UK attorney Anna de Buisseret today announced serving Notices of Liability on COVID-19 clinics and individuals administering the experimental biological agent known as the “COVID-19 vaccine” without obtaining fully informed consent, freely given in accordance with the Nuremberg Code and UK and International law.
“COVID jabs are experimental and still in phase 3 clinical trials,” de Buisseret explained. “The Nuremberg Code therefore applies. The injector MUST obtain the individuals fully informed consent freely given. All MATERIAL RISKS must be made clear to them and an individual risk assessment conducted.”
De Buisseret said among those served is Chief Medical Officer (CMO) for England, UK government’s Chief Medical Advisor, and head of the public health profession Professor Chris Whitty.
In April, Doctors for COVID Ethics served Notices of Liability for COVID-19 vaccine harms and deaths on all European Parliament Members.
In the United States, Health Impact News gave public notice that two private corporations, CVS and Rite Aid, have been issued a Safety Warning for the potential danger of indiscriminate COVID-19 “vaccination” in the naturally immune and recently COVID-19 infected, by Dr. Hooman Noorchashm, MD, Phd, on April 29th, 2021.
Many physicians have now spoken publicly about studies showing that those with natural COVID immunity will see a 2- to 3-fold increased risk of adverse reactions from the COVID shots.
When I interviewed President Reagan’s policy analyst, Jim Warner, in 1987, there was something I didn’t know: HIV had never been isolated. I did know the virus wasn’t the cause of what was being called AIDS.
Senior White House policy analyst Jim Warner first came to public attention in a November 1987 article in the New York Native. In the story, “The White House Calls the Native About Aids,” publisher Chuck Ortleb wrote: “Warner told me that the White House could be seen as divided into two groups on the issue of AIDS. One group, which he said is in the minority, wants to adopt an ‘Auschwitz model’ by quarantining all those infected with ‘the virus.’ ‘The other group,’ [Warner] said, ‘is incompetent.’”
Warner told me he wasn’t suggesting there was a White House group which was favoring “an Auschwitz model,” but that some high-risk groups might think that was so. My following interview ran in the LA Weekly on December 18, 1987.
WEEKLY: Has anyone at the White House spoken to you about the Native article and what you said in it?
WARNER: I don’t think anyone here knows there was an article in that paper. The government really hasn’t fulfilled its role in providing good information [on AIDS]. We just may not know enough. With AIDS, we’re dealing with a syndrome, not a disease. We may see a patient who has a genetic defect that’s causing his immune deficiency [instead of HIV being the causative agent]. I’m not satisfied we know all we think we do, by any means.
WEEKLY: Is your research on AIDS part of your policy work? Do you make recommendations based on what you find out? Or is it just that you’re absorbed in discovering what’s going on with AIDS?
WARNER: More of the latter than the former. I was asked to look into an Atlantic magazine article about insects and AIDS, and that’s how it started. I decided I wanted to put together a set of questions concerning the HIV virus, so that the answers would suggest its role in AIDS. I would then draft a paper and give it to the people who asked me to look into the subject.
WEEKLY: Do people at the White House get a chance to talk to scientists over at the National Institutes of Health [NIH]? I mean really talk with them, find out what they’re doing, how they’re thinking?
WARNER: There is not much communication [between people at the White House and the scientists at NIH]. I’m probably the only person here who has much interest in it. This year I determined that the [White House] working group on AIDS wasn’t adequate.
WEEKLY: Several university scientists I’ve spoken with have – off the record – criticized what they call “HIV dogma.” They feel if they speak out against the rush to judgment for HIV as the cause of AIDS they may lose money. Grants begin with the assumption that HIV has been proven as the agent of the disease.
WARNER: I’m of a mind that if no other lessons should be required of any university science curriculum, there should be a good survey course in philosophy and a grounding in logic. I’m appalled at the conceit and arrogance [of certain scientists].
WEEKLY: There has never been a performance-evaluation on the results of the NIH. NIH has balked at the idea of evaluating the worth of all their medical research over the last 20 years.
WARNER: That’s a very good idea. I’m going to see what I can do about that.
WEEKLY: The Native article mentioned that you spoke with Dr. Lo, an Army researcher on AIDS. He has his own theory about the disease, that it’s caused by a different virus. According to the Native, you had a problem getting through to him. Did they really tell you you’d have to get an okay from the Surgeon General just to talk to Lo?
WARNER: Yes. You know, although it is an honor to work at the White House, I’m not impressed that being here makes me special. But I pulled rank, and they put me through to Dr. Lo.
WEEKLY: Suppose proof emerged that HIV is not the AIDS virus. How difficult would it be to alter the course of research?
WARNER: It’s very difficult to change people’s minds. It’s not impossible, but there is a head of steam built up.
WEEKLY: What do you do if a government agency, as a whole, has been derelict?
WARNER: It may end up as a brawl. I’d sort of like to finesse that, though, I’d like to avoid a public brawl. It eats up time. It’s difficult when scientists are not open to discussing scientific issues.
WEEKLY: Robert Gallo, Max Essex, people like that, were the field commanders on the NIH war on cancer in the 70’s. They lost that war. So why are they in charge of AIDS research now? It seems odd that we don’t have other people running the show.
WARNER: If ever I’ve been tempted to believe in socialism, science has disabused me of that. These guys [at NIH] assume that it’s their show. They just assume it.
WEEKLY: Peter Duesberg, a distinguished molecular biologist at Berkeley, has said that HIV does not cause AIDS. Have you asked people at NIH what they think, specifically, of his arguments?
WARNER: Yes. I’ve been told that Peter Duesberg’s refutation of HIV has been discounted by the scientific community. I was given no explanation as to why. I was very offended. No evidence was presented to me. Just that Duesberg had been ‘discounted.’ That’s absurd. It’s not a scientific response to dismiss Duesberg as a crank.
WEEKLY: The definition of AIDS has become so broad it’s even stretching the idea of what a syndrome is, never mind a singular disease.
WARNER: A syndrome is a means of trying to understand how symptoms could be linked together. But if you do this in an atmosphere of hysteria, there is no limit to what you can attribute to a syndrome.
WEEKLY: The definition of AIDS in Africa is now becoming synonymous with starvation. They’re saying the three major symptoms are chronic diarrhea, fever, and wasting-away. Weight-loss. It certainly makes a perfect smokescreen for the aspect of hunger which is political – just call it AIDS.
WARNER: I had not considered that. There is a program to make Africa self-sufficient by the year 2000. This could certainly hinder that activity. You know, I was a prisoner of war in Vietnam. I experienced weight-loss of eighty pounds. And when I came home, I was suffering from a form of dysentery that you could call opportunistic. A number of us were. We didn’t have AIDS.
—end of interview—
In November of 1987, I found out that the journal Bio/Technology was going to hold a roundtable workshop in which HIV would be addressed. Peter Duesberg and about a dozen other researchers would attend. The purpose of the roundtable would be to formulate experiments which, once and for all, would show HIV’s role or non-role in AIDS.
I told Jim Warner about the proposed roundtable, and suggested he contact the magazine and sit in on the sessions. He did call, and to everyone’s surprise, suggested that the roundtable be held in his office at the White House.
For the next month, it was on again, off again. There were obviously pressures within the White House against sanctioning such a meeting. About a month before the scheduled January 19th date, stories about it began appearing in several newspapers.
For a brief time, it looked like the White House’s Office of Policy Development was not going to host it, but the Office of Science and Technology Policy was. Then the whole thing fell apart.
The New York Post, on January 7th, 1988, ran a story on Duesberg. The next day, the paper did a follow-up, headlined: U.S. AXES DEBATE ON TRUE CAUSE OF AIDS. After indicating that the White House meeting was canceled, medicine-science editor, Joe Nicholson, relayed a surprising quote from Gary Bauer, head of Reagan’s Office of Policy Development, and Jim Warner’s boss: “People like Dr. Duesberg need to continue to have access to research funds so that if we are heading in the wrong direction, that can be proved.”
Bauer then said he didn’t want the White House to sponsor the meeting because it would impart a political tone to a scientific event.
“I hope they have the debate elsewhere,” he said. “I’ve sort of bristled at the finality with which some have made statements about AIDS and how it is transmitted. When findings run counter to the accepted wisdom, there is a tendency to muzzle or ignore rather than have an open debate.”
The proposed debate never took place.
Given what Jim Warner told me in our 1987 interview, I’m sure, if he were still working for the government in 2021, he would have some choice comments about an NIH scientist who was a major player in the AIDS scene in 1987, and is still hogging the spotlight these days:
“Today, La Quinta Columna has made an urgent announcement that they hope will reach as many people as possible, especially those involved in health and legal services, as biostatistician Ricardo Delgado, Dr. José Luis Sevillano and the team of researchers and professors with whom they have been conducting their research have confirmed the presence of graphene oxide nanoparticles in vaccination vials.” ~ Translated by Orwell City
Since no such thing as Covid-19 has ever been separated, isolated, or identified, and not one attempt to satisfy Koch’s Postulates to determine if a novel ‘virus’ even exists has been attempted, what is really happening and why have governments worldwide shut down their countries and declared war on their citizenry? What is the real plot, and how many will die due to this fraudulent pandemic scam?
My position since very early on concerning this so-called ‘pandemic’ has been that the SARS-CoV-2 or ‘Covid-19’ was just the excuse being used as a government tool to instill great fear into the people, so as to build a system of total control over the masses. The real bioweapon evident is the poisonous injection mislabeled as the ‘Covid vaccine,’ and the tactics and mandates that have not only destroyed economic activity, but decimated the health and immune systems of the people at large. This includes every aspect of the lockdowns, quarantines, job loss due to the forced closings of businesses nationwide and worldwide, mask and false testing mandates, and the general terror purposely brought about by the controlling ‘elites’ and their government partners.
By this time, most should, but few do, understand the poisonous and toxic nature of what is being called a ‘vaccine,’ and the wide array of deadly adjuvants, live animal tissue, biological additives, metals, nano-particles, gene-altering messenger-RNA, and of course many other unknown or purposely hidden toxins in this deadly concoction. But what else is in this devil’s brew?
Just recently, reports coming from a team of doctors, scientists, researchers, and professors from the Spanish organization, La Quinta Columna, have stated emphatically that the highly toxic graphene oxide is not only present in vials of ‘Covid vaccines’ from most all pharmaceutical manufacturers, but is also being delivered in masks and through ‘Covid’ testing. This is very startling information, and answers a lot of questions about not only the symptoms present for many, but also may further expose another part of this nefarious agenda that is depopulation.
As stated by this group of researchers:
The masks being used and currently marketed contain graphene oxide. Not only the ones that were withdrawn at the time, as indicated by the media, the swabs used in both PCR and antigen tests also contain graphene oxide nanoparticles.
The COVID vaccines in all their variants, AstraZeca, Pfizer, Moderna, Sinovac, Janssen, Johnson & Johnson, etc., also contain a considerable dose of graphene oxide nanoparticles. This has been the result of their analysis by electron microscopy and spectroscopy, among other techniques used by various public universities in our country.
The anti-flu vaccine contained nanoparticles of graphene oxide and the new anti-flu vaccines and the new and supposedly intranasal anti-COVID vaccines they are preparing also contain enormous doses of graphene oxide nanoparticles. Graphene oxide is a toxic that generates thrombi in the organism, graphene oxide is a toxic that generates blood coagulation. Graphene oxide causes alteration of the immune system. By decompensating the oxidative balance in relation to the gulation reserves. If the dose of graphene oxide is increased by any route of administration, it causes the collapse of the immune system and subsequent cytokine storm.
Also, according to this study, levels of graphene oxide in certain ‘vaccine’ vials contained up to 99% graphene oxide and little else. This toxin can cause pneumonia when the nanoparticles enter the lungs. Graphene also causes a metallic taste and inflammation of the mucus membranes which can lead to a loss of taste and smell. It can as well cause strong magnetic responses inside a host organism, and can also cause red blood cell damage. When deposited on most any surface, it can be converted into an electronic conductor. This would lead one to question many ‘Covid’ symptoms and the possible uses of graphene oxide in the so-called ‘Covid-19 vaccine,’ as this study group also claims that graphene oxide actually causes what is erroneously described as ‘Covid.’ If this is the case, then the ‘vaccine’ is indeed the bioweapon.
The very many adverse effects of graphene oxide delivery into living organisms has been long studied, but virtually nothing about this has been mentioned by the pharmaceutical companies, the government, or the mainstream media. In fact, there has been express denial of any nano-particle use in the flu and ‘Covid’ injections by these same sources in the past. The information in this report is staggering, but little effort is required to understand the high risk of using these toxic nano-sized particles in ‘vaccines.’
Graphene microparticles, and therefore graphene by injection, can lead to major respiratory sickness, including lung cancer. Once these particles are inside the body, and in the cells, the human immune system has not the ability to rid itself of these deadly nano-particles, and they become permanent and can cause extreme physiological harm in the body at the cellular level.
Bioweapons can come in many forms, and this is the new tactic of war against the people by this and other governments. The powerful controlling element of society and its corrupt government partners care nothing about you or your families, but only about power and control over you. The real bioweapon is not any ‘virus,’ but is the ‘vaccine’ delivery system itself, along with masks, and testing, as perpetrated by the very entity (government) claiming to be your savior. The elimination of this government is in order.
It seems that the death of billions is sought, and a new master and slave society controlled by technocrats in a transhuman environment is the desired outcome. Today, science fiction has become reality!
The original translated article and video from La Quinta Columna can be accessed here, and also in the source links below. I would urge all to take a look at this information.
Gene research companies tend to come and go. They start out banging and popping like fireworks in the sky, and then they fade out—selling themselves to larger outfits who’ve hired better liars…
Once upon a time, it sounded easy. Start with a disease, find the gene responsible for the disease, and correct the problem.
Then, researchers wondered, was disease the result of one gene or a group of genes acting together?
Either way, the proof would be in devising cures for diseases using gene therapy. “Not yet, but soon…”
And regardless, the major need was: money. Lots and lots of money.
This need required good PR people. “We have to pump up the idea that we’re on the edge of tremendous breakthroughs. We’re always on that edge…”
This hype also needed to obscure the fact that there wasn’t (and isn’t) ANY gene cure for ANY disease.
As time passed, lack of cure could be a problem. In fact, it could mean curing disease was not a genetic undertaking at all. What about environment? Toxicity? Malnutrition? Poverty? In order to raise money, those factors would have to be pushed back out of view.
Instead, the PR people would need to flood the news with positive glow around the subject of gene research. Also known as exaggeration. Or bullshit.
You can spot the key terms in these articles. POSSIBLE, SHOULD, COULD, EXPECTED TO, SEEMS, ON THE HORIZON, MAY BE, COULD LEAD TO, EVENTUALLY, and of course, the ever-popular BREAKTHROUGH.
I dug back in my files and found a piece I wrote in 2011. As you’ll see, the “breakthroughs” touted then haven’t panned out so far. You don’t read about them in the press these days. The PR pros have moved on to other exaggerations.
The first 2011 article I cited was from Reuters, headlined: SCIENTISTS FIND “MASTER SWITCH” GENE FOR OBESITY. Here are a few choice tidbits. Note the key terms I just mentioned.
“…and say it should help the search for treatments…”
“…the regulating gene could be [a] target for drugs to treat…”
“…seems to act as a master switch…”
“We are working hard…to understand these processes and how we can use this information to improve treatment…”
Sure. You bet.
Zero results.
Next, a 2011 blockbuster piece in the Financial Times. The headline read: SCIENTISTS FIND GENETIC LINK TO DEPRESSION.
Standard trumpet blaring.
Here are the text nuggets. Again, note key terms.
“The discovery…is expected to lead to a better biological understanding of the condition and eventually to more effective antidepressants…”
“…as possibly for the first time we have found a genetic locus for depression.”
“…is likely to pin down the gene responsible…”
“…which may be the basis for designing more effective antidepressants…”
Sure. You bet.
Zero results.
Moving ahead in time—From immunology.org: “On 17 December 2015, the journal Science voted [gene-editing tool] Crispr-Cas9 ‘Breakthrough of the Year’, saying that it had ‘matured into a molecular marvel’. It is already being used in cancer immunotherapy to edit a patient’s own T-cell genome in order to remove the gene that ‘tells’ these immune cells not to target cancerous tissue.
It’s already being used—but where are the cures? Nowhere.
Anybody out there want to partner with me in launching a new company? This is a major winner. It covers a very broad area. Actually, there is no human endeavor it doesn’t cover. The name of the company? MAYBE COULD BE INC.
“We’re always on the edge and the frontier. We’re always breaking through. We’re always raising money. We’re always pumping our stock. We’re always ready to sell the company to a sucker with deep pockets.”
Let’s look at another type of gene research organization. This one happens to be the largest single medical research outfit in the world. It’s part of the US government: the National Institutes of Health (NIH). Their PR is different. They’re hedging their bets and covering their bases in every possible way. They’re saying YES, NO, AND MAYBE all at once. Of course, they can get away with it, because they run on taxpayer money. Their annual budget is a formidable $30 billion. Grit your teeth and read through their text that explains “genetic diseases”:
“A genetic disorder is a disease caused in whole or in part by a change in the DNA sequence away from the normal sequence. Genetic disorders can be caused by a mutation in one gene (monogenic disorder), by mutations in multiple genes (multifactorial inheritance disorder), by a combination of gene mutations and environmental factors, or by damage to chromosomes (changes in the number or structure of entire chromosomes, the structures that carry genes).”
“As we unlock the secrets of the human genome (the complete set of human genes), we are learning that nearly all diseases have a genetic component. Some diseases are caused by mutations that are inherited from the parents and are present in an individual at birth, like sickle cell disease. Other diseases are caused by acquired mutations in a gene or group of genes that occur during a person’s life. Such mutations are not inherited from a parent, but occur either randomly or due to some environmental exposure (such as cigarette smoke). These include many cancers, as well as some forms of neurofibromatosis.”
That is a DON’T BLAME US statement. “Don’t blame us if a disease we thought was genetic turns out to be something else. Don’t blame us if it’s 65.34 percent environmental, 4.52 percent genetic, and 30.14 percent who knows what. Don’t blame us if toxicity triggers genetic malfunctions and, in the absence of the toxicity, there would be zero cases of the disease. Don’t blame us if a disease has nothing to do with genes. We’re ready to jump in any direction. We may not know much, but we’re sitting on a pile of cash. Don’t blame us if we don’t have any solid genetic cures for anything. We’re working hard. That’s all you can ask us to do.”
If there is one disease the public tends to believe can be cured by gene therapy, it is sickle cell anemia. The PR pros have done a good job there. However, sicklecellanemianews.com states: “Gene therapy is an experimental technique that aims to treat genetic diseases by altering a disease-causing gene or introducing a healthy copy of a mutated gene to the body.”
Experimental. Aims to. Not an established cure. The confusion arises because, as with a number of diseases, the researchers and the PR flacks claim they’ve definitely traced the illness to a gene or two. They’ve struck gold. But, as you read further, you discover they’re just not ready to cure the patient. Clinical trials are underway. More work in the lab is necessary. The pudding is there, but the proof of it isn’t. They claim to know the cause; they just don’t know what to do with it.
In science, that’s known as a hypothesis. Or more simply, a speculation. You say you’ve found an answer, but you can’t apply it. This means: you don’t have an answer.
“There is no doubt. We went down into the mine and we found evidence of extraordinary amounts of gold. We just don’t know how to get it out. What’s that? You want to see the gold? No, I’m sorry. The public isn’t allowed down there. Only the professionals can enter. But don’t worry. We’re very close to a breakthrough. The gold will emerge soon. Trust us.”
Trust you? Sure. How much do you need to finish the job? Fifty million? A hundred million? Let me call my broker and sell some stock. I’ll write you a check. Just put a plaque with my name on the wall. Let me know how I’ll profit on this venture. I’m in. I’ve always wanted to invest in MAYBE COULD BE INC.
In case you need to be reminded, the RNA COVID vaccines are genetic treatments. The PR pros tell us they are working quite well. And they’re remarkably safe.
If you’re buying that line, I have electric cars for sale. And they have wings. One charge in your garage, and they’ll get you from Earth to Mars in just under two hours.
On the Connection Between Graphene Oxide Found in “Covid Vaccines”, Electromagnetic Fields, Blood Clots & Severe “Covid” Symptoms | How to Remove Graphene Oxide From the Body
Many are already aware of the work that the team of Spanish researchers that make up La Quinta Columna have been doing.
They are the ones who have had the courage to get a vial of vaccination and send it for analysis to a renowned Spanish university through Prof. Dr. Pablo Campra Madrid, who is compiling and officializing the results in a report that promises to be more conclusive than the preliminary one he prepared for the general public early last week.
However, there are people who still do not know about La Quinta Columna. If you are one of those, then the following video is especially for you. Orwell City has transcribed, translated, subtitled and edited the video to keep its message going around the world.
Ricardo Delgado, founder and director of La Quinta Columna participated with his research partner, Dr. José Luis Sevillano, in the XXVIII Humanitarian Conference organized by the World Coalition for Health and Life (COMUSAV) and the United Nations Council for Life and Truth (CONUVIVE).
Video available at Orwellito Rumble and BitChute channels.
Transcript:
“La Quinta Columna wants to make it clear from the beginning that we have the obligation, we have the obligation to be united because we are in the same battle to give the best of ourselves, because what is at stake is precisely the future of all species. Depending on the strength and momentum that we put into this task will depend on the future of all humanity. We are right now at the turning point from which things can begin to change, and in this sense La Quinta Columna is going to summarize what has been the result of its research during this year and a half, but above all and especially during the last two months. And why during the last two months? I always remember Dr. José Luis Sevillano’s words since the two of us work as a binomial and he has been accompanying me in La Quinta Columna. He said that when the vaccination started we were going to really see what he was doing and what material could be in there.
Then we realized that there was a new phenomenon that for a while we tried to deny, although today it’s evident because of the millions of videos on social media, and we have been able to even measure it with devices: teslameters, magnetometers, etc. I am referring to the magnetic or pseudo-magnetic phenomenon that people acquire after inoculation. A magnetic phenomenon on the one hand, but also one that turns inoculated people into superconductors and also stores energy that can be measured with a multimeter in certain parts, such as the forehead, for example.
So from there we started to look for what kind of materials or, better said, nanomaterials can cause those kinds of properties inside the body and we came up with some of the candidates. One of them initially was graphene. Graphene inside the body acquires magnetic properties and is a superconductor. It serves for energy storage and condensation and was a strong candidate. Without yet having any knowledge of what was inside the vial, we realized that the industry or rather the stock market of the graphene industry had high uptrend peaks just as the COVID-19 vaccination campaign was starting at the beginning of the year, late December and early January. But also, quite curious, during the flu vaccination campaign.
When we have seen the possibilities that graphene has, or rather, that graphene oxide nanoparticles have inside the body when it comes to neuromodulation and when it comes to picking up neuronal electrophysiological effects for brain mapping, we have realized the possibility that graphene is being injected. Can graphene be injected? Yes. Graphene can be injected. And, in fact, some scientific papers have already raised the possibility that it could be used as a nanoadjuvant in vaccines. With that hypothesis of suspicion, we did what anyone could have done and what I also recommend that you can do if you have access to a vial.
We had access to a sealed vial from Pfizer, and by means of a request for services to a university, specifically in my name, it was sent for an analysis of the vial, where we were looking for the material in question: graphene. After some time of investigation by Dr. Pablo Campra Madrid, Doctor in Chemical Sciences, Bachelor in Biological Sciences and member of the University of Almeria, we obtained this preliminary report where we are told that there is indeed solid evidence of graphene oxide in the sample and that it is also the main component of what they wrongly called a vaccine.
From here and with this solid evidence, which will be further complemented with other spectroscopy techniques that can be done. Those that have been used are transmission electron microscopy; EMF techniques, also, optical microscopy; and ultraviolet radiation spectroscopy, which coincide with the peak wavelength of graphene oxide. From here we began to study the toxicity or cytotoxicity that graphene oxide has on the body.
Pay attention to this finding: Graphene oxide inside the body causes thrombogenicity, thrombi. Graphene oxide inside the body causes blood clotting. Graphene oxide inside the body causes post inflammatory syndrome or systemic or multi-organ inflammations. Graphene oxide inside the body when it is above the levels of glutathione —which is the body’s natural reserve of antioxidants—, causes alteration of the immune system, collapse of the immune system and cytokine storm. Inhaled graphene oxide spreads evenly throughout the alveolar tract and causes bilateral pneumonias. Inhaled graphene oxide causes inflammation of the mucous membranes and thus loss of taste and smell, possible loss of taste and smell: anosmia.
In short, graphene oxide behaves exactly like the supposed SARS-CoV-2 of the official version, generating the same symptomatology of severe COVID-19. When installed at the neuronal level, it causes neurodegeneration or, in other words, neurological COVID-19.
So, from here we started to see what possible compounds, drugs and treatments could degrade graphene oxide. And look what we found: N-acetylcysteine or glutathione administered degrade it. Because what glutathione does is counteract free radicals and oxidants, all the toxins that can enter the body.
And we discovered that there were about 300 clinical studies where certain hospitals and certain universities were using N-acetylcysteine with incredible results. For example,100 patients with saturation levels below 50% practically dead —bluntly speaking—, with bilateral pneumonias, within an hour of intravenous glutathione or N-acetylcysteine administration they made it. They were taken off ventilators and everything.
We now fully understand why those treatments worked: because they addressed all the symptoms of the disease supposedly caused by SARS-CoV-2. Given that to date there is no scientific evidence of an actual sequencing and isolation of SARS-CoV-2, we suspect with many credible indications that COVID-19 disease is actually the side effect of the introduction of graphene oxide into the body by different ways.
And I say ‘different ways’ because, although they were withdrawn at the time, masks containing graphene oxide nanoparticles have been introduced and are still being marketed. These masks have been introduced and are still being marketed by companies such as Nanografi, so we have masks with graphene oxide, but also graphene oxide nanoparticles introduced in PCR tests; graphene oxide is also present in antigen tests; hydrogels also contain graphene oxide nanoparticles; intranasal vaccines also, since graphene oxide in aerosols is more potent, as is the supposed SARS-CoV-2. Intranasal vaccines are also prepared, for example, by Turkey. They are made by Nanografi for COVID-19 and influenza.
We know that, naturally, graphene oxide is eliminated by the levels of glutathione in the body, and that is why we suspect that they propose a second, third and even fourth dose every so often: so that you have your considerable dose of graphene oxide. In short, we are talking about the simultaneous and gradual mass poisoning of the entire world population.
Think, if the preliminary report of a professor of a public university in Almeria —and I know that the same study is being done in other European and some Latin American universities—, if it determined that there is graphene oxide in the vials, how is it possible that graphene oxide is injected if the masks were removed because it caused pulmonary affections because of this nanoparticle? We are talking about a crime against humanity with the complicity of governments or at least their participation.
When we study glutathione, we realize that it begins to fall from the age of 30 onwards, but above all it falls considerably from the age of 65 onwards. In fact, COVID-19 takes a heavier toll on older people, apart from those who are immunocompromised and have other pathologies. When we study glutathione, we realize that children have high glutathione reserves because of their youth, and the COVID-19 disease itself hardly has an impact on children. Similarly, glutathione is especially low in the obese population and we realize that it is precisely the obese who are most affected by COVID-19. We realize that glutathione is related to vitamin D. Low levels of glutathione are low levels of vitamin D and it is precisely patients with COVID-19 who have low levels of vitamin D. We realize that athletes have high levels of glutathione endogenously, which are secreted with intense exercise, and precisely athletes are hardly affected by COVID-19.
Everything that we have subsequently studied only further increases and corroborates the hypothesis that the supposed SARS-CoV-2 of the official version is precisely the graphene oxide. And that all the elements of protection, of supposed protection, that we have been given: masks, PCR tests, swabs, antigen tests and vaccine —the wrongly called vaccine— are precisely all those elements that will potentially cause the disease to develop in the future.
And why do I say ‘in the future’? When we studied the electromagnetic phenomenon we realized that graphene oxide has what is called an ‘electronic absorption band’. The electronic excitation, its magnetic resonance is precisely in the third bandwidth of the 5G technology, the one that is being tendered right now and that, remember, has been with us throughout the pandemic.
As absolutely everything started we have had three ‘nets’: The first is that 5G terrestrial antenna that never stopped being placed —because only the antenna operators worked— and that curiously 8 out of 10 of these antennas are placed near geriatrics and nursing homes, in their immediate vicinity, which has been precisely the most affected population. Another inner net: precisely of graphene, according to the preliminary report of the vial of this university. And an external net, which is the one used by space satellites to supposedly provide 5G coverage.
Incredibly, we are narrating a science fiction movie, but believe me, today nanoscience, neuroscience and biotechnology have advanced tremendously. We have only made an approximation in the realm of science and behind the back of civil society. Can a person be controlled or neurocontrolled remotely wirelessly? Yes, it can be done and it is probably being done in a disguised way, and that may explain some of the anomalous behavioral behavior of the population, especially those who have been inoculated or who have received doses of graphene oxide by different ways. As I say, I know I am drawing a science fiction movie, but at the heights we are at it can be difficult to really believe in something. In this sense we say that COVID-19 is only the collateral effect of the introduction of that nanocomposite by different ways, and we suspect that it was introduced in the 2019 anti-flu campaign.
As I was saying, graphene oxide has an absorption band from which it oxidizes much more quicklywhen a small button is turned on to provide 5G coverage or to perform a technological test. Do you think it is a coincidence that Wuhan —where the pangolin and bat soup came from as distraction elements— is the first city in the world with the 5G technology trial at the end of November 2019 and that all previous flu vaccination probably with graphene oxide started from there? When excited, graphene oxide multiplies frequencies. With a minimum signal, it oxidizes much faster and breaks the balance between glutathione levels and the toxicity of the organism, generating bilateral pneumonia, altering the behavior of the immune system, which cannot cope as soon as the neutrophils try to phagocytize it as if it were a pathogen, as if it were SARS-CoV-2.
We shared an article today, if I can screen share I’m going to try to do that, can you let me know if you’re seeing it on screen? Well, let’s see: ‘Graphene oxide is detected in the body by specialized cells (neutrophils) of the immune system.’ Just as if it were a pathogen. The body, the immune system, doesn’t care if there is a biological agent because this never behaved like a biological agent. There are incubation periods if biological. It is not possible that in residences in our country in Spain, such as Matacaz in Barcelona, half of a residence died in 4 hours. If it is a biological agent, it does not cause bilateral pneumonia, but rather asymmetric pneumonia: they usually enter through the right lung due to symmetry. But half of a residence that had previously been vaccinated against influenza could not die.
Source: Graphene Info
We observed that the higher the flu vaccination, the higher the mortality of COVID-19, and logically we saw a relationship. The other relationship was with electromagnetic fields. What we did not know is that there was a marking on each of these people to make them a target population for the electromagnetic focus. A lethal weapon that now makes people magnetic and logically you will understand that if they interact with those radiation sources at a specific frequency and quality, they cause in oxidation, they break the redox balance of the oxidative biomarkers of the organism, causing the COVID-19 disease.
We know this crystal clear, and we have all the scientific articles that prove it. One of them is this one:
‘Researchers at Karolinska Institutet, the University of Manchester and Chalmers University of Technology have shown that the human immune system handles graphene oxide in a manner similar to pathogens, possibly leading to safer biomedical applications in the future.’
What you are seeing here is graphene oxide being attacked by neutrophils which are, let’s say, cells of the immune system that try to phagocytize it, try to engulf it: to coagulate it. That’s why graphene oxide generates clots and thrombi.
‘Graphene oxide is currently being studied for use in various drug delivery methods and other medical and non-medical applications. However, it is of critical importance to understand how these materials interact with the body. The study shows that neutrophils, the most common type of white blood cell specialized in combating infections, —just like a pathogen— release so-called neutrophil extracellular traps (NETs, the most common type of white blood cells) when encountering GO (graphene oxide). NETs are made up of a “spider-web” of DNA decorated with proteins that help neutrophils to destroy microorganisms such as bacteria and fungi. The researchers found that GO causes specific changes in the lipid composition of the cell membrane of neutrophils leading to the release of NETs. They could also show that antioxidant treatment —such as with NAC and glutathione— reversed this process.’
That is why treatments with glutathione have worked, and that is why treatments with N-acetylcysteine, which is a precursor of glutathione. Because they work providing the army with antioxidant reserves to deal with a toxic substance, a poisoning, that has been introduced into the body by different ways.
‘In a companion study published in Nanoscale, it was shown that GO is degraded in NETs, much like bacteria and other pathogens.’
Taken together, these studies show that GO can be trapped and degraded in NETs just like pathogens. I want to tell you that we have published in our website at least 70 studies that reflect everything we are saying and manifesting here.
On the other hand, I have been asked about the efficacy of chlorine dioxide. That goes another way. What it does is to oxygenate the cell, it prepares it so that it is not easily destroyed by this toxicant. What glutathione would do is to provide the army with more numbers of soldiers in terms of glutathione to deal with toxins. What we have found, as I say, is that most of the treatments that have been with N-acetylcysteine or glutathione and even with other antioxidants such as astaxanthin, which is a powerful antioxidant, have been very favorable treatments for the patients.
And also, curiously and suspiciously, found that these health institutions are literally governed by evil; it is a psychopathy without previous history: we had never seen the history of such psychopathy.
By June 17 that the FDA tried to stop the marketing of N-acetylcysteine after it had been used for 57 years as a normal and ordinary mococcolytic. It was a very suspicious thing to do, wasn’t it? So this is basically my exposition. Any doubts that you may have about the studies that we have carried out at La Quinta Columna, well, there is simply something that is very conclusive, and that is the preliminary report of a renowned professor of a public university here in Spain. We are very close to providing complementary evidence to give more strength to this report in which we are already told that there is solid and proven evidence that there is graphene oxide in the sample that we sent.
Simply, for Colonel Tamayo and Judge Giorgianni: regardless of the fact that we obviously think that SARS-CoV-2 is precisely graphene oxide —and we can prove it— or at least it behaves exactly and exhaustively the same, how is it possible that graphene oxide is injected through the vials? How is it possible if the masks were really withdrawn because they caused pulmonary affections due to toxicity? What are we talking about, gentlemen?
Here I have tried to make the exposition as synthesized as possible so any doubt that may be generated by the manifestation that I have given here can be clarified throughout the time left we have.”
—Ricardo Delgado.
If you want to support La Quinta Columna, you can refer to their official website and follow them on their official channels on Telegram, Instagram, Youtube and Twitch. If you want to contact directly, send them a message to: tutoronline@hotmail.es. Don’t worry about the language barrier, they understand English and French.
Nothing illustrates the mad hysteria of pandemic theater like the bizarre “safety” measures employed by school officials. From the onset, over-zealous teachers unions and health & safety mavens have led a maximum pressure campaign which has all but destroyed any chance of children getting an adequate education experience in 2020 and 2021. As if forcing children to stay at home on Zoom, government ‘public health’ officials and school administrators have systematically abused children by forcing them to wear masks all day in school, or worse: forcing children into isolation either due to a fraudulent PCR test result, or from another child who tested PCR positive in their cohort, or because their teacher tested positive – even though the children are statistically at roughly zero risk of even getting a cough due to COVID-19. Some teachers unions are even lobbying to have children vaccinated with the unlicensed experimental jab in order for schools to be “safe for return” this fall.
But in terms of peak lunacy, nothing can match the policy of constructing plastic boxes to supposedly protect children from the virus in classrooms. In fact, there was never any actual ‘science’ to back-up this fanciful policy. While school administrators deferred to the US Centers for Disease Control (CDC) for supposed guidance, but now it’s revealed that the CDC were just making it up as they went along.
Like so many other unfounded claims and pseudo science quackery surrounding the pandemic – like social distancing and masks “in order to maintain low spread,” this ‘sneeze shield’ charade was just another elaborate farce. No science ever existed which supported caging children all day in these plastic bubbles. It was also a massive money-spinner – exploding into a multi-billion dollar school PPE industry overnight – based on a lie.
Despite any actual evidence that the plastic shields reduce the transmission of COVID, officials still recommended masks and plastic boxes anyway, in their obsession to separate and socially distance children.
Not surprisingly, the CDC also relied on spurious anecdotal evidence and widespread rumors to support its recommendation for mandatory masks – even though their own data showed 85% of supposed confirmed COVID-19 “cases” reported they either “often” or “always” wore a mask anyway.
Dystopian: President Joe Biden visits school kids wearing masks sitting behind plastic protective shields pic.twitter.com/tmfsWzVkNd
— The Post Millennial (@TPostMillennial) May 3, 2021
Mid-March 2021, the CDC released new guidelines, which reduced the social distance in schools to 3 feet and removed the recommendations for barriers between school desks. Greta Massetti leads the CDC’s community interventions task force and said about the plastic shields, “We don’t have a lot of evidence of their effectiveness” in preventing transmission.
The new recommendations triggered a variety of responses in teachers and parents, some of whom are not comfortable sending their children to school where they may be allowed within 3 feet of another child or teacher.
The fiction surrounding all the alleged ‘mitigation’ and ‘safety’ measures touted by school officials – is largely built on top of the myth of the asymptomatic spread. Despite the fact that all of the highly cited, major peer-reviewed science demonstrates that asymptomatic spreading of the virus does not exist – public health officials are still using this myth as the primary basis for all of their policies – from social distancing, to masks, plexiglass bubbles, lockdowns, travel restrictions, and even vaccinations. However, the peer-reviewed scientific literature is clear: large-scale studies have been conducted, including at the supposed epicenter of the pandemic in Wuhan, China – which show no evidence of any asymptomatic spreading of the ‘novel’ coronavirus. See the results published here, here, and here.
Vaccine “passports” being put in place by the European Union and Australia as well as some U.S. states and businesses are one of the more alarming instruments advancing the “heart and soul of Technocracy and Scientific Dictatorship.”
