‘Liberty Man’ Paul Wittenberger in conversation with Andrew Kaufman M.D:
Andrew Kaufman talks about his own path of questioning and discovery about how viruses are claimed to be identified. He goes over the key issues involved in the ongoing debate between those asserting official germ theory and those who are sharing the perspective of terrain theory.
They break down the scamdemic and share thoughts about their research into nanotech in the biomedical field.
One of the outcomes of the alleged new SARS Covid virus that publicly emerged in 2019 is that the medical specialization of virology has been raised to a stature almost Godlike in the media. Few understand the origins of virology and its elevation into a leading role in today’s medicine practice. For this we need to look at the origins and politics of America’s first medical research institute, the Rockefeller Institute for Medical Research, today Rockefeller University, and their work on what they claimed was a polio virus.
In 1907 an outbreak of a sickness in New York City gave the director of the Rockefeller Institute, Simon Flexner, MD, a golden opportunity to lay claim to discovery of an invisible “virus” caused by what was arbitrarily called poliomyelitis. The word poliomyelitis simply means inflammation of the spinal cord’s grey matter. There were some 2,500 New Yorkers, mostly children, designated with some form of poliomyelitis, including paralysis and even death, that year.
Flexner’s Fraud
The most striking aspect of the entire polio saga in the USA during the first half of the 20th Century was the fact that every key phase of the business was controlled by people tied to what became the Rockefeller medical cabal. This fraud started with claims by the Director of the Rockefeller Institute, Simon Flexner, that he and his colleague, Paul A. Lewis, had “isolated” a pathogen, invisible to the eye, smaller even than bacteria, which they claimed caused the paralyzing sickness in a series of outbreaks in the US. How did they come to this idea?
In a paper published in 1909 in the Journal of the American Medical Association, Flexner claimed he and Lewis had isolated the poliomyelitis virus responsible. He reported they had successfully “passaged” poliomyelitis through several monkeys, from monkey to monkey. They began by injecting diseased human spinal cord tissue of a young boy who had died, presumably from the virus, into the brains of monkeys. After a monkey fell ill, a suspension of its diseased spinal cord tissue was injected into the brains of other monkeys who also fell ill.
They proclaimed that the Rockefeller Institute doctors had thus proven poliomyelitis virus causality for the mysterious disease. They hadn’t done anything of the sort. Flexner and Lewis even admitted that: “We failed utterly to discover bacteria, either in film preparations or in cultures, that could account for the disease; and, since among our long series of propagations of the virus in monkeys not one animal showed, in the lesions, the cocci described by some previous investigators, and we had failed to obtain any such bacteria from the human material studied by us, we felt that they could be excluded from consideration.” What they then did was to make a bizarre supposition, a leap of faith, not a scientific claim. They took their hypothesis of viral exogenous agency and made it fact, with no proof whatever. They asserted: “Therefore, …the infecting agent of epidemic poliomyelitis belongs to the class of the minute and filterable viruses that have not thus far been demonstrated with certainty under the microscope.“ Therefore?
Simon Flexner simply asserted it “must” be a polio virus killing the monkeys, because they could find no other explanation. In fact he did not look for another source of the illnesses. This was not scientific isolation. It was wild speculation: “…not thus far been demonstrated with certainty under the microscope.” They admitted this in a December 18, 1909 follow up in JAMA, titled, THE NATURE OF THE VIRUS OF EPIDEMIC POLIOMYELITIS.
The so-called “virus” they were injecting into monkeys was hardly pure. It also contained an undetermined amount of contaminants. It included “pureed spinal cord, brain, fecal matter, even flies were ground up and injected into monkeys to induce paralysis.” Until Jonas Salk won approval from the US Government in April 1955 for a polio vaccine, no scientific proof of existence of a virus causing poliomyelitis, or infantile paralysis as it was commonly known, had been proven. That is the case to this day. The medical world all took Flexner’s word that it “must” be a virus.
Rockefeller Institute, Flexner and the American Medical Association
The Rockefeller Institute was founded from the Standard Oil fortune of John D. Rockefeller in 1901, to be America’s first biomedical institute. It was modelled on France’s Pasteur Institute (1888) and Germany’s Robert Koch Institute (1891). Its first Director, Simon Flexner, played a pivotal and most criminal role in the evolution of what became approved American medical practice. The Rockefeller goal was to completely control American medical practice and transform it into an instrument, at least initially, for promotion of medical drugs approved by the Rockefeller interests. By then they were looking to monopolize medical drugs produced from their petroleum refining, as they had done with oil.
As Rockefeller Institute head, Simon Flexner, was publishing his inconclusive but highly acclaimed studies on polio, he arranged for his brother, Abraham Flexner, a school teacher with no medical background, to head a joint study by the American Medical Association (AMA), the Rockefeller General Education Board, and the Carnegie Foundation founded by Rockefeller’s close friend Andrew Carnegie.
The 1910 study was titled, The Flexner Report, and its ostensible purpose was to investigate the quality of all US medical schools. The outcome of the report was, however, predetermined. Ties between the well-endowed Rockefeller Institute and the AMA went through the corrupt AMA head, George H. Simmons.
Simmons was also the editor of the influential Journal of the American Medical Association, a publication delivered to some 80,000 doctors across America. He reportedly wielded absolute power over the doctors’ association. He controlled the rising ad revenues for drug companies to promote their drugs to AMA doctors in his journal, a highly lucrative business. He was a key part of the Rockefeller medical coup that was to completely redefine acceptable medical practice away from remedial or preventive treatment to use of often deadly drugs and expensive surgeries. As head of the AMA Simmons realized that the competition from a proliferation of medical schools, including then-recognized chiropractic, osteopathy, homeopathy and natural medicine, was lessening income of his AMA doctors, as the number of medical schools had increased from around 90 in 1880 to over 150 in 1903.
Abraham Flexner, former headmaster of a private school, toured various US medical schools in 1909 and recommended that fully half of the 165 medical schools be closed, as what he defined as “sub-standard.” This reduced competition from other approaches to healing diseases. They ruthlessly targeted then-widespread naturopathic medical schools, chiropractic ones, osteopaths as well as independent allopathic schools unwilling to join the AMA regime. Then Rockefeller money went to the select schools with a proviso that professors be vetted by the Rockefeller Institute and the curriculum focus on drugs and surgery as treatment, not prevention, nor nutrition, nor toxicology as possible causes and solutions. They had to accept Pasteur’s germ theory of disease, which claims one germ to one disease reductionism. Rockefeller-controlled media launched a coordinated witch-hunt against all forms of alternative medicine, herbal remedies, natural vitamins and chiropractic–anything not controlled by Rockefeller patented drugs.
By 1919 the Rockefeller General Education Board and the Rockefeller Foundation had paid out more than $5,000,000 to Johns Hopkins, Yale and Washington University in St. Louis medical schools. In 1919 John D. Rockefeller granted another $20,000,000 in securities, “for the advancement of medical education in the United States.” That would be comparable to about $340 million today, a huge sum. In short the Rockefeller money interests had hijacked American medical education and medical research by the 1920’s.
Creating Virology
This medical takeover, backed by the most influential doctors’ organization, the AMA, and its corrupt head, Simmons, allowed Simon Flexner to literally create modern virology under Rockefeller rules. The highly controversial Thomas Milton Rivers, as director of The Rockefeller Institute’s virology laboratory, established virology as an independent field, separate from bacteriology, during the 1920s. They realized they could manipulate far easier when they could claim deadly pathogens that were invisible germs or “viruses.” Ironically virus comes from Latin for poison.
Virology, a reductionist medical fraud, was a creation of the Rockefeller medical cabal. That highly important fact is buried in the annals of medicine today. Diseases such as smallpox or measles or poliomyelitis were declared caused by invisible pathogens called specific viruses. If scientists could “isolate” the invisible virus, theoretically they could find vaccines to protect people from harm. So their theory went. It was a huge boon for the Rockefeller cartel of pharmaceutical companies, which at the time included American Home Products which falsely promoted drugs with no proof of effect, such as Preparation H for Hemorrhoids, or Advil for pain relief; Sterling Drug,which took over the US assets including Aspirin of German Bayer AG after World War I; Winthrop Chemical; American Cyanamid and its subsidiary Lederle Laboratories; Squibb and Monsanto.
Soon virus researchers at the Rockefeller Institute, in addition to claiming discovery of the poliomyelitis virus, claimed to discover the viruses that caused smallpox, mumps, measles and yellow fever. Then they announced “discovery” of preventive vaccines for pneumonia and yellow fever. All of these “discoveries” announced by the Institute proved false. With the control of the research in the new area of virology, the Rockefeller Institute, in collusion with Simmons at AMA and his equally corrupt successor, Morris Fishbein, could promote new patented vaccines or drug “remedies” in the influential AMA journal that went to every member doctor in America. Drug companies refusing to pay for ads in the AMA journal were blackballed by the AMA.
Controlling Polio Research
Simon Flexner and the highly-influential Rockefeller Institute succeeded in 1911 in having the symptoms that were being called poliomyelitis to be entered into the US Public Health Law as a “contagious, infectious disease caused by an air-borne virus.” Yet even they admitted they had not proven how the disease enters the body of humans. As one experienced doctor pointed out in a medical journal in 1911, “Our present knowledge of the possible methods of contagion is based almost entirely upon the work done in this city at the Rockefeller Institute.” In 1951 Dr. Ralph Scobey, a critic of the Rockefeller rush to judgment on polio contagion, noted, “This of course placed reliance on animal experiments rather than on clinical investigations…” Scobey also pointed to the lack of proof poliomyelitis was contagious: “…children afflicted with the disease were kept in general hospital wards and that not a single one of the other inmates of the wards of the hospital was affected with the disease.” The general attitude at that time was summed up in 1911: “It seems to us despite the lack of absolute proof, that the best interests of the community would be conserved by our regarding the disease from a contagious standpoint.” (sic).
By having poliomyelitis symptoms classified as a highly contagious disease caused by an invisible, alleged exogenous or external virus, the Rockefeller Institute and the AMA were able to cut off any serious research for alternative explanations such as exposure to chemical pesticides or other toxins, to explain the seasonal outbreaks of illness and paralysis, even death, mostly in very young children. That was to have fatal consequences lasting to the present.
Enter DDT
In his 1952 statement to the US House of Representatives investigating the possible dangers of chemicals in food products, Ralph R. Scobey, M.D. noted, “For almost half a century poliomyelitis investigations have been directed towards a supposed exogenous virus that enters the human body to cause the disease. The manner in which the Public Health Law is now stated, imposes only this type of investigation. No intensive studies have been made, on the other hand, to determine whether or not the so-called virus of poliomyelitis is an autochthonous chemical substance that does not enter the human body at all, but simply results from an exogenous factor or factors, for example, a food poison.” Toxins as cause were not investigated, despite huge evidence.
During the 1930s with economic depression and then war, few new major outbreaks of poliomyelitis were noted. However, immediately after the end of World War II, notably, the polio drama exploded in dimension. Beginning 1945, every summer more and more children across America were diagnosed with poliomyelitis and hospitalized. Less than 1% of the cases were actually tested via blood or urine tests. Some 99% were diagnosed by merely the presence of symptoms such as acute pain in extremities, fever, upset stomach, diarrhea.
In 1938, with the support of presumed polio victim, Franklin D. Roosevelt, the National Foundation for Infantile Paralysis (March of Dimes) was founded to solicit tax-exempt donations to fund polio research. A German doctor and researcher, Dr Henry Kumm, came to the US and joined the Rockefeller Institute in 1928 where he stayed until joining the National Foundation in 1951 as Director of Polio Research. Kumm was joined at the National Foundation by another key Rockefeller Institute veteran, the so-called “father of virology,” Thomas M. Rivers, who chaired the foundation’s vaccine research advisory committee overseeing the research of Jonas Salk. These two Rockefeller Institute key figures thus controlled funds for polio research including developing a vaccine.
During the Second World War, while still at Rockefeller Institute, Henry Kumm was a consultant to the US Army where he oversaw field studies in Italy. There Kumm directed field studies for the use of DDT against typhus and malarial mosquitoes in the marshes near Rome and Naples.DDT had been patented as an insecticide by Swiss drug firm Geigy and their US branch in 1940, and first authorized for use on US Army soldiers in 1943 as a general disinfectant against head lice, mosquitoes and many other insects. Until war’s end almost all DDT production in the US went to the military. In 1945 the chemical companies looked eagerly for new markets. They found them.
In early 1944, US newspapers triumphantly reported that typhus, “the dreaded plague that has followed in the wake of every great war in history,” was no longer a threat to American troops and their allies thanks to the army’s new “louse-killing” powder, DDT. In an experiment in Naples, American soldiers dusted more than a million Italians with DDT dissolved with kerosene (!), killing the body lice that spread typhus. Rockefeller Institute’s Henry Kumm and the US Army knew that, as one researcher put it, “DDT was a poison, but it was safe enough for war. Any person harmed by DDT would be an accepted casualty of combat.” The US Government “restricted” a report on insecticides issued by the Office of Scientific Research and Development in 1944 that warned against the cumulative toxic effects of DDT in humans and animals. Dr Morris Biskind noted in a 1949 article, “As DDT is a cumulative poison, it is inevitable that large-scale intoxication of the American population would occur. In 1944, Smith and Stohlman of the National Institutes of Health, after an extensive study of the cumulative toxicity of DDT, pointed out, “The toxicity of DDT combined with its cumulative action and absorbability from the skin places a definite health hazard on its use.” Their warnings were ignored by higher officials.
Instead, after 1945, all across America DDT was promoted as the miracle new, “safe” pesticide, much like Monsanto’s Roundup with glyphosate three decades later. DDT was said to be harmless to humans. But no one in government was seriously scientifically testing that claim. One year later in 1945 as the war ended, US newspapers praised the new DDT as a “magic” substance, a “miracle.” Time called DDT “one of the great scientific discoveries of World War II.”
Despite isolated warnings of untested side effects, that it was a persistent, toxic chemical which easily accumulates in the food chain, the US Government approved DDT for general use in 1945. The Food and Drug Administration (FDA), controlled by the Rockefeller-AMA-drug interests, established as “safe” a DDT content of up to 7 parts per million in foods, though no one had proven such. The DDT chemical companies fed the press with photos and anecdotes. Newspapers enthusiastically reported how the new miracle chemical, DDT, was being tested in the US against mosquitoes in the South believed carrying malaria, as well as “preserving Arizona vineyards, West Virginia orchards, Oregon potato fields, Illinois cornfields, and Iowa dairies.” DDT was everywhere in the USA in the late 1940s.
The US Government claimed DDT, unlike arsenic and other insecticides used before the war, was harmless to humans, even infants, and could be used liberally. Beginning 1945 cities like Chicago sprayed public beaches, parks, swimming pools. Housewives bought home aerosol spray DDT dispensers to spray the kitchen and especially childrens’ rooms, even their matrasses. Farmers were told to spray their crops and their animals, especially dairy cows, with DDT. In postwar America DDT was being promoted, above all by Rockefeller drug companies like American Home Products with its Black Flag aerosol DDT spray, and Monsanto. From 1945 through 1952 the US production of DDT increased tenfold.
As presumed cases of polio literally exploded across the USA after 1945 the theory was advanced, with no proof, that the crippling polio disease was transmitted, not by toxic pesticide chemicals like DDT, but by mosquitoes or flies to humans, most especially young children or infants. The message was that DDT can safely protect your family from the crippling polio. Officially listed polio cases went from some 25,000 in 1943 before US civilian use of DDT, to over 280,000 cases in 1952 at the peak, more than a tenfold increase.
In October 1945 DDT, which had been used by the US Army under supervision of Rockefeller Institute’s Henry Kumm as noted, was authorized by the US Government for general use as an insecticide against mosquitoes and flies. Dissenting scientists warning of toxic effects of DDT in humans and animals were silenced. Families were told DDT could save their children from the dreaded polio by killing the feared insects.
The US Department of Agriculture advised farmers to wash their dairy cows with a solution of DDT to combat mosquitoes and flies. Cornfields were aerial sprayed with DDT as well as fruit orchards. However it was incredibly persistent and its toxic effect on plants and vegetables were such it could not be washed off. Year-by-year from 1945 through 1952 the amount of DDT sprayed across the US increased. Notably, so too did the number of human cases of poliomyelitis.
Worst Polio Epidemic
By the beginning of the 1950s increasing attention was given in the US Congress and among farmers as to the possible dangers of such heavy pesticide use—not only DDT, but also the even more toxic BHC (benzene hexachloride). In 1951 Morton Biskind, a physician who had successfully treated several hundred patients with DDT poisoning, testified to the US House of Representatives on the possible link of paralytic polio to toxins, specifically DDT and BHC. He noted,
“The introduction for uncontrolled general use by the public of the insecticide “DDT” (chlorophenothane) and the series of even more deadly substances that followed, has no previous counterpart in history. Beyond question, no other substance known to man was ever before developed so rapidly and spread indiscriminately over so large a portion of the earth in so short a time. This is the more surprising as, at the time DDT was released for public use, a large amount of data was already available in the medical literature showing that this agent was extremely toxic for many different species of animals, that it was cumulatively stored in the body fat and that it appeared in the milk. At this time a few cases of DDT poisoning in human beings had also been reported. These observations were almost completely ignored or misinterpreted.”
Biskind further testified to Congress in late 1950, “Early last year I published a series of observations on DDT poisoning in man. Since shortly after the last war a large number of cases had been observed by physicians all over the country in which a group of symptoms occurred, the most prominent feature of which was gastroenteritis, persistently recurrent nervous symptoms, and extreme muscular weakness…” He described several case examples of patients whose severe symptoms including paralysis disappeared when exposure to DDT and related toxins was eliminated: “My original experience on more than 200 cases which I reported early last year has since been considerably extended. My subsequent observations have not only confirmed the view that DDT is responsible for a great deal of otherwise inexplicable human disability…” Also noted was the fact that polio cases were always most in summer months when DDT spraying against insects was maximum.
The Rockefeller Institute operatives and the AMA, via their agents in the US Government, created the 1946-1952 USA health emergency called polio. They did so by knowingly promoting the highly toxic DDT as a safe way to control the mythical insect spreaders of the feared disease. Their propaganda campaign convinced the American population that DDT was the key to stop spread of poliomyelitis.
Polio Suddenly Declines
Under leadership of the two Rockefeller Institute doctors, Henry Kumm and Thomas Rivers, the National Foundation for Infantile Paralysis (NFIP) rejected critics such as Biskind and Scobey. Natural remedial treatment, such as using intravenous Vitamin C for the infantile paralysis, were rejected out of hand as “quackery.” In April 1953, leading Rockefeller Institute DDT consultant, Dr Henry Kumm, became Director of Polio Research for NFIP. He funded the polio vaccine research of Jonas Salk.
One courageous doctor in North Carolina, Dr. Fred R. Klenner, who had also studied chemistry and physiology, had the idea to use large doses of intravenous ascorbic acid—Vitamin C—on the hypothesis that his patients were victims of toxin poisoning and that Vitamin C was a powerful detox. This was well before Dr Linus Pauling’s Nobel Prize research on Vitamin C. Klenner had remarkable success within days for more than 200 patients in the summer epidemics of 1949 to 1951. The Rockefeller Institute and the AMA had no interest in the remedial prospects. They and the Rockefeller-controlled National Foundation for Infantile Paralysis were only funding polio vaccine development, based on the unproven Flexner claim that polio was a contagious virus, not a result of environmental poison.
Then beginning sometime in 1951-1952, as polio cases were at an all-time high, something unexpected began to appear. The number of cases diagnosed as polio in the US began to decline. The decline in polio victims was dramatic, year by year until 1955, well before the National Foundation and Jonas Salk’s polio vaccine was approved for public use and was widespread.
About a year before the sudden decline in polio cases, farmers, whose dairy cows were suffering severe effects of the DDT, were advised by the US Department of Agriculture to reduce DDT use. Rising public concern about how safe DDT was for humans, including publicized US Senate hearings on DDT and Polio in 1951 also led to a significant decline in DDT exposure into 1955, even though DDT was not officially banned in the US until 1972.
So-called “polio” cases fell by some two-thirds in that 1952-1956 time, in a remarkable parallel to the decline in DDT use. It was well after that decline, in late 1955 and 1956, that the Rockefeller-developed Salk polio vaccine was first administered in large populations. Salk and the AMA gave all credit to the vaccine. Deaths and paralysis as a result of the Salk vaccine were papered over. The Government changed the definition of polio to further reduce official cases. Simultaneously, cases of similar polio-like spinal cord nerve diseases– acute flaccid paralysis, chronic fatigue syndrome, encephalitis, meningitis, Guillain-Barré syndrome, muscular sclerosis—rose notably.
Why it Matters
Over a century ago the world’s richest man, oil baron John D. Rockefeller, and his circle of advisors set about to completely reorganize how medicine was practiced in the USA and the rest of the world. The role of the Rockefeller Institute and figures like Simon Flexner literally oversaw the invention of a colossal medical fraud around claims that an invisible contagious extraneous germ, the polio virus, caused acute paralysis and even death in young people. They politically banned any efforts to link the disease to toxin poisoning, whether from DDT or arsenic pesticides or even contaminated vaccine poisoning. Their criminal project included intimate cooperation with the leadership of the AMA and control of the emerging drug industry, as well as of medical education. The same Rockefeller group financed Nazi eugenics at the Kaiser Wilhelm Institutes in Germany in the 1930s as well as the American Eugenics Society. In the 1970s they financed the creation of patented GMO seeds which were all developed by the group of Rockefeller chemical pesticide companies—Monsanto, DuPont, Dow.
Today this control of public health and the medical industrial complex is exercised by David Rockefeller’s protegé and eugenics advocate, Bill Gates, self-appointed czar over the WHO and world vaccines. Dr Tony Fauci, head of NIAID, dictates vaccine mandates without evidence. The fraud behind the polio virus scandal after World War II has been refined with use of computer models and other ruses today, to advance one alleged deadly virus after the other, from Covid19 to Monkeypox to HIV. As with polio, none of those has been scientifically isolated and proven to cause the diseases claimed. None. The same tax-free Rockefeller Foundation today, posing as a philanthropic charity, is at the heart of the global medical tyranny behind covid19 and the eugenics agenda of the World Economic Forum Great Reset. Their poliomyelitis virus model helped them create this dystopian medical tyranny. We are told, “trust the science.”
