The theory that “Covid” originated in a bio-lab has been back in the headlines over the last few weeks, serving as a prime example of the type of fake binary OffG has been warning you about.
The “lab-leak theory” – which pushes the idea Sars-Cov-2 was bio-engineered in a lab as a “gain-of-function” program, and then either accidentally or deliberately released on an unsuspecting population – first came to the front pages as early as January 2020.
At the time it was deemed a “racist” “anti-china” conspiracy theory by the vast majority of the media, and it fell away from the narrative.
It had a resurgence in 2021, suddenly & inexplicably becoming not racist anymore.
In February 2021 the World Health Organization published a report finding the lab origin for Covid19 “extremely unlikely”. But WHO chief Tedro Adhanom was obviously keen not to let the idea die completely, publicly stating “more investigation was needed”.
Overall, around this time, it suddenly became much less taboo to suggest the “virus” originated in a lab.
Then, in December 2021, the Daily Mail reported that Dr Alina Chan had told the UK’s Science Select Committee that it is ‘reasonable to believe [the] virus was engineered in China’ and that “the lab origin is more likely than not”.
But after a brief furore over that, it again faded from the front pages.
Now it’s back. And gaining momentum.
In May, 18 scientists (including Chan) published an open letter in the Science journal demanding authorities properly “investigate the origins of Covid19”.
Two weeks ago the World Health Organisation released a report that they were still investigating the origins of Covid, and that no hypothesis had been completely ruled out.
On June 15th, the WHO chief told reporters at a press conference that ruling out the lab-leak theory had been “premature” and there had been a “push” to do so. He called on China to “be transparent, open and cooperate, especially on the information, raw data that we asked for at the early days of the pandemic.”
This time China responded, dismissing the lab leak theory as “lies” and “anti-China propaganda”, whilst suggesting that the real lab leak likely came from the US bioweapons lab in Fort Detrick.
Then, on June 18th, The Daily Mail reported that despite maintaining public neutrality Tedros Adhanom “privately believed” that Covid had originated in a lab.
In short, two apparently oppositional camps are springing up – the West is laying the groundwork to blame China for the pandemic, whilst China (and probably Russia, down the line) blame the USA.
This is a textbook fake binary.
What you need to notice is that both these allegedly opposing sides agree on the most important aspect of the pandemic lie – that Covid is a unique new and dangerous disease which needs be treated with masks, lockdowns and vaccines – and only disagree violently about where this “real and deadly new disease” might have come from.
You are supposed to take your cue from them.
They want you to forget “covid” is just a meaningless new name for an old familiar cluster of “seasonal” symptoms. They want you to forget the whole thing was a scam – and to instead take a “side” in a scripted & noisy & totally phony “origin” debate.
The minute you sign up for it they have you – because by agreeing to debate where “it” comes from you have accepted “it” – ie a deadly new pathogen – exists & needs to be dealt with.
And that is all they want from you.
We think you should politely decline this staged “controversy”. Because however real the East-West divide actually is in other areas, when it comes to covid both sides are the same side & pushing the same story.
And it suits both East & West to encourage this fake binary – and “bioweapon” fear porn – at the expense of wider and more honest enquiry.
At the end of April, Dr. Jordan Grant gave a remarkable 2-part lecture breaking down the various philosophical issues related to our modern healthcare system. He deconstructed the germ theory of disease and brilliantly showcased why it is based on pseudoscience rather than natural science. Dr. Grant has been at the forefront of calling out virology for its inadherence to the scientific method and he has pinpointed the many logical fallacies surrounding the germ theory fraud.
I have been anxiously awaiting the time that I could share his presentation with you. If you know Dr. Grant, you would understand why. I am fortunate enough to call Jordan a friend. We crossed paths at the beginning of this pandemic through the Infectious Myth Facebook group created by the late David Crowe. From reading Jordan’s conversations with others in our group, I immediately realized that this was a man who carried a wealth of knowledge and he was someone from which I could learn a great deal from. He may not realize it, but Jordan has been a mentor to me in various ways and I am grateful for all of the knowledge I have gained from our conversations. My hope is that you are able to come away with many nuggets of wisdom from this excellent series! At the very least, you will learn one thing you may have never known that can kill a guinea pig.
The Philosophy of Modern Medicine
What Makes Us Ill and How Can We Optimize Health? The modern medical-industrial complex has its focus on drugs and symptom suppression. It is a “sick care” system. We need to understand this philosophy and then empower ourselves with information on true causes of “illness” in order to better understand ways to optimize our health.
The Philosophy of Modern Medicine – Dr. Jordan Grant (2022 Conference) – Delivered 04/30/2022 – Dr. Jordan Grant – Berean Bible Church –
Science, Pseudoscience, and The Germ Theory of Disease
For over 150 years, the “germ theory” of disease has dominated mainstream thought regarding many illnesses. Is this theory scientific? Are there holes in the paradigm? We will explore what “science” means, first and foremost, and then apply that to dogmas surrounding contagion and infection.
Science, Pseudoscience, and The Germ Theory of Disease – Dr. Jordan Grant (2022 Conference) – Delivered 04/30/2022 – Dr. Jordan Grant. – Berean Bible Church –
If you are interested in joining the Infectious Myth Facebook group (there are a few due to censorship) to converse with Dr. Grant and many other amazing like-minded people, you can find us here:
An active-duty senior Army official told The Defender, on condition of anonymity, the U.S. Army is strongly considering pushing the June 30 deadline for compliance with the military’s COVID-19 vaccine mandate far into the future — but will not announce the date change until closer to, or even after, the upcoming deadline.
As the June 30 deadline nears for compliance with the U.S. military’s COVID-19 vaccine mandate, U.S. Army officials publicly claim a very small percentage of its members are unvaccinated, reporting 96% or more of its members are fully vaccinated.
However, the Army’s vaccination rate is in fact significantly lower than 96%, an active-duty senior Army official with access to senior-level information told The Defender — so low, that if the Army were to enforce the deadline, the loss of up to 120,000 service members would render it “combat-ineffective.”
The official, who spoke on condition of anonymity, said the Army is strongly considering pushing the June 30 deadline much further into the future — but will not announce the date change until closer to, or even after, the upcoming deadline.
Concern about the number of unvaccinated service members was the topic of recent senior-level briefings, according to the official.
He said he’s blowing the whistle now because many service members who remain unvaccinated and/or who are “on the fence” about getting the vaccine may feel compelled to do so to meet the June 30 deadline — unaware the deadline may soon change.
He said by going public with this information now, service members who have not yet been vaccinated but who are feeling increasing pressure to get the COVID-19 vaccine may reconsider.
Real numbers of unvaccinated Army members ‘higher than anybody thought’
As far back as December 2021, an article on the U.S. Army website stated 96% of the Army’s 461,209 members were fully vaccinated.
In March 2022, as the Army began to announce the initiation of separation procedures for unvaccinated soldiers, officials again claimed 96% of its service members were fully vaccinated.
Later that month, an article on the U.S. Department of Defense (DOD) website claimed “the entire force may be vaccinated for COVID-19 by early summer.”
According to the whistleblower though, the “real numbers of unvaccinated service members are way higher than anybody thought,” adding that while “everyone thought” the number of unvaccinated in the Army was approximately 8,000-10,000 members, it is actually around 120,000.
To confirm that number, the official confidentially shared an internal U.S. Army document, dated June 2022.
According to the document, in the Army National Guard (ARNG), there are 280,678 members who are fully vaccinated (84.6%), and 7,735 who are partially vaccinated (1 dose) (2.3%) — leaving 43,269, or 13%, who have not yet received a single dose.
In some states, such as Oklahoma, the document shows the vaccination rate for members of the ARNG is as low as 74.11%. Of those, the document lists 15,698 members as “refusals” and 6,749 (2.0%) as going through an exemption process — with 6,257 (1.9%) requesting a religious exemption and 492 (0.1%) requesting a medical exemption.
The document also notes that 80% of unvaccinated soldiers in the ARNG are age 32 or younger, with an average age of 26.2 and median age of 24.
The document adds that “unvaccinated soldiers in their first 1-3 years of service and 4-7 years of service represent the greatest risk to readiness” for the ARNG, and that “Infantry, Maintenance, Engineer and Transportation career fields represent the greatest areas [of] concern for the ARNG.”
The document also states “projected losses could drive [the ARNG] below 70% available strength.”
According to the document, “Current forecasts project unprogrammed, vaccination mandate-related losses to range from … 3-6% of assigned strength,” which would require an anticipated “seven-year effort at 1,500-2,000 ramp per year to restore [the] End Strength necessary to meet required Force Structure.”
The same document also provides figures for the U.S. Army Reserve (USAR), stating that 157,390 members are fully vaccinated (87.9%), with an additional 1,411 members partially vaccinated with one dose (0.8%), leaving 19,872 members (11.3%) fully unvaccinated.
Among the unvaccinated, 7,623 members (4.3%) are listed as “refusals” and 4,100 (2.3%) are listed as undergoing an exemption process, with 3,982 members (2.2%) having requested a religious accommodation, and 118 (0.1%) having requested a medical exemption.
In some states, such as Wyoming, the vaccination rate in the USAR is as low as 80.9%, according to the document.
The document also notes 65% of unvaccinated soldiers in the USAR are age 30 or younger, with an average age of 28 and a median age of 26.
“Supply and Services, Mechanical Maintenance, Engineer and Transportation career fields represent the greatest areas [of] concern for the USAR,” the document states.
The document recommends commanders counsel “every unvaccinated Soldier,” “explore [the] impact of Bars to Reenlistment” and “publicize [the] Novavax option as [U.S. Food and Drug Administration (FDA)] approves” as it “may appeal to some seeking religious exemptions.”
The number of unvaccinated service members in the ARNG and USAR is confirmed in a second document — an internal “information” document — that the whistleblower shared with The Defender.
According to the whistleblower, this leaves approximately 56,000 unvaccinated service members in the U.S. Army itself.
These figures refer only to the Army, the whistleblower said. He does not know the figures for other branches of the armed forces, such as the Navy, Marines and Air Force.
The reason most members of the Army thought the number of unvaccinated was much smaller, aside from the information provided via the Army’s official channels, is that the Army has been “very tight-lipped” about these figures, “not leaking [them] to anybody, even internally,” according to the whistleblower.
“Those who are not vaccinated are segregated, so it is hard to find out who isn’t vaccinated,” he said. “The Army has done a very good job of not letting that information be leaked across the service.”
As a result, according to the whistleblower, “sometimes you feel you’re the only one, that there’s only a few people left” who have not received the COVID-19 vaccine.
However, those who are unvaccinated and who are privy to the real figures are, as the whistleblower described it, “re-energized and encouraged” by these numbers.
Army will be ‘combat-ineffective’ unless it moves June 30 deadline
The whistleblower told The Defender the DOD still plans to separate the unvaccinated soldiers, but instead of enforcing the June 30 deadline, “what they are going to do is hold off on separating soldiers on July 1,” and “will most likely push that into 2023 at the earliest.”
The June 2022 Army document confirms this, as it proposes that a “phased approach to involuntary separation” for unvaccinated service members would begin on October 1, 2022, with a “mandatory bar to reenlistment,” while “mandatory involuntary separations for COVID vaccine refusal” would begin January 1, 2023, and “last up to approximately 2 years.”
The document also recommends “separations for Soldiers start in FY23 [fiscal year 2023] with a phased approach.”
The whistleblower said the later date and “phased approach” are necessary because the Army is having a difficult time recruiting new troops, as “recruiting numbers have tanked over the past six months.”
The June 2022 document confirms this, describing an “extremely challenging recruiting environment.”
Moreover, the whistleblower claims that “the Army knows they cannot separate 120,000 soldiers,” as the Army would become “combat-ineffective,” which the whistleblower states is another reason why the real figures have been tightly guarded.
“Strength is in numbers,” he said.
Instead of getting the high numbers of vaccinated soldiers the DOD was hoping for, it appears the military now has to manage a larger-than-expected number of service members who have refused the COVID vaccine.
“The Pentagon knows that too many [service members] have said no and that there is not much they can do about it,” said the whistleblower.
Service members, unaware of an impending change to June 30 deadline, face a ‘very hard’ decision
While the DOD may be ready to move the June 30 COVID-19 vaccination deadline to a later date, the whistleblower said officials are keeping this information under wraps for the time being.
“Between now and July 1, nothing will change with the guidance,” he said, adding the new deadline will be announced at a later date.
However, in the period between now and June 30, unvaccinated service members who remain unaware of this possible change will “have to make a very difficult decision: Get the vaccine or be separated,” the whistleblower said.
Separately, Rep. Matt Gaetz (R-Fla.) last week called for the DOD to reinstate all troops discharged from any branch of the U.S. military, with their same rank, benefits and back pay.
And Sen. Ron Johnson (R-Wis.) last week once again demanded the DOD turn over all documents related to management of the military’s medical database between 2016 and 2020, following accusations by other DOD whistleblowers that the database was altered in order to obscure evidence of injuries related to the COVID-19 vaccines.
In this interview, French lawyer Diane Protat representing the group Navigants Libres, explains their fight in court defending pilots, flight attendants and all flight personnel who have experienced the severe and deadly effects of the Covid -19 vaccine shots and mandates.
Due to the life-threatening consequences of not just those commandeering flights but the entire population of airline passengers, it is crucial to evaluate these cases and stop the government regulations that continue to pose un-safe and grave consequences.
Serious health incidents and factual medical data coming from flight personnel is also being questioned worldwide through other international aviation organizations. The Global Aviators Coaliton, is partnering with Navigants Libres, and others who areworking to reveal that theses health risks and dangerous outcomes of the mandatory vaccines are being experienced globally within the airline industry.
Protat sites several cases where flights were forced to perform emergency landings due to pilot and co-pilot death or illness after the vaccine and the accounts of many pilots who have been grounded due to new health issues not allowing them to pass routine health examinations.
Flight crew members such as flight attendants have suffered female reproductive issues that pose serious problems and prevent them from returning to work in this sector. Because of this specific phenomenon with women, Protat has also been heard in the Senate representing the woman’s groups “Where is My Cycle” and a collective of Midwives called, “Key Woman”, where thousands of women members are reporting reproductive health issues after the Covid vaccine.
Protat argues that these mandatory vaccines present too high a risk and evidenced hazard for aviation employees and citizens around the world who embark on airplane travel, and that measures must be taken immediately to prevent any further risk.
U.S. Sen. Ron Johnson (R-Wis.) is asking the company that manages the U.S. Department of Defense’s Defense Medical Epidemiology Database to turn over records after the company failed to fully comply with a previous request seeking information about its “awareness of potential data problems” with the military’s database.
Sen. Ron Johnson (R-Wis.) is asking the company that manages the U.S. Department of Defense’s (DOD) Defense Medical Epidemiology Database (DMED) to turn over records after the company failed to fully comply with a previous request seeking information about its “awareness of potential data problems” with the military’s database.
This is the second time Johnson has requested the records from Unissant Inc.
The DMED is the military’s longstanding epidemiological database of service members.
Claiming the DMED data for 2016-2020 was incorrect, the DOD temporarily disabled the database — after whistleblowers came forward — then updated it with accurate figures, which resulted in less of an increase in medical conditions that potentially could be related to the vaccines.
The DOD said the DMED system was taken offline to “identify and correct the root cause of the data corruption.”
Given what Johnson said was the DOD’s lack of transparency, the senator asked his staff to contact Unissant to discuss its “awareness of potential data problems in DMED.”
Johnson, a ranking member of the Permanent Subcommittee on Investigations, first sent a formal letter to Unissant on March 7, requesting records related to its management of the DMED.
Unissant responded by stating it was prohibited from answering Johnson’s questions or “providing any details about the work it performs for the Defense Health Agency.”
Johnson’s staff provided Unissant with information from the DOD stating the company did not need the DOD’s consent to answer questions from Congress. A DOD contracting officer informed Unissant that “when it comes to Congressional or Senatorial inquiries, you don’t need my permission” to respond.
Despite approval to release information to Johnson’s office, Unissant requested written approval from its DOD contracting officer to release the information.
“Our letter explains why we are making this request even though you’ve stated we do not need your permission,” the email stated.
The DOD on May 2 gave Unissant permission to provide responsive documents to Johnson’s initial March 7 request, but Unissant’s letter detailing why it needed the DOD’s written permission was omitted from the records provided to his office.
“The records Unissant has provided to date as well as the company’s unclear explanation for requesting DOD’s approval to respond to Congressional inquiries raise additional questions,” Johnson said in a June 14 letter to Kenneth Bonner, president and chief growth officer of Unissant.
Johnson asked Unissant to provide the following additional information no later than June 28.
Johnson wrote:
1. Does Unissant agree with DOD’s claim that “the data in DMED was corrupt for the years 2016-2020 when accessed after September 2021?” If so, please explain why the DMED data for registered diagnoses of certain medical conditions from 2016-2020 was incorrect.
2. Please explain why registered diagnoses of myocarditis in 2021 decreased from 1,239 registered cases as of August 29, 2021, to 273 registered cases as of January 10, 2022. Please explain why the average annual registered diagnosis of myocarditis from 2016-2020 increased from 216 as of August 29, 2021, to 559 as of January 10, 2022.
3. Unissant claimed that on February 10, 2022, DOD discovered the need to “fix DMED monthly data for 2021.” However, emails produced by Unissant show that on Jan. 31, 2022, Unissant’s Vice President Stephen Gehring wrote that, “the team worked over the weekend to identify and resolve the issues” with DMED. Later that day, a DOD employee confirmed that “DMED access was restored after the data was corrected.”
Did Unissant identify the issues discussed on January 31, 2022, in its list of issues relating to DMED (see enclosure)? Were the issues discussed on January 31, 2022, different from the issue identified on February 10, 2022? Did DOD or Unissant discover the issues discussed on January 31, 2022? Please provide all communications showing this.
It does not appear that Unissant provided communications referring or relating to the DMED issue discovered on February 10, 2022 (as requested in the March 7, 2022 letter). Please provide those documents.
4. Provide a list of communications and documents discussing the “need to fix DMED monthly data for 2021” and the communications relating to the DMED issues discovered on Feb. 10, 2022, that Unissant failed to disclose with the previous request.
5. On January 31, 2022, Unissant Vice President Stephen Gehring noted that his team had “worked over the weekend to identify and resolve the issues” with DMED. He added that “the team uncovered other findings in testing that need to be addressed.” What were those “other findings”? Did those finding [sic] relate to issues with DMED? If so, were those findings identified in Unissant’s chart regarding issues relating to DMED (pursuant to the March 7, 2022 letter)?
If these findings were not identified, please provide a description of those findings, when Unissant communicated those findings to DOD, and the status of any corrective action(s).
6. In a March 3, 2022 email provided by Unissant, a Unissant representative informed Unissant officials Kenneth Bonner and Stephen Gehring that as recently as August 2021, DOD and Unissant were aware of problems with DMED but still let it “go live” with those problems. What were the problems? Why did Unissant allow DMED to “go live” if it knew it had problems?
7. On April 22, 2022, Unissant’s President Kenneth Bonner attached a letter to an email to DOD Contracting Officer Kevin Hodge regarding DOD’s permission to release information to Sen. Johnson. This attachment was not included in Unissant’s May 4, 2022 production. Please provide this letter.
8. Unissant’s May 4, 2022 production included several emails between the company’s representatives and DOD officials regarding DMED issues in August 2021. It does not appear those issues were identified in Unissant’s production Exhibit 3 or Exhibit 4 (enclosed). What were those issues, who discovered those issues and when, how long did those issues exist in DMED and when were those issues corrected?
9. Unissant’s May 4, 2022 response noted that because its employees use DOD email addresses to communicate with DOD employees referring or relating to DMED, “Unissant does not have access to these documents and communications.” Does Unissant not maintain records of its employees’ communications between and among Unissant and DOD employees regarding their contracted work?
When performing work on behalf of the federal government, how does Unissant ensure that its employees are following federal record preservation requirements if Unissant cannot access its employees’ documents and communications?
DOD changes DMED data on myocarditis after whistleblowers come forward
The first COVID-19 vaccine was authorized by the U.S. Food and Drug Administration on December 14, 2020. Secretary of Defense Lloyd Austin on Aug. 24, 2021, issued a memorandum mandating service members receive COVID-19 vaccinations.
According to downloaded data from DMED provided on Aug. 29, 2021, to Johnson’s office, there were 216 cases of myocarditis reported from 2016 to 2021 — an average of 43.2 diagnoses per year.
There were 1,239 cases of myocarditis in 2021 alone — a 2,868% increase over the 2016-2020 average.
According to a spreadsheet based on a complete DMED data set provided by whistleblowers to Johnson’s office in January 2022, figures for myocarditis had changed dramatically since the August 2021 download.
“Total myocarditis diagnoses 2016-2020 increased to 559 from 216 causing the annual average to increase to 111.8 from 43.2 diagnoses per year,” Johnson’s June letter to Unissant stated.
“For the year 2021, myocarditis diagnoses decreased from 1,239 to 263 causing the annual percentage increase to decline from 2,868% to 235% over the 2016-2020 average.”
In other words, after the DOD enforced its vaccine mandate, the database was altered to reduce the increase in myocarditis cases in 2021, compared to the previous four years.
Attorney exposes DMED data at January panel discussion led by Johnson
Attorney Thomas Renz in January told experts during a panel discussion on COVID-19 vaccines and treatment protocols that was led by Johnson, that data provided to him by three whistleblowers showed COVID-19 vaccines were causing catastrophic harm to members of the U.S. military while not preventing them from getting the virus.
Data from DMED provided by whistleblowers — who knew they would face perjury charges if they submitted false statements to the court in legal cases pending against the DOD — showed miscarriages increased 300% in 2021 over the previous five-year average, cancer increased by 300% and neurological disorders increased 1,000% in 2021 over the past five-year average — increasing from 82,000 to 863,000 in one year.
Malignant neoplasms of the esophagus: 894% increase.
Multiple sclerosis: 680% increase.
Malignant neoplasms of digestive organs: 624% increase.
Guillain–Barré syndrome: 551% increase.
Breast cancer: 487% increase.
Demyelinating: 487% increase.
Malignant neoplasms of thyroid and other endocrine glands: 474% increase.
Female infertility: 472% increase.
Pulmonary embolism: 468% increase.
Migraines: 452% increase.
Ovarian dysfunction: 437% increase.
Testicular cancer: 369% increase.
Tachycardia: 302% increase.
Renz also said DMED data showing registered diagnoses of myocarditis had been removed from the database.
Renz told the panel a “trifecta of data” from the DMED and Project SALUS, the DOD’s military-civilian integrated health database, along with human intelligence in the form of doctor-whistleblowers, suggest the DOD and the Centers for Disease Control and Prevention withheld COVID-19 vaccine surveillance data since September 2021.
Following Renz’s presentation, attorney Leigh Dundas reported evidence of the DOD doctoring data in DMED to conceal cases of myocarditis in service members vaccinated for COVID-19.
Johnson demands DOD respond to whistleblower claims
Johnson asked the DOD in February what it was doing to investigate whistleblower reports of big spikes in miscarriages, neurological disorders, cancer and other illnesses among members of the U.S. military since its rollout of COVID-19 vaccines.
Johnson also asked if the DOD had removed reports of vaccine-induced myocarditis from the DMED.
The Defense Health Agency on Jan. 26 created and preserved “a full backup of the DMED,” at Johnson’s request.
On Jan. 28, a DOD spokesman told PolitiFact there was a glitch in the DMED database that “gave the false impression that there was a huge spike in miscarriages, cancer and other medical issues among military members in 2021.”
The spokesman said the database had “been taken down to identify and correct the problem.”
In a groundbreaking article for Children of God For Life, titled “Forsaking God For the Sake of Science,” [1] [1b] Debra Vinnedge outlines how the Rockefeller-Harriman eugenics movement gave rise to the practice of medical abortions for research purposes, including live births during which the infant was murdered and its organs harvested:
“…Abortion wasn’t legal yet; this was 1936. But abortion was most certainly legal and acceptable [to eugenicists] if it meant ending the life of a child who would be born to a ‘feeble-minded’ woman, one who might end up less than perfect or who might have to rely on society to pay for their care.”
And therefore, why not perform abortions for medical research? Behind closed doors, out of view, this was happening in several countries, including the US.
Consider this research report: “Human embryos of two and one-half to five months gestation were obtained from the gynaecological department of the Toronto General Hospital…No macerated specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
Here is the citation [2]: Joan C. Thicke, Darline Duncan, William Wood, A. E. Franklin and A. J. Rhodes; Cultivation of Poliomyelitis Virus in Tissue Culture; Growth of the Lansing Strain in Human Embryonic Tissue, Canadian Journal of Medical Science, Vol. 30, pg 231-245. [June 1952]
The authors are certainly describing an infant who was taken from the womb alive, and after cells were harvested, was killed. For research on “growing virus in cell culture.”
Here is another research report that indicates the infant was born alive, its tissues taken, and then killed:
“Embryos of between 12-18 weeks gestation have been utilized. Rarely tissues were obtained from stillborn fetuses, or from premature infants at autopsy…In the experiments 3 sorts of embryonic materials were used: elements of skin, connective tissue, muscle; intestinal tissue; brain tissue…Whenever possible the embryo was removed from the amniotic sac.., transferred to a sterile towel and kept at 5 C until dissected.”
The citation [3]: Thomas H. Weller, John F. Enders, Studies on the Cultivation of Poliomyelitis Viruses in Tissue Culture : I. The Propagation of Poliomyelitis Viruses in Suspended Cell Cultures of Various Human Tissue; Journal of Immunology 1952;69;645-671. [June 1952]
Again, the infant’s tissue was used, in the lab, to “grow virus in cell culture.” The cells were from the infant.
My readers know that, for the past year, I’ve been exposing virologists’ absurd claims that they’re isolating viruses in their labs. [4] [4b] [4c]
In fact, they create soups in dishes, containing toxic drugs and chemicals, monkey cells and human cells, and a mucus sample from a patient. When the cells start dying, they claim this is proof the virus is in the mucus, in the soup, and is deadly.
Of course, this is nonsense, because the toxic drugs and chemicals are perfectly capable of killing the cells; and the cells in the soup are being starved of nutrients, which would also lead to cell-death.
The isolation of viruses is no isolation at all. It’s a fraud.
But it never occurred to me, until now, that some of these human cells in the soup in the lab came from infants, taken from the mother’s womb alive, for harvesting, who were then killed.
This completes a circle of evil.
Of course, out of the virological research fraud and infant murder come THE VACCINES, including the COVID vaccines, which are causing huge numbers of injuries and deaths across the world.
People of faith everywhere must see that declaring a religious exemption from the shots is a DUTY, whether or not the authorities allow the exemption.
The last time I looked, appealing to Pontius Pilate for an exemption didn’t work, and the status of Anthony Fauci is not higher than the Authority to whom, at minimum, four billion people of faith pray.
49 states have decided to follow the federal government’s lead in ordering COVID injections for children under 5, despite glaring evidence of a failed pharmaceutical product that doesn’t serve any benefit to them whatsoever, and has the potential to cause serious side effects.
On Friday, the FDA authorized mRNA COVID shots (both Pfizer and Moderna) under emergency use for children under 5 down to 6 months of age. The approval made its way through the halls of the federal bureaucracy, regardless of any studies showing a positive benefit for injecting young children with mRNA shots, which, even in adults, do not effectively prevent coronavirus infection.
So you’ve had your eight-month-old baby injected with the COVID vaccine.
Of course.
And the SARS-CoV-2 virus doesn’t exist.
I’ve heard that. But it’s not the issue for us.
What is the issue for you?
Making a fashion statement.
How so?
We need to stay in the forefront of trends.
Why?
Why wouldn’t we?
Have you seen the federal database that records vaccine injury and death reports?
Of course.
So you know your baby could die from the shot.
Yes.
And that doesn’t matter to you.
Not as much as being able to tell our friends we had our baby vaccinated.
You, as parents—
That’s a misunderstood term. We don’t consider ourselves parents. The State is the parent. We’re the monitors.
Monitors?
We observe, and carry out limited functions.
Even if you assume the virus exists, the chances of your baby catching it and becoming ill are incredibly tiny.
That’s right. But this isn’t what we’re about. As I said, we’re keeping pace with fashion.
Are you human?
It depends on how you define the term. Humans are biological machines. Most people believe in something beyond that, but the content of belief is predetermined by a person’s upbringing, genes, conditioning, and so on.
Have you ever questioned vaccine science?
There’s nothing to question. We understand science. I have a PhD in psychology, and my husband is a software engineer. My IQ is 141. My husband’s is 136. We’re equipped to deal with vaccine issues.
If your baby died from the shot, would you mourn?
Yes. We would post photos and statements on our Facebook page.
—No doubt, some people would take offense at this “interview.” How could I? Here’s how. I wrote it. I wrote it because the government and Pfizer and Moderna—no matter how they interpret COVID and “the virus”—are moving ahead to inject as many babies as possible—which is a crime of mass assault and mass murder. Many parents will go along with it.
While many have bought into the simplistic idea that availability of firearms is the cause of mass shootings, a number of experts have pointed out a more uncomfortable truth, which is that mass shootings are far more likely the result of how we’ve been mistreating mental illness, depression and behavioral problems
Gun control legislation has shown that law-abiding Americans who own guns are not the problem, because the more gun control laws that have been passed, the more mass shootings have occurred
97.8% of mass shootings occur in “gun-free zones,” as the perpetrators know legally armed citizens won’t be there to stop them
Depression per se rarely results in violence. Only after antidepressants became commonplace did mass shootings really take off, and many mass shooters have been shown to be on antidepressants
Antidepressants, especially selective serotonin reuptake inhibitors (SSRIs), are well-known for their ability to cause suicidal and homicidal ideation and violence
While many have bought into the simplistic idea that availability of firearms is the cause of mass shootings, a number of experts have pointed out a more uncomfortable truth, which is that mass shootings are far more likely the result of how we’ve been mistreating mental illness, depression and behavioral problems.
An article written by Molly Carter, initially published on ammo.com at an unknown date1 and subsequently republished by The Libertarian Institute in May 2019,2 and psychreg.org in late January 2021,3 noted:
“According to the Federal Bureau of Investigation (FBI), a mass murder occurs when at least four people are murdered, not including the shooter … during a single incident …
Seemingly every time a mass shooting occurs … the anti-gun media and politicians have a knee-jerk response — they blame the tragedy solely on the tool used, namely firearms, and focus all of their proposed ‘solutions’ on more laws, ignoring that the murderer already broke numerous laws when they committed their atrocity.
Facts matter when addressing such an emotionally charged topic, and more gun control legislation has shown that law-abiding Americans who own guns are NOT the problem. Consider the following: The more gun control laws that are passed, the more mass murders have occurred.
Whether or not this is correlation or causation is debatable. What is not debatable is that this sick phenomenon of mass murderers targeting ‘gun-free zones,’ where they know civilian carry isn’t available to law-abiding Americans, is happening.
According to the Crime Prevention Research Center,4 97.8% of public shootings occur in ‘gun-free zones’ – and ‘gun-free zones’ are the epitome of the core philosophical tenet of gun control, that laws are all the defense one needs against violence …
This debate leads them away from the elephant in the room and one of the real issues behind mass shootings — mental health and prescription drugs.
Ignoring what’s going on in the heads of these psychopaths not only allows mass shootings to continue, it leads to misguided gun control laws that violate the Second Amendment and negate the rights of law-abiding U.S. citizens.
As Jeff Snyder put it in The Washington Times: ‘But to ban guns because criminals use them is to tell the innocent and law-abiding that their rights and liberties depend not on their own conduct, but on the conduct of the guilty and the lawless, and that the law will permit them to have only such rights and liberties as the lawless will allow.’”
The Elephant in the Room: Antidepressants
Thoughts, emotions and a variety of environmental factors play into the manifestation of violence, but mental illness by itself cannot account for the massive rise in mass murder — unless you include antidepressants in the equation. Yet even when mental health does enter the mass shooter discussion, the issue of antidepressants, specifically, is rarely mentioned.
The fact is, depression per se rarely results in violence. Only after antidepressants became commonplace did mass shootings take off, and many mass shooters have been shown to be on antidepressants.
Prozac, released in 1987, was the first selective serotonin reuptake inhibitor (SSRI) to be approved for depression and anxiety. Only two years earlier, direct-to-consumer advertising had been legalized. In the mid-1990s, the Food and Drug Administration loosened regulations, direct-to-consumer ads for SSRIs exploded and, with it, prescriptions for SSRIs.
In 1989, just two years after Prozac came to market, Joseph Wesbecker shot 20 of his coworkers, killing nine. He had been on Prozac for one month, and the survivors of the drug-induced attack sued Eli Lilly, the maker of Prozac. Since then, antidepressant use and mass shootings have both risen, more or less in tandem.
In the two decades between 1988 and 2008, antidepressant use in the U.S. rose by 400%,5 and by 2010, 11% of the U.S. population over the age of 12 were on an antidepressant prescription.6
In 1982, pre-Prozac, there was one mass shooting in the U.S.7 In 1984, there were two incidents and in 1986 — the year Prozac was released — there was one. One to three mass shootings per year remained the norm up until 1999, when it jumped to five.
Another jump took place in 2012, when there were seven mass shootings. And while the annual count has gone up and down from year to year, there’s been a clear trend of an increased number of mass shootings post-2012. Over time, mass shootings have also gotten larger, with more people getting injured or killed per incident.8
How can we possibly ignore the connection between rampant use of drugs known to directly cause violent behavior and the rise in mass shootings? Suicidal ideation, violence and homicidal ideation are all known side effects of these drugs. Sometimes, the drugs disrupt brain function so dramatically the perpetrator can’t even remember what they did.
For example, in 2001, a 16-year-old high schooler was prescribed Effexor, starting off at 40 milligrams and moving up to 300 mg over the course of three weeks. On the first day of taking a 300-mg dose, the boy woke up with a headache, decided to skip school and went back to bed.
Some time later, he got up, took a rifle to his high school and held 23 classmates hostage at gunpoint. He later claimed he had no recollection of anything that happened after he went back to bed that morning.9
The Risks Are Clear
The risks of psychiatric disturbances are so clear, ever since mid-October 2004, all antidepressants in the U.S. must include a black box warning that the drug can cause suicidal thoughts and behaviors, especially in those younger than 25, and that:10
“Anxiety, agitation, panic attacks, insomnia, irritability, hostility (aggressiveness), impulsivity, akathisia (psychomotor restlessness), hypomania, and mania have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric.”
SSRIs can also cause emotional blunting and detachment, such that patients report “not feeling” or “not caring” about anything or anyone, as well as psychosis and hallucinations. All of these side effects can contribute to someone acting out an unthinkable violent crime.
In one review11,12 of 484 drugs in the FDA’s database, 31 were found to account for 78.8% of all cases of violence against others, and 11 of those drugs were antidepressants.
