The Great Covid Virus Debate
Drs. Andrew Kaufman and Thomas Cowan respond to their critics
by Dr. Andrew Kaufman, Weston A. Price Foundation
April 17, 2022
During crises, people ask questions, and the Covid crisis is no exception. People are asking, “Is there any real or new illness called Covid-19—apart from vaccinations and the treatments themselves?” We are not alone in proposing that we must take a cold look at the viral theory touted as the cause of this alleged disease.
Journalist Jeremy Hammond has been the most outspoken critic of our contention that the SARS-CoV-2 “virus” does not exist and therefore does not cause Covid. In a video posted in March 2021,1 he outlines the following arguments for the existence of the “virus.” We answer his arguments, point by point.
Definition of Isolation
Hammond states that people in our camp have changed the definition of isolation, but we use the actual definition of the word “isolation” in the English language. It’s the virologists who have changed the meaning of the word from “separated from other things” to meaning “combined with other things in a foreign cell culture.”
Isolation Technology
Hammond claims that scientists do not yet have the technology to purify viral particles. Actually, scientists have been able to purify particles equivalent in size to so-called viruses for decades. The traditional method, in use since at least the 1940s, involves what is called density gradient ultracentrifugation. It uses different densities of a sucrose solution spun into layers at high speeds with an ultracentrifuge, so that the densest layer ends up on the bottom. The sample will separate into bands based on different densities, and one of those bands could contain the so-called viral particles if they existed.
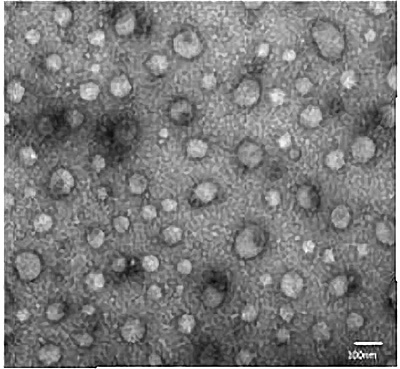
For example, a 2015 article published in Methods in Molecular Biology,2 provides electron microscopy photographs of purified exosomes (see Figure 1). Exosomes are roughly the same size as that of claimed viral particles, around fifty to one hundred nanometers, and they have the same morphology and characteristics of alleged virus particles.
If you can purify exosomes, you can purify viruses using the same techniques. Scientists take exosomes directly from a body fluid; they don’t take the exosomes and put them in a cell culture. One of the challenges the authors discuss is the fact that the exosomes are present in low numbers; also, there are many different types of extracellular particles in the bodily fluid from which to separate the exosomes. These are some of the problems that have been put forth as a reason why it’s difficult to purify virus particles, but the researchers have overcome these problems with exosomes.
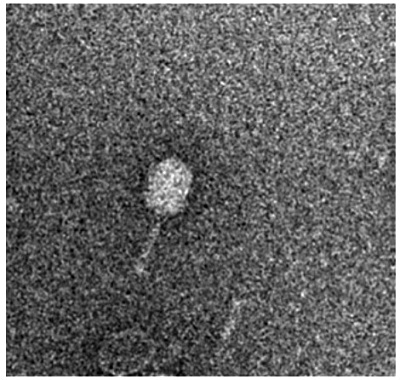
Bacteriophages, known as “the viruses of bacteria,” can also be purified, as shown in a 2018 article (again published in Methods in Molecular Biology)33 (see Figure 1). Bacteriophages are particles of similar size to viruses, and they also can be purified by chromatography and other methods. Mr. Hammond alleges that you can’t get a pure sample—a sample where you see only one thing in a vacuum. However, as you can see in the photos of exosomes and bacteriophages, all the objects are the same—they are the only thing in the microscope field because these have been isolated and purified, and there is nothing else in the sample, just exosomes or bacteriophages.
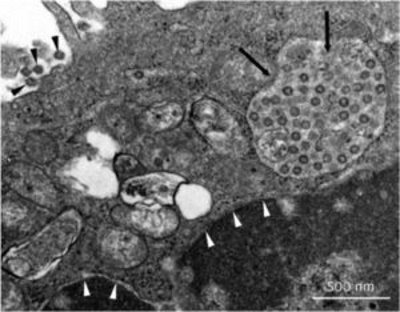
FIGURE 1. Isolated exosomes, isolated bacteriophages and “isolated” viruses
Cell Culture is the Gold Standard
Hammond admits that you need a cell culture to “isolate” a virus, because the virus needs cells in which to replicate in order to have enough virus to detect. According to the viral theory, the virus causes an infection in the lung, for example, when it invades the lung cells and then reproduces in the lung tissue, right in those cells, and then produces more viral particles. So, all we would need to do is go right to that tissue culture in the sick person, not one that we create in a laboratory with other conditions that are not natural.
In other words, why would we do this kind of indirect experiment when we have a cell culture right in the host—namely, virus-invaded lung tissue—from which we could extract the virus? Why can’t we do a proper isolation, where you go to the host, the natural source of the virus, which is a sick person with an infection, and purify the viral particles right out of that person’s bodily tissues or fluids?
