Pfizer Bullies Nations to Put Up Collateral for Lawsuits
by Dr. Joseph Mercola, Mercola.com
March 8, 2021
STORY AT-A-GLANCE
- Pfizer is demanding countries put up sovereign assets, including bank reserves, military bases and embassy buildings, as collateral for expected vaccine injury lawsuits resulting from its COVID-19 inoculation
- Argentina and Brazil have rejected Pfizer’s demands. According to legal experts, Pfizer is abusing its power
- In the U.S., vaccine makers already enjoy full indemnity against injuries occurring from the COVID-19 vaccine under the PREP Act. If you’re injured, you’d have to file a compensation claim with the Countermeasures Injury Compensation Program (CICP), which is funded by U.S. taxpayers
- A significant problem with the CICP is that it’s administered within the Department of Health and Human Services, which is also sponsoring the COVID-19 vaccination program. This conflict of interest makes the CICP less likely to admit fault with the vaccine
- The maximum CICP payout you can receive — even in cases of permanent disability or death — is $250,000 per person, and you first have to exhaust your private insurance policy before the CICP kicks in
As reported by New Delhi-based World Is One News (WION),1 Pfizer is demanding countries put up sovereign assets as collateral for expected vaccine injury lawsuits resulting from its COVID-19 inoculation. In other words, it wants governments to guarantee the company will be compensated for any expenses resulting from injury lawsuits against it.
WION reports that Argentina and Brazil have rejected Pfizer’s demands. Initially, the company demanded indemnification legislation to be enacted, such as that which it enjoys in the U.S. Argentina proposed legislation that would restrict Pfizer’s financial responsibility for injuries to those resulting from negligence or malice.
Pfizer rejected the proposal. It also rejected a rewritten proposal that included a clearer definition of negligence. Pfizer then demanded the Argentinian government put up sovereign assets — including its bank reserves, military bases and embassy buildings — as collateral. Argentina refused. A similar situation occurred in Brazil. Pfizer demanded Brazil:
- “Waive sovereignty of its assets abroad in favor of Pfizer”
- Not apply its domestic laws to the company
- Not penalize Pfizer for vaccine delivery delays
- Exempt Pfizer from all civil liability for side effects
Brazil rejected Pfizer’s demands, calling them “abusive.” As noted by WION, Pfizer developed its vaccine with the help of government funding, and now it — a private company — is demanding governments hand over sovereign assets to ensure the company won’t lose a dime if its product injures people, even if those injuries are the result of negligent company practices, fraud or malice.
Aside from Argentina and Brazil, nine other South American countries have reportedly negotiated deals with Pfizer. It’s unclear whether they actually ended up giving up national assets in return.2
Vaccine Maker Accused of Abusing Its Power
According to STAT News,3 “Legal experts have raised concerns that Pfizer’s demands amount to an abuse of power.” Lawrence Gostin, law professor at Georgetown University and director of the World Health Organization’s Collaborating Center on National and Global Health Law told STAT:4
“Pharmaceutical companies shouldn’t be using their power to limit lifesaving vaccines in low- and middle-income countries. [This] seems to be exactly what they’re doing … Some liability protection is warranted, but certainly not for fraud, gross negligence, mismanagement, failure to follow good manufacturing practices. Companies have no right to ask for indemnity for these things.”
Mark Eccleston-Turner, a lecturer in global health law at Keele University in England, added:5
“[Pfizer] is trying to eke out as much profit and minimize its risk at every juncture with this vaccine development then this vaccine rollout. Now, the vaccine development has been heavily subsidized already. So there’s very minimal risk for the manufacturer involved there.”
Don’t Expect Compensation if Injured by COVID-19 Vaccine
In the U.S., vaccine makers already enjoy full indemnity against injuries occurring from this or any other pandemic vaccine under the PREP Act. If you’re injured, you’d have to file a compensation claim with the Countermeasures Injury Compensation Program (CICP),6 which is funded by U.S. taxpayers via Congressional appropriation to the Department of Health and Human Services (DHHS).
While similar to the National Vaccine Injury Compensation Program (NVICP), which applies to nonpandemic vaccines, the CICP is even less generous when it comes to compensation. For example, while the NVICP pays some of the costs associated with any given claim, the CICP does not. This means you’ll also be responsible for attorney fees and expert witness fees.
