[Truth Comes to Light editor’s note: This presentation comes from a perspective that the “covid virus” theory is real. Even though most who find their way to this website are questioning the covid narrative, not to mention much of the “science” upon which western medicine is based (including vaccination in general), this video is well-worth watching and sharing. Dr. Mumper offers a clear and concise overview of the history of scheduled vaccinations and the large numbers of vaccine-related injuries and deaths. She talks about the toxic adjuvants found in all vaccines and dangerous ingredients that are specific to the mRNA injectables. Dr. Mumper takes a strong stance against medical mandates. ~ Kathleen]
by Children’s Health Defense
video recorded October 2020 and published January 12, 2021
Children’s Health Defense has created a video of Dr. Liz Mumper’s presentation titled “How Will We Know That a COVID-19 Vaccine is Safe?” This presentation is the result of a collaborative effort between Dr. Mumper and the team of doctors, scientists, and researchers affiliated with CHD.
Dr. Mumper carefully provides detailed answers to two questions often asked by the public: “What does a safe and effective vaccine look like?” and “How will we know that a COVID-19 vaccine is safe?” She reviews many of the reasons why vaccines, as they are currently produced, are not safe, and explains that every year there are tens of thousands of adverse events, many of them resulting in serious conditions or even death.
Video Transcript
This is Liz Mumper. I’m a pediatrician with 40 years of experience both practicing and teaching pediatrics. It’s my honor, to be asked by Children’s Health Defense to share with you some of our concerns about vaccine safety specifically regarding the safety and effectiveness of the emerging COVID vaccines. As a pediatrician, I was taught to give vaccines and over my career, I have given thousands.
Some of my patients develop significant side effects including several who developed serious enough effects that it changed the course of their lives for the worse. As a result, I spent a lot of extra time learning about vaccine side effects and the metabolic and physiologic ways by which vaccines can cause injury in certain people. Based on my clinical experience and research, I understand why the public has concerns about COVID vaccines. In August only 44% of Americans said that they would get a COVID vaccine. And 58% of those said the reason was they were primarily concerned about side effects.
When you carefully examine the history of vaccinations, it’s not all lollipops and rainbows since I’ve seen how the sausage is made and what the ingredients are, I have decided to really look carefully at vaccine safety. It’s important to realize that the process is flawed as are all human endeavors. CHD, Children’s Health Defense is in the process of carefully examining the data. And we hope to be able to share this information with you so that you can truly make an informed decision about vaccinations.
Unfortunately, with the COVID response, about 60% of small businesses have shut down. And I’m very proud that my colleagues at Children’s Health Defense were among the first to call attention to the collateral damage that can be caused by widespread economic hardship and social isolation. The amount of anxiety and depression I’m currently seeing especially in my adolescent patients is very concerning. One of the things that concerned me most this spring, was the lack of attention to potential prevention strategies.
In my community, we were told to tell patients to stay at home until they got really sick. In my opinion, this was a well-intentioned strategy, allegedly to try to preserve hospital resources. But in my opinion, we miss the obvious point of what people should be doing so that they could develop immune resiliency, so that if they did get the COVID virus they would be able to respond well. So the issue of a COVID vaccine has been considered to be central to us getting back to normal.
But why would we put all of our eggs in one basket? Why would we assume that a vaccine developed at Warp Speed is the only way to save ourselves? A public health crisis that’s unfolding with global implications should bring forth collaborative strategies to pull our collective wisdom. Now, the amygdala is a part of our brain that is ruled by fear and emotion, it’s considered the reptilian part of the brain, this very primitive response. So instant access to bad news 24/7 can have the effect of making us live in fear.
Neuroscience long ago has shown that when we are fearful, our ability to make rational decisions is compromised. We have trouble processing nuanced information. We are more likely to follow others blindly than to assess the data and make decisions for ourselves and our families. So the hijacking of the amygdala by fear, obviously a hand coming out of the grave or the scary clown face are images that would disturb most people. However, now, if we’re living in fear, the other images like the hand being presented for a handshake or the cute guy’s smile might seem threatening to some people because they’re worried about the contagion of COVID.
Now this is an important slide that most people do not realize. In the United States, disease mortality rates for vaccine preventable illnesses actually went down a lot before the vaccines were introduced. So if you think of this curve, like a ski slope, at first you start out with this very high curve where lots of people are affected and then over time you see that the curve actually levels out.
