All scientific research is built on particular dogmas including, or perhaps especially, biomedicine. It’s easier for some “scientists” to perpetuate falsehoods than it is to admit they were wrong, abandon long standing ideas, and start again from scratch. Many scientists would rather pursue trendy research areas in order to win accolades and secure grant money than question long-held beliefs and dogmas.
This is exactly what has happened with modern medicine because too much money and too many reputations are at stake. If you’re not allowed to question it, then it’s not real science.
Erroneous theories in medicine have wasted billions and caused untold harm. Imagine if they had to admit that so many years of research and countless academic careers have been wasted pursuing ideas that have no basis in reality.
Thanks to the covid pseudo pandemic, the corrupt state of the medical establishment has never been more obvious to so many people.
See No Evil, Hear No Evil, Speak No Evil
It might be difficult for some to believe that the castle of medicine is built on foundations of sand. However, Stanford scientist John P. A. Ioannidis published a study in 2005 proving that most published research findings are false.
Marcia Angell the first woman to serve as editor-in-chief of the New England Journal of Medicine has extensively investigated the corruption of medicine by drug companies.
Richard Horton, editor of The Lancet, wrote that:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
There are countless victims of iatrogenic disease in countless on-line support groups who once trusted their doctors to have their best interests at heart and to abide by the oath to “first do no harm”.
128,000 Americans die each year from correctly prescribed medications, making prescription drugs one of the leading causes of death.
Clearly, there is something rotten in the state of Denmark.
Dr. Harold Hillman Goes Renegade
In his final paper, the notorious British biologist Harold Hillman claimed that “cell biology is in dire straits”. That paper was published in 2011 and summarises his life’s work which began in the 1970s. He warned biologists and cell physiologists that something is seriously wrong with their ideas about the human body.
In the 1970s this cytologist and neurobiologist began questioning mainstream cell biology and presented evidence that the accepted model of the cell was completely wrong. He suggested that the dire straits of cell biology was the reason medical research has failed to determine the cause and provide the cure for most diseases.
“During a research career lasting more than 50 years, I have concluded that the following procedures are unsuitable for studying the biology of living cells in intact animals and plants: subcellular fractionation; histology; histochemistry; electron microscopy; binding studies; use of ligands; immunocytochemistry; tissue slices; disruptive techniques; dehydration; deep freezing; freeze-drying; boiling; use of extracellular markers; receptor studies; patch clamp measurements; inadequate calibrations. The main objections to these procedures are: (i) they change the properties of the tissues being studied grossly and significantly; (ii) they ignore the second law of thermodynamics;(iii) they produce artefacts, many of which are two-dimensional; (iv) adequate control procedures have never been published for them.”
~ Dr. Harold Hillman
He challenged the fundamental principles of biology. He was a renegade who put the quest for truth above everything else.
Unsurprisingly his views were unpopular with many in the mainstream and this took a toll on his career and reputation. He had difficulty publishing his work. Mainstream scientific journals rejected his papers without reason and refused to review his books.
“The reason I’m so determined is because they [the mainstream] won’t engage. And if they won’t engage, then to my mind it proves that I’m likely to be right.”
~ Dr Harold Hillman
Many scientists agreed with Hillmans’ compelling ideas in private but wouldn’t support him publicly for fear of losing their funding or tarnishing their reputation. Many leading biologists would refuse to meet with him to discuss his research. His goal was to start a discussion and promote a productive debate to improve and further scientific knowledge. Instead of being given a platform to share his work, he was stifled and ridiculed. Sound familiar?
Real scientists value truth above reputation and financial gain. Real scientists are willing to risk everything to expose falsities and incorrect theories. Scientists who blatantly ignore unpopular views or refuse to debate are not true scientists.
“I should like to draw attention to the fact that I regard my views as unpopular, rather than heretical, as I do not believe that scientists should talk in terms of dogma and heresy. In the best of possible worlds, good scientists who hear challenges to their beliefs, assumptions, hypotheses, procedures or conclusions, should examine such criticism with due attention. They should respond by entering into civilised dialogue with their critics. They should be prepared to admit mistakes, if necessary, and change their views. Such reactions have not occurred.”
~ Dr Harold Hillman
Hillman claimed that the routine procedures used to study the characteristics and composition of cells are completely unfit for purpose. He was adamant that these procedures would change the properties of cells more than any differences being examined so any conclusions made on the basis of these procedures were invalid.
He claimed that electron microscopy is a “waste of time and money” which goes against the vast majority of the biomedical establishment who regard the invention of the electron microscope as a pivotal point in biomedical research. Only dead tissue can be examined under an electron microscope and not living cells. Are findings based on electron microscopy relevant to living organisms?
Hillman’s work includes compelling evidence to suggest that many of the subcellular organelles that some scientists have dedicated their lives to studying are just artifacts of preparation for histology and electron microscopy. This includes both the Golgi body and the Endoplasmic Reticulum.
He also claimed that cellular receptors and transmembrane protein channels do not exist in the mainstream accepted sense. One of the reasons for this is that these cell receptors cannot be seen under an electron microscope, despite their size being within the range of visibility.
He courageously stood up for what he believed to be the truth. Despite his career and reputation taking an enormous hit, he continued to publish his ideas right up until his death.
“If I am wrong, only my reputation has been damaged. If I am right, those colleagues proved wrong may well have been wasting their time and careers and using public or charitable resources naively. They might have used their time and resources to carry out more productive research.”
~ Dr Harold Hillman
When considering the current state of medicine, it seems that “more productive research” is exactly what is needed. Research that doesn’t follow dogma and isn’t funded by the very pharma industry that has a vested interest in perpetuating erroneous ideas such as the “one germ, one disease” fallacy.
“It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing.”
~ Dr Harold Hillman
We’re led to believe that modern medicine is highly advanced but the cause of most diseases apparently remains “unknown”. Most Doctors have a mechanistic, reductionist view of disease often believing disease arises due to “genetics” or that the body is just prone to making mistakes.
“It is widely believed that medical research since the Second World War has been very successful…It is absolutely remarkable how unsuccessful this sort of research has been. If one knew the basic mechanisms, whose disarray induced disease, one could then design logical interventions to prevent them developing… it is true that the cost of failure so far has been high. The most paradoxical aspect of scientific research is that it is widely believed to be objective…”
~ Dr Harold Hillman
Hillman also criticised the lack of sufficient control experiments performed in biomedical research. Proper control experiments are the cornerstone of good science ensuring that variables, other than the one being tested, do not influence the results of the experiment.
“Control experiments for the effects of reagents and manoeuvres used on the results of experiments have been grossly inadequate.”
~ Dr Harold Hillman
Hillman also questioned the use of tissue cultures for histological analysis with compelling logic. Cells in culture have significantly different morphology, biochemistry, and environment than the cells from which they came.
“Tissue cultures are similar to the tissue from which they come in some ways and very different in other ways. It is clear that although there are a few properties in common, there are substantial differences. This is one of the most important questions, in respect of the usefulness of tissue cultures as sources of information about cells in intact animals.”
~ Dr Harold Hillman
Virology: Voodoo Scientism
Hillman’s work challenges virology as much as it does cell biology and neurobiology. The world is slowly waking up to the pseudoscientific nature of virology because of the pseudo pandemic inflicted on all of us.
“Viruses” can only be seen under an electron microscope using procedures involving heavy metals, dehydration, low pressure, electron bombardment and X-ray irradiation. Are viruses real naturally occurring structures or are they artifacts of these harsh conditions?
The effects of “viruses” are studied on cell cultures and most cell cultures are grown from embryonic tissue, cancerous tissue, stem cells, or monkey cells whose properties are completely different from that of adult human tissue. Is any of this relevant to understanding virus infectivity in humans?
Coronaviruses are supposedly assembled at the endoplasmic reticulum-Golgi interface but if Hillman is right and the endoplasmic reticulum and Golgi body are artefacts of histological preparation and electron microscopy is presumed understanding of virus assembly completely wrong?
Different cell cultures are prepared by different procedures in different chemical solutions to culture “viruses”. Could this explain why only some cells can grow “viruses” but others can’t? SARS-CoV2 cannot infect many human cell lines but can infected monkey kidney cells which is not what you would expect from a supposed human pathogen.
Viruses are supposed to bind to host cell receptors as the first step to entry but if Hillman is correct macromolecular cell receptors don’t really exist.
Adequate controls have not been performed to test the effects of lab conditions, body fluids, antibiotics, and other chemicals on cell cultures so how can virologists be sure that it is the “virus” causing any observed cytopathic effects and not the chemicals and conditions themselves?
The biomedical establishment has chosen to ignore all of these crucial questions. Sadly, Hillman’s level of critical thinking and radical questioning are rare and often completely absent in modern biomedical science.
His sharp intellect and critical thinking skills were a threat to the scientific establishment. He put his career and reputation on the line to expose the weaknesses of established biomedical knowledge.
But what if he was right? What if the castle of modern medicine really is built on foundations of sand? Will his work be forgotten, or will others be brave enough to pick up where he left off?
References
1) John P. A. Ioannidis “Why Most Published Research Findings Are False.” PLoS Med. 2005 Aug; 2(8): e124.
2) Marcia Angell M.D “The Truth About the Drug Companies-How they deceive us and what to do about it.”
3) Richard Horton “Offline: What is medicine’s 5 sigma?” Lancet Comment| Volume 385, ISSUE 9976, P1380, April 11, 2015
4) Harold Hillman “Cell Biology is Currently in Dire Straits.”
5) Harold Hillman “A Career in Neurobiology.”
6) A Biomedical Scientist “Virology’s Voodoo Scientism is Not Real Science.” The Expose.
“To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough
to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out.
This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs.
Instead of being held, rocked, and comforted in the time intervening between their birth and
their death, they have organs cut out of them alive.”
With the release of COVID vaccines, and then the mandates, we’ve seen a new resurgence of people attempting to gain religious exemptions.
Many of these attempts focus on fetal tissue obtained through abortion.
On January 19, 2021, AnnaMaria Cardinalli published an explosive article in Crisis Magazine, headlined, “Catholic Conscience and the COVID-19 Vaccine.”
Cardinalli details the collection of fetal tissue for the cell line named HEK 293.
The tissue was taken from an aborted infant in the Netherlands in 1972-3.
This cell line was used for “testing” the Moderna and Pfizer vaccines.
Cardinalli writes: “We know that the Pfizer and Moderna vaccines do not use any cells derived from abortion in the production process. That is, we know that we are not being directly injected with fetal cells or their engineered descendants (though this fact differs with other manufacturers). We hear that the abortion-derived cell lines were only used in testing, which should somehow comfort us, though it still means that the vaccines from which we seek to benefit depend on the involvement of abortion. We are told that the cell line used in testing came from one abortion, which took place decades ago. These things are all true, but they do not serve to inform us fully.”
“What we may not know follows. The most prominent cell line, called HEK 293, comes from an abortion performed in the 1970’s…”
“HEK stands for human embryonic kidney. To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out. This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs. Instead of being held, rocked, and comforted in the time intervening between their birth and their death, they have organs cut out of them alive.”
“There is no way that a spontaneous abortion could result in the cell line (as the kidneys cannot remain viable past the brief window in which they must be harvested) or that some brilliant researcher found a way for great good to come out of a rare tragedy by making use of a child’s body donated to science after it was aborted. The deliberate killing of an unwanted child (a little girl, in the case of HEK 293) took place in the tortuous manner it did precisely to obtain her organs for research. The harvest of her organs was the direct cause of her death, prior to which, she was a living child, outside the womb.”
“I fear that Pope Francis and Pope Emeritus Benedict may not have had this information when they received the vaccines. If we re-examine the Vatican statement that ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from aborted fetuses in their research and productions process,’ we see that it does not apply here. It does not imagine this scenario. To approve of the currently-available vaccines, it would have to read ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from living persons, killed by the harvest of their organs for use in medical research and productions processes,’ but the Church’s moral teachings could never truly bend so far.
Similar to the human rights abuses exposed by international tribunal in today’s China, where unwanted individuals such as religious and political dissidents are executed by the harvest of their organs for profit, the little girl whose cells gave rise to the COVID-19 vaccines was brutally sacrificed for the purpose, as were all the children whose cell lines failed before her.”
After reading Cardinalli’s analysis—not only should the granting of religious exemptions from vaccination be a foregone conclusion; the whole field of fetal tissue research, going back many years and involving many pharmaceutical products, should be put on trial.
The people who have been carrying out the murders, the people who have been using the harvested tissue, the companies—all of them—on trial.
I hope many medical professionals will take Cardinalli’s article as a springboard, and weigh in on what she is very clearly stating.
And not just doctors. All people who are shocked by her conclusions.
So far, I see one counter-claim to Cardinalli’s assertions:
The notion that the kidneys of the aborted baby must be harvested very quickly is false. The kidneys can survive for a longer period.
On that score, I refer you to a devastating video interview conducted by Robert Kennedy Jr. His guest was SOUND CHOICE PHARMACEUTICAL INSTITUTE “President and Founder, Dr. Theresa Deisher Ph.D., [with] over 30 years of pharmaceutical research and leadership experience. She discovered adult cardiac derived stem cells, has worked on their therapeutic uses as an alternative to human fetal DNA, and leads a team of scientists at AVM Biotechnology dedicated to changing what a diagnosis of cancer, autoimmunity, or chronic infectious disease means to patients and their loved ones. As a result of this work, Dr. Deisher is named as an inventor on over 47 patents.”
In the first 15 minutes of the interview, Deisher makes it quite clear that infants in the womb are taken out alive, with their blood supply functioning (essential) and then killed by cutting out their hearts or their brains. This is what is done in order to obtain tissue that will be turned into fetal cell lines.
Since this act of murder is standard practice, it would appear it was committed against the live baby whose kidney cells became cell line HEK 293, used in testing the COVID vaccines.
At the top of the interview, Kennedy said he didn’t want to get into the moral aspect of fetal cell lines. But after listening to Deisher, he was quite shaken. He said so. He said they would have to cover the moral aspect.
The whole world has to.
Here is the basic ramification: THERE IS A RELIGIOUS EXEMPTION FOR THE WHOLE WORLD.
For all people of faith. Every faith.
“According to my religious belief, the murder of an undeniably live infant for any reason is unconscionable and evil, and I refuse the vaccine.”
Here is a Force against which no government, no establishment, no secret society, no wealth can stand.
I fully understand all sorts of professionals will spout language that purports to show “the aborted infant was not alive, the lab followed all the legal guidelines, this is an old argument that has been debunked…”
But this is not just an old argument. This is the equivalent of an opening statement in a murder trial. Nothing less.
If religious leaders will read AnnaMaria Cardinalli’s article, they will see how important her charge is.
The question isn’t “will people of faith wake up and do what they should”; the question is “how can any person of faith NOT do what they should”.
If they will make a stand; if all people of faith will; the entire dire situation we are facing changes in the blink of an eye.
Solomon to God: “You have made Your servant king instead of my father David, but I am a little child; I do not know how to go out or come in…Therefore give to Your servant an understanding heart to judge Your people, that I may discern between good and evil.”
Gautama Buddha: “To cease from evil, to do good, and to purify the mind yourself, this is the teaching of all the Buddhas.”
John 10:10: “The thief comes only to steal and kill and destroy. I came that they may have life and have it abundantly.”
Would any church, any religion in the world say that God wants the killing of live infants for the purpose of medical research?
In the midst of this COVID tyranny, haven’t we all been looking for a truth that will galvanize huge numbers of people?
And not as some kind of stunt. But rather as an inevitable outcome of deep faith.
Faith and justice come from the same everlasting tree.
Yesterday I had the privilege and the honor to speak with Alec Zeck, John Blaid, Mike Donio, and Jacob Diaz about the claims made regarding the isolation and existence of “SARS-COV-2” by Dr.’s Malone, McCullough, and Cole. In this video, we address specific points they made such as whether or not:
Cultivation in cell culture is “isolation” of a “virus?”
Koch’s Postulates had been satisfied for “SARS-COV-2?”
The effect a drug has can be considered proof of the existence of a “virus?”
The electron microscopy images taken from unpurified cell cultures are proof of “virus” particles?
The particles assumed to be “viruses” are purified and isolated directly from the samples of a sick patient?
It was a pleasure to be a part of this conversation! I hope that you are able to come away with a better understanding as to why the evidence for the existence of “SARS-COV-2,” or any “virus” for the matter, is entirely lacking and unscientific.
Video available at The Truth Seeker (John Blaid) BitChute and Odysee channels.
Mike Donio, John Blaid, Jacob Diaz, Mike Stone, and Alec Zeck filmed a response to claims made by Dr. Peter McCullough, Dr. Robert Malone, and Dr. Ryan Cole regarding virus isolation and the existence of SARS-CoV-2 during an episode of The StreetMD Show hosted by Dr. Jo Yi on the Ickonic platform. The overall stance held by the speakers is simple: the claims made by these three gentlemen lack both in context and in substantial evidence to support the notion that SARS-CoV-2 exists as a pathogenic disease causing agent.
Below you will find a video presentation by Dr. Tom Cowan. The questions Dr. Cowan raises, the facts he presents, and the clarity he brings to the discussion of “viruses” and the field of virology are essential to our global conversation and quest to understand the truth. Truth Comes to Light has provided a basic transcript and added links to references for added clarity.
Over the past few years, we have shared many articles on this site related to this inquiry into the truth about “viruses” and the whole field of virology, including information on terrain theory vs germ theory. Find links here: Viruses, Vaccines & the History of Modern Medicine. At the end of this post you will find a selected list of related articles.
A few quotes from Dr. Cowan’s video:
“Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?”
“They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
“Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.”
“So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
“So I ask myself how did they do that?”
“What in the heck are these guys doing in these labs? What is gain of function research?”
“Do we really know if mRNA is in these vaccines?
“Where is the paper? Where is the evidence that there actually is mRNA in these injections?”
Okay, so before I get into talking about the question that so many people keep asking me: What about gain of function, lab-created viruses, bio labs now allegedly in the Ukraine?
So what is the science behind that?
So we’ll get into that in a minute. And before that I have a very short, little clip to play.
So that clip pretty much sums it up. That was from our friend Dr. Sam Bailey and our other good friend Stefan Lanka.
So on that note, the reason I wanted to talk about this subject is there was a recent paper that was put out by Dr. Mercola…
So let’s just read the first couple paragraphs there. So this is a summary:
“A study published February 21, 2022, (so very recently) in Frontiers in Virology claims to have discovered that a sequence of the virus’ spike protein is a 100% match to a modified messenger RNA (mRNA) sequence patented by Moderna in 2016.
The genetic sequence patented by Moderna is part of a human DNA repair gene called MSH3. This patented sequence is found in SARS-CoV-2’s furin cleavage site in the spike protein — the part that gives the virus such easy access into human cells.
According to Moderna’s patent application, the gene sequence was modified “for the production of oncology-related proteins and peptides,” ostensibly for use in cancer research.
According to the researchers, the chance that SARS-CoV-2 would have randomly acquired this furin cleavage site through natural evolution is 1 in 3 trillion.”
Okay, so why is this important? So obviously, there’s been a lot of attention in the political sphere and in the anti-vax community. There have been movies written about this.
There are many lectures, many prominent people in the “freedom” or “anti-vax” community who are investigating these patents, and saying that these patents — and as Dr. Mercola said, this study in Frontiers in Virology is literally the smoking gun proving that Moderna patented a sequence, which ended up in SARS-CoV-2, “the virus”, and the only way it could have gotten there is, not through natural evolution (that is a one in three trillion chance) but if it was introduced into the virus by some laboratory technique.
This theory is crucial to our understanding, not only of whether there were crimes committed, but the whole theory of virology and gain-of-function research and all that.
So, obviously, and this should go without saying, that the most important part of this is: Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?
The rest of the article goes on to talk about what we know about this MSH3 sequence and the protein that it allegedly codes for.
But I want to emphasize again and again and again — the whole point of this is: This sequence which was patented by Moderna in 2016 is identical to the sequence found in SARS-CoV-2.
That is the point.
If we can demonstrate that there is no SARS-CoV-2 and this is not the genome of this alleged virus, then none of the rest of this has any validity or is of any use at all.
It’s all just a sort of smokescreen or a way to throw us off the track about finding out what really is going on.
I cannot emphasize how important this is.
So for the next few minutes we’re going to actually look at how the authors of the article in Frontiers of Virology — what were they claiming was the SARS-CoV-2 genome?
What were they claiming was the evidence that there is a SARS-CoV-2 virus that they could then compare the patent to?
Again, if there’s no virus and there’s no genome then they can’t possibly have put this sequence into a virus or a genome. And it can’t possibly be the thing that’s affecting the world.
So, now let’s be clear about the next step. There is no mention in this story by Dr. Mercola of how the Frontiers in Virology authors found the genome or found the virus.
[…]
In other words, there is no information in here of how Dr. Mercola actually knows there’s a SARS-CoV-2 genome.
But the authors of the Frontiers in Virology paper said that they were comparing the sequence, the mRNA sequence patented by Moderna in 2016, to the genome found in our old friend paper by Chinese virologist Fan Wu.
So it isn’t that we picked this paper by random. It isn’t that I picked this paper to investigate how they found the genome or what their evidence for the virus was. This is the paper that the authors of the Frontiers in Virology use to compare the Moderna patent to.
So we’re using their information and this is their evidence, their proof that the virus exists.
So this is about: Did the paper by Fan Wu prove that the virus existed — the SARS-CoV-2 virus exists — and that this is the genome of the virus?
Again, in order to say that the patented sequence matches 100% to the genome of the virus, obviously, obviously, you have to know that this is actually a virus.
So, this is an old friend, we’ve been through this many times, but let’s see what they say.
So here is the paper, published in the prestigious journal, I believe, Nature — February 3, 2020.
So this is the paper, again, that was cited by the authors of Frontiers in Virology paper that is used as the reference genome.
So how did they do it?
So first we have a summary.
So how did they identify the “virus”? So I’m gonna run down the steps that they used and then we will show the clips, the actual wording from the paper, so that you know that this is actually the facts.
Okay, so we’re looking to find a virus and then find the genome of that virus — a virus that had never been found before.
So first thing they take lung fluid from one person. That’s a huge sample size (that’s a little tongue-in-cheek). That’s obviously just one person. That is a kind of ridiculous experiment to find a new virus.
Then they isolated the RNA, which is a genetic material, from the fluid in that person’s lung. They did not attempt to purify any particles that they could say you were a virus. They did not do any pictures of any virus. They did not do any maceration, filtration, ultracentrifugation to see if they had any such particles. None of that.
They took RNA from the lung fluid, of which we have many possible sources. We have bacterial sources, fungal sources, human sources, possibly viral sources, exosome sources, multivesicular body sources — many sources of RNA. We have no idea the source of that RNA.
Then they create what’s called an mRNA library, which is a catalog of all of the RNA pieces that are in that lung fluid.
This requires that they amplify these pieces of RNA with the process called RT-PCR. And, as we have demonstrated over and over again. and is completely substantiated in the literature, doing PCR amplification of RNA cycles inevitably creates new sequences of RNA which weren’t there in the original sample.
In some cases, if you do enough amplification cycles — up to even 80% of the sequences — after 45 cycles are made de novo, or anew, by the actual PCR process itself.
So now we have yet another source of our RNA. Not only do we have potential viruses, exosomes, multivesicular bodies, apoptotic bodies, human lung tissue, human epithelial lung tissue…, fungal RNA, bacterial RNA — we also have new pieces of RNA generated by the test itself.
Then they performed pair and sequencing that generates 150 base pair reads. That means they matched the sequence by pairing the ends. And you end up with sequences that are basically 150 base pairs long. That’s a fairly small amount. And this results in 56.5 million of these 150 base pair sequences known as reads.
So to be clear, they take this mass, not knowing any idea the origin of these mRNA, they chopped them up into sequences that are 150 base pairs (that’s fairly short) long by pairing the ends. They have 56.5 million of these reads. And then they start doing what’s called de novo assemble.
So there is no sequencing here. There is assembly. And, as it says, you can make a lot of genomes with that many reads.
So they put these 56 million, 150 base pair, reads in aa assembly computer program and… they actually put it in two different computer programs. And one of the computer programs generated 384,000 different sequences. The other one generated over a million sequences.
So now these sequences — all 384,000 of them — are meant to be the possible genomes of this virus. For some reason, they threw away the program that made over a million of these sequences and said the one that made 384,000 — I think that was Megahit — one of those must be the right sequence, the actual sequence of the virus.
Just to be clear, at no point did they ever find a particle. At no point did they purify or isolate a particle.
At no point did they find in any particle… an entire string of RNA, which they then sequenced one by one to find out the sequence of the genetic material of this particle.
None of that was done. All they did was chop up RNA from many different possible sources, put that in a computer program, generate 384,000 and a million in another, and then they went hunting for infectious agents and performed a search of those sequences.
The two longest sequences were a close match to a bat SARS-like coronavirus genome, found 15 years ago or so, that was made in exactly the same way — never having isolated or purified a particle, never having found an intact genome, never having sequenced the genome.
They just did the same sort of assembly, no sequencing of RNA from God knows where. And, this one, the longest one was a 89% match to the previous SARS coronavirus that they did in the same way.
And, as we say: Boom! There is the new novel human coronavirus — even though, as we’ve said over and over again, humans and chimpanzees are about a 96% match. So to say it was an 89% match is essentially like saying there’s no way this could have been anywhere similar to the previous bat SARS-like coronavirus.
In other words, they never found a virus. They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.
This is a manuscript draft and I don’t know when it will be published.
When I read this, just remember that all these articles that go into The Lancet have to pay homage to the virus god. But I will explain what they mean here.
So this is the interpretation of the entire article. I won’t go through their methods.
“The RNA code counted in PCR tests, previously attributed to SARS-CoV-2, belongs instead to a respiratory-virus-induced immune system response by human cells that liberate exosomes, and that vitiate PCR test results. PCR tests have zero specificity in vivo due to the exosome RNA.”
[…]
And they go on in this article, just as we’re saying — the reality is all of these RNA sequences, all of these reads which were assembled into a viral genome, actually when you do careful analysis, come from human epithelial lung cells.
In other words, just as we’ve been saying all along, these are not viruses. These are breakdown products of our own tissue. And the misconception in calling them a virus needs to stop.
And this idea that they put this patented sequence into a virus can’t possibly be true because, simply, there is no virus.
And all the rest of the article is for not — because nobody put a RNA sequence, patented or otherwise, into a virus.
Now just to show you that we got this from the article — so here is the one patient presenting with cough, etc. So that’s the evidence that we were correct about the one patient.
Here is the evidence that the paired and 150 base pair reads sequencing of the RNA library was performed on this computer platform. So the sequencing yields reads of only 150 base pairs. The whole SARS-CoV-2 genome is supposed to be 30,000.
That means they had to stitch it together using a computer program. This was an assembled genome, out of little bits from God knows where.
And here we see the 56.5 million reads were assembled using Megahit and Trinity. Trinity, they got over a million. They generated a total of 384,000 contigs (that’s sequences).
Trinity generated 1.3 million. They don’t like those because they weren’t long enough. They compared those with the database and compared and found that it was somewhat, although not really similar to a previous bat coronavirus. So, as he says, sequencing results in more than 56 million reads.
How can you possibly differentiate what is from a potential virus from everything else? The answer is you can’t.
And finally… The longest contig is generated by Megahits. The longest one by Trinity is 11,000. How come they didn’t use this one?
Both showed similarity to bat coronavirus. They were found at high abundance. It was only 89 percent similar. That means 11 percent didn’t match. That is a huge amount.
Then they just moved on to develop primers all from this one assay without isolating anything, and from one patient.
And, my friends, that is not science; that is propaganda, as is the entire story of a lab engineered virus.
Now, the real issue here and one of the reasons why this, to me, is so important, is if you go by this unscientific theory that there’s a lab-created virus, you actually miss what I would say are the three most important questions to be asked, and then answered, about this situation.
And so now I’m talking — I would say theory. Where everything else was what I would call simply facts.
So the question that should be asked (and it would be nice to have answers for, and which I don’t have the answers for, but I have some theories) is, to me, the most interesting thing is —
So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
So I ask myself how did they do that? How did they make — like there’s two theories, there’s two ways of looking at this.
One is: They don’t want that to happen and so it was a mistake.
But, if we think, which I’m inclined to do, that “they” (meaning Moderna and other people) wanted this to happen so that they could throw people off and essentially create a kind of patsy out there, how did they do it?
So I have three possible theories as to how they did it.
Now, let me be clear.
What I’m trying to figure out is these guys Fan Wu and others, Chinese virologists, having, I don’t think, any connection with Moderna, come up with a bogus, anti-scientific genome and for some unbelievable coincidence — let’s say for now — it actually matches exactly one of the patented sequences from the Moderna patent of four years prior. How did that happen?
So possibility number one: It was dumb luck. They just made this sequence and it just so happened to match the Moderna patent. And, frankly, I don’t think that’s actually the right answer.
The second possibility: … Somebody from Moderna or somebody — I don’t know who — calls up Fan Wu and says ‘I want you to make a genome out of nothing and I want it to have this particular sequence in it so some day people will find this out and say “you see, they genetically engineered this sequence”‘. Got it? In other words, there was collusion between the patenters (that’s Moderna) and Fan Wu and his team.
Now I gotta tell you, I actually don’t think that’s true. I would actually love to find out if it is true and if there is a phone call from doctor head of Moderna saying, you know, ‘Hey Wu, would you put this sequence in there so that we can — people find out that it was a genetically engineered sequence?’ But I just don’t think that happens.
And then I came up with a third possibility which is: Once I discovered all these people who are looking into all these patents, that there was at least 70 different patents taken out, of different sequences of RNA, that could end up in a genome. Now, my guess is … I would think it’s a good possibility that one of those sequences may end up in the final genome. And then you would then implant the story that this was a genetically engineered organism and there you go.
So you wouldn’t have to rely on luck, you wouldn’t have to actually have collusion, you could just patent a whole lot of different sequences, for instance, that came in the SARS-1 genome. You could patent all kinds of sequences knowing that, at the end of the day, when somebody makes up this new fraudulent genome it’s bound to have one of them in there. Somebody will find it some day, say it’s the smoking gun and you then implanted the story of the century which does nothing but throws people off.
So those are my three options. I’d be happy to hear about any other possible options. But those were the only three that I could come up with.
Now, the final question then is: What in the heck are these guys doing in these labs? What is gain of function research?
And, I must say, I don’t know what they’re doing in the labs and I don’t think really anybody knows — including in the Chinese labs or Ukrainian labs or North Carolina labs or any other labs.
So again, I have some possibilities.
One is the following …
Screenshot image from BrandNewTube video (specific video source unknown)
They’re doing this.
In other words, what the virologists do is they dress up in hazmat suits and they go on to their computer and start making sequences. And the hazmat suits are crucial, because, as we all know, it’s very possible for the sequences to jump from the computer into their eyes. So it’s very important, as you can see, that they wear goggles and protective head gear to prevent the computer sequences from jumping directly in their eyes.
In other words, they may be just doing nothing and it may be just a whole lot of hooey to get people to worry about things. And to implant in their minds that there is this horrible engineered virus, that we should all be scared of viruses, etc. So that’s one possibility.
Another one is they’re making some sort of proteins or genetic material which can be injected into people. In other words, they’re making toxins. And that is certainly possible.
So those are the two main categories that I came up with. Either they’re just doing nothing and they’re just a front, or a smoke screen, or they’re actually making stuff which isn’t good for people.
And that gets into my final thing that I want to point out.
… This section right here. this is something I’ve been very interested. So this is again from the Mercola article:
“For clarity, this may have nothing to do with Moderna’s patented MSH3 sequence specifically, because the RNA code in the jab is not identical to the RNA code of the actual virus. (I’m not going to get into that.) The RNA in the jab has been genetically altered yet again to resist breakdown and ensure the creation of abundant copies of the spike protein. 11“
Now, I have been asking the question now for months: Where is the paper? Where is the evidence (a) that there actually is mRNA in these injections? They say there is. That’s the whole point. But when people look there either seems to be not there or in variable amounts depending on which injection and which batch.
So it could be that even the whole mRNA in the jab is a actual smokescreen or cover for what’s really in these injections –which is a lot worse stuff like self assembling nanoparticles which we’ve heard about a lot.
So I was very interested to see that this was… stated as fact, because I can’t find a paper, and my friends can’t find a paper, that confirms that abundant copies of this protein are actually made when you inject this sequence.
And this would be like saying — if I wanted to get investors for my new pencil factory, my investors might ask me to see the pencils that we make. And so it would be natural for me to produce copies of the pencils — maybe tens or hundreds or thousands or millions of them — to show that my technology for making pencils actually works.
One would think that if the whole point of these jabs is to make you make spike proteins that, therefore, “confer immunity”, there would be scores, hundreds, thousands of papers showing here’s the amount of spike proteins in an unjabbed person. And then you jab them and then 10 minutes, half an hour, three hours, two weeks, six months, 12 years later, here’s the amount of spike protein. That would prove that the concept is real and that you can actually genetically alter a human being.
Because I have my doubts. So I’m looking for a reference to show this is true. And, lo and behold, here is the reference. Number 11. [see page 3 of Mercola article] So where is the reference from? CBS News.
Now, I could say — I would say if it was from Fox or MSNBC then I would be skeptical. But the fact it’s from CBS, that must mean it’s true. And obviously I’m kidding. Let’s see the reference.
If the whole point of this is to put RNA into injections, make you make a spike protein which is allegedly from the virus, let’s actually see that it works. And here’s a quote saying there’s at least 73 patents.
My guess is one of them was bound to show up in the imaginary sequence. Bingo! We’ve got proof that it’s there, that it was a genetically engineered virus.
And the whole thing, hopefully you now see, comes crashing down like a house of cards if, as we showed, there was no virus genetically engineered or otherwise in the first place.
[At this point in the video, Tom takes questions from the viewers.]
Question: So this one is related, but it has to do with Dr. Bush‘s reference to 10 to the 30th power of viruses within our blood, as well as in the oceans, in the soil. His purpose is to provide constant flow of updated genomic information that we need to in order to adapt and survive. And they’re not pathogens. That we need not fear, etc., etc.
Answer: So he also has said that, of course, viruses are pathogens. The real issue here is how did they find these 10 to the 30th power viruses? And I’ve gone over this, especially in reference to a paper, and I don’t remember the name, but it’s called the ….something to do with the renaming or the re-evaluating of viral…virome…viral world or something like that.
The reason people say this is because they don’t realize that they’re not talking about actual organisms or particles called viruses. They’re talking about liberated pieces of either RNA or DNA — little snippets of RNA or DNA which then get amplified in what’s called metagenomics sequencing and so there are billions and billions and billions of these breakdown products. None of them have anything to do with a virus. They’re simply little bits of genetic garbage that are coming off of our cells and tissues all the time. They have no particular meaning or function that anybody has been able to prove. They’re just little bits of garbage. And the misconception that they’re somehow actual particles and could possibly hurt you or could possibly help you is just a misunderstanding of how they found viruses in the first place.
They don’t find particles. They don’t purify particles. There haven’t been 10 to the 30th purified particles. We’re talking about little pieces of DNA or RNA that get amplified, called viruses, which is a misconception big time.
[Additional questions include speculation about the patent links to the Fan Wu team “discovery” as well as a question about allergies.]
Articles mentioned in this video presentation:
Moderna Patented Key COVID Spike Protein Sequence in 2016 by Dr. Joseph Mercola [originally published March 7, 2022 at this link — https://articles.mercola.com/sites/articles/archive/2022/03/07/moderna-patented-spike-protein.aspx — and was mirrored around the web. It can still be found at Dr. Mercola’s paid archive membership.] Dr. Cowan has provided a pdf file of the article here: https://brandfolder.com/s/fv2q4h7fp84bm5vb3ppn37
“The real purpose of the scientific method is to make sure Nature hasn’t misled you into thinking something you don’t actually know…One logical slip and an entire scientific edifice comes tumbling down. One false deduction about the machine and you can get hung up indefinitely.” – Robert Pirsig, Zen and the Art of Motorcycle Maintenance
On 11 March 2022, an article was published on The Daily Sceptic website titled “The Real Truth About Viruses”. It was written by Dr Roger Watson, a PhD-qualified registered nurse, who recently retired from the United Kingdom’s higher education sector and now has a part-time position as Academic Dean of Nursing at Southwest Medical University, China. The article was a blatant hit piece against me, typically the domain of the controlled corporate media, so it was a surprise to see it on a website that developed from Lockdown Sceptics. They have the motto “question everything” but apparently you shouldn’t question germ theory and the existence of viruses!
“Question Everything”….except germ theory and viral existence, that’s pure crazy.
Dr Watson appeared to know very little about my work and never attempted to make contact with me before he did his hit and run. We offered him the chance to come on my channel but he declined saying “I am not sure how fruitful a debate with me would be,” perhaps not feeling confident about backing up his claims or perhaps a little shaken by the derision he received in the comments section on the Sceptics website. Much of his article was ad hominem in nature and doesn’t need to be dignified with a response but I will proceed to address his inaccurate scientific claims point by point…
“I would like to hear Duesberg or Sam Bailey explain how haemophiliacs contracted AIDS from blood infusions. Somehow, I think they’ll have a stock response to that one.“ Dr Roger Watson, The Daily Sceptic
It is unclear why Watson has conflated my views with Peter Duesberg and his sentence will take some unpacking. His reference to Peter is a link to Wikipedia, a known disinformation site, which should raise a red flag for a sceptic or anyone wanting to know more about a topic. Peter does not claim that viruses don’t exist: he is one of the world’s most prominent retrovirologists after all! His position is that the HIV particle exists but that it is a harmless “passenger” virus that does not cause the clinical condition AIDS. I know he outlined the evidence of why haemophiliacs do not become “infected” through blood product transfusions here but cannot otherwise speak for him. My position is that there is no proof of the existence of a retrovirus called HIV and that the particles nominated “HIV” have never been shown to fulfil the defintion of a virus. Thus “HIV” has not been shown to cause AIDS.
In this regard, the biggest influence on both myself and my Virus Mania co-authors has been the work of The Perth Group. Watson fails to define what he means by “haemophiliacs contracted AIDS from blood” but presumably he means that the reason some haemophiliacs develop AIDS is because there is a pathogenic virus that is being transmitted to them via infected blood. (They actually receive factor VIII concentrate from pooled blood donations.) I am unaware of any research demonstrating HIV particles in blood or any human or animal models showing transmission of “infected” blood that then causes a recipient to develop AIDS. In Virus Mania we explain that “HIV” cannot be the explanation for the development of AIDS in haemophiliacs. Increased death rates did correspond to changes such as the introduction of “anti-viral” pharmaceuticals including the highly toxic AZT in “HIV positive” patients. If Watson wants to get serious about claiming that a virus is being transmitted to haemophiliacs and causing AIDS then he should have an attempt at refuting The Perth Group’s 1995 paper “Factor VIII, HIV and AIDS in haemophiliacs: an analysis of their relationship”. In my estimation it is the best I have come across and I would welcome Watson’s critique of what I’ve missed.
“Her views have been debunked regarding the existence of viruses but, possibly unknown to many who are unwilling to wade into the depths and breadths of her views, she denies germ theory completely.” Dr Roger Watson, The Daily Sceptic
Watson doesn’t let his readers know how he established I’ve been “debunked” or by who. Instead he provides a link to a small blog post written by a University of Waikato employee and Pfizer BioNTech injection enthusiast Alison Campbell. Campbell set up the blog “as a resource for secondary school biology teachers preparing students for Scholarship Biology examinations” which is probably not the level Watson should be aiming for in this debate. If he checked Campbell’s usual publications he would have realised that she has no experience in virology or medical matters. In fact, when we reached out to her she quickly retreated and would not even agree to a phone call. Watson follows in the footsteps of our state-sponsored mainstream media who also used this largely ad hominem rant as “evidence” against me. I’ve already responded to Campbell and the MSM’s little foray into virology – unfortunately, like Watson, they are limited to repeating the claims of the virologists on face value.
I’m not sure why my views on germ theory would be “unknown” to my viewers as I openly point out that I do not believe it is satisfactory model. Virus Mania is largely dedicated to dismantling germ theory and my views are closest to that of “terrain theory”. I outline why I’m in the terrain camp in much of my work, including in my video “Germ Theory vs Terrain Theory”. For those not familiar with Virus Mania, a window into the book can be found in this short essay I wrote with my co-authors.
“This essay is prompted by the most recent video from Sam Bailey: The Truth About Viruses published on March 9th 2022. She is to be congratulated for its brevity – it is only 17 minutes long – but it is presented in a typically sneering, sarcastic and patronising manner.“
Dr Roger Watson, The Daily Sceptic
Watson seems to completely miss that this video is a light-hearted and satirical take on some of the historical claims of the virologists. It was designed to engage a wider audience with material that can be a boring subject for many. If he wanted to have a serious discussion about a particular topic then he could have easily accessed my other published work or contacted me to fill in any gaps.
“It is hard to understand how Sam Bailey arrives at her views and it is not necessary to be a virus denier to be highly critical of the way the pandemic was managed.“
Dr Roger Watson, The Daily Sceptic
Watson has ignored the vast majority of my work and never bothered to converse with me so perhaps it is not surprising that he is confused. I’m not sure why anyone would decide to be a “virus denier” because they needed to criticise “pandemic” management or how this is relevant to his argument. In fact, it’s disingenuous to even suggest such a modus operandi and it slumps into the argument of the destitute.
“After all, anti (Covid) ‘vaxxer’ supreme, Dr. Mike Yeadon made it clear in his excellent interview with Neil Oliver on GB News that he believes a unique virus exists. The HART Group led by Dr. John Lee, who have mounted the most credible and well-informed responses to the UK lockdown, is not stocked with virus deniers.“
Dr Roger Watson, The Daily Sceptic
Watson has not provided any evidence for the existence of viruses here: his argument seems to be that other people believe in viruses, therefore viruses exist. Some people also believe in the tooth fairy but that would not affect my own investigations into the topic. Appeal to common opinion is a type of faulty reasoning that also plagues the medical community. Heretics like myself are prepared to examine the evidence for ourselves and reach our own conclusions, not parrot those of others. We are not motivated by the number of people who agree with us and our publications are not restricted by governments, institutions, or colleagues. Note to Dr Watson: in all the virology textbooks I’ve looked at, the method of proving the existence of a virus does not include ‘beliefs held by Dr Mike Yeadon’. (For the record: I have no problem with Dr Yeadon, we just have different thoughts on the existence of viruses.)
“It is hard to know where to start but, since she denies germ theory itself – as properly understood – I will start here with Dr Bailey’s views on whether anything exists that can cause an infection and spread between people. Louis Pasteur comes in for criticism by Bailey in her Delingpod interview. I am sure Pasteur was not perfect but he did knock the theory of spontaneous generation a body blow with his swan neck flask experiment.“
Dr Roger Watson, The Daily Sceptic
I’m unsure what Watson means by “properly understood” germ theory. My investigations into germ theory, which are dealt with in Virus Mania and videos such as “Koch’s Postulates: Germ School Dropout,” have informed me that the theory is fatally flawed. I have looked into Koch’s original work and he did not fulfil his own postulates correctly. His often uncontrolled experiments failed to take into account the traumatic effects of his procedures on animals or consider other factors that were making them ill. With regards to “infection” spreading between people, it seems that clinical experiments have struggled to demonstrated this phenomenon. Perhaps the most spectacular failure has been the inability to ever demonstrate transmission of influenza, as I outlined in this video here and ViroLIEgy’s Mike Stone detailed here. If Watson wants to send me a paper that proves the concept of microbes transmitting between humans to make them ill, then I would be happy to critique it. Pasteur’s work has been exposed as largely fraudulent, but it is unclear why Watson is bringing in his spontaneous generation and swan neck flask experiments and how that relates to anything I’ve published. Perhaps he thought terrain theory was claiming that microbes appear on the basis of spontaneous generation?
“Dr. Bailey has batted the theory of disease back into the 19th Century. Edward Jenner was another scoundrel according to Bailey and, while his experiments would not have passed muster with an NHS ethics committee, you can see where Bailey is going and leading her disciples into the realm of the ‘anti-vaxxers’, a topic which I will not explore here.“ Dr Roger Watson, The Daily Sceptic
Watson may be shocked to know that I’m not the only one who has questioned the alleged contributions Jenner has made to human health through the practice of vaccination. I would also suggest he reads the book Dissolving Illusions, or at least examine the charts that Dr Suzanne Humphries and Roman Bystrianyk have put together, if he believes that the smallpox vaccine or any other vaccine has been shown to be of benefit to the public.
The realm of “anti-vaxxers” and their bloody inconvenient, irrefutable data!
I am up front about my position on vaccines as it is clearly stated on my website FAQs that, “I am not ‘anti-vaccination’ in the sense that I don’t wish to tell other people what to do with their bodies. I’m always happy to consider new evidence, but for me personally, I don’t believe any current vaccine can provide health benefits for myself or my loved ones.” It is unclear to me why Watson thinks I am “leading disciples” into any realm. If he thinks he has sound evidence that vaccines lead to better health outcomes then he is welcome to provide it – our Virus Mania team has sought such data from major institutions such as the Robert Koch Institute for many years and they have been unable to provide it.
“She mentions, in passing, the famous TMV (tobacco mosaic virus) in a ‘that’s all very well’ kind of way. But the fact is that the TMV has been sufficiently purified for its structure to be studied by scanning electron microscopy; and that represents a very high level of both isolation and purity. A plant virus it may be, with no animal equivalent, but it is the case that disproves, in a Popperian way, the argument often repeated by the virus deniers that ‘no virus has ever been purified’. Some have been sufficiently purified for study by X-ray crystallography and that represents an extremely high level of purification.“
Dr Roger Watson, The Daily Sceptic
It’s not at all convincing in his article that Watson knows the difference between isolation and purification. He refers to a microscopy study which purports to show TMV. We may need to remind Watson that a virus is a tiny replication-competent, intracellular parasite that can infect a host and pass onto other hosts. Apart from images of tiny particles, there is nowhere in the paper he cites that any of these key properties are demonstrated. I have explained in my video “Electron Microscopy and Unidentified “Viral” Objects” the limitations of the technique and why particles that appear amongst dead tissue cannot be classified as “viruses” without further experimental steps. His reference to an x-ray crystallography paper is likewise useless. Plenty of particles can be purified Dr Watson – the issue is that they need to be shown to be viruses. In any case, you’re in for a treat as I currently have a video in production exposing the Tobacco Mosaic “Virus” story going back to Ivanovsky’s unscientific experiments considered by some to be the beginning of virology.
“But the fact is that the existence of any virus is triangulated by an array of increasingly sophisticated laboratory techniques whereby theories may be tested, cultures grown, and infectivity demonstrated. In fact, a great many viruses have been purified, often against the odds.“
Dr Roger Watson, The Daily Sceptic
Triangulation? The process of measuring distances and determining locations. Watson goes next-level cunning with his conflations to make virology look respectable again! If Watson looked at all my publications he would see that I am familiar with the historical techniques, which failed to demonstrate the existence of pathogenic viruses and how they have morphed into modern molecular detection techniques to keep the virus paradigm alive. His citation is “Virus Purification” techniques in the Encyclopedia of Virology (Fourth Edition), 2021 – I have an e-copy of this publication and am familiar with the described methods. However, Watson needs to show his hand and let us know which particles he thinks have been purified and demonstrated to be “viruses” instead of pointing at a textbook.
Dr Watson: stop keeping us in suspense and please publish your list of viruses that were purified “against the odds” with their proofs.
“The virus deniers trot out the Koch’s postulates argument repeatedly, even though Koch’s postulates were simply one way – long before the advent of amino acid and nucleotide sequencing methods – of demonstrating the presence of a bacterium. Koch’s postulates were never intended to be applied to viruses – the existence of which were not known when Koch postulated.”
Dr Roger Watson, The Daily Sceptic
Watson appears completely confused about Koch’s Postulates which relate to establishing a causative relationship between a microbe and a particular disease, and conflates it with “demonstrating the presence of a bacterium”. The postulates were designed to be applied to all microbes, but as I have stated, my investigations indicate that Koch’s Postulates have never been fulfilled and there is no sound basis to germ theory: bacteria, fungi and postulated “viruses” are not the causal agents of disease. And it doesn’t matter what nucleotide sequences or proteins you discover Dr Watson, you still need to establish where they come from – are you sure the virologists establish this or even do “sequencing”? (See below).
“The original SARS, which almost certainly jumped species, is very unusual for that very reason and, for example, bird flu does not infect humans. The jury remains out on whether SARS-CoV-2, which possibly jumped species, did so spontaneously or after a ‘gain of function’ nudge.“
Dr Roger Watson, The Daily Sceptic
Interestingly for a “sceptic”, Watson espouses most of the virology industry’s stories about viruses jumping species. Can he point to the investigations he performed to conclude something that hasn’t been shown to exist “almost certainly jumped species”? We deal with these highly speculative and sometimes baseless claims in Virus Mania and I covered the original “SARS” (and “species jumping”) in another of my videos banned by Big Tech but still available here. There is a fatal flaw regarding gain of function research with “viruses” when the pathogens themselves have not been shown to exist, as I have pointed out in more videos banned by Big Tech but still available here and here. Dr Stefan Lanka has also outlined the fallacies of “bio-weapons,” including fabricated “viruses” and how they have been used to drive fear into the public for many decades.
“I have corresponded with Siouxsie Wiles, a major debunker of the Koch’s postulates argument, at Auckland University in New Zealand over this point and over the point regarding ‘purification’ of the SARS-CoV-2 virus.“
Dr Roger Watson, The Daily Sceptic
Watson makes an appeal to “authority” here, which was the same mistake made by Steve Kirsch when he clumsily waded into the issue of the existence of “SARS-CoV-2” in January 2022. My husband Dr Mark Bailey has previously outlined why Kirsch shouldn’t rely on such “experts”. Like Watson, Kirsch started off all guns blazing against the “virus deniers”. Like Watson, Kirsch rapidly retreated when the Baileys, Dr Tom Cowan, Dr Andy Kaufman, and Dr Stefan Lanka all offered to participate in a live debate with his chosen “experts”. It is odd that our “sceptic” Watson corresponds with Wiles as she is heavily promoted by the NZ government and advised our country that “the world is on fire” and we should “all behave as they [the government] are asking us to behave” in March 2020.
“If men define situations as real, they are real in their consequences.“
William Isaac Thomas and Dorothy Swaine Thomas
She is notorious for avoiding open scientific discussions and even has a lengthy automated email reply excusing herself from such pursuits. Incidentally, in February 2022, a state-sponsored media platform was found guilty of publishing one of her false claims. Watson has referred to an article by Wiles which is a case of the blind leading the naked. In the article she provides no explanation as to how disease causation is satisfied with viruses when it is conveniently claims there are no suitable clinical experiments available. She tries to distract the reader with Falkow’s molecular postulates, and fails to inform her readers that River’s postulates were designed specifically for viruses but have not even been close to being fulfilled for SARS-CoV-2 – the first problem being that no one can show it exists. There is certainly nowhere in her article that demonstrates she can prove the existence of SARS-CoV-2 or any other virus, only excuses as to why direct proofs are lacking. I have previously addressed her false claims surrounding the application of the PCR in another video banned by Big Tech after several hundred thousand views, but still available here. New Zealanders have endured two years of state-sponsored nonsense from Wiles, who is paraded by the MSM as a go to “expert”. I’m willing to bet that a live debate with Watson & Wiles on one side and the Baileys on the other would be very revealing.
“It transpires that the purification of the novel coronavirus argument is a straw dog created by the viral deniers. In fact, nobody has claimed that it has been purified. However, it has been ‘isolated’, which is a different concept whereby studies are carried out to check it is there.“
Dr Roger Watson, The Daily Sceptic
If Watson hasn’t already indicated that he is bringing his pocketknife into a gunfight, then this is where his pocketknife falls to the floor. I suspect he didn’t know that I have already analysed Vincent Racaniello’s presentation he refers to in this video (banned by Big Tech of course). It is not clear that he even listened to Racaniello’s words: if the virologists don’t have a specific defintion of “isolation” what does Watson think it means? Can he see a problem when Racaniello says “an isolate is a virus that we have isolated…” or has he been swept up in their circular reasoning? The problem of what “isolation” means is the pivotal issue with regards to proving the existence of viruses and the virologists have a habit of playing fast and loose. As stated by The Perth Group in 2017: “The fact is that in virology, while purification retains its everyday meaning, “isolation” is an expediential term virologists assign to data they claim are proof a particular virus exists.” Watson instead chooses to cheerlead the virologists denigration of the English language: if their use of the word ‘isolation’ isn’t what everyone thinks it is, then it’s useless as a method of providing proof that a particle is a virus.
Watson, however, gives the thumbs up to ‘isolate = particles + every other bit of junk in a specimen’, perhaps oblivious to the deception of the virologists.
“According to Siouxsie Wiles, the virus has been found in hundreds of disparate samples and subsequently sequenced. The viral deniers point to the way the sequence was merely pieced together in the early stages, thus proposing a hoax. But this is how viruses are sequenced.“
Dr Roger Watson, The Daily Sceptic
How on earth this made it past the Daily Sceptic editors is a mystery to me. For his source of “truth” Watson has cited “fact-checking” organisations that are supported by Big Tech, and have financial conflicts of interest with Big Pharma. If it is not apparent at this stage of the “pandemic” that these organisations have been consistently misleading the public since day one then it is difficult to believe that he really is a “sceptic”. The fraudulent invention of the “SARS-CoV-2 genome” by Fan Wu’s lab has been exposed by Stefan Lanka’s team and it was even worse than the usual imaginary “viral genome” assembly circus. The ViroLIEgy website has one of the best collections on the many assumptions and biases involved in “genome” creation, from the collection of the crude specimen through to the hypothetical model constructed by computer software. And with regards to “viruses”, we do not call it a “hoax”, we call it fraud. “Viruses” are not really “sequenced” as you might think Dr Watson (see below).
