Senator Malcolm Roberts, Queensland, Australia: To All Who Perpetrated Covid Vaccine Injuries & Death — “We Won’t Let You Get Away With It. We Are Coming for You.”
The evidence continues to mount that these vaccines do not deserve the continuing provisional approval given to them by the TGA.
Concerns about possible adverse side effects are too big to ignore any longer, especially after my COVID Under Question inquiry which you can watch by clicking here.
Transcript
As a servant to the people of Queensland and Australia, tonight I’m speaking on this parliament’s therapeutic response to COVID-19 and the horrific medical harm and loss of life in that response.
Last week, leading Australian parliamentarians came together in an event I organised called COVID Under Question to present documented evidence and victim testimony proving a catastrophic failure of Australia’s regulatory framework.
COVID vaccine injuries are hidden behind anonymous government data, while supposed COVID virus harm is splashed across prime time.
The very least we can do for the victims of COVID vaccines is to say their names—victims like Caitlin Georgia Gotze, a healthy and vibrant 23-year-old studying at Griffith University to become a vet while working as a horse strapper. Caitlin dropped dead at work of a heart attack following a second Pfizer shot. Her death was recorded as asthma, a condition Caitlin had never had.
Reginald Shearer, a formerly healthy fit and active man, quickly went downhill and passed away from effects that began after receiving the AstraZeneca vaccine.
Daniel Perkins, a 36-year-old healthy father from Albion Park, died of a heart attack in his sleep following his second Pfizer injection.
Douglas James Roberts died after taking AstraZeneca. His family are concerned that his GP didn’t warn him of the side-effects of the vaccine. In other words, no informed consent was obtained. Neurosurgeons at the Royal Brisbane and Women’s Hospital attributed his death to a stroke, despite no family history and a clean bill of health. They refused to report his death to the TGA—refused!
The Australian Health Practitioner Regulatory Agency, Ahpra, has been bullying medical practitioners into not reporting or even for talking about the harm they’re seeing.
The TGA erased 98 per cent of the 800 vaccine deaths—98 per cent erased!—that physicians reported. The TGA did so without autopsy or suitable consideration of all the patient medical data.
TGA, ATAGI and Ahpra are the three monkeys of the pharmaceutical industry: hear no evil, see no evil, speak no evil.
Section 22D(2) of the Therapeutic Goods Act 1989 requires the Secretary of the Department of Health to ensure the quality, safety and efficacy of the vaccines were satisfactorily established for each cohort for which the provision of approval is being granted.
Data recently revealed in court papers in the United States clearly shows that vaccine harm was apparent in the clinical trials that Pfizer, BioNTech and others conducted. This information, if ATAGI had bothered to ask for it, should have resulted in a refusal of the application for provisional use.
No data was provided to the secretary regarding individual test subjects—technically, anonymized patient clinical data. No independent analysis of the fundamental issues surrounding novel mRNA vaccines was conducted in Australia—none in Australia!
Instead, the secretary took Pfizer, AstraZeneca and Moderna’s word for it.
I will say that again: the secretary took pharmaceutical companies’ word for the safety of their products.
These are the same pharmaceutical companies that have been fined over and over for criminal behaviour.
AstraZeneca got a US$355 million fine for fraud and, separately, a $550 million fine for making unfounded claims about efficacy.
Pfizer got a $430 million fine for making unfounded claims about efficacy, and a $2.3 billion fine—that’s billion dollars—for making unfounded claims about efficacy and for paying kickbacks.
This is who the Liberal-Nationals, Labor and Greens—our very own pharmaceutical lobby—want to pay more money to. That’s not on the basis of extensive local testing and inquiry, it’s simply on the basis of taking pharmaceutical companies safety assurances. There’s no testing. It’s an assurance made easy by indemnity against any damage that the vaccines cause. What deceit! What criminal incompetence!
The Labor Party and the Liberal-National Party have accepted $1 million each from the pharmaceutical establishment in this election cycle alone. Billions more are being set aside in this week’s budget to pay the pharmaceutical companies to keep the COVID-19 gravy train going. What great value this parliament provides for those electoral donations.
Mention should be made of the TGA’s decision to ban safe, fully approved and widely accepted alternatives to COVID-19 vaccines. This includes hydroxychloroquine and ivermectin; vitamins, minerals and natural antivirals; as well as proven messaging around healthy eating and lifestyles. The decision to ban proven, safe, affordable and accessible alternative treatments that are working around the world was taken to ensure the fastest and widest-possible adoption of the vaccines.
The TGA’s own customers fund the TGA. That means pharmaceutical companies fund their own product’s approval. That fails the pub test. Where are the checks and balances? There are none.
The Australian Bureau of Statistics is culpable in this scandal and cover-up. The Australian Bureau of Statistics’ annual budget is $400 million. The most recent mortality data they provide is from November last year, four months behind. The most recent breakdown of mortality by cause and age is from 2020.
The most recent data on live births is from 2020. Birth data used to be available six weeks after, not 15 months and counting. Are they hiding miscarriages?
At what point do we consider the actions of the TGA, ATAGI and the Australian Bureau of Statistics as interfering with the operation of the Senate? Peer-reviewed and soon-to-be-published data that must require the secretary to cancel the provisional approval of the vaccines has been released from outside of the government.
Let me review those quickly so the Senate fully understands the extent to which we have been misled.
Firstly, freedom of information documents indicate the TGA has failed to assess the reproductive toxicology of the COVID vaccines. Freedom of information documents indicate the TGA has failed to assess the impact of microRNA sequences and related molecular genetic issues on the human body.
Peer-reviewed and published in-vitro research shows gene based vaccine-generated spike proteins can migrate into human cell nuclei to disrupt DNA repair mechanisms. The TGA has dealt with this abysmally—murderously?
Vaccine-derived RNA can be reverse transcribed, leading to possible integration into the human genome, which the TGA denies, based only on pharmaceutical companies telling them to deny it.
Internal Pfizer data released in February indicate they accept 1,272 different adverse vaccine events, including paralysis and death.
German and US insurance actuarial data suggests the TGA’s database of adverse event notifications is underreporting side effects ninefold.
Freedom of information documents from 2018 show the TGA keeps two databases of adverse event notifications: one internal, showing all reports of harm; and one public, showing only a part of those.
This means vaccine harm is most likely significantly higher than reported.
Without honest and accurate data, the Senate has no way of deciding how much harm is too much harm.
German pathologists describe pathological aggregates of spike proteins and lymphocyte infiltrations in inflamed organs in autopsies related to death post vaccination.
In response, the TGA is failing to conduct autopsies on the 800 Australians the patients’ own doctors have reported as having died from the vaccines. What the hell is the TGA hiding?
Whistleblowers to the British Medical Journal provided reports of inadequacies, irregularities and possible fraudulent practices in the Pfizer vaccine trial—you know, the same trial for which the TGA took Pfizer’s word.
From a modern immunological perspective, two frequent vaccines for respiratory viruses run the risk of desensitising the immune responses to the virus, and that leads to hypoimmunity and worse illness than without the immunisation. To put that simply: repeated vaccination is doing more harm than good.
These are the matters I sought today to refer to the Senate Select Committee on COVID-19 without success. I thank Senators Hanson, Abetz, Rennick and Antic for their support, integrity and courage.
The truth is the Select Committee on COVID-19 has been running a protection racket for the pharmaceutical industry, and today’s vote proves it.
This unprecedented betrayal of the Australian people must be referred immediately to a royal commission. To the Prime Minister, the health minister, the federal health department and all those in the Senate and the House of Representatives—all of you who have perpetrated this crime—I direct one question: how the hell do you expect to get away with it?
We’re not going to let you get away with it. We won’t let you get away with it. We are coming for you. We have the stamina to hound you down and we damn well will.
COVID UNDER QUESTION is a cross-party inquiry into the Government’s response to COVID held on 23rd March 2022. COVID Under Question was hosted by Senator Malcolm Roberts (One Nation Federal Senator for Queensland) and attended by Stephen Andrew (One Nation Queensland State MP for Mirani), George Christensen (Federal Nationals MP for Dawson), Gerard Rennick (Federal Liberal Senator for Queensland), Alex Antic (Federal Liberal Senator for South Australia) and Craig Kelly (Federal Palmer United Australia MP for Hughes).
Parliamentarians heard from a range of Doctors, experts, economists and everyday people about how the Government’s response to COVID has affected them and at times defied belief. The absurdity of Chief Health Officer dictates and power hungry politicians is all laid bare.
The full day’s proceedings were recorded and available for public viewing.
“To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough
to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out.
This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs.
Instead of being held, rocked, and comforted in the time intervening between their birth and
their death, they have organs cut out of them alive.”
With the release of COVID vaccines, and then the mandates, we’ve seen a new resurgence of people attempting to gain religious exemptions.
Many of these attempts focus on fetal tissue obtained through abortion.
On January 19, 2021, AnnaMaria Cardinalli published an explosive article in Crisis Magazine, headlined, “Catholic Conscience and the COVID-19 Vaccine.”
Cardinalli details the collection of fetal tissue for the cell line named HEK 293.
The tissue was taken from an aborted infant in the Netherlands in 1972-3.
This cell line was used for “testing” the Moderna and Pfizer vaccines.
Cardinalli writes: “We know that the Pfizer and Moderna vaccines do not use any cells derived from abortion in the production process. That is, we know that we are not being directly injected with fetal cells or their engineered descendants (though this fact differs with other manufacturers). We hear that the abortion-derived cell lines were only used in testing, which should somehow comfort us, though it still means that the vaccines from which we seek to benefit depend on the involvement of abortion. We are told that the cell line used in testing came from one abortion, which took place decades ago. These things are all true, but they do not serve to inform us fully.”
“What we may not know follows. The most prominent cell line, called HEK 293, comes from an abortion performed in the 1970’s…”
“HEK stands for human embryonic kidney. To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out. This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs. Instead of being held, rocked, and comforted in the time intervening between their birth and their death, they have organs cut out of them alive.”
“There is no way that a spontaneous abortion could result in the cell line (as the kidneys cannot remain viable past the brief window in which they must be harvested) or that some brilliant researcher found a way for great good to come out of a rare tragedy by making use of a child’s body donated to science after it was aborted. The deliberate killing of an unwanted child (a little girl, in the case of HEK 293) took place in the tortuous manner it did precisely to obtain her organs for research. The harvest of her organs was the direct cause of her death, prior to which, she was a living child, outside the womb.”
“I fear that Pope Francis and Pope Emeritus Benedict may not have had this information when they received the vaccines. If we re-examine the Vatican statement that ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from aborted fetuses in their research and productions process,’ we see that it does not apply here. It does not imagine this scenario. To approve of the currently-available vaccines, it would have to read ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from living persons, killed by the harvest of their organs for use in medical research and productions processes,’ but the Church’s moral teachings could never truly bend so far.
Similar to the human rights abuses exposed by international tribunal in today’s China, where unwanted individuals such as religious and political dissidents are executed by the harvest of their organs for profit, the little girl whose cells gave rise to the COVID-19 vaccines was brutally sacrificed for the purpose, as were all the children whose cell lines failed before her.”
After reading Cardinalli’s analysis—not only should the granting of religious exemptions from vaccination be a foregone conclusion; the whole field of fetal tissue research, going back many years and involving many pharmaceutical products, should be put on trial.
The people who have been carrying out the murders, the people who have been using the harvested tissue, the companies—all of them—on trial.
I hope many medical professionals will take Cardinalli’s article as a springboard, and weigh in on what she is very clearly stating.
And not just doctors. All people who are shocked by her conclusions.
So far, I see one counter-claim to Cardinalli’s assertions:
The notion that the kidneys of the aborted baby must be harvested very quickly is false. The kidneys can survive for a longer period.
On that score, I refer you to a devastating video interview conducted by Robert Kennedy Jr. His guest was SOUND CHOICE PHARMACEUTICAL INSTITUTE “President and Founder, Dr. Theresa Deisher Ph.D., [with] over 30 years of pharmaceutical research and leadership experience. She discovered adult cardiac derived stem cells, has worked on their therapeutic uses as an alternative to human fetal DNA, and leads a team of scientists at AVM Biotechnology dedicated to changing what a diagnosis of cancer, autoimmunity, or chronic infectious disease means to patients and their loved ones. As a result of this work, Dr. Deisher is named as an inventor on over 47 patents.”
In the first 15 minutes of the interview, Deisher makes it quite clear that infants in the womb are taken out alive, with their blood supply functioning (essential) and then killed by cutting out their hearts or their brains. This is what is done in order to obtain tissue that will be turned into fetal cell lines.
Since this act of murder is standard practice, it would appear it was committed against the live baby whose kidney cells became cell line HEK 293, used in testing the COVID vaccines.
At the top of the interview, Kennedy said he didn’t want to get into the moral aspect of fetal cell lines. But after listening to Deisher, he was quite shaken. He said so. He said they would have to cover the moral aspect.
The whole world has to.
Here is the basic ramification: THERE IS A RELIGIOUS EXEMPTION FOR THE WHOLE WORLD.
For all people of faith. Every faith.
“According to my religious belief, the murder of an undeniably live infant for any reason is unconscionable and evil, and I refuse the vaccine.”
Here is a Force against which no government, no establishment, no secret society, no wealth can stand.
I fully understand all sorts of professionals will spout language that purports to show “the aborted infant was not alive, the lab followed all the legal guidelines, this is an old argument that has been debunked…”
But this is not just an old argument. This is the equivalent of an opening statement in a murder trial. Nothing less.
If religious leaders will read AnnaMaria Cardinalli’s article, they will see how important her charge is.
The question isn’t “will people of faith wake up and do what they should”; the question is “how can any person of faith NOT do what they should”.
If they will make a stand; if all people of faith will; the entire dire situation we are facing changes in the blink of an eye.
Solomon to God: “You have made Your servant king instead of my father David, but I am a little child; I do not know how to go out or come in…Therefore give to Your servant an understanding heart to judge Your people, that I may discern between good and evil.”
Gautama Buddha: “To cease from evil, to do good, and to purify the mind yourself, this is the teaching of all the Buddhas.”
John 10:10: “The thief comes only to steal and kill and destroy. I came that they may have life and have it abundantly.”
Would any church, any religion in the world say that God wants the killing of live infants for the purpose of medical research?
In the midst of this COVID tyranny, haven’t we all been looking for a truth that will galvanize huge numbers of people?
And not as some kind of stunt. But rather as an inevitable outcome of deep faith.
Faith and justice come from the same everlasting tree.
Yesterday I had the privilege and the honor to speak with Alec Zeck, John Blaid, Mike Donio, and Jacob Diaz about the claims made regarding the isolation and existence of “SARS-COV-2” by Dr.’s Malone, McCullough, and Cole. In this video, we address specific points they made such as whether or not:
Cultivation in cell culture is “isolation” of a “virus?”
Koch’s Postulates had been satisfied for “SARS-COV-2?”
The effect a drug has can be considered proof of the existence of a “virus?”
The electron microscopy images taken from unpurified cell cultures are proof of “virus” particles?
The particles assumed to be “viruses” are purified and isolated directly from the samples of a sick patient?
It was a pleasure to be a part of this conversation! I hope that you are able to come away with a better understanding as to why the evidence for the existence of “SARS-COV-2,” or any “virus” for the matter, is entirely lacking and unscientific.
Video available at The Truth Seeker (John Blaid) BitChute and Odysee channels.
Mike Donio, John Blaid, Jacob Diaz, Mike Stone, and Alec Zeck filmed a response to claims made by Dr. Peter McCullough, Dr. Robert Malone, and Dr. Ryan Cole regarding virus isolation and the existence of SARS-CoV-2 during an episode of The StreetMD Show hosted by Dr. Jo Yi on the Ickonic platform. The overall stance held by the speakers is simple: the claims made by these three gentlemen lack both in context and in substantial evidence to support the notion that SARS-CoV-2 exists as a pathogenic disease causing agent.
Below you will find a video presentation by Dr. Tom Cowan. The questions Dr. Cowan raises, the facts he presents, and the clarity he brings to the discussion of “viruses” and the field of virology are essential to our global conversation and quest to understand the truth. Truth Comes to Light has provided a basic transcript and added links to references for added clarity.
Over the past few years, we have shared many articles on this site related to this inquiry into the truth about “viruses” and the whole field of virology, including information on terrain theory vs germ theory. Find links here: Viruses, Vaccines & the History of Modern Medicine. At the end of this post you will find a selected list of related articles.
A few quotes from Dr. Cowan’s video:
“Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?”
“They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
“Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.”
“So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
“So I ask myself how did they do that?”
“What in the heck are these guys doing in these labs? What is gain of function research?”
“Do we really know if mRNA is in these vaccines?
“Where is the paper? Where is the evidence that there actually is mRNA in these injections?”
Okay, so before I get into talking about the question that so many people keep asking me: What about gain of function, lab-created viruses, bio labs now allegedly in the Ukraine?
So what is the science behind that?
So we’ll get into that in a minute. And before that I have a very short, little clip to play.
So that clip pretty much sums it up. That was from our friend Dr. Sam Bailey and our other good friend Stefan Lanka.
So on that note, the reason I wanted to talk about this subject is there was a recent paper that was put out by Dr. Mercola…
So let’s just read the first couple paragraphs there. So this is a summary:
“A study published February 21, 2022, (so very recently) in Frontiers in Virology claims to have discovered that a sequence of the virus’ spike protein is a 100% match to a modified messenger RNA (mRNA) sequence patented by Moderna in 2016.
The genetic sequence patented by Moderna is part of a human DNA repair gene called MSH3. This patented sequence is found in SARS-CoV-2’s furin cleavage site in the spike protein — the part that gives the virus such easy access into human cells.
According to Moderna’s patent application, the gene sequence was modified “for the production of oncology-related proteins and peptides,” ostensibly for use in cancer research.
According to the researchers, the chance that SARS-CoV-2 would have randomly acquired this furin cleavage site through natural evolution is 1 in 3 trillion.”
Okay, so why is this important? So obviously, there’s been a lot of attention in the political sphere and in the anti-vax community. There have been movies written about this.
There are many lectures, many prominent people in the “freedom” or “anti-vax” community who are investigating these patents, and saying that these patents — and as Dr. Mercola said, this study in Frontiers in Virology is literally the smoking gun proving that Moderna patented a sequence, which ended up in SARS-CoV-2, “the virus”, and the only way it could have gotten there is, not through natural evolution (that is a one in three trillion chance) but if it was introduced into the virus by some laboratory technique.
This theory is crucial to our understanding, not only of whether there were crimes committed, but the whole theory of virology and gain-of-function research and all that.
So, obviously, and this should go without saying, that the most important part of this is: Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?
The rest of the article goes on to talk about what we know about this MSH3 sequence and the protein that it allegedly codes for.
But I want to emphasize again and again and again — the whole point of this is: This sequence which was patented by Moderna in 2016 is identical to the sequence found in SARS-CoV-2.
That is the point.
If we can demonstrate that there is no SARS-CoV-2 and this is not the genome of this alleged virus, then none of the rest of this has any validity or is of any use at all.
It’s all just a sort of smokescreen or a way to throw us off the track about finding out what really is going on.
I cannot emphasize how important this is.
So for the next few minutes we’re going to actually look at how the authors of the article in Frontiers of Virology — what were they claiming was the SARS-CoV-2 genome?
What were they claiming was the evidence that there is a SARS-CoV-2 virus that they could then compare the patent to?
Again, if there’s no virus and there’s no genome then they can’t possibly have put this sequence into a virus or a genome. And it can’t possibly be the thing that’s affecting the world.
So, now let’s be clear about the next step. There is no mention in this story by Dr. Mercola of how the Frontiers in Virology authors found the genome or found the virus.
[…]
In other words, there is no information in here of how Dr. Mercola actually knows there’s a SARS-CoV-2 genome.
But the authors of the Frontiers in Virology paper said that they were comparing the sequence, the mRNA sequence patented by Moderna in 2016, to the genome found in our old friend paper by Chinese virologist Fan Wu.
So it isn’t that we picked this paper by random. It isn’t that I picked this paper to investigate how they found the genome or what their evidence for the virus was. This is the paper that the authors of the Frontiers in Virology use to compare the Moderna patent to.
So we’re using their information and this is their evidence, their proof that the virus exists.
So this is about: Did the paper by Fan Wu prove that the virus existed — the SARS-CoV-2 virus exists — and that this is the genome of the virus?
Again, in order to say that the patented sequence matches 100% to the genome of the virus, obviously, obviously, you have to know that this is actually a virus.
So, this is an old friend, we’ve been through this many times, but let’s see what they say.
So here is the paper, published in the prestigious journal, I believe, Nature — February 3, 2020.
So this is the paper, again, that was cited by the authors of Frontiers in Virology paper that is used as the reference genome.
So how did they do it?
So first we have a summary.
So how did they identify the “virus”? So I’m gonna run down the steps that they used and then we will show the clips, the actual wording from the paper, so that you know that this is actually the facts.
Okay, so we’re looking to find a virus and then find the genome of that virus — a virus that had never been found before.
So first thing they take lung fluid from one person. That’s a huge sample size (that’s a little tongue-in-cheek). That’s obviously just one person. That is a kind of ridiculous experiment to find a new virus.
Then they isolated the RNA, which is a genetic material, from the fluid in that person’s lung. They did not attempt to purify any particles that they could say you were a virus. They did not do any pictures of any virus. They did not do any maceration, filtration, ultracentrifugation to see if they had any such particles. None of that.
They took RNA from the lung fluid, of which we have many possible sources. We have bacterial sources, fungal sources, human sources, possibly viral sources, exosome sources, multivesicular body sources — many sources of RNA. We have no idea the source of that RNA.
Then they create what’s called an mRNA library, which is a catalog of all of the RNA pieces that are in that lung fluid.
This requires that they amplify these pieces of RNA with the process called RT-PCR. And, as we have demonstrated over and over again. and is completely substantiated in the literature, doing PCR amplification of RNA cycles inevitably creates new sequences of RNA which weren’t there in the original sample.
In some cases, if you do enough amplification cycles — up to even 80% of the sequences — after 45 cycles are made de novo, or anew, by the actual PCR process itself.
So now we have yet another source of our RNA. Not only do we have potential viruses, exosomes, multivesicular bodies, apoptotic bodies, human lung tissue, human epithelial lung tissue…, fungal RNA, bacterial RNA — we also have new pieces of RNA generated by the test itself.
Then they performed pair and sequencing that generates 150 base pair reads. That means they matched the sequence by pairing the ends. And you end up with sequences that are basically 150 base pairs long. That’s a fairly small amount. And this results in 56.5 million of these 150 base pair sequences known as reads.
So to be clear, they take this mass, not knowing any idea the origin of these mRNA, they chopped them up into sequences that are 150 base pairs (that’s fairly short) long by pairing the ends. They have 56.5 million of these reads. And then they start doing what’s called de novo assemble.
So there is no sequencing here. There is assembly. And, as it says, you can make a lot of genomes with that many reads.
So they put these 56 million, 150 base pair, reads in aa assembly computer program and… they actually put it in two different computer programs. And one of the computer programs generated 384,000 different sequences. The other one generated over a million sequences.
So now these sequences — all 384,000 of them — are meant to be the possible genomes of this virus. For some reason, they threw away the program that made over a million of these sequences and said the one that made 384,000 — I think that was Megahit — one of those must be the right sequence, the actual sequence of the virus.
Just to be clear, at no point did they ever find a particle. At no point did they purify or isolate a particle.
At no point did they find in any particle… an entire string of RNA, which they then sequenced one by one to find out the sequence of the genetic material of this particle.
None of that was done. All they did was chop up RNA from many different possible sources, put that in a computer program, generate 384,000 and a million in another, and then they went hunting for infectious agents and performed a search of those sequences.
The two longest sequences were a close match to a bat SARS-like coronavirus genome, found 15 years ago or so, that was made in exactly the same way — never having isolated or purified a particle, never having found an intact genome, never having sequenced the genome.
They just did the same sort of assembly, no sequencing of RNA from God knows where. And, this one, the longest one was a 89% match to the previous SARS coronavirus that they did in the same way.
And, as we say: Boom! There is the new novel human coronavirus — even though, as we’ve said over and over again, humans and chimpanzees are about a 96% match. So to say it was an 89% match is essentially like saying there’s no way this could have been anywhere similar to the previous bat SARS-like coronavirus.
In other words, they never found a virus. They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.
This is a manuscript draft and I don’t know when it will be published.
When I read this, just remember that all these articles that go into The Lancet have to pay homage to the virus god. But I will explain what they mean here.
So this is the interpretation of the entire article. I won’t go through their methods.
“The RNA code counted in PCR tests, previously attributed to SARS-CoV-2, belongs instead to a respiratory-virus-induced immune system response by human cells that liberate exosomes, and that vitiate PCR test results. PCR tests have zero specificity in vivo due to the exosome RNA.”
[…]
And they go on in this article, just as we’re saying — the reality is all of these RNA sequences, all of these reads which were assembled into a viral genome, actually when you do careful analysis, come from human epithelial lung cells.
In other words, just as we’ve been saying all along, these are not viruses. These are breakdown products of our own tissue. And the misconception in calling them a virus needs to stop.
And this idea that they put this patented sequence into a virus can’t possibly be true because, simply, there is no virus.
And all the rest of the article is for not — because nobody put a RNA sequence, patented or otherwise, into a virus.
Now just to show you that we got this from the article — so here is the one patient presenting with cough, etc. So that’s the evidence that we were correct about the one patient.
Here is the evidence that the paired and 150 base pair reads sequencing of the RNA library was performed on this computer platform. So the sequencing yields reads of only 150 base pairs. The whole SARS-CoV-2 genome is supposed to be 30,000.
That means they had to stitch it together using a computer program. This was an assembled genome, out of little bits from God knows where.
And here we see the 56.5 million reads were assembled using Megahit and Trinity. Trinity, they got over a million. They generated a total of 384,000 contigs (that’s sequences).
Trinity generated 1.3 million. They don’t like those because they weren’t long enough. They compared those with the database and compared and found that it was somewhat, although not really similar to a previous bat coronavirus. So, as he says, sequencing results in more than 56 million reads.
How can you possibly differentiate what is from a potential virus from everything else? The answer is you can’t.
And finally… The longest contig is generated by Megahits. The longest one by Trinity is 11,000. How come they didn’t use this one?
Both showed similarity to bat coronavirus. They were found at high abundance. It was only 89 percent similar. That means 11 percent didn’t match. That is a huge amount.
Then they just moved on to develop primers all from this one assay without isolating anything, and from one patient.
And, my friends, that is not science; that is propaganda, as is the entire story of a lab engineered virus.
Now, the real issue here and one of the reasons why this, to me, is so important, is if you go by this unscientific theory that there’s a lab-created virus, you actually miss what I would say are the three most important questions to be asked, and then answered, about this situation.
And so now I’m talking — I would say theory. Where everything else was what I would call simply facts.
So the question that should be asked (and it would be nice to have answers for, and which I don’t have the answers for, but I have some theories) is, to me, the most interesting thing is —
So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
So I ask myself how did they do that? How did they make — like there’s two theories, there’s two ways of looking at this.
One is: They don’t want that to happen and so it was a mistake.
But, if we think, which I’m inclined to do, that “they” (meaning Moderna and other people) wanted this to happen so that they could throw people off and essentially create a kind of patsy out there, how did they do it?
So I have three possible theories as to how they did it.
Now, let me be clear.
What I’m trying to figure out is these guys Fan Wu and others, Chinese virologists, having, I don’t think, any connection with Moderna, come up with a bogus, anti-scientific genome and for some unbelievable coincidence — let’s say for now — it actually matches exactly one of the patented sequences from the Moderna patent of four years prior. How did that happen?
So possibility number one: It was dumb luck. They just made this sequence and it just so happened to match the Moderna patent. And, frankly, I don’t think that’s actually the right answer.
The second possibility: … Somebody from Moderna or somebody — I don’t know who — calls up Fan Wu and says ‘I want you to make a genome out of nothing and I want it to have this particular sequence in it so some day people will find this out and say “you see, they genetically engineered this sequence”‘. Got it? In other words, there was collusion between the patenters (that’s Moderna) and Fan Wu and his team.
Now I gotta tell you, I actually don’t think that’s true. I would actually love to find out if it is true and if there is a phone call from doctor head of Moderna saying, you know, ‘Hey Wu, would you put this sequence in there so that we can — people find out that it was a genetically engineered sequence?’ But I just don’t think that happens.
And then I came up with a third possibility which is: Once I discovered all these people who are looking into all these patents, that there was at least 70 different patents taken out, of different sequences of RNA, that could end up in a genome. Now, my guess is … I would think it’s a good possibility that one of those sequences may end up in the final genome. And then you would then implant the story that this was a genetically engineered organism and there you go.
So you wouldn’t have to rely on luck, you wouldn’t have to actually have collusion, you could just patent a whole lot of different sequences, for instance, that came in the SARS-1 genome. You could patent all kinds of sequences knowing that, at the end of the day, when somebody makes up this new fraudulent genome it’s bound to have one of them in there. Somebody will find it some day, say it’s the smoking gun and you then implanted the story of the century which does nothing but throws people off.
So those are my three options. I’d be happy to hear about any other possible options. But those were the only three that I could come up with.
Now, the final question then is: What in the heck are these guys doing in these labs? What is gain of function research?
And, I must say, I don’t know what they’re doing in the labs and I don’t think really anybody knows — including in the Chinese labs or Ukrainian labs or North Carolina labs or any other labs.
So again, I have some possibilities.
One is the following …
Screenshot image from BrandNewTube video (specific video source unknown)
They’re doing this.
In other words, what the virologists do is they dress up in hazmat suits and they go on to their computer and start making sequences. And the hazmat suits are crucial, because, as we all know, it’s very possible for the sequences to jump from the computer into their eyes. So it’s very important, as you can see, that they wear goggles and protective head gear to prevent the computer sequences from jumping directly in their eyes.
In other words, they may be just doing nothing and it may be just a whole lot of hooey to get people to worry about things. And to implant in their minds that there is this horrible engineered virus, that we should all be scared of viruses, etc. So that’s one possibility.
Another one is they’re making some sort of proteins or genetic material which can be injected into people. In other words, they’re making toxins. And that is certainly possible.
So those are the two main categories that I came up with. Either they’re just doing nothing and they’re just a front, or a smoke screen, or they’re actually making stuff which isn’t good for people.
And that gets into my final thing that I want to point out.
… This section right here. this is something I’ve been very interested. So this is again from the Mercola article:
“For clarity, this may have nothing to do with Moderna’s patented MSH3 sequence specifically, because the RNA code in the jab is not identical to the RNA code of the actual virus. (I’m not going to get into that.) The RNA in the jab has been genetically altered yet again to resist breakdown and ensure the creation of abundant copies of the spike protein. 11“
Now, I have been asking the question now for months: Where is the paper? Where is the evidence (a) that there actually is mRNA in these injections? They say there is. That’s the whole point. But when people look there either seems to be not there or in variable amounts depending on which injection and which batch.
So it could be that even the whole mRNA in the jab is a actual smokescreen or cover for what’s really in these injections –which is a lot worse stuff like self assembling nanoparticles which we’ve heard about a lot.
So I was very interested to see that this was… stated as fact, because I can’t find a paper, and my friends can’t find a paper, that confirms that abundant copies of this protein are actually made when you inject this sequence.
And this would be like saying — if I wanted to get investors for my new pencil factory, my investors might ask me to see the pencils that we make. And so it would be natural for me to produce copies of the pencils — maybe tens or hundreds or thousands or millions of them — to show that my technology for making pencils actually works.
One would think that if the whole point of these jabs is to make you make spike proteins that, therefore, “confer immunity”, there would be scores, hundreds, thousands of papers showing here’s the amount of spike proteins in an unjabbed person. And then you jab them and then 10 minutes, half an hour, three hours, two weeks, six months, 12 years later, here’s the amount of spike protein. That would prove that the concept is real and that you can actually genetically alter a human being.
Because I have my doubts. So I’m looking for a reference to show this is true. And, lo and behold, here is the reference. Number 11. [see page 3 of Mercola article] So where is the reference from? CBS News.
Now, I could say — I would say if it was from Fox or MSNBC then I would be skeptical. But the fact it’s from CBS, that must mean it’s true. And obviously I’m kidding. Let’s see the reference.
If the whole point of this is to put RNA into injections, make you make a spike protein which is allegedly from the virus, let’s actually see that it works. And here’s a quote saying there’s at least 73 patents.
My guess is one of them was bound to show up in the imaginary sequence. Bingo! We’ve got proof that it’s there, that it was a genetically engineered virus.
And the whole thing, hopefully you now see, comes crashing down like a house of cards if, as we showed, there was no virus genetically engineered or otherwise in the first place.
[At this point in the video, Tom takes questions from the viewers.]
Question: So this one is related, but it has to do with Dr. Bush‘s reference to 10 to the 30th power of viruses within our blood, as well as in the oceans, in the soil. His purpose is to provide constant flow of updated genomic information that we need to in order to adapt and survive. And they’re not pathogens. That we need not fear, etc., etc.
Answer: So he also has said that, of course, viruses are pathogens. The real issue here is how did they find these 10 to the 30th power viruses? And I’ve gone over this, especially in reference to a paper, and I don’t remember the name, but it’s called the ….something to do with the renaming or the re-evaluating of viral…virome…viral world or something like that.
The reason people say this is because they don’t realize that they’re not talking about actual organisms or particles called viruses. They’re talking about liberated pieces of either RNA or DNA — little snippets of RNA or DNA which then get amplified in what’s called metagenomics sequencing and so there are billions and billions and billions of these breakdown products. None of them have anything to do with a virus. They’re simply little bits of genetic garbage that are coming off of our cells and tissues all the time. They have no particular meaning or function that anybody has been able to prove. They’re just little bits of garbage. And the misconception that they’re somehow actual particles and could possibly hurt you or could possibly help you is just a misunderstanding of how they found viruses in the first place.
They don’t find particles. They don’t purify particles. There haven’t been 10 to the 30th purified particles. We’re talking about little pieces of DNA or RNA that get amplified, called viruses, which is a misconception big time.
[Additional questions include speculation about the patent links to the Fan Wu team “discovery” as well as a question about allergies.]
Articles mentioned in this video presentation:
Moderna Patented Key COVID Spike Protein Sequence in 2016 by Dr. Joseph Mercola [originally published March 7, 2022 at this link — https://articles.mercola.com/sites/articles/archive/2022/03/07/moderna-patented-spike-protein.aspx — and was mirrored around the web. It can still be found at Dr. Mercola’s paid archive membership.] Dr. Cowan has provided a pdf file of the article here: https://brandfolder.com/s/fv2q4h7fp84bm5vb3ppn37
We’ve seen the unbelievable microscopy images of the experimental jabs from other investigators around the world, but we wanted to see it for ourselves! There are now 4 teams working on this in New Zealand and Dr Robin Wakeling has agreed to go public with his findings.
He compares the Pfizer jab to other vaccines and discusses the startling findings with Dr Mark Bailey.
For the past two years humanity has been under attack. And entire populations have been put under draconian restrictions under the claim that there is a pandemic.
For those of us that can see there is no evidence of a virus, the war on humanity is even more egregious.
However, within the wider circle of those questioning the covid narrative, a common theme is that something is badly wrong with the offered solution in the form of experimental vaccines.
By early 2020 globalist organizations were indicating the rollout of their touted universal vaccines and an injection in every arm.
In 2021 citizen scientists began examining the injections under the microscope and the revelations was startling.
At the forefront of the research has been the La Quinta Columna team who have produced many light and electron micrograph images, as well as detailed analysis of self-assembling particles, graphene components and potential nanotechnology.
Here in New Zealand we also have several teams who have backed up these findings.
Of course, there have been dismissals that we are just seeing artifacts or, in a sense, crystals.
That’s why we asked Dr. Robin Wakeling, a senior microbiologist and nano-emulsion delivery technology expert, to perform his own analysis of the Pfizer BioNtech product.
He joined my husband, Dr Mike Bailey, to explain the behavior of the product under the microscope. Over time and under the influence of various environmental factors, he compares his findings to known colloidal structures and other vaccines.
And, as the other investigators around the world, reaches some disturbing conclusions.
Dr. Mark Bailey
Welcome everyone. I’m doctor Mark Bailey in Christchurch, New Zealand, and it’s my pleasure to be speaking with Dr Robin Wakeling, coming in from Wellington, New Zealand.
Robin is a microbiologist, PhD and world expert in decay and mold forensics. He’s supervised polymerase chain reaction research and been a vocal critic of the pseudoscience taking place in the alleged covid pandemic.
Robin has thousands of hours of microscopy experience and has previously been involved in the development of patented nano- emulsion delivery technologies. So what better person to take a look at the Pfizer BioNTech products up close?
Now we’ve seen from some of the electromicroscopy images, coming in from other countries such as Spain and Germany, which have demonstrated that the injections contain what appear to be undeclared constituents including graphene oxide, and what could be interpreted as being nanotechnology.
Today we’re gonna take a look at the Pfizer products under the light microscope for ourselves and see how it behaves on a slightly larger scale and how perhaps that coheres to the overseas proceeds findings.
So Robin I’ll hand over to you and perhaps you can stop by telling the audience what kind of microscope you’re using and the grades of magnification we’re looking at.
Dr. Robin Wakeling
Okay, thanks Mark. Yes I use a compound light microscope with a basic magnification of 650 although the software that puts it on the computer screen sort of doubles that approximately.
I use phase contrast most of the time. A couple of the images are using bright field and polarized light.
And then I included a few images of other workers which were dark field. But most of my work was with phase contrast. And the magnification and scale, I’ll remind the audience of as we go through.
Okay, so the overarching theme of this presentation is what …. are the undisclosed ingredients in Comirnaty. We know that there are at least two declared undisclosed ingredients.
In other words they’re just coded. We don’t know what they are on the basis that they are proprietary excipients. So we know that there are some unknowns and possibly some undeclared unknowns also.
So that’s really the overarching question that we’re addressing.
[…]
There are three main findings of the microscopic images that we’re producing or suggesting — the key findings.
So the first one is that the lipid nanoparticles that are contained in Comirnaty — and I’ll explain what LNPs are in a moment — but it appears that they are continuing to self assemble in a way that forms much larger colloidal structures of some highly varied and somewhat rarefied forms.
The second main key finding was that these colloidal structures then seem to change their form in response to collision with interfaces like the glass surfaces of the microscope, preparations, or air bubbles, or other interfaces — whereby they start to take on a much more structured and unnatural formation with a lot of straight lines and right angles — sort of things that don’t usually occur in nature outside of crystallography.
And what we’re going to be showing most of the time has some profound differences to crystal structure. So we’ll cover that too.
And so the third finding, which is where the other two kind of lead to, and it’s where other workers have sort of jumped into the deep end with some of the dark field work that’s been done.
These right-angled sheets and wires seem to form colloidal structures… in some situations, where it appears that some environmental triggers are involved….
They seem to order themselves in a highly-ordered complex way — a way that is quite unusual. Certainly not something that the people who are looking at this have seen before. And these are people who should be familiar with this sort of thing…
Because some human beings care about their children, VAERS was established in 1990 as an early warning system to identify negative reactions and side effects of vaccination, which makes sense.
But there are major problems. It is managed by the FDA and the CDC, which explains why the VAERS database requires a class to learn how to find anything.
Taking the time to actually file a report is voluntary. And out of fear of losing their jobs or being considered an anti-vaxxer, nobody wants to speak ill of the all-holy vaccine, let alone make an official report.
It is estimated that only one percent of vaccine injuries ever get reported to VAERS. So that means when VAERS reports over 44,000 adverse reactions and 90 deaths, one can expect it to be as much as 4.4 million adverse reactions and 9,000 deaths.
And these numbers are only from the age 5 to 17 group.
Conservative numbers put it at 10 percent, which is half a million children that have been wounded and killed from an unneeded, unwanted, experimental gene therapy shot that we were lied to about every step of the way.
Thanks to the OpenVAERS project, which is built upon the VAERS data, the public can easily search these reports and see for themselves.
People are reporting adverse reactions such as chronic pain, loss of hearing and taste, talking gibberish, and acting out aggressively. And these are the mild cases.
There is a tsunami of major brain damage, heart disease and fatalities. Edward Dowd has analyzed the data and has reported an 84 percent increase in deaths among ages 25 through 40, which is the same amount of lives lost to the Vietnam War.
Toby Rogers estimates that Big Pharma kills twice as many people that died in World War II every single year.
The press ignores this because it’s not enough.
They want your newborn babies as well.
Pfizer is pushing to have children as young as 6 months old given a shot that we know is potentially fatal, even though children were never at risk and are still not at risk.