F. William Engdahl is strategic risk consultant and lecturer, he holds a degree in politics from Princeton University and is a best-selling author on oil and geopolitics, exclusively for the online magazine “New Eastern Outlook”.
A groundbreaking new report reveals how billionaire Bill Gates has poured hundreds of millions of dollars into media outlets all over the world.
An investigation by the outlet MintPress reports that the Bill and Melinda Gates Foundation has distributed the funds in the form of over 30,000 individual grants.
Big news organizations like CNN, NBC, The Atlantic, The Financial Times, BBC and others have all benefited from the funding.
NPR was the largest beneficiary receiving a whopping $24 million in funding. The Guardian follows with nearly $13 million.
Gates’ funding has even stretched into Germany, with the outlet Der Spiegel benefiting from $5 million in funding. Other international outlets that received millions from Gates include France’s Le Monde and South African outlet Bhekisisa.
In total, Gates has funnelled $166 million directly to media outlets while distributing the remaining money to various media centres and journalism organizations.
Here in Canada, the World University Service of Canada received $12 million from the foundation.
Gates’ money has even flowed into Chinese media, with Caixin Media receiving $250,000 from the mogul and Tsinghua University benefiting from a $450,000 grant provided by the foundation.
In June, it was revealed that Gates also gave tens of millions of dollars to various Canadian pharmaceutical and biotech companies.
The Gates Foundation provided a total of $23 million to facilities like the Institut de Cardiologie de Montreal to “provide effective, accessible, scalable treatment for COVID-19.”
Other projects under the initiative include grants to Emerging Ag Inc. to “increase awareness and understanding of possible gene drive applications for public good purposes within international policy forums.”
I remember early on in 2017, when I first started unraveling the “virus” lie through the examination of HIV/AIDS, to being introduced to the work of Dr. Stefan Lanka. If memory serves me correctly, my first encounter was through the brilliant House of Numbersdocumentary by Brent Leung. I was simply amazed that Dr. Lanka, an ex-virologist, was actually calling out the methods of his own profession. His testimony, along with that of Kary Mullis, the inventor of the misused and abused PCR technique, carried much weight with me in those early days. Their words lent credibility to the argument that the evidence for the existence of HIV and other “viruses” was entirely absent and fraudulent.
During that time of intense research where I was desperately seeking out any and all information that I could find, I fortunately stumbled onto a few of Dr. Lanka’s articles through the VirusMyth.com website. I was engrossed in his work and absorbed much of what he had to say on the subject, especially in regards to the lack of purification and isolation of any “viruses,” the faults of the cell culture method, and the problems related to electron microscope imagery. As it did for many others, Dr. Lanka’s work formed much of the foundation for my understanding of the lies of virology. It is rare to gain such critical insight from someone who was involved in the industry. It is even more rare for someone in his position to set out and actually prove what he was saying correct yet that is exactly what Dr. Lanka has done numerous times.
Without Dr. Lanka’s enormous contributions to unraveling the lies of germ theory, many of us speaking out today may not have been doing so. As his work was instrumental in helping me along on my own journey towards uncovering the truth, I want to highlight what I consider Dr. Lanka’s three biggest contributions to proving the fraud of virology along with many of the papers he has written on the subject. My hope is that you will be able to come away with a greater appreciation for Dr. Lanka’s monumental work as well as a clearer understanding of the deceptive practices used by virologists.
1. The Measles Trial
Early on in my journey, I found my way to the infamous measles trial saga while researching Dr. Lanka’s work. Back in 2017, it was difficult to find out much accurate information on what had really transpired. For those who are unaware, Dr. Lanka set forth a challenge in his own magazine calling upon anyone to come forward with a single paper providing the scientific evidence which proved the existence of a measles “virus.” If this challenge was met, the person would receive a $100,000 financial reward. A physician named David Bardens came forward with six papers spanning six decades which he claimed together proved the existence of the measles “virus.” Dr. Lanka refused to pay as he specifically requested one publication providing the entire proof necessary. Dr. Bardens sued and while Dr. Lanka lost the initial case in the lower courts, he won on appeal in the higher courts. At the time I originally came upon this story, the internet was (and still is) full of stories claiming that Dr. Lanka lost the case. However, to anyone interested in the truth, it is obvious that those lies do not hold up under scrutiny. Presented below is a great overview of how the events actually played out:
“On November 24, 2011, Dr. Lanka announced on his website that he would offer a prize of € 100,000 to anyone who could prove the existence of the measles virus. The announcement read as follows: “The reward will be paid, if a scientific publication is presented, in which the existence of the measles virus is not only asserted, but also proven and in which, among other things, the diameter of the measles virus is determined.
In January 2012, Dr. David Bardens took Dr. Lanka up on his pledge. He offered six papers on the subject and asked Dr. Lanka to transfer the € 100,000 to his bank account.
The six publications are:
Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954 Jun;86(2):277–286.
Bech V, Magnus Pv. Studies on measles virus in monkey kidney tissue cultures. Acta Pathol Microbiol Scand. 1959; 42(1): 75–85
Horikami SM, Moyer SA. Structure, Transcription, and Replication of Measles Virus. Curr Top Microbiol Immunol. 1995; 191: 35–50.
Nakai M, Imagawa DT. Electron microscopy of measles virus replication. J Virol. 1969 Feb; 3(2): 187–97.
Lund GA, Tyrell, DL, Bradley RD, Scraba DG. The molecular length of measles virus RNA and the structural organization of measles nucleocapsids. J Gen Virol. 1984 Sep;65 (Pt 9):1535–
Daikoku E, Morita C, Kohno T, Sano K. Analysis of Morphology and Infectivity of Measles Virus Particles. Bulletin of the Osaka Medical College. 2007; 53(2): 107–14.
Dr. Lanka refused to pay the money since in his opinion these publications did not provide adequate evidence. Subsequently, Dr. Bardens took Dr. Lanka to court.
On March 12, 2015, the District Court Ravensburg in southern Germany ruled that the criteria of the advertisement had been fulfilled ordering Dr. Lanka to pay up. Dr. Lanka appealed the ruling.
On February 16, 2016, the Higher Regional Court of Stuttgart (OLG) re-evaluated the first ruling, judging that Dr. Bardens did not meet the criteria since he failed to provide proof for the existence of the measles virus presented in one publication, as asked by Dr. Lanka in his announcement. Therefore, Dr. Lanka does not have to pay the prize money.
On January 16, 2017, the First Civil Senate of the German Federal Court of Justice (BGH) confirmed the ruling of the OLG Stuttgart.
Critics of the judicial verdict argue that Dr. Lanka’s victory is solely based on how he had formulated the offer of reward, namely to pay the € 100,000 for the presentation of a single publication of evidence (which Dr. Bardens was unable to provide). This argument, however, distracts the attention from the essential points.
According to the minutes of the court proceedings (page 7/ first paragraph), Andreas Podbielski, head of the Department of Medical Microbiology, Virology and Hygiene at the University Hospital in Rostock, who was one of the appointed experts at the trial, stated that even though the existence of the measles virus could be concluded from the summary of the six papers submitted by Dr. Bardens, none of the authors had conducted any controlled experiments in accordance with internationally defined rules and principles of good scientific practice (see also the method of “indirect evidence”). Professor Podbielski considers this lack of control experiments explicitly as a “methodological weakness” of these publications, which are after all the relevant studies on the subject (there are no other publications trying to attempt to prove the existence of the “measles virus”). Thus, at this point, a publication about the existence of the measles virus that stands the test of good science has yet to be delivered.
Furthermore, at the trial it was noted that contrary to its legal remit as per § 4 Infection Protection Act (IfSG) the Robert Koch Institute (RKI), the highest German authority in the field of infectious diseases, has failed to perform tests for the alleged measles virus and to publish these. The RKI claims that it made internal studies on the measles virus, however, refuses to hand over or publish the results.”
For an even more in-depth analysis of what really occured during the trial, I always recommend this article by Feli Popescu, who was actually present during the proceedings:
When I think of Dr. Lanka’s work, the measles trial stands out as the most significant moment and the most pivotal accomplishment. We had an epic head-to-head clash between he medical establishment and an ex-virologust taking place in a court of law over the legitimacy of the evidence for the measles “virus.” It was determined through this trial that the foundational paper claiming the existence and isolation of the measles “virus,” the 1954 paper by John Franklin Enders, was unworthy by itself for proving the existence of the “virus.” As all other papers and virology itself owe their evidence to the cell culture methods developed by Enders in that paper, it is an astonishingly damning admission that the evidence presented by virology is invalid.
2. The 7 Steps Proving “Viruses” Don’t Exist
More recently, Dr. Lanka put together what he felt were the main points that bring the house of cards known as virology tumbling down. These 7 steps were formulated over many years of painstaking research into the faults of virology. As he did with the measles trial, Dr. Lanka compiled a very convincing case for why “viruses” do not exist and why virology is a pseudoscience built upon fraudulent foundations.
The 7 steps to prove “viruses” do not exist:
1. Virologists interpret the death of cells in the laboratory as viral. Due to the lack of control attempts (experiments), they overlook the fact that they kill the cells in the laboratory themselves and unintentionally by starving and poisoning the cells. This misinterpretation is based on a single publication by John Franklin Enders and a colleague from June 1, 1954. This publication was ruled by the highest court in Germany in the measles virus trial that it contained no evidence of a virus. This publication became the exclusive basis not only for measles virology, but for all virology since 1954 and corona hysteria.
2. Virologists mentally assemble the shortest pieces of so-called genetic information from dying cells to form a very long genetic strand, which they output as the genetic strand of a virus. This conceptual/computational process is called alignment. In doing so, they did not make the control attempts, the attempt to conceptually/computationally construct the desired genetic strand even from short pieces of so-called genetic information from non-infected sources.
3. For the alignment of a virus, virologists always need a given genetic strand of a virus. For this, however, they always use a genetically/computationally generated genetic strand and never a real one, one found in reality. In doing so, they never attempt to check whether or not so-called genetic information could also be constructed from the existing data set, including “viral” genetic material strands of completely different viruses.
4. Virologists have never seen or isolated “viruses” in humans, animals, plants or their fluids. They only did it seemingly, indirectly, and only ever by means of very special and artificial cell systems in the laboratory. They never mentioned the control attempts or documented whether they succeeded in depicting and isolating viruses in and from humans, animals, plants or their fluids.
5. Virologists have never isolated, biochemically characterized or obtained their supposed genetic material from the supposed viruses that they photograph using electron microscope images. They have never conducted or published control experiments as to whether, after isolating these structures, it was actually possible to detect “viral” proteins (the envelope of the virus) and, above all, the viral genome, which is supposed to be the central component and characteristic of a virus.
6. Virologists report typical artifacts of dying tissue/cells and typical structures that arise when the cell’s own components such as proteins, fats and the solvents used are swirled, as viruses or viral components. Here, too, there are no control experiments with cells/tissues that were not infected but were also treated.
7. The so-called transmission attempts that virologists make to prove the transmission and pathogenicity of the suspected viruses refute the entire virology. Obviously, it is the experiments themselves that trigger the symptoms, which animal experiments provide as evidence of the existence and effectiveness of the suspected viruses. Here, too, there are no control attempts in which exactly the same thing is done, only with non-infected or sterilized materials.
Dr. Lanka explained the 7 steps himself in this short excerpt from an interview with Dr. Tom Cowan where he offered additional insight:
3. The Control Experiments
During this current “pandemic,” Dr. Lanka decided to carry out and recreate for “SARS-COV-2” the control experiments he had done during the measles trial. The experiments were conducted in three phases:
Phase 1 – The cytopathic effect
In the first control experiment, Dr. Stefan Lanka showed that what virologists attribute to the presence of a pathogenic virus can be achieved without infectious material.
Phase 2 – Construction of the SARS-CoV-2 genome
In the second control experiment, Dr. Lanka showed that what virologists call “viral genetic material actually comes from a healthy human tissue.
Phase 3 – Structural analysis of sequency data in virology
In the third control experiment, we show that with the same technique that virologists use and using nucleic acids, which are not from supposedly infectious material but from healthy human tissue, animals and plants, can construct the genome of any “virus.”
Phase 1 of Dr. Lanka’s experiments was designed to show that the cytopathogenic effect, the very criteria used to determine a “virus” is present in a cell culture, can be caused by the experimental conditions themselves without “infectious” material present. The article linked above contains the study by the independent laboratory testing the cytopathogenic effect for Dr. Lanka. It is in German but it can be easily translated into English. However, as it is a rather long study, I wanted to provide my favorite breakdown of the CPE experiments from Dr. Tom Cowan’s excellent book Breaking the Spell:
“Here is the essence of Lanka’s experiment, done by an independent professional laboratory that specializes in cell culturing. As seen in this series of photographs, each of the four vertical columns is a separate experiment. The top photo in each column was taken on day one, and the bottom photo was taken on day five.
In vertical column one, normal cells were cultured with normal nutrient medium and only a small amount of antibiotics. As you can see, on neither day one nor day five was any CPE found; the cells continued their normal, healthy growth.
In vertical column two, normal cells were again grown on normal nutrient medium and a small amount of antibiotics, but this time, 10% fetal calf serum was added to enrich the medium. Still, the cells in the culture grew normally, both on day one and day five.
The third vertical column shows what happened when Dr. Lanka’s group used the same procedures that have been used in every modern isolation experiment of every pathogenic virus that I have seen. Thisincluded changing the nutrient medium to “minimal nutrient medium”—meaning lowering the percentage of fetal calf serum from the usual 10% to 1%, which lowers the nutrients available for the cells to grow, thereby stressing them—and tripling the antibiotic concentration. As you can see, on day five of the experiment, the characteristic CPE occurred, “proving” the existence and pathogenicity of the virus—except, at no point was a pathogenic virus added to the culture. This outcome can only mean that the CPE was a result of the way the culture experiment was done and not from any virus.
The fourth and final vertical column is the same as vertical column three, except that to this culture, a solution of pure RNA from yeast was added. This produced the same result as column three, again proving that it is the culture technique—and not a virus—that is causing the CPE.”
For Dr. Lanka’s own breakdown of the phase 1 results, please see this interview with Dean Braus:
Phase 2: Construction of the “SARS-CoV-2” genome
Phase two of the control experiments looked to show that the “viral” material in the “SARS-COV-2” genome actually comes from healthy human tissue. Dr. Lanka joined Kate Sugak to discuss the findings in the below video:
Phase 3: Structural analysis of sequency data in virology
Phase 3 was designed to show that by using materials from many different sources (healthy humans, animals, plants, and synthetic nucleic acids), the PCR amplification process can create the genomes for any “virus.” I’ve provided the abstract from the study performed by the independent researchers working with Dr. Lanka to give a short overview of what was found:
Structural analysis of sequence data in virology: An elementary approach using SARS-CoV-2 as an example
“De novo meta-transcriptomic sequencing or whole genome sequencing are accepted methods in virology for the detection of claimed pathogenic viruses. In this process, no virus particles (virions) are detected and in the sense of the word isolation, isolated and biochemically characterized. In the case of SARS-CoV-2, total RNA is often extracted from patient samples (e.g.: bronchoalveolar lavage fluid (BALF) or throat-nose swabs) and sequenced. Notably, there is no evidence that the RNA fragments used to calculate viral genome sequences are of viral origin.
We therefore examined the publication “A new coronavirus associated with human respiratory disease in China” [1] and the associated published sequence data with bioproject ID PRJNA603194 dated 27/01/2020 for the original gene sequence proposal for SARS-CoV-2 (GenBank: MN908947.3). A repeat of the de novo assembly with Megahit (v.1.2.9) showed that the published results could not be reproduced. We may have detected (ribosomal) ribonucleic acids of human origin, contrary to what was reported in [1]. Further analysis provided evidence for possible nonspecific amplification of reads during PCR confirmation and determination of genomic termini not associated with SARS-CoV-2 (MN908947.3).
Finally, we performed some reference-based assemblies with additional genome sequences such as SARS-CoV, Human immunodeficiency virus, Hepatitis delta virus, Measles virus, Zika virus, Ebola virus, or Marburg virus to study the structural similarity of the present sequence data with the respective sequences. We have obtained preliminary hints that some of the viral genome sequences we have studied in the present work may be obtained from the RNA of unsuspected human samples.”
To hear Dr. Lanka’s explanation of this phase, please see this excellent interview once again with Kate Sugak:
Drs. Sam and Mark Bailey’s Tribute to Dr. Lanka
For an even greater in-depth look at the brilliant work of Dr. Lanka, please see this excellent video tribute by the Baileys. From an outline provided by Dr. Mark Bailey, in this 30 minute video they cover:
Dr. Lanka’s early discoveries that bacteriophages and giant “viruses” are able to be truly isolated but are not pathogenic
Dr. Lanka’s path as a virologist and the realization that the model was wrong
How Dr. Lanka spoke out from the very early stages against the HIV/AIDS dogma
Dr. Lanka’s discovery that the germ theory and disease entity models are incorrect
A look at Dr. Lanka’s 7 points that refute virology on their own terms
The 3 phases of the “SARS-CoV-2” control experiments performed in 2021 that were used to refute the “virus” hypothesis
And the optimism for the future as many of us are now standing on his shoulders to spread the knowledge he has given us
Sadly, it is often a lonely road for anyone willing to break away from tradition and speak out about the troubling state of their chosen profession, especially in a field with ties to a highly lucrative pharmaceutical conglomerate. More often than not, anyone who is willing to sound the alarm has their work smeared and their reputations tarnished by colleagues and the mainstream media in order to discredit the information and the charges that have been brought forth. We are fortunate enough that there were a few brave men and women who were able to see through the indoctrination of their training and push through the often painful cognitive dissonance which comes with having to change long held beliefs ingrained from birth.
Dr. Lanka helped to pave the path against virology and many of us are walking in his footsteps today. His refutation of the germ theory paradigm using their own history and methods was highly influential to myself and others. His status as an ex-virologist not only gave him an invaluable insiders look at the fraud the field is entrenched in but also the clout necessary for those hesitant about the information shared to actually listen up and to start asking the hard questions themselves. We are greatly indebted to Dr. Lanka for his trailblazing work. Without his herculean efforts, I highly doubt that we would be able to attack this fraudulent field as successfully as we are able to do so now.
Essential Reading:
I wanted to provide a list of Dr. Lanka’s work which I consider essential reading for anyone questioning the germ theory lies and/or looking to gain more knowledge of the foundational problems that the field of virology is built upon. Many of these were sources I read initially in my own journey which I found extremely helpful in broadening my own understanding. I am positive that this list will be a benefit to others as well:
A few days ago, I had the honor of being a guest on the Patrick Timpone show for the third time. As usual, the conversation was entertaining, even beyond the fact that I unknowingly wore the exact same shirt as when I was on the show a few months ago. We covered many topics in our hour long chat which was nicely listed in order on Patrick’s site:
How Can Monkey Pox Exist If the Germ Theory Is False?
Mike did video with Dr. Cowan about monkeypox. It’s on ViroLIEgy.com. Many articles there.
Monkeypox is more of the same. Nonspecific symptoms, unusual presentations, usually in genital areas, a targeted victim group, victims pegged with a faulty PCR test while presenting for other symptoms.
Monkeypox confused with herpes. Friction, sweat, stress, anxiety, immune-suppressing drugs will cause the lesions. Thin skin, lack of collagen related to herpes.
Had a drill before monkeypox outbreak similar to Event 201.
Initial victims had no travel or contact with anyone from the monkeypox endemic areas such as Africa.
Dr. Luc Montagnier said they never purified a virus.
AZT causes same symptoms as HIV/AIDs. Very toxic. Was a failed chemo drug in the 70s.
Contagion is a myth. Studies trying to transmit 1918 Flu couldn’t. Measles parties shown not to transmit measles to all exposed.
Epidemiological studies are subjective and often biased. Need to look at patient’s environment.
Bioresonance possibly explains “catching” a virus.
Virologists believe it. They don’t question because they have a lot invested in their education and position. We’re taught not to look at outside factors or to question the establishment.
Look at the information for yourself. They’re going to keep playing the same trick over and over again.
Culturing by putting in lots of other toxic substances that break down the cells, then isolating and saying it’s a virus.
7 main “coronavirus” now, and they all look the same. In a study, spikes created by a procedure that eroded the cell membrane. Can’t see a “live virus” in an electron microscope, it must be killed first. Which alters it and creates artifacts.
Can bioweapons be created? 99% of people survived COVID – it was a poor bioweapon. The real bioweapon is the jab. All they needed was the fear to induce people to get it. They can poison us though, and they are.
Gain of function – another fiction.
Shedding from the jab – another fear campaign.
Are viruses racist and homophobic? Those are identified as the target groups.
See the No Virus Challenge on viroliegy.com. Also see Debunking the Nonsense.
A photo isn’t enough because it says nothing about causality. A photo of hyenas eating a dead antelope says nothing about whether or not the hyenas killed the antelope. (A hunter might have killed it and the hyenas arrived later.)
Furthermore, reproducibility is critical, hence it being part of the Scientific Method. If the same results can’t be repeated, then the hypothesis is false. For example, if the claim that a certain type of plastic is heat resistant under certain conditions, but tests repeatedly reveal that it is not heat resistant under the said conditions, then the claim is false.
Similarly, if the claim that SARS-CoV-2 causes COVID-19, then tests must be conducted and must be reproducible.
There is nothing unusual about such logic; it is precisely how proper science works.
TNT Conversation
Mark joined me for a conversation about viruses and the aforementioned challenge. It is well worth listening to.
Podcast Conversation
A few days after our TNT conversation, Mark joined me on my podcast for an overlapping, but more free-flowing chat with coffee, craft beer, and power failures.
While walking down the darkened street late at night, have you ever had that gnawing fear as to whether or not the posse of raccoons rummaging through the trashcans nearby, staring at you with their beady yellow eyes, are ready and waiting for the right moment to pounce? Or have you ever had your fingertip accidentally pierced by the sharp fangs of a squirrel while feeding it walnuts and had to rush to the hospital on a nurses advice only to be told by the doctor that squirrels do not carry the “deadly virus?” Have you ever been bit in the very tender thin space of skin in between your thumb and index finger by a baby penguin while feeding it fish at the Omaha Zoo? Ok, the last one is obviously not related to rabies as the “virus” discriminates as to which animals it infects. Whether or not the squirrel can get or transmit rabies depends upon who you ask. In any case, these are all true experiences for me and yes, I have been bitten by numerous animals while feeding them. Like many, I have encountered the fear of being infected by a bite from a potentially rabid animal and that if I waited too long to receive treatment, it would be too late to stop the “virus” before it invades my cerebral cortex and causes me to turn into a crazed barking dog-man. Fortunately, not one of my comedically unfortunate puncture wounds left me to succumb to any disease. As I would later find out, my fears were in fact as irrational as the myths surrounding rabies which are built upon a foundation of fraud and pseudoscience.
