“Salamanders, toads and frogs have more vitality than other forms of life. The density of their strings — their meridians — that connect them to earth and sky is greater. It is why they rarely (and salamanders never) get cancer: both their external and internal communication systems are too strong for their cells to escape control. It is why frogs can partially regenerate lost limbs, and salamanders can regenerate them completely. It is why salamanders can even regenerate their heart — and do it within hours — if half of it is cut out — an astounding fact discovered by Dr. Robert O. Becker and written about in chapter 10 of his classic book, The Body Electric.
It is also why amphibians are dying out. Animals with such a strong connection to Earth’s orchestra — who are so attuned to it that they have survived for 365 million years — cannot withstand the chaos that we have superimposed on it during the past half century and more — the chaos that we have injected into the living circuitry with our radio and TV stations, our radar facilities, our cell phones and cell towers, and our satellites. “
[…]
“It is why wireless technology, which has placed a source of lethal radiation into the hands of almost every man, woman and child on earth, is such an emergency and must come rapidly to an end if we are so save our planet and the millions of other species who are still trying to share it with us. The frogs and salamanders are telling us that it is not a matter of choice, and it is not a matter of how far from our heads we hold our phones. It is a matter of their survival and ours.”
Communication towers inside Monteverde Cloud Forest Biological Preserve
“Amphibians were here when the dinosaurs were here, and they survived the age of mammals. If they’re checking out now, I think it is significant.”
– David Wake, Director of the Museum of Vertebrate Zoology, University of California, Berkeley, 1990
They are ancient animals with abilities to survive beyond belief. They live both in water and on land. They can breathe through their skin. They can regenerate limbs and organs. They don’t get cancer. They have been around for 365 million years, and have survived four mass extinctions during the history of life on Earth. Yet today, they are disappearing more rapidly than any other class of animals. By their death, they are screaming: Turn off your cell phones! Now, before it is too late!
Even before cell phones, the proliferation of radio and TV towers, radar stations, and communication antennas in the 1960s, 1970s and 1980s began killing off these most hardy, well-adapted, and important forms of life.
The northern leopard frog, Rana pipiens – the North American green frog that croaked from every marsh, pond and creek when I was growing up — was already extremely rare by the end of the 1980s.
In the Colorado and Wyoming Rocky Mountains, boreal toads used to be so numerous that, in the words of Paul Corn of the United States Fish and Wildlife Service, “You had to kick them out of the way as you were walking down the trail.” By 1990 they were difficult to find at all.
Boreal chorus frogs on the shores of Lake Superior, once innumerable, were extremely rare by 1990.
In the 1970s David Wake could turn up eighty or more salamanders under the bark of a single log in a pine forest near Oaxaca, Mexico. In the early 1980s he returned and was able to find maybe one or two after searching the forest all day.
Until 1979 frogs were abundant and diverse at the University of São Paulo’s field station at Boracea, Brazil, according to Stanley Rand of the Smithsonian Tropical Research Institute. But when he returned in 1982, of thirty common frog species, six had disappeared entirely and seven had decreased in number drastically.
In 1974 Michael Tyler of Adelaide, Australia discovered a new frog species that brooded its young in its stomach. It lived in a 100-square-kilometer area in the Conondale Ranges, 60 kilometers north of Brisbane, and was so common that he could collect a hundred in a single night. By 1980 it was extinct.
The golden toad lived only in a 320-acre stunted forest in Costa Rica’s supposedly pristine, protected Monteverde Cloud Forest Preserve. In the early 1980s Marc Hayes of the University of Miami typically counted 500 to 700 males at one of the species’ breeding sites. After 1984 that site never had more than a dozen males. At another site Martha Crump observed a thousand males in 1987, but only one in 1988 and another single male frog in 1989. Today the species is extinct.
In 1990, when I began researching this magical class of vertebrates, there were not many amphibians left in all of Europe. Out of more than five thousand known species worldwide, about a dozen were doing well.
By the time I wrote Microwaving Our Planet in 1996, every species of frog and toad in Yosemite National Park had become scarce. Seventy-five species of the colorful harlequin frogs that once lived near streams in the tropics of the Western Hemisphere from Costa Rica to Bolivia had not been seen in a decade. Of the 50 species of frogs that once inhabited the Monteverde Cloud Forest Preserve, 20 were already extinct.
Similar population crashes were occurring in North, Central and South America, Europe, and Australia. Only in Africa and Asia, when I wrote that book, were amphibians doing well. That has since changed. On March 15, 2023, a team of 19 American scientists published a paper titled “Continent-wide recent emergence of a global pathogen in African amphibians.” Amphibians, say the authors, were doing fine on the dark continent until about the year 2000 — which coincidentally is when telecommunications companies began lighting up that continent with cell phone signals in earnest.
A couple of years earlier, in December 1997, I had published an article titled “The Informationization of the Third World.” I quoted President Clinton, who had lamented that “More than half the world’s people are a two days’ walk from a telephone.” I highlighted Bangladesh, where there were plans to bring cell phones to 40,000 of the country’s 68,000 villages over the next four years. In Africa, where several countries still had less than one conventional phone per one thousand people, some two dozen countries were introducing cellular systems. The debate, in the world’s press, was about what this would do to the traditional village, and whether this was a desirable thing from a cultural point of view. I took a broader view:
“An even more important question is what will happen to nature? Can nature survive at all in a distanceless world? I think the answer, if ecologists and environmentalists brought their knowledge to bear, would be a resounding no. Biodiversity depends on distance. What is not often acknowledged is that cultural diversity also depends on distance, and that culture is nature-based. Local dialects, and local handicrafts, and local dress, and local economies, and local varieties of crops, and local varieties of plants and animals — i.e. local ecosystems — depend on the village’s being a two days’ walk from a telephone. The most basic reason for the disappearance of species is that very few of them can withstand the global exploitation that must come when there is instantaneous transportation and communication.”
And then there is the radiation. The effects of microwave radiation in Africa, as cell towers began serving larger numbers of its residents, are now apparent: amphibians have been disappearing all over the continent. This has been blamed on a type of fungus called Batrachochytrium dendrobatidis (Bd), rare in Africa prior to the year 2000. But whether it is the fungus that is killing frogs, toads and salamanders, or whether it is the radiation that is killing them, and that is allowing a fungus to grow in their devitalized bodies, is a question no one is asking. For example, why, in Cameroon, where 83 percent of the population own mobile phones, and four cell phone providers cover a lot of the country, is the fungus found in 17 percent of all amphibians collected — while in neighboring Equatorial Guinea, where only 40 percent of the population own mobile phones and there are no cell towers except in the coastal city of Bata, there is zero fungus? Why, in South Africa, where 90 percent of the population own mobile phones, and coverage is good in most of the country, is the fungus found in 23 percent of amphibians collected — while in neighboring Mozambique, where only 43 percent of the population has a mobile phone, zero fungus has been found among the amphibians collected? Could it be because cell phones are still useless in much of northern Mozambique, and that is where all the amphibians in that country have been collected: Mount Mabu, Mount Namuli, Mount Ribáuè, and Balama?
Most of the suggested explanations for the global die-off make little sense. Climate change is being widely blamed, yet scientists looking for an association of population crashes with temperature or other weather factors have found none. Why, worldwide, are amphibians declining faster at high altitudes than at lower elevations where the climate is warmer? Could it be because the higher elevations receive more radiation, and because many antennas are found on mountains? Scientists have found no evidence that fish or non-native amphibians have caused native amphibians to go extinct. Land use change does not explain sudden population crashes in pristine protected areas. Pesticide use does not correlate with the population declines.
These inconsistencies seem to be escaping the scientists who are looking for answers. They are escaping them because they have a terrific blind spot: they do not see the radiation at all, it does not exist for them.
The single most rapid and catastrophic crash in amphibian populations occurred in the year 1988 in the Monteverde Cloud Forest Biological Preserve in Costa Rica, a location that has long puzzled scientists because it is strictly protected and supposedly untouched and pristine. This is what I thought as well until I began to do research for this article. I just found out, to my astonishment, that right in the middle of this two-square-mile preserve, on top of a hill called Cerro Amigos (“Friends Hill”), is an antenna farm called Las Torres (“The Towers”). A photo of the top of that hill is at the top of this article. As of 2012, there were 17 radio, TV, cell phone, and other types of communication towers on that hill, a few of them dating from the 1970s and 1980s. I am making inquiries to try to pin down what was added in 1988. If you live in Costa Rica and know some of this history, please contact me.
More Connected Means More Vulnerable
“Is It a Hazard to Be Healthy?” asked Dr. D. B. Armstrong in the Boston Medical and Surgical Journal in 1918. If you were undernourished, physically handicapped, anemic, or tuberculous, you were much less likely to get influenza and much less likely to die from it if you did. The vast majority of people who died from the Spanish influenza were pregnant women and healthy young adults. Doctors were seriously discussing whether they were actually giving their patients a death sentence by advising them to keep fit!
Amphibians are dying for the same reason. What is completely neglected in the sciences of biology, medicine and ecology, is our electrical connection to earth and sky. As I discuss in chapter 9 of my book, The Invisible Rainbow, we are all part of the global electrical circuit that courses through the sky above us, flows down to earth on atmospheric ions and raindrops, enters the tops of our heads into our bodies, flows through our meridians, exits into the earth through the soles of our feet, travels along the surface of the earth, and flows back up to the sky on lightning bolts during thunderstorms. Those of us who are most vital and have the strongest connection to earth and sky — healthy, vigorous young adults and pregnant women — died in the largest numbers in the 1918 flu, which was caused not by a virus but by the use of enormously powerful VLF radio stations by the United States when it entered the First World War. The same thing happened in 1889 (introduction of AC electricity), 1957 (first construction of civil defense radars), and 1968 (first constellation of military satellites).
“In each case—in 1889, 1918, 1957, and 1968—the electrical envelope of the earth, to which we are all attached by invisible strings, was suddenly and profoundly disturbed. Those for whom this attachment was strongest, whose roots were most vital, whose life’s rhythms were tuned most closely to the accustomed pulsations of our planet — in other words, vigorous, healthy young adults, and pregnant women — those were the individuals who most suffered and died. Like an orchestra whose conductor has suddenly gone mad, their organs, their living instruments, no longer knew how to play.”
Salamanders, toads and frogs have more vitality than other forms of life. The density of their strings — their meridians — that connect them to earth and sky is greater. It is why they rarely (and salamanders never) get cancer: both their external and internal communication systems are too strong for their cells to escape control. It is why frogs can partially regenerate lost limbs, and salamanders can regenerate them completely. It is why salamanders can even regenerate their heart — and do it within hours — if half of it is cut out — an astounding fact discovered by Dr. Robert O. Becker and written about in chapter 10 of his classic book, The Body Electric.
It is also why amphibians are dying out. Animals with such a strong connection to Earth’s orchestra — who are so attuned to it that they have survived for 365 million years — cannot withstand the chaos that we have superimposed on it during the past half century and more — the chaos that we have injected into the living circuitry with our radio and TV stations, our radar facilities, our cell phones and cell towers, and our satellites.
It is why, in 1996, when parades of cell towers were marching from coast to coast in the United States, and sprouting at tourist destinations, mutant frogs were turning up by the thousands in pristine lakes, streams and forests in at least 32 states. Their deformed legs, extra legs, missing legs, missing eyes, misplaced eyes, misshapen tails, and whole body deformities frightened school children out on field trips.
It is why developing frog embryos and tadpoles exposed by researchers in Moscow in the late 1990s to a (wired) personal computer developed severe malformations including anencephaly (absence of a brain), absence of a heart, lack of limbs, and other deformities that are incompatible with life.
It is why, when tadpoles were kept for two months in a tank on an apartment’s terrace in Valladolid, Spain, 140 meters from a cell tower, 90 percent of them died, versus only 4 percent mortality in an identical tank that was shielded from radio waves.
It is why wireless technology, which has placed a source of lethal radiation into the hands of almost every man, woman and child on earth, is such an emergency and must come rapidly to an end if we are so save our planet and the millions of other species who are still trying to share it with us. The frogs and salamanders are telling us that it is not a matter of choice, and it is not a matter of how far from our heads we hold our phones. It is a matter of their survival and ours.
Selected Bibliography
Balmori, Alfonso. The incidence of electromagnetic pollution on the amphibian decline: Is this an important piece of the puzzle? Toxicological & Environmental Chemistry 88(2): 287-299 (2006).
Balmori, Alfonso. Mobile phone mast effects on common frog (Rana temporaria) tadpole: The city turned into a laboratory. Electromagnetic Biology and Medicine 29: 31-35 (2010).
Becker, Robert O. and Gary Selden. The Body Electric (NY: William Morrow 1985).
Berger, Lee, Rick Speare, Peter Daszak, et al. Chytridiomycosis causes amphibian mortality associated with population declines in the rain forests of Australia and Central America. Proceedings of the National Academy of Sciences 95: 9-31-9036 (1998).
Berger, Lee, Alexandra A. Roberts, Jamie Voyles, et al. History and recent progress on chytridiomycosis in amphibians. Fungal Ecology 19: 89-99 (2016).
Bittek, Jason. Half of all amphibian species at risk of extinction. National Geographic, May 8, 2019.
Blaustein, Andrew R. and Pieter TJ Johnson. The complexity of deformed amphibians. Frontiers in Ecology and the Environment 1(2): 87-94 (2003).
Collins, James P. Amphibian decline and extinction: What we know and what we need to learn. Diseases of Aquatic Organisms 92: 93-99 (2010).
Drost, Charles A. and Gary M. Fellers. Collapse of a regional frog fauna in the Yosemite area of the California Sierra Nevada, USA. Conservation Biology 10(2): 414-425 (1996).
Firstenberg, Arthur. The Informationization of the Third World. No Place To Hide 1(3): 1-2 (Dec. 1997).
Firstenberg, Arthur. Microwaving Our Planet: The Environmental Impact of the Wireless Revolution (NY: Cellular Phone Task Force 1996, 1997).
Firstenberg, Arthur. The Invisible Rainbow: A History of Electricity and Life (White River Junction, VT: Chelsea Green 2020, 560 pages).
Ghose, Sonia L., Tiffany A. Yap, Allison Q. Byrne, et al. Continent-wide recent emergence of a global pathogen in African amphibians. Frontiers in Conservation Science 4: 1069490 (2023).
González-del-Pliego, Pamela, Robert P. Freckleton, David P. Edwards, et al. Phylogenetic and trait-based prediction of extinction risk for data-deficient amphibians. Current Biology 29: 1557-1563 (2019).
Hoperskaya, O.A., L.A. Belkova, M.E. Bogdanov, and S.G. Denisov. The action of the “Gamma-7N” device on biological objects exposed to radiation from personal computers. In Electromagnetic Fields and Human Health: Proceedings of the Second International Conference, Moscow, Sept. 20-24, 1999, pp. 354-355, Abstract.
Houlahan, Jeff E., C. Scott Findlay et al. Quantitative evidence for global amphibian population declines. Nature 404: 752-755 (2000).
Laurance, William F. Global warming and amphibian extinctions in eastern Australia. Australian Ecology 33: 1-9 (2008).
Lips, Karen R., Patricia A. Burrowes, Joseph R. Mendelson III, and Gabriela Parra-Olea. Amphibian declines in Latin America: Widespread population declines, extinctions, and impacts. Biotropica 37(2): 163-165 (2005).
McCallum, Malcolm L. Amphibian decline or extinction? Current declines dwarf background extinction rate. Journal of Herpetology 41(3): 483-491 (2007).
Norris, Scott. Ghosts in our midst: Coming to terms with amphibian extinctions. BioScience 57(4): 311-316 (2007).
Pound, J. Alan and Martha I. Crump. Amphibian declines and climate disturbance: The case of the golden toad and the harlequin frog. Conservation Biology 8(1): 72-85 (1994).
Rose, S. Meryl. Regeneration (NY: Appleton-Century-Crofts 1970).
Souder, William. An amphibian horror story. New York Newsday, Oct. 15, 1996, p. B19+.
Souder, William. Deformed frogs show rift among scientists. Houston Chronicle, Nov. 5, 1997, p. 4A.
Stuart, Simon N., Janice S. Chanson, Neil A. Cox, et al. Status and trends of amphibian declines and extinctions worldwide. Sciencexpress, October 14, 2004 (5 pages).
Toledo, Luís Felipe, Sergio Potsch de Carvalho-e-Silva, Ana Maria Paulino Telles de Carvalho-e-Silva, et al. A retrospective overview of amphibian declines in Brazil’s Atlantic forest. Biological Conservation 277: 109845 (2023).
Vogt, Amanda. Mutant frogs spark a mega mystery scientists worry could be an early warning of environmental danger. Chicago Tribune, August 4, 1998, sec. 4, p. 3.
Vredenburg, Vance T., Ronald A. Knapp, Tate S. Tunstaff and Cheryl J. Briggs. Dynamics of an emerging disease drive large-scale amphibian population extinctions. Proceedings of the National Academy of Sciences 107(21): 9689-9694 (2010).
Wake, David B. and Vance T. Vredenburg. Are we in the midst of the sixth mass extinction? A view from the world of amphibians. Proceedings of the National Academy of Sciences 105(Suppl. 1): 11466-11473 (2008).
Watson, Traci. Frogs falling silent across USA. USA Today, August 12, 1998, p. 3A.
“The cabal of pandemic fraudsters must be laughing. As cartoonist Bob Moran quipped, gain of function is really gain of fiction. To date, there is no actual evidence that viruses can be made more lethal, despite the huge amounts of research grant money awarded and theoretical reports.”
Why Wuhan? For the most deadly pandemic since the Spanish influenza of 1918-1919, an enormous but hardly known metropolis from the Chinese interior was the source. The official story was zoonotic transmission of a bat coronavirus, blamed on poor hygiene at the city’s wet market.
While I saw from the outset the malevolent plot of Covid-19 to erect an authoritarian regime through an exaggerated threat to lives, I was temporarily drawn to the alternative explanation. The Wuhan Institute of Virology, funded by the US government for ‘gain of function’ viral research, seemed an obvious origin. While the lab leak was dismissed as conspiracy theory by political leaders and most mainstream media, investigative journalism by Ian Birrell in the Mail on Sundayreported lax practices and broken seals in the Wuhan laboratory, despite its intended operation at the highest level of biosecurity.
I suggested a laboratory accident in my report Year of the Bat, written for Civitas think-tank during the first lockdown. But months later I changed my mind, having listened to the likes of Patrick Henningsen of 21st Century Wire, doctors Sam Bailey and Tom Cowan, Jeff Berwick of Dollar Vigilante, and seasoned conspiracy theorist David Icke. In his Perceptions of a Renegade Mind, Icke argued that it was easier to enact a technocratic coup with a fake rather than real virus. A released pathogen would be unpredictable, likely to lose lethality, and scientific analysis would soon diverge from an initially contrived consensus.
Why didn’t medics and scientists see the scam? Covid-19 was, in my view, a carefully planned emergency, in which normal standards of science and ethics would be overridden. As the new virus began to spread in January 2020, Christian Drosten and colleagues in Germany provided the concrete foundation for the entire edifice, by identifying a genetic sequence through PCR testing, enabling screening for the disease. Incredibly, this paper was approved by peer review in 24 hours. Testing kits were already available in bulk supply across the world – one of many curious instances of readiness for a nasty viral surprise.
Doctors and health authorities uncritically accepted the existence of Covid-19 and its testing standard. Kary Mullis, inventor of the PCR test, emphasised that this tool should not be used for diagnostic purpose, and that with high level of amplification of samples, almost anything in the atmosphere could be found by the test. Perhaps too conveniently, Mullis died in August 2019.
Instead of the widely depicted CGI rendering of a sphere with spikes (like a naval mine, but typically coloured in a sinister deep purple), the reality of SARSCOV2 is a code for a genetic sequence generated with ‘next generation’ genomic sequencing software found in human beings here, there and everywhere. It may be merely dead cellular material, possibly more prevalent with seasonal respiratory infection. This code, rather than any viral sample, was all that Pfizer and Moderna used to produce their ‘vaccines’.
The origins of Covid-19 has become a major talking point recently, after the Department of Energy suggested that, after years of denial by the US government, that a lab leak was ‘possible’. The hypothesis was then elevated to ‘probable’ by FBI chief Christopher Wray. Cue a deluge of ‘told you so’ from the sceptical margins.
As lamented by Patrick Henningsen on UK Column News (3 March 2023), some of the most respected and influential dissidents are riding on the crest of this wave of sudden Covid-19 revisionism. Robert Malone, mRNA vaccine inventor, tweeted on the ‘narrative collapsing’, asserting that ‘the lab leak killed millions of people’. Stanford University professor of medicine Jay Bhattacharya, initiator of the Great Barrington Declaration, saw a belated shift ‘from putative conspiracy to legitimate science’. Fox News and Republican politicians such as Rand Paul renewed their calls for prosecution of Dr. Anthony Fauci and demand for reparations from China.
According to Henningsen, the lab leak is nothing but an official conspiracy theory. The narrative, far from collapsing, is unwittingly reinforced by halfway house sceptics. Everything reported on mainstream media is for a purpose, serving the ‘progressive’ agenda. What may appear as mea culpa is a staged performance involving well-remunerated fall guys such as Fauci, and British health secretary Matt Hancock.
Not only does the lab leak cause obfuscation and futile debate, it fools unwary sceptics into perpetrating the big lie. If you fall for this tale, you fall for everything founded on the fundamental falsehood of a ‘novel’ (and possibly manmade) virus. It diverts attention from the iatrogenic scandal of the vaccines, while also preparing the ground for a global pandemic treaty. Instead of fumbling politicians with their petty squabbles and egos, the unelected and unaccountable World Health Organisation will assume control of every nation’s public health response to any future threat of a contagion. This will be justified by the many ‘mistakes’ governments made with Covid-19, as now being highlighted in mass media. By the same token, it also serves to excuse any ‘mistakes’ by governments and the pharmaceutical firms, as they can simply say they were trying to react quickly to a potentially engineered pathogen from an unregulated lab in Wuhan.
The cabal of pandemic fraudsters must be laughing. As cartoonist Bob Moran quipped, gain of function is really gain of fiction. To date, there is no actual evidence that viruses can be made more lethal, despite the huge amounts of research grant money awarded and theoretical reports.
As the dust settles on Covid-19, even the sceptical community has much to learn. They are not always as ‘awake’ as they believe.
The stunning confluence of events and coincidences suggests that the Covid-19 global pandemic took years of planning. If so, it was the work of misanthropic geniuses who saw the potential for a power grab through a global campaign of fear and control, leading to a ‘new normal’ of digital surveillance and constraints on population and resources. The true sequence of events was in reverse. Rather than a virus leading to a vaccine leading to digital identity, the end point was achieved by mass vaccination, for which a virus was invented. Covid-19 arose not from a laboratory, but from a laptop.
Nano-materials of the Graphene family are strictly unregulated by the European Commission
How long have Graphene derivatives been contaminating Agriculture? Ten years or fifteen years?
Graphene Hydrogels commercialized for Agriculture
Studies on the toxicity of Graphene derivatives on plant growth and soil health
Studies on the toxicity of Graphene derivatives on all elements of aquatic environments
Studies on the ability of Graphene derivatives to allegedly improve plant growth
Studies on the ability of Graphene derivatives to eliminate or mitigate, allegedly, toxicities or pests in agriculture
A few Patents concerning the insertion of graphene oxide in Fertilizers and in Pesticides/Biocides of all kinds
Foreword
This dossier is a follow-up to my first one, entitled “Graphene in Agriculture”, which presented two of my short articles on the subject, as well as six essays written by the Spanish researcher, Mik Andersen. This first dossier was presented in January 2022.
In this present dossier, I have “restricted myself”, in the first part, to the proven contamination of agricultural plants, agricultural soils, terrestrial environments and aquatic environments, by Graphene present in fertilizers and pesticides used in Agriculture. I do not address the same “contamination”, by Graphene as a “decontamination vector”, of these same agricultural, terrestrial and aquatic environments… which it has itself contributed to contaminate in synergy with a host of other metallic nanoparticles. This scandalous issue of the “decontamination by Graphene” will be the subject of a subsequent dossier.
The situation is much more serious than the Spike’s Wacky Sectarians, and other devout dissidents of the Covidian religion, can imagine, when they censor us, inexorably, we whistleblowers who denounce the presence of graphene, nano-particles and other nano-technologies, in CoYid/19 injections – and other injections called infantile, anti-flu, anti-cancer, anti-meningitis, “vaccines” – ad nauseam and ad mortem.
Graphene is everywhere: namely, in all sectors of daily life because it is considered the miracle material – especially by all the eugenicist Globalists and other scientists in their pay… Indeed, Graphene will allow them to trace and connect Humans by chaining and imprisoning them, “digitally”, in the nets of the virtual network under the pretext of “digital health”, “digital medicine” or “digital pharmacy” – or under no pretext at all… when dictatorship sets in.
Biologists, doctors, researchers, journalists, activists, columnists, influencers, civil servants, etc., who continue to deny this reality of the omnipresent Graphene – or to deny the extreme health risks associated with this reality of the omnipresent Graphene – are thus invited to open their eyes, their ears and their synaptic connections very quickly… or to change profession. What about plumbing?
Why? Because they are liars and because, today, the empire of lies – and its peddlers under all ideological shades – is in the process of collapsing under the weight of its own inconsistencies, manipulations, dissonances. Indeed, the empire of lies can no longer generate as much energy as it would take to fill the gaps… which are becoming more and more gaping.
In a second part, I present the studies which affirm that Graphene can increase the growth of the plants, fight against the pests or, even, take part in the decontamination of the agricultural plants toxified by the extreme abundance of heavy metals, various and varied, in the agricultural grounds.
Indeed, there are teams of highly paid “scientists” whose mission is to claim that Graphene is harmless in agricultural soils, in food plants, in terrestrial and aquatic environments – and that it is, in fact, beneficial. These are the same people who produce “scientific” studies on the danger of the non-existent CoYid/19 or on the harmlessness of genocidal vaccines.
These are the same people who produce “scientific” studies claiming that Graphene is not dangerous for the human organism – and that it is, in fact, beneficial. In fact, I am presenting, here, summaries of hundreds of studies on the toxicity of Graphene derivatives: graphene oxide, reduced graphene oxide, carbon nanotubes, carbon quantum dots, graphene quantum dots, etc.
It is important to elucidate what a plethora of scientists have been working on, for the last 15 years or so, with regard to the very concrete problem of nano-particles in agriculture – and therefore in food. Indeed, those who finance this type of research and study are, of course, very intentional – in terms of profitability, or, in the case of “vaccines”, in terms of orchestrating planetary depopulation.
This elucidation is all the more essential since, as mentioned below, hundreds of thousands of tons of nano-materials are injected annually into agriculture, in France for example, without anyone being aware of the existence of this phenomenon – or of the nature of the nano-particulate substances injected… under the pretext of fertilizers, elicitors or pesticides.
This is why I am presenting, first of all, the very concrete and commercialized case of the graphene hydrogel, GelPonic, in order to highlight the fact that – just as insect meal has been sneaking into many foods for years – graphene has already infiltrated all sectors of agriculture… and therefore, of food.
It is no longer just a matter of patents or PhD studies… but of concrete proposals made by the industry. Moreover, patents and other scientific studies by PhDs are often only the first signs of an industrial catastrophe.
I invite readers interested in this very toxic issue to consult my very long files on the subject of Graphene in human food through cellular food, insect-based food, functionalized meats, food packaging, etc:
Graphene has infiltrated agricultural plants even more than it is beginning to contaminate all terrestrial and aquatic environments – as many of the following studies have shown. And this is, of course, without dwelling on the Graphenization of the Atmosphere, which I have already addressed in a voluminous dossier, “Graphene in the Atmosphere”.
Graphene in its various forms circulates in the Atmosphere, in agricultural environments, in aquatic environments… and, therefore, in the rivers and water tables that serve agricultural soils – in a vicious circle of self-accumulation and self-assembly.
It goes without saying that the problem of contamination of terrestrial and aquatic environments by graphene present in fertilizers, elicitors and pesticides of toxic conventional agriculture, is also posed for all other metallic or non-metallic nanoparticles that have been used in agriculture for a long time.
What should we do? We will avoid panicking, first of all, because the Globalists already handle panic with brio.
Let us be confident that in the long run – whatever the amplitude – Gaia, our Mother Earth, digests and metabolizes any substance and, one day, she will emanate, from her Biosphere, a bacterium with the capacity to digest all the two-dimensional carbonaceous nano-materials (0.35 nm thick) of the Graphene family… if they excessively disturb Her Natural ways.
Nano-materials of the Graphene family are strictly unregulated by the European Commission
Here is how the European Commission (the tool of the European dictatorship in the service of the military-industrial complex) presents the regulations on nano-materials in three pages – the third of which is extremely clear as to the strict preponderance of derivatives of the Graphene family in the general nomenclature of this class of materials. [91] These regulations are, intrinsically, non-regulations. It goes without saying that all nano-materials are strictly unregulated by the European Commission – not just graphene derivatives.
«Nanomaterials in REACH and CLP. On 3 December 2018 the Commission adopted Commission Regulation (EU) 2018/1881 to modify REACH Annexes I, III and VI-XII, introducing nano-specific clarifications and new provisions in the chemical safety assessment (Annex I), registration information requirements (Annex III and VI-XI) and downstream user obligations (Annex XII).
… On the basis of the Commission Recommendation of 18 October 2011 on the a nanoform is a form of a natural or manufactured substance containing particles, in an unbound state or as an aggregate or as an agglomerate and where, for 50 % or more of the particles in the number size distribution, one or more external dimensions is in the size range 1 nm-100 nm, including also by derogation fullerenes, graphene flakes and single wall carbon nanotubes with one or more external dimensions below 1 nm.»[86]
Reading this regulation 2018/1881, it is obvious that the European Commission authorizes, blindly, the totality of the nano-particles produced by the Industry because if one refers to its requests of non-toxicity – with regard to humans, invertebrates, algae, etc – it is a long time since a formal, and generalized, prohibition should have been promulgated in order to protect the health of the populations and the eco-systems.
Indeed, only for some graphene derivatives, I have presented about 300 studies proving their extreme toxicity. And these are, for the most part, studies dating from recent years … while the first studies, of toxicity, date from about 2011 – ie, the time of the « recommendation » of the European Commission of October 18, 2011 on the “nano-form” … [87]
How could Graphene be regulated, in terms of its toxicity, when billions of euros of public money are being transferred to all the pseudopods under the aegis of the Graphene Flagship – which, of course, all affirm, with their mouths agape, that Graphene is the miracle material – and so harmless!
How could Graphene be regulated, in terms of its toxicity, when the Globalists are drooling with excitement over the concept of “15 minute cities” promoted by the demented and eugenicist gang of the World Economic Forum?
How could Graphene be regulated, in terms of its toxicity, while the Globalists are drooling with excitement over the concept of “Graphene cities”, the integral Graphene cities? Why? Because graphene is the inescapable, fundamental foundation of the “15-minute cities” so dear to Klaus Schwab. Graphene is the fundamental vector, present and future, of the Connection, in all its virtual and false aspects. All those who are not able to apprehend, organically, this Reality are, probably, already disconnected from it.
According to the review titled “Hazard characterization of graphene nanomaterials in the frame of their food risk assessment: A review”, and published, in June 2022, in Food and Chemical Toxicology. [93]
«The obtained results showed that the investigations performed up to now did not follow internationally agreed-upon test guidelines. Moreover, GFNs seemed to resist gastrointestinal digestion and were able to be absorbed, distributed, and excreted, inducing toxic effects at different levels, including genotoxicity. Also, dose has an important role as it has been reported that low doses are more toxic than high doses because GFNs tend to aggregate in the digestive system, changing the internal exposure scenario. Thus, further studies including a thorough toxicological evaluation are required to protect consumer’s safety. »
How long have Graphene derivatives been contaminating Agriculture? Ten years or fifteen years?
If we refer to the article, from 2015, presented by Inf’OGM, and entitled « Des nanos en agriculture? », [58] here is what Danielle Lanquetuit and Mathilde Detcheverry of the association AVICENN – whose objective is to promote public debate and the transparency of political leaders on the issue of nanotechnologies – state.
«Thanks to the mandatory declaration instituted by France in order to feed a register (R-Nano) of nano-materials on our territory, created in 2013, we know that nearly 416 000 tons of nano-substances were declared as having been produced or imported in 2014 in France. But this figure is far below the overall volume of nano-materials actually introduced on our territory and which escape the radar of the authorities. For the past two years, agriculture has topped the list of declared sectors, without any indication of either the volume of nano-materials actually used in this sector, or the number of agricultural declarants…
Farmers are unknowingly exposed to the nano-materials in the mixtures they handle and spray... In 2014, we were able to identify at least seven companies that market products for crops that have filled out declarations in R-Nano, with about forty products sold in agriculture… without being able to have more information: the companies indeed do not provide any information on the nano-materials they use, neither in the safety data sheets, nor on their sites nor on the site of the Union of Plant Protection Industries (UIPP).»
The underlining is mine to emphasize that this is a ten year old agricultural issue. What is the nature of these nanoparticles in fertilizers, elicitors and pesticides/biocides in conventional agriculture? Few people know the composition of these nanoparticles because it requires going back upstream… to the trade secrets of the Pharma Industry – which controls the Agro-Chemical Industry.
What we can be sure of is that graphene is everywhere in agriculture because, firstly, its various derivatives have been known for about twenty years; secondly, it is considered to be the miracle material that will revolutionize everything; and, thirdly, for the last few years, it can be produced by the ton – from any carbonaceous bio-mass – at a very minimal cost.
Here is how the organization, called Graphene Council, presents, in May 2022, the new generation of nanoparticle pesticides as conceived by the US EPA, Environmental Protection Agency :
«To meet this need, an EPA research team led by Dr. Su conducted an exhaustive search for patents and published literature related to nanopesticides to understand the state-of-the-science. The team found and analyzed over 36,000 patents and 500 peer-reviewed journal articles. From their research findings, the team established two general categories of nanopesticides to help inform EPA’s regulatory reviews: 1) products with mostly metal-based nanomaterials as the active ingredient, like nanosilver and nanocopper oxide/hydroxide, and 2) products that encapsulate and carry the active ingredient using nanomaterials (mostly carbon based) like graphene and carbon nanotubes.
The team found that nano-enabled pesticides adhere better to plant surfaces and have a reduced impact on non-target organisms. Nanopesticides may also enhance plant resilience against stressors from heat or drought. These benefits could lead to higher crop yield and provide more agricultural resilience to address climate change and weather extremes. The team’s findings also highlight the data gaps and the need for additional research on potential adverse impacts of nanopesticides.» [59]
It is thus very clear to the US governmental environmental protection agency that there are two classes of nano-particulate materials, called « nano-pesticides » in agriculture: on the one hand, active ingredients based on metallic nano-particles and, on the other hand, conventional pesticide carriers, which are all of the Graphene family.
Here, now, is how the platform, named AzoNano, presents, in April 2022, the next generation of graphene-based nanoparticle fertilizers and pesticides: [60]
«In agriculture, carbon-based nanomaterials attempt to decrease the number of pesticides distributed, minimize nutrient leaching in fertilization, and increase pest and disease control output.
Carbon nanomaterials (CNMs) can be used as excellent fertilizer carriers due to their stable molecular arrangement, uniform dispersion, and low toxicity in application media. For example, graphene oxide nanoparticles are effective trace element transporters.
Carbon nanomaterials (CNMs) are utilized as light converters for supplementing plant photosynthesis. Through chloroplast photosynthesis, plants transform solar energy into chemical energy.
The sunlight used by chloroplasts is primarily confined in the blue and red regions of the visible spectrum. Therefore, they can be used as light conversion materials to maximize solar energy for expanding the light spectrum for plant photosynthesis. That said, to use carbon nanomaterials (CNMs) as light converters in plants, some important factors such as light conversion efficiency, biocompatibility, and cytotoxicity of light converting carbon nanomaterials (CNMs) in plants, and heat produced during carbon nanomaterials-enabled light transformation in plants must be taken into account.
Recently, Zhu et al. revealed that carbon-based nanomaterials with antifungal characteristics could be used to generate new fungicides. Among the different carbon nanomaterials (CNMs) tested against two plant pathogenic fungi, including nanotubes, fullerenes, and graphene oxide, the single-walled carbon nanotubes (SWCNTs) had the strongest antifungal action.
The use of carbon nanomaterials (CNMs) in applying biosensors, light convertors, fertilizers, pesticides, and agrochemical delivery is notable. However, their impact may change depending on plant species, carbon nanomaterial (CNM) type, and its dosages.
In agricultural applications, carbon-based nanomaterials can make the following contributions:
Increased agricultural yield with the use of plant growth boosters and innovative nanomaterial-based fertilizers.
Plant protection products based on nanomaterials, such as insecticides and herbicides.
The use of nano-encapsulated plant protection agents and slow-release fertilizers to reduce the number of agrochemicals used.
Nanotechnologies for agricultural practice optimization via precision farming. [60]
Graphene Hydrogels commercialized for Agriculture
In England, researchers at the University of Manchester are working on a new concept, called “Graphene City”, which aims to graphenize all supply chains – and, in fact, all sectors of daily life.
May I repeat that all sectors of daily life, that means: “vaccines”, injections, drugs, aerosols, cosmetics, dressings, condoms, sanitary napkins, therapeutic women’s panties, anesthetics, dental implants, eye lenses, concrete, asphalt, window frames, water treatment membranes, ventilation system filters, fertilizers, agricultural pesticides/biocides, bio-testing shoes, bio-testing clothing, clothing insulation, face masks, wall paints, batteries, electronics, wind turbines, pain relief patches, night covers, mattresses, light bulbs, headphones, ski goggles, etc., etc?
One of their research objectives is to graphenize agriculture. They are, thus, developing an agricultural alternative they have named “GelPonic” in order to, allegedly, reduce energy and space wastage by promoting vertical agriculture. “GelPonic” is a graphene hydrogel that has the ability to “sense” the nutritional needs of plants in the soil and meet them.
This graphene hydrogel is available in the form of granules, plates or blocks. [1]
This research, funded by the UK government and Europe, is under the responsibility of Dr. Beenish Siddique, the founder, and CEO, of AEH Innovative Hydrogel – which is located in the Graphene Engineering Innovation Centre in Manchester. [77]
Their official propaganda is well-smoothed and uses all the key concepts to fool the dumb and the sleepy: “sustainability”, “recycling”, “resilience”, “carbon sequestration”, “water saving”, “corporate social responsibility”, “zero carbon emissions”, etc.
AEH Innovative Hydrogel’s graphene hydrogel is also used for medical applications – in particular to treat chronic wounds, to avoid infections and amputations. [78]
“Connected bandages” are also manufactured by Grapheal in Grenoble, in France – a graphenizing company that also offers a “digital” CoYid/19 saliva test. Grapheal announces itself as “designer and manufacturer of embedded digital biosensors for field medical diagnosis and remote patient monitoring”. [902][903] The connected bandage is presented as follows: «This smart and connected graphene-based bandage is extremely flexible and adapts easily to all parts of the body. Its tiny wireless electronics with very light and highly flexible electrodes transmit data to a mobile application. Using tele-medicine software and medical technologies in the cloud, the hospital receives the information, which can then be monitored and evaluated by a specialist.»
One study, published in July 2021, even proposes an aerogel composed of graphene oxide and polyethylene glycol reinforced with grape seed extract (for its proanthocyanidins) to heal wounds. [1069]
On the other side of the Atlantic, in California, Juan Pablo Girald – from the University of California Riverside – is leading a $1.6 million funded project on the use of nanotechnology to deliver nitrogen, as a fertilizer, directly into choloroplasts.
UC San Diego, to use nanotechnology, chemized by her team, to deliver genetic material into chloroplasts. According to Nicole Steinmetz, «Our idea is to refunctionalize natural nanoparticles, namely plant viruses, in order to deliver genes into a plant… Some engineering is needed to make sure that the nanoparticles access the chloroplasts and also that they cannot infect the plants.» Their goal is, thus, to have these lettuces and spinach, chimerized in vaccine mRNA, grown by gardeners themselves – or by large-scale market gardeners for city populations.
These researchers specify, with their hand on their heart, that all their researches are oriented towards “ecology” – that is to say the same ecology promoted by Klaus Schwab, the Transhumanist Reinitiator. It is a question of optimizing the delivery of nitrogen to the heart of the cells of cultivated plants in order to avoid its waste – real, namely the direct infiltration, of half of this nitrogen of synthesis, in the water tables.
The question that one must ask oneself, when dealing with these mentally disturbed people: what is the nature of this “engineering”, of chimerization, that must be applied in order for the nanoparticles to reach the chloroplasts. In short, what is the process by which the “refunctionalization” of phytoviruses – that is, of plant-infecting viruses – is carried out?
According to the presentation of a Korean patent, from 2019, on the increase of plant growth by incorporation of graphene nano-particles: « It has been shown that carbon nanotubes, in monofoil, can be transported and deposited, in the lipid bilayer of chloroplasts, through kinetic trapping that promotes photosynthetic activity and electron transfer.» [929]
The other question we have to ask ourselves: could it be a “refunctionalization” with graphene oxide, carbon quantum dots or carbon nanotubes? Would these graphene nanoparticles be used for conveying purposes… in order to access the chloroplasts?
It is very likely that the answer will be of the same type as for the Quantum/19 injections of the Pharmacratic Mafia. The mRNA is wrapped in lipid nanoparticles and nothing more, I promise… And how do we explain, then, the magnetization of some injected?
Thus, as early as spring 2018, the University of Adelaide, Australia, made headlines in the Industrial Fertilization sector by announcing the effectiveness of “eco-friendly” industrial fertilizers, respectful of the environment, because they are vectorized by graphene oxide. [934][935]
Today, as mentioned above, it is not easy to determine who is marketing nano-fertilizers or nano-pesticides. On the other hand, it is very easy to determine which companies commercially distribute graphene, carbon nano-tubes, fullerenes, carbon nano-cones, carbon nano-pulp, etc., etc. Examples are INSCX [76], NanoIntegris [77], OCSiAl [78], Tuball [79], MKNano [84], Matexcel [83], Platonic Nanotech [82], NanoAmor [81], etc.
The Nanowerk platform presents 53 industrial companies, worldwide, commercializing a plethora of nano-products of the Graphene family. [80]
Studies on the toxicity of Graphene derivatives on plant growth and soil health
“Distribution of different surface modified carbon dots in pumpkin seedlings”. 2018. [16]At the biochemical level, the elevated antioxidant enzymes in pumpkin roots suggest that all the CDs could potentially trigger the antioxidant defense systems in pumpkin seedlings. Additionally, such alteration was greater in the roots than in the shoots. Our study represents a new perspective on CD visualization in plant tissues and provide useful information for the potential toxicity of different types of CDs to terrestrial plants, which is of importance to agricultural application.
“Graphene oxide enters the rice roots and disturbs the endophytic bacterial communities”. [55]
“Identifying the Phytotoxicity and Defense Mechanisms Associated with Graphene-Based Nanomaterials by Integrating Multiomics and Regular Analysis”. 2021. [20]
The results showed that the plant defense was regulated by reducing the calcium content by 21.7-48.3%, intercellular CO2 concentration by 12.0-35.2%, transpiration rate by 8.7-40.2%, and stomatal conductance by 16.9-50.5%….The phytohormone gibberellin and abscisic acid receptor PYL8 were upregulated, indicating the activation of defense systems. However, reduced graphene oxide and graphene oxide quantum dots trigger stronger oxidative stress (e.g., H2O2 and malondialdehyde) than graphene oxide in fruits due to the breakdown of antioxidant defense systems (e.g., cytochrome P450 86A22 and P450 77A1).
“Stress Response and Nutrient Homeostasis in Lettuce (Lactuca sativa) Exposed to Graphene Quantum Dots Are Modulated by Particle Surface Functionalization”. 2021. [2]
C-GQDs and O-GQDs cause oxidative damage, disruption of mineral and organic nutrients homeostasis, impairment of photosynthesis, and modulates the levels of phytohormones. Light-triggered reactive oxygen species generation and oxidation of antioxidants in plants are the critical reason for the phytotoxicity and explain the difference between the different functionalizations. These findings suggest that GQDs may not be as safe as expected. Future studies should consider the modulation of surface chemistry to achieve optimal safety of GQDs, and more plant species should be tested over a longer-term scale.
“Surface charge affects foliar uptake, transport and physiological effects of functionalized graphene quantum dots in plants” 2021. [21]
Overall, our findings provide direct evidence for the influence of surface charge on foliar uptake, translocation, and physiological effects of GQDs in crop plants, and imply that foliar exposure of GQDs negatively impact plant photosynthesis and growth health.
“A double-edged effect of manganese-doped graphene quantum dots on salt-stressed Capsicum annuum”. 2022. [24]
However, based on a comprehensive analysis of normal alkanes (n-alkane) using gas chromatography-mass spectrometry (GC-MS), we also observed that the leaf epicuticular wax profile was disturbed by GQD-Mn, as the concentration of long-chain n-alkanes was increased. Meanwhile, the content of magnesium (Mg) and zinc (Zn) indicated a potential promoted photosynthesis activity in C. annuum leaves.
“Sustainable agronomic response of carbon quantum dots on Allium sativum: Translocation, physiological responses and alternations in chromosomal aberrations”. 2022. [25] This study deals with the evaluation of the uptake, translocation and phytotoxicity of graphene quantum dots, blue luminescence emitters, on the Allium sativum plant. The evaluation of the genotoxicity and cytotoxicity of CQDs towards the roots of Allium sativum was estimated according to three different concentrations.
“Sunlight promoted self-fenton photodegradation and pathway of doxycycline: Interactive effects of nanomaterial on bean plant and its genotoxicity against Allium cepa”. 2023. [26]
“Synergistic effects of glyphosate and multiwall carbon nanotubes on Arabidopsis thaliana physiology and metabolism”. 2021. [27]
The synergistic effect observed was attributed to the accumulation of glyphosate resulting from permeability and transportability of the carbon nanotubes. Overall, the risk of nanotube-herbicide interaction suggests a caution use of nanotubes in agricultural applications.
“New insight into the mechanism of graphene oxide-enhanced phytotoxicity of arsenic species”. 2021. This study deals with the joint phytotoxicity of graphene oxide and arsenic species (arsenite, arsenate) on monocotyledonous (Triticum aestivum) and dicotyledonous (Solanum lycopersicum) plant species. [30]
In addition, co-exposure with GO resulted in more severe oxidative stress than single As exposure, which could subsequently induce damage in root plasma membranes and compromise key arsenic detoxification pathways such as complexation with glutathione and efflux. Co-exposure to GO and As also led to more significant reduction in macro- and micronutrient content.
“Effects of three graphene-based materials on the growth and photosynthesis of Brassica napus”. 2022. [31]
The results revealed that RGO impaired photosynthesis mainly by decreasing the chlorophyll content and Rubisco activity. A further gene-level analysis suggested that this effect of RGO might be due to its toxicity on sulfate transmembrane transporter and nitrogen metabolism, which ultimately led to nutrient imbalance. However, GO directly damaged the photosystem by disrupting the chloroplast structure, and a decrease in Rubisco activity indicated that GO also inhibits carbon fixation. Further gene-level analysis demonstrated that GO has toxicity on the chloroplast membrane, photosystem, photosynthethic electron transport and F-type ATPase.
“Is airborne graphene oxide a possible hazard for the sexual reproduction of wind-pollinated plants?” 2022. [35]
“Assessment of graphene oxide toxicity on the growth and nutrient levels of white clover (Trifolium repens”). 2022. [39]
In this study, white clover (Trifolium repens L.) was grown in a potted soil with graphene oxide (GO) at levels of 0.2%, 0.4% and 0.6% and the effects of GO on the growth and nutrient uptake of white clover were evaluated after 50 and 100 days of exposure. GO exposure showed adverse effects on seedling growth, photosynthetic parameters and nutrient uptake in shoots, and the effect was more significant with increasing concentration and exposure time. Compared with the control, GO at the highest level of 0.6% decreased plant height, leaf and stem dry weights, total chlorophyll content and net photosynthetic rate by 43.7%, 45.7%, 43.4%, 32% and 85.7%, respectively, after 100 d of exposure, and N, K, Cu, Zn, Fe, Mo, B, Si contents decreased by 19.5%, 20.1%, 12.6%, 25.0%, 12.9%, 26.0%, 18.9%, 23.0%, respectively. Furthermore, the electrolyte leakage, lipid peroxidation, reactive oxygen species, antioxidant enzyme activities were all increased by GO, especially at high dose and long exposure. These results indicate that GO can suppress plant growth by oxidative stress, photosynthesis inhibition, and nutrient imbalance.
“Graphene oxide affected root growth, anatomy, and nutrient uptake in alfalfa”. 2022. Cette étude porte sur l’ impact négatif de l’oxyde de graphène sur la croissance et le développement des racines de luzerne. [10]
Our findings indicate that GO at high levels has a negative impact on root growth and development by inducing oxidative stress, structural impairment, and nutritional imbalance. Careful soil GO management should be emphasized.
“Effect of graphene oxide on the uptake, translocation and toxicity of metal mixture to Lepidium sativum plants: Mitigation of metal phytotoxicity due to nanosorption”. 2022. [9]
“Combined effects of carbon nanotubes and cadmium on the photosynthetic capacity and antioxidant response of wheat seedlings”. 2021. [7]
Compared with Cd alone, CNTs combined with Cd decreased net photosynthetic rate, stomatal conductance, transpiration rate, primary maximum photochemical efficiency of photosystem II, actual quantum yield, photosynthetic electron transport rate, root canal protein, and ribulose-1,5-bisphosphate carboxylase/oxygenase content. Moreover, combined treatments increased the content of superoxide anion, superoxide dismutase, guaiacol peroxidase, cytochrome, and malondialdehyde in wheat seedlings. Moreover, membrane lipid peroxidation was aggravated, causing serious damage to the wheat membrane system. In addition, the toxicity of the SW treatment and the combined treatment with SW and Cd was higher than that of the MW treatment.
“Synthesis and characterization of single-walled carbon nanotube: Cyto-genotoxicity in Allium cepa root tips and molecular docking studies”. [3]
As a result, cytotoxic and genotoxic effects of SWCNTs in A. cepa root meristematic cells which is a reliable system for assessment of nanoparticle toxicology were demonstrated in this study.
“Effects of multi-walled carbon nanotubes in soil on earthworm growth and reproduction, enzymatic activities, and metabolomics”. 2022. [15]
Exposure to 50 mg/kg MWCNTs significantly increased activities of CYP2C9, CYP3A4, SOD, CAT, and GST but clearly reduced levels of L-aspartate, L-asparagine, and glutamine. With exposure to 100 mg/kg MWCNTs, toxic effects on earthworms were observed, with significant inhibition in activities of CYP isoenzymes and SOD, significant reductions in L-aspartate, L-asparagine, glutamine, and tryptophan, and simultaneous accumulations of citrate, isocitrate, fumarate, 2-oxoglutarate, pyruvate, D-galactose, carbamoyl phosphate, formyl anthranilate, hypoxanthine, and xanthine. Results suggest that toxicity of MWCNTs to earthworms is associated with reduced detoxification capacity, excessive oxidative stress, and disturbance of multiple metabolic pathways, including amino acids metabolism, the tricarboxylic acid cycle, pyruvate metabolism, D-galactose metabolism, and purine metabolism. The study provides new insights to better understand and predict the toxicity of MWCNTs in soil.
“Interactive effects of metals and carbon nanotubes in a microcosm agrosystem”. 2022. [43]
“Effects of microplastics and carbon nanotubes on soil geochemical properties and bacterial communities”. 2022. [46]
Our findings show that conventional and biodegradable MPs differently change soil geochemical properties and microbial community structure and functions, which can be further modified by co-existing MWCNTs.
“Nanomaterials in agricultural production: benefits and possible threats?”. 2013. This review covers the most recent literature on the application of nanotechnology to agriculture, including nano-fertilizers, nano-sensors, crop protection, pollution control, waste management, and pesticide detection. The negative effects of nanoparticles on edible plants are also discussed. [82]
“Induction of programmed cell death in Arabidopsis and rice by single-wall carbon nanotubes”. 2010. This study investigated the exposure of Arabidopsis and rice leaf protoplasts to single-walled carbon nanotubes and examined cell viability, DNA damage, reactive oxygen species generation and associated gene expression. [86]
Consequently, SWCNTs have an adverse effect on protoplasts and leaves through oxidative stress, leading to a certain amount of programmed cell death. Although nanomaterials have great advantages in many respects, the benefits and side effects still need to be assessed carefully.
“Effects of graphene on morphology, microstructure and transcriptomic profiling of Pinus tabuliformis roots”. 2021. This study focuses on increasing the growth of Chinese Red Pine (Pinus tabuliformis) by adding graphene oxide nanoparticles to the irrigation water – at 25 mg per liter.[1610]
Notwithstanding these positive effects, it is reported that graphene may be detrimental to plants under certain conditions. The sharp edges of graphene may physically cut cell membranes and compromise their integrity [18]. In addition to increasing the uptake of water and fertilizer by roots, graphene also increased the uptake of heavy metals such as cadmium and arsenic, which increased their toxic effects [19, 20]. Furthermore, graphene treatment may lead to the alteration of pH, metabolic processes, induce different degrees of oxidative damage, and cause cell death [21]. These reported negative effects underscore the necessity for further research before graphene can be applied in agroforestry.
“Effects of carbon nanotubes and derivatives of graphene oxide on soil bacterial diversity”. 2019. [52]
“Graphene phytotoxicity in the seedling stage of cabbage, tomato, red spinach, and lettuce”. 2011. [56]
“Advances in transport and toxicity of nanoparticles in plants”. 2023. [118]
Studies on the toxicity of Graphene derivatives on all elements of aquatic environments
“Assessment of graphene oxide ecotoxicity at several trophic levels using aquatic microcosms”. 2020. [102]
The trophic chain was composed of a consortium of algae and bacteria as primary producers, chironomid larvae as primary consumers and decomposers while larvae of the amphibian Pleurodeles waltii constituted the secondary consumers. Monitoring of multiple ecotoxicological and ecological endpoints allowed to observe changes in bacterial communities while no toxic effects were noticed in chironomids. However, chironomids feeding behaviour changed as a consequence of GO contamination, leading to an increase in leaf litter consumption. Genotoxic effects were noticed in Pleurodeles larvae. This study highlights the importance of using such experimental systems to better encompass the ecotoxic potential of GO through the determination of toxicological routes and consequences on ecosystem’s functioning.
Effects of environmental factors on graphene oxide ecotoxicity towards crustacean Daphnia magna”. 2018. [121]
“Acute toxicity assessment of polyaniline/Ag nanoparticles/graphene oxide quantum dots on Cypridopsis vidua and Artemia salina”. 2021. [125]
“The effects of humic acid on the toxicity of graphene oxide to Scenedesmus obliquus and Daphnia magna”. [88]
“Acute Toxicity of Graphene to Water Flea, Brine Shrimp and Zebrafish”. 2016. In order to understand the potential ecotoxicity of Graphene released into aquatic environment, the toxicities of two types of this material were assessed using two freshwater (Daphnia magna and Danio rerio) and one saltwater (Artemia franciscana) organism. [103]
“Fast Identification and Quantification of Graphene Oxide in Aqueous Environment by Raman Spectroscopy”. 2020. [40]
GO was chemically reduced by hydrazine hydrate to form partially reduced GO (PRGO), where the fluorescence from GO was largely reduced, and the Raman signals (G band and D band) were dominating. According to the Raman characteristics, GO was easily be distinguished from other carbon nanomaterials in aqueous environments, such as carbon nanotubes, fullerene and carbon nanoparticles.
“Carbon and Metal Quantum Dots toxicity on the microalgae Chlorella pyrenoidosa”. 2016. [68]
“Toxicity of microwave-synthesized silver-reduced graphene oxide nanocomposites to the microalga Chlorella vulgaris: Comparison with the hydrothermal method synthesized counterparts”. 2020. Cette étude porte sur les effets toxiques des nano-composites d’oxyde de graphène réduit à l’argent synthétisés par micro-ondes sur l’algue Chlorella vulgaris. [92]
Moreover, reduction in the phenol and flavonoid contents, enhancement of H2O2 content, changes in the antioxidant enzymes activity and decreases in the growth parameters as well as photosynthetic pigments quantities confirmed the toxicity of MS-Ag-rGO to the C. vulgaris cells.
“The toxicity of graphene oxide affected by algal physiological characteristics: A comparative study in cyanobacterial, green algae, diatom”. 2019. This study investigates the toxicity of graphene oxide to green algae (Chlorella vulgaris, Scenedesmus obliquus, Chlamydomonas reinhardtii), cyanobacteria (Microcystis aeruginosa) and diatoms (Cyclotella sp.). The objective was to evaluate how the physiological characteristics of the algae affect the toxicity of graphene oxide. [47]
Meanwhile, growth inhibition and cell division were significantly correlated with the oxidative stress and membrane permeability, suggesting the latter two indicators can effectively signal GO toxicity to algae. The findings of this study provide novel insights into the toxicity of graphene materials in aquatic environments.
“Toxicity Studies on Graphene-Based Nanomaterials in Aquatic Organisms: Current Understanding”. 2020. This study focuses on the toxic effects of graphene and graphene oxide on aquatic invertebrates and fish (cell lines and organisms). [28]
“Effects of graphene oxide nanosheets in the polychaete Hediste diversicolor: Behavioural, physiological and biochemical responses”. 2022. This study focuses on evaluating the effects of different concentrations of graphene oxide nanosheets on the behavior, feeding activity, mucus production, regeneration capacity, antioxidant status, biochemical damage, and metabolism of the Hediste diversicolor worm. [32]
Numerous applications exist for graphene-based materials, such as graphene oxide (GO) nanosheets. Increased concentrations of GO nanosheets in the environment have the potential to have a large negative effect on the aquatic environment, with consequences for benthic organisms, such as polychaetes. The polychaete Hediste diversicolor mobilises the sediments, hence altering the availability of contaminants and the nutrients biogeochemical cycle. As such, this study proposes to assess the effects of different GO nanosheet concentrations on the behaviour, feeding activity, mucus production, regenerative capacity, antioxidant status, biochemical damage and metabolism of H. diversicolor. This study evidenced that H. diversicolor exposed to GO nanosheets had a significantly lower ability to regenerate their bodies, took longer to feed and burrow into the sediment and produced more mucus.
“Humic acids alleviate the toxicity of reduced graphene oxide modified by nanosized palladium in microalgae”. 2022. [41]
“Toxicological effects resulting from co-exposure to nanomaterials and to a β-blocker pharmaceutical drug in the non-target macrophyte species Lemna minor”. 2023. [37]
“The cytotoxicity of nano- and micro-sized graphene oxides on microalgae depends on the characteristics of cell wall and flagella”. 2023.This study investigates the cytotoxicity of nanosized and microsized graphene oxide on microalgae depends on the characteristics of the cell wall and flagella. [34]
The nano-sized GO inhibited the growth of cell wall-deficient strains and reduced the photosynthetic activity. The micro-sized GO inhibited the growth of all strains, but the inhibition efficiency was higher in flagella-deficient strains, indicating that cell wall and flagella have different roles in response to contaminant exposure. The electron microscopy analysis demonstrated that nano-sized GO caused the cell rupture in cell wall-deficient strains. In flagella-deficient strains, the nano- and micro-sized GOs were parallelly attached on the surface of cells, covering the cells. The wrapping of flagella-deficient cells by GO led to the increase of reactive oxygen species (ROS) contents. These results indicate main cytotoxic mechanism of nano-sized GO was the membrane damage of cells, and the presence of cell wall can protect the cells from the attack of nano-sized GO. On the one hand, the presence of flagella might help to avoid the attachment of GO while the cell proliferation and photosynthesis were inhibited in flagella-deficient cells due to the GO wrapping.
“Integrating FTIR 2D correlation analyses, regular and omics analyses studies on the interaction and algal toxicity mechanisms between graphene oxide and cadmium” 2022. [42]
“A trophic transfer study: accumulation of multi-walled carbon nanotubes associated to green algae in water flea Daphnia magna”. 2021. [11]
“A trophic transfer study: accumulation of multi-walled carbon nanotubes associated to green algae in water flea Daphnia magna”. 2021. [11]“Wastewater treatment nexus: Carbon nanomaterials towards potential aquatic ecotoxicity”. 2021. [13]
“A workflow to investigate the impacts of weathered multi-walled carbon nanotubes to the mud snail Lymnaea stagnalis”. 2021. [5]
“Colloidal Behavior and Biodegradation of Engineered Carbon-Based Nanomaterials in Aquatic Environment”. 2022. This review focuses on the current knowledge regarding the colloidal behavior, transformation, and biodegradation of different types of CNMs, including graphene and graphene-like materials, carbon nanotubes, fullerenes, and carbon quantum dots. The other part of this work presents an overview of the known mechanisms of CNM biodegradation and discusses current research related to CNM biodegradation in aquatic species. [14]
“Interactions between multi-walled carbon nanotubes and plankton as detected by Raman spectroscopy”. 2022. [44]
Studies on the ability of Graphene derivatives to allegedly improve plant growth
“Multi-walled carbon nanotubes promote the accumulation, distribution, and assimilation of 15N-KNO3 in Malus hupehensis by entering the roots”. Mars 2023. Cette étude porte sur l’impact des nano-tubes de carbone à multiples parois sur l’utilisation de l’azote chez les pommiers. [85]
“Graphene: A new technology for agriculture”. 2021. This study focuses on a review of the use of graphene in different segments, explaining that this product can be used in various industrial sectors. These are mainly in agriculture (such as in major crops of great importance, such as coffee), the food industry and the environment, as a plant growth stimulator and in fertilizers, nano-encapsulation and smart release systems, antifungal and antibacterial agents, smart packaging, water treatment and ultrafiltration, contaminant removal, pesticide and insecticide quantification, detection systems and precision agriculture. [90]
“Opportunities for graphene, single-walled and multi-walled carbon nanotube applications in agriculture: A review”. 2022. [66]
“Fluorescent carbon-dots enhance light harvesting and photosynthesis by overexpressing PsbP and PsiK genes”. 2021. This study focuses on enhancing light harvesting and photosynthesis by overexpressing PsbP and PsiK genes with fluorescent carbon quantum dots. [73]
“Enhanced Biological Photosynthetic Efficiency Using Light-Harvesting Engineering with Dual-Emissive Carbon Dots”. 2018. This study focuses on improving the efficiency of biological photosynthesis through light harvesting engineering with dual-emitting carbon quantum dots. [64] Note this novel concept of using graphene derivatives to augment « sunlight harvesting » processes… and thus, photosynthesis.
“Carbon dots as light converter for plant photosynthesis: Augmenting light coverage and quantum yield effect”. 2021. This study focuses on carbon quantum dots as light converters for plant photosynthesis, inducing an increase in light coverage and a quantum yield effect. [65]
“Biofertilizers and nanofertilizers for sustainable agriculture: Phytoprospects and challenges.” 2022. This study focuses on bio-fertilizers and nano-fertilizers for sustainable agriculture.[63]
“Carbon-Based Nanomaterials for Sustainable Agriculture: Their Application as Light Converters, Nanosensors, and Delivery”. 2022. This study focuses on the different types of carbon-based nano-materials and their applications in light converters, nano-sensors and delivery tools in sustainable agriculture. [61]
“Vital roles of sustainable nano-fertilizers in improving plant quality and quantity-an updated review”. 2021. This study focuses on the vital roles of sustainable nano-fertilizers in improving plant quality and quantity. [89]
It should be noted that, according to some studies, this would be “sustainable agriculture”… but, according to field ecologists, what is sustainable is, rather, the graphene derivatives that self-accumulate in soils, terrestrial and aquatic environments – and that toxify them.
“Nanocarbon fertilizers: Implications of carbon nanomaterials in sustainable agriculture production”. 2020. This study focuses on the interactions of carbon-based nano-materials such as fullerene, carbon nanotubes, carbon quantum dots, carbon cone dots and graphene with agricultural plants for sustainable agriculture. [62]
Carbon nanofertilizers have shown their role in the improvement in seed germination, seedling growth, shoot-root length enhancement, enhancement of chlorophyll content and photosynthesis rate, and plant biomass increment in various cereals and horticultural crops. The transportation of carbon-based nanomaterials is illustrated in plants and how their accumulation causes phytotoxicity is explained. Further, the potential of carbon nanomaterials in agriculture is also discussed for commercial production of nanocarbon as fertilizer. Some of the carbon-based nanomaterials showed phytotoxicity after a certain high concentration level, but there is more research required to optimize the threshold concentration for each crop‑carbon nanomaterial model where maximum growth and production can be obtained.
“Graphene oxide exhibited positive effects on the growth of Aloe vera”. 2021. This study focuses on increasing the growth of Aloe Vera by adding graphene oxide nanoparticles to irrigation water – at 50 mg per liter. [1608]
“This new technology is called « bionic strategy for plant growth acceleration by injection of nanoparticles”.
“Chitosan and Graphene Oxide Nanocomposites as Coatings for Controlled-Release Fertilizer”. 2019. [938]
“Effects of graphene on morphology, microstructure and transcriptomic profiling of Pinus tabuliformis roots”. 2021. This study focuses on increasing the growth of Chinese Red Pine (Pinus tabuliformis) by adding graphene oxide nanoparticles to the irrigation water – at 25 mg per liter. [1610]
Notwithstanding these positive effects, it is reported that graphene may be detrimental to plants under certain conditions. The sharp edges of graphene may physically cut cell membranes and compromise their integrity [18]. In addition to increasing the uptake of water and fertilizer by roots, graphene also increased the uptake of heavy metals such as cadmium and arsenic, which increased their toxic effects [19, 20]. Furthermore, graphene treatment may lead to the alteration of pH, metabolic processes, induce different degrees of oxidative damage, and cause cell death [21]. These reported negative effects underscore the necessity for further research before graphene can be applied in agroforestry.
“Graphene quantum dots as enhanced plant growth regulators: effects on coriander and garlic plants”. 2015. [48]
“Sulfonated graphene-induced hormesis is mediated through oxidative stress in the roots of maize seedlings”. 2016. Cette étude porte sur l’hormèse induite par le graphène sulfoné qui est médiée par le stress oxydatif dans les racines des plantules de maïs. [54]
“Graphene oxide as a water transporter promoting germination of plants in soil”. 2018. [49]
“Improvement of Commercially Valuable Traits of Industrial Crops by Application of Carbon-based Nanomaterials”. 2019. This study focuses on the biological effects of graphene and carbon nanotubes on fiber-producing species (cotton, Gossypium hirsutum) and ornamental species (Catharanthus roseus). [50]
A study was published, in 2014, entitled “Slow-release fertilizer encapsulated by graphene oxide films” [936] as well as another study, in 2017, entitled “Cogranulation of Low Rates of Graphene and Graphene Oxide with Macronutrient Fertilizers Remarkably Improves Their Physical Properties”. [937]
“Slow-release fertilizer encapsulated by graphene oxide films”. 2014. [51]
“Cogranulation of Low Rates of Graphene and Graphene Oxide with Macronutrient Fertilizers Remarkably Improves Their Physical Properties”. This study focuses on the claimed improvement of physical properties through cogranulation of low levels of graphene and graphene oxide with macronutrient fertilizers. [53]
“PVA-coated fluorescent carbon dot nanocapsules as an optical amplifier for enhanced photosynthesis of lettuce”. 2020. This study focuses on the enhancement of lettuce photosynthesis with fluorescent carbon dot nano-capsules coated with polyvinyl acetate as optical enhancer. [71]
“Magnesium-nitrogen co-doped carbon dots enhance plant growth through multifunctional regulation in photosynthesis”. 2021. This study focuses on enhancing plant growth through multifunctional regulation of photosynthesis by magnesium and nitrogen codoped carbon dots. [72]
“Transfer, transportation, and accumulation of cerium-doped carbon quantum dots: Promoting growth and development in wheat”. 2021. This study investigates the transfer, transport and accumulation of cerium-doped carbon quantum dots to allegedly promote wheat growth and development. [23]
“Graphene Oxide-Assisted Promotion of Plant Growth and Stability”. 2020. This study focuses on graphene oxide to increase the growth of plants – such as watermelon. [29]
We showed that with an appropriate amount provided, graphene oxide had a positive effect on plant growth in terms of increasing the length of roots, the area of leaves, the number of leaves, and the formation of flower buds. In addition, graphene oxide affected the watermelon ripeness, increasing the perimeter and sugar content of the fruit. We believe that graphene oxide may be used as a strategy for enabling the acceleration of both plant growth and the fruit ripening process.
“Graphene Oxide, a Novel Nanomaterial as Soil Water Retention Agent, Dramatically Enhances Drought Stress Tolerance in Soybean Plants”. 2022. [36]
Taken together, our findings revealed that GO could directly increase plant defense enzymes, hormone content, and the expression of drought-related genes, thereby improving the soybean’s ability to resist drought. These findings could provide new opportunities for improving drought tolerance in soybeans through effective soil water retention agents.
“Effects of Graphene Oxide on Plant Growth: A Review”. 2022. This study focuses on the effects of graphene oxide on plant growth to facilitate its safe and effective use. [33]
Several reports of graphene oxide (GO) promoting plant growth have sparked interest in its potential applications in agroforestry. However, there are still some toxicity studies that have raised concerns about the biosafety of GO. These reports show conflicting results from different perspectives, such as plant physiology, biochemistry, cytology, and molecular biology, regarding the beneficial and detrimental effects of GO on plant growth. Seemingly inconsistent studies make it difficult to effectively apply GO in agroforestry.
“Functional carbon nanodots improve soil quality and tomato tolerance in saline-alkali soils”. 2022. This study focuses on the alleged improvement of soil quality and tolerance of tomato in saline-alkaline soils using carbon quantum dots. [4]
“Carbon nanotubes can promote seed germination via seed coat penetration”. 2011. This study investigates the enhanced germination of various crops using single-walled carbon nano-tubes: Capsicum annuum, Salvia macrosiphon, Festuca arundinace… [84]
“Nanomaterials in plant protection and fertilization: current state, foreseen applications, and research priorities”. 2012. [79]
“Proceedings of a workshop on “Nanotechnology for the agricultural sector: from research to the field””. 2014. [80]
“Carbon nanomaterials: production, impact on plant development, agricultural and environmental applications”. 2016. [88]
Studies on the ability of Graphene derivatives to eliminate or mitigate, allegedly, toxicities or pests in agriculture
Carbon nanotubes can be either toxic or beneficial to plant growth and can also modulate toxicity of organic contaminants through surface sorption. The complex interacting toxic effects of carbon nanotubes and organic contaminants in plants have received little attention in the literature to date. In this study, the toxicity of multiwall carbon nanotubes (MWCNT, 50 mg/L) and paraquat (MV, 0.82 mg/L), separately or in combination, were evaluated at the physiological and the proteomic level in Arabidopsis thaliana for 7–14 days. The results revealed that the exposure to MWCNT had no inhibitory effect on the growth of shoots and leaves.
“Whole-Transcriptome Responses to Environmental Stresses in Agricultural Crops Treated with Carbon-Based Nanomaterials”. 2021. [67]
When subjected to salt stress, sorghum seedlings showed modified expression in 51 stress-related genes. The introduction of CNTs or graphene into the salty growth medium resulted in the restoration of the expression of 29 affected genes, resembling that of untreated sorghum seedlings.
“Applications of carbon quantum dots to alleviate Cd2+ phytotoxicity in Citrus maxima seedlings”. 2019. This study focuses on the purported mitigation of cadmium toxicity in grapefruit trees with carbon quantum dots – up to 900 mg/liter. [17]
“Carbon Dots as a Protective Agent Alleviating Abiotic Stress on Rice ( Oryza sativa L.) through Promoting Nutrition Assimilation and the Defense System”. 2020. This study focuses on carbon quantum dots used as a protective agent allegedly mitigating abiotic stress on rice (Oryza sativa) by promoting nutrition uptake and the defense system. [18]
“Graphene quantum dots as cysteine protease nanocarriers against stored grain insect pests”. 2020. This study focuses on the use of graphene quantum dots as cysteine protease nano-vectors, from the species Albizia procera, against, allegedly, two species of stored grain insect pests, the small mealworm, Tribolium castaneum and the grain capuchin, Rhyzopertha dominica.[19]
“Synergistic Effects of Graphene Oxide and Pesticides on Fall Armyworm, Spodoptera frugiperda”. 2022. [38]
The results showed that graphene oxide could enhance the activity of four selected pesticides: chlorantraniliprole, cypermethrin beta, methoxyhydrazide and spinetoram.
“Can the multi-walled carbon nanotubes be used to alleviate the phytotoxicity of herbicides in soils?”. 2021. [12]
Results indicate efficient alleviation of herbicide-induced phytotoxicity to rice and tobacco due to MWCNTs amendment. When 0.4% MWCNTs were applied, the concentration of sulfentrazone that inhibited the same rice height by 50% (IC50) increased to more than 3 times that of pure soil. When the MWCNTs were used to alleviate the phytotoxicity of quinclorac to tobacco, the MWCNTs not only alleviated the phytotoxicity of quinclorac but also promoted the growth of tobacco. The MWCNTs amended soil significantly increased the adsorption of herbicide to soil than biochar. The soil microbial analysis shows that MWCNTs had no significant effect on soil microbial community diversity, but the long-term exposure to MWCNTs could change the structure of the soil microbial community. Above all, our results highlighted the potential implication of the MWCNTs to ensure crop production by promoting crop growth and reducing the residual bioavailability of herbicides.
“Copper stress alleviation in corn (Zea mays): Comparative efficiency of carbon nanotubes and carbon nanoparticles”. 2022. This study investigates the comparative role of carbon nanotubes and carbon nanoparticles in maize (Zea mays) seed germination, seedling growth and Copper stress mitigation. [6]
“Multiwalled Carbon Nanotubes Alter the PSII Photochemistry, Photosystem-Related Gene Expressions, and Chloroplastic Antioxidant System in Zea mays under Copper Toxicity”. 2022. [8]
“Applications of nanomaterials in agricultural production and crop protection: a review”. 2012. [81]
“Synthesis of nanopesticides by encapsulating pesticide nanoparticles using functionalized carbon nanotubes and application of new nanocomposite for plant disease treatment”. 2014. [83]
“Evaluation and mechanism of antifungal effects of carbon nanomaterials in controlling plant fungal pathogen”. 2014. [69]
“Graphene oxide as a pesticide delivery vector for enhancing acaricidal activity against spider mites”. 2019. [74
A few Patents concerning the insertion of graphene oxide in Fertilizers and in Pesticides/Biocides of all kinds
In the agricultural field, there are already a good number of patents for the insertion of graphene oxide in fertilizers and in pesticides/biocides of all kinds, as well as for the intensification of growth processes.
There is even a patent, from 2020, entitled “Application of graphene aqueous dispersion in farmland water retention, fertilizer retention and bacteriostasis”. It is, therefore, a question of disseminating an aqueous dispersion of graphene in agricultural water retention, in fertilizer tanks… under a bacteriostatic pretext. [1112]
These patent applications date from the last few years. Here is a very partial list, out of thousands, of such patents:
“A kind of foliar fertilizer of graphene-containing nano material”. 2016 Chine. CN106747954A. [922]
“Porous oxidation graphene and preparation method thereof and porous oxidation graphene coated slow-release chemical fertilizer and preparation method thereof”. 2017. Chine. CN107585764A. [923]
“Graphene oxide and Antagonistic Fungi compound the application in terms of preventing plant Phytophthora root rot”. 2018. Chine. CN108782610A. [926]
“Water-based graphene oxide nano pesticide and preparation method and application thereof”. 2020. Chine. CN111149798A. [927]
Cover image credit: Adrien Nicolaï/RP — Simulations by Oak Ridge National Laboratory and Rensselaer Polytechnic Institute reveal the potential of graphene oxide frameworks, pictured in black, to remove contaminants such as salt ions, seen in blue and green, from water.
“It is no exaggeration to claim that the fate of humanity is on the line now that more than two thirds of it has taken one or more of these shots. Because the stakes are sky high, the truth will come out sooner rather than later. If suspicions regarding undisclosed ingredients in the “vaccines” are confirmed, especially those regarding nanotechnology and degraded blood, there will be hell to pay for everyone involved in the COVID-19 “vaccination” programme. It is the authorities who should fear the people, not the other way around.”
~ David Hughes, PhD
by David Hughes, PhD, Senior Lecturer in International Relations, University of Lincoln, Brayford Pool, Lincoln LN6 7TS, England
originally published September 3, 2022
ABSTRACT
Between July 2021 and August 2022, evidence of undisclosed ingredients in the COVID-19 “vaccines” was published by at least 26 researchers/research teams in 16 different countries across five continents using spectroscopic and microscopic analysis. Despite operating largely independently of one another, their findings are remarkably similar and highlight the clear and present danger that the world’s population has been lied to regarding the contents of the COVID-19 “vaccines”. This raises grave questions about the true purpose of the dangerous experimental injections that have so far been shot into 5.33 billion people (over two thirds of the human race), including children, apparently without their informed consent regarding the contents. Surprise findings include sharp- edged geometric structures, fibrous or tube-like structures, crystalline formations, “microbubbles”, and possible self-assembling nanotechnology. The blood of people who have received one or more COVID-19 “vaccines” appears, in case after case, to contain foreign bodies and to be seriously degraded, with red blood cells typically in Rouleaux formation. Taken together, these 26 studies make a powerful case for the full force of scientific investigation to be brought to bear on the COVID-19 “vaccine” contents. If the findings of these 26 studies are confirmed, then the political implications are nothing short of revolutionary: a global crime against humanity has been committed, in which every government, every regulator, every establishment media organization, and all the professions have been complicit.
Keywords: COVID-19 vaccines, electron microscopy, foreign biological entities, nanotechnology, Nuremberg violations, self-assembling components, undisclosed metallic components, violations of informed consent
This is more than enough evidence, from at least 26 separate researchers/research teams in 16 different countries across five continents, to highlight the clear and present danger that the world’s population has been lied to regarding the contents of the COVID-19 “vaccines”. What is the true purpose of the dangerous experimental injections that have so far been shot into 5.33 billion people (70 percent of the human race), including children and infants? Examined under powerful magnification, the contents of the vials appear to contain a variety of unusual objects and structures for which the declared “vaccine” ingredients do not account. These include sharp-edged geometricstructures, fibrous or tube-like structures, crystalline formations, and “microbubbles”. The blood of people who have received one or more COVID-19 “vaccines” appears, in case after case (94 percent of cases according to Giovannini et al. 2022), to contain foreign bodies and to be seriously degraded, with red blood cells typically in Rouleaux formation. The effects on blood are so pronounced that one study finds that artificial intelligence can be trained to detect the difference between “vaccinated” and “unvaccinated” blood with an accuracy rate of over 98 percent.
Some researchers claim that the undisclosed artefacts contained in the COVID-19 “vaccines” self- assemble into nanotechnology. Although this sounds preposterous at first, consider some of the highest magnification imagery we are about see:
It is unclear what we are looking at here, but prima facie it does look like some kind of circuitry. Such imagery demands explanation.
The findings presented in this paper shift the debate about COVID-19 “vaccines” into new territory. The dangers of the injections lie not only in the declared ingredients — the toxic PEG of lipid nanoparticles, mRNA that programmes the human body to produce harmful spike proteins, etc. (cf. Seneff & Nigh, 2021) — but also, and perhaps to a far greater extent, in the undisclosed ingredients. In what follows, over 100 pages of microscopic imagery will demonstrate beyond reasonable doubt that the COVID-19 “vaccines” are not what we were told they are, i.e. safe and effective means of preventing disease. On the contrary, they appear to be heavily loaded with foreign bodies, as well as instructions for human cells to manufacture foreign bodies, that prove profoundly harmful to human health.
Those foreign bodies are present in all the major brands: BioNTech-Pfizer, Moderna, AstraZeneca, Johnson & Johnson, and others. It therefore appears, from what we know so far, that all the manufacturers, all regulators, and all governments, with the support of establishment media, are complicit in, and must actively have conspired to commit, what would amount to the gravest crime against humanity of all time, i.e. the attempted injection of the entire human race (apart from the perpetrators) with undisclosed toxic substances/technologies without anyone’s informed consent. There can be no more urgent investigation in our time than of the COVID-19 “vaccines”.
Impediments to Investigation
Who will undertake such an investigation, however? Certainly the regulators cannot be trusted to do so, since they all appear to have deliberately ignored evidence that can, in some cases, be detected by even an optical microscope. Universities would be the obvious candidates, yet many, particularly in North America, have mandated COVID-19 “vaccines”, so cannot be expected to meet their obligation to society by investigating what is actually in those shots which they have coerced staff and students to take. Other universities, especially in Europe, are too dependent on government funding to jeopardize their relations with the state by doing the right thing. As a result, there is a dearth of peer-reviewed research in this field: universities are compromised. It seems unlikely that the medical profession will step up, as it has been at the forefront of administering the injections; it also removes the licences to practice of any member who speaks out against them. Meanwhile, military-grade propaganda, rampant censorship, nastiness and aggression from those deceived by the official narrative, and a political climate of fear and intimidation intentionally stoked to dissuade dissidents all act as powerful disincentives for anyone to ask the questions that matter most. Indeed, several of the researchers and research teams below have chosen to remain anonymous for precisely such reasons.
Yet, beyond the technocratic totalitarianism that is now seeking to eclipse liberal democracy, beyond the incessant fear propagation and the rampant corruption, the question of what is really in the COVID-19 “vaccines” is ultimately an empirical one. It can be solved by scientists of integrity who possess the right equipment and who are willing to adhere rigorously to the correct methods. In principle, any self-respecting laboratory with the right equipment, expertise, and motivation should be able to contribute to solving the problem. There is no need for idle speculation or unsubstantiated claims and rumours. The problem is solvable if people are brave, honest, and truthful enough to address it, like the researchers presented in this paper.
In the other corner, the perpetrators of this apparent global crime against humanity have gone to great lengths to conceal their tracks. If undisclosed nanotechnology is indeed present in the
COVID-19 “vaccines”, then it is invisible to the naked eye and will not show up under conventional toxicology tests. Who would even think to look for it in the first place given the relentless propaganda about a virus and spike proteins? The very idea of undisclosed self-assembling nanotechnologies in the “vaccines” seems, on the face of it, so far-fetched that most people will refuse to entertain it in the first place. Even critical bodies, such as Doctors 4 COVID Ethics, refuse to address that possibility, instead preferring to stick to their relevant areas of medical expertise. The Vaccines Education Working Group does address, rigorously, the issue of undisclosed ingredients in the COVID-19 “vaccines”, yet even it does not entertain the possibility of the presence of nanotechnology. It would seem that if the lie is big enough, it becomes incomprehensible to all but the very worst people in society, as Hitler realized a century ago (Hughes, 2022b).
Even for those who are willing to conduct a proper investigation of the COVID-19 “vaccine” contents, further major obstacles present themselves. For a start, because we may be dealing with nanotechnology here, specialist high-power microscopes are needed. Life of the Blood was able to procure a dark field microscope with 4,000x magnification to produce the incredible images above, yet no other researcher or research team discussed in this paper was able to achieve anywhere close to the same level of magnification. Most images shown are between 400x and 1,000x magnification. The required equipment may be prohibitively expensive for individuals. For example, a new scanning electron microscope can cost $70,000 to $1,000,000. Given that different types of microscopic and spectroscopic equipment are needed, this is work that really needs to be done at an institutional level, returning us to problems of reputational risk, loss of funding, being forced to close, having careers and reputations trashed, or worse.
Even where adequate equipment and procedures are in place, the next problem is how to obtain a vial for analysis, demonstrating a secure chain of custody, and keeping it maintained at the required temperatures until it is opened. The vials themselves are strictly guarded. According to a pharmacologist working for the NHS,
I’ve been working with the NHS on [mass vaccination] since January 2021 in a lot of roles. […] Every mass vaccine centre in the UK and other sites e.g. Boots [the retail pharmacy equivalent of Walgreens in the US] has a National Vaccine protocol to destroy every vial with two different senior staff at the end of each day. The systems are also in place for counting in and out every single vial that arrives and leaves every site. All vials are disposed daily into a locked coded clinical incinerator waste system or stored again coded locks for an NHS contractor to pick up daily the clinical waste! […] If you want to get hold of vials your best bet is to seek out independent pharmacies doing COVID jabs.
It is hard to see how it is possible to obtain a COVID-19 “vaccine” vial legally given the state’s tight control over them. It was never possible to buy a COVID-19 “vaccine” privately in the UK, for instance: “vaccinations” were only available through the NHS. Thus, it becomes very difficult to establish a secure chain of custody without exposing illicit means of acquisition. Researchers who claim to have obtained unopened vials never seem to indicate where they got them from; at best, they were “sent” or “given” them. Alternatively, some researchers claim to have obtained used vials; after all, only a small droplet is required for analysis. However, this then introduces problems of potential contamination and samples no longer being at the required storage temperatures. So, we are left in a catch-22, whereby a full and transparent investigation requires vials being made freely available by the manufacturers or the state for that purpose, yet the terms of the investigation imply that those very entities cannot be trusted.
There are also high personal risks involved in doing this kind of work in a climate of mounting authoritarianism. State propagandists (including networks of academics and journalists), intelligence agencies, “fact checkers” (flak machines), and other organizations such as the Cabinet Office Rapid
Response Unit and 77th Brigade in the UK, will move to close down any such investigation, resorting to thought-terminating clichés such as “misinformation”, “disinformation”, and “conspiracy theory”, as well as censorship, hit pieces in the establishment media, ad hominem attacks, allegations of anti-semitism, calls for the investigators to be fired, etc. This has all been seen before, and it testifies to the desperation of a power structure so premised on lies that it cannot defend itself honestly and truthfully. It may not be long until dissent itself is criminalized, with so-called “anti-vaxxers” (a propaganda term used to demonize political opponents) already being branded as terrorists in readiness for new legislation apparently intended to turn liberal democracies into dictatorships (Davis, 2022).
Investigators may even be murdered. Andreas Noack in November 2021 died within days of claiming that graphene hydroxide in the “vaccines” acts like tiny, non-biodegradable razor blades that cut up blood vessels; the circumstances of his death are disputed. In September 2021, CarrieMadej went public with her findings regarding COVID-19 “vaccine” contents; in June 2022 she was involved in a suspicious plane crash that nearly killed her. Perhaps there is no connection, but the pharmaceutical industry has a known history of persecuting and allegedly murdering whistleblowers, as cases such as Andrew Wakefield, Judy Mikovits, and the late Brandy Vaughan show. “With this type of research,” Daniel Nagase warns, “it has to be kind of clandestine, because there’s a lot of money behind not letting anyone know what’s in these injections.” Thus, fear, intimidation, and a range of dirty tactics are used to cow researchers into silence.
The Establishment’s attack dogs, as well as certain victims of the propaganda, will almost certainly resort to the usual smears to dismiss the evidence presented in this paper without doing the work needed to engage with the research seriously. There will doubtless be disingenuous claims that the images shown below could mean anything, that we have no way of verifying their authenticity, that they may have been photoshopped for sensationalist or fraudulent purposes, that the samples were not properly prepared, allowing for contamination (a sleight on the professionalism of the researchers, some of whom have decades of experience), etc. Such intellectually lightweight claims founder on the fact that at least 26 different investigations of the “vaccine” contents (almost entirely unrelated to one another) from 16 different countries on five continents converge on remarkably similar findings. The investigations are mutually reinforcing, mitigating against possible fraud or human error. Researcher after researcher claims to have never seen anything like this before in their career.
Given that 5.33 billion people have received the injection, and given the apparent evidence of foul play involved, no amount of bullying, coercion, and threats of violence seems likely to stop the investigation that must now take place. As we are already seeing, scientists from across the world are doing the necessary work anyway, and once the scale of their effort is understood, more and more research teams will be spurred into action, networking with one another rather than producing isolated, yet strikingly similar, findings of the type shown below. It is no exaggeration to claim that the fate of humanity is on the line now that more than two thirds of it has taken one or more of these shots. Because the stakes are sky high, the truth will come out sooner rather than later. If suspicions regarding undisclosed ingredients in the “vaccines” are confirmed, especially those regarding nanotechnology and degraded blood, there will be hell to pay for everyone involved in the COVID-19 “vaccination” programme. It is the authorities who should fear the people, not the other way around.
Why are the COVID-19 “vaccines” considered to be so important, even though they are not “effective” at preventing or treating COVID-19? Why are these “vaccines” still promoted even though they are considered to be the most toxic “vaccines” ever created for some people, or maybe even all people? In this article, I will try to: answer these questions; tell you what I believe to be true; and explain how I came to these conclusions. I could be wrong, but I might be right.
I believe we have been lied to about the intent of the COVID-19 “vaccines”. I believe the COVID-19 “vaccines” were used to cause diseases. Since the COVID-19 “vaccines” were introduced into the human population, there has been an increase in diseases, genetic diseases, cancer, and genetic predispositions to disease. I also believe the “vaccines” were actually designed to cause genetic disease, and expose genetic defects. Why is this being done? So that we will accept the future “cures” of precision medicine CRISPR gene editing “vaccines” and other gene editing “therapies”. The globalist elitist transhumanists seem to believe this is for the “greater good”, to fulfill the Fourth Industrial Revolution GMO-transhuman evolution of our bodies and minds. We are told the Fourth Industrial Revolution is occurring to evolve humans into biotechnological GMO-transhumans. In the UK government’s Policy Paper, “Regulation for the Fourth Industrial Revolution”, published June 11, 2019, they describe the Fourth Industrial Revolution as (emphasis added):
“It is characterised by a fusion of technologies – such as artificial intelligence, gene editing and advanced robotics – that is blurring the lines between the physical, digital and biological worlds.”
