1. Every thirty seconds vivisectors around the world kill another thousand animals. They use cats, dogs, puppies, kittens, horses, sheep, rats, mice, guinea pigs, rabbits, monkeys, baboons and any other creature you can think of.
2 .While waiting to be used in laboratory experiments, animals are kept in solitary confinement in small cages. Alone and frightened they can hear the screams of the other animals being used.
3. Some of the animals used in laboratory experiments are pets which have been kidnapped, taken off the streets and sold to the vivisectors.
4. Animals used in experiments are blinded, burned, shot, injected and dissected. They have their eyes sewn up or their limbs broken. Chemicals are injected into their brains and their screams of anguish are coldly recorded.
5. Three quarters of the experiments performed by vivisectors are done without any anaesthetic.
6. Most vivisectors have no medical or veterinary training.
7. Scientists claim that animals are not sentient creatures and are incapable of suffering mental or physical pain.
8. All animals respond differently to threats of any kind depending on their circumstances (diet, cage size, etc.). None of these factors is allowed for by vivisectors. By locking an animal up in a cage, experimenters have already invalidated their experiment because by altering the animal’s surroundings, the experimenter alters the animal’s susceptibility, its habits, its instincts and its capacity to heal itself. Since these variations are not controlled (cages and surroundings differ) experiments performed on animals kept in cages are of no scientific value.
9 Many of the diseases which kill or cripple human beings do not affect any other members of the animal kingdom. It is, therefore, impossible to use different species to test drug therapies for these illnesses.
10. Doctors wouldn’t test a drug intended for old people on children (or the other way round). So why test drugs intended for pregnant women on rats? No one would test a drug for premenstrual problems on small boys and yet that would make far more sense than testing such a drug on male rats.
11. Drug tests done on animals can produce dangerously unreliable and misleading information. Thalidomide safely passed tests on animals. Penicillin and aspirin both kill cats. When Alexander Fleming discovered penicillin growing on a culture dish in 1928, he tested the drug on rabbits and discarded it when it seemed useless. Later the drug was tested on a cat and a human patient at the same time. The cat died and the human being lived. If doctors had relied upon animal experiments to decide whether or not penicillin was of any value, the drug would have been discarded long ago. Penicillin even kills guinea pigs – the classic test animal for many drugs. Aspirin can be toxic to rats, mice, dogs, monkeys and guinea pigs as well as cats. Morphine sedates human beings but excites cats, goats and horses. Digitalis, one of the best established and most effective drugs for the treatment of heart disease, is so toxic to animals that if we had relied on animal tests it would have never been cleared for use by humans.
12. Vivisectors admit that most animal experiments are unreliable and produce results which are not relevant to human patients. But they don’t know which experiments are unreliable. Logically, that means that all animal experiments are useless. If you don’t know which experiments you can rely on, you can’t rely on any of them.
13. The very unreliability and unpredictably of animal experiments is what makes them commercially valuable. Drug companies test on animals so that they can say that they have tested their drugs before marketing them. If the tests show that the drugs do not cause serious disorders when given to animals the companies say: `There you are! We have tested our drug – and have proved it to be safe!’ If, on the other hand, tests show that a drug does cause serious problems when given to animals the companies say: `The animal experiments are, of course, unreliable and cannot be used to predict what will happen when the drug is given to humans. We have, however, tested our drug.’ Tests which show that a drug causes cancer or some other serious disease when given to animals are ignored on the grounds that animals are different to people. However, tests which show that a new drug doesn’t kill animals are used as evidence that the drug is safe for human consumption. If you try a drug on enough different animals you can usually end up with at least one set of results which suggest that a drug is safe. Scores of drugs which cause cancer or other serious health problems in animals are widely prescribed for human patients. (See www.vernoncoleman.com for the names of 50).
14. Four out of ten patients who take a prescribed drug which has been tested for safety on animals can expect to suffer severe or noticeable side effects.
15. Surveys show that most practising doctors are opposed to vivisection on scientific grounds.
Taken from The Wisdom of Animals by Donna Antoinette Coleman and Vernon Coleman. Available as a paperback and an eBook.
“I would love to be able to bring back our country into a great form of unity,” Trump said. “Without a major event where people pull together, that’s hard to do. But I would like to do it without that major event because usually that major event is not a good thing.” – Donald Trump, Jan 30th 2018
By April of 2020, within two years of Donald Trump’s prophetic message, millions of people had bowed the government’s request to “unite” by “social distancing,” under a “Live Exercise” revealed by Trump’s Secretary of State Mike Pompeo. About half of the world’s population agreed to some form of lockdown. More than 3.9 billion people in more than 90 countries had been asked or ordered to stay at home by their governments. And they did.
In unison, millions donned a ritual mask to protect themselves against an invisible enemy. The effect was dubbed virtue signaling – an attempt to show other people that you are a good person, by expressing opinions that will be acceptable to them, especially on social media. How did so many people fall into lock-step to give up their freedom when they had previously been openly skeptical of government ethics and policies?
Social Engineering
The earliest social experiments had been successful using the tried-and true strategy of The Hegelian Dialectic: Problem • Reaction • Solution. Introduce a Problem and roll out the Solution! Past experiments included “The New Deal” under Franklin Roosevelt in the 1930s, and “Great Society” under Lyndon Johnson in the 1960s. Then came the “financially sound” government programs of Social Security, Medicare, and Medicaid.
Money and politics aside, why trust a government’s blanket medical solution when it comes to health, a personal responsibility?
If we understand the mechanism and motives of the group mind, it is now possible to control and regiment the masses according to our will without them knowing it. – Edward Bernays
After three years of government-induced COVID, there is still no approved government Solution to the COVID Problem because the FDA-approved vaccine is still not officially available to anyone, and may never be. Nonetheless, the Live Exercise of testing, tracking, experimentation, and restrictions, continues unabated.
While vaccine makers, such as Pfizer, insisted they need 75 years of data before releasing results to the public, the “adverse events” of the public subjects are being tracked and published in medical journals, even if not widely reported.
In any true experiment, there are two groups: the cases and the controls. All subjects who consented, received vaccine lots coded by color and number. Did they receive a vaccine with a Red cap or blue cap? Did they receive saline solution or the COVID spike protein? Did they go from a “fully vaccinated” to “double boosted? Did they opt out?
Let The Experiment Continue!
They say a picture is worth a thousand words, even if the subject matter, a spike protein, has never been officially isolated, or seen with the naked eye. As of this writing, there is no proof the cause of COVID exists.
Since no quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted… — CDC 2109 document
Even without proof, millions of people eagerly jumped aboard The Spike Protein Train to protect themselves with a mask, based on an image of a virus they believed in.
Then, by design, came the vaccines. A vaccine has always been the response to a government-declared pandemic. Recall the 1976 Swine Flu and the 1918 Spanish Flu? [See The Making of a Pandemic for more information]. Vaccine deployment is followed by the damage reports.
In any Live Exercise or Experiment, scientists cannot be expected to have any answers now, or possibly ever. Meanwhile, new symptoms to experimental mRNA vaccines create new, “rare” medical diagnoses. A quick search of Pubmed quickly shows that symptoms are the opposite of rare.
With the introduction of vaccines came the subsequent introduction of Vaccine Inflammatory Syndromes. From Autoimmune Inflammatory Syndrome Induced by Adjuvants,(ASIA), to Post Vaccination Inflammatory Syndrome (PVIS), and Multisystem Inflammatory Syndrome (MIS), all related acronyms describe one cause: Vaccine toxicity.
Since the deployment of COVID injections, the new COVID is Long COVID, ranging from back pain to sleep and digestive disorders, that go beyond 6 months. Symptoms also include postural tachycardia syndrome or POTS.
POTS affects the autonomic nervous system, or the parasympathetic nervous system that regulates voluntary and involuntary actions, as well as thinking, communication, and memory. These symptoms have been long studied as conditions of vaccine injury. Therefore, the injected spike proteins that bring on autoimmune-mediated endothelial injuries can also lead to POTS, especially in the lungs, as evidenced by this study in Clin Auton Res.
Simply go to the VAERS database to search and download the data collected from vaccine-induced injuries the government lists on its own website. VAERS data released by the CDC included a total of 7oo,ooo adverse event reports from all age groups following COVID vaccines, including 15,386 deaths between December 14, 2020, and September 17, 2021. Vaccine-injured patients become lifelong customers of pharmaceutical treatments, with doctors and scientists knowing that many will never return to their normal lifestyles.
All patients were treated with non-pharmacologic therapies, and most required pharmacologic therapies. Six to 8 months after COVID-19, 17 (85%) patients had residual autonomic symptoms, with 12 (60%) unable to return to work.
Published mRNA Vaccine Toxicity Studies: Dizziness
Whether by case study, small study, epidemiological study, or case-control study, all studies are ongoing and accumulating. Searching Pubmed by “dizziness or vertigo” and “COVID vaccine” and find dozens of studies. Here are a few:
Among all the symptoms reported, localized pain, generalized weakness, headache, myalgia, chills, fever, nausea, joint pains, sweating, localized swelling at the injection site, dizziness, itching, rash, decreased appetite, muscle spasm, decreased sleep quality, and brain fogging were the most commonly reported symptoms (in descending order of occurrence). Most of the symptoms reported were nonlife threatening.
Vestibular neuritis (VN) is an acute vestibular syndrome that causes acute and spontaneous vertigo due to unilateral vestibular deafferentiation, leading to nausea or vomiting and unsteadiness that can last from days to weeks. Reactivation of latent type 1 herpes simplex virus, autoimmune disorders, and microvascular ischemia are hypothesized to be etiologies.
We reported for the first time a case of neuromyelitis optica spectrum disorder (NMOSD) that developed after the first dose of inactivated virus vaccine for COVID-19. The patient developed mild fever, vomiting, diarrhea, and cough after receiving the first dose of inactivated virus vaccine. Two months later, she experienced dizziness and unsteady walking. MRI scanning of the brain revealed lesions in area postrema and bilateral hypothalamus, typical for NMOSD. Serum antibodies for AQP4, ANA, SSA, SSB, Ro-52, and p-ANCA were positive. The patient was diagnosed as AQP4-positive NMOSD with coexisting systemic autoimmunity.
The most frequently reported adverse events were headache, myalgia, and dizziness. Of the 835 reported deaths after COVID-19 vaccination, 2 vaccine-related deaths were confirmed.
A 67-year-old man who was medicated for hypertension and diabetes was admitted complaining of fever, maculopapular rash, diarrhea, headache, chills, and dizziness 6 days after the first vaccination of ChAdOx1 nCoV-19 in Korea. The COVID-19 test was negative but with low blood pressure, leukocytosis, skin rash, pulmonary edema, and increased inflammation markers. His lab findings and clinical course were consistent with those of MIS after COVID-19 vaccination.
The 9 patients had an evoked nystagmus pathognomonic for benign paroxysmal positional vertigo; in the remaining 17 cases, peripheral vestibular dysfunction could be excluded and central disorder may be suggested. Due to the prevalence of nystagmus of non-peripheral origin, a central nervous system involvement could not be excluded.
38% mild side effects were observed from vaccination. Following were the general side-effects: myalgia (18.2%), the feeling of sickness (16%), fever (15.6%), dizziness (7.8%), joint pain (7.4%), chills (4.8%), and flu (4.8%). Following were the common neurological side-effects reported: headache (18.2%), fatigue (16.5%), muscle pain (16%), numbness/tingling (3%), and migraine (2.6%). Nausea and diarrhoea were reported in only 3.5% of respondents.
The three most frequent AEFI recorded were vagal response (30%), anxiety reaction (24%) and dizziness (21%). AEFI were more frequently observed among women [aOR= 2.24 (95%CI= 2.00 – 2.50)], and those with at least one previous disease [aOR= 1.47 (95%CI= 1.22-1.76)].
The most common AEFI was pain/tenderness at the injection site experienced by 59.3% of those who experienced any AEFI followed by headache/dizziness (35.3%), itching/rashes at the injection site (8.1%), nausea/vomiting (5.8%) and fever/chills (4.7%).
The patient was a health care worker, aged 34-year old. Past medical history was unremarkable and had not used heparin. Over the next couple of days after the vaccination, he reported headache, nausea, and dizziness as well as abdominal pain. His general status and the laboratories studies deteriorate quickly by increasing liver enzymes and severe coagulopathy. Clinically he had presented acute hepatic failure. He had been received blood products, prednisolone pulse along with broad antibiotics without benefit. He died on the sixth day.
Herein, we describe a 48 years old man presenting with rapidly progressive cognitive decline and hyponatremia diagnosed with anti LGI1 AE, occurring shortly after the second dose of mRNA COVID -19 vaccine and possibly representing a severe adverse event related to the vaccination.
Are we living out a medical experiment or social/behavioral experiment?
Has the world been Trumped?
The government forever claims that people must plan for rising healthcare costs. In 2019, U.S. medical health spending increased by 4.6% to $3.8 trillion or $11,582 per person. If the U.S. medical system is the best in the world then shouldn’t the numbers be doing down?
Whether the crisis is called The Opioid Epidemic or The COVID Pandemic, it is a Crisis of Humanity. The conclusion is always the same when the requirement for more dollars and more research takes precedence over individual healing and freedom from government tyranny:
An estimated 21 million American adults experienced at least one major depressive episode in 2020. The highest rates reported for the past several years have consistently been among those aged between 18 and 25
The vast majority are prescribed antidepressant drugs, despite the fact there’s virtually no evidence to suggest they provide meaningful help, and plenty of evidence showing the harms are greater than patients are being told
Hundreds of thousands of toddlers are also being medicated with powerful psychiatric drugs, raising serious ethical questions, along with questions about the future mental and physical health of these children
There’s no scientific evidence to suggest depression is the result of a chemical imbalance in your brain. A lot of the evidence suggests unhealthy living conditions are at the heart of the problem
Antidepressants are not beneficial in the long term and antipsychotic drugs worsen outcomes over the long term in those diagnosed with psychotic disorders such as schizophrenia
This article was previously published September 19, 2019, and has been updated with new information.
In the U.S., an estimated 21 million American adults experienced at least one major depressive episode in 2020.1 The reported numbers for the past several years2 have consistently been highest among those aged between 18 and 25.3 However, not only is there evidence that depression is vastly overdiagnosed, but there’s also evidence showing it’s routinely mistreated.
With regard to overdiagnosis, it’s been ongoing for a long time, with one 2013 study4 finding only 38.4% of participants with clinician-identified depression actually met the DSM-4 criteria for a major depressive episode, and only 14.3% of seniors 65 and older met the criteria.
As for treatment, the vast majority are prescribed antidepressant drugs, despite the fact there’s little to no evidence to suggest they provide meaningful help, and plenty of evidence showing the harms are greater than patients are being told.
According to a 2017 study,5 1 in 6 Americans between the ages of 18 and 85 were on psychiatric drugs, most of them antidepressants, and 84.3% reported long-term use (three years or more). Out of 242 million U.S. adults, 12% were found to have filled one or more prescriptions for an antidepressant, specifically, in 2013. By 2021 in the midst of the pandemic, 1 in 4 Americans over age 18, or 50 million persons, were on prescription mental health drugs.6
According to data7 presented by a watchdog group in 2014, hundreds of thousands of toddlers are also being medicated with powerful psychiatric drugs, raising serious ethical questions, along with questions about the future mental and physical health of these children.
And, a study published in The BMJ in 20138 found that “In utero exposure to both SSRIs and non-selective monoamine reuptake inhibitors (tricyclic antidepressants) was associated with an increased risk of autism spectrum disorders, particularly without intellectual disability” in the offspring.
Studies are also shedding much needed light on the addictive nature of many antidepressants, and demonstrate that the benefits of these drugs have been overblown while their side effects — including suicidal ideation — and have been downplayed and ignored for decades, placing patients at unnecessary risk.
The Chemical Imbalance Myth
One researcher responsible for raising awareness about these important mental health issues is professor Peter C. Gøtzsche, a Danish physician-researcher and outspoken critic of the drug industry (as his book, “Deadly Medicines and Organized Crime: How Big Pharma Has Corrupted Healthcare,”9 suggests).
Gøtzsche helped found the Cochrane Collaboration in 1993 and later launched the Nordic Cochrane Centre. In 2018, he was expelled by the Cochrane governing board following the publication of a scathing critique of a Cochrane review of the HPV in which he and his coauthors pointed out several methodological flaws and conflicts of interest.
Over the past several years, Gøtzsche has published a number of scientific papers on antidepressants and media articles and a book discussing the findings. In a June 28, 2019 article,10 Gøtzsche addresses “the harmful myth” about chemical imbalances — a debunked hypothesis that continues to drive the use of antidepressants to this day. He writes, in part:11
“Psychiatrists routinely tell their patients that they are ill because they have a chemical imbalance in the brain and they will receive a drug that fixes this …
Last summer, one of my researchers and I collected information about depression from 39 popular websites in 10 countries, and we found that 29 (74%) websites attributed depression to a chemical imbalance or claimed that antidepressants could fix or correct that imbalance …
It has never been possible to show that common mental disorders start with a chemical imbalance in the brain. The studies that have claimed this are all unreliable.12
A difference in dopamine levels, for example, between patients with schizophrenia and healthy people cannot tell us anything about what started the psychosis … [I]f a lion attacks us, we get terribly frightened and produce stress hormones, but this does not prove that it was the stress hormones that made us scared.
People with psychoses have often suffered traumatic experiences in the past, so we should see these traumas as contributing causal factors and not reduce suffering to some biochemical imbalance that, if it exists at all, is more likely to be the result of the psychosis rather than its cause.13
The myth about chemical imbalance is very harmful. It makes people believe there is something seriously wrong with them, and sometimes they are even told that it is hereditary.
The result of this is that patients continue to take harmful drugs, year after year, perhaps even for the entirety of their lives. They fear what would happen if they stopped, particularly when the psychiatrists have told them that their situation is like patients with diabetes needing insulin.”
Real Cause of Depression Is Typically Ignored
According to Gøtzsche, there is no known mental health issue that is caused by an imbalance of brain chemicals. In many cases, the true cause is unknown, but “very often, it is a response to unhealthy living conditions,” he writes.14
He also cites the book,15 “Anxiety — The Inside Story: How Biological Psychiatry Got It Wrong,” written by Dr. Niall McLaren, in which the author shows that anxiety is a major factor in and trigger of most psychiatric disorders.
“A psychiatrist I respect highly, who only uses psychiatric drugs in rare cases … has said that most people are depressed because they live depressing lives,” Gøtzsche writes.
“No drug can help them live better lives. It has never been shown in placebo-controlled trials that a psychiatric drug can improve people’s lives — e.g., help them return to work, improve their social relationships or performance at school, or prevent crime and delinquency. The drugs worsen people’s lives, at least in the long run.16“
Gøtzsche rightfully points out that antipsychotic drugs create chemical imbalances; they don’t fix them. As a group, they’re also somewhat misnamed, as they do not address psychotic states. Rather, they are tranquilizers, rendering the patient passive. However, calming the patient down does not actually help them heal the underlying trauma that, in many cases, is what triggered the psychosis in the first place.
As noted in one 2012 meta-analysis17 of studies looking at childhood trauma — including sexual abuse, physical abuse, emotional/psychological abuse, neglect, parental death and bullying — and subsequent risk of psychosis:
“There were significant associations between adversity and psychosis across all research designs … Patients with psychosis were 2.72 times more likely to have been exposed to childhood adversity than controls … The estimated population attributable risk was 33% (16%-47%). These findings indicate that childhood adversity is strongly associated with increased risk for psychosis.”
Economy of Influence in Psychiatry
A related article,18 written by investigative journalist Robert Whitaker in 2017, addresses the “economy of influence” driving the use of antidepressant drugs in psychiatric treatment — and the “social injury” that results. As noted by Whitaker, mental disorders were initially categorized according to a disease model in 1980 by the American Psychiatric Association.
“We’re all familiar with the second ‘economy of influence’ that has exerted a corrupting influence on psychiatry — pharmaceutical money — but I believe the guild influence is really the bigger problem,” he writes.
Whitaker details the corruption within the APA in his book “Psychiatry Under the Influence,” one facet of which is “the false story told to the public about drugs that fixed chemical imbalances in the brain.” Other forms of corrupt behavior include:
The biased designs of clinical trials to achieve a predetermined result
Spinning results to support preconceived conclusions
Hiding poor long-term outcomes
Expanding diagnostic categories for the purpose of commercial gain
Creating clinical trial guidelines that promote drug use
In his article, Whitaker goes on to dissect a 2017 review19 published in the American Journal of Psychiatry, which Whitaker claims “defends the profession’s current protocols for prescribing antipsychotics, which includes their regular long-term use.”
As Whitaker points out, there’s ample evidence showing antipsychotic drugs worsen outcomes over the long term in those diagnosed with psychotic disorders such as schizophrenia.
The review in question, led by American psychiatrist Dr. Jeffrey A. Lieberman, was aimed at answering persistent questions raised by the mounting of such evidence. Alas, their conclusions dismissed concerns that the current drug paradigm might be doing more harm than good.
“In a subsequent press release and a video for a Medscape commentary, Lieberman has touted it as proving that antipsychotics provide a great benefit, psychiatry’s protocols are just fine, and that the critics are ‘nefarious’ individuals intent on doing harm,” Whitaker writes.20
The Scientific Bias of Psychiatric Treatment
Five of the eight researchers listed on the review have financial ties to drug companies, three are speakers for multiple drug companies and all eight are psychiatrists, “and thus there is a ‘guild’ interest present in this review, given that they are investigating whether one of their treatments is harmful over the long-term,” Whitaker notes.21
Not surprisingly, the review ignored studies showing negative effects, including studies showing antipsychotics have a detrimental effect on brain volume. What’s more, while withdrawal studies support the use of antipsychotics as maintenance therapy over the long term, these studies do not address how the drugs affect patients’ long-term health.
“They simply reveal that once a person has stabilized on the medication, going abruptly off the drug is likely to lead to relapse,” Whitaker writes.22“The focus on long-term outcomes, at least as presented by critics, provides evidence that psychiatry should adopt a selective-use protocol.
If first-episode patients are not immediately put on antipsychotics, there is a significant percentage that will recover, and this ‘spontaneous recovery’ puts them onto a good long-term course. As for patients treated with the medications, the goal would be to minimize long-term use, as there is evidence that antipsychotics, on the whole, worsen long-term outcomes.”
Vast Majority of Psychotic Patients Are Harmed, Not Helped
In his deconstruction of Lieberman’s review, Whitaker details how biased thinking influenced the review’s conclusions. It’s a rather long article, but well worth reading through if you want to understand how a scientific review can be skewed to accord with a preconceived view.
Details I want to highlight, however, include findings relating to the number needed to treat (NNT) and the percentage of patients harmed by the routine use of antipsychotic drugs as a first-line treatment.
As noted by Whitaker, while placebo-controlled studies reveal the effectiveness of a drug compared to an inert substance, they do not effectively reveal the ratio of benefit versus harm among the patient population. NNT refers to the number of patients that have to take the drug in order to get one positive response.
A meta-analysis cited in Lieberman’s review had an NNT of 6, meaning that six patients must take the drug in order for one to benefit from the treatment. The remaining five patients — 83% — are potentially harmed by the treatment. As noted by Whitaker:23
“The point … is this: reviewers seeking to promote their drug treatment as effective will look solely at whether it produces a superior response to placebo. This leads to a one-size-fits-all protocol.
Reviewers that want to assess the benefit-harm effect of the treatment on all patients will look at NNT numbers. In this instance, the NNT calculations argue for selective use of the drugs …”
Antidepressants Are Not Beneficial in the Long Term
While typically not as destructive as antipsychotics, antidepressants also leave a trail of destruction in their wake. A systematic review24 by Gøtzsche published in 2019 found studies assessing harm from selective serotonin reuptake inhibitors (SSRIs) fail to provide a clear and accurate picture of the harms, and therefore “cannot be used to investigate persistent harms of antidepressants.”
In this review, Gøtzsche and colleagues sought to assess “harms of SSRIs … that persist after end of drug intake.” The primary outcomes included mortality, functional outcomes, quality of life and core psychiatric events. In all, 22 papers on 12 SSRI trials were included. Gøtzsche found several distinct problems with these trials. For starters, only two of the 12 trials had a drop-out rate below 20%.
Gøtzsche and his team also note that “Outcome reporting was less thorough during follow-up than for the intervention period and only two trials maintained the blind during follow-up.” Importantly, though, all of the 22 papers came to the conclusion that “the drugs were not beneficial in the long term.”
Another important finding was that all trials either “reported harms outcomes selectively or did not report any,” and “Only two trials reported on any of our primary outcomes (school attendance and number of heavy drinking days).”
A few years later, in April 2022, a study using data from the United States’ Medical Expenditures Panel Survey for patients who had depression found, “The real-world effect of using antidepressant medications does not continue to improve patients” health-related quality of life (HRQoL) over time.25
Antidepressants Are More Addictive Than Admitted
In a June 4, 2019, article,26 “The Depression Pill Epidemic,” Gøtzsche writes that antidepressant drugs:
“… do not have relevant effects on depression; they increase the risk of suicide and violence; and they make it more difficult for patients to live normal lives.27 They should therefore be avoided.
We have been fooled by the drug industry, corrupt doctors on industry payroll, and by our drug regulators.28 Surely, many patients and doctors believe the pills are helpful, but they cannot know this, because people tend to become much better with time even if they are not treated.29
This is why we need placebo-controlled trials to find out what the drugs do to people. Unfortunately, virtually all trials are flawed, exaggerate the benefits of the drugs, and underestimate their harms.”30
Addictive Nature of Antidepressants Skews Results
In his article,31 Gøtzsche reviews several of the strategies used in antidepressant drug trials to exaggerate benefits and underestimate the harms. One little-known truth that helps skew study results in the drug’s favor is the fact that antidepressants tend to be far more addictive than officially admitted. He explains how this conveniently hides the skewing of results as follows:32
“Virtually all patients in the trials are already on a drug similar to the one being tested against placebo. Therefore, as the drugs are addictive, some of the patients will get abstinence symptoms … when randomized to placebo …
These abstinence symptoms are very similar to those patients experience when they try to stop benzodiazepines. It is no wonder that new drugs outperform the placebo in patients who have experienced harm as a result of cold turkey effects.
To find out how long patients need to continue taking drugs, so-called maintenance (withdrawal) studies have been carried out, but such studies also are compromised by cold turkey effects. Leading psychiatrists don’t understand this, or they pretend they don’t.
Most interpret the maintenance studies of depression pills to mean that these drugs are very effective at preventing new episodes of depression and that patients should therefore continue taking the drugs for years or even for life.”
Scientific Literature Supports Reality of User Complaints
Over the years, several studies on the dependence and withdrawal reactions associated with SSRIs and other psychiatric drugs have been published, including the following:
•In a 2011 paper33 in the journal Addiction, Gøtzsche and his team looked at the difference between dependence and withdrawal reactions by comparing benzodiazepines and SSRIs. Benzodiazepines are known to cause dependence, while SSRIs are said to not be addictive.
Despite such claims, Gøtzsche’s team found that “discontinuation symptoms were described with similar terms for benzodiazepines and SSRIs and were very similar for 37 of 42 identified symptoms described as withdrawal reactions,” which led them to conclude that:
“Withdrawal reactions to selective serotonin re‐uptake inhibitors appear to be similar to those for benzodiazepines; referring to these reactions as part of a dependence syndrome in the case of benzodiazepines, but not selective serotonin re‐uptake inhibitors, does not seem rational.”
•Two years later, in 2013, Gøtzsche’s team published a paper34 in the International Journal of Risk & Safety in Medicine, in which they analyzed “communications from drug agencies about benzodiazepine and SSRI withdrawal reactions over time.”
By searching the websites of drug agencies in Europe, the U.S., U.K. and Denmark, they found that it took years before drug regulators finally acknowledged the reality of benzodiazepine dependence and SSRI withdrawal reactions and began informing prescribers and patients about these risks.
A significant part of the problem, they found, is that drug agencies rely on spontaneous reporting of adverse effects, which “leads to underestimation and delayed information about the problems.”
In conclusion, they state that “Given the experience with the benzodiazepines, we believe the regulatory bodies should have required studies from the manufacturers that could have elucidated the dependence potential of the SSRIs before marketing authorization was granted.”
•A 2019 paper35 in the Epidemiology and Psychiatric Sciences journal notes “It took almost two decades after the SSRIs entered the market for the first systematic review to be published.” It also points out that reviews claiming withdrawal effects to be mild, brief in duration and rare “was at odds with the sparse but growing evidence base.”
In reality, “What the scientific literature reveals is in close agreement with the thousands of service user testimonies available online in large forums. It suggests that withdrawal reactions are quite common, that they may last from a few weeks to several months or even longer, and that they are often severe.”
Antidepressants Increase Your Risk of Suicide and Violence
In his June 2019 article,36 Gøtzsche also stresses the fact that antidepressants can be lethal. In one of his studies,37 published in 2016, he found antidepressants “double the occurrence of events that can lead to suicide and violence in healthy adult volunteers.”
Other research38 has shown they “increase aggression in children and adolescents by a factor of 2 to 3 — an important finding considering the many school shootings where the killers were on depression pills,” Gøtzsche writes.
In middle-aged women with stress urinary incontinence, the selective serotonin and norepinephrine reuptake inhibitor (SNRI) duloxetine, which is also used to treat incontinence, has been shown to double the risk of a psychotic episode and increase the risk of violence and suicide four to five times,39 leading the authors to conclude that harms outweighed the benefits.
“I have described the dirty tricks and scientific dishonesty involved when drug companies and leading psychiatrists try convincing us that these drugs protect against suicide and other forms of violence,”40 Gøtzsche writes.41“Even the FDA was forced to give in when it admitted in 2007, at least indirectly, that depression pills can cause suicide and madness at any age.
There is no doubt that the massive use of depression pills is harmful. In all countries where this relationship has been examined, the sharp rise in disability pensions due to psychiatric disorders has coincided with the rise of psychiatric drug usage, and depression pills are those which are used the most by far. This is not what one would expect if the drugs were helpful.”
Drugmaker Lied About Paxil’s Suicide Risk
In 2017, Wendy Dolin was awarded $3 million by a jury in a lawsuit against GlaxoSmithKline, the maker of Paxil. Dolin’s husband committed suicide six days after taking his first dose of a Paxil generic, and evidence brought forth in the case convincingly showed his suicide was the result of the drug, not emotional stress or mental illness.42
The legal team behind that victory, Baum Hedlund Aristei Goldman, also represented other victims of Paxil-induced violence and death. At the time, attorney R. Brent Wisner said:43
“The Dolin verdict sent a clear message to GSK and other drug manufacturers that hiding data and manipulating science will not be tolerated … If you create a drug and know that it poses serious risks, regardless of whether consumers use the brand name or generic version of that drug, you have a duty to warn.”
GSK’s own clinical placebo-controlled trials actually revealed subjects on Paxil had nearly nine times the risk of attempting or committing suicide than the placebo group. To gain drug approval, GSK misrepresented this shocking data, falsely reporting a higher number of suicide attempts in the placebo group and deleting some of the suicide attempts in the drug group.
An internal GSK analysis of its suicide data also showed that “patients taking Paxil were nearly seven times more likely to attempt suicide than those on placebo,” Baum Hedlund Aristei Goldman reports, adding:44
“Jurors in the Dolin trial also heard from psychiatrist David Healy, one of the world’s foremost experts on Paxil and drugs in its class … Healy told the jurors that Paxil and drugs like it can create in some people a state of extreme ’emotional turmoil’ and intense inner restlessness known as akathisia …
‘People have described it like a state worse than death. Death will be a blessed relief. I want to jump out of my skin,’ Dr. Healy said. Healthy volunteer studies have found that akathisia can happen even to people with no psychiatric condition who take the drug …
Another Paxil side effect known to increase the risk of suicide is emotional blunting … apathy or emotional indifference … [E]motional blunting, combined with akathisia, can lead to a mental state in which an individual has thoughts of harming themselves or others, but is ‘numbed’ to the consequences of their actions. Drugs in the Paxil class can also cause someone to ‘go psychotic, become delirious,’ Dr. Healy explained.”
Hundreds of Thousands of Toddlers on Psychiatric Drugs
Considering the many serious psychological and physical risks associated with psychiatric drugs, it’s shocking to learn that hundreds of thousands of American toddlers are on them. In 2014, the Citizens Commission on Human Rights, a mental health watchdog group, highlighted data showing that in 2013:45
274,000 babies aged 1 and younger were given psychiatric drugs — Of these, 249,699 were on anti-anxiety meds like Xanax; 26,406 were on antidepressants such as Prozac or Paxil, 1,422 were on ADHD drugs such as Ritalin and Adderall, and 654 were on antipsychotics such as Risperdal and Zyprexa
In the toddler category (2- to 3-year-olds), 318,997 were on anti-anxiety drugs, 46,102 were on antidepressants, 10,000 were prescribed ADHD drugs and 3,760 were on antipsychotics
Among children aged 5 and younger, 1,080,168 were on psychiatric drugs
These are shocking figures that challenge logic. How and why are so many children, babies even, on addictive and dangerously mind-altering medications? Considering these statistics are 6 years old, chances are they’re even higher today. Just what will happen to all of these youngsters as they grow up? As mentioned in the article:46
“When it comes to the psychiatric drugs used to treat ADHD, these are referred to as ‘kiddie cocaine’ for a reason. Ritalin (methylphenidate), Adderall (amphetamine) and Concerta are all considered by the federal government as Schedule II drugs — the most addictive.
ADHD drugs also have serious side effects such as agitation, mania, aggressive or hostile behavior, seizures, hallucinations, and even sudden death, according to the National Institutes of Health …
As far as antipsychotics, antianxiety drugs and antidepressants, the FDA and international drug regulatory agencies cite side effects including, but not limited to, psychosis, mania, suicidal ideation, heart attack, stroke, diabetes, and even sudden death.”
Children Increasingly Prescribed Psych Drugs Off-Label
Making matters even worse, recent research shows the number of children being prescribed medication off-label is also on the rise. An example offered by StudyFinds.org,47 which reported the findings, is “a doctor recommending antidepressant medication for ADHD symptoms.”
The study,48 published in the journal Pediatrics, looked at trends in off-label drug prescriptions made for children under the age of 18 by office-based physicians between 2006 and 2015. Findings revealed:
“Physicians ordered ≥1 off-label systemic drug at 18.5% of visits, usually (74.6%) because of unapproved conditions. Off-label ordering was most common proportionally in neonates (83%) and in absolute terms among adolescents (322 orders out of 1000 visits).
Off-label ordering was associated with female sex, subspecialists, polypharmacy, and chronic conditions. Rates and reasons for off-label orders varied considerably by age. Relative and absolute rates of off-label orders rose over time. Among common classes, off-label orders for antihistamines and several psychotropics increased over time …
US office-based physicians have ordered systemic drugs off label for children at increasing rates, most often for unapproved conditions, despite recent efforts to increase evidence and drug approvals for children.”
The researchers were taken aback by the findings, and expressed serious concern over this trend. While legal, many of the drugs prescribed off-label have not been properly tested to ensure safety and efficacy for young children and adolescents.
As noted by senior author Daniel Horton, assistant professor of pediatrics and pediatric rheumatologist at Rutgers Robert Wood Johnson Medical School, “We don’t always understand how off-label medications will affect children, who don’t always respond to medications as adults do. They may not respond as desired to these drugs and could experience harmful effects.”
In 2020 mental health experts and reviewers were still at-odds over prescribing these drugs for children, yet hesitant to call a stop to it:49
“Antidepressants are prescribed for the treatment of a number of psychiatric disorders in children and adolescents, however there is still controversy about whether they should be used in this population …
Treatment decisions should be tailored to patients on an individual basis, so we recommend clinicians, patients and policy makers to refer to the evidence provided in the present meta-review and make decisions about the use of antidepressants in children and adolescents taking into account a number of clinical and personal variables.”
Educate Yourself About the Risks
If you, your child or another family member is on a psychiatric drug, I urge you to educate yourself about the true risks and to consider switching to safer alternatives. When it comes to children, I cannot fathom a situation in which a toddler would need a psychiatric drug and I find it shocking that there are so many doctors out there that, based on a subjective evaluation, would deem a psychiatric drug necessary.
I wrote this article in 2010. It’s truer now than it was then:
DECEMBER 5, 2010. About ten years ago, I decided that the medical cartel could become the most dangerous of all power groups on the planet. I have not changed my mind.
My decision is based on looking up the road 40 or 50 years and inferring what the picture will look like then.
It’s clear to me that drug companies, as they carve up markets and create new markets, are eagerly anticipating the day when every human, from cradle to grave—actually from inside the womb—has the status of Patient.
A person is born a patient and dies a patient. And in between, he receives 40 or 50 key diagnoses of physical and mental diseases/disorders and takes prescribed drug and surgery treatments.
More than that, though, he is stamped with the label, Patient, and he learns that everyone is in the same boat. “We’re all patients, this is a medical world, and it’s normal to be disabled in some way.”
People become proud, yes, proud to be victims. They wear their diagnoses as badges of honor. If you can’t see this trend, you’re not looking.
And universal health care insurance guarantees continuous treatment all the way along the line.
Every medical diagnosis becomes an excuse not to perform, not to excel, not to pursue big goals with large ambition.
Nowhere in the search to gain recognition as a victim do circumstances conspire so well as in the medical arena. It’s perfect. There’s no argument. The doctor told you you have X disease. That’s that. It’s not political. It’s not agenda-driven. It’s science. The proof is laid out on a silver platter. You ARE a victim.
In the coming future, every move a person makes, every step he takes will come under the umbrella of the doctor.
And, again, the main supporter of this system will be the patient himself. That’s how beautiful the marketing is.
In case you’ve been living in a cave for the last 30 years, drug companies and their researchers can invent any vague disease label they want to—and then they can invent five or six sub-categories of the label—and they can set out rules on how to diagnose each sliver of the label—and of course the doctors will make these diagnoses and prescribe drugs. It’s marketing and “healing” at the same time.
Parents who don’t have a clue will submit their children to this system—especially if the government pays for it—and the children will grow up trained to think of themselves as patients/victims…and the only contest will be: who has the most drastic diagnoses and treatments? Who can most proudly wear the badge of honor as Patient?
“Last month, they had to remove my head for five minutes while they fixed my brain.”
“Wow. Well, they put me in a body cast for three months and I couldn’t move, except for my left thumb.”
Cradle to grave.
If you go back and read Huxley’s Brave New World again, you’ll notice the factor of “patient pride.” It isn’t just that the society is controlled, the citizens are idealistic about it.
That’s where the victim industry is heading.
Against it, we have, what?
A little thing called individual freedom. Which includes the right to refuse medical treatment, no matter who prescribes it under what regulations.
People imagine that this right is some arcane matter best debated in medical-ethics journals. It’s an obscure curio.
They couldn’t be more wrong.
As I’ve been writing, the ObamaCare plan contains the seeds of a future in which, by law, the citizen will have less freedom to determine his own medical fate. The walls will gradually close in.
The Founders knew what they were talking about when they warned of the incursion of government and the loss of freedom. At every crossroad, since then, the issue of freedom has resurfaced as the unavoidable key factor.
Dr. Sam Bailey: On Health Freedom Advocates Who Attack Anyone Who Dares to Question Virus & Germ Theory | How RFK, Jr. Was Recently Drawn Into the Viral Existence Debate
Truth Comes to Light editor‘s note: In the video below, Dr. Sam Bailey talks about specific attacks, coming from within the health freedom movement, on the work of those who are questioning the foundations of virus theory.
At this point, most people in the health freedom movement, not to mention the general population, don’t even know that there is a strong debate about the existence of viruses. But awareness is growing.
The so-called, ‘settled science’ of virology must be looked into carefully because, as Dr. Sam Bailey has stated, virus and germ theory “is a system that can and will be used repeatedly to promulgate fear and compliance in the population.”
Dr. Bailey is careful to emphasize that RFK, Jr. is not one of those attacking the work of those who question virology. In this video she shares a segment from a recent public Q&A session wherein Eric Coppolino asks RFK, Jr. some basic questions, pointing to the fact that SARS-C0V-2 has never been shown to exist outside of imagined computer models.
You will find a transcript below the video with links to referenced articles and papers.
RFK, Jr. has been a tireless campaigner in warning the public about the problems of vaccines. However, with regards to the viral existence problem, he has been reluctant to get involved.
Let’s find out what happened when he was drawn into the debate in a recent Q&A session…
Questioning the existence of viruses can be a risky business, as myself and others have found out. However, once you’ve seen the problems with viral theory, it’s not something that can be unseen. It becomes a realization that much of what you were told is factual is not founded in scientific evidence at all. You start to research the material and find that many of the narratives are driven by industry participants and folklore rather than organic science.
While most probably don’t have a dog in the fight, those defending the virus narrative can get pretty hostile.
However, others such as RFK, Jr. simply appear uneasy about mentioning the virus existence issue.
So let’s find out what happened when one of the champions of the health freedom movement was unexpectedly drawn into the debate.
From the start I would like to make it clear that I consider RFK Jr. an ally in promoting health freedom and autonomy. He is a world leader and raising awareness about the risks and ineffectiveness of many vaccines.
I would also say that he has not been ambiguous with regards to his public statements relating to the existence of SARS-CoV-2 or other viruses. As far as I’m aware, he has stated that he believes such viruses exist. Although, in many cases the risks to health and the necessity for a lot of vaccines have been overstated.
I’d also suggest that the virus existence debate does not mean the current health freedom movement will be fractured as some seem to fear.
I don’t mind if other people believe in viruses and germ theory. However, as we point out in ‘Virus Mania’ that is a system that can and will be used repeatedly to promulgate fear and compliance in the population. Once the fatal flaws in the contagion theory are understood, people no longer buy into any of it and don’t get distracted trying to explain different aspects of the scam.
But before we get into RFK Jr.’s recent statements, there have been a few other prominent health freedom fighters who have made forays into the virus existence debate this year.
One was Steve Kirsch. He has been very outspoken about the dangers of the Covid-19 vaccine. Kirsch has realized that many doctors, governments and pharmaceutical companies are playing a game of deception with the public.
But then, on the issue of virus existence he places his faith in the high priests of virology. In early January this year, he decided to announce in his popular blog that SARS-Cov-2 has been isolated and shown to exist.
First, he smeared Drs. Lanka, Kaufman and Cowan with completely inaccurate portrayals of their work and received a huge backlash from his followers in the comment section. Instead of realizing that he might need to conduct his own research into this topic, he then decided to include Christine Massey and myself in the smears.
In a subsequent article 11 days later, curiously Kirsch suggested that we would not front if a live debate was offered.
Well, I can tell you from a series of emails that took place, which Kirsch was part of, that Drs. Bailey times two [Drs. Mark and Samantha Bailey], along with Stefano Scoglio, Drs. Lanka, Cowan and Kaufman, all volunteered to take part in a live debate with any experts that Kirsch was able to produce.
Instead of admitting that he was in over his head, Kirsch posted a third article the following week, embarrassing himself even further with declarations such as: ‘The reason nobody has purified the virus is there is no need to do so in today’s world where gene sequencing is readily available.’ And, ‘if the virus doesn’t exist, then how can 600 labs across the country find the same sequences for the virus in infected samples.’
These kind of statements indicate he’s unaware of the fundamentals of the virus existence debate.
Kirsch doesn’t see that he relies on other “experts” to inform him on the issue. And my husband Mark has written about why this is not a good idea, outlining the nature of the evidence such experts present in his article ‘Warning Signs You’ve Been Tricked by Virologists‘.
As Kirsch has worked out that people selling vaccines may be misleading people, then we would suggest that he peel back another layer to check whether the pharmaceutical and virology establishment, who have billions of dollars of vested interests, may be misleading people with regards to viruses as well.
And some other information I can give you is that I reached out to Steve after he posted his articles offering him a chance to connect, as well as a complimentary copy of ‘Virus Mania’. But he never responded.
In any case, he seems to have gone quiet on the virus existence front, perhaps because he genuinely thinks it’s […] science. Although I would hope that he has some inkling now that there’s more to this than he thought.
Another interesting smear attack against me from a supposed health freedom fighter came from Dr. Roger Watson, writing for The Daily Sceptic in March this year.
This was surprising on a number of fronts. Firstly, because the website developed out of lockdown sceptics and has the motto “question everything”.
However, it seems that questioning the existence of SARS-CoV-2 and the existence of viruses in general is a bridge too far for the so-called ‘Sceptic’.
Secondly, along with my allies including Andy Kaufman and Kevin Corbett, Watson co-signed the viral challenge letter to Boris Johnson demanding that the British prime minister provide proof of the Covid-19 virus. And, if not, then all measures against the nonexistent virus should be dropped.
Obviously, Watson changed his mind at some point and I’m not clear on why that happened. In any case, I had some fun dismantling Watson’s various allegations in my articles ‘The COVID “Sceptics” Who Spread Viral Dogma‘.
Watson’s article was arguably worse […]
Like Kirsch, Watson did not want to enter into a debate about the topic and couldn’t find anyone to front up in his place either. But at least he responded to our emails.
So, now we get to RFK, Jr., which is a slightly different story, as he has not been involved in any smears against me.
In fact, those of you familiar with ‘Virus Mania’ will know that he wrote an important section for our book titled ‘Greed, Negligence and Deception in the Vaccine Industry’.
RFK, Jr. is certainly aware of the controversy surrounding the existence of HIV. As he outlined in his 2022 publication ‘The Real Anthony Fauci’, our friend Tom Cowan even gets a mention in the book when he says: “The first time that someone — Dr. Tom Cowan, a physician from northern California — suggested to me that HIV was not the sole cause of AIDS, I dismissed the comment as ridiculous.”
However, in Chapter 5, ‘The HIV Heresies’, RFK, Jr. goes on to explain how his own research made him realize that there were major problems with the HIV theory.
He is even aware of The Perth Group and the devastating criticisms of the very existence of an infectious HIV particle. Commenting, “In my conversations with Turner and Papadopulos, and in my reading of their paper, I find their arguments clear and convincing. However, I recognize that there are some fifty thousand articles on AIDS in the scientific literature. A casual novitiate like myself has little chance of unraveling this baroque controversy in a vacuum.”