“In any case, as explained to me by Siouxsie Wiles, it is not necessary to purify the coronavirus and as Dr. Ros Jones says in her Unity News Network interview with David Clews, this is not how it is done; the virus is cultured. This is about as close to Koch’s postulates as you could get: grow the purported virus in a cellular culture and identify it by sequencing. Introduce what you have to some other cultured cells alongside a control culture. If the one with the purported virus shows subsequent evidence for the presence of the virus and the other does not, that is about as watertight an experiment as I can think of.“
Dr Roger Watson, The Daily Sceptic
Watson has a great deal of faith in Wiles and her reassurances that purification is “not necessary” and again seems to be confused about what Koch’s Postulates is all about. He describes cell culture experiments and what he believes is “identification” of a virus. How does he know there would be a new virus in there? Apparently, by “sequencing” (I’m not sure he understands what they are actually doing – see next point.) And what does he mean by a “control culture”? Official Information Act requests have exposed that the virologists do not do valid control experiments and this has been a problem ever since Enders and Peebles started the “virus” culture technique in the 1950s. Lack of valid controls = unscientific. I can only suggest to Watson that he digs a little deeper and examines the methodology of the papers rather than simply browse their headlines.
“Bailey and co. try to debunk all the methods that are used in virology and to deny the whole field of laboratory science. The only possible retort can be that no method is perfect, and experiments often fail to show what is being hypothesised. That is an argument for rather than against science, which constantly tries to improve its methods. I recall a whole room being dedicated to a huge amino acid sequencer when I was a PhD student. Now, amino acid sequencing can be done on a microchip.”
Dr Roger Watson, The Daily Sceptic
This is so full of non sequiturs that perhaps the best advice to Watson is that he needs an editor to help him communicate what he is trying to say to his readers. He should be able to clearly see my pro-science position in the video “Science vs Dogma”. My publications analysing virology have clearly pointed out that much of it involves uncontrolled experiments and thus cannot be claimed to be scientific. He refers to Karl Popper earlier in his article but fails to see that Popper would be horrified by the reasoning used by many virologists. How is an in silico “viral genome” that is created de novo from an unpurified specimen, that has been templated to another “viral genome” which was invented in the same way, falsifiable? How is a PCR result that “diagnoses” a disease on the basis that a positive result means you have the disease, falsifiable? I also suspect he is confusing complete in silico assembly of hypothetical “viral genomes” with actual physical sequencing, such as via the Sanger method, which he may have seen when he was a student. Computer games are indeed very seductive, particularly for kids but sometimes for adults too.
“I have had Covid, despite the remarkable claims by my virus denying friends to the contrary. How do I know I had it: it hit me like an express train; I felt terrible for two days and slept for 29 of 48 hours, rather like the flu. My taste was not lost but my sense of smell became incredibly deranged, not something that I had experienced after many bouts of flu in my 66 years.“
Dr Roger Watson, The Daily Sceptic
Watson appears to include this story about his bout of illness as evidence that viruses must exist. Despite it being another non sequitur, what is his definition of “COVID”? Virus Mania co-author Dr Claus Köhnlein pointed out in 2020 that it was nothing more than an imaginary clinical condition based on a new PCR “test” with no demonstrated clinical diagnostic capability. His interview in German reached over 1 million viewers before it was quickly shut down and his interview in English with me on Youtube had 125,000 views when it was shut down. It is still available here. I produced another popular video in 2020, “What Is A Covid-19 Case?” which outlines why “COVID” is a meaningless construct – which was also banned by Big Tech. In Dr Watson’s view how do we define a case: does a person dying in intensive care and an elite athlete running a marathon both have “COVID-19”? According to the WHO they should both be counted as equal “confirmed” cases if a PCR result is positive.
“When I felt worst, I reluctantly took a lateral flow test (LFT). This showed up positive almost instantly and with a thick test line. As I felt better the test – which as it uses antibodies is highly specific but not very sensitive – took longer to show and the line became fainter. Of course, the virus deniers have this one covered under the rubric that immunology is also bogus, antibodies are not at all specific and will pick up anything. My ‘gotcha’ to this is: if I run a pregnancy test which uses antibodies to detect human chorionic gonadotropin, will it show me I am pregnant?“
Dr Roger Watson, The Daily Sceptic
It is unclear if Watson is claiming that his lateral flow test proves the existence of viruses or “COVID” or both. What does he think the test is for? Something unique to the postulated “CoV” particle or a specific bodily process? Oh dear, we are back at square one! I have dealt with “COVID” LFTs previously and they are as equally unsuitable as the PCR with regards to clinical diagnostics and proving virus existence. With the rest of his claims, I’m not aware of who said antibodies pick up “anything” and it certainly wasn’t me. The issue surrounds assigning meaning to various proteins that can be detected through in vitro chemical reactions compared to what this informs us about health in real life. This topic has been outlined in Virus Mania and I also cover it in some of my other videos. His “gotcha” with regards to human chorionic gonadotropin has nothing to do with postulated viruses and related “immunology”. β-hCG is a specific glycoprotein of known composition and provenance that has been clinically validated for diagnosing pregnancy and can be easily compared to a “gold standard”: a foetal ultrasound scan (or the actual baby). As per many of Watson’s attempts, it’s another own goal. I can also suggest to him that if he has a positive result on a pregnancy test, as a man he’s unlikely to be pregnant and should be checked for cancer.
“The virus deniers who tend to promote their views on increasingly bizarre websites and within such a deafening echo chamber that they are completely unable to hear, yet alone contemplate, alternative views. They certainly don’t listen.“
Dr Roger Watson, The Daily Sceptic
What are these “bizarre” websites that he is referring to and what’s wrong with bizarre anyway? The orthodoxy doesn’t like being challenged Dr Watson. If they played like real scientists they’d welcome views that challenge their comfy status quo and we could all go on the same URLs. It may disturb Watson but the appetite for the content we produce seems very healthy. Our audience size is mostly restricted by Big Tech censorship and I’m sure he doesn’t agree with such interference with free speech. However, despite my Youtube channel being heavily suppressed, with millions of views being removed and people informing me that my videos and articles can’t be shared on platforms such as Facebook, the audience still grows every week. Mike Stone recently put together a list of websites that challenge the virus paradigm – I am in regular contact with many of these doctors, scientists and journalists and none have indicated that lack of demand is a problem. Last year, Mark and Dr John Bevan-Smith published their essay “The COVID-19 Fraud & War on Humanity”. Not only do they explain that there is no pathogen termed “SARS-CoV-2” but also why everyone should be sceptical about everything the virologists have ever claimed. They were tracking the viewership across various internet platforms for a few months before they gave up. By that stage it had reached about 250,000 people – I would say that’s a few hundred times more than most virologists are reaching with their papers. Watson’s “deafening echo chamber” may turn out to be his own case of tinnitus…
Postscript
Perhaps Dr Watson’s annoyance stems from the fact that because people get sick and die, he thinks it is unsporting to question the methods of the hard-working virologists? They are the white knights, so if we go against them – it means we must be on the wrong side. I don’t have all the answers as to why people get sick but the extensive research I’ve done informs me that pathogenic “viruses” do not seem to exist and are not the cause of disease. The tree of virology has borne no fruit for humanity unless that fruit is a multi-billion dollar pharmaceutical industry that targets enemies that have not been shown to exist. In the last two years, virology and germ theory have brought the planet to its knees, manifesting in anti-humanity measures such as face masks, stripping of civil rights, and mandated “vaccines”. For some of us, germ theory refuted itself at its inception and we see it for what it is: a tragic misunderstanding of nature, now used as propaganda in a perpetual phoney war, like something out of Orwell’s Nineteen Eighty-Four. Dr Watson can call us whatever names he likes – we see the universe in a different light and it is a light we choose to walk in. Perhaps he’ll take a stroll with us some day?
“There are three steps in the revelation of any truth: in the first, it is ridiculed; in the second, it is resisted; in the third, it is considered self-evident.” Arthur Schopenhauer
They confess: they had no virus when they concocted the test for the virus; they “contrived” a model by pretending to find what they wanted to find; it’s called a self-fulfilling prophecy
This is the con and the crime that drove millions of lives, and economies, into ruin
Quiz: If an agency of the federal government revealed they had no basis for constructing a diagnostic test that was used on millions of people; but the test was the cornerstone of a national lockdown; and the lockdown drove the economy off a cliff; and destroyed millions of lives; however, NOW, that agency says, they DO have a basis for the test; would you buy what they’re selling?
If your answer is yes, you’re in good company; the company I call Blind, Ignorant, Denialist, Hoaxing Journalists.
The CDC issued a document that bulges with devastating admissions.
“After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives.”
Many people believe this means the CDC is giving up on the PCR test as a means of “detecting the virus.” The CDC isn’t saying that at all.
They’re saying the PCR technology will continue to be used, but they’re replacing what the test is looking FOR with a better “reference sample.” A better marker. A better target. A better piece of RNA supposedly derived from SARS-CoV-2.
CDC/FDA are confessing there has been a PROBLEM with the PCR test which has been used to detect the virus, starting in February of 2020—right up to this minute.
In other words, the millions and millions of “COVID cases” based on the PCR test in use are all suspect. Actually, that statement is too generous. Every test result of every PCR test should be thrown out.
“During the early months of the Coronavirus Disease 2019 (COVID-19) pandemic, clinical specimens [of the virus] were not readily available to developers of IVDs [in vitro diagnostics] to detect SARS-CoV-2. Therefore, the FDA authorized IVDs based on available data from contrived samples generated from a range of SARS-CoV-2 material sources (for example, gene specific RNA, synthetic RNA, or whole genome viral RNA) for analytical and clinical performance evaluation. While validation using these contrived specimens provided a measure of confidence in test performance at the beginning of the pandemic, it is not feasible to precisely compare the performance of various tests that used contrived specimens because each test validated performance using samples derived from different gene specific, synthetic, or genomic nucleic acid sources.”
Translation: We, at the CDC, did not have a specimen of the SARS-CoV-2 virus when we concocted the PCR test for SARS-CoV-2. Yes, it’s unbelievable, right? And that’s the test we’ve been using all along. So we CONTRIVED samples of the virus. We fabricated. We lied. We made up (invented) synthetic gene sequences and we SAID these sequences HAD TO BE close to the sequence of SARS-CoV-2, without having the faintest idea of what we were doing, because, again, we didn’t have an actual specimen of the virus. We had no proof THERE WAS something called SARS-CoV-2.
This amazing FDA document goes to say the Agency has granted emergency approval to 59 different PCR tests since the beginning of the (fake) pandemic. 59. And, “…it is not feasible to precisely compare the performance of various tests that used contrived specimens because each test validated performance using samples derived from different gene specific, synthetic, or genomic nucleic acid sources.”
Translation: Each of the 59 different PCR tests for SARS-CoV-2 told different lies and concocted different fabrications about the genetic makeup of the virus—the virus we didn’t have. Obviously, then, these tests would give unreliable results. THE PCR TESTS USED CONTRIVED SPECIMENS OF THE VIRUS WE DIDN’T HAVE.
BUT, don’t worry, be happy, because NOW, the CDC and the FDA say, they really do have actual virus samples of SARS-CoV-2 from patients; they have better targets for the PCR test, and labs should start gearing up for the new and improved tests.
In other words, they were lying THEN, but they’re not lying NOW. They were “contriving,” but now they’re telling the truth.
If you believe that, I have Fountain of Youth water for sale, extracted from the lead-contaminated system of Flint, Michigan.
Here, once again, I report virology’s version of “we isolated the virus”:
They have a soup they make in their labs.
This soup contains human and monkey cells, toxic chemicals and drugs, and all sorts of other random genetic material. Because the cells start to die, the researchers ASSUME a bit of mucus from a patient they dropped in the soup is doing the killing, and THE VIRUS must be the killer agent in the mucus.
This assumption is entirely unwarranted. The drugs and chemicals could be doing the cell-killing, and the researchers are also starving the cells of vital nutrients, and that starvation could kill the cells.
There is no proof that SARS-CoV-2 is in the soup, or that it is doing the cell-killing, or that it exists.
Yet the researchers call cell-death “isolation of the virus.”
To say this is a non-sequitur is a vast understatement. In their universe, “We assume, without proof, we have the virus buried in a soup in a dish in the lab” equals, “We’ve separated the virus from all surrounding material.”
Virology equals “how to spread bullshit for a living and scare the world.” Other than that, it’s perfect.
Before we get to Christine Johnson’s interview, a bit of background.
My first book, AIDS INC., was published in 1988. The research I engaged in then formed a foundation for my recent work in exposing the vast fraud called COVID-19.
In 1987-88, my main question eventually became: does HIV cause AIDS? For months, I had blithely assumed the obvious answer was yes. This created havoc in my investigation, because I was facing contradictions I couldn’t solve.
For example, in parts of Africa, people who were chronically ill and dying obviously needed no push from a new virus. All their “AIDS” conditions and symptoms could be explained by their environment: contaminated water supplies; sewage pumped directly into the drinking water; protein-calorie malnutrition; hunger, starvation; medical treatment with immunosuppressive vaccines and drugs; toxic pesticides; fertile farm land stolen by corporations and governments; wars; extreme poverty. The virus cover story actually obscured all these ongoing crimes.
Finally, in the summer of 1987, I found several researchers who were rejecting the notion that HIV caused AIDS. Their reports were persuasive.
I’m shortcutting a great deal of my 1987-8 investigation here, but once HIV was out of the picture for me, many pieces fell into place. I discovered that, in EVERY group supposedly at “high-risk” for AIDS, their conditions and symptoms could be entirely explained by factors that had nothing to do with a new virus.
AIDS was not one condition. It was an umbrella label, used to re-package a number of immunosuppressive symptoms and create the illusion of a new and unique and single “pandemic.”
Several years after the publication of AIDS INC, I became aware of a quite different emerging debate going on under the surface of research: DOES HIV EXIST?
Was the purported virus ever truly discovered?
And THAT question led to: what is the correct procedure for discovering a new virus?
The following 1997 interview, conducted by brilliant freelance journalist, Christine Johnson, delves into these questions:
How should researchers prove that a particular virus exists? How should they isolate it? What are the correct steps?
These questions, and their answers, reside at the heart of most disease research—and yet, overwhelmingly, doctors never explore them or even consider them.
Johnson interviews Dr. Eleni Papadopulos, “a biophysicist and leader of a group of HIV/AIDS scientists from Perth in Western Australia. Over the past decade and more she and her colleagues have published many scientific papers questioning the HIV/AIDS hypothesis…”
Here I’m publishing and highlighting excerpts from the interview. Technical issues are discussed. Grasping them is not the easiest exercise you’ve ever done, but I believe the serious reader can comprehend the vital essentials.
Christine Johnson: Does HIV cause AIDS?
Eleni Papadopulos: There is no proof that HIV causes AIDS.
CJ: Why not?
EP: For many reasons, but most importantly, because there is no proof that HIV exists.
… CJ: Didn’t Luc Montagnier and Robert Gallo [purportedly the co-discoverers of HIV] isolate HIV back in the early eighties?
EP: No. In the papers published in Science by those two research groups, there is no proof of the isolation of a retrovirus from AIDS patients. [HIV is said to be a retrovirus.]
CJ: They say they did isolate a virus.
EP: Our interpretation of the data differs. To prove the existence of a virus you need to do three things. First, culture cells and find a particle you think might be a virus. Obviously, at the very least, that particle should look like a virus. Second, you have to devise a method to get that particle on its own so you can take it to pieces and analyze precisely what makes it up. Then you need to prove the particle can make faithful copies of itself. In other words, that it can replicate.
CJ: Can’t you just look down a microscope and say there’s a virus in the cultures?
EP: No, you can’t. Not all particles that look like viruses are viruses.
… CJ: My understanding is that high-speed centrifugation is used to produce samples consisting exclusively of objects having the same density, a so-called “density-purified sample.” Electron microscopy is used to see if these density-purified samples consist of objects which all have the same appearance — in which case the sample is an isolate — and if this appearance matches that of a retrovirus, in terms of size, shape, and so forth. If all this is true, then you are three steps into the procedure for obtaining a retroviral isolate. (1) You have an isolate, and the isolate consists of objects with the same (2) density and (3) appearance of a retrovirus. Then you have to examine this isolate further, to see if the objects in it contain reverse transcriptase [an enzyme] and will replicate when placed in new cultures. Only then can you rightfully declare that you have obtained a retroviral isolate.
EP: Exactly. It was discovered that retroviral particles have a physical property which enables them to be separated from other material in cell cultures. That property is their buoyancy, or density, and this was utilized to purify the particles by a process called density gradient centrifugation.
The technology is complicated, but the concept is extremely simple. You prepare a test tube containing a solution of sucrose, ordinary table sugar, made so the solution is light at the top but gradually becomes heavier, or more dense, towards the bottom. Meanwhile, you grow whatever cells you think may contain your retrovirus. If you’re right, retroviral particles will be released from the cells and pass into the culture fluids. When you think everything is ready, you decant a specimen of culture fluids and gently place a drop on top of the sugar solution. Then you spin the test tube at extremely high speeds. This generates tremendous forces, and particles present in that drop of fluid are forced through the sugar solution until they reach a point where their buoyancy prevents them from penetrating any further. In other words, they drift down the density gradient until they reach a spot where their own density is the same as that region of the sugar solution. When they get there they stop, all together. To use virological jargon, that’s where they band. Retroviruses band at a characteristic point. In sucrose solutions they band at a point where the density is 1.16 gm/ml.
That band can then be selectively extracted and photographed with an electron microscope. The picture is called an electron micrograph, or EM. The electron microscope enables particles the size of retroviruses to be seen, and to be characterized by their appearance.
CJ: So, examination with the electron microscope tells you what fish you’ve caught?
EP: Not only that. It’s the only way to know if you’ve caught a fish. Or anything at all.
CJ: Did Montagnier and Gallo do this?
EP: This is one of the many problems. Montagnier and Gallo did use density gradient banding, but for some unknown reason they did not publish any Ems [photos] of the material at 1.16 gm/ml…this is quite puzzling because in 1973 the Pasteur Institute hosted a meeting attended by scientists, some of whom are now amongst the leading HIV experts. At that meeting the method of retroviral isolation was thoroughly discussed, and photographing the 1.16 band of the density gradient was considered absolutely essential.
CJ: But Montagnier and Gallo did publish photographs of virus particles.
EP: No. Montagnier and Gallo published electron micrographs of culture fluids that had not been centrifuged, or even separated from the culture cells, for that matter. These EMs contained, in addition to many other things, including the culture cells and other things that clearly are not retroviruses, a few particles which Montagnier and Gallo claimed are retroviruses, and which all belonged to the same retroviral species, now called HIV. But photographs of unpurified particles don’t prove that those particles are viruses. The existence of HIV was not established by Montagnier and Gallo — or anyone since — using the method presented at the 1973 meeting.
CJ: And what was that method?
EP: All the steps I have just told you. The only scientific method that exists. Culture cells, find a particle, isolate the particle, take it to pieces, find out what’s inside, and then prove those particles are able to make more of the same with the same constituents when they’re added to a culture of uninfected cells.
CJ: So before AIDS came along there was a well-tried method for proving the existence of a retrovirus, but Montagnier and Gallo did not follow this method?
EP: They used some of the techniques, but they did not undertake every step including proving what particles, if any, are in the 1.16 gm/ml band of the density gradient, the density that defines retroviral particles.
CJ: But what about their pictures?
EP: Montagnier’s and Gallo’s electron micrographs…are of entire cell cultures, or of unpurified fluids from cultures…
—end of interview excerpt—
If you grasp the essentials of this discussion, you’ll see there is every reason to doubt the existence of HIV, because the methods for proving its existence were not followed.
Worse yet, it appears that Robert Gallo and Luc Montagnier, the two scientists credited with the discovery of HIV—as well as other elite researchers—were aware they weren’t employing correct methods.
And so…as I’ve reported, there is every reason to doubt and reject the existence of the COVID virus, SARS-CoV-2, since correct large-scale electron microscope studies have never been done. And by large-scale, I mean: attempting to find and photograph the virus in a cohort of, say, 1000 people who are supposed to be “pandemic patients.” I’m NOT talking about one or two electron-microscope photos accompanying a study.
But even that isn’t the end of the story. There is one further potential limiting factor in virus research. I became aware of it about a year ago. Analysis of electron microscope findings is fraught with difficulty and doubt. Are scientists actually looking at what they think they’re looking at in these photos? I refer readers to the work of neurobiologist Harold Hillman, who concluded that researchers were, for the most part, looking at artifacts, not actual cells or entities within cells. Another suppressed controversy.
After more than 30 years of investigating medical research fraud, my general conclusion is, the deeper you go the stranger it gets. Or to put it another way, the worse it gets.
In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
###
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals.
“HIV is neither necessary nor sufficient to cause AIDS.” ~ Luc Montagnier, VI Int’l AIDS Conference, Jun 24 1990
If you have been following the news recently, you may have heard that there is currently a new “highly virulent strain” of HIV running around the Netherlands (I think there is a pun in there somewhere). You may also have heard that there is a brand new experimental HIV mRNA vaccine that has shown promise in animals. If you have really been paying attention, you may have even heard of French virologist Luc Montagnier, the man credited with the discovery of HIV, and his various critical statements against the dangerous use of mRNA vaccines for “Covid-19.” If so, you are also most likely aware that during this increased attention geared towards HIV and mRNA vaccines, Luc Montagnier died very recently on February 8th, 2022. While he lived to be the ripe old age of 89, many are suspicious of the timing of his death in light of the current HIV resurgence.
While I do find the timing of all of these events interesting, that is not what this article is about. I have always planned to dive into Montagnier’s original HIV paper but I have held off as the HIV/AIDS scam has been exposed brilliantly by many others before me. However, I have always felt that the HIV fraud is the perfect gateway into understanding the “Covid-19” fraud as the numerous parallels to what is going on today are uncanny. We can see the same misuse of PCR and antibody testing, the same rebranding and reuse of toxic pharmaceuticals, the same collection of various symptoms under one giant umbrella disease, the same propaganda spreading fear of the infected, and the same Anthony Fauci spearheading the whole thing. Even though it is not my intention to touch on all of these aspects in one article, the best place to start unravelling this tangled web of deceit begins with the man who was credited with unleashing the HIV monster upon the world, Luc Montagnier.
In 1983, Montagnier was sent a lymph node sample from a 33-year-old (note the age) male determined to have the symptoms of AIDS. From this sample, Montagnier and his team uncovered what they claimed was a new “retrovirus,” originally known as L.A.V., for lymphadenopathy associated “virus.” After several indirect experiments, the team concluded that further studies were needed in order to determine whether or not the new “virus” had any role in the etiology of AIDS. After this initial discovery of the potential “viral” cause of AIDS, there was a bit of drama in 1984 when American virologist Robert Gallo claimed to have uncovered the cause of AIDS himself with the discovery of HTLV-3. Long story short, it was later determined that Gallo had used/borrowed/stolen a sample from the same patient as Montagnier and uncovered the same “virus.” The “virus” was eventually renamed HIV in 1986 and in 2008, Luc Montagnier was awarded the Nobel Prize for the discovery while Robert Gallo pouted off in a dark corner somewhere.
One of the nicest aspects of writing about Montagnier’s original HIV paper now in 2022 is that in retrospect, Montagnier himself tore apart his own evidence for the existence of his “retrovirus” in the decades following the publishing of his 1983 paper. A perfect example of this is found in a 1997 interview Montagnier did with scientific journalist Djamel Tahi. I have provided highlights from this interview below yet I definitely recommend reading the whole discussion sometime. While reading, note the assumptions made by Montagnier about his “virus,” the various contradictions in his statements, and the revelations about the relation (or lack thereof) of HIV to AIDS. This interview provides an in-depth look into the illogical mindframe of a virologist stuck in unproven theories and pseudoscientific dogma:
Interview with Professor Luc Montagnier by Djamel TAHI – (Pasteur Institut, July 1997)
Djamel TAHI: A group of scientists from Australia argues that nobody up till now has isolated the AIDS virus, HIV. For them the rules of retrovirus isolation have not been carefully respected for HIV. These rules are: culture, purification of the material by ultracentrifugation, Electron Microscopic (EM) photographs of the material which bands at the retrovirus density, characterisation of these particles, proof of the infectivity of the particles.
Luc Montagnier: No, that is not isolation. We did isolation because we “passed on” the virus, we made a culture of the virus. For example Gallo said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.” But before making it emerge in immortal cell lines, we made it emerge in cultures of normal Iymphocytes from a blood donor. That is the principle criterion. One had something one could pass on serially, that one could maintain. And characterised as a retrovirus not only by its visual properties, but also biochemistry, RT [reverse transcriptase] activity which is truly specific of retroviruses. We also had the reactions of antibodies against some proteins, probably the internal proteins. I say probably by analogy with knowledge of other retroviruses. One could not have isolated this retrovirus without knowledge of other retroviruses, that’s obvious. But I believe we have answered the criteria of isolation. Totally.
Djamel TAHI: according to several published references cited by the Australian group, RT is not specific to retroviruses and moreover your work to detect RT was not done in the purified material?
Luc Montagnier: I believe we published in Science (May 1983) a gradient which showed that the RT had exactly the density of 1.16. So one had a ‘peak’ which was RT. So one has fulfilled this criterion for purification. But to pass it on serially is difficult because when you put the material in purification, into a gradient, retroviruses are very fragile, so they break each other and greatly lose their infectivity. But I think even so we were able to keep a little of their infectivity. But it was not as easy as one does it today, because the quantities of virus were nonetheless very feeble. At the beginning we stumbled on a virus which did not kill cells. The virus came from an asymptomatic patient and so was classified amongst the non-syncithia-forming, non-cytopathogenic viruses using the co-receptor ccr5 . It was the first BRU virus. One had very little of it, and one could not pass it on in an immortal cell line. We tried for some months, we didn’t succeed. We succeeded very easily with the second strain. But there lies the quite mysterious problem of the contamination of that second strain by the first. That was LAI.
Djamel TAHI: Why do the EM photographs published by you, come from the culture and not from the purification?
Luc Montagnier: There was so little production of virus it was impossible to see what might be in a concentrate of virus in the gradient. There was not enough virus to do that. Of course one looked for it, one looked for it in the tissues at the start, likewise in the biopsies. We saw some particles but they did not have the morphology typical of retroviruses. They were very different. Relatively different. So with the culture it took many hours to find the first pictures. It was a Roman effort! It’s easy to criticise after the event. What we did not have, and I have always recognised it, was that it was truly the cause of aids.
Djamel TAHI: How is it possible without EM pictures from the purification, to know whether or not these particles are viral and appertain to a retrovirus, moreover a specific retrovirus?
Luc Montagnier: Well, there were the pictures of the budding. We published images of budding which are characteristic of retroviruses. Having said that, on the morphology alone one could not say it was truly a retrovirus. For example, a French specialist of EMs of retroviruses publicly attacked me saying: “This is not a retrovirus, it is an arenavirus”. Because there are other families of virus which bud and have spikes on the surface, etc.
Djamel TAHI: Why this confusion? The EM pictures did not show clearly a retrovirus?
Luc Montagnier: At this period the best known retroviruses were those of type C, which were very typical. This retrovirus wasn’t a type C and lentiviruses were little known. I myself recognised it by looking at pictures of Equine infectious anaemia virus at the library, and later of the visna virus. But I repeat, it was not only the morphology and the budding, there was RT…it was the assemblage of these properties which made me say it was a retrovirus.
Djamel TAHI: About the RT, it is detected in the culture. Then there is purification where one finds retroviral particles. But at this density there are a lot of others elements, among others those which one calls “virus-like”.
Luc Montagnier: Exactly, exactly. If you like, it is not one property but the assemblage of the properties which made us say it was a retrovirus of the family of lentiviruses. Taken in isolation, each of the properties isn’t truly specific. It is the assemblage of them. So we had: the density, RT, pictures of budding and the analogy with the visna virus. Those are the four characteristics.
Djamel TAHI: But how do all these elements allow proof that it is a new retrovirus? Some of these elements could appertain to other things, “virus-like”…?
Luc Montagnier: Yes, and what’s more we have endogenous retroviruses which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles, in any case not in aids.
Djamel TAHI: But then how can one make out the difference?
Luc Montagnier: Because we could “pass on” the virus. We passed on the RT activity in new Iymphocytes. We got a “peak” of replication. We kept track of the virus. It is the assembly of properties which made us say it was a retrovirus. And why new? The first question put to us by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse retrovirus or an animal retrovirus?”. To that one could say no! Because we had shown that the patient had antibodies against a protein of his own virus. The assemblage has a perfect logic! But it is important to take it as an assemblage. If you take each property separately, they are not specific. It is the assemblage which gives the specificity.
Djamel TAHI: With what did you culture the lymphocytes of your patient? With the H9 cell line?
Luc Montagnier: No, because it didn’t work at all with the H9. We used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes.
Djamel TAHI: When one looks at the published electron microscope photographs, for you as a retrovirologist it is clear it’s a retrovirus, a new retrovirus?
Luc Montagnier: No, at that point one cannot say. With the first budding pictures it could be a type C virus. One cannot distinguish.
Djamel TAHI: Could it be anything else than a retrovirus?
Luc Montagnier: No…well, after all, yes…it could be another budding virus. But we have an atlas. One knows a little bit from familiarity, what is a retrovirus and what is not. With the morphology one can distinguish but it takes a certain familiarity.
Djamel TAHI: Why no purification?
Luc Montagnier: I repeat we did not purify. We purified to characterise the density of the RT, which was soundly that of a retrovirus. But we didn’t take the “peak”…or it didn’t work…because if you purify, you damage. So for infectious particles it is better to not touch them too much. So you take simply the supernatant from the culture of lymphocytes which have produced the virus and you put it in a small quantity on some new cultures of lymphocytes. And it follows, you pass on the retrovirus serially and you always get the same characteristics and you increase the production each time you pass it on.
Djamel TAHI: But there comes a point when one must do the characterisation of the virus. This means: what are the proteins of which it’s composed?
Luc Montagnier: That’s it. So then, analysis of the proteins of the virus demands mass production and purification. It is necessary to do that. And there I should say that that partially failed. J.C. Chermann was in charge of that, at least for the internal proteins. And he had difficulties producing the virus and it didn’t work. But this was one possible way, the other way was to have the nucleic acid, cloning, etc. It’s this way which worked very quickly. The other way didn’t work because we had at that time a system of production which wasn’t robust enough. One had not enough particles produced to purify and characterise the viral proteins. It couldn’t be done. One couldn’t produce a lot of virus at that time because this virus didn’t emerge in the immortal cell line. We could do it with the LAI virus, but at that time we did not know that.
Djamel TAHI: Gallo did it?
Luc Montagnier: Gallo?…I don’t know if he really purified. I don’t believe so. I believe he launched very quickly into the molecular part, that’s to say cloning. What he did do is the Western Blot. We used the RIPA technique, so what they did that was new was they showed some proteins which one had not seen well with the other technique. Here is another aspect of characterising the virus. You cannot purify it but if you know somebody who has antibodies against the proteins of the virus, you can purify the antibody/antigen complex. That’s what one did. And thus one had a visible band, radioactively labelled, which one called protein 25, p25. And Gallo saw others. There was the p25 which he calledp24, there was p41 which we saw…
Djamel TAHI: About the antibodies, numerous studies have shown that these antibodies react with other proteins or elements which are not part of HIV. And that they can not be sufficient to characterise the proteins of HIV.
Luc Montagnier: No! Because we had controls. We had people who didn’t have AIDS and had no antibodies against these proteins. And the techniques we used were techniques I had refined myself some years previously, to detect the src gene. You see the src gene was detected by immunoprecipitation too. It was the p60 [protein 60]. I was very dexterous, and my technician also, with the RIPA technique. If one gets a specific reaction, it’s specific.
Djamel TAHI: But we know AIDS patients are infected with a multitude of other infectious agents which are susceptible to induce crossreactions.
Luc Montagnier: Yes, but antibodies are very specific. They know how to distinguish one molecule in one million. There is a very great affinity. When antibodies have sufficient affinity, you fish out something really very specific. With monoclonal antibodies you fish out really ONE protein. All of that is used for diagnostic antigen detection.
Djamel TAHI: For you the p41 was not of viral origin and so didn’t belong to HIV. For Gallo it was the most specific protein of the HIV. Why this contradiction?
Luc Montagnier: We were both reasonably right. That’s to say that I in my RIPA technique…in effect there are cellular proteins that one meets everywhere – there’s a non-specific “background noise”, and amongst these proteins one is very abundant in cells, which is actin. And this protein has a molecular weight 43000kd. So, it was there. So I was reasonably right, but what Gallo saw on the other hand was the gp41 of HIV, because he was using the Western Blot. And that I have recognised.
Djamel TAHI: For you p24 was the most specific protein of HIV, for Gallo not at all. One recognises thanks to other studies that antibodies directed against p24 were often found in patients who were not infected with HIV, and even certain animals. In fact today, an antibody reaction with p24 is considered non specific.
Luc Montagnier: It is not sufficient for diagnosing HIV infection.
Djamel TAHI: No protein is sufficient.
Luc Montagnier: No protein is sufficient anyway. But at the time the problem didn’t reveal itself like that. The problem was to know whether it was an HTLV or not. The only human retrovirus known was HTLV. And we showed clearly that it was not an HTLV, that Gallo’s monoclonal antibodies against the p24 of HTLV did no recognise the p25 of HIV.
Djamel TAHI: At the density of retroviruses, 1.16, there are a lot of particles, but only 20% of them appertain to HIV. Why are 80% of the proteins not viral and the others are? How can one make out the difference?
Luc Montagnier: There are two explanations. For the one part, at this density you have what one calls microvesicles of cellular origin, which have approximately the same size as the virus, and then the virus itself, in budding, brings cellular proteins. So effectively these proteins are not viral, they are cellular in origin. So, how to make out the difference?! Frankly with this technique one can’t do it precisely. What we can do is to purify the virus to the maximum with successive gradients, and you always stumble on the same proteins.
Djamel TAHI: The others disappear?
Luc Montagnier: Let’s say the others reduce a little bit. You take off the microvesicles, but each time you lose a lot of virus, so it’s necessary to have a lot of virus to start off in order to keep a little bit when you arrive at the end. And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of viral origin or not. That’s what we began for p25, that failed…and the other technique is to do the cloning, and so then you have the DNA and from the DNA you get the proteins. You deduce the sequence of the proteins and their size and, you stumble again on what you’ve already observed with immunoprecipitation or with gel electrophoresis. And one knows by analogy with the sizes of the proteins of other retroviruses, one can deduce quite closely these proteins. So you have the p25 which was close to the p24 of HTLV, you have the p18.. in the end you have the others. On the other hand the one which was very different was the very large protein, p120.
Luc Montagnier’s 1997 interview is a highlight reel of revelations. We can see clearly, as Montagnier repeated on more than one occasion, that he himself (and Robert Gallo according to his knowledge) did not purify any “virus.” Why is this important? In order to determine whether a “virus” actually exists, the particles must be purified (freed from contaminants, pollutants, and foreign elements) so that they can be isolated (separated from everything else). Only once this occurs can the particles assumed to be “virus” then be proven pathogenic through experimentation. Only purified particles can be used to visualize as well as biochemically and molecularly characterize the “virus” in order to determine specific proteins, antibodies, genomic sequence, electron microscopy imaging, etc. Without purification, one can not determine that the “virus” exists at all and the non-specific laboratory results obtained from unpurified material are absolutely meaningless.
As most virologists do, Montagnier claimed that even though he did not purify the “virus” and therefore did not have direct evidence for its existence, he had plenty of non-specific indirect evidence that when added together, became “specific” to the “virus.” It was the accumulation of indirect evidence that proved his “virus” existed. In essence, he had a circumstantial case based upon evidence that was not drawn from direct observation. This would be considered a weak case in a court of law.
Looking at his circumstantial case, Montagnier admitted that without purification, images of particles taken from electron microscopy could not be definitively claimed to be “retroviruses” or “viruses” of any kind based on morphological appearance alone. He stated that it was necessary to have knowledge of other “retroviruses” first in order to discover a new one. He himself referred to an atlas of images of other “retroviruses” in order to claim that his unpurified particles were also “retroviruses.”
However, what Montagnier did not admit is that this atlas of “retroviruses” was also made up of images of unpurified particles. Therefore, none of the particles imaged in his atlas could be considered “retrovirus” particles until evidence of purified/isolated “retroviruses” are released. Purification would have had to have occurred with the very first “retrovirus” ever discovered and imaged in order for this method of identification to be valid. Montagnier admitted that while purification is a necessary step, it is impossible as the more you purify the sample, the more damage occurs to the particles and the less “virus” you have at the end. Since he stated that they did not purify the culture used to obtain the EM images of “HIV,” there is no proof that the random particles claimed to be HIV are in fact a “virus” at all.
Montagnier also tried to claim that antibodies/antigens, such as the p24 protein, are specific to HIV and that they can be used as part of the evidence for the existence of his “virus.” However, as Djamel expertly pointed out, these proteins are not specific to HIV as there are over 60 conditions (such as pregnancy, tuberculosis, the flu vaccine, etc.) with related proteins that can trigger positive HIV tests. Montagnier ended up admitting that no protein is sufficient for diagnosing HIV thus nullifying any claims he made about the specificity of antibodies/antigens and their value in being used as indirect evidence for the existence of an unseen “virus.”
The biggest revelation by Montagnier in this 1997 interview is his belief that HIV is not the cause of AIDS. While he believed he had discovered a new “retrovirus” based on an accumulation of weak indirect evidence, according to his statement it was not pathogenic. If we take his indirect evidence and break it down, Motagnier did not have purified “virus” particles which means his EM images are useless, his antibody tests are meaningless, and the genomic sequence is worthless. Without purified particles, he had no proof of pathogeniticity as he had no valid independent variable in order to establish cause and effect. It is amazing that Montagnier believed he had a “virus” at all as in every meaningful way possible, he did not have evidence of one.
All of that being said, for those still interested in reading Montagnier’s original 1983 paper containing no evidence of any “virus” whatsoever, here is the paper in its entirety:
Isolation of a T-Lymphotropic Retrovirus from a Patientat Risk for Acquired Immune Deficiency Syndrome (AIDS)
Abstract. A retrovirus belonging to the family of recently discovered human T-cell leukemia viruses (HTLV), but clearly distinct from each previous isolate, has been isolated from a Caucasian patient with signs and symptoms that often precede the acquired immune deficiency syndrome (AIDS). This virus is a typical type-C RNA tumor virus, buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24. Antibodies from serum of this patient react with proteins from viruses of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate. The virus from this patient has been transmitted into cord blood lymphocytes, and the virus produced by these cells is similar to the original isolate.
From these studies it is concluded that this virus as well as the previous HTLV isolates belong to a general family of T-lymphotropic retroviruses that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS.The acquired immune deficiency syndrome (AIDS) has recently been recognized in several countries (1). The disease has been reported mainly in homosexual males with multiple partners, and epidemiological studies suggest horizontal transmission by sexual routes (2) as well as by intravenous drug administration (3), and blood transfusion (4).
The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes (5) suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent. Alternatively, these modifications may result from subsequent infections. The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma (1). However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males (6) and infants (7) who may or may not develop AIDS (8).
The histological aspect of such lymph nodes is that of reactive hyperplasia. Such cases may correspond to an early or a milder form of the disease. We report here the isolation of a novel retrovirus from a lymph node of a homosexual patient with multiple lymphadenopathies. The virus appears to be a member of the human T-cell leukemia virus (HTLV) family (9).
The retrovirus was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans. Viral core proteins were not immunologically related to the p24 and p19 proteins of subgroup I of HTLV (9). However, serum of the patient reacted strongly with surface antigen (or antigens) present on HTLV-I-infected cells. Moreover, the ionic requirements of the viral reverse transcriptase were close to that of HTLV. Recently, a type-C retrovirus was also identified in T cells from a patient with hairy cell leukemia. Analysis of the proteins of this virus showed they were related to, but clearly different from, proteins of previous HTLV isolates (10).
Moreover, recent studies of the nucleic acid sequences of this new virus show it is less than 10 percent homologous to the earlier HTLV isolates (11). This virus was called HTLV-II to distinguish it from all the earlier, highly related viruses termed HTLV-I. The new retrovirus reported here appears to also differ from HTLV-II. We tentatively conclude that this virus, as well as all previous HTLV isolates, belong to a family of T-lymphotropic retroviruses that are horizontallytransmitted in humans and may be involved in several pathological syndromes, including AIDS.
The patient was a 33-year-old homosexual male who sought medical consultation in December 1982 for cervical lymphadenopathy and asthenia (patient 1). Examination showed axillary and inguinal lymphadenopathies. Neither fever nor recent loss of weight were noted. The patient had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982. During interviews he indicated that he had had more than 50 sexual partners per year and had traveled to many countries, including North Africa, Greece, and India. His last trip to New York was in 1979.
Laboratory tests indicated positive serology (immunoglobulin G) for cytomegalovirus (CMV) and Epstein-Barr virus. Herpes simplex virus was detected in cells from his throat that were cultured on human and monkey cells. A biopsy of a cervical lymph node was performed. One sample served for histological examination, which revealed follicular hyperplasia without change of the general architecture of the lymph node. Immunohistological studies revealed, in paracortical areas, numerous T lymphocytes (OKT3+). Typing of the whole cellular suspension indicated that 62 percent of the cells were T lymphocytes (OKT3+), 44 percent were T-helper cells (OKT4+), and 16 percent were suppressor cells (OKT8+).
Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon (12). The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by viruses, including retroviruses. In the mouse system, we had previously shown that antiserum to interferon could increase retrovirus production by a factor of 10 to 50 (13). After 3 days, the culture was continued in the same medium without PHA. Samples were regularly taken for assay of reverse transcriptase and for examination in the electron microscope.
After 15 days of culture, a reversetranscriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I (14). Virus production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation. Peripheral blood lymphocytes cultured in the same way were consistently negative for reverse transcriptase activity, even after 6 weeks. Cytomegalovirus could be detected, upon prolonged co-cultivation with MRC5 cells, in the original biopsy tissue, but not in the cultured T lymphocytes at any time of the culture.
Virus transmission was attempted with the use of a culture of T lymphocytes established from an adult healthy donor of the Blood Transfusion Center at the Pasteur Institute. On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions. Reverse transcriptase activity could be detected in the supernatant on day 15 of the coculture but was not detectable on days 5 and 10. The reverse transcriptase had the same characteristics as that released by the patient’s cells and the amount released remained stable for 15 to 20 days. Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks whenthe culture was discontinued.
The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml). After a lag period of 7 days, a relatively high titer of reverse transcriptase activity was detected in both of the cord lymphocyte cultures. Identical cultures, which had not been infected, remained negative. These two successive infections clearly show that the virus could be propagated on normal lymphocytes from either newborns or adults.
That this new isolate was a retrovirus was further indicated by its density in a sucrose gradient, which was 1.16, and by its labeling with [3H]uridine (Fig. 1). Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane (Fig. 2).
Virus-infected cells from the original biopsy as well as infected lymphocytes from the first and second viral passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme. The results were the same in all instances. The reverse transcriptase activity displayed a strong affinity for poly(adenylate-oligodeoxythymidylate) [poly(A) -oligo(dT)], and required Mg2+ with an optimal concentration (5 mM) slightly lower than that for HT (14) and an optimal pH of 7.8. The reaction was not inhibited by actinomycin D. This character, as well as the preferential specificity for riboseadenylate *deoxythymidylate over deoxyadenylate * deoxythymidylate, distinguish the viral enzyme from DNA-dependent polymerases.
We then determined whether or not this isolate was indistinguishable from HTLV-1 isolates. Human T-cell leukemia virus has been isolated from cultured T lymphocytes of patients with T lymphomas and T leukemias [for a review, see (9)]. The antibodies used were specific for the p19 and p24 core proteins of HTLV-I. A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytes obtained from a healthy donor and infected with the same virus. As shown in Table 1, the virus-producing cells did not react with either type of antibody, whereas two lines of cord lymphocytes chronically infected with HTLV (17) and used as controls showed strong surface fluorescence.
When serum from patient 1 was tested against infected lymphocytes from the biopsy the surface fluorescence was as ntense as that of the control HTLV-producing lines. This suggests that serum of the patient contains antibodies
that recognize a common antigen present on HTLV-I-producing cells and on the patient’s lymphocytes. Similarly, cord lymphocytes infected with the virus from patient 1 did not react with antibodies to p19 or p24. Only a minor proportion of the cells (about I percent) reacted with the patient’s serum. This may indicatethat only this fraction of the cells was infected and produced virus. Alternatively, the antigen recognized by the patient’s serum may contain cellular determinants that show less expression in T lymphocytes of newborns.
We also cultured T lymphocytes from a lymph node of another patient (patient 2) who presented with multiple adenopathies and had been in close contact with an AIDS case. These lymphocytes did not produce viral reverse transcriptase; however, they reacted in the immunofluorescence assay with serum from patient 1. Moreover, serum from patient 2 reacted strongly with control HTLV-producing lines (not shown). In order to determine which viral antigen was recognized by antibodies present in’ the two patients’ sera, several immunoprecipitation experiments were carried out. Cord lymphocytes infected with virus from patient I and uninfected controls were labeled with [35S]methionine for 20 hours. Cells were lysed with detergents, and a cytoplasmic S10 extract was made. Labeled virus released in the supernatant was banded in a sucrose gradient.
Both materials were immunoprecipitated by antiserum to HTLV- I p24, by serum from patients 1 and 2, and by serum samples from healthy donors. Immunocomplexes were analyzed by polyacrylamide gel electrophoresis under denaturing conditions. Figure 3 shows that a p25 protein present in the virus-infected cells from patient 1 and in LC1 cells infected with this virus, was specifically recognized by serum from patients I and 2 but not by antiserum to HTLV-1 p24 or serum of normal donors.
Conversely, the p24 present in control HTLV-infected cell extracts was recognized by antibodies to HTLV but not by serum from patient 1. A weak band (lane 2, Fig. 3B) could hardly be seen with serum from patient 2, suggesting some similarities of the p25 protein from this patient’s cells with HTLV-1 p24. When purified, labeled virus from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000. The 45K protein may be dueto contamination of the virus by cellular actin which was present in immunoprecipitates of all the cell extracts (Fig. 3).
These results, together with the immunofluorescence data, indicate that the retrovirus from patient 1 contains a major p25 protein, similar in size to that of HTLV-I but different immunologically. The DNA sequences of these and other members of the HTLV family are being compared. All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful.
The role of this virus in the etiology of AIDS remains to be determined. Patient 1 had circulating antibodies against the virus, and some of the latter persisted in lymphocytes of his lymph node (or nodes). The virus-producing lymphocytes seemed to have no increased growth potential in vitro compared to the uninfected cells. Therefore, the multiple lymphadenopathies may represent a host reaction against the persistent viral infection rather than hyperproliferation of virus-infected lymphocytes. Other factors, such as repeated infection by the same virus or other bacterial and viral agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity.
doi: 10.1126/science.6189183.
That’s an impressive circle. Montagnier looks quite pleased with his creation.
In Summary:
According to HIV discoverer Luc Montagnier, they did “isolate” HIV because they “passed on” the “virus” and they made a culture of the “virus”
He stated that Robert Gallo (American virologist who plagiarized Montagnier’s work) said: “They have not isolated the virus…and we (Gallo et al.), we have made it emerge in abundance in an immortal cell line.”
But before making it emerge in immortal cell lines, Montagnier claimed his team made it emerge in cultures of normal Iymphocytes from a blood donor
Montagnier stated that it is obvious one could not have isolated any retrovirus without knowledge of other “retroviruses”
To pass a “virus” on serially is difficult because when you put the material in purification, into a gradient, “retroviruses” are very fragile, so they break each other and greatly lose their infectivity
At the beginning they stumbled on a “virus” which did not kill cells
It was the first BRU “virus,” yet they had very little of it and could not pass it on in an immortal cell line
They were later successful with the second strain yet Montagnier stated that there lies the quite mysterious problem of the contamination of that second strain by the first which was LAI
Quick sidenote: BRU and LAI are considered the first strains of HIV
“The original isolate HIV-1 Bru, formerly called LAV, was derived from patient BRU. HIV-1 Lai was derived from patient LAI and contaminated a HIV-1 Bru culture between 20 July and 3 August 1983. The culture became, in effect, HIV-1 Lai, identifiable by a unique motif in the V3 loop. Because of this contamination two, rather than one, HIV-1 isolates were sent to the Laboratory of Tumor Cell Biology at the National Cancer Institute on 23 September 1983.”
When asked about the lack of purification for EM imaging of HIV, Montagnier stated that there was so little production of “virus”it was impossible to see what might be in a concentrate of “virus” in the gradient
What they saw were some particles but they did not have the morphology typical of “retroviruses” as they were very different
He claimed it was “a Roman effort” with the culture as it took many hours to find the first pictures
On the morphology alone one could not say the EM images were truly a “retrovirus”
A French specialist of EMs of “retroviruses” publicly attacked Montagnier saying: “This is not a retrovirus, it is an arenavirus” as there are other families of “virus” which bud and have spikes on the surface, etc.
He stated that it was not only the morphology and the budding, but that there was reverse transcriptase
It was not one property but the assemblage of the properties which made them say it was a “retrovirus” of the family of “lentiviruses”
Taken in isolation, each of the properties isn’t truly specific
The four properties were:
The density
Reverse Transcriptase
Pictures of budding
The analogy with the visna “virus”
Montagnier stated that we have endogenous (human origin) “retroviruses” which sometimes express particles – but of endogenous origin, and which therefore don’t have pathological roles
The first question put to them by Nature was: “Is it not a laboratory contamination? Is it perhaps a mouse “retrovirus” or an animal “retrovirus?”
Montagnier stated that it was important to take it as an assemblage as if you take each property separately, they are not specific and it is the assemblage which gives the specificity
When culturing the “virus,” they used a lot of cell lines and the only one which could produce it was the Tampon (!?) Iymphocytes
He admitted that when viewing EM images, one cannot distinguish if the particle is a “retrovirus” or not
They used an atlas of previous “retroviruses” to determine if the “virus” had the morphology of one as it takes a certain familiarity to distinguish them
Montagnier repeated they did not purify the “virus” because if you purify, you damage the “virus” particles
He stated that for infectious particles, it is better to not touch them too much
Analysis of the proteins of the “virus” demands mass production and purification and so it is necessary to do that
In that regard, Montagnier claimed that they partially failed
They did not have enough particles produced to purify and characterise the “viral” proteins as it couldn’t be done
They couldn’t produce a lot of “virus” at that time because the “virus” didn’t emerge in the immortal cell line
Montagnier stated that he believed Gallo also did not purify and he believed Gallo had launched very quickly into the molecular cloning part
He also said that you cannot purify the “virus” but if you know somebody who has antibodies against the proteins of the “virus,” you can purify the antibody/antigen complex
However, this is a complete contradiction as he claimed that purification needed to be done in order to characterise the proteins of the “virus,” so if you can’t purify the “virus” to characterise the proteins, you would be unable to know which proteins act against the “virus”as well as any specific antibodies reacting to them
Montagnier claimed antibodies are very specific and that they know how to distinguish one molecule in one million
With monoclonal antibodies you fish out really ONE protein and all of that is used for diagnostic antigen detection
There are cellular proteins that one meets everywhere – there’s a non-specific “background noise”
An antibody reaction with p24 is considered non specific and it is not sufficient for diagnosing HIV infection
Montagnier agreed that no protein is sufficient to diagnose HIV
When asked why, at the 1.16 density gradient band, 80% of the particles are “non-viral” and only 20% are HIV, Montagnier explained that at this density, there are microvesicles of cellular origin, which have approximately the same size as the “virus,” and then the “virus” itself, in budding, brings cellular proteins
Effectively these proteins are not “viral” and are cellular in origin
He stated that with this technique one can’t differentiate them precisely
If you purify the “virus” to the maximum with successive gradients, you always stumble on the same proteins
Montagnier stated that the other proteins only reduce a little bit as you can take off the microvesicles, but each time you lose a lot of “virus,” so it’s necessary to have a lot of “virus” to start off in order to keep a little bit when you arrive at the end
And then again it’s the molecular analysis, it’s the sequence of these proteins which is going allow one to say whether they are of “viral” origin or not
However, what Montagnier doesn’t seem to understand is that if you can not purify the “virus” in order to determine which proteins belong to the “virus,” sequencing proteins will not tellyou if they are “viral” or not
This “virus” is a typical type-C RNA tumor “virus,” buds from the cell membrane, prefers magnesium for reverse transcriptase activity, and has an internal antigen (p25) similar to HTLVp24
Antibodies from serum of this patient react with proteins from “viruses” of the HTLV-I subgroup, but type-specific antisera to HTLV-I do not precipitate proteins of the new isolate
Remember, Montagnier admitted they did not purify the “virus” and that purification was necessary in order to characterise the proteins of the “virus, so how would they know if the antibodies are reacting to “virus” proteins?