As must be increasingly apparent to anyone capable of digging beneath the media’s daily outpouring of Orwellian propaganda, the planet-wide changes ushered in by the conveniently timed COVID crisis have surprisingly little to do with health. Facilitated by big tech, big military, big pharma’s injectable operating systems and other tools of “biofascism,” the takeover being engineered by private central bankers and their technocratic partners represents no less than a complete end-run around human freedom.
So-called vaccine “passports” or “certificates,” being put in place by the European Union and Australia as well as some U.S. states and businesses, are one of the more alarming instruments advancing this tyrannical centralization and control agenda. Not one to mince words, author Naomi Wolf makes the case that the “passports,” if allowed to become the norm, could trigger “the end of civil society” and “literally the end of human liberty in the West.”
Why is there such a strong push to make travel and commerce contingent on vaccine passports? One important answer, well understood by Wolf as CEO of a tech company, is “location intelligence” — what technocracy expert Patrick Wood calls the “heart and soul of Technocracy and Scientific Dictatorship.” Without irony, the champions of location data rhapsodize that such data are “a powerful way to connect people to place, transactions to actions, responses to trends, and customers to where they do business and the kind of business they do” — ultimately facilitating the “digital transformation of society on the whole.”
Less cheerfully, technocrats understand, even if the general public does not, that location data permit control at the most granular levels and provide “a platform for understanding what’s going on at all scales.” This point was disturbingly illustrated in a June 21 study in JAMA Internal Medicine, which essentially denounced “small and informal social gatherings,” positing that children’s birthday parties are potential hotbeds of SARS-CoV-2 transmission.
This willingness on the part of technocracy’s foot soldiers to be party poopers — literally — would be silly were it not for the study’s baleful messaging, which confirms Wolf’s concerns that we are not only in a battle for liberty but in “a war against human beings and the qualities that make us human.”
No fun allowed
On its webpage devoted to “small gatherings,” updated May 6, the Centers for Disease Control and Prevention (CDC) addresses the topic of social gatherings with family and friends, “such as small holiday parties, family dinners and small special celebrations.” To make such events “safer,” CDC counsels hosts and attendees to limit the number of guests, wear a mask “with two or more layers…indoors and outdoors except when eating or drinking,” socially distance, avoid handshakes and hugs, supply one’s own food and dishes — and (precluding any “Happy Birthday” songs) avoid any loud cheering or singing. Better yet, CDC says, simply have a virtual gathering!
The JAMA birthday party study helpfully reinforces the CDC’s dour advice. Conducted by private-sector researchers from RAND Corporation, Harvard and “healthcare navigation” company Castlight Health, the study looked at privately insured households whose members did or did not have a birthday in the preceding two weeks and county-level COVID-19 prevalence data — but included no data from actual social gatherings.
Taken at face value, one can see how the study’s take-home message — that households in certain counties were possibly a little bit more likely to receive a COVID diagnosis subsequent to an adult or child having a birthday — could direct worriers toward the CDC’s “virtual gathering” solution. However, one needs to parse the study’s definition of risk. As has become par for the course in risk pronouncements designed to steer COVID-related behavior in a particular direction, the researchers said nothing about absolute risk, even though many consider absolute risk statistics to be “the most useful way of presenting research results to help … decision-making.”
Thus, while the study reported a 31% “relative increase” in COVID diagnoses “associated with birthdays” — a finding, moreover, that pertained solely to households in the 10% of counties with the highest background prevalence of COVID — the increased absolute risk (again, only in the 10% of high-background-prevalence counties) amounted to a flimsy 0.086 increase over the COVID “background rate” of .278/100. Nevertheless, the researchers augmented their antisocial message with the conclusion that “policy interventions designed to limit disease transmission should also focus on informal gatherings.”
Defending freedom
The heavy-handed marketing of COVID injections and COVID vaccine passports as tickets to “freedom” has brought George Orwell’s inverted “freedom is slavery” logic fully to the fore. The “appendix” to 1984 explains that while the fictional totalitarian regime Oceania could readily condone use of the word “free” in statements such as “This dog is free from lice” or “This field is free from weeds,” usages such as “politically free” or “intellectually free” had gone entirely and intentionally extinct because the concepts themselves had been erased.
The alarming rapidity with which the U.S. and once “robust” Western democracies were able to implement “elements of a locked-in, 360-degree totalitarianism” was facilitated not just by a heretofore unimaginable level of global policy coordination but also by the public’s complacency. The pressing question of the day, therefore, is whether citizens will continue to tolerate blatant efforts to memory-hole freedom.
Lobbying for COVID vaccine mandates and passports in the U.S., one of the latest darlings of vaccine coercion recently argued that the Biden administration “shouldn’t be so squeamish about vaccine verification,” openly calling mandates and “verification” desirable tools to “push [the unvaccinated] in the right direction.”
And if we are to believe Gallup poll propaganda, more than half of Americans are already on board, supporting policies such as having to show proof of vaccination to fly or attend sporting events or concerts. On the other hand, in an “unscientific” poll on independent journalist Sharyl Attkisson’s website, 97% of respondents answered “absolutely not!” to the question “Do you support requiring ‘vaccine passports’?”
The dispiriting cold water now being thrown on children’s birthday parties is part and parcel of a set of COVID-inaugurated policies that, in Naomi Wolf’s words, “seem designed to ensure that humans will have no ‘analog’ space or ‘analog’ culture left — no way to feel comfortable simply gathering in a room, touching one another as friends or allies, or joining together.”
Fortunately, as writer Allan Stevo has noted, Americans “are becoming increasingly firm and resolute” about freedom, “saying ‘Yes!’ to good things” and “saying ‘No!’ to bad things” — and that, says Stevo, “is exactly how bad times turn into good times.”
The video clip below is an excerpt from a much longer conversation between Patrick Timpone, One Radio Network, and Dr. Jennifer Daniels. Topics discussed in the full video include stretching exercise, nutritional advice and questions and answers from viewers. The full interview can be found HERE.
In this clip, Dr. Daniels shares her views on what “covid” actually is, why anti-parasitics such as Ivermectin work as “cures”, herd immunity, the “variants”, flu shots and the choice to believe in the virus and the vaccines.
Excerpts from transcript:
In response to a question about using Ivermectin for “covid”.
“Let’s get back to what covid is….What we have here is the common cold, which simply is the body attempting to dump a bunch of parasites and crap. So, of course, any anti-parasitic will work…But what’s really happening here is they have perpetrated an amazing hoax and convinced people that the common cold is the plague and it’s pretense for more government control.”
###
More from her views on “covid”:
“The death rate associated with…”the situation” (I call it the situation) is no greater than the population-wide death rate or even less… Approximately 1% of Americans die every year. That’s it. One percent drop dead. If you get “the plague”, what percent drop dead? About 1/2 percent.”
###
“The people who believe in the vaccine — who want to take and believe everyone else should take it — they don’t believe in the vaccine. If they really believed in the vaccine they would understand that it doesn’t matter if anyone else takes it. What they really believe is obedience, government control and control of other people. So we understand what the real religion is here then we can unmask that and talk about that.”
Ron Johnson (R-WI) and former Green Bay Packers player Ken Ruettgers held a press conference June 28 with families who want to ‘be seen, heard and believed by the medical community’ after suffering adverse reactions to COVID vaccines.
The group that spoke was put together by Ken Ruettgers, a former Green Bay Packers offensive lineman, whose wife suffered an adverse reaction after receiving a COVID vaccine. Ruettgers, who now lives in Oregon, started a website to bring awareness of COVID vaccine reactions to the medical community.
“We are all pro-vaccine,” Johnson said at the onset of the news conference. In fact, Johnson has had every flu shot since the Swine flu, is current on all of his vaccines and was a huge supporter of Operation Warp Speed, though he has not had a COVID vaccine because he already had COVID.
Johnson said his goal was to provide a platform for these individuals who were injured by COVID vaccines so the health community and mainstream media would acknowledge them and get to the root cause — to find a solution for these problems.
Johnson argued that while most people don’t suffer significant side effects following vaccination, he is concerned about “that small minority that are suffering severe symptoms.”
Five people from across the U.S., including a 12-year-old girl who was part of the Pfizer clinical trial, joined the conference at the federal courthouse in Milwaukee. They described their reactions to the COVID vaccines, including neurological, cardiac and gastrointestinal issues, debilitating health problems and hospitalizations.
Among them was Maddie de Garay from Ohio who volunteered for the Pfizer vaccine trial when she was 12. On Jan. 20, Maddie received her second dose of the Pfizer COVID vaccine as a participant in the clinical trial for 12- to 15-year-olds and is now in a wheelchair.
“Why is she not back to normal? She was totally fine before this,” said Stephanie de Garay, Maddie’s mother. She volunteered for the Pfizer vaccine trial “to help everyone else and they’re not helping here. Before Maddie got her final dose of the vaccine she was healthy, got straight As, had lots of friends and had a life.”
Upon receiving the second shot, Maddie immediately felt pain at the injection site and over the next 24-hours developed severe abdominal and chest pain, de Garay said at the press event.
Maddie told her mother it felt like her heart was being ripped out through her neck, and she had painful electrical shocks down her neck and spine that forced her to walk hunched over.
Maddie’s parents took her to the emergency room as instructed by the vaccine trial nurse administrator. Her labs were taken, she was checked for appendicitis, given an IV with medicine and sent home. The diagnosis in the discharge summary read “adverse effect of vaccine initial encounter.”
Maddie’s condition continued to worsen. Over the next two and a half months her abdominal, muscle and nerve pain became unbearable, her mother said.
The world has a front-row seat to a horror story in progress, a vaccine horror story that was a long time in coming. The CDC shows that it does not have an ounce of integrity, as they demonstrated in their recent meeting about the damage done to younger populations with the Pfizer and Moderna vaccines.
At the meeting, CDC scientists presented horrendous data. It showed that even without accounting for underreporting, the second dose of one of these vaccines could increase the risk of heart problems up to 200-fold in young men. But the scientists then went on to suggest the vaccines should still be given – even to kids already suffering from heart problems.
The CDC is now reporting that 6,113 people have died following COVID-19 injections, with their June 25 release of data in the Vaccine Adverse Event Reporting System (VAERS), a U.S. Government-funded database that tracks injuries and deaths caused by vaccines. Besides the 6,113 deaths reported, 5,172 permanent disabilities, 6,435 life-threatening events, and 51,558 emergency room visits.
The EudraVigilance database, which covers 27 European Union countries out of about 50 actual European countries, reports that through June 19, 2021, there are 15,472 deaths and 1,509,266 injuries from the four COVID vaccines used there. Of the total of injuries recorded, half of them (753,657) are serious injuries.
These are the official numbers, the official reports. No health official will admit that these numbers are probably ten times higher because of the historically under-reporting into ‘official’ vaccine adverse reporting systems. What every health official and governmental agency is doing is ignoring this information, these deaths. No one is dying from COVID shots. They are not lethal injections.
But we might have as many as 200,000 dead (factoring by ten because of the underreporting). If we could count the rest of the world, who do not have official vaccine reporting systems that are publically reported, we might have as many as 400,000 deaths or more. To calculate, we would need to count the vaccines administered in America and the E.U. and see how many total vaccines are given in the world.
There have been more deaths reported following COVID-19 injections, which started in December of 2020, than there have been total deaths recorded following ALL vaccinations in theprevious 30 years, from January 1, 1991, through November 30, 2020, according to the CDC’s VAERS.
Don’t you think this will catch up with other branches of government who will fry Fauci, the FDA, and the CEOs of Big Pharma who have foisted these vaccines on the public leading everyone to believe they are safe when they are not?
There have also now been 576 deaths of unborn children reported following COVID-19 shots, as the CDC continues to recommend that pregnant women should get injected with these shots, that many dissenting medical doctors and scientists are now describing as “bioweapon” injections.
Madness is infecting the world of medicine, a form of madness never seen on this scale in history. Even Hitler and his Nazi henchmen cannot compete with what is going on and the uncountable millions being harmed, killed, maimed, and driven into despair. Evil has shown its ugly face, and unfortunately, the children are suffering the most as certain adults cheer that on.
If the FDA knows what’s good for it and the public,
they will retract their emergency authorization
of all three vaccines used against COVID-19 NOW.
What Did They Do To Our Children
This week’s data for 12- to 17-year-olds show:
7,294 total adverse events, including 423 rated as serious and nine reported deaths among 12- to 17-year-olds. Four deaths (or 44%) were cardiac-related, and three were sudden, unexplained deaths.
The most recent reported death includes a 13-year-old boy (VAERS I.D. 1406840) who died two days after receiving a Pfizer vaccine. Other deaths include three 15-year-olds (VAERS I.D. 1187918, 1382906, and 1242573) and two 16-year-olds (VAERS I.D. 1225942 and 1386841), and one 17-year-old (VAERS I.D. 1199455)
What health care officials and cruel idiotic politicians have done to the children is enough to boil one’s blood. According to a new report, children in the U.K. as young as five are suffering panic attacks and other psychological trauma as a result of COVID lockdowns, leaving 1.5 million kids in need of mental health treatment. NHS leaders say that the impact of repeated lockdowns has left children fearful of leaving their homes or meeting their friends amid an explosion of “locked-in trauma.” But let us love Dr. Fauci and all the demented public health officials who will be remembered in history as the new kind of medical Nazi.
“Forecasts seen by this newspaper state that an extra 1.5 million children and young people will require mental health support “as a direct impact of the pandemic” during the next three to five years,” reports the Telegraph. “The calculations from the Centre for Mental Health, involving NHS economists, suggest demand will be as much as three times greater than the capacity of mental health services.”
Back To Nuremberg
In reality, it’s been years since pharmaceutical/medical terrorists have occupied planet Earth. Not happy with the level of terror and suffering they have accomplished, they got greedy for more evil, despicable ugliness. Fauci, the FDA, the CDC, the NIH, Google, Facebook, Twitter, and YouTube are all in trouble or will eventually be.
What does mainstream media say about all of this? “After hundreds of millions of vaccine doses administered around the world — and intense safety monitoring — few serious risks have been identified. A tiny percentage of people who got vaccines made by AstraZeneca and Johnson & Johnson reported an unusual type of blood clot. Some countries reserved those shots for older adults, but regulatory authorities say the benefits of offering them still outweigh the risks.”
VAERS’ Detection Rate Is Abysmal
It’s been established for over a decade that VAERS’ detection rate is abysmal. A report submitted to the Department of Health and Human Services (HHS) in 2010 concluded that quote “Fewer than one percent of vaccine adverse events are reported by the VAER System.”
The report mentioned was the product of a million-dollar grant the Department of Health and Human Services gave some Harvard Medical School researchers to develop a computerized “active” system that would perform better than VAERS and then run randomized trials evaluating both.
A 2013 study by researchers from the CDC itself found that almost 30% of health care professionals had never heard of the VAERS system. Among those who’d come across a potential vaccine side effect and had a jarring, 83% still failed to file any report.
Critical Race Theory Has It All Wrong
Critical Race Theory training, which pressures people not to say certain things, take a certain stance, or forces them into some segregated settings, may infringe on people’s constitutional rights and even violate civil rights laws, said Dr. Carol Swain, a former professor of political science and law at Princeton and Vanderbilt universities.
The main tenet of Critical Race Theory (CRT) is that the people of the world are divided into oppressors and oppressed. In the United States, “all white people are considered oppressors who benefit from undeserved advantages,” said Dr. Swain.
I’m afraid that’s not right, for, in the world of medicine, it is a tiny group against everyone else. The entire world, all the different races, are oppressed by pharmaceutical terrorism. It’s the super-rich against all of us. Big Pharma ended up hating us all in its lust for more money and power.
Conclusion
Fauci, Gates, the NIH, CDC, FDA, and other “authorities” killed millions by intentionally suppressing helpful information about treatments like ivermectin, which would have reduced the death rate to the point where there would have been no pandemic.
There never was a need for these deadly vaccines. What we have are thousands if not hundreds of thousands of intentionally killed vaccine dead and a cover-up barely hidden because of these ‘official’ vaccine reporting systems. Genocide? Crimes against humanity? Medical treason? Psychopathic insanity?
A top WHO official says that mask mandates
and social distancing should continue indefinitely
in order to protect against new variants of COVID-19.
So far, they are getting away with murder. But if planes start dropping out of the sky from vaccinated pilots getting blood clots or airlines having to cancel the majority of their flights because of vaccine damages to crew and pilots, I wonder what will happen.
Again our only hope is the vaccine news gets bad enough that they have to stop. However, the vaccine news is already bad enough, and look how the CDC weasels out of protecting the young.
In America you can get a free doughnut if you live in the right place and agree to have yourself jabbed with the toxic, experimental brew known as the covid-19 jab.
But there are no free doughnuts available in the UK.
Here all you get if you have a covid-19 jab is a free blood clot.
Free clots with every jab.
They should make honest adverts promoting the blood clots.
A clot for a clot. My kingdom for a clot. They could hire some of those media doctors to explain how wonderful clots can be. A clot in your leg. A clot in your lungs. A clot in your brain. Kill you quick, kill you slow.
Let’s bring some honesty into government propaganda.
Could those queues be really full of people wanting to be jabbed? Or maybe they’re all out of work actors who’ve been offered £10 to stand in a queue for three hours. For another fiver they’d hold up signs saying `jab me, jab me’. For £20 they’d say Fauci and Whitty were human. I don’t believe the number jabbed is anywhere near as many as they claim. I don’t believe anything the Government, its advisors, the BMA, the BBC or anyone working for the mainstream media has to say.
The problem is that we’re living in a world asylum controlled by psychopaths and I hardly know where to start. I don’t know about you but I feel quite pleased with myself when I manage to struggle through another day.
I have become very cautious. I tip toe round the garden to avoid falling over and breaking something because I don’t want to go to hospital. I back away from barky dogs because I don’t want one to bite me requiring a hospital visit. I’m going to buy a second hand tank so that I can drive around without worrying about being rammed by some idiot whose mask has made him drowsy. Incidentally, I realised the other day that the only time I will ever wear a mask is when the authorities tell me I must not – then we’ll know they’re necessary.
I’m terrified of needing to go to hospital. A nine hour wait in the casualty department and then, if you’re lucky, you get to see a nurse. The doctors have all disappeared and are hiding in Aberystwyth or the Colorado mountains. I don’t want to be tested. I’m terrified I’ll fall asleep and someone will creep up and jab me behind the arras with the evil poison in a syringe. You probably won’t believe this but I’ve even bought a surgical suture kit so I can sew myself up if I slice myself with the hedge-trimmer or a chain saw. Honest. I’ve got sutures and thread and lancets for tidying things up. And a nice bottle of antiseptic to splash on the wound. Do it yourself invisible mending. I’ve got a very nice bottle of malt whisky to use as an anaesthetic and a good bottle of brandy to get me through the post-op hours. You think I’m kidding but I promise you I’m not. Colin Barron’s got Lulu and a Whitty wig and I’ve got a boxful of operating theatre supplies.
The empty headed cretins who believe that we’re living through a pandemic are enjoying their days in cloud cuckoo land.
I can’t believe how many stupid, gullible people there are around. And how readily they believe the nonsense they are told. They must all have at least one foot firmly planted in the loony bin. There are battalions of bed wetting numpties around who dutifully wear their grubby masks, which they are told to wear to try to hide the Bell’s Palsy they’ll get from taking a toxic experimental jab. If the rules ever do soften for a while, millions will be so terrified they will wear their masks and do the distancing sidestep for eternity because they believe they will live for ever if they do. They might as well be immortalised in formalin like one of those hapless animals preserved in the name of what Hirst calls art and the rest of us call pointless.
There are people in the UK who still believe things they’re told by government ministers such as Johnson and Hancock when in truth the world’s politicians are about as much use a hundredweight of crisp dingle berries. I wouldn’t trust Macron to clean my car and I wouldn’t trust Biden to blow his own nose even if someone put a hanky in his hand and told him what to do. The people manipulating these sorry quarter wits, the Global Economic Forum, the Gates Foundation and so on are laughing at everyone; they’re taking the piss and no one seems to give a damn.
The only people quoted in the media these days are invertebrates such as Dr Dolly Parton and Dr Mrs Queen who, despite knowing nothing at all about anything other than wigs and corgis, are happy to assure us that the covid jabs will do us even more good than spinach. They haven’t bothered to consult the information collected by their own governments which show that the jabs have killed thousands and injured hundreds of thousands. I’ve been writing about iatrogenesis for many decades and there is no drug in history which has been promoted as hard as the covid-19 jab and no drug in history – and vaccines count as drugs – that has killed and injured as many people. I doubt if napalm has killed as many people as the covid jabs.
And then there are complete cretins who want children to be given a deadly, experimental, inadequately tested, vaccine that only has a temporary licence and that doesn’t do what the cretins think it does to protect them against a disease they probably won’t get and that almost certainly won’t kill them if they do get it. I wonder how many know what the word `experimental’ means. For the record it means that no one knows what will happen to the people who take it. That’s an experiment. If I throw Madge Hancock off the top of Big Ben I don’t know precisely what will happen. Will she die of a brain injury or blood loss? That’s the same as the covid-19 jab. The jabs have been given emergency authorisation despite the fact that the covid-19 responsible was officially downgraded and declared no deadlier than the flu.
Establishment figures are falling over themselves and each other to insist that mandatory vaccinations must be brought in. A columnist in the Daily Telegraph says that care workers must be jabbed. because they, don’t care enough. That’s what they said. The columnist, someone called Judith Woods, says that people who refuse to take the vaccine are selfish and that carers who won’t be jabbed (with junk, let us not forget that has already killed over 1,000 people in the UK – according to the Government’s own figures ) – ‘don’t care enough about their charges. `More than 30% of carers in her borough of Hackney have refused a vaccination that would she says protect them and others from a virus that she claims has laid waste to the planet. That sentence would win her applause from the BBC. The virus hasn’t laid waste to the planet. The figures show it killed no more people than the flu. And the NHS admits that the vaccine won’t necessarily stop people getting the virus or spreading it.
Do journalists know the truth, I wonder. Are they too naïve to realise that governments and their advisors know that if you tell a big enough lie no one will recognise it as a lie because no one believes anyone could lie that much and keep a straight face.
Hancock the moron says we should aim for the double jabbed cretins to be able to avoid quarantine. Wonderful. Do journalists not know that Israel says it is facing a new covid-19 outbreak despite having the world’s most vaccinated population.
Patrick Henningsen’s magnificent 21st Century Wire website contains an article from the Wall Street Journal reporting that 450 US colleges and universities have announced policies mandating that all students be fully vaccinated before the autumn term. The snag, reports the journal is that the mandated vaccinations aren’t legal or morally acceptable and violate the basic principles of medical ethics. Go to 21s Century Wire to read the report headed `WSJ: American University Vaccine Mandates Violate Medical Ethics’.
Worse still there are double, double cretins and ignorant psychopaths around who insist that 12-year-old children should be allowed to decide for themselves whether they want to be jabbed. They want children to be jabbed without parental consent. Children who aren’t considered old enough to smoke, go into pubs, vote, have sex or watch dirty movies are told they’re old enough to decide whether they want to be jabbed with stuff that is entirely experimental and so complex that not one in 100,000 adults understands it and which has, according to government figures, already killed thousands of people around the world and maimed hundreds of thousands more. How long before they start offering kids a new game console if they agree to roll up their sleeves and risk death and disablement? Alternatively, the kids will probably be told they can remain unvaccinated and be ostracised, lonely and laughed at, and will have to live in a damp, dark cellar for six months.
Adults don’t have the foggiest what they’re being jabbed with but 12–year-olds are mostly illiterate and don’t know whether to put their socks on before or after their shoes. And now we want them to decide whether or not to be jabbed.
There is no such thing as informed consent these days. And it is illegal to give this stuff to a human being without their full and informed consent. The vast majority of doctors and nurses who have been jabbing people are criminals who will, when justice is served, find themselves sitting in cells alongside world famous war criminal Tony Blair. It’s a crime to give treatment without informed consent. It’s a double crime to give treatment which is experimental without obtaining full informed consent. And it’s a triple crime to do it to children.
It was, of course, the evil Blair who gave the Brexiteers victory in the UK because every time he opened his mouth everyone knew he was lying about the Common Market. And now he’s our greatest champion. The pro-vaxxers ought to lock him up but they’re stupid and they think it helps when he opens his mouth and lets his brains dribble out. Every time he says anything promoting vaccines and death rays and mustard gas another million people decide to say no thank you very much to whatever it is the malignant bastard is selling. Blair has the eyes of the devil, the soul of a psychopath and the principles of a politician. A man who, like Bush and Powell took deceit to new depths.
Excuse my language, by the way but it is acknowledged to be impossible to mention Blair without using at least one expletive. Indeed, most people outside the UK think his first name is `Thatfuckingtwat’ because they’re so used to hearing people describe him as `Thatfuckingtwat Blair’. The odd thing is that if Blair says anything about covid-19, such as that the unvaccinated should stay in lockdown, presumably as a punishment for having working brains, the BBC clears everything to give him airtime. But if 100 independent doctors stand up and have something to say then the BBC ignores them.
Blair provides the mark for evil, of course, but the rest aren’t much better.
I hate this damned covid jab.
It is everything that is wrong with medicine. It’s deadly, not properly tested and there is a risk that the vaccinated will kill us all. The idiots who’ve let themselves be jabbed should have a big V tattooed on their foreheads so that we can identify them and keep well away. Or maybe a big I standing for Idiot.
Let me explain how much I hate it.
There is a small fish found in the river Amazon called the candiru, aka the toothpick fish. It’s a tiny fish which lives as a parasite in the gills of bigger fish. If you go swimming in the Amazon and feel the need to urinate and decide to relieve yourself in the river, something bad, really bad can happen. The little candiru will be attracted by the smell and will travel up the stream of urine into your urethra and there it will stick out its little spines and makes its home. The pain is apparently horrific. The flow of urine from the bladder will cease and serious surgery will be required if you are to be saved. This is not a fun thing to happen. It’s not something you laugh about later.
Well, I’d rather bathe in a pool full of candiru than have one of the deadly, experimental covid-19 jabs because at least with a tiny fish living inside my urethra I’ll get to keep my soul and I’ll have a better chance of staying alive.
We have to stop all this and you’re the only people who can do it. It’s no good me preaching to the converted and you’re the only people I can reach since I’m banned from anything resembling mainstream media.
Send videos and articles off my websites to everyone you know and everyone you don’t know. Everyone. It’s how we’ll win this war. Share the truth with people and they’ll be astonished at the extent of the lies they’ve been told. My websites contain up-to-date figures of the numbers who have been killed or injured by these jabs.
Encourage those who are brave enough to tell the story of how they’ve been harmed by the vaccine. Encourage them to admit they made a mistake. If you see such videos offer sympathy and support. Their courage will help us enormously.
And remember, people who rely on the mainstream media will have been lied to consistently – especially by the UK’s state broadcaster, the Government’s propaganda arm, the utterly unscrupulous, ruthless and deadly BBC. There are, remember, no proper journalists working for the BBC – just pseudo-journalists.
Remember too just how confusing everything is.
You can’t go to Spain, Guatemala or Texas or the Isle of Wight unless you’ve been to Cornwall. You can’t have you hair cut while getting married unless you’ve washed behind your ears three times and own a bicycle. If you live north of the equator you can’t hug more than three people at once and you must stay indoors between the hours of 9 am and 3 pm on Saturdays unless you’re at Ascot and there is an R in the month. You must wear a mask, socks and galoshes while eating and drinking but you can remove your mask to eructate or answer questions at the police station.
It’s hardly surprising that people get confused and frightened.
The rules about working from home are just as bad. Office workers and doctors are all working from home, and surgeons will probably soon tell patients to be prepared to perform surgery on their own kitchen table. You download a video on YouTube and a surgeon guides you through the whole procedure. The first cut isn’t necessarily the deepest by the way. Madge Hancock, who is allegedly in charge of fibbing in the UK, will probably tell us that firemen can also work from home if they wish. You ring 999 and ask for the fire brigade and one of the firemen asks you to take your fire round to his place. Alternatively, you can download an App and take pictures of the fire and the firemen will watch your home burn to the ground and make comments on what they are seeing.
The world has gone stark raving mad.
My videos on BNT are controlled and suppressed by governments, with increasingly ruthless efficiency. So spread the word far and wide. Be daring and put videos on your Twitter or Facebook. Take a chance.
And if someone you know is being threatened with a vaccination they don’t want, remember there are four ways to stop this happening.
First, tell the doctor or nurse or busy body involved that you will make an official complaint (something everyone in any bureaucracy is terrified of these days).
Second, tell them that you will send details of their perfidy to the press and all over social media – naming them personally.
Third, tell them that you will sue them personally.
And, fourth, if it’s a doctor or a nurse tell them that you will make a formal complaint to their licensing body.
And after all that hand them a loo roll because they’ll need it.
In this book, which has been a labor of love for the past decade, Seneff explains how and why glyphosate poses an existential threat to humanity, and why it’s so important to avoid it if you care about your health and the health of your family.
“It’s been a decade of learning everything I could about glyphosate,” Seneff says. “When I first heard about it I basically dropped everything else I was doing because I was so confident that I had found the answer to the autism epidemic. That was the thing I was looking for. Back in 2012, I heard a two-hour lecture by Don Huber, and it changed my focus entirely.
I already understood the symptoms of autism, a very complex disease — lots of gut problems and mineral issues — and it all came together with his lecture. Overnight I just started poring over all the papers I could find.
Shortly after that I found Séralini’s paper,1 which had not yet been retracted at that time. It was later republished, the paper by Séralini, a French toxicologist who had shown that very low doses of glyphosate over the lifespan of a rat could cause a lot of damage.
He pointed out that after three months, everything looked good, so it’s a slow kill. This is one thing I emphasize in my book. Glyphosate is subtle, and that’s really a huge problem because people don’t [make the connection]. We have diabetes, obesity, autism, Alzheimer’s. It’s a long, long list, all the gut problems.
The microbes are being very much disturbed by the chronic poisoning with glyphosate, and then the gut becomes a central starting point for many diseases, including neurological diseases and arthritis. So, you see that disruption of the gut, and glyphosate can cause exactly the things that we’re seeing.”
Glyphosate Contamination in Common Products
Before delving into glyphosate, Seneff spent five years focusing on the potential toxicities of vaccines. She still believes vaccines can play a role in the chronic diseases we’re seeing, including autism.
However, glyphosate may actually play a more significant role. Seneff believes it contributes to and worsens damage caused by vaccines, in part because it binds very efficiently to aluminum used as an adjuvant in certain vaccines. It likely binds strongly to many other toxic metals as well.
The theory is that, by being wrapped up with glyphosate molecules, the metals can more easily penetrate various barriers in your body. This is because glyphosate causes these barriers, such as your intestinal barrier and your blood-brain-barrier, to become more porous. And, as leaky gut or leaky brain set in, the toxic metals are shuttled across, along with the glyphosate.
Interestingly, Anthony Samsel, a public health research scientist, and Zen Honeycutt, founder and director of Moms Across America, have independently found glyphosate contamination in live virus vaccines that do not contain aluminum adjuvant.
Seneff suspects glyphosate may be a contaminant in many drugs as well, particularly drugs produced by genetically engineering E. coli or yeast. They’ve also found glyphosate in tampons, which may then be absorbed through your uterine lining.
Seneff also hypothesizes that, since glyphosate is found in many vegetable-based fats, such as canola and soybean oil, studies comparing the health effects of fats may be compromised since they never consider the effects of glyphosate. Interestingly, while not fat-soluble, glyphosate can still enter fats (and is found in the vegetable oils just mentioned).
Samsel suspects glyphosate acts as a phosphate analog, because it has a phosphonate unit, and fats have phosphates (phospholipids). This is something he’s investigating right now, so eventually, we may learn more about that mechanism.
Glyphosate and the Rise in Celiac Disease
In her book, Seneff details the dramatic increase in glyphosate use since its introduction in the mid-‘70s. Estimates suggest that one pound of glyphosate is applied in the U.S. every year for every man, woman and child, in America, which is an astounding amount. It’s not even enough to buy non-GMO products, as many non-GMO items have been shown to have some of the highest levels of glyphosate.
Oats, wheat, barley and legumes like chickpeas and lentils tend to be very high in glyphosate because these crops are sprayed with glyphosate right before harvest as a desiccant to speed the drying process.
“I think that’s the reason for the epidemic in celiac disease,” Seneff says. “Samsel and I wrote a paper on that. We showed there’s a strong correlation between the rise in celiac disease over time and the rise in glyphosate usage on wheat, specifically on wheat. It matches much better to wheat than it does to the other crops, which makes sense, because wheat is the source of celiac disease.”
A case study of an American woman who tried to commit suicide by drinking glyphosate reveal some of the chemical’s effects. She developed a paralyzed gut, and this may well be what’s happening to many, on a low-grade scale. In essence, people’s guts are sort of semi-paralyzed by the glyphosate in the diet, which causes small intestinal bacterial overgrowth (SIBO).
Bacteria starts festering in the upper intestine because the peristalsis is not working properly, so food remnants get stuck. Glyphosate has also been shown to accumulate in the brain, and animal studies show it causes neuro excitotoxicity due to excess glutamate in the brain. This, in turn, “is absolutely connected to autism,” Seneff says.
In her book, Seneff also discusses the importance of sulfur for optimal health, how sulfate deficiency is connected to autism, and how glyphosate can cause sulfate deficiency.
How Glyphosate Affects Your Gut and Autoimmunity
Part of what makes glyphosate so toxic has to do with the fact that it’s a very efficient metal chelator. It binds metals and minerals really well. For example, glyphosate is a million times more effective at chelating aluminum than EDTA, a chelating agent used in heavy metal chelation treatment.
This, in turn, disrupts your gut microbes because it makes minerals unavailable to the microbes. Your gut microbes need minerals, as their enzymes depend on them for proper functioning. Glyphosate also disrupts the shikimate pathway, both in plants and microbes, and beneficial microbes are particularly sensitive to glyphosate.
When lactobacillus bacteria are killed off in your gut, your ability to digest gluten and casein (milk protein) is impaired, as this bacterium carries several enzymes your body does not have that specialize in breaking down proline, an amino acid found in gluten and casein. This, in turn, can eventually lead to autoimmune problems. Seneff explains:
“We have all these allergies to gluten and casein these days, all these different food sensitivities, and I think it’s because the lactobacillus are being killed off. They can’t support the digestion of those proteins anymore. Then the protein sticks around, the peptide sequence, and that’s what causes an immune reaction.
Then you can get an autoimmune attack through molecular mimicry — the antibody mis-recognizes a human protein because it looks like the piece of gluten that they become sensitive to, so they attack a human protein instead.”
Glyphosate Makes Harmful Fat Even More Hazardous
Interestingly, glyphosate may also contribute to the harm caused by the omega-6 fat linoleic acid (LA). LA is metabolized into arachidonic acid, which is metabolized into an endogenous cannabinoid that eases pain. The enzyme that accomplishes this conversion is cytochrome P450 enzyme, which is disrupted by glyphosate.
Seneff suspects arachidonic acid is getting redirected through enzymes that convert arachidonic acid into extremely immunogenic products instead, such as leukotrienes, which act as signaling molecules that turn on an inflammatory response. A generic term for these signaling molecules is eicocanoids. She explains:
“Leukotrienes are rightfully blamed for causing all the chronic pain we’re seeing — rheumatoid arthritis, joint and bone pain, and even, probably, problems with the brain, maybe headaches.
All the different kinds of pain we’re experiencing that are connected to inflammation could be a consequence of cytochrome P450 enzymes blocking the ability to convert arachidonic acid into the endogenous cannaboid. Instead, it gets redirected towards these signaling molecules that cause all this damage.”
On top of that, LA, when oxidized, turns into highly toxic free radicals such as 4HNE, which cause direct oxidative stress damage to cell membranes, mitochondria, stem cells and DNA. In your mitochondria, a feedback loop then occurs that causes the shutdown of your energy metabolism system, resulting in an increase in adipose tissue. Translation: Excessive LA causes accumulation of belly fat.
Glyphosate Is a Biological Toxin
Its effect on the shikimate pathway is a key mechanism by which glyphosate causes biological harm in humans. The human body does not have this pathway — a fact used by Monsanto to argue for glyphosate’s safety. But the microbes in your body do have it. Research has shown over half the microbes, on average, in your gut have the shikimate pathway and can therefore be decimated by glyphosate.
These include lactobacillus and bifidobacteria, which use the shikimate pathway to produce the aromatic amino acids tryptophan, tyrosine and phenylalanine, crucial coding amino acids that go into all the proteins of your body. They’re absolutely essential for protein assembly, and your body must rely on your diet and gut microbes to produce adequate amounts of these amino acids, as your body cannot produce them any other way.
When your gut microbes are harmed, it can result in a deficiency of tryptophan, tyrosine and phenylalanine. These amino acids are also precursors to many other important biologically active molecules. For example, tryptophan is a precursor to melatonin and serotonin. Tyrosine is a precursor to thyroid hormone, dopamine and adrenaline.
“These are all really, really important hormones that control brain behavior and regulate behavior and mood,” Seneff says. “Serotonin deficiency is connected to depression, and we have an epidemic in depression. So, I think there’s a direct path there. Also, some of the B vitamins come out of the shikimate pathway, including thiamine (B1), riboflavin (B2) and niacin (B3) …
You need thiamine for augmenting your immune system. If you don’t have a lot of thiamine, you’re not going to be able to generate a healthy immune response. That’s why it’s a part of septic protocols. If you’re wrecking it with glyphosate exposure that’s disrupting the shikimate pathway in your gut microflora, you’ve got a huge problem.”
Glycine Can Help Counteract Adverse Effects of Glyphosate
One simple remedy that can help lower your glyphosate burden is to take a glycine supplement. As explained by Seneff, the way glyphosate disrupts the shikimate pathway is by affecting an enzyme called EPSP synthase. That enzyme bonds to a molecule called phosphoenolpyruvate (PEP). The “phospho” in that name stands for phosphate.
At the place where EPSB synthase binds to PEP, there’s a glycine molecule. It’s a highly-conserved glycine in the enzyme. If that glycine is swapped out for alanine, a very similar amino acid, the EPSB synthase enzyme becomes completely insensitive to glyphosate.
