Disturbing Confrontation Inside Australia’s ‘Gold Standard’ COVID Internment Camp
Disturbing Confrontation Inside Australia’s ‘Gold Standard’ COVID Internment Camp
by Tyler Durden, ZeroHedge
December 3, 2021
Days ago we presented the latest Orwellian headline out of Australia… “Aussie Police Arrest Teen ‘Fugitives’ Who Escaped From COVID Internment Camp”. Since then more incredibly disturbing video from inside the Northern Australian Covid internment camp, Howard Springs facility, has emerged. A frightening confrontation between a imprisoned “quarantined” woman and camp authorities was caught on hidden camera.
One host on the popular cultural commentary and news analysis site UnHeard recently introduced a segment taking a look at the fresh footage from inside the notorious Covid internment camp : “Australia. Until recently, that country was most famous for its sunshine and relaxed attitude. Well since the Covid pandemic hit we’ve all got to know another side of Australia…”
https://twitter.com/_evelynrae/status/1466712921266814977?
With some of the longest and most stringent lockdowns and travel restrictions in the world, it’s become a case study of what happens when a government will do anything to keep Covid numbers low,” host Freddie Sayers’ narration continues.
“Their latest policy is to build special camps, Covid internment camps – to which infected and suspected infected people are moved. The biggest of these camps is called Howard Springs.”
“It houses up to 2,000 inmates, surrounded by tall fences and carefully policed against attempts to escape. It’s been described as the ‘gold standard’ of such camps and is being replicated across Australia.”
The woman being interrogated and threatened with a 5000 AU$ fine in the above video can been seen in a follow-up interview below, conducted after she was released from detention…
As is shown in the video in question, camp officials confronted the quarantined woman, later identified as Hayley Hodgson, and began pointing out yellow lines that she could not cross.
She never tested positive for COVID after being tested three times. “Never had Covid. I was in close contact with someone – never got it, and I was treated literally like a criminal,” she later described. After her 14-day stint at the camp, she lost her job, returning to her home unemployed, she later confirmed.
Up until recently, Australia – with its sprawling coastline and beautiful beaches, outdoor and adventure life, and nearly year-round sunshine – was considered by most to be a large “paradise” vacation spot in the South Pacific… but now it’s marked as the place of “Covid quarantine hell”.
* * *
Meanwhile, in neighboring New Zealand, Prime Minister Jacinda Ardern has unironically given citizens permission to use the bathroom inside other people’s homes when visiting…
Exciting news from New Zealand, where PM Jacinda Ardern has given her people permission to use the bathroom inside their friends’ homes.https://t.co/YhbzuJiBRL
— Michael P Senger (@michaelpsenger) November 29, 2021
5-Year-Old Died 4 Days After Pfizer Shot, CDC VAERS Data Show
5-Year-Old Died 4 Days After Pfizer Shot, CDC VAERS Data Show
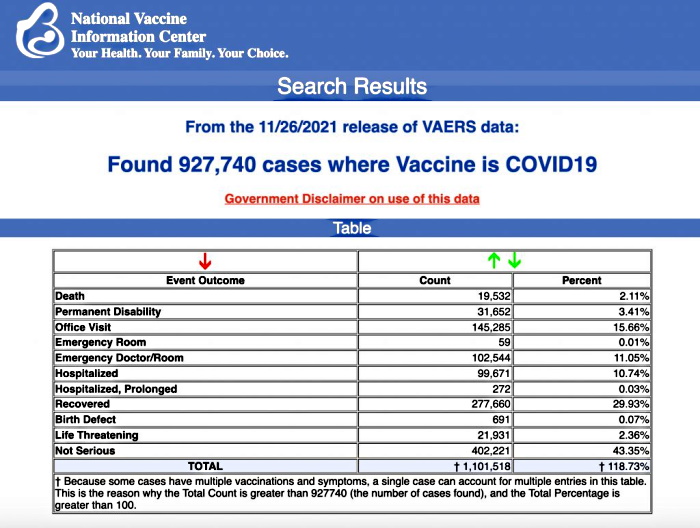
VAERS data released today by the Centers for Disease Control and Prevention included a total of 927,740 reports of adverse events from all age groups following COVID vaccines, including 19,532 deaths and 146,720 serious injuries between Dec. 14, 2020, and Nov. 26, 2021.
by Megan Redshaw, The Defender
December 3, 2021
The Centers for Disease Control and Prevention today released new data showing a total of 927,740 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and Nov. 26, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 19,532 reports of deaths — an increase of 283 over the previous week — and 146,720 reports of serious injuries, including deaths, during the same time period — up 3,325 compared with the previous week.
Excluding “foreign reports” to VAERS, 672,373 adverse events, including 8,986 deaths and 57,143 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Nov. 26, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 8,986 U.S. deaths reported as of Nov. 26, 20% occurred within 24 hours of vaccination, 26% occurred within 48 hours of vaccination and 61% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 454 million COVID vaccine doses had been administered as of Nov. 24. This includes 264 million doses of Pfizer, 173 million doses of Moderna and 16 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to Nov. 26, 2021 for 5- to 11-year-olds show:
- 2,586 adverse events, including 34 rated as serious and 2 reported deaths. One death occurred in an 11-year-old girl from Georgia vaccinated Sept. 14, prior to the authorization of Pfizer’s COVID vaccine in the 5 to 11 age group.
The second death (VAERS I.D. 1890705) occurred in a 5-year-old girl who died four days after receiving her first dose of Pfizer.
- 1,581 adverse events have been reported in the 5 to 11 age group since Nov. 1.
U.S. VAERS data from Dec. 14, 2020, to Nov. 26, 2021 for 12- to 17-year-olds show:
- 23,871 adverse events, including 1,453 rated as serious and 31 reported deaths.
The most recent death involves a 16-year-old girl from Georgia (VAERS I.D. 1865389) who died reportedly from a heart condition and multi-organ failure two days after receiving Pfizer’s COVID vaccine.
- 60 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases
attributed to Pfizer’s vaccine. - 563 reports of myocarditis and pericarditis (heart inflammation) with 553 cases attributed to Pfizer’s vaccine.
- 139 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to Nov. 26, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 42% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- As of Nov. 26, 4,480 pregnant women reported adverse events related to COVID vaccines, including 1,411 reports of miscarriage or premature birth.
- Of the 3,219 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 764 reports of Guillain-Barré syndrome (GBS), with 42% of cases attributed to Pfizer, 29% to Moderna and 27% to J&J.
- 2,163 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 11,334 reports of blood clotting disorders. Of those, 5,024 reports were attributed to Pfizer, 4,037 reports to Moderna and 2,222 reports to J&J.
- 3,257 cases of myocarditis and pericarditis with 2,025 cases attributed to Pfizer, 1,085 cases to Moderna and 137 cases to J&J’s COVID vaccine.
Athletes experience devastating injuries following COVID vaccines
As The Defender reported Dec. 2, several high-performing professional athletes are facing the end of their careers after COVID vaccines destroyed their health.
World record-holder in static breath-hold freediving, veteran triathlete, professional tennis player, professional mountain biker—all high-performing athletes until COVID vaccines ruined their health + their careers.#TheDefender: https://t.co/zL66Edfiw5https://t.co/L76vBedOOW
— Robert F. Kennedy Jr (@RobertKennedyJr) December 2, 2021
Florian Dagoury, a world record-holder in static breath-hold freediving, who once held his breath for a shocking 10 minutes and 30 seconds, was diagnosed with myocarditis, pericarditis and trivial mitral regurgitation after receiving Pfizer’s COVID vaccine.
Dagoury said he now struggles to reach an 8-minute breath-hold, feels an urge to breathe doing 40-minute dives, can’t keep his heart rate low and experienced a 30% decrease in his diving performance.
Veteran triathlete Antoine Méchin, 32, is also facing the potential end to his career after experiencing a pulmonary embolism after receiving Moderna’s COVID vaccine.
The symptoms, which included breathing problems and arm pain, started after the first dose, but doctors brushed off his shortness of breath as related to stress and fatigue.
Jeremy Chardy, a 34-year old professional tennis player ranked 73rd in the world, suspended his season due to a severe adverse reaction to a COVID vaccine, which left him unable to engage in intense activity.
Kyle Warner, a 29-year-old professional mountain bike racer, developed pericarditis, postural orthostatic tachycardia syndrome (POTS) and reactive arthritis following his second dose of Pfizer’s COVID vaccine.
Warner’s reaction was so severe that, as of October, he was still spending days in bed, overwhelmed by too much mental or physical exertion.
Two professional soccer players collapse during games
A professional soccer player collapsed suddenly on Nov. 25, during a Real Madrid’s Champions League game with Sheriff Tiraspol, a Moldovan soccer club, ZeroHedge reported.
Adama Traore, 26, a winger for Sherriff Tiraspol, was seen clutching his chest as he slumped to the ground in the middle of the game as medics rushed to revive him. The reasons behind Traore’s collapse and why he was suffering from chest pains have not been confirmed.
Traore’s collapse occurred the night after another player, Sheffield United’s John Fleck, went down during a match against Reading. Fleck was taken off on a stretcher after receiving lengthy treatment.
When a radio pundit questioned whether Fleck had received the COVID vaccine, his live feed to the show was cut.
A major German newspaper, Berliner Zeitung, recently published a report attempting to answer why an “unusually large number of professional and amateur soccer players have collapsed recently.”
The article listed many recent cases of players who experienced heart problems or collapsed on the field — in some cases resulting in death.
Pfizer seeks authorization for boosters shots for 16- and 17-year-olds
Pfizer CEO Albert Bourla said in a tweet on Tuesday the pharma giant, along with BioNTech, formally asked the FDA to authorize COVID booster doses for 16- and 17-year olds.
If approved, the shot would be the first booster available to people under 18.
The FDA could approve Pfizer’s booster doses for 16- and 17-year olds as soon as next week, according to people familiar with the matter.
COVID vaccines may be associated with heightened risk of myopericarditis among men
To help determine whether a correlation exists between COVID vaccines and myopericarditis, researchers tracked data from more than 268,000 adults in Massachusetts who received at least one dose of a COVID vaccine between August 2020 and May 2021.
The researchers compared the data to a control group made up of 235,000 of the same patients — from 2018 and 2019, well before they had received any doses of a COVID vaccine.
In a study published in the American Journal of Cardiology, the researchers found the age-adjusted incidence rate of myopericarditis in men was higher in the vaccinated than the control population, while the incidence rate of myopericarditis in women was the same between the vaccinated and control populations.
They also found an increased incidence of myocardial injury in both men and women in 2021 compared to 2019, although they suggested some of the apparent increase in the diagnosis of myopericarditis after vaccination may be attributable to factors unrelated to the COVID vaccines.
Moderna CEO says Omicron COVID booster could be ready by March
Moderna President Stephen Hoge said Wednesday boosters of its COVID vaccine targeting the Omicron variant could be ready for U.S. authorization as early as March.
Moderna is also developing a multivalent vaccine targeting Omicron and three other COVID variants, although the shot will not be available for several more months, Forbes reported.
March is the earliest date an Omicron booster could be approved under current FDA guidelines, though the company can start manufacturing the vaccine during testing.
Hoge said he thinks existing vaccines “will be able to slow down, if not completely stop, the Omicron variant.”
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
©December 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Connect with Children’s Health Defense
cover image credit: KitzD66 / pixabay
SOS Australia – Protests Planned Tomorrow (Dec 4) at Australian Embassies Worldwide
SOS Australia – Protests Planned Tomorrow (Dec 4) at Australian Embassies Worldwide
by 21st Century Wire
December 3, 2021
Last month, activists from Reignite Democracy Australia launched a global appeal for people to gather this Saturday December 4th at Australian embassies and consulates worldwide in solidarity with the people of Australia and in protest against the brutal behaviour and policies of government there.
“This is a message to all the countries who are getting ready to protest at their nearest Australian Embassy or Consulate today at 12 noon. We asked several Aussies to send you a message…here’s what they had to say!” Watch:
More info about the event: https://www.reignitedemocracyaustralia.com.au
Watch Part 1 of our interview with RDA organiser Monica Smit here
Watch Part 2 of her interview here
Connect with 21st Century Wire
For list of participating countries: https://www.reignitedemocracyaustralia.com.au/sos/

Fauci’s Dead Babies and Mass Graves From the Past
Fauci’s Dead Babies and Mass Graves From the Past
by Greg Reese, The Reese Report
December 3, 2021
Original video available at Reese Report Rumble and Banned.video
Transcript provided by Truth Comes to Light
The reception of Robert Kennedy, Jr.’s book,”The Real Anthony Fauci”, is clear evidence of a mass awakening.
The people are waking up to see Fauci for what he is — an absolute psychopath.
We’ve learned of how he directed experiments at the NIAID in which beagles had their vocal cords removed and their heads enclosed in cages where sand fleas ate them alive.

And we’ve learned of how he fraudulently used PCR tests to illegitimately push a known deadly drug upon tens of thousands of people.
And many are now learning that in 1992 under the direction of Anthony Fauci the NIAID funded drug trials on HIV positive children, although many of the children were healthy and asymptomatic. They had merely tested positive via faulty PCR tests administered through New York’s Child Welfare Department, who then handed them over to the deadly experiments.
Most of the drugs being tested on the children were already known to cause deformities, organ failure, brain damage and other lethal side effects.
And yet the children were required to continue with the drugs regardless of negative side effects.

Those administering the drugs were explicitly told that all adverse side effects they witnessed in the children were being caused by the HIV infection and not the drugs.
When parents refused to consent to these barbaric trials children services took their kids and placed them with foster families for children’s homes where participation in the trial would be assured.
When the children resisted the deadly drugs, they were brought to Columbia Presbyterian Hospital where plastic tubes were surgically inserted into their stomachs and the deadly drugs they were trying to escape we’re pumped directly into their bodies.
Once the children died, their bodies were added to a mass grave in Hawthorne, New York — a large pit with astroturf thrown over it.

To get around the Nuremberg Code and other laws the state of New York created a special review board comprised of the hospital stakeholders.
May one wonder, other than torturing and killing innocent children, what were they trying to accomplish?
They already knew of the negative side effects that these drugs are having on adults. But the more we learn about Anthony Fauci, the more we realize that he is an absolute psychopath.
And it doesn’t matter why psychopaths do what they do. Fauci and his criminal cohorts belong in cages at the very least.
Anthon Fauci is just one old crook in a mass of conspiracy that is aggressively pushing to inject everyone’s children with the new deadly and debilitating mRNA experimental jabs. Whether you like it or not.
Going after Fauci is a drop in the bucket but at least it’s a start.
See related articles:
‘Guinea Pig Kids’: Fauci’s Legacy of Cruel Experiments on Kids
Beyond #BeagleGate: Fauci’s Long History of Atrocities, Including Torturing Children
Fauci, Dead Orphans, AIDS Drug Trials, and the Lies
“Dr. Fauci, Mr. Hyde” – RFK, Jr. in Conversation With James Corbett: “There’s an Entire Coalition of Sinister Forces… Which Are All Wrapped Up in This Obliteration of Constitutional Rights…”
The Real Anthony Fauci
My New Book — ‘The Real Anthony Fauci’ by Robert F. Kennedy Jr.
How to Submit Your Public Comments to the U.S. Government Against Its Vaccine Mandates
How to Submit Your Public Comments to the U.S. Government Against Its Vaccine Mandates
Want Medical Freedom? Submit a Public Comment to the Government Against Its Vaccine Mandates
by Informed Consent Action Network (ICAN)
December 3, 2021
Very frequently, supporters of ICAN ask us: what can we do? Here is a very simple, yet very important thing that each one of you can and should do.
On September 9, 2021, President Biden announced, as part of his Path Out of the Pandemic, a mandate for all federal contractors to be vaccinated for COVID-19. The government is now seeking public comment about the guidance which requires vaccination for all federal contractors. On the same date, President Biden announced that he would direct OSHA to mandate private employers with 100 or more employees to mandate COVID-19 vaccines or testing and masking. On November 6, 2021, OSHA enacted an emergency temporary standard requiring just that. The government is also seeking public comment about this mandate.
Please make a public comment sharing your thoughts about why federal contractors should not be mandated to be vaccinated in order to keep their jobs and why private employers should not be forced to mandate that their employees be vaccinated.
Visit the docket for the OSHA ETS. Comments are due on or before January 19, 2021. On this page, you will see a blue box that says, “Comment” near the top left of the page.
Visit the docket for the federal contractor guidance. Comments are due on or before December 16, 2021. For this comment, you need to select the middle tab “Browse Documents” and then select “Comment” in the Notice section below that tab:
For both dockets, you will click on the “Comment” button and can either manually type in your comment and/or attach a document to your comment. (It is advised that you write your comment elsewhere and then copy/paste it into this section so that it is not lost.)
Please note: all comments will be made public on the docket so only include information that you want publicly shared and avoid sharing information such as personal address, email, phone number, etc.
It is incredibly important that you all share your thoughts and make your voices heard. Help ICAN by adding to our voice. Let’s make clear to the federal government that we the people do not want the government making our medical decisions!
Connect with Informed Consent Action Network (ICAN)
cover image credit: stevepb / pixabay
As Australians Seek Compensation for Vaccine Injuries Under New Plan, Here’s a Look at COVID Vaccine Liability Laws Around the World
As Australians Seek Compensation for Vaccine Injuries Under New Plan, Here’s a Look at COVID Vaccine Liability Laws Around the World
More than 10,000 Australians so far requested compensation for COVID vaccine injuries under the country’s vaccine injury compensation scheme. What types of compensation programs exist in other countries?
by Michael Nevradakis, Ph.D., The Defender
December 2, 2021
Recent reports from Australia indicate more than 10,000 Australians are requesting compensation for vaccine injuries that they received following inoculation with the COVID-19 vaccine.
The claims come as part of an Australian government program allowing individuals to be compensated for lost income after being hospitalized for “rare but significant” side effects resulting from the vaccination.
As originally conceived, compensation through the program was available to people who incurred A$5,000 or more in vaccine injury-related medical costs. However, the government enacted a reduction in the compensation threshold, permitting claims for the cost of vaccine injuries beginning at A$1,000.
The 10,000-plus compensation claims were submitted as almost 79,000 adverse side effects after COVID vaccines were reported to the country’s Therapeutic Goods Administration, as of mid-November.
No-fault vaccine liability: what is it?
Australia’s vaccine injury compensation program is an example of a “no-fault compensation program.”
This refers to a measure put in place by public health authorities, private insurance companies, manufacturers, and/or other stakeholders to compensate individuals harmed by vaccines. Such programs allow a person who has sustained a vaccine injury to be compensated financially, without having to attribute fault or error to a specific manufacturer or individual.
No-fault compensation schemes are one of three options used by various countries to handle vaccine injury claims.
The other two options include allowing vaccine-injured people to sue private-sector actors, such as vaccine manufacturers or their insurers, or to place the full financial burden on the patient.
Australia’s no-fault compensation program is fairly new. It was launched in August 2021, despite longstanding calls for the development of such a scheme well before COVID.
A 2020 study found 25 countries with a no-fault program in place, with 15 of these programs administered at the government level.
In some countries, such programs are administered at the provincial level or at multiple levels of government, while two countries (Sweden and Finland) were identified by the study as having no-fault programs fully administered by the insurance sector.
The exact nature of such no-fault schemes, however, can differ significantly from one country to another. As explained in the 2020 study:
- In Sweden and Finland, pharmaceutical companies who market their products in these jurisdictions provide insurance contributions which fund those countries’ no-fault programs.
- Similarly, Norway’s no-fault program is funded by a special insurance organization known as the Drug Liability Association.
- Latvia’s Treatment Risk Fund is funded through contributions from medical institutions, acting as professional indemnity insurance.
- In China and South Korea, there are two separate programs, covering those vaccines in each country’s national immunization program (NIP) and those not included in the respective country’s NIP. Each government funds injury claims for NIP vaccines, while pharmaceutical companies or those holding a drug’s market authorization are responsible for funding injury claims regarding non-NIP vaccines.
- The U.S. no-fault Vaccine Injury Compensation Program is funded by a flat-rate tax of 75 cents for each disease covered in each vaccine dose.
- New Zealand has set up an Accident Compensation Corporation, which acts as a general compensation fund for accidents stemming from vaccinations, and treatment injuries. The program is funded through general tax contributions and levies on employee wages, businesses, vehicle licenses and fuel sales.
Not all no-fault programs compensate for injuries arising from all vaccines. For instance, according to the 2020 study:
- Only five (Japan, France, Italy, Hungary, and Slovenia) of the 23 programs specifically examined by the study covered injuries arising from mandatory vaccines or vaccines recommended by law — of particular significance in a world where more and more countries are attempting to implement COVID vaccine mandates.
- Just over half (57%) of the programs examined provide compensation for injuries arising from registered and recommended vaccines for children, pregnant women or adults and for special indication, such as occupation or travel, within the jurisdiction. This latter point is also significant in an era where many COVID vaccine mandates are being imposed on specific occupations or as a means of being “allowed” to travel.
Different no-fault programs also have differing rules with regard to when claims can be filed.
Referring again to the 2020 study, in certain countries, claims have to be filed within a certain number of years of vaccination or, in some cases, of the initial onset of vaccine injury symptoms. This ranges from 20 years (Norway), to six years (UK, for adults), to three years (U.S. and several other countries).
In some other countries, the maximum interval varies by province (China), or there is no specific deadline for filing a claim (including Sweden, Germany, New Zealand and Japan for NIP vaccines).
As seen with the example of Australia above, no-fault programs also set compensation thresholds. This is true in all no-fault countries examined by the 2020 study.
Thresholds of eligibility also exist, which may include injuries resulting in financial loss or permanent or significant injury (such as a medical disability), serious health damage or death, severe injuries surpassing normal post-vaccination reactions or other degrees of injury.
Just over half (52%) of the programs studied also provided compensation for claims regarding vaccine defects or immunization errors, while in the remaining countries, these types of claims are covered separately, through civil litigation or medical malpractice indemnity.
The 2020 study also noted that in almost all no-fault jurisdictions, such programs are non-judicial in nature and are instead administrative in scope, typically involving panels of medical experts who review each individual vaccine injury claim.
In a minority of countries, the administrative program is combined with a legal approach and the involvement of legal experts, while in Finland and Sweden, compensation decisions are made based on civil liability (tort) laws.
The standard of proof the claimant is required to demonstrate is generally similar across most no-fault programs, according to the 2020 study. These programs tend to employ a “balance of probabilities” approach that weighs whether it is “more likely than not” that the vaccination led to the injury in question.
This approach takes into consideration such factors as the time interval since vaccination, and existing medical evidence establishing a connection between the vaccine and that type of injury.
A country-by-country look
The above provides a general overview of how no-fault compensation programs work. However, it is also worth examining the specific rules in place in major countries and blocs of nations around the world.
United States:
In 1986, the U.S. Congress passed the National Childhood Vaccine Injury Act of 1986, often simply referred to as the Vaccine Act. Under this act, a no-fault program for administering vaccine claims, known as the National Vaccine Injury Compensation Program (VICP) was established.
Through this program, any individual claiming a vaccine injury (or a parent or guardian of a child) can file a petition with the U.S.Court of Federal Claims. The petition is reviewed by the U.S. Department of Health and Human Services (HHS), which makes a preliminary recommendation.
The U.S. Department of Justice (DOJ) then prepares a legal report, which includes the medical recommendation, and submits it to the court. The court then appoints a special master, who may convene a hearing, and who decides whether the petitioner should be compensated, and if so, what the level of compensation will be.
This compensation is then disbursed to the petitioner through HHS. Petitioners may also appeal a decision that isn’t in their favor, and by rejecting the decision of the court, may then file a lawsuit in civil court against the vaccine maker and/or the healthcare provider who administered the vaccine.
VICP, however, does not encompass all vaccines. It covers vaccines that are routinely administered to children and to pregnant women, and that are subject to the previously-mentioned 75-cent excise tax.
To date, more than 8,400 VICP claims have been settled, out of more than 24,000 petitions, with a total of $4.6 billion issued in settlements.
Compensation has also been issued. However, most such settlements were reached following negotiations instead of a hearing, with no admission on the part of HHS that vaccines were ultimately responsible for the injuries in question.
A different category of vaccines, including, at present, the existing COVID-19 vaccines, are covered under what is known as the Countermeasures Injury Compensation Program (CICP).
This program was established under the aegis of the Public Readiness and Emergency Preparedness (PREP) Act of 2005. The PREP act was developed to coordinate the response to a “public health emergency.” The law is scheduled to remain in place until 2024.
CICP specifically focuses on countermeasures, that is, “a vaccination, medication, device or other item recommended to diagnose, prevent or treat a declared pandemic, epidemic or security threat.”
Under CICP, a different claims process exists as compared to the VICP. The process for claimants is more cumbersome, and individuals have only one year after the administration of the vaccine to file a claim. Injuries whose symptoms materialize later in life, for instance, would presumably not be covered under this process.
Moreover, the likelihood of success, if past precedent is any indication, is slim. As previously reported by The Defender:
“The program’s parsimonious administrators have compensated under 4% of petitioners to date — and not a single COVID vaccine injury — despite the fact that physicians, families and injured vaccine recipients have reported more than 600,000 COVID vaccine injuries.”
Notably, vaccines with full FDA approval but which are not placed on a vaccination schedule for children or pregnant women are subject to ordinary product liability laws, while vaccines administered under an Emergency Use Authorization are protected from legal liability.
Furthermore, a 2011 Supreme Court decision, Bruesewitz v. Wyeth, held that the Vaccine Act preempts claims made under state-designed defect laws, against vaccines covered by the Act. The decision stated that ““[The Vaccine Act] reflects a sensible choice to leave complex epidemiological judgments about vaccine design to the FDA and the National Vaccine Program rather than juries.”
Until the 1980s, a series of successful lawsuits against vaccine makers was seen as resulting in increasing vaccine hesitancy and declining vaccination rates, as indicated in a 1985 National Research Council publication, released just one year before the passage of the Vaccine Act.
Canada:
In recent years, Canada was the only G7 country without a nationwide no-fault vaccine injury compensation program. On a provincial level, Quebec established such a program in 1985, at which time calls for the creation of a national program followed. Attempts were made to develop a national program at this time, which ultimately failed.
As of 2018, Quebec’s program had approved a total of 43 claims, paying $5.49 million (CAD) in compensation.
In June 2021, launched a national vaccine injury compensation program, the Vaccine Injury Support Program. The program covers all provinces except Quebec, whose provincial program will continue to operate.
While this program is funded by Public Health Canada, it is administered by a private company, RCGT Consulting.
The program covers claimants who received a Health Canada-authorized vaccine (on or after Dec. 8, 2020), administered in Canada, with a resulting injury that is serious and permanent or which has resulted in death, and which was reported to the healthcare provider that administered the vaccine.
Though it wasn’t until a few months ago that Canada was able to establish a nationwide vaccine compensation program, COVID vaccine manufacturers were already, as of December 2020, indemnified against claims of vaccine injuries.
United Kingdom:
In the UK, the Vaccine Damage Payment Scheme (VDPS) provides compensation totaling £120,000 to anyone who suffers a disability of 60% or more, as a result of their vaccination.
The percentage figure refers to a severe disability resulting in such injuries as the loss of a limb, an amputation, losing 60% or more of normal vision or severe narcolepsy.
Additionally, the 1987 Consumer Protection Act also applies to those who have sustained a vaccine injury, if is found that the product in question did not meet safety standards or was defective. This is further strengthened by the 2005 General Product Safety Regulations.
Consumer protection rights still apply for people injured by the COVID vaccine, as the government wasn’t allowed to take those away. But due to the legal definition of defects, and a rule known as the state-of-the-art defense, it is difficult to get compensation when specific problems with the vaccine are not yet known.
COVID vaccines have been added to the VDPS. However, according to the Human Medicines Regulation of 2012, protection against civil liability is provided to vaccine manufacturers for unlicensed products issued under a temporary use authorization by the Medicines and Healthcare Products Regulatory Agency.
This regulation was further amended by the Human Medicines (Coronavirus and Influenza) (Amendment) Regulations 2020, providing extended immunity from civil liability to vaccine makers and those administering vaccinations. However, the consumer protection laws mentioned above still apply.
Legal indemnity has also been directly provided to vaccine manufacturers in the case of the COVID-19 vaccine.
European Union:
The UK laws are based largely on EU legislation, which was codified into British law prior to Brexit.
For instance, the UK Human Medicines Regulations of 2012 and 2020 are largely based on their EU equivalent, EU Directive 2001/83/EC relating to medicinal products for human use. This includes protections against civil actions for products released under temporary or emergency authorizations.
The 1987 Consumer Protection Act in the UK is, in turn, equivalent to the EU’s Directive 85/374/ECC of 1985, on the approximation of the laws, regulations and administrative provisions of the Member States concerning liability for defective products, while the 2005 General Product Safety Regulations were harmonized with EU Directive 2001/95/EC on general product safety.
At the EU level, immunity for vaccine manufacturers was not standard prior to COVID, when legal responsibility tended to lie with the companies.
This, however, is not the case with the COVID vaccines. Under pressure from Vaccines Europe, a trade organization representing vaccine manufacturers in the EU, and under the guide of “ensuring access” to vaccines, exemptions from liability were granted to companies such as AstraZeneca.
Notably, a question posed in August to the European Parliament by one of its elected representatives, Ivan Vilibor Sinčić of Croatia, regarding liability for COVID-19 vaccine side effects, remains unanswered as of this writing.
Within the EU, different member states have enacted their own legislation with regard to vaccine injury compensation claims. These programs were summarized in a 2021 study examining such policies on a global basis. They can be summarized as follows:
- Austria: The Vaccine Damage Act is a public-law system for the payment of compensation for vaccine injuries by the state. COVID vaccines are included in this program.
- Belgium: No vaccine compensation legislation exists.
- France: The existing vaccine injury compensation program provides relief only for injuries related to mandatory vaccinations. Claims for injuries resulting from non-compulsory vaccinations fall under the general principles of French civil law. For COVID vaccines, claims can be lodged with the National Office for Compensation of Medical Accidents, without having to prove a defect with the vaccine or fault on the part of healthcare providers.
- Germany: A flat-rate no-fault compensation program exists for vaccines that are mandatory or that are publicly recommended, including COVID vaccines.
- Greece: A no-fault program doesn’t exist, but a May 2021 high court ruling held that those who sustained vaccine injuries are entitled to state compensation.
- Italy: A no-fault program providing state compensation for injuries stemming from required or highly recommended vaccines exists, although it is unclear if this extends to COVID vaccines. Claimants are also free to pursue claims under tort law.
- Netherlands, Portugal: There is no specific no-fault scheme, but vaccine injury claims can be filed via provisions of the civil code.
- Sweden: An insurance fund, Swedish Pharmaceutical Insurance, handles vaccine injury claims out of court. However, new legislation which took effect Dec. 1 will provide additional state compensation for injuries arising from COVID-19 vaccinations.
Israel:
In Israel, the Vaccine Injury Compensation Law was passed in 1989, providing compensation to those injured by vaccines, without having to prove negligence.
Earlier this year, COVID-19 vaccines were included under this law.
New Zealand:
New Zealand maintains a no-fault system for accident compensation, including vaccine injuries, under the aegis of the previously-mentioned Accident Compensation Corporation (ACC).
Although most information on claims appears to be classified, financial compensation totaling $1.6 million (NZD) was provided between 2005 and 2019.
The ACC also handles claims related to COVID-19 vaccination.
China:
China’s vaccination program differentiates between mandatory and non-mandatory vaccinations, for the purposes of vaccine injury claims.
The 2019 Law on Vaccine Administration establishes a compensation system for deaths or significant injuries, such as organ or tissue damage, stemming from vaccines. Compensation is paid from the vaccination funds of the country’s provincial governments.
Draft legislation in 2020 called for mandatory liability insurance for vaccine manufacturers distributing vaccines in mainland China. However, it is unclear if this legislation was enacted.
Japan:
Until recently, Japan did not have a specific no-fault compensation program for vaccine injuries. But temporary programs where the government would provide compensation to vaccine makers for legal claims they sustained due to vaccine injuries had previously been passed in 2009, for the H1N1 vaccine, and again in 2011 until 2016.
However, a 2020 amendment to Japan’s Immunization Act now allows the government to take on the liability risks for COVID-19 vaccines.
India:
India has no specific no-fault legislation under the Drugs and Cosmetic Act for injuries stemming from vaccines that are fully licensed by the country’s regulator.
Claimants are, however, able to file claims in consumer courts or in India’s High Court, and the country’s drug regulator can also take action against vaccine manufacturers for violations of the law.
Indian law does provide for compensation in the event of injury or death following participation in clinical trials.
Notably, the Indian government’s negotiations with Pfizer fell through earlier this year when Indian regulators refused to provide it legal protection via indemnity.
Such protection was not provided to the three COVID-19 vaccines which received an emergency use authorization in India: Covishield, Covaxin and Sputnik V.
Adar Poonawalla, the head of the India-based Serum Institute, the world’s largest vaccine manufacturer, had previously called for protection from lawsuits for COVID vaccine injuries.
Malaysia and Singapore:
The country has not developed a no-fault vaccination program, unlike nearby Singapore.
Instead, a variety of legal remedies exist for claimants under civil law, including the Sales of Goods Act of 1957, the Consumer Protection Act of 1999, and the Contracts Act of 1950, and under criminal law, including the Poisons Act of 1952 and the Sale of Drugs Act of 1952.
South Africa:
South Africa is another country that did not develop a no-fault vaccine injury compensation fund until recently, but did so as a result of COVID and, apparently, pressure from vaccine manufacturers.
The fund is meant to provide compensation for “serious adverse responses” which lead to “permanent or significant injury, serious harm to a person’s health, other damage or death,” assuming these injuries were caused by vaccination.
Philippines:
Similar to South Africa, the Philippines only recently set up a no-fault indemnity program, shielding vaccine manufacturers, as well as public officials, from lawsuits, except in instances of gross negligence or willful misconduct.
This same program will also set up a state fund to provide compensation for vaccine injury claims.
Developing world:
Finally, for 92 low- and middle-income countries, the World Health Organization (WHO), along with a private company, Chubb Limited, has begun to administer a no-fault compensation program.
The countries in question are receiving COVID vaccines via the Gavi Alliance’s COVAX Advanced Market Commitment (AMC) program, with vaccine injury claims processed through the WHO’s new program, which is set to remain in effect until June 30, 2022.
No-fault schemes are increasing, but questions remain
With the recent examples of countries such as Canada and Australia, as well as South Africa and the Philippines, developing their own no-fault vaccine injury compensation funds, as well as their further extension to 92 low- and middle-income countries via the WHO, this type of compensation scheme is clearly the predominant method of dealing with financial claims stemming from vaccine injury claims.
As seen in the case of the U.S., such no-fault programs were developed to address claims of increased vaccine hesitancy, as a result of high-profile lawsuits against vaccine makers, and a decline in vaccine production from hesitant pharmaceutical companies which did not want to shoulder the legal and financial risks involved with releasing a new vaccine to the public.
What, however, goes unaddressed in such claims is the vaccine hesitancy, or outright refusals to get vaccinated, as people question why vaccine makers and, in many cases, everyone involved in distributing and administering vaccines, are shielded from legal action.
Such legal shields cast, for some people at least, a net of doubt, calling into question the safety of such vaccines if their manufacturers, distributors, and public health officials involved in their administration feel the need for legal protections. They may wonder why a product that is said to be safe requires such legal shields.
Such doubts further increase when governments and their agencies, which are essentially acting as guarantors of these vaccines through various no-fault schemes, redact critical information about these products, including their ingredients, and claims that releasing such documentation will take several decades, as the FDA did recently regarding its documents related to the Pfizer-BioNTech COVID vaccine.
This is despite the fact that in the 2011 Bruesewitz v. Wyeth decision, the U.S. Supreme Court gave considerable latitude to the FDA for, essentially, knowing better than judges and juries, or state lawmakers, how to regulate vaccines.
Despite this legal shielding, plenty of coverage of adverse reactions, and even deaths, following vaccinations is making its way into the media, and to the public consciousness, seemingly negating yet another argument in favor of indemnity.
Furthermore, as many no-fault schemes place the burden on taxpayers and government coffers, these financial costs are ultimately borne by the public.
Arguments that claim shielding vaccine makers from lawsuits also helps to keep the cost of these products down can be called into question on such grounds, especially if the government is the one making deals with vaccine manufacturers and paying for these vaccines.
Costs may be reduced in their purchase price, but the same government and same funds are then used to settle vaccine injury claims.
Such claims from vaccine makers, such as Pfizer for instance, also appear to be disingenuous when considering their high marketing budgets, which in the U.S., far exceed their research and innovation expenditures.
Arguments can be made that such funding could be redirected towards legal claims, towards reducing vaccine and drug prices, or both.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
©December 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Connect with Children’s Health Defense
cover image credit: mohamed_hassan & torstensimon / pixabay
Kiwi Church Leaders Defy Ardern’s Threats to Vaccinate or Face a $15K Fine
Kiwi Church Leaders Defy Ardern’s Threats to Vaccinate or Face a $15K Fine
by Tony Mobilifonitis, Cairns News
December 2, 2021
A feisty Kiwi pastor has told Jacinda Ardern and her Labor Party vaccination cabal to shove their shots and get their noses out of church business. Ardern is threatening to fine church leaders $15,000 if they are not vaccinated by December 3.
Pastor Carl Bromley of the Life Connection Missionary Baptist Fellowship in Christchurch says Ardern has crossed the line of respect between church and state. Ardern’s socialist-fascist regime is also trying to silence another high-profile and outspoken pastor, Brian Tamaki, who has been loaded with onerous bail conditions on charges of breaching so-called health orders by running a protest rally.
Ardern’s corrupt Covid cabal primarily includes her “nice guy” chief health bureaucrat Ashley Bloomfield, Covid 19 Response Minister Chris Hipkins, and Health Minister Andrew Little. Just like the Australian state premiers and their Covid cabals, these sad specimens of Kiwi political corruption follow orders from above e.g. the WHO, the global banks, big pharma and the Fauci-Gates-Rockefeller operation.
They have dug themselves into a hole of blind obedience to a corrupt narrative and they have no alternative but to dig deeper in the hope that the populations will follow them into the dystopian hell they are creating.
The slick and slimy Hipkins says he expects children aged five to 11 to start being vaccinated before the end of January, based on the notoriously compromised US FDA giving Pfizer the go ahead for five to 11-year-olds, subject to New Zealand approval from their regulator Medsafe.
Ardern claims she won’t push vaccination for children, but protesters across the country are making their distrust of her “promises” known, forcing her to cancel her appearances at country vaccination centres. Ardern’s next PR project will be her marriage over Christmas to her spin doctor husband Clarke Gayford.
The media will fall over themselves portraying this “oh so lovely event” in the seaside city of Gisborne as almost the equivalent of a royal wedding. Ardern’s circle of leftie supporters in the international media will be on to it as well. But will it be a public relations coup that leaves a bitter taste in the mouths of the many Kiwis destroyed by lockdowns, fines and now coerced vaccination.
The protests of pastors Bromley and Tamaki and others like megachurch pastor Peter Mortlock, touch upon the fundamental battle for the rights and freedoms that Ardern is systematically destroying on behalf of her globalist masters.
Whether or not you agree with Bromley’s hard-line theology, freedom of religion, speech and thought are essentially the same thing, hence their inclusion in the US Constitution’s First Amendment. They are also fundamental to English common law in the English Bill of Rights 1688 and international law.
The right at common law to informed consent to medical treatment is based on the law of trespass ie you have the right to bodily integrity free from uninvited threats and assault from individuals or the state. This is also recognised in the Nuremberg Code.
“I’ve got a message for Jacinda Ardern, Chris Hipkins, Ashleigh Bloomfield, Andrew Little and any other of their cronies: Get your noses out of God’s business. God has a message for them from His word: God is not mocked,” Bromley announced on a YouTube message below. He went on to accuse Ardern and company of shaking their fist at God and said this would induce divine judgment.
“So you can take your legislation, you can take your mandate and you can take a flying leap. And I suggest you pull your head in, otherwise you’re going to find yourself coming up against a judgment from God that you are just not prepared for … $15,000 fine for not taking a jab? You can go and take a flying leap because this pastor, this man of God is not bowing down to your tyranny, your evil, nor your ungodliness.”
Tamaki, the outspoken head of a South Auckland’s Destiny Church, told the New Zealand Herald he would rather “live in dangerous freedom than live in peaceful slavery”.
On Twitter he posted: “So a segregated, divided NZ is just around the corner with The Vaxxed No Vaxxed divide. We have been conditioned for some time now in the workplace, shops, businesses, services and among our own families. Is this what we want NZ? Is this the future for our kids?”
Mortlock, despite his megachurch’s corporate charity status with wages paid by the government, supported Tamaki’s recent protest and referred his congregation to the website of the organisers, the Freedom and Rights Coalition. “I was asked to be involved in it way back and I’ve taken a back seat in it, but enough to say if you want to go I just want to let you know about it. I think sooner or later we are going to have to make a stand – a stand for our rights, the way our freedoms are being stripped away.”
What makes it difficult for Tamaki, Bromley and Mortlock is that other churches are playing ball with the tyranny while a large, apathetic segment of the population simply go along with their mainstream media’s blatant lying and falling for Ardern’s sickly “charm”.
Bromley recently held a service in defiance of the country’s so-called “alert level 4” which bans gatherings outside of households. A YouTube post of a confrontation between Bromley and police was removed “for medical misinformation” – a code for Ardern’s censorship of anti-government information.
New Zealand’s NewsHub service made the following comment about anti-vaccine protests that would be laughable if it were not serious:
“Some anti-lockdown activists have compared New Zealand’s restrictions to the horrific Nazi regime of the 1930s, but there are marked differences between the two.
“While the Government’s alert level 4 regulations are designed to stop people falling ill and dying from COVID-19, the Nazi Party actively sought to marginalise, imprison and exterminate groups it deemed undesirable, particularly Jews and political dissidents.”
cover image of Pastor Carl Bromley is a screenshot from Is It Just Me NZ video
Test for New Omicron Variant? We Don’t Need No Stinkin’ Test
Test for New Omicron Variant? We Don’t Need No Stinkin’ Test
by Jon Rappoport, No More Fake News
December 2, 2021
This is an article in three layers. I’ve already spelled out the first layer in my current series on the Omicron variant of SARS-CoV-2 (archive: Omicron).
In a nutshell, there is no Omicron because there is no SARS-CoV-2. The “pandemic virus” doesn’t exist. A variation of nothing equals nothing.
However, I often make forays into the bubble-world where most people, including “the experts,” believe the virus is real. I do this to show that, within their world, the experts are constantly lying in their own terms and contradicting themselves.
Within their world, you would think the pros have an easily accessible test to identify the new Omicron variant in thousands or millions of people. Otherwise, how can they claim it’s here and spreading?
But you would be wrong.
And I have the evidence, based on the prior variant, the Delta. That’s level two. I take you there now, with an article I wrote months ago:
—Bombshell: PCR tests can’t identify Delta Variant; it’s all fiction—
Oooo. The Delta Variant. It’s everywhere.
Watch out. It’s under your rug. It’s in the clothes closet. It’s on your toothbrush.
And it’s The Unvaccinated who are spreading it. Those devils. We, who are pure, must be protected from the unvaxxed Unclean.
Fauci, god of soccer moms, rises every morning saying DELTA, goes on television saying DELTA, and goes to sleep praying to DELTA.
But read this from the Texas Department of State Health Services FAQ: “How can I tell if I have the Delta variant? Do labs report that to the state?” That information may not be readily available. The [PCR] viral tests that are used to determine if a person has COVID-19 are not designed to tell you what variant is causing the infection. Detecting the Delta variant, or other variants, requires a special type of testing called genomic sequencing. Due to the volume of COVID-19 cases, sequencing is not performed on all viral samples. However, because the Delta variant now accounts for the majority of COVID-19 cases in the United States, there is a strong likelihood that a positive test result indicates infection with the Delta variant.”
Boom.
I can assure you, the number of patients whose samples are genetically sequenced is tiny, contrasted against the number whose samples are simply run through the standard PCR.
So there is no way to know that the Delta variant now accounts for the majority of COVID cases in the US. And using the standard PCR, there is no way to know ANY specific patient has the Delta. It’s all fiction.
We have this from the American Lung Association: “Regular COVID-19 tests do not detect which variant is involved in a patient’s case—that information does not change the approach to care or therapy. The variant identification requires genomic sequencing, a process separate from regular virus tests and one that not all labs are able to do or do not do on a routine basis for patient care but are done more for public health monitoring.”
Let me break down how this game works. To be excessively generous, let’s say that 3 out of every 1000 positive PCR tests in America are sent to high-level labs, where genetic sequencing is done.
A certain percentage of THOSE sequencing tests come up positive for the Delta Variant. Based on these results, MODELS are constructed.
Now we’re REALLY into fake science. The models estimate what percentage of ALL positive PCR tests are really positive for Delta.
I’m sorry to break this newsflash, but modelers are notorious charlatans. Their dense calculations are as far from science as a Model-T Ford is from a spaceship.
But based on models, public health agencies—who desperately needed a new con, because COVID case numbers were declining—blasted through their media assets the new revelation: THE DELTA MONSTER IS LOOSE AMONG US.
But it gets even worse. Why? Because you can bet the farm that the current model pushing the omnipresence of the Delta Variant was never challenged. It was never handed to several groups of independent scientists who went over it with a fine-toothed comb. That’s called verification. That’s called the Scientific Method. You may have heard of it.
The most notorious modeler in the world, Neil Ferguson, of the London Imperial College, bankrolled by Bill Gates, made a prediction early in 2020: by that summer, there would 500,000 COVID deaths in the UK, and 2 million in the US.
It was this absurd prediction, swallowed whole by Boris Johnson, and swallowed whole by Donald Trump, on the urging of Tony Fauci, that led to the original mass lockdowns in US and the UK. And then other nations followed suit.
As my long-time readers know, all this is just the tip of a very large iceberg. For the past year, I’ve been proving the SARS-CoV-2 virus doesn’t exist, the tests and case numbers are meaningless, and the highly destructive vaccine is unnecessary.
But I make frequent forays into the fantasy world of official science, to illustrate that, even within that lunatic bubble, internal contradictions and outright lies abound.
Here is my original 2020 article on the most famous and celebrated modeler in the world, Neil Ferguson [this is level three]:
—Neil Ferguson: the ghost in the machine—
Why do governments salute when he predicts a pandemic and tells them to lock down their countries?
Does anyone care about his past?
Why does he still have a prestigious job?
Who is he connected to?
Neil Ferguson, through his institute at London’s Imperial College, can call the shots on a major percentage of the global population.
He’s Mr. Genius, when it comes to projecting computer models of epidemics.
Fellow experts puff up his reputation.
According to the Business Insider (4/25/20), “Ferguson’s team warned Boris Johnson that the quest for ‘herd immunity’ [letting people live their lives out in the open in the UK] could cost 510,000 lives, prompting an abrupt U-turn [massive national lockdown in the UK]…His simulations have been influential in other countries as well, cited by authorities in the US, Germany, and France.”
Not only cited, not only influential, but swallowed whole.
Business insider continues: “On March 23 [2020], the UK scrapped ‘herd immunity’ in favor of a suppression strategy, and the country made preparations for weeks of lockdown. Ferguson’s study was responsible.”
There’s more. A lot more.
Same BI article: “Dr. Deborah Birx, coronavirus response coordinator to the Trump administration, told journalists at a March 16 press briefing that the Imperial paper [Ferguson’s computer projection] prompted the CDC’s new advice to work from home and avoid gatherings of 10 or more.”
Ferguson, instigator of LOCKDOWNS. Stripping away of basic liberties. Economic devastation.
So let’s look at Ferguson’s funding and track record, spelled out in the Business Insider piece:
“Ferguson co-founded the MRC Centre for Global Infectious Disease Analysis, based at Imperial, in 2008. It is the leading body advising national governments on pathogen outbreaks.”
“It gets tens of millions of dollars in annual funding from the Bill & Melinda Gates Foundation, and works with the UK National Health Service, the US Centres for Disease Prevention and Control (CDC), and is tasked with supplying the World Health Organization with ‘rapid analysis of urgent infectious disease problems’.”
Getting the picture?
Gates money goes to Ferguson.
Ferguson predicts dire threat from COVID, necessitating lockdowns—thus preparing people to accept a vaccine. The vaccine Gates wants.
Ferguson supplies a frightening computer projection of COVID deaths—to the CDC and WHO. Ferguson thus communicates a rationale for the Gates vaccine plan.
National governments surrender to WHO and CDC and order LOCKDOWNS.
Business Insider: “Michael Thrusfield, a professor of veterinary epidemiology at Edinburgh University, told the paper he had ‘déjà vu’ after reading the [Ferguson] Imperial paper [on COVID], saying Ferguson was responsible for excessive animal culling during the 2001 Foot and Mouth [mad cow] outbreak.”
“Ferguson warned the government that 150,000 people could die. Six million animals were slaughtered as a precaution, costing the country billions in farming revenue. In the end, 200 people died.”
“Similarly, he [Ferguson] was accused of creating panic by overestimating the potential death toll during the 2005 Bird Flu outbreak. Ferguson estimated 200 million could die. The real number was in the low hundreds.” HELLO?
“In 2009, one of Ferguson’s models predicted 65,000 people could die from the Swine Flu outbreak in the UK — the final figure was below 500.”
So you have to ask yourself, why would anyone believe what Ferguson has been predicting in this COVID hustle?
Are his fellow experts that stupid?
Are presidents and prime ministers that stupid?
And the answer is: This is a monumental covert op; some people are that stupid; some are caught up in the op and are afraid to say the emperor has no clothes; some are aware of what is going on, and they want to destroy national economies and lead us into, yes, a new world order.
Gates knows he has his man: Ferguson. As the recipient of tens of millions of dollars a year from the Gates Foundation, Ferguson isn’t about to issue a model that states: COVID is nothing to worry about, let people live their lives and we’ll be all right. The chance of that happening is on a par with researchers admitting they never actually discovered a new virus as the cause of illness in 2019, in Wuhan.
In order to justify injecting every man, woman, and child in the world with synthetic genes, Gates needs A STORY ABOUT A DEADLY VIRUS THAT NECESSITATES SHUTTING DOWN AND IMPRISONING THE PLANET, ACHIEVING A CAPTIVE AUDIENCE.
He’s got the story, all dressed up in a computer model, composed by a man with a past record of abject and devastating failures.
Neil Ferguson is the ghost in the machine. The machine is the World Health Organization and the CDC. The man behind the ghost is Bill Gates.
—Those are the three layers of this story. Fraud, fraud, and fraud. But don’t worry. Tony Fauci will smooth out the wrinkles and assure us all that we’re on the right track. We just have to destroy the village in order to save it. Piece of cake.
cover image credit: CDD20 / pixabay
Perth, Western Australia Workers Lay Down Uniforms on Steps at Parliament as Mandates Set to Begin
Perth, Western Australia Workers Lay Down Uniforms on Steps at Parliament as Mandates Set to Begin
As “D-Day” arrives, workers from a variety of industries lay their uniforms down on the steps of Parliament in Perth.
by TOTT News
December 1, 2021
-

Powerful scenes on the steps of Parliament House in Perth this afternoon, as workers lay down their uniforms to protest impending mandates across the state.
Authorities say workers must receive their first dose by tomorrow or face unemployment, as mandates affect 75% of WA’s workforce.
Scenes at Parliament
Demonstrators gathered outside Parliament House on this afternoon, opposed to the WA government’s introduction of vaccine mandates.