The United States has been force-injecting infants and children with experimental vaccines for years. And now they want to add the infamous ‘clot shot’.
Thanks to virtue-signaling mothers, some children have already been getting it in the womb which is resulting in miscarriages, still births, and deaths from breast feeding on toxic genetically-modified mother’s milk.
Pfizer is planning on submitting another application for emergency use authorization in early April.
That’s about 18 million children under five who could be sacrificed to the altar of Big Pharma and political correctness.
If Pfizer can achieve permanent liability protection from the FDA, who they control, then they can add the mRNA gene therapy shot to the childhood vaccine schedule where it will enjoy permanent liability protection under the 1986 National Childhood Vaccine Injury Act.
These same crooks are putting a judge on the Supreme Court who openly defends leniency towards crimes that involve child rape.
They’re coming for your children and they will not stop.
If you still care about the human race and are looking for something you can do right now, you can go to Toby Rogers at substack and read his urgent call to action for more info.
Dr. David Martin recently filed the first in a series of lawsuits in Federal Court “to get the truth out” about COVID-19 gene therapy injections and “take back America from the COVID pandemic scare.” In what he calls a “multi-step process,” Martin explains the first lawsuit will put into the public record “that the COVID vaccine is not a vaccine.” Instead, Martin explains the Injections are experimental gene therapies “known to kill people, known to actually stay inside of the human body for over 60 days producing pathogens that are scheduled toxins.”
The lawsuit, Griner v. Biden et al., was filed on Mar. 4, 2022, in the U.S. District Court in Utah on behalf of Devan Griner, MD, a double-board certified surgeon and widely published author who has transformed the lives of hundreds of children in Utah and beyond. Besides naming Joe Biden, defendants include Xavier Becerra of the U.S. Department of Health and Human Services (HHS), as well as the Centers for Medicare and Medicaid Services (CMS) and its leaders.
Martin maintains we need to stop forcing and bribing people to get the shot, stating, “Those are illegal acts in the United States and cannot be done.” Martin explains that the first lawsuit is in part litigation for discovery—revealing the criminal conspiracy Martin has talked about for years—as much as it is a litigation for the facts, as both are equally important. Martin is confident the disclosures that will have to be filed by the Federal Government in response to the first case “are, in fact, going to be incriminating for our next case.” Looking forward to obtaining evidence of the felony, Martin explained:
“We wrote this case so that the immunity shield falls away from the manufacturers and all of the injuries and deaths become civil liabilities to the manufacturers.”
Martin, who indicated that Utah is the perfect jurisdiction to begin his campaign, pointed out that when a term like “vaccination” is used, the public believes they are getting something that will keep them from getting sick or transmitting sickness. Instead, Martin asserts that after receiving the COVID-19 injection(s), individuals turn into a biological weapons factory. Explaining further, he declares:
“And [vaccination] is actually defined in the statute exactly that it’s the ability to put something into the body that stimulates the immune system. It turns out that the mRNA that’s being injected into people is not that. In fact, specifically, what it does is take a little computer-simulated strand of mRNA, it sends it into the body, and the body becomes a biological weapons factory. It manufacturers spike proteins. The injection does not stimulate any immunity.
[Instead], it is the instructions to make a scheduled pathogen. And the scheduled pathogen is defined under three different parts of the code, but it specifically includes genetic sequences derived from—are you ready for this—SARS coronavirus. That’s actually a scheduled, known toxin on the scheduled list of biological weapons in the United States code.”
The 32-page lawsuit, with 171 pages of Exhibits, begins by highlighting that the CMS mandate requires almost every employee of any healthcare facility receiving Medicaid or Medicaid funding to “receive one of the three Injections authorized for emergency use by the Food and Drug Administration as COVID-19 vaccines (the “Injections”).”
CMS Mandate Must Be Struck Down
The suit further explains that Plaintiff, Dr. Griner—who has natural immunity and refuses to take one of the injections—is a “highly skilled and well-known plastic surgeon licensed to practice in Utah whose passion is healing children who suffer from cleft palates and other congenital defects.” The doctor has traveled the world on more than twenty medical missions, donating his time to help unfortunate children. However, the lawsuit asserts that the CMS Mandate prevents Dr. Griner from continuing to heal children—unless he takes one of the Injections. Noting that Dr. Griner enjoys robust and durable natural immunity after having recovered from COVID-19, the lawsuit explains:
Dr. Griner is subject to the CMS Mandate because the hospitals in which he has the right to practice receive CMS funding. Thus, Dr. Griner must choose not just between his “job and the jab,” as the Fifth Circuit has phrased it, he must also choose between pursuing his passion for healing children with congenital defects and taking the Injection. This despite the fact that the only justification for forcing Dr. Griner to take the injection is the assertion that doing so will prevent Dr. Griner from transmitting SARS-CoV-2 to his patients and other health care workers with whom he comes in contact, something the CDC readily admits the Injection simply does not do.
The lawsuit insists the CMS Mandate must be “struck down” because overwhelming evidence—along with admission by the CDC Director—shows that the injections do not prevent transmission, infection, or reinfection in those who receive them. And despite the windfall profits being made by the big pharma giants making the Injections, the CDC has admitted that both the “vaccinated” and “unvaccinated” are equally likely to spread COVID-19.
Regardless of CDC Definition Change, Injections Are Treatments, Not Vaccines
Furthermore, the lawsuit states the Injections fail to confer immunity “but are claimed to reduce the severity of symptoms experienced by those infected by SARS-CoV-2.” With this in mind, Plaintiff argues the shots are instead treatments and not vaccines, as that term has already been defined in the law. Displaying the CDC’s changing narrative connected to COVID “vaccines” in the brief, and the fact the CMS Mandate rests squarely on the basis that the Injection prevents transmission, the suit reveals:
In fact, the CDC has actually changed its definitions of “vaccine” and “vaccination” so that the Injections would fit within the new definition. Until recently, the Centers for Disease Control defined a “Vaccine” as: “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.
The CDC also previously defined “Vaccination” as: “The act of introducing a vaccine into the body to produce immunity to a specific disease.”
Both prior definitions fit the common understanding of those terms. To be vaccinated meant that the recipient should have lasting, robust immunity to the disease targeted by the vaccine.
But on Sept. 1, 2021, the CDC quietly rewrote these definitions. It changed the definition of a “Vaccine” to: “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease preparation that is used to stimulate the body’s immune response against diseases.” It changed the definition of “Vaccination” to: “The act of introducing a vaccine into the body to produce immunity to protection from a specific disease.”
Thus, the CDC has eliminated the word “immunity” from its definitions of “Vaccine” and “Vaccination.” Upon information and belief, the CDC did so because it recognizes that the Injections do not produce immunity to the disease known as COVID-19.
This is a critical factual and legal distinction. The Supreme Court has long held that the right to refuse medical treatment is a fundamental human right. Since the Injections do not stop the transmission of SARS-CoV-2, as a matter of fact, they are not “vaccines” as a matter of law. Instead, they are a therapeutic or medical treatment which Dr. Griner has the fundamental human right to refuse.
In great detail, the lawsuit expands on the conviction held by numerous experts that the Injections are treatments, not vaccines. The claim reminds us that the FDA categorizes the shots as “CBER-Regulated Biologics,” otherwise known as “therapeutics,” which falls under the “Coronavirus Treatment Acceleration Program.”
Indeed, among the eight professional examples offered in the suit to corroborate that the Injections do not create an immunity that prevents the transmission of COVID-19 to others, the case quoted NIAID Director Dr. Anthony Fauci’s declaration to NPR on July 27, 2021, when he stated, “We know now as a fact that [vaccinated people with COVID-19] are capable of transmitting the infection to someone else.” Additionally, the head of the Oxford vaccine team Professor Sir Andrew Pollard, is quoted in the case as saying on Oct. 8, 2021:
“We don’t have anything that will stop transmission, so I think we are in a situation where herd immunity is not a possibility, and I suspect the virus will throw up a new variant that is even better at infecting vaccinated individuals.”
Martin Insists Injections are Gene Therapy Medical Devices
Furthermore, Plaintiff declares that with rapidly waning effects, the Injections are not “vaccines,” but are instead “gene therapy medical devices” and should be appropriately classified as such. As illustrated in the screenshot below, Moderna (Pfizer uses the same technology) recognizes that its mRNA platform is not a vaccine. Instead, it is “gene therapy in the form of biological “software” developed to genetically “hack” the machinery of human cells to construct a specific protein.
Elaborating further on the role the mRNA plays in the Injections, the lawsuit summarizes that the specific protein that human cells are “hacked” to create is the spiked protein of the disease. Essentially, the Injections genetically modify human cells to make the same toxic protein that the disease itself creates—the spiked protein. With no known method to reverse the detrimental effects of the Injections, the lawsuit continues, explaining:
These spiked proteins adhere to the endothelial cells of humans, the very cells that line the entire cardiovascular system. The spike proteins adhere to the interior of the cardiovascular system like thorns on a rose bush, causing a variety of detrimental effects, the short- and long-term impact of which are currently unknown and unknowable.
According to a June 01, 2021, bio-distribution study from the Japanese Regulator Agency, the spike protein of the “…coronavirus gets into the blood where it circulates for several days post-vaccination…” and that it concentrates “…in spleen, liver, adrenals, and ovaries in high concentrations…”
Causes of Action As Campaign Gets Underway
The lawsuit lays out three Causes of Action against Defendants, the first being the “Violation of Fifth and Fourteenth Amendment Substantive Due Process.” According to Plaintiff, the CMS Mandates violates the liberty protected by the Fifth and Fourteenth Amendments to the Constitution, including “rights of personal autonomy, self-determination, bodily integrity and the right to reject medical treatment.” With no compelling interest available to Defendants to prove the necessity of mandating the shots, Plaintiff again reminds that the Injections “are simply ineffective against the current variant” and were only somewhat effective against the original SARS-CoV-2 strain.
The Second Cause of Action explains Defendant’s Violation of the Fifth and Fourteenth Amendments related to the Equal Protection Clause, which “prohibits classifications that affect some groups of citizens differently than others.” By creating two classes of healthcare workers—the injected and uninjected—the CMS Mandate dictates the members of one class (the uninjected) get terminated. These unvaccinated employees cannot advance their careers, provide for their families, or pay their mortgages. On the other hand, the injected get to keep their jobs, advance their careers, and pay their bills. Yet, the situations of these two classes are indistinguishable because vaccinated healthcare workers can become infected and reinfected with SARS-CoV-2 and can transmit the disease to fellow workers, patients, and visitors. The lawsuit asserts:
Discriminating against the uninjected controverts the goals of the Equal Protection Clause—i.e., to abolish barriers presenting unreasonable obstacles to advancement on the basis of individual merit.
Pursuant to the Fifth and Fourteenth Amendments, Plaintiff is entitled to temporary, preliminary, and permanent injunctive relief restraining Defendants from enforcing the CMS Mandate.
The Third Cause of Action insists that by issuing the CMS Mandate, Defendants are violating the Constitution of the United States “in that they invade and encroach upon sovereign powers that reside solely in the States and have never been relinquished by the States to the Federal Government.” According to the lawsuit, the CMS Mandate rests upon a general police power asserted by the Federal Government—a power it does not have. Therefore, the CMS Mandate is an ultra vires act taken by the Federal Government because the powers the Federal Government claims to assert belong to and are retained by the States.
With the filing of Griner v. Biden, Dr. Martin’s campaign to expose the illegal corruption behind the pandemic “vaccine” narrative is underway. Emphatically, Martin states that without hesitation, the vaccine needs to be called what it is—a gene therapy injection. Noting a desperate need for “truth in advertising,” he explains:
“If we start calling [the “vaccine”] the “gene therapy injection,” a lot less people will roll up their sleeves—and roll up the sleeves of their children—to actually get the shot. And by the way, if you decide to roll up your own sleeve for an experimental gene therapy, have at it, I don’t care. What I do care about is forcing other people to do it, and coercing other people to do it. And holding their jobs or their livelihoods at gunpoint to get them to do it.”
Del Bigtree: “Less than a third of the total population of the United States of America [has received a booster shot]. [The CDC] boasts that it’s about 44% of the vaccinated… That means, at the very best, there’s a 60% group of people, even that are vaccinated, that don’t listen to the CDC any longer!”
The CEOs of the nation’s largest airlines are asking the Biden administration to drop the federal mask mandate on airplanes, along with the pre-departure testing requirement for international travelers. Although COVID-19 cases in the U.S. have fallen sharply in the last two months and restrictions are being lifted across the country, the Centers for Disease Control and Prevention earlier this month extended its mass transit mask mandate by 30 days, until mid-April, and masking guidelines for airlines remain in place.
“Now is the time for the administration to sunset federal transportation travel restrictions – including the international predeparture testing requirement and the federal mask mandate – that are no longer aligned with the realities of the current epidemiological environment,” the CEOs of 10 U.S.-based passenger and cargo airlines, including Delta, American and United, wrote in a letter to President Biden.
The letter states that while the airlines and their employees supported the federal mask mandate when it was first implemented, especially because it did away with the possibility for airline-by-airline rules in the early days of the pandemic, they now feel it is no longer necessary.
After a request from the FDA to suppress vaccine data for the next 75 years, a 55,000-page set of Pfizer documents has recently been released. Vaccine efficiency aside – why has it been so hard to gain access to data about vaccines that we the public paid for?
#Pfizer #Covid #Vaccines
OTTAWA: The Justice Centre announced today that its legal team has eleven affidavits in the Federal Court lawsuit to strike down the federal government’s mandatory Covid-19 vaccine requirements for air travellers (the “Travel Ban”). The Notice of Application was initially filed on February 1, 2022 behalf of several Canadians from across Canada challenging the Travel Ban on the basis that their Charter rights and freedoms have been infringed.
The main applicant in the case is former Newfoundland Premier, The Honourable A. Brian Peckford. Mr. Peckford is the only surviving drafter and signatory to the 1982 Constitution and the Canadian Charter of Rights and Freedoms.
In his sworn affidavit, Mr. Peckford states: “What I find perhaps the most disturbing is that the federal government has mandated a two-tiered society where one group of people has benefits while another group is disadvantaged. As a person who has chosen not to receive the new medical treatment, I am all of a sudden treated as an outcast, labelled a “racist” and “misogynist”, and as an undesirable person not fit to be seated with vaccinated people on an airplane … The Covid-19 vaccinated are allowed to travel by airplane and to see their families and the unvaccinated are not. This is not the Canada I know and love, and this type of segregation causes me utmost sadness.”
In October of 2021, the federal government announced that anyone travelling by air, train, or ship, must have taken the requisite number of mRNA Covid shots (currently two).
The travel vaccination mandate has prevented approximately 6 million vaccine-free Canadians (15% of Canada’s population) from travel within Canada and prevents them from flying out of Canada. The evidence filed with the court shows how the Canadians involved in the lawsuit cannot travel to help sick loved ones, cannot get to work, cannot visit family and friends, cannot access health care outside of Canada, cannot take international vacations, and cannot live ordinary lives.
Expert medical evidence now filed with the court ranges from scientific evidence about Covid spread among both vaccinated and unvaccinated; risks associated with taking the new Covid vaccines; vaccine harms such as myocarditis and possible effects on fertility; and the superiority of natural immunity.
The Federal Court has consolidated the Justice Centre action with three other similar cases, brought by other unrelated parties, asking for the travel ban to be ruled unconstitutional. All applicants have asked the Federal Court to hear the case on an expedited basis given the serious infringement on Canadians’ mobility and other rights. The parties have agreed to the following timelines, and hope to have the matter heard in September of this year at the latest:
March 11 – Service of Applicants’ Affidavits and Documentary Exhibits April 25 – Service of Respondent’s Affidavits and Documentary Exhibits May 16 – Completion of cross-examination on Affidavits June 6 – Service and filing of Applicants’ Records June 27 – Service and filing of Respondent’s Record Fall 2022 – Hearing (proposed timeline)
“Canada is the only country in the developed world that bans unvaccinated citizens from air travel,” states Keith Wilson, Q.C., lead counsel on the case for the Justice Centre. Mr. Wilson adds, “Canada’s ban on unvaccinated flying is especially egregious given Canada is the second largest country in the world by landmass and Canadians have a far greater need to use air travel for work, family and health reasons than do the citizens of most other countries.”
“Our experts confirm that both the vaccinated and unvaccinated spread Covid. This means the government’s rationale for the ban on air travel is fatally flawed and there is no justification for the serious infringement on Canadians’ Charter rights,” notes Mr. Wilson.
“Our evidence refutes government claims that infringing the mobility, conscience, security and privacy rights of Canadians is justified,” states Justice Centre lawyer Allison Pejovic.
“Canadians have the right not to be discriminated against, and this Charter challenge seeks to enforce that right,” adds Ms. Pejovic.
The Justice Centre for Constitutional Freedoms is a non-profit national constitutional law organization funded by voluntary donations from concerned Canadians.
The Centers for Disease Control and Prevention on March 14 removed tens of thousands of deaths linked to COVID-19, including nearly a quarter of deaths it had attributed to children, blaming an algorithm for “accidentally counting deaths that were not COVID-19-related.”
The Centers for Disease Control and Prevention (CDC) on March 15 removed from its data tracker website tens of thousands of deaths linked to COVID-19, including nearly a quarter of the deaths the agency said had occurred among children.
In a statement to Reuters, the CDC said it made adjustments to the mortality data because the website’s algorithm was “accidentally counting deaths that were not COVID-19-related.”
“Data on deaths were adjusted after resolving a coding logic error,” the CDC’s website states. “This resulted in decreased death counts across all demographic categories.”
The agency also acknowledged COVID death data is not complete.
Prior to the adjustment on March 15, the CDC attributed 851,000 deaths to COVID, including 1,755 pediatric deaths, according to Kelley Krohnert, a Georgia resident who tracks CDC updates. After the change, COVID-related deaths dropped to 780,000.
The change resulted in the removal of 72,277 deaths previously reported across 26 states, including 416 pediatric deaths — a reduction of 24% to 1,341, the agency said.
The CDC’s COVID statistics, used to justify which age groups should receive vaccines, were used by U.S. health agencies to support the authorization of Pfizer’s COVID vaccine for children 5 to 11 years old.
CDC Director Dr. Rochelle Walensky referred to the tracker’s death total in November 2021, while pushing for an expert panel to advise her agency to recommend vaccination for all children 5 to 11 years old.
Children account for only 19% of all COVID cases, with .01% of childhood cases resulting in death, according to the American Academy of Pediatrics.
According to CNN, Moderna plans to report trial data in 2- to 5-year-olds in March and may seek authorization from the U.S. Food and Drug Administration “if the data is supportive and subject to regulatory consultation.”
Pfizer CEO Albert Bourla during a March 13 episode of CBS’ “Face the Nation” said he expects to have a vaccine ready for children aged 6 months to 4 years old “potentially in May if it works.”
Johnson & Johnson has a late-stage trial of its vaccine for 12- to 17-year-olds but nothing for the younger group.
It is unknown whether the pharmaceutical giants will use the CDC’s most recent COVID numbers in their risk-benefit analysis presented to U.S. health agencies to determine whether the risks of COVID outweigh the potential risks of vaccines in children.
CDC ‘cherry-picks’ COVID data for the public
Dr. Meryl Nass, physician and member of the Children’s Health Defense scientific advisory committee on March 19 wrote that the CDC cherry-picks the data it presents to the public to push its “health policies.”
The agency hides most of what it has and then “blames its ‘outdated’ IT systems for the problems if it gets caught,” Nass said.
Nass explained:
“CDC is not a public health agency. It is a public propaganda agency that collects a massive amount of data. CDC marshals its huge data library to create presentations that support the current administration’s public health policies. CDC also has state-of-the-art PR staff, as well as TV studios, and produces videos, radio spots and an enormous number of press releases that are distributed to the media. CDC hosts many journalists at its Atlanta headquarters. Free junkets successfully cultivate U.S. health reporters.”
Quoting a 2007 Senate oversight report on the CDC, Nass said the agency spends “millions of tax dollars for failed prevention efforts, international junkets and lavish facilities, but cannot demonstrate it is controlling disease.”
‘Fact-checker’ claims no evidence COVID deaths have been overcounted
Health Feedback, a fact-checking initiative under the umbrella of Science Feedback, on March 1 said there “is no evidence COVID deaths have been overcounted,” and labeled posts stating otherwise as factually inaccurate, false and misleading.
Heath Feedback focuses on “correcting misinformation about vaccine safety,” and said it “reviewed multiple false claims” that COVID cases, hospitalizations and deaths were inflated when “many public health experts believe that COVID-19 numbers are undercounted.”
Health Feedback also addressed death certificates listing COVID along with other health conditions, saying health conditions weaken a person’s resistance to disease and in “many such cases, a person with underlying health conditions wouldn’t have died at that time if it wasn’t for COVID-19.”
“This means that the cause of death is still COVID-19,” the website states.
Health Feedback did not acknowledge that deaths occurring when COVID and other health conditions are listed could be caused by underlying health conditions.
Health Feedback was established as part of the Vaccine Safety Net — a “global network of websites, created by the World Health Organization, that provides reliable information on vaccine safety.”
It also belongs to the International Fact-Checking Network, founded by the Poynter Institute and funded by the Bill & Melinda Gates Foundation, Google, Facebook, the Omidyar Network and George Soros-owned nongovernmental organizations such as the National Endowment for Democracy and Open Society Foundation.
To date, Health Feedback has not issued a correction to its fact-check reflecting the CDC’s new mortality data.
After the White House and Congress dropped their mask mandates last week, Del Bigtree said, “enough is enough” and, through his attorneys, has now sued the Centers for Disease Control and Prevention (CDC) challenging its mandate requiring masks on planes, trains, and buses.
It is incredible that our elected leaders have dropped mask mandates for themselves but yet everyday Americans must still mask. There is a term for when those that govern impose requirements on the governed but exclude themselves. Just compare the picture on the left with the those on the right:
While the science on masking should be enough for the mask mandate to disappear, the lawsuit challenges the mandate on the grounds that the CDC does not have the authority to implement or enforce the mandate.
You can read the complaint in its entirety here and we will keep you apprised of the lawsuit. Thank you for supporting ICAN’s ongoing efforts to ensure that our civil liberties are restored.
“The real purpose of the scientific method is to make sure Nature hasn’t misled you into thinking something you don’t actually know…One logical slip and an entire scientific edifice comes tumbling down. One false deduction about the machine and you can get hung up indefinitely.” – Robert Pirsig, Zen and the Art of Motorcycle Maintenance
On 11 March 2022, an article was published on The Daily Sceptic website titled “The Real Truth About Viruses”. It was written by Dr Roger Watson, a PhD-qualified registered nurse, who recently retired from the United Kingdom’s higher education sector and now has a part-time position as Academic Dean of Nursing at Southwest Medical University, China. The article was a blatant hit piece against me, typically the domain of the controlled corporate media, so it was a surprise to see it on a website that developed from Lockdown Sceptics. They have the motto “question everything” but apparently you shouldn’t question germ theory and the existence of viruses!
“Question Everything”….except germ theory and viral existence, that’s pure crazy.
Dr Watson appeared to know very little about my work and never attempted to make contact with me before he did his hit and run. We offered him the chance to come on my channel but he declined saying “I am not sure how fruitful a debate with me would be,” perhaps not feeling confident about backing up his claims or perhaps a little shaken by the derision he received in the comments section on the Sceptics website. Much of his article was ad hominem in nature and doesn’t need to be dignified with a response but I will proceed to address his inaccurate scientific claims point by point…
“I would like to hear Duesberg or Sam Bailey explain how haemophiliacs contracted AIDS from blood infusions. Somehow, I think they’ll have a stock response to that one.“ Dr Roger Watson, The Daily Sceptic
It is unclear why Watson has conflated my views with Peter Duesberg and his sentence will take some unpacking. His reference to Peter is a link to Wikipedia, a known disinformation site, which should raise a red flag for a sceptic or anyone wanting to know more about a topic. Peter does not claim that viruses don’t exist: he is one of the world’s most prominent retrovirologists after all! His position is that the HIV particle exists but that it is a harmless “passenger” virus that does not cause the clinical condition AIDS. I know he outlined the evidence of why haemophiliacs do not become “infected” through blood product transfusions here but cannot otherwise speak for him. My position is that there is no proof of the existence of a retrovirus called HIV and that the particles nominated “HIV” have never been shown to fulfil the defintion of a virus. Thus “HIV” has not been shown to cause AIDS.
In this regard, the biggest influence on both myself and my Virus Mania co-authors has been the work of The Perth Group. Watson fails to define what he means by “haemophiliacs contracted AIDS from blood” but presumably he means that the reason some haemophiliacs develop AIDS is because there is a pathogenic virus that is being transmitted to them via infected blood. (They actually receive factor VIII concentrate from pooled blood donations.) I am unaware of any research demonstrating HIV particles in blood or any human or animal models showing transmission of “infected” blood that then causes a recipient to develop AIDS. In Virus Mania we explain that “HIV” cannot be the explanation for the development of AIDS in haemophiliacs. Increased death rates did correspond to changes such as the introduction of “anti-viral” pharmaceuticals including the highly toxic AZT in “HIV positive” patients. If Watson wants to get serious about claiming that a virus is being transmitted to haemophiliacs and causing AIDS then he should have an attempt at refuting The Perth Group’s 1995 paper “Factor VIII, HIV and AIDS in haemophiliacs: an analysis of their relationship”. In my estimation it is the best I have come across and I would welcome Watson’s critique of what I’ve missed.
“Her views have been debunked regarding the existence of viruses but, possibly unknown to many who are unwilling to wade into the depths and breadths of her views, she denies germ theory completely.” Dr Roger Watson, The Daily Sceptic
Watson doesn’t let his readers know how he established I’ve been “debunked” or by who. Instead he provides a link to a small blog post written by a University of Waikato employee and Pfizer BioNTech injection enthusiast Alison Campbell. Campbell set up the blog “as a resource for secondary school biology teachers preparing students for Scholarship Biology examinations” which is probably not the level Watson should be aiming for in this debate. If he checked Campbell’s usual publications he would have realised that she has no experience in virology or medical matters. In fact, when we reached out to her she quickly retreated and would not even agree to a phone call. Watson follows in the footsteps of our state-sponsored mainstream media who also used this largely ad hominem rant as “evidence” against me. I’ve already responded to Campbell and the MSM’s little foray into virology – unfortunately, like Watson, they are limited to repeating the claims of the virologists on face value.
I’m not sure why my views on germ theory would be “unknown” to my viewers as I openly point out that I do not believe it is satisfactory model. Virus Mania is largely dedicated to dismantling germ theory and my views are closest to that of “terrain theory”. I outline why I’m in the terrain camp in much of my work, including in my video “Germ Theory vs Terrain Theory”. For those not familiar with Virus Mania, a window into the book can be found in this short essay I wrote with my co-authors.
“This essay is prompted by the most recent video from Sam Bailey: The Truth About Viruses published on March 9th 2022. She is to be congratulated for its brevity – it is only 17 minutes long – but it is presented in a typically sneering, sarcastic and patronising manner.“
Dr Roger Watson, The Daily Sceptic
Watson seems to completely miss that this video is a light-hearted and satirical take on some of the historical claims of the virologists. It was designed to engage a wider audience with material that can be a boring subject for many. If he wanted to have a serious discussion about a particular topic then he could have easily accessed my other published work or contacted me to fill in any gaps.
“It is hard to understand how Sam Bailey arrives at her views and it is not necessary to be a virus denier to be highly critical of the way the pandemic was managed.“
Dr Roger Watson, The Daily Sceptic
Watson has ignored the vast majority of my work and never bothered to converse with me so perhaps it is not surprising that he is confused. I’m not sure why anyone would decide to be a “virus denier” because they needed to criticise “pandemic” management or how this is relevant to his argument. In fact, it’s disingenuous to even suggest such a modus operandi and it slumps into the argument of the destitute.
“After all, anti (Covid) ‘vaxxer’ supreme, Dr. Mike Yeadon made it clear in his excellent interview with Neil Oliver on GB News that he believes a unique virus exists. The HART Group led by Dr. John Lee, who have mounted the most credible and well-informed responses to the UK lockdown, is not stocked with virus deniers.“
Dr Roger Watson, The Daily Sceptic
Watson has not provided any evidence for the existence of viruses here: his argument seems to be that other people believe in viruses, therefore viruses exist. Some people also believe in the tooth fairy but that would not affect my own investigations into the topic. Appeal to common opinion is a type of faulty reasoning that also plagues the medical community. Heretics like myself are prepared to examine the evidence for ourselves and reach our own conclusions, not parrot those of others. We are not motivated by the number of people who agree with us and our publications are not restricted by governments, institutions, or colleagues. Note to Dr Watson: in all the virology textbooks I’ve looked at, the method of proving the existence of a virus does not include ‘beliefs held by Dr Mike Yeadon’. (For the record: I have no problem with Dr Yeadon, we just have different thoughts on the existence of viruses.)
“It is hard to know where to start but, since she denies germ theory itself – as properly understood – I will start here with Dr Bailey’s views on whether anything exists that can cause an infection and spread between people. Louis Pasteur comes in for criticism by Bailey in her Delingpod interview. I am sure Pasteur was not perfect but he did knock the theory of spontaneous generation a body blow with his swan neck flask experiment.“
Dr Roger Watson, The Daily Sceptic
I’m unsure what Watson means by “properly understood” germ theory. My investigations into germ theory, which are dealt with in Virus Mania and videos such as “Koch’s Postulates: Germ School Dropout,” have informed me that the theory is fatally flawed. I have looked into Koch’s original work and he did not fulfil his own postulates correctly. His often uncontrolled experiments failed to take into account the traumatic effects of his procedures on animals or consider other factors that were making them ill. With regards to “infection” spreading between people, it seems that clinical experiments have struggled to demonstrated this phenomenon. Perhaps the most spectacular failure has been the inability to ever demonstrate transmission of influenza, as I outlined in this video here and ViroLIEgy’s Mike Stone detailed here. If Watson wants to send me a paper that proves the concept of microbes transmitting between humans to make them ill, then I would be happy to critique it. Pasteur’s work has been exposed as largely fraudulent, but it is unclear why Watson is bringing in his spontaneous generation and swan neck flask experiments and how that relates to anything I’ve published. Perhaps he thought terrain theory was claiming that microbes appear on the basis of spontaneous generation?
“Dr. Bailey has batted the theory of disease back into the 19th Century. Edward Jenner was another scoundrel according to Bailey and, while his experiments would not have passed muster with an NHS ethics committee, you can see where Bailey is going and leading her disciples into the realm of the ‘anti-vaxxers’, a topic which I will not explore here.“ Dr Roger Watson, The Daily Sceptic
Watson may be shocked to know that I’m not the only one who has questioned the alleged contributions Jenner has made to human health through the practice of vaccination. I would also suggest he reads the book Dissolving Illusions, or at least examine the charts that Dr Suzanne Humphries and Roman Bystrianyk have put together, if he believes that the smallpox vaccine or any other vaccine has been shown to be of benefit to the public.
The realm of “anti-vaxxers” and their bloody inconvenient, irrefutable data!
I am up front about my position on vaccines as it is clearly stated on my website FAQs that, “I am not ‘anti-vaccination’ in the sense that I don’t wish to tell other people what to do with their bodies. I’m always happy to consider new evidence, but for me personally, I don’t believe any current vaccine can provide health benefits for myself or my loved ones.” It is unclear to me why Watson thinks I am “leading disciples” into any realm. If he thinks he has sound evidence that vaccines lead to better health outcomes then he is welcome to provide it – our Virus Mania team has sought such data from major institutions such as the Robert Koch Institute for many years and they have been unable to provide it.
“She mentions, in passing, the famous TMV (tobacco mosaic virus) in a ‘that’s all very well’ kind of way. But the fact is that the TMV has been sufficiently purified for its structure to be studied by scanning electron microscopy; and that represents a very high level of both isolation and purity. A plant virus it may be, with no animal equivalent, but it is the case that disproves, in a Popperian way, the argument often repeated by the virus deniers that ‘no virus has ever been purified’. Some have been sufficiently purified for study by X-ray crystallography and that represents an extremely high level of purification.“
Dr Roger Watson, The Daily Sceptic
It’s not at all convincing in his article that Watson knows the difference between isolation and purification. He refers to a microscopy study which purports to show TMV. We may need to remind Watson that a virus is a tiny replication-competent, intracellular parasite that can infect a host and pass onto other hosts. Apart from images of tiny particles, there is nowhere in the paper he cites that any of these key properties are demonstrated. I have explained in my video “Electron Microscopy and Unidentified “Viral” Objects” the limitations of the technique and why particles that appear amongst dead tissue cannot be classified as “viruses” without further experimental steps. His reference to an x-ray crystallography paper is likewise useless. Plenty of particles can be purified Dr Watson – the issue is that they need to be shown to be viruses. In any case, you’re in for a treat as I currently have a video in production exposing the Tobacco Mosaic “Virus” story going back to Ivanovsky’s unscientific experiments considered by some to be the beginning of virology.
“But the fact is that the existence of any virus is triangulated by an array of increasingly sophisticated laboratory techniques whereby theories may be tested, cultures grown, and infectivity demonstrated. In fact, a great many viruses have been purified, often against the odds.“
Dr Roger Watson, The Daily Sceptic
Triangulation? The process of measuring distances and determining locations. Watson goes next-level cunning with his conflations to make virology look respectable again! If Watson looked at all my publications he would see that I am familiar with the historical techniques, which failed to demonstrate the existence of pathogenic viruses and how they have morphed into modern molecular detection techniques to keep the virus paradigm alive. His citation is “Virus Purification” techniques in the Encyclopedia of Virology (Fourth Edition), 2021 – I have an e-copy of this publication and am familiar with the described methods. However, Watson needs to show his hand and let us know which particles he thinks have been purified and demonstrated to be “viruses” instead of pointing at a textbook.
Dr Watson: stop keeping us in suspense and please publish your list of viruses that were purified “against the odds” with their proofs.
“The virus deniers trot out the Koch’s postulates argument repeatedly, even though Koch’s postulates were simply one way – long before the advent of amino acid and nucleotide sequencing methods – of demonstrating the presence of a bacterium. Koch’s postulates were never intended to be applied to viruses – the existence of which were not known when Koch postulated.”
Dr Roger Watson, The Daily Sceptic
Watson appears completely confused about Koch’s Postulates which relate to establishing a causative relationship between a microbe and a particular disease, and conflates it with “demonstrating the presence of a bacterium”. The postulates were designed to be applied to all microbes, but as I have stated, my investigations indicate that Koch’s Postulates have never been fulfilled and there is no sound basis to germ theory: bacteria, fungi and postulated “viruses” are not the causal agents of disease. And it doesn’t matter what nucleotide sequences or proteins you discover Dr Watson, you still need to establish where they come from – are you sure the virologists establish this or even do “sequencing”? (See below).
“The original SARS, which almost certainly jumped species, is very unusual for that very reason and, for example, bird flu does not infect humans. The jury remains out on whether SARS-CoV-2, which possibly jumped species, did so spontaneously or after a ‘gain of function’ nudge.“
Dr Roger Watson, The Daily Sceptic
Interestingly for a “sceptic”, Watson espouses most of the virology industry’s stories about viruses jumping species. Can he point to the investigations he performed to conclude something that hasn’t been shown to exist “almost certainly jumped species”? We deal with these highly speculative and sometimes baseless claims in Virus Mania and I covered the original “SARS” (and “species jumping”) in another of my videos banned by Big Tech but still available here. There is a fatal flaw regarding gain of function research with “viruses” when the pathogens themselves have not been shown to exist, as I have pointed out in more videos banned by Big Tech but still available here and here. Dr Stefan Lanka has also outlined the fallacies of “bio-weapons,” including fabricated “viruses” and how they have been used to drive fear into the public for many decades.
“I have corresponded with Siouxsie Wiles, a major debunker of the Koch’s postulates argument, at Auckland University in New Zealand over this point and over the point regarding ‘purification’ of the SARS-CoV-2 virus.“
Dr Roger Watson, The Daily Sceptic
Watson makes an appeal to “authority” here, which was the same mistake made by Steve Kirsch when he clumsily waded into the issue of the existence of “SARS-CoV-2” in January 2022. My husband Dr Mark Bailey has previously outlined why Kirsch shouldn’t rely on such “experts”. Like Watson, Kirsch started off all guns blazing against the “virus deniers”. Like Watson, Kirsch rapidly retreated when the Baileys, Dr Tom Cowan, Dr Andy Kaufman, and Dr Stefan Lanka all offered to participate in a live debate with his chosen “experts”. It is odd that our “sceptic” Watson corresponds with Wiles as she is heavily promoted by the NZ government and advised our country that “the world is on fire” and we should “all behave as they [the government] are asking us to behave” in March 2020.
“If men define situations as real, they are real in their consequences.“
William Isaac Thomas and Dorothy Swaine Thomas
She is notorious for avoiding open scientific discussions and even has a lengthy automated email reply excusing herself from such pursuits. Incidentally, in February 2022, a state-sponsored media platform was found guilty of publishing one of her false claims. Watson has referred to an article by Wiles which is a case of the blind leading the naked. In the article she provides no explanation as to how disease causation is satisfied with viruses when it is conveniently claims there are no suitable clinical experiments available. She tries to distract the reader with Falkow’s molecular postulates, and fails to inform her readers that River’s postulates were designed specifically for viruses but have not even been close to being fulfilled for SARS-CoV-2 – the first problem being that no one can show it exists. There is certainly nowhere in her article that demonstrates she can prove the existence of SARS-CoV-2 or any other virus, only excuses as to why direct proofs are lacking. I have previously addressed her false claims surrounding the application of the PCR in another video banned by Big Tech after several hundred thousand views, but still available here. New Zealanders have endured two years of state-sponsored nonsense from Wiles, who is paraded by the MSM as a go to “expert”. I’m willing to bet that a live debate with Watson & Wiles on one side and the Baileys on the other would be very revealing.
“It transpires that the purification of the novel coronavirus argument is a straw dog created by the viral deniers. In fact, nobody has claimed that it has been purified. However, it has been ‘isolated’, which is a different concept whereby studies are carried out to check it is there.“
Dr Roger Watson, The Daily Sceptic
If Watson hasn’t already indicated that he is bringing his pocketknife into a gunfight, then this is where his pocketknife falls to the floor. I suspect he didn’t know that I have already analysed Vincent Racaniello’s presentation he refers to in this video (banned by Big Tech of course). It is not clear that he even listened to Racaniello’s words: if the virologists don’t have a specific defintion of “isolation” what does Watson think it means? Can he see a problem when Racaniello says “an isolate is a virus that we have isolated…” or has he been swept up in their circular reasoning? The problem of what “isolation” means is the pivotal issue with regards to proving the existence of viruses and the virologists have a habit of playing fast and loose. As stated by The Perth Group in 2017: “The fact is that in virology, while purification retains its everyday meaning, “isolation” is an expediential term virologists assign to data they claim are proof a particular virus exists.” Watson instead chooses to cheerlead the virologists denigration of the English language: if their use of the word ‘isolation’ isn’t what everyone thinks it is, then it’s useless as a method of providing proof that a particle is a virus.
Watson, however, gives the thumbs up to ‘isolate = particles + every other bit of junk in a specimen’, perhaps oblivious to the deception of the virologists.
“According to Siouxsie Wiles, the virus has been found in hundreds of disparate samples and subsequently sequenced. The viral deniers point to the way the sequence was merely pieced together in the early stages, thus proposing a hoax. But this is how viruses are sequenced.“
Dr Roger Watson, The Daily Sceptic
How on earth this made it past the Daily Sceptic editors is a mystery to me. For his source of “truth” Watson has cited “fact-checking” organisations that are supported by Big Tech, and have financial conflicts of interest with Big Pharma. If it is not apparent at this stage of the “pandemic” that these organisations have been consistently misleading the public since day one then it is difficult to believe that he really is a “sceptic”. The fraudulent invention of the “SARS-CoV-2 genome” by Fan Wu’s lab has been exposed by Stefan Lanka’s team and it was even worse than the usual imaginary “viral genome” assembly circus. The ViroLIEgy website has one of the best collections on the many assumptions and biases involved in “genome” creation, from the collection of the crude specimen through to the hypothetical model constructed by computer software. And with regards to “viruses”, we do not call it a “hoax”, we call it fraud. “Viruses” are not really “sequenced” as you might think Dr Watson (see below).