Still, rabies seems to be one of the diseases that those who cling to the “virus” narrative love to bring up as if it is the Holy Grail of proof that “viruses” actually exist. Over the decades, the images of the mangy frothing dog snarling and ready to attack has been deeply ingrained into our subconscious through effective media fear-based propaganda.
1870’s fear propaganda.
Atticus Finch taking aim to put down a rabid dog in 1962’s To Kill A Mockingbird.
The portrayal of angry diseased animals heightened peoples fear of anything wild and undomesticated and created in their minds the living walking embodiment of an invisible “virus” coming to infect the defenseless with a slobbery bite. The fear of aquiring the deadly disease was the perfect tool to use by Louis Pasteur in the late 1800’s to ensare people into the emerging germ theory narrative. All it takes is one bite for the sneaky “virus” to find its way into the bloodstream, attacking the brain and causing a painful death. It seems, upon first glance, to be an open and shut case. However, what you will find upon researching rabies is that the presented model of the rabid animal bite transferring an infectious “virus,” which in turn causes disease, is not an accurate portrayal whatsoever and was merely a frightening myth used to propagate the delusions of a madman looking to aquire fame, fortune, and prestige.
A few months ago, I looked at the unethical and fraudulent practices Louis Pasteur employed in the 1880’s in his attempt to prove a rabies pathogen exists and causes disease in order to sell his vaccines. Pasteur openly admitted to not being able to isolate any microorganism said to cause rabies but developed his vaccine against the invisible pathogen anyways. This is also openly admitted as well by the Institut Pasteur:
“Louis Pasteur’s initial efforts to isolate the rabies virus proved unsuccessful as the virus remained invisible. Viruses could not be seen due to the poor resolution of the microscopes used. The virus was not seen until almost a century later, in 1962, with the advent of electron microscopy.
But as rabies is a disease of the nervous system, together with Emile Roux, Louis Pasteur then had the idea of inoculating part of a rabid dog’s brain directly into another dog’s brain. The inoculated dog subsequently died.”
Thus, Pasteur never worked with any purified and isolated “virus” and did what virologists still do today, which is assume an invisible entity is floating freely in the unpurified solutions of diseased animals which are then inoculated into healthy animals in attempts to cause disease and prove pathogenicity. Interestingly, as stated in the 1930 paper below, Pasteur would fail many times in his attempts to infect animals with saliva from animals claimed to be rabid, the very fluids the “virus” is supposed to reside in. Even if deemed successful, the symptoms would not appear for months, which was unheard of for any pathogen. Thus, he sought other means of infecting animals by way of injecting dogs directly in the brain with the emulsified cranial goo from animals claimed to be rabid. Once the healthy animal died from the toxic brain injection, this was considered a success:
Pasteur’s Work with Rabies
“Inoculation with saliva was found to be a method which did not always produce rabies and symptoms did not declare themselves for months. The theory that the disease virus attacks the nerve centers had already been set forth by Dr. Dubous of Paris. Pasteur accordingly inoculated a number of animals subcutaneously with some of the brain substance from other animals which had died of rabies. Most of those inoculated developed rabies, but not all.
Pasteur then conceived the idea of introducing into the brain of experimental animals some of the nerve tissue from an animal which had died of rabies. This experiment was based on the principle of providing the causal organisms with the nutritive medium best suited to their requirements. Pasteur, obliged to sacrifice so many animals, had a real dislike for vivisection; if the animal cried out a little he was full of pity. The idea of perforating the skull of the dog was repulsive to him, he wanted it done but dreaded seeing it done. So it was done one day when he was away. The next day when he was told of the intra-cranial inoculation he was moved to pity for the poor dog.”
While the exact make-up of the inoculations remain a mystery due to Pasteur’s secretive nature, the vaccine’s he utilized contained a neurotropic agent which was known to cause the exact same neurological conditions as seen in rabid animals. While injecting anything into the brain would potentially cause neurological damage and death, it is not far fetched to believe Pasteur used the same neurotropic agents in his experimental inoculations to prove pathogenicity, especially as they were said to consist of emulsified brain and nervous tissue. This created an issue in determining whether it was the invisible “virus” or the injections themselves which caused neurological damage and/or death. However, it has been admitted that the vaccines themselves led to the majority of neurological conditions rather than “wild” rabies cases as this was considered a rare occurrence in nature. This is just another in a long history of cases where the vaccine created the disease it was supposed to be preventing.
Fortunately, we can learn a lot of interesting tidbits about rabies (or the lack thereof) from the work of Gerald Geison, a leading Louis Pasteur researcher and historian who was privy to his private notebooks. In a 1978 essay he wrote on the ethics of rabies vaccination, Geison pointed out some of the pecularities of rabies such as the fact that it has always been considered a rare disease in man as well as the fact that rabies can not be transmitted from person-to-person. He also noted that, as a pathogenic disease, rabies has an unusually long incubation period. While it is said to usually last 6 to 8 weeks, Geison claimed that it can actually last for a year or more. In fact, there have been reported cases with a rabies incubation period from 6 years all the way on up to 25 years. If that wasn’t outlandish enough to make one question the validity of what we are told of the disease, Geison stated that there was a high degree of uncertainty regarding the correlation between animal bites and rabies symptoms as well as the threat of death from being bitten by a clearly rabid animal:
Pasteur’s Work on Rabies: Reexamining the Ethical Issues
“Rabies has always been rare in man. It probably never claimed more than a hundred victims in any year in France, and Fiench estimates for the years immediately preceding Pasteur’s famous work indicate an annual mortality of considerably less than fifty. In addition, rabies is not an infectious disease in the usual sense; it is not transmitted from man to man. Because of these two features, generalor compulsory vaccination has never seemed appropriate with respect to rabies.
“An even more peculiar feature of rabies is its long incubation period in the absence of detectable symptoms. No other lethal disease of rapid clinical course even approaches rabies for length of incubation-usually six to eight weeks, but sometimes a year or more.
“Unfortunately for Pasteur and his successors, there is a very high degree of uncertainty in the correlation between animal bites and the subsequent appearance of rabies-even when the biting animal is certifiably rabid. While the mortality of clinical rabies is virtually 100 percent, the threat of death from the bite of a rabid animal is vastly less. The risk depends on several factors, including the species of attacking animal (wolf and cat bites, for example, pose a much higher risk than dog bites), the location and depth of the bites, and the application or timing of cauterization. Depending on these and other circumstances, estimates of the risk of contracting rabies from the bites of animals known to be rabid range from as high as 80 percent to as low as 0.5 percent. It is perhaps futile to try to settle upon a meaningful “average” figure within this range, but Pasteur himself estimated that 16 percent of those bitten by rabid dogs would eventually die of rabies unless they submitted to his new treatment.”
In his 1995 book The Private Science of Louis Pasteur, Geison pointed out that, according to the English Commission on Rabies, there was also much uncertainty in the rabies statistics. They had suspected that at least one man had died not from rabies but from Pasteur’s vaccine instead and they actually favored animal regulations over Pasteur’s vaccination approach:
“But the English commission also drew attention to the uncertainty of all statistics on rabies, citing the difficulty of establishing that the attacking animal had in fact been rabid as well as the variable effects of the location and depth of bites, of differences in the lethality of rabid animal bites in different species and races, and of the possible prophylactic effects of cauterization or other treatments applied to bitten victims before they submitted to Pasteur’s treatment. The commission also suspected that at least one man may have died as a direct result of the Pastorian injections, and in the end it favored strict regulations on potentially rabid animals (muzzling and quarantine) over Pasteur’s more drastic remedy.”
We also find out from Geison that, in great contrast to what we are told about rabies, the great majority of rabies victims could forgo any treatment and never have any ill effects whatsoever:
“In short, the great majority of the victims of rabid animal bites could forgo Pasteur’s treatment without experiencing any untoward consequences in the future. And they had to decide whether or not to submit to the treatment at a point when they had no symptoms of the disease. For the efficacy and very possibility of Pasteur’s vaccine depended on the peculiarly long incubation period that separates the infective bites of a rabid animal from the outbreak of symptoms.”
Geison even spotlighted what was known as “false rabies,” which were cases of the exact same symptoms of disease associated with rabies that occured despite a complete lack of the victim being bitten by a rabid animal. These symptoms were said to be either induced solely based on fear alone or by alcoholism. In other words, just the mere thought of rabies could create an intense enough reaction inducing the same disease, thus no invisible microscopic pathogen is necessary. Pasteur actually emphasized these cases in defense of his vaccine as there was a growing chorus of criticism that his vaccine did not protect the victims and in fact induced the symptoms of rabies which lead to their deaths. Pasteur therefore had a vested interest in showing that these same symptoms could occur outside of animal bites and vaccination:
“Pasteur himself later pointed out some of the uncertainties surrounding the diagnosis of rabies. Two years after I’affair Girard, for example, he spoke to the Academie des sciences about several cases of “false rabies.” Relying on the authority of one Dr Trousseau, Pasteur cited two cases in which symptoms of the disease had been induced solely by fear. In one case, a man suddenly displayed several of the classic features of rabies—including throat spasms, chest pain, extreme anxiety, and other nervous symptoms—merely because the disease had become the subject of a lunchtime conversation. And this man had never even confronted a rabid animal. Presumably more common was the second case, that of a magistrate whose hand had long before been licked by a dog later suspected of rabies. Upon learning that several animals bitten by this dog had died of rabies, the magistrate became extremely agitated, even delirious, and displayed a horror of water. His symptoms disappeared ten days later, when his physician persuaded him that he would already be dead had he been afflicted with true rabies.”
In this same address, Pasteur commented upon a recently published case history of “false rabies.” Partly because it includes an arresting account of the classic symptoms of rabies, his commentary deserves quoting at length. As recorded in the Comptes rendus of the Academie des sciences for 17 October 1887, Pasteur spoke as follows:
The patient to whom Mesnet refers in his brochure was an alcoholic who, having seen some sort of deposit m his glass during lunch, was seized by a feeling of horror toward the liquid and by a constriction of the throat, followed by headache and by lameness and fatigue in all his limbs. He spent Sunday in this state.
During that night and during the day on Monday and Tuesday, no sleep, a fit of suffocation, throat spasms, and a horror of liquids, which he pushed aside in his glass. His countenance expressed disquiet. His eyes were fixed, glazed, the pupils greatly dilated. His speech was brief, jerky, rapid. He had difficulty breathing. When he was offered a glass of water, he pushed it aside with terror, and suffered fits of suffocation and of constriction of the throat. Bright objects and light were particularly disagreeable to him. He was painfully affected when the air was agitated in front of his face. He died Wednesday night after having suffered from a violent delirium, with extreme agitation, howls and cries, extremely abundant salivation, spitting, biting his bedsheets, and trying also to bite the person taking care of him. In short, this man displayed all the features of furious rabies [I’hydrophobie funeuse]. But he did not die of rabies. He had never been bitten and on several occasions, at long intervals, had already displayed symptoms analogous to false rabies.This man was an alcoholic and belonged, moreover, to a family m which one member had died of insanity [alienation mentale].
By October 1887, when he gave this address, Pasteur had a vested interest in emphasizing the difficulty of diagnosing rabies. For he was then defending himself against allegations that his rabies vaccine not only sometimes failed to protect those who submitted to it, but in some cases was itself the cause of rabies and therefore death. A few hostile critics were insisting that some people died of rabies not only despite Pasteur’s vaccine but because of it, and they tried to make Pasteur and his treatment responsible for the death of anyone who displayed any symptoms of nervous disease. In defense of his vaccine, Pasteur now emphasized the extent to which symptoms like those of rabies could appear in patients who did not have the disease. He therefore insisted that a diagnosis of rabies could only be established with confidence by experiments in which tissue from the victim’s brain was transmitted to animals susceptible to the disease.”
There is good reason for the high degree of uncertainty over the correlation between animal bites and the development of symptoms, the actual rabies statistics, as well as the ability to accurately diagnose the disease. For starters, there are many other conditions that can cause the exact same symptoms as rabies in both animals and in humans. In animals, canine distemper, encephalitis, and poisoning are a few of the conditions which can mimic rabies. In humans, this includes polio, being drunk and/or intoxicated on certain drugs, having Guillain–Barré syndrome, and as stated previously, encephalitis derived from the toxic vaccine itself.
It has been stated that it is common not to even find bite marks in cases of rabies and often, the person has had no idea that they were ever bitten to begin with. One source stated that fewer than one third of human rabies victims show evidence of bite wounds. With the vast range of conditions that mimic rabies and the lack of bite marks, it’s safe to question the existence of a specific disease known as rabies. It would be logical to conclude that rabies is nothing but the same set of symptoms that has been given a different label numerous times.
This uncertainty in rabies cases and statistics boils down to the inability to accurately diagnose a rabies case. For much of the 1800s to the mid 1900s, rabies was diagnosed upon clinical symptoms which, as previously stated, were not specific to the disease. It is also noted in the WHO’s rabies laboratory manual that the histological diagnosis for rabies, which began in the late 1800’s, was also non-specific:
When factoring in the non-specificity in diagnosis, the uncertainty in the correlation between animal bites and disease symptoms, and the vast majority of victims never needing any treatment whatsoever, it leads one to conclude that the rabies myth is vastly overstated. It is fictitious fear propaganda rather than facts based in reality. We can break this deception down even further by looking at how rabies is diagnosed in the present versus how it was in the past. According to the CDC:
Diagnosis in animals
“A diagnosis of rabies can be made after detection of rabies virus from any part of the affected brain, but in order to rule out rabies, the test must include tissue from at least two locations in the brain, preferably the brain stem and cerebellum.
The test requires that the animal be euthanized. The test itself takes about 2 hours, but it takes time to remove the brain samples from an animal suspected of having rabies and to ship these samples to a state public health or veterinary diagnostic laboratory for diagnosis.”
In order to diagnose rabies, the animal must be killed and sections must be taken from the brain in order to try and detect the “virus.” We already have a few problems here as no “virus” was ever purified and isolated in order to determine how to detect it. There is also an issue with attempting to determine anything from dead tissue as the tissue, once removed, immediately starts to change through decomposition. Biologist Harold Hillman often pointed out the faults in trying to establish credible information about what occurs inside living beings from the study of dead tissues:
“Killing an animal changes its biochemistry grossly. For example, its blood carbon dioxide, phosphate, lactate, and potassium ion concentrations, rise, while its oxygen, sodium ion, adenosine triphosphate, phosphocreatine, concentrations go down. These changes affect much of the tissue metabolism. It is hoped and normally assumed that they will reverse during incubation. There is no realistic way of testing this, since the volume and chemistry of the tissue changes during incubation. In this circumstance, it is worth asking whether cell biologists should use tissues in vitro at all. Perhaps, they should confine their experiments to working on intact animals and human beings, tissue cultures, unicellular organisms and plants.”
The current “gold standard” used to study the dead brain tissue for the diagnosis of rabies is known as the direct fluorescent antibody test. As the name implies, the test looks to detect rabies antigens on the brain by using antibodies said to be specific to the rabies “virus:”
Direct Fluorescent Antibody Test
“The dFA test is based on the observation that animals infected by rabies virus have rabies virus proteins (antigen) present in their tissues. Because rabies is present in nervous tissue (and not blood like many other viruses), the ideal tissue to test for rabies antigen is brain. The most important part of a dFA test is flouresecently-labeled anti-rabies antibody. When labeled antibody is incubated with rabies-suspect brain tissue, it will bind to rabies antigen. Unbound antibody can be washed away and areas where antigen is present can be visualized as fluorescent-apple-green areas using a fluorescence microscope. If rabies virus is absent there will be no staining.”
According to the CDC, in the 50 years that the dFA test has been used to detect rabies, it has not failed to present reliable and accurate results. This indirect method is somehow said to be more sensitive and specific than actually “isolating” the “virus,” thus the “gold standard” label. It is also stated by the CDC that the saliva of an infected animal contains millions of “virions,” making the lack of any purified and isolated “virus” and the reliance on indirect antibody testing all the more glaring of an issue:
Accuracy of the Tests
“During the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person.
Because of its high sensitivity and specificity,in comparison to virus isolation methods, the DFA test is the “gold standard” diagnostic method for rabies and has been rigorously evaluated by international, national, and state health laboratories. The DFA test is currently the only recommended diagnostic method for routine rabies determination in animals in the United States.
During clinical disease, millions of viral particles may be found intermittently in the saliva. In theory, only a single rabies particle or virion is required to result in a productive infection.”
Returning to the WHO’s rabies manual, it shows us exactly how the dFA is used and how the diagnosis is determined based on the interpretation of the person reading the results. The interpreter uses an antigen fluorescence intensity and distribution scale from +4 on down to +1 to determine one of four conclusions: positive, negative, unsatisfactory, or inconclusive. Obviously, the subjective bias of the interpreter plays no role in the accuracy of the determination as humans rarely make interpretive errors, correct?:
In fact, there are many drawbacks to using the dFA as the “gold standard” test for rabies diagnosis beyond the aforementioned use of dead tissues. For starters, due to the lack of ever properly purifying and isolating the rabies “virus” directly from the saliva said to contain millions of “virions,” any antibody result is utterly meaningless as there is no “virus” to determine a specific reaction with. We also have this same purification/isolaton problem with antibodies as these entities have also never been taken and separated directly from the fluids of a host in order to be studied independently. There is also the issue that the theoretical antibodies themselves are entirely non-specific and are regularly said to bind to proteins that are not the intended target. Thus, we once again run into the problem where one fictional entity (the rabies “virus”) is said to be detected by another fictional entity (the antibody). It is very telling that the CDC believes that the interpretive results from this indirect circular test is more accurate than actually finding and “isolating” the supposed “virus.”
Thus, we must ask ourselves if these dFA tests really are as accurate as stated by the CDC. If we do so, we find out that this is most definitely not the case according to these next three sources. This first snippet comes from a study done on bacteria which points out the obvious fault of the subjective interpretation of the dFA test results which leads to poor sensitivity and a widely varying specificity, contrary to the claims made by the CDC:
“Direct fluorescent-antibody testing (DFA) provides a much more rapid result but also has the disadvantage of poor sensitivity, and its specificity varies widely due to the subjective interpretation of test results.”
This second study also points out the flaws of the subjective interpretation of the test results as well as the need for expensive equipment and quality-controlled reagents, the varied parameters utilized for succesful results and the issues relating to the incubation times and temperatures, as well as the necessity of having well-trained personnel running and interpreting the results:
“However, DFA has several drawbacks such as the need for an expensive fluorescent microscope, well-trained personnel, and quality controlled reagents (antibodies, conjugates), and varied parameters used during microscopy, and incubation times and temperatures, not to mention the subjectivity in interpretation of the test results [27,28,29,30]. In addition, acetone used as fixative in DFA does not completely inactivate the virus, as demonstrated by the infectivity of acetone-fixed tissue for neuroblastoma cells [31], posing a potential biohazard to laboratory personnel. Indeed, complete inactivation of cell culture-derived rabies virus appears to require >30% acetone [32].”
And finally, from this 2017 study published in PLOS Neglected Tropical Diseases, we can once again see the problems with subjective interpretation of dFA test results in action. The study utilized 23 independent laboratories to aid in identifying “differences in the laboratory protocols that could explain discrepant laboratory results and provide baseline knowledge for regional standardization of protocols.” The labs were each sent 20 samples which included 17 test samples and 3 controls. The positive tissues contained major rabies “virus” variants that were circulating in the Americas while the negative samples consisted of tissues demonstrating complete absence of rabies “virus” antigen and artifacts. Each lab was asked to test the samples using their own standard protocols and to record their results (positivity, intensity, and distribution of the fluorescence staining) as well as the microscopic condition and impression quality of the tissues (Good, Acceptable, or Deficient) as evaluated by the laboratory operator. The results from this 2017 study indicated that there are substantial differences in the overall dFA results and test interpretation as the “level of concordance between the 23 participating laboratories and the CDC panel showed large variability.” Only two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories:
An inter- laboratory proficiency testing exercise for rabies diagnosis in Latin America and the Caribbean
“Our results indicate that although all laboratories can perform the direct fluorescent antibody test, there are substantial differences in the overall results and test interpretation. This study identified important gaps in standardization and/or harmonization between laboratories which could be overcome and corrected with appropriate DFA protocols standardized across the LAC, including its broad distribution and proper training.”
“Conclusive rabies diagnosis can only be achieved by appropriate laboratory testing. Clinical and epidemiological diagnosis is challenging and leads to under-reporting [1, 2, 3]. The Direct Fluorescent Antibody test (DFA) for detection of rabies virus antigen remains as the gold standard test for laboratory diagnosis of rabies in post-mortem brain tissues [3].”
“The agreement between the laboratory results and those of the CDC, as measured by the sensitivity, specificity, concordance and kappa values are shown in Table 2. Two laboratories correctly identified all samples tested (sensitivity and specificity of 1.0). However, 30% (7/23) of all laboratories reported at least one false positive and 83% (19/23) of all laboratories reported at least one false negative sample. The average sensitivity was 76% with a range of 40% to 100%. The average specificity was 88% with a range of 22% to 100%. While a majority of the laboratories had low false positive rates, there were considerable differences in the sensitivity (Fig 1).The mean concordance was 81% with a range of 50% to 100% and the mean kappa score was 0.56 with a range of 0.02 to 1.00.”
“The level of concordance between the 23 participating laboratories and the CDC panel showed large variability. Two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories.”
“The type of conjugate may also affect the sensitivity of the DFA test (monoclonal cocktail versus polyclonal, in-house made versus commercial). For the current exercise, laboratories used commercial (65%) or in-house (35%) conjugates. A study of 12 rabies reference laboratories in Europe demonstrated that the variability of conjugates could potentially lead to discordant results and influence assay sensitivity [19].”
