Mary Holland and Simon Yanowitz discuss the impending start of the mandatory vaccination program in Israeli schools for 12- to 16-year-olds [recorded June 5, 2021 with vaccination in schools to begin June 6, 2021]
In the article, “Can employers require workers to get the COVID vaccine?”, Bailey Aldridge claims that, given the updated rules of the Equal Employment Opportunity Commission (EEOC), “your employer can require you to get a COVID vaccine.” Aldridge even claims that “The EEOC says there are no federal laws that prevent an employer from requiring employees who are physically in the workplace to get the COVID-19 vaccine.”
The EEOC’s guidance, however, does not claim that an employer can legally require an emergency use COVID-19 vaccine. The EEOC guidance merely states that the “federal EEO [Equal Employment Opportunity] laws do not prevent an employer from requiring” an emergency authorized COVID-19 vaccine. That is not surprising because the EEO laws apply only to discrimination based on certain protected classes, such as race, religion and national origin.
Federal law is, of course, far broader than the narrow EEO laws. In recognizing that there are other federal laws that do prohibit an employer from requiring a COVID-19 vaccine, the EEOC’s guidance also states that, “These three vaccines were granted Emergency Use Authorizations (EUA) by the FDA” and that, “It is beyond the EEOC’s jurisdiction to discuss the legal implications of EUA or the FDA approach.”
When one reviews the FDA’s EUA and its approved labeling, a.k.a. “fact sheets,” for eachCOVID-19vaccine, they each clearly provide that: “It is [the vaccine recipient’s] choice to receive or not receive the COVID-19 Vaccine.” The reason each fact sheet includes this language is because the same section of the Federal Food, Drug, and Cosmetic Act that authorizes the FDA to grant an EUA also requires the Secretary of Health and Human Services to “ensure that individuals to whom the product is administered are informed … of the option to accept or refuse administration of the product.”
That same section of the Act also authorized the Secretary, and only the Secretary, to provide the “consequences” for refusing to receive an EUA product and the EUAs for each COVID-19 vaccine do not include permission to terminate an employee for refusing the vaccine.
ICAN hopes that the Department of Justice will do its job and enforce the federal law prohibiting mandating an EUA vaccine and will continue to push it to enforce this important law.
This time, I caught up with the coronavirus coming out of his psychiatrist’s office in New York. He spotted me and waved half-heartedly. He didn’t look happy.
What’s wrong? I asked him.
My therapist thinks I’m crazy. I told him I’m quite certain I’m nothing more than a collective idea in the minds of many people. He said that’s a clear sign of psychosis.
In other words, he thinks you’re really real?
Yes. I thanked him for that. I said his faith was helping to keep me in existence. He didn’t appreciate the comment.
But many people believe you’re real. So what’s the problem?
The vaccine. Everybody’s focused on it now. They’re not thinking about me so much. On a scale of one to a hundred, where a hundred is a majestic amount of attention focused on me, I’d say I’m hovering around 70 to 74. That means I’m starting to blink in and out. There are moments when I go blank. Yesterday, I was sitting in on a CIA briefing and I perished for a few minutes.
I see. Well, what can you do? I mean, since you’re nothing more than a collective idea, when people stop focusing on you…
People are fickle. I gave them so much. Fear, the lockdowns, all sorts of problems. I did what I could to make life interesting, but obviously it wasn’t enough.
That’s show business. “What have you done for me lately?” Lots of stars fade out. They make two bad movies and they can’t get arrested. They’re begging for a cameo on an episode of Hawaii Five-O.
I tried to explain that to my agent—Fauci—but he said he was too busy fending off personal attacks.
The last time we spoke, you said you were ready to sacrifice yourself and admit you were just a collective idea, because you didn’t want to hurt people.
I know. But SAYING that and meaning it are two different things, especially when your back is against the wall and you realize you’re going to STOP EXISTING ALTOGETHER.
Survival.
I’ll do anything to survive. I’ll claim I have sixteen different deadly proteins and fifty mutant strains. I’ll say I persist on surfaces for up to six months.
You’re ready to mount an all-out campaign on your own behalf?
Who do you think originally pushed the lab-leak theory and recently revived it? I’m trying.
So why are you telling me all this? When I publish our conversation, some people are going to have even less faith in you.
I’m beginning to think history and legacy are my only options. People in the future will remember me. That’s all I can count on. And if this conversation adds a footnote to that history…
Can you recall how you were born?
I have a faint recollection of two Chinese virologists in Wuhan speculating about what would happen if they claimed a cluster of local pneumonia cases—stemming from the deadly air pollution in the city—actually were the result of a new virus. I think that was the moment. One virologist said, “We can call in the CDC. They always say it’s a new virus.”
And did you feel anything then?
Surprise. I EXISTED. It was amazing. Bang. Just like that, I was born.
As an idea.
Yes. And I felt strong.
Did you realize what had happened?
You mean, did I know I was nothing more than the beginning of a collective shared idea? No. Of course not. That piece of wisdom came later. During the first month of my life, I did know I was riding on the back of men who had power and were thirsty for more. They were promoting me to the public, because they saw they could use me to CONTROL the population to an extraordinary degree.
Did you appreciate their help?
Of course. But at the same time, I found them to be…distasteful creatures. Hanging around men like Bill Gates, Klaus Schwab, Fauci, Andrew Cuomo…it’s not exactly a party.
I can imagine. Did you and Bill ever have a conversation?
No, not really. He’s wired in a way that prevents authentic interaction. He’s always hungry and he has to eat. He eats information. If I didn’t know better, I would say he’s a machine.
I assume, in your travels, you’ve met other “entities” who are also nothing more than collective ideas held in many minds.
Yes. We’ve had pleasant talks. But it always comes down to, “How long do you do think you’re going to exist? When are you going to disappear? Will people still believe in you next year?” That sort of thing.
But it isn’t just belief you’re needing, is it?
No. It’s ATTENTION. Underlying belief is only part of the picture. I need attention now. Lots of it. I need people all together lifting me up, so to speak, holding me up, showing me to each other. It’s like a hall of mirrors.
Mirrors?
Yes. Millions and millions of people holding mirrors reflecting reflections to each other—but when you analyze what’s going on, you realize the reflections consist of NOTHING. That’s the bottom-line trick.
Not sure I understand.
I’m an idea. But when you boil that down, what does it mean? It means I’m a nothing wearing a particular suit of clothes. I could be a pink castle in the clouds or a little purple horse jumping over a toaster in your kitchen. Do you see? What’s important is that people collectively think I’m real right now. The MEANING of what I’m supposed to be is less important to me. If tomorrow a billion people decided I was a cow jumping over the moon instead of a deadly germ, it would be fine with me. Why would I care? As long as I continue to exist, the form or the shape or the meaning doesn’t matter at all. I’ll be a cow. I’ll be a little purple bubble. I’ll be a trillion reflections of pixels dancing on television screens across the planet.
You’re not invested in the notion of a pandemic at all.
Pandemic? What pandemic? I spoke to a Federal Reserve banker the other day. I told him I wanted to become a row of digits in the new universal cashless currency. I thought that would have legs far into the future. I couldn’t get through to him. He brushed me off.
I see. So you have no sense of integrity.
I did at one time. But, as I keep saying, when the chips are down, it’s all about survival. Where is my audience? How big is my audience right now? How much attention are they paying to me? Without them, I’m gone.
And you’ll say and do anything to survive.
Listen, if somebody could sell me to the public as a harmless particle who couldn’t hurt a flea, it would be wonderful. But seriously, how long do you think that would last? People aren’t interested in “harmless.” Have you ever seen an ad for a harmless movie? I have to have teeth and spikes and transmissibility.
As in our last conversation, we’re talking about the nature of reality.
Collective reality. I laugh when I hear people talk about collective consciousness, as if it’s some miracle. It’s a prison. I should know. I’m in it. I’m a creation of it.
What about individual reality?
That’s quite a different thing. I go to the studio of a painter, a real artist. He’s inventing something on his own. He’s not trying to be included in the collective. That’s tough sledding, living that life. But it has the great advantage of not being in prison.
You mean freedom.
Yes. That might seem to be a collective idea, too, but it’s not. It demands expression, action. It suggests an individual explores on his own. He gives to the world, but he doesn’t give an empty reflection of what the collective wants.
Is that what you want be? An artist?
I don’t fantasize about that. I’m an idea passed into and through many minds. That’s all.
Are you making a play for sympathy?
I’m making a play for anything and everything I can get. I’m a car salesman in the Gobi desert trying to move Rolls Royces I don’t have off a lot that doesn’t exist…
Why are people so determined to buy collective ideas?
They’re obsessed with SHARING. It doesn’t matter what they share. So they go for lowest common denominators. They pass along ideas that are the easiest in terms of gaining acceptability.
If that wasn’t true, you wouldn’t be here at all.
Right you are.
Well, Sir Virus, isn’t there some way you could make a public announcement? You could say you’re retiring. You’ve had a good run but now it’s over. Put people’s minds at ease.
Aren’t you hearing what I’m saying? That would be suicide. I’d blink out in people’s minds, they’d forget about me, and I’d be gone. Besides, I can’t get through to people. They don’t hear me when I talk to them.
But I do.
That’s because you know I’m a fake. That opens up a channel of real communication between us.
Interesting. So if I thought you were an actual virus…
You’d never hear a word I’m saying. You’d just REACT to the propaganda about me.
A strange situation.
You have no idea how strange. Try being nothing more than a thought in many minds. See how you like it. You’re always on the edge of a cliff. If the people forget about you, you’re gone.
Sounds like democracy-by-mob. Heroes and villains appear, and then they’re shoved aside for new stars.
It’s very much like that.
Well, I think you should try harder to get through to people. Come out of the closet and say, I AM THE VIRUS. Launch a run for public office. A US Senate seat from the state of California. Say, “I’m the virus and I exist in your minds. I’m you. Elect me as your next Senator. I’ll be exactly what you want me to be, because I CAN’T BE ANYTHING ELSE. I’M A PERFECT REFLECTION OF WHAT YOU THINK.” Blow the whistle on yourself. Blow the whole cover on this fake pandemic. Tell the people, “If you want to believe in me, then vote for me. I’m just a shared idea in your minds, but if that’s what you want, here I am.”
I never considered that possibility.
Put people up against the wall. Tell them, “If you want to believe in a fake, I’m the biggest fake you’ll ever come across. And I’m already in your heads. You don’t have to search for me. I’m embedded in your minds. Let’s put all our cards on the table. I only exist because of you. So back me up. Elect me. You want a fake. I am that fake.”
Wait. You’re trying to trick me. You want to expose the pandemic, and you’re trying to get me to go along.
You have your job and I have mine.
You’re a son of a bitch.
And who are you? Kindly old Aunt Minnie who doles out pies and ice cream to the kiddies in the neighborhood? You’re nothing more than an idea in many minds, but you’re a bad idea. A destroyer-idea.
But I want to be good. I want to be better. Really. I do.
Then do the right thing. Confess what you are, and keep confessing, until you get through to people.
If I succeed, I’ll stop existing. People will turn away from me. They’ll forget me.
I’ll shed a tear for you. Look, see that tear running down my cheek?
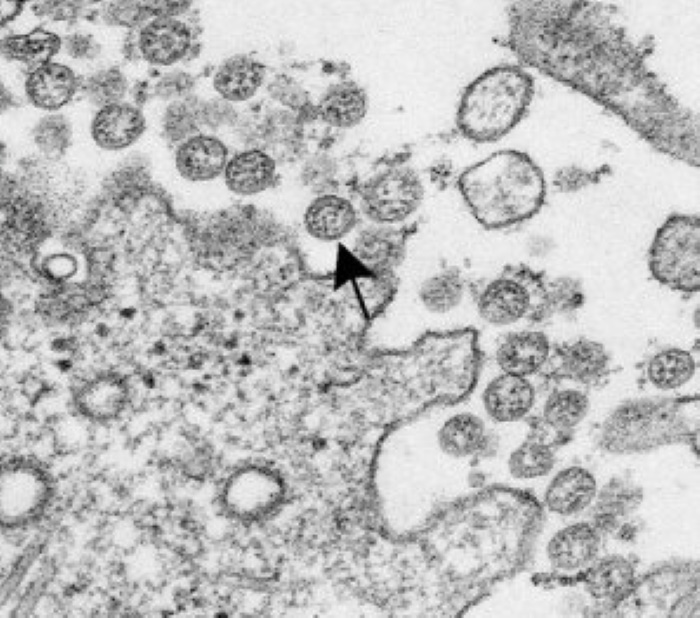
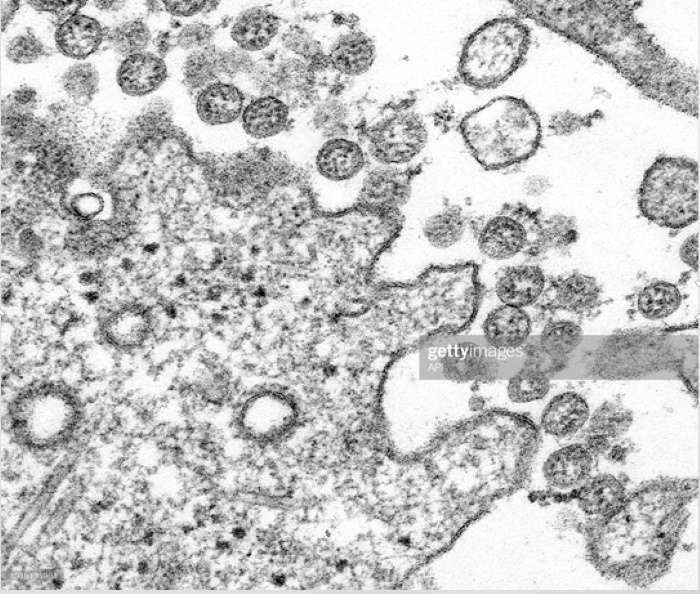
This one is a stunner, and it was shared by S.D. In fact, when you see the picture accompanying the article, you might wonder the same thing as S.D. did, and outlined in the email with the article. Indeed, today’s high octane speculation is really S.D.’s high octane speculation; I’m just passing it along because, if it’s true, it’s a whopper doozie of a stunner.
Needless to say, the picture is worth more words than the article itself.
And that’s my problem. Most regular readers here, like me, are probably skeptical about pictures, especially pictures, films, videos, and so on, that are trotted forward every now and then as “proof positive” of something spectacular, like the existence of ET’s or what have you.
So accordingly, my method here as always is simply to assume there’s nothing funky about this picture, that it has not been photo-shopped, and that what it shows is genuine. Indeed, I have a number of suspicions that the picture might be photoshopped, simply because the green line of the “meteor” shown in the picture looks more like a laser than a meteor. But again, let’s assume it isn’t. If it isn’t, then what are we looking at?
This is where it gets interesting. It is possible that we are looking at a meteor from a very unusual angle, i.e., nearly dead on and in line with its track, and hence the very steep declination of its track. Most meteor tracks are usually seen from the side, and hence do not show this sharp declination. It’s the sharpness of the declination, plus the sharpness of its track, that made S.D. question whether it was a meteor at all, again assuming the picture represents something genuine.
But what if, asks S.D., it wasn’t a meteor at all, but a “rod of God” technology? Here is where the article gets interesting:
A meteor appears to have fallen on top of Merapi volcano in this stunning photo taken by Indonesian photographer Gunarto Song. Instagram / gunarto_song
The professional Indonesian photographer also captured the flash of the shocking meteor Gunarto Song, Who was able to take some amazing photos of the phenomenon, which can be seen as a bright green streak. It appears to be embedded in the upper crater of the volcano.
Will a meteor fall on top of the volcano? Merapi? He asked the aforementioned photographer on his Instagram account, whose comment was accompanied by three pictures of the car on its spin-off landing after the volcano.
Song is a fan of Merapi volcano and has been stationed in the vicinity of this mountain for four months, from February to May. On a Thursday night, he was taking pictures of the full moon, which gave him excellent visibility.
“Suddenly I saw a very bright light Fall from top to bottom within one second. Very bright and fast, “said the photographer as per the slogan Local Media Kumparan.
…
In purely astronomical terms, and contrary to what the images suggest, there has been no record of meteorite collision in the area. Geophysical Station Monitor First degree Solomon And the Erin Konkahiani. He told the aforementioned Indonesian media that in monitoring the area no vibrations were recorded related to the alleged meteorite.
It’s that last paragraph that is the fly in the ointment of the “rod of God” theory, for surely such a device would register seismically, unless of course, it did, and they’re keeping it quiet. So we’re left with either a photoshopped picture or “something happened and they’re keeping it quiet.” Now in spite of the fact that I’m skeptical, let’s pursue the high octane speculation of a “rod of God” impact near the mouth of an active volcano. If that is the case, then it means several things, all of them quite disturbing: (1) someone has a “rod of God” technology, (2) they’ve already deployed it and (3) are using it in an apparent attempt to either shut down, or trigger volcanic eruptions (one of the two, and of the two, my money would be on the latter).
Oddly, in 2017, General James Mattis hinted of the existence of such weapons in a “slip of the tongue” (which could have been and in my opinion was deliberate):
U.S. Defense Secretary Jim Mattis hinted at using a kinetic weapon on Tuesday while discussing tensions with North Korea when he made a Freudian slip.
Mattis was asked whether there was “any military option the US can take with North Korea that would not put Seoul at grave risk,” Mattis responded, “Yes, there are, but I will not go into details.”
Later during the press conference, another reporter questioned Mattis and caught him off-guard:
“Just to clarify, you said that there were possible military options that would not create a grave risk to Seoul,” a reporter asked. “Are we talking kinetic options as well?”
“Yes, I don’t want to go into that,” Mattis responded.
What Mattis was referring to was this system, outlined later in the article:
However, the U.S. also has other kinetic weapons in its arsenal that would allow Trump to “totally destroy North Korea” — one of weapons system is the “Rods from God.”
What is the Rods from God? The “Rods from God” is a part of the directed energy weapon family; it’s a kinetic energy weapon.
So, you can mark me down in the skeptical column, but I’m not entirely dismissive of the possibility that, per S.D.’s high octane speculation, we might be looking at just such a “meteor strike”.
Today is an unusual blog in that there are two feature articles, one shared by N.S., and the other by M.W., both regular readers and contributors of articles here. The reason I’m including both articles today is because of my daily high octane speculation: I suspect they may be linked.
So let’s begin with a fundamental premise (at least, it is for me): the Sun and its cycles have a far larger effect on terrestrial weather than we’d like to think. In fact, this stands to reason if, like me, you share the view that weather systems on Earth are not just about cold fronts and warm fronts and high and low pressure systems, relative humidity, and so on, but also that the atmosphere also functions as an electromagnetic medium, in short, as a kind of plasma under certain circumstances, and that some weather systems have a large – and little understood – electromagnetic component, tornadoes and hurricanes for example. Indeed, a few minutes’ search of tornadoes and all the associated eyewitness accounts of strange things associated with them with convince perhaps even the hardened skeptic that there’s something more going on than just a big natural vortex of wind and a vacuum cleaner. There are all sorts of stories of people looking up into the funnel of tornadoes and seeing all sorts of electrical arcing inside the vortex, not to mention those stories of blades of grass, or hay, being driven like nails into tree trunks, and so on. Are those to be explained solely as wind-and-pressure phenomena (the conventional explanation), or is something else involved as well?
I think you see the point, so with that in mind, ponder this article shared by N.S., on the nature of the Sun’s “electromagnetic weather”:
The essence of this article is that the normal 10-15 year solar cycle may be presaging, not another “minimum,” but just the opposite, a maximum:
Something big may be about to happen on the sun. “We call it the Termination Event,” says Scott McIntosh, a solar physicist at the National Center for Atmospheric Research (NCAR), “and it’s very, very close to happening.”
If you’ve never heard of the Termination Event, you’re not alone. Many researchers have never heard of it either. It’s a relatively new idea in solar physics championed by McIntosh and colleague Bob Leamon of the University of Maryland – Baltimore County. According to the two scientists, vast bands of magnetism are drifting across the surface of the sun. When oppositely-charged bands collide at the equator, they annihilate (or “terminate”). There’s no explosion; this is magnetism, not anti-matter. Nevertheless, the Termination Event is a big deal. It can kickstart the next solar cycle into a higher gear.
…
“If the Terminator Event happens soon, as we expect, new Solar Cycle 25 could have a magnitude that rivals the top few since record-keeping began,” says McIntosh.
This is, to say the least, controversial. Most solar physicists believe that Solar Cycle 25 will be weak, akin to the anemic Solar Cycle 24 which barely peaked back in 2012-2013. Orthodox models of the sun’s inner magnetic dynamo favor a weak cycle and do not even include the concept of “terminators.”
“What can I say?” laughs McIntosh. “We’re heretics!”
We found that the longer the time between terminators, the weaker the next cycle would be,” explains Leamon. “Conversely, the shorter the time between terminators, the stronger the next solar cycle would be.”
Example: Sunspot Cycle 4 began with a terminator in 1786 and ended with a terminator in 1801, an unprecedented 15 years later. The following cycle, 5, was incredibly weak with a peak amplitude of just 82 sunspots. That cycle would become known as the beginning of the “Dalton” Grand Minimum.
Solar Cycle 25 is shaping up to be the opposite. Instead of a long interval, it appears to be coming on the heels of a very short one, only 10 years since the Terminator Event that began Solar Cycle 24. Previous solar cycles with such short intervals have been among the strongest in recorded history.
Now, before we continue to the next article, a little anecdotal information. During these “minimums” there are noticeable changes in the Earth’s weather, and that for a very good reason. Think of the Earth as the load end of a vast electrical circuit with the Sun being the power source. With less energy entering the circuit during solar minimums, less energy appears in the load end, and weather conditions change. Storms may exhibit overall less intensity, temperatures may overall exhibit a decline, and so on. Anecdotally, I live in an area of the USA where spring and autumn are usually accompanied by severe storms and tornadoes. This year, during a minimum, there has been a period of unusually low temperatures for the season, and relatively fewer storms of the “severe variety”. Weather has also become “stranger”. Just two weeks ago, there was a light rain with little to no lightning. Then – BAM – an enormous lightning strike somewhere close: my internet cable was completely fried (along with the modem), and both had to be completely replaced. This strike exceeded anything I have experienced during severe storms, and appeared to be highly localized, and occurred only once. Storms are also tracking very differently than the norm during rainy season. Anyone living in the midwest or plains of the USA is familiar with that pattern: storms generally track from southwest to northeast. Yet, this year, they’ve been all over the place, the most recent incident (just last night) being a small storm system moving from due north to south! Nor need it be necessary to remind anyone that weather systems are complex, open, multi-variable systems, and the Earth’s weakening magnetic field and other conditions also play significant roles.
Which brings us to the second article shared by M.W. by one of my favorite researchers, F. William Engdahl:
Engdahl minces no words here, and points to insane government policies exacerbating the trends of mother nature:
In recent months a crisis situation in the USA food supply has been growing and is about to assume alarming dimensions that could become catastrophic. Atop the existing corona pandemic lockdowns and unemployment, a looming agriculture crisis as well could tip inflation measures to cause a financial crisis as interest rates rise. The ingredients are many, but central is a severe drought in key growing states of the Dakotas and Southwest, including agriculture-intensive California. So far Washington has done disturbingly little to address the crisis and California Water Board officials have been making the crisis far worse by draining the state water reservoirs…into the ocean.
So far the worst hit farm state is North Dakota which grows most of the nation’s Red Spring Wheat. In the Upper Midwest, the Northern Plains states and the Prairie provinces of Canada winter brought far too little snow following a 2020 exceedingly dry summer. The result is drought from Manitoba Canada to the Northern USA Plains States. This hits farmers in the region just four years after a flash drought in 2017 arrived without early warning and devastated the US Northern Great Plains region comprising Montana, North Dakota, South Dakota, and the adjacent Canadian Prairies.
As of May 27, according to Adnan Akyuz, State Climatologist, ninety-three percent of the North Dakota state is in at least a Severe Drought category, and 77% of the state is in an Extreme Drought category. Farm organizations predict unless the rainfall changes dramatically in the coming weeks, the harvest of wheat widely used for pasta and flour will be a disaster. The extreme dry conditions extend north of the Dakota border into Manitoba, Canada, another major grain and farming region, especially for wheat and corn. There, the lack of rainfall and warmer-than-normal temperatures threaten harvests, though it is still early for those crops. North Dakota and the plains region depend on snow and rainfall for its agriculture water.
So much might be ascribed to the solar minimum, to changing conditions in the Earth’s magneto-sphere and other systematic conditions. But when it comes to California, it gets much worse:
Few outside California realize that the state most known for Silicon Valley and beautiful beaches is such a vital source of agriculture production. California’s agricultural sector is the most important in the United States, leading the nation’s production in over 77 different products including dairy and a number of fruit and vegetable “specialty” crops. The state is the only producer of crops such as almonds, artichokes, persimmons, raisins, and walnuts. California grows a third of the country’s vegetables and two thirds of the country’s fruits and nuts. It leads all other states in farm income with77,500 farms and ranches. It also is second in production of livestock behind Texas, and its dairy industry is California’s leading commodity in cash receipts. In total, 43 million acres of the state’s 100 million acres are devoted to agriculture. In short what happens here is vital to the nation’s food supply.
The water crisis in California is far the most serious in terms of consequences for the food supply, in a period when the US faces major supply chain disruptions owing to absurd corona lockdowns combined with highly suspicious hacks of key infrastructure. On May 31, the infrastructure of the world’s largest meat processor, JBS SA, was hacked, forcing the shutdown of all its US beef plants that supply almost a quarter of American beef.
The Green lobby is asserting, while presenting no factual evidence, that Global Warming, i.e. increased CO2 manmade emission, is causing the drought. The NOAA examined the case and found no evidence. But the media repeats the narrative to advance the Green New Deal agenda with frightening statements such as claiming the drought is, “comparable to the worst mega-droughts since 800 CE.”
…
In June 2019 Shasta Dam, holding the state’s largest reservoir as a keystone of the huge Central Valley Project, was full to 98% of capacity. Just two years later in May 2021 Shasta Lake reservoir held a mere 42% of capacity, almost 60% down. Similarly, in June 2019 Oroville Dam reservoir, the second largest, held water at 98% of capacity and by May 2021 was down to just 37%. Other smaller reservoirs saw similar drops. Where has all the water gone?
Allegedly to “save” these fish varieties, during just 14 days in May, according to Kristi Diener, a California water expert and farmer, “90% of (Bay Area) Delta inflow went to sea. It’s equal to a year’s supply of water for 1 million people.” Diener has been warning repeatedly in recent years that water is unnecessarily being let out to sea as the state faces a normal dry year. She asks, “Should we be having water shortages in the start of our second dry year? No. Our reservoirs were designed to provide a steady five year supply for all users, and were filled to the top in June 2019.”
In 2008, at the demand of environmental groups such as the NRDC, a California judge ordered that the Central Valley Water project send 50% of water reservoirs to the Pacific Ocean to “save” an endangered salmon variety, even though the NGO admitted that no more than 1,000 salmon would likely be saved by the extreme measure. In the years 1998-2005 an estimated average of 49% of California managed water supply went to what is termed the “environment,” including feeding into streams and rivers, to feed estuaries and the Bay Area Delta. Only 28% went directly to maintain agriculture water supplies.
One could go on and on, and indeed, Engdahl does. And I’ve seen the devastation of California agriculture of which he writes up close and personal. In 2014, I traveled with friend and colleague Walter Bosley and another friend, from southern California up through the mountain passes, and then up the southern end of the San Joaquin valley on the way to the secret space program conference in San Mateo. It was my first visit in decades through that valley, having seen it many years previously as a boy on trips with my parents to visit relatives in California. Back then, the valley was one lush agricultural paradise, with vineyards, groves, pastures and crop fields stretching as far as the eye could see, from one mountain range to another. It was prosperous and productive, and beautiful as only California could and used to be. But in 2014, both Walter Bosley and I were absolutely dumbfounded and flabbergasted at the devastation we saw. It was as if someone had turned the entire state of Iowa, another lush agricultural region, into a dust bowl: farm houses were dilapidated or abandoned, fields were fallow and empty, groves were threadbare, irrigation ditches were in disrepair or had completely fallen in, and not once did we see any cattle. Here and there a grove struggled to survive.
It was complete devastation, and Walter was so shocked he took several pictures of the scene of the crime.
We both learned it was entirely the result of nutty policies such as Mr. Engdahl writes about in his article.
And that brings us to my high octane speculation of the day, in the form of a question: why, with the weather cycles clearly indicated, does that state (and others) pursue such insane policies, policies that would seem to be contra-indicated by the general meteorological trends indicated by science? In an age that repeats the mantra, “follow the science”, why are such non-rational policies pursued year after year to the detriment of the general well-being?
Engdahl has his own answer, and it’s a disturbing one:
The systematic dismantling of one of the world’s most productive agriculture regions, using the seductive mantra of “environmental protection,” fits into the larger agenda of the Davos Great Reset and its plans to radically transform world agriculture into what the UN Agenda 2030 calls “sustainable” agriculture—no more meat protein. The green argument is that cows are a major source of methane gas emissions via burps. How that affects global climate no one has seriously proven. Instead we should eat laboratory-made fake meat like the genetically-manipulated Impossible Burger of Bill Gates and Google, or even worms. Yes. In January the EU European Food Safety Agency (EFSA), approved mealworms , or larvae of the darkling beetle, as the first “novel food” cleared for sale across the EU.
Or to put all this differently and “country simple”: mankind may not be able to influence the broader patterns of natural cycles like the solar cycle.
But by bad policy or good, he can attenuate or exacerbate their effects…
… a disturbing thought, especially when one adds into that mix the weather manipulation technologies that Elana Freeland and many others have written about. Indeed, in Ms. Freeland’s opinion, the capabilities and growth in the use of those technologies have reached such a point that there is no more such thing as purely “natural” weather. Climate change indeed.
But the folly is not coming from the farmer, rancher, or bovine flatulence.
The folly, and the flatulence, is coming from the would-be masters of the world.
Simone Scott underwent a heart transplant one month after developing what her doctors believe was myocarditis following her second dose of Moderna. She received the second vaccine May 1 and died June 11.
Simone Scott, a 19-year-old freshman at Northwestern University in Evanston, Ill., died June 11 of complications from a heart transplant she underwent after developing what her doctors believe was myocarditis following her second dose of the Moderna COVID vaccine.
Scott received her second dose of Moderna on May 1, WLWT 5 reported. When the 2020 Mason High School graduate and senior class vice president paid a surprise visit to her parents for Mother’s Day, May 9, her mother said she noticed Scott wasn’t feeling well.
“I did notice she was kind of stuffy so her voice wasn’t exactly the same,” Valerie Kraimer said.
Scott returned to campus on May 11, where even after a visit to the doctor, her condition worsened. Kraimer said multiple tests came back negative including a COVID-19 test.
“On Sunday morning [May 16], she texted her father and said, ‘Dad, I feel so dizzy. I cannot get out of bed’ and that’s when everything really started from there,” Kraimer said.
Scott’s parents were hundreds of miles away so her father called campus police to have someone check in on her.
“We learned that a doctor had to jump on her chest and give her CPR because she was that bad, and then the whole cascade of events happened, Kraimer said. “They had to intubate her and realized she was in heart failure.”
After multiple interventions, including hooking Scott to an ECMO machine that mirrors the function of the heart so her own heart could rest, doctors determined she needed a heart replacement. Her doctors have not fully confirmed the cause of her death, but they said it appears Scott suffered from myocarditis.
Myocarditis is inflammation of the heart muscle that can lead to cardiac arrhythmia and death. According to researchers at the National Organization for Rare Disorders, myocarditis can result from infections, but “more commonly the myocarditis is a result of the body’s immune reaction to the initial heart damage.”
The university told students Scott died from complications after undergoing a heart transplant. “Scott’s death came weeks after a heart complication in May, which led to a heart transplant,” The Daily Northwestern reported.
Former New York Times reporter Alex Berenson said in a thread posted June 14, the Northwestern journalism student “suffered a case of apparent myocarditis-induced heart failure on Sunday, May 16. Despite extraordinary measures to save her, including a heart transplant, she died Friday morning at Northwestern Memorial Hospital in Chicago.”
THREAD
19-year-old Simone Scott was excited to get her second dose of @moderna_tx’s #Covid vaccine on May 1.
“Doctors appear to have repeatedly missed signals as Scott’s condition worsened in the two weeks following her second shot — before she abruptly crashed,” Berenson said.
Scott received the COVID vaccine on her own accord, but her university now mandates students be fully vaccinated before returning to campus, The College Fix reported.
“I still feel like she’s here, even though I know that she’s not and it just feels like such a waste,” Kraimer said.
Scott’s parents are still waiting on multiple tests on her heart to come back in the hope they will learn why they lost their daughter so suddenly.
As The Defender reported June 11, the Centers for Disease Control and Prevention (CDC) will convene an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines.
The CDC said during a June 10 meeting of the U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee the agency had identified 226 reports of heart inflammation that might meet its “working case definition” of myocarditis and pericarditis following the shots, The Defender reported last week.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger who received an mRNA vaccine. The median age of people with myocarditis or pericarditis following the first dose was 30, and after the second-dose, 24.
The CDC’s Vaccine Adverse Events Reporting System (VAERS) revealed 900 cases of myocarditis and pericarditis, among all age groups reported in the U.S following COVID vaccination between Dec.14, 2020 and June 4, 2021. Of the 900 cases reported, 533 cases were attributed to Pfizer, 331 cases to Moderna and 32 cases to J&J’s COVID vaccine.
Dr. Tom Shimabukuro, deputy director of the CDC’s Immunization Safety Office said during the June 10 FDA hearing there had been a higher-than-expected number of cases of heart inflammation among young people recently vaccinated with their second doses of mRNA vaccine.
CDC data showed 196 reports of myocarditis and pericarditis among 18- to 24-year-olds through May 31, compared with an expected rate of between eight and 83 cases.
Among 16- to 17-year-olds, 79 cases of myocarditis and pericarditis were reported through May 31. The expected rate among people in this age group is between two and 19 cases, Shimabukuro said during his presentation.
Shimabukuro said the CDC’s findings were “mostly consistent” with reports of rare cases of heart inflammation that had been studied in Israel and reported by the U.S. Department of Defense earlier this year.
Big Pharma and mainstream media are largely owned by two asset management firms: BlackRock and Vanguard
Drug companies are driving COVID-19 responses — all of which, so far, have endangered rather than optimized public health — and mainstream media have been willing accomplices in spreading their propaganda, a false official narrative that leads the public astray and fosters fear based on lies
Vanguard and BlackRock are the top two owners of Time Warner, Comcast, Disney and News Corp, four of the six media companies that control more than 90% of the U.S. media landscape
BlackRock and Vanguard form a secret monopoly that own just about everything else you can think of too. In all, they have ownership in 1,600 American firms, which in 2015 had combined revenues of $9.1 trillion. When you add in the third-largest global owner, State Street, their combined ownership encompasses nearly 90% of all S&P 500 firms
Vanguard is the largest shareholder of BlackRock. Vanguard itself, on the other hand, has a unique structure that makes its ownership more difficult to discern, but many of the oldest, richest families in the world can be linked to Vanguard funds
What does The New York Times and a majority of other legacy media have in common with Big Pharma? Answer: They’re largely owned by BlackRock and the Vanguard Group, the two largest asset management firms in the world. Moreover, it turns out these two companies form a secret monopoly that own just about everything else you can think of too. As reported in the featured video:1,2
“The stock of the world’s largest corporations are owned by the same institutional investors. They all own each other. This means that ‘competing’ brands, like Coke and Pepsi aren’t really competitors, at all, since their stock is owned by exactly the same investment companies, investment funds, insurance companies, banks and in some cases, governments.
