
Montagnier’s Monster
![]()
In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
###
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals.
Montagnier’s Monster
by Mike Stone, ViroLIEgy
February 13, 2022
“HIV is neither necessary nor sufficient to cause AIDS.”
~ Luc Montagnier, VI Int’l AIDS Conference, Jun 24 1990
If you have been following the news recently, you may have heard that there is currently a new “highly virulent strain” of HIV running around the Netherlands (I think there is a pun in there somewhere). You may also have heard that there is a brand new experimental HIV mRNA vaccine that has shown promise in animals. If you have really been paying attention, you may have even heard of French virologist Luc Montagnier, the man credited with the discovery of HIV, and his various critical statements against the dangerous use of mRNA vaccines for “Covid-19.” If so, you are also most likely aware that during this increased attention geared towards HIV and mRNA vaccines, Luc Montagnier died very recently on February 8th, 2022. While he lived to be the ripe old age of 89, many are suspicious of the timing of his death in light of the current HIV resurgence.
While I do find the timing of all of these events interesting, that is not what this article is about. I have always planned to dive into Montagnier’s original HIV paper but I have held off as the HIV/AIDS scam has been exposed brilliantly by many others before me. However, I have always felt that the HIV fraud is the perfect gateway into understanding the “Covid-19” fraud as the numerous parallels to what is going on today are uncanny. We can see the same misuse of PCR and antibody testing, the same rebranding and reuse of toxic pharmaceuticals, the same collection of various symptoms under one giant umbrella disease, the same propaganda spreading fear of the infected, and the same Anthony Fauci spearheading the whole thing. Even though it is not my intention to touch on all of these aspects in one article, the best place to start unravelling this tangled web of deceit begins with the man who was credited with unleashing the HIV monster upon the world, Luc Montagnier.
In 1983, Montagnier was sent a lymph node sample from a 33-year-old (note the age) male determined to have the symptoms of AIDS. From this sample, Montagnier and his team uncovered what they claimed was a new “retrovirus,” originally known as L.A.V., for lymphadenopathy associated “virus.” After several indirect experiments, the team concluded that further studies were needed in order to determine whether or not the new “virus” had any role in the etiology of AIDS. After this initial discovery of the potential “viral” cause of AIDS, there was a bit of drama in 1984 when American virologist Robert Gallo claimed to have uncovered the cause of AIDS himself with the discovery of HTLV-3. Long story short, it was later determined that Gallo had used/borrowed/stolen a sample from the same patient as Montagnier and uncovered the same “virus.” The “virus” was eventually renamed HIV in 1986 and in 2008, Luc Montagnier was awarded the Nobel Prize for the discovery while Robert Gallo pouted off in a dark corner somewhere.
One of the nicest aspects of writing about Montagnier’s original HIV paper now in 2022 is that in retrospect, Montagnier himself tore apart his own evidence for the existence of his “retrovirus” in the decades following the publishing of his 1983 paper. A perfect example of this is found in a 1997 interview Montagnier did with scientific journalist Djamel Tahi. I have provided highlights from this interview below yet I definitely recommend reading the whole discussion sometime. While reading, note the assumptions made by Montagnier about his “virus,” the various contradictions in his statements, and the revelations about the relation (or lack thereof) of HIV to AIDS. This interview provides an in-depth look into the illogical mindframe of a virologist stuck in unproven theories and pseudoscientific dogma:
Interview with Professor Luc Montagnier by Djamel TAHI – (Pasteur Institut, July 1997)
Djamel TAHI: A group of scientists from Australia argues that nobody up till now has isolated the AIDS virus, HIV. For them the rules of retrovirus isolation have not been carefully respected for HIV. These rules are: culture, purification of the material by ultracentrifugation, Electron Microscopic (EM) photographs of the material which bands at the retrovirus density, characterisation of these particles, proof of the infectivity of the particles.
Luc Montagnier: No, that is not isolation. We did isolation because we “passed on” the virus, we made a culture of the virus. For example Gallo said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.” But before making it emerge in immortal cell lines, we made it emerge in cultures of normal Iymphocytes from a blood donor. That is the principle criterion. One had something one could pass on serially, that one could maintain. And characterised as a retrovirus not only by its visual properties, but also biochemistry, RT [reverse transcriptase] activity which is truly specific of retroviruses. We also had the reactions of antibodies against some proteins, probably the internal proteins. I say probably by analogy with knowledge of other retroviruses. One could not have isolated this retrovirus without knowledge of other retroviruses, that’s obvious. But I believe we have answered the criteria of isolation. Totally.
Djamel TAHI: according to several published references cited by the Australian group, RT is not specific to retroviruses and moreover your work to detect RT was not done in the purified material?
Luc Montagnier: I believe we published in Science (May 1983) a gradient which showed that the RT had exactly the density of 1.16. So one had a ‘peak’ which was RT. So one has fulfilled this criterion for purification. But to pass it on serially is difficult because when you put the material in purification, into a gradient, retroviruses are very fragile, so they break each other and greatly lose their infectivity. But I think even so we were able to keep a little of their infectivity. But it was not as easy as one does it today, because the quantities of virus were nonetheless very feeble. At the beginning we stumbled on a virus which did not kill cells. The virus came from an asymptomatic patient and so was classified amongst the non-syncithia-forming, non-cytopathogenic viruses using the co-receptor ccr5 . It was the first BRU virus. One had very little of it, and one could not pass it on in an immortal cell line. We tried for some months, we didn’t succeed. We succeeded very easily with the second strain. But there lies the quite mysterious problem of the contamination of that second strain by the first. That was LAI.