So Nicholas Christakis who trained at Harvard and Yale and who brings his experience from being a clinician, a research scientist and a sociologist in addition to his heritage as a Greek and the wisdom derived from that culture, reminds us about this work of Thomas Mckeown, a sociological approach to the history of medicine. This researcher showed that, for example, for the whooping cough vaccine, which is called pertussis, it was actually introduced after death from whooping cough had decreased dramatically. The same was true for measles vaccine, that vaccine was developed and introduced after the curve of mortality had greatly declined and was on this sort of flat slope, like at the end of a ski jump.
So what that tells us is that, many other factors including public health measures, like indoor toilets and water sanitation and declining poverty and increasing wealth, all those things are public health measures that make a huge difference in vaccine preventable diseases. So we should be looking at the whole picture.
Will this be a rushed vaccine? Government agencies like the CDC, basically have some political motives and conflicts of interest. And in many ways the CDC is also a vaccine distributor because about over $4 billion of their budget is spent on purchasing vaccines. And they also have the task of making vaccine recommendations and doing educational campaigns for people to get vaccines.
So we should be asking the following questions, should the same organization that’s responsible for promoting widespread use of vaccines, be the same agency that looks at safety concerns and adverse reactions? Should the same doctors and scientists who develop a vaccine, sit on the American Committee for Immunization Practices to vote on approval of that vaccine? Which they have probably been working on for over a decade. And obviously are very invested in the outcome.
As the public health officials are trying to, reassure the public about vaccine safety, Children’s Health Defense has been looking at the data. Remember public health agencies are supposed to serve you. You’ve the right to look at the data and analyze the data and to ask for transparency.
Recently, several Harvard and Yale and other esteemed researchers and scientists and physicians have written that they need more transparency in order to be able to analyze the results of the ongoing clinical trials. Ultimately, you should have the right to decide if you get the COVID vaccine or not. In my opinion, medical mandates are malpractice because by definition, they do not take into account the individual medical histories, the genetic differences of patients, nutritional choices that they make that might put them at higher risk of side effects.
There’s an emerging field of study that combines vaccinology and genomics. This is called vaccinomics. So one of the scientists that’s been working on this for a long time is Gregory Poland. He works at the Mayo Clinic for Vaccine Research and has been working on this issue for over 22 years. So for example in an era where clinicians are using genomics to develop personalized, targeted cancer chemotherapy, I don’t understand why when it comes to vaccines, we continue to push a one size, one schedule fits all vaccine strategy. Have we decided for convenience, that all infants and children should get the same set of vaccines on the same schedule? No matter what their individual circumstances and medical histories and environmental risk factors.
So what does a safe and effective vaccine look like? At Children’s Health Defense, we have many hundreds of doctors and scientists who’ve studied vaccines, their ingredients, their physiologic mechanisms. And these are the following criteria that represent the fruits of their work.
The vaccine would be tested against a true placebo, inert saline, which is salt water. So unlike drugs, which have to be tested against a true placebo, vaccines fall under the category of biologics and are not tested against a true saline placebo. As an example, Merck’s HPV vaccine was tested against an aluminum adjuvant that can trigger auto-immunity. This clinical impact of this is actually very significant since aluminum is a known neurotoxin and a known trigger for auto-immunity, having aluminum in the new vaccine and in the placebo would wash out the differences in auto-immune or neurologic disease between the two groups. The one that got the vaccine and the one that got the aluminum placebo.
A safe vaccine would be tested long enough to track adverse events. And then post approval surveillance would be conducted to measure the long-term effects. So many vaccines are just monitored for side effects for two to five days or maybe a week. And auto-immune neurodevelopmental and chronic conditions would take much longer than that to manifest. As an example, Merck’s hepatitis B vaccine, which was given to one day old infants was only safety tested for five days.
So here’s my question. Newborn babies, mostly eat and sleep. So how effective can we be at assessing if they are experiencing side effects in such a short period of time? As somebody who has studied vaccines for many years and I’ve read every single vaccine insert of every single vaccine, I’m not as worried about the short-term effects, the redness, the swelling, all those signs that show that the body has recognized the shot as foreign and is reacting to it. I’m much more concerned about potential long-term effects on brain inflammation or auto-immunity, for example.
Why is post-approval surveillance so necessary? Over the last five years, the vaccine adverse event reporting system has received an average of 45,000 adverse events reported every year. And the striking thing is that, this is expected to be only about 1% of the total real adverse reactions according to our own government’s department of health and human services. This is because it’s a volunteer reporting system and there are no measures in place to measure compliance with this system.