However, most of RFK, Jr.’s focus in the book is on the fact that Anthony Fauci has been instrumental in controlling the HIV/AIDS model and has ruthlessly suppressed dissenting voices.
My hope is that he will read The Perth Group paper ‘HIV – a virus like no other’ one more time and he’ll see there’s no evidence that a pathogenic particle termed HIV exists. And there is no need to read most of the fifty thousand AIDS articles if they fallaciously assert otherwise.
So what happened on April 24 this year — the fundraising event taking place at the Grand Hyatt Hotel in Greenwich, Connecticut?
During the Q&A session, my friend and journalist extraordinaire, Eric Coppolino, was there to put some key questions about the existence of SARS-CoV-2 to RFK Jr.
So let’s take a listen to the exchange that takes place between the two of them on that Sunday afternoon.
Eric Coppolino:
Hi Bobby. Thank you. Christine Massey in Toronto has amassed 182 responses under various Freedom of Information law requests from institutions, provincial, state, and federal, national governments which all say no one has a sample of SARS-C0V-2 taken from a human. Would you please comment on that?
RFK, Jr.:
Yeah, I really am not qualified to comment on it, but … My inclination if there are people who say that viruses don’t exist, that there is no virus… I don’t, you know, my inclination is that that simply is not, you know, that’s not true.
Dr. Sam Bailey:
At least he has admitted that he is relying on inclination, rather than having looked into the evidence himself as he has done with vaccines.
RFK, Jr.:
I can’t argue with you, and I can’t…I actually, on our list there’s a number of people who make those kind of arguments. And other people on the list server…and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.
Dr. Sam Bailey:
It’s hard to know exactly what he’s talking about here. If it’s the same virology papers we’ve been looking at, it is certainly unclear how this constitutes a lot of evidence. In my experience, they are usually reciting the paper’s title without critiquing the methodology, which is where all the problems are.
RFK, Jr.:
I am kind of amused reading the exchanges and my inclination is that viruses do exist and do make people sick. I could be wrong. It could all be a big hoax, but to me, it seems like viruses are real, and … look, I should have just shut up from the beginning and say I’m not gonna answer that question.
Eric Coppolino:
The governments have said they don’t have a sample.
RFK, Jr.:
…You know what? Actually I saw an email exchange yesterday where somebody made exactly that statement and then ten people jumped on him with examples of where that’s not true.
Dr. Sam Bailey:
This was news to me and I know it was news to Christine Massey, coordinator of the SARS-CoV-2 Freedom of Information Project, who demanded the data from the 10 people on Kennedy’s list who claim to prove that the virus had been isolated.
RFK, Jr.:
…The other thing is, I do know this, when you make a freedom of information request, the freedom of information laws do not require the government agency to do science, or to answer questions, specific questions. What they do is, they, the Freedom of Information laws make it obligatory for the government to give you existing documents. So, if you’re telling the government, “I want you to verify this.” They look at their documents and say, “There’s nothing here to verify it.” It doesn’t mean it’s not true. It means they’ve got nothing. But, listen, again, I am not a … scientist. I don’t pretend to be. I find those arguments interesting. And there’s a guy in California, who I deeply respect, Tom Cowan, who makes those arguments and it really… I can’t answer the question.
Dr. Sam Bailey:
This is another interesting statement and perhaps a chance for RFK, Jr. to reflect on the same battle he faces regarding raising awareness about vaccine problems. The mainstream could dismiss RFK Jr.’s arguments as “not being taken seriously by a lot of other people” because the majority of the medical industry still promote all vaccines. However, ‘appeal to popularity’ is a form of faulty reasoning and has no place in a scientific discussion such as this one.
My experience, and I’m sure Tom Cowan and all others in the movement can attest to, is that the majority of people are simply unaware of this debate and don’t even know that questioning the existence of a virus is a thing. And the individuals and corporations that gain from the virus theory often engage in active suppression of the debate.
Prior to widespread internet usage, dissident authors such as The Perth Group were refused publication opportunities in the medical journals. And in the modern era, material such as mine is banned on all the big tech platforms.
The virus theory was put forward in the late 1800s and, for most of us, it is a revelation to go back through the scientific literature and see the key postulants have not been fulfilled .
One of the most amusing, and perhaps tragic, things you’ll see is websites such as AIDSTruth claiming that the science is settled. In 2015 they announced that they were retiring the website because apparently their work was done. The first sentence of their self-congratulatory announcement shows just how disingenuous they are when they use the term ‘AIDS denialism’, knowing very well that what is in dispute is the HIV/AIDS theory or whether an infectious particle, termed HIV, actually exists.
The group also referred to ‘bumps in the early years of treatment’ which is an obscene way to refer to deaths caused by AZT.
In any case, I wonder if the team might consider resurrecting their website or if they are now too busy working on other projects under organizations such as the World Economic Forum and Johns Hopkins.
I think if they do decide to get back into it, they’ll find that the number of individuals and groups opposing their position on the HIV/AIDS theory has gone up dramatically.
Mike Stone of Viroliegy, put together a collection of some of the websites questioning viral theory. And many of them, including Viroliegy itself, have appeared in the last two years.
All the individuals I have personally spoken with, that have or are currently pointing out the flaws in viral theory, they share a number of things in common. Firstly, they all believed in the viral theory at some stage. But when they investigated it for themselves, something changed their minds. Secondly, they have all paid a price whether being publicly censured, smeared or blocked from working in the professions. Thirdly, they are all incredibly generous with their time and share the knowledge with everyone that is interested. And lastly, and perhaps most importantly, they have a passion for exploring the possibilities and following the scientific trail to wherever it takes them by freeing themselves from the shackles of institutional policies, industry capture and public regulatory bodies.
My feeling is that far more people are moving into the questioning the viral theory camp rather than the other way around.
Who knows. Perhaps now that the door has been opened, RFK. Jr. might take more of a look around.
So that we don’t lose touch please find me at drsambailey.com and sign up for my free newsletter.
James Corbett: I Read Bill Gates’ New Book (So You Don’t Have To!)
In an interview with the National Geographic, Tony Fauci made comments about “alternative views” of the origin of the coronavirus. But he was really talking about all unorthodox medical information:
“Anybody can claim to be an expert even when they have no idea what they’re talking about—and it’s very difficult for the general public to distinguish. So, make sure the study is coming from a reputable organization that generally gives you the truth—though even with some reputable organizations, you occasionally get an outlier who’s out there talking nonsense. If something is published in places like New England Journal of Medicine, Science, Nature, Cell, or JAMA—you know, generally that is quite well peer-reviewed because the editors and the editorial staff of those journals really take things very seriously.”
Right you are, Tony.
So, Tony, here is a very serious statement from a former editor of one of those “places,” the New England Journal of Medicine:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
And here is another one, from the editor-in-chief of the prestigious journal, The Lancet, founded in 1823:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness…”
“The apparent endemicity of bad research behaviour is alarming. In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world. Or they retrofit hypotheses to fit their data. Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours. Our acquiescence to the impact factor fuels an unhealthy competition to win a place in a select few journals. Our love of ‘significance’ pollutes the literature with many a statistical fairy-tale…Journals are not the only miscreants. Universities are in a perpetual struggle for money and talent…” (Dr. Richard Horton, editor-in-chief, The Lancet, in The Lancet, 11 April, 2015, Vol 385, “Offline: What is medicine’s 5 sigma?”)
Why stop there? Let’s consult a late public-health expert whose shoes Fauci would have been lucky to shine: Dr. Barbara Starfield, Johns Hopkins School of Public Health.
On July 26, 2000, the US medical community received a titanic shock, when Starfield revealed her findings on healthcare in America.
The Starfield review, “Is US health really the best in the world?”, published in the Journal of the American Medical Association (JAMA), came to the following conclusion, among others:
Every year in the US, correctly prescribed, FDA approved medical drugs kill 106,000 people. Thus, every decade, these drugs kill more than a MILLION people.
On the heels of Starfield’s astonishing findings, media reporting was perfunctory, and it soon dwindled. No major newspaper or television network mounted an ongoing “Medicalgate” investigation. Neither the US Department of Justice nor federal health agencies undertook prolonged remedial action.
All in all, those parties who could have made effective steps to correct this ongoing tragedy preferred to ignore it.
On December 6-7, 2009, I interviewed Dr. Starfield by email. Here is an excerpt from that interview.
Q: What has been the level and tenor of the response to your findings, since 2000?
A: The American public appears to have been hoodwinked into believing that more interventions lead to better health, and most people that I meet are completely unaware that the US does not have the ‘best health in the world’.
Q: In the medical research community, have your medically-caused mortality statistics been debated, or have these figures been accepted, albeit with some degree of shame?
A: The findings have been accepted by those who study them. There has been only one detractor, a former medical school dean, who has received a lot of attention for claiming that the US health system is the best there is and we need more of it. He has a vested interest in medical schools and teaching hospitals (they are his constituency).
Q: Have health agencies of the federal government consulted with you on ways to mitigate the [devastating] effects of the US medical system?
A: NO.
Q: Are you aware of any systematic efforts, since your 2000 JAMA study was published, to remedy the main categories of medically caused deaths in the US?
A: No systematic efforts; however, there have been a lot of studies. Most of them indicate higher rates [of death] than I calculated.
Q: Did your 2000 JAMA study sail through peer review, or was there some opposition to publishing it?
A: It was rejected by the first journal that I sent it to, on the grounds that ‘it would not be interesting to readers’!
—end of interview excerpt—
Physicians are trained to pay exclusive homage to peer-reviewed published drug studies. These doctors unfailingly ignore the fact that, if medical drugs are killing a million Americans per decade, the heraldic published studies on which those drugs are based must be fraudulent. In other words, the medical literature is completely unreliable, and impenetrable.
WHICH IS EXACTLY WHAT THE TWO ESTEEMED MEDICAL EDITORS I QUOTED ABOVE—MARCIA ANGELL AND RICHARD HORTON—ARE SAYING.
If you know a doctor who enjoys sitting up on his high horse dispensing the final word on modern medicine, you might give him the quotes from Dr. Angell and Dr. Horton, instruct him to read them, and suggest he get in touch with Angell and Horton, in order to discover what has happened to his profession.
As in: DISASTER.
But please, continue to believe everything Fauci is saying. He must be right about the “pandemic.” After all, he has a very important position, and he’s on television.
So what if his policies have torpedoed the economy and devastated and destroyed lives across the country?
So what if he accepted, without more than a glance, that fraud Neil Ferguson’s computer projection of 500,000 deaths in the UK and two million in the US? In 2005, Ferguson said 200 million people could die from bird flu. The final official tally was a few hundred.
So what?
Fauci has an important position, and he’s on television.
It is very apparent to anyone looking into the origins of antibodies that the idea of what these entities are in terms of how they look and how they function came well before any attempts to actually purify, isolate, and characterize the assumed particles. Antibodies were (and still are) nothing more than unseen theoretical constructs used to explain chemical reactions created in a lab. These fictional creations reside in the “domain of the invisible spectrum” conjured up by the “lively imagination” of a man named Paul Ehrlich. While there was no direct proof for the existence of these entities, the antibody concept was far too important to the immunological narratives forming around the growing practice of vaccination and the increased acceptance of other unseen entities known as “viruses” to just give it up. As the purification and isolation of antibodies in order to see and study them was an impossible task, researchers sought other methods to attempt to provide indirect evidence for the existence of these theoretical creations.
One man who is credited with providing such evidece is Michael Heidelberger, considered the “Founder of Immunochemistry.” He was the first to apply mathematics to the reaction of antibodies and their antigens. He is also known for “proving” that antibodies are proteins by showing that the antigens of pneumococcus bacteria are polysaccharides (or carbohydrates). Here is a brief overview of his work:
“Avery and Dochez’s initial characterization of this pneumococcal substance showed that it was resistant to both heat and trypsin—features unbefitting most proteins—but that it did contain nitrogen, a component of proteins. But its true nature was not revealed until 1923, when Michael Heidelberger—then in the chemistry department synthesizing drugs against poliomyelitis and African sleeping sickness—teamed up with Avery.
The more they purified the reactive substance the less nitrogen it contained. When it was virtually nitrogen-free, recalled Heidelberger in a 1979 article, Avery ventured a guess: “Could it be a carbohydrate?” (2). Chemical analysis confirmed its sugary character, and subsequent studies of other pneumococcal serotypes revealed that each bacterial capsule had a distinct polysaccharide signature. It was this signature that dictated the serological specificity of the organism. The duo published these findings in two articles in the Journal of Experimental Medicine (3, 4).
Their results were met with considerable skepticism, as it was then thought that only proteins could incite a specific immune response. “Nobody believed it,” says Emil Gotschlich (Rockefeller University), whose later work on polysaccharide-based vaccines stemmed in large part from Heidelberger and Avery’s discoveries. “It took them a lot of effort to convince people that the polysaccharide was the immunoreactive component.”
Antibodies solidified
Heidelberger and Avery’s discovery came at a time when antibodies were regarded—by those who believed they existed at all—as mysterious substances that floated around in serum. “It appeared to me that there was a crying need to determine the true nature of antibodies,” wrote Heidelberger in 1979, “and that until this was done there could be no end to the polemics and uncertainties that were plaguing immunology” (2). Heidelberger later purified the antibodies from his precipitin reactions and showed that they themselves were proteins. As a result, says friend and colleague Victor Nussenzweig (New York University), “there were no more mystical ideas about what antibodies were.”
Heidelberger and his postdoctoral fellow Forrest Kendall later quantitated the precipitin reaction (5), bringing much-needed mathematics to the study of antibody–antigen interactions and lifting antibodies even further out of the realm of the mysterious (see the next “From the Archive”).”
Heidelberger hard at work using his microscopic vision.
Two of Heidelberger’s papers are most often cited as the proof that antibodies are proteins. The first is a paper he did with Oswald Avery in 1923. It is used as proof that the pneumococcus antigens are carbohydrates. However, was this paper successful in drawing this conclusion? Presented here are some highlights from their collaboration:
“In 1917 Dochez and Avery (1) showed that whenever pneumococci are grown in fluid media, there is present in the cultural fluid a substance which precipitates specifically in antipneumococcus serum of the homologous type. This soluble substance is demonstrable in culture filtrates during the initial growth phase of the organisms; that is, during the period of their maximum rate of multiplication when little or no cell death or disintegration is occurring. The formation of this soluble specific material by pneumococci on growth in vitro suggested the probability of an analogous substance being formed on growth of the organism in the animal body.
Examination of the blood and urine of experimentally infected animals gave proof of the presence of this substance in considerable quantities in the body fluids following intraperitoneal infection with pneumococcus. In other words, this soluble material elaborated at the focus of the disease readily diffuses throughout the body, is taken up in the blood, passes the kidney, and appears in the urine unchanged in specificity. Similarly, a study of the serum of patients suffering from lobar pneumonia has revealed a substance of like nature in the circulating blood during the course of the disease in man. Furthermore, examination of the urine of patients having pneumonia due to pneumococci of Types I, II, and III has shown the presence of this substance in some stage of the disease in approximately two-thirds of the cases.
Recently from filtered alkaline extracts of pulverized bacteria of several varieties, including pneumococci, Zinsser and Parker have prepared substances which appear free from coagulable protein. These substances, called “residue antigens,” are specifically predpitable by homologous antisera. These observers consider these acid- and heat-resistant antigenic materials analogous to the soluble specific substance of pneumococcus described by Dochez and Avery. In spite of the fact that these “residue antigens” are precipitable by homologous sera produced by immunization with the whole bacteria, Zinsser and Parker have so far failed to produce antibodies in animals by injecting the residues.
In the earlier studies by Dochez and Avery certain facts were ascertained concerning the chemical characteristics of this substance. It was found that the specific substance is not destroyed by boiling; that it is readily soluble in water, and precipitable by acetone, alcohol, and ether; that it is precipitated by colloidal iron, and does not dialyze through parchment; and that the serological reactions of the substance are not affected by proteolytic digestion by trypsin. Since the substance is easily soluble, thermostable, and type-specific in the highest degree, it seemed an ideal basis for the beginning of a study of the relation between bacterial specificity and chemical constitution. The present report deals with the work done in this direction.
Experimental
The organism used in the present work was Pneumococcus Type II. The most abundant source of the soluble specific substance appeared to be an 8 day autolyzed broth culture; hence this material was used as the principal source of supply. For comparison dissolved pneumococci and lots of urine containing the specific substance were also worked up, with essentially the same results, as will be seen from Table I.
The process for the isolation of the soluble specific substance consisted in concentration of the broth, precipitation with alcohol, repeated re-solution and reprecipitation, followed by a careful series of fractional precipitations with alcohol or acetone after acidification of the solution with acetic acid, and, finally, repeated fractional precipitation with ammonium sulfate and dialysis of the aqueous solution of the active fractions.
Five lots of 15 liters each of 8 day cultures of Pneumococcus Type II in meat infusion phosphate broth are each concentrated on the water bath in large evaporating dishes to 1,000 to 1,200 cc. and precipitated in a separatory funnel by the gradual addition, with vigorous rotation, of 1.2 volumes of 95 per cent alcohol.The mixture separates into two layers, and is allowed to stand over night, or for several hours.
The upper layer, which is almost black and comprises the largest part of the mixture, contains only traces of the soluble specific substance, and is siphoned off and discarded. The lower, more viscous layer is run into a 250 cc. centrifuge bottle (occasionally a second will be required), capped, and rotated at high speed for ½ hour. Three layers are formed, of which the uppermost is merely a further amount of the liquid previously discarded. The middle layer consists of a compact, greenish cake of insoluble matter and gummy material, and contains most of the soluble specific substance. The bottom layer, from which salts often separate, is a brownish syrup rich in salts and nitrogenous matter and relatively poor in specific substance, and can, by careful manipulation, be poured off to a large extent.
Although a small proportion of the specific substance is lost if this syrup is discarded, its elimination represents so considerable a purification as to warrant the sacrifice of the active material contained. The gummy cake remaining in the centrifuge bottle, together with adhering salts and syrup, is now rinsed out and ultimately combined with similar material from the other lots, All of this is then dissolved as completely as possible in water, care being taken to break up the many lumps of gummy material, diluted to 1 liter, and again precipitated with alcohol. In this case about 1.3 liters are required to precipitate all but the last traces of active material from the upper layer. This is again discarded and the lower layer treated as before. At this stage there is relatively less of the bottom layer, and it is more difficult to separate it from the cake containing the specific substance, but as much as possible is removed. The remaining material is smoothed out with water, diluted to about 500 cc., and centrifuged. The precipitate is washed twice with water, and the washings are combined with the main solution. The still turbid liquid, the volume of which should be about 750 cc., is put through the alcohol purification process a third time, about 1.1 liters of alcohol being required. After having been centrifuged, the active material is again dissolved in water, made definitely acid to litmus with acetic acid, and again centrifuged. The precipitate is washed three times with water acidulated with acetic acid, and the filtrate and washings are combined in a separatory funnel and diluted again if necessary to 750 cc. Acetone (redistilled) is now added until a permanent precipitate forms, about 250 c¢. being necessary. The precipitate is allowed to settle, whereupon the lower part of the mixture containing the precipitate is drawn off and centrifuged. The clear superuatant fluid is restored to the main solution, while the precipitate, which consists largely of insoluble material and gives an aqueous solution almost devoid of activity, is discarded.
Fractional precipitation is continued, and even when the specific substance appears in quantity in the precipitate, it is occasionally possible to separate a lower, inactive, syrupy layer, as in the previous purifications by alcohol. Addition of acetone is continued until a test portion, heated on the water bath to remove acetone, diluted with saline, and neutralized, no longer gives a precipitate with immune serum, after which the upper layer may be discarded. The active precipitates are then redissolved in water, centrifuged again, and the supernatant liquid is diluted to 375 cc., reacidified with acetic acid, and again fractionated with acetone. If inactive fractions are obtained, the process is again repeated until no further purification results. Alcohol may be used for these fracfionations instead of acetone, the only difference being that a somewhat larger proportion is required. The active material is then dissolved in about 150 cc. of water and again made definitely acid with acetic acid. The solution is treated with solid ammonium sulfate until the first slight precipitate forms. This is generally inactive, and if so, may be discarded.
Finally, ammonium sulfate is added to saturation, completely precipitating the specific substance if the volume of the solution is not too great. The mixture is allowed to stand for several hours and is then centrifuged and the precipitate washed with a little saturated ammonium sulfate solution. It is redissolved in about 75 cc. of water acidified with acetic acid, centrifuged if necessary, and again precipitated by saturation with ammonium sulfate. Finally, the specific substance so obtained is dissolved in water and dialyzed first against running tap water in the presence of chloroform and toluene, and finally against distilled water until tests for sulfate and phosphate ion are negative. Addition of acetic acid during the early stages of the dialysis assists in the removal of calcium, which otherwise forms a large part of the ash.
The dialyzed solution is concentrated to dryness on the water bath and the residue redissolved in hot water. If the solution is not perfectly clear, it is centrifuged again before being evaporated to dryness, and the whole process is repeated as long as insoluble material separates. Toward the end of the final concentration absolute alcohol may be added to assist in the precipitation of the substance.
Variations in the exact volumes given are often necessary with different lots of broth, but this will occasion little difficulty if all fractionations are controlled by the specific precipitin test.
As so obtained the soluble specific substance forms an almost colorless varnish-like mass which may be broken up and dried to constant weight at 100°C. in vacuo. The yield from 75 liters of broth averages about 1 gin., although it varies within rather wide limits in individual lots.
By the method outlined above all substances precipitable with hosphotungstic acid or capable of giving the biuret reaction were eliminated. The residual material (Preparation 17, in Table I), for which no claim of purity is made, as efforts at its further purification are still under way, contained, on the ash-free basis, 1.2 percent of nitrogen. It was essentially a polysaccharide, as shown by the formation of 79 percent of reducing sugars on hydrolysis, and by the isolation and identification of glucosazone from the products of hydrolysis.”
“Table I represents a summary of the reactions of some of the earlier preparations worked with, as well as the later ones. Preparation 4 was obtained from the urine of a patient with a Type II pneumococcus infection, while No. 8 was obtained from an antiforrain solution of the pnemnococci. In both of these cases, as well as in Nos. 9, 11, and 15, the method of purification given above had not been fully worked out.
Attempts to stimulate antibody production by the immunization of animals with the purified substance yielded negative results.
Discussion.
While it has long been known that the capsular material of many microorganisms consists, at least in part, of carbohydrates, any connection between this carbohydrate material and the specificity relationships of bacteria appears to have remained unsuspected. While it cannot be said that the present work establishes this relationship, it certainly points in this direction. Evidence in favor of the probable carbohydrate nature of the soluble specific substance is the increase in specific activity with reduction of the nitrogen content, the increase in optical rotation with increase in specific activity, the parallelism between the Molisch reaction and specific activity, the high yield of reducing sugars on hydrolysis, and the actual isolation of glucosazone from a small quantity of the material. The small amounts of substance available up to the present have hindered the solution of the problem, and it is hoped that efforts at further purification of the soluble specific substance, now in progress with larger amounts of material, will definitely settle the question.
Summary.
A method is given for the concentration and purification of the soluble specific substance of the pneumococcus.
The material obtained by this method is shown to consist mainly of a carbohydrate which appears to be a polysaccharide built up of glucose molecules.
Whether the soluble specific substance is actually the polysaccharide, or occurs merely associated with it, is still undecided, although the evidence points in the direction of the former possibility.”
A beautiful mind?
Heidelberger’s original 1923 paper can hardly be claimed to be the slam-dunk proof that bacteria antigens are carbohydrates. For starters, Heidelberger admitted that he was unsure if the presumed “antigen” substance was a carbohydrate or if it was merely associated with it. Even more importantly, he could not produce any antibody response upon injecting his presumed antigen into animals. This would indicate that the substance was not an antigen whatsoever as antigens are specifically defined as “a toxin or other foreign substance which induces an immune response in the body, especially the production of antibodies.” Thus, it seems rather odd to assume antibodies are proteins based off of this work, but assume they did:
“Since the pneumococcal capsular antigen was a polysaccharide, and antibodies were thought to be proteins, Heidelberger realized that by measuring the amount of protein in specific precipitates made with the capsular antigen he could determine their antibody content. Together with Forrest Kendall, who had joined the Heidelberger lab, the protein content of immune precipitates was determined by measuring total nitrogen, using the Kjeldahl procedure that came to be the hallmark of laboratories carrying out Heidelberger-type quantitative immunochemistry.”
Since they assumed the pneumococci bacteria was a polysaccharide, that meant any nitrogen left over was the antibody content. Based on the 1923 paper, this seems to be a rather falicious premise to build from. In any case, Heidelberger carried on with his assumption and it can be seen by this second paper from 1929 how Heidelberger came to his conclusion using the precipitin test and mathematics as proof that antibodies exist. I edited out the long mathematical sections with his equations so if you are interested in Heidelberger showing his work, I recommend reading the full paper. Highlights below:
A Quantitative Study of the Precipitin Reaction Between Type III Pneumococcus Polysaccharide and Purified Homologous Antibody*
“Of all the reactions of immunity the precipitin test is perhaps the most dramatic and striking. While other immune reactions are more delicate, the precipitin test is among the most specific and least subject to errors and technical difficulties. Attempts at its quantitative interpretation and explanation have been hampered either by the difficulty of finding suitable analytical methods or by the failure to separate the reacting substances from closely related, non-specific materials with which they are normally associated.
With the aid of recent work it has been found possible to avoid these difficulties to some extent. The isolation of bacterial polysaccharides which precipitate antisera specifically and possess the properties of haptens has not only afforded one of the components of a precipitin reaction in a state of comparative purity, but has greatly simplified the analytical problem. Since many of these polysaccharides contain no nitrogen, and antibodies presumably are nitrogenous, the latter may be determined in the presence of any amount of the specific carbohydrate. Moreover, Felton’s method for the separation of pneumococcus antibodies from horse serum not only permits the isolation of a high proportion of the precipitin, freed from at least 90 percent of the serum proteins and much of the serum lipoid, but is also applicable on a sufficiently large scale to furnish the amounts of antibody solution needed to make quantitative work possible. It is realized that antibody solutions of this type do not contain pure antibodies–indeed, only 40 to 50 percent of the nitrogen is specifically precipitable–but since so small a proportion of the original serum protein remains with the antibody a far-reaching purification actually has been effected. It should thus be possible with the aid of antibodies purified by Felton’s method to obtain data of a preliminary character which should point toward the mechanism of the reaction. The present paper is concerned with such data obtained in a quantitative study of the precipitin reaction between the soluble specific substance of Type III pneumococcus and Type III pneumococcus antibody solution.
Experimental
1. Materials and Methods.–a. Solutions of Soluble Specific Substance, Type Ill Pneumococcus.–The soluble specific substance of Type III pneumococcus used was kindly supplied by Drs. O. T. Avery and W. F. Goebel of The Rockefeller Institute for Medical Research. It was ash-free, contained 0.04 percent of nitrogen, and showed a/d = -32 °. A weighed amount of anhydrous substance was suspended in 0.9 percent saline, dissolved with the aid of 0.1 normal sodium hydroxide, and the solution was diluted with saline, adjusted to pH 7.6 and made up to volume with saline to yield a 1 percent solution. This was sterilized in the autoclave and used as a stock solution for making up other dilutions. These were prepared with sterile saline under aseptic precautions, and were kept in the ice-box.
b. Type III Pneumococcus Antibody Solution.–The antibody solutions used were prepared essentially according to Felton’s procedure (loc. cit.) from Type III antipneumococcus horse serum containing no preservative and supplied by the New York State Department of Health through the courtesy of Dr. A. B. Wadsworth and Dr. Mary B. Kirkbride. 100 to 200 cc. of serum were stirred slowly into 20 volumes of ice-cold water containing 9.5 cc. of molar potassium dihydrogen phosphate and 0.5 cc. of molar dipotassium hydrogen phosPhate per liter. The final pH varied from 5.6 to 6.3. After standing over night in the cold the supernatant was decanted and the precipitate was centrifuged off in the cold and dissolved in a volume of chilled 0.9 percent saline equal to that of the serum taken. 0.1 normal hydrochloric acid was then added until a precipitate no longer formed on dilution of a test portion with two volumes of water, after which 0.1 normal sodium hydroxide solution was added until a slight precipitate again formed on dilution. In general, 5 cc. of acid and 1.5 cc. of alkali per 100 cc. of serum were satisfactory, although as Felton emphasizes, different lots vary and no absolutely definite procedure can be given. In the present work the process of purification was followed either by testing the agglutinating power of the fractions against a heat-killed Type III pneumococcus vaccine, or by the precipitin reaction, or by both methods. After addition of the alkali the opalescent solution was diluted with 2 volumes of water and centrifuged in the cold. The almost inactive precipitate was discarded and the supernatant poured into 6.7 volumes of the chilled buffer solution previously used, (equivalent to 20 times the volume of saline employed), also adding enough 0.1 normal sodium hydroxide to neutralize the remaining acid. The resulting precipitate was collected and dissolved in a volume of 0.9 percent saline equal to that of the serum taken, and the pH was adjusted to 7.6. The solution was sterilized by passage through a Berkefeld N grade filter which previously had been washed with saline containing a drop of normal sodium hydroxide, followed by saline alone.
Antibody solutions prepared in this way were found to be rather unstable under the usual conditions of the precipitin test, and it therefore was necessary to subject them to a preliminary “ageing” treatment in order that control solutions might be relied upon to remain clear. This consisted in immersing the solution in a water bath at 37 ° for 2 hours, letting stand in the ice-box over night, centrifuging off the precipitate which usually formed, readjusting the pH if necessary, and filtering through a Berkefeld candle prepared as above. This treatment was repeated as many times as necessary, but the solutions usually remained clear after the second incubation at 37 °. Much time was lost and very inconstant results were obtained until “ageing” was resorted to.
The relative antibody content of the resulting solutions was estimated by determining the agglutination titer against a single heat-killed Type III pneumococcus suspension.
It will be seen from Table I that the agglutination titer and the maximum amount of protein precipitable by the type III polysaccharide ([total N–N in supernatant] X 6.25) are approximately proportional. The latter may therefore be taken as a more definite, though not necessarily more accurate, measure of the actual antibody content of the solutions.
It is also evident that the antibody in all of these solutions has been purified to approximately the same extent, since the ratios of protein precipitable by SSS III to total protein are not very different.”
Discussion
“For purposes of discussion it will be assumed with Felton (lot. cir.) that antibody is ,modified protein, and that, in order to provide a uniform method of measurement, it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25. Since only relative values are under consideration, the actual magnitude of the factor used is of little significance so long as it be used throughout. Moreover, Table I shows a correspondence between this measure of antibody content and the agglutination titer, so that its use as a relative measure is independent of the nature of Type III pneumococcus antibodies.
doi: 10.1084/jem.50.6.809.
The Precipitin Reaction
In Summary:
Michael Heidelberger teamed up with Oswald Avery to characterize a “soluble specific substance” found in pneumococcal bacteria that fell out of solution when incubated with type-specific antisera
When it was virtually nitrogen-free, recalled Heidelberger in a 1979 article, Avery ventured a guess: “Could it be a carbohydrate?”
Chemical analysis confirmed its sugary character, and subsequent studies of other pneumococcal serotypes revealed that each bacterial capsule had a distinct polysaccharide signature
It was this signature that dictated the serological specificity of the organism
Their results were met with considerable skepticism, as it was then thought that only proteins could incite a specific immune response
According to polysaccharide-based vaccine specialist Emil Gotschlich: “Nobody believed it. It took them a lot of effort to convince people that the polysaccharide was the immunoreactive component.”
Heidelberger and Avery’s discovery came at a time when antibodies were regarded—by those who believed they existed at all—as mysterious substances that floated around in serum
“It appeared to me that there was a crying need to determine the true nature of antibodies,” wrote Heidelberger in 1979, “and that until this was done there could be no end to the polemics and uncertainties that were plaguing immunology”
Heidelberger and his postdoctoral fellow Forrest Kendall later quantitated the precipitin reaction, bringing much-needed mathematics to the study of antibody–antigen interactions and lifting antibodies even further out of the realm of the mysterious
In 1917 Dochez and Avery showed that whenever pneumococci are grown in fluid media, there is present in the cultural fluid a substance which precipitates specifically in antipneumococcus serum of the homologous type
It was assumed that the formation of this soluble specific material by pneumococci on growth in vitro suggested the probability of an analogous substance being formed on growth of the organism in the animal body
Examination of the urine of patients with pneumococci showed the substance in only approximately 2/3rds of the samples
Zinsser and Parker found similar substances with other bacteria and believe that the substances are the same as that of the pneumococci
In spite of the fact that these “residue antigens” are precipitable by homologous sera produced by immunization with the whole bacteria, Zinsser and Parker failed to produce antibodies in animals by injecting the residues.
The process for the isolation of the soluble specific substance consisted in:
Concentration of the broth
Precipitation with alcohol
Repeated re-solution and reprecipitation
A careful series of fractional precipitations with alcohol or acetone after acidification of the solution with acetic acid
Repeated fractional precipitation with ammonium sulfate and dialysis of the aqueous solution of the active fraction
For a complete step-by-step breakdown of the numerous chemical-altering procedures done to the sample, see the highlighted tan section of the paper provided above
Even with the numerous “purification” steps, the obtained soluble specific substance formed an almost colorless varnish-like mass
The residual material for which no claim of purity was made, as efforts at its further purification were still under way, contained, on the ash-free basis, 1.2 percent of nitrogen.
It was considered essentially a polysaccharide
The method of purification given had not been fully worked out for many of the preparations
Attempts to stimulate antibody production by the immunization of animals with the purified substance yielded negative results
While it had long been known that the capsular material of many microorganisms consists, at least in part, of carbohydrates, any connection between this carbohydrate material and the specificity relationships of bacteria remained unsuspected
While it could not be said that their work established this relationship, they felt it certainly pointed in that direction
The small amounts of substance available hindered the solution of the problem, and it was hoped that efforts at further purification of the soluble specific substance with larger amounts of material would definitely settle the question
Whether the soluble specific substance is actually the polysaccharide, or occurs merely associated with it, was left undecided
Heidelberger acknowledged that the precipitin test he used during this experiment has 2 drawbacks:
Quantitative interpretation/explanation is difficult due to lack of a suitable analytical method
Failure to separate out the reacting substances from non-specific material which these substances are closely related to and associated with
He stated that it was possible to avoid these failures to some extent
It is presumed that antibodies are nitrogenous
Only 90% of the precipitin can be freed from serum proteins and “much” of the lipoid
Heidelberger admitted that these are not pure antibodies and that only 40-50% of nitrogen is precipitable while small amounts of serum remain
The antibody solutions used were prepared essentially according to Felton’s procedure from Type III antipneumococcus horse serum containing no preservative and supplied by the New York State Department of Health through the courtesy of Dr. A. B. Wadsworth and Dr. Mary B. Kirkbride
100 to 200 cc. of serum were stirred slowly into 20 volumes of ice-cold water containing 9.5 cc. of molar potassium dihydrogen phosphate and 0.5 cc. of molar dipotassium hydrogen phosphate per liter
The final pH varied from 5.6 to 6.3
After standing over night in the cold the supernatant was decanted and the precipitate was centrifuged off in the cold and dissolved in a volume of chilled 0.9 percent saline equal to that of the serum taken
0.1 normal hydrochloric acid was then added until a precipitate no longer formed on dilution of a test portion with two volumes of water, after which 0.1 normal sodium hydroxide solution was added until a slight precipitate again formed on dilution
In general, 5 cc. of acid and 1.5 cc. of alkali per 100 cc. of serum were satisfactory, although as Felton emphasized, different lots vary and no absolutely definite procedure can be given
After addition of the alkali the opalescent solution was diluted with 2 volumes of water and centrifuged in the cold
The almost inactive precipitate was discarded and the supernatant poured into 6.7 volumes of the chilled buffer solution previously used, (equivalent to 20 times the volume of saline employed), also adding enough 0.1 normal sodium hydroxide to neutralize the remaining acid
The resulting precipitate was collected and dissolved in a volume of 0.9 percent saline equal to that of the serum taken, and the pH was adjusted to 7.6
The solution was sterilized by passage through a Berkefeld N grade filter which previously had been washed with saline containing a drop of normal sodium hydroxide, followed by saline alone
Antibodies were found to be unstable during testing so they were put through preliminary “ageing” processes as many times as needed until they got the result they wanted
Much time was lost and very inconstant results were obtained until “ageing” was resorted to.
The relative antibody content of the resulting solutions was estimated by determining the agglutination titer against a single heat-killed Type III pneumococcus suspension
For purposes of discussion it was assumed with Felton that antibody is modified protein, and that, in order to provide a uniform method of measurement, it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25
There is no need to spend any more time on the rest of Heidelberger’s paper as he admitted he assumed antibodies were protein and could be expressed as nitrogen thus he did not prove anything
Why would monoclonal antibodies not form a precipitate?
It is rather obvious that many assumptions were made about a substance (antibodies) for which the researchers could not see. Michael Heidelberger assumed that antibodies are modified proteins and nitrogenous. He assumed that it may be expressed as nitrogen precipitable by specific polysaccharide, multiplied by 6.25. He assumed that the failure of the precipitin test to separate out the reacting substances from non-specific material which these substances are closely related to and associated with could be somewhat avoided to some extent. He assumed that his earlier work with the pneumococcus bacteria was accurate and that he had proved the antigen component was a carbohydrate even though he was unable to produce any antibody response upon immunizing animals using his supposed antigen. Maybe this lack of any antibody response to his “antigen” has to do with the fact that, according to the WHO, the pneumococcus bacteria is regularly found in healthy people?
“Infection is acquired mainly through pneumococci contained in respiratory droplets. There are many healthy, asymptomatic carriers of the bacteria but no animal reservoir or insect vector.”
If an antigen is a toxin or foreign substance which produces an immune response creating antibodies, the pneumococci bacteria doesn’t meet that definition at all. If it isn’t an antigen, then the pneumococcus “antigen” would not be carbohydrates as described in Heidelberger’s 1923 paper. This would mean that Heidelberger’s 1929 paper measuring any of the remaining protein content, calculating the amount, and claiming the resulting protein mass as antibodies is essentially meaningless. Can you see the problem with assuming things to be true without ever proving this to be the case?
The conclusions drawn by Heidelberger were born out of chemistry experiments and reactions using the precipitin test which have no bearing on reality while using mathematical equations attempting to quantify the unquantifiable. Whether or not these indirect experiments and assumptions provide proof that antibodies exist and are proteins, I leave up to the reader. However, keep in mind that no antibodies had ever been seen nor proven to exist by proper purification and isolation up to that time and that still holds true to date. This work is based off of theoretical explanations of immunity for which nothing could be observed. Heidelberger’s indirect chemical reactions and equations provided no direct evidence for the existence of anything other than non-specific precipitate.
Dr. Tom Cowan has recently created a series of videos where he takes a close look at what some leaders in the anti-covid-vax arena are presenting as science. Dr. Cowan’s videos can be found at his Rumble and BitChute channels.
For those of you who listen to a lot of alternative “anti-vax” presentations about the origins of SARS-CoV-2 and end up feeling that you’ve just listened to a lot of faux-science gobbledygook, you’re not alone.
Below, Truth Comes to Light has clipped two key segments from the longer video where Dr. Cowan looks into Dr. Judy Mikovits’ presentations and papers related to SARS-C0V-2. Dr. Tom Cowan’s full video is also found below.
“Science has become the enterprise of people using words and concepts to make things, that everybody otherwise would understand, basically incomprehensible.”
“There are some basic ways that all of us — men, women, human beings — understand the world. It’s very clear and simple to us. And if we applied that same thinking to subjects in science and biology and medicine I think it would be fairly easy for us to find our way and to see what’s true and what isn’t true.
The problem has become that so-called scientists, especially virologists and medical doctors, have made the whole thing so confusing that most people seem to lose their bearings as far as understanding just the usual, common sense, logical, rational way of thinking and end up believing something that they wouldn’t possibly believe if they really understood the issues.”
“I’m not anti-vaccine. I just want them to be safer and more effective.”
I love that statement. It’s a lullaby. When I can’t go to sleep at night, I just repeat it to myself a few times, and I’m out cold.
It’s typical of half a revolution, which never wins.
For the past 32 years, I’ve presented overwhelming evidence that no vaccine was ever safe or effective. The whole “science” of vaccination is a rank fraud.
But stuffed-shirt journalists, who sort of go against the grain while maintaining a front of respectability, don’t want to venture that far. They know the price they’ll have to pay. They’re hedging their bets.
Occasionally, one of them will take a swipe at me. It cements their position as middle of the road. Which is where they want to be.
Except, liberty and freedom, which is what we’re fighting for, against a global coup by mass medical murders, isn’t something you win in the middle of the road.
You don’t win by trying to come off like a Washington Post reporter who just happens to have different and dissenting ideas. That’s what half-ass looks like.
That sort of person is basically saying, “I have a machine mind like other machine minds. The difference is, I’m inputting different data and therefore drawing different conclusions. If you, too, have a machine mind, read what I write and let’s establish truth and justice…”
The long-term effect of that is like pissing through a fire hose to put out a conflagration taking down a city.
This is simple. If one group of “superior” machine minds wins against another group of machine minds—regardless of which issues come out on top—there is no revolution. LIFE AND FREEDOM have been excised out of the equation.
A considerable amount of money and effort have gone into building a modern culture composed of what looks like science and rationality, but isn’t. It’s a cartoon. A fucking cartoon.
There’s no JUICE in it.
That’s why I use the phrase machine-minds. Minds that calculate and process and collate and compare and then exude “better answers.” This is your educated class. Careful, cautious. Circumspect.
“Delivery, sir. Here are flowers you ordered. I’m sorry they’re dead.”
“I don’t mind dead. But I ordered roses and you brought me tulips. I can prove it. Let me just find the receipt here on my cell phone. And then I can show you these withered blossoms are actually tulips. There are 32 differences between the two types of flowers…”
That’s your educated class.
See, I’ve been at this for 38 years. Reporting. Writing. Actually, I’ve been writing for 66 years. I’ve made the cases I wanted to make. I’ve shoved the evidence in people’s faces. The overall medical cartel is waging a VERY successful war against the people.
You have to turn that evidence with torque, with leverage, into a flamethrower. You’re not just trying to set the record straight and bring in truth, you’re using the truth to crash the gold-plated systems of machine minds.
Those minds are remote. Distant. Distant is where Big Tech domeheads operate from. They profile, they plan, they crunch trillions of pieces of data, and they develop strategies to build a civilization that looks like their minds and their computers.
When one of these high-IQ blown dry characters develops his version of a conscience, and turns whistleblower, he’s a hero to his ilk. He speaks their language. He thinks the way they do. He geeks like they geek.
If I have to guess which guy has more freedom in his belly and his brain, I’m going with the man who lives up in the hills of Tennessee with a shotgun and a dog. If he doesn’t like what I’m writing, I might think about his reasons for a half-hour. Whereas, when an “alt. journalist” claims I’m “going too far,” I know exactly what his game is. He’s spraying his usual brand of sanitizing respectable room-deodorant.
I’ll put this another way. Two men are discussing how to choose a wife. They’re looking at two different lists of characteristics a man should consider and check. But neither man mentions LOVE, so it doesn’t matter which list they decide is superior. They don’t know what love is. What they’re really discussing are machine-thoughts.
If the COVID narrative had never been launched, if we were living now as we did in 2018, we would still have a medical cartel taking away our freedom and killing and maiming an extraordinary number of people. And that will still be the case, even if all COVID mandates and restrictions are defeated.
Plus, the Brave New World on the drawing boards is fronted by medical people. Three of its main features are genetic engineering, nanotechnology, and human-computer interfaces and hybrids. If you think all possible freedom is now under fire, you haven’t seen anything yet.
Way back when, I was briefly trained in two schools. The first was formal logic, taught by a beloved college professor with an extraordinarily sophisticated mind and a huge heart. The second school consisted of two or three encounters with Ida Honorof, activist and author. She was barely five feet tall, and she had the energy, in her 70s, of ten tigers. She explained to me one afternoon, on a street corner, that officials in Los Angeles were spraying a version of deadly Agent Orange in the Angeles National Forest. She handed me a few pounds of corporate and government documents detailing the massive toxicity of a variety of pesticides. She kick-started my life as a reporter.
Neither one of these people engaged in coddling. They didn’t sit around planning their fronts and poses of respectability. They didn’t want half a revolution. They didn’t equivocate.
I’ve never been a big fan of equivocation. I’m over at the I-don’t-give-a-shit end of the spectrum.
Find answers—then shove in all your chips. At the end of the night, don’t leave anything on the table.
Fortunately for all of us, there is a life after this one. But we’re here now, so we’re fighting.
Make it COUNT.
In the wind and the rain and the storm, issue no apologies.
TORONTO: The Justice Centre has engaged lawyer Phillip Millar to represent serving members of the Canadian Armed Forces (CAF) who have declined the Covid vaccine on the basis of health concerns or conscientious objections. One of client, Warrant Officer James Topp, is a member of the CAF reserve force facing the charge of “Conduct to the Prejudice of Good Order and Discipline,” which has the potential to result in Court Martial. The Justice Centre also represents 15 other CAF members facing discipline and possible job loss over mandatory Covid vaccine policies implemented by the military.
Mr. Topp, who has been a serving member of the CAF for 28 years, has gained national headlines for his 4,293 kilometre “Canada marches” walk across the country, in protest of mandatory vaccine mandates, forced quarantines, mandatory testing, and other conditions of employment or provision of services.
Mr. Topp began his march on February 20, the same day police forces began using physical force against unarmed Freedom Convoy protesters in Ottawa. Facing job loss for refusing a Covid shot, Mr. Topp is averaging 30 km a day along the highway. His goal is to reach the Tomb of the Unknown Soldier in Ottawa by June 22.