Djamel TAHI: Why do the EM photographs published by you, come from the culture and not from the purification?
Luc Montagnier: There was so little production of virus it was impossible to see what might be in a concentrate of virus in the gradient. There was not enough virus to do that. Of course one looked for it, one looked for it in the tissues at the start, likewise in the biopsies. We saw some particles but they did not have the morphology typical of retroviruses. They were very different. Relatively different. So with the culture it took many hours to find the first pictures. It was a Roman effort! It’s easy to criticise after the event. What we did not have, and I have always recognised it, was that it was truly the cause of aids.
Djamel TAHI: How is it possible without EM pictures from the purification, to know whether or not these particles are viral and appertain to a retrovirus, moreover a specific retrovirus?
Luc Montagnier: Well, there were the pictures of the budding. We published images of budding which are characteristic of retroviruses. Having said that, on the morphology alone one could not say it was truly a retrovirus. For example, a French specialist of EMs of retroviruses publicly attacked me saying: “This is not a retrovirus, it is an arenavirus”. Because there are other families of virus which bud and have spikes on the surface, etc.
Djamel TAHI: Why this confusion? The EM pictures did not show clearly a retrovirus?
Luc Montagnier: At this period the best known retroviruses were those of type C, which were very typical. This retrovirus wasn’t a type C and lentiviruses were little known. I myself recognised it by looking at pictures of Equine infectious anaemia virus at the library, and later of the visna virus. But I repeat, it was not only the morphology and the budding, there was RT…it was the assemblage of these properties which made me say it was a retrovirus.
Djamel TAHI: About the RT, it is detected in the culture. Then there is purification where one finds retroviral particles. But at this density there are a lot of others elements, among others those which one calls “virus-like”.
Luc Montagnier: Exactly, exactly. If you like, it is not one property but the assemblage of the properties which made us say it was a retrovirus of the family of lentiviruses. Taken in isolation, each of the properties isn’t truly specific. It is the assemblage of them. So we had: the density, RT, pictures of budding and the analogy with the visna virus. Those are the four characteristics.
Djamel TAHI: But how do all these elements allow proof that it is a new retrovirus? Some of these elements could appertain to other things, “virus-like”…?
Luc Montagnier: Yes, and what’s more we have endogenous retroviruses which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles, in any case not in aids.
Djamel TAHI: But then how can one make out the difference?
Luc Montagnier: Because we could “pass on” the virus. We passed on the RT activity in new Iymphocytes. We got a “peak” of replication. We kept track of the virus. It is the assembly of properties which made us say it was a retrovirus. And why new? The first question put to us by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse retrovirus or an animal retrovirus?”. To that one could say no! Because we had shown that the patient had antibodies against a protein of his own virus. The assemblage has a perfect logic! But it is important to take it as an assemblage. If you take each property separately, they are not specific. It is the assemblage which gives the specificity.
Djamel TAHI: With what did you culture the lymphocytes of your patient? With the H9 cell line?
Luc Montagnier: No, because it didn’t work at all with the H9. We used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes.
Djamel TAHI: When one looks at the published electron microscope photographs, for you as a retrovirologist it is clear it’s a retrovirus, a new retrovirus?
Luc Montagnier: No, at that point one cannot say. With the first budding pictures it could be a type C virus. One cannot distinguish.
Djamel TAHI: Could it be anything else than a retrovirus?
Luc Montagnier: No…well, after all, yes…it could be another budding virus. But we have an atlas. One knows a little bit from familiarity, what is a retrovirus and what is not. With the morphology one can distinguish but it takes a certain familiarity.
Djamel TAHI: Why no purification?
Luc Montagnier: I repeat we did not purify. We purified to characterise the density of the RT, which was soundly that of a retrovirus. But we didn’t take the “peak”…or it didn’t work…because if you purify, you damage. So for infectious particles it is better to not touch them too much. So you take simply the supernatant from the culture of lymphocytes which have produced the virus and you put it in a small quantity on some new cultures of lymphocytes. And it follows, you pass on the retrovirus serially and you always get the same characteristics and you increase the production each time you pass it on.
Djamel TAHI: But there comes a point when one must do the characterisation of the virus. This means: what are the proteins of which it’s composed?
Luc Montagnier: That’s it. So then, analysis of the proteins of the virus demands mass production and purification. It is necessary to do that. And there I should say that that partially failed. J.C. Chermann was in charge of that, at least for the internal proteins. And he had difficulties producing the virus and it didn’t work. But this was one possible way, the other way was to have the nucleic acid, cloning, etc. It’s this way which worked very quickly. The other way didn’t work because we had at that time a system of production which wasn’t robust enough. One had not enough particles produced to purify and characterise the viral proteins. It couldn’t be done. One couldn’t produce a lot of virus at that time because this virus didn’t emerge in the immortal cell line. We could do it with the LAI virus, but at that time we did not know that.
Djamel TAHI: Gallo did it?