The “virus” from this patient has been transmitted into cord blood lymphocytes, and the “virus” produced by these cells is similar to the original isolate
From these studies it is concluded that this “virus” as well as the previous HTLV isolates belong to a general family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
The pronounced depression of cellular immunity that occurs in patients with AIDS and the quantitative modifications of subpopulations of their T lymphocytes suggest that T cells or a subset of T cells might be a preferential target for the putative infectious agent
Alternatively, these modifications may result from subsequent infections
The depressed cellular immunity may result in serious opportunistic infections in AIDS patients, many of whom develop Kaposi’s sarcoma
However, a picture of persistent multiple lymphadenopathies has also been described in homosexual males and infants who may or may not develop AIDS
The “retrovirus” was propagated in cultures of T lymphocytes from a healthy adult donor and from umbilical cord blood of newborn humans
They tentatively (i.e. subject to further confirmation; not definitely) concluded that this “virus,” as well as all previous HTLV isolates, belong to a family of T-lymphotropic “retroviruses” that are horizontally transmitted in humans and may be involved in several pathological syndromes, including AIDS
The patient the “virus” came from had a history of several episodes of gonorrhea and had been treated for syphilis in September 1982
Oddly enough, syphilis has the exact same symptoms of AIDS and the usual treatment is a series of Penicllin injections, which coincidentally (or not) can destroy a person’s “immune” system
Laboratory tests indicated positive serology (immunoglobulin G) for “cytomegalovirus” (CMV) and Epstein-Barr “virus“
Herpes simplex “virus” was detected in cells from his throat that were cultured on human and monkey cells
Cells of the same biopsied lymph node were put in culture medium with phytohemagglutinin (PHA), T-cell growth factor (TCGF), and antiserum to human a interferon
The reason for using this antiserum was to neutralize endogenous interferon which is secreted by cells chronically infected by “viruses,” including “retroviruses”
After 15 days of culture, a reverse transcriptase activity was detected in the culture supernatant by using the ionic conditions described for HTLV-I and “virus” production continued for 15 days and decreased thereafter, in parallel with the decline of lymphocyte proliferation
Quick sidenote: Montagnier stated here that the “virus” was cultured for 30 days, as it took 15 days for the reverse transcriptase activity to be detected and another 15 days for the “virus” production to decrease. Interestingly, in a paper he wrote in 2003, Montagnier stated this:
“The initial clinical isolate, unlike HTLV, had no transforming or cytopathic effects on T lymphocytes. Barré-Sinoussi notes in her commentary that the lymphocyte culture I started from the patient’s lymph node biopsy died after 4 weeks. But this was anticipated as soon as we realized that the cells were not transformed, because normal cultures of the same type also die within this time period.The need for succesive use of peripheral blood mononuclear cells to maintain a viral culture was therefore a likely hypothesis that proved to be correct. The virus would later be classified as non-syncytium-inducing, as is usually the case for viruses isolated from recently infected HIV patients who are either asymptomatic or present with lymphadenopathies. However, the first typical cytopathic effect, formation of large syncytia, was not observed until 5 months later, in a third clinical sample (HIV LAI) from a patient who had full-blown AIDS.”
It appears they cultured the “virus” for 30 days knowing full well that regular cultures of the same type die within this 4 week time frame. Montagnier stated that they did not even notice the cytopathic effect (CPE) until they had a third clinical sample 5 months later. CPE is claimed to be structural changes in host cells that are caused by “viral” invasion and yet, this was absent in their first two samples.
On day 3, half of the culture was cocultivated with lymphocytes from the biopsy after centrifugation of the mixed cell suspensions
Cells of the uninfected culture of the donor lymphocytes did not release reverse transcriptase activity during this period or up to 6 weeks when the culture was discontinued
The cell-free supernatant of the infected coculture was used to infect 3-day-old cultures of T lymphocytes from two umbilical cords, LCl and LC5, in the presence of Polybrene (2 ,ug/ml)
FYI, Polybrene was shown to negatively impact the proliferation and maintenance of growth potential of human keratinocytes here
Electron microscopy of the infected umbilical cord lymphocytes showed characteristic immature particles with dense crescent (C-type) budding at the plasma membrane
“Virus-infected” cells from the original biopsy as well as infected lymphocytes from the first and second “viral” passages were used to determine the optimal requirements for reverse transcriptase activity and the template specificity of the enzyme
A monoclonal antibody to p19 (15) and a polyclonal goat antibody to p24 (16) were used in an indirect (i.e. not directly caused by or resulting from something) fluorescence assay against infected cells from the biopsy of patient 1 and lymphocytesobtained from a healthy donor and infected with the same “virus” (why did they not use healthy donor lymphocytes without the added “virus?”)
Cord lymphocytes infected with the “virus” from patient 1 did not react with antibodies to p19 or p24
Only a minor proportion of the cells (about I percent) reacted with the patient’s serum
This may indicate that only this fraction of the cells was infected and produced “virus”
When purified, labeled “virus” from patient I was analyzed under similar conditions, three major proteins could be seen: the p25 protein and proteins with molecular weights of 80,000 and 45,000
The 45K protein may be due to contamination of the “virus” by cellular actin which was present in immunoprecipitates of all the cell extracts (i.e. “purified” with contaminants…otherwise known as not purified)
All attempts to infect other cells such as a B-lymphoblastoid cell line (Raji), immature or pre-T cell lines (CEM, HSB2), and normal fibroblasts (feline and mink lung cell lines) were unsuccessful
The role of this “virus” in the etiology of AIDS remains to be determined (ultimately, Montagnier believed his “virus” did not cause AIDS)
Other factors, such as repeated infection by the same “virus” or other bacterial and “viral” agents may, in some patients, overload this early defense mechanism and bring about an irreversible depletion of T cells involved in cellular immunity
Luc Montagnier unleashed his “retroviral” monster onto the world in 1983 and it grew into a beast of its own kind during the proceeding decades. Countless lives have been destroyed by the fear of the HIV diagnosis as well as the subsequent subjection to toxic black label pharmaceuticals. The stigma of the positive test result is the “viral” scarlet letter unfairly placed upon a person in a toxic state due to lifestyle choices and/or environmental factors. It does not matter that Montagnier attempted to steer his monster from the lethal killer it was made out to be into a harmless passenger inside the human body. It does not matter that he believed HIV did not cause AIDS. It does not matter that he believed that co-factors other than a “virus” should be examined in regards to AIDS. It does not matter that he believed HIV could be eliminated based on healthy diet/lifestyle choices. It does not matter that he admitted to not purifying any “virus.” Montagnier’s legacy is tied to the beast of his own creation. He opened Pandora’s Box and released this fraudulent curse upon the world. For that, I doubt he will rest in peace.
Truth Comes to Light editor’s note: In the following video, Spacebusters uses images to artistically highlight & add clarity to an essential part of a conversation (Merritt Medical Hour — February 2, 2022) between Dr. Lee Merritt & Dr. Tom Cowan. See the entire interview at Merritt Medical Hour on BrighteonTV.
To those of us that know that virology’s “isolation” and genomic sequencing methodologies are anti-scientific, it is still interesting to see the proponents of the nonsense offer official explanations about what they are up to.
Here in New Zealand, the Institute of Environmental Science and Research (ESR) is responsible for some of the alleged isolation experiments and genomic sequencing of the imaginary “SARS-CoV-2” particle, that they claim is responsible for the clinically undefined illness “COVID-19”. On the 9th of February 2022, they responded to questions surrounding the methodology of their cell culture and genomic sequencing experiments in relation to an Official Information Act request (which is analogous to a Freedom of Information request).
ESR couldn’t seem to find the “virus” but they featured this pretty picture.
So let’s have a look at the ESR’s “scientific” method with regards to their official records of a “SARS-CoV-2 virus”…
“Viral Culture/Experiment details –
Once the cells are 90 – 100% confluent, they are inoculated with 500 uL of diluted clinical sample (sample is diluted 1:10 in Infection media),10 mL of Infection Media is added to the flask. Infection media is made up of DMEM with 1% pen/strep/gentamycin, 1% Nystatin, 1% Glutamax, 1.5% Hepes plus 4ug/mL TPCK added.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
The “clinical sample” will be something like a crude nasopharyngeal sample taken from a patient. These specimens contain human tissue (from the host and other individuals in close contact with them), various bacterial and fungal elements, and whatever other material was in the patient’s mucosa. Amongst all this biological soup is the alleged SARS-CoV-2 virus, which of course, has never been directly found in any person. Apparently there can be 200 million copies of the virus in a sneeze but strangely they can’t find any in an “infected” individual.
Instead they resort to tissue culture experiments, as the ESR continues to explain…
“The flasks are then placed into an incubator and monitored for cytopathic effect (CPE) A SARS-CoV-2 N gene PCR is performed on the diluted 1:10 clinical sample and on the supernatant of the flask after 1 week of incubation (or sooner if 100% CPE is evident). CT values for both specimens are used as well as the CPE observed in the flask to determine if viral culture has been successful.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
Cytopathic effects are non-specific and are simply the observation that cells being stressed in a test tube eventually break down and die, with some cells producing vesicles. However, in the world of virology it is seen as evidence that a virus is at work and is somehow destroying the cells from within. “SARS-CoV-2 N gene” is a misnomer because there has never been a demonstration of a viral particle that contains this genetic sequence. Even more problematic is that there’s never been a demonstration of any viral particle. However, here we see them claiming “successful” viral culture if they detect a single short genetic sequence by PCR amplification. Note to virologists: detecting genetic sequences of unproven provenance does not equal virus.
Then we get to another interesting part…
“Viral culture/experiment details of the negative control –
The method above is also used for the negative control and the flask undergoes the same conditions as the flasks used for viral culture, however we use Infection media only.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
How on earth is this a comparable control experiment? – they added no control sample to their culture brew. In their first experiment they added a veritable biological soup containing human tissue along with various microorganisms and other organic fragments (everything present in a respiratory tract sample), and their alleged virus of course. Examples of valid control experiments would be:
The same type of sample taken from a well person.
The same type of sample taken from a person with a comparable clinical condition but said not to have “COVID-19” (without biased pre-selection in the form of a PCR result.)
Ironically, both of the above become meaningless in the case of “COVID-19” as it has no specific symptoms, signs, or investigations outside of the PCR result – a PCR result that has never been validated to a clinical condition. In fact, a priori the PCR could never be validated in this application as it is simply a tool to amplify selected genetic fragments, not determine their origin or the significance of their presence in mixed biological samples. So, in the case of (1) above, many well people are said to have “COVID-19” and in the case of (2), there is no way to distinguish a novel clinical condition. Dr Sam Bailey explained these problems back in 2020 in “What is a COVID-19 Case?” – a video banned by Big Tech after several hundred thousand views but still available here.
The wheels really fall off the ESR’s response when they are asked to explain how they purify the alleged virus sample for genomic sequencing and compare this to a control:
“’Whole Genome’ Sequencing – Purity and Control Details:
[• The degree of purity of the “virus” sample used in the sequencing experiment.] The protocols used for amplification of the SARS-CoV-2 virus consists of primers that specifically and selectively amplify the viral material, any remaining host or bacterial material is filtered out programmatically prior to data analysis.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
Either they don’t understand the question or are being disingenuous here. Their response doesn’t provide any evidence that they have a virus, let alone have attempted to purify it, in the analysis of its purported genome. They are simply using a process that amplifies sequences they have artificially selected but as it is a mixed sample they cannot demonstrate the origin of them. There is no way to claim this is “viral material” because no one has ever demonstrated that these sequences come from inside a virus, let alone belong to “SARS-CoV-2”. They are simply building on the nonsense that has spun out of control on GISAID.org where not one of the millions of deposited “genomes” has been shown to come from inside a viral particle. It’s turtles all the way down with these contrived “genomes”.
And with regards to the ESR’s “controls”?…
“[• All details of the control group that was used when comparing the results of sequencing:
o the total nucleic acid extracted from the “viral lysate” (from the experimental group), versus
o the total nucleic acid extracted from the non-viral lysate (from the control group).]
The protocols used to extract RNA from clinical samples do not yield a uniform quantity as this depends on the viral load within a sample. Details about the ranges obtained and used for further analysis are published in detail in several scientific peer-reviewed publications and can also be found on the publicly accessible protocols.io website, link provided below as requested.”
~ Jill Vintiner, Joint General Manager Health and Environment Group, ESR, 9 Feb 2022.
They appear to have dodged the question and the protocols provide no evidence of valid control experiments. The ESR have been asked to clarify this but we can already see they are not adhering to the scientific method. I also looked at the four publications that they suggested but these simply confirmed the problem: there is no evidence of any virus and the world is being duped in this war on humanity.
In fact, by definition, there has never been a demonstration of any disease-causing virus ever, full stop. Even if the ESR performed valid genomic control experiments there would still need to be further experiments to demonstrate the existence of a replication competent, obligate intracellular parasite that causes disease in a host. In other words, the actual existence of a virus. It makes me wonder whether the virologists are going to change the very definition of a virus soon in order to keep the whole façade afloat. However, once people realise that virology has never fulfilled its own postulates, they can take a major step away from this health misconception and ignore any of the related damaging measures and “treatments” coming from the medical-pharmaceutical complex.
The Covid19 narrative is broken, that battle is over. Yes, there are still pockets of token resistance, little embattled squares who aren’t ready to give up the ghost just yet, but for the most part the establishment are letting it go.
Country after country after country are “relaxing” their Covid restrictions, abandoning vaccine passport plans and attempting to “get back to normal”.
It seems every week some new “expert” who spent the last two years predicting we’re all gonna die turns up on the news claiming we should “treat Covid like the flu”.
But just because they’re giving slack on Covid does not mean the agenda behind Covid is gone. Far from it.
In fact, even as they seek to dump this pandemic in a shallow grave, they are already prepping the public for the next health scare – AIDs.
Then, just last week it was suddenly reported there was a “new variant” of HIV circulating in Europe, this new strain is allegedly “more virulent”, “more transmissable”, and “progresses to AIDS faster”.
Following hot on the heels of this fresh wave of fear is a push for everyone to get AIDS tested as soon as possible, from politicians and celebrities and everyone in between.
Prince Harry is leading the charge, in a video that caused the press invoke the spirit of his mother Princess Diana, Harry insisted we all have a “duty” to get HIV tested “to keep other people safe”, comparing it to the COVID outbreak.
“Know your status“, the video says. Which will probably be a hashtag in the near future. (I just checked, and it actually is already.)
They’re really cranking through the gears on this one.
Even while the problem and reaction are still barely out of the research and development stage, they’re already talking about the solution.
Guess what it is?
If you said “another mRNA vaccine”, well done for paying attention
Yes, Moderna has apparently learned so much from making their rushed Covid vaccine which doesn’t work that they’re already making an HIV vaccine they hope will be just as “safe and effective”.
In a truly startling coincidence, Moderna’s HIV vaccine began clinical trials the exact same day the “new variant” of HIV hit the headlines, and the same week as the NHS’s annual “HIV Testing Week”. Funny old world, isn’t it?
Anyway, everyone get ready to line up for the AIDS shot.
[Truth Comes to Light editor’s note: For the convenience of our readers, we have prepared a transcript which can be found below the information shared by Immanuel Project. This video was originally recorded in German and a voice-over has been provided by Immanuel Project.]
by Immanuel Projectwith Dr. Stefan Lanka video uploaded to Odysee August 30, 2021
Video available at Immanuel Project Odysee & BitChute channels.
The first of our extra, contributory posts “ON RELATED ISSUES” examines explosive, critical questions, rumours and theories surrounding the topic of “Corona” and everything connected with it. When new reports do the rounds in public that have the potential to fuel (additional) fear, hatred and violence, and which above all spread dangerous misinformation from the field of medicine and science, we would like to publish a special feature on this.
In contrast to our main programme, this series offers first and foremost a statement. In order to be able to publish a comment relatively quickly, we do not go into great detail and refer you to our main programme for precise evidence of our statements, where we publish a detailed list of sources for every contribution.
Since all the topics we deal with in Project Immanuel are directly related, all the contents of our special formats can also be substantiated with the sources from the main programme.
O.R.I., No. 01: “Bioweapons – the myth of the man-made pathogen”
In the first episode of our special format “On Related Issues” we deal with the topic of biological warfare/bioweapons. Due to the latest rumours surrounding the alleged “Wuhan virus” from the laboratory, we specifically address the issue of artificial “pathogens”, i.e. those modified or created in a laboratory, and explain why these are and will continue to remain, a myth.
“Project MKULTRA, the CIA’s Program of Research into Behavioral Modification – Joint Hearing before the Select Committee on Intelligence and the Subcommittee on Health and Scientific Research of the Committee on Human Resources, United State Senate, Ninety-Fifth Congress, First Session”, 03 August 1977 — https://www.nytimes.com/packages/pdf/national/13inmate_ProjectMKULTRA.pdf — published on the website of the New York Times
The following video is not intended for entertainment. It’s not a documentary report or television program.
Rather, this is an attempt to approach an explosive scientific topic in a cinematic way that is objective and respectful as possible.
We deliberately avoid staging of scenes as we’ve no intention of causing emotion in the viewer. We would like to convey factual, verifiable information.
In addition, we hereby call on all viewers to question the contents of this video and not simply to believe any information presented here. Doubt, be critical and check everything.
Only that is scientific.
Immanuel Project — “On Related Issues” (ORI).
With this video we introduce you to the first in a series of extra videos that we’ll publish in addition to our regular program.
On Related Issues focuses on pressing questions, theories and theses that are making the rounds in the public sphere, and to which we would like to respond as promptly as possible.
Most importantly, topics are discussed that are only marginally dealt with, or not dealt with at all, in the main series of our project.
No. 1 – Bioweapons: The myth of man-made pathogens
Biological warfare is a fairly complex subject. The use of biological weapons is probably as old as humanity itself.
All kinds of animals or naturally occurring toxins can be used as weapons to either attack enemies directly or in some way to make it difficult for them to survive.
Throughout history humans have been devising all kinds of biological warfare that have been as effective as they have been cruel. Time and again they have been reports about the use of supposed pathogens.
As early as the Middle Ages, and even in antiquity, allegedly transmissible diseases were claimed to be a popular means of warfare.
For instance, corpses of dead humans and animals were hurled into cities with the intention to cause epidemics in these areas.
Such stories do have a kernel of truth. Hurling decaying cadavers at enemies was certainly a proven biological weapon, but it had nothing to do with pathogens.
These days when people hear the term bioweapons, they usually think of artificial pathogens from the laboratory — bacteria and viruses that either genetically modified or even created in their entirety.
In the 21st century such ideas are more topical than ever due to the alleged progress in genetics and, equally assumed, improved understanding of biology.
Horror scenarios, wild rumors and theories, as well as adventurous novels, feature films, series and video games on this subject are dime a dozen.
But what has actually been researched and developed with regard to artificial pathogens?
Is it possible that something could really be brewed up in bioweapon laboratories that could prove dangerous to humans?
No, it’s not possible. I mean, you can see now that fear is the best bioweapon there is. You simply show some photos of coffins and corpses.
That’s the most powerful bioweapon we have: misinformation. But the most dangerous thing, of course, is the superstition associated with it.
People generally believe in the concept of dangerous viruses. Scientists also believe in them. And those working in related fields are proud that they’re working on something so dangerous and important.
They don’t see that they are being completely unscientific by not questioning the concepts in which they believe.
And it is the very first written duty of every scientist to constantly question their own findings and assumptions.
Nowadays, however, we are dealing with the reversal of science. Those who point out obvious contradictions are berated. This is really the reverse of all science.
Science is important and can contribute a lot to humanity if it’s applied with integrity. But what is happening here is pseudoscience.
In his 1956 book, Sociology Vol. 1, Eugen Rosenstock-Huessy explains why people engage in pseudoscience. He shows that, because of how science now operates, we can no longer make new discoveries. As if science have been derived from Greek criminal law, what we observe we judge and explain exclusively on the basis of what we already know. And, of course, only material explanations are permitted.
We do not want to know about any other explanations. We then say ‘they cannot be true’, ‘they are unscientific, wrong and dangerous’.
Rosenstock-Huessy clearly demonstrated that we can no longer make any developments in this way. We cannot discover anything new with our unscientific approach. And it’s a typically-human characteristic that no one likes to see their achievements and findings being thrown overboard.
Rosenstock-Huessy also shows this: He demonstrates how these unscientific principles permeate academic life and how pseudo-research has been carried out in order to somehow maintain these very principles, the models which people adhere.
For example, by doing animal experiments without any control experiments. Or killing cells in a test tube, also without any control experiments. And then simply claiming that the results of these experiments have to come about because of some virus. That’s how easy it is.
And we must not forget that this was already written in 1956.
In his book “Healing Power and Truth: Concordance of Political and Cosmic Time” — what a title — he describes how mountains of corpses, such as in genocides, can quickly pile up again if one misses the moment to recognize and correct mistakes.
Wrong decisions are made, wars escalate or whatever. This is the challenge we are facing right now — to recognize these mistakes in time. So it’s very important to deal with these things. And bioweapons is a very good example of these things.
The Russians, for example, completely abandoned their bioweapons development in the 1970s because they realize that the concept of pathogens as weapons does not work.
But the claim that dangerous bioweapons exist is very effective in order to create fear. First and foremost, of course, it’s effective in populations who are panic-stricken about contagion.
For example, historically the Israelis managed to empty the entire Palestinian refugee camps without firing a single shot. They simply claimed the wells are contaminated and soon the dangerous disease will break out here.
Nothing happened at all. No shots were fired. And voila! The Palestinians were gone. That was the starting point of Israel — an act of fear.
The Israeli population also has one of the highest cancer rates in western societies. Certainly not in all parts of the country, but in many, people live in constant fear of death. There is a constant fear of terrorism, of rockets, of bombs. Of course, such an attitude to life is anything but conducive to good health.
Didn’t the Nazis in the Third Reich also have a biological weapons program? What happened to it? Was it abandoned? The reason they never seriously worked on a bioweapons program is because nothing had ever worked in that direction. What they did was try to protect themselves from alleged germs.
In this regard, I recommend reading the book by Ludwik Fleck, “Genesis and Development of a Scientific Fact”. There are also many articles by him on the internet.
Ludwik Fleck was a bacteriologist and he was deported to Buchenwald concentration camp where he was forced to develop a vaccine for the SS. He wrote that he and his colleagues knew that all the assumptions about supposedly dangerous disease-causing bacteria were completely wrong.
He knew that things don’t work like — that this idea is just a misinterpretation. Anyone can read that for themselves. You can find a lot of material by and about Ludwik Fleck freely accessible on the internet.
Nevertheless, Ludwik Fleck and his colleagues had the task of developing a vaccine against a supposedly dangerous bacterium for the SS. And they knew that if they tried to explain to them that it wouldn’t work, they’d get their heads chopped off.
So they just made a vaccine for them as demanded. They let something or other decompose, added a few bacteria. And when the whole thing was bubbling away in the test tube, the poisonous mixture was filtered. Formaldehyde was added and that was it.
The vaccine was injected and the job was done. That’s what he describes. And he also describes how science actually operates, because he himself has experienced these undesirable developments and seen how they come about.
After the second World War, the Americans were of the opinion that the national socialists, the Nazis, might have used some kind of secret drugs to take the soldiers’ will away, so that they would happily go to war.
The Americans were investigating this to try to address the big problem that many of their soldiers who were supposed to bomb Korea deserted. Hardly any of the soldiers at that time had ever held a rifle, seen a tank, or had anything to do with weapons in the military. And suddenly they were supposed to drop bombs on another country.
Some biologists even suggested that the Russians had bred a socialist virus that could be used to render the American soldiers will-less. Such speculation really did exist. But, of course, it led no where.
What the USA did in the end, however, was to experiment with all the drugs that were available. This project, about which a great deal of information has come to light, was called MKUltra.
People were tortured and subjected to drugs to take away their will in order to program them. And this project existed solely because it was believed that at least some, if not all, of the German soldiers must have been given some kind of secret drug. It is frightening that even today speculation about bioweapons is used to scare people.
And here is another example. The virologist, professor Zhang from Shanghai, had received the order from Beijing to search for a coronavirus in bats that was harmless to humans and could then be used as a template for so-called sequence alignment.
He was under extreme time pressure because the panic of the people in Wuhan had to be brought under control. It was feared that the people there might storm the hospitals at some point, because anyone who had any kind of complaint such as asthma, cough, or fever immediately panicked and imagined that they had SARS.
Something like that can endanger public order very quickly. And it was going in that direction, triggered by the ophthalmologist Li Wenliang, whose own fear spread very quickly via social media.
That’s precisely why professor Zhang was given the task of producing a harmless bat virus as quickly as possible. It was already established that the few dozen cases of pneumonia that existed at the time had not infected anyone else.
From the beginning of December, when the first cases were tracked, until the 20th of January, no one was infected. No one else got you pneumonia.
So they assume that if, anything at all, it must be a virus that was difficult to transmit and could probably only be transmitted from animals to humans. So they looked for a virus in animals.
Then professor Zhang, from the Fan Wu et al. research group — these results were published in Nature, the first work on the so-called new coronavirus — created the genome strand of SARS-CoV-2, in the absolute record time of only 40 hours.
He got the fluid from a lung wash, obtained some nucleic acid out of the fluid, sequenced it, and then ran the puzzle called sequence alignment. But he didn’t have time to apply all the rules of virology. That’s why the genome from these 40 hours of record time looks more than bumpy.
Normally one takes at least three weeks for this process. And then a genome sequence appears really polished. But anyone who knows a bit about biochemistry can see that the genome of SARS-CoV-2 really does look very bumpy.
And this is exactly the argument. The people who claim that the virus must have come from a laboratory: ‘It must, therefore, be a bioweapon.’. Of course this then circulates on the internet again and fuels people’s primal fear of infection and of viruses.
Therefore, anyone who claims such a thing, has to be asked the question: Where has a virus ever been isolated? Where? Show me a relevant publication and show me the exact passages in which this is described.
Show me where this is described in the methods section of any scientific paper. These are only very short paragraphs. And if it cannot be shown, it must be rejected because it spreads unnecessary and dangerous fear.
Fear is always dangerous. Spreading fear is not justifiable.
The theory that there are pathogens and transmissible diseases have been perpetuated to the present day with this kind of assertion. But if you go into detail, you immediately see that none of this is tenable.
What one could say, perhaps at this point, is — what was done again and again in the so-called Middle Ages, or actually in all wars, is to make survival impossible for the enemy, and also for the civilian population, by destroying the crops, destroying the fields, killing the animals, so that simply scorched earth remains.
And by throwing carcasses into the wells. Then the water was heavily polluted with decomposing products of the proteins, that is with nitrates.
Every mother understands that. If a bottle of mineral water says it contains more than 50 milligrams of nitrates, no child is allowed to drink it because otherwise it would turn blue. And if a child were to drink this water all the time, it would get the type of buboes that were called the plague in the Middle Ages.
From 1981 onwards it was called immune deficiency in homosexuals or GRID (gay related immune deficiency) for short. And from 1983 onwards, it was called AIDS.
It’s as simple as that. It’s massive poisoning from nitrates in drinking water. It has nothing to do with pathogens producing any disease toxins.
Such toxins are produced when something decomposes, i.e. the proteins break down and turned into putrefaction. It is quite clear that it is not healthy to drink water with corpse poisons or to eat rotten food.
Already at the beginning of the corona crisis, rumors circulated very quickly that the alleged new coronavirus was not of natural origin, but came from a bioweapons laboratory.
Of course, China was first accused of having developed the virus. Later, the USA was accused. And then China again.
And, at some point in between, the French scientist Luc Montagnier, who was awarded the Nobel Prize in 2008 for the alleged proof of the HIV virus, among others, spoke out. He claimed that the virus was definitely of artificial origin because it had genetic similarities to the alleged HIV virus.
Most of these theories were dismissed after some time. And many scientists declared that there was no reason to assume that the alleged SARS-CoV-2 was a bioweapon.
In January 2021 however, the rumor of the Wuhan virus flared up again when an international group of researchers claimed to have found new evidence that strengthen the suspicion of the bioweapon. The scientists’ conclusion sounded alarming, but were also based only on suspected elements in the alleged genetic strand of SARS-CoV-2.
These observations immediately lose their significance and, above all, their threatening nature when one realizes that the same genetic genome strand of the alleged SARS-CoV-2 is, in any case, only a man-made theoretical construct. No wonder then that some of it looks artificial and man-made.
One could say SARS-CoV-2 did indeed originate in a laboratory in Wuhan, but not in the way many people believe. The genetic material of SARS-CoV-2 comes from a computer and has never left it. It is a theoretical mental construct.
The ideas of pathogens made in laboratories are all scientifically untenable. Moreover, they even contradict principles of biology that have been known for many, many years.
It’s irrelevant whether they’re supposed to be killer bacteria or killer viruses. The terrorist attack in the USA in 2001, with allegedly genetically modified anthrax pathogens, is just as unlikely as the Wuhan virus of 2020.
To understand why biological weapons in the form of pathogens have never existed in this way and never will, one must know the following:
With regard to viruses, disease-causing viruses — i.e. a dangerous genetic substance — are, to this day, nothing more than mere theory.
No scientist in the whole world has ever succeeded in providing tangible proof of such a virus.
Even if one or the other has ever been awarded the Nobel Prize for alleged proof, their work never stands up to scientific scrutiny.
So how do you make an artificial virus when you can’t even find a natural one?
The topic of viruses is dealt with in detail in the main program of Immanuel Project.
With regard to bacteria — bacteria cannot make organisms sick in the sense that we believe they can. And they are not the parasites they are made out to be. Bacteria, which are always found in our bodies, can, under certain circumstances, be involved in ailments — some of which can even be life- threatening.
But that does not mean that they are parasites and harm us in that sense. Moreover, bacteria in living bodies either produce no toxins at all or only in such small amounts that it’s impossible to become ill from them.
One must bear in mind the conditions under which … and cadaveric toxins are produced.
So how do you grow killer bacteria? By reversing their biology? That would really be a scientific sensation.
The complex topic of bacteria is not dealt with in our main program but we will return to it in one or two special formats.
Conclusion.
There are a variety of possible biological weapons. However, pathogens are definitely not one of them. All claims about genetically modified, or even artificially created, pathogens contradicts biological principles and are, therefore, inevitably doomed to failure.
There may well still be stray scientists in the world who aim to produce the ultimate killer microbe in their laboratory, but they will fail just like the people who try to make gold in earlier times.
Their scientific basis is simply incorrect, in both the cases of the alleged viruses and bacteria. All allegations, speculations, rumors and accusations revolving around artificial pathogens, therefore, only generate fear and enemy images. And we definitely do not need to either.
There is already more than enough fear and hatred, especially in this time of corona. Prolonged fear can lead to serious health problems, particularly for people who already have respiratory difficulties.
Rather than creating more fear with unfounded claims of killer viruses from a lab, we should stick to verifiable facts. Then all open questions about the alleged Wuhan virus, its latest mutations, its similarity to HIV, and other theories about bioweapons and killer viruses, will take care of themselves.
In order to complete the control experiments on SARS-CoV-2, we are still urgently looking for bioinformaticians to repeat and document the original sequence alignment. If you are a bioinformatician, are proficient in the De Novo alignment on “viruses” and have an opportunity to access the raw sequence data from Fan Wu and his colleagues please get in touch fragen @ wplus-verlag.de
Dr Robert Gallo made his famous announcement at a press conference on 23 April 1984 that “his” HIV virus was the probable cause of Acquired Immune Deficiency Syndrome (AIDS). From that moment on, the race was on to find a pharmaceutical weapon against it.
At the height of AIDS epidemic in 2005, the rhetoric about HIV danger and death penetrated every corner of the world. The rapid test for HIV was accepted as the test for AIDS, which divided people into positive and negative camps.
Flashback to June 2015, ten years after the height of the AIDS epidemic:
AIDS-related deaths have fallen by 35 percent since the peak of the epidemic in 2005 and the number of new infections continues to decline annually. That’s the good news. Nonetheless there are thought to be around 35 million people living with HIV globally; 19 million don’t currently know their HIV-positive status. Of those people who need antiretroviral drugs, only just over a third have access. That’s the bad news.
We have the scientific know-how to end AIDS and every month seems to bring news of another biomedical advance that could change the trajectory of the epidemic once and for all.
Last week the preliminary findings of the Strategic Timing of AntiRetroviral Treatment trial confirmed that early treatment is best for HIV.
No one thought that HIV might be lab-created. No one knew that just before Gallo’s April 1984 announcement, someone had filed a United States Patent number: 9499480 for HIV/AIDS Virus invention, a designer bi-product of the U.S. Special Virus program.
No one knew that Gallo, himself, was ‘Project Officer’ for the federal Special Virus Program that ran from 1962-1978. See complete list of HIV patents. No one knows that engineered evidence is found from the ‘multiply-spliced’ nature of the HIV ‘tat’ sequence in Dr. Gallo’s 1971 Special Virus paper, “Reverse Transcriptase of Type-C virus Particles of Human Origin.”
From 1985 to 1992 there were 12,000 deaths each year from AIDS. In 1992 the number increased suddenly to 15,000. Why? Because they added 5 new diseases to the AIDS definition! The actual number of cases of AIDS was on the decline until they added more diseases to the list, and still the number of new cases grew very slowly. – Dr. Robert Wilner, Deadly Deception, 1994.
HIV — it has never been found in sufficient numbers to cause disease.” –Peter Duesberg, 1991
The HIV/AIDS hypothesis is one hell of a mistake. – Kary Mullins, inventor of the PCR test.
Today, the official narrative still claims that no cure exists for AIDS, and that only toxic FDA antiretroviral drugs, including A.Z.T., D.D.I., and D.D.C., will slow down the progression of the disease.
“Why condemn a continent to death because of HIV, when you have other explanations for why people are falling sick?” – Dr John Papadimitriou, professor of pathology at the University of Western Australia in Perth and a co-author of the Journal of Nature Biotechnolgy study that found HIV tests to be inadequate.
Comparison of HIV and Coronavirus Tests. September 2020:
Sometimes testing can give you a false sense of security. That happened in the HIV epidemic, when people got a negative test and they presented it to their sex partners and spread disease, nonetheless. – Cue Mark Schlissel, M.D., Ph.D., President of University of Michigan,
The U of M president knew of the flaws of the rapid HIV test. He knew the patterns of history. And for that he received pushback for equating the COVID-19 pandemic with the AIDS epidemic to justify the University’s decision not to widely test students. He was made to apologize for unrelated reasons, but added to his response:
My comments were intended only as a critique of the effectiveness of massive testing of asymptomatic students for the virus that causes COVID-19 in an effort to prevent its spread. – Cue Mark Schlissel, M.D., Ph.D, President, U of M 2020
The COVIDIAN Age
In the COVIDIAN Age, it is accepted that Coronavirus is a virus. However, Coronavirus is a family name that includes MERS-Cov, SARS-Cov, HCoV-229E, HCoV-NL63, HCoV-OC43, HCoV-HKU1, and many others. Coronavirus is not Corona virus. It is also accepted that people with underlying diseases are more susceptible to COVID19. This is likely due to a weakened innate immune system. Immunosuppressed people no longer have a functional defense system and are more likely to suffer from any infection, whether it be called a cold, a flu, toxic overload, or ‘COVID.’
The Twist:
Ironically, new research shows the opposite; that patients with advanced stages of AIDS show less severe COVID symptoms and recover faster than others.
A July 2021 study in the Journal Immun Inflamm Dis, titled “The clinical outcomes of COVID-19 in HIV-positive patients: A systematic review of current evidence” shows evidence that the majority of HIV patients show no severe symptoms and completely recovered from COVID19 infection.
Similar to The Age of AIDS, COVID patients will soon be offered antiretroviral drugs. On December 14, 2021, Merck and Pfizer pharmaceutical companies announced the development of COVID antiretroviral drugs. The companies claimed their drugs attack different parts of the virus. Ten days later, on December 24, 2021, the FDA authorized “emergency use” of Merck’s antiviral drug to treat COVID19. FDA had previously “authorized” the first antiretroviral Molnupiravir in late November. Note: authorization does not equal approval.
Today, the FDA claims that the antiretroviral pill “should be initiated as soon as possible after diagnosis of Covid-19 and within five days of symptom onset,” – FDA Statement, December 22, 2021
In 1994, Dr. Robert Wilner wrote: “Any antiviral therapy that is immune-suppressive and aimed at treating HIV is unnecessary, dangerous, unethical and bad medicine — you are already immune to HIV!
There is no test to find out a person’s “HPV status.” Also, there is no approved HPV test to find HPV in the mouth or throat. – CDC HPV Fact Sheet, 2022
We aimed to develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus material available. – Journal of Euro Surveillance, 2020
Why blame a pandemic on innocent animals? It sounds like this: “ANIMAL X” could be hiding a deadly virus that could trigger a pandemic worse than the Black Death and kill more than 75million people. They tried to blame Ebola on a bunny.
Did the Species Barrier disappear to allow for animal research to develop profitable drug models?
After mRNA injectables, why are AIDS patients successfully fending off the worst COVID symptoms and recovering faster without an immune system?
Do HIV patients somehow recognize the lab-created Coronavirus as similar? Does the mRNA nanotech somehow protect people without an immune system? Is that why antiretroviral will be required for COVID patients?
Disclaimer: The author encourages you to consult a doctor before making any health changes, especially any changes related to a specific diagnosis or condition. No information in this article should be relied upon to determine diet, make a medical diagnosis, or to determine or prescribe a treatment for a medical condition. This information is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice. It is intended to build synapses for thinking.
A German mathematician working with Dr Stefan Lanka has just published a report titled “Structural analysis of sequence data in virology – An elementary approach using SARS-CoV-2 as an example.” It provides even more evidence that the virologists are caught up in a world of computer simulations – simulations that are unreliable even on their own terms, not to mention being disconnected from reality. The analysis is an important contribution exposing another element of the anti-science being used to sustain this fake pandemic. Further, it is a technical dismantling of how all “viruses” are being invented and then “found,” in an ongoing game of deception.
The paper is very technical and requires some understanding of how the virologists create a “genome,” starting with a crude sample from an alleged infected “COVID-19” patient. To make it easier, I’ve produced a summary of the main findings as outlined below:
None of the genetic sequences used in producing the “SARS-CoV-2” genomes were shown to come from inside any viruses. It is unclear where the genetic fragments originated from.
The original de novo “SARS-CoV-2” computer-constructed sequence published by Fan Wu, et al could not be reproduced by the methodology described in their paper, raising questions abouthow they produced itand announced the new “virus” to the world.
The PCR protocols are calibrated to sequences of unconfirmed origin that are clearly found in many humans and apparently other things as well. The PCR process was not shown to detect a “virus,” let alone diagnose an invented illness called “COVID-19”.
The virologists are fooling themselves by running amplifications at 35 to 45 cycles, as it can result in “detecting” sequences that are not even present in the sample. In effect, the methodology can result in “detecting” whatever sequences they are hoping to find.
Fan Wu, et al could have found better matches for “HIV” and “Hepatitis D virus” than “a new coronavirus” in their 41-year-old man from Wuhan, who presented with pneumonia as one of the first claimed “COVID-19” cases. If they want to find a “virus”, it all depends on what they ask the computer to look for.
Of course, it makes much more sense when you get to the root of the problem: “SARS-CoV-2” is nothing more than a computer simulation and there was never a virus to start with – the entire thing is a global fraud. Virology seems to be unaware that it is sinking further into an epistemological crisis and no more so than in the area of genomics, as outlined in this article by Mike Stone. In Stone’s article, I noticed in the comments section that Dr Valendar Turner of The Perth Group pointed out that the late Sir John Maddox, former editor of Nature, had issued a pertinent warning in 1988. It seems that those who become immersed in the world of indirect molecular detection techniques risk no longer seeing the wood for the trees as he presciently stated:
“Is there a danger, in molecular biology, that the accumulation of data will get so far ahead of its assimilation into a conceptual framework that the data will eventually prove an encumbrance? Part of the trouble is that excitement of the chase leaves little time for reflection. And there are grants for producing data, but hardly any for standing back in contemplation”.
Maddox, J. Nature 335, 11 (1998)
We will endeavour to keep exposing these anti-scientific methodologies and encourage others to ask themselves if the multi-billion dollar virology industry and the associated bogus “treatments” coming from the behemoth pharmaceutical complex are actually helping anyone with their health. For those of us that can see there is no sound basis to any of it, there is no way we would heed any advice from the doctors and scientists who promote these sick models. And perhaps more importantly, we know not to take any of the fraudulent and increasingly perverse pharmaceuticals that are products of this pseudoscience, and used as vehicles to deliver nefarious and undeclared constituents. Once again, you can avoid all of these problems by pointing out:
Where is the virus*?
*A tiny particle that is an obligate intracellular parasite (i.e. replication competent and transmissible) containing a genome surrounded by a protective, virus-coded protein coat.
This clip is from the Corona Investigative Committee’s “The Virus of Power” series of interviews , Session 90, which took place on February 4, 2022. See the entire Session 90 here (6+ hours long).
In this interview, Dr. Kaufman and Dr. Lanka challenge “germ theory” and the “science” at the foundation of virology. Of course, this is highly controversial because it shakes the foundation of modern medicine, questions the endless stream of vaccines and toxic medicines produced by big pharma — not to mention the generations of doctors, scientists and medical professionals who have dedicated careers to this “science”.
Committee member Dr. Wolfgang Wodarg, who has been invaluable in exposing the pandemic fraud and is a key source of medical insight for the committee, challenges Dr. Kaufman and Dr. Lanka, and vehemently defends the prevailing view regarding viruses as cause of disease. See Dr. Wolfgang Wodarg’s presentation during Session 90 here. His presentation occurred earlier in the session, prior to this conversation with Drs. Kaufman and Lanka.
Below the Corona Investigative Committee video, we are providing documents, videos and articles for understanding the work of Dr. Lanka, Dr. Kaufman, Dr. Tom Cowan and others.
Please do your own research and come to your own conclusions.
Video by Oval Media can be found at Corona Investigate Committee Odysee channel.
You make a list of symptoms. You say many people are experiencing this cluster of symptoms.
You give a label to this list of symptoms. A name. The name of a disease or a disorder or a syndrome.
Over time, through promotion, the name sticks.
You fund research to find the cause of the disease. This research can stretch out for a long time. Possibly forever.
Meanwhile, you develop and sell drugs to treat the disease. Money.
You keep reporting “progress” on finding the cause. “At first, we looked for environmental factors. But now we know the basis is almost certainly genetic. We’re homing in on the specific genetic dysfunction…”
Over time, what’s forgotten is this: is there really a single disease with a single cause?
And think it through; if you can’t verify a single cause, you don’t have a disease. You just have the original list of symptoms.
Alzheimer’s would be an example. Microcephaly (babies born with small heads and brain damage) would be another. The disease names seem to carry the day. “Well, if there’s a name, a label, there must be a unique disease.”
Wrong.
If there’s a name, a label, there is money.
Money for research, for drug development, money from drug and vaccine sales.
Researchers are tasked with making the list of symptoms seem compelling. “We’ve done brain studies. There are remarkable similarities among patients who have Disease X. As you can see from these scans, in Figure A…”
Still, no dice. No verified cause. Therefore, no justification for using the disease label or claiming you have found a unique disease.
But it doesn’t matter, because the business model is working well.
Here’s another example. ADHD. Has a single cause been found for this list of symptoms? No. Therefore, there is no laboratory test for ADHD. No test to confirm the diagnosis of ADHD. Because a test would detect the cause is present in the patient—and there is no cause to look for.
In fact, if you examine the complete catalog of all so-called mental disorders—about 300 of them—there is no defining lab test for ANY of them. Not a one. Each so-called disorder is simply a list of behaviors which have been clustered together by committees of psychiatrists and given a name. ADHD. Bipolar. Clinical depression. And so on.
But it doesn’t matter. Because the business model is working. Money is pouring in. Drugs are selling.
Let’s take this even further. A hundred years of Rockefeller medicine have “established” that there are thousands of separate and distinct and unique diseases, disorders, and syndromes. And each one has a cause. For many diseases, the cause “hasn’t been discovered yet.” Meaning: “We’re writing fiction. We have no justification for calling these diseases, diseases.”
For many other diseases, researchers claim, the causes have been found. The most popular type of cause? A virus.
A virus that had never been seen before. A virus that was “discovered” in a lab.
A lab—as I’ve discussed in depth—that lets in no outsiders, no truly independent observers, to see, in detail, what’s actually going on.
For that reason, and several others, there is no solid reason to believe these viruses, these causes are actually being discovered. Are actually real.
Which leaves us with thousands of lists of symptoms.
But there is always a business model. The full Rockefeller model is worth trillions of dollars. More dollars every day.
The drugs and the vaccines are the $$$ payoff.
I’ve spent decades demonstrating their toxicity.
Here’s a very interesting medical trick. A criminal trick. The researchers say a brain disorder called ABC exists but they haven’t found the cause yet. A parent has a child with severe problems and takes him to the doctor. The doctor pronounces a diagnosis: “Yes, your boy has ABC.”
The parent goes away and does some research. The list of symptoms for ABC could be the result of a vaccine. In fact, the boy developed his severe problems quite soon after vaccination.
She goes back to the doctor and says, “I think my son was damaged by the vaccine.”
The doctor says, “That’s impossible. Your boy is suffering from ABC. And you see, we’ve done studies of boys with ABC, and many of them were never vaccinated. So when you say the cause of your boy’s ABC was a vaccine, we’ve ruled that out.”
The parent doesn’t know what to do.
Of course, the trick is, ABC was never proved to be a unique disorder in the first place. It’s really the NAME of an unproven disorder. The studies the doctor is referring to are completely irrelevant.
ABC is a disorder without a proven cause. Therefore, it is no disorder at all. It’s just a list of symptoms.
The parent’s boy has many of those symptoms. He acquired them—and the damage he suffered—from a vaccine. If you wanted to put a name to what the boy has, call it what it is: vaccine damage.
Not ABC.
Part of the business model for ABC is: “We use that disease label so we can avoid having to pay out huge compensation-dollars for damage caused by a vaccine.”
If the impact of this trick isn’t getting through to you, let me give you a grossly exaggerated analogy.
Engineers claim there is a phenomenon called River Floundering. It is unique but the cause hasn’t yet been found. The basic symptom is: boats on rivers develop the propensity to sink.
Joe takes his boat out on a river. Overhead, a bridge collapses and destroys his boat. Joe barely escapes with his life. After six months, he emerges from the hospital and sues a number of parties.
But he loses his case. In court, experts testify that his boat was suffering from River Floundering. That’s why it sank. Many studies of Floundering show bridges-collapsing did not occur when “the sinking happened.” Therefore, the collapsing bridge was not the cause of Joe’s boat’s disorder, River Floundering.
What proof would I accept? What sort of proof would convince me that SARS-CoV-2 exists?
Suppose, for example, a study described how researchers actually DID separate a virus from all the material surrounding it in their cell-soup in the lab?
Would that be enough?
And the answer is no.
Why?
Because I don’t trust studies based on research conducted in elite labs where no independent outsiders are allowed. And that’s the situation, when it comes to purported virus isolation.
These labs are like the famous bunkers where key government officials are taken, in the event of a massive attack against the country.
Try getting in off the street.
And who are these researchers in the super-secret labs? To put it another way, what sort of establishment do they represent?
Is it a clean establishment with a track record of honesty? Or is it a cartel with a criminal history?
If it’s a cartel, why should I accept the “scientific methods” of these researchers or their honesty?
As my long-time readers know, I’ve spent decades exposing lies and crimes of the medical cartel. Chapter and verse. (For example this: Medical weapons of mass destruction)
When it comes to vital issues that mean the difference between life and death—drug/vaccine-fueled destruction of human life; mistreatment and errors in hospitals; faked disease case and death numbers; inaccurate, meaningless, and deceptive diagnostic tests; the fabricated existence of a whole range of phony diseases and disorders and syndromes; the true numbers of medically caused deaths—medical authorities have been lying and sliming their way out of accountability for MANY decades.
And all this doesn’t touch on the history of public health declarations of epidemics that have turned out to be duds.
Nor does it include the overall history of Rockefeller medicine, which is based on the fatuous notion that there are thousands of separate and distinct diseases, each one of which is caused by a germ that must be treated by a profit-making drug.
Nor does it include the history of vicious suppression of innovative treatments developed by individuals who’ve worked outside the mainstream.
Therefore, suspicion is warranted. Is absolutely necessary. And “suspicion” is a vast understatement.
I refuse to trust the researchers who simply claim they’re isolating viruses.
When it comes to the so-called basic building blocks of MANY so-called diseases—which ARE “the viruses”—all the discovery-research HAS BEEN conducted by insiders in their off-limit labs. Without independent witnesses. Without educated witnesses who can watch and question each and every step of “the accepted method” for isolation of new viruses.
Frankly, you would have to be crazy to accept anything coming out of these insider-club labs.
So NO. I don’t accept such findings.
Before I describe how outsiders SHOULD be allowed to witness and participate in secret lab work, let me give you two quotes to consider.
They come from decidedly mainstream and elite editors of elite medical journals. These editors have read and explored and probed and lifted the fake cover from published medical material for decades. Material they themselves have published. Therefore, these are CONFESSIONS.
ONE: “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
TWO: “The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness…”
“The apparent endemicity of bad research behaviour is alarming. In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world. Or they retrofit hypotheses to fit their data. Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours. Our acquiescence to the impact factor fuels an unhealthy competition to win a place in a select few journals. Our love of ‘significance’ pollutes the literature with many a statistical fairy-tale…Journals are not the only miscreants. Universities are in a perpetual struggle for money and talent…” (Dr. Richard Horton, editor-in-chief, The Lancet, in The Lancet, 11 April, 2015, Vol 385, “Offline: What is medicine’s 5 sigma?”)
Suspicion is warranted. It’s absolutely necessary. And again, “suspicion” is a vast understatement.
More than a year ago, I mentioned how virus-isolation research—if the word “research” applies at all—should be done.
And I issue this now, as a challenge, to the entire insider-club of virologists, all of whom claim their established method of finding and sequencing new viruses is scientific and rigorous:
Let’s have a film crew on site. As you work. In your lab. Looking over your shoulders and recording every move you make.
And with the film crew, let’s have several knowledgeable, outside, independent researchers. People whom you would ordinarily refuse to give the time of day. People who are insightful. Possibly, people like Dr. Stefan Lanka, Dr. Andrew Kaufman, Dr. Tom Cowan.
As the film crew works, and as you conduct and describe your step-by-step “isolation” of a new virus, these outsiders can stop you at any moment and question you. In depth.
“Why did you just do that?” “Why didn’t you record that step?” “Explain that answer you just gave me. It makes no sense.” “Exactly what did you just withdraw from the solution in the dish, and how do you know what it was?”
This is not a public relations exercise or an educational documentary for medical students. This is REAL. This is research about your research. No holds barred.
You give a slippery answer to a question; you evade with a vague generality; you try to pull rank; you get nailed to the wall. On film.
THIS is the procedure I want.
All the way from start to finish. Including the so-called sequencing of the “new virus.”
And then we would know a great deal more about what you’re actually doing and not doing in your labs. In the absence of what I’m proposing and demanding, THERE IS NO REASON TO ASSUME THE PROCESS OF VIRUS-ISOLATION IS LEGITIMATE.
Virologists, your work affects every human on Earth. Profoundly. To see this, all a person has to do is look around him these days, at what is called “COVID.” It proceeds from your so-called discovery of SARS-CoV-2.
I view you virologists as I would view the court magicians and soothsayers and high priests who surrounded and advised the leaders of tribes and nations in ancient times.
Those “experts” huddled with the leaders in their very private rooms and spun stories and predictions, and recommended strategies to deal with supposed ongoing and looming crises.
And then the leaders took actions that affected the lives of all the people.
So it is now. With you virologists.
So my demands are entirely within bounds. If you have a shred of honesty, and if you stop and think about it, what I’m demanding is prosaically simple:
You account for every step you take. In real time. Where you work. Right there, you submit yourselves to the detailed scrutiny of independent outsiders.
That’s my bottom line.
And I challenge any scientist, analyst, investigator, doctor, researcher, reporter, alt. reporter who says what I’m demanding is not necessary. You’re wrong. You’re dead wrong.
You either haven’t thought things through, or you’re lying.
Someone is going to tell me what I’m demanding, as proof, is impossible. It would never happen. “They” would never let it happen. They would never let independent outsiders into their holy labs.
You think I don’t know that?
If outsiders can’t get into their labs, what does that tell you?
And someone will say, “We just have to rely on the best evidence we have.”
No we don’t. Because the best available evidence is no evidence.
In a vast sea of death-dealing medical lies, a sea that has existed for more than a hundred years (actually much longer), if experts tell you they’re discovering viruses in labs you can’t enter, and they say you must believe them, and you buy that…
I have condos for sale on the far side of the moon. Full cash only, no payments.
Here it is: Virologists are saying and writing they’ve found a purple man with pink hair and green lips and four arms living a thousand miles under the surface of a planet in the next solar system over. And he causes disease.
Then they’re saying, “Prove us wrong.”
On top of that, they’re saying, “You can’t watch us work while we discover such creatures.”
Conclusion: the purple man doesn’t exist.
Virologists, text me when you’ll let my people into your lab.
Until then, get lost.
Dear reader, the elephant in the room is trust, not data.
When it comes to the “discovery of viruses,” there are no reliable data. We, on the outside, are told that what happens behind locked doors is irrefutable. Period.
We’re told we just can’t understand what the pros are doing. The problem is our lack of knowledge, our lack of training.
We’re the peasants toiling in the valley. Our better, the baron, is up in his castle on top of the mountain. He’s planning our lives, he’s taking care of us.
Sure. Of course. Uh-huh.
Sounds familiar. It’s pretty much the history of the world.
Or it was, until people who came before us finally staked out a territory called freedom, which involved opening locked doors and finding out what lay behind them.
Consider a parochial example: the mafia. They, too, plan behind closed doors. They concoct methods of carrying out crimes. They record their profits. Then, finally, a prosecutor announces, “We were able to get into their books. We saw the details. We made arrests.”
I want my independent accountants to get into the virologists’ books. But not after the fact. I want my people to BE there while the virologists are creating the books, entry by entry, in the lab.
“Why did you just make that entry? Where did your conclusion come from? Who are you trying to kid? You’re just fabricating this stuff? You know, that’s called RICO. That’s a RICO case. Continuing criminal enterprise. They’ll send you away for a long time…”
And all of a sudden, the high and mighty virologist, who’s been able to con the world with his hustle, who knows how to come off sounding superior in every way, feels a dent in his armor. A big dent. He smells his own blood.
And he starts talking.
He wants to make a deal. He’ll roll over on his colleagues. He’ll expose the whole sham.