“So, it’s black and white — either there’s a glycine there, in which case it’s incredibly susceptible to glyphosate, or there’s alanine, in which case it’s completely insensitive,” Seneff says.
Incidentally, this is how agricultural scientists create glyphosate-resistant GMO crops. They turn the glycine molecule into alanine, thereby rendering the plant impervious to glyphosate.
When glyphosate enters your system, it can take the place of the glycine molecule. While similar, (the “gly” in glyphosate stands for glycine) it’s not identical and does not work the same way as glycine. Hence, this replacement causes all sorts of trouble.
By taking a glycine supplement, you can counteract this chain of events by making sure there’s enough glycine present to fill up those glycine slots. As noted by Seneff, “If there’s lots of glycine, you’re going to be much less likely to pick up glyphosate.” She continues:
“I had thought about glyphosate being glycine, and knowing that it’s a glycine analog and that it was affecting places where glycine binds. Glycine acts as a neural transmitter. Glyphosate messes that up. I thought, ‘I wonder if it can get into the protein in place of glycine?’
My book actually centers on this idea that glyphosate substitutes for glycine in certain proteins. There’s a specific algorithm for where it would happen, and you can show that those proteins are suppressed by glyphosate experimentally.”
Importantly, glyphosate suppresses glucose-6-phosphate dehydrogenase (G6PD), a very important enzyme in red blood cells that maintains NADPH in its reduced form. If you have reduced levels of NADPH, you’re at increased risk for chronic disease, as your ability to recharge antioxidants is impaired. This is yet another mechanism by which glyphosate contributes to any number of disease states.
Glyphosate’s Impact on Collagen
Yet another protein that has a high glycine content is collagen, the primary protein for your connective tissue. It constitutes about one-quarter of your body’s proteins. Because of the presence of glycine, glyphosate has the ability to impair collagen as well.
“I feel confident that glyphosate is messing up collagen,” Seneff says. “Collagen has a beautiful triple helix structure, which gives it really special properties of tensile strength and flexibility to hold water. Collagen has long, long sequences called GXY, GXY, GXY, where every third amino acid is a glycine. Those glycines hook together to form that triple helix.
There are people who have mutations in those glycines that cause joint and bone diseases, and I think glyphosate is causing that. Ehlers-Danlos syndrome is associated with glycine mutations in collagen, and there’s an increase in the prevalence of that syndrome recently.
Of course, you have many more people getting hip replacement surgery, and people have back issues, back pain and shoulder surgery, knee and foot problems. All these different problems with the joints, I suspect, are being caused by misfolded collagen because of glyphosate messing it up.”
Glyphosate’s Impact on Your Vascular System
Another mechanism of action involves the suppression of nitric oxide (NO), primarily through the suppression of endothelial nitric oxide (eNOS), which is one of three ways your body makes NO. eNOS is a close relative to cytochrome 450 enzymes which, as mentioned, are decimated by glyphosate.
“The NO works together with sulfur dioxide to control the viscosity of your blood,” Seneff explains. “NO turns into nitrate … And sulfur dioxide turns into sulfate … Nitrate is a chaotrope, and sulfate is a kosmotrope. Kosmotropes are very interesting molecules that control the viscosity of blood. It’s all about water structuring, stuff that Gerald Pollack talks about.
Kosmotropes make the water structure more like gel and the chaotropes make it more like fluid, liquid. Those two work against each other to maintain the correct viscosity of the blood while other things are going on. If you put a bunch of lipid particles into the blood, it’s going to get more viscous, so you’ve got to make it less-viscous by adding NO.
So, there’s a back and forth between NO and sulfur dioxide that’s regulated by eNOS. This is a theory that I have, and it makes a lot of sense. I have continued to gather evidence that supports it.
If glyphosate messes up eNOS, then it messes up the blood’s ability to maintain its proper viscosity, which means your blood could be too fluid. You could end up with hemorrhaging. It could be too thick, it can’t circulate, so you end up with blood clots.”
More Information
One piece of good news is that Mexico is banning glyphosate and will phase it out entirely by 2024. There are fears Mexico may also start banning U.S. imports found to be contaminated with glyphosate, which would actually work in everyone’s favor by shining a bright light on the matter.
While the ultimate answer is to ban the use of glyphosate worldwide, in the meantime, a key strategy to protect your own health is to buy certified organic or biodynamic food. Glyphosate is not permitted in organic agriculture, and even if contamination occurs, the levels are going to be far lower than that of conventionally-grown foods.
Seneff also recommends eating a high-sulfur diet, as sulfur is crucial for the health of your metabolism and immune system. “Sulfur deficiency, I think, is a driver behind some of our health problems,” she says.
Also consider taking a glycine supplement to counteract and push out any glyphosate you might be exposed to. “Glycine is not very expensive and it is very safe, so it’s an easy thing to take as a supplement, which I think could definitely help,” Seneff says.
Other health-promoting habits include eating plenty of fermented foods and getting optimal amounts of vitamin D and K2. As noted by Seneff, your vitamin D conversion is also adversely affected by glyphosate.
As is typically the case when talking to Seneff, as she is phenomenally well-informed, we cover far more details in this interview than I’ve summarized here — including environmental effects and countermeasures to speed the cleanup of soil and water — so I encourage you to listen to the interview in its entirety.
Of course, to learn more about glyphosate, be sure to pick up a copy of “Toxic Legacy.” It’s by far the best book to date on this pernicious toxin that is robbing people everywhere of their health and quality of life.
VAERS data released today by the CDC showed a total of 387,087 reports of adverse events from all age groups following COVID vaccines, including 6,113 deaths and 31,240 serious injuries between Dec. 14, 2020 and June 18, 2021.
This week’s number of reported deaths among all age groups following COVID vaccines surpassed 6,000 according to data released today by the Centers for Disease Control and Prevention (CDC). The data comes directly from reports submitted to the Vaccine Adverse Event Reporting System (VAERS).
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date.
Data released today show that between Dec. 14, 2020 and June 18, 2021, a total of 387,087 total adverse events were reported to VAERS, including 6,113 deaths — an increase of 120 deaths over the previous week. There were 31,240 serious injury reports, up 1,369 compared with last week.
In the U.S 316.1 million COVID vaccine doses had been administered as of June 18. This includes: 131 million doses of Moderna’s vaccine, 173 million doses of Pfizer and 12 million doses of the Johnson & Johnson (J&J) COVID vaccine.
7,294 total adverse events, including 423 rated as serious and nine reported deaths among 12- to 17-year-olds. Four deaths (or 44%) were cardiac-related and three were sudden, unexplained deaths.
The most recent reported death includes a 13-year-old boy (VAERS I.D. 1406840) who died two days after receiving a Pfizer vaccine. Other deaths include three 15-year-olds (VAERS I.D. 1187918, 1382906 and 1242573) and two 16-year-olds (VAERS I.D. 1225942 and 1386841) and one 17-year-old (VAERS I.D. 1199455).
The report of a 15-year-old male (VAERS I.D. 1383620) who reportedly died after receiving a Pfizer vaccine was removed from the database on June 18. It was a duplicate of VAERS I.D. 1382096. Two of the nine deaths were suicides.
CDC finds ‘likely’ link between heart inflammation and mRNA COVID vaccines
As The Defender reported June 23, the CDC’s Advisory Committee on Immunization Practices (ACIP) said there is a “likely association” of “mild” heart inflammation in adolescents and young adults after vaccination.
Members of a CDC advisory committee acknowledged 1,200 cases of heart inflammation in 16- to 24-year-olds, mostly occurring in males, and said mRNA COVID vaccines should carry a warning statement — but physicians and other public commenters accused the CDC of exaggerating the risk to young people of COVID, and minimizing the risk of the vaccines.
Dr. Tom Shimabukuro, deputy director of the CDC’s Immunization Safety Office, said in a presentation that data from one of the agency’s safety monitoring systems — Vaccine Safety Datalink (VSD) — suggests a rate of 12.6 cases per million in 12- to 39-year-olds during the three weeks after the second shot.
The Defender has been unable to report on VSD data related to COVID vaccine adverse events, including heart inflammation, as the VSD does not make data collected through the system readily available to the public.
The VSD is a collaborative project between the CDC and “several large health plans,” according to its website. Though the public can’t access the VSD data, there is a process whereby researchers can apply to access data.
According to the VSD website: “There are several ways interested researchers can access VSD data. In 2002, the VSD established a data sharing program at the National Center for Health Statistics (NCHS) Research Data Center (RDC) to allow external Guest Analysts to (1) conduct new vaccine safety studies using VSD data files available at CDC or (2) to reanalyze study-specific datasets from published VSD studies.”
The VSD data sharing program is a three-step process:
Submission of proposals to CDC’s RDC at NCHS
Submission of proposals to VSD site Institutional Review Boards
Use of CDC’s RDC at NCHS
FDA to add warning about rare heart inflammation to Pfizer and Moderna vaccines
On June 24, The Guardian reported the U.S. Food and Drug Administration will add a warning to COVID vaccines produced by Pfizer /BioNTech and Moderna about rare cases of heart inflammation in adolescents and young adults, the agency announced Wednesday.
Health regulators in several countries have been investigating whether the Pfizer and Moderna vaccines using mRNA technology present a risk and, if so, how serious. The CDC advisory group found the inflammation in adolescents and young adults is likely linked to the vaccines, but the benefits of the shots outweigh the risk.
18-year-old has a heart attack after second dose of Pfizer vaccine
As The Defender reported June 22, 18-year-old Isaiah Harris was hospitalized after suffering a heart attack within 48 hours of his second dose of the Pfizer vaccine and is on total bed rest for six months. Isaiah Harris and his father, Justin Harris, described the traumatic ordeal in an exclusive interview.
“We took him to the hospital but they didn’t take him seriously,” Harris said. “We waited in the waiting room for over two hours and then they left him in a hallway for six hours. Things went from bad to worse while waiting in the hospital. That’s when he had his heart attack and one of his lungs filled up with fluid.”
At one point, 80% of Isaiah’s heart was inflamed and only 40% was functioning. Isaiah’s troponin levels were so high doctors said he had suffered a heart attack. According to Harris, doctors kept denying it was the vaccine until a nurse brought in a study showing the vaccine could cause myocarditis.
Harris believes his son would have been better off to have COVID versus the possible life-long issues he is now facing with his heart and the possibility of another heart attack if he overextends himself in the next three to six months. Isaiah said he would rather have COVID than a heart attack.
13-year-old Michigan boy dies three days after second dose of Pfizer vaccine
On June 24, The Defender reported a 13-year-old Michigan boy died June 16 –– three days after he received his second dose of Pfizer’s COVID vaccine. Preliminary autopsy results indicated that following his vaccination, Jacob Clynick’s heart became enlarged and was surrounded by fluid — symptoms similar to those documented in other teen boys who experienced myocarditis following COVID vaccination.
The teen’s death was reported to the CDC and is under investigation by federal health regulators to determine if there is a correlation between the death and vaccination — according to the Saginaw County Health Department.
18-year-old teen suffers ‘profuse heart damage’ after Pfizer vaccine
As The Defender reported June 23, Laura Mallozzi, whose 18-year-old son developed myocarditis two days after his second Pfizer vaccine, said she would never have connected the dots between the vaccine and her son’s symptoms if she hadn’t read about the condition in The Defender.
David (VAERS I.D 563354) was hospitalized with myocarditis on June 10 — two days after his second dose of Pfizer’s COVID vaccine. According to Mallozzi, her son felt pressured at work by his employer and co-workers to get vaccinated, so he got vaccinated without telling her.
“I shudder to think I might have sent him back to bed with an Advil and some Vicks VapoRub because I never would have guessed that an apparently healthy 18-year-old would be experiencing a serious heart injury from a vaccine,” she said.
Mallozzi took David to the emergency room and told the doctor her son was experiencing an adverse reaction to the COVID vaccine. Although hospital workers took her son’s information, the mother and son were ignored for hours. They finally left because David needed to lie down. Mallozzi ended up taking her son back to the emergency room for a second time, but didn’t mention the vaccine.
Scans showed David suffered severe heart damage and doctors acknowledged that the symptoms developed after David’s second Pfizer shot. Doctors are not sure how long it will take David to recover, but with other viruses that cause myocarditis, patients have to be monitored by a cardiologist for 18 months to two years.
Teen with previous COVID infection suffers severe myocarditis after Pfizer vaccine
In an exclusive interview with The Defender on June 21, Marie Follmer said no one warned her that her 19-year-old son — a healthy, elite athlete who had recovered from COVID — shouldn’t get the Pfizer vaccine because it would put him at greater risk of developing myocarditis.
Greyson Follmer, an Ohio State University student, was an elite athlete and member of the university’s chapter of the Reserve Officers’ Training Corps (ROTC) who developed severe heart complications following his second dose of Pfizer’s COVID vaccine and was taken three times to Nationwide Children’s Emergency Hospital.
“My son feels like he’s having a heart attack 24/7,” Follmer said. “He now has high blood pressure, severe chest pains, back pain, elevated kidney levels, hypothyroidism, inflamed lymph nodes in different areas of his body, and he can’t work or exercise.
In October 2020, Greyson got COVID and experienced mild flu symptoms, including an enlarged heart and slight inflammation. The cardiologist thought it could be related to being an elite athlete, and signed a release for Greyson to return to school. Nobody warned Follmer that her son should not get a COVID vaccine with a history of heart inflammation.
“I think what’s frustrating to me right now is that nobody told me that if you have an enlarged heart or heart inflammation, don’t get the shot,” Follmer said. “Not one person ever told us this. I never would have thought in a million years my kid would get sick.”
Dr. Hooman Noorchashm, a surgeon, immunologist and patient safety advocate said it’s a colossal error to vaccinate people who have previously had COVID and reactions like Greyson’s are a totally avoidable harm. “Why are we rushing to vaccinate people who we know are immune and don’t stand to gain any benefit? If I do anything medically unnecessary to someone as a doctor, I’m opening them up to potential harm. If you’ve had a recent infection and you have viral antigens in your tissues, you can literally and immunologically cause tissue damage.”
Pfizer vaccine linked to rare blood clot disorder, Israeli researchers say
As The Defender reported June 23, Israeli researchers discovered a link between Pfizer’s COVID vaccine and thrombotic thrombocytopenic purpura (TTP) –– a rare blood disorder that causes blood clots to form in small blood vessels throughout the body. Researchers stressed this occurred in both new patients and in patients with pre-existing TTP whose disease had been in remission but flared up soon after getting the vaccine.
Scientists with the Institute of Hematology at Shamir Medical Center said they began researching the possible link after reports of a sudden increase in TTP across Israel — four cases detected in one month compared to two or three cases per year. The Health Ministry, which is evaluating the research, asked doctors not to provide interviews until the evaluation is complete.
109 days and counting, CDC ignores The Defender’s inquiries
According to the CDC website, “the CDC follows up on any report of death to request additional information and learn more about what occurred and to determine whether the death was a result of the vaccine or unrelated.”
On March 8, The Defender contacted the CDC with a written list of questions about reported deaths and injuries related to COVID vaccines. After repeated attempts, by phone and email, to obtain a response to our questions, a health communications specialist from the CDC’s Vaccine Task Force contacted us on March 29 — three weeks after our initial inquiry.
The individual received our request for information from VAERS, but said she had never received our list of questions, even though employees we talked to several times said CDC press officers were working through the questions and confirmed the representative had received them. We provided the list of questions again along with a new deadline, but never received a response.
On May 19, a CDC employee said our questions had been reviewed and our inquiry was pending in their system, but would not provide us with a copy of the response. We were told we would be contacted by phone or email with the response.
On June 24, we contacted the CDC and were told nobody knew the specialist from the agency’s Vaccine Task Force who contacted us in March, and that our request was still pending in the system. It has been 109 days since we sent our first email inquiring into VAERS data and reports and we have yet to receive a response.
The Maine Legislature last week approved a proposal to ban aerial spraying of some herbicides, including glyphosate, in the state’s forests, Associated Press reported.
The proposal, introduced by Democratic Senate President Troy Jackson, bans the the aerial spraying of glyphosate and other synthetic herbicides as a forest management strategy.
Jackson said he was concerned the herbicides seep into rivers and streams, jeopardize ecosystems and pose threats to human health. He said the ban was a step to “protect the health and well-being of the people working and living in northern Maine, and safeguard our natural resources for future generations.”
Across the pond in Europe, the European Federation of Food, Agriculture and Tourism Trade Unions (EFFAT) recently called for an immediate ban on glyphosate-based herbicides and other harmful pesticides.
“The newly adopted position on the issue responds to EFFAT’s commitment to a more sustainable agriculture which underpins, inter alia, free trade agreements with binding requirement to respect highest environmental and social standards, investments in workers’ skills, social protection and research and development towards sustainable pest management.
“As sufficient evidence exists on the risks related to the use of glyphosate for workers, human health and biodiversity, EFFAT calls for the immediate ban of glyphosate as an active substance in herbicide products.”
Big Tech is driving a new wave of colonization in the name of sustainability and “net zero” carbon emissions
Tech billionaire Bill Gates, now the largest owner of farmland in the U.S., is at the root of the problem, pushing technology as the only mechanism to save the world, and in so doing denying real solutions
Shiva calls Gates’ book, “How to Avoid a Climate Disaster,” which pushes for the elimination of age-old farming traditions and widespread adoption of fake meat, “rubbish”
According to Shiva, in order to force the world to accept this new food and agricultural system, new conditionalities are being created through net zero “nature-based” solutions, which will only further destroy indigenous people and small farmers
Net zero does not mean zero emissions, Shiva says; it means the rich polluters will continue to pollute and also grab the land and resources of those who have not polluted
Vandana Shiva is a brilliant mind calling for inhabitants of the Earth to unite against forces that are threatening to destroy the planet, in part via a new wave of colonization in the name of sustainability.
Tech billionaire Bill Gates, now the largest owner of farmland in the U.S.,1 is at the root of the problem, pushing technology as the only mechanism to save the world, and in so doing denying real solutions. This path is not accidental but carefully orchestrated to amass wealth, power and control, while making all but the elite subservient.
In my interview with Vandana Shiva, Ph.D., she spoke about Gates Ag One,2 which is headquartered in St. Louis, Missouri, where Monsanto is also headquartered.
“Gates Ag One is one [type of] agriculture for the whole world, organized top down. He’s written about it. We have a whole section on it in our new report,3 ‘Gates to a Global Empire,'” she said. This includes digital farming, in which farmers are surveilled and mined for their agricultural data, which is then repackaged and sold back to them.
Bill Gates’ New Book Is ‘Rubbish’
In the above Under the Skin podcast with Russel Brand, Shiva takes aim at Gates’ book “How to Avoid a Climate Disaster: The Solutions We Have and the Breakthroughs We Need,” which was released in February 20214 — calling it “rubbish:”5
“Just by chance I was reading the rubbish in Bill Gates’ new book. I normally don’t read rubbish but when they want to be rulers through rubbish, I read it. And it’s lovely because he says the greenhouse gases from factory farms are not because of factory farms and putting animals in prisons … it’s because the cows were the problem. They had four stomachs and the four stomachs make the methane.”
The reason cows in concentrated animal feeding operations (CAFOs) emit methane that smells is because they’re fed an unnatural diet of grains and placed in crowded quarters. It’s not a natural phenomenon. It’s a man-made one. “You walk behind a good cow on a grazing pasture, she’s not stinking,” Shiva said.6
The strong recommendation to replace beef with fake meat is also made in Gates’ book7 — another example of replacing a whole, natural food with something engineered, heavily processed and fake. It all stems from an overreaching theme of arrogance and the desire for recolonization and a global empire.
The idea is to imply, or create the environment in which, survival isn’t possible without technology. “It is a denial of the richness of agroecological knowledges and practices that are resurging around the world,” according to one of Navdanya’s reports.8
Shiva founded Navdanya, a nonprofit organization promoting biodiversity, organic farming and seed saving, in 1994. She has also travelled the globe to warn other countries, including Africa, about plans to displace rural farmers so investors can turn the land into industrial farms to export the commodities.
Gates’ book talks about eliminating age-old farming traditions, which Shiva believes must be protected. Speaking with Brand, Shiva said:9
“He [Gates] has put the Indian plow that has existed for 10,000 years and says this primitive technology must go. I call this, as the future technology, a partnership between our bodies, the body of the Earth, and the body of the animals — realizing that we are not masters but we are there to serve through what Gandhi called bread labor, the labor of our body in the service of the Earth, in the service of community.
So we are for sure at an epic moment where everything wrong is being given a new life just at the time when the world was waking up … I think this is happening … because of arrogance … we’ve destroyed every international law, we’ve destroyed all democracy, we have locked people into fear … you know, the British empire had that arrogance.”
Breaking the Sacred Relationship With Food
Industrialization started the process of severing humans’ age-old connections to their food and the land on which it’s grown. “Now, with digitalization,” Shiva said, “they would like to end it forever.”10 Tech giants, in an effort to drive home digital agriculture, are working to reduce life to software11 while advancing digital surveillance systems.
So far, Shiva’s organization has managed to prevent Gates from introducing a seed surveillance startup, where farmers would not be allowed to grow seeds unless approved by Gates’ surveillance system. The data mining, Shiva says, is needed because they don’t actually know agriculture.
This is why Gates finances the policing of farmers. He needs to mine their data to learn how farming is actually done. In countering the tech giants’ attempts to remove humans’ sacred relationship to food, Shiva states we can fight back by remembering and focusing on a few essential principles:12
Food is the currency of life
The highest duty is to grow and give food in abundance
The worst sin is to let someone go hungry in your neighborhood, not grow food and, worse, sell bad food
“We’ve got to bring to the center of our everyday life the rituals that make life sacred,” Shiva said. “Our breath … breath is what connects us to the world … water connects us to the world. Food connects us to the world.”13
‘Net Zero’ Nonsense
Gates has been vocal that achieving “net zero” emissions will be the “most amazing thing humanity has ever done.”14 By 2030, he’s pushing for drastic, fundamental changes, including widespread consumption of fake meat, adoption of next generation nuclear energy and growing a fugus as a new type of nutritional protein.15
The deadline Gates has given to reach net zero emissions is 2050,16 likely because he wants to realize his global vision during his lifetime. But according to Shiva, in order to force the world to accept this new food and agricultural system, new conditionalities are being created through net zero “nature-based” solutions. Navdanya’s report, “Earth Democracy: Connecting Rights of Mother Earth to Human Rights and Well-Being of All,” explains:17
“If ‘feeding the world’ through chemicals and dwarf varieties bred for chemicals was the false narrative created to impose the Green Revolution, the new false narrative is ‘sustainability’ and ‘saving the planet.’ In the new ‘net zero’ world, farmers will not be respected and rewarded as custodians of the land and caregivers, as Annadatas, the providers of our food and health.
They will not be paid a fair and just price for growing healthy food through ecological processes, which protect and regenerate the farming systems as a whole.
They will be paid for linear extraction of fragments of the ecological functions of the system, which can be tied to the new ‘net zero’ false climate solution based on a fake calculus, fake science allowing continued emissions while taking control over the land of indigenous people and small farmers.
‘Net Zero’ is a new strategy to get rid of small farmers in first through ‘digital farming’ and ‘farming without farmers’ and then through the burden of fake carbon accounting.
Carbon offsets and the new accounting trick of ‘net zero’ does not mean zero emissions. It means the rich polluters will continue to pollute and also grab the land and resources of those who have not polluted — indigenous people and small farmers — for carbon offsets.”
Gates already alluded to this double-standard in responding to those who criticized him for the hypocrisy of being a serious polluter himself, with a 66,000 square-foot mansion, a private jet, 242,000 acres of farmland and investments in fossil fuel-dependent industries such as airlines, heavy machinery and cars.18
This pollution is acceptable, Gates said, because, “I am offsetting my carbon emissions by buying clean aviation fuel, and funding carbon capture and funding low-cost housing projects to use electricity instead of natural gas.”19
Carbon Colonization and Carbon Slavery
Carbon colonization and carbon slavery are two terms being used to explain the reality behind carbon trade, which is being regarded by Big Tech as the next big opportunity, Shiva says.20 Carbon trade refers to the buying and selling of credits that allow a company to emit a certain amount of carbon dioxide,21 but by buying up credits from nonpolluters, industry can continue to pollute.
Technocracy is also a resource-based economic system, which is why the World Economic Forum talks about the creation of “sustainable digital finance,”22 a carbon-based economy and carbon credit trading.23 As explained on its website:24
“Digital finance refers to the integration of big data, artificial intelligence (AI), mobile platforms, blockchain and the Internet of things (IoT) in the provision of financial services. Sustainable finance refers to financial services integrating environmental, social and governance (ESG) criteria into the business or investment decisions.
When combined, sustainable digital finance can take advantage of emerging technologies to analyze data, power investment decisions and grow jobs in sectors supporting a transition to a low-carbon economy.”
As Navdanya’s report explains, however, this will ultimately further remove the rights of small farmers, who will be forced into a new form of data slavery:25
“A global ‘seal’ of approval based on fake science, fake economics of maximizing profits through extraction will create new data slavery for farmers. Instead of using their own heads and cocreating with the Earth, they will be forced to buy ‘Big Data.’ Instead of obeying the laws of Mother Earth, they will be forced to obey algorithms created by Big Tech and Big Ag.”
Focusing solely on carbon reductionism also misses the point that “forests, lands, ecosystems are so much more than the carbon stored in them,” and putting conditionalities on small farmers will only make environmental injustices worse. The report adds:26
“Conditionalities under any condition violate democratic principles and human rights. Farmers are guided by Earth care. The culture of Earth care needs to be respected and rewarded because it is centered on rights of the Earth and rights of all her children … Conditionalities put on the nonpolluters by the polluters who want to continue to pollute is unjust and ecologically, morally and ethically bankrupt.”
‘The Universe Is Divine’
According to the ancient Vedas, the universe is divine, and everything therein — even the smallest grass — is an expression of the divine. “When I go to villages,” Shiva told Brand, “women will do sacred ceremonies with indigenous seed. They will never use a hybrid seed for a sacred ceremony … It’s quite amazing. No one told them, but they have that understanding of integrity and what the sacred means. It means to treat without violation.”27
The universe exists for the well-being of all, but her gifts must be enjoyed without greed, Shiva explained. Taking more than your share is theft, and will only backfire. The solution to true sustainability doesn’t lie with new technology, but in relying on the natural “technology” that is the universe:28
“It is by learning from the Earth that we can regenerate the Earth. We have to become students of Mother Earth, not try and dominate her. When we practice agriculture in unison with the Earth’s ecological processes aligned with the ecological laws of nature and the Earth, we evolve an agriculture of care for the land, for the soil. We participate in the process of regenerating the seed and biodiversity, soil and water.”
CHD is asking everyone who supports medical health freedom to contact all colleges and universities in their state and ask them to come down on the side of medical freedom by rejecting COVID vaccine mandates.
Children’s Health Defense (CHD) is calling on vaccine safety advocates to reach out to schools and universities with this message: No COVID vaccine mandates for children and young adults!
On June 23, the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices (ACIP) said that there is ‘likely’ a link between heart inflammation and the Pfizer and Moderna COVID Vaccines.
CDC officials acknowledged more than 1,200 cases of myocarditis or pericarditis in 16-to-24-year-olds who received an mRNA COVID vaccine. The U.S. Food and Drug Administration responded by saying warning labels will be added to the vaccines.
Still, CDC officials said the benefits of COVID vaccines outweigh the risks.
CHD is asking everyone who supports medical health freedom to send letters or emails to all colleges and universities in your state asking them to come down on the side of medical freedom by rejecting COVID vaccine mandates.
CHD has created spreadsheets containing a list of more than 300 universities that are considering mandates. The first spreadsheet is a listing of university systems with links to mandate policies, etc. The second spreadsheet provides information for emailing and mailing to more than 300 individual universities. You can also visit this page on the CHD website to learn more about this campaign.
“School and university officials should not have the ability to mandate any medical procedures including vaccinations,” said Laura Bono, CHD executive director. “In this case, the long-term effects on humans of any age from this experimental vaccine are unknown. The policy is reckless and unwarranted.”
Bono pointed to a recent op-ed in the Wall Street Journal, written by two physicians, which stated:
“Public-health authorities are making a mistake and risking the public’s trust by not being forthcoming about the possibility of harm from certain vaccine side effects. There will be lasting consequences from mingling political partisanship and science during the management of a public-health crisis.”
There is no time to wait. Colleges and universities are considering mandates now — now is the time to work for policy change. Please support this effort.
A newly published analysis in the journal Frontiers in Environmental Science argues that a toxic soup of insecticides, herbicides and fungicides is causing havoc beneath fields covered in corn, soybeans, wheat and other monoculture crops. The research is the most comprehensive review ever conducted on how pesticides affect soil health.
The study is discussed by two of the report’s authors, Nathan Donley and Tari Gunstone, in a recent article appearing on the Scientific American website.
The authors state that the findings should bring about immediate changes in how regulatory agencies like the Environmental Protection Agency (EPA) assess the risks posed by the nearly 850 pesticide ingredients approved for use in the USA.
Conducted by the Center for Biological Diversity, Friends of the Earth and the University of Maryland, the research looked at almost 400 published studies that together had carried out more than 2800 experiments on how pesticides affect soil organisms. The review encompassed 275 unique species or types of soil organisms and 284 different pesticides or pesticide mixtures.
Pesticides were found to harm organisms that are critical to maintaining healthy soils in over 70 per cent of cases. But Donley and Gunstone say this type of harm is not considered in the EPA’s safety reviews, which ignore pesticide harm to earthworms, springtails, beetles and thousands of other subterranean species.
The EPA uses a single test species to estimate risk to all soil organisms, the European honeybee, which spends its entire life above ground in artificial boxes. But 50-100 per cent of all pesticides end up in soil.
The researchers conclude that the ongoing escalation of pesticide-intensive agriculture and pollution are major driving factors in the decline of soil organisms. By carrying out wholly inadequate reviews, the regulatory system serves to protect the pesticide industry.
The study comes in the wake of other recent findings that indicate high levels of the weedkiller chemical glyphosate and its toxic breakdown product AMPA have been found in topsoil samples from no-till fields in Brazil.
Writing on the GMWatch website, Claire Robinson and Jonathan Matthews note that, despite this, the agrochemical companies seeking the renewal of the authorisation of glyphosate by the European Union in 2022 are saying that one of the greatest benefits of glyphosate is its ability to foster healthier soils by reducing the need for tillage (or ploughing).
This in itself is misleading because farmers are resorting to ploughing given increasing weed resistance to glyphosate and organic agriculture also incorporates no till methods. At the same time, proponents of glyphosate conveniently ignore or deny its toxicity to soils, water, humans and wildlife.
With that in mind, it is noteworthy that GMWatch also refers to another recent study which says that glyphosate is responsible for a five per cent increase in infant mortality in Brazil.
The new study, ‘Pesticides in a case study on no-tillage farming systems and surrounding forest patches in Brazil’ in the journal Scientific Reports, leads the researchers to conclude that glyphosate-contaminated soil can adversely impact food quality and human health and ecological processes for ecosystem services maintenance. They argue that glyphosate and AMPA presence in soil may promote toxicity to key species for biodiversity conservation, which are fundamental for maintaining functioning ecological systems.
These studies reiterate the need to shift away from increasingly discredited ‘green revolution’ ideology and practices. This chemical-intensive model has helped the drive towards greater monocropping and has resulted in less diverse diets and less nutritious foods. Its long-term impact has led to soil degradation and mineral imbalances, which in turn have adversely affected human health.
If we turn to India, for instance, that country is losing 5334 million tonnes of soil every year due to soil erosion and degradation, much of which is attributed to the indiscreet and excessive use of synthetic agrochemicals. The Indian Council of Agricultural Research reports that soil is becoming deficient in nutrients and fertility.
India is not unique in this respect. Maria-Helena Semedo of the Food and Agriculture Organization stated back in 2014 that if current rates of degradation continue all of the world’s topsoil could be gone within 60 years. She noted that about a third of the world’s soil had already been degraded. There is general agreement that chemical-heavy farming techniques are a major cause.
It can take 500 years to generate an inch of soil yet just a few generations to destroy. When you drench soil with proprietary synthetic agrochemicals as part of a model of chemical-dependent farming, you harm essential micro-organisms and end up feeding soil a limited doughnut diet of toxic inputs.
Armed with their multi-billion-dollar money-spinning synthetic biocides, this is what the agrochemical companies have been doing for decades. In their arrogance, these companies claim to have knowledge that they do not possess and then attempt to get the public and co-opted agencies and politicians to bow before the altar of corporate ‘science’ and its bought-and-paid-for scientific priesthood.
The damaging impacts of their products on health and the environment have been widely reported for decades, starting with Rachel Carson’s ground-breaking 1962 book Silent Spring.
I wrote the following piece in 2017. It details the massively successful infiltration of pharmaceutical armies among the population.
These men and women are war criminals.
Here we go:
Medical News Today reports that, in 2011, there was a modest uptick in the number of drug prescriptions written in the US. [1] [1a]
The increase brought the total to: 4.02 billion.
Yes, in 2011, doctors wrote 4.02 billion prescriptions for drugs in America.
That’s an average of roughly 13 prescriptions for each man, woman, and child.
That’s about one new prescription every month for every American. (Update: the Kaiser Family Foundation reports that in 2016, 4,065,479,343 drug prescriptions were written by US doctors—an increase of 65 million. [2])
The Medical News Today article concluded, “…the industry should be heartened by the growth of the number of prescriptions and spending.” Yes, I’m sure the drug industry popped champagne corks.
We’re talking about prescriptions here. We’re not talking about the number of pills Americans took. We’re also not counting over-the-counter drugs or vaccine shots.
Pharmacopoeia, a 2011 exhibition at the British Museum, estimated that “the average number of pills a person takes in his or her own lifetime in the UK is 14,000.” That’s as a result of prescriptions. Including over-the-counter drugs, the 14,000 number would swell to 40,000 pills taken in a lifetime. [3]
What are the effects of all these drugs?
We are looking at a supreme Trojan Horse that is rotting out America and all other countries from the inside. Wars, no wars, economic deprivation, economic prosperity, the drugs continue to do their work, debilitating and ruining and terminating lives.
Many sources can be cited to confirm this assessment.
On January 8th, 2001, the LA Times published an article by one of the best medical reporters in the business, Linda Marsa: “When Good Drugs Do Harm.” Marsa quoted researcher Dr. David Bates, who indicated that, in the US, there are 36 million serious adverse reactions to medical drugs per year. [4] [4a]
On July 26, 2000, the Journal of the American Medical Association published the most stunning mainstream estimate of medical-drug damage in history: “Is US health really the best in the world?” The author was Dr. Barbara Starfield, a respected public-health researcher at the Johns Hopkins School of Public Health. [5] [5a]
Starfield concluded that medical drugs were killing Americans at the rate of 106,000 per year.
That’s a million deaths per decade.
This is a conservative sketch of the Trojan Horse that has been placed in the center of every country in the world.
The pharmaceutical juggernaut will continue, no doubt about it. The only question is, how many people will wake up and seek another way?
The destruction of societies by medical drugs goes far beyond what some people call “over-prescribing.” This isn’t just a tilt in the wrong direction. It isn’t simply errors of judgment compounded by the number of doctors dispensing medicines.
Those are all polite terms suggesting the situation can be corrected through a show of better professional judgment. That will never happen.
Countries of the world are literally being assaulted by pharmaceutical companies and their foot-soldier doctors. It’s chemical warfare.
To even begin to see light at the end of the tunnel, hundreds of millions of people must add themselves to the rolls of those who already are pursuing better health through natural means.
Not even the Nazis and their dearly beloved cartel, the monster IG Farben, dreamed of the day when the citizenry would line up and demand to ingest more and more life-destroying chemicals.
What about the FDA, the federal agency responsible for certifying all medical drugs “safe and effective,” before release for public use in the US?
The FDA is completely aware of the monstrous death toll and the injuries stemming from the very drugs they’re approving—but they take zero responsibility.
On an FDA website page, “Preventable Adverse Drug Reactions: A Focus on Drug Interactions,” [6] the agency discusses the “problem”—but as you can see from the title, they’re framing the conversation in terms of “interactions,” as if drugs are maiming and killing people because they are accidentally combining effects. This is a gross lie.
Here are quotes from the FDA page, which come just after trying to pawn off absurdly low drug-death and injury numbers:
“However, other studies conducted on hospitalized patient populations have placed much higher estimates on the overall incidence of serious ADRs [adverse drugs reactions]. These studies estimate that 6.7% of hospitalized patients have a serious adverse drug reaction with a fatality rate of 0.32%.2 If these estimates are correct, then there are more than 2,216,000 serious ADRs in hospitalized patients, causing over 106,000 deaths annually. If true, then ADRs are the 4th leading cause of death—ahead of pulmonary disease, diabetes, AIDS, pneumonia, accidents, and automobile deaths.”
“These statistics do not include the number of ADRs that occur in ambulatory settings. Also, it is estimated that over 350,000 ADRs occur in U.S. nursing homes each year.3 The exact number of ADRs is not certain and is limited by methodological considerations. However, whatever the true number is, ADRs represent a significant public health problem that is, for the most part, preventable.”
Yes, preventable, if any government were determined to neutralize the pharmaceutical armies ravaging humanity.
University of Western Australia – home of Gates-funded researcher Christine Carson, who has spent countless hours on social media this past year insisting “YES the COVID-19 virus has been isolated” – Provided and Cited ZERO RECORDS for “SARS-COV-2” isolation/purification from a patient sample, by anyone anywhere in the World EVER!
For over a year, we’ve had mainstream reports of “unprecedented” and “illegal” DNRs – how big a role did they play in creating this “pandemic”? And are they being used to mask large-scale euthanasia?
The rise in the use of Do Not Resuscitate orders (DNRs), and the suggestion that patients are being compelled to sign them, or even having them signed on their behalf in secret, has been one of the more concerning narratives to come out of the last year of “pandemic”.