Mr. Topp says government overreach has spread into all aspects of the personal lives of Canadians. “I’m not here for profit, and I don’t want to be a celebrity, but I need to do something,” Mr. Topp told about 100 supporters in Vancouver, who came out on a cold winter day to see him off on his march. “We need to do something to repair us because we’ve been deeply fractured by what has happened…” He adds, “We have to “ensure our government upholds the laws that support Canada’s Charter of Rights and Freedoms.”
Mr. Millar will represent Mr. Topp and 15 other military members in Federal Court, seeking an injunction against the release of CAF members until their grievances are heard. The Justice Centre maintains that military members are entitled to have their constitutional freedoms such as freedom of religion and conscience protected, as CAF members have fought and served to protect the freedoms of all Canadians.
Mr. Millar is a former full-time Combat Officer in the CAF Infantry, former Assistant Crown Attorney, and experienced trial lawyer who has already successfully sued the Department of National Defence (DND) in the past.
“The mandatory vaccine is a flawed policy based on a stubborn refusal to acknowledge that the underlying justification for the mandate has changed. The government is using the Canadian Armed Forces as a policy arm to promote its vaccine mandates. The policy hurts the operational effectiveness, morale, and integrity of the system,” says Mr. Millar.
He notes that the “military chain of command is fast-tracking the release of service members who refuse to get vaccinated under administrative processes, trampling their rights and denying them due process by sidestepping the proper procedures.”
“The DND cannot claim that service members are disobeying a lawful order and then refuse to allow the issue to be tried in the military justice system where a judge can make a determination if it is in fact a “lawful order”,” adds Mr. Millar.
The government is using a “5F release,” which was never meant to be applied in this manner.
“We cannot let them get away with ruining the lives and careers of dedicated Canadians who serve their country. Our soldiers, sailors and air force personnel deserve more. They are highly trained, and many have served their country for years,” Mr. Millar concludes.
“Covid ‘vaccines’ caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.”
This week MEP Christine Anderson (AfD) gave her first speech before the European Union’s new “COVID-19 inquiry committee”. The German MEP condemned the EU’s Covid policies and demanded an investigation into the clear human rights violations under the pretext of combatting a virus.
Anderson railed against the “false claims regarding the safety of the vaccines, their alleged definitive approval, and so-called effectiveness.” The MEP pointed out that the European Medicines Agency (EMA) database shows that in seven months, the Covid “vaccines” caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.
“Why isn’t that being investigated,” questioned the MEP. She explained that the government’s Covid policies had nothing to do with public health. Instead, it seems it has been “a money-making exercise for the pharmaceutical industry.”
Why were alternative methods to fight Covid not investigated or given to the public, questioned Anderson? Instead, she exclaimed, everything in your whole Covid policy “boiled down solely to: “vaccinate, vaccinate, vaccinate.”
Issues Committee Must Address
Anderson pointed out other issues that the committee must investigate. She first zeroed in on the “implementation of vaccine contracts.” Little information is available on vaccine makers’ contracts due to the committee withholding the information. She questioned how she could “properly do her job as an elected MEP” and educate her constituents without the data.
The massive “restrictions of fundamental rights that are unworthy of a democracy” must also be investigated, exclaimed the MEP. “From job losses, discrimination and marginalization, we have experienced a redefinition of fundamental rights.” According to the new definition, our rights are now privileges to which the government picks and chooses who to grant them.
The MEP demanded answers as to why the committee is not investigating the “marginalization and criminalization of critics” who condemned their “anti-democratic measures.”
She went on to say that it is unacceptable for the World Health Organization (WHO) to sign new contracts with EU member states. As Anderson has previously explained, the WHO is fighting for de facto governing power over EU member states in the event of a pandemic:
Dr. Joseph Yi (StreetMD) with Drs. Tom Cowan, Andrew Kaufman & Mark Bailey: A Response to Claims by Drs. Robert Malone, Peter McCullough & Ryan Cole That SARS-CoV-2 Has Been Isolated & Is a Disease-Causing Virus
Dr Joseph Yi, AKA “StreetMD” asked Drs Bailey, Cowan and Kaufman to respond to Drs Malone, McCullough and Cole’s claims that SARS-CoV-2 has been isolated and shown to exist. Boom!
cover image based on creative commons work of Briam-Cute & geralt
Dr. Sam Bailey with Eric Coppolino — On the Monumental Task of Documenting & Examining the Covid-19 Chronology: “Knowledge Coming to Light Changes Things”
“Knowledge coming to light changes things.” ~ Eric Coppolino
Recently, I have been fortunate to have connected with the inspiring Eric Coppolino, who is based in New York State.
Eric has an incredible history of exposing scientific fraud and environmental pollution cover-ups. He was one of the first to start investigating the COVID-19 scam and is putting something big together to help all of us who are questioning the narrative.
GREENWICH, CT — Robert F. Kennedy, Jr. has acknowledged the controversy within his own community over whether SARS-CoV-2 physically exists, and whether any viruses exist, or make people sick. He made the comments at a fundraising event here Sunday, April 24, 2022.
Kennedy said that the issue erupts regularly on the email discussion list of Children’s Health Defense (CHD), the vaccine safety and education organization that he founded in 2016.
“On our list, there’s a number of people who make those kinds of arguments” about how viruses allegedly don’t exist, Kennedy said in his remarks. “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
He made the remarks in reply to a question about why no government can produce evidence of having a sample of SARS-CoV-2 taken from a patient, rather than artificially created using a computer model.
Kennedy, the son of Sen. Robert F. Kennedy and the nephew of Pres. John F. Kennedy, is considered one of the leading voices in the international movement against covid-related mandates, lockdowns and safety issues over covid injections. It is the first time he has publicly commented on the virus-existence issue.
Scientists on all sides of the issue agree that viral particles have not been physically
isolated (with purified samples) and then sequenced.
What is Being Used to Prime the Covid Test?
The matter of whether the SARS-CoV-2 virus physically exists has dual significance. The obvious issue is that if there is not a virus, what then is making people sick? And what are they being vaccinated against?
Second, and less obvious: If the government cannot prove that it has a sample of natural SARS-CoV-2, then what is being used to prime the PCR test that is supposed to match and find the genetic code of an actual virus in a patient?
Scientists on all sides of the issue agree that viral particles have not been physically isolated (with purified samples) and then sequenced. Rather, hypothetical viruses are assembled from mixed biological samples, and these “in silico genomes” are then assumed to not only exist in nature but come from inside a pathogenic particle. They have many names: “mimicked human specimens” and “contrived viruses” (in the words of the CDC); or “synthetic nucleotide technology” (in the words words of the authors of the WHO test for covid).
One virologist told me in July 2020 that SARS-C0V- 2 was being assembled “like pages from a book,” necessary because no natural virus particle was available to sequence. The problem is that nobody has demonstrated these pages actually belong to the proposed book.
Covid tests look for sequences attributed to the “virus” merely via computer models —
but these “found” sequences almost always originate from somewhere else (including
the testing process itself).
CDC document pertaining to detection limits in the CDC “covid” test, admitting that
purified isolates of SARS-CoV-2 are not available. Yet this long, technical paragraph
admits something else: how they go about making their contrived virus (mimicked human
specimen), rather than sequencing actual virus. Were viruses available to anyone, it would
be the federal government of the United States. What they are admitting is that the virus
has not been isolated or purified; the writer admits outright that they are using made-up
samples that mimic clinical specimens. The technical notes describe the manufacturing
process for in silico sequences that are used in the “covid” test. The notes make reference
to MN908947, a synthetic, claimed, partial metagenomic transcript (not actual sequencing)
of the “N-gene” — which was later abandoned in its entirety in the Corman-Drosten assay.
Metagenomics: The Creation of Hypothetical Sequences
These hypothetical sequences are developed using technology called metageonomics — without any reference to actual purified suspected viruses. This artificial-intelligence process assembles a hypothetical “virus” from information gathered either from a crude human body fluid sample, or by making a “cell culture” experiment by mixing the fluid with monkey cells, cervical cancer cells, fetal calf serum, antibiotics and other poisons. In all cases where covid is concerned, scientists have used the latter. Because there is no actual virus available as a reference, there is no way to verify if the proposed sequences are valid. They are all theoretical, and no two are alike.
Said another way, in the absence of a real virus specimen, covid tests look for sequences attributed to the “virus” merely via computer models — but these “found” sequences almost always originate from somewhere else. And “positive” results can emerge from nearly anywhere, including the testing process itself). Yet if someone “tests positive” for one of these claimed viral sequences, they are said to be “infected” with SARS-CoV-2.
Previously, the U.S. Centers for Disease Control and Prevention (CDC) has admitted that the polymerase chain reaction has had a 100% false positive rate and has caused several widely-documented “false epidemics.”
The claimed existence, transmissibility and pathogenicity of SARS-CoV-2 were used to declare a global pandemic that by March 31, 2020 had 4.5 billion people around the world living under a stay-at-home order or house arrest.
“On our list, there’s a number of people who make those kinds of arguments. And
other people on the list server, and these are all very brilliant people, ridicule them
and dismiss them, and have them produce a lot of evidence.” — Robert F. Kennedy, Jr.
Seeking Documents from Governments, Agencies and Institutions
At a Q-and-A session at a fundraising event here Sunday, April 24, I asked Kennedy about the work of Christine Massey in the Toronto area, a statistician who is coordinating the worldwide effort to officially query governments, agencies and institutions about whether they have a sample of the claimed virus taken from a human.
“Christine Massey in Toronto has amassed 182 responses under various Freedom of Information Law requests from institutions, provincial state, and federal, national governments, which all say that no one has a sample of SARS CoV-2 taken from a human. Would you please comment on that?”
Kennedy replied: “On our list, there’s a number of people who make those kinds of arguments. And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence. I actually saw an exchange yesterday, where somebody made that exact statement and then 10 people jumped on him on with examples, of where that’s not true.”
The issue over the nature and existence of viruses represents the single biggest split in the covid-truth and anti-mandates movements. I first documented this divide in May of 2020.
“RFK Jr. now relies on popular opinion and ridicule to evaluate science?
When did he declare incompetence with simple logic?” — Christine Massey, statistician and coordinator of the virus FOIA project
‘I Am Amused Reading These Exchanges’
He added: “I am kind of amused reading the exchanges, and my inclination is that the viruses do exist and they do make people sick. I could be wrong. It could all be a big hoax, but to me, it all seems like viruses are real.”
But Kennedy answered a different question than the one I asked. I did not present him with an argument, or ask him whether he thought viruses were real. He admits that he uses a kind of mob rule to make up his mind over critical scientific issues when he says, “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
Reading Kennedy’s response, Christine Massey said, “RFK Jr. now relies on popular opinion and ridicule to evaluate science? When did he declare incompetence with simple logic? And why is a man dedicated to protecting children from medical harm uninterested in one of the greatest medical frauds of all time?”
She also demanded the data from the 10 people on Kennedy’s list who claimed to prove that the virus had been isolated.
So far, no governments have produced a scientific paper saying that they or anyone
have such a sample, despite the claim that a contagious virus has killed more than
5 million people worldwide.
Asked About a Legal Issue — Not Scientific
Kennedy said he believed viruses exist, but I did not ask him about that. Rather, I presented him with a legal issue, asking him to comment about how someone well-known and established in covid truth circles over the past two years has collected 182 responses from top-level government agencies and institutions, all saying they do not have a sample of SARS-CoV-2 extracted from a human host.
So far, no governments have produced a scientific paper saying that they or anyone have such a sample, despite the claim that a contagious virus has killed more than 5 million people worldwide.
I followed up and said to him, “The governments have said they don’t have a sample.”
Kennedy, an attorney, responded: “Freedom Information Laws do not require the government agency to do science, or to answer specific questions. What they do is, the Freedom of Information Laws make it obligatory for the government to give you existing documents. So if you are telling the government, ‘I want you to verify these, there are documents’, they say, listen there’s nothing to verify it. It doesn’t mean it’s not true. It means they’ve got nothing.”
So far all have said no such records exist. This includes the U.S. CDC and the FDA, as
well as Health Canada and the National Health Service (NHS) of the UK. None of the
182 agencies and governments queried have replied in the affirmative.
‘Kennedy hasn’t read any of my records requests’
Massey replied to this in an email: “It appears that Kennedy hasn’t read any of my records requests. I didn’t ask governments to ‘do science’ or answer ‘specific questions’. All of my requests have been for studies/reports in the possession, custody or control of an institution.”
I asked Massey how she words her letters seeking documentation of a sample of the claimed virus from a human host.
She provided this example of what she is seeking, and what so far all governments she has queried deny having:
“All studies and/or reports in the possession, custody or control of the Centers for Disease Control and Prevention (CDC) and/or the Agency for Toxic Substances and Disease Registry (ATSDR) describing the purification of any “COVID-19 virus” (aka “SARS-COV-2”, including any alleged “variants” i.e. “B.1.1.7”, “B.1.351”, “P.1”) (for example: via filtration, ultracentrifugation and chromatography), directly from a sample taken from a diseased human where the patient sample was not first combined with any other source of genetic material (i.e. monkey kidney cells aka Vero cells; fetal bovine serum).”
And so far all have said no such records exist. This includes the U.S. CDC and the FDA, as well as Health Canada and the National Health Service (NHS) of the UK. None of the 182 agencies and governments queried have replied in the affirmative.
“It erodes popular faith in democracy when public officials insist that their arbitrary
policies are ‘science based’ and yet cannot produce a single study to support sweeping
mandates.” — Robert F. Kennedy, Jr.
‘No Records Exist’ is an Important Response
Getting a “no records exist” reply is common, and seeking such a reply is a common strategy for establishing that there has not actually been a regulatory process for a policy issue. It is one of the most important uses of open records laws.
In late 2020, the New York State Department of Health (NYS-DOH) responded to an open records request saying it had no studies to prove that masks are safe or effective at preventing the spread of viruses or other diseases. For that same kind of “sorry no documents” FOIL reply, Kennedy was much more outspoken.
At the time, he wrote to his Instagram followers, “It erodes popular faith in democracy when public officials insist that their arbitrary policies are ‘science based’ and yet cannot produce a single study to support sweeping mandates. This letter illustrates the hazard of abandoning due process.”
Previously, he had remained agnostic on the issue of masks and whether masks work. He finally took a position in response
New York State saying it had absolutely no data about whether masks are safe or effective.
“It’s a needlessly divisive issue, with people screaming, on both sides, as if it were
the key to this whole thing — which it isn’t.” — Prof. Mark Crispin Miller
“They did not isolate a virus,” Wallach said. “The reason it’s so confusing for people is that they claim to have done so in the titles of the key scientific papers, but if you read the methodology sections, it’s blatantly clear: they never isolated a virus. They never found anything. The evidence is overwhelming.”
He added: “I respect the importance of political leaders like RFK Jr. keeping an open tent, they have to. But at the same time, this is an issue that should be front and center for the world public, and nobody should be repeating this dogma about the existence of viruses.”
Mark Crispin Miller, professor of communication at New York University, said, “It’s a needlessly divisive issue, with people screaming, on both sides, as if it were the key to this whole thing — which it isn’t. What will make the whole narrative collapse is not the argument that there are no viruses, but the recognition that the authorities we’ve all been listening to — the medical establishment, Big Pharma, Academia, the media et al. — are malign, and intent on killing us.
“That’s it. Everything else is a distraction. Whether the ravages of COVID-19 have been exaggerated, or whether there’s no virus there at all, is ultimately beside the point. And since Bobby’s role is in large part political, as he attempts to keep this movement in one piece, his disinclination to take sides here ought to be respected.”
“Are all based on in-silico modeled synthetic phenomena, which has never been
scientifically proven as coming from an actual virus.” — Dr. Kevin Corbett, expert in diagnostic testing
‘This was what happened with HIV’
Dr. Kevin Corbett did his doctoral work on diagnostic testing associated with HIV and AIDS, including research into the PCR. He said this week that the existence of SARS-CoV-2 and associated tests, “Are all based on in-silico modeled synthetic phenomena, which has never been scientifically proven as coming from an actual virus.
“This was what happened with ‘HIV’, which The Perth Group of scientists [in the 1990s] first proved was never isolated or purified. Those powerful voices like Robert F. Kennedy, Jr., who sadly ignore this issue, are badly misguided, because they fail to address this fundamental caveat in ‘covid science’.”
Corbett cautioned, “Their efforts will only act to further socially embed the popular hysteria of there being a contagion, and therefore will enable further public health mandates forcing masks, social distancing and the latest covid killshot.”
On April 25th, a federal judge stuck down the mask mandate for mass transit.Part of the reasoning was based on fact that the CDC skipped the otherwise-mandatory public notice and comment period as required by the Administrative Procedures Act (APA). However, the main reasoning was to show that government officials do not recognize the limits of their power. Apparently, neither do the masses.
The ruling sent COVID doomsdayers into panic mode. Federal agencies are creatures of statute and are bound by law to operate within the law imposed by Congress. Agencies are not separate entities that may act as they wish.
Their authority is limited to what Congress grants them. So the CDC is governed by Congress – not by any President – and certainly not by career bureaucrats like Fauci. – Phillip Holloway, Esq
Up until COVID, it was illegal to wear a mask to conceal the face in public, with few exceptions. Under COVID, “the science” reversed the mask laws overnight, illegally. Few people questioned the authority of politicians practicing medicine without a license. Perhaps COVID is a lesson to understand that when “science” enters the political picture, its time to question authority. In other words, public health orders do not trump legal orders.
Science and Freedom Do Not Mix
Contrary to popular belief, the law is not based on the latest “science” because science and law are separate spheres of knowledge. Science cannot prove that something is true. Science tests theories, and explains what is observed under a specific set of conditions. Science is a tool. Like any tool, it is neither good or bad, but it can be used according to the will of the “scientist” who wields it. Science does not reveal truth.
Science cannot give you truth. All it can determine is internal self-consistency” based on data within the confines of time and distance. Everything else must be rejected. —William A. Tiller
Science does not usurp the law. Neither do mandates usurp the law. Mandates are public health policies, made by government agencies who use science and fear to manipulate behavior. Yet, federal agencies have NO authority under the law to tell people how to live when it comes to making health decisions.
For those who claim that science “raises awareness,” realize that awareness exercises do nothing to ensure freedom. Real freedom is preserved outside of science, lest people become slaves to a system that is set up to manipulate and engineer consent (as with mandates). Without true consent, there is only implied consent, the illusion of choice, based on the limited options you are provided. An illusion of choice brings an illusion of freedom.
The federal judge made clear that CDC and government officials violated the APA in issuing the mandate.
Despite the protestations by Fauci to the contrary, the CDC was created by a law, is governed by a law, and must act within the confines of that law. – Phil Holloway, Esq. Twitter
Live Exercise
The COVID exercise is a test of people’s ability to know truths from falsehoods. Did anyone investigate the legality of a mandate… or how it may differ from a man date? Did anyone question the blank package insert of the experimental injections? Did anyone know to separate the science from the law?
Early on, the Secretary of State, Mike Pompeo, disclosed, in the media, that COVID is a “live exercise.” Did anyone notice how the media then went back to its regularly scheduled programming; Tel-A-Vision?
Why did it take so long for the courts to intervene, especially when the CDC mask order was set to expire on May 3? Is this court opinion too little, too late? Many would argue the damage has already been done. People’s lives and minds have been altered. Kids breathed their own carbon dioxide to participate in school. Babies did not see the facial expressions of their parents.
What about the Covidians who continue to sport “the mask” in public places? Do they do it “to protect others” as the media tells them to do? Does the media guilt people into “taking responsibility” by wearing a mask? Is health no longer a personal responsibility? Can Fauci run a mile to help you lose weight? Can your doctor wear a life jacket to keep you afloat?
The law is supposed to protect the rights of people to decide for themselves…… but only if people know the laws! Know this: neither Congress, the CDC, nor the media can legislate choice when it comes to your body.
Stay tuned. The Department of Justice has filed a notice of appeal to the 11th Circuit Court of Appeals. This filing is expected to go nowhere, and do nothing, except to save face, since there was no motion for a stay included in the notice of appeal.
While the mask mandate may have ended, the live exercise continues…
College term paper referenced by Dr. Cowan was actually a published paper by Eleni Papadopulos-Eleopulos, et al. (Dr. Cowan made this correction at the start of a video on the snake venom controversy, streamed on 4/22/2022.)
On Saturday, Apr. 9, 2022, American Airlines (AA) flight 1067 departed Denver International Airport for its 1-hour and 46-minute flight to Dallas-Fort Worth (DFW). The nearly $100 million Airbus A321 aircraft and its 200 passengers were under the care of AA Captain Bob Snow, who has been with the company for over 31 years. Immediately after pulling into Gate 6 at DFW, Captain Snow—who was forced to get the COVID jab on Nov. 7, 2021, or lose his job—suffered a life-threatening cardiac arrest in the cockpit and almost died. If the tragic event had happened six minutes earlier, there could have been a mass casualty in the skies.
Swiftly, Captain Snow, who passed out and had to be shocked three times, was rushed to Baylor, Scott, and White Health Center ten minutes away. Thankfully, he survived. Snow, who spent time in the hospital’s Intensive Care Unit and is now home, is confident his heart attack directly resulted from the COVID-19 experimental “vaccine” he was mandated to receive. Tellingly, no one from AA or the airline union called Snow while he was in the hospital or stopped by to visit him. While in the hospital, he recorded a video, stating:
“My name is Bob Snow. I am an [American Airlines] Captain and have been a Captain for a number of years. My total service with the company is over 31 years. On Nov. 7, I was mandated to receive a vaccine. Quite literally, I was told if I did not receive the vaccination, I would be fired. This [order] was from our director of flight. So, under duress, I received the vaccine.
Now just a few days ago, after landing in Dallas, six minutes after we landed, I passed out. I coded. I required three shocks. I had to be intubated. I’m now in ICU in Dallas. This is what the vaccine has done for me. I will probably never fly again, based upon the criteria the FAA establishes for pilots. I was hoping to teach my daughter to fly; she wants to be a pilot. [Now] that will probably never happen, all courtesy of the vaccine. This is unacceptable, and I’m one of the victims.
You can see that this is an actual result of the vaccine for some of us. Mandatory, no questions asked, get the shot, or you’re fired. This is not the American way.”
American Airlines Told Captain Robert Snow to Get Vaccinated or Be Fired!
Remarkably, Captain Snow’s COVID-19 vaccine-related cardiac arrest and the myriad of pilot and flight attendant lawsuits currently underway against COVID mask and vaccine mandates are not being reported by mainstream media. Still, it is a subject that many concerned Americans, including Steve Kirsch, Executive Director of the Vaccine Safety Research Foundation, are paying attention to.
Pilots Are Speaking Up About Adverse Events From COVID Jab
Kirsch, who believes that “vaccine injury cover-up is in the interest of all affected parties (except the flying public),” recently interviewed Josh Yoder of US Freedom Flyers about AA Captain Bob Snow. Yoder, a pilot himself, has been a staunch advocate against “vaccine” mandates in the airline industries.
In the interview, Yoder shared with Kirsch that his group has received hundreds of reports about pilots flying planes while suffering from adverse side effects from the COVID jabs. He also noted that cardiologist Dr. Peter McCullough told him that if the airlines were conducting health screenings, 30 percent of the pilots currently flying would most likely be disqualified due to vaccine-induced heart conditions. Yoder told Kirsch:
“He [McCullough] said that if every vaccinated pilot were to be screened, there would be somewhere around a 30 percent loss in manpower.”
Yoder mentioned that the most prominent health issues reported include chest pains, myocarditis, and pericarditis. He noted that “three vaccinated pilots called him yesterday” and said they’re “currently flying with chest pains.” Another said a cardiologist is treating him. Yoder added that the pilots want to remain anonymous because they don’t want to lose their jobs.
Airline pilot Latane Campbell interview: A pilot’s view of COVID policies
On Dec. 15, 2021, McCullough, joined by other experts, including Robert F. Kennedy, Jr., pathologist Dr. Ryan Cole, and Lt. Col. Teresa Long, M.D., signed a 53-page letter to the Federal Aviation Administration (FAA) and major airlines, urging them to flag all vaccinated pilots and administer D-dimer tests, troponin tests, cardiac MRIs, and EKGs to assess their health.
The letter—noting that pilots have died post-vaccination—describes the side effects suffered by numerous pilots, many of whom have been afraid to report them for fear of being grounded. Some have had to seek medical attention and report their injuries due to the significance of the COVID-19 “vaccine” related adverse event. A professional agricultural pilot explained his horrible ordeal, stating in part:
“I am a 33-year-old husband and father of two young boys. I have been healthy my whole life, with no underlying conditions. I received my first dose of the Pfizer COVID Vaccine on February 1. Within thirty minutes, I developed a severe stabbing headache, which later became a burning sensation in the back of my neck. Two days after my vaccination, I got in my airplane to do a job that would only take a few hours.
Immediately after taking off, I knew that something was not right with me. I was starting to develop tunnel vision, and my headache was getting worse. Approximately two hours into flying, I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears.
Instantly, I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God, I was able to land my plane without incident, although I do not remember doing this.”
Cody Flint: 33 Y/O Airline Pilot Develops Brain Swelling, Can No Longer Fly Following Jab
Yoder argued that the overall behavior of the FAA, the airlines, and the pilots’ unions demonstrate a contempt for the safety of the flying public and the well-being of airline employees. Kirsch agrees, adding that we have seen a general tone of “belligerence” from nearly all hospitals towards patients who seek second opinions on vaccine-related injury issues. Yoder told Kirsch that the airline industry seems unwilling to address the potentially catastrophic incident.
Yoder pointed out that “AA is trying to create as much distance between themselves and this incident as possible,” adding, “so are the unions. We can’t even get a response.” Still, according to Yoder, Snow will be speaking out soon. When he does, Yoder warned:
“You’re going to hear some very interesting details that are going to be very damning for American Airlines, the Allied Pilots Association, the FAA, and everyone else involved.”
Steve Kirsch, Full Interview with Josh Yoder re: American Airlines Captain Bob Snow vax injury
The Biden administration’s vaccine mandates purporting to force U.S. military members to take the experimental Covid injections are unconstitutional and, because of the potential for genetic changes, may have implications involving patents and intellectual property, super lawyer Todd Callender tells The New American magazine’s Alex Newman in this episode of Conversations That Matter.
To protect the U.S. military, the rights of troops, and the U.S. Constitution, Callender has joined forces with other attorneys such as Tom Renz to sue the Department of Defense. The case is beyond fascinating, and you won’t want to miss this powerful interview.
Transcript of Dr. Sam Bailey’s introduction, provided by TCTL editor:
Last month, we were fortunate to have microbiologist and colloidal chemistry expert Dr. Robin Wakeling present his analysis of Pfizer Comirnaty under the microscope. Since that time Dr. Wakeling has continued to investigate the injections and is also linked up with other New Zealand teams who have shared their findings with him.
In Part 1 of his analysis, Dr. Wakeling presented the appearances of Comirnaty straight from the vial and has some new information regarding how these complexes form.
But perhaps, more importantly, in this video for the first time he is going to analyze the blood of some Pfizer-injected subjects who have suffered adverse reactions.
He’ll explain what he thinks is happening to the red blood cells and some of the most bizarre images he has ever seen in his long career.
In addition to Comirnaty, the teams have also been investigating recent influenza vaccines under the microscope, with some surprising findings that the officially disclosed ingredient don’t appear to explain.
Dr. Wakeling joins my husband, Dr. Mark Bailey, to present round two of Pfizer Under the Microscope.
This video looks at the paper cited by Dr Bryan Ardis as the main evidence that snake venom plays a role in the current plandemic. The paper purports to have found a potential association between venom-like peptides found from various animals and Covid-19. Dr. Kaufman gives an overview of the relevant issues related to the snake venom controversy and gives a critical appraisal of the experiment and conclusions.
OTTAWA: After repeatedly calling on the University of Ottawa (U of O) to end its abusive and discriminatory practices, the Justice Centre is pleased announce that the University has stated it will cancel its mandatory vaccine policy for students as of May 1, 2022.
The Justice Centre represented a pregnant student who was suspended from her university program after deciding against the Covid vaccine. Her doctor advised her that her pregnancy was at high-risk for reasons unrelated to Covid and recommended that she complete her mandatory internship virtually, which was allowed by the curriculum.
However, the University of Ottawa refused to accommodate her, falsely claiming that she was trying to circumvent the vaccination policy and that there were no places available for a virtual internship.
Throughout the process, U of O made little to no effort to find a mutually acceptable solution, the student alleges, and refused to justify its decisions in light of the facts of the case.
“It is clear that the University of Ottawa did not intend to follow the ‘reasonable accommodation’ basic criteria set out by the Supreme Court of Canada more than 15 years ago,” notes Samuel Bachand senior external counsel for the Justice Centre in the province of Québec.
After negotiations and discussions with lawyers from the Justice Centre, the student managed to find a suitable placement for virtual internship on her own, which was finally approved by the University.
“The brazenness and bad faith of the University in this matter are appalling. There are clearly, among the people in authority there, bureaucrats who are willing to sacrifice the mission of their institution to irrational health concerns,” comments Mr. Bachand,
“It is well accepted in the scientific community that the Covid vaccines do not prevent infection or transmission of the virus. There was no basis for the vaccine mandate at the University of Ottawa or any other post-secondary institution given that being vaccinated confers no special status or protection,” concludes Mr. Bachand.
“The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent
“SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and
animal “coronaviruses” created in the very same way. Attempting to claim any connections between the
random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated
into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place.
Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely
related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines,
the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have
a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a
singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial
evidence that is easily debunked.”
“My story has never been to create fear, panic, and anxiety about water.” He said he told Peters that he believes “there’s actually a snake venom connection to all of COVID-19, and I think that’s the weapon.” – Dr. Bryan Ardis
Summarizing his theory, Dr. Ardis said, “They are using Krait venom and Cobra venom, calling it Covid-19, you’re drinking it, it’s getting into your brainstem and it’s paralyzing your diaphragm’s ability to breathe.”
I really didn’t want to write this article. I was hopeful that people would easily see right through the unsubstantiated claims of Dr. Bryan Ardis that snake venom is the cause of “Covid.” I was hopeful that people would take the time to research the information presented in support of the snake venom theory to see if it held any merit at all. I thought his whirlwind alternative media tour on the who’s who of questionable sources (including the likes of Stew Peters, Mike Adams, and Infowars) would have people questioning why this theory was allowed to be so heavily promoted so quickly. I thought that the fact that the man who created the “Covid” snake venom theory was actually selling his own anti-venom line of supplements would be enough grounds to be skeptical of his motive and his claims.
It seems I was wrong. Just like the baseless vaccine shedding and gain of function/bioweapons narratives, this new snake venom theory has sadly spread through the “Truther” community like wildfire, with many who rightfully challenge the existence of “viruses” clinging to the idea of a new invisible enemy to defeat. They believe that it must be a new toxin. It can’t possibly be the same factors we have seen each and every year leading to disease. This toxin must be hiding in the vaccines, the drugs, and/or even the very water we drink. What these “Truthers” do not realize is that this very line of thinking gives credibility to the idea of a new disease which requires new treatments in order to combat it. This is exactly what the pharmaceutical companies want you to believe.
However, there is NO NEW DISEASE. There is no need for any new or even existing pharmaceutical interventions to treat the same symptoms of detoxification people go through each and every year. In fact, the current treatments can easily be shown to have led to numerous unnecessary deaths. There is no new threat known as “Covid-19” which is being caused by any one factor. The factors leading to the symptoms of disease people are experiencing are multi-causal as they are every year.
Now this is not to say that the vaccines, the drugs, or even the water supply are free of toxins. These are all sources of toxicity and should be investigated as to their composition and effects on our health. However, the theory that there is one factor in all of these sources, i.e. snake venom, and this one factor is leading to the symptoms of disease people are experiencing is, at present time, completely baseless. And it all begins at the very foundation of the fraudulent genome.
The Fradulent Genome
You take that snake or that serpent and you figure out how to isolate genes from that serpent and get those genes of that serpent to insert itself into your God-given created DNA. I think this is the plan all along, was to get the serpents’, the evil one’s DNA, into your God-created DNA.”
He also said genetic sequence testing done on sick patients in Wuhan found their genetic sequence matched two snakes, the Chinese Krait and King Cobra, not bats.”
From Dr. Ardis’ interview with Mike Adams, he supplied the article “Snakes could be the source of the Wuhan coronavirus outbreak” from CNN as his starting point for the “Covid”/snake connection. Within the article, you can see that this claim originates from the fraudulent genomes:
“The researchers used an analysis of the protein codes favored by the new coronavirus and compared it to the protein codes from coronaviruses found in different animal hosts, like birds, snakes, marmots, hedgehogs, manis, bats and humans. Surprisingly, they found that the protein codes in the 2019-nCoV are most similar to those used in snakes.” https://www.google.com/amp/s/amp.cnn.com/
To anyone who actually researched the creation of the original “SARS-COV-2” genome, it is readily apparent that it is a fraudulent computer-generated creation stemming from the unpurified lung fluid of a single patient. The sequenced material could have come from multiple sources, including host DNA/RNA, bacteria, and microbes/microorganisms. It could have even come from outside contamination. There is no way to tell what the origin of the RNA is or even if it was a single source as no particles assumed to be “SARS-COV-2” were ever properly purified and isolated directly from the fluids of the sick patient before being sequenced. Thus, any relation this fabricated sequence has to any other sequence is invalid as the source was never identified to exist as a physical entity to begin with. Considering that the bat and snake “coronavirus” sequences for which the “SARS-COV-2” sequence was then compared to also come from unpurified sources, it is easy to see that any claims as to the origins of the sequenced material is a horrible foundation to build upon for an origin theory of a nonexistent “virus” and/or disease.
Even if this snake-venom connection was valid, the enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom. These peptides are “almost identical” to the venoms of animals and yet they are regularly found in healthy humans and other mammals. From his own source:
Like Venom Coursing Through the Body: Researchers Identify Mechanism Driving COVID-19 Mortality
“Researchers from the University of Arizona, in collaboration with Stony Brook University and Wake Forest School of Medicine, analyzed blood samples from two COVID-19 patient cohorts and found that circulation of the enzyme – secreted phospholipase A2 group IIA, or sPLA2-IIA, – may be the most important factor in predicting which patients with severe COVID-19 eventually succumb to the virus.
The sPLA2-IIA enzyme, which has similarities to an active enzyme in rattlesnake venom, is found in low concentrations in healthy individuals and has long been known to play a critical role in defense against bacterial infections, destroying microbial cell membranes.”
Thus, the snake enzymes are in fact normal human enzymes that are regularly found in healthy individuals. There is no mystery as to why these would be present in a sample. We should be able to put this “Covid” snake venom nonsense to bed right here. However, let’s press on a see what else we can uncover.
Antivenom = Monoclonal Antibodies
One thing I will give Dr. Ardis credit for is spotlighting the connection between the creation of antivenoms with the creation of monoclonal antibodies. The processes for both are very similar and the desired outcome is the exact same: the creation of theoretical antibodies. In the case of snake antivenom, it is normally created by a series of injections of the venom of a snake into an animal and then collecting the blood after a period of time. This is usually done through horses but other animals can be used as the host as well. Thus, the antivenom used for a snakebite victim is typically an injection of horse blood.
Both of these therapies have their basis in animal blood and the creation of the theoretical antibodies. Both are associated with toxic side effects. Sadly, while he was originally right about the fact that monoclonal antibodies are toxic and should not be used to treat the symptoms now collectively known as “Covid,” Dr. Ardis changed his tune when another doctor texted him asking if he would use antivenom for a snake bite:
“Last December, Dr Bryan Ardis received a text message from an Emergency Room physician friend of his that sent him down an unexpected and bizarre rabbit hole that may explain the adverse events from the vaccines that we’ve been reporting. The text read: “Hey Dr Ardis…If you got bit by a rattlesnake, would you go to a hospital and get anti-venom?”
“He says, “I realized, all of a sudden, monoclonal antibodies ARE anti-venom. The Federal Government doesn’t want us using anti-venom. Why are they fighting anti-venom and why are we finding anti-venom works against COVID? Is it not a virus? Is it a venom? This is what I want to know: Is COVID a venom and is this why they don’t want you using monoclonal antibodies?”
Do you see the trick? They want you to equate monoclonal antibodies with antivenom. This is supposed to be an “aha” moment where you realize that there is no way that you would not inject antivenom (i.e. horse blood) into yourself if bitten by a snake. It’s a no-brainer, right? We have all seen the movies where a person is bitten by a venomous snake and quickly dies if not given the antivenom.
If you are willing to accept the injection of horse blood into your body to survive a snake bite, why wouldn’t you also inject the cancer-cell cultured blood of genetically altered mice in order to combat “Covid?”
As Dr. Ardis points out, monoclonal antibodies are essentially antivenom. However, he wrongly states that monoclonal antibodies are an effective therapy. According to a September 2021 Cochrane review of the available studies, they found insufficient evidence to claim that monoclonal antibodies are an effective treatment for “SARS-COV-2:”
Are laboratory-made, COVID-19-specific monoclonal antibodies an effective treatment for COVID-19?
“The evidence for each comparison is based on single studies. None of these measured quality of life. Our certainty in the evidence for all non-hospitalised individuals is low, and for hospitalised individuals is very low to moderate.We consider the current evidence insufficient to draw meaningful conclusions regarding treatment with SARS-CoV-2-neutralising mAbs.”
In other words, the evidence for the usefulness of monoclonal antibodies is non-existent. Unfortunately, the Cochrane Review failed to point out that there are various risks and adverse reactions associated with their use:
Do mAbs have risks?
“Therapeutic mAbs, typically administered by intravenous (IV) infusion, have been a valuable and generally safe treatment option for a variety of conditions for many years. However, they are also known to cause a range of side effects and reactions, which can be immediate or delayed.Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity.”
In January 2022, the FDA restricted the use of some monoclonal therapies (Bamlanivimab and Etesevimab) that are authorized against “Covid-19” as they were shown to be ineffective:
Coronavirus (COVID-19) Update: FDA Limits Use of Certain Monoclonal Antibodies to Treat COVID-19 Due to the Omicron Variant
“In light of the most recent information and data available, today, the FDA revised the authorizations for two monoclonal antibody treatments– bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
Because data show these treatments are highly unlikely to be active against the omicron variant,which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. And like other infectious organisms, SARS-CoV-2 can mutate over time, resulting in certain treatments not working against certain variants such as omicron. This is the case with these two treatments for which we’re making changes today.”
On April 16th, 2022, the FDA revoked the use of Bamlanivimab alone as it’s benefits were shown not to outweigh its risks. Somehow despite this evidence, the FDA still allows for it to be used in combination with Etesevimab, even though they previously revoked their use together in January 2022:
Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab
“Today, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate COVID-19 in adults and certain pediatric patients. Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of SARS-CoV-2 viral variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure,the FDA has determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use. Therefore, the agency determined that the criteria for issuance of an authorization are no longer met and has revoked the EUA.
On Nov. 9, 2020, based on the totality of scientific evidence available at the time, the FDA issued an EUA to Eli Lilly and Co. authorizing the emergency use of bamlanivimab alone for the treatment of mild to moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progressing to severe COVID-19 and/or hospitalization. Importantly, although the FDA is now revoking this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone. The FDA believes that these alternative monoclonal antibody therapies remain appropriate to treat patients with COVID-19 when used in accordance with the authorized labeling based on information available at this time.”
If the FDA’s confusing revoking of the EUA’s of these monoclonal antibodies has you concerned that you will not be able to use them against an imaginary “virus,” don’t worry. The FDA authorized the use of a new “Omicron-specific” monoclonal antibody called Bebtelovimab on February 11th, 2022. Granted, it still carries the same risks, adverse side effects, and uncertainty over clinical worsening listed for the previously ineffective antibody therapies. From the FDA fact sheet:
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
“Possible side effects of bebtelovimab include itching, rash, infusion-related reactions, nausea and vomiting. Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other SARS-CoV2 monoclonal antibodies and could occur with bebtelovimab. In addition, clinical worsening following administration of other SARS-CoV-2 monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19.”
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
Hypersensitivity Including Anaphylaxis and Infusion-Related Reactions: Serious hypersensitivity reactions, including anaphylaxis, have been observed with administration of other SARS-CoV-2 monoclonal antibodies and could occur with administration of bebtelovimab. If clinically significant hypersensitivity reactions occur, discontinue and initiate appropriate supportive care. Infusion-related reactions may occur up to 24 hours post injection. These reactions may be severe or life threatening. (5.1)
Clinical Worsening After SARS-CoV-2 Monoclonal Antibody Administration: Clinical worsening of COVID-19 after administration of SARS-CoV-2 monoclonal antibody treatment has been reported and may include signs or symptoms of fever, hypoxia or increased respiratory difficulty, arrhythmia (e.g., atrial fibrillation, sinus tachycardia, bradycardia), fatigue, and altered mental status. Some of these events required hospitalization. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19. (5.2)
Limitations of Benefit and Potential for Risk in Patients with Severe COVID-19: Treatment with bebtelovimab has not been studied in patients hospitalized due to COVID-19. Monoclonal antibodies, such as bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with COVID-19 requiring high flow oxygen or mechanical ventilation. (5.3)
It should be fairly clear that, unlike Dr. Ardis’ claims, monoclonal antibodies are not effective, carry numerous risky side effects, and can actually worsen the disease they are supposed to treat. Interestingly, this same risk of dangerous side effects and worsening disease outcomes is associated with snake antivenom as well. From the fact sheet of a commonly used antivenom for rattlesnake bites, we find these admitted side effects:
Rattlesnake Antivenin Side Effects Center
“Rattlesnake Antivenin (antivenin crotalidae polyvalent) is an antivenin product used only to treat envenomation caused by bites of crotalids (pit vipers) including rattlesnakes, copperhead and cottonmouth moccasins, and others. Common side effects of Rattlesnake Antivenin include allergic reactions such as flushing, itching, hives, swelling of the face/tongue/throat, cough, shortness of breath, blue color to the skin, vomiting, and anaphylaxis (severe allergic reaction).”
“Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered. An immediate reaction (e.g. shock, anaphylaxis) usually occurs within 30 minutes. Symptoms and signs may develop before the needle is withdrawn and may include apprehension, flushing, itching, urticaria; edema of the face, tongue, and throat; cough, dyspnea, cyanosis, vomiting, and collapse. There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use.”
“Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered.30 The incubation period may be less than 5 days, especially in those who have received horse-serum-containing preparations in the past. The usual symptoms and signs are malaise, fever, urticaria, lymphadenopathy, edema, arthralgia, nausea, and vomiting. Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis. Peripheral neuritis usually involves the shoulders and arms. Pain and muscle weakness are frequently present, and permanent atrophy may develop.”
Maybe the use of antivenom to treat a snakebite isn’t the super cure it has been sold to be? Is it possible that, as with many pharmaceutical products and interventions, the antivenom itself is creating the very symptoms it is said to treat? For some further insight, let’s look at a few highlights from an paper from September 2019, right before this “crisis,” which reviewed the use of antivenom and had a few revealing claims about the “anti” toxin. You will see it reiterated that the injection of antivenom created from either horse, sheep, goats, and/or rabbits can cause immediate hypersensitivity and anaphylaxis or a delayed “serum sickness” which can occur weeks after the treatment. It is stated that the antivenom has limited efficacy and can be entirely ineffective based on the geographic location. Improper use of antivenom contributes to increased servere outcomes and the production of antibodies in animals leads to a large number (70%) of immunoglobulins that do not react to snake venom:
Perspective on the Therapeutics of Anti-Snake Venom
3. Current Information in the Design of New Antivenoms
“Currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses [14,15]. Hyperimmunized animals produce antibodies against the venom proteins and serum is extracted from their blood for the treatment of envenomation [6,16]. Conventional serum therapy aims to bind and neutralize the snake venom proteins [17]. It is a fact that the antivenom allows the body to try to reverse the damage caused by the venom. However, it is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia. Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects [18];
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability;
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes;
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both.
“Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom. Around 70% of the immunoglobulins obtained do not act directly against venom toxins [26]. Despite the abovementioned facts, this is the only FDA approved therapy to treat snake venom.”
A few other studies also point out the severe reactions regularly attributed to the use of antivenom. The first is a study from 2016 which points out that not only are adverse reactions common, they occur at a high rate. It is stated that this is due to poor quality control and manufacturing problems:
Adverse reactions to snake antivenom, and their prevention and treatment
“Antivenom is the mainstay of treatment of snakebite envenoming. However, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent. Both acute (anaphylactic or pyrogenic) and delayed (serum sickness type) reactions occur. Acute reactions are usually mild but severe systemic anaphylaxis may develop, often within an hour or so of exposure to antivenom. Serum sickness after antivenom has a delayed onset between 5 and 14 days after its administration. Ultimately, the prevention reactions will depend mainly on improving the quality of antivenom.”
“The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors. This highlights the importance of addressing issues related to poor quality and potentially unsafe antivenom. Ultimately, the prevention of reactions will depend mainly on improving the quality of antivenom. Until these improvements take place, doctors will have to depend on pharmacological prophylaxis as well as careful observation of patients receiving antivenom in preparation for prompt management of acute as well as delayed reactions when they occur.”
This next source is from 2018 and it points out that early antivenoms were unsafe and caused severe life-threatening events. While they now have “acceptable” safety profiles, antivenoms still have varying quality and range from 10% adverse reactions to greater than 50%. This same variation in quality is seen in the production of monoclonal antibodies:
Antivenom therapy: efficacy of premedication for the prevention of adverse reactions
“However, in their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects [8]. The main reason was that first antivenoms were poorly purified preparations or crude sera. Over the years, for many of the original applications, heterologous serums were replaced by other drugs with better safety profiles, such as antibiotics, vaccines and homologous serums. However, in cases of envenomation by snakes, scorpions or arachnids, antivenoms remain the only effective treatment [4]. Currently, after many improvements, antivenoms exhibit acceptable safety profiles [1, 9, 10]. Nevertheless, antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50% [11, 12].”