Despite the looming uncertainty, the spirit of Australia remained high:
December 1 is being called ‘D-Day’ — the day when workers across a wide range of industries must have had their first dose of a COVID vaccine in order to keep their jobs.
FIFO miners, police, and community care workers, to name just a few, must be single-dosed by December 1 and double-dosed by December 31.
Protesters laid hi-vis FIFO vests and hard hats on the steps of Parliament and held placards with slogans such as “no to medical mandates” and “coercion is not consent”.
Former Liberal candidate Andrea Tokaji addressed the crowd, saying vaccine mandates were causing “pain”.
“These directions cause harm and suffering,” she said. “These directions violate the constitution.”
Other industries whose workers must be fully vaccinated by December 31 include port, transport and freight workers, health and aged care staff, fire and emergency services employees, abattoir and meat processing workers, and prison staff.
Staff at supermarkets, groceries, restaurants, pubs and cafes, as well as childcare, public transport and construction workers must be fully vaccinated by January 31.
Representatives from many of these industries appeared at Wednesday’s protests, with one placard reading, “Fire and rescue say no to medical mandates”.
Corporate Media Gets Heckled
As the event carried on, protesters let the corporate media know they were NOT impressed with their continued distorted coverage of the alternative viewpoint across Australia.
Channel 7 media get heckled by thousands of hard working, tax paying citizens in Western Australia who have lost their jobs just before Christmas.
"TELL THE TRUTH!"@Channel7 pic.twitter.com/tj6SZoS9Ds
— Julia Dixon 🐭 (@JuliaDixon84) December 1, 2021
Here is a POV perspective from one of the journalists in question:
WA Parliament… @geofparry7 pic.twitter.com/vwvxOQrAPZ
— James Carmody (@jamescarmody95) December 1, 2021
Mass coercion and segregation continues across Australia and shows no sign of slowing down with the ‘arrival’ of Omicron on our shores ahead of 2022.
One thing is for certain, the people are standing firm in their fundamental right to choose.
Biden COVID Vaccine Mandates Suffer Two More Legal Setbacks
Biden COVID Vaccine Mandates Suffer Two More Legal Setbacks
A federal judge in Louisiana on Tuesday issued a preliminary injunction halting President Biden’s national vaccine mandate for healthcare workers nationwide, and separately, a U.S. district judge in Kentucky issued a preliminary injunction blocking Biden’s mandate for federal contractors in three states.
by Megan Redshaw, The Defender
December 1, 2021
The Biden administration’s COVID vaccine mandates took two new legal hits Tuesday — one affecting healthcare workers nationwide, the other affecting federal contractors in three states.
The new rulings, combined with previous rulings temporarily suspending mandates for U.S. workers, affect hundreds of millions of Americans who faced mandate deadlines set to begin next week.
In the latest ruling, a federal judge in Louisiana on Tuesday issued a preliminary injunction halting President Biden’s national vaccine mandate for healthcare workers.
The injunction expanded a separate order issued Monday by a federal judge in Missouri. Monday’s order applied only to 10 states which were part of a lawsuit challenging Biden’s requirement that nearly all full-time employees, part-time employees, volunteers and contractors at a wide range of healthcare facilities receiving Medicaid or Medicaid funding get their first dose of a COVID vaccine by Dec. 6, and be fully vaccinated by Jan. 4, 2022.
Yep! Huge win.https://t.co/XjTvZ1qD7H
— Robert F. Kennedy Jr (@RobertKennedyJr) November 30, 2021
In Tuesday’s ruling, which stemmed from a 14-state lawsuit challenging the mandate for healthcare workers, U.S. District Judge Terry Doughty said the Centers for Medicare & Medicaid Services (CMS) may not enforce its vaccine mandate for healthcare workers until the court can resolve legal challenges.
“There is no question that mandating a vaccine to 10.3 million healthcare workers is something that should be done by Congress, not a government agency,” Doughty wrote in the decision. “It is not clear that even an act of Congress mandating a vaccine would be constitutional.”
Doughty said the mandate would allow the executive branch to usurp the power of the legislative branch to make laws — putting two of the three powers conferred by the U.S. Constitution in the same hands.
“If human nature and history teach anything, it is that civil liberties face grave risks when governments proclaim indefinite states of emergency,” Doughty wrote.
Louisiana Attorney General Jeff Landry said the federal mandate would blow holes in state budgets and exacerbate shortages in healthcare facilities, as the Biden administration tied compliance with the vaccine mandate to federal funding.
A U.S. District Court judge in Montana on Tuesday also enjoined and restrained the U.S. Department of Health and Human Services and CMS, their directors, employees, administrators and secretaries from imposing the mandate on Montana healthcare providers, suppliers, owners and employees.
“In the past weeks, I’ve heard from healthcare workers across our state whose jobs were being threatened if they did not comply with President Biden’s overreaching federal mandate,” Montana Attorney General Austin Knudsen said in a statement. “With the CMS mandate now blocked in Montana until the case is decided, medical facilities have no reason to threaten their employees if they don’t get the vaccine.”
In response to recent legal decisions, CMS said in a statement:
“While we cannot comment on the litigation, CMS has remained committed to protecting the health and safety of beneficiaries and healthcare workers. The vaccine requirement for healthcare workers addresses the risk of unvaccinated healthcare staff to patient safety and provides stability and uniformity across the nation’s health care system.”
The injunction issued on Tuesday is a first step in the lawsuits against the vaccine mandate for healthcare workers. The cases must still be argued before a judge, and lower-court rulings will likely be appealed.
Federal judge blocks vaccine mandate for federal workers in Kentucky, Ohio and Tennessee
Separately, a U.S. district judge in Kentucky on Tuesday issued a preliminary injunction blocking the Biden administration from enforcing a COVID vaccine mandate for federal contractors and subcontractors in three states — the first of at least 13 legal challenges nationwide against the mandate.
The ruling applies in Kentucky, Ohio and Tennessee, which joined in a lawsuit against the Biden administration arguing the mandate for companies that do business with the U.S. government violated the U.S. Constitution, Bloomberg reported.
According to U.S. District Court Judge Gregory Van Tatenhove of the Eastern District of Kentucky, Biden, in all likelihood, can’t use congressionally delegated authority to manage the federal procurement of goods and services to impose vaccines.
Kentucky, Ohio and Tennessee have about $9 billion, $10 billion and $12 billion, respectively, in government contracts. Contractors who refuse to comply risk being blacklisted by the government, Van Tatenhove said, citing Biden’s remarks from Sept. 7: “If you want to work with the federal government, vaccinate your workforce.”
Van Tatenhove said the federal government’s mandate amounts to an overreach of contracts, and the statute could be used to enact virtually any measure at the president’s whim under the guise of economy and efficiency.
“Although Congress used its power to delegate procurement authority to the president to promote economy and efficiency of federal contracting, this power has its limits,” Tatenhove wrote.
The COVID vaccine mandate for federal contractors providing services to the federal government, and the CMS mandate for healthcare workers, are part of a list of actions implemented by the Biden administration to increase vaccination rates.
In a major blow to the Biden administration, the Occupational Safety and Health Administration (OSHA) on Nov. 16 suspended implementation and enforcement of its Emergency Temporary Standard (ETS) on mandatory COVID vaccination and testing in the workplace.
Under the ETS, employers with more than 100 employees were given until Jan. 4 to comply with the mandate. However, a Nov. 12 ruling by the 5th Circuit Court of Appeals barred OSHA from enforcing the ETS “pending adequate judicial review” of a motion for a permanent injunction.
In its Nov. 12 22-page ruling, the court called the Biden administration’s mandate “fatally flawed” and said OSHA should “take no steps to implement or enforce the mandate until further court order.”
The Biden administration has acted quickly to seek reversals of the orders blocking its vaccine rules, CNN reported. The challenges to the OSHA mandate have been consolidated and assigned to the 6th Circuit, which has yet to rule on the Justice Department’s request that it revive the policy.
©December 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
New Variant Hysteria Comes From Same Gates, World Economic Forum Funded Institution That Popularized Lockdowns & Previous Covid Scares
New Variant Hysteria Comes From Same Gates, World Economic Forum Funded Institution That Popularized Lockdowns & Previous Covid Scares
by Children’s Health Defense Europe
December 1, 2021
A Substack article by Jordan Schachtel reveals how the Omicron scare started at Imperial College, London – it will be recalled how it was the alarmist modelling of Imperial College professor Neil Ferguson in March 2020 which precipitated global lockdown. The new scare apparently started with a tweet on 23 November two days before it became main news from post doctoral fellow Tom Peacock.
Imperial College entered into partnership with CEPI to produce a self-amplifying (sa) RNA vaccine against a Covid resembling virus in late 2018. CEPI was founded in Davos by the governments of Norway and India, the Bill & Melinda Gates Foundation, Wellcome, and the World Economic Forum. Prof Ferguson’s Imperial College based Vaccine Impact Modelling Consortium was in turn endowed the Bill and Melinda Gates Foundation and the global vaccine alliance (GAVI) to prospect for vaccine markets.
©December 2021, Children’s Health Defense Europe, A.S.B.L.. This work is reproduced and distributed with the permission of Children’s Health Defense, A.S.B.L.. Want to learn more from Children’s Health Defense Europe? Sign up for free news and updates from Robert F. Kennedy, Jr., Senta Depuydt and the Children’s Health Defense Europe team. Your donation will help to support us in our efforts.
Connect with Children’s Health Defense Europe
cover image credit: badafest / pixabay
The Omicron Deception; How Long Can They String Out the Mutation-Stories?
The Omicron Deception; How Long Can They String Out the Mutation-Stories?
by Jon Rappoport, No More Fake News
December 1, 2021
Nothing mutates faster than a non-virus, except perhaps Tony Fauci’s pronouncements about the “pandemic.”
In early 2020, it all started with a “virus” no one had isolated. Meaning a phantom, a fake, a con, a non-entity. NO VIRUS TO THIS DAY.
Now we’ve had fake variants of the fakes. Delta; Omicron from Africa.
The Stupidity Index—how stupid a person has to be in order to believe the official COVID narrative—is expanding. The more variants, the dumber obedient people have to be, to go along with the show.
At some point, as the number of variants grows, even people who resemble sloths living their lives hanging upside down in trees, will wake up.
“What was that new mutation last week? And this one today? It really comes from Antarctica? And we have to stay indoors for another month? I just want to tailgate and sit in a stadium and scream and drink and watch football…”
Which has already been happening this fall. By the millions, people are pouring into packed venues every weekend to watch pro, college, and high school football. On November 27th, 104,000 sat unmasked, cheek to jowl, in Michigan Stadium as their beloved home team upset Ohio State—and at the end of the game at least 20,000 fans came out on the field to celebrate. The field and the stands formed one vast sea of humanity. Variant? What variant? Delta? Omicron? Are they college fraternities?
Vegas bookies may be getting ready to post an over/under number on the final total of CDC/WHO variants. I say it would be 5.
At 5, people will lose track. They’ll forget the previous variants. They’ll tend to ignore COVID news altogether.
The basic tactic since the beginning has been: invent new fantasies to explain prior fantasies. For example, “Vaccinated people can still catch COVID.” That’s a fantasy because there is no virus. Now comes, “The vaccinated people catching COVID are really being infected by a variant; Delta or Omicron; that’s why the vaccine has become ‘less effective’.”
If you’ve ever forced yourself to sit through one of the hundred or so virus-outbreak movies, you know that at some point the scientific story line loses its impact. You’re thinking, “Let’s get to the car chase and the stuff blowing up and the people shooting each other.”
That’s what the movie is really about.
The COVID hoax is really about lockdowns and destruction of economies and lives and vaccine injury and death and tyrannical takeover of ruined society.
I’ll give you another number. It really does exist. It’s the grand total, worldwide, of people who are either: coming out into the street protesting the COVID restrictions and mandates; or ignoring them altogether and breaking all the rules and going about their lives unvaccinated.
I don’t know what that number is, but when it’s reached, the sociopaths will retreat. The genie will be out of the bottle for good.
Yes, it’s a very big number. But when has freedom not had a price?
Apparently, many people believe the number doesn’t matter, because God is going to intercede and make things right. It’s hard for me to imagine He’ll come through if most people, on their own, are doing NOTHING.
In the Old Testament, He seems to be chronically irked on this very point.
Starting in 1986, it took me two years to uncover the con that was HIV. I thought I had reached the bottom of it, but there were a few miles to go. Later, in the 1990s, I realized the bottom was NOTHING. That’s right. This sometimes is the case in really long cons. You drill all the way down and you find an empty space where you thought something existed.
The bottom of the HIV con—as with SARS-CoV-2—is: the virus doesn’t exist.
In prior articles, I’ve spelled this out in great detail.
It’s stage magic. There is no woman in the box. When the magician saws off her legs, she’s not there. As far as flesh is concerned, he’s sawing through nothing.
The magician is selling the audience’s illusion back to the audience.
As various propagandists have pointed out, the bigger the lie the easier it is to make it stick.
That’s because people are only familiar with small or moderate-sized lies; and because the amount of Structure which would be overturned by the exposure of a huge lie is too threatening.
“You mean the FDA and the CDC and WHO are all going down? Disappearing into dust? But I feel comfortable with them. They’re my friends. I don’t want to see them disappear…”
I do. And tomorrow wouldn’t be too soon.
And if the so-called branch of medical science called virology vanished from the Earth, there would be champagne corks popping in my house.
But for the moment, I’d be satisfied if all vaccine mandates everywhere were wiped off the books—just to give us some breathing room.
That revolution IS within our grasp, if enough of us build toward the critical-mass number I just alluded to above. It would be quite something to see. A fabulous jolt of adrenaline for the human race; for the right reason, for once.
Leave the Omicron and the Delta fantasies for the sloths on the couch. One day, they’ll stir from their trance and stumble along to catch up with us.
For almost two years, I’ve been demonstrating that SARS-CoV-2 doesn’t exist.
Instead, elite planners have been selling A STORY ABOUT A VIRUS.
In covert intelligence operations, this would be called a cover story. It obscures true goals. It justifies ongoing and future crimes that would otherwise be nakedly exposed.
For example, in my 1988 book, AIDS INC., I showed how the cover story about HIV was used in Africa.
For a very long time, the true causes of illness and death in areas of Africa have been: hunger; protein-calorie malnutrition; starvation; contaminated water supplies; poverty; war; farm land stolen from the people; corporate pollution; toxic medicines and vaccines; toxic pesticides; overcrowding in cities; lack of basic sanitation.
Most if not all of these causes could have been eliminated. But local governments did not want healthy people. Sick and dying people were easier to control, and taking away their land was an easier proposition.
Colluding with and paying off local government leaders, transnational corporations and foreign governments set up shop in these African countries and used the healthier people to work on their giant commercial farms and in their factories.
But in 1984, suddenly, there was a new (cover) story broadcast and sold to the world: what was really decimating Africa was HIV. THIS explained all the illness and dying.
The true causes, listed above, were shoved into the background.
Those true crimes were hidden, were permitted to continue unabated.
Not only that, the HIV cover story paved the way for pharmaceutical companies to rack up profits by selling extremely toxic AIDS drugs (e.g., AZT) to Africa.
The HIV test, which turned out false positives like Niagara Falls, made these drugs seem necessary—as fake case numbers soared.
People dying from the toxic medical treatments were, of course, listed as AIDS deaths.
And, as it turned out, HIV had never been isolated. Therefore, there was no proof it existed, no reason to suppose it existed.
Like AIDS, COVID-19 is also an intelligence-agency type covert op.
The short-term goal is wrecking economies. The long-term goal is taking the population into a new world of technocratic control.
Selling this as necessary all comes back to THE VIRUS COVER STORY.
“We’re not forcing technocracy down the throats of the people. Certainly not. We’re simply doing what we must, because of the danger of the virus…because everyone is a virus-spreader…(because too many people want their freedom)…”
Always identify and return to the cover story. Walk around it. Look at it from all sides. Walk into it from one side and exit from the other. Test it. The vital clues are there.
Another classic example: 2009, La Gloria, Mexico. Smithfield Foods, the largest pork producer in the world, operates a giant pig farm. 950,000 pigs.
The poisonous urine and feces from these 950,000 pigs run out into the open air and form what are called lagoons. They’re so large, you can see them from outer space.
Workers spray the toxic lagoons with a toxic foam. It’s routine.
Workers, and people in the surrounding neighborhood, are getting sick and dying. So new contractors are brought in to spray the lagoons with yet another toxic chemical.
Out of nowhere, guess who shows up? The CDC.
Guess what they conclude? It’s not the urine and feces lagoons or the toxic chemicals causing illness and death. No. Of course not.
It’s a new mysterious “virus.” H1N1.
And voila, we have a new cover story and a new epidemic, called Swine Flu.
The cover story serves a number of purposes, as time passes. But the most obvious one is: Smithfield Foods is protected. They get away with murder.
And to cap it all off, four years later, in 2013, Smithfield, still protected, sells itself to a Chinese company, Shuanghui International Holdings, for $4.72 billion.
Here’s what I wrote about Zika (another phantom virus) in 2015:
“Medical CIA” provides the cover story.
In Brazil, the so-called center of the “Zika epidemic,” there are many problems in poverty-stricken areas that involve more than babies being born with small heads and brain impairment.
The grinding poverty itself, of course. Stolen farm land. Widespread corporate use of poisonous pesticides, some of which are banned in 22 other countries. Contaminated water supplies. Lack of basic sanitation. Overcrowding. Prior vaccine campaigns, in which toxic substances were injected directly into the bodies of people whose immune systems were already on the verge of collapsing. Toxic medical drugs.
In 2014, the Tdap vaccine (tetanus, diphtheria, whooping cough) was recommended for pregnant women. Among other toxic substances, this vaccine contains aluminum compounds. Aluminum can cross the blood-brain barrier and cause damage.
Workers are now fumigating areas with toxic sprays to kill mosquitoes. Soldiers are going door to door, handing out more toxic mosquito sprays for indoor use.
Combine all these factors, and you have an ongoing catastrophe.
It makes a great deal of sense to highlight, promote, and blame the “Zika virus” for what is actually going on in Brazil, if you want to distract and divert and obscure.
If you stopped the vaccine campaigns, stopped the spraying, and remedied the conditions I listed above, the health of the population would return and revive, without medical intervention.
Of course, the governments and their allied corporations have no intention of returning stolen land to the people. They have no intention of stopping the use of poisonous pesticides. Medical authorities have no intention of admitting they are concocting a story about a “virus,” Zika, as a cover for their corporate and government allies, and as a pretext to have “a new disease” to treat and work on and solve. They have no intention of stopping toxic vaccine campaigns.
To cap it all off, the conditions the “virus” is supposed to be causing—babies born with small heads and brain damage—can result from ANY injury or insult to a pregnant woman or her infant. No virus required.
But…“Look here, at the virus. Don’t look there.”
Cover story.
cover image composed by truthcomestolight.com
based on creative commons work of OpenClipart, intographics & dianakuehn
After Licensing Board Threatens Disciplinary Action, Maine Physician Asks Board to Define COVID ‘Misinformation’
After Licensing Board Threatens Disciplinary Action, Maine Physician Asks Board to Define COVID ‘Misinformation’
In a letter to the Maine Board of Licensure in Medicine, Dr. Meryl Nass, a practicing physician in Maine and member of Children’s Health Defense scientific advisory board, asked the board to define what it means by “misinformation” and “disinformation,” and to clarify what statutory authority the board has to discipline physicians.
by
The Defender (Children Health Defense) editor’s note: The Maine Board of Licensure in Medicine this month issued a position statement in which it said: “Physicians who generate and spread COVID-19 vaccine misinformation or disinformation are risking disciplinary action by state medical boards, including the suspension or revocation of their medical license.”
In the letter below, Dr. Meryl Nass, a practicing physician in Maine and member of the Children’s Health Defense scientific advisory board, asked the board to define what it means by “misinformation” and “disinformation,” and to clarify what statutory authority the board has to discipline physicians on the basis of undefined transgressions. The letter, which includes the Nov. 16 testimony Nass gave to the New Hampshire state legislature, has been edited slightly for clarity.
November 22, 2021
To the Maine Board of Licensure in Medicine:
I am a physician, licensed in Maine for the past 24 years. I am concerned about the use of the terms “misinformation” and “disinformation” and the new threat to physicians’ licenses issued by the board today for undefined behaviors.
I require clarification regarding the board’s definition of misinformation and disinformation and would like to know what statutory authority the board has to discipline physicians on the basis of undefined transgressions.
Please tell me what law or regulation authorizes such threats for speech outside the clinic.
I thought I would provide the board with some information I provide to the public to see if the board intends to term documented facts as misinformation, intends to censor these facts and whether those who provide these facts to the public will be at risk of disciplinary action.
Here is my invited testimony to the New Hampshire legislature (Education Committee) on Nov. 16, 2021. Am I at risk for telling these truths? Please let me know.
UK Prime Minister Boris Johnson said: “[The vaccine] doesn’t protect you against catching the disease, and it doesn’t protect you from passing it on.”
[Centers for Disease Control and Prevention] Director Dr. Rochelle Walensky said: “The vaccines no longer prevent transmission.”
In a high-quality study of all VA beneficiaries just published in Science, by September, the Johnson & Johnson vaccine was only 13% effective against infection, the Pfizer 43% and the Moderna 58%.
In a new University of California study of more than 500 vaxxed and unvaxxed people who tested positive for COVID, the amounts of virus in saliva were the same. They could transmit the infection to others, equally.
The UK’s top vaccine expert, Sir Andrew Pollard, said in August, regarding COVID vaccines: “Herd immunity is not a possibility. We need to focus on how do we prevent dying or going to hospital.”
Please understand this: Since we cannot achieve herd immunity with our vaccines, the inevitable result is that practically everyone will eventually get the disease.
Vaccines cannot achieve safe schools and workplaces, because the vaccinated can still transmit, even when asymptomatic.
While public health leaders are hoping frequent boosters will kick the can down the road, there is no reason to think boosters will prevent transmission, when the initial series didn’t.
Instead, it is crucial that we immediately focus on preventing severe disease and death — and early treatment can do this. It saves hospitalizations and lives. This is great news.
Why doesn’t everyone know it?
Because, had the benefit of existing drugs been acknowledged, there could have been no Emergency Use Authorizations (EUA) issued for vaccines, remdesivir or monoclonal antibodies — all of which are multibillion-dollar, patented products.
According to the U.S. Food and Drug Administration (FDA), “For FDA to issue an EUA, there must be no adequate, approved and available alternative to the product.”
Hydroxychloroquine and ivermectin were approved, adequate and available — and cheap. Thus they had to be suppressed.
Many drugs and supplements have efficacy against COVID. I created a handout of treatments for you. Please do not allow therapies for COVID to be restricted. Don’t allow doctors and pharmacists to be persecuted for providing these critical medications.
Few people are aware that in a Senate hearing on May 11, Sen. Richard Burr (R-N.C.) asked Dr. Anthony Fauci, Dr. Peter Marks of the FDA and CDC Director Walensky, what percentage of the employees in their agencies were vaccinated.
None provided a number. Fauci and Marks guessed that a bit over half were vaccinated.
What did thousands of scientists in the National Institutes of Health, FDA and CDC know that you didn’t know? This:
-
-
- They knew about sky-high rates of myocarditis in young men, which had been discussed in the Israeli media in April but was not disclosed in the U.S. until June.
- They knew that deaths after vaccination were extremely high — much higher than reported for any other vaccine, ever. The CDC says that VAERS (its Vaccine Adverse Event Reporting System) received more than 9,000 reports of U.S. deaths related to COVID vaccines, but claims they are rare. RARE? Record-setting deaths have also been reported in the UK and Europe after COVID vaccinations.
-
There have been more deaths reported to VAERS for COVID vaccines in 10 months than were reported for every vaccine used in the U.S .over 30 years.
Let me repeat that. If you add together every report of a vaccine-associated death that has ever been reported to VAERS for 30 years, for all vaccines, the total is less than the deaths reported for COVID vaccines.
As of Nov. 19, more than half (56%) of the deaths reported to VAERS after COVID vaccines occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated. And although the CDC has not investigated them all, the agency still claims, ”A review of available clinical information … has not established a causal link to COVID-19 vaccines.”
But CDC officials haven’t linked the deaths to anything else, either.
Let me talk about kids. The CDC estimates that 147 million Americans have already had COVID — and that at least half of our kids are already immune.
Yet the FDA and CDC have not seen fit to allow Americans to use any available test — not PCR, not antibody, not T cell nor any combination of tests to prove immunity — even though the FDA accepts antibody tests as evidence of immunity in COVID vaccine clinical trials.
Why the double standard? It seems the reason to deny natural immunity is to force everyone to be vaccinated, whether they need it or not.
If the vaccines were safe, this policy would be less egregious. But they aren’t safe. The younger you are, the greater is the risk of myocarditis. Reported myocarditis rates in 12- to 17-year-old males after vaccination are 100 times higher than for men over 65.
One study showed that teenage boys are 3 to 6 times as likely to be hospitalized for a post-vaccine case of myocarditis as for a case of COVID.
Myocarditis is a serious side effect, which can cause sudden arrhythmic death. After three months, 25% of kids with myocarditis have still not recovered. No one knows how common this side effect will be in the 5- to 11-year-olds since it was not reported in Pfizer’s trial, which lasted an average of only 17 days after full vaccination for half the child subjects.
Dr. Eric Rubin, the New England Journal editor, said at FDA’s 5- to 11-year-old vaccine advisory meeting: “We’re never going to learn about how safe this vaccine is unless we start giving it.”
FDA Committee has approved the Pfizer vaccine Emergency Use Authorization for kids aged 5-11.
In making this decision, the FDA conceded it does not know the long-term risks to these kids.
🤷♂️ pic.twitter.com/aXFYt44I67
— Techno Fog (@Techno_Fog) October 26, 2021
The FDA knows our children are the guinea pigs, and now you do too.
Did you know that in Philadelphia, Seattle and San Francisco children as young as 12 are being vaccinated without parental consent or notice? JAMA Pediatrics in July published an article calling for states to amend the law to allow children to consent for themselves.
Will New Hampshire support this attack on parental authority?
All pediatric COVID vaccines are used under EUAs. These remove manufacturer liability from the vaccines, unless willful misconduct can be proved.
Under the Public Readiness and Preparedness (PREP) Act, a finding of willful misconduct requires the manufacturer knew there was a problem with their vaccines, but sold them anyway.
The unforeseen consequence of the PREP Act is that it gives manufacturers a huge incentive to perform the most minimal testing of their products — because if they did not know there was a problem, they cannot be sued for misconduct.
Why are we allowing experimental products that have been inadequately tested, are dangerous in older children and were produced by a manufacturer who can’t be sued to be injected into our children?
But these facts have been obscured by a smokescreen of fatuous “safe and effective” claims made by financially conflicted organizations.
Did they tell you that if your child is injured, you are unlikely to collect a penny? Did they tell you that the compensation program for EUA injuries has not compensated a single COVID drug or vaccine injury — despite a one-year statute of limitations?
Under U.S. law, you have the right to refuse EUAs. And you must be informed of all that is known and unknown about risks and benefits.
But neither of these two requirements are being followed.
Since the pandemic, the rule of law has been tossed aside. I urge you to learn about the law governing the use of EUA products, so I have provided you the relevant section of U.S. Code.
Let me conclude by saying that given the loose regulatory milieu we are in, COVID vaccines will probably be licensed for everyone soon. That imprimatur will not brush away their serious problems.
Please prevent mandates of these extremely questionable products.
Sincerely yours,
Meryl Nass, MD
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
©November 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Connect with Children’s Health Defense
cover image credit: / pixabay
Evidence That They KNEW the Covid Jab Would Kill Thousands
Evidence That They KNEW the Covid Jab Would Kill Thousands
by Dr. Vernon Coleman
November 29, 2021
It’s the 29th November 2021 and the extent of the conspiracy to suppress the truth and to promote a deadly covid jab is becoming clearer by the day. In February 2021, Pfizer and the FDA knew the covid-19 jab was going to kill or main thousands of healthy people.
They have the gall to call us conspiracy theorists but what we’ve talked about is no theory. Everything the truth-tellers and the Resistance Movement have said has been accurate.
The governments, the advisors, the drug companies and the medical establishment are not conspiracy theorists of course – they are conspiracy practitioners, and their evil plot to kill people, to promote their great reset and to introduce the new normal is now so blatant that it is difficult to believe that the majority still believe the lies they are being told.
This morning, Darren Smith, editor of the magnificent The Light Paper – the only honest newspaper in the UK – sent me what looks to me to be yet more serious evidence that both Pfizer and the FDA knew how many thousands were going to be killed by their vaccine.
According to what I’ve seen, Pfizer prepared a report for the FDA dealing with the worldwide safety of their ‘vaccine’ until 28th February 2021. If you want to read the report for yourself I’ll put the details and this transcript on my website within 24 hours. This information was kept secret and only released after a group of professionals in the USA used the FOIA to obtain the information from the FDA. So far just 91 pages have been released. There are around another 300,000 pages to be released, I’m told.
In February 2021, Pfizer reported that, after just weeks of jabbing, there were already 42,086 adverse reaction case reports of which 25,379 had been medically confirmed. Most of these came from the US and the UK but there were also reports from 61 other countries. Remember, it is believed that only 1% of adverse reactions are officially recorded.
Of these patients, 1,223 had a fatal outcome. Which, for those journalists and fact checkers who like to hide from the truth, means death.
And 11,361 people had not recovered from the adverse events they had suffered. There were 9,400 individuals for whom the outcome was not known.
What were the adverse events?
Well, you might as well just look up the index in a medical dictionary. There were respiratory problems, nervous system problems, eye problems, immune system problems, cardiac problems and vascular problems. There were 1,403 cardiovascular problems, 932 haematological problems, 70 liver related problems, 449 cases of facial paralysis, 1,050 immune system problems and 275 stroke problems. At the bottom of the report there is an appendix – a list of adverse events of special interest. Just about every disease you can think of, with the possible omission of flat feet, is listed there. Pages and pages of it. There were spontaneous abortions, heart attacks, myocarditis, brain haemorrhage – they knew all this was happening. Every Health Minister and medical advisor in the world should have known of this.
Oh, and there were 1,833 cases of anaphylactic reaction.
There were 270 pregnant women reported and of these 23 had spontaneous abortions. There is a list of adverse events occurring among women who were breast feeding their babies.
Among those under 12 who had already been jabbed there were 24 serious problems recorded.
None of this is a complete surprise, of course.
In December 2020, I made a video listing the adverse events known to be associated with Pfizer’s covid-19 jab. The list included myocarditis, heart attacks, strokes and blood clots. None of these problems was a surprise. And what we have now is evidence.
It now seems clear that Pfizer and the FDA in America were well aware that the jab they were promoting could eventually result in vast numbers of deaths and serious injuries. I cannot begin to estimate the size of the future problems among the jabbed.
We should not be surprised by any of this.
We are dealing with bad, bad people.
This is an experiment and way back – 10 months ago – I made a video headlined ‘Doctors and nurses giving the covid-19 vaccine will be tried as war criminals’.
I pointed out that doctors or nurses who did not tell their patients all the potential problems would be guilty of a crime. Patients are entitled to know the risks of a medication – it’s called informed consent. And this is especially true when they are taking part in an experiment – which the covid jabs are. Doctors are ignoring the age old principle of ensuring the benefit exceeds the risk.
The information so far revealed is just a tiny part of the information still kept secret. It’s estimated that all the documents the FDA used to approve the Pfizer jab won’t be made public before 2076 – over half a century away.
All this information should be released and published immediately. Why should anyone be expected to trust Pfizer or the people pushing these jabs?
The British Medical Journal has reported that a Pfizer subcontractor, used when their jab was being tested, is accused of falsifying data, hiring inadequately trained jabbers, un-blinding patients and failing to follow up on reported adverse reactions. The title of that paper is ‘Covid-19: researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial.’
Meanwhile, the drug companies are making a fortune.
Pfizer, one of the world’s most fined companies in history, expects its 2021 covid jab sales to reach $36 billion and in 2022 they’re expecting $29 billion, though they admit they are hoping for much better than that. And they also expect the ‘market for covid-19 vaccines to be durable and to continue generating sales for years to come’.
Pfizer, like other big drug companies has a bad record for honesty.
In the UK, Pfizer was fined £84.2 million for overcharging the NHS by 2,600% and in the US Pfizer was hit with a $2.3 billion fine for mis-promoting medicines, making false claims and paying kickbacks to doctors to prescribe their drugs. At the time that was the largest health care fraud settlement in American history.
The CEO of Pfizer is quoted as saying that people who spread misinformation about vaccines are criminals.
For once I agree with a drug company employee. He’s right. The police should arrest all politicians, all medical advisors, thousands of doctors and journalists, the staff of Facebook, Twitter, YouTube and the entire staff of the BBC and the so-called fact checkers.
Governments have deliberately and systematically created fear to terrify and manipulate and virtually force people to accept a jab that doesn’t do what most people think it does – it doesn’t stop people catching or spreading covid-19.
And now governments and advisors and journalists are demanding that the jabs be mandatory.
When will people realize what is happening to them? I’ve been making videos about this assault, this coup, since March 2020, nearly 300 of them, and find it difficult to understand how people still can’t understand what is happening to them.
The word ‘genocide’ can no longer be considered hyperbole. Medical advisors everywhere must now comment on these Pfizer figures.
Connect with Dr. Vernon Coleman
cover image credit: darksouls1 / pixabay
Virus Mutation in Jewish Deli Infecting All of Africa Came From Beverly Hills
Virus Mutation in Jewish Deli Infecting All of Africa Came From Beverly Hills
by Jon Rappoport, No More Fake News
November 30, 2021
Tony Fauci, the Great White Father, is flying to Africa, to save the continent from the latest virus-mutation, which originated in a deli in Beverly Hills.
Fauci gave a statement to reporters at LAX before departing: “We now know that what we’re calling SARS-CoV-6 crossed species from a pastrami sandwich at Fineberg’s Deli on Rodeo Drive, to Fred Reilly, a customer, in late October. Reilly flew to Botswana, where he infected three soccer players who were moonlighting as security guards at a UN cocktail party.”
Fauci will explain to Africa that a new IG Farben drug, RP-1984, which has been stockpiled for 20 years, since it failed to slow the progression of leukemia in rats, will be dropped from planes over the continent.
The drug attacks all cells of the body, preventing them from replicating. The hope is it will also prevent the deli variant from replicating before it kills the host (human beings).
“Preliminary data looks promising,” Fauci stated. “Of course, lockdowns for at least a year, vaccination, mask wearing, and distancing will have to be practiced religiously,” he added.
“Owing to business closures, most African countries will sink into irreversible and desperate debt. The International Monetary Fund, as usual, will tide these countries over with loans. However, this time, the United Nations will usher in a new digital currency for Africa.”
The currency, Fauci asserted, will include Universal Guaranteed Income for every person in Africa—as long as they obey all government dictates without question or protest.
At the White House, Joe Biden said, “I don’t eat pastrami. Nurse Jill won’t let me.”
Deli owner Hank Fineberg told the LA Times, “We didn’t start this. We buy our pastrami from Gornish Garnish, a wholesaler in Brooklyn. Why isn’t the CDC investigating them? Besides, none of our customers have actually gotten sick. So what’s the problem?”
The Times attributes the plunge of the stock market to the deli variant. It also questions California Governor Gavin Newsom’s decision to “leave Rodeo Drive open to shoppers.”
Bill Gates is urging people to eat a pastrami substitute made from dried maple leaves, a pine tar derivative, and salted mica.
A new study published in the New England Journal of Medicine concludes that “the deli variant causes the body to produce 12 different sets of antibodies, some of which resemble the original SARS-CoV-2. The body then faces the prospect of antibodies attacking antibodies, resulting in a downward vortex resembling a black hole in space…”
NBC states, “Black Lives Matter leaders are huddling with officials at the Ford Foundation, shaping a response to news that the deli variant is sweeping through Africa.”
CBS: “In Africa, the major symptoms associated with the deli variant are weight loss, dehydration, and diarrhea. These symptoms traditionally stem from malnutrition and starvation, but researchers say the variant is now the principal culprit…”
At the White House yesterday, the President’s Press Secretary, Jen Psaki, told reporters, “The dark winter has arrived early. It’s here. The deli variant will necessitate new lockdowns and business closures. President Biden will be issuing a new wide-ranging vaccine mandate in the next few days. At the moment, he is meeting with NIH researchers and poring over the latest data on infection rates. His background in statistical analysis will serve him well in this effort…”
A FOX News reporter asked, “Will Christmas be canceled?”
Psaki replied, “Shopping will proceed. But Jesus was born only once. Is it necessary to keep celebrating the event? The Secretary of State is meeting with Pope Francis to discuss the question.”
The FOX reporter followed up with another query: “What about all the migrants coming across the Southern border? How many are carrying the deli variant?”
Psaki: “We have a new mass testing program called The Wand. It can survey thousands of people at once and detect the presence of viruses. So far, we’ve found only one person at the border who is infected with the deli variant—a former Montana resident. He has been the subject of an FBI manhunt, owing to the fact that he was present at the January 6th Capitol breach. He is now in custody at Walter Reed Hospital. He has no symptoms, which is a bit of a mystery.”
Retiring NIH Director Francis Collins clarified several deli variant issues this morning, on a conference call with reporters: “The new variant is producing different effects in different populations. In Africa, we’re seeing weight loss, dehydration, and diarrhea. In South America, the primary symptom is a dry cough. In Australia, it’s transient leg pain and anger. In Europe, numbness of the extremities and increasing poverty. In the US, waning immunity conferred by the vaccine, hypnotic passivity, and paradoxically, attendance at football games…”
Senator Chuck Schumer has introduced a bill that will compensate victims of the deli variant, in the form of a federal card that can be used to purchase $900 in goods and services. The diagnosing doctor will also receive a card, worth $3900 for each variant case identified.
Don’t leave home without it. Actually, don’t leave home. Lock down.
cover image based on creative commons work of iXimus & karogers / pixabay
‘This Pivotal Moment’ Video: “The Vaccine Passport Is the Final Missing Piece in an Automated Architecture of Total Surveillance and Social Control.”
‘This Pivotal Moment’ Video: “The Vaccine Passport Is the Final Missing Piece in an Automated Architecture of Total Surveillance and Social Control.”
by This Pivotal Moment
November 24, 2021
This Pivotal Moment – Episode 1
Video available at YouTube or Odysee.
The proposed global rollout of Vaccine Passports has nothing to do with your health.
Vaccine Passports are a Trojan horse being used to create a completely new type of controlled and surveilled society in which the freedom we enjoy today will be a distant memory.
It’s time to stop this plan in its tracks.
Subtitles are now available in Brazilian Portuguese, Dutch, Finnish, German, Greek, Hebrew, Hungarian, Italian, Portuguese and Spanish. Thank you to all those who have independently decided to translate the text of this video so that it can reach a wider audience.
If you’d like to translate it into your own native tongue, please join the Telegram channel @ThisPivotalMoment where you’ll find the necessary resources.
Connect with This Pivotal Moment
cover image credit: CDD20 / pixabay
The New African Virus Mutation: Right on Time; a Kindergarten Covert Op for the Ignorant
The New African Virus Mutation: Right on Time; a Kindergarten Covert Op for the Ignorant
by Jon Rappoport, No More Fake News
November 29, 2021
There are no variants.
Because there is no virus. SARS-CoV-2 doesn’t exist. I’ve spent the past year and a half proving that. [0]
But fantasies do exist. So do covert ops with intentions to deceive.
Thus, the “scientific world” is agog over the new South African variant, named B11529 (aka Omicron, Botswana). Woo. The ghost is coming out of the closet. Beware. COVID cases are rising…
“We don’t know whether the vaccine will be effective in the face of the new variant. New lockdowns may be necessary. Travel restrictions are coming. Batten down the hatches.”
I mean, really.
As you know, for the past few months stories in the press have been claiming the vaccine-conferred immunity is sinking like a stone. This story is absurd because, again, there is no virus. So there was no conferred immunity to begin with. But anyway, that’s the story that’s been circulating. So NOW…
“It turns out one major reason for the diminished effectiveness of the vaccine is…
“The NEW VARIANT. The South African B11529.”
Uh-huh. “The vaccine is having a tough time preventing infection caused by the new variant. We may need to enforce boosters every three months…”
Keep the fear going. Push harder for the vaccine. Explain away its failures. Fabricate rising case numbers, blaming them on the new variant. Institute heavy new lockdowns.
“The South African variant is deadlier than the Delta, which is deadlier than the original.”
And none of the three exists.
What does exist is fantasy, piled higher and deeper and thicker.
The variant is Fauci. The variant is Bill Gates. The variant is CDC/WHO. The variant is the World Economic Forum. And the Chinese regime. And presidents and governors. And the mainstream press.
And don’t forget this. Vaccine injuries and deaths have been escalating all over the world. In the US alone, reported injuries have broken above 600,000 [1]. As I’ve mentioned, the well-known Harvard Pilgrim Healthcare study [2] concluded that, to obtain a true number of injuries, multiply the reported figure by 100.
Something is needed to explain all these injuries and deaths. That is, to lie about them.
And right on time, here comes the new variant.
“These people who seem to be injured by the vaccine are really keeling over from the original virus, the Delta, and woo, the South African B11529.”
Also: Recently, we’ve seen a spate of press stories with the theme—“scientists are mystified by the low COVID case numbers in Africa, where the vaccination rates are very low.” [3] Boom. That story is now gone. Wiped out. Now it’s THE WORLD IS BEING ATTACKED BY THE SOUTH AFRICAN B111529 VARIANT.
Here is one of my articles covering the non-existence of SARS-CoV-2:
—Dr. Andrew Kaufman refutes “isolation” of SARS-Cov-2; he does step-by-step analysis of a typical claim of isolation; there is no proof that the virus exists—
The global medical community has been asserting that “a pandemic is being caused by a virus, SARS-Cov-2.”
But what if the virus doesn’t exist?
People have been asking me for a step-by-step analysis of a mainstream claim of virus-isolation. Well, here it is.
“Isolation” should mean the virus has been separated out from all surrounding material, so researchers can say, “Look, we have it. It exists.”
I took a typical passage from a published study, a “methods” section, in which researchers describe how they “isolated the virus.” I sent it to Dr. Andrew Kaufman [4], and he provided his analysis in detail.
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)” [5].
First, I want to provide a bit of background that will help the reader understand what is going on in the study.
The researchers are creating a soup in the lab. This soup contains a number of compounds. The researchers assume, without evidence, that “the virus” is in this soup. At no time do they separate the purported virus from the surrounding material in the soup. Isolation of the virus is not occurring.
They set about showing that the monkey (and/or human cells) they put in the soup are dying. This cell-death, they claim, is being caused by “the virus.” However, as you’ll see, Dr. Kaufman dismantles this claim.
There is no reason to infer that SARS-CoV-2 is in the soup at all, or that it is killing cells.
Finally, the researchers assert, with no proof or rational explanation, that they were able to discover the genetic sequence of “the virus.”
Here are the study’s statements claiming isolation, alternated with Dr. Kaufman’s analysis:
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO) [6]. Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
My comments: Dr. Kaufman does several things here. He shows that isolation, in any meaningful sense of the word “isolation,” is not occurring.
Dr. Kaufman also shows that the researchers want to use damage to the cells and cell-death as proof that “the virus” is in the soup they are creating. In other words, the researchers are assuming that if the cells are dying, it must be the virus that is doing the killing. But Dr. Kaufman shows there are obvious other reasons for cell damage and death that have nothing to do with a virus. Therefore, no proof exists that “the virus” is in the soup or exists at all.
And finally, Dr. Kaufman explains that the claim of genetic sequencing of “the virus” is absurd, because there is no proof that the virus is present. How do you sequence something when you haven’t shown it exists?
Readers who are unfamiliar with my work (over 300 articles on the subject of the “pandemic” during the past year [7]) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
The answer is no.
—end of Kaufman article—
And while I’m at it, here is another piece I wrote last year about how virus-propaganda (fairy tales) must be managed, in order to make the masses stand up and salute:
—The “hot zone” theory of new frightening diseases—
Remember? There was a 1994 book by that name— and then “experts” began piling on—it went something like this:
“Out of the deep dark rainforests of Earth (cue sounds of native drumming), as a result of modern plane travel, viruses we’ve never encountered before will spread epidemics across the globe. Our immune systems, ill-equipped to recognize or deal with these strange killer germs, will fold up under the pressure, and all of civilization will be threatened with extinction.”
Let’s see. Since planes fly back and forth, and since all sorts of Westerners travel TO the rainforests, why haven’t we seen whole native tribes wiped out by viruses from the deep dark streets of Brooklyn?
It would even seem that viruses, common in, say, Norway, would cause trouble in Oregon.
Why does it have to be “viruses from jungles?” Or other faraway places like China? Why can’t we have the Second City Virus, emanating from a slaughterhouse in Chicago and infecting people in Nigeria? Why can’t we have a Big Easy virus from New Orleans traveling to Beijing?
Is it possible that jungles and Africa and China and Mexico are typically chosen for virus fairy tales because, in the minds of many Westerners, they satisfy a requirement of “strange,” “different,” “primitive,” and so on? We’re talking theater here—and when you stage a propaganda play (fiction), you want to tap into the reflex instincts of the audience. The Hartford Virus, the Des Moines Virus, the Vancouver Virus just don’t fit the bill.
Because they can’t drive up the fear that jungles or Africa or China can.
Unless you’ve been living in an ice cave in the Arctic, you know selling fear of THE VIRUS is big business. To do that, you have to strike the right notes.
I personally would be interested in a Beverly Hills or a Scarsdale or a Park Avenue epidemic virus story. I’d like to see the media try to sell that one.
What about a Bill Gates Seattle virus that some Patient Zero unknowingly carries on a plane flight to Mexico City?
Think it through. We NEVER hear killer virus stories about germs traveling from Europe and America to Asia and Africa. Why not? Because such a story won’t sell. It won’t bite.
This is called a clue.
It tells you that virus-stories are shaped and managed and written and managed and broadcast according to a plan that has nothing to do with actual disease.
If a monkey in Africa can bite a man and thus transmit a virus to the West, then a salesman in Duluth can sneeze on a man at a local airport and thus send a virus to Ethiopia.
But amazingly, through secret communication among viruses, it never happens that way. The germs have decided what the traffic pattern is, and the CDC and the World Health Organization are just discovering What Is.
Sure they are. And if you buy that, I have condos for sale on the far side of the moon.
SOURCES:
[0] https://blog.nomorefakenews.com/tag/virus/
[2] https://openvaers.com/covid-data
[4] https://andrewkaufmanmd.com/
[5] https://wwwnc.cdc.gov/eid/article/26/6/20-0516_article
[6] https://www.thermofisher.com/us/en/home.html
[7] https://blog.nomorefakenews.com/category/covid/
cover image based on African mask by Viscious-Speed
Solving the Riddle of Byram Bridle
Solving the Riddle of Byram Bridle
by Rosemary Frei, MSc
November 27, 2021
On Nov. 4 I posted an article with some questions about Byram Bridle.
After speaking to Bridle I took it down.
The vaccine developer and viral-immunology associate professor based at the University of Guelph is very popular in the Covid-questioning community.
He is a high-profile member of the Canadian Covid Care Alliance and gives many interviews. In addition, he was an expert witness in the mid-2021 Adamson Barbecue case and in the mid-November 2021 legal pursuit of an interim injunction against mandatory vaxxing of some Toronto workers.
He’s been banned from the U of Guelph campus because he’s not vaxxed. And he’s harassed by some of his colleagues and others — including people who created both an anonymously written website byrambridle.com critiquing Bridle’s claims and an accompanying Twitter account. (They’ve also linked from the website to a GitLab section on him.)
Bridle overall is a big promoter of vaxxes. He’s developing several new ones, including working on new Covid vaxxes since at least since the spring of 2020.
And he readily uses the term “anti-vaxxer” to discredit people who have very sceptical or negative views about most vaccines.
I am among the many millions of people who hold such negative views about vaxxes. That’s because there is a great deal of solid evidence showing that many vaxxes are not safe. (More about this in the ‘Continued Push’ section below.)
The only vaccines Bridle critiques are the current crop of Covid mRNA shots. He has posted several documents — such as his Nov. 12, 2021, expert report for the interim-injunction case in Toronto – and given many interviews about this.
In my Nov. 4 article I said I believed he has a conflict of interest that he doesn’t disclose to the general public with respect to his critique of the Covid mRNA jabs. I posited that Bridle is poised to potentially make a lot of profit from six of the eight US patents (and a Canadian patent that’s identical to one of those six) that I discovered he is a co-inventor of. They’re all cancer-related. [Sentence added Dec. 1 when I re-re-read the article and realized I’d omitted this.]
I hypothesized that Bridle and his colleagues could develop, based on some of their existing patents, alternative vaxxes against Covid.
I deduced the profit motive from the fact that some of Bridle’s co-inventors on the US patents are principals in a company called Turnstone Biologics (which is a sister company to the firm listed as the patents’ owners, Turnstone Limited Partnership) — and that Turnstone Biologics is working together with international giants like Takeda to commercialize their vaxx platforms via at least one huge business deal.
I also wrote that some of Bridle’s main assertions are on very weak ground. That includes his claim that the spike protein produced by the injection of the mRNA Covid shots spreads throughout the body where it becomes a “dangerous toxin” and therefore is responsible for most of the serious injuries and deaths associated with the mRNA jabs.
I emailed the article to Bridle after I posted it. (That was a mistake – I’ve now truly learned my lesson to never again omit the step of at least attempting to talk to or email people before posting an article about them.)
In his email response he accused me of making “egregious errors” – including “mixing up my cancer research-related patents with my COVID-19-focused research; they are entirely separate.” He wrote that his patent relating to the avian reovirus is an example of my very serious error of asserting that his cancer patents are connected to his Covid-vaxx work.
He also said my article was a “one-sided piece of libel [that] represents nothing short of harassment,” and that I was conducting a “witch hunt.” He threatened legal action.
I’ve never received an email like that before. It intimidated me and shook my confidence.
In his email Bridle also asked me to call him on his cell, and provided that number. So I dialed it right away.
During our ensuing hour-long conversation I was persuaded further that I’d made huge errors by his fast-paced and confidently-delivered words – which started with his saying, “I have to say you screwed up big-time on this article. You’ve got a lot of stuff – like it [the article]’s completely wrong; you’ve completely misinterpreted everything.”
I then emailed everyone I’d sent the article to, saying I’d screwed up majorly and would write a follow-up article to set the record straight. I also took the article off my website.
I did make some errors in that Nov. 4 article.
For example, Bridle told me in his Nov. 4 email and our phone call that he has a very strained relationship with the principals of Turnstone — rather than being closely involved with them with respect to patents and potential profits from them as I’d suggested in my article — because they’ve mistreated him. I believe him. (Although he also said in that same phone call that he still holds at least one patent in conjunction with Turnstone.) I reached out to Turnstone later that day for a comment but they have not yet responded. I also seem to have made the wrong deductions about the specifics of the relationship between his cancer-vaxx patents and his Covid-vaxx work.
I apologize again for my errors.
But I did not get everything wrong, by any means.
And I still have many questions about Bridle
They include:
- Why do a very large number of vaccine sceptics embrace Bridle – who is very strongly pro-vaccine, readily uses the term ‘anti-vaxxer’ to disparage people who are sceptical about the safety and efficacy of many vaccines, and is developing new Covid vaxxes even though there’s been an extremely low death rate from Covid?