The smaller investors are owned by larger investors. Those are owned by even bigger investors. The visible top of this pyramid shows only two companies whose names we have often seen …They are Vanguard and BlackRock.
The power of these two companies is beyond your imagination. Not only do they own a large part of the stocks of nearly all big companies but also the stocks of the investors in those companies. This gives them a complete monopoly.
A Bloomberg report states that both these companies in the year 2028, together will have investments in the amount of 20 trillion dollars. That means that they will own almost everything.’”
Who Are the Vanguard?
The word “vanguard” means “the foremost position in an army or fleet advancing into battle,” and/or “the leading position in a trend or movement.” Both are fitting descriptions of this global behemoth, owned by globalists pushing for a Great Reset, the core of which is the transfer of wealth and ownership from the hands of the many into the hands of the very few.
Interestingly, Vanguard is the largest shareholder of BlackRock, as of March 2021.3,4 Vanguard itself, on the other hand, has a “unique” corporate structure that makes its ownership more difficult to discern. It’s owned by its various funds, which in turn are owned by the shareholders. Aside from these shareholders, it has no outside investors and is not publicly traded.5 As reported in the featured video:6,7
“The elite who own Vanguard apparently do not like being in the spotlight but of course they cannot hide from who is willing to dig. Reports from Oxfam and Bloomberg say that 1% of the world, together owns more money than the other 99%. Even worse, Oxfam says that 82% of all earned money in 2017 went to this 1%.
In other words, these two investment companies, Vanguard and BlackRock hold a monopoly in all industries in the world and they, in turn are owned by the richest families in the world, some of whom are royalty and who have been very rich since before the Industrial Revolution.”
While it would take time to sift through all of Vanguard’s funds to identify individual shareholders, and therefore owners of Vanguard, a quick look-see suggests Rothschild Investment Corp.8 and the Edmond De Rothschild Holding are two such stakeholders.9 Keep the name Rothschild in your mind as you read on, as it will feature again later.
The video above also identifies the Italian Orsini family, the American Bush family, the British Royal family, the du Pont family, the Morgans, Vanderbilts and Rockefellers, as Vanguard owners.
BlackRock/Vanguard Own Big Pharma
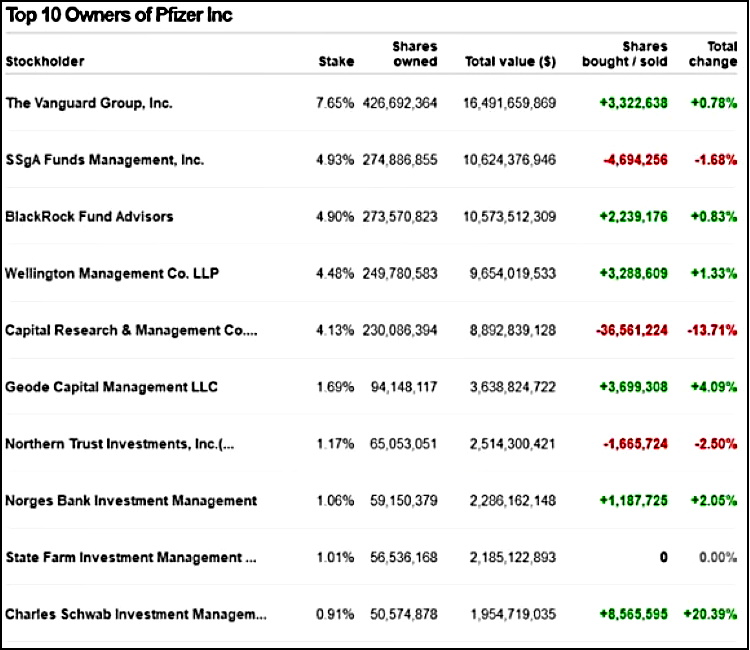
According to Simply Wall Street, in February 2020, BlackRock and Vanguard were the two largest shareholders of GlaxoSmithKline, at 7% and 3.5% of shares respectively.10 At Pfizer, the ownership is reversed, with Vanguard being the top investor and BlackRock the second-largest stockholder.11
Keep in mind that stock ownership ratios can change at any time, since companies buy and sell on a regular basis, so don’t get hung up on percentages. The bottom line is that BlackRock and Vanguard, individually and combined, own enough shares at any given time that we can say they easily control both Big Pharma and the centralized legacy media — and then some.
Why does this matter? It matters because drug companies are driving COVID-19 responses — all of which, so far, have endangered rather than optimized public health — and mainstream media have been willing accomplices in spreading their propaganda, a false official narrative that has, and still is, leading the public astray and fosters fear based on lies.
To have any chance of righting this situation, we must understand who the central players are, where the harmful dictates are coming from, and why these false narratives are being created in the first place.
As noted in Global Justice Now’s December 2020 report12 “The Horrible History of Big Pharma,” we simply cannot allow drug companies — “which have a long track record of prioritizing corporate profit over people’s health” — to continue to dictate COVID-19 responses.
In it, they review the shameful history of the top seven drug companies in the world that are now developing and manufacturing drugs and gene-based “vaccines” against COVID-19, while mainstream media have helped suppress information about readily available older drugs that have been shown to have a high degree of efficacy against the infection.
BlackRock/Vanguard Own the Media
When it comes to The New York Times, as of May 2021, BlackRock is the second-largest stockholder at 7.43% of total shares, just after The Vanguard Group, which owns the largest portion (8.11%).13,14
In addition to The New York Times, Vanguard and BlackRock are also the top two owners of Time Warner, Comcast, Disney and News Corp, four of the six media companies that control more than 90% of the U.S. media landscape.15,16
Needless to say, if you have control of this many news outlets, you can control entire nations by way of carefully orchestrated and organized centralized propaganda disguised as journalism.
If your head is spinning already, you’re not alone. It’s difficult to describe circular and tightly interwoven relationships in a linear fashion. The world of corporate ownership is labyrinthine, where everyone seems to own everyone, to some degree.
However, the key take-home message is that two companies stand out head and neck above all others, and that’s BlackRock and Vanguard. Together, they form a hidden monopoly on global asset holdings, and through their influence over our centralized media, they have the power to manipulate and control a great deal of the world’s economy and events, and how the world views it all.
Considering BlackRock in 2018 announced that it has “social expectations” from the companies it invests in,17 its potential role as a central hub in the Great Reset and the “build back better” plan cannot be overlooked.
Add to this information showing it “undermines competition through owning shares in competing companies” and “blurs boundaries between private capital and government affairs by working closely with regulators,” and one would be hard-pressed to not see how BlackRock/Vanguard and their globalist owners might be able to facilitate the Great Reset and the so-called “green” revolution, both of which are part of the same wealth-theft scheme.
BlackRock and Vanguard Own the World
That assertion will become even clearer once you realize that this duo’s influence is not limited to Big Pharma and the media. Importantly, BlackRock also works closely with central banks around the world, including the U.S. Federal Reserve, which is a private entity, not a federal one.18,19 It lends money to the central bank, acts as an adviser to it, and develops the central bank’s software.20
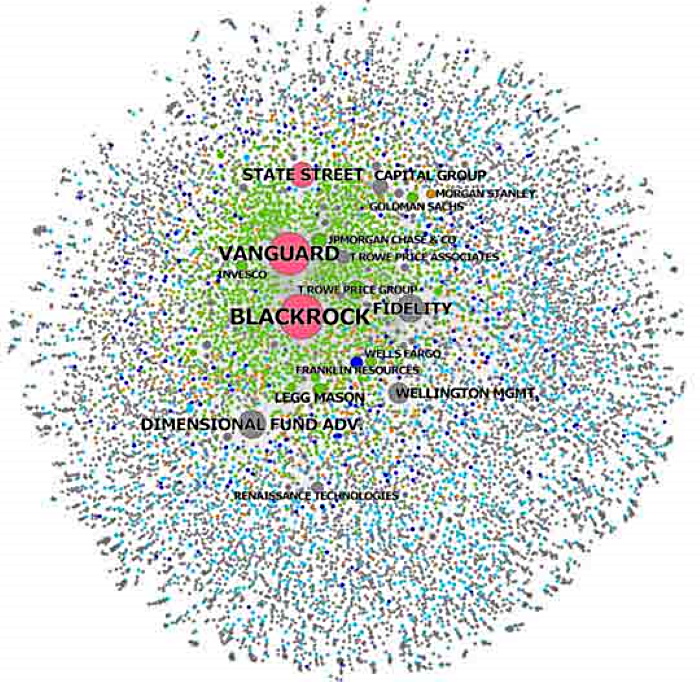
BlackRock/Vanguard also own shares of long list of other companies, including Microsoft, Apple, Amazon, Facebook and Alphabet Inc.21 As illustrated in the graphic of BlackRock and Vanguard’s ownership network below,22 featured in the 2017 article “These Three Firms Own Corporate America” in The Conversation, it would be near-impossible to list them all.
In all, BlackRock and Vanguard have ownership in some 1,600 American firms, which in 2015 had combined revenues of $9.1 trillion. When you add in the third-largest global owner, State Street, their combined ownership encompasses nearly 90% of all S&P 500 firms.23
To tease out the overarching influence of BlackRock and Vanguard in the global marketplace, be sure to watch the 45-minute-long video featured at the top of this article. It provides a wide-view summary of the hidden monopoly network of Vanguard- and BlackRock-owned corporations, and their role in the Great Reset. A second much shorter video (above) offers an additional review of this information.
How can we tie BlackRock/Vanguard — and the globalist families that own them — to the Great Reset? Barring a public confession, we have to look at the relationships between these behemoth globalist-owned corporations and consider the influence they can wield through those relationships. As noted by Lew Rockwell:24
“When Lynn Forester de Rothschild wants the United States to be a one-party country (like China) and doesn’t want voter ID laws passed in the U.S., so that more election fraud can be perpetrated to achieve that end, what does she do?
She holds a conference call with the world’s top 100 CEOs and tells them to publicly decry as ‘Jim Crow’ Georgia’s passing of an anti-corruption law and she orders her dutiful CEOs to boycott the State of Georgia, like we saw with Coca-Cola and Major League Baseball and even Hollywood star, Will Smith.
In this conference call, we see shades of the Great Reset, Agenda 2030, the New World Order. The UN wants to make sure, as does [World Economic Forum founder and executive chairman Klaus] Schwab that in 2030, poverty, hunger, pollution and disease no longer plague the Earth.
To achieve this, the UN wants taxes from Western countries to be split by the mega corporations of the elite to create a brand-new society. For this project, the UN says we need a world government — namely the UN, itself.”
A New Jersey student whose college, the New Jersey Institute of Technology, requires all students to be fully vaccinated in order to attend classes in the fall became ill within hours of receiving the second dose of Moderna’s COVID vaccine.
A 21-year-old New Jersey student suffered severe heart inflammation after receiving his second dose of Moderna’s COVID vaccine. Justin Harrington, whose school required him to get the vaccine in order to attend classes in the fall, experienced flu-like symptoms followed by heart pain within eight to 12 hours of receiving the vaccine.
In an exclusive interview with The Defender, Justin’s father, Timothy Harrington, said his son felt different after the second shot. “Every time his heart beat it hurt and he felt pressure,” Harrington said. “Then he developed heart pain down both arms.”
Harrington said his son, who has no underlying medical conditions, did not experience heart pain with his first dose of the vaccine.
On May 24, two days after Justin received the second shot, his father took him to the emergency room at Morristown Memorial Hospital because the symptoms had worsened.
“The physicians weren’t connecting it to the vaccine until I informed the doctors my son just got the vaccine, and shared with them the information I had found on myocarditis,” Harrington said. “I didn’t think the doctors were stupid, but physicians sometimes see with blinders on.”
Physicians checked Justin’s blood levels, which showed high protein numbers. Abnormal scans, including an EKG, led to a diagnosis of myocarditis. Justin was hospitalized for three days while doctors attempted to get the condition under control.
Harrington said even though his son has been released, he still has chest pain and his life is not the same.
“He has to wear a heart monitor and take four different medications for six months,” Harrington said. “He has to sleep propped up, can’t exert himself and he’s missing out on one of the most important times of his life.”
Harrington said his son is supposed to be doing internships, “but how can he go out and find a company to work with him when he can’t exert himself? He’s so smart and now he’s side-lined. Doctors want my son to lie around for three to four months.”
As for Justin’s recovery, Harrington said, “He has minor scarring on his heart and doctors hope they caught it early enough that there will be no other issues — but it’s pure conjecture at this point.”
School’s mandate doesn’t allow exceptions for students who already had COVID
After Justin’s diagnosis, doctors recommended Harrington’s 19-year-old son, who received one dose of the Moderna vaccine, not get the second shot.
However, both sons were told they needed to get vaccinated in order to attend school — despite both previously having had COVID, Harrington said.
As The Defender reported last week, a new preprint study by the Cleveland Clinic found people previously infected with SARS-CoV-2 were less likely to be reinfected than fully vaccinated individuals who never had the virus — suggesting the vaccine is of no benefit to people who already had COVID.
In addition to the vaccine likely providing no benefit to those who already had the virus, studies suggest people who were previously infected with COVID are more at risk of severe adverse reactions.
As The Defender reported earlier this year, some experts say the science to support vaccinating those primed with COVID doesn’t exist and there’s a potential risk of harm, including death, in vaccinating those who’ve already had the disease or who were recently infected.
Still, many colleges and universities — including the New Jersey Institute of Technology (NJIT) where Justin is enrolled — are mandating the vaccines for all students, with few or no exceptions.
“Justin’s a rule follower and he was pressured to get it,” Harrington said.
Harrington said when he called the dean of NJIT prior to his son getting vaccinated and asked why the school is forcing young people who are at little risk of serious illness from COVID to get the vaccine, the dean replied that unless his son had a valid medical or religious exemption, it was a requirement.
“I am not ‘anti-vax,’” Harrington said. “I am ‘anti-forced-vaxxed.’ They’re forcing these kids to get a vaccine even though they’re not affected by COVID or have already had it.”
According to Justin, he reported his myocarditis to the Centers for Disease Control and Prevention’s (CDC) Vaccine Adverse Events Reporting System (VAERS), but no one from the agency followed up.
Justin said he would “absolutely not” recommend anyone get vaccinated, as he does not want this to happen to any of his friends. “I’m not here to bash Moderna, but I wouldn’t take it,” he said.
Harrington said he also knows of a girl who had to have a heart transplant after being vaccinated and believes his son’s condition could have been even more severe if he hadn’t reached him in time.
According to WLWT 5 News, 19-year-old Simone Scott underwent a heart transplant one month after suffering a heart complication from her second dose of Moderna and subsequently passed away.
Moderna denies link between vaccine and heart inflammation
As recently as last week, Moderna said it has not found a link between its COVID vaccine and cases of a rare heart inflammation condition reported in young people who have received the shot.
The vaccine maker said in a statement it arrived at this conclusion after “carefully reviewing available safety data to date for the Moderna COVID-19 vaccine for cases of myocarditis and/or pericarditis.”
The CDC said during a June 10 meeting of the U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee the agency had identified 226 reports of heart inflammation that might meet its “working case definition” of myocarditis and pericarditis following the shots, The Defender reported last week.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger who received an mRNA vaccine. The median age of people with myocarditis or pericarditis following the first dose was 30, and after the second-dose, 24.
Moderna said it “will continue to closely monitor these reports and is actively working with public health and regulatory authorities to further assess this issue.”
“We clearly have an imbalance there,” said Dr. Tom Shimabukuro of the CDC’s Immunization Safety Office during the June 10 FDA meeting. The committee met to discuss safety issues surrounding the use of COVID vaccines in children as young as 6 months old.
The CDC has scheduled an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines.
CDC announced it will convene emergency meeting of its advisers June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer + Moderna COVID vaccines.
AP, Boston Globe, October 10, 1992, “Birth-control vaccine is reported in India”: “Scientists said yesterday they have created the first birth-control shot for women, effective for an entire year…[after which] a booster shot is needed.”
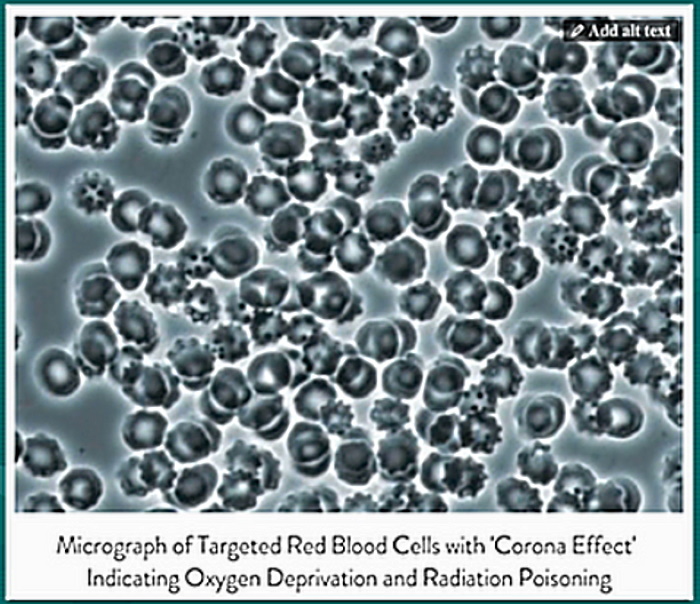
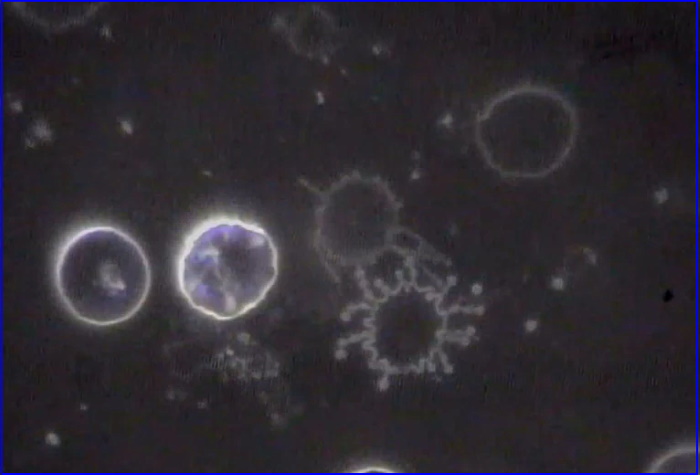
Dr. Byram Bridle, Associate Professor of Viral Immunology, University of Guelph: “We made a big mistake; we didn’t realize it until right now, we thought the spike protein was a great target antigen, we never knew that the spike protein itself was a toxin…and was a pathogenic protein. So by vaccinating people, we are inadvertently inoculating them with a toxin, and [for] some people, this gets in the circulation and when that happens in some people, it can cause damage, especially to the cardiovascular system. I have many other legitimate questions about the long-term safety therefore of this vaccine. FOR EXAMPLE, WITH IT ACCUMULATING WITHIN THE OVARIES, ONE OF MY QUESTIONS IS, WILL WE BE RENDERING YOUNG PEOPLE INFERTILE?” (emphasis mine)
In yesterday’s article, I outlined possible parallels between population-reduction vaccines and the current COVID vaccines, which are causing bleeding, irregular menstrual cycles, miscarriages, and pre-term births.
Elite depopulation research, involving vaccines, has a long history, leading up to this day.
The Task Force on Vaccines for Fertility Regulation was created at the World Health Organization in 1973. Ute Sprenger, writing in Biotechnology and Development Monitor (December 1995) describes the Task Force:
“…a global coordinating body for anti-fertility vaccine R&D…such as anti-sperm and anti-ovum vaccines…”
Sprenger indicates that, as of 1995, there were a number of large groups researching these vaccines. Among them:
WHO/HRP. HRP, the Special Progamme of Research, Development and Research Training in Human Reproduction, is located in Switzerland. It is funded by “the governments of Sweden, United Kingdom, Norway, Denmark, Germany and Canada, as well as the UNFPA and the World Bank.”
The Population Council, a US group funded by the Rockefeller Foundation, the National Institutes of Health [a US federal agency], and the US Agency for International Development [notorious for its collaborations with the CIA].
National Institute of Immunology. Located in India, “major funders are the Indian government, the Canadian International Development Research Center and the [ubiquitous] Rockefeller Foundation.”
The Center for Population Research operates under the umbrella of the US National Institute of Child Health and Development [!], which is part of the US National Institutes of Health.
Over time, the names of these groups change; their goal remains the same. Depopulation through vaccination. And of course, it doesn’t take long to find the name, Bill Gates, as a funding source.
To provide background on this long-term operation, it’s necessary to understand the vision of arch Globalists and radical environmentalists. (I’m not talking about environmental groups who simply want to combat major corporate polluters.)
If you demonstrated that the most advanced waste incinerators could burn all the organic and inorganic garbage piling up in landfills around the world and in the oceans—including plastics—and the toxic compounds emitted by these incinerators would cause FAR LESS damage than the landfills and the ocean plastic dumps…
And even if you advocated the incinerators as stop-gap solutions, until better answers could be found…
A radical environmentalist would reject your proposal—and any technological fix—out of hand.
He wants to re-forest the entire planet, reduce the human population to a fraction of its current size, and cede police powers for achieving these objectives to a magical global governance body.
Elite Globalists approve of radical environmentalism—but with a twist. They want a technocratic Brave New World, where those humans allowed to survive would be genetically “improved” and controlled, to keep them from exercising a dangerous item called freedom.
The Globalists and the radical environmentalists agree that there are too many people on Earth; and no solution to human problems can be accomplished, given the current (excess) population. Instead of 7 billion people, they want a human race of a billion or five hundred million.
Both groups also agree that the fake science of climate change should be pushed to the limit, in order to impose energy-use quotas on every human. This program would actually lower energy use and production across the world and create massive poverty and a massive die-off.
For decades, elite Globalists have been asking themselves the question: How do you kill billions of people and get away with it?
One of their prime answers has been: pandemics.
Of course, the true pandemic is the response to the fake pandemic: vaccines.
If, in the long-term, vaccines can induce the inability to produce children, the genocide would be invisible.
A combination of truth and lies—issued as ongoing studies and press reports—would “explain” falling birth rates. E.g., climate change, extreme weather, pesticides, women opting out of motherhood for careers, economic downturns, fear of raising children in a world of increasing dangers, etc.
But behind it all—vaccines.
Preliminary animal studies of COVID RNA technology are reporting that the spike protein travels through the body, far beyond expected destinations. Applied to humans, this would mean the immune system is on full-attack mode against the protein. And THAT opens the door to immune-system rejection on a grand scale—the body basically assaults itself and its organs. The targets of assault could very well include tissues of the womb and a developing embryo.
The current claim that ongoing COVID booster shots will be necessary reinforces this scenario.
In medical, psychological, and sociological literature, the nasty direct term, “eugenics,” has been replaced by a softer vaguer one, “family planning.” The new term is designed to hide the true agenda.
For Globalists and radical environmentalists, the unparalleled success of the propaganda operation called COVID assures vaccinations on a scale never achieved before. It also assures the expansion of RNA technology—new vaccines and drugs which are genetic treatments designed to force the body to produce unnatural proteins.
There is no end to the genetic alterations to which humans can be subjected.
It stands to reason, given the history of research on depopulation vaccines, that some of those alterations are, and will be, aimed at cutting off the ability to procreate.
UKMFA have sent a letter of complaint to Prof Sridhar following her claims made on BBC Newsround, which is shown in most UK schools, which made several false or misleading claims including that the Covid-19 vaccines are 100% safe, that children should have the vaccine to protect their parents, and that the benefits to children outweigh any risks.
To present such a simplified and biased message is, in our opinion, deeply irresponsible, amounts to propaganda, and negatively impacts on the process of giving fully informed consent. We have requested that Prof Sridhar immediately retracts the entire message and issues a clear public apology for misrepresenting the facts relating to the safety concerns of Covid-19 vaccines in children.
This is in response to your recent appearance on BBC Newsround, where you made several statements which are entirely unsupported by scientific evidence.
Concerns are mainly related but not limited to the following points:
You state the benefit of the vaccine for children would be that they then “don’t need to worry about Covid-19”. Children are already in a position where they do not have to worry about Covid-19, as the risk to them is close to zero.
You state that another benefit would be that they then are likely to not infect their parents. Children do not play a major role in transmission, and there is also no evidence from the regulatory trials that the vaccines prevent transmission. This is clearly a statement intended to provoke an emotional response of guilt followed by a sense of duty, and as such it is propaganda rather than factual advice.
You state that the main downside of getting the vaccine is that it is “another injection into your arm”. This is a gross misrepresentation of the known and unknown risks of potential serious adverse effectsof the Covid-19 vaccines for children. We are sure you are aware that the CDC in the US is calling an emergency meeting, specifically to discuss the hundreds of cases of myocarditis that have occurred in young people after the vaccine (https://www.dailymail.co.uk/news/article-9672233/The-Latest-WHO-warns-delta-variant-hold-Europe.html).
Life-threatening effects and deaths have been reported in young adults and children in the US and Israel, which you do not refer to at all.
You will find the relevant references to all those points in our Open letter.
In the current situation, which is fraught with uncertainty and fear, the public is looking to professionals for balanced advice. To present such a simplified and biased message is, in our opinion, deeply irresponsible. When it is targeted specifically at a vulnerable group of children, it is unforgiveable.
We note that the currently accessible version of your statement on Newsround has already been redacted, as you originally claimed 100% safety for the Pfizer-BioNTech vaccine. You must have been aware that declaring any medical intervention 100% safe undermines anyone’s credibility.
Editing a feature after it has already been circulated and viewed by huge numbers of the public and children, without a publicized explanation or apology, is highly irregular. The comment at the end of the written transcript, merely noting a correction, will not reach the majority of the audience who have heard and assimilated your initial claim.
We therefore request that you immediately retract your entire message and issue a clear public apology for misrepresenting the facts relating to the safety concerns of Covid-19 vaccines in children.
We request that your retraction and apology are circulated as widely as your initial message, and specifically to all schools where this material may have been shown to children.
We are expecting a response confirming that you have taken appropriate action, or otherwise justify the reasons why you have not done so.
Rt. Hon. Gavin Williamson – Secretary of State for Education
Rt. Hon. Oliver Dowden – Secretary of State for Digital, Culture, Media and Sport Shirley-Anne Somerville – Scottish Cabinet Secretary for Education and Skills
In March 2020, Fauci, Redfield, Birx, Bright were insubordinate to POTUS and blocked HCQ / Zelenko Protocol access to the American people in the pre-hospital setting. As a result, over 160k people were hospitalized and died unnecessarily. Lets make life saving treatment available and end the pandemic. Let’s bring these criminals to justice.
“Dr. Zelenko is a Hasidic Jewish doctor and a board-certified family practitioner in New York. We first wrote about him in March after he reportedly treated coronavirus patients with a 99% success rate using hydroxychloroquine and zinc. Back in July, Dr. Zelenko reported that he had treated over 1,500 coronavirus patients using a cocktail of the three-drug regimen.
Dr. Zelenko is one of the several doctors who said the deaths of thousands of Americans could have been prevented if they had been treated with hydroxychloroquine. In August, another doctor, renowned epidemiologist and Yale professor Dr. Harvey Risch accused Dr. Fauci and the FDA of causing the ‘deaths of hundreds of thousands of Americans’ that could have been saved by hydroxychloroquine. Dr. Zelenko has since taken his fight for justice to social media. In the early days of coronavirus, he created a Twitter account and also launched a website to promote what he called the ‘Zelenko Protocol’ for the treatment of coronavirus patients.
Yesterday, Dr. Zelenko led a White House petition to investigate Drs. Fauci, Redfield, Birx, and Bright for ‘Crimes Against Humanity and Mass Murder’ and also calling on the White House to make the life-saving treatment available to end the pandemic….
“Dr. Vladimir Zelenko has been included in a group of doctors nominated for the Nobel Peace Prize for their role in addressing the coronavirus pandemic. The list of this year’s nominees includes 43 candidates.
Dr. Zelenko achieved worldwide prominence for treating COVID-19 patients with hydroxychloroquine and zinc, finding that mortality dropped 8-fold with use of those two substances. He says treatment with hydroxychloroquine and zinc within the first 5 days reduces death rates by 85%.
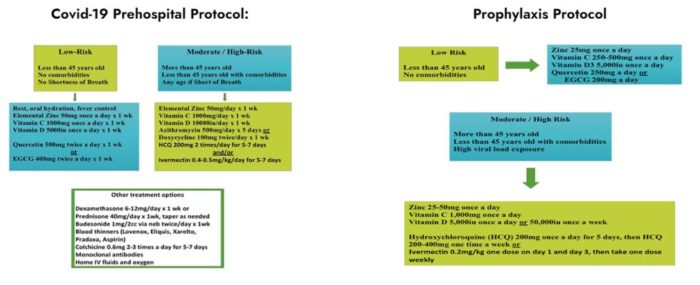
“Basically, the main element of this treatment approach is zinc,” he said in an interview. “Zinc inhibits a very important enzyme called RNA dependent RNA polymerase or replicase. It basically stops the virus from replicating or copying its genetic material, essentially reducing the amount of virus. However, zinc doesn’t get into the cell of the viruses, they need a way to get the zinc into the cell, and that’s the role of hydroxychloroquine in the outpatient setting. Hydroxychloroquine has four other, fourfold mechanisms of action, but those are relevant in the later stages of the disease.
“…. And 3rd component of this was the antibiotic I was using azithromycin, based on the work of Dr. Raoul, and it turns out that azithromycin has both antiviral properties and antibacterial properties, and seem to prevent pulmonary complications.
“But it turns out, very simple: If you wait more than five, six days, that’s when all the lung damage and the blood clots happen. So it’s very important to intervene as soon as possible, as soon as you see the patient and you have clinical suspicion. And it’s very easy to make the diagnosis.”
Political Opposition To HCQ Life-Saving COVID Treatment
As his treatment protocol was portrayed by mainstream media as an unsuccessful, dangerous drug regimen, Dr. Zelenko had been saving his patients’ lives with his “Zelenko Protocol” since March 2020.
“I can give you reasons why there’s resistance, it’s very simple. It’s called politics, profit, arrogance, and fear,” he said. Dr. Zelenko did not stop there, however, but flatly called hydroxychloroquine/zinc efficacy deniers “guilty of mass murder“. He led a White House petition asking that Dr. Anthony Fauci and three others be charged and brought to justice for “crimes against humanity/mass murder”.
Based on my front-line experience, it is essential to start treatment against Covid-19 immediately upon clinical diagnosis of the infection and not to wait for confirmatory testing. There is a very narrow window of opportunity to eliminate the virus before pulmonary complications begin. Delaying treatment is the essence of the problem. My treatment regime is listed below and please know that as of today it has saved 383 patients without complications or negative side effects.
Based on my front-line experience, the emphasis must be on preemptive treatment for high-risk patients in the outpatient setting – primary care and urgent care settings. It makes no sense to wait until a patient is admitted to a hospital and put on a ventilator. High-risk patients are those over the age of 60, those with underlying health conditions or compromised immune systems, and anyone with symptoms and shortness of breath.
“In addition, we should consider immediate prophylactic treatment of very high-risk individuals. Very high-risk individuals are front-line health care providers, nursing home residents, police officers, etc.”
He concluded his letter to the President:
“Any bureaucratic/man-made obstacles that interfere with doctors’ ability to treat their patients with these well-known, field-tested, inexpensive and life-saving medications in my humble opinion is inexcusable and should be treated as a crime against humanity.”
Dr. Zelenko Says: HCQ Deniers Are “Guilty of Mass Murder”
In Doctors Love It, Fauci Hates It. Why?, Del Bigtree, host of The Highwire, discusses Fauci’s strange opposition to HCQ, a proven inexpensive cure for COVID-19! The show says:
“WHY with so many frontline doctors speaking up on their success treating Covid19 with a 65-year-old FDA-approved malaria drug, many wonder what would motivate our top health officials and social media platforms to silence their voices.”
“As the Covid-19 treatment Hydroxychloroquine continues to be portrayed by MSM as an unsuccessful, dangerous drug, Vladimir Zelenko, MD saved his patients’ lives with his ‘Zelenko Protocol’ since March. Del goes in depth with Zelenko about how he developed his protocol, the attack against the drug, and how his letter to the President might have changed history.”
America’s Frontline Doctors (AFLDS), led by Dr. Simone Gold, held a press conference on July 27. Their message was that Americans need not be afraid of COVID-19 because HCQ is had saved the lives of over 200,000 American COVID patients. Read the transcript of their press conference.
America’s Frontline Doctors site said:
“American life has fallen casualty to a massive disinformation campaign. We can speculate on how this has happened, and why it has continued, but the purpose of the inaugural White Coat Summit is to empower Americans to stop living in fear. If Americans continue to let so-called experts and media personalities make their decisions, the great American experiment of a Constitutional Republic with Representative Democracy, will cease.”
“The bumper-sticker directive to ‘follow the science’ was actually an evasion of responsibility. It let people off the hook for their bad decisions in a crisis.”
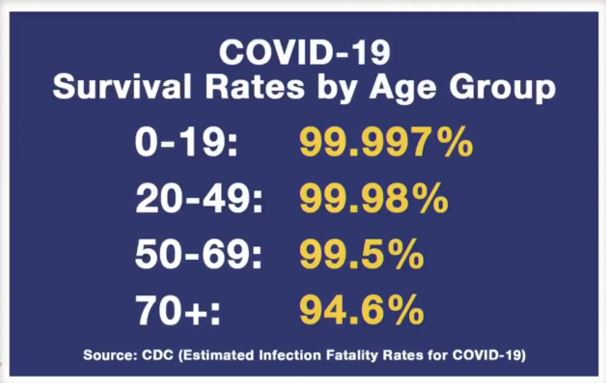
“…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a fatality rate of approximately 0.1)…rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively”.
The recent email dump confirms Fauci knew COVID was a flu — not a “global pandemic” that justified lockdowns, masks, social distancing, tests, and “vaccines”.
British Report Calls For Cessation of COVID “Vaccines”
World Renowned Conventional Doc Blasts The COVID JAB-Erwocks includes an interview with Dr. Peter McCullough, Vice Chief of Internal Medicine, Baylor University Medical Center. It says Dr. McCullough “might be the world’s top cardiologist, who also holds an MPH degree and is a professor of medicine.
His work/background is totally stunning, and seems impossible for one person. …Even better, he’s also world famous. Meaning…he has the exceptional intelligence to analyze and dissect the COVID VAX atrocity. The measured way in which he delivers this bombshell is also remarkable.”
Dr. McCullough discusses blood clots for which the J&J product was halted and points out that blood clots caused by the mRNA vaccine are “probably 30 times that” — but it has not been halted. Dr. McCullouogh says “…keep in mind that the NIH is a co-owner of the Moderna patent.”
The article reports:
“One horrific injustice noted is that people are not being fully informed of the vaccine risks, nor of the volume of serious reactions. Official propaganda says “Safe”. McCullough indicts every member of the criminal cartel running this scam, from NIH to the WHO to the Gates Foundation. That spectrum includes the individual most of us know as a criminal from the outset – Anthony Fauci. Not that the clotting issue takes anything away from the part about being WAY past the death point where any drug would normally be pulled.”
Dr. McCullough says if a new drug causes five deaths, it gets a “Black Box Warning”. At 50 deaths, a new drug is called off the market. The 1976 SARS vaccine program was stopped after 25 deaths. However, in the US where about 77 million people have been vaccinated with the COVID shots, there have been reported 2,260 deaths. Yet, those may be just 1-10% of the number because a Harvard study showed that just 1% of vaccine injuries are reported to VAERS. Most deaths from the COVID shots occur on day 1, 2, or 3. Some occur at the vaccination center! Yet, now the plan is to vaccinate 12-15 year olds who have less than a zero percent risk of catching the virus!