In is interesting to note that there are many factors that are said to influence the severity of a venomous snakebite including the age, sex, and health of the person bitten as well as the type of snake, the geographical location of the snake, the season the bite occurred in, what the snake ate, and how recently the snake released its venom. Antivenoms themselves have been shown to have varying effects in quality due to the geographical location of the snake which somehow renders the antivenom ineffective and even dangerous in different countries and continents, even against the same type of snake. It is said that this has kept locals from seeking out medical care and sticking to traditional healers:
“Snake venoms are highly complicated. At least 26 separate enzymes have been identified with 10 of these enzymes common to all snake venoms (though in different concentrations). All snake bites are not equal. The quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously.”
“A study led by Dr Fry has found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions.
Researchers tested the effectiveness of two African and two Indian saw-scaled viper antivenoms against saw-scaled vipers from 10 regions.
The results showed that the two African antivenoms were only effective against snakes from restricted ranges.
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers.
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regions. It failed completely against African saw-scaled vipers.
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry says.
“In Kenya, snakebite deaths have increased dramatically after hospitals switched supplies of a very effective African antivenom with a cheaper Indian variety.”
“This creates a knock-on effect in these communities. It’s hard enough to convince people living in these regions not to go to traditional healers to treat snakebite. And if someone does seek proper medical care but dies because of ineffective antivenom, it will be even harder to convince the next victim to seek out antivenom.”
Viper venom’s lethal evolution
It’s the variety of the saw-scaled viper’s prey, from rodents to insects, that researchers say could be the reason why antivenom from one region might not work in another.
“Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes,” UQ PhD candidate in Toxinology Bianca op den Brouw wrote in an article for The Conversation.
“Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet.
“Different saw-scaled viper populations feed on different prey. The physiology of these prey animals differs, and this dictates what makes a toxin effective.
“From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom.”
Maybe the proceeding information on how snakebite antivenoms are created as well as the high rate of adverse events from the antibodies used for antivenom now has you questioning that initial “no-brainer” thought: “Of course I would use antivenom if bit by a snake.” If so, you are on the right track as, based on information from the African Snakebite Institute, in most snake bite cases, antivenom is not used and many snake bites are often unattended and/or unreported. In fact, it is apparently a well-known “myth” (i.e. truth in this case) that the antivenom kills more people than the snake venom itself. Most people (over 80%) never receive antivenom as, like the previous sources stated, it can have disastrous side-effects. Most snake bites do not cause symptoms warranting the use of something so toxic. In fact, snake bite victims are not immediately injected with antivenom and typically are sent home after observation:
“Yet people often have a poor understanding of how it works and there are endless myths about antivenom killing more people than the snake venom itself.”
“Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite) as most victims are not severely envenomated or the bite may be from a snake that is not considered potentially deadly or is not covered by the antivenom (Rhombic Night Adder, Berg Adder and Stiletto Snake). Antivenom is relatively scarce, expensive and can have disastrous side-effects. The biggest danger is an acute allergic reaction (anaphylaxis) or, to a lesser degree, serum sickness that can affect the immune system several days after treatment.”
“Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use. The majority of snakes have control over their venom glands and are quite reluctant to waste their venom on humans. They very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious. Such patients are usually hospitalised for a day, carefully monitored and then sent home.”
“As already mentioned, some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used. Some of those victims go into anaphylactic shock which is a life-threatening medical condition and must be treated with adrenaline. This has to do with the fact that our antivenom is made from horse blood and the allergy is basically an allergy to horse proteins.”
Bill Haast – repeated snake bite victim from the world’s deadliest snakes tragically died at the young age of 100 from natural causes. ?
If snake bites regularly do not cause symptoms and do not require the use of antivenom, are snake bites really as toxic and harmful as we previously thought? Are the dangerous side effects linked to snake bites really just the reactions to having horse blood injected into the body as treatment? Is this another case where the treatment causes the symptoms of disease it was supposed to prevent? If the examples of these next few individuals are taken into consideration, it’s entirely plausible to conclude that we have been misled about the dangers stemming from snakebites in order to cover for the toxic effects of the treatment:
Repeated snake bite for recreation: Mechanisms and implications
“There is a debate in the fatality/immunity due to repeated snake bites in human beings either accidentally or incidentally. Haast and Winer[11] reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus[11] and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier.”
This snake-man got himself bitten over 200 times to become immune to venom
“Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was fatally injured about 20 times.”
“In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times as per the report published in Today I Found Out.“
Man makes deadly snakes bite him 160 times in hunt for human antidote
“An amateur scientist has deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom.
Tim Friede is obsessed by finding a human antidote to poisonous snake bites, which kill an estimated 100,000 people every year.
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra.
He said he experienced a “real throbbing sensation” but he “felt great” after the bites.
“It really hurts and it swells but that’s it,” he said.”
Poison pass: the man who became immune to snake venom
“A lot has been written about Steve Ludwin, widely known as the man who injects snake venom, and lately his life has turned into a non-stop frenzy of international journalists and film crews revelling in the seeming sheer insanity of it.”
“He’s been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years. “Snakes are fucking everywhere. The symbol for medicine is two snakes. They’re ingrained in our brain and DNA,” he tells me, proudly insisting that he hasn’t been ill for decades and has developed “a superhuman immune system”. And it’s tempting to believe him. He does look undeniably fit.”
The Photographer Who Was Bitten by a Black Mamba… and Got the Shot “After several minutes and then hours passed and Laita was still feeling fine — experts recommend heading straight for a hospital, by the way — the crew concluded that Laita didn’t have any venom in his system. The photographer believes that it was either a “dry bite,” when a snake doesn’t release any venom, or that his heavy flow of blood pushed out the venom.”
As can be seen, there are numerous examples of people being deliberately and accidentally bitten by the world’s deadliest snakes who are completely fine and do not require treatment from antivenom whatsoever. Are we to conclude that these people are the lucky few who somehow have amazing super-human “immune” systems that render snake venom ineffective? Or have snake bites and the associated symptoms of venom toxicity been blown out of proportion? Could this be a case where some have had bad reactions to a snake bite just as there are those who have severe allergic reactions to bee stings while the majority of snake bite and bee sting victims come away unscathed? Could this be similar to the supposed rabies cases where the majority of those who were bitten by “rabid” animals actually went on to be just fine without getting the rabies vaccination?
The Treatments Are Worse Than the Disease
It’s very apparent that in the case of monoclonal antibodies and anivenom, the adverse effects of the drugs are actually worse than the supposed diseases they are meant to treat. Could this be due to the fact that, like “viruses,” so-called antibodies have never been properly purified, isolated, and proven to exist? The results of studies using antibodies are regularly unreproducible and irreplicable. It is well-known that antibodies are in fact not as specific as are they are claimed to be and are said to regularly bind to the wrong proteins. Perhaps it is difficult to produce safe and effective products when the entities that are supposed to be produced and supplied in the animal blood are entirely theoretical? Maybe the ridiculous snake venom theory should be viewed in the context that it is a bad idea to be injecting anything, let alone animal blood, into our bodies in an attempt to make ourselves feel better when trusting the body and allowing it to heal is often times the best course of action we can take.
In Summary:
Dr. Bryan Ardis put forth a theory that snake venom is the cause of “Covid-19” primarily based on fraudulent genomic data
The snake connection stems from research linking proteins from the fabricated “SARS-COV-2” genome to bat and snake “coronavirus” proteins
The enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom
These peptides are “almost identical” to the venoms of animals and are regularly found in healthy humans and other mammals
Dr. Ardis pointed out that, based on a text, he uncovered the connection between antivenom and monoclonal antibodies and stated that theyare the same thing
He wrongly concluded that monoclonal antibodies are an effective treatment for snake poisons that could be in the vaccines, Remdesivir, and water
According to a Sept 2021 Cochrane Review, their certainty in the evidence for the use of monoclonal antibodies in the treatment of “Covid” for all non-hospitalised individuals was low, and for hospitalised individuals was very low to moderate
They considered the current evidence insufficient to draw meaningful conclusions regarding treatment with “SARS-CoV-2-neutralising” mAbs
Monoclonal antibodies are known to cause a range of side effects and reactions, which can be immediate or delayed
Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity
In February 2022, the FDA revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments
The data showed these treatments are highly unlikely to be active against the omicron variant which is circulating at a very high frequency throughout the United States
These treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens
In April 2022, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate “COVID-19” in adults and certain pediatric patients
Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of “SARS-CoV-2 viral” variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure, the FDA determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use
Importantly, although the FDA revoked this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone
In other words, the use of Bamlanivimab and Etesevimab was revoked as well as the use of Bamlanivimab but they can still be used together as an alternative to Bamlanivimab alone…
For the Omicron-specific Bebtelovimab authorized by the FDA in February 2022, possible side effects include
Itching
Rash
Infusion-related reactions
Nausea
Vomiting
Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other “SARS-CoV2” monoclonal antibodies and could occur with bebtelovimab
In addition, clinical worsening following administration of other “SARS-CoV-2” monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab
The FDA claims that it is not known if these events were related to “SARS-CoV-2” monoclonal antibody use or were due to progression of “COVID-19”
Treatment with Bebtelovimab has not been studied in patients hospitalized due to “COVID-19”
Monoclonal antibodies, such as Bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with “COVID-19” requiring high flow oxygen or mechanical ventilation
Antivenom carries the same risks of severe side effects and worsening condition as monoclonal antibodies
The listing for common side effects of Rattlesnake Antivenin include allergic reactions such as:
Flushing
Iitching
Hives
Swelling of the face/tongue/throat
Cough
Shortness of breath
Blue color to the skin
Vomiting, and anaphylaxis (severe allergic reaction)
Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered
There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use
Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered
The usual symptoms and signs are:
Malaise
Fever
Urticaria
Lymphadenopathy
Edema
Arthralgia
Nausea
Vomiting
Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis
Peripheral neuritis usually involves the shoulders and arms and pain and muscle weakness are frequently present, and permanent atrophy may develop
A 2019 review on antivenom stated that currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses
It is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia.
Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both
Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom
Around 70% of the immunoglobulins obtained do not act directly against venom toxins
According to a 2016 study, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent
The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors
The prevention of reactions will depend mainly on improving the quality of antivenom
According to their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects
Currently, after many improvements, antivenoms exhibit “acceptable” safety profiles yet antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50%
All snake bites are not equal and the quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously
A study led by Dr. Fry found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions
The results showed that the two African antivenoms were only effective against snakes from restricted ranges
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regionand it failed completely against African saw-scaled vipers
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry said
If someone does seek proper medical care but dies because of ineffective antivenom,it will be even harder to convince the next victim to seek out antivenom
Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes
Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet
From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom
There are endless myths about antivenom killing more people than the snake venom itself
Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite
Antivenom is relatively scarce, expensive and can have disastrous side-effects
Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use
Snakes very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious
Such patients are usually hospitalised for a day, carefully monitored and then sent home
Some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used
This has to do with the fact that antivenom is made from horse blood and the allergy is basically an allergy to horse proteins
Haast and Winer reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier
Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was seriously injured about 20 times
In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times
An amateur scientist named Tim Friede deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra
He said he experienced a “real throbbing sensation” but he “felt great” after the bites
Steve Ludwin, widely known as the man who injects snake venom, has been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years
He hasn’t been ill for decades and has developed “a superhuman immune system”
A photographer was bit by the deadliest snake, a Black Mamba, and after hours passed, he was still feeling fine and needed no treatment
The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent “SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and animal “coronaviruses” created in the very same way. Attempting to claim any connections between the random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place. Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines, the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial evidence that is easily debunked.
If we are to take the claims of Dr. Ardis seriously that the symptoms associated with snake venom is the true cause of a disease known as “Covid-19,” how does his theory explain for the fact that the antivenom and monoclonal antibody treatments cause the exact same symptoms of the disease they are supposed to treat? How would it be determined that the worsening clinical outcomes after injection are from the snake bites/venom rather than the antivenom/monoclonal antibodies given as treatment? How does his theory account for the numerous instances where people have been deliberately bitten by snakes, injected with the venom of snakes, and drank of the venom of the snakes with little to no harmful effects whatsoever? How does his theory account for the fact that the vast majority of “Covid” cases are asymptomatic and the vast majority of snake bite cases need no treatment at all? There are many holes in this theory which will easily be picked apart to make those who follow it look foolish for having done so.
There is no “SARS-COV-2.” There is no “Covid-19.” There is no new disease nor any new symptoms of disease requiring treatment from vaccines, monoclonal antibodies, Remdesivir, Hydroxychloroquine, Ivermectin, NAC, nor any other treatment. There is no need for any anti-venom supplements.
Beware those who will sell you the cause of the disease and the solution.
In a stunning move – soon to be filed under the “completely lost touch with America” folder – the Biden administration is reportedly planning to appeal the ruling that lifted the COVID mask mandate on travel, just hours after most major airlines and airports (and ground transportation) has dropped their mask rules.
It was evident this was coming earlier in the day after White House spokesperson Jen Psaki warned and Xavier Becerra, Biden’s health secretary, told reporters in Nevada, that “we are right now in the process of deciding, and we likely will appeal that ruling, but stay tuned.”
Jonathan Turley offered some insight before the actual decision was made to appeal if CDC thinks it necessary:
The Administration is going to have a hard time making this cat walks backwards. The cheering of passengers and pilots seemed as much as a communication to the Administration as it was a celebration. A large number of airlines immediately declared the mandate to be dead and unenforceable. It is like throwing a retirement party for an employee before they have decided to go. It is a tad awkward to express doubts when someone is showing you the door.
That is why those cheering videos could have a greater impact on the White House than any CDC or DOJ recommendation. The Biden Administration could still appeal as it has in past such cases. There will certainly be many DOJ lawyers asserting that they could win on appeal on the basis of agency deference. The question is who would tell the public. They may have to wait for the “ding, dong” parties to end.
But, given all that, they decided it was worth it…
Justice Department Issues Statement on Ruling in Health Freedom Defense Fund Inc, et. al. v. Biden, et. al.
WASHINGTON – The U.S. Department of Justice today released the following statement on Health Freedom Defense Fund Inc., et. al. v. Biden, et. al. from spokesman Anthony Colev:
“The Department of Justice and the Centers for Disease Control and Prevention (CDC) disagree with the district court’s decision and will appeal, subject to CDC’s conclusion that the order remains necessary for public health. The Department continues to believe that the order requiring masking in the transportation corridor is a valid exercise of the authority Congress has given CDC to protect the public health. That is an important authority the Department will continue to work to preserve.
“On April 13,2022, before the district court’s decision, CDC explained that the order w’ould remain in effect while it assessed current public health conditions, and that the Transportation Security Administration would extend its directive implementing the order until May 3 to facilitate CDC’s assessment.
“If CDC concludes that a mandatory order remains necessary for the public’s health after that assessment, the Department of Justice wall appeal the district court’s decision.“
So, if the CDC – against all the actual science – concludes that wearing a mask should remain mandatory, instead of leaving it as a personal decision, the Biden DoJ will appeal the ruling that was celebrated by most.
The more we ponder this decision, the more this smells like The DoJ throwing The CDC under the bus. The reason being that The CDC now has to come up with some “science” reason to re-mandate the masks (which we know they can’t) and therefore The DoJ is therefore covered if people try to blame them for not appealing.
And the winner of the most ironic sentence of the day goes to White House spokesperson Jen Psaki, who after relying on court ruling after court ruling to enforce varying levels of health tyranny for the last 15 months, uttered the following in her out-loud voice…
“Public health decisions shouldn’t be made by the courts. They should be made by public health experts.”
Who said the left doesn’t do humor… talking of which…
Babylon Bee has some advice for those still living in fear:
It can be difficult, though, to suddenly see all those triggering human faces after the government coddled you and fed your psychotic delusion and fear for the last two years.
Here are seven ways to cope:
Close your eyes and imagine everyone is wearing a full hazmat suit. – It’s a neat little trick that actually works.
Scream at the sky. – This is a well-known coping mechanism. It works especially well if you record your scream onto your TikTok account.
Play The Sims 4 and manage other people’s lives like you’re an all-powerful god to your heart’s content. – Now you can drown people by surrounding their swimming pools with an impenetrable wall of potted plants. You’re in charge here!
Upgrade to 3 or 4 masks, or just roll around in a giant hamster ball. – Keep upping the number of masks you wear, but if that’s not enough, go the hamster ball route.
Get your pilot’s license and start your own airline. – aIrLiNeS aRe PrIvAtE cOmPaNiEs ThEy CaN dO wHaT tHeY wAnT!
Just remember, we’re all in this together. – It’s just for a little while. It’s a small sacrifice to make. If it saves one toddler from a speech impediment it’s all worth it.
Never go outside again. – Curl up in a ball and live out the rest of your days in the corner of your home, completely safe from COVID.
Bear in mind that nothing is stopping the fearful from ‘masking up’ against the virus…
“you are free to wear masks if you like… if they work, they will protect you, if they don’t why mandate them?”
Presumably there are a number of “political science” reasons for the appeal:
1) “Trump” judge
2) Offering a bone to whatever is left on the ‘Democratic base’ amid the unhinged rantings of the blue-checks on Twitter as the dissonance suddenly strikes that they have been wearing face diapers for 2 years for no reason.
3) Making sure to maintain the role as the “party of science“…
4) …ok we couldn’t think of any more… apart from ‘scream to the sky’
Following a federal judge vacating the federal mask mandate on transportation, the TSA responded, “TSA (Transportation Security Administration) will not enforce its Security Directives and Emergency Amendment requiring mask use on public transportation and transportation hubs at this time.”
Within hours various airlines began notifying customers the mask mandate is gone:
♦ American Airlines – “In accordance with the Transportation Security Administration no longer enforcing the federal face mask mandate, face masks will no longer be required for our customers and team members at U.S. airports and on domestic flights.” (link)
♦ Southwest Airlines – “As a result of this development, effectively immediately, Southwest Employees and Customers will be able to choose whether they would like to wear a mask, and we encourage individuals to make the best decision to support their personal wellbeing.” (link)
♦ Delta Airlines – “Effective immediately, masks are optional for all airport employees, crew members and customers inside U.S. airports and on board all aircraft domestically, as well as on most international flights.” (link)
♦ Alaska Airlines – “Effective immediately, all Alaska Airlines and Horizon Air guests and employees have the option to wear a mask while traveling in the U.S. and at work. Masks are no longer required for travel and will be optional.” (link)
♦ United Airlines – No press release. “Masks are no longer required on domestic flights, select international flights (dependent upon the arrival country’s requirements) or at U.S. airports. More comfortable keeping yours on? Go right ahead… the choice is yours (you look dino-mite either way)!” ~Twitter
Various videos show airline employees in a state of jubilation cheering the announcements.
The professional political left is very sad, apoplectic and filled with anxiety. However, the overwhelming majority are happy. This example again reflects how small that minority of rabid maskers was. Easily a 4:1 ratio. Additionally, with all the major carriers and the TSA making official statements, it would be almost impossible to reinstate the mask mandate now. It’s over.
Plane applauded as the stewardess announced the end of the mandate. She broke into tears as she got to take off her mask for the first time in 2 years pic.twitter.com/WlCpZk30QM
“Ladies and gentlemen, this is your pilot speaking. This is the most important announcement I’ve ever made. The federal mask mandate is over. Take off your mask if you choose!”
A federal judge in Tampa, Florida has vacated the federal transportation mask mandate for planes, trains, buses and public Transportation. [PDF Ruling Available Here]
In essence, U.S. District Judge Kathryn Kimball Mizelle found the CDC exceeded its statutory authority with the mask mandate and violated the rules that guide CDC regulations. After Joe Biden arbitrarily announced the federal transportation mandate, the CDC triggered enforcement of the mask mandate without any required time for public feedback on a new regulation.
Within the ruling, one of the commonsense arguments against the federal mandate was noted. Prior to Joe Biden taking office there was no mask mandate. At the time Joe Biden took office and invoked the mask mandate, there was nothing substantively different in/around the spread of COVID-19 and the mitigation efforts underway.
The federal mask mandate was arbitrary and capricious with no justification from the CDC and no required time for the public to provide feedback. The government’s legal argument was that public feedback, comments on rulemaking, was irrelevant because the mandate was going to be enforced regardless of public opinion. That argument was summarily dispatched by the judge saying, just because the government has a pre-determined outcome in mind does not relinquish them from the obligation to follow the rules.
Sensing they were going to lose the case, remarkably the government lawyers argued that only the original plaintiffs in the lawsuit should be granted relief. Meaning, only the two people who filed the lawsuit should be exempt from the federal mask mandate. That didn’t work.
The federal transportation mask mandate is vacated.
Over the past week or so many people have sent us links to the documentary Watch the Water, a 50 minute interview with retired chiropractor Dr Bryan Ardis, who details his theory that “Covid” is caused by chemicals extracted from snake venom being added to the water supply.
Further, Dr Ardis claims that the same venom-based chemicals are in the vaccines and the drug remisdevir, and that researching the venom connection has already got one scientist killed.
Some notable names in the alternate media are giving it some air time, even Dr Reiner Fuellmich has said he will look into it.
He shouldn’t. It is pure nonsense.
A ridiculous theory that flies in the face of observed reality, supported only by anecdotal evidence, biblical metaphors and clips from an episode of The Blacklist.
But good news, if there IS snake venom in the water Dr Ardis can cure you – just spend 120 bucks on his antidote through his website. That’ll drive the venom right out of you.
They are literally selling snake oil.
The blurb alone tells you this is manipulation:
The plandemic continues, but its origins are still a nefarious mystery. How did the world get sick, how did Covid really spread, and did the Satanic elite tell the world about this bioweapon ahead of time?
Reality check – “The world” DIDN’T “get sick”. “Covid” was NOT a “bioweapon”. It DIDN’T “spread”.
The Powers That Be (PTB) just want you to think all this is true, and these guys are, knowingly or not, helping that along.
The whole thing looks very much like the latest attempt at introducing mainstream COVID fear porn through an “alternative” back door.
The superficial narrative in these cases may vary, but the underlying message is always the same – “Be afraid of COVID, because it is a real thing”
The PTB don’t really care if you’re afraid of a virus, a MANMADE virus, 5G…or snake venom in the water. Just so long as you believe COVID is real, new and deadly
The only really inadmissible thing has always been the truth – COVID is a scam. A pea-and-thimble game on a massive scale. Because you can’t govern through fear if no one is afraid.
Is someone dumping “snake venom” in the water?
Maybe. Who knows. The world is insane.
But it has ZERO to do with the “COVID pandemic” because the covid pandemic was made up.
“Darkness has the ability to cover up; light has the ability to uncover! Darkness is the enemy of truth; light is the friend of truth!
~ Mehet Murat ildan
Sometimes acceptance of obvious truth is so stark and thought to be fraught with treachery, that it is literally ignored by the many; making it more comfortable to remain hidden in madness amidst the shadows of deception and lies. While taking responsibility is the only way forward, fear of the truth often wins out, as reliance on collective ignorance gives the false illusion of safety. This behavior is always severely destructive over time, and any psychological relief always temporary, but much more often than not, it is the easy way out for the non-thinking and frightened societal herd. This natural flaw in the makeup of man is well known by the ruling class, and therefore taken advantage of in order to quell dissent and rebellion while gaining further control.
Considering our recent and current history, this was the tactic used for the entirety of the ‘covid’ scam. So long as voluntary acceptance of state propaganda by the masses prevails, this strategy will continually be used going forward in order to perpetuate the advancement of the takeover of humanity in the name of the “Great Reset.” That brings us to the latest threat by the purveyors of evil who have been allowed to rule without resistance. They claim, as voiced by former Trump appointed director of the CDC, Robert Redfield, that the next wave of monumental death worldwide will be due to a non-existent mystery bird flu. This approach by government to manufactured threats, has been around for a very long time, and in the past has been used to frighten the weak, but it is simply a lie.
Threats of avian bird flu, swine flu, including SARS, among many others, have been weapons of the state meant to accelerate panic where none is warranted for very many years. It is imperative to understand that these toxic concoctions are all manmade in labs using gain of function to create bio-weapons. They are not natural, or some lethal strain that just so-happened to affect birds or other animals by accident, and magically jumped to humans. Even the idea of this is ludicrous. If in fact, any such sickness or disease of these types were actually causing mass death, it would only be due to a purposeful release of a bio-weapon by the state, not any innate strain of a normal malady. Knowing this, how could entire populations continue to be so fooled by propaganda?
In 1997, the CDC said that “avian influenza A(H5N1) viruses first spread from poultry to infect humans in Hong Kong resulting in the deaths of 6 of 18 infected persons.” Because of this, the evil WHO and the U.S. sought to increase pandemic preparedness, obviously knowing that this would be useful indoctrination in order to create panic due to future plans to gain power over society. All of this was aligned with the WHO’s “global framework.”
In 2002, SARS was said to be the new disease to fear, and SARS-CoV was to be the “model for future pandemics.” In March of 2003, the ‘novel’ coronavirus, SARS-CoV, was said to be isolated, a lie, and identified and sequenced by nothing other than PCR, an impossibility. There was even the spectre of a future “catastrophic pandemic,” and investigations of live animal markets, as the supposed first case was found in Hong Kong, and said to be able to spread by infected persons traveling by airplane. Does this sound familiar or suspicious to any thinking individual? Is this not the same exact fraud that took place beginning in 2020, two decades later?
In March of 2006, Michael Chertoff, head of Homeland Security, an obvious expert on bird flu, was worried about a bird flu strike any day. “I can’t predict, but I certainly have to say that we should be prepared for the possibility that at some point in the next few months, a wild fowl will come over the migratory pathway and will be infected with H5N1.”
As far back as 1976, the H1N1 Swine Flu hoax took center stage, as the government and its controlled media propaganda campaign went into high gear in order to create a pandemic fraud so as to mass-vaccinate the U.S. population against a non-existent ‘swine flu.’ This conspiracy was also used as a way to get all ‘vaccinations’ available into every person possible. This led directly to 45 million people getting unnecessary injections. At the time, the CDC stated that 80% of the population needed to be ‘vaccinated,’ just as was sought in the ‘covid’ scam.
Again in 2009, the H1N1 fraud was revived, and another government call for mass ‘vaccination’ was issued. As always, the collusion between national and global ‘health organizations, government and government officials, pharmaceutical companies, and corporate insiders was evident. Nothing today has changed, it has only gotten worse, and in fact, the risk now due to the world takeover plot is much more sinister, and globally structured.
In the distant past, while control was a key factor, money from mass ‘vaccination’ was the primary goal. Today, money is a factor, but control of the minds and bodies of the proletariat herds is the result most desired by the ruling ‘elites.’ In addition, depopulation and eugenic transformation of the rest of society, all by way of controlling and lethal injection of a bio-weapon, is what is needed in order to finish the global takeover agenda.
This is a long-term plot to fool the public into believing and expecting that a future pandemic of epoch proportions is imminent. The very idea that ‘natural’ pandemics are inevitable has long been planned and embedded in the minds of the people. This is a multi-decade brainwashing of the common people in order to prepare them for not only mass sickness and death, but also for acceptance of a global governing body with unlimited power.
The most sought-after goal at this time is mass ‘vaccination,’ but this time is different in that the preferred injections are much more dangerous, much more able to physically and psychologically control large numbers of those who have taken the jab, and cause mass death beyond anything seen before. In order to accomplish such a deadly and evil agenda, the people will need to be fooled once again. They will have to believe the lies, and accept that all the impending deaths due to the weaponized ‘covid’ injections, are in fact due to a fraudulent and purposely crafted plot to place blame on a non-existent ‘virus’ that is being called an “avian bird flu.”
The ‘warning’, or more accurately, the foretelling of mass death by the ruling class, as outlined by the ex-CDC commandant Robert Redfield, is that 800 million to 4 billion of us will die due to some mystery bird flu. When the mass deaths occur, it will not be due to any flu or ‘virus,’ it will be due only to the toxic poison that has been previously injected into billions of unsuspecting, order-following slaves to the state.
What type of contamination might be found in a spiked COVID vaccine?
“A foreign body.”
The lot is being recalled due to a foreign body being found in one vial in the lot manufactured at the company’s contract manufacturing site, ROVI – Moderna and ROVI Pharma Industrial Services
Moderna Pharmaceutical, formerly named ModeRNA Therapeutics, became a public company in 2018, specializing in infectious diseases. Prior to the IPO, AstraZeneca was its third-largest investor.
Moderna’s coronavirus shot, known as “SPIKEVAX,” was said to have been approved by the U.S. Food and Drug Administration (FDA) for adults 18 and older on Jan. 31, 2022. But according the the FDA Factsheet, the shot is still only Emergency Use Authorized or EUA. Not approved!
Since November 2020, two of the 4 Biotech companies working to manufacture mRNA “therapies,” — Johnson & Johnson and AstraZenica — had to halt trials over safety concerns. And now the spotlight shines on Moderna’s mRNA vaccine deployment in Europe.
The contaminated lot in question was manufactured at the ROVI site in Spain, and distributed in Norway, Poland, Portugal, Spain, and Sweden from 13-14 January 2022. Reports tie the recalled batches to the Spanish company, ROVI.
Criminal Acts
Will Moderna be investigated for fraud, product safety, death by vaccine?
In February 2021, US officials investigated and acknowledged a “likely association” between Moderna and Pfizer vaccines and myocarditis in adolescents and young people. Of course, the PREP Act and CARES Act both limit liability for death or serious physical injury resulting from these products. See also Moderna’s disclosure in the SPIKEVAX package insert, referencing Myocarditis and Pericarditis, Section 5.2.
All Phase 3 COVID-19 vaccine trails are ongoing and not due to conclude until late 2022/early 2023. The treatments are currently experimental with only 1 year of short-term data and no long term safety data available.
In November 2020 Dr Andreas Noack, a German chemist and one of the EU’s top graphene experts, released a video explaining that he had discovered graphene hydroxide contained in the COVID-19 experimental treatments. He described how the graphene hydroxide nano structures injected into the human body act as ‘razor blades’ inside the veins of recipients and how they would not show up on an autopsy or normal toxicology tests given their atomic size. On 26th November 2021, just hours after publishing his latest video about graphene hydroxide, he died in suspicious circumstances. [See Summary].
Professor Dr Pablo Campra, University of Almeria, Spain also examined Covid-19 experimental treatments in November 2021 using Micro-Raman Spectroscopy, the study of frequencies. He also confirmed the presence of graphene oxide.
Today’s high drug prices show little has changed since 1963, when The Federal Trade Commission ruled that six of the nation’s largest drug companies were conspiring to fix prices on tetracycline, the most widely used antibiotic. The Kefauver drug hearings confirmed the existence of a national crime syndicate and revealed lax enforcement that continues to this day. Note, one of the “big six” criminals, Wyeth Pharmaceuticals, was absorbed by Pfizer.
Gene Therapy or Gene Reset?
Experts contend that the technology in the Pfizer/BioNTech and Moderna shots are not “gene therapy.” But that is not how the experimental products had first been marketed.
According to a November 2021 article at LifeSiteNews, during the 2021 Global Health Summit in Berlin, Bayer executive, Stefan Oelrich, told fellow “experts” that the mRNA COVID “vaccines” are actually “cell and gene therapy” that would have otherwise been rejected by the public if not for a “pandemic” and favorable marketing.
Oelrich also highlighted the term, “Bio Revolution” as:
a confluence of advances in biological science and accelerating development of computing, automation, and artificial intelligence [that] is fueling a new wave of innovation.
As part of his company’s role for “sustainability” Bayer also pledged to push contraception on 100 million women across the world. This rhetoric fits hand-in-glove with Klaus Schwab’s Socialist plan for the “Great Reset.”
Damage from the mRNA injectables are surfacing. According to an October 2021 study in the American Journal of Cardiology:
Sixty percent of the myocarditis related COVID-19 vaccine cases were associated with the Pfizer-BioNTech vaccine, 33% were associated with the Moderna vaccine, and 7% were associated with the Johnson & Johnson vaccine.
According to a November 2021 abstract published in the Journal Circulation titled, “Observational Findings of PULS Cardiac Test Findings for Inflammatory Markers in Patients Receiving mRNA Vaccines:”
…the mRNA vacs numerically increase all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle…
Ignorance Is No Excuse
Ignorance is no excuse in the Age of Information. As more information surfaces, do not expect drug companies to change their criminal ways.
The information is available and viewable for anyone who can do a Google search. Drug companies have subtly disclosed the information if you can read about it here.
If any change will come of these revelations, that change rests with each of us. There are no “good” or “bad” experiences. There is only “experience” from which we all choose to learn more.
Children today are being systematically and deliberately destroyed – both mentally and physically.
We are horrified at the way children were pushed up chimneys in the 19th century. Making children work long, arduous hours was considered normal at the time but the children abused in this way were scarred physically and mentally for life.
Today, we like to think that that sort of cruelty is today confined to those parts of the world where children are employed as slave labour in order to dig out the rare minerals needed to make batteries for electric cars.
And, of course, to the factories where slave labourers make overpriced plimsolls or manufacture mobile phones – all at such a low prices that billionaires can progress up the ladder and become even richer.
We like to think that most countries in the so-called developed world have moved on. We close our eyes to the billionaires growing ever richer on the backs of slave labour children.
Those pulling down statues of 19th century slave traders still buy the electric cars, the mobile phones and the absurd shoes and ignore the uncomfortable truths about how they were made.
In the 19th century, child labour was seen as normal and acceptable. In both physical and psychological terms what we are doing now is even worse.
For no sensible, medical reason our world has been turned upside down and millions of children will never recover. (In Africa, of course, millions of children will die as a result of the lockdowns and deliberately staged global panic.)
There is evidence that as a result of the covid hysteria many children have become withdrawn and frightened of approaching strangers – especially if they are not wearing masks.
A children’s charity has seen a massive rise in the incidence of mental and emotional problems in children under 11 years of age. Children are worried about dying, about their friends and family dying, about their future, about missing school, about loneliness, about future epidemics. The AIDS hysteria of the 20th century has become the covid hysteria of the 21st century.
As a result many are either not eating, or eating too much, and they are not sleeping. Panic attacks are becoming commonplace. A study of 10,000 parents showed that 30% of children were worried about catching the virus and 30% were worried about missing their education. Even more worrying 16% were afraid to leave their homes. More than half of the parents were worried about their children.
And yet deaths among healthy children are so rare that it has been suggested that lightning is a bigger threat to children and that it would make more sense to tell children to wear helmets to protect them against meteors than to recommend that they wore masks or practised social distancing.
Nevertheless, schools introduced masks and social distancing, and many teachers and parents want the restrictions to continue indefinitely – until the very last virus on earth has disappeared.
In Ohio, electronic beams were introduced to track school pupils and to enforce social distancing.
In China, robots have been installed to ensure that children wash their hands properly.
Some schools have installed thermal imaging cameras to see if children have a temperature. (This is entirely pointless).
One educational establishment in the US made a viral tracking app mandatory and students were constantly tracked. Students who turned off the app or tried to leave the campus without permission were expelled.
Under normal circumstances, young children touch and hug one another and derive great comfort from this.
Forcing children to remain isolated has created huge psychological problems. Children from poorer families or where there is an unhappy home life have suffered most. Also, the lack of exercise will result in health problems and obesity.
The problems have been exacerbated by threats that children who do not obey the rules `may kill granny’. (The irony is that their government wants to kill granny with blanket DNR notices in hospitals and care homes and by denying medical treatment to older citizens.) Children have seen adults frightened and as a result child terror has been exacerbated.
Many children have become socio-phobic and are developing OCD.
Figures for suicide are nigh on impossible to obtain but suicide is widely recognised to be a leading cause of death in the 5-19 age group, and one survey showed a 50% increase in suicides in 2020 compared to 2019. I suspect the figure will grow.
In an attempt to escape from reality, children are spending vast amounts of time on the internet. Gaming addiction is becoming an increasing problem with cyberbullying adding to anxiety and depression. Sports and out of school activities have been abandoned or disrupted leading to increased boredom, loneliness and depression.
Equally worrying is the fact that altered behaviour in children will frequently be diagnosed as ADHD and drugs such as Ritalin will be prescribed as a long-term remedy.
All this for an infection which children hardly ever catch and hardly ever transmit.
It’s all madness.
The whole fraud was deliberately designed by billionaires and their evil supporters.
And although politicians, their advisors and the medical establishment are guilty of mass genocide for the part they have played, parents and school teachers must also be held responsible.
If parents and teachers had done a little research, they would have known (and would know) that the covid-19 scare is fraudulent.
Their children’s lives have been sacrificed for nothing.
Last week we reported over 4000 police officers are slated to have their religious exemptions to vaccination denied and they will eventually be fired. Yesterday NYPD sources told us nearly 180 police officers had their exemptions officially denied and will be fired within 7 days if they don’t get vaccinated or voluntarily retire. If an officer is fired they give up all rights to their pension and are left with nothing.
These denials were announced the same day 18 people were shot by a gunman in NYC subways and there was not a single transit officer to be found on the scene.
The number of 4,000 we reported last week was incorrect. It is actually 4,875 cops and 1,112 civilians at NYPD that are currently unvaccinated, according to reliable sources in the NYPD. These officers and employees are currently working everyday with a weekly testing option in effect. All of these numbers are coming from NYPD Officers I am in direct contact with who are following the situation extremely closely because their careers are on the line.
Mayor Eric Adams has effectively admitted all of these NYPD officers and employees are slated to be fired. In an interview on CBS News with Marcia Kramer the following exchange occurred discussing the recent firings of NYC workers for declining covid vacciantion:
MarciaKramer: So, if the money permits, would you ever consider rehiring some of the 1,400 people who’ve lost their jobs because they refuse to get the COVID vaccine. Because it looks to me like given the fact that there’s about 5,000 others who have asked for exemptions and didn’t get them and now are appealing, that you could lose a lot more people including a large number of police, fire, and emergency service workers...
Mayor Adams: Well, people should really understand the numbers, the overwhelming number of civil service and city workers. They complied. Under the second wave that we just saw, we did not lose any police officers-
Kramer: You’re about to.
Mayor Adams: I’m sorry?
Kramer: I think you’re about to, because their appeals are now being denied.
Mayor Adams: No, I am hoping that they are smart enough to know that it is imperative to take the vaccine for themselves and their families …
Kramer: So you’re asking them to change their mind?
Mayor Adams: Yes, I am.
[emphasis added]
***
NYPD employees have no first amendment rights of free speech when it comes to their job. If they speak, they get fired. As police officers are now finally directly facing the loss of their jobs, leaks are starting to come forward:
Look at this reply to Mayor Eric Adams regarding the coming firing of nearly 200 Police Oficers due to religious exemption denials:
We need the mainstream media to hold Mayor Eric Adams accountable. The NYPD has massive staffing shortages already! The city cannot afford losing thousands of police officers.
Last November, 2021, news reports threatened that if people who die of COVID were not vaccinated, their families may not get death benefits they would otherwise have received.
If the only guarantee in life is death, then at least there is life insurance, right?
Wrong! Fast forward to the Post-COVID Era, and the fallout from Emergency Use Authorized (EUA) vaccines. According to Forbes Magazine, if today you choose to receive a COVID-19 injection, it could prevent you from receiving a death benefit from your life insurance.
Say what?
No More Death Benefit
According to an article by Brain Peckford, a recent post-Covid vaccine death in France was ruled to be “a suicide” by a judge, due to the experimental nature of the “vaccine.” The insurance company refused to pay. No death benefit. The article reads:
A wealthy elderly man with a high value Life Insurance policy to the amount of millions of euros… dies from the covid jab. His death as a consequence of being jabbed is not disputed by the doctors, nor his life insurers. The Insurance company refused to pay the policy, citing that the taking of experimental drugs, treatments, etc., is excluded from the policy. The family takes the insurance company to court and they have just lost the case.
The judge stated, “the experimental vaccine side effects are publicised and the deceased could not claim not to have known about them when he voluntarily took the jab. There is no law or mandate in France which forced him to be jabbed. Therefore, his death is essentially suicide”.
Suicide is explicitly excluded from this particular policy and in fact from all life insurance policies in general.
This has been the finding of a major western world court system and there is zero doubt that insurance companies world wide will cite this case as legal fact.
Therefore, if anyone ever challenges you on whether these jabs are experimental or not, and that neither the pharma companies, nor govts, nor anyone else but YOU are responsible for accepting them and if you die, legally you have committed suicide.
No insurance, no payouts, no refunds. You are on your own!
Listen to Dr. Pierre describe the same story and explain the view of the American Council of Life Insurers; that insurance companies may deny payment of death benefit if death results from the experimental COVID injection.
How could this possibly be? One moment the experimental vaccine and the boosters protect you against COVID, but the next moment they do not? One moment you are insured with the injection, but the next moment, you are not? As the French say, “C’est la vie. C’est la guerre!” Meaning? Such is life! That’s war. It can’t be helped!
Changing Narratives
Changing narratives happen by design. Those who own the narrative control the outcome. Moreover, in America, under the Smith-Mundt Modernization Act, the media is free to legally propagandize Americans. The EUA vaccines, once advertised to “save lives by preventing deaths” from COVID-19 coronavirus infections, are now “suicidal.”
In May 2021 it was a different story. According to the American Council of Life Insurers, life insurers could not deny a death benefit because the deceased was vaccinated against COVID-19:
A social media post appears to be behind the spread of entirely false information, suggesting a COVID-19 vaccine could be a factor a life insurer considers in the claims-paying process. The fact is that life insurers do not consider whether or not a policyholder has received a COVID vaccine when deciding whether to pay a claim. Life insurance policy contracts are very clear on how policies work, and what cause, if any, might lead to the denial of a benefit. A vaccine for COVID-19 is not one of them. Policyholders should rest assured that nothing has changed in the claims-paying process as a result of COVID-19 vaccinations.
But good propaganda shifts with the winds. Today’s America is not yesterday’s America. America has been hijacked, morally corrupted, debauched, and sold to the highest bidder.
In fact, if you received the Pfizer/BioNTech, Moderna, or Johnson & Johnson COVID-19 vaccines, you received a vaccine deemed “emergency use authorization” (EUA) from the FDA. No EUA injections are FDA-approved vaccines. Further, the first injections deployed were labelled “experimental.” Thus, participants who consented, without proper Informed Consent, became subjects in an ongoing clinical study. Note: Life insurance companies do not cover experiments.
In other news, if you are unvaccinated and hospitalized, insurance may not pay either. A news release from the University of Michigan states:
“Many insurers claim that it is justified to charge patients for COVID-19 hospitalizations now that COVID-19 vaccines are widely available,” said lead author Kao-Ping Chua, M.D., Ph.D., a health policy researcher and pediatrician at Michigan Medicine and the Susan B. Meister Child Health Evaluation Research Center. “However, some people hospitalized for COVID-19 aren’t eligible for vaccines, such as young children, while others are vaccinated patients who experienced a severe breakthrough infection. Our study suggests these patients could substantial bills.”
To recap: if you are 1) Unvaccinated and hospitalized, or 2) vaccinated pre-death, then life Insurance does not pay what you might expect, if at all.
The Double-edged Sword
Read the article Dissolving a Pandemic of Fear, to understand that this trend first began in distant lands during the summer of 2021 with unusual side effects to the globally-deployed experimental vaccines:
Because of the uncertainties from unauthorized tests and experimental vaccines, insurance companies in India and Korea are limiting what they will cover if someone becomes sick from the COVID injections:
Contrary to popular perception, existing health insurance policies are unlikely to cover the cost of vaccination and adverse reactions, if any. Only policies designed purely for the COVID vaccination process — there is none at the moment — will cover the costs.
If you consented to an EUA injection, your life insurance policy has changed. You can’t win for losing, and you can’t claim your life insurance for dying. Something that cuts both ways is known as a double-edged sword.
Justice Through the Courts?
The federal PREP Act and CARES Act prevent practically all civil litigation, ranging from COVID “vaccines” to “tests,” to doctors/pharmacists/nurses. All have blanket civil (but not criminal) protections. All prosecutions are 100.0% discretionary, meaning that even if one admits to a criminal (COVID) act, no private citizen has the power to prosecute any alleged criminal act. That power rests solely with the district attorney and attorney generals — not citizens.
What does this mean? ALL prosecutions are political. In other words, The ONLY way to legally challenge all the “COVID” treason is confined to CRIMINAL prosecutions. Evidence proving criminal fraud has been submitted to the appropriate authorities, and yet there have been no criminal prosecutions through the Department of Justice. Why not? Good question.
What about life insurance fraud? Can insurers be prosecuted in the courts if the Life Insurance Council COVID policy is against the policy holder?
In response to a FOIA request, a federal district judge recently ordered Pfizer Inc. to release 55,000 pages of documents each month, after Pfizer claimed it would not disclose any data for 75 years. That means all the Pfizer vaccine data should be made public by the end of September 2022, rather than the year 2097.
Yet, who is in charge of sifting through the flood of information? What are the consequences of learning the truth that was meant to be hidden? No one knows. What about the fact that government appears to be practicing medicine without a license? How could this possibly be?
Because the narrative is always written by those who control the pen, you must do your own research and captain your own ship. Call your insurance company directly. Ask an “expert” if getting the vaccine will affect your life insurance coverage in any way. Ask if future EUA jabs will affect your premiums or payouts.
Then ask yourself if paying those high insurance premiums is worth the outcome in The COVIDIAN Age, or if it is better to put your money elsewhere.
As the World Council for Health (WCH), our partners and allies have already sought to draw attention to, the World Health Organization (WHO) has proposed a global pandemic agreement that will give it undemocratic rights over sovereign people. See the WCH Open Letter in response to this attempted power grab here.
WHO has quietly opened the floor for comments on the agreement but has provided little time to do so ahead of the first round of hearings scheduled for April 12 and 13.
We encourage everyone to share their thoughts with World Health Organization before the deadline.
1. Go to the World Health Organization website to submit a written submission now
Written submissions are short and can be up to 250 words/1250 characters. The deadline for written submissions is 3 pm UTC on Wednesday, April 13.
Submissions must be in response to the provided guiding question: What substantive elements do you think should be included in a new international instrument on pandemic preparedness and response?