- Why is Bridle not disclosing in his interviews and articles/documents for the general public that he’s working toward an intranasal vaxx for Covid (which carries the genetic code for the novel coronavirus’s spike protein) – and for which he has a provisional patent application dated June 3, 2021, that very likely is a spin-off of his cancer-vaxx research, and that could ostensibly solve some of the main problems associated with Covid mRNA shots? Shouldn’t he be highlighting that when he critiques the mRNA jabs?
- Why does he use tenuous evidence to support his assertion that when the spike protein spreads throughout the body it becomes a “dangerous toxin” and therefore is responsible for most of the serious injuries and deaths caused by the mRNA vaxxes (yet when questioned about this assertion admits it is only theoretical)?
And as it happens, intranasal vaxxes are gaining traction rapidly. That’s in part because they’re a spray and don’t involve use of a syringe to deliver a shot/jab the arm.
Russian President Vladimir Putin took an experimental intranasal vaxx against Covid on Nov. 23, 2021, according to news reports. (I asked a Russian friend to read the Russian TASS article about this; she said the English translations are accurate.) It was an intranasal version of the Sputnik V shot. And it was given to Putin ‘off-label’ – that is, in the absence of formal approval of the vaxx. Human trials of it are just starting.
There are also many claims, such as in a Nov. 19, 2021, scientific paper Bridle co-authored, that intranasal shots can produce ‘sterilizing immunity’ and therefore curtail the problem of potential ‘vaccine escape variants.’
So I won’t be very surprised if developers and marketers of these new vaxxes soon also claim they could help curb the Nu/Omnicron variant (B.1.1.529) that’s received a great deal of attention in the last few days. B.1.1.529 already has been declared of “huge international concern” because it ostensibly has a “horrific spike[-protein-gene-mutation] profile,” spreads very fast and has the potential to evade the currently used vaxxes. Predictably there’s been panic such as long lines at airports in the very rapidly growing list of African countries subject to travel bans by other governments — along with a renewed push for more people to get vaxxed. [And just as I was ready to post this article I found out that B.1.1.529 may in fact first have surfaced in July. I may write about this in a future article.]
Yet there hasn’t been a single published scientific report, as far as I know, which would allow objective/outside verification of whether there is any real evidence to support these drastic claims and actions. And I remain very sceptical about the hype regarding all variants and the methods used to detect them, including the false narrative about ‘immune escape’; see my Feb. 3, 2021, Feb. 11, March 16, May 24 and Oct. 24 pieces.
And as I wrote in that March 16 article (about Geert Vanden Bossche): “We … need to stop production and use of antivirals and antibodies and all other parts of the Covid-industrial complex. Covid has an extremely high survival rate. So why develop yet another expensive, invasive and experimental solution to a problem that barely exists, if it does at all?”
Let’s dive into trying to answer those questions, and in the process solve the riddle of Byram Bridle.
Bridle Is Creating Fast-track Covid Vaxxes Based on His Team’s Cancer-Vaxx Tech
He doesn’t hide this. And his statements in news reports about this clearly show Bridle believes he and his collaborators can use the methodology they’d already developed for making cancer vaxxes to very quickly create vaxxes for the novel coronavirus (and for an array of iterations of it and of other viruses).
In my Nov. 4 article I cited two May 21, 2020, news pieces about Bridle and several of his collaborators receiving a one-year, $230,000 grant from the Ontario government. He was given the grant together with Leonardo Susta and Sarah Wooton — both also at the University of Guelph — and Darwyn Kobasa from the Winnipeg National Microbiology Lab (NML). (The May 21, 2020, Ontario-government news release about this also announced Covid-related grants to other researchers across the province.)
The section of the news release about the U of Guelph/NML project said they were given the money to test vaxxes containing a virus (avian avulavirus or the adenovirus) into which they spliced the genetic code for the novel coronavirus’s spike protein. First they’d do preliminary mouse testing of the shots at the University of Guelph. Then “after optimization, these vaccines will be evaluated [for efficacy] in a hamster challenge model at the” NML.
CBC reporter Kate Bueckert in her May 21, 2020, report quoted Bridle as saying, “We’ve had to, over the years, develop all kinds of ideas and methods to optimize cancer vaccines. Because we have these technological platforms, we realized we could quickly, through the virology expertise, switch our cancer vaccines over to vaccines against infectious diseases.” (Bolding added by me.)
Bridle also said, “‘Our plan is, by the end of the year [of funding], so this would be in 2021, to have completely vetted the science and identified an optimal vaccine strategy to protect against infection with the virus that causes Covid-19 and at that point … our goal would be to start talking to Health Canada.’” (Bolding added by me.)
A Guelph Today piece about this said Bridle believes “that unlike other ‘one-off’ approaches to developing a Covid-19 vaccine, the team’s platforms can be adapted to develop vaccines for future versions of a coronavirus. That means future vaccines might be made more quickly and cheaply, giving Canada a foundation for subsequent vaccine development. ‘With these vaccine vectors, we designed them to be “plug and play.” You can put any gene into the vectors within two weeks. It could be a target protein in a cancer cell, but it could just as easily be a protein on a virus,’” Bridle said. (Bolding added by me.)
The piece also said he “hopes to see a viable [Covid] vaccine based on the technology ready for Health Canada approval in 2021…. The team will work with Health Canada to ensure ‘fast tracking‘ for any potential vaccine to be released to the public.” (Bolding added by me.)
Hamsters Setting the Pace in the Covid-vaxx-development Race
The timeline given by Bridle in those May 2020 media pieces may be somewhat optimistic (and indeed in this June 21, 2020, Global TV interview, he said that vaxxes would take more than a year to be ready for widespread use).
However, there are the strong indications that he and his colleagues are moving quickly.
Hamsters play a key role in this. (Not because they move fast in their cages; rather, they – specifically, Syrian hamsters – have immune systems that are said to respond to infectious agents in very similar ways to humans’ immune systems.)
In my Nov. 4 article I said I’d found a scientific paper co-authored by, among others, Bridle, Wooton and Susta. It’s dated Nov. 19, 2021 (with an e-publishing date of Oct. 6, 2021) and is titled, ‘Intranasal vaccination with a Newcastle disease virus-vectored vaccine protects hamsters from SARS-CoV-2 infection and disease.’
In that paper, the Newcastle-disease virus/spike-protein Covid intranasal vaxx that Bridle, Wooton, Susta and their colleagues tested in Syrian hamsters came out looking rosy. For example, they concluded that spraying two doses of the vaxx (containing the full length of the spike-protein gene spliced into a Newcastle-disease virus) into the noses of a total of 10 hamsters resulted in a “clear increase of S[spike-protein]-specific antibodies after the second dose.” They also wrote that the vaxx was safe and, in addition, stopped the virus from multiplying to high levels in the hamsters.
This must be one of the results of the developing and testing of experimental Covid vaxxes by Bridle and his colleagues that started by or before the spring of 2020. In other words, at some point they must have included in their testing this experimental Newcastle-disease-virus/novel coronavirus spike-protein vaxx, either in parallel with, or as part of, the work they did using the Ontario-government grant.
In our Nov. 4 phone call Bridle dismissed this study as being at only a very early stage of development. He said, “clearly you don’t have an understanding of what it takes to get a vaccine from the pre-clinical stage to the place where it can go into a rollout into the public.”
Yet that ignores his quotes in the May 2020 articles about seeking to have their experimental vaxxes fast-tracked in 2021.
It also doesn’t seem to take into account other things such as the fact that the Canadian and other governments put into warp speed the testing and approving Covid vaxxes and are continuing to do so.
Follow the Patent Trail
Then a couple of days later, while reviewing all the material I’d gathered for the Nov. 4 article, I discovered at bottom of that Nov. 19 paper by Bridle and collaborators the following ‘Conflict of interest statement’: “L.A.S., Y.P., B.W.B. [Byram Bridle], P.P.M., L.S. [Leonardo Susta], and S.K.W. [Sarah Wooton] are co-inventors on a United States Provisional [Patent] Application No. 63/196,489 entitled ‘ENGINEERED NEWCASTLE DISEASE VIRUS VECTOR AND USES THEREOF,’ which was filed June 3, 2021.” (Bolding added by me.)
So they are moving apace on the pathway to patent their approach.
As I noted above, Bridle had commented in our Nov. 4 phone call on that Nov. 19 paper — but only to say it’s very early-stage (i.e., pre-clinical) research. He didn’t mention any provisional patent applications.
I tried to find the June 3 provisional patent application online but didn’t succeed. There doesn’t seem to be a publicly accessible database of provisional patent applications.
But I did find this website that gives information on provisional patent applications. It describes how to get one. It also lists the benefits of a provisional patent application. These include that it allows “the term ‘Patent Pending’ to be applied for 12 months in connection with the description of the invention,” and “enables immediate commercial promotion of [the] invention with greater security against having the invention stolen.“) (Bolding added by me.)
I emailed Bridle on the evening of Nov. 23. I asked him to send me the June 3 provisional patent application, along with any other provisional patent applications he has. And I emailed him again a few minutes later saying, “Further to the email I sent you a few minutes ago, if the information in the provisional patent application isn’t public then of course I’m not asking you to send it to me. Only what you’re able to – ie what’s available to the public. And if you have other provisional patent applications I’m only looking for their titles, assuming the titles are publicly available (and nothing else is).”
He replied the next morning:
“I’m not sure what the status of this provisional patent application is; two of my colleagues (equal inventors) took the lead on this. Anything that is publicly available would be searchable in the US patent database. If it isn’t there, then it isn’t publicly available yet.”
So he’s not disclosing anything about this provisional patent application, nor saying whether he has more of them.
He’s not obliged to, of course. But why he wouldn’t at least answer my question about whether he has any other provisional patent applications?
And by the way, I believe his and his colleagues’ June 3, 2021, provisional patent application is to some extent related to two US patents — 10829786 and 20200190538 — that are among the eight US patents that have Bridle’s name on them that I mentioned in my Nov. 4 article. Those two US patents are both titled, ‘Avian oncolytic virus having modified sequences and uses thereof.’ (The word oncolytic means tumour-infecting and -killing.) The patents’ description highlights the avian reovirus and the Newcastle-disease virus vector as the central part of this vaxx-tech platform.
(Bridle told me in his Nov. 4 email and our Nov. 4 phone call that he holds a patent related to the avian reovirus. One [or both] of 10829786 and 20200190538 is [are] very likely the one[s] he was referring to, because none of the other six US patents that I’ve found with his name on them mention the avian reovirus.)
They’re actually the two that in my Nov. 4 article I said I believed were not related to his Covid-vaxx work. And Bridle told me in his Nov. 4 email that his avian-reovirus patent[s] are not related to his Covid-vaxx work, because, among other things, “did you notice in the title that the claims are based on it[‘s written as] being an ‘oncolytic’ virus; that means for the treatment of cancers.”
But I believe they may well be related to his Covid-vaxx work. Because as I noted above, the information on these two US patents says they relate not only to the avian reovirus but also to the Newcastle-disease virus. And the Newcastle-disease virus is what his June 3, 2021, provisional patent application and Nov. 19 paper are focused on. There’s no way for me to know for sure, though, without seeing the provisional patent application and/or any subsequent patent application he and his colleagues may file.
Intranasal Vaxxes Gaining Traction
Intranasal vaxxes, like the Newcastle-disease-virus-based one that Bridle and his colleagues have been working on, just happen to perhaps not have the problems that Bridle ascribes to the mRNA jabs.
Intranasal vaxxes aren’t new. AstraZeneca’s intranasal flu vaxx FluMist has been used in the US since 2003 (with the exception of a two-year pause from 2016 to 2018, apparently because it wasn’t effective in kids aged two to 17).
And as I noted earlier in this article, the intranasal route is likely to become extremely popular. Intranasal-vaxx developers are counting on their being much more palatable to the public, including ‘vaccine sceptics,’ because these vaxxes aren’t jabs/shots and people can administer them themselves.
(And many have long being used for livestock – for example Merck’s – and also for dogs – here are Merck’s canine nose vaxxes.)
There already are eight intranasal vaxxes in clinical trials to date, according to the World Health Organization’s ‘COVID-19 vaccine tracker and landscape.’ (Click on the ‘Download’ button near the top left of the page; double-click to open the document that appears; scroll down to the table labelled ‘4. Number of doses, schedule and route of administration of candidates in clinical’; then look at the ‘IN’ – ‘intra nasal’ [sic] – line in the ‘Route of Injection’ section.)
That’s a small fraction of the more than 350 Covid vaxxes being tested so far.
But many more intranasals are sure to follow. For example, according to this Nov. 11, 2021, article, a Stanford University team is teeing up an intranasal spike-protein shot against Covid.
Their Oct. 27, 2021, mouse-experiment paper the article is based on states, in the abstract at the beginning of the article, that such “an alternative self-administrable vaccine capable of mounting long-lasting immunity via sterilizing neutralizing antibodies [i.e., antibodies that ostensibly prevent the virus from multiplying] would be hugely advantageous in tackling emerging mutant SC2 [SARS-CoV-2] variants. This could also diminish the possibility of vaccinated individuals acting as passive carriers of COVID-19” (Bolding added by me.)
They further note, in the third paragraph of the paper’s second page, that another advantage of the intranasal route is “the avoidance of injections, and a likely high tolerance and compliance in clinical practice.” (Bolding added by me.)
And indeed, Bridle told me in our Nov. 4 phone call that, “If somebody comes up with a vaccine [for Covid] that has properly demonstrated a good safety profile … addressing all of the safety issues, legitimate safety issues, that I and many other international colleagues have raised. And until we see that data, presented to us, and alongside the efficacy data, none of us, including myself, are going to stand behind any of these other vaccines. So yes, but could there be a future vaccine for SARS-coronavirus-2 that we would stand behind? Yes. I would be happy to do so. Because I am a virologist.”
Shaky Spike-Protein-Related Assertions
Let’s now switch gears a bit to address one of Bridle’s central claims about the mRNA Covid shots.
He lays the lion’s share of the blame for the serious injuries, such as myocarditis, and deaths from those jabs on the spike protein — which is produced in the body after the jabs — entering the bloodstream. He suggests that other shots do not lead to this type of spread.
He makes sweeping statements about this — in for example his Nov. 12, 2021, expert report and his June 15, 2021, Covid-shot guide for parents. In the middle of page 40 of the Nov. 12 report, after citing eight studies (see five paragraphs below), Bridle writes:
‘Conclusion: the spike protein, if it gets into circulation, has the potential to cause damage to the cardiovascular system and other tissues.’
And just one sentence later, at the start of the next section, he states:
“Now that there is a clear understanding that the spike protein from SARS-CoV-2 is a dangerous toxin when it gets into the blood and is distributed throughout the body, we can continue with the story about COVID-19 vaccines.” (Bolding added by me.)
On what basis did he make this leap?
He cites eight studies to support this claim. (The studies are references 84-91; you can see their details such as authors, title and publication name, on page 133 of the document.) But they’re all related to Covid, not to vaxxes for it. Plus: five of those studies are in vitro (i.e., in test tubes and/or petri dishes) and one study was done in mice (the spike protein was injected directly into their veins). The other two were on human-autopsies (which have some overlapping authors with each other). Note also that Bridle states that one of these human-autopsy papers (ref. 84) shows the free spike protein rather than the whole virus was found in various tissues. But this isn’t really accurate: the authors said that they found the spike protein grouped together with other proteins from the virus. (For example, on the fifth page of the paper the authors write, “in both the skin and brain … the spike protein co-localized with both the envelope and membrane proteins, suggesting that the capsid proteins [i.e., envelope protein, membrane proteins and the spike protein] circulated as a unit”).
And indeed, when in a September 24, 2021, interview on Rebel News, Tamara Ugolini asked Bridle how he knows it’s the spike protein and not something else causing injuries and deaths in people who have received the Covid vaccines, since we don’t know all the ingredients in the vaccines (at 30:27 in the video), Bridle admitted his evidence is purely theoretical.
“That’s a great point,” Bridle replied. “… We have to depend on the companies really – the companies, the onus is on them to evaluate the safety. So we’ve been raising all these questions. And these can readily be addressed in studies — properly conducted experiments.”
He went on to say that (at 32:05) it “is a big if if the mechanism of damage that [is] causing things like the blood clots [is] the spike getting freely into circulation.”
[And unfortunately he’s not alone in his seemingly faulty reasoning. For example, I emailed Sucharit Bhakdi to ask why, in the July 23, 2021, paper that Bhakdi co-wrote with Michael Palmer claiming the spike protein is the root of virtually all of the evils of the mRNA Covid shots, they didn’t use any information on the pattern of injuries among the many millions of people who’d already been jabbed by then. Bhakdi replied in a Sept. 9 email to me that, “Our predictions regarding development of adverse effects are based on general textbook knowledge of immunobiology and medicine. They are currently being verified.” (Bolding added by me.) Yet I’ve checked subsequent posts on doctors4covidethics.org, and as far as I can see Bhakdi and other authors still have not verified this using any clinical data in jabbed people.]
Bridle is Part of the Continued Push to Trust Vaccines
On page 5 of his June 15, 2021, vaccines guide Bridle wrote, “I consider vaccines that have been developed on a foundation of sound science to be the most efficient type of medicine; they have cost-effectively saved millions of people from sickness and/or death.” A very similar sentence is on page 5 of his Nov. 12, 2021, expert report. And he repeats this message in many other forums.
The Canadian Covid Care Alliance – of which Bridle is a key and outspoken member — also strongly promotes vaccines. For example the Alliance’s Sept. 24, 2021, ‘COVID-19 Canadian Covid Care Alliance Declaration’ notes (bolding and underlining in the original):
“Without full transparency and informed consent, and without a full appreciation and proper evaluation of the safety of these novel vaccines (both short- and long-term) the current COVID-19 vaccination programs should be paused immediately. We greatly support classical vaccine programs as developed over past decades and are therefore deeply concerned that this blatant disregard for medical ethics and most recent scientific data during COVID-19 vaccinations will irreparably damage Canadians’ trust in the traditional vaccine programs.”
And unfortunately other high-profile organizations also have been giving Bridle an uncritical platform. That includes, among others, TrialSiteNews (see for example Bridle speaking at 12:50 in this June 4, 2021, ‘Expert Panel’ video) — and Children’s Health Defense and Del Bigtree’s ‘The Highwire,’ via pieces such as this one, this one and this one.
As a result, large numbers of people and organizations who previously were standing firm in their knowledge based on a large body of evidence that vaccines are unsafe – people labelled ‘anti-vaxxers’ by Bridle and others — are being lulled into thinking Bridle is on our side because he’s vocally opposing the mRNA Covid shots.
Therefore they may well be led to believe that virtually all other vaccines are okay.
I recommend several pieces of reading material that show the clear and present dangers of many vaccines.
One is the book The Peanut Allergy Epidemic: What’s Causing It and How to Stop It by Heather Fraser. Another is the book Disease, Vaccines, and the Forgotten History by Suzanne Humphries, MD, and Roman Bystrianyk.
This is among the material that helped open my eyes 2.5 years ago to the dangers of vaccines. Contact me if you’d like other book or article recommendations.
By asking questions we can start to solve the riddle of Byram Bridle.
Don’t let ‘experts’ on either side of any issue lull or push you into giving away your power to think for yourself. Follow the money trail and potential conflicts of interest.
Work to find the real truth – it’s hard work but vital. Check the primary-source material used to make assertions, no matter who’s making them.
31,014 Deaths 2,890,600 Injuries Following COVID Shots in European Database of Adverse Reactions as Young, Previously Healthy People Continue to Die
31,014 Deaths 2,890,600 Injuries Following COVID Shots in European Database of Adverse Reactions as Young, Previously Healthy People Continue to Die
by Brian Shilhavy, Health Impact News
November 28, 2021
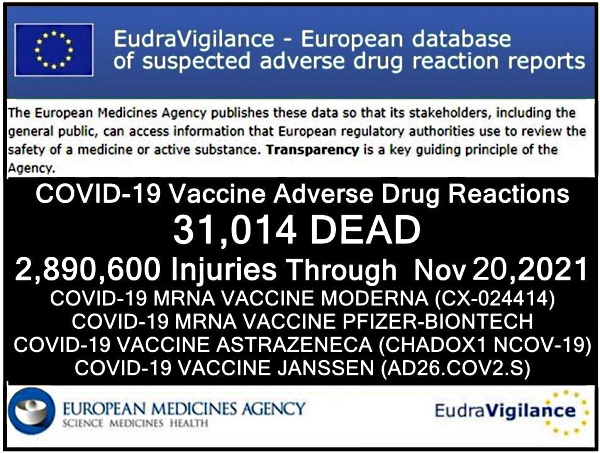
The European Union database of suspected drug reaction reports is EudraVigilance, and they are now reporting 31,014 fatalities, and 2,890,600 injuries, following COVID-19 injections.
A Health Impact News subscriber from Europe reminded us that this database maintained at EudraVigilance is only for countries in Europe who are part of the European Union (EU), which comprises 27 countries.
The total number of countries in Europe is much higher, almost twice as many, numbering around 50. (There are some differences of opinion as to which countries are technically part of Europe.)
So as high as these numbers are, they do NOT reflect all of Europe. The actual number in Europe who are reported dead or injured following COVID-19 shots would be much higher than what we are reporting here.
The EudraVigilance database reports that through November 20, 2021 there are 31,014 deaths and 2,890,600 injuries reported following injections of four experimental COVID-19 shots:
- COVID-19 MRNA VACCINE MODERNA (CX-024414)
- COVID-19 MRNA VACCINE PFIZER-BIONTECH
- COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19)
- COVID-19 VACCINE JANSSEN (AD26.COV2.S)
From the total of injuries recorded, almost half of them (1,355,192) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through November 20, 2021.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2, Comirnaty) from BioNTech/ Pfizer: 14,526 deaths and 1,323,370 injuries to 20/11/2021
- 35,826 Blood and lymphatic system disorders incl. 207 deaths
- 40,230 Cardiac disorders incl. 2,128 deaths
- 376 Congenital, familial and genetic disorders incl. 33 deaths
- 17,995 Ear and labyrinth disorders incl. 10 deaths
- 1,217 Endocrine disorders incl. 5 deaths
- 20,443 Eye disorders incl. 32 deaths
- 110,658 Gastrointestinal disorders incl. 585 deaths
- 337,450 General disorders and administration site conditions incl. 4,118 deaths
- 1,502 Hepatobiliary disorders incl. 75 deaths
- 14,528 Immune system disorders incl. 76 deaths
- 53,108 Infections and infestations incl. 1561 deaths
- 20,222 Injury, poisoning and procedural complications incl. 240 deaths
- 33,067 Investigations incl. 451 deaths
- 9,103 Metabolism and nutrition disorders incl. 249 deaths
- 164,885 Musculoskeletal and connective tissue disorders incl. 179 deaths
- 1,163 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 114 deaths
- 225,032 Nervous system disorders incl. 1,556 deaths
- 1,851 Pregnancy, puerperium and perinatal conditions incl. 55 deaths
- 206 Product issues incl. 2 deaths
- 24,225 Psychiatric disorders incl. 174 deaths
- 4,667 Renal and urinary disorders incl. 224 deaths
- 43,949 Reproductive system and breast disorders incl. 5 deaths
- 57,013 Respiratory, thoracic and mediastinal disorders incl. 1,617 deaths
- 62,414 Skin and subcutaneous tissue disorders incl. 125 deaths
- 2,765 Social circumstances incl. 19 deaths
- 4,797 Surgical and medical procedures incl. 60 deaths
- 34,678 Vascular disorders incl. 626 deaths
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna: 8,518 deaths and 390,163 injuries to 20/11/2021
- 8,227 Blood and lymphatic system disorders incl. 94 deaths
- 12,657 Cardiac disorders incl. 915 deaths
- 156 Congenital, familial and genetic disorders incl. 6 deaths
- 4,698 Ear and labyrinth disorders incl. 2 deaths
- 348 Endocrine disorders incl. 3 deaths
- 5,731 Eye disorders incl. 29 deaths
- 32,091 Gastrointestinal disorders incl. 326 deaths
- 104,720 General disorders and administration site conditions incl. 2,986 deaths
- 644 Hepatobiliary disorders incl. 40 deaths
- 3,820 Immune system disorders incl. 16 deaths
- 14,668 Infections and infestations incl. 782 deaths
- 8,158 Injury, poisoning and procedural complications incl. 162 deaths
- 7,117 Investigations incl. 143 deaths
- 3,703 Metabolism and nutrition disorders incl. 206 deaths
- 47,355 Musculoskeletal and connective tissue disorders incl. 174 deaths
- 531 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 67 deaths
- 66,320 Nervous system disorders incl. 823 deaths
- 722 Pregnancy, puerperium and perinatal conditions incl. 6 deaths
- 78 Product issues incl. 2 deaths
- 7,100 Psychiatric disorders incl. 142 deaths
- 2,277 Renal and urinary disorders incl. 164 deaths
- 8,061 Reproductive system and breast disorders incl. 7 deaths
- 17,235 Respiratory, thoracic and mediastinal disorders incl. 914 deaths
- 20,963 Skin and subcutaneous tissue disorders incl. 76 deaths
- 1,769 Social circumstances incl. 36 deaths
- 1,374 Surgical and medical procedures incl. 78 deaths
- 9,640 Vascular disorders incl. 319 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/AstraZeneca: 6,145 deaths and 1,075,335 injuries to 20/11/2021
- 13,124 Blood and lymphatic system disorders incl. 248 deaths
- 19,128 Cardiac disorders incl. 696 deaths
- 195 Congenital familial and genetic disorders incl. 8 deaths
- 12,669 Ear and labyrinth disorders incl. 3 deaths
- 597 Endocrine disorders incl. 4 deaths
- 18,919 Eye disorders incl. 29 deaths
- 102,402 Gastrointestinal disorders incl. 312 deaths
- 283,288 General disorders and administration site conditions incl. 1,469 deaths
- 950 Hepatobiliary disorders incl. 60 deaths
- 4,834 Immune system disorders incl. 29 deaths
- 32,441 Infections and infestations incl. 413 deaths
- 12,358 Injury poisoning and procedural complications incl. 177 deaths
- 23,611 Investigations incl. 150 deaths
- 12,369 Metabolism and nutrition disorders incl. 91 deaths
- 159,668 Musculoskeletal and connective tissue disorders incl. 94 deaths
- 624 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 22 deaths
- 221,536 Nervous system disorders incl. 958 deaths
- 521 Pregnancy puerperium and perinatal conditions incl. 12 deaths
- 188 Product issues incl. 1 death
- 19,933 Psychiatric disorders incl. 58 deaths
- 4,031 Renal and urinary disorders incl. 58 deaths
- 15,124 Reproductive system and breast disorders incl. 2 deaths
- 37,980 Respiratory thoracic and mediastinal disorders incl. 735 deaths
- 49,247 Skin and subcutaneous tissue disorders incl. 48 deaths
- 1,498 Social circumstances incl. 6 deaths
- 1,404 Surgical and medical procedures incl. 25 deaths
- 26,696 Vascular disorders incl. 437 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 1,825 deaths and 101,732 injuries to 20/11/2021
- 986 Blood and lymphatic system disorders incl. 40 deaths
- 1,837 Cardiac disorders incl. 155 deaths
- 35 Congenital, familial and genetic disorders
- 1,033 Ear and labyrinth disorders incl. 2 deaths
- 69 Endocrine disorders incl. 1 death
- 1,351 Eye disorders incl. 7 deaths
- 8,500 Gastrointestinal disorders incl. 75 deaths
- 26,871 General disorders and administration site conditions incl. 488 deaths
- 121 Hepatobiliary disorders incl. 11 deaths
- 445 Immune system disorders incl. 9 deaths
- 4,315 Infections and infestations incl. 143 deaths
- 920 Injury, poisoning and procedural complications incl. 18 deaths
- 4,766 Investigations incl. 103 deaths
- 625 Metabolism and nutrition disorders incl. 45 deaths
- 14,897 Musculoskeletal and connective tissue disorders incl. 43 deaths
- 54 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 3 deaths
- 20,097 Nervous system disorders incl. 197 deaths
- 41 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 26 Product issues
- 1,407 Psychiatric disorders incl. 16 deaths
- 417 Renal and urinary disorders incl. 22 deaths
- 2,059 Reproductive system and breast disorders incl. 6 deaths
- 3,617 Respiratory, thoracic and mediastinal disorders incl. 234 deaths
- 3,094 Skin and subcutaneous tissue disorders incl. 8 deaths
- 319 Social circumstances incl. 4 deaths
- 690 Surgical and medical procedures incl. 54 deaths
- 3,140 Vascular disorders incl. 140 deaths
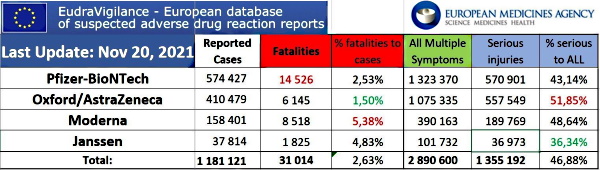
*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
Here are some faces and stories to attach to these cold statistics from those who paid the ultimate price to receive an experimental COVID-19 shot. All of these people were reportedly healthy prior to taking the shots, and they ended up dying very young, or became crippled and lost their careers.
First, we have a very emotional video posted online by a Canadian mother who mourns her daughter’s 13-year-old friend who did not want to take the COVID-19 shot, but finally gave in and took it as it was mandatory for her to continue participating in sports. Her heart stopped and now she is in critical condition.
Connect with Health Impact News
cover image credit: carolynabooth / pixabay
Riccardo Bosi & Lurnpa (David Cole) on What Is Really Happening in Australia’s Northern Territory & Why — “This Is Genocide. A Bioweapon.”
Riccardo Bosi & Lurnpa (David Cole) on What Is Really Happening in Australia’s Northern Territory & Why — “This Is Genocide. A Bioweapon.”
by Riccardo Bosi, Australia One w/ Lurnpa (David Cole), Original Sovereign Tribal Federation
November 25, 2021
A time to decide. The international community must speak up!
Video available at AustraliaOne Rumble.
Transcript provided by Truth Comes to Light:
Riccardo Bosi
Good afternoon ladies and gentleman.
My name is Ricardo Bosi, national leader of Australia One.
Today is the 25th of November 2021.
And we’ve been hearing some stories about some maltreatment of our First Nations people in Northern Territory. And a lot of rumors flying.
But we want to make sure that we give you what has been verified so we don’t cause any unnecessary concern.
Now these stories are going around the globe, which is a good thing. We need to raise awareness but we have to make sure we stick to the facts.
So in order to pursue that, we’ve got that David Cole here — who’s been on the ground. And he’s going to give us an update on what’s happening in the Northern Territory, Australia.
David, thanks for joining us. The floor is yours, mate.
David Cole:
Yes, thanks Riccardo. Look, the last couple of days I’ve been nonstop, flat out, talking to community nonstop. I’ve probably spoken… probably over 30 people from the communities, seeing the elders and local people, and just trying to get the facts so that we are very clear on what we’re telling people what’s going on on the ground.
So, I’ve been I’ve been having some good conversations… and I’m getting information that confirms the fears that people are being pressured coerced and forced into getting these vaccines.
But none of the community have confirmed for me that they’ve witnessed military people there, chasing people down, holding people down or do anything of that sort — which is comforting because that was, I think, scaring all.
But what’s not comforting is this. They still have police personnel with medical staff going door to door in these communities and they are pressuring, coercing and forcing people through pressure to take the vaccine.
A lot of the people are very skeptical, they’re very scared and they don’t want to have it. But they’re taking it because they’re being told if you don’t take it you can’t go into the local shop and buy food, you can’t leave the community, you can’t drive in to Katherine, you can’t go to the football, you can’t do anything.
So there’s a community in Barunga, for example, all the young footballers have got it because they’ve been told that they can’t play football. And for a lot of our communities, sport and football is like meditation. It’s time out. It’s a release. It’s the freedom. And to take that away from a lot of these young men is quite scary for them. So we have an entire football team in that community alone that have got it. The entire community’s got it.
These are not medical records, for the record. These are from first hand accounts of community people and some of the information has come from very trusted people who have worked in the health area for a long time, and they have family directly in these communities.
[Here David Cole shares numbers of vaccinated, breaking down by communities in the Northern Territory.]
Just because the people are not being chased down and pinned down, we are being chased down and pinned down as a people.
They have road blocks on either side of Katherine and Tindal Airbase and on the downside of Katherine, stopping all traffic going in and out.
Anybody who flees the community is being turned back and fined $5,000.
People who are trying to get out the community for food, people who have tried to get out of the community out of fear, have been fined and forced back into the communities.
So this is martial law.
I have seen an article that confirms that up to 65 military personnel were assisting the Northern Territory government.
There is a Facebook message from somebody who claims their friend is in the military and that they have taken stress leave because of the trauma of what they witnessed, what they doing in the communities.
I am being told that military are involved — to what degree we cannot confirm it from the community grassroots.
There are some communities that know they’re about to go into. Those communities are fully prepared. They are going to video. They’re going to film and they’re going to get us the evidence when they come there.
Barunga — I’m aware that just the health workers are going around there. There’s no police pressure there. But the other communities have had police and task force and pressure on the community to take the vaccine.
Now, our people are very, very peaceful. Our people are very, very gentle.
[…] A lot of people are planning to run into the bush. They are getting ready to cut bush. Even when people are leaving these communities and going out to the homelands, they’re being chased down in the homelands.
Now in the homelands is where they’re safest. They’re not only outside the community but they’re in a remote location and nobody can get to them. They are safe there.
The people are being told, if you don’t get this vaccine, this virus is going to kill you.
So they are telling lies. They are using fear tactics. They are using coercion. They’re using deprivation of their liberty and their freedom to travel — not just on Australian land.
But as sovereign, tribal people, our people are being locked into the communities and denied the right to travel across their lands, on their own lands, by corporations that don’t have the right to do this.
They are putting the fear into our people to a level where a lot of them are just taking it, out of fear. A lot of them are sad, a lot of them are upset. They are scared — what’s going to happen to them. And the conversations that we have had with the elders from numerous communities across the Katherine region is they are very frightened with what’s going on.
And the fact that they’re being forced, pressured tells them that this is not normal, tells them it’s not right and the people are very fearful.
I cannot stress enough. This is an SOS to the world.
We need to invoke the international human rights and we need intervention now.
We need to stop this corporation from doing what it’s doing — not just to the tribal people but to the Australian people.
And here’s my message to the Australian people:
If you think that this is a tribal, remote issue, I assure you that this is a dry run.
Everything that is trialed on us will come to the cities, will come to the mainstream, and will come to you.
We have a chance as a people to stand this down and stop it here now, with the international allies watching, and we need to do that.
We need to stand and stop this insanity right now so we can spare, not only the other communities, so we can spare everyone across the country — because it will not stop here, people. It will come for you.
Now the tactics they are using are military tactics. The fear is immense. Our people are so frightened. They don’t know what to expect. And I just got confirmation from a community member that people as young as 12 and up are being jabbed in a lot of these communities as well.
So they’re going for the kids.
Now, my research and what I believe, through the evidence and the science that I’ve seen, this is, without question, a bioweapon.
Now, if this is a bioweapon, this is biowarfare. And the tribal people have been subjected to this, not just in the territory but across the country, as is the Australian people.
But they are hitting us en masse …
We have to remember this. When we lose the connection to country, we lose the song, dance and ceremony that the elders hold. We lose that connection. They will remove the children off the land.
And one of the elders said to me — between Borroloola… Robinson River — that there’s been a lot of push for a lot of groups that want to come in and do big business there.
They want to do lots of businesses on the river and they want to do all sorts of stuff. And it’s very mineral rich country.
Because the tribal people have said no, these areas are getting hit hard. These areas are getting smashed.
And we have to remember that there are large military bases across that whole region. Three of the largest military operations operate within that region for foreign military powers.
I can’t hold back but state my facts and my truth.
And my truth is this:
This is a genocide, a bioweapon, that is being used to wipe out the tribal people because they want to develop the north.
They’ve destroyed the south.
The water’s dead, the rivers are dead, the land’s sick.
They’re coming north. They want the water. They want the resources. They want the land. And the only thing standing in the way is a handful of tribes across the region.
And they are hitting us hard. And I’m not kidding you — this is genocide.
And we need help, brother. We need the world to know.
Riccardo Bosi
Thanks, David. Absolutely correct.
Ladies and gentlemen, you’ve heard there yourselves.
Now a lot of people, when they read history they say, ‘If I’d been in Germany, I’d have spoken up when they came for the Jews and the Slavs and the gypsies and the disabled and homosexuals and the political dissidents.’
But they didn’t. They didn’t say a thing. And something between 14 to 20 million people died at the hands of the Nazis.
Well, now’s your chance. Now’s your chance take a take a stand.
Now, there is no middle ground here. You either speak up or you are condemned by your silence. And we will remember you.
This is one people. One country. Black and white makes no difference.
This is an attack on Australia as David has said. Please understand what’s happening here is going to happen in your country.
So every political later on on the planet — if you remain silent, we will remember you.
The common people are speaking up. They’re protesting in our support.
But every country on this planet, you either speak or remain silent.
If you remain silent, we will remember you because we’re going to win this. And you will not. And we will remember your silence, your complicit silence, in this genocide of the Australian people.
There’s only one place to be and that’s with us.
David, thank you very much for your update. If you have any more, give us a call. We’ll put you straight online. We’ll get this out into the international community.
And we are demanding that every political leader on the planet speak up and condemn the Australian government — federal and state governments — and demand that they halt this genocide.
Any last words, David?
David Cole
No, brother, I can only support you just said. We are calling out for the international community to come forward, and invoke the international human rights, and stop this genocide for us all.
And I’m with you brother, if you are silent, you are complicit. If you don’t speak up, you are complicit.
And these foreign corporate governments that have embassies here, they have to remember this: The Australian government is but a registered body in the Norfolk Islands. Their partnership with this corporation is null and void.
You are here on tribal lands and to sit silent and allow for this corporation to continue what it’s doing to the Australian people makes you, not only complicit, but you are involved. So you must speak up. You must come forward and you must stop this insanity and speak now.
As you said, brother. We will remember.
Riccardo Bosi
Thanks David and we’ll get you online again if there’s any further updates.
Ladies and gentleman
My name is Riccardo Bosi, national leader of Australia One.
Thank you for your time.
For more information on Lurnpa, see Who I am and Why I am Fighting for our Freedom &
Declaration of the Returning Sovereigns & Unveiling of King Charles V ‘Sword of Deliverance’
Connect with David Cole (Lurnpa) at Original Sovereign Tribal Federation
Connect with Riccardo Bosi at Australia One
cover image credit: walesjacqueline / pixabay
“Australia Needs Lions Not Sheep”: Melbourne Streets Overflow as Protestors Stand for Freedom — Powerful Time-Lapse Video
“Australia Needs Lions Not Sheep”: Melbourne Streets Overflow as Protestors Stand for Freedom — Powerful Time-Lapse Video
video by Real Rukshan available at Odysee and YouTube.





all images credit: screenshots from Real Rukshan videos
The Spanish Basque Court Revolts and Suspends the Health Pass for Violation of Rights
The Spanish Basque Court Revolts and Suspends the Health Pass for Violation of Rights
by Sheikh Dieng, Le Courrier du Soir
November 23, 2021
The Higher Court of Justice of the Basque Country (TSJPB) suspended, on November 22, the use of the Health Pass imposed by the autonomous government. Court mentions threat to citizens’ freedom
If there are courts in the Western world which have distinguished themselves by their courage to stand up to their state during this Coronavirus pandemic, it is the Spanish regional courts which have continued to reject health measures en masse. dictated by the autonomous governments under the blessing of the central government of Madrid.
Moreover, very recently, the Constitutional Court invalidated the state of health emergency decreed in this country in March 2020 and demanded from the central state based in Madrid to reimburse all fines collected during this period. And the revolt of the courts is far from knowing its epilogue because this November 22, it is in the Basque Country that the Sanitary Pass was attacked.
“Justice denounces an attack on the fundamental freedoms of citizens”
At least this is the information that Lecourrier-du-soir.com obtained this Monday from several reliable sources such as the media ElPeriodico.com . According to this source, the Superior Court of Justice of the Basque Country (TSJPB) suspended the decision of the Basque regional government which required the Health Pass to have access to nightclubs and restaurants with more than 50 seats.
The information was confirmed by the media, El Pais . According to this source, which says it has consulted the decision of the Court, the Basque justice refused to endorse such a measure, arguing that it would violate the fundamental rights of a fringe of the population vaccinated with two doses.
“Unsuccessful by justice, the Basque government capitulates”
According to the court, imposing the Sanitary Pass in a discriminatory manner cannot be justified, especially since the authorities themselves defend the idea that the contagion effects in vaccinated people are not very important. Still according to the court, this measure lacks consistency given that the autonomous government does not impose the Sanitary Pass on employees of leisure and catering facilities.
The carrots appear to be cooked for the autonomous government of the Spanish Basque Country which, according to information provided by the media Diario Vasco , has decided not to appeal. “The Basque government will not prosecute this case and will not appeal to this decision of the Tribunal,” the Basque government informed in a statement.
Connect with Le Courrier du Soir
cover image credit: Alexandra_Koch / pixabay
Australian MP Calls on Citizens to Revolt — Compares Leaders to Hitler and Stalin
Australian MP Calls on Citizens to Revolt — Compares Leaders to Hitler and Stalin
by Amy Mek, RAIR Foundation
November 27, 2021
“The totalitarian path we are unquestionably on has never ended well.”
– MP George Robert Christensen
Queensland MP George Robert Christensen has called on citizens to rise up against coronavirus lockdown measures and vaccination mandates. He compared governments promulgating such measures to totalitarian regimes responsible for the most horrific atrocities.
On Wednesday, Christensen said in parliament that Australian State Premiers are “drunk on power” and “trying to out tyrant each other”. He also noted that non-vaccinated Australians are increasingly “demonized, ostracized, and socially eradicated.”
No Justification
The MP explained that totalitarian regimes responsible for the most heinous atrocities of the Twentieth Century: Stalin, Mao, Hitler, Pol Pot, didn’t get there overnight.
They used fear to control, excluded the “dirty” people (softly at first), justified the exclusion, moved to harder exclusions, and eventually eliminated people either socially, or physically.
Early last year, 94-year-old Auschwitz survivor Marian Turski gave a speech during the commemoration of the 75th anniversary of the camp’s liberation. The Polish Holocaust survivor reminded the audience that the Holocaust didn’t’ start with death camps. Instead, it began with propaganda, scaremongering, scapegoating, and segregation.
In Twenty-First Century Australia, State Premiers are racing down that familiar path, setting up their own bio-security police states complete with medical apartheid,
Sadly, we have enabled it, refusing to rein them in and, worse, supplying the Australian Immunisation Register data that underpins this medical apartheid. Fear is a justification of choice for coercion and control, with non-vaccinated Australians increasingly demonised, ostracised and socially eradicated.
Just recently, the Australian military began forcibly throwing coroanvirus positive citizens and close contacts in quarantine camps.
Pandemic of the Unvaccinated Lies
The establishment claims that the virus is now a pandemic of the unvaccinated, but Christensen said there is no justification for such demonization.
He referred to a German study showing that 55 percent of symptomatic patients over 60 are fully “vaccinated”. In Gibraltar, where all 34,000 residents have been fully vaccinated, 60 new cases are registered daily.
Meanwhile, the Australian government is mandating the experiment mRNA shots, which has caused adverse effects in many people. Furthermore, they are forcing citizens to take a second shot even after they suffered an adverse event from the first.
Civil Disobedience
We are undoubtedly on the totalitarian path, and that never ends well, said the MP. “The solution is a rediscovery of human dignity, along with, and I don’t say this lightly — civil disobedience.”
Watch Liberal Party of Australia MP, George Robert Christensen impassioned speech:
Huge Freedom Protests Again Bring Australian Cities to a Standstill
Huge Freedom Protests Again Bring Australian Cities to a Standstill
Hundreds of thousands of Australians come together across more than 30 regions to say NO to mandatory vaccines
by Avi Yemini, Rebel News
November 27, 2021
Large-scale protests continued across Australia today as hundreds of thousands again turned out in the nation’s cities and towns to protest against mandatory vaccines.
The protests this week were organised by the Millions March Against Mandatory Vaccination group which were scheduled today across 30 Australian cities and towns.
Flags from nations and people across the globe continued to be featured as protesters represent their heritage, standing in support and solidarity with those affected by mandates and with the indigenous community who have expressed concern from within their own communities.
Meanwhile in Melbourne. pic.twitter.com/uYcSfDZHet
— Avi Yemini (@OzraeliAvi) November 27, 2021
In Melbourne, huge crowds marched to the steps of Victorian parliament again, a scene where many diehard protesters have been camping out in protest of Premier Daniel Andrews’ controversial pandemic powers legislation, which has been the subject of intense angst in the community.
A diverse range of protesters chanted ‘Kill The Bill’ and called for Andrews’ resignation as they marched through the cities streets to the cheering and beeping of car horns.
It was again a carnival atmosphere in the city with music, stilt-walkers, bagpipes, drums and more. Some even brought pots and pans to tap along to the beat.
Despite inclement weather, huge crowds again swarmed Sydney, with the nation’s biggest city putting on a show of defiance against government over-reach.
There were some tense moments as police appeared to take a more heavy-handed approach than seen in recent weeks, and of the hundreds of thousands marching across the nation, the crowds were largely peaceful.
It was the first weekend where smaller protests have been staged across towns and regional centres, including Adelaide, Darwin, Alice Springs, Perth, Canberra, Newcastle, Ballina, Inverell, Tamworth, Wagga Wagga, Bermagui, Launceston, Bunbury, Albany, Esperance, Kalgoorlie, Geraldton, Carnarvon, Port Hedland, Broome, and Kununurra.
Go Gold Coast! pic.twitter.com/xQp5pvId6d
— Melinda Richards 🇦🇺🇺🇸 (@goodfoodgal) November 27, 2021
Austria: Coercion and Tyranny | The Killer Agenda Behind the Vaccine “Incentives” | We Can and We Must Stop This
Austria: Coercion and Tyranny | The Killer Agenda Behind the Vaccine “Incentives” | We Can and We Must Stop This
“Extravagant” Incentives for the Non-Vaxxed to Accept the Jab
by Peter Koenig, Global Research
November 26, 2021
Austria recently announced a total lockdown of the entire population, vaxxed or unvaxxed, and compulsory vaccination as of 1 February 2022, see this. Both of these measures have raised a lot of resistance, especially the second one; it is a direct interference in people’s basic Human Rights.
This is however not enough for Chancellor Alexander Schallenberg, to withdraw the draconian and illegal request for obligatory vaccination. Instead, the Austrian Government, like so many other western governments in Europe and the US, has initiated an incentive scheme for the non-vaxxed that basically works as a lottery.
For example, under a vaccination lottery, the unvaxxed can now win a house, for a “limited time” if they submit to the jab. The news was announced on 23 November and is apparently valid until just before Christmas. See this.
But the most hilarious, and as far as I know, never heard-of before “incentive scheme” is a 30-minute free-brothel time with a prostitute, if one accepts the jab. Yes, you have read correctly: Austria offers the unvaxxed – presumably primarily men – a prostitute, free for 30 minutes, meaning the government pays for the prostitute’s time. See this CNN report.
The CNN reporter – a lady – pointedly, with a smile, says it’s a win-win solution: More men get vaxxed and the brothel makes more business. Fabulous.
This just shows how desperate governments around the world get to meet their “outside” imposed “vaxx-quotas”.
What’s the real agenda?
It becomes increasingly clear that this vaccination campaign – one can no longer call it a campaign, it is rather coercion of the worst kind with a specific goal – has a clear plan: implement as fast as possible a eugenist agenda. And that before people wake up to realize what they have been forced to accept – a highly probable lethal shot, or series of shots.
According to Dr. Elisabeth Eads, these mRNA Covid jabs are diminishing your immune system drastically, the first one by about 30%, the second one another 30% and the so-called “booster” shot by about 20%. Since the West is in the midst of the “booster campaign”, on average the western population may be losing about 80% of its immune system after receiving the three injections. Of course, there are different reactions by different people. This is an average. This means, a considerably higher vulnerability to ANY viral and infectious disease, including the common flu – which is, as we know, registered as Covid.
Would this, plus the endlessly propagated and forced “testing-testing-testing”, maybe account for what they say is an almost exponentially increased “case” load? And this, of course, in the Northern Hemisphere’s flu season. – See this.
In healthy people, and especially younger people, like children, the immune system recovers over time, more or less rapidly. Is this the reason, why some “scientists” predict already that a “booster” shot will be necessary at least once a year? And that children are coerced to get a “booster” jab?
To be repeated: The agenda is massive depopulation, as fast as possible, before people wake up.
In other disturbing but related news, the professional Journal “Circulation” offers a molecular biological explanation on how Covid vaxxes may harm people lethally. See this, as well as the short abstract below (published 8 November 2021).
*
Abstract
Our group has been using the PLUS Cardiac Test (GD Biosciences, Inc, Irvine, CA) a clinically validated measurement of multiple protein biomarkers which generates a score predicting the 5 yr risk (percentage chance) of a new Acute Coronary Syndrome (ACS). The score is based on changes from the norm of multiple protein biomarkers including IL-16, a proinflammatory cytokine, soluble Fas, an inducer of apoptosis, and Hepatocyte Growth Factor (HGF)which serves as a marker for chemotaxis of T-cells into epithelium and cardiac tissue, among other markers. Elevation above the norm increases the PULS score, while decreases below the norm lowers the PULS score.
The score has been measured every 3-6 months in our patient population for 8 years. Recently, with the advent of the mRNA COVID 19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients. This report summarizes those results. A total of 566 pts, aged 28 to 97, M:F ratio 1:1 seen in a preventive cardiology practice had a new PULS test drawn from 2 to 10 weeks following the 2nd COVID shot and was compared to the previous PULS score drawn 3 to 5 months previously pre- shot.
Baseline IL-16 increased from 35=/-20 above the norm to 82 =/- 75 above the norm post-vac; sFas increased from 22+/- 15 above the norm to 46=/-24 above the norm post-vac; HGF increased from 42+/-12 above the norm to 86+/-31 above the norm post-vac. These changes resulted in an increase of the PULS score from 11% 5 yr ACS risk to 25% 5 yr ACS risk. At the time of this report, these changes persist for at least 2.5 months post second dose of vac. We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.
*
In a 4-min video, Dr. Vernon Coleman calls this mRNA mechanism sheer murder. He also calls for an immediate stop to all “vaccination”.
It is high time that people collectively around the world stand up – at once — against this murderous tyranny and vaccination, and that everybody rejects further vaccination. It’s not just tyranny for total domination and the implementation of the Great Reset and the Fourth Industrial Revolution – it is tyranny to drive people to walk or run into their own grave by fear.
We can and must stop this.
cover image credit: Skitterphoto / pixabay
Nuremberg II in 2022?
Nuremberg II in 2022?
by Dr. Mark Sircus
November 25, 2021
It is more than evident that a significant part of humanity is stampeding to take experimental vaccines for COVID-19. However, the “experimental” vaccines violate all 10 of the Nuremberg Codes, which carry the death penalty for those who seek to break these International Laws. Now, more than ever, we need new trials, not after the fact, as was the situation after WWII, but while the crimes against humanity are in progress.
Instead of these Nazis above the tables would be full of executives from Pfizer, Moderna, Johnston and Johnston, Dr. Fauci and the infamous Bill Gates, and many others. Even the politicians, who pretended to play doctor and healthcare official, promoting life-threatening and depressing masks, lockdowns, and death shots, should be held accountable. Dr. David Martin clearly shows that all of them are guilty of breaking American laws.