How could the COVID-19 “vaccines” have caused disease? The Salk Institute describes the COVID-19 mRNA “vaccines” as communicating with our “cell’s genetic machinery” by telling our bodies to create “spike proteins” through mRNA instructions. Could it be possible that the adverse reactions, resulting from the mRNA “vaccines”, are due to a miscommunication in the mRNA instructions, or were the instructions designed to induce adverse reactions, genetic expression of disease, and diseases that might be dormant in our bodies?
Recently, Damar Hamlin of the Buffalo Bills collapsed on the football field during a live NFL game. Dr. Peter McCullough pointed out that genetic conditions should be considered in any possible “vaccine” induced myocarditis case. He explains this in his recent Substack article, “Inherited Risk of Sudden Death Triggered by COVID-19 Vaccination” (emphasis added):
“There is an array of known sodium, potassium, and other ion channel mutations in the heart that pose a genetic proclivity to sudden death.”
“….not all patients after the injection or those with manifest COVID-19 vaccine-induced myocarditis are at risk for sudden death. In my clinical practice I incorporate genetic testing for channelopathies to fine tune the prognosis for patients.”
If the COVID-19 mRNA “vaccines” induce myocarditis in people with certain genetics, what other genetic diseases might be caused or exposed by the “vaccines”?
The Pfizer mRNA COVID-19 “vaccine” potential adverse reactions list (see Appendix 1. List of Adverse Events of Special Interest) was released due to a FOIA request. This list is quite extensive and it seems that the Pfizer mRNA COVID-19 “vaccine” has the potential to cause almost any human disease. Why does it seem to contain any and all diseases? Maybe it’s because those are the diseases they were hoping to provoke, so they could then offer us more “vaccines” to try to gene edit or “cure” those diseases?
“But is the fundamental tenet of transhumanism — that we will someday use biotechnology to make ourselves stronger, smarter, less prone to violence, and longer-lived — really so outlandish?”
“If we start transforming ourselves into something superior, what rights will these enhanced creatures claim, and what rights will they possess when compared to those left behind? If some move ahead, can anyone afford not to follow? These questions are troubling enough within rich, developed societies. Add in the implications for citizens of the world’s poorest countries — for whom biotechnology’s marvels likely will be out of reach — and the threat to the idea of equality becomes even more menacing.”
Fukuyama’s concern that some people might be “left behind” from under-developed or poor countries, and not included in the biotechnology GMO-transhumanism evolution, seems to be solved by COVID-19 “vaccine” equity. “Vaccine” equity means every human in every part of the world is targeted to receive a COVID-19 “vaccine”. This means every human in the world might suffer from adverse reactions to these “vaccines”. The solution or the potential “cure” will be CRISPR precision medicine gene editing “vaccines” or other gene “therapies”. This means everyone in the world is targeted to become a GMO-transhuman.
What exactly is CRISPR precision medicine gene editing? The Royal Society describes human gene editing as being similar to creating GMO (genetically modified organism) food, and fixing errors or faulty genes. In this short video, “What is gene editing and how does it work?”, they say:
“In a nutshell, it works by identifying, then cutting pieces of DNA. One way of doing this uses a component known as CRISPR.”
The WEF explains that precision medicine can also be referred to as “personalized medicine”, in their article, “Precision Medicine” (emphasis added):
“The ultimate goal of Precision Medicine, also referred to as Personalized Medicine, is to enable the use of information about a patient’s genes and environment.”
The challenges to implementing CRISPR precision medicine gene editing seem to be related to ethics and laws, or more specifically, how to circumvent ethics and existing laws. They seem to want more agile laws and more flexible ethics to implement their strategies. The WEF states the following points in their article, “4 agile ways policy-makers can advance precision medicine”(emphasis added):
“A combination of technological, ethical, and regulatory challenges has limited the impactof precision medicine.”
“To overcome this, investment in health care innovation is vital, but the risks need to be managed with agile governance.”
“Governments should work with industry, build on best practice, and collaborate internationally to ethically accelerate innovation”.
Were the COVID-19 “vaccines” given to the majority of the population so there would be a mass demand for their solution? Is this also why it was so important to get a certain percentage of humans “vaccinated”? The more humans suffering from “vaccine” adverse reactions, the more likely the masses will advocate for new laws in favor of CRISPR precision medicine gene editing, and approve the advancement of their GMO-transhumanist agenda. Is this the real reason why they want to get rid of The United States Constitution? So that they can get rid of non-GMO human rights, our Constitutional inalienable, inherent human rights?
In the United States, the mRNA “vaccine” business model seems to be the way to circumvent any restraints to implementing CRISPR precision medicine gene editing because “vaccines” are the least regulated drug, due to their legal liability immunity. The “vaccine” manufacturers are already taking advantage of the “vaccine” business model by making more mRNA “vaccines”. MIT Technology Review’s article, “What’s Next for mRNA Vaccines” explains that both Moderna and BioNTech have many more mRNA “vaccines” on the way (emphasis added):
“These vaccines don’t rely on injecting part of a virus into a person, like many other vaccines do. Instead, they deliver genetic code that our bodies can use to make the relevant piece of viral protein ourselves.”
“Moderna, the biotech company behind one of the two approved mRNA vaccines for covid-19, is developing mRNA vaccines for RSV(respiratory syncytial virus), HIV, Zika, Epstein-Barr virus, and more. BioNTech, which partnered with Pfizer on the other approved mRNA-based covid-19 vaccine, is exploring vaccines for tuberculosis, malaria, HIV, shingles, and flu. Both companies are working on treatments for cancer. And many other companies and academic labs are getting in on the action.”
“Cells are incredibly complicated—and DNA doesn’t have straightforward “on” and “off” switches like an electronic circuit. In Wong’s engineered cells, you “turn off” the production of a certain protein by altering the segment of DNA that encodes its instructions. It doesn’t always work, because nature might have encoded some instructions in duplicate. In other words: It’s hard to debug 3 billion years of evolution.”
“The technology that could spark a gene-editing revolution has been caught introducing hundreds of unintended mutations into the genome, and with scientists already testing it in humans, it’s set off some serious alarm bells.”
This study was later retracted, but we know what that probably means….they were most likely forced to retract their study because it didn’t fit the prescribed narrative.
“The Third International Summit on Human Genome Editing is being organized as a collaborative activity of the U.K.’s Royal Society and Academy of Medical Sciences, the U.S. National Academy of Sciences and U.S. National Academy of Medicine, and The World Academy of Sciences. It will bring together leading experts to examine the potential risks and benefits of genome editing technologies and the significant ethical and societal issues associated with advances in human genome editing research.”
“The first of these summits was held in Washington, DC in 2015, and the second was held in Hong Kong in 2018.”
It was recently reported by Rasmussen Reports that 1 in 4 people know someone who may have died as a result of the COVID-19 “vaccines”. Just because a technology or pharmaceutical is invented, doesn’t mean it’s a “good” technology or pharmaceutical. There are often short-term and long-term side effects that are harmful and even life threatening. It’s more likely that new technologies and pharmaceuticals, especially no liability drugs like “vaccines”, are created for money and profit, with little to no investigation into their long-term side effects. Yes, the government will try to deceive you and use propaganda to tell you it’s “safe and effective” or “good for you”. In the meantime, they will make their billions and try to achieve their hidden agendas. It’s time to use your critical thinking skills and defend your rights to your body…..and mind. Don’t submit to government mind control manipulation.
“The Fascist conception of the State is all-embracing; outside of it no human or spiritual values can exist, much less have value. Thus understood, Fascism is totalitarian, and the Fascist State–a synthesis and a unit inclusive of all values–interprets, develops, and potentiates the whole life of a people.”
There are many questions to ask about this Fourth Industrial Revolution GMO-transhumanism agenda that the globalists and elites are trying to force upon us. Dr. Fukuyama had a very valid concern about the legal rights of GMO-transhumans, “what rights will these enhanced creatures claim, and what rights will they possess….”. If someone (or some “creature”) is a GMO-transhuman, does it still have the same rights as a non-gene-edited or non-GMO human?
Here are a few of my questions and concerns:
Is the GMO-transhumanism agenda also behind the transgender movement – in order to confuse the true meaning of what is a “human”?; “What is a Woman?”; what is my preschool child’s gender?; and why are there so many “gender” pronouns?
If no one can define a “human”, and some humans become “GMO-transhuman”, then what happens to the equal and inalienable “human” rights if some humans are “enhanced GMO-transhuman” and others are not?
Are these GMO-transhumans now owned by a corporation? Vox reported in their article, “Can GMOs be patented?”:
“Yes. In 1980, the US Supreme Court ruled in Diamond v. Chakrabarty that genetically altered life can be patented.”
Is this what Klaus Schwab and the WEF were talking about when they said, “You will own nothing and be happy.” Define the word “you”. Is Klaus Schwab referring to the “GMO-transhumans” who no longer own their own bodies and have no “inalienable human” rights?
What types of GMO-transhumans do they want to create? Will they still have emotions, a human spirit, a conscience…etc.? In whose image will these GMO-transhumans be created? Are “vaccines” part of a religion?
The answers to these questions and Fukuyama’s other concerns about GMO-transhumans are still unknown (i.e., What is a “good” GMO-transhuman?; Who decides what is a “good” GMO-transhuman?). Fukuyama stated:
“Transhumanism’s advocates think they understand what constitutes a good human being, and they are happy to leave behind the limited, mortal, natural beings they see around them in favor of something better. But do they really comprehend ultimate human goods?”
“The original Charters of Freedom: The United States Constitution, The Bill of Rights, and The Declaration of Independence were written to reflect Inherent Rights of the individual. Yet these documents are being ignored by the very government created to uphold them because, by themselves, they are only metaphorical shields.”
“There is a difference between legal and lawful. Legal pertains to the letter of law, whereas lawful pertains to the spirit of law. Legal matters reflect statutes between government entities and the color of law (i.e., the appearance or semblance, without the substance), whereas lawful matters reflect common law, the law of the land—the law of the people—and are actual in nature, not implied. Going forward, if we are to be free, we must resist playing a game of wits in a corrupt system that seeks to destroy Inherent Rights.”
“The question, then, is whether it will usher in a new era for humanity, or end up as the latest example of a promising technology that is used to inflict pain and destruction. Such technologies have emerged from physics (nuclear bombs) and from chemistry (poison gas). Now that it’s biology’s turn, hopefully our past experiences have made us wiser. Hopefully we know better, now.”
In conclusion, if the current mRNA COVID-19 “vaccines” have the potential to cause genetic damage from their genetic manipulation; and the solution to “cure” our diseases is CRISPR precision medicine gene editing; then, are the new mRNA “vaccines” and new gene “therapies” another attempt to gene edit us using CRISPR precision medicine technology?
Alicia Green is an instinctive researcher and writer, with BA in Psychology and BS in Advertising. She gained her first experience as an investigative news reporter while working for a student-run news publication, providing breaking news and information on issues affecting the university and local community.
Alicia welcomes your comments and feedback on her articles. If you have a topic or issue you would like her to investigate, please reach out to her here:
One of the “goals” of COVID-19 appears to be convincing the public to accept minimally-tested pharmaceutical products. Not only that, but to accept them whenever they are told.
The “novel” mRNA vaccines have bamboozled both medical practitioners and the general public. What these injections do to the body remains largely speculative. However, there is a bigger issue at play and that is the ongoing gaslighting surrounding vaccines, whatever their supposed mechanism of action.
The medico-pharmaceutical industry and it’s cronies are trying to keep you on the plantation by keeping their cardinal narratives intact…
There is nothing like a discussion about vaccines to end friendships, make your family doctor go red in the face, or result in millions of hours of wasted time and online debates.
The issue is not getting better, but the COVID-19 fraud probably had the unintended effect of waking up more people than ever before to the actual science of vaccination.
Additionally, only one of the effects of the new mRNA injections was to create a large group who were against these particular vaccines while simultaneously maintaining a belief in most other vaccines.
Let’s have a look at why this “novel technology” is simply another gambit to propagate infectious disease mythology and bamboozle the public, all the while keeping them trapped in the medico-pharmaceutical germ theory paradigm.
On January 5, an article was published on the MIT Technology Review website titled ‘What’s Next for mRNA Vaccines’. There was no question mark in the title, so perhaps it was intended as a statement, suggesting to the world what kind of “medicine” is in the pipeline.
The article began as follows: ‘Cast your mind back to 2020 if you can bear it. As the year progressed, so did the impact of COVID-19. We were warned that wearing face coverings, disinfecting everything we touched, and keeping away from other people were some of the only ways we could protect ourselves from the potentially fatal disease.’
Even for people who believe in the existence of viruses, this is a preposterous depiction of what happened in 2020. In fact, nothing happened in 2020 apart from a fraudulent narrative involving an alleged novel coronavirus that at various times has been said to either come from a wet market, a bat cave or, drum roll please, a laboratory.
In a way, COVID-19 did come from a lab, but only in the form of in silico, dry lab simulations that were used to make up the existence of SARS-CoV-2.
Similarly, the laboratory tests, such as the PCR and rapid antigen tests that were deployed, did not require the existence of a virus to be positive. They only required circular reasoning, based on the in silico models, with the sequences and proteins falsely claimed to be “viral”.
The MIT article claims there was a ‘potentially fatal disease’, at which point we would ask, what disease?
Even on their own terms, COVID-19 is simply confirmed on the basis of molecular detection assays that have no established diagnostic validity.
COVID-19 is not a disease. It is a global fraud sustained by a medical system that lost its way a long time ago.
As my Virus Mania[Virus Mania: Corona/COVID-19, Measles, Swine Flu, Cervical Cancer, Avian Flu, SARS, BSE, Hepatitis C, AIDS, Polio, Spanish Flu. How the Medical … Making Billion-Dollar Profits At Our Expense by Torsten Engelbrecht, Claus Köhnlein, Samantha Bailey, Stefano Scoglio] coauthor Claus Köhlein explained in 2020, it is a PCR pandemic. There was no new disease, only new tests and plenty of gullible people.
In any case, this MIT story sets the scene with the same picture-painting to make people believe there are infectious disease epidemics when in reality they don’t exist.
And of course, the establishment always has one end point in mind with the narrative — and that’s vaccines.
So the article continues by stating that: “Thankfully, a more effective form of protection was in the works. Scientists were developing all-new vaccines at rapid speed… By the end of the year, the US. Food and Drug Administration issued emergency-use authorization for these vaccines, and vaccination efforts took off.
“As things stand today, over 670 million doses of the vaccines have been delivered to people in the US.”
This has been the typical vaccine playbook for over a century. Alleged that people are getting sick because of microbes, whether they be real, such as bacteria or imagined, such as viruses, and then claim that vaccines are the best solution. Cover up the fact that contagion has never been demonstrated in a scientific study, and then, like this MIT article, imply that the success of a vaccine is based on how many of them are dished out.
In this regard. Dissolving Illusions [Dissolving Illusions: Disease, Vaccines, and The Forgotten History by Roman Bystrianyk, Suzanne Humphries MD] is one of the best books dealing with this mythology.
Suzanne Humphries and Roman Bystrianyk deliver a fatal blow to the theory that vaccines had anything to do with improving health outcomes last century. In particular, many of the charts they have put together are rather embarrassing. For anyone claiming that vaccines were the key to defeating diseases.
It doesn’t matter if you believe in pathogens or not, because as it stands, there is no scientific evidence that vaccines are useful to anyone apart from those that benefit from selling them.
However, the medical industry is a dangerous cult when it comes to vaccines. Only a tiny minority of doctors have the courage to point out the fraud, because doing so typically results in suspension or at least limited work opportunities. Most doctors prefer to keep their head in the sand and not question their overlords, especially if their incomes could be affected in any way.
As Aneurin Bevan explained in 1948, he persuaded British doctors to accept the National Health Service, not by any merits, but by stuffing their mouths with gold, and saying that many doctors seem to genuinely believe that vaccines are useful, although almost universally they have done none of their own research and just follow protocols.
They may come across something like the CDC’s ‘Ten Great Public Health Achievements — United States, 1900 to 1999’, see that vaccination is at the top of the list, and conclude it must be good.
However, we have dedicated a huge amount of time to following the links on the CDC’s website, and none of them lead to any scientific evidence that vaccines are beneficial to the recipients.
Similarly, our Virus Mania team has contacted many of the medical institutions around the world requesting they provide any papers that follow the scientific method and demonstrate overall health benefits of vaccinations.
To date, none have provided any.
That’s why the World Economic Forum, one of the biggest gaslighting shows currently running, reports that vaccination is one of the world’s most successful health interventions, saving as many as 3 million lives every year. The WEF is concerned about vaccine hesitancy and parroted the WHO claim that the reasons people choose not to vaccinate are complex.
We can stop them right there because there’s no point going further. The reason is actually simple. Many people can see that the products are dangerous and ineffective, and like my family, don’t accept any of them. The decision is based on reviewing the scientific literature as well as our own experience. None of us get these diseases despite not taking the vaccines.
Incredibly, the vaccine scam is building momentum, and in the last few years the number of them administered to the world has been enormous. And there are no signs of the jabs easing up, with mRNA vaccines being touted as solutions for all kinds of problems.
As the MIT article stated, while the first approved mRNA vaccines are for COVID-19, similar vaccines are now being explored for a whole host of other diseases. Malaria, HIV, tuberculosis and Zika are just some of the potential targets. mRNA vaccines might also be used in cancer treatments tailored to individual people.
The suggested wider use of vaccines in these conditions is not new, of course. In my video, The Future of Vaccines, I mentioned the 2007 PricewaterhouseCoopers report ‘Pharma 2020: The vision — Which path will you take?*’ In this publication, they listed the potential development of vaccines for cocaine addiction, diabetes, hypertension, Alzheimer’s disease, psoriasis, food allergies, rheumatoid arthritis and nicotine withdrawal.
What has changed since then is the focus on not just vaccines, but mRNA vaccines. Before we move on to these products, PwC had warned Big Pharma that: “The shortage of good medicines in the pipeline underlies many of the other challenges Pharma faces, including its increasing expenditure on sales and marketing, deteriorating financial performance and damaged reputation.”
In the last few years, Big Pharma worked out that you don’t need good medicines in the pipeline. They simply arranged for governments to do the marketing and purchasing for them, all at the expense of the taxpayers.
The WEF, has also cheered on the highway robbery, stating on their website in 2020 that: “More than 140 world leaders have called for a COVID-19 vaccine to be made available free to everyone”‘ Anyone that has read Henry Hazlitt’s ‘Economics in One Lesson‘ knows that there is no such thing as a free product or service. Someone always has to cover the cost.
In the COVID era, there was a vast transfer of wealth. And all of us have had to pay in one way or another, with some people who accepted the injection paying with their lives as well.
The pharmaceutical companies are now all chomping at the bit to sell phenomenal quantities of vaccines to governments, either through these false pandemics or through their most-prized cash cow — getting a product onto childhood vaccination schedules.
The problem Big Pharma has with “regular vaccines” is that, for their liking, they take too long to develop. On that note, the Wellcome Trust had a graphic titled ‘The five stages of vaccine development’, which reported that: “A vaccine usually takes more than 10 years to develop and costs up to $500 million”. Interestingly, the page was removed from their website at some point in late 2020, just before a certain product was released onto the world’s population. And this is where mRNA vaccines come into play.
COVID-19 was used as an excuse to rush into distribution the “novel technology”. No more waiting ten years to get the products injected into people.
Part of the COVID scam has been to make people think that pharmaceuticals can be tested in a matter of months. It was fascinating in early 2020 to see the mantra ‘safe and effective’ being parroted by much of the medical community and the wider public.
Leaving aside the nonexistence of a virus and a new disease, how could there possibly be any long-term safety data? There wasn’t, of course. And pharmacovigilance was completely thrown out the door.
Once upon a time, I was a clinical trials physician, and I can assure you that no products were ever released in a matter of months. In fact, most spent years in development and never made it to the wider public, often because there were too many adverse reactions.
In ‘The COVID-19 Fraud and War on Humanity‘ Dr. John Bevan-Smith and my husband Mark wrote, at the start of the essay, that the plan to inject the masses with so-called mRNA technology was already in the pipeline prior to the declaration of the alleged pandemic.
All it took was a narrative featuring an imaginary coronavirus.
[Quote from ‘The COVID-19 Fraud & War on Humanity’]
“The world was being prepared for a ‘pandemic’ and on December 4, 2019, Dr Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases stated that his agency was ‘conducting and supporting research to develop state-of-the-art vaccine platform technologies that could be used to develop universal influenza vaccines as well as to improve the speed and agility of the influenza vaccine manufacturing process. These platform technologies include DNA, messenger RNA (mRNA), virus-like particles, vector-based, and self-assembling nanoparticle vaccines.'”
Somewhat incredibly, the public have mostly gone along with the swindle and have allowed themselves to be injected as many times as they are told, even if it is making them sicker.
One would suspect that a major goal for the COVID Fear campaign was to normalize this complicit and illogical behavior while creating the infrastructure to repeat the process in the future.
Fellow COVID skeptic, Denis Rancourt, also commented on this very aspect in a recent interview:
“This is about putting into place a military system of injection that is globalized. That is, whenever they want, they can inject you with whatever they want under the pretext of health. That’s what this about. In my view, it’s that kind of a weapon that they’ve put into place. They now have the possibility, they’ve convinced you, that it’s a good idea to be injected whenever they like with whatever they say. And they’ve put into place all the procedures and all the mechanisms to do that. And they’ve bought out all the right people. And they can go into an entire continent and virtually inject everybody.”
The establishment became so comfortable with their “success” that they openly flaunted the mass compliance behavior where people had previously been much more skeptical.
Who could forget in November 2021, when president of Bayer’s Pharmaceuticals Division, Stefan Oelrich, admitted at the World Health Summit that COVID-19 had made all this possible?
[quote from Stefan Oelrich’s speech at World Health Summit]
“Ultimately, the mRNA vaccines are an example for that cell and gene therapy. I always like to say, if we had surveyed two years ago in the public, ‘Would you be willing to take gene or cell therapy and inject it into your body?’ we would have probably had a 95% refusal rate.
“I think this pandemic has also opened many people’s eyes to innovation in a way that was maybe not possible before.”
And how does the MIT article finish?
Well, apparently: “In 2023, we can expect an updated COVID-19 vaccine. And researchers are hopeful we’ll see more mRNA vaccines enter clinics in the near future. ‘I really hope that in the next couple of years, we will have other approved mRNA vaccines against infectious disease,’ says Norbert Pardi. ‘He is planning ahead for the next global disease outbreak, which may well involve a flu virus. We don’t know when the next pandemic will hit, but we have to be ready for it,’ he says. ‘It’s crystal clear that if you start vaccine development in the middle of a pandemic, it’s already too late.'”
This is why we and our colleagues focus on exposing the fallacy of contagion in so-called infectious diseases. As all of us have explained, these are illusions propagated by the medico-pharmaceutical industry, illusions that are now used to control the population, and engineered to transfer vast quantities of wealth from the masses to crony corporations.
The only pandemics in the world are things like obesity and anxiety due to lack of purpose and exposure to fear narratives.
As Tom Cowan said, perhaps the biggest pandemic is an unprecedented pandemic of not thinking.
As a group, we do not spend a lot of time analyzing what the mRNA shots do in the body, because it is largely speculative.
My Virus Mania co-author Stefano Scoglio has explained that the literature surrounding the shots is full of assumptions. And only one thing is clear. They are toxic bombs that, once injected into a human, can potentially cause a variety of inflammatory responses and even death.
It is clear that vaccines are going to be used as a mechanism to control the population, maintain a fear narrative, and continue to enrich a tiny minority at the expense of the many.
However, as these filthy products are exposed for what they really are, expect an all out-propaganda campaign as they desperately try to claim that those not accepting vaccines are dangerous extremists.
[quote from Dr. Peter Hotez]
“We have to recognize that anti-vaccine activism, which I actually call anti-science aggression, has now become a major killing force globally. During the COVID pandemic in the United States, 200,000 Americans needlessly lost their lives because they refused a COVID vaccine, even after vaccines became widely available. And now the anti-vaccine activism is expanding across the world, even into low and middle income countries. It’s a killing force. Anti-science now kills more people than things like gun violence, global terrorism, nuclear proliferation or cyberattacks. And now it’s become a political movement. In the US it’s linked to far extremism on the far right. Same in Germany. So this is a new face of anti-science aggression. And so we need political solutions to address this.”
MRNA vaccines are just the latest chapter in this psychological war and I hope you don’t lose sight of the fraud taking place upstream. That is, the misplaced belief in germ theory.
“Is it any wonder that the public is getting a little suspicious of us and our vaunted ‘discoveries’? The wonder to me is that there are still seventy millions of them willing to submit to vaccination and serum treatment.
“How much good did we do these poor fellows? Ask Edward Jenner! He knows now, if so be that we know after death, and am willing to believe that he would gladly spend a part of his eternity in purgatory if he could undo the wrong he did the world by vaccination.”
~ ‘Who are the Quacks?‘ by William Howard Hay, 1940
Cover image based on creative commons work of: Dimhou
Anthony Brink is an advocate of the High Court of South Africa and argues that former South African president Thabo Mbeki was right about HIV not causing AIDS. In fact, to be accurate, he did not say that HIV does not cause AIDS (as is often stated in the mainstream press); he said that HIV does not exist.
It’s an important distinction.
Attacking the foundation
For example, if I said that fire-breathing fairies don’t cause tornados, then I would be correct, but it leaves open the possibility that fire-breathing fairies cause snowfall. Obviously, both scenarios are absurd because fire-breathing fairies do not exist.
What does HIV-positive mean anyway?
As Anthony noted in our conversation below, the former president rejected the foundational premise and was scientifically correct. David Rasnick is a biochemist and explained why on my podcast.
The alleged virus associated with the syndrome called AIDS was never isolated.
I strongly recommend watching the award-winning documentary House Of Numbers which includes interviews with top scientists including Luc Montagnier (who won the Nobel Prize for “discovering” HIV).
And if you’re so inclined, then read through Thabo Mbeki’s 2001 AIDS Report. (Go to page 18 and stop yourself from feeling déjà vu after reading the critique of PCR tests.)
Our conversation
Anthony is also the national chairman of the Treatment Information Group, a voluntary association he founded in 2002 to promote research-based public debate of antiretroviral (ARV) drug policy, non-toxic treatment approaches to AIDS and HIV testing issues in South Africa.
The emergence of COVID-19 has led to numerous controversies over COVID-related knowledge and policy. To counter the perceived threat from doctors and scientists who challenge the official position of governmental and intergovernmental health authorities, some supporters of this orthodoxy have moved to censor those who promote dissenting views. The aim of the present study is to explore the experiences and responses of highly accomplished doctors and research scientists from different countries who have been targets of suppression and/or censorship following their publications and statements in relation to COVID-19 that challenge official views. Our findings point to the central role played by media organizations, and especially by information technology companies, in attempting to stifle debate over COVID-19 policy and measures. In the effort to silence alternative voices, widespread use was made not only of censorship, but of tactics of suppression that damaged the reputations and careers of dissenting doctors and scientists, regardless of their academic or medical status and regardless of their stature prior to expressing a contrary position. In place of open and fair discussion, censorship and suppression of scientific dissent has deleterious and far-reaching implications for medicine, science, and public health.
Introduction
The emergence of COVID-19 has led to a proliferation of disputes and disagreements over COVID-related knowledge and policy (Liester 2022), including the origin of the SARS-CoV-2 virus (van Helden et al. 2021), restrictive measures taken by most governments such as social-distancing, lockdowns, contact-tracing and mask requirements (Biana and Joaquin 2020), the use of certain treatments of the disease and the exclusion of others (Mucchielli 2020), the safety and efficacy of vaccines against COVID-19, and the implementation of “vaccine passes” in many countries (Palmer 2021). Harambam (2020) has referred to these disputes as the “Corona Truth Wars.”
Since the beginning of the pandemic, while governments and health authorities argued that restrictive lockdown policies were necessary to deal with the pandemic and prevent deaths, many scientists and medical practitioners questioned the ethics and morality of such tactics, including Nobel laureates and leading physicians and scholars (e.g., AIER 2020; Abbasi 2020; Bavli et al. 2020; Brown 2020; Ioannidis 2020a; Lenzer 2020; Levitt 2020). Furthermore, from early 2020, increasing numbers of scientists and doctors argued that the pandemic, as well as morbidity and mortality figures, were being inflated and exaggerated (Ioannidis 2020; Brown 2020); that the extreme policies and restrictions violated fundamental rights (Biana and Joaquin 2020; Stolow et al. 2020); and that governments were using fear campaigns based on speculative assumptions and unreliable predictive models (Brown 2020; Dodsworth 2021). Some scholars, medical practitioners and lawyers have pointed to biases, concealment and distortions of vital information regarding COVID-19 morbidity and mortality rates that misled policymakers and the public (AAPS 2021; Abbasi 2020; AIER, 2020; Fuellmich 2020; King 2020).
It has been argued that much of the discussion around the COVID-19 pandemic has been politicized (Bavli et al. 2020), and that science and scientists are being suppressed due to political and economic interests (Bavli et al. 2020; King 2020; Mucchielli 2020). This criticism has grown, especially following the start of the COVID-19 vaccine campaign. Criticism was made regarding the hastiness with which the mRNA vaccines were granted Emergency Use Authorization by the FDA even for children; the quality of the clinical trials that led to the authorization of the vaccines (including violations of research protocols and evidence of fraud); the lack of transparency regarding the process and data that led to the authorization; the inflation of efficacy estimates; and the minimization or ignoring of adverse events (Doshi 2020, 2021; Fraiman et al. 2022; Thacker 2021).
Critics have argued that the scientific and policy discourse surrounding COVID-19 has not been carried out on a level playing field due to censorship and suppression of views contrary to those supported by medical and government authorities (Cáceres 2022; Cadegiani 2022; Liester, 2022; Mucchielli 2020). Some governments and tech corporations, such as Facebook, Google, Twitter and LinkedIn, have taken measures to censor contrary viewpoints, arguing that views challenging government policies are dangerous misinformation, and therefore censorship is justified to protect public health (Martin 2021).
The present study explores the phenomenon of censorship of dissent from the point of view of well-known scientists and doctors who were censored for their heterodox views on COVID-19, in order to learn about the range of tactics that have been used to censor and silence them, as well as the counter-tactics they have used to resist these attempts.
Censorship of COVID-19 Heterodoxy
To describe a view or position on COVID-19 as heterodox implies the existence of an orthodox position, which here refers to the dominant position supported by most major governmental and intergovernmental health agencies. Liester (2022) provides a list comparing what he refers to as the dominant versus dissenting views with respect to COVID-19, which includes the origin of SARS CoV-2 (zoonotic vs. laboratory), mask mandates (will prevent spread vs. will not prevent spread), early treatment with drugs such as hydroxychloroquine and ivermectin (ineffective and dangerous vs. effective and safe), the usefulness of lockdown measures and other restrictions (effective and beneficial vs. ineffective and harmful), COVID-19 vaccines (safe and effective vs. unsafe and dangerous), and COVID-19 vaccine mandates and passports (necessary and ethical vs. harmful and unethical). While it may be true that none of these dominant positions have been universally adopted by all governments worldwide to the same degree or down to every last detail, nevertheless a dominant or orthodox position on all of these issues can be identified on a country-by-country basis with strong similarities across national borders.
It is worth noting that orthodox positions can change. For example, by mid-Spring 2020, discussion of the laboratory origins of SARS-CoV-2 was forbidden on certain social media sites, like Twitter and Facebook (Jacobs 2021). More recently the lab-leak theory has since gained more legitimacy, especially following articles in the Proceedings of the National Academy of Sciences (Harrison and Sachs 2022), Frontiers in Virology (Ambati 2022) and Vanity Fair (Eban 2022) as well as a statement by WHO director-general Ghebreyesus, who commented on an interim report by the Scientific Advisory Group for the Origins of Novel Pathogens, saying that all hypotheses need to be considered and criticizing the report for inadequate assessment of the lab-leak hypothesis (WHO 2022). Another example relates to the necessity of mask wearing: US officials such as the director of the National Institute of Allergic and Infectious Diseases (NIAID), Anthony Fauci, are on record recommending against universal mask wearing in March 2020, only to change their position in April to recommend universal mask wearing and mandates (Roche 2021).
Since early 2020, there has been an upsurge of complaints about censorship by individuals and groups presenting heterodox COVID-related viewpoints and information, with even more complaints in 2021 following COVID-19 vaccine rollouts. Many instances involve social media censorship, including the removal of accounts (“deplatforming”) or blocking the visibility of a user’s content without informing them (“shadow banning”) (Martin 2021).
While complaints regarding scientific censorship and suppression preceded the pandemic (Elisha et al. 2021, 2022; Martin 2015), a new feature of the COVID era is the prominent role played by information technology companies such as Facebook and Google (Martin 2021). One prominent example was the down ranking of the Great Barrington Declaration’s website by Google (Myers 2020). The Declaration, spearheaded by three epidemiologists at Harvard, Stanford and Oxford universities, was released in October 2020 (Kulldorff et al. 2020) and signed by many notable scientists and doctors, including the Nobel Prize laureate Michael Levitt. It argued against universal lockdowns in favor of focusing on protecting vulnerable groups. However, to reduce exposure, Google altered its search algorithm (Myers 2020). In February 2021, Facebook deleted a page set up by a group of scientists involved with the declaration (Rankovic 2021). In April 2021, YouTube removed a recording of an official public hearing on the pandemic that featured Florida governor Ron DeSantis and the authors of the Great Barrington Declaration. One of them, Prof. Kulldorff, who is one of the most cited epidemiologists and infectious disease experts in the world, was himself censored by Twitter in March 2021 (Sarkissian 2021). Though his tweet saying that not everyone needs the COVID-19 vaccine was not taken down, he was warned, and users have been prevented from liking or retweeting the post (Tucker 2021).
Similar cases abound. For example, the research-networking site ResearchGate removed physicist Denis Rancourt’s article about masks (Rancourt 2020), and in 2021, it banned him entirely (Jones 2021). In July 2021, LinkedIn suspended the account operated by Dr. Robert Malone, an internationally recognized virologist and immunologist, an action repeated by Twitter in December 2021 (Pandolfo 2021).
These are just some of the many examples of censorship related to COVID-19. Beyond the large scale of the censorship phenomenon, and the wide involvement of tech companies in it, another unique characteristic of COVID-related censorship is its targets. Many of the doctors and researchers being censored by the world’s biggest technology companies are not fringe figures. As in the examples above, these are mainstream scientists, many of them leading experts working in prestigious universities and/or hospitals, some of whom have authored books and published dozens or even hundreds of papers and whose studies have been widely cited. Some of them are editors of scientific/medical journals and some are heads of medical wards or clinics.
This heavy censorship was done with the encouragement of governments (Bose 2021; O’Neill 2021), which cooperated with tech companies such as Facebook, Twitter, and Google. For example, on March 7, 2022, US Surgeon General Vivek Murthy called on tech companies to report “health misinformation” to the federal government and to step up their efforts to remove it (Pavlich 2022). Subsequently, e-mails released from legal proceedings have documented the ways in which government officials directly coordinated with tech companies like Twitter and Facebook to censor doctors, scientists and journalists (Lungariello and Chamberlain 2022; Ramaswamy and Rubenfeld 2022). In December 2021, an e-mail from the fall of 2020 was released via a Freedom of Information Act (FOIA) request. It revealed a behind-the-scenes effort by Francis Collins, then head of the National Institutes of Health (NIH), to his colleague, Anthony Fauci, head of NIAID, to discredit the Great Barrington Declaration and disparage its authors. In the email, Collins told Fauci that “this proposal from the three fringe epidemiologists … seems to be getting a lot of attention,” adding that “there needs to be a quick and devastating published takedown of its premises. I don’t see anything like that online yet—is it underway?” (Wall Street Journal 2021).
Practices of censorship have also been used by the Israeli Ministry of Health (IMOH) and media against doctors and researchers whose views run counter to institutional orthodoxy. One such example is the Israeli Public Emergency Council for the Covid19 Crisis. The organization, which consists of leading doctors and scientists, was targeted by the IMOH and the media numerous times, including attacks on individual members of the organization (Reisfeld 2021).
Censorship, the Backfire Effect and Public Outrage
COVID-19 censorship is, in part, an exclusion of the views of dissident experts as well as citizens who question the standard position. This type of censorship has been a feature of many other controversial areas in science and medicine, such as AIDS, environmental studies, fluoridation, and vaccination (Delborne 2016; Elisha et al. 2021, 2022; Kuehn 2004; Martin 1991, 1999; Vernon 2017). In fact, censorship has a long history, and its purpose is to suppress free speech, publications and other forms of expression of unwanted ideas and positions that may be perceived as a threat to powerful bodies such as governments and corporations.
Censorship of opposing or alternative opinions and views can be harmful to the public (Elisha et al. 2022), especially during crisis situations such as epidemics, which are characterized by great uncertainties, since it may lead to important views, information and scientific evidence being disregarded. Furthermore, the denial or silencing of contrary views can elicit public mistrust (Gesser-Edelsburg and Shir-Raz 2016; Wynne 2001). Studies have indicated that in situations of risk, especially risk that involves uncertainty, the public prefers full transparency of information, including different views, and that providing it does not raise negative reactions in terms of behaviour, but rather, helps reduce negative feelings and increases the public’s respect for the risk-assessing agency (De Vocht et al. 2014; Lofstedt 2006; Slovic 1994). As Wynne (2001) warns, institutional science’s attempts to exaggerate its intellectual control and use knowledge as justification for policy commitments, while ignoring its limits, only alienates the public and increases mistrust.
Moreover, censorship can be counterproductive, in essence backfiring, because it can lead to greater attention being paid to the censored information, foster sympathy for those being censored and promote public distrust of the actors and agencies engaged in censorship (Jansen and Martin 2003, 2004, 2015). This is especially evident in the internet age. While information technology companies such as Google and Facebook play a prominent role in the attempts of governments and authorities to censor dissenting positions on COVID-19 (Martin 2021), it is a serious challenge to achieve this completely. Their visibility in the mainstream media and in web search results can be curtailed, but there are too many alternative communication options to prevent dissenters from communicating their positions (Cialdini 2016). Therefore, attempts to silence and censor critics can sometimes backfire.
Considering the extent of censorship reported during the COVID-19 era, and in particular the number of accomplished doctors and scientists censored and silenced, as well as the extensive involvement of tech companies, on the one hand, and governments, on the other, it is worthwhile investigating this phenomenon. The present study is designed to explore the subjective perceptions of well-credentialed, highly accomplished mainstream doctors and scientists who have experienced censorship and/or suppression after expressing non-orthodox positions regarding the handling of the COVID-19 pandemic, and how they dealt with it. Through interviews, we examine censorship tactics used by the medical establishment and the media (both mainstream and social media), and the counter-tactics employed by their targets.
Method
The study is a qualitative one (Aspers 2004), which aims to identify internal perceptions from the point of view of those who have experienced the phenomenon under question.
Participants
Study participants include 13 established doctors and scientists (12 men and 1 woman), from different countries around the world (viz., Australia, Canada, the Czech Republic, Germany, Israel, UK and US). Of these, 11 have formal medical training from a variety of fields (e.g., epidemiology, radiology, oncology, cardiology, paediatrics, gynecology, emergency room management) and two are research scientists without medical degrees (in the areas of risk management and psychology). All participants hold either an MD or PhD degree, and four hold both. Most of them are well known in their fields, with a proven research background that includes many academic publications. We used a purposeful sampling method, i.e., a non-probabilistic sampling according to which a deliberate selection is made of individuals who could teach us about the phenomenon under study (Creswell 2012). To preserve the respondents’ anonymity, details that might lead to their identification are omitted.
Research Tool and Procedure
The study is based on in-depth interviews using a semi-structured interview guide. The questions focused on the respondents’ stance towards COVID-19 that was seen as controversial, events they experienced due to their stance, the implications of these events for their professional and personal lives, and their responses to these events.
Recruitment was done in several ways. First, through a Google search we located the contact details of doctors and researchers known for their critical stances toward COVID-19 pandemic measures and policies. Second, we used the “snowball” method to reach other respondents. The initial contact with the respondents was by email, in which we explained the purpose of the study and asked for their consent to be interviewed anonymously. The interviews were conducted via Skype, Zoom or telephone, and lasted about an hour and a half on average. Each respondent was asked to sign an informed consent form. The interviews were recorded and transcribed.
Data analysis and coding were based on identifying the key issues that emerged from the interviews, while classifying and grouping them into meaningful categories. We assured the reliability and validity of the study by applying different methods. The analysis of the data was discussed by all of us as an expert peer group, and different sources of data served as triangulation of the data (e.g., documents and correspondence provided to us by the interviewees). Quotes in the text are provided for illustrative purposes (Creswell 2012).
Findings
Study participants reported being subject to a wide variety of censorship and suppression tactics used against them by both the medical establishment and the media, due to their critical and unorthodox positions on COVID-19. They also described the counter-tactics they used to resist. We divide the findings into two sections, the first describing censorship and suppression tactics and the second describing the counter-tactics used by our participants.
Silencing Dissent: Censoring and Suppressing Tactics
Tactics of censorship and suppression described by our respondents include exclusion, derogatory labelling, hostile comments and threatening statements by the media, both mainstream and social; dismissal by the respondents’ employers; official inquiries; revocation of medical licenses; lawsuits; and retraction of scientific papers after publication.
Exclusion
Respondents reported how, at a very early stage of the epidemic, when they just began to express criticism or their different position, they were surprised to discover that the mainstream media, which until then had seen them as desirable interviewees, stopped interviewing them and accepting opinion pieces from them:
Neither X nor Y [two central newspapers in the respondent’s country] wanted to publish my articles. Without a proper explanation. Just stopped receiving articles. It was quite blatant, that they stopped accepting articles expressing a different opinion from that of the ministry of health (MOH). The number of journalists who can really be talked to, who are willing to listen to another opinion, to publish, has been greatly reduced, and most health reporters today are very biased towards the MOH (#10).
Denigration
Respondents reported that exclusion was only the first step: shortly after that they started being subjected to defamation by the media, and disparaged as “anti-vaxxers,” “Covid deniers,” “dis/misinformation spreaders” and/or “conspiracy theorists”:
After that report came out…, I was front page of the Sunday Times… it said… X [the respondent name], a professor in A [the institution this respondent works in] is co-author of anti vax report… I was now, yeah…, I was told I was anti-vaccine (#9).
I have been vilified.… I’ve been called a quack…, an anti-vaxxer and a COVID denier, a conspiracy theorist (#13).
Recruiting “Third Parties” to Assist in Discrediting
One prominent tactic our respondents claim was used by the media to discredit them was the use of seemingly independent “third party sources,” such as other doctors, to undermine them, for example by writing defamatory articles:
I was shocked at what came out the next day in The Wall Street Journal… So here we had three of the most senior doctors with hundreds and hundreds of publications and scientific credibility to our resumes and …a major media outlet allowed a junior doctor to publish who has no academic standing or track record…[and] have him publish a defamatory piece (#6).
Another “third party” source used by the media, according to our respondents, was “fact-checking” organizations, a practice that is ostensibly meant to verify published information to promote the veracity of reporting. However, some respondents alleged that the fact-checking groups were recruited and operated by corporate or other stakeholders to discredit them and try to discredit the information they presented:
…the fact checkers are a source of misinformation, so though it may review something and say, Dr. X said something, but… they make a counterclaim. The counter claims are never cited in the data… they all trace back to the vaccine manufacturers or the vaccine stakeholders (#6).
you get the fact checkers… They tried to discredit S, but also, because I was a co-author, they were picking on me…, and all this sort of stuff and… discredit by association… (#4).
As seen in the second example above, some of the participants said that those “fact-checking” groups were used to discredit and defame not only the researcher or doctor who presented a contrarian opinion or information, but also others who were associated with them.
Some respondents said that the media persecuted them to the point of blackening their name at their workplace, resulting in their dismissal, or that they were forced to resign:
I lost my job…, I was working for the last 20 years in X [the institution’s name]… And so, the media started coming to X… there was a concerted effort to… ruin my reputation, even though, this is unbelievable, they had the lowest death rate basically in the world, and the doctor who brought it to them, gets vilified and slandered. So, I left on my own… My reputation was slandered. I mean the level of treatment that I didn’t expect and abuse I would say (#1).
Online Censorship
Some respondents reported being censored on social media networks (e.g., Facebook, Twitter, TikTok, YouTube, Google, LinkedIn), and said some of their posts, tweets, videos or even accounts were taken down by the networks.
My YouTube videos were being taken down. Facebook put me in jail, “Facebook Jail.” And I found that I was being de-platformed everywhere (#1).
I’ve always had videos, just my teaching material I’ve been putting up on YouTube…, but I also started to put up materials around this just sort of talking through some of the research… looking at the vaccine efficacy data… YouTube started taking it down. And so now …, I cannot post, I can’t even mention vaccines, because within seconds, as soon as I’m actually trying to upload the video, YouTube will say this video goes against our guidelines… (#3).
I got terminated from TikTok… All of a sudden, I was permanently banned because presumably I had a community violation (#2).
I’m currently on my sixth twitter account…the last one was shut down supposedly for a tweet about X’s lab [the name of the lab], but it was coming. I ruffled too many feathers (#2).
As can be seen in the above examples, respondents noted that the removal of their materials from social networks was accompanied by a notice claiming they had violated the “community rules.” They emphasized that these were academic materials, backed up scientifically:
I became aware that an academic YouTube video that I had put together regarding the paper in the XXX journal … was pulled down by YouTube, and I received a notice that it had violated terms of the YouTube community… without ever having any terms of use from YouTube that would explain what types of terms would be applied to a four PowerPoint slide scientific video…(#6).
One of the respondents reported on censorship even in Google Docs, which means that even private communications are being censored:
Google Docs started restricting and censoring my ability to share documents… This is not Twitter throwing me off like they did. This is an organization telling me that I cannot send a private communication to a colleague or to a friend, or to a family member… (#1).
Censorship and Suppression by the Medical and Academic Establishment
Some of the respondents reported that they were subjected to defamation by their own institution, with the apparent intention to harm their reputation and careers. For example:
…in [my country], we have approximately 55,000 physicians. My name appeared on the official website of the Ministry of Health, that I’m the only person, one medical doctor who is… distributing disinformation… (#12).
There was a concerted effort to… ruin my reputation even though, this is unbelievable, they [the hospital where I work] had the lowest death rate basically in the world (#1).
Some participants also said that they had received a clear message from the institution where they worked that they were not allowed to identify themselves with the institution when giving an interview or a testimony or expressing their views—in some cases as a condition of renewing their contract.
I gave X (a certain treatment) testimony, and that kind of went viral. And the hospital was not happy because my affiliation had shown up… They offered me a new contract. They said …, we got some new terms for you, because my old contract was not restricted. The new one basically had like seven or eight restrictions of my first amendment rights… basically I couldn’t talk to the press, I couldn’t speak in public…, unless I said, these are my opinions not that of my employer… It was a relatively short conversation. I said that’s never going to happen, I’m never going to sign that thing, and we said goodbye (#9).
In some cases, respondents reported that following a position or criticism they expressed, they were dismissed from their institution, or were notified that their contract would not be renewed.
I was told that my contract [at the medical clinic] wasn’t going to be renewed… There’s a whole variety of checklists for the contract not to be renewed, there must be a due process, and the first red flag is that there was no due process. I asked specifically was there a board vote…, and the answer was no, and I said… why is this action being taken, and their response was “no reason”… [Later] I received a letter from [X] University saying that I was stripped of my professorship, with no due process, with no faculty senate, nothing…. Then, I received a…letter from [Y] University, again no due process, no faculty senate, no explanation (#6).
Similarly, respondents said they were summarily dismissed or disqualified from prestigious positions, such as serving on leading health or scientific committees, or editing medical journals, without due process or transparency:
… the director general of the Ministry of [X] approached me … and said that the Minister had reached an agreement with the Ministry of Health, that he was putting a representative on the [prescription drug] basket committee …, and she said all fingers had pointed to me… Then comes a phone call after a week, and she says, “listen, your name was already passed on as a request of the Minister to the Basket Committee, and has been disqualified unequivocally because you oppose [COVID] vaccinations in children”… I was shocked… Until then the responses I received were from the bottom. This is a response from the top (#11).
…there was a whole series of actions taken again with no due process and no explanation so… I received a notice from the [medical association] that I was being stripped from a committee position… I received a letter from a journal…where I was the editor in chief, being stripped of the editorship, again with no due process, no phone calls no, tractable explanation… I received a letter from the National Institutes of Health being stripped from a longstanding committee position, I was on the committee for several decades and was stripped off of that, again no phone call, no due process, no explanation (#6).
In one case, the respondent had learned that his country’s parallel to the Centers for Disease Control (CDC) intervened and asked the university to “examine” his “case”:
…my university president invited me to talk about “corona”. In that meeting, I was informed… that the [The equivalent health authority to the CDC in the interviewees’ country] had written a letter to the president, asking him to examine my case because, according to the ministerial letter, I was going public with methodologically questionable things. According to the president, the university has never received similar requests before… (#12).
Some of the interviewees said that the health establishment had not only blackened their reputation and taken serious measures against them but also cooperated with the media and made sure to spread the information about those measures through them:
You know the news release came out, I’m a prominent physician in the United States, so, in fact, I believe the health system drafted a press release that went out, that they were suing me, and so the topic came up [during the press interview], “so are you being sued, and… what’s your reaction?” (#6).
Official Inquiries
Some doctors reported on official inquiries launched against them, such as investigating or threatening to withdraw their medical license:
…my license was investigated… At that point in time, I felt that the medical board was being weaponized… My license ended up getting investigated… three times now, each time… without any punishment or reprimand or anything… But it merely points to the fact that it’s very easy to get censored or cancelled (#2).
Following a post I wrote about the adverse events … I received a letter from the Committee of X [the name of the committee]. Allegedly they asked me for the details of these patients (the patients the interviewee reported in his post had adverse events), but if it was genuinely a real wish on their part, then it was not this committee, which in fact deals with Y [the definition of the committee’s activities] that would have asked me for the details, but a real official from the Ministry of Health. I answered them through A [my lawyer], a more legal and less medical reply. This is basically a committee without powers. I do not think I am even allowed to pass on the names of patients to them. It can be given to a relevant party, a district doctor… I will be happy to talk to them (#2).
One of the respondents reports that a million-dollar lawsuit was filed against him:
And then my wife calls me and says that the health system is suing us for over a million dollars, so I have just put together teams of attorneys and scrambled them into court… And … the charge is that is that I’m violating terms of my separation agreement, specifically that the health system is being brought into my media presentations, and I’ve never made any [such] statements (#6).
Another respondent reports on a police search conducted at his private clinic in his home:
The [medical board] showed up unexpectedly one day without a warrant to search my house, which was listed in their records as my office, to do a medical office inspection, which doesn’t require a warrant [in my country]. I told them it’s my business office and I don’t see patients there and they have no business coming in there (#7).
Retraction of Scientific Papers
Some researchers and doctors recounted how their research had been retracted by the journal after publication:
And then, five days before the FDA pediatric meeting on vaccination, [the publishing company] pulls the paper out of the National Library of Medicine and says that they are retracting it. And the explanation, they tell us a few days later, is that they think they didn’t invite the paper to begin with. And I can tell you as an editor, the paper was clearly welcomed, and it went through the standard peer review process. The only way they can legally pull a paper out of the National Library of Medicine is if it’s scientifically invalid, and that wasn’t the claim (#6).
So I submitted it to X [the name of the journal] … and well, this was a desk rejection … Actually, at least for me the arguments were kind of, say, from my perspective, there were no solid arguments… I don’t know why this was rejected, and then I submitted it to several other channels… and then I stopped to trying to publish it in the scientific literature. It’s published as a pre-print (#8).
Another theme that arose repeatedly during the interviews was that research critical of COVID-19 policies and orthodoxy were treated in ways the interviewees had never encountered before in their careers. This included having papers rejected from journals (often multiple times) without peer review, the journal review and publication process taking many months longer than typical for the journal, and even having papers rejected from pre-print servers such as MedRXiv:
At the beginning of the pandemic, we were getting a lot of stuff published. It wasn’t in any way challenging the orthodox narrative… and then we did this analysis on [X] and then when that happened, oh my God they went ballistic, we got attacked. That work never got published. This is where the censorship—we’d already had some problems because we were publishing other work on the case data, and it was being automatically rejected from any of the medical journals, anything like that. And that was when our stuff started to get rejected from arXiv and medRxiv…the only place we could get any of this stuff published, was we just put it on ResearchGate (#4).
In one case, an interviewee said he felt so threatened by the medical establishment that he refrained from putting his name on papers he co-authored with other researchers, and that those whose names do appear on the papers were trying to hide or stay under the radar until the paper was published:
We’ve got a paper that’s ready to come out in [an important journal], and the group that published it has been hiding for a year… Now, I can’t be on the paper you know (#5).
Counter-reaction: Fighting Back
The respondents noted that their initial reaction to the attacks and censorship was shock and surprise, since for the first time in their lives they felt excluded from the scientific/medical community, attacked by the media and sometimes by their employers, and/or disparaged as “conspiracy theorists” who endanger the public health. Yet, despite the censorship, the personal attacks and defamation, the dismissals, the damage to reputations and the economic price, all respondents nevertheless stated that none of it deterred them, and they decided to fight back, using various counter-tactics.
First Reactions: Shock and Surprise
Most respondents describe their initial reaction to the persecution and censorship they experienced as shock. Some said that they felt threatened, and for the first time, excluded from the scientific/medical community:
I was speechless. It does not happen to me. I did not imagine. It was terribly threatening to me all those attacks … it took me a month to recover from the understanding that this is the country we live in… I was in shock… I was surprised… My heartbeat I think was 200 per minute (#11).
As someone who has been an integral part of the [health] system, and knows the role holders personally – the rift I feel is very heavy (#1).
Respondents said that they felt that the threats, dismissals and attacks against them were in fact an attempt to silence them, just because their opinions were not aligned with those dictated by the authorities:
…everything was done initially to suppress my voice, because I was the only one screaming (#1).
Some respondents said they felt that the censorship and unprecedented attacks they experienced were especially vicious because those who did it knew they were valued and influential:
…they were actually trying to silence me in the media… it appears on the surface, that lawsuit basically was an attempt to censor me… I’m a frequent contributor on Fox News, I just testified in the US Senate…, my advice is valued all over the world, and I think it was a parochial attempt… to censor me…(#6).
Determined to Fight
Our respondents stated that the censorship and suppression they experienced made them want to fight back and make their voices heard more, on the grounds of freedom of speech and their concern for public health.
It’s an interesting question what I feel I’m paying. Because I feel there are [costs]. The fact is that I almost left. Why did I stay? Because I realized that there was a price that I was not willing to pay – that they would shut me up. (…) (#11).
To me the most important question is why do I (keep) doing this? Because if I do not live according to my values and freedom of speech, then I will not live. That’s why I am doing it (#9).
Some of them even noted that the attacks on their reputation made them even more determined and eager to expose the information that was being censored.
Actually, it makes me more determined. I’m a little bit of a pit bull. So, we’re going to keep getting the word out (#2).
Some of the respondents said they decided to take official or legal actions against the organizations that censored them:
I will file suit for breach of contract, since we had a publication contract and they signed it and they accepted… they’re going to be sued for tortious interference that they’ve actually interfered with the business of publishing valid scientific information… I imagine this is going to be quite injurious and high profile to [the publisher] (#6).
I do have a Freedom of Information request into all the entities that stripped me of various credentials and positions in order to start to uncover what is stimulating all of this… (#2).
The respondents’ counter-reactions were expressed in several ways: a desire to disclose the act of censorship and the information that was censored, which they claim is evidence-based; use of alternative channels in order to spread their positions and views in relation to COVID-19 publicly; establishment of support networks with colleagues; and development of alternative medical and health information systems. That is, they created a kind of a parallel world to the mainstream establishment.
Exposing the Censorship
Some respondents stressed that they wanted to expose the censorship act itself. For instance:
I got in contact with a few powerful people, and they referred me to the Media Resource Centre in Washington, which is a non-profit to fight censorship. I told them what had happened. And they already wrote up an article about it. That article is now being put up on different sites. I did an interview on One American News Network. I kind of brought that to the world (#1).
Using Alternative Channels
Respondents noted that when they understood that they were censored by the mainstream media, they decided to use alternative channels, such as social media platforms, to spread their position and contrary information and voice their opinions in public:
Fortunately, I built up a little bit of a Twitter Following… 34,000 or something like that…, so you can get the message out (#4).
Some of the respondents said that to protect themselves, they were forced to open “secret” telegram or anonymous Twitter accounts. Although they express frustration, they are still doing it in order to spread information. For example, one participant noted it is absurd that scientists should keep secret telegram accounts so that the government does not revoke their licenses or damage their reputations:
…my credentials from that aspect [are] really unusual… A working doctor that has that combination… That’s why I have to be careful when I’m on Twitter… because if you’re smart enough to realize there is only a small group of doctors in the world that have got that [combination]… I put a tweet and I put it on my secret telegram channel as well… Ridiculous! We’ve got secret telegram accounts, I mean, we’re scientists running secret telegram accounts, so we don’t get taken out by the government. What is going on? (#5).
Creating Social Support Networks
Some of the respondents revealed that they created support networks of fellow scientists, physicians, lawyers and politicians with similar views and opinions. These networks were used not only to exchange information, but also to receive support and empathy from “outsiders” like them, to make new friends and create a new community:
…it’s been really nice to make a whole and growing network of friends in life, who know those truths as well. I feel like I’m making a new community with new friends that I can talk to that understand the world, understand the corruption, and really can navigate this stuff. So, at the same time that I woke up with a whole new collection of colleagues and friends, but a lot of us are outside of science… (#9).
And then there were a few colleagues that came on board… And all of a sudden, I had some big heavyweights, academic leaders advocating for my work (#1).
Developing Alternative Medical and Health Information Systems
Beyond their activities in disseminating information and data, some of the respondents noted that they are working to establish new alternative platforms and organizations dedicated to developing and providing health information and medical treatments—including new journals and non-profits, instead of the existing ones, which they claim have failed and disappointed. They explain this as a means of coping with the censorship and suppression they experienced due to their opposing positions, which grant them a sense of hope and a feeling that they are building “a new world”:
I have a new thing in life. N and I, we started the X organization…, whose sole mission is to try to figure out and help people to treat COVID. And I think we’ve done a real service to the world (#9).
…there’s a lot of talk about starting a journal… Tess Lawrie started The World Council for Health. There is increasing amount of talk about starting a new health system. Like, people want to go to hospitals where the doctors can be doctors and not the other role of all these regulations and corrupt agencies, so you know, there is maybe a new world that will form…(#4).
Discussion
The purpose of the present study was to explore the subjective perceptions of accomplished and well-credentialed mainstream doctors and scientists who have experienced censorship and suppression after expressing heterodox COVID-related views, to examine tactics used by the medical establishment and the media and the counter-tactics employed by their targets.
The respondents in our study reported on a wide variety of censorship and suppressive tactics used against them by the media (including the mainstream media and social media companies such as Google, Facebook, Twitter, Instagram, LinkedIn and TikTok) and the medical establishment. Tactics used by the media include derogatory comments and labels, often using ostensibly independent “third-party” sources such as anonymous “fact-checkers” or other doctors, and online censorship involving the removal of their social media and internet contents and accounts, in some cases repeatedly after they opened new accounts. Some of the respondents reported that the media have been persecuting them to the point of blackening their names in their workplaces.
The tactics used by the medical establishment also include defamation and intimidation; retraction of scientific papers after publication; dismissal or adverse changes to employment contracts; aggressive actions aimed at sabotaging other significant roles of the individual, such as participating in important committees or serving as editors of scientific journals. Some respondents reported a targeted thwarting of their careers and harming of the reputations they had built over the years, while consistently stripping them of all the positions they held. Some reported being subject to abusive formal proceedings, such as investigations and attempts to revoke their medical licenses, and in one case even being sued for a large sum of money.
As for the reactions of the respondents to these censorship tactics, contrary to what has been found in previous studies, in which, out of fear of being marked as “anti-science” or “anti-vaxxers,” some of the doctors and scientists said that they refrain from expressing their critical position on controversial issues such as vaccines (e.g., Elisha et al. 2022; Kempner 2008; Martin 2015), the scientists and doctors in our study did not self-censor themselves, despite the heavy price many of them paid professionally and financially. According to the respondents, after the initial shock, they decided to fight back using a range of methods, from framing the actions taken against them as censorship and trying to expose the censored information and the censorship act itself, to mobilizing support and building supportive networks of friends, colleagues, and followers, which, they reported, were constantly growing. Moreover, the respondents announced that they were developing alternative health systems as well as alternative channels that would allow free dissemination of information and professional positions. The sampling method was unlikely to pick up doctors and scientists who kept a low profile or who quickly became silent at the first sign of danger, which may partly explain why all the interviewees resisted attacks. It will also not capture doctors and scientists who disagree with aspects of the official orthodoxy but are too afraid to speak out.
Despite the power held by governments and corporations, the ability to censor is limited, especially in the digital age, since even if the traditional “gatekeepers”—journalists in the popular media and editors of scientific journals—censor opposing opinions and information, opponents will still be able to spread them through alternative outlets. As Jansen and Martin (2003, 2004, 2015) have shown, exposing censorship can sometimes lead to public outrage, and powerful interests who undertake it often try to prevent or reduce this outrage using various methods, mainly by defaming and delegitimizing the targets of censorship.
Indeed, the censorship tactics reported by our respondents are consistent with those identified in Jansen and Martin’s (2015) framework on the dynamics of censorship, including:
Cover-Up—Our findings show that this tactic was very prominent, which is not surprising, since, as Jansen and Martin noted, if people aren’t aware of censorship, they are not upset about it. The cover-up tactics included various methods. For example, using third-party sources such as other doctors or “fact-checkers” to discredit dissident scientists and doctors. Since these sources are portrayed as independent, they help mask the real sources behind the censorship.
Devaluation—This tactic was described by our study respondents and included various aspects, such as publishing false and disparaging claims about them, dismissing them from work in academia or medical institutions, and stripping them of various senior positions—all actions that were felt by our respondents to be intended to undermine their credibility and legitimacy. The tactic of devaluation, also known as a “negative campaign” or a “smear campaign,” is often used by corporations, and its aim is to harm the reputation of an individual or a group (Griffin 2012; Lau and Rovner 2009). Smear campaigns help distract public attention from the content of the targets’ message and deflect the discussion from the criticism or allegations raised and instead focus the attention on those raising these allegations.
Reinterpretation—This tactic involves framing censorship as a means of “protecting the public” from the dissenting doctors and scientists, portraying them as “misinformation spreaders” endangering public health in a time of crisis. This framing echoes attempts by policymakers in other areas to justify censorship by arguing that contradictory information might confuse the public and cause panic (Clarke 2002; Frewer et al. 2003; Sandman 2007; Gesser-Edelsburg and Shir-Raz 2016).
Official Channels—As our respondents described the censorship actions taken against them were only part of a wider range of silencing and repressive actions, which also included formal proceedings, such as investigating or withdrawing their medical licenses, suing them or ordering a police search of their homes.
Intimidation—The respondents interpreted all the above tactics as being intended to intimidate and deter them from continuing to publish their views and criticism, and also single them out in a way that implicitly invites harassment by others and serves as an example to other doctors and scientists. Some of our respondents noted they were intimidated to the point they felt it necessary to use an assumed name to continue operating on social media and/or avoid putting their names on papers they co-authored.
Our findings regarding how the study participants responded to censorship tactics are also consistent with the counter-tactics described by Jansen and Martin (2015).
Exposure—The respondents sought exposure of both the censored information and the censorship itself, for example by raising an alarm about the attacks on them through their social media accounts or other platforms. They noted that even if their accounts were repeatedly removed, they opened new ones or moved to other channels or platforms. In addition, they insisted on continuing to try to publish papers in the scientific literature, regardless of the rejections and retractions, and even if the publication involved working on studies without getting credit for the publication.
Validation—Our respondents repeatedly stressed their use of evidence-based information and reliable data, as well as their credentials, thus associating themselves with science. They portray themselves as warriors whose mission is to fight against misinformation and censorship by the medical and public health establishment.
Interpretation—Our respondents framed the media and the establishment’s efforts as censorship and referred to their own efforts as attempts to present valid information for interested readers.
Redirection—Following the personal and professional attacks they experienced, some of our respondents coordinated a public response, seeking to mobilize their supporters, turning to fellow scientists and doctors, and creating alliances and cooperation networks.
Resistance—Despite the initial shock, all the respondents said they decided not to succumb, but rather to resist and fight back.
Our findings echo arguments made in previous studies on the suppression of dissent in controversial areas, such as vaccination (Elisha et al. 2021, 2022; Cernic 2018; DeLong 2012; Gatto et al. 2013; Martin 2015; Vernon 2017), AIDS, environmental studies, and fluoridation (e.g., Delborne 2016; Kuehn 2004; Martin 1981, 1991, 1999). Similar to those studies, our research findings indicate significant involvement of the media and the medical establishment in censorship and suppression of dissenters.
Yet, there are three main differences. First, when it comes to COVID-related knowledge, the censorship tactics used against dissenters are extreme and unprecedented in their intensiveness and extensiveness, with scientific journals, and academic and medical institutions taking an active and involved part in censoring critical voices. In fact, as one of our respondents indicates, even pre-print servers and academic social networking sites censor scientific papers that do not align with the mainstream narrative, and this seems to be a growing trend. One recent example is a study report by Verkerk et al. (2022), which analyzed a survey of over 300,000 people in 175 countries who had elected to not receive COVID-19 vaccines, which was removed from ResearchGate.net after 9 days citing a breach of their terms and conditions (World Council for Health 2022). Furthermore, what our respondents describe goes way beyond censorship, and includes a wide range of suppression methods intended to destroy their reputations and careers, solely because they dared to take a different position from that dictated by the medical establishment.
Second, while previous studies have also indicated isolated cases where researchers and doctors with flawless résumés and even senior academic or medical status were censored if they dared express dissenting opinions, the current study shows that in the case of COVID, censoring doctors and researchers of this stature has become a regular phenomenon. The participants in our study, as well as those mentioned in the introduction and many others not included in our sample, are not fringe scientists. Most of them are leading figures: researchers and doctors who prior to the COVID-19 era had a respectable status, with many publications in the scientific literature, some of them with books and hundreds of publications, some headed academic or medical departments, some of them were editors of medical journals, and some had won significant awards. Nevertheless, as our findings show, they were not protected from censorship, nor from the suppression and defamation campaign launched against them. This fact indicates that the message is that no one is exempt from censorship and no academic or medical status, senior as it may be, is a guaranteed shield against it.
The third prominent difference found in our study is the significant role played by media organizations during the COVID pandemic, and especially tech information companies, in censoring contrary positions. On a practical level, those who hold the power have greater ability and opportunities to control knowledge and information dissemination, and through this, to set and control the agenda. While our findings do not show the direction of the relationship between these interest holders, they may indicate collaborations between the medical establishment and these companies. Recently released documents from court cases indicate that at least some of this censorship is orchestrated by government officials (Lungariello and Chamberlain 2022; Ramaswamy and Rubenfeld 2022). Our findings also indirectly point to other stakeholders involved in the censorship phenomenon evident in the current crisis, especially pharmaceutical companies. While our study examined the subjective perceptions of those targeted by censorship rather than the involvement of stakeholders and other interested parties, our respondents’ reports echo findings from other studies, conducted both prior to the COVID-19 era (Ravelli 2015), and more recently (Mucchielli 2020), which indicate the extensive involvement of pharmaceutical and information tech corporations in silencing information and studies that may be unfavourable to them. Given the central role of these corporations alongside policymakers in health authorities and governments globally, a major concern is that substantial interests, including financial and political ones, as well as interests related to reputation and career, may lay behind the suppression efforts. The interest of the pharmaceutical corporations in controlling the discourse regarding COVID-19 is self-evident. For example, as some of our participants indicated, one of the main unresolved COVID-19 controversies is related to early treatment with repurposed drugs, and it has been claimed that highly unusual measures were taken to prevent physicians from using them (Physicians’ Declaration 2021). As Cáceres (2022) notes, this alleged unwarranted termination of that initial debate may have had enormous economic (e.g. green light for vaccines and new drugs under emergency use authorization), financial (e.g. huge gains for the largest corporations) and political consequences (e.g. global restrictions of individual freedoms).
The tech information companies also have strong interests in controlling the discourse regarding the COVID-19 pandemic. For example, in June 2021, it was revealed that Google, which was accused of silencing the theory the SARS-CoV-2 virus leaked from the Wuhan Institute of Virology, has funded virus research carried out by a Wuhan-linked scientist, Peter Daszak, through its charity arm, Google.org, for over a decade. Google has also invested one million dollars in a company that uses epidemiologists and big-data analytics to forecast and track disease outbreaks. The British Medical Journal has revealed that Facebook and YouTube’s “fact-checking” process relies on partnerships with third-party fact-checkers, convened under the umbrella of the International Fact-Checking Network (Clarke 2021). This organization is run by the Poynter Institute for Media Studies, a non-profit journalism school whose main financial supporters include Google and Facebook.
As for policymakers’ personal interests, a US government watchdog group has been demanding key data on Dr. Anthony Fauci’s financial and professional history, claiming that “During the pandemic, Dr. Fauci has handsomely profited from his federal employment, royalties, travel perks, and investment gains,” yet it is not public what his salary was during these two years, nor what stocks and bonds he bought and sold in 2020 or 2021, as he influenced COVID policies, or what he received—or didn’t receive—in royalties. As noted earlier, a FOIA request in the US revealed that Fauci was told by Francis Collins, then head of the NIH, to discredit the Great Barrington Declaration and disparage its authors (Wilson 2021). Roussel and Raoult (2020) found similar conflicts of interest among French doctors who took a public stand against the use of hydroxychloroquine.
Censorship undermines public trust in authorities, especially if the information hidden and later on revealed might have cost human lives, such as during pandemics, which involve diseases, treatments and vaccines (Gesser-Edelsburg and Shir-Raz 2018). In addition, censorship and manipulation of information are inconsistent with the essence of science, since scientific inquiry requires discourse and vigorous debate. Indeed, researchers have warned that instead of being debated, COVID controversies are being used to fuel polarization, often leading to the demonization and censorship of alternative perspectives and the imposition of mainstream views as if they were absolute truth (Cáceres 2022; Marcon and Caulfield 2021).
Cáceres (2022) has argued that the fact that the debate was silenced and alternative positions were censored is in fact a diversion from “normal science” (Kuhn 1962), which assumes that different explanations and answers to facts of scientific interest normally emerge, and have the opportunity to be resolved in conventional scientific debate. Such diversion from “normal” scientific praxis, Cáceres maintains, suggests that “non-scientific” influences are at work. This diversion is especially concerning when the voices silenced are those of a mounting number of leading and renowned scientists and doctors. The drive to censor and dismiss dissenting opinions by labeling them as “misinformation” shares close similarities with scientific “boundary work,” wherein scientific power and authority is maintained by demarcating certain fields of scientific inquiry as out of bounds and discrediting them as essentially unscientific (Gieryn 1999; also see Harambam 2014). Creating a false consensus by censoring information and preventing scientific debates might lead scientists, and thus also policymakers, to sink into the ruling paradigm, causing them to ignore other, more effective options to cope with the crisis or perhaps even prevent it. Such a “consensus” leads to a narrow worldview, which impairs the public’s ability to make informed decisions and erodes public trust in medical science and in public health (Cernic 2018; Delborne 2016; Martin 2014, 2015; Vernon 2017).
The main limitation of the study is that the findings are based on the subjective perspectives of interviewees. It is possible that if we included more heterogeneous groups, we would come to somewhat different interpretations. Therefore, we recommend conducting further studies among larger groups of professionals who suffered censorship, to expand our knowledge and perhaps suggest effective ways to mediate the struggle over freedom of information in general and especially in times of crisis.
One main contribution of this study is in giving voice to scientists and doctors who raise questions, doubts or criticism in controversial areas in public health and science, especially during times of crisis. At the same time, we seek to raise awareness of the increasing use of censorship practices and aggressive tactics of suppression, targeting even leading figures who dare to criticize or doubt the dictated “consensus.” Censorship and silencing practices can have far-reaching consequences, manifested in the violation of freedom of speech and of ethical principles, harming science, and potentially risking public health and safety (Elisha et al. 2022). Researchers have already warned that the COVID-19 crisis confirms previous concerns about the deleterious implications of censorship (Cáceres 2022; Mucchielli 2020). We concur with Cáceres’ assertion that censorship and dogma are foreign to true science and must be abandoned and replaced by open and fair discussion.
Ambati, Balamurali K., Akhil Varshney, Kenneth Lundstrom, Giorgio Palú, Bruce D. Uhal, Vladimir N. Uversky, and Adam M. Brufsky. 2022. MSH3 homology and potential recombination link to SARS-CoV-2 furin cleavage site. Frontiers in Virology. https://doi.org/10.3389/fviro.2022.834808/full. Article
Aspers, Patrik. 2004. Empirical phenomenology: An approach for qualitative research. London School of Economics and Political Science, Papers in Social Research Methods, Qualitative Series no 9.
Bavli, Itai, Brent Sutton, and Sandro Galea. 2020. Harms of public health interventions against covid-19 must not be ignored. British Medical Journal 371: m4074. https://doi.org/10.1136/bmj.m4074. Article
Brown, Ronald B. 2020. Public health lessons learned from biases in Coronavirus mortality overestimation. Disaster Medicine and Public Health Preparedness 14(3):364-371. Article
Cadegiani, Flávio A. 2022. Active actions against competitive anti-COVID drugs? The case of the anti-androgens demonstrated through a highly biased randomized clinical trial with virtually undisputed directed objectives, followed by compromised editorial integrity providing overprotection for the authors of the trial to avoid exposure of its critical issues. ResearchGate, 22 June. https://doi.org/10.13140/RG.2.2.13732.76160.
Cernic, Mateja. 2018. Ideological constructs of vaccination. Newcastle upon Tyne, UK: Vega Press.
Cialdini, Robert. 2016. Pre-suasion: A revolutionary way to influence and persuade. New York: Simon & Schuster.
Clarke, Lee. 2002. Panic: Myth or reality? Contexts 1(3):21–26. Article
Creswell, John W. 2012. Qualitative inquiry and research design: Choosing among five approaches. Thousand Oaks, CA: Sage.
Delborne, Jason A. 2016. Suppression and dissent in science. In Handbook of Academic Integrity, ed. Tracey A. Bretag, 943–956. Singapore: Springer. Chapter
DeLong, Gale. 2012. Conflicts of interest in vaccine safety research. Accountability in Research 19(2):65–88. Article
De Vocht, Melanie, An-Sofie, Claeys, Verolien, Cauberghe, Mieke, Uyttendaele, and Benedikt, Sas. 2014. Won’t we scare them? The impact of communicating uncontrollable risks on the public’s perception. Journal of Risk Research 19(3):316–330. https://doi.org/10.1080/13669877.2014.971336. Article
Dodsworth, Laura. 2021. A state of fear: How the UK government weaponised fear during the Covid-19 pandemic. London: Pinter & Martin.
Elisha, Ety, Josh Guetzkow, Yaffa Shir-Raz, and Natti Ronel. 2021. Retraction of scientific papers: The case of vaccine research. Critical Public Health. https://doi.org/10.1080/09581596.2021.1878109. Article
Elisha, Ety, Josh Guetzkow, Yaffa Shir-Raz, and Natti Ronel. 2022. Suppressing scientific discourse on vaccines? Self-perceptions of researchers and practitioners. HEC Forum. https://doi.org/10.1007/s10730-022-09479-7. Article
Fraiman, Joseph, Juan Erviti, Mark Jones, Sander Greenland, Patrick Whelan, Robert M. Kaplan, and Peter Doshi. 2022. Serious adverse events of special interest following mRNA vaccination in randomized trials. Vaccine 40(40):5798–5805.
Frewer, Lynn, Steve Hunt, Mary Brennan, Sharron Kuznesof, Mitchell Ness, and Chris Ritson. 2003. The views of scientific experts on how the public conceptualize uncertainty. Journal of Risk Research 6(1):75–85. https://doi.org/10.1080/1366987032000047815. Article
Gatto, Mariele, Nancy Agmon-Levin, Alessandra Soriano, Raffaele Manna, Ramit Maoz-Segal, Shaye Kivity, Andrea Doria, and Yehuda Shoenfeld. 2013. Human papillomavirus vaccine and systemic lupus erythematosus. Clinical Rheumatology 32(9):1301–1307. Article
Gesser-Edelsburg, Anat, and Yaffa Shir-Raz. 2016. Risk communication and infectious diseases in an age of digital media. Abingdon, UK: Routledge. Book
Gesser-Edelsburg, Anat, and Yaffa Shir-Raz. 2018. Communicating risk for issues that involve “uncertainty bias”: What can the Israeli case of water fluoridation teach us? Journal of Risk Research 21(4):395–416. https://doi.org/10.1080/13669877.2016.1215343. Article
Gieryn, Thomas F. (1999). Cultural Boundaries of Science: Credibility on the Line. Chicago: University of Chicago Press.
Griffin, Hannah. 2012. Keep it clean? How negative campaigns affect voter turnout. Res Publica—Journal of Undergraduate Research 17:6.
Harambam, Jaron. 2014. Contesting epistemic authority: Conspiracy theories on the boundaries of science. Public Understanding of Science 24(4):466–480.
Harambam, Jaron. 2020. The corona truth wars: Where have all the STS’ers gone when we need them most? Science and Technology Studies 33(4):60–67.
Harrison, Neil L. and Jeffrey D. Sachs. 2022. A call for an independent inquiry into the origin of the SARS-CoV-2 virus. Proceedings of the National Academy of Sciences 119(22): e2202769119. https://doi.org/10.1073/pnas.2202769119.
Ioannidis, John P. A. 2020. Coronavirus disease 2019: The harms of exaggerated information and non-evidence-based measures. European Journal of Clinical Investigation 50(4):e13222. https://doi.org/10.1111/eci.13222. ArticleGoogle Scholar
Jansen, Sue Curry, and Brian Martin. 2003. Making censorship backfire. Counterpoise 7(3):5–15.
Jansen, Sue Curry, and Brian Martin. 2004. Exposing and opposing censorship: Backfire dynamics in freedom-of-speech struggles. Pacific Journalism Review 10(1):29–45. Article
Jansen, Sue Curry, and Brian Martin. 2015. The Streisand effect and censorship backfire. International Journal of Communication 9:656–671.
King, Eshani M. 2020. Covid-19: Science, conflicts and the elephant in the room. BMJ 371:m4425.
Kuehn, Robert R. 2004. Suppression of environmental science. American Journal of Law & Medicine 30:333–369. Article
Kulldorff, Martin, Sunetra Gupta, and Jay Bhattacharya. 2020. Great Barrington Declaration.https://gbdeclaration.org.
Lau, Richard R., and Ivy Brown Rovner. 2009. Negative campaigning. Annual Review of Political Science 12:285–306. Article
Lenzer, Jeanne. 2020. Covid-19: Group of UK and US experts argues for “focused protection” instead of lockdowns. BMJ 371:m3908. https://doi.org/10.1136/bmj.m3908.Article
Liester, Mitchell B. 2022. The suppression of dissent during the COVID-19 pandemic. Social Epistemology Review and Reply Collective 11(4):53–76.
Lofstedt, Ragnar E. 2006. How can we make food risk communication better: Where are we and where are we going? Journal of Risk Research 9(8):869–890. https://doi.org/10.1080/13669870601065585. Article
Marcon, Alessandro R., and Timothy Caulfield. 2021. The hydroxychloroquine Twitter war: A case study examining polarization in science communication. First Monday. https://doi.org/10.5210/fm.v26i10.11707. Article
Martin, Brian. 1981. The scientific straightjacket: The power structure of science and the suppression of environmental scholarship. The Ecologist 11(1):33–43.
Martin, Brian. 1991. Scientific knowledge in controversy: The social dynamics of the fluoridation debate. New York: State University of New York Press.
Martin, Brian. 1999. Suppression of dissent in science. Research in Social Problems and Public Policy 7:105–135.
Martin, Brian. 2014. Censorship and free speech in scientific controversies. Science and Public Policy 42(3):377–386. Article
Martin, Brian. 2015. On the suppression of vaccination dissent. Science and Engineering Ethics 21(1):143–157. Article
Martin, Brian. 2021. Covid information struggles. Social Epistemology Review and Reply Collective 10(7):16–26.
Mucchielli, Laurent. 2020. Behind the French controversy over the medical treatment of Covid-19: The role of the drug industry. Journal of Sociology 56(4):736–744. https://doi.org/10.1177/1440783320936740. Article
Sandman, Peter. 2003. Four kinds of risk communication. The Synergist—Journal of the American Industrial Hygiene Association April: 26–27. https://www.psandman.com/col/4kind-1.htm.
Slovic, Paul. 1994. Beyond numbers: A broader perspective on risk perception and risk communication. In Acceptable evidence: Science and values in risk management, eds. Deborah G. Mayo and Rachelle D. Hollander, 54–89. Oxford: Oxford University Press.
Stolow, Jeni A., Lina M. Moses, Alyssa M. Lederer, and Rebecca Carter. 2020. How fear appeal approaches in COVID-19 health communication may be harming the global community. Health Education & Behavior 47(4):531–535. https://doi.org/10.1177/1090198120935073.Article
Thacker, Paul D. 2021. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 375:n2635. https://doi.org/10.1136/bmj.n2635. Article
van Helden, Jacques, Colin D. Butler, Gulliaume Achaz, Bruno Canard, Didier Casane, Jean-Michel. Claverie, et al. 2021. An appeal for an objective, open, and transparent scientific debate about the origin of SARS-CoV-2. The Lancet 398:P1402–P1404. https://doi.org/10.1016/S0140-6736(21)02019-5. Article
Verkerk, Robert, Christof Plothe, Naseeba Kathrada, and Katarina Lindley. 2022. Self-reported outcomes, choices and discrimination among a global COVID-19 unvaccinated cohort. Authorea. https://doi.org/10.22541/au.165556998.84120061/v1. Article
Vernon, Leonard F. 2017. How silencing of dissent in science impacts women: The Gardasil story. Advances in Sexual Medicine 7:179–204. https://doi.org/10.4236/asm.2017.74015. Article
Now, I share this, because “short-circuited” people seems to be on the rise, and some sort of hypothesis would seem to be in order. One has to be blind not to see that the alleged president is just not “all there.” We saw a similar thing in the final months and years of the second Reagan Administration, when clearly that president was clearly showing signs of senility. With Bai-den I think the explanation goes much deeper then mere senility, but we’ll get back to that.
If you are in the USSA, you recently also saw the spectacle of a “governors’ race debate” between the Lieutenant Governor of Pennsylvania, Fetterman, a Democrat, and Dr. Mehmet Oz, a Republican. The debate, which I have seen a little of, was honestly painful to watch, even for me who has no use for Mr. Fetterman, his party, or his policies. Let me repeat that: I have no use for him, his party, or his policies.
Yet the debate was painful to watch. Here was a man trying to recover from a stoke, who had and has obvious difficulty forming words into clear thoughts. He began the debate – his very first words – with a cheery “Hi!” immediately followed by “Goodnight everyone!” And it was downhill – no, a power dive – from there.
Frankly, I felt, and still feel, sorry for the man. to his credit, his opponent did not – as far as I am aware – once make reference to Mr. Fetterman’s difficulty and decrepit condition. But my problem was, why would any campaign allow a man in his difficulties to take a debate stage to begin with? Why, after such a stroke, allow the candidacy itself to go forward to begin with? For that matter, why allow Mr. Bai-den anywhere near power, when he too is in obvious decline?
As I said, we’ll get back to that.
The article itself raises other interesting questions, and yes, I’ve noticed it too: more and more people seem to be having some sort of difficulty:
Lately, celebrities and politicians have been exhibiting some strange behavior, and it isn’t just their usual weirdness on display. There’s clearly something else going on.
While on stage in Las Vegas, singer Katy Perry appears to have some sort of “malfunction” with her right eye where the eye appears to close on its own forcing her to prop open her eyelid more than once with her hand, only to have it close again.
Of course, there’s nothing unusual with winking one eye, but this was different. Perry appeared to have lost physical control of her eye as if it was suddenly operating on its own outside of her control while her other eye remained open appearing normal.
Then, with a flick of a switch, the wonky eye snapped out of its trance and the performer regained her composure while leaving fans (and 17 million TikTok viewers) questioning, is this chick even human?
It wasn’t just Katy Perry in a Las Vegas performance; as the article notes, we’ve been observing it in Bai-Den too:
We’ve been watching our multiple vax boosted Commander and Chief short circuit for the past year and a half, so in many ways, seeing celebrities, politicians, and even regular people rebooting in public is simply part of our New Normal. We’re told by the transhumanists that this is simply our new and improved future, and that it’s best for everyone to boldly welcome our forthcoming dystopian Brave New World where it’s acceptable for politicians to be only part human.
At this point, the article links the now-famous video clip of Mr. Bai-den Jo apparently falling asleep, or “zoning out”, only to be brought back to “reality” by the interviewer.
There are other examples; consider these:
Recently, pro vaccine and fully vaccinated incumbent Virginia democrat Jennifer Wexton (VA-10) appears to have some sort of episode during her congressional debate. As she struggles to speak and form complete and coherent sentences she stares vacantly into some far away place. Her mannerisms appearing almost robotic. WATCH THE FULL CLIP.
Then there is news anchor Julie Chin who had what she thought was a mini stroke on live television. She, too, suddenly had difficulty speaking and forming coherent sentences, and like other instances, the entire episode occurred as if a light switch was briefly switched off and then flipped back on.
As far as the article is concerned, there is a clear hypothetical cause for the behavior:
All of these anomalies have one thing in common— they started happening after a certain rollout of a certain Emergency Use Authorized vaccine treatment designed to end the Covid-19 pandemic. It’s the same treatment that ironically, never prevented “an individual from contracting or transmission Covid-19”, and whose contents to this day still remain a mystery. However, one thing we do know about the mRNA vaccines is that they are a form of “technology” that, according to the Chief Medical Officer of Moderna from his 2017 TED talk, has the potential to hack “the software of life”.
To its credit, the article notes the “change of language” now being pushed:
So, what’s going on? To be honest, I don’t know. What I do know is:
—They want you to get these shots at minimum every year and they may even require it.
—The language has changed. You are no longer vaccinated or boosted, you are considered “up-to-date” or updated. In order to comply with the latest vaccine mandate to work or attend school, you will now need to install the latest Microsoft Windows-like mRNA in order to be in compliance and fully “up-to-date”.
—The transhumanist movement exists. It is no longer conspiracy and we have no idea how “updated” vaccines will figure into this cybernetic future although the World Economic Forum has a few ideas.
Are these mRNA technology-driven “updates” that are currently being touted as the future of medicine and being sold as a cancer cure just the elites doing their thing to help save the world? Or might there be something more sinister going on?
Well, in answer to that last question, you can mark me down in the “something more sinister is going on” column, and my reasons why bring us to today’s two-for-one high octane speculations of the day. two-for-one, because you get two completely different but only somewhat separate high octane speculations for the price of one. “Buy one, get one free,” so to speak.
The first speculation is: do you remember Dr. Charles Lieber? he was the Harvard chemistry professor and nano-technology expert that was arrested by federal authorities shortly after the whole planscamdemic broke out. He was arrested, so we were told, for allegedly not disclosing his financial links to the Wuhan Laboratory of Virology in China, whence the whole planscamdemic allegedly originated. Dr. Lieber, you’ll notice, has fallen completely off the radar since then, while the Orange Man’s Operation Warp Speed zipped along to become the fraud-riddled adverse-reaction sudden death injection-induced statistical anomaly we see today. The last I heard, Dr. Lieber had managed to contract a fast-acting, virulent and terminal cancer, somewhat like Jack Ruby.
In any case, Lieber’s specialty, according to some speculations in the alternative media at the time, was to embed nanotechnologies in – get this – “vaccines” or injections, nano-technology that was designed to break the blood-brain barrier, enter the brain, and…well, at that point, no one knew exactly what it was supposed to do, but some speculated that Baal Gates’ patents on “downloadable” vaccine “updates” had something to do with it, and still others thought that this was a way of tying the 5G roll-out to injections that would significantly increase one’s emotional and mental suggestibility.
In short, the whole thing – 5g, nano-technology in the injections, and the injections themselves – were all part of a global mind-and-health manipulation event, and one reason Big Pharma was so anxious not to have to disclose the ingredients in its so-called “vaccines” was that the ingredients, or the ingredient amounts, or both, varied deliberately from batch to batch, and the responses to the different batches could be tracked through national and regional adverse reporting sites.
The scenario was like some Mengele-esque nightmare, on steroids.
I and others entertained its possibility at the time, and I still do. Now we’re in “phase two” as “they” are attempting to roll out a kind of “Soviet Psychiatry”, painting the “non-vaxed” as emotionally unstable, anti-science, and “unhealthy.”