Cytopathic Effects
Virologists claim that the pathogenic nature of viruses is evident in light microscope images of tissue cultures showing cytopathic effects (meaning cell breakdown). But what the images of “viruses” from an electron microscope show is a mixture of cellular material from the cell culture and a variety of different types of particles (see Figure 1, third image). How can we know what any of those particles actually are? And how do we know the particle didn’t come from the foreign cell culture, such as the kidney cells it was cultured in? How do we know it’s not an exosome, a particle produced inside the cell? How do we know it’s not an apoptotic body (from cellular breakdown)? How do we know it’s not another type of extracellular vesicle? How do we know it’s a virus (since it doesn’t have a label and has not been isolated and purified)? While virologists can show images of small particles, they have no way of identifying the nature or identity of any of those particles.
Genetic Sequencing
Hammond claims that scientists can do genetic sequencing of the particles found in tissue cultures. There are actually two ways of doing genetic sequencing. One way is to extract genetic material from only one organism, and then sequence the genome in its entirety. That’s how you can discover the genome sequence of a new organism.
But for viruses, scientists use a different technique, variously termed “genomic” sequencing, “next generation” sequencing or “in silico” sequencing (meaning carried out in a computer). Whatever they call it, this kind of sequencing is just piecemeal.
Hammond describes the method accurately, in that they start with lots of pieces of genetic material, and then a computer does sophisticated calculations and simulations to put them together. The problem—which Hammond does not describe—is that the starting material for these experiments is not a pure organism; it’s not just a virus. What they’re starting with is, in most cases, the lung fluid from a patient diagnosed with Covid by a PCR test. (And we know the PCR test is invalid. See sidebar page 20.)
The fluid they start with has genetic material from many different organisms—from a variety of bacteria species, probably some fungal and yeast species, as well as all of the human genetic material from the host and then anything that happened to be in the air that this person inhaled for the few breaths before they took the sample. In other words, there are many sources of genetic material. When they put those little bits of genetic material into the computer, the computer doesn’t know which organism they’re from—since they are not starting with a pure virus, there’s no way to tell.
When the computer runs the simulation and tries to fit these little strands of sequences together by overlapping ends, they don’t know whether the computer is making a real sequence of an organism, or if it’s putting little bits from different organisms together into some kind of mishmash or chimera. They have no way to check it against a reference standard, because there’s never been any true sequence of these viruses. What we end up with is just a simulation.
To give an idea of the problem, in the first sequence that they did this way with SARS-CoV-2, they actually had over fifty-six million little pieces or sequences, and they had not one but two different software programs independently take those pieces and try to construct them into a longer strand that they said was the size of a typical coronavirus genome. With one of the software programs, they just threw out the data because it didn’t give them what they wanted. So, they’re picking and choosing at each stage: “We think this is good. . . we want to use this.”
The other software program came up with over a million different possible sequences, but they just picked one. And there was no rhyme or reason to how they picked it. It was just an arbitrary selection. With all of the uncertainty about the origin of each individual piece of DNA, they just randomly select one of millions of possible combinations spit out by a computer. How could anyone believe these results represent the real genome of an actual organism? It would be impossible.
Lack of Proper Controls
Hammond states that virologists do a control experiment when they do the tissue cultures. That statement is not quite accurate. In a proper control, you have only one variable different, and as far as we know, virologists have never actually done this. The proper way to do it would be to take lung fluid from someone who is sick, but does not have Covid—sick with influenza or pneumonia, for example—or even lung fluid from someone who is healthy. Then, they would continue the experiment using the exact same methods, the same cell cultures, the same concentrations of antibiotics, the exact same nutrients, and any other additives or environmental conditions such as the same temperature, the same amount of agitation, the same protocols all around—that would be a proper control. No one is doing this type of proper control for virus identification.
Some of the papers about SARS-CoV-2 have mentioned what’s called a “mock infected culture,” but this is not the same as a control. In fact, we don’t know exactly what they do with these mock infected cultures. They’re not reported on in every paper, but in a couple they are. And curiously, they don’t describe these mock infected cultures at all. If you go to the methods sections, you don’t see any explanation of what a mock infected culture is. And they don’t mention the word “control.”
If they’re doing a true control experiment, why wouldn’t they call it a control culture? They have to use different words because they’re not really doing a proper control, but they’re trying to pass it off as one, which is why they change the words. We have read hundreds and hundreds of scientific papers on other subjects, and they always refer to the control group; they don’t say the “mock treatment group.” So, the mock infected culture is some kind of trick. We even tried to communicate with a couple of the corresponding authors on these publications. We asked an open-ended question: “Can you tell us the procedure for the mock infected cells listed in this figure?” In most cases, they didn’t reply at all.
In one case, we were unable to get a clear answer. The reply we received was, “They’re treated the same.” But what does that mean? “Can you tell us the exact conditions?” We even put our queries into a yes or no question like, “Did you use the same antibiotics at the same concentration? Did you use the same nutrition at the same concentration?” But we could not get a clear response, which suggests that they are probably hiding something.
We do have two examples of studies that included a control sample. The first comes from a 1954 article published in Proceedings of the Society for Experimental Biology and Medicine by Enders and Peebles.4 This was the first published paper to use the cell culture technique, which later became known as “virus isolation.”
In this study on measles, the authors put the patient specimen in a foreign culture of monkey kidney cells and then they got cytopathic effects—meaning they were able to show some damage to the cell culture.