Over the past years, the United States government and by that, I mean, you, the consumers of vaccines have paid out over $4.4 billion for vaccine injuries. It’s important to know that this $4 billion is paid out after a very high bar is set for families to get compensation for vaccine injuries. And it’s important to remember that that $4 billion comes not from Merck or Pfizer or Glaxo SmithKline.
Number three, experimental mRNA and DNA gene technologies should undergo years of testing before being used on consumers, mRNA vaccines have actually been used to target specific types of cancer. And if that works well for that patient, that’s fantastic. But the initial studies on COVID mRNA vaccines were done on extremely healthy patients. And since the vaccine is currently being prioritized for the most vulnerable, including the elderly, it’s crucial to assess safety for those in various states of health. And this theoretically is happening as the trials progress to phase three. mRNA vaccines have an intrinsic inflammatory effect, which could lead to auto-immune events.
Both Moderna and Pfizer and BioNTech are using mRNA technology in their vaccines. And these techniques have not been used and approved in the context of widespread use as is being contemplated now. In 1990, the first report of a successful use of In Vitro transcribed mRNA in animals was published. At that time, concerns were raised about the inherent instability of mRNA and the high innate immunogenicity of mRNA vaccines which can be a double-edged sword.
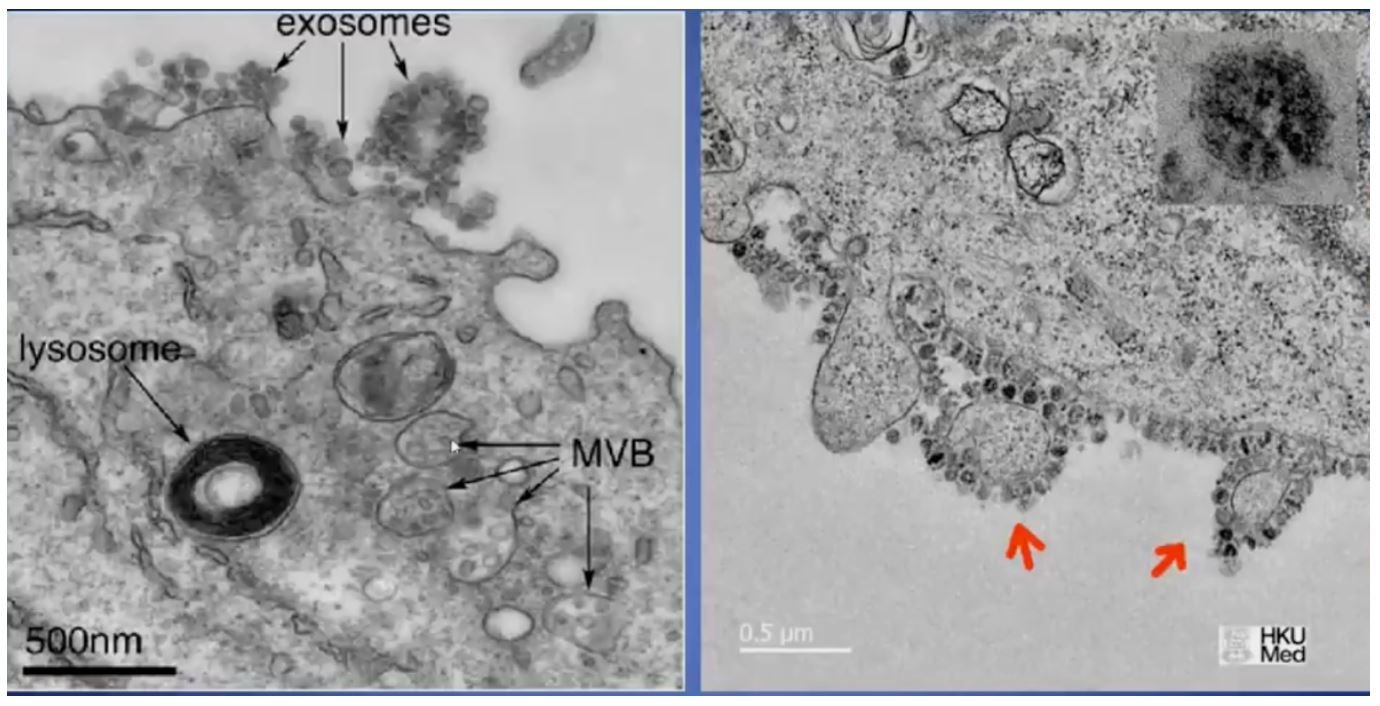
There’s been a lot of progress since then but mRNA that comes from outside a person is inherently immunostimulatory because your body recognizes that is foreign. Another concern that I have is that, in order for mRNA vaccines to penetrate into the cell membrane, they have to essentially penetrate by lipid layer, the two layers of fat that surround all our cell membranes. And this can be done through electrical measures or by using carrier proteins. And my question is, do we really wanna poke holes in our cell membrane?
