A photo isn’t enough because it says nothing about causality. A photo of hyenas eating a dead antelope says nothing about whether or not the hyenas killed the antelope. (A hunter might have killed it and the hyenas arrived later.)
Furthermore, reproducibility is critical, hence it being part of the Scientific Method. If the same results can’t be repeated, then the hypothesis is false. For example, if the claim that a certain type of plastic is heat resistant under certain conditions, but tests repeatedly reveal that it is not heat resistant under the said conditions, then the claim is false.
Similarly, if the claim that SARS-CoV-2 causes COVID-19, then tests must be conducted and must be reproducible.
There is nothing unusual about such logic; it is precisely how proper science works.
TNT Conversation
Mark joined me for a conversation about viruses and the aforementioned challenge. It is well worth listening to.
Podcast Conversation
A few days after our TNT conversation, Mark joined me on my podcast for an overlapping, but more free-flowing chat with coffee, craft beer, and power failures.
While walking down the darkened street late at night, have you ever had that gnawing fear as to whether or not the posse of raccoons rummaging through the trashcans nearby, staring at you with their beady yellow eyes, are ready and waiting for the right moment to pounce? Or have you ever had your fingertip accidentally pierced by the sharp fangs of a squirrel while feeding it walnuts and had to rush to the hospital on a nurses advice only to be told by the doctor that squirrels do not carry the “deadly virus?” Have you ever been bit in the very tender thin space of skin in between your thumb and index finger by a baby penguin while feeding it fish at the Omaha Zoo? Ok, the last one is obviously not related to rabies as the “virus” discriminates as to which animals it infects. Whether or not the squirrel can get or transmit rabies depends upon who you ask. In any case, these are all true experiences for me and yes, I have been bitten by numerous animals while feeding them. Like many, I have encountered the fear of being infected by a bite from a potentially rabid animal and that if I waited too long to receive treatment, it would be too late to stop the “virus” before it invades my cerebral cortex and causes me to turn into a crazed barking dog-man. Fortunately, not one of my comedically unfortunate puncture wounds left me to succumb to any disease. As I would later find out, my fears were in fact as irrational as the myths surrounding rabies which are built upon a foundation of fraud and pseudoscience.
Still, rabies seems to be one of the diseases that those who cling to the “virus” narrative love to bring up as if it is the Holy Grail of proof that “viruses” actually exist. Over the decades, the images of the mangy frothing dog snarling and ready to attack has been deeply ingrained into our subconscious through effective media fear-based propaganda.
1870’s fear propaganda.
Atticus Finch taking aim to put down a rabid dog in 1962’s To Kill A Mockingbird.
The portrayal of angry diseased animals heightened peoples fear of anything wild and undomesticated and created in their minds the living walking embodiment of an invisible “virus” coming to infect the defenseless with a slobbery bite. The fear of aquiring the deadly disease was the perfect tool to use by Louis Pasteur in the late 1800’s to ensare people into the emerging germ theory narrative. All it takes is one bite for the sneaky “virus” to find its way into the bloodstream, attacking the brain and causing a painful death. It seems, upon first glance, to be an open and shut case. However, what you will find upon researching rabies is that the presented model of the rabid animal bite transferring an infectious “virus,” which in turn causes disease, is not an accurate portrayal whatsoever and was merely a frightening myth used to propagate the delusions of a madman looking to aquire fame, fortune, and prestige.
A few months ago, I looked at the unethical and fraudulent practices Louis Pasteur employed in the 1880’s in his attempt to prove a rabies pathogen exists and causes disease in order to sell his vaccines. Pasteur openly admitted to not being able to isolate any microorganism said to cause rabies but developed his vaccine against the invisible pathogen anyways. This is also openly admitted as well by the Institut Pasteur:
“Louis Pasteur’s initial efforts to isolate the rabies virus proved unsuccessful as the virus remained invisible. Viruses could not be seen due to the poor resolution of the microscopes used. The virus was not seen until almost a century later, in 1962, with the advent of electron microscopy.
But as rabies is a disease of the nervous system, together with Emile Roux, Louis Pasteur then had the idea of inoculating part of a rabid dog’s brain directly into another dog’s brain. The inoculated dog subsequently died.”
Thus, Pasteur never worked with any purified and isolated “virus” and did what virologists still do today, which is assume an invisible entity is floating freely in the unpurified solutions of diseased animals which are then inoculated into healthy animals in attempts to cause disease and prove pathogenicity. Interestingly, as stated in the 1930 paper below, Pasteur would fail many times in his attempts to infect animals with saliva from animals claimed to be rabid, the very fluids the “virus” is supposed to reside in. Even if deemed successful, the symptoms would not appear for months, which was unheard of for any pathogen. Thus, he sought other means of infecting animals by way of injecting dogs directly in the brain with the emulsified cranial goo from animals claimed to be rabid. Once the healthy animal died from the toxic brain injection, this was considered a success:
Pasteur’s Work with Rabies
“Inoculation with saliva was found to be a method which did not always produce rabies and symptoms did not declare themselves for months. The theory that the disease virus attacks the nerve centers had already been set forth by Dr. Dubous of Paris. Pasteur accordingly inoculated a number of animals subcutaneously with some of the brain substance from other animals which had died of rabies. Most of those inoculated developed rabies, but not all.
Pasteur then conceived the idea of introducing into the brain of experimental animals some of the nerve tissue from an animal which had died of rabies. This experiment was based on the principle of providing the causal organisms with the nutritive medium best suited to their requirements. Pasteur, obliged to sacrifice so many animals, had a real dislike for vivisection; if the animal cried out a little he was full of pity. The idea of perforating the skull of the dog was repulsive to him, he wanted it done but dreaded seeing it done. So it was done one day when he was away. The next day when he was told of the intra-cranial inoculation he was moved to pity for the poor dog.”
While the exact make-up of the inoculations remain a mystery due to Pasteur’s secretive nature, the vaccine’s he utilized contained a neurotropic agent which was known to cause the exact same neurological conditions as seen in rabid animals. While injecting anything into the brain would potentially cause neurological damage and death, it is not far fetched to believe Pasteur used the same neurotropic agents in his experimental inoculations to prove pathogenicity, especially as they were said to consist of emulsified brain and nervous tissue. This created an issue in determining whether it was the invisible “virus” or the injections themselves which caused neurological damage and/or death. However, it has been admitted that the vaccines themselves led to the majority of neurological conditions rather than “wild” rabies cases as this was considered a rare occurrence in nature. This is just another in a long history of cases where the vaccine created the disease it was supposed to be preventing.
Fortunately, we can learn a lot of interesting tidbits about rabies (or the lack thereof) from the work of Gerald Geison, a leading Louis Pasteur researcher and historian who was privy to his private notebooks. In a 1978 essay he wrote on the ethics of rabies vaccination, Geison pointed out some of the pecularities of rabies such as the fact that it has always been considered a rare disease in man as well as the fact that rabies can not be transmitted from person-to-person. He also noted that, as a pathogenic disease, rabies has an unusually long incubation period. While it is said to usually last 6 to 8 weeks, Geison claimed that it can actually last for a year or more. In fact, there have been reported cases with a rabies incubation period from 6 years all the way on up to 25 years. If that wasn’t outlandish enough to make one question the validity of what we are told of the disease, Geison stated that there was a high degree of uncertainty regarding the correlation between animal bites and rabies symptoms as well as the threat of death from being bitten by a clearly rabid animal:
Pasteur’s Work on Rabies: Reexamining the Ethical Issues
“Rabies has always been rare in man. It probably never claimed more than a hundred victims in any year in France, and Fiench estimates for the years immediately preceding Pasteur’s famous work indicate an annual mortality of considerably less than fifty. In addition, rabies is not an infectious disease in the usual sense; it is not transmitted from man to man. Because of these two features, generalor compulsory vaccination has never seemed appropriate with respect to rabies.
“An even more peculiar feature of rabies is its long incubation period in the absence of detectable symptoms. No other lethal disease of rapid clinical course even approaches rabies for length of incubation-usually six to eight weeks, but sometimes a year or more.
“Unfortunately for Pasteur and his successors, there is a very high degree of uncertainty in the correlation between animal bites and the subsequent appearance of rabies-even when the biting animal is certifiably rabid. While the mortality of clinical rabies is virtually 100 percent, the threat of death from the bite of a rabid animal is vastly less. The risk depends on several factors, including the species of attacking animal (wolf and cat bites, for example, pose a much higher risk than dog bites), the location and depth of the bites, and the application or timing of cauterization. Depending on these and other circumstances, estimates of the risk of contracting rabies from the bites of animals known to be rabid range from as high as 80 percent to as low as 0.5 percent. It is perhaps futile to try to settle upon a meaningful “average” figure within this range, but Pasteur himself estimated that 16 percent of those bitten by rabid dogs would eventually die of rabies unless they submitted to his new treatment.”
In his 1995 book The Private Science of Louis Pasteur, Geison pointed out that, according to the English Commission on Rabies, there was also much uncertainty in the rabies statistics. They had suspected that at least one man had died not from rabies but from Pasteur’s vaccine instead and they actually favored animal regulations over Pasteur’s vaccination approach:
“But the English commission also drew attention to the uncertainty of all statistics on rabies, citing the difficulty of establishing that the attacking animal had in fact been rabid as well as the variable effects of the location and depth of bites, of differences in the lethality of rabid animal bites in different species and races, and of the possible prophylactic effects of cauterization or other treatments applied to bitten victims before they submitted to Pasteur’s treatment. The commission also suspected that at least one man may have died as a direct result of the Pastorian injections, and in the end it favored strict regulations on potentially rabid animals (muzzling and quarantine) over Pasteur’s more drastic remedy.”
We also find out from Geison that, in great contrast to what we are told about rabies, the great majority of rabies victims could forgo any treatment and never have any ill effects whatsoever:
“In short, the great majority of the victims of rabid animal bites could forgo Pasteur’s treatment without experiencing any untoward consequences in the future. And they had to decide whether or not to submit to the treatment at a point when they had no symptoms of the disease. For the efficacy and very possibility of Pasteur’s vaccine depended on the peculiarly long incubation period that separates the infective bites of a rabid animal from the outbreak of symptoms.”
Geison even spotlighted what was known as “false rabies,” which were cases of the exact same symptoms of disease associated with rabies that occured despite a complete lack of the victim being bitten by a rabid animal. These symptoms were said to be either induced solely based on fear alone or by alcoholism. In other words, just the mere thought of rabies could create an intense enough reaction inducing the same disease, thus no invisible microscopic pathogen is necessary. Pasteur actually emphasized these cases in defense of his vaccine as there was a growing chorus of criticism that his vaccine did not protect the victims and in fact induced the symptoms of rabies which lead to their deaths. Pasteur therefore had a vested interest in showing that these same symptoms could occur outside of animal bites and vaccination:
“Pasteur himself later pointed out some of the uncertainties surrounding the diagnosis of rabies. Two years after I’affair Girard, for example, he spoke to the Academie des sciences about several cases of “false rabies.” Relying on the authority of one Dr Trousseau, Pasteur cited two cases in which symptoms of the disease had been induced solely by fear. In one case, a man suddenly displayed several of the classic features of rabies—including throat spasms, chest pain, extreme anxiety, and other nervous symptoms—merely because the disease had become the subject of a lunchtime conversation. And this man had never even confronted a rabid animal. Presumably more common was the second case, that of a magistrate whose hand had long before been licked by a dog later suspected of rabies. Upon learning that several animals bitten by this dog had died of rabies, the magistrate became extremely agitated, even delirious, and displayed a horror of water. His symptoms disappeared ten days later, when his physician persuaded him that he would already be dead had he been afflicted with true rabies.”
In this same address, Pasteur commented upon a recently published case history of “false rabies.” Partly because it includes an arresting account of the classic symptoms of rabies, his commentary deserves quoting at length. As recorded in the Comptes rendus of the Academie des sciences for 17 October 1887, Pasteur spoke as follows:
The patient to whom Mesnet refers in his brochure was an alcoholic who, having seen some sort of deposit m his glass during lunch, was seized by a feeling of horror toward the liquid and by a constriction of the throat, followed by headache and by lameness and fatigue in all his limbs. He spent Sunday in this state.
During that night and during the day on Monday and Tuesday, no sleep, a fit of suffocation, throat spasms, and a horror of liquids, which he pushed aside in his glass. His countenance expressed disquiet. His eyes were fixed, glazed, the pupils greatly dilated. His speech was brief, jerky, rapid. He had difficulty breathing. When he was offered a glass of water, he pushed it aside with terror, and suffered fits of suffocation and of constriction of the throat. Bright objects and light were particularly disagreeable to him. He was painfully affected when the air was agitated in front of his face. He died Wednesday night after having suffered from a violent delirium, with extreme agitation, howls and cries, extremely abundant salivation, spitting, biting his bedsheets, and trying also to bite the person taking care of him. In short, this man displayed all the features of furious rabies [I’hydrophobie funeuse]. But he did not die of rabies. He had never been bitten and on several occasions, at long intervals, had already displayed symptoms analogous to false rabies.This man was an alcoholic and belonged, moreover, to a family m which one member had died of insanity [alienation mentale].
By October 1887, when he gave this address, Pasteur had a vested interest in emphasizing the difficulty of diagnosing rabies. For he was then defending himself against allegations that his rabies vaccine not only sometimes failed to protect those who submitted to it, but in some cases was itself the cause of rabies and therefore death. A few hostile critics were insisting that some people died of rabies not only despite Pasteur’s vaccine but because of it, and they tried to make Pasteur and his treatment responsible for the death of anyone who displayed any symptoms of nervous disease. In defense of his vaccine, Pasteur now emphasized the extent to which symptoms like those of rabies could appear in patients who did not have the disease. He therefore insisted that a diagnosis of rabies could only be established with confidence by experiments in which tissue from the victim’s brain was transmitted to animals susceptible to the disease.”
There is good reason for the high degree of uncertainty over the correlation between animal bites and the development of symptoms, the actual rabies statistics, as well as the ability to accurately diagnose the disease. For starters, there are many other conditions that can cause the exact same symptoms as rabies in both animals and in humans. In animals, canine distemper, encephalitis, and poisoning are a few of the conditions which can mimic rabies. In humans, this includes polio, being drunk and/or intoxicated on certain drugs, having Guillain–Barré syndrome, and as stated previously, encephalitis derived from the toxic vaccine itself.
It has been stated that it is common not to even find bite marks in cases of rabies and often, the person has had no idea that they were ever bitten to begin with. One source stated that fewer than one third of human rabies victims show evidence of bite wounds. With the vast range of conditions that mimic rabies and the lack of bite marks, it’s safe to question the existence of a specific disease known as rabies. It would be logical to conclude that rabies is nothing but the same set of symptoms that has been given a different label numerous times.
This uncertainty in rabies cases and statistics boils down to the inability to accurately diagnose a rabies case. For much of the 1800s to the mid 1900s, rabies was diagnosed upon clinical symptoms which, as previously stated, were not specific to the disease. It is also noted in the WHO’s rabies laboratory manual that the histological diagnosis for rabies, which began in the late 1800’s, was also non-specific:
When factoring in the non-specificity in diagnosis, the uncertainty in the correlation between animal bites and disease symptoms, and the vast majority of victims never needing any treatment whatsoever, it leads one to conclude that the rabies myth is vastly overstated. It is fictitious fear propaganda rather than facts based in reality. We can break this deception down even further by looking at how rabies is diagnosed in the present versus how it was in the past. According to the CDC:
Diagnosis in animals
“A diagnosis of rabies can be made after detection of rabies virus from any part of the affected brain, but in order to rule out rabies, the test must include tissue from at least two locations in the brain, preferably the brain stem and cerebellum.
The test requires that the animal be euthanized. The test itself takes about 2 hours, but it takes time to remove the brain samples from an animal suspected of having rabies and to ship these samples to a state public health or veterinary diagnostic laboratory for diagnosis.”
In order to diagnose rabies, the animal must be killed and sections must be taken from the brain in order to try and detect the “virus.” We already have a few problems here as no “virus” was ever purified and isolated in order to determine how to detect it. There is also an issue with attempting to determine anything from dead tissue as the tissue, once removed, immediately starts to change through decomposition. Biologist Harold Hillman often pointed out the faults in trying to establish credible information about what occurs inside living beings from the study of dead tissues:
“Killing an animal changes its biochemistry grossly. For example, its blood carbon dioxide, phosphate, lactate, and potassium ion concentrations, rise, while its oxygen, sodium ion, adenosine triphosphate, phosphocreatine, concentrations go down. These changes affect much of the tissue metabolism. It is hoped and normally assumed that they will reverse during incubation. There is no realistic way of testing this, since the volume and chemistry of the tissue changes during incubation. In this circumstance, it is worth asking whether cell biologists should use tissues in vitro at all. Perhaps, they should confine their experiments to working on intact animals and human beings, tissue cultures, unicellular organisms and plants.”
The current “gold standard” used to study the dead brain tissue for the diagnosis of rabies is known as the direct fluorescent antibody test. As the name implies, the test looks to detect rabies antigens on the brain by using antibodies said to be specific to the rabies “virus:”
Direct Fluorescent Antibody Test
“The dFA test is based on the observation that animals infected by rabies virus have rabies virus proteins (antigen) present in their tissues. Because rabies is present in nervous tissue (and not blood like many other viruses), the ideal tissue to test for rabies antigen is brain. The most important part of a dFA test is flouresecently-labeled anti-rabies antibody. When labeled antibody is incubated with rabies-suspect brain tissue, it will bind to rabies antigen. Unbound antibody can be washed away and areas where antigen is present can be visualized as fluorescent-apple-green areas using a fluorescence microscope. If rabies virus is absent there will be no staining.”
According to the CDC, in the 50 years that the dFA test has been used to detect rabies, it has not failed to present reliable and accurate results. This indirect method is somehow said to be more sensitive and specific than actually “isolating” the “virus,” thus the “gold standard” label. It is also stated by the CDC that the saliva of an infected animal contains millions of “virions,” making the lack of any purified and isolated “virus” and the reliance on indirect antibody testing all the more glaring of an issue:
Accuracy of the Tests
“During the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person.
Because of its high sensitivity and specificity,in comparison to virus isolation methods, the DFA test is the “gold standard” diagnostic method for rabies and has been rigorously evaluated by international, national, and state health laboratories. The DFA test is currently the only recommended diagnostic method for routine rabies determination in animals in the United States.
During clinical disease, millions of viral particles may be found intermittently in the saliva. In theory, only a single rabies particle or virion is required to result in a productive infection.”
Returning to the WHO’s rabies manual, it shows us exactly how the dFA is used and how the diagnosis is determined based on the interpretation of the person reading the results. The interpreter uses an antigen fluorescence intensity and distribution scale from +4 on down to +1 to determine one of four conclusions: positive, negative, unsatisfactory, or inconclusive. Obviously, the subjective bias of the interpreter plays no role in the accuracy of the determination as humans rarely make interpretive errors, correct?:
In fact, there are many drawbacks to using the dFA as the “gold standard” test for rabies diagnosis beyond the aforementioned use of dead tissues. For starters, due to the lack of ever properly purifying and isolating the rabies “virus” directly from the saliva said to contain millions of “virions,” any antibody result is utterly meaningless as there is no “virus” to determine a specific reaction with. We also have this same purification/isolaton problem with antibodies as these entities have also never been taken and separated directly from the fluids of a host in order to be studied independently. There is also the issue that the theoretical antibodies themselves are entirely non-specific and are regularly said to bind to proteins that are not the intended target. Thus, we once again run into the problem where one fictional entity (the rabies “virus”) is said to be detected by another fictional entity (the antibody). It is very telling that the CDC believes that the interpretive results from this indirect circular test is more accurate than actually finding and “isolating” the supposed “virus.”
Thus, we must ask ourselves if these dFA tests really are as accurate as stated by the CDC. If we do so, we find out that this is most definitely not the case according to these next three sources. This first snippet comes from a study done on bacteria which points out the obvious fault of the subjective interpretation of the dFA test results which leads to poor sensitivity and a widely varying specificity, contrary to the claims made by the CDC:
“Direct fluorescent-antibody testing (DFA) provides a much more rapid result but also has the disadvantage of poor sensitivity, and its specificity varies widely due to the subjective interpretation of test results.”
This second study also points out the flaws of the subjective interpretation of the test results as well as the need for expensive equipment and quality-controlled reagents, the varied parameters utilized for succesful results and the issues relating to the incubation times and temperatures, as well as the necessity of having well-trained personnel running and interpreting the results:
“However, DFA has several drawbacks such as the need for an expensive fluorescent microscope, well-trained personnel, and quality controlled reagents (antibodies, conjugates), and varied parameters used during microscopy, and incubation times and temperatures, not to mention the subjectivity in interpretation of the test results [27,28,29,30]. In addition, acetone used as fixative in DFA does not completely inactivate the virus, as demonstrated by the infectivity of acetone-fixed tissue for neuroblastoma cells [31], posing a potential biohazard to laboratory personnel. Indeed, complete inactivation of cell culture-derived rabies virus appears to require >30% acetone [32].”
And finally, from this 2017 study published in PLOS Neglected Tropical Diseases, we can once again see the problems with subjective interpretation of dFA test results in action. The study utilized 23 independent laboratories to aid in identifying “differences in the laboratory protocols that could explain discrepant laboratory results and provide baseline knowledge for regional standardization of protocols.” The labs were each sent 20 samples which included 17 test samples and 3 controls. The positive tissues contained major rabies “virus” variants that were circulating in the Americas while the negative samples consisted of tissues demonstrating complete absence of rabies “virus” antigen and artifacts. Each lab was asked to test the samples using their own standard protocols and to record their results (positivity, intensity, and distribution of the fluorescence staining) as well as the microscopic condition and impression quality of the tissues (Good, Acceptable, or Deficient) as evaluated by the laboratory operator. The results from this 2017 study indicated that there are substantial differences in the overall dFA results and test interpretation as the “level of concordance between the 23 participating laboratories and the CDC panel showed large variability.” Only two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories:
An inter- laboratory proficiency testing exercise for rabies diagnosis in Latin America and the Caribbean
“Our results indicate that although all laboratories can perform the direct fluorescent antibody test, there are substantial differences in the overall results and test interpretation. This study identified important gaps in standardization and/or harmonization between laboratories which could be overcome and corrected with appropriate DFA protocols standardized across the LAC, including its broad distribution and proper training.”
“Conclusive rabies diagnosis can only be achieved by appropriate laboratory testing. Clinical and epidemiological diagnosis is challenging and leads to under-reporting [1, 2, 3]. The Direct Fluorescent Antibody test (DFA) for detection of rabies virus antigen remains as the gold standard test for laboratory diagnosis of rabies in post-mortem brain tissues [3].”
“The agreement between the laboratory results and those of the CDC, as measured by the sensitivity, specificity, concordance and kappa values are shown in Table 2. Two laboratories correctly identified all samples tested (sensitivity and specificity of 1.0). However, 30% (7/23) of all laboratories reported at least one false positive and 83% (19/23) of all laboratories reported at least one false negative sample. The average sensitivity was 76% with a range of 40% to 100%. The average specificity was 88% with a range of 22% to 100%. While a majority of the laboratories had low false positive rates, there were considerable differences in the sensitivity (Fig 1).The mean concordance was 81% with a range of 50% to 100% and the mean kappa score was 0.56 with a range of 0.02 to 1.00.”
“The level of concordance between the 23 participating laboratories and the CDC panel showed large variability. Two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories.”
“The type of conjugate may also affect the sensitivity of the DFA test (monoclonal cocktail versus polyclonal, in-house made versus commercial). For the current exercise, laboratories used commercial (65%) or in-house (35%) conjugates. A study of 12 rabies reference laboratories in Europe demonstrated that the variability of conjugates could potentially lead to discordant results and influence assay sensitivity [19].”
A bunch of glowing green dots means…absolutely nothing.In answer to the claim by the CDC that “during the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person,” we can safely conclude that this is obviously a false statement. The dFA test has been shown to have low sensitivity and a widely varying specificity as well as major issues relating to the subjective interpretation of the results based upon the person doing the interpreting. The 23 labs participating in the 2017 study had large variability in concordance with the CDC’s own panel. Anyone looking at this indirect test with a shred of intellectual honesty can easily see that the CDC’s “golden standard” rabies test does not look so golden anymore.
While the dFA test is the “go to” diagnostic measure in modern times, there are other methods available which can be used in an attempt to claim an animal is infected with the rabies “virus.” One of these is the “isolation” of the “virus” in tissue and cell cultures, which used to be the “gold standard” method for proving a “virus” exists and is infectious. Oddly enough, the CDC stated that the supposed “isolation” of the rabies “virus” is not as sensitive nor as specific as the dFA test. How could this possibly be the case?
For one thing, it is admitted that the rabies “virus” does not actually produce the desired cytopathogenic effect (CPE) when cultured:
Detection of rabies virus replication: inoculation tests
“The other group of available techniques aim at detecting the replication of the virus on living substrates, e.g. cells. Virus isolation may be necessary to confirm inconclusive results in FAT/dRIT and for characterization of the virus strain. In neuroblastoma cells, rabies virus grows generally without cytopathic effect; once again it is necessary to use FAT to confirm the presence of rabies virus.After intracranial application, rabies induces clinical signs in mice that are relatively typical but have to be confirmed by FAT. Since cell culture is as sensitive as the mouse inoculation test, units should be established in laboratories to replace mouse inoculation tests as it avoids the use of life animals, is less expensive and gives more rapid results.”
Why is this important to note? The cytopathogenic effect (CPE) is the structural and morphological changes to the cell that are claimed to be caused by the “virus” as it enters the cell, breaking it apart as the “virus” creates more copies of itself. This effect is supposed to tell the researchers that the “virus” is present within the culture. According to their stories, without this effect, it should be a clear indicator that the host was not infected by the “virus.” However, virology loves to bend their own rules and in a clear cut case of having their cake and eating it too, virologists claim that certain “viruses” do not cause CPE in their natural host cells. They state that there are different levels of CPE based on the cell type used:
Not permissive cell – virus cannot infect
Permissive cell – virus can replicate, but does not cause obvious CPE
Highly permissive cell – virus replicates and induces an obvious CPE
Anyone looking at this logically can see that “Not permissive” and “Permissive” cells are the exact same thing. Neither of these cells produce CPE when “infected” by the “virus.” However, virologists will resort to other indirect measures in order to claim the “virus” is present in spite of the lack of any CPE observed. In the case of rabies, the dFA test is used to confirm if a “virus” is present in a culture. However, if the dFA test is considered inconclusive, the cell culture is used to confirm the dFA result. A bit circular there, don’t you think? Another confirmation is done by injecting the toxic CPE-less cell culture soup into the brain of a mouse and seeing if symptoms occur. If so, the mouse is killed and the newly damaged brain is taken and tested by dFA for confirmation. Seeing the problem yet?
Toxic cell-cultured goo injected directly into the brain causing brain damage. It must be the “virus” and not the method… ?
If neither dFA and/or cell culturing is enough satisfactory indirect evidence to claim the existence of the rabies “virus,” one can turn to the old ways of histopathology to try and build a circumstantial case against the invisible entity. Along with attempting to diagnose someone based on clinical symptoms, which thanks to Louis Pasteur and “false rabies” we know is inaccurate due to the non-specificity of the symptoms, histopathology was the main method utilized for decades for determining if an animal was in fact rabid. This consisted of staining the brain tissues with chemicals such as hematoxylin and eosin and looking for patterns of encephalopathy as well as the presence of what are called Negri bodies. Negri bodies are round or oval inclusions within the cytoplasm of nerve cells of animals which were discovered by Dr. Adelchi Negri in 1903. At the time, he claimed that these inclusions were the etiologic agent of rabies. While the rest of the virology community disagreed with Dr. Negri, his discovery was considered a tell-tale sign of rabies infection in the brain and finding these inclusions served as the basis for a rabies diagnosis for over 60 years. However, there is rather big problem for these histopathological examinations. Signs of encephalitis and finding Negri bodies are both entirely non-specific and are seen in cases that have absolutely nothing to do with rabies. In fact, Negri bodies are said to only be found in half of the cases of rabies:
Histologic examination, General histopathology
“Histologic examination of biopsy or autopsy tissues is occasionally useful in diagnosing unsuspected cases of rabies that have not been tested by routine methods. When brain tissue from rabies virus-infected animals are stained with a histologic stain, such as hematoxylin and eosin, evidence of encephalomyelitis may be recognized by a trained microscopist. This method is nonspecific and not considered diagnostic for rabies.
Before current diagnostic methods were available, rabies diagnosis was made using this method and the clinical case history. In fact, most of the significant histopathologic features (changes in tissue caused by disease) of rabies infection were described in the last quarter of the 19th century. After Louis Pasteur’s successful experiments with rabies vaccination, scientists were motivated to identify the pathologic lesions of rabies virus.
Histopathologic evidence of rabies encephalomyelitis (inflammation) in brain tissue and meninges includes the following:
Mononuclear infiltration
Perivascular cuffing of lymphocytes or polymorphonuclear cells
Lymphocytic foci
Babes nodules consisting of glial cells
Negri bodies
Negri bodies
In 1903, most of the histopathologic signs of rabies were recognized, but rabies inclusions had not yet been detected. At this time, Dr. Adelchi Negri reported the identification of what he believed to be the etiologic agent of rabies, the Negri body.In his report, he described Negri bodies as round or oval inclusions within the cytoplasm of nerve cells of animals infected with rabies. Negri bodies may vary in size from 0.25 to 27 µm. They are found most frequently in the pyramidal cells of Ammon’s horn, and the Purkinje cells of the cerebellum.
They are also found in the cells of the medulla and various other ganglia. Negri bodies can also be found in the neurons of the salivary glands, tongue, or other organs. Staining with Mann’s, giemsa, or Sellers stains can permit differentiation of rabies inclusions from other intracellular inclusions. With these stains, Negri bodies appear magenta in color and have small (0.2 µm to 0.5 µm), dark-blue interior basophilic granules.
The presence of Negri bodies is variable. Histologic staining for Negri bodies is neither as sensitive nor as specific as other tests. Some experimentally-infected cases of rabies display Negri bodies in brain tissue; others do not. Histologic examination of tissues from clinically rabid animals show Negri bodies in about 50% of the samples; in contrast, the dFA test shows rabies antigen in nearly 100% of the samples. In other cases, non-rabid tissues have shown inclusions indistinquishable from Negri bodies. Because of these problems, the presence of Negri bodies should not be considered diagnostic for rabies.”
Whoever wants to point at random circles seen in fixed and stained dead tissues and then make wild guesses about their importance, raise your hand! ️
As the Negri bodies played such a substantial role in determining the diagnosis of rabies and building the case statistics used to sell the public on a “virus” in need of vaccination and eradication, let’s look at two more studies to find out a bit more about these non-specific diagnostic blobs. In 1942, it was already well known that the Negri bodies were not specific to rabies and could be mistaken for other inclusion bodies seen in the tissues upon examination. This is a rather big deal as the mass vaccination of dogs didn’t start for another 5 years in 1947. So we can already see that the main method used for diagnosis was faulty which casts doubt on any rabies statistics generated up to that time using this method. The authors go on to admit that there were deficiencies in the method used for examining these inclusions. It is stated that every experienced microscopist encountered difficulty in deciding whether or not the bodies observed were in fact Negri bodies or whether they were instead normal or possibly distorted cytoplasmic structures. In the study of 84 mice said to be given rabies by way of injection, Negri bodies were only found in the hippocampus 8 times as well as only 4 times in the cerebral cortex. The authors concluded that there are many rabies cases without Negri bodies present upon examination and that there are various structures which resemble Negri bodies commonly found in normal animals:
Problems in the Laboratory Diagnosis of Rabies*
“THE diagnosis of rabies in the laboratory is based entirely upon the microscopic demonstration of Negri bodies and upon animal inoculation. The demonstration of Negri bodies is the method of choice since the diagnosis can be thus made in a few minutes or hours. When the technic employed demonstrates typical bodies the result is highly convincing and satisfying. However, negative and doubtful results leave much to be desired, and animal inoculation must be resorted to. The difficulties in demonstrating Negri bodies arise from two sources of error which can be enumerated as inability to differentiate them from other inclusion bodies and cell structures, and inherent deficiencies in the methods of examination.”
“However, every experienced microscopist has encountered the difficulty of deciding whether the bodies observed in some preparations are Negri bodies or cytoplasmic structures normal to the cell or if not normal at least only distorted cellular structures. Goodpasture refers to the variation in size of Negri bodies and speaks of being able to demonstrate the smallest forms. When small bodies are associated with large ones, which show the typical inner structure, no confusion is encountered. When, however, only forms so small occur that the demonstration of the “Innenkorper” is doubtful, the diagnosis is doubtful. The brain of cats, particularly, offers difficulty because of the pink staining granular material in the cells and also because the Negri bodies in the pyramidal and Purkinji cells of this animal are often very small. The failure of the microscopic diagnosis of rabies as proved by mouse inoculation is shown in Table 1.”
“Above we have mentioned the occasional occurrence of what appear to be “lyssa bodies” or small Negri bodies in the brain of some animals which did not produce rabies when injected into mice. These bodies are found most frequently in the cerebrum and medulla. Since in the study of 84 cases of rabies proved by mouse inoculation we found Negri bodies only in the hippocampus 8 times and only in the cerebral cortex 4 times (Table 2), the finding of eosinophilic bodies in any portion of a brain from an animal suspected of having had rabies creates a doubt as to the diagnosis.”
“From these results it appears that by microscopic examination of sections and in some smears we are able to demonstrate eosinophilic bodiesresembling “lyssa bodies” and atypical Negri bodies which are not associated in the brain with rabies virus. Also the results show that brain specimens in which the microscopic examination leaves the diagnosis in doubt contain rabies. The bodies that cause this confusion in the microscopic diagnosis of rabies are similar to ones found in certain parts of the brain of normal cattle and other animals and to atypical or small Negri bodies.”
doi: 10.2105/ajph.32.2.171.
While the 1942 study should have been the end of the Negri body as a diagnostic indicator of rabies, this method carried on being used over the decades. In 1975, another study emerged casting doubts on the dogma surrounding these long-held markers of the rabies disease. It’s stated that there was a universal acceptance of the Negri body as a specific indicator of rabies and that due to this widely-endorsed dogma, every time a Negri body was seen, a rabies diagnosis was made irrespective of the circumstances regarding the case.
However, in this study, a case was reported of a person who was considered rabies free by way of dFA and electron microscopy but Negri bodies were still found upon examination. This finding was inconsistent with the idea of the specificity of these bodies to rabies. The author pointed out many flaws with the use of Negri bodies as a diagnostic tool as outside of finding them upon examination, rabies is non-specific and mimics other diseases such as smallpox. It is stated that rabies encephalitis does not have any pathognomonic clinical or pathologic features distinguishing it from other diseases. The absence of Negri bodies in a substantial number of fatal cases of rabies, the lack of any inflammatory response, the absence of any history of animal contact in more than 30% of fatal cases, and the lack of specific behavioral symptoms of rabies in animals led the author to the conclusion that any association between this diagnostic method and the rabies disease is unwarranted. Thus, it is easy to see that any and all rabies case statistics based upon the clinical diagnosis and findings of Negri bodies should be thrown out:
Is the Negri Body Specific for Rabies?
“Of all viral diseases affecting the nervous systems of humans and animals, rabies seems to be the only one in which light microscopy alone can provide a definitive etiologic diagnosis. This is based on the universally accepted conviction on the specificity of the Negri body for rabies. Thus, the presence of a Negri body in the brain of a patient who did not have rabies is a matter that deserves attention.”
“Neuropathologically, the exclusion of rabies in the present case is based on the negative immunofluorescent
study results for rabies and the absence of the rabies virus within the Negri bodies (light microscope) as demonstrated by electron microscopy. Such an observation, of course, is inconsistent with the specificity of the Negri body in signifying the presence of rabies. Therefore, it is reasonable to ask: What are the other inclusion bodies that occur in sites other than the nervous system that are morphologically similar to Negri body?”
“The result of a universally accepted dogma such as this is obvious; in every instance in which a “Negri body” has been seen, a diagnosis of rabies was made irrespective of the circumstances.
To delineate some of the related aspects of the problem the following points deserve etnphasis:
Except for the occurrence of theNegri body, rabies encephalitis does not have any pathognomonic clinical or pathologic features. Variola-vaccinia virus, for example, can produce the same clinical pictures. The cutaneous manifestations can be sufficiently scanty to be missed on the physical examination, or they can be absent altogether (variole sans eruptione). There is remarkable variability in the intensity of cellular inflammatory response in rabies encephalitis. This, to some extent, may reflect the vigor with which these reactions are searched for, since the diagnostic efforts in the past have been mainly directed to the “specific” finding of the Negri body. The absence of Negri bodies in a substantial number of fatal cases of rabies and the remarkable lack of inflammatory response in some instances of the disease signify the importance of obtaining a careful history. A definitive etiologic diagnosis of rabies, however, requires obtaining positive results with immunofluorescent or electron microscopical methods or both. The former method maps the occurrence of rabies viral antigen in any morphologic form (with or without the presence of the inclusions), and the latter defines the characteristic bullet-shaped virus.
Absence of history of animal contact has been reported in more than 30% of fatal cases of rabies. Here, also, it is the unquestioned association between the Negri body and rabies that constitutes the sole ground for a definitive etiologic diagnosis. The latter report is remarkable for the absence of history of animal contact and the occurrence of the fatal illness one week after vaccination for smallpox. Even in the presence of history of animal contact, it should be remembered that such an association is unwarranted as the behavioral alterations in the animals are not pathognomonic of any one disease.
It is conceivable that the failures of antirabies therapy and the occurrence of false negative immunofluorescent results are related to the non-specificity of the Negri body for rabies.
In no other viral disease is the light microscopy alone an accepted method for the definitive etiologic diagnosis of a disease.
The validity of the present observations needs confirmation by other observers and the answer will be found “not by dogma or skepticism but by open-minded uncertainty.”
doi: 10.1001/archneur.1975.00490440025002.
In Summary:
According to the Institut Pasteur, Louis Pasteur’s initial efforts to isolate the rabies “virus” proved unsuccessful as the “virus” remained invisible
The “virus” was not seen until almost a century later, in 1962, with the advent of electron microscopy
Louis Pasteur had the idea of inoculating part of a rabid dog’s brain directly into another dog’s brain, causing the inoculated dog to subsequently die
Inoculation with saliva (where the “virus” is supposedly found) was found to be a method which did not always produce rabies and symptoms did not declare themselves for months
Pasteur accordingly inoculated a number of animals subcutaneously with some of the brain substance from other animals which had died of rabies
Most of those inoculated developed rabies, but not all
Pasteur’s idea of introducing into the brain of experimental animals some of the nerve tissue from an animal which had died of rabies was based on the principle (i.e. assumption) of providing the causal organisms with the nutritive medium best suited to their requirements
There is a very high degree of uncertainty in the correlation between animal bites and the subsequent appearance of rabies-even when the biting animal is certifiably rabid
While the mortality of clinical rabies is “virtually 100 percent,” the threat of death from the bite of a rabid animal is vastly less
Estimates of the risk of contracting rabies from the bites of animals known to be rabid range from as high as 80 percent to as low as 0.5 percent
Pasteur himself estimated that 16 percent of those bitten by rabid dogs would eventually die of rabies unless they submitted to his new treatment
In 1887, the English Commission on Rabies drew attention to the uncertainty of all statistics on rabies citing:
The difficulty of establishing that the attacking animal had in fact been rabid
The variable effects of the location and depth of bites
Differences in the lethality of rabid animal bites in different species and races
The possible prophylactic effects of cauterization or other treatments applied to bitten victims before they submitted to Pasteur’s treatment
The commission also suspected that at least one man may have died as a direct result of the Pastorian injections, and in the end it favored strict regulations on potentially rabid animals (muzzling and quarantine) over Pasteur’s more drastic remedy
The great majority of the victims of rabid animal bites could forgo Pasteur’s treatment without experiencing any untoward consequences in the future
Pasteur himself later pointed out some of the uncertainties surrounding the diagnosis of rabies
Pasteur cited two cases in which symptoms of the disease had been induced solely by fearwithout any animalbite as well as another case which was induced by alcoholism
Pasteur had a vested interest in emphasizing the difficulty of diagnosing rabies as he was then defending himself against allegations that his rabies vaccine not only sometimes failed to protect those who submitted to it, but in some cases was itself the cause of rabies and therefore death
In defense of his vaccine, Pasteur now emphasized the extent to which symptoms like those of rabies could appear in patients who did not have the disease
According to the CDC, the diagnosis of rabies can be made after detection of rabies “virus” from any part of the affected brain, preferably the brain stem and cerebellum
The test requires that the animal be euthanized
According to biologist Harold Hillman: “Killing an animal changes its biochemistry grossly. For example, its blood carbon dioxide, phosphate, lactate, and potassium ion concentrations, rise, while its oxygen, sodium ion, adenosine triphosphate, phosphocreatine, concentrations go down. These changes affect much of the tissue metabolism.”
Hillman felt that “it is worth asking whether cell biologists should use tissues in vitro at all”
The current “gold standard” test used to detect the “virus” on the brain tissue is the direct fluorescent antibody test (dFA)
The dFA test is based on the “observation” that animals infected by rabies “virus” have rabies “virus” proteins (antigen) present in their tissues
Because rabies is present in nervous tissue (and not blood like many other “viruses”), the ideal tissue to test for rabies antigen is brain
When labeled antibody is incubated with rabies-suspect brain tissue, the story goes that it will bind to rabies antigen and unbound antibody can be washed away so that areas where antigen is present can be visualized as fluorescent-apple-green areas using a fluorescence microscope
According to the CDC, during the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person
The CDC states that because of its high sensitivity and specificity, in comparison to “virus” isolation methods, the DFA test is the “gold standard” diagnostic method for rabies (way to shoot “virus” isolation in the foot there CDC…)
During clinical disease, millions of “viral” particles may be found intermittently in the saliva(which makes one wonder why they must kill an animal and do indirect antibody tests on decomposing brain tissue for diagnosis rather than properly purify and isolate the “virus” directly from the saliva supposedly containing millions of these entities)
In theory, only a single rabies particle or “virion” is required to result in a productive infection
The dFA results are based upon the opinion of an interpreter who uses an antigen fluorescence intensity and distribution scale from +4 on down to +1 to determine one of four conclusions: positive, negative, unsatisfactory, or inconclusive
The dFA test has the disadvantage of poor sensitivity, and its specificity varies widely due to the subjective interpretation of test results
The subjectivity in interpretation of the test results
According to a 2017 study testing and reviewing dFA with the help of numerous labs, the results indicated that although all laboratories can perform the direct fluorescent antibody test, there are substantial differences in the overall results and test interpretation
The authors stated that conclusive rabies diagnosis can only be achieved by appropriate laboratory testing as clinical and epidemiological diagnosis is challenging and leads to under-reporting
The agreement between the laboratory results and those of the CDC, as measured by the sensitivity, specificity, concordance and kappa values:
Only two laboratories correctly identified all samples tested (sensitivity and specificity of 1.0)
However, 30% (7/23) of all laboratories reported at least one false positive and 83% (19/23) of all laboratories reported at least one false negative sample
The average sensitivity was 76% with a range of 40% to 100%
The average specificity was 88% with a range of 22% to 100%.