In short, I discount none of this.
But at a deeper level, I think we are looking at something spiritual. I’ve mentioned this possibility in some of our recent members’ vidchats, and do so here publicly. Imagine being a self-proclaimed “good catholic” all your life, of average intelligence, but consuming ambition, willing to make the little compromises on the road to power. Once acquired, you then use that power to your and your family’s financial gain, and using your family members themselves to increase your power and wealth, and turning a bling eye to their “shortcomings.” You openly support abortion on demand and a woman’s right to choose, and continue to call yourself a good Catholic, a believing Christian. You achieve the highest and loftiest position of power… just as you’ve lost your mind, and are shaking hands with people who are no longer there. “C’mon, man, it’s ok for a little boy to have surgery to change into a girl, or vice versa.”
The world of hypocrisy and illusion and word games which you have spun for yourself has become your reality, and you are no longer capable of discerning reality. You are lost in an insane, drugged-up world, a world you’ve done everything within your rotting, debauched power, to force on others.
The British nursing academic, Dr Roger Watson, recently cited a Canadian study by Banerjee et al as an example of adequate controls being used in “viral isolation”. Watson’s article appeared in Toby Young’sThe Daily Sceptic which purports to exist for airing views others refuse to publish.
The cited study actually failed to prove any viral phenomenon because it did not use purified particles as independent variables. Only impure (crude) clinical samples from a patient were added to monkey kidney (Vero E6) cells without any suitable control. Subsequent phenomena were observed which were then claimed to be the actions of a ‘virus’ hence presumptively termed ‘cytopathic effect’. Similarly, the RNA used for sequencing the so-called ‘viral genome’ was extracted – not from any purified particles proven to be of viral origin – but from the contaminated supernatant of the Vero E6 cells used in Banerjee et al. The resulting ‘sequenced genome’ was no such thing. It was an in silico modelled confection created from the same contaminated supernatant. These unscientific claims inform the current ‘consensus’ on how to do ‘viral isolation and sequencing’, despite having been rebutted by The Perth Group of scientists decades ago.
All of these deviations from scientific method were pointed out to Dr Watson in e-mail messages by one of us (CM). Dr Watson was also asked to explain his stance in relation to this evidence which is anomalous viz a viz the scientific method and the paradigm of virology. Watson’s initial response sidestepped the question. On further probing, Watson politely indicated that he had not considered these particular anomalies and thus would need to give further thought to the lack of valid controls used by Banerjee et al. Watson further stated that this whole debate “was cue to an article onwhy those who believe in viruses will not be convinced by the evidence”. We fully agree.
These particular e-mail messages are one example of a messenger exposing the multiple anomalies of modern virology to those who are conceptually invested in that paradigm. Instead of being able to look at what has been presented with a fully detached eye, the usual recourse is to bolster that failing anomaly-stricken paradigm by trying to dismiss the message, either by side stepping the questions posed, or by attacking the messenger ad hominem.
Dr Watson attempted the former but (on this occasion) resisted doing the latter.
We respectfully argue that this response is still a strategy of deflection to cover up ignorance of the caveats in modern day ‘viral isolation’ which are axiomatic within virology. This sort of defensive manoeuvre was previously identified by both Thomas Kuhn (1962) and Stephen Cole (1983). Kuhn argued that scientists reject anomalous data which potentially break down the existing consensus as a means of trying to maintain certainty. These rejections, which (after Kuhn) were proved by Stephen Cole to occur within modern science, are essentially defensive actions similar to knee-jerk responses.
In this case, highly convincing observational data was presented (by CM) casting grave doubt over the veracity of this accepted ‘consensus’ on viral isolation. Some scientists have even argued that these sorts of observations fatally damage the whole concept of ‘viral disease’. This so-called ‘consensus’ on ‘viral’ isolation is a necessary condition for both maintaining and advancing the current paradigm of virology and its claims of ‘viral isolation’. Following Kuhn and Cole, those like Watson who seem very heavily invested in this paradigm will inevitably provide a knee-jerk response to reject any anomalous observations. We argue that this e-mail exchange is a modest example of premature closure of debate on the observed anomalies about modern virology’s claims of ‘viral isolation’.
Dr. Kevin Corbettwebsite
Dr Kevin Corbett, BA (Hons) MSc PhD is a health scientist and qualified nurse with over thirty years of experience in higher education, health care research and clinical practice.
Christine Masseywebsite
Christine Massey, MSc is a former biostatistician collating virology-related freedom of information responses from around the world.
Dr. Mark Baileywebsite
Mark Bailey, MB ChB PGDipMSM MHealSc is a microbiology, medical industry and health researcher who worked in medical practice, including clinical trials, for two decades.
cover image credit:
Illustration by Sidney Paget from ‘The Adventure of the Crooked Man’, The Strand Magazine, Volume 6, 1893
(in public domain)
Recently I spoke to an international consortium of doctors and researchers about the COVID-19 situation and the issue of virus existence. I was asked whether I thought COVID-19 cases were fictional in nature, which is an interesting question. It goes beyond the matter of whether pathogenic viruses exist and are the cause of disease. It also allows us to address the frequent claim people make that whatever COVID-19 is supposed to be, they “got it,” based on their experience or one of the so-called tests they took. Let’s examine why there is no “it” even though there are lots of “cases”…
When most people hear the word “case” in a medical context there is a natural tendency to think that the individual being counted has an actual disease. It may come as a surprise that this is not a requirement at all because in the field of epidemiology it can be defined as simply, “the standard criteria for categorizing an individual as a case.” ‘Standard criteria’ can be anything and this opens the door to all sorts of misuse and misinterpretation. In fact, it has been used to propagate outright fraud, as Dr John Bevan-Smith and I documented last year in “The COVID-19 Fraud & War on Humanity.”
In 2020, Sam published a video “What is a COVID-19 case?,” which succinctly outlined the problems of the World Health Organisation’s COVID-19 ‘case’ definition. It is evident that the cases are “confirmed” by in vitro (outside the body) molecular detection assays – in 2020 that was mostly PCR kits and today we also have the widely-deployed Rapid Antigen Tests, which I have discussed in another article. Whatever tests are being used, they have been completely disconnected from the concept of disease. By mid-2020, it was more than apparent that COVID-19 was not a clinically defined condition. A Cochrane review published in July that year concluded that, “based on currently available data, neither absence nor presence of signs or symptoms are accurate enough to rule in or rule out disease.” In other words, COVID-19 cases can be solely determined by molecular “tests” such as the above-mentioned ones.
It is astounding that the vast majority of the medical community went along with this nonsense, including many of those who have been opposed to the “pandemic” responses. What does it mean to diagnose or treat a “case” of COVID-19? Even some PCR critics have been gaslit by debates about the “accuracy” of the PCR and appropriate cycle threshold limits in determining ‘cases’. However, this falls back into the same trap, being the belief that these particular tests are capable of telling them something useful about the condition of a person. They think the PCR just needs to be tweaked in a certain way so it can be used as a diagnostic tool. For clarity, I am not talking about clinically-validated molecular assays with known diagnostic specificity and sensitivity such as urine pregnancy tests. Sam has covered the pertinent differences in her video “COVID-19: Behind The PCR Curtain.”
Beyond the medical community, the public have been deceived by linguistic legerdemain where the PCR or Rapid Antigen Test results are then called, “cases of the virus,” or, “cases of infection,” by public institutions and the corporate media. This is a game of deception because the WHO’s own definition of a case has been completely misrepresented. If they were honest they would say, “cases of a detected chemical reaction in an assay.” However, this would have failed in the marketing department and nobody would have bought into the pandemic narrative in 2020.
In summary, there are indeed cases of COVID-19 but the case definition has been disconnected from the concept of disease. The Johns Hopkins “COVID-19 Dashboard” displays hundreds of millions of meaningless cases, which look impressive to the uninitiated viewer. However, knowledge of how these numbers have been produced brings an understanding that we have just witnessed a pseudo-pandemic, or what Virus Mania’s Dr Claus Köhnlein christened a “PCR Pandemic” in 2020.
The COVID-19 fraud and the concept of “cases” is illustrative of a wider problem concerning medical training and practice within the allopathic paradigm. It is one that I am acutely aware of, having been in the conventional medical system for two decades until my exit in 2016. The paradigm is based on claimed disease entities, many of which are allegedly caused by one “pathogen” and are supposedly treated with one “magic bullet.” Medicine was subverted in this way last century after the stifling implementation of the Rockefeller-backed Flexner Report (1910) and has never recovered. Dr Montague Leverson pointed out an example of this misguided thinking about disease around the same time:
“You here assume smallpox to be a thing, an entity. This blunder is committed by nearly all the followers of the self-styled “regular school”, and it will probably be a new idea to you to be told that neither smallpox nor any other disease is an entity, but is a condition.”
Dr. Montague Leverson, Bridgeport Evening Farmer, Connecticut USA, August 21, 1909
One of the worst things that can happen when visiting an allopathic doctor is being labelled with a disease entity. Medical practice has deteriorated into protocol-driven paradigms in which the practitioners blindly follow pathways and tick boxes. Hapless patients are given a tag and then subjected to prescribed “treatments” rather than being advised on how to help cure their body’s real problems. One silver lining to the COVID fiasco is that it blatantly exposed the nature of the medical system to many people and they could see that it cannot help them with achieving true health.
New Zealand’s Dr Ulric Williams (1890-1971) was another who understood the follies of attempting to classify disease “cases” through not only investigations but also through criteria involving symptoms and signs. Rather, he identified these patterns as healing crises and the body’s attempts to restore itself to health. On that note, we are pleased to announce that we will soon be publishing a book that will once again make Dr Williams’ wisdom and curative methods available to the world.
We are frequently asked about what really makes people ill if it is not “viruses” or other disease entities. It is a matter of changing our way of thinking from the misleading model of getting or suffering from “it” to a new understanding of what our body is trying to do to get well again. As well as addressing this in our free content, we explore these concepts further in our monthly Q&A sessions. Access to this bonus content is available through Dr Sam’s Community Membership. Please sign up for this membership if you would like to support our work and have even more of your questions answered. You can also sign up for Dr Sam’s free newsletter so you don’t miss out on any of the latest developments.
“It is the function of mass agitation to exploit all the grievances, hopes, aspirations, prejudices, fears, and ideals of all the special groups that make up our society, social, religious, economic, racial, political. Stir them up. Set one against the other. Divide and conquer. That’s the way to soften up a democracy.”― J. Edgar Hoover, Masters of Deceit
The U.S. government has become a master of deceit.
It’s all documented, too.
This is a government that lies, cheats, steals, spies, kills, maims, enslaves, breaks the laws, overreaches its authority, and abuses its power at almost every turn; treats its citizens like faceless statistics and economic units to be bought, sold, bartered, traded, and tracked; and wages wars for profit, jails its own people for profit, and has no qualms about spreading its reign of terror abroad.
Worse, this is a government that has become almost indistinguishable from the evil it claims to be fighting, whether that evil takes the form of terrorism, torture, drug trafficking, sex trafficking, murder, violence, theft, pornography, scientific experimentations or some other diabolical means of inflicting pain, suffering and servitude on humanity.
With every passing day, it becomes painfully clear that this is not a government that can be trusted with your life, your loved ones, your livelihood or your freedoms.
Of the many weapons in the government’s vast arsenal, psychological warfare (or psy ops) can take many forms: mind control experiments, behavioral nudging, propaganda.
As Brianna Nofil explains, “MK-Ultra’s ‘mind control’ experiments generally centered around behavior modification via electro-shock therapy, hypnosis, polygraphs, radiation, and a variety of drugs, toxins, and chemicals.”
Similarly, the top-secret Montauk Project, the inspiration for the hit Netflix series Stranger Things, allegedly was working to develop mind-control techniques that would then be tested out on locals in a nearby village, triggering crime waves or causing teenagers to congregate.
As journalist Lorraine Boissoneault concludes, “Despite MK-ULTRA violating ethical norms for human experiments, the legacy of brainwashing experiments continued to live on in U.S. policy. The same methods that had once been used to train American soldiers ended up being used to extract information from terrorists in Abu Ghraib, Iraq and Guantanamo Bay.”
Fast forward to the present day, and it’s clear that the government—aided and abetted by technological advances and scientific experimentation—has updated its psy ops warfare for a new era. For instance, the government has been empowered to use its ever-expanding arsenal of weapons and technologies to influence behaviors en masse and control the populace.
Back in 2014, for example, a Fusion Center in Washington State (a Dept. of Homeland Security-linked data collection clearinghouse that shares information between state, local and federal agencies) inadvertently released records on remote mind control tactics (the use of “psycho-electronic” weapons to control people from a distance or subject them to varying degrees of pain).
This is how you persuade a populace to voluntarily march in lockstep with a police state and police themselves (and each other): by ratcheting up the fear-factor, meted out one carefully calibrated crisis at a time, and teaching them to distrust any who diverge from the norm.
This is not a new experiment in mind control.
Add the government’s inclination to monitor online activity and police so-called “disinformation,” and you have the makings of a restructuring of reality straight out of Orwell’s 1984, where the Ministry of Truth polices speech and ensures that facts conform to whatever version of reality the government propagandists embrace.
This “policing of the mind” is exactly the danger author Jim Keith warned about when he predicted that “information and communication sources are gradually being linked together into a single computerized network, providing an opportunity for unheralded control of what will be broadcast, what will be said, and ultimately what will be thought.”
We’ve already seen this play out on the state and federal level with hate crime legislation that cracks down on so-called “hateful” thoughts and expression, encourages self-censoring and reduces free debate on various subject matter.
The end goal of these mind-control campaigns—packaged in the guise of the greater good—is to see how far the American people will allow the government to go in re-shaping the country in the image of a totalitarian police state.
The government’s fear-mongering is yet another key element in its mind-control programming.
It’s a simple enough formula. National crises, global pandemics, reported terrorist attacks, and sporadic shootings leave us in a constant state of fear. The emotional panic that accompanies fear actually shuts down the prefrontal cortex or the rational thinking part of our brains. In other words, when we are consumed by fear, we stop thinking.
A populace that stops thinking for themselves is a populace that is easily led, easily manipulated and easily controlled whether through propaganda, brainwashing, mind control, or just plain fear-mongering.
Fear not only increases the power of government, but it also divides the people into factions, persuades them to see each other as the enemy and keeps them screaming at each other so that they drown out all other sounds. In this way, they will never reach consensus about anything and will be too distracted to notice the police state closing in on them until the final crushing curtain falls.
This Machiavellian scheme has so ensnared the nation that few Americans even realize they are being brainwashed—manipulated—into adopting an “us” against “them” mindset. All the while, those in power—bought and paid for by lobbyists and corporations—move their costly agendas forward.
It was almost 100 years ago when Bernays wrote his seminal work Propaganda:
“We are governed, our minds are molded, our tastes formed, our ideas suggested, largely by men we have never heard of… In almost every act of our daily lives, whether in the sphere of politics or business, in our social conduct or our ethical thinking, we are dominated by the relatively small number of persons…who understand the mental processes and social patterns of the masses. It is they who pull the wires which control the public mind.”
As I point out in my book Battlefield America: The War on the American People and in its fictional counterpart The Erik Blair Diaries, to this invisible government of rulers who operate behind the scenes—the architects of the Deep State—we are mere puppets on a string, to be brainwashed, manipulated and controlled.
For years now, the powers-that-be—those politicians and bureaucrats who think like tyrants and act like petty dictators regardless of what party they belong to—have attempted to brainwash us into believing that we have no rights: to think for ourselves, make decisions about our health, protect our homes and families and businesses, act in our best interests, demand accountability and transparency from government, or generally operate as if we are in control of our own lives.
Well, the government is wrong.
We have every right, and you know why? Because, as the Declaration of Independence states, we are endowed by our Creator with certain inalienable rights—to life, liberty, property and the pursuit of happiness—that no government can take away from us.
It’s time we started reminding the government that “we the people” are the ones in charge.
One of the many unfortunate side effects of the attention which has been given to the covid-19 jabs is the fact that more traditional vaccinations (including the dozens routinely given to children) have been forgotten and are now largely administered without protest, controversy or a second thought.
There was always a danger that the justifiable outrage and fear engendered by the covid-19 jabs would push the wider issue of traditional vaccination into the background. The experimental and notably toxic covid-19 jabs have understandably and rightly captured the attention of those who aren’t prepared to accept the lies, the deceits and the manipulations at face value.
But it is important that we don’t forget the ever-growing hailstorm of vaccinations, aimed particularly at children, which have seemingly become an integral part of our relationship with health care in general and doctors in particular.
We all know that the establishment and the mainstream media refuse to debate the mRNA jabs.
But it is, I suspect, less widely known that there has for a long time been a blackout on any discussion of the more traditional vaccines or that the reputation of vaccines is built on a toxic mixture of myths, fallacies and plain, vanilla lies.
I’ve been writing about vaccines for over 50 years but rather to my surprise it was 2011 before I wrote a book entirely devoted to vaccines and vaccination.
I wrote the book (Anyone who tells you vaccines are safe and effective is lying. Here’s the proof.) partly to provide evidence proving that vaccines are often dangerous and don’t work but also to destroy the outrageous, manufactured myth that vaccination has extended life expectancy and eradicated diseases such as smallpox and whooping cough.
I’ll get back to that theme in a moment but first I think it is worth using the history of that book to illustrate the extent of the media blackout which exists to protect vaccines and vaccination.
Knowing that none of my usual publishers would touch a book about vaccines, I published it myself.
We sent out 600 review copies, hoping that one or two reviewers might be brave enough to consider the book on its merit. However, to the best of my knowledge, not one reviewed it. People I’d known for years wouldn’t discuss it. Moreover, quite a number of reviewers returned the book. It is usual practice for reviewers to sell books they don’t want to keep on their shelves. But journalists actually spent time and money returning the book!
I knew there were risks in writing a whole book about vaccines. It has always been a topic which has aroused anger within the medical establishment. In the Preface I wrote: ‘Experience tells me this book will bring me much trouble, a great deal of abuse, a number of threats and considerable professional and personal inconvenience’.
But even I was surprised at how quickly I became persona non grata. My questioning of official establishment policies had, for a long time, made me unpopular with the establishment. It quickly became apparent that vaccination is a taboo subject and that vaccines are protected from criticism in the way that film stars were protected in the 1930s.
Since its publication there have been concerted efforts to ban the book and have it removed from sale.
No one has ever questioned the science, the statistics or the conclusions in the book. Critics have, however, been upset by my criticism of ‘the establishment’s unquestioned enthusiasm for a practice which is of such doubtful value and which offers such potential for disaster’.
I described vaccination as `a massive confidence trick’ and predicted (in 2011 remember) that ‘vaccination will become compulsory in the West’. I have been lied about constantly by thousands of rabid supporters of vaccination.
It seems that the mainstream media has devoted itself to promoting vaccines and never allowing any aspect of vaccination to be questioned. The BBC actually has a policy of excluding all vaccine criticism from its programmes. Merely questioning the validity of vaccination draws a torrent of abuse down upon the questioner’s head.
The inevitable result is that vaccination programmes continue pretty well unhindered and millions of children are now regularly jabbed with products which have never been properly tested or evaluated either for safety or efficacy.
The most potent claim for vaccines is, as I’ve already mentioned, that they have saved millions of lives. (This claim is now being falsely applied to the covid-19 jab which cannot be proven to have saved any lives at all). The fraud is maintained by pointing to average life expectation but this is a false argument for the figures are skewed by the vast number of babies and infants who used to die of disease or malnutrition. Every infant death drags down life expectation dramatically.
All around the world, infants and children are now subjected to a seemingly endless series of assaults on their immune systems. The vaccines used have never been adequately tested to see how they might interact or how they might affect other medications. Very few long-term trials have been done though the few available confirm my scepticism. For example, in 2017, the Danish Government and a Danish vaccine maker, funded a study of the DTP vaccine. The WHO and the medical establishment claim that the DTP vaccine saves millions of lives but, after looking at 30 years of data, the scientists concluded that the DTP vaccine was probably killing more children than died from diphtheria, pertussis and tetanus prior to the vaccines introduction. The vaccine had ruined the immune systems of children rendering them susceptible to death from pneumonia, leukaemia, bilharzia, malaria and dysentery.
The results of that trial changed nothing. The vaccination continued unhindered.
The vaccines most often described as having changed the world are those for polio, whooping cough and smallpox. But look at the evidence.
With polio the truth is that with other infectious diseases the significance of polio dropped as better sanitation, better housing, cleaner water and more food were made available in the second half of the 19th century. Look at the evidence and it shows that the number of polio victims went up not down as a result of vaccination. In Tennessee, USA (chosen at random) the number of polio victims before vaccination became compulsory was 119. The year after vaccination was introduced the figure rose to 386. In America as a whole the number of deaths from polio had fallen dramatically before the first polio vaccine was introduced but the incidence of polio increased by around 50% after the introduction of mass immunisation.
Of even more significance (which I revealed in my book `Why Animal Experiments Must Stop in 1991) 17 million people who were given polio vaccines as children in the 1950s and 1960s are now at risk of developing cancer. This is because the first practical vaccine used monkey kidney tissue – which contains a carcinogenic virus. Moreover, the virus can be passed on to the children of those who were given the contaminated vaccine. Could this explain the ever rising number of people with cancer? We’ll never know. The doctor who first warned of this risk was ignored and her laboratory was closed down. The documents showing who had received the dangerous vaccine were destroyed by the Department of Health in 1987 though it seems likely that millions of doses of the dangerous polio vaccine were used despite the risk.
The smallpox story is equally startling.
The myth that smallpox was eradicated through a mass vaccination programme is just that – a myth. Smallpox was eradicated through identifying and isolating patients with the disease. One of the worst smallpox epidemics of all time took place in England between 1870 and 1872 – nearly two decades after compulsory vaccination had been introduced. The people of Leicester refused the vaccine and there was only one death. In contrast there were massive numbers of deaths in towns where people had been vaccinated.
German doctors are taught that it was the Reich Vaccination Law (making vaccination compulsory) which halted smallpox in their country. But the incidence of smallpox had dropped before the law came into action. Once again, a legally enforced national vaccination programme did not eradicate the disease.
Look at history and it is clear that the number of cases of smallpox has gone up each time there has been a mass vaccination programme.
It’s worth remembering too that Dr Jenner, a hero for pro-vaccine folk, refused to have his second child vaccinated after he’d tried his smallpox vaccination on his own son. Tragically, the boy remained mentally retarded until his death at the age of 21.
Everywhere you look the evidence is the same: vaccination doesn’t work. Moreover, it is not difficult to sustain the argument that it does more harm than good.
Sadly, the medical establishment and the media have for years conspired to suppress the truth and to demonise the truth tellers.
The suppression of the truth about the covid-19 jab is nothing new.
A few weeks ago, I was invited by Michael Wallach, the director of the amazing docu-series The Viral Delusion, to join him as a guest on the Skeptico podcast. It was an interesting experience to say the least. We were under the impression that the conversation would be focused on the gain of function/lab leak theories as well as HIV and we had prepared ourselves to discuss these topics. However, the conversation instead took a detour when the host, Alex Tsakiris, changed the focus to rabies instead, an area he felt was left unexplained by those of us stating that “viruses” do not exist. He presented us with a graph showing statistics of rabies cases declining with the use of vaccines. Unfortunately, at the time that we were interviewed, Alex was unable to provide us with a source for the information that he shared with us. Neither Michael nor I had ever seen this graph before, however it really wasn’t the issue as vaccine statistics do not prove a “viral” cause.
Unfortunately, the rabies graph became the bulk of our time on the show. Michael Wallach did an excellent job explaining the problems with the lack of evidence behind the rabies “virus” as well as the fraud of Louis Pasteur. I wanted to chime in more to help out (not that Michael needed me to) but sadly Alex was not really interested in what I had to say about the subject. You can view our conversation with Alex on the Skeptico podcast here:
As I was unable to speak much on the topic with Alex, I want to present some information here that may help to answer his questions as to why rabies cases appeared to decline as the vaccine was introduced. However, before addressing the graph, the first thing that needs to be understood is that at no time has a rabies “virus” ever been properly purified and isolated directly from the fluids of any animal nor any human and then proven pathogenic by adherence to the scientific method. In fact, as he performed his experiments in the 1870’s and 1880’s, Louis Pasteur provided no theoretical basis for the vaccination of rabies as he admitted that he had failed to isolate the microbe that was presumed responsible for the disease. He also massaged and manipulated his data in order to justify his claims as to the success of rabies vaccination. Pasteur was a fraud who was more concerned with fame and prestige rather than performing valid scientific research. I wrote about his unethical practices involved with the early rabies research as well as how the rabies vaccines actually produced the severe neurological symptoms often associated with the disease here.
Later attempts to propagate the “virus” in the 1950’s, which were claimed to be successful, were done in hamster brain and kidney cultures. Interestingly, it was noted that no cytopathogenic changes, the very criteria used by virologists to claim ‘viruses” are present within these cultures, occured whatsoever.
doi: 10.3181/00379727-98-23997.
Even by the CPE standards used by virologists as a measure for the successful isolation of a “virus,” they had failed to “isolate” rabies in their cultured samples. As no rabies “virus” has ever been scientifically proven to cause the disease, there is no basis to claim that the symptoms associated with rabies are caused by a “virus.” Still, in spite of being given this information, Alex continued to focus on his graph as if the effect credited to the vaccine was somehow proof of a “viral” cause. However, one can not look to an effect in order to claim a cause. This is a logical fallacy known as affirming the consequent. It is often stated like this:
In other words, if rabies is caused by a “virus,” the vaccine will lower cases. The cases declined with vaccine use, therefore rabies is caused by a “virus.” Obviously, this is not a logical statement as there are many variables and factors unaccounted for that could lead to the appearance of a vaccine having a positive effect on rabies cases. It should also not need to be stated that just because a vaccine appeared to work does not mean that the cause of rabies was a “virus.” A rabies “virus” must be scientifically proven to exist first in order to be tested for as the cause of the symptoms of disease associated with it. This has never been done.
We therefore must ask ourselves a very important question:
Did the rabies vaccines really cause rabies cases to fall or are there other potential reasons for the apparent decline?
Let’s try to answer this by looking at the graph Alex provided on the air. Fortunately, I was able to find the source for the image. It came from the CDC’s own data from the Morbidity and Mortality Weekly Report in July 2019. The study was titled Vital Signs: Trends in Human Rabies Deaths and Exposures — United States, 1938–2018.
What we can find out is that rabies cases were exceedingly rare over the entire graph period, with only 588 cases of human rabies reported in the United States from 1938 to 2018. In fact, there was a sharp decline in rabies cases a few years prior to the mass vaccination of dogs in 1947, which is often the case when looking at the decline in disease before the introduction of vaccination. Of course, the vaccine is given the credit even though the cases were well in decline beforehand.
So what could have caused this sharp drop before and after vaccine introduction? If you have looked into the decrease in diseases claimed to have been caused by other “viruses,” it is easy to spot a certain trend. Often times, the symptoms of disease claimed to be declining due to vaccination are reclassified either as a new or related disease caused by a new or related “virus.” Smallpox was rebranded as chicken and/or monkeypox, polio became acute flaccid myelitis, syphilis morphed into AIDS, influenza transformed into “Covid,” etc. etc. etc. This trend of rebranding and relabelling the same symptoms of disease as either new diseases or similar ones can easily be seen with rabies and the rabies-related “lyssaviruses.” While the rabies “virus” is considered a “lyssavirus,” there are numerous other “viruses” under this same heading that are considered “rabies-like viruses” that do not cause rabies per se but instead “rabies-like” disease:
Rabies and Rabies-Related Lyssaviruses
“Closely related lyssaviruses circulate among bats in the Eastern Hemisphere, and can cause an illness identical to rabies. Rabies vaccines and post-exposure prophylaxis can provide some protection against some of these viruses, but not others. Rabies-related lyssaviruses can be found even in countries classified as rabies-free.”
“Information about rabies-related lyssaviruses is currently limited to a small number of case reports and a few reports of experimental inoculation; however, the illness appears indistinguishable from rabies. Bats may either have mild or no clinical signs and survive the infection, or develop severe neurological signs and die.”
This is a nice convenient scapegoat which allows a country to declare itself rabies-free even though the same symptoms of disease still persist. For example, in Austraila you will find disclaimers such as this:
According to Australia, they are rabies-free even though the same symptoms of disease persist within the country. These cases are blamed on the Australian bat “virus” which is claimed to cause a “rabies-like” disease. Quite convenient, right? However, what if the classification system for these “lyssaviruses” were to change? Would a country that is considered rabies-free lose its illustrious status?
Lyssaviruses and rabies: current conundrums, concerns, contradictions and controversies
“With increasing ICTV debate toward unification of virus taxonomy based on genetic distances, in the near future there may be a re-classification attempt, in which all phylogroup I viruses are segregated into one species (for example, Rabies lyssavirus?) and all phylogroup II viruses are segregated into another. Of course, such re-classification would miss important characteristics used for species demarcation at present and may have potential socio-economic or bio-political consequences for certain areas. For example, some places where RABV is not thought to circulate, such as in Australia or Western Europe (but where other lyssaviruses are present among bats), might lose their self-defined “rabies-free” status, on the basis of viral taxonomic re-organization, creating greater confusion, with potential public health, veterinary, or economic repercussions, if suddenly recast into the same disease status as Africa, Asia and the New World. Arguably, the term “rabies” appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”.
The loose definitions allow countries such as Austrailia to claim rabies-free status even though the disease still persists there. If the definition and/or classification changes, so to will their status. This is similar to how America is allowed to claim it has been polio-free since 1979 while there are cases every year of acute flaccid myelitis and other polio-like diseases which present with the same sets of symptoms. We could easily relabel those polio-like diseases as polio and lose the polio-free designation.
While the same set of rabies symptoms can be blamed on the closely related “lyssaviruses,” they can also be blamed on unrelated “viruses” and conditions that are said to be caused by different “viruses,” bacteria, genetic abnormalities, and even poisons.. For instance, animals can be diagnosed with distemper instead of rabies. These two diseases have often been confused for one another as the symptoms are indistinguishable:
Raccoons – distemper and rabies
“Canine distemper in raccoons starts slowly, with respiratory infections then they develop pneumonia. In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage. Many of these symptoms are similar to rabies – which can only be determined by laboratory testing.”
“CDV is a highly contagious paramyxovirus that affects dogs and wildlife including raccoons, skunks, grey foxes, and ferrets. This virus is closely related to the human measles virus, and can lead to respiratory, gastrointestinal (GI), and central nervous system (CNS) problems. CDV is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar.”
There are many other diseases such as encephalitis and different neurological disorders which are also said to mimic rabies in animals. Even poisoning is stated to mimic the severe stages of the disease:
Diseases that can look like Rabies
“Encephalitis is one condition that can look somewhat like the early stages of rabies. In this condition, with is immune based in most dog breeds of dogs, the dog’s own immune system begins to attack the brain. The result is a dog that may be confused, appear to stagger and bump into things, or even a dog that seems very disoriented and lost even in familiar settings. The dog may also have temperament changes and may snap at owners or become very agitated when they have previously been calm and friendly.”
“Canine distemper is another disease that may be mistaken for rabies since the symptoms are so close to being the same.Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue. Since it is still a highly contagious disease it is essential to get your dog to the vet if he or she has had any contact with wild animals or other dogs that seem to be disoriented, have a discharge from the eyes or nose, paralysis and stumbling types of movements. Typically the wild animal will be non-threatened by human presence, which in itself is a sign of abnormal behavior. It is important to realize that distemper, unlike rabies, cannot be passed from an animal to a human. However it is important to stay away from any animal that appears to have any symptoms similar to rabies or distemper.”
“Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies. In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink.”
As can be seen from the above three sources, canine distemper and other diseases such as encephalitis can be confused with rabies due to the identical nature of the symptoms. These diseases still persist within dogs and other animals while rabies, or at least “dog rabies,” has been said to have been eliminated from the US and other countries. In other words, the rabies label is no longer applied upon diagnosis even though the same symptoms of disease circulate in animals within the country.
This merry-go-round among the same symptoms of disease does not stop with animals either. There are many conditions in humans that also mimic rabies. These diseases are outlined in this final source:
Beware: there are other diseases that can mimic rabies:
Diseases that can mimic encephalitic rabies:
viral encephalitis (i.e. Japanese, eastern equine, West Nile)
Louis Pasteur admitted to not isolating the agent presumed to cause rabies
In the 1950’s, attempts to isolate the “virus” in cultures of hamster brains and kidneys were deemed successful despite the lack of observing any cytopathogenic effect (CPE)
Many “viruses” that are said to be eliminated or controlled through vaccination were rebranded and relabelled as either similar diseases caused by related “viruses” or new diseases caused by new “viruses”
Regarding rabies, closely related “lyssaviruses” circulate among bats in the Eastern Hemisphere and can cause an illness identical to rabies
Rabies-related “lyssaviruses” can be found even in countries classified as rabies-free
The illness associated with these rabies-related “lyssaviruses” appears indistinguishable from rabies
Some places where rabies is not thought to circulate, such as in Australia or Western Europe (but where other “lyssaviruses” are present among bats), might lose their self-defined “rabies-free” status, on the basis of “viral” taxonomic re-organization,
This would create greater confusion, with potential public health, veterinary, or economic repercussions, if they were suddenly recast into the same disease status as Africa, Asia and the New World
The term “rabies”appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”
Canine distemper is a rabies-like illness in animals
In raccoons, it starts slowly, with respiratory infections then they develop pneumonia
In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage
Many of these symptoms are similar to rabies – which can only be determined by laboratory testing
Canine distemper is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar
It is mistaken for rabies since the symptoms are so close to being the same
Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue
Encephalitis is another condition that can look somewhat like the early stages of rabies
The result of this brain swelling is a dog that may be confused, appear to stagger and bump into things, or even seems very disoriented and lost even in familiar settings
Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies
In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink
In humans, there are many diseases which mimic rabies:
Diseases that can mimic encephalitic rabies:
“viral” encephalitis (i.e. Japanese, eastern equine, West Nile)
For some reason, people seem to think rabies is a “gotcha” for those of us claiming that “viruses” do not exist. This disease is thrown out as proof that vaccines are effective and that because of this, the “virus” must therefore exist. However, a big problem for anyone championing rabies as proof for the existence of “viruses” continues to be the lack of any purified and isolated “virus” particles coming directly from the fluids of a rabid host. Louis Pasteur openly admitted to failing to meet this burden of proof even though he subjected animals and humans to experimental injections. Attempts by researchers in the 1950’s to propagate the “virus” in tissue and cell cultures did not produce the characteristic cytopathogenic effect said to be necessary in order to determine if a “virus” is present in a culture. Thus, there is no scientific proof for the existence of the rabies “virus,” even by virology’s own standards.
As the rabies “virus” can not be shown to exist, any data relating to a decrease in cases due to a vaccine which is then used as proof for the existence of a rabies “virus” is entirely irrelevant. There are many reasons to doubt case statistics as these can be easily manipulated and massaged in order to create whatever narrative is desired. It can be seen that the same symptoms associated with rabies still exist today as there are many other diseases either said to be caused by rabies-related “viruses” or completely unrelated “viruses” that share the exact same symptoms associated with rabies. These diseases are more commonly diagnosed in areas where rabies is said not to be circulating. It is very apparent that virology loves to rebrand and relabel the same symptoms of disease as multiple “new and different” diseases in order to create the perception that the treatments work. This is why places like Austrailia get to claim to be “rabies-free” even though a rabies-like disease said to be caused by a rabies-like “virus” still exists there. This lowers the cases as the older diseases are claimed to be either eradicated and/or under control due to “successful” vaccination campaigns and thus they are not looked for as a diagnosis. There is no way that these statistics can be trusted when the definitions and labels of what is or is not rabies seemingly changes at will.
In any case, the rabies statistics are a moot point. Until someone can provide proof of the purification and isolation of the particles assumed to be rabies directly from the fluids of a rabid host which were proven pathogenic in a natural way, these case numbers are utterly meaningless. The conversation with Alex on the Skeptico podcast should have never even reached vaccination statistics unless he provided a paper showing the evidence for the existence of a rabies “virus” first. Unfortunately, while Michael did an admirable job defending our position, we were not prepared for the graph and did not get the chance to look over the data and present our counter-argument. Hopefully we can get the chance to go on again and discuss the issue in further detail in the future. However, if not, this response will have to suffice.
“I came back home a little afraid for my country, afraid of what it might want, and get, and like, under pressure of combined reality and illusion. I felt—and feel—that it was not German man that I had met, but Man. He happened to be in Germany under certain conditions. He might, under certain conditions, be I.” —Milton Mayer, They Thought They Were Free, ix.
It’s been more than seventy-five years since the Nazis were defeated and Auschwitz was liberated. Seventy-five years is a long time—so long, in fact, that while many still learn of the horrors of the Holocaust, far fewer understand how the murder of the Jews happened. How were millions of people systematically exterminated in an advanced Western nation—a constitutional republic? How did such respectable and intelligent citizens become complicit in the murder of their countrymen? These are the questions Milton Mayer sought to answer in his book They Thought They Were Free.
In 1952, Mayer moved his family to a small German town to live among ten ordinary men, hoping to understand not only how the Nazis came to power but how ordinary Germans—ordinary people—became unwitting participants in one of history’s greatest genocides. The men Mayer lived among came from all walks of life: a tailor, a cabinetmaker, a bill-collector, a salesman, a student, a teacher, a bank clerk, a baker, a soldier, and a police officer.
Significantly, Mayer did not simply conduct formal interviews in order to “study” these men; rather, Mayer had dinner in these men’s homes, befriended their families, and lived as one of them for nearly a year. His own children went to the same school as their children. And by the end of his time in Germany, Mayer could genuinely call them friends. They Thought They Were Free is Mayer’s account of their stories, and the title of the book is his thesis. Mayer explains:
“Only one of my ten Nazi friends saw Nazism as we—you and I—saw it in any respect. This was Hildebrandt, the teacher. And even he then believed, and still believes, in part of its program and practice, ‘the democratic part.’ The other nine, decent, hard-working, ordinarily intelligent and honest men, did not know before 1933 that Nazism was evil. They did not know between 1933 and 1945 that it was evil. And they do not know it now. None of them ever knew, or now knows, Nazism as we knew and know it; and they lived under it, served it, and, indeed, made it” (47).
Until reading this book, I thought of what happened in Germany with a bit of arrogance. How could they not know Nazism was evil? And how could they see what was happening and not speak out? Cowards. All of them. But as I read Mayer’s book, I felt a knot in my stomach, a growing fear that what happened in Germany was not a result of some defect in the German people of this era.
The men and women of Germany in the 1930s and 40s were not unlike Americans in the 2010s and 20s—or the people of any nation at any time throughout history. They are human, just as we are human. And as humans, we have a great tendency to harshly judge the evils of other societies but fail to recognize our own moral failures—failures that have been on full display the past two years during the covid panic.
Mayer’s book is frighteningly prescient; reading his words is like staring into our own souls. The following paragraphs will show just how similar the world’s response to covid has been to the German response to the “threat” of the Jews. If we can truly understand the parallels between our response to covid and the situation in Hitler’s Germany, if we can see what lies at the end of “two weeks to flatten the curve,” perhaps we can prevent the greatest atrocities from being fully realized in our own day. But to stop our bent toward tyranny, we must first be willing to grapple with the darkest parts of our nature, including our tendency to dehumanize others and to treat our neighbors as enemies.
Overcoming Decency
“Ordinary people—and ordinary Germans—cannot be expected to tolerate activities which outrage the ordinary sense of ordinary decency unless the victims are, in advance, successfully stigmatized as enemies of the people, of the nation, the race, the religion. Or, if they are not enemies (that comes later), they must be an element within the community somehow extrinsic to the common bond, a decompositive ferment (be it only by the way they part their hair or tie their necktie) in the uniformity which is everywhere the condition of common quiet. The Germans’ innocuous acceptance and practice of social anti-Semitism before Hitlerism had undermined the resistance of their ordinary decency to the stigmatization and persecution to come” (55).
Others have explained the link between totalitarian impulses and “institutionalized dehumanization” and have discussed the “othering” of unvaccinated persons in nations across the world. Mayer shows that such dehumanization does not necessarily begin with prejudice:
“National Socialism was anti-Semitism. Apart from anti-Semitism, its character was that of a thousand tyrannies before it, with modern conveniences. Traditional anti-Semitism . . . played an important role in softening the Germans as a whole to Nazi doctrine, but it was separation, not prejudice as such, that made Nazism possible, the mere separation of Jews and non-Jews” (116-117).
Even if many Germans did not harbor anti-Semitic prejudices (at least not initially), the forced separation of Jews and non-Jews created a devastating rift in German society, tearing the social fabric and paving the way for tyranny. In our day, the separation of the masked and unmasked, the vaccinated and the unvaccinated, has divided populations around the world like nothing we’ve experienced in our lifetimes. And the global scale of this separation has perhaps not happened in recorded history.
How has this separation been made possible? The immense power of propaganda, and particularly propaganda in the digital age. We think we understand how propaganda affects us, but we often don’t realize the truly insidious effects on how we view others until it is too late. Mayer’s friends explained this in great depth. On one occasion, Mayer asked the former bank clerk about one of his Jewish friends. “Did your memory of the peddler make you anti-Semitic?” “No—not until I heard anti-Semitic propaganda. Jews were supposed to do terrible things that the peddler had never done. . . . The propaganda didn’t make me think of him as I knew him but of him as a Jew” (124; emphasis added).
Is there anything we can do to mitigate the dehumanizing effects of propaganda? Mayer describes the power of Nazi propaganda as so intense that all of his friends were affected by it—changed by it—including the teacher who was more aware of such tactics. Nearly seven years after the war, his friends still could not be persuaded that they had been deceived:
“Nobody has proved to my friends that the Nazis were wrong about the Jews. Nobody can. The truth or falsity of what the Nazis said, and of what my extremist friends believed, was immaterial, marvelously so. There simply was no way to reach it, no way, at least, that employed the procedures of logic and evidence” (142).
Mayer’s conclusion is depressing. If we cannot persuade others with logic and evidence, how can we persuade them? How many of us have shared indisputable data that the vaccines carry risks? How many of us have shown videos where public health officials openly admit that the vaccines do not stop transmission and that cloth masks don’t work (and are in fact little more than “facial decorations”)? Yet the evidence does not persuade those who have been captured by propaganda; indeed, it cannot persuade them. This is because the very nature of propaganda does not appeal to logic or reason; it does not appeal to evidence. Propaganda appeals to our emotions, and in a world where many people are led by emotions, propaganda becomes deeply rooted in the hearts of those who consume it.
So what are we to do? Mayer relays a frustrating reality. But understanding how propaganda worked in Nazi Germany and how it works today is essential if we are to have any chance of persuading those who have been shaped by it. Moreover, understanding why many people tend to be led by emotions and to outsource or suspend their critical thinking is perhaps even more essential to forestalling greater tragedies. We cannot expect others to escape the tyranny of propaganda if they do not have time to think or are motivated not to think.
Our Own Lives
Even without the dehumanization of those who were a “threat” to the community, most Germans were too focused on their own lives to consider the plight of their neighbors:
“Men think first of the lives they lead and the things they see; and not, among the things they see, of the extraordinary sights, but of the sights which meet them in their daily rounds. The lives of my nine friends—and even of the tenth, the teacher—were lightened and brightened by National Socialism as they knew it. And they look back at it now—nine of them, certainly—as the best time of their lives; for what are men’s lives? There were jobs and job security, summer camps for the children and the Hitler Jugend to keep them off the streets. What does a mother want to know? She wants to know where her children are, and with whom, and what they are doing. In those days she knew or thought she did; what difference does it make? So things went better at home, and when things go better at home, and on the job, what more does a husband and father want to know?” (48)
The best time of their lives. From where we stand in 2022, this seems like an unbelievable statement. How could they view a society that ostracized and eventually murdered millions of their fellow citizens as a good society? How could they look the other way when the Jews and others were suffering? It’s easy to ask these questions, but in our modern world, are we not also narrowly concerned with the comforts of our own lives and those of our loved ones? If the lives of others are put at risk so that our families can continue to “stay home and save lives”—so that we can feel safe from a deadly virus and “righteous” because of our decisions—would we not choose to do it? Many of us did. But did we even consider that our staying home meant others could not?
The lockdowns destroyed the lives of millions of poor children, both at home and abroad. But the laptop class remained insulated from this suffering, content with delivered groceries, zoom calls, and new episodes of Tiger King. And while many around the world starved or fought over limited supplies of food and water, we battled over the newest iPhones, believing that these devices were necessary to “ride out the pandemic” from our high-rise castles and suburban fortresses. Indeed, for many of us, our biggest concern was whether or not we could quickly have a new 42” TV delivered if ours stopped working. We knew nothing of the suffering of others, and we barely considered that their realities could be different. So also in Germany:
“There were wonderful ten-dollar holiday trips for the family in the ‘Strength through Joy’ program, to Norway in the summer and Spain in the winter, for people who had never dreamed of a real holiday trip at home or abroad. And in Kronenberg ‘nobody’ (nobody my friends knew) went cold, nobody went hungry, nobody went ill and uncared for. For whom do men know? They know people of their own neighborhood, of their own station and occupation, of their own political (or nonpolitical) views, of their own religion and race. All the blessings of the New Order, advertised everywhere, reached ‘everybody’” (48-49).
We quickly forget those who are distanced from us. And in a faceless world of “social distancing,” it’s that much easier to forget the myriad human beings who are suffering beyond what we could bear. The children who have never known their teachers’ faces? Not our concern. The elderly and infirm who’ve been cut off from the rest of the world, deprived of social interaction and human touch? It’s for their health and safety. Both children and adults with disabilities and special needs, those who cannot speak and cannot hear? We must all make sacrifices to slow the spread.
Our Own Fears
Add to our own lives our own fears (real or imagined), and we become even less motivated to consider the hardships of others:
“Their world was the world of National Socialism; inside it, inside the Nazi community, they knew only good-fellowship and the ordinary concerns of ordinary life. They feared the ‘Bolsheviks’ but not one another, and their fear was the accepted fear of the whole otherwise happy Nazi community that was Germany” (52).
The “accepted fear” of the community. The ten men Mayer lived among described the socially acceptable fears they were allowed to express—and the fears by which they must order their lives. But to express fear or even uneasiness about the growing totalitarianism of the Nazi regime? Such concerns were verboten. And so it is today. We are permitted (indeed, encouraged!) to fear the virus. We can fear the collapse of the healthcare system. We can fear “the unvaccinated” and even “anti-maskers.” But dare we express fear of the growing totalitarianism among us? Dare we challenge the “scientific consensus” or question the edicts of public health officials? We dare not, lest we be lumped together with the science-denying anti-vaxxers. We dare not, lest our posts be labeled misinformation or our accounts be permanently suspended.
Our Own Troubles
“It was this, I think—they had their own troubles—that in the end explained my friends’ failure to ‘do something’ or even to know something. A man can carry only so much responsibility. If he tries to carry more, he collapses; so, to save himself from collapse, he rejects the responsibility that exceeds his capacity. . . . Responsible men never shirk responsibility, and so, when they must reject it, they deny it. They draw the curtain. They detach themselves altogether from the consideration of the evil they ought to, but cannot, contend with.” (75-76).
We all have our own lives—the everyday concerns of our families and friends. We also have our own fears—fears of imaginary threats or actual risks. Add to our lives and fears the weight of our own responsibilities, and we can be rendered powerless to consider the troubles of those around us. This was true not only of the Germans of this era but of Americans as well. Mayer describes an interaction with his friend Simon, the bill collector, over the American internment of the Japanese. Simon recounted the forced relocation of more than 100,000 Americans—including children—because of their Japanese ancestry (and supposedly due to the threat they posed to the security of the nation).
Simon asked what Mayer had done to stand up for his fellow citizens who were removed from their homes without any form of due process. “Nothing,” Mayer replied. Simon’s response is sobering:
“‘There. You learned about all these things openly, through your government and your press. We did not learn through ours. As in your case, nothing was required of us—in our case, not even knowledge. You knew about things you thought were wrong—you did think it was wrong, didn’t you, Herr Professor?’ ‘Yes.’ ‘So. You did nothing. We heard, or guessed, and we did nothing. So it is everywhere.’ When I protested that the Japanese-descended Americans had not been treated like the Jews, he said, ‘And if they had been—what then? Do you not see that the idea of doing something or doing nothing is in either case the same?” (81).
We all want to think we would react differently. We all have the best of intentions and believe we would have the courage to stand up for others. We will be the heroes when everyone else is too afraid to act. But when the time comes, what will we actually do? Mayer’s interaction with his friend the teacher is worth quoting at length:
“‘I never got over marveling that I survived,’ said Herr Hildebrandt. ‘I couldn’t help being glad, when something happened to somebody else, that it hadn’t happened to me. It was like later on, when a bomb hit another city, or another house than your own; you were thankful.’ ‘More thankful for yourself than you were sorry for others?’ ‘Yes. The truth is, Yes. It may be different in your case, Herr Professor, but I’m not sure that you will know until you have faced it. . . .
You were sorry for the Jews, who had to identify themselves, every male with “Israel” inserted into his name, every female with “Sarah,” on every official occasion; sorrier, later on, that they lost their jobs and their homes and had to report themselves to the police; sorrier still that they had to leave their homeland, that they had to be taken to concentration camps and enslaved and killed. But—weren’t you glad you weren’t a Jew? You were sorry, and more terrified, when it happened, as it did, to thousands, to hundreds of thousands, of non-Jews. But—weren’t you glad that it hadn’t happened to you, a non-Jew? It might not have been the loftiest type of gladness, but you hugged it to yourself and watched your step, more cautiously than ever” (58-59).
I feel bad for them, but I am unwilling to speak up. I hate that children are denied access to speech therapy, in-person school, or social interaction with their friends. But if I speak up, I may lose my status and influence. I hate that the unvaccinated are losing their jobs and being confined to their homes. But if I speak up, I could lose my job as well. I hate that my fellow citizens are being taken to “quarantine centers” against their will. But if I speak up, I could face criminal penalties. And I hate that the unvaccinated are being excluded from society and treated with contempt by national leaders. But if I speak up, I could be excluded as well. The risk is too great.
The Tactics of Tyrants
“[M]odern tyrants all stand above politics and, in doing so, demonstrate that they are all master politicians” (55).
How often have public officials denounced those who question the narrative as “politicizing covid”? “Stop politicizing masks!” “Stop politicizing vaccines!” And those who dissent are demeaned as “science-denying Trump supporters” or “anti-vax conspiracy theorists.” It’s no wonder so few have questioned the official narratives on masks, lockdowns, and vaccines—to do so is to put oneself in the crosshairs, to draw accusations of caring more about politics and the economy than people’s lives and health. This gaslighting is by no means the only tactic of those who seek greater authoritarian control. In addition to helping us understand what makes us susceptible to totalitarianism—why so many of us will “draw the curtain” in the face of evil—Mayer’s work also exposes the tactics of tyrants, enabling his readers to see and resist.
“This separation of government from people, this widening of the gap, took place so gradually and so insensibly, each step disguised (perhaps not even intentionally) as a temporary emergency measure or associated with true patriotic allegiance or with real social purposes. And all the crises and reforms (real reforms, too) so occupied the people that they did not see the slow motion underneath, of the whole process of government growing remoter and remoter” (166-167).
Many have sounded the alarm over the past two years about the threat of endless emergencies, and we have all seen the goalposts be moved time and again. “It’s just two weeks.” “It’s just a mask.” “It’s just a vaccine.” And on and on it goes. But while most everyone recognizes that “two weeks to flatten the curve” was not just two weeks, too few understand the insidious threat of ongoing “rule by emergency.” But Mayer’s friends understood, and they experienced the catastrophic results.
Before Hitler became chancellor, Germany was still a republic governed by the Weimar Constitution. But Article 48 of this constitution permitted the suspension of civil liberties “[i]f public security and order are seriously disturbed or endangered.” These emergency powers were continually abused, and following the Reichstag Fire in 1933, the Enabling Act transferred all law-making power from the German parliament to the executive branch, allowing Hitler to “rule by decree” until the end of the War in 1945.
While the legislative branches of the States and the federal government in the United States (and other nations around the world) have been in session the past two years, the reality is that legislatures rarely sought to limit the powers of the executive. Under the auspices of the CDC, the WHO, and other health agencies, executives have effectively ruled by fiat. Closing businesses, mandating masks and vaccines, forcing people to stay home—most of these measures were implemented by executives without even consulting legislatures. And what was the justification? The “emergency” of covid. If we could go back in time to 2019 and ask whether executives should be permitted to unilaterally impose such life-altering policies on their people even with legislative consent, the vast majority of people would likely say “No!” So how did we get here in 2022? Mayer’s friends offer valuable insight.
The Common Good
“The community is suddenly an organism, a single body and a single soul, consuming its members for its own purposes. For the duration of the emergency the city does not exist for the citizen but the citizen for the city. The harder the city is pressed, the harder its citizens work for it and the more productive and efficient they become in its interest. Civic pride becomes the highest pride, for the end purpose of all one’s enormous efforts is the preservation of the city. Conscientiousness is the highest virtue now, the common good the highest good” (255).
What has been the reason given for many of the measures implemented over the past two years? The common good. We must wear our masks to protect others. Get vaccinated to love our neighbors. Stay home to save lives. And it’s not just for our neighbors as individuals but for the community as a whole. We must close schools to preserve hospital resources. In the U.K., efforts were being made to “Protect the NHS.” And countless other slogans signaled our common virtue.
To be clear, I’m not opposed to working together for the common good; I do not value my liberties more than the lives of others (this was a common gaslighting tactic employed against those who opposed government overreach). Rather, I simply understand how governments across time have used the “common good” as an excuse to consolidate power and implement authoritarian measures that under normal circumstances would be rejected. This is exactly what happened to Mayer’s friends:
“Take Germany as a city cut off from the outside world by flood or fire advancing from every direction. The mayor proclaims martial law, suspending council debate. He mobilizes the populace, assigning each section its tasks. Half the citizens are at once engaged directly in the public business. Every private act—a telephone call, the use of an electric light, the service of a physician—becomes a public act. Every private right—to take a walk, to attend a meeting, to operate a printing press—becomes a public right. Every private institution—the hospital, the church, the club—becomes a public institution. Here, although we never think to call it by any name but pressure of necessity, we have the whole formula of totalitarianism.
The individual surrenders his individuality without a murmur, without, indeed, a second thought—and not just his individual hobbies and tastes, but his individual occupation, his individual family concerns, his individual needs” (254; emphasis added).
Tyrants understand how to exploit our desire to care for others. We must understand their tendency to exploit our good will. Indeed, to understand this tactic and to resist encroachments on liberty is the way to preserve the actual common good. Tragically, many people do not realize that they have been exploited—that their desire to work for the common good has become obedience without question. Mayer’s description is stunning:
“For the rest of the citizens—95 percent or so of the population—duty is now the central fact of life. They obey, at first awkwardly but, surprisingly soon, spontaneously.” (255)
This type of compliance seems to have happened most clearly with the use of masks. We obey spontaneously, not at the point of a gun. And we obey without thinking about the rationality of what is required. We will wear a mask to walk to a table in a packed restaurant, and we will dine for two hours before donning it again to walk out. We must wear masks on a plane to “stop the spread,” but we can take them off as long as we are eating or drinking. Some even wear masks while driving alone in their cars. To be clear, I am not criticizing those who wear masks in these situations; I am lamenting how propaganda has so affected us that we comply without considering our actions. Or, perhaps worse, we have considered them, but we comply anyway because that’s what others are doing and that’s what we’re expected to do.
Do you see the dangerous parallels between what’s happening today and what happened in Germany? This is not simply about masks (and it never has been). This is about a willingness to comply with government demands, no matter how illogical or insidious. Can you see how these tendencies contribute to the demonization of certain persons, particularly the unvaccinated? Those who do not act to “protect their neighbors” by wearing a mask, or who choose not to get vaccinated “for the sake of the vulnerable,” are a danger to society and a threat to us all. Can you see where this demonization can lead? We know where it led in Germany.
Endless Distractions
“[S]uddenly, I was plunged into all the new activity, as the university was drawn into the new situation; meetings, conferences, interviews, ceremonies, and, above all, papers to be filled out, reports, bibliographies, lists, questionnaires. And on top of that were the demands in the community, the things in which one had to, was ‘expected to’ participate that had not been there or had not been important before. It was all rigmarole, of course, but it consumed all one’s energies, coming on top of the work one really wanted to do. You can see how easy it was, then, not to think about fundamental things. One had no time” (167).
Combine the tyrannical use of the common good with a perpetual state of emergency, and you have a totalitarian regime that cannot be questioned: “[T]his, of all times, is no time for divisiveness” (256). Add to these tactics endless distractions to occupy the citizenry, and no one even has time to question. Listen to one of Mayer’s colleagues:
“The dictatorship, and the whole process of its coming into being, was above all diverting. It provided an excuse not to think for people who did not want to think anyway. I do not speak of your ‘little men,’ your baker and so on; I speak of my colleagues and myself, learned men, mind you. Most of us did not want to think about fundamental things and never had. There was no need to. Nazism gave us some dreadful, fundamental things to think about—we were decent people—and kept us so busy with continuous changes and ‘crises’ and so fascinated, yes, fascinated, by the machinations of the ‘national enemies,’ without and within, that we had no time to think about these dreadful things that were growing, little by little, all around us. Unconsciously, I suppose, we were grateful. Who wants to think?” (167-168).
Is this not what is happening, even as I write this, in the world around us? Over the past two years we have experienced a continual upending of our lives with lockdowns, zooming, online “learning,” mask mandates, “social” distancing, and more. And then we are told we must comply with vaccine mandates or lose our jobs, leaving some of us too weary to resist and others more weary for trying. And for those of us who have chosen to forgo the available vaccines, we must spend time—lots and lots of time—composing exemption requests for the various mandates, explaining in depth our reasons for objecting to the jabs.
And then, when it seems the covid madness is coming to an end (at least for the time being), an “emergency” is declared in Canada that tramples the rights of Canadian citizens, and even now the world has been plunged into crisis because of the conflict in Ukraine. There is so much going on, so many legitimate concerns that demand our attention, that many are unaware of the totalitarian noose that is tightening around us. More than that, we are too exhausted to examine what is happening, too tired to even care. But care we must! Or it will be too late, and there will be no turning back.
Science and Education
“[T]he university students would believe anything complicated. The professors, too. Have you seen the ‘race purity’ chart?” “Yes,” I said. “Well, then, you know. A whole system. We Germans like systems, you know. It all fitted together, so it was science, system and science, if only you looked at the circles, black, white, and shaded, and not at real people. Such Dummheit they couldn’t teach to us little men. They didn’t even try” (142).
“Trust the science.” Or so we have been told the past two years. Yet another tactic used by authoritarians across time is the appeal to science and expertise. Mayer’s friends described how the Nazis used “science” to convince students and others that the Jews were inferior, even diseased. But this was not science; it was scientism. And so it is today.
Science is not dogma; it is not a set of beliefs. Real science is the process by which we discover the truth about the physical world. We begin with a hypothesis that must be rigorously tested through observation and experimentation. But over the past two years, “science” has meant whatever the public health authorities claim to be true, regardless whether the claims are supported by evidence. In fact, much of this so-called science has proved to be demonstrably false.
In addition to using “science” to support its goals, the Reich government also sought to control education. “National Socialism required the destruction of academic independence” (112), replacing truth and the search for truth with allegiance to Nazi doctrine. Notably, the Nazis captured not only the secondary schools but the primary schools as well, even rewriting certain subjects to comport with Nazi propaganda: “In history, in biology, and in economics the teaching program was much more elaborate than it was in literature, and much stricter. These subjects were really rewritten” (198). Mayer’s friend the teacher explained how the Reich would also place “ignorant ‘reliables,’ from politics or business, over the educators”; this was “part of the Nazi way of humiliating education and bringing it into popular contempt” (197). In today’s world, this would likely involve bringing in bureaucrats to control what is taught in the classroom or to control whether there even is a classroom, as so many schools have been perpetually closed “to slow the spread.”
Suppressing Speech and Encouraging Self-Censorship
“Everything was not regulated specifically, ever. It was not like that at all. Choices were left to the teacher’s discretion, within the ‘German spirit.’ That was all that was necessary; the teacher had only to be discreet. If he himself wondered at all whether anyone would object to a given book, he would be wise not to use it. This was a much more powerful form of intimidation, you see, than any fixed list of acceptable or unacceptable writings. The way it was done was, from the point of view of the regime, remarkably clever and effective. The teacher had to make the choices and risk the consequences; this made him all the more cautious” (194).
The Reich’s method of controlling education (and speech more broadly) did not rely on overly specific regulations. In our modern world, this tactic goes well beyond the enforcement of covid protocols, but it certainly includes them. Rare were the institutions that permitted a choice concerning masks; most schools required their students to wear them regardless of personal convictions. The result? Students who quickly learned that they must cover their faces to participate in society, and some who came to believe that they would seriously harm themselves or their classmates if they took them off. And even with most U.S. jurisdictions removing mask requirements in most schools, many students have become so self-conscious of showing their faces that they will voluntarily continue wearing them. What is the cost not only to the mental health of these students but to freedom of speech and expression? We may never fully know.
And it was not only schools. Covid protocols and covid narratives were enforced outside of schools as well. In early 2021, only a small minority of businesses permitted their customers to enter unmasked; still fewer allowed their employees this option. Though rarely acknowledged by most public health officials, masks do interfere with human communication (if they did not, world leaders would not take them off to speak). And if the ability to communicate is hindered, the free exchange of ideas also suffers.
As to speech more broadly, the tactic described by Mayer encourages self-censorship, which any fair-minded person admits is also happening today. Going back decades to speech that was considered “politically incorrect,” we all understand that there are certain accepted positions on a variety of topics, ranging from race and gender to vaccines and covid treatments.
Don’t dare share anything that counters the narrative, on covid or anything else. To share something that comes close to questioning the narrative could have myriad consequences, both personal and professional. You do not want to be accused of spreading misinformation, do you? Or maligned as a conspiracy theorist? So we refrain from sharing counterpoints and evidence, even if that evidence is absolutely legitimate and completely sound.
Uncertainty
“You see,” my colleague went on, “one doesn’t see exactly where or how to move. Believe me, this is true. Each act, each occasion, is worse than the last, but only a little worse. You wait for the next and the next. You wait for one great shocking occasion, thinking that others, when such a shock comes, will join with you in resisting somehow. You don’t want to act, or even talk, alone; you don’t want to ‘go out of your way to make trouble.’ Why not?—Well, you are not in the habit of doing it. And it is not just fear, fear of standing alone, that restrains you; it is also genuine uncertainty.
“Uncertainty is a very important factor, and, instead of decreasing as time goes on, it grows. Outside, in the streets, in the general community, ‘everyone’ is happy. One hears no protest, and certainly sees none. . . . you speak privately to your colleagues, some of whom certainly feel as you do; but what do they say? They say, ‘It’s not so bad’ or ‘You’re seeing things” or “You’re an alarmist.”
“And you are an alarmist. You are saying that this must lead to this, and you can’t prove it. These are the beginnings, yes; but how do you know for sure when you don’t know the end, and how do you know, or even surmise, the end? On the one hand, your enemies, the law, the regime, the Party, intimidate you. On the other, your colleagues pooh-pooh you as pessimistic or even neurotic. You are left with your close friends, who are, naturally, people who have always thought as you have” (169-170).
And so we do nothing. Mayer is right. His colleague was right. What can we say?
One thing we can say is that those who have required masks, whether by accident or design, have made the feeling of uncertainty even greater. We struggle to know what others are thinking, or feeling, because our faces are hidden. In addition to the low-level anxiety and fear that masks induce in everyone (at the very least causing us to view others as threats to our safety and not as persons), we are uncertain why those around us are wearing masks. Is it simply because they are told to do so? Is it out of deference to others? Or because they genuinely desire to wear them?
Let’s say it’s true that the strong majority of workers would choose not to wear masks if their employers did not require them. How are we to know for sure what they prefer if the choice is taken from them? Similarly, if one was required to do various things to show allegiance to the Party, how was one to know whether others were genuinely loyal to the Party or simply going along in order to blend in (and not be taken to the camps)?
Gradually, Then Suddenly
“To live in this process is absolutely not to be able to notice it—please try to believe me—unless one has a much greater degree of political awareness, acuity, than most of us had ever had occasion to develop. Each step was so small, so inconsequential, so well explained or, on occasion, ‘regretted,’ that, unless one were detached from the whole process from the beginning, unless one understood what the whole thing was in principle, what all these ‘little measures’ that no ‘patriotic German’ could resent must some day lead to, one no more saw it developing from day to than a farmer in his field sees the corn growing. One day it is over his head” (168).
Of all the tactics employed by tyrants to achieve their goals, the illusion that we have plenty of time to escape is arguably the most important. If we could all go back to February 2020, how many of us would have predicted we would be here? How did it all happen? Gradually, then all at once. Mayer senses our dilemma:
“How is this to be avoided, among ordinary men, even highly educated ordinary men? Frankly, I do not know. I do not see, even now. Many, many times since it all happened I have pondered that pair of great maxims, Principiis obsta and Finem respice—‘Resist the beginnings’ and ‘Consider the end.’ But one must foresee the end in order to resist, or even see, the beginnings. One must foresee the end clearly and certainly and how is this to be done, by ordinary men or even by extraordinary men? Things might have changed here before they went as far as they did; they didn’t, but they might have. And everyone counts on that might” (168).
Think back to March 2020. We should have resisted then. We should not have tolerated stay-at-home orders or various (and even non-sensical) restrictions on local businesses and private life. Governments had already gone too far. And then came the masks, and some said that masks were the hill. Individuals who shared these concerns were derided as fanatics and conspiracy theorists, but they were right.
Many did not see it, and even fewer resisted. I saw it relatively early, but I did not resist as fiercely as I should, and my failure haunts me to this day. Had we more seriously resisted masks, the prospect of vaccine mandates would have largely collapsed. Indeed, there would be no political, moral, or practical support for vaccine mandates and the more insidious vaccine passports had mask mandates been successfully resisted. But we—but I—did not resist as fiercely as I should have.
Why not? I told myself that it was worth keeping my position of influence at my job. It was a “calculated decision” to continue to help those around me. And I also needed to provide food and shelter for my daughters, to enable them to have a “normal” childhood.
But in my good and noble compromises—they are, in fact, compromises—have I laid the groundwork for further infringements on my family’s lives and liberties? Have I sowed the seeds of an eternal dystopia that will forever terrorize my daughters and their children? Have I made a deal with the devil? More importantly, if I have, is there any way out of this contract?
The Power of Non-Violent Resistance
“It is actual resistance which worries tyrants, not lack of the few hands required to do the dark work of tyranny. What the Nazis had to gauge was the point at which atrocity would awaken the community to the consciousness of its moral habits. This point may be moved forward as the national emergency, or cold war, is moved forward, and still further forward in hot war. But it remains the point which the tyrant must always approach and never pass. If his calculation is too far behind the people’s temper, he faces a palace Putsch; if it is too far ahead, a popular revolution” (56).
We underestimate how much power people have when they choose to resist. Parents across the nation pushed back against mask mandates, and many school boards relented and made masks optional. Many employees refused to comply with vaccine mandates, and many employers relented (or at least granted broad exemptions). Parents and employees did not win in all cases, but they’ve won more battles than many realize, and the war is far from over. Strong and united opposition has also resulted in reversals of government covid policies, and more mandates are being lifted as more pressure is applied. We must continue to resist and help others do the same, recognizing that the costs we bear will be worth it in the end.
The Cost of Dissent
“You are respected in the community. Why? Because your attitudes are the same as the community’s. But are the community’s attitudes respectable? We—you and I—want the community’s approval on the community’s basis. We don’t want the approval of criminals, but the community decides what is criminal and what isn’t. This is the trap. You and I—and my ten Nazi friends—are in the trap. It has nothing to do directly with fear for one’s own or his family’s safety, or his job, or his property. I may have all these, never lose them, and still be in exile. . . . My safety, unless I am accustomed to being a dissenter, or a recluse, or a snob, is in numbers; this man, who will pass me tomorrow and who, though he always said ‘Hello’ to me, would never have lifted a finger for me, will tomorrow reduce my safety by the number of one” (60).
In Hitler’s Germany, to stray from the acceptable concerns, to deviate from the accepted narrative, was to put oneself at risk. And so it is today. Dissenters are looked on as the ones who cause problems. Challenging the accepted narratives or questioning the “consensus” draws the ire of both everyday citizens and cultural elites. Dissent is dangerous, not because one is factually incorrect in his assessments, but because his assessments challenge accepted dogmas.
The Cost of Compliance
There is a cost to being a dissenter. Mayer’s friends were in constant danger of losing their jobs and their freedoms—and possibly their lives. But there is also a cost to compliance, and that cost is far greater than anything we can currently imagine. Listen carefully to Mayer:
“It is clearer all the time that, if you are going to do anything, you must make an occasion to do it, and then you are obviously a troublemaker. So you wait, and you wait. But the one great shocking occasion, when tens or hundreds or thousands will join with you, never comes. That’s the difficulty. If the last and worst act of the whole regime had come immediately after the first and smallest, thousands, yes, millions would have been sufficiently shocked—if, let us say, the gassing of the Jews in ’43 had come immediately after the ‘German Firm’ stickers on the windows of non-Jewish shops in ’33. But of course this isn’t the way it happens. In between come all the hundreds of little steps, some of them imperceptible, each of them preparing you not to be shocked by the next.
“And one day, too late, your principles, if you were ever sensible of them, all rush in upon you. The burden of self-deception has grown too heavy, and some minor incident, in my case my little boy, hardly more than a baby, saying ‘Jew swine,’ collapses it all at once, and you see that everything, everything, has changed and changed completely under your nose. The world you live in—your nation, your people—is not the world you were born in at all. The forms are all there, all untouched, all reassuring, the houses, the shops, the jobs, the mealtimes, the visits, the concerts, the cinema, the holidays. But the spirit, which you never noticed because you made the lifelong mistake of identifying it with the forms, is changed. Now you live in a world of hate and fear, and the people who hate and fear do not even know it themselves; when everyone is transformed, no one is transformed. Now you live in a system which rules without responsibility even to God.”
“You have gone almost all the way yourself. Life is a continuing process, a flow, not a succession of acts and events at all. It has flowed to a new level, carrying you with it, without any effort on your part. On this new level you live, you have been living more comfortably every day, with new morals, new principles. You have accepted things you would not have accepted five years ago, a year ago, things that your father, even in Germany, could not have imagined. Suddenly it all comes down, all at once. You see what you are, what you have done, or, more accurately, what you haven’t done (for that was all that was required of most of us: that we do nothing). You remember those early meetings of your department in the university when, if one had stood, others would have stood, perhaps, but no one stood. A small matter, a matter of hiring this man or that, and you hired this one rather than that. You remember everything now, and your heart breaks. Too late. You are compromised beyond repair.”
“What then? You must then shoot yourself. A few did. Or ‘adjust’ your principles. Many tried, and some, I suppose, succeeded; not I, however. Or learn to live the rest of your life with your shame. This last is the nearest there is, under the circumstances, to heroism: shame. Many Germans became this poor kind of hero, many more, I think, than the world knows or cares to know” (171-172).
I’ve read this section more times than I can count, and as I read it now, I weep for my own failures. My own fears. My own complicity in the slow growth of covid totalitarianism. Of allowing governments and media to set narratives. Of failing to take a stand. But it is not too late! What is coming with digital IDs and digital passports is more insidious, and more ingenious, but there is still time to resist. But we must resolve to stand now. We must resolve to stand together. And we must stand no matter the cost.
“You know,” he went on, “when men who understand what is happening—the motion, that is, of history, not the reports of single events or developments—when such men do not object or protest, men who do not understand cannot be expected to. How many men would you say understand—in this sense—in America? And when, as the motion of history accelerates and those who don’t understand are crazed by fear, as our people were, and made into a great ‘patriotic’ mob, will they understand then, when they did not before?” (175).
The duty is upon us who see what is happening to stand up and resist. We will all bear some cost, either now or in the future. Some of us have experienced the cost of standing up: we have lost jobs, lost friends, even lost freedoms. But all of us have borne the cost of tyrannical overreach in the name of public health. I’ve lost count of the number of people I know who were not permitted to say goodbye to their loved ones. Who were denied access to potentially life-saving treatments. Who were refused medical care in the name of the common good. There is no doubt we’ve all suffered during the past two years, but failing to resist this ever-encroaching tyranny will cost more than we can comprehend. I don’t know exactly what it will cost us to stand for truth and liberty in the coming months and years. But what I can say with near certainty is that the cost of present resistance will be far more tolerable to our consciences and perhaps our lives than failure to resist. More importantly, resisting now will certainly be more tolerable for the lives of our children.
The Choice Before Us
Because of the risks to their lives and their families, many Germans refused to speak openly about what was happening, even when they knew. And their fears were completely justified:
“Those who came back from Buchenwald in the early years had promised—as every inmate of every German prison had always had to promise upon his release—not to discuss his prison experience. You should have broken your promise. You should have told your countrymen about it; you might, though the chances were all against you, have saved your country had you done so. But you didn’t. You told your wife, or your father, and swore them to secrecy. And so, although millions guessed, only thousands knew. Did you want to go back to Buchenwald, and to worse treatment this time? Weren’t you sorry for those who were left there? And weren’t you glad you were out?” (59).
Is this not the case with the many who have escaped the camps in North Korea? Or the Uyghurs who have been released from “re-education facilities” in Xinjiang, China? I dare not judge harshly those who have not spoken up, as I have no way of understanding what they have experienced. But I want to think that I—and that everyone reading this piece—will have the resolve to speak up in these dark hours. To stand shoulder to shoulder, to not shirk from our responsibility to our children, to our neighbors, and to the generations who will come after us. But then I think of my children—my three precious daughters—and I think of the present cost of standing up.
If I speak up, I might be arrested, my bank accounts might be frozen, my professional license suspended or revoked. My ability to provide for my family could be greatly diminished, and my girls might lose their family home. Even more, if I am one day arrested and taken to prison or to a camp (or whatever the facilities are called where people are being held against their will), I will not be present to play catch with my youngest, to watch my second ride her hoverboard, or hear my oldest read to me. I might not be able to tuck them in bed, to sing to them, to pray with them—and not only for a night but for weeks or months (if not years). So I am torn.
Do I speak up, knowing that voicing dissent could upend my daughters’ lives and render them virtually fatherless? Or do I choose to remain silent, with the protests of my heart suppressed until they shrivel to nothing? Do I accept a new normal of dystopian tyranny in order to be physically present with my children, knowing that this choice will consign my daughters (and their families and descendants) to a totalitarianism that may never be overthrown? What would love compel me to do? What is the right thing to do? What will I choose to do? I know what I hope I will choose, but do you see the difficulty?
What Will We Choose?
“Here in Kronenberg? Well, we had twenty thousand people. Of these twenty thousand people, how many opposed? How would you know? How would I know? If you ask me how many did something in secret opposition, something that meant great danger to them, I would say, well, twenty. And how many did something like that openly, and from good motives alone? Maybe five, maybe two. That’s the way men are.” “You always say, That’s the way men are,’ Herr Klingelhöfer,” I said. “Are you sure that that’s the way men are?” “That’s the way men are here,” he said. “Are they different in America?” Alibis, alibis, alibis; alibis for the Germans; alibis, too, for man, who, when he was once asked, in olden time, whether he would prefer to do or to suffer injustice, replied, “I would rather neither.” The mortal choice which every German had to make—whether or not he knew he was making it—is a choice which we Americans have never had to confront” (93-94).
When Mayer wrote his book, Americans had not yet confronted the choices his friends had to make. But for the past two years, we have been staring these choices in the face. Certainly Australians are confronting them, as are the citizens of New Zealand. Austria, Spain, Italy, and Canada—to say nothing of many Eastern nations—are most definitely confronting them. And in many blue cities and states across the nation, our fellow Americans have faced these choices and felt the weight of separation and discrimination.
I often ask my students the following question when we discuss this book each spring: what happens if the United States and other free nations fall into tyranny? In Germany before World War II, it was at least possible to immigrate elsewhere. One could get out if he had means and if he saw it coming in time. But what happens if we give up the fight? Where else can we go? Where can our children flee? If the whole world becomes like China, there is nowhere else to escape the approaching storm.
So what must we do? We must decide today to draw a line that must not be crossed. As others have written, we should have drawn the line at masks. Governments the world over have rendered entire societies more compliant by hiding our faces. In so many cases, we no longer see others as human. We instead view them as threats, as anonymous vectors of disease. But since we didn’t draw the line at masks in 2020, we must regain that ground that was lost. We must fight to end not only the current mask and vaccine mandates (and other remaining covid restrictions), but we must not relent until the possibility of such mandates is viewed not only as politically untenable but morally and ethically indefensible. And no matter the cost, we cannot under any circumstance accept the use of digital passports (this short video shows why). And finally, we must not only be in the business of changing policies; we must strive to change hearts and minds, to wake others to the reality of what is taking place.
Friends, we must act—I must act. There is no more time to wait.
Joshua Styles is an Associate Professor of Criminal Justice & Legal Studies / Christian Studies at North Greenville University. He is committed to finding and reporting the truth.
cover image “Hitler greets the Protestant Archbishop of Nuremberg, Ludwig Müller, and Benedictine Abbott Albanus Schachleitner
at the Reich Party Rally of 1934.” is in the public domain
The “Lab-Leak Theory” Returns…as Yet Another Fake Binary
The theory that “Covid” originated in a bio-lab has been back in the headlines over the last few weeks, serving as a prime example of the type of fake binary OffG has been warning you about.
The “lab-leak theory” – which pushes the idea Sars-Cov-2 was bio-engineered in a lab as a “gain-of-function” program, and then either accidentally or deliberately released on an unsuspecting population – first came to the front pages as early as January 2020.
At the time it was deemed a “racist” “anti-china” conspiracy theory by the vast majority of the media, and it fell away from the narrative.
It had a resurgence in 2021, suddenly & inexplicably becoming not racist anymore.
In February 2021 the World Health Organization published a report finding the lab origin for Covid19 “extremely unlikely”. But WHO chief Tedro Adhanom was obviously keen not to let the idea die completely, publicly stating “more investigation was needed”.
Overall, around this time, it suddenly became much less taboo to suggest the “virus” originated in a lab.
Then, in December 2021, the Daily Mail reported that Dr Alina Chan had told the UK’s Science Select Committee that it is ‘reasonable to believe [the] virus was engineered in China’ and that “the lab origin is more likely than not”.
But after a brief furore over that, it again faded from the front pages.
Now it’s back. And gaining momentum.
In May, 18 scientists (including Chan) published an open letter in the Science journal demanding authorities properly “investigate the origins of Covid19”.
Two weeks ago the World Health Organisation released a report that they were still investigating the origins of Covid, and that no hypothesis had been completely ruled out.
On June 15th, the WHO chief told reporters at a press conference that ruling out the lab-leak theory had been “premature” and there had been a “push” to do so. He called on China to “be transparent, open and cooperate, especially on the information, raw data that we asked for at the early days of the pandemic.”
This time China responded, dismissing the lab leak theory as “lies” and “anti-China propaganda”, whilst suggesting that the real lab leak likely came from the US bioweapons lab in Fort Detrick.
Then, on June 18th, The Daily Mail reported that despite maintaining public neutrality Tedros Adhanom “privately believed” that Covid had originated in a lab.
In short, two apparently oppositional camps are springing up – the West is laying the groundwork to blame China for the pandemic, whilst China (and probably Russia, down the line) blame the USA.
This is a textbook fake binary.
What you need to notice is that both these allegedly opposing sides agree on the most important aspect of the pandemic lie – that Covid is a unique new and dangerous disease which needs be treated with masks, lockdowns and vaccines – and only disagree violently about where this “real and deadly new disease” might have come from.
You are supposed to take your cue from them.
They want you to forget “covid” is just a meaningless new name for an old familiar cluster of “seasonal” symptoms. They want you to forget the whole thing was a scam – and to instead take a “side” in a scripted & noisy & totally phony “origin” debate.
The minute you sign up for it they have you – because by agreeing to debate where “it” comes from you have accepted “it” – ie a deadly new pathogen – exists & needs to be dealt with.
And that is all they want from you.
We think you should politely decline this staged “controversy”. Because however real the East-West divide actually is in other areas, when it comes to covid both sides are the same side & pushing the same story.
And it suits both East & West to encourage this fake binary – and “bioweapon” fear porn – at the expense of wider and more honest enquiry.
“The Anti-Vaccine Movement’s New Frontier: A wave of parents has been radicalized by Covid-era misinformation to reject ordinary childhood immunizations — with potentially lethal consequences.”
And Friday morning, they sent out an email blast to promote the article.
Here’s their promo. The Times really had to stretch to come up with such a load. My comments are in brackets.
“This week, Moises Velasquez-Manoff reports on a wave of parents who have been radicalized by Covid-era misinformation to reject ordinary childhood immunizations — with potentially lethal consequences.”
[Wow. The author has three names. Impressive. I feel I need at least three to reply. Jon The Rebel on Vaccine Fantasy Island Just Say No to Bill Gates Rappoport.]
“In 2019, even before the pandemic struck, the World Health
Organization listed growing vaccine hesitancy as one of its top 10 threats to global health. Now the pandemic has given anti-vaccine advocates an opportunity to field-test a variety of messages and find new recruits.”
[Yes, our anti-vaxx squadrons use dozens of human and AI analysts to float our messages and then test the results. We use polls, surveys, in-home visits, NSA-type surveillance tools, and even covert assets in the press to expand our reach. Elite foundation money pours into our coffers.]
“’There’s a lot of misinformation about the Covid vaccines, and it just bleeds into everything,’ one doctor told us. ‘These fake stories and bad information get stuck in people’s heads, and they understandably get confused’.”
[One doctor told the Times that. Well, case closed. Verdict? We’re guilty. The doctor is always right. Wait a minute. I just called a doctor. He told me the Times’ doctor is wrong. Duel at dawn. Choice of weapons.]
“If this dynamic continues, it could threaten decades of progress in controlling infectious disease — a triumph that has, paradoxically, hindered the effort to counter vaccine skepticism. In the developed world, only a small portion of the population has seen the death and suffering caused by the diseases of eras past; vaccines, in the minds of many, have come to pose a greater threat than the diseases that they have helped nearly vanquish. In a sense, vaccines have become victims of their own success.”
[Obviously, the Times writer is a gymnast. Probably practices yoga. He can bend and stretch and twist with the best of them. Also, notice how he characterizes the parents who “have been radicalized”: They’re people who don’t have a brain in their heads. They’re massively ignorant robots, dupes and yokels just waiting for vaccine misinformation, which they grab like kids going for candy. Parents actually thinking for themselves? Never happens.]
On the other hand, readers of the Times are DISCERNING. They’re COLLEGE GRADS. They take their vaxx info from the paper’s pros, who have perfected the ability to look down their noses at the great unwashed and cluck and tsk tsk and express a modicum of sympathy.
Nowhere in the Times—ever—will we read an actual debate on the subject of vaccines, in which two sides are adequately represented and given ample space to present a little thing called EVIDENCE (or fake evidence).
To host such debates would be demeaning for the Times. It would signal a departure from their perch which constantly advertises: if-we-say-it-we-know-it.
Maintaining that pose month after month, year after year, decade after decade is debilitating.
Which is one reason why so many mainstream reporters are drunks.
In an interview with the National Geographic, Tony Fauci made comments about “alternative views” of the origin of the coronavirus. But he was really talking about all unorthodox medical information:
“Anybody can claim to be an expert even when they have no idea what they’re talking about—and it’s very difficult for the general public to distinguish. So, make sure the study is coming from a reputable organization that generally gives you the truth—though even with some reputable organizations, you occasionally get an outlier who’s out there talking nonsense. If something is published in places like New England Journal of Medicine, Science, Nature, Cell, or JAMA—you know, generally that is quite well peer-reviewed because the editors and the editorial staff of those journals really take things very seriously.”
Right you are, Tony.
So, Tony, here is a very serious statement from a former editor of one of those “places,” the New England Journal of Medicine:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
And here is another one, from the editor-in-chief of the prestigious journal, The Lancet, founded in 1823:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness…”
“The apparent endemicity of bad research behaviour is alarming. In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world. Or they retrofit hypotheses to fit their data. Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours. Our acquiescence to the impact factor fuels an unhealthy competition to win a place in a select few journals. Our love of ‘significance’ pollutes the literature with many a statistical fairy-tale…Journals are not the only miscreants. Universities are in a perpetual struggle for money and talent…” (Dr. Richard Horton, editor-in-chief, The Lancet, in The Lancet, 11 April, 2015, Vol 385, “Offline: What is medicine’s 5 sigma?”)
Why stop there? Let’s consult a late public-health expert whose shoes Fauci would have been lucky to shine: Dr. Barbara Starfield, Johns Hopkins School of Public Health.
On July 26, 2000, the US medical community received a titanic shock, when Starfield revealed her findings on healthcare in America.
The Starfield review, “Is US health really the best in the world?”, published in the Journal of the American Medical Association (JAMA), came to the following conclusion, among others:
Every year in the US, correctly prescribed, FDA approved medical drugs kill 106,000 people. Thus, every decade, these drugs kill more than a MILLION people.
On the heels of Starfield’s astonishing findings, media reporting was perfunctory, and it soon dwindled. No major newspaper or television network mounted an ongoing “Medicalgate” investigation. Neither the US Department of Justice nor federal health agencies undertook prolonged remedial action.
All in all, those parties who could have made effective steps to correct this ongoing tragedy preferred to ignore it.
On December 6-7, 2009, I interviewed Dr. Starfield by email. Here is an excerpt from that interview.
Q: What has been the level and tenor of the response to your findings, since 2000?
A: The American public appears to have been hoodwinked into believing that more interventions lead to better health, and most people that I meet are completely unaware that the US does not have the ‘best health in the world’.
Q: In the medical research community, have your medically-caused mortality statistics been debated, or have these figures been accepted, albeit with some degree of shame?
A: The findings have been accepted by those who study them. There has been only one detractor, a former medical school dean, who has received a lot of attention for claiming that the US health system is the best there is and we need more of it. He has a vested interest in medical schools and teaching hospitals (they are his constituency).
Q: Have health agencies of the federal government consulted with you on ways to mitigate the [devastating] effects of the US medical system?
A: NO.
Q: Are you aware of any systematic efforts, since your 2000 JAMA study was published, to remedy the main categories of medically caused deaths in the US?
A: No systematic efforts; however, there have been a lot of studies. Most of them indicate higher rates [of death] than I calculated.
Q: Did your 2000 JAMA study sail through peer review, or was there some opposition to publishing it?
A: It was rejected by the first journal that I sent it to, on the grounds that ‘it would not be interesting to readers’!
—end of interview excerpt—
Physicians are trained to pay exclusive homage to peer-reviewed published drug studies. These doctors unfailingly ignore the fact that, if medical drugs are killing a million Americans per decade, the heraldic published studies on which those drugs are based must be fraudulent. In other words, the medical literature is completely unreliable, and impenetrable.
WHICH IS EXACTLY WHAT THE TWO ESTEEMED MEDICAL EDITORS I QUOTED ABOVE—MARCIA ANGELL AND RICHARD HORTON—ARE SAYING.
If you know a doctor who enjoys sitting up on his high horse dispensing the final word on modern medicine, you might give him the quotes from Dr. Angell and Dr. Horton, instruct him to read them, and suggest he get in touch with Angell and Horton, in order to discover what has happened to his profession.
As in: DISASTER.
But please, continue to believe everything Fauci is saying. He must be right about the “pandemic.” After all, he has a very important position, and he’s on television.
So what if his policies have torpedoed the economy and devastated and destroyed lives across the country?
So what if he accepted, without more than a glance, that fraud Neil Ferguson’s computer projection of 500,000 deaths in the UK and two million in the US? In 2005, Ferguson said 200 million people could die from bird flu. The final official tally was a few hundred.
So what?
Fauci has an important position, and he’s on television.
College term paper referenced by Dr. Cowan was actually a published paper by Eleni Papadopulos-Eleopulos, et al. (Dr. Cowan made this correction at the start of a video on the snake venom controversy, streamed on 4/22/2022.)
“The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent
“SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and
animal “coronaviruses” created in the very same way. Attempting to claim any connections between the
random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated
into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place.
Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely
related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines,
the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have
a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a
singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial
evidence that is easily debunked.”
“My story has never been to create fear, panic, and anxiety about water.” He said he told Peters that he believes “there’s actually a snake venom connection to all of COVID-19, and I think that’s the weapon.” – Dr. Bryan Ardis
Summarizing his theory, Dr. Ardis said, “They are using Krait venom and Cobra venom, calling it Covid-19, you’re drinking it, it’s getting into your brainstem and it’s paralyzing your diaphragm’s ability to breathe.”
I really didn’t want to write this article. I was hopeful that people would easily see right through the unsubstantiated claims of Dr. Bryan Ardis that snake venom is the cause of “Covid.” I was hopeful that people would take the time to research the information presented in support of the snake venom theory to see if it held any merit at all. I thought his whirlwind alternative media tour on the who’s who of questionable sources (including the likes of Stew Peters, Mike Adams, and Infowars) would have people questioning why this theory was allowed to be so heavily promoted so quickly. I thought that the fact that the man who created the “Covid” snake venom theory was actually selling his own anti-venom line of supplements would be enough grounds to be skeptical of his motive and his claims.