Luc Montagnier: Gallo?…I don’t know if he really purified. I don’t believe so. I believe he launched very quickly into the molecular part, that’s to say cloning. What he did do is the Western Blot. We used the RIPA technique, so what they did that was new was they showed some proteins which one had not seen well with the other technique. Here is another aspect of characterising the virus. You cannot purify it but if you know somebody who has antibodies against the proteins of the virus, you can purify the antibody/antigen complex. That’s what one did. And thus one had a visible band, radioactively labelled, which one called protein 25, p25. And Gallo saw others. There was the p25 which he calledp24, there was p41 which we saw…
Djamel TAHI: About the antibodies, numerous studies have shown that these antibodies react with other proteins or elements which are not part of HIV. And that they can not be sufficient to characterise the proteins of HIV.
Luc Montagnier: No! Because we had controls. We had people who didn’t have AIDS and had no antibodies against these proteins. And the techniques we used were techniques I had refined myself some years previously, to detect the src gene. You see the src gene was detected by immunoprecipitation too. It was the p60 [protein 60]. I was very dexterous, and my technician also, with the RIPA technique. If one gets a specific reaction, it’s specific.
Djamel TAHI: But we know AIDS patients are infected with a multitude of other infectious agents which are susceptible to induce crossreactions.
Luc Montagnier: Yes, but antibodies are very specific. They know how to distinguish one molecule in one million. There is a very great affinity. When antibodies have sufficient affinity, you fish out something really very specific. With monoclonal antibodies you fish out really ONE protein. All of that is used for diagnostic antigen detection.
Djamel TAHI: For you the p41 was not of viral origin and so didn’t belong to HIV. For Gallo it was the most specific protein of the HIV. Why this contradiction?
Luc Montagnier: We were both reasonably right. That’s to say that I in my RIPA technique…in effect there are cellular proteins that one meets everywhere – there’s a non-specific “background noise”, and amongst these proteins one is very abundant in cells, which is actin. And this protein has a molecular weight 43000kd. So, it was there. So I was reasonably right, but what Gallo saw on the other hand was the gp41 of HIV, because he was using the Western Blot. And that I have recognised.
Djamel TAHI: For you p24 was the most specific protein of HIV, for Gallo not at all. One recognises thanks to other studies that antibodies directed against p24 were often found in patients who were not infected with HIV, and even certain animals. In fact today, an antibody reaction with p24 is considered non specific.
Luc Montagnier: It is not sufficient for diagnosing HIV infection.
Djamel TAHI: No protein is sufficient.
Luc Montagnier: No protein is sufficient anyway. But at the time the problem didn’t reveal itself like that. The problem was to know whether it was an HTLV or not. The only human retrovirus known was HTLV. And we showed clearly that it was not an HTLV, that Gallo’s monoclonal antibodies against the p24 of HTLV did no recognise the p25 of HIV.
Djamel TAHI: At the density of retroviruses, 1.16, there are a lot of particles, but only 20% of them appertain to HIV. Why are 80% of the proteins not viral and the others are? How can one make out the difference?
Luc Montagnier: There are two explanations. For the one part, at this density you have what one calls microvesicles of cellular origin, which have approximately the same size as the virus, and then the virus itself, in budding, brings cellular proteins. So effectively these proteins are not viral, they are cellular in origin. So, how to make out the difference?! Frankly with this technique one can’t do it precisely. What we can do is to purify the virus to the maximum with successive gradients, and you always stumble on the same proteins.
Djamel TAHI: The others disappear?
Luc Montagnier: Let’s say the others reduce a little bit. You take off the microvesicles, but each time you lose a lot of virus, so it’s necessary to have a lot of virus to start off in order to keep a little bit when you arrive at the end. And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of viral origin or not. That’s what we began for p25, that failed…and the other technique is to do the cloning, and so then you have the DNA and from the DNA you get the proteins. You deduce the sequence of the proteins and their size and, you stumble again on what you’ve already observed with immunoprecipitation or with gel electrophoresis. And one knows by analogy with the sizes of the proteins of other retroviruses, one can deduce quite closely these proteins. So you have the p25 which was close to the p24 of HTLV, you have the p18.. in the end you have the others. On the other hand the one which was very different was the very large protein, p120.
Luc Montagnier’s 1997 interview is a highlight reel of revelations. We can see clearly, as Montagnier repeated on more than one occasion, that he himself (and Robert Gallo according to his knowledge) did not purify any “virus.” Why is this important? In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
As most virologists do, Montagnier claimed that even though he did not purify the “virus” and therefore did not have direct evidence for its existence, he had plenty of non-specific indirect evidence that when added together, became “specific” to the “virus.” It was the accumulation of indirect evidence that proved his “virus” existed. In essence, he had a circumstantial case based upon evidence that was not drawn from direct observation. This would be considered a weak case in a court of law.
Looking at his circumstantial case, Montagnier admitted that without purification, images of particles taken from electron microscopy could not be definitively claimed to be “retroviruses” or “viruses” of any kind based on morphological appearance alone. He stated that it was necessary to have knowledge of other “retroviruses” first in order to discover a new one. He himself referred to an atlas of images of other “retroviruses” in order to claim that his unpurified particles were also “retroviruses.”
