care services. Government spending on healthcare, decreasing for years, spiraled down to a rate below what the WHO considered capable of offering basic health care.
These comprehensive cuts also had severe effects on the healthcare workforce and available hospital beds and equipment, effectively hampering the ability of care facilities to effectively treat patients.
The period from 2009 to 2017 saw 5.2 percent of healthcare staff cut. In the last 10 years, 70,000 beds were lost. In acute medical units bed availability dropped from 922 per 100,000 inhabitants in 1980 to 262 per 100,000.
Data from 2020 show a total of 5,179 beds in intensive care units (approx. 8.9 beds per 100,000) for all of Italy, a population of just over 60 million in 2020.
At regular operational level in 2020 the 74 Lombardy hospitals, servicing a population of 10 million, had approximately 720 ICU beds, with up to 90% of them usually occupied in the winter.
By March 10, 2020 there were 877 people hospitalized in ICUs, units in Lombardy were saturated and requests to transfer patients to other regions were prevalent.
The net effect of these radical cuts to hospital infrastructure and services in the context of the covid hysteria were predictable; for years Italian ICU physicians have been reporting that flu outbreaks cause ICU units to fill up as was the case in locations across the world.
The roaring silence from the media on these inconvenient facts kept the public in the dark on the realities of the crumbling Italian health care system.
Only “the virus.”
In light of this data, it is no surprise that individuals with routine and mostly reversible seasonal respiratory infections once admitted to hospitals might not be treated appropriately or successfully.
Iatrogenic deaths/hospital protocols
In Spring 2020 Italian health officials introduced unprecedented health protocols specifically for Covid.
These new protocols, including early intubation and accompanying sedation, were deemed necessary to protect doctors and nurses at a time when the viral load of the alleged lethal pathogen was purportedly lower.
Were these new protocols appropriate for treating upper respiratory problems?
Mechanical ventilators, that push oxygen into patients whose lungs are failing, quickly became the accepted go-to practice throughout the Italian hospital system. Doctors made extravagant claims that ventilators had “become like gold.”
Employing ventilators involves sedating the patient and placing a tube into the throat. Drugs such as midazolam, morphine sulfate and propofol are used in accompaniment with this procedure; drugs that come with contra-indications and warnings of side effects including respiratory depression and respiratory arrest. Midazolam and propofol are two drugs that are regularly used for assisted suicide and to put down death row inmates.
During the initial wave of hysteria in March 2020 the Italian government requested and received an emergency procurement of midazolam from Germany as their hospitals “suddenly needed 3-4 times the normal amount of this drug.”
The Italian Civil Protection undertook a fast-track public procurement to secure 3800 additional respiratory ventilators.
As early as April 2020 the reliance on mechanical ventilation came under fire from Italian experts. Luciano Gattinoni, a world-renowned Italian intensive care specialist suggested that “mechanical ventilation was being misused and overused.”
Marco Garrone, an emergency doctor at the Mauriziano Hospital in Turin, Italy remarked, “We started with a one-size-fits-all attitude, which didn’t pay off,” Garrone said of the practice of putting patients on ventilators right away, only to see their conditions deteriorate. “Now we try to delay intubation as much as possible.”
Even as some health officials pushed to get more ventilators to treat coronavirus patients, some doctors were moving away from using them.
Questions surrounding actual causes of “Covid deaths” of the frail and elderly placed on ventilators began to surface for the simple reason that doctors were noticing unusually high death rates for coronavirus patients on ventilators.
Could it be that it was medical malfeasance, and not a novel pathogen, that was igniting this tinderbox in the hospitals and creating a feedback loop of public panic?
Could it be that what spread through the Italian hospitals in Spring 2020 was an epidemic of iatrogenesis?
Was it possible that the Spring 2020 mortality event in Northern Italy was not an epidemiological or biological aberration but the result of an unprecedented set of administrative mandates by the Italian government and public health officials?
Emergency Measures and Lockdown Impacts on population
The Italian government, public health officials and regional doctors proclaiming a “novel virus” had landed in Northern Italy, insisted that emergency preparations be activated to prepare for this “massive” increase in Covid-19 patients. That these forecasts were speculations, using linear model forecasts, coming from doctors with conflicts of interest was of little interest to reporters.
A progressive set of restrictive decrees, including lockdowns of villages and cities, were swiftly implemented. These directives served to further terrify and disorient an already panicked populace.
Citizens were told to stay home and were banned from entering certain areas; fines were levied for those who transgressed. Most shops and businesses were ordered to shut down.
Farm owner Rosanna Ferrari said, “We’re experiencing a bit of a panic. Supermarkets have been stormed since last Friday. There are queues outside of the chemist. They said they’ll come, house to house, to collect saliva samples today.”
Angelo Caperdoni, the mayor of Somaglia, described the alarming situation, “It was difficult to contain the panic at first, especially as a lot of false news was circulating on social media that people believed to be true. There is still panic regarding food provisions. Many people went to Codogno yesterday to try and stock up.”
Franco Stefanoni, the mayor of Fombio, also under lockdown, described the harried scene in military terms as he noted the town’s two mini-markets had been “besieged”, as “people have been racing to the supermarket to buy 20kg of pasta or 30kg of bread.”
Former president of Italy’s higher health council, Roberta Siliquini, provided a more reasonable explanation for the excitement: “We have found positive cases in people who probably had few or no symptoms and who may have overcome the virus without even knowing it.”
Cooler heads advising calm were systematically buried beneath a barrage of draconian government edicts, manufactured hype from vested interests and the sustained onslaught of media agitation and deceptive reporting.
Deceptive Reporting
Mainstream news outlets and social media channels kicked into high gear warning of “waves of death” cutting across Northern Italy from a rampaging virus which was creating overcrowded emergency rooms and requiring convoys of army vehicles to transport corpses.
Television images of stacked coffins in Bergamo were catapulted across the airwaves and reported in lockstep, terrifying the Italian populace and much of the world.
A detailed inspection of these reports revealed that the media fear mongering fastidiously avoided all reasonable explanations when not outright lying.
The media kept silent on the fact that as recently as 2018 hospitals in Milan were overrun with viral lung infections. Due to the aforementioned pollution problems, decimated health infrastructure and aging population, overrun hospitals have become a seasonal feature of the national profile of Italy over the last few decades.
Mainstream news also refrained from mentioning the reality of hospital worker shortages and the reasons for this. Due to panic-mongering and the government edict of border closures the Eastern European workforce of nurses, who comprise a large portion of the labor force in Italian health care, quickly fled the country leaving the hospitals and care centers with skeleton crews.
This resulted in sudden abandonment of the fragile elderly and the disabled by those who normally attend to them leading to an avalanche of deleterious consequences as many of the abandoned elderly from care homes were shipped to already overstretched hospitals.
This vicious cycle of worker shortages in care homes leading to runs on short-staffed hospitals led to complete collapse of care for the elderly and the disabled adding to the chaos in hospital systems in regions where harsh government policies were enacted.
Covid Case Creation
Upon entry into the hospital the de facto response for incoming patients was the ubiquitous PCR swab used to determine if the patient had “Covid-19.” If deemed a “positive case” this activated the deployment of deadly hospital protocols – yet another vicious cycle of medical malfeasance which ensured the proper dosage of fear would continue.
Though it was noted as early as March 2020 that there were major problems with PCR as a diagnostic tool, the media, and general public, accepted at face value the validity of this technique as a diagnostic method.
High cycle thresholds were one of the problems cited. This created absurd numbers, as high as 97%, of “false positives”, leading to a grossly exaggerated number of Covid cases and deaths.