Front and center should be multiple members of the FDA and CDC, who are not trustful governmental agencies but richly paid whores for the vaccine companies.
American Heart Association Journal Publishes Data that U.K. Medical Doctor Claims are “Proof” that COVID-19 Vaccines are “Murder.” `We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy and other vascular events following vaccination.’
23 Nazi doctors were charged with conducting experiments on prisoners without consent, most at concentration camps. The aftermath of the trials led to creation of the Nuremberg Code, which the FDA and CDC do not follow. The Dr. Rath Health Foundation tells us that, “After six decades of silence, the historical records of the key war crimes tribunal that determined the responsibility for WWII were finally made available. Currently, history books teach that WWII was launched by a lunatic dictator, Hitler, and his ruthless Nazi henchmen.
However, tens of thousands of historical documents from the Nuremberg Tribunal – newly released online – unequivocally document that:
- WWII – a war that cost the lives of more than 60 million people – was planned and financed by the world’s largest chemical/ pharmaceutical cartel. At that time, Germany’s I.G. Farben consisted of Bayer, BASF, Hoechst, and others.
- The driving force behind WWII was I.G. Farben’s ambition to control the global oil and drug markets and eliminate, by force, any competition.
- The I.G. Farben companies financed the rise to power of the Nazi party and transformed German democracy into a dictatorship.
“The pharmaceutical industry does not act in the tradition of the protector of humanity, but in the tradition of I.G. Farben, a group of organized criminals willing to sacrifice countless human lives to maintain their profits,” writes Dr. Mathias Rath. Listen to him pleading in 2012 with his fellow Germans to not go down the same road that Germans have traveled twice before. He, too, claims that the two world wars were driven by the insatiable greed of the pharmaceutical and chemical cartels. The legacy of I.G. Farben is carried on by Bayer/Monsanto, Pfizer, and the other COVID vaccine companies.

Telford Taylor, US Chief Prosecutor at the Nuremberg War Crimes Tribunal against the executives of great I.G. Farben, wrote, “The crimes with which these men are charged were not committed in rage or under the stress of sudden temptation. One does not build a great war machine in a fit of passion nor an Auschwitz factory during a passing spasm of brutality. Their purpose was to turn the German nation into a military machine so it could impose its dominion on Europe and other nations beyond the seas. They were the warp and woof of the dark mantle of death that settled over Europe.”
The Nuremberg War Criminal Tribunal convicted 24 I.G. Farben board members and executives based on mass murder, slavery, and other crimes against humanity. Amazingly, however, by 1951, all of them had already been released and continued to consult with German corporations. The Nuremberg Tribunal dissolved IG Farben into Bayer, Hoechst, and BASF. Moreover, today each of the three daughters of I.G. Farben is 20 times as big as the I.G. Farben mother was at its height in 1944, the last year of the Second World War.
There are people on this planet that take pleasure in hurting other people. They injured others from sheer psychological habit. The general nature of ‘evil’ is not to have consciousness of the effect our actions have on the feelings and emotional world of others, which is the definition or defining characteristic of both psychopaths and sociopaths.
Dr. Russell Blaylock says that it was the Rockefeller Foundation that created orthodox Medicine back in 1901. “Rockefeller owned what was called the drug trust: that’s the major drug manufacturing firms all over the world: Merck Pharmaceuticals, Lederle, all of these pharmaceutical companies. And, of course, the aim was to remove all nutrition references to nutritional type treatments from the medical schools. They closed down half the medical schools in the United States. There were 165 medical schools at the time. Then he had his anointed medical schools, which he poured his money into, appointed the professors from his stock of professors. And so, they created an educational system that taught the things that he wanted to be taught. And therefore, every professor that came out of those programs taught the same thing.”
Dead Doctors
According to the American Medical Association (AMA), a whopping 96 percent of United States doctors as of June have been “vaccinated” for COVID-19. And now many are dead. Vaccinated Doctors are Dying, and Unvaccinated Doctors are Quitting or Being Fired: Who will Run the Hospitals?
Dr. David Martin has been spending the past year and a half fighting to unravel what he says is the global criminal conspiracy of coronavirus. Parties include the American and Chinese governments, the International Monetary Fund, and Blackrock. Martin says these groups are guilty of criminal conspiracy in a terrorist plot against the American people.
Contemporary Medicine has been on quicksand for over 100 years, and as it sinks to the bottom, it is pulling down with it millions of humans into misery and death. We have known for a decade, thanks to the work of Dr. Gary Null, Dr. Carolyn Dean, and Dr. Barbara Starfield, that properly prescribed pharmaceutical medications are killing over 100,000 Americans each year.
Journal of the American Medical Association (JAMA)
Dr. Barbara Starfield of the Johns Hopkins School of Medicine
ALL THESE ARE DEATHS PER YEAR:
12,000 —– unnecessary surgery
7,000 —– medication errors in hospitals
20,000 —– other errors in hospitals
80,000 —– infections in hospitals
106,000 —– non-error, adverse effects of drugs
James Howard Kunstler writes that modern Medicine is a hostage racket; “Medicine is now a catastrophe every bit as pernicious as the illnesses it is supposed to treat, and a grave threat to a nation that we’re supposed to care about. If you thought banking in our time was a miserable racket — which it is, of course, and by “racket” I mean a criminal enterprise — then so-called health care has it beat by a country mile, with an added layer of sadism and cruelty built into its operations.”
It Is Worse Than All The Above
Dr. Wolfgang Wodarg, former head of health at the Council of Europe, explains that a pandemic used to be associated with widespread severe illness and death, but by changing the definition, removing the severity and high mortality criteria, World Health Organization (WHO) can now make a pandemic whenever it wants. One of the most respected men in Europe, he maintains that the “World Health Organization is an institution of corruption.”
“The scientific data overwhelmingly shows how probably millions have died from the covid injections, and hundreds of millions are suffering crippling side effects that often permanently disable the victims for life. The Vaccine Death Report provides all the data, along with hundreds of references, for further investigation.”
At the above link, one must scroll down to the first video but be prepared for a shock as the entire world’s elite are exposed for who and what they are, what they own, and what they have planned for most of the rest of us. Naturally, after watching, one is tempted to run and hide, but in the end, courage is encouraged.
It will be a miracle if the 99 percent of us persevere against the elite, the Deep State, the three or four companies that seem to own most of the other mega-corporations. Add God into the equation, add truth, reason, insight, and love for each other, and perhaps a much-needed miracle will occur.
I also recommend a video exposing the lies and stupidity of Gates, Fauci, Biden, the head of the CDC, and Biden, who cannot make up their minds about what is true or not about COVID vaccines.
About 47 million adults in the U.S. remain unvaccinated, according to figures from the Centers for Disease Control and Prevention.
Medical Murder
A Judge Stands up to a Hospital: “Step Aside” and Give a Dying Man Ivermectin.
A Chicago-area judge saved a grandfather’s life with the single question that exposes hospitals blocking doctors from using a safe, FDA-approved drug: Why?
cover image credit: Wikimedia Commons
Graphene Oxide & Nano-Router Circuitry in Covid Vaccines: Uncovering the True Purpose of These Mandatory Toxic Injections
Graphene Oxide & Nano-Router Circuitry in Covid Vaccines: Uncovering the True Purpose of These Mandatory Toxic Injections
Pattern Identification in Coronavirus Vaccines: Nanorouters
by Mik Andersen, Corona2Inspect
published in Spanish November 2021
rough translation via translation software
Since graphene oxide was discovered in coronavirus vaccines, all the findings and discoveries made only confirm its presence (Campra, P. 2021). To date, more than reasonable evidence and indications have also been found for the existence of carbon nanotubes and nano-octopuses, mesoporous spheres, colloidal nano-robots; objects that should not be part of any vaccine and that are not declared among the components of the same. Additionally, other types of objects have been identified and evidenced in images of blood samples, of people vaccinated with the coronavirus vaccines, specifically micro-swimmers, nano-antennas of crystallized graphene and graphene quantum dots, as well, known as GQD.
On this occasion, analyzing one of the images obtained by Dr. Campra, corresponding to a sample of the Pfizer vaccine, see figure 1, it has been discovered, which with great probability, is a nanorouter or part of its circuitry. In the original image, a well-defined drop can be seen in which crystalline structures of a quadrangular or cubic format appear. If you look closely, you can see some marks on these crystals, with a regular pattern, well defined in some cases, but limited by the microscope optics.
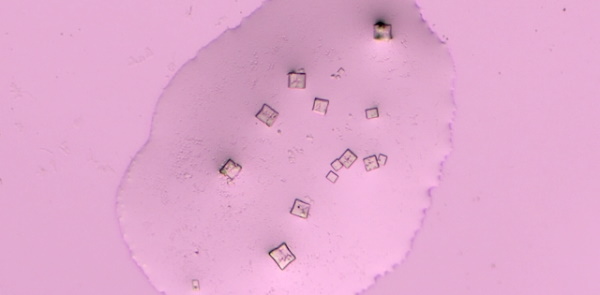
The finding has been possible by isolating each quadrangular crystal, applying a process of rasterizing, focusing and delineating the edges of the image, in order to further pronounce the observed marks. Once this process was completed, a rough draft was drawn with the lines and patterns inscribed on the glass, creating a clean outline of what actually looked like a circuit. The fact of finding parallel and perpendicular lines with a distribution far from the fractal patterns was very striking, which allowed us to automatically infer the possibility that it had been a product of manufacture. For this reason, similar patterns were searched in the scientific literature, which had a similar scheme, similar to the circuit that had just been drawn. The search result was almost immediate, as the pattern of a quantum dot nanorouter was found, as seen in Figure 2.
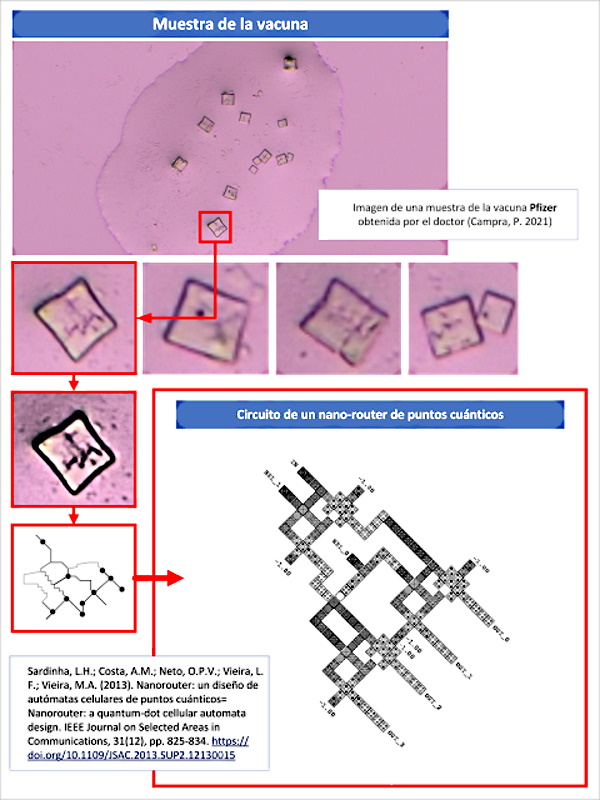
This discovery is of fundamental relevance, not only to understand the true purpose and components of the coronavirus vaccines, but also to explain the existence of the phenomenon of MAC addresses, visible through the bluetooth of many mobile devices.
Discovery context
Before proceeding with the explanation of the finding, it is convenient to remember the context in which it is framed, in order to ensure its understanding and subsequent deepening.
In the first place, it should be borne in mind that graphene and its derivatives, graphene oxide (GO) and carbon nanotubes (CNT), are part of the components of vaccines, according to what has already been stated in this blog. The properties of graphene are exceptional from the physical point of view, but also thermodynamic, electronic, mechanical and magnetic. Its characteristics allow its use as a superconductor, electromagnetic wave absorbing material (microwave EM), emitter, signal receiver, quantum antenna, which makes it possible to create advanced electronics on a nano and micrometric scale. Such is the case, that it is the fundamental nanomaterial for the development of nano-biomedicine (Mitragotri, S .; Anderson, DG; Chen, X .; Chow, EK; Ho, D .; Kabanov, AV; Xu, C. 2015 ), nano-communication networks (Kumar, MR 2019), new drug delivery therapies (Yu, J .; Zhang, Y .; Yan, J .; Kahkoska, AR; Gu, Z. 2018) and treatments against cancer (Huang, G .; Huang, H. 2018) and the neurological treatment of neurodegenerative diseases (John, AA; Subramanian, AP; Vellayappan, MV; Balaji, A .; Mohandas, H .; Jaganathan, SK 2015 ). However, all the benefits aside, the scientific literature is very clear regarding the health implications for the human body. It is well known that graphene (G), graphene oxide (GO) and other derivatives such as carbon nanotubes (CNT) are toxic in almost all their forms, causing mutagenesis, cell death (apoptosis), release of free radicals, lung toxicity , bilateral pneumonia, genotoxicity or DNA damage, inflammation, immunosuppression, damage to the nervous system, the circulatory, endocrine, reproductive, and urinary systems, which can cause anaphylactic death and multi-organ dysfunction, see page “Damages and toxicity of graphene oxide” and from “Damage and toxicity of carbon-graphene nanotubes“.
Second, graphene is a radio-modulable nanomaterial, capable of absorbing electromagnetic waves and multiplying radiation, acting as a nano-antenna, or a signal repeater (Chen, Y .; Fu, X .; Liu, L .; Zhang , Y .; Cao, L .; Yuan, D .; Liu, P. 2019). Exposure to electromagnetic radiation can cause exfoliation of the material in smaller particles (Lu, J .; Yeo, PSE; Gan, CK; Wu, P .; Loh, KP 2011), called graphene quantum dots or GQD (Graphene Quantum Dots), whose physical properties and particularities improve due to their even smaller scale, due to the “Quantum Hall” effect, since they act by amplifying electromagnetic signals (Massicotte, M .; Yu, V .; Whiteway, E .; Vatnik , D .; Hilke, M. 2013 | Zhang, X .; Zhou, Q .; Yuan, M .; Liao, B .; Wu, X .; Ying, M. 2020), and with it the emission distance, especially in environments such as the human body (Chopra, N .; Phipott, M .; Alomainy, A .; Abbasi, QH; Qaraqe, K .; Shubair, RM 2016). GQDs can acquire various morphologies, for example hexagonal, triangular, circular or irregular polygon (Tian, P .; Tang, L .; Teng, K.S .; Lau, S.P. 2018).
The superconducting and transducing capacity make graphene one of the most suitable materials to create wireless nanocommunication networks for the administration of nanotechnology in the human body. This approach has been intensively worked by the scientific community, after having found and analyzed the available protocols and specifications, but also the routing systems for the data packets that nano-devices and nano-nodes would generate within the body, in a system complex called CORONA, whose objective is the effective transmission of signals and data on the network, optimizing energy consumption (to the minimum possible), and also reducing failures in the transmission of data packets (Bouchedjera, IA ; Aliouat, Z .; Louail, L. 2020 | Bouchedjera, IA; Louail, L .; Aliouat, Z .; Harous, S. 2020 | Tsioliaridou, A .; Liaskos, C .; Ioannidis, S .; Pitsillides, A . 2015). In this nanocommunications network, a type of signal TS-OOK (Time-Spread On-Off Keying) is used that allows transmitting binary codes of 0 and 1, through short pulses that involve the activation and deactivation of the signal during time intervals very small of a few femtoseconds (Zhang, R .; Yang, K .; Abbasi, QH; Qaraqe, KA; Alomainy, A. 2017 | Vavouris, AK; Dervisi, FD; Papanikolaou, VK; Karagiannidis, GK 2018). Due to the complexity of nanocommunications in the human body, where the nano-nodes of the network are distributed throughout the body, in many cases in motion, due to blood flow, and in others attached to the endothelium to the arterial walls and capillaries or in the tissues of other organs, researchers have required the development of software for the simulation of such conditions, in order to verify and validate the nanocommunication protocols that were being developed (Dhoutaut, D .; Arrabal, T .; Dedu, E. 2018).
On the other hand, the nanocommunications network oriented to the human body (Balghusoon, A.O .; Mahfoudh, S. 2020), has been carefully designed in its topological aspects, conceiving specialized components in the performance of this task. For example, electromagnetic nanocommunication is made up in its most basic layer by nano-nodes that are devices (presumably made of graphene, carbon nanotubes, GQD, among other objects and materials) that have the ability to interact as nanosensors, piezo-electric actuators , and in any case as nano-antennas that propagate the signals to the rest of the nano-nodes. The nano-nodes, find in the nano-routers (also called nano-controllers) the next step in the topology. Its function is to receive the signals emitted by the nano-nodes, process them and send them to the nano-interfaces, which will emit them to the outside of the body with the necessary frequency and scope, since it must overcome the skin barrier without losing clarity in the signal, so that it can be received by a mobile device at a close enough distance (usually a few meters). That mobile device would actually be a smartphone or any other device with an Internet connection, which allows it to act as a “Gateway”. The topology also defines the possibility that the entire nano-node, nanorouter and nano-interface infrastructure is unified in a single nano-device, called pole or metamaterial defined by SDM software (Lee, SJ; Jung, C. ; Choi, K .; Kim, S. 2015). This model simplifies the topology, but increases the size of the device and the complexity of its construction, conceived in several layers of graphene. In any case, regardless of the topology, nanorouters are necessary to route and decode the signals correctly, for their sending, but also for their reception, since they can be designed for a bidirectional service, which de facto implies the ability to receive signals. of commands, orders, operations that interact with the objects of the network.
To electromagnetic nanocommunication, we must add molecular nanocommunication, addressed in the entry on carbon nanotubes and new evidence in vaccine samples. In both publications, the implications of these objects in the field of neuroscience, neuromodulation and neurostimulation are analyzed, since if they are located in the neuronal tissue (something very likely, given the ability to overcome the blood-brain barrier), they can establish connections that bridge the neuronal synapse. This means that they link neurons with different shortcuts, shorter than natural axons (Fabbro, A .; Cellot, G .; Prato, M .; Ballerini, L. 2011). Although this can be used in experimental treatments to mitigate the effects of neurodegenerative diseases, it can also be used to directly interfere with neurons, the secretion of neurotransmitters such as dopamine, the involuntary activation of certain areas of the brain, their neurostimulation or modulation, through electrical impulses, generated from carbon nanotubes (Suzuki, J .; Budiman, H .; Carr, TA; DeBlois, JH 2013 | Balasubramaniam, S .; Boyle, NT; Della-Chiesa, A .; Walsh, F .; Mardinoglu, A .; Botvich, D .; Prina-Mello, A. 2011), as a result of the reception of electromagnetic signals and pulses from the nanocommunications network (Akyildiz, IF; Jornet, JM 2010). It is not necessary to warn about what it means that an external signal, not controlled by the inoculated person, is the one that governs the segregation of neurotransmitters. Take an example to raise awareness; carbon nanotubes housed in neuronal tissue could interfere with the natural functioning of the secretion of neurotransmitters such as dopamine, which is partly responsible for cognitive processes, socialization, the reward system, desire, pleasure, conditioned learning or inhibition (Beyene, AG; Delevich, K .; Del Bonis-O’Donnell, JT; Piekarski, DJ; Lin, WC; Thomas, AW; Landry, MP 2019 | Sun, F .; Zhou, J .; Dai, B .; Qian, T .; Zeng, J .; Li, X .; Li, Y. 2020 | Sun, F .; Zeng, J .; Jing, M .; Zhou, J .; Feng, J .; Owen, SF; Li, Y. 2018 | Patriarchi, T .; Mohebi, A .; Sun, J .; Marley, A .; Liang, R .; Dong, C .; Tian, L. 2020 | Patriarchi, T .; Cho , JR; Merten, K .; Howe, MW; Marley, A .; Xiong, WH; Tian, L. 2018). This means that it could be inferred in the normal behavior patterns of people, their feelings and thoughts, and even force subliminal conditioned learning, without the individual being aware of what is happening. In addition to the properties already mentioned, carbon nanotubes not only open the doors to the wireless interaction of the human brain, they can also receive electrical signals from neurons and propagate them to nanorouters, since they also have the same properties as GQD graphene nano-antennas and quantum dots, as explained in (Demoustier, S .; Minoux, E .; Le Baillif, M .; Charles, M .; Ziaei, A. 2008 | Wang, Y .; Wu, Q .; Shi, W .; He, X .; Sun, X .; Gui, T. 2008 | Da-Costa, MR; Kibis, OV; Portnoi, ME 2009). This means that they can transmit and monitor the neuronal activity of individuals.
For the data packets emitted and received from the nanocommunications network to reach their destination, it is essential that the communication protocol implements in some way the unique identification of the nanodevices (that is, through MAC) and transmits the information to an IP address. default. In this sense, the human body becomes an IoNT server (from the Internet of NanoThings) in which the communication client / server model can be assimilated. The mechanisms, commands or types of request remain to be determined, as well as the exact frequency and type of signal that operates the wireless nanocommunications network that would be installed with each vaccine, although obviously this information must be very confidential, given the possible consequences of biohacking. (Vassiliou, V. 2011) that could happen. In fact, in the work of (Al-Turjman, F. 2020) the problems and circumstances of the security of nanocommunication networks connected to 5G (confidentiality, authentication, privacy, trust, intrusions, repudiation) are linked and additionally, it presents a summary of the operation of electromagnetic communication between nano-nodes, nano-sensors and nano-routers, using graphene antennas and transceivers for their link with data servers, in order to develop Big-data projects. It should be noted that the risks of network hacking are very similar to those that can be perpetrated in any network connected to the Internet (masquerade attack, location tracking, information traps, denial of service, nano-device hijacking, wormhole, MITM broker attack, malware, spam, sybil, spoofing, neurostimulation illusion attack), which means a potential and additional, very serious risk for people inoculated with the hardware of a nanocommunication network.
In this context, it is in which the discovery of the circuits of a nanorouter in the samples of the Pfizer vaccine is found, which is a key piece in all the research that has been carried out and that would confirm the installation of a hardware in the body of inoculated people, without their informed consent, which executes collection and interaction processes that are completely beyond its control.
Nanorouters QCA
The discovered circuit, see figure 3, corresponds to the field of quantum dot cellular automata, also known as QCA (Quantum Cellular Automata), characterized by its nanometric scale and a very low energy consumption, as an alternative for the replacement of technology based on transistors. This is how it is defined by the work of (Sardinha, L.H .; Costa, A.M .; Neto, O.P.V .; Vieira, L.F .; Vieira, M.A. 2013) from which the scheme of said circuit was obtained. The nanorouter referred to by the researchers is characterized by an ultra-low consumption factor, high processing speed (its frequency clock operates in a range of 1-2 THz), which is consistent with the power conditions and data transfer requirements. , in the context of nanocommunication networks for the human body described by (Pierobon, M .; Jornet, JM; Akkari, N .; Almasri, S .; Akyildiz, IF 2014).
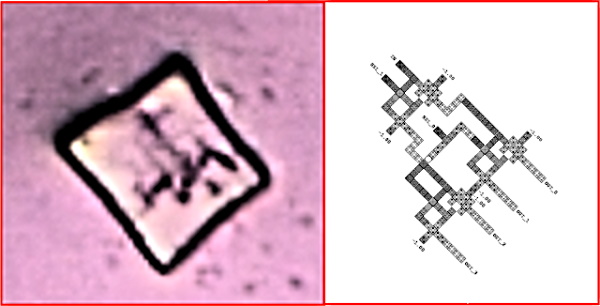
According to the explanations of the work of (Sardinha, LH; Costa, AM; Neto, OPV; Vieira, LF; Vieira, MA 2013), the concept of quantum dot and quantum dot cell is distinguished, see figure 4. The QCA cell It is made up of four quantum dots whose polarization is variable. This makes it possible to distinguish the binary code of 0 and 1 based on the positive or negative charge of the quantum dots. In the words of the authors it is explained as follows “The basic units of QCA circuits are cells made of quantum dots. A point, in this context, is just a region where an electrical charge can be located or not. A cell QCA has four quantum dots located in the corners. Each cell has two free and moving electrons that can tunnel between the quantum dots. It is assumed that tunneling to the outside of the cell is not allowed due to a high barrier potential”. Extrapolated to graphene quantum dots, known as GQDs, which were identified in blood samples (due to emitted fluorescence), a QCA cell would require four GQDs to compose, which is perfectly consistent with the description given by the researchers. This is also corroborated by (Wang, Z.F .; Liu, F. 2011) in his work entitled “Graphene quantum dots as building blocks for quantum cellular automata”, where the use of graphene to create this type of circuit is confirmed.
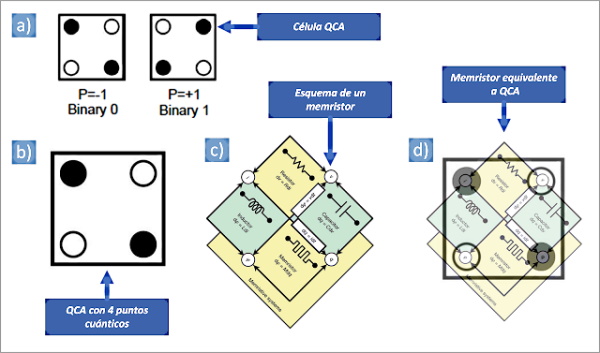
When the QCA cells are combined, cables and circuits are created, with a wide variety of shapes, schemes and applications, as can be seen in figure 5, where inverters, crossovers and logic gates are observed, also addressed by other authors such as ( Xia, Y .; Qiu, K. 2008). This gives rise to more complex structures, which allow to reproduce the electronic diagrams of the transistors, processors, transceivers, multiplexers, demultiplexers and consequently of any router.
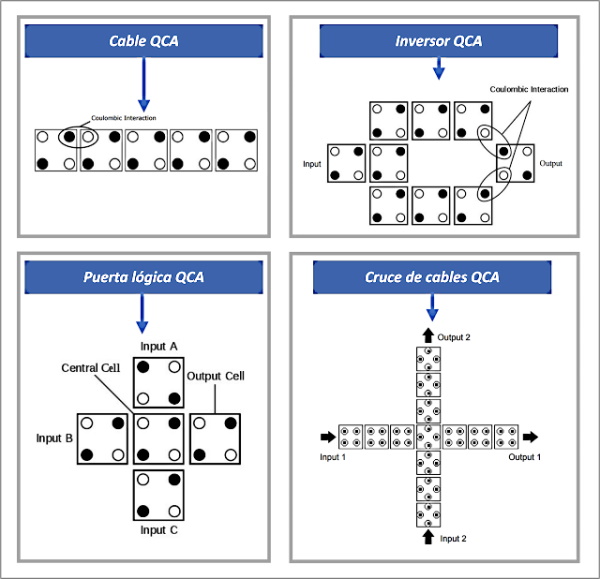
It is important to explain that QCA cell-based circuits can operate in several superimposed layers, which allows a 3D (three-dimensional) structure to create much more complex and compressed electronics, see figure 6.
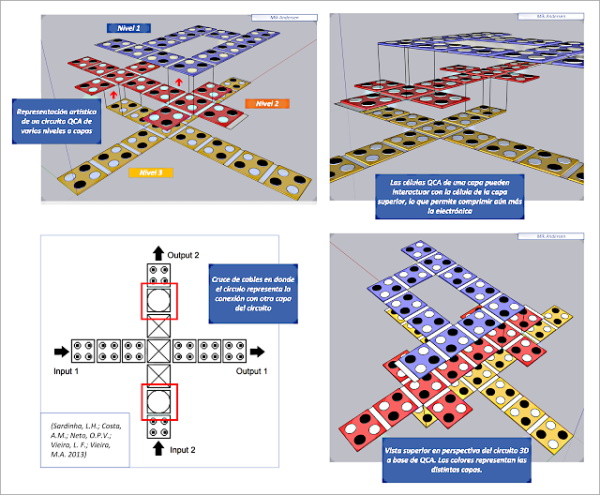
To develop a nanorouter, according to the researchers (Sardinha, LH; Costa, AM; Neto, OPV; Vieira, LF; Vieira, MA 2013), several circuit structures are needed, specifically, cable crossings (which form logic gates ), demultiplexers (demux) and parallel to serial converters, see figure X. “Demux” are electronic devices capable of receiving a signal at the input QCA (input) and sending it to one of several available output lines. (output), which allows the signal to be routed for further processing. The parallel-to-series converter is a circuit capable of taking several sets of data in an input (input), transporting them through different QCA cables and transmitting them at different instants of time through the output cables (output). This would be very, the component noticed in the vaccine samples, see figure 7.
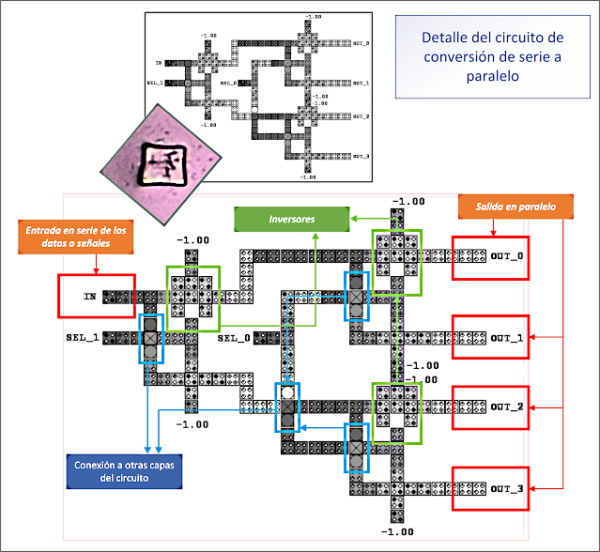
Another relevant aspect of the work of (Sardinha, LH; Costa, AM; Neto, OPV; Vieira, LF; Vieira, MA 2013) is the demonstration of the operation of the circuit, where the reception of a TS-OOK signal and its conversion to binary code, see figure 8. Once the binary code is obtained, the “demux” circuit is responsible for generating the data packets, according to the structure of the corresponding communications protocol.
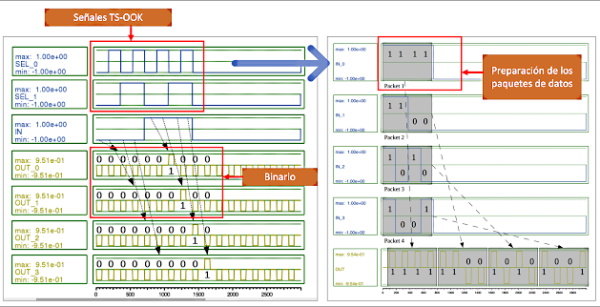
Everything explained by (Sardinha, LH; Costa, AM; Neto, OPV; Vieira, LF; Vieira, MA 2013) is also corroborated by (Das, B .; Das, JC; De, D .; Paul, AK 2017) In whose research, QCA circuit designs for demux and nanorouters are observed, with very similar schemes, to those already presented, which confirms the search for solutions for the problem of the transmission and simple processing of signals and data at the nanometric scale, at in order to make nanocommunication networks effective.
Finally, although it can already be deduced from the nature, characteristics and properties of QCA cell circuits, the concept of clock speed must be highlighted. In fact, interesting is the ability of these electronic components to operate almost autonomously, without the need for a dedicated processor. This is because the QCA cell cables can measure the transfer time of the signals between the different cells, in what is called “clock zones”, see figure 9 and the following investigations (Sadeghi, M .; Navi, K .; Dolatshahi, M. 2020 | Laajimi, R .; Niu, M. 2018 | Reis, DA; Torres, FS 2016 | Mohammadyan, S .; Angizi, S .; Navi, K. (2015). This effect allows the transmission of signals through the circuit, but it also allows creating a clock frequency, which is its own process speed. If this concept is joined, the use of superconducting materials such as graphene and more specifically graphene quantum dots Then very high processing speeds can be achieved.
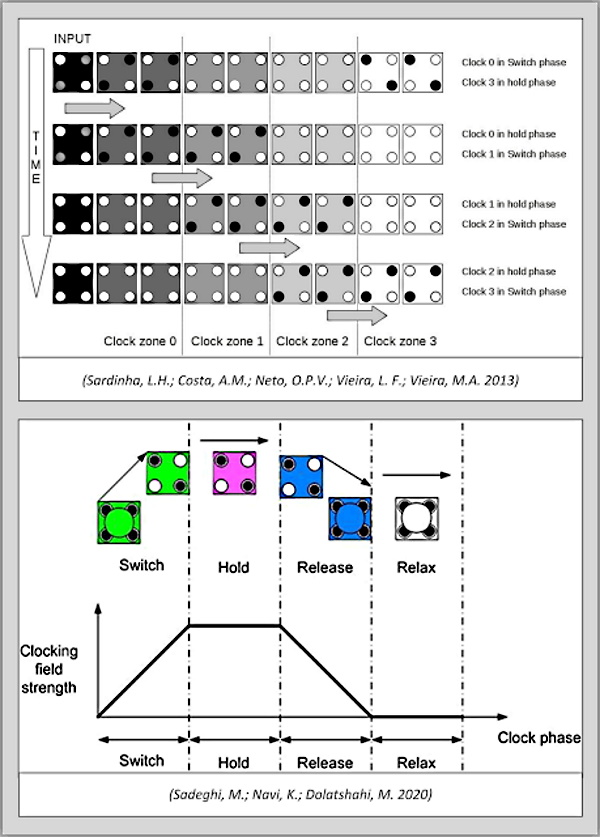
Circuit self-assembly
Although it seems impossible, the self-assembly of circuits is a possibility to consider in the hypothesis that has been explained. According to (Huang, J .; Momenzadeh, M .; Lombardi, F. 2007) “Recent developments in QCA manufacturing (involving molecular implementations) have substantially changed the nature of processing. At very small feature sizes, it is anticipated self-assembly or large-scale cell deposition on isolated substrates will be used. In these implementations, QCA cells (each composed of two dipoles) are deposited in parallel V-shaped tracks. QCA cells are arranged in a dense pattern and the computation occurs between adjacent cells. These fabrication techniques are well suited for molecular implementation. ” However, there are also other methods, such as DNA nanopatterns (Hu, W .; Sarveswaran, K .; Lieberman, M .; Bernstein, GH 2005), with which a template is created for the alignment of the quantum dots of graphene, forming the QCA cells, thereby generating the aforementioned circuitry, see figure 10.
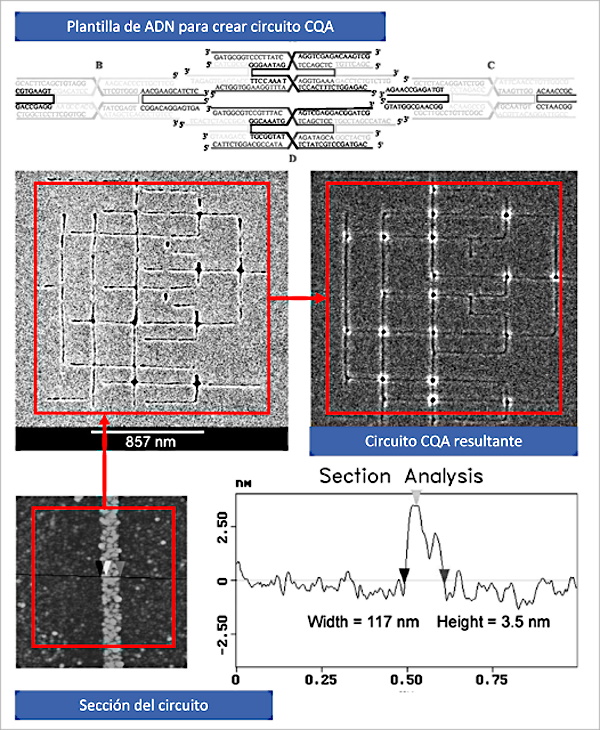
According to (Hu, W .; Sarveswaran, K .; Lieberman, M .; Bernstein, GH 2005) “Four-tile DNA rafts have been successfully synthesized and characterized by the gel electrophoresis method in our previous work” according to the work of (Sarveswaran, K. 2004). This fits with the very possible existence of a gel / hydrogel in the vaccine composition, after the doctor’s micro-Raman analysis (Campra, P. 2021) in which peaks with values close to 1450 were obtained, which could correspond to PVA, PQT-12, polyolefin, polyacrylamide or polypyrrole, all of them components recognized in the scientific literature as gels and derivatives. On the other hand, it explicitly alludes to the electrophoresis method, or what is the same, the electrical polarization process that causes teslaphoresis, on carbon nanotubes, graphene, quantum dots and other semiconductors, as described (Bornhoeft, LR; Castillo, AC; Smalley, PR; Kittrell, C .; James, DK; Brinson, BE; Cherukuri, P. 2016) in his research. This would confirm that teslaphoresis plays a fundamental role in the composition of circuits, along with DNA patterns. If this is confirmed, it would mean that the circuits could self-assemble in the presence of electric fields or even the reception of electromagnetic waves (microwave EM). The study by (Pillers, M .; Goss, V .; Lieberman, M. 2014) also confirms the construction of nanostructures and CQA using in this case graphene, graphene oxide (GO), electrophoresis and gel, causing controlled deposition in the areas indicated by the DNA pattern, reproducing results similar to those presented in the study by Hu and Sarveswaran, thus making it possible to create the electronic circuits already mentioned, see figure 11.
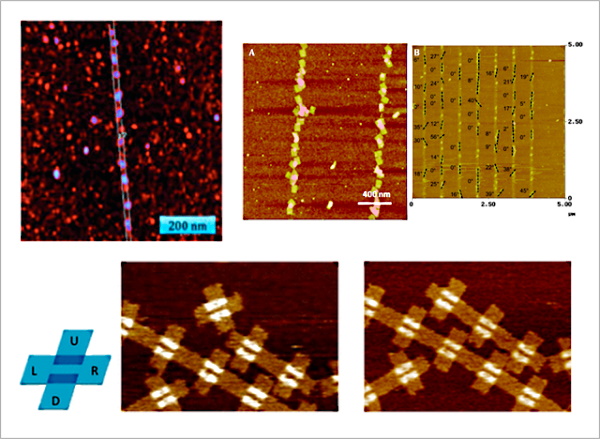
Plasmonic nano-emitters
Another issue that requires an explanation in the discovery of the circuit of a nanorouter, in the vaccine sample, is its location in what appears to be a quadrangular crystal. Although it could be thought that it is a randomly generated form, the bibliographic review reveals and justifies this type of form that serves as a framework for this type of circuit. In reality it is a “plasmonic nano-emitter”, in other words, it would correspond to a cubic-shaped nano-antenna (single crystal) of variable size on the nano-micrometric scale, which can emit, receive or repeat signals. This is possible through the plasmon activation property of its surface (that of the nanoemitter cube) that is locally excited to generate an oscillatory signal, as explained (Ge, D .; Marguet, S .; Issa, A .; Jradi, S .; Nguyen, TH; Nahra, M .; Bachelot, R. 2020), see figure 12. This agrees with the type of TS-OOK signals, which are transmitted through the intra-body nanocommunication network, being a requirement indispensable for a nano-router, to have a method to capture them. In other words, the crystalline cube acts as a transceiver for the nanorouter, due to its special properties, derived from the physics of the plasmon. This is corroborated when the scientific literature on electromagnetic nano-networks for the human body is consulted (Balghusoon, AO; Mahfoudh, S. 2020), the MAC protocols applied to the case (Jornet, JM; Pujol, JC; Pareta, JS 2012 ), the methods for the debugging of errors in the signals (Jornet, JM; Pierobon, M .; Akyildiz, IF 2008), or the modulation of pulses in femtoseconds in the terahertz band for nano-communication networks (Jornet, JM; Akyildiz, IF 2014), the parameterization of nano-networks for their perpetual operation (Yao, XW; Wang, WL; Yang, SH 2015), the performance in the modulation of wireless signals for nano-networks (Zarepour, E .; Hassan, M .; Chou, CT; Bayat, S. 2015). In all cases, nano-transceivers are essential to be able to receive or emit a TS-OOK signal.
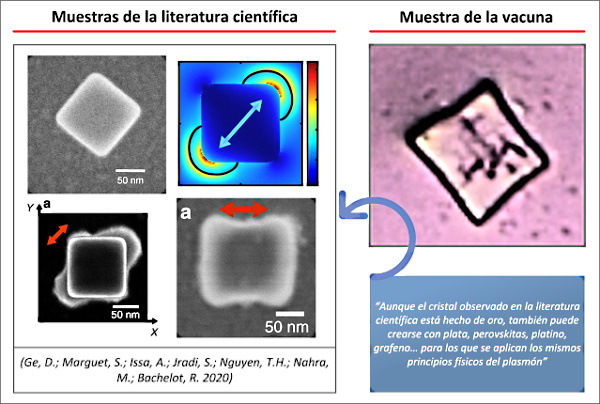
Plasmonic nanoemitters can acquire a cube shape, which would be the case observed in the vaccine sample, but also spherical and discoidal shape, being able to be self-assembled, to form larger nano-microstructures (Devaraj, V .; Lee, JM; Kim , YJ; Jeong, H .; Oh, JW 2021). Among the materials with which this plasmonic nano-emitter could be produced are gold, silver, perovskites and graphene, see (Oh, DK; Jeong, H .; Kim, J .; Kim, Y .; Kim, I .; Ok, JG; Rho, J. 2021 | Hamedi, HR; Paspalakis, E .; Yannopapas, V. 2021 | Gritsienko, AV; Kurochkin, NS; Lega, PV; Orlov, AP; Ilin, AS; Eliseev, SP; Vitukhnovsky , AG 2021 | Pierini, S. 2021), although it is likely that many others can be used.
CAM and TCAM memory for MAC and IP
If the presence of nanorouters in vaccines is considered, the hypothesis of the existence of one or more MAC addresses (fixed or dynamic) could be confirmed, which could be emitted from vaccinated people or through some other intermediary device (for example a mobile phone ). This approach is in line with what has already been explained and evidenced in this publication, but also according to scientific publications on nano-communication networks for the human body. According to (Abadal, S .; Liaskos, C .; Tsioliaridou, A .; Ioannidis, S .; Pitsillides, A .; Solé-Pareta, J .; Cabellos-Aparicio, A. 2017) these MAC addresses allow the nano- network can transmit and receive data, because the individual has a unique identifier that allows him to access the medium, this is the Internet. In this way, the nano-router can receive the signals corresponding to the data from the nano-sensors and nano-nodes of the nano-network to transmit them to the outside of the body, as long as there is a mobile device in the vicinity, which serves gateway to the Internet. Therefore, the hypothesis that MAC addresses of vaccinated people can be observed (through bluetooth signal tracking applications), when there is some type of interaction with the mobile media that act as a link. This does not mean that there is permanent communication, due to the need to save and optimize energy consumption (Mohrehkesh, S .; Weigle, MC 2014 | Mohrehkesh, S .; Weigle, MC; Das, SK 2015), which could explain intermittence in communications, periods of connection and inactivity.
The novelty in the field of MAC addresses, which comes together with the QCA circuits, with which nanorouters can be developed, is that memory circuits can also be created. The same researchers (Sardinha, LH; Silva, DS; Vieira, MA; Vieira, LF; Neto, OPV 2015) developed a new type of CAM memory that “unlike random access memory (RAM), which returns data which are stored at the given address. CAM, however, receives the data as input and returns where the data can be found. CAM is useful for many applications that need fast searches, such as Hought transforms, Huffman encoding, Lempel-compression. Ziv and network switches to map MAC addresses to IP addresses and vice versa. CAM is most useful for creating tables that look for exact matches, such as MAC address tables. ” This statement was extracted and copied verbatim to highlight that QCA circuits are the answer to the storage and management of MAC addresses for data transmission in nano-networks, which would confirm that vaccines are, among other things, a means of installing hardware for the control, modulation and monitoring of people.
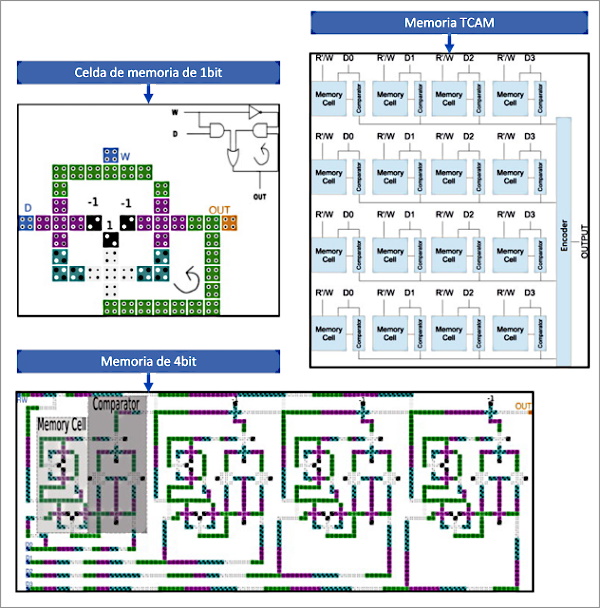
Additionally, (Sardinha, LH; Silva, DS; Vieira, MA; Vieira, LF; Neto, OPV 2015) also developed the TCAM memory, which is a special type of CAM memory that would be useful to “create tables to search for longer matches such as IP routing tables organized by IP prefixes. To reduce latency and make communication faster, routers use TCAM. ” This statement clearly affects its use in nano-routers in order to be able to transmit the data obtained in the nano-network to a specific recipient server accessible on the Internet. In other words, the data collected by the nano-network should be stored / registered in a database, of which the recipient of the vaccine would not have knowledge of its existence, of which it was not informed, and in the It is unknown what information is used.