A bunch of glowing green dots means…absolutely nothing.In answer to the claim by the CDC that “during the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person,” we can safely conclude that this is obviously a false statement. The dFA test has been shown to have low sensitivity and a widely varying specificity as well as major issues relating to the subjective interpretation of the results based upon the person doing the interpreting. The 23 labs participating in the 2017 study had large variability in concordance with the CDC’s own panel. Anyone looking at this indirect test with a shred of intellectual honesty can easily see that the CDC’s “golden standard” rabies test does not look so golden anymore.
While the dFA test is the “go to” diagnostic measure in modern times, there are other methods available which can be used in an attempt to claim an animal is infected with the rabies “virus.” One of these is the “isolation” of the “virus” in tissue and cell cultures, which used to be the “gold standard” method for proving a “virus” exists and is infectious. Oddly enough, the CDC stated that the supposed “isolation” of the rabies “virus” is not as sensitive nor as specific as the dFA test. How could this possibly be the case?
For one thing, it is admitted that the rabies “virus” does not actually produce the desired cytopathogenic effect (CPE) when cultured:
Detection of rabies virus replication: inoculation tests
“The other group of available techniques aim at detecting the replication of the virus on living substrates, e.g. cells. Virus isolation may be necessary to confirm inconclusive results in FAT/dRIT and for characterization of the virus strain. In neuroblastoma cells, rabies virus grows generally without cytopathic effect; once again it is necessary to use FAT to confirm the presence of rabies virus.After intracranial application, rabies induces clinical signs in mice that are relatively typical but have to be confirmed by FAT. Since cell culture is as sensitive as the mouse inoculation test, units should be established in laboratories to replace mouse inoculation tests as it avoids the use of life animals, is less expensive and gives more rapid results.”
Why is this important to note? The cytopathogenic effect (CPE) is the structural and morphological changes to the cell that are claimed to be caused by the “virus” as it enters the cell, breaking it apart as the “virus” creates more copies of itself. This effect is supposed to tell the researchers that the “virus” is present within the culture. According to their stories, without this effect, it should be a clear indicator that the host was not infected by the “virus.” However, virology loves to bend their own rules and in a clear cut case of having their cake and eating it too, virologists claim that certain “viruses” do not cause CPE in their natural host cells. They state that there are different levels of CPE based on the cell type used:
Not permissive cell – virus cannot infect
Permissive cell – virus can replicate, but does not cause obvious CPE
Highly permissive cell – virus replicates and induces an obvious CPE
Anyone looking at this logically can see that “Not permissive” and “Permissive” cells are the exact same thing. Neither of these cells produce CPE when “infected” by the “virus.” However, virologists will resort to other indirect measures in order to claim the “virus” is present in spite of the lack of any CPE observed. In the case of rabies, the dFA test is used to confirm if a “virus” is present in a culture. However, if the dFA test is considered inconclusive, the cell culture is used to confirm the dFA result. A bit circular there, don’t you think? Another confirmation is done by injecting the toxic CPE-less cell culture soup into the brain of a mouse and seeing if symptoms occur. If so, the mouse is killed and the newly damaged brain is taken and tested by dFA for confirmation. Seeing the problem yet?
Toxic cell-cultured goo injected directly into the brain causing brain damage. It must be the “virus” and not the method… ?
If neither dFA and/or cell culturing is enough satisfactory indirect evidence to claim the existence of the rabies “virus,” one can turn to the old ways of histopathology to try and build a circumstantial case against the invisible entity. Along with attempting to diagnose someone based on clinical symptoms, which thanks to Louis Pasteur and “false rabies” we know is inaccurate due to the non-specificity of the symptoms, histopathology was the main method utilized for decades for determining if an animal was in fact rabid. This consisted of staining the brain tissues with chemicals such as hematoxylin and eosin and looking for patterns of encephalopathy as well as the presence of what are called Negri bodies. Negri bodies are round or oval inclusions within the cytoplasm of nerve cells of animals which were discovered by Dr. Adelchi Negri in 1903. At the time, he claimed that these inclusions were the etiologic agent of rabies. While the rest of the virology community disagreed with Dr. Negri, his discovery was considered a tell-tale sign of rabies infection in the brain and finding these inclusions served as the basis for a rabies diagnosis for over 60 years. However, there is rather big problem for these histopathological examinations. Signs of encephalitis and finding Negri bodies are both entirely non-specific and are seen in cases that have absolutely nothing to do with rabies. In fact, Negri bodies are said to only be found in half of the cases of rabies:
Histologic examination, General histopathology
“Histologic examination of biopsy or autopsy tissues is occasionally useful in diagnosing unsuspected cases of rabies that have not been tested by routine methods. When brain tissue from rabies virus-infected animals are stained with a histologic stain, such as hematoxylin and eosin, evidence of encephalomyelitis may be recognized by a trained microscopist. This method is nonspecific and not considered diagnostic for rabies.
Before current diagnostic methods were available, rabies diagnosis was made using this method and the clinical case history. In fact, most of the significant histopathologic features (changes in tissue caused by disease) of rabies infection were described in the last quarter of the 19th century. After Louis Pasteur’s successful experiments with rabies vaccination, scientists were motivated to identify the pathologic lesions of rabies virus.
Histopathologic evidence of rabies encephalomyelitis (inflammation) in brain tissue and meninges includes the following:
Mononuclear infiltration
Perivascular cuffing of lymphocytes or polymorphonuclear cells
Lymphocytic foci
Babes nodules consisting of glial cells
Negri bodies
Negri bodies
In 1903, most of the histopathologic signs of rabies were recognized, but rabies inclusions had not yet been detected. At this time, Dr. Adelchi Negri reported the identification of what he believed to be the etiologic agent of rabies, the Negri body.In his report, he described Negri bodies as round or oval inclusions within the cytoplasm of nerve cells of animals infected with rabies. Negri bodies may vary in size from 0.25 to 27 µm. They are found most frequently in the pyramidal cells of Ammon’s horn, and the Purkinje cells of the cerebellum.
They are also found in the cells of the medulla and various other ganglia. Negri bodies can also be found in the neurons of the salivary glands, tongue, or other organs. Staining with Mann’s, giemsa, or Sellers stains can permit differentiation of rabies inclusions from other intracellular inclusions. With these stains, Negri bodies appear magenta in color and have small (0.2 µm to 0.5 µm), dark-blue interior basophilic granules.
The presence of Negri bodies is variable. Histologic staining for Negri bodies is neither as sensitive nor as specific as other tests. Some experimentally-infected cases of rabies display Negri bodies in brain tissue; others do not. Histologic examination of tissues from clinically rabid animals show Negri bodies in about 50% of the samples; in contrast, the dFA test shows rabies antigen in nearly 100% of the samples. In other cases, non-rabid tissues have shown inclusions indistinquishable from Negri bodies. Because of these problems, the presence of Negri bodies should not be considered diagnostic for rabies.”
Whoever wants to point at random circles seen in fixed and stained dead tissues and then make wild guesses about their importance, raise your hand! ️
As the Negri bodies played such a substantial role in determining the diagnosis of rabies and building the case statistics used to sell the public on a “virus” in need of vaccination and eradication, let’s look at two more studies to find out a bit more about these non-specific diagnostic blobs. In 1942, it was already well known that the Negri bodies were not specific to rabies and could be mistaken for other inclusion bodies seen in the tissues upon examination. This is a rather big deal as the mass vaccination of dogs didn’t start for another 5 years in 1947. So we can already see that the main method used for diagnosis was faulty which casts doubt on any rabies statistics generated up to that time using this method. The authors go on to admit that there were deficiencies in the method used for examining these inclusions. It is stated that every experienced microscopist encountered difficulty in deciding whether or not the bodies observed were in fact Negri bodies or whether they were instead normal or possibly distorted cytoplasmic structures. In the study of 84 mice said to be given rabies by way of injection, Negri bodies were only found in the hippocampus 8 times as well as only 4 times in the cerebral cortex. The authors concluded that there are many rabies cases without Negri bodies present upon examination and that there are various structures which resemble Negri bodies commonly found in normal animals:
Problems in the Laboratory Diagnosis of Rabies*
“THE diagnosis of rabies in the laboratory is based entirely upon the microscopic demonstration of Negri bodies and upon animal inoculation. The demonstration of Negri bodies is the method of choice since the diagnosis can be thus made in a few minutes or hours. When the technic employed demonstrates typical bodies the result is highly convincing and satisfying. However, negative and doubtful results leave much to be desired, and animal inoculation must be resorted to. The difficulties in demonstrating Negri bodies arise from two sources of error which can be enumerated as inability to differentiate them from other inclusion bodies and cell structures, and inherent deficiencies in the methods of examination.”
“However, every experienced microscopist has encountered the difficulty of deciding whether the bodies observed in some preparations are Negri bodies or cytoplasmic structures normal to the cell or if not normal at least only distorted cellular structures. Goodpasture refers to the variation in size of Negri bodies and speaks of being able to demonstrate the smallest forms. When small bodies are associated with large ones, which show the typical inner structure, no confusion is encountered. When, however, only forms so small occur that the demonstration of the “Innenkorper” is doubtful, the diagnosis is doubtful. The brain of cats, particularly, offers difficulty because of the pink staining granular material in the cells and also because the Negri bodies in the pyramidal and Purkinji cells of this animal are often very small. The failure of the microscopic diagnosis of rabies as proved by mouse inoculation is shown in Table 1.”
“Above we have mentioned the occasional occurrence of what appear to be “lyssa bodies” or small Negri bodies in the brain of some animals which did not produce rabies when injected into mice. These bodies are found most frequently in the cerebrum and medulla. Since in the study of 84 cases of rabies proved by mouse inoculation we found Negri bodies only in the hippocampus 8 times and only in the cerebral cortex 4 times (Table 2), the finding of eosinophilic bodies in any portion of a brain from an animal suspected of having had rabies creates a doubt as to the diagnosis.”
“From these results it appears that by microscopic examination of sections and in some smears we are able to demonstrate eosinophilic bodiesresembling “lyssa bodies” and atypical Negri bodies which are not associated in the brain with rabies virus. Also the results show that brain specimens in which the microscopic examination leaves the diagnosis in doubt contain rabies. The bodies that cause this confusion in the microscopic diagnosis of rabies are similar to ones found in certain parts of the brain of normal cattle and other animals and to atypical or small Negri bodies.”
doi: 10.2105/ajph.32.2.171.
While the 1942 study should have been the end of the Negri body as a diagnostic indicator of rabies, this method carried on being used over the decades. In 1975, another study emerged casting doubts on the dogma surrounding these long-held markers of the rabies disease. It’s stated that there was a universal acceptance of the Negri body as a specific indicator of rabies and that due to this widely-endorsed dogma, every time a Negri body was seen, a rabies diagnosis was made irrespective of the circumstances regarding the case.
However, in this study, a case was reported of a person who was considered rabies free by way of dFA and electron microscopy but Negri bodies were still found upon examination. This finding was inconsistent with the idea of the specificity of these bodies to rabies. The author pointed out many flaws with the use of Negri bodies as a diagnostic tool as outside of finding them upon examination, rabies is non-specific and mimics other diseases such as smallpox. It is stated that rabies encephalitis does not have any pathognomonic clinical or pathologic features distinguishing it from other diseases. The absence of Negri bodies in a substantial number of fatal cases of rabies, the lack of any inflammatory response, the absence of any history of animal contact in more than 30% of fatal cases, and the lack of specific behavioral symptoms of rabies in animals led the author to the conclusion that any association between this diagnostic method and the rabies disease is unwarranted. Thus, it is easy to see that any and all rabies case statistics based upon the clinical diagnosis and findings of Negri bodies should be thrown out:
Is the Negri Body Specific for Rabies?
“Of all viral diseases affecting the nervous systems of humans and animals, rabies seems to be the only one in which light microscopy alone can provide a definitive etiologic diagnosis. This is based on the universally accepted conviction on the specificity of the Negri body for rabies. Thus, the presence of a Negri body in the brain of a patient who did not have rabies is a matter that deserves attention.”
“Neuropathologically, the exclusion of rabies in the present case is based on the negative immunofluorescent
study results for rabies and the absence of the rabies virus within the Negri bodies (light microscope) as demonstrated by electron microscopy. Such an observation, of course, is inconsistent with the specificity of the Negri body in signifying the presence of rabies. Therefore, it is reasonable to ask: What are the other inclusion bodies that occur in sites other than the nervous system that are morphologically similar to Negri body?”
“The result of a universally accepted dogma such as this is obvious; in every instance in which a “Negri body” has been seen, a diagnosis of rabies was made irrespective of the circumstances.
To delineate some of the related aspects of the problem the following points deserve etnphasis:
Except for the occurrence of theNegri body, rabies encephalitis does not have any pathognomonic clinical or pathologic features. Variola-vaccinia virus, for example, can produce the same clinical pictures. The cutaneous manifestations can be sufficiently scanty to be missed on the physical examination, or they can be absent altogether (variole sans eruptione). There is remarkable variability in the intensity of cellular inflammatory response in rabies encephalitis. This, to some extent, may reflect the vigor with which these reactions are searched for, since the diagnostic efforts in the past have been mainly directed to the “specific” finding of the Negri body. The absence of Negri bodies in a substantial number of fatal cases of rabies and the remarkable lack of inflammatory response in some instances of the disease signify the importance of obtaining a careful history. A definitive etiologic diagnosis of rabies, however, requires obtaining positive results with immunofluorescent or electron microscopical methods or both. The former method maps the occurrence of rabies viral antigen in any morphologic form (with or without the presence of the inclusions), and the latter defines the characteristic bullet-shaped virus.
Absence of history of animal contact has been reported in more than 30% of fatal cases of rabies. Here, also, it is the unquestioned association between the Negri body and rabies that constitutes the sole ground for a definitive etiologic diagnosis. The latter report is remarkable for the absence of history of animal contact and the occurrence of the fatal illness one week after vaccination for smallpox. Even in the presence of history of animal contact, it should be remembered that such an association is unwarranted as the behavioral alterations in the animals are not pathognomonic of any one disease.
It is conceivable that the failures of antirabies therapy and the occurrence of false negative immunofluorescent results are related to the non-specificity of the Negri body for rabies.
In no other viral disease is the light microscopy alone an accepted method for the definitive etiologic diagnosis of a disease.
The validity of the present observations needs confirmation by other observers and the answer will be found “not by dogma or skepticism but by open-minded uncertainty.”
doi: 10.1001/archneur.1975.00490440025002.
In Summary:
According to the Institut Pasteur, Louis Pasteur’s initial efforts to isolate the rabies “virus” proved unsuccessful as the “virus” remained invisible
The “virus” was not seen until almost a century later, in 1962, with the advent of electron microscopy
Louis Pasteur had the idea of inoculating part of a rabid dog’s brain directly into another dog’s brain, causing the inoculated dog to subsequently die
Inoculation with saliva (where the “virus” is supposedly found) was found to be a method which did not always produce rabies and symptoms did not declare themselves for months
Pasteur accordingly inoculated a number of animals subcutaneously with some of the brain substance from other animals which had died of rabies
Most of those inoculated developed rabies, but not all
Pasteur’s idea of introducing into the brain of experimental animals some of the nerve tissue from an animal which had died of rabies was based on the principle (i.e. assumption) of providing the causal organisms with the nutritive medium best suited to their requirements
There is a very high degree of uncertainty in the correlation between animal bites and the subsequent appearance of rabies-even when the biting animal is certifiably rabid
While the mortality of clinical rabies is “virtually 100 percent,” the threat of death from the bite of a rabid animal is vastly less
Estimates of the risk of contracting rabies from the bites of animals known to be rabid range from as high as 80 percent to as low as 0.5 percent
Pasteur himself estimated that 16 percent of those bitten by rabid dogs would eventually die of rabies unless they submitted to his new treatment
In 1887, the English Commission on Rabies drew attention to the uncertainty of all statistics on rabies citing:
The difficulty of establishing that the attacking animal had in fact been rabid
The variable effects of the location and depth of bites
Differences in the lethality of rabid animal bites in different species and races
The possible prophylactic effects of cauterization or other treatments applied to bitten victims before they submitted to Pasteur’s treatment
The commission also suspected that at least one man may have died as a direct result of the Pastorian injections, and in the end it favored strict regulations on potentially rabid animals (muzzling and quarantine) over Pasteur’s more drastic remedy
The great majority of the victims of rabid animal bites could forgo Pasteur’s treatment without experiencing any untoward consequences in the future
Pasteur himself later pointed out some of the uncertainties surrounding the diagnosis of rabies
Pasteur cited two cases in which symptoms of the disease had been induced solely by fearwithout any animalbite as well as another case which was induced by alcoholism
Pasteur had a vested interest in emphasizing the difficulty of diagnosing rabies as he was then defending himself against allegations that his rabies vaccine not only sometimes failed to protect those who submitted to it, but in some cases was itself the cause of rabies and therefore death
In defense of his vaccine, Pasteur now emphasized the extent to which symptoms like those of rabies could appear in patients who did not have the disease
According to the CDC, the diagnosis of rabies can be made after detection of rabies “virus” from any part of the affected brain, preferably the brain stem and cerebellum
The test requires that the animal be euthanized
According to biologist Harold Hillman: “Killing an animal changes its biochemistry grossly. For example, its blood carbon dioxide, phosphate, lactate, and potassium ion concentrations, rise, while its oxygen, sodium ion, adenosine triphosphate, phosphocreatine, concentrations go down. These changes affect much of the tissue metabolism.”
Hillman felt that “it is worth asking whether cell biologists should use tissues in vitro at all”
The current “gold standard” test used to detect the “virus” on the brain tissue is the direct fluorescent antibody test (dFA)
The dFA test is based on the “observation” that animals infected by rabies “virus” have rabies “virus” proteins (antigen) present in their tissues
Because rabies is present in nervous tissue (and not blood like many other “viruses”), the ideal tissue to test for rabies antigen is brain
When labeled antibody is incubated with rabies-suspect brain tissue, the story goes that it will bind to rabies antigen and unbound antibody can be washed away so that areas where antigen is present can be visualized as fluorescent-apple-green areas using a fluorescence microscope
According to the CDC, during the 50 years the direct fluorescent antibody (DFA) test has been used in the United States, there has been no indication it has failed to provide accurate clinical information on the rabies status of an animal for the purposes of treating an exposed person
The CDC states that because of its high sensitivity and specificity, in comparison to “virus” isolation methods, the DFA test is the “gold standard” diagnostic method for rabies (way to shoot “virus” isolation in the foot there CDC…)
During clinical disease, millions of “viral” particles may be found intermittently in the saliva(which makes one wonder why they must kill an animal and do indirect antibody tests on decomposing brain tissue for diagnosis rather than properly purify and isolate the “virus” directly from the saliva supposedly containing millions of these entities)
In theory, only a single rabies particle or “virion” is required to result in a productive infection
The dFA results are based upon the opinion of an interpreter who uses an antigen fluorescence intensity and distribution scale from +4 on down to +1 to determine one of four conclusions: positive, negative, unsatisfactory, or inconclusive
The dFA test has the disadvantage of poor sensitivity, and its specificity varies widely due to the subjective interpretation of test results
The subjectivity in interpretation of the test results
According to a 2017 study testing and reviewing dFA with the help of numerous labs, the results indicated that although all laboratories can perform the direct fluorescent antibody test, there are substantial differences in the overall results and test interpretation
The authors stated that conclusive rabies diagnosis can only be achieved by appropriate laboratory testing as clinical and epidemiological diagnosis is challenging and leads to under-reporting
The agreement between the laboratory results and those of the CDC, as measured by the sensitivity, specificity, concordance and kappa values:
Only two laboratories correctly identified all samples tested (sensitivity and specificity of 1.0)
However, 30% (7/23) of all laboratories reported at least one false positive and 83% (19/23) of all laboratories reported at least one false negative sample
The average sensitivity was 76% with a range of 40% to 100%
The average specificity was 88% with a range of 22% to 100%.