Number four, vaccines should be free of mercury, aluminum and nano-metals. At Children’s Health Defense, we have over 240 studies showing that mercury is not safe. Due to safety concerns, the public health service did remove mercury for most vaccines starting in 1999 and most were phased out by 2003, 2004 but mercury is still present in many flu vaccines. Aluminum is a known neurotoxin, which is used as an adjuvant to induce immune responses in lots of vaccines.
So for example, if a two month old infant is immunized according to the CDC schedule, typically they get aluminum that exceeds the FDA’s maximal allowed dose by more than 50 times. Now, a 2017 Italian study showed that nearly all vaccines are contaminated with certain nano-metals, very, very very small metal particles. So you can go to the Children’s Health Defense website to look at peer-reviewed published studies on the adverse effects of mercury.
More than a decade ago, I testified in the national vaccine court on behalf of 5,000 children whose fate was determined by three test cases. The government experts argued that the dose makes the toxin and that the amounts of mercury in vaccines were so small that children should be able to handle that. We argued that individual children with individual capabilities for detoxification, for individual medical histories that might put them at greater risk, that we couldn’t be sure that any given dose was safe for a particular child. We lost that case.
So it appears that the Glaxo SmithKline and other vaccines may contain nano-aluminum. Christopher Exley, who is professor of bioinorganic chemistry at Keele university in the UK, he and his colleagues have done this impressive body of work about the dangers of aluminum especially with regards to neurotoxicity. His work is well worth reading, and you can find the links to his work on the Children’s Health Defense website.
Number five, vaccines should be free of adjuvants that are proven to be dangerous. This includes, but it’s not limited to squalene, aluminum and polyethylene glycol. So an adjuvant is a substance that’s deliberately added to a vaccine in order to stimulate the immune system to make a strong immune response. So squalene is one of many adjuvants that are used and it was found to be harmful in certain people by inducing, for example, auto-immune conditions or narcolepsy which is falling asleep suddenly literally while you’re on your feet sometimes. Polyethylene glycol is another adjuvant that can trigger serious auto-immune responses and anaphylaxis in certain individuals.
You’ve heard about Gulf War syndrome, Malcolm Hooper at the United Kingdom is one of the many scientists that I’ve met who’ve uncovered very concerning information about the role of vaccine adjuvants in Gulf War syndrome, which as you know, has occurred in many soldiers who were never deployed to the Persian Gulf. And basically a 100% of Gulf War syndrome soldiers who were immunized, who had symptoms of Gulf War syndrome, which can be very varied and very debilitating had antibodies to squalene and other people who got the same set of shots but didn’t develop these symptoms, did not.
This should be a cautionary tale as we move forward with COVID vaccines. Polyethylene glycol will be in the Moderna vaccine we are told and we’re concerned that polyethylene glycol can trigger serious adverse immune responses or anaphylaxis in certain people. Again, with all due respect to the vaccinologist out there and the people who are working feverishly with the best of intentions to make a vaccine in this crisis, you are not the ones who will have to take care of the patients who have significant adverse effects from the vaccines you develop, physicians, nurses, physical therapists, social workers, teachers, school administrators, first responders and most importantly families, are the ones that are going to have to deal with any potential adverse effects.
Number six, the vaccine should be free of avian, bovine, porcine, monkey and mouse viruses. So essentially many vaccines are produced in animal serums and can be contaminated with retrovirus. One such virus is known as simian virus 40 which has been shown to be associated with cancer. So in the new millennia, we have better methods for producing vaccines. And again, we need to keep safety foremost in our minds. It’s notable that SARS-CoV-2 or COVID-19 is an animal virus that allegedly originated in bats.
Number seven, vaccines should be free of human DNA and aborted human fetal tissue. So there’s a human fetal cell line dating back to the 1960s that’s been used in vaccines for many years. An Italian study identified the presence of a complete abnormal human genome of a male fetus in the MMRV vaccine, which is measles, mumps, rubella combined with chicken pox, a vaccine I have never used because of such concerns. And I invite you to go to the Children’s Health Defense website and check out the paper.