An interesting quote in this paper describes the results of the control experiment. “Monkey kidney cultures may therefore be applied for the study of these agents [referring to measles] in the same manner as cultures of human kidney. In doing so, however, it must be borne in mind that cytopathic effects which superficially resemble those resulting from infection by the measles agents may possibly be induced by other viral agents present in a monkey kidney tissue or by unknown factors.”
In other words, they saw a cytopathic effect in the cell culture that was alleged to be a result of damage from the measles virus itself—but it might not necessarily have come from the measles virus; it could have been caused by something in the kidney cells themselves, which they call viruses, or from unknown factors.
Continuing, the two authors said, “A second agent was obtained from an uninoculated culture of monkey kidney cells.” Now, that means they did not put any sample from a measles patient in the culture; they ran the cell culture without a source of virus—just the cell culture with no patient sample in it. According to the authors, “The cytopathic changes induced in the unstained preparations could not be distinguished with confidence from the viruses isolated from measles [emphasis added].” In other words, the sample with nothing added to it produced the same results as the sample containing fluid from the measles patient.
Since the control was positive, that means that the experimental procedure itself, and not the measles virus, caused the cytopathic changes.
An important recent control experiment was carried out by Dr. Stefan Lanka, who is the only virologist we are aware of who has recognized the truth about the nonexistence of a virus—and who left the field. What he did was carry out just the control experiment. There is no possible source of virus anywhere in this experiment. As you can see in Figure 2, the top row of panels is Day One and the second row is Day Five of the experiment.
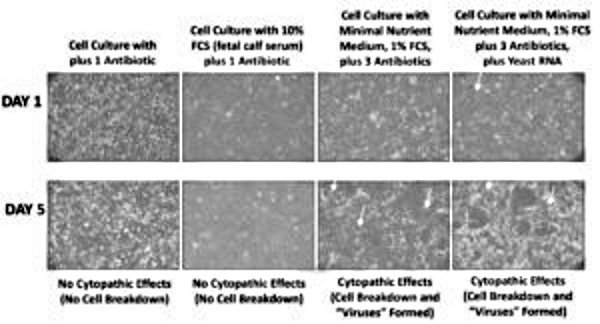
The third column simulates what they do in virus cell culture isolation experiments, using reduced nutrition while increasing the antibiotic to three times the normal concentration. (The protocols use either two times or three times the normal concentration.) You can see that on Day Five, there were cytopathic effects—the cells developed vacuoles and started to break down. Normally, virologists would give this as proof of the existence of a virus, except that there’s no virus in this experiment.
In the fourth column, Lanka added yeast RNA, which doesn’t contain any viruses—it’s a pure yeast RNA specimen bought from a laboratory supply company with good quality control. You can see even more cytopathic effects on Day Five in that culture.
So, both these control experiments show that the experimental procedure itself produces the cytopathic effects. If you took the culture materials from the two dishes with cytopathic effects and looked at them under an electron microscope, you would see particles in there that you could call a virus.
Coronavirus Fringe Pattern
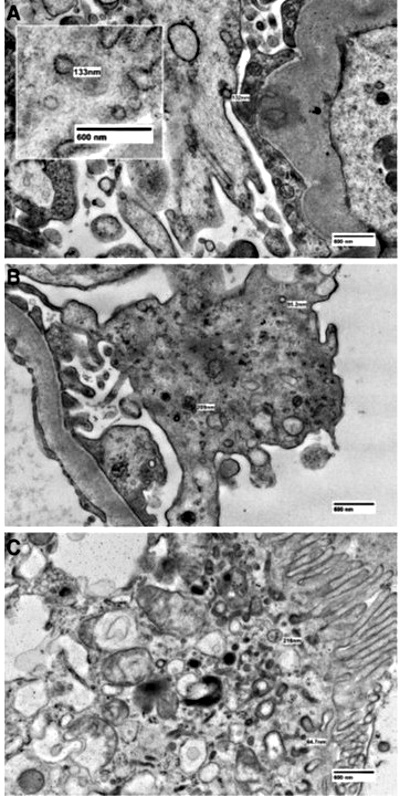
According to Hammond, virologists can see the characteristic coronavirus spikes on the particles they are calling viruses. Let’s review a couple of studies to see what is going on. The first was published in 2020 in Kidney360.5 In this study, researchers were looking at biopsies of people with kidney disease, mostly from before the Covid era. In the electron microscope photographs, they saw particles with the characteristic coronavirus spikes (see Figure 3). The researchers said that these were indistinguishable from coronavirus particles, which was a source of confusion for virologists. The authors pointed this out, and they even referenced a previous paper from the CDC that found the same thing.
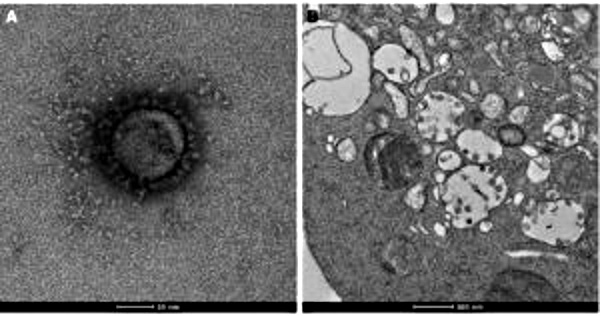
The second example comes from a “virus isolation” paper published in the Medical Journal of Australia in 2020.6 A very interesting quote occurs in this paper: “Electron micrographs. . . showed cytoplasmic membrane-bound vesicles containing coronavirus particles. Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin into the cell culture medium immediately improved virion morphology.” In other words, they didn’t see any spikes so they added the digestive enzyme trypsin, which breaks or cleaves proteins at a certain sequence, and then looked at it again under the microscope—and then saw the spikes! (See Figure 4.)