While a majority of the laboratories had low false positive rates, there were considerable differences in the sensitivity
The mean concordance was 81% with a range of 50% to 100% and the mean kappa score was 0.56 with a range of 0.02 to 1.00
The level of concordance between the 23 participating laboratories and the CDC panel showed large variability
Two laboratories had 100% concordance, while 91% of the labs had at least one discordant sample, with a total of 26 false positive and 61 false negative results among all laboratories
The type of conjugate may also affect the sensitivity of the DFA test (monoclonal cocktail versus polyclonal, in-house made versus commercial)
A study of 12 rabies reference laboratories in Europe demonstrated that the variability of conjugatescould potentially lead to discordant results and influence assay sensitivity
Another method for diagnosing rabies is the “isolation” of the “virus” by tissue or cell culture
“Virus isolation” may be necessary to confirm inconclusive results in dFA/dRIT and for characterization of the “virus” strain
In neuroblastoma cells, rabies “virus” grows generally without cytopathic effect
In a bit of cirular reasoning, it is necessary to use dFA to confirm the presence of rabies “virus” by way of cell culture whereas cell culture may also be used to confirm inconclusive dFA results
After intracranial (in the brain…some things never change)application, rabies induces clinical signs in mice that are relatively typical but have to be confirmed by dFA (i.e. the mouse that has had toxic cell culture goo injected into its brain causing symptoms must then be killed to have its cell-culture damaged brain examined by dFA to confirm the infection)
Histologic examination of biopsy or autopsy tissues looking for signs of encephalitis is occasionally useful in diagnosing unsuspected cases of rabies that have not been tested by routine methods
However, this method is nonspecific and not considered diagnostic for rabies
Before current diagnostic methods were available, rabies diagnosis was made using this method and the clinical case history(i.e. non-specific and not suited for diagnostic methods were used to identify rabies for most of the 19th and 20th century)
Histopathologic evidence of rabies encephalomyelitis (inflammation) in brain tissue and meninges includes the following:
Mononuclear infiltration
Perivascular cuffing of lymphocytes or polymorphonuclear cells
Lymphocytic foci
Babes nodules consisting of glial cells
Negri bodies
In 1903, Dr. Adelchi Negri reported the identification of what he believed to be the etiologic agent of rabies, the Negri body
In his report, he described Negri bodies as round or oval inclusions within the cytoplasm of nerve cells of animals infected with rabies
While this was the main method of diagnosing rabies for over 60 years, the presence of Negri bodies is variable
Histologic staining for Negri bodies is neither as sensitive nor as specific as other tests
Some experimentally-infected cases of rabies display Negri bodies in brain tissue; others do not
Histologic examination of tissues from clinically rabid animals show Negri bodies in about 50% of the samples
In other cases, non-rabid tissues have shown inclusions indistinquishable from Negri bodies
Because of these problems, the presence of Negri bodies should not be considered diagnostic for rabies
Despite these problems, until the mid-1960’s the diagnosis of rabies in the laboratory was based entirely upon the microscopic demonstration of Negri bodies and upon animal inoculation
According to a study from 1942, the demonstration of Negri bodies was the method of choice since the diagnosis can be thus made in a few minutes or hour
However, the authors admitted that the difficulties in demonstrating Negri bodies arose from two sources of error which could be enumerated as theinability to differentiate them from other inclusion bodies and cell structures, and inherent deficiencies in the methods of examination
Every experienced microscopist has encountered the difficulty of deciding whether the bodies observed in some preparations are Negri bodies or cytoplasmic structures normal to the cell or if not normal at least only distorted cellular structures
In the study of 84 cases of rabies proved by mouse inoculation they found Negri bodies only in the hippocampus 8 times and only in the cerebral cortex 4 times
The authors determined that the finding of eosinophilic bodies in any portion of a brain from an animal suspected of having had rabies creates a doubt as to the diagnosis
From their results it appeared that by microscopic examination of sections and in some smears, they were able to demonstrate eosinophilic bodies resembling “lyssa bodies” and atypical Negri bodies which are not associated in the brain with rabies “virus”
Also the results showed that brain specimens in which the microscopic examination leaves the diagnosis in doubt contain rabies (i.e. they determined that injecting mice in the brain caused rabies without finding Negri bodies)
The bodies that cause this confusion in the microscopic diagnosis of rabies are similar to ones found in certain parts of the brain of normal cattle and other animals and to atypical or small Negri bodies
In a 1975 study, it is stated that rabies is the only “virus” that can be diagnosed by light microscopy based on the universally accepted conviction on the specificity of the Negri body for rabies
However, the authors presented a case of a patient without rabies as determined by negative immunofluorescent study results for rabies and the absence of the rabies “virus “within the Negri bodies (light microscope) as demonstrated by electron microscopy
Such an observation was inconsistent with the specificity of the Negri body in signifying the presence of rabies
The result of this universally accepted dogma led to every instance in which a “Negri body” was seen being diagnosed as rabies irrespective of the circumstances
Except for the occurrence of the Negri body, rabies encephalitis does not have any pathognomonic clinical or pathologic features (i.e. non-specific and overlapping symptoms associated with many diseases)
Variola-vaccinia(Smallpox) “virus,” for example, can produce the same clinical pictures
There is remarkable variability in the intensity of cellular inflammatory response in rabies encephalitis
The diagnostic efforts in the past have been mainly directed to the “specific” finding of the Negri body
The absence of Negri bodies in a substantial number of fatal cases of rabies and the remarkable lack of inflammatory response in some instances of the disease signify the importance of obtaining a careful history
Absence of history of animal contact has been reported in more than 30% of fatal cases of rabies
In these cases, it is the unquestioned association between the Negri body and rabies that constitutes the sole ground for a definitive etiologic diagnosis
Even in the presence of history of animal contact, it should be remembered that such an association is unwarranted as the behavioral alterations in the animals are not pathognomonic of any one disease (i.e. there are many diseases which are said to cause the same symptoms in animals)
It is conceivable that the failures of antirabies therapy and the occurrence of false negative immunofluorescent results are related to the non-specificity of the Negri body for rabies
In no other “viral” disease is the light microscopy alone an accepted method for the definitive etiologic diagnosis of a disease
The author concludes that the answers to the observations made will be found “not by dogma or skepticism but by open-minded uncertainty.”
When one looks into the history of rabies and the methods used to diagnose the disease, it becomes undeniable that the mythical status that surrounds this fear-based fictional narrative fed to the masses throughout the centuries is entirely unjustified and unwarranted. There is literally nothing there in support of rabies as a distinct disease caused by a specific “virus” that is transmitted to humans through the bite of a sick animal. If we were to lay out the facts in front of a jury, it would be an easy conviction:
The pivotal moments of discovery in the late 19th century were built upon the fraudulent foundations laid out by Louis Pasteur, a man who manipulated and massaged his own data in order to sell his theories and his vaccine for fame and fortune.
The supposed “isolation” of the “virus” didn’t even take place until nearly a century after Pasteur admitted to never identifying a causative agent and yet it missed the necessary requirement of showing any indirect evidence of the “virus” highjacking the cell as the culture lacked any evidence of the cytopathogenic effect.
The actual correlation between animal bites and symptoms of disease was considered highly uncertain and those who were attacked and bitten by clearly rabid animals could easily forgo any treatments without any ill health effects.
The incubation period for the disease is inconsistent and is said to range anywhere from 6 weeks on up to 25 years before the development of symptoms.
The severe symptoms associated with rabies are a rare occurrence in nature and are in fact seen most frequently as an adverse reaction to the vaccine said to contain neurotropic ingredients.
The acknowledgment by Pasteur of “false rabies,” which was said to be brought about solely by FEAR of aquiring the disease as well as alcohol and/or drug use, was used to take attention away from his vaccine causing injury and death.
The statistics regarding rabies cases were considered unreliable due to the lack of any specifuc disease-defining symptoms as many diseases in animals and humans mimic the clinical picture.
The diagnosis of rabies, for much of its history, relied upon clinical symptoms and the histopathological findings related to encephalitis and Negri bodies, all of which are non-specific and are not suitable as a diagnostic measure for the disease, thus calling into question any case statistics related to rabies.
The only way to claim pathogenicity of the “virus” is by way of the completely unnatural route of intracranial inoculation of diseased brain and nervous tissues directly into the brains of dogs and mice.
The more recent modern method of direct fluorescence antibody tests, considered the “gold standard” diagnostic test, is claimed to be highly sensitive and specific, yet the results of the tests are open to human interpretation and have been shown in reviews to have low sensitivity and varied specificity.
The narrative surrounding rabies is based upon many primal fears. It plays on the fear of death, the fear of the unknown, and the fear of mutilation. Just like the rabid animal lurking in the shadows ready to strike, the “virus” hides inside the body once infected, waiting for the right moment to unleash a painful and excruciating death unless the infected leaps for the miracle cure in time. If they are a moment too late and the symptoms set in, it’s game over. This same scenario is regularly sold to the masses in our daily entertainment with the recent zombie craze. One must be afraid of the bite. Once bitten, the “virus” takes hold and the victim is condemned to certain death.
However, just as Louis Pasteur recounted tales of the fearful succumbing to the exact same symptoms in absence of any animal bite, we must realize that the real enemy here is not a “virus” but an ingrained fear that stems from outdated and unproven fictional narratives. Moreso than any of the other more common diseases of the time such as smallpox and syphilis, rabies was the perfect mascot to convince the doubting public that disease-causing pathogens exist, can be transmitted, and can be prevented by way of vaccination. The imagery of the dirty mangled dog stumbling down the road, frothing at the mouth and seeking its next victim to transfer its parasitic contents into was a powerful visual tool for pathogens that remained nothing but formless thoughts at the time.
However, the evidence consistently shows us that there is no dangerous invisible entity waiting in the wings inside the saliva of a rabid animal looking to seep into the open wound of a bite mark. There is no reason for any victim of an animal attack to subject themselves to the toxic treatments based upon the fear of an impending gruesome death. Just as there are no zombies coming for your brains, there is no frothing rabies “virus” looking to do the same. The foundation for germ theory and vaccination established by Pasteur was never built from any purified and isolated “virus” shown scientifically to exist in nature. It was built upon the only “virus” that has ever truly existed: the “virus” of fear.
For an excellent breakdown of the rabies fraud, please see Dr. Sam Bailey’s What About Rabies? video:
I’m moving on from Part 1 into a completely different area.
There is lab work in the sciences that crucially affects populations. Two examples: virologists claiming they’ve isolated SARS-CoV-2; and researchers deciding they’ve found a way to adapt RNA technology to produce a COVID vaccine.
In the first case, the purported discovery of SARS-CoV-2 enabled the launch of the global pandemic announcement, which eventually led to the lockdowns and the crashing of economies. In the second case, the RNA-vaccine “breakthrough” led to the vaccination of billions of people, and massive numbers of injuries and deaths.
These are crucial effects, to say the least.
And yet, those on the outside, who have no access to these labs AS THE WORK IS BEING DONE, those who are independent scientists and analysts and can only read the studies once they are published—
—This is an unconscionable situation, when you stop and think about it.
The whole world is changed by the research, but we can’t watch it IN PROGRESS.
People have been brainwashed into thinking this lack of access to labs is normal. Standard. Non-official persons entering these labs and tracking the work step by step would amount to a criminal invasion. That’s what we’re supposed to believe:
“Just accept our statements about our findings and shut up and obey.”
“We’re the pros. You’re the idiots.”
“We’re certified. You’re the guinea pigs.”
“Call security, call the FBI, call DHS, terrorists are trying to break into our lab.”
“This is a holy sanctum, anointed by God. You’re a mortal sinner.”
Here’s my kind of debate on the existence of SARS-Cov-2. Here’s my bottom, bottom line.
Virologists are compelled to replicate, in the lab, the so-called discovery of SARS-CoV-2. An outside team of truly independent scientists and journalists is present.
So is a camera crew. With many cameras. And many mics.
The team watches every single move the virologists make. Any member of the team can stop the work and ask a question or criticize a move.
The questions and answers and the criticisms and replies are all recorded. Ditto for every action the virologists take.
THIS is a REAL debate. The most real debate.
“Wait. That’s ridiculous. You can’t expect these highly trained virologists to submit themselves to this kind of…inspection.”
Of course I can.
For example: Our team member in the lab says, “All right, you’re observing that the monkey cells and the human cells in this soup you’ve created are dying off. You claim the killer must be ‘the virus’ in the patient’s tissue sample—the sample you dropped in the soup. You claim nothing else in the soup could be killing the cells. So let me ask you this? Where is the control experiment?”
“The what?”
“The control. My, my. You really forgot about that?”
“I don’t understand. Turn off the cameras.”
“Leave them on, boys. This is interesting. Let me explain, Dr. High Horse. You should have a second dish of soup that is absolutely identical to the first dish, except the second dish does NOT contain the tissue sample from a patient. You also keep an eye on that second dish and see whether the monkey cells and the human cells in it die off. If they do…then your contention that ‘the virus’ in the patient sample is killing those cells is worthless. And you have no evidence your virus is in the patient sample. Or that it exists.”
“Oh. Well…”
“Well, what? You don’t mean to say all those virologists in all those labs who claimed they found the new virus omitted the control experiment, do you?”
YOU KNOW, THAT KIND OF THING. THAT KIND OF INVESTIGATION.
On camera, in the lab, in person.
“That would never happen. They would never let you in there.”
Which proves what? I’m just stating what the MOST REAL DEBATE WOULD CONSIST OF, in a half-sane world. It would look exactly like that.
Here’s a parallel for you. A civilian no one ever heard of develops a car he says runs on water. He says he’s got a new process that VERY cheaply splits the water into hydrogen and oxygen, and the car runs on the hydrogen.
Over years and decades, the legend grows. Finally, major media are starting to nibble around the edges of the story.
So one day, a bunch of Saudis and oil execs and scientists and men in suits show up at this man’s garage, and express great interest in his work. THEY REALLY WANT TO KNOW WHETHER THIS CRAZY GUY HAS STUMBLED ON A REVOLUTIONARY WAY TO POWER A CAR.
So what would they ask him to do?
See, they’re the outsiders with no access, and he’s the insider.
Are they just going to ask him for assurances?
Hell no. They’re going to ask him to take the engine apart and put it back together again. They’re going to ask him to take the fuel system apart and put it back together again. They’re going to want to go through his whole car and his garage and his kitchen and his bathroom with a fine-toothed comb. BECAUSE THEY WANT TO GET TO THE BOTTOM OF THIS SITUATION, SINCE IT COULD AFFECT THE FUTURE OF CIVILIZATION, AND THEIR PROFITS, AND SO ON.
They’re not screwing around.
And neither should we.
Our lives and futures and the lives of future generations are on the line with this “virus thing.”
We should be looking at every beaker and tube and slide and instrument in the virology lab. We should be looking over the shoulders of the virologists and watching every move they make and asking pointed questions and demanding answers.
So we really know whether they’re doing science or preposterous bullshit.
And of course we wouldn’t be paying attention to random assurances from “highly qualified and respected scientists” along the way. We’d be studiously ignoring them.
If you need another parallel to the real kind of investigation I’m demanding, think of bringing a team into the Vatican and inspecting every inch of space in every building, including the basements and caverns…to see what’s really there. The whole enchilada.
All right, you get the idea. You see what I’m asking for.
Now, short of that, what do we have? What can we get access to?
Well, it’s not entirely reliable, but here it is:
We can read published studies which claim to have found SARS-CoV-2. Those studies all have methods sections. In them, the researchers describe, step by step, what they did to “isolate the virus.”
We have that.
I’m now going to republish one of those methods sections, chunk by chunk, and have Dr. Andrew Kaufman make his criticisms as we go along. I published all this about a year ago.
I want to emphasize that Dr. Kaufman’s analysis should be just the beginning of highly detailed analyses of these methods sections, from a number of other independent critics. We need much more of this.
The devil is in the details.
Here we go:
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)”.
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO). Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
Readers who are unfamiliar with my work (over 500 articles on the subject of the “pandemic” during the past two years) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
The answer is no.
As I stated, Dr. Kaufman’s analysis should be just the beginning of intense and detailed examination of studies that describe “how the virus was isolated.”
As opposed to a few hours of Zoom debate in which people summarize their opposing positions, and then submit to a vote from a panel of judges who descend from the sky with motives as pure as Superman and Wonder Woman. All this happens with Steve Kirsch in the background holding a million dollar prize. In Vegas, Steve would be called the house. And the house always wins.
One of the many unfortunate side effects of the attention which has been given to the covid-19 jabs is the fact that more traditional vaccinations (including the dozens routinely given to children) have been forgotten and are now largely administered without protest, controversy or a second thought.
There was always a danger that the justifiable outrage and fear engendered by the covid-19 jabs would push the wider issue of traditional vaccination into the background. The experimental and notably toxic covid-19 jabs have understandably and rightly captured the attention of those who aren’t prepared to accept the lies, the deceits and the manipulations at face value.
But it is important that we don’t forget the ever-growing hailstorm of vaccinations, aimed particularly at children, which have seemingly become an integral part of our relationship with health care in general and doctors in particular.
We all know that the establishment and the mainstream media refuse to debate the mRNA jabs.
But it is, I suspect, less widely known that there has for a long time been a blackout on any discussion of the more traditional vaccines or that the reputation of vaccines is built on a toxic mixture of myths, fallacies and plain, vanilla lies.
I’ve been writing about vaccines for over 50 years but rather to my surprise it was 2011 before I wrote a book entirely devoted to vaccines and vaccination.
I wrote the book (Anyone who tells you vaccines are safe and effective is lying. Here’s the proof.) partly to provide evidence proving that vaccines are often dangerous and don’t work but also to destroy the outrageous, manufactured myth that vaccination has extended life expectancy and eradicated diseases such as smallpox and whooping cough.
I’ll get back to that theme in a moment but first I think it is worth using the history of that book to illustrate the extent of the media blackout which exists to protect vaccines and vaccination.
Knowing that none of my usual publishers would touch a book about vaccines, I published it myself.
We sent out 600 review copies, hoping that one or two reviewers might be brave enough to consider the book on its merit. However, to the best of my knowledge, not one reviewed it. People I’d known for years wouldn’t discuss it. Moreover, quite a number of reviewers returned the book. It is usual practice for reviewers to sell books they don’t want to keep on their shelves. But journalists actually spent time and money returning the book!
I knew there were risks in writing a whole book about vaccines. It has always been a topic which has aroused anger within the medical establishment. In the Preface I wrote: ‘Experience tells me this book will bring me much trouble, a great deal of abuse, a number of threats and considerable professional and personal inconvenience’.
But even I was surprised at how quickly I became persona non grata. My questioning of official establishment policies had, for a long time, made me unpopular with the establishment. It quickly became apparent that vaccination is a taboo subject and that vaccines are protected from criticism in the way that film stars were protected in the 1930s.
Since its publication there have been concerted efforts to ban the book and have it removed from sale.
No one has ever questioned the science, the statistics or the conclusions in the book. Critics have, however, been upset by my criticism of ‘the establishment’s unquestioned enthusiasm for a practice which is of such doubtful value and which offers such potential for disaster’.
I described vaccination as `a massive confidence trick’ and predicted (in 2011 remember) that ‘vaccination will become compulsory in the West’. I have been lied about constantly by thousands of rabid supporters of vaccination.
It seems that the mainstream media has devoted itself to promoting vaccines and never allowing any aspect of vaccination to be questioned. The BBC actually has a policy of excluding all vaccine criticism from its programmes. Merely questioning the validity of vaccination draws a torrent of abuse down upon the questioner’s head.
The inevitable result is that vaccination programmes continue pretty well unhindered and millions of children are now regularly jabbed with products which have never been properly tested or evaluated either for safety or efficacy.
The most potent claim for vaccines is, as I’ve already mentioned, that they have saved millions of lives. (This claim is now being falsely applied to the covid-19 jab which cannot be proven to have saved any lives at all). The fraud is maintained by pointing to average life expectation but this is a false argument for the figures are skewed by the vast number of babies and infants who used to die of disease or malnutrition. Every infant death drags down life expectation dramatically.
All around the world, infants and children are now subjected to a seemingly endless series of assaults on their immune systems. The vaccines used have never been adequately tested to see how they might interact or how they might affect other medications. Very few long-term trials have been done though the few available confirm my scepticism. For example, in 2017, the Danish Government and a Danish vaccine maker, funded a study of the DTP vaccine. The WHO and the medical establishment claim that the DTP vaccine saves millions of lives but, after looking at 30 years of data, the scientists concluded that the DTP vaccine was probably killing more children than died from diphtheria, pertussis and tetanus prior to the vaccines introduction. The vaccine had ruined the immune systems of children rendering them susceptible to death from pneumonia, leukaemia, bilharzia, malaria and dysentery.
The results of that trial changed nothing. The vaccination continued unhindered.
The vaccines most often described as having changed the world are those for polio, whooping cough and smallpox. But look at the evidence.
With polio the truth is that with other infectious diseases the significance of polio dropped as better sanitation, better housing, cleaner water and more food were made available in the second half of the 19th century. Look at the evidence and it shows that the number of polio victims went up not down as a result of vaccination. In Tennessee, USA (chosen at random) the number of polio victims before vaccination became compulsory was 119. The year after vaccination was introduced the figure rose to 386. In America as a whole the number of deaths from polio had fallen dramatically before the first polio vaccine was introduced but the incidence of polio increased by around 50% after the introduction of mass immunisation.
Of even more significance (which I revealed in my book `Why Animal Experiments Must Stop in 1991) 17 million people who were given polio vaccines as children in the 1950s and 1960s are now at risk of developing cancer. This is because the first practical vaccine used monkey kidney tissue – which contains a carcinogenic virus. Moreover, the virus can be passed on to the children of those who were given the contaminated vaccine. Could this explain the ever rising number of people with cancer? We’ll never know. The doctor who first warned of this risk was ignored and her laboratory was closed down. The documents showing who had received the dangerous vaccine were destroyed by the Department of Health in 1987 though it seems likely that millions of doses of the dangerous polio vaccine were used despite the risk.
The smallpox story is equally startling.
The myth that smallpox was eradicated through a mass vaccination programme is just that – a myth. Smallpox was eradicated through identifying and isolating patients with the disease. One of the worst smallpox epidemics of all time took place in England between 1870 and 1872 – nearly two decades after compulsory vaccination had been introduced. The people of Leicester refused the vaccine and there was only one death. In contrast there were massive numbers of deaths in towns where people had been vaccinated.
German doctors are taught that it was the Reich Vaccination Law (making vaccination compulsory) which halted smallpox in their country. But the incidence of smallpox had dropped before the law came into action. Once again, a legally enforced national vaccination programme did not eradicate the disease.
Look at history and it is clear that the number of cases of smallpox has gone up each time there has been a mass vaccination programme.
It’s worth remembering too that Dr Jenner, a hero for pro-vaccine folk, refused to have his second child vaccinated after he’d tried his smallpox vaccination on his own son. Tragically, the boy remained mentally retarded until his death at the age of 21.
Everywhere you look the evidence is the same: vaccination doesn’t work. Moreover, it is not difficult to sustain the argument that it does more harm than good.
Sadly, the medical establishment and the media have for years conspired to suppress the truth and to demonise the truth tellers.
The suppression of the truth about the covid-19 jab is nothing new.
Now the people of South Africa need our help. Please see the instructions after this letter to learn how you can make your voice heard before the August 5 deadline (click here to see time remaining).
“We cannot trample upon the humanity of others without devaluing our own. The Igbo, always practical, put it concretely in their proverb Onye ji onye n’ani ji onwe ya: ‘He who will hold another down in the mud must stay in the mud to keep him down.’”
—Chinua Achebe, The Education of a British-Protected Child: Essays
“Apartness” in Afrikaans, “apartheid” is the institutionalized system of segregation. You can change the definitions of the targeted parties, but you cannot change the discriminatory rot underlying this vile legislation.
The People’s Lawctivist Sabelo Sibanda explains that under the proposed amendments:
“These regulations basically declare a scenario where everyone will end up in one of three categories where you are either deemed to be a case, or you are considered a suspect, or, alternatively, you are considered as one who has been in contact with someone who is a case.
“And once you fall into any one of those three categories, this is what this means to you. Government says, ‘You may not refuse to be medically examined,’ whereby the medical examination process is whatever government will determine.
“Second to that, you may not refuse to be put in quarantine or put in isolation. And the requirements for quarantine and isolation are such that the majority of the people of South Africa will not be able to self-quarantine so they have to be put in a state institution.
“Further to that, and most critical, is that you may not refuse to take whatever medication that the government says you should take. Your freedom—which is supposed to be guaranteed and protected by the same act in as far as the right to be informed—is taken away. You are caught in a situation whereby government has full control.