While a majority of the laboratories had low false positive rates, there were considerable differences in the sensitivity
The mean concordance was 81% with a range of 50% to 100% and the mean kappa score was 0.56 with a range of 0.02 to 1.00
The level of concordance between the 23 participating laboratories and the CDC panel showed large variability
Two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories
The type of conjugate may also affect the sensitivity of the DFA test (monoclonal cocktail versus polyclonal, in-house made versus commercial)
A study of 12 rabies reference laboratories in Europe demonstrated that the variability of conjugatescould potentially lead to discordant results and influence assay sensitivity
Another method for diagnosing rabies is the “isolation” of the “virus” by tissue or cell culture
“Virus isolation” may be necessary to confirm inconclusive results in dFA/dRIT and for characterization of the “virus” strain
In neuroblastoma cells, rabies “virus” grows generally without cytopathic effect
In a bit of cirular reasoning, it is necessary to use dFA to confirm the presence of rabies “virus” by way of cell culture whereas cell culture may also be used to confirm inconclusive dFA results
After intracranial (in the brain…some things never change)application, rabies induces clinical signs in mice that are relatively typical but have to be confirmed by dFA (i.e. the mouse that has had toxic cell culture goo injected into its brain causing symptoms must then be killed to have its cell-culture damaged brain examined by dFA to confirm the infection)
Histologic examination of biopsy or autopsy tissues looking for signs of encephalitis is occasionally useful in diagnosing unsuspected cases of rabies that have not been tested by routine methods
However, this method is nonspecific and not considered diagnostic for rabies
Before current diagnostic methods were available, rabies diagnosis was made using this method and the clinical case history(i.e. non-specific and not suited for diagnostic methods were used to identify rabies for most of the 19th and 20th century)
Histopathologic evidence of rabies encephalomyelitis (inflammation) in brain tissue and meninges includes the following:
Mononuclear infiltration
Perivascular cuffing of lymphocytes or polymorphonuclear cells
Lymphocytic foci
Babes nodules consisting of glial cells
Negri bodies
In 1903, Dr. Adelchi Negri reported the identification of what he believed to be the etiologic agent of rabies, the Negri body
In his report, he described Negri bodies as round or oval inclusions within the cytoplasm of nerve cells of animals infected with rabies
While this was the main method of diagnosing rabies for over 60 years, the presence of Negri bodies is variable
Histologic staining for Negri bodies is neither as sensitive nor as specific as other tests
Some experimentally-infected cases of rabies display Negri bodies in brain tissue; others do not
Histologic examination of tissues from clinically rabid animals show Negri bodies in about 50% of the samples
In other cases, non-rabid tissues have shown inclusions indistinquishable from Negri bodies
Because of these problems, the presence of Negri bodies should not be considered diagnostic for rabies
Despite these problems, until the mid-1960’s the diagnosis of rabies in the laboratory was based entirely upon the microscopic demonstration of Negri bodies and upon animal inoculation
According to a study from 1942, the demonstration of Negri bodies was the method of choice since the diagnosis can be thus made in a few minutes or hour
However, the authors admitted that the difficulties in demonstrating Negri bodies arose from two sources of error which could be enumerated as theinability to differentiate them from other inclusion bodies and cell structures, and inherent deficiencies in the methods of examination
Every experienced microscopist has encountered the difficulty of deciding whether the bodies observed in some preparations are Negri bodies or cytoplasmic structures normal to the cell or if not normal at least only distorted cellular structures
In the study of 84 cases of rabies proved by mouse inoculation they found Negri bodies only in the hippocampus 8 times and only in the cerebral cortex 4 times
The authors determined that the finding of eosinophilic bodies in any portion of a brain from an animal suspected of having had rabies creates a doubt as to the diagnosis
From their results it appeared that by microscopic examination of sections and in some smears, they were able to demonstrate eosinophilic bodies resembling “lyssa bodies” and atypical Negri bodies which are not associated in the brain with rabies “virus”
Also the results showed that brain specimens in which the microscopic examination leaves the diagnosis in doubt contain rabies (i.e. they determined that injecting mice in the brain caused rabies without finding Negri bodies)
The bodies that cause this confusion in the microscopic diagnosis of rabies are similar to ones found in certain parts of the brain of normal cattle and other animals and to atypical or small Negri bodies
In a 1975 study, it is stated that rabies is the only “virus” that can be diagnosed by light microscopy based on the universally accepted conviction on the specificity of the Negri body for rabies
However, the authors presented a case of a patient without rabies as determined by negative immunofluorescent study results for rabies and the absence of the rabies “virus “within the Negri bodies (light microscope) as demonstrated by electron microscopy
Such an observation was inconsistent with the specificity of the Negri body in signifying the presence of rabies
The result of this universally accepted dogma led to every instance in which a “Negri body” was seen being diagnosed as rabies irrespective of the circumstances
Except for the occurrence of the Negri body, rabies encephalitis does not have any pathognomonic clinical or pathologic features (i.e. non-specific and overlapping symptoms associated with many diseases)
Variola-vaccinia(Smallpox) “virus,” for example, can produce the same clinical pictures
There is remarkable variability in the intensity of cellular inflammatory response in rabies encephalitis
The diagnostic efforts in the past have been mainly directed to the “specific” finding of the Negri body
The absence of Negri bodies in a substantial number of fatal cases of rabies and the remarkable lack of inflammatory response in some instances of the disease signify the importance of obtaining a careful history
Absence of history of animal contact has been reported in more than 30% of fatal cases of rabies
In these cases, it is the unquestioned association between the Negri body and rabies that constitutes the sole ground for a definitive etiologic diagnosis
Even in the presence of history of animal contact, it should be remembered that such an association is unwarranted as the behavioral alterations in the animals are not pathognomonic of any one disease (i.e. there are many diseases which are said to cause the same symptoms in animals)
It is conceivable that the failures of antirabies therapy and the occurrence of false negative immunofluorescent results are related to the non-specificity of the Negri body for rabies
In no other “viral” disease is the light microscopy alone an accepted method for the definitive etiologic diagnosis of a disease
The author concludes that the answers to the observations made will be found “not by dogma or skepticism but by open-minded uncertainty.”
When one looks into the history of rabies and the methods used to diagnose the disease, it becomes undeniable that the mythical status that surrounds this fear-based fictional narrative fed to the masses throughout the centuries is entirely unjustified and unwarranted. There is literally nothing there in support of rabies as a distinct disease caused by a specific “virus” that is transmitted to humans through the bite of a sick animal. If we were to lay out the facts in front of a jury, it would be an easy conviction:
The pivotal moments of discovery in the late 19th century were built upon the fraudulent foundations laid out by Louis Pasteur, a man who manipulated and massaged his own data in order to sell his theories and his vaccine for fame and fortune.
The supposed “isolation” of the “virus” didn’t even take place until nearly a century after Pasteur admitted to never identifying a causative agent and yet it missed the necessary requirement of showing any indirect evidence of the “virus” highjacking the cell as the culture lacked any evidence of the cytopathogenic effect.
The actual correlation between animal bites and symptoms of disease was considered highly uncertain and those who were attacked and bitten by clearly rabid animals could easily forgo any treatments without any ill health effects.
The incubation period for the disease is inconsistent and is said to range anywhere from 6 weeks on up to 25 years before the development of symptoms.
The severe symptoms associated with rabies are a rare occurrence in nature and are in fact seen most frequently as an adverse reaction to the vaccine said to contain neurotropic ingredients.
The acknowledgment by Pasteur of “false rabies,” which was said to be brought about solely by FEAR of aquiring the disease as well as alcohol and/or drug use, was used to take attention away from his vaccine causing injury and death.
The statistics regarding rabies cases were considered unreliable due to the lack of any specifuc disease-defining symptoms as many diseases in animals and humans mimic the clinical picture.
The diagnosis of rabies, for much of its history, relied upon clinical symptoms and the histopathological findings related to encephalitis and Negri bodies, all of which are non-specific and are not suitable as a diagnostic measure for the disease, thus calling into question any case statistics related to rabies.
The only way to claim pathogenicity of the “virus” is by way of the completely unnatural route of intracranial inoculation of diseased brain and nervous tissues directly into the brains of dogs and mice.
The more recent modern method of direct fluorescence antibody tests, considered the “gold standard” diagnostic test, is claimed to be highly sensitive and specific, yet the results of the tests are open to human interpretation and have been shown in reviews to have low sensitivity and varied specificity.
The narrative surrounding rabies is based upon many primal fears. It plays on the fear of death, the fear of the unknown, and the fear of mutilation. Just like the rabid animal lurking in the shadows ready to strike, the “virus” hides inside the body once infected, waiting for the right moment to unleash a painful and excruciating death unless the infected leaps for the miracle cure in time. If they are a moment too late and the symptoms set in, it’s game over. This same scenario is regularly sold to the masses in our daily entertainment with the recent zombie craze. One must be afraid of the bite. Once bitten, the “virus” takes hold and the victim is condemned to certain death.
However, just as Louis Pasteur recounted tales of the fearful succumbing to the exact same symptoms in absence of any animal bite, we must realize that the real enemy here is not a “virus” but an ingrained fear that stems from outdated and unproven fictional narratives. Moreso than any of the other more common diseases of the time such as smallpox and syphilis, rabies was the perfect mascot to convince the doubting public that disease-causing pathogens exist, can be transmitted, and can be prevented by way of vaccination. The imagery of the dirty mangled dog stumbling down the road, frothing at the mouth and seeking its next victim to transfer its parasitic contents into was a powerful visual tool for pathogens that remained nothing but formless thoughts at the time.
However, the evidence consistently shows us that there is no dangerous invisible entity waiting in the wings inside the saliva of a rabid animal looking to seep into the open wound of a bite mark. There is no reason for any victim of an animal attack to subject themselves to the toxic treatments based upon the fear of an impending gruesome death. Just as there are no zombies coming for your brains, there is no frothing rabies “virus” looking to do the same. The foundation for germ theory and vaccination established by Pasteur was never built from any purified and isolated “virus” shown scientifically to exist in nature. It was built upon the only “virus” that has ever truly existed: the “virus” of fear.
For an excellent breakdown of the rabies fraud, please see Dr. Sam Bailey’s What About Rabies? video:
I’m moving on from Part 1 into a completely different area.
There is lab work in the sciences that crucially affects populations. Two examples: virologists claiming they’ve isolated SARS-CoV-2; and researchers deciding they’ve found a way to adapt RNA technology to produce a COVID vaccine.
In the first case, the purported discovery of SARS-CoV-2 enabled the launch of the global pandemic announcement, which eventually led to the lockdowns and the crashing of economies. In the second case, the RNA-vaccine “breakthrough” led to the vaccination of billions of people, and massive numbers of injuries and deaths.
These are crucial effects, to say the least.
And yet, those on the outside, who have no access to these labs AS THE WORK IS BEING DONE, those who are independent scientists and analysts and can only read the studies once they are published—
—This is an unconscionable situation, when you stop and think about it.
The whole world is changed by the research, but we can’t watch it IN PROGRESS.
People have been brainwashed into thinking this lack of access to labs is normal. Standard. Non-official persons entering these labs and tracking the work step by step would amount to a criminal invasion. That’s what we’re supposed to believe:
“Just accept our statements about our findings and shut up and obey.”
“We’re the pros. You’re the idiots.”
“We’re certified. You’re the guinea pigs.”
“Call security, call the FBI, call DHS, terrorists are trying to break into our lab.”
“This is a holy sanctum, anointed by God. You’re a mortal sinner.”
Here’s my kind of debate on the existence of SARS-Cov-2. Here’s my bottom, bottom line.
Virologists are compelled to replicate, in the lab, the so-called discovery of SARS-CoV-2. An outside team of truly independent scientists and journalists is present.
So is a camera crew. With many cameras. And many mics.
The team watches every single move the virologists make. Any member of the team can stop the work and ask a question or criticize a move.
The questions and answers and the criticisms and replies are all recorded. Ditto for every action the virologists take.
THIS is a REAL debate. The most real debate.
“Wait. That’s ridiculous. You can’t expect these highly trained virologists to submit themselves to this kind of…inspection.”
Of course I can.
For example: Our team member in the lab says, “All right, you’re observing that the monkey cells and the human cells in this soup you’ve created are dying off. You claim the killer must be ‘the virus’ in the patient’s tissue sample—the sample you dropped in the soup. You claim nothing else in the soup could be killing the cells. So let me ask you this? Where is the control experiment?”
“The what?”
“The control. My, my. You really forgot about that?”
“I don’t understand. Turn off the cameras.”
“Leave them on, boys. This is interesting. Let me explain, Dr. High Horse. You should have a second dish of soup that is absolutely identical to the first dish, except the second dish does NOT contain the tissue sample from a patient. You also keep an eye on that second dish and see whether the monkey cells and the human cells in it die off. If they do…then your contention that ‘the virus’ in the patient sample is killing those cells is worthless. And you have no evidence your virus is in the patient sample. Or that it exists.”
“Oh. Well…”
“Well, what? You don’t mean to say all those virologists in all those labs who claimed they found the new virus omitted the control experiment, do you?”
YOU KNOW, THAT KIND OF THING. THAT KIND OF INVESTIGATION.
On camera, in the lab, in person.
“That would never happen. They would never let you in there.”
Which proves what? I’m just stating what the MOST REAL DEBATE WOULD CONSIST OF, in a half-sane world. It would look exactly like that.
Here’s a parallel for you. A civilian no one ever heard of develops a car he says runs on water. He says he’s got a new process that VERY cheaply splits the water into hydrogen and oxygen, and the car runs on the hydrogen.
Over years and decades, the legend grows. Finally, major media are starting to nibble around the edges of the story.
So one day, a bunch of Saudis and oil execs and scientists and men in suits show up at this man’s garage, and express great interest in his work. THEY REALLY WANT TO KNOW WHETHER THIS CRAZY GUY HAS STUMBLED ON A REVOLUTIONARY WAY TO POWER A CAR.
So what would they ask him to do?
See, they’re the outsiders with no access, and he’s the insider.
Are they just going to ask him for assurances?
Hell no. They’re going to ask him to take the engine apart and put it back together again. They’re going to ask him to take the fuel system apart and put it back together again. They’re going to want to go through his whole car and his garage and his kitchen and his bathroom with a fine-toothed comb. BECAUSE THEY WANT TO GET TO THE BOTTOM OF THIS SITUATION, SINCE IT COULD AFFECT THE FUTURE OF CIVILIZATION, AND THEIR PROFITS, AND SO ON.
They’re not screwing around.
And neither should we.
Our lives and futures and the lives of future generations are on the line with this “virus thing.”
We should be looking at every beaker and tube and slide and instrument in the virology lab. We should be looking over the shoulders of the virologists and watching every move they make and asking pointed questions and demanding answers.
So we really know whether they’re doing science or preposterous bullshit.
And of course we wouldn’t be paying attention to random assurances from “highly qualified and respected scientists” along the way. We’d be studiously ignoring them.
If you need another parallel to the real kind of investigation I’m demanding, think of bringing a team into the Vatican and inspecting every inch of space in every building, including the basements and caverns…to see what’s really there. The whole enchilada.
All right, you get the idea. You see what I’m asking for.
Now, short of that, what do we have? What can we get access to?
Well, it’s not entirely reliable, but here it is:
We can read published studies which claim to have found SARS-CoV-2. Those studies all have methods sections. In them, the researchers describe, step by step, what they did to “isolate the virus.”
We have that.
I’m now going to republish one of those methods sections, chunk by chunk, and have Dr. Andrew Kaufman make his criticisms as we go along. I published all this about a year ago.
I want to emphasize that Dr. Kaufman’s analysis should be just the beginning of highly detailed analyses of these methods sections, from a number of other independent critics. We need much more of this.
The devil is in the details.
Here we go:
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)”.
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO). Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
Readers who are unfamiliar with my work (over 500 articles on the subject of the “pandemic” during the past two years) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
The answer is no.
As I stated, Dr. Kaufman’s analysis should be just the beginning of intense and detailed examination of studies that describe “how the virus was isolated.”
As opposed to a few hours of Zoom debate in which people summarize their opposing positions, and then submit to a vote from a panel of judges who descend from the sky with motives as pure as Superman and Wonder Woman. All this happens with Steve Kirsch in the background holding a million dollar prize. In Vegas, Steve would be called the house. And the house always wins.
On these recordings, the raw, agonized truth if this epoch emerges. A father whose son was injected against his will rages at a pharmacist, for not having let the parent know about the documented risks.
“So you don’t want to scare the parents with something that is actually happening, that’s happened to my kid. Are you out of your mind? “
Shocking phonecall recording with a pharmacist who administered the jab to a child now in hospital with myocarditis. Part 1. pic.twitter.com/q85d5s92lO
One of the many unfortunate side effects of the attention which has been given to the covid-19 jabs is the fact that more traditional vaccinations (including the dozens routinely given to children) have been forgotten and are now largely administered without protest, controversy or a second thought.
There was always a danger that the justifiable outrage and fear engendered by the covid-19 jabs would push the wider issue of traditional vaccination into the background. The experimental and notably toxic covid-19 jabs have understandably and rightly captured the attention of those who aren’t prepared to accept the lies, the deceits and the manipulations at face value.
But it is important that we don’t forget the ever-growing hailstorm of vaccinations, aimed particularly at children, which have seemingly become an integral part of our relationship with health care in general and doctors in particular.
We all know that the establishment and the mainstream media refuse to debate the mRNA jabs.
But it is, I suspect, less widely known that there has for a long time been a blackout on any discussion of the more traditional vaccines or that the reputation of vaccines is built on a toxic mixture of myths, fallacies and plain, vanilla lies.
I’ve been writing about vaccines for over 50 years but rather to my surprise it was 2011 before I wrote a book entirely devoted to vaccines and vaccination.
I wrote the book (Anyone who tells you vaccines are safe and effective is lying. Here’s the proof.) partly to provide evidence proving that vaccines are often dangerous and don’t work but also to destroy the outrageous, manufactured myth that vaccination has extended life expectancy and eradicated diseases such as smallpox and whooping cough.
I’ll get back to that theme in a moment but first I think it is worth using the history of that book to illustrate the extent of the media blackout which exists to protect vaccines and vaccination.
Knowing that none of my usual publishers would touch a book about vaccines, I published it myself.
We sent out 600 review copies, hoping that one or two reviewers might be brave enough to consider the book on its merit. However, to the best of my knowledge, not one reviewed it. People I’d known for years wouldn’t discuss it. Moreover, quite a number of reviewers returned the book. It is usual practice for reviewers to sell books they don’t want to keep on their shelves. But journalists actually spent time and money returning the book!
I knew there were risks in writing a whole book about vaccines. It has always been a topic which has aroused anger within the medical establishment. In the Preface I wrote: ‘Experience tells me this book will bring me much trouble, a great deal of abuse, a number of threats and considerable professional and personal inconvenience’.
But even I was surprised at how quickly I became persona non grata. My questioning of official establishment policies had, for a long time, made me unpopular with the establishment. It quickly became apparent that vaccination is a taboo subject and that vaccines are protected from criticism in the way that film stars were protected in the 1930s.
Since its publication there have been concerted efforts to ban the book and have it removed from sale.
No one has ever questioned the science, the statistics or the conclusions in the book. Critics have, however, been upset by my criticism of ‘the establishment’s unquestioned enthusiasm for a practice which is of such doubtful value and which offers such potential for disaster’.
I described vaccination as `a massive confidence trick’ and predicted (in 2011 remember) that ‘vaccination will become compulsory in the West’. I have been lied about constantly by thousands of rabid supporters of vaccination.
It seems that the mainstream media has devoted itself to promoting vaccines and never allowing any aspect of vaccination to be questioned. The BBC actually has a policy of excluding all vaccine criticism from its programmes. Merely questioning the validity of vaccination draws a torrent of abuse down upon the questioner’s head.
The inevitable result is that vaccination programmes continue pretty well unhindered and millions of children are now regularly jabbed with products which have never been properly tested or evaluated either for safety or efficacy.
The most potent claim for vaccines is, as I’ve already mentioned, that they have saved millions of lives. (This claim is now being falsely applied to the covid-19 jab which cannot be proven to have saved any lives at all). The fraud is maintained by pointing to average life expectation but this is a false argument for the figures are skewed by the vast number of babies and infants who used to die of disease or malnutrition. Every infant death drags down life expectation dramatically.
All around the world, infants and children are now subjected to a seemingly endless series of assaults on their immune systems. The vaccines used have never been adequately tested to see how they might interact or how they might affect other medications. Very few long-term trials have been done though the few available confirm my scepticism. For example, in 2017, the Danish Government and a Danish vaccine maker, funded a study of the DTP vaccine. The WHO and the medical establishment claim that the DTP vaccine saves millions of lives but, after looking at 30 years of data, the scientists concluded that the DTP vaccine was probably killing more children than died from diphtheria, pertussis and tetanus prior to the vaccines introduction. The vaccine had ruined the immune systems of children rendering them susceptible to death from pneumonia, leukaemia, bilharzia, malaria and dysentery.
The results of that trial changed nothing. The vaccination continued unhindered.
The vaccines most often described as having changed the world are those for polio, whooping cough and smallpox. But look at the evidence.
With polio the truth is that with other infectious diseases the significance of polio dropped as better sanitation, better housing, cleaner water and more food were made available in the second half of the 19th century. Look at the evidence and it shows that the number of polio victims went up not down as a result of vaccination. In Tennessee, USA (chosen at random) the number of polio victims before vaccination became compulsory was 119. The year after vaccination was introduced the figure rose to 386. In America as a whole the number of deaths from polio had fallen dramatically before the first polio vaccine was introduced but the incidence of polio increased by around 50% after the introduction of mass immunisation.
Of even more significance (which I revealed in my book `Why Animal Experiments Must Stop in 1991) 17 million people who were given polio vaccines as children in the 1950s and 1960s are now at risk of developing cancer. This is because the first practical vaccine used monkey kidney tissue – which contains a carcinogenic virus. Moreover, the virus can be passed on to the children of those who were given the contaminated vaccine. Could this explain the ever rising number of people with cancer? We’ll never know. The doctor who first warned of this risk was ignored and her laboratory was closed down. The documents showing who had received the dangerous vaccine were destroyed by the Department of Health in 1987 though it seems likely that millions of doses of the dangerous polio vaccine were used despite the risk.
The smallpox story is equally startling.
The myth that smallpox was eradicated through a mass vaccination programme is just that – a myth. Smallpox was eradicated through identifying and isolating patients with the disease. One of the worst smallpox epidemics of all time took place in England between 1870 and 1872 – nearly two decades after compulsory vaccination had been introduced. The people of Leicester refused the vaccine and there was only one death. In contrast there were massive numbers of deaths in towns where people had been vaccinated.
German doctors are taught that it was the Reich Vaccination Law (making vaccination compulsory) which halted smallpox in their country. But the incidence of smallpox had dropped before the law came into action. Once again, a legally enforced national vaccination programme did not eradicate the disease.
Look at history and it is clear that the number of cases of smallpox has gone up each time there has been a mass vaccination programme.
It’s worth remembering too that Dr Jenner, a hero for pro-vaccine folk, refused to have his second child vaccinated after he’d tried his smallpox vaccination on his own son. Tragically, the boy remained mentally retarded until his death at the age of 21.
Everywhere you look the evidence is the same: vaccination doesn’t work. Moreover, it is not difficult to sustain the argument that it does more harm than good.
Sadly, the medical establishment and the media have for years conspired to suppress the truth and to demonise the truth tellers.
The suppression of the truth about the covid-19 jab is nothing new.
Doctors for Covid Ethics in Europe highlighted the professional observations of Dr. Ute Kruger, Chief of Pathology at Lunds University in Sweden: Cancer went haywire when the mRNA shots began. The health of the world population is being severely compromised by mRNA/DNA injections and yet they are not stopped, underscoring TN’s claim that Technocracy is at war with humanity. ⁃- Patrick Wood, Technocracy News Editor
[In this video (26 min, Swedish with English subtitles), MD/pathologist Ute Krueger describes her findings on breast cancer and other cancers in the era of gene-based COVID vaccines. She finds increased numbers of cancers, in younger patients, which are larger in size and growing more rapidly and aggressively already at the time of the initial diagnosis.]
Dr. Ute Kruger is a researcher and senior physician at Lunds University in Sweden. She’s the Chief of Pathology, a field that she’s worked in for the last 25 years, with a specialty in breast cancer diagnosis for the past 18 years. She’s studied thousands of autopsies and breast cancer samples. She’s extremely familiar with the industry and patient age, tumor size, and malignancy grade are all within her field of expertise and have had a natural rhythm throughout her career. That natural rhythm came to a halt in 2021 once the vaccine rollout began.
Doctors for Covid Ethics posted an interview with her where she shared her concerns about unusual features that have been showing up in samples from the past year.
Age – The average ages of the samples she received dropped, with a rise in the number of samples from people in their 30’s-50’s.
Size – It used to be unusual for Dr. Kruger to find a tumor 3 cm in size. In this new environment, she’s regularly seeing tumors of 4 cm, 8 cm, 10 cm, and the occasional 12 cm. In a shocking anecdote, 2 weeks ago she found a 16 cm tumor that took up an entire breast.
Multiple Tumors – Dr. Kruger has begun to see more cases of multiple tumors growing in the same patient, sometimes even in both breasts. She had 3 cases within 3 weeks of patients who had tumors growing in multiple organs. One had tumors in his/her breast, pancreas and lungs within months of getting vaccinated.
Recurrence – There has been an uptick in patients who have been in remission from their cancer for many years, suddenly getting an aggressive recurrence of their cancer shortly after vaccination.
Speaking Out
Dr. Kruger initially thought that these turbo cancers, as she calls them, were due to delayed doctor appointments from Covid lockdowns, but that period is long over, and the tumors are still growing aggressively, and in younger patients. She reported some of these cases to the FDA, and while some higher-ups initially agreed to meet with her, they canceled the meeting with no explanation the next day and sent a phone agent to take her report instead.
Six months ago Dr. Kruger appeared at a panel in Germany to present her theory that vaccination is causing aggressive tumors, and she asked for help from the doctors at that summit in collecting data. Unfortunately, few of them have been willing to collect that data and share it with her.
Autopsies
Part of Dr. Kruger’s time is spent on autopsies, and she drew attention to numerous concerning anomalies.
A 60-year-old had multiple malignant diseases. He got 2 doses of the Covid vaccine during chemotherapy and then developed Guillain Barre Syndrome. She found inflammation in the spinal cord, brain, and blood vessels.
An 80-yr-old woman became paralyzed one month after vaccination. Dr. Kruger found a hemorrhage in the spinal cord near the neck, which is something she’s never seen before. Under the microscope, she saw inflammation in the vessel that caused the rupture and caused bleeding. She also found inflammation in the heart muscles, which is myocarditis.
Dr. Kruger was called to settle a dispute between a family of a deceased person, and the doctors who signed the autopsy. The family and their physician believed the death was a result of the Covid vaccine, yet the ones who performed the autopsy didn’t come up with any findings to support that and did not link the death to the vaccine. When Dr. Kruger performed her own autopsy, she found evidence of myocarditis and vasculitis- inflammation of blood vessels in the lungs. The original autopsy either missed those signals or didn’t look for them, and the family was correct. Dr. Kruger shared her opinion, supported by another senior-level pathologist from Germany, that the death was indeed due to the Covid vaccine.
Dr. Kruger outlined 3 major issues with the way autopsies are currently being run in practice:
Patient information is sloppy. Dr. Kruger personally had several cases where clinicians had written that the patient was unvaccinated for the autopsy, when in fact in their medical files it was documented that they were vaccinated for Covid.
The typical autopsy doesn’t run exams deep enough to diagnose the root cause of certain medical issues. They don’t do rigorous histopathological testing of the tissues where vaccine damage would likely show up, but which is necessary to detect markers of vaccine-induced injury, such as immunological infiltrates or spike proteins in myocardial tissues. Dr. Kruger ran more thorough exams and found myocarditis and inflammations that were missed by the original autopsy.
There’s a lack of experience in evaluating these findings, and a lack of desire to properly contextualize cases. In addition, most autopsy clinicians don’t report cases to the FDA.
While Dr. Kruger’s testimony is by nature anecdotal, as a top-level pathologist of many years, her concerns should be taken very seriously and investigated further. Of course, that would require an honest regulation system which seems to be sorely lacking these days.
“I’m Watching People Being Killed”
Dr. Kruger stated that she sees vaccination as a trigger for fast-growing tumors and autoimmune diseases. She’s seeing a lot of inflammation alongside tumors, and of course, it’s not only breast cancer. Many other pathologists have reported to Dr. Kruger that they’re seeing an elevation in cancers, cancers in multiple organs, and rare cancers.
She ended off by saying “I studied medicine because I wanted to help people. But now it feels like I’m watching people being killed and there’s nothing I can do”.
The first step to solving any issue is acknowledging there’s a problem. We have a huge problem, and in order to begin to resolve it, it must be acknowledged. It’s time to start pressuring doctors to speak out. Any doctor who’s aware enough to understand that something is off must begin to address the issue. An additional motivation may be the pressure of knowing that it’s all about to blow up, and they don’t want to be standing on the wrong side of the line when it does.
The pharmaceutical crime syndicate has been caught out scamming the public yet again.
This time the longstanding psychiatric con of “chemical imbalances” in the brain that can only be “rebalanced” by dishing out dangerous drugs with horrible side effects (without the “correct chemical balance” ever having been identified) has been thoroughly exposed as another overdose of mind-numbing pseudo-science.
The scam, of course, made a lot of money for the degenerates masterminding the unholy alliance of sociopathic drug manufacturers and the psychiatric control cult of drug pushers. It also incapacitated or murdered a large number of people in support of the globalist eugenics program to kill or cow the human race.
But it looks like the truth has finally penetrated the force-screens of disinformation for which the psycho-political-pharmaceutical con-plex is notorious.
This latest embarrassment for the subversives behind the pharmaceutical crime syndicate comes hot on the heels of the cash-and-burn of the covid psyop and the mounting vaxjab death toll.
The writing is on the wall for the genocidal scamsters as the number of people who still believe a ruddy word that dribbles from the forked tongues of these maniacs has dwindled almost to vanishing point.
Hopefully, heads will roll and these criminals will answer for the millions they have maimed and killed over the decades of the now vanishing Pharmaceutical Dark Age.
The following featured article from The Citizens Commission on Human Rights UK (CCHR UK) whose 60+ years of dedicated campaigning against psychopharmaceutical tyranny has now yielded a huge truth dividend, provides a cogent analysis of the “chemical imbalance” mass-drugging drive.
For decades, people have been prescribed antidepressants based on the belief that the psychiatric drugs could do something to resolve a so-called ‘chemical imbalance in the brain’.
Psychiatrists, pharmaceutical companies and their spin doctors used the idea to convince people there might be something useful in taking them, while at the same time, benefiting from increased antidepressant sales.
However, a new review of existing studies has found that depression is not likely to be caused by a chemical imbalance and has indicated people should be made aware of other options for treating it.
Consider this: if antidepressants were supposed to correct an imbalance of the brain, it would follow there would be a way of measuring when such an imbalance was corrected. For the record, there’s no way of measuring a balance or an imbalance of the brain.
Over the years, numerous requests have been made asking for data to support the claims of a chemical imbalance. The requests were never fulfilled yet psychiatrists, in an unholy alliance with pharmaceutical companies, continued to use unscientific rhetoric that resulted in a continual rise in prescriptions for the drugs. At the beginning of July, it was reported that nearly half a million more adults in England were taking antidepressants compared with the previous year.
At the end of the day, it has been indicative of an impressive marketing strategy, generating huge profits for drug companies while creating untold destruction. Since 2000, over 5 billion pounds has been spent on antidepressants in England alone. There’s no doubt this represents commercial success which has kept shareholders happy, but it has been at human expense.
There have been 151 warnings from 11 countries and the European Union warning that antidepressants cause harmful side effects. These include 37 warnings on antidepressants causing suicide risk or suicidal behaviour.
There have also been 279 studies from 35 countries showing that antidepressant drugs cause harmful side effects. These include 49 studies on antidepressants causing new-born complications and 27 studies on antidepressants causing suicide risk or suicide attempts.
The overriding factor in all of this is informed consent. By making it possible to be fully informed about the dangers of antidepressants, people can make up their own minds rather than accepting pseudoscientific claims.
Attempts will be made to protect the lucrative enterprise, but the antidepressant gravy train is like a house of cards about to fall. The time is up for the psychiatric charade.
Now the people of South Africa need our help. Please see the instructions after this letter to learn how you can make your voice heard before the August 5 deadline (click here to see time remaining).
“We cannot trample upon the humanity of others without devaluing our own. The Igbo, always practical, put it concretely in their proverb Onye ji onye n’ani ji onwe ya: ‘He who will hold another down in the mud must stay in the mud to keep him down.’”
—Chinua Achebe, The Education of a British-Protected Child: Essays
“Apartness” in Afrikaans, “apartheid” is the institutionalized system of segregation. You can change the definitions of the targeted parties, but you cannot change the discriminatory rot underlying this vile legislation.
The People’s Lawctivist Sabelo Sibanda explains that under the proposed amendments:
“These regulations basically declare a scenario where everyone will end up in one of three categories where you are either deemed to be a case, or you are considered a suspect, or, alternatively, you are considered as one who has been in contact with someone who is a case.
“And once you fall into any one of those three categories, this is what this means to you. Government says, ‘You may not refuse to be medically examined,’ whereby the medical examination process is whatever government will determine.
“Second to that, you may not refuse to be put in quarantine or put in isolation. And the requirements for quarantine and isolation are such that the majority of the people of South Africa will not be able to self-quarantine so they have to be put in a state institution.
“Further to that, and most critical, is that you may not refuse to take whatever medication that the government says you should take. Your freedom—which is supposed to be guaranteed and protected by the same act in as far as the right to be informed—is taken away. You are caught in a situation whereby government has full control.
“Once you are put in this isolation space, this quarantine space, you don’t have the ability to determine when and how you get out. It will be up to government to decide.
“So now the country of South Africa will be under a permanent state of disaster where masking will be permanent, where social distancing is permanent, through the National Health Act.”
In case you’ve forgotten what it looks like for your government to discriminate against citizens under the guise of a “state of emergency” and to demand people’s papers, here are a couple of reminders:
Today, that passport looks like a QR code on your phone.
Please take a few moments to read the following articles to understand why there is no circumstance under which it is ethically or morally acceptable to deprive individuals of their freedoms and human rights in the name of the “public good,” which can be defined according to the whims of despots and demagogues:
And if you want to understand what it feels like to be institutionalized and have medication forced on you against your will, here’s a preview of the world you would be creating:
Nurse Pilbow: Mr. McMurphy?
McMurphy: Huh?
Nurse Pilbow: Your medication.
McMurphy: What’s in the horse pill?
Nurse Pilbow: It’s just medicine, it’s good for you.
McMurphy: Yeah, but I don’t like the idea of taking something if I don’t know what it is.…
Nurse Ratched: If Mr. McMurphy doesn’t want to take his medication orally, I’m sure we can arrange that he can have it some other way.
The people of South Africa poured decades of passion, blood, and song into eradicating apartheid:
Do not let that effort be for naught. As Chinua Achebe says:
“The damage done in one year can sometimes take ten or twenty years to repair.”
Do not let fear, hatred, panic, and intolerance win. Cast out those totalitarian demons and save your people by rejecting amendments 1882, 1883, 1884, and 1885.
“Yet men were afraid, with a fear that was deep, deep in the heart, a fear so deep that they hid their kindness, or brought it out with fierceness and anger, and hid it behind fierce and frowning eyes. They were afraid because they were so few. And such fear could not be cast out, but by love.”
A few weeks ago, I was invited by Michael Wallach, the director of the amazing docu-series The Viral Delusion, to join him as a guest on the Skeptico podcast. It was an interesting experience to say the least. We were under the impression that the conversation would be focused on the gain of function/lab leak theories as well as HIV and we had prepared ourselves to discuss these topics. However, the conversation instead took a detour when the host, Alex Tsakiris, changed the focus to rabies instead, an area he felt was left unexplained by those of us stating that “viruses” do not exist. He presented us with a graph showing statistics of rabies cases declining with the use of vaccines. Unfortunately, at the time that we were interviewed, Alex was unable to provide us with a source for the information that he shared with us. Neither Michael nor I had ever seen this graph before, however it really wasn’t the issue as vaccine statistics do not prove a “viral” cause.
Unfortunately, the rabies graph became the bulk of our time on the show. Michael Wallach did an excellent job explaining the problems with the lack of evidence behind the rabies “virus” as well as the fraud of Louis Pasteur. I wanted to chime in more to help out (not that Michael needed me to) but sadly Alex was not really interested in what I had to say about the subject. You can view our conversation with Alex on the Skeptico podcast here:
As I was unable to speak much on the topic with Alex, I want to present some information here that may help to answer his questions as to why rabies cases appeared to decline as the vaccine was introduced. However, before addressing the graph, the first thing that needs to be understood is that at no time has a rabies “virus” ever been properly purified and isolated directly from the fluids of any animal nor any human and then proven pathogenic by adherence to the scientific method. In fact, as he performed his experiments in the 1870’s and 1880’s, Louis Pasteur provided no theoretical basis for the vaccination of rabies as he admitted that he had failed to isolate the microbe that was presumed responsible for the disease. He also massaged and manipulated his data in order to justify his claims as to the success of rabies vaccination. Pasteur was a fraud who was more concerned with fame and prestige rather than performing valid scientific research. I wrote about his unethical practices involved with the early rabies research as well as how the rabies vaccines actually produced the severe neurological symptoms often associated with the disease here.
Later attempts to propagate the “virus” in the 1950’s, which were claimed to be successful, were done in hamster brain and kidney cultures. Interestingly, it was noted that no cytopathogenic changes, the very criteria used by virologists to claim ‘viruses” are present within these cultures, occured whatsoever.
doi: 10.3181/00379727-98-23997.
Even by the CPE standards used by virologists as a measure for the successful isolation of a “virus,” they had failed to “isolate” rabies in their cultured samples. As no rabies “virus” has ever been scientifically proven to cause the disease, there is no basis to claim that the symptoms associated with rabies are caused by a “virus.” Still, in spite of being given this information, Alex continued to focus on his graph as if the effect credited to the vaccine was somehow proof of a “viral” cause. However, one can not look to an effect in order to claim a cause. This is a logical fallacy known as affirming the consequent. It is often stated like this:
In other words, if rabies is caused by a “virus,” the vaccine will lower cases. The cases declined with vaccine use, therefore rabies is caused by a “virus.” Obviously, this is not a logical statement as there are many variables and factors unaccounted for that could lead to the appearance of a vaccine having a positive effect on rabies cases. It should also not need to be stated that just because a vaccine appeared to work does not mean that the cause of rabies was a “virus.” A rabies “virus” must be scientifically proven to exist first in order to be tested for as the cause of the symptoms of disease associated with it. This has never been done.
We therefore must ask ourselves a very important question:
Did the rabies vaccines really cause rabies cases to fall or are there other potential reasons for the apparent decline?
Let’s try to answer this by looking at the graph Alex provided on the air. Fortunately, I was able to find the source for the image. It came from the CDC’s own data from the Morbidity and Mortality Weekly Report in July 2019. The study was titled Vital Signs: Trends in Human Rabies Deaths and Exposures — United States, 1938–2018.
What we can find out is that rabies cases were exceedingly rare over the entire graph period, with only 588 cases of human rabies reported in the United States from 1938 to 2018. In fact, there was a sharp decline in rabies cases a few years prior to the mass vaccination of dogs in 1947, which is often the case when looking at the decline in disease before the introduction of vaccination. Of course, the vaccine is given the credit even though the cases were well in decline beforehand.
So what could have caused this sharp drop before and after vaccine introduction? If you have looked into the decrease in diseases claimed to have been caused by other “viruses,” it is easy to spot a certain trend. Often times, the symptoms of disease claimed to be declining due to vaccination are reclassified either as a new or related disease caused by a new or related “virus.” Smallpox was rebranded as chicken and/or monkeypox, polio became acute flaccid myelitis, syphilis morphed into AIDS, influenza transformed into “Covid,” etc. etc. etc. This trend of rebranding and relabelling the same symptoms of disease as either new diseases or similar ones can easily be seen with rabies and the rabies-related “lyssaviruses.” While the rabies “virus” is considered a “lyssavirus,” there are numerous other “viruses” under this same heading that are considered “rabies-like viruses” that do not cause rabies per se but instead “rabies-like” disease:
Rabies and Rabies-Related Lyssaviruses
“Closely related lyssaviruses circulate among bats in the Eastern Hemisphere, and can cause an illness identical to rabies. Rabies vaccines and post-exposure prophylaxis can provide some protection against some of these viruses, but not others. Rabies-related lyssaviruses can be found even in countries classified as rabies-free.”
“Information about rabies-related lyssaviruses is currently limited to a small number of case reports and a few reports of experimental inoculation; however, the illness appears indistinguishable from rabies. Bats may either have mild or no clinical signs and survive the infection, or develop severe neurological signs and die.”
This is a nice convenient scapegoat which allows a country to declare itself rabies-free even though the same symptoms of disease still persist. For example, in Austraila you will find disclaimers such as this:
According to Australia, they are rabies-free even though the same symptoms of disease persist within the country. These cases are blamed on the Australian bat “virus” which is claimed to cause a “rabies-like” disease. Quite convenient, right? However, what if the classification system for these “lyssaviruses” were to change? Would a country that is considered rabies-free lose its illustrious status?
Lyssaviruses and rabies: current conundrums, concerns, contradictions and controversies
“With increasing ICTV debate toward unification of virus taxonomy based on genetic distances, in the near future there may be a re-classification attempt, in which all phylogroup I viruses are segregated into one species (for example, Rabies lyssavirus?) and all phylogroup II viruses are segregated into another. Of course, such re-classification would miss important characteristics used for species demarcation at present and may have potential socio-economic or bio-political consequences for certain areas. For example, some places where RABV is not thought to circulate, such as in Australia or Western Europe (but where other lyssaviruses are present among bats), might lose their self-defined “rabies-free” status, on the basis of viral taxonomic re-organization, creating greater confusion, with potential public health, veterinary, or economic repercussions, if suddenly recast into the same disease status as Africa, Asia and the New World. Arguably, the term “rabies” appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”.
The loose definitions allow countries such as Austrailia to claim rabies-free status even though the disease still persists there. If the definition and/or classification changes, so to will their status. This is similar to how America is allowed to claim it has been polio-free since 1979 while there are cases every year of acute flaccid myelitis and other polio-like diseases which present with the same sets of symptoms. We could easily relabel those polio-like diseases as polio and lose the polio-free designation.
While the same set of rabies symptoms can be blamed on the closely related “lyssaviruses,” they can also be blamed on unrelated “viruses” and conditions that are said to be caused by different “viruses,” bacteria, genetic abnormalities, and even poisons.. For instance, animals can be diagnosed with distemper instead of rabies. These two diseases have often been confused for one another as the symptoms are indistinguishable:
Raccoons – distemper and rabies
“Canine distemper in raccoons starts slowly, with respiratory infections then they develop pneumonia. In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage. Many of these symptoms are similar to rabies – which can only be determined by laboratory testing.”
“CDV is a highly contagious paramyxovirus that affects dogs and wildlife including raccoons, skunks, grey foxes, and ferrets. This virus is closely related to the human measles virus, and can lead to respiratory, gastrointestinal (GI), and central nervous system (CNS) problems. CDV is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar.”
There are many other diseases such as encephalitis and different neurological disorders which are also said to mimic rabies in animals. Even poisoning is stated to mimic the severe stages of the disease:
Diseases that can look like Rabies
“Encephalitis is one condition that can look somewhat like the early stages of rabies. In this condition, with is immune based in most dog breeds of dogs, the dog’s own immune system begins to attack the brain. The result is a dog that may be confused, appear to stagger and bump into things, or even a dog that seems very disoriented and lost even in familiar settings. The dog may also have temperament changes and may snap at owners or become very agitated when they have previously been calm and friendly.”
“Canine distemper is another disease that may be mistaken for rabies since the symptoms are so close to being the same.Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue. Since it is still a highly contagious disease it is essential to get your dog to the vet if he or she has had any contact with wild animals or other dogs that seem to be disoriented, have a discharge from the eyes or nose, paralysis and stumbling types of movements. Typically the wild animal will be non-threatened by human presence, which in itself is a sign of abnormal behavior. It is important to realize that distemper, unlike rabies, cannot be passed from an animal to a human. However it is important to stay away from any animal that appears to have any symptoms similar to rabies or distemper.”
“Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies. In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink.”
As can be seen from the above three sources, canine distemper and other diseases such as encephalitis can be confused with rabies due to the identical nature of the symptoms. These diseases still persist within dogs and other animals while rabies, or at least “dog rabies,” has been said to have been eliminated from the US and other countries. In other words, the rabies label is no longer applied upon diagnosis even though the same symptoms of disease circulate in animals within the country.