However, what Montagnier did not admit is that this atlas of “retroviruses” was also made up of images of unpurified particles. Therefore, none of the particles imaged in his atlas could be considered “retrovirus” particles until evidence of purified/isolated “retroviruses” are released. Purification would have had to have occurred with the very first “retrovirus” ever discovered and imaged in order for this method of identification to be valid. Montagnier admitted that while purification is a necessary step, it is impossible as the more you purify the sample, the more damage occurs to the particles and the less “virus” you have at the end. Since he stated that they did not purify the culture used to obtain the EM images of “HIV,” there is no proof that the random particles claimed to be HIV are in fact a “virus” at all.
Montagnier also tried to claim that antibodies/antigens, such as the p24 protein, are specific to HIV and that they can be used as part of the evidence for the existence of his “virus.” However, as Djamel expertly pointed out, these proteins are not specific to HIV as there are over 60 conditions (such as pregnancy, tuberculosis, the flu vaccine, etc.) with related proteins that can trigger positive HIV tests. Montagnier ended up admitting that no protein is sufficient for diagnosing HIV thus nullifying any claims he made about the specificity of antibodies/antigens and their value in being used as indirect evidence for the existence of an unseen “virus.”
The biggest revelation by Montagnier in this 1997 interview is his belief that HIV is not the cause of AIDS. While he believed he had discovered a new “retrovirus” based on an accumulation of weak indirect evidence, according to his statement it was not pathogenic. If we take his indirect evidence and break it down, Motagnier did not have purified “virus” particles which means his EM images are useless, his antibody tests are meaningless, and the genomic sequence is worthless. Without purified particles, he had no proof of pathogeniticity as he had no valid independent variable in order to establish cause and effect. It is amazing that Montagnier believed he had a “virus” at all as in every meaningful way possible, he did not have evidence of one.
All of that being said, for those still interested in reading Montagnier’s original 1983 paper containing no evidence of any “virus” whatsoever, here is the paper in its entirety:
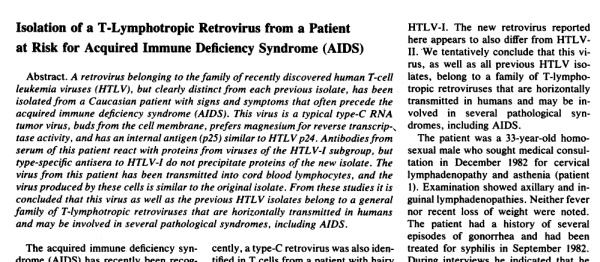
Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS)
Abstract. A retrovirus belonging to the family of recently discovered human T-cell leukemia viruses (HTLV), but clearly distinct from each previous isolate, has been isolated from a Caucasian patient with signs and symptoms that often precede the acquired immune deficiency syndrome (AIDS). This virus is a typical type-C RNA tumor virus, buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24. Antibodies from serum of this patient react with proteins from viruses of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate. The virus from this patient has been transmitted into cord blood lymphocytes, and the virus produced by these cells is similar to the original isolate.
From these studies it is concluded that this virus as well as the previous HTLV isolates belong to a general family of T-lymphotropic retroviruses that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS.The acquired immune deficiency syndrome (AIDS) has recently been recognized in several countries (1). The disease has been reported mainly in homosexual males with multiple partners, and epidemiological studies suggest horizontal transmission by sexual routes (2) as well as by intravenous drug administration (3), and blood transfusion (4).
The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes (5) suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent. Alternatively, these modifications may result from subsequent infections. The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma (1). However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males (6) and infants (7) who may or may not develop AIDS (8).
The histological aspect of such lymph nodes is that of reactive hyperplasia. Such cases may correspond to an early or a milder form of the disease. We report here the isolation of a novel retrovirus from a lymph node of a homosexual patient with multiple lymphadenopathies. The virus appears to be a member of the human T-cell leukemia virus (HTLV) family (9).
The retrovirus was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans. Viral core proteins were not immunologically related to the p24 and p19 proteins of subgroup I of HTLV (9). However, serum of the patient reacted strongly with surface antigen (or antigens) present on HTLV-I-infected cells. Moreover, the ionic requirements of the viral reverse transcriptase were close to that of HTLV. Recently, a type-C retrovirus was also identified in T cells from a patient with hairy cell leukemia. Analysis of the proteins of this virus showed they were related to, but clearly different from, proteins of previous HTLV isolates (10).
Moreover, recent studies of the nucleic acid sequences of this new virus show it is less than 10 percent homologous to the earlier HTLV isolates (11). This virus was called HTLV-II to distinguish it from all the earlier, highly related viruses termed HTLV-I. The new retrovirus reported here appears to also differ from HTLV-II. We tentatively conclude that this virus, as well as all previous HTLV isolates, belong to a family of T-lymphotropic retroviruses that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS.
The patient was a 33-year-old homosexual male who sought medical consultation in December 1982 for cervical lymphadenopathy and asthenia (patient 1). Examination showed axillary and inguinal lymphadenopathies. Neither fever nor recent loss of weight were noted. The patient had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982. During interviews he indicated that he had had more than 50 sexual partners per year and had traveled to many countries, including North Africa, Greece, and India. His last trip to New York was in 1979.