As early as April of 2020, entirely mainstream publications, such as the Health Service Journal (HSJ), were running articles expressing concern over the “unprecedented” rise in “illegal” DNR orders for those with learning disabilities.
In June 2020 the Independent picked up the story, citing some troubling examples found by charity workers and family members:
In one example, a man in his fifties with sight loss was admitted to hospital after a choking episode and was incorrectly diagnosed with coronavirus. He was discharged the next day with a DNR form giving the reason as his “blindness and severe learning disabilities” […] Marie-Anne Peters, whose brother Alistair has epilepsy but no other health conditions, overturned a DNR on her brother which included instructions for him not to be taken to hospital.
The BBC reported that, in Wales, some people were sent letters instructing them to sign DNRs, and their families not to call 999 in the event of an emergency. While, in Somerset, Sussex and Derbyshire, autism support groups were sent letters by GP surgeries telling them their members had to sign DNR orders.
As you can see, we’re not talking about people who are severely ill in the least. Autism, sight loss and epilepsy are not conditions that would ever, under normal circumstances, have patients deemed unworthy of receiving life-saving treatment.
It wasn’t just the ill or disabled who fell victim to this, either. In June last year, it was revealed that “blanket” DNRs had been applied to nursing homes by GPs all around the country.
Other surgeries and hospitals sent out letters to elderly patients, and other “at risk groups”, instructing them they needed to sign DNRs to protect the NHS.
Some care home residents were wrongly subjected to decisions ruling out attempts at cardiopulmonary resuscitation (CPR) in the early stages of the covid-19 pandemic, leading to potentially avoidable deaths
The root cause of this can be traced back to two sets of NHS guidelines, both written and published in the spring of 2020.
Then came the NICE guidelines for critical care admissions, which Dr Vernon Coleman did a video on last summer, which suggested doctors:
Sensitively discuss a possible ‘do not attempt cardiopulmonary resuscitation’ decision with all adults with capacity and an assessment suggestive of increased frailty
This was, allegedly, to protect the NHS from the influx of Covid patients and to try and keep ICU beds open. This rush, of course, never materialised, and in 2020 NHS critical care beds were actually emptier than usual.
This policy was not solely isolated to the UK either. The “Undercover Nurse” reported in Perspectives on the Pandemic, the hospital she worked at in New York had widespread abuse of the DNR system, and Rosemary Frei wrote an article breaking down the way deaths were “created” in Canadian care homes.
So, we know that people have – in all likelihood – been allowed to die during this pandemic. That has been as good as officially admitted. But does it go further? Are people being actively euthanised?
Euthanasia has already been hinted at by other whistleblowers, specifically through the use of ventilators on patients who never needed them. (The Undercover Nurse discusses that too).
It’s certainly true that the use of ventilators was pushed in guidelines from the NHS, CDC, ECDC and WHO as soon as the “pandemic” started. And it’s very probable that this did a lot more harm than good, killing huge numbers of patients who may otherwise have survived (though obviously it cannot be proven – at this stage – that this was deliberate).
In this June 10th episode of Richie Allen’s podcast, he talks to independent journalist Jacqui Deevoy about the possibility of widespread euthanasia of elderly patients in the NHS during the Covid “pandemic”. They are joined by several people who claim their parents died in as-yet-unexplained circumstances.
Listen to the testimony of the people who may have lost parents to this policy. They certainly raise a lot of important questions.
How many people, who lost family members in the last year, are in the same situation and don’t even know it? How much of the UK’s excess mortality in 2020 – currently attributed to Covid19 – was in fact caused by these callous (and potentially criminal) practices?
And, more importantly, was that all part of a plan? Were these people deliberately allowed to die in order to create an illusory “pandemic”?
You can listen to other episodes of Richie Allen’s podcast here, and follow Jacqui Deevoy’s work here.
Dr. Kelly Sutton risks losing her medical license for not strictly following CDC guidelines for writing vaccine medical exemptions. Attorney Greg Glaser, who represents Sutton, provided this eyewitness account.
A California physician could lose her medical license for not strictly following the guidelines for writing vaccine medical exemptions as outlined by the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices (ACIP).
Earlier this month, the Medical Board of California conducted a trial during which they heard testimony from witnesses in support of and those opposed to Dr. Kelly Sutton’s approach to writing vaccine medical exemptions for her patients.
The three-day trial, which ended June 16, took place in an administrative court with a single judge and no right to a jury. The judge is expected to issue a decision sometime in the fall of 2021 on whether or not to rescind Sutton’s medical license.
Sutton, an integrative physician, argued that her clinical observations confirm her unvaccinated patients are healthier than those who are vaccinated.
During her trial, Sutton was represented by health freedom attorney Rick Jaffe, who marshaled evidence from three top experts in defense of Sutton’s methods to protect patients from vaccine injury.
The state produced one expert, who lacked basic knowledge of vaccine risk, and who stated that all doctors should follow whatever the CDC’s one-size-fits-all vaccine schedule recommends at any given time.
Below are highlights from testimony provided during Sutton’s trial.
Sutton’s testimony on her behalf:
Sutton provided thoughtful discussion of how she helps and heals patients. She is a doctor member of Physicians for Informed Consent (PIC), which puts patients first. She was humble throughout the trial, going out of her way to be kind to everyone involved in the proceeding — including the state expert testifying against her. Her kindness and credibility were so strong that even the prosecuting attorney was forced to change his tone of voice to lessen the blameful nature of his scripted words.
Sutton did not need a script. She showcased her detailed scientific knowledge by explaining the biological mechanisms of disease and vaccine risk. At times the court reporter could not keep up with Sutton’s fluent use of scientific terminology.
Sutton described how California’s Senate Bill 277 removed parental rights to medical decision-making and made the doctor’s discretion the standard for medical exemptions.
Sutton discussed the process of meeting with integrative colleagues at PIC to arrive at best practices for medical exemptions.
Sutton discussed the benefit of a physical exam for patient intake, and when it is needed (i.e., diagnosing an ear infection) versus when it is not needed (i.e., taking a family history). She also discussed the reality that certain patients cannot afford the time and/or money to conduct unnecessary physical exams.
Sutton reviewed each of the relevant patient records cited by the medical board as evidence of Sutton’s non-compliance with CDC recommendations, focusing on vaccine risk based on the individual patients’ complex medical histories.
Sutton emphasized her proactive approach to protect patient privacy when writing medical exemptions.
Sutton discussed the extensive scientific citations she provided to the medical board to support her medical decisions, including Dr. Chris Exley’s findings on aluminum. The board tried to use a technical objection to prevent Sutton from introducing the science behind her decisions. However, during Jaffe’s questioning of Sutton, she was able to explain the science of vaccine risk.
Sutton testified that doctors make a lot of money by giving vaccinations, but not a lot from writing medical exemptions. Indeed, there is no profit in writing medical exemptions, only prosecution — so the doctors who write them truly care for the patient’s best interest rather than pharma’s.
Sutton testified that it is neither intelligent nor humane to force a family to continue to vaccinate after one of their children has already died or been injured by a vaccine.
Sutton said the government’s failure to compare vaccinated persons to fully unvaccinated persons is a systematic and intentional blind spot in science designed to wrongfully promote vaccines.
State’s expert witness, Dr. Deborah Lehman, infectious disease physician at the University of California, Los Angeles:
Lehman repeatedly claimed that, as a physician, her one-size-fits-all vaccine opinion was medical fact and should not be challenged.
During cross examination, Lehman was asked to quantify the risk of all vaccine injuries. Lehman responded, “I don’t think I need a number … I can’t give you a number.” She stated, “I don’t need to cite articles in my report, because the science has been decided … If you want answers to these questions, I would refer you to the CDC.” Lehman ignored that the only way to obtain the vaccine injury rate is to compare vaccinated people to fully unvaccinated people. She did not appear to know that the government refuses to study the fully unvaccinated, but instead only compares vaccinated patients to other vaccinated patients.
Lehman testified she had never heard of Dr. Peter Aaby, one of the world’s foremost vaccine experts who has published more than 400 articles on PubMed. Lehman, who has published about 15 articles on PubMed, tried to dismiss Aaby’s publications on vaccine danger by falsely claiming Aaby published in a low-impact journal. Lehman stated she would never read this type of research by Aaby, and that it is the same kind of “anti-vax” information found through a Google search.
Lehman testified she is not aware of any pertussis vaccine deaths. She claimed if there were any deaths caused by the pertussis vaccine she would have heard about them. Her callous admission proves her ignorance of even basic information from the Vaccine Adverse Event Reporting System or any other source.
Lehman admitted she has never personally written a medical exemption. At most she communicated with other doctors that all medical exemptions should adhere to the one-size-fits-all per the ACIP’s contraindications.
Lehman at one point angrily blurted out, “We’re being saved by COVID vaccines.”
Lehman repeatedly used nebulous phrases such “greater risk” and “lower risk,” yet never cited any risk value numbers with the exception of a handful of false numbers. For example, in one instance she falsely cited a 1/1,000 death rate for measles cases. This is a false number because it is based only on reported cases and ignores the fact that only about 1/10 cases are reported.
Lehman criticized Sutton’s already vaccinated patients for having some infections. Lehman did not see the self-contradicting nature of her own testimony. In other words, Lehman overlooked that vaccines are causing increased risk of infection in already vaccinated patients. She ignored published studies and Sutton’s observation that patients experience less infection over time as they stop vaccinating, and fully unvaccinated patients are the healthiest of all.
Lehman testified the standard of care is whether another physician would treat the medical issue the same or similarly. But she intentionally omitted the phrase “in the same community,” meaning that the standard of care is not simply “another physician” but “another physician in the same community.” Sutton is in the integrative medicine community, of which Lehman is not a member. It is common for conventional physicians to use one-size-fits-all thinking.
Lehman testified that before the meningococcal vaccine, she performed several lumbar punctures to treat meningitis. However, Lehman never stated how many of the meningitis patients were already vaccinated with meningococcal and other vaccines (i.e., polio vaccine).
Lehman testified that children with asthma have a higher rate of morbidity and mortality. But Lehman failed to provide any numerical risk value for her testimony. For example, she cited no studies showing health outcomes of children with asthma when vaccines are stopped versus when vaccines are continued. In fact, no such studies exist to support Lehman’s position. Moreover, Lehman didn’t cite any of the studies linking asthma to increased risk from vaccination. It is common for conventional doctors to lack knowledge that common chronic illnesses are proven to be immune-mediated and caused by vaccination.
Lehman testified “febrile seizures have no long-lasting effect.” Her testimony directly contradicts even government-accepted scientific evidence that approximately 5% of febrile seizures develop into full-blown epilepsy.
Defense expert Dr. Andrew Zimmerman, pediatric neurologist:
Zimmerman is a highly published pediatric neurology expert, with expertise in diagnosing and treating autism, mitochondrial dysfunction and many other conditions.
Zimmerman testified that Sutton followed the community standard of care to protect her patients outside the narrow CDC/ACIP guidelines. With expert attention to detail about neurodevelopmental disorders, Zimmerman agreed with Sutton’s risk assessments to protect her patients. He discussed the interaction between the immune system and the brain.
Defense expert Dr. James Neuenschwander, family physician with vaccine expertise:
Neuenschwander treats chronic illness, including autism. He attends ACIP meetings and has offered public comment. He does not administer vaccines.
Neuenschwander cited a bell curve phenomenon, which represents an inverse relationship: 10% of people who fail to respond to a vaccine compared to 10% of people who overreact to a vaccine. His example illustrates a point often overlooked by mainstream scientists.
Neuenschwander explained that vaccines cause the immune system to remain in hyperactivation, creating vaccine injuries like brain inflammation.
Neuenschwander said autoimmune conditions result when the vaccine creates antibodies against the human body itself through the mechanism of chronic immune activation. Neuenschwander cited scientific evidence to support the fact that it is logical for Sutton to ask patients about their personal and family history risk factors, such as recurring infections, asthma and autism.
Neuenschwander discussed vaccines one by one to show how conventional physicians exaggerate infection risk. Neuenschwander confirmed conventional physicians are vaccinating for rare diseases on the CDC schedule while failing to ask about vaccine injury. Neuenschwander emphasized that even common diseases have questionably effective vaccines, such as flu which has a high vaccine failure rate.
Neuenschwander said the CDC/ACIP system categorically fails to properly study vaccine injury, by comparing vaccinated individuals to unvaccinated individuals, despite the CDC’s admission in a 2016 white paper showing such a study could be done.
Neuenschwander cited numbers throughout his testimony. For example, he exposed Lehman’s above-referenced lie about 1/1000 measles deaths (where Lehman falsely only included reported measles cases rather than all measles cases). Neuenschwander cited the correct numbers.
Neuenschwander highlighted the three recent published peer-reviewed studies, Mawson 2017, Hooker 2020 and Thomas 2020, showing the unvaccinated are exponentially healthier than the vaccinated. He also explained Aaby’s findings showing a five-fold increased death rate from diphtheria vaccines in Africa.
Neuenschwander cited government admissions, for example Institute of Medicine (IOM) publications, revealing a lack of data on vaccine safety and absence of government studies on vaccinated v. fully unvaccinated patients.
Defense expert Dr. LeTrinh Hoang, pediatrician:
Hoang is an experienced integrative pediatrician in California with a busy and successful clinic.
Hoang emphasized integrative medicine’s role to protect patients in ways conventional medicine systemically fails. Hoang criticized one-size-fits-all vaccination, and the specific ways ACIP/CDC creates a ridiculously limited vaccine contraindication list that ignores entire areas of independent research and clinical findings.
Hoang criticized Lehman’s casual approach to vaccine injury.
Hoang emphasized her clinical experience that unvaccinated patients are exceptionally healthy, by contrast to vaccine-injured patients whom she must heal regularly and on an ongoing basis because of their chronic illnesses.
Society is learning valuable lessons from this trial about vaccine injury, including about the consequences of allowing biotechnology to disrupt natural human immune systems.
ICAN, through its attorneys, has sued HHS for publicly making the unsupported claim that “Vaccines do not cause autism,” in violation of the National Childhood Vaccine Injury Act of 1986. ICAN calls out the agency’s illegal behavior and pulls back the curtain on the baseless, oft-repeated claim used to silence parents who know better.
In the past four decades, no claim regarding vaccination has received more attention and publicity than the claim that vaccines cause autism. Likewise, federal health authorities claim to have studied vaccines and autism more thoroughly than any other type of alleged vaccine injury. Federal health authorities assert publicly and matter-of-factly that studies establish that vaccines do not cause autism.
Reflecting this conclusion, the Center for Disease Control and Prevention (CDC) unequivocally asserts on its website that “Vaccines Do Not Cause Autism”:
The National Childhood Vaccine Injury Act of 1986 (the Act), however, mandates that the Secretary of Health and Human Services “shall … make or assure improvements in … the … research on vaccines, in order to reduce the risks of adverse reactions to vaccines” as well as “develop and disseminate vaccine information materials … based on available data and information.”
The Act also provides that “any person may commence … a civil action on such person’s own behalf against the Secretary where there is alleged a failure of the Secretary to perform any act or duty under this part.”
Clearly there is a failure of the Secretary to uphold his duties and so ICAN sued the Secretary for his failure to perform certain acts and duties pursuant to the Act which have caused direct injuries to ICAN and the Institute for Autism Science. As long as federal health authorities claim is that “the science is settled” with regard to vaccines and autism, there will be no funding for research into this extremely alarming and important issue.
ICAN’s lawsuit lays out for the Court the lack of scientific studies supporting any such assertion that all childhood vaccines do not cause autism through the following relevant history:
1991: Institute of Medicine (“IOM”) issued a report explaining that it could not identify any studies addressing pertussis-containing vaccines and autism.
2012: IOM issues another report finding only one study that looked at the issue of pertussis-containing vaccines and autism, and that study did find a link between this vaccine and autism. The IOM could also not find any study to support that tetanus or diphtheria vaccines do not cause autism.
2014: an agency within HHS again found that there are no studies supporting a claim that these three vaccines do not cause autism and the agency was also unable to identify a study to support the assertion that Hepatitis B vaccines do not cause autism. Rather, it found only one study regarding Hepatitis B and autism and that study found that babies receiving this vaccine had autism at three times the rate as those not receiving this vaccine.
October 12, 2017: ICAN sent a demand – subscribed to by 55 organizations whose members exceed 5 million Americans – to the Secretary stating that “there are … no published studies showing that autism is not caused by Hepatitis B, Rotavirus, Hib, Pneumococcal, Inactivated Poliovirus, Influenza, … vaccines – all of which HHS recommends babies receive, typically multiple times, by one year of age.” The demand asked the Secretary to “confirm that HHS shall forthwith remove the claim that ‘Vaccines Do Not Cause Autism’ from the CDC website, or alternatively, please identify the specific studies on which HHS bases its blanket claim that no vaccines cause autism.”
January 18, 2018: The Secretary responded but failed to identify any studies that support the assertion that vaccines given to babies do not cause autism. ICAN has sent numerous unrequited follow-up requests to the Secretary asking for this science.
June 21, 2019: ICAN submitted requests pursuant to the Freedom of Information Act (“FOIA”) requesting that the CDC produce the studies it relies upon to claim that vaccines injected into babies do not cause autism .
December 31, 2019: When the CDC failed to provide any studies responsive to these requests, ICAN commenced an action against the CDC. The action requested that the Court enter an order requiring the CDC to provide the studies it relies upon to claim that the vaccines given during the first year of life do not cause autism or, in the alternative, to admit that it has no such studies.
March 2, 2020: the CDC finally identified, in a stipulated order a total of 16 studies and 4 reviews (e., a review of studies on a given topic) that it relies on to claim that the vaccines given to babies do not cause autism. Not one of these studies or reviews supports the claim that vaccines injected into babies – DTaP, Hep B, Hib, PCV13, and IPV – do not cause autism.
March 10, 2020: Plaintiffs submitted another FOIA request for “All studies supporting the claim that DTaP does not cause autism,” giving yet another chance for the CDC to provide studies to support its public assertion. In this way, the Plaintiffs asked for any studies that support that DTaP does not cause autism regardless of whether or not the CDC relies upon each one.
March 23, 2020: the CDC responded to this FOIA request by pointing to the same unresponsive and inadequate list of twenty studies it had previously pointed to in the stipulation and order of March 2, 2020.
March 27, 2020: ICAN provided the CDC yet another opportunity to provide supportive studies for the claim still being shared with the public by submitting yet another FOIA request, this time for: “Studies created or retained by CDC to support the claim that DTaP does not cause autism.” The CDC again responded by pointing to the same list of twenty studies and reviews, all of which either relate to MMR or thimerosal, a single antigen (not vaccine) study, and one review by the IOM that looked for any support that DTaP does not cause autism and could not find a shred of such evidence.
August 27, 2020: the CDC finally removed the claim that “Vaccines Do Not Cause Autism” from its webpage:
January 21, 2021: ICAN widely publicized that the CDC had removed the statement “Vaccines Do Not Cause Autism” from its webpage. Within days, the CDC restored this claim to its vaccine-autism page
ICAN, therefore, brought this action to hold the Secretary and the CDC accountable and to hold them to the same standard ICAN is held to: do not make claims that cannot be supported with science. You can read the lawsuit here.
As the Food and Agriculture Organization (FAO) Conference convened its 42nd Session on Monday, Pesticide Action Network Asia Pacific (PANAP) called on the FAO to review its desert locust program and stop the use of chlorpyrifos, a pesticide linked to brain damage and other neurodevelopmental disorders in children.
An overview of the FAO desert locust response shows the use of several Highly Hazardous Pesticides (HHPs), including chlorpyrifos. According to data available on the FAO’s website, more than half a million liters of chlorpyrifos was purchased and delivered by the FAO for desert locust control in Ethiopia (490,000 liters), Uganda (47,000 liters), Yemen (5,000 liters) and Sudan (4,800 liters).
Governments, meanwhile, separately purchased and used hundreds of thousands of liters of chlorpyrifos for desert locust response. These were the governments of Eritrea (41,250 liters), Ethiopia (145,000 liters), Kenya (38,666 liters), Sudan (80,000), Uganda (1,000 liters), and Yemen (26,740).
Overall, both the FAO and governments have used around two million liters of pesticides in desert locust affected countries since January 2020, almost half of which (879,456 liters) is chlorpyrifos.
Chlorpyrifos, an organophosphate pesticide, is a potent neurotoxin at low levels of exposure, causing delayed cognitive and motor development, reduced IQ, and attention deficit/hyperactivity disorder (ADHD). It is associated with several cancers and causes birth defects. It is also extremely toxic to fish, birds, bees and other beneficial insects.
In addition, on April 7th this year, the Council of the European Union decided to submit a proposal to the secretariat of the Stockholm Convention on Persistent Organic Pollutants (POPs) for the listing of chlorpyrifos under Annex A of the Convention, for global phase-out of its production and use. POPs are chemicals that travel long distances to cold regions of the world, particularly the Arctic and Antarctic, where they persist in the environment, bioaccumulate in the food chain and, through their toxicity, threaten both wildlife and humans. “Peristent Organic Pollutants are particularly prone to evaporating from warm regions of the world, so it is highly likely that some of the chlorpyrifos sprayed in Africa will find its way to the Inuit children living in the Arctic,” said Dr. Meriel Watts, PANAP director of science and policy.
As part of its campaign to Protect Our Children from Toxic Pesticides, PANAP is calling for a global ban on chlorpyrifos. Chlorpyrifos is currently banned in 35 countries, according to PAN’s latest consolidated list of banned pesticides.
Other HHPs used in the FAO’s desert locust response program are malathion, deltamethrin, and fenitrothion. Clorpyrifos, malathion (banned in 32 countries) and deltamethrin are also among PANAP’s Terrible 20 pesticides that are especially toxic to children.
The FAO’s Practical guidelines on pesticide risk reduction for locust control recommends a minimum buffer distance for “ecologically sensitive areas” (1,500 meters or about one mile when aerially sprayed, and 100 meters or about 330 feet when sprayed on foot). It instructs locust control staff to wear appropriate personal protective equipment, and to tell local populations to “follow precautionary measures” before control operations.
However, environmental groups have reported that communities in Kenya were not given timely warning before spraying. Pesticide drift from aerial spraying can also reach several miles and cause extensive poisoning of village inhabitants and the surrounding ecosystem.
The FAO’s Pesticide Referee Group recommends organophosphate pesticides as a “last resort” method in locust control. But the FAO insists that the current emergency status of the desert locust crisis warrants the use of these pesticides as “the most appropriate tool.”
“The FAO’s path of choosing to use Highly Hazardous Pesticides, including potential POPs, for desert locust control when more agroecological alternatives are available is alarming. It may have disastrous outcomes for succeeding generations. It should be noted that the use of these toxic pesticides occurs at a time when the UN agency has forged a controversial partnership with CropLife International, the industry association of the world’s biggest pesticide manufacturers,” Watts added.
Hundreds of civil society organisations and scientists around the world are calling on the FAO to stop its deepening collaboration with CropLife, raising concerns that it ties the FAO with manufacturers of harmful pesticides and unsustainable technologies. PANAP is co-coordinating the global campaign to stop this #ToxicAlliance.
On April 27, 2021, the Sri Lankan government decided to ban importing chemical fertilizers, pesticides and herbicides and to replace them with organic inputs and methods. This decision was supported by many, including the Global Alliance for Organic Districts, who petitioned for the President’s collaboration in order to include Sri Lanka to an international network of local organic districts. Sri Lanka’s shift towards organic farming was also heavily discussed by both local and foreign researchers and activists. On the 7th and 9th of June, Dr. Vandana Shiva, President of Navdanya International, took part in two online workshops on the Sri Lankan government’s project to go towards organic agriculture and ban agrochemicals.
The first webinar– “Regenerative Organic Farming for Economy of Permanence and Prosperity for All”, was organized by the National Institute of Plantation Management (NIPM), a Sri Lankan government institute conducting research, consultancy and training on plantation management. The webinar was on the subject of regenerative organic farming for the economy of permanence and prosperity for all. Dr. Shiva noted that organic farming is not a new method, but that it was a part of the traditional farming techniques in certain countries including Sri Lanka. According to her, Sri Lanka’s shift to become a 100% organic country means turning to an economy of permanence and prosperity for all beings, one that does not destabilise the climate and instead protects all species.
The second international webinar– “The Commitment of the Sri Lankan Government to Go Organic”, organized by IFOAM Asia, also allowed speakers to discuss the commitment of the Sri Lankan government in making a shift towards organic agriculture. Apart from Dr. Vandana Shiva, other speakers included Andre Leu, director of Regeneration International, Dr. Hans Herren, president of the Millennium Institute, and Dr. Ranil Senanayake, founder of the International Analog Forestry Network. They all endorsed Sri Lanka’s decision, albeit the remark that this huge step forward needs to be implemented according to a plan which ensures a smooth transition for farmers and the local economy. Dr. Shiva said: “The reason I am glad about the approach of the Sri Lankan government is because it connects three things, namely stopping dependency on imports, non-sustainability and the ruination of the ecosystems and of health. The minute we connect sustainability and health, organic becomes the only way we can move forward.”
A New Jersey student whose college, the New Jersey Institute of Technology, requires all students to be fully vaccinated in order to attend classes in the fall became ill within hours of receiving the second dose of Moderna’s COVID vaccine.
A 21-year-old New Jersey student suffered severe heart inflammation after receiving his second dose of Moderna’s COVID vaccine. Justin Harrington, whose school required him to get the vaccine in order to attend classes in the fall, experienced flu-like symptoms followed by heart pain within eight to 12 hours of receiving the vaccine.
In an exclusive interview with The Defender, Justin’s father, Timothy Harrington, said his son felt different after the second shot. “Every time his heart beat it hurt and he felt pressure,” Harrington said. “Then he developed heart pain down both arms.”
Harrington said his son, who has no underlying medical conditions, did not experience heart pain with his first dose of the vaccine.
On May 24, two days after Justin received the second shot, his father took him to the emergency room at Morristown Memorial Hospital because the symptoms had worsened.
“The physicians weren’t connecting it to the vaccine until I informed the doctors my son just got the vaccine, and shared with them the information I had found on myocarditis,” Harrington said. “I didn’t think the doctors were stupid, but physicians sometimes see with blinders on.”
Physicians checked Justin’s blood levels, which showed high protein numbers. Abnormal scans, including an EKG, led to a diagnosis of myocarditis. Justin was hospitalized for three days while doctors attempted to get the condition under control.
Harrington said even though his son has been released, he still has chest pain and his life is not the same.
“He has to wear a heart monitor and take four different medications for six months,” Harrington said. “He has to sleep propped up, can’t exert himself and he’s missing out on one of the most important times of his life.”
Harrington said his son is supposed to be doing internships, “but how can he go out and find a company to work with him when he can’t exert himself? He’s so smart and now he’s side-lined. Doctors want my son to lie around for three to four months.”
As for Justin’s recovery, Harrington said, “He has minor scarring on his heart and doctors hope they caught it early enough that there will be no other issues — but it’s pure conjecture at this point.”
School’s mandate doesn’t allow exceptions for students who already had COVID
After Justin’s diagnosis, doctors recommended Harrington’s 19-year-old son, who received one dose of the Moderna vaccine, not get the second shot.
However, both sons were told they needed to get vaccinated in order to attend school — despite both previously having had COVID, Harrington said.
As The Defender reported last week, a new preprint study by the Cleveland Clinic found people previously infected with SARS-CoV-2 were less likely to be reinfected than fully vaccinated individuals who never had the virus — suggesting the vaccine is of no benefit to people who already had COVID.
In addition to the vaccine likely providing no benefit to those who already had the virus, studies suggest people who were previously infected with COVID are more at risk of severe adverse reactions.
As The Defender reported earlier this year, some experts say the science to support vaccinating those primed with COVID doesn’t exist and there’s a potential risk of harm, including death, in vaccinating those who’ve already had the disease or who were recently infected.
Still, many colleges and universities — including the New Jersey Institute of Technology (NJIT) where Justin is enrolled — are mandating the vaccines for all students, with few or no exceptions.
“Justin’s a rule follower and he was pressured to get it,” Harrington said.
Harrington said when he called the dean of NJIT prior to his son getting vaccinated and asked why the school is forcing young people who are at little risk of serious illness from COVID to get the vaccine, the dean replied that unless his son had a valid medical or religious exemption, it was a requirement.
“I am not ‘anti-vax,’” Harrington said. “I am ‘anti-forced-vaxxed.’ They’re forcing these kids to get a vaccine even though they’re not affected by COVID or have already had it.”
According to Justin, he reported his myocarditis to the Centers for Disease Control and Prevention’s (CDC) Vaccine Adverse Events Reporting System (VAERS), but no one from the agency followed up.
Justin said he would “absolutely not” recommend anyone get vaccinated, as he does not want this to happen to any of his friends. “I’m not here to bash Moderna, but I wouldn’t take it,” he said.
Harrington said he also knows of a girl who had to have a heart transplant after being vaccinated and believes his son’s condition could have been even more severe if he hadn’t reached him in time.
According to WLWT 5 News, 19-year-old Simone Scott underwent a heart transplant one month after suffering a heart complication from her second dose of Moderna and subsequently passed away.
Moderna denies link between vaccine and heart inflammation
As recently as last week, Moderna said it has not found a link between its COVID vaccine and cases of a rare heart inflammation condition reported in young people who have received the shot.
The vaccine maker said in a statement it arrived at this conclusion after “carefully reviewing available safety data to date for the Moderna COVID-19 vaccine for cases of myocarditis and/or pericarditis.”
The CDC said during a June 10 meeting of the U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee the agency had identified 226 reports of heart inflammation that might meet its “working case definition” of myocarditis and pericarditis following the shots, The Defender reported last week.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger who received an mRNA vaccine. The median age of people with myocarditis or pericarditis following the first dose was 30, and after the second-dose, 24.
Moderna said it “will continue to closely monitor these reports and is actively working with public health and regulatory authorities to further assess this issue.”
“We clearly have an imbalance there,” said Dr. Tom Shimabukuro of the CDC’s Immunization Safety Office during the June 10 FDA meeting. The committee met to discuss safety issues surrounding the use of COVID vaccines in children as young as 6 months old.
The CDC has scheduled an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines.
CDC announced it will convene emergency meeting of its advisers June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer + Moderna COVID vaccines.
UKMFA have sent a letter of complaint to Prof Sridhar following her claims made on BBC Newsround, which is shown in most UK schools, which made several false or misleading claims including that the Covid-19 vaccines are 100% safe, that children should have the vaccine to protect their parents, and that the benefits to children outweigh any risks.
To present such a simplified and biased message is, in our opinion, deeply irresponsible, amounts to propaganda, and negatively impacts on the process of giving fully informed consent. We have requested that Prof Sridhar immediately retracts the entire message and issues a clear public apology for misrepresenting the facts relating to the safety concerns of Covid-19 vaccines in children.
This is in response to your recent appearance on BBC Newsround, where you made several statements which are entirely unsupported by scientific evidence.
Concerns are mainly related but not limited to the following points:
You state the benefit of the vaccine for children would be that they then “don’t need to worry about Covid-19”. Children are already in a position where they do not have to worry about Covid-19, as the risk to them is close to zero.
You state that another benefit would be that they then are likely to not infect their parents. Children do not play a major role in transmission, and there is also no evidence from the regulatory trials that the vaccines prevent transmission. This is clearly a statement intended to provoke an emotional response of guilt followed by a sense of duty, and as such it is propaganda rather than factual advice.
You state that the main downside of getting the vaccine is that it is “another injection into your arm”. This is a gross misrepresentation of the known and unknown risks of potential serious adverse effectsof the Covid-19 vaccines for children. We are sure you are aware that the CDC in the US is calling an emergency meeting, specifically to discuss the hundreds of cases of myocarditis that have occurred in young people after the vaccine (https://www.dailymail.co.uk/news/article-9672233/The-Latest-WHO-warns-delta-variant-hold-Europe.html).
Life-threatening effects and deaths have been reported in young adults and children in the US and Israel, which you do not refer to at all.
You will find the relevant references to all those points in our Open letter.
In the current situation, which is fraught with uncertainty and fear, the public is looking to professionals for balanced advice. To present such a simplified and biased message is, in our opinion, deeply irresponsible. When it is targeted specifically at a vulnerable group of children, it is unforgiveable.
We note that the currently accessible version of your statement on Newsround has already been redacted, as you originally claimed 100% safety for the Pfizer-BioNTech vaccine. You must have been aware that declaring any medical intervention 100% safe undermines anyone’s credibility.
Editing a feature after it has already been circulated and viewed by huge numbers of the public and children, without a publicized explanation or apology, is highly irregular. The comment at the end of the written transcript, merely noting a correction, will not reach the majority of the audience who have heard and assimilated your initial claim.
We therefore request that you immediately retract your entire message and issue a clear public apology for misrepresenting the facts relating to the safety concerns of Covid-19 vaccines in children.
We request that your retraction and apology are circulated as widely as your initial message, and specifically to all schools where this material may have been shown to children.
We are expecting a response confirming that you have taken appropriate action, or otherwise justify the reasons why you have not done so.
Rt. Hon. Gavin Williamson – Secretary of State for Education
Rt. Hon. Oliver Dowden – Secretary of State for Digital, Culture, Media and Sport Shirley-Anne Somerville – Scottish Cabinet Secretary for Education and Skills
Over the last several months we have requested from the Center of Disease Control (CDC) evidence for the isolation and existence for the any and all viruses, including CoV – 2 and 19, MERS, Influenza, Polio, Measles, HIV, XMRV, HTLV-1, HTLV-III/LAV, HPV, Ebola, Zika, just to name a few of the so-called viruses, disclosed under the Freedom of Information Act (FOIA).
These written requests were made by Ms. Christine Massey to CDC/ATSDR FOIA Chief Officer Mr. Robert Andoh, to locate and deliver ANY records, research and/or findings for ANY “viral” isolation and purification (by anyone, anywhere, anytime in the World) from a patient sample via maceration, filtration and/or the use of an ultracentrifuge or what is called the ‘Gold Standard’ for isolating and identifying a pathological micro or nana organism. The ‘Gold Standard’ for isolating and identifying microbes is referred to as Koch’s and Rivers Postulates which was established many years ago.
The CDC Chief FOIA, Mr. Roger Andoh provided straightforward responses to each one of our requests, admitting in writing that they have NO RECORD of ANY KIND, for the following so-called phantom “viruses”, including CoV – 2 -19, HIV, HPV, XMRV, HTMV-1, HTMV-111/LV, Measles, Influenza, MERS, EBOLA, ZIKA, POLIO:
1. June 7, 2021: CDC admits they have no record of any “COV – 2 or 19 virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever:
2. June 7, 2021: CDC admits they have no record of any “HPV virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever: (note: CDC made an error in their original response and later provided the corrected version below):
3. June 7, 2021: CDC admits they have no record of any “Measles virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever! No Isolation, No Purification and No Identification for the Measles Virus!
4. A Letter from the CDC Concerning the Childhood and Adult USA “Immunization Schedule”:
[Note: there was a reference to “influenza” in this request, but it doesn’t affect our request in any way because it was in the context of our example of the record we were looking to validate that the CDC does not have ANY record or research or findings for ANY so-called virus that is responsible for ANY sickness or disease – EVER!]
5. June 10, 2021: CDC admits they have no record of any “MERS virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever:
6. CDC June 11 2021: CDC admits they have no record of any “POLIO virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere on the planet, ever:
7. March 15, 2021 CDC FOIA response: no records of any “Ebola virus” isolation or purification from a patient sample, by anyone, anywhere on the planet, ever:
8. March 19, 2021, U.S. CDC (Centers for Disease Control and Prevention) and the Agency for Toxic Substances and Disease Registry (ATSDR) admit they have no record of any “Zika virus” isolated or purified from a patient sample, by anyone, anywhere on the planet, ever:
9. March 23, 2021 CDC admitted in a FOIA response that they have no record of any “HIV virus”, “Hepatitis viruis”, “STD virus”, and “TB bacillus bacterium” purified isolate from a patient sample, by anyone, anywhere, ever:
10. April 7th, 2021, the CDC states that they have no record of “XMRV virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
11. April 7th, 2021 the CDC states that they have no record of “HTLV-1 virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
12. April 7th, 2021, the CDC states that they have no record of “HTLV-III/LAV virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
13. April 12, 2021: CDC admits they have no record of any “influenza virus” isolated or purified from a patient sample, by anyone, anywhere on the planet, ever:
[Note: there was a reference to “influenza” in this request, but it doesn’t affect our request in any way because it was in the context of our example of the record we were looking to validate that the CDC does not have ANY record or research or findings for ANY so-called virus that is responsible for ANY sickness or disease – EVER!]
If no one any where at any time in the World has isolated and proven the existence of any such novel coronavirus or for any virus as a unique pathogen, how on earth can any pharmaceutical company provide a treatment with a vaccine for a virus that does NOT even exist?
Is the virus or pathogen a mythical virus that needs a mythical (but expensive and poisonous!) vaccine to destroy it?
Or is this phantom virus the creation of ‘bad actors’ and ‘luciferians’ for the purpose of redistributing the wealth of the world to themselves and at the same time reduce the surplus population of so-called ‘useless eaters’?
As Voltaire once warned us:
“Those who can make you believe in absurdities can make you commit atrocities.”
As stated quite clearly by Chief Officer Mr. Roger Andoh in his CDC FOIA letters:
“Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
As Rappoport has stated,
“Since that is the case, that there are no quantified virus isolates, how can one be sure of what is being determined as COVID -19 is, in fact, COVID -19?”
You cannot because you are looking for something that does not even exist!
You see the symptoms of cov – 19 are all symptoms of chemical and radiation poisoning. And the corona virus is not a virus at all but a symptom of cell membrane degeneration I call the ‘corona effect’!