Even earlier, in February of 2020, test reads from PCR results in Italy were called into question. as they were using a single SARS-CoV-2 target gene as clinical proof of a “positive” test.
Italian Nobel Prize Candidate Dr Stefan Scoglio, in noting this scientific fraud stated: “Today I discovered a new element of this real fraud, the choice to reduce the positivity to the swab by detecting only one of the three genes that would define SARS-CoV-2. If the virus were present, all 3 would have to be found, because if the virus is intact, the only case in which it can have a pathogenic role and infect, the test must find all 3 genes.”
The misuse of PCR led to the confounding issue of whether people in the Italian hospitals were
actually dying from “Covid” or from the effects of mass social breakdown and then being mislabeled as a “Covid death” as determined by this fraudulent process.
Manufacturing Covid Deaths
The answer to that question is found in later reports which made clear that nearly all of the “Covid deaths” were not in fact caused by a viral pathogen- nearly all of the individuals who died from the alleged pathogen had multiple comorbidities.
A March 17, 2020 report from the Italian Institute of Health (ISS) noted that 99.2% of Covid-related deaths were from people who had pre-existing chronic conditions.
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus.
On re-evaluation by the National Institute of Health, only 12 percent of death certificates have shown a direct causality from coronavirus, while 88 percent of patients who have died have at least one pre-morbidity – many had two or three.”
Ricciardi was citing a March 20, 2020 follow-up report from the ISS (in English here) and either misread the actual figures in the report or was misquoted. While 12% having zero comorbidities indicated a gross exaggeration of the impacts of “Covid”, the accurate figure in the report was 1.2% meaning 98.8% of the listed “Covid deaths” had pre-existing chronic conditions.
By the early summer of 2020 even the mainstream press admitted that virtually all Covid fatalities from Italy suffered from previous chronic conditions.
By October 2021 Italian newspaper Il Temporeported that the Italian Institute of Health revised the number of people who have died “from covid” rather than “with covid” from 130,468 to 3,783.
It is a well established fact that Italy labeled anyone who died with a “confirmed SARS-CoV-2 infection”, confirmed via a dubious PCR result regardless of the real causes of death, as a victim of “Covid-19.”
At the same time according to Istat (National Institute of Statistics) there was a general increase in mortality from all causes from March 1 to April 4, 2020 compared with the average for the same period in 2015-2019. Bergamo sat at the top in the growth of mortality among municipalities with a staggering 382.8% increase in deaths.
This mortality increase resulted not from a host of causes associated with alleged SARS-CoV-2 infection but from multiple other factors. Canceled cancer screenings, delayed treatments, reluctance to call ambulance services in the event of an accident or emergency became commonplace in the midst of the Corona hysteria allowing conditions to worsen beyond possible treatment.
A mere two day delay in seeking treatment of a myocardial infarction can turn a simple and treatable condition into a dangerous and life threatening defect.
Research by the Italian Society of Cardiology established that heart attack mortality more than tripled during the Covid emergency as patients fearing infection stayed away from the hospital.
Ciro Indolfi, Professor of Cardiology at the Magna Graecia University of Catanzaro, noted that, “the organization of the hospitals… in this phase was dedicated almost exclusively to Covid-19 and many cardiological wards were used for infectious patients. Furthermore, for fear of contagion, patients delay access to the emergency room and arrive at the hospital in increasingly serious conditions, often with arrhythmic or functional complications, which make therapies that have proven to be life-saving such as primary angioplasty much less effective.”
Reports of exaggerated and manipulated “deaths from covid” were kept far from public view and certainly no match for stories of military trucks hauling away human carcasses and images of piled up coffins in Bergamo that were burned into people’s brains.
Always and only “the virus.”
The Lies of Bergamo
The now infamous Bergamo image of three long rows of lined up coffins spread like wildfire and shocked the world without any investigation of the veracity of the photos by the duplicitous media hyenas who instead fanatically fanned the Covid flames at every turn.
Responsible reporting would have authenticated that the photo in question was taken in a hangar at Lampedusa Airport back on October 5, 2013.
The coffins in that photo were filled with corpses of African migrants who perished in a shipwreck, the body count was an estimated 360 deaths, off the coast of Lampedusa, an Italian island off the coast of Tunisia.
The need for trucks to haul away corpses, which the media repeated elsewhere, was readily explained by a combination of congruent factors. The dead were being removed by the military as funeral directors fearing “the killer virus” refused to pick up the bodies as they would during normal times.
The fabricated and magnified fear that made funeral directors eschew their normal duties was compounded by an emergency national law banning civil and religious ceremonies, including funerals. This unprecedented move, for an overwhelmingly Catholic country that normally relied on ritual burial, was put into effect in early March.
The danger of a “highly transmissible and deadly new disease” now firmly etched into the psyche of Italian citizens added to the frenzied situation.
Families who would normally follow the Catholic practice of burial were opting for cremation of the deceased in unprecedented numbers for fear of catching the disease from the dead.
In the north of Italy there was a 50% increase in requests for cremation which quickly overwhelmed the few small crematoria that did exist in Italy.
A Regional Curiosity
Interestingly not all of Italy was hit by the purportedly “super-spreading” virus. The excess deaths in Spring 2020 were limited to Northern Italy and to specific areas within Northern Italy.
The epicenter of the covid virus was reportedly located in the Lombardy region. The localized Lombardy crisis, portrayed to the world as the “Italian” zombie apocalypse, appeared not in the streets, shops or homes in Lombardy, but solely in hospitals and care homes situated in urban centers.
How did the alleged deadly pathogen bypass Central and Southern Italy which have similar demographics?
Data from March 26, 2020 confirms “the virus” did not migrate South honoring jurisdictional boundaries. Four regions in Northern Italy accounted for 89 percent of all Covid “cases.” This pattern would remain the same even as an onslaught of testing was rolled out across the country.
One theory that surfaced suggested that since Lombardy has a high number of Chinese workers in the garment industry the “virus” was brought to Italy by Chinese migrant workers and spread through the region. This hypothesis fell apart when it was noted that Tuscany, a region in Central Italy, which has the largest concentration of Chinese people in Italy and all of Europe, somehow wasn’t hit by the “virus.”
The fact that Southern Italy didn’t get hit by the “virus” also turned the official narrative on its head.
A significant difference in the social structures between North and South Italy entails most elderly in the South living with or very near to their children. This tradition of extended familial support is known to create conditions conducive to well-being and security.
Per capita there are more long term care facilities (LTCF’s) in the north of Italy with many more residents living in these precarious conditions.
With what we now know it is reasonable to conclude that for a large number of individuals in the north residing in LTCF’s, where conditions are often unhygienic, the nutrition is poor and the care is often negligent, a perfect storm for wholesale death was created.
The subsequent mass departure of overburdened and terrified staff and creation of mass anxiety within a disabled, fragile and abandoned populace virtually guaranteed a mass death event in this sector of the Northern Italian populace.
Critical thinking 101 informs us that with 50 percent of the “COVID deaths” in Italy occurring among nursing home residents and the average age of “Covid death” being at or above normal life expectancy, this was decidedly not an issue of “COVID deaths” per se but an issue of social conditions.
Terrorizing and isolating elderly people living in care homes, denying them visits from relatives and reducing or eliminating in-person visits from health and social carers combined with any respiratory illness could, and does, sweep through any unsanitary nursing home and wipe out a significant number of the frail.
There was no need to invent a new contagion to explain why people were dying.