The researchers concluded that violence against others was a “genuine and serious adverse drug event” and that of the drugs analyzed, SSRI antidepressants and the smoking cessation medication, varenicline (Chantix), had the strongest associations. The top-five most dangerous SSRIs were:13
Fluoxetine (Prozac), which increased aggressive behavior 10.9 times
Paroxetine (Paxil), which increased violent behavior 10.3 times
Fluvoxamine (Luvox), which increased violent behavior 8.4 times
Venlafaxine (Effexor), which increased violent behavior 8.3 times
Desvenlafaxine (Pristiq), which increased violent behavior 7.9 times
Depression Is Vastly Overdiagnosed
In her article, Carter also reviewed the clinical determinants for a diagnosis of clinical depression warranting medication. To qualify, you must experience five or more of the following symptoms, most of the day, every day, for two weeks or more, and the symptoms must be severe enough to interfere with normal everyday functioning:14
Sadness
Anxiety
Feeling hopeless
Feeling worthless
Feeling helpless
Feeling ’empty’
Feeling guilty
Irritable
Fatigue
Lack of energy
Loss of interest in hobbies
Slow talking and moving
Restlessness
Trouble concentrating
Abnormal sleep patterns, whether sleeping too much or not enough
Abnormal weight changes, either eating too much or having no appetite
Thoughts of death or suicide
The reality is that a majority of patients who receive a depression diagnosis and subsequent prescription for an antidepressant do not, in fact, qualify. In one study,15 only 38.4% actually met the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria, and among older adults, that ratio was even lower. Only 14.3% of those aged 65 and older met the diagnostic criteria. According to the authors:16
“Participants who did not meet the 12-month MDE criteria reported less distress and impairment in role functioning and used fewer services. A majority of both groups, however, were prescribed and used psychiatric medications.
Conclusion: Depression overdiagnosis and overtreatment is common in community settings in the USA. There is a need for improved targeting of diagnosis and treatments of depression and other mental disorders in these settings.”
What Role Might War Games Play?
Aside from antidepressants, another factor that gets ignored is the influence of shooting simulations, i.e., violent video games. How does the military train soldiers for war? Through simulations. With the proliferation of video games involving indiscriminate violence, should we really be surprised when this “training” is then put into practice?
As reported by World Bank Blogs, young men who experience violence “often struggle to reintegrate peacefully into their communities” when hostilities end.17 While American youth typically have little experience with real-world war, simulated war games do occupy much of their time and may over time color their everyday perceptions of life. As noted by Centrical, some of the top benefits of simulations training include:18
Allowing you to practice genuine real-life scenarios and responses
Repetition of content, which boosts knowledge retention
Personalization and diversification, so you can learn from your mistakes and evaluate your performance, thereby achieving a deeper level of learning
In short, violent mass shooter games are the perfect training platform for future mass shooters. Whereas a teenager without such exposure might not be very successful at carrying out a mass shooting due to inexperience with weapons and tactics, one who has spent many hours, years even, training in simulations could have knowledge akin to that of military personnel.
Add antidepressant side effects such as emotional blunting and loss of impulse control, and you have a perfect prescription for a mass casualty event.
On top of that, we, as a nation, also demonstrate the “righteousness” of war by engaging in them without end.19 When was the last time the U.S. was not at war someplace? It’s been ongoing for decades.
Even now, the U.S. insists on inserting itself into the dispute between Russia and Ukraine, and diplomacy isn’t the chosen conflict resolution tool. Sending weapons to Ukraine and calling for more violence against Russians are. Sen. Lindsey Graham has even called for the assassination of Russian President Vladimir Putin. Showing just how serious such a suggestion is, the White House had to publicly disavow it, stating Graham’s comment “is not the position of the U.S. government.”20
Graham, meanwhile, does not appear to understand how his nonchalant call for murder might actually incite murder. In the wake of the Uvalde school shooting, he now wants to mobilize retired service members to enhance security at schools, and while that might be a good idea, how about also vowing never to call for the murder of political opponents? Don’t politicians understand that this could translate into some kid thinking it’s acceptable to murder THEIR perceived opponents?
As far as I can tell, mass shootings have far more to do with societal norms, dangerous medications, a lack of high-quality mental health services, and the normalization of violence through entertainment and in politics, than it does with gun laws per se.
There are likely many other factors as well, but these are clearly observable phenomena known to nurture violent behavior. I’m afraid Americans are in need of a far deeper and more introspective analysis of the problem than many are capable of at the moment. But those who can should try, and make an effort to affect much-needed change locally and in their own home.
That is a TECHNICAL comment on trending claims that men can become pregnant.
Gateway Pundit has the story: “A North Carolina preschool is under fire after using LGBTQ flash cards, one of which featured a pregnant man, to teach the little kids about colors.”
“Republican State Rep. Erin Paré was emailed about the flash cards by a concerned constituent and contacted the principal at Ballentine Elementary School, part of the Wake County public school system, about the alarming email.”
“The principal searched the classroom and located the cards, according to a statement from North Carolina Speaker of the House Tim Moore.”
“’The principal found the stack of cards in a preschool classroom and verified with the teacher that they had been used by the teacher in the classroom to teach colors. The principal confirmed that the flash cards were not part of approved curriculum and that she was unaware that they were being used,’ Moore’s statement said. ‘The principal immediately took possession of the cards, contacted the WCPSS area superintendent, and engaged human resources. The principal expressed appreciation for the constituent’s information via Rep. Paré, as she would not have known about the flash cards otherwise’.”
Preschoolers. Flash cards. Pregnant man.
Does that give you a clue about the depth of re-education underway?
Follow this closely. A woman who decides to “become”—through drugs and surgery—a man, or a woman who simply identifies as a man…but in either case retains the necessary female equipment allowing pregnancy…supposedly means:
A man can become pregnant.
The best con artist on a street corner demonstrating his shell game for suckers would flush with envy at that word-game hustle.
By logical extension, a woman who identifies as a male tiger proves that male tigers can give birth to human babies.
I offer this as a warning to medical dictionaries and organizations. They’re going to be very busy with language updates.
Also, if the Supreme Court overturns Roe-Wade, many men will protest because they have to fly to distant states to obtain abortions. Right?
“We here at the Johnson Clinic are proud to announce our expanded services for men wishing to terminate their pregnancies. To show you how far we’re willing to go, last month our team handled the abortion of an apple tree. The tree, formerly a Beverly Hills banquet consultant, Marcia Crane, who identifies as a Granny Apple tree in her back yard, arrived here at the Clinic with questions, and we had answers…”
LA Times: “Apple Tree has launched her campaign for a Congressional seat in the 33rd District, after huddling with advisors, including her husband, Miriam Forever-Penelope, who sits on the board of Trans-National Sinaloa, a charity which funds several PBS wildlife series…”
This movie has been produced in many ways, in many minds.
In all cases, the theme is the same: DO NOT LIVE YOUR LIFE OUT IN THE OPEN.
Instead obey all restrictions. SHUT IT DOWN.
Believe in the dangers you’re told to believe in.
In the final analysis, this movie was a box office hit because most people gave in. Their fears may have hooked into different parts of the COVID narrative, but the deciding factor WAS fear.
A nation, a world paralyzed by fear.
And yes, lurking in the background (or in some countries, in the foreground) was the fact that the State had cops and guns and detainment facilities.
I’ve spent many hours detailing that, at one time, the citizenry would have risen up, en masse, and rebelled against the State. They would have shrugged off pandemic declarations. They would have risked everything to keep LIVING THEIR LIVES OUT IN THE OPEN.
Because at one time, freedom meant more.
The individual meant more.
People making up their own minds meant more.
Predatory groups organized to cut themselves in on a piece of the government pie meant less.
All these groups, from BLM to Climate Change, demand less freedom. That is their unspoken bottom line. And their justifications for this demand are bogus and fabricated.
They’re basically FRIENDS OF THE STATE.
Readers who have been with me for a long time know that, in 1988, I started warning people that the medical cartel was the most dangerous cartel in the world. It was seeking medical dictatorship.
I knew that in 1988, because I was meeting radical natural health advocates—tough, smart, resilient people. THEY had been warning about medical dictatorship for the previous 20, 30 years.
When I saw what my research on a phantom virus called HIV was proving, I knew civilization was in for some very rough times. All sorts of medical fantasies would be used to destroy freedom.
As Ben Franklin made clear, people WERE willing to trade that freedom for a false sense of security.
The past two years have proved it in spades.
But they’ve also proved something else. There is a limit to what people will take.
So I write this piece to say the restrictions could be coming again.
And if they do, we don’t need another two years to realize what the game really is.
We have to say NO from the get-go. We have to put fear aside and risk everything for freedom.
It wouldn’t be the first time people did, you know.
Face it, we’re all suffering from a false sense of security. Fortunately, we don’t have to succumb. We can be the individuals we dream of being, against whatever the State launches against us.
There are beasts among us. It turns out that many of them have no faces. They are the reincarnation of men and women who sat at desks and signed warrants for the death camps.
Gambling that life without freedom can still be a good life is a disastrous bet.
In the founding documents of America—the Declaration of Independence, the Articles of Confederation, the Constitution—the idea of freedom was there. Individual freedom with responsibility.
Before the ink was dry, the attacks on freedom commenced. Freedom has been dented, battered, smashed, and yes, betrayed, from all quarters. But it still stands and shines.
The U.S. Food and Drug Administration (FDA) is likely to grant Emergency Use Authorization (EUA) for Pfizer’s BioNTech SARS-CoV-2 vaccine for children ages 6 months through 4 years and Moderna’s COVID-19 mRNA vaccine for infants and children ages 6 months through 5 years and 6 years through 17 years in their upcoming meetings today and tomorrow (June 14-15).
CHD is poised to take legal action against the FDA should they grant these emergency use authorizations. We seek to hold FDA accountable for recklessly endangering our children with products that have little, no or even negative net efficacy. These products may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke, other thrombotic events and future reproductive harm.
Our children need your help! On Tuesday and Wednesday, June 14 and 15, the FDA VRBPAC committee is likely to make a catastrophic decision by voting to grant Emergency Use Authorizations (EUA) to allow for infants and young children to receive Pfizer’s and Moderna’s COVID shots.
Please take 30 seconds to tell your lawmakers to STOP the FDA from granting EUAs for COVID vaccines in babies and children by sending Robert F. Kennedy, Jr.’s letter to FDA VRBPAC committee members. His letter lays out all of the available science and data that proves vaccinating children for COVID is not only unnecessary, but will recklessly endanger their lives. There is no emergency whatsoever for children from COVID, therefore there is no justification for issuing an Emergency Use Authorization.
Time and mounting evidence have continued to prove that children have essentially zero risk of dying from COVID (99.995% recovery rate), and the vast majority of kids have little to no symptoms. There is no statistically valid evidence that shows the Pfizer and Moderna COVID injections are able to prevent severe disease or deaths in children at all. These shots have a worse safety record than all previous vaccines combined, and have been found to cause serious injuries including myocarditis, encephalopathy, blood clots, diabetes, neurological issues and death.
The United States Government, at the behest of Pharma oligarchs and government employees who own stock in the Pharma companies, hopes to approve an amendment to the EUA (Emergency Use Authorization) to inject babies 6-months-old to toddlers 4-years-old with the C19 faux-vaccine.
Before the committee meets to recommend the amendment, the FDA allows people to comment on the FDA government web site. One such comment was provided to this author and is offered to you below. The United States of America is indeed facing a government #ClotShot plot.
This comment is NOTICE of possible criminal liability to Lauren K. Roth and members of the Vaccines and Related Biological Products Advisory Committee who owe duties of care, diligence, good faith, and loyalty in recommending “for” or “against” the EUA amendment for COVID-19 mRNA vaccine in children 6 months through 4 years of age.
Only two deaths are listed herein to establish knowledge. If the amendment is approved, it will have been done by committee members “knowing” of felony crimes in context.
Your investigation of these deaths should include death certificates, autopsy records, witness interviews, and immunization records.
Massachusetts Death Certificate 2022 SFN 5980 is a 7yo girl died January 18, 2022 listed as died from U071 “COVID-19”, B49 “unspecified mycosis”, J450 “predominantly allergic asthma”, and R091 “pleurisy”.
VAERS_ID 2038120 is a 7yo girl in Massachusetts, who received her 2nd dose 1/13/2022 and was reported to VAERS 1/15/2022. PRIOR_VAX states, “Severe nausea and vomiting from 5min post vaccination and for the next 8-10 hours.” SYMPTOM_TEXT states, “Spiked a 103 fever, severe stomachache, has not had a bowel movement since the day before vaccination, which makes today 3 days without one. First vaccine caused severe nausea and vomiting from 5minutes post injection and for the next 8-10 hours.”
This little girl suffered immeasurably 4 to 5 days as her intestines shut down due likely to impeded blood vessels servicing intestines.
Massachusetts Death Certificate 2021 SFN 56611 is a 48yo man died 11/16/2021 listed as died from U071 “COVID-19” and E669 “OBESITY”.
SFN 56611 is known to have died less than 24 hours after inoculation.
In both cases, the Medical Examiners listed the cause of death as “COVID-19”, when it was clearly not COVID-19. And in both cases, the Medical Examiners omitted listing causes Y590 “Viral vaccines“ and T881 “Other complications following immunization, not elsewhere classified”, when these clearly were proximate and actual causes.
Death certificates from the state of Massachusetts are sent to the CDC, a federal entity. Thus, fraud on a state death certificate is a federal crime as it affects federal death records. Several federal felony crimes apply in this instance and are listed below.
If you dismiss this NOTICE and recommend the EUA amendment without first investigating these two deaths, you become liable for inchoate crimes and the felony crime of “misprision of felony.” If a single person subsequently dies as a result of the amendment, all the elements will have been satisfied for you to face felony murder charges or involuntary manslaughter. Qualified immunity is not a valid defense.
18 USC § 4 – Misprision of felony
“Whoever, having knowledge of the actual commission of a felony …, conceals and does not as soon as possible make known the same to some … civil or military authority …, shall be fined under this title or imprisoned not more than three years, or both.”
Felony murder is a homicide that occurs during the commission of an inherently dangerous felony, showing a conscious disregard for human life. A jury decides whether recommending an injection, that you “know” caused death, and that you refused to investigate while “knowing” it caused death, is inherently dangerous.
Here are a few federal statutes likely violated by Medical Examiners in Massachusetts. You are duty-bound to call for investigation of:
18 USC § 4 Misprision of felony
18 USC § 286 Conspiracy to defraud the government with respect to claims
18 USC § 287 False fictitious or fraudulent claims
18 USC § 371 Conspiracy to commit offense or to defraud United States
18 USC § 1035 False statements relating to health care matters
18 USC § 1040 Fraud in connection with major disaster or emergency benefits
There were found sixty likely C19 vaccine deaths in a 25-minute perusal of the 2021 and 2022 death certificates, which extrapolates to hundreds, probably thousands of C19 vaccine deaths in Massachusetts.
Refusal to investigate these fraudulent records is a crime that, because of the felony murder aspect, has no statute of limitations. Five, ten, or twenty years from now, if a federal prosecutor were to learn of this NOTICE, he or she would have significant evidence to bring charges for felony murder.
In summary, this NOTICE places you in a position requiring you to investigate these deaths prior to recommending the amendment. If you dismiss this NOTICE, you may be criminally liable for involuntary manslaughter, felony murder, and a list of federal crimes and inchoate crimes.
Please make the appropriate decision for yourselves and for the children of the United States of America.
A growing number of young healthy adults are mysteriously dying. Watch Jefferey Jaxen and Del try to make sense of, what is now being called, “Sudden Adult Death Syndrome” (SADS).
First New England Journal of Medicine Pfizer Study Reveals 80% Miscarriage Rate in Recipients in their First or Second Trimester — Dr. Christiane Northrup also reports rising number of stillbirths on ‘Friday Roundtable’ Infertility: A Diabolical Agenda Q+A
A film by award-winning filmmaker Andy Wakefield, Robert F. Kennedy, Jr. and Children’s Health Defense. Watch the chilling tale of African women whose fertility was tragically stripped away through an experimental tetanus vaccination program. Are women everywhere next?
“When they’re through with Africa, they’re coming for you.” ~ Dr. Stephan Karanja
The chilling, harrowing story of how a World Health Organization (WHO) population control experiment, under the guise of a vaccination program, resulted in the sterilization of millions of women in Africa without their knowledge or consent.
How the ability to carry a pregnancy to term has been tragically stripped away from these women as their government attempts to cover up the evidence.
About a brave, Kenyan doctor — Dr. Stephen Karanja — who warned the world that once they’re done with Africa, they’re coming for the children and everyone else.
Perspectives from leading experts expressing their concerns regarding other vaccines that could cause infertility in women around the world, including the COVID shot.
However, that is true only when the term “man” is broken down to its new definition. A re-education is now taking place because there are some common misconceptions about the term “man.”
Not all people who were assigned male at birth (AMAB) identify as men. Those who do are “cisgender” men. Conversely, some people who were assigned female at birth (AFAB) identify as men. These folks may be “transgender” men or transmasculine people.
A New Spectrum
To be clear, according to the Transnarrative, if you fall on the Transmasculine spectrum, “you may identify as a man or any number of other gender identities including nonbinary, genderqueer, or agender.”
In former times, the ability to get pregnant was based on the ability to menstruate, which only women experienced. Even today, because biologic men do not menstruate, they cannot get pregnant or birth babies. The same is true of women who pass through menopause and no longer bleed monthly.
However, in the Transgender Age, everything is reversed:
“To be a man” is now defined such that a man can get pregnant, have periods, and have biological female chromosomes. To different people, this is either an exceptional mark of progress or a symptom of rabid social and/or linguistic deterioration.” – Rory Cockshaw, The Men Who Menstruate
Do TransMen have TransWombs?
Fortunately, the Female-to-Male (FTM) Transgender has the reproductive hardware and hormones necessary to form and carry a child. And there is a recipe: Transmen taking hormones (testosterone) to stop menses will have to start up again to become pregnant.
The medical world understands all about “gender non-conforming pregnancies.” According the the December 2014 Journal of Obstetrics and Gynecology, “Transgender Men Who Experienced Pregnancy After Female-to-Male Gender Transitioning,” can and do get pregnant. This is based on a cross-sectional, web-based survey. What about underlying biology of the FTM?
Trauma-focused therapist and sex educator Aida Manduley explains that two things are needed for pregnancy (and they are not gender identify or sexual orientation):
sperm
an egg
One person needs to have testicles (where sperm is produced), prostate and bulbourethral glands (to create the other components of semen), and a urethra (for the sperm to travel through)
And another person needs to have an ovary (where eggs are produced) and a uterus (where the sperm meets the egg).
America is back to Virtue Signaling at its finest, a tactic of subtle persuasion.
It is common to hear people introduce themselves and “self-identify” by sexual, gender, racial, or ethnic classifiers. And it is becoming trendy for companies to jump on the Transgender bandwagon.
Clothing brand Calvin Klein capitalized on this trend when it aired a Mother’s day ad featuring a pregnant transgender man:
We embrace this platform as an inclusive and respectful environment for individualism and self-expression. At Calvin Klein, we tolerate everything except intolerance— any intolerant commentary will be removed, and any accounts issuing hateful statements may be blocked.
The ad generated some backlash from people who questioned the likelihood of any biologic man becoming pregnant. Calvin Klein’s response? “Bigotry!” Calvin Klein is on the record as refusing to accept all opinions different from their own. Yet, having any opinion in the “mainstream” is becoming increasingly difficult because some opinions are louder than others. It depends on who owns the megaphone.
Soon after the Calvin Klein ad, Mattel released the Transgender Barbie doll in the image of Transman Laverne Cox;emphasis on cox? The new Barbies are reported to not have genitals, but they never had genitals to begin with, as they are toys. Cox claims that it was his/her mother’s fault that he/she was denied the ability to play with a Barbie doll, which caused shame and trauma. The answer from a medical therapist? “Go out and play with a Barbie doll.” Cox claims it was playing with the Barbie dolls that inspired healing.
No one discounts that Gender Dysforia is a recognized medically diagnosed condition, where someone feels that their physical gender does not match their internal gender identity. Medical treatment includes talk therapy with a psychologist, puberty blockers, hormones, and surgery. A Spanish medical journal states:
In children and adolescents, gender identity dysphoria is a complex clinical entity. The result of entity is variable and uncertain, but in the end only a few will be transsexuals in adulthood.
Let Kids Be Kids
The inherent immaturity and vulnerability of kids, who cannot purchase cigarettes, get married, or get a tattoo without parental consent, makes them prone to being taken advantage of by others. When it comes to surgeries for minors (without parental consent), many states are taking action to safeguard children with legal protection.
On May 6, 2022, an Alabama law took effect criminalizing gender transition surgery, puberty blockers, and hormone treatments on minors, punishable by up to ten years. On June 3rd, Florida governor took steps to protect minors from transgender surgeries. While the American Academy of Pediatrics (AAP) and the Endocrine Society recommend these treatments for ‘gender affirming’ care, the Florida Agency for Health Care Administration, released a 46-page report arguing against Medicare coverage for trans surgeries. Among their reasons:
Following a review of available literature, clinical guidelines, and coverage by other insurers and nations, Florida Medicaid has determined that the research supporting sex reassignment treatment is insufficient to demonstrate efficacy and safety….
The current standards set by numerous professional organizations appear to follow a preferred political ideology instead of the highest level of generally accepted medical science
…the scientific evidence supporting these complex medical interventions is extraordinarily weak.
There are at least 16 states that have taken action to protect children from Transgender surgeries. Arkansa’s Save Adolescents From Experimentation Act, openly contradicts guidance issued by the U.S. Department of Health and Human Services under President Joe Biden and transgender rights activists. Yet, it is the State government’s role to regulate activities and issues of citizens within the boundaries of the state it governs, not the federal government’s.
Why do corporate ads fail to respond to the real consequences that these kids face in society? Do their transgender ads serve to create more division and segregation? Are Calvin Klein and Mattel virtue signaling? The truth is that girls play with GI Joe and boys play in the kitchen. Speaking out about social issues without actually acting to support the cause is called Slaktivism.
Have we reached a moment of Transanity by design, at the hands of the media?
TransHistory
Hollywood films, and international films are conduits for social change, and some would say, conduits of social engineering. Ninety percent of media is run by six corporations. This small group offers an illusion of choice. With their power, they convince a captive audience to emulate “the trends” as they see them. Some of the first films ever produced featured LBGT-themes, though they did not achieve major box office success. [See Pre-1920s, 1920s films, 1930s films, 1940s films, 1950s films, and on and on]. Today the list of Transgender movies is prolific and accepted.
In 2017, the Transgender narrative began a new cycle in the media, when Toni the Tampon made its debut to teach children that men, too, can get periods. Since 2017, a new space has been created for TransAthletes, to allow TransWomen, or Male-to-Female transgenders, to compete as equals against biological females in weightlifting, on the football field, and even in mixed martial-arts.
In 2017, writers could write their opinions even if considered “intolerant,” simply because people were still recognized to have the natural right of free speech. [See also my 2017 article, When Men Menstruate]. This all happened before Transcensorship.
In today’s Transgender Age everyone is welcome to mingle in the same genderless shower rooms and restrooms, even if athletic competitions are still segregated into “male” and “female.” And no one can say a negative word. Today, female athletes are being crushed by TransWomen who once identified as men. At least 30 Transgender athletes are now considered “famous” because the media says so. But anyone with an opposite opinion is considered prejudiced.
In the race to be “all inclusive” have we stopped long enough to recognize our biological differences? Is is not right to question the fairness or safety of biological males – with larger muscle mass, hearts and lungs, with greater strength, acceleration, power, and speed – to compete against girls and women in sports? Is it right and just that TransWomen weight lifters smash women’s world records? Is a backlash not expected from those who see the contradictions? Why must transgender athletes “pave the way?” Pave the way to what, exactly?
The Broken One-Sex Model
The One-Sex Model was the idea of Thomas Laqueur who claimed that up until 1750, all humans were seen to be different manifestations of the same sex. The difference between humans was minimal.
It was also noted that the external genitalia of a man is almost exactly the same shape, though inverted, as the internal genitalia of a woman. The testes mapped onto the ovaries, and so forth. It was therefore thought by many, Laqueur said, that if only a woman when developing in the womb of her mother were subjected to more heat, then they would have had sufficient energy to push their internal genitalia outside and become male. Cory Cockshaw, Meet the Men who Menstruate
Unfortunately, no one can corroborate Laqueur’s opinion since no one exists from his time. One historian, Pliny the Elder, killed in the eruption of Mount Vesuvius in 79AD, also claimed that men menstruate…. through the nose:
In the human race alone a flux of blood occurs in the males, in some cases at one of the nostrils, in others at both, with some people through the lower organs, with many through the mouth; it may occur at a fixed period, as recently with a man of praetorian rank named Macrinus Viscus, and every year with the City Prefect Volosius Saturninus, who actually lived to be over 90.
A famous 18th century “physician” Andreas Vesalius, a Flemish Anatomist, made illustrations of detailed human anatomy (See illustrations from Vesalius’ atlas) in 1543 including the genitalia. However, because the drawings and woodcuts proved controversial, the genitals were removed via black ink. At that time, Vesalius considered menstruation as the female equivalent of hemorrhoids in men:
a man who suffered from the complaint called haemorrhoids… at regular intervals this man used to have a flow of blood from the anal veins, in the very same way in which woman have their menstrual flux. – Cory Cockshaw
However, the MayoClinic, the 21st century medical authority, does not reference genitalia when describing hemorrhoids, also called piles, which are common in pregnant women and as a result of giving birth:
swollen veins in your anus and lower rectum, similar to varicose veins. Hemorrhoids can develop inside the rectum (internal hemorrhoids) or under the skin around the anus (external hemorrhoids). Nearly three out of four adults will have hemorrhoids from time to time. Hemorrhoids have a number of causes, but often the cause is unknown.
Certain medical drugs are known to cause the direct effects of abnormal breast growth in men, a medical condition diagnosed as gynecomastia. Likewise, some estrogen-boosting herbs, such as Saw Palmetto, which reduce the size of a swollen prostate, can also have the effect of breast swelling. See similar herbs here. It goes without saying that if you have a medical question, discuss it with your medical doctor.
Are The Sexes Being Neutered?
A new wave of uniformity is sweeping the globe to merge the separation of the sexes once and for all. Uniformity is the blending and blurring of differences into a fluid sea of ambiguity and nebulousness. The new equality movement is gender blending – to ignore the biological differences that exist between the male and female species as they were created.
Are we, as unique individuals, being made to conform to a mindless, empty, Baphomet-like shell that can be more easily controlled by the conglomerate few? Are governments, in a sense, blotting out the genitalia 500 years after Vesalius’ drawings? Are humans ultimately being neutered as vessels for something else?
In 2009, the Delhi Supreme Court instituted an official third gender in India that is neither male nor female by allowing those in the transgender community to self-identify one’s gender using legal documentation.
Since 2016, in New York City, it is illegal to discriminate against anyone whose gender is male, female. Model legislation by the NYC mayor Bill de Blasio has released a list of 31 gender pronouns approved by the New York City Commission on Human Rights. The list is a guide for businesses, which can now be fined as much as $250,000 if establishments in the state of New York refuse to address someone by their preferred gender pronoun:
BI-GENDERED • CROSS-DRESSER • DRAG KING • DRAG QUEEN • FEMME QUEEN • FEMALE-TO-MALE • FTM • GENDER BENDER GENDERQUEER • MALE-TO-FEMALE • MTF • NON-OP • HIJRA PANGENDER • TRANSEXUAL/TRANSSEXUAL • TRANS PERSON WOMAN • MAN • BUTCH • TWO-SPIRIT • TRANS • AGENDER • THIRD SEX • GENDER FLUID • NON-BINARY TRANSGENDER • ANDROGYNE • GENDER GIFTED • GENDER BLENDER • FEMME PERSON OF TRANSGENDER EXPERIENCE • ANDROGYNOUS.
Gender designations are confusing from a logical standpoint. For example, “Agender” is someone without a gender, or someone who does not believe in gender. So does an Agender person discriminate against other genders in which they do not believe? Would they be fined under this NY law? Is that legal?
Since it is now illegal in many states to discriminate on the basis of gender, how does that policy co-exist with established hiring policies under Affirmative Action Programs codified under 41 CRR Part 60-2, which falls under Executive Order 11246 – Equal Employment Opportunity, the Rehabilitation Act of 1973?
Has the world grown too complex? Will it soon be politically incorrect for women to be called menstruators? Can you play with Tonka Trucks and still call yourself female?
Where once human interactions and introductions involved sharing a name, and perhaps a vocation, people now feel obligated to express the complexities of their gender identity in different contexts and social settings. For those who see humanity in crisis, consider what Casey Chalk writes in the January, 2o20 Crisis Magazine:
These new norms, rather than facilitating more charitable and respectful human interactions, undermine them. In a world that demands hyper-sensitivity to the multivalent identities and expressions of every person—lest we offend or expose our insufficient woke credentials—it’s better not to try. It might be best to just keep one’s eyes locked on a smartphone or newspaper. The proliferation of pronouns and identities doesn’t eliminate barriers to human exchange; it raises them.
I’ve heard people say that there are no differences between male and female. Those people are idiots.”
Thus begins Daily Wire host Matt Walsh’s new “What Is a Woman?” documentary, which highlights the left’s ever-growing reluctance and inability to define gender. Think that defining the qualities of men and women is easy for most people today? Think again.
While some may struggle to “figure out” women, Walsh identifies that Western culture’s obsession with gender identity has paralyzed people from defining what a woman is. As the documentary progresses, we see further evidence that the transgender narrative has not only rejected the definitions of “man” and “woman” as insensitive and transphobic, but has dismantled the very concept of universal truth and reality.
Fittingly released on the first day of Pride Month, Walsh’s documentary is a thought-provoking, humorous, yet often emotional and disturbing film that illuminates the contradictory and dangerous narrative of the transgender agenda.
In the documentary, Walsh interviews “the experts,” such as “gender-affirming” therapists, sex-change surgeons, and gender ideology professors (most of whom are transgender themselves or members of the LGBTQ+ community), asking them, “What is a woman?”
The majority of responders say they have no idea how to define womanhood or refuse to answer the question, calling it bigoted and pointless. Not only are they unable to provide a simple definition of a woman, but they find the entire concept offensive and transphobic.
The documentary begins on a humorous note, as Walsh asks a family therapist, “How do I know if I’m a woman? I mean, I like scented candles and I watch ‘Sex and the City.’”
“What a great question!” the therapist (who has every indication of being a woman) says, nodding and smiling encouragingly.
“So, what is a woman?” Walsh asks. A disconcerted look enters the counselor’s eye: “Great question! But I’m not a woman, so I can’t really answer that.”
“I thought therapy would make me less confused,” Walsh said. Us too, Matt.
So, he takes to the streets to ask the common American if they can solve this conundrum. Surprisingly, most of the interviewees responded to the “What is a woman?” question with a blank stare and nervous laughter. Most said it couldn’t be defined and said they would accept Walsh as a woman if that’s what he believed he was.
Especially entertaining is Walsh’s trip to the Women’s March—surely they’ll know what a woman is if they’re marching for them, right? But no, the marching women either ignored Walsh or yelled, “Why are you here?”—insinuating that he was a man (without even asking his gender identity, the audacity!) and that a man had no right to attend a women’s march. “How can you have a women’s march if you don’t know what a woman is?” he asked. Touché.
What is the female gender, according to the transgender community? Walsh spoke with a transgender surgeon who differentiated between sex and gender, saying that sex-change surgery is “altering the physical characteristics of an individual to fit better with a gender identity that is female.”
In that case, what is a woman, according to this surgeon? “A woman is a combination of your physical attributes, what you’re showing to the world and the gender clues you give, and hopefully those match your gender identity.”
As if the issue couldn’t get any more confusing, Walsh speaks with a pediatrician and professor who has worked in Planned Parenthood and advocates for “gender and reproductive justice.” She provides “gender affirmation care,” saying that a good doctor is there to listen to the patient and act on what they’re expressing.
Walsh asked whether it was ethical for minors to be making life-altering decisions such as taking puberty blockers or opposite sex hormones, since children often have a fantastical, unrealistic interpretation of reality, such as believing in Santa Claus.
“Well, he’s real to them,” the pediatrician said. “But the fact that Santa exists isn’t true,” Walsh countered. “Whose truth are you talking about? It’s very real to the child,” the pediatrician responded.
The documentary makes it clear that Americans can no longer ignore the transgender movement. It is permeating every aspect of society, politics, and education and now targets children as young as preschoolers.
The push for children to define their own realities and irreversibly change their bodies is perhaps what is most disturbing about the transgender agenda. In what other sphere of medicine do patients, especially young children, prescribe both their malady and remedy to the affirmation and acceptance of a counselor or physician? As clinical psychologist Jordan Peterson said to Walsh, “It’s not my job to affirm as a therapist, you come to see me because there’s something wrong.
The fact that the transgender agenda is increasingly targeting young children is what psychiatrist Miriam Grossman finds most disturbing. Grossman explains to Walsh the history of the transgender and sex-ed movement and highlights the unethical, traumatic techniques and flawed studies that have shaped it over the years. “It’s unspeakable what these people have done to our children,” she says.
Not only is the transgender movement harming women’s sports, exposing children to inappropriate material, and encouraging them to reject science and universal truth, it is also irreparably damaging children’s bodies and destroying their futures.
The most moving and persuasive interview occurred with Scott Newgent, a biological female who transitioned to a male as an adult but passionately argues against the rise in gender surgery among children and the subjectivity of gender. “I’m a biological woman that medically transitioned to appear like a man through synthetic hormones and surgery,” Newgent said. “I will never be a man. Is it transphobic for me to tell the truth?”
Newgent describes the details and horrific side effects of gender-reassignment surgery that are so conveniently hidden from public discourse. Having undergone multiple surgeries, illnesses, and painful, permanent side effects, Newgent told Walsh, “Nobody would help me, including the doctor who did this to me, because I lost my insurance. I probably won’t live very long.”
Newgent said the possible risks and side effects were never discussed when considering gender-reassignment surgery, and warns parents and anyone considering sex-change surgery that “the truth is that medical transition is experimental.”
Revealing an arm mutilated from skin grafts, Newgent broke down in tears on camera, exclaiming in horror that minor children are regularly operated on without any discussion of the risks and permanence of the surgery, or any discussion as to whether children should ethically be allowed or able to consent to such procedures.
“We’re butchering a generation of children because no one’s willing to talk about anything,” Newgent said. “This is wrong on so many levels. Kids aren’t able to consent.”
The transgender movement is ultimately an attack on scientific fact, the concept of reality, and the meaning of language. No longer are words allowed to mean one thing. No longer is the word “truth” socially acceptable, because who are we to deny “your reality” or “your truth”?
A professor of women (whatever those are, anyway), gender, and sexuality responded to Walsh’s statement that he was seeking the truth with, “I’m really uncomfortable with that language of ‘getting to the truth’ because it sounds deeply transphobic to me. The word ‘truth’ is condescending and rude.”