The ‘Corona Effect’ Caused by Systemic Chemical and Radiation Poisoning Leading to Pathological Blood Coagulation, Hypoxia and Death
The two micrographs above show the ‘CORONA EFFECT’ on the red blood cells with the ‘SPIKED PROTEIN’ caused by decompensated acidosis of the interstitial and then vascular fluids from an acidic lifestyle and specifically, exposure to toxic pulsating electro-magnetic fields at 2.4gHz or higher, chemical poisoning from the food and water ingested, toxic acidic air pollution and chem-trails and to top-it-all-off a chemical laden inoculation! Please check your feelings and false beliefs at the door before YOU prematurely cause YOUSELF harm!
WHO report vindicates CCHR and the many groups that have fought worldwide for the recognition of psychiatric human rights violations, including involuntary commitment and forced electroshock and other biomedical, including drug treatments.
The World Health Organization (WHO) has released a damning report that lashes out against coercive psychiatric practices, which it says “are pervasive and are increasingly used in services in countries around the world, despite the lack of evidence that they offer any benefits, and the significant evidence that they lead to physical and psychological harm and even death.”[1] It points to the United Nations Convention on the Rights of Persons with Disabilities (CRPD) which in essence, calls for a ban on “forced hospitalization and forced treatment.”[2]
Citizens Commission on Human Rights International welcomes the report not just for it recognizing psychiatric abuses and torture as being rife, but also as a vindication of CCHR’s efforts since 1969 and other groups that have fought for the recognition of patents’ rights violations that WHO now acknowledges. CCHR’s Mental Health Declaration of Human Rights, written in 1969, includes many of the rights that the W.H.O. report now addresses. [3]
For example, WHO points to a series of UN guidelines and Human Rights Council resolutions that have called on countries to tackle the “unlawful or arbitrary institutionalization, overmedication and treatment practices [seen in the field of mental health] that fail to respect… autonomy, will and preferences.”[4] People who are subjected to coercive practices report feelings of dehumanization, disempowerment and being disrespected, WHO further states.[5]
CRPD says patients must not be put at risk of “torture or cruel, inhuman or degrading treatment or punishment” and recommends prohibiting “coercive practices such as forced admission and treatment, seclusion and restraint, as well as the administering of antipsychotic medication, electroconvulsive therapy (ECT) and psychosurgery without informed consent.”[6]
Coercive Practices Create Harm
Psychiatry has failed to take responsibility for the fact that its own coercive practices have caused the stigmatization which drives medical students and patients away from it, while it tries to blame this on its critics. WHO says stigmatization exists among the general population, policy makers and others when they see those with mental disabilities as being “at risk of harming themselves or others, or that they need medical treatment to keep them safe”—a psychiatric mantra—which results in a general acceptance of coercive practices such as involuntary admission and treatment or seclusion and restraint.[7]
Abusive practices CCHR has documented include:
In the U.S., children—who are too young to consent to electroshock—are subjected to it, even at the age of five or younger. American psychiatrists are administering it despite W.H.O. reporting sixteen years ago that “There are no indications for the use of ECT on minors, and hence this should be prohibited through legislation.” Yet the American Psychiatric Association has called for greater use of this brain-damaging, barbaric practice on minors.[8]
Many patients are forcibly detained and drugged under U.S. involuntary commitment laws, and with telepsychiatry now available, psychiatric hospitals are using this to incarcerate people against their will for their insurance.
Recent reports of the troubled teen industry in the U.S. highlight how coercive restraint use in psychiatric and behavioral facilities is common, despite leading to deaths of youths, without accountability. Teenagers gasping for air, crying out that they “can’t breathe” have died undergoing restraint to control their behavior.[9]
In New Zealand, a Royal Commission Inquiry into Child Abuse begins its investigation on June 14 into the torture of children with an electroshock device at the now-closed state psychiatric institution, Lake Alice. Children were not anesthetized but punitively shocked directly to various body parts, including genitalia.[10]
Despite a March 2020 Food and Drug Administration ban on a similar shock device used at the Judge Rotenberg Center in Massachusetts for behavior modification, the torturous procedure is still being used.[11]
Until recently, psychiatrists such as Patrick McGorry in Australia, pre-drugged patients in the Brave New World theory that this could prevent them from becoming psychotic, yet the antipsychotics prescribed for this list psychosis as a side effect. Similar practices are researched in the U.S.[12]
Many U.S. states allow electroshock to be given to involuntary patients against their will, constituting torture, as UN agencies have clearly stated. The WHO report specifically highlights the problem that “coercive practices are used in some cases because they are mandated in the national [or state] laws of countries.”[13]
Further, coercion is “built into mental health systems, including in professional education and training, and is reinforced through national mental health and other legislation.”[14]
These laws need to change, similar to those enacted in Australia where criminal penalties are enshrined in several mental health laws, should certain psychiatric treatments be administered, violating patients’ rights.
Countries must also ensure that “informed consent” is in place and that “the right to refuse admission and treatment is also respected.”[15] “People wishing to come off psychotropic drugs should also be actively supported to do so, and several recent resources have been developed to support people to achieve this,” WHO says.[16]
No Accountability: No Funding
WHO sees community mental health as the alternative to egregious hospitalization and the biomedical paradigm—psychotropic drugs, electroshock and psychosurgery—for treating people’s emotional and mental problems. This would require a massive injection of funds. However, the checks and balances do not exist to prevent abuses occurring in the community. Greater accountability, including criminal penalties are needed.
The same funding limitations also apply to psychiatric research, which the WHO highlights have been dominated by a biomedical model—neuroscience, genetics and psychopharmacology. It quotes the astounding admission from Thomas Insell, former director of the National Institute for Mental Health (2002 to 2015), who said: “When I look back on that, I realize that while I think I succeeded at getting lots of really cool papers published by cool scientists at fairly large costs—I think US$ 20 billion—I don’t think we moved the needle in reducing suicide, reducing hospitalizations, improving recovery for the tens of millions of people who have mental illness.”[17]
We cannot keep flooding more money into a failing and harmful mental health system, when accountability either doesn’t exist or is so ineffective that perpetrators can get away with murder.
Abolish Involuntary Hospitalization
In the U.S., in the wake of acts of senseless violence, psychiatrists have called for greater rights to involuntarily commit individuals—the antithesis of what the WHO is advocating. In fact, it debunks the idea that involuntary admission is necessary under so-called grounds such as “dangerousness” or “lack of insight.’”[18] Or that the person is “‘at risk of harming themselves or others, or that they need medical treatment to keep them safe,’” with WHO saying that such practices lead to an “over-emphasis on biomedical treatment options and a general acceptance of coercive practices such as involuntary admission and treatment or seclusion and restraint.”[19]
“Although challenging, it is important for countries…to eliminate practices that restrict the right to legal capacity, such as involuntary admission and treatment,” it says.[20]
The late Dr. Thomas Szasz, professor of psychiatry, a fellow of the American Psychiatric Association, and co-founder of CCHR, stressed this point sixty years ago. Indeed, he was more forthright in stating: “Involuntary mental hospitalization is like slavery. Refining the standards for commitment is like prettifying the slave plantations. The problem is not how to improve commitment, but how to abolish it.” Further, “The most important deprivation of human and constitutional rights inflicted upon persons said to be mentally ill is involuntary mental hospitalization….”[21]
CCHR will continue to monitor and document psychiatric abuses and with this WHO guideline against involuntary treatment, refer this to attorneys who may be able to seek charges of torture where forced treatment is administered. Until laws enact the necessary protections, more pressure is needed to bring abuses to account through the courts.
[1] “Guidance on Community Mental Health Services: Promoting Person-Centered and Rights-Based Approaches,” World Health Organization, 10 June 2021, p. 8, https://www.who.int/publications/i/item/9789240025707 (to download report)
I’m sure the grant money for this study came with the stipulation that they stick to the script that autism is a genetic disorder lots of unfortunate children are born with. It’s important that autism busywork like this continues so the public thinks that the medical community cares about autism.
How do I know this?
Everything in the piece is meant to downplay the health and humanitarian disaster that autism represents. Reporter Lauren Talarico provides the blanket definition that understates any of the horrific symptoms children and families have to live with:
Autism is a neuro-developmental disorder. It can affect speech, social interactions and the ability to communicate.
(No mention of parents changing the diapers on their non-verbal young adult son who wears a helmet because he bangs his head on the wall endlessly.)
Likewise there are no words like crisis or epidemic used. Instead Dr. Olivier Lichtarge, professor of molecular and human genetics, uses phrases like ‘a surprisingly large number of children’ to describe two percent of U.S. kids with autism.
While we are told that one in 54 children are now diagnosed with autism, there is not one word about the unstoppable increases that have preceded it: 2004: one in 166, 2007: one in 150, 2009: one in 110, 2012: one in 88, 2014: one in 68, 2018: one in 59, (also in 2018: one in 40 according to a separate study published in JAMA), one in 54, 2020.
Somehow Lichtarge thinks that looking for mutating genes will matter when the rate eventually reaches one in 10, one in 5.
Lichtarge shows no embarrassment over the complete failure of the scientific/medical community to figure out anything significant about autism despite billions of dollars in research funding and 20 years of trying.
This is how lost they are:
More and more children are being diagnosed with Autism Spectrum Disorder (ASD), and researchers are trying to figure out why.
“It is a rising fraction for reasons we do not understand,” Dr. Lichtarge said.
Doctors are not sure what causes it.
“The basis of autism is not quite clear. It’s obviously genetic. It also may have an environmental interplay,”
“There is every reason to hope that we can understand it better in the near future,” he said.
Lichtarge cleverly sidesteps the issue of an environmental trigger that marks these genetically susceptible kids for lifelong damage with the singular, vague mention of ‘an environmental interplay.’ Yet this is something he has no interest in exploring.
And don’t think the horrific number of one in 54 kids matters really. Notice the phrase is “1 in 54 kids diagnosed with Autism,” not 1 in 54 kids with autism.
This is a neat way of saying that the rate may be the result of “better diagnosing” and it’s has used for two decades as the catch phrase to mean that more kids don’t actually have autism. They’ve always been here; more are being diagnosed.
No one wants to prevent autism
We are told that the endgame of identifying those “harmful mutations….linked to autism” is merely so “scientists can develop the best treatments.”
All in all, there are no findings here that will help a single child.
Talarico also fails to ask why Lichtarge isn’t interested in adults with autism and looking at their genetics and their treatment plans.
Of course Lichtarge won’t have a problem finding kids to study; they’re on every block and in every school. Too bad he doesn’t want to use some of his funding to look for the elusive one in 54 adults with autism..
Predictably the photo companying the piece show a cute smiling girl painting a paper covered with colorful puzzle pieces. And thus it will remain: the eternal mystery of autism, the puzzle no one wants to solve.
VAERS data released today showed 329,021 reports of adverse events following COVID vaccines, including 5,888 deaths and 28,441 serious injuries between Dec. 14, 2020 and June 4, 2021.
This week’s number of reported adverse events among all age groups following COVID vaccines surpassed 329,000, according to data released today by the Centers for Disease Control and Prevention (CDC). The data comes directly from reports submitted to the Vaccine Adverse Event Reporting System (VAERS).
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Today’s data show that between Dec. 14, 2020 and June 4, a total of 329,021 total adverse events were reported to VAERS, including 5,888 deaths — an increase of 723 deaths over the previous week. There were 28,441 serious injury reports, up 3,082 compared with last week.
Among 12- to 17-year-olds, there were 59 reports of heart inflammation and 19 cases of blood clotting disorders.
In the U.S., 299.1 million COVID vaccine doses had been administered as of June 4. This includes 126 million doses of Moderna’s vaccine, 162 million doses of Pfizer and 11 million doses of the Johnson & Johnson (J&J) COVID vaccine.
Of the 3,211 cases of Bell’s Palsy reported, 53% were reported after Pfizer vaccinations, 42% following vaccination with the Moderna vaccine and 253 cases, or 8%, of Bell’s Palsy cases were reported in conjunction with J&J.
CDC to hold emergency hearing after identifying 226 cases of heart inflammation in young people
As The Defender reported today, the CDC on Thursday announced plans to convene an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines.
As The Defender reported Thursday, before the announcement, the CDC on June 1 had quietly updated its website to acknowledge a higher-than-expected number of cases of myocarditis among young teens after the second dose of an mRNA COVID vaccine.
Based on a May 24 report from the CDC’s Advisory Committee on Immunization Practices COVID-19 Vaccine Safety Technical Work Group, the CDC on June 1 added new language to its guidance:
“Data from VAERS [Vaccine Adverse Events Reporting System] show that in the 30-day window following dose 2 mRNA COVID-19 vaccination, there was a higher number of observed than expected myocarditis/pericarditis cases in 16–24-year-olds.”
The updated language differed significantly from the CDC’s statement two weeks earlier, which said rates of myocarditis were not higher among vaccinated people.
During a Thursday meeting of advisors to the U.S. Food and Drug Administration, CDC officials presented data showing a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger following mRNA vaccines.
The CDC identified 226 reports that might meet the agency’s “working case definition” of myocarditis. The majority of those affected have recovered, but 41 had ongoing symptoms, 15 are still hospitalized and three are in the intensive care unit.
On June 10, The Defender reported the Oregon Health Authority said it was aware of at least 11 cases of myocarditis or pericarditis — inflammation of the sac surrounding the heart — in all age groups following COVID vaccination.One of the cases is a 15-year-old teen in Beaverton, Oregon, who was hospitalized for heart inflammation after receiving his second dose of the Pfizer vaccine.
“The hallmark symptom of myocarditis and pericarditis is chest pain or shortness of breath,” Jonathan Modie, an Oregon Health Authority spokesperson, said in an email. “In rare cases, it can also present in the form of heart palpitations. Anyone suffering from unexplained chest pain should contact a medical provider or seek immediate emergency care.”
A search of the latest available data in VAERS revealed 900 cases of myocarditis and pericarditis, among all age groups reported in the U.S following COVID vaccination between Dec.14, 2020 and June 4, 2021. Of the 900 cases reported, 533 cases were attributed to Pfizer, 331 cases to Moderna and 32 cases to J&J’s COVID vaccine.
Experts tell FDA for kids, benefits of COVID vaccines don’t outweigh the risks
As The Defender reported June 11, an FDA advisory committee held a virtual meeting Thursday to discuss what data would be needed to vaccinate children under 12 against COVID under Emergency Use Authorization (EUA) or licensure.
Several experts spoke out against the plan, saying the benefits don’t outweigh the risks for young children. Peter Doshi, Ph,D, associate professor University of Maryland School of Pharmacy and senior editor of The BMJ, said during the open public hearing session, there is no emergency that would warrant using EUA to authorize COVID vaccines for children.
Kim Witczak, an FDA consumer representative, expressed great concerns over the premature approval of COVID vaccines for children. Witczak said data shows children are neither in danger or dangerous and questioned the timing of last Friday’s CDC announcement of the rise in children being hospitalized with COVID.
Dr. Cody Meissner, director of pediatric infectious diseases at Tufts University School of Medicine, said children are at low risk of severe disease from the virus and more study is needed about safety in younger age groups.
Witczak and Doshi were two of 27 researchers and clinicians around the world who launched a citizen’s petition demanding the FDA withhold full approval of COVID vaccines until efficacy and safety measures are met.
The members of the FDA’s Vaccines and Related Biological Products Advisory Committee were not asked to provide specific advice or to vote during the meeting.
Moderna, Pfizer push to vaccinate kids as young as 5 by September
Moderna this week asked the FDA to expand emergency use of its COVID vaccine for adolescents aged 12 to 17. The vaccine maker said its COVID vaccine was 100% effective in a study of 3,700 12-to-17-year-olds.
Moderna and Pfizer both this week said they expect to make their vaccines available to children as young as 5 by September.
As The Defender reported this week, Pfizer is advancing late-stage clinical trials of its COVID vaccine, in lower doses, on children ages 5 to 11 years old and expects to apply for approval early this fall. The study will enroll up to 4,500 children at more than 90 clinical sites in the U.S., Finland, Poland and Spain, the company said.
Based on safety, efficacy and tolerability data from the 144 children included in Pfizer’s phase 1 trial, the company will use 10 micrograms of each vaccine dose for kids between the ages of 5 and 11 in phase 2/3 trials, and 3 micrograms of each dose for those 5 and younger.
Moderna said it also expects its COVID vaccine will be available for kids as young as 5 by early fall. CEO Stéphane Bancel said Monday he thinks the data will become available sometime in September.
New Cleveland Clinic study shows vaccine provides no added benefit to those who already had COVID
A new preprint study by the Cleveland Clinic found people previously infected with SARS-CoV-2 were less likely to be reinfected than fully vaccinated individuals who never had the virus — suggesting the vaccine is of no benefit to people who already had COVID.
As The Defender reported, the study, available on medRxiv, provides insight into how the immune system protects the body once a COVID infection is confirmed.
The clinic studied 52,238 employees. Of those, 49,659 never had the virus and 2,579 had COVID and recovered. Of the 2,579 who previously were infected, 1,359, or 53%, remained unvaccinated, compared with 41%, or 22,777 who were vaccinated.
Of all infections during the study period, 99.3% occurred in participants who were not infected previously and remained unvaccinated. In contrast, 0.7% of infections occurred in participants who were not previously infected but were currently vaccinated. Significantly, not one of the 1,359 previously infected subjects who remained unvaccinated had a SARS-CoV-2 infection over the duration of the study.
Pfizer skipped critical testing, documents reveal
New documents obtained by TrialSite News suggest routine quality testing issues were overlooked in the rush to authorize use of Pfizer’s COVID vaccine, and that U.S. and other governments are conducting a massive vaccination program with an incompletely characterized experimental vaccine.
As The Defender reported June 7, regulatory documents revealed Pfizer didn’t thoroughly examine biodistribution and pharmacokinetics issues relating to its vaccine before submitting the vaccine to the European Medicines Agency (EMA) for review.
Pfizer also did not use the commercial vaccine (BNT162b2) for all of its studies, but instead relied on a “surrogate” mRNA that produced the luciferase protein.
According to TrialSite News, it’s standard practice for the EMA to disclose its assessment of investigational new drug submissions. In the case of Pfizer’s vaccine, the EMA assessment included a summary of the agency’s evaluation of the non-clinical vaccine distribution studies reported to EMA by Pfizer — but the EMA did not disclose the results of Pfizer’s biodistribution studies in its public EMA summary.
95 days and counting, CDC ignores The Defender’s inquiries
According to the CDC website, “the CDC follows up on any report of death to request additional information and learn more about what occurred and to determine whether the death was a result of the vaccine or unrelated.”
On March 8, The Defender contacted the CDC with a written list of questions about reported deaths and injuries related to COVID vaccines. After repeated attempts, by phone and email, to obtain a response to our questions, a health communications specialist from the CDC’s Vaccine Task Force contacted us on March 29 — three weeks after our initial inquiry.
The individual received our request for information from VAERS, but said she had never received our list of questions, even though employees we talked to several times said CDC press officers were working through the questions and confirmed the representative had received them. We provided the list of questions again along with a new deadline, but never received a response.
On May 19, a CDC employee said our questions had been reviewed and our inquiry was pending in their system, but would not provide us with a copy of the response. We were told we would be contacted by phone or email with the response.
On June 4, the CDC employee we contacted said nobody had responded to our inquiries. We were advised to submit our questions again, which we have done numerous times.
It has been 95 days since we sent our first email inquiring into VAERS data and reports and we have yet to receive a response.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger, but only 226 reports meet the agency’s “working case definition.”
The Centers for Disease Control and Prevention (CDC) announced Thursday it will convene an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines, CBS News reported.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger. The CDC identified 226 reports that might meet the agency’s “working case definition” of myocarditis and pericarditis following the shots, the agency disclosed Thursday during an FDA hearing.
The majority of those affected have recovered, but 41 had ongoing symptoms, 15 are still hospitalized and three are in the intensive care unit.
Dr. Tom Shimabukuro, deputy director of the CDC’s Immunization Safety Office said during Thursday’s meeting there had been a higher-than-expected number of cases of heart inflammation among young people recently vaccinated with their second doses of mRNA vaccine.
CDC data showed 196 reports of myocarditis and pericarditis among 18- to 24-year-olds through May 31, compared with an expected rate of between eight and 83 cases.
Among 16- to 17-year-olds, 79 cases of myocarditis and pericarditis were reported through May 31. The expected rate among people in this age group is between two and 19 cases, Shimabukuro said during his presentation.
Shimabukuro said the CDC’s findings were “mostly consistent” with reports of rare cases of heart inflammation that had been studied in Israel and reported by the U.S. Department of Defense earlier this year.
Myocarditis is inflammation of the heart muscle that can lead to cardiac arrhythmia and death. According to researchers at the National Organization for Rare Disorders, myocarditis can result from infections, but “more commonly the myocarditis is a result of the body’s immune reaction to the initial heart damage.”
A search in the CDC’s Vaccine Adverse Events Reporting System (VAERS) revealed 900 cases of pericarditis and myocarditis reported in the U.S., among all age groups, following COVID vaccination, between Dec. 14, 2020 and June 4, 2021.
Of the 900 cases reported, 59 cases occurred in the 12- to 17-year-old group –– all but one case was attributed to Pfizer.
On May 10, the U.S. Food and Drug Administration (FDA) expanded the EUA for Pfizer’s COVID vaccine to include children aged 12-15 years. On June 10, Moderna asked the FDA to expand emergency use of its COVID vaccine in adolescents ages 12 to 17.
The CDC had previously said it was investigating reports that some teenagers and young adults vaccinated against COVID may have experienced heart problems, according to the agency’s advisory group.
The CDC’s Advisory Committee on Immunization Practices in a statement said reports of myocarditis to date seemed to occur predominantly in adolescents and young adults, more often in males than females, more often following the second dose and typically within four days after vaccination. Most cases appeared to be “mild” and follow-up is ongoing.
The CDC’s Vaccine Safety Technical Work Group originally said its monitoring systems had not found more cases of myocarditis than would be expected in the population, but members of the committee on vaccinations said healthcare providers should be made aware of the reports of the “potential adverse event.”
But as The Defender reported June 10, the CDC subsequently acknowledged — in guidance updated on its website June 1 — a higher-than-expected number of cases of myocarditis among young teens after the second dose of an mRNA COVID vaccine. It wasn’t until Thursday’s FDA meeting that the agency publicly discussed the higher rate and followed up by announcing plans to hold an emergency meeting.
EU and Israel investigate reports of heart inflammation
On June 2, Israeli health officials found a “probable” link between Pfizer’s COVID vaccine — which the country has relied on almost exclusively in its vaccination drive — and dozens of cases of heart inflammation in young men following the second dose.
In a statement, Pfizer said there is still no indication the cases are due to its vaccine. Myocarditis is often caused by viral infections, and COVID infections have been reported to cause the condition, the drugmaker said.
Pfizer’s partner, BioNTech, said more than 300 million doses of the COVID vaccine have been administered globally and the “benefit-risk profile” of the vaccine remains positive.
On May 7, EU regulators called on Pfizer and Moderna to provide additional data related to the companies’ COVID vaccines and a potential link to heart inflammation, after the agency completed a safety review of all four COVID vaccines authorized for emergency use in the EU.
A report issued by European Medicines Agency’s Pharmacovigilance Risk Assessment Committee (PRAC) disclosed its members were aware of cases of myocarditis and pericarditis following Pfizer vaccination. Regulators said they didn’t see an indication the vaccine caused these cases, but as a prevention, PRAC requested Pfizer provide further data, including an analysis of events according to age and gender in its next pandemic summary safety report and will consider if any other regulatory action is needed.
Today my colleague from Kentucky, Chris Wiest, received an awesome ruling from the Circuit Court of Boone County declaring that all of Governor Andy Bashear’s emergency orders and actions are unconstitutional and void. The ruling was in the state-court challenge to the governor’s emergency powers executive orders, filed by Wiest on behalf of Beans Cafe’ & Bakery.
Dr. Stephen Petty, an actual expert in masks, testified at the trial about their uselessness under the circumstances in which they’re being idolized. Here’s an excerpt from the order pertaining to Dr. Petty. For those bureaucrats and social media tyrants who would censor this, this is from an actual court order issued today. Not that you care:
Stephen E. Petty, P.E., CIH, testified as an expert and was accepted as such without objection. Mr. Petty has served as an expert witness in approximately 400 cases relating to toxic or infectious exposure, personal protective equipment (“PPE”), and as a warning expert. He also served as an epidemiology expert for the plaintiffs in the Monsanto “Roundup” cases, and for those in the Dupont C8 litigation. In connection with his service as an expert, he was deposed nearly 100 times and has provided court testimony in approximately 20 trials. Mr. Petty holds nine U.S. patents, has written a book comprising nearly 1,000 pages on forensics engineering, is a certified industrial hygienist, and a recognized expert with the Occupational Safety and Health Agency. Mr. Petty helped write the rules on risk assessment for the State of Ohio and has trained Ohio’s risk assessors.
Mr. Petty explained that the field of his expertise is “to anticipate and recognize and control things that could hurt people, everything from making them sick to killing them.” He testified that, in this context, he has analyzed the use of masks and social distancing in connection with Covid-19. He testified that both the six-foot-distancing rule, and mask mandates, are wholly ineffective at reducing the spread of this virus. Masks are worthless, he explained, because they are not capable of filtering anything as small as Covid-19 aerosols. In addition, masks are not respirators and lack the limited protections that respirators can provide.
The N-95 respirator, which he states is in the bottom class of what may be classified as a respirator, is rated to filter 95% of all particles that are larger than .3 microns. However, a Covid-19 particle, which is only between .09 to .12 micron, is much smaller. Mr. Petty further explained that an N-95 will not even filter above .3 microns if it is not used in accordance with industry standards. Among the requirements, respirators must be properly fitted to seal along the face, and they also must be timely replaced. Mr. Petty stated that N-95 masks, which he said are often utilized as surgical masks, are “not intended to keep infectious disease from either the surgeon or from the patient infecting each other” but only to catch the “big droplets” from the surgeon’s mouth.”
According to Mr. Petty, masks have no standards, are not respirators, and do not even qualify as protective equipment. In contrast, respirators have standards, including rules that state respirators may not be worn by persons with facial hair, must be fitted to ensure a seal, and must be timely replaced—or, as in higher end respirators, the cartridges must be replaced to prevent saturation. In addition, standards for respirators also require users to obtain a medical clearance because the breathing restriction can impair lung function or cause other problems for persons having such limitations. Putting those persons in a respirator can harm their well-being.
Concerning the effectiveness of respirators, Mr. Petty explained that it comes down to “big stuff” versus “small stuff.” Big stuff can be taken out by the body’s defenses, such as its mucus tissue, where droplets can be caught and eliminated. The small stuff, however—like aerosols—are more dangerous. Masks cannot filter the small stuff. According to Petty, because Covid-19 particles are comprised of aerosols, it is really, really, small stuff. And, as he pointed out, an N-95 is designed to filter larger particles. Even for particles as large as .3 micron, Mr. Petty testified that an N-95’s effectiveness is in direct proportion to its seal. In fact, he stated it becomes completely ineffective if 3% or more of the contact area with the face is not sealed.
Mr. Petty testified that masks leak, do not filter out the small stuff, cannot be sealed, are commonly worn by persons with facial hair, and may be contaminated due to repetitive use and the manner of use. He emphatically stated that mask wearing provides no benefit whatsoever, either to the wearer or others.
He explained that the big droplets fall to the ground right away, the smaller droplets will float longer, and aerosols will remain suspended for days or longer if the air is stirred. Mr. Petty testified that the duration of time that particles remain suspended can be determined using “Stoke’s Law.” Based on it, for particles the size of Covid-19 (.12 to .09 micron) to fall five feet would take between 5 and 58 days in still air. Thus, particles are suspended in the air even from previous days. And so, he asks, “If it takes days for the particles to fall, how in the world does a six-foot rule have any meaning?”
Mr. Petty acknowledged that both OSHA and CDC have recommended that people wear masks. However, he called this “at best dishonest.”61 As an example on this, he pointed to CDC guidance documents where, on page 1, it recommends wearing a mask; but then on page 6, admits that “masks, do not provide . . . a reliable level of protection from . . . smaller airborne particles.”62 According to Mr. Petty, those agencies have smart individuals who know better. Mr. Petty points out that, even before March 2020, it was known that Covid-19 particles are tiny aerosols. And on this, he states that he insisted that fact early on. He also points to a more recent letter by numerous medical researchers, physicians and experts with Ph.D.s, asking the CDC to address the implications of Covid-19 aerosols. During Dr. Stack’s subsequent testimony, he also acknowledged that Covid-19 is spread “by . . . airborne transmission that could be aerosols . . . .”
Finally, Mr. Petty pointed to another recent study by Ben Sheldon of Stanford University out of Palo Alto. According to that study, “both the medical and non-medical face masks are ineffective to block human-to-human transmission of viral and infectious diseases, such as SARS, CoV-2 and COVID-19.”64 The Court finds the opinions expressed by Mr. Petty firmly established in logic. The inescapable conclusion from his testimony is that ordering masks to stop Covid-19 is like putting up chain-link fencing to keep out mosquitos. The six-foot- distancing requirements fare no better.
The judge summarizes the situation nicely:
It is obvious from even a cursory review that the orders issued over the past fifteen months “attempt to control” and seek “to form and determine future rights and duties” of Kentucky citizens. These included ordering the closure of all businesses, except those the Governor deemed essential. He ordered churches closed, prohibited social gatherings, including at weddings and funerals, prohibited travel, and through CHFS, even prohibited citizens from receiving scheduled surgeries and access to medical care. And then there is the order that everyone wear a mask. These are, undeniably, attempts to control, set policy, and determine rights and duties of the citizenry. Except in those instances where the federal courts have stepped in, Defendants assert authority to modify or re-impose these orders at their sole discretion. Consider, for example, the recent modification of the mask mandate. It orders persons who did not get vaccinated for Covid-19 to wear masks but lifts that requirement for others. That is setting policy and determining future rights and duties.
At the hearing, Defendants took exception to the Attorney General’s characterization of the Governor’s actions as a “lockdown,” and argued that prohibiting persons from entering those restaurants is not the same as ordering that they be closed. But that doesn’t minimize the impact on those who lost their businesses as a result, or those in nursing homes condemned to spend their final hours alone, deprived of the comfort from loved ones (or even any real contact with humanity), or those citizens who the Governor prohibited from celebrating their wedding day with more than ten persons, or those he forced to bury their dead alone, without the consoling presence of family and friends (and who likewise were deprived of paying their final respects), or those persons who were barred from entering church to worship Almighty God during Holy Week, and even Easter Sunday, or those persons who were denied access to health care, including cancer-screenings, or those denied entry into government buildings (which they pay for with their taxes) in order to obtain a necessary license, and who were forced to wait outside for hours in the sweltering heat, or rain, purportedly to keep them from getting sick.
What the people have endured over the past fifteen months—to borrow a phrase from United States District Judge Justin R. Walker—“is something this Court never expected to see outside the pages of a dystopian novel.” Yet, Defendants contend that the Governor’s rule by mere emergency decree must continue indefinitely, and independent of legislative limits. In effect, Defendants seek declaratory judgment that the Constitution provides this broad power so long as he utters the word, “emergency.” It does not. For this Court to accept Defendant’s position would not be honoring its oath to support the Constitution; it would be tantamount to a coup d’état against it.
Yes, life is now a dystopian novel. Let’s hope this patriot judge’s order stands up on appeal in the state appellate courts in Kentucky. And thanks to Chris Wiest and the AG of Kentucky for fighting the good fight. The order notes that the permanent injunction against the governor goes into effect on June 10, 2021 at 5:00 p.m.
“…how can you give informed consent if there’s no package insert, with no
ingredients, no test note, no anything? The words are intentionally left
blank on the package insert for the shots and there’s no long-term data,
so I can’t tell people what will happen in 2, 3, 4, 5, ten years from now,
because they took this shot. So that, by default, is the informed consent
that I’m concerned with.”
America’s Frontline Doctors (AFLDS) spoke to New York pharmacist Joel Wood about his dismissal for his refusal to administer experimental biological agents without providing his patients the ability to give their informed consent to receive them.
On May 5th, Wood called an anonymous ethics line at the Kinney Drugs corporation where he was employed to express concerns over both vaccine shedding and vaccination in youth. On May 9th he wrote an email to the corporation in which he stated: “I have been an employee for Kinneys for over 5 years. I have always felt that they have made safety for staff and patients a priority. However, I would like to know what the company is doing to address the safety concern of shedding of vaccine in the work place. It is a known phenomenon, and specifically mentioned in the Pfizer study on page 67 as a concern. It is possible to have contact thru both physical touching (which is not the concern at work) but also inhalation – this is a concern at work. The masks do not provide any safety. I would like to see this addressed in an email to the company by this weekend.”
Wood continued: “If there is not an email that addresses these concerns, I will forward my complaint to OSHA as a violation of safety.
“I am also concerned with the lack of patient safety and informed consent that involves the Moderna COVID-19 shot. I have heard from many staff and patients that they did not know that the shot was NOT FDA-approved. I know for a fact the staff who are administering this shot are not telling people that it is not an approved vaccine. This creates an issue when patients get their second shot and are informed that it is not approved and say, ‘Well, the first shot was’; no, it was not.
“I would also like to address the elephant in the room. I understand the need to follow advice from our regulatory governmental agencies. However when those agencies are wrong or make inappropriate recommendations, it is our patients that feel the brunt of this…
“I fear that Kinney is moving in a direction that is the opposite of our motto. Experience the difference means just that, if we do not change our behavior and inform the public the real science and health information that exists in the world, we do a disservice to the community and also ourselves as healthcare providers. We are now going to be administering a shot to children 12 and older for a disease that was called the common cold by the New York Times twice. We have no long-term data about this shot in children.”
Wood concluded his letter to Kinneys: “If there is not an email sent to the company that starts to address these concerns, I will be writing letters to OSHA and well as news organizations as a whistleblower for the crimes that are being committed. I do not believe that it is intentional, but we are acting against international human rights laws that discuss vaccines and discrimination. We have a responsibility to tell the public the reality about this shot, what it really does, that there is no pandemic, and that the numbers were inflated to make it appear like a pandemic. We need to inform them about the vaccine shedding that might be occurring.”
After receiving no answer to address his concerns, Wood addressed a formal complaint to the Occupational Safety and Health Administration (OSHA). On May 11th, he received an answer that read: “At this time OSHA has no standards or jurisdiction when it comes to COVID-19 concerns or complaints. We have been told to give all complainants these 3 numbers to contact if you so choose:”, listing the New York State Governor’s office, the New York State COVID-19 hotline, and the New York State Department of Labor COVID violation hotline. Wood was subsequently fired from his position at Kinney Drugs.
America’s Frontline Doctors spoke to New York pharmacist Joel Wood, who was fired after five years in his job for refusing to administer COVID-19 vaccines without informed consent.
“I’ve been a pharmacist in New York State for seven years and I’ve been working with this company in the retail setting for seven years, and ever since the coronavirus outbreak in the beginning of 2020, I’ve had my concerns as someone who works in the front line trying to make sure that my patients and the public are safe, are taken care of, to the best of the ability that we can as pharmacist and health care providers has been my number one concern.
“So I became very invested in the coronavirus outbreak and pandemic, but as time went on I started to have more concerns over what was going on with the whole story of the coronavirus pandemic and outbreak, from things like grabs for power, from different governments in with located within the United States, and I also saw abroad in the world as well. But New York State, the governor of New York, Andrew Cuomo, has had a massive power grab, and in my opinion violated a lot of concerns that I have as a health care provider, mandates and things like that.
“So it was to the forefront of my attention what was going on, and was something more going on than just what we saw at face value of ‘this is a pandemic.’
“I had my concerns about administering the coronavirus when I heard that we were going to start administering it to children.
“I also did have concerns – I’ve seen some reports of women, most likely younger women of childbearing age, having adverse reactions to either the vaccine, or potentially even the vaccine shedding – you know people who have gotten the vaccine become a vector to shed the vaccine, as noted in Pfizer’s trial.
“So the combination of both the children 12 years and up being given the vaccine, or having the ability to receive the vaccine, as well as women of childbearing age – I started to kind of have some concern what was going on with the vaccine, but also what was going on with the coronavirus pandemic, period.
“But the majority of my concerns stemmed from the lack of solid, I have to say science, backed-up evidence. I mean multiple health organizations, from the World Health Organization to the Centers for Disease Control and to some degree the FDA, in terms of their approval process for this vaccine, they’ve been all over the place. I mean multiple doctors and scientists from across the world have written into the WHO with different concerns; respiratory droplets compared to aerosol, that kind of goes into the mask detail. The CDC has published data that leads to the potential controversy for masks. I mean, I’ve read an article in which the CDC describes the masks were not statistically significant. I was taught in school that if it’s not significant, that’s not something that you look at.
“So combinations of those have led me to believe that the administration of these vaccines in any group in which the coronavirus does not have a high death rate may be unwarranted and potentially, as it is an experimental vaccine – not FDA approved – violates Nuremberg trial law.
“So my ultimate decision to stop administering these COVID-19 vaccines, as I stated, came from the combination of children 12 and up, and specifically women bleeding, menstruation issues as it relates to women specifically of childbearing age; there’s no long term data to what this vaccine does, and technically it’s impossible to give informed consent, in my opinion, because the package insert is blank. The package insert for the drug itself, for the vaccine, if it even is a vaccine, is blank, and there’s no long-term data. So I am concerned for what effects then could happen from women who take this, specifically of childbearing age, what could be the end result? I have no idea, and I’m not speculating that anything awful could happen, but we don’t know – and that’s a concern, that’s something I look at – risk versus benefit is what is what my job is all about.
“Same thing with children. Children who are less than 18 – the survival rate of the coronavirus is like 99.999. The only age group that I feel could and potentially should have concern with receiving this vaccine is 65 and older, as their survival rate was less than 99-point-x, we can just say.
“So I also was administering the shot as of January 11th when the rollout happened in New York, right along, because that was what all of the governing bodies were saying: The states, the CDC, FDA, World Health Organization – everybody was discussing the importance of the shots and need to get to herd immunity, so I was doing my part – or I thought I was doing my part – by helping us get there.
“But I noticed as we started to get there, and people started to receive the shot and get both doses, if they were getting the Pfizer and Moderna, for example, it seems like we’re never going to reach this herd immunity and they just keep pushing the vaccine.