It seems I was wrong. Just like the baseless vaccine shedding and gain of function/bioweapons narratives, this new snake venom theory has sadly spread through the “Truther” community like wildfire, with many who rightfully challenge the existence of “viruses” clinging to the idea of a new invisible enemy to defeat. They believe that it must be a new toxin. It can’t possibly be the same factors we have seen each and every year leading to disease. This toxin must be hiding in the vaccines, the drugs, and/or even the very water we drink. What these “Truthers” do not realize is that this very line of thinking gives credibility to the idea of a new disease which requires new treatments in order to combat it. This is exactly what the pharmaceutical companies want you to believe.
However, there is NO NEW DISEASE. There is no need for any new or even existing pharmaceutical interventions to treat the same symptoms of detoxification people go through each and every year. In fact, the current treatments can easily be shown to have led to numerous unnecessary deaths. There is no new threat known as “Covid-19” which is being caused by any one factor. The factors leading to the symptoms of disease people are experiencing are multi-causal as they are every year.
Now this is not to say that the vaccines, the drugs, or even the water supply are free of toxins. These are all sources of toxicity and should be investigated as to their composition and effects on our health. However, the theory that there is one factor in all of these sources, i.e. snake venom, and this one factor is leading to the symptoms of disease people are experiencing is, at present time, completely baseless. And it all begins at the very foundation of the fraudulent genome.
The Fradulent Genome
You take that snake or that serpent and you figure out how to isolate genes from that serpent and get those genes of that serpent to insert itself into your God-given created DNA. I think this is the plan all along, was to get the serpents’, the evil one’s DNA, into your God-created DNA.”
He also said genetic sequence testing done on sick patients in Wuhan found their genetic sequence matched two snakes, the Chinese Krait and King Cobra, not bats.”
From Dr. Ardis’ interview with Mike Adams, he supplied the article “Snakes could be the source of the Wuhan coronavirus outbreak” from CNN as his starting point for the “Covid”/snake connection. Within the article, you can see that this claim originates from the fraudulent genomes:
“The researchers used an analysis of the protein codes favored by the new coronavirus and compared it to the protein codes from coronaviruses found in different animal hosts, like birds, snakes, marmots, hedgehogs, manis, bats and humans. Surprisingly, they found that the protein codes in the 2019-nCoV are most similar to those used in snakes.” https://www.google.com/amp/s/amp.cnn.com/
To anyone who actually researched the creation of the original “SARS-COV-2” genome, it is readily apparent that it is a fraudulent computer-generated creation stemming from the unpurified lung fluid of a single patient. The sequenced material could have come from multiple sources, including host DNA/RNA, bacteria, and microbes/microorganisms. It could have even come from outside contamination. There is no way to tell what the origin of the RNA is or even if it was a single source as no particles assumed to be “SARS-COV-2” were ever properly purified and isolated directly from the fluids of the sick patient before being sequenced. Thus, any relation this fabricated sequence has to any other sequence is invalid as the source was never identified to exist as a physical entity to begin with. Considering that the bat and snake “coronavirus” sequences for which the “SARS-COV-2” sequence was then compared to also come from unpurified sources, it is easy to see that any claims as to the origins of the sequenced material is a horrible foundation to build upon for an origin theory of a nonexistent “virus” and/or disease.
Even if this snake-venom connection was valid, the enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom. These peptides are “almost identical” to the venoms of animals and yet they are regularly found in healthy humans and other mammals. From his own source:
Like Venom Coursing Through the Body: Researchers Identify Mechanism Driving COVID-19 Mortality
“Researchers from the University of Arizona, in collaboration with Stony Brook University and Wake Forest School of Medicine, analyzed blood samples from two COVID-19 patient cohorts and found that circulation of the enzyme – secreted phospholipase A2 group IIA, or sPLA2-IIA, – may be the most important factor in predicting which patients with severe COVID-19 eventually succumb to the virus.
The sPLA2-IIA enzyme, which has similarities to an active enzyme in rattlesnake venom, is found in low concentrations in healthy individuals and has long been known to play a critical role in defense against bacterial infections, destroying microbial cell membranes.”
Thus, the snake enzymes are in fact normal human enzymes that are regularly found in healthy individuals. There is no mystery as to why these would be present in a sample. We should be able to put this “Covid” snake venom nonsense to bed right here. However, let’s press on a see what else we can uncover.
Antivenom = Monoclonal Antibodies
One thing I will give Dr. Ardis credit for is spotlighting the connection between the creation of antivenoms with the creation of monoclonal antibodies. The processes for both are very similar and the desired outcome is the exact same: the creation of theoretical antibodies. In the case of snake antivenom, it is normally created by a series of injections of the venom of a snake into an animal and then collecting the blood after a period of time. This is usually done through horses but other animals can be used as the host as well. Thus, the antivenom used for a snakebite victim is typically an injection of horse blood.
Both of these therapies have their basis in animal blood and the creation of the theoretical antibodies. Both are associated with toxic side effects. Sadly, while he was originally right about the fact that monoclonal antibodies are toxic and should not be used to treat the symptoms now collectively known as “Covid,” Dr. Ardis changed his tune when another doctor texted him asking if he would use antivenom for a snake bite:
“Last December, Dr Bryan Ardis received a text message from an Emergency Room physician friend of his that sent him down an unexpected and bizarre rabbit hole that may explain the adverse events from the vaccines that we’ve been reporting. The text read: “Hey Dr Ardis…If you got bit by a rattlesnake, would you go to a hospital and get anti-venom?”
“He says, “I realized, all of a sudden, monoclonal antibodies ARE anti-venom. The Federal Government doesn’t want us using anti-venom. Why are they fighting anti-venom and why are we finding anti-venom works against COVID? Is it not a virus? Is it a venom? This is what I want to know: Is COVID a venom and is this why they don’t want you using monoclonal antibodies?”
Do you see the trick? They want you to equate monoclonal antibodies with antivenom. This is supposed to be an “aha” moment where you realize that there is no way that you would not inject antivenom (i.e. horse blood) into yourself if bitten by a snake. It’s a no-brainer, right? We have all seen the movies where a person is bitten by a venomous snake and quickly dies if not given the antivenom.
If you are willing to accept the injection of horse blood into your body to survive a snake bite, why wouldn’t you also inject the cancer-cell cultured blood of genetically altered mice in order to combat “Covid?”
As Dr. Ardis points out, monoclonal antibodies are essentially antivenom. However, he wrongly states that monoclonal antibodies are an effective therapy. According to a September 2021 Cochrane review of the available studies, they found insufficient evidence to claim that monoclonal antibodies are an effective treatment for “SARS-COV-2:”
Are laboratory-made, COVID-19-specific monoclonal antibodies an effective treatment for COVID-19?
“The evidence for each comparison is based on single studies. None of these measured quality of life. Our certainty in the evidence for all non-hospitalised individuals is low, and for hospitalised individuals is very low to moderate.We consider the current evidence insufficient to draw meaningful conclusions regarding treatment with SARS-CoV-2-neutralising mAbs.”
In other words, the evidence for the usefulness of monoclonal antibodies is non-existent. Unfortunately, the Cochrane Review failed to point out that there are various risks and adverse reactions associated with their use:
Do mAbs have risks?
“Therapeutic mAbs, typically administered by intravenous (IV) infusion, have been a valuable and generally safe treatment option for a variety of conditions for many years. However, they are also known to cause a range of side effects and reactions, which can be immediate or delayed.Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity.”
In January 2022, the FDA restricted the use of some monoclonal therapies (Bamlanivimab and Etesevimab) that are authorized against “Covid-19” as they were shown to be ineffective:
Coronavirus (COVID-19) Update: FDA Limits Use of Certain Monoclonal Antibodies to Treat COVID-19 Due to the Omicron Variant
“In light of the most recent information and data available, today, the FDA revised the authorizations for two monoclonal antibody treatments– bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
Because data show these treatments are highly unlikely to be active against the omicron variant,which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. And like other infectious organisms, SARS-CoV-2 can mutate over time, resulting in certain treatments not working against certain variants such as omicron. This is the case with these two treatments for which we’re making changes today.”
On April 16th, 2022, the FDA revoked the use of Bamlanivimab alone as it’s benefits were shown not to outweigh its risks. Somehow despite this evidence, the FDA still allows for it to be used in combination with Etesevimab, even though they previously revoked their use together in January 2022:
Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab
“Today, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate COVID-19 in adults and certain pediatric patients. Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of SARS-CoV-2 viral variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure,the FDA has determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use. Therefore, the agency determined that the criteria for issuance of an authorization are no longer met and has revoked the EUA.
On Nov. 9, 2020, based on the totality of scientific evidence available at the time, the FDA issued an EUA to Eli Lilly and Co. authorizing the emergency use of bamlanivimab alone for the treatment of mild to moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progressing to severe COVID-19 and/or hospitalization. Importantly, although the FDA is now revoking this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone. The FDA believes that these alternative monoclonal antibody therapies remain appropriate to treat patients with COVID-19 when used in accordance with the authorized labeling based on information available at this time.”
If the FDA’s confusing revoking of the EUA’s of these monoclonal antibodies has you concerned that you will not be able to use them against an imaginary “virus,” don’t worry. The FDA authorized the use of a new “Omicron-specific” monoclonal antibody called Bebtelovimab on February 11th, 2022. Granted, it still carries the same risks, adverse side effects, and uncertainty over clinical worsening listed for the previously ineffective antibody therapies. From the FDA fact sheet:
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
“Possible side effects of bebtelovimab include itching, rash, infusion-related reactions, nausea and vomiting. Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other SARS-CoV2 monoclonal antibodies and could occur with bebtelovimab. In addition, clinical worsening following administration of other SARS-CoV-2 monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19.”
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
Hypersensitivity Including Anaphylaxis and Infusion-Related Reactions: Serious hypersensitivity reactions, including anaphylaxis, have been observed with administration of other SARS-CoV-2 monoclonal antibodies and could occur with administration of bebtelovimab. If clinically significant hypersensitivity reactions occur, discontinue and initiate appropriate supportive care. Infusion-related reactions may occur up to 24 hours post injection. These reactions may be severe or life threatening. (5.1)
Clinical Worsening After SARS-CoV-2 Monoclonal Antibody Administration: Clinical worsening of COVID-19 after administration of SARS-CoV-2 monoclonal antibody treatment has been reported and may include signs or symptoms of fever, hypoxia or increased respiratory difficulty, arrhythmia (e.g., atrial fibrillation, sinus tachycardia, bradycardia), fatigue, and altered mental status. Some of these events required hospitalization. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19. (5.2)
Limitations of Benefit and Potential for Risk in Patients with Severe COVID-19: Treatment with bebtelovimab has not been studied in patients hospitalized due to COVID-19. Monoclonal antibodies, such as bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with COVID-19 requiring high flow oxygen or mechanical ventilation. (5.3)
It should be fairly clear that, unlike Dr. Ardis’ claims, monoclonal antibodies are not effective, carry numerous risky side effects, and can actually worsen the disease they are supposed to treat. Interestingly, this same risk of dangerous side effects and worsening disease outcomes is associated with snake antivenom as well. From the fact sheet of a commonly used antivenom for rattlesnake bites, we find these admitted side effects:
Rattlesnake Antivenin Side Effects Center
“Rattlesnake Antivenin (antivenin crotalidae polyvalent) is an antivenin product used only to treat envenomation caused by bites of crotalids (pit vipers) including rattlesnakes, copperhead and cottonmouth moccasins, and others. Common side effects of Rattlesnake Antivenin include allergic reactions such as flushing, itching, hives, swelling of the face/tongue/throat, cough, shortness of breath, blue color to the skin, vomiting, and anaphylaxis (severe allergic reaction).”
“Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered. An immediate reaction (e.g. shock, anaphylaxis) usually occurs within 30 minutes. Symptoms and signs may develop before the needle is withdrawn and may include apprehension, flushing, itching, urticaria; edema of the face, tongue, and throat; cough, dyspnea, cyanosis, vomiting, and collapse. There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use.”
“Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered.30 The incubation period may be less than 5 days, especially in those who have received horse-serum-containing preparations in the past. The usual symptoms and signs are malaise, fever, urticaria, lymphadenopathy, edema, arthralgia, nausea, and vomiting. Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis. Peripheral neuritis usually involves the shoulders and arms. Pain and muscle weakness are frequently present, and permanent atrophy may develop.”
Maybe the use of antivenom to treat a snakebite isn’t the super cure it has been sold to be? Is it possible that, as with many pharmaceutical products and interventions, the antivenom itself is creating the very symptoms it is said to treat? For some further insight, let’s look at a few highlights from an paper from September 2019, right before this “crisis,” which reviewed the use of antivenom and had a few revealing claims about the “anti” toxin. You will see it reiterated that the injection of antivenom created from either horse, sheep, goats, and/or rabbits can cause immediate hypersensitivity and anaphylaxis or a delayed “serum sickness” which can occur weeks after the treatment. It is stated that the antivenom has limited efficacy and can be entirely ineffective based on the geographic location. Improper use of antivenom contributes to increased servere outcomes and the production of antibodies in animals leads to a large number (70%) of immunoglobulins that do not react to snake venom:
Perspective on the Therapeutics of Anti-Snake Venom
3. Current Information in the Design of New Antivenoms
“Currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses [14,15]. Hyperimmunized animals produce antibodies against the venom proteins and serum is extracted from their blood for the treatment of envenomation [6,16]. Conventional serum therapy aims to bind and neutralize the snake venom proteins [17]. It is a fact that the antivenom allows the body to try to reverse the damage caused by the venom. However, it is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia. Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects [18];
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability;
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes;
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both.
“Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom. Around 70% of the immunoglobulins obtained do not act directly against venom toxins [26]. Despite the abovementioned facts, this is the only FDA approved therapy to treat snake venom.”
A few other studies also point out the severe reactions regularly attributed to the use of antivenom. The first is a study from 2016 which points out that not only are adverse reactions common, they occur at a high rate. It is stated that this is due to poor quality control and manufacturing problems:
Adverse reactions to snake antivenom, and their prevention and treatment
“Antivenom is the mainstay of treatment of snakebite envenoming. However, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent. Both acute (anaphylactic or pyrogenic) and delayed (serum sickness type) reactions occur. Acute reactions are usually mild but severe systemic anaphylaxis may develop, often within an hour or so of exposure to antivenom. Serum sickness after antivenom has a delayed onset between 5 and 14 days after its administration. Ultimately, the prevention reactions will depend mainly on improving the quality of antivenom.”
“The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors. This highlights the importance of addressing issues related to poor quality and potentially unsafe antivenom. Ultimately, the prevention of reactions will depend mainly on improving the quality of antivenom. Until these improvements take place, doctors will have to depend on pharmacological prophylaxis as well as careful observation of patients receiving antivenom in preparation for prompt management of acute as well as delayed reactions when they occur.”
This next source is from 2018 and it points out that early antivenoms were unsafe and caused severe life-threatening events. While they now have “acceptable” safety profiles, antivenoms still have varying quality and range from 10% adverse reactions to greater than 50%. This same variation in quality is seen in the production of monoclonal antibodies:
Antivenom therapy: efficacy of premedication for the prevention of adverse reactions
“However, in their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects [8]. The main reason was that first antivenoms were poorly purified preparations or crude sera. Over the years, for many of the original applications, heterologous serums were replaced by other drugs with better safety profiles, such as antibiotics, vaccines and homologous serums. However, in cases of envenomation by snakes, scorpions or arachnids, antivenoms remain the only effective treatment [4]. Currently, after many improvements, antivenoms exhibit acceptable safety profiles [1, 9, 10]. Nevertheless, antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50% [11, 12].”
In is interesting to note that there are many factors that are said to influence the severity of a venomous snakebite including the age, sex, and health of the person bitten as well as the type of snake, the geographical location of the snake, the season the bite occurred in, what the snake ate, and how recently the snake released its venom. Antivenoms themselves have been shown to have varying effects in quality due to the geographical location of the snake which somehow renders the antivenom ineffective and even dangerous in different countries and continents, even against the same type of snake. It is said that this has kept locals from seeking out medical care and sticking to traditional healers:
“Snake venoms are highly complicated. At least 26 separate enzymes have been identified with 10 of these enzymes common to all snake venoms (though in different concentrations). All snake bites are not equal. The quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously.”
“A study led by Dr Fry has found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions.
Researchers tested the effectiveness of two African and two Indian saw-scaled viper antivenoms against saw-scaled vipers from 10 regions.
The results showed that the two African antivenoms were only effective against snakes from restricted ranges.
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers.
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regions. It failed completely against African saw-scaled vipers.
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry says.
“In Kenya, snakebite deaths have increased dramatically after hospitals switched supplies of a very effective African antivenom with a cheaper Indian variety.”
“This creates a knock-on effect in these communities. It’s hard enough to convince people living in these regions not to go to traditional healers to treat snakebite. And if someone does seek proper medical care but dies because of ineffective antivenom, it will be even harder to convince the next victim to seek out antivenom.”
Viper venom’s lethal evolution
It’s the variety of the saw-scaled viper’s prey, from rodents to insects, that researchers say could be the reason why antivenom from one region might not work in another.
“Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes,” UQ PhD candidate in Toxinology Bianca op den Brouw wrote in an article for The Conversation.
“Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet.
“Different saw-scaled viper populations feed on different prey. The physiology of these prey animals differs, and this dictates what makes a toxin effective.
“From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom.”
Maybe the proceeding information on how snakebite antivenoms are created as well as the high rate of adverse events from the antibodies used for antivenom now has you questioning that initial “no-brainer” thought: “Of course I would use antivenom if bit by a snake.” If so, you are on the right track as, based on information from the African Snakebite Institute, in most snake bite cases, antivenom is not used and many snake bites are often unattended and/or unreported. In fact, it is apparently a well-known “myth” (i.e. truth in this case) that the antivenom kills more people than the snake venom itself. Most people (over 80%) never receive antivenom as, like the previous sources stated, it can have disastrous side-effects. Most snake bites do not cause symptoms warranting the use of something so toxic. In fact, snake bite victims are not immediately injected with antivenom and typically are sent home after observation:
“Yet people often have a poor understanding of how it works and there are endless myths about antivenom killing more people than the snake venom itself.”
“Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite) as most victims are not severely envenomated or the bite may be from a snake that is not considered potentially deadly or is not covered by the antivenom (Rhombic Night Adder, Berg Adder and Stiletto Snake). Antivenom is relatively scarce, expensive and can have disastrous side-effects. The biggest danger is an acute allergic reaction (anaphylaxis) or, to a lesser degree, serum sickness that can affect the immune system several days after treatment.”
“Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use. The majority of snakes have control over their venom glands and are quite reluctant to waste their venom on humans. They very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious. Such patients are usually hospitalised for a day, carefully monitored and then sent home.”
“As already mentioned, some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used. Some of those victims go into anaphylactic shock which is a life-threatening medical condition and must be treated with adrenaline. This has to do with the fact that our antivenom is made from horse blood and the allergy is basically an allergy to horse proteins.”
Bill Haast – repeated snake bite victim from the world’s deadliest snakes tragically died at the young age of 100 from natural causes. ?
If snake bites regularly do not cause symptoms and do not require the use of antivenom, are snake bites really as toxic and harmful as we previously thought? Are the dangerous side effects linked to snake bites really just the reactions to having horse blood injected into the body as treatment? Is this another case where the treatment causes the symptoms of disease it was supposed to prevent? If the examples of these next few individuals are taken into consideration, it’s entirely plausible to conclude that we have been misled about the dangers stemming from snakebites in order to cover for the toxic effects of the treatment:
Repeated snake bite for recreation: Mechanisms and implications
“There is a debate in the fatality/immunity due to repeated snake bites in human beings either accidentally or incidentally. Haast and Winer[11] reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus[11] and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier.”
This snake-man got himself bitten over 200 times to become immune to venom
“Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was fatally injured about 20 times.”
“In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times as per the report published in Today I Found Out.“
Man makes deadly snakes bite him 160 times in hunt for human antidote
“An amateur scientist has deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom.
Tim Friede is obsessed by finding a human antidote to poisonous snake bites, which kill an estimated 100,000 people every year.
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra.
He said he experienced a “real throbbing sensation” but he “felt great” after the bites.
“It really hurts and it swells but that’s it,” he said.”
Poison pass: the man who became immune to snake venom
“A lot has been written about Steve Ludwin, widely known as the man who injects snake venom, and lately his life has turned into a non-stop frenzy of international journalists and film crews revelling in the seeming sheer insanity of it.”
“He’s been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years. “Snakes are fucking everywhere. The symbol for medicine is two snakes. They’re ingrained in our brain and DNA,” he tells me, proudly insisting that he hasn’t been ill for decades and has developed “a superhuman immune system”. And it’s tempting to believe him. He does look undeniably fit.”
The Photographer Who Was Bitten by a Black Mamba… and Got the Shot “After several minutes and then hours passed and Laita was still feeling fine — experts recommend heading straight for a hospital, by the way — the crew concluded that Laita didn’t have any venom in his system. The photographer believes that it was either a “dry bite,” when a snake doesn’t release any venom, or that his heavy flow of blood pushed out the venom.”
As can be seen, there are numerous examples of people being deliberately and accidentally bitten by the world’s deadliest snakes who are completely fine and do not require treatment from antivenom whatsoever. Are we to conclude that these people are the lucky few who somehow have amazing super-human “immune” systems that render snake venom ineffective? Or have snake bites and the associated symptoms of venom toxicity been blown out of proportion? Could this be a case where some have had bad reactions to a snake bite just as there are those who have severe allergic reactions to bee stings while the majority of snake bite and bee sting victims come away unscathed? Could this be similar to the supposed rabies cases where the majority of those who were bitten by “rabid” animals actually went on to be just fine without getting the rabies vaccination?
The Treatments Are Worse Than the Disease
It’s very apparent that in the case of monoclonal antibodies and anivenom, the adverse effects of the drugs are actually worse than the supposed diseases they are meant to treat. Could this be due to the fact that, like “viruses,” so-called antibodies have never been properly purified, isolated, and proven to exist? The results of studies using antibodies are regularly unreproducible and irreplicable. It is well-known that antibodies are in fact not as specific as are they are claimed to be and are said to regularly bind to the wrong proteins. Perhaps it is difficult to produce safe and effective products when the entities that are supposed to be produced and supplied in the animal blood are entirely theoretical? Maybe the ridiculous snake venom theory should be viewed in the context that it is a bad idea to be injecting anything, let alone animal blood, into our bodies in an attempt to make ourselves feel better when trusting the body and allowing it to heal is often times the best course of action we can take.
In Summary:
Dr. Bryan Ardis put forth a theory that snake venom is the cause of “Covid-19” primarily based on fraudulent genomic data
The snake connection stems from research linking proteins from the fabricated “SARS-COV-2” genome to bat and snake “coronavirus” proteins
The enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom
These peptides are “almost identical” to the venoms of animals and are regularly found in healthy humans and other mammals
Dr. Ardis pointed out that, based on a text, he uncovered the connection between antivenom and monoclonal antibodies and stated that theyare the same thing
He wrongly concluded that monoclonal antibodies are an effective treatment for snake poisons that could be in the vaccines, Remdesivir, and water
According to a Sept 2021 Cochrane Review, their certainty in the evidence for the use of monoclonal antibodies in the treatment of “Covid” for all non-hospitalised individuals was low, and for hospitalised individuals was very low to moderate
They considered the current evidence insufficient to draw meaningful conclusions regarding treatment with “SARS-CoV-2-neutralising” mAbs
Monoclonal antibodies are known to cause a range of side effects and reactions, which can be immediate or delayed
Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity
In February 2022, the FDA revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments
The data showed these treatments are highly unlikely to be active against the omicron variant which is circulating at a very high frequency throughout the United States
These treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens
In April 2022, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate “COVID-19” in adults and certain pediatric patients
Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of “SARS-CoV-2 viral” variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure, the FDA determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use
Importantly, although the FDA revoked this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone
In other words, the use of Bamlanivimab and Etesevimab was revoked as well as the use of Bamlanivimab but they can still be used together as an alternative to Bamlanivimab alone…
For the Omicron-specific Bebtelovimab authorized by the FDA in February 2022, possible side effects include
Itching
Rash
Infusion-related reactions
Nausea
Vomiting
Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other “SARS-CoV2” monoclonal antibodies and could occur with bebtelovimab
In addition, clinical worsening following administration of other “SARS-CoV-2” monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab
The FDA claims that it is not known if these events were related to “SARS-CoV-2” monoclonal antibody use or were due to progression of “COVID-19”
Treatment with Bebtelovimab has not been studied in patients hospitalized due to “COVID-19”
Monoclonal antibodies, such as Bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with “COVID-19” requiring high flow oxygen or mechanical ventilation
Antivenom carries the same risks of severe side effects and worsening condition as monoclonal antibodies
The listing for common side effects of Rattlesnake Antivenin include allergic reactions such as:
Flushing
Iitching
Hives
Swelling of the face/tongue/throat
Cough
Shortness of breath
Blue color to the skin
Vomiting, and anaphylaxis (severe allergic reaction)
Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered
There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use
Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered
The usual symptoms and signs are:
Malaise
Fever
Urticaria
Lymphadenopathy
Edema
Arthralgia
Nausea
Vomiting
Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis
Peripheral neuritis usually involves the shoulders and arms and pain and muscle weakness are frequently present, and permanent atrophy may develop
A 2019 review on antivenom stated that currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses
It is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia.
Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both
Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom
Around 70% of the immunoglobulins obtained do not act directly against venom toxins
According to a 2016 study, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent
The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors
The prevention of reactions will depend mainly on improving the quality of antivenom
According to their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects
Currently, after many improvements, antivenoms exhibit “acceptable” safety profiles yet antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50%
All snake bites are not equal and the quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously
A study led by Dr. Fry found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions
The results showed that the two African antivenoms were only effective against snakes from restricted ranges
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regionand it failed completely against African saw-scaled vipers
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry said
If someone does seek proper medical care but dies because of ineffective antivenom,it will be even harder to convince the next victim to seek out antivenom
Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes
Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet
From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom
There are endless myths about antivenom killing more people than the snake venom itself
Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite
Antivenom is relatively scarce, expensive and can have disastrous side-effects
Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use
Snakes very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious
Such patients are usually hospitalised for a day, carefully monitored and then sent home
Some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used
This has to do with the fact that antivenom is made from horse blood and the allergy is basically an allergy to horse proteins
Haast and Winer reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier
Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was seriously injured about 20 times
In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times
An amateur scientist named Tim Friede deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra
He said he experienced a “real throbbing sensation” but he “felt great” after the bites
Steve Ludwin, widely known as the man who injects snake venom, has been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years
He hasn’t been ill for decades and has developed “a superhuman immune system”
A photographer was bit by the deadliest snake, a Black Mamba, and after hours passed, he was still feeling fine and needed no treatment
The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent “SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and animal “coronaviruses” created in the very same way. Attempting to claim any connections between the random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place. Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines, the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial evidence that is easily debunked.
If we are to take the claims of Dr. Ardis seriously that the symptoms associated with snake venom is the true cause of a disease known as “Covid-19,” how does his theory explain for the fact that the antivenom and monoclonal antibody treatments cause the exact same symptoms of the disease they are supposed to treat? How would it be determined that the worsening clinical outcomes after injection are from the snake bites/venom rather than the antivenom/monoclonal antibodies given as treatment? How does his theory account for the numerous instances where people have been deliberately bitten by snakes, injected with the venom of snakes, and drank of the venom of the snakes with little to no harmful effects whatsoever? How does his theory account for the fact that the vast majority of “Covid” cases are asymptomatic and the vast majority of snake bite cases need no treatment at all? There are many holes in this theory which will easily be picked apart to make those who follow it look foolish for having done so.
There is no “SARS-COV-2.” There is no “Covid-19.” There is no new disease nor any new symptoms of disease requiring treatment from vaccines, monoclonal antibodies, Remdesivir, Hydroxychloroquine, Ivermectin, NAC, nor any other treatment. There is no need for any anti-venom supplements.
Beware those who will sell you the cause of the disease and the solution.
What type of contamination might be found in a spiked COVID vaccine?
“A foreign body.”
The lot is being recalled due to a foreign body being found in one vial in the lot manufactured at the company’s contract manufacturing site, ROVI – Moderna and ROVI Pharma Industrial Services
Moderna Pharmaceutical, formerly named ModeRNA Therapeutics, became a public company in 2018, specializing in infectious diseases. Prior to the IPO, AstraZeneca was its third-largest investor.
Moderna’s coronavirus shot, known as “SPIKEVAX,” was said to have been approved by the U.S. Food and Drug Administration (FDA) for adults 18 and older on Jan. 31, 2022. But according the the FDA Factsheet, the shot is still only Emergency Use Authorized or EUA. Not approved!
Since November 2020, two of the 4 Biotech companies working to manufacture mRNA “therapies,” — Johnson & Johnson and AstraZenica — had to halt trials over safety concerns. And now the spotlight shines on Moderna’s mRNA vaccine deployment in Europe.
The contaminated lot in question was manufactured at the ROVI site in Spain, and distributed in Norway, Poland, Portugal, Spain, and Sweden from 13-14 January 2022. Reports tie the recalled batches to the Spanish company, ROVI.
Criminal Acts
Will Moderna be investigated for fraud, product safety, death by vaccine?
In February 2021, US officials investigated and acknowledged a “likely association” between Moderna and Pfizer vaccines and myocarditis in adolescents and young people. Of course, the PREP Act and CARES Act both limit liability for death or serious physical injury resulting from these products. See also Moderna’s disclosure in the SPIKEVAX package insert, referencing Myocarditis and Pericarditis, Section 5.2.
All Phase 3 COVID-19 vaccine trails are ongoing and not due to conclude until late 2022/early 2023. The treatments are currently experimental with only 1 year of short-term data and no long term safety data available.
In November 2020 Dr Andreas Noack, a German chemist and one of the EU’s top graphene experts, released a video explaining that he had discovered graphene hydroxide contained in the COVID-19 experimental treatments. He described how the graphene hydroxide nano structures injected into the human body act as ‘razor blades’ inside the veins of recipients and how they would not show up on an autopsy or normal toxicology tests given their atomic size. On 26th November 2021, just hours after publishing his latest video about graphene hydroxide, he died in suspicious circumstances. [See Summary].
Professor Dr Pablo Campra, University of Almeria, Spain also examined Covid-19 experimental treatments in November 2021 using Micro-Raman Spectroscopy, the study of frequencies. He also confirmed the presence of graphene oxide.
Today’s high drug prices show little has changed since 1963, when The Federal Trade Commission ruled that six of the nation’s largest drug companies were conspiring to fix prices on tetracycline, the most widely used antibiotic. The Kefauver drug hearings confirmed the existence of a national crime syndicate and revealed lax enforcement that continues to this day. Note, one of the “big six” criminals, Wyeth Pharmaceuticals, was absorbed by Pfizer.
Gene Therapy or Gene Reset?
Experts contend that the technology in the Pfizer/BioNTech and Moderna shots are not “gene therapy.” But that is not how the experimental products had first been marketed.
According to a November 2021 article at LifeSiteNews, during the 2021 Global Health Summit in Berlin, Bayer executive, Stefan Oelrich, told fellow “experts” that the mRNA COVID “vaccines” are actually “cell and gene therapy” that would have otherwise been rejected by the public if not for a “pandemic” and favorable marketing.
Oelrich also highlighted the term, “Bio Revolution” as:
a confluence of advances in biological science and accelerating development of computing, automation, and artificial intelligence [that] is fueling a new wave of innovation.
As part of his company’s role for “sustainability” Bayer also pledged to push contraception on 100 million women across the world. This rhetoric fits hand-in-glove with Klaus Schwab’s Socialist plan for the “Great Reset.”
Damage from the mRNA injectables are surfacing. According to an October 2021 study in the American Journal of Cardiology:
Sixty percent of the myocarditis related COVID-19 vaccine cases were associated with the Pfizer-BioNTech vaccine, 33% were associated with the Moderna vaccine, and 7% were associated with the Johnson & Johnson vaccine.
According to a November 2021 abstract published in the Journal Circulation titled, “Observational Findings of PULS Cardiac Test Findings for Inflammatory Markers in Patients Receiving mRNA Vaccines:”
…the mRNA vacs numerically increase all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle…
Ignorance Is No Excuse
Ignorance is no excuse in the Age of Information. As more information surfaces, do not expect drug companies to change their criminal ways.
The information is available and viewable for anyone who can do a Google search. Drug companies have subtly disclosed the information if you can read about it here.
If any change will come of these revelations, that change rests with each of us. There are no “good” or “bad” experiences. There is only “experience” from which we all choose to learn more.
Exemptions are privileges. What the government giveth, the government can taketh away.
Rights are not gifts from government. – Nature of Healing
The Ruse of Benefits & Privileges
Government laws exist to grant “BENEFITS and PRIVILEGES” to citizens who agree to be governed. Benefits and privileges do not usurp birthrights, rights that are inborn or inherent. Thus, birthrights supersede laws, mandates, and exemptions.
A government exemption is an “opt out.” By asking permission of government to opt out from any government-imposed health mandates, you agree to bypass birthrights.
Under exemptions, you are requesting permission from government to make a choice that you already possess. Remember, bodily autonomy is a BIRTHRIGHT. You come into this world alone. You leave this world alone, without government approval. Therefore, an exemption or an Exemption Act, is a form of entrapment known as Color of Law.
Color of law refers to an appearance of legal power to act that may operate in violation of law. Since the inception of the United States in 1776, both presidents and governors have been bypassing the laws through illegal Executive Orders (E.O.s) under Color of Law. Even though it might be argued that ALL federal Acts fall under the Color of Law, the chances of adjudicating an equitable solution through the court system is about as likely as isolating the Coronavirus in a lab. The CDC still admits there is no gold standard for the isolation of any virus.
So it is by the will of the people that allows government to usurp its authority and ensure the end of freedom of choice for all. In the near future, in order to attain an education, or maintain a job, to enter a hospital or clinic, to shop or travel, in order to live within any community, or function on any practical level within society, people will be made to get government shots.
The Ruse of Exemption
Have you been told to get a medical or religious exemption by your employer? Think again.
Government-granted exemptions for government-imposed health mandates are strategically designed to fail by entrapping those members of the community who sign onto them. Why?
Because here is no legal defense or enforcement for religious or medical exemptions since businesses have no legal duty of care from imposing mandates in the first place, based on the The Doctrine of Assumption of Risk.
The Doctrine of Assumption of Riskstates that no business is liable to protect others from a risk that’s widely known or believed to exist in the community.
An exemption means there has to be a legal duty of care. If there is no legal duty, there is no exemption. A legal duty is a legal obligation, the breach of which can result in liability. Businesses that impose mandates must have an insurance policy. Without one, no court will take jurisdiction. A plaintiff in court will never win. This is another reason you do not have to beg for a right you already possess.
In addition, laws cannot conflict with each other. So, for instance, when mandates, statutes, Acts, or Executive Orders conflict with the Americans with Disabilities Act (ADA), then there is a violation of the legal duty of care.
Federal (statutory) Acts attempt to protect “the public health” with “statutory rights.” Beware: A “statutory right” is an oxymoron, similar to public health, safe vaccine, and honest thief. It is meant to confuse.
All federal Acts steer “the public” into a herd by the language of legalease. In reality, there is no such thing as “Public Health.” Public Health does not exist outside of individual health. You cannot wear a life jacket to keep others afloat. So to consent to “Public Health mandates” is to give up bodily autonomy in exchange for Public Rights (i.e., Children’s rights, Gay rights, Parent rights, Women’s rights) granted by the State. State Rights can be modified, suspended, and revoked. See how California revoked all vaccine-related exemptions. By taking the Public out of Public Health, we begin to reclaim responsibility for choice and freedom.
The success of any Act depends from which perspective you view its success. From the first Act, passed in 1784, to the latest draft government Acts, ALL Acts appear to be an extension of The CIRCUS Act. From the people’s perspective, success rates are dismal thanks to exemptions and exceptions to exemptions in every Act. A few examples include:
The US PATRIOT Act of 2001 and US Patriot and Reauthorization Act of 2005 “to unite and strengthen America,” with exemptions to banking agencies which serve to divide and weaken America.
The PREP Act of 2005, allows government to bypass Rights and Freedom. The DHHS Amended Version authorizes an increased workforce to administer COVID (experimental) vaccines. And The PREP Act 2022 – limits liability for COVID countermeasures.
Note also, that any discussion of science for “public health” purposes is a purposeful distraction away from inherent rights. Do not be distracted by the vaccine debate or by the Vaxxed vs. Unvaxxed study that will never be formally approved by government. The science debate is merely a ruse to eliminate freedom.
Contagions and The American With Disabilities Act
John Jay Singleton, of TheZunga, helps people to exercise their RIGHTS to bodily autonomy under the ADA. TheZunga.com endeavors to extract people caught in the government web of exemptions under COVID19 policies. Singleton writes:
Having a contagious disease is defined as having a disability under the Americans with Disabilities Act. The Rehabilitation Act, under the standards of the Americans with Disabilities Act, precludes employers from imposing any accommodations upon employees unless they meet the criteria for establishing that the employee is a direct threat following an individualized assessment (diagnosis). Employers are prohibited by law from requiring any medical examination in this process as it is an accommodation for which the employer must advise the employee that he has the right to accept or refuse
Singleton contends that the ADA, a federal law, requires businesses to aid and encourage those with disabilities in the exercise and enjoyment of their rights. This means that not only can a business owner not impose such measures on anyone, he must actively protect everyone from any violation of this law, at least by not imposing them.
To exercise and enjoy your rights doesn’t mean you have to have a disability. It means you’re regarded as having a disability. If you’re regarded as having a disability its because the government announced a public health disaster, so the legal duties come into play with the ADA. And the legal duty of care is on anyone trying to force these measure on you. John Jay Singleton
In summary, exemptions bind people to an arbitrary, and a constantly changing, list of demands. These demands supersede basic freedoms, and thereupon deny people of their inalienable, God/life given rights to self-determination of their bodies. As the government giveth, so, too, can the government taketh away, on a whim.
No Consent
Governments have inverted inherent rights by statutes, policies, Acts, E.O.s and exemptions. In doing so, they have bound freedom, itself, to a contract. All government Acts apply to government entities and persons; not to men and women. Men and women are not subject to Acts, because they are not subjects.
Exemption or no exemptions, the power of NO always applies, as long as you can voice it. One way to say No Thank You is through a Conditional Acceptance, a lawful response to any offer to contract. Can they sign a statement agreeing to your conditions to their offer? If not, there is no contract and you remain in honor. See more at Youarelaw.org.
All Acts attempt do one thing: to allow the government to legislate choice and freedom, that is, if you consent to the offer. However, if offered an experimental product, make sure you are provided with Informed Consent (45 CFR § 46.116) before you consent, because you become a subject taking part in a clinical study.
When it comes to any mandate, it is important to appreciate that all exemptions (medical, religious, or philosophical/personal belief), are fundamentally illegal, because they transpose an inherent human RIGHT into a PRIVILEGE, on the presumption that you acknowledge, and thus sacrifice or forfeit your natural BIRTHRIGHTS to an external authority.
For instance, there is no American authority for compulsory vaccination, in the sense of forcing one to submit even if policies require compliance. When it comes to commerce, everything is an offer to contract. When it comes to Acts, All the world is a stage.
Shakespeare titled his play, As You Like It, as if to say, you always have a choice. There is no law that compels anyone to do anything related to mandated restrictions, whether COVID-related or not. The freedom to choose is non-negotiable. You always have options just like you have opinions. However, in this era, freedom must be defended and claimed as a BIRTHRIGHT.
Do you trust a government calling the shots under the ruse of exemptions? Now is the time to seize your courage, to wake up, to rise up and to find your will to act for yourself. As always, freedom lives in you!
Airplane leaving jet contrails with COVID-19 word inside. Symbolizing the global spread of the coronavirus through global air traffic.
A few months ago, I wrote an article exploring the connection between the symptoms of disease known as “Covid-19” and air pollution. While air pollution is not the only factor currently causing disease, I laid out why I believe that this is the most likely explanation for any perceived increase in respiratory symptoms of disease. I provided a general overview on the problem of air pollution and how it can impact our health and environment. Within the article, I touched upon the issue of persistent contrails, a.k.a. chemtrails, and provided information directly from Government sources admitting the impact that these trails have on our health and environment. Even though this information is readily available to anyone willing to look, there are many out there who still seem to believe that these trails are harmless. They claim that I am promoting nothing but a baseless conspiracy theory.
The fact of the matter is that these trails are admitted to be harmful to our health and environment by both sides of the “chemtrail” debate. There is no conspiracy theory here. This is a FACT. We can speculate as to who is doing this and why but that is ultimately irrelevant. While pollution from automobiles, factories, power plants, forest fires, etc. all contribute to this air pollution health crisis, the harmful effects from the aviation industry are regularly glossed over and/or omitted when this issue is discussed. However, if you dig deep enough and actually search for the information, what can be found to be admitted by official Government sources regarding the health consequences from these trails is very telling and disturbing.
To start with, I want to provide a quick breakdown of the negative health impact of just one component that is admitted to be found within these persistent trails left in the wake of aircrafts. This is known as particulate matter, the most dangerous of which is PM2.5. From the Environmental Protection Agency (EPA), you will see that PM2.5 is a known toxin potentially made up of hundreds of different chemicals that is so small that it can collect deep within the lungs and even enter the bloodstream. It has been associated with cardiovascular and respiratory disease, irritation of the eyes, throat, and lungs, and premature death:
Particulate Matter (PM) Basics
What is PM, and how does it get into the air?
“PM stands for particulate matter (also called particle pollution): the term for a mixture of solid particles and liquid droplets found in the air. Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye. Others are so small they can only be detected using an electron microscope.
Particle pollution includes:
PM10: inhalable particles, with diameters that are generally 10 micrometers and smaller; and
PM2.5: fine inhalable particles, with diameters that are generally 2.5 micrometers and smaller.
How small is 2.5 micrometers? Think about a single hair from your head. The average human hair is about 70 micrometers in diameter – making it 30 times larger than the largest fine particle.
Sources of PM
These particles come in many sizes and shapes and can be made up of hundreds of different chemicals.
Some are emitted directly from a source, such as construction sites, unpaved roads, fields, smokestacks or fires.
Most particles form in the atmosphere as a result of complex reactions of chemicals such as sulfur dioxide and nitrogen oxides, which are pollutants emitted from power plants, industries and automobiles.
What are the Harmful Effects of PM?
Particulate matter contains microscopic solids or liquid droplets that are so small that they can be inhaled and cause serious health problems. Some particles less than 10 micrometers in diameter can get deep into your lungs and some may even get into your bloodstream. Of these, particles less than 2.5 micrometers in diameter, also known as fine particles or PM2.5, pose the greatest risk to health.
Fine particles are also the main cause of reduced visibility (haze) in parts of the United States, including many of our treasured national parks and wilderness areas.”
Health and Environmental Effects of Particulate Matter (PM)
Health Effects
The size of particles is directly linked to their potential for causing health problems. Small particles less than 10 micrometers in diameter pose the greatest problems, because they can get deep into your lungs, and some may even get into your bloodstream.
Exposure to such particles can affectboth your lungs and your heart. Numerous scientific studies have linked particle pollution exposure to a variety of problems, including:
premature death in people with heart or lung disease
nonfatal heart attacks
irregular heartbeat
aggravated asthma
decreased lung function
increased respiratory symptoms, such as irritation of the airways, coughing or difficulty breathing.
People with heart or lung diseases,children, and older adults are the most likely to be affected by particle pollution exposure.
PM2.5 and other particulate matter is only part of the dangerous substances found in these persistent contrails. Other admitted substances include carbon dioxide (CO2), volatile organic compounds (VOC), nitrogen oxides (NOX), sulfur oxides (SOX), black carbon soot, and other trace metals. It is simply beyond logic and reasoning to believe that the inhalation of these substances on a daily basis is not harmful to one’s health.
Recently, some members of Congress were interested in addressing the health and environmental problems associated with aviation. On February 8th, 2022, the Congressional Research Service released a report describing the problem and how to address it. A few highlights showcase that aviation pollution is the fastest-growing pollutant over the past decade and that there are numerous toxic substances found within these trails: Aviation, Air Pollution, and Climate Change
Emissions from Aircraft
“The U.S. Environmental Protection Agency (EPA) estimates that transportation—including passenger cars and light trucks, heavy-duty trucks, buses, trains, ships, and aircraft—accounted for 35% of carbon dioxide (CO2, the principal GHG) emissions in 2018. While CO2 emissions from passenger cars and light trucks exceed those from aircraft in the United States, CO2 emissions from aviation are currently experiencing a faster rate of growth. All aircraft, including military, commercial, and privately chartered, accounted for 13% of the U.S. transportation sector’s CO2 emissions and 5% of all U.S. CO2 emissions in 2018. Commercial aircraft, including those operated by passenger and all-cargo airlines, accounted for 11% of transportation sector and 4% of all emissions. These estimates include emissions from U.S. domestic flights and emissions from international flights departing the United States, referred to as “international bunkering.”
In the United States, aggregate CO2 emissions from aircraft have fluctuated due to changes in technology, the economy, travel frequency, and military activity, among other reasons. However, since the global financial crisis in 2009,aggregate CO2 emissions from all aircraft types have grown steadily, increasing by almost 22% between 2009 and 2018. This increase makes aircraft one of the faster-growing sources of CO2 emissions in the U.S. transportation sector over the past decade. This trend is likely to be affected, at least temporarily, by reduced air travel in 2020 and 2021 due to Coronavirus Disease 2019 (COVID-19).
The effects of aircraft emissions on the atmosphere are complex, reflecting differing altitudes, geography, time horizons, and environmental conditions. Research has shown that in addition to CO2 emissions, other factors increase the climate change impacts of aviation. These factors include the contribution of aircraft emissions to ozone production; the formation of water condensation trails and cirrus clouds; the emission of various gases and particles, including water vapor, nitrous oxides, sulfates, and particulates from jet fuel combustion; and the high altitude location of the bulk of these emissions. In examining the warming and cooling influences of these factors, the United Nations’ Intergovernmental Panel on Climate Change estimated aviation’s total climate change impact could be from two to four times that of its past CO2 emissions alone.
Aside from GHG emissions, aircraft engines emit a number of criteria—or common—pollutants, including nitrogen oxides, carbon monoxide, oxides of sulfur, unburned or partially combusted hydrocarbons (also known as volatile organic compounds [VOCs]), particulates, and other trace compounds. A subset of the VOCs and particulates are considered hazardous air pollutants.”
In case you wanted a visual representation of how this pollution is said to form and impact our health.
As can be seen, the pollution coming from the aviation industry is a fast-growing problem that is impacting our health and environment in numerous ways. While this has been known for decades and solutions have been presented to try and reverse the impact, nothing is ever implemented to fix the problem. Solutions are only useful if they are enacted upon. While Congress gathers reports, there is little action taken in regards to those reports. It is one thing to acknowledge the negative health and environmental impact yet it is another thing entirely to actually shake up the industry by doing something about it. This seems not to be a major concern as these trails have become worse over time, increasingly contributing to erratic weather, disease, and premature death.
For further evidence of the impact that these trails have on our health and environment, we can turn once again to the EPA to provide more detail. In a document from January 11th, 2021, the EPA enacted standards that are supposed to combat greenhouse gas emissions from the aviation industry. In this document are findings from reports they had compiled in 2016 which call out the dangers these trails have on the public health and welfare:
Control of Air Pollution From Airplanes and Airplane Engines: GHG Emission Standards and Test Procedures
“In August 2016, the EPA issued two findings regarding GHG emissions from aircraft engines (the 2016 Findings).[7]First, the EPA found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA. Second, EPA found that emissions of GHGs from certain classes of engines used in certain aircraft are contributing to the air pollution that endangers public health and welfare under CAA section 231(a)(2)(A). Additional details of the 2016 Findings are described in Section III. As a result of the 2016 Findings, CAA sections 231(a)(2)(A) and (3) obligate the EPA to propose and adopt, respectively, GHG standards for these covered aircraft engines.”
III. Summary of the 2016 Findings
“On August 15, 2016,[46] the EPA issued two findings regarding GHG emissions from aircraft engines. First, the EPA found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA. The EPA made this finding specifically with respect to the same six well-mixed GHGs—CO2, methane, N2 O, hydrofluorocarbons, perfluorocarbons, and sulfur hexafluoride—that together were defined as the air pollution in the 2009 Endangerment Finding [47] under section 202(a) of the CAA and that together were found to constitute the primary cause of climate change. Second, the EPA found that emissions of those six well-mixed GHGs from certain classes of engines used in certain aircraft [48] cause or contribute to the air pollution—the aggregate group of the same six GHGs—that endangers public health and welfare under CAA section 231(a)(2)(A).”
In February of 2022, the EPA proposed standards that would reflect the importance of the control of PM emissions in aviation. They were looking to secure the highest practicable degree of uniformity in aviation regulations and standards. Within this proposal, the EPA provided plenty of insight into the potential health impacts of PM2.5 on human health such as cardiovascular disease, respiratory disease, neurological disorders, asthma, cancer, ferility/reproductive problems, and premature death. They also outlined the impact the chemicals in the trails have on the environment such as affecting the metabolic processes of plant foliage, altering the soil biogeochemistry and microbiology, disrupting plant and animal growth and reproduction, and the corrosion of metals and soil. They even provided more detail on the make-up of the composition of the dangerous toxins inside these trails with the addition of carcinogens such as benzene, 1,3-butadiene, formaldehyde, acetaldehyde, acrolein, polycyclic organic matter (POM), and certain metals such as chromium, manganese, and nickel. Judging by this information alone, it should be rather clear that these trails are negatively impacting our health and environment in numerous ways:
Control of Air Pollution From Aircraft Engines: Emission Standards and Test Procedures
III. Particulate Matter Impacts on Air Quality and Health
A. Background on Particulate Matter
“Particulate matter (PM) is a highly complex mixture of solid particles and liquid droplets distributed among numerous atmospheric gases which interact with solid and liquid phases. Particles range in size from those smaller than 1 nanometer (10−9 meter) to over 100 micrometers (μm, or 10−6 meter) in diameter (for reference, a typical strand of human hair is 70 μm in diameter and a grain of salt is about 100 μm). Atmospheric particles can be grouped into several classes according to their aerodynamic and physical sizes. Generally, the three broad classes of particles include ultrafine particles (UFPs, generally considered as particulates with a diameter less than or equal to 0.1 μm (typically based on physical size, thermal diffusivity or electrical mobility)), “fine” particles (PM2.5; particles with a nominal mean aerodynamic diameter less than or equal to 2.5 μm), and “thoracic” particles (PM10; particles with a nominal mean aerodynamic diameter less than or equal to 10 μm). Particles that fall within the size range between PM2.5 and PM10, are referred to as “thoracic coarse particles” (PM10-2.5, particles with a nominal mean aerodynamic diameter less than or equal to 10 μm and greater than 2.5 μm).
Particles span many sizes and shapes and may consist of hundreds of different chemicals. Particles are emitted directly from sources and are also formed through atmospheric chemical reactions between PM precursors; the former are often referred to as “primary” particles, and the latter as “secondary” particles. Particle concentration and composition varies by time of year and location, and, in addition to differences in source emissions, is affected by several weather-related factors, such as temperature, clouds, humidity, and wind. Ambient levels of PM are also impacted by particles’ ability to shift between solid/liquid and gaseous phases, which is influenced by concentration, meteorology, and especially temperature.
Fine particles are produced primarily by combustion processes and by transformations of gaseous emissions ( e.g., sulfur oxides (SOX), nitrogen oxides (NOX) and volatile organic compounds (VOCs)) in the atmosphere. The chemical and physical properties of PM2.5 may vary greatly with time, region, meteorology, and source category. Thus, PM2.5 may include a complex mixture of different components including sulfates, nitrates, organic compounds, elemental carbon, and metal compounds. These particles can remain in the atmosphere for days to weeks and travel through the atmosphere hundreds to thousands of kilometers.
Particulate matter is comprised of both volatile and non-volatile PM. PM emitted from the engine is known as non-volatile PM (nvPM), and PM formed from transformation of an engine’s gaseous emissions are defined as volatile PM.[35] Because of the difficulty in measuring volatile PM, which is formed in the engine’s exhaust plume and is significantly influenced by ambient conditions, the EPA is proposing standards only for the emission of nvPM.
B. Health Effects of Particulate Matter
Scientific studies show exposure to ambient PM is associated with a broad range of health effects. These health effects are discussed in detail in the Integrated Science Assessment for Particulate Matter (PM ISA), which was finalized in December 2019.[36]The PM ISA concludes that human exposures to ambient PM2.5 are associated with a number of adverse health effects and characterizes the weight of evidence for broad health categories ( e.g., cardiovascular effects, respiratory effects, etc.).[37] The PM ISA additionally notes that stratified analyses ( i.e., analyses that directly compare PM-related health effects across groups) provide strong evidence for racial and ethnic differences in PM2.5 exposures and in PM2.5 -related health risk. As described in Section III.D, concentrations of PM increase with proximity to an airport. Further, studies described in Section III.G report that many communities in close proximity to airports are disproportionately represented by people of color and low-income populations.
EPA has concluded that recent evidence in combination with evidence evaluated in the 2009 p.m. ISA supports a “causal relationship” between both long- and short-term exposures to PM2.5 and mortality and cardiovascular effects and a “likely to be causal relationship” between long- and short-term PM2.5 exposures and respiratory effects.[38]Additionally, recent experimental and epidemiologic studies provide evidence supporting a “likely to be causal relationship” between long-term PM2.5 exposure and nervous system effects, and long-term PM2.5 exposure and cancer. In addition, EPA noted that there was more limited and uncertain evidence for long-term PM2.5 exposure and reproductive and developmental effects ( i.e., male/female reproduction and fertility; pregnancy and birth outcomes), long- and short-term exposures and metabolic effects, and short-term exposure and nervous system effects resulting in the ISA concluding “suggestive of, but not sufficient to infer, a causal relationship.”
More detailed information on the health effects of PM can be found in a memorandum to the docket.[39]
C. Environmental Effects of Particulate Matter
Environmental effects that can result from particulate matter emissions include visibility degradation, plant and ecosystem effects, deposition effects, and materials damage and soiling. These effects are briefly summarized here and discussed in more detail in the memo to the docket cited above.
PM2.5 emissions also adversely impact visibility.[40]In the Clean Air Act Amendments of 1977, Congress recognized visibility’s value to society by establishing a national goal to protect national parks and wilderness areas from visibility impairment caused by manmade pollution.[41] In 1999, EPA finalized the regional haze program (64 FR 35714) to protect the visibility in Mandatory Class I Federal areas. There are 156 national parks, forests and wilderness areas categorized as Mandatory Class I Federal areas (62 FR 38680-38681, July 18, 1997). These areas are defined in CAA section 162 as those national parks exceeding 6,000 acres, wilderness areas and memorial parks exceeding 5,000 acres, and all international parks which were in existence on August 7, 1977. EPA has also concluded that PM2.5 causes adverse effects on visibility in other areas that are not targeted by the Regional Haze Rule, such as urban areas, depending on PM2.5 concentrations and other factors such as dry chemical composition and relative humidity ( i.e., an indicator of the water composition of the particles). EPA established the secondary 24-hour PM2.5 NAAQS in 1997 and has retained the standard in subsequent reviews.[42] This standard is expected to provide protection against visibility effects through attainment of the existing secondary standards for PM2.5 . EPA is reconsidering the 2020 decision, as announced on June 10, 2021.[43]
1. Deposition of Metallic and Organic Constituents of PM
Several significant ecological effects are associated with deposition of chemical constituents of ambient PM such as metals and organics.[44]Like all internal combustion engines, turbine engines covered by this rule may emit trace amounts of metals due to fuel contamination or engine wear. Ecological effects of PM include direct effects to metabolic processes of plant foliage; contribution to total metal loading resulting in alteration of soil biogeochemistry and microbiology, plant and animal growth and reproduction; and contribution to total organics loading resulting in bioaccumulation and biomagnification.
2. Materials Damage and Soiling
Deposition of PM is associated with both physical damage (materials damage effects) and impaired aesthetic qualities (soiling effects). Wet and dry deposition of PM can physically affect materials, adding to the effects of natural weathering processes, by potentially promoting or accelerating the corrosion of metals, by degrading paints and by deteriorating building materials such as stone, concrete and marble.[45]
D. Near-Source Impacts on Air Quality and Public Health
Airport activity can adversely impact air quality in the vicinity of airports. Furthermore, these adverse impacts may disproportionately impact sensitive subpopulations. A recent study by Yim et al. (2015) assessed global, regional, and local health impacts of civil aviation emissions, using modeling tools that address environmental impacts at different spatial scales.[46] The study attributed approximately 16,000 premature deaths per year globally to global aviation emissions, with 87 percent attributable to PM2.5 . The study concludes that about a third of these mortalities are attributable to PM2.5 exposures within 20 kilometers of an airport. Another study focused on the continental United States estimated 210 deaths per year attributable to PM2.5 from aircraft.[47] While there are considerable uncertainties associated with such estimates, these results suggest that in addition to the contributions of PM2.5 emissions to regional air quality, impacts on public health of these emissions in the vicinity of airports are an important public health concern.
A significant body of research has addressed pollutant levels and potential health effects in the vicinity of airports. Much of this research was synthesized in a 2015 report published by the Airport Cooperative Research Program (ACRP), conducted by the Transportation Research Board.[48]The report concluded that PM2.5 concentrations in and around airports vary considerably, ranging from “relatively low levels to those that are close to the NAAQS, and in some cases, exceeding the standards.” [49]
Furthermore, the report states (p. 40) that “existing studies indicate that ultrafine particle concentrations are highly elevated at an airport ( i.e., near a runway) with particle counts that can be orders of magnitude higher than background with some persistence many meters downwind ( e.g., 600 m). Finally, the report concludes that PM2.5 dominates overall health risks posed by airport emissions. Moreover, one recently published study concluded that emissions from aircraft play an etiologic role in pre-term births, independent of noise and traffic-related air pollution exposures.[50]
Since the publication of the 2015 ACRP literature review, a number of studies conducted in the U. S. have been published which concluded that ultrafine particle number concentrations were elevated downwind of commercial airports, and that proximity to an airport also increased particle number concentrations within residences.Hudda et al. investigated ultrafine particle number concentrations (PNC) inside and outside 16 residences in the Boston metropolitan area. They found elevated outdoor PNC within several kilometers of the airport. They also found that aviation-related PNC infiltrated indoors and resulted in significantly higher indoor PNC.[51] In another study in the vicinity of Logan airport, Hudda et al. analyzed PNC impacts of aviation activities.[52] They found that, at sites 4.0 and 7.3 km from the airport, average PNCs were 2 and 1.33-fold higher, respectively, when winds were from the direction of the airport compared to other directions, indicating that aviation impacts on PNC extend many kilometers downwind of Logan airport. Stacey (2019) conducted a literature survey and concluded that the literature consistently reports that particle numbers close to airports are significantly higher than locations distant and upwind of airports, and that the particle size distribution is different from traditional road traffic, with more extremely fine particles.[53] Similar findings have been published from European studies.[54 55 56 57 58 59 ] Results of a monitoring study of communities near Seattle-Tacoma International Airport also found higher levels of ultrafine PM near the airport, and an impacted area larger than at near-roadway sites.[60] The PM associated with aircraft landing activity was also smaller in size, with lower black carbon concentrations than near-roadway samples. As discussed above, PM2.5 exposures are associated with a number of serious, adverse health effects. Further, the PM attributable to aircraft emissions has been associated with potential adverse health impacts.[61 62] For example, He et al. (2018) found that particle composition, size distribution and internalized amount of particles near airports all contributed to promotion of reactive organic species in bronchial epithelial cells.
Because of these potential impacts, a systematic literature review was recently conducted to identify peer-reviewed literature on air quality near commercial airports and assess the quality of the studies.[63] The systematic review identified seventy studies for evaluation. These studies consistently showed that particulate matter, in the form of ultrafine PM (UFP), is elevated in and around airports. Furthermore, many studies showed elevated levels of black carbon, criteria pollutants, and polycyclic aromatic hydrocarbons as well. Finally, the systematic review, while not focused on health effects, identified a limited number of references reporting adverse health effects impacts, including increased rates of premature death, pre-term births, decreased lung function, oxidative DNA damage and childhood leukemia. More research is needed linking particle size distributions to specific airport activities, and proximity to airports, characterizing relationships between different pollutants, evaluating long-term impacts, and improving our understanding of health effects.
A systematic review of health effects associated with exposure to jet engine emissions in the vicinity of airports was also recently published.[64] This study concluded that literature on health effects was sparse, but jet engine emissions have physicochemical properties similar to diesel exhaust particles, and that exposure to jet engine emissions is associated with similar adverse health effects as exposure to diesel exhaust particles and other traffic emissions.A 2010 systematic review by the Health Effects Institute (HEI) concluded that evidence was sufficient to support a causal relationship between exposure to traffic-related air pollution and exacerbation of asthma among children, and suggestive of a causal relationship for childhood asthma, non-asthma respiratory symptoms, impaired lung function and cardiovascular mortality.[65]”
F. Other Pollutants Emitted by Aircraft
“In addition to particulate matter, a number of other criteria pollutants are emitted by the aircraft which are the subject of this proposed rule. These pollutants, which are not covered by the rule, include nitrogen oxides (NOX), including nitrogen dioxide (NO2), volatile organic compounds (VOC), carbon monoxide (CO), and sulfur dioxide (SO2). Aircraft also contribute to ambient levels of hazardous air pollutants (HAP), compounds that are known or suspected human or animal carcinogens, or that have noncancer health effects. These compounds include, but are not limited to, benzene, 1,3-butadiene, formaldehyde, acetaldehyde, acrolein, polycyclic organic matter (POM), and certain metals. Some POM and HAP metals are components of PM2.5 mass measured in turbine engine aircraft emissions.[70]
The term polycyclic organic matter (POM) defines a broad class of compounds that includes the polycyclic aromatic hydrocarbon compounds (PAHs). POM compounds are formed primarily from combustion and are present in the atmosphere in gas and particulate form. Metal compounds emitted from aircraft turbine engine combustion include chromium, manganese, and nickel. Several POM compounds, as well as hexavalent chromium, manganese compounds and nickel compounds are included in the National Air Toxics Assessment, based on potential carcinogenic risk.[71] In addition, as mentioned previously, deposition of metallic compounds can have ecological effects. Impacts of POM and metals are further discussed in the memorandum to the docket referenced above.”
PM stands for particulate matter – the term for a mixture of solid particles and liquid droplets found in the air
Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye while others are too small to be seen
PM10: inhalable particles, with diameters that are generally 10 micrometers and smaller
PM2.5: fine inhalable particles, with diameters that are generally 2.5 micrometers and smaller
These particles come in many sizes and shapes and can be made up of hundreds of different chemicals
Most particles form in the atmosphere as a result of complex reactions of chemicals such as sulfur dioxide and nitrogen oxides
Particulate matter contains microscopic solids or liquid droplets that are so small that they can be inhaled and cause serious health problems
Some particles less than 10 micrometers in diameter can get deep into your lungs and some may even get into your bloodstream
Fine particles are also the main cause of reduced visibility (haze) in parts of the United States
The size of particles is directly linked to their potential for causing health problems
Exposure to such particles can affect both your lungs and your heart
Numerous scientific studies have linked particle pollution exposure to a variety of problems, including:
Premature death in people with heart or lung disease
Nonfatal heart attacks
Irregular heartbeat
Aggravated asthma
Decreased lung function
Increased respiratory symptoms, such as irritation of the airways, coughing or difficulty breathing
People with heart or lung diseases,children, and older adults are the most likely to be affected by particle pollution exposure
According to a Congressional Research Service report from February 8th, 2022, CO2 emissions from aviation are currently experiencing a faster rate of growth than other sources
All aircraft, including military, commercial, and privately chartered, accounted for 13% of the U.S. transportation sector’s CO2 emissions and 5% of all U.S. CO2 emissions in 2018
Commercial aircraft, including those operated by passenger and all-cargo airlines, accounted for 11% of transportation sector and 4% of all emissions
Since the global financial crisis in 2009, aggregate CO2 emissions from all aircraft types have grown steadily, increasing by almost 22% between 2009 and 2018
This increase makes aircraft one of the faster-growing sources of CO2 emissions in the U.S. transportation sector over the past decade
The effects of aircraft emissions on the atmosphere are complex, reflecting differing altitudes, geography, time horizons, and environmental conditions
Research has shown that in addition to CO2 emissions, other factors increase the climate change impacts of aviation which include:
The contribution of aircraft emissions to ozone production
The formation of water condensation trails and cirrus clouds
The emission of various gases and particles, including water vapor, nitrous oxides, sulfates, and particulates from jet fuel combustion
The high altitude location of the bulk of these emissions
In examining the warming and cooling influences of these factors, the United Nations’ Intergovernmental Panel on Climate Change estimated aviation’s total climate change impact could be from two to four times that of its past CO2 emissions alone
Aside from GHG emissions, aircraft engines emit a number of criteria—or common—pollutants, including:
Nitrogen oxides
Carbon monoxide
Oxides of sulfur
Unburned or partially combusted hydrocarbons (also known as volatile organic compounds [VOCs])
Particulates
Other trace compounds
A subset of the VOCs and particulates are considered hazardous air pollutants
According to a 2021 report by the EPA, they found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA
Second, EPA found that emissions of GHGs from certain classes of engines used in certain aircraft are contributing to the air pollution that endangers public health and welfare under CAA section 231(a)(2)(A)
The EPA made this finding specifically with respect to the same six well-mixed GHGs—CO2, methane, N2O, hydrofluorocarbons, perfluorocarbons, and sulfur hexafluoride—that together were defined as the air pollution in the 2009 Endangerment Finding under section 202(a) of the CAA and that together were found to constitute the primary cause of climate change
The EPA found that emissions of those six well-mixed GHGs from certain classes of engines used in certain aircraft cause or contribute to the air pollution—the aggregate group of the same six GHGs—that endangers public health and welfare under CAA section 231(a)(2)(A)
Another report by the EPA from February 2022 states that particulate matter (PM) is a highly complex mixture of solid particles and liquid droplets distributed among numerous atmospheric gases which interact with solid and liquid phases
Particles span many sizes and shapes and may consist of hundreds of different chemicals
Fine particles are produced primarily by combustion processes and by transformations of gaseous emissions (e.g., sulfur oxides (SOX), nitrogen oxides (NOX) and volatile organic compounds (VOCs)) in the atmosphere
PM2.5 may include a complex mixture of different components including sulfates, nitrates, organic compounds, elemental carbon, and metal compounds
These particles can remain in the atmosphere for days to weeks and travel through the atmosphere hundreds to thousands of kilometers
Particulate matter is comprised of both volatile and non-volatile PM
PM emitted from the engine is known as non-volatile PM (nvPM), and PM formed from transformation of an engine’s gaseous emissions are defined as volatile PM
Because of the difficulty in measuring volatile PM, which is formed in the engine’s exhaust plume and is significantly influenced by ambient conditions, the EPA is proposing standards only for the emission of nvPM
In other words, there are no standards proposed by the EPA for the transformation these chemicals go through after leaving the enginewhen they become lingering trails
Scientific studies show exposure to ambient PM isassociated with a broad range of health effects
The PM ISA concludes that human exposures to ambient PM2.5 are associated with a number of adverse health effects and characterizes the weight of evidence for broad health categories ( e.g., cardiovascular effects, respiratory effects, etc.)
EPA has concluded that recent evidence in combination with evidence evaluated in the 2009 p.m. ISA supports a “causal relationship” between both long- and short-term exposures to PM2.5 and mortality and cardiovascular effects and a “likely to be causal relationship” between long- and short-term PM2.5 exposures and respiratory effects
Additionally, recent experimental and epidemiologic studies provide evidence supporting a “likely to be causal relationship” between long-term PM2.5 exposure and nervous system effects, and long-term PM2.5 exposure and cancer
In addition, EPA noted that there was more limited and uncertain evidence for long-term PM2.5 exposure and reproductive and developmental effects ( i.e., male/female reproduction and fertility; pregnancy and birth outcomes), long- and short-term exposures and metabolic effects, and short-term exposure and nervous system effects resulting in the ISA concluding “suggestive of, but not sufficient to infer, a causal relationship”
Environmental effects that can result from particulate matter emissions include:
Visibility degradation
Plant and ecosystem effects
Deposition effects
Materials damage and soiling
PM2.5 emissions also adversely impact visibility
Like all internal combustion engines, turbine engines covered by this rule may emittrace amounts of metals due to fuel contamination or engine wear
Ecological effects of PM include:
Direct effects to metabolic processes of plant foliage
Contribution to total metal loading resulting in alteration of soil biogeochemistry and microbiology, plant and animal growth and reproduction
Contribution to total organics loading resulting in bioaccumulation and biomagnification
Deposition of PM is associated with both physical damage (materials damage effects) and impaired aesthetic qualities (soiling effects)
Wet and dry deposition of PM can physically affect materials, adding to the effects of natural weathering processes, by potentially promoting or accelerating the corrosion of metals, by degrading paints and by deteriorating building materials such as stone, concrete and marble
A recent study by Yim et al. (2015) assessed global, regional, and local health impacts of civil aviation emissions, using modeling tools that address environmental impacts at different spatial scales
The study attributed approximately 16,000 premature deaths per year globally to global aviation emissions, with 87 percent attributable to PM2.5
The study concluded that about a third of these mortalities are attributable to PM2.5 exposures within 20 kilometers of an airport
Another study focused on the continental United States estimated 210 deaths per year attributable to PM2.5 from aircraft
Impacts on public health of these emissions in the vicinity of airports are an important public health concern
A 2015 report concluded that PM2.5 concentrations in and around airports vary considerably, ranging from “relatively low levels to those that are close to the NAAQS, and in some cases, exceeding the standards.”
Furthermore, the report stated (p. 40) that “existing studies indicate that ultrafine particle concentrations are highly elevated at an airport ( i.e., near a runway) with particle counts that can be orders of magnitude higher than background with some persistence many meters downwind ( e.g., 600 m)
Finally, the report concluded that PM2.5 dominates overall health risks posed by airport emissions
Hudda et al. investigated ultrafine particle number concentrations (PNC) inside and outside 16 residences in the Boston metropolitan area and found that aviation-related PNC infiltrated indoors and resulted in significantly higher indoor PNC
Stacey (2019) conducted a literature survey and concluded that the literature consistently reports that particle numbers close to airports are significantly higher than locations distant and upwind of airports, and that the particle size distribution is different from traditional road traffic, with more extremely fine particles
PM2.5 exposures are associated with a number of serious, adverse health effects and the PM attributable to aircraft emissions has been associated with potential adverse health impacts
He et al. (2018) found that particle composition, size distribution and internalized amount of particles near airports all contributed to promotion of reactive organic species in bronchial epithelial cells
A systematic review of 70 studies consistently showed that particulate matter, in the form of ultrafine PM (UFP), is elevated in and around airports
Furthermore, many studies showed elevated levels of black carbon, criteria pollutants, and polycyclic aromatic hydrocarbons as well
Finally, the systematic review, while not focused on health effects, identified a limited number of references reporting adverse health effects impacts, including increased rates of premature death, pre-term births, decreased lung function, oxidative DNA damage and childhood leukemia
A systematic review of health effects associated with exposure to jet engine emissions in the vicinity of airports found that jet engine emissions have physicochemical properties similar to diesel exhaust particles, and that exposure to jet engine emissions is associated with similar adverse health effects as exposure to diesel exhaust particles and other traffic emissions
A 2010 systematic review by the Health Effects Institute (HEI) concluded that evidence was sufficient to support a causal relationship between exposure to traffic-related air pollution and exacerbation of asthma among children, and suggestive of a causal relationship for childhood asthma, non-asthma respiratory symptoms, impaired lung function and cardiovascular mortality
Besides PM2.5, other harmful pollutants, which are not covered by the rule, include:
Nitrogen oxides (NOX)
Nitrogen dioxide (NO2)
Volatile organic compounds (VOC)
Carbon monoxide (CO)
Sulfur dioxide (SO2)
Aircraft also contribute to ambient levels of hazardous air pollutants (HAP), compounds that are known or suspected human or animal carcinogens, or that have noncancer health effects
These compounds include, but are not limited to:
Benzene,
1,3-butadiene
Formaldehyde
Acetaldehyde
Acrolein
Polycyclic organic matter (POM)
Certain metals
Some POM and HAP metals are components of PM2.5 mass measured in turbine engine aircraft emissions
The term polycyclic organic matter (POM) defines a broad class of compounds that includes the polycyclic aromatic hydrocarbon compounds (PAHs)
Metal compounds emitted from aircraft turbine engine combustion include:
Chromium
Manganese
Nickel
Several POM compounds, as well as hexavalent chromium, manganese compounds and nickel compounds are included in the National Air Toxics Assessment, based on potential carcinogenic risk
When dealing with a potential health threat, we tend to jump to the conclusion that we are facing a new “virus” as this well-orchestrated lie has been drilled into our collective consciousness since birth. It is second nature to blame the new invisible boogeyman while overlooking the old visible threats that have been plaguing us for years with no end in sight. It seems too easy to admit to ourselves that any perceived increase in respiratory disease could be attributable to the continued increase in air pollution.
Yet from the start, “Covid-19” has been linked to air pollution. The areas hit the hardest were those with the highest levels of these harmful toxins in the air. As travel died down during the lockdowns, cases fell along with subsiding smog. As travel and pollution rose up again, so too did the “Covid” cases. Even small increases in air pollution has been shown to have an impact on “Covid” case numbers and deaths.
We know for a fact that air pollution is harmful to our health and environment. We know that every single symptom of disease associated with “Covid-19” can be linked to the PM2.5 particles which make up the majority of the dirty air we breathe. We know for a fact that automobiles, factories, power plants, forest fires, volcanic eruptions, etc. all contribute to the harmful levels of toxins in the air. However, the one thing we have been told not to question as a contributor to our current problems are the lingering trails in the sky which form artificial clouds blocking out the beneficial rays of the sun. We are told that these are just regular old contrails from commercial airliners made up of ice crystals which eventually dissipate into a completely safe and harmless nothingness. Anyone questioning the trails is immediately labelled a conspiracy theorist.
It should be clear now, whether you call them chemtrails or not, that these persistent streaks in the sky are full of dangerous substances that attack the cardiovascular, respiratory, and neurological systems. Thanks to government sources such as the EPA and the Congressional Research Service, we know that these trails are the fastest growing pollutant in the air and that they are contributing to even greater levels of smog and haze. The trails and the artificial cirrus clouds they form are a near constant sight in the sky these days and the problem is only growing worse with time. The damaging effects that these lines in the sky have on our health and environment is not even debatable. It is agreed upon by both sides of the debate. That these “persistent contrails” are harmful to our health and environment is a FACT. That the chemicals and toxins found within the vapors cause the exact same symptoms of disease as “Covid-19” is not a coincidence.
Thus we are left with two choices. We can either believe the official narrative that a new “virus” of unknown origin magically leapt from animal to man or somehow escaped from a lab and infected millions of people with a disease that causes the exact same symptoms associated with allergies, the common cold, the flu, and pneumonia. And with it’s rise, it has eliminated the majority of the cases of those previous ailments and can also constantly mutate (over 10 million versions now according to GISAID.org) in order to slip by every possible measure to contain it including masks, social distancing, lockdowns, quarantines, vaccines, etc.
Or we can believe that the ever-increasing and constant daily exposure to air pollution has taken a toll on the populace damaging the health and environment of everyone living within these dangerous levels of toxic fumes. While this is not the only explanation for any perceived increase in respiratory and other diseases, it is the most logical one over an invisible “virus.” According to Occam’s Razor, the simplest of competing theories should be preferred over those that are more complex and that explanations of unknown phenomena should be sought first in terms of known quantities. We know air pollution is harmful. We know that these trails are increasing at a faster rate than any other pollutant. We know that the chemicals residing within them are associated with the exact same symptoms of disease that are ascribed to “Covid.” Unlike a “virus,” we can see this boogeyman with our own two eyes.
All we have to do is look up.
From their own sources, the trails are a threat to our health and our environment. Contrary to what they want you to believe about “persistent contrails,” a.k.a. chemtrails, this is NOT a conspiracy.
You can see more of the slides from Government sources that were presented within this article here.
“The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica…
[….]
“What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice.”
virus, infectious agent of small size and simple composition that can multiply only in living cells of animals, plants, or bacteria. The name is from a Latin word meaning “slimy liquid” or “poison.”
I have purposefully stayed away from the whole “SARS-COV-2” as a gain of function/bioweapon disinformation campaign as it is obvious to anyone who has ever read any “virus” paper, there is absolutely zero credible evidence for the existence of “SARS-COV-2” or any of these other invisible entities. At no point has any virologist ever properly purified and isolated the particles assumed to be “viruses” directly from a sick patient and then proven them pathogenic in a natural way. As this is a fact that is even admitted by virologists themselves, it should also be obvious that if they can not find the particles assumed to be “viruses” in nature, they can not tinker around and modify these fictional entities in a lab in order to create some sort of contagious bioweapon.
Somehow, this logic escapes many. Even though some have woken to the truth and accepted that “SARS-COV-2” does not exist in nature, they still believe that it must have been developed in a lab and unleashed upon the world in order to create a new contagious disease which is wrecking havoc on the elderly and immunocompromised. What they fail to realize is that there simply is no new disease and that none of the symptoms associated with “SARS-COV-2” are new, unique, or specific. There is zero proof of transmission and/or contagion beyond highly flawed epidemiological studies. There is no new “virus,” no new disease, and no contagious bioweapon. It is pure fiction based upon faulty cell culture and genomic experiments.
Before diving into the experimental evidence presented for gain of function studies, I figured it would be a good idea to get some background information on what exactly these kinds of studies entail first. From the October 2021 Nature article highlighted below, we learn that the gain of function concept earned widespread recognition in 2012 due to a pair of studies which both looked to tweak an avian influenza “virus” in order to make it transmissable by air between ferrets. Disregarding the contradictory fact that aerosol transmission is supposedly the way an upper respiratory “virus” is supposed to spread, many became concerned that this kind of work may eventually lead to the release of a super “virus” which could result in the next pandemic. These ferret studies were apparently pivotal with bringing virology into the gain of function field, even though it could be easily argued that virology has been performing these kinds of experiments throughout its existence.
The gain of function term refers to any research that improves a pathogen’s abilities to cause disease or spread from host to host. This is done by fiddling with cell culture material in a lab combined with genomic sequencing. They do this either by inserting genetic material into the cell culture or by way of animal models where the animal is said to be genetically altered in some way to be more susceptible to the “viral” material.
The article provides an example where mice were genetically modified to become susceptible to MERS. However, the mice did not become ill upon being challenged with the “virus.” Thus, the researchers resorted to passaging the “virus” between mice, which involved infecting a couple of mice, giving the “virus” two days to take hold, and then killing the mice and grinding up the lung tissue to inject into other mice. They repeated these steps at least 30 times which eventually made some mice sick. This process of culturing toxic material, injecting animals with the concoction, killing them and grinding up their remains, and then injecting this emulsified goop into other animals in an attenpt to make them sick is what GOF is all about. While this horrific process is getting recognized today, these kinds of experiments have been a staple of virology since the very beginning:
The shifting sands of ‘gain-of-function’ research
“The term first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza virus, using genetic engineering and directed evolution, until it could be transmitted between ferrets2,3. Many people were concerned that publishing the work would be tantamount to providing a recipe for a devastating pandemic, and in the years that followed, research funders, politicians and scientists debated whether such work required stricter oversight, lest someone accidentally or intentionally release a lab-created plague. Researchers around the world voluntarily paused some work, but the issue became particularly politicized in the United States.
US funding agencies, which also support research abroad, later imposed a moratorium on gain-of-function research with pathogens while they worked out new protocols to assess the risks and benefits. But many of the regulatory discussions have taken place out of the public eye.
Now, gain-of-function research is once again centre stage, thanks to SARS-CoV-2 and a divisive debate about where it came from. Most virologists say that the coronavirus probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the virus was first reported. But a group of scientists and politicians argues that a laboratory origin has not been ruled out. They are demanding investigation of the Wuhan Institute of Virology, where related bat coronaviruses have been extensively studied, to determine whether SARS-CoV-2 could have accidentally leaked from the lab or crossed into humans during collection or storage of samples.”
“The term GOF didn’t have much to do with virology until the past decade. Then, the ferret influenza studies came along. In trying to advise the federal government on the nature of such research, the US National Science Advisory Board for Biosecurity (NSABB) borrowed the term — and it stuck, says Gigi Gronvall,a biosecurity specialist at the Bloomberg School of Public Health at Johns Hopkins University in Baltimore, Maryland. From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host.
Virologists do regularly fiddle with viral genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models. “People do all of these experiments all the time,” says Juliet Morrison, a virologist at the University of California, Riverside. For example, her lab has made mouse viruses that are more harmful to mice than the originals. If only mice are at risk, should it be deemed GOF? And would it be worrying?
The answer is generally no. Morrison’s experiments, and many others like them, pose little threat to humans. GOF research starts to ring alarm bells when it involves dangerous human pathogens, such as those on the US government’s ‘select agents’ list, which includes Ebola virus and the bacteria responsible for anthrax and botulism. Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza viruses and coronaviruses. “For the most part, we’re worried about respiratory viruses because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School. GOF studies with those viruses are “a really tiny part” of virology, he adds.”
“Animal research — although fraught with its own set of ethical quandaries — allows scientists to study how pathogens work and to test potential treatments, a necessary precursor to trials in people. That’s what Perlman and his collaborators had in mind when they set out to study the coronavirus responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012. They wanted to use mice, but mice can’t catch MERS.
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells. So, the team altered the mice, giving them a human-like version of the gene for DPP4. The virus could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill. “Having a model of mild disease isn’t particularly helpful to understand why people get so sick,” says collaborator Paul McCray, a paediatric pulmonologist also at the University of Iowa.
So, the group used a classic technique called ‘passaging’ to enhance virulence. The researchers infected a couple of mice, gave the virus two days to take hold, and then transferred some of the infected lung tissue into another pair of mice. They did this repeatedly — 30 times9. By the end of two months, the virus had evolved to replicate better in mouse cells. In so doing, it made the mice more ill; a high dose was deadly, says McCray. That’s GOF of a sort because the virus became better at causing disease. But adapting a pathogen to one animal in this way often limits its ability to infect others, says Andrew Pekosz, a virologist at the Bloomberg School of Public Health.”
“With all the challenges inherent in GOF studies, why do them? Because, some virologists say, the viruses are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match. “We can either wait for something to arise, and then fight it, or we can anticipate that certain things will arise, and instead we can preemptively build our arsenals,” says Morrison. “That’s where gain-of-function research can come in handy.”
This next source is from 2015. The authors admit that virology is heavily reliant on gain or loss of function studies. They offer an alternative definition for GOF research which is any selection process involving an alteration of genotypes and their resulting phenotypes. Obviously, this definition leans far more into the genomics side of the equation. This is due to the claim that these kinds of studies are used by virologists in order to understand a “viruses” genetic make-up. It is stated that researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA. In other words, they mix genetic material from different sources, poison and/or kill lab animals by injecting them with this toxic soup, and then analyze the resulting mixture using computers so that they can claim that the generated model is a new creation. However, it is admitted that these kinds of mutations happen “naturally” with “viruses” every time a person is infected, thus confirming what we already know: virologists can not sequence the same exact “virus” every time:
Gain-of-Function Research: Background and Alternatives
“The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function. In order to understand the role of such studies in virology, Dr. Kanta Subbarao from the Laboratory of Infectious Disease at the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health (NIH) gave an overview of the current scientific and technical approaches to the research on pandemic strains of influenza and Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) coronaviruses (CoV). As discussed in greater detail later in this chapter, many participants argued that the word choice of “gain-of-function” to describe the limited type of experiments covered by the U.S. deliberative process, particularly when coupled with a pause on even a smaller number of research projects, had generated concern that the policy would affect much broader areas of virology research.
TYPES OF GAIN-OF-FUNCTION (GOF) RESEARCH
Subbarao explained that routine virological methods involve experiments that aim to produce a gain of a desired function, such as higher yields for vaccine strains, but often also lead to loss of function, such as loss of the ability for a virus to replicate well, as a consequence. In other words, any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research, even if the U.S. policy is intended to apply to only a small subset of such work.
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of viruses and added that much basic knowledge is still lacking for SARS-CoV and MERS-CoV. Subbarao introduced the key questions that virologists ask at all stages of research on the emergence or re-emergence of a virus and specifically adapted these general questions to the three viruses of interest in the symposium (see Box 3-1). To answer these questions, virologists use gain- and loss-of-function experiments to understand the genetic makeup of viruses and the specifics of virus-host interaction. For instance, researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant viruses from cloned cDNA, and deep sequencing that are critical for studying how viruses escape the host immune system and antiviral controls. Researchers also use targeted host or viral genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool.
During Session 3 of the symposium, Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments. The first category, which he called “gain of function research of concern,” includes the generation of viruses with properties that do not exist in nature. The now famous example he gave is the production of H5N1 influenza A viruses that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type. The second category deals with the generation of viruses that may be more pathogenic and/or transmissible than the wild type viruses but are still comparable to or less problematic than those existing in nature. Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates will improve their replication in mammalian cells. Finally, the third category, which is somewhere in between the two first categories, includes the generation of highly pathogenic and/or transmissible viruses in animal models that nevertheless do not appear to be a major public health concern. An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans. During the discussion, Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature.”
“Imperiale explained that, with respect to the GoF terminology, whenever researchers are working with RNA viruses, GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.” He also commented that the term GoF was understood a certain way by attendees of this symposium, but when the public hears this term “they can’t make that sort of nuanced distinction that we can make here” so the terminology should be revisited.”
Hopefully the above two sources have shown that GOF studies are nothing more than the exact same cell culture experiments utilizing the exact same genomic sequencing technologies and tricks that virologists have always used. The only difference is that they are combining different culture supernatant and genetic materials together into one in order to create a brand new synthetic computer-generated sequence. At no point in time are any purified/isolated particles ever used in these studies. In fact, there are no EM images of the new “virus” of any kind. It should therefore not be surprising that we can see the exact same pattern of unscientific methods and illogical reasoning in GOF studies as found in any of the original “virus” papers.
Seeing as to how the 2012 avian flu studies brought GOF research to the forefront, it seemed ideal to step into this area a bit more to see what actually transpired. The main study presented as evidence of GOF research was led by a man named Ron Fouchier. If that name sounds familiar, that’s because it should. Fouchier was involved in the 2003 “SARS-COV-1” study which proclaimed the satisfaction of Koch’s Postulates for proving a microorganism causes disease yet it failed miserably by not only not being able to satisfy Koch’s four original Postulates, but also Thomas River’s six revised Postulates made strictly for virology. In other words, it was an epic fail.
In Fouchier’s 2012 avian flu GOF study, he attempted to make the H5N1 “virus” infectious through the air. This was done through a process involving cell culturing combined with genetic engineering as well as passaging the material through numerous ferrets. Sounds familiar to the mice example from before, correct? You also see this same process with the early polio and influenza studies as well as in many other virology papers. The main difference is the genomic narrative and the use of modern technology such as reverse genetics to claim the insertion of specific genes.
Highlights from the below paper provide an overview of what was done during this study. It details how the material was collected from a flu strain in Indonesia, genetically altered in a Petri dish, and then transferred to ferrets in a series of experiments using the “wildtype” strain along with different modified strains. Fouchier and Co. were repeatedly unsuccessful in their endeavors of infecting ferrets until they started passaging the “virus” in the animals by injecting them with the cultured soup, grinding up their lung tissues, and injecting other ferrets in the same manner. They repeated this process 6 times and then changed up the experiment by switching to nasal turbinates for the last 4 passage attempts. The only illness said to be achieved via airborne exposure was a loss of appetite, lethargy, and ruffled fur. Upon sequencing the “viruses,” there were only two amino acid switches shared by all six “viruses.” There were several other mutations, but none that occurred in all six airborne “viruses.” In other words, they could not sequence the same “virus” at any point:
Fouchier study reveals changes enabling airborne spread of H5N1
“A study showing that it takes as few as five mutations to turn the H5N1 avian influenza virus into an airborne spreader in mammals—and that launched a historic debate on scientific accountability and transparency—was released today in Science, spilling the full experimental details that many experts had sought to suppress out of concern that publishing them could lead to the unleashing of a dangerous virus.
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 virus that can spread among ferrets without direct contact.
They say their findings show that H5N1 viruses have the potential to evolve in mammals to gain airborne transmissibility, without having to mix with other flu viruses in intermediate hosts such as pigs, and thus pose a risk of launching a pandemic.”
Indonesian H5N1 strain used
Fouchier’s team started with an H5N1 virus collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 viruses more human-like in how they bind to airway cells or in other ways. Avian flu viruses prefer to bind to alpha2,3-linked sialic acid receptors on cells, whereas human flu viruses prefer alpha2,6-linked receptors. In both humans and ferrets, alpha2,6 receptors are predominant in the upper respiratory tract, while alpha 2,6 receptors are found mainly in the lower respiratory tract.