The social contagion of government mandates and the media hysteria from social networks became a disease more dangerous than any alleged biological contagion.- but the machinery of the state can conveniently sweep these factors under the rug by curating the swirling madness of “The Virus.”
Why Italy?
To suggest that there was no aberrant viral event in N Italy in Spring 2020 and theorize that Italy was chosen as the launching pad for the Covid Operation, as the evidence indicates, we have to ask, “Why was Northern Italy chosen as the stage set for this pandemic screenplay?
Did Italy possess the means and the motive?
In order to launch the shock-and-awe phase of the Covid Operation into the Western world it was necessary to create the illusion of a viral invasion.
To conjure a post-modern Potemkin plague and the perceived need for shutting down a country’s social and economic order, Italy possessed all the ready-made ingredients. With its already soaring rates of interstitial pneumonia, panoply of pollution induced upper respiratory problems and high cancer rates, Northern Italy needed only a tiny flame to ignite a wildfire of fatalities. That spark came in the form of media generated hysteria, lockdown orders and deadly hospital protocols.
Italy also had the motivation which becomes apparent once you understand the Covid story through the lens of money, power, control, and wealth transfer.
A financially bankrupt country with a financial sector desperate for bailouts and a command structure run by central bankers made for a willing and compliant government.
For reasons unrelated to the poor health of its citizens Italy has been dubbed “the sick man in Europe” for the past decade by the EU financial sector.
Like much of Europe the Italian government was facing extreme economic pressures in 2019.
While Europe as a whole was economically stagnant Italy officially slipped into recession in early 2019. Anxieties in the Eurozone were high with concerns that the “Italian problem” would spread and trigger a meltdown across an already teetering global economy.
Italy’s government debt had mushroomed to the fourth-largest in the world and the biggest in the EU. This crushing debt was placing a strain on the EU creating tension between Rome and Brussels.
By May 2019 Italy’s financial crisis was said to be “posing major threats to the monetary targets of the European Central Bank” and if not reined in, “could shatter market confidence in the entire Euro area, putting the EU in big trouble.”
With no time to spare, the tried and true bailout scheme was proposed in order to rescue large investors. European commissioner for economy, Paolo Gentiloni, warned “A whopping €1.5 trillion ($ 1.63 trillion) could be needed to “deal with this crisis.”
All chatter about the financial industry bankrupting the nation by looting public funds, politicians destroying public services at the behest of large investors and the depredations of the casino economy were washed away with the fresh telling of a crisis sparked by the ‘outbreak of Covid-19.’
Predators who saw their financial empires coming apart at the seams resolved to shut down society and loot the world in an attempt to salvage their crumbling financial empires.
In order not to solve the problems they created these financial predators needed a cover story.
A cover story big enough to disguise the countless financial crimes they committed and suppress the social problems they created.
That cover story magically appeared in the form of a “novel virus.”
As part of the EU recovery plan the €750 billion was divided in two parts. One included €500 billion to be allocated as grants based on each country’s “recovery needs.” Italy would be getting the biggest slice of the pie.
Europe’s ‘sick man’ received a much needed infusion- strings attached.
Conclusion
Three years later the indispensable truth of the Italian story is once you scratch beneath the surface of the official narrative of the Covid Pandemic it turns out to be a bottomless snake pit of distortions, manipulations and outright lies.
Any excess deaths in Spring 2020 in Northern Italy were an artifact of already existing health conditions in an aging population, the obliteration of the existing health care infrastructure, massive industrial pollution creating chronic conditions, media generated hysteria, savage government lockdowns and administrative murder of the already fragile.
These iatrogenic deaths of fragile people were the result of the social order and public health despotism and then used to give the impression that there was “a deadly virus” circulating.
The only pandemic was one of violent government and biomedical assault against people.
The evidence from Italy in 2020 exposes the official “Covid” narrative for what it is- a cold-blooded organized deception.
Dr. Tom Cowan Responds to Derrick Broze and Dr. Peter McCullough Re McCullough’s Claim That Viruses Must Have Been Isolated Because They Use Them in Vaccines
Partial transcript provided by Truth Comes to Light. The video covers a number of subjects. This transcript is only of the first half of the video where Dr. Cowan addresses the comments made by Dr. Peter McCullough and Derrick Broze.
The introduction to this video includes a bit about Tom Cowan’s work with coherent water. He mentions dancingwithwater.com and will be doing additional interviews related to this topic in the future.
At approximately 4:58 marker he begins talking about the recent interview between Derrick Broze (founder of The Conscious Resistance and writer for The Last American Vagabond) and Dr. Peter McCullough.
“…opinion on another topic that’s related to COVID that has become the hot button issue in some corners. I’m sure you’ve come across it. But folks who believe that there are no viruses, or particularly that the COVID virus, hasn’t been isolated?
I’m not sure how much time you put in your energy into that. You know I’ve interviewed Andrew Kaufman and some of the folks who are kind of promoting that idea.
Personally, I’m not 100% sold on this idea. You know, I think there’s there’s some research needs to be done.
I do think there’s some interesting data out there about FOIA requests that have been put out trying to get governments — ‘Can you provide me proof of isolation?’.
But in general, what are your thoughts on this? Is this distraction? Division? You know? What do you think about that topic?
Dr. Peter McCullough:
I think it’s distraction. And it may even be intentional distraction.
There are standard virology lab techniques that have been used for decades, that have been used — viruses are transferred into one cell culture versus another.
They’re isolated in order to be able to make vaccines. So of course they’ve been isolated.
We can see them on electron microscopy, so we can actually physically see the viruses and we we can basically determine the entire genetic sequence of the virus. We can understand every single protein within the virus.
So the viruses clearly exist. They have clearly been isolated because we make vaccines out of them.
If they couldn’t be isolated, we could actually never make a vaccine.
The Chinese actually have — the SinoVac corona vaccine is the isolated SARS-CoV-2 virus killed and given as a vaccine.
So these claims are just, they’re not useful, claims. I don’t think they’re helping us get to any solution and they’re just, I think distractions of people who just honestly don’t understand standard virology and vaccine techniques.
Derrick Broze:
So when someone says — this is one of the arguments I’ve heard — when their argument is, when you look into the word isolation and the way virologists use it, they don’t use it in the same sense that… So if I say I’m gonna isolate the coins out of your pocket, all I have in my hand is coins. And they’re saying that the the process that’s used to isolate viruses is not as clean cut as that. And that there’s other material in there. And this is their argument. Would you say that comes from a place of total lack of understanding?
Peter McCullough:
Yeah, it’s a lack of understanding. They’re clearly isolated. I mean, the viruses are isolated and it’s actually purified in order to give us a vaccine. So they have to be isolated.
Derrick Broze:
OK. Well, thank you. Thank for addressing that.
Dr. Tom Cowan:
OK. So I made a little bit of mistake here. Derrick Broze did not ask for more tests. He called for more research so that he could verify that the ‘no virus’ so-called claim was accurate. And so again, I asked him what research or testing he would like to see. And I haven’t heard back from him.
So as you heard, Dr. McCullough made the claim that I hadn’t heard before, which is that the Chinese are making vaccines. (I’ll tell you in a minute how they’re making them.) And that this proves that the viruses have been isolated and, in fact, purified.
So even though in all our requests and all our looking at papers, we’ve not come across one example of a purified pathogenic virus including SARS-CoV-2.
So maybe Doctor McCullough can send us the reference showing us a purified virus.
But again, we’ve gone over the electron microscopy evidence for the virus.
We’ve gone over the sequencing of the virus.
And we haven’t gone over this new claim, that because the Chinese are making a vaccine of SARS-CoV-2, that must prove that the virus has been isolated and purified– or else, how could they possibly have made the vaccine?