Sensing that this concept is a purely Western phenomenon, Walsh heads to Nairobi to immerse himself in the customs of a local tribe. In this culture, gender norms and roles are crucial to the survival of the tribe. The men protect and provide, and the women maintain the home and nurture the children. It’s an honor to be a man or a woman in this tribe, and every member knows their distinct duties and privileges.
A group of men laugh in disbelief when Walsh asks what they would do if a man wanted to look and act like a woman—the entire concept is ridiculous and unheard of. “The Maasai people don’t think much about gender,” Walsh observes on the way back home to America, “but they have a firm sense of their identity.”
Instead of solving gender dysphoria and body image discomfort, Americans’ infatuation with identity has only created greater societal instability and refused to answer the most foundational of questions. “What Is a Woman?” succeeds in highlighting the inconsistencies and dangerous agenda of the transgender movement.
Walsh’s angle is particularly effective, as he gives the majority of the screentime to pro-trans activists and medical professionals. The lack of data or persuasive argument for the trans community isn’t the producers’ fault, the “experts” simply couldn’t provide any. Walsh’s sarcastic, borderline dark sense of humor in the delightfully ridiculous street interviews breaks up the more serious, unsettling information and gives a sense of hope and common sense to the insanity that’s been normalized.
Bold, humorous, thought-provoking, and undeniably chilling, “What Is a Woman?” equips its audience to better face the ever-growing reality of the transgender agenda and its far-reaching effects through civil discourse, empathy, and a firm grasp of truth, science, and reality.
At the end of the film, it’s Walsh’s wife who’s the true MVP. “Hey honey, what’s a woman?” Walsh asks. “An adult human female,” she responds.
TCTL editor’s note: “What Is a Woman” by Matt Walsh has been mirrored on various video platforms. Here it is found at Open Library of Knowledge at Odysee:
Andrew Kaufman is a Medical Doctor, Psychiatrist and Molecular Biologist who received his training and degrees from Duke University, MIT and South Carolina Medical University. He says there are no such things as “viruses” and the “Coronavirus Global Pandemic” is a “manufactured event.”
The conversation around whether or not viruses exist, appears to conjure up all kinds of emotions, and is met with resistance. My guess is because virology is a deeply entrenched paradigm, and it is what we were taught as kids.
A cult-like approach would be to dismiss dissenting views and, instead, to perpetuate a previously held belief. David Rasnick refers to this as the Tyranny Of Dogma.
Scientists are doing an awful lot of damage to the world in the name of helping it. I don’t mind attacking my own fraternity because I am ashamed of it.
The object of war is to kill or maim as many people as possible, by whatever means. However, outright killing is often less efficient than wounding because more of the enemy’s resources are consumed in caring for the wounded than burying dead bodies. The overall goal of war is to conquer and subdue a people. In the process of conquering, the enemy must be psychologically and physically broken to the point that they give up their will to fight and their will to assert self-determination.
The current pandemic war has all the markings of more traditional militaristic war except that it is still unrecognized by those who are under attack. It is the perfect stealth war. History is full of examples of stealth attacks that were extremely successful. The victims never saw the attackers until it was too late to resist.
In today’s war, the entire health system has been weaponized and turned into a giant Trojan horse. Obey, obey, obey it cries. Humiliate yourself by donning a face mask, by staying home and retreating from normal society. Mutilate yourself by giving up your job, closing your business, injecting harmful substances into your body.
Meanwhile, dead bodies are piling up in record numbers. It’s an old-fashioned genocide with a medical twist.
For a minute, forget case numbers, hospital beds and epidemiological studies. The Expose provides a back-door look at what’s going on by analyzing ambulance call-outs, all of which are nicely recorded and detailed:
The National Health Service has confirmed in response to a freedom of information request that ambulance call-outs relating to immediate care required for a debilitating condition affecting the heart nearly doubled in the whole of 2021 and are still on the rise further in 2022. But the most concerning published figures show that they have also doubled among people under the age of 30.
What group is getting hit hardest? Young people under 30 – those normally suited for military service, i.e., to build a physical army. Overall, emergency calls for heart-related incidents has skyrocketed from the first day of Emergency Use Authorization injections.
The tidal wave of propaganda – just like in any war – is designed to deceive, demoralize and confuse. Prominent medical journals spit out headlines like:
They all state that your eyes are lying to you. Rather, you should trust the propaganda that sows just enough doubt that you don’t dare open your mouth in public about such silly things as ambulance call-outs for heart-related emergencies.
This writer has continuously stated since December 18, 2015 that Technocracy declared war on the entire human population of the world. I wrote, “Technocracy is the same nefarious ideology that enabled Adolph Hitler in the 1930s. Nazi Germany used advanced technology to enslave and kill millions of its own citizens. This hasn’t happened here yet, but this is the direction we are headed.”
We have arrived.
What level of stupidity and ignorance do people have to exhibit to not see what is going on here?
Mike Stone runs viroliegy.com, easily the most powerful and persuasive critique of virology, that I’ve come across.
I’ve chatted to a number of great minds on the topic of viruses, such as Tom Cowan and Sam Bailey, and find myself convinced by their arguments.
In our conversation, Mike covers
why virology is pseudoscience;
what viruses are;
the problems with definitions;
direct evidence versus indirect evidence;
Koch’s Postulates and why they matter;
the rejection of the Scientific Method;
isolation and purification;
genomics and genome sequencing; and
the Rockefeller funding behind virology.
I strongly recommend reading Bechamp Or Pasteur, which is a biographical exposé of the fraudulent work of Louis Pasteur and the forgotten work of Antoine Béchamp.
“The Anti-Vaccine Movement’s New Frontier: A wave of parents has been radicalized by Covid-era misinformation to reject ordinary childhood immunizations — with potentially lethal consequences.”
And Friday morning, they sent out an email blast to promote the article.
Here’s their promo. The Times really had to stretch to come up with such a load. My comments are in brackets.
“This week, Moises Velasquez-Manoff reports on a wave of parents who have been radicalized by Covid-era misinformation to reject ordinary childhood immunizations — with potentially lethal consequences.”
[Wow. The author has three names. Impressive. I feel I need at least three to reply. Jon The Rebel on Vaccine Fantasy Island Just Say No to Bill Gates Rappoport.]
“In 2019, even before the pandemic struck, the World Health
Organization listed growing vaccine hesitancy as one of its top 10 threats to global health. Now the pandemic has given anti-vaccine advocates an opportunity to field-test a variety of messages and find new recruits.”
[Yes, our anti-vaxx squadrons use dozens of human and AI analysts to float our messages and then test the results. We use polls, surveys, in-home visits, NSA-type surveillance tools, and even covert assets in the press to expand our reach. Elite foundation money pours into our coffers.]
“’There’s a lot of misinformation about the Covid vaccines, and it just bleeds into everything,’ one doctor told us. ‘These fake stories and bad information get stuck in people’s heads, and they understandably get confused’.”
[One doctor told the Times that. Well, case closed. Verdict? We’re guilty. The doctor is always right. Wait a minute. I just called a doctor. He told me the Times’ doctor is wrong. Duel at dawn. Choice of weapons.]
“If this dynamic continues, it could threaten decades of progress in controlling infectious disease — a triumph that has, paradoxically, hindered the effort to counter vaccine skepticism. In the developed world, only a small portion of the population has seen the death and suffering caused by the diseases of eras past; vaccines, in the minds of many, have come to pose a greater threat than the diseases that they have helped nearly vanquish. In a sense, vaccines have become victims of their own success.”
[Obviously, the Times writer is a gymnast. Probably practices yoga. He can bend and stretch and twist with the best of them. Also, notice how he characterizes the parents who “have been radicalized”: They’re people who don’t have a brain in their heads. They’re massively ignorant robots, dupes and yokels just waiting for vaccine misinformation, which they grab like kids going for candy. Parents actually thinking for themselves? Never happens.]
On the other hand, readers of the Times are DISCERNING. They’re COLLEGE GRADS. They take their vaxx info from the paper’s pros, who have perfected the ability to look down their noses at the great unwashed and cluck and tsk tsk and express a modicum of sympathy.
Nowhere in the Times—ever—will we read an actual debate on the subject of vaccines, in which two sides are adequately represented and given ample space to present a little thing called EVIDENCE (or fake evidence).
To host such debates would be demeaning for the Times. It would signal a departure from their perch which constantly advertises: if-we-say-it-we-know-it.
Maintaining that pose month after month, year after year, decade after decade is debilitating.
Which is one reason why so many mainstream reporters are drunks.
In late 2019, I joined two other Israeli criminologists and a health risk communications expert in a research project to study the suppression of scientific dissent around the topic of vaccines. At the time, none of us could have ever imagined what was looming right around the corner.
Two of them (Natti Ronel and Ety Elisha) had written a review of a Hebrew-language book called “Turtles All The Way Down,” which was a critical review of vaccine safety science. The thing about the book is that it was published anonymously, as the author(s) feared the potential retribution that might ensue.
Their review was published in the Hebrew-language journal, Medicine (Refuah), which is the journal of the Israeli Medical Association, sort of like the Israeli equivalent of JAMA. I won’t go into how it ever got published in the book review section, but the review simply focused on the absurdity of a scientist who felt the need to publish a scientific book anonymously due to fear of the consequences. Ironically, the publication of the review caused a huge uproar (you can read more about that here where it was covered in Science), and the review itself was retracted, or more precisely it simply disappeared from the on-line version of the journal.
So we started a project to study the phenomena of scientific censorship and suppression of scientific dissent in the field of vaccines by interviewing scientists and doctors who had either had their papers retracted or who had faced attempts to suppress their views. Notably, the only retracted papers in the field of vaccinology that we could identify all raised questions about the safety of vaccines. And this was all BEFORE the COVID pandemic hit. (We’ve got another one that covers the COVID period that should be coming out fairly soon.)
In other words, everything it describes happened before the pandemic. The censorship and suppression we’ve witnessed these last two years already existed — it has only kicked into overdrive. The deliberate dismantling of science didn’t start two years ago.
If it isn’t clear why criminologists would be interested in this topic, consider the following general definition of crime: force or fraud in the pursuit of self-interest.
So without further ado, you can read both papers embedded (hopefully) below:
Symptoms may include a desire to swing from tree to tree, to pick breakfast bugs off your mate, and to screech, yell, and generally monkey around. But seriously….
According to the Centers for Disease Creation (CDC), the agency that created at least eight Genus categories of Pox Diseases, Monkeypox is called a “rare disease.” However, Monkeypox cannot be considered “rare,” if the CDC also claims that Monkeypox is spreading.
After all, where there is a will, there is a vaccine patent!
In February 2021, patent application #20210260182 was filed for RECOMBINANT POXVIRUS BASED VACCINE AGAINST SARS-CoV-2 VIRUS. This is a combination pox/COVID vaccine patent filed over a year ago:
The terms “chimeric” or “engineered” or “modified” (e.g., chimeric poxvirus, engineered polypeptide, modified polypeptide, engineered nucleic acid, modified nucleic acid) or grammatical variations thereof are used interchangeably herein to refer to a non-native sequence that has been manipulated to have one or more changes relative a native sequence.
In some embodiments, the SARS-CoV-2 protein is inserted into the Thymidine Kinase (TK) locus (Gene ID HPXV095; positions 992077-92610; SEQ ID NO: 1) of the horsepox virus or the synthetic horsepox virus.
The official story from the CDC is that “Monkeypox” was discovered in 1958 “when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research” … and injected with Smallpox.
Not too long ago, in 2018, the Horsepox virus had its heyday when researchers told the story of the”infectious virus” synthesized in a lab. Symptoms may include a desire to neigh, snort, and gallop with the herd. But seriously… Horsepox was said to be the cousin of the Smallpox virus, which health authorities claimed had been eradicated from the planet in 1980. Why eradicate one “deadly” virus only to revive its cousin? What is the purpose of Franken-science?
The official answer was “to develop cancer treatments and vaccines,” especially since the current Smallpox vaccine (Variola) has some serious adverse side effects, including death. Note: nothing is ever said about curing cancer, only about “developing treatments and vaccines.” From the 2018 paper, Synthetic viruses—Anything new?:
…it comes as no surprise that it is possible to generate infectious viruses by using synthesized DNA fragments. The first synthetic virus, poliovirus, was produced by Wimmer and colleagues and made us aware of the fact that we entered a new era of reverse genetics that allows for the generation of synthetic viruses without the need for a nucleic acid template.
Chapter 3: “A new era of reverse genetics”
Many scientific papers published since 2018 have questioned the wisdom of engineering viruses from deadly Smallpox, which they admit could lead to the reemergence of Smallpox, as well as to future pandemics. What if the lab-created monkey virus or the horse virus escaped into the wild? What then?
Previously, scientists had blamed monkeys, as well as other species, for the consequences of their genetic experiments: in monkeys (SV40); in pigs (Swine flu (H1N1)); in birds (Avian flu (H5N1) different from Chickenpox; and in insects (Zika mosquito borne virus).
Note: the same molecular signature, protein (PB1-F2), is present in both the 1918 Spanish flu virus and in the highly lethal h5N1 chicken viruses. Coincidence?
These synthesized varieties were not selected to become “epidemics,” only beta tests on behavioral dynamics; except for the Swine Flu Epidemic, which resulted in a mass vaccine campaign, and was subsequently repealed after widespread vaccine injuries and deaths [See my 2018 blog Beware the Horsepox Vaccine!].
With many stories in the media, it is important to know that there is something called The Species Barrier. Even in the Age of Ignorance, the Species Barrier still exists, and The UK Dictionary defines it as:
The natural mechanisms that prevent a virus or disease from spreading from one species to another.
In short, people cannot “catch” diseases from animals, birds, reptiles, insects, vegetables, or minerals. But, as long as people have short attention spans, and continue to be misled by the story, animals will continue to be wrongly blamed and punished for human-engineered, chimeric experiments.
Why create animalpox outbreaks that appear go viral?
The ultimate purpose of any “viral threat” is to roll out the “vaccine solution.” And what exactly is the reason to push an agenda of vaccines? To engineer consent to reengineer humanity for deeper control: Monkey see-Monkey do. Therefore, any true global “viral threat” is not complete without a patented, engineered, controllable, injectable chimeric virus, coming soon to a city near you.
Chapter 4: The Twist: Monkeypox rash
Back to the monkeys!
The media generates associations by first showing computer-generated images of microscopic cells that appear to be bacteria (not viruses). Then, they release images of raised blisters or a rash labelled as “Monkeypox.” Looking closer, any image labelled “Monkeypox” could double as an image labelled Shingles.
Is there a relationship between the pox and the rash, or is it between the COVID vaccine/boosters and the rash?
Because the world complied so quickly to the illegal Coronavirus countermeasures, brought on by governments around the world, there is no need to wait years for the next epidemic! The “flying monkeys” are here to do the bidding of their creators.
What the WHO and CDC have not disclosed is that vaccine ingredients are widely known to cause rashes, often a full body rash. A vaccine-associated rash is a consequence of an influx of toxins to the body that results in a suppressed immune system. Frequent Strep Throat infections are another indication of a suppressed immune system. A.S.I.A is not a continent when it comes to vaccine damage. A.S.I.A is Autoimmune/Inflammatory Syndrome Induced by Adjuvants, (ie, induced by toxins), where adjuvants are vaccine ingredients (eg. aluminum sulphate). Keep this in mind. Do your own research.
Prior to the COVID injections, a rash was not indicated as a symptom of “Coronavirus,” which is a family of cold/flu viruses. According to officials, Coronaviruses can produce runny nose, sore throat, headache, fever, cough, and a general feeling of being unwell. True viruses, those not engineered in a lab, cannot survive outside the cell, they cannot transmit an infection because they are not alive (like bacteria). In this way, viruses are exosomes, produced by the cell in response to a toxic exposure, to help to clean the cell to regain balance and health.
Exosome biogenesis is a mechanism of protein quality control, and once released, exosomes have activities as diverse as remodeling the extracellular matrix and transmitting signals and molecules to other cells. This pathway of intercellular vesicle traffic plays important roles in many aspects of human health and disease, including development, immunity, tissue homeostasis, cancer, and neurodegenerative diseases.
While the virus itself is not a sexually transmitted infection, which are generally spread through semen and vaginal fluids, the most recent surge in cases appears to have been spread among men who have sex with other men, WHO officials said, emphasizing that anyone can contract monkeypox.
Is that science or science fiction? Are we back to HIV-AIDS? Did we ever leave it?
“The HIV/AIDS hypothesis is one hellof a mistake”- Kary Mullis, 1996, p. 14..– Nobel Laureate in Chemistry, 1993, inventor of PCR test.
With so many stories still unfinished, has Monkeypox arrived on the scene as a hoax? A test of humanity? Another virus that divides and discriminates against bi-sexual and gay men? What about the devastation of 500,000 deaths caused by the prescription Opioid Epidemic from 1999 to 2019 that continue? What about more than 150 people who die each year from taking the OTC, FDA-approved drug Tylenol?
Chapter 6: Nature rules
Nature has always ruled and Nature will continue to rule, but only if Nature’s Law is followed. Nature does not discriminate on the basis of race, religion, politics, education, vaccine status, or sex. Only patented lab-created viruses do.
Just because the media stories report on a Monkeypox viral threat, does not mean that humans need fear monkeys or eradicate them, like they did when they agreed to put chickens into lockdown from Pennsylvania to France then exterminated them out of fear.
Fear is False Evidence Appearing Real. Fear freezes people’s ability to be reasonable and rational. Fear separates and isolates. Fear masks identity. Fear disconnects humans from Nature, from each other, and from themselves. Going forward, if choosing fear, refrain from making any decisions or they will be made for you.
Perhaps humans should fear only humans with a god-complex, those who would unleash a lab-created/patented monkeypox/Smallpox/Horsepox/SARS-CoV2 virus into the population via injection for the purpose of reverse genetics.
Forget the Horsepox and Monkeypox stories. Could humanity be looking at a re-deployment of the original Smallpox?
As you know, I’ve spent two years presenting evidence that the discovery of SARS-CoV-2 was a fake.
But I still press on. I examine the reality machine to see why people have such a problem acknowledging the virus—and by extension, all viruses—are nothing more than fairy tales.
I’ve come up with a number of explanations.
For example: DOCTORS.
Rejecting viruses is rejecting doctors. Doctors are security guards around the reality machine.
“Doctors can’t be wrong.”
“I can’t live in a world where doctors are so wrong.”
“I would never be able to stop weeping for the doctors who are so wrong.”
“If I told my doctor I didn’t believe in viruses, he would cut me off, and I couldn’t stand that.”
“I’m a journalist, and my best sources are doctors. The good doctors. And they all say viruses are real. I need my sources.”
“Without information from doctors, the world would spin into chaos.”
“My mind instructs me to believe doctors are only guilty of making mistakes up to a certain threshold. Beyond that, they simply can’t be criticized.”
OK, that takes care of the doctor fixation. But then we have what I call the world-view fixation:
“I don’t want to live in a world where there are no viruses. I would feel lonely and afraid.”
“I need the assurance that this world of ours is filled with tiny invisible killers. When I accept that, I can maintain equilibrium. You know, their threat and our response. It makes sense.”
“I love the idea of tiny killers. It comforts me.”
“I know precisely what to be afraid of in this world. Otherwise, I would start to see ghosts in closets at night again. I remember them from childhood. Those bastards were PERSONAL. They were coming for ME. Viruses are neutral. They don’t know me. To them, I’m just cells. They don’t PREFER me. They’ll take anyone. I like that.”
“Even if viruses are bullshit, they’re sophisticated bullshit. I favor that over some sort of primitive bullshit.”
“Rejecting viruses would equal rejecting my college education. I need that education to assert my superior position against the Lower Ignorant Ones.”
“The ecological chain of life includes viruses. If we remove them from the chain, Nature makes no sense. That’s what I hear.”
“The world is a dangerous place. This is good, because it helps me to explain my problems and lack of determination. Without viruses, the danger factor would be reduced, and I can’t have that.”
“The nature of reality dictates that when you’re right, you should be psychotically nasty about being right. If I’m not right about the existence of viruses, I can’t be as nasty as I want to be. And that would be a tragedy.”
“My father is a doctor, and he is a great man. At least as great as Al Capone.”
Vitamin C is a vital nutrient for human health and survival. It is not only a powerful antioxidant and immune booster, it also supports collagen, connective tissue formation, and builds the extracellular matrix – the ‘glue’ that binds the body’s cells together. It is also important for faster wound healing and the prevention of various chronic conditions. Optimum amounts of vitamin C effectively protect the body and cardiovascular system against biological rusting.
Additionally, vitamin C has several other important functions. It is a cofactor for a series of biological enzymes that are important for the improved metabolism of cholesterol, triglycerides and other risk factors for cardiovascular disease. It is also an important energy molecule needed to recharge energy carriers inside the cells. Vitamin C is essential for the production of carnitine, the molecule that carries fatty acids into the mitochondria for energy production. It participates in the biological recycling of vitamin E, glutathione, and many other cell-protective molecules. When taken together with calcium, it increases calcium absorption. Vitamin C also neutralizes various toxins in the body and protects healthy cells from harmful substances, including the effects of many pharmaceutical drugs.
As humans do not produce their own vitamin C it has to be obtained from food sources and dietary supplements. Vitamin C supplements come in several forms. These include ascorbic acid, calcium ascorbate, magnesium ascorbate, and others. However, the majority of vitamin C supplements on the market contain only a single form of vitamin C, usually ascorbic acid. Simple ascorbic acid is a water-soluble compound. Therefore, it does not remain in the body for very long and is easily excreted. Unless frequently replenished, it is difficult to obtain the benefits of vitamin C from ascorbic acid alone.
Mineral salts of ascorbic acid, such as calcium ascorbate and magnesium ascorbate, are easily absorbed and well metabolized by the body’s cells. Combining vitamin C with calcium or magnesium in this way neutralizes the acidic effect of ascorbic acid and contributes to a ‘buffering’ effect, thus making it gentler on the stomach lining.
Calcium is important for the proper contraction of muscle cells, including the heart muscle cells, and is required for the conduction of nerve impulses. This mineral is also essential for the hardening and stability of our bones and teeth. Magnesium is nature’s calcium antagonist; its benefit for the cardiovascular system is similar to that of prescription calcium channel-blocking drugs – except that magnesium is natural. Clinical studies have shown that magnesium is particularly important for helping to normalize high blood pressure and irregular heartbeat conditions.
There is a misconception that calcium ascorbate can increase the likelihood of kidney stones. However, the majority of kidney stones are made of calcium oxalate, which is present in foods such as soda, coffee, chocolate, spinach, and beets. Inadequate water intake is one of the major contributors to kidney stone formation. Well-controlled clinical studies have not been able to establish any strong correlation between supplemental vitamin C and increased kidney stones.
Another unique form of vitamin C is ascorbyl palmitate, a fat-soluble form of the nutrient. This form is better absorbed by the cells than ascorbic acid alone. Cell membranes enriched with ascorbyl palmitate are more resistant to oxidative damage, which means they are better protected against disease and aging. Ascorbyl palmitate is also an effective antioxidant and free radical scavenger.
One of the advantages of taking a nutritional supplement that contains ascorbyl palmitate is that this form of vitamin C can reach areas of the body that ascorbic acid cannot. Moreover, its effects last for longer. A well-balanced vitamin C or multinutrient supplement should contain at least 25 percent of its vitamin C in the fat-soluble, ascorbyl palmitate form. However, most vitamin C supplements contain little or no ascorbyl palmitate. Optimum supplementation with a synergistically formulated vitamin C supplement can make all the difference in protecting your health!
Thoughts of people around the world will lie with bereaved families affected by the latest school shooting at Robb Elementary School in Texas.
As the search for answers begin, the cause of violent behaviour will once again go under the spotlight, along with the gun laws in the United States.
While there is never one simple explanation for what drives a human being to commit such unspeakable acts, all too often one common denominator has surfaced in hundreds of cases—prescribed psychiatric drugs that are documented to cause mania, psychosis, violence, suicide and in some cases, homicidal ideation.
The general public remain uninformed about the well-documented links between psychiatric drugs and violence. At least 37 school shootings and or school-related acts of violence have been committed by those taking or withdrawing from psychiatric drugs resulting in 175 wounded and 82 killed. Following the latest shooting, another 21 deaths are going to be added to the abysmal death toll.
International drug regulatory warnings and studies reveal the link between psychiatric drugs and acts of violence and homicide. There are also hundreds of cases where high profile acts of violence and mass murder were committed by individuals under the influence of psychiatric drugs.
Despite 27 international drug regulatory warnings on psychiatric drugs, there has yet to be a federal investigation on the link between the drugs and acts of senseless violence.
While psychiatrists are aware of the dangers associated with their prescribing habits, they continue their routine pattern of denial while the patient is left uninformed about the dangers linked to the psychiatric drugs being recommended.
Professor David Healy, a psychiatrist and pharmacologist says, “Violence and other potentially criminal behaviour caused by prescription drugs are medicine’s best kept secret.”
We cannot allow this to be the norm and we must not remain silent on this issue. The dangers of psychiatric drugs have been known for decades so, as responsible citizens, we have to continue to repeat this message so that the populace is informed and so that school shootings become confined to the history books rather than being the headlines.
During crises, people ask questions, and the Covid crisis is no exception. People are asking, “Is there any real or new illness called Covid-19—apart from vaccinations and the treatments themselves?” We are not alone in proposing that we must take a cold look at the viral theory touted as the cause of this alleged disease.
Journalist Jeremy Hammond has been the most outspoken critic of our contention that the SARS-CoV-2 “virus” does not exist and therefore does not cause Covid. In a video posted in March 2021,1 he outlines the following arguments for the existence of the “virus.” We answer his arguments, point by point.
Definition of Isolation
Hammond states that people in our camp have changed the definition of isolation, but we use the actual definition of the word “isolation” in the English language. It’s the virologists who have changed the meaning of the word from “separated from other things” to meaning “combined with other things in a foreign cell culture.”
Isolation Technology
Hammond claims that scientists do not yet have the technology to purify viral particles. Actually, scientists have been able to purify particles equivalent in size to so-called viruses for decades. The traditional method, in use since at least the 1940s, involves what is called density gradient ultracentrifugation. It uses different densities of a sucrose solution spun into layers at high speeds with an ultracentrifuge, so that the densest layer ends up on the bottom. The sample will separate into bands based on different densities, and one of those bands could contain the so-called viral particles if they existed.
For example, a 2015 article published in Methods in Molecular Biology,2 provides electron microscopy photographs of purified exosomes (see Figure 1). Exosomes are roughly the same size as that of claimed viral particles, around fifty to one hundred nanometers, and they have the same morphology and characteristics of alleged virus particles.
If you can purify exosomes, you can purify viruses using the same techniques. Scientists take exosomes directly from a body fluid; they don’t take the exosomes and put them in a cell culture. One of the challenges the authors discuss is the fact that the exosomes are present in low numbers; also, there are many different types of extracellular particles in the bodily fluid from which to separate the exosomes. These are some of the problems that have been put forth as a reason why it’s difficult to purify virus particles, but the researchers have overcome these problems with exosomes.
Bacteriophages, known as “the viruses of bacteria,” can also be purified, as shown in a 2018 article (again published in Methods in Molecular Biology)33 (see Figure 1). Bacteriophages are particles of similar size to viruses, and they also can be purified by chromatography and other methods. Mr. Hammond alleges that you can’t get a pure sample—a sample where you see only one thing in a vacuum. However, as you can see in the photos of exosomes and bacteriophages, all the objects are the same—they are the only thing in the microscope field because these have been isolated and purified, and there is nothing else in the sample, just exosomes or bacteriophages.
FIGURE 1. Isolated exosomes, isolated bacteriophages and “isolated” viruses
Isolated, purified exosomes
Isolated, purified bacteriophages
Sample taken from human fluids and grown in a tissue culture, said to be “purified” and “isolated” virus.So, biologists clearly have this technology, and it’s been around for quite a long time. It’s just that when they tried to do isolate viral particles, back in the 1940s and 1950s, after they had electron microscopes, they were actually unable to find any particle in the tissues or fluids of anyone who was ill. The problem is that they are unable to find the viral particles, not that they don’t have the technology to isolate and purify.
Cell Culture is the Gold Standard
Hammond admits that you need a cell culture to “isolate” a virus, because the virus needs cells in which to replicate in order to have enough virus to detect. According to the viral theory, the virus causes an infection in the lung, for example, when it invades the lung cells and then reproduces in the lung tissue, right in those cells, and then produces more viral particles. So, all we would need to do is go right to that tissue culture in the sick person, not one that we create in a laboratory with other conditions that are not natural.
In other words, why would we do this kind of indirect experiment when we have a cell culture right in the host—namely, virus-invaded lung tissue—from which we could extract the virus? Why can’t we do a proper isolation, where you go to the host, the natural source of the virus, which is a sick person with an infection, and purify the viral particles right out of that person’s bodily tissues or fluids?
Cytopathic Effects
Virologists claim that the pathogenic nature of viruses is evident in light microscope images of tissue cultures showing cytopathic effects (meaning cell breakdown). But what the images of “viruses” from an electron microscope show is a mixture of cellular material from the cell culture and a variety of different types of particles (see Figure 1, third image). How can we know what any of those particles actually are? And how do we know the particle didn’t come from the foreign cell culture, such as the kidney cells it was cultured in? How do we know it’s not an exosome, a particle produced inside the cell? How do we know it’s not an apoptotic body (from cellular breakdown)? How do we know it’s not another type of extracellular vesicle? How do we know it’s a virus (since it doesn’t have a label and has not been isolated and purified)? While virologists can show images of small particles, they have no way of identifying the nature or identity of any of those particles.
Genetic Sequencing
Hammond claims that scientists can do genetic sequencing of the particles found in tissue cultures. There are actually two ways of doing genetic sequencing. One way is to extract genetic material from only one organism, and then sequence the genome in its entirety. That’s how you can discover the genome sequence of a new organism.
But for viruses, scientists use a different technique, variously termed “genomic” sequencing, “next generation” sequencing or “in silico” sequencing (meaning carried out in a computer). Whatever they call it, this kind of sequencing is just piecemeal.
Hammond describes the method accurately, in that they start with lots of pieces of genetic material, and then a computer does sophisticated calculations and simulations to put them together. The problem—which Hammond does not describe—is that the starting material for these experiments is not a pure organism; it’s not just a virus. What they’re starting with is, in most cases, the lung fluid from a patient diagnosed with Covid by a PCR test. (And we know the PCR test is invalid. See sidebar page 20.)
The fluid they start with has genetic material from many different organisms—from a variety of bacteria species, probably some fungal and yeast species, as well as all of the human genetic material from the host and then anything that happened to be in the air that this person inhaled for the few breaths before they took the sample. In other words, there are many sources of genetic material. When they put those little bits of genetic material into the computer, the computer doesn’t know which organism they’re from—since they are not starting with a pure virus, there’s no way to tell.
When the computer runs the simulation and tries to fit these little strands of sequences together by overlapping ends, they don’t know whether the computer is making a real sequence of an organism, or if it’s putting little bits from different organisms together into some kind of mishmash or chimera. They have no way to check it against a reference standard, because there’s never been any true sequence of these viruses. What we end up with is just a simulation.
To give an idea of the problem, in the first sequence that they did this way with SARS-CoV-2, they actually had over fifty-six million little pieces or sequences, and they had not one but two different software programs independently take those pieces and try to construct them into a longer strand that they said was the size of a typical coronavirus genome. With one of the software programs, they just threw out the data because it didn’t give them what they wanted. So, they’re picking and choosing at each stage: “We think this is good. . . we want to use this.”
The other software program came up with over a million different possible sequences, but they just picked one. And there was no rhyme or reason to how they picked it. It was just an arbitrary selection. With all of the uncertainty about the origin of each individual piece of DNA, they just randomly select one of millions of possible combinations spit out by a computer. How could anyone believe these results represent the real genome of an actual organism? It would be impossible.
Lack of Proper Controls
Hammond states that virologists do a control experiment when they do the tissue cultures. That statement is not quite accurate. In a proper control, you have only one variable different, and as far as we know, virologists have never actually done this. The proper way to do it would be to take lung fluid from someone who is sick, but does not have Covid—sick with influenza or pneumonia, for example—or even lung fluid from someone who is healthy. Then, they would continue the experiment using the exact same methods, the same cell cultures, the same concentrations of antibiotics, the exact same nutrients, and any other additives or environmental conditions such as the same temperature, the same amount of agitation, the same protocols all around—that would be a proper control. No one is doing this type of proper control for virus identification.
Some of the papers about SARS-CoV-2 have mentioned what’s called a “mock infected culture,” but this is not the same as a control. In fact, we don’t know exactly what they do with these mock infected cultures. They’re not reported on in every paper, but in a couple they are. And curiously, they don’t describe these mock infected cultures at all. If you go to the methods sections, you don’t see any explanation of what a mock infected culture is. And they don’t mention the word “control.”
If they’re doing a true control experiment, why wouldn’t they call it a control culture? They have to use different words because they’re not really doing a proper control, but they’re trying to pass it off as one, which is why they change the words. We have read hundreds and hundreds of scientific papers on other subjects, and they always refer to the control group; they don’t say the “mock treatment group.” So, the mock infected culture is some kind of trick. We even tried to communicate with a couple of the corresponding authors on these publications. We asked an open-ended question: “Can you tell us the procedure for the mock infected cells listed in this figure?” In most cases, they didn’t reply at all.
In one case, we were unable to get a clear answer. The reply we received was, “They’re treated the same.” But what does that mean? “Can you tell us the exact conditions?” We even put our queries into a yes or no question like, “Did you use the same antibiotics at the same concentration? Did you use the same nutrition at the same concentration?” But we could not get a clear response, which suggests that they are probably hiding something.
We do have two examples of studies that included a control sample. The first comes from a 1954 article published in Proceedings of the Society for Experimental Biology and Medicine by Enders and Peebles.4 This was the first published paper to use the cell culture technique, which later became known as “virus isolation.”
In this study on measles, the authors put the patient specimen in a foreign culture of monkey kidney cells and then they got cytopathic effects—meaning they were able to show some damage to the cell culture.
An interesting quote in this paper describes the results of the control experiment. “Monkey kidney cultures may therefore be applied for the study of these agents [referring to measles] in the same manner as cultures of human kidney. In doing so, however, it must be borne in mind that cytopathic effects which superficially resemble those resulting from infection by the measles agents may possibly be induced by other viral agents present in a monkey kidney tissue or by unknown factors.”
In other words, they saw a cytopathic effect in the cell culture that was alleged to be a result of damage from the measles virus itself—but it might not necessarily have come from the measles virus; it could have been caused by something in the kidney cells themselves, which they call viruses, or from unknown factors.