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the virus’s HA protein, the viral surface molecule that attaches to host cells. Q222L and G224S together change the binding preference of H2 and H3 subtype flu viruses, changes that contributed to the 1957 and 1968 flu pandemics, according to the report. And N182K was found in a human H5N1 case.
The scientists created three mutant H5N1 virus strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes, the report explains. They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 virus. Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type virus shed far more virus than those infected with the mutants.
In a second step, the team used a mutation in a different viral gene, PB2, the polymerase complex protein. The mutation E627K in PB2 is linked to the acquisition by avian flu viruses of the ability to grow in the human respiratory tract, which is cooler than the intestinal tract of birds, where the viruses usually reside, according to the report.
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a virus that grew more vigorously in ferrets, and the virus did not spread through the air from infected ferrets to uninfected ones.
The passaging step
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract—the move that Fouchier called “really, really stupid,” according to a report of his initial description of the research at a European meeting last September.
They inoculated one ferret with the three-mutation strain and another with the wild-type virus and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs). Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times. For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest viruses that were secreted from the upper respiratory tract.
The amount of mutant virus found in the nasal turbinate and nose swab samples increased with the number of passages, signaling that the virus was increasing its capacity to grow in the ferret upper airway. In contrast, viral titers in the samples from ferrets infected with the wild-type virus stayed the same.
The next step was to test whether the viruses produced through passaging could achieve airborne transmission. Four ferrets were inoculated with samples of the “passage-10” mutant virus, and two ferrets were inoculated with the passage-10 wild strain. Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact.
The ferrets exposed to those with the wild virus remained uninfected, but three of the four ferrets placed near those harboring the mutant virus did get infected, the researchers found. Further, they took a sample from one of the “recipient” ferrets and used it to inoculate another ferret, which then transmitted the virus to two more ferrets that were placed near it.
Thus, a total of six ferrets became infected with the mutant virus via airborne transmission. However, the level of viral shedding indicated the airborne virus didn’t transmit as efficiently as the 2009 H1N1 virus does.
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur. One of the directly inoculated ferrets died, but all those infected via airborne viruses survived.
When the scientists sequenced the genomes of the viruses that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six viruses: H103Y and T156A. They noted several other mutations, but none that occurred in all six airborne viruses.
“Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of [highly pathogenic avian flu] H5N1 virus,” the researchers wrote.
In further steps, the researchers inoculated six ferrets with high doses of the airborne-transmissible virus; after 3 days, the ferrets were either dead or “moribund.” “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia,” the report notes.”
While the proceeding article did an excellent job of providing the main points from Fouchier’s 2012 GOF study, I wanted to showcase relevant highlights directly from the paper to flesh out the methods used even further. Here you will see that Fouchier’s team claimed that they genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets. They used Influenza “virus” A/Indonesia/5/2005 (A/H5N1) which they said was isolated from a human case of HPAI “virus” infection. This was passaged once in embryonated chicken eggs which was followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000. They then used the QuickChange multisite-directed mutagenesis kit to introduce the desired amino acid substitutions. Site-directed mutagenesis is a synthetic process utilizing PCR to make artificial changes in a DNA sequence. They then took their synthetically-created cultured soup and experimented on ferrets while manipulating the methods until they achieved the results that they desired.
At no point in the paper was a “virus” of any kind ever purified and isolated. At no point were any electron microscope images of the newly mutated “viruses” ever shown. The only “evidence” of an airborne strain is genomic sequencing data from consensus genomes which did not match up. Fouchier and Co. even admitted that airborne transmission could be tested in a second mammalian model system such as guinea pigs, but even this would still not provide conclusive evidence that transmission among humans would occur. They also stated that the mutations they had identified needed further testing to determine their effect on transmission in other A/H5N1 “virus” lineages, and that further experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals. In other words, their study only told them that they could create mutated genomes and not that they created more “virulent viruses” that are transmissable by air:
Airborne Transmission of Influenza A/H5N1 Virus Between Ferrets
“Highly pathogenic avian influenza A/H5N1 virus can cause morbidity and mortality in humans but thus farhas not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”)between humans. To address the concern that the virus could acquire this ability under natural conditions,we genetically modified A/H5N1 virus by site-directed mutagenesis and subsequent serial passage inferrets. The genetically modified A/H5N1 virus acquired mutations during passage in ferrets, ultimatelybecoming airborne transmissible in ferrets. None of the recipient ferrets died after airborne infection withthe mutant A/H5N1 viruses. Four amino acid substitutions in the host receptor-binding protein hemagglutinin, and one in the polymerase complex protein basic polymerase 2, were consistently present in airborne-transmitted viruses. The transmissible viruses were sensitive to the antiviral drug oseltamivir and reacted well with antisera raised against H5 influenza vaccine strains. Thus, avian A/H5N1 influenza viruses can acquire the capacity for airborne transmission between mammals without recombination in an intermediate host and therefore constitute a risk for human pandemic influenza.
Influenza A viruses have been isolated from many host species, including humans, pigs, horses, dogs, marine mammals, and a wide range of domestic birds, yet wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the virus reservoir in nature (1). Influenza A viruses belong to the family Orthomyxoviridae; these viruses have an RNA genome consisting of eight gene segments (2, 3). Segments 1 to 3 encode the polymerase proteins: basic polymerase 2 (PB2), basic polymerase 1 (PB1), and acidic polymerase (PA), respectively. These proteins form the RNA-dependent RNA polymerase complex responsible for transcription and replication of the viral genome.”
Since the late 1990s, HPAI A/H5N1 viruses have devastated the poultry industry of numerous countries in the Eastern Hemisphere. To date, A/H5N1 has spread from Asia to Europe, Africa, and the Middle East, resulting in the death of hundreds of millions of domestic birds. In Hong Kong in 1997, the first human deaths directly attributable to avian A/H5N1 virus were recorded (11). Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 virus infections in humans have been reported from 15 countries (12). Although limited A/H5N1 virus transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 virus has not been detected (13–15). Whether this virus may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness. Although our knowledge of viral traits necessary for host switching and virulence has increased substantially in recent years (16, 17), the factors that determine airborne transmission of influenza viruses among mammals, a trait necessary for a virus to become pandemic, have remained largely unknown (18–21). Therefore, investigations of routes of influenza virus transmission between animals and on the determinants of airborne transmission are high on the influenza research agenda.
The viruses that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza viruses (22). However, given that viruses from only four pandemics are available for analyses, we cannot exclude the possibility that a futurepandemic may be triggered by a wholly avian virus without the requirement of reassortment. Several studies have shown that reassortment events between A/H5N1 and seasonal human influenza viruses do not yield viruses that are readily transmitted between ferrets (18–20, 23). In our work, we investigated whether A/H5N1 virus could change its transmissibility characteristics without any requirement for reassortment.
We chose influenza virus A/Indonesia/5/2005 for our study because the incidence of human A/H5N1 virus infections and fatalities in Indonesia remains fairly high (12), and there are concerns that this virus could acquire molecular characteristics that would allow it to become more readily transmissible between humans and initiate a pandemic. Because no reassortants between A/H5N1 viruses and seasonal or pandemic human influenza viruses have been detected in nature and because our goal was to understand the biological properties needed for an influenza virus to become airborne transmissible in mammals, we decided to use the complete A/Indonesia/5/2005 virus that was isolated from a human case of HPAI A/H5N1 infection.
We chose the ferret (Mustela putorius furo) as the animal model for our studies. Ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza viruses (24). After infection with human influenza A virus, ferrets develop respiratory disease and lung pathology similar to that observed in humans. Ferrets can also transmit human influenza viruses to other ferrets that serve as sentinels with or without direct contact (fig. S1) (25–27).”
Human-to-human transmission of influenza viruses can occur through direct contact, indirect contact via fomites (contaminated environmental surfaces), and/or airborne transmission via small aerosols or large respiratory droplets. The pandemic and epidemic influenza viruses that have circulated in humans throughout the past century were all transmitted via the airborne route, in contrast to many other respiratory viruses that are exclusively transmitted via contact. There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols. However, it is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols. Because we did not measure particle size during our experiments, we will use the term “airborne transmission” throughout this Report.”
“Using a combination of targeted mutagenesis followed by serial virus passage in ferrets, we investigated whether A/H5N1 virus can acquiremutations that would increase the risk of mammalian transmission (34). We have previously shown that several amino acid substitutions in the RBS of the HA surface glycoprotein of A/Indonesia/5/2005 change the binding preference from the avian a-2,3–linked SA receptors to the human a-2,6–linked SA receptors (35). A/Indonesia/5/2005 virus with amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S (numbers refer to amino acid positions in the mature H5 HA protein; N, Asn; Q, Gln; L, Leu; G, Gly; S, Ser) in HA display attachment patterns similar to those of human viruses to cells of the respiratory tract of ferrets and humans (35). Of these changes, we know that together, Q222L and G224S switch the receptor binding specificity of H2 and H3 subtype influenza viruses, as this switch contributed to the emergence of the 1957 and 1968 pandemics (36). N182K has been found in a human case of A/H5N1 virus infection (37).
Our experimental rationale to obtain transmissible A/H5N1 viruses was to select a mutant A/H5N1 virus with receptor specificity for a-2,6–linked SA shed at high titers from the URT of ferrets. Therefore, we used the QuickChange multisite-directed mutagenesis kit (Agilent Technologies, Amstelveen, the Netherlands) to introduce amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S in the HA of wild-type (WT) A/Indonesia/5/2005, resulting in A/H5N1HA N182K, A/H5N1HA Q222L,G224S, and A/H5N1HA N182K,Q222L,G224S. Experimental details for experiments 1 to 9 are provided in the supplementary materials (25). For experiment 1, we inoculated these mutant viruses andthe A/H5N1wildtype virus intranasally into groups of six ferrets for each virus (fig. S3). Throat and nasal swabs were collected daily, and virus titerswere determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify virus shedding from the ferret URT. Three animals were euthanized after day 3 to enable tissue sample collection. All remaining animals were euthanized by day 7 when the same tissue samples were taken. Virus titers were determined in the nasal turbinates, trachea, and lungs collected post-mortem from the euthanized ferrets. Throughout the duration of experiment 1, ferrets inoculated intranasally with A/H5N1wildtype virus produced high titers in nose and throat swabs—up to 10 times more than A/H5N1HA Q222L,G224S, which yielded the highest virus titers of all three mutants during the 7-day period (Fig. 1). However, no significant difference was observed between the virus shedding of ferrets inoculated with A/H5N1HA Q222L, G224S or A/H5N1HA N182K during the first 3 days when six animals per group were present. Thus, of the viruses with specificity for a-2,6–linked SA, A/H5N1HA Q222L,G224S yielded the highest virus titers in the ferret URT (Fig. 1).
As described above, amino acid substitution E627K in PB2 is one of the most consistent host-range determinants of influenza viruses (29–31). For experiment 2 (fig. S4), we introduced E627K into the PB2 gene of A/Indonesia/5/2005 by site-directed mutagenesis and produced the recombinant virus A/H5N1HA Q222L,G224S PB2 E627K. The introduction of E627K in PB2 did not significantly affect virus shedding in ferrets, because virus titers in the URT were similar to those seen in A/H5N1HA Q222L,G224S-inoculated animals [up to 1 × 104 50% tissue culture infectious doses (TCID50)] (Mann-Whitney U rank-sum test, P = 0.476) (Fig. 1 and fig. S5). When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously (27), A/H5N1HA Q222L,G224S PB2 E627K was not transmitted (fig. S5).
Because the mutant virus harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, we designed an experiment to force the virus to adaptto replication in the mammalian respiratory tract and to select virus variants by repeated passage (10 passages in total) of the constructedA/H5N1HA Q222L,G224S PB2 E627K virus and A/H5N1wildtype virus in the ferret URT (Fig. 2 and fig. S6). In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K. Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs. The nasal turbinates were homogenized in 3 ml of virus-transport medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate thenext ferret intranasally (passage 2). This procedure was repeated until passage 6.
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi. To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise tothe nostrils of the ferrets to induce sneezing. Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml. The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10. We changed the source of inoculum during the course of theexperiment, because passaging nasal washes may facilitate the selection of viruses that were secreted from the URT. Because influenza viruses mutate rapidly, we anticipated that 10 passages would be sufficient for the virus to adapt to efficient replication in mammals.
Virus titers in the nasal turbinates of ferrets inoculated with A/H5N1wildtype ranged from ~1 × 105 to 1 × 107 TCID50/gram tissue throughout 10 serial passages (Fig. 3A and fig. S7). In ferrets inoculated with A/H5N1HA Q222L,G224S PB2 E627K virus, a moderate increase in virus titers in the nasal turbinates was observed as the passage number increased. These titers ranged from 1 × 104 TCID50/gram tissue at the start of the experiment to 3.2 × 105 to 1 × 106 TCID50/gram tissue in the final passages (Fig. 3A and fig. S7). Notably, virus titers in the nose swabs of animals inoculated with A/H5N1HA Q222L,G224S PB2 E627K also increased during the successive passages, with peak virus shedding of 1 × 105 TCID50 at 2 dpi after 10 passages (Fig. 3B).These data indicate that A/H5N1HA Q222L,G224S PB2 E627K was developing greater capacity to replicate in the ferret URT after repeated passage, with evidence for such adaptation becoming apparent by passage number 4. In contrast, virus titers in the nose swabs of the ferrets collected at 1 to 4 dpi throughout 10 serial passages with A/H5N1wildtype revealed no changes in patterns of virus shedding.
Passaging of influenza viruses in ferrets should result in the natural selection of heterogeneous mixtures of viruses in each animal with a variety of mutations: so-called viral quasi-species (38). The genetic composition of the viral quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform (Roche, Woerden, the Netherlands) (tables S1 and S2). The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the virus population after 10 consecutive passages at a frequency >99.5% (Fig. 4 and table S1). Numerous additional nucleotide substitutions were detected in all viral gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kafter passaging, except in segment 7 (tables S1 and S2). Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions.The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kwas T156A (T, Thr; A, Ala) in HA. This substitution removes a potential N-linked glycosylation site (Asn-X-Thr/Ser; X, any amino acid) in HA and was detected in 99.6% of the A/H5N1wildtype sequences after 10 passages. T156A was detected in 89% of the A/H5N1HA Q222L,G224S PB2 E627K sequences after 10 passages, and the other 11% of sequences possessed the substitution N154K, which removes the same potential N-linked glycosylation site in HA.
In experiment 4 (see supplementary materials), we investigated whether airborne-transmissible viruses were present in the heterogeneous virus population generated during virus passaging in ferrets (fig. S4). Nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were usedin transmission experiments to test whether airborne-transmissible virus was present in the virus quasi-species. For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally: two for passage 10 A/H5N1wildtype and four for passage 10 A/H5N1HA-Q222L,G224S PB2 E627K virus.
The following day, a naïve recipient ferret was placed in a cage adjacent to each inoculated donor ferret. These cages are designed to prevent direct contact between animals but allow airflow from a donor ferret to a neighboring recipient ferret (fig. S1) (27). Although mutations had accumulated in the viral genome after passaging of A/H5N1wildtype in ferrets, we did not detect replicating virus upon inoculation of MDCKcells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype virus(Fig. 5, A and B). In contrast, we did detect virus in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627Kvirus.Three (F1 to F3) out of four (F1 to F4) naïve recipient ferrets became infected as confirmed by the presence of replicating virus in the collected nasal and throat swabs (Fig. 5, C and D). A throat-swab sample obtained from recipient ferret F2, which contained the highest virus titer among the ferrets in the first transmission experiment, was subsequently used for intranasal inoculation of two additional donor ferrets. Both of these animals, when placed in the transmission cage setup (fig. S1), again transmitted the virus to the recipient ferrets (F5 and F6) (Fig. 6, A and B). Avirus isolate was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi. The virus from F5 was inoculated intranasally into two more donor ferrets. One day later, these animals were paired with two recipient ferrets (F7 and F8) in transmission cages, one of which (F7) subsequently became infected (Fig. 6, C and D).
We used conventional Sanger sequencing to determine the consensus genome sequences ofviruses recovered from the six ferrets (F1 to F3 and F5 to F7) that acquired virus via airborne transmission (Fig. 4 and table S3). All six samples still harbored substitutions Q222L, G224S,and E627K that had been introduced by reverse genetics. Surprisingly, only two additional amino acid substitutions, both in HA, were consistently detected in all six airborne-transmissible viruses: (i) H103Y (H, His; Y, Tyr), which forms part of the HA trimer interface, and (ii) T156A, which is proximal but not immediately adjacent to the RBS (fig. S8). Although we observed severalother mutations, their occurrence was not consistent among the airborne viruses, indicating that of the heterogeneous virus populations generated by passaging in ferrets, viruses with different genotypes were transmissible. In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible viruses because, for example, the consensus sequence of virus isolated from F6 differed from the sequence of parental virus isolated from F2.
Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 virus between mammals. The airborne-transmissible virus isolate with the least number of amino acid substitutions, compared with the A/H5N1wildtype, was recovered from ferret F5. This virus isolate had a total of nine amino acid substitutions; in addition to the three mutations that we introduced (Q222L and G224S in HA and E627K in PB2), this virus harbored H103Y and T156A in HA, H99Y and I368V (I, Ile; V, Val) in PB1, and R99K (R, Arg) and S345N in NP (table S3). Reverse genetics will be needed to identify which of the five to nine amino acid substitutions in this virus are essential to confer airborne transmission.
During the course of the transmission experiments with the airborne-transmissible viruses, ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation. One of eight inoculated animals died upon intranasal inoculation (Table 1). In previously published experiments, ferrets inoculated intranasally with WTA/ Indonesia/5/2005 virus at a dose of 1 × 106 TCID50 showed neurological disease and/or death (39, 40). It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 virus and the subsequent course of disease is not representative of the natural situation in humans.Importantly, although the six ferrets that became infected via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment. Moreover, previous infections of humans with seasonal influenza viruses are likely to induce heterosubtypic immunity that would offer some protection against the development of severe disease (41, 42). It has been shown that mice and ferrets previously infected with an A/H3N2 virus are clinically protected against intranasal challenge infection with an A/H5N1 virus (43, 44).
After intratracheal inoculation (experiment 5; fig. S9), six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible virus F5 in a 3-ml volume of PBS died or were moribund at day 3. Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia (45), as is done for vaccination-challenge studies. At necropsy, the six ferrets revealed macroscopic lesions affecting 80 to 100% of the lung parenchyma with average virus titers of 7.9 × 106 TCID50/gram lung (fig. S10). These data are similar to those described previously for A/H5N1wildtype in ferrets (Table 1). Thus, although the airborne-transmissible virus is lethal to ferrets upon intratracheal inoculation at high doses, the virus was not lethal after airborne transmission.”
“Although our experiments showed that A/H5N1 virus can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear. Previous data have indicated that the 2009 pandemic A/H1N1 virus transmits efficiently among ferrets and that naïve animals shed high amounts of virus as early as 1 or 2 days after exposure (27). When we compare the A/H5N1 transmission data with that of reference (27), keeping in mind that our experimental design for studying transmission is not quantitative, the data shown in Figs. 5 and 6 suggest that A/H5N1 airborne transmission was less robust, with less and delayed virus shedding compared with pandemic A/H1N1 virus.
Airborne transmission could be tested in a second mammalian model system such as guinea pigs (59), but this would still not provide conclusive evidence that transmission among humans would occur. The mutations we identified need to be tested for their effect on transmission in other A/H5N1 virus lineages (60), and experiments are needed to quantify how they affect viral fitness and virulence in birds and mammals. For pandemic preparedness, antiviral drugs and vaccine candidates against airborne-transmissible virus should be evaluated in depth. Mechanistic studies on the phenotypic traits associated with each of the identified amino acid substitutions should provide insights into the key determinants of airborne virus transmission. Our findings indicate that HPAI A/H5N1 viruses have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in humans. Identification of the minimal requirements for virus transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness (34).”
“Influenza virus A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI virus infection and passaged once in embryonated chicken eggs followed by a singlepassage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000 (63-64). Mutations of interest (N182K, Q222L, G224S in HA and E627K in PB2) were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit (Aligent, Amstelveen, The Netherlands) according to the instructions of the manufacturer. Recombinant viruses were produced upon transfection of 293T cells and virus stocks were propagated and titrated in MDCK cells as described (63).
Cells
MDCK cells were cultured in Eagle’s minimal essential medium (EMEM, Lonza Benelux BV, Breda, the Netherlands) supplemented with 10% fetal calf serum (FCS), 100 IU/ml penicillin, 100 μg/ml streptomycin, 2 mM glutamine, 1.5 mg/ml sodium bicarbonate (Lonza), 10 mM Hepes (Lonza), and non-essential amino acids (MP Biomedicals Europe, Illkirch, France). 293T cells were cultured in Dulbecco modified Eagle’s medium (DMEM, Lonza) supplemented with 10% FCS, 100 IU/ml penicillin, 100 mg/ml streptomycin, 2mM glutamine, 1mM sodium pyruvate, and non-essential amino acids.
Virus titration in MDCK cells
Virus titrations were performed as described previously (27). Briefly, MDCK cells were inoculated with tenfold serial dilutions of virus preparations, homogenized tissues, nose swabs, and throat swabs.Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with 100 U/mlpenicillin, 100 μg/ml streptomycin, 2mM glutamine, 1.5mg/ml sodium bicarbonate, 10mM Hepes, non-essential amino acids, and 20 μg/ml trypsin (Lonza). Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of virus replication in the cells. Infectious virus titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the virus preparations by the method of Spearman-Karber (65).”
The term “Gain of Function” first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza “virus,” using genetic engineering and directed evolution, until it could be transmitted between ferrets
Most virologists say that the “coronavirus” probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the “virus” was first reported
However, a group of scientists and politicians argues that a laboratory origin has not been ruled out
The term GOF didn’t have much to do with virology until the past decade when the ferret influenza studies came along
From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host
Virologists regularly fiddle with “viral” genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models
Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza “viruses” and “coronaviruses”
“For the most part, we’re worried about respiratory “viruses” because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School
He added that GOF studies with those “viruses” are “a really tiny part” of virology
Perlman and his collaborators set out to study the “coronavirus” responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012
They wanted to use mice, but mice can’t catch MERS
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells and so the team altered the mice, giving them a human-like version of the gene for DPP4
The “virus” could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill
So, the group used a classic technique called ‘passaging’ to enhance “virulence”
The researchers infected a couple of mice, gave the “virus” two days to take hold, and then transferred some of the infected lung tissue into another pair of mice
They did this repeatedly — 30 times and by the end of two months, the “virus” had evolved to replicate better in mouse cells
In so doing, it made the mice more ill; a high dose was deadly
Some virologists say “viruses” are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match
The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function
Any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of “viruses” and added that much basic knowledge is still lacking for “SARS-CoV” and “MERS-CoV”
Virologists use gain- and loss-of-function experiments to understand the genetic makeup of “viruses” and the specifics of “virus-host” interaction
Researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA (i.e. they are synthetic lab creations)
Researchers also use targeted host or “viral” genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool
Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments:
The fisrt category is “gain of function research of concern,” includes the generation of “viruses” with properties that do not exist in nature
The now famous example he gave is the production of H5N1 influenza A “viruses” that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type
The second category deals with the generation of “viruses” that may be more pathogenic and/or transmissible than the wild type “viruses” but are still comparable to or less problematic than those existing in nature (which is odd considering no “viruses” have been found in nature…)
Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates (there are no natural isolates) will improve their replication in mammalian cells
The third category, which is somewhere in between the first two categories, includes the generation of highly pathogenic and/or transmissible “viruses” in animal models that nevertheless do not appear to be a major public health concern
An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans
Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature
GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.”
In other words, they can never sequence the same “virus” every time so what they do in the lab in GoF studies is no different than how they culture and “isolate viruses” in order to sequence the genomes in the first place
A 2012 study supposedly showed that it takes as few as five mutations to turn the H5N1 avian influenza “virus” into an airborne spreader in mammals—and this launched a historic debate on scientific accountability and transparency
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 “virus” that can spread among ferrets without direct contact
Fouchier’s team started with an H5N1 “virus” collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 “viruses” more human-like in how they bind to airway cells or in other ways
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the “virus’s” HA protein, the “viral” surface molecule that attaches to host cells
The scientists created three mutant H5N1 “virus” strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes
They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 “virus”
Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type “virus” shed far more “virus” than those infected with the mutants
In a second step, the team used a mutation in a different “viral” gene, PB2, the polymerase complex protein
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a “virus” that grew more vigorously in ferrets, and the “virus” did not spread through the air from infected ferrets to uninfected ones
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract
This was the move that Fouchier called “really, really stupid” (are we sure he wasn’t referring to the whole study?)
They inoculated one ferret with the three-mutation strain and another with the wild-type “virus” and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs)
Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times
For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest “viruses” that were secreted from the upper respiratory tract
In other words, they completely changed the source material from tissue to nasal secretions more than halfway through the experiment
It was said that the amount of mutant “virus” found in the nasal turbinate and nose swab samples increased with the number of passages while “viral” titers in the samples from ferrets infected with the wild-type “virus” stayed the same
Quick Sidenote From the Supplemtary Materials:
“After inoculation with A/H5N1wildtype, virus titers in the nasal turbinates were variable but high, ranging from 1.6 x 105 to 7.9 x 106 TCID50/gram tissue (panel A), with no further increase observed with repeated passage. After inoculation with A/H5N1HA Q222L,G224S PB2 E627K, virus titers in nasal turbinates averaged 1.6 x 104 in the first three passages, 2.5 x 105 in passage four to seven and 6.3 x 105 TCID50/gram tissue in the last three passages, suggestive of improved replication and virus adaptation. In the lungs, no apparent adaptation was observed for animals inoculated with either virus. Virus titers in lungs were highly variable; presumably it was a matter of chance whether the virus reached the lower airways.”
In other words, the “wildtype virus” titers remained and stayed high while the “mutant virus” started low and elevated throughout passaging yet was still underneath the amount seen in the “wildtype” strain. They also note that finding “virus” in the lungs was a “matter of chance” with either “virus.”
End Quick Sidenote.
The next step was to test whether the “viruses” produced through passaging could achieve airborne transmission so four ferrets were inoculated with samples of the “passage-10” mutant “virus,” and two ferrets were inoculated with the passage-10 wild strain
Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact
The ferrets exposed to those with the wild “virus” remained uninfected, but three of the four ferrets placed near those harboring the mutant “virus” did get infected (“infected” meaning they found “viral” RNA)
Thus, a total of six ferrets became “infected” with the mutant “virus” via airborne transmission
However, the level of “viral” shedding indicated the airborne “virus” didn’t transmit as efficiently as the 2009 H1N1 “virus”
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur (no consideration is given to the fact that the animals were caged, tortured, and experimented on)
One of the directly inoculated ferrets died, but all those infected via airborne “viruses” survived
When the scientists sequenced the genomes of the “viruses” that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six “viruses:” H103Y and T156A
They noted several other mutations, but none that occurred in all six airborne “viruses”
In other words, once again they were unable to sequence the exact same genome in the samples from each ferret
In further steps, the researchers inoculated intratracheallysix ferrets with high doses of the airborne-transmissible “virus;” after 3 days, the ferrets were either dead or “moribund”
They stated: “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia”
Highly “pathogenic” avian influenza A/H5N1 “virus” can cause morbidity and mortality in humans but thus far has not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”) between humans
To address the concern that the “virus” could acquire this ability under natural conditions, the researchers genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets
In other words, in order to test whether the “virus” could mutate naturally, they mutated it synthetically…
The genetically modified A/H5N1 “virus” acquired mutations during passage in ferrets, ultimately becoming airborne transmissible in ferrets (all “viruses” aquire mutations every time they are sequenced as no “viral” genome is ever the same as the original)
None of the recipient ferrets died after airborne infection with the mutant A/H5N1 “viruses”
Wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the “virus” reservoir in nature
Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 “virus” infections in humans have been reported from 15 countries
Although limited A/H5N1 “virus” transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 “virus” has not been detected
Whether this “virus” may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness
The factors that determine airborne transmission of influenza “viruses” among mammals, a trait necessary for a “virus” to become pandemic, have remained largely unknown
The “viruses” that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza “viruses”
However, given that “viruses” from only four pandemics are available for analyses, they cannot exclude the possibility that a future pandemic may be triggered by a wholly avian “virus” without the requirement of reassortment
No reassortants between A/H5N1 “viruses” and seasonal or pandemic human influenza “viruses” have been detected in nature and their goal was to understand the biological properties needed for an influenza “virus” to become airborne transmissible in mammals
They chose the ferret (Mustela putorius furo) as the animal model for the studies as ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza “viruses”
There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols
It is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols
The researchers used the QuickChange multisite-directed mutagenesis kit to introduce amino acid substitutions in the HA of wild-type “virus”
For experiment 1, they inoculated these mutant “viruses” and the A/H5N1wildtype “virus” intranasally into groups of six ferrets for each “virus”
Throat and nasal swabs were collected daily, and “virus” titers were determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify “virus” shedding from the ferret URT
When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously, A/H5N1HA Q222L,G224S PB2 E627K was not transmitted
Because the mutant “virus” harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, they designed an experiment to force the “virus” to adapt to replication in the mammalian respiratory tract and to select “virus” variants by repeated passage (10 passages in total) of the constructed A/H5N1HA Q222L,G224S PB2 E627K “virus” and A/H5N1wildtype “virus” in the ferret URT
In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K
Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs
The nasal turbinates were homogenized in 3 ml of “virus-transport” medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate the next ferret intranasally (passage 2)
This procedure was repeated until passage 6
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi
To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise to the nostrils of the ferrets to induce sneezing
Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml
The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10
They changed the source of inoculum during the course of the experiment, because passaging nasal washes may facilitate the selection of “viruses” that were secreted from the URT
Because influenza “viruses” mutate rapidly, they anticipated (i.e.guessed arbitrarily) that 10 passages would be sufficient for the “virus” to adapt to efficient replication in mammals
The genetic composition of the “viral” quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform
The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the “virus” population after 10 consecutive passages at a frequency >99.5%
Numerous additional nucleotide substitutions were detected in all “viral” gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K after passaging, except in segment 7
Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions
The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was T156A
In experiment 4, nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were used in transmission experiments to test whether airborne-transmissible “virus” was present in the “virus” quasi-species
For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally
Although mutations had accumulated in the “viral” genome after passaging of A/H5N1wildtype in ferrets, they did not detect replicating “virus” upon inoculation of MDCK cells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype “virus”
In contrast, they did detect “virus” in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627K “virus”
Three out of four naïve recipient ferrets became “infected” as confirmed by the presence of replicating “virus” in the collected nasal and throat swabs (in other words, they saw CPE in a cell culture and claimed “virus” was present)
A “virus isolate” was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi
They used conventional Sanger sequencing to determine the consensus genome sequences of viruses recovered from the six ferrets that acquired “virus” via airborne transmission and all six samples still harbored substitutions Q222L, G224S, and E627K that had been introduced by reverse genetics
In other words, they created consensus sequencing through alignment to reference genomes using computer software and algorithms from unpurified material
They observed several other mutations for which their occurrence was not consistent among the airborne “viruses,” indicating that of the heterogeneous “virus” populations generated by passaging in ferrets, “viruses” with different genotypes were transmissible
In other words, they were unable to sequence the exact same “virus” genome every time…and if that wasn’t clear
In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible “viruses” because, for example, the consensus sequence of “virus” isolated from F6 differed from the sequence of parental “virus” isolated from F2
Together, they claim that these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 “virus” between mammals
During the course of the transmission experiments with the airborne-transmissible “viruses,” ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation
It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 “virus” and the subsequent course of disease is not representative of the natural situation in humans
Importantly, although the six ferrets that became “infected” via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment
After intratracheal (in the throat) inoculation, six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible “virus” F5 in a 3-ml volume of PBSdied or were moribund at day 3
Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of “viruses” to cause pneumonia, as is done for vaccination-challenge studies
Although the airborne-transmissible “virus” is lethal to ferrets upon intratracheal inoculation at high doses, the “virus” was not lethal after airborne transmission
They openly admit that the route of injection and the amount of toxic culture goo injected causes the severity of disease, which does not require the “virus” as an explanation
They state that although experiments showed that A/H5N1 “virus” can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear
They pointed out that their experimental design for studying transmission is not quantitative (i.e. they do not know how much “virus” is required for airborne transmission and assume it occurs via PCR results)
They airborne transmission could be tested in a second mammalian model system such as guinea pigs, but this would still not provide conclusive evidence that transmission among humans would occur
The mutations they identified need to be tested for their effect on transmission in other A/H5N1 “virus” lineages, and experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals
Their findings indicate that HPAI A/H5N1 “viruses” have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in human
Of course, the only place reassortment occurs is in a lab so they never need a host…
Identification of the minimal requirements for “virus” transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness
Influenza “virus” A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI “virus” infection and passaged once in embryonated chicken eggs followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells
All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000
Mutations of interest were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit
Recombinant “viruses” were produced upon transfection of 293T cells and “virus” stocks were propagated and titrated in MDCK cells
MDCK cells (canine) were cultured in Eagle’s minimal essential medium supplemented with:
10% fetal calf serum (FCS)
100 IU/ml penicillin
100 μg/ml streptomycin
2 mM glutamine
1.5 mg/ml sodium bicarbonate
10 mM Hepes
Non-essential amino acids
293T cells (human embryonic kidney) were cultured in Dulbecco modified Eagle’s medium supplemented with:
10% FCS
100 IU/ml penicillin
100 mg/ml streptomycin
2mM glutamine
1mM sodium pyruvate
Non-essential amino acids
For “virus” titrations, MDCK cells were inoculated with tenfold serial dilutions of “virus” preparations, homogenized tissues, nose swabs, and throat swabs
Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with:
100 U/ml penicillin
100 μg/ml streptomycin
2mM glutamine
1.5mg/ml sodium bicarbonate
10mM Hepes
Non-essential amino acids
20 μg/ml trypsin
Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of “virus” replication in the cells
Infectious “virus” titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the “virus” preparations by the method of Spearman-Karber
The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica. The only way the liquid poison can potentially harm one is through injection. Cell cultured soup is not transmitted through the air nor is it infectious and/or contagious. In other words, GOF studies are not creating “viruses” in the modern sense of the word and can only be considered as such if viewed through the original Latin lens.
What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice. There will be figureheads who appear to be on the side of truth, questioning the natural existence of “SARS-COV-2,” challenging the safety of the vaccines, promoting alternative therapies, etc. who will also continue to push the idea that “viruses” exist and can be manipulated in a lab. These people are the Pied Pipers leading those who are going astray back into the fold. There is no need to create a “virus” bioweapon when all that was needed to control the masses is a PCR test and some well-designed propaganda.
To anyone who may have been taken in by this GOF/Bioweapon narrative, remember that there is no evidence of any purified and isolated “viral” particles ever coming directly from human samples that are then proven pathogenic in a natural way. Virology does not dispute this. If they can not find a “virus” in nature, they can not create one in a lab. That is truly all you need to know.
cover image based on creative commons work of 13452116/pixaby
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
Thankfully some mandates are dropping across the country, but there are still vaccine mandates that persist in schools, colleges, businesses, hospitals, and corporations. Restrictions on doctors who treat COVID, censorship by Big Tech, the unnecessary COVID-19 vaccination of children, silencing of scientific debate, and the extension of the Emergency Powers Act beyond March 1st for the coronavirus pandemic are a few of the main concerns.
In California, an aggressive slate of COVID-19-related bills—mandating vaccines for children and all employees, and allowing 12 to 17-year-olds to get the vaccine without parental consent—remain under consideration by the California state assembly.
Starting at 12:00 noon we will hold a day-long rally in the heart of Los Angeles at Grand Park where a wide range of featured guests including prominent doctors, recording artists, actors, journalists and premier thought leaders will give a series of inspiring talks and musical performances.
All scientific research is built on particular dogmas including, or perhaps especially, biomedicine. It’s easier for some “scientists” to perpetuate falsehoods than it is to admit they were wrong, abandon long standing ideas, and start again from scratch. Many scientists would rather pursue trendy research areas in order to win accolades and secure grant money than question long-held beliefs and dogmas.
This is exactly what has happened with modern medicine because too much money and too many reputations are at stake. If you’re not allowed to question it, then it’s not real science.
Erroneous theories in medicine have wasted billions and caused untold harm. Imagine if they had to admit that so many years of research and countless academic careers have been wasted pursuing ideas that have no basis in reality.
Thanks to the covid pseudo pandemic, the corrupt state of the medical establishment has never been more obvious to so many people.
See No Evil, Hear No Evil, Speak No Evil
It might be difficult for some to believe that the castle of medicine is built on foundations of sand. However, Stanford scientist John P. A. Ioannidis published a study in 2005 proving that most published research findings are false.
Marcia Angell the first woman to serve as editor-in-chief of the New England Journal of Medicine has extensively investigated the corruption of medicine by drug companies.
Richard Horton, editor of The Lancet, wrote that:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
There are countless victims of iatrogenic disease in countless on-line support groups who once trusted their doctors to have their best interests at heart and to abide by the oath to “first do no harm”.
128,000 Americans die each year from correctly prescribed medications, making prescription drugs one of the leading causes of death.
Clearly, there is something rotten in the state of Denmark.
Dr. Harold Hillman Goes Renegade
In his final paper, the notorious British biologist Harold Hillman claimed that “cell biology is in dire straits”. That paper was published in 2011 and summarises his life’s work which began in the 1970s. He warned biologists and cell physiologists that something is seriously wrong with their ideas about the human body.
In the 1970s this cytologist and neurobiologist began questioning mainstream cell biology and presented evidence that the accepted model of the cell was completely wrong. He suggested that the dire straits of cell biology was the reason medical research has failed to determine the cause and provide the cure for most diseases.
“During a research career lasting more than 50 years, I have concluded that the following procedures are unsuitable for studying the biology of living cells in intact animals and plants: subcellular fractionation; histology; histochemistry; electron microscopy; binding studies; use of ligands; immunocytochemistry; tissue slices; disruptive techniques; dehydration; deep freezing; freeze-drying; boiling; use of extracellular markers; receptor studies; patch clamp measurements; inadequate calibrations. The main objections to these procedures are: (i) they change the properties of the tissues being studied grossly and significantly; (ii) they ignore the second law of thermodynamics;(iii) they produce artefacts, many of which are two-dimensional; (iv) adequate control procedures have never been published for them.”
~ Dr. Harold Hillman
He challenged the fundamental principles of biology. He was a renegade who put the quest for truth above everything else.
Unsurprisingly his views were unpopular with many in the mainstream and this took a toll on his career and reputation. He had difficulty publishing his work. Mainstream scientific journals rejected his papers without reason and refused to review his books.
“The reason I’m so determined is because they [the mainstream] won’t engage. And if they won’t engage, then to my mind it proves that I’m likely to be right.”
~ Dr Harold Hillman
Many scientists agreed with Hillmans’ compelling ideas in private but wouldn’t support him publicly for fear of losing their funding or tarnishing their reputation. Many leading biologists would refuse to meet with him to discuss his research. His goal was to start a discussion and promote a productive debate to improve and further scientific knowledge. Instead of being given a platform to share his work, he was stifled and ridiculed. Sound familiar?
Real scientists value truth above reputation and financial gain. Real scientists are willing to risk everything to expose falsities and incorrect theories. Scientists who blatantly ignore unpopular views or refuse to debate are not true scientists.
“I should like to draw attention to the fact that I regard my views as unpopular, rather than heretical, as I do not believe that scientists should talk in terms of dogma and heresy. In the best of possible worlds, good scientists who hear challenges to their beliefs, assumptions, hypotheses, procedures or conclusions, should examine such criticism with due attention. They should respond by entering into civilised dialogue with their critics. They should be prepared to admit mistakes, if necessary, and change their views. Such reactions have not occurred.”
~ Dr Harold Hillman
Hillman claimed that the routine procedures used to study the characteristics and composition of cells are completely unfit for purpose. He was adamant that these procedures would change the properties of cells more than any differences being examined so any conclusions made on the basis of these procedures were invalid.
He claimed that electron microscopy is a “waste of time and money” which goes against the vast majority of the biomedical establishment who regard the invention of the electron microscope as a pivotal point in biomedical research. Only dead tissue can be examined under an electron microscope and not living cells. Are findings based on electron microscopy relevant to living organisms?
Hillman’s work includes compelling evidence to suggest that many of the subcellular organelles that some scientists have dedicated their lives to studying are just artifacts of preparation for histology and electron microscopy. This includes both the Golgi body and the Endoplasmic Reticulum.
He also claimed that cellular receptors and transmembrane protein channels do not exist in the mainstream accepted sense. One of the reasons for this is that these cell receptors cannot be seen under an electron microscope, despite their size being within the range of visibility.
He courageously stood up for what he believed to be the truth. Despite his career and reputation taking an enormous hit, he continued to publish his ideas right up until his death.
“If I am wrong, only my reputation has been damaged. If I am right, those colleagues proved wrong may well have been wasting their time and careers and using public or charitable resources naively. They might have used their time and resources to carry out more productive research.”
~ Dr Harold Hillman
When considering the current state of medicine, it seems that “more productive research” is exactly what is needed. Research that doesn’t follow dogma and isn’t funded by the very pharma industry that has a vested interest in perpetuating erroneous ideas such as the “one germ, one disease” fallacy.
“It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing.”
~ Dr Harold Hillman
We’re led to believe that modern medicine is highly advanced but the cause of most diseases apparently remains “unknown”. Most Doctors have a mechanistic, reductionist view of disease often believing disease arises due to “genetics” or that the body is just prone to making mistakes.
“It is widely believed that medical research since the Second World War has been very successful…It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing… it is true that the cost of failure so far has been high. The most paradoxical aspect of scientific research is that it is widely believed to be objective…”
~ Dr Harold Hillman
Hillman also criticised the lack of sufficient control experiments performed in biomedical research. Proper control experiments are the cornerstone of good science ensuring that variables, other than the one being tested, do not influence the results of the experiment.
“Control experiments for the effects of reagents and manoeuvres used on the results of experiments have been grossly inadequate.”
~ Dr Harold Hillman
Hillman also questioned the use of tissue cultures for histological analysis with compelling logic. Cells in culture have significantly different morphology, biochemistry, and environment than the cells from which they came.
“Tissue cultures are similar to the tissue from which they come in some ways and very different in other ways. It is clear that although there are a few properties in common, there are substantial differences. This is one of the most important questions, in respect of the usefulness of tissue cultures as sources of information about cells in intact animals.”
~ Dr Harold Hillman
Virology: Voodoo Scientism
Hillman’s work challenges virology as much as it does cell biology and neurobiology. The world is slowly waking up to the pseudoscientific nature of virology because of the pseudo pandemic inflicted on all of us.
“Viruses” can only be seen under an electron microscope using procedures involving heavy metals, dehydration, low pressure, electron bombardment and X-ray irradiation. Are viruses real naturally occurring structures or are they artifacts of these harsh conditions?
The effects of “viruses” are studied on cell cultures and most cell cultures are grown from embryonic tissue, cancerous tissue, stem cells, or monkey cells whose properties are completely different from that of adult human tissue. Is any of this relevant to understanding virus infectivity in humans?
Coronaviruses are supposedly assembled at the endoplasmic reticulum-Golgi interface but if Hillman is right and the endoplasmic reticulum and Golgi body are artefacts of histological preparation and electron microscopy is presumed understanding of virus assembly completely wrong?
Different cell cultures are prepared by different procedures in different chemical solutions to culture “viruses”. Could this explain why only some cells can grow “viruses” but others can’t? SARS-CoV2 cannot infect many human cell lines but can infected monkey kidney cells which is not what you would expect from a supposed human pathogen.
Viruses are supposed to bind to host cell receptors as the first step to entry but if Hillman is correct macromolecular cell receptors don’t really exist.
Adequate controls have not been performed to test the effects of lab conditions, body fluids, antibiotics, and other chemicals on cell cultures so how can virologists be sure that it is the “virus” causing any observed cytopathic effects and not the chemicals and conditions themselves?
The biomedical establishment has chosen to ignore all of these crucial questions. Sadly, Hillman’s level of critical thinking and radical questioning are rare and often completely absent in modern biomedical science.
His sharp intellect and critical thinking skills were a threat to the scientific establishment. He put his career and reputation on the line to expose the weaknesses of established biomedical knowledge.
But what if he was right? What if the castle of modern medicine really is built on foundations of sand? Will his work be forgotten, or will others be brave enough to pick up where he left off?
References
1) John P. A. Ioannidis “Why Most Published Research Findings Are False.” PLoS Med. 2005 Aug; 2(8): e124.
2) Marcia Angell M.D “The Truth About the Drug Companies-How they deceive us and what to do about it.”
3) Richard Horton “Offline: What is medicine’s 5 sigma?” Lancet Comment| Volume 385, ISSUE 9976, P1380, April 11, 2015
4) Harold Hillman “Cell Biology is Currently in Dire Straits.”
5) Harold Hillman “A Career in Neurobiology.”
6) A Biomedical Scientist “Virology’s Voodoo Scientism is Not Real Science.” The Expose.
The People’s Convoy will head back to California on Mar. 31 to protest “10 objectionable COVID-19 bills” being debated in the CA state legislature. They are leaving just a few days short of a month-long stay at the Hagerstown Speedway in Maryland. Prior to its Mar. 4 arrival in Hagerstown, the Convoy embarked on a 10-day cross-country slow roll from Adelanto, CA, beginning Feb. 23. The Convoy plans to return to the D.C. area after the protest in Sacramento.
The follow-up convoy will first stop on Apr. 10 for a Defeat the Mandates Rally with the Convoy’s partner, The Unity Project, in the Los Angeles area. They will then head to Sacramento for their protest against the proposed COVID-19 bills.
California Legislature COVID-19 Bills/The People’s Convoy/The Unity Project
The Unity Project
Contrary to some reporting, the Defeat the Mandates Rallies led by The Unity Project are not anti-vax rallies. Rather, the rallies are meant to reinforce the belief that “mandates are government overreach and that getting a vaccine should be a personal choice.”
The Unity Project/Statement of IntentionSpearheaded by several physicians and scientists, including well-respected, experienced physicians like Dr. Malone, Dr. McCullough, and Dr. Harvey Risch, the Unity Project has spoken forcefully against the vaccine mandates. Quoting Pfizer and Moderna, who state that the shots are “gene therapy” and are experimental, the participating doctors and scientists believe receiving the shots should be left to personal choice. They also think that handling the COVID-19 pandemic has subjected citizens worldwide to egregious measures that were completely unnecessary in many instances. Drs. Paul Alexander and Pierre Kory have often traveled with the Convoy and spoken at several of its rallies. Dr. Malone spoke at a Mar. 26 event in Hagerstown.
The Unity Project is now sponsoring a canvassing campaign powered by volunteers to educate Californians on the dangers of the COVID-19 bills that are currently on the floor. The website also features a series of videos to educate Californians about what is in the bills and why Californians should beware. The flier for the canvassing campaign is available in both English and Spanish. If passed, the bills will, among other things, add COVID-19 shots to the childhood immunization list for public and private schools and will classify “anti-COVID medical opinion as ‘unprofessional conduct.’”
Information on The People’s Convoy website contends that passing the bills is not only dangerous but would “set the stage for other states to introduce similar laws.”
These universally dangerous bills are about to be voted on in the California legislature! If passed, these bills will change everything for people who want to Live, Work or Learn in the State of CA while exercising their right to medical freedom.
If passed, these bills set the stage for other states to introduce similar laws. We know that what starts in CA, spreads to other blue and purple states and potentially at a federal level. This affects everyone!
The Route
A Mar. 28 press release from the Convoy explains that the trip to California represents a continuation of their mission to end emergency orders and mandates—The People’s Convoy “is in this for the long haul,” said one of its organizers, Marcus Sommers.
The truckers’ website has posted a tentative route for the Convoy. Still, specific stops and rally points will be withheld until the day of travel, just as was the protocol for their earlier cross-country trip for the safety and security of its participants. The Convoy will begin its journey on I-81 heading south, picking up I-40 to head West and then to I-20 and I-10 into California. It will then travel I-5 up to Sacramento after a brief stop in the Los Angeles area.
Map/Hagerstown to Sacramento/The People’s ConvoyPublicity for The People’s Convoy has been disappointingly scarce, and their rolls of the beltway have, at times, been met with significant resistance from authorities. However, the truckers and their allies have been undeterred. The Convoy rolled the beltway almost daily, and leadership members managed to secure meetings with Senators Ted Cruz (R-TX), Ron Johnson (R-WI), and other government officials. Senator Ted Cruz also made the trip to the Speedway on Mar. 10 to speak with the Convoy, and he then joined lead organizers Mike Landis and Brian Brase for a roll on the beltway before they delivered him to his press conference in D.C. later in the day. Several truckers were also able to make it into D.C. proper on several occasions, despite the blockades on exits to the Capitol and surrounding areas.
UncoverDC traveled with the Convoy on its initial trip. Conversations with several original truckers indicate that many in that group have had to leave to go back to work. Several truckers who have left the Convoy told UncoverDC that their “savings have been depleted,” and they have to make up for time lost; however, they will continue to work locally to ensure they are better represented in the future. Trucker Bonnie Kelly says she hopes that the convoy “will pick up steam again” along the way, just as it did with the original trip.
A compilation of videos and stills from the February/March trip shows consistent and massive support for the truckers’ mission on overpasses, highways, and cities—big and small—along the way.
CHARLOTTESVILLE, Va. — Coinciding with the second anniversary of the COVID-19 outbreak, The Rutherford Institute has issued an in-depth, follow-up report on the impact of the nation’s response to the pandemic on civil liberties.
The 2022 report, “The Right to Be Let Alone: How to Safeguard Your Freedoms in the Face of the Government’s COVID-19 Power Grabs,” posits that the government’s response to the pandemic has become a massively intrusive, coercive and authoritarian assault on the right of individual sovereignty over one’s life, self and private property. As such, concludes John W. Whitehead, these COVID-19 mandates have become the new battleground in the government’s tug-of-war over bodily autonomy and individual sovereignty.
“Right now, COVID-19 vaccines are the magic ticket for gaining access to the “privileges” of communal life,” said constitutional attorney John W. Whitehead, president of The Rutherford Institute and author of Battlefield America: The War on the American People. “Having already conditioned the population to the idea that being part of society is a privilege and not a right, such access could easily be predicated on social credit scores, the worthiness of one’s political views, or the extent to which one is willing to comply with the government’s dictates, no matter what they might be.”
In March 2020, the World Health Organization declared the novel coronavirus, COVID-19, to be a pandemic, resulting in the most widespread and disruptive public health emergency in our lifetime. Since that time, political leaders from the president to governors to mayors have subscribed to a broad range of actions aimed at limiting the spread of COVID-19, some of which have been draconian and unprecedented. On the one-year anniversary of the COVID-19 outbreak, The Rutherford Institute issued an in-depth reporting, “Civil Liberties in the Age of COVID-19,” to address the delicate balance that must be struck between security and civil liberties, the hazards of government overreach, and the long-term ramifications of an “emergency state” in which the government is increasingly empowered to declare a state of emergency and impose lockdowns, mandates and restrictions in order to address a broadening range of concerns that prioritize the government’s wide-ranging and varying institutional concerns over the individual rights of the citizenry. Coinciding with the second anniversary of the pandemic, The Rutherford Institute has issued “The Right to Be Let Alone: How to Safeguard Your Freedoms in the Face of the Government’s COVID-19 Power Grabs,” which examines the far-reaching ramifications of how the pandemic has impacted the legal, moral and political debate over who gets to decide what happens to our bodies during an encounter with government officials. As the report warns, “This merely pushes us one step further down that road towards a total control society in which the government in collusion with Corporate America gets to decide who is ‘worthy’ of being allowed to take part in society.”
The Rutherford Institute, a nonprofit civil liberties organization, provides legal assistance at no charge to individuals whose constitutional rights have been threatened or violated and educates the public on a wide spectrum of issues affecting their freedoms.
“The real purpose of the scientific method is to make sure Nature hasn’t misled you into thinking something you don’t actually know…One logical slip and an entire scientific edifice comes tumbling down. One false deduction about the machine and you can get hung up indefinitely.” – Robert Pirsig, Zen and the Art of Motorcycle Maintenance
On 11 March 2022, an article was published on The Daily Sceptic website titled “The Real Truth About Viruses”. It was written by Dr Roger Watson, a PhD-qualified registered nurse, who recently retired from the United Kingdom’s higher education sector and now has a part-time position as Academic Dean of Nursing at Southwest Medical University, China. The article was a blatant hit piece against me, typically the domain of the controlled corporate media, so it was a surprise to see it on a website that developed from Lockdown Sceptics. They have the motto “question everything” but apparently you shouldn’t question germ theory and the existence of viruses!
“Question Everything”….except germ theory and viral existence, that’s pure crazy.
Dr Watson appeared to know very little about my work and never attempted to make contact with me before he did his hit and run. We offered him the chance to come on my channel but he declined saying “I am not sure how fruitful a debate with me would be,” perhaps not feeling confident about backing up his claims or perhaps a little shaken by the derision he received in the comments section on the Sceptics website. Much of his article was ad hominem in nature and doesn’t need to be dignified with a response but I will proceed to address his inaccurate scientific claims point by point…
“I would like to hear Duesberg or Sam Bailey explain how haemophiliacs contracted AIDS from blood infusions. Somehow, I think they’ll have a stock response to that one.“ Dr Roger Watson, The Daily Sceptic
It is unclear why Watson has conflated my views with Peter Duesberg and his sentence will take some unpacking. His reference to Peter is a link to Wikipedia, a known disinformation site, which should raise a red flag for a sceptic or anyone wanting to know more about a topic. Peter does not claim that viruses don’t exist: he is one of the world’s most prominent retrovirologists after all! His position is that the HIV particle exists but that it is a harmless “passenger” virus that does not cause the clinical condition AIDS. I know he outlined the evidence of why haemophiliacs do not become “infected” through blood product transfusions here but cannot otherwise speak for him. My position is that there is no proof of the existence of a retrovirus called HIV and that the particles nominated “HIV” have never been shown to fulfil the defintion of a virus. Thus “HIV” has not been shown to cause AIDS.
In this regard, the biggest influence on both myself and my Virus Mania co-authors has been the work of The Perth Group. Watson fails to define what he means by “haemophiliacs contracted AIDS from blood” but presumably he means that the reason some haemophiliacs develop AIDS is because there is a pathogenic virus that is being transmitted to them via infected blood. (They actually receive factor VIII concentrate from pooled blood donations.) I am unaware of any research demonstrating HIV particles in blood or any human or animal models showing transmission of “infected” blood that then causes a recipient to develop AIDS. In Virus Mania we explain that “HIV” cannot be the explanation for the development of AIDS in haemophiliacs. Increased death rates did correspond to changes such as the introduction of “anti-viral” pharmaceuticals including the highly toxic AZT in “HIV positive” patients. If Watson wants to get serious about claiming that a virus is being transmitted to haemophiliacs and causing AIDS then he should have an attempt at refuting The Perth Group’s 1995 paper “Factor VIII, HIV and AIDS in haemophiliacs: an analysis of their relationship”. In my estimation it is the best I have come across and I would welcome Watson’s critique of what I’ve missed.
“Her views have been debunked regarding the existence of viruses but, possibly unknown to many who are unwilling to wade into the depths and breadths of her views, she denies germ theory completely.” Dr Roger Watson, The Daily Sceptic
Watson doesn’t let his readers know how he established I’ve been “debunked” or by who. Instead he provides a link to a small blog post written by a University of Waikato employee and Pfizer BioNTech injection enthusiast Alison Campbell. Campbell set up the blog “as a resource for secondary school biology teachers preparing students for Scholarship Biology examinations” which is probably not the level Watson should be aiming for in this debate. If he checked Campbell’s usual publications he would have realised that she has no experience in virology or medical matters. In fact, when we reached out to her she quickly retreated and would not even agree to a phone call. Watson follows in the footsteps of our state-sponsored mainstream media who also used this largely ad hominem rant as “evidence” against me. I’ve already responded to Campbell and the MSM’s little foray into virology – unfortunately, like Watson, they are limited to repeating the claims of the virologists on face value.
I’m not sure why my views on germ theory would be “unknown” to my viewers as I openly point out that I do not believe it is satisfactory model. Virus Mania is largely dedicated to dismantling germ theory and my views are closest to that of “terrain theory”. I outline why I’m in the terrain camp in much of my work, including in my video “Germ Theory vs Terrain Theory”. For those not familiar with Virus Mania, a window into the book can be found in this short essay I wrote with my co-authors.
“This essay is prompted by the most recent video from Sam Bailey: The Truth About Viruses published on March 9th 2022. She is to be congratulated for its brevity – it is only 17 minutes long – but it is presented in a typically sneering, sarcastic and patronising manner.“
Dr Roger Watson, The Daily Sceptic
Watson seems to completely miss that this video is a light-hearted and satirical take on some of the historical claims of the virologists. It was designed to engage a wider audience with material that can be a boring subject for many. If he wanted to have a serious discussion about a particular topic then he could have easily accessed my other published work or contacted me to fill in any gaps.
“It is hard to understand how Sam Bailey arrives at her views and it is not necessary to be a virus denier to be highly critical of the way the pandemic was managed.“
Dr Roger Watson, The Daily Sceptic
Watson has ignored the vast majority of my work and never bothered to converse with me so perhaps it is not surprising that he is confused. I’m not sure why anyone would decide to be a “virus denier” because they needed to criticise “pandemic” management or how this is relevant to his argument. In fact, it’s disingenuous to even suggest such a modus operandi and it slumps into the argument of the destitute.
“After all, anti (Covid) ‘vaxxer’ supreme, Dr. Mike Yeadon made it clear in his excellent interview with Neil Oliver on GB News that he believes a unique virus exists. The HART Group led by Dr. John Lee, who have mounted the most credible and well-informed responses to the UK lockdown, is not stocked with virus deniers.“
Dr Roger Watson, The Daily Sceptic
Watson has not provided any evidence for the existence of viruses here: his argument seems to be that other people believe in viruses, therefore viruses exist. Some people also believe in the tooth fairy but that would not affect my own investigations into the topic. Appeal to common opinion is a type of faulty reasoning that also plagues the medical community. Heretics like myself are prepared to examine the evidence for ourselves and reach our own conclusions, not parrot those of others. We are not motivated by the number of people who agree with us and our publications are not restricted by governments, institutions, or colleagues. Note to Dr Watson: in all the virology textbooks I’ve looked at, the method of proving the existence of a virus does not include ‘beliefs held by Dr Mike Yeadon’. (For the record: I have no problem with Dr Yeadon, we just have different thoughts on the existence of viruses.)
“It is hard to know where to start but, since she denies germ theory itself – as properly understood – I will start here with Dr Bailey’s views on whether anything exists that can cause an infection and spread between people. Louis Pasteur comes in for criticism by Bailey in her Delingpod interview. I am sure Pasteur was not perfect but he did knock the theory of spontaneous generation a body blow with his swan neck flask experiment.“
Dr Roger Watson, The Daily Sceptic
I’m unsure what Watson means by “properly understood” germ theory. My investigations into germ theory, which are dealt with in Virus Mania and videos such as “Koch’s Postulates: Germ School Dropout,” have informed me that the theory is fatally flawed. I have looked into Koch’s original work and he did not fulfil his own postulates correctly. His often uncontrolled experiments failed to take into account the traumatic effects of his procedures on animals or consider other factors that were making them ill. With regards to “infection” spreading between people, it seems that clinical experiments have struggled to demonstrated this phenomenon. Perhaps the most spectacular failure has been the inability to ever demonstrate transmission of influenza, as I outlined in this video here and ViroLIEgy’s Mike Stone detailed here. If Watson wants to send me a paper that proves the concept of microbes transmitting between humans to make them ill, then I would be happy to critique it. Pasteur’s work has been exposed as largely fraudulent, but it is unclear why Watson is bringing in his spontaneous generation and swan neck flask experiments and how that relates to anything I’ve published. Perhaps he thought terrain theory was claiming that microbes appear on the basis of spontaneous generation?
“Dr. Bailey has batted the theory of disease back into the 19th Century. Edward Jenner was another scoundrel according to Bailey and, while his experiments would not have passed muster with an NHS ethics committee, you can see where Bailey is going and leading her disciples into the realm of the ‘anti-vaxxers’, a topic which I will not explore here.“ Dr Roger Watson, The Daily Sceptic
Watson may be shocked to know that I’m not the only one who has questioned the alleged contributions Jenner has made to human health through the practice of vaccination. I would also suggest he reads the book Dissolving Illusions, or at least examine the charts that Dr Suzanne Humphries and Roman Bystrianyk have put together, if he believes that the smallpox vaccine or any other vaccine has been shown to be of benefit to the public.
The realm of “anti-vaxxers” and their bloody inconvenient, irrefutable data!
I am up front about my position on vaccines as it is clearly stated on my website FAQs that, “I am not ‘anti-vaccination’ in the sense that I don’t wish to tell other people what to do with their bodies. I’m always happy to consider new evidence, but for me personally, I don’t believe any current vaccine can provide health benefits for myself or my loved ones.” It is unclear to me why Watson thinks I am “leading disciples” into any realm. If he thinks he has sound evidence that vaccines lead to better health outcomes then he is welcome to provide it – our Virus Mania team has sought such data from major institutions such as the Robert Koch Institute for many years and they have been unable to provide it.
“She mentions, in passing, the famous TMV (tobacco mosaic virus) in a ‘that’s all very well’ kind of way. But the fact is that the TMV has been sufficiently purified for its structure to be studied by scanning electron microscopy; and that represents a very high level of both isolation and purity. A plant virus it may be, with no animal equivalent, but it is the case that disproves, in a Popperian way, the argument often repeated by the virus deniers that ‘no virus has ever been purified’. Some have been sufficiently purified for study by X-ray crystallography and that represents an extremely high level of purification.“
Dr Roger Watson, The Daily Sceptic
It’s not at all convincing in his article that Watson knows the difference between isolation and purification. He refers to a microscopy study which purports to show TMV. We may need to remind Watson that a virus is a tiny replication-competent, intracellular parasite that can infect a host and pass onto other hosts. Apart from images of tiny particles, there is nowhere in the paper he cites that any of these key properties are demonstrated. I have explained in my video “Electron Microscopy and Unidentified “Viral” Objects” the limitations of the technique and why particles that appear amongst dead tissue cannot be classified as “viruses” without further experimental steps. His reference to an x-ray crystallography paper is likewise useless. Plenty of particles can be purified Dr Watson – the issue is that they need to be shown to be viruses. In any case, you’re in for a treat as I currently have a video in production exposing the Tobacco Mosaic “Virus” story going back to Ivanovsky’s unscientific experiments considered by some to be the beginning of virology.
“But the fact is that the existence of any virus is triangulated by an array of increasingly sophisticated laboratory techniques whereby theories may be tested, cultures grown, and infectivity demonstrated. In fact, a great many viruses have been purified, often against the odds.“
Dr Roger Watson, The Daily Sceptic
Triangulation? The process of measuring distances and determining locations. Watson goes next-level cunning with his conflations to make virology look respectable again! If Watson looked at all my publications he would see that I am familiar with the historical techniques, which failed to demonstrate the existence of pathogenic viruses and how they have morphed into modern molecular detection techniques to keep the virus paradigm alive. His citation is “Virus Purification” techniques in the Encyclopedia of Virology (Fourth Edition), 2021 – I have an e-copy of this publication and am familiar with the described methods. However, Watson needs to show his hand and let us know which particles he thinks have been purified and demonstrated to be “viruses” instead of pointing at a textbook.
Dr Watson: stop keeping us in suspense and please publish your list of viruses that were purified “against the odds” with their proofs.
“The virus deniers trot out the Koch’s postulates argument repeatedly, even though Koch’s postulates were simply one way – long before the advent of amino acid and nucleotide sequencing methods – of demonstrating the presence of a bacterium. Koch’s postulates were never intended to be applied to viruses – the existence of which were not known when Koch postulated.”
Dr Roger Watson, The Daily Sceptic
Watson appears completely confused about Koch’s Postulates which relate to establishing a causative relationship between a microbe and a particular disease, and conflates it with “demonstrating the presence of a bacterium”. The postulates were designed to be applied to all microbes, but as I have stated, my investigations indicate that Koch’s Postulates have never been fulfilled and there is no sound basis to germ theory: bacteria, fungi and postulated “viruses” are not the causal agents of disease. And it doesn’t matter what nucleotide sequences or proteins you discover Dr Watson, you still need to establish where they come from – are you sure the virologists establish this or even do “sequencing”? (See below).
“The original SARS, which almost certainly jumped species, is very unusual for that very reason and, for example, bird flu does not infect humans. The jury remains out on whether SARS-CoV-2, which possibly jumped species, did so spontaneously or after a ‘gain of function’ nudge.“
Dr Roger Watson, The Daily Sceptic
Interestingly for a “sceptic”, Watson espouses most of the virology industry’s stories about viruses jumping species. Can he point to the investigations he performed to conclude something that hasn’t been shown to exist “almost certainly jumped species”? We deal with these highly speculative and sometimes baseless claims in Virus Mania and I covered the original “SARS” (and “species jumping”) in another of my videos banned by Big Tech but still available here. There is a fatal flaw regarding gain of function research with “viruses” when the pathogens themselves have not been shown to exist, as I have pointed out in more videos banned by Big Tech but still available here and here. Dr Stefan Lanka has also outlined the fallacies of “bio-weapons,” including fabricated “viruses” and how they have been used to drive fear into the public for many decades.
“I have corresponded with Siouxsie Wiles, a major debunker of the Koch’s postulates argument, at Auckland University in New Zealand over this point and over the point regarding ‘purification’ of the SARS-CoV-2 virus.“
Dr Roger Watson, The Daily Sceptic
Watson makes an appeal to “authority” here, which was the same mistake made by Steve Kirsch when he clumsily waded into the issue of the existence of “SARS-CoV-2” in January 2022. My husband Dr Mark Bailey has previously outlined why Kirsch shouldn’t rely on such “experts”. Like Watson, Kirsch started off all guns blazing against the “virus deniers”. Like Watson, Kirsch rapidly retreated when the Baileys, Dr Tom Cowan, Dr Andy Kaufman, and Dr Stefan Lanka all offered to participate in a live debate with his chosen “experts”. It is odd that our “sceptic” Watson corresponds with Wiles as she is heavily promoted by the NZ government and advised our country that “the world is on fire” and we should “all behave as they [the government] are asking us to behave” in March 2020.
“If men define situations as real, they are real in their consequences.“
William Isaac Thomas and Dorothy Swaine Thomas
She is notorious for avoiding open scientific discussions and even has a lengthy automated email reply excusing herself from such pursuits. Incidentally, in February 2022, a state-sponsored media platform was found guilty of publishing one of her false claims. Watson has referred to an article by Wiles which is a case of the blind leading the naked. In the article she provides no explanation as to how disease causation is satisfied with viruses when it is conveniently claims there are no suitable clinical experiments available. She tries to distract the reader with Falkow’s molecular postulates, and fails to inform her readers that River’s postulates were designed specifically for viruses but have not even been close to being fulfilled for SARS-CoV-2 – the first problem being that no one can show it exists. There is certainly nowhere in her article that demonstrates she can prove the existence of SARS-CoV-2 or any other virus, only excuses as to why direct proofs are lacking. I have previously addressed her false claims surrounding the application of the PCR in another video banned by Big Tech after several hundred thousand views, but still available here. New Zealanders have endured two years of state-sponsored nonsense from Wiles, who is paraded by the MSM as a go to “expert”. I’m willing to bet that a live debate with Watson & Wiles on one side and the Baileys on the other would be very revealing.
“It transpires that the purification of the novel coronavirus argument is a straw dog created by the viral deniers. In fact, nobody has claimed that it has been purified. However, it has been ‘isolated’, which is a different concept whereby studies are carried out to check it is there.“
Dr Roger Watson, The Daily Sceptic
If Watson hasn’t already indicated that he is bringing his pocketknife into a gunfight, then this is where his pocketknife falls to the floor. I suspect he didn’t know that I have already analysed Vincent Racaniello’s presentation he refers to in this video (banned by Big Tech of course). It is not clear that he even listened to Racaniello’s words: if the virologists don’t have a specific defintion of “isolation” what does Watson think it means? Can he see a problem when Racaniello says “an isolate is a virus that we have isolated…” or has he been swept up in their circular reasoning? The problem of what “isolation” means is the pivotal issue with regards to proving the existence of viruses and the virologists have a habit of playing fast and loose. As stated by The Perth Group in 2017: “The fact is that in virology, while purification retains its everyday meaning, “isolation” is an expediential term virologists assign to data they claim are proof a particular virus exists.” Watson instead chooses to cheerlead the virologists denigration of the English language: if their use of the word ‘isolation’ isn’t what everyone thinks it is, then it’s useless as a method of providing proof that a particle is a virus.
Watson, however, gives the thumbs up to ‘isolate = particles + every other bit of junk in a specimen’, perhaps oblivious to the deception of the virologists.
“According to Siouxsie Wiles, the virus has been found in hundreds of disparate samples and subsequently sequenced. The viral deniers point to the way the sequence was merely pieced together in the early stages, thus proposing a hoax. But this is how viruses are sequenced.“
Dr Roger Watson, The Daily Sceptic
How on earth this made it past the Daily Sceptic editors is a mystery to me. For his source of “truth” Watson has cited “fact-checking” organisations that are supported by Big Tech, and have financial conflicts of interest with Big Pharma. If it is not apparent at this stage of the “pandemic” that these organisations have been consistently misleading the public since day one then it is difficult to believe that he really is a “sceptic”. The fraudulent invention of the “SARS-CoV-2 genome” by Fan Wu’s lab has been exposed by Stefan Lanka’s team and it was even worse than the usual imaginary “viral genome” assembly circus. The ViroLIEgy website has one of the best collections on the many assumptions and biases involved in “genome” creation, from the collection of the crude specimen through to the hypothetical model constructed by computer software. And with regards to “viruses”, we do not call it a “hoax”, we call it fraud. “Viruses” are not really “sequenced” as you might think Dr Watson (see below).
“In any case, as explained to me by Siouxsie Wiles, it is not necessary to purify the coronavirus and as Dr. Ros Jones says in her Unity News Network interview with David Clews, this is not how it is done; the virus is cultured. This is about as close to Koch’s postulates as you could get: grow the purported virus in a cellular culture and identify it by sequencing. Introduce what you have to some other cultured cells alongside a control culture. If the one with the purported virus shows subsequent evidence for the presence of the virus and the other does not, that is about as watertight an experiment as I can think of.“
Dr Roger Watson, The Daily Sceptic
Watson has a great deal of faith in Wiles and her reassurances that purification is “not necessary” and again seems to be confused about what Koch’s Postulates is all about. He describes cell culture experiments and what he believes is “identification” of a virus. How does he know there would be a new virus in there? Apparently, by “sequencing” (I’m not sure he understands what they are actually doing – see next point.) And what does he mean by a “control culture”? Official Information Act requests have exposed that the virologists do not do valid control experiments and this has been a problem ever since Enders and Peebles started the “virus” culture technique in the 1950s. Lack of valid controls = unscientific. I can only suggest to Watson that he digs a little deeper and examines the methodology of the papers rather than simply browse their headlines.
“Bailey and co. try to debunk all the methods that are used in virology and to deny the whole field of laboratory science. The only possible retort can be that no method is perfect, and experiments often fail to show what is being hypothesised. That is an argument for rather than against science, which constantly tries to improve its methods. I recall a whole room being dedicated to a huge amino acid sequencer when I was a PhD student. Now, amino acid sequencing can be done on a microchip.”
Dr Roger Watson, The Daily Sceptic
This is so full of non sequiturs that perhaps the best advice to Watson is that he needs an editor to help him communicate what he is trying to say to his readers. He should be able to clearly see my pro-science position in the video “Science vs Dogma”. My publications analysing virology have clearly pointed out that much of it involves uncontrolled experiments and thus cannot be claimed to be scientific. He refers to Karl Popper earlier in his article but fails to see that Popper would be horrified by the reasoning used by many virologists. How is an in silico “viral genome” that is created de novo from an unpurified specimen, that has been templated to another “viral genome” which was invented in the same way, falsifiable? How is a PCR result that “diagnoses” a disease on the basis that a positive result means you have the disease, falsifiable? I also suspect he is confusing complete in silico assembly of hypothetical “viral genomes” with actual physical sequencing, such as via the Sanger method, which he may have seen when he was a student. Computer games are indeed very seductive, particularly for kids but sometimes for adults too.
“I have had Covid, despite the remarkable claims by my virus denying friends to the contrary. How do I know I had it: it hit me like an express train; I felt terrible for two days and slept for 29 of 48 hours, rather like the flu. My taste was not lost but my sense of smell became incredibly deranged, not something that I had experienced after many bouts of flu in my 66 years.“
Dr Roger Watson, The Daily Sceptic
Watson appears to include this story about his bout of illness as evidence that viruses must exist. Despite it being another non sequitur, what is his definition of “COVID”? Virus Mania co-author Dr Claus Köhnlein pointed out in 2020 that it was nothing more than an imaginary clinical condition based on a new PCR “test” with no demonstrated clinical diagnostic capability. His interview in German reached over 1 million viewers before it was quickly shut down and his interview in English with me on Youtube had 125,000 views when it was shut down. It is still available here. I produced another popular video in 2020, “What Is A Covid-19 Case?” which outlines why “COVID” is a meaningless construct – which was also banned by Big Tech. In Dr Watson’s view how do we define a case: does a person dying in intensive care and an elite athlete running a marathon both have “COVID-19”? According to the WHO they should both be counted as equal “confirmed” cases if a PCR result is positive.
“When I felt worst, I reluctantly took a lateral flow test (LFT). This showed up positive almost instantly and with a thick test line. As I felt better the test – which as it uses antibodies is highly specific but not very sensitive – took longer to show and the line became fainter. Of course, the virus deniers have this one covered under the rubric that immunology is also bogus, antibodies are not at all specific and will pick up anything. My ‘gotcha’ to this is: if I run a pregnancy test which uses antibodies to detect human chorionic gonadotropin, will it show me I am pregnant?“
Dr Roger Watson, The Daily Sceptic
It is unclear if Watson is claiming that his lateral flow test proves the existence of viruses or “COVID” or both. What does he think the test is for? Something unique to the postulated “CoV” particle or a specific bodily process? Oh dear, we are back at square one! I have dealt with “COVID” LFTs previously and they are as equally unsuitable as the PCR with regards to clinical diagnostics and proving virus existence. With the rest of his claims, I’m not aware of who said antibodies pick up “anything” and it certainly wasn’t me. The issue surrounds assigning meaning to various proteins that can be detected through in vitro chemical reactions compared to what this informs us about health in real life. This topic has been outlined in Virus Mania and I also cover it in some of my other videos. His “gotcha” with regards to human chorionic gonadotropin has nothing to do with postulated viruses and related “immunology”. β-hCG is a specific glycoprotein of known composition and provenance that has been clinically validated for diagnosing pregnancy and can be easily compared to a “gold standard”: a foetal ultrasound scan (or the actual baby). As per many of Watson’s attempts, it’s another own goal. I can also suggest to him that if he has a positive result on a pregnancy test, as a man he’s unlikely to be pregnant and should be checked for cancer.
“The virus deniers who tend to promote their views on increasingly bizarre websites and within such a deafening echo chamber that they are completely unable to hear, yet alone contemplate, alternative views. They certainly don’t listen.“
Dr Roger Watson, The Daily Sceptic
What are these “bizarre” websites that he is referring to and what’s wrong with bizarre anyway? The orthodoxy doesn’t like being challenged Dr Watson. If they played like real scientists they’d welcome views that challenge their comfy status quo and we could all go on the same URLs. It may disturb Watson but the appetite for the content we produce seems very healthy. Our audience size is mostly restricted by Big Tech censorship and I’m sure he doesn’t agree with such interference with free speech. However, despite my Youtube channel being heavily suppressed, with millions of views being removed and people informing me that my videos and articles can’t be shared on platforms such as Facebook, the audience still grows every week. Mike Stone recently put together a list of websites that challenge the virus paradigm – I am in regular contact with many of these doctors, scientists and journalists and none have indicated that lack of demand is a problem. Last year, Mark and Dr John Bevan-Smith published their essay “The COVID-19 Fraud & War on Humanity”. Not only do they explain that there is no pathogen termed “SARS-CoV-2” but also why everyone should be sceptical about everything the virologists have ever claimed. They were tracking the viewership across various internet platforms for a few months before they gave up. By that stage it had reached about 250,000 people – I would say that’s a few hundred times more than most virologists are reaching with their papers. Watson’s “deafening echo chamber” may turn out to be his own case of tinnitus…
Postscript
Perhaps Dr Watson’s annoyance stems from the fact that because people get sick and die, he thinks it is unsporting to question the methods of the hard-working virologists? They are the white knights, so if we go against them – it means we must be on the wrong side. I don’t have all the answers as to why people get sick but the extensive research I’ve done informs me that pathogenic “viruses” do not seem to exist and are not the cause of disease. The tree of virology has borne no fruit for humanity unless that fruit is a multi-billion dollar pharmaceutical industry that targets enemies that have not been shown to exist. In the last two years, virology and germ theory have brought the planet to its knees, manifesting in anti-humanity measures such as face masks, stripping of civil rights, and mandated “vaccines”. For some of us, germ theory refuted itself at its inception and we see it for what it is: a tragic misunderstanding of nature, now used as propaganda in a perpetual phoney war, like something out of Orwell’s Nineteen Eighty-Four. Dr Watson can call us whatever names he likes – we see the universe in a different light and it is a light we choose to walk in. Perhaps he’ll take a stroll with us some day?
“There are three steps in the revelation of any truth: in the first, it is ridiculed; in the second, it is resisted; in the third, it is considered self-evident.” Arthur Schopenhauer
I told you this part wasn’t going to be pretty. The collapse of fascist ideological movements and fanatical death cults never is. The New Normal is proving to be no exception.
After three weeks of non-violent civil disobedience outside the Canadian parliament in Ottawa by truckers and other Canadian citizens struggling to uphold their right to not be subjected to forced “vaccination,” Justin Trudeau unleashed the goon squads. Thousands of militarized riot police (and other unidentified heavily-armed operatives) swarmed the area, surrounded the protesters, started breaking into trucks and arresting people, and beating them with batons and the butts of their rifles.
Despite an abundance of video evidence clearly depicting exactly what happened, the Ottawa Police tried to spin it this way …
Here’s an overhead photo of the incident …
The big red arrow (courtesy of The Marie Oakes) points to the lady’s walker, or the alleged “horse-assaulting bicycle.” Presumably, the face of the gentlemen above her also caused the horse “to trip,” or was in the process of causing the horse “to trip,” at the moment that this photo was taken.
And that wasn’t all. Oh no, far from it. The “show of force” was just getting started. After all, this was not a “mostly peaceful” outbreak of rioting, looting, and arson. This was non-violent civil disobedience, with children’s bouncy castles, makeshift saunas, honking, dancing, illegal barbecuing, and other forms of “terrorist” activity, which had to be crushed with an iron fist.
Before he turned the goon squads loose on Friday, Trudeau invoked the Emergencies Act, suspending the Canadian constitution, which he had already suspended back in 2020 due to the “apocalyptic pandemic,” which is why the protesters were protesting in the first place. Parliament was scheduled to debate his authority to declare another “state of emergency,” but, of course, the debate was abruptly suspended due to the massive “police operation” that his invocation of the Act had enabled.
Acting under the Emergencies Act, he immediately cancelled the right of assembly, outlawed the protests, and started threatening to kill people’s dogs and take away their kids. Then he and his fascist New Normal lieutenants started freezing the bank accounts of anyone and everyone even vaguely connected to the trucker protest. According to a Bloomberg report:
“The emergency orders require virtually every participant in the Canadian financial system — banks, investment firms, credit unions, loan companies, securities dealers, fundraising platforms and payment and clearing services — to determine whether they possess or control property of a person who’s attending an illegal protest or providing supplies to demonstrators.”
I have been describing the New Normal as a new form of totalitarianism (or fascism, if you prefer) for the past two years, and I have been documenting it from the very beginning (see, e.g., these Twitter threads from March 2020 and April 2020, which the OffGuardian editors have preserved for posterity). It has been there all along, right out in the open, but rendered invisible by the official Covid narrative.
The official narrative is rapidly dissolving, rendering the fascism of the New Normal visible. This is happening now because those of us who have seen it from the beginning — and have been resisting it all along — have held out long enough to run out the clock. GloboCap can’t keep the narrative going, so all they have left is brute fascist force.
We need to make GloboCap deploy that force, and to shine a big, bright spotlight on it, as the truckers and protesters in Ottawa have just done. In case anyone is confused about the tactic, it’s called classic non-violent civil disobedience. I described it in a recent column:
“In other words, we need to make GloboCap (and its minions) go openly totalitarian … because it can’t. If it could, it would have done so already. Global capitalism cannot function that way. Going openly totalitarian will cause it to implode … no, not global capitalism itself, but this totalitarian version of it. In fact, this is starting to happen already. It needs the simulation of ‘reality,’ and ‘democracy,’ and ‘normality,’ to keep the masses docile. So we need to attack that simulation. We need to hammer on it until it cracks, and the monster hiding within in appears. That is the weakness of the system … New Normal totalitarianism will not work if the masses perceive it as totalitarianism, as a political/ideological program, rather than as a response to a deadly pandemic.”
The official narrative is dead, or dying. The Covidian Cult is coming apart. No one but the most fanatical New Normals believes there is any real justification for imposing mandatory “vaccination,” “quarantine camps,” segregation of “the Unvaccinated,” or any of the other “Covid restrictions.” “The virus” is no longer an excuse for mindlessly following ridiculous orders and persecuting those of us who refuse.
Apocalyptic Pandemic Theater is over. It is a purely political fight from now on.
Ottawa is not the end. It is just the beginning. Protests and other forms of civil disobedience are growing all around the world … yes, even here in New Normal Germany. That does not mean it is time to relax. On the contrary, it is time to step up the pressure. It is time to make the monster show itself, in all its naked fascist ugliness, and to force everyone to pick a side.
Before we get to Christine Johnson’s interview, a bit of background.
My first book, AIDS INC., was published in 1988. The research I engaged in then formed a foundation for my recent work in exposing the vast fraud called COVID-19.
In 1987-88, my main question eventually became: does HIV cause AIDS? For months, I had blithely assumed the obvious answer was yes. This created havoc in my investigation, because I was facing contradictions I couldn’t solve.
For example, in parts of Africa, people who were chronically ill and dying obviously needed no push from a new virus. All their “AIDS” conditions and symptoms could be explained by their environment: contaminated water supplies; sewage pumped directly into the drinking water; protein-calorie malnutrition; hunger, starvation; medical treatment with immunosuppressive vaccines and drugs; toxic pesticides; fertile farm land stolen by corporations and governments; wars; extreme poverty. The virus cover story actually obscured all these ongoing crimes.
Finally, in the summer of 1987, I found several researchers who were rejecting the notion that HIV caused AIDS. Their reports were persuasive.
I’m shortcutting a great deal of my 1987-8 investigation here, but once HIV was out of the picture for me, many pieces fell into place. I discovered that, in EVERY group supposedly at “high-risk” for AIDS, their conditions and symptoms could be entirely explained by factors that had nothing to do with a new virus.
AIDS was not one condition. It was an umbrella label, used to re-package a number of immunosuppressive symptoms and create the illusion of a new and unique and single “pandemic.”
Several years after the publication of AIDS INC, I became aware of a quite different emerging debate going on under the surface of research: DOES HIV EXIST?
Was the purported virus ever truly discovered?
And THAT question led to: what is the correct procedure for discovering a new virus?
The following 1997 interview, conducted by brilliant freelance journalist, Christine Johnson, delves into these questions:
How should researchers prove that a particular virus exists? How should they isolate it? What are the correct steps?
These questions, and their answers, reside at the heart of most disease research—and yet, overwhelmingly, doctors never explore them or even consider them.
Johnson interviews Dr. Eleni Papadopulos, “a biophysicist and leader of a group of HIV/AIDS scientists from Perth in Western Australia. Over the past decade and more she and her colleagues have published many scientific papers questioning the HIV/AIDS hypothesis…”
Here I’m publishing and highlighting excerpts from the interview. Technical issues are discussed. Grasping them is not the easiest exercise you’ve ever done, but I believe the serious reader can comprehend the vital essentials.
Christine Johnson: Does HIV cause AIDS?
Eleni Papadopulos: There is no proof that HIV causes AIDS.
CJ: Why not?
EP: For many reasons, but most importantly, because there is no proof that HIV exists.
… CJ: Didn’t Luc Montagnier and Robert Gallo [purportedly the co-discoverers of HIV] isolate HIV back in the early eighties?
EP: No. In the papers published in Science by those two research groups, there is no proof of the isolation of a retrovirus from AIDS patients. [HIV is said to be a retrovirus.]
CJ: They say they did isolate a virus.
EP: Our interpretation of the data differs. To prove the existence of a virus you need to do three things. First, culture cells and find a particle you think might be a virus. Obviously, at the very least, that particle should look like a virus. Second, you have to devise a method to get that particle on its own so you can take it to pieces and analyze precisely what makes it up. Then you need to prove the particle can make faithful copies of itself. In other words, that it can replicate.
CJ: Can’t you just look down a microscope and say there’s a virus in the cultures?
EP: No, you can’t. Not all particles that look like viruses are viruses.
… CJ: My understanding is that high-speed centrifugation is used to produce samples consisting exclusively of objects having the same density, a so-called “density-purified sample.” Electron microscopy is used to see if these density-purified samples consist of objects which all have the same appearance — in which case the sample is an isolate — and if this appearance matches that of a retrovirus, in terms of size, shape, and so forth. If all this is true, then you are three steps into the procedure for obtaining a retroviral isolate. (1) You have an isolate, and the isolate consists of objects with the same (2) density and (3) appearance of a retrovirus. Then you have to examine this isolate further, to see if the objects in it contain reverse transcriptase [an enzyme] and will replicate when placed in new cultures. Only then can you rightfully declare that you have obtained a retroviral isolate.
EP: Exactly. It was discovered that retroviral particles have a physical property which enables them to be separated from other material in cell cultures. That property is their buoyancy, or density, and this was utilized to purify the particles by a process called density gradient centrifugation.
The technology is complicated, but the concept is extremely simple. You prepare a test tube containing a solution of sucrose, ordinary table sugar, made so the solution is light at the top but gradually becomes heavier, or more dense, towards the bottom. Meanwhile, you grow whatever cells you think may contain your retrovirus. If you’re right, retroviral particles will be released from the cells and pass into the culture fluids. When you think everything is ready, you decant a specimen of culture fluids and gently place a drop on top of the sugar solution. Then you spin the test tube at extremely high speeds. This generates tremendous forces, and particles present in that drop of fluid are forced through the sugar solution until they reach a point where their buoyancy prevents them from penetrating any further. In other words, they drift down the density gradient until they reach a spot where their own density is the same as that region of the sugar solution. When they get there they stop, all together. To use virological jargon, that’s where they band. Retroviruses band at a characteristic point. In sucrose solutions they band at a point where the density is 1.16 gm/ml.
That band can then be selectively extracted and photographed with an electron microscope. The picture is called an electron micrograph, or EM. The electron microscope enables particles the size of retroviruses to be seen, and to be characterized by their appearance.
CJ: So, examination with the electron microscope tells you what fish you’ve caught?
EP: Not only that. It’s the only way to know if you’ve caught a fish. Or anything at all.
CJ: Did Montagnier and Gallo do this?
EP: This is one of the many problems. Montagnier and Gallo did use density gradient banding, but for some unknown reason they did not publish any Ems [photos] of the material at 1.16 gm/ml…this is quite puzzling because in 1973 the Pasteur Institute hosted a meeting attended by scientists, some of whom are now amongst the leading HIV experts. At that meeting the method of retroviral isolation was thoroughly discussed, and photographing the 1.16 band of the density gradient was considered absolutely essential.
CJ: But Montagnier and Gallo did publish photographs of virus particles.
EP: No. Montagnier and Gallo published electron micrographs of culture fluids that had not been centrifuged, or even separated from the culture cells, for that matter. These EMs contained, in addition to many other things, including the culture cells and other things that clearly are not retroviruses, a few particles which Montagnier and Gallo claimed are retroviruses, and which all belonged to the same retroviral species, now called HIV. But photographs of unpurified particles don’t prove that those particles are viruses. The existence of HIV was not established by Montagnier and Gallo — or anyone since — using the method presented at the 1973 meeting.
CJ: And what was that method?
EP: All the steps I have just told you. The only scientific method that exists. Culture cells, find a particle, isolate the particle, take it to pieces, find out what’s inside, and then prove those particles are able to make more of the same with the same constituents when they’re added to a culture of uninfected cells.
CJ: So before AIDS came along there was a well-tried method for proving the existence of a retrovirus, but Montagnier and Gallo did not follow this method?
EP: They used some of the techniques, but they did not undertake every step including proving what particles, if any, are in the 1.16 gm/ml band of the density gradient, the density that defines retroviral particles.
CJ: But what about their pictures?