Laboratory tests indicated positive serology (immunoglobulin G) for cytomegalovirus (CMV) and Epstein-Barr virus. Herpes simplex virus was detected in cells from his throat that were cultured on human and monkey cells. A biopsy of a cervical lymph node was performed. One sample served for histological examination, which revealed follicular hyperplasia without change of the general architecture of the lymph node. Immunohistological studies revealed, in paracortical areas, numerous T lymphocytes (OKT3+). Typing of the whole cellular suspension indicated that 62 percent of the cells were T lymphocytes (OKT3+), 44 percent were T-helper cells (OKT4+), and 16 percent were suppressor cells (OKT8+).
Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon (12). The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by viruses, including retroviruses. In the mouse system, we had previously shown that antiserum to interferon could increase retrovirus production by a factor of 10 to 50 (13). After 3 days, the culture was continued in the same medium without PHA. Samples were regularly taken for assay of reverse transcriptase and for examination in the electron microscope.
After 15 days of culture, a reverse transcriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I (14). Virus production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation. Peripheral blood lymphocytes cultured in the same way were consistently negative for reverse transcriptase activity, even after 6 weeks. Cytomegalovirus could be detected, upon prolonged co-cultivation with MRC5 cells, in the original biopsy tissue, but not in the cultured T lymphocytes at any time of the culture.
Virus transmission was attempted with the use of a culture of T lymphocytes established from an adult healthy donor of the Blood Transfusion Center at the Pasteur Institute. On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions. Reverse transcriptase activity could be detected in the supernatant on day 15 of the coculture but was not detectable on days 5 and 10. The reverse transcriptase had the same characteristics as that released by the patient’s cells and the amount released remained stable for 15 to 20 days. Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks when the culture was discontinued.
The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml). After a lag period of 7 days, a relatively high titer of reverse transcriptase activity was detected in both of the cord lymphocyte cultures. Identical cultures, which had not been infected, remained negative. These two successive infections clearly show that the virus could be propagated on normal lymphocytes from either newborns or adults.
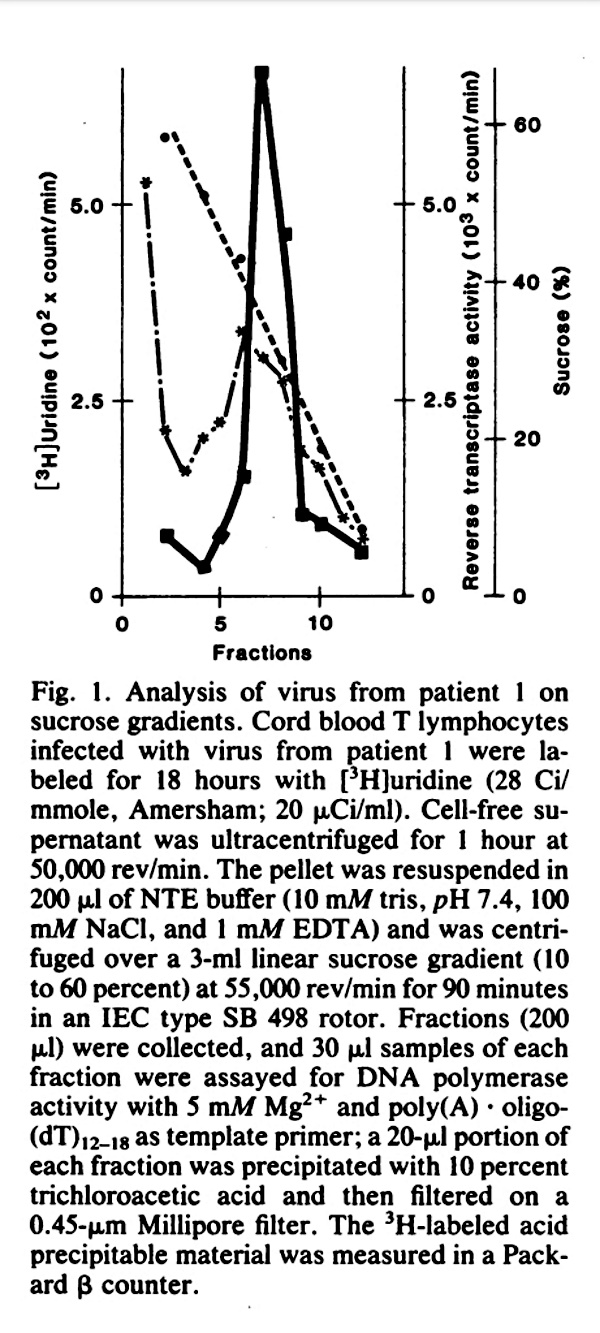
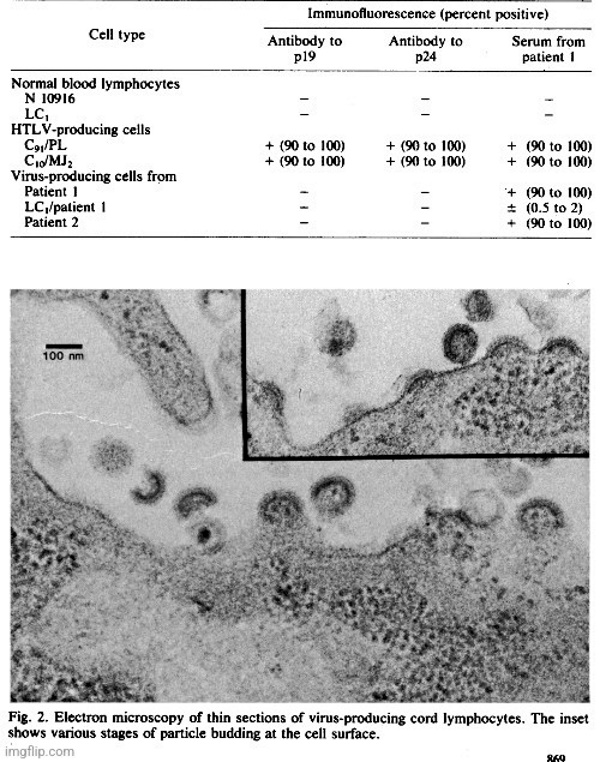
That this new isolate was a retrovirus was further indicated by its density in a sucrose gradient, which was 1.16, and by its labeling with [3H]uridine (Fig. 1). Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane (Fig. 2).