Continuing, the two authors said, “A second agent was obtained from an uninoculated culture of monkey kidney cells.” Now, that means they did not put any sample from a measles patient in the culture; they ran the cell culture without a source of virus—just the cell culture with no patient sample in it. According to the authors, “The cytopathic changes induced in the unstained preparations could not be distinguished with confidence from the viruses isolated from measles [emphasis added].” In other words, the sample with nothing added to it produced the same results as the sample containing fluid from the measles patient.
Since the control was positive, that means that the experimental procedure itself, and not the measles virus, caused the cytopathic changes.
An important recent control experiment was carried out by Dr. Stefan Lanka, who is the only virologist we are aware of who has recognized the truth about the nonexistence of a virus—and who left the field. What he did was carry out just the control experiment. There is no possible source of virus anywhere in this experiment. As you can see in Figure 2, the top row of panels is Day One and the second row is Day Five of the experiment.
FIGURE 2. Control experiment by Dr. Stefan LankaDay One is when they changed the cell culture conditions. Previous to Day One, all of these cell cultures were kept healthy with normal cell culture procedures; then, on Day One, they changed the condition. In the first column, they used the full nutrition (GlutaMAX plus 10 percent fetal calf serum) and antibiotics at the normal concentration. In the second column, they reduced the nutrition and kept the same concentration of antibiotics. There was no change on Day Five for either of these two procedures, no cytopathic effects.
The third column simulates what they do in virus cell culture isolation experiments, using reduced nutrition while increasing the antibiotic to three times the normal concentration. (The protocols use either two times or three times the normal concentration.) You can see that on Day Five, there were cytopathic effects—the cells developed vacuoles and started to break down. Normally, virologists would give this as proof of the existence of a virus, except that there’s no virus in this experiment.
In the fourth column, Lanka added yeast RNA, which doesn’t contain any viruses—it’s a pure yeast RNA specimen bought from a laboratory supply company with good quality control. You can see even more cytopathic effects on Day Five in that culture.
So, both these control experiments show that the experimental procedure itself produces the cytopathic effects. If you took the culture materials from the two dishes with cytopathic effects and looked at them under an electron microscope, you would see particles in there that you could call a virus.
Coronavirus Fringe Pattern
According to Hammond, virologists can see the characteristic coronavirus spikes on the particles they are calling viruses. Let’s review a couple of studies to see what is going on. The first was published in 2020 in Kidney360.5 In this study, researchers were looking at biopsies of people with kidney disease, mostly from before the Covid era. In the electron microscope photographs, they saw particles with the characteristic coronavirus spikes (see Figure 3). The researchers said that these were indistinguishable from coronavirus particles, which was a source of confusion for virologists. The authors pointed this out, and they even referenced a previous paper from the CDC that found the same thing.
FIGURE 3. “Viral-like particles in non-COVID19 patients’ biopsies. Electron microscopy images of viral-like particles within podocytes in a case of thrombotic microangiopathy in a (A) native kidney biopsy specimen and (B) acute cellular rejection in an allograft. Note the presence in both cases of single vesicles with an electrondense rim likely representing endocytic coated vesicles, as well as larger multivesicular bodies (arrows), which could be confounded with vesicle packets containing virions. Inset in (A): the individual small coated pits in the exterior of the vesicle bear resemblance to a viral corona. (C) Similar intracytoplasmic vesicles within tubules in an allograft with changes suspicious for acute cellular rejection.”They also said that they identified the protein that made up the spikes, and it was not the spike protein, but a protein called clathrin. So, seeing the characteristic spikes is completely meaningless; it doesn’t identify something as a coronavirus. Remember that these kidney biopsies were from people who had no disease that anyone thought was related to a virus, and it was before even the “discovery” of so-called SARS-CoV-2.
The second example comes from a “virus isolation” paper published in the Medical Journal of Australia in 2020.6 A very interesting quote occurs in this paper: “Electron micrographs. . . showed cytoplasmic membrane-bound vesicles containing coronavirus particles. Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin into the cell culture medium immediately improved virion morphology.” In other words, they didn’t see any spikes so they added the digestive enzyme trypsin, which breaks or cleaves proteins at a certain sequence, and then looked at it again under the microscope—and then saw the spikes! (See Figure 4.)
FIGURE 4: “Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin into the cell culture medium immediately improved virion morphology.”Now, isn’t that convenient? In other words, they put a spike suit on the particles so they could look like they’re supposed to look, instead of saying, “Hey, maybe there is no coronavirus in the sample.” If we have to digest a protein to make it look a certain way, then how could we say that’s what it is? It’s like having a cat but really wanting a dog, so you put a little microphone around the cat’s neck that makes a barking sound and then call it a dog. We would call this cheating.
Genome Sequencing
As Hammond and other adherents of viral theory have often stated, genome sequencing has been repeated thousands of times, and the results are published in international databases, so they can’t be a hoax. Actually, the in silico genome-sequencing procedure that we have described has been repeated over two million times—far more than Hammond claims. And of course, each time they get different results, because they can’t repeat results in an invalid experiment, so the different results are all published.
As described earlier, the way they do this is to take a bunch of pieces of unknown origin, which they run through different software simulations, and then pick out the one they like. And then they do some further magic on it by just popping things in or taking things out somewhat arbitrarily to make it look more like what they think a coronavirus genome should look like. Then they claim that this sequence is a “reference sequence” and against all of those couple of million experiments that they have repeated, they can template a reference genome. So, of course, the computer is able to put things together in such a way that it matches the so-called reference sequence somewhat closely, because the sequences that make this up are probably mostly just human sequences of non-coding RNA. (A recent analysis shows this and will soon be published.) Thus, you should be able to have similar enough sequences that you can put something together that’s close, but not exactly identical—which they then call “variants.”
Now Hammond claims that if the procedures were fraudulent, then tens of thousands of scientists all over the world would be participating together in a conspiracy; but that’s not the case at all because almost none of these scientists realizes that what they’re doing is not good science—they never question it. Doctors rarely question the things they’re taught; they just learn them and accept them as true. That’s why I (Andrew Kaufman) was recommending vaccines and using antibiotics earlier in my career, because I also just accepted those things and did them without question. Now I realize that they’re quite lethal, so I don’t do them anymore. There was a kind of individual process that I went through for that.
But the scientists involved in “virus isolation” don’t realize that they’re doing fraudulent science because they’ve never looked at it carefully. And one of the ways that science allows this kind of thing to happen is by a high degree of compartmentalization, where they don’t collaborate or talk with other people in different fields. They don’t learn how other scientists do their experiments and also how they do control experiments. And they don’t seem to talk to exosome scientists, often because they would then see that exosome scientists are able to extract and purify exosomes right from the source. And then they would try to do that and fail, because there aren’t any viruses, and then they would have to have a different conclusion and change their opinion.
But the truth is, it doesn’t matter whether all of the thousands of scientists doing “virus isolation” are in a conspiracy, and it doesn’t matter whether they’re completely ignorant, because the only thing that’s important is to look at the actual science itself—the experiments—and ask the question, can you learn something from this? Can you conclude anything from this experiment? And if the answer is no, it doesn’t matter how many people think you’re wrong, it only matters that the answer is no. It shouldn’t be terribly surprising that the virologists have gotten this wrong, because in medicine this happens frequently. Take the example of beta blockers and heart failure. For many decades, it was an absolute contraindication to prescribe a beta blocker to someone with heart failure, because beta blockers make your heart beat less strongly and less rapidly. So, that was seen to make your heart weaker. But then research showed that actually, adding a beta blocker slows the progression of heart failure and allows people to live longer. It took some time for that scientific finding to be integrated into medicine, but there was no truth to the notion that doctors everywhere were in a conspiracy to hasten the death of heart failure patients. They were just ignorant to the truth of the scientific relationship between that drug in that condition. We could interpret “virus isolation” as a similar phenomenon; virologists who are doing these experiments are not able to actually show the results or provide the conclusive evidence because they are just ignorant of that fact, because they haven’t looked at it. It’s quite as simple as that.
Response to Mercola
Entering the virus debate on January 17, 2022, Dr. Joseph Mercola published a “fact-checked” article entitled, “Yes, SARS-CoV-2 is a Real Virus,”1 in which he insisted that SARS-CoV-2 has been isolated, photographed, genetically sequenced, and exists as a pathogenic entity.
Mercola cites studies from Italy, Germany, India, Columbia, Canada, Australia, Korea and the U.S., which claim to have isolated SARS-CoV-2 and characterized it by genome sequencing. However, none of these studies isolated any virus from the fluids of the patient; all of these studies used culturing techniques that can lead to tissue breakdown and the creation of exosomes (identical in form to “viruses”); none of these studies had a meaningful control; and all used questionable computer techniques to generate a genome in silico. Remember that these tissue cultures would also contain genetic material from the kidney cells of the culture and the bovine serum used as a nutrient medium. Even if the tissue cultures did contain viral particles, how can anyone know that the DNA the computer is analyzing comes from the virus?
As Mercola states, “Another sticking point for some is whether or not SARS-CoV-2 has ever been isolated from a human subject without passing it through animal cells, as such media could be contaminated and therefore the source of the virus.”
Indeed, this is the “sticking point!” All of the studies that Mercola cites as proof passed the sample through animal cells—cultures contaminated with fetal bovine serum and toxic antibiotics, and starved with a minimal nutrient medium.
Furthermore, no paper has proven that an isolated or pure virus obtained from a cell culture has ever made an animal or human sick in any way. Therefore, it is illogical, irrational and anti-scientific to claim that the “virus” is a pathogen.
According to Mercola, “At least part of the confusion appears to be rooted in how the term ‘isolated’ is defined. Some insist a virus is not isolated unless it’s also purified, while others say a virus doesn’t have to be purified in order to be ‘isolated.’” Actually, as we have pointed out, the confusion—deliberate confusion—results from virologists using the word “isolated” to mean “not isolated,” and insisting that “purified” and “isolated” do not mean the same thing.
More Genome Sequencing
One study Mercola highlights is a “genome sequencing” study published in January 2021 in Gut Pathology.7 In this study, the genetic material (RNA) was extracted directly from stool samples of a patient identified as having Covid-19 using the meaningless PCR test.
This paper relies on an in silico genome-sequencing procedure whereby they extract all of the RNA that is present in a body fluid or tissue sample, which would include a number of different sources of genetic material, including the person’s own. The material would include non-coding DNA that has been transcribed, spliced and recombined to make all sorts of novel sequences.
They then throw out the long fragments and just look at the short ones. This is a really important point, because the longer the sequence, the more you can be sure that it came from one source; whereas if you have short sequences, when they put them together in a longer sequence, parts of it could have come from different sources. It’s more reliable to have longer sequences, but then they can’t do the sequencing as fast. So, they put all those short sequences into the computer and let various computer software programs put them together, mapping them to the “reference” standard genome—which has been done in the same way—and then give you a result. The result is a little bit different each time, which is why they have over two million “variants.”
In this 2021 paper, they used fecal material, which they said contained the same genetic material as that extracted from the nose using a nasal swab. And interestingly, in this case, they did use a control group, which is very unusual—they actually used a purchased heat-inactivated SARS-CoV-2 toxic cell culture that served as a negative control.
The other unusual procedure was that they used shorter strands of RNA than normal. Usually, they look at strands of up to one hundred fifty base pairs, but in this study, they limited the length to seventy-six base pairs. This would result in even more error in terms of the source of each particular little strand.
They also skipped an important step, which they call making “contigs” (from the word contiguous). Usually, what they do is take all those little sequences of short strands—there are often over fifty million of them—and put them into software number-crunching programs that try to pair up overlapping sequences on the ends to make longer and longer strands—this is what they call “contig.” Then they pick one of the longest strands and use that as the base genome.
In this case, they didn’t do that. They just took the sequence strands and templated them right away against the reference standard from the database. In other words, they chose the pieces that would fit into the puzzle and entered them into the program, and then the software filled in the gaps and rearranged things as necessary. In this way, they made sure that the genome looked the way they wanted it to look.
All of the studies Mercola lists as proving the existence of the SARS-CoV-2 virus are done in similar fashion to come up with a computer simulation, not a real genome taken intact from a real organism.
When Hammond talks about finding a genome of twenty-eight to twenty-nine thousand base pairs, it’s important to understand that they have never found this genome in any bodily fluid, just like they have never found anything they could call a virus. They have never found a strand of twenty-nine thousand base pairs; instead, they have created it in the computer by matching pieces together based on a template. In other words, they find the sequence only because that’s the sequence they’re telling it to find. This is not science!
More Covid-19 Virus Studies
Another paper cited by Mercola comes from Italy, published in the Annals of Internal Medicine in August 2020.8 The researchers took a sputum sample from a sixty-five-year-old woman and diagnosed her with Covid-19 using a PCR test. Then they cultured the sample in kidney cells, followed by genome sequencing as described above. It’s the same in all the studies that Mercola cites. Nobody isolates the virus from the patient directly; nobody takes that virus and determines the genetic material in that virus; nobody takes that virus and exposes somebody else to it and shows that it causes disease.
Mercola cites a study from Colombia that is the same exact experiment—a nose swab cultured in a toxic cell culture, followed by genetic sequencing and electron microscopy.9 According to the researchers, “Electron microscopy images obtained from infected cells showed the presence of structures compatible with SARS-CoV-2”—not structures that are, but that are compatible.
These structures are also “compatible” with kidney failure and probably many other things. The authors state that the genetic composition of their isolates was consistent with the predominant variant—not saying it was the predominant variant. In other words, they are hedging at every turn.
At the end of his article, Mercola mentions “antibody dependent enhancement (ADE),” but there is absolutely no scientific evidence to support something called ADE. Virus theory posits that we make antibodies against viral diseases. In July 2020, the head of the Bulgarian Pathology Association stated that they had found no monoclonal (coming from the same cell) antibodies in any of the people said to have died of Covid.10
This is like saying that no one has died of Covid, because since they haven’t found antibodies, they must conclude that the patients didn’t have Covid.
Does It Matter?
Hammond dismisses those who question the viral theory of disease as his “pet peeve” and “divisive” of the health freedom movement. According to Mercola, “Getting too far into the weeds of theories that refute the existence of viruses altogether will only slow down and hamper the truth movement rather than aid it along, and I would strongly discourage anyone from engaging in this highly unproductive narrative.” In other words, if you question the viral theory, you are the bad guy, hindering the movement for health freedom. One virus advocate has referred to “virus-deniers” as domestic terrorists!
And yet the virus debate has immense importance to the health freedom movement. All the objectionable “public health” measures— masks, social distancing, isolation, testing and above all toxic vaccines—are predicated on the belief that we are threatened by a virulent, contagious virus. If there is no virus—not for Covid-19, not for any disease—then the justification for forcing these measures on the public disappears.
SIDEBARS
Electron Microscopy
Scientists use an electron microscope in order to see the structures inside a cell. To view a sample under the electron microscope, they must prepare it using special procedures. One reason is that the beams of the electron microscope are extremely powerful and can heat the sample up to 150 degrees C. The preparation method requires the following steps:
FIXATION: The sample is placed in some kind of chemical fixative, such as formalin, glutaraldehyde or osmium tetroxide. This preserves the structure of the tissue.
DEHYDRATION: This step requires bathing the tissue many times in alcohol (ethanol or acetone) to remove all water from the tissue.
EMBEDDING: The tissue is put inside a small mold that is filled with paraffin wax or epoxy resin, which is then cooled to harden.
SLICING: The hardened resin is sliced into extremely thin pieces.
STAINING: The tissue is stained with some type of heavy metal, such as uranyl acetate, another name for uranium, or lead acetate, so you can have more contrast when you’re viewing the tissue through the electron microscope.
These methods will obviously have effects on biological samples. For example, formalin in the staining process is formaldehyde, a known human carcinogen and neurotoxin; glutaraldehyde is specifically dangerous for the gastrointestinal tract and the lungs, and osmium tetroxide causes pulmonary edema. Ethanol used in the alcohol baths can cause severe liver damage, and acetone damages the kidneys, the lungs and the brain. Paraffin wax and epoxy resin used for embedding can also affect biological tissues.
Most toxic are the heavy metals uranium and lead used for staining; they are bound to have toxic effects on biological samples. The result is that what you see using the electron microscope has little resemblance to living tissue—it is an artifact and a distortion, from which no conclusions about cell structure can be made.
A Mouse Study
Recently, Dr. Robert Malone stated that the omicron variant is not as dangerous as the others and that we should rethink our vaccines. One of the papers he cited was “Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model,” published in December 2021 in Emerging Microbes and Infections.11
In the abstract of this paper we read, “Older individuals are at higher risk of SARS-CoV-2 infection and severe outcomes, but the underlying mechanisms are incompletely understood. In addition, how age modulates SARS-CoV-2 re-infection and vaccine breakthrough infections remain largely unexplored. Here, we investigated age-associated SARS-CoV-2 pathogenesis, immune responses, and the occurrence of re-infection and vaccine breakthrough infection utilizing a wild-type C57BL/6N mouse model. We demonstrated that interferon and adaptive antibody response upon SARS-CoV-2 challenge are significantly impaired in aged mice compared to young mice, which results in more effective virus replications and severe disease manifestations in the respiratory tract. Aged mice also showed increased susceptibility to re-infection due to insufficient immune protection acquired during the primary infection.”
Now, when well-known spokesmen such as Dr. Robert Malone comment on the importance of a study like this, it works to convince the public that SARS-CoV-2 is real and the omicron variant is real. Maybe omicron is not so bad, maybe it is worse in the elderly, but in any event, the new “variant” is real.
According to Malone, the reason this study is important is that it explains the significant adverse event profile of the vaccines. We would agree that these adverse events combined with a milder disease profile of omicron raise the possibility that boosters may not be good medicine, even for the elderly, but the suggestion that viruses have anything to do with this only perpetuates the kind of misinformation that justifies everything that is wrong with how the health authorities have handled the pandemic—masks, social distancing, isolation, hand sanitizing and vaccinations.
According to the authors, the antibody response was severely impaired in aged mice leading to more severe disease. In the Materials and Methods section, we see that the SARS-CoV-2 variant was “isolated” from a confirmed Covid-19 patient in Hong Kong and that the virus was cultured in Vero (kidney) cells and stored at negative 80 degrees C.
Now, the important part: they expose the mice to a “variant” of the “virus”—to what they think is the omicron variant. One would expect that what scientists would do is take purified virus and expose the mice in the way that humans are exposed, by breathing it in the air. But what did these scientists do? They did a standard viral culture, meaning they inoculated monkey kidney cells (Vero cells) with fetal calf serum and an unpurified sample from a person with alleged “Covid.” (Fetal bovine serum, by the way, is taken from live aborted slaughterhouse calves whose blood is sucked directly from their hearts.) So, they didn’t, in fact, use a virus—that is a flat-out lie. Instead of a virus, they used a culture of kidney cells that contained some of the primers allegedly from a variant strain, a variant that has never been isolated.
Now, you would think that they must have sprayed this culture onto the mice, or gently into their noses, but that’s not what they did. Instead, they anesthetized the mice with toxic drugs—essentially poisoning them—and then squirted a mixture of phosphate-buffered saline and the toxic kidney culture under high pressure down their noses through an intranasal cannula directly into their lungs. No rational person would say that this type of experiment has any relation to what happens in old or young people or to anybody exposed to a “virus.” It’s ridiculous to call this science.
And then they found out whether the young mice did better than the old mice. Upon intranasal inoculation, the young mice transiently lost a maximum of 5 percent body weight for a short period. In contrast, the older mice lost 12 percent of body weight, and they didn’t recover. Moreover, the young mice did not show any sign of disease. The older mice showed hunched postures and labored breathing, which was more severe at higher doses of toxic cell culture injection into their lungs.
If you wanted to be precise in your language, you would say that young mice—injected, anesthetized and subjected to high-pressure squirts of toxins directly into their lungs—seemed to be okay; they just lost a little weight. That’s probably the definition of a bad day for a mouse. But they seemed to recover, whereas the older mice didn’t do as well. That’s what they found.
And then they did all kinds of biochemical histological genetic studies, analyzing the tissue after they ground up the nasal turbinates, the lungs and so forth. They then concluded, “Yep,” these mice have a lot more antibodies than they should—which means they are trying to protect themselves against being poisoned with toxic cell cultures injected right into their lungs.
The authors found that the staining of the nucleocapsid protein was more intense at higher doses of the stuff squirted up the mice’s lungs. Later, they say these findings indicate that SARS-CoV-2 “replicates more effectively in the respiratory tract of aged mice than young mice upon virus exposure.” We would submit that they never actually took out any virus and never saw any replication of any virus in any lung of any mouse.
In other words, the researchers essentially said, “This study does not prove what we thought it was proving, but is just another way to convince us that there is a virus and that the virus is the cause of disease.” When in fact, all this study really tells us is that older, poorly-fed mice do worse when exposed to poisons than younger ones.
Does it matter whether this disease is caused by a virus or not? When the Chief Medical Officer of the World Health Organization predicts that half of the United States is going to get sick in the next six to eight weeks, yes, it does matter. The problem with all this talk about viruses is that it completely obscures the reasons why people are getting sick. We know that a lot of people are getting sick from the injections, but they are not the only people getting sick. Unfortunately, as long as we stick to this nonsense called the viral narrative, we will never ask the right questions, and we will never get any answers as to what otherwise is making people sick.
Rapid Tests for Covid-19 Virus
Recently, the CDC announced—quietly and without explanation—that as of January 1, 2022, they were no longer going to use PCR tests for “diagnosing Covid.” Many people saw this as a kind of capitulation by the CDC, as if to say they had finally seen the light; or perhaps there was enough pressure on CDC that they realized they had to back down quietly from the PCR test. Many people interpreted the CDC’s move as an end to testing, and since this pandemic is really a pandemic of testing, they believed this would go a long way toward ending the pandemic. After all, if they stopped doing the test, nobody would test positive. However, the CDC didn’t say they were going to end testing.
The problem is that these people are playing chess, while the rest of us are playing checkers—if they’re playing chess, we need to play chess, too, and understand the motivations and the rationale behind some of the moves we’re hearing about. And this is particularly true in the case of things that seem to be small victories—sometimes even fairly large victories—because upon closer examination, they don’t all turn out to be the victories that we imagined.
The PCR (Polymerase Chain Reaction) is not a diagnostic test, it’s a manufacturing tool, and it does not test whether or not anybody has any virus. Rather, the PCR is a method to rapidly make millions to billions of copies (complete copies or partial copies) of a specific DNA sample, allowing scientists to take a very small sample of DNA and amplify it (or a part of it) to a large enough amount to study in detail. The inventor, Kary Mullis, was emphatic that his test could not be used to diagnose or determine disease.
The PCR amplifies the DNA sample anywhere from twenty to forty cycles in order to get enough genetic material to detect—the test does this by showing a color change. To use the PCR as a diagnostic test requires two assumptions. The first is that you know that the genetic sequence you are amplifying comes from the virus you are looking for; the second is that there are no other biological organisms in the sample—no microbes, bacteria, fungi or human DNA. To repeat, the premise of using the PCR for diagnosis is that you already know the sequence of the virus, and you know that this primer sequence is one of the pieces of the entire virus genome, and that no other biological organism has that same sequence of DNA. We know that both these premises are not true with PCR Covid tests. Actually, one of the people who came up with the original primer sequences was Christian Drosten, who admitted in a paper that they never had a copy of any virus.12
Now, just think about that for a minute. If you never had a copy of the virus, how can you possibly know that this piece of the genome is a piece of the virus, that it actually came from a virus? If we gave you a sentence and asked you whether this sentence came from a certain book, the obvious common-sense question that any rational human being would ask is, can you show me the book? How can you know whether a sentence comes from a certain book if you don’t have the book?
Furthermore, how can you prove that no other living being has this same sequence? You can determine this by doing what is called a BLAST search, which searches the database of all the genome sequences of all the organisms that have ever been sequenced. Scientists have done this and found out that the same sequence used in the PCR test primers for SARS-CoV-2 is found in at least ninety human sequences and ninety microbial sequences (meaning bacterial or fungal sequences).
Thus, the second premise, that a sequence is unique to a specific virus, is also not true. The sequence is found in humans and in bacteria. If you start with a sample that has sequences that come from humans and that has bacteria and fungus in it, there is no way of knowing whether the positive match—the sticking of the primer to a sequence in the sample that will then be amplified—comes from a virus, the person, bacteria, fungus or maybe from something else.
So, the PCR test is invalid—there are no “false positives,” there are no “false negatives,” there are just false results. So, shouldn’t we applaud when the CDC finally acknowledges that they are not going to do a PCR test anymore?
The question is, what are they going to replace it with? According to government announcements, they are going to use a “higher throughput and multiplexed assay with biotinylated primers.” To explain further: “This developed invention is multiplex and uses the Luminex bead-based liquid assay, which contains one hundred different unique bead oligonucleotide probes with sequences complementary to the target sequences covalently coupled to these unique beads. These capture beads are mixed with viral samples obtained from the patient via cheek swabbing or throat wash and subjected to PCR in a conventional thermocycler. The amplified target sequences then hybridize to complementary capture oligonucleotide probes via forward biotinylated primers; if this bead probe amplicon unit contains the target nucleic acid, it will be bound by the reporter molecule and fluorescence will be detected by flow site cytometer. This multiplex assay would thus be able to detect and identify respiratory pathogens present in hospital and clinical settings.”
English translation: Instead of the old PCR test, they are going to use one hundred different unique beads. These beads contain the primer sequences, and they’re all attached to the other beads. These beads are mixed with viral samples from the patient, and then they are put into PCR amplification cycles.
Now, the only real difference between this and the normal PCR test is that there are more of the primer sequences—like one hundred more—attached to a compound called biotin. These biotinylated primers stick easily to the sequences in the sample, which then get put into the old-fashioned PCR thermocycler, so that they can be amplified. And then you get a result. Now, instead of a PCR test for Covid, one test will test for all the “viruses.”
The upshot of this is that now they will be able to say that you have many different viruses, all at the same time. Since all these viruses can make you sick (so they will argue), you may need a vaccine for each one of them.
This is a checkmate: They now are able to find the code for the original “virus” as well as the delta variant and the lambda variant, right on through the Greek alphabet, because they can make it look like you have multiple different sequences. These sequences amplify more easily because they figured out a way to make the primer sequences stick more readily to whatever is in your sample. And this is not a single-plex test. This is a multiplex assay, which means they can find any number they want, just by increasing the amplifications. And checkmate, they got us.
So, they replaced the old-fashioned PCR with something that will make the whole thing even worse. The lesson is that we should not be fooled by false minor victories, because they are not necessarily good news.
The Seven U.S. Government Payoffs to Kill You in Hospitals
by Dr. Peterson Pierre13
If you have Covid, and you end up in the hospital, you’re put on a rigid protocol. There’s a high mortality rate in the hospital, and your family is kept in the dark about what is happening. So, what’s going on here?
The CARES Act is providing bonus payments to hospitals whenever they have a diagnosis of Covid, while the Center for Medicare and Medicaid Services is waiving patient rights. This is a deadly combination.
The hospital gets the first payment when they offer a free Covid test in the emergency room, and they get another payment if they can come up with a diagnosis of Covid. Number three, they get another bonus payment if they admit a patient with Covid. Number four, they get another bonus payment if the patient is put on remdesivir. Number five, another bonus payment if the patient is put on a mechanical ventilator. Number six, another 20 percent bonus if the diagnosis on your death certificate says Covid, even though you may not have died from Covid. And then number seven, there are bonus payments for the coroners.
Does the public understand the gravity of what’s happening right now? The government is literally paying hospitals to kill you. That’s what’s happening. These are real human lives we’re talking about, priceless human lives. It’s estimated that about one hundred thousand dollars per patient is what the hospital is getting. Think about that.
Rai A, Fang H, Fatmous M, et al. A protocol for isolation, purification, characterization, and functional dissection of exosomes. Methods Mol Biol. 2021;2261:105-149.
Vanderheuvel D, Rombouts S, Adriaenssens EM. Purification of bacteriophages using anion-exchange chromatography. Methods Mol Biol. 2018;1681;59-69.
Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954;86(2):277-286.
Cassol CA, Gokden N, Larsen CP, et al. Appearances can be deceiving – Viral-like inclusions in COVID-19 negative renal biopsies by electron microscopy. Kidney360. 2020;1(8):824-828.
Caly L, Druce J, Roberts J, et al. Isolation and rapid sharing of the 2019 novel coronavirus (SARS-CoV-2) from the first patient diagnosed with COVID-19 in Australia. Med J Aust. 2020;212(10):459-462.
Papoutsis A, Borody T, Dolai S, et al. Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing. Gut Pathog. 2021;13(1):7.
Colavita F, Lapa D, Carletti F, et al. SARS-CoV-2 isolation from ocular secretions of a patient with COVID-19 in Italy with prolonged viral RNA detection. Ann Intern Med. 2020;173(3):242-243.
Díaz FJ, Aguilar-Jiménez W, Flórez-Álvarez L, et al. Isolation and characterization of an early SARS-Cov-2 isolate from the 2020 epidemic in Medillin, Colombia. Biomedica. 2020;40(Supl. 2):148-158.
Chen Y, Li C, Liu F, et al. Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model. Emerg Microbes Infect. 2022;11(1):368-383.
Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):2000045.
1. Normal people have no interest in killing children, especially ones they do not know, especially in large numbers.
2. In my view, only people subject to mind control (please investigate Sirhan Sirhan or read about US intelligence agency attempts to create mind controlled assassins beginning in the 1950s) or people taking certain drugs, or special trained assassins are even capable of carrying out such an act. [In the case of Sirhan Sirhan, who did fire wildly on a crowd, but did not kill Kennedy, the actual assassin was an intelligence asset. From the WaPo in 2018:
Though Sirhan admitted at his trial in 1969 that he shot Kennedy, he claimed from the start that he had no memory of doing so. And midway through Sirhan’s trial, prosecutors provided his lawyers with an autopsy report that launched five decades of controversy: Kennedy was shot at point-blank range from behind, including a fatal shot behind his ear. But Sirhan, a 24-year-old Palestinian immigrant, was standing in front of him.
3. School shootings are the most provocative and effective way to initiate a change in gun laws, which means taking away the guns from some or all of the people who privately own them.
4. The large number of American gun owners pose a daunting challenge to the globalists who wish to control them. Police and military will not be willing to enter the homes of gun owners to remove their guns or for other purposes.
5. Few Europeans, Canadians, Australians, New Zealanders own guns, and it is believed by many that the imposition of much harsher lockdowns on the citizens of these nations, compared to the US, was enabled by this fact.
6. There have been shortages of guns and ammunition in the US since the onset of the pandemic. Whether this is due to supply-demand, including increased purchases by the federal government, or to other market forces, is not clear.
7. There has been very little exploration into the past history of those who committed mass murders in the US in recent years, especially in schools. I want to know if any or all of these mass murderers may have been enrolled in black mind control projects.
8. I want a full accounting of the mind control programs paid for with taxpayer dollars in the US and elsewhere.
9. I want an investigation into the many thousands of self-reported “targeted individuals” (TIs) who complain of voices beamed into their heads and other forms of what can only be termed torture.
10. I want an investigation into the implants some of these people claim were introduced into their bodies.
11. A reader sent me this piece by David Swanson, revealing that at least a third of mass US shooters have been trained in the US military. Were they put through mind control programs while serving their country?
12. Why have so many assassins and mass shooters appeared to be in an altered state of consciousness immediately after the event, and/or at other times? Think Sirhan Sirhan, Mark David Chapman, Reagan’s attempted assassin whose father was having dinner with GHW Bush the week of the attempt? Has anyone analyzed their behaviors systematically? Their histories and connections to the powerful?
13. We are being attacked in many perverse ways, and we must open our eyes, take our power back, or the attacks will continue and will destroy us.
“A pill with a tiny chip that sends a signal to relevant authorities when [the pill] has been digested…imagine the implications…the compliance…”
Patient compliance is a very big deal in the pharma/medical universe. The patient gets his orders. He follows them.
From a purely $$ perspective, the chip is a major advance. No pills left in bottles. People finish their meds. They go back to the doctor. He authorizes a new script or changes the drug. More pills taken, more money rolls in.
But of course, the larger bonus is control.
“You see, Mr. Jones, we know you didn’t finish taking the meds you were prescribed. So we can’t keep treating you. It’s a waste of time if you won’t follow orders…”
And this is just the first phase of ultimate control. Over time, it gets heavier. Cancelation of health insurance for non-compliance. Mandates.
COVID has been a training ground for citizen obedience. But the medical dictatorship wants more. Always more. And they’ll dream up one occasion after another to secure more.
Bird flu. Monkeypox. Smallpox. Whatever STORYTELLING it takes.
The medical cartel is in the business of making horror movies and promoting them as real.
A pill with a chip is the soft version of nanotech—by which tiny transmitters and receivers are placed in the body and brain. The nanos are also sensors. They report on all sorts of ongoing body processes—which leads to medical diagnoses, toxic drugs, and toxic vaccines in an endless parade.
This is not science fiction. This is not a hundred years in the future. We’re almost there.
Don’t make the mistake of thinking that humans are going to be on the receiving end of all the reports which the nano sensors issue from inside humans. This operation is planned as AI. Eventually, algorithms will interpret those reports and make decisions about treatment.
Many doctors will eventually take on roles as comforting guides, PR flacks, pitchmen, counselors. “Of course this is all for your benefit, Jim. It’s a good diagnosis. The treatment is standard. Think of Carol and the kids and what they need you to do. We caught it in time. You’ll be fine. But for God sakes, stop reading that nonsense online about toxic side effects. What do you think clinical trials are for? We did the prep work. The FDA approved this drug. It’s safe. I looked at your chart myself. The Pfizer antiviral is the preferred choice in your case. This is routine. If you need a human therapist, rather than the AI psychologist, I can recommend a good man. He lives in your town. Your insurance will cover it. But just suck it up and take the medicine. Believe me, you don’t want to progress to the stage where surgery is necessary. Then we would be talking hospitalization and recovery…”
Some of your children will be talking about earning a PhD in Bedside Manner.
Health Freedom and Medical Freedom are the alternative.
Everything coming down the medical pipeline makes this freedom absolutely vital. YOU decide what’s good for your body and mind, and what’s bad.
You assert that right, come hell or high water.
No matter how many court cases are won or lost, FREEDOM to say yes or no to medical treatment is the ultimate back up. This is what I kept writing and saying early on in the COVID hustle.
Meanwhile, the Pfizer CEO, Albert Boura, is a shark. In every sense of the word.
Moderna CEO Stéphane Bancel is complaining about having to ‘throw away’ 30 million doses of Covid-19 vaccine because ‘nobody wants them.’
“It’s sad to say, I’m in the process of throwing 30 million doses in the garbage because nobody wants them. We have a big demand problem,” Bancel told an audience at the World Economic Forum, adding that attempts to contact various governments to see if anyone wants to pick up the slack was a total fail.
“We right now have governments – we tried to contact … through the embassies in Washington. Every country, and nobody wants to take them.”