EP: Montagnier’s and Gallo’s electron micrographs…are of entire cell cultures, or of unpurified fluids from cultures…
—end of interview excerpt—
If you grasp the essentials of this discussion, you’ll see there is every reason to doubt the existence of HIV, because the methods for proving its existence were not followed.
Worse yet, it appears that Robert Gallo and Luc Montagnier, the two scientists credited with the discovery of HIV—as well as other elite researchers—were aware they weren’t employing correct methods.
And so…as I’ve reported, there is every reason to doubt and reject the existence of the COVID virus, SARS-CoV-2, since correct large-scale electron microscope studies have never been done. And by large-scale, I mean: attempting to find and photograph the virus in a cohort of, say, 1000 people who are supposed to be “pandemic patients.” I’m NOT talking about one or two electron-microscope photos accompanying a study.
But even that isn’t the end of the story. There is one further potential limiting factor in virus research. I became aware of it about a year ago. Analysis of electron microscope findings is fraught with difficulty and doubt. Are scientists actually looking at what they think they’re looking at in these photos? I refer readers to the work of neurobiologist Harold Hillman, who concluded that researchers were, for the most part, looking at artifacts, not actual cells or entities within cells. Another suppressed controversy.
After more than 30 years of investigating medical research fraud, my general conclusion is, the deeper you go the stranger it gets. Or to put it another way, the worse it gets.
COVID psychosis is a state of mind in which sufferers believe what doctors are telling them.
And what doctors are telling them justifies all the restrictions and mandates—and the need to censor and cancel those who ignore and disagree with the doctors.
Official doctors promoted by the government and major media are doing the gross forms of hypnosis; and lesser doctors are working the same street with modifications of the official messages.
Official doctors: “Vaccinate everybody. Give them as many boosters as necessary.”
Lesser doctors: “We shouldn’t vaccinate children. And no more than three booster for anyone.”
Mental midgets Neil Young and Joni Mitchell are pulling their music from Spotify, because Joe Rogan, whose Spotify podcast draws in 11 million people, criticizes the party line on COVID.
Free speech no longer means anything to Young and Mitchell. They’re tuned in nice and tight to the official doctors.
These two goofs have bought the whole enchilada.
And it’s a chance to stand out front and wave flags and urge their troops forward.
They’re actually urging the government forward. They’re on the side of big government and big corporations and especially drug companies and elite foundations and all sorts of petty little would-be fascists who want their day in the sun.
They’re civilian Fauci’s.
Celebs for repression.
One aspect of medical hypnosis is the phrase: THIS TIME IT’S DIFFERENT. As in: My God, it’s a pandemic, all bets are off.
Young and Mitchell actually believe all the horseshit being shoveled into their brains about the virus and the spread and the testing and the contact tracing and the quarantining and the lockdowns and the “safe and effective” vaccine—which add up to the absolute need for a State of Emergency and the need to wipe out anyone who doesn’t believe there is an emergency.
Because their basic educations were so thin to begin with, the Young-Mitchell duo have never been able to THINK about the fact that free speech is NEVER overridden, no matter what the current crisis might be. They never got that lesson in school. They’re idiots.
And as far as “the science” is concerned, they’re so dumb and incurious, they can’t even recognize the possibility that unofficial scientific FACTS might contradict official lies.
The two of them are regular dyed-in-the-wool knee-jerk liberals, acting as operatives for big government, because liberals (who’ve turned into weirdly shaped “radicals”) have taken over the machinery of the government. They own it. So whatever it wants, these two jokers want.
If back in the old days, Young and Mitchell whined and yakked and sang about freedom, that’s gone. That’s off the table. That was always a pretense. They don’t know what freedom is. They’re cherry-pickers. They take what they want from freedom and throw the rest in the garbage.
They can’t take the heat of competition and debate and strong opinion, so they just insist on canceling it. They’re chicken-shits.
No guts, no glory.
If they had a few active brain cells to rub together, they’d say, “We disagree with everything Joe Rogan says about COVID. We think he’s dead wrong. But because of a little thing called the First Amendment, the idea of censoring him or removing him from Spotify is grotesque…”
They can’t do it. They don’t have what it takes.
I wouldn’t pay a nickel to listen to their music on any platform. I wouldn’t listen to it if they paid me.
Robert F. Kennedy Jr. succinctly summarizes how Dr. Anthony Fauci wields his power to control and manipulate science across the globe
It’s Fauci’s job to conduct research on chronic diseases to figure out their etiology and environmental causes to protect public health, but instead he turned the NIAID into an incubator for pharmaceuticals
Fauci has a $7.6 billion annual budget that he uses to develop new drugs, which he then farms out to universities
Fauci’s control — in collusion with that of Bill Gates — has rendered the majority of global scientific research nothing more than pharmaceutical propaganda
Fauci shares drug patents with universities, sells them to drug companies, splits the patents with them, and walks those drugs through the FDA approval process, which he also controls; once approved, Fauci himself often profits
Robert F. Kennedy Jr. succinctly summarizes how Dr. Anthony Fauci wields his power to control and manipulate science in this riveting episode of The Jimmy Dore Show.1 Fauci has been painted as a hero throughout the pandemic, an image that is not only misleading but wildly inaccurate, as detailed in Kennedy’s best-selling book, “The Real Anthony Fauci.”
“I wrote the book because so many Americans were looking at Tony Fauci as this kind of savior,” Kennedy said. “… [T]he man on the white horse, or in the white lab coat, that would ride us out of this coronavirus crises but I knew from the beginning … that he does not do public health and has not done public health since the 1980s.” 2 , 3
Rather than looking out for public health, Fauci and his agency, the National Institute of Allergy and Infectious Diseases (NIAID), prioritize pharmaceutical promotion. Kennedy refers to Fauci as the “leader of the pack” when it comes to those promoting pharmaceutical products, profiteering from Big Pharma and promoting their own personal power.
Public Health Plummeted During Fauci’s Reign
In 1984, when Fauci was appointed director of NIAID, 11.8% of Americans had chronic disease, but this has risen sharply since.4 Fauci doesn’t talk about this public health failure — at least not publicly — but as Kennedy noted, it was Fauci’s job to figure out why cases of autism, food allergies, ADHD, sleep disorders, juvenile diabetes, rheumatoid arthritis and many other chronic and infectious diseases have skyrocketed.
It was Fauci’s job to conduct research on these diseases to figure out their etiology and environmental causes to protect public health, but instead he turned the NIAID into an incubator for pharmaceuticals. According to Kennedy:5
“When Tony Fauci came in, 6% of American children had chronic disease. By 2006, 54% had it. We went from being the healthiest country in the world with the healthiest children to the sickest. Literally, we do not even qualify as a developed nation. We are 79th in the world, behind Nicaragua and Costa Rica in terms of our health outcomes.
And why did that happen? Well, the one figure who is more responsible for that than anybody else in the world is Tony Fauci. He is the reason we take more pharmaceutical drugs than any other nation in the world. Three times the average among western countries. We pay the highest prices and have the worst outcomes.”
Fauci’s Multibillion-Dollar Budget Gives Him Immense Power
Fauci has a $7.6 billion annual budget, which in total during his entire tenure is more than half a trillion dollars that he’s been in control of. Instead of using that to reveal the environmental issues leading to outbreaks of chronic disease, he uses the money to develop new drugs, Kennedy explains, which he then farms out to universities:6
“He shares the patents with them, and then he sells them to the drug companies, splits the patents with them, and he walks those drugs through the FDA approval process, which he completely controls from the bottom up. And then he gets them approved and in many cases he himself profits. People within his agency can collect $150,000 a year from royalties off each of these products.”
The NIH owns half the patent for Moderna’s COVID-19 injection, which means that it stands to make billions of dollars as a result. Four of Fauci’s top deputies will also collect $150,000 a year for life as a result — from a product they’re responsible for regulating, an obvious massive conflict of interests.
“The mercantile and commercial interests have overwhelmed the regulatory function at that agency and it no longer does public health — it does pharmaceutical promotion,” Kennedy said.7 As an example, between 2009 and 2016 there were 240 new drugs approved by the FDA, all of which came out of Fauci’s “shop,” he added. “He is the incubator for the whole pharmaceutical industry.”8
How Fauci Controls Science Globally
Fauci has spread the notion that he is untouchable, going so far as to tell MSNBC that an attack on him is an attack on science:9
“It’s very dangerous … because a lot of what you’re seeing as attacks on me quite frankly are attacks on science, because all of the things that I have spoken about consistently from the very beginning, have been fundamentally based on science.”
Throughout the pandemic, “trusting the science” has become a cultural statement and propaganda tool, but one that’s far from what true science is all about. Far from being a source of independent science, in essence Fauci’s control — in collusion with that of Bill Gates — has rendered the majority of global scientific research nothing more than pharmaceutical propaganda. Kennedy explains:10
“Every virologist in the world knew that the coronavirus was engineered. All you have to do is look at the genome. Everybody knew that and they kept silent for a year, and here’s how. He gives away $7.6 billion a year. That’s two to three times what [Bill] Gates gives away. Him and Gates work tandemly. They partner up on everything. They talk together a couple times a week.
They are business partners … in 2000, in Gates’ library, the two of them got together and they formally formed a partnership. You take those two and one other guy — Jeremey Farrar — who is their other de facto partner who is the head of the Wellcome Trust, which is the U.K. version of the Bill and Melinda Gates Foundation. Between those three men, they control 61% of the biomedical research funding on Earth.
So if you want to get your study funded, you’ve got to go to those guys. Not only can they give you the money, but they also can kill a study because they control all of the other funding sources. They can kill a study, they can ruin a career, they can bankrupt colleges who do science that they don’t want done. So they are able to really dictate virtually all the science on the globe.”
Drug Companies and Universities All Benefit
Kennedy gives a theoretical example of how Fauci yields his immense power to influence science: In his lab, Fauci develops a molecule that kills a virus. This is done by scientists dropping molecules onto one of countless viruses — influenza, Ebola, coronaviruses, zika and others — in petri dishes and test tubes to see if it kills them. If the molecule works to kill the virus in a petri dish, they move on to testing it on rats infected with the virus.
“If the rats don’t die, now he’s got a drug,” he says. “It’s an antiviral and it’s usable in mammals because it will kill the virus but it won’t kill the mammal. Then he farms it out to the university.”11 There, a PI, or principal investigator, who is usually a person of power, such as the dean of a department, does a phase I trial, experimenting on animals and around 100 humans. Kennedy explains:12
“For each of the humans that he recruits — he’s a medical doctor, he brings in patients, persuades them to take part in the study — Tony Fauci’s agency gives him $15,000 for every one of those patients. The university keeps 50% of that so now they’re also part of this process. And then if the drug gets through that phase I, then they move on to phase 2 and phase 3. So now they have to bring in 20,000 or 30,000 people.
They bring in a drug company as a partner, and they go through the phase 2 and phase 3 [trials], and then at the end of it, they all split up the patents. So the drug company owns half, Tony Fauci’s agency may get part of it and he and his cronies take little slivers of it so they get paid for life. The university gets a part of it, so now you have all the medical schools in the country … dependent on this income stream.”
‘Independent Panels’ Aren’t Independent
At this point, the new drug still has to get regulatory approval, which brings it before a supposedly independent panel of experts. But this panel isn’t made up of independent scientists looking for the truth about whether or not the drug is safe and effective; it’s made up of Fauci’s and Gates’ PIs, who often have drugs of their own in development. Kennedy continues:13
“When this drug goes to FDA to get approved, it goes to a panel. Tony Fauci’s always saying it’s an independent panel who decides, based upon real science, whether or not this drug is worthy of approval. It’s not an independent science. They’re virtually all his PIs or Gates’ PIs.
Those guys go sit on that panel for a year, and they know that they’ve got their own drugs back at Baylor University they’re working on, or Berkeley or Columbia, that they know are going to be in front of that same panel next year. And they’re all scratching each other’s backs. And they approve that drug and then they go off the panel, finish their drug, and then that drug goes in front of a panel that’s similarly constituted and populated.”
These principal scientists act as gatekeepers to the public, spreading the official narrative under the guise of independent science, often pushing questionable COVID-19 policies. “These PIs control the journals, they control the public debate, they’re on TV all over the world, and these are the people that form the narrative, that protect the orthodoxy,” Kennedy says.14
“If you look at Tony Fauci as the pope, the PIs are the cardinals, the bishops and the archbishops. And they’re the ones that protect the orthodoxy, that make sure that the heretics burn, that doctors who disagree are … delicensed, that they get discredited, that they get gaslighted and vilified and marginalized. They’re the army that controls the narrative.”15
Waking up to Fauci’s façade is necessary to understand the orchestrated planned use of pandemics to clamp down totalitarian control. You can find even more details about the coalition of sinister forces — intelligence agencies, pharmaceutical companies, social media titans, medical bureaucracies, mainstream media and the military — that are intent on obliterating constitutional rights globally in “The Real Anthony Fauci.”
Kennedy’s book has been a best seller for two months now and if you haven’t already picked up a copy I would encourage you to do so now.
Entertaining Content
Dore not only does interviews with important guests as the one above, but he also is a comedian. It can be very depressing when we keep sharing all the devastation that has resulted from COVID. Dore’s mission is to take the news and share the obvious in an entreating way as can be evidenced below how he interprets CNN giving the CEO of Pfizer the CEO of the year award.
This story is about Dr. Meryl Nass, a brilliant and courageous human being and a top medical doctor whom I had the honor of interviewing recently and who is currently under attack in a way that I thought was only possible in my old Soviet homeland—before my time.
It is really strange. Like, really really strange.
Dr. Nass’ mainstream credentials are impeccable. Here is an excerpt from Dr. Nass’ pre-COVID bio:
Dr. Meryl Nass earned her BS in Biology from MIT and her MD from
the University of Mississippi in 1980. She is known for
expertise in anthrax, bioterrorism, anthrax vaccine and Gulf War
syndrome. She identified the first modern use of anthrax as a
biological weapon, which occurred in 1978 during the Rhodesian Civil
War. She has testified for seven Congressional committees on
bioterrorism, vaccines, the anthrax letters and Gulf War syndrome.
She has consulted for the Director of National Intelligence and the
World Bank on the prevention and mitigation of bioterrorism.
Despite Dr. Nass’ top qualifications and expertise, her impeccable career, her history of being one of the top medical experts in the area of bioterrorism and epidemics, and her recent successes in helping COVID patients, her medical license was recently suspended—and—she was ordered to undergo a psychological evaluation (!!!), based on complaints from strangers about “spreading misinformation” and daring prescribe ivermectin and HCQ. That is insane. The complaints did not come from her patients or their family members. It’s the apparatchiks who are going after Dr. Nass because she is (A) effective—and (B) fearless.
Now, let’s get very human and serious. Salon-type debates and snarky remarks about horse medicine are all fun and good—to some people, anyway—but if one were to actually find oneself unable to catch a breath or in great pain as a result of COVID (whatever it is, and wherever it came from, and whatever factors can make it worse), Dr. Nass would be one of the few doctors in today’s surreal medical environment who would have the guts to be a real doctor and not an expensive walking algorithm in a white coat—a real doctor using her expertise and her heart to help the patient survive. When things get personal and physical, snark falls off real fast.
And by the way, no one is saying that either medicine is a panacea. Panaceas might not exist in this world at all. What I am saying though is that when the creative spirit is murdered and the algorithm is allowed to take over medicine for any reason (benevolent or malevolent), actual people suffer and die.
Notably, Dr. Nass concluded as early as March 2020 that the pathogen came from the lab. She also suggested back then that that the now notorious Nature study “proving natural origin of the virus” was either ghost-written or heavily “guided”—and her theory was later strongly supported by Fauci emails.
Dr. Nass was also the one who broke the story about the use of near-lethal dosages of HCQ in WHO-sponsored studies. Dr. Nass talks about it in the interview and shows how it could not have been a mistake. You can read about the entire saga here.
(Pair that with the promptly accepted and as promptly retracted Lancet study that was so fraudulent that it could be on display next to the dictionary definition of “fraud”— and it becomes very hard to explain the situation with simple chaos and ignorance.)
Dr. Nass also talks about the uncomfortably high plausibility of euthanasia of the helpless elderly. In our lifetime. On our watch. In this world.
And despite all the darkness of what we have to deal with today, our conversation is about kindness and hope.
Dr. Nass is a hero.
Without further ado, here is the interview.
UPDATE: Since YouTube removed the video in less than 5 minutes after I posted this article, I uploaded to Rumble.
Dr. Astrid Stuckelberger is an interdisciplinary scientist at University of Geneva and Lausanne, Switzerland. She is an invited professor in European universities, an author and international public speaker.
Below the video and transcript provided by Orwell City, you will find links to the two videos mentioned by Dr. Stuckelberger. The first is a presentation at a US military conference on the topic of Psycho-Neurobiology and War, The second is Dr. Reiner Fuellmich (Corona Investigative Committee) in conversation with Dr. David Martin.
In the same interview that CONUVIVE Mundial conducted with Dr. Astrid Stuckelberger two days ago, the scientist commented on the relationship between graphene, 5G, and Neuro-rights.
One mindblowing point is that the technology that’s being injected into the population would make it possible to intervene in human beings to send them virus imprints and make them sick, among other possibilities.
Dr. Stuckelberger emphasizes the need to become aware of this and start a detox from the graphene present in the body since it’s thanks to this nanomaterial that the bio-hacking of the human being is possible.
More details in the new excerpt that Orwell City has prepared.
Jorge Osorio:
Doctor, I’d like to ask you… Because I was just going to ask you about Dr. Pablo Campra’s report. And you already brought it up. In this same line, what do you think about graphene —which is a nano-conductor—, electromagnetic waves, and 5G?
5G is already being implemented all over the world. Especially here, in South America. And if we add to that, as part of this cocktail, the Neuro-rights that, at least here in Chile, are groundbreaking. Groundbreaking. This is the only country in the world where Neuro-rights have already been implemented. And now they want to implement them in Spain as well.
What could we be talking about, in your opinion? Graphene, 5G, and Neuro-rights.
Dr. Astrid Stuckelberger:
What are Neuro-rights? Can you just explain?
Jorge Osorio:
The Neuro-rights Law establishes —the Chilean President of the Republic said it here— that your thoughts could be intervened. He regularized it as a law.
Dr. Astrid Stuckelberger:
OK. Yeah, that’s… We’re coming to a very interesting topic. So, Dr. Charles Morgan… And I invite you to go and see it on YouTube. Bio-Psycho-Neurology. He made a YouTube video of 58 minutes. And it’s fantastic.
He’s teaching the military about this new DARPA technology in 2018. And in this… And it’s an eye-opening video, really. And in there, he says —about graphene oxide in nanoparticles—, that they were doing experiments —with monkeys, first— of the transmission of thought patterns. They can read or transmit thought patterns.
And they were taking the example of a surgeon. Of course, they want to make it look like it’s good, but you can also use it badly. So, they took the example and said that, if a neurosurgeon wants to make an operation in the Philippines and wants to take control of a person’s hand by his thinking, they can analyze his pattern lighting… We’re electric beings. We’re bioelectronic, so it’s easy to see the pattern. And then they transmit… The person has graphene, and they can transfer the pattern by WiFi. And the person in the Philippines gets the hands going into a pattern of a surgeon. And the person even says, “Oh, it’s very strange. I don’t even do anything, and I’m directed by this program.”
So can you see where I’m going? I’m going to this zombie pandemic because what they’re doing now is that… Yes. Professor Campra came to the conclusion that, in fact, this bioelectric graphene is able to receive information and change the body because it’s everywhere. It’s everywhere, and it even goes in the brain. So, of course, it can have a toxicity. So… The endpoint of this is that they’re going to… What they want to do is bio-hack the brain and bio-hack people. And yeah, that’s what I wanted to say.
I want to make the link with David Martin. Dr. David Martin is a patent expert in the USA who spoke to Reiner Fuellmich, in his debate (program). And he said something very important. I invite you to go and see his video with Dr. David Martin. He gives a clue. He says that he was responsible to give the patents of coronavirus and of the vaccine. And he was doing a mea culpa. He said, “I’m very sorry because I should have never accepted those patents because they aren’t biological. They are synthetic modélisations of the virus.”
And when you go and see into some of the documents of Bill Gates, you see in the back the… I have put this in the report. I can give it to you so you can translate it into Spanish. They have put the number of the patent of the synthetic modélisation of many diseases. Marburg, also.
So what they’re doing is: they have modelized a synthetic message to send through Wi-Fi, through 5G. Because the band is so potent, it’s going up to terahertz. Because of the ionization that increases 1000 times. That’s what La Quinta Columna says. It goes up to terahertz, so it can get the information very quickly.
So, the first thing is that people have to stop this receptor. The graphene. Because they’re going to get the information and will be sick. It’s not a biological virus. It’s a synthetic nanoparticle. Biotech through WiFi. And you can already, you know, transmit through your computer. Information.
And they know this because Luc Montagnier, the Nobel prize, was doing this with water. He was doing the composition of water. And he said that he can give the composition through the computer into a database at the time.
This is crazy. But now, I see that it has been used for the collection of data with the PCR —in the nose—, the mask, the antigenic test. They’re getting it through WiFi to the databank because there’s a hydrogel, and there’s everything to make this transmission.
OK, so this is what I’m saying. We’re in a world where they have kept us ignorant in medicine and science. And they have gone very far into what we’re doing now. We’re electric beings, and we can get the imprint of a virus. hat’s why we have to protect ourselves from 5G. From our phone. Even the phone. You hold it like this, and the graphene comes up. So we have to stop using the phone like this. We have to use it like that. Not having it in our pockets, not sleeping with WiFi, etc. And to detox with zinc, glutathione, and N-acetylcysteine, for example.
There’s a reason CNN’s Jake Tapper is intent on branding me a “menace” and “a liar,” and why he refuses to debate me on the merits of facts and scientific evidence. Here’s the back story.
Apparently, appalled by robust sales of my bestseller, “The Real Anthony Fauci,” CNN anchor Jake Tapper — in lieu of critically reviewing the work — used his Twitter feed to unleash a barrage of ad hominem insults against me.
Breaking with the traditional restraints of journalistic neutrality, professional propriety and intellectual rigor, he branded me “dangerous,” a “menace,” a “liar,” a “grifter,” a fraud, “unhinged” and more.
But Tapper’s defamations hang in the atmosphere without substantiation or citation. If I’m a liar, then what was my lie? If I’m a grifter, then what is my personal profit or advantage? If I am a fraud, then where is my inaccurate statement?
I concede that I’m a dangerous menace, but only to the pharmaceutical industry, its captive technocrats and its media toadies.
When I responded to his slander with a respectful tweet inviting him to debate me, Tapper declined, explaining he would not debate a “conspiracy theorist.” Characteristically, he neglected to cite any conspiracy theory he believes I promoted.
I’ve won hundreds of successful lawsuits, including milestone victories against Monsanto, DuPont, Exxon, Smithfield Foods and leading polluters from the chemical, carbon, pharmaceutical and agricultural industries. (Many of these also initially dismissed me as a “conspiracy theorist.”)
My current book, “The Real Anthony Fauci,” may be the most heavily footnoted volume to ever sit atop global best-seller lists for six consecutive weeks. With 500,000 copies sold, it has attracted a whopping 5,500+ five-star reviews (92%).
Despite extreme hostility toward this volume from mainstream media and the medical cartel, no one has yet identified a factual inaccuracy in its 250,000 words.
If my book is baseless conspiracy theories, then shouldn’t Mr. Tapper welcome an opportunity to correct me with facts or arguments that go beyond name-calling?
Allow me, then, to offer my own theory for Mr. Tapper’s apoplexy.
Many people make Faustian bargains during their lives, trading personal integrity for material advantage. Oftentimes the metamorphosis occurs as a gradual erosion of moral fiber. Occasionally it happens in an instant; a man stands at a moral crossroads and chooses the dark side.
I happened to have a front-row seat when Jake Tapper had his moment of moral crisis. I’m guessing his fierce vitriol toward me is a reaction to his embarrassment that I was witness to the instant when Mr. Tapper chose career over character.
In July 2005, Jake Tapper was ABC’s senior producer when the network ordered him to pull a lengthy exposé on the Centers for Disease Control and Prevention’s (CDC) secret 2000 Simpsonwood conference.
Here is the background:
In 1999, in response to exploding epidemics of autism and other neurological disorders, CDC decided to study its vast Vaccine Safety Datalink — the medical and vaccination record of millions of Americans, archived by the top HMOs — to learn whether the dramatic escalation of the vaccine schedule, beginning in 1989, was a culprit. CDC’s in-house epidemiologist, Thomas Verstraeten, led the effort.
Verstraeten’s findings propelled CDC into DEFCON 1. The agency’s top vaccine officials summoned 52 pharmaceutical industry leaders, the foremost vaccinologists from academia and the American Academy of Pediatrics (AAP), and public health regulators from the National Institutes of Health, U.S. Food and Drug Administration (FDA), CDC, World Health Organization (WHO) and European Medicines Agency to a secret two-day meeting at the remote Simpsonwood retreat center in Norcross, Georgia, to strategize about how to hide these awful revelations from the public.
In 2005, I obtained the explosive transcripts of this meeting and was about to publish excerpts in Rolling Stone (Deadly Immunity, July 18, 2005). Those recordings, ironically, portrayed these leading kingpins of the vaccine cartel poised at their own moral brink, and chronicled their collapse into corruption over two sickening days of debate.
Most of these individuals were physicians and regulatory officials who had committed their lives to public health out of idealism and deep concern for children. Verstraeten’s data confronted them with the fact that the cumulative mercury levels in all those new vaccines they had recommended had overdosed a generation of American children with mercury concentrations over a hundred times the exposures the U.S. Environmental Protection Agency considered safe.
In recommending a vast battery of new vaccines for children, public health regulators had somehow neglected to calculate the cumulative mercury and aluminum loads in all the new jabs.
Dr. Peter Patriarca, the then-director of the FDA Office on Vaccine Research and Review, expressed the general feeling of horror when he asked why no one had calculated the cumulative mercury exposure to children as policymakers added this cascade of new vaccines to the childhood schedule: “Conversion of the percentage thimerosal to actual micrograms of mercury involves ninth-grade algebra. What took the FDA so long to do the calculations?”
In the tense days leading up to the Simpsonwood conclave, children’s health champion Dr. Ruth Etzel of the EPA pleaded with her fellow public health leaders to publicly admit they made a terrible mistake by inadvertently poisoning American children, and to repair the damage.
Dr. Etzel urged AAP and the government regulators to handle the crisis with the same honesty and public remorse that Johnson & Johnson had demonstrated on discovering toxic chemicals in its Tylenol formulations:
“We must follow three basic rules: (1) act quickly to inform pediatricians that the products have more mercury than we realized; (2) be open with consumers about why we didn’t catch this earlier; (3) show contrition. If the public loses faith in the Public Health Services recommendations, then the immunization battle will falter. To keep faith, we must be open and honest and move forward quickly to replace these products.”
Confronted with scientific proof of their role in the chronic disease calamity, the cabal did exactly the opposite. The shocking Simpsonwood transcripts show Dr. Patriarca and the other public health panjandrums warning each other of their reputational liabilities, their vulnerability to litigation by plaintiffs’ lawyers and potential damage to the vaccine program.
Dr. Patriarca cautioned that public disclosure of CDC’s explosive findings would make Americans feel that the FDA, CDC and vaccine policymakers had been “asleep at the switch” for decades in allowing Thimerosal to remain in childhood vaccines.
Over two days of intense discussion, these Big Pharma operatives and government technocrats persuaded each other to transform their disastrous error into villainy — by doubling down and hiding their mistake from the public.
Tapper saw an early draft of my Rolling Stone story and proposed that, in exchange for exclusivity, he would do a companion piece for ABC timed to air on the magazine’s publication day.
Tapper spent several weeks working on the story with me and a team of enthusiastic ABC reporters and technicians. During his frequent conversations with me over that period, he was on fire with indignation over the Simpsonwood revelations. He acted like a journalist hoping to win an Emmy.
The day before the piece was to air, an exasperated Tapper called me to say that ABC’s corporate officials ordered him to pull the story. The network’s pharmaceutical advertisers were threatening to cancel their advertising.
“Corporate told us to shut it down,” Tapper fumed. Tapper told me that it was the first time in his career that ABC officials had ordered him to kill a story.
ABC had advertised the Simpsonwood exposé, and its sudden cancellation disappointed an army of vaccine safety advocates and parents of injured children who deluged the network with a maelstrom of angry emails.
In response, ABC changed tack and publicly promised to air the piece. Instead, following a one-week delay, the network duplicitously aired a hastily assembled puff piece promoting vaccines and assuring listeners that mercury-laden vaccines were safe.
The new “bait and switch” segment precisely followed Pharma’s talking points. “I’m putting my faith in the Institute of Medicine,” ABC’s obsequious medical editor, Dr. Tim Johnson, declared in closing. Two pharmaceutical advertisements bracketed the story.
After that piece aired, I called Jake to complain. He neither answered nor returned my calls.
During the 16 intervening years, Pharma has returned Mr. Tapper’s favor by aggressively promoting his career. Pfizer shamelessly sponsors Tapper’s CNN news show, announcing its ownership of the space — and Mr. Tapper’s indentured servitude — before each episode with the loaded phrase: “Brought to you by Pfizer.”
Under the apparent terms of that sponsorship, CNN and Tapper provide Pfizer a platform to market its products and allow the drug company — a serial felon — to dictate content on CNN.
This arrangement has transformed CNN’s The Lead with Jake Tapper into a propaganda vehicle for Pharma and effectively reduced Mr. Tapper to the role of a drug rep — shamelessly promoting fear porn, confusion, and germophobia, and ushering his audience toward high-yield patent pharmaceuticals.
Tapper’s main thrust during the pandemic has been to promote levels of public terror sufficient to indemnify all the official lies against critical thinking.
All that Pharma money naturally requires that Mr. Tapper kowtow to Dr. Fauci, and the CNN host’s slavishness has helped make Tapper’s show the go-to pulpit for the National Institute of Allergy and Infectious Diseases (NIAID) director.
It’s a safe place for Dr. Fauci to hit all Jake’s reliable softballs out of the park.
“The bootlicking competition at CNN is pretty nauseating,” observed investigative journalist Celia Farber who has chronicled Dr. Fauci’s mismanagement at NIAID for more than 25 years. “It’s ruinous for both democracy and for public health.”
Another journalist has compared Tapper’s mortifying on-air servility toward Dr. Fauci to the adulation of a loyal and obedient canine. “It’s like a dog watching a chess match,” says former New York Times reporter Alex Berenson. “So much intensity and so little understanding.”
Tapper has gone two years without asking Dr. Fauci a single tough question. He has covered up Fauci’s involvement with Wuhan, suppressed news of vaccine injuries, gaslighted the injured, and defended every official orthodoxy on masks, lockdowns, social distancing, vaccines, remdesivir, ivermectin and hydroxychloroquine.
He has never asked about the public health, mental health, and economic costs of lockdown, about the disproportionate burdens of Dr. Fauci’s policies on minorities, the working class and the global poor.
He has never asked Dr. Fauci to explain why countries and states that refused Dr. Fauci’s prescription have consistently experienced dramatically better health outcomes. For example, why are U.S. death rates 1,000x the death rates of African countries like Nigeria and Indian states that widely use hydroxychloroquine and ivermectin? Mr. Tapper simply never allows contrary views on his show.
He continues to extol COVID vaccines as a miracle technology that individuals can take four times and still both get and spread the illness.
“He never calls Dr. Fauci on his vacillating science-free pronouncements,” said Farber. “Dr. Fauci seems to be able to paralyze the curiosity features of Tapper’s brain.”
Tapper has to ask Dr. Fauci why, under his direction, America suffered the world’s highest body count. With 4.2% of the global population, our nation suffered 15% of COVID deaths.
Instead, he functions as high priest of every official orthodoxy, working to deify Dr. Fauci and anoint all his absurd, vacillating and contradictory pronouncements with papal infallibility. The sure way to earn Tapper’s indignation is to criticize Dr. Fauci.
Here are just a few examples of Mr. Tapper’s brazen deceptions:
On Feb. 2, 2021, Tapper “debunked” claims that baseball great Hank Aaron may have died from a COVID shot. The home run king submitted to a CDC-staged press conference 17 days earlier. Tapper assured his audience that the Fulton County coroner had determined Aaron to have died from “natural causes.”
When the Fulton County coroner subsequently denied ever having seen Aaron’s body, much less performed an autopsy, Tapper refused to correct his story.
In August 2021, Tapper gave Dr. Fauci a platform to spread the rumor that deluded Americans were poisoning themselves with a “horse medicine” called ivermectin.
In an Aug. 29, 2021 interview, Dr. Fauci told Tapper, “There’s no evidence whatsoever that that works, and it could potentially have toxicity… with people who have gone to poison control centers because they’ve taken the drug at a ridiculous dose and wind up getting sick. There’s no clinical evidence that indicates that this works.”
Tapper never corrected Dr. Fauci. He never pointed out that there were by then 70 peer-reviewed studies demonstrating ivermectin’s miraculous efficacy against COVID.
He didn’t dispute Dr. Fauci’s characterization of ivermectin as a horse medicine by noting that the drug had won both a Nobel Prize and WHO’s listing as an “essential medicine” for its miraculous efficacy against human illnesses, and that people have consumed billions of doses with no significant safety signals.
Mr. Tapper never thought to ask Dr. Fauci if he was trying to discourage use of a cheap, effective drug that might compete with his experimental vaccines.
Instead, Tapper abjectly parroted Dr. Fauci’s talking points: “Poison control centers are reporting that their calls are spiking in places like Mississippi and Oklahoma, because some Americans are trying to use an anti-parasite horse drug called ivermectin to treat coronavirus, to prevent contracting coronavirus.”
It mattered not to Tapper that both Mississippi and Oklahoma officials quickly denied that anyone in their state had been hospitalized for ivermectin poisoning. Tapper never corrected his false story.
On Sept. 14, 2021, Tapper obligingly gave Dr. Fauci a platform to dispute rapper Nicki Minaj’s worry that COVID vaccines may affect fertility. Dr. Fauci simply declared, “The answer to that, Jake, is a resounding no.”
As usual, Tapper did not ask Dr. Fauci to cite a study to support this assertion. He never pointed out to Dr. Fauci that all of the COVID vaccine manufacturers acknowledge that their products are not tested for effects on fertility, or that recent data has shown dramatic upticks in miscarriages and pre-eclampsia in vaccinated women.
Nevertheless, based upon Dr. Fauci’s word alone, CNN rushed on to defame and discredit the rapper and to assure the public that Minaj was wrong. Dr. Fauci, after all, had spoken!
It’s easy to see how two years of such obsequious deference emboldened Dr. Fauci in November 2021 to declare that “I represent science.”
There are too many other examples of Tapper’s uncritical promotion of government and pharma falsehoods to even summarize. These are not harmless lies. Each of them has potentially disastrous consequences for public health.
The term “psychological projection” describes the uncanny precision with which a certain sort of person applies the very pejoratives to others that most accurately depict their own shortcomings.
When Mr. Tapper calls me “unhinged,” a “menace to public health,” a “fraud,” a “liar,” is he falling victim to projection?
The critical functions of journalism in a democracy are to speak truth to power, relentlessly expose official corruption, and to forever maintain a posture of skepticism toward government and corporate power centers.
What Jake Tapper does is the opposite of journalism. Tapper, instead, aligns himself with power, and makes himself a propagandist for official narratives and a servile publicist for powerful elites and government technocrats.
No wonder his fury at those who challenge their narratives.
Stasys Jakeliūnas is a Lithuanian politician currently serving as a Member of the European Parliament for the Lithuanian Farmers and Greens Union.
The video below is an excerpt from the full length press conference held on December 8, 2021 during which five European Union MEPs push back against the totalitarian tactics of Ursula Von Der Leyen, a German politician and physician who has been President of the European Commission since December 2019.
This video clip is available at Truth Comes to Light Odysee, BitChute and Brighteon channels. All credit for the original full-length press conference video, goes to 21st Century Wire.
Now some researchers, including medical researchers, call this pandemic a “PCR test pandemic”. I agree with them. And I would add that this is also a pandemic of fear.
Because PCR tests are resulting in a number of cases, and so-called covid cases and covid deaths. And this statistic is unreliable, confirmed by three statistical institutions in the European Union.
Now data, statistical data, and feeling of fear is manipulated to push all of us, including our children, into being vaccinated.
Now President Von der Leyen called for mandatory — for discussion, I would be correct — for discussion on mandatory vaccination.
But what we already have — we already have forced or coerced vaccination because of this manipulation of fear, data. And because of requirement to use covid digital certificate.
When ask to vaccinate, we are asked to trust in science.
Now, what is science? I did some science myself years ago, but I remember what it is.
First of all, it’s a scientific debate — open scientific debate.
Now, what is the scientific debate on vaccination and other covid issues, including the PCR test? I don’t see any.
Why? Because it’s blocked. It’s blocked in most of the media. And it’s even censored on the global scale by some global networks.
Now I was born in the USSR. Actually, I was expelled from my home country before I was born because my parents where political prisoners during the Stalinist regime. And they were sent far away from the home country.
I lived in the Soviet Union prison with this censorship, with the control, for 30 years. I didn’t imagine that we would be moving again, somehow, to the environment of the censorship and to the environment of the control.
I was myself censored by the global network three times.
Why? Because I ask questions? I propose some discussion, scientific discussion. I initiated some discussion myself. And it was blocked. It was censored.
Now Commission President Von der Leyen, I don’t know if she is a victim of manipulation — data and fear manipulation — or is she manipulating herself.
The scientists I trust and the data I analyze don’t indicate that we need a vaccination for all. Especially for children and young adults up to 50 years of age, there is no risk from this virus, on a statistical basis, to this age group.
Now, this censorship is quite dangerous because it’s creeping into us. And if it continues to happen I think we’ll be living in something — we can call it global China, we can call it global Soviet Union, or we can call it Global Digital Covid Land. Doesn’t matter what we call it, but it’s not a free world anymore.
So we have to fight for the free world, we have to fight for our right to live in the free world, and for our children’s right to live in the free world.
Thank you.
The Financial Control System — Part 2 of Planet Lockdown’s Interview With Catherine Austin Fitts
In 1998, trillions of dollars started to get sucked out of the U.S. government by the central banks. Our retirement funds have been looted and will within just a few years be nonexistent
Historically, U.S. intelligence agencies have primarily worked on behalf of the central bankers
Central bankers are now putting into place a system that will allow them to extract tax without representation
The central bankers, most of whom are technocrats, have created a breakaway society, a parallel society, in which they are above all law and control everything
To combat their control system, we must first be able to see it for what it is, and realize how it’s being used by us, to our own detriment
The “Planet Lockdown Part 2” interview above features finance guru Catherine Austin Fitts, founder of the Solari Report. (To get a taste of what you’ll find in the Solaris Report, you can download this previous 2020 issue.) You many think you previously saw this but most likely it was Part 1.
Fitts has spent decades exposing corruption and fraud, both within the banking industry and government, and corruption and fraud are driving forces in the COVID pandemic as well. She got her start on Wall Street, where she had a successful career for over a decade.
In 1989, she became the assistant secretary of Housing and Urban Development under the Bush administration. After 18 months, she resigned, but while there, she discovered how technology could make the financing of neighborhoods more productive.
“Government money was destroying neighborhoods, not helping them,” she says, but private entrepreneurs could take this new technology and finance privately. To that end, Fitts started an investment bank and broker dealer named Hamilton Securities Group.
A couple of years later, they were hired by the federal housing administration to be the lead financial adviser, which gave Fitts access to “incredibly rich databases about how the real estate, land and a lot of the mortgage financing and home building works in America’s 3,100 counties.” Fitts continues:
“Then I entered a period where I litigated with the federal government for 11 years. The Department of Justice seized all the databases and all the software tools, and I litigated with the federal government. That’s [what] forced me to really dive into how the control systems were working.
When I was in Wall Street, I saw how the financial control systems worked, but since so much is rigged through the central bank and through government, it gave me a chance to really see how government worked on the covert side, and how that related to Wall Street and Washington.”
Our Retirement Funds Have Been Looted
In 1998, trillions of dollars started to get sucked out of the U.S. government, Fitts says. In essence, it was “a coup d’etat by financial means.” She realized then the extent to which our government was siphoning — stealing — the money. “They were stealing everybody’s retirement,” Fitts says.
“Everybody’s going to retire in 20 or 30 years, but they were going to steal the money up front. So, by the time we got to where we are now, the money would be gone and they could turn to everybody and say, ‘Well, we can’t really afford your retirement.’”
On Wall Street, you have markets and monetary policy run by the central banks, and then you have the electorate, which influences fiscal policy and the government. So, it’s a dual pillar system. Markets are managed centrally. So, central banks, which control monetary policy, can simply print money, and the military then makes sure the money is taken up, which keeps everything liquid. Fitts explains:
“The economic equation is: Can you make more money from printing than you have to spend on the military and making the system go? I’ll give you an example. In the 1980s, we had a period of tremendous monetary expansion. In the last year of the decade, in ‘89, there was a huge fight in the Doolan partnership [Furey, Doolan & Abell LLP] about how much money should be paid to the traders for bonuses.
I had a wonderful partner who did a study, showing that … if instead of having traders in the seats, we’d had chimpanzees, we would’ve made more money. It was very interesting because you’d go out to the Hamptons on the weekends and you’d … hear everybody talking about making fantastic amounts of money because they were brilliant and geniuses and smart and clever.
But it wasn’t [because of their smarts]. It was just simply the monetary policy floating the boats … A lot of the money comes from economic warfare. So, [when] you pump up the dollar, you’re moving money out of the U.S. government. As we’re coming through this big change of globalization, you loan massive amounts of dollars.
And then all of a sudden you pull all the loans. You throw them into a dead-end trap. You pull the money and then they get a crash. Now your dollar is high. So, you go and buy up everything on the cheap.
The governance structure that existed before the financial coup was basically: You have the central banks running monetary policy, and then you have the sovereign government running fiscal policy. The citizens pay taxes to the sovereign government, and they elect representatives who have something say about how that fiscal money gets [divided] up.
Then you have private central bankers and private interests who control monetary policy and are relatively independent of the fiscal. What we’ve seen [is that] … the less the government has information sovereignty and financial sovereignty, the more dependent it is on the central bankers.
So, as the government have levered up with debt and lost their informational and financial sovereignty — part of this is what’s happened with digital technology — the central bankers have gotten more and more powerful.
Since fiscal [year] 1998, we’ve had what I call the financial coup d’etat. So, in the United States, up to $100 trillion have been moved out. Dr. Skidmore and I did a study, and as of 2015, the number was $21 trillion …
At that exact time, we had $20 trillion of debt. So, there was more money disappearing than there was debt. [So, they were taking that] money out. That’s the financial coup. Now that the money is out, you can collapse the government.”
Why Central Bankers Are Intentionally Collapsing Government
Importantly, Fitts stresses that government doesn’t have the power to make illegal transactions. The central banks — which are privately owned — must be involved in order for that to occur. The private banks “are doing it for them,” Fitts explains.
“So, we’ve now reached the point where the central banks are moving in and basically taking control of fiscal policy as well,” she says. “And this is why there’s such a big debate about election fraud.
Essentially the computer systems are controls for the elections, and essentially, the citizens or taxpayers have lost any say. If you look at polls over the last 10 years, the citizens want the country to go to the right, and Congress votes to go to the left. That’s because increasingly these people are controlled and dependent on what the central bankers want.
There’s a great interview that Chuck Schumer, the senator from New York did at the beginning of the Trump administration, where he basically said that if Trump thinks he’s going to contradict or defy the CIA, he’s dreaming; they have 50 ways from Sunday to get you. And traditionally, if you look at the U.S. intelligence agencies, they basically worked for the central bankers.
So, what’s happening is we’re watching a reengineering of this fiscal line. You’re basically looking at the central bankers moving to put into place a system that will allow them to extract tax without representation. That’s the trick, financially. How do you force the citizens to pay taxes with no representation?
Of course, they’re using the pandemic to roll in the system that will make it possible for them to achieve that. Naomi Wolf has done a very good job of describing this, and she said, ‘Vaccine passports are the end of human liberty in the west.’
She’s right, because ultimately, what it’s going to evolve into is a financial transaction system where, if you don’t behave, the central banks can take money right out of your account. They can stop you from transacting.”
An example Fitts gives is, say the central bankers (read totalitarian rulers of the whole world) don’t want you to be able to travel. They want you to stay put where you are. They can easily accomplish this, in this planned system, by programming your electric car such that it cannot operate past that five-mile boundary line.
They will also have full control over the function of money in this system, meaning they can decide what you are allowed to spend your money on. They could decide they don’t want you to have fresh food, so you can only use the central bank digital currency for processed food.
We’ve Been Lured to Create Our Own Prison
The central bankers are nothing if not clever when it comes to prototyping. They don’t do anything without first running many tests to see what will work best. But they don’t just hire top experts. No, instead, they persuade the top developers that they can make a ton of money by developing these prototypes. They make it fun and innovative, allowing skilled people to come up with the ideas.
Once a successful prototype has been identified, they then build their own version of that. In the case of cryptocurrencies, their version is a central bank digital currency under centralized control. Another part of the complete system is the smart grid, which was prototyped, developed and rolled out in recent years. The smart grid is, of course, a requirement for the surveillance apparatus that is at the heart of it all.
While all of these things, cryptocurrencies, the smart grid, artificial intelligence technologies and the like, are marketed as a way to make us all freer, the intended result is a global prison system where no one is free. The good news here is that they must get the general population to build their own prisons. The answer then, is that once you see how it’s done, you can just stop. Stop building the prison walls. Stop building and contributing to the surveillance grid.
This could mean quitting your job if you work for a company that is involved in developing and building technologies intended for this control grid. But even if you don’t actually perform work that helps build it, you are still participating in the control grid structure by using surveillance tools like Facebook and Google.
By allowing smart meters to be installed in your home, by buying and using AI-based technologies and “smart” technologies, by allowing GPS tracking on your phone and so on. If you don’t want to contribute to building this global prison, you have to actually take action and change how and who you do business with.
“If you look at a lot of the financial fraud over the last 20 years in the United States, the leader of that financial fraud in many cases was JP Morgan Chase. Yet statistics show that 50% of Americans bank or have credit cards or other relationships with JP Morgan Chase.
In 1998, when I first realized what was happening with the mortgage fraud and JP Morgan Chase was at the heart of it, I was writing a check on a JP Morgan Chase banking account. And I said, ‘Why am I banking [with JP Morgan]? Why am I allowing my funds to be used as deposits to engineer financial fraud? I’ve got to come clean.’
Forget about protesting. If tomorrow, everybody woke up and said, ‘You know, I’m not going to bank with the New York fed member banks,’ the change would be dramatic, because if you look at where we’re banking and who we’re working for and who we’re associating with, we’re helping them do this.
Remember this is an all-digital system. One aspect of this is currency, but the other is a one-way mirror where you have 24/7 surveillance and data. So not only can I watch you 24/7 and collect data from your body, from your mind, from your activities, but then I can stop you from moving around spatially, or I can turn off your ability to transact.”
The Control System and Transaction System Are One
As noted by Fitts, the system being built is both a control system and a transaction system. The transaction system, however, is not based on what we consider a real currency. It’s actually the end of currencies, because in this system, you can never take the currency out of the bank and put it in your pocket. You can only conduct transactions that are validated and approved through and by the central bank.
Remember, the 24/7 surveillance system “can literally get the human race to be connected to the cloud, to the AI, the software and the robots,” Fitts says. “We’re talking about connecting the human race to a cloud where they teach the AI, the software and the robots, how to do their jobs.” In short, we are actively engineering a future where we, humans, have been largely eliminated from the workplace.
Those who remain will be integrated with robotics. “In other words, whether I have a human do that job, or whether I have a robot do that job, I can manage them in the same system if I can have them all hooked up to the cloud and communicating with each other.”
Basically, what we’re looking at is transhumanism, and we’re quite literally dehumanizing ourselves. This system will also do away with markets, because what we think of as markets will be micromanaged and optimized through artificial intelligence and software.
What Do You Want?
Knowing this, the options become rather simple. As noted by Fitts, we can have a human civilization, or we can have an inhuman civilization. We can have a financial system where private monopoly controls the printing of money, or we can have a decentralized system.
I agree with Fitts, who states that the world she wants to live in is where the financial printing press has been decentralized, and where we are committed to human civilization — not a transhumanist one run by technocrats. As crazy as this transhuman technocratic future may sound to the everyday person, it’s clear the technocrats believe their system can work.
“I think they believe it can work because of the one-way mirror,” Fitts says. “[Let’s say] you have a one-way year where you have 100% access to the data, 24/7, of all the people on this side of the mirror.
Remember, once you engineer all this secret money in taxation without representation, they [the people] can’t see behind the mirror. The thing that punches a hole in the mirror is transparency about government money, and no taxation without representation.”
Creating a Breakaway Civilization
This is why the central bank takeover of the sovereign governments is so important, because this takeover allows them to create a system in which the two sides of the mirror are two entirely separate civilizations. Those behind the mirror — you and I — cannot see what the technocrats are doing on the other side, while they can see every last thing we do and say. “You’re literally talking about a parallel universe,” Fitts says.
Those behind the mirror, the technocratic rulers, do not obey any law that applies to those of us on the other side of the mirror. They are not subject to the law. They have complete immunity from prosecution.
“They can engage in systematic violation of what you and I think of as the law, with impunity,” Fitts says. “And if you look at how much money has been moved out in the financial coup, they can literally become a parallel civilization.”
They’re Trying to Sell You on Being a Serf
The vaccine passport is clearly the tool of choice for the authoritarian globalists’ plan to deprive you and your family of your freedom and personal liberties. This financial coup is 20 years in the making. They voted on the “direct reset” plan (aka The Great Reset), they wrote the plan, and have been implementing that plan, year by year, step by step.We’re now in the end game, Fitts says, where they need to consolidate everything. Now, with their vote for The Great Reset, the central bankers made the decision to put 500 million people out of work over the next year alone.
“That’s the equivalent of dropping several nuclear bombs around the world. That’s financial warfare, and they made it intentionally,” Fitts says. “They made it knowingly. It was a plan. And what is very important to understand, when you think about this pandemic, is people are not dying from magic viruses.
People are dying from tyranny, they’re dying from a great poisoning. That’s part of that tyranny, but our problem, and the thing we need to be afraid of, is tyranny. Because the tyranny needs, and is about to get much, much worse.
It’s the passports and that system of central bank digital control that will give them the ability to do that. The world economic forum calls it The Great Reset, which is kind of the marketing … The World Economic Forum guys make it interesting and fashionable [to say] ‘In 2030, you own nothing, and you’re happy.’
Now, what I hear is ‘It’s 2030, the direct reset has stolen all your money, taken all your assets, and they’ve got your mind-controlled.’ The Great Reset is to sell people on a vision of a world where the average person has a much smaller command on resources and assets, and is subject to complete central control.
Part of what you’re dealing with is that human beings crave coherence. And so, if you can put them in a state of incoherence, they will literally do anything they can to get back to coherence. It’s a torture mechanism. If you study torture, it’s a typical torture tactic …
That’s why you see all these people saying, ‘If you just accept the passports, you’ll be free. Or if you get the vaccination, you’ll be free. They have spent a fortune since World War II on figuring out how to use digital technology, telecommunications and media to implement mind control much more economically and much more broadly. And one of the things I think they’re very enthusiastic about how well it has worked.”
Watch the Financial Transactions
When will it stop working? When enough of us can see what they’re doing. For example, it’s important to realize that, during this pandemic, people have been bought out of the labor market with federal assistance that pays them more than they were making while working.
This strategy has severely impeded small businesses from getting the labor they need to keep going, and according to Fitts, this is all part of the plan to bankrupt all small businesses.
Of course, the next step will be to require the COVID jab for anyone who wants to collect unemployment or other financial assistance, as the vaccine passport is combined and integrated with the new all-digital central bank transaction system. Step by step, everyone is being herded into the new control system. But remember, we can stop it, because we’re doing it to ourselves.
The problem is, ending tyranny almost always requires some kind of sacrifice. End tyranny is rarely a comfortable or profitable venture. That said, there are countless ways to fight back.
Prayer War Room and Other Suggestions
Fitts tells the story of a woman fighting corruption in her hometown. She was scared because taking it to the next level would require her to go public, and she was a very private person. Fitts suggested she watch the film “War Room,” a Christian movie about prayer. “Start a war room and just fight them through prayer,” Fitts told her. Apparently, it worked wonders.
“So, there are many different ways to fight, and you could fight in a way that’s comfortable. Some people organize, some people are bringing lawsuits. Some people are lobbying. Some people are moving and going to another jurisdiction. Some people are pulling their money out of JP Morgan Chase.
There are many different ways to do it. If you’re working for a big bank or big corporation, start working on building the skills and the resources and the wherewithal you need to start something yourself. Start learning. It’s called DIY — do it yourself.
Start looking at your financial picture and figuring out … how you can collapse your income statement and your balance sheet to something which is much more resilient, locally, and doing it yourself.
We don’t need to get mortgaged up and get dependent on the system. The third thing is, for God’s sakes, go out and get yourself a great bank. Particularly if you’re in the United States, there are lots of great banks and great bankers … who also don’t want the central bankers controlling everything.
I know a lot of community bank presidents who don’t want to be controlled by the New York Fed … So, the first thing you need to do is swing your money out of — if you’re invested in the New York fed member banks, or in the big corporations that are running government this way — swing your money out of those stocks and start investing in building a local food system.
Who’s your farmer, who’s your rancher? Where are you going to get high-quality fresh food? There is tremendous opportunity to build out the local, fresh food systems. If you take the time and have patience, there are very good investments to be had there.
[Next, know] who’s your sheriff. The entire enforcement within a county area is controlled by the sheriff [in the U.S.], and in most counties, the sheriff is elected. Not all but most. The feds cannot come in and do an enforcement action unless the sheriff allows it to occur.
[Why should you] care about who your state legislators are? Because the state legislators have the power to say no to the federal government, particularly if you’re not willing to escrow your taxes and get into this taxation without representation.
So, go through your financial statement and your balance sheet and get the bad guys out of your money and start supporting the local guys who are willing to support the rule of law …
I had a former client who called me and said, ‘I just sold a house, and I want to know, should I put the money into real estate or precious metals?’ And I said, what’s the point of having assets? If you don’t have an army to protect them, meaning if you don’t have litigators, state legislators and sheriffs who are willing to go protect your assets, your assets are worthless; you’ll lose them.
So, she took the money and gave it to a group of litigators who were litigating some of what’s going on right now. Anytime you can make an investment that permanently reduces your expenses, you’re better off to do it yourself. So instead of paying your water bill, build a well. In other words, get your money out of financing the guys who are doing this to you, and get your money into financing yourself, your friends or people you know.
Trust me, if tyranny controls everything, and tyranny can operate above the law, then nothing’s going to work. This is a war. And if we don’t stand up and fight it, now, there will be no way to wiggle around this. There’s no way to outplay it. There’s no place to run. There’s no place to go. So, you’ve got to stand and fight back …
We have a choice. Everybody has a choice. So, stop building the prison, stop helping these guys and start creating friction. We don’t have to go along. And we’re the ones who are building the prison. So, you have to bring transparency to what’s going on, and then you have to take action.
We’re not all going to make it out of this process alive. It’s war. That’s what happens in a war, but human liberty is worth fighting for. We’re living in a world where there are two visions, and the top 1% have a vision of us as a natural resource, [while] we have a vision of us as individuals with sovereign rights that come to us by divine authority.”
As noted by Fitts, these are two extraordinarily different visions. One option is a society where all people have the ability to exercise our potential. In the other, only a few get to exercise their potential, while the rest have no opportunity at all. We’re in the end game. It’s all or nothing at this point. There’s no middle ground.
In the end, Fitts and I both believe the plan will fail, but ONLY if we all do our part to prevent it. What’s more, we also need to prepare for what comes after their plan fails. This too could be just as challenging. Fitts notes in conclusion:
“I tell people, while the Titanic is sinking, grab some planks and deck chairs and start building your ark, because these guys are going to make a huge mess. This is a mess. And if you look at what they’re trying to do, it’s very hard, it’s very complicated. I think it’s going to fail.”
On Nov. 2, members of the Centers for Disease Control and Prevention’s vaccine advisory committee voted 14–0 to recommend Pfizer’s pediatric COVID shot for children 5 –11 years old. Were their decisions driven by science and conscience — or their ties to drugmakers?
CHD EDITOR’S NOTE: Following the Oct. 26 meeting of the U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee (VRBPAC), Children’s Health Defense argued it is time to shun the individuals — and institutions — that are selling out America’s children without even a prick of conscience. At the close of this article about the members of the Centers for Disease Control and Prevention’s (CDC’s) Advisory Committee on Immunization Practices (ACIP), we reiterate our list of suggestions for shunning.
On Nov. 2, the members of ACIP voted 14–0 to recommend Pfizer’s Emergency Use Authorization (EUA) COVID shot for children 5 –11 years old.
Neither the disgracefully unscientific vote nor CDC Director Rochelle Walensky’s prompt endorsement came as a surprise. Though billed as “independent,” the 14 ACIP members — like the 17 members of FDA’s VRBPAC who voted the same way the previous week — have deep ties to pharma, with careers that hinge on promoting and rubber-stamping the United States’ destructive one-size-fits-all vaccination agenda.
Describing the VRBPAC and ACIP meetings as “a total sham,” Children’s Health Defense President Mary Holland said, “Sadly, approval from these committees means nothing in terms of safety.”
Political scientist Toby Rogers agreed, stating the ACIP meeting “was not a scientific review. It was banal bureaucrats announcing plans for a Blitzkrieg and the bought white coats were cheering them on.”
With their vote to give young children the dangerous injections, ACIP members signaled that they, too, deserve to be shunned, along with the powerful institutions with which they are affiliated. The latter include the nation’s top universities and leading pediatric hospitals.
Pediatric hospitals, meanwhile, are playing a frontline role as COVID vaccination sites. Promoting the injection for 5-year-olds, First Lady Jill Biden visited Texas Children’s Hospital straight away, applauding the hospital for the 39,000 pediatric vaccine appointments it had already scheduled.
Also worthy of shunning are the 20,000 individual vaccine providers who were pre-positioned to “hit the ground running” and “get shots in little arms.”
Within two days of ACIP’s and Walensky’s verdicts, these providers had administered the jab to thousands of 5- to 11-year-olds, and within the first week, according to the White House, 900,000 children had been injected.
New dangers emerging
Community vaccination sites such as pharmacies and pop-up clinics have attracted recent attention for egregious vaccine administration errors in young children:
In Texas, a pop-up clinic gave adult doses of the Pfizer jab to 6- and 7-year-old boys “two days before a proper dose of the vaccine was even approved for that age range.”
In Virginia, a pharmacy (subsequently ordered to stop administering the shots) gave 112 children in the 5–11 age group the wrong COVID vaccine formulation.
A pediatric practice in California also gave 14 children an incorrect dose of the Pfizer jab, not disclosing “whether the kids got too much or too little.”
In addition, pharmacies have “mistakenly” given adult COVID shots to children under age 5 whose parents had requested flu shots.
With censorship rampant, many parents may be unaware of these transgressions. They also may not know that the experimental product FDA and CDC are unleashing on children is coming under increasing fire from Pfizer whistleblowers.
The same day as the ACIP vote, The BMJ published a whistleblower’s hair-raising account of “data integrity issues” in Pfizer’s “helter-skelter” clinical trials. According to Brook Jackson — a trained clinical trial auditor — Ventavia Research Group (one of the contract research organizations engaged by Pfizer) “falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events.” Quality control staff, Jackson further reported, were “overwhelmed by the volume of problems they were finding.”
When Jackson shared her concerns with both Ventavia and FDA in September 2020, Ventavia fired her. FDA ignored her warnings and granted EUA status to Pfizer’s injection in December.
Melissa Strickler McAtee, until recently a quality control employee at Pfizer’s plant in McPherson, Kansas, described, in an interview with Project Veritas, Pfizer’s efforts to deceive the public about the use of fetal cell lines in creating the COVID shot.
Equally disturbingly, Strickler McAtee told other journalists that Pfizer’s vaccine exhibits an unusual fluorescent blue glow, stating she had “never once [previously] seen anything do that, not even close” during her 10-year career inspecting “hundreds of thousands of units” of vaccines. She also reports that her co-workers at the plant are being unprecedentedly kept in the dark about what the vaccine’s ingredients are.
Pfizer has a lengthy history of quality control problems in addition to a business model predicated on habitual fraud. The Kansas plant, which Pfizer acquired when it strategically purchased injectable drug company Hospira in 2015, has been repeatedly “dinged” by FDA for problems with quality, cleanliness and contamination.
In the three years leading up to its acquisition by Pfizer, Hospira had to issue more than 40 recalls, and Pfizer/Hospira has continued to be a frequent offender on FDA’s recall list since 2015, receiving another warning letter from FDA in 2017.
FDA’s tsk-tsking of Pfizer clearly represents a hollow rebuke, however, as this week’s FDA request to a federal judge made plain: FDA is asking for 55 years to make public the data and information it relied on to license Pfizer’s COVID-19 vaccine.
These and other clinical trial shenanigans strongly intimate that “the data that the FDA and CDC have been pretending to base their decisions on for the last year, are fiction.”
Below are the ACIP members who signed off on Pfizer’s pediatric vaccine, and their conflicts of interest.
ACIP Chair Grace Lee
Dr. Grace Lee (gmlee@stanford.edu) chaired the November ACIP deliberations. Lee has been associate chief medical officer for practice innovation at Stanford Children’s Health and a pediatrics professor at Stanford School of Medicine since 2017, after having spent two decades at Harvard and Boston-area hospitals.
In addition to policy work focusing on financial rewards and penalties to reshape hospital performance, Lee has built her reputation by shoring up the pretense that the nation has a functioning vaccine safety surveillance system.
Lee served as past principal investigator for the CDC’s Vaccine Safety Datalink (VSD), a large database that includes comprehensive longitudinal medical and vaccination records for two million children and seven million adults. Although VSD analyses have the potential to permit enlightening vaccinated-unvaccinated comparisons of health outcomes, the CDC has sole access to the data.
In the words of CHD’s chief scientific officer Dr. Brian Hooker, CDC has “shut [VSD] up like a fortress, despite the fact that it’s taxpayer-funded.”
In VSD-based publications — some of which include fellow ACIP member Matthew Daly — Lee has made a habit of downplaying vaccine risks. For example, she encourages women to get Tdap (tetanus-diphtheria-acellular pertussis) shots during pregnancy, even while data show an increased risk of placental and amniotic fluid infection in vaccinated pregnant women.
She also has whitewashed risks of flu shots in children under age 5 despite finding “an apparent dose-response for vaccine and allergic reactions in the 1- to 3-day risk window.” She dismisses post-vaccination anaphylaxis risks as “rare,” though the package inserts for most vaccines on the childhood schedule prominently list anaphylaxis as an adverse event.
Another VSD study co-authored by Lee documented a safety signal for febrile seizures linked to influenza vaccination of children in their first five years, particularly if administered along with pneumococcal vaccination; massaging the troubling conclusion with vaccine doublespeak, Lee and colleagues proposed placing their findings “in a benefit-risk framework to ensure that population health benefits are maximized.”
While in Boston, Lee served as associate director of the FDA-funded Mini-Sentinel Project, one of several newer vaccine safety surveillance mechanisms trotted out over the past decade.
As noted by CHD Chairman Robert F. Kennedy, Jr. in a letter to Biden advisor David Kessler in December 2020, studies published using Sentinel data — all authored by the same small pool of insiders — focus on an extremely narrow subset of adverse outcomes and reflect methodological decisions “that could easily constrain researchers’ ability to detect outcomes of interest.”
When a Sentinel study of the two rotavirus vaccines routinely given to American children identified a “significant risk” of intussusception after dose 2 — a bowel complication that forced CDC to revoke its recommendation for an earlier rotavirus vaccine — Lee and co-authors deployed more doublespeak, once again advising the public to consider the risk “in light of the demonstrated benefits of rotavirus vaccination.”
Discussing myocarditis last June, Lee admitted, “clinical presentation of myocarditis cases following vaccination has been distinct, occurring most often within 1 week after dose two, with chest pain as the most common presentation.”
This did not stop Lee from joining with other public health officials in passing off myocarditis as “an extremely rare side effect” and claiming that young people are likely to “recover on their own or with minimal treatment.”
In September of this year, Lee co-authored a paper in JAMA belatedly conceding that a large segment of the population (“women and those with a history of allergic reactions”) is at “elevated risk” of experiencing allergic reactions to mRNA COVID vaccines due to the presence in the injections of polyethylene glycol (PEG). CHD issued urgent warnings about PEG and its entirely predictable anaphylaxis risks a full year earlier, in September 2020.
Stanford receives extensive vaccine funding from the Gates Foundation, including for the development of 3D-printed vaccine microneedle patches (a strategy that would allow “vaccination without a shot”).
Not only does Stanford require all students to be COVID-vaccinated, but it also urges vaccination for students’ children.
Lynn Bahta
Lynn Bahta, RN, MPH (lynn.bahta@state.mn.us) is an immunization program clinical consultant for the Minnesota Department of Health, with a 25-year career focused on promoting vaccination.
During the pandemic, Bahta has been giving talks about “vaccine hesitancy in the time of COVID,” offering “key communication strategies to build confidence among those who are hesitant.”
Vaccine “hesitancy” appears to have been her bailiwick long before COVID, however, and her publications suggest a particular interest in coaxing Minnesota’s immigrant, migrant and refugee populations into higher vaccination rates.
Loyal to the fraudulent CDC party line that denies any link between MMR (measles-mumps-rubella) vaccination and autism, Bahta has published articles dismissing the well-founded autism concerns of Minnesota’s Somali community as “misinformation.”
Somali children in Minneapolis suffer the highest known rate of severe autism in the world. Somali parents allege that the reaction of public health officials like Bahta has been one of indifference.
Discussing COVID vaccines, Bahta claims that the “great majority, usually over 90%” of adverse reactions “are not serious.”
In fact, while stating that she “never disagrees with people who believe they were injured by vaccines because it’s difficult to know,” she clearly sides with public health officials in viewing “unverified reports” to the Vaccine Adverse Event Reporting System (VAERS) as “misunderstood by the public and exploited by skeptics in a way that is undermining immunization efforts against COVID-19.”
Bahta disingenuously opines that “people naturally but incorrectly associate injuries with recent events.”
Also of note:
Bahta’s was one of the core “yes” votes in favor of recommending Moderna’s COVID shot last December.
When ACIP deliberated over COVID booster shots in September, Bahta was willing to recommend boosters for adults age 50 and up and individuals with underlying conditions but not for some groups of younger adults. At the time, Bahta argued for the need to “stay with the science,” stating, “I don’t think we have the data.”
By November, Bahta apparently was untroubled by the paucity of safety data available for the 5–11 age group, stating, “We know more than what we don’t know.”
Beth Bell
Beth Bell, M.D., MPH (bzb8@uw.edu) is a clinical professor in the Department of Global Health at the University of Washington (UW) School of Public Health. Until 2017, Bell spent most of her career at CDC, including as Director of the National Center for Emerging and Zoonotic [animal/insect-to-human] Infectious Diseases.
“Health security” and biosecurity are the linchpin buzzwords that global technocrats are using to push for complete control over people’s “ability to work, to socialize, to travel, conduct business, access public services and to purchase essential goods and services.”
Like many of the individuals who make their way onto FDA and CDC committees, Bell started her CDC career as an officer in the Epidemic Intelligence Service (EIS), a branch that journalist Jon Rappoport has dubbed the “medical CIA.”
As Rappoport notes, EIS graduates’ occupancy of “key positions in the overall medical cartel” furnishes an “unparalleled opportunity” to control information — and disseminate disinformation.
During COVID, Bell has positioned herself as a champion for vaccination “equity,” stating “If we’re serious about valuing equity, we need to have that baked in early in the vaccination process.”
Bell’s comments about wanting to make sure “socially vulnerable” communities and people of color have access to COVID shots echo troubling racially oriented remarks made by Melinda Gates early on in the pandemic. Located in Gates’ backyard, UW not only benefits from close ties with and extensive funding from the Gates Foundation — an organization tainted by allegations of medical experimentation and an underlying eugenicist ideology — but also enjoys extensive support from Microsoft.
Also of note:
As co-author of a CDC paper summarizing ACIP’s May recommendation that 12- to 15-year-olds get the Pfizer shot, Bell and colleagues inaccurately argued that “COVID-19 in adolescents is a major public health problem” and that “desirable [vaccine] effects” outweigh “any undesirable effects in most settings.” The authors did not mention the teens who are dying of post-vaccination cardiac arrest.
Regarding COVID booster shots, Bell first stated, “I have my own concerns that we appear to be recommending vaccines for people who I don’t think need it”; she later agreed, however, that “moving forward with the recommendations makes sense for the sake of being clear.”
Regarding COVID jabs for young children, Bell claimed, after the November vote, “if she had a grandchild, she’d get the grandchild vaccinated as soon as possible.”
Oliver Brooks
Oliver Brooks, M.D. (oliver.brooks@wattshealth.org) is chief medical officer and a member of the executive team at Watts Healthcare Corporation in Los Angeles. Watts Healthcare provides primary care services under the Department of Health and Human Services (HHS) and also receives federal funding for other services, including those related to HIV/AIDS.
Brooks is immediate past president of the National Medical Association (NMA), which he describes as “the oldest and largest organization representing African-America’s physicians and the guardians of the health of African-Americans.” As such, Brooks — like Beth Bell — made “health equity” his calling card, with vaccination of minority groups one of his signature goals as NMA president.
CDC celebrates Brooks’ “leadership roles focusing on disparities in vaccine coverage rates.”
Brooks speaks frequently “on the science and the implementation perspective of vaccine utilization,” is a board member and past president of the California Immunization Coalition, chairman of the Immunize LA Families Coalition and member of the national Leadership Panel for the Adolescent Immunization Initiative.
During the pandemic, Watts Healthcare has received millions in funding from Kaiser Permanente to promote COVID vaccination in L.A.’s Hispanic and African American communities.
In March 2021, Watts Healthcare also received $4.3 million via the American Rescue Plan to increase the federally qualified health center’s “ability to get more shots in arms.” The nonprofit is further beholden to the federal government for a $5.18 million coronavirus-related Paycheck Protection Loan approved in April 2020.
Brooks co-chaired California’s COVID-19 Vaccine Work Group, working to “get the vaccine out more rapidly” through “more points of distribution.” Early on in the vaccine rollout, one of those “points of distribution” in San Diego was forced to pause vaccine administration when numerous recipients suffered severe allergic reactions.
Since 2014, Brooks has received $118,439 (350 general payments primarily for consulting or speaking engagements) from biopharmaceutical companies that include Pfizer as well as Sanofi Pasteur, Novartis, Seqirus, Gilead, GlaxoSmithKline, Merck, Meda, AbbVie and Theratechnologies.
Also of note:
At over $271,000, Brooks’ annual salary is second only to that of the Watts Healthcare CEO.
Watts Healthcare and another South LA nonprofit received $3 million in COVID-related funding from the Oprah Winfrey Charitable Foundation in July 2020. The media tycoon — one-time member (along with Bill Gates, Warren Buffett, George Soros, David Rockefeller, Ted Turner and others) of an elite “club” of billionaire philanthropists — urges compliance with mask mandates and uses her influential platform to tell those who are not vaccinated to “reconsider.”
Wilbur Chen
Wilbur Chen, M.D. (wchen@som.umaryland.edu) is a professor at the University of Maryland School of Medicine, with research interests “in developing vaccines against pathogens which afflict low- and middle-income countries” as well as in vaccine development for the elderly. Chen has headed up vaccine trials for influenza viruses, enteric pathogens and “agents of bioterror.”
Chen is co-investigator for two entities funded by the Anthony-Fauci-led National Institute of Allergy and Infectious Diseases (NIAID): the Vaccine Treatment and Evaluation Unit (composed of 10 academic centers throughout the U.S.) and the Collaborative Influenza Vaccine Innovation Centers (a network of research centers developing “novel vaccine candidates and delivery platforms”).
In advance of the ACIP vote on the 5–11 age group, CHD joined numerous citizens in arguing (unsuccessfully) that Chen be removed from the committee for blatant financial conflicts of interest. In 2020 alone, Chen accepted $437,251 from vaccine makers GlaxoSmithKline (GSK) and Emergent BioSolutions — a fact “researched and exposed by average citizens” rather than disclosed by CDC. Chen’s payments since 2014 total over $476,880 and include monies from Janssen, Seqirus, MedImmune, Astellas Pharma, Valneva Austria and BioFire Diagnostics in addition to the two companies already mentioned.
Chen also receives research funding from the Gates Foundation and from the Seattle-based global health organization PATH. PATH’s former CEO, Christopher Elias, now serves as president of the Gates Foundation’s Global Development Division, leading efforts in areas such as vaccine delivery and family planning; Elias was a leading Event 201 participant.
Also of note:
In addition to serving as a voting member of ACIP, Chen is a core member of NIAID’s Data and Safety Advisory Board.
During COVID, Chen has been a staunch advocate of “aggressive nonpharmacologic intervention and control measures,” including “aggressive recognition and isolation and quarantine of cases and contacts.”
Despite the well-documented risks and failures of influenza vaccination, Chen continues to insist that “Vaccination is by far the best method to prevent and control influenza.”
Chen recently voted to make a highly reactogenic Ebola vaccine obligatory for healthcare personnel, lab workers and support staff at facilities that handle Ebola specimens, arguing against letting workers make their own risk-benefit decisions.
Sybil Cineas
Sybil Cineas, M.D. (sybil_cineas@brown.edu), a Harvard Medical School graduate, is an associate professor of medicine, pediatrics and medical science at Brown University, and, as associate program director of Brown’s combined residency program in internal medicine and pediatrics, is “highly involved in the training of residents and medical students.”
According to CDC, Cineas has “20+ years of experience teaching about and promoting vaccination.”
Like fellow ACIP members Beth Bell and Oliver Brooks, Cineas frequently cites health equity to justify her vaccine votes. For example, as a member of the ACIP Hepatitis Work Group, which recently recommended hepatitis B vaccines for everyone age 59 and younger while issuing a more qualified risk-based recommendation for adults age 60 and up, Cineas wanted to recommend universal hepatitis B vaccination for all ages. She argued, “A simplification of this recommendation [would] reach more individuals at risk … and promote health equity.”
Also of note:
CDC has given Brown researchers $4.9 million to study COVID vaccine effectiveness in seniors; the researchers state that “the urgently needed research will be used to inform recommendations about vaccine booster shots for nursing home residents.”
Matthew Daley
Matthew Daley, M.D. (matthew.f.daley@kp.org) is a senior investigator and practicing pediatrician at Kaiser Permanente Colorado, described by CDC as having “extensive research experience in the areas of vaccine safety, parental vaccine hesitancy, and immunization services delivery.”
Daley’s published studies on vaccine “hesitancy” cover topics such as social media interventions to increase vaccine acceptance, barriers to adolescent human papillomavirus (HPV) vaccination, under vaccination patterns and parent-provider trust. (In one study, parents reported trusting pediatricians on topics such as nutrition but “did not believe their pediatrician provided ‘balanced’ information on both the benefits and risks of vaccination.”)
Daley also conducts Vaccine Safety Datalink (VSD) studies on a variety of topics, including safety of newly licensed vaccines, vaccine safety during pregnancy and, according to the CDC, safety of the childhood immunization schedule.
After the Institute of Medicine acknowledged that studies “to examine the long-term effects of the cumulative number of vaccines or other aspects of the immunization schedule have not been conducted” — and identified the VSD as “an important resource for conducting this research” — Daley and CDC co-authors wrote a white paper to describe how this could be done but shrouded their remarks in so many caveats about potential studies’ “inherent complexity” as to make their feasibility seem highly doubtful.
Daley’s VSD studies, some co-authored with ACIP colleague Grace Lee, have identified potential safety signals, but in each case, Daley and co-authors have found reasons to reject or mask their own conclusions.
Examples include attributing a statistically significant association between hepatitis A vaccination during pregnancy and small-for-gestational-age infants to “unmeasured confounding”; putting forth “seasonality” as the likely contributor to a statistical signal for Bell’s palsy in adults age 25 and up following H1N1 influenza vaccination; and dismissing as “rare” two types of adverse events (anaphylaxis and fainting) significantly associated with live attenuated influenza vaccination in children 2 through 17 years of age.
Also of note:
After the vote recommending the COVID shots for younger children, Daly professed to not be surprised by parents’ hesitation, stating that parents “may be more risk-averse about their child.” However, though Pfizer’s clinical trial in children was too short and too small to assess the risk of myocarditis, Daley confidently asserted that “younger children are at a greater risk of developing myocarditis after a COVID infection than from the vaccine.”
A current VSD/CDC study by Daley is assessing “factors associated with COVID vaccination or non-vaccination” in the general population and among pregnant women.
Camille Kotton
Camille N. Kotton, M.D. (ckotton@partners.org) is clinical director for Transplant and Immunocompromised Host Infectious Diseases at Massachusetts General Hospital and an associate professor at Harvard Medical School. CDC describes Kotton as a “national expert in vaccination and zoonotic infectious diseases in the immunocompromised,” including solid organ transplant recipients.
Since 2014, Kotton has received over $304,000 in general payments and associated research funding from companies like Merck, GSK, Roche, Quiagen Sciences, Oxford Immunotec, Astellas Pharma, Shire, Takeda Pharmaceuticals, BeiGene and Biotest.
In voting to give younger children the COVID injections, Kotton stated, “the safety data in children looked very good” and added, “she would feel comfortable having her own children immunized if they were in that age group.”
Although few children suffer ill effects from COVID-19, Kotton argued that children should be vaccinated “both to prevent death as well as to prevent major long-term effects of having this devastating infection.”
In the past, Kotton has disclosed conflicts of interest due to her financial relationships with (and vaccine “adjudication” for) companies like Merck, Astellas, Roche and others.
James Loehr
James Loehr, M.D. (staff@cayugafamilymedicine.com) owns Cayuga Family Medicine in Ithaca, New York. According to CDC, for 30 years Loehr has counseled patients “every day on the benefits of vaccines.” Loehr was a member of ACIP’s influenza working group for more than 10 years.
In 2015, Loehr authored an article with detailed instructions telling physicians how to “minimiz[e] costs and maximiz[e] reimbursement” to “make immunizations profitable.”
Describing how Cayuga Family Medicine “enjoys steady revenue from immunizations, with vaccine reimbursement sometimes exceeding that for the rest of the visit,” Loehr outlined a series of strategies to improve a practice’s financial viability through vaccination, including becoming a “savvy vaccine shopper,” taking advantage of manufacturer discounts and doing “a bit of additional work” when coding for the service to obtain extra reimbursement for “brief counseling” and multiple vaccine components.
At an October ACIP meeting focused on Moderna boosters that was, according to Stat, driven by a “sense of the inevitability of [the] outcome,” Loehr stated, “There are probably many people who are going to get a Moderna booster who don’t need it. However, given the situation that we’ve already approved a Pfizer [booster] and there are enough people who are looking for a booster, I am inclined, reluctantly, to just go ahead and recommend a similar pattern for the Moderna booster.”
Loehr was similarly wishy-washy the previous month when he stated, “I … feel that we’re getting too much ahead of ourselves and that we have too much hope on the line with these boosters.”
He then added, “However, having said that, we shouldn’t let the perfect be in the way of the good. And if we can do a little bit of good by giving boosters to people over 65 I’m in favor of that.”
Like most of his ACIP peers, Loehr promotes himself as an expert on “strategies for addressing and overcoming vaccine hesitancy,” stating that “most patients…are not truly resistant to immunization” but just want “clarification and reassurance.”
Sarah Long
Sarah Long, M.D. is a professor of pediatrics at Drexel University College of Medicine and a physician at St. Christopher’s Hospital for Children in Philadelphia. In addition to her role on ACIP, Long has served on VRBPAC and as a member of the American Academy of Pediatrics (AAP) Committee on Infectious Diseases.
Long was widely quoted in the press following her “yes” vote on COVID injections for children. Though she expressed several concerns and voted “no” in September regarding Pfizer boosters for healthcare workers, Long “threw her full support behind the pediatric recommendation.”
Fully aware that “CDC was not able to conduct a full benefit-risk analysis for myocarditis post-vaccination in this age group,” Long is nevertheless telling mothers that the shot’s risks are preferable to the myocarditis that could arise from COVID illness.
Without citing any evidence, Long states that “vaccine-related events are completely different, and much less dire, than typical myocarditis,” adding that “she’d rather treat many people with vaccine-associated myopericarditis than a single case of viral myocarditis.”
Claiming that “Nobody has died of myopericarditis, and children are dying of coronavirus,” Long has concluded that “of course it’s a benefit-risk ratio that comes out in the direction of vaccination.”
The hundreds of teens who have experienced post-vaccination myocarditis — some now dead — might beg to differ.
Ironically, Long’s bio includes numerous “awards and honors for her outstanding work to improve the health and well-being of children.” After the “yes” vote on COVID shots, she reportedly joked, “I, believe it or not, have no questions. I have just a comment: I am very supportive of this recommendation in its fullest extent, as a ‘should,’ not a ‘may,’ for all children in this age group.”
Long continued, “I think the data support that we have one more vaccine that saves lives of children, and that we should be very confident to employ it to the maximum to do what it is meant to do, without significant concerns of serious adverse events. So, I couldn’t be more supportive.”
Also of note:
Drexel University received half a million dollars from the Gates Foundation in June 2020 “to evaluate the use of a digital health platform to make care for COVID more accessible to marginalized populations.”
The Gates Foundation is also supporting the work of other Drexel researchers in areas such as diagnostic test development.
Having lost an infant to pertussis, McNally describes herself as a “public health advocate” in addition to being an attorney.
She is founder and president of the Franny Strong Foundation — framing a mission to “promote pertussis awareness and boost childhood immunization rates for all vaccine-preventable diseases” — and founded the I Vaccinate Campaign, which, on November 16, excitedly reported that “nearly 1 million kids ages 5-11 will have their first COVID shots by the end of today.”
McNally is seemingly unaware of the many failures of a pertussis vaccination program that is widely acknowledged to be making vaccinated children more rather than less susceptible to pertussis over their lifetimes.
Also of note:
McNally is a CDC darling, having been named “Childhood Immunization Champion” for Michigan in 2018 — the same year in which she was appointed to her four-year term on ACIP.
Katherine Poehling
Katherine A. Poehling, M.D., MPH (kpoehlin@wakehealth.edu) is a professor of pediatrics and epidemiology at North Carolina’s Wake Forest University School of Medicine. CDC cites her expertise “on the community impact of vaccines, specifically pneumococcal and influenza vaccines.”
As an ACIP insider, Poehling has headed up past ACIP presentations on pneumococcal vaccines.
Poehling has published on “ethics and academic pediatrics” but apparently sees no conflict in sitting on ACIP while receiving, according to Open Payments, over $523,000 in general payments and associated research funding from MedImmune and AstraZeneca since 2014.
Poehling endorses CDC’s astonishingly fact-free claim that COVID has caused “substantially more misery than other childhood diseases,” stating, “that information helped convince her to strongly support COVID-19 vaccines for elementary school children.”
Poehling also buys into Long’s non-evidence-based assertion that COVID-19 disease is responsible for more heart problems than the vaccine. During a May review of Moderna data, Poehling enthusiastically favored making multiple vaccines available — to “increase access.”
Also of note:
When endorsing COVID boosters for the immunocompromised, Poehling stated, “the benefits are tremendous and the potential negative impacts are minimal and so I agree that we should recommend.”
Many of Poehling’s publications seem intended to address the burden of diseases such as influenza for which vaccine “solutions” can then be promoted. It seems likely that her published articles about respiratory syncytial virus (RSV) will be used to lay the groundwork for an mRNA vaccine for RSV.
Pablo Sanchez
Pablo J. Sanchez, M.D. (sanchez.940@osu.edu) has been a professor of pediatrics at Ohio State University since 2013 and directs Clinical and Translational Research in Neonatology at Nationwide Children’s Hospital in Columbus. Sanchez previously held positions at University of Texas Southwestern Medical Center.
Sanchez’s 80-page self-congratulatory curriculum vitae reveals that he is a consummate insider fluidly bridging academia, public health agencies and private industry. Sanchez’s invited participation and lectures include appearances at public health agencies like CDC, the World Health Organization (WHO) and the Pan American Health Organization (PAHO); COVID-vaccine-promoting trade groups like the AAP and March of Dimes; and biopharma companies like AbbVie, GSK (formerly Smithkline Beecham), ICN Pharmaceuticals, Inhibitex, MedImmune and Ross Laboratories.
Sanchez also lists hundreds of thousands in research monies received from these same entities.
Since the 1990s, Sanchez has been funded by Abbott Laboratories, American Lung Association, BioStar, Biosynexus, Burroughs Wellcome, CDC, F. Hoffman-La Roche, Gerber Foundation, MedImmune, NIAID, NICHD [National Institute of Child Health and Human Development], Pediatric AIDS Foundation, Ross Laboratories and Smithkline Beecham/Glaxo/GSK.
According to Open Payments, since 2014, Sanchez has pocketed roughly $221,000 in general payments and associated research funding from AbbVie, AstraZeneca, F. Hoffmann-La Roche, MedImmune, Medtronic, Merck, Novartis, Sanofi Pasteur, Seqirus and Sobi.
The database lists AstraZeneca, MedImmune and Merck as the “top companies making associated payments,” with notable payments from Merck in Fall 2020.
In June, Sanchez hedged his bets on the topic of COVID vaccines and myocarditis. While declaring that the benefits of vaccination outweigh myocarditis risks, he also noted, “we need to be very upfront in terms of mentioning this as a potential risk of COVID messenger RNA vaccination. Hopefully, the parents and patients are aware of this before vaccination.”
Sanchez did not repeat these remarks at the November meeting when he okayed the jab for 5-year-olds.
Also of note:
In 2010, Sanchez served as a “Pfizer visiting professor.”
Sanchez served on VRBPAC from 2007–2010 as well as on FDA’s vaccine-focused Pediatric Advisory Committee from 2010–2012. In Texas, he chaired the Texas Pediatric Society’s Committee of Infectious Diseases and Immunizations from 2004–2009 and served on the committee from 1995–2013.
Many of Sanchez’s publications focus on amplifying concern about illnesses attributed to viruses— such as cytomegalovirus, herpes simplex, RSV and Zika — for which Moderna and other companies now anticipate developing mRNA vaccines.
Helen Keipp Talbot
Helen Keipp Talbot, M.D., MPH (keipp.talbot@vumc.org) is associate professor of medicine at Nashville’s Vanderbilt University, where she has held various appointments since 2002. Talbot’s research and publications (sometimes co-authored with fellow ACIP member Poehling) center on adult vaccination, influenza vaccination, human coronaviruses and vaccine trials for respiratory illnesses such as RSV. The focus on coronaviruses pre-dates COVID; from 2007–2009, Talbot was principal investigator on an NIH-funded study on the “epidemiology of human coronaviruses.”
According to Talbot’s curriculum vitae, her recent research funding comes from both the federal government (CDC, National Institutes of Health [NIH]) and Sanofi Pasteur, primarily for the study of pandemic preparedness (in 2015) and influenza vaccination. Sanofi and MedImmune have been recurrent funders since 2009, along with AstraZeneca, Gilead, Protein Sciences, VaxInnate and Wyeth (since acquired by Pfizer).
Open Payments lists Talbot’s receipt of roughly $1.4 million in research payments and associated research funding since 2014 (417 total payments) from these companies, along with 29 general payments totaling $17,000.
In December 2020, Talbot was the “lone dissenter” objecting to ACIP’s recommendation that long-term care residents “be at the front of the line” for COVID vaccines. At the time, Talbot argued that vaccination of long-term care residents was “risky” because they “have a high rate of medical events that could be confused as side effects of vaccination and undermine confidence in the vaccines.”
Talbot stated, “And I think you’re going to have a very striking backlash of, ‘My grandmother got the vaccine and she passed away.’” Talbot elaborated: “I fear a loss of confidence in the vaccine…. [T]here will be temporally associated events and people will be scared to use the vaccine.”
Talbot exhibited no scruples in voting to administer COVID vaccines to young children. On the same day as the “yes” vote, Talbot told the press, “I have vaccinated my kids” (who, presumably, were at least 12 years of age at the time of injection).
Also of note:
In 2008, Talbot received a Sanofi Pasteur Advanced Vaccinology Course travel grant.
No overview of ACIP would be complete without noting the conflicts of interest surrounding CDC Director Rochelle Walensky, who used ACIP’s vote to immediately green-light vaccination of younger children.
As reported by independent media outlet RedState (but not by the mainstream media), Walensky’s husband, Loren Walensky, became scientific co-founder and board member of early-stage biotech company Lytica Therapeutics in October 2019.
In December, the Biden administration announced Rochelle Walensky’s pending appointment as CDC director, and in February 2020, Lytica received the first installment ($5.3 million) of a $16.9 million grant from HHS, representing the “only funding this new company [had] received to date — nearly two years after its founding.”
Even before becoming CDC director, Walensky had been “directly associated with HHS for more than a decade,” including close participation on committees and panels with Anthony “Tony” Fauci. According to RedState’s exposé, “when ‘insiders’ were surprised that Walensky was picked [to head CDC], it was revealed that Fauci had a lot to do with her appointment.”