“Once you are put in this isolation space, this quarantine space, you don’t have the ability to determine when and how you get out. It will be up to government to decide.
“So now the country of South Africa will be under a permanent state of disaster where masking will be permanent, where social distancing is permanent, through the National Health Act.”
In case you’ve forgotten what it looks like for your government to discriminate against citizens under the guise of a “state of emergency” and to demand people’s papers, here are a couple of reminders:
Today, that passport looks like a QR code on your phone.
Please take a few moments to read the following articles to understand why there is no circumstance under which it is ethically or morally acceptable to deprive individuals of their freedoms and human rights in the name of the “public good,” which can be defined according to the whims of despots and demagogues:
And if you want to understand what it feels like to be institutionalized and have medication forced on you against your will, here’s a preview of the world you would be creating:
Nurse Pilbow: Mr. McMurphy?
McMurphy: Huh?
Nurse Pilbow: Your medication.
McMurphy: What’s in the horse pill?
Nurse Pilbow: It’s just medicine, it’s good for you.
McMurphy: Yeah, but I don’t like the idea of taking something if I don’t know what it is.…
Nurse Ratched: If Mr. McMurphy doesn’t want to take his medication orally, I’m sure we can arrange that he can have it some other way.
The people of South Africa poured decades of passion, blood, and song into eradicating apartheid:
Do not let that effort be for naught. As Chinua Achebe says:
“The damage done in one year can sometimes take ten or twenty years to repair.”
Do not let fear, hatred, panic, and intolerance win. Cast out those totalitarian demons and save your people by rejecting amendments 1882, 1883, 1884, and 1885.
“Yet men were afraid, with a fear that was deep, deep in the heart, a fear so deep that they hid their kindness, or brought it out with fierceness and anger, and hid it behind fierce and frowning eyes. They were afraid because they were so few. And such fear could not be cast out, but by love.”
Let me be clear. I’m speaking for myself here, as a reporter who says SARS-CoV-2 doesn’t exist. I’m not speaking for Andrew Kaufman, Stefan Lanka, Tom Cowan, Christine Massey, Sam Bailey, or anyone else who has come to the same conclusion.
OK. Steve Kirsch frames the debate (see also here) this way: There are a set of facts about COVID you can lay on the table. Then you decide which hypothesis best explains those facts.
In his case, he chooses: “SARS-CoV-2 exists.”
This approach is an elementary mistake.
I’m not challenging any hypothesis. I’m ATTACKING A STRAIGHT-OUT LABORATORY PROCEDURE.
My attack is on the level of: “You poured the liquid from beaker A into beaker B. Wrong. You should have poured it into beaker C.”
Virologists employ a lab procedure to discover a virus they’ve never seen before. They claim this procedure ISOLATES the virus from all the surrounding material in a soup they create. I say their procedure doesn’t produce that result at all. Period.
I say there is no isolation.
That’s it in a nutshell.
Arguing about hypotheses is entirely beside the point.
But I will write a few words on that subject, just to clear the air.
If a real scientist laid a whole collection of facts on the table, he would then do a hard examination of each one, to make sure it is a true fact. When satisfied, he might sit and think and ask himself, “What hypothesis would explain these facts?”
Let’s say he comes up with one. That’s just the beginning of doing actual science. Why? Because the only scientific value of a hypothesis is its ability to PREDICT.
And by that I mean, MAKE A SPECIFIC AND VERY USEFUL PREDICTION THAT CAN BE VERIFIED OR DENIED BY ACTUAL EXPERIMENT.
Claiming a hypothesis which explains a set of facts as a reason to pop champagne corks signals a gross misconception about what science is.
Forming a debate on that basis would be futile, irrelevant, and a waste of time.
Finally, for now, carrying out a debate on video may impart useful information to viewers, but there is a reason why medical and science journals stubbornly persist in presenting studies as words on the page—as opposed to having the authors dress up and describe their work on camera instead.
Words on the page are much better.
They allow other scientists, journalists, and civilians to go over a study very carefully, phrase by phrase. They allow other scientists to REPLICATE the authors’ work, in order to discover whether the results and conclusions stand up.
Of course, in this “fast moving world, with people on the go, living the active lifestyle,” we should perhaps adopt Easier and Quicker as the mode of scientific decision-making.
“OK, Fred, are the cameras set up, are we ready to roll? Are all the debaters online? Have you got the poll screen in place, so the viewers can vote and decide what’s science and what isn’t when we’re done?”
I’m breathless with anticipation.
On the other hand, if we have “a panel of independent experts” on hand to make that ruling, we can rent them out, in the future, to The New England Journal and The Lancet. Yes, a roving panel making all sorts of judgment calls. They’ll spice up science, which is badly in need of instant melodrama and boffo box office.
Hell, let’s make this debate a game show.
“Great idea, Jim. A couple of tall models in bikinis walking around with big signs, and a host like, oh, Chris Wallace or that guy who keeps talking about laying down a bet for a million dollars. What’s his name? Kirsch. Steve Kirsch.”
Stevie, baby, nobody cares about your money. Nobody cares about your million dollars.
A few weeks ago, I was invited by Michael Wallach, the director of the amazing docu-series The Viral Delusion, to join him as a guest on the Skeptico podcast. It was an interesting experience to say the least. We were under the impression that the conversation would be focused on the gain of function/lab leak theories as well as HIV and we had prepared ourselves to discuss these topics. However, the conversation instead took a detour when the host, Alex Tsakiris, changed the focus to rabies instead, an area he felt was left unexplained by those of us stating that “viruses” do not exist. He presented us with a graph showing statistics of rabies cases declining with the use of vaccines. Unfortunately, at the time that we were interviewed, Alex was unable to provide us with a source for the information that he shared with us. Neither Michael nor I had ever seen this graph before, however it really wasn’t the issue as vaccine statistics do not prove a “viral” cause.
Unfortunately, the rabies graph became the bulk of our time on the show. Michael Wallach did an excellent job explaining the problems with the lack of evidence behind the rabies “virus” as well as the fraud of Louis Pasteur. I wanted to chime in more to help out (not that Michael needed me to) but sadly Alex was not really interested in what I had to say about the subject. You can view our conversation with Alex on the Skeptico podcast here:
As I was unable to speak much on the topic with Alex, I want to present some information here that may help to answer his questions as to why rabies cases appeared to decline as the vaccine was introduced. However, before addressing the graph, the first thing that needs to be understood is that at no time has a rabies “virus” ever been properly purified and isolated directly from the fluids of any animal nor any human and then proven pathogenic by adherence to the scientific method. In fact, as he performed his experiments in the 1870’s and 1880’s, Louis Pasteur provided no theoretical basis for the vaccination of rabies as he admitted that he had failed to isolate the microbe that was presumed responsible for the disease. He also massaged and manipulated his data in order to justify his claims as to the success of rabies vaccination. Pasteur was a fraud who was more concerned with fame and prestige rather than performing valid scientific research. I wrote about his unethical practices involved with the early rabies research as well as how the rabies vaccines actually produced the severe neurological symptoms often associated with the disease here.
Later attempts to propagate the “virus” in the 1950’s, which were claimed to be successful, were done in hamster brain and kidney cultures. Interestingly, it was noted that no cytopathogenic changes, the very criteria used by virologists to claim ‘viruses” are present within these cultures, occured whatsoever.
doi: 10.3181/00379727-98-23997.
Even by the CPE standards used by virologists as a measure for the successful isolation of a “virus,” they had failed to “isolate” rabies in their cultured samples. As no rabies “virus” has ever been scientifically proven to cause the disease, there is no basis to claim that the symptoms associated with rabies are caused by a “virus.” Still, in spite of being given this information, Alex continued to focus on his graph as if the effect credited to the vaccine was somehow proof of a “viral” cause. However, one can not look to an effect in order to claim a cause. This is a logical fallacy known as affirming the consequent. It is often stated like this:
In other words, if rabies is caused by a “virus,” the vaccine will lower cases. The cases declined with vaccine use, therefore rabies is caused by a “virus.” Obviously, this is not a logical statement as there are many variables and factors unaccounted for that could lead to the appearance of a vaccine having a positive effect on rabies cases. It should also not need to be stated that just because a vaccine appeared to work does not mean that the cause of rabies was a “virus.” A rabies “virus” must be scientifically proven to exist first in order to be tested for as the cause of the symptoms of disease associated with it. This has never been done.
We therefore must ask ourselves a very important question:
Did the rabies vaccines really cause rabies cases to fall or are there other potential reasons for the apparent decline?
Let’s try to answer this by looking at the graph Alex provided on the air. Fortunately, I was able to find the source for the image. It came from the CDC’s own data from the Morbidity and Mortality Weekly Report in July 2019. The study was titled Vital Signs: Trends in Human Rabies Deaths and Exposures — United States, 1938–2018.
What we can find out is that rabies cases were exceedingly rare over the entire graph period, with only 588 cases of human rabies reported in the United States from 1938 to 2018. In fact, there was a sharp decline in rabies cases a few years prior to the mass vaccination of dogs in 1947, which is often the case when looking at the decline in disease before the introduction of vaccination. Of course, the vaccine is given the credit even though the cases were well in decline beforehand.
So what could have caused this sharp drop before and after vaccine introduction? If you have looked into the decrease in diseases claimed to have been caused by other “viruses,” it is easy to spot a certain trend. Often times, the symptoms of disease claimed to be declining due to vaccination are reclassified either as a new or related disease caused by a new or related “virus.” Smallpox was rebranded as chicken and/or monkeypox, polio became acute flaccid myelitis, syphilis morphed into AIDS, influenza transformed into “Covid,” etc. etc. etc. This trend of rebranding and relabelling the same symptoms of disease as either new diseases or similar ones can easily be seen with rabies and the rabies-related “lyssaviruses.” While the rabies “virus” is considered a “lyssavirus,” there are numerous other “viruses” under this same heading that are considered “rabies-like viruses” that do not cause rabies per se but instead “rabies-like” disease:
Rabies and Rabies-Related Lyssaviruses
“Closely related lyssaviruses circulate among bats in the Eastern Hemisphere, and can cause an illness identical to rabies. Rabies vaccines and post-exposure prophylaxis can provide some protection against some of these viruses, but not others. Rabies-related lyssaviruses can be found even in countries classified as rabies-free.”
“Information about rabies-related lyssaviruses is currently limited to a small number of case reports and a few reports of experimental inoculation; however, the illness appears indistinguishable from rabies. Bats may either have mild or no clinical signs and survive the infection, or develop severe neurological signs and die.”
This is a nice convenient scapegoat which allows a country to declare itself rabies-free even though the same symptoms of disease still persist. For example, in Austraila you will find disclaimers such as this:
According to Australia, they are rabies-free even though the same symptoms of disease persist within the country. These cases are blamed on the Australian bat “virus” which is claimed to cause a “rabies-like” disease. Quite convenient, right? However, what if the classification system for these “lyssaviruses” were to change? Would a country that is considered rabies-free lose its illustrious status?
Lyssaviruses and rabies: current conundrums, concerns, contradictions and controversies
“With increasing ICTV debate toward unification of virus taxonomy based on genetic distances, in the near future there may be a re-classification attempt, in which all phylogroup I viruses are segregated into one species (for example, Rabies lyssavirus?) and all phylogroup II viruses are segregated into another. Of course, such re-classification would miss important characteristics used for species demarcation at present and may have potential socio-economic or bio-political consequences for certain areas. For example, some places where RABV is not thought to circulate, such as in Australia or Western Europe (but where other lyssaviruses are present among bats), might lose their self-defined “rabies-free” status, on the basis of viral taxonomic re-organization, creating greater confusion, with potential public health, veterinary, or economic repercussions, if suddenly recast into the same disease status as Africa, Asia and the New World. Arguably, the term “rabies” appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”.
The loose definitions allow countries such as Austrailia to claim rabies-free status even though the disease still persists there. If the definition and/or classification changes, so to will their status. This is similar to how America is allowed to claim it has been polio-free since 1979 while there are cases every year of acute flaccid myelitis and other polio-like diseases which present with the same sets of symptoms. We could easily relabel those polio-like diseases as polio and lose the polio-free designation.
While the same set of rabies symptoms can be blamed on the closely related “lyssaviruses,” they can also be blamed on unrelated “viruses” and conditions that are said to be caused by different “viruses,” bacteria, genetic abnormalities, and even poisons.. For instance, animals can be diagnosed with distemper instead of rabies. These two diseases have often been confused for one another as the symptoms are indistinguishable:
Raccoons – distemper and rabies
“Canine distemper in raccoons starts slowly, with respiratory infections then they develop pneumonia. In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage. Many of these symptoms are similar to rabies – which can only be determined by laboratory testing.”
“CDV is a highly contagious paramyxovirus that affects dogs and wildlife including raccoons, skunks, grey foxes, and ferrets. This virus is closely related to the human measles virus, and can lead to respiratory, gastrointestinal (GI), and central nervous system (CNS) problems. CDV is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar.”
There are many other diseases such as encephalitis and different neurological disorders which are also said to mimic rabies in animals. Even poisoning is stated to mimic the severe stages of the disease:
Diseases that can look like Rabies
“Encephalitis is one condition that can look somewhat like the early stages of rabies. In this condition, with is immune based in most dog breeds of dogs, the dog’s own immune system begins to attack the brain. The result is a dog that may be confused, appear to stagger and bump into things, or even a dog that seems very disoriented and lost even in familiar settings. The dog may also have temperament changes and may snap at owners or become very agitated when they have previously been calm and friendly.”
“Canine distemper is another disease that may be mistaken for rabies since the symptoms are so close to being the same.Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue. Since it is still a highly contagious disease it is essential to get your dog to the vet if he or she has had any contact with wild animals or other dogs that seem to be disoriented, have a discharge from the eyes or nose, paralysis and stumbling types of movements. Typically the wild animal will be non-threatened by human presence, which in itself is a sign of abnormal behavior. It is important to realize that distemper, unlike rabies, cannot be passed from an animal to a human. However it is important to stay away from any animal that appears to have any symptoms similar to rabies or distemper.”
“Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies. In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink.”
As can be seen from the above three sources, canine distemper and other diseases such as encephalitis can be confused with rabies due to the identical nature of the symptoms. These diseases still persist within dogs and other animals while rabies, or at least “dog rabies,” has been said to have been eliminated from the US and other countries. In other words, the rabies label is no longer applied upon diagnosis even though the same symptoms of disease circulate in animals within the country.
This merry-go-round among the same symptoms of disease does not stop with animals either. There are many conditions in humans that also mimic rabies. These diseases are outlined in this final source:
Beware: there are other diseases that can mimic rabies:
Diseases that can mimic encephalitic rabies:
viral encephalitis (i.e. Japanese, eastern equine, West Nile)
Louis Pasteur admitted to not isolating the agent presumed to cause rabies
In the 1950’s, attempts to isolate the “virus” in cultures of hamster brains and kidneys were deemed successful despite the lack of observing any cytopathogenic effect (CPE)
Many “viruses” that are said to be eliminated or controlled through vaccination were rebranded and relabelled as either similar diseases caused by related “viruses” or new diseases caused by new “viruses”
Regarding rabies, closely related “lyssaviruses” circulate among bats in the Eastern Hemisphere and can cause an illness identical to rabies
Rabies-related “lyssaviruses” can be found even in countries classified as rabies-free
The illness associated with these rabies-related “lyssaviruses” appears indistinguishable from rabies
Some places where rabies is not thought to circulate, such as in Australia or Western Europe (but where other “lyssaviruses” are present among bats), might lose their self-defined “rabies-free” status, on the basis of “viral” taxonomic re-organization,
This would create greater confusion, with potential public health, veterinary, or economic repercussions, if they were suddenly recast into the same disease status as Africa, Asia and the New World
The term “rabies”appears to garner greater weight and seriousness than the less familiar designation “bat lyssavirus”
Canine distemper is a rabies-like illness in animals
In raccoons, it starts slowly, with respiratory infections then they develop pneumonia
In the final stage of the disease, the raccoon may begin to wander aimlessly in a circle with bizarre behaviour as a result of brain damage
Many of these symptoms are similar to rabies – which can only be determined by laboratory testing
Canine distemper is often confused with other infectious diseases, including rabies, because the organ systems affected and clinical signs are similar
It is mistaken for rabies since the symptoms are so close to being the same
Even wild animals such as raccoons, foxes and coyotes can have distemper that can even further confuse the issue
Encephalitis is another condition that can look somewhat like the early stages of rabies
The result of this brain swelling is a dog that may be confused, appear to stagger and bump into things, or even seems very disoriented and lost even in familiar settings
Other neurological conditions, some which are fatal and contagious and some that are strictly a result of a genetic or inherited condition can mimic the early signs of rabies
In rare cases animals that are poisoned and those with neurological conditions can exhibit the same signs as advanced stages of rabies including paralysis, drooling, sensitively to light and sound, dramatic changes in behavior and even refusal to eat or drink
In humans, there are many diseases which mimic rabies:
Diseases that can mimic encephalitic rabies:
“viral” encephalitis (i.e. Japanese, eastern equine, West Nile)
For some reason, people seem to think rabies is a “gotcha” for those of us claiming that “viruses” do not exist. This disease is thrown out as proof that vaccines are effective and that because of this, the “virus” must therefore exist. However, a big problem for anyone championing rabies as proof for the existence of “viruses” continues to be the lack of any purified and isolated “virus” particles coming directly from the fluids of a rabid host. Louis Pasteur openly admitted to failing to meet this burden of proof even though he subjected animals and humans to experimental injections. Attempts by researchers in the 1950’s to propagate the “virus” in tissue and cell cultures did not produce the characteristic cytopathogenic effect said to be necessary in order to determine if a “virus” is present in a culture. Thus, there is no scientific proof for the existence of the rabies “virus,” even by virology’s own standards.
As the rabies “virus” can not be shown to exist, any data relating to a decrease in cases due to a vaccine which is then used as proof for the existence of a rabies “virus” is entirely irrelevant. There are many reasons to doubt case statistics as these can be easily manipulated and massaged in order to create whatever narrative is desired. It can be seen that the same symptoms associated with rabies still exist today as there are many other diseases either said to be caused by rabies-related “viruses” or completely unrelated “viruses” that share the exact same symptoms associated with rabies. These diseases are more commonly diagnosed in areas where rabies is said not to be circulating. It is very apparent that virology loves to rebrand and relabel the same symptoms of disease as multiple “new and different” diseases in order to create the perception that the treatments work. This is why places like Austrailia get to claim to be “rabies-free” even though a rabies-like disease said to be caused by a rabies-like “virus” still exists there. This lowers the cases as the older diseases are claimed to be either eradicated and/or under control due to “successful” vaccination campaigns and thus they are not looked for as a diagnosis. There is no way that these statistics can be trusted when the definitions and labels of what is or is not rabies seemingly changes at will.
In any case, the rabies statistics are a moot point. Until someone can provide proof of the purification and isolation of the particles assumed to be rabies directly from the fluids of a rabid host which were proven pathogenic in a natural way, these case numbers are utterly meaningless. The conversation with Alex on the Skeptico podcast should have never even reached vaccination statistics unless he provided a paper showing the evidence for the existence of a rabies “virus” first. Unfortunately, while Michael did an admirable job defending our position, we were not prepared for the graph and did not get the chance to look over the data and present our counter-argument. Hopefully we can get the chance to go on again and discuss the issue in further detail in the future. However, if not, this response will have to suffice.
Yesterday, I had the absolute pleasure and honor of being on Dr. Tom Cowan’s Wednesday webinar to discuss a follow-up on the No “Virus” Challenge. We addressed a paper that was supplied by Steve Kirsch and Co. as the “irrefutable evidence” for the existence of “SARS-COV-2.” The paper, a June 2022 non peer-reviewed preprint written by Dr. Sin Lee, is nothing but meaningless genomic data based on a fraudulent “SARS-COV-2” genome from January 2020. For some reason, the Fan Wu paper supplying the original fraudulent genome was not presented as “irrefutable evidence.”
Also discussed are cyro-EM images said to be considered evidence of live “virus.”
Please watch the webinar and find out why neither the genomic data nor the EM images constitute “irrefutable evidence” of a “virus” that was never purified and isolated.
Live Webinar With Dr. Andrew Kaufman, Mike Stone, and Mike Donio – Recorded on July 27th, 2022
In this webinar, along with Dr. Andrew Kaufman, Mike Stone & Mike Donio, we discussed the Virus Challenge in further detail.
Note: In a number of articles, I’ve offered compelling evidence that the deaths attributed to COVID-19 can be explained without reference to a virus. Furthermore, whatever merits “alternative treatments” may have, I see no convincing evidence their action has anything to do with “neutralizing a virus.”
The entire tragic, criminal, murderous, stupid, farcical COVID fraud is based on a hundred years of Rockefeller medicine—a pharmaceutical tyranny in which the enduring headline is:
ONE DISEASE, ONE GERM.
That’s the motto engraved on the gate of the medical cartel.
—Thousands of so-called separate diseases, each caused by an individual germ.
“Kill each germ with a toxic drug, prevent each germ with a toxic vaccine.”
In the absence of those hundred years of false science and propaganda, COVID-19 promotion would have gone over like a bad joke. A few sour laughs, and then nothing, except people going on with their lives.
The overall health of an individual human being has to do with factors entirely unrelated to “one disease, one germ.”
As I quoted, for example, at the end of a recent article—
“The combined death rate from scarlet fever, diphtheria, whooping cough and measles among children up to fifteen shows that nearly 90 percent of the total decline in mortality between 1860 and 1965 had occurred before the introduction of antibiotics and widespread immunization. In part, this recession may be attributed to improved housing and to a decrease in the virulence of micro-organisms, but by far the most important factor was a higher host-resistance due to better nutrition.” Ivan Illich, Medical Nemesis, Bantam Books, 1977
And Robert F Kennedy, Jr.: “After extensively studying a century of recorded data, the Centers for Disease Control and Prevention and Johns Hopkins researchers concluded: ‘Thus vaccinations does not account for the impressive declines in mortality from infectious diseases seen in the first half of the twentieth century’.”
“Similarly, in 1977, Boston University epidemiologists (and husband and wife) John and Sonja McKinlay published their seminal work in the Millbank Memorial Fund Quarterly on the role that vaccines (and other medical interventions) played in the massive 74% decline in mortality seen in the twentieth century: ‘The Questionable Contribution of Medical Measures to the Decline of Mortality in the United States in the Twentieth Century’.”