“The issue in many countries is that people don’t want vaccines.”
Watch:
Stéphane Bancel, CEO of Moderna:
“it’s sad to say, I’m in the process of throwing 30 million doses in the garbage because nobody wants them. We have a big demand problem.”
— Efron Monsanto ???? (@realmonsanto) May 23, 2022
Bancel’s comments come days after Bloomberg reported that EU health officials want to amend contracts with Pfizer and other vaccine makers in order to reduce supplies.
During a virtual meeting organized by Polish Health Minister Adam Niedzielski, governments shared a joint letter to the EU Commission which reads: “We hope that the discussion with the commission and among member states will allow flexibility in the vaccine agreements,” adding “We are also counting on vaccine producers to show understanding to the exceptional challenges that Poland is facing supporting Ukraine and giving shelter to millions of Ukrainian citizens fleeing the war.”
Some countries are seeking to amend so-called advanced purchase agreements signed with producers, as demand for shots wanes and budgets come under strain from the fallout of the war in Ukraine and the costs of accommodating refugees.
Adjusting deals with suppliers could grant member states the right to “re-phase, suspend or cancel altogether vaccine deliveries with short shelf life,” Estonia, Latvia and Lithuania’s prime ministers wrote in a joint letter to Commission President Ursula Von Der Leyen late last month.
Meanwhile, in a separate letter the health ministry of Bulgaria called for an “open dialog” with the commission and pharmaceutical companies, arguing that the current arrangement forces member states to “purchase quantities of vaccines they don’t need.”
“Monkeypox” – who could have seen it coming? Well, apparently the organisation founded by Ted Turner in 2001 called the ‘Nuclear Threat Initiative’ (NTI) saw it coming when they published a report in November 2021 called, “Strengthening Global Systems to Prevent and Respond to High-Consequence Biological Threats.” The report states that in March 2021, they partnered with the Munich Security Conference to run an exercise scenario involving a, “deadly, global pandemic involving an unusual strain of monkeypox virus that emerged in the fictional nation of Brinia and spread globally over 18 months…the fictional pandemic resulted in more than three billion cases and 270 million fatalities worldwide.”
The Nuclear Threat Initiative introduces Plandemic 2.0? This time it is even bigger and monkeypox takes centre stage.
Amazingly, the scenario had the monkeypox outbreak emerging as a result of an act of bioterrorism in May 2022, right where we are now. We have dealt with gain of function garbage involving non-existent viruses in several other videos, while Dr Stefan Lanka has also dismantled such fallacies. Regardless, the NTI’s report suggests that what is required in a fantasy outbreak is, “aggressive measures to slow virus transmission by shutting down mass gatherings, imposing social-distancing measures, and implementing mask mandates”. The winning countries, in their hallucination implemented, “large-scale testing and contact-tracing operations and scaled-up their health care systems.”
Their charts, which seem to be produced by Neil Ferguson’s calculator, show that countries that don’t comply with their restrictions and medical interventions will be far worse off. The report goes on to state, “both the exercise scenario and the COVID-19 response demonstrate that early actions by national governments have significant, positive impacts in managing the impact of the disease”. When they say “positive impacts” it is not quite clear who is on the receiving end, although they note that “the COVID vaccine market will exceed $150 billion in 2021.” All in all the NTI’s report reads like Event 201 on Ritalin. (Event 201 took place on 18 October, 2019. It was an exercise involving a, “coronavirus pandemic” just months before the COVID-19 “pandemic” was declared.)
Monkeypox attacks right on cue!
As with COVID-19 it appears that other parties have also been eagerly awaiting a market such a “pandemic” would present. Likewise, these fortune-tellers were preparing vaccines to go where no vaccine had gone before. In this case the biotech company Bavarian Nordic gained approval from the FDA in 2019 to market JYNNEOS, a smallpox and monkeypox vaccine. Other health authorities were also primed to react to a previously rare condition that has been of no concern for their nations…until now apparently. For example, on May 20, 2022, the UK Health Security Agency published a document titled, “Recommendations for the use of pre and post exposure vaccination during a monkeypox incident”. Like COVID-19, it’s starting to feel like all roads lead to vaccines again…
Just a matter of time before the “rare” monkeypox vaccine comes to your neighbourhood.
So now that the scene has been set we can get into the “science” of monkeypox starting with an official description of the alleged viral disease. The CDC states that, “Monkeypox was first discovered in 1958 when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research, hence the name ‘monkeypox.’ The first human case of monkeypox was recorded in 1970 in the Democratic Republic of Congo.” They go on to state that, “in humans, the symptoms of monkeypox are similar to but milder than the symptoms of smallpox.” The illness is said to be flu-like with the addition of lymph node swelling and then development of a rash, and then lesions that progress from macules to vesicles to scabs.
In terms of the lethality of monkeypox, the CDC state that, “in Africa, monkeypox has been shown to cause death in as many as 1 in 10 persons who contract the disease.” This 10% fatality rate has already stoked the fear narrative and was also used as the case fatality rate in the NTI’s monkeypox pipe dream. It should be noted that historically monkeypox has been virtually unheard of in first world countries and the rare cases are usually in people that have recently arrived from Africa.
Indeed, one of the only recorded “outbreaks” of monkeypox in the first world was in the United States in April 2003. Cases were declared in 6 states and said to be caused by rodents that were imported to Texas from Ghana. This was the first time monkeypox had been reported outside of Africa and the CDC published a paper in 2006 analysing the incident. The paper states that, “person-to-person spread of the virus is thought to occur principally via infectious oropharyngeal exudates” although it is clear that this has never been scientifically established. They continue to say that, “the virus is thought to have been transmitted from African animals” – in other words, it’s another species-jumping pathogen tale.
Blaming it on minority groups, when have we seen that before?
They reported that, “individuals who had illness onset within 21 days after exposure to MPXV [Monkeypox virus] who experienced fever (defined as a body temperature greater 37.4°C) and vesicular pustular rash or rash (potentially uncharacterized) plus orthopox IgM antibodies were classified as having probable cases of infection.” Now 37.4°C is not a fever in our book, it is a normal body temperature and we would suggest 37.6°C and above qualifies as a fever. We noted in their chart that they were using the classification ≥39.4°C, but this appears to be an error as in another paper, we’ll get to soon, it was once again 37.4°C. The second paper even said the “fever” could be subjective, so they appear to be using this loose criteria and pathologising a normal state. Additionally, the CDC’s weekly report from the 11th of July 2003, stated that from a total of 71 cases, only “two patients, both children, had serious clinical illness; both of these patients have recovered.” The remainder had a variety of respiratory and gastrointestinal symptoms.
The CDC’s cases were confirmed on the basis of specimens that showed: “monkeypox virus isolation, detection of monkeypox-specific nucleic acid signatures, positive electron-microscopy findings, or positive immunohistochemical findings”. We had a look at the electron micrographs presented by the CDC including the image shown below of a skin sample from one of the patients. The caption informs us that the round particles on the right are immature monkeypox virions, while the oval particles on the left are mature viruses. However, all they have is a static image of dead tissue and no conclusions can be made about the biological role of the imaged particles. None of them have been shown to be replication-competent disease-causing intracellular parasites and so should not be called ‘viruses’.
Looking at the CDC’s weekly report from 2003 again, it appears that the 35 “laboratory-confirmed cases” all involved polymerase chain reaction (PCR) “tests”, so we investigated the scientific evidence behind this claim. One of the citations for the development of PCR detection of monkeypox is a 2004 paper titled “Real-Time PCR System for Detection of Orthopoxviruses and Simultaneous Identification of Smallpox Virus”. Now a PCR protocol requires them to know the genetic sequences of the alleged monkeypox virus, which takes us to this 2001 paper titled, “Human monkeypox and smallpox viruses: genomic comparison”. The paper claimed to have “isolated” the monkeypox virus in a rhesus monkey kidney cell culture from a scab of a monkeypox patient. Here the virologists are up to their old tricks again by asserting that: (a) the patient’s scab contains the monkeypox virus, and (b) it is now in their culture brew. They claimed to have sequenced the “viral genome” by referring to a process described for sequencing an alleged variola virus in 1993.
But when we look at this paper there is no virus demonstrated either, simply an assertion that it was “isolated” from, “the material from a patient from India” in 1967. They go on to make the claim that, “the virions were purified by differential centrifugation and viral DNA was isolated” – however, there is no demonstration of what they purified or how they were determined to be virions. In none of these experiments did they perform any controls by seeing what sequences can be detected from other human-derived scabs or similar specimens from unwell individuals. This is where we need to remind the virologists of what a virus is supposed to be – that is a replication-competent intracellular parasite that infects and causes disease in a host. It is not detecting genetic sequences contained within scabs and claiming that it belongs to a virus.
So returning to the CDC’s paper describing the 2003 “outbreak”, it is unclear how they established they could be diagnosing anyone with monkeypox by using the PCR. Their PCR can only have been calibrated to sequences of unproven provenance. Additionally, it doesn’t matter what kind of analytical specificity their PCR protocol had, there was no established diagnostic specificity – in other words it was not a clinically-validated test, an issue that goes beyond whether the “virus” exists or not. (From the MIQE Guidelines: Analytical specificity refers to the qPCR assay detecting the appropriate target sequence rather than other, nonspecific targets also present in a sample. Diagnostic specificity is the percentage of individuals without a given condition whom the assay identifies as negative for that condition.)
The 47 US cases they ended up describing were all in some sort of contact with imported African prairie dogs and the CDC’s paper concludes that, “individuals contracted MPXV infections from infected prairie dogs; no human-to-human transmission was documented, but there were many different potential scenarios of infection involving respiratory and/or muco-cutaneous exposures, percutaneous and/or inoculation exposures”. Now there were some problems with the study design which they admitted to including that, “the analyses were limited by incomplete reporting or recall of information by patients. And, because of the retrospective nature of the study, we were unable to obtain highly detailed data”.
However, even allowing some wriggle room for them here, the inconsistencies go further still. Firstly, no one in the US incident died from the disease which is said to have a 10% fatality rate in Africa. No doubt, the inconsistent lethality rates will be attributed to different “variants”, but there can’t be variants of something that doesn’t exist.
There were few images available of the skin lesions that were reported in the 2003 incident but two of the US cases are depicted below and an image from a monkeypox case in Africa is shown for comparison. The reader can make up their own mind but those skin reactions do not look remotely comparable to us.
Next, the CDC claim that, “the natural reservoir of monkeypox remains unknown. However, African rodents and non-human primates (like monkeys) may harbor the virus and infect people” – in other words it’s all rather vague and remains an unproven hypothesis. Now, obviously some people became unwell in the US in 2003 but with the viral theory we are supposed to believe that it jumped from some prairie dogs to some humans and the latter became infected with the alleged virus…but then no human could pass it on to another human. The theory falls flat – a virus needs to spread, if it can’t spread, it’s dead and thus it’s not a virus. And the historical patterns of alleged monkeypox virus outbreaks make no sense – why did it pass to these people so easily and yet it can go a decade between alleged “outbreaks”?
Unfortunately, the 2003 incident was investigated as though the viral contagion theory had already been established and other explanations were ignored. If people were allegedly getting sick from these African rodents, wouldn’t it be a good idea to check the animals for other toxicities, particularly in their faeces and also for any ticks or parasites? We did note another reference state that with regards to the US cases, “many of the people had initial and satellite lesions on palms, soles, and extremities”. However, according to the CDC, monkeypox usually starts on the face so the clinical picture in the US cases was not consistent with cases that are typically described in Africa.
In any case, a review of the scientific evidence revealed that with regards to monkeypox: (a) there is no evidence of a physical particle that meets the definition of a virus, (b) there is no evidence of anything transmitting between humans, and (c) there is no way to confirm a diagnosis of monkeypox unless you believe in clinically-unvalidated tests such as the PCR kits that have been produced. In other words, if we see a monkeypox “pandemic” that is used as an excuse to role out more globalist terrorism, it will be on the back of another PCR pandemic, not one that has any basis in nature.
For those of you wanting to explore more problems with the various monkeypox claims, Mike Stone of ViroLIEgy has written a couple of interesting commentaries. The first article is, “Was Smallpox Really Eradicated?”, which among other things deals with the convenient emergence of monkeypox while smallpox was apparently being eradicated. The second article is, “Did William Heberden Distinguish Chickenpox From Smallpox in 1767?” This outlines the fact that the pox conditions are not as readily distinguishable from each other as the text books suggest and appear to relate more to the severity of a similar disease process. You can also watch our video, “Chickenpox Parties and Varicella Zoster Virus?” to see why there is no evidence of a virus in that related condition either.
From the perspective of terrain theory it is a fundamental mistake to attribute a person’s illness to a supposed virus, as the subsequent “treatments” don’t address the underlying issues. If someone is unwell, then they are usually deficient in nutrients and need to restore balance, or they have been exposed to environmental toxins and need to help the body detoxify. Wars against alleged pathogens that involve treating everyone the same way with civil rights restrictions and vaccines are certainly not about heath. It is good to see more people waking up to the COVID-19 fraud so there is hope that a monkeypox scamdemic, if attempted, will bring even more light to the situation. As always, your best health is in your own hands, not in the hands of a globalist cult and their cronies.
If you have been outsourcing your health, there has never been a better time to free yourself from the virus fear narrative and begin manifesting your full potential instead.
The doctors, scientists and journalists featured in THE VIRAL DELUSION examine in detail the scientific papers that were used to justify the pandemic, and what they find is shattering. In this shocking, five-part, seven hour documentary series, they explode every single major claim, from the “isolation” of the virus to its so-called genetic sequencing, from the discovery of how to “test” for SARS-CoV2 to the emergence of “variants” that in reality, they explain, exist only on a computer. Their point: that the so-called SARS-CoV2 virus exists only as a mental construct whose existence in the real world has been disproven by the science itself.
They then go back through history to reveal how the birth and growth of virology has led to massive misunderstanding and misdiagnosis of disease: from Smallpox to the Spanish Flu, Polio to AIDS, to COVID itself – putting the pandemic in a whole new context better understood not as settled science, but the tragic culmination of misunderstood biology by the growing cult of virology, built on pseudo-science, to which much of the rest of the medical profession defers without understanding or examination, and the tragic consequences that have been wrought in its name.
In 2019, the virologists took center stage, and for the first time on film, their methods, miscues and tragedy they have wrought are put under the spotlight, revealing the extraordinary leaps of fantasy buried in their methodology, the contradictions quietly acknowledged in their papers, their desperate effort to change language to justify their findings, the obvious incongruence of their conclusions and the extraordinary stakes for our entire society in whether we continue to blindly follow their lead into a full-scale war against nature itself.
Featuring: Andrew Kaufman, MD; Tom Cowan, MD; Stefan Lanka, Virologist; Torsten Engelbrecht, journalist; Claus Kohnlein, MD; Kevin Corbett, PhD RN; David Rasnick, Biochemist PhD; Mark Bailey, MD; Dawn Lester and David Parker, Authors; Stefano Scoglio, Biochemist PhD; Saeed Qureeshi, Chemist PhD; Celia Farber, Journalist; Harold Wallach, PhD; Pam Popper, PhD, ND; Charles Geshekter, PhD; Amandha Vollmer ND, Jim West, Author; Larry Palevsky MD; and more.
The Viral Delusion (2022) Episode 1:The Tragic Pseudoscience of SARS-CoV-2
When doctor Andrew Kaufman began reading the first virology papers out of Wuhan in December 2019, he was shocked to discover that the scientists had come nowhere close to proving that a new virus had emerged… yet saw the media and authorities already claiming a viral pandemic was on it’s way.
In this extraordinarily revealing opening episode, a group of biologists, chemists, doctors and journalists take apart the SARS-COV-2 narrative piece by piece — from the non-isolation of the virus, to the hidden problems with purported photographs of the virus, to the claims that it has been genetically sequenced, to the invalidity of the PCR “covid-test.”
From the treatment protocols for COVID to the assumption of its transmission, Episode One unpacks the science of the claims that changed the world – in which these doctors and scientists make the case that every single claim the authorities made about the so-called SARS-COV2 virus has been based not on evidence, but pseudoscience.
The Viral Delusion (2022) Episode 2: Monkey Business: Polio, Measles And How It All Began
How did it all begin?
How could the scientific establishment have possibly gotten so big a story so wrong?
Everyone knows the story of Polio…or do they?
What from that story is actual history and what is medical marketing?
How did a small branch of the scientific establishment come to convince the world polio was the result of a virus and not from environmental toxins?
Learn what the actual experiments were upon which this theory was based — and how shockingly unconvincing they are.
Discover too how the medical establishment’s efforts to squeeze the symptoms of polio into a virus model formed the very foundation of modern virology, and how that commercially successful model has steered modern science ever since, evidence be damned.
The Viral Delusion (2022) Episode 3: The Mask of Death – The Plague, Smallpox and The Spanish Flu
What about Smallpox?
The Spanish Flu?
The Black Plague?
Go back, back, back in time to examine the claims and counter-claims as to what truly caused these deadly epidemics.
Are the rats of Europe innocent? Turns out they have to be…
And in that discovery we see how the superstitions of our time have clouded the eyes of “science” to avoid the most obvious of insights about disease.
The Viral Delusion (2022) Episode 4: AIDS, The Deadly Deception
AIDS. It was the defining epidemic of a generation.
But it was also the coming of age for many leading scientists and doctors who came to realize that blaming the illnesses known as AIDS on a virus was not only unsupported by science, it was downright nonsensical.
What were the true causes of the many illnesses labelled AIDS around the world?
How many suffered from their misdiagnosis?
How the scientific establishment fell into the deadly AIDS delusion is crucial to understanding the pandemic, and health, today.
The Viral Delusion (2022) Episode 5: Sequencing The Virus, Without The Virus
With the rise of computing and genetic research in the 90’s the virologists go high-tech.
They move away from experiments altogether and into genetic modeling — but do the models have any connection to reality?
The wonders of genetic sequencing have been pointed to as the proof of virology’s explanatory power — but when the claimed sequencing of SARS-COV2 is put under the microscope, has the game changed from the realm of science, to science fiction?
What’s really going on the claim of genetically identifying the SARS-CoV-2 virus is made?
Monkeypox – it’s the hip new disease sweeping the globe. Allegedly appearing almost simultaneously in over a dozen different countries on four different continents.
As we wrote in the early days of the Covid “pandemic”, the only thing spreading faster than the disease is fear.
The media reported the first UK case of monkeypox on the 7th of May. Less than two weeks later, we’re seeing some very familiar headlines. Just like that…Pandemic 2: Monkey Pox!! begins playing at all your favorite fear porn outlets.
The BBC went real subtle with it, blaring: “Monkeypox: Doctors concerned over impact on sexual health”
The New Scientist has actually used the P-word, asking “Can Monkeypox become a new pandemic?”, before answering, essentially, “probably no, but also maybe yes!”. Keeping their options open.
Sciencewarns that“Monkeypox outbreak questions intensify as cases soar”
The Mirror has gone full paranoid already, headlining:
Russia looked into using monkeypox as biological weapon, claims ex soviet scientist
So that’s one direction the story might go.
To be clear, “monkeypox” (whatever that even means in this context), is NOT a Russian bio-weapon. It’s not a Western bio-weapon either. Or Chinese bio-weapon. It’s just another scare story. And a rushed, half-hearted one at that.
One of the signs that marked the Covid “pandemic” as a psy-op from an early stage was the sheer speed with which the hysteria spread. Far from learning from their mistakes, the powers-that-be have decided to go even faster this time.
Despite “cases” numbering barely in the dozens, the World Health Organization has called an emergency meeting, a strange thing to do when their annual Assembly starts literally tomorrow. But I guess when your launching a new product you need to do everything you can to get the hype going.
Despite just two “cases” in the entire United States (and indeed the fact they still don’t work), New York is bringing back mask recommendations.
Nobody has said “lockdown”…yet. But Hans Kluge, WHO regional director for Europe, is “concerned” that transmission could accelerate if people attend mass gatherings:
as we enter the summer season … with mass gatherings, festivals and parties, I am concerned that transmission could accelerate”.
(As inflation soars and the cost of living crisis only gets worse, it’s probably handy for them to have a new “public health” reason to ban protests or clampdown on civil unrest. Just a thought.)
There’s some good news though…for vaccine manufacturers, anyway. As Whitney Webb reports, two struggling pharmaceutical companies have already seen a big stock boost from the “outbreak”:
Regardless of how the monkeypox situation plays out, two companies are already cashing in. As concern over monkeypox has risen, so too have the shares of Emergent Biosolutions and SIGA Technologies. Both companies essentially have monopolies in the US market, and other markets as well, on smallpox vaccines and treatments. Their main smallpox-focused products are, conveniently, also used to protect against or treat monkeypox as well. As a result, the shares of Emergent Biosolutions climbed 12% on Thursday, while those of SIGA soared 17.1%.
Just as with Covid, and despite rumours they would be leaving the World Health Organization, Russia appears to be lining up with the WHO agenda. Already they are “tightening border quarantine” rules, vaccinating healthcare workers and supplying quick bedside tests internationally.
Looks like we might be in for an epic summer of scare-mongering, panic-buying & bucketloads of cringe.
Are the new jabs already prepped & ready to go?
Are the “our hospitals are overwhelmed videos” being filmed as we speak, complete with “monkey pox” moulage and crying nurses who turn out to have IMDB pages & multiple acting credits?
Are the sleepy masses going to be fooled yet again?
Children’s Health Defense seeks help from parents in 13 Texas counties, after a U.S. District Court on Tuesday granted CHD 45 days to amend its lawsuit against the U.S. Food and Drug Administration’s Emergency Use Authorization of COVID-19 vaccines for children ages 5 to 11.
A U.S. District Court on Tuesday gave Children’s Health Defense (CHD) 45 days to amend its lawsuit against the U.S. Food and Drug Administration’s (FDA) Emergency Use Authorization (EUA) of COVID-19 vaccines for children ages 5 to 11.
CHD’s lawsuit, filed Jan. 24 in the U.S. District Court for the Western District of Texas, alleges, among other things, that the FDA — under pretext of EUA powers — “authorized a dangerous drug for minor children as young as 5 years old to address COVID-19, which poses less risk to a 5-year-old than the ordinary flu.”
CHD last month filed a motion to stay asking the court to suspend the FDA’s authorization of the vaccine for young children pending judicial review of the lawsuit.
During Tuesday’s hearing Judge Alan Albright heard arguments on CHD’s motion to stay and also on the FDA’s motion to dismiss CHD’s lawsuit.
Judge Alan Albright denied CHD’s request to suspend authorization of the vaccines until the lawsuit is resolved, stating he was skeptical of CHD’s organizational standing and the standing of the two parents named in the suit, given the lack of any children’s COVID-19 vaccine mandate in the district at this time.
Judge Albright said for CHD to have standing, it must show “diversion of resources.”
For the parents named in the complaint — Deborah L. Else and Sacha Dietrich — to have standing, they must show their children are at demonstrable risk of vaccination against the parents’ wishes.
Attorney Robert Barnes, arguing for CHD, said if the FDA’s interpretation of standing were correct, then no one could sue the FDA because it would mean the FDA is completely insulated from judicial scrutiny.
Barnes also argued the harm to plaintiffs is not simply the threat of vaccination, but includes the FDA’s false assertions that the vaccines are safe, effective and actually vaccines, i.e. products that prevent infection and transmission.
U.S. Department of Justice attorney James Harlow, arguing on behalf of the FDA, said the agency cannot mandate products and that products authorized for emergency use clearly permit patients to accept or reject them.
Harlow also argued that Texas Gov. Greg Abbott issued an executive order prohibiting COVID-19 mandates at schools, thus undermining an argument for any threat.
After hearing arguments from both sides, Judge Albright said given the importance of the case, he wanted to give CHD and plaintiffs Else and Dietrich the opportunity to assert standing, and would give them 45 days to amend their lawsuit.
The judge also provided a roadmap for how to amend the case.
CHD is seeking help from the public in order to provide the court the necessary evidence to prove standing in its case against the FDA.
Parents in 13 counties in the Western District of Texas who have information about coercive COVID-19 vaccine policies for children or adolescents are asked to submit that information to chd@childrenshealthdefense.org with subject line “CHD v. FDA.”
The 13 counties are: Bell, Bosque, Coryell, Falls, Freestone, Hamilton, Hill, Leon, Limestone, McLennan, Milam, Robertson and Somervell.
CHD is especially interested in these types of situations occurring in the counties listed above:
Hospitals or medical facilities that require COVID-19 vaccination for treatment
Children in foster care, correctional settings or other institutional settings who are required to receive COVID-19 vaccinations
Vaccination clinics or vaccination stations in schools or youth facilities promoting COVID-19 vaccines for kids
Evidence of school pressure to vaccinate children even without an explicit mandate
After-school programs or extra-curricular activities requiring COVID-19 vaccines.
CHD in May 2021 filed a citizen petition with the FDA and the U.S. Department of Health and Human Services outlining the arguments against EUA and/or licensing of COVID-19 vaccines.
The FDA on Tuesday granted Pfizer’s request for EUA of a third COVID-19 shot for children ages 5 to 11, and the Centers for Disease Control and Prevention on Thursday signed off on the shots.
hey, let’s play a pandemic wargame and blame leopards!
NOW – German health minister Lauterbach at G7 meeting: "We will do a very realistic exercise in which a smallpox pandemic results from a leopard bite." pic.twitter.com/j0l9poJwxn
i was going to do a piece on it, but igor beat me to it and i really have nothing much to add apart from the idea that i doubt that it was paid or even coordinated.
it’s just another topic the media all grabbed onto because it might turn into something and it will sell a few papers in the meantime. they all have the same 4 sources, so it’s not like it’s hard to see how it propagates.
there is no need to suspect a conspiracy.
it’s just the emergent property of “scary thing sells papers!”
but even reuters, despite their alarmist “worst ever” and “WHO emergency meeting” headlines is calling this a nothingburger.
(this is a classic practice BTW. alarming headline that few will read past that is actually refuted/disarmed in the body of the piece if you actually read it. only scanning headline nearly always leaves one with a vastly inflated sense of crisis.)
i suspect this is more about clamoring attention, the WHO trying to look useful/needed while they try to push through their massive power grab and posing for the papers, and left leaning media seeking to distract from some other matters like this:
and this:
but as of now, apart from more of this aggravatingly consistent policy of maligning felines for the world’s woes, i suspect the odds are in our favor to ignore monkeypox and media alike.
and just remember, when the gang whose reckless ineptitude broke the world for 2 years and brought you this asks for more unaccountable, technocratic power,
“Here’s another fun fact. The entire medical cartel thrives on the insane proposition—launched
with fervor more than a hundred years ago—that people suffer from thousands of distinct
diseases, each of which is caused by a single germ, which must be treated by a toxic drug and
prevented by a toxic vaccine.
It is this great lie that that has killed millions upon millions upon millions of people.”
The headline of this article has become a battle cry among some “alternative journalists,” activists, lawyers, and doctors.
As my readers know, I’ve devoted considerable space, over the past two years, to presenting evidence that SARS-CoV-2 is a scientific fairy tale, a con, and the virus doesn’t exist.
So when I hear this battle cry, I’m motivated to mention a few significant points.
Let me start by countering the claim that debating the existence of the virus is wasting time.
Here’s a shocker. A person can do more than one thing at the same time. For example, he can expose/oppose the toxic vaccine. He can expose the murderous COVID treatments (ventilators, sedatives, antiviral drugs). He can expose using simple flu-like illness to create fraudulent COVID case numbers.
And he can ALSO expose the fact that the virus has never been isolated (discovered) or sequenced.
So highlighting the non-existence of the virus doesn’t rule out dealing with other vital concerns.
This may come as a surprise, but it’s even possible to go to court to challenge a vaccine mandate, while ALSO arguing elsewhere that the virus doesn’t exist. I know. Amazing, right?
Those alarmed by “the virus doesn’t exist” also say: making that statement leaves us open to being called whackos, and leaves us unable to convince people that all our other criticisms of the pandemic are true.
I would counter that in two ways. Millions of people already believe we’re whackos, even those of us who take a sacred blood oath that the virus is real.
And second, people going against the grain, when their vital issue is still in the budding stage, are always called nuts. Trust me, there was a time when criticizing vaccines made people look like total whackos in the eyes of the general public—and it took decades of fighting the consensus to bring that criticism into the open, where many people saw the truth about jabs.
Here’s another fun fact. The entire medical cartel thrives on the insane proposition—launched with fervor more than a hundred years ago—that people suffer from thousands of distinct diseases, each of which is caused by a single germ, which must be treated by a toxic drug and prevented by a toxic vaccine.
It is this great lie that that has killed millions upon millions upon millions of people.
Therefore, the very real question about the existence of viruses in general is more than a weird preoccupation.
Next, those who claim, “OF COURSE viruses exist,” don’t know what the hell they’re talking about. They’re merely PARROTING what they learned in school or what researchers baldly claim in studies.
“Well, all virologists can’t be wrong.”
Yes, Virginia, they can all be wrong. Just as vaccinologists can all be wrong about “the remarkable safety and efficacy of vaccines.”
Some of the OF COURSE VIRUSES EXIST people are new to the way blogs and videos work. They’ve never encountered commenters in any great numbers before. So when a few dozen committed people suddenly tell them they should examine their premises more carefully and consider what really goes on in virology labs, these OF COURSE people are annoyed and irritated. They don’t like being challenged on basic issues. They don’t like feeling that the floor might suddenly shift under their feet. So they turn on their arrogance machines.
So be it.
The issue isn’t going away. Nor should it.
Despite growing digital censorship, the internet is still the Wild West in certain respects. People are going to say THE VIRUS DOESN’T EXIST, and VIRUSES DON’T EXIST.
And foundations will shake.
Foundations of the medical cartel, and foundations underlying people’s cherished assumptions.
In any area of human life, there are conflicts between “this is strategy” and “this is the truth.” There always will be.
Trying to shortchange the truth or casually say the truth is a lie doesn’t work.
NO ONE who is reading this article has ever been in a virology lab and witnessed the step by step process of “discovering a new virus.” I find that stunning. And yet all sorts of people are quite ready to assert with great finality that they know all about isolating viruses.
If by chance, someone reading this article HAS actually been in a lab and “discovered a virus,” you can bet your bottom dollar he won’t let you or me in there with a full film crew and our outlier experts asking very pointed questions about each “scientific” move he makes, as he “isolates a virus.”
To which somebody might reply: “Well, I’ve never seen a car being made in a factory, but I drive one with full confidence.”
Yes, but when the “virus discovered in a lab” results in you or someone you love being dosed with a drug or vaccine that maims you or kills your family member, you damn well should want to get into “that factory where the car is made.”
But you can’t. They won’t let you…
…Despite the fact that, as I’ve documented many times, the US medical system kills, by a very conservative estimate, 225,000 people a year, or 2.25 million people per decade. [0]
Chew on THAT for a while.
Here is one of my articles on the subject of virus isolation:
The global medical community has been asserting that “a pandemic is being caused by a virus, SARS-Cov-2.”
But what if the virus doesn’t exist?
People have been asking me for a step-by-step analysis of a mainstream claim of virus-isolation. Well, here it is.
“Isolation” should mean the virus has been separated out from all surrounding material, so researchers can say, “Look, we have it. It exists.”
I took a typical passage from a published study, a “methods” section, in which researchers describe how they “isolated the virus.” I sent it to Dr. Andrew Kaufman [1], and he provided his analysis in detail.
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)” [2].
First, I want to provide a bit of background that will help the reader understand what is going on in the study.
The researchers are creating a soup in the lab. This soup contains a number of compounds. Human cells, monkey cells, antibiotics, other chemicals, random genetic material.
The researchers assume, without evidence, that “the virus” is in this soup, because they’re dropped a mucus sample from a patient in the soup. At no time do they separate the purported virus from the surrounding material in the soup. Isolation of the virus is not occurring.
They set about showing that the monkey (and/or human cells) they put in the soup are dying. This cell-death, they claim, is being caused by “the virus.” However, as you’ll see, Dr. Kaufman dismantles this claim.
There is no reason to infer that SARS-CoV-2 is in the soup at all, or that it is killing cells.
Finally, the researchers assert, with no proof or rational explanation, that they were able to discover the genetic sequence of “the virus.”
Here are the study’s statements claiming isolation, alternated with Dr. Kaufman’s analysis:
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO) [3]. Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
My comments: Dr. Kaufman does several things here. He shows that isolation, in any meaningful sense of the word “isolation,” is not occurring.
Dr. Kaufman also shows that the researchers want to use damage to the cells and cell-death as proof that “the virus” is in the soup they are creating. In other words, the researchers are assuming that if the cells are dying, it must be the virus that is doing the killing. But Dr. Kaufman shows there are obvious other reasons for cell damage and death that have nothing to do with a virus. Therefore, no proof exists that “the virus” is in the soup or exists at all.
And finally, Dr. Kaufman explains that the claim of genetic sequencing of “the virus” is absurd, because there is no proof that the virus is present. How do you sequence something when you haven’t shown it exists, and you don’t have an isolated specimen of it?
Readers who are unfamiliar with my work (over 375 articles on the subject of the “pandemic” during the past year [4]) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
I came across this Facebook post recently by Dr Tom Cowan. He is yet another qualified and intelligent voice of reason steadfastly and dedicatedly censored by the corporate media in an ongoing and increasingly desperate effort to prevent the People getting wise to things they don’t want you to know.
The truth of the matter is these highly qualified a voices of reason are growing in number and ubiquity at an accelerating rate and the enemies of Humanity are having dickens of a job keeping lid on the volcano.
The entire biochemical paradigm of the pharmaceutical-industrial complex that results in the systemic poisoning of Man, which itself is intended to render human beings tired, sick and introverted on their health – and thus neutralised as potential sources of trouble (ie liberty) -is now in jeopardy.
All we have to do is keep going, keep speaking out, keep right on advocating Reason and common sense and keep on bringing to the attention of the People the huge reservoir of wisdom and more workable paradigms that are being kept from them by those with a vested interest in prolonging the Dark Age 0f their barbarism.
In other words, simply REFUSE to shut up.
And the more we can unite and work together, the sooner the Dark Age will be over and the Age of Reason begun.
Dr Tom Cowan is a highly recommended voice of reason.
And here by way of a taster is his post from Facebook
As you can see from this blockbuster article published on Aug. 9, 2016, in the prestigious journal Nature, researchers conclusively demonstrated that whenever fetal calf serum is added to any cell culture (as is done in virtually all modern virology studies, including those used during the past two years), it is simply impossible to use the results of this culture to determine the RNA sequence of any new vîru$. As they demonstrate, fetal calf serum itself is a rich source of many types of RNA sequences. Once this is introduced into the cell culture, from then on, there is no way to determine the origin of the RNA that researchers find.
The significance of this study cannot be overstated and validates what we’ve been saying for many months. Virologists use cell cultures to prove the existence of a new vîru$ and its cytopathic effect. If the culture is contaminated, as this study demonstrates, any claims about a new vîru$ and its genetic makeup are meaningless.