“In any case, as explained to me by Siouxsie Wiles, it is not necessary to purify the coronavirus and as Dr. Ros Jones says in her Unity News Network interview with David Clews, this is not how it is done; the virus is cultured. This is about as close to Koch’s postulates as you could get: grow the purported virus in a cellular culture and identify it by sequencing. Introduce what you have to some other cultured cells alongside a control culture. If the one with the purported virus shows subsequent evidence for the presence of the virus and the other does not, that is about as watertight an experiment as I can think of.“
Dr Roger Watson, The Daily Sceptic
Watson has a great deal of faith in Wiles and her reassurances that purification is “not necessary” and again seems to be confused about what Koch’s Postulates is all about. He describes cell culture experiments and what he believes is “identification” of a virus. How does he know there would be a new virus in there? Apparently, by “sequencing” (I’m not sure he understands what they are actually doing – see next point.) And what does he mean by a “control culture”? Official Information Act requests have exposed that the virologists do not do valid control experiments and this has been a problem ever since Enders and Peebles started the “virus” culture technique in the 1950s. Lack of valid controls = unscientific. I can only suggest to Watson that he digs a little deeper and examines the methodology of the papers rather than simply browse their headlines.
“Bailey and co. try to debunk all the methods that are used in virology and to deny the whole field of laboratory science. The only possible retort can be that no method is perfect, and experiments often fail to show what is being hypothesised. That is an argument for rather than against science, which constantly tries to improve its methods. I recall a whole room being dedicated to a huge amino acid sequencer when I was a PhD student. Now, amino acid sequencing can be done on a microchip.”
Dr Roger Watson, The Daily Sceptic
This is so full of non sequiturs that perhaps the best advice to Watson is that he needs an editor to help him communicate what he is trying to say to his readers. He should be able to clearly see my pro-science position in the video “Science vs Dogma”. My publications analysing virology have clearly pointed out that much of it involves uncontrolled experiments and thus cannot be claimed to be scientific. He refers to Karl Popper earlier in his article but fails to see that Popper would be horrified by the reasoning used by many virologists. How is an in silico “viral genome” that is created de novo from an unpurified specimen, that has been templated to another “viral genome” which was invented in the same way, falsifiable? How is a PCR result that “diagnoses” a disease on the basis that a positive result means you have the disease, falsifiable? I also suspect he is confusing complete in silico assembly of hypothetical “viral genomes” with actual physical sequencing, such as via the Sanger method, which he may have seen when he was a student. Computer games are indeed very seductive, particularly for kids but sometimes for adults too.
“I have had Covid, despite the remarkable claims by my virus denying friends to the contrary. How do I know I had it: it hit me like an express train; I felt terrible for two days and slept for 29 of 48 hours, rather like the flu. My taste was not lost but my sense of smell became incredibly deranged, not something that I had experienced after many bouts of flu in my 66 years.“
Dr Roger Watson, The Daily Sceptic
Watson appears to include this story about his bout of illness as evidence that viruses must exist. Despite it being another non sequitur, what is his definition of “COVID”? Virus Mania co-author Dr Claus Köhnlein pointed out in 2020 that it was nothing more than an imaginary clinical condition based on a new PCR “test” with no demonstrated clinical diagnostic capability. His interview in German reached over 1 million viewers before it was quickly shut down and his interview in English with me on Youtube had 125,000 views when it was shut down. It is still available here. I produced another popular video in 2020, “What Is A Covid-19 Case?” which outlines why “COVID” is a meaningless construct – which was also banned by Big Tech. In Dr Watson’s view how do we define a case: does a person dying in intensive care and an elite athlete running a marathon both have “COVID-19”? According to the WHO they should both be counted as equal “confirmed” cases if a PCR result is positive.
“When I felt worst, I reluctantly took a lateral flow test (LFT). This showed up positive almost instantly and with a thick test line. As I felt better the test – which as it uses antibodies is highly specific but not very sensitive – took longer to show and the line became fainter. Of course, the virus deniers have this one covered under the rubric that immunology is also bogus, antibodies are not at all specific and will pick up anything. My ‘gotcha’ to this is: if I run a pregnancy test which uses antibodies to detect human chorionic gonadotropin, will it show me I am pregnant?“
Dr Roger Watson, The Daily Sceptic
It is unclear if Watson is claiming that his lateral flow test proves the existence of viruses or “COVID” or both. What does he think the test is for? Something unique to the postulated “CoV” particle or a specific bodily process? Oh dear, we are back at square one! I have dealt with “COVID” LFTs previously and they are as equally unsuitable as the PCR with regards to clinical diagnostics and proving virus existence. With the rest of his claims, I’m not aware of who said antibodies pick up “anything” and it certainly wasn’t me. The issue surrounds assigning meaning to various proteins that can be detected through in vitro chemical reactions compared to what this informs us about health in real life. This topic has been outlined in Virus Mania and I also cover it in some of my other videos. His “gotcha” with regards to human chorionic gonadotropin has nothing to do with postulated viruses and related “immunology”. β-hCG is a specific glycoprotein of known composition and provenance that has been clinically validated for diagnosing pregnancy and can be easily compared to a “gold standard”: a foetal ultrasound scan (or the actual baby). As per many of Watson’s attempts, it’s another own goal. I can also suggest to him that if he has a positive result on a pregnancy test, as a man he’s unlikely to be pregnant and should be checked for cancer.
“The virus deniers who tend to promote their views on increasingly bizarre websites and within such a deafening echo chamber that they are completely unable to hear, yet alone contemplate, alternative views. They certainly don’t listen.“
Dr Roger Watson, The Daily Sceptic
What are these “bizarre” websites that he is referring to and what’s wrong with bizarre anyway? The orthodoxy doesn’t like being challenged Dr Watson. If they played like real scientists they’d welcome views that challenge their comfy status quo and we could all go on the same URLs. It may disturb Watson but the appetite for the content we produce seems very healthy. Our audience size is mostly restricted by Big Tech censorship and I’m sure he doesn’t agree with such interference with free speech. However, despite my Youtube channel being heavily suppressed, with millions of views being removed and people informing me that my videos and articles can’t be shared on platforms such as Facebook, the audience still grows every week. Mike Stone recently put together a list of websites that challenge the virus paradigm – I am in regular contact with many of these doctors, scientists and journalists and none have indicated that lack of demand is a problem. Last year, Mark and Dr John Bevan-Smith published their essay “The COVID-19 Fraud & War on Humanity”. Not only do they explain that there is no pathogen termed “SARS-CoV-2” but also why everyone should be sceptical about everything the virologists have ever claimed. They were tracking the viewership across various internet platforms for a few months before they gave up. By that stage it had reached about 250,000 people – I would say that’s a few hundred times more than most virologists are reaching with their papers. Watson’s “deafening echo chamber” may turn out to be his own case of tinnitus…
Postscript
Perhaps Dr Watson’s annoyance stems from the fact that because people get sick and die, he thinks it is unsporting to question the methods of the hard-working virologists? They are the white knights, so if we go against them – it means we must be on the wrong side. I don’t have all the answers as to why people get sick but the extensive research I’ve done informs me that pathogenic “viruses” do not seem to exist and are not the cause of disease. The tree of virology has borne no fruit for humanity unless that fruit is a multi-billion dollar pharmaceutical industry that targets enemies that have not been shown to exist. In the last two years, virology and germ theory have brought the planet to its knees, manifesting in anti-humanity measures such as face masks, stripping of civil rights, and mandated “vaccines”. For some of us, germ theory refuted itself at its inception and we see it for what it is: a tragic misunderstanding of nature, now used as propaganda in a perpetual phoney war, like something out of Orwell’s Nineteen Eighty-Four. Dr Watson can call us whatever names he likes – we see the universe in a different light and it is a light we choose to walk in. Perhaps he’ll take a stroll with us some day?
“There are three steps in the revelation of any truth: in the first, it is ridiculed; in the second, it is resisted; in the third, it is considered self-evident.” Arthur Schopenhauer
This week has seen several timely reminders that the Covid narrative is not done. It may have lost its number 1 spot at the top of the “news” charts, but it’s not dead. It’s just resting.
While the big red numbers at the top of every front page are now casualties instead of “cases”, the pandemic is simmering on the backburner and can be brought back to boil at a moment’s notice.
In China they are reporting huge spikes in “cases”, numbers not seen since the halcyon days of March 2020. Millions of Chinese citizens are already back on lockdowns, many now need police permission to travel from one province to another.
Giant multinationals are halting production for the near future at least, with the BBC warning that:
The lockdowns have raised concerns that crucial supply chains may be disrupted.
Yes, more supply chain disruption. Just like the war.
Funny how that works out.
It’s not just China either, according to Bloomberg Europe is seeing a “Covid Resurgence” after a “rushed exit” from restrictions, with Germany, Switzerland and the Netherlands all reporting spikes in cases.
Germany’s “Covid resurgence” comes just days before the government’s emergency powers are due to expire, and just as they are planning to ease all restrictions.
Funny how that works out.
The alleged “resurgence” is the work of a not one but two “new” variants.
Firstly, Deltacron is back. They’re calling it a “new variant”, but the truth is the recombinant virus was first “discovered” back in early January.
Why Everyone’s Talking About The Deltacron Variant Again
Why indeed. It’s a real puzzler.
Perhaps aware that “Deltacron” sounds like a villain from Transformers, they’re also pushing another new variant: “Omicron BA.2”.
Now, while that name definitely isn’t silly, it also isn’t very catchy – so they’ve got a cool scary sounding name for it too: “Stealth Omicron”.
It’s called “stealth omicron”, because it’s lacks markers that can be picked up on by PCR tests, meaning testing positive for this strain of the virus will look just like testing positive for the other strains.
Oh, and this variant isn’t actually new either, it was first discovered back in December, to very little fanfare.
But that was then, and this is now, and now experts are “worried”, apparently.
The press are already reporting that it might be the “most infectious disease on Earth”
All this just serves as a reminder that the Covid story is still there, and they can (and probably will) bring it back whenever they want. Maybe the very moment Ukraine and Russia agree on a peace deal.
Game of Thrones famously used to alternate their season finales, in an odd-numbered season the show would end with a shocking plot twist, and in even numbered seasons it would be an epic battle.
Maybe this will be our new reality, lurching from pandemic to war to pandemic to war, and around and around.
A perpetual cycle of different grand narratives, linked only in their shared consequences: More power for them, less freedom for us.
VAERS data released Friday by the Centers for Disease Control and Prevention included a total of 1,168,894 reports of adverse events from all age groups following COVID vaccines, including 25,158 deaths and 203,888 serious injuries between Dec. 14, 2020, and March 4, 2022.
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,168,894 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and March 4, 2022, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 11,505 U.S. deaths reported as of March 4, 17% occurred within 24 hours of vaccination, 22% occurred within 48 hours of vaccination and 60% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 554 million COVID vaccine doses had been administered as of March 4, including 327 million doses of Pfizer, 209 million doses of Moderna and 18 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to March 4, 2022, for 5- to 11-year-olds show:
The most recent death involves a 7-year-old boy (VAERS I.D. 2152560) from Washington who died 13 days after receiving his first dose of Pfizer’s COVID vaccine when he went into shock and suffered cardiac arrest. He was unable to be resuscitated and died in the emergency department.
17 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department.
The most recent death involves a 14-year-old boy (VAERS I.D. 2148498) who experienced a cerebral aneurysm leading to death one day after receiving his first dose of Pfizer’s COVID vaccine.
69 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
650 reports of myocarditis and pericarditis with 631 cases attributed to Pfizer’s vaccine.
161 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to March 4, 2022, for all age groups combined, show:
19% of deaths were related to cardiac disorders.
54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
CDC study concludes COVID vaccine adverse events ‘mild’
A study funded by the CDC and published Monday in The Lancet concluded most COVID vaccine-related adverse events reported during the first six months of the rollout in the U.S were “mild and short in duration,” despite thousands of deaths reported to VAERS.
For the study, researchers analyzed data captured between Dec. 14, 2020, and June 14, 2021, by VAERS and v-safe, both of which are overseen by the CDC. Nearly 300 million doses of COVID vaccines were administered during the study period.
The authors found that of the 340,522 adverse events reported to VAERS, 27,023 (8%) were serious, 4,496 were deaths. The authors said the cause of the increased reporting of deaths during the first few days after vaccination might represent “reporting bias.”
The authors suggested that deaths occurring soon after vaccination were more likely to be reported than deaths that occurred later. This, they believe, is why the number of deaths asymptotically approaches zero as more time elapses since vaccination.
Jessica Rose, Ph.D., attempted to duplicate the Lancet authors’ findings through her independent analysis of the VAERS data. Despite filtering the database using three different date stamps, Rose was unable to duplicate the Lancet study’s results.
Florida surgeon general breaks with CDC, recommends against shots for healthy kids
Florida’s surgeon general on Monday said he will issue guidance formally recommending against COVID vaccines for healthy children. Florida is the first state to break with official guidance from the CDC, which recommends all children over age 5 get the vaccine.
Dr. Joseph Ladapo made the announcement at a roundtable, hosted by Gov. Ron DeSantis, featuring physicians and other medical experts who criticized CDC and government policies, including mask mandates and lockdowns, which they said were ineffective and harmful.
Ladapo and DeSantis said the new guidance had to do with lingering questions about the vaccines’ potential health risks for young people and the fact that children are in a low-risk category for severe COVID.
COVID vaccines may be enhancing disease
COVID vaccines may be causing enhanced disease because they target an old version of the coronavirus, Dr. Robert Malone told the Epoch Times in a recent interview.
“The data are showing that vaccination can actually increase the risk of being infected with the Omicron version of this virus,” Malone said, referring to how in some areas, including Scotland and New Zealand, patients hospitalized with COVID are more likely to have received a COVID vaccine.
U.S. drug regulators identified vaccine-associated enhanced diseases (VAED) as an “important potential risk” of COVID vaccines, along with enhanced respiratory disease.
Some adverse events reported following COVID vaccination “could indicate” VAED, according to a CDC team.
VAED refers to disease “resulting from infection in individuals primed with non-protective immune responses against the respective wild-type viruses,” researchers said last year.
“Given that these enhanced responses are triggered by failed attempts to control the infecting virus, VAED typically presents with symptoms related to the target organ of the infection pathogen,” they added.
Vaccine researcher develops tinnitus after COVID shot, calls for further study
Dr. Gregory Poland, director of the Mayo Clinic’s Vaccine Research Group in Rochester, Minnesota, developed life-altering tinnitus, or ringing in the ear, after receiving his second dose of a COVID vaccine.
“It was like someone suddenly blew a dog whistle in my ear,” Poland told MedPage Today. “It has been pretty much unrelenting.”
Poland then received a booster, after which his tinnitus briefly disappeared but then returned at a slightly higher pitch. Poland realized his life may never be the same and says he has received emails from people across the world struggling with the same condition to the point they’re considering taking their own lives.
Poland, who said he supports COVID vaccines, believes there may be tens of thousands of people affected in the U.S. and is calling for more research to be done to provide help to people desperate for relief.
Michigan woman files claim over mom’s COVID vaccine-related death
Tatum Strieter-Byron is asking the federal government to compensate her for the death in April of her mother Sandra Jacobs. An autopsy confirmed Jacobs died from a blood-clotting disorder caused by J&J’s COVID vaccine.
Strieter-Byron received confirmation Monday her claim to the Countermeasures Injury Compensation Program (CICP) had been received. The program was established to give pharmaceutical companies blanket liability protection from harm caused by their COVID vaccines.
In 2020, the U.S. Health and Human Services secretary invoked the Public Readiness and Emergency Preparedness (PREP) Act and declared COVID-19 a public health emergency, providing J&J other COVID vaccine makers immunity from lawsuits.
The only exception under the PREP Act is if a plaintiff can prove a vaccine-related death or serious physical injury was caused by “willful misconduct.” The protections, unless amended or rescinded, extend through Oct. 1, 2024.
Claims to the CICP must be made within one year of the date the vaccine was received.
Jacobs, 60, received the single-shot vaccine at a CVS pharmacy on April 8, 2021, just five days before federal health agencies temporarily paused the vaccine to examine numerous reports of a serious and potentially fatal blood-clotting disorder.
Jacobs died on April 21 of “complications of cerebral venous sinus thrombosis,” a type of stroke caused by the vaccine.
Dr. José Luis Sevillano is conducting research based on the observation and evolution of different possible unidentified life forms in the most detailed way possible.
In a recent program, he identified some structures that look like long leaves and others that are more vermiform and frightening.
Orwell City brings Dr. Sevillano’s observations and theories to English.
Transcript:
Dr. Sevillano: These are the ones I was telling you about. They’re all of this kind and look alike. And I don’t know if it’s contamination or something else. I don’t know if they’re plants or something else. That’s why I was saying that if there’s someone who’s an expert in these things, please tell me.
Ricardo Delgado: A botanical expert. A botanist.
Dr. Sevillano: Exactly. And there are many of them. I have observed this in the first sample that I took, and I have left it to dry. Let’s see if it dries completely. But these things have appeared so far. This doesn’t look like pollen or anything like that. So I wondered, is this contamination or what? I have my doubts about this, but there it is. Just in case, I’ll confirm it for you. Look at the shape of it. And look, this is what makes me suspect that the famous carbon deposits are releasing that sort of tube-like…
Ricardo Delgado: Filaments?
Dr. Sevillano: Filaments or I don’t know what is born from them. And that’s why I took the picture because I said I thought: “Couldn’t all this come out of the charcoals and then come to life? Or what’s that?”
There are more pictures, see? Another one again. That one looks like… These are… Anyway, I’ll confirm it when I see I look at tonight’s sample again. These are from the first sample. These things have been popping up over the last few of the last few days.
I have to confirm if this is contamination or something else that comes up after a few days in the sample.
Ricardo Delgado: My goodness.
Dr. Sevillano: It looks like a plant, right? Like it’s some kind of plant. You can see that when you leave it there on its side. And now, this is from the new sample that I have with the coverslip, on the drop. So, there’s no possibility of contamination there.
This is one of the famous microchips. This is a photo at 10X. And the previous one was at 40X. Look at this… 40X. So you can see that this previous structure isn’t crystal of any kind. Neither of sucrose. It’s not a crystal. It’s a plate of the kind we’ve already seen. A microchip or what has also been seen as a nanochip.
Ricardo Delgado: Look at that.
Dr. Sevillano: See? See the indentations that form there? That’s so you can see the self-assembly.
Ricardo Delgado: Unbelievable. All of this is seen in Pfizer’s vaccine.
Dr. Sevillano: Another one of the indentations. You can see that from a distance it looks like a crystal, maybe, but up close you realize that it’s nanotechnology. This is a strange structure that I have seen that was shaped like a pyramid with several… It’s very strange. And I took a picture of it. I don’t know exactly what that is.
Ricardo Delgado: Another one.
Dr. Sevillano: It’s another microchip. And this is something else. A ribbon that in the enlargement loops around. I took the screenshot of the two ends because then it kind of loops around, and it looks like it could make a… This isn’t a droplet, but it’s the ends extending.
Ricardo Delgado: Yes.
Dr. Sevillano: That’s where I took the starting photo because it was so big that I couldn’t capture it all in the same capture. And there is another one of the supposed plants. I’m sure it’s not contamination because I’ve made from this new sample that’s covered with a coverslip on the slide. Here is another one of these famous plants, like the ones I showed you the other days. That one. And now comes the most frightening one. This is a small one.
And then the next one and the one after that are the scariest ones I’ve ever seen. There you see it. This has appeared the day after I made the sample. I prepared it last night. And this afternoon, looking through the microscope, I spotted it. That hasn’t grown, but it was already in the drop. Here it is seen with less magnification. From far away. That’s seen at 10X. And then there’s another one. Let’s see if we can see another. That one is terrifying. That’s seen at 40X.
Ricardo Delgado: This one.
Dr. Sevillano:Yes. And now you’ll see it from far away. It’s too big too. There you can see the folds that make those… I don’t know if they’re leaves or what the heck is that. And now you’ll see it from far away. Horrible.
Ricardo Delgado: There.
Dr. Sevillano: That’s it.
Ricardo Delgado: Holy crap!
Dr. Sevillano: Those aren’t microchips, you know. That’s something else. So if people complain about things happening to them, how do they want nothing to happen? How do you want nothing to happen?
So far we’ve identified graphene, a microchip, they can go nanochips, this thing, what I showed you at the beginning, which is that sort of thing that looks like… I don’t even know what that is. We’re going to consider like that was contamination, but this thing that you just saw isn’t contamination for sure. I’m sure it’s not because I covered the sample as soon as I prepared it to avoid contamination. And that’s protected. The first thing you’ve seen looks to me like it’s no contamination. But until I see how this drop evolves now, I can’t guarantee it. I’ll be monitoring to see if the same shape appears, because those little ones that we saw at the beginning, I have the feeling that they’re also going to appear over time.
IMAGE: The guided missile destroyer USS Arleigh Burke (DDG 51) steams through the Mediterranean Sea. Arleigh Burke is currently
deployed in the Mediterranean Sea conducting missions in support of Operation Enduring Freedom (U.S. Navy photo by Journalist
2nd Class Patrick Reilly)
More than any other recent pandemic story, this one really demonstrates the complete farce which the Biden Administration is still clinging to in order to save face after two years of completely fraudulent Covid and vaccine policies.
“After a briefing involving dozens of sailors in close quarters on the ship, the Navy commander admitted to his boss that he had a sore throat.”
And it all went down hill from there.
Well, it was only a matter of time before Covid paranoia and vaccine fanaticism would begin to cripple the US military.
An ongoing legal battle over whether the military can force troops to get vaccinated against COVID-19 has left the Navy with a warship they say they can’t deploy because it is commanded by an officer they cannot fire.
It’s a standoff the brass are calling a “manifest national security concern,” according to recent federal court filings.
The issues stem from a lawsuit filed in the U.S. District Court for the Middle District of Florida late last year alleging service members’ rights are being infringed upon by the COVID vaccine mandate because their religious beliefs prevent them from taking the vaccine.
Judge Steven D. Merryday issue an order last month banning the Navy and Marine Corps from taking any disciplinary action against the unnamed Navy warship commander and a Marine Corps lieutenant colonel for refusing the vaccine.
In the process, the case has raised questions about the lines between military good order and discipline, and the legal rights of service members as American citizens.
Merryday’s injunction is “an extraordinary intrusion upon the inner workings of the military” and has essentially left the Navy short a warship, according to a Feb. 28 filing by the government.
“With respect to Navy Commander, the Navy has lost confidence in his ability to lead and will not deploy the warship with him in command,” the filing states…
They confess: they had no virus when they concocted the test for the virus; they “contrived” a model by pretending to find what they wanted to find; it’s called a self-fulfilling prophecy
This is the con and the crime that drove millions of lives, and economies, into ruin
Quiz: If an agency of the federal government revealed they had no basis for constructing a diagnostic test that was used on millions of people; but the test was the cornerstone of a national lockdown; and the lockdown drove the economy off a cliff; and destroyed millions of lives; however, NOW, that agency says, they DO have a basis for the test; would you buy what they’re selling?
If your answer is yes, you’re in good company; the company I call Blind, Ignorant, Denialist, Hoaxing Journalists.
The CDC issued a document that bulges with devastating admissions.
“After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives.”
Many people believe this means the CDC is giving up on the PCR test as a means of “detecting the virus.” The CDC isn’t saying that at all.
They’re saying the PCR technology will continue to be used, but they’re replacing what the test is looking FOR with a better “reference sample.” A better marker. A better target. A better piece of RNA supposedly derived from SARS-CoV-2.
CDC/FDA are confessing there has been a PROBLEM with the PCR test which has been used to detect the virus, starting in February of 2020—right up to this minute.
In other words, the millions and millions of “COVID cases” based on the PCR test in use are all suspect. Actually, that statement is too generous. Every test result of every PCR test should be thrown out.
“During the early months of the Coronavirus Disease 2019 (COVID-19) pandemic, clinical specimens [of the virus] were not readily available to developers of IVDs [in vitro diagnostics] to detect SARS-CoV-2. Therefore, the FDA authorized IVDs based on available data from contrived samples generated from a range of SARS-CoV-2 material sources (for example, gene specific RNA, synthetic RNA, or whole genome viral RNA) for analytical and clinical performance evaluation. While validation using these contrived specimens provided a measure of confidence in test performance at the beginning of the pandemic, it is not feasible to precisely compare the performance of various tests that used contrived specimens because each test validated performance using samples derived from different gene specific, synthetic, or genomic nucleic acid sources.”
Translation: We, at the CDC, did not have a specimen of the SARS-CoV-2 virus when we concocted the PCR test for SARS-CoV-2. Yes, it’s unbelievable, right? And that’s the test we’ve been using all along. So we CONTRIVED samples of the virus. We fabricated. We lied. We made up (invented) synthetic gene sequences and we SAID these sequences HAD TO BE close to the sequence of SARS-CoV-2, without having the faintest idea of what we were doing, because, again, we didn’t have an actual specimen of the virus. We had no proof THERE WAS something called SARS-CoV-2.
This amazing FDA document goes to say the Agency has granted emergency approval to 59 different PCR tests since the beginning of the (fake) pandemic. 59. And, “…it is not feasible to precisely compare the performance of various tests that used contrived specimens because each test validated performance using samples derived from different gene specific, synthetic, or genomic nucleic acid sources.”
Translation: Each of the 59 different PCR tests for SARS-CoV-2 told different lies and concocted different fabrications about the genetic makeup of the virus—the virus we didn’t have. Obviously, then, these tests would give unreliable results. THE PCR TESTS USED CONTRIVED SPECIMENS OF THE VIRUS WE DIDN’T HAVE.
BUT, don’t worry, be happy, because NOW, the CDC and the FDA say, they really do have actual virus samples of SARS-CoV-2 from patients; they have better targets for the PCR test, and labs should start gearing up for the new and improved tests.
In other words, they were lying THEN, but they’re not lying NOW. They were “contriving,” but now they’re telling the truth.
If you believe that, I have Fountain of Youth water for sale, extracted from the lead-contaminated system of Flint, Michigan.
Here, once again, I report virology’s version of “we isolated the virus”:
They have a soup they make in their labs.
This soup contains human and monkey cells, toxic chemicals and drugs, and all sorts of other random genetic material. Because the cells start to die, the researchers ASSUME a bit of mucus from a patient they dropped in the soup is doing the killing, and THE VIRUS must be the killer agent in the mucus.
This assumption is entirely unwarranted. The drugs and chemicals could be doing the cell-killing, and the researchers are also starving the cells of vital nutrients, and that starvation could kill the cells.
There is no proof that SARS-CoV-2 is in the soup, or that it is doing the cell-killing, or that it exists.
Yet the researchers call cell-death “isolation of the virus.”
To say this is a non-sequitur is a vast understatement. In their universe, “We assume, without proof, we have the virus buried in a soup in a dish in the lab” equals, “We’ve separated the virus from all surrounding material.”
Virology equals “how to spread bullshit for a living and scare the world.” Other than that, it’s perfect.
The U.S. Environmental Protection Agency approved the world’s largest release of genetically engineered mosquitoes, despite warnings by public health experts.
In defiance of science and public health concerns, Monday the Environmental Protection Agency (EPA) approved the mass release of billions of experimental genetically engineered (GE) mosquitoes into the U.S.’ most populous and agriculturally significant states.
The British biotechnology company Oxitec was granted an experimental use permit for the release of a genetically engineered version of the species Aedes aegypti across Fresno, Tulare, San Bernadino and Stanislaus Counties in California and in Monroe County in Florida.
This will be the biggest release of GE insects in the world.
EPA’s approval came despite growing concerns raised by scientists, public health experts and environmental groups about potential impacts of the experimental releases on public health, the environment and endangered species.
No publicly available data supports Oxitec’s claims that GE mosquitoes will reduce incidence of mosquito-borne diseases.
An independent peer-reviewed study from Yale University scientists revealed that over two years of continual releases of the GE mosquitoes at a test site in Brazil failed to reduce populations of Aedes aegypti.
The Yale study also found that the GE mosquitoes bred with local Aedes aegypti, resulting in hybrid mosquitoes in the wild that may be more aggressive, more difficult to eradicate and may increase the spread of mosquito-borne disease.
“Scientists have found genetic material from GE mosquitoes in wild populations at significant levels, which means GE mosquitoes are not sterile. GE mosquitoes could result in far more health and environmental problems than they would solve,” said Dana Perls, food and technology program manager at Friends of the Earth, and a California resident.
“EPA needs to do a real review of potential risks and stop ignoring widespread opposition in the communities where releases will happen.”
The experimental release will purportedly investigate whether the GE mosquito can reduce the population of Aedes aegypti mosquitoes — one species that can carry yellow fever, dengue, chikungunya and Zika.
However, California does not have any cases of these diseases, as reported by the Centers for Disease Control and Prevention. In addition, the Aedes aegypti mosquito is not prevalent in California.
“This experiment is unnecessary and even dangerous, as there are no locally acquired cases of dengue, yellow fever, chikungunya or Zika in California,” said Jaydee Hanson, policy director for the International Center for Technology Assessment and Center for Food Safety.
”Releasing billions of GE mosquitoes makes it likely that female GE mosquitoes will get out and create hybrid mosquitoes that are more virulent and aggressive. Other public health strategies, including the use of Wolbachia infected mosquitoes, could better control the Aedes aegypti in California and Florida.”
The EPA did not publicly release any data from Oxitec field trials in Florida or Brazil and key information about health effects, including allergenicity and toxicity, was redacted from the company’s application for a permit.
EPA did not require key scientific assessments, including an endangered species assessment, public health impact analysis or caged trials ahead of any environmental release. The EPA declined to convene a Scientific Advisory Panel as it does for other new pesticides.
“Once released into the environment, genetically engineered mosquitoes cannot be recalled,” said Dr. Robert Gould, president of San Francisco Bay Physicians for Social Responsibility and California resident. “Rather than forge ahead with an unregulated open-air genetic experiment, we need precautionary action, transparent data and appropriate risk assessments.”
Despite strong public opposition, in April 2021, Oxitec and the Florida Keys Mosquito Control Board began the release of half a billion genetically engineered mosquitoes into Monroe County, Florida.
Neither the mosquito control board nor Oxitec informed community residents about the locations of release until three days beforehand, and there was no informed consent by affected community members prior to release.
Following the EPA’s approval, California’s Department of Pesticide Regulation and local mosquito abatement districts will also decide whether to approve the permit for release.
If approved, billions of GE mosquitoes will be released over a 2-year period in 4 counties in California, beginning in 2022, and the current GE mosquito release in Monroe County, Florida, will be extended for another 2 years.
Center for Food Safety‘s mission is to empower people, support farmers and protect the earth from the harmful impacts of industrial agriculture.
As the news cycle continues to focus on the Ukraine situation, the FDA complied with a court order to begin releasing 55,000 pages of Pfizer data per month that was used to authorize their COVID-19 vaccine produced with BioNTech, with the first batch quietly released yesterday, March 1st.
There are 150 documents that the public can now download here.
One of the documents released was the “Prescription Drug User Fee Payment” that BioNTech paid to the FDA on 4/20/2021 for the “COMIRNATY COVID-19 mRNA Vaccine” which the FDA subsequently approved in August of 2021.
That “Prescription Drug User Fee Payment” was $2,875,842.00. (Source.)
Another interesting document I found was the “EXTERNAL DATA MONITORING COMMITTEE” found here.
Here is the stated purpose of this “External Data Monitoring Committee”:
This External Data Monitoring Committee (E-DMC) (hereafter referred to as “the committee”) is a single, external, independent, expert advisory group established to oversee safety and efficacy data from the BNT162 Vaccine Program. The primary rationale for establishing the committee is to make certain that appropriate external safeguards are in place to help ensure the safety of subjects and to maintain scientific rigor and study integrity while the trial is on-going.
The committee will review accumulating safety data across all studies, as well as efficacy data in the Phase 2/3 portion of the C4591001 study. The committee will advise Pfizer regarding the safety of current participants and those yet to be recruited, as well as the continuing scientific validity of the trial. In addition to safety review by the committee, qualified Pfizer personnel will review safety data as specified in the safety surveillance review plan and will inform the committee of significant findings. Efficacy data from the C4591001 study will be available to the committee when there is a planned interim analysis of efficacy or if this is considered necessary to conduct a risk-benefit assessment.
And to make sure that this Committee is doing their job properly to ensure “the safety of subjects and to maintain scientific rigor,” who at the FDA is responsible to make sure this happens?
Well, that would be no one. Pfizer is the one who was responsible, and BioNTech funded it.
“Pfizer is responsible for conducting this study. BioNTech is the regulatory sponsor of this study.”
The committee members are to be free from “conflicts of interest.”
The committee members will complete a CT22-GSOP-RF01 Independent Oversight Committee Member Conflict of Interest Form. Committee members should be free of apparent significant conflicts of interest. Any potential conflict of interest that develops during a member’s tenure on the committee must be disclosed by the committee member.
And who at the FDA is responsible for assuring that this committee who is overseeing “safety and efficacy data” is free from conflicts of interest?
Well, that would be no one. Again, Pfizer is responsible for that.
“Pfizer will determine if any potential conflict requires termination of committee membership.”
The question that then begs to be answered here is, what role did the FDA play, if any, in the “external” monitoring of the data to ensure integrity and safety of a new vaccine about to be injected into hundreds of millions people in the U.S.?
It would appear that all they did was rubber stamp the process that was completely managed by Pfizer, and funded by BioNTech.
Here are the members of the “External Data Monitoring Committee” that apparently were chosen by Pfizer, monitored by Pfizer, and investigated by Pfizer to make sure they were doing their job and that there were no “conflicts of interest.”
The other interesting thing this document reveals is that a significant number of people compiling the data for this committee to review were located in China.
Rong Zhang: Senior Statistical Programming Lead
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Rong.Zhang@pfizer.com
Chen Xu*: Senior Statistical Programmer
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Chen.Xu4@pfizer.com
Huan Liu* Senior Statistical Programmer
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Huan.Liu@pfizer.com
Jiyang Chen*: Senior Statistical Programmer
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Jiyang.Chen@pfizer.com
Bochen Zhu*: Senior Statistical Programmer
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Bochen.Zhu@pfizer.com
Ran Xiong*: Senior Statistical Programmer
4/F, Building 3, Lotus Business Park, Lane
60, Naxian Road,
Pudong ZhangJiang Hi-tech. Park, Shanghai,
China, 201203
Ran.Xiong@pfizer.com
I wonder if the raw data is also located in China?
There is a lot more data I am still reviewing, and tens of thousands of more pages of data still to be released by the FDA.
But with everyone watching what is happening in the Ukraine right now, I wonder if anyone is even noticing this?
U.S. health officials continue to say blood-clotting disorders like the one that killed 52-year-old Monica Melkonianare two weeks after the J&J vaccine are rare — despite thousands of vaccine-induced blood-clotting events reported to the Centers for Disease Control and Prevention.
The husband of an Oregon woman who died last year from a blood-clotting disorder — two weeks after receiving Johnson & Johnson’s (J&J) COVID vaccine — spoke out publicly this week about his wife’s death.
Stan Thomas told NBC News he’s fighting to ensure his wife’s sacrifice is not forgotten.
“When it’s 8 million doses and two people are going to die from it,” Thomas said, “who thinks it’s going to be you?”
NBC News characterized the risk of harm in general from COVID vaccines as “a 1-in-a-million risk.”
And U.S. health officials continue to say blood-clotting disorders like the one that killed Thomas’ wife are rare — despite thousands of vaccine-induced blood-clotting events reported to the Centers for Disease Control and Prevention (CDC).
Monica Melkonian, 52, received her J&J shot at a vaccination clinic on April 7, 2021 — the same day the CDC and U.S. Food and Drug Administration (FDA) temporarily paused the vaccine while they investigated numerous reports of a rare blood-clotting disorder called vaccine-induced thrombotic thrombocytopenia (VITT).
VITT is a sometimes fatal condition characterized by simultaneous acute thrombosis and thrombocytopenia that presents after receiving a COVID vaccine.
Melkonian’s most notable symptoms included a persistent headache and pain behind her left eye. But Thomas said she and her husband continued to work around their home and carry out their daily activities.
Her headache was mostly gone by April 17, but at 4 a.m the next day, Thomas heard his wife call out as she hit the floor. She experienced a seizure and could not move her right arm. Thomas, who immediately suspected a stroke caused by the shot, called 9-1-1.
“The progression of this was just lightning-fast,” Thomas said, “which I am tragically grateful for.”
At the emergency room, Thomas asked his wife to squeeze his hand once for “yes” and twice for “no” in an effort to communicate with her.
“The last thing that I said to her was that I loved her and asked her to squeeze my hand twice,” Thomas said. “She did.”
“This blood clot was seen in combination with very low platelets,” the Oregon Health Authority wrote in a statement. “Prior to the issuance of the pause, cases of this serious blood clot had been identified among six women around the country who received the vaccine.”
Both Melkonian and her husband were “experts in the field of occupational health and safety” and were directly involved in the COVID pandemic response, Thomas said.
Both were aware of risks associated with COVID vaccines, but they believed the risks paled in comparison to the risks associated with the virus.
Thomas said he is steadfastly “pro-vax,” but questions whether health authorities have done enough to help people understand their options.
U.S. acknowledges only nine deaths from blood clots following J&J shot
During the CDC vaccine advisory panel’s most recent benefit and risk assessment meeting, on Dec. 16, 2021, the agency acknowledged only 54 cases of blood-clotting conditions among J&J recipients, including nine deaths.
Thirty-nine of the 54 reported cases occurred before the CDC and FDA paused the vaccine in April to investigate its link to blood clots.
The CDC’s COVID-19 Vaccine Task Force said it excluded “reports where [the] only thrombosis is ischemic stroke or myocardial infarction” — a move that significantly reduced the number of blood-clotting cases included in the task force’s analysis.
According to the CDC website, most strokes (87%) are ischemic strokes. An ischemic stroke occurs when blood flow through the artery that supplies oxygen-rich blood to the brain becomes blocked — a condition often caused by blood clots.
Myocardial infarction is a heart attack that occurs when the heart muscle doesn’t get enough blood due to a blockage — such as a blood clot — in the arteries that supply blood to the heart.
Because rates were still higher than previously estimated among both men and women, the panel voted 15 – 0 to “preferentially recommend” mRNA COVID vaccines Pfizer and Moderna over the J&J shot for adults 18 years and older.
However, both the Pfizer and Moderna vaccines also are associated with blood-clotting disorders.
According to data compiled by “Our World In Data,” between Dec. 14, 2021, and Feb. 18, 2022, 18.36 million doses of the J&J vaccine had been given.
Data from VAERS show there were 2,275 reports of blood-clotting disorders following J&J’s COVID vaccine between Dec. 14, 2020, and Dec. 10, 2021 — a far greater number than the 54 cases acknowledged by the CDC during its December advisory meeting.
The Defender has reported on numerous cases of blood clots following COVID vaccination with the J&J shot:
Jessica Berg Wilson, a 37-year-old mother died from VITT after she received J&J’s COVID vaccine as a condition of volunteering at her child’s school.
Emma Burkey, an 18-year-old teen was put on a respirator and underwent three brain surgeries from blood clots after receiving J&J’s vaccine.
Anne VanGeest, a healthy 35-year-old, died of a brain hemorrhage 11 days after receiving J&J’s COVID vaccine.
Brad Malagarie, a healthy 43-year-old father of seven experienced a stroke from blood clots hours after receiving J&J’s COVID vaccine. The stroke left him unable to walk, talk and with paralysis on the right side of his body.
A 30-year-old man from California on April 8, 2021, was hospitalized and treated for a blood clotting disorder he developed after receiving J&J’s vaccine.
Barbara Buchanan developed blood clots in her lungs, stomach, brain and throat 6 to 8 days after receiving J&J’s COVID vaccine. She chose J&J because it was a one-dose shot, and because experts declared the vaccine was safe after they lifted a 10-day pause.
Kendra Lippy, a healthy 38-year old woman, was diagnosed with severe blood clots that subsequently sent most of her organs into failure after receiving J&J’s COVID vaccine. She also was left without most of her small intestine — and with crippling medical bills.
Sandra Jacobs, a 60-year-old woman died from blood clots after receiving the J&J shot, according to an autopsy report released Sept. 20, 2021, by a forensic pathologist for Michigan Medicine.
On April 13, 2021, federal agencies paused J&J’s COVID vaccine, marketed under its Janssen subsidiary, while they investigated the vaccine’s possible link to dangerous and potentially fatal blood clots.
During the April 23, 2021 meeting, the CDC’s vaccine advisory panel said it had identified 15 women diagnosed with rare blood clots, including three who died.
Only two of the women were older than 50, with the risk highest in women ages 30 to 39.
The CDC’s advisory panel said the link between blood clots and J&J’s COVID vaccine was “plausible,” but concluded the vaccine’s “benefits outweighed the risks” and recommended the vaccine for persons 18 and older in the U.S. under the FDA’s Emergency Use Authorization.