Virus-infected cells from the original biopsy as well as infected lymphocytes from the first and second viral passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme. The results were the same in all instances. The reverse transcriptase activity displayed a strong affinity for poly(adenylate-oligodeoxythymidylate) [poly(A) -oligo(dT)], and required Mg2+ with an optimal concentration (5 mM) slightly lower than that for HT (14) and an optimal pH of 7.8. The reaction was not inhibited by actinomycin D. This character, as well as the preferential specificity for riboseadenylate *deoxythymidylate over deoxyadenylate * deoxythymidylate, distinguish the viral enzyme from DNA-dependent polymerases.
We then determined whether or not this isolate was indistinguishable from HTLV-1 isolates. Human T-cell leukemia virus has been isolated from cultured T lymphocytes of patients with T lymphomas and T leukemias [for a review, see (9)]. The antibodies used were specific for the p19 and p24 core proteins of HTLV-I. A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytes obtained from a healthy donor and infected with the same virus. As shown in Table 1, the virus-producing cells did not react with either type of antibody, whereas two lines of cord lymphocytes chronically infected with HTLV (17) and used as controls showed strong surface fluorescence.
When serum from patient 1 was tested against infected lymphocytes from the biopsy the surface fluorescence was as ntense as that of the control HTLV-producing lines. This suggests that serum of the patient contains antibodies
that recognize a common antigen present on HTLV-I-producing cells and on the patient’s lymphocytes. Similarly, cord lymphocytes infected with the virus from patient 1 did not react with antibodies to p19 or p24. Only a minor proportion of the cells (about I percent) reacted with the patient’s serum. This may indicate that only this fraction of the cells was infected and produced virus. Alternatively, the antigen recognized by the patient’s serum may contain cellular determinants that show less expression in T lymphocytes of newborns.
We also cultured T lymphocytes from a lymph node of another patient (patient 2) who presented with multiple adenopathies and had been in close contact with an AIDS case. These lymphocytes did not produce viral reverse transcriptase; however, they reacted in the immunofluorescence assay with serum from patient 1. Moreover, serum from patient 2 reacted strongly with control HTLV-producing lines (not shown). In order to determine which viral antigen was recognized by antibodies present in’ the two patients’ sera, several immunoprecipitation experiments were carried out. Cord lymphocytes infected with virus from patient I and uninfected controls were labeled with [35S]methionine for 20 hours. Cells were lysed with detergents, and a cytoplasmic S10 extract was made. Labeled virus released in the supernatant was banded in a sucrose gradient.
Both materials were immunoprecipitated by antiserum to HTLV- I p24, by serum from patients 1 and 2, and by serum samples from healthy donors. Immunocomplexes were analyzed by polyacrylamide gel electrophoresis under denaturing conditions. Figure 3 shows that a p25 protein present in the virus-infected cells from patient 1 and in LC1 cells infected with this virus, was specifically recognized by serum from patients I and 2 but not by antiserum to HTLV-1 p24 or serum of normal donors.
Conversely, the p24 present in control HTLV-infected cell extracts was recognized by antibodies to HTLV but not by serum from patient 1. A weak band (lane 2, Fig. 3B) could hardly be seen with serum from patient 2, suggesting some similarities of the p25 protein from this patient’s cells with HTLV-1 p24. When purified, labeled virus from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000. The 45K protein may be due to contamination of the virus by cellular actin which was present in immunoprecipitates of all the cell extracts (Fig. 3).

These results, together with the immunofluorescence data, indicate that the retrovirus from patient 1 contains a major p25 protein, similar in size to that of HTLV-I but different immunologically. The DNA sequences of these and other members of the HTLV family are being compared. All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful.
The role of this virus in the etiology of AIDS remains to be determined. Patient 1 had circulating antibodies against the virus, and some of the latter persisted in lymphocytes of his lymph node (or nodes). The virus-producing lymphocytes seemed to have no increased growth potential in vitro compared to the uninfected cells. Therefore, the multiple lymphadenopathies may represent a host reaction against the persistent viral infection rather than hyperproliferation of virus-infected lymphocytes. Other factors, such as repeated infection by the same virus or other bacterial and viral agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity.
doi: 10.1126/science.6189183.