“In this article, which was formerly required reading in U.S. medical schools, the McKinlays pointed out that 92.3% of the mortality rate decline happened between 1900 and 1950, before most vaccines existed, and that all medical measures, including antibiotics and surgeries, ‘appear to have contributed little to the overall decline in mortality in the United States since about 1900 — having in many instances been introduced several decades after a marked decline had already set in and having no detectable influence in most instances’.”
How the immune system (if it is a system) actually operates is beyond current medical hypotheses.
“T-cells, B-cells, neutrophils, monocytes, natural killer cells, proteins,” are welded into a breathless story about a military machine that attacks germ invaders. Push-pull. Search and destroy.
The notion that THIS is what creates health is fatuous.
Positive vitality is what keeps us healthy.
A few factors of positive vitality are on the tyrannical COVID list of what-should-be-squashed: financial survival; open mingling of friends and family; people looking (unmasked) at people; open communication without fear of censorship.
Nutrition and basic sanitation are key vitality factors, of course.
And then we have Purpose in Life: where are people pouring their creative energies?
Obviously, freedom from harmful medical treatment is necessary for vitality to flourish.
Suppression of LIFE, in order to stop a purported germ, is institutionalized death.
Modern medicine is sensationally exposed in a review I’ve mentioned dozens of time over the past 10 years: Authored by the late famous public health doctor at Johns Hopkins, Barbara Starfield, it is titled, “Is US Health Really the Best in the World?” It was published in the Journal of the American Medical Association on July 26, 2000.
It found that, every year in the US, the medical system kills 225,000 people.
Per decade, the death toll would come to 2.25 million people.
You won’t find that in CDC reports.
In 2009, I interviewed Dr. Starfield. I asked her whether the federal government had undertaken a major effort to remedy medically caused death in America, and whether she had been sought to consult with the government in such an effort.
Recently I joined a group of 20 doctors and scientists around the world who put their names to the “Settling the Virus Debate” statement. In this two-page document we suggested, “rather than engaging in wasteful verbal sparring, let us put this argument to rest by doing clear, precise, scientific experiments that will, without any doubt, show whether these claims are valid.” Some of the individuals who believe that the existence of pathogenic viruses is an established fact, proceeded to immediately disagree. One was Steve Kirsch, who attempted to distract from the central tenet of our statement, being that virology had failed to carry out scientific control experiments. In reality, it is clear that the virologists have not shown that their techniques of “viral” cultures, genomics, and clinical diagnostics are valid even on their own terms. Indeed, I have not seen Kirsch or anyone else provide evidence that the appropriately-controlled experiments we suggested in the statement have been performed.
Kirsch admitted, “this is not my field of expertise at all. I rely on other people around me who I trust.” I have written a previous article about why I think Kirsch should be careful about trusting other “experts.” However, he continues to favour this approach and one of his trusted parties includes the pathologist/virologist Dr Sin Lee. Lee wrote, “Tom Cowan claimed the virus has not been isolated. But the virus has been isolated by the CDC and marketed by ATCC as the control materials. I bought the virus as the control for my CLIA tests. Many others do.” We have covered the follies concerning these claims of “isolation” many times and the CDC certainly have no studies demonstrating the existence of a pathogenic particle termed ‘SARS-CoV-2’. The ATCC simply repeat the claim by the CDC that their listed product contains a “virus” – however as I outlined in my first “Warning Signs” article, following the trail back to the start does not lead to any evidence of a virus in the biological potions being passed around.
On 18 July 2022, Lee sent the following email to Dr Tom Cowan:
I have a Preprint manuscript currently under peer review as follows. ://www.preprints.org/manuscript/202206.0192/v1 There is irrefutable Sanger sequencing evidence that the virus exists and keeps mutating. If Dr. Tom Cowan disagrees, please write a critique to challenge my data and interpretation online in the open. I will respond. Other scientists can join in for the debate.
Dr Sin H. Lee, 18 July 2022
The preprint paper is titled, “Implementation of the eCDC/WHO Recommendation for Molecular Diagnosis of SARS-CoV-2 Omicron Subvariants and Its Challenges.” To expose the problems of virology it is crucial to examine the methodology section of any publication and in this case it is no different. In the “material and methods” section Lee stated that, “five (5) selective nasopharyngeal swab specimens collected from non-hospitalized patients with respiratory infection, which were confirmed to be true-positive for SARS-CoV-2 Omicron variant by Sanger sequencing.” Here we are straight into the deep end of virology’s circular reasoning: the “virus” has been confirmed to exist on the basis of detected sequences from some nasopharyngeal swabs. There is nowhere in the paper that any evidence is provided for the existence of an actual virus, that is, a tiny particle that acts as an obligate intracellular parasite and is capable of causing disease in a host.
The claim that the specimens were, “true-positive[s] for SARS-CoV-2 Omicron variant,” simply means some sequences that were previously deposited on genetic databases, and fraudulently declared to be “viral,” were being detected again. It doesn’t make any difference which sequencing technique is used, in this case bidirectional Sanger sequencing because the crucial issue is the provenance and clinical relevance of these detected sequences. This is the foundational issue in the entire COVID-19 fraud: there is no virus, simply sequences falsely claimed to be evidence of an actual virus. The World Health Organisation helped orchestrate the deception when it declared that a confirmed ‘case’ of infection with the invented virus is simply the detection of some of these sequences. We have covered this absurd circular reasoning in much of our work including in Sam’s 2020 video “What Is A Covid-19 Case?” (And rapid antigen tests are covered here.)
Back to Lee’s paper and in the following paragraph of the “material and methods” section, he described the, “RNA Extraction from Nasopharyngeal Swab Specimens,” as follows:
As previously reported [25-27], the cellular pellet derived from about 1 mL of the nasopharyngeal swab rinse along with 0.2 mL supernatant after centrifugation was first digested in a buffered solution containing sodium dodecyl sulfate and proteinase K. The digestate was extracted with phenol. The nucleic acid was precipitated by ethanol and redissolved in 50 μL of DEPC-treated water.
In other words, there was no step to demonstrate: (a) there were any “viral” particles contained within the samples, or (b) that the RNA came from such imagined viral particles. A reverse transcription polymerase chain reaction was then applied to these undifferentiated samples to generate amplicons ranging from 398 to 707 nucleotides in length. Most of these sequences spanned the so-called ‘Spike protein’ gene of the alleged SARS-CoV-2 genome, as that was the area of interest for the study. In the next step it was stated:
The crude nested PCR products showing an expected amplicon at agarose gel electrophoresis were subjected to automated Sanger sequencing without further purification.
In fact, at no stage was an attempt undertaken to purify any entity from the crude nasopharyngeal specimens. The entire basis of the study was built on the unestablished premise that the genetic sequences detected were already known to come from inside a pathogenic particle.
The “results” section then detailed the nucleotide sequences of the various amplicons that were generated from the crude samples. Some of the codons (three-nucleotide units that encode a particular amino acid or stop signal) were described as “mutated” on the basis of comparisons to other sequences previously deposited on the genetic databanks. The use of the word ‘mutation’ is problematic in itself, because it implies that a genome has been altered. A genome must belong to a discrete biological entity, so virology is once again misusing terminology to imply that a certain proof has been established. Lee’s study was simply looking at RNA sequences in uncontrolled experiments.
Those of us that dispute the virus narrative point out that no RNA (or DNA) sequences have ever been shown to come from inside any specific identifiable particle that fulfils the definition of a virus. Thus all RNAs can only be said to be expressed by a known organism, introduced artificially (e.g. synthetic mRNA injections) or be of unknown provenance. The “mutations” only exist within in silico models that have not been shown to be independent entities in nature. There are other reasons why RNA sequences can and do vary in dynamic biological systems and I can’t imagine that any virologist would disagree with this fact. Simply detecting RNAs is not enough to draw conclusions about their provenance. Other experiments are required to make this determination.
In our first COVID-19 Fraud essay we documented the original invention of SARS-CoV-2 by Fan Wu’s team who assembled an in silico “genome” from genetic fragments of unknown provenance, found in the crude lung washings of a single ‘case’ and documented in, “A new coronavirus associated with human respiratory disease in China.” Their in silico construct served as a reference for others to then “find” the same “virus” around the world, without evidence that such a particle actually existed.
In our soon to be published follow-up COVID-19 Fraud essay we will provide a more detailed explanation as to why detecting nucleic acid sequences per se in crude specimens or cell cultures does not provide the required evidence for “viruses.” In the essay we will also follow the trail back to the first ever declarations of “coronavirus genomes” in the 1980s and show that no viruses were demonstrated in any part of the trail. However, such sequence data is used to promulgate the illusion of “virus” family trees, or claimed “mutations” as discussed above.
Dr Lee’s paper does not even appear to be designed to demonstrate the existence of a postulated disease-causing particle. I sent him several questions including, “I have read the preprint and there does not appear to be a hypothesis presented – is that correct?”, “In your study there did not appear to be any controls (e.g. checking for selected sequences in other nasopharyngeal specimens from humans said not to have the alleged virus) – presumably that was by design?” and “What is your definition of a ‘virus’ in the paper?” Lee responded, “your questions are irrelevant to you [sic] intention to write a comment or critique on the manuscript involved,” and suggested I write something in the preprint website’s comment section.
Lee has provided a descriptive paper that omits a falsifiable hypothesis so it is unclear why he would present it as experimental evidence, let alone “irrefutable” evidence of the existence of SARS-CoV-2. His paper is inappropriately designed for this purpose and his claim engages in a circular reasoning fallacy: the genetic sequences are proffered as evidence of the virus, because it was presupposed that they come from the virus. We are asking, “where is the virus?”
Virology has a problem: It needs to show that “A” actually exists
It’s back to the drawing board for virology: it invented the theory of viruses, so whatever method it employs to prove their existence, it must satisfy that definition. In fact, do the virologists even have a theory? The definition of a scientific theory is:
an explanation of an aspect of the natural world and universe that has been repeatedly tested and corroboratedin accordance with the scientific method, using accepted protocols of observation, measurement, and evaluation of results.
Our “Settling the Virus Debate” statement proposes that the virologists need to employ the required scientific method as a starting point. It is not looking good for them because they have not even demonstrated any internal validity on their own terms. According to science they may not even have a theory. If they have a hypothesis, they need to specify an independent variable (in this case the postulated “virus”) and a dependent variable for analysis. Moreover, to even get started, the independent variable must first be shown to physically exist. I would implore Steve Kirsch to reconsider taking advice from these “experts” and to commence his own investigations into the house of virology. By scientific accounts, it is a house of cards.
Postscript
(Derived from: A. F. Chalmers, What is this thing called Science?, 2nd ed, 1982)
‘Observational statements are frequently presupposed by theory. Such statements are always made in the language of some theory and will be as precise as the theoretical or conceptual framework that they utilise is precise’. In this instance, a virus particle was not observed first and subsequently viral theory and pathology developed. Scientists of the mid and late nineteenth century were preoccupied with the identification of imagined contagious pathogenic entities.
‘The observations of the naïve inductionist did not identify a virus a priori, and then set about studying its properties and characteristics. The extant presupposition of the time was that a very small germ particle existed that may explain contagion. What came thereafter arose to fulfil the presuppositional premise’.
‘A popular view of scientific knowledge is that it is proven knowledge and scientific theories are derived in some righteous way from the facts of experience acquired by observation and experiment. Science is based upon what we can see, hear, measure and touch. Science is objective and explicit. Scientific knowledge is reliable knowledge because it is objectively proven knowledge’.
‘A realistic scientific theory will consist of a complex of universal statements rather than a single statement. Further a theory will need to be augmented by auxiliary assumptions, such as laws and theories governing the use of any instruments used, for instance’.
‘The premises from which the prediction is derived must also include the interconnected statements that constitute the theory under test, the initial conditions, and the auxiliary assumptions. Falsification of the theory also indicates the possibility of a failure of any number of the associated assumptions and conditions, and not necessarily of the theory itself’.
Acknowledgement
I would like to express my gratitude to Dr M. C. McGrath (New Zealand) for his constructive criticisms and inspiration for the postscript.
After years of hearing about the planet’s overpopulation as a young woman, I made a very clear and conscious decision not to have children. I considered this my “contribution” to the earth, not to add an additional burden upon our natural resources.
Little did I know that I may have been duped like many other women I know who made a similar decision. Now, if I had known the truth, that our planet, particularly the US birth rates, have been in decline for… well, decades now, I may have made a very different decision.
A lagging US birthrate continues to be a little-known fact. Ask the average American, and they would swear to you that we are on a massive overpopulation curvature.
Dr. Carrie Madej tipped me off a year ago that the US was utilizing the tetanus shots as an undercover sterilization campaign. She told me that she knew firsthand that the more a woman receives a tetanus shot, the more likely she will be unable to conceive.
I had always suspected a host of reasons for the global population decline, most of which are environmental. However, it never dawned on me that tetanus shots could play a huge role.
Official U.S. birth data for 2020 showed that births have been falling almost continuously for over a decade. For 50 years now, the U.S. total fertility rate has remained near or below the “replacement” level of 2.1. The total fertility rate estimates the average number of babies a woman would have in her lifetime; 2.1 is the level needed for a generation to replace itself.
It wasn’t just Dr. Carrie Madej pointing out a correlation between infertility and tetanus shots.
A brouhaha had been stewing in Africa in the early 1990s when the Kenya Conference of Catholic Bishops and the Kenyan Health Ministry were going head to head in a battle over the safety of a tetanus vaccine administered to women in the country.
In November 1993, a Catholic publication appeared claiming an abortifacient vaccine was being used as tetanus prophylactic. Catholic church leaders began accusing the WHO and UNICEF of nefariously lacing tetanus shots they had given to girls and women of childbearing age containing the anti-fertility drug human chorionic gonadotropin (hCG).
We have been led to believe that one tetanus injection should protect for at least ten years. Yet, these tetanus protocols in Mexico and Africa targeted childbearing women to be injected every six months.
Continuously denying the accusation, in 2014, the WHO and UNICEF made a public statement expressing “their deep concern about the misinformation circulating in the media on the quality of the Tetanus Toxoid (TT) Vaccine in Kenya.”
They neglected to include in their statement that the WHO announced a “birth-control vaccine” for “family planning” in 1976 when WHO researchers had “conjugated tetanus toxoid (TT) with human chorionic gonadotropin (hCG), producing a “birth-control” vaccine. Conjugating TT with hCG causes pregnancy hormones to be attacked by the immune system. Expected results are [spontaneous] abortions in pregnant females and/or infertility in recipients not yet impregnated. Repeated inoculations prolong infertility.”
Pub med article here, Tetanus vaccine may be laced with an anti-fertility drug. International / developing countries
Similar tetanus vaccines laced with hCG have been uncovered in the Philippines and Nicaragua. In addition to the WHO, other organizations involved in the development of an anti-fertility vaccine using hCG include the Bill and Melinda Gates Foundation, the Rockefeller Foundation, the UN Population Fund, the UN Development Programme, the World Bank, the Population Council, the All India Institute of Medical Sciences, the US National Institute of Child Health and Human Development, and Ohio State universities.
(I know that “correlation does not imply causation,” but knowing what we know now, we need to consider this explanation as a possibility)
Once again, we have another criminal case of uninformed consent. Women who have no clue these shots have been preventing pregnancies or causing spontaneous abortions. The tetanus shots are possibly another example of medical malfeasance of the highest order.
How do we respond? First of all, know that the risk of a person contracting tetanus is very low unless he/she is an agricultural worker and working near animal manure. It’s not rust that gives us tetanus; it’s manure. The medical establishment never tells us this. If you are a young woman or girl that intends on becoming a mother someday, perhaps think twice about the tetanus shot. The more shots you receive, the higher the risk of not being able to conceive.
If you want more in-depth information, I recommend watching (and sharing) the newly released 30-minute documentary, “Infertility: A Diabolical Agenda.”
Lastly, spread the word. At the very least, let women know they should seriously investigate before deciding whether or not to take a tetanus shot. Knowledge is power.
I’ve just interviewed the one and only Jon Rappoport, who launched his website nomorefakenews.com over 20 years ago. Jon is now 84 years old but continues with his prolific output and is always at the forefront of exposing global scams.
We talked about:
identifying the COVID-19 fraud in early 2020
why he started investigating virology 35 years ago
why people need the virus narrative
the state of the health freedom movement
plus much more!
Over the past few weeks, I have had the privilege of working with some brilliant people on establishing a challenge to virology in order to finally put their (pseudo)scientific methods to the test. Stemming from the mind of Dr. Tom Cowan and meticulously crafted by Dr. Mark Bailey and Dr. Kevin Corbett, theNo “Virus” Challengeis designed to meet virology halfway. We want virology to show us, using their own methods, that they can actually independently reproduce and replicate the exact same results while blinded to the different samples that they will be working with.
I will leave the exact details of the challenge to be explained by the document linked below, but we are offering a first step to finally settle this debate once and for all. Whether the virology community (and those who back them) will accept this challenge (which Dr. Cowan has already received financial backing for) remains to be seen. However, if the virologists are truly interested in science and performing the proper control experiments that should have been carried out from the very beginning, there is absolutely no reason for them not to accept.
“A small parasite consisting of nucleic acid (RNA or DNA) enclosed in a protein coat that can replicate only in a susceptible host cell.”1
It has been more than two years since the onset of the “corona” crisis, which changed the trajectory of our world. The fundamental tenet of this crisis is that a deadly and novel “virus”, SARS-CoV-2, has spread around the world and negatively impacted large segments of humanity. Central to this tenet is the accepted wisdom that viruses, defined as replicating, protein-coated pieces of genetic material, either DNA or RNA, exist as independent entities in the real world and are able to act as pathogens. That is, the so-called particle with the protein coating and genetic interior is commonly believed to infect living tissues and cells, replicate inside these living tissues, damage the tissues as it makes its way out, and, in doing so, is also believed to create disease and sometimes death in its host – the so-called viral theory of disease causation. The alleged virus particles are then said to be able to transmit to other hosts, causing disease in them as well.
After a century of experimentation and studies, as well as untold billions of dollars spent toward this “war against viruses”, we must ask whether it’s time to reconsider this theory. For several decades, many doctors and scientists have been putting forth the case that this commonly-accepted understanding of viruses is based on fundamental misconceptions. Fundamentally, rather than seeing “viruses” as independent, exogenous, pathogenic entities, these doctors and scientists have suggested they are simply the ordinary and inevitable breakdown particles of stressed and/or dead and dying tissues. They are therefore not pathogens, they are not harmful to other living beings, and no scientific or rationale reasons exist to take measures to protect oneself or others against them. The misconceptions about “viruses” appears to largely derive from the nature of the experiments that are used as evidence to argue that such particles exist and act in the above pathological manner. In essence, the publications in virology are largely of a descriptive nature, rather than controlled and falsifiable hypothesis-driven experiments that are the heart of the scientific method.
Perhaps the primary evidence that the pathogenic viral theory is problematic is that no published scientific paper has ever shown that particles fulfilling the definition of viruses have been directly isolated and purified from any tissues or bodily fluids of any sick human or animal. Using the commonly accepted definition of “isolation”, which is the separation of one thing from all other things, there is general agreement that this has never been done in the history of virology. Particles that have been successfully isolated through purification have not been shown to be replication-competent, infectious and disease-causing, hence they cannot be said to be viruses. Additionally, the proffered “evidence” of viruses through “genomes” and animal experiments derives from methodologies with insufficient controls.
The following experiments would need to be successfully completed before the viral theory can be deemed factual:
1. a unique particle with the characteristics of a virus is purified from the tissues or fluids of a sick living being. The purification method to be used is at the discretion of the virologists but electron micrographs must be provided to confirm the successful purification of morphologically-identical alleged viral particles;
2. the purified particle is biochemically characterized for its protein components and genetic sequence;
3. the proteins are proven to be coded for by these same genetic sequences;
4. the purified viral particles alone, through a natural exposure route, are shown to cause identical sickness in test subjects, by using valid controls;
5. particles must then be successfully re-isolated (through purification) from the test subject at 4 above, and demonstrated to have exactly the same characteristics as the particles found in step 1.
However, we realize that the virologists may not take the steps outlined above, likely because all attempts to date have failed. They now simply avoid this experiment, insisting that what they say are “viruses” cannot be found in sufficient amounts in the tissues of any sick person or animal to allow such an analysis. Therefore, we have decided to meet the virologists half way. In the first instance, we propose that the methods in current use are put to the test. The virologists assert that these pathogenic viruses exist in our tissues, cells and bodily fluids because they claim to see the effects of these supposed unique particles in a variety of cell cultures. This process is what they call “isolation” of the virus. They also claim that, using electron microscopy, they can see these unique particles in the results of their cell cultures. Finally, they claim that each “species” of pathogenic virus has its unique genome, which can be sequenced either directly from the bodily fluids of the sick person or from the results of a cell culture. We now ask that the virology community prove that these claims are valid, scientific and reproducible. Rather than engaging in wasteful verbal sparring, let us put this argument to rest by doing clear, precise, scientific experiments that will, without any doubt, show whether these claims are valid.
We propose the following experiment as the first step in determining whether such an entity as a pathogenic human virus exists…
STEP ONE
5 virology labs worldwide would participate in this experiment and none would know the identities of the other participating labs. A monitor will be appointed to supervise all steps. Each of the 5 labs will receive five nasopharyngeal samples from four categories of people (i.e. 20 samples each), who either:
1) are not currently in receipt of, or being treated for a medical diagnosis;
2) have received a diagnosis of lung cancer;
3) have received a diagnosis of influenza A (according to recognized guidelines); or who
4) have received a diagnosis of ‘COVID-19’ (through a PCR “test” or lateral flow assay.)
Each person’s diagnosis (or “non-diagnosis”) will be independently verified, and the pathology reports will be made available in the study report. The labs will be blinded to the nature of the 20 samples they receive.
Each lab will then attempt to “isolate” the viruses in question (Influenza A or SARS-CoV-2) from the samples or conclude that no pathogenic virus is present. Each lab will show photographs documenting the CPE (cytopathic effect), if present, and explain clearly each step of the culturing process and materials used, including full details of the controls or “mock-infections”. Next, each lab will obtain independently verified electron microscope images of the “isolated” virus, if present, as well as images showing the absence of the virus (presumably, in the well people and people with lung cancer). The electron microscopist will also be blinded to the nature of the samples they are analyzing. All procedures will be carefully documented and monitored.