The prompt provided by the WHO does not ask the people of the world whether or not they believe a global agreement is necessary. Instead, the organization has decided for itself that this measure is warranted and is asking for input on what people believe should be included in it.
Refrain from making any statements unrelated to the topic at hand; and
Be presented in a respectful manner, free of any profanity, ad hominem attacks, vulgarity, or other inappropriate language.
If participation, spoken or written, does not conform with these requirements, as determined solely by WHO, the participation will not be receivable. This means that WHO may call speakers to order, and/or discontinue speakers’ connections, and elect to not post written statements.
Why do I need to frame my submission using WHO’s provided context?
Because the WHO reserves the right to judge the relevancy of submissions, it is important to respond to the prompt in an appropriate yet constructive manner. As such, the World Council for Health suggests the following elements be addressed:
National and local leadership retain full autonomy, reserving the right to make decisions based on what is best for their own people.
The ability of nations and local municipalities to opt out of any and all portions of the agreement as they see fit, without consequence.
An open and transparent process with the ability for all people of the world to vote on including failsafe measures that will prevent the application of the global agreement in places where a majority of the people do not want it.
Measures that do not allow for influence in the process by any and all pharmaceutical companies or other global health profiteers.
The hearing will be livestreamed here on Tuesday, April 12.
cover image based on creative commons work of Caniceus
Dr. Naomi Wolf at Defeat the Mandates Rally: “You Hurt Our Kids & Watch Out. Because You Have Never Faced the Rage of Thousands of Mothers & Stepmothers”
In an exclusive interview with The Defender, Jeffrey Beauchine said his mother, Carol, knew her Creutzfeldt-Jakob Disease was related to the Moderna shot. Watching her death was like “something you see out of a movie,” he said.
In an exclusive interview with The Defender, Carol’s son, Jeffrey Beauchine, said it was excruciating to watch his 70-year-old mother — who was healthy until she got the vaccine — die from a disease he believes the vaccine caused.
“I’ve seen a lot in my 20 years as a police officer,” Beauchine said. “I’ve seen hundreds of people shot and this affected me more than anything.”
Beauchine said Carol received her first dose of Moderna on Feb. 16, 2021, and didn’t report any complaints. After getting the second dose on March 17, Carol immediately said she “felt different.”
Beauchine said:
“On March 17, she got her second dose and immediately started having reactions to the second dose. She just had this malaise. She just didn’t feel right and said she just felt ‘off.’ She had what she described as pain and burning at the injection site — like someone was tying a hot rope around her arm. Then she explained it as this numbness setting in around the injection site.”
Beauchine said he and his family members didn’t think it was a usual side effect, but they also didn’t think it was unusual.
“We just thought it was a result of the jab working through the system,” Beauchine said. “Then the numbness spread up through her neck and down her left arm.”
The numbness altered Carol’s hearing and spread “down through her hands” until the left hand lost sensation and mobility.
Beauchine said:
“At this point, it was her entire left arm. She started to develop insomnia. She would go a couple of days at a time without sleep and then she was fatigued. This numbness continued to spread. It went down to her hip and moved to her knees, then the entire left side. You could almost bisect her body and the left side was numb and the right side was normal.”
Beauchine said Carol went to the doctors — who initially thought she had suffered a stroke — but her MRI scans were completely normal.
“Nobody could find anything wrong with her so they sent her home,” Beauchine said. “It was almost like reassurance, while at the same time I wondered why they couldn’t.”
Carol then developed tremors in her left arm.
“It was almost like her arm would start jerking involuntarily,” Beauchine said. “Then the tremors moved on to the left leg.”
Beauchine added:
“My mother began to complain that something was wrong with her brain. She said she couldn’t put thoughts together or make sense of things but she could still communicate. Over the phone, you wouldn’t see the altered version of my mom I knew for 44 years.”
Then Carol developed double vision that ultimately led to blindness, and she began to hallucinate.
“She would see herself falling out of the chair and she would physically see herself on the ground,” Beauchine said. “It was weird to understand. She developed a fear of water and would become scared she was near a body of water.”
Doctors believed Carol was suffering from anxiety because of the shot and started treating her for anxiety. Meanwhile, Carol lost the ability to walk.
Beauchine said:
“She was still at home at this time because the hospital couldn’t find anything wrong with her. She was pretty much in a wheelchair. She went from the one who takes care of everybody to my 70-year-old father taking care of her. Then it got too hard for him and during one doctor’s visit they admitted her to see if they could dive into it further.
Beauchine said doctors ran every test “under the sun,” including an MRI, but couldn’t find anything. The only things doctors noticed were the obvious mobility problems on the left side of her body and balance problems.
The doctors also said there was “something off with her cerebellum but they didn’t know what it was,” he added. Carol tried to explain to the doctors that there was something “internally” wrong with her.
“She was then released to a nursing home,” Beauchine said. “It was the first time I saw my mom really sick.”
He said:
“She was in a nursing home where all this COVID was going on and we had to stand outside the window and yell through the air conditioner hole to talk to my mom. She felt defeated and scared, and my father cared for her 18 hours a day — spoon-feeding her — until the end. It just happened so fast.”
Eventually, Carol was able to get into a skilled nursing home, but she deteriorated rapidly.
“She lost the ability to feed herself because she couldn’t get the food on her fork to put it in her mouth,” Beauchine said. “It crushed me because I could see in her eyes without us having any convo, the fear and like she was defeated.”
Beauchine said there were no more good days and his mother lost the ability to communicate.
“By mid-end of July my mom was just a complete rigid person,” he said. “Lips stopped moving. She could only get a couple of syllables out. She would almost be falling out of a wheelchair in a forward position. She couldn’t tell if she was sitting up.”
Beauchine said his mother knew from the very beginning her condition was related to the shot.
“We all knew from the very beginning it was related to the shot, but we didn’t know the future significance of how bad this would get,” Beauchine said. “People have bad reactions all the time but you get over them. She didn’t get over them.”
Beauchine said the doctors didn’t know what to do because “it was just so new.”
“I’m more content with a doctor telling me they don’t know if it’s the shot because there’s no research than the doctors who say it’s definitely not the shot,” he said. “I got more ‘I don’t knows’ than denials.”
By the end of July, Carol’s husband couldn’t wake her up at the nursing home and the family had a meeting and decided their mother needed to go back to the hospital.
Beauchine said:
“When I rounded the corner, I saw my mom and it was like she was like yelling or howling. Her eyes were completely fixed in the open position. Her mouth was stuck in the open position and she had violent tremors that wouldn’t stop. She didn’t understand what was going on. The only way I can put it is a bomb went off inside of her head.
“It was excruciating for all of us. My dad was like a deer in the headlights — a blank look I had never seen before. And I’ve seen a lot of stuff in my life with my job but this was like … a bomb went off in my mom’s head and all of her limbs were convulsing and tremoring.
“It’s like something you see out of a movie. They say with this disease you come to the cliff and it’s just a drop-off and once you drop off you’re able to physically see that dropping point — and you could see it that night.”
Doctors sent Carol to Strong Memorial in Rochester, New York, and within weeks they confirmed she had CJD.
“We didn’t know what CJD was, but we were told it was like mad cow disease but like a different variant or different mode of getting it,” Beauchine said. “Same disease but a different way of getting it.”
Carol’s prognosis was fatal and the family was told she had only days left. Beauchine said a panel consisting of doctors and students who were overseeing Carol’s case were open to the fact they did not know what caused her CJD.
“People were learning and they said ‘we don’t know if this is related to the vaccine or not. We don’t know because the vaccine is new and there weren’t a lot of studies on the vaccine. We won’t know until the long-term.’”
Carol passed away on Aug. 2, 202, from CJD — a condition she did not have prior to receiving her second dose of Moderna a few months earlier. Her doctors filed a report with the Centers for Disease Control and Prevention’s Vaccine Adverse Event Reporting System (VAERS I.D. 2180699).
VAERS is the primary government-funded system for reporting vaccine adverse vaccine reactions in the U.S. According to the CDC’s website, “CDC and [U.S. Food and Drug Administration] clinicians review reports of death to VAERS including death certificates, autopsy and medical records.”
Beauchine confirmed the family has never received any contact from the CDC regarding his mother’s death, and to his knowledge, her doctors haven’t either.
Beauchine said Carol was a relatively healthy person with no previous history of COVID. Her only underlying condition was arthritis.
“She was always taking care of other people and when the whole COVID thing broke out in the media, she wanted to stay protected so she could see her kids and grandkids,” Beauchine said. “She didn’t want to be hindered by the virus, so when the opportunity arose for her age group, she got the first dose with no complaints.”
Beauchine said he also received the COVID vaccine because it was required for his job.
“At the time, there was a little smidgeon of excitement because they had you so feared over COVID-19 and finally there was a little light at the end of the tunnel,” he said. “And it was going to be okay.”
He added:
“I got the vax. My wife got the vax. My father got the vax. My children will never get the vax. I’m not against a COVID-19 vaccine but it takes years and years and years of clinical trials and studies to deem something safe to put in the human body, and that wasn’t done. We all turned a blind eye to it at the time in moments of hope.
“I didn’t know any of this stuff that we know now, and then you come to find out that hydroxychloroquine and ivermectin have been used off label for years, but to get the Emergency Use Authorization (EUA), you have to show there’s no treatment available to be able to give that authorization, so they killed the treatments, gave the EUA, but there’s no liability on their end.
“It’s just scary nobody knew that at the time. If somebody wants to make an informed decision, let them know what they’re up against.”
Beauchine said when he talks to people, or his mother comes up in conversation, everyone seems to know someone who had a very serious reaction to a COVID vaccine.
“I am not an anti-vaxxer. I’m not crazy or anything like that,” Beauchine said. “But if I or my family can do anything to help somebody or inform somebody or even be a statistic that could come to some sort of positive resolution in all of this, so be it.”
He added:
“Watching someone slowly walk this path and their health degrading right before your eyes from day to day over a few months is terrible. It’s awful. No one should have to go through this. We all just felt for my mom the whole time. It affected us all.”
The Defender has received numerous reports of people who died from sporadic CJD after receiving a COVID vaccine — all women who were between the ages of 60 and 70. This includes Cheryl Cohen and Jennifer Deason Sprague.
According to the latest data from VAERS, between December 14, 2020, and April 1, 2022, there were 19 reported deaths due to CJD attributed to COVID vaccines. The majority of cases occurred in the 65 to 75 age range and involved a sudden onset of symptoms.
That should be everyone’s starting point – with everything, really – assume the media is lying and wait for them to prove they’re not.
Always doubt the press.
Always.
Especially when the fates seem to converge and every single item in the “news” herds public opinion in the same direction and serves the same agenda
…which bird flu definitely does.
Food shortages. Soaring poverty. Rationing. The cost of living crisis. They’re all part of the Great Reset agenda.
In pursuit of that agenda, over the last two years, they destroyed small businesses and wrecked the economy, they have driven truckers out of work and broken supply lines, they have started a war between two of the biggest exporters of wheat in the world and driven up the price of petrol and natural gas.
Bird flu fits this pattern perfectly. The price of poultry and eggs is set to skyrocket…and just days before Easter.
We know they just faked a pandemic in humans. You think they can’t – or won’t – do the same for chickens?
Now, maybe some of you still have faith in the headlines, maybe you haven’t developed that spidey sense that lets you just know when something is total bollocks. And maybe we should make an argument, lest we fall victim to the “fact-checkers”.
So, let’s talk evidence for a quick minute.
*
First, let’s talk about how the US government “detects” bird flu outbreaks.
To detect [avian influenza], the US Department of Agriculture oversees routine testing of flocks done by farmers and carries out federal inspection programs to ensure that eggs and birds are safe and free of virus […] using molecular diagnostics such as polymerase chain reaction (PCR) tests – the same method labs use to detect COVID-19 infections.
The USDA does routine testing of poultry farms using PCR tests.
Remind you of anything?
Second, let’s talk about how world governments are handling the “crisis”.
The mainstream media are reporting a “deadly” bird flu outbreak, The Guardian claims [emphasis added]:
US officials believe nearly 24m poultry birds, mostly chickens and turkeys, have died of flu since virus strain identified in February
All mainstream outlets are taking the same line – reporting million of birds dying of flu.
However, The Conversation article quoted above says [emphasis added]:
As of early April, the outbreak had CAUSED THE CULLING of some 23 million birds from Maine to Wyoming”
And this article in The Scientist claims [again, emphasis added]…
So far this season, tens of millions of birds have died of disease OR BEEN CULLED
So, there is some inconsistency here. Essentially, we don’t know how many died of “bird flu”, or how many were culled with “bird flu”.
Sound familiar?
Now, let’s do some simple math to try and clear up the confusion.
We know the press are reporting roughly 24 million poultry deaths in the US.
Well, that’s already 16 million out of our 24 million. Or 67% of the alleged total “killed by the flu” in the US.
So, at least two thirds of the dead birds – and potentially all of them – were killed in culls, and NOT by the flu at all.
And that’s just the US numbers. Other countries are culling too.
France has had two huge culls of poultry, totalling over 11 million birds.
The UK has culled at least 2 million since October, despite detecting just 108 cases by late March.
Governments are killing millions of birds, and these deaths are being blamed on the flu.
*
To sum up, the backbone of this “bird flu” outbreak is:
Routine testing done using unreliable PCR tests, which can be manipulated to create false-positive results.
Linguistic ambiguity over causes of death, and unreliable reporting of casualty numbers.
Governmental over-reactions which “accidentally” make the problem worse.
…seriously, any of this ringing a bell yet?
Bird flu is just like Covid. The same people, telling the same lies, for the same reasons.
We all know where it goes from here.
Just as with everything else, this will lead to more talk of a food crisis. France is already warning of poultry shortages, and since the US is the worlds biggest exporter of eggs and chicken any disruption there has huge knock effects. The price of eggs and chicken is already going up.
Just as with lockdowns, the bird flu “crisis” will hit small local businesses harder and faster than Big Farma giants (we’re already seeing reports of family farms being destroyed).
They are reporting that free-range birds are more at risk from bird flu (what with being allowed to go outside and live like normal birds), so organic sustainable and ethical farming practices will be hit with new rules that don’t apply to corporate meat factories who treat animals as inanimate objects.
Meanwhile, this will be used to further advance the war on meat, boosting both veganism and backers of lab-grown “meat”.
Inevitably they are already talking about a new bird flu vaccine for people and/or birds. In fact, a UK firm announced a new bird flu vaccine for chicks just three days ago. That’s some well-timed research, great work.
Good luck being an “anti-vaxxer” when they make it law to literally inject all your food with spike proteins or experimental mRNA modifiers or who knows what else.
And, of course, if they ever need it to, the “bird flu” can jump from chickens to humans, and we can have a brand new pandemic, just as the former head of the CDC predicted the other day.
Like I said at the beginning, there is no “bird flu” outbreak, it’s just Covid for chickens. Just more building back better. Just more new normal.
It’s all the Great Reset. That’s all there is these days.
The Bill and Melinda Gates Foundation have funded the development and distribution of polio vaccines in developing regions like Asia and Africa (Image Source: GRAIN)
Current NHS information describes it as a ‘serious viral infection’ but adds that most people won’t even know they are infected. While some will experience ‘flu-like’ symptoms, others may become temporarily or permanently paralysed.
The term ‘polio’ is a description of spinal pathology: an inflammation of the grey marrow (polio muelos) of the brain stem and spinal cord. Symptoms vary wildly from none to fever, vomiting, bowel irritation, back pain, neck stiffness, problems with swallowing and breathing, paralysis, and death.
Poliovirus is an enterovirus that is activated in the human gut. The corporate science machine maintains that it is a dangerous pathogen spread by infected faecal matter but Dr Suzanne Humphries explains in her book, Dissolving Illusions, that it is a naturally occurring common bowel irritant that existed for millennia before it began crippling people — which poses the question: what changed?
One factor is pesticide usage, which is implicated in other neurological conditions such as Parkinson’s disease. Polio incidence and pesticide usage closely correlate; if you plot them on a graph, they follow the same lines.
What came to be known as polio was once called ‘summer diarrhoea’ because local outbreaks occurred after crop spraying had taken place in the spring. Children played in contaminated soils and ate unwashed fruit; their parents reported finding them paralysed in apple orchards.
High consumption of sugary foods in the summer lowered immunity by suppressing white blood cell activity, creating the perfect environment for toxic pesticides to interact with viruses in the gut and cause illness.
Doctors noted that symptoms of polio resembled food poisoning.
Poor diet increased susceptibility to poliovirus infection – especially a diet full of refined sugar, white flour, and processed foods, which were introduced to the public during the industrial revolution, around the time that polio began to emerge.
British physician Michael Underwood first observed ‘debility of the lower extremities’ in children in 1789. It was the height of the industrial and agricultural revolutions in Europe and pesticide use skyrocketed. Most pesticides contained toxic metals such as lead and arsenic.
Lead and arsenic bind tightly to soil and do not deteriorate; they remain within the first 12-18 inches of topsoil for generations and contaminate waterways. Redevelopment of former rural sites without proper clearance of toxic soil has the potential to poison whole areas of people.
Crops were heavily sprayed with pesticides that were designed to attack the nervous systems of insects — unfortunately they had the same effect on humans. They were inhaled and absorbed through the skin and oral cavity, causing nausea, vomiting, diarrhoea, brain dysfunction, and bone malformation – all of which are common symptoms of heavy metal poisoning and polio.
Heavy metals were present in everyday products in the 18th, 19th, and early 20th centuries. Arsenic was used in synthetic dyes and syphilis treatments; mercury was used in teething powders, dental fillings, and medical preparations.
Lead, arsenic, and mercury are neurotoxic environmental poisons – all are fat-soluble and therefore can affect fatty areas of the body such as the brain and nerves.
Orthopaedist Jacob von Heine observed ‘infantile spinal paralysis’ in 1840 and speculated that it was a contagious disease. It was named ‘acute anterior poliomyelitis’ by Wilhelm Heinrich Erb in 1875, by which time outbreaks had started to occur.
Regional patterns of disease led physicians to believe that polio was a contagious virus, but it was an unproven assumption. Scientists had no idea what a virus was in the nineteenth century — nobody had seen one because the electron microscope, which enabled observation of viruses, was not invented until 1931.
A study of 2,000 case histories carried out by Harvard Infantile Paralysis Commission concluded that tonsillectomies (introduced in 1909 and carried out routinely as a preventative measure) provoked respiratory paralysis due to bulbar polio. This was known at the time as authorities prohibited removal of tonsils and adenoids during epidemics. Bulbar polio was the type that required use of an iron lung and had the highest death rate.
The case fatality rate in the early 1900s was very high. England and Wales made polio a notifiable disease in 1912, and it was endemic from then on. The New York epidemic of 1916 saw patients experimented on with spinal injections of disinfectant and adrenaline. Roughly half of those treated died and were recorded as polio deaths.
A new pesticide, DDT — labeled ‘the killer of killers’ — was introduced just as WW2 began. People were led to believe it was good for them and even sprayed it on their children’s lunches. It is a cumulative poison and can be absorbed through the skin and mucosa. Governments started to ban DDT in the early 1950s, but the damage was done. The UK outlawed it in 1986, and it was banned worldwide in 2001, though it continues to be used in areas with high malaria incidence.
Epidemics peaked in the 1940s and 50s and physicians began to notice a correlation between certain medical interventions and polio paralysis. Children treated for congenital syphilis with arsenic-based Salvarsan often developed paralysis in their injected limbs.
Cases of polio rose in line with the expansion of vaccination programmes for diphtheria, pertussis, and tetanus.
The diphtheria vaccine was introduced in the UK in 1942 and was noted for its adverse effects. The British Medical Association published news on the 10th of April 1950 that the diphtheria vaccine was responsible for childhood paralysis attributed to polio.
A doctor at Guy’s Hospital in London found that 80 children developed paralysis within a month of receiving the shots; a health ministry doctor reported that another 65 children had developed paralysis within a fortnight; the St. Pancras medical officer found 40 more cases. Some children recovered from the paralysis, but others were still paralysed 18 months after onset. Two of the cases followed injection of penicillin.
Anne McLaren, writing for Cambridge University Press in 1957, stated that, “It is now well established that intramuscular inoculation with combined diphtheria-pertussis prophylactics can affect the course of poliomyelitic infection in children. Localisation of paralysis in the limb injected with vaccines was reported by McCloskey, Martin, Geffen, Hill & Knowelden, and Benjamin in 1950.”
In 1951, Dr Ralph Scobey and Dr Mortind Biskind testified in front of the U.S Congress that the paralysis around the country known as ‘polio’ was being caused by industrial poisons, and that a virus theory was purposely fabricated by the chemical industry and the government to deflect litigation away from both parties.
The diagnostic criteria for polio were very loose prior to trials for the vaccine in 1954.Only after the vaccine was introduced was there any effort to distinguish polio from other types of paralytic disease.
The first polio vaccine, created by Jonas Salk in 1955, caused a great deal of controversy. The ‘Cutter Incident’ happened when 120,000 children were injected with a live virus instead of a weakened one: 40,000 developed polio, 200 were paralysed, and ten died. When the immunisation program was eventually rolled out to the public, a different, untested, rapidly approved formula was used.
Salk later admitted that live virus vaccines against influenza or poliomyelitis might produce the diseases they intended to prevent (Science, 4th March 1977).
In 1956, the American Medical Association ordered that doctors could no longer diagnose paralysis as polio – it had to be called ‘acute flaccid paralysis’. This reduced polio statistics dramatically and gave the appearance that the vaccine programme had succeeded, when really the definition of the disease had just changed.
Simple, timely changes to diagnostic criteria meant the number of paralytic cases dropped irrespective of the vaccine programme.
Laboratory testing for polio wasn’t introduced until 1958. Before then, all manner of other diseases could be classed as polio, including other enteroviruses, lead, arsenic, and DDT poisoning, Guillain-Barré syndrome, transverse myelitis, post-polio syndrome, viral or aseptic meningitis, traumatic neuritis, and Reye’s syndrome. How many were misdiagnosed and put on the wrong path of treatment as a result?
It is claimed that the polio vaccine eradicated polio due to overblown, tightly controlled propaganda campaigns, but the truth is that cases plummeted because of changes in pesticide use, elimination of toxic metals in everyday products, improved diets and sanitary behaviour, and redefinition of the disease.
There is no convincing evidence of polio as a contagious viral disease. Naturally occurring polio is all but obsolete in the modern world and the only ‘polio’ we see nowadays is vaccine-induced, courtesy of immunisation programmes run by the World Health Organisation.
There has been a huge rise in vaccine-induced polio paralysis in India. In 2011 there were an extra 47,000 cases, which were directly proportionate to the amount of oral vaccines administered. In 2018 a vaccine tainted with eradicated type-2 polio was given to children in Uttar Pradesh. The country remains vulnerable to polio due to its continued use of DDT, intramuscular injection of antibiotics, and diets high in sugar and low in vitamins.
Research scientist Viera Scheibner says that modern day vaccine advocates have forgotten the ‘polio provocation’ of the past. She believes that vaccines represent a assault on the immune system, which seems to be clearly implicated in the shadowy history of polio.
Vaccines were not needed to combat polio. Dr Fred Klenner published results of a study that used intravenous vitamin C to cure polio and other viral diseases 73 years ago — six years before the vaccine was introduced. With a success rate of 100%, we have to ask why this simple, non-toxic, affordable cure was completely overlooked and ignored by the medical community. Why is it still ignored?
The answer may lie in the criminal deceptions peddled by medical-industrial-pharmaceutical cartels that control the narrative of disease in order to sustain their gravy train of ill-gotten gain. A customer cured is a customer lost and there is no profit to be made from a healthy population.
Over the past year-plus, athletes across the world have been dropping like flies as they compete in games. If they aren’t passed out cold, they are seen gripping their chests in agony, unable to breathe due to sudden cardiac events that hit in the heat of the competition.
This wave of heart issues is unprecedented, to say the least. Never before have we seen young, healthy, world-class athletes experiencing heart issues en masse like this. It has never happened, ever. Furthermore, the timing of this sweeping phenomenon could not be more relevant, coinciding perfectly with the rollout of the experimental Covid-19 vaccines.
In December nearly 300 athletes reportedly collapsed or suffered cardiac arrests after taking the COVID vaccines.
But it gets worse. Thanks to a new explosive report by OAN that pegs the number of affected athletes in the hundreds.
In all, their investigation found a jaw-dropping 769 men and women who collapsed with heart issues during competition over the past year (between March 2021 and March 2022).
Most shockingly, the average age of those who experienced full-blown cardiac arrest was just 23.
Considering the timing of this never-before-seen issue in healthy athletes, and the universal push for Covid jabs, all signs point to one culprit: the experimental vaccine.
After detailing two recent high-profile cases, in which two tennis players were forced to recuse themselves from last month’s Miami Open, OAN’s Pearson Sharp reviewed their shocking investigation and asked a few pressing questions that should be answered if you are still questioning what is driving these heart issues in young individuals:
“These are just two o more than 769 athletes who have collapsed during a game on the field over the last year. From March of 2021 to March of this year. The average age of the players suffering cardiac arrest is just 23-years-old.
How many 23-year-old athletes were collapsing and suffering heart attacks before this year? Do you know any 23-year-old people who had heart attacks before now?
And these are just the ones we know about. How many have gone unreported? Nearly 800 athletes – young, fit people in the prime of life falling down on the field. In fact, 500% more soccer players in the EU are dropping dead from heart attacks than just one year ago.”
Just in case there is any lingering inclination to call this a coincidence, Sharp sets the record straight.
“Coincidence? When the Pfizer vaccine is known to cause heart inflamation? No. In fact, many doctors treating these players list their injuries and deaths as being directly caused by the vaccine…
This is not a coincidence – healthy teenagers dying after getting the Pfizer injection. Doctors warned the FDA before they released the experimental vaccine that it would ‘almost certainly cause terrible organ damage.’”
The only question left is: when do we see some accountability?
This video taken yesterday in Shanghai, China, by the father of a close friend of mine. She verified its authenticity: People screaming out of their windows after a week of total lockdown, no leaving your apartment for any reason.
Videos circulating on social media show an eerie cityscape at night filled with the anguished screams of residents forcibly quarantined in their apartment buildings for over a week.
Haunting video out of Shanghai shows thousands of frustrated residents screaming from apartment buildings after being locked down again following another alleged COVID-19 outbreak.
What the?? This video taken yesterday in Shanghai, China, by the father of a close friend of mine. She verified its authenticity: People screaming out of their windows after a week of total lockdown, no leaving your apartment for any reason. pic.twitter.com/iHGOO8D8Cz
‘It’s Shanghai, everyone is screaming, started with a couple now everyone is screaming, after a week of lockdown, something is going to happen, no one knows when this is going to end.’ He says they can’t even step outside their apartments.”
Another dystopian video shows a drone hovering around the buildings with a prerecorded message discouraging residents from crying for help: “Please comply with COVID restrictions. Control your soul’s desire for freedom. Do not open the window or sing.”
As seen on Weibo: Shanghai residents go to their balconies to sing & protest lack of supplies. A drone appears: “Please comply w covid restrictions. Control your soul’s desire for freedom. Do not open the window or sing.” https://t.co/0ZTc8fznaVpic.twitter.com/pAnEGOlBIh
The Chinese Communist Party extended its citywide “zero tolerance” lockdown for 26 million residents in Shanghai earlier this week after thousands of new COVID cases were detected in the city.
“The city will continue to implement seal and control management and strictly implement ‘staying at home,’ except for medical treatment,” the city wrote in its official WeChat account.
The People’s Liberation Army has deployed 2,000 medical personnel to Shanghai with an additional 38,000 medical workers to carry out a mass mitigation effort to test all 26 million city residents for COVID.
Authorities had initially locked down Shanghai, China’s largest city, on March 28 amid a surge of mostly asymptomatic COVID cases.
Former CDC Director Robert Redfield has stated that Bird Flu will jump to humans and be highly fatal in the coming “Great Pandemic,” for which C19 was a mere warm-up.
Airplane leaving jet contrails with COVID-19 word inside. Symbolizing the global spread of the coronavirus through global air traffic.
A few months ago, I wrote an article exploring the connection between the symptoms of disease known as “Covid-19” and air pollution. While air pollution is not the only factor currently causing disease, I laid out why I believe that this is the most likely explanation for any perceived increase in respiratory symptoms of disease. I provided a general overview on the problem of air pollution and how it can impact our health and environment. Within the article, I touched upon the issue of persistent contrails, a.k.a. chemtrails, and provided information directly from Government sources admitting the impact that these trails have on our health and environment. Even though this information is readily available to anyone willing to look, there are many out there who still seem to believe that these trails are harmless. They claim that I am promoting nothing but a baseless conspiracy theory.
The fact of the matter is that these trails are admitted to be harmful to our health and environment by both sides of the “chemtrail” debate. There is no conspiracy theory here. This is a FACT. We can speculate as to who is doing this and why but that is ultimately irrelevant. While pollution from automobiles, factories, power plants, forest fires, etc. all contribute to this air pollution health crisis, the harmful effects from the aviation industry are regularly glossed over and/or omitted when this issue is discussed. However, if you dig deep enough and actually search for the information, what can be found to be admitted by official Government sources regarding the health consequences from these trails is very telling and disturbing.
To start with, I want to provide a quick breakdown of the negative health impact of just one component that is admitted to be found within these persistent trails left in the wake of aircrafts. This is known as particulate matter, the most dangerous of which is PM2.5. From the Environmental Protection Agency (EPA), you will see that PM2.5 is a known toxin potentially made up of hundreds of different chemicals that is so small that it can collect deep within the lungs and even enter the bloodstream. It has been associated with cardiovascular and respiratory disease, irritation of the eyes, throat, and lungs, and premature death:
Particulate Matter (PM) Basics
What is PM, and how does it get into the air?
“PM stands for particulate matter (also called particle pollution): the term for a mixture of solid particles and liquid droplets found in the air. Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye. Others are so small they can only be detected using an electron microscope.
Particle pollution includes:
PM10: inhalable particles, with diameters that are generally 10 micrometers and smaller; and
PM2.5: fine inhalable particles, with diameters that are generally 2.5 micrometers and smaller.
How small is 2.5 micrometers? Think about a single hair from your head. The average human hair is about 70 micrometers in diameter – making it 30 times larger than the largest fine particle.
Sources of PM
These particles come in many sizes and shapes and can be made up of hundreds of different chemicals.
Some are emitted directly from a source, such as construction sites, unpaved roads, fields, smokestacks or fires.
Most particles form in the atmosphere as a result of complex reactions of chemicals such as sulfur dioxide and nitrogen oxides, which are pollutants emitted from power plants, industries and automobiles.
What are the Harmful Effects of PM?
Particulate matter contains microscopic solids or liquid droplets that are so small that they can be inhaled and cause serious health problems. Some particles less than 10 micrometers in diameter can get deep into your lungs and some may even get into your bloodstream. Of these, particles less than 2.5 micrometers in diameter, also known as fine particles or PM2.5, pose the greatest risk to health.
Fine particles are also the main cause of reduced visibility (haze) in parts of the United States, including many of our treasured national parks and wilderness areas.”
Health and Environmental Effects of Particulate Matter (PM)
Health Effects
The size of particles is directly linked to their potential for causing health problems. Small particles less than 10 micrometers in diameter pose the greatest problems, because they can get deep into your lungs, and some may even get into your bloodstream.
Exposure to such particles can affectboth your lungs and your heart. Numerous scientific studies have linked particle pollution exposure to a variety of problems, including:
premature death in people with heart or lung disease
nonfatal heart attacks
irregular heartbeat
aggravated asthma
decreased lung function
increased respiratory symptoms, such as irritation of the airways, coughing or difficulty breathing.
People with heart or lung diseases,children, and older adults are the most likely to be affected by particle pollution exposure.
PM2.5 and other particulate matter is only part of the dangerous substances found in these persistent contrails. Other admitted substances include carbon dioxide (CO2), volatile organic compounds (VOC), nitrogen oxides (NOX), sulfur oxides (SOX), black carbon soot, and other trace metals. It is simply beyond logic and reasoning to believe that the inhalation of these substances on a daily basis is not harmful to one’s health.
Recently, some members of Congress were interested in addressing the health and environmental problems associated with aviation. On February 8th, 2022, the Congressional Research Service released a report describing the problem and how to address it. A few highlights showcase that aviation pollution is the fastest-growing pollutant over the past decade and that there are numerous toxic substances found within these trails: Aviation, Air Pollution, and Climate Change
Emissions from Aircraft
“The U.S. Environmental Protection Agency (EPA) estimates that transportation—including passenger cars and light trucks, heavy-duty trucks, buses, trains, ships, and aircraft—accounted for 35% of carbon dioxide (CO2, the principal GHG) emissions in 2018. While CO2 emissions from passenger cars and light trucks exceed those from aircraft in the United States, CO2 emissions from aviation are currently experiencing a faster rate of growth. All aircraft, including military, commercial, and privately chartered, accounted for 13% of the U.S. transportation sector’s CO2 emissions and 5% of all U.S. CO2 emissions in 2018. Commercial aircraft, including those operated by passenger and all-cargo airlines, accounted for 11% of transportation sector and 4% of all emissions. These estimates include emissions from U.S. domestic flights and emissions from international flights departing the United States, referred to as “international bunkering.”
In the United States, aggregate CO2 emissions from aircraft have fluctuated due to changes in technology, the economy, travel frequency, and military activity, among other reasons. However, since the global financial crisis in 2009,aggregate CO2 emissions from all aircraft types have grown steadily, increasing by almost 22% between 2009 and 2018. This increase makes aircraft one of the faster-growing sources of CO2 emissions in the U.S. transportation sector over the past decade. This trend is likely to be affected, at least temporarily, by reduced air travel in 2020 and 2021 due to Coronavirus Disease 2019 (COVID-19).
The effects of aircraft emissions on the atmosphere are complex, reflecting differing altitudes, geography, time horizons, and environmental conditions. Research has shown that in addition to CO2 emissions, other factors increase the climate change impacts of aviation. These factors include the contribution of aircraft emissions to ozone production; the formation of water condensation trails and cirrus clouds; the emission of various gases and particles, including water vapor, nitrous oxides, sulfates, and particulates from jet fuel combustion; and the high altitude location of the bulk of these emissions. In examining the warming and cooling influences of these factors, the United Nations’ Intergovernmental Panel on Climate Change estimated aviation’s total climate change impact could be from two to four times that of its past CO2 emissions alone.
Aside from GHG emissions, aircraft engines emit a number of criteria—or common—pollutants, including nitrogen oxides, carbon monoxide, oxides of sulfur, unburned or partially combusted hydrocarbons (also known as volatile organic compounds [VOCs]), particulates, and other trace compounds. A subset of the VOCs and particulates are considered hazardous air pollutants.”
In case you wanted a visual representation of how this pollution is said to form and impact our health.
As can be seen, the pollution coming from the aviation industry is a fast-growing problem that is impacting our health and environment in numerous ways. While this has been known for decades and solutions have been presented to try and reverse the impact, nothing is ever implemented to fix the problem. Solutions are only useful if they are enacted upon. While Congress gathers reports, there is little action taken in regards to those reports. It is one thing to acknowledge the negative health and environmental impact yet it is another thing entirely to actually shake up the industry by doing something about it. This seems not to be a major concern as these trails have become worse over time, increasingly contributing to erratic weather, disease, and premature death.
For further evidence of the impact that these trails have on our health and environment, we can turn once again to the EPA to provide more detail. In a document from January 11th, 2021, the EPA enacted standards that are supposed to combat greenhouse gas emissions from the aviation industry. In this document are findings from reports they had compiled in 2016 which call out the dangers these trails have on the public health and welfare:
Control of Air Pollution From Airplanes and Airplane Engines: GHG Emission Standards and Test Procedures
“In August 2016, the EPA issued two findings regarding GHG emissions from aircraft engines (the 2016 Findings).[7]First, the EPA found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA. Second, EPA found that emissions of GHGs from certain classes of engines used in certain aircraft are contributing to the air pollution that endangers public health and welfare under CAA section 231(a)(2)(A). Additional details of the 2016 Findings are described in Section III. As a result of the 2016 Findings, CAA sections 231(a)(2)(A) and (3) obligate the EPA to propose and adopt, respectively, GHG standards for these covered aircraft engines.”
III. Summary of the 2016 Findings
“On August 15, 2016,[46] the EPA issued two findings regarding GHG emissions from aircraft engines. First, the EPA found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA. The EPA made this finding specifically with respect to the same six well-mixed GHGs—CO2, methane, N2 O, hydrofluorocarbons, perfluorocarbons, and sulfur hexafluoride—that together were defined as the air pollution in the 2009 Endangerment Finding [47] under section 202(a) of the CAA and that together were found to constitute the primary cause of climate change. Second, the EPA found that emissions of those six well-mixed GHGs from certain classes of engines used in certain aircraft [48] cause or contribute to the air pollution—the aggregate group of the same six GHGs—that endangers public health and welfare under CAA section 231(a)(2)(A).”
In February of 2022, the EPA proposed standards that would reflect the importance of the control of PM emissions in aviation. They were looking to secure the highest practicable degree of uniformity in aviation regulations and standards. Within this proposal, the EPA provided plenty of insight into the potential health impacts of PM2.5 on human health such as cardiovascular disease, respiratory disease, neurological disorders, asthma, cancer, ferility/reproductive problems, and premature death. They also outlined the impact the chemicals in the trails have on the environment such as affecting the metabolic processes of plant foliage, altering the soil biogeochemistry and microbiology, disrupting plant and animal growth and reproduction, and the corrosion of metals and soil. They even provided more detail on the make-up of the composition of the dangerous toxins inside these trails with the addition of carcinogens such as benzene, 1,3-butadiene, formaldehyde, acetaldehyde, acrolein, polycyclic organic matter (POM), and certain metals such as chromium, manganese, and nickel. Judging by this information alone, it should be rather clear that these trails are negatively impacting our health and environment in numerous ways:
Control of Air Pollution From Aircraft Engines: Emission Standards and Test Procedures
III. Particulate Matter Impacts on Air Quality and Health
A. Background on Particulate Matter
“Particulate matter (PM) is a highly complex mixture of solid particles and liquid droplets distributed among numerous atmospheric gases which interact with solid and liquid phases. Particles range in size from those smaller than 1 nanometer (10−9 meter) to over 100 micrometers (μm, or 10−6 meter) in diameter (for reference, a typical strand of human hair is 70 μm in diameter and a grain of salt is about 100 μm). Atmospheric particles can be grouped into several classes according to their aerodynamic and physical sizes. Generally, the three broad classes of particles include ultrafine particles (UFPs, generally considered as particulates with a diameter less than or equal to 0.1 μm (typically based on physical size, thermal diffusivity or electrical mobility)), “fine” particles (PM2.5; particles with a nominal mean aerodynamic diameter less than or equal to 2.5 μm), and “thoracic” particles (PM10; particles with a nominal mean aerodynamic diameter less than or equal to 10 μm). Particles that fall within the size range between PM2.5 and PM10, are referred to as “thoracic coarse particles” (PM10-2.5, particles with a nominal mean aerodynamic diameter less than or equal to 10 μm and greater than 2.5 μm).
Particles span many sizes and shapes and may consist of hundreds of different chemicals. Particles are emitted directly from sources and are also formed through atmospheric chemical reactions between PM precursors; the former are often referred to as “primary” particles, and the latter as “secondary” particles. Particle concentration and composition varies by time of year and location, and, in addition to differences in source emissions, is affected by several weather-related factors, such as temperature, clouds, humidity, and wind. Ambient levels of PM are also impacted by particles’ ability to shift between solid/liquid and gaseous phases, which is influenced by concentration, meteorology, and especially temperature.
Fine particles are produced primarily by combustion processes and by transformations of gaseous emissions ( e.g., sulfur oxides (SOX), nitrogen oxides (NOX) and volatile organic compounds (VOCs)) in the atmosphere. The chemical and physical properties of PM2.5 may vary greatly with time, region, meteorology, and source category. Thus, PM2.5 may include a complex mixture of different components including sulfates, nitrates, organic compounds, elemental carbon, and metal compounds. These particles can remain in the atmosphere for days to weeks and travel through the atmosphere hundreds to thousands of kilometers.
Particulate matter is comprised of both volatile and non-volatile PM. PM emitted from the engine is known as non-volatile PM (nvPM), and PM formed from transformation of an engine’s gaseous emissions are defined as volatile PM.[35] Because of the difficulty in measuring volatile PM, which is formed in the engine’s exhaust plume and is significantly influenced by ambient conditions, the EPA is proposing standards only for the emission of nvPM.
B. Health Effects of Particulate Matter
Scientific studies show exposure to ambient PM is associated with a broad range of health effects. These health effects are discussed in detail in the Integrated Science Assessment for Particulate Matter (PM ISA), which was finalized in December 2019.[36]The PM ISA concludes that human exposures to ambient PM2.5 are associated with a number of adverse health effects and characterizes the weight of evidence for broad health categories ( e.g., cardiovascular effects, respiratory effects, etc.).[37] The PM ISA additionally notes that stratified analyses ( i.e., analyses that directly compare PM-related health effects across groups) provide strong evidence for racial and ethnic differences in PM2.5 exposures and in PM2.5 -related health risk. As described in Section III.D, concentrations of PM increase with proximity to an airport. Further, studies described in Section III.G report that many communities in close proximity to airports are disproportionately represented by people of color and low-income populations.
EPA has concluded that recent evidence in combination with evidence evaluated in the 2009 p.m. ISA supports a “causal relationship” between both long- and short-term exposures to PM2.5 and mortality and cardiovascular effects and a “likely to be causal relationship” between long- and short-term PM2.5 exposures and respiratory effects.[38]Additionally, recent experimental and epidemiologic studies provide evidence supporting a “likely to be causal relationship” between long-term PM2.5 exposure and nervous system effects, and long-term PM2.5 exposure and cancer. In addition, EPA noted that there was more limited and uncertain evidence for long-term PM2.5 exposure and reproductive and developmental effects ( i.e., male/female reproduction and fertility; pregnancy and birth outcomes), long- and short-term exposures and metabolic effects, and short-term exposure and nervous system effects resulting in the ISA concluding “suggestive of, but not sufficient to infer, a causal relationship.”
More detailed information on the health effects of PM can be found in a memorandum to the docket.[39]
C. Environmental Effects of Particulate Matter
Environmental effects that can result from particulate matter emissions include visibility degradation, plant and ecosystem effects, deposition effects, and materials damage and soiling. These effects are briefly summarized here and discussed in more detail in the memo to the docket cited above.
PM2.5 emissions also adversely impact visibility.[40]In the Clean Air Act Amendments of 1977, Congress recognized visibility’s value to society by establishing a national goal to protect national parks and wilderness areas from visibility impairment caused by manmade pollution.[41] In 1999, EPA finalized the regional haze program (64 FR 35714) to protect the visibility in Mandatory Class I Federal areas. There are 156 national parks, forests and wilderness areas categorized as Mandatory Class I Federal areas (62 FR 38680-38681, July 18, 1997). These areas are defined in CAA section 162 as those national parks exceeding 6,000 acres, wilderness areas and memorial parks exceeding 5,000 acres, and all international parks which were in existence on August 7, 1977. EPA has also concluded that PM2.5 causes adverse effects on visibility in other areas that are not targeted by the Regional Haze Rule, such as urban areas, depending on PM2.5 concentrations and other factors such as dry chemical composition and relative humidity ( i.e., an indicator of the water composition of the particles). EPA established the secondary 24-hour PM2.5 NAAQS in 1997 and has retained the standard in subsequent reviews.[42] This standard is expected to provide protection against visibility effects through attainment of the existing secondary standards for PM2.5 . EPA is reconsidering the 2020 decision, as announced on June 10, 2021.[43]
1. Deposition of Metallic and Organic Constituents of PM
Several significant ecological effects are associated with deposition of chemical constituents of ambient PM such as metals and organics.[44]Like all internal combustion engines, turbine engines covered by this rule may emit trace amounts of metals due to fuel contamination or engine wear. Ecological effects of PM include direct effects to metabolic processes of plant foliage; contribution to total metal loading resulting in alteration of soil biogeochemistry and microbiology, plant and animal growth and reproduction; and contribution to total organics loading resulting in bioaccumulation and biomagnification.
2. Materials Damage and Soiling
Deposition of PM is associated with both physical damage (materials damage effects) and impaired aesthetic qualities (soiling effects). Wet and dry deposition of PM can physically affect materials, adding to the effects of natural weathering processes, by potentially promoting or accelerating the corrosion of metals, by degrading paints and by deteriorating building materials such as stone, concrete and marble.[45]
D. Near-Source Impacts on Air Quality and Public Health
Airport activity can adversely impact air quality in the vicinity of airports. Furthermore, these adverse impacts may disproportionately impact sensitive subpopulations. A recent study by Yim et al. (2015) assessed global, regional, and local health impacts of civil aviation emissions, using modeling tools that address environmental impacts at different spatial scales.[46] The study attributed approximately 16,000 premature deaths per year globally to global aviation emissions, with 87 percent attributable to PM2.5 . The study concludes that about a third of these mortalities are attributable to PM2.5 exposures within 20 kilometers of an airport. Another study focused on the continental United States estimated 210 deaths per year attributable to PM2.5 from aircraft.[47] While there are considerable uncertainties associated with such estimates, these results suggest that in addition to the contributions of PM2.5 emissions to regional air quality, impacts on public health of these emissions in the vicinity of airports are an important public health concern.