Genome Sequencing
As Hammond and other adherents of viral theory have often stated, genome sequencing has been repeated thousands of times, and the results are published in international databases, so they can’t be a hoax. Actually, the in silico genome-sequencing procedure that we have described has been repeated over two million times—far more than Hammond claims. And of course, each time they get different results, because they can’t repeat results in an invalid experiment, so the different results are all published.
As described earlier, the way they do this is to take a bunch of pieces of unknown origin, which they run through different software simulations, and then pick out the one they like. And then they do some further magic on it by just popping things in or taking things out somewhat arbitrarily to make it look more like what they think a coronavirus genome should look like. Then they claim that this sequence is a “reference sequence” and against all of those couple of million experiments that they have repeated, they can template a reference genome. So, of course, the computer is able to put things together in such a way that it matches the so-called reference sequence somewhat closely, because the sequences that make this up are probably mostly just human sequences of non-coding RNA. (A recent analysis shows this and will soon be published.) Thus, you should be able to have similar enough sequences that you can put something together that’s close, but not exactly identical—which they then call “variants.”
Now Hammond claims that if the procedures were fraudulent, then tens of thousands of scientists all over the world would be participating together in a conspiracy; but that’s not the case at all because almost none of these scientists realizes that what they’re doing is not good science—they never question it. Doctors rarely question the things they’re taught; they just learn them and accept them as true. That’s why I (Andrew Kaufman) was recommending vaccines and using antibiotics earlier in my career, because I also just accepted those things and did them without question. Now I realize that they’re quite lethal, so I don’t do them anymore. There was a kind of individual process that I went through for that.
But the scientists involved in “virus isolation” don’t realize that they’re doing fraudulent science because they’ve never looked at it carefully. And one of the ways that science allows this kind of thing to happen is by a high degree of compartmentalization, where they don’t collaborate or talk with other people in different fields. They don’t learn how other scientists do their experiments and also how they do control experiments. And they don’t seem to talk to exosome scientists, often because they would then see that exosome scientists are able to extract and purify exosomes right from the source. And then they would try to do that and fail, because there aren’t any viruses, and then they would have to have a different conclusion and change their opinion.
But the truth is, it doesn’t matter whether all of the thousands of scientists doing “virus isolation” are in a conspiracy, and it doesn’t matter whether they’re completely ignorant, because the only thing that’s important is to look at the actual science itself—the experiments—and ask the question, can you learn something from this? Can you conclude anything from this experiment? And if the answer is no, it doesn’t matter how many people think you’re wrong, it only matters that the answer is no. It shouldn’t be terribly surprising that the virologists have gotten this wrong, because in medicine this happens frequently. Take the example of beta blockers and heart failure. For many decades, it was an absolute contraindication to prescribe a beta blocker to someone with heart failure, because beta blockers make your heart beat less strongly and less rapidly. So, that was seen to make your heart weaker. But then research showed that actually, adding a beta blocker slows the progression of heart failure and allows people to live longer. It took some time for that scientific finding to be integrated into medicine, but there was no truth to the notion that doctors everywhere were in a conspiracy to hasten the death of heart failure patients. They were just ignorant to the truth of the scientific relationship between that drug in that condition. We could interpret “virus isolation” as a similar phenomenon; virologists who are doing these experiments are not able to actually show the results or provide the conclusive evidence because they are just ignorant of that fact, because they haven’t looked at it. It’s quite as simple as that.
Response to Mercola
Entering the virus debate on January 17, 2022, Dr. Joseph Mercola published a “fact-checked” article entitled, “Yes, SARS-CoV-2 is a Real Virus,”1 in which he insisted that SARS-CoV-2 has been isolated, photographed, genetically sequenced, and exists as a pathogenic entity.
Mercola cites studies from Italy, Germany, India, Columbia, Canada, Australia, Korea and the U.S., which claim to have isolated SARS-CoV-2 and characterized it by genome sequencing. However, none of these studies isolated any virus from the fluids of the patient; all of these studies used culturing techniques that can lead to tissue breakdown and the creation of exosomes (identical in form to “viruses”); none of these studies had a meaningful control; and all used questionable computer techniques to generate a genome in silico. Remember that these tissue cultures would also contain genetic material from the kidney cells of the culture and the bovine serum used as a nutrient medium. Even if the tissue cultures did contain viral particles, how can anyone know that the DNA the computer is analyzing comes from the virus?
As Mercola states, “Another sticking point for some is whether or not SARS-CoV-2 has ever been isolated from a human subject without passing it through animal cells, as such media could be contaminated and therefore the source of the virus.”
Indeed, this is the “sticking point!” All of the studies that Mercola cites as proof passed the sample through animal cells—cultures contaminated with fetal bovine serum and toxic antibiotics, and starved with a minimal nutrient medium.
Furthermore, no paper has proven that an isolated or pure virus obtained from a cell culture has ever made an animal or human sick in any way. Therefore, it is illogical, irrational and anti-scientific to claim that the “virus” is a pathogen.