On April 26, 2021, the FDA amended its EUA for the J&J vaccine to reflect the risk of rare blood clots and said vaccinations could resume immediately.
Countries all over the world are totally scrubbing their Covid measures, mask mandates and social distancing rules.
The CDC has changed their guidance on vaccine doses, and said people don’t need to wear masks anymore. Boris has done the same, and (some) of the UK’s emergency powers are going to expire soon.
It seems like Covid is over, and the good guys won, right?
Well, not exactly.
The pandemic narrative may be fading away, but certainly not without a trace. Covid might be dying, but vaccine passports are still very much alive.
This week, while the eyes of the world are fixed on Ukraine and the next wave of propaganda, the World Health Organization is launching an initiative to create a “trust network” on vaccination and international travel.
According to a report in Politico published last week:
WHO making moves on international vaccine ‘passport’”
The article quotes Brian Anderson, co-founder of the Vaccination Credential Initiative, which describes itself as:
a voluntary coalition of public and private organizations committed to empowering individuals with access to verifiable clinical information including a trustworthy and verifiable copy of their vaccination records in digital or paper form using open, interoperable standards.
They are, to take the PR agency sheen off this phrase, a corporate/government joint project researching and promoting digital medical identification papers.
In short, vaccine passports.
The VCI has existed since January 2021, and its list of “members” is very revealing, including Google, Amazon, dozens of insurance companies, hospitals, “bio-security firms” and seemingly every major university in the US.
It’s run by a steering committee made up of representatives from Apple, Microsoft, the MAYO Clinic and the MITRE Corporation, a multi-billion-dollar government-funded research organization.
Anderson – who was an employee of MITRE before founding the VCI – tells Politico that the current system of international travel and vaccine records is:
piecemeal, not coordinated and done nation to nation…It can be a real challenge.”
Discussion of an international “Pandemic Treaty” gets underway today in Geneva, and any eventual agreement will doubtless include provisions on the matter of international vaccine certification.
If the VCI is involved – and with their backers, they doubtless will be – any international system will likely be based on their SMART Health Cards system.
Smart Cards in the US – a Covert Federal Vaccine Passport
VCI’s SMART Health Cards are the dominant tech in the emerging field of biosurveillance and “inoculation certification”. They are already implemented by 25 different US states, plus Puerto Rico and DC, and have become the US’s de-facto national passport
According to this article from Forbes (a puff piece which is little more than an advertisement):
While the United States government has not issued a federal digital vaccine pass, a national standard has nevertheless emerged.
They use the word “emerged” as if it’s a natural, organic process. But it’s not.
The US government, unlike many European countries, has not issued their own official vaccine passport, knowing such a move would rankle with the more Libertarian-leaning US public, not to mention get tangled in the question of state vs federal law.
The SMART cards allow them to sidestep this issue. They are technically only implemented by each state individually via agreements with VCI, which is technically a private entity.
However, since the SMART cards are indirectly funded by the US government, their implementation across every state makes them a national standard in all but name.
The Politico article repeats the claim the US has no national system, adding that the US doesn’t have a federal vaccine database either:
The Biden administration has said it wouldn’t issue digital credentials and hasn’t rolled out standards for vaccine credentials it said it would issue. Complicating the situation is that the U.S. doesn’t have a national inoculation database.
The propaganda message here is underlining what the government doesn’t have and doesn’t know. The suggestion being that the SMART system is totally separate from the government, that it’s a private company that would never share your medical records with the state.
But only the terminally naive would believe that.
SMART Health Cards are run by VCI, which was created by the MITRE Corporation, which is funded by the United States government.
If you give SMART access to your medical records, you’d better believe the US government and its agencies will get their hands on them. They might not have their own database, but they would have access to MITRE’s database when and if they needed or wanted it.
And so would Apple, Amazon, Google and Microsoft.
That’s how private-public partnerships work. Symbiosis.
Corporate giants serve as fronts for government programs and, in return, they get a big cut of the profits, bailouts if they’re needed, and regulatory “reforms” that cripple their smaller competitors.
We’ve seen this social media already.
Quasi-monopolies like Facebook and Twitter harvest data for the government and censor anyone they are told to, then they are rewarded with “regulation” that barely hurts them whilst targeting smaller companies such as Gab, Parler or Telegram.
The Smart Health Cards clearly fall into this model.
Microsoft, Google et al. take government money to help create the tech, they then run the program, harvest and store the data, and make it available to the government when they want it.
This allows the federal government “truthfully” claim to not be implementing a federal passport system, OR keeping a vaccination database, all the while they are sub-contracting tech giants to do it for them.
This system of backdoor government surveillance via corporate veneer is already spreading across the US, and it looks like it will play some part in any future “pandemic treaty” too.
They may have stopped talking about Covid for now, but they got a good chunk of what they wanted out of it.
And if they don’t get the rest of what they want out of the war in Ukraine, they’ll just bring Covid back.
Think what you will about Pastor Artur, love him or hate him, he is gong to continue feeding the homeless and preaching his convictions regardless. When Pastor Artur’s eldest son was very young, he nearly passed away, doctors had essentially given up hope. Artur in those challenging times turned to God and said if you save my son, I will commit myself wholly to you. His son, defying all odds, survived, and Artur true to his word has been feeding and caring for the homeless and living out his vocation as a Pastor without compromise ever since.
His steadfast adherence to his sworn mission has garnered the ire of politicians and authorities who have had Pastor Artur sitting behind bars for several weeks awaiting trial, with bail being denied as he is supposedly to great a liability to be let out.
In the last two years, Artur has been arrested five times and incarcerated three times. All of this as a result of feeding the poor, preaching and opening his church in contravention of mandates and restrictions that are presently being dropped? Pastor Artur’s actions would be considered laudable at any other time, but with COVID-19 restrictions in place, they suddenly merit jailing?
People seem to forget that the homeless people who rely on Pastor Artur’s help don’t stop being cold or hungry just because a COVID-19 restriction is dictates by some myopic health bureaucrat. While others are being let off with warnings and tickets, or in the case of politicians in the sky-palace no consequences at all, Pastor Artur has been made into public enemy number one.
I was fortunate to be able to arrange an exclusive interview with Pastor Artur over the phone from within the Calgary Remand Centre where he is being held. He talked about life behind bars, the challenges he is facing at the hands of jail guards, his interactions with inmates in his brief times outside of solitary confinement and about how deeply he misses his family.
Please consider making a tax receipt eligible donation to Pastor Artur’s legal defence by visiting SaveArtur.com today. Your donation will help pay for the incredible legal team at JSS Barristers, including Sarah Miller, who are working tirelessly to secure Artur’s release.
Chile now has a law for mutants and genetically altered individuals. It’s a rather peculiar law, in addition to the neuro-rights law, which also exists in that country.
What could be the reason for the enactment of this new law?
Obviously, the reason for the origin of this law —which will probably soon be replicated in other countries— is because there’s already a considerable number of people in the population who are no longer human, but transgenic beings.
Orwell City brings into English a summary of this rare yet real law that Chile now has to prevent people from being discriminated in their jobs because they are mutants or have their genome altered in some way.
Narrator:
After becoming the first country to add neuro-rights to its Constitution, Chile now also becomes the first country in the world not to discriminate against mutants and genetically altered individuals after publishing Law 21.422 on February 16, 2022.
Specifically, this law forbids “employment discrimination in the face of mutations or alterations of genetic material.”
The question everyone is asking now is, what’s the reason for this law?
Since Chile is one of the most inoculated countries in the world, it’s not surprising that such a law has been enacted. As dissident doctors warned from the beginning, these inoculums contain secret materials and components that alter the human genome. Of course, this genetic modification is inheritable.
And well, What does the new Chilean law establish?
1. No employer may condition the hiring of workers, their permanence or renewal of their contract, or promotion or mobility in their employment, to the absence of mutations or alterations in their genome.
2. The worker may give his free and informed consent to undergo a genetic test.
3. If these examinations are required by the employer, the employer shall bear the cost thereof.
4. The health establishments and laboratories that carry out this type of test, as well as the employers who have access to this information, shall adopt all security measures to protect the privacy of the worker and guarantee reserved handling of the data.
5. The worker will always have the right to access the information resulting from a genetic test.
With all these laws that are appearing, do you still believe that these inoculums are vaccines?
The paper by Aldén, et al, titled “Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line,” published on 25 February 2022, reveals what some of us have been warning about since the experimental mRNA injections were released onto largely unsuspecting populations. That is, the mechanisms do indeed exist for the genetic injections to change and/or damage the recipient’s genome.
In New Zealand, Medsafe approved the Pfizer injections for wholesale use in the country despite minimal safety data being available. In 2021 they engaged their “experts,” Professor Peter McIntyre from the University of Otago and Dr Ian Town, Chief Science Advisor for the Ministry of Health to address any “concern that permanent alteration of DNA may occur.” Bizarrely, they went way out on a limb in a few sentences in the following letter to NZDSOS:
“Messenger RNA is unstable, which is why it must be stored at very low temperatures prior to use. As mRNA does not enter the nucleus and is rapidly broken down by the cell after protein transcription has occurred, it is unable to alter DNA (Ref 10) . This is shown in the graphic below (Ref 11).”
~ Report for Medsafe: Professor P McIntyre & Dr Ian Town, 14 June 2021
Nature is not directed by colourful man-made cartoons.
NZDSOS were concerned that this was an over-simplification of the state of the science and thus presented a paper to Medsafe the following week, specifically addressing the potential problems:
“The science on this is still unfolding and we are concerned that the authors claim a definitive statement on this topic. The first reference the authors provide is the Centers for Disease Control and Prevention website which is aimed at providing the public with a simple overview of the mRNA injection. The second reference (and diagram) only shows the ‘proposed sequence of events leading to the generation of adaptive immune responses upon mRNA vaccination’. From this the authors appear to conclude that it would be impossible for the injected mRNA to become integrated into our DNA because mRNA does not work that way.”
~ NZDSOS to Medsafe, 21 June 2021
The mechanism for the conversion of RNA to DNA is possible through reverse transcriptase enzymes. Although some virologists have suggested that reverse transcriptase is specific to “retroviruses” it has long been known that the enzymes can be found in normal mammalian cells. This has been well documented by The Perth Group and has gained more mainstream attention in recent years including in this SciTechDaily article in 2021:
“Thomas Jefferson University researchers provide the first evidence that RNA segments can be written back into DNA, which potentially challenges the central dogma in biology and could have wide implications affecting many fields of biology. ‘This work opens the door to many other studies that will help us understand the significance of having a mechanism for converting RNA messages into DNA in our own cells,’ says Richard Pomerantz, PhD, associate professor of biochemistry and molecular biology at Thomas Jefferson University.”
~ New Discovery Shows Human Cells Can Write RNA Sequences Into DNA – Challenges Central Principle in Biology. THOMAS JEFFERSON UNIVERSITY JUNE 12, 2021
I’m not sure why they think the central dogma of biology is only now being “potentially challenged” as it was never proven to be relevant from the day that Francis Crick first suggested it in 1958, but at least they are opening their eyes.
In any case, what did Aldén et al’s recent paper demonstrate? I’ll outline some of the highlights:
“Our results indicate a fast up-take of BNT162b2 into human liver cell line Huh7, leading to changes in LINE-1 expression and distribution. We also show that BNT162b2 mRNA is reverse transcribed intracellularly into DNA in as fast as 6 h upon BNT162b2 exposure.“
“BNT162b2 DNA amplicons were detected in all three time points (6, 24, and 48 h). Sanger sequencing confirmed that the DNA amplicons were identical to the BNT162b2 sequence flanked by the primers.”
“In the BNT162b2 toxicity report, no genotoxicity nor carcinogenicity studies have been provided [26]. Our study shows that BNT162b2 can be reverse transcribed to DNA in liver cell line Huh7, and this may give rise to the concern if BNT162b2-derived DNA may be integrated into the host genome and affect the integrity of genomic DNA, which may potentially mediate genotoxic side effects.”
~ Alden, M. et al. (2022.) Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr. Issues Mol. Biol. 2022, 44(3), 1115-1126.
NZ Ministry of Health’s Infomercial for Pfizer: so many things wrong here, where should we start?
Now, to be clear this does not mean that those who have been injected with the Pfizer BioNTech product have had their DNA modified – but it raises very significant concerns. The study was carried out in vitro (in a test tube) with Huh-7 cells which are of human origin but derived from an abnormal (liver cancer) cell line.
Therefore, the next logical step would be to assess whether those that have been injected with the product have evidence that the sequence has been integrated into their DNA.
The authors didn’t proceed to test this themselves although suggested that genomic sequencing and integrity should be checked in “human subjects who received BNT162b2 vaccination.” Who will (be allowed to) take up the challenge?
This paper comes hot on the heels of another major revelation related to these mRNA injections. Dr Mikolaj Raszek has recently highlighted a potential problem that is apparent in the Australian Therapeutic Goods Administration’s (TGA) own “Nonclinical Evaluation Report” on Pfizer’s Comirnaty (BNT162b2). Dr Raszek has previously discussed how the spike protein can circulate in the blood of the injected for months, which considering the recent Aldén et al paper, may be explained by the integration of the genetic sequence into the host’s DNA. In effect, the jabbed may produce the spike protein indefinitely or at least have the potential to do so. His latest revelation from the TGA’s report adds more weight to his theory that the spike proteins themselves are entering the nucleus of the cell and once it is inside it “could be a mutagen because it prevents the fixing of our DNA.”
All in all it makes the Australian TGA look like a complicit partner in this COVID-19 Fraud & War on Humanity as they gamble on their citizens lives under the influence of Pfizer:
“Neither the mRNA nor the lipid excipients of the LNP formulation are expected to have genotoxic potential. However, the potential of the LNP or the vaccine formulation for complement activation or stimulation of cytokine release was not adequately assessed in nonclinical studies. Further investigation (i.e., analysis of complement activation and cytokine stimulation) is recommended unless this particular concern is addressed by clinical data. The absence of a repeat dose toxicity study in a second species and genotoxicity studies with the novel excipients was adequately justified by the Sponsor…Short term protection studies, lack of pharmacokinetic data for the S antigen-encoding mRNA (BNT162b2 V9), suboptimal dosing interval in the repeat dose study, lack of repeat dose toxicity studies in a second species and genotoxicity studies with the novel excipients, and lack of studies investigating potential for autoimmune diseases were noted. However, these deficiencies are either adequately justified by the Sponsor or addressable by clinical data.”
~ Nonclinical Evaluation Report BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATY™). Australian Government Therapeutic Goods Administration. January 2021.
Pfizer’s Comirnaty brought their corporation around US$36 billion in revenue in 2021, and they expect to top that in 2022. Their product can’t possibly protect anyone from an undefined clinical entity and a “virus” that does not exist. What we can see is that entire countries are being swindled out of billions of dollars while their hapless citizens are at risk of becoming genetically modified organisms in addition to the barrage of other toxic effects they are enduring from these injections.
Wall Street investors are dumping their Moderna and Pfizer stock faster than the world can drop the mandates. Moderna is down 70 percent from its high, while Pfizer is off 19 percent. Former Blackrock Executive and investment adviser Edward Dowd calls for Moderna to go to zero and Pfizer to end under ten dollars per share.
How is this possible given that Pfizer now enjoys record earnings per share and a market capitalization of some $270 billion, making it the 29th largest corporation globally? With nothing but profits in sight for the Pharmaceutical giant, what could be the problem?
After all, in December, a Forbes’ headline read, “The Vaccine Maker Can Dominate The Covid Market For Years to Come, Wells Fargo Predicts.” In addition to the enormously profitable mRNA vaccines, Pfizer is rolling out potent antivirals like Paxlovid, which could earn $22 billion in 2022.
Compared to the $81 billion in 2021 revenue, the earnings from the vaccines and the antivirals could top $102 billion for 2022, which is music to shareholders’ ears. However some are hearing shrieks, and these happen to be Wall Street’s finest, the smart money that beats the rest of the herd to the exits like clockwork.
These sophisticated investors make it their business to not go with the conventional wisdom but to do their own research, which often pays spectacular dividends.
Edward Dowd is one such investor. He saw the dot com bubble ready to burst and acted accordingly. But, unfortunately, other not-so-savvy investors later saw their dot com heavy portfolios collapse as the NASDAQ Composite Index lost 40% of its value in 2000.
Dowd, a graduate of Notre Dame University and former Portfolio Manager at Blackrock, grew his fund from $2 billion to $14 billion and commanded the respect of his investment community peers.
Today, after semi-retiring to the shores of South Maui, he remains a voice of stock market wisdom that many hedge funds continue to rely upon. LinkedIn lists him as a Consultant to Founder & Partner of Symphonic Capital, LLC.
But the dot com collapse is not the only one Dowd successfully navigated. While many other portfolio managers placed their client’s money in highly rated and lucrative mortgage-backed securities, Dowd hesitated and questioned. He considered that those might be grossly over-rated, and he was correct.
It turns out that the mortgage rating system was corrupted by the high profitability of predatory financial products tied to home mortgages. According to Edward Dowd, a large portion of the blame was shouldered by the rating agencies, those trusted organizations whose job it was to judge the risk of these subprime mortgage-backed securities – agencies like Moody’s, Standard & Poor’s and Fitch.
Dowd says they turned a blind eye to the true risk because it was profitable. So, in essence, these rating agencies were captured by the institutions backing these risky subprime securities.
Joseph Stiglitz, a Nobel Prize-winning economist, put it this way, “The incentive structure of the ratings agencies also proved perverse. Agencies such as Moody’s and Standard & Poor’s are paid by the very people they are supposed to grade. As a result, they’ve had every reason to give companies high ratings, in a financial version of what college professors know as grade inflation.”
Dowd has sounded the alarm on Moderna and Pfizer as sinking ships that investors need to abandon. So what does the man who foresaw the dot com and the subprime mortgage crisis have to say about Moderna and Pfizer, and what trouble could exist in the paradise of COVID vaccine profits?
Here are Dowd’s words:
I want to liken here to what’s gone on in the Great Financial Crisis. We had rating agencies, third-party verification sources that were able to perpetuate the fraud because the money got too big, their institutions became corrupted with the institutional imperative, and they got triple-A ratings which we all know in hindsight were not triple-A ratings – let’s move forward to today.
The FDA is the trusted third-party verification of pharmaceutical products. 50% of their budget comes from Pharma…due to the institutional imperative that was in place at the time and the speed with which they tried to approve these unproven products with this unproven technology, fraud did occur, and what’s my proof of that? The FDA, together with Pfizer, were trying to hide the clinical data.
And it’s come out recently…that the all-cause mortality for the Pfizer product failed – that means there were more deaths in the vaccine group than the placebo group. Normally in such a case, you have NO drug approval for such drugs. It’s the gold standard. I’ve been told by all my people in the Biotech Industry they were horrified… See mark 25:10.
And unfortunately, that is not all. Dowd feels that although he has successfully predicted three large frauds in his career, he now expects a global financial market collapse with the debt bubble getting ready to burst.
“So I’ve seen three frauds; the corporate fraud of the dot com boom, the bank fraud of the Great Financial Recession, and I believe the fraud has moved on to central banks and governments – because that’s the nature of our monetary system – you have to constantly create credit to keep this thing going.” See mark 2:22.
“The global debt bubble is at its peak…we are at the end…we are going to see lots of crazy things in the financial markets…we are going to see the credit markets become unhinged, the equity markets become unhinged. The Fed got a reprieve…under the cover of COVID, they were able to print 65% more money to keep this thing afloat, but we are at the end days here.” See mark 3:41.
He clarifies that the emergence of global totalitarianism is not purely about power and profit. Instead Dowd feels it is to control the masses when they realize the economy is collapsing – the ramifications of which may be the loss of pensions and social security income.
“A lot of what you are seeing in the response of global governments is setting up a system – under the guise of medical tyranny – to prevent the riots that are going to ensue once this thing all unwinds – that’s my personal belief…” See mark 4:04.
For the skeptics, consider that Pfizer stock lost $20 billion in market capitalization on February 8, 2022, when their record earnings fell short of more optimistic expectations.
Dowd predicts Moderna will drop to zero with bankruptcy as fraud related to concealing the COVID vaccine dangers surfaces, and he predicts Pfizer will become a sub-ten-dollar stock. Dowd explains that the smart money has already left Moderna and will soon be exiting Pfizer.
Dowd foresees an avalanche of lawsuits coming as the insurance industry continues to uncover the legions of mounting deaths coming from the complications of the mRNA COVID-19 vaccines.
Dowd teamed up with an insurance industry analyst and researched the life insurance claims. They found that since OneAmerica shocked the world by announcing a 40% rise in non-COVID deaths in younger working-class employees, multiple other insurance companies worldwide have seen the same thing – massive rises in non-COVID deaths. And the evidence inescapably points to the vaccines as the cause. See mark 13:16.
Meanwhile, the funeral company stocks have outperformed the S&P. “Funeral Home companies are growth stocks. They had a great year in 2021 compared to 2020, and they outperformed the S&P 500. The peer group of Funeral Home stocks was up 40 plus percent while the S&P was up 26 percent – and they started accelerating price-wise in 2021 during the roll-out of the vaccines – You don’t need to be a rocket scientist to connect the dots here.” See mark 5:55.
Other insurance companies have reported the same or worse death numbers as OneAmerica. For example, “Unum Insurance is up 36%, Lincoln National plus 57%, Prudential plus 41%, Reinsurance Group of America plus 21%, Hartford plus 32%, Met Life plus 24%, and Aegon – which is a Dutch insurer – saw in their US arm plus 57% in the 4th quarter – in the 3rd quarter they saw a 258% increase in death claims.” See mark 07:55.
“They raised (mortality) expectations 300,000 for 2022 over 2021 due to COVID plus ‘indirect COVID,’ which I think we know what that’s code for… They (Aegon) did a
$1.4 billion reinsurance deal with Wilton Reinsurance…what they were reinsuring were high face amount individual policies from 1 million to 10 million… (So) I think there is an asymmetric information situation going on in the insurance industry where some people have figured out something’s going on. They are off-loading their risk – they are not going to say what it is as they don’t want that information to get out as they unload the risk.” See mark 08:49.
“Someone is going to be the bag holder here.” And Dowd is confident it won’t be the insurance industry. A court in France has already held that a life insurance company cannot be held liable for a death because of the mRNA vaccine.
But that does not explain how mRNA manufacturers can be held responsible for an emergency product they were told was liability-free. Aren’t the vaccine manufacturers immunized from lawsuits?
After all, they were granted EUA, the specialized Emergency Use Authorization, which means they cannot be held legally accountable for deaths or adverse effects stemming from the experimental vaccines.
The idea is that no company – upon government request – should have to pay for unforeseen complications resulting from an emergency product that they released to the world out of their goodness of the hearts, with the best of intentions. Right?
Wrong – not when your company accomplishes this through deceit, also known as fraud.
Fraud undoes all these protections. If a company or person intentionally deceives another to profit, we have fraud. If Pfizer’s data showed increased all-cause mortality and hid this to motivate people to take the vaccine while claiming it was safe, then fraud exists.
Under common law, the required elements to prove fraud amount to:
#1. A materially false statement or purposeful failure to state or release material facts which non-disclosure makes other statements misleading.
#2. The false statement is made to induce Plaintiff to act.
#3. The Plaintiff relied upon the false statement, and the injury resulted from this reliance.
#4. Damages include a punitive award as a punishment that serves as a public example to discourage any future similar fraud. Punitive damages are generally proportional to the Defendant’s assets.
Dowd has been researching the COVID-19 vaccines and what he considers obvious evidence of knowing concealment of the actual risks of death – and he points to the Herculean efforts of Pfizer with FDA in withholding their data despite legal challenges to release it. He likens the FDA today to the rating agencies during the Mortgage Crisis.
“FDA is the trusted third party, just like the rating agencies were. And a lot of doctors in this country, a lot of local governments are placing their trust in the FDA which gets 50 percent of its budget from large cap pharma. It wasn’t any one person…I think they overlooked things…An all-cause mortality end-point should have stopped this thing in its tracks – and it didn’t.” See mark 1:51.
There were more deaths in the vaxxed group than in the unvaxxed. Dowd assumes fraud based upon the FDA backing Pfizer in not releasing their data. He believes this is a knowing attempt to conceal the deaths.
“When one party enters into a contract…and fraud was occurring when they entered into that contract, and the other party did not know that – the contract is void and null. There’s no indemnity if this can be proven, and I think it will be.” See mark 4:45.
“Pfizer got blanket immunity with EUA. If fraud occurred, to my mind and what I’m seeing from their refusal to release the data – if there is fraud and it comes out – and we need whistleblowers – and it’s looking more apparent that this product is deadly –
fraud eviscerates all contracts – that’s case law. So you go down the daisy chain, and that’s liability – that’s bankruptcy for Moderna, definitely Pfizer.” See mark 00:51.
He notes that the deaths skyrocketed after the vaccine rollout when they should have dropped. And the deaths are what distinguished the 2021-2022 vaccine scandal as far worse than what happened with Enron.
“People are dying and being maimed. This is a fraud that goes beyond the pale…We have the VAERS data…We have the DoD leak…And now we have the insurance company results and the funeral home results…We don’t need to think too hard about this…Deaths should have gone down after the vaccines rolled out. This is the most egregious fraud in history of the nation – and it’s global…Pfizer’s involved, and they committed fraud,” Dowd explained. See mark 10:25.
“My job is to be ahead of the news and be a lead steer…when I use my stock picking skills outside the realm of stock picking, I am called a conspiracy theorist.” See mark 6:45.
Dowd emphasized that he is not short on Pfizer or Moderna stock. He explained that he does not profit from their share prices dropping. He also points out that his predictions are not the cause of the steep declines as these occurred before he came out with this analysis. See mark 13:45.
“So we don’t need the mainstream media…And I want you to know – Wall Street is rallying to this – I’m getting lots of inquiries from former colleagues. Nothing will convince a sleeping public more than red stocks or collapsing stocks. My goal is to awaken the country by seeing something is going on. And Wall Street is AWAKE!” See mark 2:33.
If money is any indicator, Edward Dowd is correct that insurance will win a fight between the insurance and the vaccine industries. The life insurance market in the US is worth some $900 billion, while the vaccine market pales in comparison.
If someone is left holding the bag, it will not be the insurance industry, but it just might be you and me, the average citizen. However, there is one major caveat – if Edward Dowd succeeds in awakening the citizens, then they – the oligarchs – cannot get away with this – the Vaccine Fraud, the Great Reset, the Fourth Industrial Revolution and Global Totalitarianism.
“There’s lots of people who got the jabs that didn’t understand what was going on. A lot of them are in the investment world. A lot of them are smart people – they were duped too. Some of these people that got the jab are doing the work on shorting these stocks because – you know, you can guess – because they are mad as hell – and you’ve awakened the sleeping giant known as Wall Street. And Wall Street is on the move. The smart money is moving first – as always there’s lead steers. Nothing gets going faster than a red momentum down-trending stock.” See mark 3:26.
Those of you who still think nothing’s going on, you don’t want to be – what I call – the bag holder. You don’t want to be the guy taking the fourth jab booster and holding these stocks (on their way) down – Moderna’s going to zero – I think Pfizer goes sub ten dollars once the lawsuits come out. ” See mark 4:06.
Dowd’s forecast can awaken not only Wall Street but the ordinary citizen. We are those sleeping giants of the world, those who can move mountains with the force of our stock sales and non-violent protests, the great silent majority who can remove dictators from power and elect new and fair leaders.
There is power in numbers, as the Canadian Truckers recently found. Courage is contagious as freedom convoys have sprung up everywhere. We hold the power if we choose to exercise it while we lose that power if we passively comply.
As this Freedom Trucker fireman said, “I don’t know what happened to our country. It’s disgusting. There’s nothing that’s going to be taken from us here today that they’re not going to take anyways – And people need to stand. With enough of us, they can’t do this.” See mark 1:58:10.
If enough of us speak out NOW, collectively, we have the power to not only end the mandates, but to restore ALL freedoms in Canada, Australia, the UK, Europe and the United States, and we will win the day. We will never consent to authoritarian rule.
We will not leave a world of slavery to our children and grandchildren. We will protest every single day until the government realizes who truly is in charge. We believe in government of the people, by the people, and for the people. The cure for 1984 remains 1776.
Edward Dowd cautions those who continue to slumber, “If you are long these two stocks, you are long mandates, you are long government control, and you are long the selling of your freedoms.” Let us get everyone on board the freedom train. See mark 15:16.
Catherine Austin Fitts With Dr. Mark Skidmore: How Many People Died from the Covid-19 Inoculation? An Estimate Based on a Survey of the United States Population
[Video available at Solari Report BitChute channel.]
“[S]he lost her baby.”
“[O]ur daughter, her whole body shut down after 2nd shot. If her brother were not there she would not have survived.”
“She had a stroke within days of #2 Moderna vaccine. She has to use a walker and has speech issues. She was in her 40s. She is a registered nurse.”
“Cousin 47-stroke Cousin 28-blood clots Aunt 63-death Friend 41-death”
~ Covid-19 Survey, Appendix 3 (Respondents’ comments regarding the health condition of “the person they know best” who experienced an adverse event from a Covid-19 injection)
There is a wide range of opinion about the scale of injuries related to the Covid-19 injections. An unprecedented number of adverse events are being reported to official surveillance systems, but because these systems are known for their significant underreporting, it is difficult to know the true extent of injuries and fatalities. A well-designed survey of people’s beliefs and experiences can provide a useful estimate of what is actually happening on the ground.
The online survey, conducted in December 2021, included about 3,000 respondents representative of the general U.S. population, who described their own adverse-event-related experiences—and, equally importantly, the experiences of people in their social circles. Almost half of the respondents had received Covid shots themselves—with more than one in six experiencing health issues afterwards—and about one-fourth reported knowing others who had experienced significant post-injection health issues.
Dr. Skidmore notes that if one were to abide by the CDC’s count of “rare” injection-related fatalities (CDC acknowledges only nine Covid-vaccine-related deaths), then statistically, “in a survey of 3,000 people we should see ZERO (or close to zero) fatalities.” The survey provided a different picture, however. One in twelve respondents reported knowing someone who had died post-injection—a total of 55 fatalities—and the people described as likely vaccine-related deaths were, on average, 48 years old. Respondents also described numerous non-fatal but severe adverse events like heart-related issues, blood clotting, strokes, and paralysis.
Dr. Skidmore presented his survey results at the February 2022 Doctors for Covid Ethics Symposium III, and they are also available in his working paper titled “How Many People Died from the Covid-19 Inoculations? An Estimate Based on a Survey of the United States Population” posted at Dr. Skidmore’s Lighthouse Economics website. The working paper’s Appendix 3 includes respondents’ verbatim descriptions of the adverse events witnessed in their social circles.
The central question raised by Dr. Skidmore’s survey is this: What if the survey results, rather than CDC numbers, reflect the true ratio for fatalities and serious injuries following Covid injections? This would yield an estimated 260,000 to 300,00 fatalities and 1.1 million potentially life-threatening or life-shortening serious injuries—estimates that must be taken seriously by anyone still debating the injections’ safety.
by Jon Rappoport, No More Fake News
February 24, 2022
Two breaking developments—
File the first one under: WHEN YOU SPIN A CONVENTIONAL FAKE NARRATIVE, YOU KNOW EXACTLY WHERE YOU’RE GOING TO END UP.
Iceland cancels all COVID restrictions. Not because case numbers are dropping, but because, as I’ve written several times, once you (falsely) accept the existence of a new spreading virus, you’re committed to a narrative which can only end with EVERYONE INFECTED—and THAT’S called herd immunity.
Done. Finished. Forget vaccines, masks, distancing, lockdowns. Just live. Live out in the open.
Get a load of this:
Reuters: “Iceland will lift all remaining COVID-19 restrictions on Friday…the Ministry of Health said on Wednesday.”
“’Widespread societal [immune system] resistance to COVID-19 [meaning the development of natural immunity] is the main route out of the epidemic,’ the ministry said…”
“’To achieve this [immunity], as many people as possible need to be infected with the virus’…”
BANG. BOOM. POW.
The Ministry of Health just announced the end game, in alignment with the (false) assumptions which have been in place since January of 2020. Again, once you say a virus is on the loose all over the world, you’re committed to the only response there is:
GET INFECTED. DEVELOP NATURAL IMMUNITY. GO ABOUT YOUR LIVES.
That’s how the story wraps up. Humpty Dumpty fell off the wall and no one could put him back together again. You tell the virus tale, and that’s your predestined conclusion.
Of course there is no new virus, and the whole virus story is a fraud, as I’ve proved numerous times over the past 2 years. I’ve already described, in detail, all the ins and outs of the con called COVID.
But here, with Iceland, we see the beginning of sane national responses within the context of a completely insane scenario.
THAT’S what we’re looking at. Nothing more, nothing less.
“Well, we pretended there was a new unstoppable virus…and so here we are, exactly where we knew we would be. Get infected. Develop herd immunity. That is all. Goodbye.”
And all the major medical liars slowly back away from the general population…very slowly…hoping no one notices what just happened…hoping no one realizes this wrap-up was always in the cards…hoping no one will say: YOU RUINED AND KILLED UNTOLD MILLIONS OF PEOPLE AND YOU KNEW ALL ALONG THIS WAS GOING TO BE YOUR CLIMAX: “GET INFECTED.”
Shocking story number two—
The health/life insurance company tidal wave is breaking.
Well, of course it is. Who did you think was going to be left holding the bag for all the unreported injuries and deaths stemming from the COVID vaccines?
These life insurance companies employ actuaries, and these smart guys predict the number of claims they’re going to pay out…and THAT’S how they decide what the policy holders must pay…in order for the companies to maintain their profits…
Except, the actuaries had no idea what was going to happen.
They didn’t realize how many injury/death claims were going to be filed, once the COVID killshots were unleashed on the world.
But NOW THEY KNOW.
Former NY Times reporter, Alex Berenson: “Welt, a major German newspaper, just ran an interview with Andreas Schofbeck, a board member for a Bavarian insurer called BKK Provita.”
“By itself, BKK Provita has 120,000 members. But it is a much larger consortium of so-called BKK insurers that are affiliated with German companies and collectively have 10.9 million members.”
“Here’s how Schofbeck described the [injury] claims in the BKK [company] database, according to one of the reporters who interviewed him:…‘a violent warning signal’.”
Schofbeck is reacting, with great alarm, to all the vaccine injury claims that have been filed—looking at data from 10.9 MILLION policy holders.
In other words, it’s OVERWHELMING.
Another Humpty Dumpty just fell off the wall and broke into pieces.
Obviously, health/life insurance companies around the world are looking at similar horrific numbers.
What are these companies going to do? Just sit there and suck up their huge losses?
No. For starters, they’re going to blame the vaccine manufacturers. That’s already quite interesting, even if news outlets aren’t reporting it. Because, as Edward Dowd, former portfolio manager for BlackRock, has been saying, WALL STREET will take notice.
430 to 144. Can you guess what those numbers represent? The all-time high peak of the Moderna share price, and the most recent closing price, as of this writing.
BANG.
61 to 46. The first number is the high, over the past year, for the Pfizer share price, and the second number is the most recent close, as of this writing.
These insurance-vaccine company developments were also inevitable, from the beginning of the fake pandemic.
Anyone who knows the real history of vaccines would have seen it in a second.
You rapidly shoot up the whole world with a new vaccine, and the injury-death numbers are going to go through the roof.
Insurance companies don’t like to be left holding the bag and absorbing the consequences of both the jab and the lies the vaccine front men have been telling.
Insurance companies are wired up to, heavily influence, and control all sorts of politicians and bureaucrats and public health officials. You can bet your bottom dollar these companies have been reading the riot act to their government puppets.
“You [FDA] morons…you’re supposed to be protecting the public from dangerous drugs and vaccines. And now people all over the world are dropping like flies from the COVID shot, and those people are our POLICY HOLDERS.”
“What did you want us to do? For chrissakes, we work for the pharmaceutical companies.”
“We’re not interested in excuses. We want money. Lots of it, to make up for our losses.”
“Don’t look at us. We don’t do bailouts. Go to Treasury, or the President.”
“The President can’t even find his way from the shower to the bedroom in the White House residence.”
“Talk to nurse Jill or Susan Rice…”
And word of these conversations leaks out to Wall Street.
Look for new bailouts, and a plethora of cover stories to explain why insurance companies are suddenly inhaling hundreds of billions of government dollars (or more.)
Cover stories only the most naïve fools will believe.
Serial liar Tony Fauci may be able to tap dance with his media partners every Sunday morning on the news talk shows; but when giant insurance companies want him to pay for his sins, that’s a whole different story.
Tony could become yet another Humpty Dumpty…
All we need now—among all the insurance companies in the world—are five or six OUTRAGED big-time insurance execs to step out of the shadows with their hair on fire, completely fed up with the grand cover-up of vaccine injuries, and talking their heads off.
Knowing my regular readers can handle more than one major point in an article, I start with this: Justin Trudeau is not serving the interests of Canadians; he is loyal to the World Economic Forum (WEF) and the brand of Globalism it represents.
Meaning: global governance; the submerging of nations in a scheme of external top-down control; the expansion of poverty; wall to wall surveillance; a currency reset; and other totalitarian transformations.
If you watch these two brief videos (here and here), you’ll see Klaus Schwab confirm, in Trudeau’s presence, the prime minister’s loyalty to the WEF, as well as the penetration of Trudeau’s cabinet with WEF agents.
Schwab, the head of WEF, also mentions a new dawn of entrepreneurs who lead corporations dedicated to social responsibility.
And THAT is a test for Schwab. Because he certainly backs major pharmaceutical companies. Do those businesses display social responsibility?
I’m not talking about their pricing of drugs or their equitable distribution of drugs. I’m talking about killing and maiming people with the drugs. Many people.
And so I return to citations I’ve published a number of times. By the way, virtually no one takes these devastating references and runs with them.
I can only conclude journalists and doctors who otherwise criticize medical policies don’t want to admit the medical cartel has a very long track record of destroying populations.
These journalists and doctors only want to cherry pick their targets. In fact, they support the overall performance of the medical system. Why? You would have to ask them.
Here, I’m testing Klaus Schwab. Does he really think he can get away with his talk about “social responsibility” and his simultaneous support of Pharma?
Buckle up—
ONE: Journal of the American Medical Association, April 15, 1998: “Incidence of Adverse Drug Reactions in Hospitalized Patients.”
The authors, led by Jason Lazarou, culled 39 previous studies on patients in hospitals. These patients, who received drugs in hospitals, or were admitted to hospitals because they were suffering from the drugs doctors had given them, met the following fate:
Every year, in the US, between 76,000 and 137,000 hospitalized patients die as a direct result of the drugs.
Beyond that, every year 2.2 million hospitalized patients experience serious adverse reactions to the drugs.
The authors write: “…Our study on ADRs [Adverse Drug Reactions], which excludes medication errors, had a different objective: to show that there are a large number of ADRs even when the drugs are properly prescribed and administered.”
So this study had nothing to do with doctor errors, nurse errors, or improper combining of drugs. And it only counted people killed or maimed who were admitted to hospitals. It didn’t begin to tally all the people taking pharmaceuticals who died as consequence of the drugs, at home.
TWO: July 26, 2000, Journal of the American Medical Association; author, Dr. Barbara Starfield, revered public health expert at the Johns Hopkins School of Public Health; “Is US health really the best in the world?”
Starfield reported that the US medical system kills 225,000 Americans per year. 106,000 as a result of FDA-approved medical drugs, and 119,000 as a result of mistreatment and errors in hospitals. Extrapolate the numbers to a decade: that’s 2.25 million deaths. You might want to read that last number again.
I interviewed Starfield in 2009. I asked her whether she was aware of any overall effort by the US government to eliminate this holocaust. She answered a resounding NO. She also said her estimate of medically caused deaths in America was on the conservative side.
THREE: BMJ June 7, 2012 (BMJ 2012:344:e3989). Author, Jeanne Lenzer. Lenzer refers to a report by the Institute for Safe Medication Practices: “It [the Institute] calculated that in 2011 prescription drugs were associated with two to four million people in the US experiencing ‘serious, disabling, or fatal injuries, including 128,000 deaths.’”
The report called this “one of the most significant perils to humans resulting from human activity.”
The report was compiled by outside researchers who went into the FDA’s own database of “serious adverse [medical-drug] events.”
Therefore, to say the FDA isn’t aware of this finding would be absurd. The FDA knows. The FDA knows and it isn’t saying anything about it, because the FDA certifies, as safe and effective, all the medical drugs that are routinely maiming and killing Americans. Every public health agency knows the truth.