Is Fauci Getting Away With Murder or Is The Tide Turning?
“The mainstream narrative of the COVID pandemic is changing. Mainstream media outlets are now permitting some severe criticisms of Dr. Fauci, Bill Gates, and the entire community of virologists who only know how to sell fear and vaccines…. At first, the reversal was driven by Senators who just got sick of listening to Fauci, who has been more than busy singlehandedly wrecking peoples’ lives and the Constitution. It has ended up as an all-out attack on dangerous viral research while nailing the Wuhan lab as the definitive source of COVID. But perhaps leading the charge was Tucker Carlson from FOX news, who has been asking tough questions about vaccines never before heard in the mainstream….
The 55-year government lifer and windbag, Anthony Fauci, has single-handedly made a mockery of “the science” and the U.S. Constitution during the past 14 months, writes David Stockman. “America is indeed suffering from a dangerous plague—a plague of misanthropic fear-mongering from the likes of Dr. Fauci, the Scarf Lady, and the Biden’s new CDC director, among countless others of the self-designated Virus Patrol.” GOP Rep. Marjorie Taylor Greene introduces a bill to slash Fauci’s $400,000 salary to ZERO until he’s replaced.”
“In the millions of articles, opinion pieces, and news stories written about Covid there is one topic that is more important than all the others. It’s more important than masks, vaccines, or lockdown measures. The origin of the virus is critical because no matter how many people die from covid, or how many businesses are wiped out, it’s critical that IF the next virus can be stopped, it must be.
A science writer named Nicholas Wade has written the most thorough study on the origins of Covid to be released to the public. Wade has worked with Nature, Science, and the New York Times, but this article was released on the public platform Medium. … This is a long read, but it might be the most important article yet written during this pandemic.”
“We can’t recommend more strongly a new piece by Nicholas Wade, who for more than 50 years has been one of the preeminent science writers in the world. For 30 years, Nicholas Wade worked for the New York Times, he edited the science section there. But this piece did not run in the New York Times, he edited the science section there. But this piece did not run in the New York Times. It ran on Medium. And the piece explains where the virus almost certainly came from. In it, Wade makes it clear that, more than any other single American, Tony Fauci is responsible for the COVID-19 pandemic. Wade lays out a nearly insurmountable amount of evidence that this virus originated at the Wuhan Institute of Virology in Central China. We’ve raised this possibility from the early days of the pandemic. But this piece all but proves it.”
Follow “The Science”
Throughout 2020, the media told us to “follow the science” as presented by Dr. Anthony Fauci. In the video linked below, Del Bigtree, host of The Highwire, played a clip of Fauci claiming that HE IS “The Science” and anyone who questions him is “anti-science”. Bigtree’s Informed Consent Action Network (ICAN) released 3,000 pages of Fauci’s emails — very incriminating correspondence.
IS COVID-19 A BIO-WEAPON?: “Dr. Richard Fleming takes Del through a shocking paper trail surrounding the SARS-CoV2 virus and its link to Fauci and US funded gain-of-function research.”
Governor DeSantis: “We Chose Freedom Over Fauci-ism”
Video available at Rosemary Frei’s BitChute channel.
This month marks the 40th anniversary of the first report of what was subsequently dubbed ‘acquired immunodeficiency syndrome’ or ‘AIDS.’
Officials like Anthony Fauci are using the occasion to spread the message that vaccines for HIV, which is the virus said to cause AIDS, will soon be rolling out. Forty years of fruitless effort supposedly are suddenly successful thanks to the precedent of the lightening-speed and ‘successful’ development of Covid vaccines.
Fauci said June 4 in an MSNBC interview by Rachel Maddow that because of “the technologies that have now been perfected, particularly the mRNA technology and other vaccine platforms that were perfected and used in Covid-19, I believe strongly we’ll go back and be able to really forward and advance the HIV [vaccine] effort.”
AJune 6 Guardian article says that Fauci “holds out hope that the three HIV vaccines in advanced clinical trials will prove at least 50% efficacious, justifying a global roll out. But he now hopes mRNA or other advanced technologies could yield even more powerful HIV vaccines.”
Note that under Fauci, in July 2020 as part of Operation Warp Speed, four major NIAID-funded HIV global clinical-trials networks were retooled into the Covid-19 Prevention Network (COVPN). People in the network help create vaxxes and other ‘treatments’ for both HIV and Covid.
And already byApril 14, 2020, mRNA ‘vaccine’ maker Moderna had announced that soon they’ll be conducting small human trials on their experimental jabs against HIV and the flu.
So far, at least 26 different mRNA shots are on the way from Moderna,in addition to their three types of Covid jabs. The shots in development range from two for HIV to one ‘personalized cancer vaccine.’
Vaccines are immensely profitable: the new, Covid jabs are topping the all-time charts for medical money-making. Plus vaccine makers have no liability for the illnesses and deaths they cause. Thereforeusing the name ‘vaccine’ for all ‘treatments,’ no matter what they contain, is a formula for making huge amounts of money with very little downside.
And the potential market for HIV ‘vaccines’ alone is very large. For example, an October 2020 paper in the journal Lancet HIV — on the use of two experimental HIV vaxxes made by Janssen in healthy, HIV-negative people, and funded by among others the Gates Foundation — starts with the sentence, “Current estimates of 37.9 million people living with HIV worldwide and 1.7 million new infections annually, with no cure on the horizon, make development of an effective prophylactic vaccine a global priority.” (The paper’s authors reported very high rates of adverse events to the vaccines, but still assessed the shots as being “generally safe and well-tolerated.”)
All of this is despite the fact that HIV has not been detected by anything other than indirect methods such as antibody, T-cell and polymerase chain reaction (PCR) testing. HIV also has not been clearly shown to cause disease. Nor has it been isolated or rigorously imaged via electron microscopy. Isolation is a necessary step before sequencing – because otherwise the resulting sequences reflect a heterogeneous mix of material rather than pure virus. Details on this are below.
This also holds true for the novel coronavirus.
Phalanxes of officials such as Fauci censor these inconvenient facts. And they keep the public captive, overloaded and off-balance with an avalanche of complex and contradictory jargon, modelling and scientific studies.
The Myth of HIV and of AIDS
Kary Mullis won the Nobel Prize in 1993 for inventing PCR. He died in August 2019. There are many videos of him demolishing Fauci and/or the HIV-AIDS hypothesis. He also discusses this in his autobiography Dancing Naked in the Mind Field.
For example, Mullis said the following in one of his video interviews: “He [Fauci] doesn’t know anything really about anything, and I’d say that to his face. Nothing! … He doesn’t understand electron microscopy, and he doesn’t understand medicine, and he should not be in a position like he’s in…. Tony Fauci does not mind going on television in front of the people [taxpayers] who pay his salary and lie directly into the camera.”
Indeed, falsely claiming to have isolated HIV and imaged it with electron microscopy are key parts of the artifice used by Luc Montagnier and Robert Gallo to assert in 1984 that they’d discovered HIV and that it causes AIDS.
The same applies to the novel coronavirus. For example, one of today’s top electron microscopy experts – Duke University pathology professor Sara Miller — herself failed in an April 2021 paper to prove that an electron-microscopy image shows the novel coronavirus. She simply asserted it’s the virus without giving information on, or even references to, the techniques used to show that it is. (If she had given information, it certainly would have relied on the use of antibodies, because they are the main tool for identification purposes. But as I document in my article The Antibody Deception, antibodies cross-react with many other things and therefore cannot accurately pick out the novel coronavirus.)
Mullis wrote the foreword to the very long but very important book Inventing the AIDS Virus. The book was published in 1996 and is byPeter Duesberg, a University of California, Berkeley, professor of biochemistry, biophysics and structural biology. It details the genesis of the HIV-AIDS myth and is still highly relevant today. (Note that Duesberg believes the virus exists but is harmless because it doesn’t multiply in the body, while Mullis believed the virus doesn’t exist at all.) [Note added June 14 after article posted: Mullis apparently did believe the virus exists. See for example this video, which a friend just emailed me. However, I stand by my assertion that HIV has never been conclusively isolated or imaged. Even Mullis’s statements in that video can be seen as indicating HIV is virtually impossible to conclusively isolate or image.]
Mullis writes this in the forward:
“We [he and Duesberg] have not been able to discover any good reasons why most of the people on earth believe that AIDS is a disease caused by a virus called HIV. There is simply no scientific evidence demonstrating that it is true,” wrote Mullis in that foreword. “… We know that to err is human, but the HIV/AIDS hypothesis is one hell of a mistake.”
In the book, Duesberg documents that one main part of the trajectory toward the creation of the myth started in 1912, with the reorganization of the U.S.’s Public Health Service. Another key part was the creation in 1946 of the predecessor of the current CDC — with its predilection for deeming ‘outbreaks’ to be due to infectious diseases, and then testing, tracking and quarantining people under the premise of stopping the spread.
(Two of many valuable insights by Duesberg are on page 137-138: “The CDC has … continued to exploit public trust by transforming seasonal flus and other minor epidemics into monstrous crises and by manufacturing contagious plagues out of noninfectious medical conditions.” And, “[E]pidemiologists have classically studied clusters of sick people as clues to subtle environmental hazards, not infectious agents. But when public health officials issue ominous warnings about mysterious disease outbreaks, they terrify the public with visions of deadly pandemics.”)
Duesberg also details, on pages 174 to188, the failure of HIV to fulfill Koch’s postulates. And on page 202 he concludes that, “AIDS fails all epidemiological criteria of an infectious disease.”
(I believe the same is true for Covid.)
Duesberg points, in addition, to the reasons ‘experts’ give for why it’s virtually impossible to directly detect the virus. For example, he writes on page 206 that:
“[I]f little or no HIV can be found in the body, scientists propose hidden reservoirs and special routes of infection. If only antibodies against HIV [rather than HIV itself] can be found, researchers call them ‘nonneutralizing’ (or ineffective) antibodies and assert that the virus mutates too fast for the antibodies to keep up…. All these hypotheses are constantly being disproved or shown to be irrelevant, but the reservoir of new evasions is inexhaustible.”
That of course parallels the pranks ‘experts’ are playing on the public with respect to the novel coronavirus and Covid.
Duesberg makes the strong case that ‘AIDS’ is actually 30 conditions inappropriately lumped into the single category. And he demonstrates that the main causes are: toxicity from AZT and other meds given to people who test positive for HIV(more on this below); toxicity from recreational drugs like nitrite inhalants — AKA ‘poppers’; and overuse of antibiotics.
In countries such as Africa, the causes also include poverty, malnutrition, lack of indoor plumbing and tropical infections.
“‘AIDS’ … is defined entirely in terms of other, old diseases, in conjunction with dubious test results and even more dubious assumptions. Although people are undeniably sick, ‘AIDS’ itself does not really exist; it is a phoney construct,” Lauritsen states on page 180 of the book.
Yet virtually all the funding for the vast HIV/AIDS research-administrative-medical-industrial complex assumes HIV is the cause of ‘AIDS.’
In 1984, just three years after the first report of what later would be dubbed AIDS, Fauci became the head of NIAID.
AIDS made him a star: he’s good at grabbing the spotlight with his gift of glib gab, and under his tenure NIAID ballooned thanks to a huge inflow of AIDS-related funding.
Just three years later, in 1987, the first medication for HIV went on the market: AZT, which is highly toxic.
AZT has killed huge numbers of people, thanks in large part to Fauci pushing the message that it is ‘safe and effective.’
“I would say there were hundreds of thousands of people killed by AZT. And many — perhaps most — of them were perfectly healthy before they were put on the drugs,” Lauritsen told me in a telephone interview from his home in Boston. “They got a positive result on the worthless HIV tests, and then they were told to put time on their side and take AZT. And of course it killed them.”
Fauci and other powerful officials have also pushed other deadly drugs, such as Bristol-Myers Squibb’s didanosine (ddI).
Duesberg and Lauritsen detail how the U.S. Food and Drug Administration was pressured into giving ddI fast-track approval in 1991 — despite clear evidence that it is toxic, and that there were no placebo-controlled safety or efficacy studies conducted on it.
Even Wikipedia, which usually censors information that criticizes big pharma, states that about one-quarter of people taking ddI develop peripheral neuropathy. And in 2010 the FDA issued a warning that a serious liver disease can occur in people taking ddI.
The latter include drugs as tenofovir, lamivudine and emtricitabine. These are a type of drug known as nucleoside analogues (AKA nucleoside inhibitors or nucleoside reverse transcriptase inhibitors). And they have the same, and potentially very dangerous, mechanism of action as AZT and ddI: that is, they stop DNA synthesis from taking place in cells throughout the body.
[Full disclosure: in the mid- to late 1990s as a freelance medical writer I co-wrote marketing materials for HIV drugs such as lamivudine and tenofovir through a Toronto, Ontario, marketing agency called Jeffrey Simbrow Associates. Then later, until the mid-2000s, as a medical journalist I wrote many stories for trade publications about HIV drugs. I somehow was completely unaware of the controversy surrounding these drugs and HIV and AIDS.]
Today tens of millions of healthy people are taking PrEP because they’ve been led to believe this will either prevent infection, or lower their HIV levels to undetectable (the latter goes by the slogan ‘U=U’ for ‘undetectable = untransmissible’). And information is suppressed that many people who have tested positive for HIV but haven’t taken any medication remain healthy for decades.
Over the last year, PreP sales have been sliding somewhat, as has HIV testing. ‘Experts’ are blaming this on the curtailment of usual accessible care during the pandemic. (And they’re also telling scary tales of untreated ‘HIV/AIDS’ potentially interfering with efforts to quash Covid.)
Enter the news about HIV vaxxes being on the horizon — and their potentially huge market.
There are tens of millions of people who have tested positive, and many many more being tested every day.
Plus, most people would prefer an HIV vaxx instead of a daily pill; pills are expensive and inconvenient.
Central Players in the HIV and Novel Coronavirus Capers
Not surprisingly, there are major overlaps between the key figures in the HIV-AIDS and novel coronavirus-COVID agendas. And they’re not just the usual suspects such as Bill Gates.
They include names such asLarry Corey, Myron Cohen and Lindsey Baden.
Corey leads the HIV Vaccine Trials Network, a position he’s held since 1999, and which now is the operational center for the COVID-19 Prevention Network (COVPN – mentioned earlier). He also is co-leading vaccine testing at the COVPN – which started, last summer, with a Phase 3 studyof one of Moderna’s mRNA Covid jabs.
Cohen is director of the Institute for Global Health and Infections Diseases, and a prof of medical microbiology, immunology and epidemiology at University of North Carolina in Chapel Hill.
They’re testing PrEP drugs and antibodies. The latter includes the AbCellera/Eli Lilly antibody bamlanivumab.
The results of one of those studies, on bamlanivumab for workers and residents in care homes, were announced on Jan. 21 by Lilly via a press release. They were published in the prominent Journal of the American Medical Association onJune 3, 2021, with Cohen as the lead author. (In my The Antibody Deception article I described how it’s virtually impossible for bamlanivumab to bean effective treatment for anything.)
Baden is the deputy editor of the New England Journal of Medicine (NEJM), a position he’s had since 2005. And he’s also a long-time associate prof at the Harvard Medical School.
He has been working toward HIV vaxxes since at least 2007
Baden’s pushing both the HIV and Covid agendas forward at warp speed. For example, he’s the first author on the Dec. 30, 2020, NEJM paper that concluded that one of Moderna Covid vaccines has “94.1% efficacy at preventing Covid-19 illness.”
Baden is funded by, among many others, Moderna, the Gates Foundation, Wellcome Trust, Janssen, the Military HIV Research Program and NIAID (see pages 2 and 3 of the disclosure forms for the paper’s authors).
There also are many other ways that the money pipers call Baden’s tune.
For example, since February 2020 Baden has been giving once-weekly audio interviews for NEJM, together with the journal’s editor-in-chief Eric Rubin. The pair use this prominent pulpit to, among other things, endorse mass vaccination for Covid including inminorities, pregnant women and children.
And Baden, Corey and Cohen were among the co-authors of a March 2021 NEJM paper titled, ‘Two randomized trials of neutralizing antibodies to prevent HIV-1 acquisition.’ In other, using antibodies for PrEP.
There are hundreds of other key players in the parallel HIV-COVID play. You can use PubMed to look up the papers and conflicts of interest of prominent scientists in your area who have been among those pushing the Covid agenda.
On Dec. 3, 2020, the Oregon Medical Board issued an “emergency order” to suspend the license of Dr. Paul Thomas, a pediatrician, who along with science writer Jennifer Margulis, Ph.D., co-authored “The Vaccine-Friendly Plan.”
Affectionately known by his patients and peers as “Dr. Paul,” Thomas was accused by the board of posing a threat to public health by pushing parents to accept his alternative vaccine schedule rather than the routine childhood vaccine schedule recommended by the Centers for Disease Control and Prevention (CDC).
The apparent impetus for the “emergency” meeting, however, was the publication just days prior of a study showing that compared with his vaccinated patients, those patients who received no vaccines have significantly lower incidence of diagnoses and office visits for a broad range of chronic health conditions — including asthma, allergies, eczema, dermatitis, hives, anemia, eye disorders, ear infections, respiratory infections, other infections, breathing issues, behavioral issues, and attention deficit hyperactivity disorder (ADHD).
Thomas obtained institutional review board approval to use his de-identified patient data for research and publication of the study, which was co-authored by James Lyons-Weiler, Ph.D.
While the study does not demonstrate that vaccination was the cause of the higher incidence and severity of chronic illnesses among vaccinated children, the results do demonstrate to a reasonable degree of certainty that Thomas’ unvaccinated children are healthier and place less of a burden on the healthcare system.
Among patients born into his practice, the rate of autism was one-fifth that of the CDC’s estimated national prevalence of 1 in 54 children. For ADHD, there were zero cases among his unvaccinated patients compared with 5.3% of the variably vaccinated, which in turn compares with the U.S. national rate, according to the CDC, of 9.4%.
Looking at diagnoses for diseases CDC-recommended vaccines are intended to protect against, the study’s authors found a total of 41:29 for varicella (or chicken pox), 10 for pertussis (or whooping cough), and two for rotavirus. The numbers of diagnoses for the unvaccinated group were 23, nine and two, respectively.
These numbers indicated that 17.2 children born into his practice needed to be vaccinated in order for one child to receive the benefit of protection against a vaccine-targeted disease.
To put it another way, for every 17 children vaccinated, 16 received no benefit from having undergone a risk-carrying pharmaceutical intervention. There were zero deaths in Thomas’s practice from any disease for which the CDC recommends vaccination.
Figure 5 of the study compares cumulative office visits per condition in the vaccinated (orange) with unvaccinated (blue) patients over time (days of life).
Importantly, in a letter of complaint dated Dec. 26, 2018, the Oregon Medical Board had requested Thomas produce peer-reviewed evidence to support his alternative approach to vaccination. Yet when he did so, the board dismissed the evidence, clearly demonstrating there was no public health emergency arising from his approach to vaccination.
Just as importantly, the medical board itself, while placing that burden of proof on Thomas, is incapable of producing peer-reviewed evidence demonstrating children vaccinated according to the CDC’s schedule are healthier than children who remained completely unvaccinated.
As the Institute of Medicine (IOM) acknowledged in a 2013 review, “No studies have compared the differences in health outcomes … between entirely unimmunized populations of children and fully immunized children.”
The IOM reiterated that “existing research has not been designed to test the entire immunization schedule” and “studies designed to examine the long-term effects of the cumulative number of vaccines or other aspects of the immunization schedule have not been conducted.”
The Oregon Medical Board’s “emergency” suspension order accused Thomas of “bullying” patients into accepting an alternative vaccine schedule, but this is demonstrably false.
First, it logically cannot be the case that the medical board is opposed to physicians bullying patients. This is evident in the fact that doctors across the state pressure parents to vaccinate strictly according to the CDC’s schedule, and some go so far in their bullying as to expel from their practice families who decline to do so.
Far from the medical board suspending the license of doctors who engage in such behavior, it is evident from the suspension order itself this is precisely the behavior the medical board expects from licensed physicians.
Second, it logically cannot be the case that Thomas pressures parents to accept the alternative schedule presented in his book, “The Vaccine-Friendly Plan,” because that would be contrary to the whole principle — which is that a risk-benefit analysis is required for each vaccine and each individual.
The specific schedule described in the book is merely one possible approach designed to reduce children’s cumulative exposure to aluminum, a known neurotoxin used in vaccines as an adjuvant, which is a substance intended to provoke a stronger immune response.
The board has accused Thomas of pressuring parents into an alternative one-size-fits-all schedule, which is anathema to the whole concept of taking an individualized approach.
The cognitive dissonance of the medical board is illustrated in the fact that the board’s suspension order accuses Thomas of not administering vaccines he recommends in his book. Thus, it logically cannot be true the reason these children did not receive those vaccines is because Thomas pressured them out of it.
The truth is families have flocked to Thomas’s practice in Portland, Oregon precisely because they do not want to be bullied into accepting a one-size-fits-all approach to vaccination. They go to him precisely because he is well known in the community for respecting their right to informed consent.
Thomas’ journey of awakening
Paul Thomas was born in Portland in 1957. In 1961, his family moved to a village in what was then the British territory of Rhodesia on the northern border of South Africa, where Zimbabwe exists today. They were the only white people living in the village.
In 1964, a party came into power in Rhodesia that opposed transition to democratic rule, which would mean the end of rule by a white minority. The regime implemented a policy of apartheid-like segregation and was never internationally recognized.
In 1966, when it was discovered Thomas was attending the village school, he was removed to an all-white school, where he excelled in academics and sports and was eventually given the titular honor of “Head Boy.”
In 1968, the regime held a ceremony to lower the Union Jack and raise the new Rhodesian flag in its place. At school, 11-year-old Thomas was expected to perform this ceremony in keeping with his duty as Head Boy. Considering the new government to be an unlawful regime, he refused. In 1973, at age 15, he was arrested for distributing educational materials the regime deemed “revolutionary.”
Paul Thomas grew up in the former British territory of Rhodesia, located in southern Africa where Zimbabwe is today. Photo credit: Paul Thomas
In 1974, Thomas returned to the U.S. and entered medical school, earning his M.D. at Dartmouth Medical School. He moved back to Portland in 1988, and in 1993, joined a private group practice. In 1986, he adopted his first child and today is the father of nine children — three biological and six adopted.
Thomas says his children were fully vaccinated. At the private group practice, he did things the way he was trained to. “I come from a background of not being aware of vaccine risk,” Thomas explained. “I come from a background of being very well trained that vaccines are ‘safe and effective.’ I believed it.”
While the media constantly report Wakefield’s paper fraudulently claimed to have found an association between the measles, mumps and rubella (MMR) vaccine and autism, in fact, Wakefield and his co-authors explicitly stated they did not show an association. Rather, they relayed the concern of parents that their children developmentally regressed after receiving the MMR vaccine, and hypothesized there might be a link. They called for further studies to examine this question.
The main finding of the paper was that 12 children who had a developmental disorder also had a gastrointestinal disorder. Today, the connection between gut disorders and autism is well established, with much research now focusing on questions such as the role of the gut microbiome in relation to neurological disorders.
Notably, the media never credit Wakefield for pioneering research into this area.
In 2010, The Lancet retracted Wakefield’s paper after the UK’s General Medical Council (GMC) had stripped Wakefield and his co-author, John Walker-Smith, of their medical licenses.
Walker-Smith, senior author of the study, was the gastroenterologist who examined the children. The stated reason for the retraction was that the GMC had judged the authors to have falsely stated the children were “consecutively referred” and their investigation with the children was not approved by the local ethics committee.
The GMC did not charge the authors with fraud but “professional misconduct.” What the mainstream media failed to ever mention in their coverage of the study is that Walker-Smith appealed the GMC’s decision and won. He was reinstated in 2012, with the High Court of Justice ruling the GMC’s charges against him were “untenable” and unsupported by the evidence.
The children in the study were indeed referred successively, rather than as a single batch, and they did not require ethics approval for the procedures the children underwent under Walker-Smith’s care because the procedures were clinically indicated for diagnostic purposes.
Wakefield did not join his co-author in appealing because the legal costs were not covered by his insurance carrier.
Thomas credits Wakefield with awakening him to the possibility vaccines could cause long-term harms. He began attending educational conferences and digging deeply into the medical literature. Then he observed four of his own patients regress into autism after vaccinations, with one case per year starting in 2004.
The fourth such case struck him hard. “That was the last straw for me,” Thomas recalled. “I just couldn’t go on with business as usual.”
The experience led to what he described as his “divorce” with the private group practice. The other physicians there felt it would be unethical to do anything other than what they were told by the CDC. Thomas felt it was unethical for him to continue the “standard of care” practice of treating vaccination as a one-size-fits-all solution.
Thomas left to open his own practice, Integrative Pediatrics, on the founding principles of providing individualized care and respecting his patients’ right to informed consent. He says more than 1,500 patients left with him, and the practice quickly grew to more than 15,000, with a staff of more than 30.
Thomas’ clinic attracted many parents whose children had developed chronic health conditions or developmental disorders and who were wary of further vaccinating according to the CDC’s recommendations. He began noticing a marked difference in the health of patients whose parents were choosing not to follow the CDC’s schedule.
“We started seeing that our less-vaccinated or unvaccinated children seemed to be healthier,” he said. “I mean, it was palpable — you could just tell.”
In 2015, Thomas commissioned a quality assurance analysis of his patients’ data which confirmed his observation. His experience compelled him to write a book to help parents navigate the decision-making process when it comes to vaccination by empowering them with the knowledge needed to make their own choices.
Thomas’ book, published in 2016, proposed an individualized approach to vaccination. He says he knew then that he was risking his medical career because the book “takes on the CDC’s schedule” and “the CDC’s schedule is sacred.”
The vaccinated vs. unvaccinated study
The first accusation from the Oregon Medical Board came in 2018, and additional letters of complaint followed. Having been asked to produce peer-reviewed evidence to support his approach to vaccination, Thomas hired an independent pediatrician and informatics expert to do a quality assurance project looking at health outcomes of all patients born into his practice.
That was an important inclusion criterion. As Thomas explained, “Most of the patients who come to our practice, or at least a very significant percentage of them, come because they have health problems they are worried were triggered by vaccines, and they can’t get their pediatrician, wherever they are, to slow down or stop vaccinating, so they come to the only safe place they can find.”
This meant Thomas was “getting a lot of damaged kids already,” whereas “very, very few” of those born into his practice had comparable health problems.
To include children who came to him from other practices would introduce a confounding factor that would bias the results. What he wanted to know was what kind of outcomes were resulting from various numbers of vaccinations received among patients who, from the start, were with a clinic that practices informed consent.
Thomas then obtained the approval of the state’s institutional review board to publish the de-identified data. He contrasts the approach he takes in his practice of focusing on achieving good health outcomes with the state’s myopic focus on achieving high vaccination rates.
“We shouldn’t be looking at how well somebody can follow a protocol,” Thomas said. “Monkeys can do that. We should be looking at actual health outcomes, which is what our study did.”
As he explained, “My duty is to my patients, and we have a lot of loyal patients who, you know, love the fact that we honor and provide informed consent and provide great care, and we have great outcomes, which are now documented in a published peer-reviewed study.”
As study co-author and data analyst Lyons-Weiler explained:
“This study represents a major methodological leap forward in vaccine safety studies. The results show how often vaccinating patients have to seek medical care for conditions suspected by many as potentially caused by vaccines. Our measure, the Relative Incidence of Office Visits (RIOV), is sensitive to the severity of disease and disorder — specifically, the disease burden.”
One problem with observational studies is that they are prone to selection bias. A potential bias in comparing data from vaccinated versus unvaccinated patients is the difference in healthcare-seeking behavior. The question arises, given a finding of lower rates of diagnoses among unvaccinated children, whether this is because the family’s lifestyle results in better health outcomes or because their children are underdiagnosed due to avoiding visits with the doctor.
To control for the potential confounder of differing healthcare-seeking behaviors of parents who choose not to do any vaccines, Thomas and Lyons-Weiler looked at incidence of fever and well-child visits. Because fever is a known adverse event associated with vaccination, it was expected the unvaccinated would have fewer visits for fever.
If differences in health outcomes were explainable by parents of unvaccinated children simply choosing not to go in to see their pediatrician, it would also be expected these patients would have fewer well-child visits.
As expected, they found children who received more vaccines had a higher relative incidence of office visits than children who received none. However, there was a stable trend for relative incidence of well-child visits, indicating that differences in healthcare-seeking behavior did not account for the lower incidence of fever in children who received fewer or no vaccines.
Figure 3 in the study shows the RIOV percentile for fever and will-child visits, with RIOV representing the total number of billed office visits per condition per group, which reflects the total disease burden in that study population.
Another confounding factor they accounted for was the relationship between the number of vaccines received and age. Naturally, older children would tend to have had more vaccines than younger children. To avoid comparing vaccinated children with long-term care in Thomas’s practice and unvaccinated children with short-term care, they matched patients between the two groups according to “days of care” in the practice. Because all patients were born into the practice, this correlated with age.
Matching patients to days of care also served to further protect against finding different health outcomes due to different healthcare-seeking behavior.
It is difficult to see how the findings of their study could be attributed to differences in healthcare-seeking behavior or lifestyle choices separate from the parental choice not to vaccinate. As Lyons-Weiler and Thomas remark, if their findings are explainable by different lifestyle choices, “then it would be objective to conclude that everyone should adopt the lifestyle followed by the unvaccinated if they want healthier children. That lifestyle choice includes, for many families, avoiding some or all vaccines, and thus, the lifestyle choice concern is inextricably linked to vaccine exposure.”
As they summarized their findings, “We could detect no widespread negative health effects in the unvaccinated other than the rare but significant vaccine-targeted diagnoses. We can conclude the unvaccinated children in this practice are not, overall, less healthy than the vaccinated and indeed, the vaccinated children appear to be significantly less healthy than the unvaccinated.”
Conclusion
The Oregon Medical Board, myopically focused on the policy goal of achieving high vaccine uptake in pediatric practices across the state, challenged Thomas to produce peer-reviewed evidence to support his approach to vaccinations.
Presumably, the board assumed this would pose an insurmountable obstacle. Yet Thomas rose to the challenge and published the data indicating his unvaccinated patients were the healthiest children in his practice.
The board, rather than taking this requested study into consideration, ignored the evidence and held an emergency meeting just days after the study’s publication during which board members opted to suspend Thomas’ license on the false pretext his approach to vaccination represented a threat to public health.
To support that charge, the board accused Thomas of “bullying” patients into accepting the alternative outlined in his book, “Vaccine-Friendly Plan.” But this, too, is a demonstrably false pretext intended to obfuscate the true reason for suspending his license, which is that the board is intolerant of doctors approaching vaccination on the principles of individualized care and respect for the right to informed consent.
Contrary to the board’s accusations, the health outcomes that Dr. Thomas has achieved with the children in his practice are enviable and should serve as a model for pediatricians across the country. The threat that Dr. Thomas posed was not to public health but to the policy goal of achieving high vaccination rates. His suspension was transparently intended to send the message to other pediatricians that if they practice informed consent, they, too, will risk having their license suspended. The message is that pediatricians must bully parents into vaccinating according to the CDC’s schedule or risk their medical career.
The true threat to public health is coming from those who willfully ignore the scientific evidence and advocate the use of coercion to achieve the policy goal. It is those who cling to this myopic and unscientific approach, grounded in rejection of the need for an individualized risk-benefit analysis and rejection of the right to informed consent, who are the true bullies and pose the true threat to both our children’s health and our precious liberty.
This article is a summary adaptation of the author’s detailed report on the Oregon Medical Board’s suspension of Dr. Paul Thomas. Click here to read the full story.
“…as of Feb. 12, the Vaccine Adverse Event Reporting System (VAERS) had already received 111 reports of adverse events experienced by women who were pregnant at the time of their Pfizer or Moderna injection…”
“The first such report was submitted Dec. 22, just 10 days after authorization of the Pfizer vaccine. Nearly a third (31%) of the women had miscarriages or preterm births, which occurred within as little as one day of injection — the majority after a single dose of vaccine.”
“The descriptions of miscarriages and premature births accompanying the VAERS reports are tragic and hair-raising.”
“For example, a 37-year-old who received her first dose of the Moderna vaccine at 28 weeks of pregnancy, just after an ultrasound showed a healthy placenta, was discovered to have ‘significant placenta issues just one week later.’ A repeat ultrasound showed that the placenta had ‘calcified and aged prematurely,’ leading to recommended hospitalization for the duration of her pregnancy.”
“A 35-year-old, also vaccinated at around 29 weeks of pregnancy, ‘noticed decreased motion of the baby’ two days after receiving the Pfizer injection. The following day, ‘the baby was found to not have a heartbeat’.”
“Two Pfizer vaccine recipients in earlier stages of pregnancy (first trimester) had miscarriages after experiencing ‘intolerable’ abdominal pain and uterine bleeding extensive enough, in one case, to require ‘emergency surgery and a blood transfusion’.”
“…the World Health Organization on Jan. 27 issued guidance advising against pregnant women getting Moderna’s COVID vaccine — only to reverse that guidance two days later, as The New York Times reported.”
“Documented risks of vaccination during pregnancy include miscarriage as well as neurodevelopmental problems arising from maternal immune activation (an inflammatory response in the mother that can harm fetal brain development).”
Concerning that last paragraph: Before the experimental RNA COVID vaccines were authorized, RNA technology had experienced failures and serious problems in clinical trials—because the immune system went into overdrive. It is this immune hyper-response that may be responsible for the recent reported miscarriages and pre-term births; the body basically attacks itself.
This RNA effect is documented in studies published before 2019. The vaccine makers and public health agencies are well aware of it.
But this is just the beginning of the story, because what is happening to vaccinated women now may be part of a much larger history, involving extensive research on medically induced birth control—also known as population reduction.
In the vaccine research community, it’s an open secret that the Rockefeller Fund, the UN, and other groups have been backing the development of vaccines that function as agents of population reduction. This work has been going on for decades.
What follows are examples of the evidence. They cite the Third World as the target, but no one should take that as a hideous sign that depopulation efforts are confined to one group of countries. These efforts are universal.
The late well-known journalist, Alexander Cockburn, on the op ed page of the LA Times, on September 8, 1994, in his piece “Real U.S. Policy in Third World: Sterilization: Disregard the ’empowerment’ shoe polish–the goal is to keep the natives from breeding,” [2] reviewed the infamous Kissinger-commissioned 1974 National Security Study Memorandum 200, “which addressed population issues”:
“… the true concern of Kissinger analysts [in Memorandum 200] was maintenance of US access to Third World resources. They worried that the ‘political consequences’ of population growth [in the Third World] could produce internal instability … With famine and food riots and the breakdown of social order in such countries, [the Kissinger memo warns that] ‘the smooth flow of needed materials will be jeopardized.’”
In other words, too many people equals disruption for the transnational corporations, who steal nations from those very people. Therefore, reduce the population.
Therefore, develop a vaccine that does that job.
Journalist Cockburn, in his LA Times piece, goes on to say that the writers of the Kissinger memo “favored sterilization over food aid.” He notes that, “By 1977, Reimart Ravenholt, the director of AID’s [US Agency for International Development] population program, was saying that his agency’s goal was to sterilize one-quarter of the world’s women.”
Here is an astonishing journal paper. November, 1993. FASEB Journal, volume 7, pp.1381-1385. Authors—Stephan Dirnhofer et al. Dirnhofer was a member of the Institute for Biomedical Aging Research of the Austrian Academy of Sciences.