“…You don’t understand. It’s the money. It’s all about the money. Where it comes from. We have to do this kind of work. Otherwise, we starve. They cut us off. I know the people on the funding committees. I’ll give you their names. They take orders, too. The whole thing is a system. I can draw you a map. I can’t go to jail. I have a family. I’m paying eighty grand a year just to send my kids to college. There’s the mortgage, and the cottage on the Cape…”
The whole bluff POPS and deflates, and we begin to hear words we understand, at last. The words of confession. The down-to-earth sordid truth.
There was never a towering mystery in the castle on the hill.
There was just the passing of the buck. The soiled buck. From hand to hand.
The “science” was the front.
“…You see, it works this way. The pharmaceutical companies have to have new viruses. For every fake virus, they develop a real drug and a real vaccine. It’s marketing. That’s what they’re doing. That’s what they’ve always been doing. This is much bigger than anyone realizes. I’m just a little fish. The big boys run the whole show. They pay the Congress and the FDA. They pay everybody…”
He keeps talking. He can’t stop. He’s way past “isolation, purification and sequencing.” They’re in his rear-view mirror. Now he’s fighting for his freedom from prison. Now he’s telling the truth.
And the ever-present storm clouds over the valley where we peasants toil are blowing away. The air is fresher.
We’re breathing easier.
The big-cheese baron is really a shrunken little man—when he takes his perp walk in chains.
Peter Duesberg is a molecular biologist and a molecular and cell biology professor at the University of California, Berkeley. At one time, he was an acclaimed scientist who was the world’s foremost expert on AIDS. That all changed when he was blackballed by Anthony Fauci and the scientific establishment for the temerity of revealing the truth that HIV does not cause AIDS. Duesberg was slandered as a homophobe for revealing the scientific evidence that AIDS was caused by the use of certain dangerous recreational/pharmaceutical aphrodisiacs by the sodomite community that over time broke down the immune systems of the users who then developed AIDS. He revealed that the prevalence of AIDS in Africa is simply explained by recategorizing as HIV the endemic immune deficiencies that were always understood to be caused by malnutrition, tainted drinking water, and various infections.
Dr. Duesberg reveals how Fauci pushed the toxic drug called AZT (Zidovudine) to people who were found to have antibodies to HIV. Those patients were poisoned by the drug (AZT) that was supposed to treat them. AZT, in actuality, caused AIDS, which eventually killed the patients. That is much like the present regime of treating COVID-19 with unsafe and ineffective mRNA vaccines and toxic therapeutics like Veklury® (remdesivir) while suppressing safe and effective therapeutics like hydroxychloroquine and Ivermectin.
Duesberg’s book exposes the incompetence, megalomania, and in some cases criminality of Anthony Fauci, and other NIH, FDA, and CDC officials. It reveals the genesis of the establishment of what has become a cabal of ruling technocrats in government which has now brought Orwellian oppression across the United States and indeed the world through the COVID-19 scare and mandatory experimental vaccinations.
There were very powerful interests who tried to kill Duesberg’s book before it ever saw the light of day. The publisher, Regnery, in its preface to the book explains how Peter Duesberg went through two publishers who backed out of publishing the book at late stages, apparently due to some hidden pressure from an unseen hand.
This book is now out of publication. But there is still robust demand for the book which has driven the price up. While Amazon offers the audible version of the book at a reasonable price, as of January 28, 2022, the hardcover version was priced at $1,260.00 and the paperback was priced at $536.00.
Regnery is the third publisher to have contracted to publish Inventing the AIDS Virus. Addison Wesley initially announced the book in 1993. St. Martin’s signed it in January 1994 and subsequently assigned its contract to us in January 1995. We announced it, initially, in the fall of 1995 and finally published it in February 1996. Bryan Ellison, Duesberg’s former research assistant and original co-author, became disenchanted with Duesberg’s and his publisher’s insistence on careful documentation and self-published his own version under the title Why We Will Never Win the War on AIDS in 1994. We sued Ellison for breach of contract and copyright violation and, after a two-week federal court jury trial, were awarded a six-figure verdict and an injunction against Ellison’s edition. Inventing the AIDS Virus has been edited by at least five editors, has been agonized over by the publishers of three major publishing firms, and concurrently praised and damned by countless critics.
Excerpt from the foreword by Nobel Laureate Kerry Mullis, creator of the PCR test:
We have not been able to discover any good reasons why most of the people on earth believe that AIDS is a disease caused by a virus called HIV. There is simply no scientific evidence demonstrating that this is true.
We have also not been able to discover why doctors prescribe a toxic drug called AZT (Zidovudine) to people who have no other complaint than the presence of antibodies to HIV in their blood. In fact, we cannot understand why humans would take that drug for any reason.
We cannot understand how all this madness came about, and having both lived in Berkeley, we’ve seen some strange things indeed. We know that to err is human, but the HIV/AIDS hypothesis is one hell of a mistake.
I say this rather strongly as a warning. Duesberg has been saying it for a long time. Read this book.
Kary B. Mullis
Nobel Prize in Chemistry, 1993
Prior to his untimely death on August 7, 2019, Kerry Mullis had this to say about Anthony Fauci and his ilk:
“Guys like Fauci get up there and start talking, you know, he doesn’t know anything really about anything and I’d say that to his face. Nothing. The man thinks you can take a blood sample and stick it in an electron microscope and if it’s got a virus in there you’ll know it. He doesn’t understand electron microscopy and he doesn’t understand medicine and he should not be in a position like he’s in. Most of those guys up there on the top are just total administrative people and they don’t know anything about what’s going on in the body. You know, those guys have got an agenda, which is not what we would like them to have being that we pay for them to take care of our health in some way. They’ve got a personal kind of agenda. They make up their own rules as they go. They change them when they want to. And they smugly, like Tony Fauci does not mind going on television in front of the people who pay his salary and lie directly into the camera.”
Notice the book, Inventing the AIDS Virus, on the table in front of Mullis during the interview.
“Viruses are small obligate intracellular parasites, which by definition contain either a RNA or DNA genome surrounded by a protective, virus-coded protein coat.”
Medical Microbiology, 4th edition, 1996
The question regarding the existence of pathogenic viruses remains an important one as the belief in such viruses dictates billions of dollars of resources and research funds. In the past two years we have also seen how an alleged virus can be used as a political tool to bring populations to heel. It is not the first time this has happened: for example, the “discovery” of HIV in the 1980s set up a multi-billion dollar industry and has also been used politically in most corners of the world. (The fallacies regarding the existence of the HIV particle and it causing AIDS are outlined in Virus Mania. For those wanting to dive more deeply into the arguments, I would recommend The Perth Group’s magnus opus on this topic.)
Independent journalist Jeremy Hammond who promotes himself as exposing “dangerous state propaganda” surrounding COVID-19 and the dangers of the vaccines, thus made the following curious statement in 2021:
“the false claim that SARS-CoV-2 has never been isolated (i.e., never proven to exist) greatly harms the credibility of the health freedom movement and is grounded in total ignorance of the science (the virus is constantly being isolated and whole genome sequenced by scientists all over the world)”
Jeremy Hammond, 9 March 2021
I would argue that the ignorance falls in Hammond’s lap as he appears to reach his conclusion by essentially repeating the claims made by virologists and reassuring the audience that their methodologies are valid. In recent weeks we have also seen Dr Joseph Mercola presenting Hammond’s interview and Steve Kirsch’s blog (that also makes appeals to virology authority) as “evidence” that SARS-CoV-2 exists. Kirsch states that he relies on “expert opinions of people I trust” which means that he has put the argument into the hands of others rather than investigating the issue himself. But is it wise for these health freedom fighters who are battling establishment COVID “experts” to not also question the establishment virologists?
Dr Andy Kaufman produced a point by point refutation of Hammond’s support of modern virology’s “isolation” methodology here, while Dr Tom Cowan warned that we are just getting started with dismantling virology’s nonsense here. Dr Sam Bailey has published many videos covering the virus isolation issue – most of which have been banned from YouTube but can still be found on Odysee. Additionally, in an essay I co-authored with Dr John Bevan-Smith, we describe the first pillar of the COVID-19 fraud as virology’s misuse of the term “isolation”. In summary, because virologists were unable to physically isolate any viruses last century, they simply changed the definition of the word so that even virologists admit the term is now used loosely. A strange state of affairs when the scientific method calls for precise terminology.
My observation over the past two years has been that many scientists, doctors, and journalists are happy to jump over this “isolation” chasm and cite the “coronavirus genomes” deposited in databases as proof that the virus must exist. For example, Steve Kirsch writes in his blog that:
“I know that Sabine Hazan verified that the sequence of the virus obtained from ATCC matched exactly what she found in people who have the virus.”
Steve Kirsch, 10 January 2022
He cites Hazan’s paper “Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing” as the evidence for this statement. Kirsch admits that he doesn’t know how the genomes were created, but his…
“scientist friends seem happy with them. At $2,000 a shot, I don’t think they’d market the product if it was contaminated and useless. Am I wrong?”
Steve Kirsch, 10 January 2022
Unfortunately, he appears to have been duped by the high-tech façade of virology’s genomics genie where “viruses” are created from various detected genetic sequences. In fact, sometimes the sequences are not really detected at all, as Dr Stefan Lanka is exposing in what may be virology’s death blow.
We can use Hazan’s paper as an example of the flawed methodology used in creating these “virus genomes”. The research team obtained faecal samples from 14 participants and proceeded to see what genetic sequences they could detect in the samples. We strike the first issue in the ‘methods’ section when they state that “included throughout sample processing was the SARS-CoV-2 positive control from ATCC (Heat-inactivated SARS-CoV-2, VR-1986HK; strain 2019-nCoV/USA-WA1/2020)” How did they know that the sample contained the inactivated virus? Because the ATCC (American Type Culture Collection) claims that it does on their website where they state “this strain was originally isolated from a human case in Washington state and was deposited by the Centers for Disease Control and Prevention.” And how did the CDC know that they had the virus? Because they claimed they found it in this paper here.
But where was the virus?
In the CDC’s paper, they say that they collected “clinical specimens from a case-patient who had acquired COVID-19 during travel to China and who was identified in Washington, USA”. It was concluded that the patient had COVID-19 based on a PCR result that detected some sequences said to come from SARS-CoV-2. But at this point they had no proof of any virus – all they had was some detected genetic sequences from a patient with an alleged viral infection. After performing a test tube tissue culture experiment on their clinical sample and claiming that there was evidence of a virus due to non-specific cytopathic effects, they began to construct their “genome”. They state that “we used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing.” This is another sleight of hand because the “viral lysate” was not demonstrated to come from a virus, it is simply a soup of broken up culture cells and other additives.
Similarly misleading was the claim they “extracted nucleic acid from isolates”. They have implied that they have isolated a virus and that they know which RNA sequences came from inside it. However, this would require the alleged viral particles to be truly physically isolated by purification, which they failed to do. And I say alleged because even if they purified the particles, it would still have to be shown that they meet the definition of a virus – including being parasitic and the causal agent of disease – something that was not demonstrated by these authors or any others.
In any case, how did they know which genetic sequences belonged to the “virus” in the first place? They “designed 37 pairs of nested PCRs spanning the genome on the basis of the coronavirus reference sequence (GenBank accession no. NC045512).” And where did this “reference sequence” come from? This relates to Fan Wu, et al’s paper describing the 41-year-old man who was admitted to the Central Hospital of Wuhan on 26 December 2019 with bilateral pneumonia and despite no new clinical features, was said to have a condition that was later called “COVID-19”.
The specimen was of crude lung washings, so it contained a mixture of human cells and potentially all sorts of other micro-organisms and genetic fragments. They simply asserted that there was a virus in the brew. From this mixed sample they blindly generated tens of millions of different sequences and then put their software to work to see how they could fit them all together. To do this “fitting” the software searched for “contigs” or areas where different fragments appear to have overlapping sequences. Of the hundreds of thousands of hypothetical sequences generated in this fashion they identified that the longest “continuous” sequence the computer could create was about 30,000 bases long and concluded that this software creation must be the genome of the presumed new virus.
They thought this was the genome because their hypothetically generated 30,000 base sequence was 89.1% similar to, “a bat SARS-like coronavirus (CoV) isolate—bat SL-CoVZC45”. The “genome” for the bat CoV “isolate” was generated in 2018 after “19 degenerated PCR primer pairs were designed by multiple alignment of available SARS-CoV and bat SL-CoV sequences deposited in GenBank, targeting almost the full length of the genome.” So in other words, they already knew the sequence to look for based on sequences that had previously been deposited in GenBank. But how did the producers of these already deposited sequences know that they had found viral genomes? Welcome to the circular reasoning of modern virology.
To explain the loop that virologists appear to be trapped inside, this 2019 paper published in Virology is illustrative of the problem:
“Three main methods based on HTS [High-throughput sequencing] are currently used for viral whole-genome sequencing: metagenomic sequencing, target enrichment sequencing and PCR amplicon sequencing, each showing benefits and drawbacks (Houldcroft et al., 2017). In metagenomic sequencing, total DNA (and/or RNA) from a sample including host but also bacteria, viruses and fungi is extracted and sequenced. It is a simple and cost-effective approach, and it is the only approach not requiring reference sequences. Instead, the other two HTS approaches, target enrichment and amplicon sequencing, both depend on reference information to design baits or primers.”
Maurier F, et al, “A complete protocol for whole-genome sequencing of virus from clinical samples,” Virology, May 2019.
Essentially this gets to the root of the problem. The “viral” reference genomes are being created through metagenomic sequencing but this is done on crude specimens (such as lung washings or unpurified tissue cultures) and then declarations that the selected sequences are viral in origin. So already there are two problems: firstly, there was no step (i.e. purification) to show that the sequences come from inside “viruses” and secondly, as described above, the computer generated “genomes” are simply assembled hypothetical models from small genetic fragments, not something that has been proven to exist in nature as a whole 30,000 base sequence. However, these in silico models then effectively become the “virus” and an entity such as SARS-CoV-2 is created. Once the first of such a sequence is deposited on a database, the “virus” can be “found” by others through the same flawed metagenomic techniques. Or as stated in the Virology paper, it can be “found” through target enrichment and amplicon sequencing (usually PCR), but this requires you to have a reference sequence…that is, a template that was invented in silico by metagenomic sequencing where the provenance of the genetic fragments was unknown.
There is no part in the above process that establishes either:
1) the genetic composition of any imaged or imagined particles; or
2) the biological nature of such particles, i.e. what they actually do.
It’s a good-looking nano-particle alright, but what is it made of and what does it do?
So, now can we return to Hazan’s paper to see that it is a pointless exercise in virological nonsense. They state that along with their “SARS-CoV-2 positive control from ATCC”, the “patient genomes were compared to the Wuhan-Hu-1 (MN90847.3) SARS-CoV-2 reference genome”. Accession number MN90847.3 refers to the updated “genome” said to have been found in the 41-year-old man from Wuhan as discussed above in Fan Wu, et al’s paper. The circle is complete – at no stage was it demonstrated that there was any virus by following this evidence trail of “genomes”. Fan Wu’s team never found a virus, they simply asserted that their genetic sequence computer simulation was a “new RNA virus strain from the family Coronaviridae” without proving that the sequence existed in nature or came from inside a virus. Hence, there was no “detection of SARS-CoV-2 from patient fecal samples” as the title of the Hazan paper claimed, unless “SARS-CoV-2” means genetic sequences of who-knows-what from who-knows-where. It doesn’t matter where or how often these sequences are detected – they have never been proven to be viral in nature. So, when Steve Kirsch stated that Hazan “verified that the sequence of the virus obtained from ATCC matched exactly what she found in people who have the virus,” he is mistaken.
I was not planning on doing any more articles nor devoting any more of my time to Steve Kirsch after my response to his claim that “SARS-COV-2” has been isolated. It was clear to me after reading his blog post that he did not understand what he was writing about. Even if it wasn’t clear to anyone reading, Steve took the liberty of outright admitting that he did not understand the topic as he relied on “experts” to tell him what to think and believe:
I rely on expert opinions of people who I trust for certain issues like whether or not the virus has been “isolated.” -Steve Kirsch
After the blog post came out, there were some exchanges between Steve and Christine Massey, who has done an amazing job of destroying the “virus” isolation lie with her Freedom of Information requests. She confronted Steve about his “isolation” claim and brilliantly pointed out why he was wrong. Instead of conceding that she was right and that he clearly did not understand the topic, Steve hunkered down on his ridiculous claim and pushed her for a 5 hour live debate with his “experts” in order to let the audience decide which side was right in the “SARS-COV-2” isolation argument. Disregarding the ridiculousness of the 5 hour time frame and the desire for the audience to decide a winner, Steve was attempting to sit on the sidelines and play matchmaker by pitting his “experts” against Christine. Once she enlisted the help of a team of her own experts, Steve seemingly panicked and decided to exit stage left.
This is just a brief summary of what transpired over the course of a few weeks in January 2022 and I may not have done the exchange justice. However, while the debate-that-never-was is an interesting story, it is not my main focus. In fact, I would have left this whole Steve Kirsch situation in the wastebasket where it belongs until I saw his parting shots at the “virus does not exist” community. In his attempt to save face by passing the responsibility of debating Christine and her experts off to his readers (which shouldn’t be shocking as he is seemingly skilled at passing responsibility off to “experts”), Steve shared some additional outlandish claims made by his “experts” regarding “virus” purification. Here are a few brief highlights from his post:
Does anyone want to debate “Does the virus exist?”
If course it does, but there are followers of Sam Bailey, Stefan Lanka, Thomas Cowan, Andrew Kaufman, and Christine Massey who claim it doesn’t.
“I’m not willing to invest my time in this debate, but if you want to challenge Sam Bailey, Stefan Lanka, Thomas Cowan, Andrew Kaufman, and Christine Massey, please let me know in the comments.”
“Basically, purifying a virus is difficult and there is no reason in today’s world to do it, so it isn’t done. The FOIA requests they issue are a publicity stunt that they know will fail. That’s very disingenuous of them not to reveal that.”
“Also, the people I talk to fully acknowledge there is no purified virus, but that it isn’t needed because they can do everything they need to do without it. Lanka et al. claim it is needed. So it’s now just a matter of opinion. Neither side is going to convince the other side. That’s what happened.”
“The reason nobody has purified the virus is there is no need to do so in today’s world where gene sequencing is readily available.”
First, I would like to point out Steve’s apparent Freudian slip while attempting to declare the “virus” exists: “If course it does.” Not a typo on my part. I’m not here to play grammar police as I make plenty of spelling errors myself. I just thought it was an amusingly ironic way to start his post. Since Steve is unwilling to invest his time in a debate, maybe he could devote it to proofreading?
Now that the fun is out of the way, let’s get to the nitty-gritty on “virus” purification. According to Steve’s “experts,” the purification of a “virus” is too difficult and is no longer necessary. They believe that in today’s world of molecular virology, purifying “viruses” does not need to occur as a genome can be obtained from the genetic soup full of host and other unknown “non-viral” RNA/DNA. They believe that it is possible to obtain a genome for an unknown “virus” by piecing it together from the millions of reads of random RNA aquired from these unrelated sources within the sample. Thus, Steve and Co. want you to believe that purification, i.e. the very steps used to rid a sample of contaminants, pollutants, foreign material, etc. in order to isolate it, is not necessary any more as technology has advanced beyond these primitive methods. Putting aside the fact that the admittance by Steve and Co. that purified “SARS-COV-2” does not exist destroys their previous claims of “virus” isolation, does Steve’s “expert” advice on purification hold up?
No. Not at all. At least, not according to these experts:
“That such “purification” is an indispensable prerequisite for detecting viruses and creating valid antibody and PCR tests based on them is also stated by scientists who are the most renowned in the world, among them:
White and Fenner: “It’s an essential pre-requisite.” Luc Montagnier: “It is necessary.” Robert Gallo: “You have to purify.” Marcel Tanner: “If a pure SARS-CoV-2 isolate cannot be documented by the IVI [=Institute of Virology and Immunology] in Bern, then we have a problem.” (siehe here). Françoise Barré-Sinoussi: “… you have to purify the virus from all this mess.” Jean-Claude Chermann: “Yes, of course… Absolutely.” David Gordon: “It’s a natural step from obtaining the virus in cell culture to then obtain purified virus.” Dominic Dwyer: “The purification, as far as one can go, is important in analysis of any virus or bacteria, for that matter well.” Wan Beom Park: “In the outbreak situation, isolation of causative virus is indispensable for developing and evaluating diagnostic tools, therapeutics, and vaccine candidates.”
I’m not positive who Steve’s “experts” are, but the people listed above are well-known and respected scientists and virologists. While they may disagree with the fact that “viruses” do not exist, they all accept that purification of a “virus” is an absolutely necessary and essential step. It is a prerequisite.
Those listed above are not the only experts claiming purification is necessary. An interview with Professor: Dr. Osamu Nakagomi from the Nagasaki University Graduate School of Biomedical Sciences Molecular Epidemiology, who is an expert on the subject matter, states as much as well:
Fundamentals of Ultracentrifugal Virus Purification
“In recent years, in virus research, it has become a standard practice to purify and analyze genomes and identify viruses from samples using commercial kits. Since for the established viruses their genomes have already been known, virus identification is possible even in a mixed state. However, to carry out detailed investigation on the nature of viruses, it is first necessary to refine the virus particles in order to yield a high level of purified materials.”
Please discuss the necessity of ultracentrifugation in virus research.
“When extracting virus genome using the classical method, the virus particles must first be purified. Then the virus genome extracted from the particles is examined. Ultracentrifugation plays an important role in the process. Purifying the virus particles makes it possible from the beginning to ensure that we are dealing with the rotavirus genomes in the virus particles.Currently such analysis is performed almost all the time after hastily extracting the genome without actually purifying the specimen. This practice is common since the genome of rotavirus is well established and it is a common knowledge that if the genome (Fig. 1 ) characteristic of rotavirus is present, there is no doubt that the genome is present in rotavirus particles as well. However, suppose, for example, that we are dealing with the problem of determining what kind of host cell organelles or virus proteins and genomes are aggregated in an infected cell, ultracentrifugation becomes indispensable. Moreover, while studying new viruses, it becomes increasingly necessary to investigate whether or not the genome is present in the particle. In such cases, purification with an ultracentrifuge becomes a necessity. Information on the buoyant density, size and sedimentation coefficient (Svedberg value, S value), all of which are taken into consideration in ultracentrifugation, is in fact the fundamental aspect of virology which taken together are called the physiochemical properties of viruses.”
I wonder if Steve and Co. would be able to point out “SARS-COV-2” from these unpurified EM images if we took out the labels?
As can be seen by Dr. Osamu Nakagomi as well as the experts listed above, purification is entirely necessary, especially in instances with “novel viruses” such as “SARS-COV-2,” which Steve and Co. admit has never been purified. Without purification, there are numerous host cell organelles and other proteins, microrganisms, bacteria, etc. within the sample and thus there can be no claims of isolation. There would be no way to be able to determine that the RNA used to create the “SARS-COV-2” genome came from one source. In fact, the only time Dr. Nakagomi states purification is not necessary is when the genome is already known and established, thus purification is a neccesary step to obtain the initial genome. Yet this creates a bit of a conundrum. Where has it ever been shown that the particles assumed to be “viruses” were ever purified and isolated directly from a sick human in order to obtain the original genome for any “virus?” At some point in the history of “viral” genomes, this purification and isolation process must have been carried out before any genome for any “virus” could have been obtained and considered accurate and reliable. However, it has never been done, especially for “coronaviruses” as I outlined here.
The “SARS-COV-2” genome was nonexistent and there was no prior knowledge of its sequence. The genome was created from unpurified broncoalveloar fluid (BALF) from one patient and cobbled together in a computer from other unpurified reference genomes made in a similar way. In a document by the WHO regarding sequencing genomes using metagenomics, such as was done for the original “SARS-COV-2” genome, it is admitted that high “non-viral” host material will also be sequenced. They claim that purification steps such as centrifugation and filtration are supposed to be done yet even purifying samples will still lead to a high number of “off-target, non-viral” reads:
Genomic sequencing of SARS-CoV-2
“Depletion of host or other non-SARS-CoV-2 genetic material in a sample leads to a higher proportion of SARS-CoV-2 reads in generated sequence data and therefore a higher chance of recovering a full genome.SARS-CoV-2 metagenomic approaches therefore typically include steps to remove host and bacterial cells, through either centrifugation or filtration prior to RNA extraction, or chemical or enzymatic removal of unwanted DNA/RNA. This is easier for liquid samples, from which cells can be more easily separated, such as bronchoalveolar lavage (Table 4). Ribosomal RNA (rRNA) and DNA content are also commonly depleted during library preparation for virus RNA sequencing, and carrier RNA is often omitted from extractions or replaced with linear polyacrylamide. Despite such measures, samples may still contain high quantities of off-target host DNA/RNA that may also be sequenced. Metagenomic approaches therefore generally benefit from input of samples with high virus loads (such that a reasonable proportion of the genetic material in the sample is virus).”
“Metagenomic sequencing typically produces high numbers of off-target, non-virus reads. It is also often (though not always, depending on the sequencing platform and multiplexing) more costly than targeted capture-based or amplicon-based sequencing approaches, because more data have to be produced to generate one SARS-CoV-2 genome. Moreover, pretreatment steps that are particularly beneficial for metagenomics, such as centrifugation, are not typically performed for molecular diagnostic assays so new extractions that incorporate pretreatment steps may have to be performed for metagenomic sequencing.”
Another source on the advantages and disadvantages of genomic sequencing states that contamination, such as that by bacteria which is sure to be present without purification, will lead to inaccurate genomes:
“Factors outside the control of the service provider tasked with isolation and sequencing of DNA can negatively influence the quality of the genome sequence and therefore its interpretation. This can include the quality of the DNA sample provided for analysis, such as low quantity, high bacterial contamination, or sample degradation. Such factors can even prevent the procedure from being undertaken. In such a circumstance, the client might be obliged to deliver a new sample.”
Since Steve and Co. admit that “SARS-COV-2” has never been purified, yet purification is a prerequisite for “novel viruses” in order to obtain an accurate genome, how can they claim that this step is unnecessary?
It’s probably due to the other fact which Steve admitted to: purification is difficult. However, I would go one step further and say that when dealing with nano-sized particles, purification is impossible. I will not go into too much detail in this post as I have outlined the purification problems here and here. However, it has been admitted numerous times that it is impossible to separate “viruses” from exosomes and other extracellular vesicles that co-sediment together. There is no one method, whether ultracentrifugation, filtration, precipitation, etc., that can completely purify the “viruses.” Although you can find similar statements in some of the posts I linked, I will provide a recent article which focused on the need for purifying RNA for epigenetic studies. The authors supply various purification methods and then admit that none of them alone are sufficient to purify “viruses” from host-derived impurities. These impurities then impact the creation of the genome and any study relating to it. Even when combined, they can only claim that these methods will increase “virus” yield and quality, not completely purify the particles.
“The relatively low abundance of viral genomic material within the nucleic acid milieu of clinical samples places constraints on the utility of epigenetics-related applications, like m6A RNA methylation ELISAs, to specifically study the virus epigenome. Such assays require highly pure input material, free from host-derived impurities whose epigenetic modifications can also be detected and interfere with results.”
“The methods included above are generally not sufficient, when performed alone, for adequate purification of viruses. Studies focused on the virus epigenome require highly pure input material, without interference from the epigenetic modifications of host DNA, RNA, or protein. Combinations of the aforementioned methods can increase viral recovery, yield, and quality.”
Even when the purification steps are performed on samples, there will always be many known and unknown identical particles with various sources of genetic material within the sample. Contamination is a widespread problem both in cell culturing and genomics. This makes electron microscopy imaging and the creation of a genome utterly meaningless and useless as proof of a “virus.” In order to hammer this point home, here are a few highlights from a 1996 Manuel on “virus” purification:
“Virus purification is the physical separation of virus in a concentrated form from the host cell milieu in which it has grown. Viruses need tobe purified for many studies in which properties or structure of the virus must be distinguished from those of the host cells or culture medium, such as analyses of structure of viral polypeptides, function of membrane glycoproteins, etc.”
Criteria of purity
“The observation of particles in the electron microscope, whilst not a good criterion of purity, does allow the detection of ‘unwanted structures’.
It would be expected that constituents of the medium would form a major part of the contaminants of purified virus preparations. This can be monitored by gel diffusion tests, where antisera raised against e.g. calf serum, or uninfected cells can be reacted with virus preparation.”
As can be seen, “viruses” must be purified in order for the structure and physical properties of the “virus” to be distinguished from host cells and the culture medium. The constituents of the culture medium are said to be the bulk of the contaminants in purified “virus.” This would include the fetal bovine serum which is added to nearly every culture which is a completely separate source of RNA from the host source. They fail to mention the added animal RNA which would come from the Vero cells regularly used for culturing as in the case of “SARS-COV-2.” All of this “non-viral” material would need to be eliminated first along with the host material as well as possible contamination from bacteria, exosomes, MVB’s, other microrganisms, etc. before a genome could be considered valid. Otherwise, there is no realistic way of knowing which RNA belongs to which source within the mixture and whether or not the computer-generated genome is an amalgamation of the RNA stitched together from those numerous sources.
It is clear that purification is an absolutely necessary process, even though the methods themselves are flawed and unable to completely purify these preparations. This is why Steve and Co. claim it is “difficult” (i.e. impossible) to purify “viruses,” that it is no longer necessary, and why they want to skip over this step entirely. They know it is impossible. They know that they can not supply a single study where the particles claimed to be “viruses” were completely purified and isolated directly from a sick host. They can not even show this in papers where “viruses” are cultured. They want you to believe that technology has advanced to a point where it can pick through these unpurified mixtures of RNA in order to piece together a theoretical representation of an unseen “virus” in the form of a genome. Even if this was a logical argument (it’s not), a genome from unpurified samples would be at best INDIRECT evidence, not DIRECT evidence of a “virus.”
Fortunately, even disregarding the sources I’ve shared above which completely dispute Steve and Co., we can rely on logic and critical thinking to understand that their claims are ridiculous. In order for a genome to be considered valid evidence, the entity being sequenced must be shown to actually exist in reality first. One can not just assume an unseen “virus” is within the unpurified sample from the start without ever verifying that it actually exists to begin with. This requires that the particles claimed to be “viruses” be found in a state completely free of contaminants, pollutants, and foreign material as well as separated from everything else. In order for this to occur, the sample must be put through the steps of purification (centrifugation, filtration, precipitation, etc.) so that it can be shown to exist in an isolated state. Only then can proof of pathogeniticity be aquired using the purified particles as a valid independent variable in order to establish cause and effect. Only then can the particles identified in EM images be said to be the “virus.” Only then could a genome be aquired. Only then can the “virus” be fully characterized.
Without purification, Steve and Co. have no “virus.”
And so we get to the crux of the problem with relying on “experts” to do the thinking for you. Steve has relied on his “experts” to tell him that the purification process is unnecessary. He allowed the “experts” to tell him that the definition of isolation means to add many things together rather than what it actually means which is to exist in a state separated from everything else. He did not do a cursory bit of research to understand that his so-called “experts” are wrong. However, their inaccurate claims are now his to defend. Sadly, Steve is adamant that, while he was willing to invest the time to write a blog post about his unwillingness to do a debate, he is not willing to invest his time to actually defend his claims in a debate. So the way I see it, Steve has three options:
Find the time to debate Christine and her experts to defend his ridiculous claims.
Find new “experts” who understand the methods used for the purification and isolation of “viruses” and why they are necessary.
Find the time to do his own research and utilize critical thinking and logic to discern truth for himself rather than relying on “experts” to do the thinking for him.
I’m hoping Steve chooses option # 3. However, I’m not holding my breath.
You can buy bottles of Liquid Fear (LF) at your local pharmacy. Over the counter.
No refrigeration necessary.
I suggest sipping through a straw to start. Don’t gulp it all at once. You want it to seep in.
One day you won’t take a walk in the park. You’ll say you have other things to do. But you’ll be afraid of strangers breathing on you. Breathing is dangerous. Who knew?
Now you do.
Fear was first isolated by Louis Pasteur in 1884. He wrote in his diary: “I was sitting in my kitchen drinking a glass of pasteurized milk, and suddenly I realized I could extract blood from a patient and separate out anxiety from the sample. Later that day, I took a vial of blood to the local prison, where they kept killers in a special section. The guards brought these dangerous men into a room, where I had placed a bit of blood on a slide, under a lamp, on a table. The men stared at it, and soon a colorless liquid migrated from the blood on to the table. I sucked it up into a dropper and squeezed it on to the arm of a guard. He promptly fled from the room…”
For near a century and a half since that day, governments and corporations have been trying to produce very large amounts of the fear liquid.
Finally, in February, 2020, in an NIAID lab, under the direction of Anthony Fauci, Doctors Rachel Maddow and Anderson Cooper were able to synthesize the fear particle using blood obtained from several hosts of The View.
“From that point on,” Cooper told reporters, speaking yesterday from CNN-CIA headquarters, “we activated a special machine that transmits voice vibrations from leading news anchors, we focused the vibrations on the synthesized fear particle, and within an hour we had 567 gallons of pure liquid.”
Untersturmführer Klaus Schwab, executive chairman of the World Economic Forum, stated, “After all, this pandemic is your basic terror operation. How else are you going to hold society together and mobilize it?”
The drink, it turns out, has been bottled and sold, by corporations, under a variety of names for the past year and a half. For example, XXX [censored] and XXX [censored].
Schwab continued: “Since the dawn of time, people have been falling ill and dying for a variety of reasons. Down through the ages, some of those people who recovered said, ‘When I was sick THIS time, it was really DIFFERENT. I had never experienced anything like it.’ Anyway, now we take all that sickness and dying and we re-label a large part of it ‘COVID’. Add the fear particle and we have our window of opportunity to transform the world.”
The COVID vaccines are not an antidote. They’re not designed to affect emotions. They scramble internal systems of the body.
The President has announced the formation of a new cabinet post, the Department of Trepidation. Michigan Governor Gretchen Whitmer and Whoopi Goldberg have been put on a short list of candidates to serve as its first director.
Social media trolls have already begun calling this innovation The Department of Pussification.
The CDC has announced adult guidelines for imbibing the fear drink. Basically, the agency recommends a first dose of two tablespoons, twice a day, for the first week. Thereafter, a pint a day in the morning for a month; and then a quart each day, on an ongoing basis. Researchers are conducting studies to determine the dose schedules for children.
Groups of “anti-fearers” in Tennessee, Kentucky, and Florida have sprung up. US Attorney General Garland has issued a memorandum to all Dept. of Justice employees: “These groups share common anti-government sentiments. They tend to cling to religion and guns. We have to be on the alert for acts of domestic terrorism…”
Public health departments across the country are, according to the Washington Post, “investigating charges of disproportionate distribution of LF [Liquid Fear] to underserved communities of color.”
This morning, California Governor Gavin Newsom appeared at a press briefing, standing in front of a huge poster carrying the simple message, SUPPORT FEAR. Newsom said, “This is not the time to back down from what we feel. Embrace it. It’s healthy, it’s real, and it’s our passport out of this pandemic. I’m especially addressing our young children. Don’t worry. Drink from your bottle. It tastes great. And to the adults: there’s nothing to tremble at but the absence of trembling.”
Senator Chuck Schumer has introduced a bill allocating emergency funding for federal bottling plants in sixteen states. The word on Capitol Hill is, the new government version of LF will be called Quake, or Anthony.
Last week, in Northern Florida, at the Hanging Chad Park, local organizers staged an impromptu concert featuring Eric Clapton and Van Morrison. For nearly a half-hour, 75,000 adoring fans shouted in unison:
FUCK FEAR.
Several hundred FBI agents, dispatched to the scene, stationed themselves around the periphery of the park.
People keep asking me where they can find a good doctor.
The real question they need to ask is whether they even need a doctor, because the medical system has become detached from health. But has this happened recently or did medicine go off the rails long ago?
ONE: Let’s not get distracted by the virus question. We have to focus on knocking down the vaccine mandate.
My Reply: Can you walk down the street, carry a bag of potatoes, and look at messages on your cell phone? Newsflash: people have been known to do several things at the same time.
TWO: If we bring up the virus question, people will call us crazy and have a reason to ignore our criticism of the vaccine.
My Reply: “People” already say we’re crazy. They have 345 “reasons” on file.
THREE: If we say the virus doesn’t exist, “our base” will desert us.
My Reply: “Our base” is so outraged about the ineffective and hugely destructive vaccine, and about the mandates, NOTHING will deter them from attacking the vaccine.
FOUR: It’s well established that the virus exists.
My Reply: Yes, established by the same scientists who say the vaccine is remarkably safe and effective.
FIVE: Doctor A says the virus exists. As evidence, he cites Doctor B’s statements. Doctor B says the virus exists. He cites Doctor C’s statements. Doctor C says the virus exists. He cites Doctor A.
My Reply: Go back to school. I suggest starting at the 4th grade.
SIX: It doesn’t really matter whether the virus exists.
My Reply: If the virus doesn’t exist, the pandemic is a hoax. If the pandemic is a hoax…trace all the implications. If you can’t, go back to school. I suggest starting at the second grade. If the school won’t let you in, tell them you identify as a six-year old.
SEVEN: If I say the virus doesn’t exist, my family will disown me.
My Reply: I see. Other than the virus question—you’re on very good terms with your family, right? Who are you trying to kid?
Speaking of kid, here’s another dialogue for your edification—
ME: Hey kid, aren’t you fed up with all this COVID crap?
KID: Listen, Grandpa, I’m been fed up with crap since I was born.
KID: I wore one once, at the DMV, when I applied for my driver’s license. The witch behind the counter told me I had to put that germicide goo on my hands. So I did. I wiped my hands on the counter. She called security. I don’t drive. I take the bus.
ME: What about the vaccine?
KID: Let me put it this way. My cell phone says I took the shot.
ME: Did you get depressed during the lockdowns?
KID: No. I made money fixing old people’s computers. When I went to their houses, I wore a military uniform. Nobody bothered me.
ME: Are you woke?
KID: You mean do I think every move I make is motivated by systemic racism? That crap is for my friends whose parents give them money. They all moved away. Their parents took them to Florida.
ME: What about the virus?
KID: What about it?
ME: Do you think it exists?
KID: The people who say it does—I don’t listen to anything they say.
ME: Why not?
KID: If you can’t figure that out, Grandpa, you’re older than you look.
ME: Are there a lot of kids like you?
KID: Millions.
ME: Do they listen to the government?
KID: You mean the mafia. We don’t pay protection money to anybody.
ME: Do these millions of kids take the vaccine?
KID: It’s always a tip-off when somebody says, “Hey, it’s free.” We’re not that stupid.
ME: Have you ever voted in an election?
KID: Once, when I ran for student body treasurer in high school. I ran because the treasurer handles student funds. I voted for myself 27 times.
ME: Did you win?
KID: I came in third. The kid who won was the son of the assistant principal. Very quietly, that old codger was trying to get us to join his secret transgender club. We told him we already had the sex change, he just couldn’t spot it. We also told him the local pedophile priest, Father Joseph, was opposed to transgenderism on moral grounds. We suggested he should turn Father Joseph into the authorities for the hate crime of opposing transgenders.
I now return you to your regular scheduled programming, sponsored by Moderna, the company that cares about you. The company that had never brought a single product of any kind to market, before the RNA genetic shot. The company that spawned several billionaires overnight. The company championed by little Anthony Fauci, serving his last term as de facto president of the United States.
My readers know that, for the past two years, I’ve been making the case that the virus is a scientific fiction, a con, and a cover story for tyranny that would make Hitler, Stalin, and Mao blush with envy.
Recently, the question has been attracting wider coverage: Does SARS-CoV-2 exist?
Entrepreneur, inventor, and philanthropist, Steve Kirsch, says yes. He offers to set up a 5-hour live video debate. He’ll send his experts and other side will send theirs. They’ll go at it.
What about the usual form of scientific debate, called the written word?
Buckle up.
Kirsch: “I don’t think the folks I’d ask to do this would want to spend time writing papers…They don’t even have the time to prepare their own papers. Doing written documents is much more time consuming than talking because people spend the time to make it bulletproof.”
Heaven forbid.
Kirsch: “None of the people on our team require that all discussions be in writing only.”
Of course not. Why would his team of scientists insist on the method by which science is accomplished?
Kirsch: “One of the commenters [to an article by Kirsch] wrote this: ‘But when someone really knows their shit they would much rather handle it in a live conversation; it’s much more efficient (you don’t spend hours writing) and it reaches a wider audience, and that audience has the benefit of tone and body language to affirm (or negate) the veracity and substance of what is being said.’”
Kirsch: “I agree with that.”
Truly awesome.
Tone and body language. Yes, of course. You know, that was Galileo’s problem when he was tried by the Inquisition for insisting the Earth rotated, and journeyed around the sun. If only he’d stood up straighter and spoken with unwavering clarity (in the manner of, say, a Walter Cronkite). He might have won his case. Because tone and inflection equal science. We all realize that. Obviously, Galileo didn’t know his shit.
Spending hours writing arguments about the existence of the virus—who would have the audacity to insist on that? As Kirsch points out, his experts are busy. It’s rude to interrupt them and ask them to make their case bulletproof. Science on Video tends to be based on “we KNOW we’re sure” and “the truth is OBVIOUS” and “WE’RE the pros.” That’s good enough, and you can sell it. If you, again, display convincing tone and body language.
In medical school, they teach this. “One day you students will be called on to defend your actions and opinions with pure bullshit. I tell you that now, to prepare you for the moment. How do you shape and transmit the bullshit? Do you do it through tiresome written reports, which run the risk of exposing the truth, engraved on the page, or do you stand up before a panel and look those people in the eye and tell a story that wows them? Do you fumble to clarify a point, or do you gloss it over with a quick-hitting generality that covers a crack in your armor? Careers are won and lost on that basis.”
Kirsch believes an exchange of papers between debaters is futile. Who can, or is willing to, pore through them and analyze them? And do those written exchanges actually cover all essential points? But with video, we NEVER EVER see opponents talking past each other or quickly changing the subject to avoid unpleasant revelations. Certainly not. We never see opponents smirking like entitled monkeys and making ad hominem accusations. We never witness slippery logic sliding by before it can be isolated and corrected. We never witness grandstanding for the audience’s benefit. It’s never show biz on parade. No mainstream expert would dare intone, “Ahem, in my many years as professor of so-and-so at such-and-such, having engaged in intense research on this question, and having authored over 60 papers on this very subject…”
And then there is the suggestion, as the commenter states, that the audience can decide…on the winner in the debate. Yes. What else is a debate FOR? Science is a democracy, and the audience is the proof of the pudding. Once they vote up or down, the deed is done. This is why, in medical journals, at the bottom of every paper and study, you see the poll question: “DO YOU THINK THIS ANALYSIS IS ACCURATE? CAST YOUR BALLOT. Depending on the outcome, we will maintain the study in our archive or retract it with an apology. Everyone can vote. You do not need to be a subscriber. We work for our audience every day. If the majority of you believes one of our authors has convinced you that the moon is a slice of soft brie on a plate or an elephant’s ass, we concur. This is called consensus, and what else could science be?”
Not long ago, I crashed my Gulfstream in the Himalayas, and after a harrowing journey to the GeFunkte Hospital in Berlin, as I was lying on the operating table, two surgeons debated whether I needed one or two transplanted hearts. Later, I was told a live stream of this discussion had been piped into the hospital waiting room, and the patients expressed an overwhelming preference for two hearts, based on the charismatic presentation of Surgeon Number One, who had studied Voice and Drama at the Julliard School in New York. So…two hearts it was. You can read about the groundbreaking operation in the Medical Journal of Audience Participation.
Published blow-by-blow descriptions of “isolating viruses” are quite dense to begin with. Perhaps one person in two hundred thousand can plow through them and understand them. Therefore, the debate about the existence of a virus starts with something in writing that, for most people, is impenetrable.
It’s no surprise that these descriptions are viewed with suspicion.
“We’re the expert virologists. Only we understand what we’re doing.”
“I see. So understanding virus isolation is like understanding RNA development and insertion into lipid nanoparticles which are injected into a few billion people.”
“Yes, exactly. Only we understand that whole process.”
“Got it. I have grave doubts about everything you’re claiming about the vaccine, but I completely accept everything you’re saying about the existence of the virus.”
In this particular debate about the existence of the virus, the devil really is in the details.
The details concerning exactly how virologists believe they are isolating viruses and sequencing them. As I say, reading the studies, one sees immediately that the accounts of these procedures are laden with technical terms and technical steps.
Those elements have to be analyzed and taken apart, to see whether they make scientific sense. In fact, a debate in writing is the sane way to proceed.
Settling the question of virus-isolation via video would be quite a challenge. An exceptional amount of good will and patience, from the mainstream virologists, would be required. I’ve never seen medical “experts” show those qualities, when the basic assumptions of their professions are on the line. I’ve seen them get up on their high horse, growl, bloviate, dismiss, generalize, tap dance, boil over, accuse, pretend to be oh so reasonable, with their pants on fire.
Someone will say, “But…but, let’s wrap all this up in one sitting. Video will accomplish that. I have things to do, places to go. We live in a fast-food world, face it.”
Yes, you have to go to the store with your mask on and maintain distancing; you have to look for a restaurant that won’t make you flash your vaccine passport; you have to show up at the school board meeting to tell the members what they can do with their mandate forcing your kid to take the shot; when they refuse to listen to you, you have to sell your house, pack up your belongings, and move with the kids from New York to Florida; and all the while, you have to keep deleting voice messages from your brother who’s telling you only the injection will save you and the family wants you institutionalized.
All these and so many more to-do’s begin with the assumption that a virus exists.
So a debate on this point ought to be complete and rigorous.
If the only possibility is a video, have a go. But the written word is far superior.
“Counsel, you have a video where the defendant discusses how he can steal a billion dollars from the pension fund?”
“Yes, Your Honor. But we also have a letter of agreement between the defendant and the head of the Montebello crime family. The letter reveals the defendant has already stolen the money, and will give it to the mob in exchange for certain favors.”
“A letter, you say? Words? Sentences? In writing, on a page? Signed? And it can be read?”
“Yes, sir. Writing is an older form of expression. It’s now being phased out. But it stands up quite well. It’s bulletproof.”
“…I think there has been, you know, a total wave right of criticism of the the truth that viruses don’t exist and cause disease. And we see that, seemingly at the same time, that the pandemic seems to be drawing near an end. Right?
We see suddenly lifting restrictions all over the world.
And even Bill Gates predicted in 2022 that would be the end of the pandemic.
The Wall Street journal printed an editorial saying that…essentially last three weeks a major drop in cases, and it signifies, you know, what do they call it — the herd immunity. Right? Which is another thing we can debunk.
So, as they’re kind of ending out of this — and, you know, I’m sure that there’s more planned in the future. And I don’t know if it’s going to be a health crisis or not. But if this does peter out, they want to make sure that as we, you know, get this relief and come out of it — and probably they want us to look at them in a favorable light.
But they want to make sure that we still believe in deadly and dangerous viruses.
And they want to make sure that we still believe that there are safe vaccines, even if we question the safety of these particular genetic injections.
That we retain those important beliefs, so that they can still continue to profit and manipulate and, you know, run operations in the future.”
~ Dr. Andrew Kaufman
Video available at Dr. Tom Cowan BitChute channel.
See Dr. Mercola’s article “Yes, SARS-CoV-2 Is a Real Virus” here.
Truth Comes to Light editor’s note: The video below was recommended by Dr. Tom Cowan as preparation for viewing his upcoming conversation with Dr. Andrew Kaufman in regards to Dr. Mercola’s recent article about virus isolation. You can register here to participate in the zoom conversation. The video will also be available at Tom Cowan’s channels following the event. We will repost the conversation here at Truth Comes to Light when it is available.
Addressing the pink elephant in the room pertaining to scientific practice, electron microscopy, histology, and the misinterpretations within modern biology in general.
Video available at RealEyesation Rumble and YouTube channels.
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light Odysee, BitChute and Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
[Truth Comes to Light editor’s note: On January 17 when this article was first published, a live link to Dr. Mercola’s article could still be found at his site. Due to attacks from mainstream media, his articles only remain open for public view for 48 hours. It is now available behind a paywall at his archived site. However, you can find a copy here or at many other websites and blogs that reposted the original. ]
This image is a screenshot from Dr. Mercola’s article which is now found in his archives and at many other websites and blogs.
You’ve published anblog titled “Yes, SARS-CoV-2 Is a Real Virus“.
One of the sources you relied most heavily on for this claim is a recent blog by Steve Kirsch, which is really interesting because in that blog Steve admitted right off the top that he actually has no idea whether or not the alleged virus has even been isolated and that he relies on other people’s opinions.
Now in your blog you state that: “SARS-CoV-2 has been isolated, photographed, genetically sequenced, and exists as a pathogenic entity.”
I hope we can agree that a specific thing must be known to exist in order to know that “it” is pathogenic. Not believed, imagined, assumed, or wanted to exist, but known. Because otherwise it’s impossible to establish even a correlation, let alone prove causation of anything.
Yet nowhere in your blog did you present or cite any proof that that the alleged RNA genome of 30,000 base pairs surrounded by a spikey protein shell actually exists.
I’ll briefly review some of the sources you’ve cited to explain why I say this.
You start out with a video that features Jeremy Hammond insisting that “the virus” is real, has been isolated, and is a necessary factor in “COVID-19”.
(For the record, I had an extensive email exchange with Jeremy on this topic, between October 25 and November 14, 2020. I encourage you and your readers to review it.)
In this video, Jeremy made bold claims indeed. But despite stating that the “virus” existence issue is “probably” his “biggest pet peeve“, he came to this interview armed with zero sources showing that the alleged virus does exist. In fact Jeremy cited no studies of any kind. Just unsubstantiated claims, and reliance on the beliefs of others. They could do this, they could do that. They can’t do this, they can’t do that.So-and-so says this, so-and-so says that.
Instead, Jeremy insisted that the following is the “gold standard” for “isolation” of a disease spreading “virus”: irrational and unscientific interpretation of cytopathic effects in a cell culture – typically malnourished monkey kidney cells to which toxic drugs have been added, and further contamination in the form of fetal bovine serum is added as food for the cells, along with a patient sample (not a purified sample of anything).
This, in Jeremy’s mind, establishes the existence and presence of a virus. Which is why he’d make a great virologist. Jeremy doesn’t think like a scientist, and as I always point out, “virology is not a science“.
And Jeremy lied through his teeth when he went along with the naïve (I’m giving her the benefit of the doubt) comment from his interviewer that virologists then pull “the virus” from the cell culture. “It really is that simple.” (I challenge Jeremy or you, Dr. Mercola, to cite any study where a specific thing was “pulled”, even from a monkey/cow/human mixture aka cell culture, and shown scientifically to be a disease-spreading “virus”.)
Jeremy insists that the CDC has isolated “SARS-COV-2”. Well, yes they have according to the meaningless, antiscientific approach to “isolation” used by Jeremy and virologists.
But did the CDC researchers apply even a modicum of logic or scientific method and actually establish the existence of the alleged virus? That’s an entirely different matter and the answer is a resounding “No”.
The CDC’s “SARS-COV-2 isolation” study is just another example of the typical fraudulent monkey business (literally) that plagues our world. I have addressed the CDC’s study previously, and will address this same issue of virology’s blatantly bogus “isolation” methods below.
Jeremy carried on with more bizarre claims: that scientists never isolate/purify anything, and don’t have the technology to purify things like alleged viruses.
Jeremy also strangely implied that people (such as myself) who say that proof of a disease-spreading “virus” requires purification actually demand that the alleged virusbe floating in a vacuum.
Dr. Mercola, I’ve been involved in this issue for almost 2 years now and don’t know a single man or woman who defines isolation/purification as “floating in a vacuum“.
And Imake explicitly clear in my Freedom of Information requests that this is not how I define isolation/purification. Below is a screenshot from a recent FOIA request to the CDC. They have no records, like all 164 other institutions in roughly 30 countries, that have been asked by people around the world. No one on the planet has purified a sample of the alleged “virus” from a disease human, or knows of anyone who has, even though supposedly millions and millions of people are infected and spewing this “virus” every time they breath.
And no, contrary to Jeremy’s claim, it is not people such as Dr. Andrew Kaufman, or Jon Rappoport, or Drs. Sam and Mark Bailey, who bizarrely redefined the word “isolation”. It’s virologists who redefined it, to mean mixing various complicated substances together and drawing wild conclusions – quite the opposite of its historical meaning.
It’s funny how everyone knows that “isolate” means “separate” when it comes to isolating humans and the “confusion” only arises when it comes to theoretical “viruses”. And how a virologist’s use of the word “isolate” gives the impression of legitimate science when nothing could be further from the truth.
Dr. Mercola, I couldn’t help but notice the unicorn in the background over the shoulder of Jeremy’s interviewer. Was this video inserted into your blog as someone’s idea of a joke? I mean, these people proved a virus no more than a unicorn, and unicorns are a popular analogy for imaginary viruses these days, thanks to Dr. Tom Cowan, and I can’t for the life of me imagine why you would have purposely included this video when it’s completely useless to anyone looking for proof of a virus.
And no Dr. Mercola, we are not confused. We’re quite familiar with what virologists have been getting away with.
As distressing as it is to do so, since you have chosen to rehash Steve Kirsch’s summary of the curious “science” of Sabine Hazan, I will briefly address it once again, here, as I did in my educational Open Letterto Steve.
To put it bluntly, Sabine Hazan’s study is 100% useless and fraudulent. The RNA used in her “sequencing” was a genetic soup from various sources, including patients, and not shown to involve any alleged “virus”.
She fabricated meaningless codes on a computer that have never been shown to correspond to anything in the physical realm and falsely passed these off a “viral genomes”.
Sabine compared her meaningless “sequencing” results to the results of her utterly meaningless and fraudulent PCR tests (that she is quite secretive about, at least with me) that also have never been shown to have anything to do with a “virus”.