“I mean, now in New York State, you can win anywhere from $20 to $5 million with the lottery, just for signing up and getting the vaccine. For me, that’s a huge concern on multiple different levels. I mean one, on the very face value, the government of New York under the leadership of Governor Cuomo, and along with the federal government as well, at least for part of this, is using our federal and state tax dollars to get the money for this vaccine, which my question is may or may not be causing more harm, and also now we are using tax money that should be going towards schools, is my is my understanding of what the New York State lottery was supposed to be for when it was revamped believe over a decade ago, now we’re using that money to give people for getting the vaccine? It’s just highly irregular. I’ve never seen anything like that before in my life. It’s a concern.
“I also have concerns, as I previously mentioned, about violations of the Nuremberg trial, human rights as it pertains to the Geneva conference in the Nuremberg trials. This is an experimental vaccine, it’s not FDA approved.
“And from there, my concerns go out to: Is this coronavirus pandemic a real pandemic? No more people died from it month over month in 2020 than in previous years. The CDC has come out that 6% of deaths were attributed specifically to coronavirus, meaning that the other 94% had underlying comorbid diseases, which we would generally assume similar to like the flu, we don’t say that everyone just died from the flu if you had the flu, something else helped you get there. That’s how that’s how it presents itself.
“The CDC has been, in my opinion, manipulating and shifting how they are counting deaths and cases to establish a point that if anyone believes that we are not in a pandemic, there is a massive issue and concern with that. So moving forward, if we are actually not in a pandemic, there is fraud and deceit associated with receiving this experiment which both violate the Nuremberg trial.
“The other part of the Nuremberg trial that concerns me is coercion. It’s also stated in the Nuremberg trials that you have to have free, informed consent to be able to have someone sign up for your experiment. And we are coercing people now to have to get the vaccine to be able to take their mask off. So it’s also a false pretense that you have to get the vaccine to take the mask off, but that’s not how we should be doing an experiment, it gives a false sense of reality to people that were not truly informed as to what could be happening.”
Just for the record, what has been your stance on vaccines in general, prior to the emergence of COVID-19, and what has been your experience regarding the whole issue of informed consent? Has there not been a problem until now?
“I don’t have a concern with vaccines in general. I mean, I do have some minor concerns, specifically as it pertains to the pediatric administration of vaccines, but it’s not necessarily the vaccines itself as much it is the tenacity to which we give all these vaccines. I mean, just for example, the amount of aluminum in a child’s vaccine series could be more than what the FDA allows to have in an adult’s i.v. So just as a quick example of where my concerns for vaccines stem from, that’s pretty much my only concern with vaccines, like the current childhood immunization schedule I think is a little over the top. But otherwise no, I don’t have a problem with other vaccines, I don’t have a problem with administering other vaccines. The informed consent has never come up as a major issue for me, in general because they’re all FDA approved. In the very least, every other vaccine that I have ever administered has been FDA approved. So then from there, it’s more of the informed consent of like, ‘these are the side effects, this is to look what to look out for, what could happen; if this happens, do this,’ which is common for any and all medications, new medications, or any and all medications that I would be giving in a pharmacy. Letting people know what the risks and benefits are from the shots that are given.
“The informed consent is a massive concern this time because the package insert is blank. So if someone were to ask me, ‘Hey Dr. Wood, what’s in this?’ I couldn’t tell you. I do know some of the things, I do know some of what’s in it, but I couldn’t give you specific details from the package insert. And then also, ‘What could happen to me?’ I can tell you what has happened to people previously to this point; I can tell you adverse reactions that I have seen from the VAERS reporting, including all of the deaths, the rashes; I can tell you what I have seen up to this point, but I can’t tell you what’s going to happen to you a year from now or two years from now, five, seven, ten years – I have no idea. So informed consent is for me the biggest concern, as it pertains to this coronavirus shot.
“In New York, and in I believe most of the rest of the United States, pharmacists are administering vaccines and have been quite a while, typically in the very least the influenza, maybe the pneumonia or shingles vaccine. But since the beginning of January, retail pharmacies of which I was working for have been administering the coronavirus shot – I will call it a shot, it’s not a vaccine in my opinion. So I have been giving the coronavirus shot probably upwards of over at least 500 people, if not more, and I’ve expressed what my concern is. I went to my employer and said I don’t feel comfortable giving this. We can’t give the people full, informed consent.
“When I told people it wasn’t FDA-approved, people didn’t even know it wasn’t FDA-approved. Or people would say, ‘Well, the first one was.’ That by itself indicates that pharmacists were not telling people that it was not even an FDA-approved shot yet. And second to that, how can you give informed consent if there’s no package insert, with no ingredients, no test note, no anything? The words are intentionally left blank on the package insert for the shots and there’s no long-term data, so I can’t tell people what will happen in 2, 3, 4, 5, ten years from now, because they took this shot. So that, by default, is the informed consent that I’m concerned with.”
Can you tell us about your complaint to OSHA? What is their jurisdiction? What were you hoping to achieve? And what did they finally answer?
“So I had reached out to OSHA after I had reached out to my employer about concerns of vaccine shedding. The vaccine shedding phenomenon is a well-documented concern, and specifically for the coronavirus shot: Pfizer’s own study mentions they were worried about environmental spreading of the vaccine, specifically to pregnant women through both inhalation and skin-to-skin contact. So that leads me to believe that it’s at least possible, or they were worried about it, that vaccine shedding could be a thing.
“I reached out to OSHA because my employer ignored my concerns of vaccine shedding. I have not received the shot yet, so I was concerned about other people, both employees who have received it, and patients and customers who have received it, shedding the vaccine, and what my company was going to do to protect me and other people like me who have not received it. They said nothing.
“I reached out to OSHA and said, ‘What can be done? I have a concern in my own position, job, business, as well as any other retail pharmacy in the country – if you chose not to get the shot, but you are around people who have gotten it, and they are shedding the vax, they are shedding parts of the shot, that’s a concern. So I reached out to OSHA, and OSHA emailed me back and said that they currently have no jurisdiction over the coronavirus shot, there’s nothing in place, there’s no policies or procedures as it pertains to the coronavirus, and that I needed to reach out to New York State, both the New York State governor’s office and the Department of Labor as a means to get an answer, which I was not happy with, I did not accept. My concern for OSHA’s complaint is, how can a federal body not have something in place for after a brand-new experimental shot is released from big pharma, and the only people that have the answers are the same people that I am potentially concerned with are violating human rights set forth in the Geneva laws put forth after the Nuremberg trials?
“Her response indicates exactly what I think it says: We don’t have any jurisdiction, we don’t know anything about this; reach out to the New York Department of Labor and the governor’s office. That is a huge concern for anyone who is worried about his safety and health in the office. Anyone across the country right now could have a concern over whether someone is or is not vaccinated, and that’s part of the debate, I believe, that’s going on in the country. Before, it meant forcing vaccines, or forcing masks, or all of this stuff – and if OSHA’s response is to just default to whatever the state says, then you are potentially at the mercy of whoever your state governor is. And I don’t I don’t mean to turn it into a political, Republican/Democrat, red versus blue concern, but in the very least both certain Democrats and certain Republicans have taken opposite stances. So just that being said alone, it’s very concerning that in one state, for example, you can eliminate the mask mandates and there’s no vaccine passports, but in other states, that’s the only way we’re operating. So OSHA’s response is very concerning to me. That’s part of the federal government that in my opinion is supposed to be watching out for workplace safety concerns, and I agree 100% – I think her answer is kind of just wool over the eyes, the programmed response to say ‘we don’t have any jurisdiction, here’s who you can talk to…’ and then guess what? It’s not OSHA’s problem anymore, they have addressed it, they emailed me back. I mean, it’s so bizarre and terrifying.”
You said risk versus benefit is what your job is all about. Could you elaborate on that more, and explain to us how that specifically relates to your responsibilities as a pharmacist vis-à-vis COVID-19?
“Yes, the risk versus benefit: One of the great conundrums of how all healthcare works. That’s the basis for my job as a pharmacist, and I believe that’s the basis for almost every other health care profession out there. We have the knowledge through teaching, training, education, to assess the risk versus disease state, or the risk versus treatment, versus the benefit of not having treatment, or the benefit of getting treatment, so whether it’s triple bypass surgery, your doctor, your cardiologist, your surgeon looks and measures and decides what’s going to be the healthiest outcome, the best outcome for you.
“Same thing for me, it just happens for me, as a pharmacist, drugs is what I look at and evaluate. And then when it came to the COVID-19, initially I was under the impression that this was the only thing that was going to get us over this, over the hump, through this awful time in history, was to give these vaccines, give these shots.
“But as time went on, I started to be concerned more with what the shots were doing to people, that’s when I started to change my opinion. And I noticed the risk/benefit may not be the same. It appears to me the risk of the coronavirus itself COVID-19 in most age groups less than 65, maybe even 50, the negative outweighs the risk of the shot. Getting COVID-19 in someone less than 50 poses almost zero health risk to you.
“So the benefit of the shot, we don’t know. All the shot does, at this point, technically, is prevent you from getting severe disease. You can still pass the coronavirus, you can still get the coronavirus, it just prevents you from getting severe disease. So that’s the risk/benefit that I look at. What is the benefit to this shot? Just getting severe just preventing severe disease? When 80% of cases are asymptomatic, the coronavirus itself kind of prevents severe disease. Coronavirus has been around for decades, they are part of what causes the common cold.”
Do you believe that there is a code of silence among pharmacists regarding this issue?
“I do not believe that there is a code of silence among pharmacists. I’m more inclined to believe that there is a very deep-rooted psychological hand at play by certain groups of people or certain bodies or certain powers, I don’t know, but I don’t think it’s a silence code.
“And it was hard for myself to do it, too. We are trained – why would we ever think that any one of the federal governing bodies or even worldly, in the example of the World Health Organization, why would we believe that they would be telling us lies? So I don’t think it’s a code of silence, I just think we’re trained and taught to think the CDC, FDA, and the World Health Organization are all quality, upstanding government bodies that aim to solve public health crises.
“And that is not to say that they are not those things and that they do not do that. I don’t want to sound like a complete martyr. Again, I’m not saying that they do. My concern is, I don’t know what’s going on, and that’s why I have concerns over the administration of this shot.”
Have you received feedback from your colleagues? What did they think about the stand you’ve taken?
“I have reached out to a few colleagues and expressed my concerns. Most of them think that I have a decent case, or that the case that I am making isn’t necessarily completely left-field bizarre, even though it is kind of left-field. I don’t know that they’re willing to take a stand, I mean, I was fired from my position. I could only imagine that in any other pharmacy, company, corporation, chain – or most, I would say, for a pharmacist who is not willing to do an aspect of their job, as in giving shots and vaccinations, whether it’s COVID or any vaccine, but specifically the COVID one, it’s going to be hard for a company to keep them on or want to keep them on because there’s a lot of other pharmacists out there who will do it because they need a job, they need the paycheck. So it’s hard for someone to risk it all unless they feel strongly about it.”
At what point did you understand that making this stand may mean the termination of your employment, and when you did realize that, what was it that pushed you to decide to go on anyway?
“I had always known that by taking the stance of not doing a role in your job, when you choose not to do something in your position or your job that is what is expected, you always risk being fired, terminated, reprimanded, what have you. So I always knew that would be a concern, at any point I had decided to take the stance.
“But what officially gave me the courage to decide to do this was when my wife agreed with me that being able to vaccinate children 12 and up was just not right and we needed to do something, I needed to do something. We needed to take a stand and express our concerns for the health and safety of, most importantly, children, and I think potentially even everyone who is eligible to get this shot 12 and up, and it’s going to get younger soon I imagine, they’re going to try for it. So it was my wife who gave me the encouragement and kind of the okay to be like, ‘Yeah, this is a possibility, if you do get fired we’ll do whatever we have to, but it’s the right thing to do.”
Does this move and does the termination of your job represent financial hardship for your family?
“The move does represent financial hardship for my family, my wife and I have a lot of student loan debt; just that alone is a huge concern as a means of bills we have to pay, and now I’m losing a very good salaried job, so it will it will be difficult to weather the storm…”
What does your family say? Are they supportive?
“My family is supportive. I would say for the most part I think the majority of my family is supportive because they support me, and first and foremost that’s what families do, that’s what that’s what blood is, but I think parts of my family Also question, ‘what is he talking about? What is he thinking? How can you know?’ But that kind of goes back to the pharmacists keeping a code of silence and other health care providers – why would anyone question health authorities like the CDC, FDA, World Health Organization? It just sounds so bizarre, and I don’t disagree with him, I mean it does sound bizarre, but for me, I’m educated as a pharmacist and I’ve also been keeping track of all things related to coronavirus because I wanted to make sure that first and foremost my family was safe when the outbreak happened, and then secondly, it’s my job to make sure that people in the public are taken care of, and in the public scene as a pharmacist, in the pharmacy we’re a store that’s open, so anyone could be a patient of mine, anyone could come in off the streets and ask me a question and that could be anyone from around the world. I’ve worked in cities where I see people and meet people who are from around the world who don’t speak English, don’t speak English very well, so for me it’s the real undertaking I needed to do, because anyone and everyone could be one of my patients and I took an oath to protect and serve and make sure that people received quality health care with no harm.”
Do you think that you’ll be able to identify another source of employment?
“I definitely believe that I would be able to find another source for employment from someone who is like-minded, like myself, and has made commitments to protecting health in the public eye. I think the biggest concern is just kind of waiting when that will happen kind of the who, what, where, why, when will that job happen I’m not sure, but I’ve also decided I wasn’t happy as I could be as a pharmacist in my previous job, just from what I was seeing happening in the whole healthcare landscape.
“So the next job that I hopefully get will be where I can feel more impactful that I’m actually creating and changing people’s health and health outcomes in as in as dynamic away as possible. But yes, I do believe that there are people, companies, employers out there who, whether or not they are specifically concerned with whether I am or I’m not vaccinated, or if they’re concerned with the stance that I’ve taken, I think there are employers out there who are looking for someone who is willing and wanting to provide quality health care and that has always been my goal.”
Over the years the medical establishment has acquired a well-deserved reputation for ignoring good discoveries (which would make a dramatic difference to human health) and continuing with useless practices (which do more harm than good) long after they should have abandoned them. The medical profession, or, rather, perhaps I should say ‘the medical establishment’ has always been slow to accept and assimilate new ideas – and slow to see the obvious.
I have long thought that the main problem with modern medical education is that it is largely based upon learning by rote and upon eliminating all original thought. This is deliberate since the aim of an orthodox modern medical education is to help maintain the status quo (and preserve the position of the pharmaceutical industry). Right from the very beginning, young students are made to learn long lists of information. They learn the names of the bones, the arteries, the nerves and the veins in the body. They learn the names of the muscles and they learn the histology of the various organs. They then learn lists of clinical signs and symptoms. And they learn lists of drugs. At no point are students encouraged to think for themselves.
As a result it is not surprising that after graduation most doctors continue to do as they are told. The average doctor is strangely incapable of critical thought. Given the indoctrination they have undergone it is hardly surprising that doctors readily accept everything they are told by the drug companies (which more or less control post graduate education) and equally readily reject alternative medicine – something which never makes much of an appearance in the undergraduate syllabus.
There is nothing new about this.
The greatest thinkers – the ones who have, in the end, contributed most to medicine and human health – have always been scorned or ignored (or preferably both) by the medical establishment. The establishment has always manipulated the truth to suit its own political, religious or commercial purposes. Simple truths which are inconvenient have always been suppressed. It happened in the past, it will happen in the future and it is happening now.
Few medical stories illustrate the way the medical establishment works better than the story of how scurvy was discovered and how the treatment for it was ignored for centuries.
In 1535, Jacques Cartier sailed from France to Newfoundland with a crew of 110 men. Within six weeks a hundred of his men had developed scurvy. Luckily for Cartier and his men a native told them to drink the juice from the fruit of local trees. The men recovered in days. From that time on wise sea captains made sure that their men were given regular supplies of orange or lemon juice. In a book called The Surgeons Mate, published in 1636 John Woodall recommended that these juices be used to prevent scurvy. But the medical establishment was slow to accept this sensible suggestion.
It wasn’t until two centuries later, in 1747, that the idea was reintroduced by James Lind, who conducted a proper clinical trial and proved that scurvy could be prevented with the right diet. It was Lind’s work which enabled Captain Cook (he was a Lieutenant at the time) to sail around the world without a single case of scurvy.
The admiralty and the medical establishment continued to ignore all this. In the Seven Years War, from 1756 to 1763, approximately half of the 185,000 sailors involved died of scurvy. In 1779 the Channel Fleet had 2,400 cases of scurvy after a single ten week cruise.
Eventually, in 1795 the medical establishment (and the navy) succumbed to common sense and lemon juice became a compulsory part of every sailor’s diet. This breakthrough took well over two centuries to be accepted.
Then there is Paracelsus.
There is no doubt that Paracelsus (Aureolus Theophrastus Bombastus von Hohenheim to his friends) is the father of modern medicine. He tore into the precepts of established medical thinking with all the zeal of a missionary. He revolutionised medical thinking throughout Europe and scandalised the medical establishment by claiming to have learned more from his contact with witches and midwives than from his study of ancient and well-revered medical texts. No idea or theory was too bizarre to be studied and considered and no belief, no practice and no concept too sacred to be rejected. He was the first man to associate mining with chest disease, to use mercury in the treatment of syphilis, to advocate allowing wounds to drain instead of smothering them with layers of dried dung and to argue that some foods contained poisons which harmed the human body. Paracelsus scandalised the establishment by claiming that he was interested more in pleasing the sick than his own profession. He was, not surprisingly, rejected by the medical establishment and widely and persistently persecuted for his beliefs. It was years after his death that his ideas were recognised.
And there is Vesalius.
In the sixteenth century Andreas Vesalius achieved contemporary notoriety and eternal fame as the author of the first textbook of human anatomy, ‘De Humanis Corporis Fabrica’. Up until Vesalius medical students had studied anatomy using texts prepared by Galen. Since Galen used pigs not human corpses for his studies his anatomical notes were, to say the least, rather misleading.
Vesalius’s frank rejection of many of Galen’s anatomical claims earned him considerable disapproval. The medical establishment still firmly believed that Galen could do no wrong. They weren’t interested in anything as superficial and irrelevant as evidence.
Like so many original thinkers before and after him, Vesalius was unable to cope with the outcry. He burnt his remaining manuscripts, abandoned his study of anatomy and took a job as court physician to Charles V in Madrid.
Vesalius wasn’t the only anatomist whose work was rejected. In the 17th century, British doctor William Harvey spent eight years researching the circulation of the blood – and getting it right. His patience was rewarded with ridicule. He received nothing but abuse. He lost many friends and his practice shrank.
When Ambrose Pare, the great French surgeon, first started work as an army surgeon it was accepted practice to stop a haemorrhage by sealing a wound with a red hot iron. Amputations were performed with a red hot knife and the wounds which were left were sealed with boiling oil. One day Pare ran out of boiling oil and used a mild emollient to dress the wounds of the men he was treating. He worried all night about what he had done but the next day he found that his patients were not only healthy but that they were also in less pain than the men whose wounds had been sealed with boiling oil. Pare was wise enough to learn from this and from that day on he started dressing wounds with an emollient rather than boiling oil. He also introduced ligatures, artificial limbs and many surgical instruments. Inevitably, Pare met the usual fate of innovators and reformers (who get a rougher ride within the world of medicine than anywhere else). He was denounced by other surgeons as dangerous and unprofessional. Older surgeons banded together to oppose him and in their attempts to discredit him they attacked him for all sorts of things – for example, his ignorance of Latin and Greek. Pare eventually succeeded because the soldiers he treated trusted him and wanted to be treated by him. They weren’t interested in the views of the French medical establishment.
A look back at hospitals is also revealing.
When Tsar Paul came to power in Russia in 1796 he was so horrified at the state of the hospital in Moscow that he ordered it to be rebuilt. In Frankfurt in the 18th century physicians considered working in hospital to be equivalent to a sentence of death.
In 1788, Jacobus-Rene Tenon published a report on the hospitals of Paris which shocked city officials. He described how the Hotel Dieu (the magnificent looking hospital next to Notre Dame) contained 1200 beds but up to 7,000 patients – with up to six patients crammed into each bed. The stench in the hospital was so foul that people who entered would do so holding a vinegar soaked sponge to their noses. Very few patients escaped from the hospital with their lives. When reformer John Howard toured European hospitals he angrily reported that no fresh air, no sunlight, straw as bedding, no bandages and a milk and water diet supplemented with weak soup were standard. The reports of Tenon and Howard were ignored and dismissed for years and it took decades for the medical establishment to make any real changes.
In the 18th century the treatment of the mentally ill was abysmal. Daniel Defoe, best remembered for his story of the adventures of Robinson Crusoe, wrote a vicious attack on mental hospitals. ‘Is it not enough to make anyone mad,’ he asked, ‘ to be suddenly clap’d up, stripp’d, whipp’d, ill fed and worse us’d? To have no reason assigned for such treatment, no crime alleged or accusers to confront? And what is worse, no soul to appeal to but merciless creatures who answer but in laughter, surliness, contradiction and too often stripes?’
No one took much notice and medical practitioners continued to treat mentally ill patients without respect or care.
At the Bethlem Royal Hospital half naked patients were kept chained in irons. Physicians bled their patients once a year and the more troublesome patients were put on a tranquillising wheel. Until 1770 visitors could pay a penny to see the ‘fun’ at Bedlam. John Wesley, founder of the Wesleyan Church, who considered himself a benefactor of the mentally ill, suggested pouring water onto the heads of the mentally ill and forcing them to eat nothing but apples for a month. Wesley was one of the first men to use electricity in the attempted treatment of the mentally ill. Despite the protests of reformers such as Philippe Pinel (who shocked the establishment in the late 18th century by claiming that the mentally ill were sick and needed treatment) mental hospitals were, well into the 19th century, still quite unsuitable for people needing medical treatment.
There was never any evidence to show that it did any good but blood-letting was a favourite therapeutic tool for centuries. The fact that removing blood from a patient made him or her quieter was regarded as proof that it was doing some good. (This is no dafter than the rationale used to explain some modern treatments.) Blood-letting was easy to perform and it was something to do. Doctors have always felt the need to do something to their patients. (Possibly because it is difficult to explain away a big fee if all you do is give advice.) Leeches were hugely popular in the 19th century. In 1824, two million leeches were imported into France. In 1832, the figure had risen to 57 million a year.
In 1843, the American poet, novelist and anatomist, Oliver Wendell Holmes, read to the Boston Society for Medical Improvement a paper entitled ‘On The Contagiousness of Puerperal Fever’. He argued that the disease could be carried from patient to patient by doctors. He suggested that surgeons should consider changing their clothes and washing their hands after leaving a patient with puerperal fever. His lecture annoyed the medical establishment and his advice was ignored completely.
A similar fate befell Ignaz Philipp Semmelweiss who, in 1846, at the age of 28, became an assistant in an obstetric ward at the Allgemeines Krankenhaus in Vienna. Semmelweiss noticed that the number of women dying in his ward was higher than the number dying in other wards. It wasn’t difficult to notice this. Women would beg, in tears, not to be taken into Semmelweiss’s ward.
Deciding that he wasn’t that bad a doctor, Semmelweiss looked for an explanation and came to the conclusion that the major difference was that patients on his ward were looked after by medical students whereas the patients on other wards were looked after by midwives. Semmelweiss then discovered that the students came straight to the ward from the dissecting room where they had had their hands stuck into the corpses of women who had died from puerperal fever. The midwives never went near to the dissecting room. Semmelweiss instructed the medical students that they should start washing their hands in a solution of calcium chloride after coming from the dissecting room. The remedy produced a dramatic drop in the death rate on his ward.
Predictably the medical establishment was not well pleased – even though Semmelweiss had proved his point very dramatically. The unfortunate young doctor couldn’t cope with the rejection. He became an outcast and died in a mental hospital a few years later. The medical establishment had scored another hollow victory. Once again the patients were the losers.
You might have thought that the medical establishment would have welcomed anaesthesia. After all, before anaesthetics were available, surgeons had to get their patients drunk or knock them out with a blow to the head. Surgeons would often operate with the patient held down by four strong men. The first operation under anaesthesia was performed at the Massachusetts General Hospital in 1846. But the establishment was not going to accept this new-fangled nonsense lying down. The main objection was that anaesthetics were being used to help women who were in labour. And that, said the establishment, just wasn’t acceptable. It was, said the wise men, unnatural and unhealthy for women to deliver babies without suffering pain. ‘In sorrow thou shalt bring forth children,’ says the Bible. However, the religious barbarians were eventually overcome by Dr James Simpson who trumped the Bible quoters with this quote: ‘And the Good Lord caused a deep sleep to fall upon Adam and he slept; and He took one of his ribs and closed up the flesh instead thereof.’ The opposition to anaesthesia was finally quelled when Queen Victoria gave birth to Prince Leopold while under the influence of chloroform.
In 1867 Joseph Lister published a paper in The Lancet entitled ‘On the Antiseptic Principle in the Practice of Medicine’. Lister had found a solution to the age old problem of post-operative infection. But the medical establishment doesn’t like change, even if it means keeping patients alive. And Lister found himself being attacked by doctors who ignored the evidence but disapproved of his new techniques simply because they were new. It was decades before the ‘antiseptic principle’ was accepted.
One of the reasons why hospital infections are so commonplace today is that doctors and nurses seem to believe that they can use antibiotics instead of washing their hands. Incompetence, carelessness and ignorance mean that the quality of cleanliness in the average modern hospital is little better than it was in a hospital in the Middle Ages.
Until surprisingly recently, it was routine for surgery on babies to be performed without anaesthesia on the grounds that babies are incapable of feeling pain. There was no evidence for this claim (one which any mother would be able to oppose with credible if anecdotal evidence) but anaesthetists were taught that babies had immature nervous systems and so didn’t need painkillers.
Above I have described just a few of the hundreds (probably thousands) of examples I could give to illustrate the way that the medical establishment, in recent years allied with the drug industry, has always opposed original thought and has protected the status quo – regardless of the effect on patients.
The medical establishment has acted in the interests of the profession but against the interests of patients, and thoughtful and creative individuals have always had a hard time. The value of serendipity has also been ignored, of course. Both penicillin and X-rays were the result of serendipity.
The real tragedy is that absolutely nothing has changed for the better. Indeed, things have arguably got worse.
The medical establishment is still responsible for protecting and promoting medical procedures which do not work and have never worked (and which expose patients to great risk) while at the same time it opposes and suppresses treatments which do work and have been proved to work.
Today, anyone in the medical profession who dares to offer thoughts or warnings which don’t fit in with the specific requirements of the medical establishment will get the Semmelweiss treatment. They will be laughed at and suppressed.
[Original video is available at Dr. Vernon Coleman BrandNewTube channel. As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute and Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Dr. Andrew Kaufman with Dr. Sam Bailey: “Hunting for Viruses”
They’re called the College of Physicians and Surgeons of Ontario (CPSO).
As their home page states, they “regulate the practice of medicine in Ontario. Physicians are required to be members to practice medicine in Ontario.”
In other words, CPSO is THE medical board. They run the show. If practicing doctors make a wrong move or say the wrong thing, CPSO is there to step on their faces and discipline them and even cancel their licenses to practice.
But now a new rebel group of Canadian MDs has emerged. Why? Because CPSO has issued a fascist edict threatening practicing doctors. Read the threat carefully.
College of Physicians and Surgeons of Ontario [CPSO] Statement on Public Health Misinformation (4/30/21): [1]
“The College is aware and concerned about the increase of misinformation circulating on social media and other platforms regarding physicians who are publicly contradicting public health orders and recommendations. Physicians hold a unique position of trust with the public and have a professional responsibility to not communicate anti-vaccine, anti-masking, anti-distancing and anti-lockdown statements and/or promoting unsupported, unproven treatments for COVID-19. Physicians must not make comments or provide advice that encourages the public to act contrary to public health orders and recommendations. Physicians who put the public at risk may face an investigation by the CPSO and disciplinary action, when warranted. When offering opinions, physicians must be guided by the law, regulatory standards, and the code of ethics and professional conduct. The information shared must not be misleading or deceptive and must be supported by available evidence and science.”
WE’RE YOUR BOSSES. YOU DO WHAT WE TELL YOU TO DO. SHUT YOUR MOUTHS. MARCH STRAIGHT AHEAD. KILL YOUR PATIENTS IF YOU HAVE TO, BUT OBEY US.
The new rebels against this monster call themselves the Canadian Physicians for Science and Truth. This is a brief excerpt from their response: [2]
“On April 30, 2021, Ontario’s physician licensing body, the College of Physicians and Surgeons of Ontario (CPSO), issued a statement forbidding physicians from questioning or debating any or all of the official measures imposed in response to COVID-19.”
“We regard this recent statement of the CPSO to be unethical, anti-science and deeply disturbing.”
“As physicians, our primary duty of care is not to the CPSO or any other authority, but to our patients.”
“The CPSO statement orders us to violate our duty and pledge to our patients…”
I wondered what medical treatments, in general, CPSO supports and tolerates. It took me three minutes to find a Toronto outfit called the Centre for Addiction and Mental Health Foundation (CAMH). They promote electro-convulsive therapy. In other words, shock treatment.
In other words, delivering electric shocks to the brain. As a cure for “mental illness.” I call it torture.
Apparently, this treatment is just fine and dandy, but telling patients the COVID lockdowns are criminal is forbidden by the Nazi bureaucrats at CPSO. Saying the vaccine is dangerous is forbidden. Saying masks are useless and harmful is forbidden.
What would happen if these medical rebels, the Canadian Physicians for Science and Truth—say, 10,000 of them—took this war to the wall?
Practiced non-harmful medicine, kept warning their patients about the sociopathic COVID regulations and the vaccine, refused to knuckle under to the Nazi bureaucrats, even to the point of having their licenses stripped and going to jail?
What would happen, as many thousands/millions of Canadians rallied to their side?
I’ll tell you what would happen. Sanity. Revolution. The downfall of the scum.
We’re at Nuremberg 2.0, people. If you don’t know what that means, look it up.
Doctors clear their vision and their brains and do their level best to HEAL, or they follow orders of the Commandants and maim and kill. It’s one side or the other.
In my 83 years, I’ve known a few very good doctors, and a number of The Cold Ones. The Cold Ones administer, without feeling or remorse, the Book of Death.
They’re ice on the outside, and rotting fungus and stench within.
Many of them sit at the top of medical boards.
They turn open societies into concentration camps.
On 25 May 2021, the Indian Bar Association (IBA) served a 51-page legal notice on Dr Soumya Swaminathan, the Chief Scientist at the World Health Organisation (WHO), for:
“[H]er act of spreading disinformation and misguiding the people of India, in order to fulfil her agenda.”
The Mumbai-based IBA is an association of lawyers who strive to bring transparency and accountability to the Indian justice system. It is actively involved in the dissemination of legal knowledge and provides guidance and support to advocates and ordinary people in their fight for justice.
The legal notice says Dr Swaminathan has been:
“Running a disinformation campaign against Ivermectin by deliberate suppression of effectiveness of drug Ivermectin as prophylaxis and for treatment of COVID-19, despite the existence of large amounts of clinical data compiled and presented by esteemed, highly qualified, experienced medical doctors and scientists,”
And:
“Issuing statements in social media and mainstream media, thereby influencing the public against the use of Ivermectin and attacking the credibility of acclaimed bodies/institutes like ICMR and AIIMS, Delhi, which have included ‘Ivermectin’ in the ‘National Guidelines for COVID-19 management’.”
The IBA states that legal action is being taken against Dr Swaminathan in order to stop her from causing further damage to the lives of citizens of India.
The IBA says that Dr Swaminathan has ignored these studies and reports and has deliberately suppressed the data regarding the effectiveness of Ivermectin, with an intent to dissuade the people of India from using it.
However, two key medical bodies, the Indian Council for Medical Research (ICMR) and the All India Institute of Medical Sciences (AIIMS) Delhi, have refused to accept her stand and have retained the recommendation for Ivermectin, under a ‘May Do’ category, for patients with mild symptoms and those in home isolation, as stated in ‘The National Guidelines for COVID-19 management’.
It is interesting to note that the content of several web links to news articles and reports included in the notice served upon Dr Swaminathan, which was visible before issuing the notice, has either been removed or deleted.
It seems that the vaccine manufacturers and many governments are desperate to protect their pro-vaccine agenda and will attempt to censor information and news regarding the efficacy of Ivermectin.
Colin Todhunter is an independent journalist who writes on development, environmental issues, politics, food and agriculture. In August 2018 he was named as one of 400 Living Peace and Justice Leaders and Models by Transcend Media Services, in recognition of his journalism.
Thanks to the diligent efforts of one of my listeners, I received a paper yesterday that puts another nail in the coffin for the existence of SARS-CoV-2. The paper is titled “Appearances Can be Deceiving – Viral-like Inclusions in Covid-19 Negative Renal Biopsies by Electron Microscopy.” The authors are Clarrisa A. Cassol, et al., and the citation is Kidney360 1:824-828, 2020. This is a peer-reviewed journal affiliated with the American Society of Nephrology; in other words, this paper comes squarely from what is called acceptable, mainstream science.
Many of you have probably seen the electron-micrograph pictures of SARS-CoV-2, the ones in black and white, with the black dots within the faint outline of the circle. I have attached two such images from papers that claim these photos show direct evidence of the existence of the virus. These are the pictures that virologists show us, not the computer-generated, colorful images that you see in magazines and on the internet. These are the “real” pictures of the virus, and they are offered as “proof” that the virus exists.
However, it turns out these photos are actually NOT corona viruses, and the CDC, among others, has known this fact since at least 2004. The above paper examines the evidence used to claim that these images represent viruses, rather than normal “structures” within a cell, particularly sick cells. Here is what the paper says:
“We have observed morphologically indistinguishable inclusions within podocytes and tubular epithelial cells both in patients negative for coronavirus disease 2019 (COVID-19) as well as in renal biopsies from the pre-COVID-19 era” (emphasis added).
In other words, the researchers saw these same structures in people with no evidence of Covid and in samples they took before Covid even happened, before the virus was said to even exist.
In addition, they say:
“We postulated that endogenous mimickers could be present that are morphologically indistinguishable from SARS-CoV-2 virions ultrastructurally.”
And:
“Viral-like inclusions, consisting both of single vesicles with diameters between 50 and 138 nm, as well as packed groups within larger vesicles, were found in all 15 cases, either in podocytes. Tubular epithelia, or vascular epithelial cells (figure 1).”
In all 15 cases that they examined, they found structures identical to what is being called SARS-CoV-2. They were scattered all over the kidneys and blood vessels; they are not viruses, but normal parts of the cells.
Then they go on to describe how these particles come about:
“A number of potential natural mimickers that can generate intracellular groups of round vesicles mimicking
SARS-CoV-2 virions could be listed, the most likely being endocytic vesicles and endosomal components such as microvesicular bodies containing exosomes, among others. Endocytosis leads to the formation of 60-120 nm vesicles, which is within the size range described for SARS-CoV-2 (60-140nm). These endocytic vesicles may be coated by different proteins, one of the most common being clathrin. The presence of coating proteins may be responsible for the presence of an electron-dense area surrounding these vesicles, giving the appearance of a viral corona.”
In other words, remember the famous “corona” on the corona virus? It turns out it’s just a common protein coating on normal vesicles, picking up the dyes in the electron-microscope preparation. The corona appearance is just another creative fiction, dreamed up by virologists and their graphic design teams.
Finally, the paper goes on to say that, naturally, you see more of these particles in sick people than in healthy people, which is exactly what I have been suggesting this past year. Dead and dying cells make these particles in the dying process and partly to get rid of poisons.
But the final nail comes in this quote:
“The potential for confusion of coronavirus particles with normal cellular components was in fact highlighted in a detailed ultrastructural study by the Centers for Disease Control and Prevention (CDC) of SARS-CoV responsible for the 2003 SARS outbreak.”[1]
In other words, the CDC in 2004 knew that researchers couldn’t reliably know these particles were coronavirus particles. Not a word has been heard about this since. All virologists use these pictures as proof of the existence of this virus. It is a fraud, based on junk science, like everything else connected with “Covid 19.”
Scientific propaganda about vaccines has reached dizzying heights, as officials point the uninformed public toward the Day of Liberation, when a COVID shot, otherwise known as God, will rescue Earth.
Here, from a chapter in my 1988 book, AIDS INC., is an excerpt exposing some of the infamous moments in vaccination history—hidden by the press, or simply forgotten.
For those denialists who cling to the notion that vaccines are remarkably safe and effective, this article is a pill you can swallow, bitter to be sure, but immunizing against the effects of bald lies from the bent medical establishment.
Understand: this is only a partial history of disasters and revelations, and it stops at 1988.
“The combined death rate from scarlet fever, diphtheria, whooping cough and measles among children up to fifteen shows that nearly 90 percent of the total decline in mortality between 1860 and 1965 had occurred before the introduction of antibiotics and widespread immunization. In part, this recession may be attributed to improved housing and to a decrease in the virulence of micro-organisms, but by far the most important factor was a higher host-resistance due to better nutrition.” Ivan Illich, Medical Nemesis, Bantam Books, 1977
“In a recent British outbreak of whooping cough, for example, even fully immunized children contracted the disease in fairly large numbers; and the rates of serious complications and death were reduced only slightly. In another recent outbreak of pertussis, 46 of the 85 fully immunized children studied eventually contracted the disease.”
“In 1977, 34 new cases of measles were reported on the campus of UCLA, in a population that was supposedly 91% immune, according to careful serological testing. Another 20 cases of measles were reported in the Pecos, New Mexico, area within a period of a few months in 1981, and 75% of them had been fully immunized, some of them quite recently. A survey of sixth-graders in a well-immunized urban community revealed that about 15% of this age group are still susceptible to rubella, a figure essentially identical with that of the pre-vaccine era.”