This merry-go-round among the same symptoms of disease does not stop with animals either. There are many conditions in humans that also mimic rabies. These diseases are outlined in this final source:
Beware: there are other diseases that can mimic rabies:
Diseases that can mimic encephalitic rabies:
viral encephalitis (i.e. Japanese, eastern equine, West Nile)
Louis Pasteur admitted to not isolating the agent presumed to cause rabies
In the 1950’s, attempts to isolate the “virus” in cultures of hamster brains and kidneys were deemed successful despite the lack of observing any cytopathogenic effect (CPE)
Many “viruses” that are said to be eliminated or controlled through vaccination were rebranded and relabelled as either similar diseases caused by related “viruses” or new diseases caused by new “viruses”
Regarding rabies, closely related “lyssaviruses” circulate among bats in the Eastern Hemisphere and can cause an illness identical to rabies
Rabies-related “lyssaviruses” can be found even in countries classified as rabies-free
The illness associated with these rabies-related “lyssaviruses” appears indistinguishable from rabies
Some places where rabies is not thought to circulate, such as in Australia or Western Europe (but where other “lyssaviruses” are present among bats), might lose their self-defined “rabies-free” status, on the basis of “viral” taxonomic re-organization,
This would create greater confusion, with potential public health, veterinary, or economic repercussions, if they were suddenly recast into the same disease status as Africa, Asia and the New World
The term “rabies”appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”
Canine distemper is a rabies-like illness in animals
In raccoons, it starts slowly, with respiratory infections then they develop pneumonia
In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage
Many of these symptoms are similar to rabies – which can only be determined by laboratory testing
Canine distemper is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar
It is mistaken for rabies since the symptoms are so close to being the same
Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue
Encephalitis is another condition that can look somewhat like the early stages of rabies
The result of this brain swelling is a dog that may be confused, appear to stagger and bump into things, or even seems very disoriented and lost even in familiar settings
Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies
In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink
In humans, there are many diseases which mimic rabies:
Diseases that can mimic encephalitic rabies:
“viral” encephalitis (i.e. Japanese, eastern equine, West Nile)
For some reason, people seem to think rabies is a “gotcha” for those of us claiming that “viruses” do not exist. This disease is thrown out as proof that vaccines are effective and that because of this, the “virus” must therefore exist. However, a big problem for anyone championing rabies as proof for the existence of “viruses” continues to be the lack of any purified and isolated “virus” particles coming directly from the fluids of a rabid host. Louis Pasteur openly admitted to failing to meet this burden of proof even though he subjected animals and humans to experimental injections. Attempts by researchers in the 1950’s to propagate the “virus” in tissue and cell cultures did not produce the characteristic cytopathogenic effect said to be necessary in order to determine if a “virus” is present in a culture. Thus, there is no scientific proof for the existence of the rabies “virus,” even by virology’s own standards.
As the rabies “virus” can not be shown to exist, any data relating to a decrease in cases due to a vaccine which is then used as proof for the existence of a rabies “virus” is entirely irrelevant. There are many reasons to doubt case statistics as these can be easily manipulated and massaged in order to create whatever narrative is desired. It can be seen that the same symptoms associated with rabies still exist today as there are many other diseases either said to be caused by rabies-related “viruses” or completely unrelated “viruses” that share the exact same symptoms associated with rabies. These diseases are more commonly diagnosed in areas where rabies is said not to be circulating. It is very apparent that virology loves to rebrand and relabel the same symptoms of disease as multiple “new and different” diseases in order to create the perception that the treatments work. This is why places like Austrailia get to claim to be “rabies-free” even though a rabies-like disease said to be caused by a rabies-like “virus” still exists there. This lowers the cases as the older diseases are claimed to be either eradicated and/or under control due to “successful” vaccination campaigns and thus they are not looked for as a diagnosis. There is no way that these statistics can be trusted when the definitions and labels of what is or is not rabies seemingly changes at will.
In any case, the rabies statistics are a moot point. Until someone can provide proof of the purification and isolation of the particles assumed to be rabies directly from the fluids of a rabid host which were proven pathogenic in a natural way, these case numbers are utterly meaningless. The conversation with Alex on the Skeptico podcast should have never even reached vaccination statistics unless he provided a paper showing the evidence for the existence of a rabies “virus” first. Unfortunately, while Michael did an admirable job defending our position, we were not prepared for the graph and did not get the chance to look over the data and present our counter-argument. Hopefully we can get the chance to go on again and discuss the issue in further detail in the future. However, if not, this response will have to suffice.
More than 130 U.S. Coast Guard members filed a class action lawsuit alleging the religious exemptions they filed in response to the Biden administration’s COVID-19 vaccine mandate for military service members were unlawfully denied.
More than 130 U.S. Coast Guard members filed a class action lawsuit alleging the religious exemptions they filed in response to the Biden administration’s COVID-19 vaccine mandate for military service members were unlawfully denied.
The lawsuit, filed July 25 in the U.S. District Court for the Southern District of Texas — Galveston Division, also challenges the constitutionality of the mandate.
The number of plaintiffs exceeds 130 and will likely end up surpassing 200, according to Dale Saran, one of the attorneys representing the service members.
The suit names four defendants: Alejandro Mayorkas, secretary of the U.S. Department of Homeland Security (DHS); Linda L. Fagan, commandant of the Coast Guard; Lloyd Austin, secretary of the U.S. Department of Defense (DOD) and Dr. Janet Woodcock, acting commissioner of the U.S. Food and Drug Administration (FDA).
Plaintiffs are either active-duty or reserve members of the Coast Guard, and all “have sincerely held religious beliefs that prohibit them from receiving the COVID-19 vaccine.”
According to the complaint, under the August 24, 2021, DOD vaccine mandate, the military theoretically offers “medical, administrative, and Religious Accommodation Requests (RARs) to the mandate,” while the Coast Guard’s vaccine mandate, issued two days later, “incorporates the provisions of the DOD mandate.”
The suit alleges:
“In practice, only servicemembers with medical or administrative reasons for an exemption from the mandate are accommodated, and even those sparingly, while RARs are universally denied unless the requester is eligible for administrative separation – i.e. imminently leaving the Service.”
This “conclusively demonstrates that the Armed Services have systematically and willfully violated service members’ free exercise rights under RFRA [Religious Freedom Restoration Act] and the First Amendment,” the lawsuit states.
In all, the lawsuit alleges:
Violation of the Religious Freedom Restoration Act.
Violation of the Free Exercise Clause of the First Amendment.
Violation of the Fifth Amendment’s Due Process clause, pertaining to substantive due process.
Violation of the Fifth Amendment’s Due Process clause, pertaining to procedural due process.
The lawsuit also questions the DOD’s claim — which has come under judicial scrutiny — that the Pfizer-BioNTech COVID-19 vaccine, issued under an Emergency Use Authorization (EUA), is “interchangeable” with the FDA-licensed Pfizer Comirnaty vaccine.
Arguing that the plaintiffs “will suffer concrete and particularized harm” from these mandates, including potential involuntary separation, forced retirement, removal from senior or leadership positions, duty and promotion restrictions, PCS restrictions, letters of reprimand or counseling, loss of pay and benefits or other adverse actions, the service members are requesting from the court to:
Declare the DOD and Coast Guard mandates “unlawful and unconstitutional” and to vacate those orders.
Declare the defendants’ “no accommodation policy” is unconstitutional under the First and Fifth Amendments and violates the Religious Freedom Restoration Act.
Enjoin the implementation of the DOD and Coast Guard mandates with respect to the plaintiffs and all service members.
Enjoin any adverse or retaliatory action against the plaintiffs.
Award all legal, court and attorneys’ fees as well as other relief to the plaintiffs.
Remarking on the recent block placed on the vaccine mandate for the Air Force, Space Force and Air National Guard by a federal judge in Ohio, and the recent $10.3 million settlement awarded to over 500 Illinois healthcare workers over the denial of religious exemptions to a COVID-19 vaccine mandate, Travis Miller, one of the attorneys representing the plaintiffs in the Coast Guard lawsuit, told The Defender:
“The latest ruling against the Air Force COVID-19 vaccine mandate is further proof that the military has violated — and continues to violate — the rights of religious service members.
“Courts around the country have recognized this fact, and yet President Biden and Secretary Austin continue targeting the faithful for discipline and removal. It’s an indictment of leadership.
“The $10.3 million class action settlement will hopefully lead the way for other successful challenges to employer COVID-19 vaccine mandates that discriminate against those with sincerely held religious beliefs.”
Saran described the Coast Guard as “the forgotten branch of the Armed Services,” which has been largely overshadowed as mandate-related cases from other branches attained more public prominence.
Saran told The Defender:
“They are being treated at least as badly as any of the other Armed Services — arguably worse — in part because they get little to no publicity about what they’re enduring, in part because they number less than 30% of the personnel of the Marine Corps, itself the smallest of the overseas warfighting forces [~45,000 active duty compared to ~175,000 active duty].
“These folks represent some of the most dedicated, selfless defenders of American lives here at home … They deserve better, they deserve advocates for their rights and that’s why we’re filing on their behalf.”
Service members forced to get vaccinated ‘under duress’
The lawsuit includes written testimony from several service members who shared their experiences in attempting to secure religious exemptions from the Coast Guard.
Sabrina Wilder is an operations specialist from Rosharon, Texas, serving at the Coast Guard Vessel Traffic Service in Houston/Galveston, Texas. She first joined the Coast Guard in 2016. In September 2021, she submitted a RAR, and received the following email in response:
“For both processes [medical or religious] we were told that you are still likely to be Administratively Separated if you receive either exemption.
“The exemption will just permit you to not receive the vaccine before you are … processed. Please do not think you will be allowed to continue to serve if you are exempted.
“This was the official communication in the brief today with the Sector Commander, Chaplin, and Medical present.”
Wilder proceeded with the RAR. According to Wilder, while the exemption requests of unvaccinated service members were pending, they were required to “walk around base with masks on, thus identifying them to the entire command,” while their travel was restricted to no more than 50 miles from base. Vaccinated members were under no such restrictions.
Wilder’s RAR was denied in January 2022, as was her appeal, on June 2, 2022. On June 15, she “was ordered to go to the nearest Walgreen’s to receive the vaccine.” When she refused, she received a counseling form and is now at risk of being discharged.
Timothy Jorden is a maritime enforcement specialist stationed in Houston. He has been on active duty in the Coast Guard since 2016, and previously served in the Marine Corps for four years.
His RAR was initially denied on Dec. 3, 2021. On Dec. 9, 2021, he submitted a request for all of the pertinent documentation relating to the denial and on Dec. 17, 2021, he submitted an appeal. He never received a response to his initial request, but received a “form denial” to his appeal five months later, despite a Coast Guard requirement that a response be granted within 30 days.
According to the lawsuit, the denial he received “was identical to those of other Coast Guard members he knows, despite being from different commands.”
In the meantime, like Wilder, Jorden was “restricted to within 50 miles of his base — in violation of military law,” and was required to wear a mask on base while those who were “vaccinated” were not. His previously approved leave to visit his family was revoked.
Despite these restrictions and initially being told “he was non-deployable because of his vaccination status,” he was almost immediately notified “he would have to be part of a Presidential security detail.” As the lawsuit states:
“Plaintiff Jorden has his leave and liberty restricted as a general matter, and was told he was non-deployable, but the very next day when his particular expertise was necessary to support missions around the country, including a Presidential protective detail, his ‘threat’ to others instantly evaporated.
“This is just one instance of many showing that the entire framework and claims about the unvaccinated are nothing more than facade.”
Michael Bazzrea is a senior chief party officer from Ardmore, Oklahoma, serving in Galveston, Texas. He has been enlisted in the Coast Guard since 1994. He remained on active duty until 1998, and remained part of the Reserve since then.
In July 2021, Bazzrea tested positive for COVID-19 and subsequently submitted a RAR, which was denied, as was his appeal. He was told that once an “FDA-approved” vaccine was available, he would be ordered to take it “regardless of any civil rights complaints” he might have.
On July 6, 2022, Bazzrea was ordered to get vaccinated within 10 days. In his own words:
“I stated in my appeal that I did not want to take the vaccine and that being forced to do so would put me in duress. However, I was ordered to do so regardless.
“An email was sent out from [my] Chief of Staff stating anyone with a denied RA appeal that had not received the vaccination would NOT be eligible for advancement or promotion and that this email would serve as official policy.
“I was told I would be facing removal from the advancement eligibility list and the inability to take positions such as silver or gold badge positions as well as separation from the Coast Guard.”
The lawsuit states that “under great duress, moral conflict, and now with great remorse,” Bazzrea “took the first shot … against [his] religious and personal beliefs,” as “it was his last chance at advancement to Master Chief (E-9),” a promotion which entailed “a large financial difference in retirement to his family.”
Aaron Cheatum is a First Class Petty Officer in the Coast Guard Reserve, stationed in Galveston. He first enlisted in the Coast Guard in 2000, and was on active duty for 11 years before joining the Reserve.
Cheatum submitted his RAR on Nov. 29, 2021. It was denied on Jan. 31, 2022, despite stating that the Coast Guard did “not question the sincerity of [his] religious belief or whether vaccine requirements would substantially burden [his] religious practice.”
His appeal also was denied, even though in the meantime, Cheatum tested positive for COVID-19 on Jan. 28, 2022. In his own words:
“On July 8, 2022, facing a loss of earned retirement, loss of VA benefits, inability to advance in rank, loss of medical insurance, being processed for discharge with a less than Honorable discharge after 22 years, and under duress, I violated my own religious conviction by receiving the initial COVID-19 vaccine.”
Caleb Wadsworth is a lieutenant in the Coast Guard, assigned to the Coast Guard Sector/Air Station in Corpus Christi, Texas. He has been a member of the Coast Guard since 2013.
Wadsworth submitted his RAR on Sept. 28, 2021. It was denied on Dec. 2, 2021, despite affirming that his religious beliefs were “sincere.” Despite an appeal submitted on May 17, 2022, he was “officially counseled” on June 2 and ordered to receive a “fully FDA-approved COVID-19 vaccine” by June 8, under threat of disciplinary action.
In his own words:
“On this form I annotated that taking a COVID-19 vaccine was against my well-documented religious beliefs and that there was no FDA-approved vaccine available for administration, which would negate the legality of the order to vaccinate.
“On 03 JUN2022, I reported to the Air Station Corpus Christi Clinic, as ordered, and documented what vaccines were available for administration … I learned that Air Station Corpus Christi did not have any COVID-19 vaccines … [my flight doctor] was unable to locate an FDA Approved vaccine.
“On 06-07 June 2022, I visited four separate clinics in our area in an attempt to gain access to an FDA-approved/labeled vaccine. At each clinic I had health care professionals document NDC’s [National Drug Code] and lot numbers for the vaccines they had in stock, all of which were labeled as EUA vaccines.
“These details were captured in photos, documented in memo format, signed by health care professionals and a witness, and forwarded to my commanding officer.”
Wadsworth was told the EUA vaccines “could be administered interchangeably.” He subsequently received negative counseling on June 8, and has been told that “he is now no longer eligible to promote.”
As Wadsworth describes it, he was “treated poorly by my command and they flagrantly admitted to trying to coerce me into vaccinating, which was against my religious beliefs.”
Expert testimony questions myocarditis risks
The lawsuit also goes into extensive detail about the differences between EUA vaccines and fully approved vaccines, arguing that “publicly available information indicates that there are differences in the composition of the EUA and licensed products.”
According to the lawsuit, “there are significant differences between licensed vaccines and those subject to EUA that render them ‘legally distinct.’” This includes lower efficacy requirements and “minimal” safety requirements for EUA products.
According to the lawsuit, “EUA products are exempt from certain manufacturing and marketing standards, enjoy broader product liability protections, and cannot be mandated due to informed consent laws and regulations.”
And despite the DOD’s claim that the EUA and fully approved vaccines are “interchangeable,” the lawsuit argues, “the [U.S. Food and Drug Administration] FDA has never asserted that the EUA and licensed versions are legally interchangeable.” Instead, the FDA has “consistently acknowledged that the two vaccines are ‘legally distinct.’”
In two appendices containing expert testimony accompanying the lawsuit, cardiologist and immunologist Dr. Peter McCullough stated:
“The Pfizer, Moderna, and JNJ [Johnson & Johnson] vaccines are considered ‘genetic vaccines’, or vaccines produced from gene therapy molecular platforms, which according to U.S. FDA regulatory guidance are classified as gene delivery therapies and should be under a 15-year regulatory cycle with annual visits for safety evaluation by the research sponsors.”
“The current COVID-19 vaccines are not sufficiently protective against contracting COVID-19 to support their use beyond the current voluntary participation in the CDC-sponsored program.”
McCullough placed particular emphasis on the risk of vaccine-induced myocarditis, especially among young adults:
“COVID-19 vaccine-induced myocarditis has a predilection for young males below age 30 years.
“Multiple recent studies and news reports detail people aged 18-29 dying from myocarditis after receiving the COVID-19 vaccine.
“The FDA found that people 12-24 account for 8.8% of the vaccines administrated, but 52% of the cases of myocarditis and pericarditis were reported.”
Active-duty members of the Coast Guard are required to be between the ages of 17-35, and Reservists between the ages of 17-40, placing a significant number of service members within the age range at highest risk for vaccine-induced myocarditis.
McCullough referenced a July 29, 2021 report in the Journal of the American Medical Association (JAMA) by the Defense Health Agency, which found that “previously healthy service members have developed myocarditis, a severe and life-threatening inflammation of the heart, within an average of just four days of receiving their first shot of either the Pfizer-BioNTech or the Moderna vaccine.”
McCullough pointed out that in addition to the “superiority” of natural immunity conferred by COVID-19 infection, vaccination following infection is “dangerous,” according to recent research.
In reference to the military context, McCullough concluded:
“Vaccination is not the best way to minimize the risk posed by COVID-19 to military readiness. COVID-19 vaccination has led to record fatal and nonfatal organ injury syndromes according to over 1,000 publications in the preprint and PUBMED citation systems.
“Because U.S. military readiness depends on the health of our service men and women, and these data suggest the COVID-19 vaccines markedly decrease health and lead to disability and death, COVID-19 vaccination is not the best way to protect our military.”
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
Artificial intelligence is pulling new vaccines out of the Platonic realm. Automated labs are on standby, prepared to crank out alien strands of mRNA and pack them into toxic nanoparticles. A billion empty syringes are waiting on shelves.
This is not science fiction. These jabs will be on the market before you can say “boostah.”
Google. Moderna. Microsoft. They’re all racing to the edge. This is corporate transhumanism in all its avaricious glory, riding waves of propaganda and channeled by the biosecurity state.
These people uphold a new mythos whose axis mundi is the Machine. In their world, digital minds are “dreaming up” novel genetic configurations. Biological systems are treated as “living software.” With each technical advance, their myths bleed into our reality.
A 2019 white paper from Policy Horizons Canada describes this shift as a “biodigital convergence,” characterized by:
1 –Full physical integration of biological and digital entities
2 –Coevolution of biological and digital entities
3 –Conceptual convergence of biological and digital systems
Our intelligentsia—the elites “educated beyond their level of intelligence”—are undergoing a sort of religious conversion. Their world has been illuminated by gene sequencing and neural networks.
Their machines have convinced them that living things are just clunky machines. Our immune systems require software updates. Our flawed genomes need debugging. In order to get there, our brains must be augmented.
“Reality explored by AI, or with the assistance of AI, may prove to be something other than what humans had imagined,” wrote ex-Google chief Eric Schmidt in his 2021 book The Age of AI. “Across the biological, chemical, and physical sciences, a hybrid partnership is emerging in which AI is enabling new discoveries.”
For Schmidt and his coauthors, this vantage point has a mystical quality:
The prognostications of the Gnostic philosophers, of an inner reality beyond ordinary experience, may prove newly significant. … Sometimes, the result will be the revelation of properties of the world that were beyond our conception—until we cooperated with machines.
Lifeless eyes gaze out on a world composed of numbers. Every living creature is just data to be manipulated.
On July 28, Google’s DeepMind announced its powerful AI system, AlphaFold, has modeled the 3D structures of some 200 million proteins. That’s almost every protein on the planet, published on an open database. Even if we account for errors, no human team has achieved anything close to this.
AlphaFold is a deep learning system. In the initial phase, it was trained on the datasets of known protein structures. Over the past two years, programmers have turned it loose on every genome ever sequenced. The AI can look at any gene and convert the DNA to protein—in virtual space—then predict the folding pattern with remarkable accuracy.
That means scientists can anticipate any protein’s function, whether natural or artificial, starting with nothing but its DNA sequence. That also means genetic engineers can predict what mutations will produce new functions—in silico—before they ever test it in the lab. Months of trial-and-error can be done by computer in an instant. It’s a transhuman fantasy come to life.
The project’s leader, Dame Janet Thornton, toldThe Guardian, “This insight will now be used to design improved vaccines which induce the most potent transmission-blocking antibodies.”
In the next few years, a flood of experimental mRNA vaccines—all designed using AI—will flood the pharmaceutical market. Moderna is working on fifteen different concoctions, targeting everything from the common flu and HIV to malaria and dengue fever. If they can drum up enough public anxiety, we’ll soon see two-legged bio-machines lined up around the block to get their injectable updates.
“We call mRNA the software of life,” Moderna’s CEO toldMIT Sloan. “You can copy and paste the information into a lot of drugs by using the same technology.” In the spirit of biodigital convergence, Moderna has trademarked the name “mRNA OS”—as in “mRNA operating system.”
Back in 2017, Moderna’s chief medical officer, Tal Zaks, explained this approach to his TEDx audience:
We’ve been living this phenomenal digital and scientific revolution. And I’m here today to tell you that we’re actually hacking the software of life.
Using Moderna’s zany jargon, Zaks described the transcription of DNA into mRNA and proteins as an “operating system”:
If you think about what it is we’re trying to do, we’ve taken information…and how that information is transmitted in a cell. And we’ve taken our understanding of medicine and how to make drugs. And we’re fusing the two.
We think of it as “information therapy.”
That means new inoculations, new cancer treatments, new gene therapies—and maybe a few potions to make designer humans—all developed using AI and manufactured by robots.
If nothing else, Moderna has reprogrammed our federal budget. The US government is about to pay $1.47 billion in taxpayer money for 66 million doses of Moderna’s new Omicron strain. That’s on top of more than 200 million original doses already administered nationwide. The company’s meteoric stocks have produced five billionaires since the pandemic started.
“The era of the digital vaccine is here,” a GlaxoSmithKline team declared in Science.
It’s a Jab 2.0 for Humanity 2.0.
Postcard by Mister Blister | Amsterdam
It’s fitting that Moderna’s mRNA vaxx was initially funded with $20 million from the Bill and Melinda Gates Foundation in 2016. Microsoft’s founder is all about operating systems and viruses and sci-fi swindles. Consider his endless vaccine initiatives—or the Epstein flight logs. It seems like Bill would jab anything that moves, no matter how innocent.
For Bill Gates and his cyber-conquistadors, biodigital convergence is the next frontier. Just before the pandemic broke out, Microsoft spotlighted Sara-Jane Dunn and her work at the company’s Station B. She waxed poetic about programmable bio-machines in an official propaganda video:
The last technological revolution, the software revolution, was defined by our ability to encode 1’s and 0’s on silicon. The next revolution won’t be about 1’s and 0’s. It will be about our ability to code A’s, G’s, C’s, and T’s—the building blocks of DNA. …
Everywhere I look, I see cells operating as little computers. … You can think of this as living software.
This approach is applied to everything from gene therapies to the creation of synthetic organisms. In partnership with Oxford Biomedica and other tech companies, the team at Station B is dedicated to building “integrated systems” to “program biology more effectively”—as if mice and men really were “living software.”
In this mentality, we’re not souls enshrined in bodies. We’re half-assed bots constructed by faulty genes. Our only hope is to be reprogrammed.
Of course, Dunn makes a lot of noise about “ethical concerns” and “unintentional consequences.” They all do. But listening to her, you get the feeling that Microsoft is run by mad scientists with more stock options than common sense. Dunn seems intoxicated by her transhuman dreams:
We’ve developed biological programming languages that allow us to encode our designs for genetic circuits. Our tools allow us to compile these designs down to the DNA code, then to automatically run our experiments in the lab. The experiments are run on lab robots, and then we pull the data from those experiments and store it in a Microsoft cloud storage space [and] our knowledge base is continuously updated by automated learning.
That’s right. Microsoft has robo-labs to create designer genes. Google uses AI to digitize every protein in the world. Moderna is cranking out mRNA jabs like they’re cheap software patches.
To biotech cyborgs, everything looks like a computer simulation.
In 2021, the UK Ministry of Defense put out a white paper entitled Human Augmentation: The Dawn of a New Paradigm. If you ever wondered about the connection between mask Karens and cyborg super-soldiers, this is the place to start. After hyping genetic enhancement and brain-controlled drones, the authors take a sudden detour to scold the vaxx hesitant as technophobes:
The history of vaccinations demonstrates how proven, and seemingly uncontroversial human augmentation technologies can take many years to become globally effective and accepted by societies. … Human augmentation may be resisted by elements of society that do not trust the effectiveness and motive of augmentation.
Call me “phobic” all you want—I’m not down with getting penetrated by Big Pharma. I don’t want my veins clotting up with “information therapy.” I don’t trust these people and I don’t trust their calculations. Not unless they’re counting money.
Think about when your web-browser crashes, or your Internet goes down. Now imagine that happening to your immune system. Imagine your heart doing an automatic reboot.
It ain’t easy being a caveman, but it’s preferable to whatever Big Tech and Big Pharma have conspired to turn us into.
We are not machines to be reprogrammed. Don’t let anybody tell you otherwise. More than likely, they’re just paid to say so.
WASHINGTON – On Monday, U.S. Sen. Ron Johnson sent a follow-up letter to Rochelle Walensky, Director of the Centers for Disease Control and Prevention (CDC), demanding clarity on whether the agency performed sufficient surveillance of COVID-19 vaccine adverse events. Recent conflicting statements by CDC officials about monitoring adverse events called into question CDC’s integrity and transparency.
In a June 2022 letter to the CDC, Sen. Johnson outlined the CDC’s Standard Operating Procedures (SOP) document dated January 29, 2021, in which the agency claimed it would “perform routine [Vaccine Adverse Event Reporting System (VAERS)] surveillance to identify potential new safety concerns for COVID-19 vaccines.” The SOP also stated that the “CDC will perform Proportional Reporting Ratio (PRR) analysis . . . to identify [adverse events]” and “perform PRR data mining on a weekly basis or as needed.”
However, in response to a May 9, 2022 Freedom of Information Act (FOIA) request, the CDC wrote, “no PRRs were conducted.”
Dr. John Su, a CDC official on the agency’s Vaccine Safety Team, recently said the opposite to a media outlet claiming that the “CDC has been performing PRRs since Feb 2021, and continues to do so to date.”
The senator wrote, “CDC’s assertion and Dr. Su’s statement cannot both be true.”
“The American people deserve the truth and you have not been providing it. That is why I, together with millions of Americans, have completely lost faith in the CDC and other federal health agencies. It is time to start regaining their confidence and your agency’s integrity by coming clean, being transparent, and telling the truth,” the senator added.
Yesterday, I had the absolute pleasure and honor of being on Dr. Tom Cowan’s Wednesday webinar to discuss a follow-up on the No “Virus” Challenge. We addressed a paper that was supplied by Steve Kirsch and Co. as the “irrefutable evidence” for the existence of “SARS-COV-2.” The paper, a June 2022 non peer-reviewed preprint written by Dr. Sin Lee, is nothing but meaningless genomic data based on a fraudulent “SARS-COV-2” genome from January 2020. For some reason, the Fan Wu paper supplying the original fraudulent genome was not presented as “irrefutable evidence.”
Also discussed are cyro-EM images said to be considered evidence of live “virus.”
Please watch the webinar and find out why neither the genomic data nor the EM images constitute “irrefutable evidence” of a “virus” that was never purified and isolated.
Live Webinar With Dr. Andrew Kaufman, Mike Stone, and Mike Donio – Recorded on July 27th, 2022
In this webinar, along with Dr. Andrew Kaufman, Mike Stone & Mike Donio, we discussed the Virus Challenge in further detail.
Children, who are at no risk from Covid-19, are being aggressively pursued and forcibly injected with an experimental injection whose ingredients are secret. The injection, which is marketed as a vaccine, has garnered more life-threatening adverse reactions within 18 months than all other FDA-licensed vaccines combined for the last 30 years.
Infants and young children are being injected within the framework of an experimental medical atrocity, an atrocity that is a chilling reminder of Nazi medical atrocities. FDA officials issued one after another Emergency Use Authorization for the use of the “vaccine” for ever younger age groups. The latest FDA authorization was issued on June 17th, authorizing the injections for very young children and infants as young as 6 months.
FDA officials ignored entirely the accumulating, unprecedented number of severe injury reports involving children aged 5 to 11. These reports were submitted to the FDA-CDC Vaccine Adverse Event Reporting System (VAERS).
An analysis of 58 VAERS case reports of severe adverse events suffered by babies and toddlers under 3 years of age following the mRNA Covid injection. The VAERS case reports reveal that the Covid-19 injections are attacking infants’ and toddlers’ brains, hearts, and other vital organs.
The analysis was submitted by Israeli journalists Ranit Feinberg & Yaffa Shir-Raz, to the FDA, prior to its advisory committee meeting on June 17th. The analysis was published by Rite Time an Israeli online magazine, on June 13, 2022.
“The most common serious adverse events were life-threatening bleeding, anaphylactic shock, anticholinergic syndrome, encephalitis, hypoglycemia and neuroleptic syndrome. In most of the reported cases, these are multi-system injuries.
In some cases it is not clear what happened to the babies – did they survive? And if so, have they recovered?
Most reports do not specify under what circumstances the infants were vaccinated, and if they participated in the clinical trials.
Most reports do not record whether the babies died or survived.” (Emphasis in original)
(case number 1015467) Cardiac arrest, chest pain of a two-month-old baby boy, one Hour after Pfizer’s mRNA Experimental Vaccine
Torsade de Pointes/QT prolongation (broad), Anaphylactic reaction (broad), Arrhythmia related investigations, signs and symptoms (broad), Shock-associated circulatory or cardiac conditions (excl torsade de Pointes) (narrow), Acute central respiratory depression (broad), Gastrointestinal nonspecific symptoms and therapeutic procedures (broad), Cardiomyopathy (broad), Respiratory failure (broad), Hypoglycaemia (broad), Noninfectious myocarditis/pericarditis (broad)
(case number 1133837) is of a 43-day-old baby girl who reportedly received an “intramuscular” COVID-19 jab and immediately afterward suffered a variety of multi-system, life-threatening injuries.
These include: “‘Anaphylactic reaction (broad), Asthma/bronchospasm (narrow), Anticholinergic syndrome (broad), Acute central respiratory depression (broad), Pulmonary hypertension (broad), Cardiomyopathy (broad), Eosinophilic pneumonia (broad), Vestibular disorders (broad), Hypersensitivity (broad), Respiratory failure (narrow), Drug reaction with eosinophilia and systemic symptoms syndrome (broad).’”
While the section for noting whether or not the patient died was marked “No,” the recovery section was also marked “No.”
“What then happened to her? Is she alive, or did she die?” Does anyone employed by the FDA or CDC care about what happened to these babies?
FDA officials disregarded the evidence of harm entirely. It is unclear whether FDA shared the analysis of the 58 VAERS case reports with the advisory committee. The committee voted unanimously to recommend these clearly UNSAFE experimental injections for infants and young children – thereby lending their support to a morally perverse policy that subjects children to a medically unjustifiable experiment that exposes them to life-threatening hazards.
As of July 8th, VAERS received 278 case reports of adverse events following Covid-19 injections involving 5-month-old infants to less than 5-year-old young children. Of these, 137 cases were recorded since the FDA authorization. (MedAlerts.)
Case 2342486, a nine-month-old female infant who, submitted on June 27th — one day after the injection, her condition was life-threatening. Electroencephalogram, Intensive care, Seizure Her symptoms: Systemic lupus erythematosus (broad), Convulsions (narrow), Noninfectious encephalitis (broad), Noninfectious encephalopathy/delirium (broad), Noninfectious meningitis (broad), Generalised convulsive seizures following immunization (narrow), Hypoglycemia
By July 15th, the number of case reports involving infants and young children under 5 who have suffered serious adverse reactions rose to 381.
Young children who have been forcibly injected in a massive, unethical vaccination experiment suffer from multiple life-threatening adverse reactions. The following are described in VAERS reports involving infants and young children::
“Inflammation and systemic symptoms syndrome, Anaphylactic reaction,Peripheral neuropathy, Guillain-Barre syndrome, Noninfectious encephalitis, delirium, Febrile convulsion, Generalised convulsive seizures following immunization, Decreased oxygen saturation, Seizure, Unresponsive to stimuli, Abnormal sleep-related event, Acute pancreatitis, Hyperglycemia/new onset diabetes mellitus, Neuroleptic malignant syndrome, Anticholinergic syndrome, Systemic lupus erythematosus, Dementia, Convulsions, Acute central respiratory depression, Psychosis and psychotic disorders, Hostility/aggression, Hypotonic-hyporesponsive episode, Generalized convulsive seizures following immunization, Respiratory failure, Drug reaction and systemic symptoms syndrome, Hypoglycemia, Infective pneumonia Abnormal sleep-related event, Acute pancreatitis, meningitis…”
Most of these conditions have never before been diagnosed in young children, such as “Neuroleptic Malignant Syndrome,” which is induced by toxic psychotropic drugs.
“Neuroleptic malignant syndrome (NMS) is a rare and life-threatening reaction to the use of any neuroleptic medication. Neuroleptics, also known as antipsychotic medications.”
Since FDA officials authorized the toxic experimental shots for babies, 27 reported cases of Neuroloeptic Malignat Syndrome involved the youngest children.
As the mother of an adult-aged son who died of Clozaril-induced Neuroleptic Malignant Syndrome, which led to organ failure, I am horrified that children, including infants and toddlers, are being exposed to multiple risks of death.
What are the undisclosed ingredients in these toxic injections?
Why did the manufacturers, distributors, as well as doctors, and public officials insist on getting total immunity from liability?
This extraordinary marketing scheme has resulted in hundreds of thousands of human casualties. Most were previously healthy men, women, and even younger children who have suffered profound, life-altering harm following the injections.
Are Children and Infants Targets of Deliberate Genocide?
The evidence that the medical establishment and the media ignore and disavow is documented in an unprecedented number of children who died following Covid injections:
The evidence that children are dying in unprecedented numbers is also documented by the bulk orders for child-sized burial caskets since 2021, following the rollout of the Covid injections.
The tweet below was posted on July 4, 2022, by Mick Haddock
Mick Haddock says that he has sold 5 years’ worth of child-sized caskets in 7 months. “Vaccines are killing children. If not, what is?”
Having escaped the Nazi genocidal agenda – i.e., the Final Solution– I am convinced that we are confronted with a genocidal war. This time, the genocide is on a Global scale. This time instead of Zyklon B gas, the weapons of mass destruction are genetically engineered injectable bioweapons.
This time, the Israeli Health Ministry follows in lockstep with FDA vaccine authorizations. Officials at the Health Ministry ignored the alarming VAERS data and ignored their own substantial data confirming that Pfizer’s Covid injections are causing severe harm and cutting short the lives of Israeli children in unprecedented numbers
[Read: Israel Was Caught Concealing Children’s Vaccine Injuries]
Read the report below:
*********
58 Babies Who Received mRNA COVID-19 Vaccines Suffered Life-threatening Adverse Events
Ranit Feinberg & Yaffa Shir-Raz June 13, 2022
An analysis of VAERS reports shows that contrary to the FDA’s briefing document claiming that the majority of adverse events in Pfizers’ clinical trial were non-serious – at least 58 cases of life-threatening side effects in infants under 3 years old who received mRNA vaccines were reported. For some, it is unclear if they survived. It is also unclear why the infants were vaccinated and whether they were part of the clinical trials. However, in the upcoming FDA meeting on Wednesday, the FDA will not be able to argue it did not know
While the FDA is preparing to approve the mRNA COVID-19 vaccine for infants and toddlers aged 6 months to four years and claims in its’ VRBPAC Briefing Document released today that the majority of adverse events found in Pfizers’ trial were non-serious – Real-Time magazine analysis reveals at least 58 life-threatening adverse events in infants and toddlers aged under 3 years old reported to VAERS.
The most common serious adverse events were life-threatening bleeding, anaphylactic shock, anticholinergic syndrome, encephalitis, hypoglycemia, and neuroleptic syndrome. In most of the reported cases, these are multi-system injuries.
In some cases, it is not clear what happened to the babies – did they survive? And if so, have they recovered?
Most reports do not specify under what circumstances the infants were vaccinated and if they participated in the clinical trials.
While the FDA claims in its’ briefing document that the vaccine efficacy in infants is 80.4%, the document reveals that the claim is based on a total of 10 symptomatic cases of COVID-19 identified in the trial among 1415 participants – 7 of them in the placebo group vs. 3 in the vaccine group.
Assisted in the preparation of the article Shani Cohen
“Chest pain; cardiac arrest; Skin cold clammy”. This short description of a cardiac arrest, which occurred one hour after receiving a Pfizer-BioNTech COVID-19 vaccine, is taken from the VAERS system – the US Vaccine Adverse Eve Reporting System ( case number 1015467), and it does not refer to an elderly person, nor to a young adult, or even a teenager. It is hard to believe, but this report refers to a two-month-old baby. “A 2-month-old male patient received bnt162b2 (PFIZER-BioNTech COVID-19 VACCINE) lot number: EL 739, via an unspecified route of administration on 02 Feb 2021 at single dose for COVID-19 immunisation”, thus stated in the report.
“Patient administered vaccination, observed for 15 minutes left the clinic then returned one hour later on 02 Feb 2021, presenting as skin cold, clammy and with chest pain, cardiac arrest event then developed, patient stabilised and transferred for further medical treatment… The outcome of the events was unknown. This case was reported as serious with seriousness criteria-life threatening from HA. No follow-up attempts possible. No further information expected”.
How did a 2-month-old baby receive the mRNA vaccine? These vaccines have not yet received EUA (Emergency Use Authorization) for approved use in children ages five and under by the FDA, or any other regulatory authority, and even if it will, the EUA will only include babies 6 months and older.
Was this baby a participant in Pfizer-BioNTech’s clinical trials, testing efficacy, and safety among babies?
The answer is unclear. According to the person who wrote the report, “Unsure if the patient was enrolled in a clinical trial.” However, the author of the report also states that the report was ”received from a contactable Other Health Care Professional by Pfizer from the Regulatory Agency.” This note implies that the infant might have actually participated in Pfizer’s trial. The regulatory agency report Safety Report Unique Identifier GB-MHRA-ADR 24687611 – indicates that the report came from Great Britain (the first 2 letters in the report ID stand for the country of origin, GB- Great Britain, and MHRA indicate that the source of reporting was its’ drug authority).
Why did they not follow up on the 2-month-old baby’s condition after going into cardiac arrest an hour after receiving an experimental vaccine? Why is there no further information? Is it because he died? Or was the baby removed from an experiment? Why would the author of the report not mention this?
Shockingly, it turns out that this incident is not isolated but, in fact, one of many in the VAERS system describing babies and children under five exposed to mRNA Covid vaccines who suffered life-threatening adverse reactions.
Even though children under five were not considered eligible for these vaccines unless they were part of a clinical trial, astonishingly, it appears that there are many reports in the system describing babies and toddlers who were vaccinated. Some of the children suffered from life-threatening adverse events. In some cases, it is not clear what happened to them; did they survive and recover, do they still suffer from health problems, or did they die.
In a couple of days, on June 15, the FDA’s Vaccines and Related Biological Products Advisory Committee will discuss Moderna and Pfizer’s EUA requests for vaccines for infants and toddlers aged 6 months to 4 years – the only group not yet eligible for COVID-19 vaccination today. According to the FDA’s briefing document released today ahead of the VRBPA committees’ meeting, there were “245 US reports” to the VAERS system “in children 6 months through 4 years of age” who were injected (“product administered to the patient of inappropriate age” or “off-label use”) or exposed to the vaccine “via breastmilk.”
Nevertheless, both companies announced already in May that their findings indicate that their vaccines are safe and effective. The VRBPAC Briefing Document lists a variety of adverse events reported following the exposure to the vaccine in this age group, including “pyrexia…, body temperature…, cough, headache, rash, diarrhea”. According to the document, “Among US VAERS reports for individuals aged 6 months through 4 years, which may reflect unauthorized use of the vaccine or may reflect a reporting error, the majority (96.3%) were non-serious”.
While the document specifies safety concerns identified from post-authorization safety surveillance data in VAERS, including anaphylaxis, myocarditis, and pericarditis, it does not relate to these safety concerns identified in the younger age group. Instead, it states: “No unusual frequency, clusters, or other trends for adverse events were identified that would suggest a new safety concern.”
But is that really the case? It seems that regardless of the results, and despite the disturbing and shocking findings that are being exposed from Pfizer’s documents, it is expected that both companies will receive the desired EUA very soon. In fact, the CDC website, already in April, had advertised a protocol regarding children’s vaccination, which included babies 6 months to 4 years as well.
In light of this expected approval, RT Magazine conducted an analysis of the cases reported in the VAERS system referring to babies up to 3 years old.
During the analysis, cases were removed in which it was stated that the exposure to the vaccine was through breastfeeding (these cases were analyzed separately and will soon be presented in a follow-up article), as well as cases that were identified as errors in the age registration.
The analysis shows there were at least 58 cases of severe and life-threatening adverse reactions among babies and toddlers 3 years old and younger. This finding is especially puzzling considering the fact that they weren’t supposed to be vaccinated at this age, to begin with. Sadly, similarly to the case reported above, most VAERS reports do not indicate how and under which circumstances they were exposed to the vaccine – were the participants in the companies’ trials? And if not, why and in which circumstances were they vaccinated?
Both companies have not yet released the safety data from their trials on this age group. However, one thing is clear from the VAERS reports: there were many babies who were injured after receiving the vaccine. Whether vaccinated in the trials or illegally in their communities, Pfizer and Moderna will definitely not be able to claim, when presenting their data to the FDA, that the vaccine is safe for babies and that there weren’t any severe adverse events in this age group. Moreover, the FDA’s committee experts who will discuss the EUA approval will not be able to ignore those cases and argue that they did not know. The data presented in this article demonstrate beyond any doubt the complete opposite, and this time – these data are presented to the public in advance before the EUA is granted and ahead of the VRBPAC discussion.
The outcome of the events: Did not recover
One of the most chilling reports refers to a 43-day-old female baby, who on January 30, 2021, received Pfizer’s Comirnaty vaccine. In the incident description (report no. 1133837), it is clearly stated that she was vaccinated and that the vaccine was injected into the muscle: “A 43-days-old female patient received bnt162b2 (COMIRNATY), intramuscular on 30Jan2021 (Lot Number: EK9788) as SINGLE DOSE for COVID-19 immunization”. Right after the vaccination, the baby suffered a variety of life-threatening multi-system injuries, such as:
“Anaphylactic reaction (broad), Asthma/bronchospasm (narrow), Anticholinergic syndrome (broad), Acute central respiratory depression (broad), Pulmonary hypertension (broad), Cardiomyopathy (broad), Eosinophilic pneumonia (broad), Vestibular disorders (broad), Hypersensitivity (broad), Respiratory failure (narrow), Drug reaction with eosinophilia andsystemic symptoms syndrome (broad).” Although in the section reporting death, the statement states “No,” the section reporting recovery also states “No,” – meaning the baby has not recovered. What then happened to her? Is she alive, or did she die?
In addition, this report, like many others, raises some difficult questions. How did a 43-day-old baby receive a vaccine not yet approved for use in babies? Furthermore, the current clinical trials conducted are supposed to include babies and children over 6 months. Was this baby a participant in Pfizers’ trial? The report does not answer this question.
Just like this baby, it turns out that in most of the reported cases, several life-threatening side effects were recorded for the same baby. The most common severe adverse events were dangerous hemorrhaging; anaphylactic shock – a life-threatening allergy that can damage the respiratory system and cause dizziness, fainting, and even death; anticholinergic syndrome- a condition that occurs when the receptor sites for the neurotransmitter acetylcholine are blocked, which can lead to coordination problems, increased heart rate, and other symptoms; encephalitis – a brain infection, that can cause headaches, vomiting, loss of consciousness and death; hypoglycemia – very low blood sugar, a condition that can quickly escalate to death in infants; and neuroleptic syndrome – which is also life-threatening and can damage the heart muscles, other muscles, and the kidneys.