So let’s take a look at this claim. So I pulled this from somewhere but I think it’s sort of standard stuff. So I think we can basically rely on it because it’s pretty much accurate for the standard response.
[Here Tom reads from a paper by Anne Moore, a senior lecturer in biochemistry and cell biology at University College Cork.]
So are all vaccines the same? So the answer is no.
And then they go on to say, the Chinese vaccines, which are ones he’s referring to from Sinovac and Sinopharm. Not sure if it’s Sino or Sino are the main ones using this platform.
This platform means they’re using an inactivated vaccine because it “contains a dead virus”. The virus is still whole. It has all its parts in the correct shape that can stimulate a response from the immune system, what we call antigens. The immune response can be against multiple antigens.
And so that is the platform that he’s referring to. It is an inactivated viral vaccine.
They say it’s a great technology. It works for human and veterinary vaccines, used for the seasonal flu vaccine some years ago.
And then they go on to talk about other types of vaccines. So we’re not so interested. And then of course, there’s the obligatory computer pictures.
So then we get down to the important point, which is how do you make these vaccines? And I’m going to read most of this.
It depends on the platform.
So we we’re not talking about the viral vectored vaccines. But let me just go over this because they say it’s the same for inactivated vaccines. The process is similar.
So then you have — you’ll have this bulking up of the virus over course of a few days, anywhere from four liters of cell culture to maybe 20 to 30 liters. Really high-scale production can be carried out in steel tank. The manufacturing environment can look a bit similar to super clean, sterile brewery. You have to make sure that your cells are in the best environment possible for them to live and to allow the virus to grow. This requires monitoring many environmental factors in and around the cell culture, temperature, oxygen, CO2 levels, acidity, and so on.
You end up with this liquid that is full of the virus you’re interested in, but it’s also full of materials you don’t want. So then you have what we call downstream processing, where you’re purifying the virus vaccine away from all the components that you’re not interested in.
This downstream process is very important and highly controlled and evaluated. It involves a lot of filtration and chromatography. In the end, you have a very safe and sterile product that contains only what you want.
There are multiple steps and in each step you’re taking samples and running experiments to show that you’re purifying your product as you go along. Even though it can take a few days to grow a batch of virus it can take a long time to purify it, and it’s pure, sterile and that’s what you say it is. The vaccine will only be released when you can prove that it’s the exact purity, sterility and composition you’re claiming.
So here we get to the inactivated vaccines. The process is similar. You grow up liters of the virus itself, and then you kill it in a specific way so that you maintain the structure of that dead virus. And then you take that and you inject it into people.
So again you grow liters of the virus. Then you kill it in a specific way.
As far as I can tell, the two usual ways that the “virus” is killed is by heat iactivation. In other words, you heat it up. Or they use a chemical called formaldehyde, which they say kills the virus, but it maintains the structure of the now dead virus.
And then you take that brew, that culture material, and you inject that into people, sometimes with some amount of filtration or centrifugation or so-called purification.
Now let’s go through these steps again.
And the question that I want to ask is:
At which step in this process did the people who are making the inactivated vaccine prove there was a virus in this and then prove that it was the virus that was growing in their cell culture?
That is actually the only question that we’re interested in right now.
At which step, which part of this method was there the proof, or even I would say the possible proof, that you’re dealing with an actual virus.
So let’s go through all the steps very clearly, and with that methodically, with those questions in mind.
Which step is showing us the virus?
So they take a person who is sick and they say this looks like whatever illness they’re talking about. In this case, we say that they have COVID.
Now you could say that the proof that they have COVID is — because we all know at this point that COVID has no particular pathognomonic symptoms.
Let me just show you that just to make sure everybody is on the same page. These are the symptoms of cold, flu, COVID and RSV. And you can see they’re basically identical. I won’t spend a lot of time on this.
Here’s another one that says from the CDC. No particular set of signs or symptoms can reliably discriminate COVID-19 from other respiratory viral illnesses, such as the flu.
So there is no possible way by looking at a person, examining the person, that you can say they have COVID.
Even if you could do that, which you can’t, that certainly doesn’t demonstrate that the reason they’re sick is because they have a virus.
I certainly hope everybody would agree with that. All you know at this point is this person is sick with a non-specific respiratory illness.
OK, so then you take a sample of liquid or fluid from that patient, either a bronchial sample or mucus from their nose, or maybe something else. But those are the usual ones.
And let’s look at that. So there’s no examination done on that specimen. So there’s no possible way that could show you that there’s a virus there, because actually nothing is investigated.
So then they put it through some, I would say not purification steps, but they clarify it by putting it either through a filter that filters out the dead cells and the bacteria. And so all you have then is whatever is liquid from the person’s mucus or lungs.
And I would think that there is nobody who knows anything about this who would say that is a purified virus or it even shows you the existence of a virus.
Sometimes they do a different clarification process which is called centrifuging it, again not looking for a virus but just to get rid of the cells and the bacteria.
And then they have the supernatant, the liquid part. And importantly, and this is a crucial part of this analysis, there is no test done on this that could demonstrate the existence of a virus.
They might do a PCR test, which is not a test. But we have to remember that these are PCR processes that can never show the existence of a virus. And the PCR process that is being used for SARS-CoV-2, we all remember was made by Christian Drosten who said “We made this PCR without having access to any viral material.”
So nobody could possibly claim that the PCR examination of this centrifuged or filtered fluid could possibly prove the existence of a virus.
There is no ultracentrifugation done at this step. There’s no electron microscopy analysis of the fluid. So we have no idea whether or not there’s a virus, a particle that you could call a virus, in this supernatant or filtered fluid.
And importantly, nobody at this point is looking for a virus or claiming that somehow these steps have found or demonstrated the existence of a virus.
So that should be clear.
So now let’s say they filtered it. So we have all the liquid parts that come from the mucus or lung fluid of a sick person.
We don’t know why they’re sick. We haven’t seen any virus. We have the liquid, which contains probably hundreds, maybe more types of things. It has proteins, nucleic acids, minerals, lots of maybe poisons, toxins if they’re in there.
Lots of things are in there. I dare say nobody would claim that is a pure virus.
So they take this fluid and they mix that into these big vats that contain cell cultures, mostly some type of Vero cells. Then they add antibiotics, like usually gentamicin, antifungals like amphotericin, both of which we have presented papers that are showing both of these are toxic to kidney cells and other types of cells. Therefore could be the reason for the breakdown of these cells.
They change the nutrient blend and they also add fetal calf serum to this. They change the temperature a little bit and maybe the pH. So they add some other chemicals. And then to this they add this mixture of many different substances, which may or may not include a virus — but the virus has never been seen.
Now, if you’re doing a scientific experiment, as we all again know by now, you have a dependent variable, which is the effect you’re looking for.
Which in this case then you’re looking for: Do these cells die? That’s called the cytopathic effect. And then you’re testing an independent variable, which is meant to be one thing that you’re trying to investigate whether it caused this effect that you’re looking for.
So if we’re trying to prove that only a virus caused the death of these cells, only the virus grew in this culture and caused the death of these cells, then by definition, the virus would have to be the independent variable.
But in fact, what is the independent variable here?
So the independent variable is a combination of antibiotics, change in nutrients and all the things that are soluble from the bronchial fluid of a sick person.
There is at no point up till now any even attempt to establish that there’s a virus. All we can say is that some component of that of that mix — the soluble part of what’s in somebody who’s sick, the antibiotics, antifungals, change in nutrients, fetal bovine serum — some part of that broke down the cells, made it so that these broken-down cells created, essentially, cellular debris, which as we’ve said over and over again are then misinterpreted as viruses. So the cells breakdown into all this debris.