1. Every thirty seconds vivisectors around the world kill another thousand animals. They use cats, dogs, puppies, kittens, horses, sheep, rats, mice, guinea pigs, rabbits, monkeys, baboons and any other creature you can think of.
2 .While waiting to be used in laboratory experiments, animals are kept in solitary confinement in small cages. Alone and frightened they can hear the screams of the other animals being used.
3. Some of the animals used in laboratory experiments are pets which have been kidnapped, taken off the streets and sold to the vivisectors.
4. Animals used in experiments are blinded, burned, shot, injected and dissected. They have their eyes sewn up or their limbs broken. Chemicals are injected into their brains and their screams of anguish are coldly recorded.
5. Three quarters of the experiments performed by vivisectors are done without any anaesthetic.
6. Most vivisectors have no medical or veterinary training.
7. Scientists claim that animals are not sentient creatures and are incapable of suffering mental or physical pain.
8. All animals respond differently to threats of any kind depending on their circumstances (diet, cage size, etc.). None of these factors is allowed for by vivisectors. By locking an animal up in a cage, experimenters have already invalidated their experiment because by altering the animal’s surroundings, the experimenter alters the animal’s susceptibility, its habits, its instincts and its capacity to heal itself. Since these variations are not controlled (cages and surroundings differ) experiments performed on animals kept in cages are of no scientific value.
9 Many of the diseases which kill or cripple human beings do not affect any other members of the animal kingdom. It is, therefore, impossible to use different species to test drug therapies for these illnesses.
10. Doctors wouldn’t test a drug intended for old people on children (or the other way round). So why test drugs intended for pregnant women on rats? No one would test a drug for premenstrual problems on small boys and yet that would make far more sense than testing such a drug on male rats.
11. Drug tests done on animals can produce dangerously unreliable and misleading information. Thalidomide safely passed tests on animals. Penicillin and aspirin both kill cats. When Alexander Fleming discovered penicillin growing on a culture dish in 1928, he tested the drug on rabbits and discarded it when it seemed useless. Later the drug was tested on a cat and a human patient at the same time. The cat died and the human being lived. If doctors had relied upon animal experiments to decide whether or not penicillin was of any value, the drug would have been discarded long ago. Penicillin even kills guinea pigs – the classic test animal for many drugs. Aspirin can be toxic to rats, mice, dogs, monkeys and guinea pigs as well as cats. Morphine sedates human beings but excites cats, goats and horses. Digitalis, one of the best established and most effective drugs for the treatment of heart disease, is so toxic to animals that if we had relied on animal tests it would have never been cleared for use by humans.
12. Vivisectors admit that most animal experiments are unreliable and produce results which are not relevant to human patients. But they don’t know which experiments are unreliable. Logically, that means that all animal experiments are useless. If you don’t know which experiments you can rely on, you can’t rely on any of them.
13. The very unreliability and unpredictably of animal experiments is what makes them commercially valuable. Drug companies test on animals so that they can say that they have tested their drugs before marketing them. If the tests show that the drugs do not cause serious disorders when given to animals the companies say: `There you are! We have tested our drug – and have proved it to be safe!’ If, on the other hand, tests show that a drug does cause serious problems when given to animals the companies say: `The animal experiments are, of course, unreliable and cannot be used to predict what will happen when the drug is given to humans. We have, however, tested our drug.’ Tests which show that a drug causes cancer or some other serious disease when given to animals are ignored on the grounds that animals are different to people. However, tests which show that a new drug doesn’t kill animals are used as evidence that the drug is safe for human consumption. If you try a drug on enough different animals you can usually end up with at least one set of results which suggest that a drug is safe. Scores of drugs which cause cancer or other serious health problems in animals are widely prescribed for human patients. (See www.vernoncoleman.com for the names of 50).
14. Four out of ten patients who take a prescribed drug which has been tested for safety on animals can expect to suffer severe or noticeable side effects.
15. Surveys show that most practising doctors are opposed to vivisection on scientific grounds.
Taken from The Wisdom of Animals by Donna Antoinette Coleman and Vernon Coleman. Available as a paperback and an eBook.
“I would love to be able to bring back our country into a great form of unity,” Trump said. “Without a major event where people pull together, that’s hard to do. But I would like to do it without that major event because usually that major event is not a good thing.” – Donald Trump, Jan 30th 2018
By April of 2020, within two years of Donald Trump’s prophetic message, millions of people had bowed the government’s request to “unite” by “social distancing,” under a “Live Exercise” revealed by Trump’s Secretary of State Mike Pompeo. About half of the world’s population agreed to some form of lockdown. More than 3.9 billion people in more than 90 countries had been asked or ordered to stay at home by their governments. And they did.
In unison, millions donned a ritual mask to protect themselves against an invisible enemy. The effect was dubbed virtue signaling – an attempt to show other people that you are a good person, by expressing opinions that will be acceptable to them, especially on social media. How did so many people fall into lock-step to give up their freedom when they had previously been openly skeptical of government ethics and policies?
Social Engineering
The earliest social experiments had been successful using the tried-and true strategy of The Hegelian Dialectic: Problem • Reaction • Solution. Introduce a Problem and roll out the Solution! Past experiments included “The New Deal” under Franklin Roosevelt in the 1930s, and “Great Society” under Lyndon Johnson in the 1960s. Then came the “financially sound” government programs of Social Security, Medicare, and Medicaid.
Money and politics aside, why trust a government’s blanket medical solution when it comes to health, a personal responsibility?
If we understand the mechanism and motives of the group mind, it is now possible to control and regiment the masses according to our will without them knowing it. – Edward Bernays
After three years of government-induced COVID, there is still no approved government Solution to the COVID Problem because the FDA-approved vaccine is still not officially available to anyone, and may never be. Nonetheless, the Live Exercise of testing, tracking, experimentation, and restrictions, continues unabated.
While vaccine makers, such as Pfizer, insisted they need 75 years of data before releasing results to the public, the “adverse events” of the public subjects are being tracked and published in medical journals, even if not widely reported.
In any true experiment, there are two groups: the cases and the controls. All subjects who consented, received vaccine lots coded by color and number. Did they receive a vaccine with a Red cap or blue cap? Did they receive saline solution or the COVID spike protein? Did they go from a “fully vaccinated” to “double boosted? Did they opt out?
Let The Experiment Continue!
They say a picture is worth a thousand words, even if the subject matter, a spike protein, has never been officially isolated, or seen with the naked eye. As of this writing, there is no proof the cause of COVID exists.
Since no quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted… — CDC 2109 document
Even without proof, millions of people eagerly jumped aboard The Spike Protein Train to protect themselves with a mask, based on an image of a virus they believed in.
Then, by design, came the vaccines. A vaccine has always been the response to a government-declared pandemic. Recall the 1976 Swine Flu and the 1918 Spanish Flu? [See The Making of a Pandemic for more information]. Vaccine deployment is followed by the damage reports.
In any Live Exercise or Experiment, scientists cannot be expected to have any answers now, or possibly ever. Meanwhile, new symptoms to experimental mRNA vaccines create new, “rare” medical diagnoses. A quick search of Pubmed quickly shows that symptoms are the opposite of rare.
With the introduction of vaccines came the subsequent introduction of Vaccine Inflammatory Syndromes. From Autoimmune Inflammatory Syndrome Induced by Adjuvants,(ASIA), to Post Vaccination Inflammatory Syndrome (PVIS), and Multisystem Inflammatory Syndrome (MIS), all related acronyms describe one cause: Vaccine toxicity.
Since the deployment of COVID injections, the new COVID is Long COVID, ranging from back pain to sleep and digestive disorders, that go beyond 6 months. Symptoms also include postural tachycardia syndrome or POTS.
POTS affects the autonomic nervous system, or the parasympathetic nervous system that regulates voluntary and involuntary actions, as well as thinking, communication, and memory. These symptoms have been long studied as conditions of vaccine injury. Therefore, the injected spike proteins that bring on autoimmune-mediated endothelial injuries can also lead to POTS, especially in the lungs, as evidenced by this study in Clin Auton Res.
Simply go to the VAERS database to search and download the data collected from vaccine-induced injuries the government lists on its own website. VAERS data released by the CDC included a total of 7oo,ooo adverse event reports from all age groups following COVID vaccines, including 15,386 deaths between December 14, 2020, and September 17, 2021. Vaccine-injured patients become lifelong customers of pharmaceutical treatments, with doctors and scientists knowing that many will never return to their normal lifestyles.
All patients were treated with non-pharmacologic therapies, and most required pharmacologic therapies. Six to 8 months after COVID-19, 17 (85%) patients had residual autonomic symptoms, with 12 (60%) unable to return to work.
Published mRNA Vaccine Toxicity Studies: Dizziness
Whether by case study, small study, epidemiological study, or case-control study, all studies are ongoing and accumulating. Searching Pubmed by “dizziness or vertigo” and “COVID vaccine” and find dozens of studies. Here are a few:
Among all the symptoms reported, localized pain, generalized weakness, headache, myalgia, chills, fever, nausea, joint pains, sweating, localized swelling at the injection site, dizziness, itching, rash, decreased appetite, muscle spasm, decreased sleep quality, and brain fogging were the most commonly reported symptoms (in descending order of occurrence). Most of the symptoms reported were nonlife threatening.
Vestibular neuritis (VN) is an acute vestibular syndrome that causes acute and spontaneous vertigo due to unilateral vestibular deafferentiation, leading to nausea or vomiting and unsteadiness that can last from days to weeks. Reactivation of latent type 1 herpes simplex virus, autoimmune disorders, and microvascular ischemia are hypothesized to be etiologies.
We reported for the first time a case of neuromyelitis optica spectrum disorder (NMOSD) that developed after the first dose of inactivated virus vaccine for COVID-19. The patient developed mild fever, vomiting, diarrhea, and cough after receiving the first dose of inactivated virus vaccine. Two months later, she experienced dizziness and unsteady walking. MRI scanning of the brain revealed lesions in area postrema and bilateral hypothalamus, typical for NMOSD. Serum antibodies for AQP4, ANA, SSA, SSB, Ro-52, and p-ANCA were positive. The patient was diagnosed as AQP4-positive NMOSD with coexisting systemic autoimmunity.
The most frequently reported adverse events were headache, myalgia, and dizziness. Of the 835 reported deaths after COVID-19 vaccination, 2 vaccine-related deaths were confirmed.
A 67-year-old man who was medicated for hypertension and diabetes was admitted complaining of fever, maculopapular rash, diarrhea, headache, chills, and dizziness 6 days after the first vaccination of ChAdOx1 nCoV-19 in Korea. The COVID-19 test was negative but with low blood pressure, leukocytosis, skin rash, pulmonary edema, and increased inflammation markers. His lab findings and clinical course were consistent with those of MIS after COVID-19 vaccination.
The 9 patients had an evoked nystagmus pathognomonic for benign paroxysmal positional vertigo; in the remaining 17 cases, peripheral vestibular dysfunction could be excluded and central disorder may be suggested. Due to the prevalence of nystagmus of non-peripheral origin, a central nervous system involvement could not be excluded.
38% mild side effects were observed from vaccination. Following were the general side-effects: myalgia (18.2%), the feeling of sickness (16%), fever (15.6%), dizziness (7.8%), joint pain (7.4%), chills (4.8%), and flu (4.8%). Following were the common neurological side-effects reported: headache (18.2%), fatigue (16.5%), muscle pain (16%), numbness/tingling (3%), and migraine (2.6%). Nausea and diarrhoea were reported in only 3.5% of respondents.
The three most frequent AEFI recorded were vagal response (30%), anxiety reaction (24%) and dizziness (21%). AEFI were more frequently observed among women [aOR= 2.24 (95%CI= 2.00 – 2.50)], and those with at least one previous disease [aOR= 1.47 (95%CI= 1.22-1.76)].
The most common AEFI was pain/tenderness at the injection site experienced by 59.3% of those who experienced any AEFI followed by headache/dizziness (35.3%), itching/rashes at the injection site (8.1%), nausea/vomiting (5.8%) and fever/chills (4.7%).
The patient was a health care worker, aged 34-year old. Past medical history was unremarkable and had not used heparin. Over the next couple of days after the vaccination, he reported headache, nausea, and dizziness as well as abdominal pain. His general status and the laboratories studies deteriorate quickly by increasing liver enzymes and severe coagulopathy. Clinically he had presented acute hepatic failure. He had been received blood products, prednisolone pulse along with broad antibiotics without benefit. He died on the sixth day.
Herein, we describe a 48 years old man presenting with rapidly progressive cognitive decline and hyponatremia diagnosed with anti LGI1 AE, occurring shortly after the second dose of mRNA COVID -19 vaccine and possibly representing a severe adverse event related to the vaccination.
Are we living out a medical experiment or social/behavioral experiment?
Has the world been Trumped?
The government forever claims that people must plan for rising healthcare costs. In 2019, U.S. medical health spending increased by 4.6% to $3.8 trillion or $11,582 per person. If the U.S. medical system is the best in the world then shouldn’t the numbers be doing down?
Whether the crisis is called The Opioid Epidemic or The COVID Pandemic, it is a Crisis of Humanity. The conclusion is always the same when the requirement for more dollars and more research takes precedence over individual healing and freedom from government tyranny:
An estimated 21 million American adults experienced at least one major depressive episode in 2020. The highest rates reported for the past several years have consistently been among those aged between 18 and 25
The vast majority are prescribed antidepressant drugs, despite the fact there’s virtually no evidence to suggest they provide meaningful help, and plenty of evidence showing the harms are greater than patients are being told
Hundreds of thousands of toddlers are also being medicated with powerful psychiatric drugs, raising serious ethical questions, along with questions about the future mental and physical health of these children
There’s no scientific evidence to suggest depression is the result of a chemical imbalance in your brain. A lot of the evidence suggests unhealthy living conditions are at the heart of the problem
Antidepressants are not beneficial in the long term and antipsychotic drugs worsen outcomes over the long term in those diagnosed with psychotic disorders such as schizophrenia
This article was previously published September 19, 2019, and has been updated with new information.
In the U.S., an estimated 21 million American adults experienced at least one major depressive episode in 2020.1 The reported numbers for the past several years2 have consistently been highest among those aged between 18 and 25.3 However, not only is there evidence that depression is vastly overdiagnosed, but there’s also evidence showing it’s routinely mistreated.
With regard to overdiagnosis, it’s been ongoing for a long time, with one 2013 study4 finding only 38.4% of participants with clinician-identified depression actually met the DSM-4 criteria for a major depressive episode, and only 14.3% of seniors 65 and older met the criteria.
As for treatment, the vast majority are prescribed antidepressant drugs, despite the fact there’s little to no evidence to suggest they provide meaningful help, and plenty of evidence showing the harms are greater than patients are being told.
According to a 2017 study,5 1 in 6 Americans between the ages of 18 and 85 were on psychiatric drugs, most of them antidepressants, and 84.3% reported long-term use (three years or more). Out of 242 million U.S. adults, 12% were found to have filled one or more prescriptions for an antidepressant, specifically, in 2013. By 2021 in the midst of the pandemic, 1 in 4 Americans over age 18, or 50 million persons, were on prescription mental health drugs.6
According to data7 presented by a watchdog group in 2014, hundreds of thousands of toddlers are also being medicated with powerful psychiatric drugs, raising serious ethical questions, along with questions about the future mental and physical health of these children.
And, a study published in The BMJ in 20138 found that “In utero exposure to both SSRIs and non-selective monoamine reuptake inhibitors (tricyclic antidepressants) was associated with an increased risk of autism spectrum disorders, particularly without intellectual disability” in the offspring.
Studies are also shedding much needed light on the addictive nature of many antidepressants, and demonstrate that the benefits of these drugs have been overblown while their side effects — including suicidal ideation — and have been downplayed and ignored for decades, placing patients at unnecessary risk.
The Chemical Imbalance Myth
One researcher responsible for raising awareness about these important mental health issues is professor Peter C. Gøtzsche, a Danish physician-researcher and outspoken critic of the drug industry (as his book, “Deadly Medicines and Organized Crime: How Big Pharma Has Corrupted Healthcare,”9 suggests).
Gøtzsche helped found the Cochrane Collaboration in 1993 and later launched the Nordic Cochrane Centre. In 2018, he was expelled by the Cochrane governing board following the publication of a scathing critique of a Cochrane review of the HPV in which he and his coauthors pointed out several methodological flaws and conflicts of interest.
Over the past several years, Gøtzsche has published a number of scientific papers on antidepressants and media articles and a book discussing the findings. In a June 28, 2019 article,10 Gøtzsche addresses “the harmful myth” about chemical imbalances — a debunked hypothesis that continues to drive the use of antidepressants to this day. He writes, in part:11
“Psychiatrists routinely tell their patients that they are ill because they have a chemical imbalance in the brain and they will receive a drug that fixes this …
Last summer, one of my researchers and I collected information about depression from 39 popular websites in 10 countries, and we found that 29 (74%) websites attributed depression to a chemical imbalance or claimed that antidepressants could fix or correct that imbalance …
It has never been possible to show that common mental disorders start with a chemical imbalance in the brain. The studies that have claimed this are all unreliable.12
A difference in dopamine levels, for example, between patients with schizophrenia and healthy people cannot tell us anything about what started the psychosis … [I]f a lion attacks us, we get terribly frightened and produce stress hormones, but this does not prove that it was the stress hormones that made us scared.
People with psychoses have often suffered traumatic experiences in the past, so we should see these traumas as contributing causal factors and not reduce suffering to some biochemical imbalance that, if it exists at all, is more likely to be the result of the psychosis rather than its cause.13
The myth about chemical imbalance is very harmful. It makes people believe there is something seriously wrong with them, and sometimes they are even told that it is hereditary.
The result of this is that patients continue to take harmful drugs, year after year, perhaps even for the entirety of their lives. They fear what would happen if they stopped, particularly when the psychiatrists have told them that their situation is like patients with diabetes needing insulin.”
Real Cause of Depression Is Typically Ignored
According to Gøtzsche, there is no known mental health issue that is caused by an imbalance of brain chemicals. In many cases, the true cause is unknown, but “very often, it is a response to unhealthy living conditions,” he writes.14
He also cites the book,15 “Anxiety — The Inside Story: How Biological Psychiatry Got It Wrong,” written by Dr. Niall McLaren, in which the author shows that anxiety is a major factor in and trigger of most psychiatric disorders.
“A psychiatrist I respect highly, who only uses psychiatric drugs in rare cases … has said that most people are depressed because they live depressing lives,” Gøtzsche writes.
“No drug can help them live better lives. It has never been shown in placebo-controlled trials that a psychiatric drug can improve people’s lives — e.g., help them return to work, improve their social relationships or performance at school, or prevent crime and delinquency. The drugs worsen people’s lives, at least in the long run.16“
Gøtzsche rightfully points out that antipsychotic drugs create chemical imbalances; they don’t fix them. As a group, they’re also somewhat misnamed, as they do not address psychotic states. Rather, they are tranquilizers, rendering the patient passive. However, calming the patient down does not actually help them heal the underlying trauma that, in many cases, is what triggered the psychosis in the first place.
As noted in one 2012 meta-analysis17 of studies looking at childhood trauma — including sexual abuse, physical abuse, emotional/psychological abuse, neglect, parental death and bullying — and subsequent risk of psychosis:
“There were significant associations between adversity and psychosis across all research designs … Patients with psychosis were 2.72 times more likely to have been exposed to childhood adversity than controls … The estimated population attributable risk was 33% (16%-47%). These findings indicate that childhood adversity is strongly associated with increased risk for psychosis.”
Economy of Influence in Psychiatry
A related article,18 written by investigative journalist Robert Whitaker in 2017, addresses the “economy of influence” driving the use of antidepressant drugs in psychiatric treatment — and the “social injury” that results. As noted by Whitaker, mental disorders were initially categorized according to a disease model in 1980 by the American Psychiatric Association.
“We’re all familiar with the second ‘economy of influence’ that has exerted a corrupting influence on psychiatry — pharmaceutical money — but I believe the guild influence is really the bigger problem,” he writes.
Whitaker details the corruption within the APA in his book “Psychiatry Under the Influence,” one facet of which is “the false story told to the public about drugs that fixed chemical imbalances in the brain.” Other forms of corrupt behavior include:
The biased designs of clinical trials to achieve a predetermined result
Spinning results to support preconceived conclusions
Hiding poor long-term outcomes
Expanding diagnostic categories for the purpose of commercial gain
Creating clinical trial guidelines that promote drug use
In his article, Whitaker goes on to dissect a 2017 review19 published in the American Journal of Psychiatry, which Whitaker claims “defends the profession’s current protocols for prescribing antipsychotics, which includes their regular long-term use.”
As Whitaker points out, there’s ample evidence showing antipsychotic drugs worsen outcomes over the long term in those diagnosed with psychotic disorders such as schizophrenia.
The review in question, led by American psychiatrist Dr. Jeffrey A. Lieberman, was aimed at answering persistent questions raised by the mounting of such evidence. Alas, their conclusions dismissed concerns that the current drug paradigm might be doing more harm than good.
“In a subsequent press release and a video for a Medscape commentary, Lieberman has touted it as proving that antipsychotics provide a great benefit, psychiatry’s protocols are just fine, and that the critics are ‘nefarious’ individuals intent on doing harm,” Whitaker writes.20
The Scientific Bias of Psychiatric Treatment
Five of the eight researchers listed on the review have financial ties to drug companies, three are speakers for multiple drug companies and all eight are psychiatrists, “and thus there is a ‘guild’ interest present in this review, given that they are investigating whether one of their treatments is harmful over the long-term,” Whitaker notes.21
Not surprisingly, the review ignored studies showing negative effects, including studies showing antipsychotics have a detrimental effect on brain volume. What’s more, while withdrawal studies support the use of antipsychotics as maintenance therapy over the long term, these studies do not address how the drugs affect patients’ long-term health.
“They simply reveal that once a person has stabilized on the medication, going abruptly off the drug is likely to lead to relapse,” Whitaker writes.22“The focus on long-term outcomes, at least as presented by critics, provides evidence that psychiatry should adopt a selective-use protocol.
If first-episode patients are not immediately put on antipsychotics, there is a significant percentage that will recover, and this ‘spontaneous recovery’ puts them onto a good long-term course. As for patients treated with the medications, the goal would be to minimize long-term use, as there is evidence that antipsychotics, on the whole, worsen long-term outcomes.”
Vast Majority of Psychotic Patients Are Harmed, Not Helped
In his deconstruction of Lieberman’s review, Whitaker details how biased thinking influenced the review’s conclusions. It’s a rather long article, but well worth reading through if you want to understand how a scientific review can be skewed to accord with a preconceived view.
Details I want to highlight, however, include findings relating to the number needed to treat (NNT) and the percentage of patients harmed by the routine use of antipsychotic drugs as a first-line treatment.
As noted by Whitaker, while placebo-controlled studies reveal the effectiveness of a drug compared to an inert substance, they do not effectively reveal the ratio of benefit versus harm among the patient population. NNT refers to the number of patients that have to take the drug in order to get one positive response.
A meta-analysis cited in Lieberman’s review had an NNT of 6, meaning that six patients must take the drug in order for one to benefit from the treatment. The remaining five patients — 83% — are potentially harmed by the treatment. As noted by Whitaker:23
“The point … is this: reviewers seeking to promote their drug treatment as effective will look solely at whether it produces a superior response to placebo. This leads to a one-size-fits-all protocol.
Reviewers that want to assess the benefit-harm effect of the treatment on all patients will look at NNT numbers. In this instance, the NNT calculations argue for selective use of the drugs …”
Antidepressants Are Not Beneficial in the Long Term
While typically not as destructive as antipsychotics, antidepressants also leave a trail of destruction in their wake. A systematic review24 by Gøtzsche published in 2019 found studies assessing harm from selective serotonin reuptake inhibitors (SSRIs) fail to provide a clear and accurate picture of the harms, and therefore “cannot be used to investigate persistent harms of antidepressants.”
In this review, Gøtzsche and colleagues sought to assess “harms of SSRIs … that persist after end of drug intake.” The primary outcomes included mortality, functional outcomes, quality of life and core psychiatric events. In all, 22 papers on 12 SSRI trials were included. Gøtzsche found several distinct problems with these trials. For starters, only two of the 12 trials had a drop-out rate below 20%.
Gøtzsche and his team also note that “Outcome reporting was less thorough during follow-up than for the intervention period and only two trials maintained the blind during follow-up.” Importantly, though, all of the 22 papers came to the conclusion that “the drugs were not beneficial in the long term.”
Another important finding was that all trials either “reported harms outcomes selectively or did not report any,” and “Only two trials reported on any of our primary outcomes (school attendance and number of heavy drinking days).”
A few years later, in April 2022, a study using data from the United States’ Medical Expenditures Panel Survey for patients who had depression found, “The real-world effect of using antidepressant medications does not continue to improve patients” health-related quality of life (HRQoL) over time.25
Antidepressants Are More Addictive Than Admitted
In a June 4, 2019, article,26 “The Depression Pill Epidemic,” Gøtzsche writes that antidepressant drugs:
“… do not have relevant effects on depression; they increase the risk of suicide and violence; and they make it more difficult for patients to live normal lives.27 They should therefore be avoided.
We have been fooled by the drug industry, corrupt doctors on industry payroll, and by our drug regulators.28 Surely, many patients and doctors believe the pills are helpful, but they cannot know this, because people tend to become much better with time even if they are not treated.29
This is why we need placebo-controlled trials to find out what the drugs do to people. Unfortunately, virtually all trials are flawed, exaggerate the benefits of the drugs, and underestimate their harms.”30
Addictive Nature of Antidepressants Skews Results
In his article,31 Gøtzsche reviews several of the strategies used in antidepressant drug trials to exaggerate benefits and underestimate the harms. One little-known truth that helps skew study results in the drug’s favor is the fact that antidepressants tend to be far more addictive than officially admitted. He explains how this conveniently hides the skewing of results as follows:32
“Virtually all patients in the trials are already on a drug similar to the one being tested against placebo. Therefore, as the drugs are addictive, some of the patients will get abstinence symptoms … when randomized to placebo …
These abstinence symptoms are very similar to those patients experience when they try to stop benzodiazepines. It is no wonder that new drugs outperform the placebo in patients who have experienced harm as a result of cold turkey effects.
To find out how long patients need to continue taking drugs, so-called maintenance (withdrawal) studies have been carried out, but such studies also are compromised by cold turkey effects. Leading psychiatrists don’t understand this, or they pretend they don’t.
Most interpret the maintenance studies of depression pills to mean that these drugs are very effective at preventing new episodes of depression and that patients should therefore continue taking the drugs for years or even for life.”
Scientific Literature Supports Reality of User Complaints
Over the years, several studies on the dependence and withdrawal reactions associated with SSRIs and other psychiatric drugs have been published, including the following:
•In a 2011 paper33 in the journal Addiction, Gøtzsche and his team looked at the difference between dependence and withdrawal reactions by comparing benzodiazepines and SSRIs. Benzodiazepines are known to cause dependence, while SSRIs are said to not be addictive.
Despite such claims, Gøtzsche’s team found that “discontinuation symptoms were described with similar terms for benzodiazepines and SSRIs and were very similar for 37 of 42 identified symptoms described as withdrawal reactions,” which led them to conclude that:
“Withdrawal reactions to selective serotonin re‐uptake inhibitors appear to be similar to those for benzodiazepines; referring to these reactions as part of a dependence syndrome in the case of benzodiazepines, but not selective serotonin re‐uptake inhibitors, does not seem rational.”
•Two years later, in 2013, Gøtzsche’s team published a paper34 in the International Journal of Risk & Safety in Medicine, in which they analyzed “communications from drug agencies about benzodiazepine and SSRI withdrawal reactions over time.”
By searching the websites of drug agencies in Europe, the U.S., U.K. and Denmark, they found that it took years before drug regulators finally acknowledged the reality of benzodiazepine dependence and SSRI withdrawal reactions and began informing prescribers and patients about these risks.
A significant part of the problem, they found, is that drug agencies rely on spontaneous reporting of adverse effects, which “leads to underestimation and delayed information about the problems.”
In conclusion, they state that “Given the experience with the benzodiazepines, we believe the regulatory bodies should have required studies from the manufacturers that could have elucidated the dependence potential of the SSRIs before marketing authorization was granted.”
•A 2019 paper35 in the Epidemiology and Psychiatric Sciences journal notes “It took almost two decades after the SSRIs entered the market for the first systematic review to be published.” It also points out that reviews claiming withdrawal effects to be mild, brief in duration and rare “was at odds with the sparse but growing evidence base.”
In reality, “What the scientific literature reveals is in close agreement with the thousands of service user testimonies available online in large forums. It suggests that withdrawal reactions are quite common, that they may last from a few weeks to several months or even longer, and that they are often severe.”
Antidepressants Increase Your Risk of Suicide and Violence
In his June 2019 article,36 Gøtzsche also stresses the fact that antidepressants can be lethal. In one of his studies,37 published in 2016, he found antidepressants “double the occurrence of events that can lead to suicide and violence in healthy adult volunteers.”
Other research38 has shown they “increase aggression in children and adolescents by a factor of 2 to 3 — an important finding considering the many school shootings where the killers were on depression pills,” Gøtzsche writes.
In middle-aged women with stress urinary incontinence, the selective serotonin and norepinephrine reuptake inhibitor (SNRI) duloxetine, which is also used to treat incontinence, has been shown to double the risk of a psychotic episode and increase the risk of violence and suicide four to five times,39 leading the authors to conclude that harms outweighed the benefits.
“I have described the dirty tricks and scientific dishonesty involved when drug companies and leading psychiatrists try convincing us that these drugs protect against suicide and other forms of violence,”40 Gøtzsche writes.41“Even the FDA was forced to give in when it admitted in 2007, at least indirectly, that depression pills can cause suicide and madness at any age.
There is no doubt that the massive use of depression pills is harmful. In all countries where this relationship has been examined, the sharp rise in disability pensions due to psychiatric disorders has coincided with the rise of psychiatric drug usage, and depression pills are those which are used the most by far. This is not what one would expect if the drugs were helpful.”
Drugmaker Lied About Paxil’s Suicide Risk
In 2017, Wendy Dolin was awarded $3 million by a jury in a lawsuit against GlaxoSmithKline, the maker of Paxil. Dolin’s husband committed suicide six days after taking his first dose of a Paxil generic, and evidence brought forth in the case convincingly showed his suicide was the result of the drug, not emotional stress or mental illness.42
The legal team behind that victory, Baum Hedlund Aristei Goldman, also represented other victims of Paxil-induced violence and death. At the time, attorney R. Brent Wisner said:43
“The Dolin verdict sent a clear message to GSK and other drug manufacturers that hiding data and manipulating science will not be tolerated … If you create a drug and know that it poses serious risks, regardless of whether consumers use the brand name or generic version of that drug, you have a duty to warn.”
GSK’s own clinical placebo-controlled trials actually revealed subjects on Paxil had nearly nine times the risk of attempting or committing suicide than the placebo group. To gain drug approval, GSK misrepresented this shocking data, falsely reporting a higher number of suicide attempts in the placebo group and deleting some of the suicide attempts in the drug group.
An internal GSK analysis of its suicide data also showed that “patients taking Paxil were nearly seven times more likely to attempt suicide than those on placebo,” Baum Hedlund Aristei Goldman reports, adding:44
“Jurors in the Dolin trial also heard from psychiatrist David Healy, one of the world’s foremost experts on Paxil and drugs in its class … Healy told the jurors that Paxil and drugs like it can create in some people a state of extreme ’emotional turmoil’ and intense inner restlessness known as akathisia …
‘People have described it like a state worse than death. Death will be a blessed relief. I want to jump out of my skin,’ Dr. Healy said. Healthy volunteer studies have found that akathisia can happen even to people with no psychiatric condition who take the drug …
Another Paxil side effect known to increase the risk of suicide is emotional blunting … apathy or emotional indifference … [E]motional blunting, combined with akathisia, can lead to a mental state in which an individual has thoughts of harming themselves or others, but is ‘numbed’ to the consequences of their actions. Drugs in the Paxil class can also cause someone to ‘go psychotic, become delirious,’ Dr. Healy explained.”
Hundreds of Thousands of Toddlers on Psychiatric Drugs
Considering the many serious psychological and physical risks associated with psychiatric drugs, it’s shocking to learn that hundreds of thousands of American toddlers are on them. In 2014, the Citizens Commission on Human Rights, a mental health watchdog group, highlighted data showing that in 2013:45
274,000 babies aged 1 and younger were given psychiatric drugs — Of these, 249,699 were on anti-anxiety meds like Xanax; 26,406 were on antidepressants such as Prozac or Paxil, 1,422 were on ADHD drugs such as Ritalin and Adderall, and 654 were on antipsychotics such as Risperdal and Zyprexa
In the toddler category (2- to 3-year-olds), 318,997 were on anti-anxiety drugs, 46,102 were on antidepressants, 10,000 were prescribed ADHD drugs and 3,760 were on antipsychotics
Among children aged 5 and younger, 1,080,168 were on psychiatric drugs
These are shocking figures that challenge logic. How and why are so many children, babies even, on addictive and dangerously mind-altering medications? Considering these statistics are 6 years old, chances are they’re even higher today. Just what will happen to all of these youngsters as they grow up? As mentioned in the article:46
“When it comes to the psychiatric drugs used to treat ADHD, these are referred to as ‘kiddie cocaine’ for a reason. Ritalin (methylphenidate), Adderall (amphetamine) and Concerta are all considered by the federal government as Schedule II drugs — the most addictive.
ADHD drugs also have serious side effects such as agitation, mania, aggressive or hostile behavior, seizures, hallucinations, and even sudden death, according to the National Institutes of Health …
As far as antipsychotics, antianxiety drugs and antidepressants, the FDA and international drug regulatory agencies cite side effects including, but not limited to, psychosis, mania, suicidal ideation, heart attack, stroke, diabetes, and even sudden death.”
Children Increasingly Prescribed Psych Drugs Off-Label
Making matters even worse, recent research shows the number of children being prescribed medication off-label is also on the rise. An example offered by StudyFinds.org,47 which reported the findings, is “a doctor recommending antidepressant medication for ADHD symptoms.”
The study,48 published in the journal Pediatrics, looked at trends in off-label drug prescriptions made for children under the age of 18 by office-based physicians between 2006 and 2015. Findings revealed:
“Physicians ordered ≥1 off-label systemic drug at 18.5% of visits, usually (74.6%) because of unapproved conditions. Off-label ordering was most common proportionally in neonates (83%) and in absolute terms among adolescents (322 orders out of 1000 visits).
Off-label ordering was associated with female sex, subspecialists, polypharmacy, and chronic conditions. Rates and reasons for off-label orders varied considerably by age. Relative and absolute rates of off-label orders rose over time. Among common classes, off-label orders for antihistamines and several psychotropics increased over time …
US office-based physicians have ordered systemic drugs off label for children at increasing rates, most often for unapproved conditions, despite recent efforts to increase evidence and drug approvals for children.”