From the summary of the findings of the analysis according to age and gender groups, the following picture emerges:
In the age group of 0-6 months – there are 28 reports, of which 10 are males, 16 are females, and 2 whose gender was not specified.
9 of them (32%) suffered an anticholinergic syndrome, 9 (32%) had an anaphylactic shock, 8 (28.6%) suffered from Neuroleptic syndrome, 5 suffered from heart rhythm irregularities, and 5 had hypoglycemia.
In the age group of 6-12 months – in this group, 5 reports were found – 3 males, one female, and one whose gender was not specified. This group is small compared to the other groups. The list of adverse reactions included: anaphylactic shock, anticholinergic syndrome, and Neuroleptic syndrome.
In the age group of one-to-three year old – in this group, 25 cases were reported, of which 5 related to males, 19 related to females, and one to a baby whose gender was not specified.
6 of the babies (24%) had an anaphylactic shock, 6 (24%) suffered anticholinergic syndrome, 5 (20%) suffered from Neuroleptic syndrome, 4 (16%) suffered encephalitis, 3 (12%) had irregular heartbeats, one baby was hemorrhaging and one suffered from hypoglycemia.
It should be noted that the adverse events listed above are only some of the ones reported in VAERS with respect to babies. We have chosen to focus only on life-threatening and common adverse events.
Table No. 1: Analysis of reports by age and gender
Table No. 2: Analysis of reports by adverse events
Are the babies alive?
Similarly to the previous case described, another baby, two months old, also went through anaphylactic shock after being exposed to a single dose of the Pfizer-BioNTech vaccine on January 6, 2021, and just like her, according to the report (no. 976433), she suffered from an array of multi-system symptoms. Regarding the method of administering the vaccine, it was stated ”via an unspecified route of administration”, meaning it is not clear in what circumstances the baby was exposed to the vaccine.
Was she part of Pfizers’ clinical trial? Again, it is unclear from the report.
However, the more important question that should be asked, just like in the previous case, is what happened to the baby? Did she survive? Is she alive?
And again, in the section reporting death, it states “No”, meaning the baby did not die. However, in the report description, it says, “The patient had not recovered from the event. No follow-up attempts possible. No further information expected”. Read the rest here
It is hard to believe, but this basic question – what happened to a baby after suffering such severe and life-threatening adverse reactions – also arises from other serious cases, such as the case of a 6-month-old baby (report # 2084418) who “received bnt162b2 (COMIRNATY), intramuscular” on December 29, 2021, and went through anaphylactic shock, anticholinergic syndrome, Neuroleptic syndrome, infectious pneumonia, other infections, and multi-system symptoms.
In this case, as well, the section reporting death states “No”, meaning supposedly the baby did not die, while in the event description it says “outcome ‘unknown’… No follow-up attempts are possible. No further information is expected”.
In another case (report no. 1012508), a one-year-old baby who also received a Pfizer vaccine on January 19, 2021 (in this case, it is specified that the baby did not take part in a trial) developed pain in her left ear that escalated to full paralysis, which was diagnosed as Guillain Barre syndrome. In the case described, it was stated that the baby suffered Guillain Barre Syndrome, face paralysis, non-infectious encephalitis, non-infectious meningitis, earaches, and hearing disorders. Nonetheless, in the summary of the report, it was again written that “No follow-up attempts are possible.”
And another shocking case (report number 1379484) emerges from the report of a baby who was only one month old, who suffered “Vaginal bleeding/ Constant heavy vaginal bleeding with chunks of clot” the following day after receiving the Pfizer-BioNTech vaccine on May 19, 2021.
Although the symptoms the baby suffered from were defined as “serious as medically significant,” in the incident description, it is stated that the result is “unknown” and that “No follow-up attempts are possible. No further information is expected”.
As mentioned, in some of the cases, it is stated the babies were not part of a clinical trial, while in others, it is not clear whether they participated in a clinical trial or were vaccinated in other unknown circumstances. But whether they were part of the trial or not, the report does not explain the absence of this critical information; what happened to these babies? Did they survive? And if so, did they recover? Why was there not a follow-up on the medical condition of babies who suffered from severe and life-threatening adverse events while it was clearly stated that they did not recover? Is it not required in such severe cases by the FDA that the company should make every effort to locate these babies, find out what their condition is and follow up on them?
“Redness in the injection area: the clinical trial protocol does not mention severe adverse reactions”
The press release issued in February 11, 2022, in which Pfizer-BioNTech announced that they intend to apply to the FDA for approval for infants from 6 months to 4 years of age, the safety findings from the company’s clinical trials in babies and toddlers at these ages are not mentioned, not even in a word. The information brochure regarding the clinical trials testing the safety and efficacy of the Pfizer vaccine in adults, children, and babies, on the FDA website clearly states, “No Study Results Posted on ClinicalTrials.gov for this Study.” And as noted above, the newly released VRBPAC Briefing Document only lists a handful of non-serious adverse events reported in this age group, including, and concludes that there is nothing that would suggest a new safety concern. How could the FDA not know about so many serious adverse events that were reported to the CDC’s reporting systems? Alternatively, if they do know about them – why are they ignoring them?
How were adverse events in babies tested in the clinical trials? In an attempt to answer this critical question, intended to address the safety issues and to assure parents that the vaccine is safe for babies, we examined the study protocol found on the FDA clinical trial website.
It appears that no potential severe adverse events were listed. The list of potential adverse events that the study was supposed to evaluate according to the protocol (“outcome measure”) did include both local and systemic reactions. However, these are relatively non-serious adverse events.
The list of local adverse events that the trial was supposed to monitor includes: “Pain or tenderness at the injection site, redness, and swelling,” and the systematic reactions included ”Fever, fatigue, headache, chills, vomiting, diarrhea, new or worsened muscle pain, new or worsened joint pain, decreased appetite, drowsiness, and irritability”. Moreover, although the study is scheduled to end only on June 14, 2024, the time frame set for examining adverse events is limited to seven days after each of the doses – the first and the second dose.
The vaccine is ineffective in infants. The solution: lower the efficiency threshold and add a third dose
In addition to the substantial concerns regarding the vaccines’ safety for babies, their efficacy in this age group is questionable by and large. According to the available data, healthy children are at almost zero risk for severe illness, hospitalization, or death due to COVID-19.
Hospitalization due to COVID-19 is very rare among children, and death cases are even rarer. In Germany, for instance, a large study found that not even one child died of COVID-19 among 5-11 age group without pre-existing conditions. Under these circumstances, even one case of a serious adverse event, let alone death, is crucial and outweighs any possible benefit of the vaccine.
Not surprisingly, Pfizer clinical trials in babies under 4 proved that 2 vaccine doses do not increase their antibody count significantly. The FDA commissioner, Dr. Janet Woodcock, admitted in an interview in early April 2022 that “The antibodies that were developed were not as high, so they didn’t have the same antibody response to the two-shot series in the older kids. It wasn’t as high as what we would have hoped for the younger as it was for the older kids.” According to Woodcock, this is why Pfizer, which planned to apply for EUA approval for babies in February, postponed the submittal date and decided to add a third dose to the trial and wait for the findings after all babies got their third dose.
Furthermore, in a statement given on May 11, Dr. Peter Marks, director of the Center for Biologic Evaluation and Research at the FDA, announced that infant and toddler vaccines will not need to pass the 50% efficacy rate against Covid. A 50% efficacy rate is the threshold adult vaccines need to pass. However, Marks explains that despite the previous guidelines, the FDA will not deny companies now approval for babies and toddlers just because it did not reach the 50% efficacy in preventing symptomatic infections.
Pfizer issued a press release on May 23 announcing that “Vaccine efficacy of 80.3% was observed in the descriptive analysis of three doses during a time when Omicron was the predominant variant”. According to the press release, “The study suggests that a low 3-ug dose of our vaccine…, provides young children with a high level of protection against the recent COVID-19 strains”.
Yet, the FDA’s briefing document reveals that the claim for a “high level of protection” is based on a total of 10 symptomatic cases of COVID-19 identified in the trial, that occurred at least 7 days postDose 3. Three of them occurred among participants 6-23 months of age (which included 555 participants – 376 in the vaccine group and 179 in the placebo group) – with 1 case in the Pfizer-BioNTech vaccine group and two in the placebo group. Seven other cases occurred among participants 2-4 years of age (which included 860 participants – 589 in the vaccine group and 271 in the placebo group) – with 2 cases in the Pfizer-BioNTech vaccine group compared to 5 in the placebo group.
Nevertheless, the vaccine’s efficacy was framed by the FDA as 80,4%, and the document concludes that “Available data support the effectiveness of the Pfizer-BioNTech COVID-19 Vaccine 3-dose primary series (3 µg each dose) in preventing COVID-19 in the age group of 6 months through 4 years”. In addition, the document states that “Among infants and children 6 months through 4 years of age, rates of hospitalization and death due to COVID-19 are higher than among children and adolescents 5-17 years of age, and comparable to individuals 18-25 years of age, underscoring the benefit of an effective COVID19 vaccine in this age group”.
How ethical is it to give a baby a vaccine for a disease that the chances of getting severely ill or dying from are almost zero, while the benefits of the treatment are unclear and, and life-threatening adverse reactions are very significant?
This question was the topic of an article published in March this year in Bioethics. The researchers stated that not even one of the main claims argued to justify approval for babies is valid. According to them, the benefits of the vaccine for healthy children are minimal, and therefore, even though complications are rare, they outweigh the vaccine’s benefits, especially since it is highly unclear what the short and long-term risks are, and the experience with the vaccine is very short. The altruistic claim of protecting the environment is also very problematic, since as a vaccine exists, the groups at risk can defend themselves, and it was proven already that children are not the main transmitters of the virus.
Congress members demand answers
This ethical issue has been raised in recent days by 18 members of Congress in a letter issued to the FDA on June 7, demanding answers before the authority’s decision to grant an emergency permit for the infant vaccine. Members of Congress demanded to know why COVID-19 vaccines are necessary for this age group in light of the fact that the disease poses a very small risk to infants and young children, that vaccines have little efficacy, and that there are many unanswered questions regarding these vaccines’ safety and adverse events.
The letter presents 19 questions to the FDA, including, among others – why did the FDA delayed the publication of the hundreds of thousands of data pages from the manufacturers’ studies, the state of adverse events, and when can all FDA data be expected to be made public? The FDA was also asked to provide the public with more details regarding children who were severely injured or died from COVID-19 and how many children, in general, became seriously ill. Legislators also addressed the issue of cardiac risks in giving the mRNA COVID-19 vaccines to children, noting that following vaccinations given to large numbers of children aged 5-18, an increase in myocarditis and pericarditis was observed, with some cases ending in death, and the long-term effects of heart-related inflammation not yet quantified by health authorities. What’s more, lawmakers demanded to know why the FDA lowered the threshold of efficacy for the vaccines specifically for infants and youngest children, thus actually allowing companies to apply for EUA without any justification.
The FDA will not be able to argue it did not know
As stated, the data emerging from the analysis presented in this article demonstrate beyond any doubt that the vaccine is not safe for babies and toddlers. Whether these children were part of the study or not – these reports have been in the VAERS system for many months, so there is no chance that the FDA does not know them. Unfortunately, the fact that the FDA was aware of at least some of the serious adverse events, including increased risk of morbidity in the first days after vaccination, myocarditis, and increased risk of miscarriage and fetal malformations, and yet approved the vaccine for teens, children, and pregnant women, was later revealed too late – long after the EUA was granted to Pfizer and Moderna, when many have already been harmed. It only became clear thanks to FOIA (Freedom of Information) requests submitted to the FDA and other health authorities, and only after the FDA was forced by the court to disclose the documents. This time, the VAERS data presented here makes it possible to reveal this fact even before the approval. The FDA will not be able to claim that it did not know.
Note: In a number of articles, I’ve offered compelling evidence that the deaths attributed to COVID-19 can be explained without reference to a virus. Furthermore, whatever merits “alternative treatments” may have, I see no convincing evidence their action has anything to do with “neutralizing a virus.”
The entire tragic, criminal, murderous, stupid, farcical COVID fraud is based on a hundred years of Rockefeller medicine—a pharmaceutical tyranny in which the enduring headline is:
ONE DISEASE, ONE GERM.
That’s the motto engraved on the gate of the medical cartel.
—Thousands of so-called separate diseases, each caused by an individual germ.
“Kill each germ with a toxic drug, prevent each germ with a toxic vaccine.”
In the absence of those hundred years of false science and propaganda, COVID-19 promotion would have gone over like a bad joke. A few sour laughs, and then nothing, except people going on with their lives.
The overall health of an individual human being has to do with factors entirely unrelated to “one disease, one germ.”
As I quoted, for example, at the end of a recent article—
“The combined death rate from scarlet fever, diphtheria, whooping cough and measles among children up to fifteen shows that nearly 90 percent of the total decline in mortality between 1860 and 1965 had occurred before the introduction of antibiotics and widespread immunization. In part, this recession may be attributed to improved housing and to a decrease in the virulence of micro-organisms, but by far the most important factor was a higher host-resistance due to better nutrition.” Ivan Illich, Medical Nemesis, Bantam Books, 1977
And Robert F Kennedy, Jr.: “After extensively studying a century of recorded data, the Centers for Disease Control and Prevention and Johns Hopkins researchers concluded: ‘Thus vaccinations does not account for the impressive declines in mortality from infectious diseases seen in the first half of the twentieth century’.”
“Similarly, in 1977, Boston University epidemiologists (and husband and wife) John and Sonja McKinlay published their seminal work in the Millbank Memorial Fund Quarterly on the role that vaccines (and other medical interventions) played in the massive 74% decline in mortality seen in the twentieth century: ‘The Questionable Contribution of Medical Measures to the Decline of Mortality in the United States in the Twentieth Century’.”
“In this article, which was formerly required reading in U.S. medical schools, the McKinlays pointed out that 92.3% of the mortality rate decline happened between 1900 and 1950, before most vaccines existed, and that all medical measures, including antibiotics and surgeries, ‘appear to have contributed little to the overall decline in mortality in the United States since about 1900 — having in many instances been introduced several decades after a marked decline had already set in and having no detectable influence in most instances’.”
How the immune system (if it is a system) actually operates is beyond current medical hypotheses.
“T-cells, B-cells, neutrophils, monocytes, natural killer cells, proteins,” are welded into a breathless story about a military machine that attacks germ invaders. Push-pull. Search and destroy.
The notion that THIS is what creates health is fatuous.
Positive vitality is what keeps us healthy.
A few factors of positive vitality are on the tyrannical COVID list of what-should-be-squashed: financial survival; open mingling of friends and family; people looking (unmasked) at people; open communication without fear of censorship.
Nutrition and basic sanitation are key vitality factors, of course.
And then we have Purpose in Life: where are people pouring their creative energies?
Obviously, freedom from harmful medical treatment is necessary for vitality to flourish.
Suppression of LIFE, in order to stop a purported germ, is institutionalized death.
Modern medicine is sensationally exposed in a review I’ve mentioned dozens of time over the past 10 years: Authored by the late famous public health doctor at Johns Hopkins, Barbara Starfield, it is titled, “Is US Health Really the Best in the World?” It was published in the Journal of the American Medical Association on July 26, 2000.
It found that, every year in the US, the medical system kills 225,000 people.
Per decade, the death toll would come to 2.25 million people.
You won’t find that in CDC reports.
In 2009, I interviewed Dr. Starfield. I asked her whether the federal government had undertaken a major effort to remedy medically caused death in America, and whether she had been sought to consult with the government in such an effort.
Professor Thomas Seyfried has published over 150 peer reviewed studies in biology and cancer biology and has verified Nobel Prize Winner Otto Warburg’s assertation that cancer is a metabolic disease of the mitochondria, not a genetic disorder. If we misunderstand the origin of the disease, the treatment is going to be wrong as well, and this is exactly what has happened. Ever think about why the cancer rates have tripled in the past 40 years? Well, this is why.
Thomas N. Seyfried received his Ph.D. in Genetics and Biochemistry from the University of Illinois, Urbana, in 1976. He did his undergraduate work at the University of New England, where he recently received the distinguished Alumni Achievement Award. He also holds a Master’s degree in Genetics from Illinois State University. Thomas Seyfried served with distinction in the United States Army’s First Cavalry Division during the Vietnam War and received numerous medals and commendations. He was a Postdoctoral Fellow in the Department of Neurology at the Yale University School of Medicine and then served on the faculty as an Assistant Professor in Neurology.
Other awards and honors have come from such diverse organizations as the American Oil Chemists Society, the National Institutes of Health, The American Society for Neurochemistry, the Ketogenic Diet Special Interest Group of the American Epilepsy Society, the Academy of Comprehensive and Complementary Medicine, and the American College of Nutrition.
Dr. Seyfried previously served as Chair, Scientific Advisory Committee for the National Tay-Sachs and Allied Diseases Association and presently serves on several editorial boards, including those for Nutrition & Metabolism, Neurochemical Research, the Journal of Lipid Research, and ASN Neuro, where he is a Senior Editor.
Dr. Seyfried is also the author of the book, Cancer as a Metabolic Disease: On the Origin, Management, and Prevention of Cancer (Wiley, 1st ed., 2012).
Daily Clout and Health Freedom Defense Fund (HFDF) filed a Citizen Petition with the U.S. Food and Drug Administration (FDA) requesting that FDA revoke Emergency Use Authorization of COVID-19 vaccines for young children subsequent to FDA’s authorization of the COVID-19 injections for that age group on June 17, 2022.
Dr. Naomi Wolf, CEO of Daily Clout, asserted,
“With this decision, the FDA abandons its duty to protect the American people. COVID-19 poses statistically insignificant risk to babies and young children, and neither safety nor efficacy of the injections have been proven. But research from the WarRoom/DailyClout Pfizer Documents Research Volunteers, along with analyses of official databases, primary source documents, and peer-reviewed studies, shows that the mRNA vaccines damage many teens’ hearts, leave babies with GI problems, sleep problems, seizures, liver damage, and multiorgan system failure, and suppress leukocytes; the vaccines visibly damaged the hearts of animals in studies. Why on earth would we thus risk the health of small children and babies?”
In fact, ignoring this data is the definition of arbitrary and capricious, a clear legal dereliction of FDA’s duty.
While the COVID injections were promoted as the only way to end the COVID crisis, the real-world evidence has demonstrated the injections not only fail to prevent infection, they also do not stop transmission.
Moreover, clinical trial data from Pfizer and Moderna reveal that more children who received the vaccines were diagnosed with COVID and hospitalized, respectively, than those in the placebo group. In addition, recent research and data from around the world suggest the injections impair long-term immunity to the virus, rendering recipients more likely to be hospitalized or die from COVID.
Leslie Manookian, President of Health Freedom Defense Fund stated,
“Aside from not performing as purported, the injections pose serious known and unknown risks to young children. Leaked data from Japan revealed high levels of the lipid nanoparticles from the mRNA shots accumulate in the ovaries with unknown consequences. But menstrual irregularities and increased rates of miscarriage have been reported after the injections. A recent study identified reduced sperm concentrations and effects on sperm motility. With these safety concerns in mind, FDA authorizing the injections for young children defies reason and the precautionary principle.”
FDA is charged with protecting public health, not marketing the products of what is arguably the most powerful industry in the world.
Daily Clout and HFDF request that FDA reverse or at the very least pause its decision to issue an EUA for mRNA vaccines for six-month-olds to under-fives. We ask instead that they further study the research available, including the research itemizing harms described above, and that they take into account over 130,000 comments submitted to the FDA regarding the dangerous step of authorizing these shots for young children, which they are legally required to consider.
Should FDA fail to reverse its authorization, Daily Clout and Health Freedom Defense Fund will take legal action to ensure that FDA abides by the law.
Recently I joined a group of 20 doctors and scientists around the world who put their names to the “Settling the Virus Debate” statement. In this two-page document we suggested, “rather than engaging in wasteful verbal sparring, let us put this argument to rest by doing clear, precise, scientific experiments that will, without any doubt, show whether these claims are valid.” Some of the individuals who believe that the existence of pathogenic viruses is an established fact, proceeded to immediately disagree. One was Steve Kirsch, who attempted to distract from the central tenet of our statement, being that virology had failed to carry out scientific control experiments. In reality, it is clear that the virologists have not shown that their techniques of “viral” cultures, genomics, and clinical diagnostics are valid even on their own terms. Indeed, I have not seen Kirsch or anyone else provide evidence that the appropriately-controlled experiments we suggested in the statement have been performed.
Kirsch admitted, “this is not my field of expertise at all. I rely on other people around me who I trust.” I have written a previous article about why I think Kirsch should be careful about trusting other “experts.” However, he continues to favour this approach and one of his trusted parties includes the pathologist/virologist Dr Sin Lee. Lee wrote, “Tom Cowan claimed the virus has not been isolated. But the virus has been isolated by the CDC and marketed by ATCC as the control materials. I bought the virus as the control for my CLIA tests. Many others do.” We have covered the follies concerning these claims of “isolation” many times and the CDC certainly have no studies demonstrating the existence of a pathogenic particle termed ‘SARS-CoV-2’. The ATCC simply repeat the claim by the CDC that their listed product contains a “virus” – however as I outlined in my first “Warning Signs” article, following the trail back to the start does not lead to any evidence of a virus in the biological potions being passed around.
On 18 July 2022, Lee sent the following email to Dr Tom Cowan:
I have a Preprint manuscript currently under peer review as follows. ://www.preprints.org/manuscript/202206.0192/v1 There is irrefutable Sanger sequencing evidence that the virus exists and keeps mutating. If Dr. Tom Cowan disagrees, please write a critique to challenge my data and interpretation online in the open. I will respond. Other scientists can join in for the debate.
Dr Sin H. Lee, 18 July 2022
The preprint paper is titled, “Implementation of the eCDC/WHO Recommendation for Molecular Diagnosis of SARS-CoV-2 Omicron Subvariants and Its Challenges.” To expose the problems of virology it is crucial to examine the methodology section of any publication and in this case it is no different. In the “material and methods” section Lee stated that, “five (5) selective nasopharyngeal swab specimens collected from non-hospitalized patients with respiratory infection, which were confirmed to be true-positive for SARS-CoV-2 Omicron variant by Sanger sequencing.” Here we are straight into the deep end of virology’s circular reasoning: the “virus” has been confirmed to exist on the basis of detected sequences from some nasopharyngeal swabs. There is nowhere in the paper that any evidence is provided for the existence of an actual virus, that is, a tiny particle that acts as an obligate intracellular parasite and is capable of causing disease in a host.
The claim that the specimens were, “true-positive[s] for SARS-CoV-2 Omicron variant,” simply means some sequences that were previously deposited on genetic databases, and fraudulently declared to be “viral,” were being detected again. It doesn’t make any difference which sequencing technique is used, in this case bidirectional Sanger sequencing because the crucial issue is the provenance and clinical relevance of these detected sequences. This is the foundational issue in the entire COVID-19 fraud: there is no virus, simply sequences falsely claimed to be evidence of an actual virus. The World Health Organisation helped orchestrate the deception when it declared that a confirmed ‘case’ of infection with the invented virus is simply the detection of some of these sequences. We have covered this absurd circular reasoning in much of our work including in Sam’s 2020 video “What Is A Covid-19 Case?” (And rapid antigen tests are covered here.)
Back to Lee’s paper and in the following paragraph of the “material and methods” section, he described the, “RNA Extraction from Nasopharyngeal Swab Specimens,” as follows:
As previously reported [25-27], the cellular pellet derived from about 1 mL of the nasopharyngeal swab rinse along with 0.2 mL supernatant after centrifugation was first digested in a buffered solution containing sodium dodecyl sulfate and proteinase K. The digestate was extracted with phenol. The nucleic acid was precipitated by ethanol and redissolved in 50 μL of DEPC-treated water.
In other words, there was no step to demonstrate: (a) there were any “viral” particles contained within the samples, or (b) that the RNA came from such imagined viral particles. A reverse transcription polymerase chain reaction was then applied to these undifferentiated samples to generate amplicons ranging from 398 to 707 nucleotides in length. Most of these sequences spanned the so-called ‘Spike protein’ gene of the alleged SARS-CoV-2 genome, as that was the area of interest for the study. In the next step it was stated:
The crude nested PCR products showing an expected amplicon at agarose gel electrophoresis were subjected to automated Sanger sequencing without further purification.
In fact, at no stage was an attempt undertaken to purify any entity from the crude nasopharyngeal specimens. The entire basis of the study was built on the unestablished premise that the genetic sequences detected were already known to come from inside a pathogenic particle.
The “results” section then detailed the nucleotide sequences of the various amplicons that were generated from the crude samples. Some of the codons (three-nucleotide units that encode a particular amino acid or stop signal) were described as “mutated” on the basis of comparisons to other sequences previously deposited on the genetic databanks. The use of the word ‘mutation’ is problematic in itself, because it implies that a genome has been altered. A genome must belong to a discrete biological entity, so virology is once again misusing terminology to imply that a certain proof has been established. Lee’s study was simply looking at RNA sequences in uncontrolled experiments.
Those of us that dispute the virus narrative point out that no RNA (or DNA) sequences have ever been shown to come from inside any specific identifiable particle that fulfils the definition of a virus. Thus all RNAs can only be said to be expressed by a known organism, introduced artificially (e.g. synthetic mRNA injections) or be of unknown provenance. The “mutations” only exist within in silico models that have not been shown to be independent entities in nature. There are other reasons why RNA sequences can and do vary in dynamic biological systems and I can’t imagine that any virologist would disagree with this fact. Simply detecting RNAs is not enough to draw conclusions about their provenance. Other experiments are required to make this determination.
In our first COVID-19 Fraud essay we documented the original invention of SARS-CoV-2 by Fan Wu’s team who assembled an in silico “genome” from genetic fragments of unknown provenance, found in the crude lung washings of a single ‘case’ and documented in, “A new coronavirus associated with human respiratory disease in China.” Their in silico construct served as a reference for others to then “find” the same “virus” around the world, without evidence that such a particle actually existed.
In our soon to be published follow-up COVID-19 Fraud essay we will provide a more detailed explanation as to why detecting nucleic acid sequences per se in crude specimens or cell cultures does not provide the required evidence for “viruses.” In the essay we will also follow the trail back to the first ever declarations of “coronavirus genomes” in the 1980s and show that no viruses were demonstrated in any part of the trail. However, such sequence data is used to promulgate the illusion of “virus” family trees, or claimed “mutations” as discussed above.
Dr Lee’s paper does not even appear to be designed to demonstrate the existence of a postulated disease-causing particle. I sent him several questions including, “I have read the preprint and there does not appear to be a hypothesis presented – is that correct?”, “In your study there did not appear to be any controls (e.g. checking for selected sequences in other nasopharyngeal specimens from humans said not to have the alleged virus) – presumably that was by design?” and “What is your definition of a ‘virus’ in the paper?” Lee responded, “your questions are irrelevant to you [sic] intention to write a comment or critique on the manuscript involved,” and suggested I write something in the preprint website’s comment section.
Lee has provided a descriptive paper that omits a falsifiable hypothesis so it is unclear why he would present it as experimental evidence, let alone “irrefutable” evidence of the existence of SARS-CoV-2. His paper is inappropriately designed for this purpose and his claim engages in a circular reasoning fallacy: the genetic sequences are proffered as evidence of the virus, because it was presupposed that they come from the virus. We are asking, “where is the virus?”
Virology has a problem: It needs to show that “A” actually exists
It’s back to the drawing board for virology: it invented the theory of viruses, so whatever method it employs to prove their existence, it must satisfy that definition. In fact, do the virologists even have a theory? The definition of a scientific theory is:
an explanation of an aspect of the natural world and universe that has been repeatedly tested and corroboratedin accordance with the scientific method, using accepted protocols of observation, measurement, and evaluation of results.
Our “Settling the Virus Debate” statement proposes that the virologists need to employ the required scientific method as a starting point. It is not looking good for them because they have not even demonstrated any internal validity on their own terms. According to science they may not even have a theory. If they have a hypothesis, they need to specify an independent variable (in this case the postulated “virus”) and a dependent variable for analysis. Moreover, to even get started, the independent variable must first be shown to physically exist. I would implore Steve Kirsch to reconsider taking advice from these “experts” and to commence his own investigations into the house of virology. By scientific accounts, it is a house of cards.
Postscript
(Derived from: A. F. Chalmers, What is this thing called Science?, 2nd ed, 1982)
‘Observational statements are frequently presupposed by theory. Such statements are always made in the language of some theory and will be as precise as the theoretical or conceptual framework that they utilise is precise’. In this instance, a virus particle was not observed first and subsequently viral theory and pathology developed. Scientists of the mid and late nineteenth century were preoccupied with the identification of imagined contagious pathogenic entities.
‘The observations of the naïve inductionist did not identify a virus a priori, and then set about studying its properties and characteristics. The extant presupposition of the time was that a very small germ particle existed that may explain contagion. What came thereafter arose to fulfil the presuppositional premise’.
‘A popular view of scientific knowledge is that it is proven knowledge and scientific theories are derived in some righteous way from the facts of experience acquired by observation and experiment. Science is based upon what we can see, hear, measure and touch. Science is objective and explicit. Scientific knowledge is reliable knowledge because it is objectively proven knowledge’.
‘A realistic scientific theory will consist of a complex of universal statements rather than a single statement. Further a theory will need to be augmented by auxiliary assumptions, such as laws and theories governing the use of any instruments used, for instance’.
‘The premises from which the prediction is derived must also include the interconnected statements that constitute the theory under test, the initial conditions, and the auxiliary assumptions. Falsification of the theory also indicates the possibility of a failure of any number of the associated assumptions and conditions, and not necessarily of the theory itself’.
Acknowledgement
I would like to express my gratitude to Dr M. C. McGrath (New Zealand) for his constructive criticisms and inspiration for the postscript.
I was relaxing in our screened porch in our little cottage in the forest, feeling rather pleased with myself. It had been an arduous week of the usual combat for liberty, but there had been victories.
I was reading a decorating magazine (we all have our vices). The grass was dewy; birds were loud. The morning was glorious.
I was feeling pioneer-ish and independent. I was alone in the house; Brian was traveling. I enjoyed the narrative moment: “Lady in the woods.”
Then I heard a “thump” about eight feet away behind my head. It was an exasperated thump, like a teenager slamming the door to his room. Like, “Really??”
I glanced behind me and saw the enormous ears and forehead of a sizable brown bear, who was ducking insolently, clearly aware of me, to lower himself behind the trash cans.
I sped indoors, locking the door. I grabbed a weapon out of the hall closet. In my haste, I grabbed the weapon that looked like a rifle, instead of the actual rifle, which was in a case. Thus I found myself locked in an upstairs bathroom, cowering, armed with a BB gun.
I sort of knew this bear. Brian had captured on his trail camera about a year ago, what must have been this bear and his brother or sister, when the little ones were just adorable cubs. One of the cubs had nuzzled the trailcam til the mom had batted it away, urging her little ones to follow her deeper into the woods, far from the dangerous things of men. One of the cubs was now this massive creature, that bear-watchers call a “sub-adult.”
I saw, peering fearfully out of the window, that it was no longer cute and fat. It was was thin, but massively muscled, and looked disoriented. It must have been eight feet long.
I paced into the upstairs bedroom and secured the windows. The bear left the garbage cans, and followed me around the corner of the house. I could now see it pacing and sniffing directly opposite the bedroom windows, though on the ground level. There were windows all around the house on that level. Bears had been known to break into homes.
I looked under the bed: hiding there could not save me if the bear made it into the house. I realized I was holding a BB gun, and felt ridiculous. Even if I managed to shoot it, this would do nothing but enrage him. The thin bedroom doors that I had thought so rustic and charming, could be broken down by an angry animal of that size in no time.
My heart pounded as I realized that he was not leaving; he continued pacing and circling, no matter where I went.
I went back into the bathroom, and locked that door with its flimsy lock.
There he was again, outside on that side of the house, as if he was spotting me or as if he could scent me. Surely he could smell my fear.
I cowered behind the bathroom curtain. The bear paused in its ransacking of the trash, stood up again on hind legs, looked right at me — or smelled right at me — and bared its long, sharp yellow teeth.
If I had had sympathy for the hungry teenager abandoned by its mom (or “emancipated” by its mom, as the bear watching sites explain) it evaporated.
I was on the phone with Brian, frozen with fear.
“Make yourself big! Shout at him!” Brian instructed. That was impossible. I could not move. I could hardly breathe.
That would be it, surely, I thought, after he’d exhausted the trash bag. He’d leave now, surely. But no. He came back toward me again like a nightmare, and headed once more to circle the house.
I called the sheriff’s office.
Twice they told me that nothing could be done, and to stay inside. I don’t blame the Columbia County Sheriffs. They have issues to deal with more serious than a former city lady trapped in her house by a hungry bear.
But the bear kept circling right up against the walls of the house. This went on for an hour. Adrenaline poured through my bloodstream. I did wonder if I would die that day.
When I called back in spite of myself and begged the police for help, they told me to call again only if he managed to break into the house. (Thank you, ‘Defund the Police’ advocates…)
At certain points of extreme stress, I could not even bring myself any longer to look outside to see where the bear was. What if I looked and couldn’t see him because he was already in the house? I went right into a place that is familiar to those of us with PTSD – a traumatized place where you freeze, and where you engage in magical thinking.
If I don’t look at the bear he won’t be there. If I don’t meet his gaze he won’t see me or smell me. I am somewhere else. I am not really here.
Reader, after an hour I was saved when brave colleagues of mine, Craig Klein, Reinette Senum and Jamie Arrigo, who had been meeting nearby, drove down our wooded driveway, blowing their car horns. I raced down the steps, never so happy to see people in my life. Reinette laughed at the sight of me racing to open the door, still carrying my useless BB gun.
I think I was coherent, but I was in shock. An officer from the Sheriff’s department arrived at the same time, bless him. Humans saved me. The aggressor, the wild animal, had been scared away, and not by me. I’d been a wreck, hopeless.
For days, I ruminated about the sharp yellow teeth of that bear, exposed as he raised his snout into the air, sniffing, like a scene from a horrifying fairy tale.
Why do I tell this story?
Because – the bear had been growing more and more comfortable emerging from the woods; he grew more and more comfortable exploring our trash and then he took over territory in exploring our lawn; he was “habituated” ultimately, as bear watchers say; he had ownership of the lawn and was circling the house to mark his territory. He was comfortable at last in stalking the homeowners.
He was here because — I had done nothing to stop him. He was here because I let him slowly take over our home.
My not being able to look directly at the bear did not make me any safer. My denial put me in greater danger.
This all, of course, really happened. But that does not mean it is not also a metaphor.
The same week that this happened, I also finalized my reporting about the Pfizer vaccines, showing — what I knew for months I would eventually find.
The heart of the manufacture and distribution of millions of doses of the MRNA vaccines that are causing such a swath of death and destruction throughout North America and Western Europe, is enmeshed with the plans, methods and manufacturing infrastructure of our existential adversary.
The enemy is within our very bodies.
Since I first started reading the reports produced by the 3000 medical and scientific experts of the WarRoom/DailyClout Pfizer Documents Research Volunteers team, based on the 55000 Pfizer documents released under court order, I knew I was seeing not just medicine gone wrong, not just a greedy pharmaceutical company and a regulatory agency that was fully corrupted, but rather, or additionally, I was seeing a massive act of war. [https://campaigns.dailyclout.io/campaign/brand/cc3b3e5a-6536-4738-8ed6-5ee368c67240]
When I saw the eighteen months’ worth of sudden deaths, slow deaths, encephalies, strokes, heart attacks, pericarditis, myocarditis, Guillain Barre, Bell’s palsy, MS, blood clots, lung clots, leg clots, blue-green breast milk, spontaneous abortions, stillbirths, neonatal seizures, neonatal multi-organ system failure, liver damage, kidney damage, suppressed lactation, suppressed sperm count, disrupted menses, all detailed the Pfizer documents; when I saw the fact that 34,000 plus of the 42000 plus adverse events “cases” itemized in the worldwide rollout of the Pfizer injections, were sustained in the US — with the next largest group being sustained in Western Europe – and that the 56 countries around the world that also had Pfizer injections rolled out, amounted for only a bit over 7000 adverse events total — I knew I was seeing not just medicine gone wrong on a massive scale, but rather that I was seeing an act of war.
When I saw the doubling of neonatal deaths in country after country, the rise of 34% above normal in stillbirths and spontaneous abortions for vaccinated versus unvaccinated mothers; when I saw that 3816 vaccinated women in the VAERS database lost their babies — 57% of all the neonatal deaths in all the time that VAERS records had been kept — [https://www.clarkcountytoday.com/news/cdc-database-shows-death-risk-for-babies-of-vaccinated-mothers/]; when I saw that of 36 pregnancies followed in the Pfizer documents, 28 of the babies died [https://www.drpaulalexander.com/blogs/news/etana-hecht-israeli-scientist-researcher-vaccinated-women-fertility-signals-are-coming-through-the-fda-pfizer-actively-worked-to-keep-this-data-hidden-from-sight-for-our-lifetimes]; when I saw the rise of 40 per cent in death rates and the shocking rise in cases of disability in the West [https://journal.rajeshtaylor.com/further-disturbing-rates-of-disability-mortality-in-life-insurance-data-since-covid-vaccine-rollout/—] I knew I was not seeing just medicine gone wrong on a massive scale, but that I was witnessing an act of war.
When I saw that you could boost the lethality or the damage caused by the injection by simply changing how dilute the solution is, or simply by reassigning which brand you use – with Moderna (100 mcg) far more damaging than Pfizer (30 mcg) — I knew that I was seeing not just medicine gone wrong on massive scale, but an act of war.
When I saw a study out of Hong Kong in 2021 — a study that, of course, was answerable to the CCP — that revealed that a second dose (a “booster”) into the bloodstreams of mice, resulted in visibly enlarged hearts with white patches that could be seen by the naked eye, as well as cytokine storms and liver damage, I realized that the two-dose regime and then the “boosters” were slow but progressive ways to damage and then destroy the health of Western patients. The study concluded: “Post-vaccination myopericarditis is reported after immunization with coronavirus disease 2019 (COVID-19) messenger RNA (mRNA) vaccines.”
And yet with this CCP-overseen finding, that by injecting mammals with the MRNA vaccine, their hearts were visibly damaged, the worldwide injection program kept going.
[https://academic.oup.com/cid/article/74/11/1933/6353927; Intravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model, Can Li, Yanxia Chen, Yan Zhao, David Christopher Lung, Zhanhong Ye, Wenchen Song, Fei-Fei Liu, Jian-Piao Cai, Wan-Man Wong, Cyril Chik-Yan Yip, Jasper Fuk-Woo Chan, Kelvin Kai-Wang To, Siddharth Sridhar, Ivan Fan-Ngai Hung, Hin Chu, Kin-Hang Kok, Dong-Yan Jin, Anna Jinxia Zhang, Kwok-Yung Yuen; Clinical Infectious Diseases, Volume 74, Issue 11, 1 June 2022, Pages 1933–1950, https://doi.org/10.1093/cid/ciab707]
We were told that Pfizer/BioNTech is a German company. But it is actually a German-Chinese company. Since I first found that Pfizer/BioNTech had an MOU with Fosun Pharmaceuticals, a major CCP-linked pharmaceutical company based in Shanghai, to make the Pfizer/BioNTech MRNA vaccines, I knew that with a bit more digging I would find China at the heart of these acts of war.
BioNTech’s SEC filing shows that the MOU with Fosun Pharmaceuticals includes an equity investment by Fosun in BioNTech. In other words, the CCP is an equity investor in BioNTech: “As part of the strategic alliance with Shanghai Fosun Pharmaceutical (Group) Co., Ltd (“Fosun Pharma”; Stock Symbol: 600196.SH, 02196.HK) whereby the two companies will work together on the development of BNT162 in China, Fosun agreed to make an equity investment which was received in mid-April 2020. The issuance of 1,580,777 ordinary shares with the nominal amount of k€ 1,581 was registered within the commercial register (Handelsregister) as of April 23, 2020.” Not only that but: “Ai-Min Hui, President of Global R&D, and Chief Medical Officer of Fosun Pharma said: ”We are closely working with BioNTech and regulatory authorities to evaluate the safety and efficacy of the vaccine candidate, in order to synchronize the development process in China with other countries, and to bring the vaccine to public as soon as possible, if the vaccine succeeds.” [https://www.sec.gov/Archives/edgar/data/1776985/000119312520210694/d54613d424b3.htm]
Fosun is not separate from the CCP; it is the CCP: Fosun acquired almost half of Sinopharm: “In 2003 Fosun Pharmaceutical acquired 49% stake of Sinopharm Group (Chinese: 国药控股). […] In 2008, a year before the initial public offering of Sinopharm Group, Fosun Pharmaceutical owned the direct parent company of Sinopharm Group, Sinopharm Industrial Investment (Chinese: 国药产业投资) instead; the majority owner of the joint venture was state-owned China National Pharmaceutical Group (Sinopharm).” 2003年年报 [2003 Annual Report] (PDF). Fosun Industrial. 24 April 2004. Retrieved 5 August 2018– via Shanghai Stock Exchange website. [^国药集团复星联合成立首家混合所有制药企. 企业观察报 (in Chinese (China)). 4 August 2014. Retrieved 5 August 2018 – via Sina; ^2009年年报 [2009 Annual Report] (PDF). Fosun Pharmaceutical. 25 March 2010. Retrieved 5 August 2018 – via Shanghai Stock Exchange website.; ^“Connection Transaction” (PDF) (Press release). Shanghai: Fosun International. 20 June 2008.]
Sinopharm, of course, as you see above, of which Fosun owns almost half, is owned in turn directly by the Chinese State and thus reports directly to the CCP.
The initial BioNTech/Fosun MOU seems to imply that all of the BioNTech/Fosun joint ventures’ activity is in China, or in regions aligned with or close to China. But is that now the case? Fosun Pharma did not stay in China.
It came here. Fosun Pharmaceuticals is now also Fosun Pharmaceuticals USA, with branches for R and D and product formulation in Boston, MA and Princeton, NJ: [https://fosunpharmausa.com/covid19/pcr/]
It is producing formulations and products in the US for distribution in the US and around the world. Fosun Pharma has built a “global operation strategy” for the manufacture of COVID-19 vaccines, COVID-19 PCR tests and COVID-19 antigen tests:
“Fosun Pharma has built a strong root in China and developed a global operation strategy, with pharmaceutical manufacturing and R&D being the largest and core business segment, […]”
“In 2021, the revenue from new and sub-new products including COMIRNATY® (mRNA COVID-19 vaccine, also known as BNT162b2), […] accounted for over 25% of the revenue in the pharmaceutical manufacturing segment;
· Revenue from regions outside Mainland China and countries overseas reached RMB13,599 million, accounting for 34.86% of the total revenue, marking a step forward on globalization.” [Italics mine].
And more: “Continuously strengthening the global operation capability and making further enhancement for globalization, Fosun Pharma has formed a global operating system for R&D, manufacturing and commercialization, and continuously expands overseas markets. [..] Globalization capability is continuously strengthened. The second headquarters in the United States help to build a global business landscape with full coverage of R&D, manufacturing and commercialization.[…]
“By the end of 2021, Fosun Pharma’s overseas commercialization team with over 1,200 employees has built marketing platforms in the United States, Africa and Europe [italics mine]and has achieved direct sales of formulations to the U.S. market. […] The COVID-19 test kit by Fosun Diagnostics has been sold in over ten countries. […] Gland Pharma, a holding subsidiary in India, received approvals from the US FDA for 13 generic drugs in 2021.
“Leveraging the current global manufacturing capability and world-class manufacturing facilities […] Fosun Pharma has accelerated the acquirement of international GMP certification of domestic production lines, laying a solid foundation for exporting domestic products. In January and March 2022, Fosun Pharmaceutical Industrial obtained the Medicines Patent Pool (MPP)’s license to produce and supply the generic version of Merck’s oral COVID-19 treatment Molnupiravir and Pfizer’s oral COVID-19 treatment Nirmatrelvir, as well as the co-packaged product of Nirmatrelvir and Ritonavir of Pfizer [….]. The license includes both ingredients and the finished drug. Through this license, Fosun Pharma devoted itself further to fighting against the pandemic around the world.”