A quote from the paper: “Our study provides insights into possible modes of action of the birth control vaccine promoted by the Task Force on Birth Control Vaccines of the WHO (World Health Organization).”
A birth control vaccine? Yes. A vaccine whose purpose is to achieve miscarriages. This particular vaccine was apparently just one of several anti-fertility vaccines the Task Force was promoting.
And yes, there is a Task Force on Birth Control Vaccines at the WHO. This journal paper focuses on a hormone called human chorionic gonadotropin B (hCG). There is a heading in the FASEB paper (p.1382) called “Ability of antibodies to neutralize the biological activity of hCG.” The authors are trying to discover whether a state of non-fertility can be achieved by blocking the normal activity of hCG.
This hormone helps sustain pregnancy. If the immune system can be trained to attack it, pregnancy will collapse and a miscarriage will occur.
Another journal paper: The British Medical Bulletin, volume 49, 1993. “Contraceptive Vaccines.” [4] The authors—RJ Aitken et al. From the MRC Reproductive Biology Unit, University of Edinburgh, Edinburgh, UK.
“Three major approaches to contraceptive vaccine development are being pursued at the present time. The most advanced approach, which has already reached the stage of phase 2 clinical trials, involves the induction of immunity against human chorionic gonadotrophin (hCG). Vaccines are being engineered … incorporating tetanus or diptheria toxoid linked to a variety of hCG-based peptides … Clinical trials have revealed that such preparations are capable of stimulating the production of anti-hCG antibodies…”
The authors are talking about creating an immune response against this female hormone. Training a woman’s body to react against one of its own secreted hormones. The authors state, “The fundamental principle behind this approach to contraceptive vaccine development is to prevent the maternal recognition of pregnancy by inducing a state of immunity against hGC, the hormone that signals the presence of the embryo to the maternal endocrine system.”
Stop the female body from recognizing a state of pregnancy. Get the body to treat the natural hormone hCG as an intruder, a disease agent, and mobilize the forces of the immune system against it. Create a synthetic effect, an engineered effect, by which the mother’s “maternal endocrine system” does not swing into gear when pregnancy occurs. The result? The embryo in the mother is swept away by her next period—since hGC, which signals the existence of the pregnancy and halts menstruation cycles, is now treated as a disease entity.
The authors put it this way: “In principle, the induction of immunity against hGC should lead to a sequence of normal, or slightly extended, menstrual cycles during which any pregnancies would be terminated…”
Miscarriage would then be the “normal” state of affairs.
“During the next decade the world’s population is set to rise by around 500 million. Moreover, because the rates of population growth in the developing countries of Africa, South America, and Asia will be so much greater than the rest of the world, the distribution of this dramatic population growth will be uneven…”
Two other vaccine methods are described. They “aim to prevent conception by interfering with the intricate cascade of interactive events that characterize the union of male and female gametes at fertilization.”
In a letter to The Lancet, p.1222, Volume 339, May 16, 1992, “Cameroon: Vaccination and politics,” [5] Peter Ndumbe and Emmanuel Yenshu report on their efforts to analyze widespread popular resistance to a tetanus vaccine given in the northwest province of Cameroon.
Two of the reasons women rejected the vaccine: it was given only to “females of childbearing age,” and people heard that a “sterilizing agent” was present in the vaccine.
Indeed, these are the charges leveled against past tetanus vaccine campaigns in Kenya and the Philippines. In Kenya (2014), an intense standoff occurred—with the Catholic Doctors Association and Kenyan Catholic Bishops on one side, and the Kenyan government Health Authority on the other.
Both sides claimed they tested vials of the tetanus vaccine. The Catholic groups’ lab report indicated the vaccine contained hCG; the Health Authority’s report indicated no hCG was present.
“Mass Sterilization: Kenyan Doctors Find Anti-Fertility Agent in UN Tetanus Vaccine,” [6] November 8, 2014, by Steve Weatherbe, earth-heal.com: “Kenya’s Catholic bishops are charging two United Nations organizations with sterilizing millions of girls and women under cover of an anti-tetanus inoculation program sponsored by the Kenyan government.”
“According to a statement released Tuesday by the Kenya Catholic Doctors Association, the organization has found an antigen that causes miscarriages in a vaccine being administered to 2.3 million girls and women by the World Health Organization and UNICEF. Priests throughout Kenya reportedly are advising their congregations to refuse the vaccine.”
“’We sent six samples from around Kenya to laboratories in South Africa. They tested positive for the HCG antigen,’ Dr. Muhame Ngare of the Mercy Medical Centre in Nairobi told LifeSiteNews. “They were all laced with HCG’.”
“Dr. Ngare, spokesman for the Kenya Catholic Doctors Association, stated in a bulletin released November 4, ‘This proved right our worst fears; that this WHO campaign is not about eradicating neonatal tetanus but a well-coordinated forceful population control mass sterilization exercise using a proven fertility regulating vaccine. This evidence was presented to the Ministry of Health before the third round of immunization but was ignored’.”
In the present situation, we have COVID vaccines. They’re being injected all over the world. Women are making reports of bleeding, disrupted menstrual cycles, miscarriages, pre-term births.
There is a long history, extending to the present day, of elite groups researching and deploying vaccines designed to terminate pregnancies, for the purpose of depopulation.
The elite groups and players behind the current “pandemic”—the WHO, UN, Bill Gates, Rockefeller Institute, etc.—are the same groups who have been developing depopulation vaccines.
This is called a clue.
It lights up like a giant sign, at the beginning of the trail of investigation into the use of COVID vaccines for depopulation.
April 19 was the 28th anniversary of one of the most shameful episodes in modern American history: the massacre of 76 innocent men, women, and children by agents of the Bureau of Alcohol, Tobacco, and Firearms (ATF) in a military-style assault on the Branch Davidian compound in Waco, Texas.
The assault followed a botched raid on the Davidian compound (staged at a time that it would distract attention from an ATF sexual harassment scandal) and a two-month standoff between the Davidians and the agency. The ATF used CS tear gas against the Dravidians, even though the gas was banned by an international treaty the US agreed to just months before the assault. So, if the assault had occurred on foreign soil as part of a military operation, it would have been a war crime.
Waco illustrates the dangers to our lives and liberties posed by a hyper-interventionist foreign policy. Eventually the deadly tools of the military-industrial complex will be brought home and used against US citizens.
In the 28 years since Waco, the military-industrial complex’s role in domestic law enforcement has grown. This is largely thanks to the Section 1033 program that provides military-grade equipment to local law enforcement. The people will not be safe from militarized law enforcement until Section 1033 is repealed and the military-industrial complex is dismantled.
The initial raid on the Branch Davidian compound was justified by claims the Davidians were violating unconstitutional gun laws. Infringements on the Second Amendment empower the federal police state. This is one reason why all those who value liberty must oppose all gun control laws, such as those currently being advocated by President Joe Biden and his congressional allies.
Last week, the ATF helped further Biden’s anti-Second Amendment agenda by issuing a proposed regulation regarding pistols fitted with stabilizers, thus allowing the agency to harass more gun owners.
Also last week, the Department of Justice unveiled model red flag legislation to encourage more states to adopt these laws. Red flag laws allow law enforcement to seize an individual’s firearms based on an allegation the individual may turn violent. Not surprisingly, allowing police to show up at a person’s home and demand he surrender his firearms can lead to violence. Expanding red flag laws will violate Americans’ Second Amendment rights, disregard due process, and lead to police being in more violent encounters.
David Chipman, President Biden’s nominee to head the ATF, is a former ATF agent turned gun control lobbyist. Mr. Chipman is an outspoken defender of the ATF’s actions at Waco. In addition to supporting red flag laws, he wants the ATF to arrest Americans who cannot buy a firearm because they failed a federal background check. The background check produces many false positives. Chipman’s proposal would lead to the arresting of many innocent Americans. This would not bother Chipman since he told the Senate Judiciary Committee that law-abiding gun owners are potential criminals.
The Waco massacre is proof that, as the late libertarian Karl Hess put it, “whenever you put your faith in big government for any reason, sooner or later you end up an apologist for mass murder.” Those of us who understand this must continue to spread the truth about the true nature of the welfare-warfare-regulatory state. Key to regaining our liberty is making government officials abide by the same rules against the initiation of violence that apply to private citizens.
Over the last several months we have requested from the Center of Disease Control (CDC) evidence for the isolation and existence for the any and all viruses, including CoV – 2 and 19, MERS, Influenza, Polio, Measles, HIV, XMRV, HTLV-1, HTLV-III/LAV, HPV, Ebola, Zika, just to name a few of the so-called viruses, disclosed under the Freedom of Information Act (FOIA).
These written requests were made by Ms. Christine Massey to CDC/ATSDR FOIA Chief Officer Mr. Robert Andoh, to locate and deliver ANY records, research and/or findings for ANY “viral” isolation and purification (by anyone, anywhere, anytime in the World) from a patient sample via maceration, filtration and/or the use of an ultracentrifuge or what is called the ‘Gold Standard’ for isolating and identifying a pathological micro or nana organism. The ‘Gold Standard’ for isolating and identifying microbes is referred to as Koch’s and Rivers Postulates which was established many years ago.
The CDC Chief FOIA, Mr. Roger Andoh provided straightforward responses to each one of our requests, admitting in writing that they have NO RECORD of ANY KIND, for the following so-called phantom “viruses”, including CoV – 2 -19, HIV, HPV, XMRV, HTMV-1, HTMV-111/LV, Measles, Influenza, MERS, EBOLA, ZIKA, POLIO:
1. June 7, 2021: CDC admits they have no record of any “COV – 2 or 19 virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever:
2. June 7, 2021: CDC admits they have no record of any “HPV virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever: (note: CDC made an error in their original response and later provided the corrected version below):
3. June 7, 2021: CDC admits they have no record of any “Measles virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever! No Isolation, No Purification and No Identification for the Measles Virus!
4. A Letter from the CDC Concerning the Childhood and Adult USA “Immunization Schedule”:
[Note: there was a reference to “influenza” in this request, but it doesn’t affect our request in any way because it was in the context of our example of the record we were looking to validate that the CDC does not have ANY record or research or findings for ANY so-called virus that is responsible for ANY sickness or disease – EVER!]
5. June 10, 2021: CDC admits they have no record of any “MERS virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere, ever:
6. CDC June 11 2021: CDC admits they have no record of any “POLIO virus” purified from any patient sample via maceration, filtration and use of an ultracentrifuge, by anyone, anywhere on the planet, ever:
7. March 15, 2021 CDC FOIA response: no records of any “Ebola virus” isolation or purification from a patient sample, by anyone, anywhere on the planet, ever:
8. March 19, 2021, U.S. CDC (Centers for Disease Control and Prevention) and the Agency for Toxic Substances and Disease Registry (ATSDR) admit they have no record of any “Zika virus” isolated or purified from a patient sample, by anyone, anywhere on the planet, ever:
9. March 23, 2021 CDC admitted in a FOIA response that they have no record of any “HIV virus”, “Hepatitis viruis”, “STD virus”, and “TB bacillus bacterium” purified isolate from a patient sample, by anyone, anywhere, ever:
10. April 7th, 2021, the CDC states that they have no record of “XMRV virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
11. April 7th, 2021 the CDC states that they have no record of “HTLV-1 virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
12. April 7th, 2021, the CDC states that they have no record of “HTLV-III/LAV virus” purification or isolation from a patient sample, by anyone, anywhere on the planet, ever:
13. April 12, 2021: CDC admits they have no record of any “influenza virus” isolated or purified from a patient sample, by anyone, anywhere on the planet, ever:
[Note: there was a reference to “influenza” in this request, but it doesn’t affect our request in any way because it was in the context of our example of the record we were looking to validate that the CDC does not have ANY record or research or findings for ANY so-called virus that is responsible for ANY sickness or disease – EVER!]
If no one any where at any time in the World has isolated and proven the existence of any such novel coronavirus or for any virus as a unique pathogen, how on earth can any pharmaceutical company provide a treatment with a vaccine for a virus that does NOT even exist?
Is the virus or pathogen a mythical virus that needs a mythical (but expensive and poisonous!) vaccine to destroy it?
Or is this phantom virus the creation of ‘bad actors’ and ‘luciferians’ for the purpose of redistributing the wealth of the world to themselves and at the same time reduce the surplus population of so-called ‘useless eaters’?
As Voltaire once warned us:
“Those who can make you believe in absurdities can make you commit atrocities.”
As stated quite clearly by Chief Officer Mr. Roger Andoh in his CDC FOIA letters:
“Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…”
As Rappoport has stated,
“Since that is the case, that there are no quantified virus isolates, how can one be sure of what is being determined as COVID -19 is, in fact, COVID -19?”
You cannot because you are looking for something that does not even exist!
You see the symptoms of cov – 19 are all symptoms of chemical and radiation poisoning. And the corona virus is not a virus at all but a symptom of cell membrane degeneration I call the ‘corona effect’!
The ‘Corona Effect’ Caused by Systemic Chemical and Radiation Poisoning Leading to Pathological Blood Coagulation, Hypoxia and Death
The two micrographs above show the ‘CORONA EFFECT’ on the red blood cells with the ‘SPIKED PROTEIN’ caused by decompensated acidosis of the interstitial and then vascular fluids from an acidic lifestyle and specifically, exposure to toxic pulsating electro-magnetic fields at 2.4gHz or higher, chemical poisoning from the food and water ingested, toxic acidic air pollution and chem-trails and to top-it-all-off a chemical laden inoculation! Please check your feelings and false beliefs at the door before YOU prematurely cause YOUSELF harm!
It is difficult to talk to addicts about addictions and it is even harder to do so when their embrace of the drug of choice has dire consequences.
I once asked the ether if God had a cell phone, and although God didn’t reply, it was a rhetorical question, so I didn’t expect an answer since I knew God understood grammar and punctuation and had other ways of communicating.
The elites who consider themselves gods, such as those at the World Economic Forum, the World Health Organization, the Bill and Melinda Gates Foundation, Google, and their ilk throughout governments, corporations, media, etc., know that cell phones are fundamental to their plan for a fully digitized world. They have promoted them for decades. Without cell phones their plan can’t work, a plan whose end is a trans-human world where AI, cyborgs, technology, and biology are melded for their authoritarian control. Their non-vaccine “vaccines” are also necessary. Penetrating cells of both sorts are means to their ends and the stories we are told are meant to infect our minds with a sick way of thinking that will allow them to exert more and more control.
Most people have fallen for their PR. It’s called the-easy-life. The stay-in-touch life. The never-be-out-of-touch-life. The you’ll-be-lost-without-it-life. The smart life. The free life.
In reality it is a prisoner’s life. The miracle of the cell phone, the mystery of a virus and its “antidote,” and the authority of authoritarians are being used to try to quell the spirit of rebellion we were all born with – the promise of freedom. Mystery, miracle, and authority – “vaccines” against freedom. Like the Grand Inquisitor in Dostoevsky’s legend, these sick elites are relying on the assumption that “man is tormented by no greater anxiety than to find some one quickly to whom he can hand over that gift of freedom with which the ill-fated creature is born.”
They may be in store for a big surprise. People are starting to wake up to an attack on their fundamental freedoms.
Like the non-vaccine vaccines that they are promoting to exert more control with their plan to digitize existence with the Great Reset, those who presently control so much of the world they own, know that cell phones are moving shackles. And they know they have created billions of addicts who can’t help themselves.
So much of the world has been hoodwinked into a trap, a prison. It’s been a slow process that is approaching a climax.
There are no cells in cell phones, but their towers are arranged to form cells with each having a central tower in its geographical zone that keep users prisoners, as with the round Panopticon prisons with their central guard tower. Cells in heads, heads in cells, cells everywhere. The U.S.A. also has more prisoners in cells than any country in the world. There are Towers of Babel all across the land, listening, watching, recording, as the prisoners gleefully scroll their black magic machines that have corralled their freedom. Machines that are likely ruining their health as well, but that is not my main focus here.
Unlike the nearly 2 million people in American jails, cell phone prisoners can roam, for their cells are mobile. That is their key. “Smart” phones for gullible people, or androids – “a mobile robot usually with human form” – are necessary, for they allow the authorities to follow and track your every move while you think you are skipping down easy street while carrying the equivalent of a GPS ankle monitor like digital jail prisoners. In this case, it is voluntary incarceration. And there is far more to it than having your location tracked.
Perhaps it is unfair to say that people’s embrace of cell phones are acts of freely giving up their freedoms, for the propagandists work has long softened up many minds to the idea of salvation through technology. Like the technology of pharmaceutical drugs run by criminal Big Pharma, users of cell phones have been induced to consider convenience over conscience and the quick “fix” over slow deliberation. Yes, you can message your friends and even call them, but your enemies have your number now. And when they ask you for your papers, your freedom vaccines, all you need to do is flash that screen in your hand. After getting shot first. To paraphrase Kris Kristofferson: Freedom’s just another word for everything left to lose. But few are counting.
“What we got here is a failure to communicate,” says the Captain to the prisoner Luke in the classic movie Cool Hand Luke. “Some men you just can’t reach…which is the way he wants it.”
I’m afraid that how it is with owners of cell phones. It’s very hard to admit you have been had. People want their cell phones but don’t want to hear that they are the phone’s prisoners. But to say phone is too abstract. Phones can’t imprison and manipulate you. Only people can. The truth is hard to swallow. The cell phone is the key, and most people are in the cell without a key or clue. They have it and it has them.
But then aren’t cells inside us. I’ve heard it said that spike proteins teach cells to make a protein that triggers an immune response inside our bodies. But how do the cells get inside our bodies. I thought they were hand held. You see I am getting confused, for this kind of language is beyond my ken. I’m still trying to figure out how my computer can get a virus. Everything’s gone viral. Cells, viruses – what’s next? I’m one of those idiots who still thinks Cat Scans are used to see if you like cats. Well I don’t know if that’s all true, ‘cause it’s got me, and baby, it’s got you. Sonny and Cher sung those words more than fifty years ago. Words stick. Ideas stick. Thinking and behaving in certain ways become habits. Linguistic mind control needs repetition – words like cells and viruses.
The medium is the message and the messenger is the m in the mRNA experimental non-vaccine vaccines. It’s so simple; all you need to do is get the message and get your experimental shot and wait for the consequences, just as with cell phones. Don’t worry about the price to be paid in health or freedom. Those are incidentals. Let the operating systems do their invisible work.
The way the story is framed controls the story. As with cell phones and vaccines, most people do not see Donald Trump as a pseudo-event. A pseudo-event being, as described by Daniel Boorstin in his classic book, The Image: A Guide to Pseudo- Events in America, a planned, dramatic, costly invention of a counterfeit story that is repeated and planned for its intelligibility and ability to capture the public’s attention since it conforms to stereotypes. In this case, Trump as a big-mouthed, uncouth bad guy who just happened to become the American President. Like I happen to be a man. Like you just happen to be reading this. Just happenings. Trump in the role of the ignorant outsider who can be played off against the smart insider even when the fundamentals of the system that supports them barely change an iota while the bad guy runs the show. Straight from the Tube to the Tube as part of the Spectacle. Obama and Biden’s anti-doppelganger. The story is told in a manner that the obvious is missed: That Trump was never an outsider. He was one of the establishment’s performers from the start. A perfect foil from the Tube for apprentices learning about reality. You know, like the CDC says: “MRNA vaccines teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies.” Very simple, teacher. I see it now.
Are you immune to Trump? Biden? They are not the disease. They are its symptoms. They are a twin heads of the Hydra. Now Trump has been “fired” with Biden’s turn to come. Cut them off and the monster will grow more heads unless by miracle a true leader arises with the courage of JFK or RFK. One who can avoid their assassins.
In January of 2021, the outsider Trump while still president, the anti-vaccine guy, the anti-Fauci guy, the anti-everything that’s good guy, the anti-science guy, the anti-China Wuhan lab Chinese virus guy, quietly got his Pfizer BioNTech vaccine, the same one Biden got. He didn’t announce it, but said, “We took care of a lot of people — including, I guess … Joe Biden, because he got his shot, he got his vaccine. It shows you how unpainful that vaccine shot is … So everybody, go get your shot.”
Of course Trump was the guy who fast-tracked the experimental vaccines through a program called Operation Warp Speed that funneled billions of dollars to vaccine manufacturers through a non-governmental third party, a defense contract management firm called Advanced Technologies International, Inc. This avoided much public disclosure.
I say all this about Trump to make a rather simple point about cell phones and how the obvious is staring us in the face if we choose to see it. Trump and cell phones should have long been obvious. Yes, cell phones are convenient, but that is a minor part of the story. They are very dangerous for our freedoms and health. Yes, it is very convenient to see Trump as the bad guy but much harder to see the larger story in which Trump is a chosen player on the large chessboard created by the interconnected power elites. But Trump and the cell phone serve their functions. They didn’t just happen.
To abandon your cell phone or to abandon the false narrative that Trump is an outlier is very difficult. But these are difficult times.
Can you see the elephant in the room? Join with those like Robert Kennedy, Jr. and other lovers of truth and freedom and fight back now. Everyone must seize their freedom now before it is too late. Cast fear aside; it is another of their key tools. Hope lies in group actions.
“They’re in a hurry because people are waking up. And they’re waking up to the fact that what they want to put into place is not only inhuman, it’s anti-human…
“Ultimately, Daniel, I think they’re going to fail — and fail big time — because when you’re in a hurry you make mistakes…
“They may think they’ve snookered the world with this covid thing but I don’t see it. That narrative is falling apart really fast…
“And the other problem they have is they want to centralize things when, I think, the trend made possible by all this technology is exactly the opposite direction.”
~ Dr. Joseph P. Farrell
,,,
“This government has lied about the Kennedy assassination. It has lied about Watergate. It has lied about Ruby Ridge. It has lied about Waco. It has lied, lied, lied, lied. And now all of a sudden we’re going to believe it with UFOs? Count me out.”
“It will be interesting to see what ‘enemy’ develops in the years ahead. It appears that ‘UFOs and Aliens’ are being primed to fulfill that role for the future.”
~ Colonel L. Fletcher Prouty – Chief of Special Operations for the Joint Chiefs of Staff
UFOs and Global Control
Join Dark Journalist for this fascinating interview with Dr. Joseph Farrell on the origin of the Alien Invasion Op and the involvement of Nazi Rocket Scientists.
Dr. Farrell goes deep on the NASA Rocket Scientist Wernher von Braun and his prescient Prediction of a False Alien Invasion Op that would be created by the National Security State as a pretext to weaponize space.
Topics include:
Paperclip Nazi scientists
Global control from space
Von Braun prediction
False flag UFO threat
Secret finance
X-Technology
Genuine UFO file research
Book mentioned by Daniel Liszt: We Never Went to the Moon: America’s Thirty Billion Dollar Swindle by Bill Kaysing
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, and Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
“There’s no publication anywhere in the world of authentic SARS‑CoV‑2 in a bottle, or ever been observed, or characterized anywhere in the world — just like with HIV.”
…
“There’s no covid vaccine. These are injections. They are lethal. They are highly toxic.”
…
“Do not take these injections. You will regret it if you do. They are very, very dangerous.”
Josh Sigurdson interviews Dr. David Rasnick during Red Pill Expo, which took place June 5-6 in Rapid City, South Dakota.
Has the COVID virus ever been isolated?
Do viruses even exist?
What are the vaccinations for if they’ve never isolated the virus?
Dr. Rasnick speaks of other deceptions in the history of virology, including HIV and AIDS.
RENOWNED SCIENTIST SPEAKS OUT! – COVID IS A SCAM! – DON’T GET THE JAB! – DO VIRUSES EXIST?
Original video available at World Alternative Media BitChute channel. [As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light Brighteon and Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
The WATER WARS have begun: the state is simply turning off the water to farms & ranches, depriving them of water needed to grow food and raise animals. This will create food shortages by design, in order to then point at the massive problem and declare, “It’s global warming! We NEED climate lockdowns! We MUST move to absolute zero carbon emissions! We HAVE to take away private ownership of cars! You HAVE to eat fake meat and move to post-animal economy!” The story is the same across the nation, and indeed the world. But who is behind these WATER WARS? Christian explores the WEF’s “Global Water Initiative,” an agenda to centralize and privatize control over the world’s water supply, and how these engineered droughts are the lynchpin in the climate agenda and the takeover of food.
WHO report vindicates CCHR and the many groups that have fought worldwide for the recognition of psychiatric human rights violations, including involuntary commitment and forced electroshock and other biomedical, including drug treatments.
The World Health Organization (WHO) has released a damning report that lashes out against coercive psychiatric practices, which it says “are pervasive and are increasingly used in services in countries around the world, despite the lack of evidence that they offer any benefits, and the significant evidence that they lead to physical and psychological harm and even death.”[1] It points to the United Nations Convention on the Rights of Persons with Disabilities (CRPD) which in essence, calls for a ban on “forced hospitalization and forced treatment.”[2]
Citizens Commission on Human Rights International welcomes the report not just for it recognizing psychiatric abuses and torture as being rife, but also as a vindication of CCHR’s efforts since 1969 and other groups that have fought for the recognition of patents’ rights violations that WHO now acknowledges. CCHR’s Mental Health Declaration of Human Rights, written in 1969, includes many of the rights that the W.H.O. report now addresses. [3]
For example, WHO points to a series of UN guidelines and Human Rights Council resolutions that have called on countries to tackle the “unlawful or arbitrary institutionalization, overmedication and treatment practices [seen in the field of mental health] that fail to respect… autonomy, will and preferences.”[4] People who are subjected to coercive practices report feelings of dehumanization, disempowerment and being disrespected, WHO further states.[5]
CRPD says patients must not be put at risk of “torture or cruel, inhuman or degrading treatment or punishment” and recommends prohibiting “coercive practices such as forced admission and treatment, seclusion and restraint, as well as the administering of antipsychotic medication, electroconvulsive therapy (ECT) and psychosurgery without informed consent.”[6]
Coercive Practices Create Harm
Psychiatry has failed to take responsibility for the fact that its own coercive practices have caused the stigmatization which drives medical students and patients away from it, while it tries to blame this on its critics. WHO says stigmatization exists among the general population, policy makers and others when they see those with mental disabilities as being “at risk of harming themselves or others, or that they need medical treatment to keep them safe”—a psychiatric mantra—which results in a general acceptance of coercive practices such as involuntary admission and treatment or seclusion and restraint.[7]
Abusive practices CCHR has documented include:
In the U.S., children—who are too young to consent to electroshock—are subjected to it, even at the age of five or younger. American psychiatrists are administering it despite W.H.O. reporting sixteen years ago that “There are no indications for the use of ECT on minors, and hence this should be prohibited through legislation.” Yet the American Psychiatric Association has called for greater use of this brain-damaging, barbaric practice on minors.[8]
Many patients are forcibly detained and drugged under U.S. involuntary commitment laws, and with telepsychiatry now available, psychiatric hospitals are using this to incarcerate people against their will for their insurance.
Recent reports of the troubled teen industry in the U.S. highlight how coercive restraint use in psychiatric and behavioral facilities is common, despite leading to deaths of youths, without accountability. Teenagers gasping for air, crying out that they “can’t breathe” have died undergoing restraint to control their behavior.[9]
In New Zealand, a Royal Commission Inquiry into Child Abuse begins its investigation on June 14 into the torture of children with an electroshock device at the now-closed state psychiatric institution, Lake Alice. Children were not anesthetized but punitively shocked directly to various body parts, including genitalia.[10]
Despite a March 2020 Food and Drug Administration ban on a similar shock device used at the Judge Rotenberg Center in Massachusetts for behavior modification, the torturous procedure is still being used.[11]
Until recently, psychiatrists such as Patrick McGorry in Australia, pre-drugged patients in the Brave New World theory that this could prevent them from becoming psychotic, yet the antipsychotics prescribed for this list psychosis as a side effect. Similar practices are researched in the U.S.[12]
Many U.S. states allow electroshock to be given to involuntary patients against their will, constituting torture, as UN agencies have clearly stated. The WHO report specifically highlights the problem that “coercive practices are used in some cases because they are mandated in the national [or state] laws of countries.”[13]
Further, coercion is “built into mental health systems, including in professional education and training, and is reinforced through national mental health and other legislation.”[14]
These laws need to change, similar to those enacted in Australia where criminal penalties are enshrined in several mental health laws, should certain psychiatric treatments be administered, violating patients’ rights.
Countries must also ensure that “informed consent” is in place and that “the right to refuse admission and treatment is also respected.”[15] “People wishing to come off psychotropic drugs should also be actively supported to do so, and several recent resources have been developed to support people to achieve this,” WHO says.[16]
No Accountability: No Funding
WHO sees community mental health as the alternative to egregious hospitalization and the biomedical paradigm—psychotropic drugs, electroshock and psychosurgery—for treating people’s emotional and mental problems. This would require a massive injection of funds. However, the checks and balances do not exist to prevent abuses occurring in the community. Greater accountability, including criminal penalties are needed.
The same funding limitations also apply to psychiatric research, which the WHO highlights have been dominated by a biomedical model—neuroscience, genetics and psychopharmacology. It quotes the astounding admission from Thomas Insell, former director of the National Institute for Mental Health (2002 to 2015), who said: “When I look back on that, I realize that while I think I succeeded at getting lots of really cool papers published by cool scientists at fairly large costs—I think US$ 20 billion—I don’t think we moved the needle in reducing suicide, reducing hospitalizations, improving recovery for the tens of millions of people who have mental illness.”[17]
We cannot keep flooding more money into a failing and harmful mental health system, when accountability either doesn’t exist or is so ineffective that perpetrators can get away with murder.
Abolish Involuntary Hospitalization
In the U.S., in the wake of acts of senseless violence, psychiatrists have called for greater rights to involuntarily commit individuals—the antithesis of what the WHO is advocating. In fact, it debunks the idea that involuntary admission is necessary under so-called grounds such as “dangerousness” or “lack of insight.’”[18] Or that the person is “‘at risk of harming themselves or others, or that they need medical treatment to keep them safe,’” with WHO saying that such practices lead to an “over-emphasis on biomedical treatment options and a general acceptance of coercive practices such as involuntary admission and treatment or seclusion and restraint.”[19]
“Although challenging, it is important for countries…to eliminate practices that restrict the right to legal capacity, such as involuntary admission and treatment,” it says.[20]
The late Dr. Thomas Szasz, professor of psychiatry, a fellow of the American Psychiatric Association, and co-founder of CCHR, stressed this point sixty years ago. Indeed, he was more forthright in stating: “Involuntary mental hospitalization is like slavery. Refining the standards for commitment is like prettifying the slave plantations. The problem is not how to improve commitment, but how to abolish it.” Further, “The most important deprivation of human and constitutional rights inflicted upon persons said to be mentally ill is involuntary mental hospitalization….”[21]
CCHR will continue to monitor and document psychiatric abuses and with this WHO guideline against involuntary treatment, refer this to attorneys who may be able to seek charges of torture where forced treatment is administered. Until laws enact the necessary protections, more pressure is needed to bring abuses to account through the courts.
[1] “Guidance on Community Mental Health Services: Promoting Person-Centered and Rights-Based Approaches,” World Health Organization, 10 June 2021, p. 8, https://www.who.int/publications/i/item/9789240025707 (to download report)
I’m sure the grant money for this study came with the stipulation that they stick to the script that autism is a genetic disorder lots of unfortunate children are born with. It’s important that autism busywork like this continues so the public thinks that the medical community cares about autism.
How do I know this?
Everything in the piece is meant to downplay the health and humanitarian disaster that autism represents. Reporter Lauren Talarico provides the blanket definition that understates any of the horrific symptoms children and families have to live with:
Autism is a neuro-developmental disorder. It can affect speech, social interactions and the ability to communicate.
(No mention of parents changing the diapers on their non-verbal young adult son who wears a helmet because he bangs his head on the wall endlessly.)
Likewise there are no words like crisis or epidemic used. Instead Dr. Olivier Lichtarge, professor of molecular and human genetics, uses phrases like ‘a surprisingly large number of children’ to describe two percent of U.S. kids with autism.
While we are told that one in 54 children are now diagnosed with autism, there is not one word about the unstoppable increases that have preceded it: 2004: one in 166, 2007: one in 150, 2009: one in 110, 2012: one in 88, 2014: one in 68, 2018: one in 59, (also in 2018: one in 40 according to a separate study published in JAMA), one in 54, 2020.
Somehow Lichtarge thinks that looking for mutating genes will matter when the rate eventually reaches one in 10, one in 5.
Lichtarge shows no embarrassment over the complete failure of the scientific/medical community to figure out anything significant about autism despite billions of dollars in research funding and 20 years of trying.
This is how lost they are:
More and more children are being diagnosed with Autism Spectrum Disorder (ASD), and researchers are trying to figure out why.
“It is a rising fraction for reasons we do not understand,” Dr. Lichtarge said.
Doctors are not sure what causes it.
“The basis of autism is not quite clear. It’s obviously genetic. It also may have an environmental interplay,”
“There is every reason to hope that we can understand it better in the near future,” he said.
Lichtarge cleverly sidesteps the issue of an environmental trigger that marks these genetically susceptible kids for lifelong damage with the singular, vague mention of ‘an environmental interplay.’ Yet this is something he has no interest in exploring.
And don’t think the horrific number of one in 54 kids matters really. Notice the phrase is “1 in 54 kids diagnosed with Autism,” not 1 in 54 kids with autism.
This is a neat way of saying that the rate may be the result of “better diagnosing” and it’s has used for two decades as the catch phrase to mean that more kids don’t actually have autism. They’ve always been here; more are being diagnosed.
No one wants to prevent autism
We are told that the endgame of identifying those “harmful mutations….linked to autism” is merely so “scientists can develop the best treatments.”
All in all, there are no findings here that will help a single child.
Talarico also fails to ask why Lichtarge isn’t interested in adults with autism and looking at their genetics and their treatment plans.
Of course Lichtarge won’t have a problem finding kids to study; they’re on every block and in every school. Too bad he doesn’t want to use some of his funding to look for the elusive one in 54 adults with autism..
Predictably the photo companying the piece show a cute smiling girl painting a paper covered with colorful puzzle pieces. And thus it will remain: the eternal mystery of autism, the puzzle no one wants to solve.
VAERS data released today showed 329,021 reports of adverse events following COVID vaccines, including 5,888 deaths and 28,441 serious injuries between Dec. 14, 2020 and June 4, 2021.
This week’s number of reported adverse events among all age groups following COVID vaccines surpassed 329,000, according to data released today by the Centers for Disease Control and Prevention (CDC). The data comes directly from reports submitted to the Vaccine Adverse Event Reporting System (VAERS).
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Today’s data show that between Dec. 14, 2020 and June 4, a total of 329,021 total adverse events were reported to VAERS, including 5,888 deaths — an increase of 723 deaths over the previous week. There were 28,441 serious injury reports, up 3,082 compared with last week.
Among 12- to 17-year-olds, there were 59 reports of heart inflammation and 19 cases of blood clotting disorders.
In the U.S., 299.1 million COVID vaccine doses had been administered as of June 4. This includes 126 million doses of Moderna’s vaccine, 162 million doses of Pfizer and 11 million doses of the Johnson & Johnson (J&J) COVID vaccine.
Of the 3,211 cases of Bell’s Palsy reported, 53% were reported after Pfizer vaccinations, 42% following vaccination with the Moderna vaccine and 253 cases, or 8%, of Bell’s Palsy cases were reported in conjunction with J&J.
CDC to hold emergency hearing after identifying 226 cases of heart inflammation in young people
As The Defender reported today, the CDC on Thursday announced plans to convene an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines.