The researchers were taken aback by the findings, and expressed serious concern over this trend. While legal, many of the drugs prescribed off-label have not been properly tested to ensure safety and efficacy for young children and adolescents.
As noted by senior author Daniel Horton, assistant professor of pediatrics and pediatric rheumatologist at Rutgers Robert Wood Johnson Medical School, “We don’t always understand how off-label medications will affect children, who don’t always respond to medications as adults do. They may not respond as desired to these drugs and could experience harmful effects.”
In 2020 mental health experts and reviewers were still at-odds over prescribing these drugs for children, yet hesitant to call a stop to it:49
“Antidepressants are prescribed for the treatment of a number of psychiatric disorders in children and adolescents, however there is still controversy about whether they should be used in this population …
Treatment decisions should be tailored to patients on an individual basis, so we recommend clinicians, patients and policy makers to refer to the evidence provided in the present meta-review and make decisions about the use of antidepressants in children and adolescents taking into account a number of clinical and personal variables.”
Educate Yourself About the Risks
If you, your child or another family member is on a psychiatric drug, I urge you to educate yourself about the true risks and to consider switching to safer alternatives. When it comes to children, I cannot fathom a situation in which a toddler would need a psychiatric drug and I find it shocking that there are so many doctors out there that, based on a subjective evaluation, would deem a psychiatric drug necessary.
I wrote this article in 2010. It’s truer now than it was then:
DECEMBER 5, 2010. About ten years ago, I decided that the medical cartel could become the most dangerous of all power groups on the planet. I have not changed my mind.
My decision is based on looking up the road 40 or 50 years and inferring what the picture will look like then.
It’s clear to me that drug companies, as they carve up markets and create new markets, are eagerly anticipating the day when every human, from cradle to grave—actually from inside the womb—has the status of Patient.
A person is born a patient and dies a patient. And in between, he receives 40 or 50 key diagnoses of physical and mental diseases/disorders and takes prescribed drug and surgery treatments.
More than that, though, he is stamped with the label, Patient, and he learns that everyone is in the same boat. “We’re all patients, this is a medical world, and it’s normal to be disabled in some way.”
People become proud, yes, proud to be victims. They wear their diagnoses as badges of honor. If you can’t see this trend, you’re not looking.
And universal health care insurance guarantees continuous treatment all the way along the line.
Every medical diagnosis becomes an excuse not to perform, not to excel, not to pursue big goals with large ambition.
Nowhere in the search to gain recognition as a victim do circumstances conspire so well as in the medical arena. It’s perfect. There’s no argument. The doctor told you you have X disease. That’s that. It’s not political. It’s not agenda-driven. It’s science. The proof is laid out on a silver platter. You ARE a victim.
In the coming future, every move a person makes, every step he takes will come under the umbrella of the doctor.
And, again, the main supporter of this system will be the patient himself. That’s how beautiful the marketing is.
In case you’ve been living in a cave for the last 30 years, drug companies and their researchers can invent any vague disease label they want to—and then they can invent five or six sub-categories of the label—and they can set out rules on how to diagnose each sliver of the label—and of course the doctors will make these diagnoses and prescribe drugs. It’s marketing and “healing” at the same time.
Parents who don’t have a clue will submit their children to this system—especially if the government pays for it—and the children will grow up trained to think of themselves as patients/victims…and the only contest will be: who has the most drastic diagnoses and treatments? Who can most proudly wear the badge of honor as Patient?
“Last month, they had to remove my head for five minutes while they fixed my brain.”
“Wow. Well, they put me in a body cast for three months and I couldn’t move, except for my left thumb.”
Cradle to grave.
If you go back and read Huxley’s Brave New World again, you’ll notice the factor of “patient pride.” It isn’t just that the society is controlled, the citizens are idealistic about it.
That’s where the victim industry is heading.
Against it, we have, what?
A little thing called individual freedom. Which includes the right to refuse medical treatment, no matter who prescribes it under what regulations.
People imagine that this right is some arcane matter best debated in medical-ethics journals. It’s an obscure curio.
They couldn’t be more wrong.
As I’ve been writing, the ObamaCare plan contains the seeds of a future in which, by law, the citizen will have less freedom to determine his own medical fate. The walls will gradually close in.
The Founders knew what they were talking about when they warned of the incursion of government and the loss of freedom. At every crossroad, since then, the issue of freedom has resurfaced as the unavoidable key factor.
Dr. Sam Bailey: On Health Freedom Advocates Who Attack Anyone Who Dares to Question Virus & Germ Theory | How RFK, Jr. Was Recently Drawn Into the Viral Existence Debate
Truth Comes to Light editor‘s note: In the video below, Dr. Sam Bailey talks about specific attacks, coming from within the health freedom movement, on the work of those who are questioning the foundations of virus theory.
At this point, most people in the health freedom movement, not to mention the general population, don’t even know that there is a strong debate about the existence of viruses. But awareness is growing.
The so-called, ‘settled science’ of virology must be looked into carefully because, as Dr. Sam Bailey has stated, virus and germ theory “is a system that can and will be used repeatedly to promulgate fear and compliance in the population.”
Dr. Bailey is careful to emphasize that RFK, Jr. is not one of those attacking the work of those who question virology. In this video she shares a segment from a recent public Q&A session wherein Eric Coppolino asks RFK, Jr. some basic questions, pointing to the fact that SARS-C0V-2 has never been shown to exist outside of imagined computer models.
You will find a transcript below the video with links to referenced articles and papers.
RFK, Jr. has been a tireless campaigner in warning the public about the problems of vaccines. However, with regards to the viral existence problem, he has been reluctant to get involved.
Let’s find out what happened when he was drawn into the debate in a recent Q&A session…
Questioning the existence of viruses can be a risky business, as myself and others have found out. However, once you’ve seen the problems with viral theory, it’s not something that can be unseen. It becomes a realization that much of what you were told is factual is not founded in scientific evidence at all. You start to research the material and find that many of the narratives are driven by industry participants and folklore rather than organic science.
While most probably don’t have a dog in the fight, those defending the virus narrative can get pretty hostile.
However, others such as RFK, Jr. simply appear uneasy about mentioning the virus existence issue.
So let’s find out what happened when one of the champions of the health freedom movement was unexpectedly drawn into the debate.
From the start I would like to make it clear that I consider RFK Jr. an ally in promoting health freedom and autonomy. He is a world leader and raising awareness about the risks and ineffectiveness of many vaccines.
I would also say that he has not been ambiguous with regards to his public statements relating to the existence of SARS-CoV-2 or other viruses. As far as I’m aware, he has stated that he believes such viruses exist. Although, in many cases the risks to health and the necessity for a lot of vaccines have been overstated.
I’d also suggest that the virus existence debate does not mean the current health freedom movement will be fractured as some seem to fear.
I don’t mind if other people believe in viruses and germ theory. However, as we point out in ‘Virus Mania’ that is a system that can and will be used repeatedly to promulgate fear and compliance in the population. Once the fatal flaws in the contagion theory are understood, people no longer buy into any of it and don’t get distracted trying to explain different aspects of the scam.
But before we get into RFK Jr.’s recent statements, there have been a few other prominent health freedom fighters who have made forays into the virus existence debate this year.
One was Steve Kirsch. He has been very outspoken about the dangers of the Covid-19 vaccine. Kirsch has realized that many doctors, governments and pharmaceutical companies are playing a game of deception with the public.
But then, on the issue of virus existence he places his faith in the high priests of virology. In early January this year, he decided to announce in his popular blog that SARS-Cov-2 has been isolated and shown to exist.
First, he smeared Drs. Lanka, Kaufman and Cowan with completely inaccurate portrayals of their work and received a huge backlash from his followers in the comment section. Instead of realizing that he might need to conduct his own research into this topic, he then decided to include Christine Massey and myself in the smears.
In a subsequent article 11 days later, curiously Kirsch suggested that we would not front if a live debate was offered.
Well, I can tell you from a series of emails that took place, which Kirsch was part of, that Drs. Bailey times two [Drs. Mark and Samantha Bailey], along with Stefano Scoglio, Drs. Lanka, Cowan and Kaufman, all volunteered to take part in a live debate with any experts that Kirsch was able to produce.
Instead of admitting that he was in over his head, Kirsch posted a third article the following week, embarrassing himself even further with declarations such as: ‘The reason nobody has purified the virus is there is no need to do so in today’s world where gene sequencing is readily available.’ And, ‘if the virus doesn’t exist, then how can 600 labs across the country find the same sequences for the virus in infected samples.’
These kind of statements indicate he’s unaware of the fundamentals of the virus existence debate.
Kirsch doesn’t see that he relies on other “experts” to inform him on the issue. And my husband Mark has written about why this is not a good idea, outlining the nature of the evidence such experts present in his article ‘Warning Signs You’ve Been Tricked by Virologists‘.
As Kirsch has worked out that people selling vaccines may be misleading people, then we would suggest that he peel back another layer to check whether the pharmaceutical and virology establishment, who have billions of dollars of vested interests, may be misleading people with regards to viruses as well.
And some other information I can give you is that I reached out to Steve after he posted his articles offering him a chance to connect, as well as a complimentary copy of ‘Virus Mania’. But he never responded.
In any case, he seems to have gone quiet on the virus existence front, perhaps because he genuinely thinks it’s […] science. Although I would hope that he has some inkling now that there’s more to this than he thought.
Another interesting smear attack against me from a supposed health freedom fighter came from Dr. Roger Watson, writing for The Daily Sceptic in March this year.
This was surprising on a number of fronts. Firstly, because the website developed out of lockdown sceptics and has the motto “question everything”.
However, it seems that questioning the existence of SARS-CoV-2 and the existence of viruses in general is a bridge too far for the so-called ‘Sceptic’.
Secondly, along with my allies including Andy Kaufman and Kevin Corbett, Watson co-signed the viral challenge letter to Boris Johnson demanding that the British prime minister provide proof of the Covid-19 virus. And, if not, then all measures against the nonexistent virus should be dropped.
Obviously, Watson changed his mind at some point and I’m not clear on why that happened. In any case, I had some fun dismantling Watson’s various allegations in my articles ‘The COVID “Sceptics” Who Spread Viral Dogma‘.
Watson’s article was arguably worse […]
Like Kirsch, Watson did not want to enter into a debate about the topic and couldn’t find anyone to front up in his place either. But at least he responded to our emails.
So, now we get to RFK, Jr., which is a slightly different story, as he has not been involved in any smears against me.
In fact, those of you familiar with ‘Virus Mania’ will know that he wrote an important section for our book titled ‘Greed, Negligence and Deception in the Vaccine Industry’.
RFK, Jr. is certainly aware of the controversy surrounding the existence of HIV. As he outlined in his 2022 publication ‘The Real Anthony Fauci’, our friend Tom Cowan even gets a mention in the book when he says: “The first time that someone — Dr. Tom Cowan, a physician from northern California — suggested to me that HIV was not the sole cause of AIDS, I dismissed the comment as ridiculous.”
However, in Chapter 5, ‘The HIV Heresies’, RFK, Jr. goes on to explain how his own research made him realize that there were major problems with the HIV theory.
He is even aware of The Perth Group and the devastating criticisms of the very existence of an infectious HIV particle. Commenting, “In my conversations with Turner and Papadopulos, and in my reading of their paper, I find their arguments clear and convincing. However, I recognize that there are some fifty thousand articles on AIDS in the scientific literature. A casual novitiate like myself has little chance of unraveling this baroque controversy in a vacuum.”
However, most of RFK, Jr.’s focus in the book is on the fact that Anthony Fauci has been instrumental in controlling the HIV/AIDS model and has ruthlessly suppressed dissenting voices.
My hope is that he will read The Perth Group paper ‘HIV – a virus like no other’ one more time and he’ll see there’s no evidence that a pathogenic particle termed HIV exists. And there is no need to read most of the fifty thousand AIDS articles if they fallaciously assert otherwise.
So what happened on April 24 this year — the fundraising event taking place at the Grand Hyatt Hotel in Greenwich, Connecticut?
During the Q&A session, my friend and journalist extraordinaire, Eric Coppolino, was there to put some key questions about the existence of SARS-CoV-2 to RFK Jr.
So let’s take a listen to the exchange that takes place between the two of them on that Sunday afternoon.
Eric Coppolino:
Hi Bobby. Thank you. Christine Massey in Toronto has amassed 182 responses under various Freedom of Information law requests from institutions, provincial, state, and federal, national governments which all say no one has a sample of SARS-C0V-2 taken from a human. Would you please comment on that?
RFK, Jr.:
Yeah, I really am not qualified to comment on it, but … My inclination if there are people who say that viruses don’t exist, that there is no virus… I don’t, you know, my inclination is that that simply is not, you know, that’s not true.
Dr. Sam Bailey:
At least he has admitted that he is relying on inclination, rather than having looked into the evidence himself as he has done with vaccines.
RFK, Jr.:
I can’t argue with you, and I can’t…I actually, on our list there’s a number of people who make those kind of arguments. And other people on the list server…and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.
Dr. Sam Bailey:
It’s hard to know exactly what he’s talking about here. If it’s the same virology papers we’ve been looking at, it is certainly unclear how this constitutes a lot of evidence. In my experience, they are usually reciting the paper’s title without critiquing the methodology, which is where all the problems are.
RFK, Jr.:
I am kind of amused reading the exchanges and my inclination is that viruses do exist and do make people sick. I could be wrong. It could all be a big hoax, but to me, it seems like viruses are real, and … look, I should have just shut up from the beginning and say I’m not gonna answer that question.
Eric Coppolino:
The governments have said they don’t have a sample.
RFK, Jr.:
…You know what? Actually I saw an email exchange yesterday where somebody made exactly that statement and then ten people jumped on him with examples of where that’s not true.
Dr. Sam Bailey:
This was news to me and I know it was news to Christine Massey, coordinator of the SARS-CoV-2 Freedom of Information Project, who demanded the data from the 10 people on Kennedy’s list who claim to prove that the virus had been isolated.
RFK, Jr.:
…The other thing is, I do know this, when you make a freedom of information request, the freedom of information laws do not require the government agency to do science, or to answer questions, specific questions. What they do is, they, the Freedom of Information laws make it obligatory for the government to give you existing documents. So, if you’re telling the government, “I want you to verify this.” They look at their documents and say, “There’s nothing here to verify it.” It doesn’t mean it’s not true. It means they’ve got nothing. But, listen, again, I am not a … scientist. I don’t pretend to be. I find those arguments interesting. And there’s a guy in California, who I deeply respect, Tom Cowan, who makes those arguments and it really… I can’t answer the question.
Dr. Sam Bailey:
This is another interesting statement and perhaps a chance for RFK, Jr. to reflect on the same battle he faces regarding raising awareness about vaccine problems. The mainstream could dismiss RFK Jr.’s arguments as “not being taken seriously by a lot of other people” because the majority of the medical industry still promote all vaccines. However, ‘appeal to popularity’ is a form of faulty reasoning and has no place in a scientific discussion such as this one.
My experience, and I’m sure Tom Cowan and all others in the movement can attest to, is that the majority of people are simply unaware of this debate and don’t even know that questioning the existence of a virus is a thing. And the individuals and corporations that gain from the virus theory often engage in active suppression of the debate.
Prior to widespread internet usage, dissident authors such as The Perth Group were refused publication opportunities in the medical journals. And in the modern era, material such as mine is banned on all the big tech platforms.
The virus theory was put forward in the late 1800s and, for most of us, it is a revelation to go back through the scientific literature and see the key postulants have not been fulfilled .
One of the most amusing, and perhaps tragic, things you’ll see is websites such as AIDSTruth claiming that the science is settled. In 2015 they announced that they were retiring the website because apparently their work was done. The first sentence of their self-congratulatory announcement shows just how disingenuous they are when they use the term ‘AIDS denialism’, knowing very well that what is in dispute is the HIV/AIDS theory or whether an infectious particle, termed HIV, actually exists.
The group also referred to ‘bumps in the early years of treatment’ which is an obscene way to refer to deaths caused by AZT.
In any case, I wonder if the team might consider resurrecting their website or if they are now too busy working on other projects under organizations such as the World Economic Forum and Johns Hopkins.
I think if they do decide to get back into it, they’ll find that the number of individuals and groups opposing their position on the HIV/AIDS theory has gone up dramatically.
Mike Stone of Viroliegy, put together a collection of some of the websites questioning viral theory. And many of them, including Viroliegy itself, have appeared in the last two years.
All the individuals I have personally spoken with, that have or are currently pointing out the flaws in viral theory, they share a number of things in common. Firstly, they all believed in the viral theory at some stage. But when they investigated it for themselves, something changed their minds. Secondly, they have all paid a price whether being publicly censured, smeared or blocked from working in the professions. Thirdly, they are all incredibly generous with their time and share the knowledge with everyone that is interested. And lastly, and perhaps most importantly, they have a passion for exploring the possibilities and following the scientific trail to wherever it takes them by freeing themselves from the shackles of institutional policies, industry capture and public regulatory bodies.
My feeling is that far more people are moving into the questioning the viral theory camp rather than the other way around.
Who knows. Perhaps now that the door has been opened, RFK. Jr. might take more of a look around.
So that we don’t lose touch please find me at drsambailey.com and sign up for my free newsletter.
James Corbett: I Read Bill Gates’ New Book (So You Don’t Have To!)
In an interview with the National Geographic, Tony Fauci made comments about “alternative views” of the origin of the coronavirus. But he was really talking about all unorthodox medical information:
“Anybody can claim to be an expert even when they have no idea what they’re talking about—and it’s very difficult for the general public to distinguish. So, make sure the study is coming from a reputable organization that generally gives you the truth—though even with some reputable organizations, you occasionally get an outlier who’s out there talking nonsense. If something is published in places like New England Journal of Medicine, Science, Nature, Cell, or JAMA—you know, generally that is quite well peer-reviewed because the editors and the editorial staff of those journals really take things very seriously.”
Right you are, Tony.
So, Tony, here is a very serious statement from a former editor of one of those “places,” the New England Journal of Medicine:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
And here is another one, from the editor-in-chief of the prestigious journal, The Lancet, founded in 1823:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness…”
“The apparent endemicity of bad research behaviour is alarming. In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world. Or they retrofit hypotheses to fit their data. Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours. Our acquiescence to the impact factor fuels an unhealthy competition to win a place in a select few journals. Our love of ‘significance’ pollutes the literature with many a statistical fairy-tale…Journals are not the only miscreants. Universities are in a perpetual struggle for money and talent…” (Dr. Richard Horton, editor-in-chief, The Lancet, in The Lancet, 11 April, 2015, Vol 385, “Offline: What is medicine’s 5 sigma?”)
Why stop there? Let’s consult a late public-health expert whose shoes Fauci would have been lucky to shine: Dr. Barbara Starfield, Johns Hopkins School of Public Health.
On July 26, 2000, the US medical community received a titanic shock, when Starfield revealed her findings on healthcare in America.
The Starfield review, “Is US health really the best in the world?”, published in the Journal of the American Medical Association (JAMA), came to the following conclusion, among others:
Every year in the US, correctly prescribed, FDA approved medical drugs kill 106,000 people. Thus, every decade, these drugs kill more than a MILLION people.
On the heels of Starfield’s astonishing findings, media reporting was perfunctory, and it soon dwindled. No major newspaper or television network mounted an ongoing “Medicalgate” investigation. Neither the US Department of Justice nor federal health agencies undertook prolonged remedial action.
All in all, those parties who could have made effective steps to correct this ongoing tragedy preferred to ignore it.
On December 6-7, 2009, I interviewed Dr. Starfield by email. Here is an excerpt from that interview.
Q: What has been the level and tenor of the response to your findings, since 2000?
A: The American public appears to have been hoodwinked into believing that more interventions lead to better health, and most people that I meet are completely unaware that the US does not have the ‘best health in the world’.
Q: In the medical research community, have your medically-caused mortality statistics been debated, or have these figures been accepted, albeit with some degree of shame?
A: The findings have been accepted by those who study them. There has been only one detractor, a former medical school dean, who has received a lot of attention for claiming that the US health system is the best there is and we need more of it. He has a vested interest in medical schools and teaching hospitals (they are his constituency).
Q: Have health agencies of the federal government consulted with you on ways to mitigate the [devastating] effects of the US medical system?
A: NO.
Q: Are you aware of any systematic efforts, since your 2000 JAMA study was published, to remedy the main categories of medically caused deaths in the US?
A: No systematic efforts; however, there have been a lot of studies. Most of them indicate higher rates [of death] than I calculated.
Q: Did your 2000 JAMA study sail through peer review, or was there some opposition to publishing it?
A: It was rejected by the first journal that I sent it to, on the grounds that ‘it would not be interesting to readers’!
—end of interview excerpt—
Physicians are trained to pay exclusive homage to peer-reviewed published drug studies. These doctors unfailingly ignore the fact that, if medical drugs are killing a million Americans per decade, the heraldic published studies on which those drugs are based must be fraudulent. In other words, the medical literature is completely unreliable, and impenetrable.
WHICH IS EXACTLY WHAT THE TWO ESTEEMED MEDICAL EDITORS I QUOTED ABOVE—MARCIA ANGELL AND RICHARD HORTON—ARE SAYING.
If you know a doctor who enjoys sitting up on his high horse dispensing the final word on modern medicine, you might give him the quotes from Dr. Angell and Dr. Horton, instruct him to read them, and suggest he get in touch with Angell and Horton, in order to discover what has happened to his profession.
As in: DISASTER.
But please, continue to believe everything Fauci is saying. He must be right about the “pandemic.” After all, he has a very important position, and he’s on television.
So what if his policies have torpedoed the economy and devastated and destroyed lives across the country?
So what if he accepted, without more than a glance, that fraud Neil Ferguson’s computer projection of 500,000 deaths in the UK and two million in the US? In 2005, Ferguson said 200 million people could die from bird flu. The final official tally was a few hundred.
So what?
Fauci has an important position, and he’s on television.
It is very apparent to anyone looking into the origins of antibodies that the idea of what these entities are in terms of how they look and how they function came well before any attempts to actually purify, isolate, and characterize the assumed particles. Antibodies were (and still are) nothing more than unseen theoretical constructs used to explain chemical reactions created in a lab. These fictional creations reside in the “domain of the invisible spectrum” conjured up by the “lively imagination” of a man named Paul Ehrlich. While there was no direct proof for the existence of these entities, the antibody concept was far too important to the immunological narratives forming around the growing practice of vaccination and the increased acceptance of other unseen entities known as “viruses” to just give it up. As the purification and isolation of antibodies in order to see and study them was an impossible task, researchers sought other methods to attempt to provide indirect evidence for the existence of these theoretical creations.
One man who is credited with providing such evidece is Michael Heidelberger, considered the “Founder of Immunochemistry.” He was the first to apply mathematics to the reaction of antibodies and their antigens. He is also known for “proving” that antibodies are proteins by showing that the antigens of pneumococcus bacteria are polysaccharides (or carbohydrates). Here is a brief overview of his work:
“Avery and Dochez’s initial characterization of this pneumococcal substance showed that it was resistant to both heat and trypsin—features unbefitting most proteins—but that it did contain nitrogen, a component of proteins. But its true nature was not revealed until 1923, when Michael Heidelberger—then in the chemistry department synthesizing drugs against poliomyelitis and African sleeping sickness—teamed up with Avery.
The more they purified the reactive substance the less nitrogen it contained. When it was virtually nitrogen-free, recalled Heidelberger in a 1979 article, Avery ventured a guess: “Could it be a carbohydrate?” (2). Chemical analysis confirmed its sugary character, and subsequent studies of other pneumococcal serotypes revealed that each bacterial capsule had a distinct polysaccharide signature. It was this signature that dictated the serological specificity of the organism. The duo published these findings in two articles in the Journal of Experimental Medicine (3, 4).
Their results were met with considerable skepticism, as it was then thought that only proteins could incite a specific immune response. “Nobody believed it,” says Emil Gotschlich (Rockefeller University), whose later work on polysaccharide-based vaccines stemmed in large part from Heidelberger and Avery’s discoveries. “It took them a lot of effort to convince people that the polysaccharide was the immunoreactive component.”
Antibodies solidified
Heidelberger and Avery’s discovery came at a time when antibodies were regarded—by those who believed they existed at all—as mysterious substances that floated around in serum. “It appeared to me that there was a crying need to determine the true nature of antibodies,” wrote Heidelberger in 1979, “and that until this was done there could be no end to the polemics and uncertainties that were plaguing immunology” (2). Heidelberger later purified the antibodies from his precipitin reactions and showed that they themselves were proteins. As a result, says friend and colleague Victor Nussenzweig (New York University), “there were no more mystical ideas about what antibodies were.”
Heidelberger and his postdoctoral fellow Forrest Kendall later quantitated the precipitin reaction (5), bringing much-needed mathematics to the study of antibody–antigen interactions and lifting antibodies even further out of the realm of the mysterious (see the next “From the Archive”).”
Heidelberger hard at work using his microscopic vision.
Two of Heidelberger’s papers are most often cited as the proof that antibodies are proteins. The first is a paper he did with Oswald Avery in 1923. It is used as proof that the pneumococcus antigens are carbohydrates. However, was this paper successful in drawing this conclusion? Presented here are some highlights from their collaboration:
“In 1917 Dochez and Avery (1) showed that whenever pneumococci are grown in fluid media, there is present in the cultural fluid a substance which precipitates specifically in antipneumococcus serum of the homologous type. This soluble substance is demonstrable in culture filtrates during the initial growth phase of the organisms; that is, during the period of their maximum rate of multiplication when little or no cell death or disintegration is occurring. The formation of this soluble specific material by pneumococci on growth in vitro suggested the probability of an analogous substance being formed on growth of the organism in the animal body.
Examination of the blood and urine of experimentally infected animals gave proof of the presence of this substance in considerable quantities in the body fluids following intraperitoneal infection with pneumococcus. In other words, this soluble material elaborated at the focus of the disease readily diffuses throughout the body, is taken up in the blood, passes the kidney, and appears in the urine unchanged in specificity. Similarly, a study of the serum of patients suffering from lobar pneumonia has revealed a substance of like nature in the circulating blood during the course of the disease in man. Furthermore, examination of the urine of patients having pneumonia due to pneumococci of Types I, II, and III has shown the presence of this substance in some stage of the disease in approximately two-thirds of the cases.
Recently from filtered alkaline extracts of pulverized bacteria of several varieties, including pneumococci, Zinsser and Parker have prepared substances which appear free from coagulable protein. These substances, called “residue antigens,” are specifically predpitable by homologous antisera. These observers consider these acid- and heat-resistant antigenic materials analogous to the soluble specific substance of pneumococcus described by Dochez and Avery. In spite of the fact that these “residue antigens” are precipitable by homologous sera produced by immunization with the whole bacteria, Zinsser and Parker have so far failed to produce antibodies in animals by injecting the residues.
In the earlier studies by Dochez and Avery certain facts were ascertained concerning the chemical characteristics of this substance. It was found that the specific substance is not destroyed by boiling; that it is readily soluble in water, and precipitable by acetone, alcohol, and ether; that it is precipitated by colloidal iron, and does not dialyze through parchment; and that the serological reactions of the substance are not affected by proteolytic digestion by trypsin. Since the substance is easily soluble, thermostable, and type-specific in the highest degree, it seemed an ideal basis for the beginning of a study of the relation between bacterial specificity and chemical constitution. The present report deals with the work done in this direction.
Experimental
The organism used in the present work was Pneumococcus Type II. The most abundant source of the soluble specific substance appeared to be an 8 day autolyzed broth culture; hence this material was used as the principal source of supply. For comparison dissolved pneumococci and lots of urine containing the specific substance were also worked up, with essentially the same results, as will be seen from Table I.
The process for the isolation of the soluble specific substance consisted in concentration of the broth, precipitation with alcohol, repeated re-solution and reprecipitation, followed by a careful series of fractional precipitations with alcohol or acetone after acidification of the solution with acetic acid, and, finally, repeated fractional precipitation with ammonium sulfate and dialysis of the aqueous solution of the active fractions.
Five lots of 15 liters each of 8 day cultures of Pneumococcus Type II in meat infusion phosphate broth are each concentrated on the water bath in large evaporating dishes to 1,000 to 1,200 cc. and precipitated in a separatory funnel by the gradual addition, with vigorous rotation, of 1.2 volumes of 95 per cent alcohol.The mixture separates into two layers, and is allowed to stand over night, or for several hours.
The upper layer, which is almost black and comprises the largest part of the mixture, contains only traces of the soluble specific substance, and is siphoned off and discarded. The lower, more viscous layer is run into a 250 cc. centrifuge bottle (occasionally a second will be required), capped, and rotated at high speed for ½ hour. Three layers are formed, of which the uppermost is merely a further amount of the liquid previously discarded. The middle layer consists of a compact, greenish cake of insoluble matter and gummy material, and contains most of the soluble specific substance. The bottom layer, from which salts often separate, is a brownish syrup rich in salts and nitrogenous matter and relatively poor in specific substance, and can, by careful manipulation, be poured off to a large extent.
Although a small proportion of the specific substance is lost if this syrup is discarded, its elimination represents so considerable a purification as to warrant the sacrifice of the active material contained. The gummy cake remaining in the centrifuge bottle, together with adhering salts and syrup, is now rinsed out and ultimately combined with similar material from the other lots, All of this is then dissolved as completely as possible in water, care being taken to break up the many lumps of gummy material, diluted to 1 liter, and again precipitated with alcohol. In this case about 1.3 liters are required to precipitate all but the last traces of active material from the upper layer. This is again discarded and the lower layer treated as before. At this stage there is relatively less of the bottom layer, and it is more difficult to separate it from the cake containing the specific substance, but as much as possible is removed. The remaining material is smoothed out with water, diluted to about 500 cc., and centrifuged. The precipitate is washed twice with water, and the washings are combined with the main solution. The still turbid liquid, the volume of which should be about 750 cc., is put through the alcohol purification process a third time, about 1.1 liters of alcohol being required. After having been centrifuged, the active material is again dissolved in water, made definitely acid to litmus with acetic acid, and again centrifuged. The precipitate is washed three times with water acidulated with acetic acid, and the filtrate and washings are combined in a separatory funnel and diluted again if necessary to 750 cc. Acetone (redistilled) is now added until a permanent precipitate forms, about 250 c¢. being necessary. The precipitate is allowed to settle, whereupon the lower part of the mixture containing the precipitate is drawn off and centrifuged. The clear superuatant fluid is restored to the main solution, while the precipitate, which consists largely of insoluble material and gives an aqueous solution almost devoid of activity, is discarded.
Fractional precipitation is continued, and even when the specific substance appears in quantity in the precipitate, it is occasionally possible to separate a lower, inactive, syrupy layer, as in the previous purifications by alcohol. Addition of acetone is continued until a test portion, heated on the water bath to remove acetone, diluted with saline, and neutralized, no longer gives a precipitate with immune serum, after which the upper layer may be discarded. The active precipitates are then redissolved in water, centrifuged again, and the supernatant liquid is diluted to 375 cc., reacidified with acetic acid, and again fractionated with acetone. If inactive fractions are obtained, the process is again repeated until no further purification results. Alcohol may be used for these fracfionations instead of acetone, the only difference being that a somewhat larger proportion is required. The active material is then dissolved in about 150 cc. of water and again made definitely acid with acetic acid. The solution is treated with solid ammonium sulfate until the first slight precipitate forms. This is generally inactive, and if so, may be discarded.
Finally, ammonium sulfate is added to saturation, completely precipitating the specific substance if the volume of the solution is not too great. The mixture is allowed to stand for several hours and is then centrifuged and the precipitate washed with a little saturated ammonium sulfate solution. It is redissolved in about 75 cc. of water acidified with acetic acid, centrifuged if necessary, and again precipitated by saturation with ammonium sulfate. Finally, the specific substance so obtained is dissolved in water and dialyzed first against running tap water in the presence of chloroform and toluene, and finally against distilled water until tests for sulfate and phosphate ion are negative. Addition of acetic acid during the early stages of the dialysis assists in the removal of calcium, which otherwise forms a large part of the ash.
The dialyzed solution is concentrated to dryness on the water bath and the residue redissolved in hot water. If the solution is not perfectly clear, it is centrifuged again before being evaporated to dryness, and the whole process is repeated as long as insoluble material separates. Toward the end of the final concentration absolute alcohol may be added to assist in the precipitation of the substance.
Variations in the exact volumes given are often necessary with different lots of broth, but this will occasion little difficulty if all fractionations are controlled by the specific precipitin test.
As so obtained the soluble specific substance forms an almost colorless varnish-like mass which may be broken up and dried to constant weight at 100°C. in vacuo. The yield from 75 liters of broth averages about 1 gin., although it varies within rather wide limits in individual lots.
By the method outlined above all substances precipitable with hosphotungstic acid or capable of giving the biuret reaction were eliminated. The residual material (Preparation 17, in Table I), for which no claim of purity is made, as efforts at its further purification are still under way, contained, on the ash-free basis, 1.2 percent of nitrogen. It was essentially a polysaccharide, as shown by the formation of 79 percent of reducing sugars on hydrolysis, and by the isolation and identification of glucosazone from the products of hydrolysis.”
“Table I represents a summary of the reactions of some of the earlier preparations worked with, as well as the later ones. Preparation 4 was obtained from the urine of a patient with a Type II pneumococcus infection, while No. 8 was obtained from an antiforrain solution of the pnemnococci. In both of these cases, as well as in Nos. 9, 11, and 15, the method of purification given above had not been fully worked out.
Attempts to stimulate antibody production by the immunization of animals with the purified substance yielded negative results.
Discussion.
While it has long been known that the capsular material of many microorganisms consists, at least in part, of carbohydrates, any connection between this carbohydrate material and the specificity relationships of bacteria appears to have remained unsuspected. While it cannot be said that the present work establishes this relationship, it certainly points in this direction. Evidence in favor of the probable carbohydrate nature of the soluble specific substance is the increase in specific activity with reduction of the nitrogen content, the increase in optical rotation with increase in specific activity, the parallelism between the Molisch reaction and specific activity, the high yield of reducing sugars on hydrolysis, and the actual isolation of glucosazone from a small quantity of the material. The small amounts of substance available up to the present have hindered the solution of the problem, and it is hoped that efforts at further purification of the soluble specific substance, now in progress with larger amounts of material, will definitely settle the question.
Summary.
A method is given for the concentration and purification of the soluble specific substance of the pneumococcus.
The material obtained by this method is shown to consist mainly of a carbohydrate which appears to be a polysaccharide built up of glucose molecules.
Whether the soluble specific substance is actually the polysaccharide, or occurs merely associated with it, is still undecided, although the evidence points in the direction of the former possibility.”
A beautiful mind?