No attempt is made by these Chinese manufacturers then to identify any virus or prove that any virus is in that vat of broken-down-now cells, antibiotics, filtrate from the person who is sick, et cetera. No attempt.
They put that into vials and that’s the vaccine.
So the question for Doctor McCullough is:
Which step in there proved the existence of a virus?
Which step in there was the so-called isolation of the virus?
Now let’s define isolation. As Derrick Broze said, isolation means to take something out of its environment so that you only have that single thing.
If I have a bunch of things on my desk and I take the pencil, I have now isolated the pencil and only the pencil from my desk.
In which step up till now did they “isolate” the virus?
Because, as far as I can see, not only did they fail to isolate the virus. At this point nobody has even attempted to demonstrate there’s even a virus in this process — at any point in the process.
The importance of this is, if you haven’t isolated and, therefore, seen and proven the virus to exist, any further evaluation — such as pictures with an electron microscopy or evaluating parts of it like proteins or nucleic acids — you have no idea the origin of those nucleic acids, proteins, antibodies or anything else in there, because at no point in this process did you obtain a pure sample.
So let’s be very clear what we’re asking you.
We’re asking you to present proof, evidence, that at some point in this process, you have obtained a pure virus. You’ve seen it on an electron microscopy. There’s nothing else in there but the virus. You’ve proven that that virus came from the original person. You’ve then proved that all of the nucleic acids come from that particle, which you have purified. That there’s no chance those particles came from the cells or the fetal bovine calf serum, or anything else part of that mix.
That’s what we’re asking you.
Not whether they say they isolated it. Not whether they say there’s electron microscopy pictures. Not whether they say that the PCR proves that there’s a virus even though they got the PCR test, essentially without even having an isolated or purified virus, which is their own words.
We are asking for validating the methodology of that vaccine production process which you stated should be considered proof that they isolated the virus.
I’m hoping that this is very clear. And in any future discussions we have about the existence of the virus, it has to start with:
Did you find the virus in its natural ecosystem?
The answer, of course, is no.
And then, if you isolate the virus, as you say, through the cell culture process, how did you prove that the virus existed in the first place in order to do an experiment with it?
And how have you proven that the cytopathic effect could have only come from the virus?
Because every experiment that we’ve looked at has shown just the opposite.
“Our instincts led us to go beyond our medical textbooks and establishment microbiology training, and we were soon immersed in the second English edition of Virus Mania.
“The book shocked us. Biology wasn’t just a bit dodgy, it was fraudulent.
“Pathogenic viruses were invented boogeymen that had never been shown to exist in scientific experiments, let alone cause disease.”
People around the world are becoming more aware of the ‘no virus’ argument as the “science” of virology has been exposed. However, there is often a language barrier when it comes to reaching some countries. Many of the best-known critics of virology are in the English-speaking world and have developed strong alliances with large followings.
The good news is that the movement for truth is truly international and this video will look at some of the advancements being made in regions that are perhaps lesser known to most of our English-speaking audience.
And could the madness of COVID-19 end up bringing the world closer together?…
I’ll be the first to admit that those of us in the English-speaking world can be in the dark when it comes to literature and interviews and other languages. This affects all manner of topics, of course. But this video will focus on the international spread of the ‘no virus’ issue. And while English material is often translated into other languages — for example, Virus Mania is now available in seven languages, with more in development — translations are often less available in the other direction.
I’m also going to give a shout out to perhaps one of the lesser-known teams that has been hammering their country’s government for years over the lack of evidence for SARS-CoV-2 and COVID-19.
Let’s find out who they are and how they have exposed their public office holders on every aspect of the alleged science of virology and pandemics.
For my husband Mark and I, our first introduction to the ‘no virus’ position was in early 2020. The COVID-19 production alerted us that something was badly wrong with virology. Our instincts led us to go beyond our medical textbooks and establishment microbiology training, and we were soon immersed in the second. English edition of Virus Mania.
The book shocked us. Biology wasn’t just a bit dodgy, it was fraudulent.
Pathogenic viruses were invented boogeymen that had never been shown to exist in scientific experiments, let alone cause disease.
Virus Mania led us to the work of the Perth Group and their detailed scholarship and essays — such as HIV: A Virus Like No Other — showed us that the ‘no virus’ arguments had not only been put forward decades earlier, but were very advanced.
To us, the question became ‘Why have we never seen this before?’ and the inspiration to start our own work into the virus existence issue, as well as going wider into the flawed germ theory and allopathic medical models.
In 2020, my online platforms grew quickly, as did those of Tom Cowan and Andy Kaufman, across the ditch as we say in New Zealand.
Tom Barnett also called out the fraud in 2020 in Australia.
Seasoned campaigners such as Kevin Corbett, David Crowe, Jim West and Amandha Vollmer found a resurgence in interest in their work questioning viruses.
Meanwhile, Mike Stone’s pent-up issues with germ theory and so-called viruses came flooding out in the Viroliegy website.
Christine Massey paused her fluoride work and began publishing the FOIA requests, revealing that no institution in the world had isolated SARS-CoV-2 or any other “virus” for that matter.
Steve Falconer of Spacebusters, pivoted his channel in 2020, and his videos calling out the COVID fraud and contagion myth gained millions of views.
Documentary maker Mike Wallach had known for years that much of allopathic medicine was fraudulent and produced the massive Viral Delusion series in the middle of the scamdemic.
Mark decided to write a fully-referenced, formal refutation of the entire virus model and published the 29,000 word essay, A Farewell to Virology.
These examples show we are spoilt for choice in the English speaking world.
But there are, of course, other prominent members around the world.
In Germany we have the incomparable Dr. Stefan Lanka, the trained biologist who worked out in the 1990s that there were no pathogenic viruses.
Also in Germany are my original inspirations, Torsten Engelbrecht and Dr. Claus Köhnlein, the first person to be on the Dr. Sam Bailey channel.
I was honoured when they asked me to become part of the Virus Mania team in 2020.
Then in Italy, we have the 4th Virus Mania co-author, the one and only Stefano Scoglio.
And the Spanish-speaking world La Quinta Columna have been at the forefront of investigating the contents of the COVID-19 vaccines. And as far as I know, also take the ‘no virus’ position.
When the “Settling the Virus Debate” statement was launched in July 2022, we had an international alliance of doctors and scientists.
For most of our audience, three of the lesser-known names were likely to be Mufassil Dingankar, Jitendra Banjara, and Sachin Pethkar. These are our friends from India and they have been doing an incredible amount of work with their team to show to India and the world that the Emperor has no virus when it comes to COVID-19 or any other alleged viral disease.
They have collected hundreds of pages of documents with responses from so-called health institutions and politicians in India. They have documented the uncontrolled and unscientific experiments related to alleged virus isolation, electron microscopy and genome sequencing. Starting with Fan Wu, whose infamous 2020 paper they had pointed out that the PCR was not clinically validated, and couldn’t be in any case, Because of the failed biological science upstream from the test.
They have even pointed out the financial fraud with the government of India taking out a loan of 1 billion U.S. dollars on the 2nd of April 2020, in the name of the pandemic, placing a further burden on Indian citizens.
Not only this, but the public purse has been used to fund the necessary medical drugs and vaccines and run marketing campaigns of fear.
They have pointed out that cases of COVID-19 are defined by preposterous circular reasoning, due to its non-specific symptoms and flawed testing kits.