“Finally, although the overall incidence of typical acute measles in the U.S. has dropped sharply from about 400,000 cases annually in the early 1960s to about 30,000 cases by 1974-76, the death rate remained exactly the same; and, with the peak incidence now occurring in adolescents and young adults, the risk of pneumonia and demonstrable liver abnormalities has actually increased substantially, according to one recent study, to well over 3% and 2%, respectively.” Richard Moskowitz, MD, The Case Against Immunizations, 1983, American Institute of Homeopathy.
“Of all reported whooping cough cases between 1979 and 1984 in children over 7 months of age – that is, old enough to have received the primary course of the DPT shots (diphtheria, pertussis, tetanus) – 41% occurred in children who had received three or more shots and 22% in children who had one or two immunizations.”
“Among children under 7 months of age who had whooping cough, 34% had been immunized between one and three times…”
“… Based on the only U.S. findings on adverse DPT reactions, an FDA-financed study at the University of California, Los Angeles, one out of every 350 children will have a convulsion; one in 180 children will experience high-pitched screaming [can indicate brain damage]; and one in 66 will have a fever of 105 degrees or more.” Jennifer Hyman, Democrat and Chronicle, Rochester, New York, special supplement on DPT, dated April, 1987.
“A study undertaken in 1979 at the University of California, Los Angeles, under the sponsorship of the Food and Drug Administration, and which has been confirmed by other studies, indicates that in the U.S.A. approximately 1,000 infants die annually as a direct result of DPT vaccinations, and these are classified as SIDS (Sudden Infant Death Syndrome) deaths. These represent about 10 to 15% of the total number of SIDS deaths occurring annually in the U.S.A. (between 8,000 and 10,000 depending on which statistics are used).” Leon Chaitow, Vaccination and Immunization, CW Daniel Company Limited, Saffron Walden, Essex, England, 1987.
“Assistant Secretary of Health Edward Brandt, Jr., MD, testifying before the U.S. Senate Committee on Labor and Human Resources, rounded… figures off to 9,000 cases of convulsions, 9,000 cases of collapse, and 17,000 cases of high-pitched screaming for a total of 35,000 acute neurological reactions occurring within forty-eight hours of a DPT shot among America’s children every year.” DPT: A Shot in the Dark, by Harris L. Coulter and Barbara Loe Fischer, Harcourt Brace Jovanovich.
“While 70-80% of British children were immunized against pertussis in 1970-71, the rate is now 39%. The committee predicts that the next pertussis epidemic will probably turn out to be more severe than the one in 1974/75. However, they do not explain why, in 1970/71, there were more than 33,000 cases of pertussis with 41 fatal cases among the very well immunized British child population; whereas in 1974/75, with a declining rate of vaccination, a pertussis epidemic caused only 25,000 cases with 25 fatalities.” Wolfgang Ehrengut, Lancet, Feb. 18, 1978, p. 370.
“… Barker and Pichichero, in a prospective study of 1232 children in Denver, Colorado, found after DTP that only 7% of those vaccinated were free from untoward reactions, which included pyrexia (53%), acute behavioral changes (82%), prolonged screaming (13%), and listlessness, anorexia and vomiting. 71% of those receiving second injections of DTP experienced two or more of the reactions monitored.” Lancet, May 28, 1983, p. 1217
“Publications by the World Health Organization show that diphtheria is steadily declining in most European countries, including those in which there has been no immunization. The decline began long before vaccination was developed. There is certainly no guarantee that vaccination will protect a child against the disease; in fact, over 30,000 cases of diphtheria have been recorded in the United Kingdom in fully immunized children.” Leon Chaitow, Vaccination and Immunization, p. 58.
“Pertussis (whooping cough) immunization is controversial, as the side effects have received a great deal of publicity. The counter claim is that the effectiveness and protection offered by the procedure far outweigh the possible ill effects… annual deaths, per million children, from this disease over the period from 1900 to the mid-nineteen seventies, shows that from a high point of just under 900 deaths per million children (under age 15) in 1905, the decline has been consistent and dramatic. There had been a lowering of mortality rates of approximately 80% by the time immunization was introduced on a mass scale, in the mid-nineteen fifties. The decline has continued, albeit at a slower rate, ever since. No credit can be given to vaccination for the major part of the decline since it was not in use.” Chaitow, Vaccination and Immunization, p. 63.
“… the swine-flu vaccination program was one of its (CDC) greatest blunders. It all began in 1976 when CDC scientists saw that a virus involved in a flu attack outbreak at Fort Dix, N.J., was similar to the swine-flu virus that killed 500,000 Americans in 1918. Health officials immediately launched a 100-million dollar program to immunize every American. But the expected epidemic never materialized, and the vaccine led to partial paralysis in 532 people. There were 32 deaths.” U.S. News and World Report, Joseph Carey, October 14, 1985, p. 70, “How Medical Sleuths Track Killer Diseases.”
“Despite (cases) in which (smallpox) vaccination plainly failed to protect the population, and despite the rampant side-effects of the methods, the proponents of vaccination continued their attempts to justify the methods by claims that the disease had declined in Europe as a whole during the period of its compulsory use. If the decline could be correlated with the use of the vaccination, then all else could be set aside, and the advantage between its current low incidence could be shown to outweigh the periodic failures of the method, and to favour the continued use of vaccination. However, the credit for the decline in the incidence of smallpox could not be given to vaccination. The fact is that its incidence declined in all parts of Europe, whether or not vaccination was employed.” Chaitow, Vaccination and Immunization, pp. 6-7.
“Smallpox, like typhus, has been dying out (in England) since 1780. Vaccination in this country has largely fallen into disuse since people began to realize how its value was discredited by the great smallpox epidemic of 1871-2 (which occurred after extensive vaccination).” W. Scott Webb, A Century of Vaccination, Swan Sonnenschein, 1898.
“In this incident (Kyoto, Japan, 1948) – the most serious of its kind – a toxic batch of alum-precipitated toxoid (APT) was responsible for illness in over 600 infants and for no fewer than 68 deaths.”
“On 20 and 22 October, 1948, a large number of babies and children in the city of Kyoto received their first injection of APT. On the 4th and 5th of November, 15,561 babies and children aged some months to 13 years received their second dose. One to two days later, 606 of those who had been injected fell ill. Of these, 9 died of acute diphtheritic paralysis in seven to fourteen days, and 59 of late paralysis mainly in four to seven weeks.” Sir Graham Wilson, Hazards of Immunization, Athone Press, University of London, 1967.
“Accidents may, however, follow the use of this so-called killed (rabies) vaccine owing to inadequate processing. A very serious occurrence of this sort occurred at Fortaleza, Ceara, Brazil, in 1960. No fewer than 18 out of 66 persons vaccinated with Fermi’s carbolized (rabies ) vaccine suffered from encephalomyelitis and every one of the eighteen died.” Sir Graham Wilson, Hazards of Immunization.
“At a press conference in Washington on 24 July, 1942, the Secretary of War reported that 28,585 cases of jaundice had been observed in the (American) Army between 1 January and 4 July after yellow fever vaccination, and of these 62 proved fatal.” Wilson, Hazards of Immunization.
“The world’s biggest trial (conducted in south India) to assess the value of BCG tuberculosis vaccine has made the startling revelation that the vaccine ‘does not give any protection against bacillary forms of tuberculosis.’ The study said to be ‘most exhaustive and meticulous,’ was launched in 1968 by the Indian Council of Medical Research (ICMR) with assistance from the World Health Organization (WHO) and the U.S. Centers for Disease Control in Atlanta, Georgia.”
“The incidence of new cases among the BCG vaccinated group was slightly (but statistically insignificantly) higher than in the control group, a finding that led to the conclusion that BCG’s protective effect ‘was zero.’” New Scientist, November 15, 1979, as quoted by Hans Ruesch in Naked Empress, Civis Publishers, Switzerland, 1982.
“Between 10 December 1929 and 30 April 1930, 251 of 412 infants born in Lubeck received three doses of BCG vaccine by the mouth during the first ten days of life. Of these 251, 72 died of tuberculosis, most of them in two to five months and all but one before the end of the first year. In addition, 135 suffered from clinical tuberculosis but eventually recovered; and 44 became tuberculin-positive but remained well. None of the 161 unvaccinated infants born at the time was affected in this way and none of these died of tuberculosis within the following three years.” Hazards of Immunization, Wilson.
“We conducted a randomized double-blind placebo-controlled trial to test the efficacy of the 14-valent pneumococcal capsular polysaccharide vaccine in 2295 high-risk patients… Seventy-one episodes of proved or probable pneumococcal pneumonia or bronchitis occurred among 63 of the patients (27 placebo recipients and 36 vaccine recipients)… We were unable to demonstrate any efficacy of the pneumococcal vaccine in preventing pneumonia or bronchitis in this population.” New England Journal of Medicine, November 20, 1986, p. 1318, Michael Simberkoff et al.
In the spring of 1955, Cutter Labs started selling their standard polio vaccine. The vaccine was infective, and 200 cases of polio resulted among recipients. Of these, there were eleven deaths. About 100 cases of paralysis resulted. JR
“But already before Salk developed his vaccine, polio had been constantly regressing; the 39 cases out of every 100,000 inhabitants registered in 1942 had gradually diminished from year to year until they were reduced to only 15 cases in 1952… according to M. Beddow Baylay, the English surgeon and medical historian.” Slaughter of the Innocent, Hans Reusch, Civitas Publish ers, Switzerland, and Swain, New York, 1983.
“Many published stories and reports have stated, implied and otherwise led professional people and the public to believe that the sharp reduction of cases (and of deaths) from poliomyelitis in 1955 as compared to 1954 is attributable to the Salk vaccine…That it is a misconception follows from these considerations. The number of children inoculated has been too small to account for the decrease. The sharp decrease was apparent before the inoculations began or could take effect and was of the same order as the decrease following the immediate post-inoculation period.” Dr. Herbert Ratner, Child and Family, vol. 20, no. 1, 1987.
“So far it is hardly possible to gain insight into the extent of the immunization catastrophe of 1955 in the United States. It may be considered certain that the officially ascertained 200 cases (of polio) which were caused directly or indirectly by the (polio) vaccination constitute minimum figures… It can hardly be estimated how many of the 1359 (polio) cases among vaccinated persons must be regarded as failures of the vaccine and how many of them were infected by the vaccine. A careful study of the epidemiologic course of polio in the United States yields indications of grave significance. In numerous states of the U.S.A., typical early epidemics developed with the immunizations in the spring of 1955…The vaccination incidents of the year 1955 cannot be exclusively traced back to the failure of one manufacturing firm.” Dr. Herbert Ratner, Child and Family, 1980, vol. 19, no. 4, “Story of the Salk Vaccine (Part 2).”
“Suffice it to say that most of the large (polio) epidemics that have occurred in this country since the introduction of the Salk vaccine have followed the wide-scale use of the vaccine and have been characterized by an uncommon early seasonal onset. To name a few, there is the Massachusetts epidemic of 1955; the Chicago epidemic of 1956; and the Des Moines epidemic of 1959.” Dr. Herbert Ratner, Child and Family, 1980 vol. 19, no. 4.
“The live (Sabin) poliovirus vaccine has been the predominant cause of domestically arising cases of paralytic poliomyelitis in the United States since 1972. To avoid the occurrence of such cases, it would be necessary to discontinue the routine use of live poliovirus vaccine.” Jonas Salk, Science, March 4, 1977, p. 845.
“By the (U.S.) government’s own admission, there has been a 41% failure rate in persons who were previously vaccinated against the (measles) virus.” Dr. Anthony Morris, John Chriss, BG Young, “Occurrence of Measles in Previously Vaccinated Individuals,” 1979; presented at a meeting of the American Society for Microbiology at Fort Detrick, Maryland, April 27, 1979.
“Prior to the time doctors began giving rubella vaccinations, an estimated 85% of adults were naturally immune to the disease (for life). Because of immunization, the vast majority of women never acquire natural immunity (or lifetime protection).” Dr. Robert Mendelsohn, Let’s Live, December 1983, as quoted by Carolyn Reuben in the LA WEEKLY, June 28, 1985.
“Adminstration of KMV (killed measles vaccine) apparently set in motion an aberrant immunologic response that not only failed to protect children against natural measles, but resulted in heightened susceptibility.” JAMA Aug. 22, 1980, vol. 244, p. 804, Vincent Fulginiti and Ray Helfer. The authors indicate that such falsely protected children can come down with “an often severe, atypical form of measles. Atypical measles is characterized by fever, headache… and a diverse rash (which)… may consist of a mixture of macules, papules, vesicles, and pustules… ”
The above quotes reflect only a mere fraction of an available literature.
It is criminally deceiving to say, “Vaccines are simple; they stimulate the immune system and confer immunity against specific germ agents.”
Official reports on vaccine reactions are often at odds with unofficial estimates because of the method of analysis used. If adverse vaccine-reaction is defined as a small set of possible effects experienced within 72 hours of an inoculation, then figures will be smaller. But doctors like G.T. Stewart, of the University of Glasgow, have found through meticulous investigation, including visits to hospitals and interviews with parents of children vaccinated, that reactions as severe as brain-damage (e.g., from the DPT vaccine) can be overlooked, go unreported and can be assumed to have come from other causes.
—Well, that was my finding, in 1988, when I looked beneath the surface of the vaccine question.
Now we are in very deep waters. COVID-19 hysteria has been tuned up to the NEED for a vaccine.
WE need to slough off this promoted bad dream and stand firm against the little gods who traffic their vials in every doctor’s office, hospital, school, drug store, and tented parking lot—making them into shooting galleries.
We already have natural immune systems. They work.
On June 13, 2021, Swiss citizens are called to vote for the outlawing of synthetic pesticides. A citizens’ initiative, turned referendum, supported and endorsed by Navdanya International on the path towards a true agrofood systems transition. In case the ‘Yes’ vote should win, the ban would extend from agriculture, to private use, and to the import and marketing of foodstuffs containing synthetic chemicals. Voters will also have to decide on the proposal to remove public subsidies for farmers who are not willing to convert to ecological production practices.
The initiative holds significant symbolic value as Switzerland is home to one of the most powerful agribusiness corporations in the world, Syngenta. Recently acquired by ChemChina, Syngenta was recently at the center of the Paraquat Papers scandal, named after the herbicide produced by the company and considered one of the most toxic and dangerous in the world.
The Swiss initiative is intended to inspire similar actions in other countries.
The president of Navdanya International, Vandana Shiva, commented: “We are members of one Earth family. Poisons and pesticides kill insects and biodiversity, they are destroying the infrastructure of life. Poisons are causing a health emergency, as chronic diseases such as cancer, autism, infertility are connected to toxins in food and environmental pollution. Through knowledge manipulation and propaganda, the Poison Cartel also undermines independent science and threatens democracy by trying to silence citizens’ efforts towards pesticide-free communities. The health of the planet, her biodiversity, our health makes poison-free food and farming a survival imperative. As our work in Navdanya over 3 decades has shown, we can grow more and better food through biodiversity-intensive, chemical-free organic farming. I congratulate and support the Swiss Referendum as a significant step towards Earth Democracy to defend the rights of the biodiversity of species, including all human beings. Poison free food and farming is our birthright.”
Navdanya International
Good news: Vandana Shiva supports our initiative! «We are members of One Earth Family. Poisons and Pesticides kill insects and biodiversity, they are destroying the infrastructure of life. Poisons are causing a health emergency. (…) (1/6) pic.twitter.com/Pg0G7ovxDH
— #PestizidinitiativeJA am 13. Juni (@LebenstattGift) June 4, 2021
Today James talks to Christian Westbrook (aka the Ice Age Farmer) about the problems facing the global food supply—from the coming global solar minimum to the globalist plan to “reset the table” and transform global food systems. More importantly, we discuss what can be done about these problems.
Let’s say a minor religion emerges in Ohio. Its basis is a story about a miraculous tree growing in an arid desert.
The only problem is, if the members of this Church bothered to check, they would discover the exact place where the tree supposedly grew was no desert. Instead, it was an ocean. The ocean had been there for a billion years.
But no one bothers to check. They collectively INVENT AND ACCEPT the notion of the tree in the desert. They’re not aware that this is what they’re doing, but they ARE doing it.
They build rituals and ceremonies and art—“data banks”—around the idea of the tree.
The same factors are present in the case of promoting a new virus. In this situation—the virus is collectively dreamed up and accepted by virologists—the “checking” would occur by doing a retrospective step-by-step analysis of what happened in the lab where the virus was “discovered.”
But no analysis is carried out. None of the professionals believes it’s necessary. The traditional methods of virus-discovery are beyond reproach.
And if an outsider, a skeptic demands an inquiry into the process of discovery, he is labeled a sinner. The lab is an inner sanctum. The mere presence of an outsider looking over the shoulders of the researchers (priests) at work would be an offense against the Church.
What we’re left with is a collective idea whose content is: “new virus.”
That’s all.
“Would you like to look at our line of hats that go with your new virus?”
“How about a mutant strain?”
“The vaccine, of course, is free.”
Another collective idea: the 300 official mental disorders, promoted by the American Psychiatric Association. The truth is, the so-called disorders have no accompanying definitive lab tests, for diagnosis.
Collective ideas give rise to data banks and data sets that bolster and expand the original ideas.
“25% of all college students [2] have at least one mental disorder.” Here are the studies and surveys and confirmations from leading researchers—data sets.
“Three major public health organizations have formed a task force to study solutions to the growing mental illness problem among college students.” More data sets will be created and deposited in data banks.
“MIT and Harvard, cooperating in a federally funded program, are developing AI software that will predict future trends in mental illness among college students, in an effort to identify preventive measures which might head off this growing problem…” More data sets placed in data banks—but this time, all the work, and its logic, are hidden behind walls of automatic AI.
Collectivism=collective ideas=data banks filled with supposed confirmation of the truth of the ideas.
The whole op involves creating more and more layers between the data sets and the original collective ideas, until no one considers examining those ideas.
As IoT (Internet of Things), enabled by 5G tech, makes more of the functions of society automatic, successive generations of the populations are pushed farther and farther away from the collective ideas which form the basis of AI programs.
Here is a passage from John Klyczek’s article, “From UNESCO Study 11 to UNESCO 2050: Project BEST and the Forty-Year Plan to Reimagine Education for the Fourth Industrial Revolution,” [3] published at unlimitedhangout.com. Consider the sheer number of layers, data sets, and AI involved in the monster project Klyczek is describing:
“…UNESCO’s Study 11 was carried out through international public-private partnerships between communist, socialist, and capitalist countries coordinating efforts between multinational telecommunications and computer corporations. Working in concert with academic institutions and national government agencies, Study 11 affiliates lobbied to restructure laws in order to globalize school systems through proto-internet technologies manufactured by Big Tech companies, such as Microsoft, IBM, and Apple, which are now steering the Fourth Industrial Revolution into a new political system of communitarian technocracy driven by a new economic system of ‘stakeholder capitalism’ through ‘community-based’ public-private partnerships that are managed by Big Data.”
“…schools around the entire world are forced to rely on the technocratic IT infrastructure that has been set up by Study 11 and Project BEST through their public-private partnerships with Microsoft, Apple, and IBM. These partnerships are now converting brick-and-mortar schoolhouses into virtual classrooms that digitally data-mine students through computer hardware devices, such as Apple iPads and Macbooks, which transmit video teleconferencing through software programs, including Microsoft Teams, supplemented by adaptive-learning courseware and other artificial-intelligence applications like IBM’s Watson Education.”
Getting the picture? Imagine how many parents are hypnotized and baffled by the total load of data sets which establish this new global education system, vs. the number of parents who will see through the layers of the con to the collectivist root.
Want a parallel? Try the current debate over the origin of the “pandemic virus.” It jumped from bat to human. No, perhaps other animals carried it. No, it was born in a Wuhan lab. Fauci and his agency funded gain-of function research at the lab. Well, perhaps they did, but the total amount of money was really an insignificant pittance. What did Fauci know, and when did he know it? Layer after layer, built higher and higher.
And at bottom, the virus was never isolated (never discovered), and it was never authentically sequenced. It was an idea, collectively concocted. [4]
Every death from, and case of, COVID virus infection can be explained (as I have, over the past year) without the need for, or reference to, a virus. [5]
In the old days, a stage magician would show his empty hands, then start pulling the edge of a colored handkerchief from one closed fist. A whole string of handkerchiefs would appear. But now, the magician presents 12 empty cabinets stacked on top of one another, and he seems to make those handkerchiefs ascend from the lowest to the highest cabinet.
Each cabinet is a data bank, and he isn’t even on the stage. He’s a hundred miles away talking to the audience via Zoom.
And soon, he won’t be a he. He’ll be a constructed image of a human.
And the image won’t be transporting handkerchiefs. It’ll be notifying people they have a disease; and the drugs will arrive promptly at their door.
The drugs will be toxic and won’t heal. The diagnosis will be flawed or completely irrelevant. The standard cause of the so-called disease will be false. The research on which the cause was based will be fake.
Just like now. But the layers of AI data all along the line will transmit a more powerful illusion.
Responding to Freedom of Information Requests, 69 Health/Science Institutions Failed to Provide Proof of “SARS-Cov-2” Isolation — by Anyone, Anywhere, Ever
69 health/science FOI’s institutions globally had all failed to provide or cite even 1 record of “SARS-COV-2” isolation/purification, by anyone, anywhere, ever.
6/10/2021 — Update by Truth Comes to Light editor:
See related Freedom of Information Act response from Melbourne, Victoria, Department of Health and Human Services as shared with us by a reader. The closing statement is most relevant:
Texas Wine Grape Growers Sue Bayer-Monsanto Over Dicamba Drift Damage
The volatile nature of the pesticide dicamba has meant that it can wind up miles away from where it was sprayed.
Dicamba, and dicamba-resistant seeds, were meant to be the next huge product for Monsanto, which was bought by agrochemical giant Bayer back in 2018. But “dicamba drift,” the name for the phenomenon in which dicamba particles float through the air onto plants that have no protection against it, has affected farmers and forests across the country. Most often, we’ve seen dicamba drift pegged as a damaging agent on unprotected soybean fields, but soy is far from the only victim. A new lawsuit claims that dicamba drift leveled extensive damage on vineyards—in Texas.
When we think of American wine production we tend to think of California first, then maybe Washington state, Oregon and the Finger Lakes region of New York. But grapes are grown just about everywhere and many wine grape varieties are well suited for non-coastal environments as well. In the High Plains region of Texas, just south of the Texas Panhandle, wine grape (and wine) production has been a recent local success story; Texas wines have even won awards held elsewhere.
In the larger wine-grape-growing regions of the United States, like in Northern California, dicamba drift has not been a substantial problem. Dicamba can drift for about three miles from where it was applied, which means that any affected crops need to be within that range to be hit. Napa and Sonoma counties in California, just for example, don’t have substantial dicamba-treated crops that close to the vineyards; there’s much more money to be made in growing grapes in those counties than growing cotton or soy.
But in Texas, cotton is a major crop and can be very close to the vineyards. Those vineyards’ owners, according to a press release from the law firm that filed the case, “saw their highly productive vineyards wither and, in some cases, die as a result of the dicamba-resistant seed system’s use on over two million surrounding acres of cotton.” That release says that 57 Texas wine grape growers have filed suit against Bayer-Monsanto and BASF (which also sells dicamba products) for “hundreds of millions of dollars.”
The suit alleges that some grape growers saw a truly insane 90 percent reduction in their yield owing to dicamba drift. And grapevines, unlike some other crops, cannot simply be replanted the next year for a similar yield; they require decades to mature and produce the right quality of fruit for some wines.
The European Federation of Food, Agriculture and Tourism Trade Unions (EFFAT) has called for an immediate ban on glyphosate-based herbicides and other harmful pesticides.
In a press release on Friday EFFAT stated “Protecting agri-workers’ health is EFFAT’s number one priority. EFFAT calls for an immediate ban on glyphosate in the renewal process, which ends in 2022. EFFAT also calls for more investments in the promotion of alternatives to the use of glyphosate and other harmful pesticides and urges a clear governance in charge of a smooth transition with the involvement of Trade Unions. Existing jobs must be protected and new quality ones created.
“The newly adopted position on the issue responds to EFFAT’s commitment to a more sustainable agriculture which underpins, inter alia, free trade agreements with binding requirement to respect highest environmental and social standards, investments in workers’ skills, social protection and research and development towards sustainable pest management.
“As sufficient evidence exists on the risks related to the use of glyphosate for workers, human health and biodiversity, EFFAT calls for the immediate ban of glyphosate as an active substance in herbicide products in the renewal process which is expected to end in 2022. The precautionary principle should guide EFSA and ECHA assessments.
Glyphosate Box
Glyphosate Residue Free Certification for Food Brands – Click Here
Test Your Food and Water at Home for Glyphosate – Click Here
Test Your Hair for Glyphosate and other Pesticides – Click Here to Find Out Your Long-Term Exposure
“If a transition period is to be set, it should be as short as possible and only apply for limited cases in professional use, whilst for uses in public areas, private gardens, railway tracks, desiccation, and all cases where Integrated Pest management (IPM) can be used, the ban should apply immediately. In any case, there should be no more use of glyphosate in Europe from 2024.
“EFSA, ECHA and the European Commission should carry out their assessment in atransparent and reliable way, free of the influence of the agro-chemical industry. The protection of agricultural workers’ health and safety must be considered as one of the main priorities throughout the scientific evaluation that will guide the process. The use of Personal protective equipment (PPE) should not be given a prominent position in the scientific assessment, as evidence shows that PPE is not always available, and its effectiveness is often over-estimated.
“Alternatives to the use of glyphosate and other harmful chemicals already exist and must be further promoted. This includes agronomic practices, mechanical and biological weed control, animal grazing and natural herbicides.
“A 13-week pilot study run by the Ramazzini Institute in Bologna in 2019 demonstrates that exposure to glyphosate-based herbicides from prenatal period to adulthood induced endocrine disruptive effects and altered reproductive developmental parameters in male and female rats. A recent study has proven glyphosate acts as an endocrine disruptor in the case of exposure during pregnancy.
“EFFAT supports the ambitious environmental objectives of the Green Deal and the Farm to Fork strategy, including the 50% reduction target for use and risk of pesticides by 2030.1 However, acting solely at a European level will not be sufficient to protect consumers’ health, safeguard our ecosystems and biodiversity and prevent soil erosion. On the contrary, it may affect jobs and the competitiveness of the EU agriculture sector. A vision towards a more sustainable agriculture without glyphosate and other hazardous chemical must be pursued at a global level. The EU should be at the forefront of this radical change, since the decisions taken in the EU will also have a substantial impact in other countries.
“It is not acceptable that harmful pesticides already banned in the EU keep being produced and exported by European agro-chemical companies. Foodstuff produced using pesticides banned in Europe should not enter the EU market.
“If the EU were to adopt a different approach to Free Trade Agreements (FTAs), this could contribute to building a more sustainable vision for the agriculture sector. Agriculture and food always require specific attention in the negotiation of FTAs, as the economic, social and environmental sustainability of these sectors is fragile and easily disrupted. Moreover, the respect of equal environmental and social standards must be a precondition to engage in negotiations.”
Chalk up a victory vs. public health tyranny! In the face of massive public resistance, so-called ‘officials’ have retreated from their unscientific and misanthropic propaganda tactics.
Another round of record protests across in London (barely acknowledged in corporate media) has served as a bellwether for the surging distaste against several forms of public health Covid edicts.
After more than a year ignoring the data and science to lockdown the world, public health officials have begun reluctantly abandoning many of their heavy-handed tactics. Taking a “carrot and stick” approach, global populations have been continually beaten with a medical stick to force compliance. Yet few doing the ‘beating’ cared to look at history or do a simple cost-benefit analysis to examine the erroneous plan for their populations.
Continued analysis of the data behind lockdowns shows epic failures that have set society back in unimaginable ways. Forcing public health edicts illogically has forever weakened confidence in governmental and global health bodies.
Canadian economist Douglas W. Allen recently published an examination of over 80 Covid-19 studies, taking a critical look at the literature to assess the lockdown Cost vs. Benefits:
“There are about 45 stringency points from the least stringent country (Russia: 40.28) to the most stringent (Ireland: 84.26). Over this range, moving from the least to most stringent lockdown increases the cumulative deaths per million by 630 deaths. Contrary to the popular understanding, lockdown is not associated with fewer deaths per million, but more. “
Despite the false assertion by public health officials that the limited, available science pointed to lockdowns being the only solution, Allen refutes this, stating:
“By August there was enough information available to show that any reasonable cost/benefit analysis would show that lockdown was creating more harm than good. It is unreasonable to suggest that a proper decision could not have been made in the fall when the second wave of infections hit.”
The public is emboldened like never before to both return to normal and disobey public health officials pushing irrational, unscientific orders whose only roots stem from virtue signaling, political jockeying and/or petty power plays. It’s over. And would-be government employees refusing to see the writing on the wall will be voted out of office.
Established in April 2020 and composed by a group of multi-disciplinary professionals, the Pandemics Data & Analytics (or PANDA) organization understands this. PANDA stands for open science, rational debate about replacing flawed science, and for retrieving liberty and prosperity from the clutches of a dystopian “new normal”.
The organization recently released its 17-page analysis and Declaration for the Protection of Children and Young People. It states:
“Evidence already shows serious damage to the physical, mental and social wellbeing of children and young people, as well as their educational attainment and future prospects (Lewis et al., 2021). There was never a reason to disrupt the lives of children and young people and there is every reason to restore normality to this population. Policymakers should take immediate action to protect children and young people from further harm and injustice, now and in the future.”
Meanwhile, the U.S. Centers For Disease Control and Prevention (CDC) is facing down a scandal from several directions. First, internal emails revealed the agency relied upon politically motivated actors, rather than science, to craft its school reopening policy. Secondly, the agency’s mask guidance was peppered with confusion and questionable science.
Research examining mitigation practices and Covid-19 rates in Florida, New York and Massachusetts’ schools continued to drive home the CDC’s scientific misadventures. After looking at all the data encompassing public schools and districts for the 2020-2021 school year, the authors concluded “…we do not see a correlation between mask mandates and COVID-19 rates among students…”
Even at this advanced stage of public revelation and transparency to the failed policies of some tone-deaf public health officials, some are still desperately trying to move the goalposts. For example: After the goal of lowering case counts in an effort to return to normal was reached, officials in Australia and New Zealand demanded a zero-Covid approach! Good luck with that.
Meanwhile, Ontario has announced a three-step plan to reopen the province, starting with outdoor recreational amenities, as it gradually prepares to ease pandemic restrictions. But wait! Hold on! Forget about lower case counts or mortality rates, Ontario must wait at least two weeks after 60 per cent of adults have received one dose of the vaccine!
In the U.S., the reopening has happened too rapidly for power-hungry public officials still not ready to give up their ill-gotten fiefdoms. The vaccine passport idea continues to be a non-starter in the USA as many governors checkmated the idea with a slew of early executive orders and bills.
Defaulting to individual businesses, a few governors have resorted to making weary frontline business owners manually violate their patron’s health privacy by asking them to check the vaccine status of everyone who enters their establishment. This is the textbook definition of fascism, by the way: The marriage of government and industry.
Other businesses have simply removed their “face masks mandatory” signs and replaced them with masking suggestions for the unvaccinated. How many people are complying no one knows for sure.
A month ago, headlines told of an impending U.K. domestic vaccine passport despite widespread public distaste. It manifested in the form of an NHS app which had some concerning additional features as exposed during an interview on U.K.’s Talk Radio:
The NHS app has been updated to include far more than vaccine jabs.
Julia: “Data relating to mental health, lifestyle, ethnic origin, biometric data and alleged criminal behaviour; what the hell does that have to do with proving you’ve had two jabs!?”@JuliaHB1 | @silkiecarlopic.twitter.com/TFztDpoMpq
In a surprising plot twist, following this weekend’s capacity protests, plans for the U.K. vaccine passport have reportedly been scrapped. In a Telegraph exclusive, ‘officials’ working on Covid-19 status certification believe there is no chance the law will be changed to mandate vaccine passports’ use within the U.K. Called a “well-placed source” by The Telegraph stated, “No one is talking about it still as a potential thing … It has been killed off really.”
As travel and employment appear to be the new chokepoints to ram through vaccine certificates, are governments defaulting to private business to finish the op? Or will something happen that gives officials a rejuvenated push in the near future?
The following is a slightly shortened version of a BBC Portuguese-language report on a carefully conducted study published in 2020, which has been largely overlooked till now. The study shows that glyphosate contamination of water, driven by expanded GM soy production, leads to a large increase in infant mortality, as well as a higher probability of low birth weight and a higher probability of premature births.
Glyphosate is the most popular pesticide in Brazil. It represents 62% of the total herbicides used in the country and, in 2016, sales of this chemical in thousands of tons were higher than the sum of the seven other pesticides most commercialised in the national territory.
Used on GM glyphosate-tolerant soybeans, the herbicide contributed to Brazil becoming the largest producer of the grain in the world, surpassing the United States.
As a result, the GDP (Gross Domestic Product) of soy-producing states has grown far above the economy of the country as a whole in recent decades. And the income generated by agricultural activity has stimulated other economic sectors in the producing regions.
But the new study, carried out by researchers at the universities of Princeton, FGV (Fundação Getulio Vargas) and Insper, reveals that this generation of wealth has a high cost. According to the study, the spraying of glyphosate on soybean crops led to a 5% increase in infant mortality in southern and central-western municipalities that receive water from soybean regions.
This represents a total of 503 more infant deaths per year associated with the use of glyphosate in soy production.
“There is great concern about the effects of herbicides on populations that are not directly involved in agriculture, who are not directly exposed to pesticides,” Rodrigo Soares, full professor at the Lemann Foundation Chair at Insper and one of the authors of the study, alongside Mateus Dias (Princeton) and Rudi Rocha (FGV), told the BBC.
“Although these substances are present in the body of more than 50% of the western population, we do not know if this is harmful or not,” added the researcher.
“Our article is one of the first to credibly show that this should indeed be a concern, as it demonstrates contamination through watercourses in areas far from the areas of use, in a way that has never been done before.”
Bayer, owner of Monsanto since 2018 – the company that launched glyphosate on the market in 1974, under the trade name Roundup – assesses the study as “unreliable and poorly conducted” and says the safety of its products is the highest priority of the company.
Aprosoja (Brazilian Association of Soy Producers), in turn, states that “the conclusions pointed out in the study do not seem to be supported by the scientific facts and reality found in the practice of Brazilian agriculture”.
Finally, CropLife Brasil, which represents the pesticide sector in the country, said that “for more than 40 years, glyphosate has undergone extensive safety tests, including 15 studies to assess the potential toxicity to human development and 10 studies to assess potential reproductive toxicity”.
“Regulatory authorities in Brazil, Europe, the USA and around the world have reviewed these studies and concluded that glyphosate does not pose a risk to human development or human reproduction,” said the organisation.
The use of glyphosate in Brazil
The most widely used herbicide in the world today, glyphosate was discovered by Monsanto in 1970. The pesticide is used to eliminate weeds in agriculture, acting by blocking an enzyme that is part of the synthesis of essential amino acids for plant development.
Glyphosate is a non-selective herbicide – that is, it kills most plants. Because of this, it became widely used on crops genetically modified to resist the chemical, such as GM soybeans, marketed by Monsanto under the name Roundup Ready. Glyphosate herbicides were first sold by the company under the name Roundup. In 2000, however, the glyphosate patent expired, and the product is currently offered by several manufacturers under different trade names.
Genetically modified soy was first marketed by Monsanto in the United States in 1996.
In Brazil, a first authorization for use was granted in 1998, but was almost immediately suspended by the courts. In 2003, the government granted a temporary marketing authorization, which required the incineration of the remaining seeds to prevent their reuse in the following year.
In September of that year, a provisional measure allowed producers to reuse the seeds and, in October 2004, the temporary sale concession was renewed. Finally, in March 2005, the Biosafety Law permanently authorized the production and sale of transgenic soybean seeds.
The use of genetically modified soy has spread rapidly in Brazil since 2004, representing 93% of the grain-planted area in the mid-2010s, according to data from the United States Department of Agriculture (USDA), cited by the study of researchers from Princeton, FGV and Insper.
Along with the productivity gain of the soybean crop, the use of glyphosate grew strongly in the country, more than tripling in volume between 2000 and 2010, from 39,500 tons to 127,600 tons.
Differences between Brazil and other countries
In the European Union, since 2015, there has been a wide debate about the possibility of banning the use of glyphosate, after a report by the International Cancer Research Agency (Iarc) that year classified the substance as “probable human carcinogen”, that is, as a possible cancer-causing agent.
In the United States, Bayer has already disbursed billions of dollars in deals to settle lawsuits over allegations that glyphosate causes cancer.
“In the European Union, unlike Brazil, the registration of pesticides is always for a finite time. Here, when a pesticide is registered, this registration is eternal, until it eventually comes to be questioned”, explains Alan Tygel, member of the coordination of the Permanent Campaign Against Pesticides and For Life.
In Europe, currently, the authorization for the use of glyphosate is valid until December 2022. Austria became the first country in the region to ban the product in 2019, while Germany plans to do without the herbicide from 2024.
Another important difference, according to the activist, concerns the maximum allowed value of concentration of the pesticide in water, so that it is considered suitable for human consumption.
“Brazilian water can be considered potable containing up to 500 micrograms of glyphosate per litre, while water in the European Union can have a maximum of 0.1 micrograms of glyphosate,” said Tygel. “So, the Brazilian limit is 5,000 times higher than the European Union limit.”
If these existing regulatory differences were not enough, Brazilian agribusiness has been pressing in recent years for the approval of the Bill of Law 6,299/2002, which eases the rules for inspection and application of pesticides.
In addition, within the federal government there has been a change in the correlation between forces opposed to and in favour of the use of pesticides.
“Until 2016, there was within the government a certain balance of forces between agribusiness, family farming and public policies to encourage agroecology,” said Tygel.
“From that year on, one of the first actions of the Michel Temer government [MDB] was to end the Ministry of Agrarian Development, which developed these organic agriculture policies. Since then, we have seen an exponential increase in the number of pesticide registrations,” he said.