FOUR: “The Epidemic of Sickness and Death from Prescription Drugs.” The author is Donald Light, who teaches at Rowan University, and was the 2013 recipient of ASA’s [American Sociological Association’s] Distinguished Career Award for the Practice of Sociology. Light is a founding fellow of the Center for Bioethics at the University of Pennsylvania. In 2013, he was a fellow at the Edmond J. Safra Center for Ethics at Harvard. He is a Lokey Visiting Professor at Stanford University.
Donald Light: “Epidemiologically, appropriately prescribed, prescription drugs are the fourth leading cause of death, tied with stroke at about 2,460 deaths each week in the United States. About 330,000 patients die each year from prescription drugs in the United States and Europe. They [the drugs] cause an epidemic of about 20 times more hospitalizations [6.6 million annually], as well as falls, road accidents, and [annually] about 80 million medically minor problems such as pains, discomforts, and dysfunctions that hobble productivity or the ability to care for others. Deaths and adverse effects from overmedication, errors, and self-medication would increase these figures.” (ASA publication, “Footnotes,” November 2014)
FIVE: None of the above reports factor in death or injury by vaccine.
Medical crimes.
Medically caused deaths of friends, family members, loved ones, who are buried along with the truth.
No criminal investigations, no prosecutions, no guilty verdicts, no prison sentences.
But of course, you can believe everything leading lights of the US medical system tell you about COVID.
You can believe everything the press—who buries the truth about this medical holocaust—tells you about COVID.
Given the reports on medically caused death and maiming I’ve just cited and described in this article, it’s obvious that…
Leading medical journals around the world, which routinely publish glowing accounts of clinical trials of medical drugs…
Are spilling over with rank fraud, on page after page.
Indeed, here is a stunning quote from an editor who has quite probably read and analyzed more medical-drug studies than any doctor in the world:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
Compare that quote with one from “the father of COVID science,” Anthony Fauci. In an interview with the National Geographic, Fauci stated:
“Anybody can claim to be an expert even when they have no idea what they’re talking about…If something is published in places like New England Journal of Medicine, Science, Nature, Cell, or JAMA—you know, generally that is quite well peer-reviewed because the editors and the editorial staff of those journals really take things very seriously.”
They take things so seriously, they routinely publish glowing studies of medical drugs that are killing people in great numbers.
—So, Mr. Schwab, which is it? You support corporate social responsibility, and therefore you condemn, in the strongest possible way, the ongoing death-and-maiming count achieved by beloved pharmaceutical companies? Or you maintain your unwavering support for Pharma, and admit your pose of “social responsibility” is a complete fraud.
And to journalists and doctors who refuse to pick up the citations in this article and DO something with them, I ask: what’s holding you back? What’s been holding you back? I’ve been publishing and speaking about this information for more than 10 years.
What are you afraid of? Where do YOUR loyalties lie?
La Quinta Columna has shared with the world a very particular observation about the filament-like structures they have found when looking at vials of Pfizer vaccines under an optical microscope.
Dr. Sevillano noticed that within the particulate composition, there are some crystals that appear to be microcircuitry, but are actually some other material that would be a kind of food for the Morgellons-like filaments to grow. They don’t know what kind of crystals these are, but they continue in their research to try to unravel as many mysteries as possible.
Ricardo Delgado: So I’m going to move the microscope, and let’s go down. Here is the “hair.” See?
Dr. Sevillano: Here’s the hair. Yes.
Ricardo Delgado: Let’s see, I’m going to move it a little bit. There it is. See that you can even see… This sample is more dried out now. But look at the size of it.
Dr. Sevillano: And how it attracts the crystals. If you notice, you can see how it’s attracting them.
Ricardo Delgado: This one has been growing too. Here I’m going to focus it now to…
Dr. Sevillano: Let’s see if you find the generator pole. We have to look for the generator pole. Let’s see if we can see the deflection and the cubes generating around it. Let’s see if we can find the extreme.
Ricardo Delgado: This is incredible. Come on. Look at this. It’s still here. This is where I think it ends, right?
Dr. Sevillano: Yeah, it looks like this is where it ends.
Ricardo Delgado: This is where it ends. What happens is that in, here, there’s no longer any kind of aqueous suspension. I mean, it’s completely dried out.
Dr. Sevillano: It’s completely dried out. Maybe, for that reason, it has stopped… By not having… Maybe, it lacks something to… But look how it attracts all the material. How it’s full of crystals all over the place.
Ricardo Delgado: Surely, there must be more around here. Let’s see, I’m going to look around. Well, this is the content of the Pfizer vaccine. It’s crazy!
Dr. Sevillano: There… I’m beginning to think, Ricardo, that most of the stuff we see there is circuitry. And probably, there’s also material that we’re talking about that’s used for the growth of that.
Ricardo Delgado: Yes.
Dr. Sevillano: The ones that don’t have “drawings” or that don’t have printed circuitry, those ones have to be the material that uses that to grow. That’s all.
Ricardo Delgado: This is the edge of the drop, which is already dry. This is where it ends.
Dr. Sevillano: Yes, more mysteries that we understand nothing about in all this.
Ricardo Delgado: Look what’s here.
Dr. Sevillano: There’s another one. Yes. It’s quite huge.
Autopsies of two teenage boys who died days after receiving Pfizer’s COVID vaccine prove the vaccine caused their deaths. Pathological findings suggest there may be a way to distinguish SARS-COV-2 infection-induced myo/pericarditis from vaccine-induced cardiac injury. Vaccine-induced heart injury can be sub-clinical, but how often?
Pathologists who examined the autopsies of two teenage boys who died days after receiving Pfizer’s COVID-19 vaccine concluded the vaccine caused the teens’ deaths.
The three pathologists, two of whom are medical examiners, published their findings Feb. 14 in an early online release article, “Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose,” in the Archives of Pathology and Laboratory Medicine.
The authors’ findings were conclusive. Two teenage boys were pronounced dead in their homes three and four days after receiving the second Pfizer-BioNTech COVID-19 dose.
There was no evidence of active or previous COVID-19 infection. The teens had negative toxicology screens (i.e. no drugs or poisons were present in their bodies).
These boys died from the vaccine.
Histopathological examination of their cardiac tissue revealed an important new finding: Neither heart demonstrated evidence of typical myocarditis.
Instead, the authors found evidence of microscopic changes consistent with a different form of heart injury called toxic cardiomyopathy. They wrote:
“The myocardial injury seen in these post-vaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy.”
The authors further explained what they observed under the microscope:
“Their histopathology does not demonstrate a typical myocarditis… In these two post-vaccination instances, there are areas of contraction bands and hypereosinophilic myocytes distinct from the inflammation.
“This injury pattern is instead similar to what is seen in the myocardium of patients who are clinically diagnosed with Takotsubo, toxic, or ‘stress’ cardiomyopathy, which is a temporary myocardial injury that can develop in patients with extreme physical, chemical, or sometimes emotional stressors.
“Stress cardiomyopathy is a catecholamine-mediated ischemic process seen in high catecholamine states in the absence of coronary artery disease or spasm. It has also been called ‘neurogenic myocardial injury’ and ‘broken heart syndrome.’”
The pathologists determined there was a different mechanism of heart injury at play in these two boys, distinct from a purely infectious process that would result directly from a viral infection like COVID-19.
This is an important finding. There may be a way to distinguish cardiac injury resulting from a SARS-COV-2 infection from cardiac injury where the vaccine predisposes the patient to stress cardiomyopathy before contracting COVID-19.
However, the authors are careful not to assume that cardiac injuries from COVID-19 and COVID-19 vaccines can always be sorted out under the microscope.
They explain that stress cardiomyopathy, or “broken heart syndrome,” may also occur in a rare hyperinflammatory state that is known to occur in COVID-19 infection as well:
“This post-vaccine reaction may represent an overly exuberant immune response and the myocardial injury is mediated by similar immune mechanisms as described with SARS-COV-2 and multisystem inflammatory syndrome (MIS-C) cytokine storms.”
The authors admit this pathological finding may also occur as a result of MIS-C, a known complication of SARS-COV2 infection.
Learning more about this condition requires a biopsy of heart tissue, or in this case an autopsy. We know very little about the nature of myocarditis in people who are clinically stable because heart biopsies are not conducted on them and autopsies are rarely done on patients who die from COVID-19.
There still is no practical way of screening for cardiac injury beyond assessing symptoms.
Unfortunately, the two boys did not have symptoms of myocarditis (fever, chest pain, palpitations, or dyspnea) prior to their cardiac arrest and death. One complained of a headache and gastric upset which resolved. The other had no complaints.
This is extremely concerning. These boys had smoldering, catastrophic heart injuries with no symptoms.
How many others have insidious cardiac involvement from vaccination that won’t manifest until they get a serious case of COVID-19 or the flu? Or perhaps when they subject themselves to the physical stress of competitive sports?
These findings suggest a significant subset of COVID-19 deaths in the vaccinated could be due to the vaccines themselves.
Furthermore, it raises this question: How often does this condition exist in a latent form in vaccinated individuals?
The CDC believes the risk of vaccine-induced myocarditis not significant
The Centers for Disease Control and Prevention (CDC) says the risk of myocarditis and pericarditis in adolescents who get the COVID-19 vaccine is “extremely rare” and “most cases are mild.”
But those assurances conflict with the agency’s own data.
The CDC’s Advisory Committee on Immunization Practices (ACIP) presented this disquieting information (see chart below) during its June 23, 2021 meeting convened specifically to address the risks of myo/pericarditis in 12- to 15-year-olds who received Pfizer’s COVID vaccine:
This slide is important for two reasons.
First, the incidence of this potentially lethal condition is significantly higher in the vaccinated (“Observed” column) compared to the background rate (“Expected” column), especially in males in the 18- to 24-year-old age range.
In the 12- to 17-year-old male cohort, the risk of myo/pericarditis is at least 11 times higher than the background rate.
With more than 2 million doses administered at the time when these cases of myo/pericarditis were identified, we can be confident these data represent an undeniable safety signal.
The second reason this slide is important is this: The CDC is drawing directly from the Vaccine Adverse Event Reporting System (VAERS), a system specifically designed to monitor for safety signals when vaccines are administered to the public.
As of Feb. 15, the CDC continues to assure the public that “Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem.”
In essence, the CDC is acknowledging that reports of deaths and other adverse events following vaccination exist in VAERS but do not comprise any risk because causality has not been verified.
Then why did the ACIP choose to accept VAERS as a legitimate source of information on myo/pericarditis in their calculations?
The CDC released its conclusions immediately following the ACIP meeting:
“The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination. Importantly, for the young people who do, most cases are mild, and individuals recover often on their own or with minimal treatment.”
But how do they know this?
One month after this comforting statement from the CDC, the U.S. Food and Drug Administration (FDA) admitted in this letter to Pfizer that the agency was not able to adequately assess the risk of myocarditis from Pfizer’s product:
“We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA [Federal Food, Drug and Cosmetic Act] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
“Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.”
Commenting on the FDA’s letter, Dr. Meryl Nass said, “The FDA is saying that neither an analysis of the data in VAERS or of any of the other taxpayer-funded databases will provide sufficient assessment of the risk of this product.”
“This is a joke,” said Nass, adding:
“All this data, plus software, plus a team of analysts, and the FDA says it can’t assess the risk of myocarditis, despite identifying thousands of cases?
“Furthermore, unsaid, but implied by the FDA, is that if the FDA is incapable of assessing the risk of myocarditis despite thousands of reported cases, it cannot or will not be capable of assessing the other serious adverse events that have been reported in conjunction with COVID vaccines.”
If the FDA is not able to perform adequate surveillance of safety signals around vaccine-induced myocarditis, who will?
The FDA assigns this unenviable but essential task to Pfizer itself (again, from the FDA’S letter to Pfizer):
“Therefore, based on appropriate scientific data, we have determined that you are required to conduct the following studies…”
Is myocarditis ‘extremely rare’ after COVID-19 vaccination?
As of Feb. 4, VAERS reported 495 cases of myo/pericarditis in 12- to 17-year-olds. VAERS data show that as of Feb. 10, there were 2,239 reported cases of myocarditis in people under the age of 30.
However, a widely cited CDC-sponsored study (Lazarus et al) concluded the incidence of adverse events is 10 to 100 times higher than are reported to VAERS.
More recent calculations estimate that adverse events are underreported by a factor of approximately 41.
From these estimates, we can conclude there may have been approximately 20,000 cases of myocarditis in 12- to 17-year-olds since Pfizer’s COVID-19 vaccine received Emergency Use Authorization and was rolled out to this age group..
The VAERS data from June 11, 2021 from the table above show 132 cases of myo/pericarditis were observed in 2,039,000 doses given to 12- to 17-year-old males. This is approximately 6.5 cases in 100,000 doses.
This study from Hong Kong found the incidence of myo/pericarditis after two doses with Pfizer’s Comirnaty vaccine was 37 in 100,000. This incidence matches nearly exactly with findings from this study that used the Vaccine Safety DataLink (VSD) system (37.7 12-17 year olds per 100,000 suffered myo/pericarditis after their second dose). This is more evidence that significant underreporting is in play in the VAERS system.
Will most of these teens “recover on their own”? How many other vaccinated people have varying degrees of “broken heart” syndrome that remain asymptomatic, undiagnosed and unreported?
These new findings indicate that no one can answer these questions right now — especially not the CDC and the FDA.
If the FDA has admitted it cannot assess the risk of myocarditis using the surveillance systems in place, how then is the CDC able to assure us that the risk is low enough to continue to proceed with a vaccination campaign that now includes 5- to 11-year-old children?
The FDA has abdicated its responsibility for monitoring the safety of these vaccines to the vaccine manufacturers.
The CDC is using VAERS data in its own analyses while urging the public to discount all adverse events, including deaths, that appear in the very same database.
There isn’t any regulation happening here. Our regulatory agencies have become mouthpieces for the very industry they are tasked to oversee.
Madhava Setty, M.D. is senior science editor for The Defender.
Before we get to Christine Johnson’s interview, a bit of background.
My first book, AIDS INC., was published in 1988. The research I engaged in then formed a foundation for my recent work in exposing the vast fraud called COVID-19.
In 1987-88, my main question eventually became: does HIV cause AIDS? For months, I had blithely assumed the obvious answer was yes. This created havoc in my investigation, because I was facing contradictions I couldn’t solve.
For example, in parts of Africa, people who were chronically ill and dying obviously needed no push from a new virus. All their “AIDS” conditions and symptoms could be explained by their environment: contaminated water supplies; sewage pumped directly into the drinking water; protein-calorie malnutrition; hunger, starvation; medical treatment with immunosuppressive vaccines and drugs; toxic pesticides; fertile farm land stolen by corporations and governments; wars; extreme poverty. The virus cover story actually obscured all these ongoing crimes.
Finally, in the summer of 1987, I found several researchers who were rejecting the notion that HIV caused AIDS. Their reports were persuasive.
I’m shortcutting a great deal of my 1987-8 investigation here, but once HIV was out of the picture for me, many pieces fell into place. I discovered that, in EVERY group supposedly at “high-risk” for AIDS, their conditions and symptoms could be entirely explained by factors that had nothing to do with a new virus.
AIDS was not one condition. It was an umbrella label, used to re-package a number of immunosuppressive symptoms and create the illusion of a new and unique and single “pandemic.”
Several years after the publication of AIDS INC, I became aware of a quite different emerging debate going on under the surface of research: DOES HIV EXIST?
Was the purported virus ever truly discovered?
And THAT question led to: what is the correct procedure for discovering a new virus?
The following 1997 interview, conducted by brilliant freelance journalist, Christine Johnson, delves into these questions:
How should researchers prove that a particular virus exists? How should they isolate it? What are the correct steps?
These questions, and their answers, reside at the heart of most disease research—and yet, overwhelmingly, doctors never explore them or even consider them.
Johnson interviews Dr. Eleni Papadopulos, “a biophysicist and leader of a group of HIV/AIDS scientists from Perth in Western Australia. Over the past decade and more she and her colleagues have published many scientific papers questioning the HIV/AIDS hypothesis…”
Here I’m publishing and highlighting excerpts from the interview. Technical issues are discussed. Grasping them is not the easiest exercise you’ve ever done, but I believe the serious reader can comprehend the vital essentials.
Christine Johnson: Does HIV cause AIDS?
Eleni Papadopulos: There is no proof that HIV causes AIDS.
CJ: Why not?
EP: For many reasons, but most importantly, because there is no proof that HIV exists.
… CJ: Didn’t Luc Montagnier and Robert Gallo [purportedly the co-discoverers of HIV] isolate HIV back in the early eighties?
EP: No. In the papers published in Science by those two research groups, there is no proof of the isolation of a retrovirus from AIDS patients. [HIV is said to be a retrovirus.]
CJ: They say they did isolate a virus.
EP: Our interpretation of the data differs. To prove the existence of a virus you need to do three things. First, culture cells and find a particle you think might be a virus. Obviously, at the very least, that particle should look like a virus. Second, you have to devise a method to get that particle on its own so you can take it to pieces and analyze precisely what makes it up. Then you need to prove the particle can make faithful copies of itself. In other words, that it can replicate.
CJ: Can’t you just look down a microscope and say there’s a virus in the cultures?
EP: No, you can’t. Not all particles that look like viruses are viruses.
… CJ: My understanding is that high-speed centrifugation is used to produce samples consisting exclusively of objects having the same density, a so-called “density-purified sample.” Electron microscopy is used to see if these density-purified samples consist of objects which all have the same appearance — in which case the sample is an isolate — and if this appearance matches that of a retrovirus, in terms of size, shape, and so forth. If all this is true, then you are three steps into the procedure for obtaining a retroviral isolate. (1) You have an isolate, and the isolate consists of objects with the same (2) density and (3) appearance of a retrovirus. Then you have to examine this isolate further, to see if the objects in it contain reverse transcriptase [an enzyme] and will replicate when placed in new cultures. Only then can you rightfully declare that you have obtained a retroviral isolate.
EP: Exactly. It was discovered that retroviral particles have a physical property which enables them to be separated from other material in cell cultures. That property is their buoyancy, or density, and this was utilized to purify the particles by a process called density gradient centrifugation.
The technology is complicated, but the concept is extremely simple. You prepare a test tube containing a solution of sucrose, ordinary table sugar, made so the solution is light at the top but gradually becomes heavier, or more dense, towards the bottom. Meanwhile, you grow whatever cells you think may contain your retrovirus. If you’re right, retroviral particles will be released from the cells and pass into the culture fluids. When you think everything is ready, you decant a specimen of culture fluids and gently place a drop on top of the sugar solution. Then you spin the test tube at extremely high speeds. This generates tremendous forces, and particles present in that drop of fluid are forced through the sugar solution until they reach a point where their buoyancy prevents them from penetrating any further. In other words, they drift down the density gradient until they reach a spot where their own density is the same as that region of the sugar solution. When they get there they stop, all together. To use virological jargon, that’s where they band. Retroviruses band at a characteristic point. In sucrose solutions they band at a point where the density is 1.16 gm/ml.
That band can then be selectively extracted and photographed with an electron microscope. The picture is called an electron micrograph, or EM. The electron microscope enables particles the size of retroviruses to be seen, and to be characterized by their appearance.
CJ: So, examination with the electron microscope tells you what fish you’ve caught?
EP: Not only that. It’s the only way to know if you’ve caught a fish. Or anything at all.
CJ: Did Montagnier and Gallo do this?
EP: This is one of the many problems. Montagnier and Gallo did use density gradient banding, but for some unknown reason they did not publish any Ems [photos] of the material at 1.16 gm/ml…this is quite puzzling because in 1973 the Pasteur Institute hosted a meeting attended by scientists, some of whom are now amongst the leading HIV experts. At that meeting the method of retroviral isolation was thoroughly discussed, and photographing the 1.16 band of the density gradient was considered absolutely essential.
CJ: But Montagnier and Gallo did publish photographs of virus particles.
EP: No. Montagnier and Gallo published electron micrographs of culture fluids that had not been centrifuged, or even separated from the culture cells, for that matter. These EMs contained, in addition to many other things, including the culture cells and other things that clearly are not retroviruses, a few particles which Montagnier and Gallo claimed are retroviruses, and which all belonged to the same retroviral species, now called HIV. But photographs of unpurified particles don’t prove that those particles are viruses. The existence of HIV was not established by Montagnier and Gallo — or anyone since — using the method presented at the 1973 meeting.
CJ: And what was that method?
EP: All the steps I have just told you. The only scientific method that exists. Culture cells, find a particle, isolate the particle, take it to pieces, find out what’s inside, and then prove those particles are able to make more of the same with the same constituents when they’re added to a culture of uninfected cells.
CJ: So before AIDS came along there was a well-tried method for proving the existence of a retrovirus, but Montagnier and Gallo did not follow this method?
EP: They used some of the techniques, but they did not undertake every step including proving what particles, if any, are in the 1.16 gm/ml band of the density gradient, the density that defines retroviral particles.
CJ: But what about their pictures?
EP: Montagnier’s and Gallo’s electron micrographs…are of entire cell cultures, or of unpurified fluids from cultures…
—end of interview excerpt—
If you grasp the essentials of this discussion, you’ll see there is every reason to doubt the existence of HIV, because the methods for proving its existence were not followed.
Worse yet, it appears that Robert Gallo and Luc Montagnier, the two scientists credited with the discovery of HIV—as well as other elite researchers—were aware they weren’t employing correct methods.
And so…as I’ve reported, there is every reason to doubt and reject the existence of the COVID virus, SARS-CoV-2, since correct large-scale electron microscope studies have never been done. And by large-scale, I mean: attempting to find and photograph the virus in a cohort of, say, 1000 people who are supposed to be “pandemic patients.” I’m NOT talking about one or two electron-microscope photos accompanying a study.
But even that isn’t the end of the story. There is one further potential limiting factor in virus research. I became aware of it about a year ago. Analysis of electron microscope findings is fraught with difficulty and doubt. Are scientists actually looking at what they think they’re looking at in these photos? I refer readers to the work of neurobiologist Harold Hillman, who concluded that researchers were, for the most part, looking at artifacts, not actual cells or entities within cells. Another suppressed controversy.
After more than 30 years of investigating medical research fraud, my general conclusion is, the deeper you go the stranger it gets. Or to put it another way, the worse it gets.
“Above all we should not forget, that government is an evil, a usurpation upon the private judgment and individual conscience of mankind.”
~ William Godwin (1793) “An enquiry concerning political justice, and its influence on general virtue and happiness”, p.143
Lest we forget, it is not a fake or mysterious disease or ‘virus’ that is responsible for the unnecessary death and destruction that has befallen mankind, it is the deliberate elimination of those thought to be undesirables by the controlling class of monsters and their pawns in government. This is not ‘conspiracy theory,’ as espoused by the powerful and their media, it is an actual conspiracy.
There is method to the madness of this ruling cabal, as the older among us were heavily targeted initially, followed by the breakdown and dividing of society, the assault against young men, and now the children are being threatened and targeted with the experimental bio-weapon injection in order to solidify the control of the future. To understand this progression only requires logic, and of course an open mind.
The old and established, those who are also thought by the state to be a drain on society, are considered to be a danger to the rulers because they have lived and understand history, and history and historical accounting are meant to be destroyed by those attempting to create a new paradigm based on what might be labeled as progressive postmodernism. The division of societies is necessary in order keep the people distracted and fighting amongst themselves enough so that they are not a threat to the state. The apparent attack against young men by adverse effects due to poisonous injection, is an effort to disable current or future insurrection by men of ‘fighting age,’ as evidenced by the government’s aggression against the current trucker’s freedom rebellion in Canada and other parts of the world, most of whom are younger men. Destroying the bodies and minds of all the children, at least from the state’s perspective, is the ultimate goal sought, because to capture and control the children today, as well as the youngest generation, is to control the future.
With this background in mind, it is important to understand that no pandemic has occurred, and claimed deaths due to ‘Covid’ are historically unique in that certain areas over others had substantially higher death counts due to so-called’ Covid;’ so much so as to be very suspicious in nature, because this has never happened before this wrongly claimed ‘pandemic.’ New York and the Southern states are prime examples of these contradictory claims. It actually makes no sense, and there is no validity concerning the ‘Covid’ explanation for these unheard-of anomalies, other than fraud and deceit. One thing is for certain, the state response to this fake pandemic has been responsible for much harm, and untold numbers of deaths; these deaths having been purposely used to bolster ‘Covid’ mortality numbers in order to advance a false narrative bent on creating and generating even more public fear.
The obvious contradictions are most always explained away by conjecture, false excuses, and lies, but why should that be any surprise to any thinking individual? The pattern of deaths reported today, considering any ‘viral’ respiratory illness, has never once occurred, which should immediately trigger hard questions, and very critical analysis of all the un-substantiated hogwash that passes for ‘news’ reporting in this environment of deception.
To provide even more fuel to the fire for the indifferent and obedient fools, and those in the manipulative media, it is distinctly apparent that the depopulation agenda is alive and well. While many will scoff at this claim, why else would the ruling class and government be willing to murder so many people by nefarious means, who either stand in the way of state totalitarianism, or are a threat to the desired status quo that would consist of a population made up of ignorant and voluntarily compliant citizens?
Consider the fact that this communistic takeover coup was initially based on a fake ‘virus,’ requiring the most anti-freedom, liberty-destroying, and deadly response ever undertaken here in this country and globally. We will never know exactly how many have and will die due to this evil draconian response to a world-changing, terroristic, and false flag event meant to achieve a totalitarian outcome.
Many have said that the response was worse than the threat, but this is a smoke and mirrors and hypocritical reaction, because there was never any legitimate threat in the first place, other than the democidal tendencies of the state against the people. This is literally a war against the common man, and an eager willingness by those in power to destroy or genocide certain individuals, groups, ethnicities, select members of certain demographic makeups, the poor and disadvantaged, the entire middle class, the psychologically weak, and the most vulnerable among us; simply to gain total power and control of all monetary, financial, economic, geopolitical, and societal systems worldwide. With this end in sight, the next obvious step is to gain complete control of all children by bio-weapon injections meant to subdue the minds and bodies of future generations. This plot is already underway.
By simply looking at the treatment protocols demanded and implemented, one can only come to the certain conclusion that the death of many in this population due to the response to a fake ‘virus,’ has not only been planned and sought by the powerful and their pawns, but has been intentionally put into place over the past two years. This is a long-planned scheme meant to achieve a particular outcome of death and control. To argue this is to ignore reality, and to assume a position based on fallacy.
Consider Remdesivir, a killer drug promoted knowingly by the evil Fauci. It became basically the only hospital treatment for the fraud called ‘Covid-19’ early on in this scam. It was well known to be extremely toxic and deadly. It was approved for emergency use by the FDA on May 1, 2020, and was subsequently fully approved by the FDA to treat ‘Covid-19’ on October 22, 2020. Just recently on January 22, 2022, the FDA granted expedited approval of a new supplemental drug application for Remdesivir, based on the recommendation of Fauci and the NIH. Nine of the people at NIH who recommended this poison, had financial ties to the maker of Veklury (Remdesivir), Gilead Sciences.
Consider the mass use of ventilators, especially in New York. Most so-called ‘Covid’ patients put on these machines for ‘Covid’ treatment died. According to a study done early on by the American Medical Association Network: “Mortality rates for those who received mechanical ventilation in the 18-to-65 and older-than-65 age groups were 76.4% and 97.2%, respectively. Mortality rates for those in the 18-to-65 and older-than-65 age groups who did not receive mechanical ventilation were 19.8% and 26.6%, respectively.”
Consider that stress is a known major killer, and extreme stress brought on by the bogus response to a non-existent ‘virus,’ caused many deaths; not only in the U.S., but all around the world. This was due to lockdowns, quarantine, loss of family and friend contact, suicide, isolation, distancing, mask-wearing, job loss, bankruptcy, business closures, travel restrictions, and much more tyranny aimed at the general population.
Consider the restriction of treatments for all sickness due to the fact that most every ill and every symptom was co-opted and said to be ‘Covid.” Hospitals refused to treat patients, medical facilities closed their doors, certain drugs and natural treatments were outlawed, necessary surgeries were cancelled, and eventually, many, if not most, medical services were eliminated for those who refused to take an experimental bio-weapon injection. People died in their home prisons or nursing homes without any sympathy or loosening of restrictions by the evil state.
The government and its bosses were and are willing to commit murder, and their enforcement goons and political allies are willing to assist in this murder of innocents, all in the name of state control and tyranny, but there has been a change of heart recently by larger numbers of people, much due to those willing to fight back to regain some freedom. This is happening worldwide by not only truckers but by others as well.
The government and its bosses were and are willing to commit murder, and their enforcement goons and political allies are willing to assist in this murder of innocents, all in the name of state control and tyranny, but there has been a change of heart recently by larger numbers of people, much due to those willing to fight back to regain some freedom. This is happening worldwide by not only truckers but by others as well.
FDA Executive Officer Exposes Close Ties Between Agency and Pharmaceutical Companies: ‘Almost a Billion Dollars a Year Going into FDA’s Budget from the People we Regulate’
• FDA Executive Officer Chris Cole: “The drug companies, the food companies, the vaccine companies. So, they pay us hundreds of millions of dollars a year to hire and keep the reviewers to approve their products.”
• Cole on FDA fees: “Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers which will speed up the approval process. So, they [pharmaceutical companies] make more money.”
• Cole: “They [FDA] tone down the impact of the user fees on their operations because they know they’re dependent on the drug companies, and the vaccine companies, and these other companies for their agency to operate.”
• Cole on blowing the whistle: “There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it.”
• Cole on retaliation in government: “You’ll be marked from getting other jobs because another office is not going to want to hire you if you’ve spoken out about something, right or wrong. They don’t look at what you’ve spoken out about. They’re just not willing to- government’s about rocking the boat and they don’t want to- which is the problem I have with- one of the problems I have with government is, like, they don’t like people rocking the boat, for right or wrong, at all costs. They want to hire a safe person that can do the job but doesn’t necessarily- is a great hire.”
[WASHINGTON, D.C. – Feb. 16, 2022] Project Veritas published Part Two of its series on the FDA on Wednesday night which featured FDA Executive Officer, Christopher Cole, speaking about the inner workings of the agency including the FDA’s conflicts of interest, overspending, and why it’s hard for those within the agency to speak out on such abuses.
In the footage, Cole talks about the impact that pharmaceutical companies have on the agency including the process for approving drugs.
“A long time ago, Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers, which will speed up the approval process, so they make more money,” Cole says in the hidden camera footage.
He then reveals that the FDA tones down the impact that these user fees have on the agency’s operations because, “they’re dependent on the drug companies, and the vaccine companies and these other companies for their agency to operate.”
The incendiary footage, which features Cole talking about how the additional money the FDA brings in “gets banked” to be spent on “whatever you can, whether it’s right or wrong,’’ also features Cole discussing reasons why it’s difficult for anyone in government to speak out about practices he sees as “probably excessive.”
“I don’t think there’s enough people saying — they’re, like, ‘Look, that’s fine, but that’s not right. So, we’re not going to charge that.’ You don’t want to be that person. You’re not going to have a long shelf life in the agency if you’re always that person,” Cole said.
“There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it. The whistleblower, well, it’s high-profile whistleblower statutes and everything, that’s kind of ridiculous,” Cole said before adding “it’s better to just stay quiet and accept.”
Cole’s LinkedIn page lists him as an Executive Officer within the agency’s Countermeasures Initiatives, which plays a critical role in ensuring that drugs, vaccines, and other measures to counter infectious diseases and viruses are safe. He made these revelations on a hidden camera to an undercover Project Veritas reporter.
A spokesperson for FDA issued a statement yesterday saying, “The person purportedly in the video does not work on vaccine matters and does not represent the views of the FDA.”
This statement appears to contradict a phone call released Wednesday afternoon by Project Veritas wherein Cole reiterated, during the conversation with Project Veritas Founder and CEO, James O’Keefe, that he is “a manager in the office that helps oversee the approval of the COVID vaccines for emergency approval.”
See Part 1:
Project Veritas videos are available at Odysee and YouTube
Despite a 28% decrease in 0- to 5-year-old U.S. children taking psychostimulants since 2017, new changes to an international mental disorders manual could revert this and put them at risk. Watchdog relaunches PSAs for parents warning “Childhood is not a mental disorder.”
by CCHR International, The Mental Health Industry Watchdog
February 14, 2022
CCHR International warns there could be an increase in the number of children and adolescents prescribed powerful, addictive stimulants for Attention Deficit Hyperactivity Disorder (ADHD) with the new insurance billing codes released this month in the 11th edition of the International Classification of Diseases (ICD), Mental Disorders Section. For years, CCHR International, based in Los Angeles, has conducted a “Fight for Kids” public awareness campaign about the risks of childhood and teen behavior being mis-diagnosed as disorders and “medicated.”
However, changes to ICD-11 reinforce this and as such, it relaunched two Public Service Announcements (PSAs) reminding parents that “Childhood is not a Mental Disorder.”
CCHR welcomes a 28% decrease in U.S. children aged 0-5 years old being prescribed psychostimulants between 2017 and 2020. According to the IQVia Total Patient Tracker database that CCHR obtained for 2017 and 2020, there were 80,235 children in this age group in 2017 prescribed stimulants compared to 58,091 in 2020. Overall, for the 0-17 age group, there was a 14% decrease in the numbers taking psychostimulants.
The U.S. Diagnostic & Statistical Manual of Mental Disorders (DSM-5, being updated in March 2022) and ICD-11 have redefined and categorized ADHD as a “neurodevelopmental disorder,” making it appear to be a neurological or brain-based physical disease when scientific evidence does not substantiate this.
Dr. Fred Baughman, Jr., a retired pediatric neurologist and author of The ADHD Fraud: How Psychiatry Makes “Patients” of Normal Children, said that psychiatric associations representing ADHD as a biologic abnormality of the brain is “neurobiological propaganda” because “psychiatry has never validated ADHD as a biologic entity.”[1]
Prof. Allen Frances, the former Chairman of the DSM-IV Task Force said that the DSM-IV, published in 1994, already created “false epidemics” of ADHD.[2] He wrote that twenty years later, “The rate of ADHD in the U.S. has tripled to a ridiculously inflated 11%. Sales of ADHD medications are approaching an obscenely profitable $10 billion a year.” Frances was forthright about how diagnoses such as ADHD are determined: “There are no objective tests in psychiatry—no X-ray, laboratory or exam finding that says definitively that someone does or does not have a mental disorder….”[3] Inclusion of a disorder in the DSM is by consensus vote.
As such, the fact that ICD-11 and DSM-5 claim ADHD is neurobiological is misleading for parents who could erroneously believe that their child has a faulty brain requiring “medication” rather than an issue which can be handled with behavioral, dietary and educational solutions. Dr. Baughman adds that children have also been led to “believe they have something wrong with their brains that makes it impossible for them to control themselves without a pill.”[4] In saying that, he is not saying that children do not sometimes have trouble with their behavior, focusing, or their emotions; it just simply isn’t neurobiological.
March 21 this year marks the 22nd anniversary of 14-year-old Matthew Smith’s death from a cardiac arrest while skateboarding. Oakland County (Michigan) Medical Examiner Ljubisa Dragovic determined that the skateboarding did not kill Matthew but rather the damage done to his heart from 10 years of taking prescribed methylphenidate, an ADHD psychostimulant that caused a “chronic change of the heart muscle and the small blood vessels in the heart.”[5] Michael’s tragic death was part of the impetus that started CCHR’s Fight for Kids campaign and PSAs.
In 2014, researchers from the University of Delaware and Drexel University College of Medicine reviewed research on the effects of psychostimulants like methylphenidate. They found the drug can impact the brain’s plasticity, interfering with a person’s ability to plan, switch between tasks, and be overall flexible in their behaviors. For a drug that’s supposed to offer better mental performance, they found that the long-term effects appear to do the opposite.[6]
“All proposed ADD and ADHD treatments” are “aimed at modifying observable behaviors rather than in treating their underlying causes,” say other researchers, including Dr. Howard Glasser, writing in Ethical Human Psychology and Psychiatry.[7]
In his last interview before his death in 2009, Dr. Leon Eisenberg, the “scientific father of ADHD” and a leader in child psychiatry for more than 40 years, admitted “ADHD is a prime example of a fictitious disease.”[8] The symptoms are so common that anyone could believe they have ADHD: fails to give close attention to details or may make careless mistakes; work is often messy or disorganized; has problems staying focused on tasks or activities; fails to complete schoolwork, chores or other duties; often fidgets with hands or feet or squirms in seat; often talks excessively and interrupts or intrudes on others (e.g., cuts into conversations).
The consequences of the drugs prescribed to quell such symptoms are telling: The U.S. Drug Enforcement Administration reports methylphenidate can lead to addiction and “psychotic episodes, violent behavior and bizarre mannerisms have been reported” with its use.[9] The manufacturer admits it is a drug of dependency.[10] Suicide is a major complication of withdrawal from it and similar amphetamine-like drugs.[11] FDA also warns of the risks of heart-related problems.
CCHR says the direction ICD-11 and DSM-5 have taken is not in sync with current thinking. Former United Nations Special Rapporteur Dainius Pūras, M.D., in a June 2021 interview with Psychiatric Times, said there is too much reliance upon “the biomedical model and biomedical interventions” for people with mental health or behavioral issues and this represents a “biased use of knowledge and evidence.” In 2017, he also called for a revolution in mental health care around the world, writing: “There is now unequivocal evidence of the failures of a system that relies too heavily on the biomedical model of mental health services, including the front-line and excessive use of psychotropic medicines, and yet these models persist.”[12]
CCHR brought their concerns about the worldwide mass diagnosing of ADHD and prescribing of stimulants to the attention of the UN Committee on the Rights of the Child, which responded with hearings and a recommendation for the establishment of a system for “monitoring of the excessive use of psychostimulants to children.” It also said that governments should “take the necessary measures to prevent any pressure on children and parents to accept treatment with psychostimulant drugs.”[13]
ICD-11 says it changed the category under which ADHD has been placed from “hyperkinetic” to “neurodevelopmental disorders” so that it is not equated as being “disruptive behavior,” but conveys the idea that a child has a deficiently developed brain disease, which experts say it is not. [14]
Child and adolescent video-gamers will also be a potential market under ICD-11 with “gaming disorder.”[15] This has been included in a newly added diagnostic grouping under ICD-11 called “disorders due to addictive behaviors,” again not in response to any scientific evidence but “to global concerns about the impact of problematic gaming, especially the online form.”
As for nebulous “conduct disorders,” such as oppositional defiant disorder and conduct‐dissocial disorder, these are grouped into a new label, “disruptive behavior and dissocial disorder.” ICD‐11 also expanded these from being limiting to children to include across the lifespan.[16] Disorders are no longer grouped by age but reflect a continuous lifespan approach[17]—anyone can be labeled and stigmatized.
Moreover, ICD‐10’s so-called gender identity disorders have been renamed as “gender incongruence” (the condition of not matching or being in agreement) in the ICD‐11 and moved from the mental disorders chapter to the new “sexual health chapter,” meaning that a transgender identity is no longer to be considered a mental disorder.[18] Under DSM, gender identity was called gender dysphoria (unwanted emotional state).[19]
Such arbitrary and capricious diagnosing has come under earlier criticism when in 1973, the American Psychiatric Association committee members voted—5,584 to 3,810—to delete homosexuality as a mental disorder from DSM after gay activists picketed the APA conferences.[20] As The Atlantic reported, “It’s not always that explicit, and the votes are not public. In the case of the DSM-5, committee members were forbidden to talk about it, so we’ll never really know what the deliberations were. They all signed non-disclosure agreements.”[21]
Lawrence Stevens, a former Assistant District Attorney in California, commented: “If mental illness were really an illness in the same sense that physical illnesses are illnesses, the idea of deleting homosexuality or anything else from the categories of illness by having a vote would be as absurd as a group of physicians voting to delete cancer or measles from the concept of disease.”[22]
The late Dr. Keith Conners, who “put ADHD on the medical map,” conducted the first formal trials on the use of methylphenidate. But in 2013, when he was asked to address the American Professional Society of ADHD and Related Disorders, he was so appalled at how many children had been saddled with ADHD, he called it “a national disaster of dangerous proportions.”[23]
The ICD-11 and DSM-5 update can only exacerbate the disaster. Parents, pediatricians, family doctors, and educators should be informed that ADHD is not a proven neurobiological disorder. The behavioral symptoms could be representative of any normal childhood behavior. In an article that has been widely quoted in literature, James T. Webb, Ph.D., reviewed the symptoms of ADHD and noted “almost all of these behaviors are found in bright, talented, creative, gifted children.”[24] Dr. Mary Ann Block, author of No More ADHD advises to look for and treat the underlying causes; don’t just cover symptoms with drugs but “find the cause and fix the problem.”[25]
All of which adds up to: Childhood, including ADHD, is not a mental disorder.