A significant body of research has addressed pollutant levels and potential health effects in the vicinity of airports. Much of this research was synthesized in a 2015 report published by the Airport Cooperative Research Program (ACRP), conducted by the Transportation Research Board.[48]The report concluded that PM2.5 concentrations in and around airports vary considerably, ranging from “relatively low levels to those that are close to the NAAQS, and in some cases, exceeding the standards.” [49]
Furthermore, the report states (p. 40) that “existing studies indicate that ultrafine particle concentrations are highly elevated at an airport ( i.e., near a runway) with particle counts that can be orders of magnitude higher than background with some persistence many meters downwind ( e.g., 600 m). Finally, the report concludes that PM2.5 dominates overall health risks posed by airport emissions. Moreover, one recently published study concluded that emissions from aircraft play an etiologic role in pre-term births, independent of noise and traffic-related air pollution exposures.[50]
Since the publication of the 2015 ACRP literature review, a number of studies conducted in the U. S. have been published which concluded that ultrafine particle number concentrations were elevated downwind of commercial airports, and that proximity to an airport also increased particle number concentrations within residences.Hudda et al. investigated ultrafine particle number concentrations (PNC) inside and outside 16 residences in the Boston metropolitan area. They found elevated outdoor PNC within several kilometers of the airport. They also found that aviation-related PNC infiltrated indoors and resulted in significantly higher indoor PNC.[51] In another study in the vicinity of Logan airport, Hudda et al. analyzed PNC impacts of aviation activities.[52] They found that, at sites 4.0 and 7.3 km from the airport, average PNCs were 2 and 1.33-fold higher, respectively, when winds were from the direction of the airport compared to other directions, indicating that aviation impacts on PNC extend many kilometers downwind of Logan airport. Stacey (2019) conducted a literature survey and concluded that the literature consistently reports that particle numbers close to airports are significantly higher than locations distant and upwind of airports, and that the particle size distribution is different from traditional road traffic, with more extremely fine particles.[53] Similar findings have been published from European studies.[54 55 56 57 58 59 ] Results of a monitoring study of communities near Seattle-Tacoma International Airport also found higher levels of ultrafine PM near the airport, and an impacted area larger than at near-roadway sites.[60] The PM associated with aircraft landing activity was also smaller in size, with lower black carbon concentrations than near-roadway samples. As discussed above, PM2.5 exposures are associated with a number of serious, adverse health effects. Further, the PM attributable to aircraft emissions has been associated with potential adverse health impacts.[61 62] For example, He et al. (2018) found that particle composition, size distribution and internalized amount of particles near airports all contributed to promotion of reactive organic species in bronchial epithelial cells.
Because of these potential impacts, a systematic literature review was recently conducted to identify peer-reviewed literature on air quality near commercial airports and assess the quality of the studies.[63] The systematic review identified seventy studies for evaluation. These studies consistently showed that particulate matter, in the form of ultrafine PM (UFP), is elevated in and around airports. Furthermore, many studies showed elevated levels of black carbon, criteria pollutants, and polycyclic aromatic hydrocarbons as well. Finally, the systematic review, while not focused on health effects, identified a limited number of references reporting adverse health effects impacts, including increased rates of premature death, pre-term births, decreased lung function, oxidative DNA damage and childhood leukemia. More research is needed linking particle size distributions to specific airport activities, and proximity to airports, characterizing relationships between different pollutants, evaluating long-term impacts, and improving our understanding of health effects.
A systematic review of health effects associated with exposure to jet engine emissions in the vicinity of airports was also recently published.[64] This study concluded that literature on health effects was sparse, but jet engine emissions have physicochemical properties similar to diesel exhaust particles, and that exposure to jet engine emissions is associated with similar adverse health effects as exposure to diesel exhaust particles and other traffic emissions.A 2010 systematic review by the Health Effects Institute (HEI) concluded that evidence was sufficient to support a causal relationship between exposure to traffic-related air pollution and exacerbation of asthma among children, and suggestive of a causal relationship for childhood asthma, non-asthma respiratory symptoms, impaired lung function and cardiovascular mortality.[65]”
F. Other Pollutants Emitted by Aircraft
“In addition to particulate matter, a number of other criteria pollutants are emitted by the aircraft which are the subject of this proposed rule. These pollutants, which are not covered by the rule, include nitrogen oxides (NOX), including nitrogen dioxide (NO2), volatile organic compounds (VOC), carbon monoxide (CO), and sulfur dioxide (SO2). Aircraft also contribute to ambient levels of hazardous air pollutants (HAP), compounds that are known or suspected human or animal carcinogens, or that have noncancer health effects. These compounds include, but are not limited to, benzene, 1,3-butadiene, formaldehyde, acetaldehyde, acrolein, polycyclic organic matter (POM), and certain metals. Some POM and HAP metals are components of PM2.5 mass measured in turbine engine aircraft emissions.[70]
The term polycyclic organic matter (POM) defines a broad class of compounds that includes the polycyclic aromatic hydrocarbon compounds (PAHs). POM compounds are formed primarily from combustion and are present in the atmosphere in gas and particulate form. Metal compounds emitted from aircraft turbine engine combustion include chromium, manganese, and nickel. Several POM compounds, as well as hexavalent chromium, manganese compounds and nickel compounds are included in the National Air Toxics Assessment, based on potential carcinogenic risk.[71] In addition, as mentioned previously, deposition of metallic compounds can have ecological effects. Impacts of POM and metals are further discussed in the memorandum to the docket referenced above.”
PM stands for particulate matter – the term for a mixture of solid particles and liquid droplets found in the air
Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye while others are too small to be seen
PM10: inhalable particles, with diameters that are generally 10 micrometers and smaller
PM2.5: fine inhalable particles, with diameters that are generally 2.5 micrometers and smaller
These particles come in many sizes and shapes and can be made up of hundreds of different chemicals
Most particles form in the atmosphere as a result of complex reactions of chemicals such as sulfur dioxide and nitrogen oxides
Particulate matter contains microscopic solids or liquid droplets that are so small that they can be inhaled and cause serious health problems
Some particles less than 10 micrometers in diameter can get deep into your lungs and some may even get into your bloodstream
Fine particles are also the main cause of reduced visibility (haze) in parts of the United States
The size of particles is directly linked to their potential for causing health problems
Exposure to such particles can affect both your lungs and your heart
Numerous scientific studies have linked particle pollution exposure to a variety of problems, including:
Premature death in people with heart or lung disease
Nonfatal heart attacks
Irregular heartbeat
Aggravated asthma
Decreased lung function
Increased respiratory symptoms, such as irritation of the airways, coughing or difficulty breathing
People with heart or lung diseases,children, and older adults are the most likely to be affected by particle pollution exposure
According to a Congressional Research Service report from February 8th, 2022, CO2 emissions from aviation are currently experiencing a faster rate of growth than other sources
All aircraft, including military, commercial, and privately chartered, accounted for 13% of the U.S. transportation sector’s CO2 emissions and 5% of all U.S. CO2 emissions in 2018
Commercial aircraft, including those operated by passenger and all-cargo airlines, accounted for 11% of transportation sector and 4% of all emissions
Since the global financial crisis in 2009, aggregate CO2 emissions from all aircraft types have grown steadily, increasing by almost 22% between 2009 and 2018
This increase makes aircraft one of the faster-growing sources of CO2 emissions in the U.S. transportation sector over the past decade
The effects of aircraft emissions on the atmosphere are complex, reflecting differing altitudes, geography, time horizons, and environmental conditions
Research has shown that in addition to CO2 emissions, other factors increase the climate change impacts of aviation which include:
The contribution of aircraft emissions to ozone production
The formation of water condensation trails and cirrus clouds
The emission of various gases and particles, including water vapor, nitrous oxides, sulfates, and particulates from jet fuel combustion
The high altitude location of the bulk of these emissions
In examining the warming and cooling influences of these factors, the United Nations’ Intergovernmental Panel on Climate Change estimated aviation’s total climate change impact could be from two to four times that of its past CO2 emissions alone
Aside from GHG emissions, aircraft engines emit a number of criteria—or common—pollutants, including:
Nitrogen oxides
Carbon monoxide
Oxides of sulfur
Unburned or partially combusted hydrocarbons (also known as volatile organic compounds [VOCs])
Particulates
Other trace compounds
A subset of the VOCs and particulates are considered hazardous air pollutants
According to a 2021 report by the EPA, they found that elevated concentrations of GHGs in the atmosphere endanger the public health and welfare of current and future generations within the meaning of section 231(a)(2)(A) of the CAA
Second, EPA found that emissions of GHGs from certain classes of engines used in certain aircraft are contributing to the air pollution that endangers public health and welfare under CAA section 231(a)(2)(A)
The EPA made this finding specifically with respect to the same six well-mixed GHGs—CO2, methane, N2O, hydrofluorocarbons, perfluorocarbons, and sulfur hexafluoride—that together were defined as the air pollution in the 2009 Endangerment Finding under section 202(a) of the CAA and that together were found to constitute the primary cause of climate change
The EPA found that emissions of those six well-mixed GHGs from certain classes of engines used in certain aircraft cause or contribute to the air pollution—the aggregate group of the same six GHGs—that endangers public health and welfare under CAA section 231(a)(2)(A)
Another report by the EPA from February 2022 states that particulate matter (PM) is a highly complex mixture of solid particles and liquid droplets distributed among numerous atmospheric gases which interact with solid and liquid phases
Particles span many sizes and shapes and may consist of hundreds of different chemicals
Fine particles are produced primarily by combustion processes and by transformations of gaseous emissions (e.g., sulfur oxides (SOX), nitrogen oxides (NOX) and volatile organic compounds (VOCs)) in the atmosphere
PM2.5 may include a complex mixture of different components including sulfates, nitrates, organic compounds, elemental carbon, and metal compounds
These particles can remain in the atmosphere for days to weeks and travel through the atmosphere hundreds to thousands of kilometers
Particulate matter is comprised of both volatile and non-volatile PM
PM emitted from the engine is known as non-volatile PM (nvPM), and PM formed from transformation of an engine’s gaseous emissions are defined as volatile PM
Because of the difficulty in measuring volatile PM, which is formed in the engine’s exhaust plume and is significantly influenced by ambient conditions, the EPA is proposing standards only for the emission of nvPM
In other words, there are no standards proposed by the EPA for the transformation these chemicals go through after leaving the enginewhen they become lingering trails
Scientific studies show exposure to ambient PM isassociated with a broad range of health effects
The PM ISA concludes that human exposures to ambient PM2.5 are associated with a number of adverse health effects and characterizes the weight of evidence for broad health categories ( e.g., cardiovascular effects, respiratory effects, etc.)
EPA has concluded that recent evidence in combination with evidence evaluated in the 2009 p.m. ISA supports a “causal relationship” between both long- and short-term exposures to PM2.5 and mortality and cardiovascular effects and a “likely to be causal relationship” between long- and short-term PM2.5 exposures and respiratory effects
Additionally, recent experimental and epidemiologic studies provide evidence supporting a “likely to be causal relationship” between long-term PM2.5 exposure and nervous system effects, and long-term PM2.5 exposure and cancer
In addition, EPA noted that there was more limited and uncertain evidence for long-term PM2.5 exposure and reproductive and developmental effects ( i.e., male/female reproduction and fertility; pregnancy and birth outcomes), long- and short-term exposures and metabolic effects, and short-term exposure and nervous system effects resulting in the ISA concluding “suggestive of, but not sufficient to infer, a causal relationship”
Environmental effects that can result from particulate matter emissions include:
Visibility degradation
Plant and ecosystem effects
Deposition effects
Materials damage and soiling
PM2.5 emissions also adversely impact visibility
Like all internal combustion engines, turbine engines covered by this rule may emittrace amounts of metals due to fuel contamination or engine wear
Ecological effects of PM include:
Direct effects to metabolic processes of plant foliage
Contribution to total metal loading resulting in alteration of soil biogeochemistry and microbiology, plant and animal growth and reproduction
Contribution to total organics loading resulting in bioaccumulation and biomagnification
Deposition of PM is associated with both physical damage (materials damage effects) and impaired aesthetic qualities (soiling effects)
Wet and dry deposition of PM can physically affect materials, adding to the effects of natural weathering processes, by potentially promoting or accelerating the corrosion of metals, by degrading paints and by deteriorating building materials such as stone, concrete and marble
A recent study by Yim et al. (2015) assessed global, regional, and local health impacts of civil aviation emissions, using modeling tools that address environmental impacts at different spatial scales
The study attributed approximately 16,000 premature deaths per year globally to global aviation emissions, with 87 percent attributable to PM2.5
The study concluded that about a third of these mortalities are attributable to PM2.5 exposures within 20 kilometers of an airport
Another study focused on the continental United States estimated 210 deaths per year attributable to PM2.5 from aircraft
Impacts on public health of these emissions in the vicinity of airports are an important public health concern
A 2015 report concluded that PM2.5 concentrations in and around airports vary considerably, ranging from “relatively low levels to those that are close to the NAAQS, and in some cases, exceeding the standards.”
Furthermore, the report stated (p. 40) that “existing studies indicate that ultrafine particle concentrations are highly elevated at an airport ( i.e., near a runway) with particle counts that can be orders of magnitude higher than background with some persistence many meters downwind ( e.g., 600 m)
Finally, the report concluded that PM2.5 dominates overall health risks posed by airport emissions
Hudda et al. investigated ultrafine particle number concentrations (PNC) inside and outside 16 residences in the Boston metropolitan area and found that aviation-related PNC infiltrated indoors and resulted in significantly higher indoor PNC
Stacey (2019) conducted a literature survey and concluded that the literature consistently reports that particle numbers close to airports are significantly higher than locations distant and upwind of airports, and that the particle size distribution is different from traditional road traffic, with more extremely fine particles
PM2.5 exposures are associated with a number of serious, adverse health effects and the PM attributable to aircraft emissions has been associated with potential adverse health impacts
He et al. (2018) found that particle composition, size distribution and internalized amount of particles near airports all contributed to promotion of reactive organic species in bronchial epithelial cells
A systematic review of 70 studies consistently showed that particulate matter, in the form of ultrafine PM (UFP), is elevated in and around airports
Furthermore, many studies showed elevated levels of black carbon, criteria pollutants, and polycyclic aromatic hydrocarbons as well
Finally, the systematic review, while not focused on health effects, identified a limited number of references reporting adverse health effects impacts, including increased rates of premature death, pre-term births, decreased lung function, oxidative DNA damage and childhood leukemia
A systematic review of health effects associated with exposure to jet engine emissions in the vicinity of airports found that jet engine emissions have physicochemical properties similar to diesel exhaust particles, and that exposure to jet engine emissions is associated with similar adverse health effects as exposure to diesel exhaust particles and other traffic emissions
A 2010 systematic review by the Health Effects Institute (HEI) concluded that evidence was sufficient to support a causal relationship between exposure to traffic-related air pollution and exacerbation of asthma among children, and suggestive of a causal relationship for childhood asthma, non-asthma respiratory symptoms, impaired lung function and cardiovascular mortality
Besides PM2.5, other harmful pollutants, which are not covered by the rule, include:
Nitrogen oxides (NOX)
Nitrogen dioxide (NO2)
Volatile organic compounds (VOC)
Carbon monoxide (CO)
Sulfur dioxide (SO2)
Aircraft also contribute to ambient levels of hazardous air pollutants (HAP), compounds that are known or suspected human or animal carcinogens, or that have noncancer health effects
These compounds include, but are not limited to:
Benzene,
1,3-butadiene
Formaldehyde
Acetaldehyde
Acrolein
Polycyclic organic matter (POM)
Certain metals
Some POM and HAP metals are components of PM2.5 mass measured in turbine engine aircraft emissions
The term polycyclic organic matter (POM) defines a broad class of compounds that includes the polycyclic aromatic hydrocarbon compounds (PAHs)
Metal compounds emitted from aircraft turbine engine combustion include:
Chromium
Manganese
Nickel
Several POM compounds, as well as hexavalent chromium, manganese compounds and nickel compounds are included in the National Air Toxics Assessment, based on potential carcinogenic risk
When dealing with a potential health threat, we tend to jump to the conclusion that we are facing a new “virus” as this well-orchestrated lie has been drilled into our collective consciousness since birth. It is second nature to blame the new invisible boogeyman while overlooking the old visible threats that have been plaguing us for years with no end in sight. It seems too easy to admit to ourselves that any perceived increase in respiratory disease could be attributable to the continued increase in air pollution.
Yet from the start, “Covid-19” has been linked to air pollution. The areas hit the hardest were those with the highest levels of these harmful toxins in the air. As travel died down during the lockdowns, cases fell along with subsiding smog. As travel and pollution rose up again, so too did the “Covid” cases. Even small increases in air pollution has been shown to have an impact on “Covid” case numbers and deaths.
We know for a fact that air pollution is harmful to our health and environment. We know that every single symptom of disease associated with “Covid-19” can be linked to the PM2.5 particles which make up the majority of the dirty air we breathe. We know for a fact that automobiles, factories, power plants, forest fires, volcanic eruptions, etc. all contribute to the harmful levels of toxins in the air. However, the one thing we have been told not to question as a contributor to our current problems are the lingering trails in the sky which form artificial clouds blocking out the beneficial rays of the sun. We are told that these are just regular old contrails from commercial airliners made up of ice crystals which eventually dissipate into a completely safe and harmless nothingness. Anyone questioning the trails is immediately labelled a conspiracy theorist.
It should be clear now, whether you call them chemtrails or not, that these persistent streaks in the sky are full of dangerous substances that attack the cardiovascular, respiratory, and neurological systems. Thanks to government sources such as the EPA and the Congressional Research Service, we know that these trails are the fastest growing pollutant in the air and that they are contributing to even greater levels of smog and haze. The trails and the artificial cirrus clouds they form are a near constant sight in the sky these days and the problem is only growing worse with time. The damaging effects that these lines in the sky have on our health and environment is not even debatable. It is agreed upon by both sides of the debate. That these “persistent contrails” are harmful to our health and environment is a FACT. That the chemicals and toxins found within the vapors cause the exact same symptoms of disease as “Covid-19” is not a coincidence.
Thus we are left with two choices. We can either believe the official narrative that a new “virus” of unknown origin magically leapt from animal to man or somehow escaped from a lab and infected millions of people with a disease that causes the exact same symptoms associated with allergies, the common cold, the flu, and pneumonia. And with it’s rise, it has eliminated the majority of the cases of those previous ailments and can also constantly mutate (over 10 million versions now according to GISAID.org) in order to slip by every possible measure to contain it including masks, social distancing, lockdowns, quarantines, vaccines, etc.
Or we can believe that the ever-increasing and constant daily exposure to air pollution has taken a toll on the populace damaging the health and environment of everyone living within these dangerous levels of toxic fumes. While this is not the only explanation for any perceived increase in respiratory and other diseases, it is the most logical one over an invisible “virus.” According to Occam’s Razor, the simplest of competing theories should be preferred over those that are more complex and that explanations of unknown phenomena should be sought first in terms of known quantities. We know air pollution is harmful. We know that these trails are increasing at a faster rate than any other pollutant. We know that the chemicals residing within them are associated with the exact same symptoms of disease that are ascribed to “Covid.” Unlike a “virus,” we can see this boogeyman with our own two eyes.
All we have to do is look up.
From their own sources, the trails are a threat to our health and our environment. Contrary to what they want you to believe about “persistent contrails,” a.k.a. chemtrails, this is NOT a conspiracy.
You can see more of the slides from Government sources that were presented within this article here.
As avian influenza runs through the nation’s poultry flocks, with the current extermination of about 28 million laying hens and turkeys, I can’t help but wonder why we aren’t putting beak masks on the chickens.
If masks are so effective against viruses in the human population, why don’t we just make a chicken mask to stop this virus? Seems like a better fix than exterminating all these animals.
The problem is that Dr. Fauci isn’t in the chicken business. Rats. What a shame. If only he were in charge of chickens, he’d have this thing under control in a day. I think we need to expand his authority to the animals of America so he can take care of them like he’s taken care of the humans of America.
When avian flu broke out in our part of Virginia many years ago, two of the federal veterinarians sent in to exterminate chickens visited me just to chat. The independent visits shared an identical assessment: too many chickens crammed in too tight a space in too small a geographic area. Both said if they mentioned that publicly they would be fired.
Hmmmm, I wonder if decentralization of poultry would be better than centralization. Notice that on one farm, 5.8 million laying hens were destroyed—ON ONE FARM!
It’s all blamed on wildlife. Folks, whenever a culture views wildlife as a liability rather than asset, you know everything is wonky. It’s like blaming babies for drug addiction. Or blaming churches for drunkards. When wildlife is the enemy, something is out of whack in the culture’s thinking.
I don’t trust the tests. I don’t trust the experts. I don’t trust the bureaucrats. Isn’t it amazing that as a culture, we’re fixated on prolonging human life for a week or two with ultra-expensive, painful, and invasive intervention but at the first sign of sniffles in a chicken, the “only” cure, according to the experts, is mass extermination. Perhaps the wrong beings are being exterminated. Just sayin’.
The biggest tragedy is that these government gumshoes will come onto a property, without a warrant and unannounced, demanding to pull blood from pastured chickens. They’ll take that sample to a lab driven by political agendas and industrial paradigms (chickens locked in houses are healthier than chickens roaming on a pasture) to determine positive or negative.
Does this sound like incestuous fraternal collusion shenanigans to you?
In a World First on Maria Zeee Uncensored, Australian Senator Malcolm Roberts exposes the Nanotech found in the COVID-19 Vaccines, declaring this is genocide.
We discuss the incoming Digital Identity and the government’s plan to enslave humanity through their plans for a New World Order.
Dr. Naomi Wolf discusses the war on children and on Western values. Forcing children to wear masks is abusive because new studies show that this prevents them from developing normal facial recognition and the practice has a now-measurable effect on their IQ levels.
With all the new information surfacing from the WarRoom/DailyClout volunteers regarding the formerly secret Pfizer documents, and with attorney Stevan Looney’s new essay on the redacted documents in the secret Pfizer tranche now published on DailyClout.io, it is becoming clear that informed consent before receiving the vaccine was never even possible.
Bombshell: in order to process just the paperwork from the “large number of adverse events” — Pfizer’s own words — Pfizer had to hire 2,400 new, full-time employees and the company proudly informed the FDA of these thousands of new hires to grapple with the flood of adverse events they saw as early as February 28, 2021. Yet they did not disclose these adverse events to the public and neither did the FDA.
“The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica…
[….]
“What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice.”
virus, infectious agent of small size and simple composition that can multiply only in living cells of animals, plants, or bacteria. The name is from a Latin word meaning “slimy liquid” or “poison.”
I have purposefully stayed away from the whole “SARS-COV-2” as a gain of function/bioweapon disinformation campaign as it is obvious to anyone who has ever read any “virus” paper, there is absolutely zero credible evidence for the existence of “SARS-COV-2” or any of these other invisible entities. At no point has any virologist ever properly purified and isolated the particles assumed to be “viruses” directly from a sick patient and then proven them pathogenic in a natural way. As this is a fact that is even admitted by virologists themselves, it should also be obvious that if they can not find the particles assumed to be “viruses” in nature, they can not tinker around and modify these fictional entities in a lab in order to create some sort of contagious bioweapon.
Somehow, this logic escapes many. Even though some have woken to the truth and accepted that “SARS-COV-2” does not exist in nature, they still believe that it must have been developed in a lab and unleashed upon the world in order to create a new contagious disease which is wrecking havoc on the elderly and immunocompromised. What they fail to realize is that there simply is no new disease and that none of the symptoms associated with “SARS-COV-2” are new, unique, or specific. There is zero proof of transmission and/or contagion beyond highly flawed epidemiological studies. There is no new “virus,” no new disease, and no contagious bioweapon. It is pure fiction based upon faulty cell culture and genomic experiments.
Before diving into the experimental evidence presented for gain of function studies, I figured it would be a good idea to get some background information on what exactly these kinds of studies entail first. From the October 2021 Nature article highlighted below, we learn that the gain of function concept earned widespread recognition in 2012 due to a pair of studies which both looked to tweak an avian influenza “virus” in order to make it transmissable by air between ferrets. Disregarding the contradictory fact that aerosol transmission is supposedly the way an upper respiratory “virus” is supposed to spread, many became concerned that this kind of work may eventually lead to the release of a super “virus” which could result in the next pandemic. These ferret studies were apparently pivotal with bringing virology into the gain of function field, even though it could be easily argued that virology has been performing these kinds of experiments throughout its existence.
The gain of function term refers to any research that improves a pathogen’s abilities to cause disease or spread from host to host. This is done by fiddling with cell culture material in a lab combined with genomic sequencing. They do this either by inserting genetic material into the cell culture or by way of animal models where the animal is said to be genetically altered in some way to be more susceptible to the “viral” material.
The article provides an example where mice were genetically modified to become susceptible to MERS. However, the mice did not become ill upon being challenged with the “virus.” Thus, the researchers resorted to passaging the “virus” between mice, which involved infecting a couple of mice, giving the “virus” two days to take hold, and then killing the mice and grinding up the lung tissue to inject into other mice. They repeated these steps at least 30 times which eventually made some mice sick. This process of culturing toxic material, injecting animals with the concoction, killing them and grinding up their remains, and then injecting this emulsified goop into other animals in an attenpt to make them sick is what GOF is all about. While this horrific process is getting recognized today, these kinds of experiments have been a staple of virology since the very beginning:
The shifting sands of ‘gain-of-function’ research
“The term first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza virus, using genetic engineering and directed evolution, until it could be transmitted between ferrets2,3. Many people were concerned that publishing the work would be tantamount to providing a recipe for a devastating pandemic, and in the years that followed, research funders, politicians and scientists debated whether such work required stricter oversight, lest someone accidentally or intentionally release a lab-created plague. Researchers around the world voluntarily paused some work, but the issue became particularly politicized in the United States.
US funding agencies, which also support research abroad, later imposed a moratorium on gain-of-function research with pathogens while they worked out new protocols to assess the risks and benefits. But many of the regulatory discussions have taken place out of the public eye.
Now, gain-of-function research is once again centre stage, thanks to SARS-CoV-2 and a divisive debate about where it came from. Most virologists say that the coronavirus probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the virus was first reported. But a group of scientists and politicians argues that a laboratory origin has not been ruled out. They are demanding investigation of the Wuhan Institute of Virology, where related bat coronaviruses have been extensively studied, to determine whether SARS-CoV-2 could have accidentally leaked from the lab or crossed into humans during collection or storage of samples.”
“The term GOF didn’t have much to do with virology until the past decade. Then, the ferret influenza studies came along. In trying to advise the federal government on the nature of such research, the US National Science Advisory Board for Biosecurity (NSABB) borrowed the term — and it stuck, says Gigi Gronvall,a biosecurity specialist at the Bloomberg School of Public Health at Johns Hopkins University in Baltimore, Maryland. From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host.
Virologists do regularly fiddle with viral genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models. “People do all of these experiments all the time,” says Juliet Morrison, a virologist at the University of California, Riverside. For example, her lab has made mouse viruses that are more harmful to mice than the originals. If only mice are at risk, should it be deemed GOF? And would it be worrying?
The answer is generally no. Morrison’s experiments, and many others like them, pose little threat to humans. GOF research starts to ring alarm bells when it involves dangerous human pathogens, such as those on the US government’s ‘select agents’ list, which includes Ebola virus and the bacteria responsible for anthrax and botulism. Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza viruses and coronaviruses. “For the most part, we’re worried about respiratory viruses because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School. GOF studies with those viruses are “a really tiny part” of virology, he adds.”
“Animal research — although fraught with its own set of ethical quandaries — allows scientists to study how pathogens work and to test potential treatments, a necessary precursor to trials in people. That’s what Perlman and his collaborators had in mind when they set out to study the coronavirus responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012. They wanted to use mice, but mice can’t catch MERS.
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells. So, the team altered the mice, giving them a human-like version of the gene for DPP4. The virus could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill. “Having a model of mild disease isn’t particularly helpful to understand why people get so sick,” says collaborator Paul McCray, a paediatric pulmonologist also at the University of Iowa.
So, the group used a classic technique called ‘passaging’ to enhance virulence. The researchers infected a couple of mice, gave the virus two days to take hold, and then transferred some of the infected lung tissue into another pair of mice. They did this repeatedly — 30 times9. By the end of two months, the virus had evolved to replicate better in mouse cells. In so doing, it made the mice more ill; a high dose was deadly, says McCray. That’s GOF of a sort because the virus became better at causing disease. But adapting a pathogen to one animal in this way often limits its ability to infect others, says Andrew Pekosz, a virologist at the Bloomberg School of Public Health.”
“With all the challenges inherent in GOF studies, why do them? Because, some virologists say, the viruses are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match. “We can either wait for something to arise, and then fight it, or we can anticipate that certain things will arise, and instead we can preemptively build our arsenals,” says Morrison. “That’s where gain-of-function research can come in handy.”
This next source is from 2015. The authors admit that virology is heavily reliant on gain or loss of function studies. They offer an alternative definition for GOF research which is any selection process involving an alteration of genotypes and their resulting phenotypes. Obviously, this definition leans far more into the genomics side of the equation. This is due to the claim that these kinds of studies are used by virologists in order to understand a “viruses” genetic make-up. It is stated that researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA. In other words, they mix genetic material from different sources, poison and/or kill lab animals by injecting them with this toxic soup, and then analyze the resulting mixture using computers so that they can claim that the generated model is a new creation. However, it is admitted that these kinds of mutations happen “naturally” with “viruses” every time a person is infected, thus confirming what we already know: virologists can not sequence the same exact “virus” every time:
Gain-of-Function Research: Background and Alternatives
“The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function. In order to understand the role of such studies in virology, Dr. Kanta Subbarao from the Laboratory of Infectious Disease at the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health (NIH) gave an overview of the current scientific and technical approaches to the research on pandemic strains of influenza and Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) coronaviruses (CoV). As discussed in greater detail later in this chapter, many participants argued that the word choice of “gain-of-function” to describe the limited type of experiments covered by the U.S. deliberative process, particularly when coupled with a pause on even a smaller number of research projects, had generated concern that the policy would affect much broader areas of virology research.
TYPES OF GAIN-OF-FUNCTION (GOF) RESEARCH
Subbarao explained that routine virological methods involve experiments that aim to produce a gain of a desired function, such as higher yields for vaccine strains, but often also lead to loss of function, such as loss of the ability for a virus to replicate well, as a consequence. In other words, any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research, even if the U.S. policy is intended to apply to only a small subset of such work.
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of viruses and added that much basic knowledge is still lacking for SARS-CoV and MERS-CoV. Subbarao introduced the key questions that virologists ask at all stages of research on the emergence or re-emergence of a virus and specifically adapted these general questions to the three viruses of interest in the symposium (see Box 3-1). To answer these questions, virologists use gain- and loss-of-function experiments to understand the genetic makeup of viruses and the specifics of virus-host interaction. For instance, researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant viruses from cloned cDNA, and deep sequencing that are critical for studying how viruses escape the host immune system and antiviral controls. Researchers also use targeted host or viral genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool.
During Session 3 of the symposium, Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments. The first category, which he called “gain of function research of concern,” includes the generation of viruses with properties that do not exist in nature. The now famous example he gave is the production of H5N1 influenza A viruses that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type. The second category deals with the generation of viruses that may be more pathogenic and/or transmissible than the wild type viruses but are still comparable to or less problematic than those existing in nature. Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates will improve their replication in mammalian cells. Finally, the third category, which is somewhere in between the two first categories, includes the generation of highly pathogenic and/or transmissible viruses in animal models that nevertheless do not appear to be a major public health concern. An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans. During the discussion, Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature.”
“Imperiale explained that, with respect to the GoF terminology, whenever researchers are working with RNA viruses, GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.” He also commented that the term GoF was understood a certain way by attendees of this symposium, but when the public hears this term “they can’t make that sort of nuanced distinction that we can make here” so the terminology should be revisited.”
Hopefully the above two sources have shown that GOF studies are nothing more than the exact same cell culture experiments utilizing the exact same genomic sequencing technologies and tricks that virologists have always used. The only difference is that they are combining different culture supernatant and genetic materials together into one in order to create a brand new synthetic computer-generated sequence. At no point in time are any purified/isolated particles ever used in these studies. In fact, there are no EM images of the new “virus” of any kind. It should therefore not be surprising that we can see the exact same pattern of unscientific methods and illogical reasoning in GOF studies as found in any of the original “virus” papers.
Seeing as to how the 2012 avian flu studies brought GOF research to the forefront, it seemed ideal to step into this area a bit more to see what actually transpired. The main study presented as evidence of GOF research was led by a man named Ron Fouchier. If that name sounds familiar, that’s because it should. Fouchier was involved in the 2003 “SARS-COV-1” study which proclaimed the satisfaction of Koch’s Postulates for proving a microorganism causes disease yet it failed miserably by not only not being able to satisfy Koch’s four original Postulates, but also Thomas River’s six revised Postulates made strictly for virology. In other words, it was an epic fail.
In Fouchier’s 2012 avian flu GOF study, he attempted to make the H5N1 “virus” infectious through the air. This was done through a process involving cell culturing combined with genetic engineering as well as passaging the material through numerous ferrets. Sounds familiar to the mice example from before, correct? You also see this same process with the early polio and influenza studies as well as in many other virology papers. The main difference is the genomic narrative and the use of modern technology such as reverse genetics to claim the insertion of specific genes.
Highlights from the below paper provide an overview of what was done during this study. It details how the material was collected from a flu strain in Indonesia, genetically altered in a Petri dish, and then transferred to ferrets in a series of experiments using the “wildtype” strain along with different modified strains. Fouchier and Co. were repeatedly unsuccessful in their endeavors of infecting ferrets until they started passaging the “virus” in the animals by injecting them with the cultured soup, grinding up their lung tissues, and injecting other ferrets in the same manner. They repeated this process 6 times and then changed up the experiment by switching to nasal turbinates for the last 4 passage attempts. The only illness said to be achieved via airborne exposure was a loss of appetite, lethargy, and ruffled fur. Upon sequencing the “viruses,” there were only two amino acid switches shared by all six “viruses.” There were several other mutations, but none that occurred in all six airborne “viruses.” In other words, they could not sequence the same “virus” at any point:
Fouchier study reveals changes enabling airborne spread of H5N1
“A study showing that it takes as few as five mutations to turn the H5N1 avian influenza virus into an airborne spreader in mammals—and that launched a historic debate on scientific accountability and transparency—was released today in Science, spilling the full experimental details that many experts had sought to suppress out of concern that publishing them could lead to the unleashing of a dangerous virus.
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 virus that can spread among ferrets without direct contact.
They say their findings show that H5N1 viruses have the potential to evolve in mammals to gain airborne transmissibility, without having to mix with other flu viruses in intermediate hosts such as pigs, and thus pose a risk of launching a pandemic.”
Indonesian H5N1 strain used
Fouchier’s team started with an H5N1 virus collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 viruses more human-like in how they bind to airway cells or in other ways. Avian flu viruses prefer to bind to alpha2,3-linked sialic acid receptors on cells, whereas human flu viruses prefer alpha2,6-linked receptors. In both humans and ferrets, alpha2,6 receptors are predominant in the upper respiratory tract, while alpha 2,6 receptors are found mainly in the lower respiratory tract.
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the virus’s HA protein, the viral surface molecule that attaches to host cells. Q222L and G224S together change the binding preference of H2 and H3 subtype flu viruses, changes that contributed to the 1957 and 1968 flu pandemics, according to the report. And N182K was found in a human H5N1 case.
The scientists created three mutant H5N1 virus strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes, the report explains. They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 virus. Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type virus shed far more virus than those infected with the mutants.
In a second step, the team used a mutation in a different viral gene, PB2, the polymerase complex protein. The mutation E627K in PB2 is linked to the acquisition by avian flu viruses of the ability to grow in the human respiratory tract, which is cooler than the intestinal tract of birds, where the viruses usually reside, according to the report.
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a virus that grew more vigorously in ferrets, and the virus did not spread through the air from infected ferrets to uninfected ones.
The passaging step
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract—the move that Fouchier called “really, really stupid,” according to a report of his initial description of the research at a European meeting last September.
They inoculated one ferret with the three-mutation strain and another with the wild-type virus and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs). Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times. For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest viruses that were secreted from the upper respiratory tract.
The amount of mutant virus found in the nasal turbinate and nose swab samples increased with the number of passages, signaling that the virus was increasing its capacity to grow in the ferret upper airway. In contrast, viral titers in the samples from ferrets infected with the wild-type virus stayed the same.
The next step was to test whether the viruses produced through passaging could achieve airborne transmission. Four ferrets were inoculated with samples of the “passage-10” mutant virus, and two ferrets were inoculated with the passage-10 wild strain. Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact.
The ferrets exposed to those with the wild virus remained uninfected, but three of the four ferrets placed near those harboring the mutant virus did get infected, the researchers found. Further, they took a sample from one of the “recipient” ferrets and used it to inoculate another ferret, which then transmitted the virus to two more ferrets that were placed near it.
Thus, a total of six ferrets became infected with the mutant virus via airborne transmission. However, the level of viral shedding indicated the airborne virus didn’t transmit as efficiently as the 2009 H1N1 virus does.
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur. One of the directly inoculated ferrets died, but all those infected via airborne viruses survived.
When the scientists sequenced the genomes of the viruses that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six viruses: H103Y and T156A. They noted several other mutations, but none that occurred in all six airborne viruses.
“Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of [highly pathogenic avian flu] H5N1 virus,” the researchers wrote.
In further steps, the researchers inoculated six ferrets with high doses of the airborne-transmissible virus; after 3 days, the ferrets were either dead or “moribund.” “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia,” the report notes.”
While the proceeding article did an excellent job of providing the main points from Fouchier’s 2012 GOF study, I wanted to showcase relevant highlights directly from the paper to flesh out the methods used even further. Here you will see that Fouchier’s team claimed that they genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets. They used Influenza “virus” A/Indonesia/5/2005 (A/H5N1) which they said was isolated from a human case of HPAI “virus” infection. This was passaged once in embryonated chicken eggs which was followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000. They then used the QuickChange multisite-directed mutagenesis kit to introduce the desired amino acid substitutions. Site-directed mutagenesis is a synthetic process utilizing PCR to make artificial changes in a DNA sequence. They then took their synthetically-created cultured soup and experimented on ferrets while manipulating the methods until they achieved the results that they desired.
At no point in the paper was a “virus” of any kind ever purified and isolated. At no point were any electron microscope images of the newly mutated “viruses” ever shown. The only “evidence” of an airborne strain is genomic sequencing data from consensus genomes which did not match up. Fouchier and Co. even admitted that airborne transmission could be tested in a second mammalian model system such as guinea pigs, but even this would still not provide conclusive evidence that transmission among humans would occur. They also stated that the mutations they had identified needed further testing to determine their effect on transmission in other A/H5N1 “virus” lineages, and that further experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals. In other words, their study only told them that they could create mutated genomes and not that they created more “virulent viruses” that are transmissable by air:
Airborne Transmission of Influenza A/H5N1 Virus Between Ferrets
“Highly pathogenic avian influenza A/H5N1 virus can cause morbidity and mortality in humans but thus farhas not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”)between humans. To address the concern that the virus could acquire this ability under natural conditions,we genetically modified A/H5N1 virus by site-directed mutagenesis and subsequent serial passage inferrets. The genetically modified A/H5N1 virus acquired mutations during passage in ferrets, ultimatelybecoming airborne transmissible in ferrets. None of the recipient ferrets died after airborne infection withthe mutant A/H5N1 viruses. Four amino acid substitutions in the host receptor-binding protein hemagglutinin, and one in the polymerase complex protein basic polymerase 2, were consistently present in airborne-transmitted viruses. The transmissible viruses were sensitive to the antiviral drug oseltamivir and reacted well with antisera raised against H5 influenza vaccine strains. Thus, avian A/H5N1 influenza viruses can acquire the capacity for airborne transmission between mammals without recombination in an intermediate host and therefore constitute a risk for human pandemic influenza.
Influenza A viruses have been isolated from many host species, including humans, pigs, horses, dogs, marine mammals, and a wide range of domestic birds, yet wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the virus reservoir in nature (1). Influenza A viruses belong to the family Orthomyxoviridae; these viruses have an RNA genome consisting of eight gene segments (2, 3). Segments 1 to 3 encode the polymerase proteins: basic polymerase 2 (PB2), basic polymerase 1 (PB1), and acidic polymerase (PA), respectively. These proteins form the RNA-dependent RNA polymerase complex responsible for transcription and replication of the viral genome.”
Since the late 1990s, HPAI A/H5N1 viruses have devastated the poultry industry of numerous countries in the Eastern Hemisphere. To date, A/H5N1 has spread from Asia to Europe, Africa, and the Middle East, resulting in the death of hundreds of millions of domestic birds. In Hong Kong in 1997, the first human deaths directly attributable to avian A/H5N1 virus were recorded (11). Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 virus infections in humans have been reported from 15 countries (12). Although limited A/H5N1 virus transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 virus has not been detected (13–15). Whether this virus may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness. Although our knowledge of viral traits necessary for host switching and virulence has increased substantially in recent years (16, 17), the factors that determine airborne transmission of influenza viruses among mammals, a trait necessary for a virus to become pandemic, have remained largely unknown (18–21). Therefore, investigations of routes of influenza virus transmission between animals and on the determinants of airborne transmission are high on the influenza research agenda.
The viruses that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza viruses (22). However, given that viruses from only four pandemics are available for analyses, we cannot exclude the possibility that a futurepandemic may be triggered by a wholly avian virus without the requirement of reassortment. Several studies have shown that reassortment events between A/H5N1 and seasonal human influenza viruses do not yield viruses that are readily transmitted between ferrets (18–20, 23). In our work, we investigated whether A/H5N1 virus could change its transmissibility characteristics without any requirement for reassortment.
We chose influenza virus A/Indonesia/5/2005 for our study because the incidence of human A/H5N1 virus infections and fatalities in Indonesia remains fairly high (12), and there are concerns that this virus could acquire molecular characteristics that would allow it to become more readily transmissible between humans and initiate a pandemic. Because no reassortants between A/H5N1 viruses and seasonal or pandemic human influenza viruses have been detected in nature and because our goal was to understand the biological properties needed for an influenza virus to become airborne transmissible in mammals, we decided to use the complete A/Indonesia/5/2005 virus that was isolated from a human case of HPAI A/H5N1 infection.
We chose the ferret (Mustela putorius furo) as the animal model for our studies. Ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza viruses (24). After infection with human influenza A virus, ferrets develop respiratory disease and lung pathology similar to that observed in humans. Ferrets can also transmit human influenza viruses to other ferrets that serve as sentinels with or without direct contact (fig. S1) (25–27).”
Human-to-human transmission of influenza viruses can occur through direct contact, indirect contact via fomites (contaminated environmental surfaces), and/or airborne transmission via small aerosols or large respiratory droplets. The pandemic and epidemic influenza viruses that have circulated in humans throughout the past century were all transmitted via the airborne route, in contrast to many other respiratory viruses that are exclusively transmitted via contact. There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols. However, it is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols. Because we did not measure particle size during our experiments, we will use the term “airborne transmission” throughout this Report.”
“Using a combination of targeted mutagenesis followed by serial virus passage in ferrets, we investigated whether A/H5N1 virus can acquiremutations that would increase the risk of mammalian transmission (34). We have previously shown that several amino acid substitutions in the RBS of the HA surface glycoprotein of A/Indonesia/5/2005 change the binding preference from the avian a-2,3–linked SA receptors to the human a-2,6–linked SA receptors (35). A/Indonesia/5/2005 virus with amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S (numbers refer to amino acid positions in the mature H5 HA protein; N, Asn; Q, Gln; L, Leu; G, Gly; S, Ser) in HA display attachment patterns similar to those of human viruses to cells of the respiratory tract of ferrets and humans (35). Of these changes, we know that together, Q222L and G224S switch the receptor binding specificity of H2 and H3 subtype influenza viruses, as this switch contributed to the emergence of the 1957 and 1968 pandemics (36). N182K has been found in a human case of A/H5N1 virus infection (37).
Our experimental rationale to obtain transmissible A/H5N1 viruses was to select a mutant A/H5N1 virus with receptor specificity for a-2,6–linked SA shed at high titers from the URT of ferrets. Therefore, we used the QuickChange multisite-directed mutagenesis kit (Agilent Technologies, Amstelveen, the Netherlands) to introduce amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S in the HA of wild-type (WT) A/Indonesia/5/2005, resulting in A/H5N1HA N182K, A/H5N1HA Q222L,G224S, and A/H5N1HA N182K,Q222L,G224S. Experimental details for experiments 1 to 9 are provided in the supplementary materials (25). For experiment 1, we inoculated these mutant viruses andthe A/H5N1wildtype virus intranasally into groups of six ferrets for each virus (fig. S3). Throat and nasal swabs were collected daily, and virus titerswere determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify virus shedding from the ferret URT. Three animals were euthanized after day 3 to enable tissue sample collection. All remaining animals were euthanized by day 7 when the same tissue samples were taken. Virus titers were determined in the nasal turbinates, trachea, and lungs collected post-mortem from the euthanized ferrets. Throughout the duration of experiment 1, ferrets inoculated intranasally with A/H5N1wildtype virus produced high titers in nose and throat swabs—up to 10 times more than A/H5N1HA Q222L,G224S, which yielded the highest virus titers of all three mutants during the 7-day period (Fig. 1). However, no significant difference was observed between the virus shedding of ferrets inoculated with A/H5N1HA Q222L, G224S or A/H5N1HA N182K during the first 3 days when six animals per group were present. Thus, of the viruses with specificity for a-2,6–linked SA, A/H5N1HA Q222L,G224S yielded the highest virus titers in the ferret URT (Fig. 1).
As described above, amino acid substitution E627K in PB2 is one of the most consistent host-range determinants of influenza viruses (29–31). For experiment 2 (fig. S4), we introduced E627K into the PB2 gene of A/Indonesia/5/2005 by site-directed mutagenesis and produced the recombinant virus A/H5N1HA Q222L,G224S PB2 E627K. The introduction of E627K in PB2 did not significantly affect virus shedding in ferrets, because virus titers in the URT were similar to those seen in A/H5N1HA Q222L,G224S-inoculated animals [up to 1 × 104 50% tissue culture infectious doses (TCID50)] (Mann-Whitney U rank-sum test, P = 0.476) (Fig. 1 and fig. S5). When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously (27), A/H5N1HA Q222L,G224S PB2 E627K was not transmitted (fig. S5).