According to Mercola, “At least part of the confusion appears to be rooted in how the term ‘isolated’ is defined. Some insist a virus is not isolated unless it’s also purified, while others say a virus doesn’t have to be purified in order to be ‘isolated.’” Actually, as we have pointed out, the confusion—deliberate confusion—results from virologists using the word “isolated” to mean “not isolated,” and insisting that “purified” and “isolated” do not mean the same thing.
More Genome Sequencing
One study Mercola highlights is a “genome sequencing” study published in January 2021 in Gut Pathology.7 In this study, the genetic material (RNA) was extracted directly from stool samples of a patient identified as having Covid-19 using the meaningless PCR test.
This paper relies on an in silico genome-sequencing procedure whereby they extract all of the RNA that is present in a body fluid or tissue sample, which would include a number of different sources of genetic material, including the person’s own. The material would include non-coding DNA that has been transcribed, spliced and recombined to make all sorts of novel sequences.
They then throw out the long fragments and just look at the short ones. This is a really important point, because the longer the sequence, the more you can be sure that it came from one source; whereas if you have short sequences, when they put them together in a longer sequence, parts of it could have come from different sources. It’s more reliable to have longer sequences, but then they can’t do the sequencing as fast. So, they put all those short sequences into the computer and let various computer software programs put them together, mapping them to the “reference” standard genome—which has been done in the same way—and then give you a result. The result is a little bit different each time, which is why they have over two million “variants.”
In this 2021 paper, they used fecal material, which they said contained the same genetic material as that extracted from the nose using a nasal swab. And interestingly, in this case, they did use a control group, which is very unusual—they actually used a purchased heat-inactivated SARS-CoV-2 toxic cell culture that served as a negative control.
The other unusual procedure was that they used shorter strands of RNA than normal. Usually, they look at strands of up to one hundred fifty base pairs, but in this study, they limited the length to seventy-six base pairs. This would result in even more error in terms of the source of each particular little strand.
They also skipped an important step, which they call making “contigs” (from the word contiguous). Usually, what they do is take all those little sequences of short strands—there are often over fifty million of them—and put them into software number-crunching programs that try to pair up overlapping sequences on the ends to make longer and longer strands—this is what they call “contig.” Then they pick one of the longest strands and use that as the base genome.
In this case, they didn’t do that. They just took the sequence strands and templated them right away against the reference standard from the database. In other words, they chose the pieces that would fit into the puzzle and entered them into the program, and then the software filled in the gaps and rearranged things as necessary. In this way, they made sure that the genome looked the way they wanted it to look.
All of the studies Mercola lists as proving the existence of the SARS-CoV-2 virus are done in similar fashion to come up with a computer simulation, not a real genome taken intact from a real organism.
When Hammond talks about finding a genome of twenty-eight to twenty-nine thousand base pairs, it’s important to understand that they have never found this genome in any bodily fluid, just like they have never found anything they could call a virus. They have never found a strand of twenty-nine thousand base pairs; instead, they have created it in the computer by matching pieces together based on a template. In other words, they find the sequence only because that’s the sequence they’re telling it to find. This is not science!
More Covid-19 Virus Studies
Another paper cited by Mercola comes from Italy, published in the Annals of Internal Medicine in August 2020.8 The researchers took a sputum sample from a sixty-five-year-old woman and diagnosed her with Covid-19 using a PCR test. Then they cultured the sample in kidney cells, followed by genome sequencing as described above. It’s the same in all the studies that Mercola cites. Nobody isolates the virus from the patient directly; nobody takes that virus and determines the genetic material in that virus; nobody takes that virus and exposes somebody else to it and shows that it causes disease.
Mercola cites a study from Colombia that is the same exact experiment—a nose swab cultured in a toxic cell culture, followed by genetic sequencing and electron microscopy.9 According to the researchers, “Electron microscopy images obtained from infected cells showed the presence of structures compatible with SARS-CoV-2”—not structures that are, but that are compatible.
These structures are also “compatible” with kidney failure and probably many other things. The authors state that the genetic composition of their isolates was consistent with the predominant variant—not saying it was the predominant variant. In other words, they are hedging at every turn.
At the end of his article, Mercola mentions “antibody dependent enhancement (ADE),” but there is absolutely no scientific evidence to support something called ADE. Virus theory posits that we make antibodies against viral diseases. In July 2020, the head of the Bulgarian Pathology Association stated that they had found no monoclonal (coming from the same cell) antibodies in any of the people said to have died of Covid.10
This is like saying that no one has died of Covid, because since they haven’t found antibodies, they must conclude that the patients didn’t have Covid.
Does It Matter?
Hammond dismisses those who question the viral theory of disease as his “pet peeve” and “divisive” of the health freedom movement. According to Mercola, “Getting too far into the weeds of theories that refute the existence of viruses altogether will only slow down and hamper the truth movement rather than aid it along, and I would strongly discourage anyone from engaging in this highly unproductive narrative.” In other words, if you question the viral theory, you are the bad guy, hindering the movement for health freedom. One virus advocate has referred to “virus-deniers” as domestic terrorists!
And yet the virus debate has immense importance to the health freedom movement. All the objectionable “public health” measures— masks, social distancing, isolation, testing and above all toxic vaccines—are predicated on the belief that we are threatened by a virulent, contagious virus. If there is no virus—not for Covid-19, not for any disease—then the justification for forcing these measures on the public disappears.