References:
[1] Samantha Gluck, “Does ADHD Exist?” Healthy Place, interview with Dr. Fed Baughman, https://aws.healthyplace.com/adhd/articles/does-adhd-exist
[2] “Watchdog Group Alerts Parents and Teachers About Gifted Children Being Mislabeled ‘ADHD’ and Given Stimulant Drugs,” CCHR International, 9 Aug. 2017, https://www.cchrint.org/2017/08/09/watchdog-group-alerts-parents-and-teachers-about-gifted-children-being-mislabeled-adhd-and-given-stimulant-drugs/, citing: Allen Frances, “DSM 5 Will Further Inflate The ADD Bubble,” Psychology Today, 2 Aug. 2011, https://www.psychologytoday.com/us/blog/dsm5-in-distress/201108/dsm-5-will-further-inflate-the-add-bubble
[3] Allen Frances, “Most Active Kids Don’t Have ADHD,” Psychology Today, 11 Mar. 2014, https://www.psychologytoday.com/us/blog/saving-normal/201403/most-active-kids-don-t-have-adhd; Allen Frances, “Psychiatric Fads and Overdiagnosis,” Psychology Today, 2 June 2010, https://www.psychologytoday.com/us/blog/dsm5-in-distress/201006/psychiatric-fads-and-overdiagnosis
[4] Fred A. Baughman, Jr., MD, “Treatment of Attention-Deficit Hyperactivity Disorder,” Journal of the American Medical Association, Vol. 269, No. 18, 12 May 1993, p. 2369
[5] Caroline Kern, “Death of 14-year-old Caused by Ritalin,” 14 Apr. 2000, http://www.drugfreechild.org/article/Death_of_14-year-old_Caused_by_Ritalin.html
[6] “Bad News For Ivy Leaguers: ADHD Drugs Hurt Your Memory,” TIME Health, 13 May 2014, http://time.com/97448/bad-news-for-ivy-leaguers-adhd-drugs-hurt-your-memory/
[7] Dr. Howard Glasser, et al., “The Online Nurtured Heart Approach to Parenting: A Randomized Study to Improve ADHD Behaviors in Children Ages 6–8,” Ethical Human Psychology and Psychiatry, Vol. 22, 1 Nov. 2020
[8] “New Federal Statistics Show Teen Overdose Deaths From ADHD & Anti-Anxiety Drugs On The Rise,” CCHR International, 22 Aug. 2017, https://www.cchrint.org/2017/08/23/teen-overdose-deaths-from-adhd-anti-anxiety-drugs-on-the-rise/, citing: “Father of ADHD calls himself a liar,” WND, 23 May, 2013 http://www.wnd.com/2013/05/father-of-adhd-calls-himself-a-liar/#SAe7LssguLIzLtry.99
[9] “Methylphenidate (A Background Paper),” U.S. Drug Enforcement Administration, Oct. 1995, p. 16
[11] DSM-III-R, (American Psychiatric Association, Washington, D.C., 1987), p. 136
[12] “UN Special Rapporteur Dainius Pūras Addresses Psychiatry’s Global Coercion & Crisis,” CCHR International, 7 June 2021, https://www.cchrint.org/2021/06/07/un-special-rapporteur-dainius-puras-addresses-psychiatrys-global-coercion-crisis/, citing: Awais Aftab, MD, “Global Psychiatry’s Crisis of Values: Dainius Pūras, MD,” Psychiatric Times, 3 June 2021, https://www.psychiatrictimes.com/view/global-psychiatry-crisis-values; “World needs ‘revolution’ in mental health care – UN rights expert,” United Nations Human Rights, Office of the High Commissioner, 6 June 2017, https://ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=21689
[14] Michael B. First, Steven H. Hyman, Wolfgang Gaebel, “Innovations and changes in the ICD‐11 classification of mental, behavioural and neurodevelopmental disorders,” et al., World Psychiatry, 2 Jan. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6313247/
[15] Tolu Ajiboye, “3 Major Changes to Look for with ICD-11,” Pollen, 9 Oct. 2019, https://www.simplepractice.com/blog/3-major-changes-to-look-for-with-icd-11/
[17] “ICD 11 Takes Centre Stage,” Journal of Psychiatry Reform, 21 June 2019, https://journalofpsychiatryreform.com/2019/06/21/icd-11-takes-centre-stage/
[21] Hope Reese, “The Real Problems with Psychiatry,” The Atlantic, 2 May 2013, https://www.theatlantic.com/health/archive/2013/05/the-real-problems-with-psychiatry/275371/
[23] “New Federal Statistics Show Teen Overdose Deaths From ADHD & Anti-Anxiety Drugs On The Rise,” CCHR International, 22 Aug. 2017, https://www.cchrint.org/2017/08/23/teen-overdose-deaths-from-adhd-anti-anxiety-drugs-on-the-rise/, citing: Gareth Cook, “Big Pharma’s Manufactured Epidemic: The Misdiagnosis of ADHD,” Scientific American, 11 Oct. 2016, https://www.scientificamerican.com/article/big-pharma-s-manufactured-epidemic-the-misdiagnosis-of-adhd; “ADHD: the statistics of a ‘national disaster’” Significance, Dec. 2016 https://rss.onlinelibrary.wiley.com/doi/pdf/10.1111/j.1740-9713.2016.00979.x
[24] James T. Webb, Misdiagnosis And Dual Diagnoses Of Gifted Children And Adults: Adhd, Bipolar, Ocd, Asperger’s, Depression, And Other Disorders, (Great Potential Press Inc., Scottsdale, AZ, 2004), p. 195
A White House email, obtained on behalf of ICAN, shows Facebook, Merck, and the CDC Foundation, whose corporate partners includes Pfizer, have formed an alliance “to use social media and digital platforms to build confidence in and drive uptake of vaccines.” No conflict there.
On August 12, 2021, ICAN, through its attorneys, submitted a Freedom of Information Act request for communications between White House staff and Facebook, Google, and YouTube. In response to this request, ICAN received a June 15, 2021 email sent by Facebook’s then-Public Policy Manager, Nkechi “Payton” Iheme, to several White House employees.
In it, Iheme announces a new initiative, the “Alliance for Advancing Health Care,” between Facebook and several major companies and organizations, including Merck, the Vaccine Confidence Project, the Sabin Vaccine Institute, and the CDC Foundation. Significantly, one of the CDC Foundation’s corporate partners is Pfizer. In the email, Iheme explains that the Alliance is “focused on advancing public understanding of how social media and behavioral sciences can be leveraged to improve the health of communities around the world” and states that its first project is to “provide grants to researchers and organizations for projects that explore how to use social media and digital platforms to build confidence in and drive uptake of vaccines.” Facebook announced this new initiative on June 9, 2021 here.
The conflict of interest is astonishing. This email shows without a doubt that, through the CDC Foundation created “to support the [CDC’s] work,” the federal government, which is in charge of ensuring the safety of vaccines, has teamed up with Big Pharma and Big Tech to push a liability-free product on the world, while attempting to stomp out anyone who questions this arrangement.
Just as the pharmaceutical companies will never rest when it comes to promoting and selling their vaccine products, and the federal government will not rest in its efforts to assist them, we will never rest in exposing the truth regarding these products or in demanding full transparency and full informed consent for any and all vaccines.
The video below was recorded by Australian aboriginal leader Lurnpa, also known as David Cole. He is joined by Northern Territory aboriginal leaders Keith Rory (elder) and Gadrian Hoosan.
Here we share a few key excerpts from Lumpa’s message:
“Everything all governments do on this continent is all about minerals and resources. All interaction and dealings with aboriginal, original, people is about control, oppression and land grabbing — since 1788 to today.
The state, territory and federal quasi-governments are really corporations, vying to steal the land for multinational and national corporations.
The Intervention was nothing but a land grab. It allowed for the removal of the Racial Discrimination Act which resulted in the removal of the land permit system.
Once The Intervention started, 273 exploration permits for uranium mining were approved within the first 6 months of The Intervention. And our communities witnessed a large number of planes and helicopters flying in grid formation across their lands, across the entire territory, mapping out the land, the resources and the minerals.
The current fraudulent pandemic is also being used as an opportunity to steal the land and take as much resources and minerals for the government and private corporations.
I’ve said it from the start, this is not about our health. It is an attempt to remove the tribal people of the land and steal everything. The only thing standing in the way is the tribal people.
This corporate genocide is a war crime. And all involved are complicit.
As the Nuremberg 2 trials [Grand Jury model proceeding] begin, led by Reiner Fuellmich, it is evident through evidence available to all, that this pandemic is a lie. And this experimental vaccine they are forcing upon humanity is nothing but a bioweapon, designed to kill people.”
###
“The planned and approved sell-off of the land contradicts the people’s wishes to not have any businesses on their lands that destroy the land any further.”
###
“It is my belief, through evidence and the mistreatment of our tribal people, that this absolute agenda of all quasi- governments, national and international corporations, is to steal the land and rid the land of the one thing stopping them from completely taking everything — and that’s the sovereign original tribal people of the lands.
The Deagel military website states that the Australian population will decrease to 9 million people by 2025. That’s 16 million people gone.
So these multinational corporations are happy to genocide 15 million non-tribal people in order to convince 1 million tribal people to take this bioweapon — so they can be left with 9 million obedient slaves to mine all these lands and resources they are stealing off the sovereign tribal people through this process.
This is genocide on a grand scale.
These corporate governments and the land councils are trying to eradicate the sovereign tribal people, for the greed of multinational corporate conglomerates and private shareholders, in order to steal the land and resources at the expense of killing off the oldest living culture on the planet.
…
All parties, domestic and foreign, should cease and desist in these actions immediately. This is an evil agenda.
The international community needs to intervene immediately and stop the genocide.”
###
“This is a once-in-a-lifetime opportunity for us to stand together — black and white — to unite, to take back our country and to stop this genocide against all people. And to keep the land healthy, to keep the land safe for future generations.
We can do this. We can work together. We just have to unite and stand together as one.
Please, work with us. Let’s stand together. Let’s free us aa.
In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
###
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals.
“HIV is neither necessary nor sufficient to cause AIDS.” ~ Luc Montagnier, VI Int’l AIDS Conference, Jun 24 1990
If you have been following the news recently, you may have heard that there is currently a new “highly virulent strain” of HIV running around the Netherlands (I think there is a pun in there somewhere). You may also have heard that there is a brand new experimental HIV mRNA vaccine that has shown promise in animals. If you have really been paying attention, you may have even heard of French virologist Luc Montagnier, the man credited with the discovery of HIV, and his various critical statements against the dangerous use of mRNA vaccines for “Covid-19.” If so, you are also most likely aware that during this increased attention geared towards HIV and mRNA vaccines, Luc Montagnier died very recently on February 8th, 2022. While he lived to be the ripe old age of 89, many are suspicious of the timing of his death in light of the current HIV resurgence.
While I do find the timing of all of these events interesting, that is not what this article is about. I have always planned to dive into Montagnier’s original HIV paper but I have held off as the HIV/AIDS scam has been exposed brilliantly by many others before me. However, I have always felt that the HIV fraud is the perfect gateway into understanding the “Covid-19” fraud as the numerous parallels to what is going on today are uncanny. We can see the same misuse of PCR and antibody testing, the same rebranding and reuse of toxic pharmaceuticals, the same collection of various symptoms under one giant umbrella disease, the same propaganda spreading fear of the infected, and the same Anthony Fauci spearheading the whole thing. Even though it is not my intention to touch on all of these aspects in one article, the best place to start unravelling this tangled web of deceit begins with the man who was credited with unleashing the HIV monster upon the world, Luc Montagnier.
In 1983, Montagnier was sent a lymph node sample from a 33-year-old (note the age) male determined to have the symptoms of AIDS. From this sample, Montagnier and his team uncovered what they claimed was a new “retrovirus,” originally known as L.A.V., for lymphadenopathy associated “virus.” After several indirect experiments, the team concluded that further studies were needed in order to determine whether or not the new “virus” had any role in the etiology of AIDS. After this initial discovery of the potential “viral” cause of AIDS, there was a bit of drama in 1984 when American virologist Robert Gallo claimed to have uncovered the cause of AIDS himself with the discovery of HTLV-3. Long story short, it was later determined that Gallo had used/borrowed/stolen a sample from the same patient as Montagnier and uncovered the same “virus.” The “virus” was eventually renamed HIV in 1986 and in 2008, Luc Montagnier was awarded the Nobel Prize for the discovery while Robert Gallo pouted off in a dark corner somewhere.
One of the nicest aspects of writing about Montagnier’s original HIV paper now in 2022 is that in retrospect, Montagnier himself tore apart his own evidence for the existence of his “retrovirus” in the decades following the publishing of his 1983 paper. A perfect example of this is found in a 1997 interview Montagnier did with scientific journalist Djamel Tahi. I have provided highlights from this interview below yet I definitely recommend reading the whole discussion sometime. While reading, note the assumptions made by Montagnier about his “virus,” the various contradictions in his statements, and the revelations about the relation (or lack thereof) of HIV to AIDS. This interview provides an in-depth look into the illogical mindframe of a virologist stuck in unproven theories and pseudoscientific dogma:
Interview with Professor Luc Montagnier by Djamel TAHI – (Pasteur Institut, July 1997)
Djamel TAHI: A group of scientists from Australia argues that nobody up till now has isolated the AIDS virus, HIV. For them the rules of retrovirus isolation have not been carefully respected for HIV. These rules are: culture, purification of the material by ultracentrifugation, Electron Microscopic (EM) photographs of the material which bands at the retrovirus density, characterisation of these particles, proof of the infectivity of the particles.
Luc Montagnier: No, that is not isolation. We did isolation because we “passed on” the virus, we made a culture of the virus. For example Gallo said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.” But before making it emerge in immortal cell lines, we made it emerge in cultures of normal Iymphocytes from a blood donor. That is the principle criterion. One had something one could pass on serially, that one could maintain. And characterised as a retrovirus not only by its visual properties, but also biochemistry, RT [reverse transcriptase] activity which is truly specific of retroviruses. We also had the reactions of antibodies against some proteins, probably the internal proteins. I say probably by analogy with knowledge of other retroviruses. One could not have isolated this retrovirus without knowledge of other retroviruses, that’s obvious. But I believe we have answered the criteria of isolation. Totally.
Djamel TAHI: according to several published references cited by the Australian group, RT is not specific to retroviruses and moreover your work to detect RT was not done in the purified material?
Luc Montagnier: I believe we published in Science (May 1983) a gradient which showed that the RT had exactly the density of 1.16. So one had a ‘peak’ which was RT. So one has fulfilled this criterion for purification. But to pass it on serially is difficult because when you put the material in purification, into a gradient, retroviruses are very fragile, so they break each other and greatly lose their infectivity. But I think even so we were able to keep a little of their infectivity. But it was not as easy as one does it today, because the quantities of virus were nonetheless very feeble. At the beginning we stumbled on a virus which did not kill cells. The virus came from an asymptomatic patient and so was classified amongst the non-syncithia-forming, non-cytopathogenic viruses using the co-receptor ccr5 . It was the first BRU virus. One had very little of it, and one could not pass it on in an immortal cell line. We tried for some months, we didn’t succeed. We succeeded very easily with the second strain. But there lies the quite mysterious problem of the contamination of that second strain by the first. That was LAI.
Djamel TAHI: Why do the EM photographs published by you, come from the culture and not from the purification?
Luc Montagnier: There was so little production of virus it was impossible to see what might be in a concentrate of virus in the gradient. There was not enough virus to do that. Of course one looked for it, one looked for it in the tissues at the start, likewise in the biopsies. We saw some particles but they did not have the morphology typical of retroviruses. They were very different. Relatively different. So with the culture it took many hours to find the first pictures. It was a Roman effort! It’s easy to criticise after the event. What we did not have, and I have always recognised it, was that it was truly the cause of aids.
Djamel TAHI: How is it possible without EM pictures from the purification, to know whether or not these particles are viral and appertain to a retrovirus, moreover a specific retrovirus?
Luc Montagnier: Well, there were the pictures of the budding. We published images of budding which are characteristic of retroviruses. Having said that, on the morphology alone one could not say it was truly a retrovirus. For example, a French specialist of EMs of retroviruses publicly attacked me saying: “This is not a retrovirus, it is an arenavirus”. Because there are other families of virus which bud and have spikes on the surface, etc.
Djamel TAHI: Why this confusion? The EM pictures did not show clearly a retrovirus?
Luc Montagnier: At this period the best known retroviruses were those of type C, which were very typical. This retrovirus wasn’t a type C and lentiviruses were little known. I myself recognised it by looking at pictures of Equine infectious anaemia virus at the library, and later of the visna virus. But I repeat, it was not only the morphology and the budding, there was RT…it was the assemblage of these properties which made me say it was a retrovirus.
Djamel TAHI: About the RT, it is detected in the culture. Then there is purification where one finds retroviral particles. But at this density there are a lot of others elements, among others those which one calls “virus-like”.
Luc Montagnier: Exactly, exactly. If you like, it is not one property but the assemblage of the properties which made us say it was a retrovirus of the family of lentiviruses. Taken in isolation, each of the properties isn’t truly specific. It is the assemblage of them. So we had: the density, RT, pictures of budding and the analogy with the visna virus. Those are the four characteristics.
Djamel TAHI: But how do all these elements allow proof that it is a new retrovirus? Some of these elements could appertain to other things, “virus-like”…?
Luc Montagnier: Yes, and what’s more we have endogenous retroviruses which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles, in any case not in aids.
Djamel TAHI: But then how can one make out the difference?
Luc Montagnier: Because we could “pass on” the virus. We passed on the RT activity in new Iymphocytes. We got a “peak” of replication. We kept track of the virus. It is the assembly of properties which made us say it was a retrovirus. And why new? The first question put to us by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse retrovirus or an animal retrovirus?”. To that one could say no! Because we had shown that the patient had antibodies against a protein of his own virus. The assemblage has a perfect logic! But it is important to take it as an assemblage. If you take each property separately, they are not specific. It is the assemblage which gives the specificity.
Djamel TAHI: With what did you culture the lymphocytes of your patient? With the H9 cell line?
Luc Montagnier: No, because it didn’t work at all with the H9. We used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes.
Djamel TAHI: When one looks at the published electron microscope photographs, for you as a retrovirologist it is clear it’s a retrovirus, a new retrovirus?
Luc Montagnier: No, at that point one cannot say. With the first budding pictures it could be a type C virus. One cannot distinguish.
Djamel TAHI: Could it be anything else than a retrovirus?
Luc Montagnier: No…well, after all, yes…it could be another budding virus. But we have an atlas. One knows a little bit from familiarity, what is a retrovirus and what is not. With the morphology one can distinguish but it takes a certain familiarity.
Djamel TAHI: Why no purification?
Luc Montagnier: I repeat we did not purify. We purified to characterise the density of the RT, which was soundly that of a retrovirus. But we didn’t take the “peak”…or it didn’t work…because if you purify, you damage. So for infectious particles it is better to not touch them too much. So you take simply the supernatant from the culture of lymphocytes which have produced the virus and you put it in a small quantity on some new cultures of lymphocytes. And it follows, you pass on the retrovirus serially and you always get the same characteristics and you increase the production each time you pass it on.
Djamel TAHI: But there comes a point when one must do the characterisation of the virus. This means: what are the proteins of which it’s composed?
Luc Montagnier: That’s it. So then, analysis of the proteins of the virus demands mass production and purification. It is necessary to do that. And there I should say that that partially failed. J.C. Chermann was in charge of that, at least for the internal proteins. And he had difficulties producing the virus and it didn’t work. But this was one possible way, the other way was to have the nucleic acid, cloning, etc. It’s this way which worked very quickly. The other way didn’t work because we had at that time a system of production which wasn’t robust enough. One had not enough particles produced to purify and characterise the viral proteins. It couldn’t be done. One couldn’t produce a lot of virus at that time because this virus didn’t emerge in the immortal cell line. We could do it with the LAI virus, but at that time we did not know that.
Djamel TAHI: Gallo did it?
Luc Montagnier: Gallo?…I don’t know if he really purified. I don’t believe so. I believe he launched very quickly into the molecular part, that’s to say cloning. What he did do is the Western Blot. We used the RIPA technique, so what they did that was new was they showed some proteins which one had not seen well with the other technique. Here is another aspect of characterising the virus. You cannot purify it but if you know somebody who has antibodies against the proteins of the virus, you can purify the antibody/antigen complex. That’s what one did. And thus one had a visible band, radioactively labelled, which one called protein 25, p25. And Gallo saw others. There was the p25 which he calledp24, there was p41 which we saw…
Djamel TAHI: About the antibodies, numerous studies have shown that these antibodies react with other proteins or elements which are not part of HIV. And that they can not be sufficient to characterise the proteins of HIV.
Luc Montagnier: No! Because we had controls. We had people who didn’t have AIDS and had no antibodies against these proteins. And the techniques we used were techniques I had refined myself some years previously, to detect the src gene. You see the src gene was detected by immunoprecipitation too. It was the p60 [protein 60]. I was very dexterous, and my technician also, with the RIPA technique. If one gets a specific reaction, it’s specific.
Djamel TAHI: But we know AIDS patients are infected with a multitude of other infectious agents which are susceptible to induce crossreactions.
Luc Montagnier: Yes, but antibodies are very specific. They know how to distinguish one molecule in one million. There is a very great affinity. When antibodies have sufficient affinity, you fish out something really very specific. With monoclonal antibodies you fish out really ONE protein. All of that is used for diagnostic antigen detection.
Djamel TAHI: For you the p41 was not of viral origin and so didn’t belong to HIV. For Gallo it was the most specific protein of the HIV. Why this contradiction?
Luc Montagnier: We were both reasonably right. That’s to say that I in my RIPA technique…in effect there are cellular proteins that one meets everywhere – there’s a non-specific “background noise”, and amongst these proteins one is very abundant in cells, which is actin. And this protein has a molecular weight 43000kd. So, it was there. So I was reasonably right, but what Gallo saw on the other hand was the gp41 of HIV, because he was using the Western Blot. And that I have recognised.
Djamel TAHI: For you p24 was the most specific protein of HIV, for Gallo not at all. One recognises thanks to other studies that antibodies directed against p24 were often found in patients who were not infected with HIV, and even certain animals. In fact today, an antibody reaction with p24 is considered non specific.
Luc Montagnier: It is not sufficient for diagnosing HIV infection.
Djamel TAHI: No protein is sufficient.
Luc Montagnier: No protein is sufficient anyway. But at the time the problem didn’t reveal itself like that. The problem was to know whether it was an HTLV or not. The only human retrovirus known was HTLV. And we showed clearly that it was not an HTLV, that Gallo’s monoclonal antibodies against the p24 of HTLV did no recognise the p25 of HIV.
Djamel TAHI: At the density of retroviruses, 1.16, there are a lot of particles, but only 20% of them appertain to HIV. Why are 80% of the proteins not viral and the others are? How can one make out the difference?
Luc Montagnier: There are two explanations. For the one part, at this density you have what one calls microvesicles of cellular origin, which have approximately the same size as the virus, and then the virus itself, in budding, brings cellular proteins. So effectively these proteins are not viral, they are cellular in origin. So, how to make out the difference?! Frankly with this technique one can’t do it precisely. What we can do is to purify the virus to the maximum with successive gradients, and you always stumble on the same proteins.
Djamel TAHI: The others disappear?
Luc Montagnier: Let’s say the others reduce a little bit. You take off the microvesicles, but each time you lose a lot of virus, so it’s necessary to have a lot of virus to start off in order to keep a little bit when you arrive at the end. And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of viral origin or not. That’s what we began for p25, that failed…and the other technique is to do the cloning, and so then you have the DNA and from the DNA you get the proteins. You deduce the sequence of the proteins and their size and, you stumble again on what you’ve already observed with immunoprecipitation or with gel electrophoresis. And one knows by analogy with the sizes of the proteins of other retroviruses, one can deduce quite closely these proteins. So you have the p25 which was close to the p24 of HTLV, you have the p18.. in the end you have the others. On the other hand the one which was very different was the very large protein, p120.
Luc Montagnier’s 1997 interview is a highlight reel of revelations. We can see clearly, as Montagnier repeated on more than one occasion, that he himself (and Robert Gallo according to his knowledge) did not purify any “virus.” Why is this important? In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
As most virologists do, Montagnier claimed that even though he did not purify the “virus” and therefore did not have direct evidence for its existence, he had plenty of non-specific indirect evidence that when added together, became “specific” to the “virus.” It was the accumulation of indirect evidence that proved his “virus” existed. In essence, he had a circumstantial case based upon evidence that was not drawn from direct observation. This would be considered a weak case in a court of law.
Looking at his circumstantial case, Montagnier admitted that without purification, images of particles taken from electron microscopy could not be definitively claimed to be “retroviruses” or “viruses” of any kind based on morphological appearance alone. He stated that it was necessary to have knowledge of other “retroviruses” first in order to discover a new one. He himself referred to an atlas of images of other “retroviruses” in order to claim that his unpurified particles were also “retroviruses.”
However, what Montagnier did not admit is that this atlas of “retroviruses” was also made up of images of unpurified particles. Therefore, none of the particles imaged in his atlas could be considered “retrovirus” particles until evidence of purified/isolated “retroviruses” are released. Purification would have had to have occurred with the very first “retrovirus” ever discovered and imaged in order for this method of identification to be valid. Montagnier admitted that while purification is a necessary step, it is impossible as the more you purify the sample, the more damage occurs to the particles and the less “virus” you have at the end. Since he stated that they did not purify the culture used to obtain the EM images of “HIV,” there is no proof that the random particles claimed to be HIV are in fact a “virus” at all.
Montagnier also tried to claim that antibodies/antigens, such as the p24 protein, are specific to HIV and that they can be used as part of the evidence for the existence of his “virus.” However, as Djamel expertly pointed out, these proteins are not specific to HIV as there are over 60 conditions (such as pregnancy, tuberculosis, the flu vaccine, etc.) with related proteins that can trigger positive HIV tests. Montagnier ended up admitting that no protein is sufficient for diagnosing HIV thus nullifying any claims he made about the specificity of antibodies/antigens and their value in being used as indirect evidence for the existence of an unseen “virus.”
The biggest revelation by Montagnier in this 1997 interview is his belief that HIV is not the cause of AIDS. While he believed he had discovered a new “retrovirus” based on an accumulation of weak indirect evidence, according to his statement it was not pathogenic. If we take his indirect evidence and break it down, Motagnier did not have purified “virus” particles which means his EM images are useless, his antibody tests are meaningless, and the genomic sequence is worthless. Without purified particles, he had no proof of pathogeniticity as he had no valid independent variable in order to establish cause and effect. It is amazing that Montagnier believed he had a “virus” at all as in every meaningful way possible, he did not have evidence of one.
All of that being said, for those still interested in reading Montagnier’s original 1983 paper containing no evidence of any “virus” whatsoever, here is the paper in its entirety:
Isolation of a T-Lymphotropic Retrovirus from a Patientat Risk for Acquired Immune Deficiency Syndrome (AIDS)
Abstract. A retrovirus belonging to the family of recently discovered human T-cell leukemia viruses (HTLV), but clearly distinct from each previous isolate, has been isolated from a Caucasian patient with signs and symptoms that often precede the acquired immune deficiency syndrome (AIDS). This virus is a typical type-C RNA tumor virus, buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24. Antibodies from serum of this patient react with proteins from viruses of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate. The virus from this patient has been transmitted into cord blood lymphocytes, and the virus produced by these cells is similar to the original isolate.
From these studies it is concluded that this virus as well as the previous HTLV isolates belong to a general family of T-lymphotropic retroviruses that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS.The acquired immune deficiency syndrome (AIDS) has recently been recognized in several countries (1). The disease has been reported mainly in homosexual males with multiple partners, and epidemiological studies suggest horizontal transmission by sexual routes (2) as well as by intravenous drug administration (3), and blood transfusion (4).
The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes (5) suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent. Alternatively, these modifications may result from subsequent infections. The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma (1). However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males (6) and infants (7) who may or may not develop AIDS (8).
The histological aspect of such lymph nodes is that of reactive hyperplasia. Such cases may correspond to an early or a milder form of the disease. We report here the isolation of a novel retrovirus from a lymph node of a homosexual patient with multiple lymphadenopathies. The virus appears to be a member of the human T-cell leukemia virus (HTLV) family (9).
The retrovirus was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans. Viral core proteins were not immunologically related to the p24 and p19 proteins of subgroup I of HTLV (9). However, serum of the patient reacted strongly with surface antigen (or antigens) present on HTLV-I-infected cells. Moreover, the ionic requirements of the viral reverse transcriptase were close to that of HTLV. Recently, a type-C retrovirus was also identified in T cells from a patient with hairy cell leukemia. Analysis of the proteins of this virus showed they were related to, but clearly different from, proteins of previous HTLV isolates (10).
Moreover, recent studies of the nucleic acid sequences of this new virus show it is less than 10 percent homologous to the earlier HTLV isolates (11). This virus was called HTLV-II to distinguish it from all the earlier, highly related viruses termed HTLV-I. The new retrovirus reported here appears to also differ from HTLV-II. We tentatively conclude that this virus, as well as all previous HTLV isolates, belong to a family of T-lymphotropic retroviruses that are horizontallytransmitted in humans and may be involved in several pathological syndromes, including AIDS.
The patient was a 33-year-old homosexual male who sought medical consultation in December 1982 for cervical lymphadenopathy and asthenia (patient 1). Examination showed axillary and inguinal lymphadenopathies. Neither fever nor recent loss of weight were noted. The patient had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982. During interviews he indicated that he had had more than 50 sexual partners per year and had traveled to many countries, including North Africa, Greece, and India. His last trip to New York was in 1979.
Laboratory tests indicated positive serology (immunoglobulin G) for cytomegalovirus (CMV) and Epstein-Barr virus. Herpes simplex virus was detected in cells from his throat that were cultured on human and monkey cells. A biopsy of a cervical lymph node was performed. One sample served for histological examination, which revealed follicular hyperplasia without change of the general architecture of the lymph node. Immunohistological studies revealed, in paracortical areas, numerous T lymphocytes (OKT3+). Typing of the whole cellular suspension indicated that 62 percent of the cells were T lymphocytes (OKT3+), 44 percent were T-helper cells (OKT4+), and 16 percent were suppressor cells (OKT8+).
Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon (12). The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by viruses, including retroviruses. In the mouse system, we had previously shown that antiserum to interferon could increase retrovirus production by a factor of 10 to 50 (13). After 3 days, the culture was continued in the same medium without PHA. Samples were regularly taken for assay of reverse transcriptase and for examination in the electron microscope.
After 15 days of culture, a reversetranscriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I (14). Virus production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation. Peripheral blood lymphocytes cultured in the same way were consistently negative for reverse transcriptase activity, even after 6 weeks. Cytomegalovirus could be detected, upon prolonged co-cultivation with MRC5 cells, in the original biopsy tissue, but not in the cultured T lymphocytes at any time of the culture.
Virus transmission was attempted with the use of a culture of T lymphocytes established from an adult healthy donor of the Blood Transfusion Center at the Pasteur Institute. On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions. Reverse transcriptase activity could be detected in the supernatant on day 15 of the coculture but was not detectable on days 5 and 10. The reverse transcriptase had the same characteristics as that released by the patient’s cells and the amount released remained stable for 15 to 20 days. Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks whenthe culture was discontinued.
The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml). After a lag period of 7 days, a relatively high titer of reverse transcriptase activity was detected in both of the cord lymphocyte cultures. Identical cultures, which had not been infected, remained negative. These two successive infections clearly show that the virus could be propagated on normal lymphocytes from either newborns or adults.
That this new isolate was a retrovirus was further indicated by its density in a sucrose gradient, which was 1.16, and by its labeling with [3H]uridine (Fig. 1). Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane (Fig. 2).
Virus-infected cells from the original biopsy as well as infected lymphocytes from the first and second viral passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme. The results were the same in all instances. The reverse transcriptase activity displayed a strong affinity for poly(adenylate-oligodeoxythymidylate) [poly(A) -oligo(dT)], and required Mg2+ with an optimal concentration (5 mM) slightly lower than that for HT (14) and an optimal pH of 7.8. The reaction was not inhibited by actinomycin D. This character, as well as the preferential specificity for riboseadenylate *deoxythymidylate over deoxyadenylate * deoxythymidylate, distinguish the viral enzyme from DNA-dependent polymerases.
We then determined whether or not this isolate was indistinguishable from HTLV-1 isolates. Human T-cell leukemia virus has been isolated from cultured T lymphocytes of patients with T lymphomas and T leukemias [for a review, see (9)]. The antibodies used were specific for the p19 and p24 core proteins of HTLV-I. A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytes obtained from a healthy donor and infected with the same virus. As shown in Table 1, the virus-producing cells did not react with either type of antibody, whereas two lines of cord lymphocytes chronically infected with HTLV (17) and used as controls showed strong surface fluorescence.
When serum from patient 1 was tested against infected lymphocytes from the biopsy the surface fluorescence was as ntense as that of the control HTLV-producing lines. This suggests that serum of the patient contains antibodies
that recognize a common antigen present on HTLV-I-producing cells and on the patient’s lymphocytes. Similarly, cord lymphocytes infected with the virus from patient 1 did not react with antibodies to p19 or p24. Only a minor proportion of the cells (about I percent) reacted with the patient’s serum. This may indicatethat only this fraction of the cells was infected and produced virus. Alternatively, the antigen recognized by the patient’s serum may contain cellular determinants that show less expression in T lymphocytes of newborns.
We also cultured T lymphocytes from a lymph node of another patient (patient 2) who presented with multiple adenopathies and had been in close contact with an AIDS case. These lymphocytes did not produce viral reverse transcriptase; however, they reacted in the immunofluorescence assay with serum from patient 1. Moreover, serum from patient 2 reacted strongly with control HTLV-producing lines (not shown). In order to determine which viral antigen was recognized by antibodies present in’ the two patients’ sera, several immunoprecipitation experiments were carried out. Cord lymphocytes infected with virus from patient I and uninfected controls were labeled with [35S]methionine for 20 hours. Cells were lysed with detergents, and a cytoplasmic S10 extract was made. Labeled virus released in the supernatant was banded in a sucrose gradient.
Both materials were immunoprecipitated by antiserum to HTLV- I p24, by serum from patients 1 and 2, and by serum samples from healthy donors. Immunocomplexes were analyzed by polyacrylamide gel electrophoresis under denaturing conditions. Figure 3 shows that a p25 protein present in the virus-infected cells from patient 1 and in LC1 cells infected with this virus, was specifically recognized by serum from patients I and 2 but not by antiserum to HTLV-1 p24 or serum of normal donors.
Conversely, the p24 present in control HTLV-infected cell extracts was recognized by antibodies to HTLV but not by serum from patient 1. A weak band (lane 2, Fig. 3B) could hardly be seen with serum from patient 2, suggesting some similarities of the p25 protein from this patient’s cells with HTLV-1 p24. When purified, labeled virus from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000. The 45K protein may be dueto contamination of the virus by cellular actin which was present in immunoprecipitates of all the cell extracts (Fig. 3).
These results, together with the immunofluorescence data, indicate that the retrovirus from patient 1 contains a major p25 protein, similar in size to that of HTLV-I but different immunologically. The DNA sequences of these and other members of the HTLV family are being compared. All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful.
The role of this virus in the etiology of AIDS remains to be determined. Patient 1 had circulating antibodies against the virus, and some of the latter persisted in lymphocytes of his lymph node (or nodes). The virus-producing lymphocytes seemed to have no increased growth potential in vitro compared to the uninfected cells. Therefore, the multiple lymphadenopathies may represent a host reaction against the persistent viral infection rather than hyperproliferation of virus-infected lymphocytes. Other factors, such as repeated infection by the same virus or other bacterial and viral agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity.
doi: 10.1126/science.6189183.
That’s an impressive circle. Montagnier looks quite pleased with his creation.
In Summary:
According to HIV discoverer Luc Montagnier, they did “isolate” HIV because they “passed on” the “virus” and they made a culture of the “virus”
He stated that Robert Gallo (American virologist who plagiarized Montagnier’s work) said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.”
But before making it emerge in immortal cell lines, Montagnier claimed his team made it emerge in cultures of normal Iymphocytes from a blood donor
Montagnier stated that it is obvious one could not have isolated any retrovirus without knowledge of other “retroviruses”
To pass a “virus” on serially is difficult because when you put the material in purification, into a gradient, “retroviruses” are very fragile, so they break each other and greatly lose their infectivity
At the beginning they stumbled on a “virus” which did not kill cells
It was the first BRU “virus,” yet they had very little of it and could not pass it on in an immortal cell line
They were later successful with the second strain yet Montagnier stated that there lies the quite mysterious problem of the contamination of that second strain by the first which was LAI
Quick sidenote: BRU and LAI are considered the first strains of HIV
“The original isolate HIV-1 Bru, formerly called LAV, was derived from patient BRU. HIV-1 Lai was derived from patient LAI and contaminated a HIV-1 Bru culture between 20 July and 3 August 1983. The culture became, in effect, HIV-1 Lai, identifiable by a unique motif in the V3 loop. Because of this contamination two, rather than one, HIV-1 isolates were sent to the Laboratory of Tumor Cell Biology at the National Cancer Institute on 23 September 1983.”
When asked about the lack of purification for EM imaging of HIV, Montagnier stated that there was so little production of “virus”it was impossible to see what might be in a concentrate of “virus” in the gradient
What they saw were some particles but they did not have the morphology typical of “retroviruses” as they were very different
He claimed it was “a Roman effort” with the culture as it took many hours to find the first pictures
On the morphology alone one could not say the EM images were truly a “retrovirus”
A French specialist of EMs of “retroviruses” publicly attacked Montagnier saying: “This is not a retrovirus, it is an arenavirus” as there are other families of “virus” which bud and have spikes on the surface, etc.
He stated that it was not only the morphology and the budding, but that there was reverse transcriptase
It was not one property but the assemblage of the properties which made them say it was a “retrovirus” of the family of “lentiviruses”
Taken in isolation, each of the properties isn’t truly specific
The four properties were:
The density
Reverse Transcriptase
Pictures of budding
The analogy with the visna “virus”
Montagnier stated that we have endogenous (human origin) “retroviruses” which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles
The first question put to them by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse “retrovirus” or an animal “retrovirus?”
Montagnier stated that it was important to take it as an assemblage as if you take each property separately, they are not specific and it is the assemblage which gives the specificity
When culturing the “virus,” they used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes
He admitted that when viewing EM images, one cannot distinguish if the particle is a “retrovirus” or not
They used an atlas of previous “retroviruses” to determine if the “virus” had the morphology of one as it takes a certain familiarity to distinguish them
Montagnier repeated they did not purify the “virus” because if you purify, you damage the “virus” particles
He stated that for infectious particles, it is better to not touch them too much
Analysis of the proteins of the “virus” demands mass production and purification and so it is necessary to do that
In that regard, Montagnier claimed that they partially failed
They did not have enough particles produced to purify and characterise the “viral” proteins as it couldn’t be done
They couldn’t produce a lot of “virus” at that time because the “virus” didn’t emerge in the immortal cell line
Montagnier stated that he believed Gallo also did not purify and he believed Gallo had launched very quickly into the molecular cloning part
He also said that you cannot purify the “virus” but if you know somebody who has antibodies against the proteins of the “virus,” you can purify the antibody/antigen complex
However, this is a complete contradiction as he claimed that purification needed to be done in order to characterise the proteins of the “virus,” so if you can’t purify the “virus” to characterise the proteins, you would be unable to know which proteins act against the “virus”as well as any specific antibodies reacting to them
Montagnier claimed antibodies are very specific and that they know how to distinguish one molecule in one million
With monoclonal antibodies you fish out really ONE protein and all of that is used for diagnostic antigen detection
There are cellular proteins that one meets everywhere – there’s a non-specific “background noise”
An antibody reaction with p24 is considered non specific and it is not sufficient for diagnosing HIV infection
Montagnier agreed that no protein is sufficient to diagnose HIV
When asked why, at the 1.16 density gradient band, 80% of the particles are “non-viral” and only 20% are HIV, Montagnier explained that at this density, there are microvesicles of cellular origin, which have approximately the same size as the “virus,” and then the “virus” itself, in budding, brings cellular proteins
Effectively these proteins are not “viral” and are cellular in origin
He stated that with this technique one can’t differentiate them precisely
If you purify the “virus” to the maximum with successive gradients, you always stumble on the same proteins
Montagnier stated that the other proteins only reduce a little bit as you can take off the microvesicles, but each time you lose a lot of “virus,” so it’s necessary to have a lot of “virus” to start off in order to keep a little bit when you arrive at the end
And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of “viral” origin or not
However, what Montagnier doesn’t seem to understand is that if you can not purify the “virus” in order to determine which proteins belong to the “virus,” sequencing proteins will not tellyou if they are “viral” or not
This “virus” is a typical type-C RNA tumor “virus,” buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24
Antibodies from serum of this patient react with proteins from “viruses” of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate
Remember, Montagnier admitted they did not purify the “virus” and that purification was necessary in order to characterise the proteins of the “virus, so how would they know if the antibodies are reacting to “virus” proteins?