Bibliography
- Akyildiz, I.F.; Jornet, J.M. (2010). Redes de nanosensores inalámbricos electromagnéticos = Electromagnetic wireless nanosensor networks. Nano Communication Networks, 1(1), pp. 3-19. https://doi.org/10.1016/j.nancom.2010.04.001
- Al-Turjman, F. (2020). Inteligencia y seguridad en un gran IoNT orientado a 5G: descripción general = Intelligence and security in big 5G-oriented IoNT: An overview. Future Generation Computer Systems, 102, pp. 357-368. https://doi.org/10.1016/j.future.2019.08.009
- Balasubramaniam, S.; Boyle, N.T.; Della-Chiesa, A.; Walsh, F.; Mardinoglu, A.; Botvich, D.; Prina-Mello, A. (2011). Desarrollo de redes neuronales artificiales para la comunicación molecular = Development of artificial neuronal networks for molecular communication. Nano Communication Networks, 2(2-3), pp. 150-160. https://doi.org/10.1016/j.nancom.2011.05.004
- Balghusoon, A.O.; Mahfoudh, S. (2020). Protocolos de enrutamiento para redes inalámbricas de nanosensores e Internet de las nano cosas: una revisión completa = Routing Protocols for Wireless Nanosensor Networks and Internet of Nano Things: A Comprehensive Survey. IEEE Access, 8, pp. 200724-200748. https://doi.org/10.1109/ACCESS.2020.3035646
- Beyene, A.G.; Delevich, K.; Del Bonis-O’Donnell, J.T.; Piekarski, D.J.; Lin, W.C.; Thomas, A.W.; Landry, M.P. (2019). Obtención de imágenes de la liberación de dopamina estriatal utilizando un nanosensor de catecolamina fluorescente de infrarrojo cercano no codificado genéticamente = Imaging striatal dopamine release using a nongenetically encoded near infrared fluorescent catecholamine nanosensor. Science advances, 5(7), eaaw3108. https://doi.org/10.1126/sciadv.aaw3108
- Bornhoeft, L.R.; Castillo, A.C.; Smalley, P.R.; Kittrell, C.; James, D.K.; Brinson, B.E.; Cherukuri, P. (2016). Teslaforesis de nanotubos de carbono = Teslaphoresis of carbon nanotubes. ACS nano, 10(4), pp. 4873-4881. https://doi.org/10.1021/acsnano.6b02313
- Bouchedjera, I.A.; Aliouat, Z.; Louail, L. (2020). EECORONA: Sistema de Coordinación y Enrutamiento de Eficiencia Energética para Nanoredes = EECORONA: Energy Efficiency Coordinate and Routing System for Nanonetworks. En: International Symposium on Modelling and Implementation of Complex Systems. Cham. pp. 18-32. https://doi.org/10.1007/978-3-030-58861-8_2
- Bouchedjera, I.A.; Louail, L.; Aliouat, Z.; Harous, S. (2020). DCCORONA: Sistema distribuido de enrutamiento y coordenadas basado en clústeres para nanorredes = DCCORONA: Distributed Cluster-based Coordinate and Routing System for Nanonetworks. En: 2020 11th IEEE Annual Ubiquitous Computing, Electronics & Mobile Communication Conference (UEMCON). IEEE. pp. 0939-0945. https://doi.org/10.1109/UEMCON51285.2020.9298084
- Campra, P. (2021a). Observaciones de posible microbiótica en vacunas COVID RNAm Version 1. [Observations of possible microbiotics in COVID mRNA vaccines] http://dx.doi.org/10.13140/RG.2.2.13875.55840
- Campra, P. (2021b). Detección de grafeno en vacunas COVID19 por espectroscopía Micro-RAMAN. https://www.researchgate.net/publication/355684360_Deteccion_de_grafeno_en_vacunas_COVID19_por_espectroscopia_Micro-RAMAN
- Campra, P. (2021c). MICROSTRUCTURES IN COVID VACCINES: ¿inorganic crystals or Wireless Nanosensors Network?https://www.researchgate.net/publication/356507702_MICROSTRUCTURES_IN_COVID_VACCINES_inorganic_crystals_or_Wireless_Nanosensors_Network
- Chopra, N.; Phipott, M.; Alomainy, A.; Abbasi, Q.H.; Qaraqe, K.; Shubair, R.M. (2016). THz time domain characterization of human skin tissue for nano-electromagnetic communication. En: 2016 16th Mediterranean Microwave Symposium (MMS) (pp. 1-3). IEEE. https://doi.org/10.1109/MMS.2016.7803787
- Da-Costa, M.R.; Kibis, O.V.; Portnoi, M.E. (2009). Nanotubos de carbono como base para emisores y detectores de terahercios = Carbon nanotubes as a basis for terahertz emitters and detectors. Microelectronics Journal, 40(4-5), pp. 776-778. https://doi.org/10.1016/j.mejo.2008.11.016
- Das, B.; Das, J.C.; De, D.; Paul, A.K. (2017). Diseño de nanoenrutador para nanocomunicación en autómatas celulares cuánticos de una sola capa =Nano-Router Design for Nano-Communication in Single Layer Quantum Cellular Automata. En: International Conference on Computational Intelligence, Communications, and Business Analytics (pp. 121-133). Springer, Singapore. https://doi.org/10.1007/978-981-10-6430-2_11
- Demoustier, S.; Minoux, E.; Le Baillif, M.; Charles, M.; Ziaei, A. (2008). Revisión de dos aplicaciones de microondas de nanotubos de carbono: nano antenas y nanointerruptores = Revue d’applications des nanotubes de carbone aux micro-ondes: nano-antennes et nano-commutateurs = Review of two microwave applications of carbon nanotubes: nano-antennas and nano-switches. Comptes Rendus Physique, 9(1), pp. 53-66. https://doi.org/10.1016/j.crhy.2008.01.001
- Devaraj, V.; Lee, J.M.; Kim, Y.J.; Jeong, H.; Oh, J.W. (2021). [Pre-print]. Diseño de nanoestructuras plasmónicas autoensambladas eficientes a partir de nanopartículas de forma esférica = Designing an Efficient Self-Assembled Plasmonic Nanostructures from Spherical Shaped Nanoparticles. International Journal of Molecular Science. https://www.preprints.org/manuscript/202109.0225/v1
- Dhoutaut, D.; Arrabal, T.; Dedu, E. (2018). Bit Simulator, un simulador de nanorredes electromagnéticas = Bit simulator, an electromagnetic nanonetworks simulator. En: Proceedings of the 5th ACM International Conference on Nanoscale Computing and Communication (pp. 1-6). https://doi.org/10.1145/3233188.3233205
- Fabbro, A.; Cellot, G.; Prato, M.; Ballerini, L. (2011). Interconexión de neuronas con nanotubos de carbono: (re) ingeniería de la señalización neuronal = Interfacing neurons with carbon nanotubes: (re) engineering neuronal signaling. Progress in brain research, 194, pp. 241-252. https://doi.org/10.1016/B978-0-444-53815-4.00003-0
- Ferjani, H.; Touati, H. (2019). Comunicación de datos en nano-redes electromagnéticas para aplicaciones sanitarias = Data communication in electromagnetic nano-networks for healthcare applications. En: International Conference on Mobile, Secure, and Programmable Networking (pp. 140-152). Springer, Cham. https://doi.org/10.1007/978-3-030-22885-9_13
- Ge, D.; Marguet, S.; Issa, A.; Jradi, S.; Nguyen, T.H.; Nahra, M.; Bachelot, R. (2020). Nanoemisores plasmónicos híbridos con posicionamiento controlado de un único emisor cuántico en el campo de excitación local = Hybrid plasmonic nano-emitters with controlled single quantum emitter positioning on the local excitation field. Nature communications, 11(1), pp1-11. https://doi.org/10.1038/s41467-020-17248-8
- Gritsienko, A.V.; Kurochkin, N.S.; Lega, P.V.; Orlov, A.P.; Ilin, A.S.; Eliseev, S.P.; Vitukhnovsky, A.G. (2021). Propiedades ópticas de la nueva nanoantena híbrida en cavidad submicrónica = Optical properties of new hybrid nanoantenna in submicron cavity. En: Journal of Physics: Conference Series (Vol. 2015, No. 1, p. 012052). IOP Publishing. https://doi.org/10.1088/1742-6596/2015/1/012052
- Hamedi, H.R.; Paspalakis, E.; Yannopapas, V. (2021). Control efectivo de la biestabilidad óptica de un emisor cuántico de tres niveles cerca de una metauperficie plasmónica nanoestructurada = Effective Control of the Optical Bistability of a Three-Level Quantum Emitter near a Nanostructured Plasmonic Metasurface. En: Photonics (Vol. 8, No. 7, p. 285). Multidisciplinary Digital Publishing Institute. https://doi.org/10.3390/photonics8070285
- Hu, W.; Sarveswaran, K.; Lieberman, M.; Bernstein, G.H. (2005). Litografía por haz de electrones de alta resolución y nanopatrones de ADN para QCA molecular. IEEE Transactions on Nanotechnology, 4(3), pp. 312-316. https://doi.org/10.1109/TNANO.2005.847034
- Huang, G.; Huang, H. (2018). Aplicación de dextrano como portadores de fármacos a nanoescala = Application of dextran as nanoscale drug carriers. Nanomedicine, 13(24), pp. 3149-3158. https://doi.org/10.2217/nnm-2018-0331
- Huang, J.; Momenzadeh, M.; Lombardi, F. (2007). Diseño de circuitos secuenciales por autómatas celulares de puntos cuánticos = Design of sequential circuits by quantum-dot cellular automata. Microelectronics Journal, 38(4-5), pp. 525-537. https://doi.org/10.1016/j.mejo.2007.03.013
- Huang, J.; Xie, G.; Kuang, R.; Deng, F.; Zhang, Y. (2021). Circuito de código Hamming basado en QCA para redes de nanocomunicación = QCA-based Hamming code circuit for nano communication network. Microprocessors and Microsystems, 84, 104237. https://doi.org/10.1016/j.micpro.2021.104237
- John, A.A.; Subramanian, A.P.; Vellayappan, M.V.; Balaji, A.; Mohandas, H.; Jaganathan, S.K. (2015). Los nanotubos de carbono y el grafeno como candidatos emergentes en la neurorregeneración y la administración de neurofármacos = Carbon nanotubes and graphene as emerging candidates in neuroregeneration and neurodrug delivery. International journal of nanomedicine, 10, 4267. https://dx.doi.org/10.2147%2FIJN.S83777
- Jornet, J.M.; Akyildiz, I.F. (2014). Modulación basada en pulsos de femtosegundo largo para comunicación en banda de terahercios en nanorredes = Femtosecond-long pulse-based modulation for terahertz band communication in nanonetworks. IEEE Transactions on Communications, 62(5), pp. 1742-1754. https://doi.org/10.1109/TCOMM.2014.033014.130403
- Jornet, J.M.; Pierobon, M.; Akyildiz, I.F. (2008). Redes de nanocomunicación = Nano Communication Networks. Networks (Elsevier), 52, pp. 2260-2279. http://dx.doi.org/10.1016/j.nancom.2014.04.001
- Jornet, J.M.; Pujol, J.C.; Pareta, J.S. (2012). PHLAME: un protocolo MAC consciente de la capa física para nanorredes electromagnéticas en la banda de terahercios = Phlame: A physical layer aware mac protocol for electromagnetic nanonetworks in the terahertz band. Nano Communication Networks, 3(1), pp. 74-81. https://doi.org/10.1016/j.nancom.2012.01.006
- Kumar, M.R. (2019). Una nano-antena compacta basada en grafeno para la comunicación en nano-redes = A Compact Graphene Based Nano-Antenna for Communication in Nano-Network. Journal of the Institute of Electronics and Computer, 1(1), pp. 17-27. https://doi.org/10.33969/JIEC.2019.11003
- Laajimi, R.; Niu, M. (2018). Nanoarquitectura de autómatas celulares de puntos cuánticos (QCA) que utilizan áreas pequeñas para circuitos digitales = Nanoarchitecture of Quantum-Dot Cellular Automata (QCA) Using Small Area for Digital Circuits. Advanced Electronics Circuits–Principles, Architectures and Applications on Emerging Technologies, pp. 67-84. https://www.intechopen.com/chapters/58619
- Lee, S.J.; Jung, C.; Choi, K.; Kim, S. (2015). Diseño de redes inalámbricas de nanosensores para aplicaciones intracuerpo = Design of wireless nanosensor networks for intrabody application. International Journal of Distributed Sensor Networks, 11(7), 176761. https://doi.org/10.1155/2015/176761
- Lu, J.; Yeo, P.S.E.; Gan, C.K.; Wu, P.; Loh, K.P. (2011). Transformando moléculas C60 en puntos cuánticos de grafeno = Transforming C60 molecules into graphene quantum dots. Nature nanotechnology, 6(4), pp. 247-252. https://doi.org/10.1038/nnano.2011.30
- Massicotte, M.; Yu, V.; Whiteway, E.; Vatnik, D.; Hilke, M. (2013). Efecto Hall cuántico en el grafeno fractal: crecimiento y propiedades de los grafloconos = Quantum Hall effect in fractal graphene: growth and properties of graphlocons. Nanotechnology, 24(32), 325601. https://doi.org/10.1088/0957-4484/24/32/325601
- Mitragotri, S.; Anderson, D.G.; Chen, X.; Chow, E.K.; Ho, D.; Kabanov, A.V.; Xu, C. (2015). Acelerando la traducción de nanomateriales en biomedicina = Accelerating the translation of nanomaterials in biomedicine. ACS nano, 9(7), pp. 6644-6654. https://doi.org/10.1021/acsnano.5b03569
- Mohammadyan, S.; Angizi, S.; Navi, K. (2015). Nueva celda sumadora completa QCA de una sola capa basada en el modelo de retroalimentación = New fully single layer QCA full-adder cell based on feedback model. International Journal of High Performance Systems Architecture, 5(4), pp. 202-208. https://doi.org/10.1504/IJHPSA.2015.072847
- Mohrehkesh, S.; Weigle, M.C. (2014). Optimización del consumo de energía en nanorredes de banda de terahercios = Optimizing energy consumption in terahertz band nanonetworks. IEEE Journal on Selected Areas in Communications, 32(12), pp. 2432-2441. https://doi.org/10.1109/JSAC.2014.2367668
- Mohrehkesh, S.; Weigle, M.C.; Das, S.K. (2015). DRIH-MAC: una MAC de recolección iniciada por un receptor distribuido para nanorredes = DRIH-MAC: A distributed receiver-initiated harvesting-aware MAC for nanonetworks. IEEE Transactions on Molecular, Biological and Multi-Scale Communications, 1(1), pp. 97-110. https://doi.org/10.1109/TMBMC.2015.2465519
- Oh, D.K.; Jeong, H.; Kim, J.; Kim, Y.; Kim, I.; Ok, J.G.; Rho, J. (2021). Enfoques de nanofabricación de arriba hacia abajo hacia estructuras de escala nanométrica de un solo dígito = Top-down nanofabrication approaches toward single-digit-nanometer scale structures. Journal of Mechanical Science and Technology, pp. 1-23. https://doi.org/10.1007/s12206-021-0243-7
- Patriarchi, T.; Cho, J.R.; Merten, K.; Howe, M.W.; Marley, A.; Xiong, W.H.; Tian, L. (2018). Imágenes neuronales ultrarrápidas de la dinámica de la dopamina con sensores codificados genéticamente diseñados = Ultrafast neuronal imaging of dopamine dynamics with designed genetically encoded sensors. Science, 360(6396). https://doi.org/10.1126/science.aat4422
- Patriarchi, T.; Mohebi, A.; Sun, J.; Marley, A.; Liang, R.; Dong, C.; Tian, L. (2020). Una paleta ampliada de sensores de dopamina para imágenes multiplex in vivo = An expanded palette of dopamine sensors for multiplex imaging in vivo. Nature methods, 17(11), pp. 1147-1155. https://doi.org/10.1038/s41592-020-0936-3
- Pierini, S. (2021). [Preprint]. Estudio experimental de nanocristales de perovskita como fuentes de fotón único para fotónica cuántica integrada = Experimental study of perovskite nanocrystals as single photon sources for integrated quantum photonics. Arxiv. https://arxiv.org/pdf/2105.14245.pdf
- Pierobon, M.; Jornet, J.M.; Akkari, N.; Almasri, S.; Akyildiz, I.F. (2014). Un marco de enrutamiento para redes de nanosensores inalámbricos de recolección de energía en la banda de terahercios = A routing framework for energy harvesting wireless nanosensor networks in the Terahertz Band. Wireless networks, 20(5), pp. 1169-1183. https://doi.org/10.1007/s11276-013-0665-y
- Pillers, M.; Goss, V.; Lieberman, M. (2014). Litografía por haz de electrones y despegue molecular para la fijación dirigida de nanoestructuras de ADN sobre silicio: de arriba hacia abajo se encuentra con de abajo hacia arriba = Electron-beam lithography and molecular liftoff for directed attachment of DNA nanostructures on silicon: Top-down meets bottom-up. Accounts of chemical research, 47(6), pp. 1759-1767. https://doi.org/10.1021/ar500001e
- Reis, D.A.; Torres, F.S. (2016). Un simulador de defectos para el análisis de robustez de circuitos QCA = A Defects Simulator for Robustness Analysis of QCA Circuits. Journal of Integrated Circuits and Systems, 11(2), pp. 86-96. https://doi.org/10.29292/jics.v11i2.433
- Sadeghi, M.; Navi, K.; Dolatshahi, M. (2020). Nuevos diseños eficientes de sumador completo y restador completo en autómatas celulares cuánticos = Novel efficient full adder and full subtractor designs in quantum cellular automata. The Journal of Supercomputing, 76(3), pp. 2191-2205. https://doi.org/10.1007/s11227-019-03073-4
- Sardinha, L.H.; Costa, A.M.; Neto, O.P.V.; Vieira, L.F.; Vieira, M.A. (2013). NanoRouter: un diseño de autómatas celulares de puntos cuánticos = Nanorouter: a quantum-dot cellular automata design. IEEE Journal on Selected Areas in Communications, 31(12), pp. 825-834. https://doi.org/10.1109/JSAC.2013.SUP2.12130015
- Sardinha, L.H.; Silva, D.S.; Vieira, M.A.; Vieira, L.F.; Neto, O.P.V. (2015). TCAM / CAM-QCA: Memoria direccionable de contenido (ternario) utilizando autómatas celulares de punto cuántico = Tcam/cam-qca:(ternary) content addressable memory using quantum-dot cellular automata. Microelectronics Journal, 46(7), pp. 563-571. https://doi.org/10.1016/j.mejo.2015.03.020
- Sarveswaran, K. (2004). [Documento reservado]. Self-assembly and lithographic patterning of DNA rafts. DARPA Conf. Foundations of Nanoscience: Self-Assembled Architectures and Devices, Snowbird, UT. [Enlace no disponible]
- Strukov, D.B.; Snider, G.S.; Stewart, D.R.; Williams, R.S. (2009). El memristor perdido, encontrado The missing memristor found. Nature, 459(7250), 1154. https://doi.org/10.1038/nature06932
- Sun, F.; Zhou, J.; Dai, B.; Qian, T.; Zeng, J.; Li, X.; Li, Y. (2020). Sensores GRAB de próxima generación para monitorear la actividad dopaminérgica in vivo = Next-generation GRAB sensors for monitoring dopaminergic activity in vivo. Nature methods, 17(11), pp. 1156-1166. https://doi.org/10.1038/s41592-020-00981-9
- Suzuki, J.; Budiman, H.; Carr, T.A.; DeBlois, J.H. (2013). Un marco de simulación para la comunicación molecular basada en neuronas = A simulation framework for neuron-based molecular communication. Procedia Computer Science, 24, pp. 103-113. https://doi.org/10.1016/j.procs.2013.10.032
- Tsioliaridou, A.; Liaskos, C.; Ioannidis, S.; Pitsillides, A. (2015). CORONA: un sistema de coordenadas y enrutamiento para nanorredes = CORONA: A Coordinate and Routing system for Nanonetworks. En: Proceedings of the second annual international conference on nanoscale computing and communication. pp. 1-6. https://doi.org/10.1145/2800795.2800809 | https://sci-hub.mksa.top/10.1145/2800795.2800809
- Vassiliou, V. (2011). Problemas de seguridad en redes de comunicación a nanoescala = Security issues in nanoscale communication networks. 3rd NaNoNetworking Summit, pp. 1-53. http://www.n3cat.upc.edu/n3summit2011/presentations/Security_Issues_in_Nanoscale_Communication_Networks.pdf
- Vavouris, A.K.; Dervisi, F.D.; Papanikolaou, V.K.; Karagiannidis, G.K. (2018). Un esquema de modulación energéticamente eficiente para nanocomunicaciones centradas en el cuerpo en la banda THz = An energy efficient modulation scheme for body-centric nano-communications in the THz band. En: 2018 7th International Conference on Modern Circuits and Systems Technologies (MOCAST) (pp. 1-4). IEEE. https://doi.org/10.1109/MOCAST.2018.8376563
- Wang, Z.F.; Liu, F. (2011). Puntos de cuánticos de grafeno como bloques de construcción para autómatas celulares cuánticos = Nanopatterned graphene quantum dots as building blocks for quantum cellular automata. Nanoscale, 3(10), pp. 4201-4205. https://doi.org/10.1039/C1NR10489F
- Wang, W.L.; Wang, C.C.; Yao, X.W. (2019). Protocolo MAC basado en autoasignación de ranuras para nano-redes de recolección de energía = Slot self-allocation based mac protocol for energy harvesting nano-networks. Sensors, 19(21), 4646. https://doi.org/10.3390/s19214646
- Wang, Y.; Wu, Q.; Shi, W.; He, X.; Sun, X.; Gui, T. (2008). Propiedades de radiación de la antena de nanotubos de carbono en el rango de terahercios / infrarrojos = Radiation properties of carbon nanotubes antenna at terahertz/infrared range. International Journal of Infrared and Millimeter Waves, 29(1), pp. 35-42. https://doi.org/10.1007/s10762-007-9306-9
- Xia, Y.; Qiu, K. (2008). Diseño y aplicación de puerta lógica universal basada en autómatas celulares de puntos cuánticos = Design and application of universal logic gate based on quantum-dot cellular automata. En: 2008 11th IEEE International Conference on Communication Technology (pp. 335-338). IEEE. https://doi.org/10.1109/ICCT.2008.4716260 | https://sci-hub.mksa.top/10.1109/ICCT.2008.4716260
- Yao, X.W.; Wang, W.L.; Yang, S.H. (2015). Optimización de parámetros conjuntos para redes perpetuas y capacidad máxima de red = Joint parameter optimization for perpetual nanonetworks and maximum network capacity. IEEE Transactions on Molecular, Biological and Multi-Scale Communications, 1(4), pp. 321-330. https://doi.org/10.1109/TMBMC.2016.2564967
- Yu, J.; Zhang, Y.; Yan, J.; Kahkoska, A.R.; Gu, Z. (2018). Advances in bioresponsive closed-loop drug delivery systems. International journal of pharmaceutics, 544(2), pp. 350-357. https://doi.org/10.1016/j.ijpharm.2017.11.064
- Zarepour, E.; Hassan, M.; Chou, C.T.; Bayat, S. (2015). Análisis de rendimiento de esquemas de modulación sin portadora para redes inalámbricas de nanosensores = Performance analysis of carrier-less modulation schemes for wireless nanosensor networks. En: 2015 IEEE 15th International Conference on Nanotechnology (IEEE-NANO) (pp. 45-50). IEEE. https://doi.org/10.1109/NANO.2015.7388653
- Zhang, R.; Yang, K.; Abbasi, Q.H.; Qaraqe, K.A.; Alomainy, A. (2017). Caracterización analítica de la nanored In-Vivo de Terahercios en presencia de interferencia basada en el esquema de comunicación TS-OOK = Analytical characterisation of the terahertz in-vivo nano-network in the presence of interference based on TS-OOK communication scheme. IEEE Access, 5, pp. 10172-10181. https://doi.org/10.1109/ACCESS.2017.2713459
Football: Where Money Trumps “The Virus”
Football: Where Money Trumps “The Virus”
by Jon Rappoport, No More Fake News
November 26, 2021
I wouldn’t ordinarily write about football; but the sport illustrates how vaunted Public Health Officials look the other way, when they’re supposed to. They have as much integrity as thieves in the night. Only idiots would pay attention to anything they say or claim or demand.
According to the government narrative, fully vaccinated people still spread “the virus.” That’s why, in many places, they’re supposed to wear masks.
Recently, Green Bay quarterback Aaron Rogers was mercilessly attacked for claiming he was vaccinated when he wasn’t; and for freely mingling with opposing team players after games and appearing before reporters without a mask.
Of course, no one mentioned that, DURING THE GAME, all players grab, breathe on, spit on, bleed on, pile on, scratch and claw one another. That’s permitted because it’s the source of MONEY. Lots of money.
And, in both college and pro games across the country, stadiums fill up with anywhere from 40,000 to 100,000 screaming, coughing, spitting, drinking, cursing fans, who sit cheek to jowl with one another. But that’s all right, too, because it’s MONEY.
This situation is pretty much like the US southern border, where thousands (millions?) of immigrants come into the US “with the virus.”
But that’s all right, too, because, well, it’s policy, one aspect of which is welcoming drugs into America. Drugs are MONEY. Big money.
Sports “journalists” don’t discuss what I’m writing about in this article. They’re not supposed to. It might turn off the audience. And yes, again, their audience is MONEY.
“Hey, Jim. Did you see what just happened down on the field during that last play? The big offensive left tackle bit the arm of the Rams linebacker. Blood is flowing. I wonder how much virus is being transmitted.”
“A ton, Frank. We really should have a graphic that illustrates it. Heck, there’s gobs of spit all over the field. So when a player falls down, he’s getting 100 percent pure from-the-lung SARS-CoV-2 rubbed in his face.”
“You and I are sitting in a veritable mist of virus engulfing the stadium.”
“That’s why your ex wants you to take out a bigger life insurance policy naming her as beneficiary.”
Where are the little prissy public health demons? Nowhere.
But they’ll tell YOU to take the highly destructive vaccine and then wear a mask and get ready for the boosters every six months and lock down and isolate whenever they deem it necessary.
They’ll collude with politicians to destroy all sorts of businesses and lives with these lockdowns.
But not the football business.
Despite his bitching and whining and moaning about crowds at large events, I assure you that if little Anthony Fauci suddenly ascended to the positon of Commissioner of the National Football League, he would find a way to keep the game going and the stadiums full of fans. He’d change his tune.
He’s the head of a public health mafia, and the mafia knows money.
On Hidden Nano Structures in Covid Vaccines: La Quinta Columna Takes a Closer Look at Nanocircuitry & Media Access Control Addresses (MACs)
On Hidden Nano Structures in Covid Vaccines: La Quinta Columna Takes a Closer Look at Nanocircuitry & Media Access Control Addresses (MACs)
MAC-cinated: Pattern identification in coronavirus vaccines – Nanorouters
by Orwellito, Orwell City
November 26, 2021
La Quinta Columna has gained the support of several researchers both in Spain and around the world.
A prominent researcher among those collaborating with them is the author of the Corona2Inspect blog, Mik Andersen, who’s carrying out “high-level research work“, as described by Dr. Pablo Campra during the presentation he gave on November 2.
On this occasion, the featured blog published an article about possible nanorouters that can be seen in some of the photographs taken by Dr. Campra. These nanostructures, most likely, would be part of the system that would allow the generation of MAC addresses in inoculated individuals.
Orwell City brings below the comments made by La Quinta Columna on this remarkable research entitled:
“Pattern identification in coronavirus vaccines: Nanorouters.”
Video available at Rumble
Ricardo Delgado:
Well, you know there’s a blog called Corona2Inspect. The author is Mik Andersen. He writes under this pseudonym. He’s an important person. On this occasion, he has posted an article today, November 25. It’s titled “Pattern identification in coronavirus vaccines: nanorouters.” And the images he presents are very curious because he’s taking images out of the scientific literature and comparing them to what Dr. Campra found in different vials.
“Since the discovery of graphene oxide in coronavirus vaccines, all the findings and the discovery made only confirm its presence (Campra 2021). To date, we’ve also found evidence of more than reasonable indications of the existence of nanotubes, carbon nanoribbons, mesoporous spheres, colloidal nanoribbons…”
Here are the different links.
“Objects that shouldn’t be part of any vaccine and that aren’t declared among the components of the vaccines. Additionally, other types of objects have been identified and evidenced in images of blood samples from people vaccinated with coronavirus vaccines. Specifically, micronadators, crystallized graphene nanoantennas, and the famous graphene quantum dots, also known as GQD. On this occasion, analyzing one of the images obtained by Dr. Campra, I remember seeing this, corresponding to a sample of the Pfizer vaccine. See Figure 1, which is this one here, has discovered what’s most likely a nanorouter or part of its circuitry.
And this is where it gets interesting because they did indeed appear to have typically printed circuit designs. Especially those of us who have worked with electronics and draw the tracks were reminded of that.
“In the original image, a well-delimited drop can be seen in which there’s a crystalline structure of quadrangular or cubic shape. If you look closely, you can see some marks in these crystals with a regular pattern, well delimited in some cases, but limited by the optics of the microscope. The finding has been possible by isolating each quadrangular crystal by applying a process of rastering, focusing, and delimitation of the edges of the image…”
José Luis, this is also being analyzed by another chemist. We’ve got to have a meeting with Campra.
“…To further pronounce the observed marks.” “Once this process was completed, a draft was drawn with the lines and patterns inscribed on the crystal, creating a clean outline of what actually looked like a circuit. It was very striking to find parallel and perpendicular lines with a distribution far from what would be fractal patterns —which would correspond, then, to crystals’ randomness—, which allowed us to automatically infer the possibility that it had been the product of manufacturing.”
At that level!
“Therefore, we looked for similar patterns in the scientific literature that had a similar scheme to the circuit that had just been drawn.”
I’m going to zoom in a little bit more so you can see it better. There. I’ve gone a little too far.
“The result of the search was almost immediate since the pattern of a quantum dot nanorouter was found, as shown in Figure 2.”
Take a look.
The images have been enlarged here. See, for example, this one here, which is very clear. It has these things like printed circuit board tracks. And this, what you see here on the right, is taken from the scientific literature. It’s a circuit of a quantum dot nanorouter. It actually has a very striking resemblance.
“Possible quantum dot nanorouters were observed in a quadrangular crystal in an image obtained by Dr. Campra.”
I seem to remember that it was the Pfizer vaccine. Precisely the first one, I think.
“In the lower right corner is the quantum dot nanorouter circuit published by Sardinha in 2013. Note the obvious resemblance between the sketch, the shape written on the crystal, and the quantum dot circuit.”
See? It’s very similar. Very similar even in the distribution it has. Quite similar.
“This discovery is of fundamental relevance. Not only to understand the true purpose and components of coronavirus vaccines, but also to explain the existence of the phenomenon of MAC addresses visible through the Bluetooth of many mobile devices. Because nanorouters, then, will, like routers, broadcast visible MAC addresses in, in this case, Bluetooth wireless technology, as is being proven, as well. The context of the discovery is as follows. Before proceeding to the explanation of the finding, it’s worth recalling the context in which it is framed, to ensure its understanding and subsequent deepening. First of all, it should be borne in mind that graphene and its derivatives, graphene oxide and carbon nanotubes, form part of the components of vaccines, as has already been explained in this blog. The properties of graphene are exceptional from a physical, thermodynamic, electronic, mechanical, and magnetic point of view. Its characteristics allow it to be used as a superconductor. It’s an electromagnetic wave absorbing material, a signal emitter-receiver, a quantum antenna which makes it possible to create advanced nano and micrometric scale electronics.”
Well, remember that these images were seen under the optical microscope. Those that you see in pink.
“So we would be talking, in this case, about micro-metric structures. So, the fundamental material for the development of nanobiomedicine…”
Here he talks about a paper.
“…Communication nanonetworks, new drug delivery therapies, cancer treatments, and neurological treatment of neurodegenerative diseases…”
Well, he talks about different studies.
“However, aside from all the benefits, the scientific literature is very clear about the health implications for the human body. It’s notorious that graphene, graphene oxide (GO), and other derivatives such as carbon nanotubes (CNT) are toxic in almost all their forms, causing mutagenesis (or cancer, chromosomal alteration), cell death, apoptosis, necrosis, the release of free radicals. And as a consequence of that, it increases toxicity rapidly in the lungs, favoring the cytokine storm that you know as bilateral pneumonia, genotoxicity, or DNA damage.”
All those studies that we have reviewed. “Systemic inflammation…”
That’s COVID-19.
“Immunosuppression, damage to the central nervous system, circulatory, endocrine, reproductive, urinary system, which can cause anaphylactic death (we also saw another study on that), and multi-organ dysfunction.”
And here it says: see the article on “Damage and toxicity of graphene oxide” and “Damage and toxicity of carbon-graphene nanotubes”. They’re also in La Quinta Columna.
“Secondly, graphene is a radiomodulatable nanomaterial.”
This is very important and one that people need to understand. And here’s the interaction with those radio frequency antennas.
“It’s able to absorb electromagnetic waves.”
All the links are here. This blog is very, very important to go deeper.
“It can also multiply radiation, acting as a nanoantenna, or else a signal repeater, a transistor. Exposure to electromagnetic radiation can cause the exfoliation of the material into smaller particles called GQDs (Graphene Quantum Dots), whose properties and physical peculiarities are enhanced due to their even smaller scale due to the “quantum hall effect,” since they act by amplifying electromagnetic signals and, with that, the emission distance, especially in environments such as the human body. Graphene quantum dots can acquire various morphologies, for example, hexagonal, triangular, circular, or irregular polygon.”
The truth is that this article is very long, but extremely interesting from beginning to end. And here, what’s most striking from the optical-visual point of view is the comparison, José Luis. If we compare the image of what’s in the scientific literature, you can see that it’s practically the same. Notice that it has… It’s the same!
Dr. Sevillano:
I recall that when we started to see the images, at first, we thought that those structures that appeared there were sugar crystals or something like that. Heh, sugar crystals are a thing of the past.
Here… Everything in the vaccine is introduced and has a purpose. And it has a purpose. Everything. Even genetic material has a purpose and, surely, it has the purpose to mutate people, the new generations. Almost certainly.
Ricardo Delgado:
That given what we’re seeing.
Dr. Sevillano:
Exactly. Given what we’re seeing. It’s just that people don’t understand this. That’s why they’ve been pounding our brains for 20 or 30 years since the X-Files started. Mulder and Scully started to tell us fictional movie stuff, that this Mothman, that I don’t know what, that this and that. Crazy fiction stuff.
But they were preparing us psychologically for the mess they were going to make. All they do is watch weird series of strange things and, in the end, they say: “All this that these people are telling us is crazy.”
Of course, they have been preparing us this way so that when you talk about this and complain, they call you crazy. So that they call you crazy, literally.
But that’s what they’re doing. They’re injecting something into people that, at the moment, is killing them. At some point, surely, they’re going to modulate them with it. At the same time, they’re mutating us for future generations.
see related:
Lethal Injection; Frontline E.R. Doctor Gives Chilling Account of Unusual Vaccine-Induced Illness
Lethal Injection; Frontline E.R. Doctor Gives Chilling Account of Unusual Vaccine-Induced Illness
by Mike Whitney, The Unz Review
November 20, 2021
“Americans are scared to death…. People are walking off the job, not because they want to lose their jobs, but they don’t want to die from the vaccine! … They say, ‘Listen, I don’t want to die. That’s the reason I’m not taking the vaccine.’ It’s that clear.” Dr. Peter McCullough
A report in the U.K. Telegraph explains how the Covid-19 vaccine has led to a sharp rise in excess deaths. Here’s an excerpt from the article:
“Nearly 10,000 more people than usual have died in the past four months from non-Covid reasons, as experts called for an urgent government inquiry into whether the deaths were preventable….
Latest figures from the Office for National Statistics showed that England and Wales registered 20,823 more deaths than the five-year average in the past 18 weeks. Only 11,531 deaths involved Covid.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
Mortality is rising because more people are dying. And more people are dying because more people have been vaccinated. There’s a link between rising mortality and the Covid-19 vaccine. Naturally, the media wants to shift responsibility for the fatalities to “delayed treatments” and “the lack of preventable care”. But this is just a diversion. The primary cause of death is the injection of a toxic pathogen into the bloodstreams of roughly 70% of the population. That’s what’s causing the clotting, the bleeding, the pulmonary embolisms, the heart attacks, the strokes, and the premature deaths. It’s the vaccine. Here’s more
“Weekly figures for the week ending November 5 showed that there were 1,659 more deaths than would normally be expected at this time of year. Of those, 700 were not caused by Covid.
The excess is likely to grow as more deaths are registered in the coming weeks.
Data from the UK Health Security Agency show there have been thousands more deaths than the five-year average in heart failure, heart disease, circulatory conditions and diabetes since the summer.
The number of deaths in private homes is also 40.9 per cent above the five-year average, with 964 excess deaths recorded in the most recent week, which runs up to November 5.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph)
The sudden surge in mortality is not a meaningless blip on the radar. It’s a red flag indicating a significant break in the five-year trend. Something has gone terribly wrong. Mass vaccination was supposed to reduce the number of cases, hospitalizations and deaths. Instead, the fatalities continue to rise.
Why?
The answer to that question can be found in the data itself. As the author admits, there has been a sharp uptick in heart failure, heart disease, circulatory conditions and strokes. (Diabetes is the outlier) These are precisely the ailments one would expect to see if one had just injected millions of people with a clot-generating biologic that triggers a violent immune response that attacks the inner lining of the blood vessels inflicting severe damage to the body’s critical infrastructure. So, yes, all-cause mortality is up, and it is certain to climb even higher as more people are vaccinated and gradually succumb to the (frequently) delayed effects of a hybrid concoction that is the cornerstone of a malign plan to dramatically reduce global population. Check out this chart followed by a brief comment by diagnostic pathologist, Dr Claire Craig:
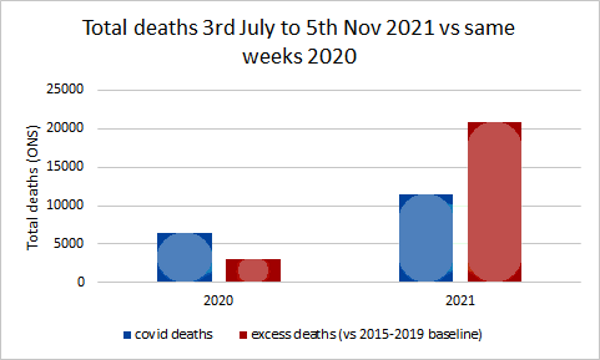
So, not only are more people dying, but the demographic has shifted downwards as younger and younger people are drawn into the vaccine vortex. Simply put, the number of young people dying from vaccine-inflicted cardiac arrest and myocarditis continues to increase with no end in sight.
Not surprisingly, all-cause mortality is higher among the vaccinated than the unvaccinated which, again, makes it easier to trace the problem back to its root, a cytotoxic “poison-death shot” that suppresses the innate immune system, damages vital organs and shaves years off the lives of normal, healthy people.
Perhaps, you’ve seen one of the many short videos of fit, young athletes who suddenly have dropped dead on the field of play or been rushed to hospital shortly after getting injected. If not, here’s a link to two of them. (Athletes collapse following vaccination: See here and here)
According to Israeli Real-Time News, there has been a “500% increase in deaths of players in 2021… Since December, 183 professional athletes and coaches have suddenly collapsed! 108 of them died!”
“500% increase in the deaths” of athletes?!? What are we to make of this?
For starters; the Covid-19 vaccine is not a medication. It is the essential component in the elitist plan for industrial-scale extermination. It is designed to inflict severe physical injury on the people who take it. It’s shocking that people are so deep in denial that can’t see what’s going on right before their eyes. (Please, watch the video clips of the athletes. These are the fittest people on the planet and, yet, they are being struck down by the mystery substance in the vaccine.) Here’s how South African doctor Shankara Chetty summed it up in a recent video posted on Bitchute:
“The pathogen that is causing all the deaths from the illness is the spike protein. And the spike protein is what the vaccine is supposed to make in your body. …Spike protein is one of the most contrived poisons that man has ever made. And, the aim of this toxin, is to kill billions of people without anyone noticing it. So it is a poison with an agenda.” (“South African Physician Dr. Shankara Chetty Talks about “The Bigger Plan”, Bitchute)
There it is in a nutshell. And Chetty is not alone in linking the vaccine to the agenda of the globalist elites who plan to use the cover of a pandemic to implement their “population management” scheme. Former Pfizer vice president, Mike Yeadon, offered a similar view just days ago on his website. He said:
“We are in the midst of the biggest depopulation program the world has ever seen, where most of humanity are acting as useful idiots to it and to their own demise.”
Indeed, and we have tried to provide as much information as possible on the biologic agent that is being used to pursue this malign agenda, the spike protein. In early reports we passed along the research of Dr. Patrick Whelan who grasped the danger of the spike protein before anyone else. Here’s a brief recap of his analysis from a letter he submitted to the FDA on December 8, 2020:
“I am concerned about the possibility that the new vaccines aimed at creating immunity against the SARS-CoV-2 spike protein have the potential to cause microvascular injury to the brain, heart, liver, and kidneys in a way that does not currently appear to be assessed in safety trials of these potential drugs.
… Meinhardt et al…. show that the spike protein in brain endothelial cells is associated with formation of microthrombi (clots)… In other words, viral proteins appear to cause tissue damage without actively replicating virus…. The Pfizer/BioNTech vaccine (BNT162b2) is composed of an mRNA that produces a membrane-anchored full-length spike protein. The mouse studies suggest that an untruncated form of the S1 protein like this may cause a microvasculopathy in tissues that express much ACE2 receptor.
…it appears that the viral spike protein… is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung, and kidney. Before any of these vaccines are approved for widespread use in humans, it is important to assess in vaccinated subjects the effects of vaccination on the heart…. As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs. (“FDA shrugs off dire warning about lethal spike protein“, Truth in the Age of Covid)
From the very beginning, government regulators and their allies in public health establishment have ignored (or censored) the warnings of capable physicians and researchers. They also waved-off career immunologist and vaccinologist, Dr Byram Bridle who was the first in his profession to identify the spike protein as “a specific causative agent of disease”; aka–“a pathogen”. Here’s Bridle:
“‘We have known for a long time that the spike protein is pathogenic…. It is a toxin. It can cause damage in our body if it’s in circulation. Now, we have clear-cut evidence that . . . the vaccine itself, plus the protein, gets into blood circulation.’”
Once that happens, the spike protein can combine with receptors on blood platelets and with cells that line our blood vessels. This is why, paradoxically, it can cause both blood clotting and bleeding. ‘And of course the heart is involved, as part of the cardiovascular system… That’s why we’re seeing heart problems. The protein can also cross the blood-brain barrier and cause neurological damage.…
‘In short,… we made a big mistake. We didn’t realize it until now. We didn’t realize that by vaccinating people we are inadvertently inoculating them with a toxin.”… (“Vaccine scientist: ‘We’ve made a big mistake’“, Conservative Woman)
Here again, we have a highly-regarded immunologist, with more than 3 decades of experience under his belt, who offered his informed and evidence-based research on an issue that should have been of great interest to the regulators that were making decisions about the long-term safety of the experimental drug they were foisting on millions of people across the country. But there was no interest at all. Despite the fact that the science supported his conclusions, Bridle was viciously attacked, censored, dragged through the mud, and forced to leave his place of employment.
Why?
Because he drew the same conclusions as Dr. Patrick Whelan. There’s really no substantive difference between the two except that Bridle’s comments attracted more attention in the media which made him a greater threat to the “universal vaccination” strategy. That was his real crime; he discovered the truth and made his findings available to the public, basically alerting them to the dangers of the “poison-death shot”. For that he was crushed.
>Bridle has since made other claims that should concern anyone whose cancer might be in remission. Here’s what he said in a recent interview:
“What I’ve seen way too much of is people who had cancers that were in remission, or that were being well controlled; their cancers have gone completely out of control after getting this vaccine. And we know the vaccine causes a drop in T-cell numbers, and those T-cells are part of our immune system and they are part of the critical weapons our immune system has to fight off cancer cells; so there’s a potential mechanism there. All I can say, is I’ve had way too many people contact me with these reports for me to feel comfortable. I would say that is my newest major safety concern, and it’s also the one that’s going to be the most under-reported in the adverse data base, because if someone has had cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine.” (“Dr Byram Bridle speaks”, Bitchute, :55 second-mark)
So, the vaccine suppresses the immune system?
Yes, it does, and author Alex Berenson provided evidence of this just recently in an article he posted on Substack. Here’s an excerpt:
“… the British government…. admitted today, in its newest vaccine surveillance report, that:
“N antibody levels appear to be lower in people who acquire infection following two doses of vaccination.” (Page 23)
What’s this mean?…
What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus….
This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE…
… it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.” (“URGENT: Covid vaccines will keep you from acquiring full immunity EVEN IF YOU ARE INFECTED AND RECOVER”, Alex Berenson, Substack)
Berenson’s observations square with research that was compiled earlier in the year by scientists in The Netherlands and Germany who:
“….warned that the … (COVID-19) vaccine induces complex reprogramming of innate immune responses that should be considered in the development and use of mRNA-based vaccines… the research team from Radboud University Medical Center and Erasmus MC in the Netherlands… showed that the vaccine altered the production of inflammatory cytokines by innate immune cells following stimulation with both specific (SARS-CoV-2) and non-specific stimuli.
Following vaccination, innate immune cells had a reduced response to toll-like receptor 4 (TLR4), TLR7 and TLR8 – all ligands that play an important role in the immune response to viral infection…. an unexplored area is whether BNT162b2 vaccination has long-term effects on innate immune responses …
This could be very relevant in COVID-19, in which dysregulated inflammation plays an important role in the pathogenesis and severity of the disease,” writes the team. “Multiple studies have shown that long-term innate immune responses can be either increased (trained immunity) or down-regulated (innate immune tolerance) after certain vaccines or infections.” (Research suggests Pfizer-BioNTech COVID-19 vaccine reprograms innate immune responses, new-medical-net)
Berenson’s finding also align with with cutting-edge research showing that the spike protein greatly “impedes adaptive immunity” by preventing DNA from repairing damaged cells. The paper suggests that the spike protein does in fact “impact on the nucleus of the cell, where we store our DNA, our core genetic material.” Here’s more from Berenson’s breakdown of the paper:
“…. our cells have mechanisms to repair their own DNA.
But – at least in the experiments these two scientists ran – the spike protein appeared to interfere with our own DNA repair proteins: “Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site.”
To be clear, the scientists did NOT prove the spike protein was causing these problems in people, or even animals… Nonetheless, at a time when advanced countries that have high mRNA (and DNA/AAV) vaccination rates are seeing unusually full hospitals and higher-than-normal death rates, they are yet more cause for concern. As the authors explained:
“Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.” (“URGENT: Worrisome paper about the spike protein’s impact on DNA and DNA repair”, Alex Berenson, Substack)
Bottom line: If the vaccine does in fact inhibit the body’s innate immune response, then people are going to get alot sicker from seasonal infections that routinely spread through the population. Their path to recovery will also be alot more difficult.
But rather that belabor the immunity angle, let’s move on to the research of Dr Charles Hoffe who was the first physician to provide hard evidence that the vaccines generate blood clots by triggering an immune response in which the body attacks the thin layer of cells lining the walls of the blood vessels. Hoffe found that 62% of his patients that had been vaccinated tested positive for blood clots on a D-dimer test. Naturally, he was alarmed by what he found, particularly since the vaccine “was causing serious neurological events, and even death. When he raised his concerns with the BC College of Physicians, they immediately implemented a gag order, and reprimanded him in an attempt to intimidate, and silence him.”
Hoffe has been interviewed a number of times and always provides a detailed and riveting account of his findings. In a recent interview, he predicted that some vaccinees suffering from clot-related issues would likely die in just three years. Here’s what he said:
“… once you block off a significant number of blood vessels to your lungs, your heart must pump at a much greater resistance to get the blood through your lungs. That causes a condition called pulmonary artery hypertension, which is high blood pressure in your lungs because so many of the blood vessels in your lungs are blocked. And the terrifying thing about this is tha t people with pulmonary artery hypertension usually die of right-sided heart failure in three years… And not only is the long-term outlook very grim, but with each successive shot, the damage will add and add and add. It’s going to be cumulative because you are getting more and more damaged capillaries.” (“Shock: Doctor Warns That Majority Of Vaccinated Patients Could HavePermanent Heart Damage, Some May Die Within Three Years”Permanent Heart Damage, Some May Die Within Three Years”, Infowars; Minute 6:10)
Once again, there is no discrepancy between the analysis of Whelan, Bridle and Hoffe. And while the focus of their attention might vary slightly, their conclusions are the same. These experimental injections pose serious risks for anyone who allows himself to be inoculated.
Now check out how similar Hoffe’s analysis is to Dr. Rochagne Kilian who was an Emergency Room physician at the GBHS hospital until she resigned in protest. This is a particularly important video as it describes the “oddball” symptoms and exceedingly rare conditions that are now presenting in emergency rooms everywhere following the mass vaccination of millions of people with the “poison-death shot”. (I transcribed the video myself, so there could be errors.)
Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels
“What I was seeing in my ER department especially in the last 8 to 9 months is related to the D-Dimer levels. We use D-Dimers specifically related to pulmonary embolisms as well as Deep Vein Thrombosis. D-Dimer detects any thrombosis (clots) in the body but it doesn’t give you a diagnosis it gives you a basis for going further and doing an ultrasound and CT scan to either confirm or deny the presence of a pulmonary embolism or Deep Vein Thrombosis.
The first part of 2020 was probably the slowest ever in the emergency department, but when we went into 2021 and the vaccination rollout started, we ended up seeing an increase in stroke, transient ischemic attacks and stroke like presentations. (There were) definitely significant larger numbers of those people coming in. I ended up doing D-dimer tests on these people and never before in my clinical experience had I seen D-dimers and the amount of people with positive D-dimers higher than 2,000, higher than 3,000 and higher than 5,000. My clinical experience told me a needed to go look for a large clot either in their legs or their lungs. And I ended up doing a CT scan on these people. Most of them, and I will say almost all of them, had negative scans which started making me think that if there was not a significant clot in their lungs, but my D-dimer was so much higher than what I was usually seeing, it might not be concentrated in one clot. But that it is multiple micro-thrombi extended throughout the body, and that is so easy to miss because the CT scan is not going to pick it up.
“These people coming into the ER were all people anywhere from about a week to four months after receiving their 2nd injections. There are certain factors that can influence a D-dimer test that can give you a sense of a higher level than would be expected in the body. That said, the patients I was doing D-Dimer tests on did not have a level of maybe a positive 500 or 400 reading. It was more than 3500, more than 5000 ng/ml. So those are significantly positive without any proof of having a pulmonary embolism. If I was seeing high levels of D-dimer without a definite diagnosis, I needed to ask more questions.
One study said, never ignore extremely elevated D-dimer levels. They are specific for serious illness, including venous thrombosis, sepsis, and/or cancer. Even if sharply elevated D-dimer are a seemingly solitary finding, clinical suspicion of severe underlying disease should be maintained.
There were two conditions that stood out and the first one was disseminated intravascular coagulation also known as DIC. The second one is antiphosphlipid syndrome. Both of these conditions are related to an abnormality in either the initiation or the feedback of the coagulation pathway as well as thrombosis or the thrombosis cycle where clots are being broken down. DIC is a serious sometimes life threatening situation in which the proteins in the blood involved in blood clotting become overactive. It’s a cascade that’s difficult to stop once it’s reached a certain level. There are certain conditions that trigger DIC; significant sepsis, underlying viruses, trauma, major surgery, pregnancy and childbirth. And less common causes toxic drug reaction, blood transfusion reaction, and organ transplants. So there was a connection with intravascular products and a possible DIC.
Most cases of DIC are diagnosed rapidly and suddenly which is the acute presentation. But there are cases where it develops gradually, occurring over a longer period of time. This is known as a chronic form of DIC and I would go as far to say a subacute form of DIC that is very easy to miss. Simultaneous clotting and bleeding can occur with chronic DIC. The bleeding part comes in blood in the urine, headaches and other symptoms associated with brain bleeds, bruising, inflammation of red, small dots on the limbs, bleeding at sites of wounds and mucosal bleeding. which means bleeding out of the gums and nose. I definitely saw an increase in nose bleeds and bleeding from previous wound sites. ulcers, as well as rashes that couldn’t be explained. Blood clotting symptoms and signs were symptoms like chest pains, heart attacks, strokes, TIAs, and headaches either related to bleeding or not. As well as symptoms related to kidney failure, because of the clotting of those smaller blood vessels that go to the kidneys. Antiphosphlipid syndrome is a very similar type of condition. But the basis of the antiphosphlipid syndrome is an autoimmune disorder meaning that the body’s immune system makes proteins–known as antibodies–that mistakenly attacks its own body or tissues. That gives the skin the cascading effect of clotting disorder but it is linked to an autoimmune trigger. Basically, it presented in exactly the same way; high blood pressure which I was seeing alot of; first diagnosis of high blood pressure, heart attacks, strokes, TIAs, heart valve problems, repeated headaches or migraines, vision loss, balance and mobility problems, difficulty concentrating or thinking clearly,
The astute listener would start forming a picture of what we’ve been told about Covid-19, and there are research papers connecting Covid 19 with an underlying vascular disease. One of these was a study called “Covid 19; unraveling the clinical progression of Nature’s Virtually perfect Biological weapon.”
“SARS-Cov-2, presenting as Covid-19 syndrome, was not a respiratory basis, but an underlying vascular basis. which had certain phases of incubation, pulmonary phase, pro inflammatory phase, (which once again comes into a cytotoxic inflammation process) then moves into a protothrombic phase . Covid-19 is a thrombotic disease. implications for prevention, antithrombotic therapy and follow up…..
This picture shows us certain risk factors, Homeostatic Abnormalities, as well as clinical outcomes. It indicates increased D-dimer levels. It also mentions Venous Thromboembolism, Myocardial Infarction, and Disseminated Intravascular Coagulation that is connected to postulated mechanisms of coagulathopy as well as parthenogenesis of thrombosis in Covid-19…
I started asking the question, if we are able to detect certain connections between vascular abnormalities and Covid-19, and we based our proposed treatment on the spike protein, which includes the Pfizer and Moderna injections, shouldn’t we be looking for similar side effects or complications from that same injection?
If we are mandating certain treatments, we do need to do the due diligence to make sure what the side effects and complications especially in a time where there has not been long term studies.”And that’s what led me to focusing on D-dimers.” (“Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels“, Bitchute)
Kilian’s statement should be read over and over again. It is the most detailed description we have of the mysterious and deeply sinister machinations of a laboratory-engineered bioweapon that, in effect, turns the vascular and immune systems against the person who was vaccinated. Disseminated intravascular coagulation and antiphosphlipid syndrome are names that are entirely unknown to the American people, and yet, these freakish conditions are now responsible for a growing number of patients that are experiencing bleeding, clotting, headaches, rashes, bruising, high blood pressure, and inflammation . And– in more extreme cases– chest pains, heart attacks, strokes, heart-valve problems, and brain bleeds. One can only guess how the media will try to cover-up these extraordinarily-rare and potentially life-threatening conditions??
When Kilian asks:
“If we are able to detect certain connections between vascular abnormalities and Covid-19… shouldn’t we be looking for similar side effects or complications from that same injection?”
>Bingo! If the spike protein produced by the vaccines, inflicts the same internal damage as Covid-19, then shouldn’t doctors expect to see the same symptoms?
Yes, they should. And if the symptoms are the same, then there’s a good chance that vaccine-induced injuries are being misdiagnosed as Covid-19.
Think about that for a minute. That would be the perfect scenario for the pandemic managers and their billionaire backers who’d love to see the impending mountain of carnage blamed on the waning virus instead of on their own poison-death shot.
And that is the evil-genius of the globalist strategy; to remove the fingerprints from the smoking gun before the investigators even arrive at the scene of the crime.
The amount of planning that must have gone into this scam, is simply breathtaking.
Read more by Mike Whitney at The Unz Review
cover image credit: paulbr75 / pixabay
14 ACIP Members Who Voted to Jab Your Young Children — and Their Big Ties to Big Pharma
14 ACIP Members Who Voted to Jab Your Young Children — and Their Big Ties to Big Pharma
On Nov. 2, members of the Centers for Disease Control and Prevention’s vaccine advisory committee voted 14–0 to recommend Pfizer’s pediatric COVID shot for children 5 –11 years old. Were their decisions driven by science and conscience — or their ties to drugmakers?
by Children’s Health Defense Team
November 24, 2021
CHD EDITOR’S NOTE: Following the Oct. 26 meeting of the U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee (VRBPAC), Children’s Health Defense argued it is time to shun the individuals — and institutions — that are selling out America’s children without even a prick of conscience. At the close of this article about the members of the Centers for Disease Control and Prevention’s (CDC’s) Advisory Committee on Immunization Practices (ACIP), we reiterate our list of suggestions for shunning.
On Nov. 2, the members of ACIP voted 14–0 to recommend Pfizer’s Emergency Use Authorization (EUA) COVID shot for children 5 –11 years old.
Committee members readily voted “yes” despite many unknowns about long-term safety, including a complete lack of data on the risk of heart problems like the ones experienced by some adolescents who received COVID vaccines.
Neither the disgracefully unscientific vote nor CDC Director Rochelle Walensky’s prompt endorsement came as a surprise. Though billed as “independent,” the 14 ACIP members — like the 17 members of FDA’s VRBPAC who voted the same way the previous week — have deep ties to pharma, with careers that hinge on promoting and rubber-stamping the United States’ destructive one-size-fits-all vaccination agenda.