SIDEBARS
Electron Microscopy
Scientists use an electron microscope in order to see the structures inside a cell. To view a sample under the electron microscope, they must prepare it using special procedures. One reason is that the beams of the electron microscope are extremely powerful and can heat the sample up to 150 degrees C. The preparation method requires the following steps:
FIXATION: The sample is placed in some kind of chemical fixative, such as formalin, glutaraldehyde or osmium tetroxide. This preserves the structure of the tissue.
DEHYDRATION: This step requires bathing the tissue many times in alcohol (ethanol or acetone) to remove all water from the tissue.
EMBEDDING: The tissue is put inside a small mold that is filled with paraffin wax or epoxy resin, which is then cooled to harden.
SLICING: The hardened resin is sliced into extremely thin pieces.
STAINING: The tissue is stained with some type of heavy metal, such as uranyl acetate, another name for uranium, or lead acetate, so you can have more contrast when you’re viewing the tissue through the electron microscope.
These methods will obviously have effects on biological samples. For example, formalin in the staining process is formaldehyde, a known human carcinogen and neurotoxin; glutaraldehyde is specifically dangerous for the gastrointestinal tract and the lungs, and osmium tetroxide causes pulmonary edema. Ethanol used in the alcohol baths can cause severe liver damage, and acetone damages the kidneys, the lungs and the brain. Paraffin wax and epoxy resin used for embedding can also affect biological tissues.
Most toxic are the heavy metals uranium and lead used for staining; they are bound to have toxic effects on biological samples. The result is that what you see using the electron microscope has little resemblance to living tissue—it is an artifact and a distortion, from which no conclusions about cell structure can be made.
A Mouse Study
Recently, Dr. Robert Malone stated that the omicron variant is not as dangerous as the others and that we should rethink our vaccines. One of the papers he cited was “Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model,” published in December 2021 in Emerging Microbes and Infections.11
In the abstract of this paper we read, “Older individuals are at higher risk of SARS-CoV-2 infection and severe outcomes, but the underlying mechanisms are incompletely understood. In addition, how age modulates SARS-CoV-2 re-infection and vaccine breakthrough infections remain largely unexplored. Here, we investigated age-associated SARS-CoV-2 pathogenesis, immune responses, and the occurrence of re-infection and vaccine breakthrough infection utilizing a wild-type C57BL/6N mouse model. We demonstrated that interferon and adaptive antibody response upon SARS-CoV-2 challenge are significantly impaired in aged mice compared to young mice, which results in more effective virus replications and severe disease manifestations in the respiratory tract. Aged mice also showed increased susceptibility to re-infection due to insufficient immune protection acquired during the primary infection.”
Now, when well-known spokesmen such as Dr. Robert Malone comment on the importance of a study like this, it works to convince the public that SARS-CoV-2 is real and the omicron variant is real. Maybe omicron is not so bad, maybe it is worse in the elderly, but in any event, the new “variant” is real.
According to Malone, the reason this study is important is that it explains the significant adverse event profile of the vaccines. We would agree that these adverse events combined with a milder disease profile of omicron raise the possibility that boosters may not be good medicine, even for the elderly, but the suggestion that viruses have anything to do with this only perpetuates the kind of misinformation that justifies everything that is wrong with how the health authorities have handled the pandemic—masks, social distancing, isolation, hand sanitizing and vaccinations.
According to the authors, the antibody response was severely impaired in aged mice leading to more severe disease. In the Materials and Methods section, we see that the SARS-CoV-2 variant was “isolated” from a confirmed Covid-19 patient in Hong Kong and that the virus was cultured in Vero (kidney) cells and stored at negative 80 degrees C.
Now, the important part: they expose the mice to a “variant” of the “virus”—to what they think is the omicron variant. One would expect that what scientists would do is take purified virus and expose the mice in the way that humans are exposed, by breathing it in the air. But what did these scientists do? They did a standard viral culture, meaning they inoculated monkey kidney cells (Vero cells) with fetal calf serum and an unpurified sample from a person with alleged “Covid.” (Fetal bovine serum, by the way, is taken from live aborted slaughterhouse calves whose blood is sucked directly from their hearts.) So, they didn’t, in fact, use a virus—that is a flat-out lie. Instead of a virus, they used a culture of kidney cells that contained some of the primers allegedly from a variant strain, a variant that has never been isolated.
Now, you would think that they must have sprayed this culture onto the mice, or gently into their noses, but that’s not what they did. Instead, they anesthetized the mice with toxic drugs—essentially poisoning them—and then squirted a mixture of phosphate-buffered saline and the toxic kidney culture under high pressure down their noses through an intranasal cannula directly into their lungs. No rational person would say that this type of experiment has any relation to what happens in old or young people or to anybody exposed to a “virus.” It’s ridiculous to call this science.
And then they found out whether the young mice did better than the old mice. Upon intranasal inoculation, the young mice transiently lost a maximum of 5 percent body weight for a short period. In contrast, the older mice lost 12 percent of body weight, and they didn’t recover. Moreover, the young mice did not show any sign of disease. The older mice showed hunched postures and labored breathing, which was more severe at higher doses of toxic cell culture injection into their lungs.
If you wanted to be precise in your language, you would say that young mice—injected, anesthetized and subjected to high-pressure squirts of toxins directly into their lungs—seemed to be okay; they just lost a little weight. That’s probably the definition of a bad day for a mouse. But they seemed to recover, whereas the older mice didn’t do as well. That’s what they found.