In 2020 alone, Brazil approved the registration of 493 pesticides, the largest number ever documented by the Ministry of Agriculture, which has compiled this data since 2000.
Glyphosate and infant mortality
The authors of the study “Down the River: Glyphosate Use in Agriculture and Birth Outcomes of Surrounding Populations” say that they decided to study the relationship between pesticide and infant mortality due to the heated debate over the use of genetically modified seeds and their combination with herbicides.
“We thought the debate was very passionate and very uninformed,” says Rodrigo Soares, from Insper. “Then we realized that the expansion of GM soy in Brazil, mainly in the Midwest and the South, as it was very fast and very marked after the introduction of the GM seeds, could be an interesting context for analysis.”
The regulatory change that allowed the use of transgenic soybean seeds in Brazil has generated what is called in economics a “natural experiment” – an event brought about by external causes, which changes the environment in which individuals, families, companies or cities operate, and that makes it possible to compare groups affected and not affected by this event.
“One concern that existed is that there could be water contamination, since toxicological studies in the United States, Argentina and Brazil detected the presence of glyphosate in rivers, but in a one-off, non-systematic way,” says Soares.
“To evaluate this, we used information about the hydrographic basins in the country and the relative position of the municipalities – above or below areas of intensive use of glyphosate,” explained the researcher.
“It was a way of understanding how the expansion of the use of transgenic soy and glyphosate in a given municipality could affect the municipalities that receive water that passes through that region where pesticides are used.”
What the researchers did then was to analyze, for the period between 2004 and 2010, when the greatest expansion of transgenic soybean production occurred in Brazil and the use of glyphosate tripled, the birth statistics of these municipalities “downstream” from areas of use intensive herbicide.
“What we have shown is that there is a deterioration in health conditions at birth in these municipalities downstream from the municipalities that expanded soy production,” said the professor at Insper.
Within this deterioration in health conditions at birth are: a higher probability of low birth weight, a higher probability of premature births and – the most serious – an increase in infant mortality.
“We have also produced a series of other empirical analyzes to show that this was in fact associated with water and that this in fact appears to be associated with the expansion of soy.”
Isolating the effect of glyphosate
For example, comparing data from municipalities “downstream” with municipalities “upstream” – which therefore do not receive water that has passed through areas of use of glyphosate – the researchers find that municipalities “upstream” are not affected by this worsening of birth statistics.
The researchers also demonstrate that the negative effects on health outcomes at birth are particularly strong for pregnancies most exposed to the period of application of glyphosate, which in Brazil typically occurs between October and March, since soybeans are planted in the country between October and January.
The worsening of birth data is also greater when it rains more in the glyphosate application season, which the researchers showed by crossing health statistics with rainfall data. This finding is in line with the idea that more of the product reaches the rivers when soil erosion by rain is most significant.
Mateus Dias, a doctoral student at Princeton University and coauthor of Soares in the study, explained the researchers’ decision to analyse municipalities downstream and upstream, instead of the municipalities that apply the glyphosate itself.
“Glyphosate use has an impact on soybean productivity, and this may end up affecting child mortality in that municipality in other ways – for example, higher productivity can generate higher income and this will reduce child mortality,” he said.
The researchers also assessed whether the expansion of soybeans affected soil erodibility due to the advancement of agriculture over forested areas.
“We showed that this did not happen, because these areas that started to plant soy seem to have been pastures before, so there was no radical change in vegetation and consequently, there was no significant change in soil erodibility,” says Dias.
Study results may contribute to better regulation
According to the researchers, the objective of the study is not to “demonise” glyphosate, but to contribute to an improvement in public policies to regulate the use of pesticides in the country.
“We know what the use of agricultural substances in general has meant throughout human history – fertilizers, herbicides, pesticides. They have indeed enabled a revolution in terms of agricultural production and, in the net result, I believe that the effect was very positive,” said Soares, from Insper.
“We only have the production we have today, with its impact on the price of food and on the populations involved in agriculture that benefit from productivity gains, because of these substances,” he adds.
“This does not mean that we should not be aware of the potential negative effects,” he saod, defending changes in the regulations for the use and management of pesticides and the protection of water courses and water tables.
Alan Tygel, of the Permanent Campaign Against Pesticides and For Life – created in 2011 and composed of more than a hundred social movements, trade unions and class entities, NGOs, cooperatives, universities and research institutions, has a more radical opinion.
“We believe that the central objective is in fact to end the use of these substances, especially since today there is no doubt about the technical capacity to produce food without the use of chemical and synthetic pesticides,” the activist said.
According to him, the campaign’s proposals are contained in a bill (PL 6670/2016), which institutes a National Pesticide Reduction Policy, with measures that range from the ban on aerial spraying, through state support for agroecology, to the ban on pesticides banned in their countries of origin and the end of tax exemptions for pesticides.
“We will fight for every small gain that we may have, because we know that each percentage less of pesticides used results in lives saved,” says Tygel.
“But we know that there is no possible coexistence between organic production and the massive use of pesticides. The path that we envision is a production model that can be adopted nationally and is totally free of pesticides and transgenics.”
— The study:
Down the river: Glyphosate use in agriculture and birth outcomes of surrounding populations
Mateus Dias, Rudi Rocha, Rodrigo R. Soares
Latin American and the Caribbean Economic Association
Dec 2020 http://vox.lacea.org/files/Working_Papers/lacea_wps_0024_dias_rocha_soares.pdf
As I’ve been demonstrating for a year, SARS-CoV-2 was never discovered, never isolated, never legitimately sequenced.
In yesterday’s article, I laid out how this fake pandemic story, focusing on Wuhan, obscured Wuhan’s role as the number-one global launch-point for opioid trafficking.
Synthetic opioids—especially fentanyl, which is a hundred times more potent than morphine—are killing and addicting and maiming millions of people worldwide. That’s the scope of what we’re talking about.
Understand that one of the cardinal effects of opioids is suppression of breathing. During the so-called COVID pandemic, you’ve heard this referred to as “hypoxia.”
Yes, hypoxia is listed as a COVID symptom. It has a number of causes that have nothing to do with a virus. But of course, in the rush to diagnose as many people as possible with COVID—and with a PCR test that spits out false-positives like water from a fire hose—opioid users suffering from hypoxia are labeled “victims of the coronavirus.”
Drugabuse.com: “…opiate [opioid] drugs also slow your breathing…and in case of an overdose, your breathing is slowed to a virtually non-existent and lethal level.”
“The opioids depress your breathing, bring on heavy sedation and make it impossible to wake up.”
For many months in 2020, New York was touted as the global “epicenter of the pandemic.”
Patients in New York mystified ER doctors because they showed up with hypoxia.
2018 estimate of deaths from opioid overdoses in New York: 3000. Many more people in the New York area are addicted to these drugs. In New York State, in 2017, the number of people discharged from hospitals, after treatment for opioid overdose or dependency: 25,000.
In 2020-21, people who have developed opioid hypoxia have been misdiagnosed with “COVID-19 lung problems.” A large number of these people are sedated further, in order to be put on ventilators—ignoring the need to deal with their overdose, their addiction, their withdrawal—and they die.
Backing up a few steps from all this, you can see how a diagnosis of COVID functions as a cover story, to conceal the destruction-and-death-toll resulting from opioids.
How convenient that the whole COVID fairy tale was launched in Wuhan, the city that is the number-one source for global opioid trafficking. The fairy tale obscured the real Wuhan story.
City-journal.org, May 12, 2020, “Wuhan’s other epidemic,” Christopher F. Rufo: “…many don’t know that Wuhan is also the source of another deadly epidemic: America’s fentanyl overdoses… Over the past decade, Wuhan has emerged as the global headquarters for fentanyl production. The city’s chemical and pharmaceutical manufacturers hide production of the drug within their larger, licit manufacturing operations, then ship it abroad using deliberately mislabeled packaging, concealment techniques, and a complex network of forwarding addresses. According to a recent ABC News report, ‘huge amounts of these mail-order [fentanyl] components can be traced to a single, state-subsidized company [Yuancheng] in Wuhan.’”
And history matters:
Do you think the current Chinese political leadership has forgotten the two notorious 19th-century Opium Wars China lost? (Opium is the original natural opioid.)
In the 19th century, selling opium to China was very big business for England. Of course, addictive opium was devastating to China, who tried to stop the trade. Two Opium Wars against China (1839-42 and 1856-60) resulted. The Encyclopedia Britannica states:
“In each case the foreign powers were victorious and gained commercial privileges and legal and territorial concessions in China [including the uninterrupted sale of opium]. The conflicts marked the start of the era of unequal treaties and other inroads on Qing sovereignty that helped weaken and ultimately topple the dynasty [which had ruled since 1644]…”
It would be hard to overstate the lasting fury and resentment of Chinese rulers against the foreign powers who defeated and humiliated them in the Opium Wars.
The UK Daily Mail [2017]: “[a new drug coming into the UK is] not just heroin. It had been mixed with two lethal man-made opioids – fentanyl, a painkiller 100 times more potent than morphine; and carfentanyl, an elephant tranquilliser 10,000 times stronger than street heroin.”
“Now the drugs have arrived in Britain – and a spate of sudden deaths in Hull, the worst incident in the UK so far, shows their devastating impact. Just a few grains of carfentanyl – 0.00002g – can be fatal.”
“These lethal drugs have begun cropping up across the country – first found in Blyth, Northumberland, then suspected in deaths and drug busts from Leeds to London, St Albans to Southampton, Wakefield to Winchester, and Wales to Northern Ireland.” [In 2021, the UK government states that opioid addiction and death aren’t overwhelming concerns. I find it hard to believe these assurances.]
FOX Business, March 31, 2017. Headline: “DEA: Made in China Lethal Opioid Fueling US Drug Epidemic.”
“A homemade designer version of fentanyl, the highly addictive opioid which is similar to morphine but is 50 to 100 times more potent, has been the center of drug busts across the country this month—with law enforcement pinpointing its origin from underground labs in China. The DEA says the China-U.S. supply is further fueling the country’s drug epidemic.”
“’This [Chinese] stuff is unbelievably potent. It is so powerful that even a tiny amount can kill you,’ DEA spokesman Rusty Payne tells FOX Business. ‘China is by far the most significant manufacturer of illicit designer synthetic drugs. There is so much manufacturing of new drugs, [it’s] amazing what is coming out of China. Hundreds of [versions], including synthetic fentanyl and fentanyl-based compounds’.”
“China only made the drug [fentanyl] illegal in 2015, and at that point black market Chinese labs began increasing production of their own versions, including the one turning up recently across the country [the US] called furanyl fentanyl.”
“’While heroin gets harder to buy on the street or from a dealer, fentanyl comes via FedEx,’ Brad Lamm, CEO of Intervention.com, tells FOX Business.”
“Brooklyn District Attorney Eric Gonzalez announced this week details on a mail-order furanyl fentanyl smuggling ring bust. The operation had been bringing the drug — which has been dubbed ‘White China’ — into the U.S from Asia. NYPD Chief of Detective Bob Boyce said that this was the first time investigators have seen this type of fentanyl in New York City.”
“Also this week, Cincinnati Customs and Border Protection agents said they seized 83 shipments of illegal synthetic drugs, including 36 pounds of furanyl fentanyl, from China.”
The Boston Globe [2017]: “An extremely powerful drug used as an elephant tranquilizer has quickly become a new killer in the nation’s opioid epidemic, and New England authorities and health workers are bracing for its arrival.”
“The drug, carfentanil, is a synthetic opioid that is 10,000 times stronger than morphine and 100 times more potent than fentanyl, another deadly synthetic opioid.”
“The Drug Enforcement Administration has issued a nationwide alert about the drug, which its acting chief called ‘crazy dangerous.’ In Massachusetts, State Police have warned their crime lab staff about how to handle carfentanil during analysis. Even inhaling the drug or absorbing it through a cut can be fatal.”
“Law enforcement and health officials believe most users do not know they are ingesting carfentanil, which apparently is often mistakenly thought to be heroin or a mixture of heroin and fentanyl, a weaker but still lethal synthetic opioid.”
“If carfentanil’s trade route is similar to that of fentanyl, the path stretches from Chinese manufacturers to Mexican processors to smugglers who supply dealers in the United States, law enforcement officials said.”
“’There’s no quality control, so when it gets here the distributors don’t know what they have and the user has no idea,’ said Timothy Desmond, a special agent with the New England division of the DEA. ‘That’s where it’s a game of Russian roulette’.”
“Hamilton County officials are baffled by the marketing strategy behind such a lethal drug. ‘It doesn’t really make sense that you would want to kill your customers’,” Fallon said.
“Law enforcement officials also are concerned that carfentanil will harm first responders. The DEA has warned police not to conduct field tests on seized drugs that might contain carfentanil. Instead, the agency urged officers to secure their samples and deliver them only to colleagues with training and equipment to handle the drug.”
In 2020-21, the opioid catastrophe continues.
And its number-one trafficking source, Wuhan, is famous only for birthing a pandemic that doesn’t exist because the virus causing it has never been proven to exist.
This article takes off from the work of investigative reporter, Whitney Webb. Much of what I’m laying out here confirms her exposure of “the other Wuhan.” Webb writes at Unlimited Hangout and The Last American Vagabond.
When I put together Webb’s findings with my own COVID research, startling new dimensions of the false “pandemic” story come to light.
Who would have thought that, in less than a year, the image of the opioid drug, fentanyl, would undergo a face lift, enhancing it from “most destructive killer drug in the world” to “lifesaver in the treatment of COVID patients?”
And if this PR miracle is not a sufficient stunner, it just so happens that Opioid Central for illegally trafficking fentanyl to the planet is Wuhan, now the focus of claims that COVID was born in a lab there.
(Fake) pandemic transforms fentanyl into “vital COVID medication.”
(Fake) pandemic starts in Wuhan.
Wuhan is the city where killer drug fentanyl is shipped out to dealers all over the world.
High-level operators, focusing on Wuhan, manage to obscure, from the broad public, the city’s global role in killing millions of people with opioids…by claiming a pandemic was born in Wuhan. “The ONLY thing you have to know about Wuhan is the virus broke out there.”
This has the earmarks of a highly successful cover story.
Here’s a prime illustration of fentanyl’s PR facelift:
NJ [New Jersey] Spotlight News, April 14, 2020, “No Longer a Scourge, Fentanyl Is Now Most-Needed Drug in COVID-19 War.”
“…fentanyl, one of the drugs given to patients so they can withstand the pain of having a breathing tube inserted, is in short supply along with a handful of other crucial drugs.”
“The first wave of critical shortages exposed by the coronavirus was medical masks and gowns. Then it was ventilators. Now, a handful of crucial drugs are in short supply in overrun ICUs throughout northern New Jersey and New York City, many of which are needed to use the ventilators.”
“At the top of the list is fentanyl, the deadly synthetic painkiller — 100 times more powerful than morphine — the very drug that has become public enemy No. 1 in the nation’s war on opioid addiction. Demand for fentanyl has doubled nationwide and shot up more than 500% in the New York/New Jersey metropolitan region, the current global epicenter of the pandemic.”
“Fentanyl may have been killing people in record numbers on the streets of New Jersey in recent years, but in our hospitals, it is now saving lives.”
“Demand for fentanyl is followed by Propofol, a sedative also used with ventilators, according to Soumi Saha, Premier’s senior director of advocacy…Close behind those two is a new category of drugs to face shortages — neuromuscular blockers, which are also being used for ventilator patients because they keep them from involuntarily coughing on the healthcare worker inserting the vent tube.”
“During normal times, patients stay on ventilators for three or four days. Now, not only has the number of ventilated patients spiked, but the time they remain on the device is two to three weeks.”
I gave you an extended quote from that New Jersey article, because I’ll cover the real story behind ventilators later in this piece.
Right now, here are a few references pointing to Wuhan as Opioid Central.
City-journal.org, May 12, 2020, “Wuhan’s other epidemic,” Christopher F. Rufo: “…many don’t know that Wuhan is also the source of another deadly epidemic: America’s fentanyl overdoses… Over the past decade, Wuhan has emerged as the global headquarters for fentanyl production. The city’s chemical and pharmaceutical manufacturers hide production of the drug within their larger, licit manufacturing operations, then ship it abroad using deliberately mislabeled packaging, concealment techniques, and a complex network of forwarding addresses. According to a recent ABC News report, ‘huge amounts of these mail-order [fentanyl] components can be traced to a single, state-subsidized company in Wuhan.’”
The Atlantic, August 18, 2019, “The Brazen Way a Chinese Company Pumped Fentanyl Ingredients Into the US,” by Ben Westhoff: “According to Bryce Pardo, a fentanyl expert at the Rand Corporation, the two most commonly used fentanyl precursors—think of them as ingredients—are chemicals called NPP and 4-ANPP. When I first started researching them, in early 2017, advertisements for the chemicals were all over the internet, from a wide variety of different companies. Later, I determined that the majority of those companies were under the Yuancheng [company] umbrella.”
“Posing as a buyer, I answered an online advertisement for fentanyl precursors and was put in touch with a Yuancheng salesman who called himself Sean. We arranged to meet at the company’s main office in Wuhan, in the Wuchang district, near a busy subway station in a blue-collar neighborhood…”
LA Times, April 24, 2020: “For drug traffickers interested in getting in on the fentanyl business, all roads once led to Wuhan.”
“The sprawling industrial city built along the Yangtze River in east-central China is known for its production of chemicals, including the ingredients needed to cook fentanyl and other powerful synthetic opioids.”
“Vendors there shipped huge quantities around the world. The biggest customers were Mexican drug cartels, which have embraced fentanyl in recent years because it is cheaper and easier to produce than heroin.”
The Times article cites the pandemic as the reason for a decline in the fentanyl business. But lockdowns increased people’s desires for drugs. And of course, since economies have started loosening up, fentanyl trafficking operations are certainly booming again.
The highly successful cover story I described above…were there reasons for this cover, other than an attempt to conceal, from the broad public, Wuhan as the global center of opioid trafficking?
I can think of two other reasons. The first one I would introduce this way: “We’re killing people in the streets with fentanyl, but that’s not enough. We want to kill them in the hospitals, too.”
Heavy hitters, intent on getting rid of the elderly on a wide scale, saw an opportunity. And now we come to the ventilator story.
There is no doubt that, globally speaking, there has been a mad and destructive rush to put people diagnosed with COVID on breathing ventilators.
To deploy these devices in hospitals requires intubation, which is painful and very disruptive. Patients must be sedated. They must be kept sedated, while they’re hooked up to the breathing machines— for days and weeks.
Enter fentanyl and other opioids.
Since the whole story of the COVID virus was a fake from the get-go, some group would have to bear the burden of dying, in order to inflate death numbers; in order to make it appear that the “pandemic” was a fire sweeping through the world.
The group was and is the elderly, and in a series of articles on this gruesome subject a year ago, I left no doubt about the truth staring us in the face. (Note: CDC, May 14, 2021: “8 out 10 COVID-19 deaths reported in the US have been in adults 65 years old and older.”)
COVID is old people. Their premature deaths are forced. Their statistical numbers are gold for the planners of the operation. And this has nothing to do with a virus.
The Hill, (undated, late April 2020), reports on “data…gathered at Northwell Health, New York state’s largest hospital system. The study, published in the Journal of the American Medical Association (JAMA) examines 5,700 patients hospitalized with coronavirus infections in the New York City region, with final outcomes recorded for 2,634 patients. The average patient age was 63 years old… For the next oldest age group, ages 66 years and older, patients receiving mechanical [breathing] ventilation recorded a 97.2 percent mortality rate.”
97.2 percent of elderly patients put on breathing ventilators died.
Just in case other obvious strategies failed to produce premature death in the elderly, ventilators provided the method:
VENTILATORS PLUS SEDATION WITH OPIOIDS.
THE OPIOIDS CAUSE SUPPRESSION OF BREATHING AND DEATH.
OF COURSE, THAT SUPPRESSION OF BREATHING (“HYPOXIA”) IS CALLED A CARDINAL SYMPTOM OF COVID.
Don’t even think of saying, “Well, you see, those old people put on ventilators were already very sick and close to dying.” NO medical treatment that kills 97.2 percent of patients in a well-defined group is continued, unless there are orders mandating it. Unless there is insurance money to be saved. Unless the doctors are willing to follow orders and keep using the treatment, despite the results.
So yes, opioids were transformed, by a cover story, from a killer street drug to a “lifesaving treatment” for COVID—but at the deepest level, that meant murdering the elderly with the drugs.
The second reason for the cover story would have involved moving up the time table for launching the fake pandemic story in Wuhan.
Was there some sort of accident, in which the people of Wuhan were exposed to fentanyl, with deadly consequences? Desperately needing a phony cover-up explanation—was “THE VIRUS” story invoked?
I can only speculate about that possibility. However, China is famous for loose enforcement of safety regulations in factories, and it’s possible that some sort of accident occurred, which blew fentanyl or its components through the city of Wuhan, killing people on the spot.
There are analogous recent incidents in China.
The Wikipedia page for the 2019 Xiangshui chemical plant explosion, which killed 78 people and injured 617, mentions other events as well:
“On 27 November 2007, an explosion occurred in one of the chemical factories in Chenjiagang Chemical Zone, with seven killed and around 50 injured…In the early morning of 11 February 2011, rumors of toxic chemical release and potential imminent explosions in the Chenjiagang Chemical Industry Park led over ten thousand residents to evacuate in panic from the towns of Chenjiagang and Shuanggang during which four people died and many were injured. On the afternoon of May 18 and again on July 26 in 2011, there were explosions at local factories.”
As I keep reminding readers, the whole “pandemic” is a covert op. Such operations always deploy cover stories, in order to hide what is really being done, how it’s being done, and why.
Speaking of which, there are several major pharmaceutical companies who’ve faced heavy exposure for their roles in the opioid criminal trafficking business. For example, Purdue, and Johnson & Johnson. A third one is (Mossad-connected) Teva.
If you could offer Warren Buffet an ice cream cone with a truth-serum cherry on top, it would be interesting to ask him whether the PR campaign to push opioids as life-saving COVID treatments helped stabilize his 42,789,295 shares of beleaguered Teva, worth $412,916,000.
To connect one more dot (for now,) the Bill & Melinda Gates Foundation holds 50 million shares, worth $11 billion, in Buffett’s company, Berkshire Hathaway. It is the Gates Foundation’s top investment.



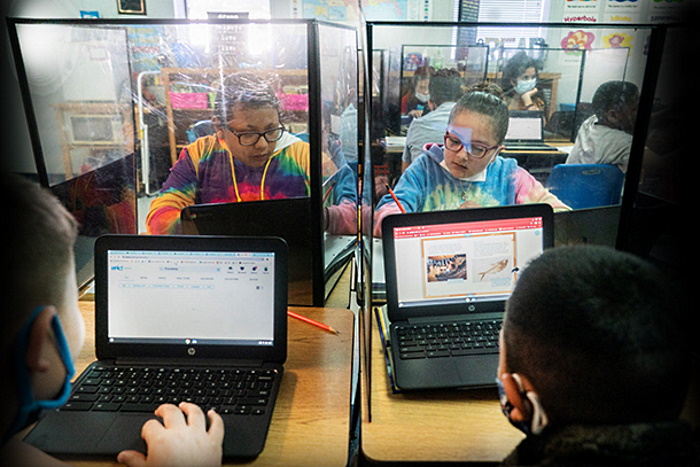
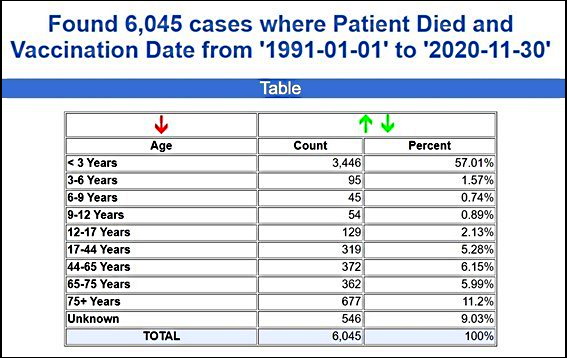
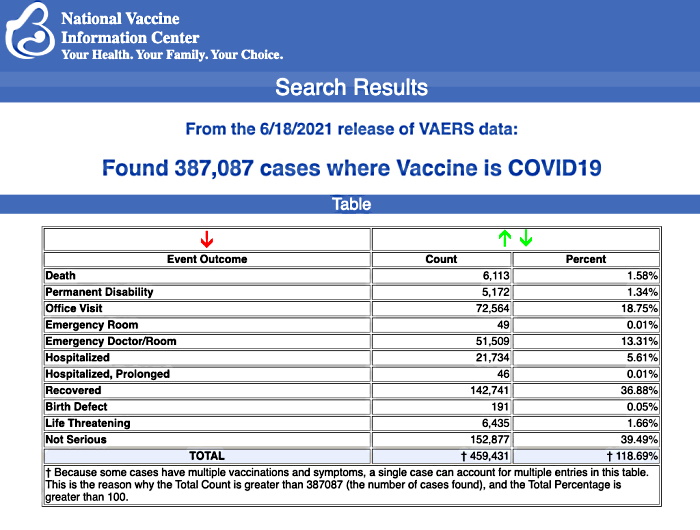


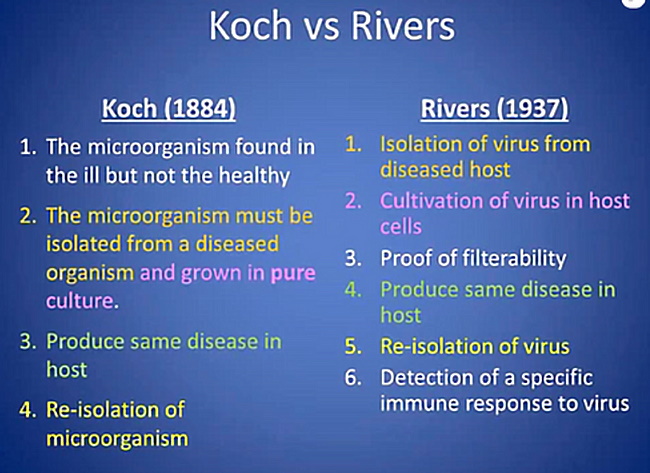
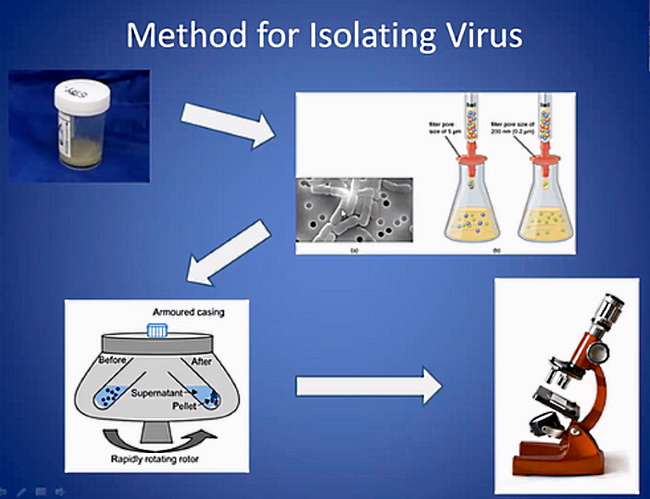

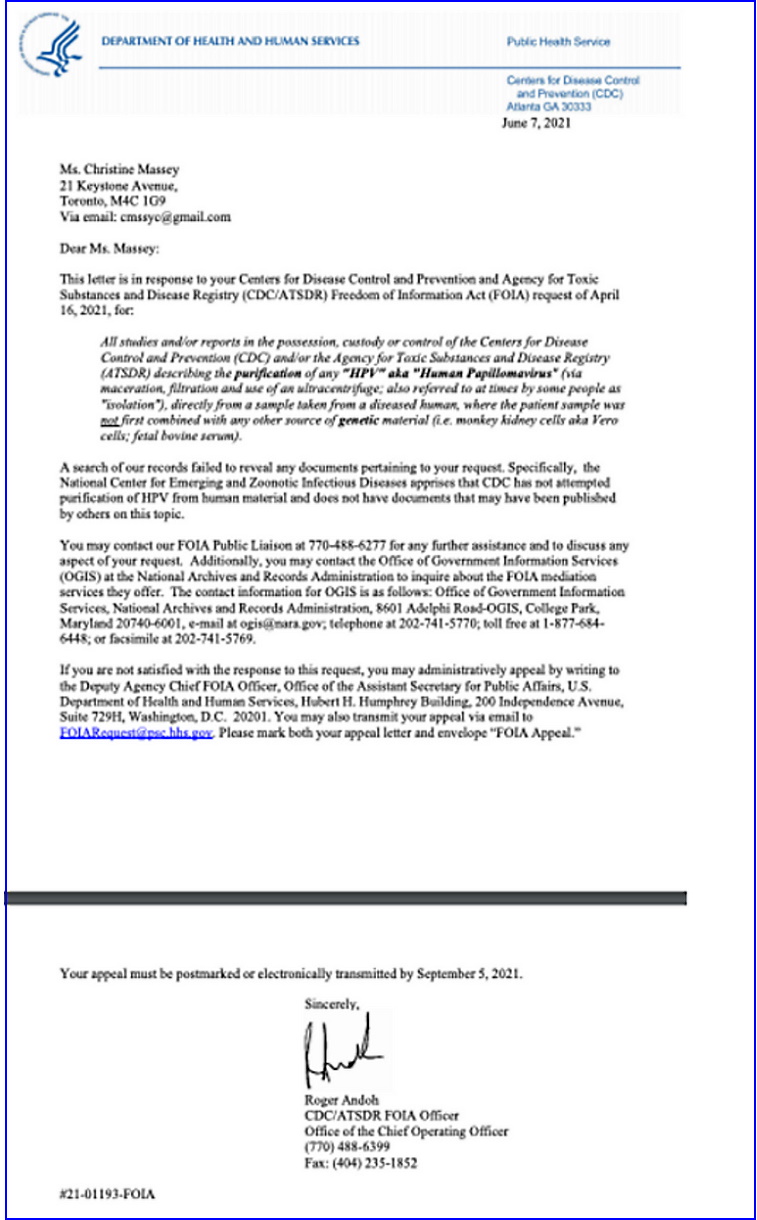
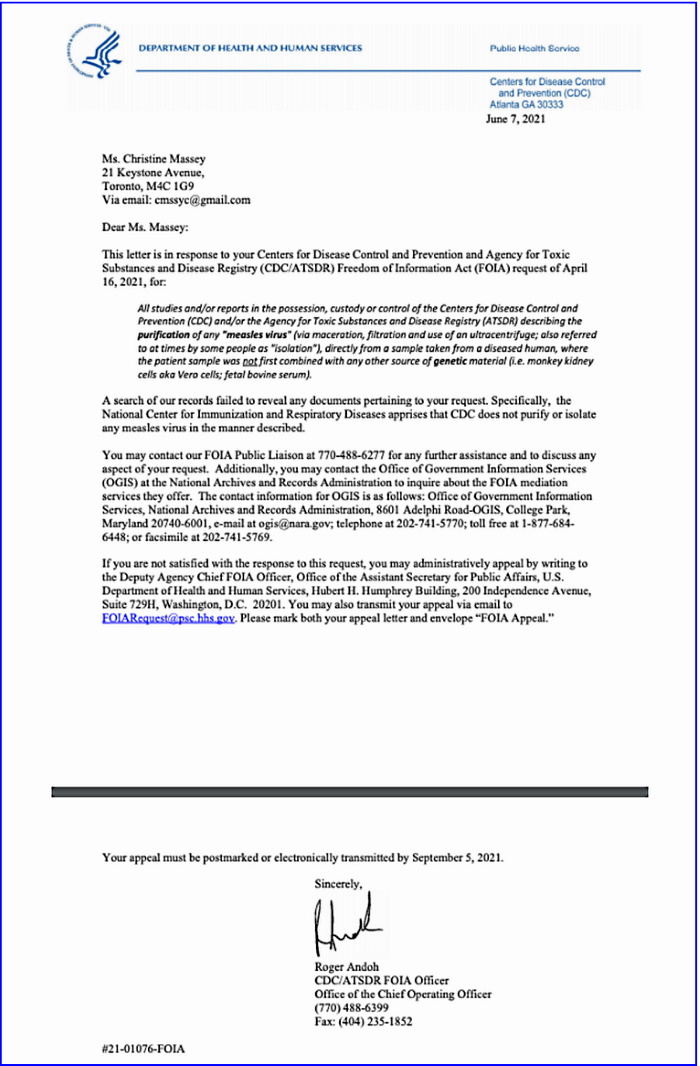
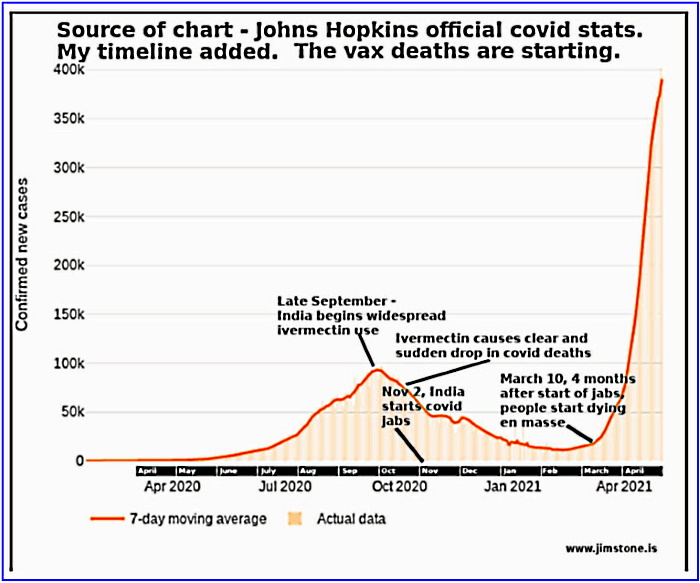

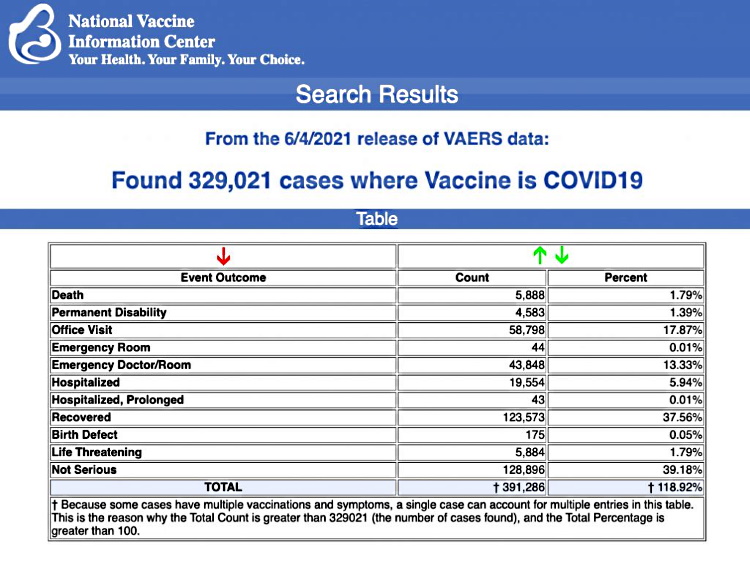


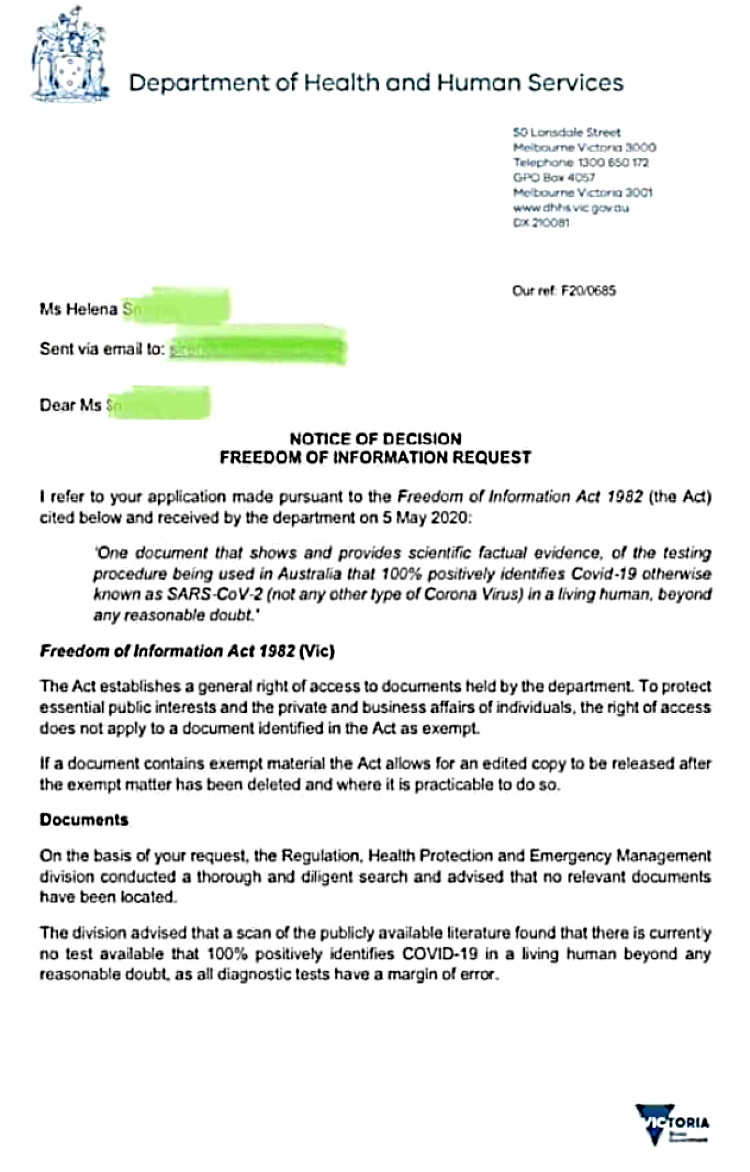
_Wellcome_L0073696.jpg){kind=link}