Heidelberger’s original 1923 paper can hardly be claimed to be the slam-dunk proof that bacteria antigens are carbohydrates. For starters, Heidelberger admitted that he was unsure if the presumed “antigen” substance was a carbohydrate or if it was merely associated with it. Even more importantly, he could not produce any antibody response upon injecting his presumed antigen into animals. This would indicate that the substance was not an antigen whatsoever as antigens are specifically defined as “a toxin or other foreign substance which induces an immune response in the body, especially the production of antibodies.” Thus, it seems rather odd to assume antibodies are proteins based off of this work, but assume they did:
“Since the pneumococcal capsular antigen was a polysaccharide, and antibodies were thought to be proteins, Heidelberger realized that by measuring the amount of protein in specific precipitates made with the capsular antigen he could determine their antibody content. Together with Forrest Kendall, who had joined the Heidelberger lab, the protein content of immune precipitates was determined by measuring total nitrogen, using the Kjeldahl procedure that came to be the hallmark of laboratories carrying out Heidelberger-type quantitative immunochemistry.”
Since they assumed the pneumococci bacteria was a polysaccharide, that meant any nitrogen left over was the antibody content. Based on the 1923 paper, this seems to be a rather falicious premise to build from. In any case, Heidelberger carried on with his assumption and it can be seen by this second paper from 1929 how Heidelberger came to his conclusion using the precipitin test and mathematics as proof that antibodies exist. I edited out the long mathematical sections with his equations so if you are interested in Heidelberger showing his work, I recommend reading the full paper. Highlights below:
A Quantitative Study of the Precipitin Reaction Between Type III Pneumococcus Polysaccharide and Purified Homologous Antibody*
“Of all the reactions of immunity the precipitin test is perhaps the most dramatic and striking. While other immune reactions are more delicate, the precipitin test is among the most specific and least subject to errors and technical difficulties. Attempts at its quantitative interpretation and explanation have been hampered either by the difficulty of finding suitable analytical methods or by the failure to separate the reacting substances from closely related, non-specific materials with which they are normally associated.
With the aid of recent work it has been found possible to avoid these difficulties to some extent. The isolation of bacterial polysaccharides which precipitate antisera specifically and possess the properties of haptens has not only afforded one of the components of a precipitin reaction in a state of comparative purity, but has greatly simplified the analytical problem. Since many of these polysaccharides contain no nitrogen, and antibodies presumably are nitrogenous, the latter may be determined in the presence of any amount of the specific carbohydrate. Moreover, Felton’s method for the separation of pneumococcus antibodies from horse serum not only permits the isolation of a high proportion of the precipitin, freed from at least 90 percent of the serum proteins and much of the serum lipoid, but is also applicable on a sufficiently large scale to furnish the amounts of antibody solution needed to make quantitative work possible. It is realized that antibody solutions of this type do not contain pure antibodies–indeed, only 40 to 50 percent of the nitrogen is specifically precipitable–but since so small a proportion of the original serum protein remains with the antibody a far-reaching purification actually has been effected. It should thus be possible with the aid of antibodies purified by Felton’s method to obtain data of a preliminary character which should point toward the mechanism of the reaction. The present paper is concerned with such data obtained in a quantitative study of the precipitin reaction between the soluble specific substance of Type III pneumococcus and Type III pneumococcus antibody solution.
Experimental
1. Materials and Methods.–a. Solutions of Soluble Specific Substance, Type Ill Pneumococcus.–The soluble specific substance of Type III pneumococcus used was kindly supplied by Drs. O. T. Avery and W. F. Goebel of The Rockefeller Institute for Medical Research. It was ash-free, contained 0.04 percent of nitrogen, and showed a/d = -32 °. A weighed amount of anhydrous substance was suspended in 0.9 percent saline, dissolved with the aid of 0.1 normal sodium hydroxide, and the solution was diluted with saline, adjusted to pH 7.6 and made up to volume with saline to yield a 1 percent solution. This was sterilized in the autoclave and used as a stock solution for making up other dilutions. These were prepared with sterile saline under aseptic precautions, and were kept in the ice-box.
b. Type III Pneumococcus Antibody Solution.–The antibody solutions used were prepared essentially according to Felton’s procedure (loc. cit.) from Type III antipneumococcus horse serum containing no preservative and supplied by the New York State Department of Health through the courtesy of Dr. A. B. Wadsworth and Dr. Mary B. Kirkbride. 100 to 200 cc. of serum were stirred slowly into 20 volumes of ice-cold water containing 9.5 cc. of molar potassium dihydrogen phosphate and 0.5 cc. of molar dipotassium hydrogen phosPhate per liter. The final pH varied from 5.6 to 6.3. After standing over night in the cold the supernatant was decanted and the precipitate was centrifuged off in the cold and dissolved in a volume of chilled 0.9 percent saline equal to that of the serum taken. 0.1 normal hydrochloric acid was then added until a precipitate no longer formed on dilution of a test portion with two volumes of water, after which 0.1 normal sodium hydroxide solution was added until a slight precipitate again formed on dilution. In general, 5 cc. of acid and 1.5 cc. of alkali per 100 cc. of serum were satisfactory, although as Felton emphasizes, different lots vary and no absolutely definite procedure can be given. In the present work the process of purification was followed either by testing the agglutinating power of the fractions against a heat-killed Type III pneumococcus vaccine, or by the precipitin reaction, or by both methods. After addition of the alkali the opalescent solution was diluted with 2 volumes of water and centrifuged in the cold. The almost inactive precipitate was discarded and the supernatant poured into 6.7 volumes of the chilled buffer solution previously used, (equivalent to 20 times the volume of saline employed), also adding enough 0.1 normal sodium hydroxide to neutralize the remaining acid. The resulting precipitate was collected and dissolved in a volume of 0.9 percent saline equal to that of the serum taken, and the pH was adjusted to 7.6. The solution was sterilized by passage through a Berkefeld N grade filter which previously had been washed with saline containing a drop of normal sodium hydroxide, followed by saline alone.
Antibody solutions prepared in this way were found to be rather unstable under the usual conditions of the precipitin test, and it therefore was necessary to subject them to a preliminary “ageing” treatment in order that control solutions might be relied upon to remain clear. This consisted in immersing the solution in a water bath at 37 ° for 2 hours, letting stand in the ice-box over night, centrifuging off the precipitate which usually formed, readjusting the pH if necessary, and filtering through a Berkefeld candle prepared as above. This treatment was repeated as many times as necessary, but the solutions usually remained clear after the second incubation at 37 °. Much time was lost and very inconstant results were obtained until “ageing” was resorted to.
The relative antibody content of the resulting solutions was estimated by determining the agglutination titer against a single heat-killed Type III pneumococcus suspension.
It will be seen from Table I that the agglutination titer and the maximum amount of protein precipitable by the type III polysaccharide ([total N–N in supernatant] X 6.25) are approximately proportional. The latter may therefore be taken as a more definite, though not necessarily more accurate, measure of the actual antibody content of the solutions.
It is also evident that the antibody in all of these solutions has been purified to approximately the same extent, since the ratios of protein precipitable by SSS III to total protein are not very different.”
Discussion
“For purposes of discussion it will be assumed with Felton (lot. cir.) that antibody is ,modified protein, and that, in order to provide a uniform method of measurement, it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25. Since only relative values are under consideration, the actual magnitude of the factor used is of little significance so long as it be used throughout. Moreover, Table I shows a correspondence between this measure of antibody content and the agglutination titer, so that its use as a relative measure is independent of the nature of Type III pneumococcus antibodies.
doi: 10.1084/jem.50.6.809.
The Precipitin Reaction
In Summary:
Michael Heidelberger teamed up with Oswald Avery to characterize a “soluble specific substance” found in pneumococcal bacteria that fell out of solution when incubated with type-specific antisera
When it was virtually nitrogen-free, recalled Heidelberger in a 1979 article, Avery ventured a guess: “Could it be a carbohydrate?”
Chemical analysis confirmed its sugary character, and subsequent studies of other pneumococcal serotypes revealed that each bacterial capsule had a distinct polysaccharide signature
It was this signature that dictated the serological specificity of the organism
Their results were met with considerable skepticism, as it was then thought that only proteins could incite a specific immune response
According to polysaccharide-based vaccine specialist Emil Gotschlich: “Nobody believed it. It took them a lot of effort to convince people that the polysaccharide was the immunoreactive component.”
Heidelberger and Avery’s discovery came at a time when antibodies were regarded—by those who believed they existed at all—as mysterious substances that floated around in serum
“It appeared to me that there was a crying need to determine the true nature of antibodies,” wrote Heidelberger in 1979, “and that until this was done there could be no end to the polemics and uncertainties that were plaguing immunology”
Heidelberger and his postdoctoral fellow Forrest Kendall later quantitated the precipitin reaction, bringing much-needed mathematics to the study of antibody–antigen interactions and lifting antibodies even further out of the realm of the mysterious
In 1917 Dochez and Avery showed that whenever pneumococci are grown in fluid media, there is present in the cultural fluid a substance which precipitates specifically in antipneumococcus serum of the homologous type
It was assumed that the formation of this soluble specific material by pneumococci on growth in vitro suggested the probability of an analogous substance being formed on growth of the organism in the animal body
Examination of the urine of patients with pneumococci showed the substance in only approximately 2/3rds of the samples
Zinsser and Parker found similar substances with other bacteria and believe that the substances are the same as that of the pneumococci
In spite of the fact that these “residue antigens” are precipitable by homologous sera produced by immunization with the whole bacteria, Zinsser and Parker failed to produce antibodies in animals by injecting the residues.
The process for the isolation of the soluble specific substance consisted in:
Concentration of the broth
Precipitation with alcohol
Repeated re-solution and reprecipitation
A careful series of fractional precipitations with alcohol or acetone after acidification of the solution with acetic acid
Repeated fractional precipitation with ammonium sulfate and dialysis of the aqueous solution of the active fraction
For a complete step-by-step breakdown of the numerous chemical-altering procedures done to the sample, see the highlighted tan section of the paper provided above
Even with the numerous “purification” steps, the obtained soluble specific substance formed an almost colorless varnish-like mass
The residual material for which no claim of purity was made, as efforts at its further purification were still under way, contained, on the ash-free basis, 1.2 percent of nitrogen.
It was considered essentially a polysaccharide
The method of purification given had not been fully worked out for many of the preparations
Attempts to stimulate antibody production by the immunization of animals with the purified substance yielded negative results
While it had long been known that the capsular material of many microorganisms consists, at least in part, of carbohydrates, any connection between this carbohydrate material and the specificity relationships of bacteria remained unsuspected
While it could not be said that their work established this relationship, they felt it certainly pointed in that direction
The small amounts of substance available hindered the solution of the problem, and it was hoped that efforts at further purification of the soluble specific substance with larger amounts of material would definitely settle the question
Whether the soluble specific substance is actually the polysaccharide, or occurs merely associated with it, was left undecided
Heidelberger acknowledged that the precipitin test he used during this experiment has 2 drawbacks:
Quantitative interpretation/explanation is difficult due to lack of a suitable analytical method
Failure to separate out the reacting substances from non-specific material which these substances are closely related to and associated with
He stated that it was possible to avoid these failures to some extent
It is presumed that antibodies are nitrogenous
Only 90% of the precipitin can be freed from serum proteins and “much” of the lipoid
Heidelberger admitted that these are not pure antibodies and that only 40-50% of nitrogen is precipitable while small amounts of serum remain
The antibody solutions used were prepared essentially according to Felton’s procedure from Type III antipneumococcus horse serum containing no preservative and supplied by the New York State Department of Health through the courtesy of Dr. A. B. Wadsworth and Dr. Mary B. Kirkbride
100 to 200 cc. of serum were stirred slowly into 20 volumes of ice-cold water containing 9.5 cc. of molar potassium dihydrogen phosphate and 0.5 cc. of molar dipotassium hydrogen phosphate per liter
The final pH varied from 5.6 to 6.3
After standing over night in the cold the supernatant was decanted and the precipitate was centrifuged off in the cold and dissolved in a volume of chilled 0.9 percent saline equal to that of the serum taken
0.1 normal hydrochloric acid was then added until a precipitate no longer formed on dilution of a test portion with two volumes of water, after which 0.1 normal sodium hydroxide solution was added until a slight precipitate again formed on dilution
In general, 5 cc. of acid and 1.5 cc. of alkali per 100 cc. of serum were satisfactory, although as Felton emphasized, different lots vary and no absolutely definite procedure can be given
After addition of the alkali the opalescent solution was diluted with 2 volumes of water and centrifuged in the cold
The almost inactive precipitate was discarded and the supernatant poured into 6.7 volumes of the chilled buffer solution previously used, (equivalent to 20 times the volume of saline employed), also adding enough 0.1 normal sodium hydroxide to neutralize the remaining acid
The resulting precipitate was collected and dissolved in a volume of 0.9 percent saline equal to that of the serum taken, and the pH was adjusted to 7.6
The solution was sterilized by passage through a Berkefeld N grade filter which previously had been washed with saline containing a drop of normal sodium hydroxide, followed by saline alone
Antibodies were found to be unstable during testing so they were put through preliminary “ageing” processes as many times as needed until they got the result they wanted
Much time was lost and very inconstant results were obtained until “ageing” was resorted to.
The relative antibody content of the resulting solutions was estimated by determining the agglutination titer against a single heat-killed Type III pneumococcus suspension
For purposes of discussion it was assumed with Felton that antibody is modified protein, and that, in order to provide a uniform method of measurement, it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25
There is no need to spend any more time on the rest of Heidelberger’s paper as he admitted he assumed antibodies were protein and could be expressed as nitrogen thus he did not prove anything
Why would monoclonal antibodies not form a precipitate?
It is rather obvious that many assumptions were made about a substance (antibodies) for which the researchers could not see. Michael Heidelberger assumed that antibodies are modified proteins and nitrogenous. He assumed that it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25. He assumed that the failure of the precipitin test to separate out the reacting substances from non-specific material which these substances are closely related to and associated with could be somewhat avoided to some extent. He assumed that his earlier work with the pneumococcus bacteria was accurate and that he had proved the antigen component was a carbohydrate even though he was unable to produce any antibody response upon immunizing animals using his supposed antigen. Maybe this lack of any antibody response to his “antigen” has to do with the fact that, according to the WHO, the pneumococcus bacteria is regularly found in healthy people?
“Infection is acquired mainly through pneumococci contained in respiratory droplets. There are many healthy, asymptomatic carriers of the bacteria but no animal reservoir or insect vector.”
If an antigen is a toxin or foreign substance which produces an immune response creating antibodies, the pneumococci bacteria doesn’t meet that definition at all. If it isn’t an antigen, then the pneumococcus “antigen” would not be carbohydrates as described in Heidelberger’s 1923 paper. This would mean that Heidelberger’s 1929 paper measuring any of the remaining protein content, calculating the amount, and claiming the resulting protein mass as antibodies is essentially meaningless. Can you see the problem with assuming things to be true without ever proving this to be the case?
The conclusions drawn by Heidelberger were born out of chemistry experiments and reactions using the precipitin test which have no bearing on reality while using mathematical equations attempting to quantify the unquantifiable. Whether or not these indirect experiments and assumptions provide proof that antibodies exist and are proteins, I leave up to the reader. However, keep in mind that no antibodies had ever been seen nor proven to exist by proper purification and isolation up to that time and that still holds true to date. This work is based off of theoretical explanations of immunity for which nothing could be observed. Heidelberger’s indirect chemical reactions and equations provided no direct evidence for the existence of anything other than non-specific precipitate.
Dr. Tom Cowan has recently created a series of videos where he takes a close look at what some leaders in the anti-covid-vax arena are presenting as science. Dr. Cowan’s videos can be found at his Rumble and BitChute channels.
For those of you who listen to a lot of alternative “anti-vax” presentations about the origins of SARS-CoV-2 and end up feeling that you’ve just listened to a lot of faux-science gobbledygook, you’re not alone.
Below, Truth Comes to Light has clipped two key segments from the longer video where Dr. Cowan looks into Dr. Judy Mikovits’ presentations and papers related to SARS-C0V-2. Dr. Tom Cowan’s full video is also found below.
“Science has become the enterprise of people using words and concepts to make things, that everybody otherwise would understand, basically incomprehensible.”
“There are some basic ways that all of us — men, women, human beings — understand the world. It’s very clear and simple to us. And if we applied that same thinking to subjects in science and biology and medicine I think it would be fairly easy for us to find our way and to see what’s true and what isn’t true.
The problem has become that so-called scientists, especially virologists and medical doctors, have made the whole thing so confusing that most people seem to lose their bearings as far as understanding just the usual, common sense, logical, rational way of thinking and end up believing something that they wouldn’t possibly believe if they really understood the issues.”
“I’m not anti-vaccine. I just want them to be safer and more effective.”
I love that statement. It’s a lullaby. When I can’t go to sleep at night, I just repeat it to myself a few times, and I’m out cold.
It’s typical of half a revolution, which never wins.
For the past 32 years, I’ve presented overwhelming evidence that no vaccine was ever safe or effective. The whole “science” of vaccination is a rank fraud.
But stuffed-shirt journalists, who sort of go against the grain while maintaining a front of respectability, don’t want to venture that far. They know the price they’ll have to pay. They’re hedging their bets.
Occasionally, one of them will take a swipe at me. It cements their position as middle of the road. Which is where they want to be.
Except, liberty and freedom, which is what we’re fighting for, against a global coup by mass medical murders, isn’t something you win in the middle of the road.
You don’t win by trying to come off like a Washington Post reporter who just happens to have different and dissenting ideas. That’s what half-ass looks like.
That sort of person is basically saying, “I have a machine mind like other machine minds. The difference is, I’m inputting different data and therefore drawing different conclusions. If you, too, have a machine mind, read what I write and let’s establish truth and justice…”
The long-term effect of that is like pissing through a fire hose to put out a conflagration taking down a city.
This is simple. If one group of “superior” machine minds wins against another group of machine minds—regardless of which issues come out on top—there is no revolution. LIFE AND FREEDOM have been excised out of the equation.
A considerable amount of money and effort have gone into building a modern culture composed of what looks like science and rationality, but isn’t. It’s a cartoon. A fucking cartoon.
There’s no JUICE in it.
That’s why I use the phrase machine-minds. Minds that calculate and process and collate and compare and then exude “better answers.” This is your educated class. Careful, cautious. Circumspect.
“Delivery, sir. Here are flowers you ordered. I’m sorry they’re dead.”
“I don’t mind dead. But I ordered roses and you brought me tulips. I can prove it. Let me just find the receipt here on my cell phone. And then I can show you these withered blossoms are actually tulips. There are 32 differences between the two types of flowers…”
That’s your educated class.
See, I’ve been at this for 38 years. Reporting. Writing. Actually, I’ve been writing for 66 years. I’ve made the cases I wanted to make. I’ve shoved the evidence in people’s faces. The overall medical cartel is waging a VERY successful war against the people.
You have to turn that evidence with torque, with leverage, into a flamethrower. You’re not just trying to set the record straight and bring in truth, you’re using the truth to crash the gold-plated systems of machine minds.
Those minds are remote. Distant. Distant is where Big Tech domeheads operate from. They profile, they plan, they crunch trillions of pieces of data, and they develop strategies to build a civilization that looks like their minds and their computers.
When one of these high-IQ blown dry characters develops his version of a conscience, and turns whistleblower, he’s a hero to his ilk. He speaks their language. He thinks the way they do. He geeks like they geek.
If I have to guess which guy has more freedom in his belly and his brain, I’m going with the man who lives up in the hills of Tennessee with a shotgun and a dog. If he doesn’t like what I’m writing, I might think about his reasons for a half-hour. Whereas, when an “alt. journalist” claims I’m “going too far,” I know exactly what his game is. He’s spraying his usual brand of sanitizing respectable room-deodorant.
I’ll put this another way. Two men are discussing how to choose a wife. They’re looking at two different lists of characteristics a man should consider and check. But neither man mentions LOVE, so it doesn’t matter which list they decide is superior. They don’t know what love is. What they’re really discussing are machine-thoughts.
If the COVID narrative had never been launched, if we were living now as we did in 2018, we would still have a medical cartel taking away our freedom and killing and maiming an extraordinary number of people. And that will still be the case, even if all COVID mandates and restrictions are defeated.
Plus, the Brave New World on the drawing boards is fronted by medical people. Three of its main features are genetic engineering, nanotechnology, and human-computer interfaces and hybrids. If you think all possible freedom is now under fire, you haven’t seen anything yet.
Way back when, I was briefly trained in two schools. The first was formal logic, taught by a beloved college professor with an extraordinarily sophisticated mind and a huge heart. The second school consisted of two or three encounters with Ida Honorof, activist and author. She was barely five feet tall, and she had the energy, in her 70s, of ten tigers. She explained to me one afternoon, on a street corner, that officials in Los Angeles were spraying a version of deadly Agent Orange in the Angeles National Forest. She handed me a few pounds of corporate and government documents detailing the massive toxicity of a variety of pesticides. She kick-started my life as a reporter.
Neither one of these people engaged in coddling. They didn’t sit around planning their fronts and poses of respectability. They didn’t want half a revolution. They didn’t equivocate.
I’ve never been a big fan of equivocation. I’m over at the I-don’t-give-a-shit end of the spectrum.
Find answers—then shove in all your chips. At the end of the night, don’t leave anything on the table.
Fortunately for all of us, there is a life after this one. But we’re here now, so we’re fighting.
Make it COUNT.
In the wind and the rain and the storm, issue no apologies.
TORONTO: The Justice Centre has engaged lawyer Phillip Millar to represent serving members of the Canadian Armed Forces (CAF) who have declined the Covid vaccine on the basis of health concerns or conscientious objections. One of client, Warrant Officer James Topp, is a member of the CAF reserve force facing the charge of “Conduct to the Prejudice of Good Order and Discipline,” which has the potential to result in Court Martial. The Justice Centre also represents 15 other CAF members facing discipline and possible job loss over mandatory Covid vaccine policies implemented by the military.
Mr. Topp, who has been a serving member of the CAF for 28 years, has gained national headlines for his 4,293 kilometre “Canada marches” walk across the country, in protest of mandatory vaccine mandates, forced quarantines, mandatory testing, and other conditions of employment or provision of services.
Mr. Topp began his march on February 20, the same day police forces began using physical force against unarmed Freedom Convoy protesters in Ottawa. Facing job loss for refusing a Covid shot, Mr. Topp is averaging 30 km a day along the highway. His goal is to reach the Tomb of the Unknown Soldier in Ottawa by June 22.
Mr. Topp says government overreach has spread into all aspects of the personal lives of Canadians. “I’m not here for profit, and I don’t want to be a celebrity, but I need to do something,” Mr. Topp told about 100 supporters in Vancouver, who came out on a cold winter day to see him off on his march. “We need to do something to repair us because we’ve been deeply fractured by what has happened…” He adds, “We have to “ensure our government upholds the laws that support Canada’s Charter of Rights and Freedoms.”
Mr. Millar will represent Mr. Topp and 15 other military members in Federal Court, seeking an injunction against the release of CAF members until their grievances are heard. The Justice Centre maintains that military members are entitled to have their constitutional freedoms such as freedom of religion and conscience protected, as CAF members have fought and served to protect the freedoms of all Canadians.
Mr. Millar is a former full-time Combat Officer in the CAF Infantry, former Assistant Crown Attorney, and experienced trial lawyer who has already successfully sued the Department of National Defence (DND) in the past.
“The mandatory vaccine is a flawed policy based on a stubborn refusal to acknowledge that the underlying justification for the mandate has changed. The government is using the Canadian Armed Forces as a policy arm to promote its vaccine mandates. The policy hurts the operational effectiveness, morale, and integrity of the system,” says Mr. Millar.
He notes that the “military chain of command is fast-tracking the release of service members who refuse to get vaccinated under administrative processes, trampling their rights and denying them due process by sidestepping the proper procedures.”
“The DND cannot claim that service members are disobeying a lawful order and then refuse to allow the issue to be tried in the military justice system where a judge can make a determination if it is in fact a “lawful order”,” adds Mr. Millar.
The government is using a “5F release,” which was never meant to be applied in this manner.
“We cannot let them get away with ruining the lives and careers of dedicated Canadians who serve their country. Our soldiers, sailors and air force personnel deserve more. They are highly trained, and many have served their country for years,” Mr. Millar concludes.
“Covid ‘vaccines’ caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.”
This week MEP Christine Anderson (AfD) gave her first speech before the European Union’s new “COVID-19 inquiry committee”. The German MEP condemned the EU’s Covid policies and demanded an investigation into the clear human rights violations under the pretext of combatting a virus.
Anderson railed against the “false claims regarding the safety of the vaccines, their alleged definitive approval, and so-called effectiveness.” The MEP pointed out that the European Medicines Agency (EMA) database shows that in seven months, the Covid “vaccines” caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.
“Why isn’t that being investigated,” questioned the MEP. She explained that the government’s Covid policies had nothing to do with public health. Instead, it seems it has been “a money-making exercise for the pharmaceutical industry.”
Why were alternative methods to fight Covid not investigated or given to the public, questioned Anderson? Instead, she exclaimed, everything in your whole Covid policy “boiled down solely to: “vaccinate, vaccinate, vaccinate.”
Issues Committee Must Address
Anderson pointed out other issues that the committee must investigate. She first zeroed in on the “implementation of vaccine contracts.” Little information is available on vaccine makers’ contracts due to the committee withholding the information. She questioned how she could “properly do her job as an elected MEP” and educate her constituents without the data.
The massive “restrictions of fundamental rights that are unworthy of a democracy” must also be investigated, exclaimed the MEP. “From job losses, discrimination and marginalization, we have experienced a redefinition of fundamental rights.” According to the new definition, our rights are now privileges to which the government picks and chooses who to grant them.
The MEP demanded answers as to why the committee is not investigating the “marginalization and criminalization of critics” who condemned their “anti-democratic measures.”
She went on to say that it is unacceptable for the World Health Organization (WHO) to sign new contracts with EU member states. As Anderson has previously explained, the WHO is fighting for de facto governing power over EU member states in the event of a pandemic:
Dr. Joseph Yi (StreetMD) with Drs. Tom Cowan, Andrew Kaufman & Mark Bailey: A Response to Claims by Drs. Robert Malone, Peter McCullough & Ryan Cole That SARS-CoV-2 Has Been Isolated & Is a Disease-Causing Virus
Dr Joseph Yi, AKA “StreetMD” asked Drs Bailey, Cowan and Kaufman to respond to Drs Malone, McCullough and Cole’s claims that SARS-CoV-2 has been isolated and shown to exist. Boom!

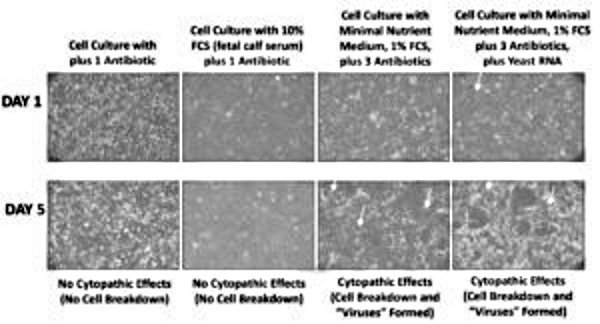
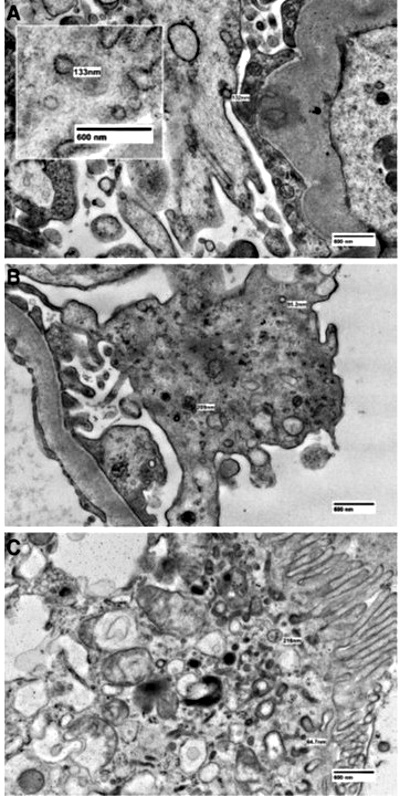
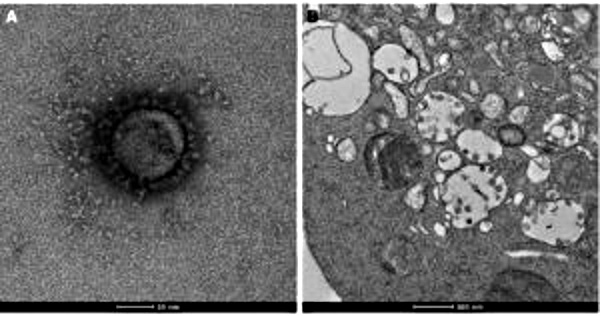

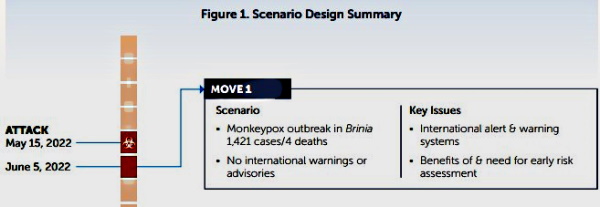

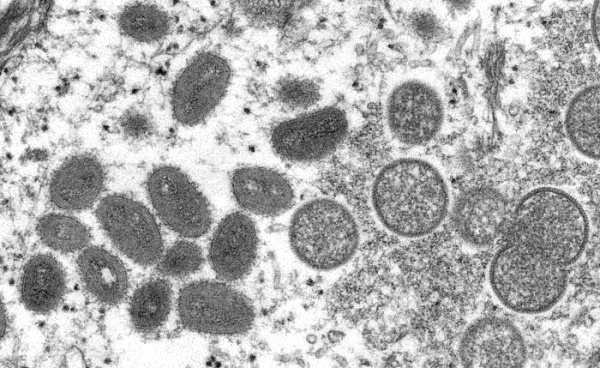
 Next, the
Next, the 
 Are the new jabs already prepped & ready to go?
Are the new jabs already prepped & ready to go?

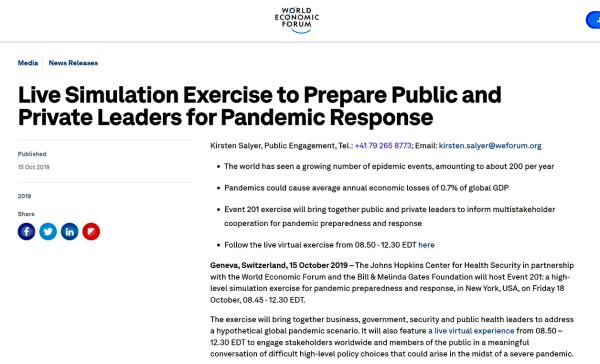




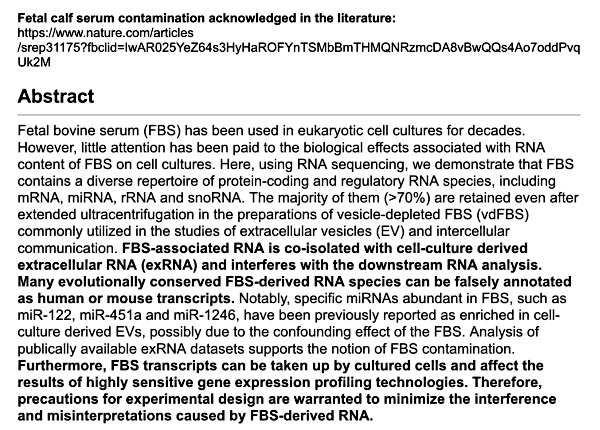
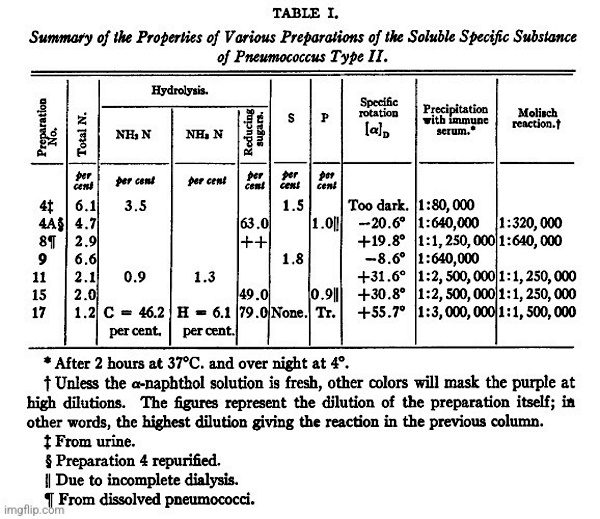
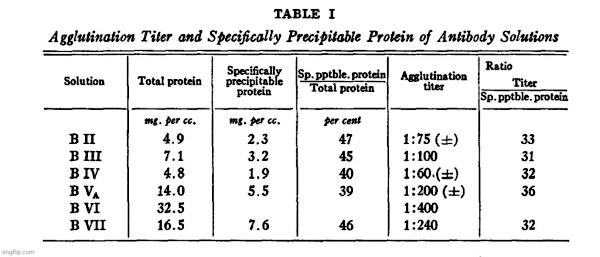
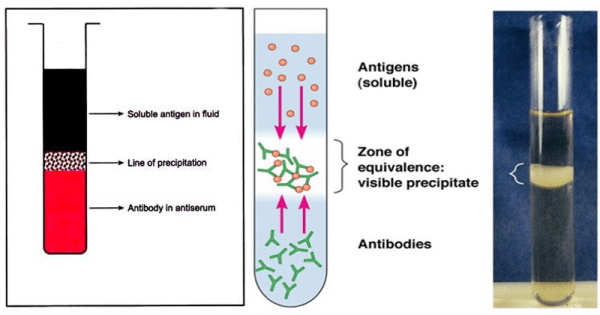
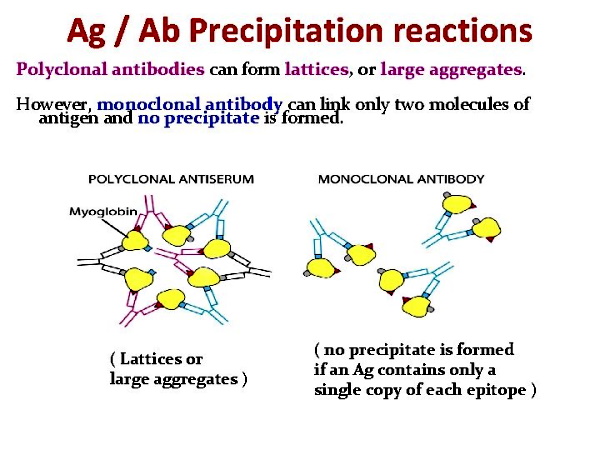
{kind=link}