In Summary:
- According to HIV discoverer Luc Montagnier, they did “isolate” HIV because they “passed on” the “virus” and they made a culture of the “virus”
- He stated that Robert Gallo (American virologist who plagiarized Montagnier’s work) said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.”
- But before making it emerge in immortal cell lines, Montagnier claimed his team made it emerge in cultures of normal Iymphocytes from a blood donor
- Montagnier stated that it is obvious one could not have isolated any retrovirus without knowledge of other “retroviruses”
- To pass a “virus” on serially is difficult because when you put the material in purification, into a gradient, “retroviruses” are very fragile, so they break each other and greatly lose their infectivity
- At the beginning they stumbled on a “virus” which did not kill cells
- It was the first BRU “virus,” yet they had very little of it and could not pass it on in an immortal cell line
- They were later successful with the second strain yet Montagnier stated that there lies the quite mysterious problem of the contamination of that second strain by the first which was LAI
Quick sidenote: BRU and LAI are considered the first strains of HIV
“The original isolate HIV-1 Bru, formerly called LAV, was derived from patient BRU. HIV-1 Lai was derived from patient LAI and contaminated a HIV-1 Bru culture between 20 July and 3 August 1983. The culture became, in effect, HIV-1 Lai, identifiable by a unique motif in the V3 loop. Because of this contamination two, rather than one, HIV-1 isolates were sent to the Laboratory of Tumor Cell Biology at the National Cancer Institute on 23 September 1983.”
https://pubmed.ncbi.nlm.nih.gov/2035026/
- When asked about the lack of purification for EM imaging of HIV, Montagnier stated that there was so little production of “virus” it was impossible to see what might be in a concentrate of “virus” in the gradient
- What they saw were some particles but they did not have the morphology typical of “retroviruses” as they were very different
- He claimed it was “a Roman effort” with the culture as it took many hours to find the first pictures
- On the morphology alone one could not say the EM images were truly a “retrovirus”
- A French specialist of EMs of “retroviruses” publicly attacked Montagnier saying: “This is not a retrovirus, it is an arenavirus” as there are other families of “virus” which bud and have spikes on the surface, etc.
- He stated that it was not only the morphology and the budding, but that there was reverse transcriptase
- It was not one property but the assemblage of the properties which made them say it was a “retrovirus” of the family of “lentiviruses”
- Taken in isolation, each of the properties isn’t truly specific
- The four properties were:
- The density
- Reverse Transcriptase
- Pictures of budding
- The analogy with the visna “virus”
- Montagnier stated that we have endogenous (human origin) “retroviruses” which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles
- The first question put to them by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse “retrovirus” or an animal “retrovirus?”
- Montagnier stated that it was important to take it as an assemblage as if you take each property separately, they are not specific and it is the assemblage which gives the specificity
- When culturing the “virus,” they used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes
- He admitted that when viewing EM images, one cannot distinguish if the particle is a “retrovirus” or not
- They used an atlas of previous “retroviruses” to determine if the “virus” had the morphology of one as it takes a certain familiarity to distinguish them
- Montagnier repeated they did not purify the “virus” because if you purify, you damage the “virus” particles
- He stated that for infectious particles, it is better to not touch them too much
- Analysis of the proteins of the “virus” demands mass production and purification and so it is necessary to do that
- In that regard, Montagnier claimed that they partially failed
- They did not have enough particles produced to purify and characterise the “viral” proteins as it couldn’t be done
- They couldn’t produce a lot of “virus” at that time because the “virus” didn’t emerge in the immortal cell line
- Montagnier stated that he believed Gallo also did not purify and he believed Gallo had launched very quickly into the molecular cloning part
- He also said that you cannot purify the “virus” but if you know somebody who has antibodies against the proteins of the “virus,” you can purify the antibody/antigen complex
- However, this is a complete contradiction as he claimed that purification needed to be done in order to characterise the proteins of the “virus,” so if you can’t purify the “virus” to characterise the proteins, you would be unable to know which proteins act against the “virus”as well as any specific antibodies reacting to them
- Montagnier claimed antibodies are very specific and that they know how to distinguish one molecule in one million
- With monoclonal antibodies you fish out really ONE protein and all of that is used for diagnostic antigen detection
- There are cellular proteins that one meets everywhere – there’s a non-specific “background noise”
- An antibody reaction with p24 is considered non specific and it is not sufficient for diagnosing HIV infection
- Montagnier agreed that no protein is sufficient to diagnose HIV
- When asked why, at the 1.16 density gradient band, 80% of the particles are “non-viral” and only 20% are HIV, Montagnier explained that at this density, there are microvesicles of cellular origin, which have approximately the same size as the “virus,” and then the “virus” itself, in budding, brings cellular proteins
- Effectively these proteins are not “viral” and are cellular in origin
- He stated that with this technique one can’t differentiate them precisely
- If you purify the “virus” to the maximum with successive gradients, you always stumble on the same proteins
- Montagnier stated that the other proteins only reduce a little bit as you can take off the microvesicles, but each time you lose a lot of “virus,” so it’s necessary to have a lot of “virus” to start off in order to keep a little bit when you arrive at the end
- And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of “viral” origin or not
- However, what Montagnier doesn’t seem to understand is that if you can not purify the “virus” in order to determine which proteins belong to the “virus,” sequencing proteins will not tell you if they are “viral” or not
- This “virus” is a typical type-C RNA tumor “virus,” buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24
- Antibodies from serum of this patient react with proteins from “viruses” of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate
- Remember, Montagnier admitted they did not purify the “virus” and that purification was necessary in order to characterise the proteins of the “virus, so how would they know if the antibodies are reacting to “virus” proteins?