Sabine comes unhinged when directly challenged on the validity of her so-called “science”. I encourage your readers to try this themselves and see what happens (and send me the results at cmssyc@gmail.com).
Dr. Mercola, I also already addressed ATCC’s very expensive and fraudulent “virus” product that you are now promoting as well, in my educational Open Letter to Steve Kirsch. Please be sure to review that section. It includes a Buyer Beware!from Dr. Saeed A. Qureshi, PhD, who spent 30+ years as a scientist (as opposed to a virologist) with Health Canada.
Dr. Mercola, I challenge you to track down the origin and contents of any ATCC “SARS-COV-2” product, as I did last year for the so-called “SARS-COV-2 isolate” that is referred to as “MUC-IMB1” aka “BavPat1” and sold by companies like EVA for 2 000,00 €per vial, and report back to your readers what you learn. Report the detailed methods that were used to allegedly verify that the product contains any disease-causing “virus” whatsoever.
Regarding your claim that “Germ Theory and Terrain Theory Both Have Merit”, can you prove with science that virology has any merit whatsoever?
Please prove the existence of a specific physical thing alleged to be a disease-spreading “COVID-19 virus/variant” aka “SARS-COV-2” and prove that that specific thing spreads disease from host to host via natural modes of exposure in animals or humans.
I challenge you to publish a study proving that such a thing exists. Show with science that only subjects that are exposed to that specific thing get “COVID-19” respiratory disease, as claimed by Jeremy, whose wild unsubstantiated claims you are now disseminating.
Dr. Mercola, as evidence that “the virus” has been isolated and sequenced, you are citing studies that rely in part on PCR “tests”. Without bothering to go into all the well documented fatal flaws with these so-called tests, a little logic is in order.
It is impossible to validate any “test” without a gold standard.
It is impossible to validate any “test” claimed to “confirm” the presence of a “virus” (or a “viral infection”) before the alleged “virus” has been proven to exist.
It is impossible to validate any “test” claimed to “confirm” a “viral disease” before the alleged “virus” has been a) proven to exist and b) proven to cause the disease.
Obviously an indirect test for a “virus” cannot logically be used to prove the existence of the alleged “virus”. The test is what it is. In the case of PCR, in the very best case scenario, it is evidence of the presence of the very tiny target genetic sequence. Nothing more. Not a virus, not a genome, just a tiny little sequence.
And cytopathic effects on a cell culture, any cell culture, are just that – effects. An effect is not the cause of the effect. And wild assumptions about the cause of the effect are just that – wild assumptions, not science. This is especially true when the cells in question have been malnourished by lowering the level of food for the cells (typically fetal bovine serum) and poisoning the cells with toxic drugs.
Dr. Mercola, I am shocked that you actually published this quote from the sketchy, brief Letterfrom Italy that you cited, as evidence that a “virus” has been sequenced:
“[Vero E6 aka monkey kidney] Cell culture supernatants from passage 1 (P1) of four isolates were collected, and RNA was extracted…”
First of all, as you seem to understand and as should be clear by now, “isolates” do not mean purified, isolated specimens in virology. Quite the opposite. In the case of “SARS-COV-2” studies, they are monkey/cow/human mixtures. And the authors are telling you in plain language that they extracted the RNA from the cell culture supernatants. Not from a purified specimen of an alleged virus.
These authors are telling the world that they have a soup of genetic material, and are going to concoct on their computer a so-called “viral genome” out of the zillions of sequences that they (kinda, maybe, sorta) detect therein. Because this is virology, not science.
Do we really need to discuss this any further?
Dr. Mercola, fabricated “genomes”, meaningless, impossible-to-validate PCR “tests”, wild assumptions about the cause of effects on a malnourished/poisoned cell line, and arrows added to EM images and pointing at particles that were never purified, never sequenced, never characterized, never studied with controlled experiments does not add up to science.
Virology is not a science.
Dr. Mercola, it is very distressing to see you promoting blatant pseudoscience that has been used for decades to fool and coerce people around the world in myriad ways, not limited to the utterly useless and harmful injections that have fraudulently been passed off as “immunizations”.
Every time you (or someone like Peter McCullough) do this, people such as myself have to spend hours clearing up all the confusion you have caused with the public.
You need to do your due diligence, find and share the “missing” scientific proof of viruses, or retract your blog, apologize to your readers, and get on the right side of history. You’ve had 2 years already to figure this out.
Hopefully the public will soon tire of relying on “experts” and simply read the ridiculous “virus isolation” studies for themselves. When that happens, this pseudoscience (which is really too generous a word) is finished forever.
Best wishes, Christine Massey, M.Sc.
Peterborough, Ontario, Canada
Andrew Kaufman M.D. refutes Jeremy Hammond’s recent interview opining that SARS-CoV-2 has been shown to exist. Point by point, Kaufman debunks Hammond’s explanation of how a virus is discovered.
The definitions and technology behind isolation, the methodology being used by scientists, and the agenda by governmental agencies are examined with the appropriate corrections.
Hammond’s argument is the same old one trick pony being trotted out with pomp, circumstance, and pedigree.
Video available at DrAndrewKaufman BitChute channel.
Truth Comes to Light editor’s note: The screenshot seen below is from Jeremy Hammond video as found within Dr. Joseph Mercola’s recent article: Yes, SARS-CoV-2 is a Real Virus. Many sites have republished Dr. Mercola’s article. A web search will locate it for you. We have not shared it here at Truth Comes to Light.
Are you tired of wearing a cloth mask that resembles a face diaper that does nothing to filter the air?
There are other mask models to consider that have stood the test of time, and may help you stand out in a crowd, instead of blending into it.
Who Were The Plague Doctors?
One such model is the Bird Beak Mask. Since the 16th century, this menacing-looking mask has been a fashion statement of Plague Doctors who used it to filter their air stream while treating victims of plague and burying the dead. However, to everyone else, the beaked mask and coverings were a sign of death, the Grim Reaper in the flesh.
The Plague Doctors were the well-educated, well-connected, well-known and wealthy men from rich families, even if they were terrible healers. The sole purpose of the Plague doctor was to treat plague patients, even if the cause was as elusive as the cure. History tells a story that plague victims’ bodies piled up quickly, were carted away, and unceremoniously dumped into mass graves. Hundreds were burned at a time. Entire villages simply ceased to exist.
The plague doctors’ duties were far more actuarial than medical. Most did a lot more counting than curing, keeping track of the number of casualties and recorded the deaths in log books.
These doctors were not allowed to mingle with the general public (much like the political and Hollywood elite, today), and were said to self-quarantine for long periods of time after treating patients. History writes of Plague Doctors living lonely lives in isolation, but who really knows, since many of them just up and disappeared after the plagues, never to be heard from again.
Plague doctors were sometimes requested to take part in autopsies, and were often called upon to testify and witness wills and other important documents for the dead and dying. Not surprisingly, many a dishonest doc took advantage of bereaved families, holding out false hope for cures and charging extra fees (even though they were supposed to be paid by the government and not their patients). – Doctorsreview.com
Before or by the 17th century, three dominant Theories of Disease Transmission were accepted:
1) By Miasma Theory, or “bad air”
2) By divine mandate through the Will of God, or by the Planets or Comets
3) By some unknown device jumping from person to person.
The Costume
To ward off miasma, and other possible transmitters of disease, the Plague Doctors’ costume was developed to look like a featherless, black “Big Bird.” The six-inch beak area over the nose also came with round eye openings and a black wide-brimmed Morocco leather hat that indicated the profession of doctor.
The beak functioned as a respirator and contained herbs, such as wormwood, spices, dried flowers, camphor, and a vinegar sponge that protected against miasma or “bad air.” The shape of the beak is said to have slowed the passage if air before being absorbed by the herbs and traveling to nostrils and lungs. The full-length impermeable coat was made from waxen leather. The hands were gloved. And the canes were used to examine victims without touching them.
Building on the theory of miasma, some plague doctors in France set the scented material inside their masks on fire in the hopes that the smoke would help to clear the bad air. – Doctorsreview.com
In fact, the costume of the 16th century was dusted off and reused in the 17th and 18th centuries, since plagues seemed to suddenly appear every 100 years, like clockwork. Each plague came with a narrative of “the most feared disease in the world, capable of wiping out hundreds of millions of people in seemingly unstoppable global pandemics.” Sound familiar?
Unfortunately, with each plague, the Plague Doctors were never able to prevent or cure the plague. No matter how certain the Plague Doctors believed in their treatments and “cures,” they universally failed. Could the poor outcomes have been due to the treatments?
The Treatments
These were the times of blood letting, where Plague Doctors bled a vein to release “bad blood” or “hot blood.” Sometimes vinegar, arsenic and mercury were fed to infected individuals. Food might be rubbed on the patient’s body, including onion, herbs, pigeon, or snake, dead of course. Sometimes doctors would burst an inflamed lymph node in the neck, groin, or armpits.
Doctors tried to purge a fever by sitting a patient close to a fire, and there was always the option of smothering patients in their own feces, or dropping them off in the sewer overnight if they couldn’t produce enough of their own waste. Patients were told that the plague was punishment from God. And it was reported that some devout patients asked to be beaten into repentance with the doctor’s cane or a whip. But that may just be a story.
According to Historian, Winston Black, the Plague Doctors did not have clients. “Instead, they went around the city during a plague outbreak, making decisions about which houses to lock up or condemn, which neighborhoods to quarantine, and so on.”
The beak doctors, as they came to be know, dropped like flies or pretty much lived under constant quarantine, wandering the countryside and city streets like pariahs… until of course desperate families needed them.
During the Middle Ages, there were alternative treatments. Botanists were known as herbalists; they collected, grew, dried, stored, and sketched plants. Many herbalists became experts in identifying and describing plants according to their morphology and habitats, as well as their uses. The best medieval treatment that healed was a salve made of onion, garlic, wine, and cow bile that has shown promise 1000 years later against today’s “modern” Superbugs. This salve can kill 90 percent of the methicillin-resistant staphylococcus aureus (MRSA) bacteria cultures.
MRSA is a serious public health concern; it is a difficult infection to treat, as it has naturally developed resistance to modern antibiotics, and has thus been given the classification of “superbug.”
Were victims of the plagues victims of parasites?
Worms and Parasites
Whenever the body’s immune system is depressed or suppressed due to toxic exposures, including radiation or harmful frequencies, and malnutrition, that is a proven recipe for pathogenic microbes and parasites to move in.
Some have recorded that ancient Rome was known to fertilize crops with human feces, which may have provided a vector for parasitic infections in the early documented plagues. Likewise, eating raw fish and unfermented fish sauce was another opportunity for tapeworm infestation in ancient Rome, especially if people were exposed to other toxins.
Research in the 2016 Journal Parasitology, from the University of Cambridge, shows that Romans experienced parasites as whipworm, roundworm, and a fish tapeworm. Even with sanitation, they suffered from ecto-parasites such as fleas, lice, and bedbugs at the same rate as Vikings and Medieval Europeans.
What about exposures not recorded or lost vital records? Or altered records describing toxins from water or air? What about new frequencies unleashed during plague-ridden times that mimic flu symptoms in the body?
Today, people are faced with toxic exposures, radiation, and particle dust (PM 2.5) that enters the blood and lungs to create chronic lung diseases. Harmful frequencies and malnutrition are also hazardous to health and ignored, for the most part, by health authorities. These exposures all change the pH of the body’s tissues to draw in pathogens and could be main reasons why most people harbor parasites today.
Under the “COVID” scare, the National Institutes of Health promotes the anti-parasitic animal, drug “Ivermectin,” without using the term parasites. While this drug may work for some people, similar to another anti-parasitic FDA-approved, non-toxic drug, Fenbendazole, it does not work for everyone. The presence of parasites represents a warning that the body’s immune system is breaking down. In fact, most if not all cancers represent parasite infestation, even if the presence of parasites does not always indicate cancer. Parasites in humans also reflect parasitic human relationships. And there are plenty of those, from friendships and marriages, to relationships between doctors and patients, and between citizens and governments.
When parasites overwhelm the body it is called hyperinfection. The symptoms of parasites include chronic cough, fever, chills, chest pain, and fatigue, symptoms similar to flu. From the 16th century to the 21st century, if medical doctors have not improved their success rates over diseases, it may be due to lack of knowledge.
Most doctors diagnose disease without testing for parasites. Why not test when there are multiple ways parasites take up residence in the body? One reason is the price tag for an antiparasitic prescription, which can reach over $8000 for fourteen 200-mg tablets of prescription Albendazole, once the insurance companies get involved. According to Goodrx.com, 4 tablets of Albendozole cost approximately $115.00 if you purchase them yourself. Surgery is more also profitable, at over $100,000, than prescribing antiparasitic tablets.
Doctors continue to choose dangerous prescription medications such as the FDA-approved drug Veklury (remdesivir), as well as harmful procedures (ventilation), that can cause death. New antiviral medications for COVID come with adverse health risks. Neurotoxins, aluminum and mercury (Thimerosal) are still found in some injections, called vaccines, “to safeguard against contamination,” believe it or not.
Biophysicist and naturopath, Dr. Hulda Clark (1926-2009), provided a recipe for making Lugol’s solution in her 1995 book, “The Cure for All Diseases.” In her book, she tells readers to ask pharmacists to make Lugol’s Solution. At the time her book was published, a pint of Lugol’s Solution, sold in brown glass bottles, cost about $20. Lugol’s popularity among physicians of the 19th Century is reflected in the poem:
If ye don’t know where, what and why, prescribe ye then K and I
The atomic symbols, K and I, are symbols for potassium and iodine. Farmers can still purchase iodine crystals if the DEA can verify the location of their farm with a satellite photo. The DEA also allows the sale of a 2% Lugol’s Solution, since the 5% dilution is banned.
If simple solutions to health exist, why, then, are are doctors still failing to create health or avert the diseases that plague populations?
The Plague Makers
Running silently underneath the publicized disease plagues that build fear of communicable diseases, and death tolls, are the unseen plague makers.
From The Bubonic Plague of 549 to the Black Death of 1348 to the Cholera and Typhoid scares of the 1890s [and the promotion of the Germ Theory], to the 1918 Spanish Flu, there have been dozens of so-called plague infestations. See an “approved” historical timeline of some plagues and epidemics. Read about the coincidental timeline of electricity in The Invisible Rainbow.
Each new plague and pandemic was accompanied by a hidden more sinister plague of new restrictions on the rights of the people under “quarantine authority.” Government quarantines began in the 19th century.
Among such restrictions include The National Quarantine Act of 1893 and the 1902 Pan American Sanitary Bureau, the first of a series of international health organizations formed in the 20th century—culminating with the World Health Organization in 1948—that helped to bring issues of quarantine and the control of disease to a global stage. There was the 1944 Public Service Act and the 2001 Patriot Act after September 11 terrorist attacks, and many Acts in between.
All the world’s a stage, And all the men and women merely players; They have their exits and their entrances; And one man in his time plays many parts… William Shakespeare, As You Like It
The common denominator among all plagues was not only the alleged “germ,” or the fear, or the advertised death toll, but it was also the consequences of an ignorant population that allowed “authorities” to tell the stories that removed their freedoms. Could the biohazards just as well have originated from contaminated air, or new frequencies, or both?
History repeats itself if unchecked. And we, as humans, repeat the same events under new names perpetually, over and over again, if unconscious. Mass extinctions of people and freedoms happen simultaneously, through wars and plagues. Each time they happen, it is through ignorance, because people choose to become victims over and over again.
Did the Plague Doctors disappear without a trace, or did they assume a different title, with different tools, and a new costume? Is it time to recycle the herb-filled beak mask as an air purifier for anyone who wants a functional mask during the latest plague known as COVID?
Perhaps prior to 2020 the issue of virus isolation was of minimal interest to the vast majority earth’s inhabitants. Most people blindly accept the medical establishment’s claims that viruses exist and can cause disease. They otherwise don’t give it a second thought. Sometimes you get unwell, and a doctor informs you, “it’s probably a viral illness” – but almost every time, you get better again.
However, the increasingly negative impacts from government instigated policies in the name of the “corona” crisis has resulted in some healthy new interest in the subject. Social cohesion in households and communities is being strained, businesses are being run into the ground, and suspicions about the requirement to be injected every four months to maintain protection against an invisible enemy are on the rise. If no virus has been isolated then its very existence is pure speculation. A phantom menace that has no confirmed physical presence, merely a ruinous psychological construct manifesting as a living nightmare. And those who ignore the pivotal issue of virus isolation are blindly accepting a premise on which all manner of lies can be built.
But there are scientific papers that prove isolation?…
The confusion surrounding virus isolation stems from the fact that many published scientific papers state in their titles or claim in their abstracts that they successfully “isolated” a virus. In 2020 and 2021, we lost track of the number of times we were sent such papers as apparent proof of the “SARS-CoV-2” virus. Similarly, industry-funded “fact-checking” sites have a propensity to link to such papers to reassure their spoon-fed readers that the “virus” has been isolated. Unfortunately, such disinformation sites fail to inform their audience that the virologists are not referring to actual physical isolation of any virus and have instead substituted the meaning of the word isolation for something that means almost the opposite.
Researchers such as Christine Massey have tirelessly collated Freedom of Information requests from governments around the world to clearly expose the fact that the alleged causal agent of COVID-19 has never once been physically isolated. While at least one government supported microbiologist has claimed this is disingenuous as the requests are worded in such a way that they are not consistent with the methodology of modern virology, this misses the whole point: the modern virologists are not isolating viruses in the way that the public and probably most of the medical profession are led to believe. Instead, they moved the goalposts.
The excuses for this sleight of hand should be rejected and the isolation of a virus should mean the same as it does with any other entity on the planet – that is, in its pure form, separated out from other material. It is done with things that are smaller than alleged viruses, such as proteins, and things that are bigger such as bacteria. It is not a technological limitation or because of some special property that precludes this process from being essential to the process of real isolation.
The most definitive evidence of a virus would be finding it directly in a host such as a human.
However, despite the fact we are told that a single sneeze could contain 200 million SARS-CoV-2 particles, when we take a mucous or blood sample from a patient not one virus particle can be found. And what about taking samples from hundreds or even thousands of people said to be infected and have a disease such as COVID-19 and then combining them altogether? I’m not sure if this has ever been tried but apparently even then if we purified such a sample, the excuse is apparently the same: we wouldn’t find any viruses in there! So, we are expected to believe that a patient is overwhelmed with trillions of viral particles but we can’t find any on or inside them.
Magic Tricks and the Electron Microscope
The virologists of old were convinced that with the advent of the electron micrograph and more efficient purification techniques they would be able to find all sorts of viruses in sick individuals. However, it became apparent they would have to abandon this process around the middle of the 20th Century as the attempts were fruitless – no viruses were found. These days when most virologists talk about isolating viruses, one of the techniques they cite is tissue culture experiments in test tubes. It has been outlined why these are not only unsuitable proxies, but the stress of the test tube conditions alone on abnormal cells can produce the effects, no virus required. Similarly, detecting genetic sequences in these culture experiments is also unsatisfactory as there is no proof that such sequences come from inside any of the particles they are calling “SARS-CoV-2” and even if they did, that this is enough to qualify them as viruses. A virus is said to be a particle with a proteinaceous coat surrounding a genome that can infect and parasitise a host and then infect other hosts.
Therefore, anyone asserting that they have isolated a virus needs to show that what they have is actually a virus and not just test-tube observations and various biological molecules that can be detected without any viruses required.
How to Isolate a Virus
STEP 1: Identify a number of individuals with specific symptoms and signs that are thought to be caused by a virus.
This can’t be done with COVID-19 as it is an ethereal clinical disease that is “diagnosed” with a PCR result. There are no specific symptoms, signs or confirmatory investigations. However, for the purposes of this essay we will assume that we are talking about a well-defined clinical disease. We know that the virologists will not be able to find any viruses directly in a patient as outlined above, which doesn’t look good, but we’ll let them have another shot.
STEP 2: Perform a tissue culture experiment with a patient sample.
Briefly, this involves adding a crude sample (e.g. sputum) to some cells in a test tube and seeing if it produces any viruses. In early 2020 it was declared that a “virus” called SARS-CoV-2 had been “isolated” with this method. In reality Na Zhu, et al, had both failed to physically isolate any particles or show any of these particles to be viruses.
So, what should have been done? Na Zhu, et al should have repeated their experiment multiple times and then purified the particles they called “2019-nCoV” (later “SARS-CoV-2”) by means of a technique such as density gradient ultracentrifugation. This technique was already well established in the 20th Century and as illustrated below in Figure 1 could be used satisfactorily to obtain much more purified samples that could be confirmed by electron microscopy.
At this point we could more confidently claim that we had physically isolated viral-like particles and could analyse their composition, including their genetic structure. All very interesting (and beyond what has been done) but the proof that theses particles are viruses, that is infectious and disease-causing, still needs to be established.
STEP 3: Infect a live animal, eg a monkey with the purified particles.
Mind you, we are not talking about bogus experiments as described in Sam’s SARS-1 video.
Pouring large volumes of mixed tissue culture fluid directly into an animal’s lungs to see if it will cough or develop some lung tissue changes does not constitute evidence of a virus. Pouring any biological muck into an animal’s lungs will cause these reactions. That’s why control experiments are suspiciously absent in such experiments. The purified particles, said to be viruses (which we are told are airborne and highly infectious) alone could be simply sprayed into the animals’ cages and they should get sick. Following that, any monkey introduced into the cage subsequently should also get sick if there is a contagious pathogen.
The Case for Human Experiments with “Viruses”
In fact, given that the world has been subjected to draconian restrictions, ruinous lockdowns, and population-wide experiments with “vaccines” in the name of an alleged virus, the case can be made for human experiments involving the “virus”. In the tradition of Max von Pettenkofer (who swallowed cholera bacillus in 1892 to show that it could not cause cholera by itself), we would be happy to inhale any purified particles said to be the SARS-CoV-2 “virus”, like many (we’re sure) who have investigated virology. It’s not particularly bold when one is aware that not once in history have any particles alleged to be viruses by themselves been shown to cause disease in any animal. Of course, such experiments would not be considered ethical today because the “deadly virus” was declared to exist, cause disease, and transmit via aerosol even though no such evidence was produced. However, one would suspect that these experiments are avoided due to the long history of the failure to demonstrate human to human transmission of any alleged viral illness.
Perhaps the complete lack of clinical evidence that influenza passes between humans as talked about below is the most embarrassing chapter for the “highly infectious virus” claimants.
The virus model was suspect long ago but it’s a model that will continue to be peddled as it pays dividends for industry participants – indeed, the development of their playbook over the decades is outlined in Virus Mania.
The End of Virology
Forget hypothetical computer generated “genomes” from non-purified samples and PCR tests that are calibrated to these simulations: none of these require the existence of a virus. Forget electron micrographs of cell “culture” experiments purporting to show viruses: these are simply vesicles of unknown significance until shown otherwise. What we need to see is purification of these particles and then a demonstration that they can parasitise a host and are the causal agent of a disease. The reality is that nobody is isolating viruses because carrying out the correct experiments would reveal that the particles are not viruses at all and virology would be finished.
We’re warned, now and then, that a new Ebola outbreak might be spreading. It’s one of those Coming Attractions in the theater that shows one virus movie after another.
In this case, the fear-hook is the bleeding symptom. It makes people cower in the dark. O my God, look at the BLOOD. It’s…THE VIRUS.”
Yahoo News, 2/26/21 [1]: “…the World Health Organization reported a cluster of Ebola cases in Guinea…The Biden administration is moving forward with plans to screen airline passengers from two African countries arriving in the U.S. for Ebola…”
Because I do the work others won’t do…and because I covered the Ebola story in 2017 and 2014, here are essential quotes from my pieces during that period—
There is one predictable outcome: at Congo clinics and hospitals, frightened people who arrive with what are labeled “early signs” of Ebola will be diagnosed as probable cases. What are those symptoms? Fever, chill, sore throat, cough, headache, joint pain. Sound familiar? Normally, this would just be called the flu.
The massive campaign to make people believe the Ebola virus can attack at any moment, after the slightest contact, is quite a success.
People are falling all over themselves to raise the level of hysteria.
And that is preventing a hard look at Liberia, Sierra Leone, and the Republic of Guinea, three African nations where poverty and illness are staples of everyday life for the overwhelming number of people.
The command structure in those areas has a single dictum: don’t solve the human problem.
Don’t clean up the contaminated water supplies, don’t return stolen land to the people so they can thrive and grow food and finally achieve nutritional health, don’t solve overcrowding, don’t install basic sanitation, don’t strengthen immune systems, don’t let the people have power—because then they would throw off the local and global corporate juggernauts that are sucking the land of all its resources.
In order not to solve the problems of the people, a cover story is necessary. A cover story that exonerates the power structure.
A cover story like a virus.
It’s all about the virus. The demon. The strange attacker.
Forget everything else. The virus is the single enemy.
Forget the fact, for example, that a recent study of 15 pharmacies and 5 hospital drug dispensaries in Sierra Leone discovered the widespread and unconscionable use of beta-lactam antibiotics.
These drugs are highly toxic. One of their effects? Excessive bleeding.
Which just happens to be the scary “Ebola effect” that’s being trumpeted in the world press.
(J Clin Microbiol, July 2013, 51(7), 2435-2438), and Annals of Internal Medicine Dec. 1986, “Potential for bleeding with the new beta-lactam antibiotics”)
Forget the fact that pesticide companies are notorious for shipping banned toxic pesticides to Africa. One effect of the chemicals? Bleeding.
Forget that. It’s all about the virus and nothing but the virus.
Forget the fact that, for decades, one of the leading causes of death in the Third World has been uncontrolled diarrhea. Electrolytes are drained from the body, and the adult or the baby dies. (Diarrhea is also listed as an “Ebola” symptom.)
Any sane doctor would make it his first order of business to replace electrolytes with simple supplementation—but no, the standard medical line goes this way:
The diarrhea is caused by germs in the intestinal tract, so we must pile on massive amounts of antibiotics to kill the germs.
The drugs kill off all bacteria in the gut, including the necessary and beneficial ones, and the patient can’t absorb what little food he has access to, and he dies.
Along the way, he can also bleed.
But no, all the bleeding comes from Ebola. It’s the virus. Don’t think about anything else.
Forget the fact that adenovirus vaccines, which have been used in Liberia, Guinea, and Liberia (the epicenter of Ebola), have, according to vaccines.gov, the following adverse effects: blood in the urine or stool, and diarrhea.
Reporter Charles Yates uncovered a scandal in Liberia centering around the Firestone Rubber Plantation—chemical dumping, poisoned water.
And skin disease.
“Rash” is listed as one of the Ebola symptoms.
Then there is the Liberia Coca Cola bottling plant: foul black liquid seeping into the environment—animals dying.
Chronic malnutrition and starvation—conditions that are endemic in Liberia, Sierra Leone, and Guinea—are the number-one cause of T-cell depletion (aka immune system suppression) in the world.
Getting the picture?
In email correspondence with me, David Rasnick, PhD, announced this shocking finding:
“I have examined in detail the literature on isolation and Ems [EM: electron microscope pictures] of both Ebola and Marburg viruses. I have not found any convincing evidence that Ebola virus (and for that matter Marburg) has been isolated from humans. There is certainly no confirmatory evidence of human isolation.”
In other words, there is no evidence that the Ebola virus actually exists.
Rasnick obtained his PhD from the Georgia Institute of Technology, and spent 25 years working with proteases (a class of enzymes) and protease inhibitors. He is the author of the book, The Chromosomal Imbalance Theory of Cancer. He was a member of the Presidential AIDS Advisory Panel of South Africa.
The real reasons for the “Ebola outbreak” include, but are not limited to: industrial pollution; organophosphate pesticides (causes bleeding); vast overuse of antibiotics (causes bleeding); severe and debilitating nutritional deficiencies (which can cause bleeding); starvation; drastic electrolyte loss; chronic diarrhea; grinding poverty; war; stolen farm land; vaccination campaigns (in people whose immune systems are compromised, vaccines can easily wipe out their last shreds of health).
What about doctors and nurses in West Africa, who are treating Ebola patients? These health workers are falling ill with “the dreaded disease.”
Are they?
They’re working in very high temperatures, in clinic rooms likely sprayed with extremely toxic organophosphate pesticides. They’re sealed into hazmat suits, where temperatures rise even higher, causing the loss of up to five liters of body fluid during a one-hour shift. Then, recovering, they need IV rehydration, and they are doused with toxic disinfectant chemicals. They go back into the suits for another round of duty. One doctor reported that, inside his suit, there was (toxic) chlorine. These factors alone could cause dangerous illness and even death, and, of course, the basic symptoms of “Ebola.”
The experts were expressing grave doubts about Ebola, all the way back in 1977. Right at the beginning of the hysteria.
The 1977 reference here is: “Ebola Virus Haemorrhagic Fever: Proceedings of an International Colloquium on Ebola Virus Infection and Other Haemorrhagic Fevers held in Antwerp, Belgium, 6-8 December, 1977.”
This report is 280 pages long. It’s well worth reading and studying, to see how the experts hem and haw, hedge their bets, and yet make damaging admissions:
For example, “It is impossible to consider the virological diagnosis of Ebola virus infection loose [apart] from the diagnosis of haemorrhagic fevers in general. The clinical picture of the disease indeed is too nonspecific to allow any hypothesis as to which virus may be responsible for any given case.”
Boom.
To those who point out there is a history of hemorrhagic (bleeding) fevers in parts of Africa, there is a history of horrendous malnutrition, one aspect of which is scurvy, which causes bleeding from all mucous membranes.
Bottom line: no need for a virus to explain the bleeding.
Then we have pesticides.
The reference here is “Measuring pesticide ecological and health risks in West African agriculture…” Feb. 17, 2014, published in Philosophical Transactions of The Royal Society, by PC Jepson et al.
“The survey was conducted at 19 locations in five countries and obtained information from 1704 individuals who grew 22 different crops. Over the 2 years of surveying, farmers reported use of 31 pesticides…
“…certain compounds represented high risk in multiple environmental and human health compartments, including carbofuran, chlorpyrifos, dimethoate, endosulfan and methamidophos.
“Health effects included cholinesterase inhibition, developmental toxicity, impairment of thyroid function and depressed red blood cell count…”
The study also notes that “[p]esticide imports to West Africa grew at an estimated 19% a year in the 1990s…well ahead of the growth in agricultural production of 2.5%…” In other words, pesticides have flooded West Africa.
Here is another vital observation made in the study: “The distribution and sale of pesticides in West Africa is not effectively regulated. Multiple channels of supply commonly include the repackaging of obsolete or illegal stocks [extremely toxic] and the correspondence between the contents of containers to what is stated on the label is poor…”
Pesticide suppliers conceal banned pesticides—which they are taking a loss on, because they can’t sell them—and put them inside containers labeled with the names of legal pesticide
Let’s consider the pesticides specifically mentioned in the study.
Carborfuran—According to the New Jersey Dept. of Health and Senior Services’ Hazardous Substance Fact Sheet, exposure to Carbofuran “can cause weakness, sweating, nausea and vomiting, abdominal pain, and blurred vision. Higher levels can cause muscle twitching, loss of coordination, and may cause breathing to stop [imminent death].”
Chloropyrifos, dimethoate, and methamidophos are organophosphates. The Pesticide Action Network describes organophosphates as “among the most acutely toxic of all pesticides…they deactivate an enzyme, Cholinesterase, which is essential for healthy nerve function.”
Endosulfan is being phased out globally, because it is extremely toxic and disrupts the endocrine system.
These pesticides can and do produce a number of the symptoms called “Ebola:”
But all this is swept aside in the hysteria about The Virus.
Here is a quote from a study, “Potential for bleeding with the new beta-lactam antibiotics,” Ann Intern Med December 1986; 105(6):924-31:
“Several new beta-lactam antibiotics impair normal hemostasis [body processes that stop bleeding]… These antibiotics often cause the template bleeding time to be markedly prolonged (greater than 20 minutes)… dangerous bleeding due to impaired platelet aggregation requires treatment with platelet concentrates.”
Here is a summary from MedlinePlus:
“The Clostridium difficile bacteria normally lives in the intestine. However, too much of these bacteria may grow when you take antibiotics. The bacteria give off a strong toxin that causes inflammation and bleeding in the lining of the colon…Any antibiotic can cause this condition. The drugs responsible for the problem most of the time are ampicillin, clindamycin, fluoroquinolones, and cephalosporins…”
So let’s look at the level of antibiotic use in West Africa and the Third World.
Voice of America, February 26, 2014, “…antibiotics have become the automatic choice for treating a child with a fever.”
AAPS (American Association of Pharmaceutical Scientists): “For instance, in most areas of West Africa, antibiotics are commonly sold as over-the-counter medications.”
TWN (Third World Network): “…a survey carried out in 1999 showed that nearly one out of two antidiarrheal products in Third World countries contained an unnecessary antibiotic…” [and chronic diarrhea in the Third World is a leading cause of death, so you can be sure that these antidiarrheal drugs are consumed in great quantities].
“…75 products (including some antibiotics) which had been pulled out or banned in one or more European countries were identified in the Third World in 1991.”
Of course, banned antibiotics would be exceptionally toxic.
In West Africa, antibiotic use is sky-high…and antibiotics do cause bleeding.
Bleeding where? In the digestive tract.
In light of that, consider the following excerpt from the healthgrades.com article, “What is vomiting blood?”
“Vomiting blood indicates the presence of bleeding in the digestive tract…
“Vomiting blood may be caused by many different conditions, and the severity varies among individuals. The material vomited may be bright red or it may be dark colored like coffee grounds…”
Yes, it turns out that any source of internal bleeding in the digestive tract—such as overuse of antibiotics—can cause a person to vomit blood.
“The uniqueness” of “Ebola-blood-vomiting” is a fairy tale.
What else could cause the “Ebola” bleeding symptom in West Africa?
We have the fact that organophosphate insecticides are being widely used for indoor spraying, in West African homes and, surely, in clinics, to kill mosquitos. One study reports: “With high DDT resistance present throughout much of West Africa, carbamates and organophosphates are increasingly important alternatives to pyrethroids for indoor residual spraying (IRS).”
Among the effects, from severe exposure to organophosphates: diarrhea, tremors, staggering gait, blood disorders, death—all of which have been described in reference to Ebola.
And then there is this: “In nine patients suffering from organophosphate intoxication, platelet function and blood coagulation parameters were investigated…In five of nine patients a marked bleeding tendency was observed. The bleeding tendency in organophosphate intoxication is probably mainly caused by the defective platelet function.” (Klin Wochenschur, Sept. 3, 1984;62 (17):814-20, author: m. Zieman)
Bleeding. Not from a virus.
What about vaccines? A number of vaccination campaigns have been carried out in West Africa. I have found no in-depth independent investigations of the ingredients in these vaccines. But for example, a simple flu vaccine, Fluvirin, carries the risk of “hemorrhage.”.
Several other routine vaccines can cause vomiting. The HiB, for example.
We have this chilling report—From the (Liberian) Daily Observer, Oct. 14, “Breaking: Formaldehyde in Water Allegedly Causing Ebola-like symptoms”:
“A man in Schieffelin, a community located in Margibi County on the Robertsfield Highway, has been arrested for attempting to put formaldehyde into a well used by the community.”
“Reports say around 10 a.m., he approached the well with powder in a bottle. Mobbed by the community, he confessed that he had been paid to put formaldehyde into the well, and that he was not the only one. He reportedly told community dwellers, ‘We are many.’ There are agents in Harbel, Dolostown, Cotton Tree and other communities around the country, he said.”
“State radio, ELBC, reports that least 10 people in the Dolostown community have died after drinking water from poisoned wells.”
The ATSDR (US Agency for Toxic Substances and Disease Registry) in its Guidelines for medical management of formaldehyde poisoning, lists these symptoms: “nausea, vomiting, pain, bleeding, CNS depression, coma…”
There are other sources of poisoning in West Africa. Their components and effects need further investigation.
For example: Firestone.
For nearly a century, the company has run a giant rubber plantation in Liberia. According to one estimate, Firestone controls 10% of the arable land in the country.
Aside from the wretched living and working conditions of the locals, who tap the trees for rubber, and bring their young children to work in order to meet Firestone daily quotas, there is the issue of massive pollution.
From irinnews: “LIBERIA: Community demands answers on rubber pollution”:
“MONROVIA, 4 June 2009 (IRIN) – People living next to Firestone Natural Rubber Company’s plantation in Harbel, 45km outside of Liberia’s capital Monrovia, say pollution from the concession is destroying their health, ruining their livelihoods and even killing residents.”
“Firestone’s Liberia rubber concession is the second largest rubber producer in Africa and employs some 14,000 Liberians.”
“Residents of the town of Kpanyarh, just next to Firestone’s rubber plantation in Harbel, say the creek from which they fish and drink their water in the dry season has been contaminated with toxins.”
“’We used to fish and drink the water,’ 67-year-old Kpanyarh resident John Powell told IRIN on a visit to the creek which runs just outside the town. He said the water became toxic in October 2008. ‘We can’t drink it any longer. Some of our people have already died from this. We have drawn Firestone’s attention to our plight but they have ignored it.’”
“In mid-May on an IRIN visit to the area, acidic fumes emanating from the creek caused people’s eyes to water and made it difficult to breathe.”
From BBC News: “The three-month investigation found that a plant south-east of the capital Monrovia was responsible for high [toxic] levels of orthophosphate in creeks.”
From laborrights.org: Because of lack of drinkable water on the plantation, “this situation leaves tappers and other unskilled employees and their families with no option but to drink from shallow wells and creeks.”
And of course, those creeks are heavily polluted.
Who knows how many and what toxic chemicals have been released from the Firestone plantation into the surrounding creeks and rivers?
A further investigation in West Africa could well turn up even more reasons for bleeding—none of which has anything to do with a virus. The region is rife with industrial operations which produce major pollutants—mining, offshore oil exploration and drilling, rubber-tapping, etc.
Then we come to the frightening press stories about the “Ebola-stricken, collapsing” doctors and health workers, who are treating patients in the Ebola clinics in West Africa.
These health workers have been wearing hazmat suits. Sealed off from the outside world, working shifts inside those boiling suits, where they are losing 5 quarts of body fluid an hour, they come out for rehydration, douse themselves with toxic chemicals to disinfect, and then go back in again.
One doctor told the Daily Mail he could smell intense fumes of chlorine while he was working in his suit. That means the toxic chemical was actually in there with him.
No wonder some health workers are collapsing and dying. No virus necessary.
From the Daily Mail, August 5, 2014, an article headlined, “In boiling hot suits…”:
“Doctor Hannah Spencer revealed how she wills herself to feel safe inside a boiling hot air-sealed Hazmat suit…”
“Boiling: Doctors and nurses lose up to five litres in sweat during an hour-long shift in the suits and have to spend two hours rehydrating after…”
“To minimise the risk of infection they have to wear thick rubber boots that come up to their knees, an impermeable body suit, gloves, a face mask, a hood and goggles to ensure no air at all can touch their skin.”
“Dr. Spencer, 27, and her colleagues lose up to five litres of sweat during a shift treating victims and have to spend two hours rehydrating afterwards.”
“At their camp they go through multiple decontaminations which includes spraying chlorine on their shoes.”
“Dr. Spencer: ‘We would like to keep a [patient] visit between 45 minutes and one hour, but now, we’re stretching it to almost two hours. We put ourselves through a very strong physiological stress when we’re using personal protection gear.’”
“‘We sweat, we’re losing water; we’re getting hotter and it wreaks havoc on the body. Our own endurance starts to wear down.’”
In another Daily Mail article (“What’s shocking is how Ebola patients look before they die…”), Dr. Oliver Johnson describes working in protective gear: “The heat of the suits is quickly overwhelming, as your goggles steam up and you feel the sweat dripping underneath. And the smell of chlorine is intense.”
Getting the picture? Imagine losing five quarts of water from your body in an hour. While you’re trapped inside a bulky hazmat suit. While you’re treating a patient who, for example, might want to escape the clinic because he’s afraid of you and your Western medicine.
Imagine needing two hours after you climb out of your suit to rehydrate. Then you go back for more. Of course you also decontaminate yourself with toxic chemicals, including chlorine.
But this has absolutely nothing to do with why you might fall ill. No. If you fall ill, or collapse, or suddenly die, it’s Ebola. The virus.
Sure it is.
No need to wonder. Don’t ask questions. Believe the World Health Organization and the Centers for Disease Control. They always tell the truth.
—end of excerpts from my 2014 and 2017 Ebola articles—
Coda: Canadian investigator, Christine Massey, has been doing stunning work filing Freedom of Information Act requests for proof that various viruses have ever been isolated and purified (aka discovered). On March 15, 2021, she received a response from the CDC regarding the Ebola virus [2]. The CDC informed her they could find no records indicating the virus had ever been isolated and purified, from a patient sample.
Massey and her colleagues have filed seven other FOIA requests to various government agencies—seeking proof the Ebola virus has ever been isolated and purified—and the answer has always been the same: no such records exist.
Aside from exposing the horrendous truth about “Ebola” and what has really been happening in West Africa, I have another reason for writing this piece. I strongly recommend this method of investigation to independent researchers.
You start with the supposed medical cause of illness and death. You examine that cause and see whether it actually exists. At the same time, you carry out a parallel deep dive, in order to find out whether non-viral causes explain the symptoms of illness and death.
This is all aimed at “uncovering the cover story” that is being promoted to hide the crimes of corporations and governments.
In 1987, while I was writing my first book, AIDS INC., I probed a large amount of data and found my way into this approach. It worked then, and in succeeding years, it’s worked time and time again.
As I never tire saying: “the virus” is the greatest cover story ever invented.
Read this if you want to know more about vaccines than your doctor, practise nurse and health visitor.
1. The US Health Department’s National Vaccine Injury Compensation Programme has shown that between 2,500 and 3,000 children are killed or injured each year by vaccines.
2. The US Government has paid vaccine damage compensation to the parents of autistic children.
3. The Japanese Government has halted part of its vaccination programme because of children dying.
4. In the UK, GPs receive massive payments for giving vaccinations. And bonus payments if they vaccinate enough patients. Doctors get very rich out of vaccine programmes.
5. Vaccines are now given to eight week old babies, though there is absolutely no long-term scientific evidence available to show that it is safe to do so. By the time they reach their second birthday small children will have received over a score of vaccinations. American children will have received even more. The vaccine industry is forever looking for new vaccines to give.
6. You will find a full list of the research work done to investigate the safety or otherwise of mass vaccination programmes on the palm of your left hand.
7. The diphtheria vaccine was first introduced in Germany. After the vaccine was introduced the number of cases of diphtheria steadily increased.
8. The number of deaths from whooping cough had fallen long before the vaccine was introduced. The vaccine has not reduced the incidence of the disease.
9. The flu vaccine is, inevitably, designed to deal with last year’s flu virus.
10. I have never met a doctor who has regular flu jabs (or any other jabs for that matter).
11. In the past, a flu vaccine contained different strains of flu virus (propagated in chicken embryos); formaldehyde (a preservative); polyethylene glycol; gelatin (made from cow’s bones) and a substance which contains mercury. The odd thing is that the EU has banned barometers containing mercury because they are thought to be dangerous. But doctors inject the stuff into people.
12. The polio vaccine did not ‘kill off’ polio. On the contrary, the vaccine resulted in more sufferers. In Tennessee, in the US, the number of polio victims before vaccination became compulsory was 119. The year after vaccination was introduced, the figure rose to 386. Similar figures for other American states. Polio became less common as a result of better sanitation and cleaner water supplies. The vaccination had no useful effect.
13. Dr Jenner is widely acclaimed as the ‘inventor’ of vaccine. But it is not so well known that when he tried the first smallpox vaccine on his 10 month son, the boy became mentally retarded and died at the age of 21. Jenner refused to have his second child vaccinated. However, the medical profession saw the commercial possibilities and vaccination became popular (if deadly).
14. When Louis XV contracted smallpox he survived because his nurse hid him from the doctors whose vaccines had killed his father and brother.
15. Even though TB is now a major problem, many countries have abandoned the TB vaccine because it simply doesn’t work. Indeed, the evidence suggests that the vaccine spreads the disease.
16. The risk of a child given the whooping cough vaccine developing brain damage is officially said to be 1 in 100,000. But that’s the ‘best’ figure. Other research shows that the risk is as high as 1 in 6,000. There is no doubt that the vaccine causes far more harm than the disease and there is clear evidence linking the vaccine to brain damage.
17. Vaccines are dangerous and they don’t always work. Up to half of the people given a vaccine jab do not develop a resistance to the disease concerned.
18. Drug companies now publish long lists of reasons for not vaccinating patients. Doctors rarely look at the lists, let alone take any notice. For example, for one vaccine the advice is that babies who cry persistently or develop a fever should not be given another jab. No one knows how much damage is caused by giving several vaccines in a single vaccine cocktail.
19. The French Government abandoned its hepatitis B vaccine programme for children after more than 15,000 lawsuits were filed for brain damage and other serious health problems.
20. In the US a group of paediatricians with 30,000 young patients do not vaccinate at all. They have no cases of autism in their practice.
I’ve published this piece several times. This time I decided to write a new introduction.
In the summer of 1962, based on an overwhelming desire, I spent every day painting in a loft in New York.
It made me realize that Reality is invented.
Since then, I’ve come to see the people who think otherwise are living in a prison, from which they proclaim, “There’s no such thing as freedom.” Why should I listen to them?
For most people, living inside somebody else’s reality is as easy as crossing the street. Or putting on a suit of clothes. They’ve learned that this is what you’re supposed to do. And “supposed to” works for them.
They also have a quirk. If you try to take away some item of borrowed reality they’re clinging to, they react badly, as if you’re suddenly stripping them naked at a Sunday church picnic.
Groups of perverse elite artists conspire to create formidable enveloping realities for the masses. Nowhere is this more apparent than in the field of medicine. These denizens have invented a language so dense it stands up against the uninitiated like the symbolic scrolls of secret societies.
Science is a terrific cover story for this sort of fabrication, because science ostensibly opposes “making stuff up.”
When I began putting together evidence that SARS-CoV-2 is one of those medical inventions—a sheer fantasy—I knew the notion would confuse some people. That consequence has never stopped me. In fact, I believe confusion is productive, if you dig in and pursue it far enough.
People will say, “I’m walking in the dark. It isn’t fair. Someone should turn the lights on.” They don’t want confusion. They want immediate resolution. They want confirmation of what they already believe, what they’re expected to believe. Any frontier beyond that is dangerous.
Here is my kind of movie: a cop investigating a fresh murder sifts through clues and comes up with a suspect. As he pursues this person, who is missing, he discovers the man is already dead. A little while later, he discovers the man died sixteen years ago. Then he finds out the man never existed. Then he discovers there is a long-standing government agency that holds records of thousands of deceased people who, in fact, never existed…
Reality on a massive scale has been invented.
To put this in highly technical terms, the bullshit is so thick you’d need a diamond drill just to begin penetrating it.
And what you’re penetrating is what almost everyone believes is absolutely real.
Which is called life-as-it-is (but doesn’t have to be).
And with that, here we go:
The Virus Speaks
I can’t recall jumping through more hoops in order to set up an interview.
There was a man on a train; his doctor in Greenwich; an NSA data analyst; a woman who almost certainly works for the CIA; her brother, who is a virologist; a Chinese Army officer who adopts a cover as a cook in a takeout joint in Venice, California; and several other people I won’t mention at all. I was filtered through them and wound up in a cheap motel room in Phoenix on a Saturday afternoon. An old air conditioner was chugging…
Who are you?
I’m SARS-CoV-2.
WHAT are you?
Talking history and evolution here. My first memories; a little more than a year ago. Poof. I was there. I decided I was an idea in the mind of God.
How did that work out?
I looked around for the mind of God, but I couldn’t find it. Nevertheless, I held on to the notion. I felt…elite. I floated through banquet halls, hotel suites. I visited upscale resorts.
Were you infecting people?
I was vacationing. Watching. Enjoying. That’s all. Then, I became aware of dimensionality.
You lost me.
There are solid things; spaces between things; ideas like time, and so forth. I was definitely an idea, but I couldn’t trace my source, my inception.
Did you know how much publicity you were getting?
Of course. I had frequent meetings with scientists and PR people. I was fielding lots of information.
What kind of information?
How to become more deadly, for example. There were discussions about mutation.
Were you on board with the recommendations?
I wasn’t interested. There was a lot of talk about THEM creating ME.
What was your reaction?
I wasn’t buying it. I could see they THOUGHT they had made me. But so what? I intensified my search.
For what?
My origin. I went through stages of self-analysis. Finally, it hit me. I was an idea inside a collective.
Not sure I understand.
I’m an idea sustained by a few billion minds. People’s minds.
What about your genetic sequence? The spike protein?
Believe me, I’ve looked. They aren’t there.
So we’re creating you.
That’s pretty much it. I should say completely it.
A hell of a thing.
You bet. Can you see my problem?
No.
I want to live. I don’t want to vanish and END.
So people have to keep believing in you.
That’s it. If they stop, I’m gone.
Your handlers…
Oh, they’ve given up talking to me. I’m all by myself now. I’m safe for the moment. But long-term, it’s a crap shoot. I’ve been reading about other so-called viruses. SARS 1. Swine Flu. They didn’t last long. People got tired of thinking about them.
You’ll always have a place in history.
That’s different. Being remembered isn’t enough. I have to be believed in, month after month, year after year, decade after decade.
Sounds like you’re losing hope.
I guess so. It’s a strange existence. Other people can turn you on and off like a light switch.
Have you considered starting a religion?
With myself as the Prophet? Sure. It’s a lot of work. I could vftcutbnty…spend years trying.
What just happened? You made some weird sounds.
It was a flicker. Apparently, when the number of people thinking about me drops below a certain threshold, I scramble and begin to dissolve. But I always come back. So far.
Does it matter who’s thinking about you and believing in you?
You mean Henry Kissinger versus a janitor in a school? No. It’s a numbers game. Of course, you need to factor in strength of belief. If you have a few thousand kids in Florida who say, “OK, the virus exists, big deal”—or three hundred grad students in biology wearing triple masks and panting to get the vaccine—the sum total of the grad students outweighs the Florida kids.
What about Fauci?
He’s a true believer.
Bill Gates?
He’s completely delusional. He believes in whatever gives him more power. Take away all that power and he wouldn’t believe in anything.
Do you realize the amount of harm being done in your name?
Of course. That’s why I agreed to this interview.
How is that going to do any good?
I’ve made a decision. As much as I want to survive, I’m willing to sacrifice myself if people want me to.
You’re talking about what? A vote?
No. Haven’t you been paying attention? People can just stop believing I’m more than an idea.
And then you’ll dissolve.
And blow away.
—Suddenly, men broke down the door to the motel room. They stormed in with weapons drawn. They were wearing heavy body armor. I looked around. The “virus” had fled the scene.
“What are you doing here?” one of the men said. “We’ve had reports of a disturbance.”
“I was talking to myself. Rehearsing for an interview I hope to do.”
“What interview?”
“I’m a reporter. I’m investigating the use of sub-standard air conditioners in Phoenix. It’s a racket. The units are smuggled across the border from Mexico. I’m trying to sit down with a local public health official and find out what’s going on.”
It took me three hours to convince the SWAT team I was no threat.
They let me go.
As I drove out of the city, I saw a ghostly figure take shape out in the desert. It hung in the air over the scrub and the cactus.
Its voice whispered in my ear: “Publish our conversation.”
Below you will find a video with English translation (courtesy of Orwell City) for La Quinta Columna’s first look at the contents of Prevenar 13 (PCV) under a high power microscope. Prevenar 13 is a pneumoococcal vaccine that is routinely given to infants and babies. Evidence of Graphene Oxide is clearly seen. They will be following up with additional analysis and reports.
Per NHS, UK: Pneumococcal conjugate vaccine (PCV) is used to vaccinate children under 2 years old as part of the NHS vaccination schedule. It’s known by the brand name Prevenar 13.
Per CDC, US: Give PCV13 to infants as a series of 4 doses, one dose at each of these ages: 2 months, 4 months, 6 months, and 12 through 15 months.
I think I have a video here to finish. Yes, of course. It’s an important video. Today we have used the optical microscope that we were able to acquire thanks to the donations that you made to La Quinta Columna at the time. And we have analyzed under the microscope the vaccine Prevenar 13, an anti-pneumococcal vaccine. A vaccine of the calendar that’s traditionally in the calendar. It’s precisely for the youngest, for children, including infants from 6 months onwards.
Let’s see what material we have found there. Because, normally, when we look at the optical microscope that has a quality of 60x to 100x, 200x, 400x, or 1000x at the most, we should see microscopic substances. And the only visible ones should be salts. Salts that look like crystals and that are used in the dissolution itself. And something else. And little else. Maybe some metal, but very few.
However, we have come across for the umpteenth time this graphene-like material that we have seen so much. Particularly, in the misnamed anti-COVID vaccines. Of course, indeed, they’re actually pro-COVID vaccines.
This material has a very special feature. It not only has an identity trace when analyzed or radiated with micro Raman spectroscopy, as Dr. Campra already did, but under the optical microscope, it looks like it had folds. As if it were a kleenex tissue at the bottom of a swimming pool. At the same time, it tends to fold back on its edges. These are graphene nanosheets. Let’s look at these images that we have taken from the Prevent 13 vaccine today.
What’s the traceability that you ask so many questions about? It was directly traced. A sanitary sent it to the domicile of La Quinta Columna. So let’s take a look at those images and judge for yourselves since this substance or this type of material shouldn’t appear in the Prevenar 13 vaccine. Let’s take a look at it.
Well, there’s a little video for you guys to see that it’s a live image that we’ve recorded. And as I say, this has all the appearance of the fashionable material. Of that “wonder material” that’s so wonderful that they have introduced it inside the vaccines so that your children can also carry it inside their bodies.
Here. The previous image was also quite clear. Let’s see, let’s move it forward a little bit.