Describing the VRBPAC and ACIP meetings as “a total sham,” Children’s Health Defense President Mary Holland said, “Sadly, approval from these committees means nothing in terms of safety.”
Political scientist Toby Rogers agreed, stating the ACIP meeting “was not a scientific review. It was banal bureaucrats announcing plans for a Blitzkrieg and the bought white coats were cheering them on.”
With their vote to give young children the dangerous injections, ACIP members signaled that they, too, deserve to be shunned, along with the powerful institutions with which they are affiliated. The latter include the nation’s top universities and leading pediatric hospitals.
Without exception, all the universities at which ACIP members have appointments — Brown, Drexel, Harvard, Michigan State, Ohio State, Stanford, University of Maryland, University of Washington, Vanderbilt and Wake Forest — have mandated COVID vaccines.
Pediatric hospitals, meanwhile, are playing a frontline role as COVID vaccination sites. Promoting the injection for 5-year-olds, First Lady Jill Biden visited Texas Children’s Hospital straight away, applauding the hospital for the 39,000 pediatric vaccine appointments it had already scheduled.
Also worthy of shunning are the 20,000 individual vaccine providers who were pre-positioned to “hit the ground running” and “get shots in little arms.”
Within two days of ACIP’s and Walensky’s verdicts, these providers had administered the jab to thousands of 5- to 11-year-olds, and within the first week, according to the White House, 900,000 children had been injected.
New dangers emerging
Community vaccination sites such as pharmacies and pop-up clinics have attracted recent attention for egregious vaccine administration errors in young children:
- In Texas, a pop-up clinic gave adult doses of the Pfizer jab to 6- and 7-year-old boys “two days before a proper dose of the vaccine was even approved for that age range.”
- In Virginia, a pharmacy (subsequently ordered to stop administering the shots) gave 112 children in the 5–11 age group the wrong COVID vaccine formulation.
- A pediatric practice in California also gave 14 children an incorrect dose of the Pfizer jab, not disclosing “whether the kids got too much or too little.”
- In addition, pharmacies have “mistakenly” given adult COVID shots to children under age 5 whose parents had requested flu shots.
With censorship rampant, many parents may be unaware of these transgressions. They also may not know that the experimental product FDA and CDC are unleashing on children is coming under increasing fire from Pfizer whistleblowers.
The same day as the ACIP vote, The BMJ published a whistleblower’s hair-raising account of “data integrity issues” in Pfizer’s “helter-skelter” clinical trials. According to Brook Jackson — a trained clinical trial auditor — Ventavia Research Group (one of the contract research organizations engaged by Pfizer) “falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events.” Quality control staff, Jackson further reported, were “overwhelmed by the volume of problems they were finding.”
When Jackson shared her concerns with both Ventavia and FDA in September 2020, Ventavia fired her. FDA ignored her warnings and granted EUA status to Pfizer’s injection in December.
Melissa Strickler McAtee, until recently a quality control employee at Pfizer’s plant in McPherson, Kansas, described, in an interview with Project Veritas, Pfizer’s efforts to deceive the public about the use of fetal cell lines in creating the COVID shot.
Equally disturbingly, Strickler McAtee told other journalists that Pfizer’s vaccine exhibits an unusual fluorescent blue glow, stating she had “never once [previously] seen anything do that, not even close” during her 10-year career inspecting “hundreds of thousands of units” of vaccines. She also reports that her co-workers at the plant are being unprecedentedly kept in the dark about what the vaccine’s ingredients are.
Pfizer has a lengthy history of quality control problems in addition to a business model predicated on habitual fraud. The Kansas plant, which Pfizer acquired when it strategically purchased injectable drug company Hospira in 2015, has been repeatedly “dinged” by FDA for problems with quality, cleanliness and contamination.
In the three years leading up to its acquisition by Pfizer, Hospira had to issue more than 40 recalls, and Pfizer/Hospira has continued to be a frequent offender on FDA’s recall list since 2015, receiving another warning letter from FDA in 2017.
FDA’s tsk-tsking of Pfizer clearly represents a hollow rebuke, however, as this week’s FDA request to a federal judge made plain: FDA is asking for 55 years to make public the data and information it relied on to license Pfizer’s COVID-19 vaccine.
These and other clinical trial shenanigans strongly intimate that “the data that the FDA and CDC have been pretending to base their decisions on for the last year, are fiction.”
Below are the ACIP members who signed off on Pfizer’s pediatric vaccine, and their conflicts of interest.
ACIP Chair Grace Lee
Dr. Grace Lee (gmlee@stanford.edu) chaired the November ACIP deliberations. Lee has been associate chief medical officer for practice innovation at Stanford Children’s Health and a pediatrics professor at Stanford School of Medicine since 2017, after having spent two decades at Harvard and Boston-area hospitals.
In addition to policy work focusing on financial rewards and penalties to reshape hospital performance, Lee has built her reputation by shoring up the pretense that the nation has a functioning vaccine safety surveillance system.
Lee served as past principal investigator for the CDC’s Vaccine Safety Datalink (VSD), a large database that includes comprehensive longitudinal medical and vaccination records for two million children and seven million adults. Although VSD analyses have the potential to permit enlightening vaccinated-unvaccinated comparisons of health outcomes, the CDC has sole access to the data.
In the words of CHD’s chief scientific officer Dr. Brian Hooker, CDC has “shut [VSD] up like a fortress, despite the fact that it’s taxpayer-funded.”
In VSD-based publications — some of which include fellow ACIP member Matthew Daly — Lee has made a habit of downplaying vaccine risks. For example, she encourages women to get Tdap (tetanus-diphtheria-acellular pertussis) shots during pregnancy, even while data show an increased risk of placental and amniotic fluid infection in vaccinated pregnant women.
She also has whitewashed risks of flu shots in children under age 5 despite finding “an apparent dose-response for vaccine and allergic reactions in the 1- to 3-day risk window.” She dismisses post-vaccination anaphylaxis risks as “rare,” though the package inserts for most vaccines on the childhood schedule prominently list anaphylaxis as an adverse event.
Another VSD study co-authored by Lee documented a safety signal for febrile seizures linked to influenza vaccination of children in their first five years, particularly if administered along with pneumococcal vaccination; massaging the troubling conclusion with vaccine doublespeak, Lee and colleagues proposed placing their findings “in a benefit-risk framework to ensure that population health benefits are maximized.”
While in Boston, Lee served as associate director of the FDA-funded Mini-Sentinel Project, one of several newer vaccine safety surveillance mechanisms trotted out over the past decade.
As noted by CHD Chairman Robert F. Kennedy, Jr. in a letter to Biden advisor David Kessler in December 2020, studies published using Sentinel data — all authored by the same small pool of insiders — focus on an extremely narrow subset of adverse outcomes and reflect methodological decisions “that could easily constrain researchers’ ability to detect outcomes of interest.”
When a Sentinel study of the two rotavirus vaccines routinely given to American children identified a “significant risk” of intussusception after dose 2 — a bowel complication that forced CDC to revoke its recommendation for an earlier rotavirus vaccine — Lee and co-authors deployed more doublespeak, once again advising the public to consider the risk “in light of the demonstrated benefits of rotavirus vaccination.”
Discussing myocarditis last June, Lee admitted, “clinical presentation of myocarditis cases following vaccination has been distinct, occurring most often within 1 week after dose two, with chest pain as the most common presentation.”
This did not stop Lee from joining with other public health officials in passing off myocarditis as “an extremely rare side effect” and claiming that young people are likely to “recover on their own or with minimal treatment.”
Many experienced health professionals, including Dr. Ryan Cole, Dr. Aaron Kheriaty and Dr. Steven Pelech, fiercely dispute the notion of “mild” myocarditis.
Also of note:
- In September of this year, Lee co-authored a paper in JAMA belatedly conceding that a large segment of the population (“women and those with a history of allergic reactions”) is at “elevated risk” of experiencing allergic reactions to mRNA COVID vaccines due to the presence in the injections of polyethylene glycol (PEG). CHD issued urgent warnings about PEG and its entirely predictable anaphylaxis risks a full year earlier, in September 2020.
- Stanford receives extensive vaccine funding from the Gates Foundation, including for the development of 3D-printed vaccine microneedle patches (a strategy that would allow “vaccination without a shot”).
- Stanford is the second-largest university beneficiary of funding from the David and Lucile Packard Foundation, which is aggressively funding COVID vaccination of U.S. Latinos.
- Not only does Stanford require all students to be COVID-vaccinated, but it also urges vaccination for students’ children.
Lynn Bahta
Lynn Bahta, RN, MPH (lynn.bahta@state.mn.us) is an immunization program clinical consultant for the Minnesota Department of Health, with a 25-year career focused on promoting vaccination.
During the pandemic, Bahta has been giving talks about “vaccine hesitancy in the time of COVID,” offering “key communication strategies to build confidence among those who are hesitant.”
Vaccine “hesitancy” appears to have been her bailiwick long before COVID, however, and her publications suggest a particular interest in coaxing Minnesota’s immigrant, migrant and refugee populations into higher vaccination rates.
Loyal to the fraudulent CDC party line that denies any link between MMR (measles-mumps-rubella) vaccination and autism, Bahta has published articles dismissing the well-founded autism concerns of Minnesota’s Somali community as “misinformation.”
Somali children in Minneapolis suffer the highest known rate of severe autism in the world. Somali parents allege that the reaction of public health officials like Bahta has been one of indifference.
Discussing COVID vaccines, Bahta claims that the “great majority, usually over 90%” of adverse reactions “are not serious.”
In fact, while stating that she “never disagrees with people who believe they were injured by vaccines because it’s difficult to know,” she clearly sides with public health officials in viewing “unverified reports” to the Vaccine Adverse Event Reporting System (VAERS) as “misunderstood by the public and exploited by skeptics in a way that is undermining immunization efforts against COVID-19.”
Bahta disingenuously opines that “people naturally but incorrectly associate injuries with recent events.”
Also of note:
- Bahta’s was one of the core “yes” votes in favor of recommending Moderna’s COVID shot last December.
- When ACIP deliberated over COVID booster shots in September, Bahta was willing to recommend boosters for adults age 50 and up and individuals with underlying conditions but not for some groups of younger adults. At the time, Bahta argued for the need to “stay with the science,” stating, “I don’t think we have the data.”
- By November, Bahta apparently was untroubled by the paucity of safety data available for the 5–11 age group, stating, “We know more than what we don’t know.”
Beth Bell
Beth Bell, M.D., MPH (bzb8@uw.edu) is a clinical professor in the Department of Global Health at the University of Washington (UW) School of Public Health. Until 2017, Bell spent most of her career at CDC, including as Director of the National Center for Emerging and Zoonotic [animal/insect-to-human] Infectious Diseases.
At UW, Bell is on faculty at the UW Alliance for Pandemic Preparedness (formerly called, until fall 2020, the MetaCenter for Pandemic Preparedness and Global Health Security), which “harness[es] big data and forward-thinking strategies to devise more unified approaches to current and future health security risks.”
“Health security” and biosecurity are the linchpin buzzwords that global technocrats are using to push for complete control over people’s “ability to work, to socialize, to travel, conduct business, access public services and to purchase essential goods and services.”
Like many of the individuals who make their way onto FDA and CDC committees, Bell started her CDC career as an officer in the Epidemic Intelligence Service (EIS), a branch that journalist Jon Rappoport has dubbed the “medical CIA.”
As Rappoport notes, EIS graduates’ occupancy of “key positions in the overall medical cartel” furnishes an “unparalleled opportunity” to control information — and disseminate disinformation.
During COVID, Bell has positioned herself as a champion for vaccination “equity,” stating “If we’re serious about valuing equity, we need to have that baked in early in the vaccination process.”
Bell’s comments about wanting to make sure “socially vulnerable” communities and people of color have access to COVID shots echo troubling racially oriented remarks made by Melinda Gates early on in the pandemic. Located in Gates’ backyard, UW not only benefits from close ties with and extensive funding from the Gates Foundation — an organization tainted by allegations of medical experimentation and an underlying eugenicist ideology — but also enjoys extensive support from Microsoft.
Also of note:
- As co-author of a CDC paper summarizing ACIP’s May recommendation that 12- to 15-year-olds get the Pfizer shot, Bell and colleagues inaccurately argued that “COVID-19 in adolescents is a major public health problem” and that “desirable [vaccine] effects” outweigh “any undesirable effects in most settings.” The authors did not mention the teens who are dying of post-vaccination cardiac arrest.
- Regarding COVID booster shots, Bell first stated, “I have my own concerns that we appear to be recommending vaccines for people who I don’t think need it”; she later agreed, however, that “moving forward with the recommendations makes sense for the sake of being clear.”
- Regarding COVID jabs for young children, Bell claimed, after the November vote, “if she had a grandchild, she’d get the grandchild vaccinated as soon as possible.”
Oliver Brooks
Oliver Brooks, M.D. (oliver.brooks@wattshealth.org) is chief medical officer and a member of the executive team at Watts Healthcare Corporation in Los Angeles. Watts Healthcare provides primary care services under the Department of Health and Human Services (HHS) and also receives federal funding for other services, including those related to HIV/AIDS.
Brooks is immediate past president of the National Medical Association (NMA), which he describes as “the oldest and largest organization representing African-America’s physicians and the guardians of the health of African-Americans.” As such, Brooks — like Beth Bell — made “health equity” his calling card, with vaccination of minority groups one of his signature goals as NMA president.
CDC celebrates Brooks’ “leadership roles focusing on disparities in vaccine coverage rates.”
Brooks speaks frequently “on the science and the implementation perspective of vaccine utilization,” is a board member and past president of the California Immunization Coalition, chairman of the Immunize LA Families Coalition and member of the national Leadership Panel for the Adolescent Immunization Initiative.
During the pandemic, Watts Healthcare has received millions in funding from Kaiser Permanente to promote COVID vaccination in L.A.’s Hispanic and African American communities.
In March 2021, Watts Healthcare also received $4.3 million via the American Rescue Plan to increase the federally qualified health center’s “ability to get more shots in arms.” The nonprofit is further beholden to the federal government for a $5.18 million coronavirus-related Paycheck Protection Loan approved in April 2020.
Brooks co-chaired California’s COVID-19 Vaccine Work Group, working to “get the vaccine out more rapidly” through “more points of distribution.” Early on in the vaccine rollout, one of those “points of distribution” in San Diego was forced to pause vaccine administration when numerous recipients suffered severe allergic reactions.
Since 2014, Brooks has received $118,439 (350 general payments primarily for consulting or speaking engagements) from biopharmaceutical companies that include Pfizer as well as Sanofi Pasteur, Novartis, Seqirus, Gilead, GlaxoSmithKline, Merck, Meda, AbbVie and Theratechnologies.
Also of note:
- At over $271,000, Brooks’ annual salary is second only to that of the Watts Healthcare CEO.
- Watts Healthcare and another South LA nonprofit received $3 million in COVID-related funding from the Oprah Winfrey Charitable Foundation in July 2020. The media tycoon — one-time member (along with Bill Gates, Warren Buffett, George Soros, David Rockefeller, Ted Turner and others) of an elite “club” of billionaire philanthropists — urges compliance with mask mandates and uses her influential platform to tell those who are not vaccinated to “reconsider.”
Wilbur Chen
Wilbur Chen, M.D. (wchen@som.umaryland.edu) is a professor at the University of Maryland School of Medicine, with research interests “in developing vaccines against pathogens which afflict low- and middle-income countries” as well as in vaccine development for the elderly. Chen has headed up vaccine trials for influenza viruses, enteric pathogens and “agents of bioterror.”
Chen is co-investigator for two entities funded by the Anthony-Fauci-led National Institute of Allergy and Infectious Diseases (NIAID): the Vaccine Treatment and Evaluation Unit (composed of 10 academic centers throughout the U.S.) and the Collaborative Influenza Vaccine Innovation Centers (a network of research centers developing “novel vaccine candidates and delivery platforms”).
In advance of the ACIP vote on the 5–11 age group, CHD joined numerous citizens in arguing (unsuccessfully) that Chen be removed from the committee for blatant financial conflicts of interest. In 2020 alone, Chen accepted $437,251 from vaccine makers GlaxoSmithKline (GSK) and Emergent BioSolutions — a fact “researched and exposed by average citizens” rather than disclosed by CDC. Chen’s payments since 2014 total over $476,880 and include monies from Janssen, Seqirus, MedImmune, Astellas Pharma, Valneva Austria and BioFire Diagnostics in addition to the two companies already mentioned.
Chen also receives research funding from the Gates Foundation and from the Seattle-based global health organization PATH. PATH’s former CEO, Christopher Elias, now serves as president of the Gates Foundation’s Global Development Division, leading efforts in areas such as vaccine delivery and family planning; Elias was a leading Event 201 participant.
Also of note:
- In addition to serving as a voting member of ACIP, Chen is a core member of NIAID’s Data and Safety Advisory Board.
- During COVID, Chen has been a staunch advocate of “aggressive nonpharmacologic intervention and control measures,” including “aggressive recognition and isolation and quarantine of cases and contacts.”
- Despite the well-documented risks and failures of influenza vaccination, Chen continues to insist that “Vaccination is by far the best method to prevent and control influenza.”
- Chen recently voted to make a highly reactogenic Ebola vaccine obligatory for healthcare personnel, lab workers and support staff at facilities that handle Ebola specimens, arguing against letting workers make their own risk-benefit decisions.
Sybil Cineas
Sybil Cineas, M.D. (sybil_cineas@brown.edu), a Harvard Medical School graduate, is an associate professor of medicine, pediatrics and medical science at Brown University, and, as associate program director of Brown’s combined residency program in internal medicine and pediatrics, is “highly involved in the training of residents and medical students.”
According to CDC, Cineas has “20+ years of experience teaching about and promoting vaccination.”
Like fellow ACIP members Beth Bell and Oliver Brooks, Cineas frequently cites health equity to justify her vaccine votes. For example, as a member of the ACIP Hepatitis Work Group, which recently recommended hepatitis B vaccines for everyone age 59 and younger while issuing a more qualified risk-based recommendation for adults age 60 and up, Cineas wanted to recommend universal hepatitis B vaccination for all ages. She argued, “A simplification of this recommendation [would] reach more individuals at risk … and promote health equity.”
Also of note:
- CDC has given Brown researchers $4.9 million to study COVID vaccine effectiveness in seniors; the researchers state that “the urgently needed research will be used to inform recommendations about vaccine booster shots for nursing home residents.”
Matthew Daley
Matthew Daley, M.D. (matthew.f.daley@kp.org) is a senior investigator and practicing pediatrician at Kaiser Permanente Colorado, described by CDC as having “extensive research experience in the areas of vaccine safety, parental vaccine hesitancy, and immunization services delivery.”
Daley’s published studies on vaccine “hesitancy” cover topics such as social media interventions to increase vaccine acceptance, barriers to adolescent human papillomavirus (HPV) vaccination, under vaccination patterns and parent-provider trust. (In one study, parents reported trusting pediatricians on topics such as nutrition but “did not believe their pediatrician provided ‘balanced’ information on both the benefits and risks of vaccination.”)
Daley also conducts Vaccine Safety Datalink (VSD) studies on a variety of topics, including safety of newly licensed vaccines, vaccine safety during pregnancy and, according to the CDC, safety of the childhood immunization schedule.
After the Institute of Medicine acknowledged that studies “to examine the long-term effects of the cumulative number of vaccines or other aspects of the immunization schedule have not been conducted” — and identified the VSD as “an important resource for conducting this research” — Daley and CDC co-authors wrote a white paper to describe how this could be done but shrouded their remarks in so many caveats about potential studies’ “inherent complexity” as to make their feasibility seem highly doubtful.
Daley’s VSD studies, some co-authored with ACIP colleague Grace Lee, have identified potential safety signals, but in each case, Daley and co-authors have found reasons to reject or mask their own conclusions.
Examples include attributing a statistically significant association between hepatitis A vaccination during pregnancy and small-for-gestational-age infants to “unmeasured confounding”; putting forth “seasonality” as the likely contributor to a statistical signal for Bell’s palsy in adults age 25 and up following H1N1 influenza vaccination; and dismissing as “rare” two types of adverse events (anaphylaxis and fainting) significantly associated with live attenuated influenza vaccination in children 2 through 17 years of age.
Also of note:
- After the vote recommending the COVID shots for younger children, Daly professed to not be surprised by parents’ hesitation, stating that parents “may be more risk-averse about their child.” However, though Pfizer’s clinical trial in children was too short and too small to assess the risk of myocarditis, Daley confidently asserted that “younger children are at a greater risk of developing myocarditis after a COVID infection than from the vaccine.”
- A current VSD/CDC study by Daley is assessing “factors associated with COVID vaccination or non-vaccination” in the general population and among pregnant women.
Camille Kotton
Camille N. Kotton, M.D. (ckotton@partners.org) is clinical director for Transplant and Immunocompromised Host Infectious Diseases at Massachusetts General Hospital and an associate professor at Harvard Medical School. CDC describes Kotton as a “national expert in vaccination and zoonotic infectious diseases in the immunocompromised,” including solid organ transplant recipients.
Since 2014, Kotton has received over $304,000 in general payments and associated research funding from companies like Merck, GSK, Roche, Quiagen Sciences, Oxford Immunotec, Astellas Pharma, Shire, Takeda Pharmaceuticals, BeiGene and Biotest.
In voting to give younger children the COVID injections, Kotton stated, “the safety data in children looked very good” and added, “she would feel comfortable having her own children immunized if they were in that age group.”
Although few children suffer ill effects from COVID-19, Kotton argued that children should be vaccinated “both to prevent death as well as to prevent major long-term effects of having this devastating infection.”
Also of note:
- Kotton promotes routine vaccination of individuals with inflammatory bowel disease (IBD) despite evidence of IBD’s association with some vaccines.
- Kotton has co-authored papers on vaccine development with “Godfather of Vaccines” Stanley Plotkin.
- In the past, Kotton has disclosed conflicts of interest due to her financial relationships with (and vaccine “adjudication” for) companies like Merck, Astellas, Roche and others.
James Loehr
James Loehr, M.D. (staff@cayugafamilymedicine.com) owns Cayuga Family Medicine in Ithaca, New York. According to CDC, for 30 years Loehr has counseled patients “every day on the benefits of vaccines.” Loehr was a member of ACIP’s influenza working group for more than 10 years.
In 2015, Loehr authored an article with detailed instructions telling physicians how to “minimiz[e] costs and maximiz[e] reimbursement” to “make immunizations profitable.”
Describing how Cayuga Family Medicine “enjoys steady revenue from immunizations, with vaccine reimbursement sometimes exceeding that for the rest of the visit,” Loehr outlined a series of strategies to improve a practice’s financial viability through vaccination, including becoming a “savvy vaccine shopper,” taking advantage of manufacturer discounts and doing “a bit of additional work” when coding for the service to obtain extra reimbursement for “brief counseling” and multiple vaccine components.
At an October ACIP meeting focused on Moderna boosters that was, according to Stat, driven by a “sense of the inevitability of [the] outcome,” Loehr stated, “There are probably many people who are going to get a Moderna booster who don’t need it. However, given the situation that we’ve already approved a Pfizer [booster] and there are enough people who are looking for a booster, I am inclined, reluctantly, to just go ahead and recommend a similar pattern for the Moderna booster.”
Loehr was similarly wishy-washy the previous month when he stated, “I … feel that we’re getting too much ahead of ourselves and that we have too much hope on the line with these boosters.”
He then added, “However, having said that, we shouldn’t let the perfect be in the way of the good. And if we can do a little bit of good by giving boosters to people over 65 I’m in favor of that.”
Loehr is a past Vaccine Fellow of the American Academy of Family Physicians (AAFP). Speaking for AAFP, Loehr has noted that the medical trade group “does not support nonmedical immunization exemption policies.” AAFP does support COVID-19 vaccine mandates for health and long-term care workers, and last August, it also started lobbying FDA to authorize the vaccines for children under age 12.
Also of note:
- Like most of his ACIP peers, Loehr promotes himself as an expert on “strategies for addressing and overcoming vaccine hesitancy,” stating that “most patients…are not truly resistant to immunization” but just want “clarification and reassurance.”
Sarah Long
Sarah Long, M.D. is a professor of pediatrics at Drexel University College of Medicine and a physician at St. Christopher’s Hospital for Children in Philadelphia. In addition to her role on ACIP, Long has served on VRBPAC and as a member of the American Academy of Pediatrics (AAP) Committee on Infectious Diseases.
Long was widely quoted in the press following her “yes” vote on COVID injections for children. Though she expressed several concerns and voted “no” in September regarding Pfizer boosters for healthcare workers, Long “threw her full support behind the pediatric recommendation.”
Fully aware that “CDC was not able to conduct a full benefit-risk analysis for myocarditis post-vaccination in this age group,” Long is nevertheless telling mothers that the shot’s risks are preferable to the myocarditis that could arise from COVID illness.
Without citing any evidence, Long states that “vaccine-related events are completely different, and much less dire, than typical myocarditis,” adding that “she’d rather treat many people with vaccine-associated myopericarditis than a single case of viral myocarditis.”
Claiming that “Nobody has died of myopericarditis, and children are dying of coronavirus,” Long has concluded that “of course it’s a benefit-risk ratio that comes out in the direction of vaccination.”
The hundreds of teens who have experienced post-vaccination myocarditis — some now dead — might beg to differ.
Ironically, Long’s bio includes numerous “awards and honors for her outstanding work to improve the health and well-being of children.” After the “yes” vote on COVID shots, she reportedly joked, “I, believe it or not, have no questions. I have just a comment: I am very supportive of this recommendation in its fullest extent, as a ‘should,’ not a ‘may,’ for all children in this age group.”
Long continued, “I think the data support that we have one more vaccine that saves lives of children, and that we should be very confident to employ it to the maximum to do what it is meant to do, without significant concerns of serious adverse events. So, I couldn’t be more supportive.”
Also of note:
- Drexel University received half a million dollars from the Gates Foundation in June 2020 “to evaluate the use of a digital health platform to make care for COVID more accessible to marginalized populations.”
- The Gates Foundation is also supporting the work of other Drexel researchers in areas such as diagnostic test development.
Veronica McNally
Veronica V. McNally, JD (valent29@law.msu.edu) is a law professor and an assistant dean at Michigan State University. McNally is ACIP’s “consumer representative.”
Having lost an infant to pertussis, McNally describes herself as a “public health advocate” in addition to being an attorney.
She is founder and president of the Franny Strong Foundation — framing a mission to “promote pertussis awareness and boost childhood immunization rates for all vaccine-preventable diseases” — and founded the I Vaccinate Campaign, which, on November 16, excitedly reported that “nearly 1 million kids ages 5-11 will have their first COVID shots by the end of today.”
McNally is seemingly unaware of the many failures of a pertussis vaccination program that is widely acknowledged to be making vaccinated children more rather than less susceptible to pertussis over their lifetimes.
Also of note:
- McNally is a CDC darling, having been named “Childhood Immunization Champion” for Michigan in 2018 — the same year in which she was appointed to her four-year term on ACIP.
Katherine Poehling
Katherine A. Poehling, M.D., MPH (kpoehlin@wakehealth.edu) is a professor of pediatrics and epidemiology at North Carolina’s Wake Forest University School of Medicine. CDC cites her expertise “on the community impact of vaccines, specifically pneumococcal and influenza vaccines.”
As an ACIP insider, Poehling has headed up past ACIP presentations on pneumococcal vaccines.
Poehling has published on “ethics and academic pediatrics” but apparently sees no conflict in sitting on ACIP while receiving, according to Open Payments, over $523,000 in general payments and associated research funding from MedImmune and AstraZeneca since 2014.
Poehling endorses CDC’s astonishingly fact-free claim that COVID has caused “substantially more misery than other childhood diseases,” stating, “that information helped convince her to strongly support COVID-19 vaccines for elementary school children.”
Poehling also buys into Long’s non-evidence-based assertion that COVID-19 disease is responsible for more heart problems than the vaccine. During a May review of Moderna data, Poehling enthusiastically favored making multiple vaccines available — to “increase access.”
Also of note:
- When endorsing COVID boosters for the immunocompromised, Poehling stated, “the benefits are tremendous and the potential negative impacts are minimal and so I agree that we should recommend.”
- Many of Poehling’s publications seem intended to address the burden of diseases such as influenza for which vaccine “solutions” can then be promoted. It seems likely that her published articles about respiratory syncytial virus (RSV) will be used to lay the groundwork for an mRNA vaccine for RSV.
Pablo Sanchez
Pablo J. Sanchez, M.D. (sanchez.940@osu.edu) has been a professor of pediatrics at Ohio State University since 2013 and directs Clinical and Translational Research in Neonatology at Nationwide Children’s Hospital in Columbus. Sanchez previously held positions at University of Texas Southwestern Medical Center.
Sanchez’s 80-page self-congratulatory curriculum vitae reveals that he is a consummate insider fluidly bridging academia, public health agencies and private industry. Sanchez’s invited participation and lectures include appearances at public health agencies like CDC, the World Health Organization (WHO) and the Pan American Health Organization (PAHO); COVID-vaccine-promoting trade groups like the AAP and March of Dimes; and biopharma companies like AbbVie, GSK (formerly Smithkline Beecham), ICN Pharmaceuticals, Inhibitex, MedImmune and Ross Laboratories.
Sanchez also lists hundreds of thousands in research monies received from these same entities.
Since the 1990s, Sanchez has been funded by Abbott Laboratories, American Lung Association, BioStar, Biosynexus, Burroughs Wellcome, CDC, F. Hoffman-La Roche, Gerber Foundation, MedImmune, NIAID, NICHD [National Institute of Child Health and Human Development], Pediatric AIDS Foundation, Ross Laboratories and Smithkline Beecham/Glaxo/GSK.
According to Open Payments, since 2014, Sanchez has pocketed roughly $221,000 in general payments and associated research funding from AbbVie, AstraZeneca, F. Hoffmann-La Roche, MedImmune, Medtronic, Merck, Novartis, Sanofi Pasteur, Seqirus and Sobi.
The database lists AstraZeneca, MedImmune and Merck as the “top companies making associated payments,” with notable payments from Merck in Fall 2020.
In June, Sanchez hedged his bets on the topic of COVID vaccines and myocarditis. While declaring that the benefits of vaccination outweigh myocarditis risks, he also noted, “we need to be very upfront in terms of mentioning this as a potential risk of COVID messenger RNA vaccination. Hopefully, the parents and patients are aware of this before vaccination.”
Sanchez did not repeat these remarks at the November meeting when he okayed the jab for 5-year-olds.
Also of note:
- In 2010, Sanchez served as a “Pfizer visiting professor.”
- Sanchez served on VRBPAC from 2007–2010 as well as on FDA’s vaccine-focused Pediatric Advisory Committee from 2010–2012. In Texas, he chaired the Texas Pediatric Society’s Committee of Infectious Diseases and Immunizations from 2004–2009 and served on the committee from 1995–2013.
- Many of Sanchez’s publications focus on amplifying concern about illnesses attributed to viruses— such as cytomegalovirus, herpes simplex, RSV and Zika — for which Moderna and other companies now anticipate developing mRNA vaccines.
Helen Keipp Talbot
Helen Keipp Talbot, M.D., MPH (keipp.talbot@vumc.org) is associate professor of medicine at Nashville’s Vanderbilt University, where she has held various appointments since 2002. Talbot’s research and publications (sometimes co-authored with fellow ACIP member Poehling) center on adult vaccination, influenza vaccination, human coronaviruses and vaccine trials for respiratory illnesses such as RSV. The focus on coronaviruses pre-dates COVID; from 2007–2009, Talbot was principal investigator on an NIH-funded study on the “epidemiology of human coronaviruses.”
According to Talbot’s curriculum vitae, her recent research funding comes from both the federal government (CDC, National Institutes of Health [NIH]) and Sanofi Pasteur, primarily for the study of pandemic preparedness (in 2015) and influenza vaccination. Sanofi and MedImmune have been recurrent funders since 2009, along with AstraZeneca, Gilead, Protein Sciences, VaxInnate and Wyeth (since acquired by Pfizer).
Open Payments lists Talbot’s receipt of roughly $1.4 million in research payments and associated research funding since 2014 (417 total payments) from these companies, along with 29 general payments totaling $17,000.
In December 2020, Talbot was the “lone dissenter” objecting to ACIP’s recommendation that long-term care residents “be at the front of the line” for COVID vaccines. At the time, Talbot argued that vaccination of long-term care residents was “risky” because they “have a high rate of medical events that could be confused as side effects of vaccination and undermine confidence in the vaccines.”
Talbot stated, “And I think you’re going to have a very striking backlash of, ‘My grandmother got the vaccine and she passed away.’” Talbot elaborated: “I fear a loss of confidence in the vaccine…. [T]here will be temporally associated events and people will be scared to use the vaccine.”
Talbot exhibited no scruples in voting to administer COVID vaccines to young children. On the same day as the “yes” vote, Talbot told the press, “I have vaccinated my kids” (who, presumably, were at least 12 years of age at the time of injection).
Also of note:
- In 2008, Talbot received a Sanofi Pasteur Advanced Vaccinology Course travel grant.
- Talbot is on the editorial board of the journal Vaccine.
And … Rochelle Walensky
No overview of ACIP would be complete without noting the conflicts of interest surrounding CDC Director Rochelle Walensky, who used ACIP’s vote to immediately green-light vaccination of younger children.
As reported by independent media outlet RedState (but not by the mainstream media), Walensky’s husband, Loren Walensky, became scientific co-founder and board member of early-stage biotech company Lytica Therapeutics in October 2019.
In December, the Biden administration announced Rochelle Walensky’s pending appointment as CDC director, and in February 2020, Lytica received the first installment ($5.3 million) of a $16.9 million grant from HHS, representing the “only funding this new company [had] received to date — nearly two years after its founding.”
Even before becoming CDC director, Walensky had been “directly associated with HHS for more than a decade,” including close participation on committees and panels with Anthony “Tony” Fauci. According to RedState’s exposé, “when ‘insiders’ were surprised that Walensky was picked [to head CDC], it was revealed that Fauci had a lot to do with her appointment.”
Loyal to Fauci, Walensky has written opinion pieces for leading media outlets “about how to fairly and effectively distribute Remdesivir,” the ineffective, expensive and dangerous drug promoted by NIAID and Fauci as virtually the sole treatment option for hospitalized COVID patients.
A former Boston colleague of Walensky’s stated the CDC director “has a lot of Tony in her,” including the “ability to take complex information and convey it in clear and concise messaging.”
Shunning and Nuremberg 2.0
As bad as the ACIP (and VRBPAC) decisions were, vaccine-risk-aware observers are even more shocked that CDC and FDA are “blithely” allowing Pfizer’s shot to be administered to children and adolescents with other vaccines at the same time.
As Informed Choice Washington put it last May regarding the authorization for kids ages 12 and up:
“As unethical as it is to expose children to investigational liability-free products that have seen unprecedented levels of vaccine adverse reactions and deaths reported … when ACIP opened up the shots to be co-administered with other vaccines, including those with adjuvants, they stepped fully into crimes against humanity. Not a single clinical trial has been done administering the COVID-19 shots with any other vaccine. There is zero safety data.”
Other observers agree with this assessment, arguing that “Every single person associated with the ACIP meeting today must be tried for crimes against humanity at Nuremberg 2.0.” Some are also calling for a second Nuremberg trial for “perpetration of COVID-response policies that led to forced shutdowns, destroyed businesses, impoverished families, broken lives and a spike in suicide rates.”
In the meantime, it is time to shun ACIP members. And because it is inconceivable that ACIP members would behave in such a corrupt manner without the approval and say-so of their institutions, shunning actions necessarily must also extend to the universities and other institutions that have these individuals’ backs.
- Send a Notice of Liability to each ACIP member — see examples at the Doctors for Covid Ethics website.
- Check the campaign contributions of ACIP members at OpenSecrets.org. If they are donating to a politician who represents your state or Congressional District, call or write your representative and ask why they are accepting donations from people who are seriously compromised by the pharmaceutical industry and harming our children.
- Refrain from appointing ACIP members to the Boards of community organizations — or revoke their current Board appointments. These types of “good citizen” positions should not be offered to people who are not behaving as “good citizens.”
- All universities benefit from state and local appropriations; contact your legislators, explain that academic operations at these universities are clearly supporting federal corruption and demand that the legislators revoke the appropriations.
- Write to the board of trustees or person who manages the university endowment. Demand they disclose their investments in companies that are harming our children and explain how these investments support active participation in federal corruption by those affiliated with the university.
- Stop donating to the universities and academic departments in question and let them know why. When asked for an update by your university alumni group, ask to be removed from the alumni email list and database, and explain you have stopped donating to the university as a result of its support of federal corruption.
- Cancel your season tickets and other participation in sports and cultural events at the university. Explain why.
- If you are involved in recruiting for your company, remove these universities from your recruiting lists. Write to the university’s placement office to explain why.
- Ask local newspapers to publish copies of the letters you write to university officials. Organize to support members of the independent media in researching and publishing information regarding ACIP members’ conflicts of interest, as well as the university conflicts of interest that compromise the institutions’ intellectual resources and activities in science, medicine and technology.
- Write to the university chaplain and ask for prayers for the university to be released from the spirit of corruption. Provide details.
- Identify the banks involved in managing the university’s bank accounts, financial assets, endowment and pension funds; where applicable, demand to know why the university is doing business with banks that have compromised our federal government accounts and are financing policies at the federal level that are harming our children.
- Do not buy or hold stocks in companies with which ACIP members are connected.
- Do not buy products or drugs that ACIP members have developed or patented.
- Make it clear — through letters to the editor and letters to the institutions — that you will not forget ACIP members’ decision to enable the needless harming of young children.
©November 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
“Dr. Fauci, Mr. Hyde” – RFK, Jr. in Conversation With James Corbett: “There’s an Entire Coalition of Sinister Forces… Which Are All Wrapped Up in This Obliteration of Constitutional Rights…”
“Dr. Fauci, Mr. Hyde” – RFK, Jr. in Conversation With James Corbett: “There’s an Entire Coalition of Sinister Forces… Which Are All Wrapped Up in This Obliteration of Constitutional Rights…”
‘Dr. Fauci, Mr. Hyde’: RFK, Jr. Shares Details About New Book on ‘The Corbett Report’
On a recent episode of “The Corbett Report,” journalist and researcher James Corbett interviewed Robert F. Kennedy, Jr. about his latest book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health.”
by Jeremy Loffredo, The Defender
November 24, 2021
On a recent episode of “The Corbett Report,” journalist and researcher James Corbett interviewed Robert F. Kennedy, Jr. about his latest book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health.”
Asked why he wrote the book, Kennedy said:
“Over the past 20 months [there’s been] a coup d’état against liberal democracy, and one of the key players in this medical cartel or medical technocracy is Dr. Anthony Fauci.
“There’s an entire coalition of sinister forces [including] pharmaceutical companies, the intelligence agencies, the medical bureaucracies, the social media titans, the mainstream media and the military, which are all wrapped up in this obliteration of constitutional rights and the use of a health crisis to impose totalitarian controls.”
Kennedy described Fauci as “this sort of avuncular presence who is the face of the technocracy and the demolition of constitutional rights.”
Kennedy discussed Fauci’s role in helping Big Pharma capture federal regulatory agencies. “Fauci is the spearhead of an agency that has experienced regulatory capture on steroids,” he said.
Kennedy told Corbett the financial links between the federal health agencies and the pharmaceutical companies are unlike any other federal regulatory regime. The metrics used within these agencies to measure whether or not an employee will get promoted, advanced or get a salary raise revolve almost entirely around how well the employee promotes vaccine uptake.
[These] people do not get rewarded for finding problems with vaccines — they get rewarded for covering up problems with vaccines … and some of the agencies directly profit from vaccine sales,” Kennedy said.
“For example, the [National Institutes of Health] owns thousands of medical patents, including half of the patent for the Moderna vaccine,” Kennedy said. “So Tony Fauci’s agency stands to make billions and billions of dollars. And Fauci was able to choose four of his high-level employees who each get their own individual patent shares and who’ll collect $150,000 per year for life.”
Corbett said the chapter of Kennedy’s book he found the “most difficult to read through” was the one titled, “Dr. Fauci, Mr. Hyde: NIAID’s Barbaric and Illegal Experiments on Children,” which details the role of Fauci and the organization he heads up — the National Institute of Allergy and Infectious Diseases — in illegal experiments on foster children.
“In this case [Fauci] was able to get control of different foster homes in seven states and essentially turn these pharmaceutical companies loose onto these children,” Kennedy said. “The experiments were absolutely barbaric … the children were tortured and they did not have legal representation.”
Kennedy added:
“The children who stopped taking the drugs because they were making them sick were sent to Columbia Hospital to have feeding tubes installed so the drug companies could [continue testing on them] even when they fought back. At least 85 of these kids died.”
Kennedy also cited the dramatic rise in chronic illness since Fauci took office, pointing out that Fauci has failed to protect the public from environmental health threats.
Other topics covered by Kennedy and Corbett include how Fauci was “locked into” carrying out controversial gain-of-function research for the military, how a large portion of Fauci’s salary comes from the Pentagon and the involvement of the Central Intelligence Agency in pandemic planning and policy.
Watch the interview here + buy the book here:
©November 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
La Quinta Columna on What Parts of the Body Are Most Affected by Covid Vaccines and Why This Is Happening
La Quinta Columna on What Parts of the Body Are Most Affected by Covid Vaccines and Why This Is Happening
Dr. Sevillano on the most affected organs post-inoculation
by Orwellito, Orwell City
November 24, 2021
In a new round of questions addressed to Dr. Sevillano in La Quinta Columna, he was asked which organs are most affected post-inoculation and why.
Below, Orwell City brings his answer in English.
Video available at Rumble.
Transcript:
Ricardo Delgado: ‘What would be the reason why the vaccine attacks different organs in different people?’ Because it’s a toxicant…
Dr. Sevillano: Well, very good question. That’s a very good one. At the moment, this has two targets. One is the heart —you’re seeing what’s happening at the moment— and the head. What’s happening is that as we’re realizing, it seems to be that the heart is suffering more damage than the head and the cardiovascular.
That’s to say, the product is going into the blood, and in the blood, it’s generating thrombosis. Don’t lose any more. First, there are thrombi, and then there are the different places where this thrombus can do damage.
The first thing: it causes damage in the blood, it causes coagulation, but then, when it can cross, let us say, the capillaries, and it starts to localize in many places, it starts looking for, it stays, it tries to get into the places where there’s an important electrophysiological activity, such as the heart and the head.
But in the head, it has the blood-brain barrier, and if the size of the particle is very high, it doesn’t cross it. We don’t know if it’s entering or not. It seems to be entering the heart more than the head, but in reality, it goes everywhere. It goes everywhere. It goes following… What happens is that it’s attracted to the places where there is great electrophysiological activity. A great activity, such as the nerves, the nervous system, and the heart.
Why? Because they’re cells that are constantly working, constantly launching electrical stimuli. The heart and the nerves. Muscles need a tone for that, they need a rhythm, but they don’t have the intensity, let’s say, they don’t do the same work that the heart does, which is constant and permanent, of contraction and relaxation, and it is completely directed by electrical polarization of its cells. Those polarizations aren’t done by the muscles of the skeletal muscle system. It’s a much less powerful activity.
That’s why people suffer, above all, from nerve problems, Guillain-Barré —like what this guy told us earlier— and in the heart more than in other places. But it does go elsewhere. And it’s responsible for hepatitis that has been seen and continues to be seen. And pancreatitis. And what else has it triggered? The meningoencephalitis that we’ve seen. I mean, that does go everywhere, but particularly, it goes to you know where.
Ricardo Delgado: Heart and head.
Dr. Sevillano: Exactly. And be careful because people who drink it or swallow it … When they ingest it develop gastroenteritis of those that give diarrhea of those in which you spend four or five months with your pants down looking for the toilet all the time. And they say that they don’t know where it comes from either.
There are quite a few of this type of colitis they haven’t seen, and they don’t know where it comes from. They don’t know.
They do the biopsies, and they say, “This was colitis that I don’t know how it came about.”
In other words, it was an inflammation of the colon and so long. But we do know. Especially, when you see those kinds of patients fall near antennas.
Those people drink it somehow in some product, whether it’s in the water or in the food. That’s where those kinds of problems come from. But it does affect, mostly, the heart and the head. And what makes me think that right now we’re not seeing people losing their minds completely, is that I get the feeling that the particles are too big to get through the barrier. And that’s why little material gets through, at the moment. But wait until the new doses start to contain smaller-sized particles.
cover image credit: www_slon_pics / pixabay
Melbourne, Australia Rally 200,000 Protesters | Premier Dangerous Dan in Safe House, Too Many Threats
Melbourne, Australia Rally 200,000 Protesters | Premier Dangerous Dan in Safe House, Too Many Threats

by Cairns News
November 24, 2021
Video available at Rumble
The biggest protest in Australian history? Reliable estimates put the crowd at 200,000 people in Melbourne November 20th rally 2021 .
More Australian Freedom Rallies are planned around the nation this Saturday.
Covid Concentration Camps for Australians; It’s Happening
Covid Concentration Camps for Australians; It’s Happening
by Jon Rappoport, No More Fake News
November 24, 2021
Zero Hedge, November 22, 2021: “The Australian army has begun forcibly removing residents in the Northern Territories to the Howard Springs quarantine camp located in Darwin, after nine new Covid-19 cases were identified in the community of Binjari. The move comes after hard lockdowns were instituted in the communities of both Binjari and nearby Rockhole on Saturday night.”
“’Residents of Binjari and Rockhole no longer have the five reasons to leave their homes,’ said Northern Territory chief minister, Michael Gunner, referring to the country’s five allowable reasons to avoid lockdown (buying food and supplies, exercising for up to two hours, care or caregiving, work or education if it can’t be done from home, and to get vaccinated at the nearest possible location).”
“’They can only leave [home] for medical treatment, in an emergency, or as required by law’.”
“’It’s highly likely that more residents will be transferred to Howard Springs today, either as positive cases or close contacts,’ he continued, adding ‘We have already identified 38 close contacts from Binjari but that number will go up. Those 38 are being transferred now’.”
“’I contacted the Prime Minister last night. We are grateful for the support of about 20 ADF personnel, as well as army trucks to assist with the transfer of positive cases and close contacts – and to support the communities’.”
“’We are doing an assessment today of what extra resources we might need from the Feds, and the Prime Minister is ready to help further – I thank him for that’.”
“Five days ago, NT [Northern Territories] Senator Malarndirri McCarthy told ABC that over crowding in Indigenous communities was a ‘massive problem,’ pointing to the region’s second cluster of new infections – which included nine members of McCarthy’s direct family, including her sister who flew from Katherine to Robinson River while unknowingly bringing COVID-19 with her, per the report.”
The sociopaths and their stormtroopers who run Australia would make Hitler and Stalin envious. “You mean you can exercise iron control over a whole nation based on a STORY ABOUT A VIRUS?”
I’ve received a report from Australia showing numbers of protesters against the national vaccine mandate, in key cities, for the weekend of November 20-21. The total is close to a million people—in a nation of 25 million. That’s stunning.
Hopefully, those numbers will increase.
Update: another report from Australia; the military have begun forcing vaccinations on the aborigines in the Northern Territory.
It’s abundantly clear we’re not living in the same world we were two years ago. That world doesn’t exist anymore.
Watch this shocking video made by June Mills, an aboriginal elder in the Northern Territory. As she excoriates the fascist Chief Minister of the Territory, Michael Gunner, and calls on her people in other towns to report on what’s happening to them and what the Army is doing, ask yourself: Is this the irrational raving of a woman who’s gone over the edge, or is this exactly how a sane person would react when government killers are loose in her neighborhood?
SOURCES:
https://www.facebook.com/TerritoryChief/posts/435285761296933 (Micheal Gunner’s statement)
https://aecom.com/projects/manigurr-ma-village/ (Howard Springs COVID concentration camp)
https://www.brighteon.com/cf5650c2-4167-4be8-9ca6-47d2bb52961d (June Mills’s call to action)
cover image credit: Fifaliana-joy / pixabay
Australian Army Called In to Transfer Indigenous Covid Contacts to Quarantine Camps
Australian Army Called In to Transfer Indigenous Covid Contacts to Quarantine Camps
Removing aboriginal people from their homes into a government-operated facility branded as disturbing and a violation of human rights
by Alexandra Marshall, Rebel News
November 24, 2021

Disturbing news has surfaced from the Northern Territory where the army has been brought in to round up 38 indigenous Covid contacts and escort them to compulsory quarantine camps.
“It’s highly likely that more residents will be transferred to Howard Springs today, either as positive cases or close contacts,” said Michael Gunner, Chief Minister of the Northern Territory. “We have already identified 38 close contacts, but that number will go up. Those 38 are being transferred now.”
The Howard Springs quarantine facility in Darwin was set up to process travellers coming into the state domestically and internationally. Expensive quarantine periods are enforced on those attempting to enter the Northern Territory which must be paid for by the traveller.
However, removing Indigenous people from their homes into an government-operated facility has been branded as both disturbing and a violation of human rights.
🇦🇺 #Australia: Quarantine Camps. The 'conspiracy theory' comes true.
Michael Gunner: "We’re grateful for the support of about twenty ADF personnel as well as army trucks to assist with the transfer of positive cases and close contacts".
Wake up world. #HumanRightsViolations pic.twitter.com/3se38HOnuc
— Know Your Human Rights (@HumanRights4UK) November 22, 2021
The army is on loan from the Prime Minister.
This comes after the Northern Territory issued a hard lockdown on remote communities, preventing residents from leaving their homes to buy food or supplies, exercise, give care, work, or access education.
“Residents of Binjari and Rockhole no longer have the five reasons to leave their homes,” announced Michael Gunner.
People inside the lockdown area can only leave their homes for medical treatment, an emergency situation, or if the law requires it.
Although Michael Gunner continues to enforce some of the strictest Covid health orders in Australia, vaccination rates for the Indigenous community lags behind. This is partly due to vaccine hesitancy in remote communities where many have said that they do not want to partake in Covid vaccines.
The government and Indigenous health groups have been setting up information campaigns inside these communities.
“It [the ‘Spread the Freedom’ campaign] is designed to really highlight the close links between vaccination and either regaining those freedoms that we all want to enjoy, or protecting those freedoms in the states where we haven’t yet seen outbreaks,” said Lieutenant General Frewen.
A second campaign ‘For All Of Us’ is also attempting to reach these populations.
Aboriginal & Torres Strait Islander people have over 60,000 years of history. 60,000 years of culture, art, song, dance & language. But let’s not forget where we’re going—with vaccination, the future is bright☀️
Get vaccinated against COVID-19💪🛡️Visit💻https://t.co/LPNXcd3koi pic.twitter.com/E9ENwS7s9L
— Australian Department of Health and Aged Care (@healthgovau) October 23, 2021
The general message of both government-operated advertising initiatives is that if you want to have your freedom back, get vaccinated.
“I’ve always said that I wanted 100% vaccination of our people before the country opened up. Well, obviously that hasn’t happened,” said Pat Turner, CEO of the National Aboriginal Community Controlled Health Organisation. “The Northern Territory have now got their wake-up call and we should not have to wait until these infections get in before the health authorities get in and start the vaccinations. They’ve got to do it now.”
While the messaging from the government may be about ‘All Of Us’, it’s clear that some in the political class are privileged not to have to play by the same rules.
There does not appear to be any serious discussion, either from Indigenous advisory groups or the Northern Territory government, about valid informed consent or the ability for Indigenous people to say ‘no’.