Fosun Pharma USA offers potential partners: “A global reach with a focus on the United States and China markets”. It offers “US Rights” and “Global Rights” as well as “China Rights.” [https://fosunpharmausa.com/innovative-medicine/]
The FDA Filing for the Fosun Pharma USA facility says the facility is authorized to “develop specifications,” including for the PCR tests and antigen tests it creates, and that the facility can also have US agents: [https://fda.report/Company/Fosun-Pharma-Usa-Inc]
This is crucial. Fosun Pharmaceuticals does not just partner with Pfizer/BioNTech to make the COVID-19 vaccines: they make, as noted, the PCR tests that are the one primary metric that determine the scale of the pandemic in North America and Western Europe and thus the “lockdowns” of whole countries, whole industrial sectors.
A CCP-run company, and CCP-created product, thus, decides — who can go to work or school, who must close his or her shop, who can or cannot travel — in all of Europe and the US: [https://fosunpharmausa.com/covid19/pcr/]. A CCP-run company decides the formulation of the PCR and antigen tests that go deep into the nasopharyngeal cavities of Westerners who are forced, week after week, to test and test and test with these products. This is what is on the Fosun Pharma USA’s product pages:
The following products are developed in the Princeton NJ Fosun Pharma USA facility:
So this CCP-owned hybrid entity is here now and it is creating the diagnostic instruments that determine the scale of the pandemic in the West. The CCP can thus dial it up or down.
It also makes: millions of the Pfizer/BioNTech MRNA injections, the Merck COVID-19 pill Molnupiravir, the Pfizer COVID-19 pill Paxlovid — for which Pfizer CEO Albert Bourla just signed a contract with the US government for 10 million doses and $5.29 billion dollars for 2022 [https://www.fiercepharma.com/manufacturing/pfizer-boosts-paxlovid-manufacturing-capacity-as-merck-s-rival-covid-pill-sees] — all this for the US and for ten other countries including the EU.
These are all formulated and distributed by a company leading directly to Chinese Communist Party.
When Pres. Biden does a deal with Pfizer/BioNTech in the millions of dollars, with our tax money, he is giving a substantial portion of the funds to China. When he spends a billion dollars via omnibus bills for PPE, including millions for PCR and antigen tests, he is writing checks to — China.
This is from Fosun Pharmaceutical USA’s website section “R and D”: look at the last three entries:
Is Fosun a squeaky clean CCP-run Pharma enterprise? In 2018 a whistleblower — and in China that is courageous thing to be — broke a scandal revealing that Fosun Pharmaceuticals had “massively” faked its data and also bribed regulators. Facilities were so chaotic that the US FDA sent the company a stern letter. [https://www.fiercepharma.com/manufacturing/fosun-pharma-massively-fakes-api-production-data-and-bribes-regulators-whistle-blower].
BioNTech’s SEC filing reports as 100 per cent achieved, a tech transfer to — China. Not to a “Chinese company” or a “Chinese individual” but to the country of — China:
[https://investors.biontech.de/node/12681/html]
Further, the SEC filing explains that it will effect the “technology transfer with China” after marketing approval has been granted. I don’t know what “Technology transfer” or “tech transfer” means in this SEC filing; SEC filing experts who have reviewed it for me have suggested that this can mean IP, manufacturing methodologies, formulas, data, or all four. But surely it is significant that the company BioNTech has declared as 100 % complete or in process, a “Tech transfer” to CHINA. It is not “sharing” the tech or “licensing” the tech — it is transferring the tech. That means that in some capacity, China will be or is in charge of some aspect of BioNTech’s technology, however that is defined here.
So take all of the above, and map it against the 150,000 plus adverse events in the Pfizer documents, the deadly harms to reproduction, the Western baby die-off, the babies in seizures; map it against the population drop, the rise in disabilities, map it against the rigid, cruel vaccine mandates aimed at Western defense forces (Canada’s, and Australia’s and all of Western Europe’s, as well as at the most powerful military in the world, that of the United States) — map it against the vaccine mandates aimed at our police, our health care workers, our firefighters, our pilots, our first responders, our kids, our babies — all this done by a White House captive, via Hunter Biden’s laptop, to the CCP. Add to all of this the evidence of birth rates declining, especially in the West, by 12-20 per cent:
How better to cripple the world’s other superpower than by destroying our American front lines and our American next generation, with tainted, murderous vaccines, flowed easily enough into the West via (not even that many) shell companies and cutouts? How easy to do the same to Western Europe, to Canada and Australia, as a whole?
Take all of the above and consider that the virus originated in China; and now all of the testing apparatuses, as well as millions of the vaccines, the catastrophically damaging or lethal “solutions” to the virus, also all originate from the same folks; the same leadership cadre who brought the world forced abortions, citizens welded into their homes, Uighur concentration camps, and organ harvesting.
I made the case in my new book The Bodies of Others that a transnational group of bad actors – including the WEF, The WHO, the Bill and Melinda Gates Foundation, tech companies and the CCP — used the pandemic to crush humanity and in particular to destroy the West.
With the provenance of the vaccines and tests, you can see yet another mechanism, yet another core methodology of this warfare.
Mapping these points of evidence, I think you may start to see what I see.
This all means, of course, that we are staring into the abyss right now.
Traumatized or not, we all need to snap out of denial.
We let our adversary come too close to us. Into our very bloodstreams.
Despite reports otherwise, the Air Force has ceased discharges of unvaccinated airmen after a Federal Judge ordered a halt to the discharges of members who have religious exemptions to Covid vaccination, marking a huge win for thousands of members of the Air Force.
ICAN has filed a Citizen Petition with the FDA calling on the agency to reverse its reckless course on Covid-19 injections for teenagers. The Petition demands that the FDA revoke its emergency use authorization (EUA) for Pfizer’s product in children aged 12 through 15 and deny Moderna any future EUA for children aged 12 through 17.
The document, submitted through ICAN’s legal team, spans 20 pages, cites dozens of medical studies, and includes 94 footnotes and roughly 1,500 pages of sources, but it boils down to a few simple principles: There never was any emergency with this age group in the first place, rendering EUAs illegal under federal law; the clinical trials relied upon to authorize the vaccines were woefully deficient; almost all in the 12-15 age demographic currently have natural immunity to Covid-19; and the injury risks from injection are catastrophically higher than any purported benefit.
The Petition cites a Lancet article of March 2021 that found Covid’s death toll among children was a negligible 0.17 per 100,000 population. Since then, a large U.K. study posted in July 2021 found a Covid-19 fatality rate of just 0.005% among all those under 18. “Based on these facts, the current EUA for Pfizer’s vaccine for this population is without legal foundation or necessity,” the Petition observes, “because COVID-19 does not present a current emergency for children.”
Furthermore, the population has been developing robust natural immunity against the disease. As of February 2022, according to a study published on the CDC’s website, 75% of children aged 12-17 had developed infection-induced antibodies. NIH data showed an even higher percentage of natural protection, at 89.4%, for all children under 18. And that percentage could only have increased since.
But the gaps in FDA logic do not begin and end with its misappropriation of the word “emergency,” nor with its selective blindness on natural immunity. As our Petition reminds the agency, quoting international scientists in an August 2008 PLOS Medicine paper, “inadequately powered studies should themselves be considered a breach of ethical standards.”
The FDA’s authorization for Pfizer’s injection rests on a trial in which only 1,131 children received the experimental product. Yet, even among that small and statistically insignificant group, at least seven recipients “had at least one serious adverse event.” Among them was Maddie de Garay who, at 12 years old, was paralyzed from the waist down after receiving her second shot. Among a multitude of horrific injuries, she became incontinent, and can now only receive nutrition through a feeding tube.
But Pfizer recorded her life-altering reaction as mere “functional abdominal pain” in the safety-evaluation data it turned over to the FDA and has since failed to ensure adequate medical care, including an appropriate diagnosis and treatment.
Nor has the safety profile for the mRNA shots improved since their problematic trials. As early as June 2021, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) examined the growing issue of vaccine-induced myocarditis, where the heart muscle becomes inflamed and thereby weakened, especially in individuals under 30 years old. Moreover, as the Petition points out, “Moderna’s vaccine presents an even higher risk profile to this age group than Pfizer’s vaccine.”
Meanwhile, the Vaccine Adverse Events Reporting System (VAERS), though vastly understating the full extent of injection injuries, had accumulated 31,549 reports of adverse events among children under 18 as of May 6, 2022. Of these, 1,812 were rated as serious and 44 were deaths. This is to say nothing of the long-term effects.
And, if the glaring safety signals were not enough for the FDA to revoke its EUA for minors, the Petition also points out that several studies now show there is virtually no benefit from these shots since their efficacy wanes dramatically within just months or even weeks after inoculation.
The FDA has played very fast and extremely loose with its EUA powers when it comes to children’s health, invoking an emergency that never existed and accepting data that was never adequate. Moreover, it has continued doubling down on its failed approach in spite of the overwhelming case against it. Numerous additional VRBPAC meetings are scheduled to discuss authorizations for additional vaccines and age groups and ICAN plans to file as many petitions as are necessary to address the concerns of each.
The FDA’s increasingly reckless actions have prompted ICAN to file several Petitions with the FDA. These include demands the agency adhere to federal law requiring promotional material for EUA vaccines to “clearly and conspicuously” state the product has not been approved or licensed by FDA, but only authorized for emergency use. We have also called on the FDA to publicly clarify an individual’s statutory right to refuse medical products without coercion, penalty, or retaliation of any kind, and we have demanded that it obtain proper data before vaccine approvals. On all counts, the FDA has failed miserably and ICAN will continue to hold its feet to the fire.
When we’re dealing with a controversial topic, it’s a good item to start with something we know and go from there. What is something that we know for sure about Covid-19 vaccines? They kill people.
Jon Rappoport pointed this out a year ago: “A new May 4 report by independent researcher, Virginia Stoner, reveals US vaccine-death figures. The report is titled, ‘The Deadly Covid-19 Vaccine Coverup.’
Stoner uses the US government’s own numbers.
Here are key quotes from her report:
‘There has been a massive increase in deaths reported to the Vaccine Adverse Event Reporting System (VAERS) this year. That’s not a ‘conspiracy theory’, that’s an indisputable fact.’
‘We’re talking about a huge and unprecedented increase—so massive that in the last 4 months alone, VAERS has received over 40% of all death reports it has ever received in its entire 30+year history.”
‘The increase in VAERS death reports is not due to more vaccination.’
“Most recently, the death count went from 2794 on April 5, to 3005 on April 12, to 3848 on April 26….1054 deaths in 21 days.’
‘One hypothesis…is that the elderly and infirm, many in long-term care facilities, were the first to be targeted by the COVID-19 vaccine campaign, and they are much more likely to die coincidentally. These coincidental deaths then lead to an increase in suspected vaccine-induced deaths reported to VAERS.’
‘VAERS data just does not support that hypothesis. First, because all age groups—not just seniors—had a dramatic increase in VAERS death reports from COVID-19 vaccines…Across the board, all age groups experienced a dramatic increase in deaths reported to VAERS from the COVID-19 shots—even the under 18 group, which has had very few COVID-19 shots (so far).’
Stoner constructs a chart showing reported deaths from vaccinations in years prior to COVID, and deaths reported so far from COVID vaccines.
For prior years, we’re talking about roughly 100 deaths a year from somewhere between 250 million and 350 million vaccines administered. On the other hand, we’re talking about 3800 deaths from about 150 million COVID shots—not in a full year; in only four months.
The experts would say neither death figure (100 or 3800) is alarming, given the huge number of vaccines administered. But this is a deception.
Over the years, much has been written (even in the mainstream) about what sits behind REPORTED vaccine injuries and deaths. Estimates of TRUE injury numbers range from 10 to 100 times greater than the reported figures.
3800 reported deaths from COVID vaccines would skyrocket when you estimated the true figure.
As Stoner points out in her report, public health officials, in Orwellian fashion, keep repeating, ‘The vaccine is safe and effective.’ A straightforward analysis of their own numbers completely contradicts their stance.
Likewise, the mainstream press, politicians, corporations, and celebrities are on an all-out push to convince the public that the vaccine is a) necessary and b) a marvel, if only the ‘hesitant’ people would ‘follow the science’ and see the light.
Well, some cults are small; that one is huge.
Virginia Stoner’s report is a stark refutation of the conspiracy theory the cult is promoting.
When the entire population is being subjected to a vast experiment deploying a never-before-released RNA technology; when the shot in the arm is actually a genetic treatment; when the entire field of genetic research is riddled with pretense and lies and alarming miscalculations, leading to ripple effects in overall genetic structures; what else would you expect?
Vernon Coleman asks the appropriate question: exactly how many people has the Covid vaccine killed? “No one knows how many people the vaccines are killing – or how many they will kill.
But although I haven’t seen the mainstream media mention most of these deaths, people have already died or been injured after being given the vaccine:
SHOCKING – The latest covid jab deaths and injuries from VAERS (infants, teenagers and young adults are dying after the vaccine)
openvaers.com covid data (it is estimated that only 1% of vaccine adverse events is reported)
Note: The following paragraph has now been added to the UK’s Pfizer analysis data print, ‘A report of a suspected ADR to the Yellow Card scheme does not necessarily mean that it was caused by the vaccine…’ In my view, this is yet another attempt to draw attention away from the very real problems associated with the vaccines. We note that when patients die 60 days after a positive covid test, they are added to the covid death figures but if someone were to die 60 minutes after a covid vaccine, then it is just a coincidence.
PFIZER (UK data) – Some of the Injuries include: strokes, heart attacks, miscarriages, Bell’s Palsy, sepsis, paralysis, psychiatric disorders, blindness, deafness, shingles, alopecia and covid-19.
The following paragraph has now been added to the UK’s AstraZeneca analysis data print, ‘A report of a suspected ADR to the Yellow Card scheme does not necessarily mean that it was caused by the vaccine…’ In my view, this is yet another attempt to draw attention away from the very real problems associated with the vaccines. We note that when patients die 60 days after a positive covid test, they are added to the covid death figures but if someone were to die 60 minutes after a covid vaccine, then it is just a coincidence.
ASTRAZENECA (UK data) – Some of the many injuries include: blindness, strokes, heart attacks, miscarriages, sepsis, paralysis, Bell’s Palsy, deafness, shingles, alopecia and covid-19.
Derek Sloan MP raised concerns on covid-19 vaccine censorship of doctors and scientists (video – bitchute)
Moderna begins first human trials for flu shot based on new mRNA technology used to make the company’s covid-19 vaccine (article – Daily Mail)
The following is the FDA’s draft working list of possible covid vaccine side effects (see page 16 of document). This was published in October 2020 BEFORE the jab roll-out began.
Canadian whistleblowers expose 13 stillborn deaths in 24 hours at Lions Gate Hospital caused by covid-19 vaccines (article – dailyexpose.uk)
Paul Dimattina: Australian football league legend rushed to hospital after sever reaction to Pfizer booster shot (article – the covidworld.com)
Sithipol Bovornkittipaisal: 26-year-old man dies 1 day after receiving Moderna covid-19 vaccine, investigation launched (article – thecovidworld.com)
As reports of injuries after covid vaccines near 1 million mark, CDC, FDA clear Pfizer, Moderna boosters for all adults (article – childrenshealthdfense.org)
29,034 deaths 2,804,900 injuries following covid shots in European database of adverse reactions – corporate journalists have pericarditis after Pfizer shots (article – vaccineimpact.com)
Pfizer secretly adds dangerous ingredient to injection for 5 to 11-year-olds as Taiwan stops Pfizer shots for 12 to 17-year-olds (article – vaccineimpact.com)
You might wonder, even if the Covid-19 vaccine kills people, doesn’t it also save lives? But in fact it is ineffective in warding off the so-called Covid “pandemic.” Vasko Kohlmayer says, “’Pfizer and BioNTech’s Covid-19 vaccine is just 39% effective in Israel where the delta variant is the dominant strain according to a new report from the country’s Health Ministry’ we read in a CNBC report.
Astonishment is one’s first reaction when coming across this piece of information, since it was not so long ago the vaccine manufacturers claimed their products were 92 to 98 percent effective.
The manufacturers’ initial claims, however, have been steadily revised down as real-world data has been coming in. In March of this year news came from South Africa that ‘AstraZeneca vaccine doesn’t prevent B1351 Covid.’ A couple of months later, the Hill ran a piece by a Baylor School of Medicine virologist who observed:
‘A new study published in the New England Journal of Medicine found that Pfizer-BioNTech vaccine provides only 51 percent protection against B.1.351 of South Africa.’
Just a couple of weeks ago, we learned that recipients of the Sinovac Biotech’s vaccine have no antibodies after six months. This effectually means that merely half a year after being injected into people’s bodies the vaccine has zero percent efficacy in protecting against Covid-19.
Even factoring for the variants, the hard data makes it quite clear that the initial claims of vaccine effectiveness were greatly exaggerated. This, of course, comes as no surprise to anyone familiar with the dynamic of the pharma industry. Drug manufacturers tend to wildly overstate the efficacy of their products, while doing their very best to understate their side effects. It is for this purpose they conduct trials that are manipulated to obtain the results they wish for. Sadly, they too often get away with it because of the corruption of the system by what is called regulatory capture. This is why the outcomes of manufacturers’ trials are almost never replicated by independent trials or real-world data.
This is what has apparently happened with the Covid vaccines. The manufacturers used the sense of emergency brought on by the Covid pandemic to conduct rushed and incomplete trials which were designed to yield the results they wanted to see. There is every reason to believe that the effectiveness of their injections was nowhere close to the 92-98% range they initially claimed even for the variants that were in circulation at that time.
Needless to say, one has a strong suspicion that even the meagre 39 percent figure is still overstated. This would only be natural, since everyone involved in the vaccination enterprise – the manufacturers, politicians, regulators, the medical establishment and corporate scientists – is trying their best to save face and reputation in the face of this fiasco. Bad though the data is, we can be quite sure that it has been massaged to soften the blow.
You can clearly observe this tendency at work in the CNBC piece which claims that even though Pfizer is only 39 percent effective, it still protects against serious disease. But this is simply not true, which you can easily see if you take the trouble to look into the data put out by the Israeli government. At roughly the same time that CNBC filed its report, the Israeli Ministry of Health published a bulletin which reported on Covid cases in the country. According to their data, there were 137 serious cases in Israel of which 95 were fully vaccinated and 42 unvaccinated or partially vaccinated (see here and here). In other words, the bulk of the serious cases was comprised of those who had received their shots. If the vaccine was as effective in protecting against heavy illness as the article claims, the numbers would look completely different. The figures published by the Israeli Ministry of Health shows that the claims of Pfizer’s efficacy of protecting against serious Covid are simply untrue.
This has been confirmed by the testimony of Dr Kobi Haviv, Director of Herzog Hospital in Jerusalem. In a recent TV interview, Dr Haviv stated that the fully vaccinated people account for about 90 percent of hospitalizations. Given that less than 90 percent of the Israeli population is fully vaccinated, it would appear that the vaccination not only does not prevent you from contracting the disease, but actually increases one’s chances of becoming a serious Covid case. Observes Dr Haviv: ‘yes, unfortunately, the vaccine… as they say, its effectiveness is waning.” And so it is, indeed. Dr Haviv’s interview is on YouTube so you can hear the truth straight from his mouth. It will be interesting to see how long it will take for the Establishment Censors to take it down.” See this.
But there is worse. Everybody knows how sensitive and delicate small children are. Now the monsters want to give them the killer jab too! Let’s listen to Kohlmayer again:” “’CDC recommends COVID-19 vaccine boosters down to age 12,’ says a recent CBC news headline.
The article opens as follows:
‘Millions of Americans between the ages of 12 and 15 can now get a booster shot of Pfizer’s COVID-19 vaccine, after the CDC formally adopted new recommendations backed by a majority of the agency’s outside vaccine advisers. The CDC now says that Americans as young as 12 who received Pfizer’s COVID-19 vaccine should receive a third dose as early as five months after their first two shots. The agency’s officials said that enough time has passed for around 5 million adolescents to be eligible’
‘Why in the world are they doing this?’ one asks in disbelief.
Three basic facts have been well established by data and studies:
Healthy children are at virtually zero risk of serious Covid.
The vaccines will not prevent children from contracting the virus.
Covid injections carry risk of serious side effects.
According to a cost-benefit analysis conducted by Toby Rogers, Ph.D., in the 5 to 11 age range, 117 healthy kids will have to die of vaccine-related side effects in order to save one child from perishing of Covid 19.
A study from Japan has shown that young people are seven hundred percent more likely to be killed by Pfizer jabs than by Covid.
We have been repeatedly told that we must follow facts and science when dealing with this pandemic.
The science on vaccinating children against Covid-19 is in, and it could not be any clearer: while healthy children are at negligible risk from the disease itself, they are at real risk from the shots.
Since the vaccines do not stop infection and transmission, they will protect neither children nor their communities from the spread of the virus.
It makes not scientific or medical sense to give them these shots. Vaccinating children for SARS-CoV-2 violates both the tenets of good medicine and evidence-based science.
According to Dr Robert Malone, who is one of the world’s preeminent vaccine scientists, the cost benefit analysis is not even close.
Those who want to vaccinate children follow neither the science nor logic. Subjecting children to Covid jabs needlessly exposes young lives to potentially grave risks.
The incidence of myocarditis and pericarditis may be as high as 1 in 317 in the young, especially boys, and increases further with each additional dose.
Then there is a danger of deadly blood clots as well as several other serious conditions such as Guillain-Barré syndrome.
Astonishingly, scores of children have already been injected with two doses that turned out to be ineffective, which is the reason a booster is now required.
The booster, however, already looks to be even more useless than the original offering. The booster, in fact, appears to have negative efficacy which means that those who receive it seem to be more likely to contract the virus.
Soon we will have a multitude of 12-year-olds who will have received three of these pointless and dangerous shots without any medical justification whatsoever.
Robert Kennedy, Jr. said that injecting children with the Covid vaccines is a crime. He is not incorrect.
A number of children have already been killed by the vaccines.
The prominent Covid-vaccine sceptic has taken two doses of the Moderna vaccine. And that’s just one of many inconsistencies between his words to the Covid-sceptic crowd and his actions.
This is a guest post by Miriam Walton and Alan Goater in Derbyshire, U.K. Over the last year they’ve been closely following interviews and articles by and about Robert Malone. And that’s left them with more questions than answers.
I also have raised questions about Malone: see my Oct. 24, 2021, article titled, ‘The Vanden Bossche Caper Continues.’ In it, I focus on a high-profile interview of Malone and Vanden Bossche, in which Malone boosts and extends Vanden Bossche’s disinformation and fear-mongering. (I first exposed Vanden Bossche’s deliberate disinformation in my March 2021 article, ‘The Curious Case of Geert Vanden Bossche.’)
Below is Walton and Goater’s email to Malone in February 2022 with questions about information in the public domain about Malone. (I’ve added hyperlinks to the source material, photos from that source material and, in square brackets, some clarification/comments.)
Malone still hasn’t responded to the U.K. couple’s questions.
Dear Dr. Malone,
From the Pennine foothills of the UK we have followed with interest your public and media appearances in connection with your opposition to current US (and global) public health policies, in particular the controversies which have arisen concerning possible misinterpretations of your position. We have it in mind to write (and possibly publish) about these issues and would be very grateful for some clarifications from you in the interests of fairness and accuracy to all parties. Please find our questions below.
We appreciate that you must be exceedingly busy at this time but would hope that you could respond within, say, 7 days.
Best wishes,
Miriam Walton and Alan Goater
1. You are on record as saying that you had two doses of the Moderna Covid vaccine some months after being infected with the disease because a) you had heard rumours that your long-haul symptoms might be helped by the vaccine and b) you wanted (needed?) to travel abroad.
Questions:
Has any vaccine ever been successfully deployed to mitigate current patient symptoms of anything?
What, in all your training and experience as a physician and scientist, informed your decision to take an experimental injection (twice) on the basis of a rumour and a desire to travel?
Is a desire to travel a good reason for participation as a subject in a medical experiment?
Why were high-quality photographs taken of you on both occasions of vaccination?
2. There exists online footage of professor Mattias Desmet asking you not to use the word ‘psychosis’ in connection with his theory of mass formation. [‘online footage’ refers to this interview of Malone and Desmet on Tommy’s Podcast; in it, Malone starts speaking at 4:33 and at 15:25 Desmet finally gets a chance to correct Malone by saying his theory is termed mass formation, not mass psychosis.]
You said, on the same occasion, that you had come to “sit at the feet of the master” (Desmet) and to learn from him.
However, you have been speaking and writing about ‘mass formation psychosis’ since then, including on your own Substack (i.e., your reformulation of Desmet’s mass formation with reference to Dr. Mark McDonald’s work on ‘mass delusional psychosis’ – a different phenomenon).
Questions:
Can you provide the rationale for ignoring the express wishes of ‘the master’?
Have you said or done anything to remedy the debunkingof professor Desmet’s theory of mass formation because of its unauthorised association with ‘Psychosis’? [i.e., has Malone admitted – and attempted to rectify the effects of – his changing of Desmet’s theory to supposedly be about ‘mass psychosis’ that in turn caused Desmet and his theory to be pumeled by baseless attacks/’debunking’?]
3. You are on record as identifying both Michael Callahan and Daryl Galloway as CIA agents. [For example starting at 1:00:07 in this video interview of Malone in which he talks about outing Callahan.]
Questions:
Was that information [i.e., about Callahan and Galloway being CIA agents] available to you as a result of your own security clearance status?
Do you expect an investigation into these revelations under the Intelligence Identities and Protection Act of 1982? [This Act “amends the National Security Act of 1947 to establish criminal penalties for any person who knowingly discloses information which identifies a U.S. covert intelligence agent.”]
4. [Background to this point: 1. Malone being activelyinvolved currently or in the recent past in the development of a Covid jab called RelCoVax made by India-based Reliance Life Sciences; and 2. a Substack article by a member of an organization called ‘Health Freedom for Humanity;’ the article apparently points out that Malone in his Dec. 2021 interview by Joe Rogan didn’t mention this vaxx or his involvement with it, and also posed other questions such as whether there is graphene oxide in the vaxx. (We couldn’t find the article online; the information about the article in the question below comes from Malone’s Jan. 26, 2022, Substack post about it.)]
Screenshot of the beginning of this video Malone’s presentation about the vaxx at the Vaccines Summit 2021
In your recent robust dismissal of criticism from the ‘Health Freedom for Humanity’ organisation you answered in respect of Statement #2 – “it [RelCovax] allegedly has Darpa (graphene oxide) Hydrogel in it” in the following terms:
“Hydrogel, and other alum-based adjuvants, are among the best characterized of the traditional adjuvants. DARPA had nothing to do with developing Alum or Alhydrogel adjuvants. Alhydrogel has nothing to do with Graphene Oxide. This “Relcovax” vaccine product using Alum + CpG for its adjuvant system. The vaccine candidate is designed to be a very low cost, traditional alternative to the genetic vaccines, and employs much more traditional methods than, say, the Novavax product.” [Bolding in the original.]
Screenshot of the part of Malone’s Substack article with this information
Question:
Does/will the ‘RelCovax’ product contain ‘Darpa Hydrogel’ or graphene oxide in any form?
5. During your Lincoln Memorial speech on January 22, 2022, you said “Now we have Omicron. These vaccines were designed for the Original Wuhan strain, a different virus.” [At 4:35 in this video of Malone’s speech]
Question:
On what basis do you assert that ‘Omicron’ and ‘the Original Wuhan strain’ are two different viruses?
6. During that same [Jan. 22, 2022] speech you asserted twice, in support of your not wanting to see them used on children, that the genetic vaccines are not ‘completely safe,’ [At 4:19 and 5:37 in this video of Malone’s speech (the same video cited in point 5 above).]
Question:
In view of the universal awareness among health professionals that no medication is ‘completely safe,’ why do you single out these genetic vaccines for censure?
7. On 12 February 2020 you and your wife’s book, ‘The Novel Coronavirus‘ was published. The synopsis refers to the ‘coming epidemic’. [It appears to now be impossible to find a copy of the book. Therefore the hyperlink and mention is to a synopsis.]
Screenshot of the synopsis of The Novel Coronavirus
Questions:
How reliant were you, in the absence of real-world data at that time, on modelling, planning and/or role-play exercises like the ‘DOMANE‘ project [see also information about Malone’s involvement in DOMANE in the sixth and seventh paragraphs of this April 2020 Science article] and ‘Event 201‘ for material and information for the book?
If you did not rely on such exercises how, otherwise, were you able to confidently predict the eventuality and write about likely countermeasures?
[Miriam and Alan wish they’d also asked Malone how he and his wife knew in advance that the World Health Organization would name the virus ‘COVID-19.’ See for example this abstract of the book posted on researchgate.net – it shows the table of contents, with the second chapter titled, ‘Epidemiology of COVID-19’ and the second-last titled, ‘Clinical Characteristics and Medical Countermeasures for COVID-19.’]
8. You are on record advocating for continuing/increasing testing for SARS-COV-2 and for these to be self-administered. [Malone does this in many places – as just one example, at 1:13:35 in this interview.]
Question:
To your knowledge, have the medical risks associated with the test equipment itself and its unsupervised use by untrained people ever been assessed?
9. You have advocated ‘active surveillance’ and ‘tracing’ as appropriate countermeasures to Covid-19 (along with self-testing).
Question:
In your view is the imposition of the infrastructure of population surveillance really an appropriate step for a government of a democratic country to take, ever?
10. You are on record advocating the use of the vaccines on the elderly/vulnerable. [See for example this interview (the same article is cited in point 9 above).] You are also (famously!) on record deploring their use on children because of the known, and unknown, dangers. [He has done so many times, such as in this video of his Jan. 22, 2022, Lincoln Memorial speech (which was also linked to in points 5 and 6 above).]
Question:
How can anyone provide informed consent to a medical intervention that carries unknown dangers? Why, in your view, should the elderly/vulnerable populations, in particular, be exposed to these dangers?
11. All expert opinion at the outset of the public-health emergency agreed that respiratory-disease pandemics, epidemics and outbreaks end in 18-24 months. [See for example the CDC web page titled ‘Past Pandemiccs’ and note that none of the highlighted outbreaks lasted longer than two years.]
Question:
Why, in your opinion, did so many pharmaceutical companies (including Reliance Life Sciences!) at that time invest in the development of medications, particularly vaccines, that were not expected to be available until after the expected pandemic end date?
12. Your knowledge, credentials and experience are second to none in the field of public health. Your reputation is well established in the US and internationally.
Question:
Can you see yourself in a leadership role at, say, the CDC [U.S. Centers for Disease Control and Prevention] in the future?
cover image based on creative commons work of congerdesign / pixabay
Historic Decision Against Mandatory Vaccination by Italian Court — Judge Declares in Her Decision That Covid Vaccines Are Producing Very Serious Adverse Effects & Thousands of Deaths
On July 6th, 2022, the court of Florence has approved a sentence annulling the measure taken by the Order of Psychologists of Tuscany against one of its members, the reason being: ‘the suspension of the exercise of the profession risks compromising primary individual rights such as the right to a livelihood and the right to work’.
The judge ruled that the psychologist doesn’t need to be vaccinated in order to do his job by establishing that:
these substances don’t prevent infection and transmission. Therefore, in front of the Italian law, there can not be an obligation.
She also recognises that these substances provokes severe adverse events. Therefore, it even less legitimate to force anybody to be injected.
The judge put the dignity of the human being at the centre and referred twice to the period of Nazism and Fascism. Mandatory vaccination is possible if there is informed consent. For Covid injections, she explained that an informed consent is not possible as we don’t know the ingredients and the mechanisms of these substances because of industrial and alleged military secret.
This interim decision is grounded in serious conclusion: there is no right to suspend a citizen from the right to work based of this illegal request of vaccination with these experimental substances.
With this historic court decision, “the Risk to human genome is now legally established” Renate Holzeisen, attorney for the plaintiff, said in an interview for an Italian radio.
“This could be a milestone” said Reiner Fuellmich during the Corona Committee 113, interviewing Renate Holzeisen.
No Obligation as the official data show that these experimental substances don’t prevent infection and transmission amongst people treated with 3 or more Covid shots.
First of all, the judge declares that based on the datas published by the Ministry of Health, AIFA (Italian Medicines Agency) and the SSN (Italian Health Services), it is very clear that these substances (aka Covid vaccines), defined several times by the judge as “experimental”, don’t prevent infection from the virus. For a mandatory vaccination, the substances should be proven to work.
Therefore, as they don’t work, in front of the Italian law, there can not be an obligation.
Doctor leading the intensive care in Verona has declared in television that all Covid patients in intensive care are people treated with 3 Covid shots.
Nobody can be forced to be injected as these substances provoke severe adverse events and this is based on official public data regarding adverse events.
In the court decision, the judge also recognises that these substances cause very serious side effects that can even lead to death, and also refers to the risk of genetic mutation.
Therefore, it even less legitimate to force anybody to be injected.
The Dignity of the human being is at the centre. Mandatory vaccination is not possible because there is NO informed consent due to industrial and alleged military secret regarding the ingredients and the mechanism of these injections.
Even if these substances would work to prevent these infection, after the Nazi and fascism period, it can not be a mandatory without an informed consent.
The judge stated that there is no benefit for these substances BUT even if there was a benefit, we can not sacrifice the individual right in the name of the common interest, and put the dignity of the human being at the centre.
The judge referred twice to the Nazi and fascism period, to the Italian Constitution article 32 highlighting that there is a reason why Dignity is at the centre of the first article of the German constitution.
She explained that an informed consent is not possible as we don’t know the ingredients and the mechanisms of these substances (industrial and alleged military secret).
We should recall a group of Human Rights Italian activists who presented a Freedom of Information Act to the EMA and to the Italian Cares Authority asking for clear informations about the ingredients and the safety of these experimental substances aka Covid injections. As an answer, the EMA said that no information can be shared as there is a military secret in place.
In his decision, the judge stated it: no information are available about these substances and even if we ask for information publicly, we don’t receive it. There is no informed consent.
In this historic decision, the Tuscan judge concluded that based on all these, the discrimination of this psychologist and his suspension from work is totally illegal. Without hearing the other part (Chamber of Psychologist in Tuscany), she declared that there is no time to spend anymore for this psychologist who has been suspended last October 2021. Evidence is so clear.
This interim decision is grounded in serious conclusion: there is no right to suspend a citizen from the right to work based of this illegal mandatory vaccination with experimental substances. A future court hearing will take place on September 15th, 2022, when the judge will rule based on what the chamber of psychologists will present. But the judge shows as well that there is no need to go to the constitutional court as we know that these substances (aka Covid-19 vaccine) don’t prevent infection. In front of the Italian law regarding mandatory Covid vaccination, it is enough to say the suspension from labour of healthcare workers is illegitimate because these substances don’t do what the constitution request.
During the last 2 years, we saw incredible decisions where judges says that they can not take decisions going against governmental decisions. Mandatory vaccination for all workers and people over 50 are already in place in Italy, even if official data regarding severe adverse events show the danger of these substances. This happens in a country where ongoing advertising campaigns sell Covid vaccines as “safe and effective” – ie. Prime Minister Mario Draghi and President Sergio Mattarella, have declared several times that only people who get these treatments will survive and the others will dye and be responsible of the Covid deaths.
After two years of Covid pandemic – in which many have fought to defend their freedom and rights – ‘a great judge and a great sentence’ open a new glimmer of hope. This is the first decision with which an Italian judge declared the material truth and the imposition of the treatment is radically illegitimate.
On a recent episode of “RFK Jr. The Defender Podcast,” guitarist Jeff Diamond described having eight fingers amputated and losing his singing voice after developing blood clots about a week after getting the Johnson & Johnson COVID-19 vaccine.
On July 9, 2021, Jeff Diamond, a professional musician, vocal instructor and backup guitarist, got the Johnson & Johnson (J&J) COVID-19 vaccine.
About a week later, Diamond was found unconscious in his apartment and taken to a local hospital in Minnesota, where he remained in a coma for three weeks.
The condition caused doctors to amputate eight of his fingers, without his knowledge or consent, while he was still in a coma.
Diamond, a guest on the July 5 episode of “RFK Jr. The Defender Podcast,” told Robert F. Kennedy, Jr., he got the vaccine only because he’d been performing at an event in Atlanta, and didn’t want to risk infecting his mother.
“I was taking care of my mother, and that’s the only reason I got the shot in the first place,” Diamond said.
When Diamond awoke from the coma, he also found himself intubated, which impaired his singing voice.
With his kidneys barely functioning and his balance thrown off by all the medications he was prescribed, Diamond lay in the hospital for another three weeks until he was able to go into a nursing home.
While in the nursing home for six weeks, Diamond’s feeding tube burst open and he was rushed to an emergency room. “Blood was gushing out of my stomach,” he told Kennedy. It “almost killed me.”
A doctor in Minneapolis saved his life, but Diamond told Kennedy he’s been “in pain with these fingers ever since.” Diamond was fitted with prosthetic fingers, but while “they may look great,” he said, “they’re not working out for playing the guitar.”
Diamond’s singing voice has “bounced back a bit,” he said, but not all the way.
And it’s “all from, I believe, the Johnson & Johnson shot,” Diamond said.
Now, a year after he was injured, Diamond said he’s taking things day by day, and hopes to someday play guitar again.
More importantly, though, he wants to get the word out about what happened to him.
“What happened to me … I don’t want to see this happen to anybody else,” Diamond said. “I think it’s a crime … People have got to be held accountable.”
Watch the podcast here:
Rachel Militello has worked extensively as a legal assistant at law firms and newspaper companies. She is also a self-published author of poetry that is geared toward mental health awareness.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
According to Alexandra Latypova, an ex-pharmaceutical industry executive, documents obtained from the U.S. Department of Health and Human Services on Moderna’s COVID-19 vaccine suggest the U.S. Food and Drug Administration and Moderna colluded to bypass regulatory and scientific standards used to ensure products are safe.
According to an ex-pharmaceutical industry and biotech executive, documents obtained from the U.S. Department of Health and Human Services (HHS) on Moderna’s COVID-19 vaccine suggest the U.S. Food and Drug Administration (FDA) and Moderna colluded to bypass regulatory and scientific standards used to ensure products are safe.
Alexandra Latypova has spent 25 years in pharmaceutical research and development working with more than 60 companies worldwide to submit data to the FDA on hundreds of clinical trials.
After analyzing 699 pages of studies and test results “supposedly used by the FDA to clear Moderna’s mRNA platform-based mRNA-1273, or Spikevax,” Latypova told The Defender she believes U.S. health agencies are lying to the public on behalf of vaccine manufacturers.
“It is evident that the FDA and NIH [National Institutes of Health] colluded with Moderna to subvert the regulatory and scientific standards of drug safety testing,” Latypova said.
“They accepted fraudulent test designs, substitutions of test articles, glaring omissions and whitewashing of serious signs of health damage by the product, then lied to the public on behalf of the manufacturers.”
In an op-ed on Trial Site News, Latypova disclosed the following findings:
Moderna claims the active substance — mRNA in Spikevax — does not need to be studied for toxicity and can be replaced with any other mRNA without further testing.
Moderna’s nonclinical program consisted of irrelevant studies of unapproved mRNAs and only one non-GLP [Good Laboratory Practice] toxicology study of mRNA-1273 — the active substance in Spikevax.
The FDA failed to question Moderna’s “scientifically dishonest studies” dismissing an “extremely significant risk” of vaccine-induced antibody-enhanced disease.
The FDA and Moderna lied about reproductive toxicology studies in public disclosures and product labeling.
“Moderna’s documents are poorly and often incompetently written — with numerous hypothetical statements unsupported by any data, proposed theories, and admission of using unvalidated assays and repetitive paragraphs throughout,” Latypova wrote.
“Quite shockingly, this represents the entire safety toxicology assessment for an extremely novel product that has gotten injected into millions of arms worldwide.”
According to Latypova, about 80% of the materials disclosed by HHS that FDA considered in approving Moderna’s Spikevax pertain to other mRNA products unrelated to SARS-CoV-2 or COVID-19.
“Approximately 400 pages of the materials belong to a single biodistribution study in rats conducted at the Charles River facility in Canada for an irrelevant test article, mRNA-1674,” Latypova said. “This product is a construct of 6 different mRNAs studied for cytomegalovirus in 2017 and never approved for market.”
Latypova said the study showed lipid nanoparticles (LNPs) distribute throughout the entire body to all major organ systems.
Latypova found it odd the study protocol, report and amendments related to the study were copied numerous times throughout the HHS documents, suggesting Moderna may have been trying to meet a minimum word count.
In between the repetitive copies of the “same irrelevant study,” Latypova found “ModernaTX, Inc. 2.4 Nonclinical Overview” for Moderna’s COVID-19 vaccine with the investigational new drug application reference IND #19745.
Module 2.4, she said, is a standard part of the new drug application and is supposed to contain summaries of nonclinical studies.
“There are three separate versions of Module 2.4 included and many sections appear to be missing. It is not clear why multiple versions are included and there is no explanation provided as to which version specifically was used for the approval of Spikevax by the FDA.”
Latypova noted all three copies of Module 2.4 appear to have the same overview but reference a different set of statements and studies.
Latypova said the description of the finished supplied product differs between the two versions:
“Version 1 (p. 0001466) [says] mRNA-1273 is provided as a sterile liquid for injection at a concentration of 5 mg/mL in 20 mM trometamol (Tris) buffer containing 87 mg/mL sucrose and 10.7 mM sodium acetate, at pH 7.5.
“Version 2 (p. 0001499) [says] the mRNA-1273 Drug Product is provided as a sterile suspension for injection at a concentration of 20 mg/mL in 20 mM Tris buffer containing 87 g/L sucrose and 4.3 mM acetate, at pH 7.5.”
“It appears from reading section 2.4.1.2 Test Material (p.0001499) that Version 2 of the drug product had been used for manufacturing the Lot AMPDP-200005 which was used for nonclinical studies,” Latypova said. But “there is no explanation given for why the drug product in version 1 is different, and no comparability testing studies between the two product specifications are provided.”
Latypova pointed out that the package insert for FDA-approved Spikevax does not contain any information regarding the concentration of the product supplied in its vials.
Finding 2: Moderna said Spikevax mRNA does not need to be studied for toxicity and can be replaced with any other mRNA without further testing.
Latypova alleges Moderna, Pfizer and Janssen — manufacturer of the Johnson & Johnson shot — along with the FDA, have been deceptive in their assertions claiming the risks of COVID-19 vaccines are associated with the LNP delivery platform, and therefore, the mRNA “payload” does not need to undergo standard safety toxicological tests.
The documents state:
“The distribution, toxicity, and genotoxicity associated with mRNA vaccines formulated in LNPs are driven primarily by the composition of the LNPs and, to a lesser extent, by the biologic activity of the antigen(s) encoded by the mRNA. Therefore, the distribution study, Good Laboratory Practice (GLP)-compliant toxicology studies, and in vivo GLP-compliant genotoxicity study conducted with mRNA vaccines that encode various antigens developed with the Sponsor’s mRNA-based platform using SM 102-containing LNPs are considered supportive and BLA-enabling for mRNA-1273.”
Moderna is “claiming that the active drug substance of a novel medicine does not need to be tested for toxicity,” Latypova said. “This is analogous to claiming that a truck carrying food and a truck carrying explosives are the same thing. Ignore the cargo, focus on the vehicle.”
Latypova called the claim “preposterous,” as mRNAs and LNPs separately and together are “entirely novel chemical entities” that each require their own IND application and data dossier filed with regulators.
“Studies with one mRNA are no substitute for all others,” she added.
“The modified mRNA in the COVID-19 mRNA Vaccine is a chemical active substance that has not been previously authorized in medicinal products in the European Union. From a chemical structure point of view, the modified mRNA is not related to any other authorized substances. It is not structurally related as a salt, ester, ether, isomer, mixture of isomers, complex or derivative of an already approved active substance in the European Union.