The “virus” from this patient has been transmitted into cord blood lymphocytes, and the “virus” produced by these cells is similar to the original isolate
From these studies it is concluded that this “virus” as well as the previous HTLV isolates belong to a general family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent
Alternatively, these modifications may result from subsequent infections
The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma
However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males and infants who may or may not develop AIDS
The “retrovirus” was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans
They tentatively (i.e. subject to further confirmation; not definitely) concluded that this “virus,” as well as all previous HTLV isolates, belong to a family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
The patient the “virus” came from had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982
Oddly enough, syphilis has the exact same symptoms of AIDS and the usual treatment is a series of Penicllin injections, which coincidentally (or not) can destroy a person’s “immune” system
Laboratory tests indicated positive serology (immunoglobulin G) for “cytomegalovirus” (CMV) and Epstein-Barr “virus“
Herpes simplex “virus” was detected in cells from his throat that were cultured on human and monkey cells
Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon
The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by “viruses,” including “retroviruses”
After 15 days of culture, a reverse transcriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I and “virus” production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation
Quick sidenote: Montagnier stated here that the “virus” was cultured for 30 days, as it took 15 days for the reverse transcriptase activity to be detected and another 15 days for the “virus” production to decrease. Interestingly, in a paper he wrote in 2003, Montagnier stated this:
“The initial clinical isolate, unlike HTLV, had no transforming or cytopathic effects on T lymphocytes. Barré-Sinoussi notes in her commentary that the lymphocyte culture I started from the patient’s lymph node biopsy died after 4 weeks. But this was anticipated as soon as we realized that the cells were not transformed, because normal cultures of the same type also die within this time period.The need for succesive use of peripheral blood mononuclear cells to maintain a viral culture was therefore a likely hypothesis that proved to be correct. The virus would later be classified as non-syncytium-inducing, as is usually the case for viruses isolated from recently infected HIV patients who are either asymptomatic or present with lymphadenopathies. However, the first typical cytopathic effect, formation of large syncytia, was not observed until 5 months later, in a third clinical sample (HIV LAI) from a patient who had full-blown AIDS.”
It appears they cultured the “virus” for 30 days knowing full well that regular cultures of the same type die within this 4 week time frame. Montagnier stated that they did not even notice the cytopathic effect (CPE) until they had a third clinical sample 5 months later. CPE is claimed to be structural changes in host cells that are caused by “viral” invasion and yet, this was absent in their first two samples.
On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions
Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks when the culture was discontinued
The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml)
FYI, Polybrene was shown to negatively impact the proliferation and maintenance of growth potential of human keratinocytes here
Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane
“Virus-infected” cells from the original biopsy as well as infected lymphocytes from the first and second “viral” passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme
A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect (i.e. not directly caused by or resulting from something) fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytesobtained from a healthy donor and infected with the same “virus” (why did they not use healthy donor lymphocytes without the added “virus?”)
Cord lymphocytes infected with the “virus” from patient 1 did not react with antibodies to p19 or p24
Only a minor proportion of the cells (about I percent) reacted with the patient’s serum
This may indicate that only this fraction of the cells was infected and produced “virus”
When purified, labeled “virus” from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000
The 45K protein may be due to contamination of the “virus” by cellular actin which was present in immunoprecipitates of all the cell extracts (i.e. “purified” with contaminants…otherwise known as not purified)
All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful
The role of this “virus” in the etiology of AIDS remains to be determined (ultimately, Montagnier believed his “virus” did not cause AIDS)
Other factors, such as repeated infection by the same “virus” or other bacterial and “viral” agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals. The stigma of the positive test result is the “viral” scarlet letter unfairly placed upon a person in a toxic state due to lifestyle choices and/or environmental factors. It does not matter that Montagnier attempted to steer his monster from the lethal killer it was made out to be into a harmless passenger inside the human body. It does not matter that he believed HIV did not cause AIDS. It does not matter that he believed that co-factors other than a “virus” should be examined in regards to AIDS. It does not matter that he believed HIV could be eliminated based on healthy diet/lifestyle choices. It does not matter that he admitted to not purifying any “virus.” Montagnier’s legacy is tied to the beast of his own creation. He opened Pandora’s Box and released this fraudulent curse upon the world. For that, I doubt he will rest in peace.
Truth Comes to Light editor’s note: In the following video, Spacebusters uses images to artistically highlight & add clarity to an essential part of a conversation (Merritt Medical Hour — February 2, 2022) between Dr. Lee Merritt & Dr. Tom Cowan. See the entire interview at Merritt Medical Hour on BrighteonTV.
To those of us that know that virology’s “isolation” and genomic sequencing methodologies are anti-scientific, it is still interesting to see the proponents of the nonsense offer official explanations about what they are up to.
Here in New Zealand, the Institute of Environmental Science and Research (ESR) is responsible for some of the alleged isolation experiments and genomic sequencing of the imaginary “SARS-CoV-2” particle, that they claim is responsible for the clinically undefined illness “COVID-19”. On the 9th of February 2022, they responded to questions surrounding the methodology of their cell culture and genomic sequencing experiments in relation to an Official Information Act request (which is analogous to a Freedom of Information request).
ESR couldn’t seem to find the “virus” but they featured this pretty picture.
So let’s have a look at the ESR’s “scientific” method with regards to their official records of a “SARS-CoV-2 virus”…
“Viral Culture/Experiment details –
Once the cells are 90 – 100% confluent, they are inoculated with 500 uL of diluted clinical sample (sample is diluted 1:10 in Infection media),10 mL of Infection Media is added to the flask. Infection media is made up of DMEM with 1% pen/strep/gentamycin, 1% Nystatin, 1% Glutamax, 1.5% Hepes plus 4ug/mL TPCK added.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
The “clinical sample” will be something like a crude nasopharyngeal sample taken from a patient. These specimens contain human tissue (from the host and other individuals in close contact with them), various bacterial and fungal elements, and whatever other material was in the patient’s mucosa. Amongst all this biological soup is the alleged SARS-CoV-2 virus, which of course, has never been directly found in any person. Apparently there can be 200 million copies of the virus in a sneeze but strangely they can’t find any in an “infected” individual.
Instead they resort to tissue culture experiments, as the ESR continues to explain…
“The flasks are then placed into an incubator and monitored for cytopathic effect (CPE) A SARS-CoV-2 N gene PCR is performed on the diluted 1:10 clinical sample and on the supernatant of the flask after 1 week of incubation (or sooner if 100% CPE is evident). CT values for both specimens are used as well as the CPE observed in the flask to determine if viral culture has been successful.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
Cytopathic effects are non-specific and are simply the observation that cells being stressed in a test tube eventually break down and die, with some cells producing vesicles. However, in the world of virology it is seen as evidence that a virus is at work and is somehow destroying the cells from within. “SARS-CoV-2 N gene” is a misnomer because there has never been a demonstration of a viral particle that contains this genetic sequence. Even more problematic is that there’s never been a demonstration of any viral particle. However, here we see them claiming “successful” viral culture if they detect a single short genetic sequence by PCR amplification. Note to virologists: detecting genetic sequences of unproven provenance does not equal virus.
Then we get to another interesting part…
“Viral culture/experiment details of the negative control –
The method above is also used for the negative control and the flask undergoes the same conditions as the flasks used for viral culture, however we use Infection media only.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
How on earth is this a comparable control experiment? – they added no control sample to their culture brew. In their first experiment they added a veritable biological soup containing human tissue along with various microorganisms and other organic fragments (everything present in a respiratory tract sample), and their alleged virus of course. Examples of valid control experiments would be:
The same type of sample taken from a well person.
The same type of sample taken from a person with a comparable clinical condition but said not to have “COVID-19” (without biased pre-selection in the form of a PCR result.)
Ironically, both of the above become meaningless in the case of “COVID-19” as it has no specific symptoms, signs, or investigations outside of the PCR result – a PCR result that has never been validated to a clinical condition. In fact, a priori the PCR could never be validated in this application as it is simply a tool to amplify selected genetic fragments, not determine their origin or the significance of their presence in mixed biological samples. So, in the case of (1) above, many well people are said to have “COVID-19” and in the case of (2), there is no way to distinguish a novel clinical condition. Dr Sam Bailey explained these problems back in 2020 in “What is a COVID-19 Case?” – a video banned by Big Tech after several hundred thousand views but still available here.
The wheels really fall off the ESR’s response when they are asked to explain how they purify the alleged virus sample for genomic sequencing and compare this to a control:
“’Whole Genome’ Sequencing – Purity and Control Details:
[• The degree of purity of the “virus” sample used in the sequencing experiment.] The protocols used for amplification of the SARS-CoV-2 virus consists of primers that specifically and selectively amplify the viral material, any remaining host or bacterial material is filtered out programmatically prior to data analysis.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
Either they don’t understand the question or are being disingenuous here. Their response doesn’t provide any evidence that they have a virus, let alone have attempted to purify it, in the analysis of its purported genome. They are simply using a process that amplifies sequences they have artificially selected but as it is a mixed sample they cannot demonstrate the origin of them. There is no way to claim this is “viral material” because no one has ever demonstrated that these sequences come from inside a virus, let alone belong to “SARS-CoV-2”. They are simply building on the nonsense that has spun out of control on GISAID.org where not one of the millions of deposited “genomes” has been shown to come from inside a viral particle. It’s turtles all the way down with these contrived “genomes”.
And with regards to the ESR’s “controls”?…
“[• All details of the control group that was used when comparing the results of sequencing:
o the total nucleic acid extracted from the “viral lysate” (from the experimental group), versus
o the total nucleic acid extracted from the non-viral lysate (from the control group).]
The protocols used to extract RNA from clinical samples do not yield a uniform quantity as this depends on the viral load within a sample. Details about the ranges obtained and used for further analysis are published in detail in several scientific peer-reviewed publications and can also be found on the publicly accessible protocols.io website, link provided below as requested.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
They appear to have dodged the question and the protocols provide no evidence of valid control experiments. The ESR have been asked to clarify this but we can already see they are not adhering to the scientific method. I also looked at the four publications that they suggested but these simply confirmed the problem: there is no evidence of any virus and the world is being duped in this war on humanity.
In fact, by definition, there has never been a demonstration of any disease-causing virus ever, full stop. Even if the ESR performed valid genomic control experiments there would still need to be further experiments to demonstrate the existence of a replication competent, obligate intracellular parasite that causes disease in a host. In other words, the actual existence of a virus. It makes me wonder whether the virologists are going to change the very definition of a virus soon in order to keep the whole façade afloat. However, once people realise that virology has never fulfilled its own postulates, they can take a major step away from this health misconception and ignore any of the related damaging measures and “treatments” coming from the medical-pharmaceutical complex.
In an October, 2021 Forbes article, AstraZeneca marketed an experimental “injectable antibody therapy cocktail” to a fearful public. Without valid research, or proof, it claimed its cocktail to be effective at preventing severe illness or death in people with mild or moderate Covid-19 infections. It claimed its therapy cut the risk of death or severe illness by two-thirds (67%) if given within five days of showing symptoms.
The cocktail was marked as experimental for a reason.
Neither AstraZeneca, nor any vaccine maker, has ever revealed the ingredients of its experimental antibody or mRNA cocktail to the public. Neither have they provided informed consent as part of the offer.
Everything is an offer to contract, whether it be a personal, medical, or a business relationship. Every vaccinated subject must sign that they take full responsibility. Because no one else will.
According to the AMA, Informed Consent is required in all medical contracts in order to provide the nature, purpose, burdens, and risks of the proposed medical intervention so the patient can formally consent. The informed consent process falls under 45 CFR 46, for human subjects in research, which sounds a lot like conducting human experimentation. Americans were warned by the Secretary of State in March of 2020 that COVID is a live exercise.
In the beginning, COVID injectables were deployed as Emergency Use Authorized, or EUA, meaning, Off-label, Experimental Research, Unapproved, and without Informed Consent. In other words, use at your own discretion. Until recently, if you wanted to know what was inside the injectable mRNA cocktails, you were handed a blank piece of paper. However, what was hidden is now being revealed.
In November 2020 Dr Andreas Noack, a German chemist and one of the EU’s top graphene experts, released a video explaining that he had discovered graphene hydroxide contained in the COVID-19 experimental treatments. He described how the graphene hydroxide nano structures injected into the human body act as ‘razor blades’ inside the veins of recipients and how they would not show up on an autopsy or normal toxicology tests given their atomic size. On 26th November 2021, just hours after publishing his latest video about graphene hydroxide, he died in suspicious circumstances.
Professor Dr Pablo Campra, University of Almeria, Spain also examined Covid-19 experimental treatments in November 2021 using Micro-Raman Spectroscopy, the study of frequencies. He too confirmed the presence of graphene.
The charges center around the nano-ingredient, graphene hydroxide (GHO), discovered in EUA COVID injections. Considered to be a trade secret, GHO is not found on any label. Therefore, no one would be the wiser, except that GHO can be identified for its polymeric signature properties using Micro-Raman Spectroscopy. Other methods used to verify the serums morphologies and contents include: Optical Microscope, Dark-Field Microscope, UV absorbance and fluorescence spectroscope, Scanning Electron Microscopes, Transmission Electron Microscope, Energy Dispersive Spectroscope, X-ray Diffractometer, and Nuclear Magnetic Resonance instruments.
Damage Report
Trade secrets aside, Graphene hydroxide is well known in the world of science. A Pubmed database search generates over 18,000 published studies on ‘Graphene oxide’. Whether called graphene oxide (GO), or graphene hydroxide, (GOH), it is nanotechnology invisible to the human eye. Graphene has optical, thermal, mechanical, and electrical properties, with applications in silicon-based semi-conductor devices. Once inside the human body, graphene acquires magnetic properties and becomes a superconductor. The human superconductor.
Graphene is isolated from crystalline graphite. It is a flat monolayer composed of single-atom-thick, two-dimensional sheets of a hexagonally arranged honeycomb lattice. A summary of the findings detailed in the attached toxicology report reveals that Graphene nanomaterials (GFNs) can penetrate the body’s natural barriers and damage the central nervous system.
Summary of Graphene hydroxide (GOH) in biological systems:
Epigenetic toxicity comes from toxic environmental exposures which exert undesirable genetic effects on living organisms. Epigenetic toxins are found in water, air, food, and medical drugs, including nanotech. The current focus of graphene nanotech utilizes its electromagnetic properties as a carrier and adjuvant in vaccines. For instance, UV Fluorescence test results from the Pfizer BioNanoTech vaccine, show nanomaterial present in the vial that corresponds perfectly to that of graphene oxide (340 nm).
Due to its magnetic properties, Graphene oxide nanoparticles have the ability to absorb radiation from frequency 5G technology. Unfortunately, most MSDS sheets ignore contact by injection, and electromagnetic effects. If injected into the body, these nanoparticles have the ability to not only cause biological harm, but also to absorb radiation and convert gigahertz signals to terahertz signals, thousands of times higher than those created by silicon, alone. The European Union research group called EUCALL states:
What makes this feat possible is the highly efficient non-linear interaction between light and matter that occurs in graphene. The researchers used graphene containing a large number of free electrons that originated from the interaction between graphene and the substrate onto which it was deposited. When these electrons became excited by an oscillating electric field in room-temperature conditions, they rapidly shared their energy with bound electrons in the material.
It is best to lower expectations for justice to prevail in the UK case, or any case, of criminal corporations who geo-engineer humanity using experimental cocktails. After all, it is the individuals hidden behind the “corporate entity” who write history. For as long as humans have lived on earth, biology, along with history, has been altered. (See Arthur Firstenberg’s book, The Invisible Rainbow). Nothing changes when criminal defendants are identified as “corporate entities,” without names and insurance bonds. It becomes impossible stop the interconnected crimes, let alone stop the madness.
History and biology continue to be rewritten and transformed. While fraud is allowed to continue under the guise of ineffective public shaming rituals that pass for justice, humanity is entering a new Transhuman Age. With so many corporate criminals protected by bubble indemnity, there is a question that must be asked. Is the Corporate Manslaughter and Corporate Homicide Act of 2007 and other Acts like it, a distraction, established to legalize the Act of Corporate Homicide, rather than deter it?
The way to rewrite history and biology is an individual process of knowing who you are and of rejecting The Transhuman Agenda.
Disclaimer: The author encourages you to consult your health care practitioner before making any health changes, especially any changes related to a specific diagnosis or condition. No information in this article should be relied upon to determine diet, make a medical diagnosis, or to determine or prescribe a treatment for a medical condition. This information is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice. It is intended to build synapses for thinking.
Through a Freedom of Information Request, a watchdog organization revealed that the National Institutes for Health spent $2.3 million of taxpayer money injecting puppies with cocaine.
The point of the experiment was to see how a certain prescription drug reacted with cocaine.
The dogs were then euthanized, or used in further experiments.
This is the second recent example of the NIH funding cruel experiments using puppies.
In October, we talked about an experiment from Anthony Fauci’s National Institute of Allergy and Infectious Diseases (a sub agency of the NIH) which forced beagle puppies into mesh cages to allow sand flies to attack their heads, and spread parasites.
Some of the dogs’ vocal cords were removed so that Fauci’s researchers did not have to hear them cry.
At the time, FDA officials clarified that none of these experiments require testing on dogs.
These are the totally ethical health experts we are supposed to trust.
And the answer to that question is obvious. Throwing babies into a volcano makes no money for Pfizer.
On Feb. 15, the FDA will decide whether to approve the Pfizer COVID shot for children between the ages of six months and four years. The press and gov’t. spokespeople predict it’s a GO.
This is murder.
The FDA approval committee members will come in several categories: those who’ve been paid off; those who’ve been threatened; straight-out cold Nazi bureaucrats; those who’ve been blackmailed; and those who WANT TO murder babies.
You can’t get around this. Given the mainstream view of COVID, these FDA/CDC people KNOW the risk of the disease to babies is non-existent, and risks of the vaccine are absolutely devastating.
—Over a million vaccine injuries have already been reported to the US federal database; and this number represents vast UNDER-REPORTING.
Nevertheless, the FDA deciders are ready to say, unless exposed for what they are: inject the babies; kill the babies.
If you still think the government COVID response had anything to do with science or public health or human concern, if you’re still making excuses for Fauci and the whole rogue crew of predators and maniacs at the FDA and CDC, you’re an automatic robot; you just don’t know it.
Get a load of this. CNBC: “Pfizer amended its clinical trial in December to evaluate a third dose after two shots did not induce an adequate immune response in children 2- to 4-years-old. Pfizer and BioNTech said they will submit data on the third dose to the FDA in the coming months.”
I see. The vaccine didn’t work after 2 shots, but it’ll be approved anyway in few days, and Pfizer will let us know IN A FEW MONTHS how the third shot worked.
And that’s science. That’s the bullshit the educated class believes in. That’s the bullshit the deaf, dumb, and blind believe in.
And THE TRUCKERS are the terrorists. Sure. The government is righteous and just. Of course.
People “who spread misinformation about COVID” are terrorists. The government is righteous and just.
Love the government. Hate the terrorists.
Memo to parents: if you’ve been crazy enough to take the shots yourselves, are you ready to deliver your innocent babies into the hands of doctors and nurses who’ll spin the roulette wheel of death and inject their bodies? Is that what you’re going to do?
If so, why? Do you think it’ll make a nice talking point when you get together with friends? Do you think it’s a potent virtue signal? Do you think it proves you’re a loyal subject of the king?
Perhaps you can show up at a local school board meeting, with your infant in your arms; and you can look at the doughy morbid faces of the low-rent grifters sitting behind their long table, and you can say, “Look! I just had my baby shot with the vaccine! It’s wonderful!” And they’ll nod approvingly.
And some piece of dreck who picks up a paycheck as a city public health official will speak at the meeting. He might say vaccinated babies should wear masks. Ask him and find out. Look at his eyes. His brother-in-law, who knows the mayor, rescued him from a career as a gravedigger.
I want to know what the Pope thinks. He’s already stated taking the vaccine is a loving gift to God. What about the babies? Does Popius Maximus Jesuiticus believe The Lord wants infants injected? Let’s get this Pontiff on the record.
Would Mary, in her hut, have told the local doc to inject baby Jesus? Perhaps her husband Joseph, a minor character in the story up to that point, would have brandished a Glock and motioned the sawbones to the door.
Speaking of guns, I think four or five Secret Service agents, their weapons drawn, should usher Nurse Jill to the White House residence, where she will speak candidly and starkly to old Joe—spending as much time as necessary informing him about what the FDA is ready to do, until he UNDERSTANDS.
Then, the agents will force Joe in front of a camera—going live on major channels—where he will unambiguously declare his position on injecting babies.
If he supports the program, he will take full responsibility for the consequences.
After all, the FDA is an agency in the Executive Branch, under the President.
The buck stops with him. It should stop under harsh television spotlights, where no tap-dancing is permitted.
Of course, you parents will have the last word. Unless the guns of the State are pointed at you. If that comes to pass, are you ready to die fighting for your children?
Or will you sacrifice them on the altar of your own passivity and cowardice?
I STRONGLY suggest you make your position clear now.
Publically.
Leave no doubt.
Before it’s too late.
WE NEED AN UPROAR.
Are you standing up? Or are you grinning and virtue signaling—down on your knees?
The Covid19 narrative is broken, that battle is over. Yes, there are still pockets of token resistance, little embattled squares who aren’t ready to give up the ghost just yet, but for the most part the establishment are letting it go.
Country after country after country are “relaxing” their Covid restrictions, abandoning vaccine passport plans and attempting to “get back to normal”.
It seems every week some new “expert” who spent the last two years predicting we’re all gonna die turns up on the news claiming we should “treat Covid like the flu”.
But just because they’re giving slack on Covid does not mean the agenda behind Covid is gone. Far from it.
In fact, even as they seek to dump this pandemic in a shallow grave, they are already prepping the public for the next health scare – AIDs.
Then, just last week it was suddenly reported there was a “new variant” of HIV circulating in Europe, this new strain is allegedly “more virulent”, “more transmissable”, and “progresses to AIDS faster”.
Following hot on the heels of this fresh wave of fear is a push for everyone to get AIDS tested as soon as possible, from politicians and celebrities and everyone in between.
Prince Harry is leading the charge, in a video that caused the press invoke the spirit of his mother Princess Diana, Harry insisted we all have a “duty” to get HIV tested “to keep other people safe”, comparing it to the COVID outbreak.
“Know your status“, the video says. Which will probably be a hashtag in the near future. (I just checked, and it actually is already.)
They’re really cranking through the gears on this one.
Even while the problem and reaction are still barely out of the research and development stage, they’re already talking about the solution.
Guess what it is?
If you said “another mRNA vaccine”, well done for paying attention
Yes, Moderna has apparently learned so much from making their rushed Covid vaccine which doesn’t work that they’re already making an HIV vaccine they hope will be just as “safe and effective”.
In a truly startling coincidence, Moderna’s HIV vaccine began clinical trials the exact same day the “new variant” of HIV hit the headlines, and the same week as the NHS’s annual “HIV Testing Week”. Funny old world, isn’t it?
Anyway, everyone get ready to line up for the AIDS shot.
by Global Research
first published by Global Research on January 28, 2022
.
UK Law Enforcement procedures have been initiated against the architects of the Covid-19 crisis.
This initiative sets a precedent Worldwide.
Should a Criminal Investigation be contemplated in regards to Canada’s Trudeau Government Covid-19 Mandates?
****
Metropolitan Police Crime Number: 6029679/21
International Criminal Court (The Hague) case number: OTP‐CR‐473/21
The world’s largest‐ever international criminal investigation is now under‐way, involving Hammersmith Police, The Metropolitan Police, and The International Criminal Court. The UK police accepted the supporting information and agreed there is enough evidence to proceed under the above crime number.
The case was lodged on 20th December 2021 by Sam White MD, Philip Hyland (PJH Law), Lois Bayliss (Broad Yorkshire Law) and retired policeman Mark Sexton.
Requests for further assistance have been made to international lawyer Robert F Kennedy Jnr (nephew of J F Kennedy), Dr Reiner Fuellmich (German corporate lawyer who won the emissions scandal case against Volkswagen Audi), Dr. Michael Yeadon (Former Pfizer Vice President), plus countless other doctors, professors, virologists, biologists, data experts and lawyers nationally and internationally; some of whom have already made direct contact with the police and have been acknowledged by Superintendent Simpson (Assistant to Cressida Dick, Head of The Metropolitan Police).
The complaints allege numerous serious crimes including misfeasance and misconduct in public office; gross negligence manslaughter; corporate manslaughter, murder, conspiracy to murder, genocide and crimes against humanity.
The evidence submitted by Philip Hyland and Dr Sam White against the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) is damning and shows they did not carry out due diligence surrounding the vaccine data, trials and studies; and that they continued to ignore the death, harm and injury the vaccines cause.
Mark Sexton says:
“This is now a live criminal investigation. We were forced to act due to the complacency of the UK Government, despite them being fully aware of the catastrophic death and injury figures to adults and children alike. This is nothing short of genocide; once again it seems that profit over people is the overriding motive. There is a deliberate blanket campaign of misinformation underway. Many don’t even realise that the covid Vaccine is still an experimental product. This is the most far-reaching criminal inquiry ever undertaken. A national scandal that threatens the lives and the livelihoods of every person in the UK. If people want unassailable current evidence, I’d suggest in the interim they look at: ”
“In years to come this will be the equivalent of another Thalidomide scandal, but for now we have to act on a united front to get the truth out to the public and stop the unsafe covid vaccine rollout. We have several thousand pieces of evidence to discredit the safety and efficacy of this vaccine, but we are still encouraging members of the public to contact us to further support our claim. We therefore appeal to anyone who has suffered the death of a loved one following a Covid vaccine and anyone who has been injured by it, e.g. blindness, heart issues, blood clots, stroke, myocarditis etc”.
“We’d also like to hear from those illegally threatened with ‘No jab, no job’”.
We must act now. If you have information to assist the police inquiry, please contact Lois Bayliss of Broad Yorkshire Law: loisbayliss@broadyorkshirelaw.co.uk
[Truth Comes to Light editor’s note: For the convenience of our readers, we have prepared a transcript which can be found below the information shared by Immanuel Project. This video was originally recorded in German and a voice-over has been provided by Immanuel Project.]
by Immanuel Projectwith Dr. Stefan Lanka video uploaded to Odysee August 30, 2021
Video available at Immanuel Project Odysee & BitChute channels.
The first of our extra, contributory posts “ON RELATED ISSUES” examines explosive, critical questions, rumours and theories surrounding the topic of “Corona” and everything connected with it. When new reports do the rounds in public that have the potential to fuel (additional) fear, hatred and violence, and which above all spread dangerous misinformation from the field of medicine and science, we would like to publish a special feature on this.
In contrast to our main programme, this series offers first and foremost a statement. In order to be able to publish a comment relatively quickly, we do not go into great detail and refer you to our main programme for precise evidence of our statements, where we publish a detailed list of sources for every contribution.
Since all the topics we deal with in Project Immanuel are directly related, all the contents of our special formats can also be substantiated with the sources from the main programme.
O.R.I., No. 01: “Bioweapons – the myth of the man-made pathogen”
In the first episode of our special format “On Related Issues” we deal with the topic of biological warfare/bioweapons. Due to the latest rumours surrounding the alleged “Wuhan virus” from the laboratory, we specifically address the issue of artificial “pathogens”, i.e. those modified or created in a laboratory, and explain why these are and will continue to remain, a myth.
“Project MKULTRA, the CIA’s Program of Research into Behavioral Modification – Joint Hearing before the Select Committee on Intelligence and the Subcommittee on Health and Scientific Research of the Committee on Human Resources, United State Senate, Ninety-Fifth Congress, First Session”, 03 August 1977 — https://www.nytimes.com/packages/pdf/national/13inmate_ProjectMKULTRA.pdf — published on the website of the New York Times
The following video is not intended for entertainment. It’s not a documentary report or television program.
Rather, this is an attempt to approach an explosive scientific topic in a cinematic way that is objective and respectful as possible.
We deliberately avoid staging of scenes as we’ve no intention of causing emotion in the viewer. We would like to convey factual, verifiable information.
In addition, we hereby call on all viewers to question the contents of this video and not simply to believe any information presented here. Doubt, be critical and check everything.
Only that is scientific.
Immanuel Project — “On Related Issues” (ORI).
With this video we introduce you to the first in a series of extra videos that we’ll publish in addition to our regular program.
On Related Issues focuses on pressing questions, theories and theses that are making the rounds in the public sphere, and to which we would like to respond as promptly as possible.
Most importantly, topics are discussed that are only marginally dealt with, or not dealt with at all, in the main series of our project.
No. 1 – Bioweapons: The myth of man-made pathogens
Biological warfare is a fairly complex subject. The use of biological weapons is probably as old as humanity itself.
All kinds of animals or naturally occurring toxins can be used as weapons to either attack enemies directly or in some way to make it difficult for them to survive.
Throughout history humans have been devising all kinds of biological warfare that have been as effective as they have been cruel. Time and again they have been reports about the use of supposed pathogens.
As early as the Middle Ages, and even in antiquity, allegedly transmissible diseases were claimed to be a popular means of warfare.
For instance, corpses of dead humans and animals were hurled into cities with the intention to cause epidemics in these areas.
Such stories do have a kernel of truth. Hurling decaying cadavers at enemies was certainly a proven biological weapon, but it had nothing to do with pathogens.
These days when people hear the term bioweapons, they usually think of artificial pathogens from the laboratory — bacteria and viruses that either genetically modified or even created in their entirety.
In the 21st century such ideas are more topical than ever due to the alleged progress in genetics and, equally assumed, improved understanding of biology.
Horror scenarios, wild rumors and theories, as well as adventurous novels, feature films, series and video games on this subject are dime a dozen.
But what has actually been researched and developed with regard to artificial pathogens?
Is it possible that something could really be brewed up in bioweapon laboratories that could prove dangerous to humans?
No, it’s not possible. I mean, you can see now that fear is the best bioweapon there is. You simply show some photos of coffins and corpses.
That’s the most powerful bioweapon we have: misinformation. But the most dangerous thing, of course, is the superstition associated with it.
People generally believe in the concept of dangerous viruses. Scientists also believe in them. And those working in related fields are proud that they’re working on something so dangerous and important.
They don’t see that they are being completely unscientific by not questioning the concepts in which they believe.
And it is the very first written duty of every scientist to constantly question their own findings and assumptions.
Nowadays, however, we are dealing with the reversal of science. Those who point out obvious contradictions are berated. This is really the reverse of all science.
Science is important and can contribute a lot to humanity if it’s applied with integrity. But what is happening here is pseudoscience.
In his 1956 book, Sociology Vol. 1, Eugen Rosenstock-Huessy explains why people engage in pseudoscience. He shows that, because of how science now operates, we can no longer make new discoveries. As if science have been derived from Greek criminal law, what we observe we judge and explain exclusively on the basis of what we already know. And, of course, only material explanations are permitted.
We do not want to know about any other explanations. We then say ‘they cannot be true’, ‘they are unscientific, wrong and dangerous’.
Rosenstock-Huessy clearly demonstrated that we can no longer make any developments in this way. We cannot discover anything new with our unscientific approach. And it’s a typically-human characteristic that no one likes to see their achievements and findings being thrown overboard.
Rosenstock-Huessy also shows this: He demonstrates how these unscientific principles permeate academic life and how pseudo-research has been carried out in order to somehow maintain these very principles, the models which people adhere.
For example, by doing animal experiments without any control experiments. Or killing cells in a test tube, also without any control experiments. And then simply claiming that the results of these experiments have to come about because of some virus. That’s how easy it is.
And we must not forget that this was already written in 1956.
In his book “Healing Power and Truth: Concordance of Political and Cosmic Time” — what a title — he describes how mountains of corpses, such as in genocides, can quickly pile up again if one misses the moment to recognize and correct mistakes.
Wrong decisions are made, wars escalate or whatever. This is the challenge we are facing right now — to recognize these mistakes in time. So it’s very important to deal with these things. And bioweapons is a very good example of these things.
The Russians, for example, completely abandoned their bioweapons development in the 1970s because they realize that the concept of pathogens as weapons does not work.
But the claim that dangerous bioweapons exist is very effective in order to create fear. First and foremost, of course, it’s effective in populations who are panic-stricken about contagion.
For example, historically the Israelis managed to empty the entire Palestinian refugee camps without firing a single shot. They simply claimed the wells are contaminated and soon the dangerous disease will break out here.
Nothing happened at all. No shots were fired. And voila! The Palestinians were gone. That was the starting point of Israel — an act of fear.
The Israeli population also has one of the highest cancer rates in western societies. Certainly not in all parts of the country, but in many, people live in constant fear of death. There is a constant fear of terrorism, of rockets, of bombs. Of course, such an attitude to life is anything but conducive to good health.
Didn’t the Nazis in the Third Reich also have a biological weapons program? What happened to it? Was it abandoned? The reason they never seriously worked on a bioweapons program is because nothing had ever worked in that direction. What they did was try to protect themselves from alleged germs.
In this regard, I recommend reading the book by Ludwik Fleck, “Genesis and Development of a Scientific Fact”. There are also many articles by him on the internet.
Ludwik Fleck was a bacteriologist and he was deported to Buchenwald concentration camp where he was forced to develop a vaccine for the SS. He wrote that he and his colleagues knew that all the assumptions about supposedly dangerous disease-causing bacteria were completely wrong.
He knew that things don’t work like — that this idea is just a misinterpretation. Anyone can read that for themselves. You can find a lot of material by and about Ludwik Fleck freely accessible on the internet.
Nevertheless, Ludwik Fleck and his colleagues had the task of developing a vaccine against a supposedly dangerous bacterium for the SS. And they knew that if they tried to explain to them that it wouldn’t work, they’d get their heads chopped off.
So they just made a vaccine for them as demanded. They let something or other decompose, added a few bacteria. And when the whole thing was bubbling away in the test tube, the poisonous mixture was filtered. Formaldehyde was added and that was it.
The vaccine was injected and the job was done. That’s what he describes. And he also describes how science actually operates, because he himself has experienced these undesirable developments and seen how they come about.
After the second World War, the Americans were of the opinion that the national socialists, the Nazis, might have used some kind of secret drugs to take the soldiers’ will away, so that they would happily go to war.
The Americans were investigating this to try to address the big problem that many of their soldiers who were supposed to bomb Korea deserted. Hardly any of the soldiers at that time had ever held a rifle, seen a tank, or had anything to do with weapons in the military. And suddenly they were supposed to drop bombs on another country.
Some biologists even suggested that the Russians had bred a socialist virus that could be used to render the American soldiers will-less. Such speculation really did exist. But, of course, it led no where.
What the USA did in the end, however, was to experiment with all the drugs that were available. This project, about which a great deal of information has come to light, was called MKUltra.
People were tortured and subjected to drugs to take away their will in order to program them. And this project existed solely because it was believed that at least some, if not all, of the German soldiers must have been given some kind of secret drug. It is frightening that even today speculation about bioweapons is used to scare people.
And here is another example. The virologist, professor Zhang from Shanghai, had received the order from Beijing to search for a coronavirus in bats that was harmless to humans and could then be used as a template for so-called sequence alignment.
He was under extreme time pressure because the panic of the people in Wuhan had to be brought under control. It was feared that the people there might storm the hospitals at some point, because anyone who had any kind of complaint such as asthma, cough, or fever immediately panicked and imagined that they had SARS.
Something like that can endanger public order very quickly. And it was going in that direction, triggered by the ophthalmologist Li Wenliang, whose own fear spread very quickly via social media.
That’s precisely why professor Zhang was given the task of producing a harmless bat virus as quickly as possible. It was already established that the few dozen cases of pneumonia that existed at the time had not infected anyone else.
From the beginning of December, when the first cases were tracked, until the 20th of January, no one was infected. No one else got you pneumonia.
So they assume that if, anything at all, it must be a virus that was difficult to transmit and could probably only be transmitted from animals to humans. So they looked for a virus in animals.
Then professor Zhang, from the Fan Wu et al. research group — these results were published in Nature, the first work on the so-called new coronavirus — created the genome strand of SARS-CoV-2, in the absolute record time of only 40 hours.
He got the fluid from a lung wash, obtained some nucleic acid out of the fluid, sequenced it, and then ran the puzzle called sequence alignment. But he didn’t have time to apply all the rules of virology. That’s why the genome from these 40 hours of record time looks more than bumpy.
Normally one takes at least three weeks for this process. And then a genome sequence appears really polished. But anyone who knows a bit about biochemistry can see that the genome of SARS-CoV-2 really does look very bumpy.
And this is exactly the argument. The people who claim that the virus must have come from a laboratory: ‘It must, therefore, be a bioweapon.’. Of course this then circulates on the internet again and fuels people’s primal fear of infection and of viruses.
Therefore, anyone who claims such a thing, has to be asked the question: Where has a virus ever been isolated? Where? Show me a relevant publication and show me the exact passages in which this is described.
Show me where this is described in the methods section of any scientific paper. These are only very short paragraphs. And if it cannot be shown, it must be rejected because it spreads unnecessary and dangerous fear.
Fear is always dangerous. Spreading fear is not justifiable.
The theory that there are pathogens and transmissible diseases have been perpetuated to the present day with this kind of assertion. But if you go into detail, you immediately see that none of this is tenable.
What one could say, perhaps at this point, is — what was done again and again in the so-called Middle Ages, or actually in all wars, is to make survival impossible for the enemy, and also for the civilian population, by destroying the crops, destroying the fields, killing the animals, so that simply scorched earth remains.
And by throwing carcasses into the wells. Then the water was heavily polluted with decomposing products of the proteins, that is with nitrates.
Every mother understands that. If a bottle of mineral water says it contains more than 50 milligrams of nitrates, no child is allowed to drink it because otherwise it would turn blue. And if a child were to drink this water all the time, it would get the type of buboes that were called the plague in the Middle Ages.
From 1981 onwards it was called immune deficiency in homosexuals or GRID (gay related immune deficiency) for short. And from 1983 onwards, it was called AIDS.
It’s as simple as that. It’s massive poisoning from nitrates in drinking water. It has nothing to do with pathogens producing any disease toxins.
Such toxins are produced when something decomposes, i.e. the proteins break down and turned into putrefaction. It is quite clear that it is not healthy to drink water with corpse poisons or to eat rotten food.
Already at the beginning of the corona crisis, rumors circulated very quickly that the alleged new coronavirus was not of natural origin, but came from a bioweapons laboratory.
Of course, China was first accused of having developed the virus. Later, the USA was accused. And then China again.
And, at some point in between, the French scientist Luc Montagnier, who was awarded the Nobel Prize in 2008 for the alleged proof of the HIV virus, among others, spoke out. He claimed that the virus was definitely of artificial origin because it had genetic similarities to the alleged HIV virus.
Most of these theories were dismissed after some time. And many scientists declared that there was no reason to assume that the alleged SARS-CoV-2 was a bioweapon.
In January 2021 however, the rumor of the Wuhan virus flared up again when an international group of researchers claimed to have found new evidence that strengthen the suspicion of the bioweapon. The scientists’ conclusion sounded alarming, but were also based only on suspected elements in the alleged genetic strand of SARS-CoV-2.
These observations immediately lose their significance and, above all, their threatening nature when one realizes that the same genetic genome strand of the alleged SARS-CoV-2 is, in any case, only a man-made theoretical construct. No wonder then that some of it looks artificial and man-made.
One could say SARS-CoV-2 did indeed originate in a laboratory in Wuhan, but not in the way many people believe. The genetic material of SARS-CoV-2 comes from a computer and has never left it. It is a theoretical mental construct.
The ideas of pathogens made in laboratories are all scientifically untenable. Moreover, they even contradict principles of biology that have been known for many, many years.
It’s irrelevant whether they’re supposed to be killer bacteria or killer viruses. The terrorist attack in the USA in 2001, with allegedly genetically modified anthrax pathogens, is just as unlikely as the Wuhan virus of 2020.