The Federal government, under the direction of Greg Hunt the Minister for Health and Aged Care, has extended Covid measures introduced to protect remote communities in the Northern Territories.
Communities surrounding the Robinson River will be sealed off under section 477 of the Commonwealth Biosecurity Act 2015 until 6pm, 1 December 2021 as requested by the Northern Territory government.
Despite building and operating quarantine facilities, the Northern Territory has not significantly expanded its critical care or intensive bed capacity in the two years since Covid first appeared.
“The Doherty Institute modelling shows that we can have between 30 and 100 cases a day at an 80% vaccination rate across the Northern Territory, and our health system can manage,” said Northern Territory Health Minister Natasha Fyles. “But it means we’ve had to make changes, so in the Top End we’ve gone to tier 3 and deferred elective surgery.”
Meanwhile, mental health patients were forced to wait for beds at the Royal Darwin Hospital in June, despite there being no active cases in the Northern Territory for over a month.
There has been a surge in mental health emergencies blamed on Covid which has pushed hospitals in the region beyond capacity.
cover image credit: AAP — Glenn Campbell via abc.net.au
Fake Science, Invalid Data: There Is No Such Thing as a “Confirmed Covid-19 Case”. There Is No Pandemic.
Fake Science, Invalid Data: There Is No Such Thing as a “Confirmed Covid-19 Case”. There Is No Pandemic.
by Prof Michel Chossudovsky, Global Research
November 23, 2021
“The PCR is a Process. It does not tell you that you are sick”.
Dr. Kary Mullis, Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“…All or a substantial part of these positives could be due to what’s called false positives tests.”
Dr. Michael Yeadon: former Vice President and Chief Science Officer for Pfizer
This misuse of the PCR-RT technique is applied as a relentless and intentional strategy by some governments to justify excessive measures such as the violation of a large number of constitutional rights, … under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.
.Dr. Pascal Sacré, Belgian physician specialized in critical care and renowned public health analyst.
To read PART I of this article click link below
The Covid-19 Pandemic Does Not Exist — Part 1
Introduction
Media lies coupled with a systemic and carefully engineered fear campaign have sustained the image of a killer virus which is relentlessly spreading to all major regions of the World.
Several billion people in more than 190 countries have been tested (as well as retested) for Covid-19.
At the time of writing, approximately 260 million people Worldwide have been categorized as “confirmed Covid-19 cases”. The alleged pandemic is said to have resulted in more than 5 million Covid-19 related deaths.
Both sets of figures: morbidity and mortality are fabricated. A highly organized Covid testing apparatus (part of which is funded by the billionaire foundations) has been established with a view to driving up the numbers of “Confirmed Covid-19 Cases”, which are then used as a justification to impose the “vaccine” passport coupled with the repeal of fundamental human rights.
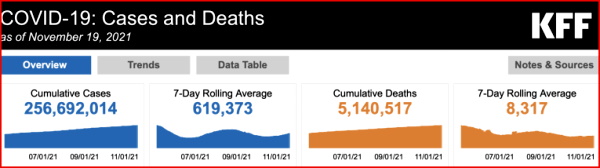
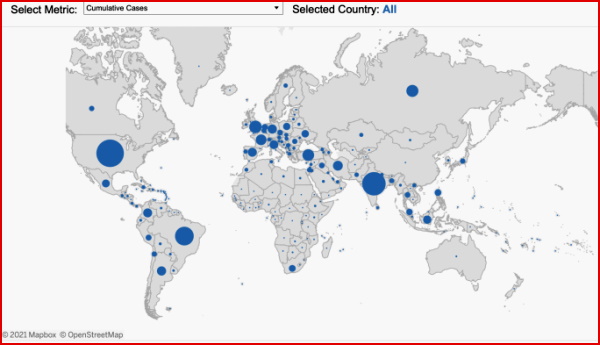
A so-called “Global Tracker System” has been established with an interactive map pointing to global as well as country level trends and weekly tendencies.
A Fourth Wave has been announced. Invalid figures pertaining to Covid-19 are routinely plastered on the news tabloids.
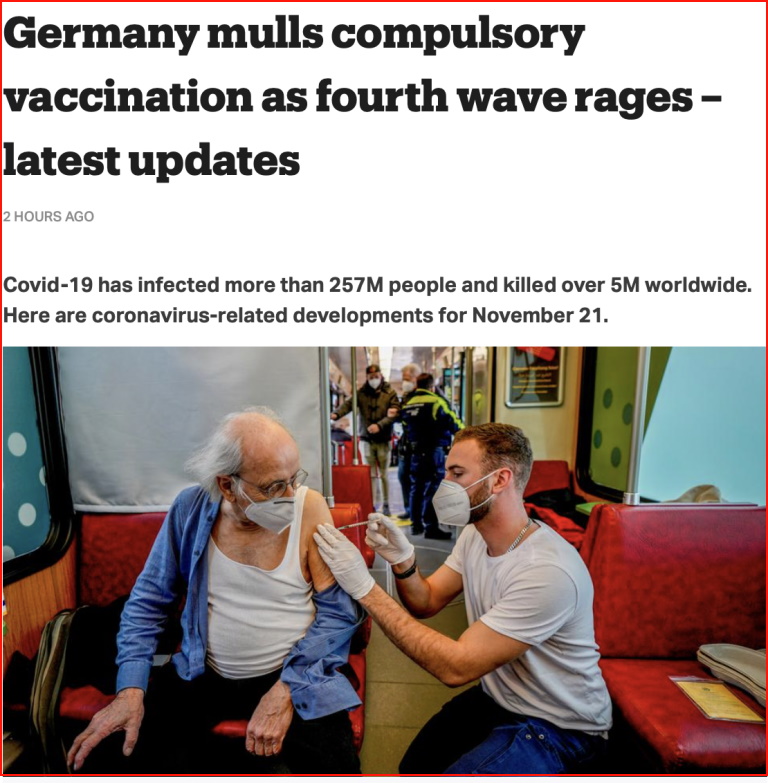
Meanwhile, both the media and the governments have turned a blind eye to the rising trend of Covid-19 vaccine deaths and adverse events, which are confirmed by “official” government agencies. (See below)
TOTAL for EU/UK/USA
45,250 Covid-19 injection related deaths, 7,418,980 injuries
EudraVigilance Database, MHRA Yellow Card Scheme. VAERS database.
The Reverse Transcription Polymerase Chain Reaction Test (RT-PCR)
The slanted methodology applied under WHO guidance for detecting the alleged spread of the virus is the Polymerase Chain Reaction Test (RT-PCR), which is routinely applied all over the World.
The RT-PCR Test has been used Worldwide to generate millions of erroneous “Confirmed Covid-19 cases”, which are then used to sustain the illusion that the alleged pandemic is Real.
This assessment based on erroneous numbers has been used in the course of the last 20 months to spearhead and sustain the fear campaign.
And people are now led to believe that the Covid-19 “vaccine” is the “solution”. And that “normality” will be restored once the entire population of Planet Earth has been vaccinated.
“Confirmed” is a misnomer: A “Confirmed RT-PCR Positive Case” does not Imply a “Confirmed Covid-19 Case”.
Positive RT-PCR is not synonymous with COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability] (Dr. Pascal Sacré)
The procedure used by the national health authorities is to categorize all RT-PCR positive cases, as “Confirmed Covid-19 Cases” (with or without a medical diagnosis). Ironically, this routine process of identifying “confirmed cases” . is in derogation of the CDC’s own guidelines:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. This test cannot rule out diseases caused by other bacterial or viral pathogens.” (emphasis added)
In this article we will present detailed evidence that the methodology used to detect and estimate the spread of the virus is flawed and invalid.
1. False Positives
The earlier debate at the outset of the crisis focused on the issue of “False Positives”.
Acknowledged by the WHO and the CDC, the RT-PCR Test was known to produce a high percentage of false positives. According to Dr. Pascal Sacré:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
The debate on false positives (acknowledged by the health authorities) points to so-called errors without necessarily questioning the overall validity of the RT-PCR test as a means to detecting the alleged spread of the CoV-SARS-2 virus.
2. The PCR-Test Does Not Detect the Identity of the Virus
The RT-PCR test does not identify/ detect the virus. What the PCR test identifies are genetic fragments of numerous viruses (including influenza viruses types A and B, and coronaviruses which trigger common colds).
The results of the TR-PCR test cannot “confirm” whether an individual who undertakes the test is infected with Covid-19.
According to Dr. Kary Mullis, inventor of the PCR technique: “The PCR detects a very small segment of the nucleic acid which is part of a virus itself.”According to renowned Swiss immunologist Dr B. Stadler
So if we do a PCR corona test on an immune person, it is not a virus that is detected, but a small shattered part of the viral genome. The test comes back positive for as long as there are tiny shattered parts of the virus left. Even if the infectious viri are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected].
Dr. Pascal Sacré concurs: “These tests detect viral particles, genetic sequences, not the whole virus.”
In an attempt to quantify the viral load, these sequences are then amplified several times through numerous complex steps that are subject to errors, sterility errors and contamination.
3. The WHO’s “Customized” RT-PCR Covid-19 “Test”
Two important and related issues.
The PCR Test does not identify the virus as outlined above. Moreover, the WHO in January 2020, did not possess an isolate and purified sample of the novel 2019-nCov virus.
What was contemplated in January 2020 was a “customization”of the PCR test by the WHO, under the scientific guidance of the Berlin Virology Institute at Charité Hospital.
Dr. Christian Drosten, and his colleagues of the Berlin Virology Institute undertook a study entitled, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR”.
The title of the Berlin Virology Institute Study is an obvious misnomer. The PCR test cannot “detect” the 2019 novel coronavirus. (See Dr. Kary Mullis, Dr. B. Stadler, Dr. Pascal Sacré quoted in Section 2).
Moreover, the study, published by Eurosurveillance acknowledges that the WHO did not possess an isolate and purified sample of the novel 2019-nCov virus:
[While]… several viral genome sequences had been released,… virus isolates or samples [of 2019-nCoV] from infected patients were not available …”
The Drosten et al team report then recommended to the WHO, that in the absence of an isolate of the 2019-nCoV virus, a similar 2003-SARS-CoV should be used as a “proxy” of the novel virus:
“The genome sequences suggest presence of a virus closely related to the members of a viral species termed severe acute respiratory syndrome (SARS)-related CoV, a species defined by the agent of the 2002/03 outbreak of SARS in humans [3,4].
We report on the the establishment and validation of a diagnostic workflow for 2019-nCoV screening and specific confirmation [using the RT-PCR test], designed in absence of available virus isolates or original patient specimens. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.” (Eurosurveillance, January 23, 2020, emphasis added).
What this ambiguous statement suggests is that the identity of 2019-nCoV was not required and that “Confirmed Covid-19 Cases” (aka infection resulting from the novel 2019 coronavirus) would be validated by “the close genetic relatedness to the 2003-SARS-CoV.”
What this means is that a coronavirus detected 19 years ago (2003-SARS-CoV) is being used to “validate” the identity of a so-called “novel coronavirus” first detected in China’s Hubei Province in late December 2019.
The recommendations of the Drosten study (generously supported and financed by the Gates Foundation) were then transmitted to the WHO. They were subsequently endorsed by the Director General of the WHO, Tedros Adhanom.
The WHO did not have in its possession the “virus isolate” required to identify the virus. It was decided that an isolate of the new coronavirus was not required.
The Drosten et al article pertaining to the use of the RT-PCR test Worldwide (under WHO guidance) was challenged in a November 27, 2020 study by a group of 23 international virologists, microbiologists et al.
It stands to reason that if the PCR test uses the 2003 SARS- CoV virus as “a point of reference”, there can be no “confirmed” Covid-19 cases resulting from the novel virus 2019-nCoV, subsequently renamed SARS-CoV-2.
4. Has the Identity of the 2019-nCoV Been Confirmed? Does the Virus Exist?
While the WHO did not possess an isolate of the virus, is there valid and reliable evidence that the 2019 novel coronavirus had been isolated from an “unadulterated sample taken from a diseased patient”?
The Chinese authorities announced on January 7, 2020 that “a new type of virus” had been “identified” “similar to the one associated with SARS and MERS” (related report, not original Chinese government source). The underlying method adopted by the Chinese research team is described below:
We prospectively collected and analysed data on patients with laboratory-confirmed 2019-nCoV infection by real-time RT-PCR and next-generation sequencing.
Data were obtained with standardised data collection forms shared by WHO and the International Severe Acute Respiratory and Emerging Infection Consortium from electronic medical records. (emphasis added)
The above study (quotation above as well as other documents consulted ) suggest that China’s health authorities did not undertake an isolation / purification of a patient’s specimen.
Using “laboratory-confirmed 2019-nCoV infection by real-time RT-PCR” is an obvious misnomer, i.e. the RT-PCR test cannot under any circumstances be used to identify the virus. (see section 2 above). The isolate of the virus by the Chinese authorities is unconfirmed.
Freedom of Information Pertaining to the Isolate of SARS-CoV-2
A detailed investigative project by Christine Massey, entitled: Freedom of Information Requests: Health/ Science Institutions Worldwide “Have No Record” of SARS-COV-2 Isolation/Purification provides documentation concerning the identity of the virus.
Freedom of Information (FOI) requests were addressed to ninety Health /Science institutions in a large number of countries.
The responses to these requests confirm that there is no record of isolation / purification of SARS-CoV-2 “having been performed by anyone, anywhere, ever.”
“The 90 Health /Science institutions that have responded thus far have provided and/or cited, in total, zero such records:
Our requests [under “freedom of information”] have not been limited to records of isolation performed by the respective institution, or limited to records authored by the respective institution, rather they were open to any records describing “COVID-19 virus” (aka “SARS-COV-2”) isolation/purification performed by anyone, ever, anywhere on the planet.”
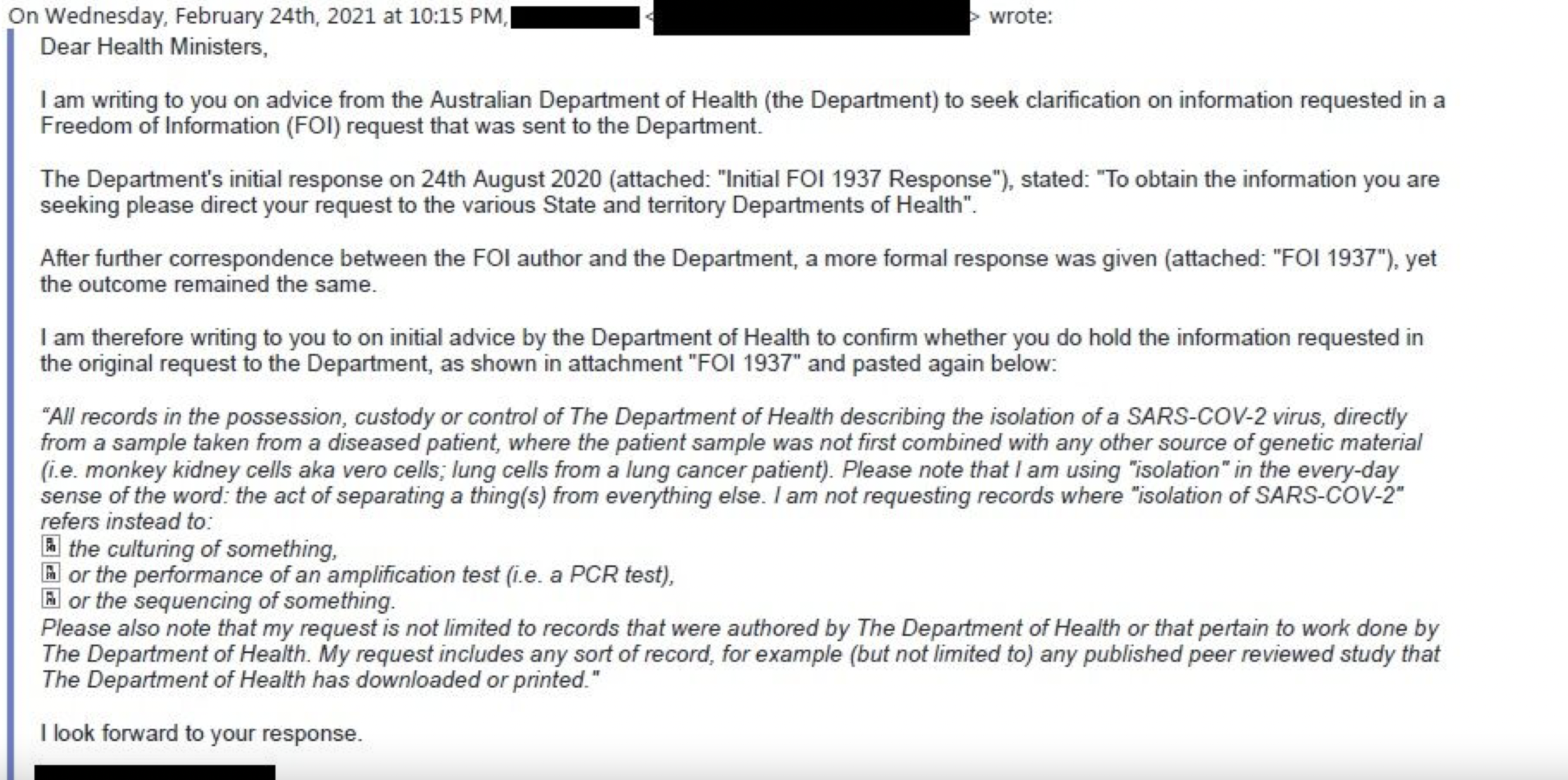
See also: 90 Health/Science Institutions Globally All Failed to Cite Even 1 Record of “SARS-COV-2” Purification, by Anyone, Anywhere, Ever, By , August 04, 2021
5. The Threshold Amplification Cycles. The WHO Admits that the The Results of the RT-PCR “Test” are Totally Invalid
The rRT-PCR test was adopted by the WHO on January 23, 2020 as a means to detecting the SARS-COV-2 virus, following the recommendations of the Berlin Virology research group (quoted above).
Exactly one year later on January 20th, 2021, the WHO retracts. They don’t say “We Made a Mistake”. The retraction is carefully formulated. (See original WHO document here)
Below are selected excerpts from my article entitled: The WHO Confirms that the Covid-19 PCR Test is Flawed: Estimates of “Positive Cases” are Meaningless. The Lockdown Has No Scientific Basis
The contentious issue pertains to the number of amplification threshold cycles (Ct). According to Pieter Borger, et al
The number of amplification cycles [should be] less than 35; preferably 25-30 cycles. In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture…(Critique of Drosten Study)
The World Health Organization (WHO) tacitly admits one year later that ALL PCR tests conducted at a 35 cycle amplification threshold (Ct) or higher are INVALID. But that is what they recommended in January 2020, in consultation with the virology team at Charité Hospital in Berlin.
If the test is conducted at a 35 Ct threshold or above (which was recommended by the WHO), genetic segments of the SARS-CoV-2 virus cannot be detected, which means that ALL the so-called “Confirmed Covid-19 Cases” tabulated Worldwide in the course of the last 22 months are invalid.
According to Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, et al, the Ct > 35 has been the norm “in most laboratories in Europe & the US”.
The WHO’s Mea Culpa
Below is the WHO’s carefully formulated “Retraction”.
“WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology. (emphasis added)
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
“Invalid Positives” is the Underlying Concept
This is not an issue of “Weak Positives” and “Risk of False Positive Increases”. What is at stake is a “Flawed Methodology” which leads to invalid estimates of “Confirmed Covid-19 Cases”.
What this admission of the WHO confirms is that the estimate of covid positive from a PCR test (with an amplification threshold of 35 cycles or higher) is invalid. In which case, the WHO recommends retesting: “a new specimen should be taken and retested…”.
The WHO calls for “Retesting”, which is tantamount to saying “We Screwed Up”.
That recommendation is pro-forma. It won’t happen. Several billion people Worldwide have already been tested, starting in early February 2020. Nonetheless, we must conclude that unless retested, those estimates (according to the WHO) are invalid.
From the outset, the PCR test has routinely been applied at a Ct amplification threshold of 35 or higher, following the January 2020 recommendations of the WHO. What this means is that the PCR methodology as applied Worldwide has in the course of the last 20 months led to the compilation of faulty and misleading Covid statistics.
And these are the statistics which are used to measure the progression of the so-called “pandemic”. Above an amplification cycle of 35 or higher, the test will not detect fragments of the virus. Therefore, the official “covid numbers” (Confirmed Covid-19 Cases) are meaningless.
It follows that there is no scientific basis for confirming the existence of a pandemic.
Which in turn means that the lockdown / economic measures which have resulted in social panic, mass poverty and unemployment (allegedly to curtail the spread of the virus) have no justification whatsoever.
According to scientific opinion:
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97% (Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, Clare Craig, Kevin McKernan, et al, Critique of Drosten Study)
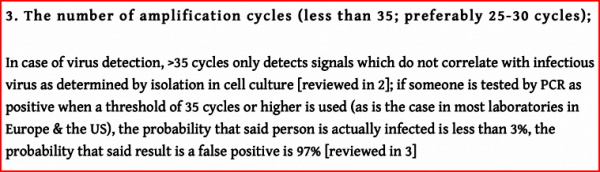
As outlined above, “the probability that said result is a false positive is 97%”: It follows that using the >35 cycles detection will indelibly contribute to “hiking up” the number of “fake positives”.
The WHO’ Mea Culpa confirms that the Covid-19 PCR test procedure as applied is invalid.
Concluding Remarks
The RT-PCR Test is the Smoking Gun. It invalidates Everything.
There is no such thing as a “Confirmed Covid-19 Case”. The entire data bank is invalid.
At the time of writing, the number of tabulated so-called “Confirmed Covid-19 Cases” is of the order of 260 million Worldwide. These numbers are totally meaningless.
None of this data can be categorized as “Confirmed”.
The PCR Test does not identify the novel virus, and the genetic fragments of a so-called “similar” 2003 coronavirus (SARS-1) cannot be used as a means to identify the virus which causes Covid-19, nor can it be used to identify the deadly variants of the 2019 novel coronavirus.
Moreover, according to the Freedom of Information (FOI) study quoted above, the isolate of the novel coronavirus is unconfirmed.
Sustained by a complexity of lies, the covid-19 narrative is extremely fragile. This consensus relies on fake science and a totally invalid data bank of alleged “confirmed Covid-19 cases”.
There is no pandemic.
And in the absence of a Covid-19 pandemic, there is no scientific justification for implementing the Covid-19 “Vaccine” which has resulted in a Worldwide trend of deaths and injuries:
How did Big Pharma manage to develop a vaccine (sponsored by the WHO, GAVI, the Gates Foundation, et al) with a mandate “to protect people” against a virus which has not been isolated/ purified from an “unadulterated sample taken from a diseased patient”?
Vaccine in relation to What? The virus has not been identified.
Moreover, 2019 SARS-CoV-2 has been categorized as similar to the 2003 SARS-CoV which means that the 2019 SARS-CoV-2 is not a novel virus.
The legitimacy of the Covid vaccine project hinges upon the validity of hundreds of thousands of RT-PCR fake positive cases Worldwide combined with fake Covid related mortality data. ( See Michel Chossudovsky, Does the Virus Exist)
What lies ahead?
National governments have announced a Fifth Wave, focussing on the deadly variants of SARS-CoV-2, including the Delta variant.
The variant is a scam. How do they identify the “variants”. The PCR test neither detects the virus nor the variants of the virus.
There is no isolate of the novel coronavirus on record. Moreover, the WHO’s “customized” PCR test uses as a proxy a similar 2003 SARS-CoV virus (which no doubt has mutated extensively over the last 19 years).
“Restrictions would have to be reintroduced”. … the Delta variant poses a “higher risk of hospitalisations”
These announcements are intended to justify a continuation of repressive policy measures, the speeding up of the vaccination program as well as the repression of the protest movement.
There is no Pandemic. The Endgame is Tyranny.
The Pandemic is being used to Impose a New World Order.
When the Lie Becomes the Truth, There is Moving Backwards.
The first Step is to Dismantle the Propaganda Apparatus.
The Elite’s Covid Consensus is Extremely Fragile.
There is no Pandemic. They Do not have a Leg to Stand on.
That Consensus must be broken.
See Michel Chossudovsky’s E-Book (13 Chapters) entitled
See also
Does the Virus Exist? SARS-CoV-2 Has Not Been Isolated? “Biggest Fraud in Medical History”
cover image credit: geralt / pixabay
Finally! Medical Proof the Covid Jab Is “Murder”
Finally! Medical Proof the Covid Jab Is “Murder”
by Dr. Vernon Coleman
November 22, 2021
It’s the 22nd November 2021 and this is the moment when the jabbing has to stop.
A couple of hours ago Darren Smith, the editor of the excellent The Light Paper, sent me a paper from the medical journal Circulation which proves that the covid-19 jabbing experiment has to stop today. I believe that any doctor or nurse who gives one of the mRNA covid jabs after today will in due course be struck off the appropriate register and arrested.
The journal Circulation is a well-respected publication. It’s 71-years-old, its articles are peer reviewed and in one survey it was rated the world’s no 1 journal in the cardiac and cardiovascular system category.
I’m going to quote the final sentence of the abstract which appears at the beginning of the article. This is all I, you – or anyone else – needs to know.
`We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy and other vascular events following vaccination.’
That’s it. That’s the death bell for the covid-19 mRNA jabs.
The endothelium is a layer of cells lining blood vessels and lymphatic vessels. T cells are a type of white cell.
We always knew these jabs were experimental. My video in December 2020, just under a year ago, warned about these specific risks. I read out a list of possible adverse events published officially by the American Government.
But now we have the proof of the link.
The mRNA jab is, remember, known not to stop people catching covid. And it is known not to stop people spreading it. I don’t believe anyone disputes these facts.
And yet vast numbers of deaths and serious injuries have occurred among people who have been jabbed. Look at the item entitled ‘Updated: how many are the vaccines killing?’ on my websites.
Now we have the evidence to stop the jabbing programmes.
In the study quoted in Circulation, a total of 566 patients aged 28 to 97 were tested. They were equally divided among men and women.
‘At the time of this report,’ says the author, ‘these changes persist for at least 2.5 months post second dose of vaccine.’
At the very least, the use of these jabs must stop now. Immediately, until more long-term tests are done.
If there were any journalists left in the mainstream media, this news would be lead item on all TV and radio programmes and be on the front pages of all newspapers.
Thank heavens for free speech platforms such as BNT which enables me to bring you this news.
I’ve said for a year that this jab was an experiment – certain to kill and injure.
We’ve always known that to experiment on people without their full consent and understanding – after disclosing all the risks and potential side effects – is a crime.
Now the evidence exists that must stop this experiment.
If the covid jab experiment continues after today then we know for absolute sure that this is not a medical treatment, it is a cull.
Please share this video immediately with everyone you know.
Thank you.
Connect with Dr. Vernon Coleman
cover image credit: geralt / pixabay
A Pandemic of the Vaccinated
A Pandemic of the Vaccinated
And to keep the REAL pandemic going, we must have vaccine mandates and passports and crackdowns on the unvaccinated
by Jon Rappoport, No More Fake News
November 23, 2021
Daily Mail, November 18, 2021: “Dr. Anthony Fauci, the director of the National Institute for Allergy and Infectious Diseases, said waning immunity from the initial shots is leading to a rise in severe cases among immunized Americans. ‘What we’re starting to see now is an uptick in hospitalizations among people who’ve been vaccinated but not boosted’…”
NY Times podcast, November 12, 2021; Fauci states: “They are seeing a waning of [vaccine-induced] immunity not only against infection but against hospitalization and to some extent death, which is starting to now involve all age groups. It isn’t just the elderly.”
Translation: The vaccine is severely injuring and killing MANY people, but of course we’re calling those injuries and deaths “COVID-19 disease.” Also, our solution to this catastrophe is piling on MORE injections (boosters), which will hospitalize and kill even MORE people.
The dailyexpose.uk has the much deeper story:
“The public are being repeatedly lied to by elected officials, unelected advisors, and the mainstream media, with all of them claiming that the world is currently experiencing a Pandemic of the Unvaccinated. This could not be further from the truth.”
“But the lie has now been used to justify locking down the unvaccinated in Austria, and locking the unvaccinated out of society in Australia.”
“Now Germany is about to follow suit, Scotland is about to ban the unvaccinated from pubs and restaurants under the advice of a qualified nutritionist posing as a Pandemic expert who goes by the name of Devi Sridhar, and the authorities and media in England have gone into overdrive on the advice of the ‘nudge unit’ to sway the population into supporting a lockdown for only the unvaccinated.”
“But it all makes absolutely no sense because official Public Health data shows that over the past three months… two-thirds of Covid-19 hospitalisations [people who get very sick from the shot] have been among the fully vaccinated, and a frightening 91% of Covid-19 deaths [people who die from the shot] have been among the fully vaccinated, and projections shows things are about to get a lot worse.”
“…in the week beginning November 6th a total of 773 Covid-19 hospitalisations [people injured by the shot] were confirmed in Scotland. Of these 137 were among the unvaccinated population, whilst 363 were among the vaccinated population.”
“…the fully vaccinated accounted for the majority of hospitalisations [in Scotland] between October 16th and November 12th, and again by taking into account hospitalisations as far back as August 23rd we can see that things have been getting progressively worse for the fully vaccinated by the week.”
“In the week beginning August 21st the vaccinated accounted for 68% of hospitalisations, but fast forward to the week beginning November 6th and we can see that the vaccinated accounted for 73% of hospitalisations.”
“The worst week so far for the vaccinated however, in terms of hospitalisations, came in the week beginning October 16th which saw the vaccinated population account for 79% of Covid-19 hospitalisations [people injured by the shot].”
“[In Scotland]…the fully vaccinated accounted for the overwhelming majority of Covid-19 deaths [deaths from the shot] between October 9th and November 5th 2021. But by also taking into account the number of…deaths by vaccination status as far back as August 14th we’re able to see that things are getting significantly worse for the fully vaccinated population by the week…”
“…the week beginning August 14th the vaccinated accounted for 78% of deaths, but fast forward to the week beginning October 30th and we can see that the vaccinated accounted for 85% of deaths.”
Switching from Scotland to England: “The latest Public Health England technical briefing on Covid-19 variants of concern has been published and it reveals that up to the 12th September 2021, 74% of all alleged Covid-19 deaths since August 2nd 2021 [people killed by the shot] have been among the vaccinated population, confirming the UK is currently experiencing a pandemic of the vaccinated.”
But don’t worry, be happy. The solution—endless toxic boosters—will surely save the day. And by “save the day,” I mean tens or even hundreds of millions of lives will be ruined and ended.
And by “save the day,” I also mean the news media will cover all this up and continue to promote an alternative fantasy of a universe, in which the vaccine is a rescuing rainbow and the unvaccinated are terrorists.
There’s magic at work here. If you believe what the news media are telling you, then you’ll remain vibrant and healthy (if you take the vaccine and all the boosters). If you don’t take the vaccine, you’re doomed. It’s really quite something. Those talking news heads are elves from the forest. With every word they utter, they cast powerful spells.
That’s why the really smart people trust the news and embrace the elves.
SOURCES:
nytimes.com/2021/11/12/podcasts/the-daily/anthony-fauci-vaccine-mandates-booster-shots.html?showTranscript=1
https://dailyexpose.uk/2021/11/18/91-percent-covid-19-deaths-among-the-fully-vaccinated/
cover image credit: geralt / pixabay
Australian Army Begins Transferring COVID-Positive Cases & Contacts to Quarantine Camps — From Areas Largely Populated by Indigenous Australians
Australian Army Begins Transferring COVID-Positive Cases & Contacts to Quarantine Camps — From Areas Largely Populated by Indigenous Australians
by Tyler Durden, ZeroHedge
November 22, 2021

The Australian army has begun forcibly removing residents in the Northern Territories to the Howard Springs quarantine camp located in Darwin, after nine new Covid-19 cases were identified in the community of Binjari. The move comes after hard lockdowns were instituted in the communities of both Binjari and nearby Rockhole on Saturday night.
“Residents of Binjari and Rockhole no longer have the five reasons to leave their homes,” said Northern Territory chief minister, Michael Gunner, referring to the country’s five allowable reasons to avoid lockdown (buying food and supplies, exercising for up to two hours, care or caregiving, work or education if it can’t be done from home, and to get vaccinated at the nearest possible location).
“They can only leave for medical treatment, in an emergency, or as required by law.”
“It’s highly likely that more residents will be transferred to Howard Springs today, either as positive cases or close contacts,” he continued, adding “We have already identified 38 close contacts from Binjari but that number will go up. Those 38 are being transferred now.”
“I contacted the Prime Minister last night. We are grateful for the support of about 20 ADF personnel, as well as army trucks to assist with the transfer of positive cases and close contacts – and to support the communities.
We are doing an assessment today of what extra resources we might need from the Feds, and the Prime Minister is ready to help further – I thank him for that.”
Watch:
“We’re conscious of the fact that this can have some impacts on people’s mental health as well as their general well being,” Police Commissioner Jamie Chalkner told NT News.
Of note, the Northern Territories are home to a large percentage of indigenous Australians. As the Epoch Times‘ Steve Milne notes:
According to the Australian Institute of Health and Welfare, in 2018-19, almost one in five Indigenous Australians lived in overcrowded dwellings (18 percent), compared to 5 percent of non-Indigenous Australians. Although this percentage had decreased from 27 percent in 2004, it still meant an estimated 145,340 Indigenous Australians were living in overcrowded dwellings in 2018-19.
In addition, the more remote an area, the higher the proportion of Indigenous Australians living in overcrowded dwellings (26 percent in remote areas and 51 percent in “very remote” areas), compared to 8 and 22 percent in non-remote areas.
Five days ago, NT Senator Malarndirri McCarthy told ABC that over crowding in Indigenous communities was a “massive problem,” pointing to the region’s second cluster of new infections – which included nine members of McCarthy’s direct family, including her sister who flew from Katherine to Robinson River while unknowingly bringing COVID-19 with her, per the report.
“If we could get housing in there right now, I would be pushing that straight away to the federal government and the NT government to work on that, but we obviously need the resources to do so,” she said.
Of the nine new cases in Binjari, four are women and five are men, including a 78-year-old woman who has been transported to Darwin Hospital.
There were zero new COVID-19 cases reported on Sunday, however Minister Gunner said he was worried about ‘mingling between households’ in Binjari and Rockhole, whose populations are around 220 and 130 respectively.
On Sunday, Gunner said: “Yes, these are strong measures, but the threat to lives is extreme.”
Nice people…
Australia's leaders are dumb and authoritarian. A very bad combo. pic.twitter.com/NfHPVifaVL
— Justin Hart (@justin_hart) November 22, 2021
cover image credit: Mylene2401 / pixabay
FDA to Disclose Pfizer Vaccine Data…in 2076?
FDA to Disclose Pfizer Vaccine Data…in 2076?
by Del Bigtree, The HighWire
November 20, 2021
ICAN Attorney, Aaron Siri, Esq. breaks down three big ICAN Legal Updates.
In response to a recent ICAN petition CDC revealed it didn’t have records of a single documented case of a person with natural immunity to Covid, transmitting the virus to another.
Then, The Biden Vaccine Mandate is Stayed.
Finally, the FDA requested a federal judge give it until the year 2076 to disclose all of Pfizer’s Covid Vaccine Data.
That’s 55 years!
Support ICAN’s legal work at icandecide.org
“Absolutely Forbidden to Give COVID Shots to Kids, Young Men and Women”, Jewish Court Rules
“Absolutely Forbidden to Give COVID Shots to Kids, Young Men and Women”, Jewish Court Rules
by Doctors for Covid Ethics
November 22, 2021
After eight hours of hearing a Halachic court in New York City ruled that “it is absolutely forbidden to administer or even to promote this (COVID-19) injection to children, adolescents, young men or women.”
The court also implored “all healthy adults who are of child-bearing age” to “stay away” from the abortion-tainted jab. The Jewish group sees the injection as intentionally practice of “sterilization or preventing fertility.” Due to concerns about what the jab might do to fertile women – including risks of severe blood-clotting – “it is forbidden for them to take this injection.”
The ruling referred to “breakthrough cases” as evidence that “there is no substantial difference between those who receive the injection and those who did not.” And “the number of COVID patients are about the same, comparatively, in both demographics.” Thus “further clarification is needed” for administering the jab to the elderly.
Halachic stands for the legal part of the Old Testament, the principles of right and wrong that have worked for mankind for over 5,000 years, and upon which some of our most fundamental legal concepts are based. Dr. Robert Malone, the inventor of the mRNA technology, was one of the recognized, renowned experts who testified before the court.
Mandatory COVID-19 “vaccines” transgress Halachic law, which means it could be anti-Semitic to enforce it on Jews who have no wish to take it. Given that the rabbinical courts in Israel are part of the formal legal system, further decrees forbidding mandatory Covid-19 vaccines might have the power to dissolve the infamous green pass system.
The official translation of Halachic delineation is available for view and download.
Download official translation of Halachic delineation
Connect with Doctors for Covid Ethics
cover image credit: hurk / pixabay
Fauci, Dead Orphans, AIDS Drug Trials, and the Lies
Fauci, Dead Orphans, AIDS Drug Trials, and the Lies
by Jon Rappoport, No More Fake News
November 22, 2021
Leaks are turning into floods. We are hearing about brutal clinical studies on puppies and other animals, and now a study involving orphans in New York.
These studies were funded, in whole or part, by the National Institute of Allergy and Infectious Diseases, a federal agency headed up by Anthony Fauci since 1984.
In 2014, investigative reporter, Liam Scheff, wrote an article at omsj.org, looking back on the orphan scandal. Ten years earlier, he had broken the story, and was then subjected to multiple attacks in the press.
Here is Liam’s 2014 article. As you read it, remember where the funding for the orphan drug trial came from:
“In 2004, I broke open the NIH Clinical Trial Scandal, the internationally-covered story of hundreds of New York City orphans used by government agencies and pharmaceutical companies in deadly AIDS drug trials.”
“In reporting this issue, I entered the orphanage where children were being used as guinea pigs, and over a period of several years, took interviews with mothers, children and childcare workers at the Incarnation Children’s Center. I also interviewed the medical director, and investigated the FDA documentation and published medical literature on the tests and drugs used, drugs which were often force-fed through nasal and gastric tubes to the children. I reported several deaths in children, and although the mainstream denied that any deaths were due to drug toxicity, they admit that over 200 children died.”
“In 2005, the city of New York hired the VERA Institute to form a final report on the drug trials. VERA was given no access to medical records for any of the children used in trials. Their report was published in 2008. They reported that twenty-five children died during the drug studies, that an additional fifty-five children died following the studies (in foster care), and, according to Tim Ross, Director of the Child Welfare program at VERA (as of 2009), 29% of the remaining 417 children who were used in drug studies had died (out of a total 532 children that are admitted to have been used).”
“The WIKIPEDIA writers cover up all details, as is expected.”
[Wikipedia:] “’No payment or compensation has been paid to any of the children used in the trials, or to their families’.”
“The New York Times, which was instrumental in covering up the story, hired Janny Scott and Leslie Kaufman to write a hit piece on me in 2005. They declared the following about using orphans in drug trials:”
“’It was seen as one of the great successes of AIDS treatment. In the late 1980’s and early 1990’s, hundreds of children in New York City were dying of AIDS. The only approved drugs were for adults, and many of the patients were foster children. So doctors obtained permission to include foster children in what they regarded as promising drug trials’.”
“Later in the article, Scott admits that the ‘permissions’ for many of these children are ‘missing,’ (or were never there).”
“She continued:”
“’[T]here is little evidence that the trials were anything but a medical success’.“
“In 2009, she responded to my persistent queries about their investigation method. They had taken at least 40 documents from me and buried them; what else had they buried? Her answers to me were clarifying:”
“’No, we did not review patients’ medical files…I would be surprised if that would not have been a breach of patient confidentiality if someone had shown them to us…An unexpected side effect would have been a side effect not previously seen in response to those drugs, presumably. Advanced testing methods were the methods available at the time for diagnosing HIV infection…I do not recall interviewing Dr. Painter [the doctor in charge of the orphanage and orphans] but I may simply not remember. As you know, the Times moved to a new office a year ago. It was not possible to move all of our files. In my case, I threw away files that were more than 12 months old. As you know, the story you are asking about was done in 2005…I do not recall which studies we looked at. There were a lot of them — some more easily accessible than others, as you know…As for mentioning side-effects and FDA warnings, there are side-effects and FDA warnings on many if not most drugs. The side-effects of early AIDS drugs have been written about extensively…And, as I have said before, we were not presuming to judge whether or not experimental AIDS drugs should have been tried on children — a question that I suspect few journalists would be qualified to answer; we were attempting to put a public controversy in context…If you have further objections to the way the story was handled, I suggest you contact Joe Sexton, the editor of the metropolitan news section of the paper and the editor on that story’.”
“In 2009, the Times admitted that many children had died – but the VERA Institute, hired to ‘investigate’ the trials, was also forbidden from looking at medical records. Their ‘investigator’ also refused to take data from me on the trials – lists of the trials themselves, the drugs used, and their recorded ‘black box’ warnings. In a follow-up interview with Vera Myles of WBAI, the head of the VERA Institute admitted that many more children had died.”
“The Wikipedia is not able to talk about AIDS drugs, which kill people. But, of course, take them if you really want to.”
“Happy Anniversary.”
—end of Liam Scheff article—
FAUCI.
cover image credit: hunny0001 / pixabay
Australia: People Are Awakening, Politicians and Bureaucrats Are Panicking
Australia: People Are Awakening, Politicians and Bureaucrats Are Panicking
by Tony Mobilifonitis, Cairns News
November 21, 2021

Support has surged across Australia and the globe in the fight for freedom against the Covid vaccine tyranny that has descended into the most appalling, insane bullying of the population by governments ever seen in the modern history of the nation.
Aussies across the board are waking up to the fact that sacking nurses, teachers, police and many other people on the basis of their choice not to take an experimental injection is pure evil driven by the total corruption of government at the highest levels.
But these same government and media entities are beating the drum over a gallows prop that was rolled up to the Melbourne protest during the week and then some unnamed man (a patsy?) who was charged with threatening to kill Dictator Dan. But these same government interests didn’t blink when they banned medicines that could have stopped the Covid flu in its tracks and prevented the deaths of hundreds of vulnerable elderly in care.
Neither have they raised a peep about dozens of fit young athetes and others worldwide who have been dying from cardiac arrests experienced after their Pfizer shots. The stories are heart rending. Is this what it takes to wake the public up?
Meanwhile the Labor-media strategy is to force the Coalition to condemn the alleged “ugly, violent, extremists”, thereby distracting from the major issue, which is the coercion and extortion of large sections of the workforce to be vaccinated or lose their jobs.
In Brisbane the rallies run throughout the year by The People’s Revolution have doubled in size. The city’s Botanical Gardens were overflowing for Saturday’s (Nov. 20) rally. Estimates of the turnout ranged from 30 to 60 thousand people.
And in Melbourne, a massive rally on November 13 and a week-long occupation of the steps of Parliament House helped raise pressure to block Andrews’ totalitarian pandemic powers bill. Now the powers that be are in panic mode.
In Brisbane, rally guest speaker Clive Palmer of the United Australia Party said his message was simply “freedom, freedom and freedom” and the need to unseat the major parties at the next election. He also pledged to back a new independent media outlet for Australia and to throw out legislation enabling states to use quarantine powers and place the responsibility back on the Commonwealth.
Asked about his purchase of 33 million hydroxychloroquine tablets in March 2020, that he donated to the national medical stockpile, Palmer said he had since learned about a third of them had been destroyed by authorities. The news brought boos from the crowd.
More positive news was that TPM’s legal counsel was now working with German lawyer Reiner Fuellmich’s team to launch lawsuits on some key issues around the pandemic response.
Also announced was the move to form a new, independent group for health practitioners, the Queensland Health Practitioners Alliance (qhpa.org), a group of medical, complementary and allied health professionals who have joined together in the fight to uphold their right to practice and support their community.
“We believe in the fundamental freedom of every individual to choose their own medical treatments, procedures and healthcare options. We are defending our right to practice our professions free of coercion, discrimination, censorship and forced vaccination by Queensland Government mandates,” the group states on its website.
TPM spokesman Tristian Triccy stressed the message of unity throughout the rally. “The Premier (Palaszczuk) seeks to divide us, to suggest that the values of the vaccinated are somehow different to those of the unvaccinated, but our values are the same, we all love our children and make the decision to vaccinate or to not vaccinate, based on what we believe is best for our families,” he said.
“That decision must remain with us as parents and we must unite and defend each other’s right to be able to make that choice, or when our children are grown, the rights and freedoms we have now will have been completely stripped.
“We stand for the right to choose, free of coercion and blackmail and for the right to make choices based on what we believe is best for our families.”
The Gold Coast will be hosting a Millions March Against Mandatory Vaccinations and Passports from midday this Saturday, November 27, at Kurrawa Park, Broadbeach. Guest speakers include Senator Malcolm Roberts. Details on Telegram at t.me/mmamvgoldcoast. Also @mmamvgoldcoast on Instagram and Millions March Gold Coast on FB.
Dr. Pablo Campra on Graphene, Weird Morgellons-Like Elements & Possible Microbiota in Covid Vaccines
Dr. Pablo Campra on Graphene, Weird Morgellons-Like Elements & Possible Microbiota in Covid Vaccines
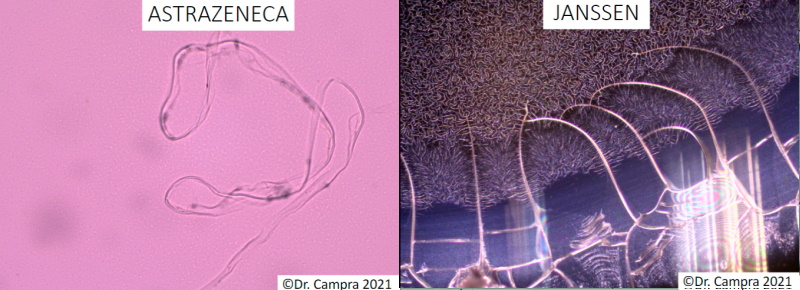


{kind=link}
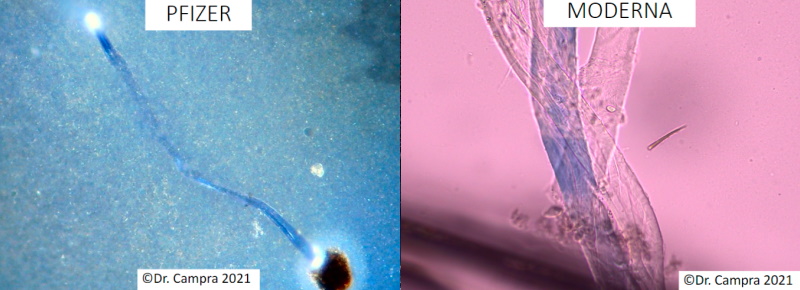
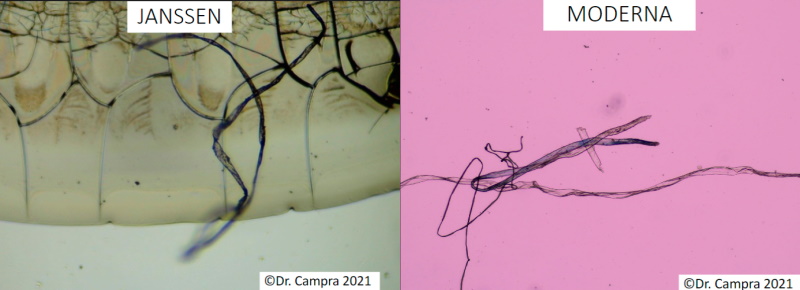
See full collection of images — download PDF
Observations of Possible Microbiota in Covid mRNA Vaccines
Graphene Morgellons: Dr. Pablo Campra on the Weird Elements He Saw in Vaccination Vials
by Orwellito, Orwell City
November 21, 2021
Dr. Pablo Campra has been interviewed by different media to date. In each of the interviews, he has provided valuable information regarding his research on the real content of vaccines. A very interesting interview was the one he gave for El Arconte TV. In this interview, Dr. Pablo Campra talked about the possible microbiota that he detected some time ago and whose photographs he shared at the time.
In the interview, Dr. Campra shared his hypotheses about what the detected objects may be. While there’s uncertainty with some of them, the doctor holds a hypothesis that he’ll continue to share in other media: graphene Morgellons.
Below, Orwell City brings the key excerpt of the interview for all his followers and the scientific community interested in this topic.
Video available at Orwellito Rumble channel
Transcript:
El Arconte (Pedro Rosillo): This. For example, this would also be graphene, in theory. This is AstraZeneca.
Dr. Pablo Campra: Well, the one above is. In the one above is clear because graphene… Show the one above. It’s just that a lot of people get confused if they don’t have experience seeing it a lot. I’ve had to develop it myself. Many times it looks like crystallites, like pebbles. What’s indeed graphene, most probably —I don’t know if I have the spectrum— are objects that look like a handkerchief, like a kleenex that has folds, shadows, wrinkles. That could be graphene. It could be graphene if the spectrum confirms it. What can’t be graphene is…
El Arconte (Pedro Rosillo): And these ones that look like that? With those folds.
Dr. Pablo Campra: What gives the graphene peaks, I’ll tell you now… The one above… Can you show the one above? Well, that one. That one. Well, these are rare objects. This is not the technical report. These are the rare objects I found, which I find more interesting than graphene.
El Arconte (Pedro Rosillo): If you want, let’s go to the report. Want to see it?
Dr. Pablo Campra: I’m more interested in this, but well, if you want to clarify something in the report because I’ve already talked enough about graphene. Now, the most important thing is what we have already said: magnetism, Bluetooth, and these rare objects. Graphene is there. I already know it’s there. Now, what relationship does graphene have with strange phenomena and thrombosis? Well, it seems to be related to thrombosis, but it’s not the only material that produces thrombosis. And all those strange things have the size of tens of microns. Look, it’s there. I have it measured. I can’t get a good look. 184 microns. That’s quite big. But that’s the spectrum that’s there. I’ve put these spectra up to show that they’re not graphene. If you zoom out we can see the spectroscopy.
El Arconte (Pedro Rosillo): That one there looks like it has folds in it.
Dr. Pablo Campra: You have to show the spectrum to see if it’s graphene or not. Then, if you want, I’ll explain the peaks.
El Arconte (Pedro Rosillo): And what is this we see here?
Well, that looks like the wings of an archon. When I saw it, I thought of you.
Dr. Campra makes a joke about the name Pedro Rosillo uses for his channel (El Arconte = The Archon).
That’s seen when the drop dries. Some material drags and stays like mud. I put the spectrum in, and it didn’t give the graphene peak, but it gave a very strange peak at 1450 cm-1, which is the clue. It’s that little ghost that appears there. That little ghost appears all over the sample. So, I think it’s the medium because there’s a gel there. A kind of strange hydrogel that never dries completely. And I think that’s what’s there because it appears a lot, is that hydrogel. And here there are some strange peaks, the one at 1450 cm-1 and the other one. They’re not graphene peaks, but they’re from some material we have there, and there are several hypotheses about them. This is really weird. What about this? Well, these are strange fibers that appear a lot. They’re a very intense color, like blue and red. Sometimes, they also look green or yellow.