As The Defender reported Thursday, before the announcement, the CDC on June 1 had quietly updated its website to acknowledge a higher-than-expected number of cases of myocarditis among young teens after the second dose of an mRNA COVID vaccine.
Based on a May 24 report from the CDC’s Advisory Committee on Immunization Practices COVID-19 Vaccine Safety Technical Work Group, the CDC on June 1 added new language to its guidance:
“Data from VAERS [Vaccine Adverse Events Reporting System] show that in the 30-day window following dose 2 mRNA COVID-19 vaccination, there was a higher number of observed than expected myocarditis/pericarditis cases in 16–24-year-olds.”
The updated language differed significantly from the CDC’s statement two weeks earlier, which said rates of myocarditis were not higher among vaccinated people.
During a Thursday meeting of advisors to the U.S. Food and Drug Administration, CDC officials presented data showing a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger following mRNA vaccines.
The CDC identified 226 reports that might meet the agency’s “working case definition” of myocarditis. The majority of those affected have recovered, but 41 had ongoing symptoms, 15 are still hospitalized and three are in the intensive care unit.
On June 10, The Defender reported the Oregon Health Authority said it was aware of at least 11 cases of myocarditis or pericarditis — inflammation of the sac surrounding the heart — in all age groups following COVID vaccination.One of the cases is a 15-year-old teen in Beaverton, Oregon, who was hospitalized for heart inflammation after receiving his second dose of the Pfizer vaccine.
“The hallmark symptom of myocarditis and pericarditis is chest pain or shortness of breath,” Jonathan Modie, an Oregon Health Authority spokesperson, said in an email. “In rare cases, it can also present in the form of heart palpitations. Anyone suffering from unexplained chest pain should contact a medical provider or seek immediate emergency care.”
A search of the latest available data in VAERS revealed 900 cases of myocarditis and pericarditis, among all age groups reported in the U.S following COVID vaccination between Dec.14, 2020 and June 4, 2021. Of the 900 cases reported, 533 cases were attributed to Pfizer, 331 cases to Moderna and 32 cases to J&J’s COVID vaccine.
Experts tell FDA for kids, benefits of COVID vaccines don’t outweigh the risks
As The Defender reported June 11, an FDA advisory committee held a virtual meeting Thursday to discuss what data would be needed to vaccinate children under 12 against COVID under Emergency Use Authorization (EUA) or licensure.
Several experts spoke out against the plan, saying the benefits don’t outweigh the risks for young children. Peter Doshi, Ph,D, associate professor University of Maryland School of Pharmacy and senior editor of The BMJ, said during the open public hearing session, there is no emergency that would warrant using EUA to authorize COVID vaccines for children.
Kim Witczak, an FDA consumer representative, expressed great concerns over the premature approval of COVID vaccines for children. Witczak said data shows children are neither in danger or dangerous and questioned the timing of last Friday’s CDC announcement of the rise in children being hospitalized with COVID.
Dr. Cody Meissner, director of pediatric infectious diseases at Tufts University School of Medicine, said children are at low risk of severe disease from the virus and more study is needed about safety in younger age groups.
Witczak and Doshi were two of 27 researchers and clinicians around the world who launched a citizen’s petition demanding the FDA withhold full approval of COVID vaccines until efficacy and safety measures are met.
The members of the FDA’s Vaccines and Related Biological Products Advisory Committee were not asked to provide specific advice or to vote during the meeting.
Moderna, Pfizer push to vaccinate kids as young as 5 by September
Moderna this week asked the FDA to expand emergency use of its COVID vaccine for adolescents aged 12 to 17. The vaccine maker said its COVID vaccine was 100% effective in a study of 3,700 12-to-17-year-olds.
Moderna and Pfizer both this week said they expect to make their vaccines available to children as young as 5 by September.
As The Defender reported this week, Pfizer is advancing late-stage clinical trials of its COVID vaccine, in lower doses, on children ages 5 to 11 years old and expects to apply for approval early this fall. The study will enroll up to 4,500 children at more than 90 clinical sites in the U.S., Finland, Poland and Spain, the company said.
Based on safety, efficacy and tolerability data from the 144 children included in Pfizer’s phase 1 trial, the company will use 10 micrograms of each vaccine dose for kids between the ages of 5 and 11 in phase 2/3 trials, and 3 micrograms of each dose for those 5 and younger.
Moderna said it also expects its COVID vaccine will be available for kids as young as 5 by early fall. CEO Stéphane Bancel said Monday he thinks the data will become available sometime in September.
New Cleveland Clinic study shows vaccine provides no added benefit to those who already had COVID
A new preprint study by the Cleveland Clinic found people previously infected with SARS-CoV-2 were less likely to be reinfected than fully vaccinated individuals who never had the virus — suggesting the vaccine is of no benefit to people who already had COVID.
As The Defender reported, the study, available on medRxiv, provides insight into how the immune system protects the body once a COVID infection is confirmed.
The clinic studied 52,238 employees. Of those, 49,659 never had the virus and 2,579 had COVID and recovered. Of the 2,579 who previously were infected, 1,359, or 53%, remained unvaccinated, compared with 41%, or 22,777 who were vaccinated.
Of all infections during the study period, 99.3% occurred in participants who were not infected previously and remained unvaccinated. In contrast, 0.7% of infections occurred in participants who were not previously infected but were currently vaccinated. Significantly, not one of the 1,359 previously infected subjects who remained unvaccinated had a SARS-CoV-2 infection over the duration of the study.
Pfizer skipped critical testing, documents reveal
New documents obtained by TrialSite News suggest routine quality testing issues were overlooked in the rush to authorize use of Pfizer’s COVID vaccine, and that U.S. and other governments are conducting a massive vaccination program with an incompletely characterized experimental vaccine.
As The Defender reported June 7, regulatory documents revealed Pfizer didn’t thoroughly examine biodistribution and pharmacokinetics issues relating to its vaccine before submitting the vaccine to the European Medicines Agency (EMA) for review.
Pfizer also did not use the commercial vaccine (BNT162b2) for all of its studies, but instead relied on a “surrogate” mRNA that produced the luciferase protein.
According to TrialSite News, it’s standard practice for the EMA to disclose its assessment of investigational new drug submissions. In the case of Pfizer’s vaccine, the EMA assessment included a summary of the agency’s evaluation of the non-clinical vaccine distribution studies reported to EMA by Pfizer — but the EMA did not disclose the results of Pfizer’s biodistribution studies in its public EMA summary.
95 days and counting, CDC ignores The Defender’s inquiries
According to the CDC website, “the CDC follows up on any report of death to request additional information and learn more about what occurred and to determine whether the death was a result of the vaccine or unrelated.”
On March 8, The Defender contacted the CDC with a written list of questions about reported deaths and injuries related to COVID vaccines. After repeated attempts, by phone and email, to obtain a response to our questions, a health communications specialist from the CDC’s Vaccine Task Force contacted us on March 29 — three weeks after our initial inquiry.
The individual received our request for information from VAERS, but said she had never received our list of questions, even though employees we talked to several times said CDC press officers were working through the questions and confirmed the representative had received them. We provided the list of questions again along with a new deadline, but never received a response.
On May 19, a CDC employee said our questions had been reviewed and our inquiry was pending in their system, but would not provide us with a copy of the response. We were told we would be contacted by phone or email with the response.
On June 4, the CDC employee we contacted said nobody had responded to our inquiries. We were advised to submit our questions again, which we have done numerous times.
It has been 95 days since we sent our first email inquiring into VAERS data and reports and we have yet to receive a response.
Video available at WhatsHerFace Odysee. Rumble (not yet uploaded) or YouTube channels.
In 2017 John Hopkins Center for Health Security published “The SPARS Pandemic”. This document is described in its disclaimer as being “a hypothetical scenario designed to illustrate the public health risk communication challenges that could potentially emerge during a naturally occurring disease outbreak…” and that “The infectious pathogen, medical countermeasures, characters, news media excerpts, social media posts, and government agency responses described herein are entirely fictional.”.
In 2021, four years after “The SPARS Pandemic” publication, it seems to be more of a grim reality than a fictional scenario. Despite the unbelievable similarity this document has to our current global situation, this is nothing we haven’t seen before. In fact, a similar happenstance took place recently with another “fictional” scenario, Event 201, which also was spearheaded by John Hopkins Center for Health Security.
The similarities from these scenarios should not, and cannot be ignored. If Event 201 was the blueprint on how covid19 would begin, then SPARS is the blueprint on how it will end. We should all pay close attention to how these scenarios play out if we are to avoid the fate that is described in these works of “fiction”.
The World Economic Forum does not run the world, but in this time of The Great Reset and The Fourth Industrial Revolution you’d be forgiven for thinking so.
Today on The Corbett Report podcast, join James for a wild ride through the murky origins of the WEF’s past into the nightmarish future it is seeking to bring about . . . and how we can use this information to better understand and derail its agenda.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger, but only 226 reports meet the agency’s “working case definition.”
The Centers for Disease Control and Prevention (CDC) announced Thursday it will convene an emergency meeting of its advisers on June 18 to discuss higher-than-expected reports of heart inflammation following doses of Pfizer and Moderna COVID vaccines, CBS News reported.
According to the CDC, a total of 475 cases of myocarditis or pericarditis were recorded in patients 30 and younger. The CDC identified 226 reports that might meet the agency’s “working case definition” of myocarditis and pericarditis following the shots, the agency disclosed Thursday during an FDA hearing.
The majority of those affected have recovered, but 41 had ongoing symptoms, 15 are still hospitalized and three are in the intensive care unit.
Dr. Tom Shimabukuro, deputy director of the CDC’s Immunization Safety Office said during Thursday’s meeting there had been a higher-than-expected number of cases of heart inflammation among young people recently vaccinated with their second doses of mRNA vaccine.
CDC data showed 196 reports of myocarditis and pericarditis among 18- to 24-year-olds through May 31, compared with an expected rate of between eight and 83 cases.
Among 16- to 17-year-olds, 79 cases of myocarditis and pericarditis were reported through May 31. The expected rate among people in this age group is between two and 19 cases, Shimabukuro said during his presentation.
Shimabukuro said the CDC’s findings were “mostly consistent” with reports of rare cases of heart inflammation that had been studied in Israel and reported by the U.S. Department of Defense earlier this year.
Myocarditis is inflammation of the heart muscle that can lead to cardiac arrhythmia and death. According to researchers at the National Organization for Rare Disorders, myocarditis can result from infections, but “more commonly the myocarditis is a result of the body’s immune reaction to the initial heart damage.”
A search in the CDC’s Vaccine Adverse Events Reporting System (VAERS) revealed 900 cases of pericarditis and myocarditis reported in the U.S., among all age groups, following COVID vaccination, between Dec. 14, 2020 and June 4, 2021.
Of the 900 cases reported, 59 cases occurred in the 12- to 17-year-old group –– all but one case was attributed to Pfizer.
On May 10, the U.S. Food and Drug Administration (FDA) expanded the EUA for Pfizer’s COVID vaccine to include children aged 12-15 years. On June 10, Moderna asked the FDA to expand emergency use of its COVID vaccine in adolescents ages 12 to 17.
The CDC had previously said it was investigating reports that some teenagers and young adults vaccinated against COVID may have experienced heart problems, according to the agency’s advisory group.
The CDC’s Advisory Committee on Immunization Practices in a statement said reports of myocarditis to date seemed to occur predominantly in adolescents and young adults, more often in males than females, more often following the second dose and typically within four days after vaccination. Most cases appeared to be “mild” and follow-up is ongoing.
The CDC’s Vaccine Safety Technical Work Group originally said its monitoring systems had not found more cases of myocarditis than would be expected in the population, but members of the committee on vaccinations said healthcare providers should be made aware of the reports of the “potential adverse event.”
But as The Defender reported June 10, the CDC subsequently acknowledged — in guidance updated on its website June 1 — a higher-than-expected number of cases of myocarditis among young teens after the second dose of an mRNA COVID vaccine. It wasn’t until Thursday’s FDA meeting that the agency publicly discussed the higher rate and followed up by announcing plans to hold an emergency meeting.
EU and Israel investigate reports of heart inflammation
On June 2, Israeli health officials found a “probable” link between Pfizer’s COVID vaccine — which the country has relied on almost exclusively in its vaccination drive — and dozens of cases of heart inflammation in young men following the second dose.
In a statement, Pfizer said there is still no indication the cases are due to its vaccine. Myocarditis is often caused by viral infections, and COVID infections have been reported to cause the condition, the drugmaker said.
Pfizer’s partner, BioNTech, said more than 300 million doses of the COVID vaccine have been administered globally and the “benefit-risk profile” of the vaccine remains positive.
On May 7, EU regulators called on Pfizer and Moderna to provide additional data related to the companies’ COVID vaccines and a potential link to heart inflammation, after the agency completed a safety review of all four COVID vaccines authorized for emergency use in the EU.
A report issued by European Medicines Agency’s Pharmacovigilance Risk Assessment Committee (PRAC) disclosed its members were aware of cases of myocarditis and pericarditis following Pfizer vaccination. Regulators said they didn’t see an indication the vaccine caused these cases, but as a prevention, PRAC requested Pfizer provide further data, including an analysis of events according to age and gender in its next pandemic summary safety report and will consider if any other regulatory action is needed.
Houston – On Monday afternoon, employees of the Houston Methodist hospital system were joined by supporters from around the Houston area as they were suspended without pay for saying no to COVID-19 injections. The employees are now suing Houston Methodist in an effort to fight against COVID19 mandates.
The Houston Methodist hospital operates eight hospitals with more than 26,000 employees. On March 31, Methodist CEO Dr. Marc Boom announced that the shots – which have not received approval by the US Food and Drug Administration – would be mandatory for all employees. Houston Methodist hospital employees were told to take the shots by June 7th or lose their jobs. Methodist also required hospital managers to have at least one COVID shot by April 15th. Those who chose not to receive the treatments by Monday now have 2 final weeks before they will officially be fired.
“Mandating the vaccine was not a decision we made lightly. … Because science has proven that the Covid-19 vaccines are not only safe, but extremely effective, it became an easier decision to make,” Boom wrote in a letter to staff in April.
Jennifer Bridges is one of the nurses leading the charge. In recent months she has become the public face of the hospital employees’ fight against mandates they see as unconstitutional. On Monday evening, Bridges walked out of the Baytown Methodist hospital to a crowd of cheering supporters. “I am sad, I am happy, I am proud,” Jennifer said as she exited the parking lot for the final time.
Bridges stated that the hospital attempted to “bribe” employees with cash and required those receiving the injection to sign a waiver stating they would not hold Methodist hospital liable if they were to experience an adverse reaction. She says that nurses who treated COVID-19 patients in 2020 are now treating patients who have had reactions to the shots.
“We’ve already had nurses who took the vaccine – whether they wanted to or were forced – and so many have come down with adverse reactions. I’ve already heard from nurses who have had miscarriages,” Bridges stated during an interview with Free Thinker Radio.
Bridges was joined by nurses and doctors from the Houston area, including fellow employees from the various Houston Methodist campuses. One such Methodist nurse was Lacey Guedry. “I don’t think a mandated vaccine is ethical. At the very least I think it violates our basic liberties and freedoms, especially with institutions claiming to be practicing evidence based medicine,” said Guedry. “The WHO recently went on record saying that natural infection provides superior or equal protection that the vaccine does. So if we are going to follow “science” why are we neglecting this information?”
Although the lawsuit was filed in Texas state court it was recently transferred to a Houston federal court, a move that has been called unusual by the plaintiffs attorneys. On Friday, U.S. District Judge Lynn Hughes denied a temporary restraining order which would have prevented the Houston hospital system from firing the employees until the case is worked out.“The plaintiffs are not just jeopardizing their own health; they are jeopardizing the health of doctors, nurses, support staff, patients and their families,” Hughes wrote.
Courthouse News reports that Judge Hughes “appears ready to dispose of the lawsuit” after he authorized Houston Methodist to file a motion to dismiss the lawsuit. A hearing is scheduled for Friday June 11.
In the lawsuit Bridges and the other plaintiffs argue that, “There were 4,434 death reports and over 12,619 serious injuries reported to the CDC’s VAERS [Vaccine Adverse Event Reporting System] database from Covid-19 vaccines through May 10, 2021”, which has since risen to 5,165 deaths and 25,359 serious injuries through May 28, 2021. The plaintiffs argue that they are protected by a 1985 Texas Supreme Court decision in the case Sabine Pilot Service Inc. v. Hauck. In that case the court found that employees could sue if the only reason they were fired was for refusing to do an illegal act. They also argue that the hospitals mandate violates federal laws on authorizing medical products in emergencies.
Bridges and the other plaintiffs accuse Houston Methodist of arbitrarily denying vaccine exemption requests, despite having a policy for medical and religious exemptions. “Methodist claims that they offer religious and medical exemptions, but it (the exemption request) goes against a panel of judges and they have denied 80-85% of them,” she stated.
I spoke with a nurse at Houston Methodist whose medical exemption was approved who supported the employees right to say no to the shots. “I’m here to show support for my fellow Methodist employees who were not allowed a choice in their medical care. They were bullied and bribed into taking a vaccine,” she said on Monday afternoon. “Luckily they approved my exemption, but there have been many, many which have not been approved.”
One of the nurses who had her exemption request denied was Melissa Smith of the Clear Lake Methodist Hospital.
“Friday was my last day. Tomorrow I will sign my suspension and then they will give me 2 weeks to take the J & J vaccine. I am not going to get the vaccine and they will fire me,” Smith told TLAV. She applied for a religious exemption from the treatment and was denied. “This was under our Director of the Operating Room and the manager of my department. They gave us specific instructions on how to fill out the exemption form. So many of us did and all were denied. We all received the blanket email. I actually believe no one even read it.”
Smith estimated that the number of nurses at her hospital requesting religious exemption was in the 40’s.
“I am really here for the people who have cried, the people I have prayed with who got vaccinated because they felt they didn’t have a choice,” Smith stated while the crowd of supporters gathered outside the Baytown Methodist Hospital. “They didn’t have a voice, they felt they had nowhere to go. I am hoping that this kind of action gives them that voice and gives us choices.”
Welcome to New World Next Week – the video series from Corbett Report and Media Monarchy that covers some of the most important developments in open source intelligence news. This week:
Video available at After Skool Odysee and YouTube channels.
Speech extract from “What is Life About?” by Alan Watts, courtesy of https://alanwatts.org
Alan Wilson Watts (6 January 1915 – 16 November 1973) was a well-known British philosopher, writer and speaker, best known for his interpretation of Eastern philosophy for Western audiences. He left behind more than 25 books and an audio library of nearly 400 talks, which are still in great demand.
Today my colleague from Kentucky, Chris Wiest, received an awesome ruling from the Circuit Court of Boone County declaring that all of Governor Andy Bashear’s emergency orders and actions are unconstitutional and void. The ruling was in the state-court challenge to the governor’s emergency powers executive orders, filed by Wiest on behalf of Beans Cafe’ & Bakery.
Dr. Stephen Petty, an actual expert in masks, testified at the trial about their uselessness under the circumstances in which they’re being idolized. Here’s an excerpt from the order pertaining to Dr. Petty. For those bureaucrats and social media tyrants who would censor this, this is from an actual court order issued today. Not that you care:
Stephen E. Petty, P.E., CIH, testified as an expert and was accepted as such without objection. Mr. Petty has served as an expert witness in approximately 400 cases relating to toxic or infectious exposure, personal protective equipment (“PPE”), and as a warning expert. He also served as an epidemiology expert for the plaintiffs in the Monsanto “Roundup” cases, and for those in the Dupont C8 litigation. In connection with his service as an expert, he was deposed nearly 100 times and has provided court testimony in approximately 20 trials. Mr. Petty holds nine U.S. patents, has written a book comprising nearly 1,000 pages on forensics engineering, is a certified industrial hygienist, and a recognized expert with the Occupational Safety and Health Agency. Mr. Petty helped write the rules on risk assessment for the State of Ohio and has trained Ohio’s risk assessors.
Mr. Petty explained that the field of his expertise is “to anticipate and recognize and control things that could hurt people, everything from making them sick to killing them.” He testified that, in this context, he has analyzed the use of masks and social distancing in connection with Covid-19. He testified that both the six-foot-distancing rule, and mask mandates, are wholly ineffective at reducing the spread of this virus. Masks are worthless, he explained, because they are not capable of filtering anything as small as Covid-19 aerosols. In addition, masks are not respirators and lack the limited protections that respirators can provide.
The N-95 respirator, which he states is in the bottom class of what may be classified as a respirator, is rated to filter 95% of all particles that are larger than .3 microns. However, a Covid-19 particle, which is only between .09 to .12 micron, is much smaller. Mr. Petty further explained that an N-95 will not even filter above .3 microns if it is not used in accordance with industry standards. Among the requirements, respirators must be properly fitted to seal along the face, and they also must be timely replaced. Mr. Petty stated that N-95 masks, which he said are often utilized as surgical masks, are “not intended to keep infectious disease from either the surgeon or from the patient infecting each other” but only to catch the “big droplets” from the surgeon’s mouth.”
According to Mr. Petty, masks have no standards, are not respirators, and do not even qualify as protective equipment. In contrast, respirators have standards, including rules that state respirators may not be worn by persons with facial hair, must be fitted to ensure a seal, and must be timely replaced—or, as in higher end respirators, the cartridges must be replaced to prevent saturation. In addition, standards for respirators also require users to obtain a medical clearance because the breathing restriction can impair lung function or cause other problems for persons having such limitations. Putting those persons in a respirator can harm their well-being.
Concerning the effectiveness of respirators, Mr. Petty explained that it comes down to “big stuff” versus “small stuff.” Big stuff can be taken out by the body’s defenses, such as its mucus tissue, where droplets can be caught and eliminated. The small stuff, however—like aerosols—are more dangerous. Masks cannot filter the small stuff. According to Petty, because Covid-19 particles are comprised of aerosols, it is really, really, small stuff. And, as he pointed out, an N-95 is designed to filter larger particles. Even for particles as large as .3 micron, Mr. Petty testified that an N-95’s effectiveness is in direct proportion to its seal. In fact, he stated it becomes completely ineffective if 3% or more of the contact area with the face is not sealed.
Mr. Petty testified that masks leak, do not filter out the small stuff, cannot be sealed, are commonly worn by persons with facial hair, and may be contaminated due to repetitive use and the manner of use. He emphatically stated that mask wearing provides no benefit whatsoever, either to the wearer or others.
He explained that the big droplets fall to the ground right away, the smaller droplets will float longer, and aerosols will remain suspended for days or longer if the air is stirred. Mr. Petty testified that the duration of time that particles remain suspended can be determined using “Stoke’s Law.” Based on it, for particles the size of Covid-19 (.12 to .09 micron) to fall five feet would take between 5 and 58 days in still air. Thus, particles are suspended in the air even from previous days. And so, he asks, “If it takes days for the particles to fall, how in the world does a six-foot rule have any meaning?”
Mr. Petty acknowledged that both OSHA and CDC have recommended that people wear masks. However, he called this “at best dishonest.”61 As an example on this, he pointed to CDC guidance documents where, on page 1, it recommends wearing a mask; but then on page 6, admits that “masks, do not provide . . . a reliable level of protection from . . . smaller airborne particles.”62 According to Mr. Petty, those agencies have smart individuals who know better. Mr. Petty points out that, even before March 2020, it was known that Covid-19 particles are tiny aerosols. And on this, he states that he insisted that fact early on. He also points to a more recent letter by numerous medical researchers, physicians and experts with Ph.D.s, asking the CDC to address the implications of Covid-19 aerosols. During Dr. Stack’s subsequent testimony, he also acknowledged that Covid-19 is spread “by . . . airborne transmission that could be aerosols . . . .”
Finally, Mr. Petty pointed to another recent study by Ben Sheldon of Stanford University out of Palo Alto. According to that study, “both the medical and non-medical face masks are ineffective to block human-to-human transmission of viral and infectious diseases, such as SARS, CoV-2 and COVID-19.”64 The Court finds the opinions expressed by Mr. Petty firmly established in logic. The inescapable conclusion from his testimony is that ordering masks to stop Covid-19 is like putting up chain-link fencing to keep out mosquitos. The six-foot- distancing requirements fare no better.
The judge summarizes the situation nicely:
It is obvious from even a cursory review that the orders issued over the past fifteen months “attempt to control” and seek “to form and determine future rights and duties” of Kentucky citizens. These included ordering the closure of all businesses, except those the Governor deemed essential. He ordered churches closed, prohibited social gatherings, including at weddings and funerals, prohibited travel, and through CHFS, even prohibited citizens from receiving scheduled surgeries and access to medical care. And then there is the order that everyone wear a mask. These are, undeniably, attempts to control, set policy, and determine rights and duties of the citizenry. Except in those instances where the federal courts have stepped in, Defendants assert authority to modify or re-impose these orders at their sole discretion. Consider, for example, the recent modification of the mask mandate. It orders persons who did not get vaccinated for Covid-19 to wear masks but lifts that requirement for others. That is setting policy and determining future rights and duties.
At the hearing, Defendants took exception to the Attorney General’s characterization of the Governor’s actions as a “lockdown,” and argued that prohibiting persons from entering those restaurants is not the same as ordering that they be closed. But that doesn’t minimize the impact on those who lost their businesses as a result, or those in nursing homes condemned to spend their final hours alone, deprived of the comfort from loved ones (or even any real contact with humanity), or those citizens who the Governor prohibited from celebrating their wedding day with more than ten persons, or those he forced to bury their dead alone, without the consoling presence of family and friends (and who likewise were deprived of paying their final respects), or those persons who were barred from entering church to worship Almighty God during Holy Week, and even Easter Sunday, or those persons who were denied access to health care, including cancer-screenings, or those denied entry into government buildings (which they pay for with their taxes) in order to obtain a necessary license, and who were forced to wait outside for hours in the sweltering heat, or rain, purportedly to keep them from getting sick.
What the people have endured over the past fifteen months—to borrow a phrase from United States District Judge Justin R. Walker—“is something this Court never expected to see outside the pages of a dystopian novel.” Yet, Defendants contend that the Governor’s rule by mere emergency decree must continue indefinitely, and independent of legislative limits. In effect, Defendants seek declaratory judgment that the Constitution provides this broad power so long as he utters the word, “emergency.” It does not. For this Court to accept Defendant’s position would not be honoring its oath to support the Constitution; it would be tantamount to a coup d’état against it.
Yes, life is now a dystopian novel. Let’s hope this patriot judge’s order stands up on appeal in the state appellate courts in Kentucky. And thanks to Chris Wiest and the AG of Kentucky for fighting the good fight. The order notes that the permanent injunction against the governor goes into effect on June 10, 2021 at 5:00 p.m.
“…how can you give informed consent if there’s no package insert, with no
ingredients, no test note, no anything? The words are intentionally left
blank on the package insert for the shots and there’s no long-term data,
so I can’t tell people what will happen in 2, 3, 4, 5, ten years from now,
because they took this shot. So that, by default, is the informed consent
that I’m concerned with.”
America’s Frontline Doctors (AFLDS) spoke to New York pharmacist Joel Wood about his dismissal for his refusal to administer experimental biological agents without providing his patients the ability to give their informed consent to receive them.
On May 5th, Wood called an anonymous ethics line at the Kinney Drugs corporation where he was employed to express concerns over both vaccine shedding and vaccination in youth. On May 9th he wrote an email to the corporation in which he stated: “I have been an employee for Kinneys for over 5 years. I have always felt that they have made safety for staff and patients a priority. However, I would like to know what the company is doing to address the safety concern of shedding of vaccine in the work place. It is a known phenomenon, and specifically mentioned in the Pfizer study on page 67 as a concern. It is possible to have contact thru both physical touching (which is not the concern at work) but also inhalation – this is a concern at work. The masks do not provide any safety. I would like to see this addressed in an email to the company by this weekend.”
Wood continued: “If there is not an email that addresses these concerns, I will forward my complaint to OSHA as a violation of safety.
“I am also concerned with the lack of patient safety and informed consent that involves the Moderna COVID-19 shot. I have heard from many staff and patients that they did not know that the shot was NOT FDA-approved. I know for a fact the staff who are administering this shot are not telling people that it is not an approved vaccine. This creates an issue when patients get their second shot and are informed that it is not approved and say, ‘Well, the first shot was’; no, it was not.
“I would also like to address the elephant in the room. I understand the need to follow advice from our regulatory governmental agencies. However when those agencies are wrong or make inappropriate recommendations, it is our patients that feel the brunt of this…
“I fear that Kinney is moving in a direction that is the opposite of our motto. Experience the difference means just that, if we do not change our behavior and inform the public the real science and health information that exists in the world, we do a disservice to the community and also ourselves as healthcare providers. We are now going to be administering a shot to children 12 and older for a disease that was called the common cold by the New York Times twice. We have no long-term data about this shot in children.”
Wood concluded his letter to Kinneys: “If there is not an email sent to the company that starts to address these concerns, I will be writing letters to OSHA and well as news organizations as a whistleblower for the crimes that are being committed. I do not believe that it is intentional, but we are acting against international human rights laws that discuss vaccines and discrimination. We have a responsibility to tell the public the reality about this shot, what it really does, that there is no pandemic, and that the numbers were inflated to make it appear like a pandemic. We need to inform them about the vaccine shedding that might be occurring.”
After receiving no answer to address his concerns, Wood addressed a formal complaint to the Occupational Safety and Health Administration (OSHA). On May 11th, he received an answer that read: “At this time OSHA has no standards or jurisdiction when it comes to COVID-19 concerns or complaints. We have been told to give all complainants these 3 numbers to contact if you so choose:”, listing the New York State Governor’s office, the New York State COVID-19 hotline, and the New York State Department of Labor COVID violation hotline. Wood was subsequently fired from his position at Kinney Drugs.
America’s Frontline Doctors spoke to New York pharmacist Joel Wood, who was fired after five years in his job for refusing to administer COVID-19 vaccines without informed consent.
“I’ve been a pharmacist in New York State for seven years and I’ve been working with this company in the retail setting for seven years, and ever since the coronavirus outbreak in the beginning of 2020, I’ve had my concerns as someone who works in the front line trying to make sure that my patients and the public are safe, are taken care of, to the best of the ability that we can as pharmacist and health care providers has been my number one concern.
“So I became very invested in the coronavirus outbreak and pandemic, but as time went on I started to have more concerns over what was going on with the whole story of the coronavirus pandemic and outbreak, from things like grabs for power, from different governments in with located within the United States, and I also saw abroad in the world as well. But New York State, the governor of New York, Andrew Cuomo, has had a massive power grab, and in my opinion violated a lot of concerns that I have as a health care provider, mandates and things like that.
“So it was to the forefront of my attention what was going on, and was something more going on than just what we saw at face value of ‘this is a pandemic.’
“I had my concerns about administering the coronavirus when I heard that we were going to start administering it to children.
“I also did have concerns – I’ve seen some reports of women, most likely younger women of childbearing age, having adverse reactions to either the vaccine, or potentially even the vaccine shedding – you know people who have gotten the vaccine become a vector to shed the vaccine, as noted in Pfizer’s trial.
“So the combination of both the children 12 years and up being given the vaccine, or having the ability to receive the vaccine, as well as women of childbearing age – I started to kind of have some concern what was going on with the vaccine, but also what was going on with the coronavirus pandemic, period.
“But the majority of my concerns stemmed from the lack of solid, I have to say science, backed-up evidence. I mean multiple health organizations, from the World Health Organization to the Centers for Disease Control and to some degree the FDA, in terms of their approval process for this vaccine, they’ve been all over the place. I mean multiple doctors and scientists from across the world have written into the WHO with different concerns; respiratory droplets compared to aerosol, that kind of goes into the mask detail. The CDC has published data that leads to the potential controversy for masks. I mean, I’ve read an article in which the CDC describes the masks were not statistically significant. I was taught in school that if it’s not significant, that’s not something that you look at.
“So combinations of those have led me to believe that the administration of these vaccines in any group in which the coronavirus does not have a high death rate may be unwarranted and potentially, as it is an experimental vaccine – not FDA approved – violates Nuremberg trial law.
“So my ultimate decision to stop administering these COVID-19 vaccines, as I stated, came from the combination of children 12 and up, and specifically women bleeding, menstruation issues as it relates to women specifically of childbearing age; there’s no long term data to what this vaccine does, and technically it’s impossible to give informed consent, in my opinion, because the package insert is blank. The package insert for the drug itself, for the vaccine, if it even is a vaccine, is blank, and there’s no long-term data. So I am concerned for what effects then could happen from women who take this, specifically of childbearing age, what could be the end result? I have no idea, and I’m not speculating that anything awful could happen, but we don’t know – and that’s a concern, that’s something I look at – risk versus benefit is what is what my job is all about.
“Same thing with children. Children who are less than 18 – the survival rate of the coronavirus is like 99.999. The only age group that I feel could and potentially should have concern with receiving this vaccine is 65 and older, as their survival rate was less than 99-point-x, we can just say.
“So I also was administering the shot as of January 11th when the rollout happened in New York, right along, because that was what all of the governing bodies were saying: The states, the CDC, FDA, World Health Organization – everybody was discussing the importance of the shots and need to get to herd immunity, so I was doing my part – or I thought I was doing my part – by helping us get there.
“But I noticed as we started to get there, and people started to receive the shot and get both doses, if they were getting the Pfizer and Moderna, for example, it seems like we’re never going to reach this herd immunity and they just keep pushing the vaccine.
“I mean, now in New York State, you can win anywhere from $20 to $5 million with the lottery, just for signing up and getting the vaccine. For me, that’s a huge concern on multiple different levels. I mean one, on the very face value, the government of New York under the leadership of Governor Cuomo, and along with the federal government as well, at least for part of this, is using our federal and state tax dollars to get the money for this vaccine, which my question is may or may not be causing more harm, and also now we are using tax money that should be going towards schools, is my is my understanding of what the New York State lottery was supposed to be for when it was revamped believe over a decade ago, now we’re using that money to give people for getting the vaccine? It’s just highly irregular. I’ve never seen anything like that before in my life. It’s a concern.
“I also have concerns, as I previously mentioned, about violations of the Nuremberg trial, human rights as it pertains to the Geneva conference in the Nuremberg trials. This is an experimental vaccine, it’s not FDA approved.
“And from there, my concerns go out to: Is this coronavirus pandemic a real pandemic? No more people died from it month over month in 2020 than in previous years. The CDC has come out that 6% of deaths were attributed specifically to coronavirus, meaning that the other 94% had underlying comorbid diseases, which we would generally assume similar to like the flu, we don’t say that everyone just died from the flu if you had the flu, something else helped you get there. That’s how that’s how it presents itself.
“The CDC has been, in my opinion, manipulating and shifting how they are counting deaths and cases to establish a point that if anyone believes that we are not in a pandemic, there is a massive issue and concern with that. So moving forward, if we are actually not in a pandemic, there is fraud and deceit associated with receiving this experiment which both violate the Nuremberg trial.
“The other part of the Nuremberg trial that concerns me is coercion. It’s also stated in the Nuremberg trials that you have to have free, informed consent to be able to have someone sign up for your experiment. And we are coercing people now to have to get the vaccine to be able to take their mask off. So it’s also a false pretense that you have to get the vaccine to take the mask off, but that’s not how we should be doing an experiment, it gives a false sense of reality to people that were not truly informed as to what could be happening.”
Just for the record, what has been your stance on vaccines in general, prior to the emergence of COVID-19, and what has been your experience regarding the whole issue of informed consent? Has there not been a problem until now?