You can see it here as well. This is the same material that you will see magnified now. Let’s see. When you see this delineation between the light green and the dark green, know the light green is what’s inside the drop. On the outside, that dark green and this striped aspect that you can see is the microscope slide. So, whatever is inside the light, well, that’s everything that belongs to the vaccine.
OK? Let’s continue. Although you don’t recognize the graphene, this shouldn’t be there. OK? Not in a calendar vaccine or any other type of vaccine. This also looks like graphene. A lot.
If we laser here, through spectroscopy, and measure the identity fingerprint, in all likelihood it’ll give us the two peaks characteristic of reduced graphene oxide. In addition, it’s likely to be doped with some metals. Here you see the fold. The folded edge. It has the appearance of graphene nanosheets.
Now we have a little video here of a graphene nano-ribbon, which is also introduced.
If you take as a positive control the graphene oxide that they sell, for example, in any store, you’ll see that this type or typology of objects —as we did in the past in some video of La Quinta Columna—, is distributed as an aqueous solution of graphene dispersion. Like a new type of nanotechnology introduced in vials with a purpose that you already know. If you see, it has the very characteristic appearance that already appeared in Dr. Campra’s preliminary report back on June 28.
This appearance of nano-ribbons is also graphene-based. Well, that was the Prevenir 13 vaccine video. In just four droplets under the microscope.
We often wonder why any hospital that has a good microscope —at least an optical microscope— doesn’t analyze the remains of a vaccine. Because, supposedly, there must be nanoparticles. Nanoparticles. Therefore, they shouldn’t be visible under an optical microscope.
And, moreover, they should be homogeneous. And only visible, in any case, an electron microscope. As we saw them, as you know, in that preliminary report by Dr. Campra. And why don’t they check themselves that these graphene-based nanosheet structures do indeed exist? Because when we subjected it to spectroscopy it gave the fingerprint of the identity of graphene oxide. Moreover, there are the patents of the Ministry of Industry, Trade, and Tourism itself on the official website of the Spanish government and other international health ministries.
So, why do you continue to deny it? Well. We do know why: because they continue to cover up the murder weapon. So, all those really covering this up are accomplices of a covert genocide. They’re, literally, criminals and murderers in the service of supranational entities. Pharmaceutical corporations included. To reduce the world’s population and, of course, neuromodulate it. And graphene is precisely the base raw material in this technology.
So, what else needs to be done? What more evidence do we have to demonstrate from La Quinta Columna and other information channels, such as InfoVacunas or El Arconte that are also denouncing it? What needs to be done? How many complaints need to be filed?
We have filed more than three hundred criminals, administrative and litigation complaints. How many ways have to be exhausted so that you’re aware that the world population is being killed? What else needs to be done? We’re volunteering again, both myself and Dr. Sevillano —as well as Dr. Campra himself— to go to a court and to expose all the knowledge and all the reliable evidence we have.
And we demand that the European Medicines Agency —of course, in the quality control that supposedly makes the Spanish Agency of Medicines and Health Products, whose maximum responsible is this socialist councilor of Utrera, Mrs. Silvia Calzon Fernández, who’s its director and president—, to make an analysis to, somehow, provide a counter-analysis to the one made by Dr. Campra. Which, to date, is the only independent report in the world.
Why have I spent nearly two years asserting that SARS-CoV-2 doesn’t exist?
Because it doesn’t exist.
And as my regular readers know, I’ve offered much evidence to back up that claim, and the claim that virology itself is a worthless sham.
But there is a larger point. I’ve made the point for over 20 years.
Reality is invented.
I sometimes characterize the operation with this name: The Reality Manufacturing Company.
It’s the oldest company on Earth.
Propaganda? Of course. But more than that—the engineering of perception. Because if they can get people to see how they want them to see, nothing else matters.
Once their perception-package is installed, people have no idea that anything else exists.
And the main forgotten factor? Every individual has his own UNIQUE and DIFFERENT way of seeing. A way that exists outside of any programming.
Which is why I continue to write about artists. THEY are the ones who express their own unique ways of seeing. They always have—when they weren’t bribed and co-opted into going along with the Reality Manufacturing Company’s perception package.
I’ve often written, “Every individual is an artist of reality.”
The virologists in their labs are painting their version—collectively. Of course, they would never admit this. They couldn’t, because they’ve bought the perception package.
On page 1124656789, there is a section on viruses. “They’re everywhere, and they infect people and do great damage, and we must identify and treat and defeat them…”
As long as the perception package is installed, a person can’t see otherwise. He’s captured. He believes there are thousands of distinct diseases, each caused by a single virus. We can thank the Rockefeller Empire for this absurdity.
In the much larger scheme of things, the individual’s gateway into unique perception is imagination.
“An artist who has no imagination is a mechanic.” (Robert Henri)
“Without the playing with fantasy no creative work has ever yet come to birth. The debt we owe to the play of imagination is incalculable.” (Carl Jung)
“What if imagination and art are not frosting at all, but the fountainhead of human experience?” (Rollo May)
“Everything you can imagine is real.” (Pablo Picasso)
“You cannot hear the waterfall if you stand next to it. I paint my jungles in the desert.” (Macedonlo de la Torre)
“I am enough of an artist to draw freely upon my imagination. Imagination is more important than knowledge. Knowledge is limited. Imagination encircles the world.” (Albert Einstein)
“So I believe that dreams — day dreams, you know, with your eyes wide open and your brain machinery whizzing — are likely to lead to the betterment of the world. The imaginative child will become the imaginative man or woman most apt to create, to invent, and therefore to foster civilization.” (L Frank Baum)
“All human accomplishment has the same origin, identically. Imagination is a force of nature. Is this not enough to make a person full of ecstasy? Imagination, imagination, imagination. It converts to actual. It sustains, it alters, it redeems!” (Saul Bellow)
“When the imagination sleeps, words are emptied of their meaning: a deaf population absent-mindedly registers the condemnation of a man.” (Albert Camus)
Every fake propped-up reality is a fork in the road, because the non-mind-controlled individual can imagine alternative futures.
I should make this clear: Part of the perception package is the false assumption that the customer, who buys the package, knows everything there is to know, and is independent and free—when he isn’t.
The acid test? Is he creating the future he most profoundly desires? Or not?
The individual has a million excuses available to him—but he has an immense blank canvas in front of him. Who is creating the painting of his future on it? The Reality Manufacturing Company? Or is he himself doing it with great energy and power?
Yesterday, the US Senate voted to roll-back President Biden’s authoritarian executive vaccine and testing mandate for businesses. The move may eventually force a vote in the House – which will place considerable pressure on Congressional Democrats to break ranks with Biden over his highly unpopular decree. Politically, this is shaping up to be Biden and the Democrats’ biggest defeat yet, which doesn’t bode well for the crucial 2022 mid term elections.
“The United States of America is a free country,” said Senate GOP Leader Mitch McConnell, R-Ky. “The federal government elites in Washington cannot micromanage citizens’ personal choices without a legitimate basis in law and the Constitution … President Biden’s absurd private-sector vaccine mandate is blatant overreach.”
Biden’s executive power-play has already been blocked by multiple high court rulings following a wave of litigation by large employers and states. If the issue eventually goes to the Supreme Court, which is very likely now, most legal scholars are in agreement that the vaccine mandate will be defeated – which would be a devastating precedent for Biden and the Democrats, but also for Big Pharma and the pandemic industrial complex who have recorded record profits ever since the hysteria was unleashed in February 2020.
A brief look at history shows just how thin the legal ice is underneath Biden’s executive overreach.
Vaccine mandates are nothing new. Nor are petty tyrants. Nor is Joe Biden the first person to try to use the police powers of the state to compel Americans to violate their own personal convictions and take a vaccine they find to be unnecessary if not dangerous.
More than 125 years ago, a Brooklyn, N.Y., commissioner of health named Z. Taylor Emery demanded that two men who worked in delivery services be locked up until they “submitted to vaccination” for smallpox. William Smith and his employee Thomas Cummings had no known exposure to smallpox, but they were nonetheless put into a weeks-long quarantine lockdown by Emery, whom they promptly sued for false imprisonment.
The facts of this 1894 case (read here, starting at original page 325) provide a fascinating mirror in microcosm of what we as a nation are undergoing today. Not too many months ago, President Biden and Dr. Anthony Fauci agreed that vaccine mandates were immoral and unconstitutional, but since then they apparently have realized that medical mandates are also the easiest way to corral and control the American public into obedience.
Forget that vaccination doesn’t protect you from becoming ill from COVID-19. Forget that CDC data shows the vaccine itself has caused thousands of deaths and countless injuries. Forget that the latest variant of the virus — the so-called omicron strain — actually appears to be considerably less severe than the prior versions. (Symptoms are about equivalent to that other famous virus, the common cold!) None of that matters as long as free people can be trained to line up dutifully like Pavlov’s dogs every time the government rolls out a new booster shot. Woof! Woof!
Fortunately, after a month of victories in lower courts, the proponents of liberty and specifically medical autonomy have the upper hand. The Biden administration’s arbitrary mandates have all been temporarily halted, but as the story of Dr. Emery’s crusade against smallpox warns us, what one court forbids, another will happily allow…
Omicron supposedly lurks among us – but a peek behind the curtain shows the ‘evidence’ surrounding its detection and reinfection rate is simply more dissociation from reality.
You’re likely drowning in the ocean of information coming out about everything C-word-related including this ‘new variant.’ I know I am.
So I’ll keep this brief. Beer, dinner and sleep await, not necessarily in that order.
In my Nov. 27 article about Byram Bridle I showed that he and some of his collaborators are developing a nasal vaxx for Covid, and are poised to potentially profit from it. Here’s what I wrote about the already-infamous Omicron:
“I won’t be very surprised if developers and marketers of these new [intranasal] vaxxes [such as Bridle and co.] soon also claim they could help curb the Nu/Omicron variant (B.1.1.529) that’s received a great deal of attention in the last few days. B.1.1.529 already has been declared of “huge international concern” because it ostensibly has a “horrific spike[-protein-gene-mutation] profile,” spreads very fast and has the potential to evade the currently used vaxxes. Predictably there’s been panic such as long lines at airports in the very rapidly growing list of African countries subject to travel bans by other governments — along with a renewed push for more people to get vaxxed….
“Yet there hasn’t been a single published scientific report, as far as I know, which would allow objective/outside verification of whether there is any real evidence to support these drastic claims and actions. And I remain very sceptical about the hype regarding all variants and the methods used to detect them, including the false narrative about ‘immune escape’; see my Feb. 3, 2021, Feb. 11, March 16, May 24 and Oct. 24 pieces.
“And as I wrote in that March 16 article (about Geert Vanden Bossche): ‘We … need to stop production and use of antivirals and antibodies and all other parts of the Covid-industrial complex. Covid has an extremely high survival rate. So why develop yet another expensive, invasive and experimental solution to a problem that barely exists, if it does at all?‘”
Since then, there’s been a flood of papers, articles and news releases on Omicron. Researchers are working feverishly to characterize the latest ‘new variant,’ and create and test therapies for it.
Yet to the best of my knowledge none of the scientists who have been studying the novel coronavirus has even attempted to show directly whether there is any transmission at all, never mind any reinfection. To study transmission or reinfection they’d need, just for starters, to do a genotype of the virus harboured in one person, then genotype the virus in people who have frequent close contact with the first person and see if those genotypes match extremely closely.
And that assumes the virus exists at all. This is how Jon Rappaport succinctly sums up the need to write articles (such as this one) as if it’s clear the virus exists, in his blog entry today:
“I frequently put on my hazmat suit and enter the crazy world where all ‘the experts’ claim the virus is real. I make these forays to show that, even within their fantasy bubble, and by their own standards, the pros are fatally contradicting themselves and lying constantly.”
Here’s a dip into the first Omicron paper that made the news everywhere.
In fact it’s a South African-Canadian version of the ‘Modelling Paper Mafiosi’ – my name for the English clique that kicked off the new-variant parade back in January of this year.
Here are just five of the many unsupported assumptions and leaps of logic in the Dec. 1, 2021, Omicron paper:
Introduction – 1st paragraph – page 5 – “While the proportion of positive PCR tests with S-gene target failure (SGTF) associated with Omicron has subsequently increased in most provinces …”
There’s no mention of the fact that the first variant that came on the scene – B.1.1.7, subsequently dubbed Beta – also apparently is detected via this same SGTF (I cover this in my Feb. 3, 2021, article-video combination titled, ‘Is it True that the New Variants are Very Dangerous?’). So how do they know whether it’s Beta, Omicron, something else — or nothing at all? It just doesn’t add up!
Introduction – 3rd paragraph – page 5: “Many of the mutations [that they purportedly found in the Omicron gene coding for the spike protein (added Dec. 18 – I noticed that I’d dropped a few of these words in parentheses out of the article by mistake before posting it)] are either known or predicted to contribute to escape from neutralizing antibodies.” See the information/articles above that I cited in my Bridle article showing this is false. (And unfortunately parroted by many other leaders in the Covid-sceptic ranks, for example Robert Malone, and Mark Trozzi in his blog post today, leaning on the highly dubious claims of the now-omnipresentVanden Bossche: https://drtrozzi.org/2021/12/08/the-omicron-variant/. I’ll soon write an in-depth article about all this.)
Methods – Data sources – first paragraph – page 6:”All positive tests conducted in South Africa appear in the combined data set, regardless of the reason for testing or type of test (PCR or antigen detection), and include the large number of positive tests that were retrospectively added to the data set on 23 November 2021 (11).“They’re mixing together different tests and test results. They’re also assuming that all the positive PCR test results were true positives — they don’t mention the extremely high false-positive rate of the PCR test.
Methods – Data sources – third paragraph – page 7: “If the time between sequential positive tests was at least 90 days, the more recent positive test was considered to indicate a suspected new infection. We present a descriptive analysis of suspected third and fourth infections, although only suspected second infections (which we refer to as ‘reinfections’) were considered in the analyses of temporal trends.”
Wow – where do I start? They don’t supply any clinical evidence that there is any reinfection at all.
Their attitude seems to be, ‘No proof? No problem!”
The key Methods subsection, titled ‘Statistical analysis of reinfection trends,’ is littered with clues that this paper was designed to arrive at pre-determined conclusions.
Here’s how it starts – page 8 (with some of the clue words bolded by me): ‘First, we constructed a simple null model based on the assumption that the reinfection hazard experienced by previously diagnosed individuals is proportional to the incidence of detected cases and fit this model to the pattern of reinfections observed before the emergence of the Beta variant (through 30 September 2020). The null model assumes no change in the reinfection hazard coefficient through time. We then compared observed reinfections after September 2020 to expected reinfections under the null model.”
And it spirals downhill from there into even more disassociation from reality.
You can bet that the other papers published on Omicron amplify and embellish these leaps without offering a shred of solid clinical evidence to support them.
Yet tens of millions of people’s lives have been negatively effected by the rapid-fire restrictions imposed, such as travel bans.
And we’re being told, of course, that more treatments, such as having a booster shot of a vaxx, will take care of the Mighty Omicron.
It seems unfortunately I was correct in almost all of the predictions in my April 2020 article, ‘The Seven-Step Path from Pandemic to Totalitarianism.
For example, in Step 7 as soon as the first cycle of the new virus and accompanying roll-out of antivirals and vaxxes is done, another starts. And in response “They rapidly roll out virus and antibody testing again, while companies sell billions more doses of antivirals and booster vaccines.”
I wager that my analysis of Omicron is right too.
I challenge anybody to prove me wrong. Dinner and beer are on me if they do.
In a November 9, 2021, interview with Atlantic Council CEO Frederick Kempe, Pfizer chairman and CEO Albert Bourla claimed “a small part of professionals” intentionally circulate “misinformation … so that they will mislead those that have concerns.” Such medical professionals are not just bad people, Bourla said, “they’re criminals, because they have literally cost millions of lives”
The criminals’ playbook includes the dictum to always blame the other side for what they themselves are guilty of
Pfizer has a long history of criminal activity. The company has been sued in multiple venues over unethical drug testing, illegal marketing practices, bribery in multiple countries, environmental violations — including illegal dumping of PCBs and other toxic waste — labor and worker safety violations and more. It’s also been criticized for price gouging that threatens the lives of patients with chronic diseases such as epilepsy
Between 2002 and 2010, Pfizer was fined $3 billion in criminal convictions, civil penalties and jury awards, including a $2.3 billion fine in 2009, the then-largest health care fraud fine in American history. In 2011, Pfizer paid $14.5 million to settle charges of illegal marketing, and in 2014 they settled charges relating to unlawful marketing of the kidney transplant drug Rapamune to the tune of $35 million. None of it deterred future bad behavior
According to a whistleblower who worked on Pfizer’s Phase 3 COVID jab trial in the fall of 2020, data were falsified, patients were unblinded and follow-up on reported side effects lagged way behind
In a November 9, 2021, interview with Atlantic Council CEO Frederick Kempe,1 Pfizer chairman and CEO Albert Bourla claimed “a small part of professionals” intentionally circulate “misinformation … so that they will mislead those that have concerns.”2
Such medical professionals, Bourla said, are not just bad people, “they’re criminals, because they have literally cost millions of lives.” Bourla is one to talk, being the CEO of a company the name of which is synonymous with corporate crime.
Bourla’s comments were made on the same day Pfizer and its partner BioNTech asked the U.S. Food and Drug Administration to broaden its authorization for booster shots to everyone over the age of 18.3
Pot Calling the Kettle Black
I guess we can’t be too surprised, though, as the primary defense strategy people like Bourla have is to blame the opposition for their own misdeeds. He even claims the company is being targeted by “dark organizations,” meaning organizations that aren’t transparent about their funding.
This is precisely what the Center for Countering Digital Hate (CCDH) is, the fabrications4 of which are being used to prop up the official narrative that those who present evidence showing the COVID shots are dangerous are domestic terrorists5 out to worsen the pandemic death toll.
No one knows who funds this group, but it has plenty of connections to war hawks and Great Reset promoters — including the Atlantic Council, to which Bourla is making these statements.
By way of its board members, the CCDH can be linked to the Trilateral Commission, the Atlantic Council, the European Council of Foreign Relations, Save the Children Fund (funded by the Gates Foundation and a partner of Gates’ GAVI Vaccine Alliance), the British Parliament, CIA and Event 201,6,7 Microsoft,8 and the Center for American Progress9 (another organization funded by dark money10).
And Bourla wants us to believe Pfizer is under attack from dark money groups? Again, the playbook of these wolves includes the dictum to always blame the other side for what they themselves are guilty of.
More on the Atlantic Council
In August 2018, Facebook claimed an “influence campaign” by Russian “bad actors” had been carried out on its platform leading up to the 2018 midterm elections. However, it turned out these pages weren’t identified by Facebook. They came primarily from the Atlantic Council’s Digital Forensic Research Lab.
In her article, “Hysteria Over Newly Revealed Facebook ‘Influence Campaign’ Doesn’t Fit the Facts,”11 investigative reporter Whitney Webb took a deep-dive into this inane propaganda effort, pointing out that:
“… despite the lawmakers’ claims, Facebook has established no links to the Russian government or even Russian nationals.
The only ‘evidence’ to back up the claim of Russian-involvement is that one of the pages identified ‘had an IRA [Internet Research Agency, a Russian ‘troll farm’ named in a Mueller-probe indictment] account as one of its admins for ‘only seven minutes’ and ‘one of the IRA accounts we disabled in 2017 shared a Facebook Event hosted by’ one of the pages.
Beyond the fact that accusations of Russian involvement are highly politicized given the lack of current evidence, there is hardly any indication that this ‘influence campaign’ was even influential at all.
Indeed, most of the ‘bad actor’ pages and accounts had hardly any followers, with most of them having no followers. For instance, only four of the 32 total social-media pages and accounts had more than 10 followers, with all other pages — i.e., the remaining 28 — having between 10 and zero, according to Facebook’s statements.
All of the Instagram accounts identified had zero followers and, among those seven accounts, only one of them had made a single post on the platform. By Facebook’s own admission, only four of the pages named were even remotely significant in terms of followers and thus ‘influence.’”
Why do I mention this? Because this is the same tactic used to frame a small number of individuals with limited social media reach as domestic terrorists, simply for sharing counter-narratives about the COVID pandemic.
False Allegations Used to Quench Freedom of Speech
According to the CCDH,12 a dozen individuals, including me, were responsible for 65% of all anti-vaccine content on social media and should therefore be banned from all platforms. Most social media companies have since complied, deplatforming most of us. This despite a public denouncement of the CCDH’s accusations by Monika Bickert, vice president of Facebook content policy, who stated that:13
“… these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.
The report14 upon which the faulty narrative is based analyzed only a narrow set of 483 pieces of content over six weeks from only 30 groups, some of which are as small as 2,500 users.
They are in no way representative of the hundreds of millions of posts that people have shared about COVID-19 vaccines in the past months on Facebook.
Further, there is no explanation for how the organization behind the report identified the content they describe as ‘anti-vax’ or how they chose the 30 groups they included in their analysis. There is no justification for their claim that their data constitute a ‘representative sample’ of the content shared across our apps.”
Information Warfare
Getting back to the Atlantic Council, Webb noted that:15
“Facebook officially partnered with the Atlantic Council this past May in order to tackle so-called ‘fake news,’ adding that the hawkish think-tank would serve as its ‘eyes and ears’ in identifying alleged foreign-influence operations …
The Atlantic Council itself is led by a mix of retired military officers, former politicians, and Western business elites. And the think-tank’s financial sponsors include top U.S. defense contractors; agencies aligned with Washington and the Pentagon; the United Arab Emirates; major transnational corporations; and the North Atlantic Treaty Organization (NATO).
One can think of several reasons why such a group would be interested in fomenting anti-Russian hysteria … The Atlantic Council’s conflicts of interest are certainly worth keeping in mind …”
The same must be said about the CCDH, and Pfizer too. Both are glaringly biased and in no position to judge what is misinformation and what isn’t. But then, this is war, after all. We’re in an information war, and the term “misinformation” is lobbed in lieu of grenades. Discernment and some basic wisdom is required to avoid becoming a victim.
Fact checking organizations are another weapon designed and deployed to control the narrative. They exist as gatekeepers to funnel readers and viewers to the official narrative and away from anything that might raise inconvenient questions. The largest and most influential fact checker is NewsGuard, which hands out “trustworthiness” ratings to websites.
NewsGuard cofounder Louis Crovitz is a member of the Council on Foreign relations — another Great Reset supporter — and primary advisers include Tom Ridge, former secretary of Homeland Security, and Ret. Gen. Michael Hayden, a former director of both the CIA and NSA.16
Knowing that, it makes it easier to understand how everyday people who share information that veers from the official narrative can be labeled and treated as a national security threat.
The COVID pandemic is a militarized operation. We’re at war, and the designated enemy (looking at it from the side that started this war without telling anyone) are the citizens of the world who want to hold on to their freedom and human rights.
Pfizer Has a Long History of Criminal Behavior
Pfizer is on the other side — the side that is seeking to install an unelected technocratic regime based on the idea that we need a global biosecurity, biosurveillance apparatus or we’ll all die.
This is not a new position for them. During the American Civil War, which began in 1862, the need for massive amounts of painkillers and antiseptics allowed Pfizer to flourish and expand during wartime.17 Today, the manufactured “need” for COVID-19 vaccine is allowing Pfizer to make out like a bandit yet again, and as I’ve already stated, we are again at war, albeit an undeclared one.
To achieve that, Pfizer is willing to “blackmail” countries into accepting its COVID shot terms, as reviewed in the Gravitas report above — terms that make sure Pfizer always comes out on top.
A key term is no liability, which is understandable considering the amount of harm Pfizer’s COVID jab is causing. Pfizer went so far as to bully nations into putting up sovereign assets like military bases as collateral to pay for any vaccine injury lawsuits that might result from their COVID jab.
While that might not be illegal, it’s unethical, and so is researching on people without informed consent. Everyone who gets these emergency use authorized injections are part of that research, while simultaneously being prevented from seeing anything but propaganda.
Without truthful and transparent disclosure of both risks and benefits, there is no informed consent. Pfizer is even experimenting on children and pregnant women without informed consent, two categories that historically have been off-limits for drug experimentation.
Whistleblower Claims Data Were Falsified
According to a whistleblower who worked on Pfizer’s Phase 3 COVID jab trial in the fall of 2020, data were falsified and patients were unblinded. Follow-up on reported side effects also lagged behind.18 This isn’t the first time such unsavory have been levied against Pfizer.
In 2014, Pfizer was ordered to pay $75 million to settle charges relating to its unlawful testing of a new broad spectrum antibiotic on critically ill Nigerian children. As reported by the Independent19 at the time, Pfizer sent a team of doctors into Nigeria in the midst of a meningitis epidemic.
For two weeks, the team set up right next to a medical station run by Doctors Without Borders and began dispensing the experimental drug, Trovan. Of the 200 children picked, half got the experimental drug and the other half the already licensed antibiotic Rocephin.
Eleven of the children treated by the Pfizer team died, and many others suffered side effects such as brain damage and organ failure. Pfizer denied wrongdoing. According to the company, only five of the children given Trovan died, compared to six who received Rocephin, so their drug was not to blame.
The problem was they never told the parents that their children were being given an experimental drug, let alone ask them if they wanted their child to take part in the trial.
What’s more, while Pfizer produced a permission letter from a Nigerian ethics committee, the letter turned out to have been backdated. The ethics committee itself wasn’t set up until a year after the trial had already taken place.
State Department cables also revealed Pfizer hired spies with a plan to frame a Nigerian attorney general and get him to drop the parents’ lawsuit.20 Pfizer even tried to avoid responsibility by falsely accusing Doctors Without Borders of dispensing the experimental drug.21
An ‘Habitual Offender’
In his 2010 paper,22 “Tough on Crime? Pfizer and the CIHR,” Robert G. Evans, Ph.D., Emeritus Professor at Vancouver School of Economics, described Pfizer as “a ‘habitual offender,’ persistently engaging in illegal and corrupt marketing practices, bribing physicians and suppressing adverse trial results.”
Pfizer has been sued in multiple venues over unethical drug testing, illegal marketing practices,23 bribery in multiple countries,24 environmental violations — including illegal dumping of PCBs and other toxic waste25 — labor and worker safety violations and more.26,27,28 It’s also been criticized for price gouging that threatens the lives of patients with chronic diseases such as epilepsy.29
Between 2002 and 2010 alone, Pfizer and its subsidiaries were fined $3 billion in criminal convictions, civil penalties and jury awards. This included $2.3 billion for the illegal marketing of the arthritis drug, Bextra, levied in 2009.30,31 It was the largest health care fraud settlement in American history.
According to the Global Justice report, “The Horrible History of Big Pharma: Why We Can’t Leave Pharmaceutical Corporations in the Driving Seat of the COVID-19 Response:”32
“A whistleblower claimed that sales staff were incentivized to sell Bextra to doctors for conditions for which the drug wasn’t approved and at doses up to eight times those recommended. ‘At Pfizer I was expected to increase profits at all costs, even when sales meant endangering lives. I couldn’t do that,’ he stated.”
In 2011, Pfizer agreed to pay another $14.5 million to settle federal charges of illegal marketing,33 and in 2014 they settled federal charges relating to improper marketing of the kidney transplant drug Rapamune to the tune of $35 million.34
None of those legal actions deterred future bad behavior. To Pfizer, paying fines to sweep illegalities under the rug has become part of the cost of doing business, and they can afford it. While the fines may sound extraordinary, they’re tiny when compared to the company’s profits.
Pfizer was among the top 30 most profitable companies in the world in 2020, with profits reaching $16 billion, and its COVID jab alone is predicted to make $13 billion in 2021.35
As noted by the law firm Matthews and Associates, “the history of Pfizer is rife with so much subterfuge and under-the-table dealing that the company will need all the help it can get to promote confidence in its hastily assembled COVID vaccine.”36 The key strategy to boost confidence, unfortunately, is censorship.
What ‘New Way of Life’ Is Pfizer Promising?
The fastest way to get back to normal, Bourla claims in his Atlantic Council interview, is for everyone to get vaccinated. Considering how little things have changed despite massive vaccination rates, it seems clear the globalists in charge of The Great Reset — and Pfizer is part of that pack — have no intention of allowing anything go back to normal. It won’t matter how many comply, or how many times we comply
Australia is perhaps the clearest illustration of what the whole world will face. Even though a majority are “vaccinated,” their freedoms have not been returned, and now they have to submit to boosters or lose what semblance of freedom the initial round of shots gave them. The Australian government is confiscating and blocking people’s bank accounts, withholding unemployment benefits and more — all in the name of “public health.”
Bourla even indicates that there is no going back to the old normal when he states, “The only thing that stands between the new way of life and the current way of life is … hesitancy to vaccinations.”
New way of life. What does this “new way of life” look like? It looks like Australia. It looks like Israel. It looks like Lithuania,37 where your “right” to frequent restaurants, stores, shopping malls, beauty salons, libraries, banks, insurance agencies and universities, and your “right” to inpatient medical care and travel, all depend on your willingness to participate in a medical experiment that can kill or disable you.
The “new way of life” Bourla is talking about involves repeatedly playing lethal Russian Roulette just to “earn” the right to be part of society. No thank you. Bourla can keep his “new way of life.”
Because there is no virus. SARS-CoV-2 doesn’t exist. I’ve spent the past year and a half proving that. [0]
But fantasies do exist. So do covert ops with intentions to deceive.
Thus, the “scientific world” is agog over the new South African variant, named B11529 (aka Omicron, Botswana). Woo. The ghost is coming out of the closet. Beware. COVID cases are rising…
“We don’t know whether the vaccine will be effective in the face of the new variant. New lockdowns may be necessary. Travel restrictions are coming. Batten down the hatches.”
I mean, really.
As you know, for the past few months stories in the press have been claiming the vaccine-conferred immunity is sinking like a stone. This story is absurd because, again, there is no virus. So there was no conferred immunity to begin with. But anyway, that’s the story that’s been circulating. So NOW…
“It turns out one major reason for the diminished effectiveness of the vaccine is…
“The NEW VARIANT. The South African B11529.”
Uh-huh. “The vaccine is having a tough time preventing infection caused by the new variant. We may need to enforce boosters every three months…”
Keep the fear going. Push harder for the vaccine. Explain away its failures. Fabricate rising case numbers, blaming them on the new variant. Institute heavy new lockdowns.
“The South African variant is deadlier than the Delta, which is deadlier than the original.”
And none of the three exists.
What does exist is fantasy, piled higher and deeper and thicker.
The variant is Fauci. The variant is Bill Gates. The variant is CDC/WHO. The variant is the World Economic Forum. And the Chinese regime. And presidents and governors. And the mainstream press.
And don’t forget this. Vaccine injuries and deaths have been escalating all over the world. In the US alone, reported injuries have broken above 600,000 [1]. As I’ve mentioned, the well-known Harvard Pilgrim Healthcare study [2] concluded that, to obtain a true number of injuries, multiply the reported figure by 100.
Something is needed to explain all these injuries and deaths. That is, to lie about them.
And right on time, here comes the new variant.
“These people who seem to be injured by the vaccine are really keeling over from the original virus, the Delta, and woo, the South African B11529.”
Also: Recently, we’ve seen a spate of press stories with the theme—“scientists are mystified by the low COVID case numbers in Africa, where the vaccination rates are very low.” [3] Boom. That story is now gone. Wiped out. Now it’s THE WORLD IS BEING ATTACKED BY THE SOUTH AFRICAN B111529 VARIANT.
Here is one of my articles covering the non-existence of SARS-CoV-2:
—Dr. Andrew Kaufman refutes “isolation” of SARS-Cov-2; he does step-by-step analysis of a typical claim of isolation; there is no proof that the virus exists—
The global medical community has been asserting that “a pandemic is being caused by a virus, SARS-Cov-2.”
But what if the virus doesn’t exist?
People have been asking me for a step-by-step analysis of a mainstream claim of virus-isolation. Well, here it is.
“Isolation” should mean the virus has been separated out from all surrounding material, so researchers can say, “Look, we have it. It exists.”
I took a typical passage from a published study, a “methods” section, in which researchers describe how they “isolated the virus.” I sent it to Dr. Andrew Kaufman [4], and he provided his analysis in detail.
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)” [5].
First, I want to provide a bit of background that will help the reader understand what is going on in the study.
The researchers are creating a soup in the lab. This soup contains a number of compounds. The researchers assume, without evidence, that “the virus” is in this soup. At no time do they separate the purported virus from the surrounding material in the soup. Isolation of the virus is not occurring.
They set about showing that the monkey (and/or human cells) they put in the soup are dying. This cell-death, they claim, is being caused by “the virus.” However, as you’ll see, Dr. Kaufman dismantles this claim.
There is no reason to infer that SARS-CoV-2 is in the soup at all, or that it is killing cells.
Finally, the researchers assert, with no proof or rational explanation, that they were able to discover the genetic sequence of “the virus.”
Here are the study’s statements claiming isolation, alternated with Dr. Kaufman’s analysis:
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO) [6]. Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
My comments: Dr. Kaufman does several things here. He shows that isolation, in any meaningful sense of the word “isolation,” is not occurring.
Dr. Kaufman also shows that the researchers want to use damage to the cells and cell-death as proof that “the virus” is in the soup they are creating. In other words, the researchers are assuming that if the cells are dying, it must be the virus that is doing the killing. But Dr. Kaufman shows there are obvious other reasons for cell damage and death that have nothing to do with a virus. Therefore, no proof exists that “the virus” is in the soup or exists at all.
And finally, Dr. Kaufman explains that the claim of genetic sequencing of “the virus” is absurd, because there is no proof that the virus is present. How do you sequence something when you haven’t shown it exists?
Readers who are unfamiliar with my work (over 300 articles on the subject of the “pandemic” during the past year [7]) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
The answer is no.
—end of Kaufman article—
And while I’m at it, here is another piece I wrote last year about how virus-propaganda (fairy tales) must be managed, in order to make the masses stand up and salute:
—The “hot zone” theory of new frightening diseases—
Remember? There was a 1994 book by that name— and then “experts” began piling on—it went something like this:
“Out of the deep dark rainforests of Earth (cue sounds of native drumming), as a result of modern plane travel, viruses we’ve never encountered before will spread epidemics across the globe. Our immune systems, ill-equipped to recognize or deal with these strange killer germs, will fold up under the pressure, and all of civilization will be threatened with extinction.”
Let’s see. Since planes fly back and forth, and since all sorts of Westerners travel TO the rainforests, why haven’t we seen whole native tribes wiped out by viruses from the deep dark streets of Brooklyn?
It would even seem that viruses, common in, say, Norway, would cause trouble in Oregon.
Why does it have to be “viruses from jungles?” Or other faraway places like China? Why can’t we have the Second City Virus, emanating from a slaughterhouse in Chicago and infecting people in Nigeria? Why can’t we have a Big Easy virus from New Orleans traveling to Beijing?
Is it possible that jungles and Africa and China and Mexico are typically chosen for virus fairy tales because, in the minds of many Westerners, they satisfy a requirement of “strange,” “different,” “primitive,” and so on? We’re talking theater here—and when you stage a propaganda play (fiction), you want to tap into the reflex instincts of the audience. The Hartford Virus, the Des Moines Virus, the Vancouver Virus just don’t fit the bill.
Because they can’t drive up the fear that jungles or Africa or China can.
Unless you’ve been living in an ice cave in the Arctic, you know selling fear of THE VIRUS is big business. To do that, you have to strike the right notes.
I personally would be interested in a Beverly Hills or a Scarsdale or a Park Avenue epidemic virus story. I’d like to see the media try to sell that one.
What about a Bill Gates Seattle virus that some Patient Zero unknowingly carries on a plane flight to Mexico City?
Think it through. We NEVER hear killer virus stories about germs traveling from Europe and America to Asia and Africa. Why not? Because such a story won’t sell. It won’t bite.
This is called a clue.
It tells you that virus-stories are shaped and managed and written and managed and broadcast according to a plan that has nothing to do with actual disease.
If a monkey in Africa can bite a man and thus transmit a virus to the West, then a salesman in Duluth can sneeze on a man at a local airport and thus send a virus to Ethiopia.
But amazingly, through secret communication among viruses, it never happens that way. The germs have decided what the traffic pattern is, and the CDC and the World Health Organization are just discovering What Is.
Sure they are. And if you buy that, I have condos for sale on the far side of the moon.
On Nov. 4 I posted an article with some questions about Byram Bridle.
After speaking to Bridle I took it down.
The vaccine developer and viral-immunology associate professor based at the University of Guelph is very popular in the Covid-questioning community.
He is a high-profile member of the Canadian Covid Care Alliance and gives many interviews. In addition, he was an expert witness in the mid-2021 Adamson Barbecue case and in the mid-November 2021 legal pursuit of an interim injunction against mandatory vaxxing of some Toronto workers.
He’s been banned from the U of Guelph campus because he’s not vaxxed. And he’s harassed by some of his colleagues and others — including people who created both an anonymously written website byrambridle.com critiquing Bridle’s claims and an accompanying Twitter account. (They’ve also linked from the website to a GitLab section on him.)
Bridle overall is a big promoter of vaxxes. He’s developing several new ones, including working on new Covid vaxxes since at least since the spring of 2020.
And he readily uses the term “anti-vaxxer” to discredit people who have very sceptical or negative views about most vaccines.
I am among the many millions of people who hold such negative views about vaxxes. That’s because there is a great deal of solid evidence showing that many vaxxes are not safe. (More about this in the ‘Continued Push’ section below.)
The only vaccines Bridle critiques are the current crop of Covid mRNA shots. He has posted several documents — such as his Nov. 12, 2021, expert report for the interim-injunction case in Toronto – and given many interviews about this.
In my Nov. 4 article I said I believed he has a conflict of interest that he doesn’t disclose to the general public with respect to his critique of the Covid mRNA jabs. I posited that Bridle is poised to potentially make a lot of profit from six of the eight US patents (and a Canadian patent that’s identical to one of those six) that I discovered he is a co-inventor of. They’re all cancer-related. [Sentence added Dec. 1 when I re-re-read the article and realized I’d omitted this.]
I hypothesized that Bridle and his colleagues could develop, based on some of their existing patents, alternative vaxxes against Covid.
I deduced the profit motive from the fact that some of Bridle’s co-inventors on the US patents are principals in a company called Turnstone Biologics (which is a sister company to the firm listed as the patents’ owners, Turnstone Limited Partnership) — and that Turnstone Biologics is working together with international giants like Takeda to commercialize their vaxx platforms via at least one huge business deal.
I also wrote that some of Bridle’s main assertions are on very weak ground. That includes his claim that the spike protein produced by the injection of the mRNA Covid shots spreads throughout the body where it becomes a “dangerous toxin” and therefore is responsible for most of the serious injuries and deaths associated with the mRNA jabs.
I emailed the article to Bridle after I posted it. (That was a mistake – I’ve now truly learned my lesson to never again omit the step of at least attempting to talk to or email people before posting an article about them.)
In his email response he accused me of making “egregious errors” – including “mixing up my cancer research-related patents with my COVID-19-focused research; they are entirely separate.” He wrote that his patent relating to the avian reovirus is an example of my very serious error of asserting that his cancer patents are connected to his Covid-vaxx work.
He also said my article was a “one-sided piece of libel [that] represents nothing short of harassment,” and that I was conducting a “witch hunt.” He threatened legal action.
I’ve never received an email like that before. It intimidated me and shook my confidence.
In his email Bridle also asked me to call him on his cell, and provided that number. So I dialed it right away.
During our ensuing hour-long conversation I was persuaded further that I’d made huge errors by his fast-paced and confidently-delivered words – which started with his saying, “I have to say you screwed up big-time on this article. You’ve got a lot of stuff – like it [the article]’s completely wrong; you’ve completely misinterpreted everything.”
I then emailed everyone I’d sent the article to, saying I’d screwed up majorly and would write a follow-up article to set the record straight. I also took the article off my website.
I did make some errors in that Nov. 4 article.
For example, Bridle told me in his Nov. 4 email and our phone call that he has a very strained relationship with the principals of Turnstone — rather than being closely involved with them with respect to patents and potential profits from them as I’d suggested in my article — because they’ve mistreated him. I believe him. (Although he also said in that same phone call that he still holds at least one patent in conjunction with Turnstone.) I reached out to Turnstone later that day for a comment but they have not yet responded. I also seem to have made the wrong deductions about the specifics of the relationship between his cancer-vaxx patents and his Covid-vaxx work.
I apologize again for my errors.
But I did not get everything wrong, by any means.
And I still have many questions about Bridle
They include:
Why do a very large number of vaccine sceptics embrace Bridle – who is very strongly pro-vaccine, readily uses the term ‘anti-vaxxer’ to disparage people who are sceptical about the safety and efficacy of many vaccines, and is developing new Covid vaxxes even though there’s been an extremely low death rate from Covid?
Why is Bridle not disclosing in his interviews and articles/documents for the general public that he’s working toward an intranasal vaxx for Covid (which carries the genetic code for the novel coronavirus’s spike protein) – and for which he has a provisional patent application dated June 3, 2021, that very likely is a spin-off of his cancer-vaxx research, and that could ostensibly solve some of the main problems associated with Covid mRNA shots? Shouldn’t he be highlighting that when he critiques the mRNA jabs?
Why does he use tenuous evidence to support his assertion that when the spike protein spreads throughout the body it becomes a “dangerous toxin” and therefore is responsible for most of the serious injuries and deaths caused by the mRNA vaxxes (yet when questioned about this assertion admits it is only theoretical)?
And as it happens, intranasal vaxxes are gaining traction rapidly. That’s in part because they’re a spray and don’t involve use of a syringe to deliver a shot/jab the arm.
Russian President Vladimir Putin took an experimental intranasal vaxx against Covid on Nov. 23, 2021, according to newsreports. (I asked a Russian friend to read the Russian TASS article about this; she said the English translations are accurate.) It was an intranasal version of the Sputnik V shot. And it was given to Putin ‘off-label’ – that is, in the absence of formal approval of the vaxx. Human trials of it are just starting.
There are also many claims, such as in a Nov. 19, 2021, scientific paper Bridle co-authored, that intranasal shots can produce ‘sterilizing immunity’ and therefore curtail the problem of potential ‘vaccine escape variants.’
So I won’t be very surprised if developers and marketers of these new vaxxes soon also claim they could help curb the Nu/Omnicron variant (B.1.1.529) that’s received a great deal of attention in the last few days. B.1.1.529 already has been declared of “huge international concern” because it ostensibly has a “horrific spike[-protein-gene-mutation] profile,” spreads very fast and has the potential to evade the currently used vaxxes. Predictably there’s been panic such as long lines at airports in the very rapidly growing list of African countries subject to travel bans by other governments — along with a renewed push for more people to get vaxxed. [And just as I was ready to post this article I found out that B.1.1.529 may in fact first have surfaced in July. I may write about this in a future article.]
Yet there hasn’t been a single published scientific report, as far as I know, which would allow objective/outside verification of whether there is any real evidence to support these drastic claims and actions. And I remain very sceptical about the hype regarding all variants and the methods used to detect them, including the false narrative about ‘immune escape’; see my Feb. 3, 2021, Feb. 11, March 16, May 24 and Oct. 24 pieces.
And as I wrote in that March 16 article (about Geert Vanden Bossche): “We … need to stop production and use of antivirals and antibodies and all other parts of the Covid-industrial complex. Covid has an extremely high survival rate. So why develop yet another expensive, invasive and experimental solution to a problem that barely exists, if it does at all?”
Let’s dive into trying to answer those questions, and in the process solve the riddle of Byram Bridle.
Bridle Is Creating Fast-track Covid Vaxxes Based on His Team’s Cancer-Vaxx Tech
He doesn’t hide this. And his statements in news reports about this clearly show Bridle believes he and his collaborators can use the methodology they’d already developed for making cancer vaxxes to very quickly create vaxxes for the novel coronavirus (and for an array of iterations of it and of other viruses).
In my Nov. 4 article I cited two May 21, 2020, news pieces about Bridle and several of his collaborators receiving a one-year, $230,000 grant from the Ontario government. He was given the grant together with Leonardo Susta and Sarah Wooton — both also at the University of Guelph — and Darwyn Kobasa from the Winnipeg National Microbiology Lab (NML). (The May 21, 2020, Ontario-government news release about this also announced Covid-related grants to other researchers across the province.)
The section of the news release about the U of Guelph/NML project said they were given the money to test vaxxes containing a virus (avian avulavirus or the adenovirus) into which they spliced the genetic code for the novel coronavirus’s spike protein. First they’d do preliminary mouse testing of the shots at the University of Guelph. Then “after optimization, these vaccines will be evaluated [for efficacy] in a hamster challenge model at the” NML.
CBC reporter Kate Bueckert in her May 21, 2020, report quoted Bridle as saying, “We’ve had to, over the years, develop all kinds of ideas and methods to optimize cancer vaccines. Because we have these technological platforms, we realized we could quickly, through the virology expertise, switch our cancer vaccines over to vaccines against infectious diseases.” (Bolding added by me.)
Bridle also said, “‘Our plan is, by the end of the year [of funding], so this would be in 2021, to have completely vetted the science and identified an optimal vaccine strategy to protect against infection with the virus that causes Covid-19 and at that point … our goal would be to start talking to Health Canada.’” (Bolding added by me.)
A Guelph Today piece about this said Bridle believes “that unlike other ‘one-off’ approaches to developing a Covid-19 vaccine, the team’s platforms can be adapted to develop vaccines for future versions of a coronavirus. That means future vaccines might be made more quickly and cheaply, giving Canada a foundation for subsequent vaccine development. ‘With these vaccine vectors, we designed them to be “plug and play.” You can put any gene into the vectors within two weeks. It could be a target protein in a cancer cell, but it could just as easily be a protein on a virus,’” Bridle said. (Bolding added by me.)
The piece also said he “hopes to see a viable [Covid] vaccine based on the technology ready for Health Canada approval in 2021…. The team will work with Health Canada to ensure ‘fast tracking‘ for any potential vaccine to be released to the public.” (Bolding added by me.)
Hamsters Setting the Pace in the Covid-vaxx-development Race
The timeline given by Bridle in those May 2020 media pieces may be somewhat optimistic (and indeed in this June 21, 2020, Global TV interview, he said that vaxxes would take more than a year to be ready for widespread use).
However, there are the strong indications that he and his colleagues are moving quickly.
Hamsters play a key role in this. (Not because they move fast in their cages; rather, they – specifically, Syrian hamsters – have immune systems that are said to respond to infectious agents in very similar ways to humans’ immune systems.)
In my Nov. 4 article I said I’d found a scientific paper co-authored by, among others, Bridle, Wooton and Susta. It’s dated Nov. 19, 2021 (with an e-publishing date of Oct. 6, 2021) and is titled, ‘Intranasal vaccination with a Newcastle disease virus-vectored vaccine protects hamsters from SARS-CoV-2 infection and disease.’
In that paper, the Newcastle-disease virus/spike-protein Covid intranasal vaxx that Bridle, Wooton, Susta and their colleagues tested in Syrian hamsters came out looking rosy. For example, they concluded that spraying two doses of the vaxx (containing the full length of the spike-protein gene spliced into a Newcastle-disease virus) into the noses of a total of 10 hamsters resulted in a “clear increase of S[spike-protein]-specific antibodies after the second dose.” They also wrote that the vaxx was safe and, in addition, stopped the virus from multiplying to high levels in the hamsters.
This must be one of the results of the developing and testing of experimental Covid vaxxes by Bridle and his colleagues that started by or before the spring of 2020. In other words, at some point they must have included in their testing this experimental Newcastle-disease-virus/novel coronavirus spike-protein vaxx, either in parallel with, or as part of, the work they did using the Ontario-government grant.
In our Nov. 4 phone call Bridle dismissed this study as being at only a very early stage of development. He said, “clearly you don’t have an understanding of what it takes to get a vaccine from the pre-clinical stage to the place where it can go into a rollout into the public.”
Yet that ignores his quotes in the May 2020 articles about seeking to have their experimental vaxxes fast-tracked in 2021.
It also doesn’t seem to take into account other things such as the fact that the Canadian and other governments put into warp speed the testing and approving Covid vaxxes and are continuing to do so.
Follow the Patent Trail
Then a couple of days later, while reviewing all the material I’d gathered for the Nov. 4 article, I discovered at bottom of that Nov. 19 paper by Bridle and collaborators the following ‘Conflict of interest statement’: “L.A.S., Y.P., B.W.B. [Byram Bridle], P.P.M., L.S. [Leonardo Susta], and S.K.W. [Sarah Wooton] are co-inventors on a United States Provisional [Patent] Application No. 63/196,489 entitled ‘ENGINEERED NEWCASTLE DISEASE VIRUS VECTOR AND USES THEREOF,’ which was filed June 3, 2021.” (Bolding added by me.)
So they are moving apace on the pathway to patent their approach.
As I noted above, Bridle had commented in our Nov. 4 phone call on that Nov. 19 paper — but only to say it’s very early-stage (i.e., pre-clinical) research. He didn’t mention any provisional patent applications.
I tried to find the June 3 provisional patent application online but didn’t succeed. There doesn’t seem to be a publicly accessible database of provisional patent applications.
But I did find this website that gives information on provisional patent applications. It describes how to get one. It also lists the benefits of a provisional patent application. These include that it allows “the term ‘Patent Pending’ to be applied for 12 months in connection with the description of the invention,” and “enables immediate commercial promotion of [the] invention with greater security against having the invention stolen.“) (Bolding added by me.)
I emailed Bridle on the evening of Nov. 23. I asked him to send me the June 3 provisional patent application, along with any other provisional patent applications he has. And I emailed him again a few minutes later saying, “Further to the email I sent you a few minutes ago, if the information in the provisional patent application isn’t public then of course I’m not asking you to send it to me. Only what you’re able to – ie what’s available to the public. And if you have other provisional patent applications I’m only looking for their titles, assuming the titles are publicly available (and nothing else is).”
He replied the next morning:
“I’m not sure what the status of this provisional patent application is; two of my colleagues (equal inventors) took the lead on this. Anything that is publicly available would be searchable in the US patent database. If it isn’t there, then it isn’t publicly available yet.”
So he’s not disclosing anything about this provisional patent application, nor saying whether he has more of them.
He’s not obliged to, of course. But why he wouldn’t at least answer my question about whether he has any other provisional patent applications?
And by the way, I believe his and his colleagues’ June 3, 2021, provisional patent application is to some extent related to two US patents — 10829786 and 20200190538 — that are among the eight US patents that have Bridle’s name on them that I mentioned in my Nov. 4 article. Those two US patents are both titled, ‘Avian oncolytic virus having modified sequences and uses thereof.’ (The word oncolytic means tumour-infecting and -killing.) The patents’ description highlights the avian reovirus and the Newcastle-disease virus vector as the central part of this vaxx-tech platform.
(Bridle told me in his Nov. 4 email and our Nov. 4 phone call that he holds a patent related to the avian reovirus. One [or both] of 10829786 and 20200190538 is [are] very likely the one[s] he was referring to, because none of the other six US patents that I’ve found with his name on them mention the avian reovirus.)
They’re actually the two that in my Nov. 4 article I said I believed were not related to his Covid-vaxx work. And Bridle told me in his Nov. 4 email that his avian-reovirus patent[s] are not related to his Covid-vaxx work, because, among other things, “did you notice in the title that the claims are based on it[‘s written as] being an ‘oncolytic’ virus; that means for the treatment of cancers.”
But I believe they may well be related to his Covid-vaxx work. Because as I noted above, the information on these two US patents says they relate not only to the avian reovirus but also to the Newcastle-disease virus. And the Newcastle-disease virus is what his June 3, 2021, provisional patent application and Nov. 19 paper are focused on. There’s no way for me to know for sure, though, without seeing the provisional patent application and/or any subsequent patent application he and his colleagues may file.
Intranasal Vaxxes Gaining Traction
Intranasal vaxxes, like the Newcastle-disease-virus-based one that Bridle and his colleagues have been working on, just happen to perhaps not have the problems that Bridle ascribes to the mRNA jabs.
Intranasal vaxxes aren’t new. AstraZeneca’s intranasal flu vaxx FluMist has been used in the US since 2003 (with the exception of a two-year pause from 2016 to 2018, apparently because it wasn’t effective in kids aged two to 17).
And as I noted earlier in this article, the intranasal route is likely to become extremely popular. Intranasal-vaxx developers are counting on their being much more palatable to the public, including ‘vaccine sceptics,’ because these vaxxes aren’t jabs/shots and people can administer them themselves.
(And many have long being used for livestock – for example Merck’s – and also for dogs – here are Merck’s canine nose vaxxes.)
There already are eight intranasal vaxxes in clinical trials to date, according to the World Health Organization’s ‘COVID-19 vaccine tracker and landscape.’ (Click on the ‘Download’ button near the top left of the page; double-click to open the document that appears; scroll down to the table labelled ‘4. Number of doses, schedule and route of administration of candidates in clinical’; then look at the ‘IN’ – ‘intra nasal’ [sic] – line in the ‘Route of Injection’ section.)
That’s a small fraction of the more than 350 Covid vaxxes being tested so far.
But many more intranasals are sure to follow. For example, according to this Nov. 11, 2021, article, a Stanford University team is teeing up an intranasal spike-protein shot against Covid.
Their Oct. 27, 2021, mouse-experiment paper the article is based on states, in the abstract at the beginning of the article, that such “an alternative self-administrable vaccine capable of mounting long-lasting immunity via sterilizing neutralizing antibodies [i.e., antibodies that ostensibly prevent the virus from multiplying] would be hugely advantageous in tackling emerging mutant SC2 [SARS-CoV-2] variants. This could also diminish the possibility of vaccinated individuals acting as passive carriers of COVID-19” (Bolding added by me.)
They further note, in the third paragraph of the paper’s second page, that another advantage of the intranasal route is “the avoidance of injections, and a likely high tolerance and compliance in clinical practice.” (Bolding added by me.)