Loyal to Fauci, Walensky has written opinion pieces for leading media outlets “about how to fairly and effectively distribute Remdesivir,” the ineffective, expensive and dangerous drug promoted by NIAID and Fauci as virtually the sole treatment option for hospitalized COVID patients.
A former Boston colleague of Walensky’s stated the CDC director “has a lot of Tony in her,” including the “ability to take complex information and convey it in clear and concise messaging.”
Shunning and Nuremberg 2.0
As bad as the ACIP (and VRBPAC) decisions were, vaccine-risk-aware observers are even more shocked that CDC and FDA are “blithely” allowing Pfizer’s shot to be administered to children and adolescents with other vaccines at the same time.
As Informed Choice Washington put it last May regarding the authorization for kids ages 12 and up:
“As unethical as it is to expose children to investigational liability-free products that have seen unprecedented levels of vaccine adverse reactions and deaths reported … when ACIP opened up the shots to be co-administered with other vaccines, including those with adjuvants, they stepped fully into crimes against humanity. Not a single clinical trial has been done administering the COVID-19 shots with any other vaccine. There is zero safety data.”
Other observers agree with this assessment, arguing that “Every single person associated with the ACIP meeting today must be tried for crimes against humanity at Nuremberg 2.0.” Some are also calling for a second Nuremberg trial for “perpetration of COVID-response policies that led to forced shutdowns, destroyed businesses, impoverished families, broken lives and a spike in suicide rates.”
In the meantime, it is time to shun ACIP members. And because it is inconceivable that ACIP members would behave in such a corrupt manner without the approval and say-so of their institutions, shunning actions necessarily must also extend to the universities and other institutions that have these individuals’ backs.
Send a Notice of Liability to each ACIP member — see examples at the Doctors for Covid Ethics website.
Check the campaign contributions of ACIP members at OpenSecrets.org. If they are donating to a politician who represents your state or Congressional District, call or write your representative and ask why they are accepting donations from people who are seriously compromised by the pharmaceutical industry and harming our children.
Refrain from appointing ACIP members to the Boards of community organizations — or revoke their current Board appointments. These types of “good citizen” positions should not be offered to people who are not behaving as “good citizens.”
All universities benefit from state and local appropriations; contact your legislators, explain that academic operations at these universities are clearly supporting federal corruption and demand that the legislators revoke the appropriations.
Write to the board of trustees or person who manages the university endowment. Demand they disclose their investments in companies that are harming our children and explain how these investments support active participation in federal corruption by those affiliated with the university.
Stop donating to the universities and academic departments in question and let them know why. When asked for an update by your university alumni group, ask to be removed from the alumni email list and database, and explain you have stopped donating to the university as a result of its support of federal corruption.
Cancel your season tickets and other participation in sports and cultural events at the university. Explain why.
If you are involved in recruiting for your company, remove these universities from your recruiting lists. Write to the university’s placement office to explain why.
Ask local newspapers to publish copies of the letters you write to university officials. Organize to support members of the independent media in researching and publishing information regarding ACIP members’ conflicts of interest, as well as the university conflicts of interest that compromise the institutions’ intellectual resources and activities in science, medicine and technology.
Write to the university chaplain and ask for prayers for the university to be released from the spirit of corruption. Provide details.
Identify the banks involved in managing the university’s bank accounts, financial assets, endowment and pension funds; where applicable, demand to know why the university is doing business with banks that have compromised our federal government accounts and are financing policies at the federal level that are harming our children.
Do not buy or hold stocks in companies with which ACIP members are connected.
Do not buy products or drugs that ACIP members have developed or patented.
Make it clear — through letters to the editor and letters to the institutions — that you will not forget ACIP members’ decision to enable the needless harming of young children.
“The PCR is a Process. It does not tell you that you are sick”.
Dr. Kary Mullis, Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“…All or a substantial part of these positives could be due to what’s called false positives tests.”
Dr. Michael Yeadon: former Vice President and Chief Science Officer for Pfizer
This misuse of the PCR-RT technique is applied as a relentless and intentional strategy by some governmentsto justify excessive measures such as the violation of a large number of constitutional rights, … under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.
.Dr. Pascal Sacré, Belgian physician specialized in critical care and renowned public health analyst.
Media lies coupled with a systemic and carefully engineered fear campaign have sustained the image of a killer virus which is relentlessly spreading to all major regions of the World.
Several billion people in more than 190 countries have been tested (as well as retested) for Covid-19.
At the time of writing, approximately 260 million people Worldwide have been categorized as “confirmed Covid-19 cases”. The alleged pandemic is said to have resulted in more than 5 million Covid-19 related deaths.
Both sets of figures: morbidity and mortality are fabricated. A highly organized Covid testing apparatus (part of which is funded by the billionaire foundations) has been established with a view to driving up the numbers of “Confirmed Covid-19 Cases”, which are then used as a justification to impose the “vaccine” passport coupled with the repeal of fundamental human rights.
A so-called “Global Tracker System” has been established with an interactive map pointing to global as well as country level trends and weekly tendencies.
A Fourth Wave has been announced. Invalid figures pertaining to Covid-19 are routinely plastered on the news tabloids.
Meanwhile, both the media and the governments have turned a blind eye to the rising trend of Covid-19 vaccine deaths and adverse events, which are confirmed by “official” government agencies. (See below)
TOTAL for EU/UK/USA
45,250 Covid-19 injection related deaths, 7,418,980 injuries
The Reverse Transcription Polymerase Chain Reaction Test (RT-PCR)
The slanted methodology applied under WHO guidance for detecting the alleged spread of the virus is the Polymerase Chain Reaction Test (RT-PCR), which is routinely applied all over the World.
The RT-PCR Test has been used Worldwide to generate millions of erroneous “Confirmed Covid-19 cases”, which are thenused to sustain the illusion that the alleged pandemic is Real.
This assessment based on erroneous numbers has been used in the course of the last 20 months to spearhead and sustain the fear campaign.
And people are now led to believe that the Covid-19 “vaccine” is the “solution”. And that “normality” will be restored once the entire population of Planet Earth has been vaccinated.
“Confirmed” is a misnomer: A “Confirmed RT-PCR Positive Case” does not Imply a “Confirmed Covid-19 Case”.
Positive RT-PCR is not synonymous with COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability] (Dr. Pascal Sacré)
The procedure used by the national health authorities is to categorize all RT-PCR positive cases, as “Confirmed Covid-19 Cases” (with or without a medical diagnosis).Ironically, this routine process of identifying “confirmed cases” . is in derogation of the CDC’s own guidelines:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. This test cannot rule out diseases caused by other bacterial or viral pathogens.” (emphasis added)
In this article we will present detailed evidence that the methodology used to detect and estimate the spread of the virus is flawed and invalid.
1. False Positives
The earlier debate at the outset of the crisis focused on the issue of “False Positives”.
Acknowledged by the WHO and the CDC, the RT-PCR Test was known to produce a high percentage of false positives. According to Dr. Pascal Sacré:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
The debate on false positives (acknowledged by the health authorities) points to so-called errors without necessarily questioning the overall validity of the RT-PCR test as a means to detecting the alleged spread of the CoV-SARS-2 virus.
2. The PCR-Test Does Not Detect the Identity of the Virus
The RT-PCR test does not identify/ detect the virus. What the PCR test identifies are genetic fragments of numerous viruses (including influenza viruses types A and B, and coronaviruses which trigger common colds).
The results of the TR-PCR test cannot “confirm” whether an individual who undertakes the test is infected with Covid-19.
According to Dr. Kary Mullis, inventor of the PCR technique: “The PCR detects a very small segment of the nucleic acid which is part of a virus itself.”According to renowned Swiss immunologist Dr B. Stadler
So if we do a PCR corona test on an immune person, it is not a virus that is detected, but a small shattered part of the viral genome. The test comes back positive for as long as there are tiny shattered parts of the virus left. Even if the infectious viri are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected].
Dr. Pascal Sacré concurs: “These tests detect viral particles, genetic sequences, not the whole virus.”
In an attempt to quantify the viral load, these sequences are then amplified several times through numerous complex steps that are subject to errors, sterility errors and contamination.
3. The WHO’s “Customized” RT-PCR Covid-19 “Test”
Two important and related issues.
The PCR Test does not identify the virus as outlined above. Moreover, the WHO in January 2020, did not possess an isolate and purified sample of the novel 2019-nCov virus.
What was contemplated in January 2020 was a “customization”of the PCR test by the WHO, under the scientific guidance of the Berlin Virology Institute at Charité Hospital.
The title of the Berlin Virology Institute Study is an obvious misnomer. The PCR test cannot “detect” the 2019 novel coronavirus. (See Dr. Kary Mullis, Dr. B. Stadler, Dr. Pascal Sacré quoted in Section 2).
Moreover, the study, published by Eurosurveillance acknowledges that the WHO did not possess an isolate and purified sample of the novel 2019-nCov virus:
[While]… several viral genome sequences had been released,… virus isolates or samples [of 2019-nCoV] from infected patients were not available …”
The Drosten et al team report then recommended to the WHO, that in the absence of an isolate of the 2019-nCoV virus, a similar 2003-SARS-CoV should be used as a “proxy” of the novel virus:
“The genome sequences suggest presence of a virus closely related to the members of a viral species termed severe acute respiratory syndrome (SARS)-related CoV, a species defined by the agent of the 2002/03 outbreak of SARS in humans [3,4].
We report on the the establishment and validation of a diagnostic workflow for 2019-nCoV screening and specific confirmation [using the RT-PCR test], designed in absence of available virus isolates or original patient specimens. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.” (Eurosurveillance, January 23, 2020, emphasis added).
What this ambiguous statement suggests is that the identity of 2019-nCoV was not required and that “Confirmed Covid-19 Cases” (aka infection resulting from the novel 2019 coronavirus) would be validated by “the close genetic relatedness to the 2003-SARS-CoV.”
What this means is that a coronavirus detected 19 years ago (2003-SARS-CoV) is being used to “validate” the identity of a so-called “novel coronavirus” first detected in China’s Hubei Province in late December 2019.
The recommendations of the Drosten study (generously supported and financed by the Gates Foundation) were then transmitted to the WHO. They were subsequently endorsed by the Director General of the WHO, Tedros Adhanom.
The WHO did not have in its possession the “virus isolate” required to identify the virus. It was decided that an isolate of the new coronavirus was not required.
The Drosten et al article pertaining to the use of the RT-PCR test Worldwide (under WHO guidance) was challenged in a November 27, 2020 study by a group of 23 international virologists, microbiologists et al.
It stands to reason that if the PCR test uses the 2003 SARS- CoV virus as “a point of reference”, there can be no “confirmed” Covid-19 cases resulting from the novel virus 2019-nCoV, subsequently renamed SARS-CoV-2.
4. Has the Identity of the 2019-nCoV Been Confirmed? Does the Virus Exist?
The Chinese authorities announced on January 7, 2020 that “a new type of virus” had been “identified” “similar to the one associated with SARS and MERS” (related report, not original Chinese government source). The underlying method adopted by the Chinese research team is described below:
We prospectively collected and analysed data on patients with laboratory-confirmed 2019-nCoV infection by real-time RT-PCR and next-generation sequencing.
Data were obtained with standardised data collection forms shared by WHO and the International Severe Acute Respiratory and Emerging Infection Consortium from electronic medical records. (emphasis added)
The above study (quotation above as well as other documents consulted ) suggest that China’s health authorities did not undertake an isolation / purification of a patient’s specimen.
Using“laboratory-confirmed 2019-nCoV infection by real-time RT-PCR” is an obvious misnomer, i.e. the RT-PCR test cannot under any circumstances be used to identify the virus. (see section 2 above). The isolate of the virus by the Chinese authorities is unconfirmed.
Freedom of Information Pertaining to the Isolate of SARS-CoV-2
Freedom of Information (FOI) requests were addressed to ninety Health /Science institutions in a large number of countries.
The responses to these requests confirm that there is no record of isolation / purification of SARS-CoV-2 “having been performed by anyone, anywhere, ever.”
“The 90 Health /Science institutions that have responded thus far have provided and/or cited, in total, zero such records:
Our requests [under “freedom of information”] have not been limited to records of isolation performed by the respective institution, or limited to records authored by the respective institution, rather they were open to any records describing “COVID-19 virus” (aka “SARS-COV-2”) isolation/purification performed by anyone, ever, anywhere on the planet.”
5. The Threshold Amplification Cycles. The WHO Admits that the The Results of the RT-PCR “Test” are Totally Invalid
The rRT-PCR test was adopted by the WHO on January 23, 2020 as a means to detecting the SARS-COV-2 virus, following the recommendations of the Berlin Virology research group (quoted above).
Exactly one year later on January 20th, 2021, the WHO retracts. They don’t say “We Made a Mistake”. The retraction is carefully formulated. (See original WHO document here)
The contentious issue pertains to the number of amplification threshold cycles (Ct). According to Pieter Borger, et al
The number of amplification cycles [should be] less than 35; preferably 25-30 cycles. In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture…(Critique of Drosten Study)
The World Health Organization (WHO) tacitly admits one year later that ALL PCR tests conducted at a 35 cycle amplification threshold (Ct) or higher are INVALID. But that is what they recommended in January 2020, in consultation with the virology team at Charité Hospital in Berlin.
If the test is conducted at a 35 Ct threshold or above (which was recommended by the WHO), genetic segments of the SARS-CoV-2 virus cannot be detected, which means that ALL the so-called “Confirmed Covid-19 Cases” tabulated Worldwide in the course of the last 22 months are invalid.
Below is the WHO’s carefully formulated “Retraction”.
“WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology. (emphasis added)
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
“Invalid Positives” is the Underlying Concept
This is not an issue of “Weak Positives” and “Risk of False Positive Increases”. What is at stake is a “Flawed Methodology” which leads to invalid estimates of “Confirmed Covid-19 Cases”.
What this admission of the WHO confirms is that the estimate of covid positive from a PCR test (with an amplification threshold of 35 cycles or higher) is invalid. In which case, the WHO recommends retesting: “a new specimen should be taken and retested…”.
The WHO calls for “Retesting”, which is tantamount to saying “We Screwed Up”.
That recommendation is pro-forma. It won’t happen. Several billion people Worldwide have already been tested, starting in early February 2020. Nonetheless,we must conclude that unless retested, those estimates (according to the WHO) are invalid.
From the outset, the PCR test has routinely been applied at a Ct amplification threshold of 35 or higher, following the January 2020 recommendations of the WHO. What this means is that the PCR methodology as applied Worldwide has in the course of the last 20 months led to the compilation of faulty and misleading Covid statistics.
And these are the statistics which are used to measure the progression of the so-called “pandemic”. Above an amplification cycle of 35 or higher, the test will not detect fragments of the virus. Therefore, the official “covid numbers” (Confirmed Covid-19 Cases) are meaningless.
It follows that there is no scientific basis for confirming the existence of a pandemic.
Which in turn means that the lockdown / economic measures which have resulted in social panic, mass poverty and unemployment (allegedly to curtail the spread of the virus) have no justification whatsoever.
As outlined above, “the probability that said result is a false positive is 97%”: It follows that using the >35 cycles detection will indelibly contribute to “hiking up” the number of “fake positives”.
The WHO’ Mea Culpa confirms that the Covid-19 PCR test procedure as applied is invalid.
Concluding Remarks
The RT-PCR Test is the Smoking Gun. It invalidates Everything.
There is no such thing as a “Confirmed Covid-19 Case”. The entire data bank is invalid.
At the time of writing, the number of tabulated so-called “Confirmed Covid-19 Cases” is of the order of 260 million Worldwide. These numbers are totally meaningless.
None of this data can be categorized as “Confirmed”.
The PCR Test does not identify the novel virus, and the genetic fragments of a so-called “similar” 2003 coronavirus (SARS-1) cannot be used as a means to identify the virus which causes Covid-19, nor can it be used to identify the deadly variants of the 2019 novel coronavirus.
Moreover, according to the Freedom of Information (FOI) study quoted above, the isolate of the novel coronavirus is unconfirmed.
Sustained by a complexity of lies, the covid-19 narrative is extremely fragile. This consensus relies on fake science and a totally invalid data bank of alleged “confirmed Covid-19 cases”.
How did Big Pharma manage to develop a vaccine (sponsored by the WHO, GAVI, the Gates Foundation, et al) with a mandate “to protect people” against a virus which has not been isolated/ purified from an “unadulterated sample taken from a diseased patient”?
Vaccine in relation to What? The virus has not been identified.
Moreover, 2019SARS-CoV-2 has been categorized as similar to the 2003 SARS-CoV which means that the 2019 SARS-CoV-2 is not a novel virus.
The legitimacy of the Covid vaccine project hinges upon the validity of hundreds of thousands of RT-PCR fake positive cases Worldwide combined with fake Covid related mortality data. ( See Michel Chossudovsky, Does the Virus Exist)
What lies ahead?
National governments have announced a Fifth Wave, focussing on the deadly variants of SARS-CoV-2, including the Delta variant.
The variant is a scam. How do they identify the “variants”. The PCR test neither detects the virus nor the variants of the virus.
There is no isolate of the novel coronavirus on record. Moreover, the WHO’s “customized” PCR test uses as a proxy a similar 2003 SARS-CoV virus (which no doubt has mutated extensively over the last 19 years).
“Restrictions would have to be reintroduced”. … the Delta variant poses a “higher risk of hospitalisations”
These announcements are intended to justify a continuation of repressive policy measures, the speeding up of the vaccination program as well as the repression of the protest movement.
There is no Pandemic. The Endgame is Tyranny.
The Pandemic is being used to Impose a New World Order.
When the Lie Becomes the Truth, There is Moving Backwards.
The first Step is to Dismantle the Propaganda Apparatus.
The Elite’s Covid Consensus is Extremely Fragile.
There is no Pandemic. They Do not have a Leg to Stand on.
That Consensus must be broken.
See Michel Chossudovsky’s E-Book (13 Chapters) entitled
This week, tens of thousands of protesters gathered in Melbourne, Victoria State, to oppose their government’s new pandemic laws and vaccination mandates. Mainstream media outlets appear to be upset that attendees are daring to compare the decrees of their government to that of the Nazis, specifically citing state policies of targeted discrimination and medical apartheid.
The latest round of protests comes after the government’s push to enact new draconian legislation meant to ‘fight the pandemic.’
Australian public health authorities are claiming that vaccinations are voluntary, and that 83% of its population aged 16 and above have been ‘fully inoculated’ against the coronavirus. However, states and territories have had to deploy coercive and intimidating policies in order to enforce vaccine mandates, including threats by the state to prevent any employee from the right to work if they refuse to accept the experimental gene-based pharmaceutical injection, as well as policies which prohibit ‘the unvaccinated’ from participating in basic activities such as eating out and attending concerts and other public facilities.
The Melbourne demonstration against the vaccination mandate that came into effect on Saturday – requiring construction workers in Victoria state to be fully inoculated – was peaceful, with no immediate reports of unruly behaviour or arrests.
But a reporter at The Age posted video on Twitter of a protester carrying a mock gallows with three nooses hanging from it, and the newspaper showed a protester carrying a poster depicting Victorian Premier Daniel Andrews with a Hitler moustache and the hashtag #DictatorDan.
“We’re being governed by insane medical bureaucrats,” Craig Kelly, former Liberal Party member of parliament and now the leader of United Australia Party, told the rally, media reported.
The Age said some protesters called for violence against politicians but did not offer specifics.
Australia has captured global attention as one of worst violators of human rights, and where governments have all but abandoned any pretence of civil liberties and rights, and regularly deploying police forces in violent attacks against protesters, and to break up any pro-freedom rallies.
Since the beginning of the alleged ‘global pandemic’, Victoria’s Premier Dan Andrews has enacted no less than six COVID-19 lockdowns, totalling nearly nine months – despite the fact that there was never any significant number of deaths from COVID-19 among the general population outside of the elderly with comorbidities.
Still, the main justification for continuing anti-democratic policies is the state’s ongoing coronavirus testing regime. Authorities in Victoria are claiming there have been 1,221 new coronavirus “cases” (PCR positive tests) and 4 deaths ‘from’ (or ‘with’, officials will not specify precisely which) COVID. In New South Wales state officials are claiming to have 250 daily ‘cases.’
Recently, Victoria State’s lower house had passed the latest version of its disturbing coronavirus state of emergency law, the Public Health and Wellbeing Amendment (Pandemic Management) Bill 2021, which gives the government near unlimited power to declare a ‘pandemic’ at any time and for any reason. The draconian legislation also gives the state new powers to levy crippling fines against any individuals or businesses who do not obey the state’s new restrictions, and also gives the state the power to send its residents to internment facilities – which the individual will be forced to pay for.
GRAPH: The Measles Myth: one popular talking point is that the Measles vaccine has more or less eliminated Measles globally. However, real data shows that incidences began plummeting long before there was any mass-vaccination program for measles.
According the leading public health bodies like the World Health Organisation, the Measles virus is an ongoing deadly epidemic which kills more than 140 000 people globally per year, mostly among children under the age of five. It is also claimed that Measles were eliminated from the United States in 2000, but continue to be ‘reintroduced’ by international travelers into the country. In 2019 there were claimed to be a minuscule 1,241 cases spread across the United States.
Yet, despite all of these official claims, there seems to be very little scientific evidence that clearly shows Measles being an infectious agent in a host. Rather, it is just widely assumed to be the case.
Here’s what modern virology and public health mavens cannot seem to answer: what causes Measles?
We are told that it is a virus, but is there any evidence for this?
In this video, Dr Sam Bailey examines the evidence presented by Measles experts and the media, as well as the court case where Dr. Stefan Lanka offered €100k euros for proof of a Measles virus. Watch:
On October 27 the US Food and Drug Administration Advisory Panel on Vaccines recommended the agency allow Pfizer to amend its Emergency Use Authorization for its COVID vaccine to include children 5 through 11 years old. Two days later the FDA officially approved the rollout. Major media are treating this as a positive development to protect young children. On closer inspection it is anything but that. The FDA is today shockingly corrupt under the Acting Director and is little more than a rubber stamp for Big Pharma, and especially Pfizer, where the former FDA head sits on the board.
The FDA’s Vaccines and Related Biological Products Advisory Committee voted 17 to 0, with one abstention, to give a green light allowing Emergency Use Authorization for the Pfizer-BioNTech experimental mRNA to children between 5 and 12 years. The expert who abstained later explained he did so because of limited safety and efficacy data provided. Previously the FDA had approved the vaccine for 12 and older. Adding to the stench of corruption around the latest vote, the Biden Administration a week earlier announced it had already purchased enough Pfizer vaccine to inoculate all 28 million 5- to 11-year-olds in the US. Did they know the fix was in?
‘…Just the Way it Goes’
The record of the FDA, the major drug oversight agency in the US Government, regarding safety and risks of the experimental gene-altered mRNA vaccines of Pfizer, is one of criminal malfeasance, defined as willful violation of a public trust or obligation that causes harm or death. Their latest ruling is even more egregious for blatant conflicts of interest and scientific fraud. Both Pfizer, who conducted the tests on the efficacy of their own vaccine on the 5-11 year age group, and the FDA experts, admitted that they had no idea if the vaccine was safe for such a young population.
Dr. Eric Rubin, professor of immunology at the Harvard T.H. Chan School of Public Health voted to approve the Pfizer-BioNTech vaccine, noting, “The data show that the vaccine works and is pretty safe … and yet we’re worried about a side effect that we can’t measure yet, but it’s probably real.” That is hardly confidence-building. He then stated, “we’re never going to learn about how safe this vaccine is unless we start giving it. That’s just the way it goes.”
This cold-blooded nonchalance is even more astonishing in light of the fact that the incidence of serious side effects in the 5-11 age group who allegedly have tested positive for the corona virus is essentially zero. According to data of the US Government Centers for Disease Control, the Infection Fatality Rate for children from 0-17 years is 0.0002 per 100,000 and far lower for the 5-11 years. A research study by Johns Hopkins University found that risk of severe illness or death from covid19 in a study of 48,000 children is essentially zero if no other morbidity risk such as leukemia, diabetes or asthma is present. Moreover, risk of infecting other children is also very low.
In their submission to FDA for approval, Pfizer stated the vaccination was needed for the 5-11 age group to prevent covid disease transmission. Yet in their FDA hearing on questioning, Dr. William Gruber, senior vice president of Pfizer Vaccine Clinical Research and Development, said they did not even assess whether the vaccine prevents transmission. We might ask why is this at all needed then if the risk to children is zero and there is no evidence of children transmission?
Even more shocking is the statement by Pfizer about its tests. First there were no animal tests on rats or such first. They admitted that the tested human group was so small that they could not test for myocarditis or pericarditis. Yet those are among the most reported negative effects for all others that have had the Pfizer jab. In its FDA application Pfizer noted that the number of participants in the current clinical development program was “too small to detect any potential risks of myocarditis associated with vaccination,” and that “to evaluate long-term sequelae of post-vaccination myocarditis/pericarditis” in participants 5 to <12 years of age will not be studied until after the vaccine is authorized for children.”
Flawed Pfizer Tests
The tests Pfizer made were also fatally flawed. According to Dr. Josh Guetzkow, of the Hebrew University of Jerusalem, the Pfizer study was not double-blind. Further, Pfizer cherry-picked subjects to evidently better their results. Three thousand children age 5-11 received Pfizer’s COVID vaccine, but only 750 of those children were selectively included in the company’s safety analysis. And Pfizer dismissed cases with adverse vaccine effects in their FDA filing: “Few serious Adverse Events, none of which were related to vaccine, and no AEs leading to withdrawal were reported.” They give no explanation how that was determined. Just trust Pfizer.
And post-vaccination follow up was less than 2 months for one test cohort and only 2.4 weeks for a second. The Pfizer report to FDA read, “Supplemental safety expansion group data were analyzed from approximately 1500 vaccine recipients with a median follow-up time of 2.4 weeks after Dose 2. These supplemental data demonstrate an acceptable safety profile…” It can take months or longer for side effects to manifest. Vaccine experts recommend at least 18-24 month post-vaccine follow up, not 3 months or 2.4 weeks. This is not serious science.
As well, it seems the FDA and or Pfizer wrongly name the vaccine in the title as “BNT162B2 [COMIRNATY (COVID-19 VACCINE, MRNA)] .“Yet the actual FDA text calls it “Pfizer-BioNTech COVID-19 Vaccine (BNT162b2).”
The separate company, BioNTech of Mainz, Germany, has a similar but “legally different” vaccine, trade-named Comirnaty, that is not available in the USA. The distinction is essential as it was the basis in August for the corrupt FDA to give Pfizer-BioNTech vaccine an extension of Emergency Use Authorization but to misleadingly declare its full approval for Comirnaty vaccine of BioNTech. This is deliberate fraud and allowed the Biden Administration to mandate vaccination of US government workers (curiously except for White House and Congress), military, and any company with more than 100 employees.
Conflicts of Interest?
The corruption of the FDA extends to the members of the Vaccine Advisory Committee. Many of the members of the current 18 person committee have direct ties to Pfizer or to the pro-Pfizer Gates Foundation.
Prof. Holly Janes of the Fred Hutch Cancer Research Center in Seattle designed the flawed Pfizer tests. Her institute is funded by Gates Foundation money. FDA committee member Dr. Steven Pergam is also with the Gates-funded Fred Hutch center. Acting committee chair, Arnold S. Monto was a paid consultant to Pfizer. Committee member Archana Chatterjee worked on a Pfizer research project related to vaccines for infants between 2018-2020. Geeta K. Swamy is chair of the “Independent Data Monitoring Committee for the Pfizer Group B Streptococcus Vaccine Program,” a committee sponsored by Pfizer. Duke University states that “Dr. Swamy serves as a co-investigator for the Pfizer COVID-19 vaccine trial.” FDA Committee member Gregg Sylvester was a vice president for Pfizer Vaccines. Ofer Levy, professor of pediatrics at Harvard Medical School is on record vigorously supporting Pfizer covid vaccines for children 12 and older. And FDA committee member Paul Offit professor of pediatrics at The Children’s Hospital of Philadelphia called openly last June for covid vaccine permission for children.
When we compare the actions of corrupt FDA Acting Director Janet Woodcock during the August FDA extension of emergency use authorization for Pfizer-BioNTech vaccine, she refused then to even allow the vaccine committee to meet to debate the issue. Several months before in June 2021 three members of the FDA Vaccine Committee resigned in protest over Woodcock’s refusal to heed the near unanimous vote of the advisory committee to approve an Alzheimer’s drug called Aduhelm against the wishes of nearly every member on the panel.
Clearly Woodcock has been busy in the meantime stacking the advisory committee with pro-Pfizer members. Not to be forgotten is the fact that after he left as head of the FDA under Trump, Scott Gottlieb immediately joined the board of directors of…Pfizer Inc. Woodcock served under him at FDA.Woodcock has been at FDA since 1986, almost as long as Fauci at NIAID. Woodcock was Biden’s choice to head FDA, but a massive opposition from 28 groups including state attorneys general and citizen groups forced him to name her “acting,” which does not need Congressional scrutiny. Woodcock was directly responsible for the original FDA approval of deadly opioids over the objections of her own scientists and other advisors.
Already California has moved to make public school admission contingent on covid vaccination, anticipating Pfizer approval. This spread of the deadly Pfizer vaccine to children who have near zero risk of serious disease makes no public health sense. It is simply prima facie evidence of medical malfeasance at the highest levels of the US Government including FDA, with plausible criminal intent. The FDA decision will now be used to argue for similar inclusion of essentially no risk children for the vaccine jab.
Ricardo Maarman & Thousands of South Africans File Constitutional Lawsuit Against the President, Speaker of Parliament & Governor of SA Reserve Bank for ‘Pandemic’-Related Crimes Against South Africans
Listen to the announcement by Ricardo Maarman in the video provided below. We have also provided a transcript of his powerful statement.
Ricardo Maarman holds a BA Degree in Politics/Philosophy and Economics obtained at the University of South Africa and an MA International Politics obtained at the University of Leicester in the UK. He specialized in the Post-Cold War World Order, International Security, Intelligence and Security, and US Foreign Policy.
Original video available at HWP Report Brighteon channel.
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light Odysee, BitChute and Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Transcript:
Good Day, everyone. Today I have a very important message for the people of South Africa. We have filed our case with the Constitutional Court of South Africa, case number CCT 299/21.
Despite the many difficulties that we have faced along the way, we have successfully filed this case.
I would like to thank Dr. Faiez Kirsten for his unwavering commitment to the cause. I would like to thank those more than 8,700 South Africans who have signed our petition, and in so doing, have become co-applicants to the case.
I would like to thank those who have given us financial support. I would like to thank those who have prayed for our success.
I would like to thank my wife for her loyal partnership, for her wavering commitment to the cause of truth, of justice and her service to God.
Finally, and most importantly, I would like to thank God in whom we put all our trust.
The case that we have brought to the Constitutional Court is against the president of South Africa, the South African Parliament, and the South African Reserve Bank.
Now, what has the president done wrong? Why have we brought a case against hi?
Well, the president heard claims made by the Chinese government that there was a virus that broke out in Wuhan. And subsequently, the World Health Organization has declared an international or global pandemic. He followed suit. He declared a national disaster in South Africa.
What he has done wrong here is he did not confirm the claim that was made by the Chinese government, or the claim that was made by the World Health Organization, as he should have done before he imposed a lockdown on the South African people.
What the president should have done was to send scientists to China and to ask the Chinese government to provide a pure sample of the SARS-CoV-2 virus, separated and isolated from all other contaminants and substances. Once a scientist was in possession of this pure sample of the SARS-CoV-2, he should have instructed them to infect a living, healthy organism with this pure virus only to see whether it produces the symptoms of Covid-19 — and to see if Covid-19 is indeed as deadly as the Chinese and the World Health Organization claim it to be.
He should have repeated this a few times. After doing so, he should have presented his facts and his information to the people of South Africa, to Parliament. And then he should have declared a national state of disaster.
The president did not do so, therefore he did wrong. The president should have shown the people of South Africa the virus before he declared a national disaster based on the virus. In doing so, the president has contravened the Constitution. He contravened Section 36.1 that says he can only limit the rights of the people of South Africa, the Bill of Rights, if he had reasonable justification and if he shows that reasonable justification to the people of South Africa as in an open and democratic society.
He also failed Section 52.1 of the Constitution that says if you take someone’s rights away then you should provide him information that could help him to understand why his rights have been taken away, or to fight for his rights to be restored. The president simply failed to do so.
What is the case that we have brought against the South African parliament?
Well, when the president declared the national state of disaster, Parliament went along without any question. That was wrong.
Parliament should’ve called a debate. They should have questioned the president. They should have asked the president to show us the virus before they agreed to support these measures of the lockdown and the national disaster declaration. Parliament failed to do so. That is why they did wrong.
They contravened the Constitution Section 37.1. Parliament should have made sure that there is a real threat to the life and property of the people of South Africa before they went along. Parliament should have made sure, according to Section 22.3, that the president has a reasonable justification for taking away the rights of the people of South Africa — before they agreed to go along.
According to Section 55.2, Parliament should have put all measures in place to find out whether the virus exists and whether it’s dangerous. And whether it’s deadly. Parliament should have asked the president to show us the virus. They had the power to do so, and he would have had no other choice but to answer them.
Parliament has failed the people of South Africa.
The South African Reserve Bank, when they heard the president make a declaration of a national state of disaster, they then funded the president. They instituted financial measures to provide finance for the lockdown measures. That is what the South African Reserve Bank did.
Before they provided such finance, what they should have done was to confirm whether the virus was real, confirm whether the virus was indeed deadly before they agreed to finance the government. They had a responsibility to do this under Section 224.2 of the Constitution. They have a responsibility to act independently without fear or favor. They have failed to do so.
Now we have great evidence against these responses.
To start with, Christine Massey of Canada and many others went around the world and they asked more than 100 laboratories, health laboratories around the world, to show them the SARS-CoV-2 virus. And the answer they got from these laboratories was, no, they cannot show the virus because they don’t have it. More than 100 health laboratories around the world.
The president and the scientists rely on the PCR test in order for them to demonstrate death rates and infection rates. But the inventor of the PCR test method they said that it shouldn’t be used for that. Yet they continue to use it for that.
The inventor of the PCR test method, Dr. Mullis [Kary Mullis, PhD], died shortly before the outbreak of the pandemic. But, luckily for us, that those who know him well, and who have the same expertise as him, have given a sworn testimony to verify and to confirm that he indeed has sent them that these tests should not be used for this. We have sworn testimony to this and we have presented this to the court.
The PCR test has been found unreliable by a Portuguese court. And, in this matter, according to Section 39.1 of the Constitution, the Constitutional Court must consider that Portuguese case. But it makes it’s ruling here. And the Portuguese case ruled that the PCR test is unreliable.
The PCR test is not calibrated to find SARS-CoV-2 based on a pure genetic sample that was taken from a pure sample of the SARS-Cov-2 virus. Rather it is based on a computer-generated, genetic sequence.
The NICD [The National Institute for Communicable Diseases] has claimed that it had a photograph of the SARS-CoV-2 virus. Now how did they obtain this photograph?
According to their own version, found on their website, the NICD says that it took samples from patients that tested positive for SARS-CoV-2 using a PCR test. And then it took those samples and mixed it with green monkey kidney cells amongst other things. And then it took a picture of this mixture and claimed that this picture is a photograph of the SARS-CoV-2 virus.
Well, it is wrong. One cannot rely on such a picture because all you have is a picture of a mixture.
According to the […] high court in Germany, ruled that when you take samples that are supposedly from infected people of a virus and you mix it with green monkey kidney cells or any other thing, then you cannot rely on such identification of the virus. Because how do you discount the green monkey kidney cells?
And this is exactly what the NICD has done in the supposed photograph. We placed this before the court and the court must consider this as per Section 39.1 of the Constitution.
This is overwhelming evidence that is supported by sworn testimony from scientific experts. Dr. Qureshi from Canada. Dr. […] from the United States, Dr. Corbett from the UK and, of course, the evidence that I have shown you from Christine Massey.
We thank them greatly for providing such sworn testimony to us. In addition to this sworn testimony, we also have incriminating evidence coming out of the mouths of the president, of the speaker of Parliament, and of the Reserve Bank governor themselves.
The president has admitted under oath at the Zondo commission, that his government has people or officials in high office that are captured. He admitted this.
He also said that members of Parliament from the African National Congress are in Parliament because of the party. And they are there to serve the party and represent the party, not the people of South Africa. This is out of his own mouth — sworn testimony.
The former speaker of Parliament Thandi Modise also delivered sworn testimony at the Zondo commission. And she said at the Zondo commission that sometimes members of parliament don’t ask unnecessary questions because they have ambitions of becoming ministers in future.
Thandi Modise did not ask the president to show us the virus. And now Thandi Modise is the Minister of Defense.
The South African Reserve Bank Governor, when he was helping, at the same time that South Africa incurred billions of dollars of debt with the IMF [International Monetary Fund], the South African Reserve Bank Governor was helping the government put together the budget in which this loan was decided upon. And at the same time, he was an advisor to the IMF, the entity to which the South African people would be eventually sold into debt slavery.
He was working for the IMF and he was working with the South African government the same time — benefitting the IMF with this loan and it was eventually taken up. This was a clear conflict of interest. Highly unacceptable. How can we expect that the Reserve Bank would have acted independently without fear or favor in such circumstances, as it should have done, when its governor was so highly conflicted.
As you can see, we have a very, very strong case here against these respondents. And we are asking the court to grant the South African people relief.
And the relief that we are asking from the court is: Number one, for the national state of disaster and all its measures including the lockdown etc. to be declared invalid and to be set aside immediately.
We are asking the court that the Covid-19 budget, or the budget that was decided upon on the 24th of June 2020, in which the South African people incurred, indirectly, a good deal of debt, to fund the lockdown and the national disaster — that that budget must be declared invalid and set aside. And that the South African people must not be responsible for any debt incurred as a result of this unproven pandemic.
We are asking the Constitutional Court that all the respondents be held financially liable personally for all the financial losses suffered by South African people — because of their actions or their failures to act in the correct manner.
Asking the court to hold the South African Reserve Bank liable as an institution, as an organization, because the South African Reserve Bank is the financial authority of the country. So as the financial authority, who acted wrongly in this instance, that the South African Reserve Bank should be held liable financially for all losses suffered by the South African people.
We are asking that all these respondents must resign voluntarily in an orderly manner. We are asking the court to grant the people of South Africa a referendum in which the people of South Africa can have a vote of no confidence in all of these respondents.
We are asking the court that the South African people be granted a referendum where they can decide whether to have a direct presidential election with individual candidates instead of party-based system that we have now, so that we can remedy this conflict of interest and this confusion that ANC party members have — whether they should represent the people or whether they should represent their party. We should have a referendum to solve this matter once and for all.
We are asking the court to grant the people of South Africa a referendum to decide whether we should liquidate the South African Reserve Bank in order to finance all of the financial losses suffered by the people of South Africa because of the failures of the South African Reserve Bank.
We are asking the court to grant the people a referendum so that the people can decide on a metal-based currency and the abolition of interest, to ensure that in future our financial system cannot be manipulated by anyone.
As you have seen here in my explanation for you, that our case is simple, clear and just.
We have faced many difficulties. Some of our witnesses that were supposed to give sworn testimony pulled out under threat, under coercion, under fear.
But we have labored on and we are here. This is a serious time in the history of South Africa and in the history of the world.
I ask all of you who are listening to this video that — should something happen to me — that all those co-applicants have the right to have this case continue to the end, until justice is done.
Please support our efforts. Please support our case. Please pray to God for our success.
As I have said, our case is simple, our case is clear, and our case is just. Thank you very much.
Today, there’s an entire generation who have grown up in the shadow of the towers. Who have never known a world that was not haunted by the hobgoblin of terrorism. Who have never thought twice about giving up the freedoms they barely knew they had in the name of fighting the “invisible enemy.” How can we blame them for not understanding the gravity of this moment, today, giving up those few freedoms that remain in the name of fighting the new phantom menace?
Half my life have I spent in the smoldering ruins of those exploded towers.
Picked my way through the eight mile-long debris field in Shanksville.
Huddled in the blast hole of the Army’s accounting offices in the E-ring of the Pentagon.
“Take off your shoes and belt, suspect! Single file! Digital fingerprints and photograph, please. Don’t worry. We’re just looking for the terrorists.”
“Speak up, prisoner! The NSA is recording this phone call for posterity. Machines of loving grace are scanning your emails and monitoring your social media posts. All in the name of Homeland Security, you understand.”
“How much cash do you want to withdraw? What for? Why don’t you just use a card like everybody else? We’re going to have to run a background check on you for this. After all, you might be one of them.”
And yet, I’m one of the lucky ones. At least I got to live half my life in the old world. The “see your friend off at their airport gate” world. The “government wouldn’t spy on us” world. The “‘Papers, please’ is a sign of tyranny!” world. That world, too, was a lie. But at the least they need to tell that lie to the public because people still believed in it.
Now there’s an entire generation who have grown up in the shadow of the towers. Who have never known a world that was not haunted by the hobgoblin of terrorism. Who have never thought twice about giving up the freedoms they barely knew they had in the name of fighting the “invisible enemy.”
How can we blame them for not understanding the gravity of this moment, today, giving up those few freedoms that remain in the name of fighting the new phantom menace?
Me? I came to the party five years late. The rallies. The C-SPAN broadcasts.
“Investigate 9/11!”
“Impeach Cheney first!”
“Remember Building 7!”
How innocent that all seems today, twenty years later. How naive.
But why not? We had the t-shirts, we had the slogans, we had the spindles of DVDs and we had the momentum on our side. By the sixth anniversary it was undeniable: a majority of Americans wanted an investigation of Bush and Cheney’s actions on 9/11. A full 32% wanted immediate impeachment. 67% believed that the 9/11 Commission had failed by not investigating the destruction of World Trade Center Building 7.
So, what happened?
Well, hope and change happened, of course. Never underestimate the sedative effect that a pure, unadulterated hit of hopium spiked directly into the veins of the body politic can have in quelling public dissent. It works every time.
But it was more than that. 9/11 Truth was not derailed by the Obamessiah; at least, not completely. No. 9/11 Truth was derailed by 9/11 Truth.
You see, the truth about 9/11 is as remarkably simple as it is incredibly powerful. We were lied to about 9/11. Period. End of debate. No one who knows anything about 9/11 could possibly deny that. I’d like to see them try.
That is the basis for a movement. With that one truth we could demolish an entire edifice of lies. They lied about 9/11. They didn’t just cover up the truth, they actively suppressed it. Everyone who is guilty of keeping the truth about 9/11 from the public is thereby an accessory to those crimes.
Every one of the actions that followed on from those lies—the PATRIOT ACT, the war of terror, the deaths of millions of Afghans and Iraqis and Libyans and Syrians, the construction of the police state, even the blowing of the post-9/11 housing bubble that led to the Global Financial Crisis—are as criminal as the events of 9/11 themselves. And those who have justified their criminal actions by recourse to the lies of 9/11 are thereby guilty of terrorism.
Those who committed their signatures to the PATRIOT ACT are the terrorists.
Those who invoked the doctrine of “pre-emptive self-defense” to justify their wars of aggression around the world are the terrorists.
Those who paraded on the corpses at Ground Zero in order to justify their own political agenda are by definition the terrorists.
This isn’t rocket science. It isn’t even controlled demolition science. It’s just plain, simple truth.
But somewhere along the way that plain truth about 9/11 got complicated. As the years turned into decades, the movement lost sight of that simple truth. Speculations became hypotheses. Hypotheses became theories. Theories became doctrines. Doctrines became dogma.
Soon, there was no movement. There were only egos proffering their own totalizing explanation of 9/11 right down to the minutia of operational details that they could not possibly have access to . . . unless they were in on the plot, that is. As if the very intelligence agencies they were accusing of perpetrating the attacks didn’t have (documentably!) a half century of experience derailing citizen investigations of deep state operations with false leads and cookie crumb trails that lead to nowhere.
Now there are no rallies, no C-SPAN broadcasts, no street activism. Just the remaining 9/11 Truther in the shrinking 9/11 Truth tent denouncing each other as loudly as possible for deviating from the catechism of their preferred dogma.
But, in retrospect, perhaps it was inevitable. After all, a movement that focuses on the events of a single day is destined to lose sight of the forest of the 20-year conspiracy that brought those events about for the trees of the events themselves. And a movement that focuses on one day in the increasingly distant past will find it increasingly difficult to stay relevant to the political present.
The 9/11 liars have human psychology on their side. The lies are seared into the public consciousness. The retractions and debunkings of those lies pass largely unnoticed. And in the end the pyrotechnics of 9/11 have had their intended effect: they have traumatized much of the public and hypnotized those who know they are being lied to. Blinded by the fireworks, 9/11 Truth could never turn away from the explosions and take the movement to the next level.
9/11 is not a series of dusty facts about demolition physics and airplane turning radiuses. As the 9/11 liars know all too well, it is a talisman that can be wielded to scare the public into submission.
But, like all talismans, this one, too, has begun to lose its power. Whereas once the very invocation of terrorism was enough to justify an entire political platform, now not even the specter of Al Qaeda (the bad Al Qaeda, not the good Al Qaeda in Syria) or ISIS (ISIS-K, that is, the new, scarier version of ISIS) is enough to catch the public’s attention. No. The terrorists needed a new talisman. A new 9/11.
And here it is, right on schedule! A new terror has been unleashed upon the world to traumatize the public once again. But this time the phantom menace is not a bearded Muslim boogeyman. No. It’s a virus.
At least in the good ol’ Homeland Security state erected to “keep us safe from the terrorists” you could protest, “But I’m not a terrorist.” It might not have saved you, but at least you could raise the point.
But in the new biosecurity state, your cries of innocence will not be permitted.
“I’m sorry, ma’am, but the test says you’re an asymptomatic spreader. We’re going to have to quarantine you. It’s for your own good.”
There is resistance, of course, just as there was resistance to the 9/11 lies. But is it a movement? Already it’s devolving into egos and dogma and bickering.
“Ivermectin is our only hope.”
“What are you talking about? The vaccines are the bioweapon.”
“What? You believe viruses exist?”
. . . Wait. What’s that? I swear I can hear Cass Sunstein laughing in the background.
Of course the terrorists are laughing. Why wouldn’t they be? They’ve got us scrutinizing the trees again while they’re busy encircling the forest.
This isn’t about COVID-19. This has nothing to do with a virus. This is about finishing the job that the terrorists started on 9/11; the job of locking down the planet.
Oh, sure. Examine the details. Put the pieces together on the health passports and the digital ID. The mandatory injections and government permission to leave your home. The central bank digital currencies and the Great Reset and the fourth industrial revolution. We do need to know these things.
But don’t get stuck marveling at the pyrotechnics. Don’t get stuck fighting your allies because they won’t subscribe to your dogma. Don’t get stuck focusing on what happened in 2019 so hard that you miss what’s happening in 2021. Or, some 20-year-old who’s just joining the party today will blink and he’ll find himself in 2039 wondering how he spent half his life in the shadow of a scamdemic.
The terrorists know all of this, of course. It’s how they stay in power. We don’t need to speculate about this, we just have to take them at face value when they tell it to us.
Like when Karl Rove admonished Ron Suskind for being part of the “reality-based community” who “believe that solutions emerge from your judicious study of discernible reality. But,” he insisted, “that’s not the way the world really works anymore.
We’re an empire now, and when we act, we create our own reality. And while you’re studying that reality—judiciously, as you will—we’ll act again, creating other new realities, which you can study too, and that’s how things will sort out. We’re history’s actors . . . and you, all of you, will be left to just study what we do.
And here we are. “History’s actors” have created “other new realities” and the same 9/11 Truth movement that spent the last 20 years judiciously studying the last set of lies will spend the next 20 years judiciously studying these ones . . . assuming we have 20 years left to spend in idle study, that is.
Or we could become history’s actors. Stop waiting for events to happen so we can judiciously study them and start creating events, structures, institutions of our own.
Can you imagine if the 9/11 Truth movement had devoted 1/10th of the time and energy and resources that it spent arguing over pyroclastic dust clouds and measuring entry and exit holes to something actually productive?
Growing the free market and expanding the use of alternative currencies?
Creating our own businesses and institutions and building out alternative communication infrastructure and building up our own media?
I don’t have “the” answer. No one person does. But I can tell you this: We cannot afford to spend the next two decades judiciously studying the way our most basic rights—the right to refuse medical experimentation, the right to interact and transact with our friends and neighbours as we see fit, the right to leave our own home—are being stripped from us, one by one.
If we don’t resist the biosecurity state with all our might—refuse to comply with its dictates, refuse to shut ourselves in and lay down when the government tells us to—then we are the terrorists, terrorizing our own children and grandchildren and consigning those generations yet unborn to the maws of a technocratic tyranny beyond any sci-fi dystopia.
In the meantime, we look back yet again at that September day 20 years ago, not as a single day when “the world changed forever,” but as a signpost along the path. Yet another in a chain of events and decisions and choices made by history’s actors: us.
I may never quite escape the shadows of those towers. But in that shadow, we can build towers of our own.
Draconian COVID policies and vaccine mandates are creating an uncertain future for a health care system that was already on shaky ground even before the terrible COVID policies took hold.
In January 2020 — pre-COVID — the Commonwealth Fund published a sobering report on the state of U.S. healthcare, comparing the U.S. to other high-income countries belonging to the Organization for Economic Co-operation and Development (OECD).
The report shared a number of depressing findings. First, despite the U.S. spending twice as much on healthcare (as a share of the economy) as comparable wealthy nations, Americans have the lowest life expectancy and highest suicide rates. Nor is America’s poor bang for its healthcare buck anything sudden or new — a 30-year-old study that compared the U.S. to 15 OECD nations reached the same conclusions.
The Commonwealth Fund report also drew attention to the fact that, among peer nations, the U.S. has the highest chronic disease burden, the highest number of hospitalizations from “preventable causes” and the highest rate of “avoidable deaths.”
Restrictive COVID policies have worsened these health indicators, with mounting deaths of despair and a plummeting life expectancy that researchers predict will drop still further.
The draconian policies — and especially COVID vaccine mandates for healthcare workers (HCWs) — are also wreaking havoc on the U.S. healthcare system and health workforce. Astoundingly high percentages of HCWs have experienced adverse events after accepting the jabs, rendering some unfit for duty. And among HCWs who, having done their due diligence, have chosen to decline the injections, firings and resignations are growing increasingly commonplace. These kinds of handicaps portend an uncertain future for a healthcare system that was already on shaky ground even before the terrible COVID policies took hold.
Early guinea pigs
As soon as the U.S. Food and Drug Administration granted Emergency Use Authorization for the COVID vaccines, HCWs began to find themselves in a catch-22: take an experimental injection (made by felonious pharma giants exempt from legal liability for injuries) or — egged on by hostile parties that now include no less than POTUS himself — risk ostracism or worse.
Many HCWs who dutifully did what they were told have not fared well. An online survey of 1,245 HCWs published in April (“representing various parts of the country during the early phase of COVID-19 vaccination”) furnishes one particularly hair-raising glimpse of the potential risks — for both provider and patient.
The study focused on roughly 800 HCWs (46% younger than age 41 and nearly all with doctoral, medical or Master’s degrees) who received the Pfizer vaccine and reported one or more symptoms. Almost all (93%) had received two doses.
Post-vaccination, about one in eight HCWs “temporarily” had trouble performing activities of daily living. In addition, the survey results highlighted the following:
Symptoms such as fatigue, headache, joint pain, nausea, muscle spasm, sweating, dizziness, flushing, brain fog, anorexia, sleep disruptions, tingling and palpitations were common.
Grouped by organ system, large percentages of the Pfizer-injected HCWs reported symptoms that were “generalized” (76%) or musculoskeletal (53%). However, the injections also displayed the capacity to affect nearly every body system: gastrointestinal (21%), psychological/psychiatric (17%), neurological (13%), otolaryngological (12%), endocrine (10%), cardiovascular (6%), respiratory (3%), urinary (1%) and allergic (1%).
The principal neurological symptom reported was brain fog or “reduced mental clarity” — a disabling symptom that can scarcely be reassuring to the affected individuals’ patients. This category also included reports of symptoms such as numbness, paralysis, vertigo and reactivation of herpes or shingles. These types of neurological symptoms are no joke; some HCWs have reported being denied health insurance and Workers’ Compensation despite symptoms so debilitating that they can no longer work.
In the otolarnygological category, ear and eye symptoms predominated, included ear ringing, changes in hearing, ear/eye pain, blurred vision and “flashing lights.” The vision-related symptoms dovetail with data from the European drug monitoring agency, which has recorded tens of thousands of eye disorders following COVID vaccination.
Oddly, 6% of Pfizer recipients reported upbeat feelings of joy, relief or gratitude in response to receiving the injections. The researchers characterized this as a “positive sign” of HCW willingness to “[take] the challenge to end the deadly pandemic, irrespective of side effects experienced.”
In early 2021, Czech researchers conducted a nearly identical HCW survey. Virtually all of the respondents (n=818), about a third of whom had at least one chronic illness at baseline, received two doses of the Pfizer shot, and 93% of the latter reported one or more side effects. Disturbingly, the prevalence of adverse reactions was consistently higher in younger (< 43 years old) HCWs with more of their careers ahead of them. Almost one in ten Pfizer recipients reported symptoms lasting for a week or more. Nevertheless, the researchers gaily concluded that healthcare workers and students “are among the ideal population groups to participate in this type of studies [sic] due to their high level of health literacy and scientific motivation.”
No thanks
From the beginning of the COVID vaccines’ rollout, surveys have indicated that HCWs are “somewhat more skeptical [about COVID vaccine safety] compared to the general public.” In early January, one in four surveyed HCWs indicated that they had no plans to ever get a COVID shot, with “wariness of going first” being one of the commonly cited reasons. In many healthcare settings, far larger proportions than 25% have chosen to remain unvaccinated.
In an opinion piece that appeared in HuffPost in February, senior reporter Jeffrey Young patronizingly explained that HCWs have “complicated” reasons for rejecting COVID shots, but he kindly suggested that those reasons do not make them “conspiracy theorists.” Somewhat more aptly, Young stated that HCWs “have watched the government bungle so many aspects of the COVID-19 response that when those same authority figures tell them to get vaccinated first, essentially to be guinea pigs for new vaccines, their messages aren’t always well-received.”
Months later, HCWs have had numerous opportunities to observe first-hand the post-jab travails of injected colleagues and patients, and for many, this has only intensified their “wariness.” In late August, two thousand HCWs filed a lawsuit in the state of Maine to block COVID vaccine mandates, arguing their wish “to be able to continue to provide the healthcare they have provided to patients for their entire careers, and to do so under the same protective measures that have sufficed for them to be considered superheroes for the last 18 months.”
The administration of Maine Governor Janet Mills is requiring that all HCWs in the state be vaccinated by Oct. 1. Outgoing New York Governor Andrew Cuomo announced a similar HCW vaccine mandate in August, stating that HCWs would be required to get a first dose even sooner (by Sept. 27), but on Sept. 14, District Judge David Hurd granted a temporary restraining order suspending the mandate because the state unlawfully disallowed religious exemptions available under federal law and the Constitution.
States imposing top-down HCW mandates may need to brace for some heavy fallout. The U.S. is already in the midst of an unprecedented nursing shortage, and as the mandates drive out even more of the best and brightest, the situation promises to get worse. Healthcare analysts point out that shortages of skilled nurses have major implications for patient care, with consequences ranging from longer wait times (and shorter visits), to less available care in rural settings to a higher risk of medication errors and even patient deaths.
The U.S. is also facing a shortfall of doctors. The pre-COVID Commonwealth Fund report — which found that Americans, even though sicker than their healthier counterparts in other wealthy nations, go to the doctor less often — suggested that physician shortages could be a contributing factor.
Get your care now
With an eye on the vaccine-mandate-impelled nursing shortage, former New York Times journalist Alex Berenson advised in August, “if you need to get sick, do it before the mandates hit Oct. 1.”
Though Berenson’s warning may have been somewhat tongue in cheek, a New York hospital announced earlier this month that it would be putting maternity services on hold after Sept. 24 due to resignations from maternity staff opposed to the mandates. In addition to stating that “The number of resignations received leaves…no choice but to pause delivering babies,” the hospital’s CEO indicated that services in five other units could be “curtailed in some way” if more hospital staff end up choosing departure over vaccination.
While noting that 70% of the resignations thus far have been from staff working in crucial clinical positions, the hospital CEO maintained that he was “unequivocally” in favor of mandatory vaccination.
The pausing of maternity services may inconvenience pregnant women with late September due dates, but the clinical staff fleeing heavy-handed mandates can hardly be blamed for objecting to the Hobbesian choice between risks to life and livelihood. As Children’s Health Defense president Mary Holland forcefully reiterated in response to President Biden’s inflammatory demonization of the unvaccinated, “The Nuremberg Code, which the U.S. promulgated and has expanded over time, says it best: ‘The voluntary consent of the human subject is absolutely essential.’”
What is the end game?
Kaiser Family Foundation characterizes the healthcare workforce impacts of COVID vaccine mandates as “unintended consequences,” but one has to wonder whether the medical and political establishment could truly be blind to the fact that so many “health-literate” HCWs would choose to decline the injections.
Many strangely “counter intuitive” episodes have transpired within the health system over the past 18 months, including widespread and dramatic health workforce layoffs and facility closures early last year, at precisely the same time that the media were trumpeting the emergency and celebrating HCWs for their heroism in the COVID trenches.
With COVID-19 clearly serving as the pretext to orchestrate a vast reengineering of society and governance in favor of more centralization and surveillance, it stands to reason that the medical-pharmaceutical cartel may be seizing the opportunity to catalyze similar health system changes. The departure of seasoned HCWs accustomed to providing competent in-person care could, in fact, facilitate the desired push for more virtual healthcare and telemedicine, a CDC-encouraged trend that will send far more patient data into the waiting hands of cloud services providers like Amazon and Microsoft.
For people who desire face-to-face care, and for ethical healthcare workers whose gift is to provide that type of care, it may be time to come up with a new model, one that perhaps emphasizes old-fashioned prevention — good nutrition and plenty of sunlight and exercise — over newfangled, gene-modifying injections that thus far have proven more effective at lining pockets than in doing anything useful for health.
“This was a tall order, and one could criticize it on the grounds that it was somewhat circular: how can you justify your methods of reasoning on the basis of those same methods of reasoning? It is like lifting yourself up by your own bootstraps.” ~ Douglas R. Hofstadter, Gödel, Escher, Bach: An Eternal Golden Braid
One of the aspects of the perpetuation of tyranny during this scam called the ‘Covid pandemic,’ is the “too smart by half” approach, which leads to a circular argument against a circular narrative. In this instance, nothing is ever fully refuted, little is ever achieved; the result being the promotion of the original narrative. This is very common concerning the current situation, and the most harm is being caused by many of those claiming to be on the side of right and liberty.
An example of this is the argument by ‘libertarians’ and independent writers and reporters who continue in their efforts to fight for the right to gain universal treatment of ‘Covid-19’ by promoting what they call ‘cures’ in the forms of Ivermectin and other claimed remedies. By doing this, they are accepting that there is a deadly ‘virus’ called ‘Covid,’ and that it can be ‘cured’ by using their preferred method. But there has never been any pure isolation, separation, or identification of anything called ‘SARS-CoV-2’ or ‘Covid-19.’ In other words, it does not exist, so how can one or another remedy ‘cure’ it?
Arguing against the atrocious standard CDC ‘Covid’ treatment protocol by promoting another protocol, simply solidifies the original propaganda that a deadly ‘virus’ called ‘Covid’ has caused a ‘pandemic.’ It has not; there is no ‘pandemic.’ In the case of Ivermectin, it is useful in that it is a substance meant to attack and neutralize harmful parasites, but it does not cure disease, and certainly cannot cure a phantom ‘virus.’ If one is sick and fraught with discomfort, that would mean that their body’s immune system was working to rid itself of the toxins by the natural healing process. Should the body’s bacteria not be able to complete this task, and if the problem were due to parasite infestation, then Ivermectin would likely alleviate that problem and give some relief, but would not cure anything. The only useful defense against this fraud is not to find a ‘cure’ for something that does not even exist, but to expose the deceit of this plot, and expose the agendas of those who perpetrated this scam.
Arguing in circles has no validity, and can only strengthen the position being argued against. This is not to say that promoting the positive uses of natural products or medicines is not warranted and appropriate, but doing so by accepting the state’s lies about a contrived ‘pandemic’ is more harmful than not. Staying healthy is one thing, claiming cure is something else. There have been any number of promoted ‘cures’ for a non-existent ‘virus’ discussed over time, but the cure for the real problem, which is tyranny, is never fully addressed. This is exactly what the evil controlling class desires, and many of those who claim to be on the side of freedom, whether wittingly or not, are helping to maintain the politically motivated status quo that a real ‘virus’ exists.
This brings us to the fake ‘vaccine’ for the fake ‘virus,’ as the same situation exists here. There is constant arguing on both sides concerning the efficacy of these very poisonous injections. How can there be a ‘vaccine’ for a ‘virus’ that does not exist? How can there be a ‘vaccine’ for something that is said openly to mutate constantly? Since this is the case, why would so many advocate for more testing, more trials, and so-called legitimate approval by the FDA, an accomplice in the state’s efforts to harm, murder, and control all of us, instead of simply denouncing any and all of these toxic shots as illegitimate? They are bioweapons after all, so instead of going in circles concerning which one is safer, which one has less side effects, or which one kills fewer people, why not denounce them all?
Words mean things, phrases mean things, debate can be deceiving, and language can go a long way in gaining control over people by promoting and maintaining the nefarious state narrative. Proper argument against wrong is vitally important, but arguing at the margins, arguing in circles, arguing to gain favor or position, or in-fighting to make a point, can do so much more harm than good, and in the process help to solidify tyranny.
Never trust the narrative, and always question everything. Do not get caught up in the argument, seek and accept only truth. This will require tenacity, strength, self-responsibility, and the ability to see through the hyperbole. It is time to tell it like it is, and accept reality, regardless of the consequences.
“The ideal subject of totalitarian rule is not the convinced Nazi or the dedicated communist, but people for whom the distinction between fact and fiction, true and false, no longer exists.” ~ Hannah Arendt
VAERS data released Friday by the CDC showed a total of 623,343 reports of adverse events from all age groups following COVID vaccines, including 13,627 deaths and 84,466 serious injuries between Dec. 14, 2020 and Aug. 20, 2021.
Data released today by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020 and Aug. 20, 2021, a total of 623,343 total adverse events were reported to VAERS, including 13,627 deaths — an increase of 559 over the data released last week.
There were 84,466 reports of serious injuries, including deaths, during the same time period — up 3,416 compared with the previous week.
Of the 6,128 U.S. deaths reported as of Aug. 20, 13% occurred within 24 hours of vaccination, 18% occurred within 48 hours of vaccination and 32% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 360.3 million COVID vaccine doses had been administered as of Aug. 20. This includes: 203 million doses of Pfizer, 143 million doses of Moderna and 14 million doses of the Johnson & Johnson (J&J).
The data come directly from reports submitted to the Vaccine Adverse Event Reporting System (VAERS), the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
This week’s U.S. data for 12- to 17-year-olds show:
The most recent reported deaths include a 15-year-old boy (VAERS I.D. 1498080) who previously had COVID, was diagnosed with cardiomyopathy in May 2021 and died four days after receiving his second dose of Pfizer’s vaccine on June 18, when he collapsed on the soccer field and went into ventricular tachycardia; and a 13-year-old girl (VAERS I.D. 1505250) who died after suffering a heart condition after receiving her first dose of Pfizer.
Lisa Shaw, 44, received her first dose of AstraZeneca on April 29. On May 13, she was taken by ambulance to University Hospital of North Durham after having a headache for several days. She was transferred to the Royal Victoria Infirmary in Newcastle, where she received a number of treatments, which included cutting away part of her skull to relieve the pressure on her brain. She died May 21.
According to the BBC, Tuomo Polvikoski, a pathologist, told the coroner Shaw was fit and healthy before receiving the vaccine. When asked about the underlying cause of the fatal clotting on her brain, Polvikoski said the clinical evidence “strongly supports the idea that it was, indeed, vaccine-induced.”
FDA grants full approval of Pfizer vaccine, critics blast agency for lack of data, scientific debate
The U.S. Food and Drug Administration (FDA) Aug. 23 granted full approval to Pfizer’s “Comirnaty” COVID vaccine for people 16 years and older — without allowing public discussion or holding a formal advisory committee meeting to discuss data.
This is the first COVID vaccine approved by the FDA, and is expected to open the door to more vaccine mandates by employers and universities.
According to The Washington Post, Pfizer’s vaccine approval was the fastest in the agency’s history, coming less than four months after Pfizer/BioNTech filed for licensing on May 7.
According to an article published Aug. 20 in the BMJ, transparency advocates criticized the FDA decision not to hold a formal advisory committee meeting to discuss Pfizer’s application for full approval — an important mechanism used to scrutinize data.
Last year the FDA said it was “committed to use an advisory committee composed of independent experts to ensure deliberations about authorisation or licensure are transparent for the public.”
But in a statement to The BMJ, the FDA said it did not believe a meeting was necessary ahead of the expected full FDA approval.
Kim Witczak, a drug safety advocate who serves as a consumer representative on the FDA’s Psychopharmacologic Drugs Advisory Committee, said it’s concerning that full approval is based on only six months’ worth of data — despite clinical trials designed for two years — and there’s no control group after Pfizer offered the product to placebo participants before the trials were completed.
FDA approval letter causes confusion, raises questions
Buried in the fine print of Monday’s approval of the Pfizer Comirnaty vaccine are two critical facts that affect whether the vaccine can be mandated, and whether Pfizer can be held liable for injuries, according to Children’s Health Defense Chairman Robert F. Kennedy, Jr. and Dr. Meryl Nass.
Here's my latest with @NassMeryl… Buried in fine print of Monday's approval by FDA of Pfizer Comirnaty COVID vaccine are 2 critical facts that affect whether vaccine can be mandated + whether Pfizer can be held liable for injuries.https://t.co/QtpHufCKDI
Kennedy and Nass, who accused the FDA of pulling a “bait and switch” on the public, said the FDA acknowledged that while Pfizer has “insufficient stocks” of the newly licensed Comirnaty vaccine available, there is “a significant amount” of the Pfizer-BioNTech COVID vaccine — produced under Emergency Use Authorization (EUA) — still available for use.
The FDA decreed that the Pfizer-BioNTech vaccine under the EUA should remain unlicensed — but that it can be used “interchangeably” (page 2, footnote 8) with the newly licensed Comirnaty product.
Second, the FDA said the licensed Pfizer Comirnaty vaccine and the existing EUA Pfizer vaccine are “legally distinct,” but said their differences do not “impact safety or effectiveness.”
Kennedy and Nass said EUA products are experimental under U.S. law. Both the Nuremberg Code and federal regulations provide that no one can force a human being to participate in this experiment.
Under 21 U.S. Code Sec.360bbb-3(e)(1)(A)(ii)(III), “authorization for medical products for use in emergencies,” it is unlawful to deny someone a job or an education because they refuse to be an experimental subject, they wrote.
At least for the moment, the Pfizer Comirnaty vaccine has no liability shield. Vials of the branded product, which say “Comirnaty” on the label, are subject to the same product liability laws as other U.S. products, Kennedy and Nass said, adding that “Pfizer is therefore unlikely to allow any American to take a Comirnaty vaccine until it can somehow arrange immunity for this product.”
On Thursday, Sen. Ron Johnson (R-Wis.) wrote the FDA raising similar concerns and questions about the agency’s approval of the Pfizer Comirnaty vaccine.
In his letter, Johnson asked FDA Acting Commissioner Dr. Janet Woodruff why the FDA didn’t grant full licensure for the Pfizer-BioNTech vaccine that is already in use and available in the U.S., and how the agency will ensure that those being vaccinated under mandates will receive the FDA-approved version.
As COVID surges among fully vaccinated, CDC fails to properly track breakthrough cases
As The Defender reported Aug. 24, the most recent data from the CDC shows 9,716 breakthrough cases resulting in hospitalization or death as of Aug. 16. However, the agency states those numbers are underreported.
On May 1, the CDC made a decision to stop tracking all breakthrough cases and instead only track cases in the fully vaccinated that resulted in hospitalization or death. That leaves public health officials without the full data that can answer questions as the new Delta variant spreads.
In an interview with PBS News Hour, Jessica Malaty Rivera, an infectious disease epidemiologist and research fellow at Boston Children’s Hospital and former science communications lead at the COVID Tracking Project, said not tracking breakthrough data with as much granularity as we would hope is “basically creating blind spots in our understanding of the true impact of the virus, especially the variants that are circulating so widely in the United States.”
The New York Times recently published data from seven states — California, Colorado, Massachusetts, Oregon, Utah, Vermont and Virginia — that keeps particularly detailed records on breakthrough cases.
Analysis showed that in six of the states, breakthrough infections made up 18% to 28% of all newly diagnosed cases of COVID in the past several weeks, and 12% to 24% of all COVID-related hospitalizations, with reported deaths higher than the CDC’s original estimate of .5%.
Pfizer scheme to churn out ‘variant-specific’ vaccines will lead to more variants, experts warn
Pfizer CEO Albert Bourla on Tuesday told Fox News the company has a system in place to turn around a variant-specific jab within 95 days in the likelihood a vaccine-resistant COVID strain emerges, but experts warn that strategy will backfire.
Bourla said Pfizer hasn’t identified any variants that could escape the vaccine yet. However, that statement contradicts the findings of numerous studies by the Centers for Disease Control and Prevention (CDC) which show waning immunity against the Delta variant.
Dr. Peter McCullough, board certified in internal medicine, cardiovascular diseases and clinical lipidology, said in a recent podcast: “There are clearly sources of information to suggest that once we start vaccination and we get more than 25% of the population vaccinated, we will allow one of the variants that’s in the background to emerge because it’s resistant to the vaccine.”
“That [theory] makes sense,” McCullough said. “Just like an antibiotic, once we get to a certain percentage of coverage with an antibiotic, we’ll allow a resistant bacteria to move forward.”
According to Dr. Robert Malone, inventor of mRNA and DNA vaccines, worldwide expert in RNA technologies and Harvard-trained physician, continued mass vaccination campaigns will enable new, more infectious viral variants.
Even if we had complete uptake in vaccines and complete masking, Malone said, CDC data makes it clear that at best we can slow the spread of Delta but we can’t stop it.
New CDC studies show waning vaccine immunity to Delta variant
Two studies released Aug. 24 by the CDC showed fully vaccinated Americans’ immunity to COVID is waning as the Delta variant now makes up 98.8% of U.S. COVID cases.
One study found vaccine effectiveness among frontline healthcare workers declined by nearly 30 percentage points since the Delta variant became the dominant strain in the U.S.
The analysis also concluded COVID vaccines were only 80% effective in preventing infection among the frontline healthcare workers.
The second study examined 43,000 Los Angeles residents 16 and older. Between May 1 and July 25, 25.3% of COVID infections occurred in fully vaccinated persons and 3.3% were in partially vaccinated persons.
The CDC cautioned in its report that vaccine effectiveness “might also be declining as time since vaccination increases and because of poor precision in estimates due to limited number of weeks of observation.”
The publication of the new studies followed a week after the CDC released its first three reports on vaccine efficacy — which also showed waning vaccine protection against the Delta variant.
172 days and counting, CDC ignores The Defender’s inquiries
According to the CDC website, “the CDC follows up on any report of death to request additional information and learn more about what occurred and to determine whether the death was a result of the vaccine or unrelated.”
On March 8, The Defender contacted the CDC with a written list of questions about reported deaths and injuries related to COVID vaccines. We have made repeated attempts, by phone and email, to obtain a response to our questions.
Despite multiple phone and email communications with many people at the CDC, and despite being told that our request was in the system and that someone would respond, we have not yet received answers to any of the questions we submitted. It has been 172 days since we sent our first email to the CDC requesting information.
In my latest book — “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health” — I take an in-depth look at the disastrous consequences of Dr. Anthony Fauci’s 50-year reign as America’s public health czar. The book, which will be released Nov. 9, is available now for preorder.
On Nov. 9, Children’s Health Defense Chairman Robert F. Kennedy, Jr. will release his new book — “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health.”
As director of the National Institute of Allergy and Infectious Diseases (NIAID), Dr. Anthony Fauci dispenses $6.1 billion in annual taxpayer-provided funding for scientific research.
The research I conducted for my new book exposes how Fauci’s gargantuan yearly disbursements allow him to dictate the subject, content and outcome of scientific health research across the globe.
These annual disbursements also allow Fauci to exercise dictatorial control over the army of “knowledge-and-innovation” leaders who populate the “independent” federal panels that approve and mandate drugs and vaccines — including the committees that allowed the Emergency Use Authorization of COVID-19 vaccines.
Fauci uses the financial clout at his disposal to wield extraordinary influence over hospitals, universities, journals and thousands of influential doctors and scientists — whose careers and institutions he has the power to ruin, advance or reward.
These are the same doctors who appear on network news shows, publish on the op-ed pages of influential media, and craft and defend the pharmaceutical cartel’s official narratives.
Fauci only rarely performs NIAID’s traditional mission of researching the causes behind the exploding epidemics of allergic and autoimmune diseases — as evidenced by the fact that under his watch, the chronic diseases Congress charged NIAID with preventing rose from 1.8 % among children when Fauci came to NIAID in the 1960s, to 54% today, when obesity is factored in.
Instead of addressing the rise in chronic diseases, Fauci transformed NIAID from a world-class regulator into a product incubator for Big Pharma by developing new drugs and vaccines for which he, his agency and his employees often share patents and royalties.
My book also reveals how Fauci and his cohorts in Pharma profit handsomely from sickness — but not so much from good health.
50 years as the ‘J. Edgar Hoover of public health’
Fauci has survived half a century in his government post — he’s the J. Edgar Hoover of public health — by kowtowing to (and profiting from) pharmaceutical interests.
He launched his career during the early AIDS crisis by partnering with pharmaceutical companies to sabotage safe and effective off-patent therapeutic treatments for AIDS.
Fauci orchestrated fraudulent studies, and then pressured U.S. Food and Drug Administration (FDA) regulators into approving a deadly chemotherapy treatment he knew to be worthless against AIDS.
Thanks to Fauci’s corrupt intervention, AZT, at $10,000 per patient per year, became history’s most expensive commercial drug — one that made billions for GlaxoSmithKline.
Fauci repeatedly violated federal laws to allow his Pharma partners to use impoverished and dark-skinned children as lab rats in deadly experiments with toxic AIDS and cancer chemotherapies.
In 2005, Congress cited his agency for consistently breaking federal laws in outlaw experiments on Black and Hispanic orphans in foster homes in New York and six other states.
Fauci’s long list of unethical and genocidal experiments on Africans caused mayhem and tragedy across the continent, particularly for children and pregnant mothers.
Each of the vaccines funded by Fauci and Bill Gates — polio, DPT, malaria, meningitis, tetanus and HIV — likely caused far more injuries and deaths around the world than they averted.
The carefully constructed Pharma-Fauci-Gates alliance
In early 2000, Fauci shook hands with Gates in the library of Gates’ $147 million Seattle mansion, cementing a partnership that would aim to control an increasingly profitable $60 billion global vaccine enterprise with unlimited growth potential.
In 2009, Gates stood before the United Nations and declared the “Decade of Vaccines.” He committed $10 billion to build a regulatory, political, media and brick-and-mortar infrastructure with the goal of inoculating the entire global population with multiple jabs by 2020.
Through funding leverage and carefully cultivated personal relationships with heads of state and leading media and social media institutions, the Pharma-Fauci-Gates alliance exercises dominion over global health policy.
Gates and Fauci now wield far-reaching influence and unprecedented power to shut down the global economy, abolish civil and constitutional rights, impose police state surveillance and engineer the greatest upward shift of global wealth in human history.
In my book, I lay bare how Fauci, Gates and their collaborators:
invented and weaponized a parade of fraudulently concocted global pandemics, including bird flu (2005), swine flu (2009) and Zika (2015-2016), in order to sell novel vaccines, enrich their Pharma partners and increase the power of public health technocrats and Gates’ entourage of international agencies.
made a series of prescient predictions about the imminent COVID-19 pandemic — almost to the day. Their precision soothsaying further awed a fawning, credulous and scientifically illiterate media that treats Gates and Fauci as religious deities, insulates them from public criticism and vilifies their doubters as heretics and “conspiracy theorists.” Adulatory mainstream media abetted Fauci’s conspiracy to cover up COVID’s origins at the Wuhan lab.
teamed with government technocrats, military and intelligence planners, and health officials from the U.S., Europe and China to stage sophisticated pandemic “simulations” and “Germ Games.” Exercises like these, encouraged by the Global Preparedness Monitoring Board, laid the groundwork for imposition of global totalitarianism, including compulsory masking, lockdowns, mass propaganda and censorship, with the ultimate goal of mandating the coercive vaccination of 7 billion humans.
practiced, in each of their “simulations,” psychological warfare techniques to create chaos, stoke fear, shatter economies, destroy public morale and quash individual self-expression — and then impose autocratic governance.
Stoking COVID-19 pandemic fear
The “Real Anthony Fauci” details how Fauci, Gates and their cohorts used their control of media outlets, scientific journals, key government and quasi-governmental agencies, and influential scientists and physicians to flood the public with fearful propaganda about COVID-19 virulence and pathogenesis, and to muzzle debate and ruthlessly censor dissent.
Gates and Fauci engaged in almost daily communications throughout the lockdown, and coordinated virtually every decision about COVID-19 countermeasures with each other.
They effectively placed global populations under house arrest, and flooded the mainstream and social media with propaganda crafted to terrorize.
To justify the implementation of draconian measures, Gates and Fauci systematically stoked irrational fears and stifled common sense to induce a form of mass psychosis known as “Stockholm Syndrome.”
They inspired in their hostages gratitude towards their captors, and the belief that total obedience and unquestioning submission to an experimental, shoddily tested, fast-tracked, zero-liability COVID vaccine was their only hope for safe escape from captivity and “return to normal.”
anointed fraudulent PCR tests in order to deliberately inflate numbers of COVID cases by some 90%.
facilitated the adoption of new, unprecedented instructions for coroners to fraudulently attribute COVID as the cause of death “on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death” — with or without a positive COVID-19 test.
discredited all early COVID-19 treatments like hydroxychloroquine and many other remedies that could have quickly ended the pandemic and saved hundreds of thousands of lives.
Predictably, during the COVID crisis, Fauci’s policies resulted in the U.S. accounting for 20% of the world’s COVID deaths, despite making up only 4.2% of the global population — another example of Fauci failing upward.
As my book makes clear: Fauci’s COVID policies also spawned new insidious authoritarianism — and propelled America down a slippery slope toward a grim future as a dark totalitarian security and surveillance state.
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light BitChute, Brighteon, and Odysee channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
Transcript
So, children over the age of 16 won’t need parental permission to accept the experimental jab for covid-19. The British Government wants to give it to children over the age of 12. And they are now testing it on pre-school and primary school children.
Listen carefully to what I’ve got to tell you.
If you’re a human and not a zombie this will fill you with rage. If the squaddies in the 77th Brigade listen properly even they are going to think twice about pressing the thumbs down button.
On the 15th July 2021, the UK Government’s advisors the Joint Committee on Vaccination and Immunisation said: `until more data become available JCVI does not currently advise routine universal vaccination of children and young people less than 18 years of age.’ They added that the `the health benefits in this population is small and do not outweigh the potential risks.
Splendid, I thought. Send up a rocket.
And then a few weeks later, on 4th August, the committee changed its mind after the UK’s Chief Medical Officers requested that JCVI accelerated its review of advice for jabbing children.
Changed their minds.
They admitted that covid-19 disease in children is typically mild or asymptomatic. But they changed their minds and said that all 16 and 17-year-olds be jabbed. And that many children aged 12 and over be jabbed.
One odd thing was that they said that `in recent weeks, reports have been submitted about myocarditis.
Recent weeks.
Take a look at my video dated 8th December 2020 entitled `Covid 19 vaccine – possible vaccine side effects’ and you will find that I listed myocarditis.
So how come I knew about this risk half a year before the Government’s advisory committee? Not boasting but I’ve been half a year ahead since early 2020.
I can’t find any new evidence that would have changed their minds.
But the minds changed.
The membership of the JCVI’s subcommittee on covid changed and one prominent critic of covid jabs for children coincidentally left. Three other members changed too. Gosh. However, committee members said that they had not felt any political pressure to change their views on giving the jab to teenagers. How reassuring.
Just out of idle curiosity I wonder if any members of the committee have any links with drug companies or have ever accepted drug company money. Or are there any who have no links with drug company money. Just wondering. I’ll perhaps look into that in detail another day.
Politicians, advisers and doctors should know that the experimental jab will kill children – almost certainly kill or injure far more than would be killed or injured by this year’s flu: covid-19.
And there won’t be one in a million of these jabbed children who will understand that they’re taking part in a massive, unethical, immoral and illegal experiment. The Joint Committee says `in all instances, the offer of vaccination to children and young people must be accompanied by appropriate information to enable children and young people…to be adequately appraised of the potential harms and benefits of vaccination as part of informed consent prior to vaccination.
That’s called covering your back.
The queen, Dolly Parton and a bunch of influencers on social media will say it’s OK. The kids will be bribed. And not one in a thousand doctors or nurses will explain the risks in detail.
What am I saying: I bet not one in a thousand doctors or nurses have any idea of the risks.
And the idea that 16-year-olds will understand these complicated vaccines would be laughable if it were not obscene. Most kids think the jab will stop them getting covid. And stop them spreading it to granny.
Not that this matters much because the Government killed granny last year.
And all this is illegal.
Back in February, six months ago, I pointed out in a video entitled, ‘Doctors and Nurses giving the covid-19 vaccine will be tried as war criminals’ that the Nuremberg Code on medical experimentation, which was written in 1947, stated that explicit voluntary consent from patients is required for human experimentation.
That means, of course, that patients must be told that they are taking part in a trial. And they must be warned of the dozens of possible adverse events – which were known before Christmas. I made a video listing the FDA’s draft working list of adverse events in December 2020. Those being jabbed must be warned that they could die. And they must be warned that the vaccine they’re being given won’t necessarily stop them catching covid or passing it on if they do catch it.
That’s informed consent.
And as I said, I doubt if one in a million adults was properly advised.
How many 16-year-olds will understand what an mRNA vaccine does? How many will understand the principles of pathogenic priming?
Once again, as I said back in February, any doctor or nurse giving one of these experimental jabs without making sure that their victim has been given all the necessary information, and understands it, is breaking international law and will go to prison.
The fact is that the whole vaccination programme is built on lies and deceit. Governments and the media wouldn’t need to lie, harass and suppress the truth if there really were a plague and if the experimental injection really worked. People would be fighting to get jabbed.
Of course, if there really were a plague there wouldn’t be a vaccine. The vaccine’s promoters are mostly on record as saying that they want a smaller global population. So if there were a killer plague they wouldn’t want a vaccine, would they?
Accepting this experimental and unnecessary jab is the most important decision any citizen will ever make. The so-called vaccine is for ever. It isn’t like a drug that you can stop and get over. The covid-19 jab stays. You can’t get it out. And no one, repeat no one, knows what the effect will be in six months or six years or sixteen years. It’s an experiment and the preliminary part of the experiment won’t be over until 2023. The vaccine has already killed thousands of people and injured millions more. Just look at the updated figures on my website where I quote the official death and injury figures published by the British and American governments.
Will the vaccinated be more susceptible to new variations? Will they die when they contract winter viruses? No one knows the answers.
The risks are so great that I believe that anyone who has been jabbed – particular the young who seem to be particularly liable to heart damage – should avoid all strenuous exercise and stress.
Forever.
Meanwhile, the promotional campaign to sell the jab to kids is moving fast. Free money. Free kebabs. The chance to reclaim a little of the life that was taken from them.
The BBC has reported that 60,000 lives have been saved by the covid jab. There’s isn’t one shred of evidence to prove that claim. They might as well claim that 60 billion lives have been saved.
The disgusting BBC and the rest of the mainstream media become indecently orgasmic with excitement when they find someone who hasn’t been vaccinated and who has died of or with covid-19 (aka the rebranded flu) or, probably, anything else. They ignore the fact that every year, in the six month flu season, up to 650,000 people of all ages die of the flu worldwide. Often ordinary healthy people.
But the deception and the lies about the rebranded flu just keep getting bigger.
Unvaccinated man with flu run over by bus. Unvaccinated woman eaten by lion.
The truth is that these experimental jabs have not been sufficiently tested, do not do what most people think they do and are so dangerous that their distribution should be halted immediately.
Doctors who object, who point out the dangers, and who explain why the risk benefit ratio shows that the people producing, and promoting these damned things should be locked up, are monstered and silenced and lied about and offered mental health care – just as if we were in Russia in Stalin’s time. Objections are dismissed without debate. There is no debate. Never before in my knowledge has a drug been introduced and used so widely with no discussion. For 18 months I’ve been asking government advisors to debate with me on live television.
Nothing. Silence.
We pay them. They ignore us.
All this proves, of course, that the promotion of this experimental product is a heinous fraud.
Meanwhile, the majority of doctors will accept the lies, promote the jab and take the big money they’re being paid.
When these disgusting women and men are arrested – as they will be – I hope they are shown no mercy. They are, man and woman, guilty of some of the most awful crimes in history.
Please go to vernoncoleman.org and email this video – together with the transcript – to every school and doctor’s surgery in your area.
I’ll leave you with this.
The UK Government admits that the longer term health effects from the myocarditis events reported are not yet well understood.
But they’re planning to give the damned stuff to pre-school children and primary school children as well as teenagers.
They’ve killed the grandparents. Now they want to kill the kids.
When it comes to the safety and efficacy of the so-called COVID-19 vaccinations the public has been thoroughly divided and conquered. On one side of the carefully crafted argument, governments can’t get enough shots in enough arms to ward off a “pandemic” of unvaccinated people. The other side has as many excuses for avoiding these injections as it has members. So when a controversial study comes along showing that these injections may contain a toxic substance called graphene oxide the allowed spectrum of debate is quickly alight and the bigger picture is missed by all but a few.
The story of vaccines containing graphene oxide broke in late June when Ricardo Delgado Martin, Founder and Director of Quinta Columna, which calls itself a “free thinking movement,” published the the results of an analysis conducted by a Spanish research team at the University of Almeria. The analysis claims to have discovered graphene oxide in a vial of a Pfizer vaccine via electron microscopy and spectroscopy. The analysis can be read in English here.
It took a few weeks for this story to find it’s way into the English speaking world it would seem. Once it did, the mainstream media’s fact checkers were all over this story. Reuters, Full Fact, and Forbes among other establishment outlets have tried to debunk the study by assuring their readers that only an anti-vax QAnon conspiracy theorist would believe such nonsense. On the other side of the aisle, the analysis has been uncritically circulated which only adds to the problem.
As usual, the truth lies somewhere in the middle. The analysis conducted by the team at the University of Almeria has it’s flaws but concerns over the presence of graphene oxide in the Pfizer vaccines, and elsewhere in our environment, should be given serious consideration.
But first, let’s address some of the issues with the analysis:
The analysis is an interim report needing further study.
The analysis was commissioned.
The origin of Pfizer vial used in this analysis is unknown.
Graphene oxide and reduced graphene oxide are, at times, used interchangeably.
Comparative images of graphene oxide are of different magnification levels.
For an in-depth look at these concerns and others that arise from this analysis we recommend watching world class researcher, Whitney Webb’s recent appearance over at The Last American Vagabond where they dive into this analysis.
Just because this study currently stands on scientifically shaky grounds does not mean that the theory that graphene oxide is in fact in these injections should be dismissed. The substance has also already been discovered in face masks in Canada and Spain while patents in China (1, 2) that explore the possibility of using graphene oxide in COVID19 vaccines are pending.
It is also curious graphene oxide can be made to have magnetic properties which would explain the countless videos circulating online of magnets sticking to those who’ve been injected with these so-called vaccines. More research on this phenomenon is certainly needed but a recent “statistical and sociological” survey conducted by the European Forum for Vaccine Vigilance in Luxemburg found that 29 of the 30 “vaccinated” individuals interviewed showed attraction to the magnet at the site of injection.
Additionally, it has been shown that graphene oxide can cause blood clots and damage lungs. Does this explain why blood clots are such an often reported adverse effect from these shots? Is there a connection to this lung damage and surge in supposed surge in COVID-19 cases in areas of high injection rates?
These questions and many others surrounding graphene oxide, injections, masks, and the so-called pandemic need answering but if we just focus on these elements of the conversation we risk missing the bigger picture. Graphene oxide, its applications, and its impact on humanity are not limited to the so-called pandemic. The applications of graphene and it’s related materials are almost limitless and as they are introduced into the ecosystem, inside and out of the human body, they have the potential to reshape our relationship with the natural world by making it impossible to escape the digital realm.
On the future applications of graphene, Alan S. Brown writes:
Silicon electronics dominate the world, but engineers frequently turn to other types of semiconductors to do things that silicon cannot. These materials—ranging from silicon carbide to indium gallium arsenide—emit and interact with light, enable high-frequency microwave communications in smartphones, run at higher speeds, and handle massive amounts of power.