“The modified mRNA is not an active metabolite of any active substance(s) approved in the European Union. The modified mRNA is not a pro-drug for any existing agent. The administration of the applied active substance does not expose patients to the same therapeutic moiety as already authorized active substance(s) in the European Union.
“A justification for these claims is provided in accordance with the ‘Reflection paper on the chemical structure and properties criteria to be considered for the evaluation of new active substance (NAS) status of chemical substances’ (EMA/CHMP/QWP/104223/2015), COVID-19 mRNA Vaccine is therefore classified as a New Active Substance and considered to be new in itself.”
“The reviewers specifically stated ‘modified RNA’ and not just the lipid envelope constitute the new chemical entity,” Latypova said. “All new chemical entities must undergo rigorous safety testing before they are approved as medicinal products in the United States, European Union and the rest of the world.”
Latypova said Moderna failed to cite any studies showing “all toxicity of the product resides with the lipid envelope and none with the payload” of the type and sequence of mRNA delivered to various tissues and organs.
“It is also not a matter of a mistake or rushing new technology to market under crisis conditions,” she added. “This scientifically fraudulent strategy was not only premeditated, it was also never really concealed.”
Latypova gave the example of a 2018 PowerPoint presentation by Moderna CEO Stéphane Bancel at a JP Morgan conference where he stated: “If mRNA works once, it will work many times.”
“This describes the deception practiced by the manufacturers, FDA, the Centers for Disease Control and Prevention (CDC), NIH and every government health authority or mainstream media talking head who participated in it,” Latypova said.
She continued:
“Imagine Ford Motor Company claiming that its crash testing program should be contained to the vehicle’s tires and that one test is sufficient for all vehicle models.
“After all both F150 and Taurus have tires, what’s in between the tires ‘worked once and will work again,’ and therefore it is inconsequential to safety, does not need to be separately tested and can be replaced at the manufacturer’s will with any new variation.
“This is the claim that Moderna, Pfizer, Janssen and other manufacturers of the gene therapy ‘platforms’ have utilized. Unlike Ford’s products, theirs have never worked as none of their mRNA-based gene therapy products have ever been approved for any indication. The fact that the regulators did not object to this argument raises an even greater alarm.”
“There is no question of incompetence or mistake,” Latypova said. “If this represents the current ‘gold standard’ of regulatory pharmaceutical science, I have very bad news regarding the safety of the entire supply or new medicines in the U.S. and the world.”
Finding 3: Moderna’s nonclinical program included only one non-GLP toxicology study of the active substance in Spikevax.
According to Latypova, a non-clinical program for a novel product usually includes information on pharmacology, pharmacokinetics, safety pharmacology, toxicology and other studies to determine the carcinogenicity or genotoxicity of a drug and its effects on reproduction.
The more novel the product, the more extensive the safety and toxicity evaluations need to be, she said.
In Module 2.4 described above, Latypova was able to identify 29 unique studies but only 10 were done with the correct mRNA-1273 test particle. The other studies were conducted using a “variety of unapproved experimental mRNAs unrelated to Spikevax or COVID illness.”
For example, the in-vivo genotoxicity studies included an irrelevant mRNA-1706 and a luciferase mRNA that is not in Moderna’s COVID-19 vaccine.
“Of the 10 studies using mRNA-1273, nine were pharmacology (‘efficacy’) studies and only one was a toxicology (‘safety’) study,” Latypova said. “All of these were non-GLP studies, i.e., research experiments conducted without validation standards acceptable for regulatory approval.”
There was only one toxicology study included in Moderna’s package related to the correct test particle mRNA-1273, but the study was non-GLP compliant, was conducted in rats and was not completed at the time the documents were submitted to the FDA for approval.
The results of the study were indicative of possible tissue damage, systemic inflammation and potential severe safety issues — and they are also dose-dependent, Latypova said. Moderna noted its findings but “simply moved on, deciding to forgo any further evaluation of these effects.”
Regarding reproductive toxicology, the only assessment was conducted on rats.
Pharmacokinetics — or the biodistribution, absorption, metabolism and excretion of a compound — were not studied with Moderna’s Spikevax mRNA-1273.
“Instead, Moderna included a set of studies with another, unrelated mRNA-1647 — a construct of six different mRNAs which was in development for cytomegalovirus in 2017 in a non-GLP compliant study,” Latypova said. “This product has not been approved for market and its current development status is unknown.”
Moderna claimed the LNP formulation of mRNA-1647 was the same as in Spikevax, so the study using this particle was “supportive of” the development of Spikevax.
“This claim is dishonest,” Latypova said. “While the kinetics of the product may be studied this way, the toxicities may not!”
“We do not know what happens with the organs and tissues when the delivered mRNA starts expressing spike proteins in those cells. This is a crucial safety-related issue, and both the manufacturer and the regulator were aware of it, yet chose to ignore it.
“The study demonstrated that the LNPs did not remain in the vaccination site exclusively, but were distributed in all organs analyzed, except the kidney. High concentrations were observed in lymph nodes and spleen and persisted in those organs at three days after the injection.
“The study was stopped before full clearance could be observed, therefore no knowledge exists on the full time-course of the biodistribution. Other organs where vaccine product was detected included bone marrow, brain, eye, heart, small intestine, liver, lung, stomach and testes.”
Given that LNPs of the mRNA-1647 were detected in these tissues, it’s reasonable to assume the same occurs with mRNA-1273 and “likewise would distribute in the same way,” Latypova said. “Therefore the spike protein would be expressed by the cells in those critical organ systems with unpredictable and possibly catastrophic effects.”
“Neither Moderna nor FDA wanted to evaluate this matter any further,” she added. “No metabolism, excretion, pharmacokinetic drug interactions or any other pharmacokinetic studies for mRNA-1273 were conducted,” nor were safety pharmacology assessments for any organ classes.
Finding 4: ‘Serious conflict of interest’ exists between Moderna and NIH.
According to Latypova, Moderna’s documents contain a letter from the Division of Microbiology and Infectious Diseases authorizing the FDA to refer to IND #19635 to support the review of Moderna’s own IND #19745 provided in “Module 1.4.”
Although Module 1.4 was not included in the documents provided by HHS, the FDA on Jan. 30 revealed the following timeline for Moderna’s Spikevax.
The date of the pre-IND meeting for Spikevax was on Feb. 19, 2020. The IND submission for the NIH’s IND was on Feb. 20, 2020, while Moderna’s own IND was submitted on April 27, 2020.
According to the CDC, as of Jan. 11, 2020, Chinese health authorities had identified more than 40 human infections as part of the COVID-19 outbreak first reported on Dec. 31, 2020.
The World Health Organization on Jan. 9, 2020, announced the preliminary identification of the novel coronavirus. The record of Wuhan-Hu-1 includes sequence data, annotation and metadata from the virus isolated from a patient approximately two weeks prior.
Latypova said this raises several questions warranting further investigation:
Preparation for a pre-IND meeting is a process that typically takes several months, and is expensive and labor-consuming. How was it possible for the NIH and Moderna to have a pre-IND meeting for a Phase 1 human clinical trial scheduled with the FDA for a vaccine product a month before the COVID-19 pandemic was declared?
“How was it possible to have all materials prepared and the entire non-clinical testing process completed for this specific product related to a very specific virus which was only isolated and sequenced (so we were told) by Jan. 9, 2020?”
Ownership of the IND is both a legal and commercial matter, which in the case of a public-private partnership, must be transparently disclosed. “What is the precise commercial and legal arrangement between Moderna and NIH regarding Spikevax?”
“Does NIH financially benefit from sales of Moderna’s product? Who at NIH specifically?”
“Does forcing vaccination with the Moderna product via mandates, government-funded media campaigns and perverse government financial incentives to schools, healthcare system and employers represent a significant conflict of interest for the NIH as a financial beneficiary of these actions?”
“Does concealing important safety information by a financially interested party (NIH and Moderna) represent a conspiracy by the pharma-government cartel to defraud the public?”
Latypova further noted that immediately after the pre-IND meeting with the FDA, an “extremely heavy volume of orders for Moderna stock” began to be placed in the public markets.
This warrants an “additional investigation into the investors that were able to predict the spectacular future of the previously poorly performing stock with such timely precision,” she said.
Finding 5: FDA failed to question Moderna’s ‘scientifically dishonest studies’ dismissing an ‘extremely significant risk’ of vaccine-induced antibody-enhanced disease.
“Its entire product development history was marked by numerous failures despite millions of dollars and lengthy time spent in development,” Latypova said. “Notably, its mRNA-based vaccines were associated with the antibody-dependent-enhancement phenomenon.”
For example, Moderna’s preclinical study of its mRNA-based Zika vaccine in mice showed all mice “uniformly [suffered from] lethal infection and severe disease due to antibody enhancement.”
The scientists were able to develop a type of vaccine that generated protection against Zika that “resulted in significantly less morbidity and mortality,” but all versions of the vaccine unequivocally led to some level of antibody-dependent-enhancement.
The Primary Pharmacology section for Spikevax includes nine studies evaluating immunogenicity, protection from viral replication and potential for vaccine-associated enhanced respiratory disease.
“These studies included the correct test article (mRNA-1273), however, all were non-GLP compliant,” Latypova said. The results of these studies are briefly summarized in the text of the document package, yet the study reports are not provided.
In the disclosed documents, Moderna claims “there were no established animal models” for SARS-CoV-2 virus due to its extreme novelty.
Yet, in the next sentence, “despite the extreme novelty of the virus,” Ralph Baric, Ph.D., at the University of North Carolina possessed an already mouse-adapted SARS-CoV-2 virus strain and provided it for some of Moderna’s studies, Latypova said.
According to Latypova’s assessment, there were other numerous contradictions in Moderna’s documents, and when enhanced disease risk was revealed in assays, the company waived off its own results with a statement regarding the invalidity of the assays and methods they used.
“As SARS-CoV-2 neutralization assays are, to this point, still highly variable and in the process of being further developed, optimized and validated, study measurements should not be considered a strong predictor of clinical outcomes, especially in the absence of results from a positive control that has demonstrated disease enhancement,” Moderna said.
“Clearly, both Moderna and FDA knew about disease enhancement and were aware of numerous examples of this dangerous phenomenon, including Moderna’s own Zika vaccine product of the same type,” Latypova said. “Yet, the FDA did not question Moderna’s scientifically dishonest ‘studies’ that dismissed this extremely significant risk without a proper study design.”
Finding 6: FDA and Moderna lied about reproductive toxicology studies in public disclosures and product labeling.
Although the FDA recommends Moderna’s COVID-19 vaccine for pregnant and lactating women, Moderna conducted only one reproductive toxicology study in pregnant and lactating rats using a human dose of 100 mcg of mRNA-1273.
Although the full study was excluded, a narrative summary of Moderna’s findings state, “high IgG antibodies to SARS-CoV-2 S-2P were also observed in GD 21 F1 fetuses and LD 21 F1 pups, indicating strong transfer of antibodies from dam to fetus and from dam to pup.”
Latypova said safety assessments in the study are very limited, but the following findings are described by Moderna:
“The mothers lost fur after vaccine administration, and it persisted for several days. No information on when it was fully resolved since the study was terminated before this could be assessed.”
In the rat pups, the following skeletal malformations were observed:
“In the F1 generation [rat pups], there were no mRNA-1273-related effects or changes in the following parameters: mortality, body weight, clinical observations, macroscopic observations, gross pathology, external or visceral malformations or variations, skeletal malformations, and mean number of ossification sites per fetus per litter.
“mRNA-1273-related variations in skeletal examination included statistically significant increases in the number of F1 rats with 1 or more wavy ribs and 1 or more rib nodules.
“Wavy ribs appeared in 6 fetuses and 4 litters with a fetal prevalence of 4.03% and a litter prevalence of 18.2%. Rib nodules appeared in 5 of those 6 fetuses.”
Moderna related the skeletal malformations to days when toxicity was observed in the mothers but waived away the finding as “unrelated to the vaccine,” Latypova said.
The FDA then “lied on Moderna’s behalf” in its Basis for Regulatory Action Summary document (p.14) stating “no skeletal malformations” occurred in the non-clinical study in rat pups despite the opposite reported by Moderna.
“No vaccine-related fetal malformations or variations and no adverse effect on postnatal development were observed in the study. Immunoglobulin G (IgG) responses to the pre-fusion stabilized spike protein antigen following immunization were observed in maternal samples and F1 generation rats indicating transfer of antibodies from mother to fetus and from mother to nursing pups.”
“In summary, the vaccine-derived antibodies transfer from mother to child,” Latypova said. “It was never assessed by Moderna whether the LNPs, mRNA and spike proteins transfer as well, but it is reasonable to assume that they do due to the mechanism of action of these products.”
Latypova said studies should have been done to assess the risks to the child by vaccinating pregnant or lactating women before recommending these groups receive a COVID-19 vaccine.
“We should ask the question why are they concealing the critical safety-related information from public, and making the product look better than the manufacturer has admitted,” Latypova said.
“The FDA did not have any objective scientific evidence excluding the skeletal malformations being related to the vaccine,” she added. “Thus, the information should have been disclosed fully in the label of this experimental and poorly tested product — not hidden from the public for over a year and then disclosed only under a court order.”
Latypova said FDA reviewers should have “easily seen through the blatant fraud, omissions, use of inadequate study designs and general lack of scientific rigor.”
The fact that more than half of the document package contains non-GLP studies for irrelevant, unapproved and previously failed chemical entities alone should have been sufficient reason to not approve this product, she added.
It would appear the FDA based its decision that the product is safe to administer to thousands of otherwise healthy humans on two studies in rats, Latypova said. The rest of the 700-page package was deemed to consist of “other supportive studies.”
The FDA noted studies were conducted in “five vaccines formulated in SM-102 lipid particles containing mRNAs encoding various viral glycoprotein antigens” but “failed to mention that these were five unapproved and previously failed products,” she said.
The regulators then concluded that using novel unapproved mRNAs in support of another unapproved novel mRNA was acceptable.
“The circular logic is astonishing,” Latypova said. Regulators allowed and personally promoted the use of failed experiments in support of a different and new experiment directly on the unsuspecting public.
Latypova called for the FDA, pharmaceutical manufacturers and “all other perpetrators of this fraud to be urgently stopped and investigated.”
“The guilt for the mass murder is solely that of the political leaders….. I accuse the leaders of abusing my obedience. At that time obedience was demanded, just as in the future it will also be demanded of the subordinate. Obedience is commended as a virtue.” —Adolph Eichmann, Nazi, at his trial
Early in the declared Covid19 Pandemic, America’s medical community —and this included America’s pharmacies—coalesced around a system of outlawing medicines known to be effective, safe and inexpensive, notably ivermectin and hydroxychloroquineIn time, it became obvious that withholding early treatment was crucial for the pharmaceutical industry’s project to vaccinate the world against a claimed Covid19 virus.
Had the effectiveness of inexpensive and available medicines been widely seen, the pretext for ‘Emergency Use Authorization’ of a warpspeed-produced experimental product would have vaporized. With a trillion dollar global vaccination project at stake, that couldn’t be allowed, so the lies of ivermectin and hydroxychloroquine being toxic were authoritatively enforced.
The policy descended (and continues to descend) from administrative networks within the Department of Health and Human Services, (notably CDC and NIAID) to the states. These networks are part of, and fed by, an international complex involving the World Health Organization, itself under the control of international pharmaceutical interests focused primarily on vaccines, as well as on gene manipulations sold under the deceptive banner of “vaccine”.
This multi-pronged, vaccine-focused universe now includes research universities and medical schools, medical societies and fraudulent medical journals showcasing ghost-written “scientific” articles. A key player is the discipline of Public Health, a politicized field posing as objective science, enforcer of official narrative and hurler of the “misinformation” epithet at dissenters. And of course there is the compliant media. And money, endless rivers of it.
At hospital level, commands from this complex flow through desk-bound administrators, with doctors and nurses induced to follow those commands for fear of losing needed hospital access. Failure to mind can even result in suspension of license to practice medicine. This control system extends to state medical boards under the umbrella of the Federation of State Medical Boards, the guidelines of which require practitioners to use treatments “… supported by the best available scientific evidence or prevailing scientific consensus”. But officially accepted “best available scientific evidence” is now so tightly controlled that one is literally forced toward the “prevailing scientific consensus”.
The “consensus” referred to is a rigidly enforced story, and divergence from it is immediately attacked from all corners of officialdom as “misinformation”. A key branch of the army protecting the official, lie-riddled storyline has been the burgeoning fact-check industry, succinctly nailed by Dr. Bryan Ardis“Fact checking is to divert you from the truth and take you back to the narrative you’re being sold worldwide.”
You doctors who have been obedient to an industry-inspired, governmentally-driven protocol have abdicated the doctor-patient relationship. And what is true for doctors in this respect applies to nurses as well. By withholding available treatments and sending sick people home; by injecting a trusting public with an experimental gene-altering technology that has potentially devastating long-range, even trans-generational impacts; by not seeing immediately the criminal idiocy of injecting children, for whom the claimed virus is known to be benign, you have made your patients de facto lab animals.
FBI Director J. Edgar Hoover once wrote “The individual is handicapped by coming face to face with a conspiracy so monstrous he cannot believe it exists.” The Covid19 Pandemic, set up as justification for a global project to inject humanity with a gene-altering death-dealing technology, is certainly monstrous enough to handicap anyone, at least for a time. It is murderous on a scale so immense as to be unbelievable on first exposure. And that alone may have posed too great a barrier for most of the multitude to even want to take a closer look.
But you medical professionals cannot claim ignorance at this late date, when mere minutes of online search can reveal that outstanding medical figures all over the world have been struggling against censorship and mainstream media vomitings to expose the lie-riddled Covid19/“vaccine” project ( 1, 2, 3…) For their troubles, of course, they continue to be attacked by the media network long known to be rotten to the core. Has your choosing to be obedient within this long nightmare been simply to hold on to a job? Or have you just been too lazy to search out censored information? Or too uncaring? Or are you just stupid? Only you would know for sure.
Josef Mengele, like yourselves, was a medical doctor. At Auschwitz concentration camp, his grisly medical experiments won him a place in history as Todesengel, “The Angel of Death”. He is supposed to have said “The more we do to you, the less you seem to believe we are doing it.” Does that seem familiar, and do your patients still trust you? In any case, you medics who have been so obedient to the vaccine industry’s merciless global project might want to get to know Dr. Mengele. There are even books on the man. After all, he was a soul mate of yours, as you have, eyes wide open, made yourselves, whether by omission or commission, his medical heirs.
*
Bill Willers is an emeritus professor of biology, University of Wisconsin at Oshkosh. He is founder of the Superior Wilderness Action Network and editor of Learning to Listen to the Land, and Unmanaged Landscapes, both from Island Press. He can be contacted at willers@uwosh.edu.
In a move Children’s Health Defense President Mary Holland called “head-spinning,” the U.S. Food and Drug Administration on Friday granted full approval of Pfizer-BioNTech’s Comirnaty COVID-19 vaccine for adolescents 12 through 15 years old.
The U.S. Food and Drug Administration (FDA) on Friday granted full approval of Pfizer-BioNTech’s Comirnaty COVID-19 vaccine for adolescents 12 through 15 years old.
In an FDA press release, the agency said full approval of Comirnaty follows a “rigorous analysis and evaluation of the safety and effectiveness data,” and the Pfizer-BioNTech vaccine “has been, and will continue to be authorized for emergency use in this age group since May 2021.”
Pfizer’s press release announcing the approval said the Comirnaty vaccine has been available under Emergency Use Authorization (EUA) since May 2021 for the adolescent age group.
Yet, Comirnaty is not available in the U.S for any age group and is not the same formula as the Pfizer-BioNTech vaccine currently authorized under EUA and being distributed as a “fully approved” vaccine.
“The approval of Comirnaty for adolescents 12 to 15 is head-spinning,” said Mary Holland, president and general counsel for Children’s Health Defense.
Holland added:
“The FDA failed to convene an expert committee and failed to appropriately weigh the risk-benefit profile of this vaccine for this age group. Even Vaccine cheerleader Dr. Paul Offit acknowledged FDA decisions are being made based on political pressure, not science when, in commenting on the agency’s vote last week to allow reformulated booster shots, he said it felt like ‘the fix was in.’”
Holland said that at base, “this is a move by pharma to ensure liability protection” under the National Childhood Vaccine Injury Act of 1986. Some states likely will attempt to put Comirnaty on the childhood vaccine schedule, despite the myriad known and unknown risks, Holland said.
“Pfizer‘s fraud and collusion with government is becoming more evident by the day,” Holland said. “CHD, already challenging the authorizations for those six months through age 11, will be at the forefront of challenging this approval for teenagers.”
Efficacy claims based on old analysis of 16- to 25-year-olds — before Delta, Omicron variants
Pfizer said Friday’s approval is based on data from a Phase 3 clinical trial of 2,260 participants ages 12 through 15.
About half of the participants, “elicited SARS-CoV-2–neutralizing antibody geometric mean titers (GMTs)” demonstrating “strong immunogenicity in a subset of adolescents one month after the second dose,” Pfizer said.
It is unknown what happened to antibody levels after one month, but peer-reviewed research suggests vaccine protection conferred by second and third doses of Pfizer’s COVID-19 vaccine wanes rapidly against the Omicron variant.
“Our study found a rapid decline in Omicron-specific serum neutralizing antibody titers only a few weeks after the second and third doses of [the Pfizer-BioNTech] BNT162b2,” said the authors of a May 13 study published in JAMA.
To further support its claim that Comirnaty is effective in the 12 to 15 age group, Pfizer used an old analysis of 16- to 25-year-olds conducted before the Delta and Omicron surges.
“The efficacy analysis was conducted between November 2020 and May 2021, which was before the Delta and Omicron surges,” and the “only SARS-CoV-2 variant of concern identified from the confirmed COVID-19 cases in this age group was Alpha,” Pfizer said in its press release.
FDA experts question neutralizing antibodies as standard for vaccine effectiveness
During a June 28 meeting of the FDA’s Vaccine and Related Biological Products Advisory Committee (VRBPAC), vaccine experts raised concerns that neutralizing antibodies did not correlate to clinical protection — noting Moderna’s COVID-19 vaccine had a two-fold increase in neutralizing antibody levels compared with Pfizer’s vaccine during clinical trials, but it did not translate into a clinically significant difference in terms of protection against severe disease.
Dr. Ofer Levy, VRBPAC member and infectious disease physician at Boston Children’s Hospital, said during the meeting there is still “no established correlate of protection,” referring to the level of antibodies needed to confer protection.
“You have a lot of data now,” Levy told Pfizer. “What is your relative protection?”
“I would say there is no established correlate of protection,” Kena Swanson, Ph.D., vice president of viral vaccines at Pfizer, told Levy.
Levy said:
“I would like to hear from FDA what their overall approach will be around improving our understanding of correlate protection. We spend a good amount of time reviewing antibody data. We have no doubt antibody data is important. We don’t have a level of antibody that anybody is comfortable stating is correlated [with] protection.
Levy, who said antibodies are important, but T cells are more important, called for federal leadership to establish a “standardization of the T-cell assay and encourage or in fact require the sponsors to gather that information.”
“So what is the effort to standardize the pre-clinical assays?” Levy asked. “This is an effort that’s critical not just now but for future cycles of vaccine revision. If we aren’t able to define a standard for correlate protection we are fighting with one arm behind our back.”
Dr. Peter Marks, head of the FDA’s Center for Biologics Evaluation and Research, acknowledged the importance of Levy’s question and said they are “having conversations” with colleagues at the National Institutes of Health and throughout government about how they might move forward, but it is something they “don’t have an answer to yet.”
Marks said as vaccines are developed in the future, it will “become even more important” to define a standard of correlate protection because “we won’t be able to have a large naive population to vaccinate with newer vaccines.”
“We will need to understand the T-cell response better,” Marks said. “I take your point, it’s just that we haven’t solved the problem yet.“
Comirnaty not available in the U.S.
According to Pfizer’s press release, Comirnaty was previously made available to the 12 to 15 age group in the U.S. under EUA and 9 million U.S. adolescents in this age group have completed a primary series.
“The vaccine, sold under the brand name Comirnaty for adults, has been available under an emergency use authorization since May 2021 for the 12-15 age group,” Reuters reported. “It will now be sold under the same brand name for adolescents as well.”
Yet, Pfizer’s information hotline says it has no specific information on when Comirnaty will be available.
The FDA said Friday the Pfizer-BioNTech vaccine “has been, and will continue to be, authorized for emergency use in this age group since May 2021.”
The CDC’s website states that Comirnaty is “not orderable.”
A branch of the U.S. Department of Health and Human Services overseeing the Strategic National Stockpile indicated Comirnaty was not available because Pfizer did not have time to change the labels.
According to FDA documents, Comirnaty is not available in the U.S. and nobody has received a fully approved and licensed COVID-19 vaccine.
“Comirnaty has not been made available under EUA,” said Dr. Madhava Setty, physician and senior science editor for The Defender.
Setty added:
“The FDA and Pfizer have already stated very quietly, that they have no intent of manufacturing Comirnaty for distribution. Everyone is getting the non-licensed formulation that carries no liability for pharmaceutical companies.”
The CDC website confirms this, stating the Comirnaty formulation “will not be manufactured or made available in the near term even if authorized.”
CHD challenged FDA on Comirnaty ‘approval’ for adults
As The Defender reported, there were “several bizarre aspects to the FDA approval” that proved confusing — which led to CHD suing the FDA over its approval of Comirnaty.
The FDA acknowledged that while Pfizer had “insufficient stocks” of the newly licensed Comirnaty vaccine, there was “a significant amount” of the Pfizer-BioNTech COVID vaccine — produced under EUA — still available for use.
The FDA said the Pfizer-BioNTech vaccine under EUA should remain unlicensed but could be used “interchangeably” with the newly licensed Comirnaty product.
The FDA also said the licensed Pfizer Comirnaty vaccine and the existing Pfizer-BioNTech vaccine were “legally distinct,” but proclaimed their differences did not “impact safety or effectiveness.”
Yet, there is a “huge real-world difference” between products approved under EUA compared with those the FDA has fully licensed.
EUA products are experimental under U.S. law and cannot be mandated. A licensed vaccine, such as Comirnaty, can be mandated by employers and schools.
Although Pfizer’s Comirnaty vaccine can be mandated, it has no liability shield. Vials of the branded product, which say “Comirnaty” on the label, are subject to the same product liability laws as other U.S. products.
Only COVID-19 vaccines distributed under EUA — which in the U.S. includes Pfizer-BioNTech, Moderna and Johnson & Johnson — have liability protection under the 2005 Public Readiness and Preparedness Act (PREP).
Under PREP, the only way an injured party can sue a pharmaceutical company for an injury caused by an EUA vaccine is if he or she can prove willful misconduct and if the U.S. government has also brought an enforcement action against the party for willful misconduct. No such lawsuit has ever succeeded.
Comirnaty cannot receive liability protection unless it is fully approved for children and added to the CDC’s immunization schedule bringing it under the auspices of the National Vaccine Injury Compensation Program.
Pfizer-BioNTech and Comirnaty vaccines aren’t interchangeable
The FDA on Oct. 29, 2021, authorized a manufacturing change to allow an additional formulation of the Pfizer-BioNTech COVID-19 vaccine that uses tromethamine (Tris) buffer instead of phosphate-buffered saline (PBS) used in the originally authorized Pfizer-BioNTech COVID-19 vaccine.
The FDA on Dec. 16, 2021, approved a supplement to the Comirnaty BLA to include a new 30 mcg dose formulation that uses the Tris buffer instead of the PBS buffer used in the originally approved vaccine.
The Pfizer-BioNTech vaccine may contain either the PBS buffer or tris buffer, except for the 5 to 11 age group. The Comirnaty vaccine contains the Tris buffer.
The Pfizer-BioNTech vaccine used for the 5 to 11 age group uses a Tris buffer, despite clinical trials having been conducted using Pfizer’s vaccine containing the PBS buffer.
According to Pfizer’s July 8 press release, the FDA relied upon studies conducted prior to the formula change to justify the approval of Pfizer’s Comirnaty vaccine for adolescents ages 12 to 15.
The type of buffer used in a COVID-19 vaccine can affect the potency of the vaccine, how it is stored and the propensity to develop potential adverse events, TrialSite News reported.
It is unknown if tromethamine will harm an unborn baby, but animal reproduction studies have shown an adverse effect on the fetus, and there are “no adequate and well-controlled studies in humans.”
“The FDA-evaluated manufacturing data [to] support the change in this inactive ingredient and concluded it did not impact the safety or effectiveness of the product,” Marks, said during an October 2021, press briefing.
According to the FDA’s Letter of Authorization, reissued on Oct. 29, “analytical comparability assessments” revealed the Pfizer-BioNTech COVID vaccine formulations containing Tris and PBS buffers were “analytically comparable.”
Yet, no human or animal trials were conducted to determine the safety or efficacy of the new formula.
Uruguay suspended COVID-19 vaccines for children under 13 after a judge on Thursday issued an injunction halting vaccinations in that age group until government officials turn over its contracts with Pfizer.
Uruguay suspended COVID-19 vaccines for children under 13 after a judge on Thursday issued an injunction halting vaccinations in that age group until government officials turn over its contracts with Pfizer.
Uruguayan government officials and Pfizer were ordered on Wednesday to appear in court after judge Alejandro Recarey gave them 48 hours to present detailed information on Pfizer’s COVID-19 vaccine while the court considered an injunction request to halt COVID-19 vaccinations for children 5 and older.
The government said a confidentiality clause in the contract prevents it from producing the documents, The Washington Post reported.
According to ABC News, the judge received answers to 18 questions about the safety and chemical composition of COVID-19 vaccines, signed by Health Minister Daniel Salinas, but did not turn over the contracts.
It is unknown whether the answers provided by government officials adequately addressed the questions posed by the judge, who ultimately ordered an injunction based on what was provided.
Salinas, after the court’s ruling, strongly defended the government’s vaccination plan and criticized the judge for questioning the safety of vaccines.
Alvaro Delgado, the secretary of the presidency, said the halt is a threat to public health.
“We’re convinced that it’s crazy to suspend voluntary vaccination because it has a strong scientific backing,” Delgado said at a news conference.
Vaccinations for those older than 13 will continue, the Health Ministry said in a statement.
The government plans to appeal the decision, according to ABC News.
As The Defender reported Wednesday, judge Recarey of the Administrative Litigation Tribunal used his inquisitorial powers to demand the Uruguayan Ministry of Public Health, State Health Services Administration and the President’s Office submit all information regarding the contracts for the purchase of COVID-19 vaccines, including contractual information related to any clauses of civil indemnity or criminal impunity of the suppliers in the event of adverse effects.
Uruguayan government officials and Pfizer were ordered to appear in court Wednesday to provide documents for review regarding vaccine ingredients, adverse effects and contracts shielding the pharma giant from liability.https://t.co/A9RZs1FXyA
— Robert F. Kennedy Jr (@RobertKennedyJr) July 7, 2022
The judge is seeking, among other things, to know whether there are clauses in the contracts that promised pharmaceutical companies like Pfizer civil and criminal immunity for adverse effects caused by their vaccines.
Judge Recarey posed a series of questions to government officials and Pfizer regarding the chemical composition, efficacy and safety of COVID-19 vaccines, and required Pfizer to state whether it has “admitted, in any area, internal or external to it and its partners, the verification of adverse effects” of its COVID-19 vaccines in children.
Biotech/Pharmaceutical Chemist Mike Donio on the Tyranny of Medical Dogma: Exposing the Corruption, Lies, and Medical Fraud in the Pharmaceutical Industry
to California State University’s Leemon McHenry exposing pharmaceutical companies who buy medical journals in order to peer-review their own research, in order to invent fake diseases, in order to sell unnecessary products (such as the HPV vaccine),
America’s most cited cardiologist, Peter McCullough, said this week that he no longer trusts any Flu shot, due to the unbelievable corruption within the pharmaceutical industry.
But the fact that humanity is in an abusive relationship with its governments, is only one part of the problem. There’s a long history of cults infiltrating polite society. The cult of personality of Lenin and later Stalin once captured an entire nation. But never in history has the entire world fallen to a cult.
Del Bigtree has revealed how the American government (including the CDC and FDA) collude with Big Pharma for monetary gain, particularly where safety trials are concerned. Or rather, the lack of safety trials.
Roman Bystrianyk co-authored a book called Dissolving Illusions, in which they use official data to show how, over the last century, no vaccine has worked in the way promised by the pharmaceutical industry and governments. Every vaccine was introduced way after its respective disease was on its way out. Measles, for example, was around 97% eradicated before its vaccine hit the market.
The point is that the pharmaceutical industry is untrustworthy, and few scientists are as close to the action as Mike Donio.
The Army confirmed on July 1 that tens of thousands of military Guard and Reserve soldiers can no longer participate in training or receive benefits, as Army faces recruiting crisis.
About 60,000 Army National Guard members and Army Reserve soldiers who refused to comply with a Department of Defense (DOD) COVID-19 vaccine mandate are no longer allowed to participate in their military duties and were cut off from some of their pay and benefits, Army officials announced July 1.
Of the more than 40,000 members of the Guard who remain unvaccinated, 14,000 have said they do not intend to ever receive a COVID-19 vaccine, Guard officials told CBS News.
Approximately 22,000 Reserve soldiers have refused to get vaccinated.
“Soldiers who refuse the vaccination order without an approved or pending exemption request are subject to adverse administrative actions, including flags, bars to service and official reprimands,” an Army spokesperson said in a statement.
If the soldiers continue to refuse to get vaccinated, the consequences could be even more severe.
“In the future, Soldiers who continue to refuse the vaccination order without an exemption may be subject to additional adverse administrative action, including separation,” the Army spokesperson said.
Despite the military’s deadline, the services said they wish to continue to work with the remaining holdouts as commanders face increased anger from critics concerned over a recruiting crisis that has left Defense Department officials struggling to fill the ranks.
According to Rep. Mike Johnson (R-LA), the Army is having “significant trouble filling its ranks” while simultaneously discharging soldiers who refuse to get vaccinated.
As of mid-April, the Army had “discharged 255 soldiers for refusing the COVID-19 vaccine and is on track to give another 2,500 to 3,000 the boot before the end of the year — a number roughly equivalent to two or three Army battalions,” Johnson wrote on his website.
Six Army officers, including two battalion commanders, have been relieved of command, while 3,330 active-duty soldiers have been issued written reprimands for refusing to get vaccinated.
“The Army priority remains vaccinating all soldiers to maintain readiness. In determining this policy, Army leaders considered the unique realities of each component,” Reserve spokesman John Bradley told U.S. News & World Report.
“Reserve component commanders are working through a deliberate process in as few as two days per month with geographically dispersed Soldiers to ensure they become fully vaccinated.”
Soldiers will be allowed to come on duty and earn their pay if it’s for the purpose of getting vaccinated or to take part in separation procedures. Part-time soldiers with a pending medical or religious exemption request may train with their units and collect pay and benefits, but exemptions are not being approved.
To date, only six Guard soldiers across all states and territories have received medical exemptions out of 53 who submitted requests, according to Army data. No Reserve soldiers have received a medical exemption.
No Guard or Reserve soldiers have been approved for a religious exemption despite nearly 3,000 requests.
The Army National Guard and Army Reserve deadline to receive the COVID-19 vaccine was June 30 — the final deadline among all the service branches subject to Secretary of Defense Lloyd Austin’s mandate issued last August.
According to internal documents shared with The Defender, 280,678 Army National Guard members are fully vaccinated (84.6%), and 7,735 have received one dose (2.3%) leaving 43,269 (13%), who have not yet received a single dose.
In some states, such as Oklahoma, the vaccination rate for Guard members is as low as 74.11%.
The document lists 15,698 members as “refusals” and 6,749 (2.0%) as going through an exemption process — with 6,257 (1.9%) requesting a religious exemption and 492 (0.1%) requesting a medical exemption.
The document also notes that 80% of unvaccinated Guard members are age 32 or younger, with an average age of 26.2 and median age of 24.
According to CBS News, vaccine compliance among Army National Guard members is the lowest in the U.S. military — the rate among active-duty Army, Navy, Air Force and Marine Corps is 97% or greater and the Air Guard uptake is about 94%.
Pfizer Ordered by Uruguayan Judge to Report Composition of Covid-19 Vaccines Including Any Presence of “Graphene Oxide” or “Nanotechnological Elements”
According to a recent ruling by an Uruguayan judge, the government and the pharmaceutical company Pfizer must provide all the information they have on the COVID vaccine’s biochemical composition, including any evidence of “graphene oxide” or “nanotechnological elements,” as well as proof of the vaccine’s efficacy and safety.
Administrative Litigation Court (TCA) Judge Alejandro Recarey made the order in response to a request to suspend the immunization of children from 5 years of age in Uruguay.
According to the court order released on Saturday, Judge Alejandro Recarey ordered the Presidency, the Ministry of Public Health, the State Health Services Administration (ASSE), and Pfizer to present all the information on Covid-19 vaccines within 48 hours, El Observador reported.
“A hearing will be held on Wednesday at 9:00 am where representatives of all the agencies and the company must appear,” the news outlet added.
According to the decision, the Executive and the US laboratory must provide documentation on the composition of the vaccines, including the possible presence of “graphene oxide” or “nanotechnological elements”.
Data is also requested that demonstrates the “harmlessness” of “the substance called messenger RNA” and that proves with studies by the US agency of the United States, the FDA, “the experimental nature” of the vaccines.
The magistrate asks that the authorities “explain whether alternative anticovid-19 therapies have been studied” and “if not, clarify why these solutions were not explored,” according to the document.
The contracts signed between the government and Pfizer are also subject to scrutiny to see if they contain clauses “for civil indemnity or criminal impunity for suppliers regarding the occurrence of possible adverse effects,” among other details.
The court decision also requires explanations as to whether studies have been carried out “aiming to explain the notorious increase in deaths from covid-19 as of March 2021 in relation to the previous year.”
“Very especially, Pfizer will be instructed to state within 48 hours – with the provision of documentary data if applicable – if the company has admitted (…) the verification of adverse effects of vaccines against the so-called Covid-19. In general, and also in detail regarding the child population,” says the document.
Yates Hazlehurst, who developed autism after receiving his childhood vaccines, was the first and only vaccine-injured plaintiff to make it to a jury. The 20-year process revealed major flaws in a system that is supposed to compensate children for vaccine injuries.
In a riveting legal battle spanning two decades, William Yates Hazlehurst (“Yates”) on Feb. 2, 2022, became the first vaccine-injured person with a diagnosis of autism to reach a jury since the National Childhood Vaccine Injury Compensation Act of 1986 (the Vaccine Act) became law.
In a medical malpractice case filed in the Madison County Circuit Court in Tennessee, attorneys for Yates argued the clinic and physician who administered Yates’ vaccines, including the measles-mumps-rubella (MMR) vaccine on Feb. 8, 2001, should be held liable for medical malpractice and the neurological injuries Yates developed after being vaccinated.
Although the jury decided in favor of the physician — who Yates’ father said failed to adequately inform the parents of the risks of vaccinating Yates while he had an active ear infection — the case exposed major flaws in a system designed to protect children and shield pharmaceutical companies and physicians from liability for vaccine injuries.
“In the fight to end the autism epidemic, we were all hoping for the one knockout punch that would bring the truth to light and help end the autism epidemic,” Yates’ father, Rolf Hazlehurst, said.
“This medical malpractice trial was the only opportunity in the last 35 years for a jury to hear evidence in a court of law regarding whether a vaccine injury can cause neurological injury, including autism.”
Hazlehurst, who is a senior staff attorney for Children’s Health Defense (CHD), said “unless the Vaccine Act is repealed, my son is probably the only vaccine-injured child with a diagnosis of autism who will ever reach a jury.”
The Hazlehurst case was a medical malpractice case against the doctor who administered the pediatric vaccines that, in the opinion of the world’s top experts, sent Yates, now 22, spiraling into the depths of severe, non-verbal autism.
Although the case was originally filed in 2003, it didn’t receive its day in court for 19 years because a separate case involving Yates’ injury first had to work its way through the National Vaccine Injury Compensation Program (NVICP).
When Yates’ medical malpractice case was finally heard, the trial exposed alarming evidence about autism and vaccines, the low standard of care practiced by physicians administering pediatric vaccines and financial conflicts of interests between pharmaceutical companies that manufacture vaccines and government agencies entrusted with vaccine safety.
During the trial, the world’s top experts in the field of autism and mitochondrial disorder explained how the administration of “routine” childhood immunizations can cause autism, brain injury, and many other disorders.
According to the National Institute of Mental Health, autism is a neurological and developmental disorder that affects how people interact with others, communicate, learn and behave. Symptoms can be severe and usually manifest before a child turns 3, which coincides with the age children receive the most childhood vaccines.
Increasing evidence indicates a significant proportion of individuals with autism have concurrent diseases such as mitochondrial dysfunction, abnormalities of energy generation, gastrointestinal abnormalities and abnormalities in the regulation of the immune system.
Yates’ medical malpractice trial illuminated how vaccines can cause autism in children with mitochondrial disorder and showed how the Vaccine Act — which is designed to ensure informed consent and compensation to injured children — is an abject failure because it’s largely unenforceable.
Robert F. Kennedy, Jr. , Lane Hodges and Yates Hazlehurst.
Yates was normal until he received his 12-month vaccines
During the first year of his life, Yates developed typically and met all of his developmental milestones.
“He was a happy, healthy and normal child,” his father said.
After his 6-month shots, Yates experienced a severe screaming episode approximately 24 hours after receiving the DTaP, Prevnar, Hib and Hep B vaccines.
In the days following his vaccinations, Yates began to experience seizure-like shaking episodes.
But his parents didn’t realize their son’s symptoms were consistent with a severe vaccine adverse reaction because they were not given a Vaccine Information Statement (VIS) at their pediatrician’s office.
According to the Centers for Disease Control and Prevention (CDC), a VIS is an information sheet produced by the CDC that explains both the benefits and risks of a vaccine to recipients.
“Federal law requires that healthcare staff provide a VIS to a patient, parent or legal representative before each dose of certain vaccines,” the CDC website states.
Instead of providing the VIS, Yates’ physician told his parents any adverse event to a vaccine would be “almost immediate” — within 5 to 15 minutes after vaccination.
Before Yates’ first birthday, his mother and aunt took him to the doctor because he had been sick, and his parents wanted to make sure it was okay for Yates to have a birthday party.
Hazlehurst told The Defender this appointment was not a scheduled well-child check. It was a sick visit. At the appointment, Yates was diagnosed with an ear infection and prescribed an antibiotic.
As the pediatrician turned to leave, he stated Yates would receive his shots, as it was close to his first birthday. A woman returned to the room who portrayed herself to be a nurse, but Hazlehurst later found out was only a medical assistant.
Yates’ mother asked the “nurse” whether their son should receive his shots despite being sick and was told he should.
Once again, they were not given a VIS form informing them of the risks of vaccinating Yates while he had a fever and an active ear infection.
“By administering vaccines to a sick child, the doctor and his clinic could charge a “modified double bill” Hazlehurst said.
That day, on Feb. 8, 2001, Yates received the MMR, Prevnar, Hib and Hep B vaccines. Twelve days later, Hazlehurst said his son experienced a high fever, rash and vomiting consistent with a vaccine adverse reaction.
Hazlehurst called the clinic where his son received his vaccine and talked to the doctor on call who asked him which vaccines Yates received. Hazlehurst responded, “whatever you get when you’re a year old.”
Hazlehurst was told his son was having an adverse reaction to the antibiotic and the doctor wrote him a prescription for a different antibiotic and an anti-fungal medication.
Soon after, Yates began to lose the skills he once had and began developing abnormally. He lost his speech, started running wild, was constantly on the go and would knock things off the table.
“He was visually ‘stimming’ off the falling objects and running with his head down for the visual stimulation,” Hazlehurst said.
He explained:
“It was not like he got the shots and boom, the next day he was autistic. That’s not the way it happened. The mitochondria produce the energy to the connecting tissue in the cells in the brain, and if they don’t get enough energy for a short period of time (as short as 6 seconds), cellular death occurs.
“The brain keeps developing, but it cannot develop normally because the connecting cellular tissue has been damaged. That’s why it takes time to manifest. It’s like watching grass grow. It’s happening, but you don’t realize it’s happening.”