A significant problem with the CICP is that it’s administered within the DHHS, which is also sponsoring the COVID-19 vaccination program. This conflict of interest makes the CICP less than likely to find fault with the vaccine.
Your only route of appeal is within the DHHS, where your case would simply be reviewed by another employee. The DHHS is also responsible for making the payment, so the DHHS effectively acts as judge, jury and defendant. As reported by Dr. Meryl Nass,7 the maximum payout you can receive — even in cases of permanent disability or death — is $250,000 per person; however, you’d have to exhaust your private insurance policy before the CICP gives you a dime.
CICP will only pay the difference between what your insurance covers and the total payout amount established for your case. For permanent disability, even $250,000 won’t go far. The CICP also has a one year statute of limitations, so you have to act quickly.
This too is a significant problem, as no one really knows what injuries might arise from the COVID-19 vaccine, or when, and this makes tying the injury to the vaccination a difficult prospect. Employers that mandate the COVID-19 vaccine will also be indemnified from liability for side effects. Instead, claims will be routed through worker’s compensation programs.
If the COVID-19 vaccines are as safe as the manufacturers claim, why do they insist on so much indemnification? Do they suspect or know something they’re refusing to admit publicly?
Side Effects Are Inevitable
Of course, those of us who have been looking at the science behind the mRNA technology used to create these novel “vaccines” have long since realized there are tremendous risks involved. For starters, mRNA vaccines are most accurately referred to as gene therapies, as this is what they are.
They effectively turn your cells into bioreactors that churn out viral proteins to incite an immune response, and there’s no off-switch.8 Based on historical and preliminary evidence, significant short- and long-term side effects are, quite frankly, inevitable.
For starters, your body sees the synthetic mRNA as “non-self,” which can cause autoantibodies to attack your own tissues. Judy Mikovits, Ph.D., explained this in her interview, featured in “How COVID-19 ‘Vaccines’ May Destroy the Lives of Millions.”
Free mRNA also drive inflammatory diseases, which is why making synthetic mRNA thermostable — i.e., slowing the breakdown of the RNA by encasing it in lipid nanoparticles — is likely to be problematic. The nanoparticles themselves also pose a risk. COVID-19 vaccines use PEGylated lipid nanoparticles, which is known to cause allergic reactions and anaphylaxis.9,10
What’s more, previous attempts to develop an mRNA-based drug using lipid nanoparticles failed and had to be abandoned because when the dose was too low, the drug had no effect, and when dosed too high, the drug became too toxic.11 An obvious question is: What has changed that now makes this technology safe enough for mass use?
As detailed in my interview with Mikovits, the synthetic RNA influences the gene syncytin, which can result in:
- Brain inflammation
- Dysregulated communication between the microglia in your brain, which are critical for clearing toxins and pathogens
- Dysregulated immune system
- Dysregulated endocannabinoid system (which calms inflammation)
Pathogenic Priming and Antibody-Dependent Enhancement
Another significant problem is that we don’t know whether antibody production is protective or pathogenic in coronavirus infections. If pathogenic, vaccinated individuals may be at increased risk of severe illness if they’re exposed to SARS-CoV-2 in the future. As reported in a December 11, 2020, Vaccine: X paper:12
“The first SARS-CoV-2 vaccine(s) will likely be licensed based on neutralizing antibodies in Phase 2 trials, but there are significant concerns about using antibody response in coronavirus infections as a sole metric of protective immunity.
Antibody response is often a poor marker of prior coronavirus infection, particularly in mild infections, and is shorter-lived than virus-reactive T-cells … Strong antibody response correlates with more severe clinical disease while T-cell response is correlated with less severe disease; and antibody-dependent enhancement of pathology and clinical severity has been described.
Indeed, it is unclear whether antibody production is protective or pathogenic in coronavirus infections. Early data with SARS-CoV-2 support these findings. Data from coronavirus infections in animals and humans emphasize the generation of a high-quality T cell response in protective immunity.”
A number of reports in the medical literature have indeed highlighted the risk of pathogenic priming and antibody-dependent enhancement (ADE). As explained in “Out of the Frying Pan and Into the Fire? Due Diligence Warranted for ADE in COVID-19”:13
“ADE is an immunological phenomenon whereby a previous immune response to a virus can render an individual more susceptible to a subsequent analogous infection.