Because the mutant virus harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, we designed an experiment to force the virus to adaptto replication in the mammalian respiratory tract and to select virus variants by repeated passage (10 passages in total) of the constructedA/H5N1HA Q222L,G224S PB2 E627K virus and A/H5N1wildtype virus in the ferret URT (Fig. 2 and fig. S6). In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K. Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs. The nasal turbinates were homogenized in 3 ml of virus-transport medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate thenext ferret intranasally (passage 2). This procedure was repeated until passage 6.
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi. To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise tothe nostrils of the ferrets to induce sneezing. Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml. The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10. We changed the source of inoculum during the course of theexperiment, because passaging nasal washes may facilitate the selection of viruses that were secreted from the URT. Because influenza viruses mutate rapidly, we anticipated that 10 passages would be sufficient for the virus to adapt to efficient replication in mammals.
Virus titers in the nasal turbinates of ferrets inoculated with A/H5N1wildtype ranged from ~1 × 105 to 1 × 107 TCID50/gram tissue throughout 10 serial passages (Fig. 3A and fig. S7). In ferrets inoculated with A/H5N1HA Q222L,G224S PB2 E627K virus, a moderate increase in virus titers in the nasal turbinates was observed as the passage number increased. These titers ranged from 1 × 104 TCID50/gram tissue at the start of the experiment to 3.2 × 105 to 1 × 106 TCID50/gram tissue in the final passages (Fig. 3A and fig. S7). Notably, virus titers in the nose swabs of animals inoculated with A/H5N1HA Q222L,G224S PB2 E627K also increased during the successive passages, with peak virus shedding of 1 × 105 TCID50 at 2 dpi after 10 passages (Fig. 3B).These data indicate that A/H5N1HA Q222L,G224S PB2 E627K was developing greater capacity to replicate in the ferret URT after repeated passage, with evidence for such adaptation becoming apparent by passage number 4. In contrast, virus titers in the nose swabs of the ferrets collected at 1 to 4 dpi throughout 10 serial passages with A/H5N1wildtype revealed no changes in patterns of virus shedding.
Passaging of influenza viruses in ferrets should result in the natural selection of heterogeneous mixtures of viruses in each animal with a variety of mutations: so-called viral quasi-species (38). The genetic composition of the viral quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform (Roche, Woerden, the Netherlands) (tables S1 and S2). The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the virus population after 10 consecutive passages at a frequency >99.5% (Fig. 4 and table S1). Numerous additional nucleotide substitutions were detected in all viral gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kafter passaging, except in segment 7 (tables S1 and S2). Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions.The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kwas T156A (T, Thr; A, Ala) in HA. This substitution removes a potential N-linked glycosylation site (Asn-X-Thr/Ser; X, any amino acid) in HA and was detected in 99.6% of the A/H5N1wildtype sequences after 10 passages. T156A was detected in 89% of the A/H5N1HA Q222L,G224S PB2 E627K sequences after 10 passages, and the other 11% of sequences possessed the substitution N154K, which removes the same potential N-linked glycosylation site in HA.
In experiment 4 (see supplementary materials), we investigated whether airborne-transmissible viruses were present in the heterogeneous virus population generated during virus passaging in ferrets (fig. S4). Nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were usedin transmission experiments to test whether airborne-transmissible virus was present in the virus quasi-species. For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally: two for passage 10 A/H5N1wildtype and four for passage 10 A/H5N1HA-Q222L,G224S PB2 E627K virus.
The following day, a naïve recipient ferret was placed in a cage adjacent to each inoculated donor ferret. These cages are designed to prevent direct contact between animals but allow airflow from a donor ferret to a neighboring recipient ferret (fig. S1) (27). Although mutations had accumulated in the viral genome after passaging of A/H5N1wildtype in ferrets, we did not detect replicating virus upon inoculation of MDCKcells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype virus(Fig. 5, A and B). In contrast, we did detect virus in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627Kvirus.Three (F1 to F3) out of four (F1 to F4) naïve recipient ferrets became infected as confirmed by the presence of replicating virus in the collected nasal and throat swabs (Fig. 5, C and D). A throat-swab sample obtained from recipient ferret F2, which contained the highest virus titer among the ferrets in the first transmission experiment, was subsequently used for intranasal inoculation of two additional donor ferrets. Both of these animals, when placed in the transmission cage setup (fig. S1), again transmitted the virus to the recipient ferrets (F5 and F6) (Fig. 6, A and B). Avirus isolate was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi. The virus from F5 was inoculated intranasally into two more donor ferrets. One day later, these animals were paired with two recipient ferrets (F7 and F8) in transmission cages, one of which (F7) subsequently became infected (Fig. 6, C and D).
We used conventional Sanger sequencing to determine the consensus genome sequences ofviruses recovered from the six ferrets (F1 to F3 and F5 to F7) that acquired virus via airborne transmission (Fig. 4 and table S3). All six samples still harbored substitutions Q222L, G224S,and E627K that had been introduced by reverse genetics. Surprisingly, only two additional amino acid substitutions, both in HA, were consistently detected in all six airborne-transmissible viruses: (i) H103Y (H, His; Y, Tyr), which forms part of the HA trimer interface, and (ii) T156A, which is proximal but not immediately adjacent to the RBS (fig. S8). Although we observed severalother mutations, their occurrence was not consistent among the airborne viruses, indicating that of the heterogeneous virus populations generated by passaging in ferrets, viruses with different genotypes were transmissible. In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible viruses because, for example, the consensus sequence of virus isolated from F6 differed from the sequence of parental virus isolated from F2.
Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 virus between mammals. The airborne-transmissible virus isolate with the least number of amino acid substitutions, compared with the A/H5N1wildtype, was recovered from ferret F5. This virus isolate had a total of nine amino acid substitutions; in addition to the three mutations that we introduced (Q222L and G224S in HA and E627K in PB2), this virus harbored H103Y and T156A in HA, H99Y and I368V (I, Ile; V, Val) in PB1, and R99K (R, Arg) and S345N in NP (table S3). Reverse genetics will be needed to identify which of the five to nine amino acid substitutions in this virus are essential to confer airborne transmission.
During the course of the transmission experiments with the airborne-transmissible viruses, ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation. One of eight inoculated animals died upon intranasal inoculation (Table 1). In previously published experiments, ferrets inoculated intranasally with WTA/ Indonesia/5/2005 virus at a dose of 1 × 106 TCID50 showed neurological disease and/or death (39, 40). It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 virus and the subsequent course of disease is not representative of the natural situation in humans.Importantly, although the six ferrets that became infected via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment. Moreover, previous infections of humans with seasonal influenza viruses are likely to induce heterosubtypic immunity that would offer some protection against the development of severe disease (41, 42). It has been shown that mice and ferrets previously infected with an A/H3N2 virus are clinically protected against intranasal challenge infection with an A/H5N1 virus (43, 44).
After intratracheal inoculation (experiment 5; fig. S9), six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible virus F5 in a 3-ml volume of PBS died or were moribund at day 3. Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia (45), as is done for vaccination-challenge studies. At necropsy, the six ferrets revealed macroscopic lesions affecting 80 to 100% of the lung parenchyma with average virus titers of 7.9 × 106 TCID50/gram lung (fig. S10). These data are similar to those described previously for A/H5N1wildtype in ferrets (Table 1). Thus, although the airborne-transmissible virus is lethal to ferrets upon intratracheal inoculation at high doses, the virus was not lethal after airborne transmission.”
“Although our experiments showed that A/H5N1 virus can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear. Previous data have indicated that the 2009 pandemic A/H1N1 virus transmits efficiently among ferrets and that naïve animals shed high amounts of virus as early as 1 or 2 days after exposure (27). When we compare the A/H5N1 transmission data with that of reference (27), keeping in mind that our experimental design for studying transmission is not quantitative, the data shown in Figs. 5 and 6 suggest that A/H5N1 airborne transmission was less robust, with less and delayed virus shedding compared with pandemic A/H1N1 virus.
Airborne transmission could be tested in a second mammalian model system such as guinea pigs (59), but this would still not provide conclusive evidence that transmission among humans would occur. The mutations we identified need to be tested for their effect on transmission in other A/H5N1 virus lineages (60), and experiments are needed to quantify how they affect viral fitness and virulence in birds and mammals. For pandemic preparedness, antiviral drugs and vaccine candidates against airborne-transmissible virus should be evaluated in depth. Mechanistic studies on the phenotypic traits associated with each of the identified amino acid substitutions should provide insights into the key determinants of airborne virus transmission. Our findings indicate that HPAI A/H5N1 viruses have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in humans. Identification of the minimal requirements for virus transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness (34).”
“Influenza virus A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI virus infection and passaged once in embryonated chicken eggs followed by a singlepassage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000 (63-64). Mutations of interest (N182K, Q222L, G224S in HA and E627K in PB2) were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit (Aligent, Amstelveen, The Netherlands) according to the instructions of the manufacturer. Recombinant viruses were produced upon transfection of 293T cells and virus stocks were propagated and titrated in MDCK cells as described (63).
Cells
MDCK cells were cultured in Eagle’s minimal essential medium (EMEM, Lonza Benelux BV, Breda, the Netherlands) supplemented with 10% fetal calf serum (FCS), 100 IU/ml penicillin, 100 μg/ml streptomycin, 2 mM glutamine, 1.5 mg/ml sodium bicarbonate (Lonza), 10 mM Hepes (Lonza), and non-essential amino acids (MP Biomedicals Europe, Illkirch, France). 293T cells were cultured in Dulbecco modified Eagle’s medium (DMEM, Lonza) supplemented with 10% FCS, 100 IU/ml penicillin, 100 mg/ml streptomycin, 2mM glutamine, 1mM sodium pyruvate, and non-essential amino acids.
Virus titration in MDCK cells
Virus titrations were performed as described previously (27). Briefly, MDCK cells were inoculated with tenfold serial dilutions of virus preparations, homogenized tissues, nose swabs, and throat swabs.Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with 100 U/mlpenicillin, 100 μg/ml streptomycin, 2mM glutamine, 1.5mg/ml sodium bicarbonate, 10mM Hepes, non-essential amino acids, and 20 μg/ml trypsin (Lonza). Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of virus replication in the cells. Infectious virus titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the virus preparations by the method of Spearman-Karber (65).”
The term “Gain of Function” first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza “virus,” using genetic engineering and directed evolution, until it could be transmitted between ferrets
Most virologists say that the “coronavirus” probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the “virus” was first reported
However, a group of scientists and politicians argues that a laboratory origin has not been ruled out
The term GOF didn’t have much to do with virology until the past decade when the ferret influenza studies came along
From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host
Virologists regularly fiddle with “viral” genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models
Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza “viruses” and “coronaviruses”
“For the most part, we’re worried about respiratory “viruses” because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School
He added that GOF studies with those “viruses” are “a really tiny part” of virology
Perlman and his collaborators set out to study the “coronavirus” responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012
They wanted to use mice, but mice can’t catch MERS
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells and so the team altered the mice, giving them a human-like version of the gene for DPP4
The “virus” could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill
So, the group used a classic technique called ‘passaging’ to enhance “virulence”
The researchers infected a couple of mice, gave the “virus” two days to take hold, and then transferred some of the infected lung tissue into another pair of mice
They did this repeatedly — 30 times and by the end of two months, the “virus” had evolved to replicate better in mouse cells
In so doing, it made the mice more ill; a high dose was deadly
Some virologists say “viruses” are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match
The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function
Any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of “viruses” and added that much basic knowledge is still lacking for “SARS-CoV” and “MERS-CoV”
Virologists use gain- and loss-of-function experiments to understand the genetic makeup of “viruses” and the specifics of “virus-host” interaction
Researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA (i.e. they are synthetic lab creations)
Researchers also use targeted host or “viral” genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool
Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments:
The fisrt category is “gain of function research of concern,” includes the generation of “viruses” with properties that do not exist in nature
The now famous example he gave is the production of H5N1 influenza A “viruses” that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type
The second category deals with the generation of “viruses” that may be more pathogenic and/or transmissible than the wild type “viruses” but are still comparable to or less problematic than those existing in nature (which is odd considering no “viruses” have been found in nature…)
Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates (there are no natural isolates) will improve their replication in mammalian cells
The third category, which is somewhere in between the first two categories, includes the generation of highly pathogenic and/or transmissible “viruses” in animal models that nevertheless do not appear to be a major public health concern
An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans
Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature
GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.”
In other words, they can never sequence the same “virus” every time so what they do in the lab in GoF studies is no different than how they culture and “isolate viruses” in order to sequence the genomes in the first place
A 2012 study supposedly showed that it takes as few as five mutations to turn the H5N1 avian influenza “virus” into an airborne spreader in mammals—and this launched a historic debate on scientific accountability and transparency
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 “virus” that can spread among ferrets without direct contact
Fouchier’s team started with an H5N1 “virus” collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 “viruses” more human-like in how they bind to airway cells or in other ways
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the “virus’s” HA protein, the “viral” surface molecule that attaches to host cells
The scientists created three mutant H5N1 “virus” strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes
They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 “virus”
Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type “virus” shed far more “virus” than those infected with the mutants
In a second step, the team used a mutation in a different “viral” gene, PB2, the polymerase complex protein
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a “virus” that grew more vigorously in ferrets, and the “virus” did not spread through the air from infected ferrets to uninfected ones
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract
This was the move that Fouchier called “really, really stupid” (are we sure he wasn’t referring to the whole study?)
They inoculated one ferret with the three-mutation strain and another with the wild-type “virus” and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs)
Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times
For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest “viruses” that were secreted from the upper respiratory tract
In other words, they completely changed the source material from tissue to nasal secretions more than halfway through the experiment
It was said that the amount of mutant “virus” found in the nasal turbinate and nose swab samples increased with the number of passages while “viral” titers in the samples from ferrets infected with the wild-type “virus” stayed the same
Quick Sidenote From the Supplemtary Materials:
“After inoculation with A/H5N1wildtype, virus titers in the nasal turbinates were variable but high, ranging from 1.6 x 105 to 7.9 x 106 TCID50/gram tissue (panel A), with no further increase observed with repeated passage. After inoculation with A/H5N1HA Q222L,G224S PB2 E627K, virus titers in nasal turbinates averaged 1.6 x 104 in the first three passages, 2.5 x 105 in passage four to seven and 6.3 x 105 TCID50/gram tissue in the last three passages, suggestive of improved replication and virus adaptation. In the lungs, no apparent adaptation was observed for animals inoculated with either virus. Virus titers in lungs were highly variable; presumably it was a matter of chance whether the virus reached the lower airways.”
In other words, the “wildtype virus” titers remained and stayed high while the “mutant virus” started low and elevated throughout passaging yet was still underneath the amount seen in the “wildtype” strain. They also note that finding “virus” in the lungs was a “matter of chance” with either “virus.”
End Quick Sidenote.
The next step was to test whether the “viruses” produced through passaging could achieve airborne transmission so four ferrets were inoculated with samples of the “passage-10” mutant “virus,” and two ferrets were inoculated with the passage-10 wild strain
Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact
The ferrets exposed to those with the wild “virus” remained uninfected, but three of the four ferrets placed near those harboring the mutant “virus” did get infected (“infected” meaning they found “viral” RNA)
Thus, a total of six ferrets became “infected” with the mutant “virus” via airborne transmission
However, the level of “viral” shedding indicated the airborne “virus” didn’t transmit as efficiently as the 2009 H1N1 “virus”
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur (no consideration is given to the fact that the animals were caged, tortured, and experimented on)
One of the directly inoculated ferrets died, but all those infected via airborne “viruses” survived
When the scientists sequenced the genomes of the “viruses” that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six “viruses:” H103Y and T156A
They noted several other mutations, but none that occurred in all six airborne “viruses”
In other words, once again they were unable to sequence the exact same genome in the samples from each ferret
In further steps, the researchers inoculated intratracheallysix ferrets with high doses of the airborne-transmissible “virus;” after 3 days, the ferrets were either dead or “moribund”
They stated: “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia”
Highly “pathogenic” avian influenza A/H5N1 “virus” can cause morbidity and mortality in humans but thus far has not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”) between humans
To address the concern that the “virus” could acquire this ability under natural conditions, the researchers genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets
In other words, in order to test whether the “virus” could mutate naturally, they mutated it synthetically…
The genetically modified A/H5N1 “virus” acquired mutations during passage in ferrets, ultimately becoming airborne transmissible in ferrets (all “viruses” aquire mutations every time they are sequenced as no “viral” genome is ever the same as the original)
None of the recipient ferrets died after airborne infection with the mutant A/H5N1 “viruses”
Wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the “virus” reservoir in nature
Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 “virus” infections in humans have been reported from 15 countries
Although limited A/H5N1 “virus” transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 “virus” has not been detected
Whether this “virus” may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness
The factors that determine airborne transmission of influenza “viruses” among mammals, a trait necessary for a “virus” to become pandemic, have remained largely unknown
The “viruses” that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza “viruses”
However, given that “viruses” from only four pandemics are available for analyses, they cannot exclude the possibility that a future pandemic may be triggered by a wholly avian “virus” without the requirement of reassortment
No reassortants between A/H5N1 “viruses” and seasonal or pandemic human influenza “viruses” have been detected in nature and their goal was to understand the biological properties needed for an influenza “virus” to become airborne transmissible in mammals
They chose the ferret (Mustela putorius furo) as the animal model for the studies as ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza “viruses”
There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols
It is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols
The researchers used the QuickChange multisite-directed mutagenesis kit to introduce amino acid substitutions in the HA of wild-type “virus”
For experiment 1, they inoculated these mutant “viruses” and the A/H5N1wildtype “virus” intranasally into groups of six ferrets for each “virus”
Throat and nasal swabs were collected daily, and “virus” titers were determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify “virus” shedding from the ferret URT
When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously, A/H5N1HA Q222L,G224S PB2 E627K was not transmitted
Because the mutant “virus” harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, they designed an experiment to force the “virus” to adapt to replication in the mammalian respiratory tract and to select “virus” variants by repeated passage (10 passages in total) of the constructed A/H5N1HA Q222L,G224S PB2 E627K “virus” and A/H5N1wildtype “virus” in the ferret URT
In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K
Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs
The nasal turbinates were homogenized in 3 ml of “virus-transport” medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate the next ferret intranasally (passage 2)
This procedure was repeated until passage 6
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi
To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise to the nostrils of the ferrets to induce sneezing
Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml
The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10
They changed the source of inoculum during the course of the experiment, because passaging nasal washes may facilitate the selection of “viruses” that were secreted from the URT
Because influenza “viruses” mutate rapidly, they anticipated (i.e.guessed arbitrarily) that 10 passages would be sufficient for the “virus” to adapt to efficient replication in mammals
The genetic composition of the “viral” quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform
The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the “virus” population after 10 consecutive passages at a frequency >99.5%
Numerous additional nucleotide substitutions were detected in all “viral” gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K after passaging, except in segment 7
Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions
The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was T156A
In experiment 4, nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were used in transmission experiments to test whether airborne-transmissible “virus” was present in the “virus” quasi-species
For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally
Although mutations had accumulated in the “viral” genome after passaging of A/H5N1wildtype in ferrets, they did not detect replicating “virus” upon inoculation of MDCK cells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype “virus”
In contrast, they did detect “virus” in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627K “virus”
Three out of four naïve recipient ferrets became “infected” as confirmed by the presence of replicating “virus” in the collected nasal and throat swabs (in other words, they saw CPE in a cell culture and claimed “virus” was present)
A “virus isolate” was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi
They used conventional Sanger sequencing to determine the consensus genome sequences of viruses recovered from the six ferrets that acquired “virus” via airborne transmission and all six samples still harbored substitutions Q222L, G224S, and E627K that had been introduced by reverse genetics
In other words, they created consensus sequencing through alignment to reference genomes using computer software and algorithms from unpurified material
They observed several other mutations for which their occurrence was not consistent among the airborne “viruses,” indicating that of the heterogeneous “virus” populations generated by passaging in ferrets, “viruses” with different genotypes were transmissible
In other words, they were unable to sequence the exact same “virus” genome every time…and if that wasn’t clear
In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible “viruses” because, for example, the consensus sequence of “virus” isolated from F6 differed from the sequence of parental “virus” isolated from F2
Together, they claim that these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 “virus” between mammals
During the course of the transmission experiments with the airborne-transmissible “viruses,” ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation
It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 “virus” and the subsequent course of disease is not representative of the natural situation in humans
Importantly, although the six ferrets that became “infected” via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment
After intratracheal (in the throat) inoculation, six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible “virus” F5 in a 3-ml volume of PBSdied or were moribund at day 3
Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of “viruses” to cause pneumonia, as is done for vaccination-challenge studies
Although the airborne-transmissible “virus” is lethal to ferrets upon intratracheal inoculation at high doses, the “virus” was not lethal after airborne transmission
They openly admit that the route of injection and the amount of toxic culture goo injected causes the severity of disease, which does not require the “virus” as an explanation
They state that although experiments showed that A/H5N1 “virus” can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear
They pointed out that their experimental design for studying transmission is not quantitative (i.e. they do not know how much “virus” is required for airborne transmission and assume it occurs via PCR results)
They airborne transmission could be tested in a second mammalian model system such as guinea pigs, but this would still not provide conclusive evidence that transmission among humans would occur
The mutations they identified need to be tested for their effect on transmission in other A/H5N1 “virus” lineages, and experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals
Their findings indicate that HPAI A/H5N1 “viruses” have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in human
Of course, the only place reassortment occurs is in a lab so they never need a host…
Identification of the minimal requirements for “virus” transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness
Influenza “virus” A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI “virus” infection and passaged once in embryonated chicken eggs followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells
All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000
Mutations of interest were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit
Recombinant “viruses” were produced upon transfection of 293T cells and “virus” stocks were propagated and titrated in MDCK cells
MDCK cells (canine) were cultured in Eagle’s minimal essential medium supplemented with:
10% fetal calf serum (FCS)
100 IU/ml penicillin
100 μg/ml streptomycin
2 mM glutamine
1.5 mg/ml sodium bicarbonate
10 mM Hepes
Non-essential amino acids
293T cells (human embryonic kidney) were cultured in Dulbecco modified Eagle’s medium supplemented with:
10% FCS
100 IU/ml penicillin
100 mg/ml streptomycin
2mM glutamine
1mM sodium pyruvate
Non-essential amino acids
For “virus” titrations, MDCK cells were inoculated with tenfold serial dilutions of “virus” preparations, homogenized tissues, nose swabs, and throat swabs
Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with:
100 U/ml penicillin
100 μg/ml streptomycin
2mM glutamine
1.5mg/ml sodium bicarbonate
10mM Hepes
Non-essential amino acids
20 μg/ml trypsin
Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of “virus” replication in the cells
Infectious “virus” titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the “virus” preparations by the method of Spearman-Karber
The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica. The only way the liquid poison can potentially harm one is through injection. Cell cultured soup is not transmitted through the air nor is it infectious and/or contagious. In other words, GOF studies are not creating “viruses” in the modern sense of the word and can only be considered as such if viewed through the original Latin lens.
What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice. There will be figureheads who appear to be on the side of truth, questioning the natural existence of “SARS-COV-2,” challenging the safety of the vaccines, promoting alternative therapies, etc. who will also continue to push the idea that “viruses” exist and can be manipulated in a lab. These people are the Pied Pipers leading those who are going astray back into the fold. There is no need to create a “virus” bioweapon when all that was needed to control the masses is a PCR test and some well-designed propaganda.
To anyone who may have been taken in by this GOF/Bioweapon narrative, remember that there is no evidence of any purified and isolated “viral” particles ever coming directly from human samples that are then proven pathogenic in a natural way. Virology does not dispute this. If they can not find a “virus” in nature, they can not create one in a lab. That is truly all you need to know.
cover image based on creative commons work of 13452116/pixaby
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
Thankfully some mandates are dropping across the country, but there are still vaccine mandates that persist in schools, colleges, businesses, hospitals, and corporations. Restrictions on doctors who treat COVID, censorship by Big Tech, the unnecessary COVID-19 vaccination of children, silencing of scientific debate, and the extension of the Emergency Powers Act beyond March 1st for the coronavirus pandemic are a few of the main concerns.
In California, an aggressive slate of COVID-19-related bills—mandating vaccines for children and all employees, and allowing 12 to 17-year-olds to get the vaccine without parental consent—remain under consideration by the California state assembly.
Starting at 12:00 noon we will hold a day-long rally in the heart of Los Angeles at Grand Park where a wide range of featured guests including prominent doctors, recording artists, actors, journalists and premier thought leaders will give a series of inspiring talks and musical performances.
Ever since the beginning of the Covid saga, people have speculated about a possible link between increased illness and the rollout of 5G networks around the world.
And while “Covid-19” has hardly been the apocalyptic death storm that the media made it out to be, there have been excess deaths recorded in certain areas. The question is: are the excess deaths solely attributable to “pandemic” measures (i.e. lockdowns, masks, toxic medications, etc) or did electromagnetic radiation have a more significant role to play?
And if so, was it due to 5G or the use of some other covert, as yet unknown, technology? That is what this investigation aims to uncover.
This article will also focus mostly on excess mortality. For, if there were no excess deaths, it would be difficult to argue that there was some kind of EMF (electromagnetic fields) weapon being deployed as that would surely increase deaths above the regular threshold. In certain areas, in certain countries, there undoubtedly were excess deaths, and, as this article will demonstrate, these can be explained without the need for a new, infectious pathogen (as I have argued elsewhere).
In fact, there are several independent lines of evidence to suggest that it was not “Sars-Cov-2”, or any alleged virus for that matter, that caused these excess deaths. While the reasons advanced by other researchers as to the real cause are all valid – and probably, to some extent, all true – in this article, I argue for the EMF cause.
I am simply making the case for EMFs, in one capacity or another, having contributed to excess mortality throughout the Covid period. I will also argue that EMFs were responsible for some of the more peculiar symptoms expressed by so-called “Covid” patients.
Also, when I refer to “EMFs” (electromagnetic fields/electromagnetic radiation), I am not referring solely to 5G (although that is important), I am also willing to consider other, covert EMF influences, possibly in the form of weaponry of some kind. And as we shall see, there is evidence to suggest that this type of weaponry exists and has been used.
Make no mistake, much of what I propose here is speculation. However, it is argued speculation, with evidence to back it up.
Evidence for “Other Factors” Contributing to Excess Mortality During the Covid Saga
Here we will examine four lines of evidence that clearly suggest there were other, possibly unknown, factors causing increased ill health during the Covid period. There is more that could be discussed here but for the sake of keeping this article to a readable length, I have chosen just four.
1. The Testimony of Dr Cameron Kyle-Sidell
Early on during the Covid pandemic, a New York doctor named Cameron Kyle-Sidell posted a video on YouTube where he revealed some shocking information about the nature of “Covid-19” and the standard of care that all hospitals in the US were working under.
The video was removed from YouTube (who would have guessed?) but you can still view it here on Bitchute.
Dr Kyle-Sidell is an E.R and critical care doctor working in New York City (Brooklyn to be exact). His testimony was posted online in early April 2020. As the original video was taken down by YouTube, I couldn’t pinpoint the exact date of publishing, but it was likely posted around the 6th.
Dr Kyle-Sidell begins his statement rather harrowingly:
“Nine days ago I opened an intensive care unit to care for the sickest COVID positive patients in the city, and in these nine days I’ve seen things I’ve never seen before.”
This should already give us cause for concern. An experienced critical care doctor seeing things “he’s never seen before”? If Covid-19 were a typical viral pneumonia (AKA a cold), then he surely would have seen it before, countless times in fact. So we can already be certain that there is something different going on here.
And that, in fact, is exactly what Dr. Sidell himself asserts:
“COVID-19 lung disease, as far as I can see, is not a pneumonia and should not be treated as one.”
He then goes on to comment on what he thinks may be the real cause of the condition (emphasis added):
“Rather, it appears as some kind of viral induced disease, most resembling high altitude sickness. It is as if tens of thousands of my fellow New Yorkers are on a plane at 30,000 feet in the cabin pressure is slowly being let out. These patients are slowly being starved of oxygen.”
So Dr Sidell still claims the bizarre condition to be “viral induced”, but let’s face it, his medical training combined with the Wuhan virus propaganda would compel him to do so. What he says next is more interesting for he compares his patients’ condition to high altitude sickness and claims they are being starved of oxygen. Keep this in mind as we move forward.
Dr Sidell goes on to stress the fact that the use of ventilators is the incorrect way to treat such a condition.
“I fear that we are using a false paradigm to treat a new disease…”
He then makes the bold suggestion that ARDS (Acute Respiratory Distress Syndrome), reported as being caused by “Covid-19”, is actually being caused by the use of ventilators.
“…the ARDS that we are seeing, that the whole world is seeing, may be nothing more than lung injury caused by the ventilator.”
Dr Sidell says a lot more in his testimony, I have just pulled out some key extracts so as to keep this section concise. However, feel free to watch the full video yourself.
Here are the key takeaways from Dr Sidell’s testimony:
Patients were being admitted to Dr Sidell’s Covid ward with symptoms that he had never seen before.
The symptoms these patients were experiencing (alleged to be “Covid-19”) were not characteristic of a typical viral pneumonia, but rather something more akin to high altitude sickness, causing oxygen deprivation.
Ventilators were the incorrect treatment for such a condition and were likely doing more harm than good. This last point is highly significant, for it means that hospitals may have intentionally been directed to use ventilators precisely to increase “Covid-19” death rates. In fact, later on, evidence did come out suggesting that ventilators were ineffective and harmful. In fact, according to the above-cited study, “88% of patients who received invasive mechanical ventilation died, including 97% of those aged >65”.
It is the first and second point that interests us most here. In other words, some patients in the New York City area (and possibly elsewhere) were exhibiting symptoms foreign to anything regularly observed by experienced doctors and this condition resembled high altitude sickness.
As it turns out, this strange condition can be rationalized by examining the effects of certain electromagnetic frequencies. We will explore this later in the article.
And there is something else to note. It is highly relevant that Dr Sidell observed this strange high altitude sickness-like condition in New York City, for, as we shall see, at one point during the pandemic, NYC had by far the highest Covid-19 death rate, indicating that something strange was happening there that may not have been happening elsewhere.
This anomaly in NYC was also reported by Dr Denis Rancourt, whose research we will now examine.
2. The Research of Dr Denis Rancourt
Dr Denis Rancourt is a Canadian physicist, with highly impressive academic credentials. He has written a number of papers concerning Covid-19 excess mortality in various countries around the world and his findings are rather illuminating.
His first paper concerning this phenomenon was published on June 2nd 2020 titled “All-cause mortality during COVID-19 – No plague and a likely signature of mass homicide by government response”.
In the abstract of the paper, he states that
“The latest data of all-cause mortality by week does not show a winter-burden mortality that is statistically larger than for past winters. There was no plague. However, a sharp “COVID peak” is present in the data, for several jurisdictions in Europe and the USA.”
It’s this sharp peak that is most interesting, for, as Rancourt notes, this is an anomaly, never having occurred before in the majority of jurisdictions; the data is simply not consistent with a viral cause (the same conclusion was reached by another team of researchers whose research we will analyse later).
Rancourt hypothesizes the anomalous “COVID peak” to be a signature of mass homicide by government response. In other words, according to Rancourt, the original sharp increase in deaths in various areas in the US and EU was a direct result of pandemic measures, including the use of ventilators.
However, important to note here is that the “COVID peak” in the USA arises from certain hot spots, and New York City is the main one. In fact, New York City’s “COVID Peak” is virtually off the charts (see the below graph taken from Rancourt’s paper).
“Figure 8: All-cause mortality by week for NYC, starting in 2013, in black. The red vertical line indicates the date at which the WHO declared the COVID-19 pandemic. The grey line is simply the same data on a vertically expanded and shifted scale, for visualization.”
So here we can clearly see an anomalous increase in all-cause mortality in NYC beginning just before Dr Sidell posts his video testifying to the fact that his patients are experiencing symptoms he’s never seen that are entirely uncharacteristic of any viral pneumonia. Coincidence? I think not.Rancourt’s next paper, co-written with Marine Baudin and Jérémie Mercier, titled “Evaluation of the virulence of SARS-CoV-2 in France, from all-cause mortality 1946-2020” was published on the 20th October 2020. In the paper, the researchers analyse all-cause mortality in France, with a focus once again on the strange “COVID Peak”.In the abstract the researcher state that
“We prove that the “COVID-peak” feature that is present in the all-cause mortality data of certain mid-latitude Northern hemisphere jurisdictions, including France, cannot be a natural epidemiological event occurring in the absence of a large non-pathogenic perturbation.”
The conclusion they reach is that the “COVID peak” was artificial, i.e., caused by deliberate intervention rather than the result of some naturally occurring, novel respiratory virus. The researchers note several reasons for this conclusion, one of which is that the COVID peak
“is absent in many jurisdictions (34 of the USA States have no “COVID-peak”).”
This is highly anomalous, for if there were a novel virus going around, we’d expect to see some level of consistency with regards to the rise in all-cause mortality in different states (and indeed, different countries). Instead what we see is huge increases in all-cause mortality in certain jurisdictions (e.g. NYC) and nothing in others.
Although arrived at differently, Rancourt’s conclusion and Dr Sidell’s are the same – if something new is killing people, it’s not a novel viral pneumonia.
Rancourt & Co’s latest paper dealing with excess mortality is titled “Nature of the COVID-era public health disaster in the USA, from all-cause mortality and socio-geo-economic and climatic data.”
In this paper, the researchers seek to investigate why the USA suffered a sustained, exceedingly large mortality during the Covid period, while Canada and Western European countries did not. Once again, their research indicates that a viral pandemic did not occur (emphasis added):
“The behaviour of the USA all-cause mortality by time (week, year), by age group, by sex, and by state is contrary to pandemic behaviour caused by a new respiratory disease virus for which there is no prior natural immunity in the population. Its seasonal structure (summer maxima), age-group distribution (young residents), and large state-wise heterogeneity are unprecedented and are opposite to viral respiratory disease behaviour, pandemic or not.”
Rancourt & Co conclude that government-imposed measures combined with societal risk factors (obesity, poverty, etc) were responsible for the excess mortality. While I absolutely agree with their findings, I think they may have missed another, important contributing factor: EMFs.
But that’s not all. Rancourt & Co found something else which is highly relevant to Dr. Sidell’s statement:
“We also find a large COVID-era USA pneumonia epidemic that is not mentioned in the media or significantly in the scientific literature, which was not adequately addressed. Many COVID-19-assigned deaths may be misdiagnosed bacterial pneumonia deaths.”
In other words, cases of “pneumonia” increased, but it wasn’t treated properly and it wasn’t being caused by a novel virus. This finding is similar to what Dr Sidell observed, only he referred to cases of “high altitude sickness” (rather than pneumonia). In each case, it is the lungs being affected and it is not hard to see how some kind of novel EMF-induced lung disorder could have been mislabelled as merely “pneumonia”.
3. The Research of Torsten Engelbrecht and Dr. Claus Kohnlein
The next line of evidence we will examine is that of the research of journalist Torsten Engelbrecht and physician, Claus Kohnlein.
On the 1st of October, the two researchers co-authored an article titled “COVID-19 (excess) mortalities: viral cause impossible—drugs with key role in about 200,000 extra deaths in Europe and the US alone”, in which they reach a similar conclusion to Dr Rancourt – excess mortality was not caused by a novel virus.
Engelbrecht and Kohnlein focused their analysis mostly on EU countries, noting that most of the countries reporting excess mortality instituted stringent lockdowns (a total contradiction of the virus hypothesis). In their analysis, they highlight the same, anomalous “COVID peak” uncovered by Rancourt & Co.
“Z-score for various European countries, Dec. 2019 – Sept. 2020”
But it’s not only this anomalous “COVID peak” (which occurred outside the regular flu season), they also note the fact that neighbouring countries often exhibited a completely different pattern of excess mortality. For example, Belgium had a rather noticeably peak while Germany (its neighbour), did not.
With regards to the viral theory, this kind of wildly inconsistent pattern of excess mortality simply does not make sense.
The conclusion reached by Engelbrecht and Kohnlein is that the “COVID peaks” were caused by the increased use of highly toxic medications.
“Highly toxic and also potentially lethal drugs were used excessively, especially in all of the above-mentioned countries with excess mortality, both experimentally and off-label, meaning that the drugs were used outside of their regulatory approval—and this in people, most of whom were old and had serious illnesses, before being tested “positive” for COVID-19.”
Their article is persuasive and I agree with their conclusions. However, once again, their conclusions do not rule out a contributing EMF-related cause.
4. Wildly Inconsistent Covid-19 Death Rates
Finally, the official COVID death data, as recorded by the WHO, provides yet another line of evidence to suggest that any recorded excess mortality was not due to a novel virus.
For example, take a look at the graph below created by Andrew Mather, a British mathematician in September 2020.
Covid-19 deaths by country per 100m population (Sept. 2020).
The graph shows the number of recorded COVID deaths in different countries, normalised to account for the difference in population sizes. Once again, the data is highly anomalous. New York City has by far the highest COVID death rate, higher than any other country in the world at that time! Belgium, Peru, the UK and Spain are also high on the list, while African countries, South East Asia and Japan barely feature.
So either, we’re dealing with a far deadlier virus in New York City, Western Europe and parts of South America, or there’s another factor at play.
Let’s summarise our findings thus far:
Shortly after the WHO declared a pandemic, an experienced New York City doctor came forward explaining that his so-called “COVID” patients were not suffering from a typical viral pneumonia, but were instead showing signs of something akin to high altitude sickness.
Dr Denis Rancourt and his co-researchers analysed all-cause mortality in various countries and jurisdictions, reaching the conclusion that a pandemic did not occur. They noted an anomalous “COVID peak” which was especially prominent in New York City.
Journalist Torsten Engelbrecht and physician, Dr Claus Kohnlein analyzed European mortality data and came to the exact same conclusion – the data simply did not support the virus theory.
Six months into the Covid “pandemic”, Covid death rates were differing wildly across different countries and jurisdictions. New York City had by far the highest death rate, more than any other country in the world. The data, once again, did not fit a viral cause and instead pointed to an alternate factor at play, localised to NYC and possibly some other countries.
In the next part of this investigation, we’ll build a case for that “other factor” having been EMF-related and likely linked to the 5G rollout.
Symptoms of “Covid-19” Related to EMF Exposure
In this section, we will examine a groundbreaking study published in September of 2021. The study, published in the Journal of Clinical and Translational Research, is titled “Evidence for a connection between coronavirus disease-19 and exposure to radiofrequency radiation from wireless communications including 5G”.
The title says it all, for the paper presents a wide range of evidence pointing to a connection between what has been called “Covid-19” and EMF exposure, including 5G.
For anyone unaware of the harms caused by EMF exposure, I suggest reading my two previous articles dealing with this topic, as they provide an overview of the evidence linking EMF exposure to various chronic illnesses as well as environmental devastation.
In order to keep this section short, we’ll dive straight into the aforementioned paper. Here it is worth quoting the study at length. The researchers begin by noting that
“There is a large body of peer reviewed literature, since before World War II, on the biological effects of WCR [wireless communications radiation] that impact many aspects of our health. In examining this literature, we found intersections between the pathophysiology of SARS-CoV-2 and detrimental bioeffects of WCR exposure. Here, we present the evidence suggesting that WCR has been a possible contributing factor exacerbating COVID-19.”
In other words, these researchers found that reported symptoms of Covid-19 were also symptoms of WCR exposure. The researchers go on to summarise some of the epidemiological evidence linking the 5G rollout to the Covid-19 “outbreak”.
“COVID-19 began in Wuhan, China in December 2019, shortly after city-wide 5G had “gone live,” that is, become an operational system, on October 31, 2019. COVID-19 outbreaks soon followed in other areas where 5G had also been at least partially implemented, including South Korea, Northern Italy, New York City, Seattle, and Southern California. In May 2020, Mordachev [4] reported a statistically significant correlation between the intensity of radiofrequency radiation and the mortality from SARS-CoV-2 in 31 countries throughout the world. During the first pandemic wave in the United States, COVID-19 attributed cases and deaths were statistically higher in states and major cities with 5G infrastructure as compared with states and cities that did not yet have this technology [5].”
Here are some maps that I compiled (not from the paper quoted above) showing, visually, the Covid-5G association.
Note that New York City features on the list of areas where, according to the researchers, “5G had been at least partially implemented”. We can now note the following about NYC:
The “COVID peak” was “off the charts” compared to other areas in the US and the COVID death rate was abnormally high.
So-called “COVID-19” patients there suffered from some unknown condition akin to high altitude sickness.
A 5G network had been at least partially implemented shortly before the COVID “outbreak” occurred.
The researchers go on to present the following table, showing a clear relationship between the effects of WCR (Wireless Communications Radiation) exposure and various symptoms associated with “COVID-19”.
Table reproduced from Rubik & Brown, 2021.
They then conclude by summing up the known effects of WCR exposure and how they relate to COVID-19 (emphasis added):
“Specifically, evidence presented here supports a premise that WCR and, in particular, 5G, which involves densification of 4G, may have exacerbated the COVID-19 pandemic by weakening host immunity and increasing SARS-CoV-2 virulence by (1) causing morphologic changes in erythrocytes including echinocyte and rouleaux formation that may be contributing to hypercoagulation; (2) impairing microcirculation and reducing erythrocyte and hemoglobin levels exacerbating hypoxia; (3) amplifying immune dysfunction, including immunosuppression, autoimmunity, and hyperinflammation; (4) increasing cellular oxidative stress and the production of free radicals exacerbating vascular injury and organ damage; (5) increasing intracellular Ca2+ essential for viral entry, replication, and release, in addition to promoting pro-inflammatory pathways; and (6) worsening heart arrhythmias and cardiac disorders.”
What interests us most here is point number 2 (italicised/bolded). The researchers claim that WCR can impair microcirculation and reduce erythrocyte and haemoglobin levels, exacerbating hypoxia. Another name for “hypoxia” is “altitude sickness” (i.e. a severe lack of oxygen). In other words, here we have a potential explanation for the “high altitude sickness” like condition described by Dr Sidell in NYC.
Note also that some of the COVID-19 related manifestations listed in the table such as organ failure, myocarditis, cardiac failure, arrhythmia, etc (effects not generally associated with the flu or any viral pneumonia), may be explainable when one considers the effects of EMF exposure.
In his book “The Contagion Myth”, Dr Thomas Cowan provides more evidence for the deleterious effects of radiofrequency radiation, especially 5G. After noting that “hypoxia” is reported as a frequent symptom of COVID-19 and that this is caused by the release of iron from the haemoglobin molecule, he goes to comment as follows (emphasis added):
“The conventional explanation for the release of iron from hemoglobin is the action of glycoproteins in the coronavirus—but the action of 5G’s millimeter waves is an equally good explanation, especially those at 60GHz, which disrupt oxygen molecules. An interesting observation about lung malfunction in Covid-19 patients is that it is bilateral (both lungs at the same time), whereas ordinary pneumonia typically affects only one lung. What kind of virus knows to attack both lungs?”
Dr Cowan then goes on to comment on the nature of “COVID-19” as experienced by patients in Wuhan (a city that also rolled out its 5G network mere days before the “outbreak”):
“A study from Wuhan showed that more than one-third of coronavirus patients had neurologic symptoms including dizziness, headaches, impaired consciousness, skeletal-muscle injury, and loss of smell and taste—and more rarely seizures and stroke. This is not your normal flu, this is a serious disease.”
When Cowan says, “This is not your normal flu, this is a serious disease.” He is right in one sense and wrong in another. You see, as has been my thesis throughout, “COVID-19” is not and never has been, a single disease, rather, it has been used as an “umbrella term” to include everything from mild flu symptoms to life-threatening, EMF-induced hypoxia.
In light of this evidence, we must ask ourselves – What role did EMFs/5G play in the COVID charade? Was it 5G alone that caused the anomalous “COVID peak” we see in certain areas? If so, why was the death rate in NYC so much higher than anywhere else? Was “Sars-Cov-2″ used as a cover for the rollout of dangerous radiofrequencies?
Or… Was there some sort of covert, EMF-related weaponry being used in select areas?
Speculating on the Existence and Possible Use of Advanced Electromagnetic Weapons
The reader should be advised that this section of the article is mostly speculation. However, the case for the intentional deployment of some kind of EMF-related weaponry, is, I believe, a solid one. After all, if you were part of a group looking to feign the signs of a viral respiratory pandemic, blasting people with hypoxia-inducing radiofrequencies is one way you could do it. And as we discovered, that appears to be what happened in NYC (and possibly other areas).
However, the only evidence for this theory is the rollout of a 5G network in key pandemic “hotspots” around the world (including NYC). The problem, of course, is that there were plenty of countries that had 5G networks and yet did not showcase the same dramatic “COVID peak” as NYC did.
While there are many factors that would have contributed to this COVID peak besides EMFs, including lockdown stringency, care home laws, population age and health status, etc, three other possibilities exist:
5G networks in certain areas were covertly used (or possibly hijacked) to “blast” the local population with dangerous radiofrequencies (such as 60Ghz millimetre-wave 5G which can disrupt oxygen molecules).
The increased density of radiofrequencies, brought about by the 5G rollout interacted with something that was already present within people’s bodies, “activating” a disease state.
An altogether separate EMF technology was in use.
As it turns out, there is evidence to support all three possibilities.
Evidence for the Existence of EMF-Related Weapons
The Spanish research group “La Quinta Columna” (the fifth column) have also argued that there is an EMF-related component to the Covid-19 “pandemic”.
La Quinta Columna was founded by Ricardo Delgado Martín, a biostatistician from Seville university. Quinta Columna says its main objective is to
“Show THE REALITY, no matter how uncomfortable the TRUTH may be due to the nature of the events or news in which it participates, without being subject to prejudice and conflicts of economic, moral, ethical, political, religious, ideological or otherwise.”
Most of the information regarding Quinta Columna online is in Spanish and as such, I lack the necessary information to make an informed judgement regarding their thesis. However, as they are one of the few research groups brave enough to investigate the link between Covid-19, vaccines and 5G/EMFs, it’s important to consider what they have to say.