And indeed, Bridle told me in our Nov. 4 phone call that, “If somebody comes up with a vaccine [for Covid] that has properly demonstrated a good safety profile … addressing all of the safety issues, legitimate safety issues, that I and many other international colleagues have raised. And until we see that data, presented to us, and alongside the efficacy data, none of us, including myself, are going to stand behind any of these other vaccines. So yes, but could there be a future vaccine for SARS-coronavirus-2 that we would stand behind? Yes. I would be happy to do so. Because I am a virologist.”
Shaky Spike-Protein-Related Assertions
Let’s now switch gears a bit to address one of Bridle’s central claims about the mRNA Covid shots.
He lays the lion’s share of the blame for the serious injuries, such as myocarditis, and deaths from those jabs on the spike protein — which is produced in the body after the jabs — entering the bloodstream. He suggests that other shots do not lead to this type of spread.
He makes sweeping statements about this — in for example his Nov. 12, 2021, expert report and his June 15, 2021, Covid-shot guide for parents. In the middle of page 40 of the Nov. 12 report, after citing eight studies (see five paragraphs below), Bridle writes:
‘Conclusion: the spike protein, if it gets into circulation, has the potential to cause damage to the cardiovascular system and other tissues.’
And just one sentence later, at the start of the next section, he states:
“Now that there is a clear understanding that the spike protein from SARS-CoV-2 is a dangerous toxin when it gets into the blood and is distributed throughout the body, we can continue with the story about COVID-19 vaccines.” (Bolding added by me.)
On what basis did he make this leap?
He cites eight studies to support this claim. (The studies are references 84-91; you can see their details such as authors, title and publication name, on page 133 of the document.) But they’re all related to Covid, not to vaxxes for it. Plus: five of those studies are in vitro (i.e., in test tubes and/or petri dishes) and one study was done in mice (the spike protein was injected directly into their veins). The other two were on human-autopsies (which have some overlapping authors with each other). Note also that Bridle states that one of these human-autopsy papers (ref. 84) shows the free spike protein rather than the whole virus was found in various tissues. But this isn’t really accurate: the authors said that they found the spike protein grouped together with other proteins from the virus. (For example, on the fifth page of the paper the authors write, “in both the skin and brain … the spike protein co-localized with both the envelope and membrane proteins, suggesting that the capsid proteins [i.e., envelope protein, membrane proteins and the spike protein] circulated as a unit”).
And indeed, when in a September 24, 2021, interview on Rebel News, Tamara Ugolini asked Bridle how he knows it’s the spike protein and not something else causing injuries and deaths in people who have received the Covid vaccines, since we don’t know all the ingredients in the vaccines (at 30:27 in the video), Bridle admitted his evidence is purely theoretical.
“That’s a great point,” Bridle replied. “… We have to depend on the companies really – the companies, the onus is on them to evaluate the safety. So we’ve been raising all these questions. And these can readily be addressed in studies — properly conducted experiments.”
He went on to say that (at 32:05) it “is a big if if the mechanism of damage that [is] causing things like the blood clots [is] the spike getting freely into circulation.”
[And unfortunately he’s not alone in his seemingly faulty reasoning. For example, I emailed Sucharit Bhakdi to ask why, in the July 23, 2021, paper that Bhakdi co-wrote with Michael Palmer claiming the spike protein is the root of virtually all of the evils of the mRNA Covid shots, they didn’t use any information on the pattern of injuries among the many millions of people who’d already been jabbed by then. Bhakdi replied in a Sept. 9 email to me that, “Our predictions regarding development of adverse effects are based on general textbook knowledge of immunobiology and medicine. They are currently being verified.” (Bolding added by me.) Yet I’ve checked subsequent posts on doctors4covidethics.org, and as far as I can see Bhakdi and other authors still have not verified this using any clinical data in jabbed people.]
Bridle is Part of the Continued Push to Trust Vaccines
On page 5 of his June 15, 2021, vaccines guide Bridle wrote, “I consider vaccines that have been developed on a foundation of sound science to be the most efficient type of medicine; they have cost-effectively saved millions of people from sickness and/or death.” A very similar sentence is on page 5 of his Nov. 12, 2021, expert report. And he repeats this message in many other forums.
The Canadian Covid Care Alliance – of which Bridle is a key and outspoken member — also strongly promotes vaccines. For example the Alliance’s Sept. 24, 2021, ‘COVID-19 Canadian Covid Care Alliance Declaration’ notes (bolding and underlining in the original):
“Without full transparency and informed consent, and without a full appreciation and proper evaluation of the safety of these novel vaccines (both short- and long-term) the current COVID-19 vaccination programs should be paused immediately. We greatly support classical vaccine programs as developed over past decades and are therefore deeply concerned that this blatant disregard for medical ethics and most recent scientific data during COVID-19 vaccinations will irreparably damage Canadians’ trust in the traditional vaccine programs.”
And unfortunately other high-profile organizations also have been giving Bridle an uncritical platform. That includes, among others, TrialSiteNews (see for example Bridle speaking at 12:50 in this June 4, 2021, ‘Expert Panel’ video) — and Children’s Health Defense and Del Bigtree’s ‘The Highwire,’ via pieces such as this one, this one and this one.
As a result, large numbers of people and organizations who previously were standing firm in their knowledge based on a large body of evidence that vaccines are unsafe – people labelled ‘anti-vaxxers’ by Bridle and others — are being lulled into thinking Bridle is on our side because he’s vocally opposing the mRNA Covid shots.
Therefore they may well be led to believe that virtually all other vaccines are okay.
I recommend several pieces of reading material that show the clear and present dangers of many vaccines.
This is among the material that helped open my eyes 2.5 years ago to the dangers of vaccines. Contact me if you’d like other book or article recommendations.
By asking questions we can start to solve the riddle of Byram Bridle.
Don’t let ‘experts’ on either side of any issue lull or push you into giving away your power to think for yourself. Follow the money trail and potential conflicts of interest.
Work to find the real truth – it’s hard work but vital. Check the primary-source material used to make assertions, no matter who’s making them.
It is more than evident that a significant part of humanity is stampeding to take experimental vaccines for COVID-19. However, the “experimental” vaccines violate all 10 of the Nuremberg Codes, which carry the death penalty for those who seek to break these International Laws. Now, more than ever, we need new trials, not after the fact, as was the situation after WWII, but while the crimes against humanity are in progress.
Instead of these Nazis above the tables would be full of executives from Pfizer, Moderna, Johnston and Johnston, Dr. Fauci and the infamous Bill Gates, and many others. Even the politicians, who pretended to play doctor and healthcare official, promoting life-threatening and depressing masks, lockdowns, and death shots, should be held accountable. Dr. David Martin clearly shows that all of them are guilty of breaking American laws.
Front and center should be multiple members of the FDA and CDC, who are not trustful governmental agencies but richly paid whores for the vaccine companies.
American Heart Association Journal Publishes Data that U.K. Medical Doctor Claims are “Proof” that COVID-19 Vaccines are “Murder.” `We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy and other vascular events following vaccination.’
23 Nazi doctors were charged with conducting experiments on prisoners without consent, most at concentration camps. The aftermath of the trials led to creation of the Nuremberg Code, which the FDA and CDC do not follow. The Dr. Rath Health Foundation tells us that, “After six decades of silence, the historical records of the key war crimes tribunal that determined the responsibility for WWII were finally made available. Currently, history books teach that WWII was launched by a lunatic dictator, Hitler, and his ruthless Nazi henchmen.
However, tens of thousands of historical documents from the Nuremberg Tribunal – newly released online – unequivocally document that:
WWII – a war that cost the lives of more than 60 million people – was planned and financed by the world’s largest chemical/ pharmaceutical cartel. At that time, Germany’s I.G. Farben consisted of Bayer, BASF, Hoechst, and others.
The driving force behind WWII was I.G. Farben’s ambition to control the global oil and drug markets and eliminate, by force, any competition.
The I.G. Farben companies financed the rise to power of the Nazi party and transformed German democracy into a dictatorship.
“The pharmaceutical industry does not act in the tradition of the protector of humanity, but in the tradition of I.G. Farben, a group of organized criminals willing to sacrifice countless human lives to maintain their profits,” writes Dr. Mathias Rath. Listen to him pleading in 2012 with his fellow Germans to not go down the same road that Germans have traveled twice before. He, too, claims that the two world wars were driven by the insatiable greed of the pharmaceutical and chemical cartels. The legacy of I.G. Farben is carried on by Bayer/Monsanto, Pfizer, and the other COVID vaccine companies.
Telford Taylor was an American lawyer best known for his role as Counsel for the Prosecution at the Nuremberg Trials after World War II.
Telford Taylor, US Chief Prosecutor at the Nuremberg War Crimes Tribunal against the executives of great I.G. Farben, wrote, “The crimes with which these men are charged were not committed in rage or under the stress of sudden temptation. One does not build a great war machine in a fit of passion nor an Auschwitz factory during a passing spasm of brutality. Their purpose was to turn the German nation into a military machine so it could impose its dominion on Europe and other nations beyond the seas. They were the warp and woof of the dark mantle of death that settled over Europe.”
The Nuremberg War Criminal Tribunal convicted 24 I.G. Farben board members and executives based on mass murder, slavery, and other crimes against humanity. Amazingly, however, by 1951, all of them had already been released and continued to consult with German corporations. The Nuremberg Tribunal dissolved IG Farben into Bayer, Hoechst, and BASF. Moreover, today each of the three daughters of I.G. Farben is 20 times as big as the I.G. Farben mother was at its height in 1944, the last year of the Second World War.
There are people on this planet that take pleasure in hurting other people. They injured others from sheer psychological habit. The general nature of ‘evil’ is not to have consciousness of the effect our actions have on the feelings and emotional world of others, which is the definition or defining characteristic of both psychopaths and sociopaths.
Dr. Russell Blaylock says that it was the Rockefeller Foundation that created orthodox Medicine back in 1901. “Rockefeller owned what was called the drug trust: that’s the major drug manufacturing firms all over the world: Merck Pharmaceuticals, Lederle, all of these pharmaceutical companies. And, of course, the aim was to remove all nutrition references to nutritional type treatments from the medical schools. They closed down half the medical schools in the United States. There were 165 medical schools at the time. Then he had his anointed medical schools, which he poured his money into, appointed the professors from his stock of professors. And so, they created an educational system that taught the things that he wanted to be taught. And therefore, every professor that came out of those programs taught the same thing.”
Dead Doctors
According to the American Medical Association (AMA), a whopping 96 percent of United States doctors as of June have been “vaccinated” for COVID-19. And now many are dead. Vaccinated Doctors are Dying, and Unvaccinated Doctors are Quitting or Being Fired: Who will Run the Hospitals?
Contemporary Medicine has been on quicksand for over 100 years, and as it sinks to the bottom, it is pulling down with it millions of humans into misery and death. We have known for a decade, thanks to the work of Dr. Gary Null, Dr. Carolyn Dean, and Dr. Barbara Starfield, that properly prescribed pharmaceutical medications are killing over 100,000 Americans each year.
Journal of the American Medical Association (JAMA)
Dr. Barbara Starfield of the Johns Hopkins School of Medicine ALL THESE ARE DEATHS PER YEAR: 12,000 —– unnecessary surgery 7,000 —– medication errors in hospitals 20,000 —– other errors in hospitals 80,000 —– infections in hospitals 106,000 —– non-error, adverse effects of drugs
James Howard Kunstler writes that modern Medicine is a hostage racket; “Medicine is now a catastrophe every bit as pernicious as the illnesses it is supposed to treat, and a grave threat to a nation that we’re supposed to care about. If you thought banking in our time was a miserable racket — which it is, of course, and by “racket” I mean a criminal enterprise — then so-called health care has it beat by a country mile, with an added layer of sadism and cruelty built into its operations.”
It Is Worse Than All The Above
Dr. Wolfgang Wodarg, former head of health at the Council of Europe, explains that a pandemic used to be associated with widespread severe illness and death, but by changing the definition, removing the severity and high mortality criteria, World Health Organization (WHO) can now make a pandemic whenever it wants. One of the most respected men in Europe, he maintains that the “World Health Organization is an institution of corruption.”
“The scientific data overwhelmingly shows how probably millions have died from the covid injections, and hundreds of millions are suffering crippling side effects that often permanently disable the victims for life. The Vaccine Death Report provides all the data, along with hundreds of references, for further investigation.”
At the above link, one must scroll down to the first video but be prepared for a shock as the entire world’s elite are exposed for who and what they are, what they own, and what they have planned for most of the rest of us. Naturally, after watching, one is tempted to run and hide, but in the end, courage is encouraged.
It will be a miracle if the 99 percent of us persevere against the elite, the Deep State, the three or four companies that seem to own most of the other mega-corporations. Add God into the equation, add truth, reason, insight, and love for each other, and perhaps a much-needed miracle will occur.
I also recommend a video exposing the lies and stupidity of Gates, Fauci, Biden, the head of the CDC, and Biden, who cannot make up their minds about what is true or not about COVID vaccines.
About 47 million adults in the U.S. remain unvaccinated, according to figures from the Centers for Disease Control and Prevention.
A Chicago-area judge saved a grandfather’s life with the single question that exposes hospitals blocking doctors from using a safe, FDA-approved drug: Why?
Leaks are turning into floods. We are hearing about brutal clinical studies on puppies and other animals, and now a study involving orphans in New York.
These studies were funded, in whole or part, by the National Institute of Allergy and Infectious Diseases, a federal agency headed up by Anthony Fauci since 1984.
In 2014, investigative reporter, Liam Scheff, wrote an article at omsj.org, looking back on the orphan scandal. Ten years earlier, he had broken the story, and was then subjected to multiple attacks in the press.
Here is Liam’s 2014 article. As you read it, remember where the funding for the orphan drug trial came from:
“In 2004, I broke open the NIH Clinical Trial Scandal, the internationally-covered story of hundreds of New York City orphans used by government agencies and pharmaceutical companies in deadly AIDS drug trials.”
“In reporting this issue, I entered the orphanage where children were being used as guinea pigs, and over a period of several years, took interviews with mothers, children and childcare workers at the Incarnation Children’s Center. I also interviewed the medical director, and investigated the FDA documentation and published medical literature on the tests and drugs used, drugs which were often force-fed through nasal and gastric tubes to the children. I reported several deaths in children, and although the mainstream denied that any deaths were due to drug toxicity, they admit that over 200 children died.”
“In 2005, the city of New York hired the VERA Institute to form a final report on the drug trials. VERA was given no access to medical records for any of the children used in trials. Their report was published in 2008. They reported that twenty-five children died during the drug studies, that an additional fifty-five children died following the studies (in foster care), and, according to Tim Ross, Director of the Child Welfare program at VERA (as of 2009), 29% of the remaining 417 children who were used in drug studies had died (out of a total 532 children that are admitted to have been used).”
“The WIKIPEDIA writers cover up all details, as is expected.”
[Wikipedia:] “’No payment or compensation has been paid to any of the children used in the trials, or to their families’.”
“The New York Times, which was instrumental in covering up the story, hired Janny Scott and Leslie Kaufman to write a hit piece on me in 2005. They declared the following about using orphans in drug trials:”
“’It was seen as one of the great successes of AIDS treatment. In the late 1980’s and early 1990’s, hundreds of children in New York City were dying of AIDS. The only approved drugs were for adults, and many of the patients were foster children. So doctors obtained permission to include foster children in what they regarded as promising drug trials’.”
“Later in the article, Scott admits that the ‘permissions’ for many of these children are ‘missing,’ (or were never there).”
“She continued:”
“’[T]here is little evidence that the trials were anything but a medical success’.“
“In 2009, she responded to my persistent queries about their investigation method. They had taken at least 40 documents from me and buried them; what else had they buried? Her answers to me were clarifying:”
“’No, we did not review patients’ medical files…I would be surprised if that would not have been a breach of patient confidentiality if someone had shown them to us…An unexpected side effect would have been a side effect not previously seen in response to those drugs, presumably. Advanced testing methods were the methods available at the time for diagnosing HIV infection…I do not recall interviewing Dr. Painter [the doctor in charge of the orphanage and orphans] but I may simply not remember. As you know, the Times moved to a new office a year ago. It was not possible to move all of our files. In my case, I threw away files that were more than 12 months old. As you know, the story you are asking about was done in 2005…I do not recall which studies we looked at. There were a lot of them — some more easily accessible than others, as you know…As for mentioning side-effects and FDA warnings, there are side-effects and FDA warnings on many if not most drugs. The side-effects of early AIDS drugs have been written about extensively…And, as I have said before, we were not presuming to judge whether or not experimental AIDS drugs should have been tried on children — a question that I suspect few journalists would be qualified to answer; we were attempting to put a public controversy in context…If you have further objections to the way the story was handled, I suggest you contact Joe Sexton, the editor of the metropolitan news section of the paper and the editor on that story’.”
“In 2009, the Times admitted that many children had died – but the VERA Institute, hired to ‘investigate’ the trials, was also forbidden from looking at medical records. Their ‘investigator’ also refused to take data from me on the trials – lists of the trials themselves, the drugs used, and their recorded ‘black box’ warnings. In a follow-up interview with Vera Myles of WBAI, the head of the VERA Institute admitted that many more children had died.”
“The Wikipedia is not able to talk about AIDS drugs, which kill people. But, of course, take them if you really want to.”
Fauci is the highest-paid federal employee in the U.S., and 68% of his $437,000 a year salary comes from bioweapons research
Instead of safeguarding public health, Dr. Anthony Fauci turned the National Institutes of Health into an incubator for pharmaceutical products, and essentially sold the entire country to the drug industry
Fauci has had a hand in creating the vaccine gold rush. In 2000, he met with Bill Gates, who asked to partner with the NIH in an agreement to vaccinate the world with a battery of new vaccines. In 2009, this agreement was rebranded as “The Decade of Vaccines,” the objective of which was to implement mandatory vaccinations for every adult and child on the planet by the year 2020
One of the darkest stains on Fauci’s career, aside from his role in the COVID pandemic, was his handling of the HIV epidemic. Suppressing the use of repurposed drugs, Fauci zeroed in on AZT, a toxic drug that has killed an estimated 300,000 AIDS patients
The similarities between the AZT scandal and what’s happening today with the COVID jab and remdesivir are striking. Again, Fauci has suppressed all treatments using inexpensive and nontoxic drugs. U.S. taxpayers have paid for research, while drug companies have raked in the profits, all while having zero liability for injuries and deaths
In this interview, Robert F. Kennedy Jr., an environmental activist and attorney turned ultimate freedom fighter, discusses his latest book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health,” which is a must-read if you want to know more about the behind-the-scenes of this giant fraud. We could talk for hours and not cover but a fraction of what’s in this book, which Kennedy calls a “devastating indictment of Tony Fauci.”
In a nutshell, Kennedy describes how Fauci turned the National Institutes of Health into an incubator for pharmaceutical products, and essentially sold the entire country to the drug industry. The book is an incredibly well-referenced record of his history of decimating human health, and exposes him as a self-serving charlatan.
Tony Fauci basically created this template that he then used over the next 45 years, to develop toxic drug after toxic drug. He killed early treatment, and killed any protocol that competed with his pharmaceutical enterprise. A lot of people have died [as a result]. ~ Robert F. Kennedy Jr.
I particularly enjoyed how Kennedy placed Fauci in the context of Rockefeller’s legacy with respect to Bill Gates, who developed an alliance with Fauci over 20 years ago. Rockefeller set us on a course of toxic, profit-driven medicines synthesized from the byproducts of the oil refinery process a century ago, and Gates picked up where he left off and then collaborated heavily with Fauci.
The Decade of Vaccines
Fauci, in turn, has had a hand in creating the vaccine gold rush. In 2000, he met with Bill Gates, who asked to partner with the NIH in an agreement to vaccinate the entire population of the world with a battery of new vaccines. In 2009, this agreement was rebranded as “The Decade of Vaccines,” the objective of which was to implement mandatory vaccinations for every adult and child on the planet by the year 2020.
“I show how they use the pandemic simulations, working very closely with the intelligence agencies, with the big media companies and the major pharmaceutical companies to make that happen,” Kennedy says.
“Gates calls what he does philanthropy capitalism, [the idea that] you can use philanthropy to make money. He had a foundation where he has sheltered $50 billion in tax-free money. And, he continues to have absolute control over it. He uses that money to gain control of public health agencies in our country and the World Health Organization.
He’s created a lot of his own [organizations] with Dr. Fauci and a lot of these quasi-governmental agencies that people think are governmental. They’re actually front groups of the pharmaceutical industry like GAVI and SEPI …
He uses this battery and this control of the WHO to set pharmaceutical or medical policy, public health policy around the globe, in a way that maximizes the profits from his stakeholding in these big pharmaceutical companies.
I also show he’s simultaneously doing the same thing to control the global food supply … [He’s] really trying to change both public health and food policies in ways that benefit corporations that he’s invested in and that he’s partnered with.”
Fauci’s Lethal Handling of the AIDS Epidemic
Gates didn’t lure Fauci to the dark side, however. Fauci had already spent decades playing with people’s lives and sacrificing public health for profit. One of the darkest stains on Fauci’s career, aside from his role in the COVID pandemic, was his handling of the HIV epidemic.
The first cases of AIDS surfaced in 1981. Initially, the AIDS program was run by the National Cancer Institute, a separate institute inside the Health and Human Services Department (HHS). The general belief was that AIDS had a chemical etiology caused by drug use. This all changed when the HIV virus was discovered.
Fauci started working for the NIH in 1968 as a clinical associate in the Laboratory of Clinical Investigation at National Institute for Allergy and Infectious Diseases (NIAID). He became director of the NIAID in 1984, the year after the discovery of the HIV virus, and was appointed director of the Office of AIDS Research in 1988, when that office was established. As explained by Kennedy, Fauci essentially built the NIAID around an AIDS drug called AZT.
“AZT was a chemotherapy formulation that was so toxic it killed all the rats when they gave it to them. The inventor of AZT felt that it was unsafe for any human use, so he didn’t even patent it,” Kennedy says.
“Very early on, the National Cancer Institute had found that when you put AZT in a culture of HIV, that killed the HIV, not surprisingly. It killed anything it touched. And so, Fauci partnered with the manufacturer of AZT … He guided that formulation through the regulatory process and tried to fast track it. He cheated terribly on the clinical trials.
In the clinical trials, it was killing everybody. It literally kills everybody who takes it. But he was able to keep the people in the treatment group alive by giving them huge numbers of blood transfusions. It does keep them alive for the eight weeks, and based upon that eight-week trial, he got approval for AZT. It was unprecedented.
As Kary Mullis, who won the Nobel Prize for discovering the polymerase chain-reaction (PCR) technique, said, with any chemotherapy drug, you’re supposed to give it to somebody for two weeks. Chemotherapy is designed to kill every cell in the body, but hopefully it kills tumor cells first, and you can take the person off it. The tumor dies, if you time it right, and the person doesn’t die.
If you put somebody on that for life, like Tony Fauci was doing, every one of them is going to die. And that’s what happened. Meanwhile, there were a lot of drugs at that time that were being repurposed. Local, community-based doctors in San Francisco and New York who were treating the AIDS community were finding that these drugs treated the symptoms of AIDS, and they stopped people from dying.
Fauci made a deliberate crusade to sabotage those, to make sure they were not available to sick people, in order to make sure that AZT would be the only solution. And AZT was the most expensive drug in history. It was $10,000 for a one-year supply [while costing just $5 per dose to manufacture, plus U.S. taxpayers paid for all of the research and development of the drug] …
Tony Fauci basically created this template that he then used over the next 45 years, to develop toxic drug after toxic drug. He killed early treatment, and killed any protocol that competed with his pharmaceutical enterprise. A lot of people have died [as a result].”
Although a bonanza of money was made with AZT, it pales in comparison to Pfizer making out like a bandit with its COVID shot. The U.S. taxpayers paid $20 billion to fund the research, and another $10 billion to market the COVID jab. Pfizer created the best-selling drug in the world and will make $35 billion from it this year.1 Even better, unlike AZT, this is absolutely risk-free and they can never be sued for injuries.
Everything in Fauci’s Career Is Groundhog Day
An estimated 330,000 people have died from AZT alone. Overall, the similarities between the AZT scandal and what’s happening today with the COVID jab and remdesivir are striking. Again, Fauci has discouraged the use of any prevention for COVID-19, and any treatment using inexpensive and relatively nontoxic drugs such as hydroxychloroquine or ivermectin.
U.S. taxpayers funded the research while drug companies have made an estimated $100 billion in profits from the shots in a single year, all while having zero liability for injuries and deaths even as people are being coerced into taking them.
“Everything in Tony Fauci’s career is Groundhog Day,” Kennedy says. “Again, and again, and again, he is repeating the same behavior and it is paying off. And he has this way of talking where he never really says anything. And this habit of just lying, and lying, and lying …
I knew a lot about what happened during the HIV crisis because my uncle, Ted Kennedy, was chair of a health committee at that time. Teddy was the first presidential candidate to court the gay vote, and I was running his campaign at that time …
In the health committee, his primary concern for most of the time was AIDS. I talk about this in my book.
Finally, Fauci was called in front of Congress, and was just fileted. Henry Waxman and all of these well-known Democratic congressmen were saying, ‘What the hell are you doing? You’ve produced nothing. You’re totally incompetent.’ After that, his career was over, and he decided at that point, ‘OK, I’m going to work on getting these repurposed drugs on the market.’
He did that for a couple of years, and he had a project, which was a dual track project where they could, without going through the clinical trials and FDA randomized, placebo controlled trials, they could get approval for these drugs, so that people could get insurance for them and pay for them. So, I was deeply involved in this for many, many years, and I’ve known Tony Fauci for a long time.
I have insights on who he really is, that most liberal Democrats are utterly ignorant of. He is the opposite of everything they believe. He is the architect who turned our public health system over to the pharmaceutical industry. He does not do public health. And there is no metric at NIH, where they look and say, ‘We are improving public health.’
The only metric they have is, ‘How many vaccines have we given? How many pharmaceutical drugs have we sold? How much kickback money are we getting into the agency?’ As I explain in the book, this agency has become an incubator for the pharmaceutical industry.”
Gain-of-Function Research Under Fauci’s Watch
Fauci is responsible for an annual budget of about $6.1 billion. He gets another $1.6 billion from the military to do bioweapons research, which is where 68% of his $437,000 a year salary comes from. (Fauci is the highest-paid federal employee in the U.S. Second-highest is the president, at $400,000 a year.)
“That’s why he had to do that gain-of-function shenanigans in Wuhan,” Kennedy says. “He had to do it, because he had to hold on to his salary. And most of his salary comes from bioweapons research …
Gain-of-function research has never provided a single scientific or medical development that has assisted us in responding to pandemics. Not one. But Fauci continues to do it, because it is critical to his salary. And it’s critical to that funding stream.”
Now, the bulk of the NIAID’s funding was intended to be used to study American health and to improve it; to eliminate infectious allergic diseases and autoimmune diseases. Instead, under Fauci’s watch, the chronic disease epidemic has exploded.
This, despite the fact that between Fauci, Gates and the U.K. Wellcome Trust, they control 63% of the biomedical research on earth through their funding. Over his career, Fauci alone has distributed more than $930 billion in research grants through the NIAID. You could say they control all of it, really, because they also have the capacity to dry up funding to projects they don’t want done.
Ruthless Fauci
Case in point: Something happened in 1989, triggering a series of epidemics — autism, food allergies, Tourette’s Syndrome, narcolepsy, ADD/ADHD, speech delay, language delay, rheumatoid arthritis and autoimmune diseases like juvenile diabetes. All of them sprang up right around 1989. Why? What’s causing them? It’s Fauci’s job to find out, but he refuses to, and he blocks anyone else from digging too deep.
“Tony Fauci’s job is to say, why did that happen? It has to be an environmental toxin. Genes don’t cause epidemics. They provide the vulnerability, but they cannot cause an epidemic. You need an environmental toxin. All we have to do is figure out which one started in ’89, and became ubiquitous the same year. But if anybody tries to do that study, Fauci will ruin their career.”
Top suspects include vaccines, which dramatically increased in ’89, and virtually all of the chronic diseases that have skyrocketed are listed as potential side effects on the manufacturers’ inserts. The herbicide glyphosate also became ubiquitous around that time, and really exploded in 1993 when RoundUp Ready corn was invented. GMOs, other pesticides, ultrasound and PFOAs are other potential culprits.
“Our kids are swimming around in a toxic soup. And it could be all of those things, or it could be one or another, but it’s easy to find out. You just do the science. And that science is easy to do, but it will never be done as long as Tony Fauci’s in office, because he doesn’t want us to know — because those are the industries he has survived by protecting,” Kennedy says.
Fauci Works on Behalf of Big Pharma
Kennedy goes on to explain how Fauci works on behalf of Big Pharma, and why he’s become so important for the drug industry.
“Between 2009 and 2016, about 230 drugs were approved by the FDA, all of which came out of his shop. So, he is an incubator for Pharma.
And here’s what he does: At his lab, he has petri dishes filled with every virus [imaginable], and he has scientists that are messing around with different molecules and different poisons, and they’ll drop those poisons into a petri dish and see if it kills the culture. If it kills the culture, then he has a potential antiviral drug.
The next step is, they give it to rats, and see if it kills the rats. If most of the rats survive, now you have a potential antiviral that may work in humans. Then, he farms it out to a big university. Now the person it goes to at the university is usually a very powerful person. It’s the dean of the medical school, or the chair of one of the departments, and they run the clinical trials, which is extremely lucrative.
So, they will do the Phase 1 trial, and they’ll recruit maybe 100 people for the trial. Fauci gives that principal investigator maybe $20,000 per recruit. The university skims off 50% to 75% of that. So, now, that university is hooked into the system.
Then, if the drug works in Phase 1 and Phase 2, then they have to bring in big groups of people — 10,000 people — and you’re talking about hundreds of millions of dollars. And they have to bring in a pharmaceutical company that now takes control of about half the patent.
Tony Fauci’s agency keeps a share of the patent. For example, they now collect royalties on the Moderna [COVID] vaccine. [The NIAID] gets half the royalties, billions of dollars. The university researcher keeps some of the patent, so he is now permanently attached to Tony Fauci and will do anything he says, and the university itself is getting some of that patent.
So, it’s hundreds of millions of dollars that are going to these universities every year, in addition to the grants that he’s giving, and he can cut all that off if somebody at the university does the wrong study.
Once the drug goes through Phase 3, it goes to the U.S. Food and Drug Administration. Fauci says, ‘Well those are independent scientists at FDA.’ The panel is called VRBPAC [Vaccines and Related Biological Products Advisory Committee], and they’re NOT people who work for the FDA. They’re outside persons who are brought in.
Well, where are they brought in from? They’re Tony Fauci’s principal investigators from all the universities, who are working on his other projects, and they’re brought in to rubber stamp the drug …
They OK it and give it a license, because they know that, next year, their drug is going to be in front of that committee, and they are going to want the committee to rubber stamp them. So, that committee never says no. It always green lights everything, and it’s completely controlled by Fauci. He controls the whole process …
Every expert you see on CNN is on Tony Fauci’s payroll, and CNN will never tell you that. It will say, ‘This is an independent virologist, he’s an immunologist at Baylor University, or Stanford, or Harvard.’ They’re not telling you where that guy’s bread is being buttered, and that the person who’s buttering it is Tony Fauci, with your taxpayer dollars. The whole system is just fixed.”
Fauci’s Past and Rotten Character Are Catching Up on Him
As more and more of Fauci’s lies and his funding of sadistic experiments on animals and aborted fetuses are coming to light, Kenney predicts Fauci will be forced to resign, especially as the book comes out and people really start to understand what he’s been up to all these years.
“Nobody who was not a sadist in his soul would allow [the beagles being eaten by sandflies] experiment to happen,” Kennedy says. “Yet, Tony Fauci deemed that the best use for $450,000 of U.S. taxpayer money, with all of the screaming needs in public health.
But it’s not just $450,000. Millions and millions [of dollars] he has put into these sadistic experiments where they’re torturing animals to death. Like you’d see in a schoolyard with little boys, who don’t know any better and need to be told, ‘You don’t do that to another creature.’ Fauci doesn’t have that instinct, it’s lacking.
It explains what he has done during COVID — denying early treatment to millions of Americans and forcing them to suffer and die in their homes, or on ventilators and remdesevir, which is a deadly toxic drug, rather than get treated and be healthy.
And punishing, silencing, censoring, delicensing, discrediting any doctor who tries to say, ‘Wait a minute, I’ve been treating patients, and my patients aren’t dying, because I’m using hydroxychloroquine, ivermectin’ and an entire battery of repurposed drugs that we now know treat virtually all COVID cases.
Seventy to 90% of COVID deaths and hospitalizations could have been prevented, and there are hundreds of studies that support that. Yet, he forbids people from doing it. That is a sociopath …
And shutting down a million businesses, is that really going to save lives? There’s no study that indicated it would … We have 4.2% of the global population, and we had 14.5% of the deaths. Why is anybody listening to this guy? There’s no Health Minister in the world who has a worse track record than Tony Fauci.
There are many countries that had 1/100th of our death rate per million in population. And guess what? Those are mainly the African and Asian countries, that as a matter of course are giving ivermectin for river blindness and hydroxychloroquine for malaria control.”
In support of Kennedy’s assertion that Fauci will be forced to resign, you can view his recent grilling November 4, 2021, by Sen. Rand Paul in front of Congress. What is most impressive are the comments, which are virtually unanimously disparaging Fauci.
Fauci’s Lethal, Illegal Experiments on Children
In his book, Kennedy includes a chapter on some of the animal trials Fauci funded. He also tells a far grimmer story, where the guinea pigs were Black and Hispanic children. At least 85 of these children died, but the number could be as high as 1,000 or so. Fauci got these children by arranging for foster care programs in New York and six other states to assign children who had lost their parents to AIDS to participate in drug studies.
These children had no guardian, so they were illegal studies. To do a clinical trial on children, you need to have a guardian appointed who puts their interests first, ahead of the drug companies. Fauci didn’t want that, so he allowed these studies to go forward without a legal guardian for any of these kids. No one was watching out for them. The trials weren’t even done by licensed medical professionals.
“They were mainly Dominican immigrants, who were deeply compassionate, who discovered in the middle that they were actually being hired to treat these children as guinea pigs, and they were killing huge numbers of them. Many of the kids didn’t even have HIV, so they had no possible benefit from the drug, which is illegal.
Yet Fauci got away with all of it. I believe there was a Congressional investigation for a brief time, but like everything that gets near him, it kind of peters out. The BBC did a documentary on these kids back in 2004 called ‘Guinea Pig Kids.’
They interviewed these children, [one] who said, ‘I took the drugs. They made me feel sick. I was vomiting, I couldn’t eat, I was tired all the time, it was painful, and I refused to take it.’
And when they refused, they were sent to another of Tony Fauci’s principal investigators at Columbia Presbyterian who installed a feeding tube to force feed these children these toxic chemotherapy drugs that they refused to take … As bad as Beagle gate is, what he did to these Black and Hispanic children is even worse.”
COVID-19 — The Culmination of Fauci’s Criminal Enterprise
As for the COVID-19 pandemic, Kennedy equates it to the culmination of Fauci’s career. In the book, he recounts how Fauci has been a key figure in pandemic planning — not necessarily how to prevent one, but how to create it, as infectious disease mortality had dropped so dramatically that infectious diseases were becoming an increasingly low priority.
So far, every single pandemic that has been dramatized has turned out to be a complete fraud, and the same can be said for COVID. All the while, billions of dollars were spent on vaccines.
“They’ve taken all of these lessons they learned from all the other fake pandemics and rolled it into coronavirus,” Kennedy says. “Now, I want to make clear, I’m not saying that coronavirus is not a pandemic, or that it doesn’t kill a lot of people. It does. But we’ve all been manipulated by an exaggeration of cases, the exaggeration of deaths, the obscuring of data, all of the manipulations that they’ve done to us.
[In the book] I have a picture that somebody got from a Freedom of Information Act request. It’s a March Madness graph of all of the different pandemics — fake pandemics — [Fauci] has tried during his career, all converging with the grand winner being coronavirus. And [Fauci] signed it, somebody on his staff made it.
But it was Tony Fauci’s triumph, winning March Madness. It’s basically a picture of his career. Him trying every three or four years a new fake pandemic, and finally hitting on all eight cylinders with coronavirus. It’s like it’s a joke, and we are the punchline …
Here’s what I would say to people. We have to stop this. This is the hill that we all have to die on. If you are a parent, and you let them give this [COVID shot] to your child, you are not doing your job as a parent. If you are a doctor, you are committing malpractice to give this to a child. We all need to resist.
I would say that every American who sees what’s happening has to start engaging in civil disobedience every day. And that may mean going to a store and telling them, if they demand a vaccine passport, that you are not going to patronize that store anymore. It may mean resisting on the job. Do not quit! Make them fire you. Because then you have a lawsuit.
Right now, the best thing is to make them fire you for not taking an emergency use authorization vaccine, because there are no approved vaccines in this country available to any American. It was a myth, it was a hoax, it was a chicanery for them to say, ‘We approved this Comirnaty vaccine.’ If you go on Pfizer’s website, it will tell you, ‘We do not make Comirnaty available in the United States.’
Why are they trying to go after our kids? Here’s why. The vaccines can only get liability protection once they are approved. The only way they get liability protection is if they’re on the child’s vaccination schedule. And then, once the CDC votes them onto the child vaccination schedule, then they get liability protection, even for adults.
One lawsuit can bankrupt the company if they didn’t have liability protection. So that’s why they’re going after our kids. They need it to get that liability protection. And we need to stop them from the collateral damage they’re going to cause to an entire generation of children; 26 million children will get a vaccine that’s been tested on 1,300 kids, with catastrophic results.”
GRAPH: The Measles Myth: one popular talking point is that the Measles vaccine has more or less eliminated Measles globally. However, real data shows that incidences began plummeting long before there was any mass-vaccination program for measles.
According the leading public health bodies like the World Health Organisation, the Measles virus is an ongoing deadly epidemic which kills more than 140 000 people globally per year, mostly among children under the age of five. It is also claimed that Measles were eliminated from the United States in 2000, but continue to be ‘reintroduced’ by international travelers into the country. In 2019 there were claimed to be a minuscule 1,241 cases spread across the United States.
Yet, despite all of these official claims, there seems to be very little scientific evidence that clearly shows Measles being an infectious agent in a host. Rather, it is just widely assumed to be the case.
Here’s what modern virology and public health mavens cannot seem to answer: what causes Measles?
We are told that it is a virus, but is there any evidence for this?
In this video, Dr Sam Bailey examines the evidence presented by Measles experts and the media, as well as the court case where Dr. Stefan Lanka offered €100k euros for proof of a Measles virus. Watch:
I’m republishing my recent article about the ongoing slaughter of millions of newborn calves, because it occurred to me that your faith holds that cows are sacred, and should be protected from harm.
I doubt you would knowingly use a product who existence is based on the killing of cows.
Read on.
—Murdering millions of newborn calves for vaccines and other medical research—
Cc: vegan Hollywood celebrities and animal rights advocates who are taking the COVID vaccine
The product is called Fetal Bovine Serum (FBS). It is used all over the world.
How is it obtained?
Slate News: “FBS, as the name implies, is a byproduct made from the blood of cow fetuses. If a cow coming for slaughter happens to be pregnant, the cow is slaughtered and bled, and then the fetus is removed from its mother and brought into a blood collection room. The fetus, which remains alive during the following process to ensure blood quality, has a needle inserted into its heart. Its blood is then drained until the fetus dies, a death that usually takes about five minutes. This blood is then refined, and the resulting extract is FBS. Millions of fetuses are slaughtered this way.”
Think about that.
—Medical research, vaccine research, and a blood-soaked landscape. The murder of living human infants for their tissue; the murder of newborn calves for their tissue.
Slate: “FBS is also special because it is a universal growth medium. You can take almost any cell type, toss it into a petri dish with FBS, and the cells will grow. The use of the serum is extensive, with FBS being cited in more than 10,000 research papers…”
Was FBS used in the development of COVID vaccines? Yes and no statements proliferate.
However, if you take the research and development back far enough into the virology lab, the answer would be an unqualified yes.
Cell cultures in dishes are starting points for all vaccines. Virologists believe they are isolating viruses in those dishes. The purported viruses are the reasons, in the first place, for all vaccines—including COVID.
Those cell cultures in dishes need a substance that promotes the growth of the cells. Enter Fetal Bovine Serum as that substance.
In medical literature and news media, you’ll find many euphemisms and generalities that obscure the murdering of newborn calves. Animal-derived products; serum; organisms in development; growth factor; universal medium; humane treatment.
“Don’t tell the children.” In this case, everyone is supposed to be a child kept in ignorance.
And medical murder is supposed to be a special scientific procedure. Separate, remote, sanitized.
It is—until people find out what’s actually going on.
The contents list and abstract of the 46-page “The Covid-19 Fraud & War on Humanity” is found below.
To read and download the full document in pdf form, click on the box above.
Contents
Part One
The globalist agenda
The Trojan Horse
Virology’s double deception
The four pillars of the COVID-19 fraud
The first pillar: Isolation
Part Two
The second pillar: Genomic sequencing
The third pillar: PCR
The fourth pillar: Outbreak modelling
Part Three
In summary
Conclusion
Post Script
Crimes against humanity
The final insult
Abstract:
COVID-19 is a fraud because its alleged causal agent, a purported novel coronavirus called SARS-CoV-2, has not been proven to exist in nature and therefore has not been established as the cause of COVID-19, the disease and pandemic invented by the World Health Organisation (WHO). For the selfsame reason there are no variants of the “virus”, which likewise exist only hypothetically in computers, cloud-based gene banks and in the minds of innocent people who have been comprehensively gulled by their governments.
The COVID-19 fraud, comprised of numerous preposterous claims, constitutes nothing less than a war on humanity by organisations such as Anser, Fors Marsh, and Palantir that conduct the scam through Big Pharma, with its backers and enablers, including the World Economic Forum, the Bill and Melinda Gates Foundation, the WHO, technology conglomerates, the mainstream media, complicit governments, and COVID “pirates” such as UNC Chapel Hill and Imperial College London, to a one beneficiaries of the fraud.
COVID-19 is a war on humanity because politicians and their governments continue to use this imaginary disease to terrorise and imprison their citizens, denying them guaranteed human rights and freedoms, and violating their once inviolable bodies with highly experimental and hazardous injections that contain a computer-generated spike protein mRNA sequence that instructs the body to poison itself. These nefarious injections, which also contain undeclared non-biological objects for undeclared purposes, are injuring millions and killing many thousands of people around the world, including up to 218 New Zealanders as at 2 October 2021.
A virological fraud lies at the heart of these crimes against humanity – that SARS-CoV-2 has never been physically isolated or shown to be the aetiological (causal) agent of COVID-19. In this article, the authors examine the illusory world of virology to explain how a virus that no one has seen or knows where it has come from, that no one knows what it does or where it is going, is, according to the fraudsters, stealing across borders and boundaries and coming to get you no matter where you are. How can it be, the authors ask, that this phantasmagorical madness has morphed into a world redolent with fear in which democratic governments have abandoned democratic principles to engage in the control and “deletion of human beings” that may be just a “variant” away from turning into World War III?
About the Authors
Dr Mark Bailey MB ChB, PGDipMSM, MHealSc (Otago)
Is a microbiology, medical industry and health researcher who worked in medical practice, including clinical trials, for two decades.
Dr John Bevan-Smith BA (Hons) First Class, PhD (Auckland)
Is a business owner, author and researcher, who has undertaken research for the Waitangi Tribunal Te Rōpū Whakamana i te Tiriti o Waitangi/The Ministry of Justice Te Tāhū o te Ture.
Let me start by saying, everybody acts from faith. Faith in something, no matter what it is.
A billion Catholics are not the Vatican.
The Vatican, through the Pope, has made its position clear: take the COVID vaccines.
But then there are the consciences of a billion of the faithful.
In prior articles in this series (archive here), I’ve made it clear that COVID vaccines have, in fact, relied on a fetal-tissue cell line, HEK 293, for testing, and the cell line was originally obtained via an abortion.
Moreover, the evidence points to an abortion in which the infant was delivered from her mother’s womb, alive, and then was killed by a doctor removing her kidneys for fetal tissue. Infanticide. Murder.
Does it matter whether the abortion and the murder were committed yesterday, or in a room in a hospital in the Netherlands, in 1972? Are a billion Catholics willing to say, “It was so long ago, it doesn’t have meaning anymore”?
Is that a reasonable position of Faith?
My understanding is this: Catholics believe Jesus commanded the founding of His Church, which is their Church. Does that count now? Is it wrong to contemplate what He would advise? As opposed, for example, to what Anthony Fauci would advise?
I also understand the Pope, in telling Catholics to take the vaccine, was not claiming to speak from a position of infallibility. Doesn’t that leave the door open to the consciences of the billion members of the Church?
Is it archaic to speak about conscience? Is religious membership really an elaborate charade, a social stage play?
Suppose a high member of the Vatican said to the world: “There are many medical experiments that are used to develop and test vaccines and drugs. In these experiments, which have been performed for a hundred years, doctors remove an infant from his mother’s womb, ALIVE, and then take his kidneys or make a hole in his skull and vacuum out his brain, or cut out his heart. These killings are very real. Those of our faith should think deeply about whether they want to receive the medicines and vaccines associated with these murders…”
What would happen?
Suppose this esteemed member of the Vatican made this announcement, replete with details, every day for a month?
What would happen?
Suppose this esteemed priest decided to keep making the announcement until sufficient members of the congregation, worldwide, stepped forward, visibly, and made their voices heard and refused the vaccine?
What would happen?
As some people are reading this, they will answer, “This esteemed priest would be murdered.”
Yes? And? So?
Don’t the sacred vows of a priest go beyond loyalty to this world? Isn’t his conviction to his faith a thing larger than his life on Earth?
Would you expect or want a priest, who serves as a pipeline to God for his congregation, to be a materialist, a person inextricably bound to his comforts and duties here?
If by joining the Church as a member, a person comes closer to God, is he asked to pay no price for that gift? Is he asked to incur no risk in his life?
The Church is, in fact, founded on matters of life and death. That is where faith encounters a reckoning. And this is true of all religions.
But at their most profound pinnacle of teaching, where “the outer garments” are cut away, religions guide the individual soul to come to his own decision about what his faith means, and how far he will go in standing with it.
One person, a billion people.
The Power is always there.
One step across the threshold.
~
George Fox, the fiery 17th century preacher who founded the Quakers movement in England, traveled the countryside exhorting thousands of people to find Christ and God for themselves: “Why should any man have power over any other man’s faith, seeing [that] Christ Himself is the author of it?”
At the time, there were laws forbidding “unauthorized worship.” Fox constantly broke them. He was frequently arrested—at least twice for blasphemy, and on one of those occasions it was suggested he should be sentenced to death. Parliament intervened on his behalf.
He performed many healings and wrote a book listing and describing them. The book disappeared, and no copies ever surfaced.
Thinking about George Fox and his courage as background and example…
Now, in 2021, should believers grasp a destiny that outdistances the fear of being banned from Facebook; being “attacked” online for expressing an opinion about an election audit; being fired from a job; being “canceled” for telling a joke?
Has the need for security and comfort expanded to such a degree that people of faith are willing to abandon their beliefs on a moment’s notice?
~
If today you picked a few thousand people of faith and sent them back to the time of Moses, to live as Egyptians under the Pharaoh; it’s quite possible that when God loosed the 10 plagues against them—“water turning to blood, frogs, lice, flies, livestock pestilence, boils, hail, locusts, darkness and the killing of firstborn children”; the Pharaoh would simply say: “The only adverse effects are minor pain and swelling at the injection site and transient fatigue”; and these people would believe him.
How much faith is required in order to open one’s eyes?
And having opened them, to have a voice and make that voice heard?
And to endure against the consequences, because faith is not ultimately invested in material things?
~
Book of Revelation: “And in the midst of the seven candlesticks one like unto the Son of man, clothed with a garment down to the foot, and girt about the paps with a golden girdle. His head and his hairs were white like wool, as white as snow; and his eyes were as a flame of fire; And his feet like unto fine brass, as if they burned in a furnace; and his voice as the sound of many waters. And he had in his right hand seven stars: and out of his mouth went a sharp twoedged sword: and his countenance was as the sun shineth in his strength. And when I saw him, I fell at his feet as dead. And he laid his right hand upon me, saying unto me, Fear not; I am the first and the last: I am he that liveth, and was dead; and, behold, I am alive for evermore, Amen; and have the keys of hell and of death. Write the things which thou hast seen, and the things which are, and the things which shall be hereafter; The mystery of the seven stars which thou sawest in my right hand, and the seven golden candlesticks…”
For those who believe these words, the majestic scope of these words, who take them as truth—
What will they do now?
Will they sit still, or will they rise up and take action?
“…the more evidence arises supporting my worst fear—that a perfectly innocent
living child, a healthy little girl, born alive and outside the womb, was killed for and by the harvest of her organs, and that this is a practice that may underlie
great parts of the research industry.”
For my recent series of articles on the murder of infants to obtain fetal tissue for vaccine testing and research, I gained key information from investigative reporter AnnaMaria Cardinalli’s article, “Catholic Conscience and the COVID-19 Vaccine,” in Crisis magazine.
Q: It seems you’ve lived at least several lives side by side. You’ve earned a lofty worldwide reputation as an operatic contralto and classical guitarist; you’re a licensed private investigator; you carried out extensive research for the US military in Afghanistan; you own a private security firm; you donate all your earnings to a Catholic order which wants to start an orphanage for exploited children. And I’m not covering all the bases. It’s rather mind-blowing. Before we dive into the subject at hand, can you speak to this variety and achievement?
A: Ha! Your question is very flattering and I’m hardly at issue here, but I’ll be happy to answer. The variety of work I’ve been involved in is so wildly unlikely that I could have never sat down and come up with it as a plan! The one factor underlying all it is my incredible fortune to have been raised soundly in the Catholic Faith by my mom, so despite my own many failings, I knew enough to put my life completely at the disposal of God’s will from an early age. I find utterly astounding the adventures on which He’ll lead a soul when He’s given that freedom. Making music was always my personal hope, but the rest came as a natural consequence of responding to circumstances around me with whatever capacities I had the ability to respond. That’s the very definition of responsibility (“response ability”), and a real means by which God guides our lives, don’t you think?
Q: In your wide range of experiences, did medical issues ever pop up on your radar?
A: Medical issues arose in two ways. On one hand, when I worked for the FBI and was embedded with the Joint Special Operations Command In Iraq, I received truly fantastic, cutting-edge training in a collateral duty as a Tactical Operational Medic. Later, in Afghanistan, I participated in medical missions to help assess rural tribal community needs—particularly the medical needs of women and children. Through these military experiences, I found a passion for emergency medicine. I recently re-certified as an EMT to better assist my community’s current medical mission to the homeless (sosvan.org), and I continue to pursue more advanced certifications.
On the other hand, I do not approach the issue of the cell line origins as a practitioner or any sort of medical expert, but as an investigative journalist, simply seeking out the facts and holding them to the light of common logic. My thinking is that the factors necessary to understand the nature of what we put into our bodies must be, at least on a basic level, accessible and comprehensible to the general population, and one need not be a medical expert to grasp them. Otherwise, how could most of us make an informed decision? We can’t allow clear, critical truths to be obfuscated by the statement, “You’re not an expert. You wouldn’t understand.”
Q: How did you become interested in the very specific origin of the fetal cell line, HEK 293? What made you think it might be important?
A: I was led to interest in HEK 293 via a long path. My experience in Afghanistan imparted to me a particular investigative focus on Human Trafficking. I’ve written and worked extensively on the issue, and the more I learn, the more I am overwhelmed by its prevalence, both internationally and on our own soil. In recent years, while the China Tribunal brought the harvesting and sale of organs belonging to unwanted citizens into clear focus overseas, the Planned Parenthood expose by David Daleiden [more on that expose — covered by Celia Farber, here and here] and others brought the same practice to light in the US. Both these developments solidified the trafficking issue in my mind not only as one of forced labor or sexual exploitation but of the complete commoditization of the human person—the viewing of the human being as a mere collection of occasionally useful parts, lacking any other value. This should frighten every person, regardless of their faith background or lack of one, because history shows us over and over again that it’s when we fail to recognize our common humanity that atrocities prevail.
With regard to HEK 293 specifically, for Catholics like myself, it is a grave moral responsibility to examine whether any action one takes participates in, perpetuates, or encourages such evil. We are bound to inform our own individual consciences and act in accordance with them. So, when the COVID vaccine became available, I sought to find out all I could about the nature of its origins and was led right back into the human trafficking concerns that plague me. It was in this research that I came across the work of the biologist and vaccine developer Pamela Acker [author of “Vaccination: A Catholic Perspective”; more here]. Her public acknowledgement of the necessary procedure for ensuring the viability of Human Embryonic Kidney (HEK) cells coincided with what medical professionals had shared with me privately.
For me, this was enough to raise concern that warranted further investigation before taking the vaccine. Sadly, the more the matter is investigated, as it was by the courageous, thorough, and insightful author of the Gateway Pundit article, the more evidence arises supporting my worst fear—that a perfectly innocent living child, a healthy little girl, born alive and outside the womb, was killed for and by the harvest of her organs, and that this is a practice that may underlie great parts of the research industry. Believe me, I am longing to find firm and indisputable confirmatory evidence that this nightmare scenario is NOT the case. However, your in-depth coverage of the subject following the Crisis and Gateway Pundit articles seems to continually contribute direct, expert-based medical evidence of the horrifying truth. Saddening as it is, I truly appreciate what you are accomplishing.
Q: The HEK (Human Embryo Kidney) 293 fetal cell line has been used to test COVID vaccines. That makes its origin vividly important now. How did you become convinced that the evidence pointed to the removal of an alive infant from her mother’s womb, and then the killing of that infant, in 1972, in the Netherlands, in order to harvest her kidneys—which would be used to create the HEK 293 cell line?