So it seems like we’re phasing out use of fetal tissue but I wanna remind you that one of the most basic roles of the immune system is to determine the difference between self and non-self. So vaccine developers and biologists are human. So by definition, they are not infallible. And we must remain very humble in my opinion, about the limitations of our knowledge. As Donald Rumsfeld said, there is what we know, what we don’t know and what we don’t know, we don’t know. Or if you prefer Mark Twain, he said, the trouble with the world is not that people know too little, it’s that they know so many things that just aren’t so. Another thing he said that I find inspiring is whenever you find yourself on the side of the majority, it’s time to pause and reflect.
So I want you to look more carefully at this new data that shows DNA from aborted fetal cell lines in vaccines, and notably there are some errors in this genomic DNA that potentially can have great consequences. And it’s important to understand that this is data that’s independent of the religious, philosophical or political views on aborted fetal tissue in vaccines that some officials might dismiss on the argument of the greater good for mankind. So the potential implications need to be taken very seriously.
Number eight, vaccine should be free of bio chips and nano-technology agents. So it’s important to know that bio-chips and nano-technology agents can be introduced into the body through vaccines. This would allow communication between a person’s biology physiology or psychology and outside technology. This is a new frontier but you need to know that it is being examined by tech companies as well as by the defense advanced research projects agency. I’m not saying this will be done with COVID vaccines as Yogi Berra said, it’s tough to make predictions especially about the future, but we need to have our eyes wide open so that those of us who have backgrounds in history and sociology and theology and the humanities and medicine can temper the momentum of big tech as these options are explored.
Here’s your slide for the FDA, looking at approval of injectable bio-chip implants for COVID. Even though we’ve all become addicted to our technology and I assure you that the big tech companies have very carefully studied our psyches in order to figure out how to addict us, it’s actually imperative that we make thoughtful choices about the interface between humanity and technology and make informed risk versus benefit decisions.
Dr. Morgan, in a 2020 JAMA article points out that to use the term risks emphasizes that the unfavorable outcome may not happen. There is no parallel language for benefits that acknowledges that the benefits might not happen also. So he argues that we should talk about harms versus potential benefits. Independent testing would be needed to determine the presence of these bio-chips or nano-technology agents in a vaccine. It’s highly unlikely that those agents would be listed under the ingredients.
So people at Children’s Health Defense who are much less naive than I am, are really concerned about this. So whether you’re a Republican, a Democrat, an independent or whether you live outside the United States, I urge you to listen to Bobby Kennedy Junior’s perspective on history and the role of authoritarianism. This is available at the CHD website.
Number nine, the liability protection provided to vaccine makers actually creates a perverse incentive to rush the vaccine and potentially downplay safety concerns. So at Children’s Health Defense, we argue that vaccine makers need to bear responsibility and financial liability for ensuring that their products are safe. Again, many people are not aware that vaccine injuries and deaths do occur. And again, that the consumers of vaccines paid over $4.4 billion to compensate the vaccine injured.
So as you think about the billions of dollars being invested in these vaccines, think about what Bobby Kennedy Jr. calls the perfect business model, where you get government funding for research and then you avoid liability for any defects. Due to the public readiness and preparedness act, the PREP Act of 2005, even if someone develops a serious reaction to the COVID vaccine, or even dies as a direct result, there is no liability for the people that manufactured that vaccine. They have been granted immunity from the federal government when COVID was declared an emergency. How many of you knew that?
Again, think about potentially good intentions, potentially unanticipated consequences of actions. Right now public health authorities are trying to assure us that COVID vaccines will be safe and effective. So it’s very important that our leaders maintain credibility and really take vaccine safety very, very seriously.