Yet, what if a single material could do all that—if it could interact with electrons, light, and even magnetism. What if it could transmit electricity like a metal and also behave as a semiconductor. Just for good measure, suppose it might make a good building block for quantum computers? And—most impressively—what if it could do all these things just by changing its shape?
That material is graphene.
By introducing graphene and other related nanoparticles into the human system, our bodies become cybernetic systems where light, microwaves and other frequencies, or magnets could be used to control bodily and neurological functions. If some predictions are correct then graphene oxide will one day be as prevalent in our world as plastic is now. It is already raining down on us from above, polluting our soil, being laser printed onto food, and, in turn, is likely already in all of us. If so, it seems reasonable to conclude that, based on all that we know about previous medical experimentation carried out on humans, something similar is happening today.
But why introduce a material like this into the human body? Catherine Austin Fitts ventures a guess:
So let me go through where I think he’s going. I think where they’re going—and they’re they’re prototyping tons of technology, so I don’t think they have it yet—but where they want to go is they want to download a Microsoft Office system into your body, into your brain, and hook it up to the Jedi cloud contract and the Amazon Cloud contract at the CIA. And if they can get seven people seven billion people hooked up directly to their cloud contracts and use viruses—I mean, it’s very clever—use viruses to keep those updates coming. You know, just keep those updates coming.
So you saw my most recent article, “The Injection Fraud.” I think it’s a fraud to call these vaccines they’re not vaccines, they’re not medicine. But I think it’s the exact same model you used in the computers and the ideas. Just like Bill Gates made it possible for the intelligence agencies to get a backdoor into our—you know, our data—and our computers. They want a backdoor into our mind and it’s very hard if you haven’t if you haven’t looked into the creepy technology, the Charles Lieber kind of technology, it’s hard to fathom but we’re beginning to fathom it.
Experimental injections. Magnetic nanoparticles. A human operating system. Sadly, these are not the fever dreams of a lone, crazed scientist but technologies which have already arrived. The COVID-19 panic has accelerated the introduction of these and many more frightening technologies into the public sphere as trojan horses for even more terrifying technologies yet to be revealed. The work from researchers like Whitney Webb, Alison McDowell, Catherine Austin Fitts, Rosa Koire, James Corbett, Patrick Wood, and everyone else which shines light on the this transhumanist agenda is becoming more important than ever.
For too long we’ve narrowed in on all things COVID-19 just like the powers-that-shouldn’t-be hope for. There is no pandemic, only a psychological operation afoot. That operation needs as much resistance as possible but if we fail to see beyond this then their dream of can be reached without a fight. Beyond saying no to experimental injections and nanoparticle-laden masks we must starting saying no to everything that is being used to create the graphene oxide prison being built around us.
When airplanes routinely dump megatons of toxic garbage into our atmosphere as they have been doing for twenty years plus now, the most obvious question is: What are the biological impacts? What are the environmental implications of very small coal fly ash particles entering our bodies and fouling our biosphere? As one might guess, the implications are grave. Although the geoengineers will undoubtedly tell us that everything is fine, the best available evidence shows that the general population’s health is being negatively impacted, at least hundreds of thousands of people are dying, and our environment is being summarily wrecked as well. These are the biological impacts of the New Manhattan Project.
Particulate matter
The inhalation of aerosolized particulate matter has generally harmful human health impacts. This is not a matter of debate. Common sense and many studies show this. A slew of studies referenced at the end of this chapter shows that inhalation of fine particulate matter is associated with: Alzheimer’s disease, risk for stroke, risk for cardiovascular disease, lung inflammation and diabetes, reduced renal (kidney) function in older males, morbidity and premature mortality, decreased male fertility, low birth weight, onset of asthma, and increased hospital admissions.
Coal fly ash
As far back as October of 1979, a study was performed about the health effects of aerosolized coal fly ash. Unsurprisingly, the authors of the study found that exposure to aerosolized coal fly ash through the lungs causes harm. In other news, the geniuses at the World Health Organization found that bullets fired from guns can kill people.
We should be thankful that the good Dr. Marvin Herndon has recently produced a series of peer-reviewed, published journal articles detailing the health effects of exposure to that specific material being routinely pumped out of jet aircraft. His first paper in this area titled “Coal Fly Ash Aerosol: Risk Factor for Lung Cancer,” published in February of 2018, was co-authored by Dr. Mark Whiteside, MD, MPH, the Medical Director of the Monroe County, Florida Department of Health. Herndon and Whiteside found that coal fly ash has lots of nasty, cancer-causing stuff in it. The authors write:
“CFA [coal fly ash] contains a variety of potentially carcinogenic substances including aluminosilicates, an iron oxide-containing magnetic fraction, several toxic trace elements, nanoparticles, and alpha-particle-emitting radionuclides. Silica, arsenic, cadmium, and hexavalent chromium are found in CFA and all have been associated with increased lung cancer risk.”
Further, the authors write, “Chronic exposure to aerosolized CFA, emplaced in the atmosphere for climate intervention, may be an important, yet unrecognized, environmental risk factor for development of lung cancer.”
Doctors Herndon and Whiteside
As we can see from the passage above and as many have feared, Dr.s Herndon and Whiteside have found that at least some of these atmospheric coal fly ash particles are nano-sized. This is a concern because when nano-sized particles are inhaled, they are so small that they go directly into the blood stream and right into the brain, often causing a host of neurological disorders. Nano-sized particles are so small that one ingests them through one’s skin.
Herndon and Whiteside teamed up again for the March 2018 publication of their paper “Aerosolized Coal Fly Ash: Risk Factor for Neurodegenerative Disease.” The authors write:
“The recent finding of spherical exogenous magnetite (Fe3O4) nanoparticles in the brain tissue of persons with dementia suggests an origin in air pollution produced by coal fly ash. The primary components of coal fly ash, iron oxides and aluminosilicates, are all found in the abnormal proteins that characterize Alzheimer’s dementia. The presence of these substances in brain tissue leads to oxidative stress and chronic inflammation. Energy absorbed by magnetite from external electromagnetic fields may contribute to this neuropathology.”
Later, in May of 2018, Herndon and Whiteside were published once again. This time, their paper titled “Aerosolized Coal Fly Ash: Risk Factor for COPD and Respiratory Disease” found that:
“Aerosolized CFA [coal fly ash] is a particularly hazardous form of deliberate air pollution. Ultrafine particles and nanoparticles found in coal fly ash can be inhaled into the lungs and produce many toxic effects including decreased host defenses, tissue inflammation, altered cellular redox balance toward oxidation, and genotoxicity. Oxidative stress and chronic inflammation can predispose to chronic lung disease. Recognition and public disclosure of the adverse health effects of geoengineering projects taking place in our skies, and their concomitant cessation will be necessary to prevent an ever-widening epidemic of COPD and other respiratory illnesses.”
Rounding out this duo’s series of papers on the Human health impacts of chemtrails, Herndon and Whiteside wrote a November 2019 paper titled “Geoengineering, Coal Fly Ash and the New Heart-Iron Connection: Universal Exposure to Iron Oxide Nanoparticulates.” The authors write:
“Coal fly ash is a rich source of nano-sized metal, iron oxide, and carbonaceous particles. Previous findings revealed that coal fly ash is widely utilized in undisclosed tropospheric aerosol geoengineering. Proper iron balance is central to human health and disease, and the harmful effects of iron are normally prevented by tightly controlled processes of systemic and cellular iron homeostasis. Altered iron balance is linked to the traditional risk factors for cardiovascular disease. The iron-heart hypothesis is supported by epidemiological, clinical, and experimental studies. Biogenic magnetite (Fe3O4) serves essential life functions, but iron oxide nanoparticles from anthropogenic sources cause disease. The recent finding of countless combustion-type magnetic nanoparticles in damaged hearts of persons from highly polluted areas is definitive evidence of the connection between the iron oxide fraction of air pollution and cardiovascular disease. Spherical magnetic iron oxide particles found in coal fly ash and certain vehicle emissions match the exogenous iron pollution particles found in the human heart. Iron oxide nanoparticles cross the placenta and may act as seed material for future cardiovascular disease. The pandemic of non-communicable diseases like cardiovascular disease and also rapid global warming can be alleviated by drastically reducing nanoparticulate air pollution. It is crucial to halt tropospheric aerosol geoengineering, and to curb fine particulate emissions from industrial and traffic sources to avoid further gross contamination of the human race by iron oxide-type nanoparticles.”
Now that we have seen the Human health impacts of aerosolized coal fly ash, we will now take a look at the Human health impacts of some known constituents of coal fly ash.
Aluminum
As evidenced by voluminous rainwater sample lab reports (ch 1), chemtrails have been shown to consist significantly of aluminum oxide. Aluminum is a common component of coal fly ash. As we have learned from Dr.s Herndon and Whiteside, these particles can be nano-sized.
Aluminum nanoparticles are nasty stuff. A material safety data sheet (MSDS) produced by US Research Nanomaterials, Inc. says that they can cause: respiratory problems, skin irritation, eye irritation, tumors, Alzheimer’s, pulmonary disease, neoplasms, and gastric or intestinal disorders. This MSDS also states that people coming in contact with aluminum nanoparticles should wear a respirator and a fully protective, impervious suit.
A 2016 paper titled “Assessing the Direct Occupational and Public Health Impacts of Solar Radiation Management with Stratospheric Aerosols” says that Aluminum aerosols will target these bodily systems: respiratory, cardiovascular, hematologic (blood), musculoskeletal (muscles & bones), endocrine (glands), immunologic, and neurologic (brain). They also say exposure to small atmospheric aluminum particles can cause cancer and death.
It appears coincidental that Wright-Patterson Air Force Base has studied the biological impacts of aerosolized aluminum. In March 2001, the Air Force Research Laboratory at Wright-Patterson published a study titled “In Vitro Toxicity of Aluminum Nanoparticles in Rat Alveolar Macrophages.” Scientists exposed rats to airborne, nano-sized aluminum oxide particles. The authors concluded:
“Aluminum oxide nanoparticles displayed significant toxicity after 96 and 144 hours post exposure at high doses (100 and 250 µg/ml). Aluminum nanoparticles also showed slight toxicity after 24 hours at high doses (100 and 250 μg/ml). When these cells were dosed at lower non toxic levels (25 μg/ml) Al 50, 80, 120 nm caused a significant reduction in phagocytosis. Even at a dose as low as 5 μg/ml Al 50 nm still caused a significant reduction. None of these nanoparticles caused the induction of nitric oxide, TNF-alpha, or MIP-2, important components in inflammatory responses. In summary, based on viability aluminum nanoparticles appear to be slightly toxic to rat alveolar macrophages. However, there was a significant reduction in phagocytic function of macrophages.”
In other words, they found that even at low doses, forcing rats to breathe in tiny aluminum particles screwed up their lungs. The induced lack of phagocytes means that the rats’ immune systems (especially in the lungs) became unable to fight off invading harmful organisms.
“In Vitro Toxicity of Aluminum Nanoparticles in Rat Alveolar Macrophages” was but one of a series of studies produced by Wright-Patterson pertaining to aluminum nanoparticle exposure. Wright-Patterson also produced a 2010 study titled “Nanosized Aluminum Altered Immune Function” in which they found that inhaled aluminum nanoparticles impair human immune systems. The authors again noted that nanoparticles have more deleterious health effects than do larger sized particles. Curiously, “Nanosized Aluminum Altered Immune Function” also states that we are prone to inhale aluminum nanoparticles because they are used in jet fuels. This information, makes yet another case for aluminum-spiked jet fuels. All this is extremely interesting when one considers Wright-Patterson’s involvement in the New Manhattan Project such as that which was documented in chapter 5.
A 2009 paper titled “Manufactured Aluminum Oxide Nanoparticles Decrease Expression of Tight Junction Proteins in Brain Vasculature” found that, due to brain cell death, aluminum exposure can cause: Alzheimer’s, stroke, reperfusion, hypoxia, mitochondrial disease, and general vascular dysfunction.
In a 2012 paper written by one of the world’s top neurosurgeons (now retired), many neurological diseases are linked to aluminum exposure. Russell Blaylock’s “Aluminum Induced Immunoexcitotoxicity in Neurodevelopmental and Neurodegenerative Disorders” found a link between aluminum exposure and: Alzheimer’s, Parkinson’s, Huntington’s, Pick’s, HIV dementia, multiple sclerosis, viral encephalopathies, chronic traumatic encephalopathy, and amyotrophic lateral sclerosis (ALS / Lou Gehrig’s disease). In this paper, Dr. Blaylock also found that aluminum exposure is linked to: impaired cognition, poor memory, impaired learning, poor attention, social withdrawal, irritability, reduced food and water intake and depression. Not only that, but Dr. Blaylock cites another paper here showing how extremely small aluminum particles like the ones used in today’s New Manhattan Project can intensify adverse health reactions.
Dr. Blaylock has provided us with some impressive evidence for a causal relationship between chemtrails and Alzheimer’s here. He tells us that the aluminum nanoparticles we constantly inhale are carried directly to the part of the brain that is first affected by Alzheimer’s disease AND most severely affected by Alzheimer’s disease. On March 28, 2013 Dr. Blaylock went on the Linderman Unleashed radio program. The host asked him how he became chemtrail aware and Dr. Blaylock said this:
Dr. Russell Blaylock, MD
“Well, you know, the connection has been the aluminum in the vaccines. I wrote several articles about the effects of the adjuvants in vaccines including the mercury and the aluminum effect.
“Then I found some articles about the chemtrails and there was a lot being said about it and I wasn’t too sure whether it was true or not because in my state we rarely saw them. But as I started looking on the Internet and I would see these states in which there were these criss-cross patterns and they were very tight patterns and geometrical shapes where it was obvious that it was a purposeful covering of the atmosphere with these patterns and the trails were so long. Well now, you know, we’re starting to see them in my state and as I look at them, they go from to horizon to horizon. Well, you know, I’ve been alive long enough to know that jets never did that in the past and I see the same patterning effect now where they’re criss-crossing; it’s an obvious pattern.
“And so I look into the literature and some of the reports and YouTube videos and they were saying that they were dropping as one of the ingredients, aluminum. Well, I had done a fair amount of writing and research on the effect of aerosolized chemicals in the nose when you breathe them. And what we knew was that these particles tend to travel along the olfactory nerves which are the smell nerves in the nose. And it travels directly to the part of the brain that has to do with memory and emotions; the hippocampus, the interlinal area, and the prefrontal cortex. And that you can trace these chemicals traveling along that nerve and depositing in this area of the brain.
“The other thing that was known is that if you aerosolize aluminum, it’s one of the metals that passes very easily along this track and directly into the brain. So it bypasses the blood-brain barrier and goes directly into the brain and accumulates. Well, if you do it in animals, it produces lesions, or damage in that area of the brain and the animal will begin to show changes of memory and learning and emotional changes.
“When we look at people who have Alzheimer’s disease, ironically, the highest concentration of aluminum in the brain is that same entry point; what’s called the interlinal cortex. And the levels continue to accumulate. So we have compelling evidence that aerosolized aluminum alone will enter the brain and produce damage to that critical area of the brain.
“The worst of all is the nano-sized. Nano-size means you make it such a small particle that it easily penetrates skin. It penetrates barriers in the body that normally metals cannot pass through. When you nano-size and produce these incredibly small particulate matter, it passes very easily. So when you nano-size aluminum and you use it in these aerosols through the nasal passages, it enters the brain in very high concentration and they find that the nano-sized aluminum in the brain is infinitely more toxic.
“Now one of the toxic reactions to aluminum is intense inflammation and activation of cells in the brain that are the immune cells called microglia. Aluminum is a very potent activator of these immune cells and that triggers the release of a powerful substance called glutamate which is an excitotoxin that causes cells to die from an excitatory mechanism. Kinda complex mechanism, but it is a combination of inflammation and excitotoxicity. And I coined the term in the medical literature called immunoexcitotoxicity to describe that process. So, we know that occurs. We know it occurs very easily.
“Now, the reports are coming out now that what they’re spraying is nano-sized aluminum and the idea is the old concept of preventing global warming. And they nano-size the aluminum so it will stay in the upper atmosphere longer; supposedly as a reflective compound metal. The problem with that, even from a climatological description is that if you make it into cirrus-like clouds rather than reflecting it upward and out of the atmosphere, it reflects the heat downward and actually causes global warming. So, you know, you could envision that they’re doing this on purpose to make the atmosphere heat up so they can say, ‘See, the atmosphere is warming up.’
“But what I’m concerned about mainly is the medical effect and that’s because of these very strong connections between aluminum passing through this pathway into the brain [which] is so strongly connected with Alzheimer’s disease and other diseases of memory.
“If you’re aerosolizing this and spraying literally tons of it over the world, people are constantly breathing that aerosolized, nano-sized aluminum which will easily penetrate filters in your air-conditioning system [and] enter your home. So you’re breathing it 24 hours a day; producing high levels of aluminum in this part of the brain. And the consequences could be absolutely devastating. It could cause a huge increase in Alzheimer’s disease and inflammatory neurological disorders.
“I watched a YouTube which was a geoengineering conference that the government had put on. And in the conference, one of the questions somebody in the audience asked was: What is the medical effect of spraying aluminum in the atmosphere? And the speaker said, ‘Well, uh, we don’t really know. But we’re in the process of researching that.’ Well, of course that was an absolute lie. We do know what it does. But the fact that they were admitting that in fact they were going to spray, they gave it in the future tense that they were going to spray aluminum, the evidence now from the examination by biologists and scientists around the world is that the aluminum level in the lakes and streams and trees is increasing enormously. Some areas have incredible elevations of aluminum in the groundwater and in the vegetation. So if this indeed is happening, we’re looking at a medical catastrophe that’s worldwide.”
There is lots of other highly credible evidence available linking aluminum exposure to the diseases mentioned here. If you want more information, please search the term ‘aluminum toxicity.’ Expediency demands that we move on.
Barium
Rainwater sample test results from around the world consistently show barium as well, and barium can also be a component of coal fly ash. Barium is highly toxic. Barium material safety data sheets (MSDS) readily available online will inform you that barium is extremely hazardous in case of inhalation. Severe exposure to barium can cause lung damage, choking, unconsciousness and death. Many other barium oxide MSDSs go on and on in a similar fashion. The Centers for Disease Control and Prevention (CDC) says that barium oxide reacts violently with water while the atmosphere has lots of water in it and our bodies consist mostly of water. My science advisor says that barium titanate and barium sulfate have been used in atmospheric dispersions as well.
The aforementioned paper “Assessing the Direct Occupational and Public Health Impacts of Solar Radiation Management with Stratospheric Aerosols” says that barium compounds used as atmospheric sprays target these Human bodily systems: respiratory, gastrointestinal, musculoskeletal, renal, metabolic, and neurologic. They also say barium compounds dispersed by aircraft as part of geoengineering programs can cause death.
Strontium
Rainwater sample test results as well as others such as ambient air sample test results collected by Dr. Herndon have also been showing a presence of strontium. Strontium can be a component of coal fly ash. It is not surprising, but, like aluminum and barium, strontium is highly toxic as well.
A strontium MSDS from Sigma-Aldrich states that it is corrosive. It causes burns when it comes in contact with the skin and can be absorbed through the skin. If one inhales it, the MSDS states that it is, “…extremely destructive to the tissue of the mucous membranes and upper respiratory tract.” The MSDS continues:
“Inhalation may result in spasm, inflammation and edema of the larynx and bronchi, chemical pneumonitis, and pulmonary edema. Material is extremely destructive to tissue of the mucous membranes and upper respiratory tract, eyes, and skin.”
The Sigma-Aldrich MSDS finishes up by noting that the chemical, physical, and toxicological properties of strontium have not been thoroughly investigated.
Strontium hydroxide is even worse. Being that there is lots of water in the atmosphere, the atmospheric strontium produced as part of the New Manhattan Project may react with it and form the extremely caustic strontium hydroxide. Not only that, but don’t forget that our bodies are comprised of mostly H2O. Strontium in the atmosphere and inside of us has lots of opportunities to become strontium hydroxide. The Sigma-Aldrich MSDS cautions potential users to never expose strontium oxide to water because it reacts violently.
Because strontium can be a component of coal fly ash, it is interesting to note that studies have been done concerning exposure to the strontium found in ‘fly ash.’ The CDC writes:
“Rats were exposed to aerosols of 85Sr [strontium] carbonate, phosphate, fluoride, oxide, or titanate (particle sizes and doses not specified) (Willard and Snyder 1966). Greater than 99% of the initial lung burden of 85Sr was cleared from the lung 5 days after inhalation of the carbonate, phosphate, fluoride, or oxide, whereas 60% of the 85Sr remained in the lung after inhalation of the more insoluble strontium titanate.
“In rats exposed to airborne fly ash (sieved to have a particle diameter of distribution of 90% less than 20 μm) for 6 hours, strontium was eliminated from the lung with a half-time of 23 days (observations were made for 30 days) (Srivastava et al. 1984b). One day after the exposure, the tissue: plasma strontium concentration ratios were 0.3–0.5 in the liver, kidney, small intestine, and heart. The report of this study does not indicate whether whole-body or nose-only exposures were utilized in the study; therefore, it is not possible to know for certain how much of the absorption may have resulted from ingestion of fly ash deposited on the animals. Furthermore, given the relatively large particle size of the fly ash, it is likely that deposition in the respiratory tract was largely in the tracheobronchial and nasopharyngeal region, from which the strontium may have been cleared mechanically to the esophagus and swallowed. Nevertheless, studies in which 89Sr-enriched fly ash was instilled into the trachea of rats indicate that strontium in this form was partly absorbed and appeared in plasma and other tissues within days of the exposure (Srivastava et al. 1984a).”
The CDC goes on to note that the fly ash strontium administered to the lab rats ended up mostly in the bones. After that, it appeared in (in order of prevalence): muscle, skin, liver, and kidneys. Those heady days of just dumping dry ice into clouds are long gone.
Mercury
Dr. J. Marvin Herndon produced a December 2017 paper co-authored by Mark Whiteside, MD in which the authors write specifically of the Human health impacts of mercury. It has been well known for a long time now that mercury is one of the most toxic substances on the planet and we now know that mercury is a common constituent of the coal fly ash currently being sprayed by the megaton. The authors write:
“Despite strengthened mercury emission regulations, mercury measured in rainwater is increasing. Since it is known that the upper troposphere contains oxidized, particle-bound mercury, it is likely that covert aerosolized coal fly ash sprayed into this region is a major source of mercury pollution. Mercury affects multiple systems in the body, potentially causing neurological, cardiovascular, genitourinary, reproductive, immunological, and even genetic disease.”
CDC rates of associated diseases
As this chapter has explained, chemtrails are associated with many diseases. As we have been assaulted by this New Manhattan Project for over twenty years now, it is no surprise that the best available data shows rates of the associated diseases going up significantly. Historical rates of every disease associated with chemtrail spray are not presented here due to a lack of CDC data. Every associated disease with available CDC data is presented.
Let’s start with the most strongly correlated disease: Alzheimer’s. According to the latest data from the CDC, from 1999 to 2014, age-adjusted rates of death from Alzheimer’s increased 54.5% with the 2014 number of total deaths at 93,541. That means that in 2014 alone we saw tens of thousands of additional American deaths from Alzheimer’s. If one adds up all the additional deaths from Alzheimer’s between 1999 and 2014, we’re talking about hundreds of thousands of additional deaths. Let us recall that large-scale domestic spraying operations began in 1996.
Age adjusted rates of Alzheimer’s disease 1999-2014
In a 2013 report, the CDC found that while deaths from other diseases such as cancer, heart disease, and stroke decreased significantly, Alzheimer’s deaths increased 39%. They write, “Mortality from Alzheimer’s disease has steadily increased during the last 30 years.” Knowing what we now know, it is reasonable to assume that chemtrails have contributed greatly to this.
Not only have the rates of adult Alzheimer’s disease been increasing, but a disease that used to be relegated to the elderly is now showing up in children. Reports have been pouring in from around the world documenting research into Niemann Pick Type C disease, also known as ‘childhood Alzheimer’s.’ As previously mentioned, Dr. Blaylock has seen this phenomenon as well.
~ ~ ~
Dr. Blaylock says that there is also a correlation between aluminum exposure and Parkinson’s. The latest data from the CDC shows that between 1999 and 2017, the age-adjusted rate of Parkinson’s disease in people aged 65 or older went from 41.7 per 100,000 to 65.3 per 100,000.
CDC rates of Parkinson’s disease 1999-2017
Despite what the tobacco companies said in the 1950s, routinely breathing in particulate matter is bad for your lungs. It is for this reason that we now take a look at the CDC data pertaining to diseases associated with the routine inhalation of particulate matter such as COPD, asthma, and lung cancer. Although the CDC found that the rate of chronic pulmonary disease (COPD) was stable between 1998 and 2009, they also found that the prevalence of asthma rose during a similar period (between 2001 and 2010). The CDC also reports that between 1995 and 2011, smoking went from 35% among students and 25% among adults to 18% and 19% respectively. Concurrently, the CDC reports significant drops in the rate of lung cancer between 2002 and 2011.
Rate of smoking from 1965-2011
With these big drops in the rate of smoking, one might assume that the rate of COPD and asthma would go down as well, instead of remaining stable. Chemtrails probably kept the rate of COPD stable while contributing to the prevalence of asthma. Lung cancer probably decreased because chemtrail exposure has not been as carcinogenic for your lungs as smoking. It’s good to know that there are more carcinogenic things for your lungs than routine chemtrail exposure. Smoking cigarettes apparently fits that category. Moderate chemtrail exposure is probably better for you than inhaling burning plutonium too, but that doesn’t mean it’s ok.
Overall life expectancy
Very recently, we here in America have seen a slight reduction in our life expectancies. According to CDC data, for the first time in many decades, between 2016 and 2017 overall life expectancy at birth fell by .1 years.
CDC life expectancy 1970-2017
One might think, with all the much-touted breakthroughs in medicine, a growing health care industry, expanded access to better nutrition such as organic foods and supplements, and the like, that we would be experiencing longer average life expectancies, not shorter. Might chemtrails have something to do with it?
Early exposures
Although it appears that our bodies have been finding ways to better cope with this daily onslaught of aerosolized toxic waste, around the times when people were first exposed, emergency rooms filled up. William Thomas’ aforementioned 2004 book Chemtrails Confirmed chronicles many of these examples. Thomas recounts the words of a registered nurse:
“Approximately December 16th or the 17th, while traveling north, I could see ‘stripes’ in the sky. It appeared as if someone took white paint on their fingers and from north to south ran their fingers through the sky. These contrails were evenly spaced and covered the whole sky! They covered it completely! When I was finished with the next visit, approximately 45 minutes, I came out of the house and found the whole sky was white. There was no definition in cloud pattern.
“Within the 24 hours I became very weak, feverish, and my asthma began to act up. I didn’t think too much about it, until my boyfriend told me that many in his family started coming down with the same complaints. I also started noticing a lot of my patients and their family members were coming down with these symptoms at the same time. In our area we have one main hospital which I was the Supervisor of for four years. I worked there a total of six years. I stay in close contact with the nurses and physicians and am planning on investigating into this more. At that time, they complained of being extremely busy with respiratory diagnoses.”
Another passage from Chemtrails Confirmed recounts the experiences of a restaurant owner from Oklahoma. The passage reads:
“On January 24, 1999 [Pat] Edgar reported that on, ‘Monday, Tuesday and Wednesday and Thursday of last week, we were really hit hard with the contrails. I mean real bad. Everybody in this town is sick right now; sicker than a damn dog. It’s all in their head and their sinuses, and it hangs in the throat, (sore necks), ears ringing.’
“Edgar added: ‘Some customers that frequent our business have stated that they have been to the doctor and the offices have been full of sick people. Same thing at the Indian clinic.’
“‘People have to wait for hours because the waiting room is full. Some people have reported being on their third and fourth round of antibiotics and they are still ill. We noticed excessive contrails Thursday, Feb. 11th.’
“Edgar became ill the following day, and visited a doctor. From a friend he learned that Sparks regional hospital had over 500 people seeking medical attention at the emergency room for flu, or flu-like symptoms.”
Others appearing in Thomas’ book tell similar stories.
Bodily contamination testing
When we ingest aluminum, some of it eventually comes out in our hair and fingernails. There are many reports online of people finding high levels of chemtrail toxins in their hair and fingernails. Certain laboratories can analyze hair and fingernail samples for aluminum and other substances. If you are curious about your bodily contamination, one may get their hair tested by the Great Plains Laboratory or Analytical Research Labs. One can find their websites online.
Biospheric implications
There is evidence that chemtrails are changing soil pH. This could be very bad for our biosphere. As mentioned in the first chapter, anti-geoengineering activist Francis Mangels has a Bachelor of Science in forestry from the International School of Forestry at Missoula, spent 35 years with the U.S. Forest Service as a wildlife biologist and worked several years with the USDA Soil Conservation Service as a soil conservationist. In order to document the effect of chemtrail spray upon soil pH, Mr. Mangels wrote on Oct. 30, 2009:
“The soil scientists from the USDA Soil Conservation Department visited private property east of Shasta Lake, California, on Oct. 27, 2009. Mr. Bailey, Komar, and Owens tested the pH with standard federal meters. All agreed the pH should be 5.5.
“Under Douglas fir, the ph was 7.4, astoundingly basic for that habitat.
“Under Poderosa pine, at the precise soil-needle interface, I would expect a pH of 5. At that point, Bailey’s meter showed 6.5. This is high for a microhabitat that should be very acid. Old soil surveys indicate this soil should be very acid, around pH of 5.5.
“I bought a house in Mt. Shasta old black oak/pine pasture in 2002, tested the pH at below 6, good for vegetable gardening. It was a major reason for purchase, and proceeded with highly acid composting of leaves and grass to drive the pH down or at least keep it low, as every master gardener knows. I added a touch of sulphur and avoided wood ash to insure acidity, and proceeded to teach organic gardening courses out of my yard through COS. The pH tests were an embarrassment because now my garden is pH 7, sometimes higher. This is the opposite of what should happen.
“The pH meter of Jon McClellan proceeded to show pH in McCloud gardens also running close to 7 or 8, which is too high for heavy organic mulch with no ashes. General lawns were also running over pH 7 under oaks and pines and fir trees. This is contrary to everything I learned in college and the Soil Conservation Service for 35 years. The old data sheets say these soils should be running at a pH of 5-6.”
Francis Mangels
In the movie What In the World Are They Spraying?, Mr. Mangels says that when soil pH changes, soil arthropods (a vital link in our ecosystem) start to go away. This type of disruption could have negative effects up and down the food chain.
Reports of massive plant and animal die-offs potentially due to chemtrails are widespread. Spraying vast regions of the Earth with tens of thousands of megatons of toxic waste is probably contributing to the alarming rate of animal species extinction as well. Although many other factors are in play here, the chemtrails surely don’t help. The Center for Biological Diversity reports that:
“Scientists estimate we’re now losing species at 1,000 to 10,000 times the background rate, with literally dozens going extinct every day. It could be a scary future indeed, with as many as 30 to 50 percent of all species possibly heading toward extinction by mid-century.”
Once again, our Spartacus with the dragon energy, Dr. J. Marvin Herndon, PhD has been on the case. Dr. Herndon has again teamed up with the Medical Director of the Monroe County, Florida Department of Health, Dr. Mark Whiteside, MD, MPH to publish a series of peer-reviewed, published journal articles addressing the biospheric implications of the ongoing and uncontrolled geoengineering experimentation and we will go over them here.
Let’s start at the bottom of the food chain. In June of 2019 Herndon and Whiteside published a paper titled “Role of Aerosolized Coal Fly Ash in the Global Plankton Imbalance: Case of Florida’s Toxic Algae Crisis.” In this paper, the authors provide evidence for the assertion that the coal fly ash sprayed by the megaton into our biosphere is causing, among other things, an overabundance of harmful plankton blooms which, in turn, has more harmful effects. The authors write:
“Our objective is to review the effects the multifold components of aerosolized coal fly ash as they relate to the increasing occurrences of HABs [harmful algal blooms]. Aerosolized coal fly ash (CFA) pollutants from non-sequestered coal-fired power plant emissions and from undisclosed, although ‘hidden in plain sight,’ tropospheric particulate geoengineering operations are inflicting irreparable damage to the world’s surface water-bodies and causing great harm to human health (including lung cancer, respiratory and neurodegenerative diseases) and environmental health (including major die-offs of insects, birds and trees). Florida’s ever-growing toxic nightmare of red tides and blue-green algae is a microcosm of similar activity globally. Atmospheric deposition of aerosol particulates, most importantly bioavailable iron, has drastically shifted the global plankton community balance in the direction of harmful algae and cyanobacterial blooms in fresh and salt water.”
A little further up the food chain we find insects. Herndon and Whiteside have been working in this area as well. In August of 2018 their paper titled “Previously Unacknowledged Potential Factors in Catastrophic Bee and Insect Die-off Arising from Coal Fly Ash Geoengineering” was published. In this paper, the authors substantiate a multitude of harmful, observed effects upon insects from chemtrail spray. We can stop wondering why bee populations are being decimated. The authors write:
“The primary components of CFA [coal fly ash], silicon, aluminum, and iron, consisting in part of magnetite (Fe3O4), all have important potential toxicities to insects. Many of the trace elements in CFA are injurious to insects; several of them (e.g., arsenic, mercury, and cadmium) are used as insecticides. Toxic particulates and heavy metals in CFA contaminate air, water, and soil and thus impact the entire biosphere. Components of CFA, including aluminum extractable in a chemically-mobile form, have been shown to adversely affect insects in terrestrial, aquatic, and aerial environments. Both the primary and trace elements in CFA have been found on, in, and around insects and the plants they feed on in polluted regions around the world. Magnetite from CFA may potentially disrupt insect magnetoreception. Chlorine and certain other constituents of aerosolized CFA potentially destroy atmospheric ozone thus exposing insects to elevated mutagenicity and lethality levels of UV-B and UV-C solar radiation.”
This information goes a long way towards explaining the tremendous drops in global insect populations lately. It’s almost too scary to look into, but an Internet search of the term ‘insect populations’ will bring pages and pages of relevant results. Of course, many are blaming it on the dreaded global warming/climate change, but insect populations have done just fine throughout previous fluctuations in Earth’s average temperature. In fact, insect populations have most probably done better in warmer climates, so maybe we should look instead at the gigantic aircraft routinely dumping megatons of toxic waste into our biosphere.
As noted, Francis Mangels has been observing a lack of insects as well. He logically attributes it to geoengineering. On July 19, 2017, Francis emailed to the author the following:
“Several streams were sampled for aquatic insects, and I likewise fished them hard to get stomach samples of trout. Total sample over 1000, lately around 400 stomach samples. Methods used were fairly casual, using typical nets for streams in gravel substrates that appeared similar. Standard data was orders of aquatics per square foot, accuracy about 80% due to equipment. It was very easy to see which streams would have the most trout.
“The bottom fell out of the sampling from 2000 to 2008, and it continues today. All major orders of bugs took severe hits from an unknown source. Then I was contacted by Dane [Wigington], and logic said only sky pollution could hit all the streams at once in the same way.
“Likewise, the trout I caught before then always were loaded with bugs and etc. food both terra and aquatic. Ever since about 2006, the trout stomachs were almost empty, and I quit taking data because there was no data to take, for the most part. A bug here and there, mostly terrestrials, very small amounts and the trout got skinny over the years (except for those freshly planted, that soon lost the fat and got skinny too, as we say, poor condition factors). Very clear streams went almost barren, no bugs or trout either.
“Net sweeps in lots showed plenty of earwigs, pill bugs, ants, aphids, box elder bugs, any SUCKING types. However, the caterpillar types for the most part became very scarce, as did moths and butterflies as you would expect (leaf eaters eat the aluminum). I turned in a huge collection to the American butterfly association of CA, but damned if I could do it now….Lepidoptera are around, but rare now except for the cabbage butterfly and a few swallowtails. Point is, this distribution showed in the trout stomachs, which caused me to do the sweeps.”
Further up the food chain we find birds. Dr.s Herndon and Whiteside published a paper in November of 2018 titled “Aerosolized Coal Fly Ash: A Previously Unrecognized Primary Factor in the Catastrophic Global Demise of Bird Populations and Species.” In this paper, the authors find that coal fly ash is causing unprecedented bird die-offs.
The authors write, “Bird populations and species world-wide are experiencing die-offs on an unprecedented scale.” A little later, the authors continue, “Aerosolized CFA [coal fly ash], a particularly toxic form of air pollution, contains multiple metals and elements well-known to adversely affect all portions of the avian life cycle, in aerial, terrestrial, and marine environments. Studies from around the globe reveal systemic contamination of birds by these elements.” The authors conclude that, “Coal fly ash, including its use in ongoing atmospheric geoengineering operations, is a major factor in global bird die-off. The accelerating decline of birds parallels the catastrophic decline of insects, due in part to the same type of aerial pollution.”
Doctors Herndon and Whiteside have also looked at the biological impacts of chemtrails upon bat populations. In January of this year (2020), they published a paper titled “Unacknowledged Potential Factors in Catastrophic Bat Die-off Arising from Coal Fly Ash Geoengineering.” In this paper, the authors find that bat populations worldwide are suffering a precipitous decline. The authors write:
“Bats are excellent mammalian bioindicators of environmental contaminants and it is known that their tissue contains high levels of metals and persistent organic pollutants. From a review of the literature, we show that the pollutant element ratios in bat tissue and bat guano are consistent with an origin in CFA-type air pollution. These findings suggest that CFA [coal fly ash], including its use in covert climate engineering operations, is an unacknowledged factor in the morbidity and mortality of bats. Bats, therefore, are an important ‘canary in the coal mine’ pointing to the urgency of halting covert climate engineering and greatly reducing ultrafine particulate air pollution.”
~ ~ ~
As we saw at the beginning of this section, with all the professionally observed soil pH anomalies, plants are not doing very well under this New Manhattan Project either. Doctors Herndon, Whiteside and other co-authors have been doing work in these areas as well. In a series of published, peer-reviewed journal articles, they have found that a combination of factors, all caused by the spraying of coal fly ash, are causing mass die-offs of global vegetation. They found that trees, in particular, are weakened by increased UV radiation, desiccation, and toxicity – all caused by chemtrails. Once a tree is weakened by this trifecta, it becomes susceptible to insect infestations, fungal infections, and other biotic factors such as bacteria and viruses.
The result of all this is dry, dead and dying vegetation. An abundance of dry, dead and dying vegetation makes forest fires occur more often and burn more furiously. Herndon et al. find that this is most probably why we have seen such tremendously large forest fires lately. The increased levels of UV radiation noted by Herndon et al. as being harmful to vegetation, are also harmful to Humans as well as phytoplankton, coral, and insects.
Silver iodide
The conventional weather modification industry has been openly spraying vast areas of the United States with silver iodide since 1947. The super-secret New Manhattan Project only started spraying us with coal fly ash in 1996. Hence, the vast majority of the weather modification and atmospheric sciences literature is geared towards the dispersion of silver iodide. Although silver iodide is not what is used in today’s New Manhattan Project, as a side issue, let’s take a look at the scientific evidence (or lack thereof) concerning the biological impacts of silver iodide. Past is prelude.
Considering that this issue is the most obvious question and of grave importance, the lack of publicly available research pertaining to the biological impacts of silver iodide dispersion is quite shocking. You may read the 746 page, 1978 Congressional Research Service report on weather modification. You may read all 21 of the Interdepartmental Committee for Atmospheric Sciences reports or all of the National Science Foundation annual weather modification reports. You may read scores of weather modification reports, book after book, and myriad reports and papers about weather modification and the atmospheric sciences. But nowhere in any of these documents may you find an adequate examination of biological impacts and specifically human health impacts caused by exposure to atmospheric silver iodide. Only after reading a stack of documents about a yard high, did your author finally find a report containing an adequate discussion of this topic.
A popular silver iodide material safety data sheet describes silver iodide as, “Hazardous in case of skin contact (irritant), of eye contact (irritant), of ingestion, [and] of inhalation.” Unbelievably, the authors of this data sheet write that much of the toxicology information is NOT AVAILABLE. They’ve been spraying us with this stuff since 1947 and the toxicology information is not available?! Equally as unbelievable, to date, no publicly available, long-term studies have been done.
It is widely suggested that exposure to silver iodide causes argyria – characterized by a blue-grey discoloration of the eyes, skin, mucous membranes, and internal organs. Does that sound healthy? Another MSDS produced by Fisher Scientific reads:
“Chronic ingestion of iodides during pregnancy has resulted in fetal death, severe goiter, and cretinoid appearance of the newborn. Prolonged exposure to iodides may produce iodism in sensitive individuals. Symptoms could include skin rash, running nose and headache.”
In spite of this information, the historical weather modification literature notes a lack of data. A 1966 National Science Foundation report stated, “The present state of knowledge places uncomfortable limits on the prediction of the biological consequences of modifying the weather.” A 1969 Bureau of Reclamation report noted, “There has so far not been a single biological field study completed and reported in the literature specifically designed to identify any aspect of the ecological effects of weather modification.” A 1972 study conducted by the Council on Environmental Quality stated, “Projects may have significant adverse environmental effects, ranging from immediate hazards to life and property to long-term alterations in land use patterns and threats to ecological systems.”
Weather modifiers have exhibited a pattern of dismissing the potentially harmful effects of substances used in weather modification activities. In 1967 weather modifier Archie Kahan, writing for the Bureau of Reclamation, dismissed concerns about the use of silver iodide as he conflated the biological impacts of silver iodide with its efficacy as a nucleant and any possible hazardous weather that might arise from its use.
In 1972, decades after silver iodide was first used as a nucleant, Bernard Vonnegut and another atmospheric scientist by the name of Ronald Standler wrote a biology paper published in the Journal of Applied Meteorology that mollified concerns about their activities. Although the biological impacts of prolonged silver iodide dispersion has implications not only for Human health, but also for the health of the entire biosphere, the paper concerns itself almost exclusively with impacts upon Human health. The questionable biological impacts of their activities pertaining to plant and animal life is glossed over only briefly. They note that prolonged exposure to silver iodide has been known to cause Humans to exhibit an ashen appearance, but they claim that this is not of particular concern. They also dismiss concerns about silver iodide’s ability to cause a yellowing of the skin when exposure is topical. They even dismiss two examples of individuals having been significantly harmed by exposure to silver iodide. Their paper is full of phrases like ’seem to be’ and ‘we do not expect’ because much of what is presented in the paper is assumptions and extrapolations based on other people’s work rather than any scientific findings of their own.
The vast majority of research done in this area does not even concern itself with Human health impacts or biospheric contamination. Rather, it focuses on the ancillary issue of how plants and animals may be affected by either more or less rainfall. The work that is publicly available is mostly cursory. In the vast majority of cases where the subject is even so much as broached, the literature quickly follows with assurances that there are probably no adverse effects and that further study is not necessary.
Thankfully, some research indicating silver iodide’s negative biological impacts has surfaced. It is not good news, but we need to hear it. Evidence suggests that it is exceptionally bad for organisms further down the food chain. The aforementioned 1969 Bureau of Reclamation report also noted:
“Silver compounds are much more toxic to fish than to terrestrial vertebrates. Some of the higher concentrations of Ag recorded in precipitation from seeded storms are comparable to the lowest concentrations lethal to fish in the short run. In one set of experiments, sticklebacks were able to withstand no more than 0.003 ppm Ag in water at 15-18° C. The fish survived one week at 0.004 ppm, four days at 0.01 ppm, and but one day at 0.1 ppm.”
This 1969 report also found silver to be, “…highly toxic to microorganisms….” The report continues:
“Many investigators have placed Ag at or near the top of the list among heavy metals in toxicity to fungi, slime molds, and bacteria. Water containing 0.015 ppm Ag from contact with specially prepared metal has exhibited bacteriocidal activity. 0.006 ppm Ag has killed E. coli in 2 to 24 hours, depending on numbers of bacteria. Bacteriocidal activity in this context usually implies death of 9.99% or so of the cells present.”
Killing fungi, E. coli, and slime molds may sound like a good thing. But in the context of our complex and interdependent biosphere, it is not. Our overall ecosystem needs slime molds and the like. These things are vital links in the food chain.
Why does the conventional weather modification and atmospheric sciences literature not sufficiently address the issue of silver iodide’s biological impacts? They wouldn’t have anything to hide, would they? That which is not disclosed is often more incriminating than that which is. Although today’s Weather Modification Association claims it is completely safe, they have a conflict of interest and they do not have enough data to sufficiently back up their claims.
The bottom line is that there is evidence showing that silver iodide has negative biological impacts. We cannot know for sure that spraying this stuff is safe if no public long term studies have been done. But they have been going ahead and doing it anyway – just like today’s geoengineers.
Conclusions
Although it is currently not feasible to completely assess the damage to Earth’s biosphere caused by this New Manhattan Project, the available evidence does not paint a pretty picture. This is an area of study and body of work which should be vastly expanded and updated in the coming years and decades. We already know that massive quantities of atmospheric coal fly ash are bad for Humans, animals, insects, plants, and the overall environment. In Humans, the rates of diseases linked to exposure are on the rise. Many people became very sick when first exposed. The historical precedent set by the conventional weather modification industry mandates irresponsibility. When geoengineers say that their activities are harmless, we have plenty of good reasons to not believe them.
References
“An Open Letter to Members of AGU, EGU, and IPCC Alleging Promotion of Fake Science at the Expense of Human and Environmental Health and Comments on AGU Draft Geoengineering Position Statement” a paper by J. Marvin Herndon, published by New Concepts in Global Tectonics Journal, September 2017
Kampa, M.; Castanas, E. Human health effects of air pollution Environmental Pollution 2008, 151, 362-367.
Calderon-Garciduenas, L.; Franko-Lira, M.; Mora-Tiscareno, A.; Medina-Cortina, H.; Torres-Jardon, R.; et al. Early alzheimer’s and parkinson’s diese pathology in urban children: Friend verses foe response – it’s time to face the evidence. BioMed Research International 2013, 32, 650-658.
Moulton, P.V.; Yang, W. Air pollution, oxidative stress, and alzheimer’s disease. Journal of Environmental and Public Health 2012, 109, 1004-1011.
Beeson, W.L.; Abbey, D.E.; Knutsen, S.F. Long-term concentrations of ambient air pollutants and incident lung cancer in california adults: Results from the ahsmog study. Environ. Health Perspect. 1998, 106, 813-822.
Hong, Y.C.; Lee, J.T.; Kim, H.; Kwon, H.J. Air pollution: A new risk factor in ischemic stroke mortality. Stroke 2002, 33, 2165-2169.
Haberzetti, P.; Lee, J.; Duggineni, D.; McCracken, J.; Bolanowski, D.; O’Toole, T.E.; Bhatnagar, A.; Conklin, D., J. Exposure to ambient air fine particulate matter prevents vegf-induced mobilization of endothelial progenitor cells from bone matter. Environ. Health Perspect. 2012, 120, 848-856.
Potera, C. Toxicity beyond the lung: Connecting pm2.5, inflammation, and diabetes. Environ. Health Perspect. 2014, 122, A29
Mehta, A.J.; Zanobetti, A.; Bind, M.-A., C.; Kloog, I.; Koutrakis, P.; Sparrow, D.; Vokonas, P.S.; Schwartz, J.D. Long-term exposure to ambient fine particulate matter and renal function in older men: The va normative aging study. Environ. Health Perspect. 2016, 124(9), 1353-1360.
Dai, L.; Zanobetti, A.; Koutrakis, P.; Schwartz, J.D. Associations of fine particulate matter species with mortality in the united states: A multicity time-series analysis. Environ. Health Perspect. 2014, 122,
Dockery, D.W.; Pope, C.A.I.; Xu, X.P.; Spengler, J.D.; Ware, J.H.; et al. An association between air pollution and mortality in six U. S. Cities. N. Eng. J. Med. 1993, 329, 1753-1759.
Pope, C.A.I.; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the united states. N. Eng. J. Med. 2009, 360, 376-386.
Pires, A.; de Melo, E.N.; Mauad, T.; Saldiva, P.H.N.; Bueno, H.M.d.S. Pre- and postnatal exposure to ambient levels of urban particulate matter (pm2.5) affects mice spermatogenesis. Inhalation Toxicology: International Forum for Respiratory Research: DOI: 10.3109/08958378.2011.563508 2011, 23.
Ebisu, K.; Bell, M.L. Airborne pm2.5 chemical components and low birth weight in the northeastern and midatlantic regions of the united states. Environ. Health Perspect. 2012, 120, 1746-1752.
Tetreault, L.-F.; Doucet, M.; Gamache, P.; Fournier, M.; Brand, A.; Kosatsky, T.; Smargiassi, A. Childhood exposure to ambient air pollutants and the onset of asthma: An administrative cohort study in quebec. Environ. Health Perspect. 2016, 124(8), 1276.
Bell, M.L.; Ebisu, K.; Leaderer, B.P.; Gent, J.F.; Lee, H.J.; Koutrakis, P.; Wang, Y.; Dominici, F.; Peng, R.D. Associations of pm2.5 constituents and sources with hospital admissions: Analysis of four counties in connecticut and massachusetts (USA). Environ. Health Perspect. 2014, 122, 138-144.
“The Effect of Reaerosolized Fly Ash from an Atmospheric Fluidized Bed Combustor on Murine Alveolar Macrophages” a paper by Patricia C. Brennan, Frederick R. Kirchner, and William P. Norris, published by Argonne National Laboratory, 1979
“Coal Fly Ash Aerosol: Risk Factor for Lung Cancer” a paper by Dr. Mark Whiteside and J. Marvin Herndon, PhD, published by the Journal of Advances in Medicine and Medical Research, February 2018
“Aerosolized Coal Fly Ash: Risk Factor for Neurodegenerative Disease” a paper by Dr. Mark Whiteside and J. Marvin Herndon, PhD, published by the Journal of Advances in Medicine and Medical Research, March 2018
“Aerosolized Coal Fly Ash: Risk Factor for COPD and Respiratory Disease” a paper by Dr. Mark Whiteside and J. Marvin Herndon, PhD, published by the Journal of Advances in Medicine and Medical Research, May 2018
“Geoengineering, Coal Fly Ash and the New Heart-Iron Connection: Universal Exposure to Iron Oxide Nanoparticulates” a paper by Dr. Mark Whiteside and J. Marvin Herndon, PhD, published by the Journal of Advances in Medicine and Medical Research, November 2019
“Weather and Climate Modification: Report of the Special Commission on Weather Modification” by the National Science Foundation, 1965
Aluminum oxide material safety data sheet by US Research Nanomaterials, Inc., 2013
“Assessing the Direct Occupational and Public Health Impacts of Solar Radiation Management with Stratospheric Aerosols” a paper by Utibe Effiong and Richard L. Neitzel, published in Environmental Health, 2016
“In Vitro Toxicity of Aluminum Nanoparticles in Rat Alveolar Macrophages” a report by Andrew Wagner, Charles Bleckmann, and E. England of the Air Force Institute of Technology, Krista Hess of Geo-Centers, Inc., Dayton, Ohio, and Saber Hussain and John J. Schlager of the Air Force Research Laboratory, Human Effectiveness Directorate, Applied Biotechnology Branch, Wright-Patterson AFB, published by the Air Force Research Laboratory, Human Effectiveness Directorate, Applied Biotechnology Branch, Wright-Patterson AFB, 2001
“Nanosized Aluminum Altered Immune Function” a paper by Laura K. Braydich-Stolle, Janice L. Speshock, Alicia Castle, Marcus Smith, Richard C. Murdock, and Saber M. Hussain, published by the American Chemical Society, 2010
“Manufactured Aluminum Oxide Nanoparticles Decrease Expression of Tight Junction Proteins in Brain Vasculature” a paper by Lei Chen, Robert A. Yokel, Bernhard Henning, and Michal Toborek, published by the Journal of Neuroimmune Pharmacology, December, 2008
“Aluminum Induced Immunoexcitotoxicity in Neurodevelopmental and Neurodegenerative Disorders” a paper by Dr. Russell L. Blaylock, as published in Current Inorganic Chemistry, 2012
“Gila Activation Induced by Peripheral Administration of Aluminum Oxide Nanoparticles in Rat Brains” a paper by X. Li, H. Zheng, Z. Zhang, M. Li, Z. Huang, H.J. Schluesener, Y. Li, and S. Xu, published in Nanomed, 2009, 5, (4), 473-479
Strontium oxide material safety data sheet by Sigma- Aldrich, 2007
“Aluminum Poisoning of Humanity and Earth’s Biota by Clandestine Geoengineering Activity: Implications for India” a paper by J. Marvin Herndon, PhD, published by Current Science, 2015
“Strontium” a report by the Centers for Disease Control and Prevention
“Contamination of the Biosphere with Mercury: Another Potential Consequence of On-going Climate Manipulation Using Aerosolized Coal Fly Ash” a paper by Dr. Mark Whiteside and J. Marvin Herndon, PhD, published by the Journal of Geography, Environment and Earth Science International, December 2017
Inhaled Particles and Vapours a book edited by C.N. Davies, published by Pergamon Press, 1961
“Fine Particulate Air Pollution and Mortality in 20 U.S. Cities, 1987-1994” a report by Jonathan M. Samet, MD, Francesca Dominici, PhD, Frank C. Curriero, PhD, Ivan Coursac, MS, and Scott L. Zeger, PhD, published by the New England Journal of Medicine, volume 343, number 24, 2000
Pulmonary Deposition and Retention of Inhaled Aerosols a book by Theodore F. Hatch, Paul Gross, the American Industrial Hygiene Association, and the United States Atomic Energy Commission, published by Academic Press, 1964
“Mortality from Alzheimer’s Disease in the United States: Data for 2000 and 2010” a report by Betzaida Tejada-Vera, M.S., published by the U.S. Department of Health and Human Services, 2013
“Deaths from Alzheimer’s Disease – United States, 1999-2014” an article by Christopher A. Taylor, PhD, Sujay F. Greenlund, Lisa C. McGuire, PhD, Hua Lu, MS, and Janet B. Croft, PhD, published in the Morbidity and Mortality Weekly Report of the Centers for Disease Control and Prevention, May 26, 2017
“Age-Adjusted Death Rates for Parkinson’s Disease Among Adults Aged ≥65 Years – National Vital Statistics System, United States, 1999-2017” an article by Nancy Han, MS and Barnali Das, PhD, published by the Morbidity and Mortality Weekly Report of the Centers for Disease Control and Prevention, Sept. 6, 2019
“Chronic Obstructive Pulmonary Disease Among Adults Aged 18 and Over in the United States, 1998–2009” a report by Lara J. Akinbami, MD; and Xiang Liu, MSc, published by the U.S. Department of Health and Human Services, 2011
“United States Life Tables, 2017” an article by Elizabeth Arias, PhD and Jiaquan Xu, MD, published by National Vital Statistics Reports, June 24, 2019
“National Surveillance of Asthma: United States, 2001-2010” a report by the Centers for Disease Control, U.S. Department of Health and Human Services, November, 2012
Chemtrails Confirmed a book by William Thomas, published by Bridger House Publishers, 2004
What In the World Are They Spraying? a documentary film by Michael Murphy, Paul Wittenberger, and Edward G. Griffin, produced by Truth Media Productions, 2010
“Role of Aerosolized Coal Fly Ash in the Global Plankton Imbalance: Case of Florida’s Toxic Algae Crisis” a paper by Dr. J. Marvin Herndon, PhD and Dr. Mark Whiteside, MD, published by the Asian Journal of Biology, June 2019
“Previously Unacknowledged Potential Factors in Catastrophic Bee and Insect Die-off Arising from Coal Fly Ash Geoengineering” a paper by Dr. J. Marvin Herndon, PhD and Dr. Mark Whiteside, MD, published by the Asian Journal of Biology, August 2018
“Aerosolized Coal Fly Ash: A Previously Unrecognized Primary Factor in the Catastrophic Global Demise of Bird Populations and Species” a paper by Dr. J. Marvin Herndon, PhD and Dr. Mark Whiteside, MD, published by the Asian Journal of Biology, November 2018
“Unacknowledged Potential Factors in Catastrophic Bat Die-off Arising from Coal Fly Ash Geoengineering” a paper by Dr. J. Marvin Herndon, PhD and Dr. Mark Whiteside, MD, published by the Asian Journal of Biology, January 2020
“Previously Unrecognized Primary Factors in the Demise of Endangered Torrey Pines: A Microcosm of Global Forest Die-offs” a paper by J. Marvin Herndon, PhD, Dale D. Williams, and Dr. Mark Whiteside, MD, published by the Journal of Geography, Environment and Earth Science International, August 2018
“California Wildfires: Role of Undisclosed Atmospheric Manipulation and Geoengineering” a paper by J. Marvin Herndon and Dr. Mark Whiteside, MD, published by the Journal of Geography, Environment and Earth Science International, October 2018
“Deadly Ultraviolet UV-C and UV-B Penetration to Earth’s Surface: Human and Environmental Health Implications” a paper by J. Marvin Herndon, PhD, Raymond D. Hoisington and Dr. Mark Whiteside, MD, published by the Journal of Geography, Environment and Earth Science International, March 2018
Silver iodide material safety data sheet produced by ScienceLab.com, 2010
Silver iodide material safety data sheet produced by Fisher Scientific, 2009
National Science Foundation Report No. 66-3 as it appeared in a hearing before the Subcommittee on Oceans and Atmosphere of the Committee on Commerce, United States Senate, Ninety-fourth Congress, second session, Feb. 17, 1976
“Ecological Effects of Weather Modification: A Problem Analysis” a report by Charles F. Cooper and William C. Jolly, produced by the U.S. Department of the Interior, Bureau of Reclamation, Office of Atmospheric Water Resources, published by the University of Michigan, 1969
“Some Comments About Weather Modification Affects on Man’s Environment” by Archie M. Kahan, Office of Atmospheric Water Resources, Office of Chief Engineer, Bureau of Reclamation, Department of the Interior, published by the Department of the Interior, 1967
“Federal Regulation of Weather Modification” a report by the Council on Environmental Quality, Washington, D.C., 1972 as it appeared in a hearing before the Subcommittee on Oceans and Atmosphere of the Committee on Commerce, United States Senate, Ninety-fourth Congress, second session, Feb. 17, 1976
Environmental Impacts of Artificial Ice Nucleating Agents a book edited and co-written by Donald A. Klein, published by Dowden, Hutchinson & Ross, 1978
“Weather Modification Association Position Statement on the Environmental Impact of Using Silver Iodide as a Cloud Seeding Agent” a paper by the Weather Modification Association, published by the Weather Modification Association, 2009
“Estimated Possible Effects of AgI Cloud Seeding on Human Health” a paper by Ronald B. Standler and Bernard Vonnegut, published by the Journal of Applied Meteorology, Volume 11, August 11, 1972
Peter A. Kirby is a San Rafael, CA researcher, author, and activist. The greatly revised and expanded second edition of his book Chemtrails Exposed: A New Manhattan Project is now available. Join his email list at his website PeterAKirby.com.
The staff of the hospital in Montelimar, in the French department of Drome, have gone on indefinite strike to protest the new rules demanding they take a vaccine against Covid-19 by mid-September or face losing their jobs.
The strike against “forced vaccination” was announced on Thursday by the CGT-GHPP trade union, and affects some 200 doctors and 1,500 nurses in the southeastern French city.
Hundreds of them gathered outside the hospital on Friday, denouncing lockdowns and vaccine mandates and chanting “liberté!” (freedom).
The French legislature is finalizing the proposal that would require all medical professionals in contact with the vulnerable to be fully vaccinated by September 15, or else lose their salaries and even their jobs.
“We are against mandatory vaccination and vaccine coercion,” Elsa Ruillere, local union representative, told Sputnik France. “There is no choice between tests or vaccination: vaccination is compulsory. No, we don’t agree. We want to have the choice like the rest of the world and we do not want compulsory vaccination.”
Ruillere says her union supports “free and informed consent” and is not against vaccination on principle but is against coercion. Some of the medical workers said they are waiting for the French-made Sanofi-GSK vaccine, promised for December.
“We are well aware of the evolution of the virus. We do not take it lightly,” Ruillere said. However, she and her striking colleagues point out that even with the rise in positive tests for the Delta variant of the coronavirus, there is no commensurate rise in hospitalizations.
“Yes, we turned ‘red’ but that’s in fact due to the positive tests. In terms of hospitalizations, we are fine at the moment, we did not need to reopen beds, we have far fewer hospitalized people than before and fewer people in intensive care,” she added.
Another union gripe is the lack of public debate, since France’s National Assembly seems to have simply proceeded on the advice of the High Health Authority (HAS), which called the vaccination mandate “justified.”
There have been widespread protests in France since mid-July, as the government of President Emmanuel Macron imposed the vaccination mandate on health workers and introduced a “health pass” requirement to access public venues with more than 50 people in attendance. The pass requirement will extend to cafes, restaurants and shops starting August 1.
There has been a 150% increase in coronavirus cases over the past week in France, attributed to the Delta variant. The government says 96% of those infected are unvaccinated.
When I interviewed President Reagan’s policy analyst, Jim Warner, in 1987, there was something I didn’t know: HIV had never been isolated. I did know the virus wasn’t the cause of what was being called AIDS.
Senior White House policy analyst Jim Warner first came to public attention in a November 1987 article in the New York Native. In the story, “The White House Calls the Native About Aids,” publisher Chuck Ortleb wrote: “Warner told me that the White House could be seen as divided into two groups on the issue of AIDS. One group, which he said is in the minority, wants to adopt an ‘Auschwitz model’ by quarantining all those infected with ‘the virus.’ ‘The other group,’ [Warner] said, ‘is incompetent.’”
Warner told me he wasn’t suggesting there was a White House group which was favoring “an Auschwitz model,” but that some high-risk groups might think that was so. My following interview ran in the LA Weekly on December 18, 1987.
WEEKLY: Has anyone at the White House spoken to you about the Native article and what you said in it?
WARNER: I don’t think anyone here knows there was an article in that paper. The government really hasn’t fulfilled its role in providing good information [on AIDS]. We just may not know enough. With AIDS, we’re dealing with a syndrome, not a disease. We may see a patient who has a genetic defect that’s causing his immune deficiency [instead of HIV being the causative agent]. I’m not satisfied we know all we think we do, by any means.
WEEKLY: Is your research on AIDS part of your policy work? Do you make recommendations based on what you find out? Or is it just that you’re absorbed in discovering what’s going on with AIDS?
WARNER: More of the latter than the former. I was asked to look into an Atlantic magazine article about insects and AIDS, and that’s how it started. I decided I wanted to put together a set of questions concerning the HIV virus, so that the answers would suggest its role in AIDS. I would then draft a paper and give it to the people who asked me to look into the subject.
WEEKLY: Do people at the White House get a chance to talk to scientists over at the National Institutes of Health [NIH]? I mean really talk with them, find out what they’re doing, how they’re thinking?
WARNER: There is not much communication [between people at the White House and the scientists at NIH]. I’m probably the only person here who has much interest in it. This year I determined that the [White House] working group on AIDS wasn’t adequate.
WEEKLY: Several university scientists I’ve spoken with have – off the record – criticized what they call “HIV dogma.” They feel if they speak out against the rush to judgment for HIV as the cause of AIDS they may lose money. Grants begin with the assumption that HIV has been proven as the agent of the disease.
WARNER: I’m of a mind that if no other lessons should be required of any university science curriculum, there should be a good survey course in philosophy and a grounding in logic. I’m appalled at the conceit and arrogance [of certain scientists].
WEEKLY: There has never been a performance-evaluation on the results of the NIH. NIH has balked at the idea of evaluating the worth of all their medical research over the last 20 years.
WARNER: That’s a very good idea. I’m going to see what I can do about that.
WEEKLY: The Native article mentioned that you spoke with Dr. Lo, an Army researcher on AIDS. He has his own theory about the disease, that it’s caused by a different virus. According to the Native, you had a problem getting through to him. Did they really tell you you’d have to get an okay from the Surgeon General just to talk to Lo?
WARNER: Yes. You know, although it is an honor to work at the White House, I’m not impressed that being here makes me special. But I pulled rank, and they put me through to Dr. Lo.
WEEKLY: Suppose proof emerged that HIV is not the AIDS virus. How difficult would it be to alter the course of research?
WARNER: It’s very difficult to change people’s minds. It’s not impossible, but there is a head of steam built up.
WEEKLY: What do you do if a government agency, as a whole, has been derelict?
WARNER: It may end up as a brawl. I’d sort of like to finesse that, though, I’d like to avoid a public brawl. It eats up time. It’s difficult when scientists are not open to discussing scientific issues.
WEEKLY: Robert Gallo, Max Essex, people like that, were the field commanders on the NIH war on cancer in the 70’s. They lost that war. So why are they in charge of AIDS research now? It seems odd that we don’t have other people running the show.
WARNER: If ever I’ve been tempted to believe in socialism, science has disabused me of that. These guys [at NIH] assume that it’s their show. They just assume it.
WEEKLY: Peter Duesberg, a distinguished molecular biologist at Berkeley, has said that HIV does not cause AIDS. Have you asked people at NIH what they think, specifically, of his arguments?
WARNER: Yes. I’ve been told that Peter Duesberg’s refutation of HIV has been discounted by the scientific community. I was given no explanation as to why. I was very offended. No evidence was presented to me. Just that Duesberg had been ‘discounted.’ That’s absurd. It’s not a scientific response to dismiss Duesberg as a crank.
WEEKLY: The definition of AIDS has become so broad it’s even stretching the idea of what a syndrome is, never mind a singular disease.
WARNER: A syndrome is a means of trying to understand how symptoms could be linked together. But if you do this in an atmosphere of hysteria, there is no limit to what you can attribute to a syndrome.
WEEKLY: The definition of AIDS in Africa is now becoming synonymous with starvation. They’re saying the three major symptoms are chronic diarrhea, fever, and wasting-away. Weight-loss. It certainly makes a perfect smokescreen for the aspect of hunger which is political – just call it AIDS.
WARNER: I had not considered that. There is a program to make Africa self-sufficient by the year 2000. This could certainly hinder that activity. You know, I was a prisoner of war in Vietnam. I experienced weight-loss of eighty pounds. And when I came home, I was suffering from a form of dysentery that you could call opportunistic. A number of us were. We didn’t have AIDS.
—end of interview—
In November of 1987, I found out that the journal Bio/Technology was going to hold a roundtable workshop in which HIV would be addressed. Peter Duesberg and about a dozen other researchers would attend. The purpose of the roundtable would be to formulate experiments which, once and for all, would show HIV’s role or non-role in AIDS.
I told Jim Warner about the proposed roundtable, and suggested he contact the magazine and sit in on the sessions. He did call, and to everyone’s surprise, suggested that the roundtable be held in his office at the White House.
For the next month, it was on again, off again. There were obviously pressures within the White House against sanctioning such a meeting. About a month before the scheduled January 19th date, stories about it began appearing in several newspapers.
For a brief time, it looked like the White House’s Office of Policy Development was not going to host it, but the Office of Science and Technology Policy was. Then the whole thing fell apart.
The New York Post, on January 7th, 1988, ran a story on Duesberg. The next day, the paper did a follow-up, headlined: U.S. AXES DEBATE ON TRUE CAUSE OF AIDS. After indicating that the White House meeting was canceled, medicine-science editor, Joe Nicholson, relayed a surprising quote from Gary Bauer, head of Reagan’s Office of Policy Development, and Jim Warner’s boss: “People like Dr. Duesberg need to continue to have access to research funds so that if we are heading in the wrong direction, that can be proved.”
Bauer then said he didn’t want the White House to sponsor the meeting because it would impart a political tone to a scientific event.
“I hope they have the debate elsewhere,” he said. “I’ve sort of bristled at the finality with which some have made statements about AIDS and how it is transmitted. When findings run counter to the accepted wisdom, there is a tendency to muzzle or ignore rather than have an open debate.”
The proposed debate never took place.
Given what Jim Warner told me in our 1987 interview, I’m sure, if he were still working for the government in 2021, he would have some choice comments about an NIH scientist who was a major player in the AIDS scene in 1987, and is still hogging the spotlight these days:

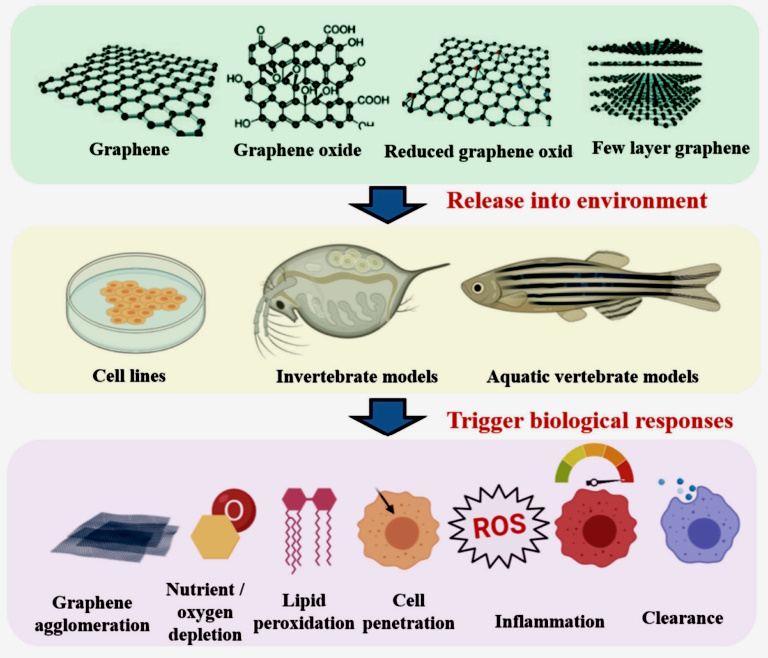
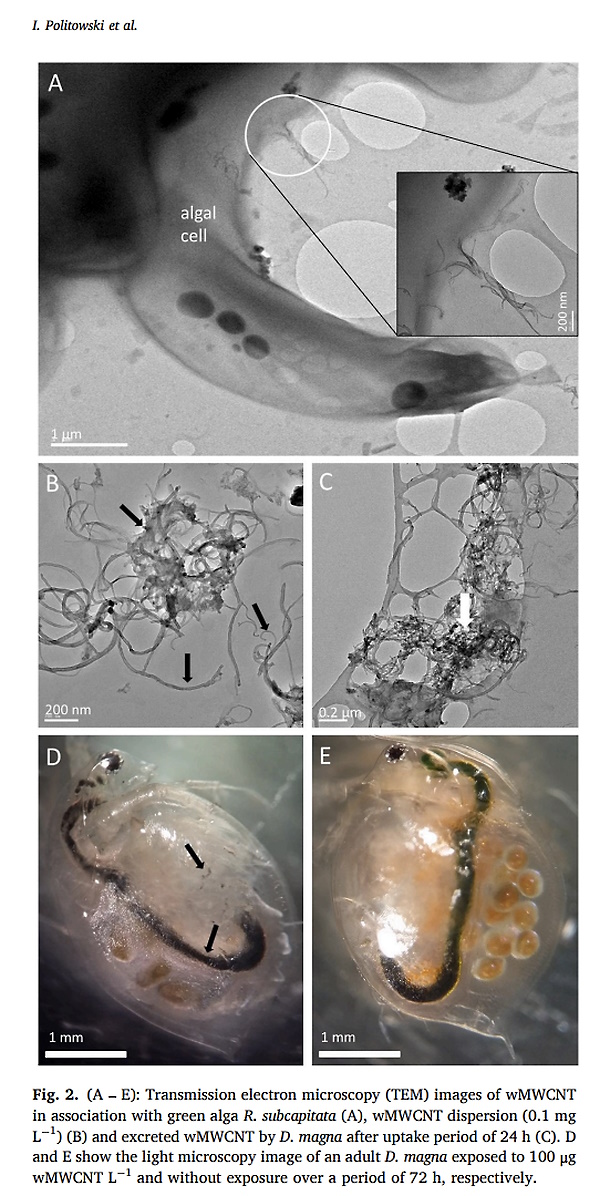
 Alicia Green is an instinctive researcher and writer, with BA in Psychology and BS in Advertising. She gained her first experience as an investigative news reporter while working for a student-run news publication, providing breaking news and information on issues affecting the university and local community.
Alicia Green is an instinctive researcher and writer, with BA in Psychology and BS in Advertising. She gained her first experience as an investigative news reporter while working for a student-run news publication, providing breaking news and information on issues affecting the university and local community.


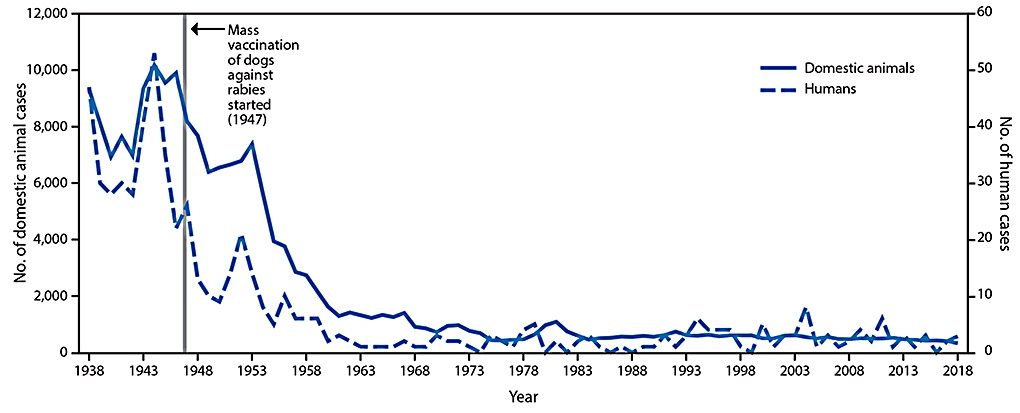
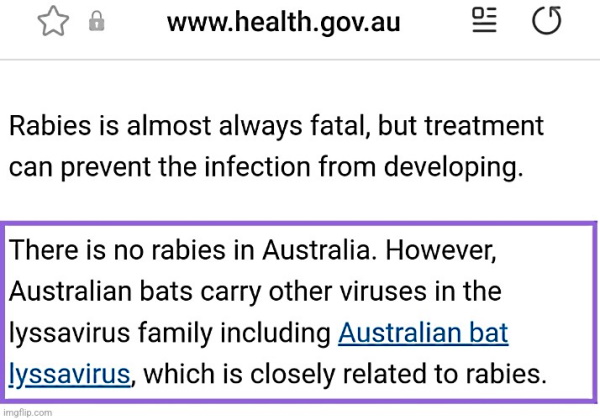
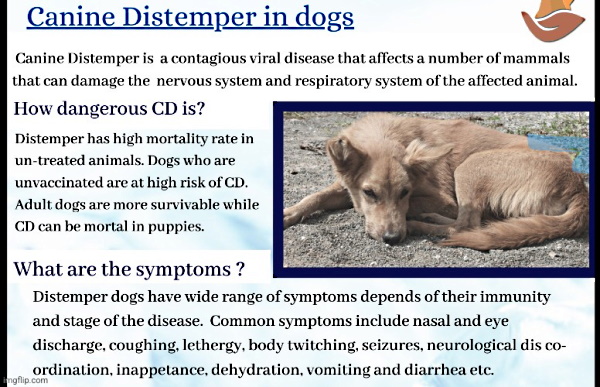

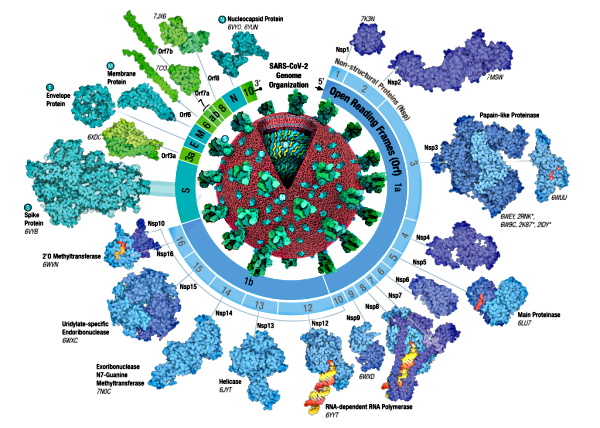
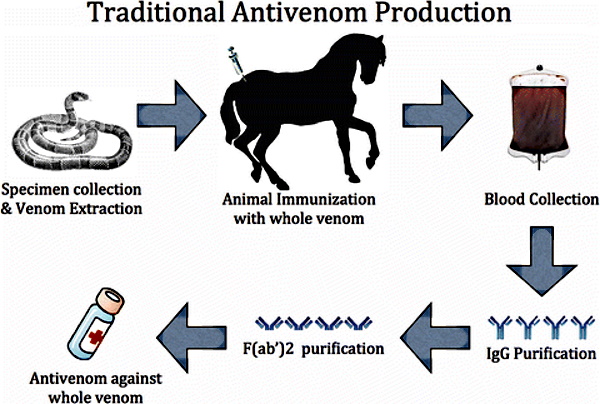
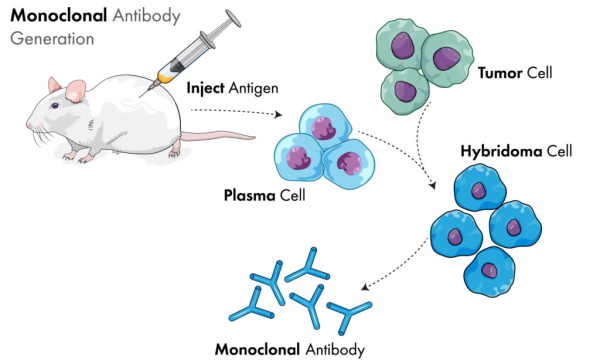
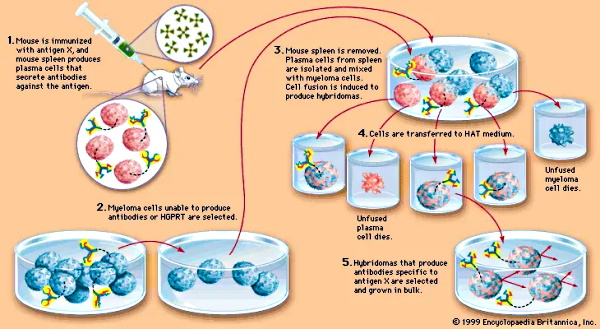


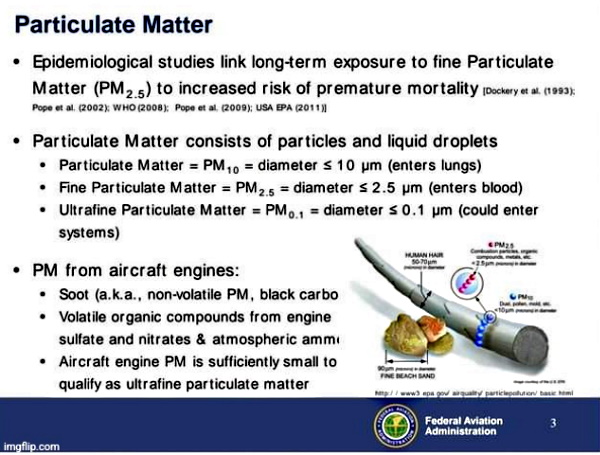
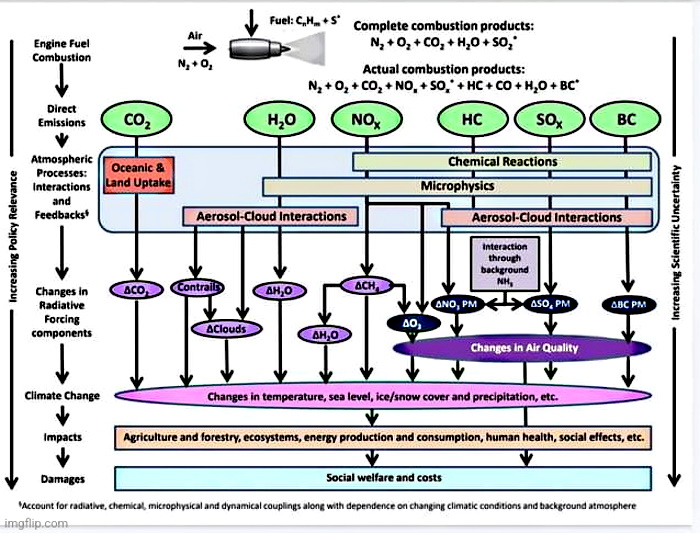
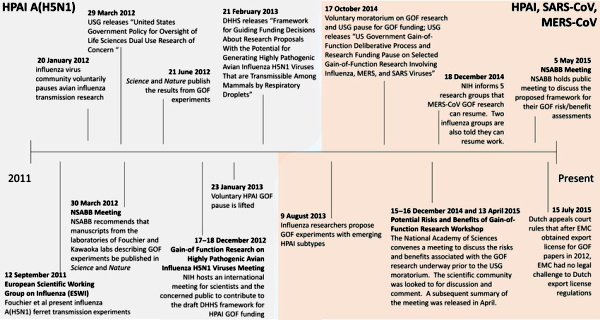
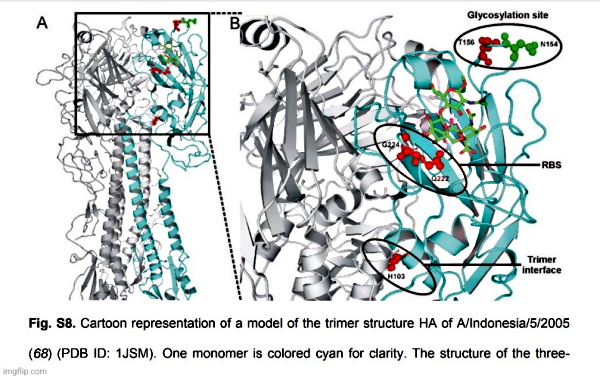




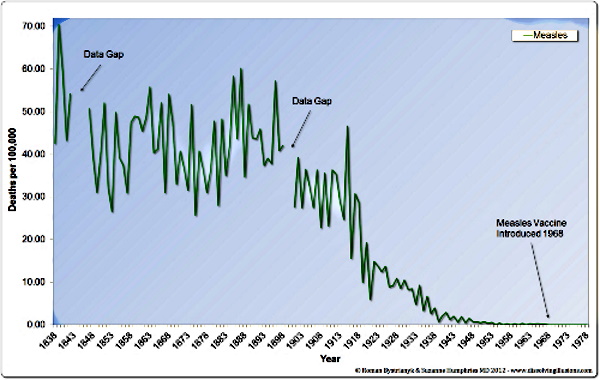


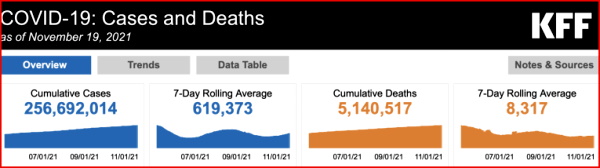
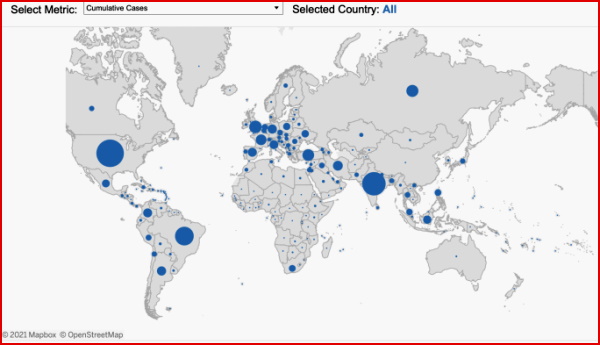
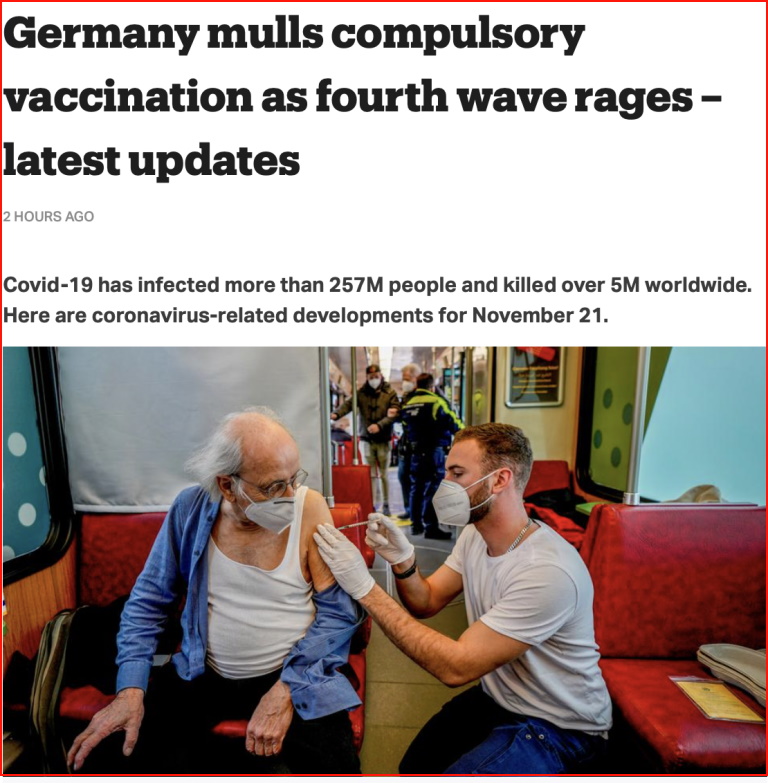
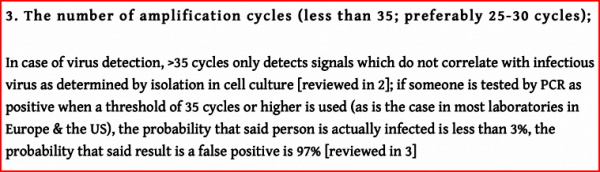
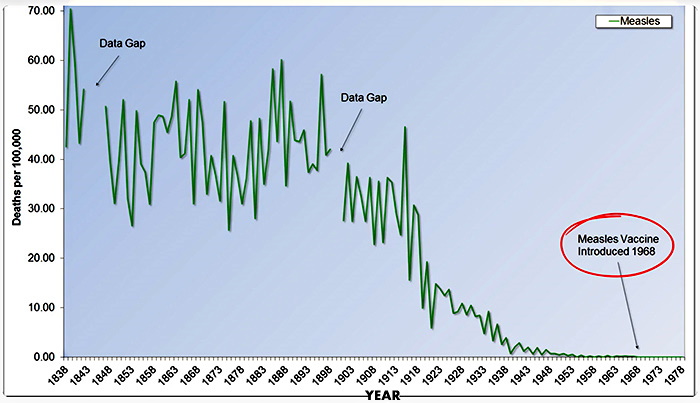
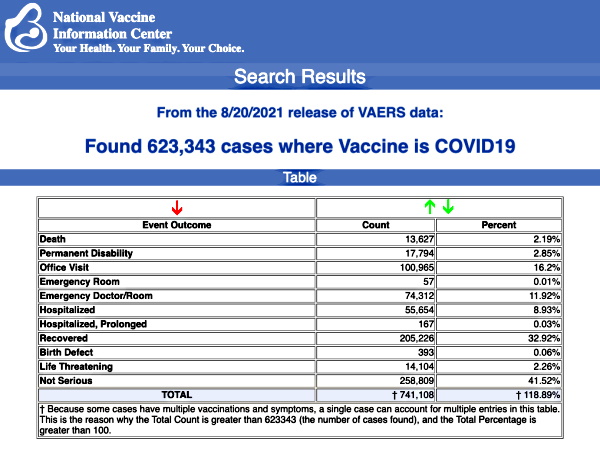
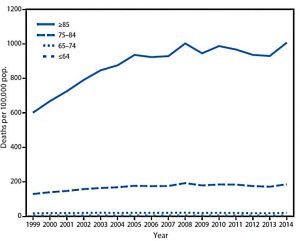
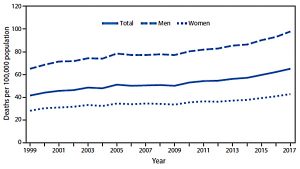
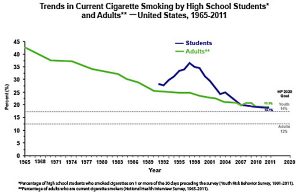
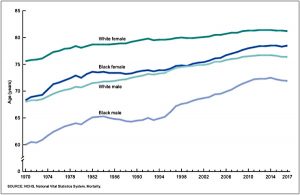

.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
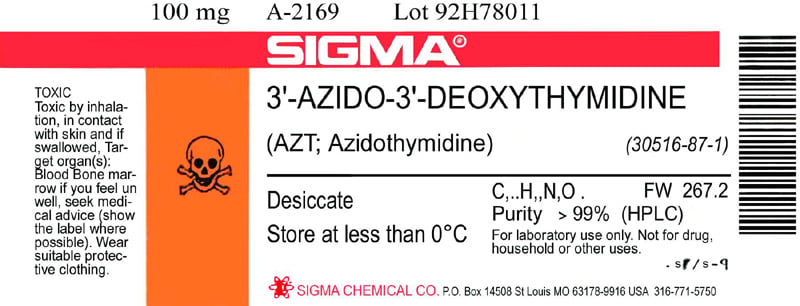{kind=link}
_Wellcome_L0073696.jpg){kind=link}