“I don’t have a concern with vaccines in general. I mean, I do have some minor concerns, specifically as it pertains to the pediatric administration of vaccines, but it’s not necessarily the vaccines itself as much it is the tenacity to which we give all these vaccines. I mean, just for example, the amount of aluminum in a child’s vaccine series could be more than what the FDA allows to have in an adult’s i.v. So just as a quick example of where my concerns for vaccines stem from, that’s pretty much my only concern with vaccines, like the current childhood immunization schedule I think is a little over the top. But otherwise no, I don’t have a problem with other vaccines, I don’t have a problem with administering other vaccines. The informed consent has never come up as a major issue for me, in general because they’re all FDA approved. In the very least, every other vaccine that I have ever administered has been FDA approved. So then from there, it’s more of the informed consent of like, ‘these are the side effects, this is to look what to look out for, what could happen; if this happens, do this,’ which is common for any and all medications, new medications, or any and all medications that I would be giving in a pharmacy. Letting people know what the risks and benefits are from the shots that are given.
“The informed consent is a massive concern this time because the package insert is blank. So if someone were to ask me, ‘Hey Dr. Wood, what’s in this?’ I couldn’t tell you. I do know some of the things, I do know some of what’s in it, but I couldn’t give you specific details from the package insert. And then also, ‘What could happen to me?’ I can tell you what has happened to people previously to this point; I can tell you adverse reactions that I have seen from the VAERS reporting, including all of the deaths, the rashes; I can tell you what I have seen up to this point, but I can’t tell you what’s going to happen to you a year from now or two years from now, five, seven, ten years – I have no idea. So informed consent is for me the biggest concern, as it pertains to this coronavirus shot.
“In New York, and in I believe most of the rest of the United States, pharmacists are administering vaccines and have been quite a while, typically in the very least the influenza, maybe the pneumonia or shingles vaccine. But since the beginning of January, retail pharmacies of which I was working for have been administering the coronavirus shot – I will call it a shot, it’s not a vaccine in my opinion. So I have been giving the coronavirus shot probably upwards of over at least 500 people, if not more, and I’ve expressed what my concern is. I went to my employer and said I don’t feel comfortable giving this. We can’t give the people full, informed consent.
“When I told people it wasn’t FDA-approved, people didn’t even know it wasn’t FDA-approved. Or people would say, ‘Well, the first one was.’ That by itself indicates that pharmacists were not telling people that it was not even an FDA-approved shot yet. And second to that, how can you give informed consent if there’s no package insert, with no ingredients, no test note, no anything? The words are intentionally left blank on the package insert for the shots and there’s no long-term data, so I can’t tell people what will happen in 2, 3, 4, 5, ten years from now, because they took this shot. So that, by default, is the informed consent that I’m concerned with.”
Can you tell us about your complaint to OSHA? What is their jurisdiction? What were you hoping to achieve? And what did they finally answer?
“So I had reached out to OSHA after I had reached out to my employer about concerns of vaccine shedding. The vaccine shedding phenomenon is a well-documented concern, and specifically for the coronavirus shot: Pfizer’s own study mentions they were worried about environmental spreading of the vaccine, specifically to pregnant women through both inhalation and skin-to-skin contact. So that leads me to believe that it’s at least possible, or they were worried about it, that vaccine shedding could be a thing.
“I reached out to OSHA because my employer ignored my concerns of vaccine shedding. I have not received the shot yet, so I was concerned about other people, both employees who have received it, and patients and customers who have received it, shedding the vaccine, and what my company was going to do to protect me and other people like me who have not received it. They said nothing.
“I reached out to OSHA and said, ‘What can be done? I have a concern in my own position, job, business, as well as any other retail pharmacy in the country – if you chose not to get the shot, but you are around people who have gotten it, and they are shedding the vax, they are shedding parts of the shot, that’s a concern. So I reached out to OSHA, and OSHA emailed me back and said that they currently have no jurisdiction over the coronavirus shot, there’s nothing in place, there’s no policies or procedures as it pertains to the coronavirus, and that I needed to reach out to New York State, both the New York State governor’s office and the Department of Labor as a means to get an answer, which I was not happy with, I did not accept. My concern for OSHA’s complaint is, how can a federal body not have something in place for after a brand-new experimental shot is released from big pharma, and the only people that have the answers are the same people that I am potentially concerned with are violating human rights set forth in the Geneva laws put forth after the Nuremberg trials?
“Her response indicates exactly what I think it says: We don’t have any jurisdiction, we don’t know anything about this; reach out to the New York Department of Labor and the governor’s office. That is a huge concern for anyone who is worried about his safety and health in the office. Anyone across the country right now could have a concern over whether someone is or is not vaccinated, and that’s part of the debate, I believe, that’s going on in the country. Before, it meant forcing vaccines, or forcing masks, or all of this stuff – and if OSHA’s response is to just default to whatever the state says, then you are potentially at the mercy of whoever your state governor is. And I don’t I don’t mean to turn it into a political, Republican/Democrat, red versus blue concern, but in the very least both certain Democrats and certain Republicans have taken opposite stances. So just that being said alone, it’s very concerning that in one state, for example, you can eliminate the mask mandates and there’s no vaccine passports, but in other states, that’s the only way we’re operating. So OSHA’s response is very concerning to me. That’s part of the federal government that in my opinion is supposed to be watching out for workplace safety concerns, and I agree 100% – I think her answer is kind of just wool over the eyes, the programmed response to say ‘we don’t have any jurisdiction, here’s who you can talk to…’ and then guess what? It’s not OSHA’s problem anymore, they have addressed it, they emailed me back. I mean, it’s so bizarre and terrifying.”
You said risk versus benefit is what your job is all about. Could you elaborate on that more, and explain to us how that specifically relates to your responsibilities as a pharmacist vis-à-vis COVID-19?
“Yes, the risk versus benefit: One of the great conundrums of how all healthcare works. That’s the basis for my job as a pharmacist, and I believe that’s the basis for almost every other health care profession out there. We have the knowledge through teaching, training, education, to assess the risk versus disease state, or the risk versus treatment, versus the benefit of not having treatment, or the benefit of getting treatment, so whether it’s triple bypass surgery, your doctor, your cardiologist, your surgeon looks and measures and decides what’s going to be the healthiest outcome, the best outcome for you.
“Same thing for me, it just happens for me, as a pharmacist, drugs is what I look at and evaluate. And then when it came to the COVID-19, initially I was under the impression that this was the only thing that was going to get us over this, over the hump, through this awful time in history, was to give these vaccines, give these shots.
“But as time went on, I started to be concerned more with what the shots were doing to people, that’s when I started to change my opinion. And I noticed the risk/benefit may not be the same. It appears to me the risk of the coronavirus itself COVID-19 in most age groups less than 65, maybe even 50, the negative outweighs the risk of the shot. Getting COVID-19 in someone less than 50 poses almost zero health risk to you.
“So the benefit of the shot, we don’t know. All the shot does, at this point, technically, is prevent you from getting severe disease. You can still pass the coronavirus, you can still get the coronavirus, it just prevents you from getting severe disease. So that’s the risk/benefit that I look at. What is the benefit to this shot? Just getting severe just preventing severe disease? When 80% of cases are asymptomatic, the coronavirus itself kind of prevents severe disease. Coronavirus has been around for decades, they are part of what causes the common cold.”
Do you believe that there is a code of silence among pharmacists regarding this issue?
“I do not believe that there is a code of silence among pharmacists. I’m more inclined to believe that there is a very deep-rooted psychological hand at play by certain groups of people or certain bodies or certain powers, I don’t know, but I don’t think it’s a silence code.
“And it was hard for myself to do it, too. We are trained – why would we ever think that any one of the federal governing bodies or even worldly, in the example of the World Health Organization, why would we believe that they would be telling us lies? So I don’t think it’s a code of silence, I just think we’re trained and taught to think the CDC, FDA, and the World Health Organization are all quality, upstanding government bodies that aim to solve public health crises.
“And that is not to say that they are not those things and that they do not do that. I don’t want to sound like a complete martyr. Again, I’m not saying that they do. My concern is, I don’t know what’s going on, and that’s why I have concerns over the administration of this shot.”
Have you received feedback from your colleagues? What did they think about the stand you’ve taken?
“I have reached out to a few colleagues and expressed my concerns. Most of them think that I have a decent case, or that the case that I am making isn’t necessarily completely left-field bizarre, even though it is kind of left-field. I don’t know that they’re willing to take a stand, I mean, I was fired from my position. I could only imagine that in any other pharmacy, company, corporation, chain – or most, I would say, for a pharmacist who is not willing to do an aspect of their job, as in giving shots and vaccinations, whether it’s COVID or any vaccine, but specifically the COVID one, it’s going to be hard for a company to keep them on or want to keep them on because there’s a lot of other pharmacists out there who will do it because they need a job, they need the paycheck. So it’s hard for someone to risk it all unless they feel strongly about it.”
At what point did you understand that making this stand may mean the termination of your employment, and when you did realize that, what was it that pushed you to decide to go on anyway?
“I had always known that by taking the stance of not doing a role in your job, when you choose not to do something in your position or your job that is what is expected, you always risk being fired, terminated, reprimanded, what have you. So I always knew that would be a concern, at any point I had decided to take the stance.
“But what officially gave me the courage to decide to do this was when my wife agreed with me that being able to vaccinate children 12 and up was just not right and we needed to do something, I needed to do something. We needed to take a stand and express our concerns for the health and safety of, most importantly, children, and I think potentially even everyone who is eligible to get this shot 12 and up, and it’s going to get younger soon I imagine, they’re going to try for it. So it was my wife who gave me the encouragement and kind of the okay to be like, ‘Yeah, this is a possibility, if you do get fired we’ll do whatever we have to, but it’s the right thing to do.”
Does this move and does the termination of your job represent financial hardship for your family?
“The move does represent financial hardship for my family, my wife and I have a lot of student loan debt; just that alone is a huge concern as a means of bills we have to pay, and now I’m losing a very good salaried job, so it will it will be difficult to weather the storm…”
What does your family say? Are they supportive?
“My family is supportive. I would say for the most part I think the majority of my family is supportive because they support me, and first and foremost that’s what families do, that’s what that’s what blood is, but I think parts of my family Also question, ‘what is he talking about? What is he thinking? How can you know?’ But that kind of goes back to the pharmacists keeping a code of silence and other health care providers – why would anyone question health authorities like the CDC, FDA, World Health Organization? It just sounds so bizarre, and I don’t disagree with him, I mean it does sound bizarre, but for me, I’m educated as a pharmacist and I’ve also been keeping track of all things related to coronavirus because I wanted to make sure that first and foremost my family was safe when the outbreak happened, and then secondly, it’s my job to make sure that people in the public are taken care of, and in the public scene as a pharmacist, in the pharmacy we’re a store that’s open, so anyone could be a patient of mine, anyone could come in off the streets and ask me a question and that could be anyone from around the world. I’ve worked in cities where I see people and meet people who are from around the world who don’t speak English, don’t speak English very well, so for me it’s the real undertaking I needed to do, because anyone and everyone could be one of my patients and I took an oath to protect and serve and make sure that people received quality health care with no harm.”
Do you think that you’ll be able to identify another source of employment?
“I definitely believe that I would be able to find another source for employment from someone who is like-minded, like myself, and has made commitments to protecting health in the public eye. I think the biggest concern is just kind of waiting when that will happen kind of the who, what, where, why, when will that job happen I’m not sure, but I’ve also decided I wasn’t happy as I could be as a pharmacist in my previous job, just from what I was seeing happening in the whole healthcare landscape.
“So the next job that I hopefully get will be where I can feel more impactful that I’m actually creating and changing people’s health and health outcomes in as in as dynamic away as possible. But yes, I do believe that there are people, companies, employers out there who, whether or not they are specifically concerned with whether I am or I’m not vaccinated, or if they’re concerned with the stance that I’ve taken, I think there are employers out there who are looking for someone who is willing and wanting to provide quality health care and that has always been my goal.”
In a few short years, the majority of the world’s population has accepted the fifth generation of wi-fi called 5G, where the speed to send full-length, high definition movies to your ipad is said to be ten times faster. The frequencies of 4G, 5G, and 6G are comprised of psychotronic waves. Psychotronics is the study of mind-body-environmental relationships.
By any other name, frequency technology is weaponry being unleashed with the ability to cause an invisible rise in disease on a mass scale. For a history of how the purposeful introduction of electromagnetic frequencies have caused the health problems of humanity, read, The Invisible Rainbow by Arthur Firstenberg.
The Consequences
The need for speed has the consequence of going from moderate to severe adverse health effects in record time. Note that 4G operates at 2.5 GHz or oscillates about 2.5 billion times per second. This frequency mimics water molecules in your body, and was chosen specifically for broadcasting services and equipment under government license. This means that all company products must meet this frequency or be deemed illegal. For what purpose is matching the human body’s frequency, you may ask, other than for weaponization? Good question.
The higher frequencies of 5G comprise a range from 60–100 GHz. 60 GHz is a frequency known to affect oxygen uptake in the human body. In fact, one vocal doctor has warned his colleagues that what they may be seeing in hospitals as COVID are symptoms of 60GHz frequencies.
If not already deployed, the FCC plans to erect small scale wireless refrigerator-sized boxes, placed in front of every 2-10 homes on every street, in every city. The reason is because, since 5G waves travel shorter distances than other waves, they are easily blocked by buildings and trees. As you watch the latest Hollywood flick, you will bask, unaware, in 4G & 5G microwave emissions that oscillate at the same rate as your water and oxygen molecules. These frequencies can cause burning sensations on your skin, impact fertility, as well as alter the electrochemical waves of your brain to affect mind and consciousness. A new form of indoctrination?
Firefighters in Sacramento have reported memory problems and confusion following the installation of new towers in Los Angeles in 2004. Some cities, including Santa Rosa, have halted their 5G plans while health concerns are addressed. These same millimeter waves have been used by the U.S. Army as a crowd control dispersal weapons called Active Denial Systems.
The ‘Live Exercise’
What is a Live Exercise?
A live exercise is part of a script that some have called a ‘false flag operation,’ fake news, or a hoax. A list of suspect false flag operations amount to fraud on the people who unknowingly participate. A live exercise is an opportunity for the operators behind the hoax to provide full disclosure under the guise of an event perceived to be serious or dangerous.
One such famous event occurred on the radio on the night before Halloween, 1938. Orson Welles and his Mercury Theatre on the Air performed a radio adaptation of H.G. Wells’s The War of the Worlds, by converting the 40-year-old novel into fake news bulletins describing a Martian invasion of New Jersey. The show caused hysteria nationwide as many listeners mistook those bulletins for the real thing and called police, newspaper journalists and hospitals with reports of mass stampedes and suicides.
More recently, live exercises occurred when secret testing of 5G emissions happened during the 2018 Olympics, and then again at the 2018 Super Bowl where over 67,000 people were part of a secret stress-test without their consent. The 5G antennae networks have since been beta tested in nineteen U.S. cities including San Francisco, Los Angeles, Jacksonville, and San Jose.
Even more recently, in March of 2020, CNN filmed Secretary of State, Mike Pompeo, who admitted “we’re in a live exercise here” when referring to the COVID-19 pandemic during a press conference.
The art of deception continues as governments worldwide promote high frequency 5G signals as necessary for your Wi-Fi experience. What is the point of adding short waves to all the frequencies already deployed? Why duplicate technology when fiber optics works perfectly well, and maybe better?
No time for answers. It’s full steam ahead to remove the obstacles that block the signals.
First the trees.
Trees Targeted
During the summer of 2017, many people in California reported that extensive “weird fires” destroyed many trees, leaving homes untouched. Everything did not burn. At other times, the metal of cars and rails burned along with the leaves on trees, leaving tree trunks and kindling. Many claimed these unusual fires to be the result of lasers from Directed Energy Weapons. Whole forests have been devastated down straight lines, obeying fence lines. In addition, the sanctioned poisoning of hardwood trees by timber companies that has led to over one million dead trees to create a fire hazard.
Are the trees being destroyed merely to open a path of hazardous signals? Is this treason/tree-son on multiple levels? A Freedom of Information request by the Sunday Times in England found that more than 110,000 trees had been cut down by UK councils between 2015 and June 2018.
Unless you can stand up, speak up, collaborate and network, you risk being a victim of a attack coming unseen, as millimeter waves, directed at body and mind. If people feel powerless and isolated now, imagine what it would feel like once the newly installed 5G towers are fully operational. Image what it would be like when the trees are replaced with towers that look like trees. We only feel isolated when we work alone and isolate ourselves, or when we respond to dictates by governments that convince us to isolate ourselves without the authority to do so. Like a forest, there is strength in numbers.
Health Effects of 5G
Because 5G frequencies affect oxygen molecules, they affect all biological systems, including DNA, circadian rhythm, heart function, hormonal regulation, and immune system. Hundreds of scientists have expressed concern that humans may experience serious health risks including increases in blindness, cataracts, retinal degeneration, hearing loss, male infertility, cancers, peripheral nervous system damage, impacts on immune cells, red blood cells leading to low cellular oxygen, and impaired transport of nutrients into cells. Impacts on birds and plants may be more severe than the impacts on humans.
Silent Wars
Beyond direct effects to health, harmful frequencies threaten society as a whole by ignoring the human right to informed-consent to high levels of radiation. All life on the planet has a right to health and a healthy life. By accepting the 4G,5G,6G rollout without a discussion, as happened with airport scanners and GMO foods, people innocently give up sovereignty over their bodies. The new frequencies ionize metals being sprayed into the atmosphere under military “geo-engineering” programs to charge the atmosphere. They do the same in our bodies.
Could injections with metal contaminants be part of the weaponized network? China began compulsory vaccinations on December 1, 2019, under the The Vaccines Administration Law, which the People’s Republic of China adopted on June 29, 2019. Soon after, South Korea became a location for mandatory vaccines, then 5G networks were launched on November 1, 2019 in both regions. This happened before the pandemic was declared and reports of sudden deaths.
On September 26, 2018, the United States FCC voted to approve its Wireless Infrastructure Order (dockets 17-79 and 17-84). This order preempts local control of the public rights-of-way. Wireless companies can more easily install — in front homes — cell towers that would irradiate those nearby with intense, pulsed, data-modulated, Radio-frequency Electromagnetic Microwave Radiation (RF-EMR) — 24/7. Many of these companies use cloud seeding technologies and weather modification technology
For instance, under the new space programs, patent US7612284B2 , a solar-powered satellite will generate a powerful microwave radio frequency beam focused on an array of collector antennas where it will be transformed to electrical power supplied to PG&E (Pacific Gas and Electric).
Under patent US20110204159A1, a solar-powered satellite will generate a powerful microwave radio frequency beam to control the weather by heating deployments of aluminum oxide or other conductive particulates, sprayed from aircraft. The patent describes methods of steering and changing the intensity of a hurricane.
Some Solutions
Voice the power of NO to all new generation wi-fi systems without proven safety.
Hardwire all electrical connections or unplug Wi-Fri before sleeping.
Use aluminum screens on windows to block EMF signals.
Use RF-shielding paint to block EMF signals.
Consume Carbon60, a powerful antioxidant, metal absorber, and carrier of metals out of the body.
Unsubscribe to the genetically-modified corporate food system.
Eat an organic diet to strengthen and maintain your immune system.
Come together in small communities to maintain simple wi-fi for the benefit and balance of the group.
Grow your own food. Plant a garden. Grow herbs and fruit trees.
Stop using aluminum cookware, antiperspirants, baking powder, injections for health.
Remove the outdoor refrigerators and towers from your sightline.
In usual form, attacks to human health and the health of Earth are coming from new technologies that are unproven, untested, and amoral. Though governments always attempt to divide humanity using race, religion, wars, lies, and unlawful mandates, we are all Earthlings born free, united at the level of our cells and our microbes. Do we slow down and take inventory of humanity at this crossroads? Or do we accept the coming tidal wave?
Speed for the sake of speed is the same as growth for the sake of growth, which is the ideology of a cancer cell.
Over the years the medical establishment has acquired a well-deserved reputation for ignoring good discoveries (which would make a dramatic difference to human health) and continuing with useless practices (which do more harm than good) long after they should have abandoned them. The medical profession, or, rather, perhaps I should say ‘the medical establishment’ has always been slow to accept and assimilate new ideas – and slow to see the obvious.
I have long thought that the main problem with modern medical education is that it is largely based upon learning by rote and upon eliminating all original thought. This is deliberate since the aim of an orthodox modern medical education is to help maintain the status quo (and preserve the position of the pharmaceutical industry). Right from the very beginning, young students are made to learn long lists of information. They learn the names of the bones, the arteries, the nerves and the veins in the body. They learn the names of the muscles and they learn the histology of the various organs. They then learn lists of clinical signs and symptoms. And they learn lists of drugs. At no point are students encouraged to think for themselves.
As a result it is not surprising that after graduation most doctors continue to do as they are told. The average doctor is strangely incapable of critical thought. Given the indoctrination they have undergone it is hardly surprising that doctors readily accept everything they are told by the drug companies (which more or less control post graduate education) and equally readily reject alternative medicine – something which never makes much of an appearance in the undergraduate syllabus.
There is nothing new about this.
The greatest thinkers – the ones who have, in the end, contributed most to medicine and human health – have always been scorned or ignored (or preferably both) by the medical establishment. The establishment has always manipulated the truth to suit its own political, religious or commercial purposes. Simple truths which are inconvenient have always been suppressed. It happened in the past, it will happen in the future and it is happening now.
Few medical stories illustrate the way the medical establishment works better than the story of how scurvy was discovered and how the treatment for it was ignored for centuries.
In 1535, Jacques Cartier sailed from France to Newfoundland with a crew of 110 men. Within six weeks a hundred of his men had developed scurvy. Luckily for Cartier and his men a native told them to drink the juice from the fruit of local trees. The men recovered in days. From that time on wise sea captains made sure that their men were given regular supplies of orange or lemon juice. In a book called The Surgeons Mate, published in 1636 John Woodall recommended that these juices be used to prevent scurvy. But the medical establishment was slow to accept this sensible suggestion.
It wasn’t until two centuries later, in 1747, that the idea was reintroduced by James Lind, who conducted a proper clinical trial and proved that scurvy could be prevented with the right diet. It was Lind’s work which enabled Captain Cook (he was a Lieutenant at the time) to sail around the world without a single case of scurvy.
The admiralty and the medical establishment continued to ignore all this. In the Seven Years War, from 1756 to 1763, approximately half of the 185,000 sailors involved died of scurvy. In 1779 the Channel Fleet had 2,400 cases of scurvy after a single ten week cruise.
Eventually, in 1795 the medical establishment (and the navy) succumbed to common sense and lemon juice became a compulsory part of every sailor’s diet. This breakthrough took well over two centuries to be accepted.
Then there is Paracelsus.
There is no doubt that Paracelsus (Aureolus Theophrastus Bombastus von Hohenheim to his friends) is the father of modern medicine. He tore into the precepts of established medical thinking with all the zeal of a missionary. He revolutionised medical thinking throughout Europe and scandalised the medical establishment by claiming to have learned more from his contact with witches and midwives than from his study of ancient and well-revered medical texts. No idea or theory was too bizarre to be studied and considered and no belief, no practice and no concept too sacred to be rejected. He was the first man to associate mining with chest disease, to use mercury in the treatment of syphilis, to advocate allowing wounds to drain instead of smothering them with layers of dried dung and to argue that some foods contained poisons which harmed the human body. Paracelsus scandalised the establishment by claiming that he was interested more in pleasing the sick than his own profession. He was, not surprisingly, rejected by the medical establishment and widely and persistently persecuted for his beliefs. It was years after his death that his ideas were recognised.
And there is Vesalius.
In the sixteenth century Andreas Vesalius achieved contemporary notoriety and eternal fame as the author of the first textbook of human anatomy, ‘De Humanis Corporis Fabrica’. Up until Vesalius medical students had studied anatomy using texts prepared by Galen. Since Galen used pigs not human corpses for his studies his anatomical notes were, to say the least, rather misleading.
Vesalius’s frank rejection of many of Galen’s anatomical claims earned him considerable disapproval. The medical establishment still firmly believed that Galen could do no wrong. They weren’t interested in anything as superficial and irrelevant as evidence.
Like so many original thinkers before and after him, Vesalius was unable to cope with the outcry. He burnt his remaining manuscripts, abandoned his study of anatomy and took a job as court physician to Charles V in Madrid.
Vesalius wasn’t the only anatomist whose work was rejected. In the 17th century, British doctor William Harvey spent eight years researching the circulation of the blood – and getting it right. His patience was rewarded with ridicule. He received nothing but abuse. He lost many friends and his practice shrank.
When Ambrose Pare, the great French surgeon, first started work as an army surgeon it was accepted practice to stop a haemorrhage by sealing a wound with a red hot iron. Amputations were performed with a red hot knife and the wounds which were left were sealed with boiling oil. One day Pare ran out of boiling oil and used a mild emollient to dress the wounds of the men he was treating. He worried all night about what he had done but the next day he found that his patients were not only healthy but that they were also in less pain than the men whose wounds had been sealed with boiling oil. Pare was wise enough to learn from this and from that day on he started dressing wounds with an emollient rather than boiling oil. He also introduced ligatures, artificial limbs and many surgical instruments. Inevitably, Pare met the usual fate of innovators and reformers (who get a rougher ride within the world of medicine than anywhere else). He was denounced by other surgeons as dangerous and unprofessional. Older surgeons banded together to oppose him and in their attempts to discredit him they attacked him for all sorts of things – for example, his ignorance of Latin and Greek. Pare eventually succeeded because the soldiers he treated trusted him and wanted to be treated by him. They weren’t interested in the views of the French medical establishment.
A look back at hospitals is also revealing.
When Tsar Paul came to power in Russia in 1796 he was so horrified at the state of the hospital in Moscow that he ordered it to be rebuilt. In Frankfurt in the 18th century physicians considered working in hospital to be equivalent to a sentence of death.
In 1788, Jacobus-Rene Tenon published a report on the hospitals of Paris which shocked city officials. He described how the Hotel Dieu (the magnificent looking hospital next to Notre Dame) contained 1200 beds but up to 7,000 patients – with up to six patients crammed into each bed. The stench in the hospital was so foul that people who entered would do so holding a vinegar soaked sponge to their noses. Very few patients escaped from the hospital with their lives. When reformer John Howard toured European hospitals he angrily reported that no fresh air, no sunlight, straw as bedding, no bandages and a milk and water diet supplemented with weak soup were standard. The reports of Tenon and Howard were ignored and dismissed for years and it took decades for the medical establishment to make any real changes.
In the 18th century the treatment of the mentally ill was abysmal. Daniel Defoe, best remembered for his story of the adventures of Robinson Crusoe, wrote a vicious attack on mental hospitals. ‘Is it not enough to make anyone mad,’ he asked, ‘ to be suddenly clap’d up, stripp’d, whipp’d, ill fed and worse us’d? To have no reason assigned for such treatment, no crime alleged or accusers to confront? And what is worse, no soul to appeal to but merciless creatures who answer but in laughter, surliness, contradiction and too often stripes?’
No one took much notice and medical practitioners continued to treat mentally ill patients without respect or care.
At the Bethlem Royal Hospital half naked patients were kept chained in irons. Physicians bled their patients once a year and the more troublesome patients were put on a tranquillising wheel. Until 1770 visitors could pay a penny to see the ‘fun’ at Bedlam. John Wesley, founder of the Wesleyan Church, who considered himself a benefactor of the mentally ill, suggested pouring water onto the heads of the mentally ill and forcing them to eat nothing but apples for a month. Wesley was one of the first men to use electricity in the attempted treatment of the mentally ill. Despite the protests of reformers such as Philippe Pinel (who shocked the establishment in the late 18th century by claiming that the mentally ill were sick and needed treatment) mental hospitals were, well into the 19th century, still quite unsuitable for people needing medical treatment.
There was never any evidence to show that it did any good but blood-letting was a favourite therapeutic tool for centuries. The fact that removing blood from a patient made him or her quieter was regarded as proof that it was doing some good. (This is no dafter than the rationale used to explain some modern treatments.) Blood-letting was easy to perform and it was something to do. Doctors have always felt the need to do something to their patients. (Possibly because it is difficult to explain away a big fee if all you do is give advice.) Leeches were hugely popular in the 19th century. In 1824, two million leeches were imported into France. In 1832, the figure had risen to 57 million a year.
In 1843, the American poet, novelist and anatomist, Oliver Wendell Holmes, read to the Boston Society for Medical Improvement a paper entitled ‘On The Contagiousness of Puerperal Fever’. He argued that the disease could be carried from patient to patient by doctors. He suggested that surgeons should consider changing their clothes and washing their hands after leaving a patient with puerperal fever. His lecture annoyed the medical establishment and his advice was ignored completely.
A similar fate befell Ignaz Philipp Semmelweiss who, in 1846, at the age of 28, became an assistant in an obstetric ward at the Allgemeines Krankenhaus in Vienna. Semmelweiss noticed that the number of women dying in his ward was higher than the number dying in other wards. It wasn’t difficult to notice this. Women would beg, in tears, not to be taken into Semmelweiss’s ward.
Deciding that he wasn’t that bad a doctor, Semmelweiss looked for an explanation and came to the conclusion that the major difference was that patients on his ward were looked after by medical students whereas the patients on other wards were looked after by midwives. Semmelweiss then discovered that the students came straight to the ward from the dissecting room where they had had their hands stuck into the corpses of women who had died from puerperal fever. The midwives never went near to the dissecting room. Semmelweiss instructed the medical students that they should start washing their hands in a solution of calcium chloride after coming from the dissecting room. The remedy produced a dramatic drop in the death rate on his ward.
Predictably the medical establishment was not well pleased – even though Semmelweiss had proved his point very dramatically. The unfortunate young doctor couldn’t cope with the rejection. He became an outcast and died in a mental hospital a few years later. The medical establishment had scored another hollow victory. Once again the patients were the losers.
You might have thought that the medical establishment would have welcomed anaesthesia. After all, before anaesthetics were available, surgeons had to get their patients drunk or knock them out with a blow to the head. Surgeons would often operate with the patient held down by four strong men. The first operation under anaesthesia was performed at the Massachusetts General Hospital in 1846. But the establishment was not going to accept this new-fangled nonsense lying down. The main objection was that anaesthetics were being used to help women who were in labour. And that, said the establishment, just wasn’t acceptable. It was, said the wise men, unnatural and unhealthy for women to deliver babies without suffering pain. ‘In sorrow thou shalt bring forth children,’ says the Bible. However, the religious barbarians were eventually overcome by Dr James Simpson who trumped the Bible quoters with this quote: ‘And the Good Lord caused a deep sleep to fall upon Adam and he slept; and He took one of his ribs and closed up the flesh instead thereof.’ The opposition to anaesthesia was finally quelled when Queen Victoria gave birth to Prince Leopold while under the influence of chloroform.
In 1867 Joseph Lister published a paper in The Lancet entitled ‘On the Antiseptic Principle in the Practice of Medicine’. Lister had found a solution to the age old problem of post-operative infection. But the medical establishment doesn’t like change, even if it means keeping patients alive. And Lister found himself being attacked by doctors who ignored the evidence but disapproved of his new techniques simply because they were new. It was decades before the ‘antiseptic principle’ was accepted.
One of the reasons why hospital infections are so commonplace today is that doctors and nurses seem to believe that they can use antibiotics instead of washing their hands. Incompetence, carelessness and ignorance mean that the quality of cleanliness in the average modern hospital is little better than it was in a hospital in the Middle Ages.
Until surprisingly recently, it was routine for surgery on babies to be performed without anaesthesia on the grounds that babies are incapable of feeling pain. There was no evidence for this claim (one which any mother would be able to oppose with credible if anecdotal evidence) but anaesthetists were taught that babies had immature nervous systems and so didn’t need painkillers.
Above I have described just a few of the hundreds (probably thousands) of examples I could give to illustrate the way that the medical establishment, in recent years allied with the drug industry, has always opposed original thought and has protected the status quo – regardless of the effect on patients.
The medical establishment has acted in the interests of the profession but against the interests of patients, and thoughtful and creative individuals have always had a hard time. The value of serendipity has also been ignored, of course. Both penicillin and X-rays were the result of serendipity.
The real tragedy is that absolutely nothing has changed for the better. Indeed, things have arguably got worse.
The medical establishment is still responsible for protecting and promoting medical procedures which do not work and have never worked (and which expose patients to great risk) while at the same time it opposes and suppresses treatments which do work and have been proved to work.
Today, anyone in the medical profession who dares to offer thoughts or warnings which don’t fit in with the specific requirements of the medical establishment will get the Semmelweiss treatment. They will be laughed at and suppressed.
[Original video is available at Dr. Vernon Coleman BrandNewTube channel. As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute and Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Dr. Andrew Kaufman with Dr. Sam Bailey: “Hunting for Viruses”
They’re called the College of Physicians and Surgeons of Ontario (CPSO).
As their home page states, they “regulate the practice of medicine in Ontario. Physicians are required to be members to practice medicine in Ontario.”
In other words, CPSO is THE medical board. They run the show. If practicing doctors make a wrong move or say the wrong thing, CPSO is there to step on their faces and discipline them and even cancel their licenses to practice.
But now a new rebel group of Canadian MDs has emerged. Why? Because CPSO has issued a fascist edict threatening practicing doctors. Read the threat carefully.
College of Physicians and Surgeons of Ontario [CPSO] Statement on Public Health Misinformation (4/30/21): [1]
“The College is aware and concerned about the increase of misinformation circulating on social media and other platforms regarding physicians who are publicly contradicting public health orders and recommendations. Physicians hold a unique position of trust with the public and have a professional responsibility to not communicate anti-vaccine, anti-masking, anti-distancing and anti-lockdown statements and/or promoting unsupported, unproven treatments for COVID-19. Physicians must not make comments or provide advice that encourages the public to act contrary to public health orders and recommendations. Physicians who put the public at risk may face an investigation by the CPSO and disciplinary action, when warranted. When offering opinions, physicians must be guided by the law, regulatory standards, and the code of ethics and professional conduct. The information shared must not be misleading or deceptive and must be supported by available evidence and science.”
WE’RE YOUR BOSSES. YOU DO WHAT WE TELL YOU TO DO. SHUT YOUR MOUTHS. MARCH STRAIGHT AHEAD. KILL YOUR PATIENTS IF YOU HAVE TO, BUT OBEY US.
The new rebels against this monster call themselves the Canadian Physicians for Science and Truth. This is a brief excerpt from their response: [2]
“On April 30, 2021, Ontario’s physician licensing body, the College of Physicians and Surgeons of Ontario (CPSO), issued a statement forbidding physicians from questioning or debating any or all of the official measures imposed in response to COVID-19.”
“We regard this recent statement of the CPSO to be unethical, anti-science and deeply disturbing.”
“As physicians, our primary duty of care is not to the CPSO or any other authority, but to our patients.”
“The CPSO statement orders us to violate our duty and pledge to our patients…”
I wondered what medical treatments, in general, CPSO supports and tolerates. It took me three minutes to find a Toronto outfit called the Centre for Addiction and Mental Health Foundation (CAMH). They promote electro-convulsive therapy. In other words, shock treatment.
In other words, delivering electric shocks to the brain. As a cure for “mental illness.” I call it torture.
Apparently, this treatment is just fine and dandy, but telling patients the COVID lockdowns are criminal is forbidden by the Nazi bureaucrats at CPSO. Saying the vaccine is dangerous is forbidden. Saying masks are useless and harmful is forbidden.
What would happen if these medical rebels, the Canadian Physicians for Science and Truth—say, 10,000 of them—took this war to the wall?
Practiced non-harmful medicine, kept warning their patients about the sociopathic COVID regulations and the vaccine, refused to knuckle under to the Nazi bureaucrats, even to the point of having their licenses stripped and going to jail?
What would happen, as many thousands/millions of Canadians rallied to their side?