Of major concern to the team has been the suppression of natural therapies for illnesses. I love the way they reject the allopathic medical system and state:
“A serious issue is, if any disease/symptom cannot be cured by Allopathy (or the alternate) Medical System, it is declared an incurable disease/symptom or epidemic or pandemic by ignoring the other mainstream medicinal systems such as Ayurveda, Yoga, Naturopathy, Homeopathy, Unani, Siddha etc. at the outset.”
I think we should all take up this approach and describe Rockefeller and Pasteur medicine as alternative rather than true medicine.
Much of the overall strategy from our Indian colleagues has been to focus on the legal aspects of COVID-19 in their country. For example, under the Indian Evidence Act, 1872, the burden of proof is on the government to establish the existence of the alleged SARS-CoV-2 virus in human samples, and its pathogenicity with that sample.
It has become clear that, like virologists around the world, the Indian medical authorities cannot deliver the evidence with any papers that follow the scientific method.
The conclusion from our Indian colleagues and their politely-worded statement:
“This is nothing but a serious medical experiment which is likely a crime against humanity and this act clearly shows that health authorities may have no intention of public health and welfare of citizens of India.”
And while the highest level institution, the Indian Council of Medical Research, claimed they have proof of existence of SARS-CoV-2, they have yet to provide any document to back this up. Hence a demand letter is now being sent to them, as well as the National Institute of Virology and various politicians. It calls on them to provide a public demonstration showing the existence of a virus.
They’ve even opened it up further and have suggested that the demonstration could involve providing the evidence for ANY alleged disease-causing microbe.
So here’s how their demand letter reads.
SUBJECT:
Demand to prove the existence of the alleged SARS-CoV-2 virus (or disease-causing virus). In other words, to prove that the alleged SARS-CoV-2 and the alleged variants (or disease-causing viruses) are real physical entities that are supported with real-time research via public demonstration and peer reviewed scientific papers. Additionally, to prove that there was a real scientific basis behind this COVID-19 pandemic.
Dear Public Servant,
At the outset, we are very disheartened and unsatisfied with your response. We are referring herewith to your response, which lacks sincerity and shows great negligence/disrespect towards the public. Moreover, it also lacks rationality and scientificity.
YOUR UNSATISFACTORY RESPONSE:
If you diligently read our Open Legal Notice, you would have noticed that we asked you for valid scientific experimental research papers/records/documents to prove the existence of alleged SAR-CoV-2 or disease-causing viruses. However, the scientific research papers that you provided against the RTIs and our correspondences fail to prove the existence of any ‘disease-causing virus’, including the alleged SAR-CoV-2 virus or its variants, that we showed in our Open Legal Notice (based on scientific principles/methods and rationality.
Furthermore, without providing any valid scientific papers/records/documents to prove your claim (i.e. existence of any disease-causing virus and/or the alleged SAR-CoV-2 virus), you have given a poor logical reply. This, to our surprise, was a kind of response never expected from an esteemed scientific institution such as yours. Therefore, we are now forced-obligated to mandate scientific, rational, and clear-cut answers to our questions.”
Therefore, unless you can provide us with a valid scientific proof and/or research papers to prove the existence of the alleged SARS-CoV-2 or its alleged variants, we demand an explicit statement mentioning that you do not have any such evidence; as you clearly mentioned that you do not have any scientific evidence for disease-causing germs, i.e. disease-causing bacteria, fungi, protozoa, parasites, or any kind of disease-causing microorganism against the RTI attached.
ONE. Your Reply Failed the Scientific Temperament:
As per our present observation/experience and doubt, the absence of valid scientific evidence and the lack of submission of proper science principles/methods in the research work of Virology show that: Through imagination, theory and fear-generating tools like the PPE kit, as well as masks and heavy sophisticated machineries/tools etc, an atmosphere has been created by the virologists fabricating an imaginary entity to be a real one for others.
Virologists are the victim of a misconception (i.e. existence of disease-causing virus), which has been conceived by them and is further spread/propagated by the medical doctors/professionals across the society/public. As a result, people are now suffering from the fear of an imaginary entity. This misconception has been made the basis of almost all the alleged epidemic and pandemics since hundreds of years.
The truth revealed through proper scientific investigation has never been done yet.
Also, after interacting with various scientists/experts from over the world their statements further clarified that existence of disease-causing virus is a misconception:
For instance:
“When cells die, they are broken down into submicroscopic particles, some of which biologists arbitrarily label viruses.”
“Anyone who closely analyzes what virologists actually do in the laboratory to ‘prove’ that these particles they call ‘viruses’ cause disease will easily see the absurdity of their conclusions”
~ Dr. Stefan Lanka, virologist
[mention of paper COVID-19 the virus does not exist. It is confirmed. by Dr. Saeed A. Queshi, PhD.]
Secondly, regarding the PCR/RT-PCR, we already showed in our Open Legal Notice why and how the test is totally irrelevant for the purpose and it’s a misuse of this test that was/is being used for the alleged COVID-19 pandemic purpose. However, you could not clarify our inquiry in your response.
Additionally, we also present herewith excerpts of the laboratory experiment conducted by Dr. Biswaroop Roy Chowdhury and his team to validate the government- approved RT-PCR test for COVID-19.
Excerpts:
Recently from June 15-17, 2022, I and my medical team conducted an experiment wherein we took some fruits, some vegetables, and some animals like rabbit and dog and a few birds like chicken and pigeon. We collected samples of each of them and went to a government- authorised COVID Test Laboratory to run them through the test to understand which of the samples are COVID positive and which of them are COVID negative.
Dr. Biswaroop Roy Chowdhury demonstrated and explained the invalid and irrelevant usage of RT-PCR test kit to detect the unclear nucleic acid and proved that the RT-PCR testing is non-specific for the purpose of diagnosis.
Now it is your responsibility to prove your claim via practical demonstration. You have claimed in your response that you can prove practically the existence of the alleged SARS-CoV-2 virus (or disease-causing viruses). Therefore, we are eager to participate and witness your practical demonstration, as it is the only way to prove your claim.
If you claim the existence of the disease-causing germ (microbes) we demand to prove your claim via practical demonstration by providing us with the below.
– Date, time and schedule of your practical experimental demonstration.
– Name and location of the laboratory (including wet and dry lab).
-Names of the virologist/scientist/committee who will perform and participate in the demonstration.
Please mention all details of the procedure(s)/steps that you will perform and demonstrate during the practical demonstration.
So, there you have it.
Rest assured that the ‘no virus’ arguments are being advanced in many countries around the world, including by our friends in India.
Keep the conversation going in the comments. And if you know of other individuals or teams around the world that are doing this work, then let us know.
One of the best things to come out of the plandemic was linking up with people around the world to make new alliances and often friendships.
Let’s see if waking more of the world up to the virus fraud might bring even more of us together.
Children’s Health Defense is funding a lawsuit by a D.C. mother alleging a doctor vaccinated two of her children for COVID-19 without her consent after falsely telling the teens the shots were required for school.
The mother of two children who were given COVID-19 vaccines without the mother’s consent is suing the doctor who administered the vaccines.
An attorney representing NaTonya McNeil last week filed a lawsuit in Superior Court for the District of Columbia against Janine A. Rethy, M.D., M.P.H.
According to the complaint, on Sept. 2, 2022, McNeil took her two older children, ages 15 and 17, to the KIDS Mobile Medical Clinic/Ronald McDonald Care Mobile clinic, operated by Georgetown Hospital, to complete their required annual physical exam for the 2022-2023 school year.