Rather than viral recognition and clearance, the prior development of virus-specific antibodies at a non-neutralizing level can facilitate viral uptake, enhancing replication; a possible immune evasion strategy avoiding intracellular innate immune sensors, or pattern recognition receptors …
ADE of SARS-CoV has also been described14 through a novel FcγRII-dependent and ACE2-independent cell entry mechanism. The authors state15 that this warrants concern in the safety evaluation of any candidate human vaccines against SARS-CoV.”
Similarly, “Pathogenic Priming Likely Contributes to Serious and Critical Illness and Mortality in COVID-19 Via Autoimmunity,” published in the Journal of Translational Autoimmunity, warns that:16
“Failure of SARS and MERS vaccines in animal trials involved pathogenesis consistent with an immunological priming that could involve autoimmunity in lung tissues due to previous exposure to the SARS and MERS spike protein. Exposure pathogenesis to SARS-CoV-2 in COVID-19 likely will lead to similar outcomes.”
So, to be clear, what all of this means is that if you get vaccinated, you may actually be at increased risk for serious illness if/when you’re exposed to any number of mutated SARS-CoV-2 strains in the future.
This is why the recommendation to vaccinate individuals who have previously been infected with SARS-CoV-2, or who have an active SARS-CoV-2 infection, may actually be quite dangerous. Dr. Hooman Noorchashm recently sent a public letter17 to the U.S. Food and Drug Administration Commissioner detailing these risks.
How mRNA Injections May Trigger Prion Disease
What’s more, in a paper18 titled, “COVID-19 RNA Based Vaccines and the Risk of Prion Disease,” published in Microbiology & Infectious Diseases, Dr. Bart Classen warns there are also troubling evidences suggesting some of the mRNA shots may cause prion diseases such as Alzheimer’s and ALS. He writes:
“In the current paper, the concern is raised that the RNA based COVID vaccines have the potential to cause more disease than the epidemic of COVID-19. This paper focuses on a novel potential adverse event mechanism causing prion disease which could be even more common and debilitating than the viral infection the vaccine is designed to prevent …
Analysis of the Pfizer vaccine against COVID-19 identified two potential risk factors for inducing prion disease is humans. The RNA sequence in the vaccine contains sequences believed to induce TDP-43 and FUS to aggregate in their prion based conformation leading to the development of common neurodegerative diseases.
In particular it has been shown that RNA sequences GGUA, UG rich sequences, UG tandem repeats, and G Quadruplex sequences, have increased affinity to bind TDP-43 and or FUS and may cause TDP-43 or FUS to take their pathologic configurations in the cytoplasm.
In the current analysis a total of sixteen UG tandem repeats were identified and additional UG rich sequences were identified. Two GGΨA sequences were found. G Quadruplex sequences are possibly present but sophisticated computer programs are needed to verify these.
The spike protein encoded by the vaccine binds angiotensin converting enzyme 2 (ACE2), an enzyme which contains zinc molecules. The binding of spike protein to ACE2 has the potential to release the zinc molecule, an ion that causes TDP-43 to assume its pathologic prion transformation.”
mRNA Technology Has Potential to Cause Microvascular Injury
Additionally, Dr. J. Patrick Whelan, a pediatric rheumatologist specializing in multisystem inflammatory syndrome, submitted a public comment19 to the FDA back in December 2020, in which he expressed concern that mRNA vaccines have “the potential to cause microvascular injury to the brain, heart, liver and kidneys in ways that were not assessed in safety trials.”
He cited research showing that “the spike protein in brain endothelial cells is associated with formation of microthrombi (clots),” and that since no viral RNA has been found in brain endothelium, “viral proteins appear to cause tissue damage without actively replicating virus.”
“Is it possible the spike protein itself causes the tissue damage associated with Covid-19?” he asks. “In 13/13 brains from patients with fatal COVID-19, pseudovirions (spike, envelope, and membrane proteins) without viral RNA are present in the endothelia of cerebral microvessels …
It appears that the viral spike protein that is the target of the major SARS-CoV-2 vaccines is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung, and kidney.