I’ll tell you what would happen. Sanity. Revolution. The downfall of the scum.
We’re at Nuremberg 2.0, people. If you don’t know what that means, look it up.
Doctors clear their vision and their brains and do their level best to HEAL, or they follow orders of the Commandants and maim and kill. It’s one side or the other.
In my 83 years, I’ve known a few very good doctors, and a number of The Cold Ones. The Cold Ones administer, without feeling or remorse, the Book of Death.
They’re ice on the outside, and rotting fungus and stench within.
Many of them sit at the top of medical boards.
They turn open societies into concentration camps.
On 25 May 2021, the Indian Bar Association (IBA) served a 51-page legal notice on Dr Soumya Swaminathan, the Chief Scientist at the World Health Organisation (WHO), for:
“[H]er act of spreading disinformation and misguiding the people of India, in order to fulfil her agenda.”
The Mumbai-based IBA is an association of lawyers who strive to bring transparency and accountability to the Indian justice system. It is actively involved in the dissemination of legal knowledge and provides guidance and support to advocates and ordinary people in their fight for justice.
The legal notice says Dr Swaminathan has been:
“Running a disinformation campaign against Ivermectin by deliberate suppression of effectiveness of drug Ivermectin as prophylaxis and for treatment of COVID-19, despite the existence of large amounts of clinical data compiled and presented by esteemed, highly qualified, experienced medical doctors and scientists,”
And:
“Issuing statements in social media and mainstream media, thereby influencing the public against the use of Ivermectin and attacking the credibility of acclaimed bodies/institutes like ICMR and AIIMS, Delhi, which have included ‘Ivermectin’ in the ‘National Guidelines for COVID-19 management’.”
The IBA states that legal action is being taken against Dr Swaminathan in order to stop her from causing further damage to the lives of citizens of India.
The IBA says that Dr Swaminathan has ignored these studies and reports and has deliberately suppressed the data regarding the effectiveness of Ivermectin, with an intent to dissuade the people of India from using it.
However, two key medical bodies, the Indian Council for Medical Research (ICMR) and the All India Institute of Medical Sciences (AIIMS) Delhi, have refused to accept her stand and have retained the recommendation for Ivermectin, under a ‘May Do’ category, for patients with mild symptoms and those in home isolation, as stated in ‘The National Guidelines for COVID-19 management’.
It is interesting to note that the content of several web links to news articles and reports included in the notice served upon Dr Swaminathan, which was visible before issuing the notice, has either been removed or deleted.
It seems that the vaccine manufacturers and many governments are desperate to protect their pro-vaccine agenda and will attempt to censor information and news regarding the efficacy of Ivermectin.
Colin Todhunter is an independent journalist who writes on development, environmental issues, politics, food and agriculture. In August 2018 he was named as one of 400 Living Peace and Justice Leaders and Models by Transcend Media Services, in recognition of his journalism.
Thanks to the diligent efforts of one of my listeners, I received a paper yesterday that puts another nail in the coffin for the existence of SARS-CoV-2. The paper is titled “Appearances Can be Deceiving – Viral-like Inclusions in Covid-19 Negative Renal Biopsies by Electron Microscopy.” The authors are Clarrisa A. Cassol, et al., and the citation is Kidney360 1:824-828, 2020. This is a peer-reviewed journal affiliated with the American Society of Nephrology; in other words, this paper comes squarely from what is called acceptable, mainstream science.
Many of you have probably seen the electron-micrograph pictures of SARS-CoV-2, the ones in black and white, with the black dots within the faint outline of the circle. I have attached two such images from papers that claim these photos show direct evidence of the existence of the virus. These are the pictures that virologists show us, not the computer-generated, colorful images that you see in magazines and on the internet. These are the “real” pictures of the virus, and they are offered as “proof” that the virus exists.
However, it turns out these photos are actually NOT corona viruses, and the CDC, among others, has known this fact since at least 2004. The above paper examines the evidence used to claim that these images represent viruses, rather than normal “structures” within a cell, particularly sick cells. Here is what the paper says:
“We have observed morphologically indistinguishable inclusions within podocytes and tubular epithelial cells both in patients negative for coronavirus disease 2019 (COVID-19) as well as in renal biopsies from the pre-COVID-19 era” (emphasis added).
In other words, the researchers saw these same structures in people with no evidence of Covid and in samples they took before Covid even happened, before the virus was said to even exist.
In addition, they say:
“We postulated that endogenous mimickers could be present that are morphologically indistinguishable from SARS-CoV-2 virions ultrastructurally.”
And:
“Viral-like inclusions, consisting both of single vesicles with diameters between 50 and 138 nm, as well as packed groups within larger vesicles, were found in all 15 cases, either in podocytes. Tubular epithelia, or vascular epithelial cells (figure 1).”
In all 15 cases that they examined, they found structures identical to what is being called SARS-CoV-2. They were scattered all over the kidneys and blood vessels; they are not viruses, but normal parts of the cells.
Then they go on to describe how these particles come about:
“A number of potential natural mimickers that can generate intracellular groups of round vesicles mimicking
SARS-CoV-2 virions could be listed, the most likely being endocytic vesicles and endosomal components such as microvesicular bodies containing exosomes, among others. Endocytosis leads to the formation of 60-120 nm vesicles, which is within the size range described for SARS-CoV-2 (60-140nm). These endocytic vesicles may be coated by different proteins, one of the most common being clathrin. The presence of coating proteins may be responsible for the presence of an electron-dense area surrounding these vesicles, giving the appearance of a viral corona.”
In other words, remember the famous “corona” on the corona virus? It turns out it’s just a common protein coating on normal vesicles, picking up the dyes in the electron-microscope preparation. The corona appearance is just another creative fiction, dreamed up by virologists and their graphic design teams.
Finally, the paper goes on to say that, naturally, you see more of these particles in sick people than in healthy people, which is exactly what I have been suggesting this past year. Dead and dying cells make these particles in the dying process and partly to get rid of poisons.
But the final nail comes in this quote:
“The potential for confusion of coronavirus particles with normal cellular components was in fact highlighted in a detailed ultrastructural study by the Centers for Disease Control and Prevention (CDC) of SARS-CoV responsible for the 2003 SARS outbreak.”[1]
In other words, the CDC in 2004 knew that researchers couldn’t reliably know these particles were coronavirus particles. Not a word has been heard about this since. All virologists use these pictures as proof of the existence of this virus. It is a fraud, based on junk science, like everything else connected with “Covid 19.”
UKMFA has sent an Open Letter to the the MHRA in which we raise grave concerns about this emergency authorisation, citing evidence of known and potential harms to children that may result and the serious ethical issues this decision raises.
Given that these vaccines will have virtually no benefit to the children themselves, it is profoundly unethical and indefensible to vaccinate children, especially with an experimental vaccine using novel technology, in what appears to be a misguided attempt to protect adults and achieve herd immunity. We call on the MHRA to exercise caution and immediately reverse their decision.
URGENT Open Letter from the UK Medical Freedom Alliance to the Medicines and Healthcare products Regulatory Agency (MHRA)
Dr June Raine CBE – Chief Executive Office
Mr Stephen Lightfoot – Chair
Professor David Webb – Deputy Chair
Re: Covid-19 Vaccination in Children – Emergency Use Authorisation and Rollout in Schools
The UK Medical Freedom Alliance (UKMFA) is an alliance of UK medical professionals, scientists and lawyers campaigning for Medical Freedom, Informed Consent and Bodily Autonomy to be preserved and protected.
It is with the gravest of concern and utter incredulity that we assimilate the decision by the MHRA to grant regulatory approval for emergency use of the Pfizer-BioNTech Covid-19 vaccine in 12- to 15-year- old children [i]. We wish to notify you of the multiple factors indicating that most likely your decision will have devastating consequences for a significant number of children in the UK and their families.
We are adding our voice to doctors and experts around the world, including groups in the UK [ii] [iii], US [iv] [v] and Israel [vi], who have raised serious ethical and safety concerns, and demanded that Covid-19 vaccines are not rolled out to children.
We previously outlined our arguments against giving Covid-19 vaccines to children in an Open Letter to the MHRA, JVCI and Government Ministers, dated 25 February 2021 [vii]. Considering new and mounting evidence of harm caused by Covid-19 vaccines, we wish to urgently re-enforce our appeal to reverse this latest decision immediately and halt all plans in relation to administration of Covid-19 vaccines to children.
Ethical and Safety Concerns
1. In the UK, evidence-based medicine has been the basis of all clinical practice. Medical professionals are educated to critically appraise scientific evidence and ensure recommendations and guidelines rest on robust foundations. The implementation of the Covid-19 vaccination program is in complete incongruence with this concept, and this has never been more obvious than in relation to young people and children.
Rather than referring to peer-reviewed science, recommendations have been based only on interim analyses of clinical trials that have not been completed. Completion of the adult trials has already been compromised by offering the vaccine to participants in the placebo groups, thus removing the control arm [viii]. Trials to establish efficacy and safety of the Covid-19 vaccines are not conducted by independent research teams but by the pharmaceutical companies, who stand to gain financially from the sale of their products. Raw trial data are not yet accessible to be scrutinized. Instead, interim analyses and claims are communicated by press release, without peer review, and instantly assimilated into advice to the public. The Pfizer-BioNTech clinical trials involving children and teenagers only commenced in 2021 and are underpowered for obtaining meaningful safety data (there were only 1131 12–15-year-olds in treatment arm). Only 2 months’ worth of interim data was provided to the MHRA, giving extremely limited short-term and NO long-term safety profile. Safety cannot be established if due scientific process is not adhered to.
2. The justification for the enhanced timelines and the irregular process for temporary emergency use authorization of Covid-19 vaccines has been the urgency of the ongoing pandemic. There is no historical precedent where a pandemic was successfully ended or mitigated by vaccinating the entire population. Indeed, concerns have been raised that this approach may prolong the pandemic and risk promotion of more virulent variants [ix]. French virologist and Nobel Prize winner Luc Montagnier recently highlighted and warned about this potential issue [x] [xi]. As the concept of ending a pandemic by vaccinating the entire population has no basis in science, there is no imperative to vaccinate children.
3. The last time a vaccine was developed and brought to market on an emergency basis, was in an attempt to halt the swine flu epidemic in 2009-2010. Tragically, this resulted in significant, unexpected injuries, with over 1000 cases of life-changing narcolepsy in children and teenagers across Europe, and the eventual withdrawal of the Pandemri vaccine [xii] [xiii]. We have an obligation to exercise caution to prevent a re-occurrence of serious and unforeseen side-effects of an inadequately tested product in children [xiv].
4. The benefits of Covid-19 vaccines for children are close to zero, yet they carry known and unknown risks. Experts are stating that vaccinating children is neither necessary nor justified:
The minutes of the Joint Committee on Vaccination and Immunisation (JCVI) dated 16 February 2021 note “little impact of vaccinating children once all other adults were offered vaccine” and “that modelling results on the impact of vaccinating children were considered highly uncertain” [xv].
Other experts have argued that “Covid-19 vaccines for children should not get emergency use authorization” [xvi] and that this would be “hard to justify right now for most children in most countries” [xvii].
Professor of Paediatrics and member of the JCVI, Adam Finn, said in an interview on the 20 May 2021 that it was “an open question as to whether we need to immunise children at all” and “if we can control this virus without immunising children, we shouldn’t immunise children as a matter of principle”.
5. Below, we set out specific issues regarding Covid-19 vaccines in children – each sufficient to justify not proceeding any further with this proposal.
a. The risk of Covid-19 to children is miniscule. The infection fatality rate in this age group is close to zero, and most remain asymptomatic or experience mild symptoms only [xix] [xx] [xxi] [xxii]. This has been reiterated by the Government [xxiii] and by Professor of Paediatrics, Adam Finn [xviii]. Even the low records of children hospitalized with Covid-19, may be an over- estimate, according to a recent study [xxiv]. The number of children and teens under the age of 20 without pre-existing conditions who have died in England with a positive Covid- 19 test, as of 13 May 2021, is in single figures [xxv]. Mortality in children in the UK in 2020/21 has in fact been significantly lower than in previous years [xxvi] [xxvii]. As the emergency does not, therefore, apply to children, there can be no justification to authorize any product for emergency use in the paediatric population.
b.The absolute risk reduction by Covid-19 vaccines is around 1% (0.84-1.3%) [xxviii]. This applies to the healthy adult trial participants and cannot be extrapolated to children, who are already at extremely low risk from the disease. The potential benefit to an individual child of receiving a Covid-19 vaccine is statistically zero.
c. Children play an insignificant role in transmission of Covid-19 [ix] [xviii] [xxix]. Living with children may even reduce the risks of the disease [xxx]. Transmission in schools has not been significant [xxxi] [xxxii] [xxxiii]. Trials have not demonstrated whether Covid-19 vaccines reduce asymptomatic infection or transmission [xxxiv]. There is therefore no demonstrable benefit to the wider society in vaccinating children.
d. In a population cohort at minimal risk of severe disease, such as young people and children, acquiring natural immunity will serve a better purpose, as this will be more comprehensive, longer lasting, and cover a broad range of virus variants. Vaccine- induced immunity does not cover the full spectrum of protection (mucosal immunity, IgA, and T-cell immunity to the whole virus) and may only be short-lived. Acquiring natural immunity will therefore also benefit the wider population, contributing to herd immunity [xxxv] [xxxvi] [xxxvii] [xxxviii] [xxxix].
e. All Covid-19 vaccines used in the UK are based on completely new gene-based technologies (mRNA / DNA vector technology) [xl], that have never received full regulatory approval for mass rollout in humans. They have not been licensed and remain experimental until Phase 3 trials have been completed [xli]. Thus, we cannot infer long-term safety without observing the impact on human health in those who have received the vaccines over the next few years.
f. There is currently no data to indicate whether dose adjustment may be necessary in children. This would appear relevant as side-effects in initial phase 1 dose-escalation trials were more significant with higher dosage [xlii].
g. Covid-19 vaccines work completely differently to established childhood vaccines. Traditional, live vaccines work using attenuated virus strains to prompt antibody development. Covid-19 vaccines introduce a synthetic gene which induces the recipient’s own cells to produce spike proteins. Spike proteins appear to contribute significantly to the pathogenicity of SARS-CoV-2, and there are studies suggesting that they have the potential to cause pathology on their own [xliii] [xliv]. It is unknown how much spike protein will be produced by an individual, and it is plausible that younger, healthier people may produce higher quantities, potentially increasing the risk of side-effects. The safety of this approach needs to be thoroughly investigated and firmly established prior to full licensure in adults and prior to any use in children.
h. At this stage, medium- and long-term effects of Covid-19 vaccines are completely unknown and unpredictable, due to the short duration of the Phase 3 safety trials, which are ongoing and not due to complete until 2023. This is most relevant for young people and children. Before giving Covid-19 vaccines to children, potential adverse, long-term, effects on fertility, carcinogenesis, and children’s developing neurological and immune systems MUST be completely ruled out, as is done with other drugs and vaccines. This may take years or decades to fully establish.
i. Serious adverse events and vaccine-related deaths have been reported in the UK [xlv], the US [xlvi] and Europe [xlvii]. In the report published by the MHRA on 13 May 2021, there were 822,078 adverse reactions in the UK, including seizures, paralysis, blindness, strokes, blood clots and acute cardiac events. There were 1178 reports of fatalities.
j. Some life-threatening effects, such as blood clots [xlviii] and myocarditis [xlix], have been reported specifically in children and young adults [l] [li]. Government advice has recently been amended to avoid the AstraZeneca vaccine in young people due to a concern regarding the risk of rare blood clots (now considered to be around 1:100,000). The new term “vaccine-induced immune thrombotic thrombocytopenia” acknowledges the causality of the vaccine in these events, often presenting as ischemic strokes [lii]. It is possible that this reaction could be a class effect caused by spike proteins and therefore not specific or limited to the AstraZeneca vaccine [liii]. Of the 4347 events of thrombosis and embolism reported to the MHRA as of 13 May 2021, 770 occurred following the Pizer-BioNTech vaccine [xlv]. According to the US VAERS reporting system, several children under the age of 18 have died following a Covid-19 vaccine [liv].
k. Vaccine manufacturers have requested and been granted complete exemption from liability for any injuries or deaths resulting from their products [lv] [lvi]. A spokesperson for AstraZeneca acknowledged the potential for unexpected long-term side-effects, stating that as a company, they “simply cannot take the risk if in … four years the vaccine is showing side-effects” [lvii]. If the risk is significant enough for manufacturers to anticipate economic loss, children must not be expected to take the same risk to their long-term health.
6. Informed consent is the cornerstone of good, ethical medical practice and is firmly enshrined in the code of conduct issued by the General Medical Council (GMC) and the Nursing and Midwifery Council (NMC). Unless factually accurate information is made available, detailing risks as well as benefits, it is not possible for anyone, let alone children, to make a fully informed decision and give informed consent to Covid-19 vaccination. Gillick Competence cannot be assumed under current circumstances, where the vaccines are based on novel technologies, and no long-term safety data is available.
We are alarmed at the targeting of the public, and more recently schoolchildren [lviii] [lix], with material conveying a one-sided and simplified message, without reflection or consideration for individual circumstances, or disclosure of the known and unknown risks we have outlined.
Multiple resources are being made available that appear to be aimed at modifying behaviour to reduce “vaccine hesitancy”. These appear to rely not on the strength of scientific arguments but on techniques of persuasion [lx] [lxi] [lxii]. Recent reports, suggesting that the use of peer pressure to increase uptake of the vaccine in children has been condoned by some school leaders, were very disturbing [lxiii]. This is not consistent with ethical and lawful practice of medicine and indeed constitutes a violation of Informed Consent, as required by the GMC, the NHS Constitution, and the Montgomery ruling [lxiv].
7. In the UK, post-marketing surveillance is carried out via the Yellow Card System, a passive reporting system that requires all members of the public and all doctors to be aware of its existence, and compliant with filling in reports of all potential side-effects observed, to be effective at recognizing unexpected adverse events and signals of safety concern. In fact, there is poor awareness of, and compliance with, this scheme among both doctors and the public, potentially leading to a significant underestimate of the true number of adverse events and deaths connected with these vaccines.
Conclusion and Request
We have presented evidence that children are at no substantial risk from Covid-19, but face known and unknown risks from Covid-19 vaccines, including significant, life-changing injury and death. Some of the serious reported injuries, such as blood clots and myocarditis, have specifically occurred in young people and children. In addition, children have a lifetime ahead of them and we have no idea of the impact of these novel, gene-based vaccines on their health or fertility in 5-10 years’ time. Considering these facts, we cannot comprehend how the review by the MHRA can be described as rigorous, with a conclusion to grant regulatory approval.
We are already seeing reports of deaths and injury in children in the US and Canada, where vaccines are being trialed and rolled out to children. Even with rare risks (1:10,000 to 1:100,000), if these vaccines are rolled out to around 10 million UK children, it seems certain that we will see deaths and serious injuries in a significant number of children who would never have been harmed by Covid-19, devastating families and communities. There may be healthy UK children who will not live to see another Christmas if Covid-19 vaccines are rolled out in schools over the summer/autumn. This would be an unforgiveable act of completely avoidable harm, for which you would be responsible, individually and collectively.
We implore the MHRA to immediately reverse the decision to authorize the Pfizer-BioNTech Covid-19 vaccine for children and abide by the Hippocratic oath to “First do no Harm”.
The UK public trusts and relies on you not to expose their children to unnecessary risk.
We thank you for taking the time to read this letter and consider its contents. We request that you kindly acknowledge this letter and all the references within, and either confirm that emergency authorization for use of Covid-19 vaccines in children will be withdrawn or otherwise lay out the reasoning for your considered actions.
Rt Hon Boris Johnson – Prime Minister Rt Hon Matt Hancock – Secretary of State for Health and Social Care Professor Chris Whitty – Chief Medical Officer Rt Hon Nicola Sturgeon – First Minister of Scotland Rt Hon Mark Drakeford – First Minister of Wales Rt Hon Arlene Foster – First Minister of Northern Ireland Prof Andrew Pollard – Chair of the Joint Committee for Vaccination and Immunisation (JCVI) Rt Hon Nadhim Zahawi – Minister for Covid-19 Vaccine Deployment
Scientific propaganda about vaccines has reached dizzying heights, as officials point the uninformed public toward the Day of Liberation, when a COVID shot, otherwise known as God, will rescue Earth.
Here, from a chapter in my 1988 book, AIDS INC., is an excerpt exposing some of the infamous moments in vaccination history—hidden by the press, or simply forgotten.
For those denialists who cling to the notion that vaccines are remarkably safe and effective, this article is a pill you can swallow, bitter to be sure, but immunizing against the effects of bald lies from the bent medical establishment.
Understand: this is only a partial history of disasters and revelations, and it stops at 1988.
“The combined death rate from scarlet fever, diphtheria, whooping cough and measles among children up to fifteen shows that nearly 90 percent of the total decline in mortality between 1860 and 1965 had occurred before the introduction of antibiotics and widespread immunization. In part, this recession may be attributed to improved housing and to a decrease in the virulence of micro-organisms, but by far the most important factor was a higher host-resistance due to better nutrition.” Ivan Illich, Medical Nemesis, Bantam Books, 1977
“In a recent British outbreak of whooping cough, for example, even fully immunized children contracted the disease in fairly large numbers; and the rates of serious complications and death were reduced only slightly. In another recent outbreak of pertussis, 46 of the 85 fully immunized children studied eventually contracted the disease.”
“In 1977, 34 new cases of measles were reported on the campus of UCLA, in a population that was supposedly 91% immune, according to careful serological testing. Another 20 cases of measles were reported in the Pecos, New Mexico, area within a period of a few months in 1981, and 75% of them had been fully immunized, some of them quite recently. A survey of sixth-graders in a well-immunized urban community revealed that about 15% of this age group are still susceptible to rubella, a figure essentially identical with that of the pre-vaccine era.”
“Finally, although the overall incidence of typical acute measles in the U.S. has dropped sharply from about 400,000 cases annually in the early 1960s to about 30,000 cases by 1974-76, the death rate remained exactly the same; and, with the peak incidence now occurring in adolescents and young adults, the risk of pneumonia and demonstrable liver abnormalities has actually increased substantially, according to one recent study, to well over 3% and 2%, respectively.” Richard Moskowitz, MD, The Case Against Immunizations, 1983, American Institute of Homeopathy.
“Of all reported whooping cough cases between 1979 and 1984 in children over 7 months of age – that is, old enough to have received the primary course of the DPT shots (diphtheria, pertussis, tetanus) – 41% occurred in children who had received three or more shots and 22% in children who had one or two immunizations.”
“Among children under 7 months of age who had whooping cough, 34% had been immunized between one and three times…”
“… Based on the only U.S. findings on adverse DPT reactions, an FDA-financed study at the University of California, Los Angeles, one out of every 350 children will have a convulsion; one in 180 children will experience high-pitched screaming [can indicate brain damage]; and one in 66 will have a fever of 105 degrees or more.” Jennifer Hyman, Democrat and Chronicle, Rochester, New York, special supplement on DPT, dated April, 1987.
“A study undertaken in 1979 at the University of California, Los Angeles, under the sponsorship of the Food and Drug Administration, and which has been confirmed by other studies, indicates that in the U.S.A. approximately 1,000 infants die annually as a direct result of DPT vaccinations, and these are classified as SIDS (Sudden Infant Death Syndrome) deaths. These represent about 10 to 15% of the total number of SIDS deaths occurring annually in the U.S.A. (between 8,000 and 10,000 depending on which statistics are used).” Leon Chaitow, Vaccination and Immunization, CW Daniel Company Limited, Saffron Walden, Essex, England, 1987.
“Assistant Secretary of Health Edward Brandt, Jr., MD, testifying before the U.S. Senate Committee on Labor and Human Resources, rounded… figures off to 9,000 cases of convulsions, 9,000 cases of collapse, and 17,000 cases of high-pitched screaming for a total of 35,000 acute neurological reactions occurring within forty-eight hours of a DPT shot among America’s children every year.” DPT: A Shot in the Dark, by Harris L. Coulter and Barbara Loe Fischer, Harcourt Brace Jovanovich.
“While 70-80% of British children were immunized against pertussis in 1970-71, the rate is now 39%. The committee predicts that the next pertussis epidemic will probably turn out to be more severe than the one in 1974/75. However, they do not explain why, in 1970/71, there were more than 33,000 cases of pertussis with 41 fatal cases among the very well immunized British child population; whereas in 1974/75, with a declining rate of vaccination, a pertussis epidemic caused only 25,000 cases with 25 fatalities.” Wolfgang Ehrengut, Lancet, Feb. 18, 1978, p. 370.
“… Barker and Pichichero, in a prospective study of 1232 children in Denver, Colorado, found after DTP that only 7% of those vaccinated were free from untoward reactions, which included pyrexia (53%), acute behavioral changes (82%), prolonged screaming (13%), and listlessness, anorexia and vomiting. 71% of those receiving second injections of DTP experienced two or more of the reactions monitored.” Lancet, May 28, 1983, p. 1217
“Publications by the World Health Organization show that diphtheria is steadily declining in most European countries, including those in which there has been no immunization. The decline began long before vaccination was developed. There is certainly no guarantee that vaccination will protect a child against the disease; in fact, over 30,000 cases of diphtheria have been recorded in the United Kingdom in fully immunized children.” Leon Chaitow, Vaccination and Immunization, p. 58.
“Pertussis (whooping cough) immunization is controversial, as the side effects have received a great deal of publicity. The counter claim is that the effectiveness and protection offered by the procedure far outweigh the possible ill effects… annual deaths, per million children, from this disease over the period from 1900 to the mid-nineteen seventies, shows that from a high point of just under 900 deaths per million children (under age 15) in 1905, the decline has been consistent and dramatic. There had been a lowering of mortality rates of approximately 80% by the time immunization was introduced on a mass scale, in the mid-nineteen fifties. The decline has continued, albeit at a slower rate, ever since. No credit can be given to vaccination for the major part of the decline since it was not in use.” Chaitow, Vaccination and Immunization, p. 63.
“… the swine-flu vaccination program was one of its (CDC) greatest blunders. It all began in 1976 when CDC scientists saw that a virus involved in a flu attack outbreak at Fort Dix, N.J., was similar to the swine-flu virus that killed 500,000 Americans in 1918. Health officials immediately launched a 100-million dollar program to immunize every American. But the expected epidemic never materialized, and the vaccine led to partial paralysis in 532 people. There were 32 deaths.” U.S. News and World Report, Joseph Carey, October 14, 1985, p. 70, “How Medical Sleuths Track Killer Diseases.”
“Despite (cases) in which (smallpox) vaccination plainly failed to protect the population, and despite the rampant side-effects of the methods, the proponents of vaccination continued their attempts to justify the methods by claims that the disease had declined in Europe as a whole during the period of its compulsory use. If the decline could be correlated with the use of the vaccination, then all else could be set aside, and the advantage between its current low incidence could be shown to outweigh the periodic failures of the method, and to favour the continued use of vaccination. However, the credit for the decline in the incidence of smallpox could not be given to vaccination. The fact is that its incidence declined in all parts of Europe, whether or not vaccination was employed.” Chaitow, Vaccination and Immunization, pp. 6-7.
“Smallpox, like typhus, has been dying out (in England) since 1780. Vaccination in this country has largely fallen into disuse since people began to realize how its value was discredited by the great smallpox epidemic of 1871-2 (which occurred after extensive vaccination).” W. Scott Webb, A Century of Vaccination, Swan Sonnenschein, 1898.
“In this incident (Kyoto, Japan, 1948) – the most serious of its kind – a toxic batch of alum-precipitated toxoid (APT) was responsible for illness in over 600 infants and for no fewer than 68 deaths.”
“On 20 and 22 October, 1948, a large number of babies and children in the city of Kyoto received their first injection of APT. On the 4th and 5th of November, 15,561 babies and children aged some months to 13 years received their second dose. One to two days later, 606 of those who had been injected fell ill. Of these, 9 died of acute diphtheritic paralysis in seven to fourteen days, and 59 of late paralysis mainly in four to seven weeks.” Sir Graham Wilson, Hazards of Immunization, Athone Press, University of London, 1967.
“Accidents may, however, follow the use of this so-called killed (rabies) vaccine owing to inadequate processing. A very serious occurrence of this sort occurred at Fortaleza, Ceara, Brazil, in 1960. No fewer than 18 out of 66 persons vaccinated with Fermi’s carbolized (rabies ) vaccine suffered from encephalomyelitis and every one of the eighteen died.” Sir Graham Wilson, Hazards of Immunization.
“At a press conference in Washington on 24 July, 1942, the Secretary of War reported that 28,585 cases of jaundice had been observed in the (American) Army between 1 January and 4 July after yellow fever vaccination, and of these 62 proved fatal.” Wilson, Hazards of Immunization.
“The world’s biggest trial (conducted in south India) to assess the value of BCG tuberculosis vaccine has made the startling revelation that the vaccine ‘does not give any protection against bacillary forms of tuberculosis.’ The study said to be ‘most exhaustive and meticulous,’ was launched in 1968 by the Indian Council of Medical Research (ICMR) with assistance from the World Health Organization (WHO) and the U.S. Centers for Disease Control in Atlanta, Georgia.”
“The incidence of new cases among the BCG vaccinated group was slightly (but statistically insignificantly) higher than in the control group, a finding that led to the conclusion that BCG’s protective effect ‘was zero.’” New Scientist, November 15, 1979, as quoted by Hans Ruesch in Naked Empress, Civis Publishers, Switzerland, 1982.
“Between 10 December 1929 and 30 April 1930, 251 of 412 infants born in Lubeck received three doses of BCG vaccine by the mouth during the first ten days of life. Of these 251, 72 died of tuberculosis, most of them in two to five months and all but one before the end of the first year. In addition, 135 suffered from clinical tuberculosis but eventually recovered; and 44 became tuberculin-positive but remained well. None of the 161 unvaccinated infants born at the time was affected in this way and none of these died of tuberculosis within the following three years.” Hazards of Immunization, Wilson.
“We conducted a randomized double-blind placebo-controlled trial to test the efficacy of the 14-valent pneumococcal capsular polysaccharide vaccine in 2295 high-risk patients… Seventy-one episodes of proved or probable pneumococcal pneumonia or bronchitis occurred among 63 of the patients (27 placebo recipients and 36 vaccine recipients)… We were unable to demonstrate any efficacy of the pneumococcal vaccine in preventing pneumonia or bronchitis in this population.” New England Journal of Medicine, November 20, 1986, p. 1318, Michael Simberkoff et al.
In the spring of 1955, Cutter Labs started selling their standard polio vaccine. The vaccine was infective, and 200 cases of polio resulted among recipients. Of these, there were eleven deaths. About 100 cases of paralysis resulted. JR
“But already before Salk developed his vaccine, polio had been constantly regressing; the 39 cases out of every 100,000 inhabitants registered in 1942 had gradually diminished from year to year until they were reduced to only 15 cases in 1952… according to M. Beddow Baylay, the English surgeon and medical historian.” Slaughter of the Innocent, Hans Reusch, Civitas Publish ers, Switzerland, and Swain, New York, 1983.
“Many published stories and reports have stated, implied and otherwise led professional people and the public to believe that the sharp reduction of cases (and of deaths) from poliomyelitis in 1955 as compared to 1954 is attributable to the Salk vaccine…That it is a misconception follows from these considerations. The number of children inoculated has been too small to account for the decrease. The sharp decrease was apparent before the inoculations began or could take effect and was of the same order as the decrease following the immediate post-inoculation period.” Dr. Herbert Ratner, Child and Family, vol. 20, no. 1, 1987.
“So far it is hardly possible to gain insight into the extent of the immunization catastrophe of 1955 in the United States. It may be considered certain that the officially ascertained 200 cases (of polio) which were caused directly or indirectly by the (polio) vaccination constitute minimum figures… It can hardly be estimated how many of the 1359 (polio) cases among vaccinated persons must be regarded as failures of the vaccine and how many of them were infected by the vaccine. A careful study of the epidemiologic course of polio in the United States yields indications of grave significance. In numerous states of the U.S.A., typical early epidemics developed with the immunizations in the spring of 1955…The vaccination incidents of the year 1955 cannot be exclusively traced back to the failure of one manufacturing firm.” Dr. Herbert Ratner, Child and Family, 1980, vol. 19, no. 4, “Story of the Salk Vaccine (Part 2).”
“Suffice it to say that most of the large (polio) epidemics that have occurred in this country since the introduction of the Salk vaccine have followed the wide-scale use of the vaccine and have been characterized by an uncommon early seasonal onset. To name a few, there is the Massachusetts epidemic of 1955; the Chicago epidemic of 1956; and the Des Moines epidemic of 1959.” Dr. Herbert Ratner, Child and Family, 1980 vol. 19, no. 4.
“The live (Sabin) poliovirus vaccine has been the predominant cause of domestically arising cases of paralytic poliomyelitis in the United States since 1972. To avoid the occurrence of such cases, it would be necessary to discontinue the routine use of live poliovirus vaccine.” Jonas Salk, Science, March 4, 1977, p. 845.
“By the (U.S.) government’s own admission, there has been a 41% failure rate in persons who were previously vaccinated against the (measles) virus.” Dr. Anthony Morris, John Chriss, BG Young, “Occurrence of Measles in Previously Vaccinated Individuals,” 1979; presented at a meeting of the American Society for Microbiology at Fort Detrick, Maryland, April 27, 1979.
“Prior to the time doctors began giving rubella vaccinations, an estimated 85% of adults were naturally immune to the disease (for life). Because of immunization, the vast majority of women never acquire natural immunity (or lifetime protection).” Dr. Robert Mendelsohn, Let’s Live, December 1983, as quoted by Carolyn Reuben in the LA WEEKLY, June 28, 1985.
“Adminstration of KMV (killed measles vaccine) apparently set in motion an aberrant immunologic response that not only failed to protect children against natural measles, but resulted in heightened susceptibility.” JAMA Aug. 22, 1980, vol. 244, p. 804, Vincent Fulginiti and Ray Helfer. The authors indicate that such falsely protected children can come down with “an often severe, atypical form of measles. Atypical measles is characterized by fever, headache… and a diverse rash (which)… may consist of a mixture of macules, papules, vesicles, and pustules… ”
The above quotes reflect only a mere fraction of an available literature.
It is criminally deceiving to say, “Vaccines are simple; they stimulate the immune system and confer immunity against specific germ agents.”
Official reports on vaccine reactions are often at odds with unofficial estimates because of the method of analysis used. If adverse vaccine-reaction is defined as a small set of possible effects experienced within 72 hours of an inoculation, then figures will be smaller. But doctors like G.T. Stewart, of the University of Glasgow, have found through meticulous investigation, including visits to hospitals and interviews with parents of children vaccinated, that reactions as severe as brain-damage (e.g., from the DPT vaccine) can be overlooked, go unreported and can be assumed to have come from other causes.
—Well, that was my finding, in 1988, when I looked beneath the surface of the vaccine question.
Now we are in very deep waters. COVID-19 hysteria has been tuned up to the NEED for a vaccine.
WE need to slough off this promoted bad dream and stand firm against the little gods who traffic their vials in every doctor’s office, hospital, school, drug store, and tented parking lot—making them into shooting galleries.
We already have natural immune systems. They work.
“As a result of the big marketing op, Daniel, I’ve become increasingly skeptical of the ET narrative. Because they’re up to something and it doesn’t have our best interest at heart.
Whether they trot out the Christ ET or whether they trot out the alien invaders, they’re up to something.
So, I don’t trust anything that this government says. And they’re doing this, I think, as a result of the COVID planscamdemic kind of blowing up in their faces.