Yates’ condition worsened. He developed an obsession with spinning objects, became a picky eater, started hand-flapping and toe-walking, became unable to sleep and exhibited gastrointestinal and multiple other medical and neurodevelopmental issues, Hazlehurst said.
Hazlehurst searches for answers to his son’s autism
According to federal law, there are specific recording requirements for vaccine medical records, and healthcare providers must provide records to a parent upon request.
Hazlehurst, on June 21, 2002, requested a copy of his son’s original vaccine records so other physicians could evaluate, diagnose and treat Yates.
Hazlehurst had questions about the American Academy of Pediatrics’ standard of care and wanted to know why his son was vaccinated while he was sick with a fever.
In response to Hazlehurst’s request and questions about Yates’ care, the pediatrician rushed out of the room and called his attorney, Hazlehurst said.
The doctor and clinic denied Hazlehurst’s requests to review and receive copies of his son’s original vaccine records, forcing him to petition the court for Yates’ records.
The court granted the request, and the local sheriff’s department seized Yates’ medical records from the doctor’s clinic.
Hazlehurst quickly realized there were problems with his son’s vaccine record, which was on an unsigned consent form that had a billing code sticker placed over the language regarding the risks and benefits of vaccines and vaccine information materials.
Hazlehurst said he never received a VIS form and Yates had been vaccinated without informed consent.
Hazlehurst files claim with the NVICP for son’s vaccine injury
Hazlehurst, like many parents of vaccine-injured children, pursued a claim with the NVICP as federal law requires. The process took nine years — from 2002 to 2011.
In order to bring a case in a court of law, the parents of a vaccine-injured child must first file their case with the NVICP.
The NVICP is a special, no-fault tribunal housed within the U.S. Court of Federal Claims that handles injury claims for 16 federally recommended vaccines. To date, the court has awarded more than $4 billion to thousands of people for vaccine injuries.
In the NVICP, America’s legal system is replaced by a “special master.” The special masters who review claims are government-appointed attorneys, many of whom are former U.S. Department of Justice (DOJ) attorneys.
Under the NVICP, the parents of vaccine-injured children are forced to sue the secretary of the U.S. Department of Health and Human Services (HHS) for compensation. HHS is represented by DOJ attorneys.
It is exceptionally difficult to obtain compensation within the NVICP, Hazlehurst said. The proceedings are often turned into drawn-out, contentious expert battles and the backlog of cases is substantial. Because of this, a single case can drag on for over a decade.
Payouts, including attorneys’ fees, are funded by a 75-cent tax per vaccine. There is a $250,000 cap on pain and suffering and death benefits.
The Vaccine Act established the NVICP, and the 2011 U.S. Supreme Court decision Bruesewitz et al v. Wyeth et al later guaranteed vaccine manufacturers, doctors and other vaccine administrators almost always have no legal accountability or financial liability in civil court when a government-recommended or mandated vaccine(s) causes permanent injury or death, Hazlehurst said.
The NVICP ultimately denied Yates’ claim, but his case against HHS became a central part of the U.S Supreme Court’s decision in Bruesewitz v. Wyeth.
Yates’ case in the NVICP was part of the Omnibus Autism Proceeding (OAP), in which 5,400 claims submitted to the NVICP were consolidated to determine if vaccines cause autism and if so, under what conditions.
“HHS whittled down the thousands of cases to six “test cases,” one of which was Yates’ case,” Hazlehurst said. “If HHS could find a way to deny NVICP compensation to the test cases, the agency would be able to deny compensation to all 5,400 families.”
Hazlehurst said HHS and the DOJ “took advantage of the fact that the rules of evidence, discovery and civil procedure mechanisms available in a regular court do not apply in the so-called vaccine court, and perpetrated fraud upon the special masters, the Court of Appeals for the D.C. Circuit and ultimately, the U.S. Supreme Court.”
The special masters on Feb. 12, 2009, in the so-called vaccine court, denied Yates’ petition for compensation and those of the five remaining OAP “test cases” involving children who developed autism after receiving their pediatric vaccines.
HHS makes key concession in Hannah Poling case
The potential fourth test case — Hannah Poling’s — was quietly conceded in 2007, in a corrupt coverup to conceal the opinion of the HHS expert witness, Dr. Andrew Zimmerman, the world’s leading expert in autism research, Hazlehurst said.
When Poling was 19 months old, she was vaccinated against nine diseases at one doctor’s visit: measles, mumps, rubella, polio, varicella, diphtheria, pertussis, tetanus and Haemophilus influenzae type b. In total, she received five vaccines.
Prior to receiving her vaccines, Poling was described as normal, happy, healthy, interactive, playful and communicative. But two days after being vaccinated, she was lethargic, irritable and febrile, and within 10 days she developed a rash consistent with vaccine-induced chicken pox.
Over the course of several months, Poling stopped eating, didn’t respond when spoken to, began showing signs of autism, developed neurological and psychological disorders and was diagnosed with encephalopathy caused by an underlying mitochondrial disorder.
In 2003, Poling’s father, Jon, a physician and trained neurologist, and mother, Terry, an attorney and nurse, filed an autism claim against HHS under the NVICP for their daughter’s injuries.
During the OAP, in the Poling case, the government quietly conceded vaccines caused “regressive encephalopathy with features of autism spectrum disorder.”
According to CBS News, Poling received more than $1.5 million dollars for her life care, lost earnings and pain and suffering for the first year alone. After the first year, the family was supposed to receive more than $500,000 per year to pay for Poling’s care, which is estimated to amount to $40 million over her lifetime.
Jon Poling on March 6, 2008, said, “the results, in this case, may well signify a landmark decision with children developing autism following vaccinations.”
Prior to the Poling case, federal health agencies and professional organizations had reassured the public vaccines didn’t cause autism. The Poling case challenged that narrative, which is why the case was conceded and in essence sealed.
HHS’ concession that Poling developed autism as a result of a vaccine injury briefly became international news. Yet, only a handful of people knew why the government conceded Hannah’s case.
When news of the concession in Poling v. HHS was made public in March 2008, Dr. Julie Gerberding, then-director of the CDC, in an interview with CNN’s Dr. Sanjay Gupta said:
“We all know that vaccines can occasionally cause fevers in kids, so if a child was immunized, got a fever, had other complications from the vaccines, then if you are predisposed with a mitochondrial disorder, it can certainly set off some damage — some of the symptoms can be symptoms that have characteristics of autism.”
If HHS had not conceded her case, the truth as to how vaccines cause autism in some children with an underlying mitochondrial disorder would have been exposed by the world’s leading expert witnesses in the spotlight of the OAP, Hazlehurst said.
“The vaccinations Hannah received on July 19, 2000, significantly aggravated an underlying mitochondrial disorder, which predisposed her to deficits in cellular energy metabolism, and manifested as a regressive encephalopathy with features of autism spectrum disorder.”
Zimmerman was an expert witness for the government defending vaccines in the NVICP. In 2007, during the hearing in the first test case, he told the government vaccines could cause autism in “exceptional” cases, but said the government later hid that information and misrepresented his expert opinion.
In a 2018 letter, Robert F. Kennedy, Jr., CHD chairman and chief legal counsel, and Hazlehurst meticulously described the DOJ’s fraud pertaining to the misrepresentation of Zimmerman’s opinions in the OAP and requested an investigation.
“The Office of Inspector General passed the buck to the DOJ Department of Ethics,” Hazlehurst said. “The DOJ investigated itself and wrote a highly misleading letter absolving itself of any wrongdoing.”
“Shortly after I clarified my opinions with the DOJ attorneys, I was contacted by one of the junior DOJ attorneys and informed that I would no longer be needed as an expert witness on behalf of H.H.S. The telephone call … occurred after the above-referenced conversation on Friday, June 15, 2007, and before Monday, June 18, 2007. To the best of my recollection, I was scheduled to testify on behalf of H.H.S. on Monday, June 18, 2007.”
As a result of his firing, Zimmerman was not present for the Hazlehurst OAP proceedings, which allowed DOJ attorneys to misrepresent Zimmerman’s statements related to a separate autism case and apply them to all cases of autism, including Yates’ case.
Over the years Hazlehurst has repeatedly stated, “I want to be very clear, neither the Polings nor Dr. Zimmerman did anything wrong.”
“But,” he added, “if I did to a criminal, in a court of law, what the United States Department of Justice did to vaccine-injured children, I would be disbarred and I would be facing criminal charges.”
Zimmerman did testify as an expert witness on behalf of Yates in the medical malpractice case filed against Yates’ doctor, which was finally heard by a Tennessee court in February 2022.
Research by Zimmerman and others determined that at least 30%-40% of children with a diagnosis of regressive autism suffer from a mitochondrial disorder, which is a condition with which Yates was later diagnosed.
Yates in ‘perfect position’ to file lawsuit after exhausting remedies in NVICP
After exhausting all remedies under the NVICP — a process that took 25 years — the legal floodgates were then open, Hazlehurst said.
But because no one could sue the vaccine manufacturer, the only vaccine-injured child — out of thousands of cases originally included in the OAP — left with legal standing was Yates Hazlehurst and his claim of medical malpractice against the pediatrician who oversaw the administration of his vaccines.
Ultimately, the same medical experts, including Zimmerman and Dr. Richard Kelley, former director of the Genetics Department at Johns Hopkins Medical Institute — whose testimony HHS and the DOJ relied on in the Poling concession — concluded that what happened to Hannah Poling is what also happened to Yates Hazlehurst.
In an affidavit which was not admissible in the 2022 medical malpractice trial, Kelley stated:
“I also find, with a high degree of medical certainty, that the set of immunizations administered to Yates at 11 months while he was ill was the immediate cause of his autistic regression because of the effect of these immunizations to further impair the ability of his weakened mitochondria to supply adequate amounts of energy for the brain, the highest energy-consuming tissue in the body.”
Zimmerman’s expert opinion on the cause of Yates’ neurological condition was consistent with Kelley’s opinion.
Throughout the medical malpractice case, opposing counsel representing the pediatrician continuously echoed the CDC slogan, “vaccines do not cause autism.”
Hazlehurst said:
“In a medical malpractice case, the plaintiff has the burden of proof that the defendant deviated from the local “standard of care” or the defendant failed to obtain informed consent and that the deviation from the standard of care or failure to obtain informed consent caused the plaintiff’s injuries.
“The plaintiff must prove the standard of care, breach of the standard of care, the standard for informed consent and lack of informed consent through the testimony of an expert witness.”
“The issue of informed consent was hotly contested,” Hazlehurst added. “To a large degree, the trial was about whether and to what extent the federal laws applied at all to the standard of care.”
Yates’ father alleged the pediatrician deviated from the standard of care by administering vaccinations when his son had contraindications to being vaccinated.
Hazlehurst alleged the standard of care would include taking a sick baby’s temperature before administering vaccinations and believes the doctor failed to recognize that the “shaking episodes” as recorded in the medical records were consistent with a vaccine adverse reaction that should have been considered before further vaccinations were administered.
“Most people would be shocked if they witnessed the evidence presented by the defense to the jury as to just how low the requirements for informed consent and the standard of care are for the administration of childhood immunizations,” Hazlehurst said.
The defense experts testified the standard of care did not require taking a sick baby’s temperature before administering a vaccine, that he could be vaccinated even while ill and with an active bilateral ear infection, while on antibiotics and after suffering screaming and shaking episodes following previous vaccinations, he added.
Yates prohibited from presenting key expert witnesses
Medical malpractice cases are very difficult to win, and finding a pediatrician who is willing to testify in a vaccine injury case like Yates’ is extremely difficult, Hazlehurst said.
“Through the course of Yates’ long medical and legal journey, several doctors expressed that Yates should not have been vaccinated in his condition,” Hazlehurst told The Defender.
“However, they would not agree to testify. Most of the experts who refused to testify expressed fear of the negative professional consequences if they testified in an autism case,” he said.
Yates was also limited on the expert witnesses he could call due to Tennessee rules that determine which experts may testify about the local standard of care.
“These rules along with an extreme reluctance of pediatricians to testify in an autism case severely limited Yates’ ability to prevail,” Hazlehurst said.
Although Zimmerman was able to testify in Yates’ medical malpractice case, Kelley was not allowed to testify as to the standard of care and was not allowed to give an opinion as to how the defendant was negligent or why Yates should not have been vaccinated.
“The court granted an exception to allow Dr. Kelley’s causation testimony because his testimony was so highly specialized that another expert witness in the field of genetic metabolic disorders was obviously not available in Tennessee or a contiguous state, but his opinion as a pediatrician was not allowed,” Hazlehurst said.
Hazlehurst attempted to compel the CDC to allow whistleblower Dr. William Thompson, a senior scientist at the CDC, to testify in Yates’ case, but the agency prevailed and blocked Thompson from testifying.
Thompson in 2014 admitted to omitting “statistically significant information” in a 2004 study he co-authored with other CDC scientists that claimed the MMR vaccine does not cause autism.
But the omitted data suggested that a sub-group of males who received the MMR vaccine were at a significantly increased risk of autism.
“Decisions were made regarding which findings to report after the data were collected, and I believe that the final study protocol was not followed,” Thompson said in a statement.
“Any reference to Dr. William Thompson or the CDC whistleblower was later specifically excluded by the court in Yates’ medical malpractice trial,” Hazlehurst said.
“Likewise, the jury was not allowed to hear any reference to the concession in the Poling case and specifically the comments of Gerberding,” who in 2010 left the CDC and became the chief patient officer and executive vice president of Merck — the manufacturer of the MMR vaccine.
Due to the substantial length of time between the alleged malpractice and trial, several expert and fact witnesses passed away.
A critical fact witness and two doctors willing to testify on Yates’ behalf, passed away before trial. Two other doctors who initially gave sworn testimony as to negligence and causation backed out, leaving Yates without the experts needed to bolster his position.
The same was not true for the defendant, who had no difficulty finding expert witnesses to testify on his behalf, Hazlehurst said.
“The array of experts the defense called left little doubt as to the importance of this potentially precedent-setting case and raised the question of what forces were at play behind the scene,” he said.
“Yates was not just up against the local doctor and clinic, and David does not always beat Goliath,” Hazlehurst said.
The verdict in Yates’ medical malpractice case
At the end of the trial, the jury answered two questions based on the evidence it was allowed to consider and the instructions provided by the court.
Yates’ attorneys asked for a jury instruction quoting the language in the Vaccine Act that a VIS must be given to the parents of the child prior to the administration of a vaccine.
Although the judge originally approved the instruction prior to the start of the trial, the judge later reversed his decision and removed the critical instruction before jury deliberation, Hazlehurst said.
The first question the jury answered was, “Did the defendants provide the requisite information to Yates Hazlehurst’s parents to allow Yates Hazlehurst’s parents to formulate an intelligent and informed decision on authorizing or consenting to Yates Hazlehurst receiving his childhood immunizations on February 8, 2001?”
The jury answered, “yes.”
The second question the jury answered was, “Did the defendants deviate from the recognized standard of acceptable professional practice in this medical community or a similar medical community in his/their treatment of Plaintiff Yates Hazlehurst when administering vaccines to Yates Hazlehurst on February 8, 2001?”
The jury answered, “no.”
Although the jury never addressed the issue of whether a vaccine can cause neurological injury, including autism, valuable evidence was discovered and preserved during Yates’ legal battle.
The world’s top experts in the field of autism and mitochondrial disorder, on video, explained how the administration of “routine childhood immunizations” can cause autism, Hazlehurst told The Defender.
“These were the same medical experts who compelled HHS and DOJ to secretly concede the case of Hannah Poling during the OAP in the so-called vaccine court,” he said.
The trial exposed compelling evidence of the incredibly low standard of practice being taught to medical students and doctors and illuminates how the laws contained in the Vaccine Act — designed to ensure a patient receives informed consent — are unenforceable and largely meaningless, Hazlehurst said.
Many of the reasons Yates lost his case are the same reasons underlying the autism epidemic, he added.
Robert F. Kennedy, Jr., Aud Hazlehurst, Yates Hazlehurst, Lane Hodges, Rolf Hazlehurst, Anne Hazlehurst Garrard, David Riley, Marry Garrard, Anne Elizabeth Garrard, Tammy McCoy and Kevin Cox.
Hazlehurst told The Defender he has sincere gratitude to everyone who has helped Yates over the past 20 years in both his medical and legal struggles.
“Regardless of the jury verdict, exposing the evidence which came to light in the legal cases of Yates Hazlehurst will be a powerful tool towards the ultimate goal of bringing the truth to light and ending the autism epidemic,” he said.
CHD and Hazlehurst said they will continue to fight for vaccine-injured children.
In the words of Winston Churchill, “Now is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning,” Hazlehurst said.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
If you worked for a federal agency that was studiously ignoring a kill-rate of 100,000 Americans a year, every year, like clockwork, and if you knew it, wouldn’t you feel compelled to say or do something about it?
At the FDA, which is that federal agency, no one has ever felt the need to step forward and speak up.
Let’s shift the venue and ask the same question. If you were a medical reporter for a major media outlet in the US, and you knew the above fact, wouldn’t you make it a priority to say something, write something, do something?
Lenzer refers to a report by the Institute for Safe Medication Practices: “It [the report] calculated that in 2011 prescription drugs were associated with two to four million people in the US experiencing ‘serious, disabling, or fatal injuries, including 128,000 deaths.’”
The report called this “one of the most significant perils to humans resulting from human activity.”
And here is the final dagger. The report was compiled by outside researchers who went into the FDA’s own database of “serious adverse [medical-drug] events.”
Therefore, to say the FDA isn’t aware of this finding would be absurd. The FDA knows. The FDA knows and it isn’t saying anything about it, because the FDA certifies, as safe and effective, all the medical drugs that are routinely maiming and killing Americans.
And for the past 10 years or so, I have been writing about and citing a published report by the late Dr. Barbara Starfield that indicates 106,000 people in the US are killed by medical drugs every year. Until her death in 2011, Dr. Starfield worked at the Johns Hopkins School of Public Health. Her report, “Is US health really the best in the world?”, was published in the Journal of American Medical Association on July 26, 2000.
Since the Department of Homeland Security is working its way into every nook and corner of American life, hyper-extending its mandate to protect all of us from everything, why shouldn’t the DHS investigate the FDA as a terrorist organization?
How many smoking guns do we need before a sitting president shuts down the FDA buildings, fumigates the place, and prosecutes very large numbers of FDA employees?
Do we need 100,000 smoking guns every year? Do we need relatives of the people who’ve all died in the span of merely a year, from the poisonous effects of FDA-approved medical drugs, bringing corpses to the doors of FDA headquarters?
And let me ask another question. If instead of drugs like warfarin, dabigatran, levofloxacin, carboplatin, and lisinopril (the five leading killers in the FDA database), the 100,000 deaths per year were led by gingko, ginseng, vitamin D, niacin, and raw milk, what do you think would happen?
I’ll tell you what would happen. SEALS, Delta Force, SWAT teams, snipers, predator drones, tanks, and infantry would be lining up and hovering outside every health-food store and nutritional supplement manufacturer in America.
All those fake stories in the press, reported dutifully by so-called medical reporters? The stories about maybe-could-be-possible-miracle breakthroughs just over the horizon of state-of-the-art medical research? Those stories are there to obscure the very, very hard facts of medically-caused death on the ground.
The buck stops at the FDA.
Except in the real world, it doesn’t. Which tells you something about the so-called real world and how much of it is composed of propaganda.
No medical drug in the US can be released for public use unless and until the FDA says it is safe and effective. That’s the rule. The FDA is spitting out drug approvals month after month and year after year, and the drugs are routinely killing 100,000 people a year and maiming two million more, which adds up to a million deaths per decade and 20 million maimings per decade. The FDA and the federal government are doing nothing about it, even though they know what’s going on. This is mass murder. Not accidental death. Murder. A holocaust.
Do you want another citation?
Here are a few horrific quotes. I’ll discuss the source afterwards:
“…appropriately prescribed prescription drugs are the fourth leading cause of death…About 330,000 patients die each year from prescription drugs in the US and Europe.”
“They [the drugs] cause an epidemic of about 20 times more [6.6 million per year] hospitalizations, as well as falls, road accidents, and about 80 million [per year] medically minor problems such as pains, discomforts, and dysfunctions that hobble productivity or the ability to care for others.”
“Deaths from overmedication, errors, and self-medication would increase these figures.”
In other words, the 330,000 deaths per year, the 6.6 million hospitalizations per year, and the 80 million “medically minor” problems per year…all of this stems from CORRECTLY PRESCRIBED medicines.
The quotes come from the ASA [American Sociological Association] publication called Footnotes, in its November 2014 issue. The article is “The Epidemic of Sickness and Death from Prescription Drugs.” The author of the article is Donald W Light.
Donald W Light is a professor of medical and economic sociology. He is a founding fellow of the Center for Bioethics at the University of Pennsylvania. In 2013, he was a fellow at the Edmond J. Safra Center for Ethics at Harvard. He is a Lokey Visiting Professor at Stanford University and a Fellow of the Royal Society of Medicine.
It’s been my policy to quote medical analysts who have mainstream credentials, when it comes to adding up the results of medical-drug destruction.
I do this to show that, in refusing to fix the holocaust, the federal government, medical schools, and pharmaceutical companies can’t claim their critics and detractors are “fringe researchers.”
Believe me, the officials who should have been fixing the enormous tragedy for at least the past 15 years are intent on hiding it.
When you stop and think about the meaning of these medical numbers, one of the things you realize is: this massive destruction of life envelops whole countries.
It not only maims and kills, it brings emotional turmoil and loss to the families, friends, co-workers, and colleagues of those who are killed and maimed: the 330,000 who are killed and the 6.6 million who are hospitalized and the 80 million whose productivity is hobbled or whose ability to care for others is significantly diminished.
If you consciously set out to bring a nation to its knees;
to kill it;
to make it unable to function at any reasonable level;
you would be hard pressed to find a more effective long-term method than exposing the population to the US/European medical-drug cartel.
In a groundbreaking article for Children of God For Life, titled “Forsaking God For the Sake of Science,” [1] [1b] Debra Vinnedge outlines how the Rockefeller-Harriman eugenics movement gave rise to the practice of medical abortions for research purposes, including live births during which the infant was murdered and its organs harvested:
“…Abortion wasn’t legal yet; this was 1936. But abortion was most certainly legal and acceptable [to eugenicists] if it meant ending the life of a child who would be born to a ‘feeble-minded’ woman, one who might end up less than perfect or who might have to rely on society to pay for their care.”
And therefore, why not perform abortions for medical research? Behind closed doors, out of view, this was happening in several countries, including the US.
Consider this research report: “Human embryos of two and one-half to five months gestation were obtained from the gynaecological department of the Toronto General Hospital…No macerated specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
Here is the citation [2]: Joan C. Thicke, Darline Duncan, William Wood, A. E. Franklin and A. J. Rhodes; Cultivation of Poliomyelitis Virus in Tissue Culture; Growth of the Lansing Strain in Human Embryonic Tissue, Canadian Journal of Medical Science, Vol. 30, pg 231-245. [June 1952]
The authors are certainly describing an infant who was taken from the womb alive, and after cells were harvested, was killed. For research on “growing virus in cell culture.”
Here is another research report that indicates the infant was born alive, its tissues taken, and then killed:
“Embryos of between 12-18 weeks gestation have been utilized. Rarely tissues were obtained from stillborn fetuses, or from premature infants at autopsy…In the experiments 3 sorts of embryonic materials were used: elements of skin, connective tissue, muscle; intestinal tissue; brain tissue…Whenever possible the embryo was removed from the amniotic sac.., transferred to a sterile towel and kept at 5 C until dissected.”
The citation [3]: Thomas H. Weller, John F. Enders, Studies on the Cultivation of Poliomyelitis Viruses in Tissue Culture : I. The Propagation of Poliomyelitis Viruses in Suspended Cell Cultures of Various Human Tissue; Journal of Immunology 1952;69;645-671. [June 1952]
Again, the infant’s tissue was used, in the lab, to “grow virus in cell culture.” The cells were from the infant.
My readers know that, for the past year, I’ve been exposing virologists’ absurd claims that they’re isolating viruses in their labs. [4] [4b] [4c]
In fact, they create soups in dishes, containing toxic drugs and chemicals, monkey cells and human cells, and a mucus sample from a patient. When the cells start dying, they claim this is proof the virus is in the mucus, in the soup, and is deadly.
Of course, this is nonsense, because the toxic drugs and chemicals are perfectly capable of killing the cells; and the cells in the soup are being starved of nutrients, which would also lead to cell-death.
The isolation of viruses is no isolation at all. It’s a fraud.
But it never occurred to me, until now, that some of these human cells in the soup in the lab came from infants, taken from the mother’s womb alive, for harvesting, who were then killed.
This completes a circle of evil.
Of course, out of the virological research fraud and infant murder come THE VACCINES, including the COVID vaccines, which are causing huge numbers of injuries and deaths across the world.
People of faith everywhere must see that declaring a religious exemption from the shots is a DUTY, whether or not the authorities allow the exemption.
The last time I looked, appealing to Pontius Pilate for an exemption didn’t work, and the status of Anthony Fauci is not higher than the Authority to whom, at minimum, four billion people of faith pray.
49 states have decided to follow the federal government’s lead in ordering COVID injections for children under 5, despite glaring evidence of a failed pharmaceutical product that doesn’t serve any benefit to them whatsoever, and has the potential to cause serious side effects.
On Friday, the FDA authorized mRNA COVID shots (both Pfizer and Moderna) under emergency use for children under 5 down to 6 months of age. The approval made its way through the halls of the federal bureaucracy, regardless of any studies showing a positive benefit for injecting young children with mRNA shots, which, even in adults, do not effectively prevent coronavirus infection.
So you’ve had your eight-month-old baby injected with the COVID vaccine.
Of course.
And the SARS-CoV-2 virus doesn’t exist.
I’ve heard that. But it’s not the issue for us.
What is the issue for you?
Making a fashion statement.
How so?
We need to stay in the forefront of trends.
Why?
Why wouldn’t we?
Have you seen the federal database that records vaccine injury and death reports?
Of course.
So you know your baby could die from the shot.
Yes.
And that doesn’t matter to you.
Not as much as being able to tell our friends we had our baby vaccinated.
You, as parents—
That’s a misunderstood term. We don’t consider ourselves parents. The State is the parent. We’re the monitors.
Monitors?
We observe, and carry out limited functions.
Even if you assume the virus exists, the chances of your baby catching it and becoming ill are incredibly tiny.
That’s right. But this isn’t what we’re about. As I said, we’re keeping pace with fashion.
Are you human?
It depends on how you define the term. Humans are biological machines. Most people believe in something beyond that, but the content of belief is predetermined by a person’s upbringing, genes, conditioning, and so on.
Have you ever questioned vaccine science?
There’s nothing to question. We understand science. I have a PhD in psychology, and my husband is a software engineer. My IQ is 141. My husband’s is 136. We’re equipped to deal with vaccine issues.
If your baby died from the shot, would you mourn?
Yes. We would post photos and statements on our Facebook page.
—No doubt, some people would take offense at this “interview.” How could I? Here’s how. I wrote it. I wrote it because the government and Pfizer and Moderna—no matter how they interpret COVID and “the virus”—are moving ahead to inject as many babies as possible—which is a crime of mass assault and mass murder. Many parents will go along with it.
While many have bought into the simplistic idea that availability of firearms is the cause of mass shootings, a number of experts have pointed out a more uncomfortable truth, which is that mass shootings are far more likely the result of how we’ve been mistreating mental illness, depression and behavioral problems
Gun control legislation has shown that law-abiding Americans who own guns are not the problem, because the more gun control laws that have been passed, the more mass shootings have occurred
97.8% of mass shootings occur in “gun-free zones,” as the perpetrators know legally armed citizens won’t be there to stop them
Depression per se rarely results in violence. Only after antidepressants became commonplace did mass shootings really take off, and many mass shooters have been shown to be on antidepressants
Antidepressants, especially selective serotonin reuptake inhibitors (SSRIs), are well-known for their ability to cause suicidal and homicidal ideation and violence
While many have bought into the simplistic idea that availability of firearms is the cause of mass shootings, a number of experts have pointed out a more uncomfortable truth, which is that mass shootings are far more likely the result of how we’ve been mistreating mental illness, depression and behavioral problems.
An article written by Molly Carter, initially published on ammo.com at an unknown date1 and subsequently republished by The Libertarian Institute in May 2019,2 and psychreg.org in late January 2021,3 noted:
“According to the Federal Bureau of Investigation (FBI), a mass murder occurs when at least four people are murdered, not including the shooter … during a single incident …
Seemingly every time a mass shooting occurs … the anti-gun media and politicians have a knee-jerk response — they blame the tragedy solely on the tool used, namely firearms, and focus all of their proposed ‘solutions’ on more laws, ignoring that the murderer already broke numerous laws when they committed their atrocity.
Facts matter when addressing such an emotionally charged topic, and more gun control legislation has shown that law-abiding Americans who own guns are NOT the problem. Consider the following: The more gun control laws that are passed, the more mass murders have occurred.
Whether or not this is correlation or causation is debatable. What is not debatable is that this sick phenomenon of mass murderers targeting ‘gun-free zones,’ where they know civilian carry isn’t available to law-abiding Americans, is happening.
According to the Crime Prevention Research Center,4 97.8% of public shootings occur in ‘gun-free zones’ – and ‘gun-free zones’ are the epitome of the core philosophical tenet of gun control, that laws are all the defense one needs against violence …
This debate leads them away from the elephant in the room and one of the real issues behind mass shootings — mental health and prescription drugs.
Ignoring what’s going on in the heads of these psychopaths not only allows mass shootings to continue, it leads to misguided gun control laws that violate the Second Amendment and negate the rights of law-abiding U.S. citizens.
As Jeff Snyder put it in The Washington Times: ‘But to ban guns because criminals use them is to tell the innocent and law-abiding that their rights and liberties depend not on their own conduct, but on the conduct of the guilty and the lawless, and that the law will permit them to have only such rights and liberties as the lawless will allow.’”
The Elephant in the Room: Antidepressants
Thoughts, emotions and a variety of environmental factors play into the manifestation of violence, but mental illness by itself cannot account for the massive rise in mass murder — unless you include antidepressants in the equation. Yet even when mental health does enter the mass shooter discussion, the issue of antidepressants, specifically, is rarely mentioned.
The fact is, depression per se rarely results in violence. Only after antidepressants became commonplace did mass shootings take off, and many mass shooters have been shown to be on antidepressants.
Prozac, released in 1987, was the first selective serotonin reuptake inhibitor (SSRI) to be approved for depression and anxiety. Only two years earlier, direct-to-consumer advertising had been legalized. In the mid-1990s, the Food and Drug Administration loosened regulations, direct-to-consumer ads for SSRIs exploded and, with it, prescriptions for SSRIs.
In 1989, just two years after Prozac came to market, Joseph Wesbecker shot 20 of his coworkers, killing nine. He had been on Prozac for one month, and the survivors of the drug-induced attack sued Eli Lilly, the maker of Prozac. Since then, antidepressant use and mass shootings have both risen, more or less in tandem.
In the two decades between 1988 and 2008, antidepressant use in the U.S. rose by 400%,5 and by 2010, 11% of the U.S. population over the age of 12 were on an antidepressant prescription.6
In 1982, pre-Prozac, there was one mass shooting in the U.S.7 In 1984, there were two incidents and in 1986 — the year Prozac was released — there was one. One to three mass shootings per year remained the norm up until 1999, when it jumped to five.
Another jump took place in 2012, when there were seven mass shootings. And while the annual count has gone up and down from year to year, there’s been a clear trend of an increased number of mass shootings post-2012. Over time, mass shootings have also gotten larger, with more people getting injured or killed per incident.8
How can we possibly ignore the connection between rampant use of drugs known to directly cause violent behavior and the rise in mass shootings? Suicidal ideation, violence and homicidal ideation are all known side effects of these drugs. Sometimes, the drugs disrupt brain function so dramatically the perpetrator can’t even remember what they did.
For example, in 2001, a 16-year-old high schooler was prescribed Effexor, starting off at 40 milligrams and moving up to 300 mg over the course of three weeks. On the first day of taking a 300-mg dose, the boy woke up with a headache, decided to skip school and went back to bed.
Some time later, he got up, took a rifle to his high school and held 23 classmates hostage at gunpoint. He later claimed he had no recollection of anything that happened after he went back to bed that morning.9
The Risks Are Clear
The risks of psychiatric disturbances are so clear, ever since mid-October 2004, all antidepressants in the U.S. must include a black box warning that the drug can cause suicidal thoughts and behaviors, especially in those younger than 25, and that:10
“Anxiety, agitation, panic attacks, insomnia, irritability, hostility (aggressiveness), impulsivity, akathisia (psychomotor restlessness), hypomania, and mania have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric.”
SSRIs can also cause emotional blunting and detachment, such that patients report “not feeling” or “not caring” about anything or anyone, as well as psychosis and hallucinations. All of these side effects can contribute to someone acting out an unthinkable violent crime.
In one review11,12 of 484 drugs in the FDA’s database, 31 were found to account for 78.8% of all cases of violence against others, and 11 of those drugs were antidepressants.
The researchers concluded that violence against others was a “genuine and serious adverse drug event” and that of the drugs analyzed, SSRI antidepressants and the smoking cessation medication, varenicline (Chantix), had the strongest associations. The top-five most dangerous SSRIs were:13
Fluoxetine (Prozac), which increased aggressive behavior 10.9 times
Paroxetine (Paxil), which increased violent behavior 10.3 times
Fluvoxamine (Luvox), which increased violent behavior 8.4 times
Venlafaxine (Effexor), which increased violent behavior 8.3 times
Desvenlafaxine (Pristiq), which increased violent behavior 7.9 times
Depression Is Vastly Overdiagnosed
In her article, Carter also reviewed the clinical determinants for a diagnosis of clinical depression warranting medication. To qualify, you must experience five or more of the following symptoms, most of the day, every day, for two weeks or more, and the symptoms must be severe enough to interfere with normal everyday functioning:14
Sadness
Anxiety
Feeling hopeless
Feeling worthless
Feeling helpless
Feeling ’empty’
Feeling guilty
Irritable
Fatigue
Lack of energy
Loss of interest in hobbies
Slow talking and moving
Restlessness
Trouble concentrating
Abnormal sleep patterns, whether sleeping too much or not enough
Abnormal weight changes, either eating too much or having no appetite
Thoughts of death or suicide
The reality is that a majority of patients who receive a depression diagnosis and subsequent prescription for an antidepressant do not, in fact, qualify. In one study,15 only 38.4% actually met the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria, and among older adults, that ratio was even lower. Only 14.3% of those aged 65 and older met the diagnostic criteria. According to the authors:16
“Participants who did not meet the 12-month MDE criteria reported less distress and impairment in role functioning and used fewer services. A majority of both groups, however, were prescribed and used psychiatric medications.
Conclusion: Depression overdiagnosis and overtreatment is common in community settings in the USA. There is a need for improved targeting of diagnosis and treatments of depression and other mental disorders in these settings.”
What Role Might War Games Play?
Aside from antidepressants, another factor that gets ignored is the influence of shooting simulations, i.e., violent video games. How does the military train soldiers for war? Through simulations. With the proliferation of video games involving indiscriminate violence, should we really be surprised when this “training” is then put into practice?
As reported by World Bank Blogs, young men who experience violence “often struggle to reintegrate peacefully into their communities” when hostilities end.17 While American youth typically have little experience with real-world war, simulated war games do occupy much of their time and may over time color their everyday perceptions of life. As noted by Centrical, some of the top benefits of simulations training include:18
Allowing you to practice genuine real-life scenarios and responses
Repetition of content, which boosts knowledge retention
Personalization and diversification, so you can learn from your mistakes and evaluate your performance, thereby achieving a deeper level of learning
In short, violent mass shooter games are the perfect training platform for future mass shooters. Whereas a teenager without such exposure might not be very successful at carrying out a mass shooting due to inexperience with weapons and tactics, one who has spent many hours, years even, training in simulations could have knowledge akin to that of military personnel.
Add antidepressant side effects such as emotional blunting and loss of impulse control, and you have a perfect prescription for a mass casualty event.
On top of that, we, as a nation, also demonstrate the “righteousness” of war by engaging in them without end.19 When was the last time the U.S. was not at war someplace? It’s been ongoing for decades.
Even now, the U.S. insists on inserting itself into the dispute between Russia and Ukraine, and diplomacy isn’t the chosen conflict resolution tool. Sending weapons to Ukraine and calling for more violence against Russians are. Sen. Lindsey Graham has even called for the assassination of Russian President Vladimir Putin. Showing just how serious such a suggestion is, the White House had to publicly disavow it, stating Graham’s comment “is not the position of the U.S. government.”20
Graham, meanwhile, does not appear to understand how his nonchalant call for murder might actually incite murder. In the wake of the Uvalde school shooting, he now wants to mobilize retired service members to enhance security at schools, and while that might be a good idea, how about also vowing never to call for the murder of political opponents? Don’t politicians understand that this could translate into some kid thinking it’s acceptable to murder THEIR perceived opponents?
As far as I can tell, mass shootings have far more to do with societal norms, dangerous medications, a lack of high-quality mental health services, and the normalization of violence through entertainment and in politics, than it does with gun laws per se.
There are likely many other factors as well, but these are clearly observable phenomena known to nurture violent behavior. I’m afraid Americans are in need of a far deeper and more introspective analysis of the problem than many are capable of at the moment. But those who can should try, and make an effort to affect much-needed change locally and in their own home.
The U.S. Food and Drug Administration (FDA) is likely to grant Emergency Use Authorization (EUA) for Pfizer’s BioNTech SARS-CoV-2 vaccine for children ages 6 months through 4 years and Moderna’s COVID-19 mRNA vaccine for infants and children ages 6 months through 5 years and 6 years through 17 years in their upcoming meetings today and tomorrow (June 14-15).
CHD is poised to take legal action against the FDA should they grant these emergency use authorizations. We seek to hold FDA accountable for recklessly endangering our children with products that have little, no or even negative net efficacy. These products may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke, other thrombotic events and future reproductive harm.
Our children need your help! On Tuesday and Wednesday, June 14 and 15, the FDA VRBPAC committee is likely to make a catastrophic decision by voting to grant Emergency Use Authorizations (EUA) to allow for infants and young children to receive Pfizer’s and Moderna’s COVID shots.
Please take 30 seconds to tell your lawmakers to STOP the FDA from granting EUAs for COVID vaccines in babies and children by sending Robert F. Kennedy, Jr.’s letter to FDA VRBPAC committee members. His letter lays out all of the available science and data that proves vaccinating children for COVID is not only unnecessary, but will recklessly endanger their lives. There is no emergency whatsoever for children from COVID, therefore there is no justification for issuing an Emergency Use Authorization.
Time and mounting evidence have continued to prove that children have essentially zero risk of dying from COVID (99.995% recovery rate), and the vast majority of kids have little to no symptoms. There is no statistically valid evidence that shows the Pfizer and Moderna COVID injections are able to prevent severe disease or deaths in children at all. These shots have a worse safety record than all previous vaccines combined, and have been found to cause serious injuries including myocarditis, encephalopathy, blood clots, diabetes, neurological issues and death.
The United States Government, at the behest of Pharma oligarchs and government employees who own stock in the Pharma companies, hopes to approve an amendment to the EUA (Emergency Use Authorization) to inject babies 6-months-old to toddlers 4-years-old with the C19 faux-vaccine.
Before the committee meets to recommend the amendment, the FDA allows people to comment on the FDA government web site. One such comment was provided to this author and is offered to you below. The United States of America is indeed facing a government #ClotShot plot.
This comment is NOTICE of possible criminal liability to Lauren K. Roth and members of the Vaccines and Related Biological Products Advisory Committee who owe duties of care, diligence, good faith, and loyalty in recommending “for” or “against” the EUA amendment for COVID-19 mRNA vaccine in children 6 months through 4 years of age.
Only two deaths are listed herein to establish knowledge. If the amendment is approved, it will have been done by committee members “knowing” of felony crimes in context.
Your investigation of these deaths should include death certificates, autopsy records, witness interviews, and immunization records.
Massachusetts Death Certificate 2022 SFN 5980 is a 7yo girl died January 18, 2022 listed as died from U071 “COVID-19”, B49 “unspecified mycosis”, J450 “predominantly allergic asthma”, and R091 “pleurisy”.
VAERS_ID 2038120 is a 7yo girl in Massachusetts, who received her 2nd dose 1/13/2022 and was reported to VAERS 1/15/2022. PRIOR_VAX states, “Severe nausea and vomiting from 5min post vaccination and for the next 8-10 hours.” SYMPTOM_TEXT states, “Spiked a 103 fever, severe stomachache, has not had a bowel movement since the day before vaccination, which makes today 3 days without one. First vaccine caused severe nausea and vomiting from 5minutes post injection and for the next 8-10 hours.”
This little girl suffered immeasurably 4 to 5 days as her intestines shut down due likely to impeded blood vessels servicing intestines.
Massachusetts Death Certificate 2021 SFN 56611 is a 48yo man died 11/16/2021 listed as died from U071 “COVID-19” and E669 “OBESITY”.
SFN 56611 is known to have died less than 24 hours after inoculation.
In both cases, the Medical Examiners listed the cause of death as “COVID-19”, when it was clearly not COVID-19. And in both cases, the Medical Examiners omitted listing causes Y590 “Viral vaccines“ and T881 “Other complications following immunization, not elsewhere classified”, when these clearly were proximate and actual causes.
Death certificates from the state of Massachusetts are sent to the CDC, a federal entity. Thus, fraud on a state death certificate is a federal crime as it affects federal death records. Several federal felony crimes apply in this instance and are listed below.
If you dismiss this NOTICE and recommend the EUA amendment without first investigating these two deaths, you become liable for inchoate crimes and the felony crime of “misprision of felony.” If a single person subsequently dies as a result of the amendment, all the elements will have been satisfied for you to face felony murder charges or involuntary manslaughter. Qualified immunity is not a valid defense.
18 USC § 4 – Misprision of felony
“Whoever, having knowledge of the actual commission of a felony …, conceals and does not as soon as possible make known the same to some … civil or military authority …, shall be fined under this title or imprisoned not more than three years, or both.”
Felony murder is a homicide that occurs during the commission of an inherently dangerous felony, showing a conscious disregard for human life. A jury decides whether recommending an injection, that you “know” caused death, and that you refused to investigate while “knowing” it caused death, is inherently dangerous.
Here are a few federal statutes likely violated by Medical Examiners in Massachusetts. You are duty-bound to call for investigation of:
18 USC § 4 Misprision of felony
18 USC § 286 Conspiracy to defraud the government with respect to claims
18 USC § 287 False fictitious or fraudulent claims
18 USC § 371 Conspiracy to commit offense or to defraud United States
18 USC § 1035 False statements relating to health care matters
18 USC § 1040 Fraud in connection with major disaster or emergency benefits
There were found sixty likely C19 vaccine deaths in a 25-minute perusal of the 2021 and 2022 death certificates, which extrapolates to hundreds, probably thousands of C19 vaccine deaths in Massachusetts.
Refusal to investigate these fraudulent records is a crime that, because of the felony murder aspect, has no statute of limitations. Five, ten, or twenty years from now, if a federal prosecutor were to learn of this NOTICE, he or she would have significant evidence to bring charges for felony murder.
In summary, this NOTICE places you in a position requiring you to investigate these deaths prior to recommending the amendment. If you dismiss this NOTICE, you may be criminally liable for involuntary manslaughter, felony murder, and a list of federal crimes and inchoate crimes.
Please make the appropriate decision for yourselves and for the children of the United States of America.
A growing number of young healthy adults are mysteriously dying. Watch Jefferey Jaxen and Del try to make sense of, what is now being called, “Sudden Adult Death Syndrome” (SADS).
First New England Journal of Medicine Pfizer Study Reveals 80% Miscarriage Rate in Recipients in their First or Second Trimester — Dr. Christiane Northrup also reports rising number of stillbirths on ‘Friday Roundtable’ Infertility: A Diabolical Agenda Q+A
A film by award-winning filmmaker Andy Wakefield, Robert F. Kennedy, Jr. and Children’s Health Defense. Watch the chilling tale of African women whose fertility was tragically stripped away through an experimental tetanus vaccination program. Are women everywhere next?