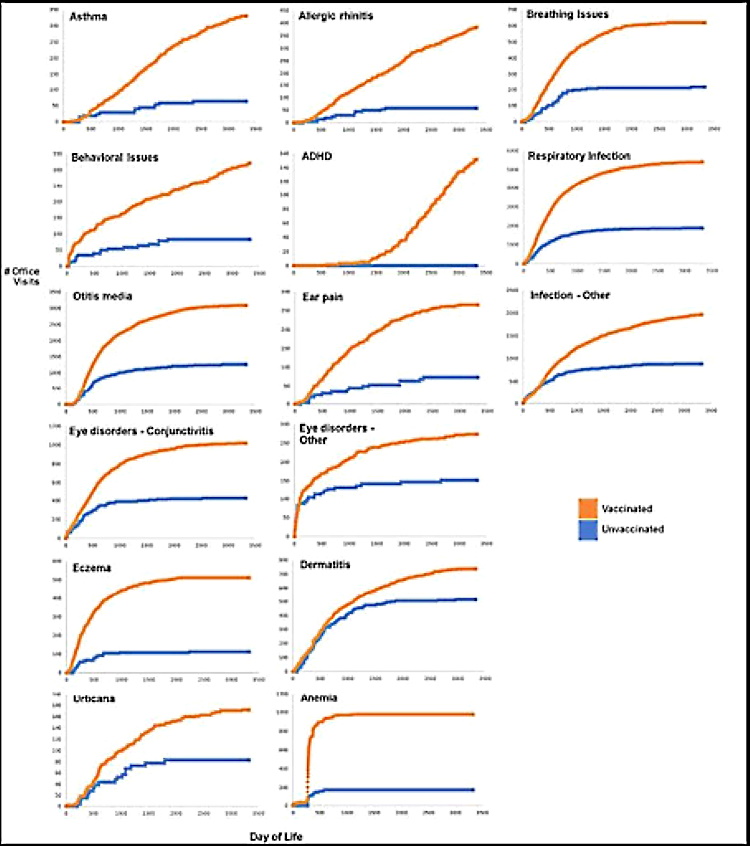
According to a 2011 peer-reviewed study in academic pediatrics, 54% of American children now have at least one of 20 different chronic health conditions. A chronic health condition is one that you don’t get over but it tracks you for many years typically that’s different from an acute illness, like a strep throat or an earache where typically with treatment, you get better. So there’s a strong possibility that the role of the vaccine schedule developed by the CDC is very important in the genesis of all this chronic illness.
Now for our detractors, and there will be many, yes, we know that correlation is not causality, but we have tried to analyze the emerging scientific evidence about the mechanisms of vaccine injury. And I’m particularly worried about the fact that any vaccine stresses the mitochondria which are the powerhouses of ourselves that essentially run our cellular biochemistry. So the public should know that the current vaccine schedule has never really been tested in its entirety. As new vaccines were developed and added to the schedule there was an assumption that it would be safe to give them in combination.
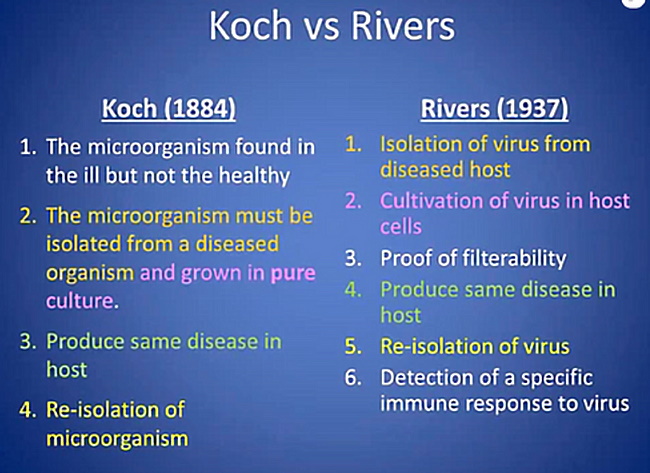
My father was a history professor. So I was taught from an early age that we should try to gain insights from previous history when we’re making complicated decisions. For example, here’s some people who were mocked for their ideas, which later turned out to be quite true. Dr. Semmelweis was kicked out of his hospital, put in an insane asylum and actually died in mysterious circumstances two weeks later because he had the audacity to suggest that doctors should wash their hands between the time they did an autopsy and then went to deliver a baby. Obviously germ theory later was shown to be very true.
Another example, Dr. Barry Marshall, who was the one who proved that Helicobacter pylori was associated with ulcers, reports that he was widely mocked by his colleagues at the University of Virginia which coincidentally is where I did my chief residency in pediatrics. And that drove him to actually swallow the organism and then proved by biopsy that he’d gotten an ulcer. Of course later when he won a Nobel prize, UVA had that information all over their website. So sometimes people in the minority are worth listening to.
So let’s look at some of the COVID vaccine candidates and we’re going to have this information available to you on the Children’s Health Defense website so that you can examine it more carefully. At this stage there’s actually very little transparency regarding the vaccines being tested and their ingredients. And it’s possible that we won’t really know until we get the package inserts out about everything that’s in the vaccines.
Candidate number one from Moderna is currently in phase three trials where it’s being more widely used so that we can assess safety and efficacy. It is based on mRNA technology and it contains the adjuvant polyethylene glycol. It’s important to know that about 21% of the participants in the first round of these vaccine trials had very significant adverse events. And that’s why we do vaccine trials. And it’s important to identify those but it reminds us of the potential power of the vaccines that are being developed.
Candidate two, also uses mRNA technology and contains PEG. And these companies are working on about four different vaccine trials concurrently and some have had to be paused for unsatisfactory intolerability problems.