Before any of these vaccines are approved for widespread use in humans, it is important to assess in vaccinated subjects the effects of vaccination on the heart … Vaccinated patients could also be tested for distant tissue damage in deltoid area skin biopsies …”
Reports of Side Effects Are Rapidly Mounting
Around the world, reports are now pouring in of people dying shortly after receiving the COVID-19 vaccine. In many cases, they die suddenly within hours of getting the shot. In others, death occurs within the span of a couple of weeks.
In the wake of 29 senior citizen deaths,20 Norway is reportedly considering excluding the very old and terminally ill from getting the AstraZeneca vaccine. According to the Norwegian Medicines Agency:21
“Most people have experienced the expected side effects of the vaccine, such as nausea and vomiting, fever, local reactions at the injection site, and worsening of their underlying condition.”
The Norwegian Institute of Public Health further noted that “for those with the most severe frailty, even relatively mild vaccine side effects can have serious consequences,” and that “For those who have a very short remaining life span anyway, the benefit of the vaccine may be marginal or irrelevant.”22
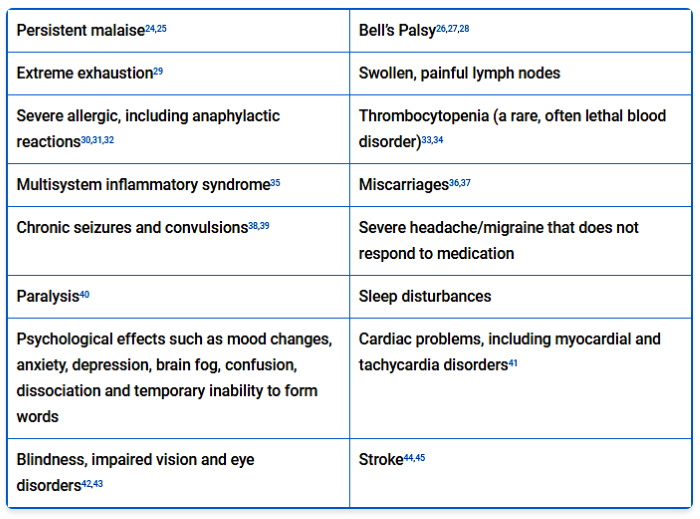
In Sweden, hospitals in Sörmland and Gävleborg suspended the AstraZeneca vaccine in mid-February 2021 after a full quarter of the vaccinated hospital staff reported side effects. To prevent staff shortages and conduct an investigation, the vaccination push was temporarily paused.23 Examples of side effects reported after vaccination with Pfizer’s, Moderna’s and AstraZeneca’s vaccines from around the world include:
In the U.K., there were 49,472 reported side effects to the Pfizer vaccine and 21,032 reactions to the AstraZeneca vaccine as of January 24, 2021. As reported by Principia Scientific International,46 “For both vaccines this equates to 1 in every 333 people suffering an adverse reaction. This rate could actually be higher as some cases may have not been reported …”
Greatest Risk of All: Sudden Death
Perhaps most concerning of all are rapidly mounting reports of sudden death,47,48,49,50,51,52 mostly in the elderly but also in much younger, healthy individuals. In the U.S., COVID-19 vaccines accounted for 70% of vaccine-related deaths between January 2020 and January 2021.
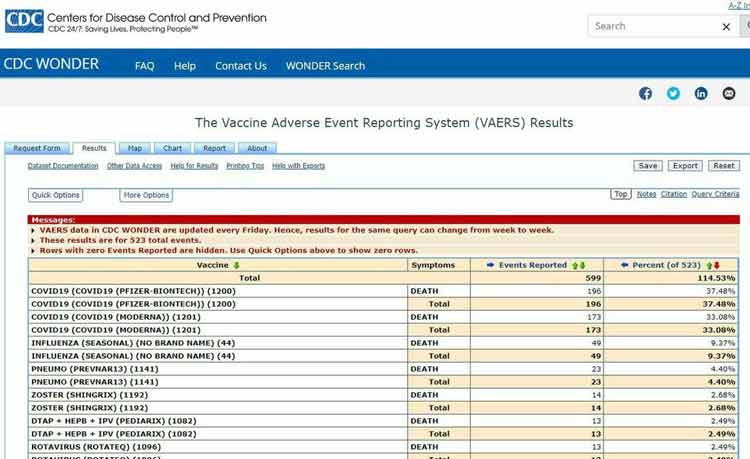
As of February 12, 2021, the number of side effects reported to VAERS totaled 15,923, including 929 deaths.53 Of the 799 deaths reported within the U.S., one-third occurred within 48 hours of vaccination and 21% of them were cardiac-related.