“When they’re through with Africa, they’re coming for you.” ~ Dr. Stephan Karanja
The chilling, harrowing story of how a World Health Organization (WHO) population control experiment, under the guise of a vaccination program, resulted in the sterilization of millions of women in Africa without their knowledge or consent.
How the ability to carry a pregnancy to term has been tragically stripped away from these women as their government attempts to cover up the evidence.
About a brave, Kenyan doctor — Dr. Stephen Karanja — who warned the world that once they’re done with Africa, they’re coming for the children and everyone else.
Perspectives from leading experts expressing their concerns regarding other vaccines that could cause infertility in women around the world, including the COVID shot.
VAERS data released Friday by the Centers for Disease Control and Prevention show 1,287,595 reports of adverse events from all age groups following COVID-19 vaccines, including 28,532 deaths and 235,041 serious injuries between Dec. 14, 2020, and May 27, 2022.
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,287,595 reports of adverse events following COVID-19 vaccines were submitted between Dec. 14, 2020, and May 27, 2022, to the Vaccine Adverse Event Reporting System (VAERS). That’s an increase of 9,615 adverse events over the previous week.
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 28,532 reports of deaths — an increase of 220 over the previous week — and 235,041 serious injuries, including deaths, during the same time period — up 2,347compared with the previous week.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 13,150 U.S. deaths reported as of May 27, 16% occurred within 24 hours of vaccination, 20% occurred within 48 hours of vaccination and 59% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 586 million COVID-19 vaccine doses had been administered as of May 27, including 346 million doses of Pfizer, 221 million doses of Moderna and 19 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
22 reports of myocarditis and pericarditis (heart inflammation).The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department.The Defender has noticed over previous weeks that reports of myocarditis and pericarditis have been removed by the CDC from the VAERS system in this age group. No explanation was provided.
62 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine. VAERS reported 63 reports in the 12- to 17-year-old age group last week.
654 reports of myocarditis and pericarditis with 642 cases attributed to Pfizer’s vaccine.
167 reports of blood clotting disorders with all cases attributed to Pfizer. VAERS reported 168 cases of blood clotting disorders in the 12- to 17-year-old age group last week.
U.S. VAERS data from Dec. 14, 2020, to May 27, 2022, for all age groups combined, show:
20% of deaths were related to cardiac disorders.
54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
COVID-19 shots for kids under 5 could begin by June 21, White House says
COVID-19 vaccines could be available for children younger than 5 as early as June 21 if U.S. health regulators clear the shots, White House coronavirus response coordinator Ashish Jha said Thursday.
According to The Washington Post, states can start ordering vaccines today, with 10 million initially available. The FDA vaccine advisors are scheduled to meet June 14 and 15 to discuss pediatric vaccines. The CDC will meet shortly after to sign off on the decision.
There are about 19 million children under 5 in the U.S.
Young males have highest risk of heart damage from COVID vaccines
Young males are more likely to report heart damage following vaccination with an mRNA COVID-19 vaccine, and the damage is more likely to be reported after the second dose, according to researchers who reviewed the scientific literature and vaccine injury databases in the U.K., EU and U.S.
Research published May 25 in The BMJ showed 18,204 reports of myocarditis and pericarditis were submitted to U.K., U.S. and EU regulators during the study period, beginning when the mRNA vaccines first rolled out until mid-March 2022.
In the U.S., 2,986 events following Pfizer’s vaccine and 1,640 events following Moderna’s vaccine were reported to VAERS.
According to the CDC, 124.12 million people were fully vaccinated with Pfizer and 75.57 million people fully vaccinated with Moderna during the study period.
For Pfizer, the reporting rate was 14.70 cases of myocarditis and 9.36 cases of pericarditis per 1 million fully vaccinated individuals. The combined rate of myocarditis and pericarditis is 12.03 cases reported per 1 million fully vaccinated individuals.
For Moderna, there were 12.35 cases of myocarditis and 9.36 cases of pericarditis reported per 1 million fully vaccinated recipients. The combined reporting rate of both myocarditis and pericarditis is 10.86 per 1 million.
There were 13,573 events of myocarditis and/or pericarditis reported in observational studies included in the systematic review of the literature, but these cannot help to calculate the overall rate of these adverse events.
Vaccine injury compensation programs overwhelmed by thousands of reports
Federal programs compensating people who suffered injuries from vaccines or COVID-19 pandemic treatment are facing so many claims that thousands of people may not receive payment for their injuries for a long time, Politico reported.
The first program, the Vaccine Injury Compensation Program (VICP), has too little staff to handle the number of reported injuries resulting from pediatric vaccines such as polio and MMR, leaving thousands of patients waiting years for their cases to be heard.
The second program, the Countermeasure Injuries Compensation Program (CICP), designed to compensate people for injuries caused by COVID-19 vaccines and countermeasures, has seen unsustainable growth.
Between 2010 and 2020, the CICP received only 500 complaints. Since the start of the pandemic, it has received more than 8,000 complaints — 5,000 of which are related to COVID-19 vaccines.
To date, the CICP has paid zero claims, although it did approve one in December 2021.
Should COVID-19 vaccines become routine, any injuries would be handled by the already overwhelmed VICP. There are fears the public will mistake the situation for “too many injuries flooding the program,” which will lead to vaccine hesitancy.
In late 2019, I joined two other Israeli criminologists and a health risk communications expert in a research project to study the suppression of scientific dissent around the topic of vaccines. At the time, none of us could have ever imagined what was looming right around the corner.
Two of them (Natti Ronel and Ety Elisha) had written a review of a Hebrew-language book called “Turtles All The Way Down,” which was a critical review of vaccine safety science. The thing about the book is that it was published anonymously, as the author(s) feared the potential retribution that might ensue.
Their review was published in the Hebrew-language journal, Medicine (Refuah), which is the journal of the Israeli Medical Association, sort of like the Israeli equivalent of JAMA. I won’t go into how it ever got published in the book review section, but the review simply focused on the absurdity of a scientist who felt the need to publish a scientific book anonymously due to fear of the consequences. Ironically, the publication of the review caused a huge uproar (you can read more about that here where it was covered in Science), and the review itself was retracted, or more precisely it simply disappeared from the on-line version of the journal.
So we started a project to study the phenomena of scientific censorship and suppression of scientific dissent in the field of vaccines by interviewing scientists and doctors who had either had their papers retracted or who had faced attempts to suppress their views. Notably, the only retracted papers in the field of vaccinology that we could identify all raised questions about the safety of vaccines. And this was all BEFORE the COVID pandemic hit. (We’ve got another one that covers the COVID period that should be coming out fairly soon.)
In other words, everything it describes happened before the pandemic. The censorship and suppression we’ve witnessed these last two years already existed — it has only kicked into overdrive. The deliberate dismantling of science didn’t start two years ago.
If it isn’t clear why criminologists would be interested in this topic, consider the following general definition of crime: force or fraud in the pursuit of self-interest.
So without further ado, you can read both papers embedded (hopefully) below:
The European (EEA and non-EEA countries) database of suspected drug reaction reports is EudraVigilance, verified by the European Medicines Agency (EMA), and they are now reporting 44,821 fatalities, and 4,351,483 injuries following injections of five experimental COVID-19 shots:
From the total of injuries recorded, almost half of them (1,972,105) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through May 21, 2022.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2, Comirnaty) from BioNTech/ Pfizer: 21,070 deaths and 2,207,919 injuries to 21/05/2022
67,512 Blood and lymphatic system disorders incl. 303 deaths
78,229 Cardiac disorders incl. 3,061 deaths
694 Congenital, familial and genetic disorders incl. 63 deaths
29,164 Ear and labyrinth disorders incl. 16 deaths
41,462 General disorders and administration site conditions incl. 816 deaths
191 Hepatobiliary disorders incl. 17 deaths
713 Immune system disorders incl. 11 deaths
12,281 Infections and infestations incl. 246 deaths
1,425 Injury, poisoning and procedural complications incl. 31 deaths
7,093 Investigations incl. 154 deaths
950 Metabolism and nutrition disorders incl. 77 deaths
19,497 Musculoskeletal and connective tissue disorders incl. 63 deaths
123 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 11 deaths
26,795 Nervous system disorders incl. 274 deaths
110 Pregnancy, puerperium and perinatal conditions incl. 1 death
34 Product issues
2,205 Psychiatric disorders incl. 31 deaths
666 Renal and urinary disorders incl. 43 deaths
3,864 Reproductive system and breast disorders incl. 6 deaths
5,401 Respiratory, thoracic and mediastinal disorders incl. 358 deaths
4,636 Skin and subcutaneous tissue disorders incl. 13 deaths
546 Social circumstances incl. 7 deaths
1,119 Surgical and medical procedures incl. 96 deaths
4,266 Vascular disorders incl. 188 deaths
Total reactions for the COVID-19 vaccine NUVAXOVID (NVX-COV2373) from Novavax: 0 deaths and 2,101 injuries to 21/05/2022
44 Blood and lymphatic system disorders
116 Cardiac disorders
26 Ear and labyrinth disorders
1 Endocrine disorders
46 Eye disorders
154 Gastrointestinal disorders
463 General disorders and administration site conditions
3 Hepatobiliary disorders
8 Immune system disorders
102 Infections and infestations
19 Injury, poisoning and procedural complications
57 Investigations
13 Metabolism and nutrition disorders
275 Musculoskeletal and connective tissue disorders
2 Neoplasms benign, malignant and unspecified (incl cysts and polyps)
373 Nervous system disorders
1 Pregnancy, puerperium and perinatal conditions
1 Product issues
36 Psychiatric disorders
11 Renal and urinary disorders
39 Reproductive system and breast disorders
105 Respiratory, thoracic and mediastinal disorders
142 Skin and subcutaneous tissue disorders
3 Social circumstances
9 Surgical and medical procedures
52 Vascular disorders
These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
Here are some faces and names to put on these cold, hard statistics.
Horrible: A Mom Films Her Daughter Receiving The Jab – The Young Girl Ends Up Puking, Then Dying (Brazil)
Listening to her mom cry over the phone is one of the saddest things I’ve ever heard.
These are unspeakable atrocities against children and it needs to stop now. I don’t like sharing these types of videos but as a truth seeker it’s my duty to warn others.
Symptoms may include a desire to swing from tree to tree, to pick breakfast bugs off your mate, and to screech, yell, and generally monkey around. But seriously….
According to the Centers for Disease Creation (CDC), the agency that created at least eight Genus categories of Pox Diseases, Monkeypox is called a “rare disease.” However, Monkeypox cannot be considered “rare,” if the CDC also claims that Monkeypox is spreading.
After all, where there is a will, there is a vaccine patent!
In February 2021, patent application #20210260182 was filed for RECOMBINANT POXVIRUS BASED VACCINE AGAINST SARS-CoV-2 VIRUS. This is a combination pox/COVID vaccine patent filed over a year ago:
The terms “chimeric” or “engineered” or “modified” (e.g., chimeric poxvirus, engineered polypeptide, modified polypeptide, engineered nucleic acid, modified nucleic acid) or grammatical variations thereof are used interchangeably herein to refer to a non-native sequence that has been manipulated to have one or more changes relative a native sequence.
In some embodiments, the SARS-CoV-2 protein is inserted into the Thymidine Kinase (TK) locus (Gene ID HPXV095; positions 992077-92610; SEQ ID NO: 1) of the horsepox virus or the synthetic horsepox virus.
The official story from the CDC is that “Monkeypox” was discovered in 1958 “when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research” … and injected with Smallpox.
Not too long ago, in 2018, the Horsepox virus had its heyday when researchers told the story of the”infectious virus” synthesized in a lab. Symptoms may include a desire to neigh, snort, and gallop with the herd. But seriously… Horsepox was said to be the cousin of the Smallpox virus, which health authorities claimed had been eradicated from the planet in 1980. Why eradicate one “deadly” virus only to revive its cousin? What is the purpose of Franken-science?
The official answer was “to develop cancer treatments and vaccines,” especially since the current Smallpox vaccine (Variola) has some serious adverse side effects, including death. Note: nothing is ever said about curing cancer, only about “developing treatments and vaccines.” From the 2018 paper, Synthetic viruses—Anything new?:
…it comes as no surprise that it is possible to generate infectious viruses by using synthesized DNA fragments. The first synthetic virus, poliovirus, was produced by Wimmer and colleagues and made us aware of the fact that we entered a new era of reverse genetics that allows for the generation of synthetic viruses without the need for a nucleic acid template.
Chapter 3: “A new era of reverse genetics”
Many scientific papers published since 2018 have questioned the wisdom of engineering viruses from deadly Smallpox, which they admit could lead to the reemergence of Smallpox, as well as to future pandemics. What if the lab-created monkey virus or the horse virus escaped into the wild? What then?
Previously, scientists had blamed monkeys, as well as other species, for the consequences of their genetic experiments: in monkeys (SV40); in pigs (Swine flu (H1N1)); in birds (Avian flu (H5N1) different from Chickenpox; and in insects (Zika mosquito borne virus).
Note: the same molecular signature, protein (PB1-F2), is present in both the 1918 Spanish flu virus and in the highly lethal h5N1 chicken viruses. Coincidence?
These synthesized varieties were not selected to become “epidemics,” only beta tests on behavioral dynamics; except for the Swine Flu Epidemic, which resulted in a mass vaccine campaign, and was subsequently repealed after widespread vaccine injuries and deaths [See my 2018 blog Beware the Horsepox Vaccine!].
With many stories in the media, it is important to know that there is something called The Species Barrier. Even in the Age of Ignorance, the Species Barrier still exists, and The UK Dictionary defines it as:
The natural mechanisms that prevent a virus or disease from spreading from one species to another.
In short, people cannot “catch” diseases from animals, birds, reptiles, insects, vegetables, or minerals. But, as long as people have short attention spans, and continue to be misled by the story, animals will continue to be wrongly blamed and punished for human-engineered, chimeric experiments.
Why create animalpox outbreaks that appear go viral?
The ultimate purpose of any “viral threat” is to roll out the “vaccine solution.” And what exactly is the reason to push an agenda of vaccines? To engineer consent to reengineer humanity for deeper control: Monkey see-Monkey do. Therefore, any true global “viral threat” is not complete without a patented, engineered, controllable, injectable chimeric virus, coming soon to a city near you.
Chapter 4: The Twist: Monkeypox rash
Back to the monkeys!
The media generates associations by first showing computer-generated images of microscopic cells that appear to be bacteria (not viruses). Then, they release images of raised blisters or a rash labelled as “Monkeypox.” Looking closer, any image labelled “Monkeypox” could double as an image labelled Shingles.
Is there a relationship between the pox and the rash, or is it between the COVID vaccine/boosters and the rash?
Because the world complied so quickly to the illegal Coronavirus countermeasures, brought on by governments around the world, there is no need to wait years for the next epidemic! The “flying monkeys” are here to do the bidding of their creators.
What the WHO and CDC have not disclosed is that vaccine ingredients are widely known to cause rashes, often a full body rash. A vaccine-associated rash is a consequence of an influx of toxins to the body that results in a suppressed immune system. Frequent Strep Throat infections are another indication of a suppressed immune system. A.S.I.A is not a continent when it comes to vaccine damage. A.S.I.A is Autoimmune/Inflammatory Syndrome Induced by Adjuvants, (ie, induced by toxins), where adjuvants are vaccine ingredients (eg. aluminum sulphate). Keep this in mind. Do your own research.
Prior to the COVID injections, a rash was not indicated as a symptom of “Coronavirus,” which is a family of cold/flu viruses. According to officials, Coronaviruses can produce runny nose, sore throat, headache, fever, cough, and a general feeling of being unwell. True viruses, those not engineered in a lab, cannot survive outside the cell, they cannot transmit an infection because they are not alive (like bacteria). In this way, viruses are exosomes, produced by the cell in response to a toxic exposure, to help to clean the cell to regain balance and health.
Exosome biogenesis is a mechanism of protein quality control, and once released, exosomes have activities as diverse as remodeling the extracellular matrix and transmitting signals and molecules to other cells. This pathway of intercellular vesicle traffic plays important roles in many aspects of human health and disease, including development, immunity, tissue homeostasis, cancer, and neurodegenerative diseases.
While the virus itself is not a sexually transmitted infection, which are generally spread through semen and vaginal fluids, the most recent surge in cases appears to have been spread among men who have sex with other men, WHO officials said, emphasizing that anyone can contract monkeypox.
Is that science or science fiction? Are we back to HIV-AIDS? Did we ever leave it?
“The HIV/AIDS hypothesis is one hellof a mistake”- Kary Mullis, 1996, p. 14..– Nobel Laureate in Chemistry, 1993, inventor of PCR test.
With so many stories still unfinished, has Monkeypox arrived on the scene as a hoax? A test of humanity? Another virus that divides and discriminates against bi-sexual and gay men? What about the devastation of 500,000 deaths caused by the prescription Opioid Epidemic from 1999 to 2019 that continue? What about more than 150 people who die each year from taking the OTC, FDA-approved drug Tylenol?
Chapter 6: Nature rules
Nature has always ruled and Nature will continue to rule, but only if Nature’s Law is followed. Nature does not discriminate on the basis of race, religion, politics, education, vaccine status, or sex. Only patented lab-created viruses do.
Just because the media stories report on a Monkeypox viral threat, does not mean that humans need fear monkeys or eradicate them, like they did when they agreed to put chickens into lockdown from Pennsylvania to France then exterminated them out of fear.
Fear is False Evidence Appearing Real. Fear freezes people’s ability to be reasonable and rational. Fear separates and isolates. Fear masks identity. Fear disconnects humans from Nature, from each other, and from themselves. Going forward, if choosing fear, refrain from making any decisions or they will be made for you.
Perhaps humans should fear only humans with a god-complex, those who would unleash a lab-created/patented monkeypox/Smallpox/Horsepox/SARS-CoV2 virus into the population via injection for the purpose of reverse genetics.
Forget the Horsepox and Monkeypox stories. Could humanity be looking at a re-deployment of the original Smallpox?
Thoughts of people around the world will lie with bereaved families affected by the latest school shooting at Robb Elementary School in Texas.
As the search for answers begin, the cause of violent behaviour will once again go under the spotlight, along with the gun laws in the United States.
While there is never one simple explanation for what drives a human being to commit such unspeakable acts, all too often one common denominator has surfaced in hundreds of cases—prescribed psychiatric drugs that are documented to cause mania, psychosis, violence, suicide and in some cases, homicidal ideation.
The general public remain uninformed about the well-documented links between psychiatric drugs and violence. At least 37 school shootings and or school-related acts of violence have been committed by those taking or withdrawing from psychiatric drugs resulting in 175 wounded and 82 killed. Following the latest shooting, another 21 deaths are going to be added to the abysmal death toll.
International drug regulatory warnings and studies reveal the link between psychiatric drugs and acts of violence and homicide. There are also hundreds of cases where high profile acts of violence and mass murder were committed by individuals under the influence of psychiatric drugs.
Despite 27 international drug regulatory warnings on psychiatric drugs, there has yet to be a federal investigation on the link between the drugs and acts of senseless violence.
While psychiatrists are aware of the dangers associated with their prescribing habits, they continue their routine pattern of denial while the patient is left uninformed about the dangers linked to the psychiatric drugs being recommended.
Professor David Healy, a psychiatrist and pharmacologist says, “Violence and other potentially criminal behaviour caused by prescription drugs are medicine’s best kept secret.”
We cannot allow this to be the norm and we must not remain silent on this issue. The dangers of psychiatric drugs have been known for decades so, as responsible citizens, we have to continue to repeat this message so that the populace is informed and so that school shootings become confined to the history books rather than being the headlines.
1. Normal people have no interest in killing children, especially ones they do not know, especially in large numbers.
2. In my view, only people subject to mind control (please investigate Sirhan Sirhan or read about US intelligence agency attempts to create mind controlled assassins beginning in the 1950s) or people taking certain drugs, or special trained assassins are even capable of carrying out such an act. [In the case of Sirhan Sirhan, who did fire wildly on a crowd, but did not kill Kennedy, the actual assassin was an intelligence asset. From the WaPo in 2018:
Though Sirhan admitted at his trial in 1969 that he shot Kennedy, he claimed from the start that he had no memory of doing so. And midway through Sirhan’s trial, prosecutors provided his lawyers with an autopsy report that launched five decades of controversy: Kennedy was shot at point-blank range from behind, including a fatal shot behind his ear. But Sirhan, a 24-year-old Palestinian immigrant, was standing in front of him.
3. School shootings are the most provocative and effective way to initiate a change in gun laws, which means taking away the guns from some or all of the people who privately own them.
4. The large number of American gun owners pose a daunting challenge to the globalists who wish to control them. Police and military will not be willing to enter the homes of gun owners to remove their guns or for other purposes.
5. Few Europeans, Canadians, Australians, New Zealanders own guns, and it is believed by many that the imposition of much harsher lockdowns on the citizens of these nations, compared to the US, was enabled by this fact.
6. There have been shortages of guns and ammunition in the US since the onset of the pandemic. Whether this is due to supply-demand, including increased purchases by the federal government, or to other market forces, is not clear.
7. There has been very little exploration into the past history of those who committed mass murders in the US in recent years, especially in schools. I want to know if any or all of these mass murderers may have been enrolled in black mind control projects.
8. I want a full accounting of the mind control programs paid for with taxpayer dollars in the US and elsewhere.
9. I want an investigation into the many thousands of self-reported “targeted individuals” (TIs) who complain of voices beamed into their heads and other forms of what can only be termed torture.
10. I want an investigation into the implants some of these people claim were introduced into their bodies.
11. A reader sent me this piece by David Swanson, revealing that at least a third of mass US shooters have been trained in the US military. Were they put through mind control programs while serving their country?
12. Why have so many assassins and mass shooters appeared to be in an altered state of consciousness immediately after the event, and/or at other times? Think Sirhan Sirhan, Mark David Chapman, Reagan’s attempted assassin whose father was having dinner with GHW Bush the week of the attempt? Has anyone analyzed their behaviors systematically? Their histories and connections to the powerful?
13. We are being attacked in many perverse ways, and we must open our eyes, take our power back, or the attacks will continue and will destroy us.
“A pill with a tiny chip that sends a signal to relevant authorities when [the pill] has been digested…imagine the implications…the compliance…”
Patient compliance is a very big deal in the pharma/medical universe. The patient gets his orders. He follows them.
From a purely $$ perspective, the chip is a major advance. No pills left in bottles. People finish their meds. They go back to the doctor. He authorizes a new script or changes the drug. More pills taken, more money rolls in.
But of course, the larger bonus is control.
“You see, Mr. Jones, we know you didn’t finish taking the meds you were prescribed. So we can’t keep treating you. It’s a waste of time if you won’t follow orders…”
And this is just the first phase of ultimate control. Over time, it gets heavier. Cancelation of health insurance for non-compliance. Mandates.
COVID has been a training ground for citizen obedience. But the medical dictatorship wants more. Always more. And they’ll dream up one occasion after another to secure more.
Bird flu. Monkeypox. Smallpox. Whatever STORYTELLING it takes.
The medical cartel is in the business of making horror movies and promoting them as real.
A pill with a chip is the soft version of nanotech—by which tiny transmitters and receivers are placed in the body and brain. The nanos are also sensors. They report on all sorts of ongoing body processes—which leads to medical diagnoses, toxic drugs, and toxic vaccines in an endless parade.
This is not science fiction. This is not a hundred years in the future. We’re almost there.
Don’t make the mistake of thinking that humans are going to be on the receiving end of all the reports which the nano sensors issue from inside humans. This operation is planned as AI. Eventually, algorithms will interpret those reports and make decisions about treatment.
Many doctors will eventually take on roles as comforting guides, PR flacks, pitchmen, counselors. “Of course this is all for your benefit, Jim. It’s a good diagnosis. The treatment is standard. Think of Carol and the kids and what they need you to do. We caught it in time. You’ll be fine. But for God sakes, stop reading that nonsense online about toxic side effects. What do you think clinical trials are for? We did the prep work. The FDA approved this drug. It’s safe. I looked at your chart myself. The Pfizer antiviral is the preferred choice in your case. This is routine. If you need a human therapist, rather than the AI psychologist, I can recommend a good man. He lives in your town. Your insurance will cover it. But just suck it up and take the medicine. Believe me, you don’t want to progress to the stage where surgery is necessary. Then we would be talking hospitalization and recovery…”
Some of your children will be talking about earning a PhD in Bedside Manner.
Health Freedom and Medical Freedom are the alternative.
Everything coming down the medical pipeline makes this freedom absolutely vital. YOU decide what’s good for your body and mind, and what’s bad.
You assert that right, come hell or high water.
No matter how many court cases are won or lost, FREEDOM to say yes or no to medical treatment is the ultimate back up. This is what I kept writing and saying early on in the COVID hustle.
Meanwhile, the Pfizer CEO, Albert Boura, is a shark. In every sense of the word.
Moderna CEO Stéphane Bancel is complaining about having to ‘throw away’ 30 million doses of Covid-19 vaccine because ‘nobody wants them.’
“It’s sad to say, I’m in the process of throwing 30 million doses in the garbage because nobody wants them. We have a big demand problem,” Bancel told an audience at the World Economic Forum, adding that attempts to contact various governments to see if anyone wants to pick up the slack was a total fail.
“We right now have governments – we tried to contact … through the embassies in Washington. Every country, and nobody wants to take them.”
“The issue in many countries is that people don’t want vaccines.”
Watch:
Stéphane Bancel, CEO of Moderna:
“it’s sad to say, I’m in the process of throwing 30 million doses in the garbage because nobody wants them. We have a big demand problem.”
— Efron Monsanto ???? (@realmonsanto) May 23, 2022
Bancel’s comments come days after Bloomberg reported that EU health officials want to amend contracts with Pfizer and other vaccine makers in order to reduce supplies.
During a virtual meeting organized by Polish Health Minister Adam Niedzielski, governments shared a joint letter to the EU Commission which reads: “We hope that the discussion with the commission and among member states will allow flexibility in the vaccine agreements,” adding “We are also counting on vaccine producers to show understanding to the exceptional challenges that Poland is facing supporting Ukraine and giving shelter to millions of Ukrainian citizens fleeing the war.”
Some countries are seeking to amend so-called advanced purchase agreements signed with producers, as demand for shots wanes and budgets come under strain from the fallout of the war in Ukraine and the costs of accommodating refugees.
Adjusting deals with suppliers could grant member states the right to “re-phase, suspend or cancel altogether vaccine deliveries with short shelf life,” Estonia, Latvia and Lithuania’s prime ministers wrote in a joint letter to Commission President Ursula Von Der Leyen late last month.
Meanwhile, in a separate letter the health ministry of Bulgaria called for an “open dialog” with the commission and pharmaceutical companies, arguing that the current arrangement forces member states to “purchase quantities of vaccines they don’t need.”
The doctors, scientists and journalists featured in THE VIRAL DELUSION examine in detail the scientific papers that were used to justify the pandemic, and what they find is shattering. In this shocking, five-part, seven hour documentary series, they explode every single major claim, from the “isolation” of the virus to its so-called genetic sequencing, from the discovery of how to “test” for SARS-CoV2 to the emergence of “variants” that in reality, they explain, exist only on a computer. Their point: that the so-called SARS-CoV2 virus exists only as a mental construct whose existence in the real world has been disproven by the science itself.
They then go back through history to reveal how the birth and growth of virology has led to massive misunderstanding and misdiagnosis of disease: from Smallpox to the Spanish Flu, Polio to AIDS, to COVID itself – putting the pandemic in a whole new context better understood not as settled science, but the tragic culmination of misunderstood biology by the growing cult of virology, built on pseudo-science, to which much of the rest of the medical profession defers without understanding or examination, and the tragic consequences that have been wrought in its name.
In 2019, the virologists took center stage, and for the first time on film, their methods, miscues and tragedy they have wrought are put under the spotlight, revealing the extraordinary leaps of fantasy buried in their methodology, the contradictions quietly acknowledged in their papers, their desperate effort to change language to justify their findings, the obvious incongruence of their conclusions and the extraordinary stakes for our entire society in whether we continue to blindly follow their lead into a full-scale war against nature itself.
Featuring: Andrew Kaufman, MD; Tom Cowan, MD; Stefan Lanka, Virologist; Torsten Engelbrecht, journalist; Claus Kohnlein, MD; Kevin Corbett, PhD RN; David Rasnick, Biochemist PhD; Mark Bailey, MD; Dawn Lester and David Parker, Authors; Stefano Scoglio, Biochemist PhD; Saeed Qureeshi, Chemist PhD; Celia Farber, Journalist; Harold Wallach, PhD; Pam Popper, PhD, ND; Charles Geshekter, PhD; Amandha Vollmer ND, Jim West, Author; Larry Palevsky MD; and more.
The Viral Delusion (2022) Episode 1:The Tragic Pseudoscience of SARS-CoV-2
When doctor Andrew Kaufman began reading the first virology papers out of Wuhan in December 2019, he was shocked to discover that the scientists had come nowhere close to proving that a new virus had emerged… yet saw the media and authorities already claiming a viral pandemic was on it’s way.
In this extraordinarily revealing opening episode, a group of biologists, chemists, doctors and journalists take apart the SARS-COV-2 narrative piece by piece — from the non-isolation of the virus, to the hidden problems with purported photographs of the virus, to the claims that it has been genetically sequenced, to the invalidity of the PCR “covid-test.”
From the treatment protocols for COVID to the assumption of its transmission, Episode One unpacks the science of the claims that changed the world – in which these doctors and scientists make the case that every single claim the authorities made about the so-called SARS-COV2 virus has been based not on evidence, but pseudoscience.
The Viral Delusion (2022) Episode 2: Monkey Business: Polio, Measles And How It All Began
How did it all begin?
How could the scientific establishment have possibly gotten so big a story so wrong?
Everyone knows the story of Polio…or do they?
What from that story is actual history and what is medical marketing?
How did a small branch of the scientific establishment come to convince the world polio was the result of a virus and not from environmental toxins?
Learn what the actual experiments were upon which this theory was based — and how shockingly unconvincing they are.
Discover too how the medical establishment’s efforts to squeeze the symptoms of polio into a virus model formed the very foundation of modern virology, and how that commercially successful model has steered modern science ever since, evidence be damned.
The Viral Delusion (2022) Episode 3: The Mask of Death – The Plague, Smallpox and The Spanish Flu
What about Smallpox?
The Spanish Flu?
The Black Plague?
Go back, back, back in time to examine the claims and counter-claims as to what truly caused these deadly epidemics.
Are the rats of Europe innocent? Turns out they have to be…
And in that discovery we see how the superstitions of our time have clouded the eyes of “science” to avoid the most obvious of insights about disease.
The Viral Delusion (2022) Episode 4: AIDS, The Deadly Deception
AIDS. It was the defining epidemic of a generation.
But it was also the coming of age for many leading scientists and doctors who came to realize that blaming the illnesses known as AIDS on a virus was not only unsupported by science, it was downright nonsensical.
What were the true causes of the many illnesses labelled AIDS around the world?
How many suffered from their misdiagnosis?
How the scientific establishment fell into the deadly AIDS delusion is crucial to understanding the pandemic, and health, today.
The Viral Delusion (2022) Episode 5: Sequencing The Virus, Without The Virus
With the rise of computing and genetic research in the 90’s the virologists go high-tech.
They move away from experiments altogether and into genetic modeling — but do the models have any connection to reality?
The wonders of genetic sequencing have been pointed to as the proof of virology’s explanatory power — but when the claimed sequencing of SARS-COV2 is put under the microscope, has the game changed from the realm of science, to science fiction?
What’s really going on the claim of genetically identifying the SARS-CoV-2 virus is made?

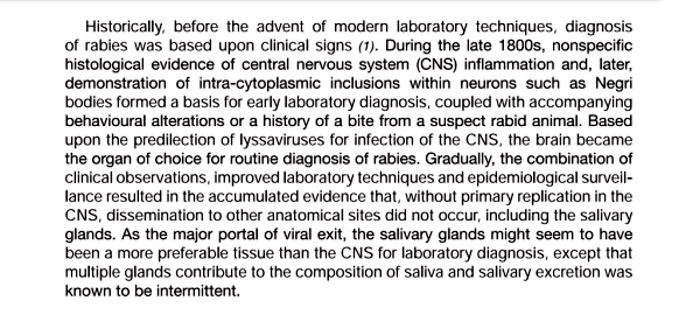
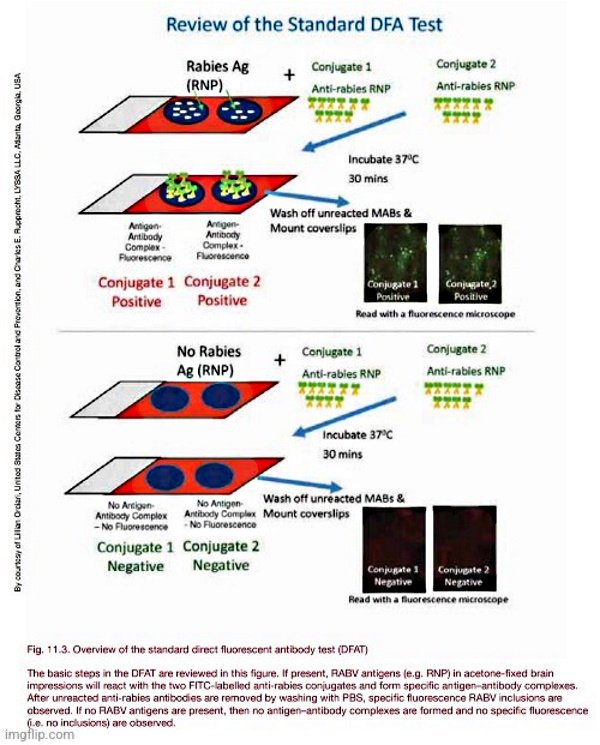
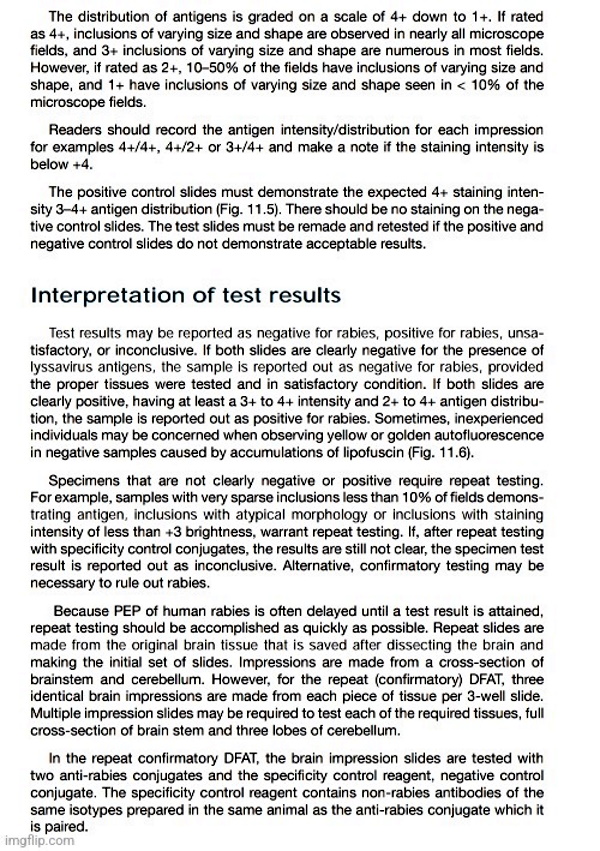
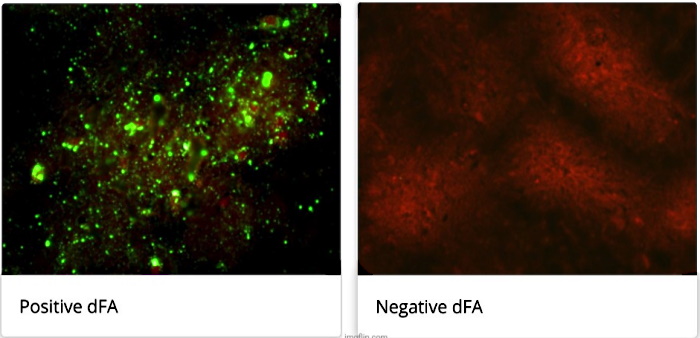
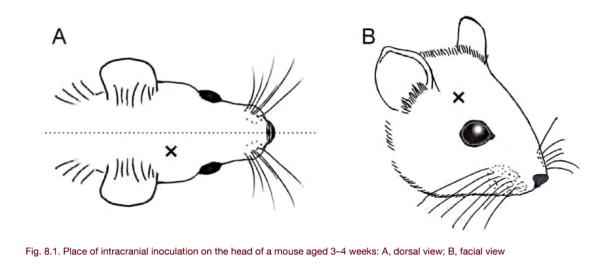
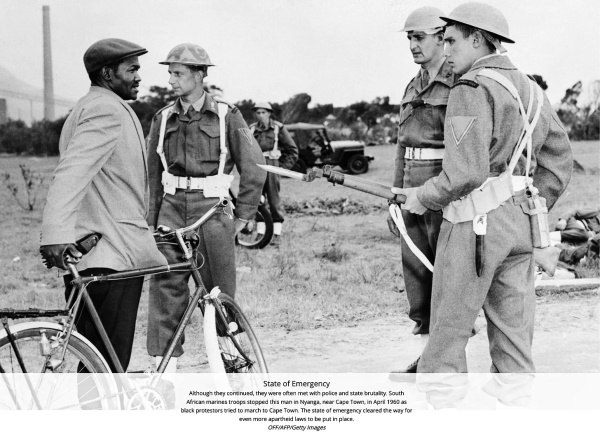
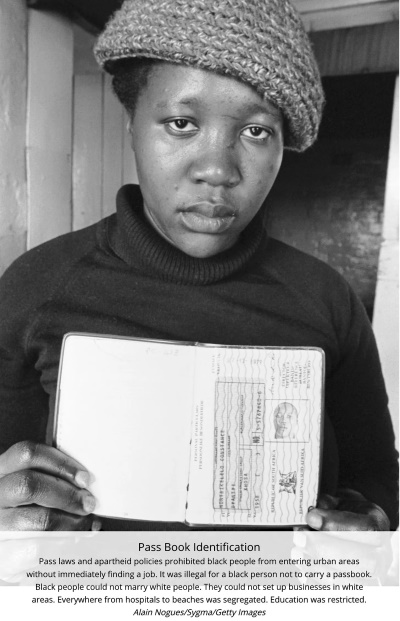
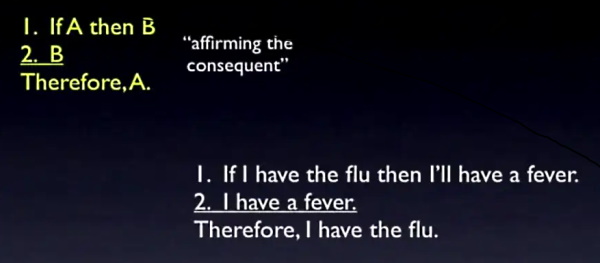
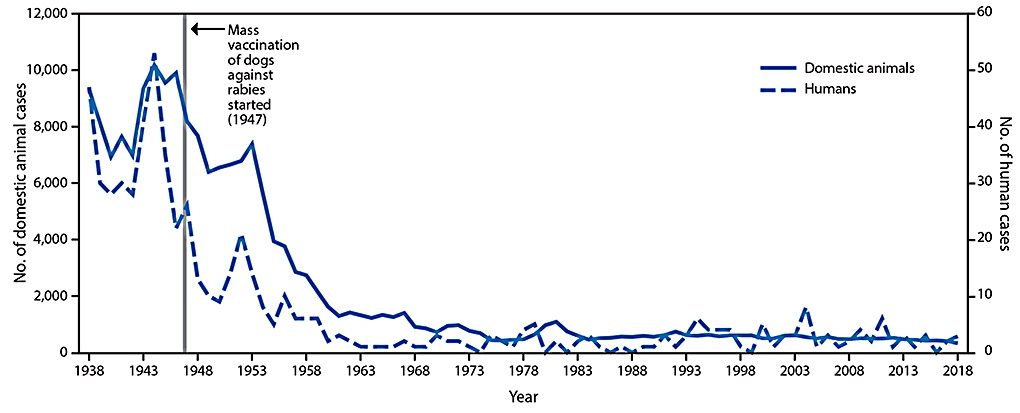


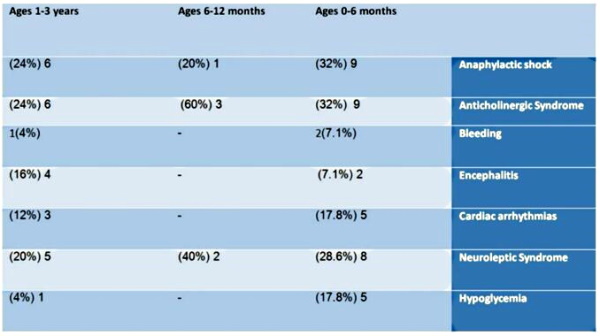
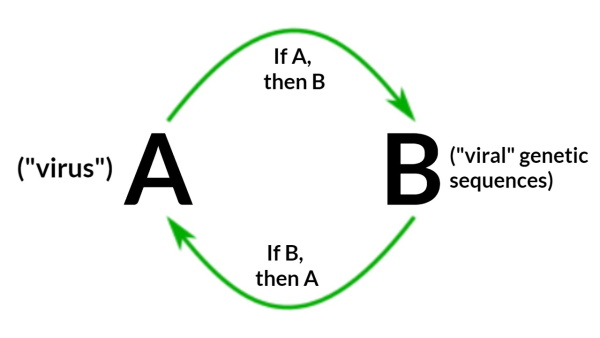
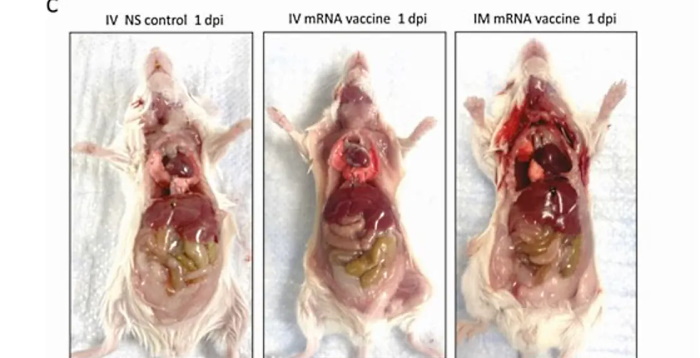




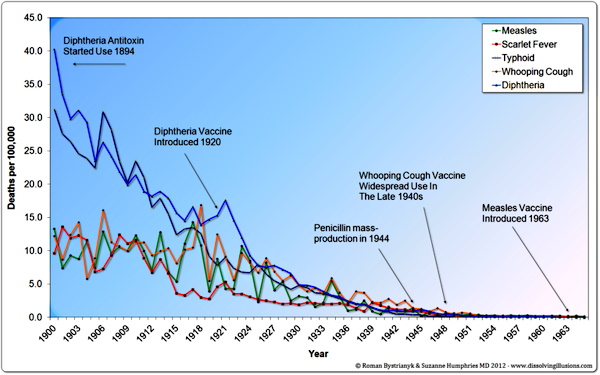


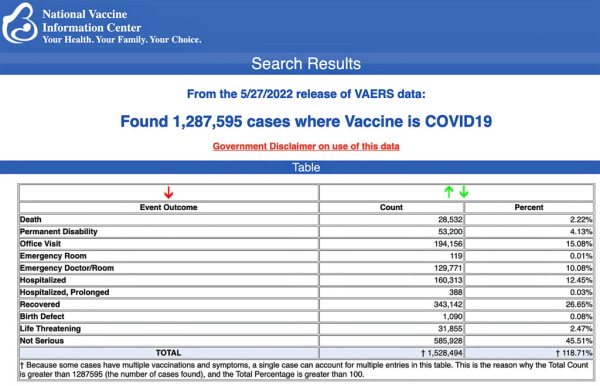

 (Brazil)
(Brazil) 
{kind=link}
{kind=link}