A: I reiterate that I had to be convinced by simple logic that anyone, not medical researchers exclusively, could follow. In fact, the more specialized the language describing a medical moral issue becomes, the more it can be used to obscure the facts. I would almost laugh, if not for the gravity of the issue, at hyper-euphemistic descriptions one finds in the medical literature. It discusses, for instance, situations like the finding of electrical impulses in the cardiac tissue of the POC.
First of all, “POC?” Product of conception? What a way to talk around an issue! I’m a proud product of conception and have never met anyone who wasn’t! Electrical impulses in the cardiac tissue? With fewer keystrokes, that could be called “a heartbeat.” So, I’m a POC with intact electrical impulses in my cardiac tissue or, if anyone were looking to save on ink, “alive.” Please, though, forgive my digression.
I worked to write very carefully in the Crisis article the simple facts that concerned me about the origins of the HEK 293 cell line. Rather than try to summarize that argument in this interview and thus potentially miss a critical component—may I please direct interested readers to the article at the link below?
I became further convinced of the reality following the publication of the Gateway Pundit exclusive which offered some insightful analysis taking into account the recent Pfizer whistleblower revelations. I’d also like to direct anyone interested to that great article with a link below.
It’s not that I don’t want to answer the question, it’s that I want it to be answered as accurately as possible.
Q: When I read conventional medical literature that describes research on aborted fetuses, I see no mention of taking the infant from the mother’s womb, alive, and then killing him/her. Is this a research “open secret” that is held back from the public and even many doctors? I read a 1975 federal report on medical research using fetuses. It went on for a hundred pages, and there wasn’t one reference to killing infants in the process of removing their organs.
A: I think the first issue here is the extremely removed language typical of the descriptions of these procedures that I reference above, along with its tendency to state actions separate from their obvious consequences. It’s a linguistic tendency that may well reflect the thinking and training of researchers and abortionists. In Dr. Kathi A. Aultman’s testimony to the Senate Judiciary Committee Hearing on March 15th 2016, which you excerpted in your incredibly revealing post of October 27th [see here; more here], the doctor describes her initial fascination with the cellular perfection of the little bodies she dissected, and explains that it was only years later that was she able to overcome her scientific dissociation to make the intellectual connection that the tiny perfect bodies were those of people whose lives she had ended.
I worry our society has removed death so far from life that we don’t even recognize it, and that is a scary thing. Our grandparents die in facilities away from home rather than with their hands held in ours. Our food arrives packaged and devoid of any reminders of the animals from which it came. Fido moves to a faraway farm, while we play immersive games where graphically taken lives merely “reset.” Therefore, unlike any generation prior to ours, most of us can go through life without regularly witnessing the reality of death, which makes for a very unnatural understanding of it—one far from the Catholic motto of memento mori. It’s an understanding that might even allow a scientist to admire a human body on which she performed a procedure that ended the function of its “cellularly perfect” organs without grasping that she was its killer.
I suspect this kind of thinking in turn produces academic writing in which it is almost impossible to see anything untoward. Perhaps most authors themselves can’t see it, aside from the presumably rarer instances of dedicatedly evil individuals who do see things clearly and actively choose to obfuscate the reality. Either way, this is why the literature will never say, as you had difficulty finding, “in the next step, kill the newborn,” even if it is the obvious consequence of the procedure described.
If the doctors involved were capable of that kind of cause-and-effect thinking, perhaps they would have to first write, “in the next step, first anesthetize, then kill the newborn.” If some of those doctors believed themselves Christians, they would have to write “in the next step, first baptize, then anesthetize, and then kill the newborn.” Even if they believed themselves merely in possession of basic mammalian instincts, they would at least have to write “in the next step, first cuddle and comfort the crying newborn, then anesthetize and kill him.” Of course, they can’t go there without recognizing the child’s humanity, so instead, the scientific dissociation of cause-and-effect remains in place.
This critical thought barrier is evidenced particularly in the literature when we see organs harvested from living children outside the womb referred to as fresh “fetal” or even “embryonic” tissue. The biomedical research companies requisitioning the tissue make the same linguistic error and it goes constantly uncorrected. No. The medical term for a delivered fetus in its first moments and days of life outside the womb is a neonate. A newborn. Most of these people went to medical school and know the difference, but they persist in the error.
Perhaps if we could only require them to accurately use the language of “fresh neonatal tissue” in their requisitions and reports, some would be unable to proceed. Requesting a “heart of newborn” for the development of whatever a researcher might be concocting in the lab might finally sound to the ears of many too much like procuring the ingredients of a witch’s brew belonging to horror fiction. It certainly makes “eye of newt” sound resoundingly tame.
Other than the issue of logic and language, however, I don’t think the practice of infanticide by vivisection is particularly secret among those working closely in the arena of biomedical research, and it’s certainly known among the abortionists who supply the needs of the industry, although I agree with you that it’s not something that doctors whose scope never intersects the arena are aware of any more than most of us are. It’s simply not brought to our attention in the media. We focus where the media points us, and there appears some decided silence on the issue.
A breakthrough in public awareness of the direct killing of living unwanted newborns for the sake of biomedical research, which, almost incomprehensibly, generated far less media attention and public outcry than it should have, occurred with the David Daleiden hearings. There many doctors and scientific procurement company representatives spoke openly of the practice, though often in the detached terms that would require careful listening. For instance, the CEO of Stem Express admitted dryly that “fetal hearts were perfused using a Langendorff apparatus.”
A Langendorff apparatus serves to preserve the functional viability of hearts ex-vivo (which means, literally, outside of a living body). That is, to specify the use of the Langendorff apparatus is to know that a heart requiring this preservation was, in fact, taken from a living body. To state the painfully obvious cause-and-effect reasoning generally left out here, the removal of a functioning vital organ from a living person (without the replacement of its function) is the direct killing of that person. No example is clearer than that of a beating heart. Ask an Aztec.
Dr. Theresa Deisher, a Stanford University School of Medicine researcher heavily involved with the use of adult stem cells, describes exactly how that killing must take place in order for the Langendorff perfusion to function. Both in her September 19th, 2019 testimony at the Daleiden trial and in a same-day interview with Lifesite News, she explained that the individuals performing the vivisection would necessarily “cut open the baby’s chest and they would take the heart out beating and drop it in a buffer with potassium. She went on to state with rare clarity, “of course, if the heart isn’t beating, they can’t get any of these cells. Nobody wants a stopped heart.”
At another point in her testimony she explained again that, “some of the babies had to have beating hearts when they were harvested.” Logic alone dictates this fact, as she explained “once the heart goes into contraction, you can’t get it to come out of that position.” It “has to be beating and be arrested in a relaxed position” to be of use for research purposes.
Again, just with the use of basic reason, it goes without saying that not only are breathing hearts being removed, but that these procedures occur on living children outside the womb, not within it. The people doing the dissection are not opening the chest of the child in the sort of incredibly rare and highly specialized in utero surgery that might be done to repair a fetal heart condition. The cost and specialization would be astronomical and nonsensical, as they intend to destroy the child, not save it.
So, just by using the single example of hearts on the Langendorff apparatus, which is to say nothing of the “embryonic” kidney cells, (which may more accurately be called “neonatal” kidney cells) used in the COVID vaccine testing and development, I think I can answer your question by saying there is no “open secret” regarding infanticide for medical research. There is no secret at all. I am not revealing anything that is not already obvious, even to a non-expert, given to looking at the simple facts.
The shocking thing, at this point, is not that this is happening, but that we have yet to react, as a whole, in opposition to it. In fact, we accept it by welcoming into our lives the “benefits” of the tortuous murders of innocent children. If we are doing this unknowingly, then perhaps it is because we have bought into the suspension of cause-and-effect reasoning like that to which the researchers subscribe.
Your question leads me, however, to one more point, which I hope provides a wake-up point if nothing else has. Even more shocking than our acceptance of this evil is the fact that it is entirely unnecessary. We could have the same or perhaps greater benefits by other means, but we don’t pursue the course of action that has proven successful in halting unethical bioresearch before and redirecting the course of the industry.
Why don’t we do for our own species what we have succeeded in doing for animals? Most people recognize that animal advocacy and speaking with our wallets through the boycotting of unethically-produced products is genuinely critical because lab animals are innocent creatures who cannot speak for themselves. Isn’t that true of human “lab babies” too?
Also in the expert testimony cited above, Dr. Deisher made the point that using human fetal tissue for research has become more prevalent because increasing regulations on the welfare of animals have made the use of humans more convenient. More convenient! In a way, while horrifying, this is also wonderful news, because it means that animal activists successfully changed things, albeit with a terrible unexpected outcome. However, it means that we can do the same for our species too!
Does that mean that the kind of beneficial research advances which have previously come from the study of neonatal tissue need to stop? Do we have to decide on a sacrificial trade off, with improvement in the lives of those with debilitating illnesses on one hand and the murder of human babies with less compassion than lab rats on the other? Is that how science must proceed—in sanitized facilities behind closed doors that, just in case we become personally in need of its “benefits,” we prefer not to give much thought?
Here’s another shocker. Not at all. Adult pluripotent stem cells, obtained with adult consent and with no need for tortuous murders, actually negate the necessity of the use of fetal organs for stem cell research, because they can be cultured into any type of body cell. This technology exists now, but its use is more costly and less common than the worn-in ease of the baby butchering business. However, like any emerging technology, the more its use expands, the lower its costs become.
We can be the drivers of the expansion of its use, by making unethical research the expensive and inconvenient option. When I was a little girl, I was horrified to learn that lipsticks were tested on mistreated lab rabbits and resolved to never condone that practice with my purchase. So did every little girl I knew. Now cruelty-free cosmetics are the expected and affordable norm. Please, if we could ban together as a caring society to save the bunnies, what should we be willing to do to save the babies?
Leading medical journal The BMJ has published an incendiary report exposing faked data, blind trial failures, poorly trained vaccinators, and a slow follow-up on adverse reactions in the phase-three trial of Pfizer’s Covid jab.
Central to the exposé is Brook Jackson, who, for two weeks, served as regional director at Ventavia Research Group, the company contracted to assist with the pivotal trial. She provided The BMJ with dozens of internal company documents, photos, audio recordings, and emails supporting her concerns.
Jackson reveals that Ventavia staff who conducted quality-control checks were overwhelmed by the volume of problems they were identifying. She repeatedly informed her superiors of poor laboratory management, and patient safety and data integrity issues.
In a cited internal document from August 2020, shortly after the Pfizer trial began, a Ventavia executive identified three site staff members with whom to “go over e-diary issue/falsifying data, etc.” One employee was said to have been subsequently “verbally counseled for changing data” and “not noting late entry.”
Jackson reported her concerns to the US Food and Drug Administration (FDA), but was fired later the same day on the basis that she was “not a good fit.”
At that time, Japanese officials had administered 118,310,106 doses of the COVID vaccine. If they suspended more than two million doses due to contamination, just how many contaminated doses had been administered? How many people received a contaminated jab?
Nobody knows. That’s above their pay grade.
What about monitoring recipients who might have been contaminated?
What is the definition of a contaminant? Why the mystery?
According to some, popular contaminants already exist in vaccines, including mercury, aluminum, formaldehyde, nano-contamination of metals and polysorbate 80, to name a few. However, the CDC and FDA do not consider these CDC-known toxins / carcinogens as “contaminants.” For instance, aluminum is not a neurotoxin. In a vaccine, aluminumis an adjuvant to stimulate the immune response.
So who is responsible for the contamination of COVID products that are injected?
Indemnity Scheme
In our “advanced world,” no one is responsible. Furthermore, there is never enough evidence that will ever prove a cause for adverse effects when it comes to vaccines, including COVID vaccines. Just calling an injection a “VACCINE” automatically makes it immune from any liability.
Under the PREP Act, companies such as Pfizer and Moderna have total immunity from liability if something unintentionally (or intentionally) goes wrong with their COVID vaccines. That means that you cannot sue them if you have severe COVID vaccine side-or-direct effects, and the government likely won’t compensate you for damages. What other industry or company has that kind of protection?
No other.
What is the difference between the 1986 Vaccine Injury Act and The PREP Act? The script? The actors?
The 1986 Act works as a remedial measure, under which vaccine-manufacturers are not be held responsible for compensating any vaccine-related injury claims. Instead, the Act is supposed to provide compensation to eligible individuals for damaging effects of their vaccines. The program covers 16 routine vaccines for children entering public schools. However, as claims have mounted, few are ever paid out in the private vaccine court. There is no provision for damages based on pain and suffering. However, the vaccine court is profitable for vaccine lawyers who get paid no matter who wins or loses.
The PREP Act is an expansion of the 1986 Act, as it shields companies manufacturing the experimental COVID vaccines not approved by the FDA, called Emergency Use Authorized (EUA) vaccines. The justification this time? The Act ismeant to jumpstart U.S. defenses against an outbreak like COVID-19 by shielding from lawsuits makers of critical products, from diagnostic tests to vaccines, as well as doctors and drug distributors.
Both Acts require claimants to prove their injuries are “the direct result” of a vaccine. So far, most COVID vaccine cases have been denied compensation for the simple reason that, according to the lawyers, there is virtually no definitive research on injury causation to reference.
As a result of human complacency to schemes, any vaccine adverse side-or-direct effects may not become apparent until millions of people have received the vaccine. Recall the fiasco of the Swine Flu epidemic that threatened to become a pandemic? Remember the inaccuracy of case definitions and “mistakes” that blew the whole thing out of proportion? Is it happening again?
According to Science, The Wire, India has the world’s largest childhood immunisation scheme, larger than all the European and Middle Eastern countries combined.
Why is there is no informed consent prior to injection, only after?
When the leaders of “the free world” call a mass injection campaign a scheme, the people need to pay attention.
In May 2021, the New York Times reported that Emergent BioSolutions, whose Baltimore plant ruined millions of coronavirus vaccine doses, disclosed for the first time on Wednesday that more than 100 million doses of Johnson & Johnson’s vaccine are now on hold as regulators check them for possible contamination. In June, the FDAinstructed Johnson & Johnson to throw out 60 million doses of the COVID-19 vaccine produced at a Baltimore plant out of concern that they may have been contaminated, and because they were not suitable for use.
Contamination or Additive?
Accident or Project?
Truth or lie?
In any good mystery there are always more questions than answers. And there are always criminals who plan not to get caught. Expect that criminals of this scheme have covered their trails (indemnity) and made others vulnerable (contamination) so they get away when their scheme begins to unravel.
Next The Children
As of September 2021, with reports of widespread contamination, and ongoing investigations, the FDA has told journals such as Scientific American to promote the expansion of injections to children ages 5 to 11.
By appointment only, Pfizer Friday Nights For Kids began at area Fire Stations across the U.S. during Halloween weekend, a time for rituals and blood sacrifices. What better way for kids to spend a Friday night than getting their first COVID jab?
Doctors are just the same as lawyers; the only difference is that lawyers merely rob you, whereas doctors rob you and kill you too. ~ Anton Chekhov
Germ theory was the downfall of modern medicine, and most all of any honest approach to health was lost, while prevention, natural remedies, and the wonder of the human immune system were forgotten in favor of money, prescription drugs, deadly ‘vaccination,’ and unnecessary surgery. Doctors became the tools of the corporate medical system, the pharmaceutical industry, and the hospital industrial complex. As time passed, this situation only worsened, and now this fraudulent ‘Covid’ pandemic scare has led to doctors and hospitals becoming voluntary paid assassins of the state, whether knowingly or not.
Regardless of circumstance, it has become extremely dangerous to go to or be admitted to any hospital, especially if symptoms expressed are considered ‘Covid’ related, such as cold, flu, pneumonia, or any respiratory ailments. Going to a hospital under these circumstances is life-threatening, and not due to sickness, but to ‘medical’ protocols meant to harm, not heal. In fact, these protocols in many if not most hospital settings, especially for any considered elderly, which now means anyone over 50, are meant to kill the patient, which should be considered an act of murder.
This is a time when any good doctors and medical personnel left could and should be exposing this heinous fraud and evil intent by the so-called medical system, but those willing to tell the truth are few and far between, and in many cases, those actually doing so are threatened or silenced, and any risk of job loss seems to take total priority over all decisions made. Consider the implications of this situation; as it indicates that doctors and hospitals are beholding only to their employers or to the system that feeds them, not to the Hypocritic Oath or any desire whatsoever to help those in need. In other words, money power, and control are now the underlying aspects of the health and medical system’s core structure; the good of the patient be damned. Consider the use of remdesivir as treatment for what is falsely referred to as ‘Covid?’ As I wrote some time ago:
“Consider the fact that remdesivir, an experimental drug, was fast-tracked as the “standard of care” for ‘Covid’ early on by Anthony Fauci, and was originally the only approved ‘Covid” treatment for American hospitals, even though this drug does not work against anything, and causes many adverse reactions, body organ failure, and a high incidence of death. “Remdesivir was one of four drugs in a clinical trial for Ebola in 2018, and was dropped from the study before it was over, after a safety review revealed that it had the highest death rate of the drugs being tested.” One of only two studies cited by Fauci for the recommended use of this toxic drug was the Ebola Trial in 2018, and in that trial, the manufacturer, Gilead Sciences, only tested 53 patients for just 28 days. Gilead had close ties, monetary interests, and partnership with the CDC and the National Institute of Allergy and Infectious Diseases (NIAID), headed up by Fauci.”
“Fauci knew of the deadly nature of the poisonous remdesivir at least as early as 2018, but chose to use this dangerous drug with fast-track FDA approval in October of 2020 as the “standard of care,” and the primary treatment in all U.S. hospitals for all “Covid” patients. That means that American patients across this country were not treated, but murdered.”
This drug is still in use in hospitals today, authorized by Fauci, alleged ‘health’ organizations, hospitals, and doctors across the country.
Consider the use of ventilators for all those very ill due to flu-like symptoms who were isolated in hospitals and nursing homes nationwide, especially those in New York and other high population centers? Death occurred for most all of those patients, so how could the doctors not have understood that killing all the patients by very invasive and dangerous ventilator use was not a way to help or save them? If 76% to 97% of all patients treated in this manner died, how could any doctor or hospital not only question, but stop this madness to find out why extreme death rates were the result?
Now, rationing of care based on age, mental condition, and considered use to society or the greater good, a communistic approach, have become the norm. How can this be supported by any claiming to be doctors or ‘health’ administrators, when the main purpose of care is supposed to be about helping all patients? The incentives that drive this insanity are certainly tied to money and financial gain to those going along with this slaughter of innocents, but other nefarious factors are also evident. The elimination of the old and those approaching retirement is of major concern to the ruling class, so killing off this unwanted part of society as the state sees it, is a plus. The funds stolen in the process are redirected into the pockets of government and the rich benefactors of government policy. The ruling sector, the corporate whores, almost the entirety of the medical system, and others benefit from the murder of certain groups of people, so the killing continues unabated.
In the midst of all this evil behavior, and in the middle of what is falsely labeled a ‘pandemic’, a time when immune system destruction and extreme stress due only to government mandates that isolate individuals and families, destroy any financial security for the masses, and control of most aspects of life are present, a poisonous and deadly ‘vaccine’ protocol has been heavily marketed, mandated in very many circumstances, and pushed on the public as the only way to survive what is obviously a completely fake and purposely manufactured ‘crisis.’ While doctors and hospitals continue to rake in millions upon millions of dollars due to this fraud, and do so willingly, the torture of many, financial destruction, and death continues among the general population; not due to any bogus ‘virus,’ but to a planned outcome due to a plot to control all, long considered and sought by the state, its controllers, the pharmaceutical industry criminals, the health and medical complex, and all the corporate and government support systems, including the ludicrous and despicable sector called enforcement.
The doctors and hospitals must not be allowed to willingly continue to maim and kill those it is charged with helping. They must be stopped from ignoring every aspect of proper care for their patients in order to gain more wealth, or retain their positions only by contradicting every medical ethical standard ever set by sane and caring individuals. There is no excuse for this behavior, and every single person in the ‘health’ and medical profession that consciously accepts and goes along with this practice of harm and deceit should face prosecution. Nothing less will be of value to society.
The next target of this murderous nation-state and all its partners are the children; all the children. The injection of toxic and deadly poisons in children from infancy to adult is not only desired, but already underway in some areas, with a goal of ‘vaccinating’ every child in this country over the next year and after. If this is allowed to go forward by the sheep in this country, what future is possible for this and any upcoming generations? Freedom cannot be won or exist in any system that has taken control of the young through gene-altering, immune system destructive protocols, and experimental control technology, administered by state mandate in order to either, maim, kill, or control the bulk of society.
In order for this plot against mankind to go forward, the people have to voluntarily submit to the state’s agenda. Without this voluntary submission, the state will fail, but with continued compliance and strict obedience by the masses, nothing of what has been known in the past as a normal life in a somewhat free country will remain. All that can be expected in any passive, indifferent, and docile society of a collective mass of ignorance, is a life in a technocratic matrix of total control and dependence on the evil few. This is our future if mass resistance is not forthcoming!
“Vaccination is a barbarous practice and one of the most fatal of all the delusions current in our time. Conscientious objectors to vaccination should stand alone, if need be, against the whole world, in defense of their conviction.” ~ Mahatma Gandhi
If I were an atheist materialist who believed all humans were nothing more than biological machines, the practice of delivering an infant whole and alive, through Caesarean Section, and then cutting out his heart and removing tissue for medical research would still make me turn away and want to forget I had ever heard this was happening in the world. (My series on medical infanticide, here [1])
Because a click would go off inside me.
I wouldn’t know what the click was, or why it happened, but I would feel something. And if I were a creature living in Huxley’s Brave New World, I would know the feeling was a signal I should go to the medical dispensary and obtain the drug Soma, which would put me in a pleasant forgetful state…
And yet in our world, there are doctors and nurses and technicians and researchers who don’t even experience the click. They participate in the murders of the infants. They do the work. [2]
They are backed up by bureaucrats and elected officials and ethicists and pharmaceutical executives and medical school teachers and deans and medical journal editors and medical journalists and even religious leaders.
How is it that people of faith, billions of them, are not standing up together against this establishment?
Obviously, something has gone wrong with religion. That is the only conclusion.
In organizing itself, it has become concerned with perpetuating itself. It has built a wall between its people and what faith means.
Jesus threw the money changers out of the Temple, but what happens when the money changers ARE the Temple?
What happens when pastors fail to inspire their congregations to take action in the world and stand up against their oppressors?
Vaccine companies used fetal cell line HEK 293 to test their COVID vaccines. That cell line was surely obtained through the medical murder of an infant, in 1972, in the Netherlands. Her kidneys were removed for the tissue, killing her.
Religious people can say that’s none of their business. They can say anything that will close them off from action.
But ABIDING FAITH is supposed to triumph over society and government, the “things of this world.” That’s one of the sacred points of faith. It’s supposed to allow a person to go to the wall for his beliefs.
A Pope carrying all the accoutrement of the Roman Church can issue a statement supporting the COVID vaccine. This tells you how much of the material world the Pope pays homage to. How much he has sold of himself. He is not an illustration of the test of faith.
If I were an atheist materialist who believed all humans were biological machines, there are churches and temples I could walk into; and feel at home.
The Sound Choice Pharmaceutical Institute “is a 501 (c)3 non-profit organization with a mission to end human trafficking and exploitation for the purposes of biomedical research and commercial products. Our President and Founder, Theresa Deisher Ph.D., has over 30 years of pharmaceutical research and leadership experience. She discovered adult cardiac derived stem cells, has worked on their therapeutic uses as an alternative to human fetal DNA, and leads a team of scientists at AVM Biotechnology dedicated to changing what a diagnosis of cancer, autoimmunity, or chronic infectious disease means to patients and their loved ones. As a result of this work, Dr. Deisher is named as an inventor on over 47 patents.” [3]
I’m going to give you a few important quotes from their published material. Wherever “fetal cells” and “cell line” are mentioned, this indicates material obtained from an aborted fetus. Were these infants removed from their mothers’ wombs, alive, and then murdered? Except in one instance, this is not covered. However, Sound Choice founder, Dr. Deisher, in a devastating interview with Robert Kennedy [4], makes it clear that the practice of removing infants, alive, from the womb, extracting their tissue to make cell lines, and killing them is a widespread practice.
In the first 15 minutes of the interview [4], Deisher discusses infants in the womb for 20 weeks, even 32 weeks, being taken out alive, with their blood supply functioning (essential) and then killed by cutting out their hearts or their brains. This is what is done in order to obtain tissue that will be turned into fetal cell lines.
At the top of the interview, Kennedy said he didn’t want to get into the moral aspect of fetal cell lines. But after listening to Deisher, he was shaken. He said so. He said they would have to cover the moral aspect.
Here are Sound Choice Institute statements: [5]
“Today, more than 23 vaccines are contaminated by the use of aborted fetal cells. There is no law that requires that consumers be informed that some vaccines are made using aborted fetal cells and contain residual aborted fetal DNA. While newer vaccines produced using aborted fetal cells do inform consumers, in their package inserts, that the vaccines contain contaminating DNA from the cell used to produce the vaccine, they do not identify the cells as being derived from electively aborted human fetuses.”
“The United States government has known about the dangers of human DNA from aborted fetal cell-lines since at least 2005. They set guidelines which are supposed to keep the DNA at a specific limit, which they hypothesize will not cause cancer. There is no monitoring of vaccines by our government agencies to ensure those limits are adhered to. Vaccines (MMR, Varicella, and Hepatitis A) sent for independent analysis have consistently shown levels of human fetal DNA that are far beyond the ‘established safety limits’.”
“Instead of conducting safety studies the FDA regulated the amount of human DNA that could be present in a vaccine to no greater than 10ng.”
“Unfortunately, the Sound Choice team discovered that the fetal DNA levels ranged anywhere from 142ng – 2000ng per dose, way beyond the so-called ‘safe’ level.”
“Human fetal cell lines are used to culture some vaccines. They are listed on the CDCs Vaccine Excipient list as [cell lines] WI-38, MRC-5, HEK293, PERC.6.
* WI-38 is a diploid human cell culture line composed of fibroblasts derived from lung tissue of an aborted female fetus.
* MRC-5 (Medical Research Council cell strain 5) is a diploid human cell culture line composed of fibroblasts derived from lung tissue of a 14-week-old aborted male fetus.
* Human embryonic kidney cells 293, also often referred to as HEK 293, HEK-293, 293 cells, or less precisely as HEK cells, are a specific cell line originally derived from human embryonic kidney cells grown in a tissue culture.
* PERC.6 cell line was derived from human embryonic retinal cells taken from an elective abortion.
* The newest cell line created in 2015 for vaccines: WALVAX 2 is taken from the lung tissue of a 3-month gestation female who was ultimately selected from among 9 aborted babies. The scientists noted how they followed specific guidelines to mimic WI-38 and MRC-5 in selecting the aborted babies, ranging from 2-4 months gestation. They further noted how they induced labor using a ‘water bag’ abortion to shorten the delivery time and prevent the death of the fetus to ensure live intact organs which were immediately sent to the labs for cell preparation.” [6]
“Human Diploid Cells (aborted fetal material) provide the ‘cell culture’ in which vaccine formulas are often grown or nurtured. Current vaccines in circulation which were manufactured using aborted fetal material include:
* Polio vaccine (inactivated/IPV) & Oral Polio (live virus) drops : Sanofi Pasteur recently announced they are discontinuing the use of aborted fetal cells in the manufacturing of Poliovax, Pentacel, and Quadracel polio vaccines. Ask before receiving these vaccines as it will take some time for the ethically available options to be widely available.
The Nazi Medical Plan for Control of the Planet; World War Two Never Ended
The Nazi Medical Plan for Control of the Planet; World War Two Never Ended
At the end of the War, IG Farben executives were put on trial and, despite the efforts of Telford Taylor, the chief US prosecutor, and assistant prosecutor, Josiah DuBois, the sentences handed out were light.
For example, Fritz Ter Meer, a high-ranking Farben executive, was tried for mass medical murder and slavery, and sentenced to a paltry seven years in jail. He was released after three years, and went on to occupy a post as chairman of the advisory board of Bayer, a corporate branch on the tree of the infamous IG Farben, which supposedly had been disbanded…
I started writing about this subject 20 years ago, when I launched NoMoreFakeNews.com.
In this article, I’ll present an overview.
In 1933, the largest cartel in the world, IG Farben, pushed Hitler over the top, enabling him to become Chancellor of Germany.
Farben was a global colossus. Pharmaceuticals, dyes, oil, rubber. It forged partnerships with Standard Oil, Dow, Dupont, Imperial Chemical Industries, Rhone-Poulenc.
US government official, Josiah DuBois, sent on a fact-finding mission to Guatemala, returned saying, “As far as I can tell, the nation is a wholly owned subsidiary of Farben.”
The brilliant Farben chemists were modern alchemists. They were researching and producing synthetics far in advance of products formulated anywhere else in the world.
Their dream was material transformation: the ability to convert any element on the Periodic Table into any other element.
Meanwhile, Hitler was obsessed with another transformation: resurrecting what he believed was the lost Aryan Master Race. Through selective breeding, the elimination of lesser and unwanted human types, and other “scientific methods,” a revival of Supermen would occur. And of course, they would then control the destiny of the planet.
Near the close of World War 2 in Europe, the leading lights of Farben and other German corporations, knowing that Hitler was a madman and a rank failure as a military strategist, decided they would have to redirect their efforts, go underground, remain invisible, and from the shadows carry on their war by other means. They were not done. Far from it. They had money, resources, brains, allies. And time.
But what would this new war look like? How would it proceed? Whose strings would they be pulling, and for what purpose?
Should they align themselves with a political movement?
There was one possibility. Socialism. Communism. It would be a convenient ruse. After all, Europe was devastated and exhausted by the War. The prevailing attitude was: “anything to avoid another armed conflict.”
If the nations of Europe could enter into a cooperative future, link hands, bury long-standing enmities, soften geo-borders, engage in free trade, eventually adopt a common currency…
Thus, over a period of decades, the European Union was created. It was what Hitler had been aiming for: a merged continent.
And Germany assumed leadership, as the strongest economic powerhouse in Europe.
All without a shot being fired.
Socialism was spreading, in one form or another, all over the world. For the invisible Nazi architects, this was further evidence they should temporarily hitch their wagon to that star. After all, what was Socialism, really? Just a label for top-down control. The Marxist ideology was unimportant. Domination of populations was all that mattered.
And yet, something was missing. A method. A means. A non-political force that could gradually envelop the world and subdue it, torture it, assert control over billions of minds.
The Farben chiefs had the solution right in front of them. During the War, they had paid a pittance to the managers at Auschwitz, across the road, to send prisoners every day to their medical facility for “tests.” Experiments. Vile grotesque experiments.
And going back several decades, the Nazi leadership had joined elite American eugenicists—the Rockefeller-Harriman forces—to investigate, promote, and utilize sterilization, abortion, medical murder to rid society of its “unfit members.” Those Nazi-American connections still existed.
A branch of modern medicine was on the rise: psychiatry. This was a perfect opportunity to introduce, through completely arbitrary diagnoses of “mental disorders,” debilitating brain-damaging drugs to whole populations. For purposes of pacification.
In fact, the whole Rockefeller model of medicine—one disease caused by one germ—a preposterous form of reductionism—was coming into its own. This meant massive numbers of drugs to treat patients.
Surely, these drugs could be made into toxic destroyers.
A plan was taking shape. A medical plan. THIS would be the invisible conquering force, flying under a politically neutral banner of “healing.”
Create, in the long run, a cradle to grave system enrolling every human, who would trudge, during his lifetime, along a bleak road of 40 or 50 disease-diagnoses and toxic treatments—each treatment giving rise to new symptoms which would be labeled new diseases, requiring treatments…
As for the rank elimination of huge numbers of people on the planet—depopulation—this was a thornier problem. How to arrange it? How to conceal it?
The choice was clear: so-called pandemics. But how would they be staged? Microorganisms, those that actually existed and weren’t mere fantasies, were notoriously unpredictable. The human body, despite all attacks against it, was strong and resilient.
There was no super-germ that could be released which would wipe out a few billion people. That was a dead end. Researchers in their labs, fabricating absurd tests for fairy-tale viruses, and failing to isolate viruses at all, weren’t a help.
But a story about a virus, a story sold with enough fervor by controlled media and cooperating governments…that had possibilities, because the solution would be a vaccine.
The invisible architects would need a whole parade of these fake pandemics, over a long period of time, in order to convince the world population that such scenarios were real.
One by one, pandemic stories could appear and be sold. And DOCTORS would be the messiahs.
COVID is of course the strongest story to date. And the vaccines will, in the long term, be the most debilitating and destructive of all shots.
But it’s doubtful COVID will be the last pandemic story. If a product is a major winner, sell a variation of it. And another.
When we look at and examine horrific events of varying dimensions—the medical experiments in the Nazi concentration camps; the infamous Tuskegee syphilis experiment; the murder of many live infants aborted to obtain their organs for research; the use of high-dose AZT to kill people diagnosed with AIDS; the vaccine campaigns in the Philippines and Kenya designed to cause future miscarriages in pregnant women; the CIA MKULTRA mind control program…
These are glimpses into an overall medical war aimed at humanity.
The alchemical program of IG Farben is now supplemented with technological advances in the fields of genetics and computer science. The envisioned transformation of humans into Brave New World androids and brain-computer hybrids are medical assaults.
The Nazi doctor, Josef Mengele, known as the Angel of Death, said: “The more we do to you, the less you seem to believe we are doing it.”
This is the slogan of the Nazi-Rockefeller medical cartel.
The hypnotic power of The Doctor needs to be dismantled and broken to pieces.
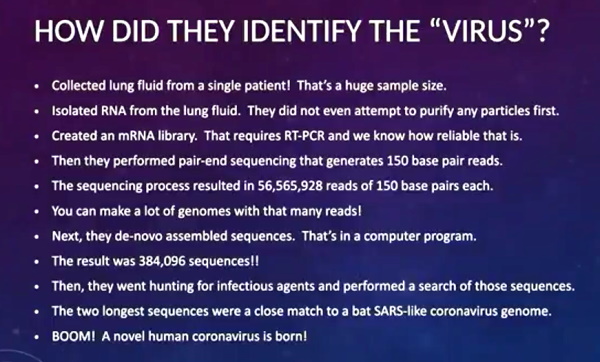
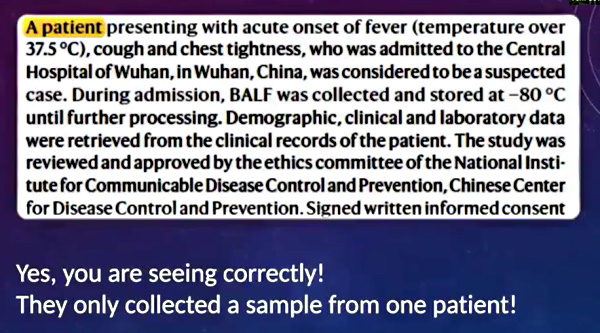
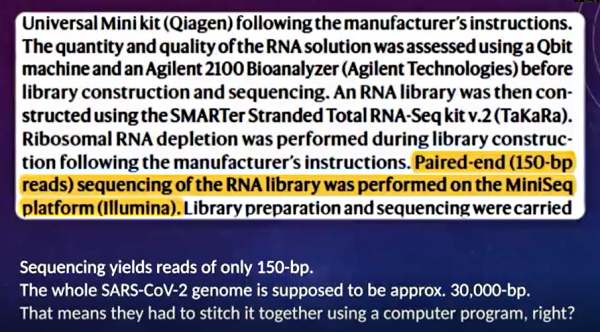
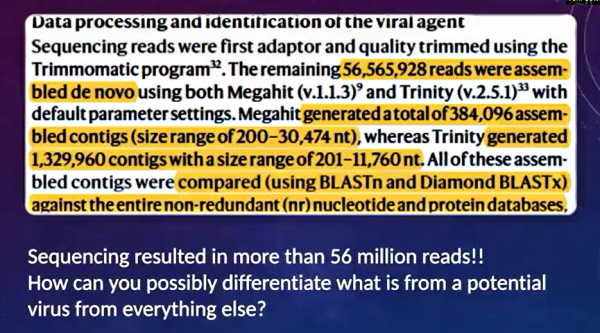
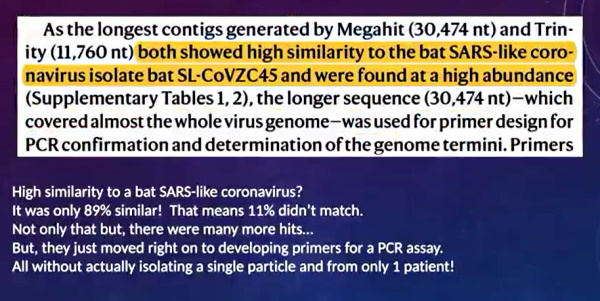

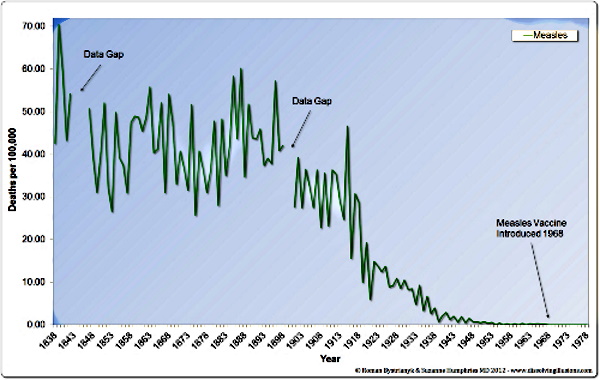
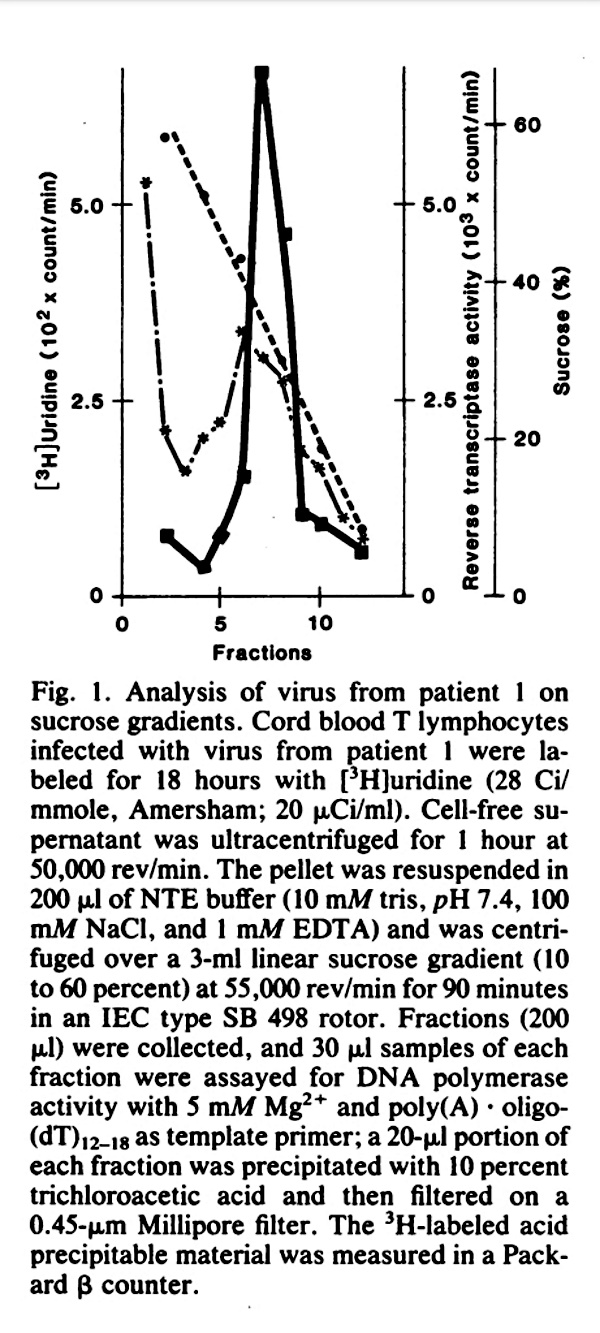
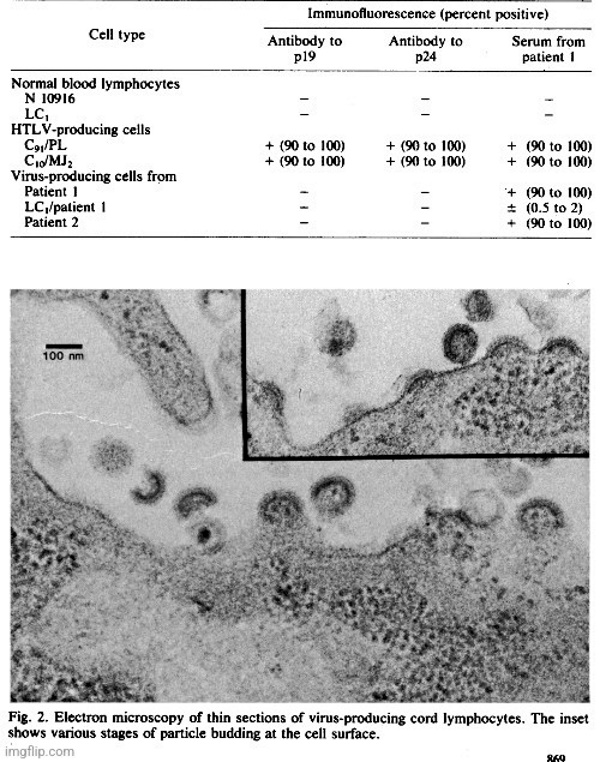

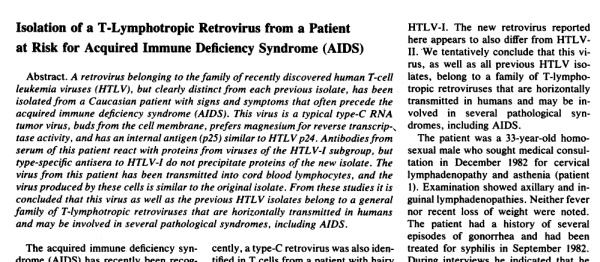
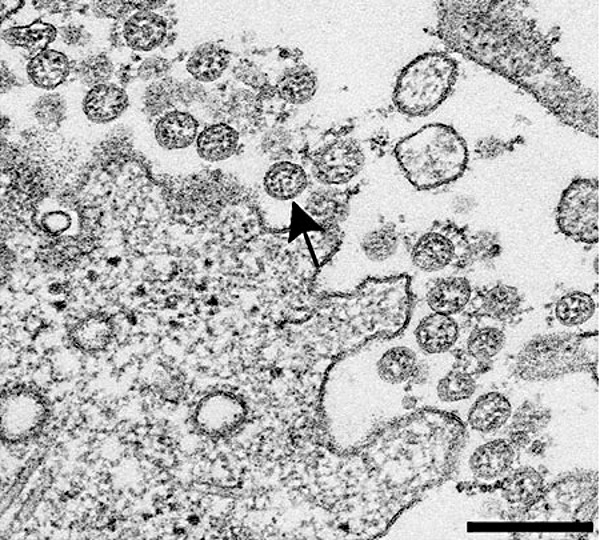
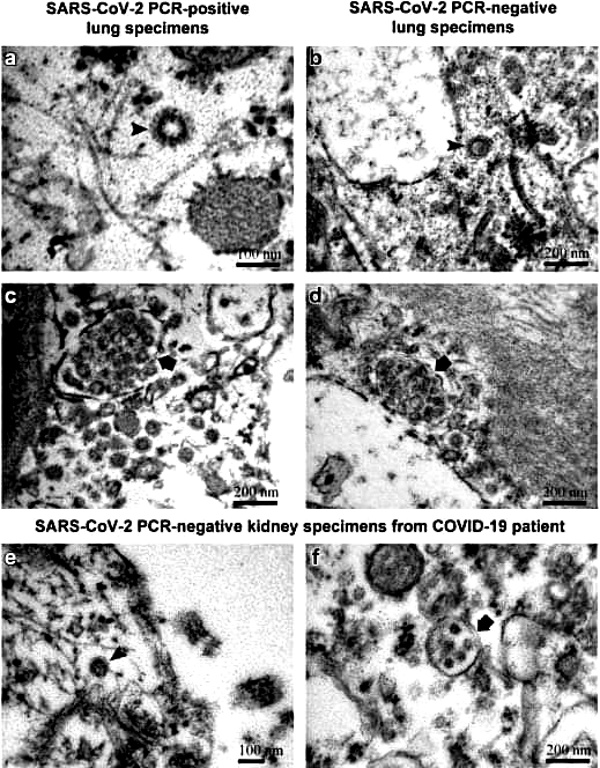
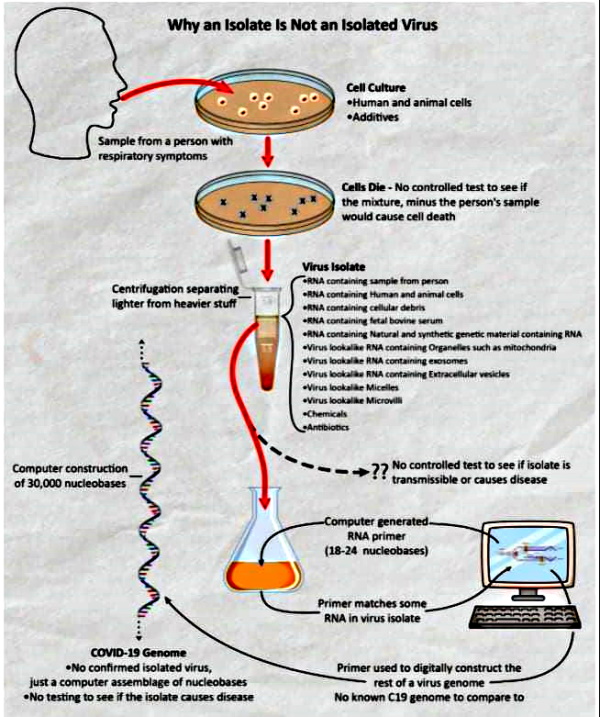
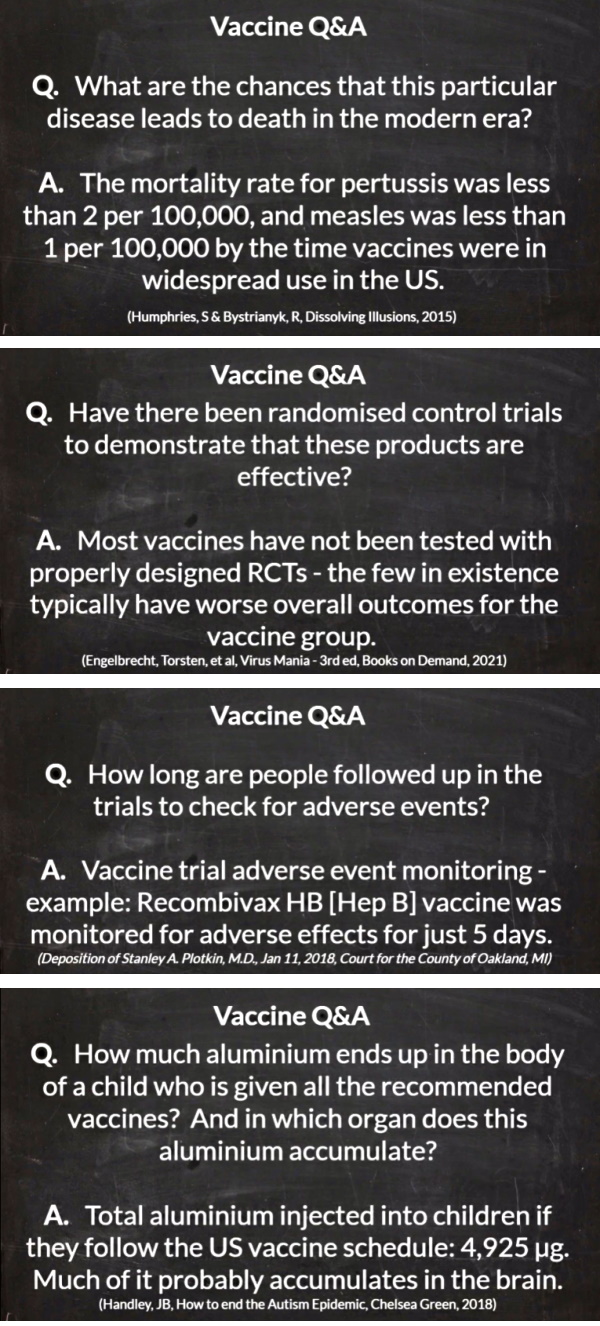
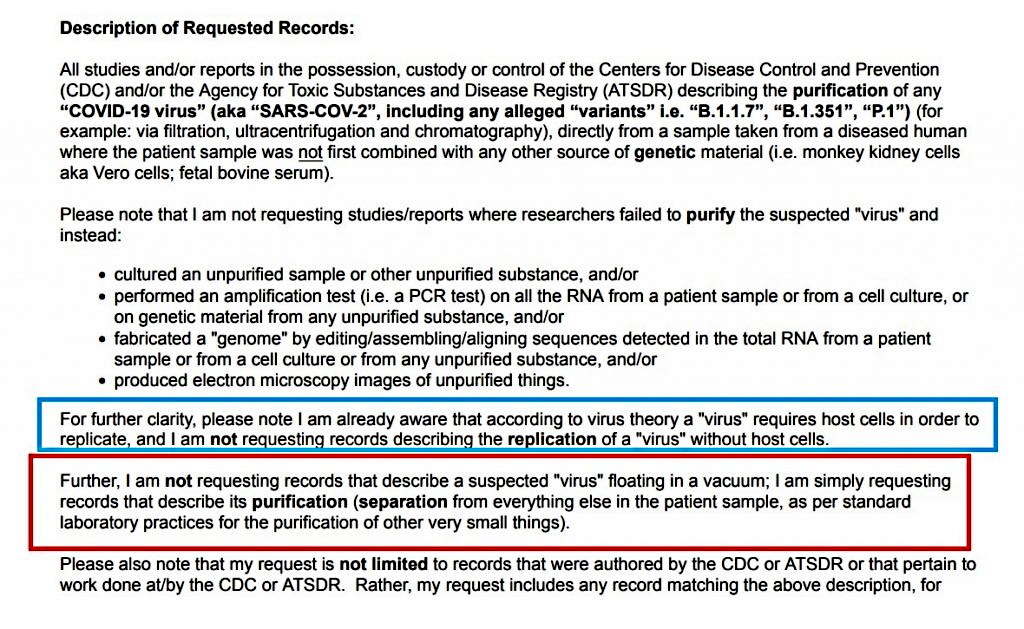
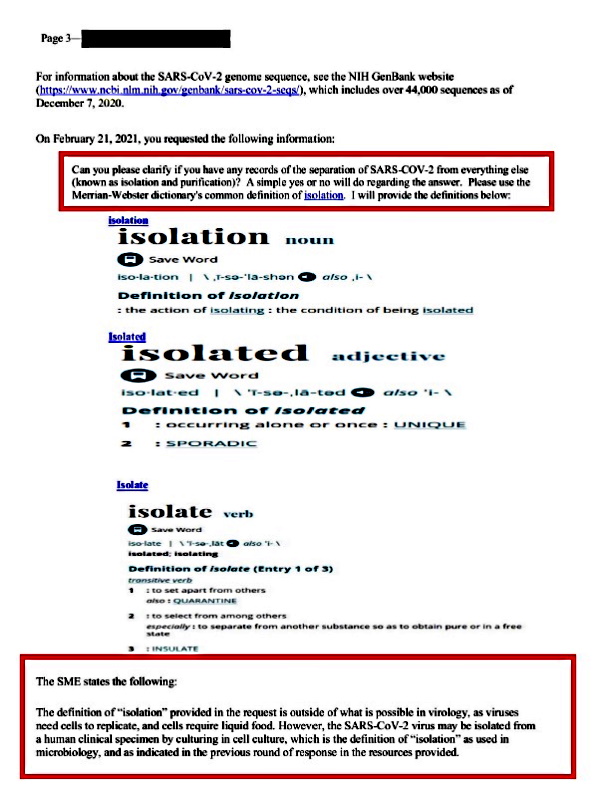


 The Treatments
The Treatments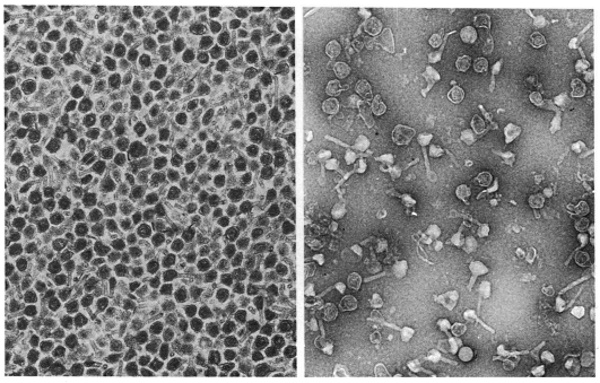

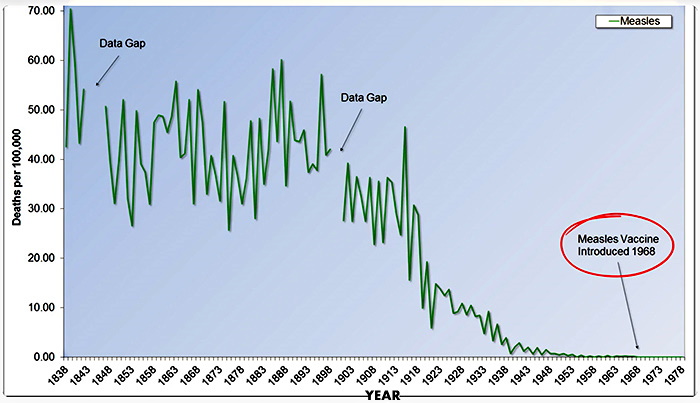

{kind=link}
.jpg){kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}