And then they did all kinds of biochemical histological genetic studies, analyzing the tissue after they ground up the nasal turbinates, the lungs and so forth. They then concluded, “Yep,” these mice have a lot more antibodies than they should—which means they are trying to protect themselves against being poisoned with toxic cell cultures injected right into their lungs.
The authors found that the staining of the nucleocapsid protein was more intense at higher doses of the stuff squirted up the mice’s lungs. Later, they say these findings indicate that SARS-CoV-2 “replicates more effectively in the respiratory tract of aged mice than young mice upon virus exposure.” We would submit that they never actually took out any virus and never saw any replication of any virus in any lung of any mouse.
In other words, the researchers essentially said, “This study does not prove what we thought it was proving, but is just another way to convince us that there is a virus and that the virus is the cause of disease.” When in fact, all this study really tells us is that older, poorly-fed mice do worse when exposed to poisons than younger ones.
Does it matter whether this disease is caused by a virus or not? When the Chief Medical Officer of the World Health Organization predicts that half of the United States is going to get sick in the next six to eight weeks, yes, it does matter. The problem with all this talk about viruses is that it completely obscures the reasons why people are getting sick. We know that a lot of people are getting sick from the injections, but they are not the only people getting sick. Unfortunately, as long as we stick to this nonsense called the viral narrative, we will never ask the right questions, and we will never get any answers as to what otherwise is making people sick.
Rapid Tests for Covid-19 Virus
Recently, the CDC announced—quietly and without explanation—that as of January 1, 2022, they were no longer going to use PCR tests for “diagnosing Covid.” Many people saw this as a kind of capitulation by the CDC, as if to say they had finally seen the light; or perhaps there was enough pressure on CDC that they realized they had to back down quietly from the PCR test. Many people interpreted the CDC’s move as an end to testing, and since this pandemic is really a pandemic of testing, they believed this would go a long way toward ending the pandemic. After all, if they stopped doing the test, nobody would test positive. However, the CDC didn’t say they were going to end testing.
The problem is that these people are playing chess, while the rest of us are playing checkers—if they’re playing chess, we need to play chess, too, and understand the motivations and the rationale behind some of the moves we’re hearing about. And this is particularly true in the case of things that seem to be small victories—sometimes even fairly large victories—because upon closer examination, they don’t all turn out to be the victories that we imagined.
The PCR (Polymerase Chain Reaction) is not a diagnostic test, it’s a manufacturing tool, and it does not test whether or not anybody has any virus. Rather, the PCR is a method to rapidly make millions to billions of copies (complete copies or partial copies) of a specific DNA sample, allowing scientists to take a very small sample of DNA and amplify it (or a part of it) to a large enough amount to study in detail. The inventor, Kary Mullis, was emphatic that his test could not be used to diagnose or determine disease.
The PCR amplifies the DNA sample anywhere from twenty to forty cycles in order to get enough genetic material to detect—the test does this by showing a color change. To use the PCR as a diagnostic test requires two assumptions. The first is that you know that the genetic sequence you are amplifying comes from the virus you are looking for; the second is that there are no other biological organisms in the sample—no microbes, bacteria, fungi or human DNA. To repeat, the premise of using the PCR for diagnosis is that you already know the sequence of the virus, and you know that this primer sequence is one of the pieces of the entire virus genome, and that no other biological organism has that same sequence of DNA. We know that both these premises are not true with PCR Covid tests. Actually, one of the people who came up with the original primer sequences was Christian Drosten, who admitted in a paper that they never had a copy of any virus.12
Now, just think about that for a minute. If you never had a copy of the virus, how can you possibly know that this piece of the genome is a piece of the virus, that it actually came from a virus? If we gave you a sentence and asked you whether this sentence came from a certain book, the obvious common-sense question that any rational human being would ask is, can you show me the book? How can you know whether a sentence comes from a certain book if you don’t have the book?
Furthermore, how can you prove that no other living being has this same sequence? You can determine this by doing what is called a BLAST search, which searches the database of all the genome sequences of all the organisms that have ever been sequenced. Scientists have done this and found out that the same sequence used in the PCR test primers for SARS-CoV-2 is found in at least ninety human sequences and ninety microbial sequences (meaning bacterial or fungal sequences).
Thus, the second premise, that a sequence is unique to a specific virus, is also not true. The sequence is found in humans and in bacteria. If you start with a sample that has sequences that come from humans and that has bacteria and fungus in it, there is no way of knowing whether the positive match—the sticking of the primer to a sequence in the sample that will then be amplified—comes from a virus, the person, bacteria, fungus or maybe from something else.
So, the PCR test is invalid—there are no “false positives,” there are no “false negatives,” there are just false results. So, shouldn’t we applaud when the CDC finally acknowledges that they are not going to do a PCR test anymore?
The question is, what are they going to replace it with? According to government announcements, they are going to use a “higher throughput and multiplexed assay with biotinylated primers.” To explain further: “This developed invention is multiplex and uses the Luminex bead-based liquid assay, which contains one hundred different unique bead oligonucleotide probes with sequences complementary to the target sequences covalently coupled to these unique beads. These capture beads are mixed with viral samples obtained from the patient via cheek swabbing or throat wash and subjected to PCR in a conventional thermocycler. The amplified target sequences then hybridize to complementary capture oligonucleotide probes via forward biotinylated primers; if this bead probe amplicon unit contains the target nucleic acid, it will be bound by the reporter molecule and fluorescence will be detected by flow site cytometer. This multiplex assay would thus be able to detect and identify respiratory pathogens present in hospital and clinical settings.”