To understand why biological weapons in the form of pathogens have never existed in this way and never will, one must know the following:
With regard to viruses, disease-causing viruses — i.e. a dangerous genetic substance — are, to this day, nothing more than mere theory.
No scientist in the whole world has ever succeeded in providing tangible proof of such a virus.
Even if one or the other has ever been awarded the Nobel Prize for alleged proof, their work never stands up to scientific scrutiny.
So how do you make an artificial virus when you can’t even find a natural one?
The topic of viruses is dealt with in detail in the main program of Immanuel Project.
With regard to bacteria — bacteria cannot make organisms sick in the sense that we believe they can. And they are not the parasites they are made out to be. Bacteria, which are always found in our bodies, can, under certain circumstances, be involved in ailments — some of which can even be life- threatening.
But that does not mean that they are parasites and harm us in that sense. Moreover, bacteria in living bodies either produce no toxins at all or only in such small amounts that it’s impossible to become ill from them.
One must bear in mind the conditions under which … and cadaveric toxins are produced.
So how do you grow killer bacteria? By reversing their biology? That would really be a scientific sensation.
The complex topic of bacteria is not dealt with in our main program but we will return to it in one or two special formats.
Conclusion.
There are a variety of possible biological weapons. However, pathogens are definitely not one of them. All claims about genetically modified, or even artificially created, pathogens contradicts biological principles and are, therefore, inevitably doomed to failure.
There may well still be stray scientists in the world who aim to produce the ultimate killer microbe in their laboratory, but they will fail just like the people who try to make gold in earlier times.
Their scientific basis is simply incorrect, in both the cases of the alleged viruses and bacteria. All allegations, speculations, rumors and accusations revolving around artificial pathogens, therefore, only generate fear and enemy images. And we definitely do not need to either.
There is already more than enough fear and hatred, especially in this time of corona. Prolonged fear can lead to serious health problems, particularly for people who already have respiratory difficulties.
Rather than creating more fear with unfounded claims of killer viruses from a lab, we should stick to verifiable facts. Then all open questions about the alleged Wuhan virus, its latest mutations, its similarity to HIV, and other theories about bioweapons and killer viruses, will take care of themselves.
In order to complete the control experiments on SARS-CoV-2, we are still urgently looking for bioinformaticians to repeat and document the original sequence alignment. If you are a bioinformatician, are proficient in the De Novo alignment on “viruses” and have an opportunity to access the raw sequence data from Fan Wu and his colleagues please get in touch fragen @ wplus-verlag.de
The wireless future is here. The model ostensibly turns human beings, via nano-implants, into antennas that can transmit information. They’re turning human beings into quasi-machines. Under this transhumanist agenda, the idea is to place nanotech inside our bodies we can communicate in real-time with the Smart Grid powered by way of 5G.
The 4th Industrial Transhumanist IOB Graphene Nanobot Revolution.
It’s called the ‘internet of bodies’ (IoB) or the ‘nanotech of things,’ (NToT), and it connects with the Internet of Things (IOT). One way this is accomplished is to embed graphene-made sensors into fabrics. Another is to implant or ingest the nanotech matter into the body, creating an internal technology platform.
For instance, Pfizer CEO Albert Bourla described the first-ever FDA-approved ‘electronic pill,’ which will invite ‘compliance,’ by sending a signal to your ‘doctor’ that you have indeed swallowed your ‘medication.’
“What we will see is a kind of fusion of the physical, digital, and biological world,” says Klaus Schwab of the World Economic Forum.
Oh Klausy!
In order for all this connectivity to occur, these particles must contain GRAPHENE, a superconductive material that integrates with neurons in the body and brain. Nanotech, pioneered by Nanotech King Charles Lieber, is completely unregulated. Arguably, it already exists in food, drugs, vaccines, water., and the air we breathe. While there is no shortage of studies devoted to graphene-based nanomaterials (GBNs), systematic research on human health or environmental effects is severely lacking.
And yet integrating humans with hardware is supposedly being sold to us for our safety and health. In fact, on a site called Nano Robot Inventor, a 2008 paper titled Nanorobots to improve health care states:
“Recent developments in the field of nanoelectronics, with transducers progressively shrinking down to smaller sizes through nanotechnology and carbon nanotubes, are expected to result in innovative biomedical instrumentation possibilities, with new therapies and efficient diagnosis methodologies.”
“A transistor also allows the application of a voltage pulse, such devices might one day provide hybrid biological-digital computation, or deep-brain stimulation for Parkinson’s patients, or serve as an interface for a prosthetic that requires information processing at the point where it attaches to its owner.”
By the way, Lieber worked for communist China. Lieber has also worked on highly sensitive research projects for the US government Department of Defense (DOD).
Back in the 1930s, the CCP invented what is now known as “brainwashing.” The term is a literal translation of the Chinese term, Xi Nau, or “wash brain.” Arguably, Lieber has helped China and others upgrade to a modern version of mind control.
“ I was one of the first people — in 1998 — to figure out how to grow these nanoscale wires,” Lieber has stated.
If you do not believe me, just do a search for his brain-controlled mouse. And yet, Lieber went from supposed spy to a convicted tax evader. Who has explored the ethics of his inventions? It has already been proven that Lieber’s “injectable electronics” can be integrated within the brain with ‘minimal invasions,’ and can continue to function for at least a year. Who knows what happens after that?
The Purpose of AI: Brain-Computer Interface
At Code Conference 2016, Elon Musk stated publicly that given the current rate of artificial intelligence (AI) advancement, humans could ultimately expect to be left behind cognitively, intellectually “by a lot.” His solution to this unappealing fate is a novel brain-computer interface.
The internet of bodies (IoB) will tell us a lot, too. The sensors placed inside each person’s body will collect data…and that data has been determined to be more precious than oil.
To put things in perspective, ‘Big Harma’, with the help of Big Tech, began usurping the medical data of millions of Americans as early as 2019. You can read my article titled Dr. Google Will See You Now. Alphabet, Google’s parent company, acquired FitBit for a cool $2.1 billion. Now, in Year Three of the Rona Regime, they are coming after us.
Imagine how much information they can technically collect by giving us a ‘viability score.’ In the Netherlands, their biometric mass surveillance practices are increasingly being used to control people’s access to healthcare, sports venues, travel, shopping, and other everyday activities. Activists actually have a campaign called ‘reclaim your face.’
While globalists aim to vaccinate the world and watch as our fellow man turns into ‘Magneto Man’, evidence indicates that Big Harma, aided and abetted by VERY sick Rockefeller hospitals, are injecting us with nanoparticles meant to respond to signals while –oops – changing our very nature and DNA.
I understand, this sounds conspiratorial. If you haven’t gotten the memo that some of these jabs contain saline, why others have been sullied with microscopic nanoparticles that are conductive, consider:
In 2017, in a now-scrubbed-off-the-internet was a study from taly looking at adjuvants. Researchers found that 15 traditional vaccines (and 44 variations of these), all manufactured by leading global companies, shared a previously unreported and troubling similarity: the vaccines were “heavily contaminated with a variety of nanoparticles.”
This is an indisputable fact. You just can’t see them. A nanometer is 1/80000th the diameter of an eyelash, one-millionth the size of a pinhead.
“If your nanoparticles self-assemble correctly with Harvard’s Charles Lieber injectable nano meshes, you can actually get a nice little wireless nano network going in the target,” says Investigative Journalist George Webb, who has looked into Lieber and the Wuhan origin story since 2020. “Corona didn’t just launch DARPA’s mRNA technology, Corona also launched nanotechnology for immunology. Gold, silver, iron oxide, silicon dioxide, and graphene are all nanoparticles being researched for COVID applications.”
It’s all part of the Covid Industrial Complex.
Cinco Geo Your Existence
In January 2020, when people in Wuhan began dropping like flies, I surmised that maybe nanotech — brought to us by Charlie Lieber via a mandated experimental injection or sprayed via drones – was parlaying with the Internet of Things. Interestingly, Wuhan, the capital of China’s Hubei Province was the first 5G demonstration zone in the Central Business District (CBD), according to a 5G cooperation agreement signed between China Mobile and local authorities on September 3, 2019.
That’s how I uncovered the connection between Lieber to 5G. It was taboo to talk about 5G back in 2020, so I coined the code words, Cinco Geo, to ward off censorship. For the record, I lived across the street from a test cell tower in Beachwood, Los Angeles. I developed a fever for 65 days and couldn’t sleep. While I could not prove it was the radiation, a meter endorsed by Dr. Mercola proved the 5G technology was definitely turned ON. That was 2019.
Fast forward to 2020.
As we were locking down over the virus, cell towers across the country were going up. In fact, 5G cell tower installation was the only industry that was thriving during the early to mid-2020.
When it came to appealing net neutrality, Ajit Pai, the former Trump-appointed chairman of the U.S. Federal Communications Commission (FCC) said that the government had no place in the private sector. However, when it came to 5G, the government wasn’t only a necessity, it was a requirement. For example, when I recently called Miami-Dade County to try to find out whether they had amplified the 5G signal, I was referred to the federal government.
In fact, in 2018, the FCC initiated the “5G Fast Plan” to establish the United States’ superiority in the tech race. They intended to blanket the ENTIRE country with 5G small cells placed between every 2 to 10 homes. The industry claims they need so many towers because 5G uses millimeter waves that travel small distances and can be easily blocked by walls and even foliage. To compensate for this, engineers found ways to convert the waves to beams and intentionally direct them.
For the record, the CEO of Verizon helped bust the myth of millimeter waves and said that indeed the signals could penetrate through foliage and that the waves can cross 2000 feet from transmitter to receiver. And yet small cells continued to be built.
The 5G Fast Plan
As part of the 5G Fast Plan, the FCC reformed rules that had been designed decades ago to accommodate small cells. The reforms were designed to ban ‘short-sighted’ municipalities who tried to block the deployment of the 5G technology. Local governments were given a reasonable deadline to approve or disapprove small-cell tower applications.
Small groups of people throughout the nation have attended local meetings to fight these eyesores but they don’t really stand a chance. At best, if the municipalities have money, the 5G poles are moved to another neighborhood. Of course, health studies on 5G have not been conducted.
On January 19, the day I got sick with what felt like radiation exposure, flights were suspended to the U.S., including to Miami, over 5G concerns. I threw up three times. I had watery stools. I felt anxious. I almost fainted in yoga class. And, I lost my sense of smell. I thought it was the Rona. But I wasn’t sick with the flu or cold symptoms. I had no cough or respiratory issues. My symptoms didn’t match the Moronic variant. One friend told me, ‘you must have gotten the Delta.’ I laughed to myself. Upon doing research, I also learned that the CDC acknowledges something called Acute Radiation Syndrome.
Can You See The (Smart) Light?
Did you know that every lighting installation can be a data infrastructure? Two-way communication can also be done via light signals.
Think cellphones and streetlights.
Analysts predict the smart lighting market will grow more than 21% a year between 2018 and 2023. Much of this growth will be driven by wireless installations – and the exciting new applications they support. That’s why one company is putting Bluetooth low energy (BLE) technology in their connected components, enabling every fixture to communicate wirelessly with nearby Bluetooth-enabled smartphones.
Will wireless lighting controls soon be the new normal, making the benefits of smart lighting more accessible to organizations everywhere?
Ping, Collect, Ping, Ping
Let’s recap how all this connects (pun intended).
Seamless human-machine interaction is increasing rapidly.
What if these injections were never “vaccines” against a virus? What if instead, the jabs have been a secret nanotech project developed to control the brains of the human population? (Until now, we don’t know specifically how they can modify our DNA via 5G).
Seemingly, some jabs were manufactured using nanotechnology. In Spain, it was even described as “secret nanoparticles.” These nanoparticles become magnetic when they reach the same temperature as the human body. When they remain in an under-zero-degree environment, they remain non-magnetic. Maybe one of the reasons they use the injections?
The graphene hydroxide works as an antenna for the electronic circuits they are injecting. If they can create transistors, they can also make an identifier like an RFID chip that can ping a number back, once the person is near a radiofrequency (RF) field. Graphene oxide in the brain creates transistors, and ostensibly its own network.
Thanks in big part to Lieber, molecules of GRAPHENE can interact with neurons in the brain in a remote mode using different radiofrequencies (5G could be one of these). Can they also map the brain and transmit and receive INSTRUCTIONS remotely? Do these nano devices and smart biosensors become programmable? Yes!
“… In the proposed platform architecture, different programs and commands can be sent and information retrieved from inside [the] body through wireless communication, providing important aspects on the interface and medical instrumentation of nanorobots.”
“The proposed model uses electromagnetic radio waves to command and detect the current status of nanorobots inside the body. Therefore, the cell phone is applied for the medical nanorobotics platform. This occurs as the cell phone emits a magnetic signature to the passive CMOS sensors embedded in the nanorobot, which enables sending and receiving data through electromagnetic fields. From the last set of events recorded in pattern arrays, information can be reflected back by wave resonance.”
What happens when you integrate communication with nanorobots using RFID, mobile phones, and satellites and apply it to long-distance ubiquitous surveillance and health monitoring?
The jury is still not out.
“We are in a live exercise here …. to get this right!” Sec. Mike Pompeo stated during a presser back in January 2020.
“You should have let us know,” President Trump murmured back.
Maryam Henein is an investigative journalist, and founder, and editor-in-chief of the health magazine and marketplace HoneyColony. She is also a functional medicine consultant/coach, and the director of the award-winning documentary film Vanishing of the Bees, narrated by Elliot Page. Follow her on Gab: @ladybee. Email her: maryam @ honeycolony.com.
Dr Robert Gallo made his famous announcement at a press conference on 23 April 1984 that “his” HIV virus was the probable cause of Acquired Immune Deficiency Syndrome (AIDS). From that moment on, the race was on to find a pharmaceutical weapon against it.
At the height of AIDS epidemic in 2005, the rhetoric about HIV danger and death penetrated every corner of the world. The rapid test for HIV was accepted as the test for AIDS, which divided people into positive and negative camps.
Flashback to June 2015, ten years after the height of the AIDS epidemic:
AIDS-related deaths have fallen by 35 percent since the peak of the epidemic in 2005 and the number of new infections continues to decline annually. That’s the good news. Nonetheless there are thought to be around 35 million people living with HIV globally; 19 million don’t currently know their HIV-positive status. Of those people who need antiretroviral drugs, only just over a third have access. That’s the bad news.
We have the scientific know-how to end AIDS and every month seems to bring news of another biomedical advance that could change the trajectory of the epidemic once and for all.
Last week the preliminary findings of the Strategic Timing of AntiRetroviral Treatment trial confirmed that early treatment is best for HIV.
No one thought that HIV might be lab-created. No one knew that just before Gallo’s April 1984 announcement, someone had filed a United States Patent number: 9499480 for HIV/AIDS Virus invention, a designer bi-product of the U.S. Special Virus program.
No one knew that Gallo, himself, was ‘Project Officer’ for the federal Special Virus Program that ran from 1962-1978. See complete list of HIV patents. No one knows that engineered evidence is found from the ‘multiply-spliced’ nature of the HIV ‘tat’ sequence in Dr. Gallo’s 1971 Special Virus paper, “Reverse Transcriptase of Type-C virus Particles of Human Origin.”
From 1985 to 1992 there were 12,000 deaths each year from AIDS. In 1992 the number increased suddenly to 15,000. Why? Because they added 5 new diseases to the AIDS definition! The actual number of cases of AIDS was on the decline until they added more diseases to the list, and still the number of new cases grew very slowly. – Dr. Robert Wilner, Deadly Deception, 1994.
HIV — it has never been found in sufficient numbers to cause disease.” –Peter Duesberg, 1991
The HIV/AIDS hypothesis is one hell of a mistake. – Kary Mullins, inventor of the PCR test.
Today, the official narrative still claims that no cure exists for AIDS, and that only toxic FDA antiretroviral drugs, including A.Z.T., D.D.I., and D.D.C., will slow down the progression of the disease.
“Why condemn a continent to death because of HIV, when you have other explanations for why people are falling sick?” – Dr John Papadimitriou, professor of pathology at the University of Western Australia in Perth and a co-author of the Journal of Nature Biotechnolgy study that found HIV tests to be inadequate.
Comparison of HIV and Coronavirus Tests. September 2020:
Sometimes testing can give you a false sense of security. That happened in the HIV epidemic, when people got a negative test and they presented it to their sex partners and spread disease, nonetheless. – Cue Mark Schlissel, M.D., Ph.D., President of University of Michigan,
The U of M president knew of the flaws of the rapid HIV test. He knew the patterns of history. And for that he received pushback for equating the COVID-19 pandemic with the AIDS epidemic to justify the University’s decision not to widely test students. He was made to apologize for unrelated reasons, but added to his response:
My comments were intended only as a critique of the effectiveness of massive testing of asymptomatic students for the virus that causes COVID-19 in an effort to prevent its spread. – Cue Mark Schlissel, M.D., Ph.D, President, U of M 2020
The COVIDIAN Age
In the COVIDIAN Age, it is accepted that Coronavirus is a virus. However, Coronavirus is a family name that includes MERS-Cov, SARS-Cov, HCoV-229E, HCoV-NL63, HCoV-OC43, HCoV-HKU1, and many others. Coronavirus is not Corona virus. It is also accepted that people with underlying diseases are more susceptible to COVID19. This is likely due to a weakened innate immune system. Immunosuppressed people no longer have a functional defense system and are more likely to suffer from any infection, whether it be called a cold, a flu, toxic overload, or ‘COVID.’
The Twist:
Ironically, new research shows the opposite; that patients with advanced stages of AIDS show less severe COVID symptoms and recover faster than others.
A July 2021 study in the Journal Immun Inflamm Dis, titled “The clinical outcomes of COVID-19 in HIV-positive patients: A systematic review of current evidence” shows evidence that the majority of HIV patients show no severe symptoms and completely recovered from COVID19 infection.
Similar to The Age of AIDS, COVID patients will soon be offered antiretroviral drugs. On December 14, 2021, Merck and Pfizer pharmaceutical companies announced the development of COVID antiretroviral drugs. The companies claimed their drugs attack different parts of the virus. Ten days later, on December 24, 2021, the FDA authorized “emergency use” of Merck’s antiviral drug to treat COVID19. FDA had previously “authorized” the first antiretroviral Molnupiravir in late November. Note: authorization does not equal approval.
Today, the FDA claims that the antiretroviral pill “should be initiated as soon as possible after diagnosis of Covid-19 and within five days of symptom onset,” – FDA Statement, December 22, 2021
In 1994, Dr. Robert Wilner wrote: “Any antiviral therapy that is immune-suppressive and aimed at treating HIV is unnecessary, dangerous, unethical and bad medicine — you are already immune to HIV!
There is no test to find out a person’s “HPV status.” Also, there is no approved HPV test to find HPV in the mouth or throat. – CDC HPV Fact Sheet, 2022
We aimed to develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus material available. – Journal of Euro Surveillance, 2020
Why blame a pandemic on innocent animals? It sounds like this: “ANIMAL X” could be hiding a deadly virus that could trigger a pandemic worse than the Black Death and kill more than 75million people. They tried to blame Ebola on a bunny.
Did the Species Barrier disappear to allow for animal research to develop profitable drug models?
After mRNA injectables, why are AIDS patients successfully fending off the worst COVID symptoms and recovering faster without an immune system?
Do HIV patients somehow recognize the lab-created Coronavirus as similar? Does the mRNA nanotech somehow protect people without an immune system? Is that why antiretroviral will be required for COVID patients?
Disclaimer: The author encourages you to consult a doctor before making any health changes, especially any changes related to a specific diagnosis or condition. No information in this article should be relied upon to determine diet, make a medical diagnosis, or to determine or prescribe a treatment for a medical condition. This information is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice. It is intended to build synapses for thinking.
ONE: Billboard (8/2/21): “Sir Paul McCartney is spreading one simple message for his fans: ‘BE COOL. GET VAX’D’.”
Well, that’s it then. You can tell Paul dug deep to do his research on the injection. Be cool.
“The beanie- and face-mask-wearing 79-year-old rocker wrote this message on Instagram, while signing off as ‘Paul,’ underneath a picture of himself getting his COVID shot from a health care professional on Monday (Aug. 2).”
As opposed to getting his shot from a health care amateur, or a shoe salesman?
“’The vaccine will get us out of this. I think we’ll come through it, I know we’ll come through, and it’s great news about the vaccine’,” he [McCartney] said in the interview.”
Sir Paul has obviously bought the whole enchilada. Virus spreads, infects, makes people sick and kills them, get tested, isolate if necessary, lock down a whole country if necessary, the vaccine will stop the virus in its tracks, we’ll be OK.
No need to look at contrary evidence. The official doctors and the political authorities know what they’re doing.
Obey. Comply. Was that always the secret message of Paul’s music, hidden amidst the vinyl grooves?
Since God knows when, famous Brits have issued consoling messages to the lower classes. “We’ll get through it. We’ll pull together.”
It turns out lots of famous ones aren’t doing any of the pulling.
A reasonable person would realize a vaccine mandated for the whole population should be scrutinized down to it core. It’s cool, and we’ll get through it, don’t cut it.
A breezy cavalier attitude is a sign of a mental midget.
I wonder whether a hypnotic medical blind spot will turn up on a brain-scan. “You see this dark area, Paul? The neurons aren’t firing. When I shine this ray of light at your skull and it penetrates and hits that area, a message pops up: ‘Don’t think. The doctors know everything’. If I were you, I’d get that checked out. But not by a doctor.”
Judging from his Billboard quote, Paul seems to realize he’s being enlisted by the National Health Service and the government to assure the public the vaccine is safe; and he’s willing to go along.
If he were working a steady job, and a SINGER told him it was cool to take the shot, would he go along?
Having amassed fame and fortune, he’s not able to imagine that reverse-scenario anymore. That’s not the fault of his career, his composing, his singing, or his earning pounds and dollars. It’s his fault for surrendering to his elevated status.
He wouldn’t admit it, but he’s detached himself to a sufficiently remote area, from which he can shrug and support a government edict affecting millions of people without a second thought.
His stupidity is towering.
TWO: Howard Stern is a bunch of ugly sticks glued together with dried semen from one of his old wet dreams.
Once upon a time an abject failure as a broadcaster, he glimpsed a possible way out of Doom by taking on the role of psychological pornographer.
He’d assume everyone was obsessed by sex, and he’d force their inner dog to drool when he rang the bell.
Now, from a political perch, he’s decreed that all unvaccinated people should be locked in their homes and die.
That’s his style. Cut to the extreme chase. And also: see nothing, say something.
The mental midget status applies to Stern in spades. He knows zero about vaccines. He listens to the official doctors and the federal government like the kind of good little boy he hates.
As a young awkward schlub, he decided to rebel and burn down normal people by illustrating they were nothing more than prurient fish waiting to be shot in a barrel.
It was an easy choice. Once he found his radio style, he opened fire. His ratings soared; fame and fortune arrived.
He knows his success is nothing to be proud of. But success is all he has to hang his hat on. So he pretends it means something about his character.
It only means he’s one more person who’s tapped into a lowest common denominator and found dollars.
If Howard Stern tells you, you need to get vaccinated, you pretty much know it’s the wrong thing to do, on that basis alone. Directing people down bad alleys turns out to be one of Stern’s skills.
His notion of free speech is entirely self-serving. He wants to elevate his tired half-baked porn into a Constitutional issue.
He possesses a high degree of intelligence. He’s used it to recreate himself as mental midget. The only interesting moments in his career arrive when he laughs at himself because he knows what he’s done to himself.
He probably, on occasion, dreams he’s Field Marshal Fauci. And Fauci occasionally dreams he’s Howard Stern.
Coda: Now here is the REAL WORLD. LOOK AT THE PEOPLE. WATCH THIS BRIEF CLIP ALL THE WAY TO THE END. Canberra, Australia, Feb 7th, 2022
A German mathematician working with Dr Stefan Lanka has just published a report titled “Structural analysis of sequence data in virology – An elementary approach using SARS-CoV-2 as an example.” It provides even more evidence that the virologists are caught up in a world of computer simulations – simulations that are unreliable even on their own terms, not to mention being disconnected from reality. The analysis is an important contribution exposing another element of the anti-science being used to sustain this fake pandemic. Further, it is a technical dismantling of how all “viruses” are being invented and then “found,” in an ongoing game of deception.
The paper is very technical and requires some understanding of how the virologists create a “genome,” starting with a crude sample from an alleged infected “COVID-19” patient. To make it easier, I’ve produced a summary of the main findings as outlined below:
None of the genetic sequences used in producing the “SARS-CoV-2” genomes were shown to come from inside any viruses. It is unclear where the genetic fragments originated from.
The original de novo “SARS-CoV-2” computer-constructed sequence published by Fan Wu, et al could not be reproduced by the methodology described in their paper, raising questions abouthow they produced itand announced the new “virus” to the world.
The PCR protocols are calibrated to sequences of unconfirmed origin that are clearly found in many humans and apparently other things as well. The PCR process was not shown to detect a “virus,” let alone diagnose an invented illness called “COVID-19”.
The virologists are fooling themselves by running amplifications at 35 to 45 cycles, as it can result in “detecting” sequences that are not even present in the sample. In effect, the methodology can result in “detecting” whatever sequences they are hoping to find.
Fan Wu, et al could have found better matches for “HIV” and “Hepatitis D virus” than “a new coronavirus” in their 41-year-old man from Wuhan, who presented with pneumonia as one of the first claimed “COVID-19” cases. If they want to find a “virus”, it all depends on what they ask the computer to look for.
Of course, it makes much more sense when you get to the root of the problem: “SARS-CoV-2” is nothing more than a computer simulation and there was never a virus to start with – the entire thing is a global fraud. Virology seems to be unaware that it is sinking further into an epistemological crisis and no more so than in the area of genomics, as outlined in this article by Mike Stone. In Stone’s article, I noticed in the comments section that Dr Valendar Turner of The Perth Group pointed out that the late Sir John Maddox, former editor of Nature, had issued a pertinent warning in 1988. It seems that those who become immersed in the world of indirect molecular detection techniques risk no longer seeing the wood for the trees as he presciently stated:
“Is there a danger, in molecular biology, that the accumulation of data will get so far ahead of its assimilation into a conceptual framework that the data will eventually prove an encumbrance? Part of the trouble is that excitement of the chase leaves little time for reflection. And there are grants for producing data, but hardly any for standing back in contemplation”.
Maddox, J. Nature 335, 11 (1998)
We will endeavour to keep exposing these anti-scientific methodologies and encourage others to ask themselves if the multi-billion dollar virology industry and the associated bogus “treatments” coming from the behemoth pharmaceutical complex are actually helping anyone with their health. For those of us that can see there is no sound basis to any of it, there is no way we would heed any advice from the doctors and scientists who promote these sick models. And perhaps more importantly, we know not to take any of the fraudulent and increasingly perverse pharmaceuticals that are products of this pseudoscience, and used as vehicles to deliver nefarious and undeclared constituents. Once again, you can avoid all of these problems by pointing out:
Where is the virus*?
*A tiny particle that is an obligate intracellular parasite (i.e. replication competent and transmissible) containing a genome surrounded by a protective, virus-coded protein coat.
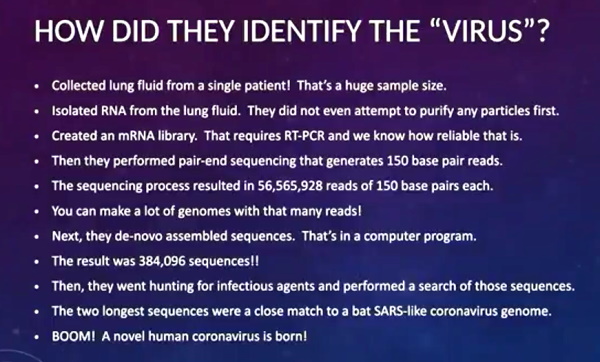
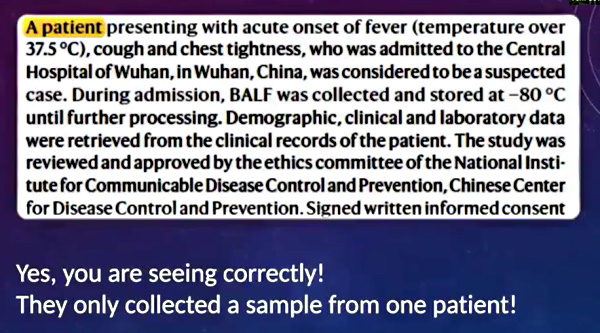
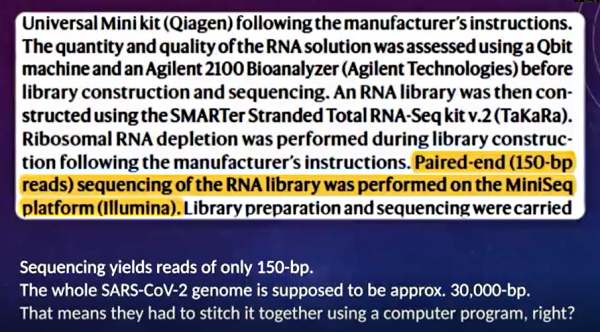
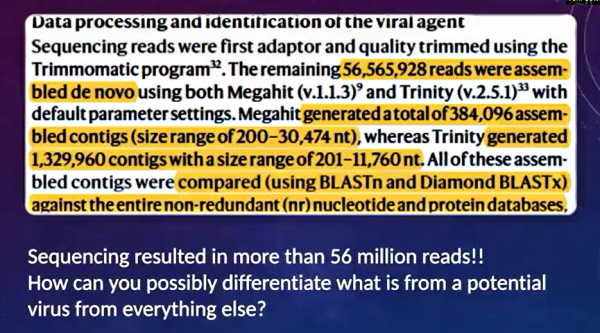
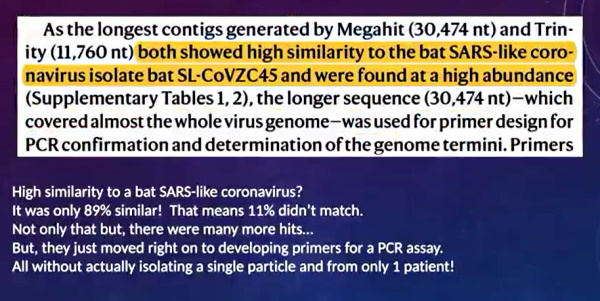

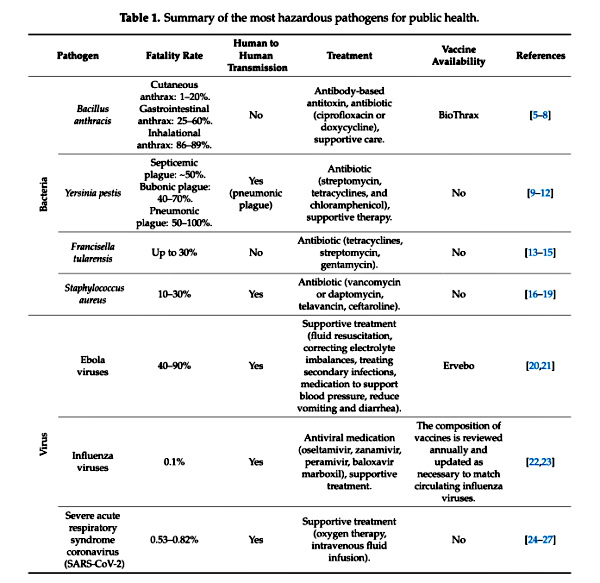
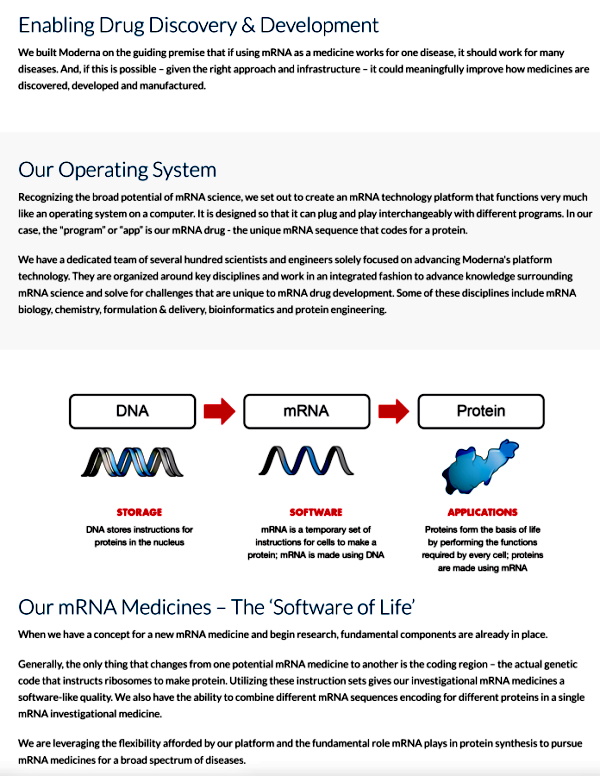 Screenshot /
Screenshot / 
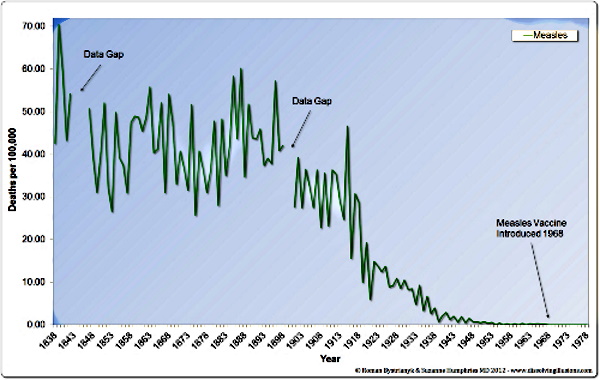
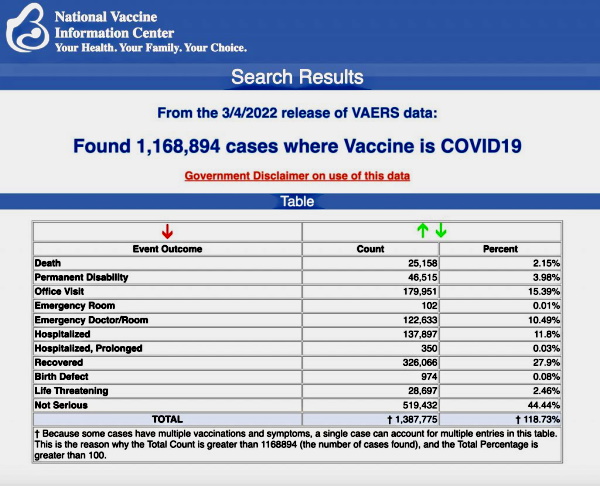

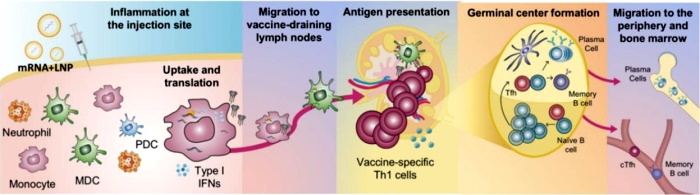
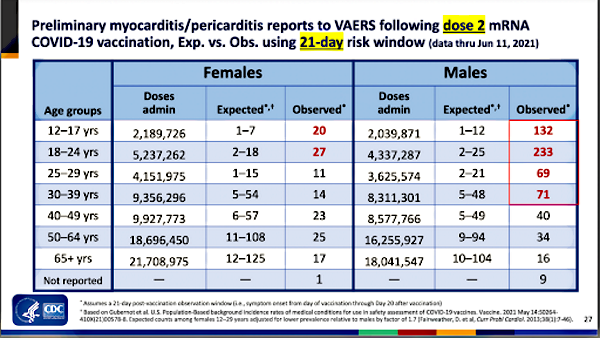
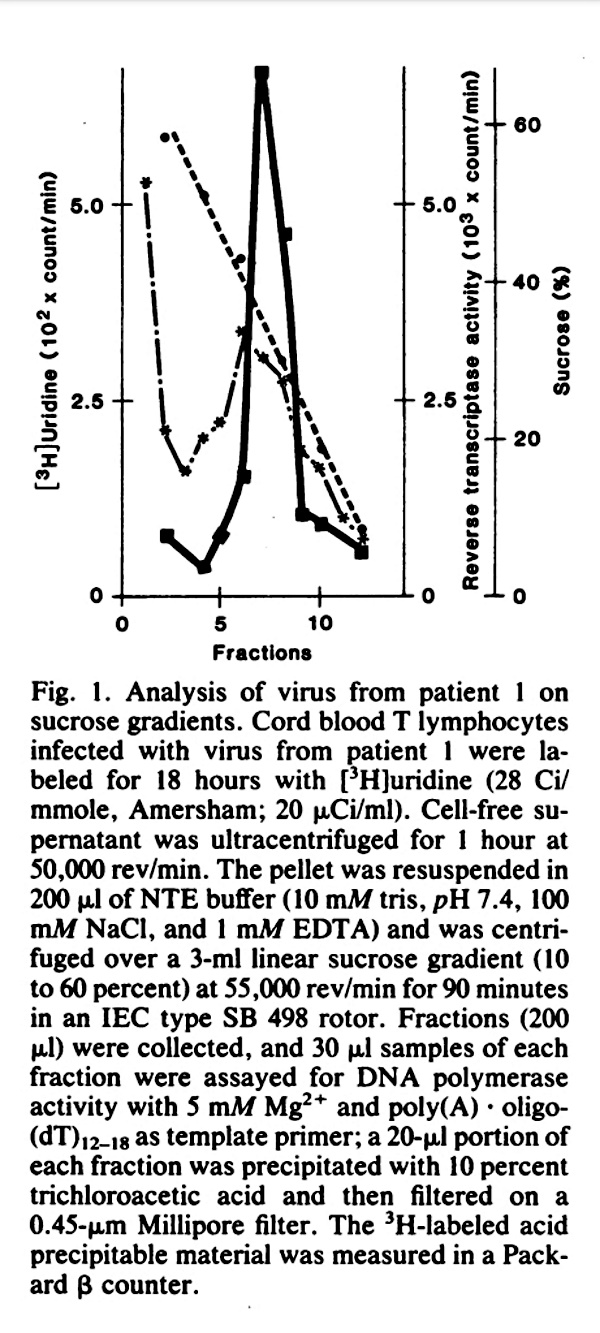
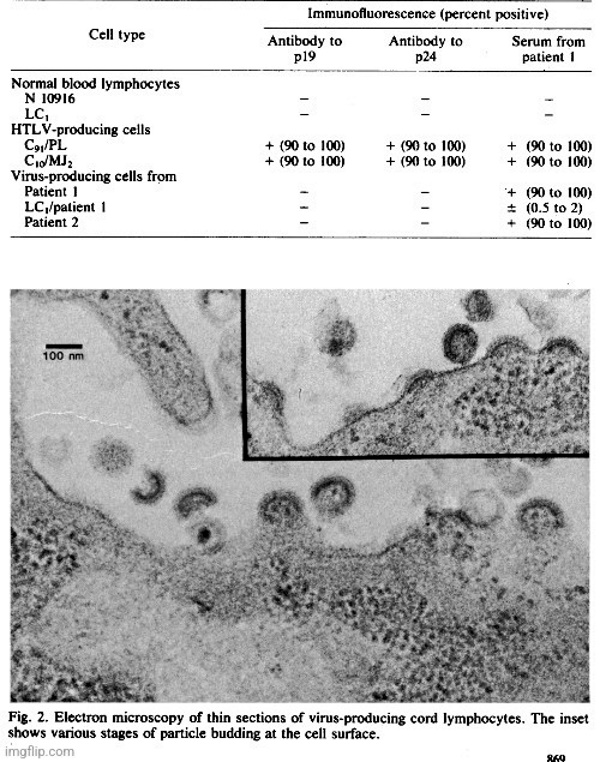

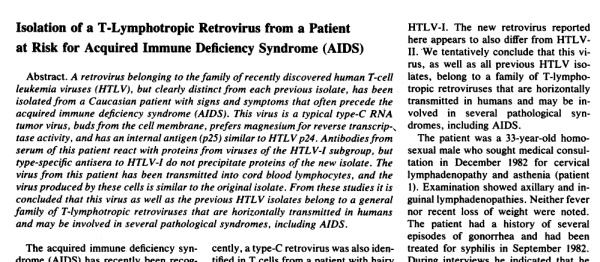
_J.jpg){kind=link}
_G.jpg){kind=link}
{kind=link}
{kind=link}