Candidate three, these trials were suspended temporarily due to severe adverse events. One was a case of transverse myelitis. And one was a case of multiple sclerosis that was deemed to be coincidental, that was dismissed as coincidental.
Now let me clarify that it’s not at all unusual for a trial to be paused while what seemed to be adverse events are investigated. In an ideal world, those doing the investigations would be unbiased and make excellent decisions, deciding between correlation and causality. However, it’s really important to remember that there are human lives at stake here and there’s a different perspective from a clinician like me, who actually takes care of children who have vaccine injuries versus the perspective of those developing the vaccines.
So I wanna tell you a little bit about transverse myelitis. This is an inflammatory disease that affects the spinal cord, and it’s actually a pretty common vaccine side effect that’s reported in the package inserts of about 10 different vaccines. Three different hepatitis B vaccines and Merck’s HPV vaccine both lists transverse myelitis as a possible side effect.
I was very concerned about the case of transverse myelitis when I heard it on the news because Children’s Health Defense has a case involving a young teenage boy who was healthy and very athletic before he was given the Gardasil vaccine. Within two weeks he developed symptoms and ultimately became wheelchair bound and ventilator dependent. Eventually he disconnected himself from the ventilator when he was at home alone as a result of vaccine side effects. So Children’s Health Defense has a very gripping video that talks about Colton’s case and shows before and after pictures of how his life changed so dramatically. I would encourage you to look at that.
So in the last two decades, the vaccine injury compensation program has actually awarded compensation for many transverse myelitis cases. Johnson and Johnson has candidate 4, in which adenovirus will be spliced to a coronavirus.
Candidate 5 is currently in phase one trials, may have moved on to phase two soon which is the use of a genetically-engineered virus. And it also has an adjuvant in it that contains nano-aluminum, very tiny particles of aluminum.
So there are another eight manufacturers who have vaccines in the pipeline. Four of those are using this mRNA technology. So the other thing that concerned me about COVID vaccine development is that the typical animal trials that we used to look for adverse events were skipped over because of the urgency. This is where we would typically find problems like inflammation or what’s called pathogenic priming. Pathogenic priming by a vaccine is also known as immune enhancement or an antibody dependent phenomenon that causes enhancement of the inflammatory process.
So the PREP Act went into effect this spring when COVID was deemed an emergency. And so that prohibits us from suing vaccine makers. But I do worry that we will see a phenomenon in humans that may be like this pathogenic priming that was identified in animals during the other SARS virus vaccine trials.
Now, Children’s Health Defense opposes mandates for vaccines. The Nuremberg Code of 1947 is very explicit that even if an action is for the greater good of society, individuals still have the right for voluntary consent which they deemed absolutely essential. It is clear that we can’t be guaranteed that the COVID vaccine will be safe, but it will be protected from liability under the PREP Act. Children’s Health Defense would argue that in order for individuals to be asked to give up sovereignty over their bodies, the evidence must be crystal clear, that the greater good would be served. Even then the Nuremberg Code requires voluntary consent.
I think this is one of the important civil rights issues of our times. The immune system is complex and redundant. We need to be very humble about our abilities to manipulate immune mechanisms. We need to acknowledge the possibility of unforeseen consequences. So for those of you who are not physicians or immunologists basically there are two arms to the immune system. There’s the innate immune system that is like our first line of defense.
It’s a generalized response and very sensitive to things like the foods we eat and the vitamins that we take. Adaptive immunity is the traditional target of vaccines. It essentially creates very specific immunity and it remembers the infection. It can remember the infection if you get it. Like I got measles in the 1950s and have immunity now or it can remember it from a vaccine that induces this memory. But it’s specific, so we need to think as we’re dealing with COVID not just that the vaccine that targets this one arm of the immune system is going to be the answer, we need to honor mother nature. And this very exquisite system that we have that really defies our complete understanding.
So how do we develop immune resiliency? There are things that aren’t expensive that we can do. For example, we would recommend that you maintain an optimal vitamin D level, not just one that barely sufficient to keep you from getting rickets, but one that actually helps your immune system and your brain. Vitamin D acts to increase something called interleukin 10 which acts to regulate inflammation. It dampens down inflammation much like an aspirin, acetaminophen or ibuprofen would. But it also has an important role in consolidating memories in the hippocampus. So that what you learned today after you sleep tonight, you’ll be able to remember tomorrow. This might have some value for the COVID long haulers who are dealing with horrible brain fog.