English translation: Instead of the old PCR test, they are going to use one hundred different unique beads. These beads contain the primer sequences, and they’re all attached to the other beads. These beads are mixed with viral samples from the patient, and then they are put into PCR amplification cycles.
Now, the only real difference between this and the normal PCR test is that there are more of the primer sequences—like one hundred more—attached to a compound called biotin. These biotinylated primers stick easily to the sequences in the sample, which then get put into the old-fashioned PCR thermocycler, so that they can be amplified. And then you get a result. Now, instead of a PCR test for Covid, one test will test for all the “viruses.”
The upshot of this is that now they will be able to say that you have many different viruses, all at the same time. Since all these viruses can make you sick (so they will argue), you may need a vaccine for each one of them.
This is a checkmate: They now are able to find the code for the original “virus” as well as the delta variant and the lambda variant, right on through the Greek alphabet, because they can make it look like you have multiple different sequences. These sequences amplify more easily because they figured out a way to make the primer sequences stick more readily to whatever is in your sample. And this is not a single-plex test. This is a multiplex assay, which means they can find any number they want, just by increasing the amplifications. And checkmate, they got us.
So, they replaced the old-fashioned PCR with something that will make the whole thing even worse. The lesson is that we should not be fooled by false minor victories, because they are not necessarily good news.
The Seven U.S. Government Payoffs to Kill You in Hospitals
by Dr. Peterson Pierre13
If you have Covid, and you end up in the hospital, you’re put on a rigid protocol. There’s a high mortality rate in the hospital, and your family is kept in the dark about what is happening. So, what’s going on here?
The CARES Act is providing bonus payments to hospitals whenever they have a diagnosis of Covid, while the Center for Medicare and Medicaid Services is waiving patient rights. This is a deadly combination.
The hospital gets the first payment when they offer a free Covid test in the emergency room, and they get another payment if they can come up with a diagnosis of Covid. Number three, they get another bonus payment if they admit a patient with Covid. Number four, they get another bonus payment if the patient is put on remdesivir. Number five, another bonus payment if the patient is put on a mechanical ventilator. Number six, another 20 percent bonus if the diagnosis on your death certificate says Covid, even though you may not have died from Covid. And then number seven, there are bonus payments for the coroners.
Does the public understand the gravity of what’s happening right now? The government is literally paying hospitals to kill you. That’s what’s happening. These are real human lives we’re talking about, priceless human lives. It’s estimated that about one hundred thousand dollars per patient is what the hospital is getting. Think about that.
References
- https://amos37.com/mercola-yes-sars-cov-2-is-real-virus/
- Rai A, Fang H, Fatmous M, et al. A protocol for isolation, purification, characterization, and functional dissection of exosomes. Methods Mol Biol. 2021;2261:105-149.
- Vanderheuvel D, Rombouts S, Adriaenssens EM. Purification of bacteriophages using anion-exchange chromatography. Methods Mol Biol. 2018;1681;59-69.
- Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954;86(2):277-286.
- Cassol CA, Gokden N, Larsen CP, et al. Appearances can be deceiving – Viral-like inclusions in COVID-19 negative renal biopsies by electron microscopy. Kidney360. 2020;1(8):824-828.
- Caly L, Druce J, Roberts J, et al. Isolation and rapid sharing of the 2019 novel coronavirus (SARS-CoV-2) from the first patient diagnosed with COVID-19 in Australia. Med J Aust. 2020;212(10):459-462.
- Papoutsis A, Borody T, Dolai S, et al. Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing. Gut Pathog. 2021;13(1):7.
- Colavita F, Lapa D, Carletti F, et al. SARS-CoV-2 isolation from ocular secretions of a patient with COVID-19 in Italy with prolonged viral RNA detection. Ann Intern Med. 2020;173(3):242-243.
- Díaz FJ, Aguilar-Jiménez W, Flórez-Álvarez L, et al. Isolation and characterization of an early SARS-Cov-2 isolate from the 2020 epidemic in Medillin, Colombia. Biomedica. 2020;40(Supl. 2):148-158.
- Frei R, Corbett P. Bombshell! “No one has died from the coronavirus” says leading pathologist. James Fetzer, July 11, 2020. https://jamesfetzer.org/2020/07/bombshell-no-one-has-died-from-the-coronavirus-says-leading-pathologist/
- Chen Y, Li C, Liu F, et al. Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model. Emerg Microbes Infect. 2022;11(1):368-383.
- Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):2000045.
- Pierre P. The seven US government payoffs to kill you in hospitals. Jan. 16, 2022. https://www.bitchute.com/video/rzcEVrVaA9jY/
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Spring 2022
Connect with Weston A. Price Foundation
Connect with Dr. Andrew Kaufman
cover image credit: geralt


Truth Comes to Light highlights writers and video creators who ask the difficult questions while sharing their unique insights and visions.
Everything posted on this site is done in the spirit of conversation. Please do your own research and trust yourself when reading and giving consideration to anything that appears here or anywhere else.