Pfizer’s vaccine was the most dangerous in terms of death, being responsible for 58% of deaths while Moderna’s vaccine accounted for 41% of deaths. Pfizer’s vaccine was also responsible for 75% of Bell’s Palsy cases, compared to Moderna’s at 25%.54
Curiously, based on the data submitted to the FDA, Moderna’s vaccine has a death rate 5.41 times higher than Pfizer’s, yet both are dramatically lower than the national average. As noted by The Defender, the dramatic discrepancy in death rates “deserves notice and requires explanation,” adding:55
“If Moderna’s on-vaccine death rate is so far below the national death rate and also simultaneously more than five times greater than Pfizer’s on-vaccine death rate, then Pfizer’s study sample appears even less representative of the entire population …
Moderna’s screening process and exclusion criteria in the trial led to evidence that the general population is dying at a rate 6.3 times greater than the death rate in the Moderna trial — which means the Moderna study, including its estimated efficacy rate and the vaccine’s alleged safety profile — cannot possibly be relevant to most of the U.S. population.
The super-healthy cohorts studied by Moderna are in no way representative of the U.S. population. Most deaths from COVID-19 involve pre-existing health conditions of the types excluded from both Pfizer and Moderna trials …
Those enrolling in the post-market surveillance studies deserve to know the abject absence of any relevant information on efficacy and risk for them. In their zeal to help humanity, or to help themselves, these people may very well be walking into a situation that will cause autoimmunity due to pathogenic priming, potentially leading to disease enhancement should they become infected following vaccination.”
Do a Risk-Benefit Analysis Before Making Up Your Mind
To avoid becoming a sad statistic, I urge you to review the science very carefully before making up your mind about this experimental gene therapy. Also remember that the lethality of COVID-19 is actually surprisingly low. It’s lower than the flu for those under the age of 60.56
If you’re under the age of 40, your risk of dying from COVID-19 is just 0.01%, meaning you have a 99.99% chance of surviving the infection. And you could improve that to 99.999% if you’re metabolically flexible, insulin sensitive, and vitamin D replete.
So, really, what are we protecting against with a COVID-19 vaccine? These mRNA vaccines aren’t even designed to prevent infection, only to reduce the severity of symptoms. Meanwhile, they could potentially make you sicker once you’re exposed to the virus, and/or cause persistent serious side effects such as those reviewed above.
While I won’t tell anyone what to do, I would urge you to take the time to review the science and weigh the potential risks and benefits based on your individual situation before you make a decision that you may regret for the rest of your life, which can actually be shortened with this vaccine. Undoubtedly, Pfizer and other vaccine makers suspect this as well, which is why Pfizer is bullying nations into covering for any and all of its mistakes.
The National Vaccine Information Center (NVIC) recently posted more than 50 video presentations from the pay-for-view Fifth International Public Conference on Vaccination held online October 16 to 18, 2020, and made them available to everyone for free.
The conference’s theme was “Protecting Health and Autonomy in the 21st Century” and it featured physicians, scientists and other health professionals, human rights activists, faith community leaders, constitutional and civil rights attorneys, authors and parents of vaccine injured children talking about vaccine science, policy, law and ethics and infectious diseases, including coronavirus and COVID-19 vaccines.
In December 2020, a U.K. company published false and misleading information about NVIC and its conference, which prompted NVIC to open up the whole conference for free viewing. The conference has everything you need to educate yourself and protect your personal freedoms and liberties with respect to your health.
Don’t miss out on this incredible opportunity. I was a speaker at this empowering conference and urge you to watch these video presentations before they’re censored and taken away by the technocratic elite.
Link to Protecting Health and Autonomy in the 21st Century videos.
Connect with and support the work of Dr. Joseph Mercola


Truth Comes to Light highlights writers and video creators who ask the difficult questions while sharing their unique insights and visions.
Everything posted on this site is done in the spirit of conversation. Please do your own research and trust yourself when reading and giving consideration to anything that appears here or anywhere else.