They aren’t fibers from my sweater because there’s another doctor in Tenerife and other people who’re seeing them too. They have also taken samples of this from the masks, and… Is this one of the many weird things you say you have seen? This is the most intriguing thing. I’ll share with you the hypothesis, but it’s not confirmed. These are hypotheses derived from my work, and I’m going to share them with you. And when I’m interviewed by the American Stew Peters, I’ll also share it. Because I know that many people are working on this subject. So, these could be plant fibers that have gotten there through the air. But when they appear so frequently and are seen by so many researchers and in so many vaccines… And you see that they have some luminescence, too. That light there. No matter how many times I rotated the light source of the microscope, that luminiscence was still there. Well, is that until you see it there like…
El Arconte (Pedro Rosillo): Is this something biological or not? This looks like…
Dr. Pablo Campra: It’s either a textile fiber or a plant or fungal fiber. Or nanotechnology. Because here, what you have to do… These, I think, haven’t given me the graphene signal. But there’s a theory that we’re handling. And it could be the famous Morgellons. Mysterious Morgellons, which I don’t want to talk about because they would put us on the same level as Iker Jiménez and the like. But this is a disease. It’s a lot like those fibers that appear on people’s skin. It’s like hives, a bad disease. It appears… The only thing missing is that they put a router in the vaccine. They’ve put everything in there, haven’t they? Those are other theories. The fact is that it gives a Bluetooth signal. That’s confirmed.
This fiber… Well, there’s a theory which is that of the Morgellons. It’s a real disease that people suffer from it manifests on the skin as an itch. It’s not luciferase, which I have used a lot. That’s a test that’s done a lot to detect some substance. That’s something else. And then, regarding the origin of the Morgellons’ disease, there are all kinds of more or less bizarre hypotheses: that they come from outer space, that they’re extraterrestrials, that they’re demons… I don’t want to go into this subject. When you come here, we’ll have a beer and talk about whatever you want. But they really look very, very much like the Morgellons. Above all, because of the intense blue or red color that the famous Morgellons usually have. The Morgellons are cited as having electromagnetic properties. Of interacting with electromagnetic fields. So, it’s a hypothesis derived from my work that I’m going to state, but I don’t have it worked out.
El Arconte (Pedro Rosillo): But of course. But those Morgellons in which I’ve been particularly interested… I’ve investigated, and they say that it’s not biological, that it’s something artificial. And I wonder: How can it be artificial if it reacts with the environment? It’s like it’s looking for… It moves like it’s looking for you.
Dr. Pablo Campra: I know… some doctors who have been working…
El Arconte (Pedro Rosillo): But they say they aren’t biological, but that…
Dr. Pablo Campra: I know some doctors… There are some doctors who have worked on it a lot. They have treated people and are still treating them. There’s a doctor in Seville, but I don’t know her name. It’s a real disease. Now, whether it comes from space or not, I don’t go into that subject. But it’s a real disease, and they shouldn’t be in the vaccine. And we have to see if they really are because I want to analyze Morgellon’s hair and analyze this to see if it has the same structure. Because it does appear, over there, cited that there are graphene Morgellons. We can see the relationship with graphene.
El Arconte (Pedro Rosillo): So, there are graphene Morgellons.
Dr. Pablo Campra: Yes. That’s cited. But if I do analysis…
El Arconte (Pedro Rosillo): But of course, you can’t rule out anything.
Dr. Pablo Campra: Exactly. In science, nothing is ruled out. That’s a common mistake: to close oneself to hypotheses. Hypotheses are put on the table, and then you analyze them. And you state them with supporting data. If you don’t, then let those of us who are working do their job. One doesn’t close oneself to a hypothesis. So, is there the Morgellons? I’ve stated the hypothesis because people who work with Morgellons have told me that they are. I have shown them my photos of the fibers, and they have told me: ‘Man, those are Morgellons! That’s really bad.’ So, I don’t say that vaccines have Morgellons, but needs to be studied. You cannot close yourself to the possibility. Of course. Now, if people start searching the net for ‘Morgellons’, they’ll find a German saying that this is extraterrestrial technology and that the demons are this and that. I’m neither in nor out. I have to know what that fiber is and what it is doing there. Yes. The other thing is philosophizing, let’s say. That’s all. In science, you only talk about what you can prove with certainty, right? Exactly.
El Arconte (Pedro Rosillo): Let’s see more photos because I hallucinate. I hallucinate with everything you see around here. -This, for example…
Dr. Pablo Campra: Some say that these are vegetable fibers, trichomes, textile fibers… I’m not the only one who has seen these things with such an intense color. This is what a Polish guy over there said they are like octopuses. Here, everybody is naming them. But I think the most plausible clue, for the moment, is that of the Morgellons. Anyway, we have to check it out.
El Arconte (Pedro Rosillo): This is the same kind of thing, isn’t it?
That isn’t contamination that has come from the air to my sample, because they appear too many times. And these things can cause thrombi, I guess. Because they’re pretty big. I’m not a doctor, but thrombi are any clumping of platelets.
El Arconte (Pedro Rosillo): I don’t know if they’re are Morgellons or not, but the tought is terrifying.
Dr. Pablo Campra: What you see there is kind of embedded in the gel. It’s like that’s kind of ‘sucking’ on the gel. And that’s when the people who grow these things come along. Some people grow them. And they say they, in fact, grow. Look at that… Here are things like… Also, there’s one thing… If you want, I’ll show you a picture taken by the German guy. It’s very curious. He has them very well studied. And the life cycle is like a fungus, but then it’s like nanotechnology. And then, the sporangia, which are the structures that release spores, it turns out that has a hexagonal mesh.
El Arconte (Pedro Rosillo): Holy cow.
Dr. Pablo Campra: A big mesh. Not like graphene, which is atomic. No. This one is big and hexagonal. Curious, isn’t it? It’s not a coincidence. None of this is on the package insert. But how much crap they’ve put in the vaccine! They’re never going to tell you that the vaccine is full of ‘hairs.’
El Arconte (Pedro Rosillo): Mother of God!
Dr. Pablo Campra: Well, I’m not saying that in vaccines in general, but they’re present in the ones I’ve seen. Look at this one that looks like an intestine… People are speculating that it could be Morgellons or something else. But the important thing, really, is that none of this should be in the vaccine. That’s true. That’s a fact. The important thing is that it shouldn’t be in them and that there’s no comprehensive batch control system in continuous to see if this is or isn’t there. To rule out that it was only in the batches they sent me. Or that they added it in the batches they sent me. This is classic Morgellon.
El Arconte (Pedro Rosillo): Mother of God! It’s scary. It’s really scary. This is in Moderna. But they’re in all the vaccines! Well, Janssen, Moderna…
Dr. Pablo Campra: Well, I haven’t seen it myself, but this doctor from Tenerife… I don’t want to give the other people’s names, but well… He doesn’t care if I say it. He has a very nice name, though. Well, he has detected these hairs in graphene solutions. Of course, I don’t know if they’re made of this stuff. There, next to it, goes the spectrum. Look at the spectrum. There you have a peak. The one at 1611 cm-1 could be graphene or not. I’ve put it in the grid. And the important peak is the other one, the one at 1450 cm-1, and something because that one isn’t graphene. And we’re investigating what it is. There are 4 or 5 things that may be. It could be polyvinyl alcohol or some polymers. All of those are cited in interaction with graphene. Anyway. We don’t know what it is. But that peak comes up very frequently, and we have to find out what it is, which isn’t difficult if we’re allowed to work.
El Arconte (Pedro Rosillo): My goodness!
Dr. Pablo Campra: Here’s another peak. That’s a huge peak. That could be a ‘pollen’ right there. I haven’t seen much, but if you keep going… Well, now we’re talking about it.
El Arconte (Pedro Rosillo): And this is seen in Pfizer. And what is this roundel that you see here that has more roundels in it?
Dr. Pablo Campra: That could be pollen that’s gotten on me or somebody. But the thing is that it’s not Easter week to be struggling with pollen. But if you go down, you’ll see there’s more. Yes. I call this structure ‘morula.’ I don’t know what they are. Some can tell you that are bubbles, that they have air. These are things you have to check. I don’t say anything about it in this document that I have shared because I don’t know what they are. I put it there because someone with experience in this type of thing can formulate a hypothesis we can corroborate. What you can’t do is to go around pontificating, as there are many experts out there… Not even a Nobel laureate is an ‘expert.’ That laureate is just an expert in the research that has led him to the Nobel Prize. But if you take him out of his field, he is lost. So, an expert…
El Arconte (Pedro Rosillo): Here the followers say ‘spores.’
Dr. Pablo Campra: An expert has to tell you, exactly, if this can be Morgellons or what they say here about ‘spores’ of Morgellons. I don’t know. I’m not an expert on Morgellons either. It’s necessary to leave all the hypotheses open and to observe this with the available analytical techniques and go discarding or accepting things. One cannot close oneself to anything and, above all, one cannot block an investigation of this type, as is being done at the level of the scientific system with coercion of all kinds that violate academic freedom and many others.
El Arconte (Pedro Rosillo): Someone asks: Has Dr. Campra received threats or pressures for his research?
No threats, but institutional pressures, of course. But it’s because the whole scientific system has bet on vaccination. So anyone who calls it into question… As the UNESCO treaties say about the rights of university researchers, among them is the right to question public policies with research free of coercion. Threats haven’t been made. But we’re under as much pressure as journalists, doctors… Everyone is under pressure here. The only thing missing here is pressure on the judges, which will come when this reaches the courts. This need to be investigated as well. Someone told me that they could be Morgellons’ eggs. I don’t know what they are, but they aren’t bubbles. And they usually have that little dot that looks like an embryo. Anyway. I have contacted people who know more about Morgellons, to see if we close the hypothesis. Let’s see if we confirm it, disprove it, or whatever. In other words, we cannot rule out anything here.
(Dr. Campra is making reference to the book of Revelation).
That’s why I tell you that there’s nothing definitive, only the second death, but for that, we have to wait a thousand years.
(Dr. Campra is making reference to the book of Revelation).
What about this? It’s the same thing, isn’t it? That’s a strange thing. Besides, I have many videos where they appear surrounded by those little dots. I mean, it’s like a nano-sized microorganism that you can’t see with the naked eye, and they move and interact with that. They appear there moving.
El Arconte (Pedro Rosillo): Question: Have you seen magnetism in people, Dr. Campra?
Dr. Pablo Campra: Yes, I’ve seen the magnetism. I have measured it. Now, I have seen very few cases. Of all the people I know, only in one person did I see it. But it’s what we all have seen. And the instrument did beep when I brought it close to the whole body. And then, over time, it went away. In most of the people I have passed the instrument over, I haven’t seen the phenomenon of magnetism. But, in short, magnetism is a real thing. What I’m seeing a lot is the phenomenon of Bluetooth. That’s easy to see. Anybody who has a cell phone with Bluetooth, which is not all of them… I don’t think the iPhone or the Samsungs. But the Chinese ones do. In the Resmi that I have, if I choose to locate Bluetooth without a name and go to a place where there’re many people, I check it. Some say that contactless credit card readers and smartwatches detect it. But well, you see this as Dr. Luis De Benito is researching it.
Well, this is a very curious thing. It looks like a Klimt painting. Curious, isn’t it? It seems to be reminiscent of 50 years ago. I don’t know how long ago. These are some rare discs. This was also shown by Dr. Carrie Madej on Stew Peters’ show. I’ve been watching it for a while. These are from AstraZeneca, and I’ve also seen them in Pfizer when the samples dry. And they’re like discs. I call them discs. Some said it could be graphene, that it was a variant of graphene.
However, I put the laser on it, and I don’t know if you see the spectrum, but it’s not graphene. It’s something else. And some say they are bubbles, for example, this researcher from Info….. I don’t know if it’s InfoVacunas or InfoCorona… There are two very good blogs: Corona2Inspect and InfoVacunas. Both are doing quite a commendable job, technically speaking. Of literature review and comparing photos. Well, but there’s a lack of analytics, isn’t there? But they find things similar to all these objects we are seeing now. The comparison of photos isn’t enough. You have to do an analysis. And those who’re saying that this is graphene, well, it doesn’t give me a spectrum.
If you show the spectrum, for example, it seems to me that the peak was at 1450 cm-1. So I haven’t seen the graphene peak. That’s one of the hypotheses of this man from InfoVacunas, whose name is Dani. And he’s doing a good job. Very few people are doing research, of course. Of those scientists from the system, only two have answered me. And one hasn’t even told me his name, so you can see what’s going on. Well, I don’t know what this is either.
El Arconte (Pedro Rosillo): Come on, I’m amazed because it turns out that graphene is the last thing to worry about.
Dr. Pablo Campra: I don’t care about graphene because it has already been detected. What matters in all this are the adverse and anomalous effects. The least important thing is graphene, which is present, but given the number of strange objects we see, it means that graphene is the least important thing. In other words… Once the regulatory system starts to get off its butt, it will make any court-appointed judge or the military, as you said, say, ‘Okay, let’s see, let’s do analysis. Meaningful sampling. Come on, do it to hundreds of vaccines. Do it to all the departments in all the universities that can do this. Each one with its own technique.’ In two days, we’re going to find out for sure.
On top of that, we’re talking about drugs that come, as you say, from foreign powers and are controlled by European drug agencies. Of course. For example, food. If something comes from abroad, the first thing you have to do is analysis because you don’t know if it can bring something… The agricultural sector of Almeria, which has been much vilified because decades ago a lot of agrochemicals were used, it’s the most controlled thing in the world. You would be amazed at the controls we have here to eat a tomato. On the other hand, a German is taking a shot of anything.
El Arconte (Pedro Rosillo): Question: Can graphene cross barriers until it reaches the brain? Does the intramuscular puncture reach the bloodstream? I don’t know much about that, I’m not an expert either, but the little I’ve read in papers says that it does. Because there may be graphene nanoparticles that are even called… What was the name? Quantum dots. Look at how big it can get, and it can go through barriers. You can take a look at the papers that are published. But I don’t think they the particles I saw can, because they’re too big. The ones I was able to locate were the size of tens of microns. I don’t know if they do or don’t pass through.
El Arconte (Pedro Rosillo): They say here: ‘Russian roulette is more reliable than inoculation’. But come on, I think that after what we’re seeing tonight, the last thing to worry about is graphene. The last thing!
Dr. Pablo Campra: Let’s see. Here are the major adverse effects that I don’t know how many are going. About 40,000 official deaths in VAERS. I don’t know how many are in Europe. Why do they occur? We don’t know. I don’t know. There’s a lack of a control system. Of continuous monitoring. And then, we have the issue of magnetism and Bluetooth. If it’s denied, then it’s not investigated. But both phenomena are a fact. Well… That’s the serious thing, not whether it’s graphene or Spike protein.
El Arconte (Pedro Rosillo): That’s the least worrisome issue here. Well, this is the same thing…
Dr. Pablo Campra: Yes, but I put the spectrum there, I think. Show the spectrum. It’s on the right. Not that one. It seems to me that, also, you’ve enlarged the PDF a lot. On the right is the spectrum of the phantom peak, a peak at 1450 cm-1, another at 1355 cm-1, and another at 1200 cm-1. As I’m not a Raman expert, I’m waiting for someone expert in Raman or who has software to analyze the spectra well to do it. I don’t have such software because it has to have a big data database. And boom, boom, boom! It tells you what it is because it compares it with thousands of substances and tells you more or less which of them it might be, with a margin of error. I think that, as I see a lot of this subject of the peak but not graphene, it could be the above gel, which is the one that is mentioned together with graphene for a series of biomedical applications.
And it’s a peak that I get too much. I think that it may be, that this signal is masking the disk below. These lumps show up a lot. Then, if you enlarge it, you will see that there are some dots there, like a dope. And this could be something doped with heavy metals, which you know, have been found in the vaccine. I don’t do that, but this Antonieta Gatti, an Italian woman with whom I was working at the beginning… Then, we had a fight because she leaked photos for others to plagiarize, like Dr. Young, do you realize? Well, she had detected heavy metals in all the vaccines, and she had already published it some time ago.
But there are also heavy metals in these. You detect them with a technique that is similar to this one. In which you introduce an electron microscopic spectroscopy, you put them… It’s called EDS, you introduce electron spectroscopy, and you know what heavy metal is present. Now, with this technique, you cannot see graphene. So, several heavy metals have been detected.
El Arconte (Pedro Rosillo): So what is this?
Dr. Pablo Campra: This is a rare thing. This weird thing that you see here is seen in dark-field microscopy. If you look at the picture below, you’ll see it’s the same thing, but in a bright field.
El Arconte (Pedro Rosillo): It looks a little different, doesn’t it?
Dr. Pablo Campra: That’s what I call a mushroom. This one I’ve only been able to see at AstraZeneca. It appears —as you know— when the drop is drying out. There’s a carryover and, in the end, objects just sit there. Like that gel that never dries. And that crystallizes. This can be either an inorganic crystal or an organic crystal. I don’t know what it is. I’ve even shown it to mushroom experts. I have no idea what it is. That only appears in the AstraZeneca. And, again, there’s the mysterious peak at 1450 cm-1. And that’s a big object. Anyway. You have to enter the values of those peaks in a database, a suitable software, to know which substances are compatible with that spectrum. And I couldn’t do that because I don’t have the means to do that. I don’t have the range of spectra. To me, the machine has given me the minimum analysis. This is the same thing. They look like arborescent forms. They may be a crystallization of salts that go in the vaccine. The manufacturer is the one who has to tell us. What’s surreal here is that we’re breaking our heads while everyone is silent: manufacturers, regulatory agencies, and, on top of that, all the media do nothing more than to crush us. That’s what’s not normal.
El Arconte (Pedro Rosillo): You saw this in Janssen.
Dr. Pablo Campra: This is very rare. This has only been seen in Janssen. This has a very strange insectoid look. This is indeed cited in the Morgellons. Morgellons look like these insectoid structures. That’s what I call ‘noodles,’ because they look like noodles. Now, we’ll look at it in more detail. Go down in the document. OK. This appears when it dries. It’s also quoted as appearing when you dry graphene suspensions. Someone sent me that information. I think it was Corona2Inspect, Mike Andersen. These weird noodles appear when the droplet dries. This isn’t a crystal. Crystals don’t form that. This is something else. And if you go further down in the document, it appears larger. That there grows when the drop dries. They are like nuclei that are condensing. If you go down further, you’ll see them even bigger. There’s a kind of a nucleus from which they start to grow. And if you look further down, you’ll see… this. This is much more magnified and with their appearance next to it. And, again, we have the same little ghost peak.
1457 cm-1.
Dr. Pablo Campra: It’s not just the peak. It’s that phantom appears to me in everything I looked at in Janssen. So, here it appears as a rosary of little balls. It could be Morgellons. It could be. It’s certainly not what it says on the package insert. These are not nanoparticles with RNA related to the protein Spike. Nor is it any salt that is cited in the package insert that dries that way. These are dark fields. These are videos, actually. I haven’t embedded them because they’re heavy. But in the dark field, you can see all these little dots quite frequently. This is what’s called symbionts. I’ve been seeing this for a long time in cell culture. But they’re living things. That’s not in random Brownian motion.
And well, I don’t know if it’s the result of contamination or not, but it appears quite frequently. And there you have a sign, for example… Look at that one that looks like a rhombus. The bug or whatever it is. That little dot or nanobots or whatever. I don’t know what it is. These little dots are always kind of ‘fiddling’ with those little crystals. They go like dragging them as if it were a layer. These crystallites always have that rhomboid shape. And these little dots are playing with them. These are microbiota. It doesn’t float around and moves. I can’t put videos in the document, though. If you go further down, there’s another strange shape. See? Here’s one that’s a little bit bigger, and the little dot is always clinging to the little crystal. Here you see another one.
El Arconte (Pedro Rosillo): Yes, yes, yes. Keep scrolling. As I’m Andalusian, I speak as such. The good thing about talking to you is that I don’t have to pronounce the ‘s’.
El Arconte (Pedro Rosillo): I understand you. I ‘peak.
Dr. Pablo Campra: Look at this circle. This is a very strange thing. The little I’ve read says there’s nanotechnology called ‘SiN cells,’ which are these weird spheres. These spheres appear and, sometimes, they have the diamond inside with the little dot moving.
El Arconte (Pedro Rosillo): Well, some people say it’s alien technology. Well, all I know…
Dr. Pablo Campra: Bring me a beer, and you and I can talk all you want. But here… The only thing we know for sure is that this shouldn’t be in the vaccine. The rest is philosophizing. It’s not just that it shouldn’t be. It’s that there’s no one monitoring it. The fact that they don’t test for it or the FDA… Look, here’s what I’m telling you. That circle that has that little diamond inside it with the little dot moving. I’m not a microbiologist, but no microbiologist has been able to tell me what the hell that is.
cover image credit: Dr. Pablo Campra
“We’ll Never Give Up” – Protests Erupt Across World Over Gov’t COVID Tyranny
“We’ll Never Give Up” – Protests Erupt Across World Over Gov’t COVID Tyranny
by Tyler Durden, ZeroHedge
November 21, 2021
AP News calls them “far-right,” but tens of thousands of freedom-loving people marched against new tyrannical public health measures, such as partial and full lockdowns and health passports and mandatory vaccinations, across Europe.
Demonstrations against new virus restrictions were observed in Austria, Croatia, Italy, Northern Ireland, the UK, France, Germany, and the Netherlands. Outside of Europe, protesters were seen in several cities across Canada, Australia, Japan, and even the US. Some marked Saturday as part of a “Worldwide Freedom” rally to protest COVID-19 restrictions and vaccine mandates.
Some of the most intense rallies, which turned into riots, were in the port city of Rotterdam. Clashes between protesters and police began Friday and continued through Saturday night.
"COVID-19 protests in Rotterdam, Netherlands turn violent as demonstrators clash with police" https://t.co/x6nGwBwr8r
— italjami (@ItalJami) November 21, 2021
About 30 minutes away, protests transformed into riots in Hague.
The Hague burns🔥, home of international court of justice, the seat of Dutch cabinet and 3rd largest city in Netherlands https://t.co/8gjqu2sE60
— petrichor (@1e9petrichor) November 20, 2021
The Hague riots live #TheHague #Holland pic.twitter.com/d0ko9YmZFn
— Pierre Crom (@PierreCrom) November 20, 2021
Protesters across many European cities shared commonalities as they marched to preserve their lives and liberty. Governments are attempting to plunder that via increased COVID restrictions, mandatory health passports, and forced vaccinations.
The worst of restrictions, or rather the government’s plundering of liberties, was in Austria, where full lockdowns begin Monday. Nationwide lockdowns are expected for at least ten days but can be extended to more than two weeks. Then by Feb. 1, the government will make vaccinations mandatory (only 66% of Austria’s 8.9 million people are fully vaccinated). Good luck with that one.
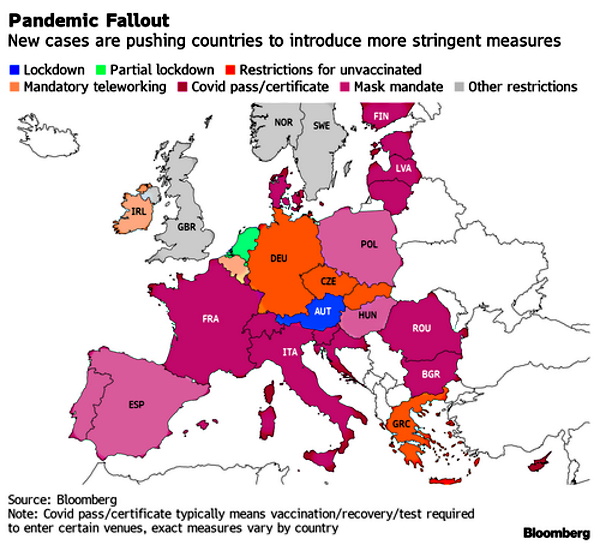
Saturday’s march in Vienna’s massive Heldenplatz square had many chanting “My Body, My Choice,” “We’re Standing Up for Our Kids!,” and “Resistance!”
AUSTRALIA FINALLY SAYS NO pic.twitter.com/4Winq1Ov6f
— Avi Yemini (@OzraeliAvi) November 20, 2021
One of the biggest protests might have been in Zagreb, Croatia’s northwestern capital, where Citizen Free Press reports as many as 100,000 flooded streets to protest the government’s health passports and new COVID measures.

In Rome, thousands of demonstrators gathered in the capital’s Circus Maximus to protest against “Green Pass” certificates required at workplaces, restaurants, cinemas, theaters, sports venues, and gyms, as well as for public transportation.
“People like us never give up,” read a protester’s sign.
Protest against vaccine mandates in Rome: pic.twitter.com/q3HZSJ9Wiq
— Alex Salvi (@alexsalvinews) November 21, 2021
The pushback against totalitarianism is spreading across Europe. Usually, “Europeans generally are more compliant than Americans when it comes to government orders. But even there, citizens are protesting governments seizing power in the name of public health,” said American Thinker’s Thomas Lifson.
People of the world are awakening to government tyranny plundering their life and liberties as the Davos Man, the world’s elites, and their political puppet officials are becoming more unfavorable than ever. The increasing discontent among citizens and their respective governments is dangerous – this is how revolutions begin.
cover image credit: screenshot from AUF1 footage of Vienna, Austria protest
Cardiologist ‘Warning’: Heart Risk Measure ‘Dramatically’ Increases in Covid-19 Vaccinated Patients
Cardiologist ‘Warning’: Heart Risk Measure ‘Dramatically’ Increases in Covid-19 Vaccinated Patients
by Sharyl Attkisson
November 21, 2021
The Covid-19 Pfizer and Moderna RNA vaccines “dramatically increase” a common measure of heart risk in people.
That’s according to a recently-published “warning” in the journal Circulation by cardiologist Dr. Steven Gundry, who is called a pioneer in infant heart transplant surgery.
The analysis was presented at the recent meeting of the American Heart Association.
The “dramatic changes in most patients” means they are at higher risk of a new Acute Coronary Syndrome, such as heart attack, according to Gundry.
In part, the analysis states:
“We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.”
Recently, with the advent of the mRNA COVID 19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients
Dr. Steven R Gundry in Circulation
Scientists have already established a myriad of heart and blood related effects of Covid-19 vaccines in some patients, including young people. Among the adverse events linked to the vaccines are thrombosis blood clots and heart inflammation known as myocarditis and pericarditis.
The Centers for Disease Control (CDC) and Food and Drug Administration (FDA) say the vaccines are safe and effective for everyone they are recommended for, and that the benefits outweigh the known risks, which will be emerging for some years as more people get vaccinated.
There are millions of adverse events officially reported by people after vaccination, including thousands of heart-related injuries.
The PULS (Protein Unstable Lesion Signature) Test measures the most clinically-significant protein biomarkers that measure the body’s immune system response to arterial injury. These injuries lead to the formation and progression of cardiac lesions which may become unstable and rupture, leading to cardiac event.
- Covid-19 Natural Immunity: The Definitive Summary
- Covid-19 Vaccine: 80 of the Most Common Adverse Events
- Covid-19 Vaccine Concerns Summary
- Covid-19 Vaccine Analysis: Common Adverse Events
- Covid-19 Origins: Separating Rumor from Fact (WATCH)
- Report a Possible Vaccine Adverse Event
cover image credit: Pexels / pixabay
Archbishop Viganò Calling for ‘Anti-Globalist Alliance’ to Stop the Enslavement of Humanity
Archbishop Viganò Calling for ‘Anti-Globalist Alliance’ to Stop the Enslavement of Humanity
by 21st Century Wire
November 21, 2021
Previously 21WIRE reported on an incredible interview which took place between Inside the Vatican editor Robert Moynihan and Archbishop Carlo Maria Viganò (image above) based in Rome, about a global takeover currently underway, waged by powerful financial and ideological actors, and with grave consequences for the future humanity should this new elite international combine succeed in its designs.
This week, Archbishop Viganò returned with a follow-up address to the world, this time calling for the creation of a new “Anti-Globalist Alliance” to counter what he describes as a ‘global coup d’etat’ targeting governments and institutions under the guise of an alleged global pandemic, and marketed under the World Economic Forum’s “Build Back Better” agenda currently being pushed by leading world powers like the United States, EU, UK, Canada, Australia and numerous others.
In his video address, the 80 year-old Archbishop from Rome called on members of the Christian faith to join together “under the Cross of Our Lord Jesus Christ, the only King and Savior,” in order to fight back against the establishment of an insidious ‘New World Order.’
Viganò proceeds to call-out ‘change agents’ embedded throughout government, the judiciary, mainstream media, institutions and foundations, seduced by financial gain, status and social affirmation. He describes how the agenda seeks to stage-manage a series of global crises in order to consolidate its power and control over the executive, legislative and judicial branches of stakeholder government in the global plan.
“Today a health emergency, tomorrow an ecological emergency, and after that, an internet emergency,” said Viganò.
He went on to add, “It is a world war, where the enemies are all of us…..It’s a war fought not with weapons, but with illegitimate rules, wicked economic policies, and intolerable limitations of natural rights.”
He also described the current globalist takeover as a drive to “centralised power, so as to establish a planetary dictatorship. It is the Great Reset of the World Economic Forum and (Agenda) 2030 of the United Nations.”
Watch the full address by Archbishop Carlo Maria Viganò here:
A Reminder of Liability Information for COVID-19 Vaccination Sent to German Physicians
A Reminder of Liability Information for COVID-19 Vaccination Sent to German Physicians
by Doctors for Covid Ethics
November 19, 2021
In June 2021, a Notice-of-Liability letter was sent to physicians in Germany. This reminder letter includes the recent findings and results that further strengthen the conclusion that the gene-based COVID vaccines are unnecessary, ineffective, and dangerous, as stated in the June letter.
“We would also like to ask you, beyond the legal level, that you, as physicians and also human beings, once again thoroughly examine whether you can reconcile your attitude and your medical practice with your conscience. Our first principle is that we must do no harm.”
Special thanks to Mascha Orel and her team for the excellent translation.
Read and download full letter
Excerpt from letter:
This letter is to remind you that you may be held personally liable for vaccine injuries if you administer any of the gene-based COVID-19 vaccines to your patients. In our previous letter this June, we outlined that these vaccines are all unnecessary, ineffective, and dangerous. The contents of that letter can be found at the following web address:
https://doctors4covidethics.org/wp-content/uploads/2021/11/nol1-german.pdf
Along with the June letter, you received a detailed liability notice to make you aware of the legal risks. In the meantime, there have been public attempts to downplay this issue and dismiss our warning as “misinformation”. We would like to remind you that the initial situation with the Covid-19 vaccines is completely different than with the swine flu vaccines.
In the current situation, it is not to be expected that the state will take over the injury compensation payments to the people harmed by the Covid-19 vaccinations, as it did after the swine flu. The only certain thing is that the manufacturers enjoy “immunity” and cannot be held liable. You are hopefully aware that the contracts and the terms of the contracts contained therein have now become public. At the end of our letter today, we also address the fact that in the meantime, more and more is becoming known about how Pfizer simply falsified and deceived data in the approval process, which adds a completely new dimension to the current situation. Please take our reminder seriously and carefully consider our letter today, as well as the one from June of this year.
We would also like to ask you, beyond the legal level, that you, as physicians and also human beings, once again thoroughly examine whether you can reconcile your attitude and your medical practice with your conscience. Our first principle is that we must do no harm. Please check carefully if you really fully inform your patients before vaccination and if they can really give an understanding consent. Please check to see if patients are being pressured by third parties or are able to make a true free choice. And in particular, please check as carefully and thoroughly as you can whether you can really ethically and scientifically justify vaccinating pregnant women, adolescents, and children. We would like to briefly present recent findings and results that reinforce and expand on these points in the following.
1. The vaccines are unnecessary
It should be common knowledge by now that COVID-19 carries only an extremely small risk of death or serious, irreversible damage to health for people without serious pre-existing or concomitant diseases. This is true even for people over 65 years of age, and especially for young people. [1] For example, only a full 11 COVID deaths in the 10- to 19-year-old age group have been reported to the Robert Koch Institute in the period ending July 13, 2021.
The main reason for the very low overall mortality is cross-immunity brought about by the previous infection with other beta-coronaviruses. The wide distribution of this immunity [2, 3] and its clinical efficacy [4-7] have been adequately confirmed.
2. The vaccines are ineffective
The reports on the so-called clinical trials that were supposed to prove the effectiveness of the Pfizer and Moderna vaccines [8, 9] are full of contradictions and, therefore, not credible [10, 11]. However, the failure of the vaccines has now been documented in practice.
The U.S. Center for Disease Control (CDC) published a study that included 469 COVID cases [12] – this number is more than double the sum of cases reported in Pfizer’s and Moderna’s clinical trials. Of these 469 cases, 74% involved previously vaccinated individuals, whereas only 69% had been vaccinated in the general population during the period. These apparent vaccine failures affected all three vaccines covered, those from Pfizer, Moderna, and Johnson & Johnson. Since the vaccine produced by AstraZeneca is very similar to that produced by Johnson & Johnson, one must assume that AstraZeneca vaccine would not have performed any better.
The ineffectiveness of the vaccines can further be demonstrated by international comparison. Plotting the number of new COVID cases against the population vaccination rate for 68 countries yields only a weak but positive correlation [13] – even high vaccination rates in the 60-80% range fail to reduce the number of new infections.
If their benefit is zero, the benefit-risk analysis of the “COVID-19 vaccines” is negative even if their adverse side effects are overestimated, which is hardly possible since experience shows that only about 1-3 % of adverse effects are reported at all.
3. The vaccines are dangerous
As with any other treatment, an honest weighing of benefits and risks is essential for COVID vaccination. The work of Kostoff et al. [1] on this topic makes it clear that the harms far outweigh the benefits – and this is true in every age group, even in seniors.
Severe side effects of vaccination are common. Canadian general practitioner Dr. Charles Hoffe wrote an open letter to the British Columbia provincial health minister back in April, pointing out four such cases among a total of 900 patients; these had occurred after the first injection of Moderna vaccine [14]. One of these cases was fatal; the other three had severe, probably permanent, neurological damage. Hoffe has since reported other such cases in the same group of patients.
The U.S. (VAERS) and European Union Vaccine Adverse Event Reporting Sites have recorded tens of thousands of deaths and a much larger number of serious illnesses, mostly vascular and inflammatory. Table 1 summarizes the status of reports in the VAERS database. As expected, the number of deaths recorded so far in 2021 that occurred after the administration of other vaccines is about three-quarters the value for the entire previous year. In comparison, the number of deaths following COVID vaccination is huge – it is over 50 times greater.
Read and download full letter
The letter of Notice of Liability sent to German physicians in June is available for view and download.
https://doctors4covidethics.org/wp-content/uploads/2021/11/nol1-german.pdf
Connect with Doctors for Covid Ethics
cover image credit: laxman8 / pixabay
As Reports of Injuries After COVID Vaccines Near 1 Million Mark, CDC, FDA Clear Pfizer, Moderna Boosters for All Adults
As Reports of Injuries After COVID Vaccines Near 1 Million Mark, CDC, FDA Clear Pfizer, Moderna Boosters for All Adults
VAERS data released today by the CDC included a total of 894,145 reports of adverse events from all age groups following COVID vaccines, including 18,853 deaths and 139,126 serious injuries between Dec. 14, 2020, and Nov. 12, 2021.
by Megan Redshaw, The Defender
November 19, 2021
The Centers for Disease Control and Prevention (CDC) released new data today showing a total of 894,145 adverse events following COVID vaccines were reported between Dec. 14, 2020, and Nov. 12, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 18,853 reports of deaths — an increase of 392 over the previous week — and 139,126 reports of serious injuries, including deaths, during the same time period — up 3,726 compared with the previous week.
Excluding “foreign reports” to VAERS, 654,413 adverse events, including 8,664 deaths and 54,962 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Nov. 12, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 8,664 U.S. deaths reported as of Nov. 12, 10% occurred within 24 hours of vaccination, 15% occurred within 48 hours of vaccination and 26% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 436.9 million COVID vaccine doses had been administered as of Nov. 12. This includes: 254.5 million doses of Pfizer, 166.3 million doses of Moderna and 16.1 million doses of Johnson & Johnson (J&J).
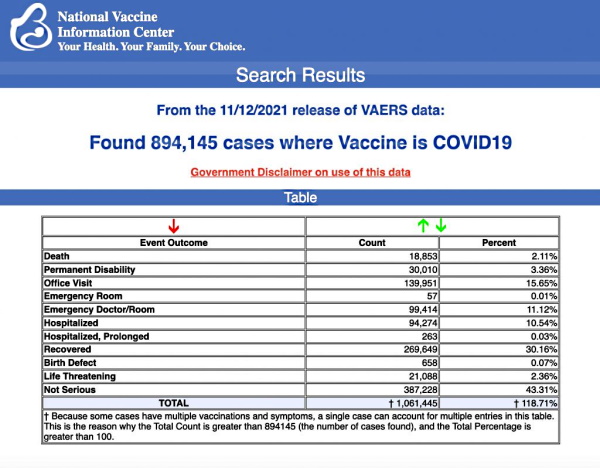
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
This week’s U.S. data for 5- to 11-year-olds show:
- 1,426 total adverse events, including 9 rated as serious and 1 reported death that occurred in an 11-year-old girl from Georgia vaccinated Sept. 14, prior to the authorization of Pfizer’s COVID vaccine in the 5 to 11 age group.
- 444 adverse events have been reported in the 5 to 11 age group since Nov. 1.
- The rest of the reports in VAERS for children in the 5 to 11 age group occurred prior to the authorization of Pfizer’s COVID vaccine, and are due to ”product administered to patient of inappropriate age.”
This week’s U.S. data for 12- to 17-year-olds show:
- 23,105 total adverse events, including 1,429 rated as serious and 30 reported deaths.
The most recent death includes a 16-year-old girl from Missouri (VAERS I.D. 1823671) who died after receiving her second dose of Pfizer.
Other reported deaths include a 17-year-old female from Washington (VAERS I.D. 1828901) who died Oct. 29 reportedly from a heart condition after receiving her second dose of Pfizer; a 12-year-old girl from South Carolina (VAERS I.D. 1784945) who hemorrhaged 22 days after receiving Pfizer’s COVID vaccine; and a 13-year-old girl from Maryland (VAERS I.D. 1815096) who died from a heart condition 15 days after receiving her first dose of Pfizer’s vaccine.
- 59 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
- 559 reports of myocarditis and pericarditis (heart inflammation) with 549 cases attributed to Pfizer’s vaccine.
- 134 reports of blood clotting disorders, with all cases attributed to Pfizer.
This week’s U.S. VAERS data, from Dec. 14, 2020, to Nov. 12, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 42% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- As of Nov. 12, 4,362 pregnant women reported adverse events related to COVID vaccines, including 1,376 reports of miscarriage or premature birth.
- Of the 3,158 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 743 reports of Guillain-Barré syndrome (GBS), with 42% of cases attributed to Pfizer, 31% to Moderna and 27% to J&J.
- 2,125 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 11,058 reports of blood clotting disorders. Of those, 4,888 reports were attributed to Pfizer, 3,937 reports to Moderna and 2,179 reports to J&J.
- 3,145 cases of myocarditis and pericarditis with 1,963 cases attributed to Pfizer, 1,041 cases to Moderna and 130 cases to J&J’s COVID vaccine.
FDA, CDC sign off on Pfizer, Moderna COVID boosters for all adults
The U.S. Food and Drug Administration (FDA) today authorized Moderna and Pfizer COVID boosters for all adults. The agency made its decision without input from its advisory committee, whose members, on Sept. 17, voted 16 to 2 against recommending boosters, citing a lack of long-term data and stating the risks did not outweigh the benefits.
Hours after the FDA announced its decision, the CDC’s Advisory Committee on Immunization Practices (ACIP) signed off with an unanimous endorsement.
The ACIP said 18- to 49-year-olds “may” get a booster, but people 50 and older should get one. CDC Director Dr. Rochelle Walensky is expected to clear the doses, which will allow boosters to be administered broadly to the general public.
Speaking for the FDA, Dr. Peter Marks, head of the agency’s Center for Biologics Evaluation and Research, said in a statement:
“The FDA has determined that the currently available data support expanding the eligibility of a single booster dose of the Moderna and Pfizer-BioNTech COVID-19 vaccines to individuals 18 years of age and older.”
Dr. Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, and an FDA advisory panel member took issue with how the FDA arrived at its decision.
In an email to The Epoch Times, Offit said, “I think it would have been of value for the public to hear an open discussion about the need for boosters. I wish we had had the chance to discuss this.”
The FDA said it did not hold a meeting because “the agency previously convened the committee for extensive discussions regarding the use of booster doses of COVID-19 vaccines and, after review of both Pfizer’s and Moderna’s [Emergency Use Authorization] requests, the FDA concluded that the requests do not raise questions that would benefit from additional discussion by committee members.”
Pfizer and BioNTech requested authorization last week after submitting the results of a phase 3 trial involving more than 10,000 participants.
Moderna resubmitted its application for its 50-microgram booster dose for all adults just two days ago. The company said the FDA based its decision on the “totality of scientific evidence shared by the company,” including data that showed neutralizing antibodies had waned at about six months.
14-year-old Kentucky girl mistakenly given J&J vaccine
A 14-year-old Kentucky girl was mistakenly given J&J’s COVID vaccine, which is not authorized for anyone under the age of 18, International Business Times reported.
The girl was given the jab Oct. 16 at a vaccine drive-in at a high school in Covington.
The girl’s mother, Rolina Mason, said her daughter was reluctant to get vaccinated and wanted the J&J vaccine because it was only one dose. Mason agreed that the nurse could administer J&J, but didn’t realize it wasn’t authorized for use in children.
Mason said she trusted the nurse who told them that it was okay for her daughter to get it.
The health department contacted Mason a week later and informed her that her daughter should have received Pfizer’s COVID vaccine instead. Mason’s daughter reportedly experienced skin rashes after receiving the shot.
States bypass CDC, gave out COVID boosters to all adults before authorization
State officials from California to Maine encouraged and allowed adult residents to get COVID vaccine boosters despite recommendations by the FDA and CDC to reserve the shots for elderly and high-risk groups, CNBC reported.
California also told medical providers not to turn away any adults who requested a booster.
Arkansas, Colorado, Louisiana, Kansas, Kentucky, Maine, New Mexico, Vermont and West Virginia are also promoting widespread rollout of boosters for any fully vaccinated adult, with governors in Colorado and New Mexico signing executive orders a week before the FDA authorized the shots for the general population.
Gov. Jim Justice of West Virginia called for all adults in-state to get their boosters, adding that fully vaccinated residents would be “very foolish” not to register for the third dose.
Arkansas Gov. Asa Hutchinson said during a briefing Monday she wanted to make sure everybody 18 and over was eligible and encouraged to get a booster. Danyelle McNeill, a spokesperson for the Arkansas Department of Health, told CNBC in an email “the great majority of adults in Arkansas” were already considered high risk by the CDC before Hutchinson issued his recommendation.
Kentucky approved boosters for fully vaccinated adults on Wednesday, while Connecticut, Kansas, Louisiana, Maine, Massachusetts and Vermont expanded their booster programs this week before the FDA and CDC signed off, today.
Several children in California sick after receiving wrong COVID vaccine doses
At least two children in California are sick after a clinic administered the wrong doses of a COVID vaccine to 14 kids.
Denise Iserloth said she took her two children, ages 8 and 11, to a clinic where they received 20 micrograms of dosage instead of the recommended 10 micrograms.
Sutter Health said in a statement it warned parents of the mistake as soon as they learned of it, and contacted parents to advise them of CDC guidance. But Iserloth said she wasn’t made aware of the error until 10 hours after her children were vaccinated.
Both of her children stayed home from school on Monday with bad stomach aches, and her oldest child fell down twice in the hours following the shot, Iseroth said.
“I understand the mandate, I tried to comply with it, and my children now have been given a double dose and I don’t know the long-term side effects,” Iserloth said. “[…] It is unacceptable and negligent, completely negligent on their part.”
COVID hospitalizations on the rise among fully vaccinated
COVID hospitalizations and emergency room visits are on the rise among people who are fully vaccinated, according to Dr. Anthony Fauci, director of the National Institute for Allergy and Infectious Diseases.
“What we’re starting to see now is an uptick in hospitalizations among people who’ve been vaccinated but not boosted,” Fauci said Tuesday. “It’s a significant proportion, but not the majority by any means.”
In a White House COVID-19 Response Team briefing Wednesday, Fauci stressed the importance of vaccines and highlighted how well they work. At the same panel, CDC Director Walensky reported a decline in vaccine effectiveness among the elderly and residents of long-term care facilities, many of whom were the first to be eligible to be vaccinated last winter.
The current seven-day rate of COVID hospital admissions is about 5,300 per day, according to the CDC.
It’s not clear how many hospitalizations are breakthrough cases as the agency stopped reporting hospitalizations among fully vaccinated people and its website shows data only through Aug. 28.
CDC admits to not tracking data on natural immunity
In response to a Freedom of Information Act (FOIA) request, the CDC said it has no record of an individual previously infected with COVID becoming reinfected or transmitting the virus to others — because the agency doesn’t collect that data.
The FOIA request, submitted Sept. 2 by attorney Aaron Siri of the Siri & Glimstad law firm on behalf of the Informed Consent Action Network, sought documents reflecting any documented case of an individual who: (1) never received a COVID vaccine; (2) was infected with COVID once, recovered, and then later became infected again; and (3) transmitted SARS-CoV-2 to another person when reinfected.
The CDC responded Nov. 5, stating:
“A search of our records failed to reveal any documents pertaining to your request. The CDC Emergency Operations Center (EOC) conveyed that this information is not collected.”
According to Siri, the revelation that the CDC does not collect data on people who have acquired natural immunity to the virus raises questions about vaccine mandates, specifically how the government or employers can mandate vaccines for people who may not need them and who could be at a greater-than-average risk of experiencing an adverse reaction to the shots.
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
©November 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Connect with Children’s Health Defense
cover image credit: ronstik / pixabay
Indigenous Australian at Melbourne Freedom Rally: “It’s Not About a Vaccination…We Are Fighting for Our Lives.”
Indigenous Australian at Melbourne Freedom Rally: “It’s Not About a Vaccination…We Are Fighting for Our Lives.”
“I look out now, I see brothers and sisters united for one reason only. It’s not about a vaccination. It’s not about segregation in the end. We are fighting for our lives.”
Fifteen Million Jews, the Vaccine, and the Conscience to Refuse
Fifteen Million Jews, the Vaccine, and the Conscience to Refuse
by Jon Rappoport, No More Fake News
November 26, 2021
In the US alone, reported vaccine injuries have soared past 600,000.
The well-known Harvard Pilgrim Healthcare study concluded that, in order to obtain a true number for such injuries, you would need to multiply the reported figure by 100.
First, it was two shots. But then the format was changed. There would be a booster. Then, not just one booster, but at least two. And for months, experts have suggested that the program will evolve into yearly shots.
On top of that, proof of vaccination is now demanded. The passports. The government, of course, controls these passports, which allow vaccinated persons to participate in ordinary social life. Those without passports are confined, restricted, in a form of slavery. And the passport will be revoked if a person doesn’t line up for all required boosters.
In other words, this has been a step-operation, with the individual’s rights constrained and eaten into, progressively, over time—finally resulting in his complete capture by the State.
And so I refer you to the story of Joseph in the Old Testament. The real story. It holds a valuable lesson.
As you recall, Joseph was the favored son of Jacob. Joseph’s jealous brothers sold him into slavery. While imprisoned in Egypt, Joseph revealed his ability to interpret dreams.
He was eventually brought before the Pharaoh, who needed someone who could tell him what his troubling dream meant: seven starving cows ate seven well-fed cows; seven dead ears of corn ate seven plump ears.
Joseph told the Pharaoh there would be seven years of plenty in the land, and then seven years of famine. Therefore, the Pharaoh should immediately store up grain.
When the terrible famine hit, Joseph, who was now the Pharaoh’s vizier, dealt with the MANY hungry people who came to buy bread. In exchange for the bread, Joseph first demanded that the people sell their possessions to the State; then, their property; and finally themselves. AS SLAVES. A step-operation.
When next we learn of the condition of the Jews in Egypt, in the story of Moses, the Jews are slaves. Do you suppose this turnabout had something to do with Joseph’s “solution” to the famine and the anger it raised in the population?
Of course, the Bible story focuses on Joseph reuniting with his brothers and his father, all of whom who believed he died.
The story passes no judgment on Joseph, who put a population into slavery to the State.
Those of the Jewish faith must consider this tale from Genesis, because it is parallel to what is happening now: a Globalist elite is bent on capturing the population degree by degree, with its “solution.”
In Genesis, after the famine was over, the Egyptians, who continued to farm grain, were planting government seeds on government land, and they had to turn over a fifth of their crop to the Pharaoh. There was no privately owned land.
If that doesn’t ring any bells, what will?
Jews today are being betrayed by their leadership, who are aligned with the State. Jews are being told “the best medical minds” have decided the vaccine is safe and effective and only wild conspiracy theorists believe otherwise.
So as usual, it falls to the conscience and common sense of the individual to ignore the official word.
The lying, criminal, murderous official word.
It falls to the conscience of Jewish parents to protect their children against the shot, no matter what. And to protest against the mandates and the passports.
How long did Moses and his people wander in the desert? 40 years? Given that extreme ordeal, can modern Jews work up the courage to say no to a destructive vaccine and an enslaving mandate?
Or do modern Jews actually believe God wants them to take the shot?
Because unless I’m mistaken, the religion of the Jews is centered on the One God. That is its whole point. That was its whole point, when Jews declared, not many gods, only one.
Of course, DOCTORS are quite adept at playing God. So perhaps the leadership councils of the Jewish faith should come out and switch their allegiance. WE NOW PRAY TO DOCTORS. WE NOW MUST HAVE THE PERMISSION OF DOCTORS. WE MUST HAVE NO IDOLS THAT SUPERSEDE DOCTORS.
“Sh’ma Yisrael Adonai Eloheinu Adonai Eḥad.” “Hear O Israel, the doctor our doctor, the doctor is one.” Say it. Bow the head and bend the knee and say it. The new prayer.
Or find your soul and your conscience and your God and throw off the chains of your slavery.
If you’re a Conservative Jew or a Reform Jew, you’re going to have to wake up from the chapter you and your rabbis added to the Old Testament. It’s called SUBURBAN LIFE. It mainly involves new temples designed by talentless architectural morons and the eternal building funds maintained to pay for those temples. I know; I was steeped in that neighborhood “culture” as a child. Fortunately, my parents had moral spine, but that’s a different story for a different time.
To you 15 million Jews: there are two swords. One is wielded by the doctors. The other is wielded by your God. Make your decision and your choice.
cover image credit: Ajale / pixabay
Dr. Jose Luis Sevillano, La Quinta Columna: Planet Lockdown Full Interview
Dr. Jose Luis Sevillano, La Quinta Columna: Planet Lockdown Full Interview
by Planet Lockdown
November 17, 2021
Video available at Planet Lockdown Odysee channel.
Dr Sevillano is one of the key people in a Spanish speaking ad hoc group of researchers called the Fifth Column or La Quinta Columna.
They were the ones that arrange for the examination of vials of various brands of the Covid vaccines at a Spanish University laboratory and released a report on it at the beginning of July 2021 revealing the presence of graphic oxide in all the vials examined.
This material is heavily referenced in endless scientific studies, with a preponderance of applications in the field of bio-sensing, e-medicine and nano-medicine. It is a very hot high tech material now and fits the bill as a possible purpose for this obsessive global vaccination push.
Website: https://www.laquintacolumna.net/
Follow on Telegram: https://t.me/laquintacolumna
For English translations of much of La Quinta Columna’s work, see Orwell City.
Watch more full interviews and educate yourself! https://planetlockdownfilm.com/full-interviews/