Delgado’s thesis is that increased illness due to “COVID-19” is actually a result of the excitation, by radio-frequency signals, of graphene oxide already present within the body. Delgado briefly outlines his hypothesis in a July 2021 interview:
“…we are convinced that precisely the graphene oxide was the cause of the COVID-19 disease that was introduced, silently and stealthily in the 2019 anti-flu campaign globally. And they caused, with the subsequent electromagnetic bidding that everyone knows —with the famous 5G switch-on, the tests— the fashionable disease.”
In other words, Delgado believes that graphene oxide was introduced into people’s bodies via the 2019 flu vaccine and then excited by 5G radiofrequencies, causing hypoxia (i.e. “Covid-19”) which was then propagandized as a viral pandemic.
Noteworthy is that flu vaccine uptake was highest among the elderly population.
Delgado goes on to remind us that many surgical masks were also found to contain graphene and hypothesizes that Covid “waves” (i.e. the observed “COVID peaks”) are actually the result of 5G antenna activations:
“And by pressing a little button that activates the 5G, that is why they know when a wave is coming, the 2nd, the 3rd… The Delta variant, the Lambda… The Delta variant is the next 5G antennas activation, and that’s why we have to be careful.”
Delgado claims that NAC (n-acetylcysteine) and Glutathione were successful treatments for Covid patients suffering from hypoxia. The reason for this, he claims, is because, along with inhibiting or reducing the cytokine storm, “glutathione reduces and oxidizes, that is, eliminates the graphene oxide.”
Their research has claimed to find graphene oxide present in Covid-19 vaccines, which they say interacts with radio frequencies causing a number of severe health effects, including cardiac events.
Their research is controversial and their claims are not supported by all on the alternative side. However, in light of everything presented in this article thus far, it is worth considering.
And there is one more interesting piece of evidence that they have brought forward, possibly indicating the existence of a powerful EMF-related weapons capability. This will be more persuasive when we examine other anomalous happenings later on.
In this video, Ricardo Delgado and Jose Luis discuss a recording (seemingly captured by a CCTV camera, though it’s hard to tell) showing what appears to be the sudden death of a cyclist. The most interesting aspect of the video is the split-second glitch in the recording at the precise moment the cyclist collapses to the ground.
According to Delgado and Luis, this constitutes evidence of an electromagnetic “pulse” of some kind. I have embedded the video below.
A disclaimer is in order: I have not been able to verify the original footage. I don’t know where it comes from, I don’t know if the cyclist actually died and I don’t know whether it’s a legitimate recording. However, I include it here because, if real, this odd phenomenon seems to fall in line with another perplexing phenomenon that has increased in recent years: mass, sudden bird deaths.
Mass Sudden Die-Offs of Birds: Evidence of EMF Weaponry?
While not common knowledge, there have been a number of recorded mass sudden bird deaths in recent years. Not much digging was needed on my part to uncover these cases, for many of them have been catalogued by Dr Joseph Farrell on his blog at gizadeathstar.com.
Here is a brief overview of some of these strange cases, along with Dr Farrell’s enlightening commentary:
“On June 27, 2015, a road in Kuna, Idaho, was found covered with dead songbirds. This follows the mass deaths earlier this year of over 2,000 migrating snow geese that dropped to the ground dead or dying in eastern Idaho.”
“Now you’ll note that in this version of the story, in the comments section, there’s a brief exchange between two commenters, one of whom notes strange intereference with his bluetooth signal as he was driving through Idaho.”
(I haven’t been able to find the comment he refers to but then again, the article is almost 7 years old so it may have been removed).
Dr Farrell then speculates as follows
“Could these events be caused by some sort of secret human technology, or could they be the unintended consequence of its use or other secret activity? Maybe. Again, I don’t know.”
“About a week ago at The Hague, many birds died spontaneously, falling dead in a park. You likely haven’t heard a lot about this because it seems keeping it quiet was the plan all along. However, when about 150 more suddenly died – bringing the death toll to 297 – some started to take notice.”
“…And if you are looking around that park you might have seen what is on the corner of the roof across the street from where they died: a new 5G mast, where they had done a test, in connection with the Dutch railway station, to see how large the range was and whether no harmful equipment would occur on and around the station.”
The interesting thing about this story is that Snopes was quick to publish a “fact check” claiming that no such 5G test took place (although they did admit that one such test had taken place in that area in June of that year).
More interesting is Dr Farrell’s commentary on the incident. After outlining his thoughts regarding the use of microwave interferometry technologies, he goes on to offer his usual “high octane speculation”:
“It is a short step from that basic concept to a similar use of microwave technologies – perhaps again involving interferometry – to produce beat frequencies which could interfere with, or actually shut down, the electrical functioning of organisms’ nervous systems, including organs such as the heart. And that’s what is so alarming here: birds might be resonant to certain such frequencies, other organisms to other frequencies. All one needs to do, so to speak, is to “dial in” the right frequency, and one could eradicate a regional population of dogs, cats… or even humans.”
“Wildlife experts in New Mexico say birds in the region are dropping dead in alarming numbers, potentially in the “hundreds of thousands.””
NBC goes on to note that
“Multiple agencies are investigating the occurrences, including the Bureau of Land Management and the White Sands Missile Range, a military testing area.”
And here is Dr Farrell’s commentary (emphasis added):
“You don’t say… the military at the White Sands Missile Range is investigating? Well, it makes sense… if one suspected an unknown fast-acting pathogen, biowarfare, or some completely different cause, or maybe even some version of my bio-electromagnetically activated pathogen.”
And now for two more interesting cases that also occurred during the Covid scamdemic…
“As if we didn’t have enough weird things going on, now birds are suddenly dropping dead in large numbers all across the eastern half of the country. Before they die, a lot of these birds are exhibiting very strange symptoms… If scientists understood what was causing this to happen, that would be one thing. But at this point they have no idea why this is taking place, and that is quite alarming.”
Dr Farrell offers no speculation about what might be causing this round of mass bird deaths but finds the timing of the event, and the symptoms experienced by the birds, to be overly suspicious.
“What I do know is that birds going blind, or not being able to fly away from approaching humans, or shivering and shaking as if they’re having a seizure, is not normal… And what I strongly suspect is that someone knows why, and isn’t talking…”
“Hundreds of birds dropped dead from the sky in Wales on Thursday, after witnesses reported hearing a “’huge electrical-type bang’.”
“Ian Mccaffrey, who works in Waterston, reported hearing a large electrical-type bang as he left work on Thursday night. He says following the shocking noise, dozens of birds fell from the sky and landed on his car. Mccaffrey said the loud sound was similar to lightning.”
Here it is the reports of a “large electrical-type bang” that is most interesting as it seems to corroborate the idea of the existence of a powerful EMF weapons technology. Dr Farrell recognizes this too, offering the following commentary:
“When that flock of crows (I believe) first died in Tennessee many years ago, I’ve thought that this electro-magnetic “pressure field” was perhaps the best explanation. And now we have an odd video, and reports of “electrical bangs”, to go with it. And yes, that means in my opinion the case for that speculation just became a small bit stronger.”
It is to be noted that the cases of strange sudden bird deaths reviewed here constitute only a portion of the total reported incidents. It is also highly relevant that EMF signals can penetrate into a bird’s nervous system, disrupting its ability to navigate. I covered this in a previous article on environmental crises.
Let’s sum up:
Recent years have seen increasing reports of mass, sudden bird deaths.
In many of these cases, there is some sort of link to electromagnetic technology. In the Idaho case, one person complained of bluetooth interference around the time of the incident; in the Netherlands case, 5G tests were being carried out in the vicinity of the mass die-offs, and in the latest Wales case, a “huge electrical-type bang” was heard prior to the die-offs. In one case, even the military began investigating.
Dr Joseph Farrell, a scholar who has been tracking strange animal deaths has speculated that the cause may be due to some kind of “electromagnetic pressure field”.
And finally, a recent video posted online captured the apparent sudden death of a cyclist at the exact time there was a split-second glitch in the video recording. Some have argued that this points to an electromagnetic “pulse” of some sort, perhaps hinting at a similar technology as proposed above.
And with that, we are ready to conclude our investigation.
Conclusions
Although the Covid-19 death rate is more or less akin to seasonal flu, not warranting the need for special vaccines or preventatives, lurking beneath the fraudulent testing and dubious death reporting were the reports of strange symptoms resembling high altitude sickness.
The all-cause mortality data for certain areas, NYC in particular, also exhibited a highly anomalous “COVID peak”, certainly not explainable in terms of a novel respiratory pathogen.
A recent peer-reviewed study provided compelling evidence that many of the symptoms associated with “COVID-19” are also effects of EMF exposure. This, together with the compelling epidemiological data, suggests a link between the rollout of 5G and areas that exhibited a pronounced “COVID peak”.
Finally, in recent years there has been a flurry of mass sudden bird deaths in various places around the world. Many of these incidents exhibited some sort of connection to electromagnetic interference or radiofrequencies of some sort.
Spanish researchers from Quinta Columna have also analysed a video purported to show the sudden death of a cyclist that they believe occurred due to an EMF pulse of some kind.
They further maintain that “COVID peaks” occurred as a result of the excitation of graphene oxide by EMF bombardment which they believe can cause hypoxia (explaining the strange reports of “high altitude sickness” in NYC) and cardiac events (which have increased since the COVID vaccine roll out).
The volume of research linking EMF exposure with ill health is far too great to ignore, meaning that, regardless of the data put forth here, EMFs undoubtedly contributed to ill health during the COVID-19 “pandemic” and continue to do so. However, the evidence presented here may also point to the deliberate use of a covert, EMF-related weapons technology.
If that is the case, then, considering the massive effort to flood low earth orbit with EMF-beaming satellites and the ever-expanding 5G rollout, a lot more research is needed… and fast.
“‘Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“To obtain embryo cells [for research on vaccines and other pharma products], embryos from spontaneous abortions cannot be used, nor can those obtained by means of abortions performed via the vagina: in both cases, the embryo will be contaminated by micro-organisms.”
“The correct way consists in having recourse to Caesarian section or to the removal of the uterus. Only in this way can bacteriological sterility be guaranteed.”
“In either case, then, to obtain embryo cells for culture a programmed abortion must be adopted, choosing the age of the embryo and dissecting it while still alive, in order to remove tissues to be placed in culture media.”
“Given these premises, we face the dilemma of whether the deliberate systematic destruction of a human creature to obtain cell material can be justified, when it is recognized that this is of great interest to fundamental research and for the diagnosis of some human diseases. Are research and diagnosis of such great value that they justify the destruction of human beings?”
“The Geneva Declaration affirms that the doctor has the duty to take the greatest care to safeguard the life of a human being from its conception and will not, even under threat, use his knowledge to infringe humanitarian laws.” (1986-04-26; Herranz, Gonzalo; Il Sabato, no.15…Professor Herranz was, at the time, president of the Committee of Medical Ethics of Spanish Doctors and vice-president of the Permanent Committee of Medical Ethics of the European Community.)”
What exactly happened in 1972 or 1973, in the Netherlands, where an infant girl was aborted, and her kidneys used to make a cell line that would be used, going forward, in the testing of vaccines?
That cell line is called HEK 293, and it has been used to test COVID vaccines.
I have already presented evidence for concluding the abortion involved removing the living infant from her mother’s womb, and taking her kidneys, which of course killed her.
This evidence rests on the realization that, in order to extract viable and useful kidney tissue, the baby had to have a functioning blood supply, which meant she was alive.
But the evidence ALSO comes from knowing many other abortions have been carried out, in order to harvest tissue for medical research, by murdering living babies.
I have found a very informative article (2/9/2021) at the Centre for Bio-Ethical Reform UK, by Christian Hacking, titled, “What the HEK?!” by Christian Hacking. Quoting from the article:
“HEK 293 is a human cell line created using a kidney from a dissected unborn baby in the Netherlands between 1972 and 1973. It is the second most common cell line and is used extensively in ‘pharmaceutical and biomedical research’. It is also used in vaccine creation and cancer research.”
“It was used, along with other human cell lines, to develop a genetically engineered spike protein (that the mRNA vaccine codes for) in the original development stage of the vaccine. The ‘new technology’ Pfizer vaccine and the Moderna Vaccine were tested on HEK 293 before they began human trials. This testing is ongoing for all new batches. Finally the ‘old technology’ Oxford AstraZeneca vaccine grew a weakened viral strain in HEK 293 cell culture…”
“The kidney in question was dissected from a healthy Dutch baby girl of unknown origin by the team at Leiden University in the Netherlands in 1972. Despite the inclusion of the term ‘embryonic’ in the title, the baby in question was probably 12-13 weeks old when she was killed so as to secure functioning kidney cells. The man in charge of the research was named Alex Jan Van der Eb; he is still alive and still based in Holland.”
“When questioned on the matter by the FDA in 2001, Dr Van der Eb confirmed it was an intentional abortion of a ‘fetus’ but gave hazy details of the exact experiments.”
“’So the kidney material, the fetal kidney material was as follows: the kidney of the fetus was, with an unknown family history, obtained in 1972 probably. The precise date is not known anymore. The fetus, as far as I can remember, was completely normal. Nothing was wrong. The reasons for the abortion were unknown to me. I probably knew it at that time, but it got lost, all this information’.”
Author Hacking continues: “…extracting and growing living cells is incredibly difficult. In order to give oneself the best chance of success you need to ensure the child is healthy, fresh, intact and sterile. As one embryologist and Emeritus Professor of Anatomy confirms:”
“’In order to sustain 95% of the cells, the live tissue would need to be preserved within 5 minutes of the abortion. Within an hour the cells would continue to deteriorate, rendering the specimens useless’.”
[That statement was made by “Dr C Ward Kischer, embryologist and Emeritus Professor of Anatomy; specialist in Human Embryology, University of Arizona College of Medicine…”]
[My comment: This suggests the abortion, in the Netherlands, in 1972, was planned and technicians were standing by. I would say that, to ensure the viability of the tissue, the infant had a functioning blood supply and was alive when her kidneys were removed, killing her.]
Hacking:
“In order for the organs to be at ‘optimal viability’, the child needs to be dissected and organs extracted within 5 minutes of delivery. Anaesthetic also cannot be used so as to not change the cellular activity of the organs the researcher wants to obtain.”
“Acclaimed Doctor, Ian Donald, the pioneer of the ultrasound scanner, also claims to have witnessed the WI-38 [another cell-line] dissections [1962], conducted at the Karolinska Institute; he described them such:
“’Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“In his dense book ‘The Foetus As Transplant Donor the Scientific, Social, and Ethical Perspectives’, immunologist Dr Peter McCullagh relays detailed descriptions of the methods used on dozens of ‘fetal tissue donors’ from the 1970’s onward, including the deaths of babies between 7 and 26 weeks gestation by decapitations, exposure, dissection and drug testing. Gynaecologist and ex-abortionist Dr Bernard Nathanson, relaying his own understanding of abortion, and citing McCullagh’s book claims the Swedish experiments took place thus:
“’…in Sweden they have been puncturing the sac of a pregnant woman at let us say 14 to 16 weeks, and then they put a clamp on the head of the baby, pull the head down into the neck of the womb, drill a hole into the baby’s head, and then put a suction machine into the brain and suck out the brain cells….. Healthy human fetuses from 7 to 21 weeks from legal abortions were used. This is in Sweden. The conception age was estimated from crown rump length and so on. Fetal liver and kidney were rapidly removed and weighed. Now at 21 weeks, what they were doing, or 18 weeks, or 16 weeks, was what is called prostaglandin abortions. They would inject a substance into the womb. The woman would then go into mini-labor and pass this baby. 50% of the time, the baby would be born alive, but that didn’t stop them. They would just simply open up the abdomen of the baby with no anesthesia, and take out the liver and kidneys, etc.’”
“A research paper from the University of Toronto from June 1952 commenting on the method of their experiments suggests that these techniques were universal with researchers working in close proximity to the abortions.”
“’No macerated [softened after death] specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
“According to Gonzalo Herranz, former head of the Committee of Medical Ethics of Spanish doctors, the best way to prevent ‘contamination by microorganisms’ is to deliver the child by caesarean section or the removal of the uterus.”
“A 1982 review of a history of tissue donation affirms this, and much of the above evidence:”
“’Fetal tissue for transplantation must be “harvested” within a few minutes of delivery. Ideally this is by hysterectomy, with the fetus delivered in utero. Drugs which reduce fetal physiological activity need to be avoided. The fetus is therefore in as alive and aware a state as possible when being opened’.”
From Hacking’s article, it’s quite clear how the standard procedure of infant-murder is carried out.
It’s entirely reasonable to assume fetal cell line HEK 293—used for COVID vaccine testing—was originally produced, in 1972, by the murder of an infant. Refusal to take a COVID vaccine on the basis of conscience and religion is more than justified.
Given the weight of the circumstantial case, I would say that for all people of faith, refusal is essential.
Lunatic medical murderers and their allies will say anything to avoid blame and the application of true justice to themselves. They will invent “science” at the drop of a hat and couch it in humanitarian terms. They will claim the ends justify the means. They will commit gross forgery to pretend those ends are vital.
But we don’t have to stand by and passively believe them.
Billions of people of faith can stand against them.
If you are looking for one of the most masterful takedowns of virology to date, this presentation by Alec Zeck, Dr. Jordan Grant, Mike Donio,Jacob Diaz, and John Blaid is one of the best out there. When I first watched it a month ago, I was blown away and I had intended to share it here but, as often happens, I got sidetracked and sadly forgot to upload it. I hope you can take away a great deal of value from this presentation as the guys delve into the numerous fallacies and assumptions related to this fraudulent field.
In this presentation, you will find:
A break down of the ridiculous cell culture experiments
The lack of adhering to the scientific method
The foundational issues with virology from the very beginning
The inherent problems with and the limitations of electron microscopy imaging
The lack of any purified and isolated physical “viral” particles found directly in human samples
The issues related to the creation of the theoretical genome
The fabrication and lack of validation of the PCR test for “SARS-COV-2”
A thorough explanation of the Stefan Lanka control experiments
The myths of contagion and other possible explanations for dis-ease
The FOI requests and the burden of proof
As I said, a masterful takedown of the pseudoscience called virology!
Virology’s Unproven Assumptions
In this episode, Alec Zeck has a discussion with Mike Donio, Jacob Diaz, Dr. Jordan Grant MD, and John Blaid on the fallacious reasoning, unproven assumptions, and lack of proof for virus theory.
The implementation of a digital passport system is a crucial element in this plan, which would go on to enable the creation of a Central Bank Digital Currency (CBDC) that eventually will be able strip you of your assets and turn them into a credit courtesy of governments led by authoritarian technocrats. You can not use money any longer unless someone “higher up” agrees to it. Together with plans to turn dissentic voices into “domestic terrorists” that would be the end of all of the freedoms our forefathers paid with their lives to defend.
One of these systems that could be turned into a didgital concentration camp is the Digital Green Certificate introduced by the European Union in June 2021 under the pretext of “enabling freedom of travel”. It turned out to be quite the opposite.
Consequently, brave parliamentarians such as Mr Roos have started an initiative to block the EU commission’s attempt to extend the “Covid Pass”/Green Certificate until at least 2023.
While CHD is not endorsing political platforms but focuses on advocacy for Children’s Health and Fundamental Human Rights, we kindly ask you to please take 90 seconds and listen to this video which Mr Roos has put out, and also follow the link to object to these plans of the EU Commission’s website:
“The European Commission, wants to extend the covid pass until June 2023. In one and a half minutes, I will explain to you why you should care, and what you can do to stop this.
The covid pass was introduced by the European Union in June 2021. They claimed it would make travel within the European Union easier. But that never worked. Countries still kept introducing their own restrictions. Within just a few months, member states transformed the covid pass into something much bigger. All of a sudden, you needed a QR code to enter a restaurant or even to go to work. But it was never introduced for that.
Now, Omicron is the dominant strain of the virus. To most people, it’s not dangerous anymore. The vaccine doesn’t stop the spread. Science shows that the QR system does not come with any health benefit anymore, while undermining fundamental rights.
This is the moment to abolish the covid pass once and for all.
But the European Commission wants to extend it until at least June 2023, an extremely bad idea.
Together with several colleagues in the Parliament, I will do everything I can to stop this. But we have to do it together.
We need your help, please follow this link to the European Commission website and tell them that you oppose this extension. Please do it as soon as possible, because conditional freedom is NO freedom!”
All scientific research is built on particular dogmas including, or perhaps especially, biomedicine. It’s easier for some “scientists” to perpetuate falsehoods than it is to admit they were wrong, abandon long standing ideas, and start again from scratch. Many scientists would rather pursue trendy research areas in order to win accolades and secure grant money than question long-held beliefs and dogmas.
This is exactly what has happened with modern medicine because too much money and too many reputations are at stake. If you’re not allowed to question it, then it’s not real science.
Erroneous theories in medicine have wasted billions and caused untold harm. Imagine if they had to admit that so many years of research and countless academic careers have been wasted pursuing ideas that have no basis in reality.
Thanks to the covid pseudo pandemic, the corrupt state of the medical establishment has never been more obvious to so many people.
See No Evil, Hear No Evil, Speak No Evil
It might be difficult for some to believe that the castle of medicine is built on foundations of sand. However, Stanford scientist John P. A. Ioannidis published a study in 2005 proving that most published research findings are false.
Marcia Angell the first woman to serve as editor-in-chief of the New England Journal of Medicine has extensively investigated the corruption of medicine by drug companies.
Richard Horton, editor of The Lancet, wrote that:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
There are countless victims of iatrogenic disease in countless on-line support groups who once trusted their doctors to have their best interests at heart and to abide by the oath to “first do no harm”.
128,000 Americans die each year from correctly prescribed medications, making prescription drugs one of the leading causes of death.
Clearly, there is something rotten in the state of Denmark.
Dr. Harold Hillman Goes Renegade
In his final paper, the notorious British biologist Harold Hillman claimed that “cell biology is in dire straits”. That paper was published in 2011 and summarises his life’s work which began in the 1970s. He warned biologists and cell physiologists that something is seriously wrong with their ideas about the human body.
In the 1970s this cytologist and neurobiologist began questioning mainstream cell biology and presented evidence that the accepted model of the cell was completely wrong. He suggested that the dire straits of cell biology was the reason medical research has failed to determine the cause and provide the cure for most diseases.
“During a research career lasting more than 50 years, I have concluded that the following procedures are unsuitable for studying the biology of living cells in intact animals and plants: subcellular fractionation; histology; histochemistry; electron microscopy; binding studies; use of ligands; immunocytochemistry; tissue slices; disruptive techniques; dehydration; deep freezing; freeze-drying; boiling; use of extracellular markers; receptor studies; patch clamp measurements; inadequate calibrations. The main objections to these procedures are: (i) they change the properties of the tissues being studied grossly and significantly; (ii) they ignore the second law of thermodynamics;(iii) they produce artefacts, many of which are two-dimensional; (iv) adequate control procedures have never been published for them.”
~ Dr. Harold Hillman
He challenged the fundamental principles of biology. He was a renegade who put the quest for truth above everything else.
Unsurprisingly his views were unpopular with many in the mainstream and this took a toll on his career and reputation. He had difficulty publishing his work. Mainstream scientific journals rejected his papers without reason and refused to review his books.
“The reason I’m so determined is because they [the mainstream] won’t engage. And if they won’t engage, then to my mind it proves that I’m likely to be right.”
~ Dr Harold Hillman
Many scientists agreed with Hillmans’ compelling ideas in private but wouldn’t support him publicly for fear of losing their funding or tarnishing their reputation. Many leading biologists would refuse to meet with him to discuss his research. His goal was to start a discussion and promote a productive debate to improve and further scientific knowledge. Instead of being given a platform to share his work, he was stifled and ridiculed. Sound familiar?
Real scientists value truth above reputation and financial gain. Real scientists are willing to risk everything to expose falsities and incorrect theories. Scientists who blatantly ignore unpopular views or refuse to debate are not true scientists.
“I should like to draw attention to the fact that I regard my views as unpopular, rather than heretical, as I do not believe that scientists should talk in terms of dogma and heresy. In the best of possible worlds, good scientists who hear challenges to their beliefs, assumptions, hypotheses, procedures or conclusions, should examine such criticism with due attention. They should respond by entering into civilised dialogue with their critics. They should be prepared to admit mistakes, if necessary, and change their views. Such reactions have not occurred.”
~ Dr Harold Hillman
Hillman claimed that the routine procedures used to study the characteristics and composition of cells are completely unfit for purpose. He was adamant that these procedures would change the properties of cells more than any differences being examined so any conclusions made on the basis of these procedures were invalid.
He claimed that electron microscopy is a “waste of time and money” which goes against the vast majority of the biomedical establishment who regard the invention of the electron microscope as a pivotal point in biomedical research. Only dead tissue can be examined under an electron microscope and not living cells. Are findings based on electron microscopy relevant to living organisms?
Hillman’s work includes compelling evidence to suggest that many of the subcellular organelles that some scientists have dedicated their lives to studying are just artifacts of preparation for histology and electron microscopy. This includes both the Golgi body and the Endoplasmic Reticulum.
He also claimed that cellular receptors and transmembrane protein channels do not exist in the mainstream accepted sense. One of the reasons for this is that these cell receptors cannot be seen under an electron microscope, despite their size being within the range of visibility.
He courageously stood up for what he believed to be the truth. Despite his career and reputation taking an enormous hit, he continued to publish his ideas right up until his death.
“If I am wrong, only my reputation has been damaged. If I am right, those colleagues proved wrong may well have been wasting their time and careers and using public or charitable resources naively. They might have used their time and resources to carry out more productive research.”
~ Dr Harold Hillman
When considering the current state of medicine, it seems that “more productive research” is exactly what is needed. Research that doesn’t follow dogma and isn’t funded by the very pharma industry that has a vested interest in perpetuating erroneous ideas such as the “one germ, one disease” fallacy.
“It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing.”
~ Dr Harold Hillman
We’re led to believe that modern medicine is highly advanced but the cause of most diseases apparently remains “unknown”. Most Doctors have a mechanistic, reductionist view of disease often believing disease arises due to “genetics” or that the body is just prone to making mistakes.
“It is widely believed that medical research since the Second World War has been very successful…It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing… it is true that the cost of failure so far has been high. The most paradoxical aspect of scientific research is that it is widely believed to be objective…”
~ Dr Harold Hillman
Hillman also criticised the lack of sufficient control experiments performed in biomedical research. Proper control experiments are the cornerstone of good science ensuring that variables, other than the one being tested, do not influence the results of the experiment.
“Control experiments for the effects of reagents and manoeuvres used on the results of experiments have been grossly inadequate.”
~ Dr Harold Hillman
Hillman also questioned the use of tissue cultures for histological analysis with compelling logic. Cells in culture have significantly different morphology, biochemistry, and environment than the cells from which they came.
“Tissue cultures are similar to the tissue from which they come in some ways and very different in other ways. It is clear that although there are a few properties in common, there are substantial differences. This is one of the most important questions, in respect of the usefulness of tissue cultures as sources of information about cells in intact animals.”
~ Dr Harold Hillman
Virology: Voodoo Scientism
Hillman’s work challenges virology as much as it does cell biology and neurobiology. The world is slowly waking up to the pseudoscientific nature of virology because of the pseudo pandemic inflicted on all of us.
“Viruses” can only be seen under an electron microscope using procedures involving heavy metals, dehydration, low pressure, electron bombardment and X-ray irradiation. Are viruses real naturally occurring structures or are they artifacts of these harsh conditions?
The effects of “viruses” are studied on cell cultures and most cell cultures are grown from embryonic tissue, cancerous tissue, stem cells, or monkey cells whose properties are completely different from that of adult human tissue. Is any of this relevant to understanding virus infectivity in humans?
Coronaviruses are supposedly assembled at the endoplasmic reticulum-Golgi interface but if Hillman is right and the endoplasmic reticulum and Golgi body are artefacts of histological preparation and electron microscopy is presumed understanding of virus assembly completely wrong?
Different cell cultures are prepared by different procedures in different chemical solutions to culture “viruses”. Could this explain why only some cells can grow “viruses” but others can’t? SARS-CoV2 cannot infect many human cell lines but can infected monkey kidney cells which is not what you would expect from a supposed human pathogen.
Viruses are supposed to bind to host cell receptors as the first step to entry but if Hillman is correct macromolecular cell receptors don’t really exist.
Adequate controls have not been performed to test the effects of lab conditions, body fluids, antibiotics, and other chemicals on cell cultures so how can virologists be sure that it is the “virus” causing any observed cytopathic effects and not the chemicals and conditions themselves?
The biomedical establishment has chosen to ignore all of these crucial questions. Sadly, Hillman’s level of critical thinking and radical questioning are rare and often completely absent in modern biomedical science.
His sharp intellect and critical thinking skills were a threat to the scientific establishment. He put his career and reputation on the line to expose the weaknesses of established biomedical knowledge.
But what if he was right? What if the castle of modern medicine really is built on foundations of sand? Will his work be forgotten, or will others be brave enough to pick up where he left off?
References
1) John P. A. Ioannidis “Why Most Published Research Findings Are False.” PLoS Med. 2005 Aug; 2(8): e124.
2) Marcia Angell M.D “The Truth About the Drug Companies-How they deceive us and what to do about it.”
3) Richard Horton “Offline: What is medicine’s 5 sigma?” Lancet Comment| Volume 385, ISSUE 9976, P1380, April 11, 2015
4) Harold Hillman “Cell Biology is Currently in Dire Straits.”
5) Harold Hillman “A Career in Neurobiology.”
6) A Biomedical Scientist “Virology’s Voodoo Scientism is Not Real Science.” The Expose.
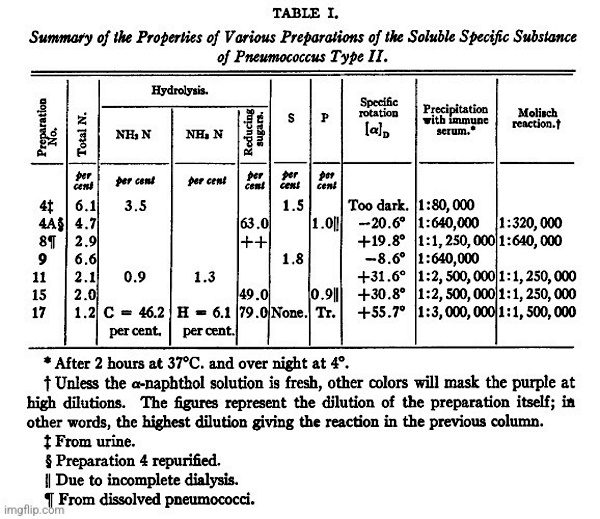
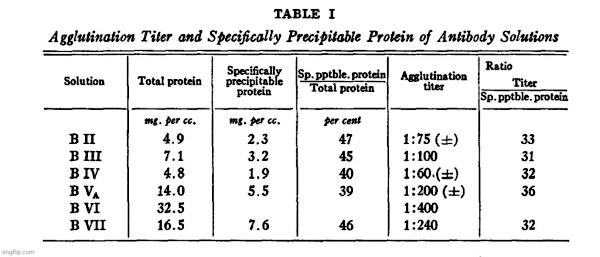
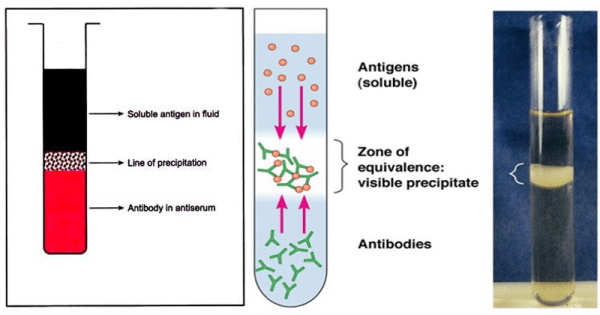
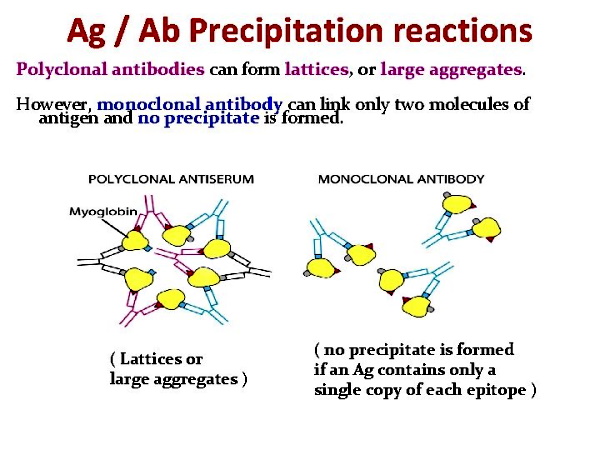
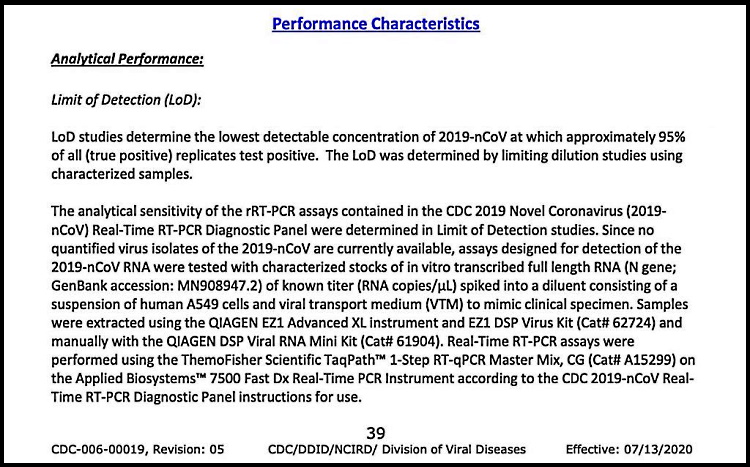
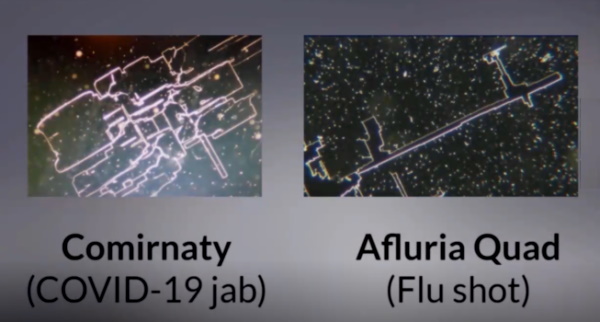
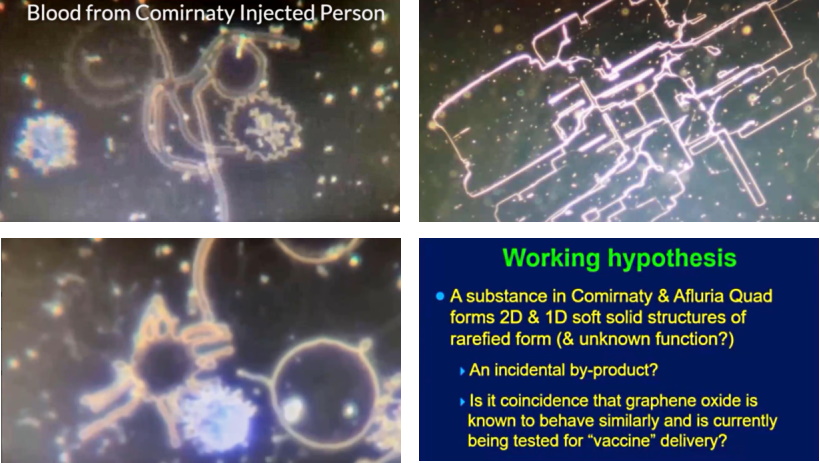
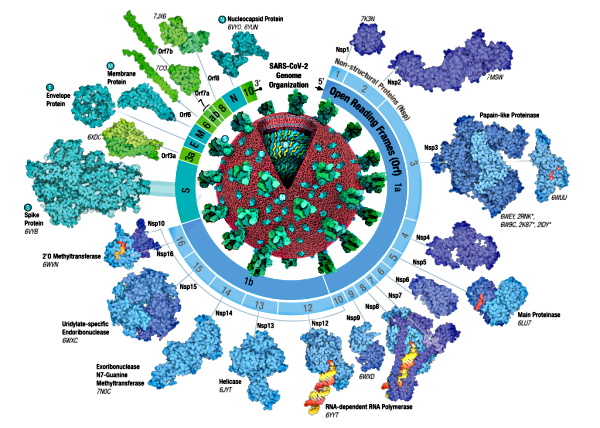
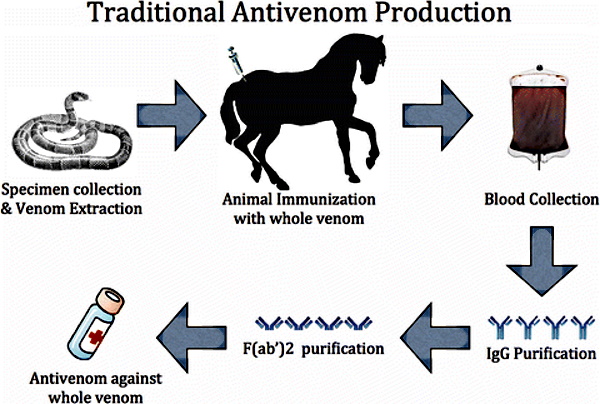
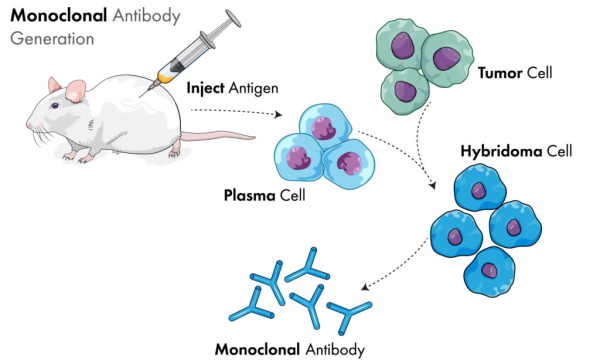
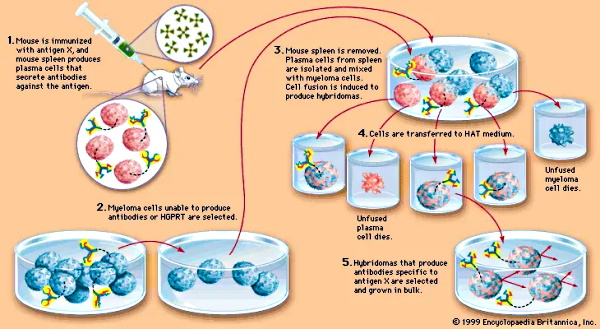


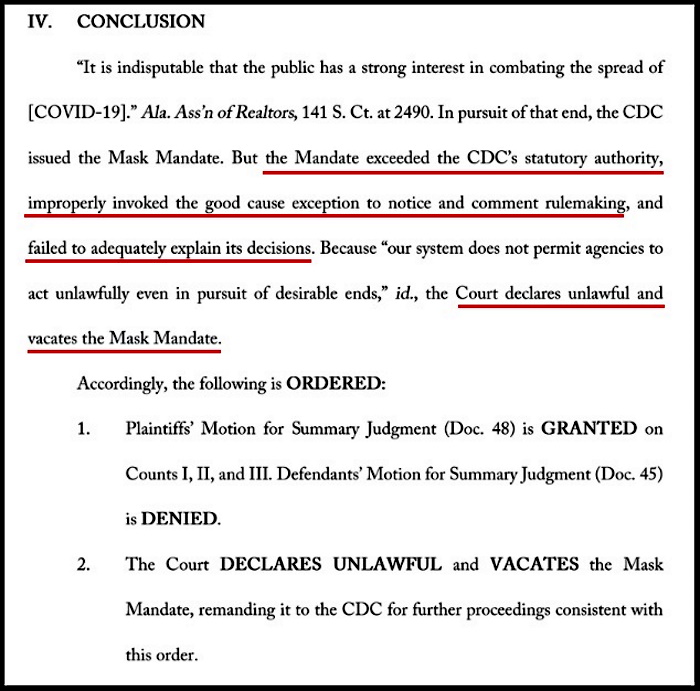




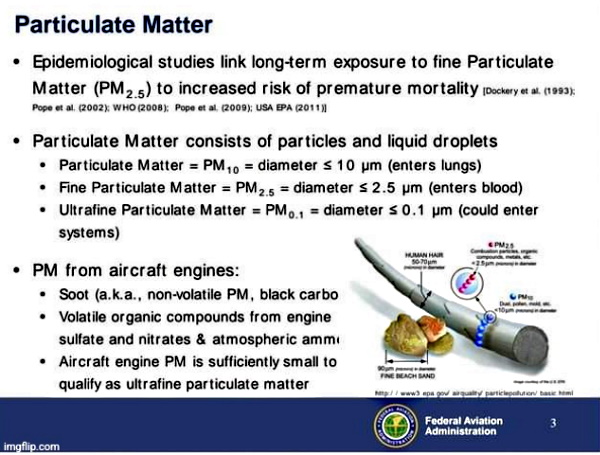
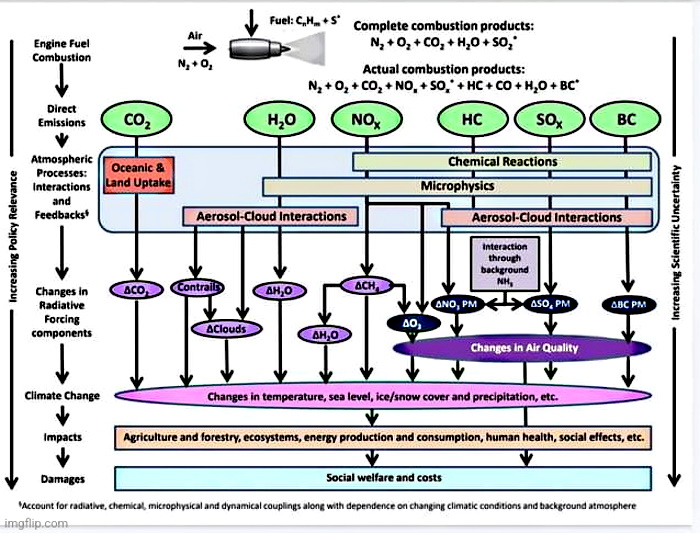
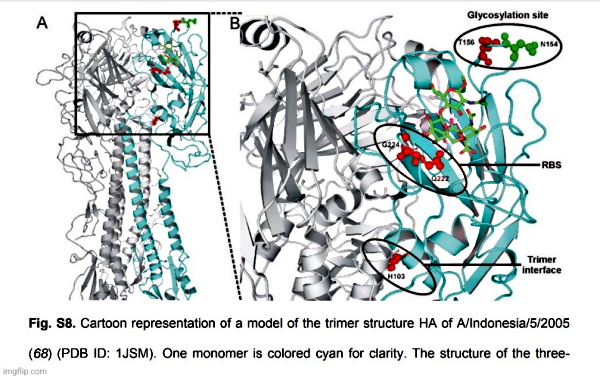


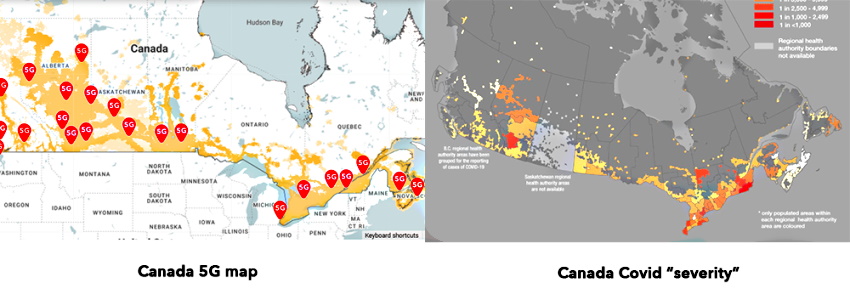
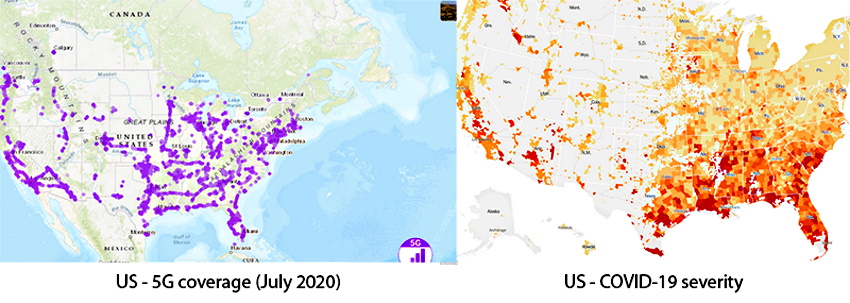
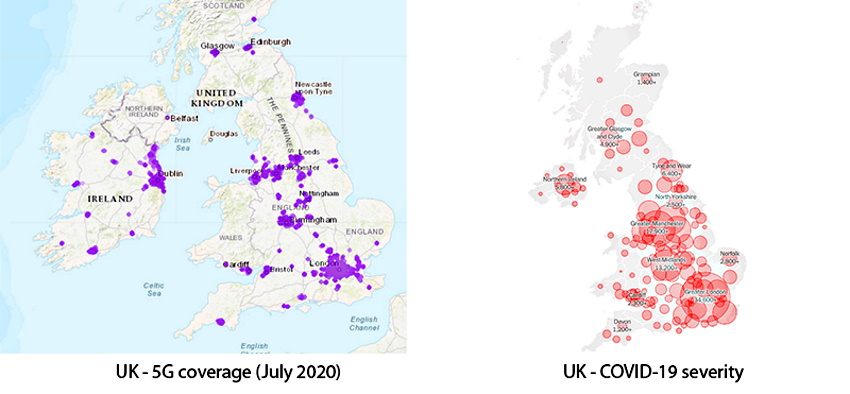

{kind=link}
{kind=link}
{kind=link}