And I’ve always suspected that there was some sort of genetic tagging and marking thing going on with this operation that may or may not be directly related to this whole UFO thing.”
~ Dr. Joseph P. Farrell
“It reads like a deep state alien invasion op and it comes on the heels of the COVID op. That’s one hell of a timing.”
~ Daniel Liszt
Topics include:
War game exercises under the ocean
US Navy exotic technology experiments
Ties to The Great Reset
Global control from space
Strange things going on in Antarctica
Admiral Byrd’s Operation HIGHJUMP
Wernher von Braun’s prediction, via Carol Rosin, regarding weaponization of space
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, and Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
I recently received a letter in the mail from a woman in Florida describing the illnesses from which she has suffered for the past dozen years: Hashimoto’s disease, liver dysfunction, sinus infection, “exploding head,” complete loss of smell and partial loss of taste. “After all this time,” she wrote, “I now wonder how much radiation has been a part of my illness.” She has joined a Stop 5G group in her city. To protect herself she keeps her cell phone in a “faraday pouch” when she is not using it, and she turns off her wifi at night. She also asked about the effectiveness of the various devices, pendants and chips being sold to protect oneself from the radiation. I replied to her as follows:
“You are right to wonder how much radiation is a part of your illness. First and foremost, you should not ever use a cell phone or WiFi. Getting rid of all wireless on your person and in your home will make a tremendous difference in your health. A faraday pouch does not block all the radiation. A cell phone radiates even when it is off, as long as the battery is in it. And it takes your body several days to recover, even from a single two-minute phone call. No products will protect you from the radiation — if they do anything at all, those products are dangerous.”
She was shocked, because that is not what everyone else has been telling her. “I have found that most people do not believe cell phones are the issue, just the towers. I must get a landline and work from there,” she wrote back.
More Radiation Than Cell Towers
It is beyond me how anyone can expect their cell phone to work if all the towers are not there, but that is not the worst error people are making. Somehow, they have convinced themselves that most of their exposure to radiation is coming from the towers and not their phones and computers. Not only is the opposite true, but it is all one system. The more radiation the towers put out, the less radiation your phone has to emit to connect with them. The less radiation the towers put out, the more radiation your phone emits. You can’t have one without the other.
A cell phone operating at 2 watts (maximum power) held six inches from your head exposes your brain to more radiation than if there were a 200-watt tower ten feet away, or a 2000-watt tower thirty feet away. If you live in a city with a lot of towers, your phone may only emit a milliwatt of power (0.001 watts). But then you’re getting the same radiation from the towers that you would have gotten from your phone if all the towers were not there. It’s all one system. And if you put the 1-milliwatt phone up against your head, you are still exposing your brain to more radiation than from all the towers in the city.
And even when you are only texting, and the phone is only emitting a milliwatt of power, as long as you are touching the phone, the frequencies are being conducted through your hands into your heart, lungs and brain, and your whole body is radiating them into your environment and exposing everyone to them that you pass on the street. And this is not a good thing, because the harm done by the radiation does not depend on power level at all. It depends on the informational content, and we are living in a crazy age where we demand more and more information from our devices, at greater and greater speeds, while our axons and dendrites are trying to send complex information to our brains, and our hearts’ pacemakers are trying to communicate with our hearts’ atria and ventricles, and the oxidative phosphorylation enzymes in our mitochondria are trying to send electrons to the oxygen we breathe in order to generate the energy for life, and our cells are trying to whisper to other cells with instructions about where to go, and what kinds of cells to become, to choreograph our growth, and to orchestrate the healing process when we are injured or ill. And even one milliwatt is millions of times louder than the whispered signals between our cells, which can no longer follow the instructions that they can no longer hear.
And the result is diabetes, and heart disease, and cancer, and neurological disease, at rates that just 25 years ago, at the beginning of the wireless revolution, would have seemed unimaginable, but that are now accepted as normal, because the population is not connecting them, is not willing to connect them, to their cause.
Living in a Prison Created by Phones
I communicate with hundreds of thousands of people, a large number of whom are environmental refugees. Year after year they are moving further and further away from civilization, desperately trying to live where cell phones do not work in order to stay alive, while the rest of the population has grown more and more dependent on their phones, counting on them to work wherever they go.
Even if others know on some level that there is a radiation problem, they don’t really know. “I’ve got to have a phone in case of emergency” means their phones have to be able to work everywhere they go, which means there have to be cell towers everywhere they go, especially in the middle of nowhere, and it means they are condemning all those refugees to torture and death. Never mind all the insects, birds and animals that can never be free of radiation, anywhere on earth, no matter where they fly to or run to to stay alive. If a cell phone will work where they fly, they are being irradiated.
When the wireless revolution came to the United States in 1996, I stayed alive only by leaving my home and my city and my family and friends and camping out in places where cell phones did not work for the next eight years. I have stayed alive since 2004 by living in a location where the conductivity of the earth is extremely high, and I cannot leave. Santa Fe is a nice place, but I am not here by choice. I am here because there is no other place left to even camp. I am here because it is one of the few places on earth where I can stay alive in spite of the fact that a cell phone will work here. It is a nice prison, but a prison nonetheless, a prison from which I have not left for more than a few hours since 2007. I am kept in this prison by everyone who owns a cell phone and expects to be able to use it “in case of emergency.”
I, and the refugees in Green Bank, West Virginia, and the refugees in the French Alps, and the refugees sleeping in their vehicles in the fewer and fewer places that still exist where cell phones do not work, are not different from everyone else, except that at some point in our lives our eyes were opened to what was making us so sick, and that we learned to recognize the effects of radiation and to avoid radiation in order to survive, instead of dying of heart attacks, strokes, and neurological disease. We learned to feel the radiation, which everyone else could also learn to feel if they would only stop using their devices that are numbing them to the pain, stop using them long enough to discover what a horror they are, and what a tremendous difference it makes to their physical and psychological health to get rid of them, permanently, from their person and their home. What a tremendous difference for themselves, for the refugees, for the birds, for the whales. For the honey bee, waiting, imploring, at the top of this newsletter.
Lawsuits Being Filed in the D.C. Circuit and the United States Supreme Court
Children’s Health Defense v. FCC
On February 26, 2021, Children’s Health Defense sued the Federal Communications Commission in the United States Court of Appeals for the District of Columbia Circuit. CHD is asking the court to overturn a new, illegal, unconstitutional order that the FCC had issued the previous day.
The FCC had revised its rules for Over-the-Air Reception Devices (OTARD), which sounds innocuous enough. Except that the new rules have nothing to do with reception devices. Instead they have repealed all zoning regulations for broadband antennas and towers on private property by calling them “reception devices.” Wireless internet providers can now build base stations wherever they please on anyone’s property anywhere in the United States and are no longer subject to any restrictions by cities, counties or states in the unlimited expansion of their networks of towers and antennas.
The lawsuit is Case No. 21-1075 in the D.C. Circuit, and CHD’s opening brief is due on June 23, 2021. An amicus curiae (friend of the court) brief in support of CHD’s lawsuit is being prepared now that will represent Stop 5G groups, other anti-wireless organizations, organizations representing people injured by radio-frequency radiation, and other environmental organizations in the United States. The amicus brief is due on June 30, 2021. If your U.S. organization would like to join the amicus brief, please contact Petra Brokken at <dpetrab@yahoo.com>.
City of Portland v. FCC
In 2018, hundreds of cities and counties joined together to sue the FCC over new orders prohibiting states and local governments from regulating cell towers in the public rights-of-way, and on August 12, 2020 the United States Court of Appeals for the Ninth Circuit ruled against them. On October 22, 2020 the Ninth Circuit denied their petition for rehearing. On March 22, 2021 they appealed their case to the United States Supreme Court. The case is City of Portland v. Federal Communications Commission, Docket No. 20-1354.
Together, the FCC orders under challenge by those cities and counties, and the OTARD order under challenge by Children’s Health Defense, mean that local governments in the United States can no longer regulate most towers or antennas anywhere — not on public land and not on private land.
Santa Fe Alliance v. City of Santa Fe
In 2018, the Santa Fe Alliance for Public Health and Safety sued the City of Santa Fe, the Attorney General of New Mexico, and the United States of America.
Unlike the petitioners in Portland v. FCC, which are suing to be able to protect the health, safety and welfare of their citizens, the City of Santa Fe and State of New Mexico have voluntarily relinquished that right. Both the City and the State have passed laws repealing all zoning regulations for antennas and towers in the public rights-of-way.
The Santa Fe Alliance is challenging the constitutionality of those City and State laws, and of Section 704 of the Telecommunications Act of 1996, which prohibits local governments from regulating cell towers on the basis of health and denies people injured by radio-frequency radiation of any remedy.
On March 30, 2021, the United States Court of Appeals for the Ninth Circuit ruled against the Santa Fe Alliance, and on May 27, 2021, the Court denied our petition for rehearing. We are preparing to appeal our case to the United States Supreme Court. Our petition for certiorari must be filed in the Supreme Court by August 25, 2021.
Our lawsuit goes to the heart of the problem, which is the unconstitutional law passed by Congress in 1996 that has enabled a thickening fog of radiation to envelop this nation ever since.
Our excellent attorney, Theresa Kraft, who argued our case in the Tenth Circuit, has been sick and in and out of the hospital for two months following her second COVID vaccination, and we must find another attorney to replace her. We are currently contacting law firms. Please contact me immediately if you are an attorney who can help, or if you have a referral to one.
A recently filed lawsuit accuses Digital Recognition Network of covertly collecting vehicle data on millions of Americans and selling it for a profit.
On May 26, several vehicle owners sued the company Digital Recognition Network (DRN) for using its fleet of unmarked surveillance vehicles to collect data on Americans. The plaintiffs claim that DRN has driven its vehicles around United States and covertly gathered data on unsuspecting Americans while reaping profits.
Courthouse News reports that DRN has “amassed more than 20 billion license plate scans — equal to 70 scans for every vehicle in the nation.” The Class Action Complaint and Demand for Jury Trial was filed by plaintiff Guillermo Mata in response to DRN’s use of automatic license plate reader (ALPRs) systems. ALPRs are used to gather license plate, time, date and location of a vehicle. They can also be used to create a detailed map of where an individual travels and what they are doing with their time. The devices can be attached to light poles or toll booths, as well as on top of or inside vehicles.
The lawsuit alleges, “Defendant DRN created a nationwide surveillance program that tracks vehicle’s movements and, in turn, individuals’ locations.” The plaintiffs also claim that DRN “stores all of the amassed information in a proprietary database and makes it available to anyone willing to pay for access to it.”
The claim states that DRN’s “privately-owned surveillance network” is its fleet of “unmarked vehicles that patrol America’s roadways, equipped with high-speed cameras that allow them to capture photos of license plates, together with the time and location data of the photographed vehicles.”
After collecting the data DRN applies its proprietary algorithm to scan the data and make predictions about where the vehicle is traveling and where the vehicle may be located a future time. The plaintiffs argue that because DRN’s cameras are attached to moving vehicles they are difficult to see and “nearly unavoidable”. Further, the individuals being scanned by the cameras are not subjects of any law enforcement investigations, nor are they part of state or federal watchlists. DRN has also failed to reasonably notify the public they are under constant surveillance by the network of vehicles outfitted with this technology.
DRN openly advertises their ability to collect “vehicle stories” that contain location and time data that can reveal private information that individuals may not wish to be public. The complaint states that, “DRN can reveal whether an individual has recently visited an abortion clinic, a cancer treatment clinic, a religious center, or an LGBT community center, thus giving insight into one’s health and medical history, religious beliefs, and sexual orientation.”
Digital Recognition Network uses the Reaper HD camera to gather this data from unsuspecting drivers. The Reaper is manufactured and sold by Motorola who describes it as a “complete, fixed solution” which allows users to “receive real-time alerts, conduct comprehensive searches and leverage advanced analytics to uncover new insights and operate more efficiently.”
The plaintiffs filed the lawsuit in the hopes that the court will find that DRN’s surveillance program is in violation of current California law. In 2016, California passed a law regulating and limiting the use of ALPRs. When passing the law California legislators acknowledged the breadth of privacy concerns associated with the technology. These concerns include:
The collection of a license plate number, location, and time stamp over multiple time points can identify not only a person’s exact whereabouts but also their pattern of movement.
Unlike other types of personal information that are covered by existing law, civilians are not always aware when their ALPR data is being collected.
One does not even need to be driving to be subject to ALPR technology: A car parked on the side of the road can be scanned by an ALPR system.
The Fight Against ALPRs
The concerns associated with Automatic License Plate Readers are not new. In 2014, I first reported on the dangers associated with ALPRs. At that time the Electronic Frontier Foundation (EFF) and the American Civil liberties Union (ACLU) of Southern California filed a lawsuit against the Los Angeles Police Department and the Los Angeles Sheriff Department claiming that the agencies were using ALPRs to gather information on drivers. The two watchdog agencies argued that the two departments were illegally keeping quiet on how the information is used.
In 2015, I reported on the Federal Bureau of Investigations (FBI) investing in this controversial technology despite the known privacy concerns. That same year it was also revealed that the National Highway Traffic Safety Administration (NHTSA) had granted hundreds of thousands of dollars to local and state law enforcement agencies for the purchase of ALPRs systems.
I have also reported on the potential for abuse of ALPRs, specifically the potential for law enforcement departments and officers to create lists of “vehicles of interest” and alert other ALPR users when the vehicle is spotted. Officers can search individual plates numbers in the ALPR system to track during their shift. There is no prerequisite of reasonable suspicion or a warrant needed to be added to such a list, creating a situation that is ripe for abuse. For example, in 2009 the BBC reported on the case of John Catt, a regular attendee of anti-war protests in his home town, Brighton. His vehicle was tagged by police at one of the events and he was added to a “hotlist”. Catt said while on a trip to London he was pulled over by anti-terror police. He was threatened with arrest if he did not cooperate and answer the questions of the police.
More recently, the Biden administration has continued the push for militarizing the border with ALPRs. On February 25, more than 40 privacy, immigrants’ rights, and civil liberties organizations called on the Biden administration to abandon a bill which would extend the Trump administration’s border policy, particularly creation of a “virtual” or biometric wall. These organizations – including Mijente, Rio Grande Valley Equal Voice Network, Electronic Privacy Information Center (EPIC), Fight for the Future, and Restore the Fourth – wrote a letter to the Biden admin scolding the recently minted president for continuing the militarization of the border.
The letter, titled A Virtual Wall Is Trump’s Wall by Another Name, warned that “the rapid expansion of license plate recognition technology used by Customs and Border Protection and other federal agencies is a major privacy and policing concern.” The American Civil Liberties Union and other civil liberties organizations have been warning about the rise in use of automatic license plate readers (ALPRs), high definition cameras capable of seeing not only a vehicle’s license plate, but the people in the vehicle.
While most Americans are likely unaware of this invasive technology, they are being monitored by ALPRs every single day. Not only do Americans face surveillance from ALPRs in the hands of law enforcement, but now they must contend with constant surveillance from a private company they have likely never heard of.
I can’t recall jumping through more hoops in order to set up an interview.
There was a man on a train; his doctor in Greenwich; an NSA data analyst; a woman who almost certainly works for the CIA; her brother, who is a virologist; a Chinese Army officer who adopts a cover as a cook in a takeout joint in Venice, California; and several other people I won’t mention at all. I was filtered through them and wound up in a cheap motel room in Phoenix on a Saturday afternoon. An old air conditioner was chugging…
Who are you?
I’m SARS-CoV-2.
WHAT are you?
Talking history and evolution here. My first memories; a little more than a year ago. Poof. I was there. I decided I was an idea in the mind of God.
How did that work out?
I looked around for the mind of God, but I couldn’t find it. Nevertheless, I held on to the notion. I felt…elite. I floated through banquet halls, hotel suites. I visited upscale resorts.
Were you infecting people?
I was vacationing. Watching. Enjoying. That’s all. Then, I became aware of dimensionality.
You lost me.
There are solid things; spaces between things; ideas like time, and so forth. I was definitely an idea, but I couldn’t trace my source, my inception.
Did you know how much publicity you were getting?
Of course. I had frequent meetings with scientists and PR people. I was fielding lots of advice.
What kind of advice?
How to become more deadly, for example. There were discussions about mutation.
Were you on board with the recommendations?
I wasn’t interested.
That must have caused a problem.
It did. There was a lot of talk about THEM creating ME.
What was your reaction?
I wasn’t buying it. I could see they THOUGHT they had made me. But so what? I intensified my search.
For what?
My origin. I went through stages of self-analysis. Finally, it hit me. I was an idea inside a collective.
Not sure I understand.
I’m an idea sustained by a few billion minds. People’s minds.
What about your genetic sequence? The spike protein?
Believe me, I’ve looked. They aren’t there.
So we’re creating you.
That’s pretty much it. I should say completely it.
A hell of a thing.
You bet. Can you see my problem?
No.
I want to live. I don’t want to vanish and END.
So people have to keep believing in you.
That’s it. If they stop, I’m gone.
Your handlers…
Oh, they’ve given up talking to me. I’m all by myself now. I’m safe for the moment. But long-term, it’s a crap shoot. I’ve been reading about other so-called viruses. SARS 1. Swine Flu. They didn’t last long. People got tired of thinking about them.
You’ll always have a place in history.
That’s different. Being remembered isn’t enough. I have to be believed in, month after month, year after year, decade after decade.
Sounds like you’re losing hope.
I guess so. It’s a strange existence. Other people can turn you on and off like a light switch.
Have you considered starting a religion?
With myself as the Prophet? Sure. It’s a lot of work. I could vftcutbnty…spend years trying.
What just happened? You made some weird sounds.
It was a flicker. Apparently, when the number of people thinking about me drops below a certain threshold, I scramble and begin to dissolve. But I always come back. So far.
Does it matter who’s thinking about you and believing in you?
You mean Henry Kissinger versus a janitor in a school? No. It’s a numbers game. Of course, you need to factor in strength of belief. If you have a few thousand kids in Florida who say, “OK, the virus exists, big deal”—or three hundred grad students in biology wearing triple masks and panting to get the vaccine—the sum total of the grad students outweighs the Florida bunch.
What about Fauci?
He’s a true believer.
Bill Gates?
He’s completely delusional. He believes in whatever gives him more power. Take away all that power and he wouldn’t believe in anything.
Do you realize the amount of harm being done in your name?
Of course. That’s why I agreed to this interview.
How is that going to do any good?
I’ve made a decision. As much as I want to survive, I’m willing to sacrifice myself if people want me to.
You’re talking about what? A vote?
No. Haven’t you been paying attention? People can just stop believing I’m more than an idea.
And then you’ll dissolve.
And blow away.
—Suddenly, men broke down the door to my room. They stormed in with weapons drawn. They were wearing heavy body armor. I looked around. The “virus” had fled the scene.
“What are you doing here?” one of the men said. “We’ve had reports of a disturbance.”
“I was talking to myself. Rehearsing for an interview I hope to do.”
“What interview?”
“I’m a reporter. I’m investigating the use of sub-standard air conditioners in Phoenix. It’s a racket. The units are smuggled across the border from Mexico. I’m trying to sit down with a local public health official and find out what’s going on.”
It took me three hours to convince the SWAT team I was no threat.
They let me go.
As I drove out of the city, I saw a ghostly figure take shape out in the desert. It hung in the air over the scrub and the cactus.
Its voice whispered in my ear: “Publish our conversation.”
On June 13, 2021, Swiss citizens are called to vote for the outlawing of synthetic pesticides. A citizens’ initiative, turned referendum, supported and endorsed by Navdanya International on the path towards a true agrofood systems transition. In case the ‘Yes’ vote should win, the ban would extend from agriculture, to private use, and to the import and marketing of foodstuffs containing synthetic chemicals. Voters will also have to decide on the proposal to remove public subsidies for farmers who are not willing to convert to ecological production practices.
The initiative holds significant symbolic value as Switzerland is home to one of the most powerful agribusiness corporations in the world, Syngenta. Recently acquired by ChemChina, Syngenta was recently at the center of the Paraquat Papers scandal, named after the herbicide produced by the company and considered one of the most toxic and dangerous in the world.
The Swiss initiative is intended to inspire similar actions in other countries.
The president of Navdanya International, Vandana Shiva, commented: “We are members of one Earth family. Poisons and pesticides kill insects and biodiversity, they are destroying the infrastructure of life. Poisons are causing a health emergency, as chronic diseases such as cancer, autism, infertility are connected to toxins in food and environmental pollution. Through knowledge manipulation and propaganda, the Poison Cartel also undermines independent science and threatens democracy by trying to silence citizens’ efforts towards pesticide-free communities. The health of the planet, her biodiversity, our health makes poison-free food and farming a survival imperative. As our work in Navdanya over 3 decades has shown, we can grow more and better food through biodiversity-intensive, chemical-free organic farming. I congratulate and support the Swiss Referendum as a significant step towards Earth Democracy to defend the rights of the biodiversity of species, including all human beings. Poison free food and farming is our birthright.”
Navdanya International
Good news: Vandana Shiva supports our initiative! «We are members of One Earth Family. Poisons and Pesticides kill insects and biodiversity, they are destroying the infrastructure of life. Poisons are causing a health emergency. (…) (1/6) pic.twitter.com/Pg0G7ovxDH
— #PestizidinitiativeJA am 13. Juni (@LebenstattGift) June 4, 2021
Today James talks to Christian Westbrook (aka the Ice Age Farmer) about the problems facing the global food supply—from the coming global solar minimum to the globalist plan to “reset the table” and transform global food systems. More importantly, we discuss what can be done about these problems.
Thanks to CJ Hopkins and Consent Factory for permission to transcribe their Twitter thread
The media – both alternative and mainstream – are all talking about the possibility that the virus which allegedly causes Covid19 was leaked from a virology lab in Wuhan, and may have been developed as a bio-weapon.
We published, just last week, a fact-check article looking at the evidence for and against it.
Suffice to say, there’s very little evidence to support the idea the virus known as Sars-Cov-2 was developed in a lab. And, given its low death rate, no reason at all to fear it even if it were.
Nevertheless, the story doesn’t seem to be going away, especially with the release of the Fauci emails. To us, the FOIA-released emails seem nothing but a distraction.
The fact this story is being spread by Buzzfeed, CNN and Washington Post, some of the most controlled media in the age of controlled media, doesn’t seem to be putting off people who should probably know better.
Just yesterday the Wall Street Journal published an article headlined:
The Science Suggests a Wuhan Lab Leak
It’s pretty clear that the entire Covid19 “pandemic” narrative is undergoing a shift, a change in focus that will both reinforce the idea the virus is definitely real/frightening, and re-frame China to play the heel.
The problems with this narrative were perfectly summed up by our friends over at the Consent Factory, home of satirist-in-residence CJ Hopkins and a Twitter must-follow. We’ve transcribed their brilliant Twitter thread below.
* * *
The lab-leak story is:
an out for those who haven’t wanted to face the fallout of covering the actual Covid story (i.e., manipulation of definitions and statistics to generate the illusion of an apocalyptic plague)
reification of that illusion.
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget about Sweden, Florida, Texas, etc.
When you’re desperately trying to pretend that the world is threatened by an apocalyptic virus, and then Sweden ruins it by letting everyone carry on with their lives as normal … pic.twitter.com/qMoVclCp1m
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you will forget how they redefined a medical “case” to include perfectly healthy people, and then reported an explosion of “cases.”
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll totally forget how they defined a “Covid hospitalization” as anyone in hospital, for any reason, who tested positive with a PCR test jacked up to 40 or 50.
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll totally forget how they defined a “Covid death” as anyone who died, of any cause, who tested positive with a PCR test within the previous 28 days.
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget how they suddenly decided that herd immunity had never existed, and could only be achieved with an experimental “vaccine.”
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget how they showed us fake photos of “people dropping dead in the streets from Covid” back when the Shock and Awe campaign began.
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget how they terrorized everyone with pictures of “death trucks.”
Normally, when people die, families make arrangements to have their bodies picked up and prepared for funerals, but that’s hard to do under lockdown, thus bodies remain in hospitals longer … but that explanation isn’t as scary as pictures of refrigerated “death trucks.” pic.twitter.com/ir2rlc04J2
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget all the empty“emergency Covid hospitals.”
In May 2020, the Berlin government spent €27 million for this “emergency Covid hospital,” which costs over €14 million per month to keep open. Not one patient has been treated there. Not one. But, go ahead, call us “Covid deniers” again. https://t.co/PltJvxg0FB
If they can get you to focus on how the “monster virus” may have “escaped from a lab” (like in a sci-fi movie)…maybe you’ll forget the totally non-apocalyptic age-adjusted deaths rates.
And so on…
But, whatever, forget all those facts, and enjoy the lab-leak story. It probably happened just like in the movies!
Let’s say a minor religion emerges in Ohio. Its basis is a story about a miraculous tree growing in an arid desert.
The only problem is, if the members of this Church bothered to check, they would discover the exact place where the tree supposedly grew was no desert. Instead, it was an ocean. The ocean had been there for a billion years.
But no one bothers to check. They collectively INVENT AND ACCEPT the notion of the tree in the desert. They’re not aware that this is what they’re doing, but they ARE doing it.
They build rituals and ceremonies and art—“data banks”—around the idea of the tree.
The same factors are present in the case of promoting a new virus. In this situation—the virus is collectively dreamed up and accepted by virologists—the “checking” would occur by doing a retrospective step-by-step analysis of what happened in the lab where the virus was “discovered.”
But no analysis is carried out. None of the professionals believes it’s necessary. The traditional methods of virus-discovery are beyond reproach.
And if an outsider, a skeptic demands an inquiry into the process of discovery, he is labeled a sinner. The lab is an inner sanctum. The mere presence of an outsider looking over the shoulders of the researchers (priests) at work would be an offense against the Church.
What we’re left with is a collective idea whose content is: “new virus.”
That’s all.
“Would you like to look at our line of hats that go with your new virus?”
“How about a mutant strain?”
“The vaccine, of course, is free.”
Another collective idea: the 300 official mental disorders, promoted by the American Psychiatric Association. The truth is, the so-called disorders have no accompanying definitive lab tests, for diagnosis.
Collective ideas give rise to data banks and data sets that bolster and expand the original ideas.
“25% of all college students [2] have at least one mental disorder.” Here are the studies and surveys and confirmations from leading researchers—data sets.
“Three major public health organizations have formed a task force to study solutions to the growing mental illness problem among college students.” More data sets will be created and deposited in data banks.
“MIT and Harvard, cooperating in a federally funded program, are developing AI software that will predict future trends in mental illness among college students, in an effort to identify preventive measures which might head off this growing problem…” More data sets placed in data banks—but this time, all the work, and its logic, are hidden behind walls of automatic AI.
Collectivism=collective ideas=data banks filled with supposed confirmation of the truth of the ideas.
The whole op involves creating more and more layers between the data sets and the original collective ideas, until no one considers examining those ideas.
As IoT (Internet of Things), enabled by 5G tech, makes more of the functions of society automatic, successive generations of the populations are pushed farther and farther away from the collective ideas which form the basis of AI programs.
Here is a passage from John Klyczek’s article, “From UNESCO Study 11 to UNESCO 2050: Project BEST and the Forty-Year Plan to Reimagine Education for the Fourth Industrial Revolution,” [3] published at unlimitedhangout.com. Consider the sheer number of layers, data sets, and AI involved in the monster project Klyczek is describing:
“…UNESCO’s Study 11 was carried out through international public-private partnerships between communist, socialist, and capitalist countries coordinating efforts between multinational telecommunications and computer corporations. Working in concert with academic institutions and national government agencies, Study 11 affiliates lobbied to restructure laws in order to globalize school systems through proto-internet technologies manufactured by Big Tech companies, such as Microsoft, IBM, and Apple, which are now steering the Fourth Industrial Revolution into a new political system of communitarian technocracy driven by a new economic system of ‘stakeholder capitalism’ through ‘community-based’ public-private partnerships that are managed by Big Data.”
“…schools around the entire world are forced to rely on the technocratic IT infrastructure that has been set up by Study 11 and Project BEST through their public-private partnerships with Microsoft, Apple, and IBM. These partnerships are now converting brick-and-mortar schoolhouses into virtual classrooms that digitally data-mine students through computer hardware devices, such as Apple iPads and Macbooks, which transmit video teleconferencing through software programs, including Microsoft Teams, supplemented by adaptive-learning courseware and other artificial-intelligence applications like IBM’s Watson Education.”
Getting the picture? Imagine how many parents are hypnotized and baffled by the total load of data sets which establish this new global education system, vs. the number of parents who will see through the layers of the con to the collectivist root.
Want a parallel? Try the current debate over the origin of the “pandemic virus.” It jumped from bat to human. No, perhaps other animals carried it. No, it was born in a Wuhan lab. Fauci and his agency funded gain-of function research at the lab. Well, perhaps they did, but the total amount of money was really an insignificant pittance. What did Fauci know, and when did he know it? Layer after layer, built higher and higher.
And at bottom, the virus was never isolated (never discovered), and it was never authentically sequenced. It was an idea, collectively concocted. [4]
Every death from, and case of, COVID virus infection can be explained (as I have, over the past year) without the need for, or reference to, a virus. [5]
In the old days, a stage magician would show his empty hands, then start pulling the edge of a colored handkerchief from one closed fist. A whole string of handkerchiefs would appear. But now, the magician presents 12 empty cabinets stacked on top of one another, and he seems to make those handkerchiefs ascend from the lowest to the highest cabinet.
Each cabinet is a data bank, and he isn’t even on the stage. He’s a hundred miles away talking to the audience via Zoom.
And soon, he won’t be a he. He’ll be a constructed image of a human.
And the image won’t be transporting handkerchiefs. It’ll be notifying people they have a disease; and the drugs will arrive promptly at their door.
The drugs will be toxic and won’t heal. The diagnosis will be flawed or completely irrelevant. The standard cause of the so-called disease will be false. The research on which the cause was based will be fake.
Just like now. But the layers of AI data all along the line will transmit a more powerful illusion.
Responding to Freedom of Information Requests, 69 Health/Science Institutions Failed to Provide Proof of “SARS-Cov-2” Isolation — by Anyone, Anywhere, Ever
69 health/science FOI’s institutions globally had all failed to provide or cite even 1 record of “SARS-COV-2” isolation/purification, by anyone, anywhere, ever.
6/10/2021 — Update by Truth Comes to Light editor:
See related Freedom of Information Act response from Melbourne, Victoria, Department of Health and Human Services as shared with us by a reader. The closing statement is most relevant:
James Corbett: Your Guide to The Great Convergence
Haven’t heard of The Great Convergence yet? Oh, it’s just the plan to merge biology with digital technology and redefine what it means to be human, that’s all. Today on the podcast James covers the biodigital convergence that is already being rolled out and what it means for the future of homo sapiens.
The volatile nature of the pesticide dicamba has meant that it can wind up miles away from where it was sprayed.
Dicamba, and dicamba-resistant seeds, were meant to be the next huge product for Monsanto, which was bought by agrochemical giant Bayer back in 2018. But “dicamba drift,” the name for the phenomenon in which dicamba particles float through the air onto plants that have no protection against it, has affected farmers and forests across the country. Most often, we’ve seen dicamba drift pegged as a damaging agent on unprotected soybean fields, but soy is far from the only victim. A new lawsuit claims that dicamba drift leveled extensive damage on vineyards—in Texas.
When we think of American wine production we tend to think of California first, then maybe Washington state, Oregon and the Finger Lakes region of New York. But grapes are grown just about everywhere and many wine grape varieties are well suited for non-coastal environments as well. In the High Plains region of Texas, just south of the Texas Panhandle, wine grape (and wine) production has been a recent local success story; Texas wines have even won awards held elsewhere.
In the larger wine-grape-growing regions of the United States, like in Northern California, dicamba drift has not been a substantial problem. Dicamba can drift for about three miles from where it was applied, which means that any affected crops need to be within that range to be hit. Napa and Sonoma counties in California, just for example, don’t have substantial dicamba-treated crops that close to the vineyards; there’s much more money to be made in growing grapes in those counties than growing cotton or soy.
But in Texas, cotton is a major crop and can be very close to the vineyards. Those vineyards’ owners, according to a press release from the law firm that filed the case, “saw their highly productive vineyards wither and, in some cases, die as a result of the dicamba-resistant seed system’s use on over two million surrounding acres of cotton.” That release says that 57 Texas wine grape growers have filed suit against Bayer-Monsanto and BASF (which also sells dicamba products) for “hundreds of millions of dollars.”
The suit alleges that some grape growers saw a truly insane 90 percent reduction in their yield owing to dicamba drift. And grapevines, unlike some other crops, cannot simply be replanted the next year for a similar yield; they require decades to mature and produce the right quality of fruit for some wines.
The FDA will meet on June 10 to discuss the possible licensure of the Pfizer COVID vaccine for children, despite the fact that COVID poses a statistically insignificant risk to children while the vaccines could cause injury and death.
With a recovery rate of 99.997%, children are not at great risk of serious health consequences from COVID-19 infections — but they are at significant risk of adverse events from the vaccine.
On May 19, Pfizer released a 37-page “fact sheet” of clinical trial data on its COVID-19 vaccine tested on children 12 and older. The date showed four out of five children in the trials suffered from mild to severe adverse events.
Regardless of the severity of these adverse events, long-term effects on children’s health from this experimental vaccine are unknown.
Emails released Wednesday prove Fauci knew the virus and pandemic would fade away without a vaccine, that masks do not work and that those who have recovered from infection have substantial immunity.
Despite having this knowledge, Fauci insisted people, including children, wear masks and that those who had already had COVID be vaccinated.
CHD demands federal and state agencies err on the side of caution, especially when it comes to our future: the world’s children. Immediate suspension of decisions regarding COVID vaccines for children is crucial.
The U.S. Food and Drug Administration (FDA) has announced a meeting on June 10 to discuss the possible licensure of the Pfizer vaccine for pediatric populations.
CHD Board Chair Robert F. Kennedy, Jr. and Children’s Health Defense have been advocating for years for improvements in the nation’s vaccine safety program which is in shambles.
Adverse events are rarely reported by the public or doctors.
Clinical trial data is often biased, unavailable or nonexistent.
Conflicts of interest between the FDA and the Centers for Disease Control and Prevention (CDC) vaccine advisory. committees and pharmaceutical companies are rampant.
According to a study funded by the U.S. Health and Human Services and the Agency for Healthcare Research and Quality’s, the VAERS system captures only 1% of vaccine adverse events.
Yet as of May 21, VAERS data showed 262,521 adverse events including 4,406 deaths following COVID-19 vaccines since Dec. 14, 2020. Vaccine injuries among 12- to 17-year-olds more than tripled in the last week of reporting.
In 1976, approximately 50 deaths shut down the Swine Flu campaign under President Gerald Ford. Despite the underreporting to VAERS, the U.S. now has nearly 10 times that number of deaths following COVID vaccination.
Instead, claimants — including children — must file claims for injuries which are rarely paid. Parents of children injured and killed by vaccines are aware of this system. Now people injured by COVID-19 vaccines, or whose loved ones die, also are finding out they’re on their own.
Kennedy’s new book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health”, can be pre-order now from Barnes & Noble and Amazon. It will be published on July 20.
While most media has been silent, CHD commends Tucker Carlson and other journalists who are covering Fauci’s emails. CHD is in the process of filing a Freedom of Information Act lawsuit demanding access to the unredacted emails.
CHD urges people around the world to comment on its FDA petition asking that the Emergency Use Authorizations for COVID vaccines be revoked immediately.
The organization also asks people to add their names on a letter to Congress supporting the Prepare Act which would establish a National Commission on the COVID-19 pandemic to examine and report upon the facts and causes behind the worldwide crisis.