- The “virus” from this patient has been transmitted into cord blood lymphocytes, and the “virus” produced by these cells is similar to the original isolate
- From these studies it is concluded that this “virus” as well as the previous HTLV isolates belong to a general family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
- The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent
- Alternatively, these modifications may result from subsequent infections
- The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma
- However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males and infants who may or may not develop AIDS
- The “retrovirus” was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans
- They tentatively (i.e. subject to further confirmation; not definitely) concluded that this “virus,” as well as all previous HTLV isolates, belong to a family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
- The patient the “virus” came from had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982
- Oddly enough, syphilis has the exact same symptoms of AIDS and the usual treatment is a series of Penicllin injections, which coincidentally (or not) can destroy a person’s “immune” system
- Laboratory tests indicated positive serology (immunoglobulin G) for “cytomegalovirus” (CMV) and Epstein-Barr “virus“
- Herpes simplex “virus” was detected in cells from his throat that were cultured on human and monkey cells
- Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon
- The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by “viruses,” including “retroviruses”
- After 15 days of culture, a reverse transcriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I and “virus” production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation
Quick sidenote: Montagnier stated here that the “virus” was cultured for 30 days, as it took 15 days for the reverse transcriptase activity to be detected and another 15 days for the “virus” production to decrease. Interestingly, in a paper he wrote in 2003, Montagnier stated this:
“The initial clinical isolate, unlike HTLV, had no transforming or cytopathic effects on T lymphocytes. Barré-Sinoussi notes in her commentary that the lymphocyte culture I started from the patient’s lymph node biopsy died after 4 weeks. But this was anticipated as soon as we realized that the cells were not transformed, because normal cultures of the same type also die within this time period. The need for succesive use of peripheral blood mononuclear cells to maintain a viral culture was therefore a likely hypothesis that proved to be correct. The virus would later be classified as non-syncytium-inducing, as is usually the case for viruses isolated from recently infected HIV patients who are either asymptomatic or present with lymphadenopathies. However, the first typical cytopathic effect, formation of large syncytia, was not observed until 5 months later, in a third clinical sample (HIV LAI) from a patient who had full-blown AIDS.”
https://www.nature.com/articles/nm1003-1235a
It appears they cultured the “virus” for 30 days knowing full well that regular cultures of the same type die within this 4 week time frame. Montagnier stated that they did not even notice the cytopathic effect (CPE) until they had a third clinical sample 5 months later. CPE is claimed to be structural changes in host cells that are caused by “viral” invasion and yet, this was absent in their first two samples.
- On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions
- Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks when the culture was discontinued
- The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml)
- FYI, Polybrene was shown to negatively impact the proliferation and maintenance of growth potential of human keratinocytes here
- Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane
- “Virus-infected” cells from the original biopsy as well as infected lymphocytes from the first and second “viral” passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme
- A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect (i.e. not directly caused by or resulting from something) fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytes obtained from a healthy donor and infected with the same “virus” (why did they not use healthy donor lymphocytes without the added “virus?”)
- Cord lymphocytes infected with the “virus” from patient 1 did not react with antibodies to p19 or p24
- Only a minor proportion of the cells (about I percent) reacted with the patient’s serum
- This may indicate that only this fraction of the cells was infected and produced “virus”
- When purified, labeled “virus” from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000
- The 45K protein may be due to contamination of the “virus” by cellular actin which was present in immunoprecipitates of all the cell extracts (i.e. “purified” with contaminants…otherwise known as not purified)
- All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful
- The role of this “virus” in the etiology of AIDS remains to be determined (ultimately, Montagnier believed his “virus” did not cause AIDS)
- Other factors, such as repeated infection by the same “virus” or other bacterial and “viral” agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals. The stigma of the positive test result is the “viral” scarlet letter unfairly placed upon a person in a toxic state due to lifestyle choices and/or environmental factors. It does not matter that Montagnier attempted to steer his monster from the lethal killer it was made out to be into a harmless passenger inside the human body. It does not matter that he believed HIV did not cause AIDS. It does not matter that he believed that co-factors other than a “virus” should be examined in regards to AIDS. It does not matter that he believed HIV could be eliminated based on healthy diet/lifestyle choices. It does not matter that he admitted to not purifying any “virus.” Montagnier’s legacy is tied to the beast of his own creation. He opened Pandora’s Box and released this fraudulent curse upon the world. For that, I doubt he will rest in peace.
cover image credit: Wikimedia Commons


Truth Comes to Light highlights writers and video creators who ask the difficult questions while sharing their unique insights and visions.
Everything posted on this site is done in the spirit of conversation. Please do your own research and trust yourself when reading and giving consideration to anything that appears here or anywhere else.









{kind=link}