Another thing we would advocate is generous amounts of vitamin C. Vitamin C is an excellent antiviral. It’s also an excellent antioxidant. Humans don’t make their own vitamin C. So we need to get it in our foods or in supplements. When animals face an infection, they are able to make their vitamin C and they immediately ratchet up their production of vitamin C by a factor of about 10 or more. So we need to consider using vitamin C both to help us be ready for an infection and prevent COVID severe side effects. And also to think about high doses of vitamin C to rescue people that do get COVID.
Zinc is very important for the sense of smell. And you may remember that one of the very unique characteristics of COVID infection is that people lose their sense of smell and therefore their sense of taste. So we would recommend that the population take zinc supplements or food sources of zinc, so that they are not deficient as they encounter COVID in their communities. There are other integrative and functional strategies for your lifestyle supplements, including selenium, Omega 3 essential fatty acids, bioflavonoids all these things are anti-inflammatory.
Very importantly, you want to avoid pro-inflammatory foods. Sugar and processed foods are pro-inflammatory meaning that they drive inflammation. Very healthy diets like Mediterranean diets that emphasize lots of fruits and vegetables are anti-inflammatory. And fruits and vegetables and high quality proteins, and good fats are what essentially tell ourselves what to do. So let’s try to optimize those interventions.
And then very critically, the field of psycho neuroimmunology has very clearly demonstrated for decades the vital connections between our immune system and the way that we’re feeling, the supportive relationships that we either have or lack whether or not we get to spend time in nature and whether or not we have good coping mechanisms for stress. If you are inside and stressed out and fearful and alone, your immune system by definition is not going to be functioning well. So if you wanna find out more, you can look at one of the many research compilations of non-prescription, non-vaccine options to consider to keep yourself safe.
I worry incessantly about elderly people, our grandmothers and grandfathers who are locked down often in their rooms without visitors, without sunshine or nature. I really wonder how many deaths could we have prevented by making sure that all these people in nursing homes and assisted living had adequate sources of vitamin C and vitamin D. And how many doses of vitamin C, at a cost of 10 or 20 cents a dose could we have given them for 10 to $18 billion? Which is what we spent on vaccine development so far. And very poignantly, how many of those people died a death of despair alone without their families?
So we have a proposal for safer vaccines. What we can do in six steps. Our premise is that the public demands a safe COVID vaccine but importantly, they also deserve one. Many of us want a safer vaccination program for all vaccines and for all people. This is common to us, whether you identify as pro-vaccine or have concerns about safety of vaccines, which by the way does not make one an anti-vaxxer. We need to know that we’re developing the health of our children as best we can. So we could work together and make us safer vaccine program. Children’s Health Defense has been looking at this for years, and we have a lot of resources.
So the six steps that we advocate; vaccines should be subjective to scientifically rigorous approval processes. We need to remove conflicts of interest so that those involved in the vaccine approval process are not going to directly or indirectly benefit from approving a vaccine. We need acknowledgement from both medical and public health authorities that vaccine injury exists and that they will take this seriously and take steps to investigate the causes of vaccine injuries.
We need systems that can actually measure the safety of vaccines and their adverse events after the vaccine is deployed. So the existing systems that we have, VAERS which is the vaccine adverse event reporting system and VSD, which is the vaccine safety data link, these need to be automated and updated. Government needs to support fully-informed consent. And this does involve potentially the individual right to refuse vaccination, obviously, a topic for much debate. We at Children’s Health Defense welcome civil debate among people who disagree. Number six, government-granted immunity for vaccine makers needs to be rescinded. We need to restore some liability for people who are profiting from vaccines. At Children’s Health Defense, we are working with like-minded organizations around the globe to push for these safety changes and for vaccine safety reform.
So please remember there are outstanding safety concerns that need to be addressed. There are tens of millions of people who may have concerns that you have, and ultimately you have the right to decide about getting this vaccine. So we’re asking that you join our vaccine safety movement, visit Children’s Health Defense. You’ll see the website listed. We will provide this PowerPoint and the links to the research that we have referenced.
And I know I’ve given you a lot to think about today. We ask that you keep an open mind and remember some of the themes we talked about today. Number one, learning from our prior history of previous vaccines. Number two, recognizing that your ability to process information and think clearly is impaired when you’re living in fear. Number three, the law of unintended consequences, number four, the principles in the Nuremberg Code. And number five, remember that we as humans by definition are fallible and that we need to be very humble when we try to manipulate genetics and manipulate cellular machinery that comes from a complex system from nature that we do not fully understand. Thank you very much.
©January 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.