The lawsuit alleges Rethy, director of the mobile clinic, held the children in the examination room longer than necessary for a regular check-up and vaccinated them against COVID-19 over their objections and without consulting their mother
In order to attempt to obtain the children’s consent — which they are not legally able to provide without a parent or guardian — the doctor falsely informed the children the COVID-19 vaccine was mandatory for school attendance and told them they could not lawfully decline it if they wanted to attend school.
The suit, filed by D.C. Attorney Matthew Hardin, seeks damages for false imprisonment, battery and fraud.
Children’s Health Defense (CHD) is financing the lawsuit because, according to CHD President and General Counsel Mary Holland, “CHD couldn’t just sit still and not allow this wrong to go unpunished and not bring this to the public’s attention.”
In an exclusive conversation with The Defender, McNeil explained why she is suing the the doctor:
“I just feel like people shouldn’t be able to do whatever they want to do to other people and especially not to children. As a mother, I feel like, ‘You all just took all my rights away from me to do what you wanted to do to my kids.’
“I do want justice to be done in this case. I feel like something needs to be done. This can’t just continue to happen.”
‘I feel violated’
According to the complaint, Rethy’s stated goal is to vaccinate all children against COVID-19. The complaint quotes her statement to the press:
“Our goal is to increase vaccination rates in children here in D.C. . . . For more than 30 years our role has been to be in the community to help address the problem of health disparities, bringing families care where they are.
“For this particular effort, we are glad to be partnering with DC Health to provide both regular childhood vaccines and COVID-19 vaccines to all children.”
In addition to her role as director of the mobile clinic, Rethy is chief of MedStar Georgetown University Hospital’s Division of Community Pediatrics and assistant professor of pediatrics at Georgetown University School of Medicine.
McNeil said that when she took her older children to the clinic, she stayed outside the examination room to care for her infant. As soon as the children entered the doctor’s office, she called her daughter’s cellphone to let Rethy know she was just outside the door if the doctor needed to consult her for anything.
According to McNeil, the doctor did not ask or inform her about any vaccinations, and did not ask her to sign anything. At the end of the physical, Rethy came out to talk to her.
McNeil said the doctor explained her son’s asthma treatment plan, but that’s all they discussed.
As they were heading home, McNeil said she was shocked when her daughter complained that her arm hurt “pretty bad.” When McNeil asked her why it hurt, her daughter said she was given the COVID-19 shot, even though she told the doctor she didn’t want it.
When McNeil asked her why she allowed the doctor to administer the shot, her daughter said:
“When she had the needle in her hand and she was coming towards me, I backed up and I asked her what is that needle, and she said it was the COVID shot and I … told her I didn’t want it and she said, ‘Well it is mandatory, you have to get it in order to go to school.’”
Rethy allegedly administered the shot to her daughter, and then to her son. McNeil said:
“He’s 14 and he said they didn’t even ask him if he wanted it or not, but when they gave it to him, he said he thought he had to get it because his sister got it.”
According to the complaint, both children received the Pfizer/BioNTech vaccine, authorized for emergency use, and the meningococcal vaccine. Her son was also injected with TDaP.
Both children were upset and angry they had been coerced into vaccination, the complaint says.
No school mandate, despite what clinic and doctor alleged
When she got home, McNeil said she called the doctor’s office, and asked them why they vaccinated her children without her consent.
“I would have never consented to you all vaccinating my children,” she said. “I’m not vaccinated and I’m not getting vaccinated and my kids were never supposed to be vaccinated for COVID period, under no circumstances.”
She said the person on the phone said they were supposed to get them for school.
After hanging up, McNeil said she was “so irritated I even started crying” because she couldn’t believe “they put this poison” into her children’s bodies.
In July 2022, D.C. public schools imposed a vaccine mandate for schoolchildren ages 12 and up for the 2022-2023 school year. But on Aug. 26, just weeks after imposing the mandate, officials walked it back, postponing it until 2023.
That means when McNeil’s children saw the doctor, there was no school vaccine mandate in place, despite what the Rethy allegedly told the children.
The age of consent
The District of Columbia in March 2021 enacted the D.C. Minor Consent for Vaccination Amendment Act of 2020 (D.C. Minor Consent Act), allowing children 11 and older to consent to the administration of any vaccine — including COVID-19 shots — recommended by the Advisory Committee on Immunization Practices (ACIP) — without parental knowledge or consent if the medical provider believed “the minor is capable of meeting the informed consent standard.”
The law also required healthcare personnel to provide accurate immunization records to the Department of Health and to the student’s school, but not to parents with religious exemptions.
CHD and Parental Rights Foundation filed a lawsuit seeking a court order to declare the D.C. Act unconstitutional.
A judge for the U.S. District Court for the District of Columbia on March 18, 2022, granted a preliminary injunction prohibiting the D.C. mayor, Department of Health and public schools from enforcing the law.
That means at the time McNeil’s children visited the clinic, they could not legally provide consent to be vaccinated without their mother’s consent.
McNeil said:
“To do that to my little children, my innocent children. They took her rights. When she backed away from you [the doctor] and said she didn’t want it, that should have been the end of it.
“Or you [the doctor] should have called me on the phone to find out what I feel about the situation. But you [the doctor] basically told my child a lie so you [she] could do what you [she] wanted to do to my kid.”







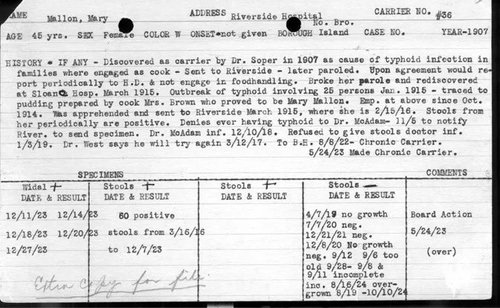


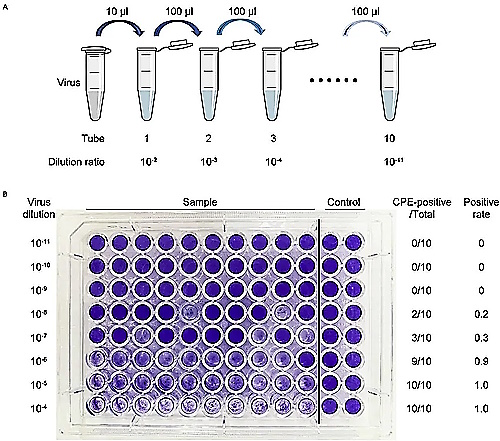

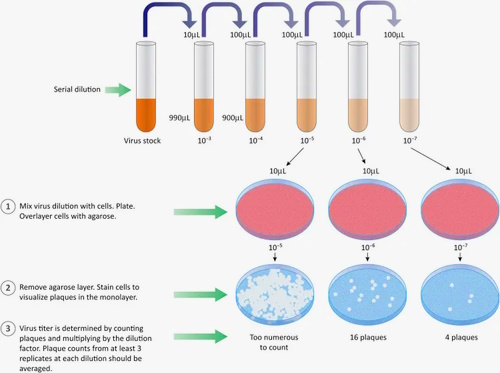
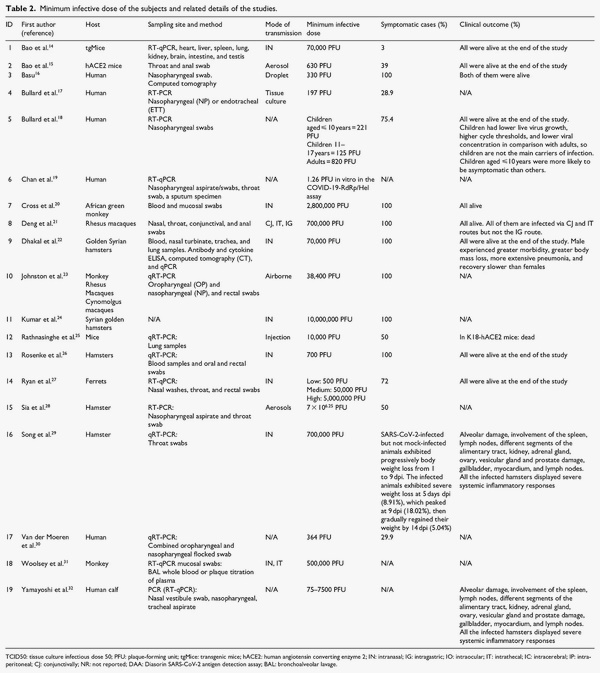
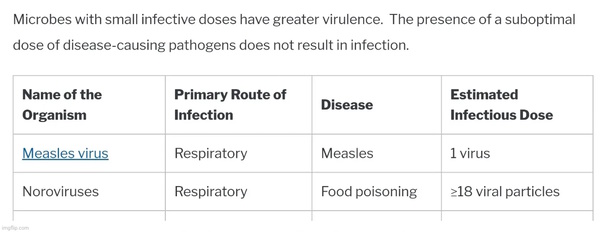
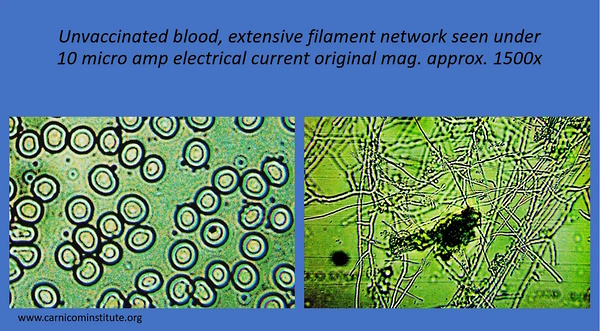
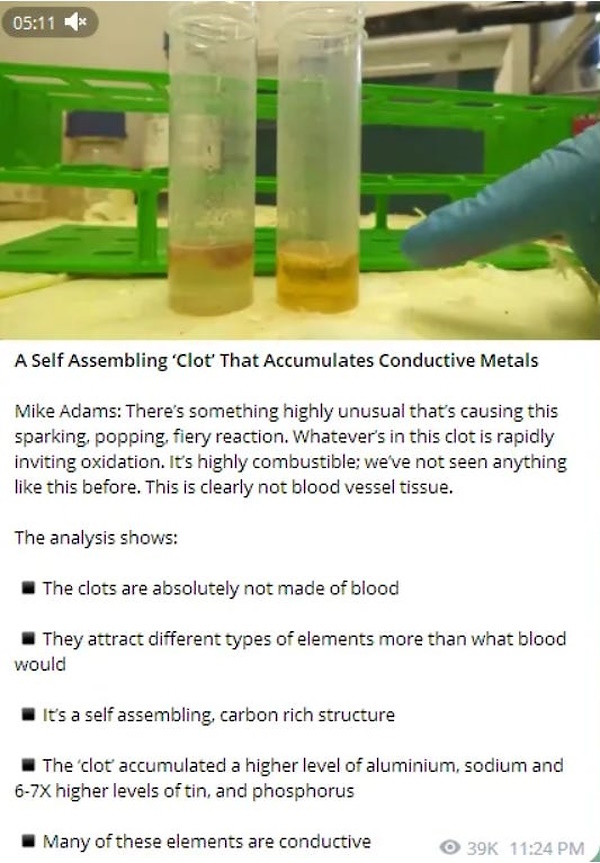
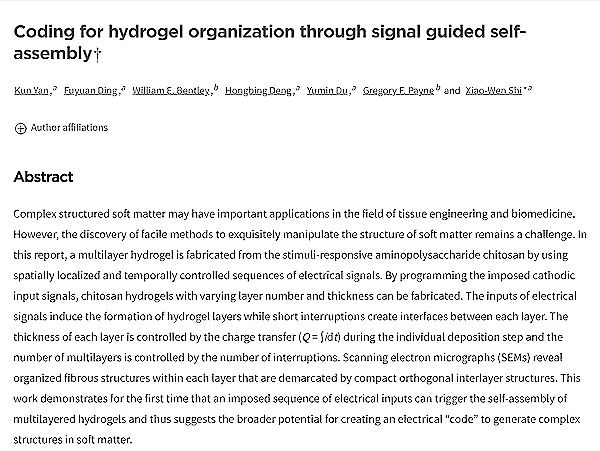
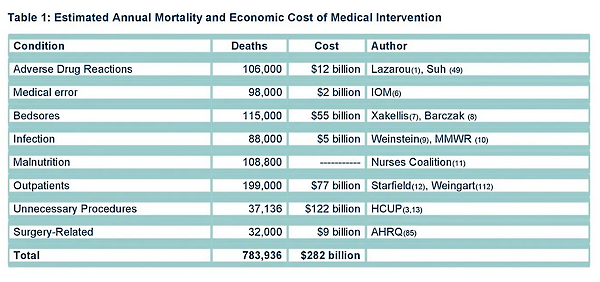
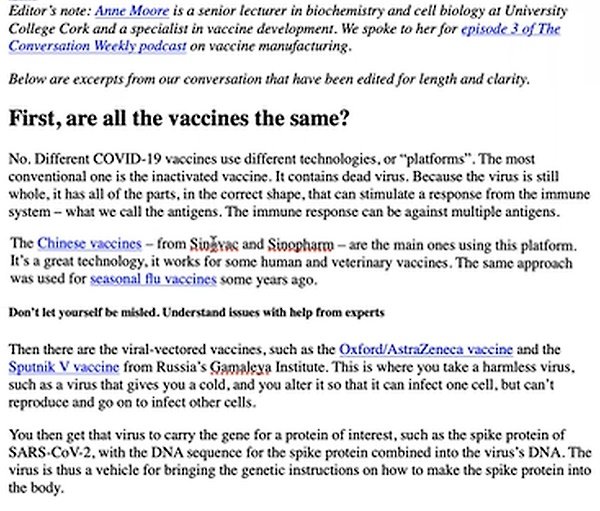


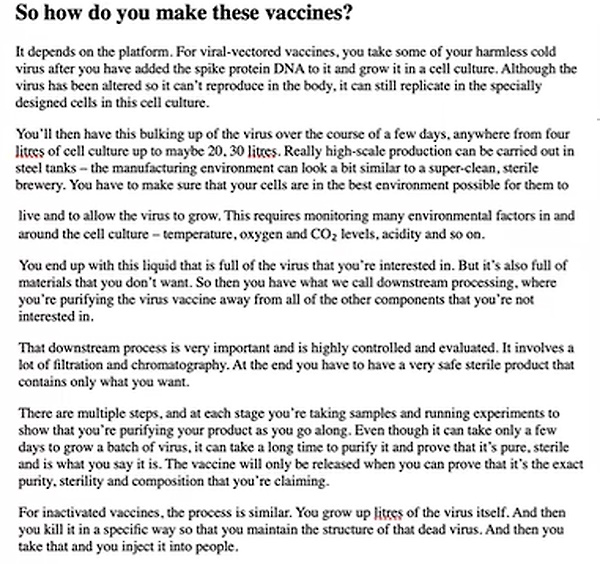


{kind=link}
{kind=link}
{kind=link}