STEP TWO
ALL of the samples will then be sent for genomic sequencing and once again the operators will remain blinded to the nature of their samples. It would be expected that if 5 labs receive material from the same sample of a patient diagnosed with COVID-19, each lab should report IDENTICAL sequences of the alleged SARS-CoV-2 genome. On the other hand, this genome should not be found in any other samples. (Note: this statement is a brief outline of the suggested experiments – a fully detailed protocol would obviously need to be developed and agreed upon by the laboratories and signatories.)
If the virologists fail to obtain a satisfactory result from the above study, then their claims about detecting “viruses” will be shown to be unfounded. All of the measures put in place as a result of these claims should be brought to an immediate halt. If they succeed in this first task then we would encourage them to proceed to the required purification experiments to obtain the probative evidence for the existence of viruses.
It is in the interest of everyone to address the issue of isolation, and the very existence, of alleged viruses such as SARS-CoV-2. This requires proof that the entry of morphologically and biochemically, virus-like particles into living cells is both necessary and sufficient to cause the appearance of the identical particles, which are contagious and disease causing.
We welcome your support and feedback for this initiative.
Signatories,
Thomas Cowan, MD Mark Bailey, MD Samantha Bailey, MD Jitendra Banjara, MSc
Kelly Brogan, MD
Kevin Corbett, PhD
Mufassil Dingankar, BHMS
Michael Donio, MS
Jordan Grant, MD Andrew Kaufman, MD
Valentina Kiseleva, MD
Christine Massey, MSc
Paul McSheehy, PhD
Prof. Timothy Noakes, MD
Sachin Pethkar, BAMS Saeed Qureshi, PhD
Stefano Scoglio, PhD
Mike Stone, BEXSc Amandha Vollmer, NDoc
Michael Yeadon, PhD
Biotech/Pharmaceutical Chemist Mike Donio on the Tyranny of Medical Dogma: Exposing the Corruption, Lies, and Medical Fraud in the Pharmaceutical Industry
to California State University’s Leemon McHenry exposing pharmaceutical companies who buy medical journals in order to peer-review their own research, in order to invent fake diseases, in order to sell unnecessary products (such as the HPV vaccine),
America’s most cited cardiologist, Peter McCullough, said this week that he no longer trusts any Flu shot, due to the unbelievable corruption within the pharmaceutical industry.
But the fact that humanity is in an abusive relationship with its governments, is only one part of the problem. There’s a long history of cults infiltrating polite society. The cult of personality of Lenin and later Stalin once captured an entire nation. But never in history has the entire world fallen to a cult.
Del Bigtree has revealed how the American government (including the CDC and FDA) collude with Big Pharma for monetary gain, particularly where safety trials are concerned. Or rather, the lack of safety trials.
Roman Bystrianyk co-authored a book called Dissolving Illusions, in which they use official data to show how, over the last century, no vaccine has worked in the way promised by the pharmaceutical industry and governments. Every vaccine was introduced way after its respective disease was on its way out. Measles, for example, was around 97% eradicated before its vaccine hit the market.
The point is that the pharmaceutical industry is untrustworthy, and few scientists are as close to the action as Mike Donio.
In the world of healing and opposite extremes, The Terrain Theory is contrasted to The Germ Theory.
Are these opposing theories working for us? Are people healing on all levels, physical, mental, emotional, spiritual? Or are opposites set up to cause friction, division, and separation?
In a world of duality, are people coerced into making a choice between two extremes when there is always a third option: balance? If balance is where healing, peace, and unity are found, then shouldn’t we move past duality toward a One consciousness existence?
In a world of opposing forces, does one force eventually rise to truth, thus proving the opposite to be counterfeit? Or are both valid options in a world of free will and free choice? Let’s break these theories down to discern if we must be held to a dual reality standard or if another reality works better.
diseases are results of our internal environment and its ability to maintain homeostasis against outside threats. Terrain theory believes if an individual maintains a healthy terrain, it can handle outside invaders or threats (microbes), which cause diseases. When terrain is weak, it favors the microbes.
specific microscopic organisms are the cause of specific diseases. The theory was developed, proved, and popularized in Europe and North America between about 1850 and 1920. Because its implications were so different from the centuries–old humoral theory, germ theory revolutionized the theory and practice of medicine and the understanding of disease.
Disease arises from micro-organisms outside the body.
Micro-organisms are generally to be guarded against.
The function of micro-organisms is constant.
The shapes and colors of micro-organisms are constant.
Every disease is associated with a particular micro-organism.
Micro-organisms are primary causal agents.
Disease can “strike” any body.
Koch’s Postulates are used to prove both that specific germs cause specific diseases and that disease germs transmit disease from one body to another, which is fundamental to the germ theory. Read more below.
TERRAIN THEORY or MICROZYMIAN THEORY or CELLULAR THEORY (By BERNARD & BÉCHAMP)
Microbes exist naturally in the body.
Disease arises from microorganisms within the cells of the body.
These intracellular microbes normally function to build and assist in the metabolic processes of the body.
The function of these organisms changes to assist in the catabolic (disintegration) processes of the host organism when that organism dies or is injured, which may be chemical as well as mechanical.
Microbes are pleomorphic (having many forms): they change their shapes and colors (shape-shift) to reflect the condition of the host.
Every disease is associated with a particular condition.
Disease results when microbes change form, function, and toxicity according to the terrain of the host. Hence, the condition of the host organism is the primary causal agent.
Disease is built by unhealthy conditions.
To prevent disease we have to create health.
Disease reversal proves that changing the internal terrain heals the body.
Each theory isset up as an offer to consider. Whether you consider yourself to be a left-brained or right-brained human, whether you identify as a man, a woman, or something in between, you can choose what best resonates with you. Such is life in duality reality!
If you choose The Germ Theory, you believe in an invisible germ as the causative agent of disease. The germ is an external agent. The agent is thwarted by using harsh FDA-approved solutions, such as chemicals and injections to kill the agent, by medical gatekeepers who are licensed by government officials. In the process, these solutions suppress your symptoms with its direct effects.
If, on the other hand, you choose The Terrain Theory, you might also recognize the concept of balance. You might experience ‘As Within So Without,’ the universal law of correspondence, and see the One consciousness, where everything is connected. To kill a microbe inside your body is to kill a part of yourself, since you know you are 10:1 more microbe than human. In choosing Terrain Theory, you chose to regain balance using Nature’s medicine in the form of herbs, plants, clays, clean water, clean air, homeopathic remedies, Earthing, meditation, exercise, and good sleep. These natural solutions serve to support and enhance your immune system, your natural defense system.
Meanwhile, pay no attention to the man who recanted his Germ Theory on his deathbed, Louis Pasteur, who said:
The microbe (germ) is nothing. The terrain (milieu) is everything.” – Louis Pasteur, 1895
Two Laws In Duality
The main difference between these two theories? The Germ Theory falls under Human-made law, while the Terrain Theory falls under Natural Law.
What is Natural Law?
Thomas Jefferson wrote, “We hold these truths to be self-evident…” Here, Jefferson was referring to Natural Law, a universal standard that directly reflects human nature.
Natural Law is determined by the human condition. Jefferson considered the equality of man, and life, liberty, and the pursuit of happiness to be born directly from the nature of humanity.
Natural Law is the embodiment of Universal Spiritual Laws, which governs Consciousness. Consciousness creates reality through each of us using free will, which is inborn and, therefore, a birthright.
Natural law describes the universal Laws on which both Spiritual and Natural Order are based. It is the mathematics and sacred geometry expressed by all life, connected to everything in nature under the sun.
The Power of Free Will
Where there is a will there is a way!
Everyone conceived and born in this dimension is granted free will by the Creator. Free to obey or disobey the Natural Laws, your choice determines the consequences. By your choice, you become responsible for the outcome.
Nobody ever did or ever will escape the consequences of his choices.”- Alfred A. Montapert
Natural Law honors personal responsibility.
Natural Law holds true regardless of a population’s belief systems. Therefore, it does not matter how many people agree that a “Wrong can be turned into a Right” or that “a Right can be turned into a Wrong.” It does not matter if you believe in a Germ Theory or a Terrain Theory. Natural law equals the freedom to choose.
For instance, most of humanity erroneously believes that it is morally possible for governments to “create” and “delegate” Rights, and to take away “Rights.” [See Roe v. Wade]. Neither is accurate.
“Government Rights” is an oxymoron. These “Rights” are a way that government claims rights over your body. No one considers the fact that governments cannot create rights at all. Governments are established to protect natural human rights, rights that are inborn. Governments are limited to granting “benefits and privileges,” that are taken away as easily as they are granted. [See the driver’s license or any license or law].
In reality, Natural Law is a system of natural justice, a level of understanding held to be common among all humans, derived from Nature rather than from human-made law. The Law of Terrain is all about bringing the ecosystem back into balance, internal and external. Government has no jurisdiction over Nature.
If a human-made law is in harmony with Natural Law, it logically follows that it is redundant since it states a truth that is inherent, pre-existing, and self-evident. Such human-made laws are both irrelevant and unnecessary.
If a particular human-made law is in opposition to Natural Law, then it follows logically that it is both false (incorrect) and immoral (harmful), or in other words, wrong. Such a law can neither be legitimate, nor binding upon anyone.
Why would natural healers choose to believe The Germ theory after watching people heal themselves and reverse disease, using Nature’s tools and their innate immune systems?
To Prove A Cause
To choose The Germ Theory narrative nets the cause to the ills of the Coronavirus pandemic. Germ Theorists accept an external cause hypothesis as the reason for global disease outbreaks. Yet only one group of “approved scientists” are ever able to identify this cause. The cause is never self-evident.
Perhaps the real plague of humanity is the 100-year pandemic cycle (of coercion) that removes freedoms through individual choice and action.
Under COVID, pro-Germ Theorists subscribe to a virus called Coronavirus as the cause of the condition called “COVID”, much like HIV was ascribed as the cause of the condition called AIDS. [See How COVID is like AIDS].
Up until recently, the world of science suggested a fool-proof way to prove a causal relationship between an infectious agent and a disease through a process known as Koch’s Postulates. Koch’s postulates include four criteria that must be fulfilled to prove a true cause. These 4 criteria are:
(1) it must be found in all cases of the disease;
(2) it must be isolated from the host and grown in pure culture;
(3) it must reproduce the original disease when introduced into a susceptible host;
(4) it must be found present in the experimental host so infected
Kochs Postulates Obsolete
Unfortunately, Coronavirus does not meet any of the above 4 criteria. Some official sources claim that Coronavirus has never been isolated. This makes sense since a virus cannot reproduce on its own. A virus is not alive. It cannot be found in a host since it hides inside cells, and it has not been found in all cases of disease. Some say the virus is really an exosome that has been demonized and inverted. Does the body create exosomes as part of the natural healing process? Are exosomes as individual as the host?
...exosomes have activities as diverse as remodeling the extracellular matrix and transmitting signals and molecules to other cells. This pathway of intercellular vesicle traffic plays important roles in many aspects of human health and disease, including development, immunity, tissue homeostasis, cancer, and neurodegenerative diseases. –Annu Rev Biochem, 2019
Back to the killer virus! The pro-Germ Theorists have an answer to why viruses cannot be found, except in a lab.
The entire fabric of the germ theory of disease rests upon assumptions which not only have not been proved, but which are incapable of proof, and many of them can be proved to be the reverse of truth. The basic one of the unproven assumptions, wholly due to Pasteur, is the hypothesis that all the so-called infections and contagious disorders are caused by germs. – M.L. Leverson, M.D
We live in a world of contradictions because we live in a world of duality where you get to make a choice from what is offered.
If Koch’s Postulates are rendered obsolete, then a new standard appears, the PCR test!
Unfortunately, a virus cannot be proven through the use of a PCR test either, since the test’s inventor, Dr. Kary B. Mullis, specifically warned against its use to identify any virus since the amplification necessary to run the test means the results are nonspecific and test positive for everything. This is the same PCR test used to “prove” HIV/AIDS.
It uses ‘amplification’ which means taking a very very tiny amount of DNA and growing it exponentially until it can be analysed. Obviously any minute contaminations in the sample will also be amplified leading to potentially gross errors of discovery.
I don’t think they understand what they’re doing; I think it’s out of control. They don’t know how to end this. This is what I think what happened: They have built a pandemic machine over many years and, and as you know, there was a pandemic exercise not long before this whole thing started. – Kary Mullis, TruthinPlainSight.com
Dr. Kary B. Mullis died on August 7, 2019 at age 74. He emphatically stated that no infection or illness can be accurately diagnosed with the PCR-RT. Mullis also questioned the validity of the HIV/ AIDS theory.
Patenting Nature
Coronavirus cannot be proven as a causative agent to any disease using the existing science. It must be taken on “scientific faith,” an oxymoron. This is known as Scientism, the religion of Science. Scientism is based in a material view that the hard sciences—chemistry, physics, virology, astronomy—provide the only genuine knowledge and truth of reality. Everything else is labelled as bigotry, demonized, or censored.
The Germ Theory and pandemic serve a purpose in leading people to lose identity and choose the path of a material world. By choosing Germs, people accept government-approved experts to provide the scientific truth of healing. In the process, people give up responsibility for self-healing and, in the process, suppress their true Nature.
The Germ Theory further serves as a tool to patent Nature. The patents for Coronavirus are numerous, and net lucrative vaccine deals. The patents go back to 2015, well before the causative “Coronavirus” agent was named. Well before billions in profit could be realized by vaccine makers. Now, “new and improved” recombinant patented vaccines containing Monkeypox,Smallpox and Horsepox are being introduced to those who choose this science.
However, Nature can never be patented by manipulation since the result is a mere simulation; a false, immoral, and illegitimate representative of Nature, with matching consequences.
The time will come – and it may not be far off – … The soul will be made non-existent with the aid of a drug. Taking a ‘sound point of view,’ people will invent a vaccine to influence the organism as early as possible, preferably as soon as it is born, so that this human body never even gets the idea that there is a soul and spirit. The heirs of modern materialism will look for the vaccine to make the body ‘healthy,’ that is, make its constitution such that this body no longer talks of such rubbish as soul and spirit, but takes a ‘sound’ view of the forces which live in engines and in chemistry and let planets and suns arise from nebulae in the cosmos. –Rudolf Steiner, October 7, 1917, . The Fall of the Spirits of Darkness, A Future Vaccine to Prevent Knowledge of Soul and Spirit, Rudolf Steiner Press, Bristol, 1993, GA 177, p. 85
Questioning Duality
Terrain Theorists don’t want to argue. They like to question the status quo. They support free will and the freedom to choose as all important.
Free will is the gift that keeps on giving. The gift is also engaging in the disease process to find answers, your answers. Dis-ease is a spiritual offer to evolve and heal on many levels, in many layers, and in many dimensions. Owning your immune system makes you responsible for yourself. This is Natural Law, to claim responsibility for your individual part of the greater whole… not the greater good. For, as you change from within, your world changes.
Perhaps it is in accepting an Earth Suit and meeting the challenge of the dis-ease process, through finding balance, that is the full exbodiment of Natural Law in action.
The media platform that pits one theory against another is an artifact of duality reality. Media is a distraction away from seeking Nature and balance.
Make Your Choice
It’s time to choose the best offer. Door #1 or Door #2? The Universe of Nature, or the Metaverse of Cyborgs?
The Metaverse is a Transhuman reality that connects human minds to an artificial neural net. The Star Trek Series disclosed the center of the Metaverse as The Borg.The Borg are cyborgs. Their mission? To remove the human from human consciousness.
They’re made up of organic and artificial life which has been developing for thousands of centuries.” – Guinan, 2365 (“Q Who”)
“Interesting, isn’t it? Not a he, not a she. Not like anything you’ve ever seen. An enhanced humanoid.” – Q, 2365 (“Q Who”)
Does Star Trek reveal a timeline for humanity that already exists? What if beyond our universe, in the higher dimensions, we are offered something different than what we know here, an existence without free will?
If there is no free will anywhere beyond this universal reality, called Nature, then, here, we experience something special, indeed. In truth, we may need the challenges we face through disease to discover what humanity is made of …. to move humanity forward in the direction of healing.
While here, we are each responsible for our own healing through the gift of choice. Each choice affects “the whole” because we are connected to everything through consciousness, i.e., Spirit. Here, we can each choose to believe what we want; to be good or bad, to be sick or healthy, to experience freedom or slavery, to live in a Universe or a Metaverse. We can choose to believe the Germ theory or the Terrain theory because we have free will.
We can live in a duality consciousness or a One consciousness.
Although originally ignored as cell debris, it is increasingly evident that exosome release is regulated and occurs via an energy-dependent pathway. Exosomes are believed to ferry proteins, mRNA, and miRNA cargos through the bloodstream and other body fluids, shielding them from enzymatic degradation—a process that some retroviruses may hijack to travel beneath the immune system’s radar.”
During the past two plus years, exosomes have become a hotly discussed topic among those questioning the “virus” lie. This is primarily due to Dr. Andrew Kaufman bringing them to prominence in his original video questioning the existence of “SARS-COV-2.” Even though these entities have been known about for the last 40 years, many people, including myself, had either never heard of these particles or had not paid much attention to them. Dr. Kaufman did a great job showcasing how the particles known as exosomes are the exact same particles associated with “SARS-COV-2” as seen in EM images. They were just given different names and functions.
With this new spotlight on exosomes, many people who had begun questioning the “viral” narrative replaced the “virus” concept with the exosome concept. It appeared to them that this was just a case of mistaken identity. The harmful pathogenic “viruses” were being misidentified this whole time and were in fact just beneficial exosomes carrying information between the cells.
While they rightfully questioned the evidence for the existence of “viruses” and also understood that the same particles are used as representation for both “viruses” and exosomes, these people latched on to the belief that the evidence for the existence of exosomes somehow passed the scientific smell test. They believe that, unlike “viruses,” exosomes have been purified, isolated, characterized, and that their functions have been scientifically proven. However, nothing could be further from the truth.
Exosomes/”Viruses:” Same Particles, Same Faulty “Science”
I have written many articles on the inability to completely purify and isolate exosomes from “viruses” and other particles of similar size and density. This is a fundamental problem for exosome and “viral” research as without being able to separate the particles assumed to be exosomes from those claimed to be “viruses,” there is no way to be able to study either independently, distinguish them from any of the other particles, nor to characterize the particles properly. This problem was expressed in the article Extracellular Vesicles and Viruses – Two Sides of the Same Coin?:
“How can we be sure that we are isolating and quantifying extracellular vesicles rather than enveloped viruses present in thesample? Equally, how can viral researchers know that they are not detecting similarly sized non-viral vesicles or empty vectors during vaccine production?”
Somehow, people are under the impression that exosomes can be completely separated from everything else. While it is true that exosome researchers will put their samples through greater purification steps than those seen in “virus” research, it is admitted regularly by these researchers that complete separation can not be achieved by the current methods, even with the “gold standard” ultracentrifugation:
“Unless more specifically defined, it is currently virtually impossible to specifically separate and identify EVs that carry viral proteins, host proteins, and viral genomic elements from enveloped viral particles that carry the same molecules.”
“Nowadays, it is an almost impossible mission to separate EVs and viruses by means of canonical vesicle isolation methods, such as differential ultracentrifugation, because they are frequently co-pelleted due to their similar dimension [56,57]. To overcome this problem, different studies have proposed the separation of EVs from virus particles by exploiting their different migration velocity in a density gradient or using the presence of specific markers that distinguish viruses from EVs [56,58,59]. However, to date, a reliable method that can actually guarantee a complete separation does not exist.”
“Since it is near impossible to separate EV from virions by biochemical methods, the absence of EV is typically demonstrated by the absence of EV protein markers.”
Even if the researchers combine purification methods, they are unable to entirely separate the particles claimed to be exosomes from everything else. If they are unable to get the particles they claim are exosomes away from “viruses” and other similar particles of the same size, density, and morphology, this would mean any electron microscope image of the particles in question are useless as they could potentially be anything, as I have shown in numerous articles discussing these problematic images. Yet an even bigger problem is that due to the nature of EM, the particles called exosomes can only be seen in a dead state. As we can not peer into the body to see these particles at work, their functioning can not be observed. What they do or if they even float around in the body as presented is anyone’s best guess, as pointed out in the opening quote to this article as well as in numerous other sources:
“Exosomes, once thoughtto be biomarkers of a diseased state are now thought to be biologically active and some of the paracrine effects of stem cell therapy.”
“First, they are thought to provide a means of intercellular communication and of transmission of macromolecules between cells. Second, in the past decade, exosomes have been attributed roles in the spread of proteins, lipids, mRNA, miRNA and DNA and as contributing factors in the development of several diseases. And third, they have been proposed to be useful vectors for drugs because they are composed of cell membranes, rather than synthetic polymers, and as such are better tolerated by the host.”
“Yet despite 20 years of research, the very basics of exosome biology are in their infancy and we know little of the part they play in normal cellular physiology.”
As can be seen from the above sources, the role that the particles claimed to be exosomes play in the human body is thought to be one of intercellular communication and transport. They have been attributed roles and have had functions proposed. However, even after decades of research, researchers still do not know what these particles do. They only have guesses, assumptions, and hypotheses. In fact, the particles now called exosomes were originally regarded as nothing more than cellular debris created through the process of cell death known as apoptosis:
“They were initially thought to be “cellular dust” or served as a mechanism by which cells actively dispose of their own waste [3].”
When cells die, they go into a programmed cell death known as apoptosis where the cell begins to break apart and collapse which then releases tiny particles of cellular debris and waste. This process is separated into 5 main steps:
The last step listed above is the release of what are called apoptotic bodies. What are apoptotic bodies?
“Apoptotic bodies, “little sealed sacs” containing information and substances from dying cells, were previously regarded as garbage bags until they were discovered to be capable of delivering useful materials to healthy recipient cells (e.g., autoantigens) [23].”
The particles called apoptotic bodies, which can range in size anywhere from 50 to 5000 nm, were considered “garbage bags” containing information from dying cells until they were “discovered” to carry useful materials to healthy cells. Where have I seen this description before?
Exosomes: Revisiting their role as “garbage bags”
“Fifteen years ago, we proposed that one physiological function of exosomes could be a clearance process, whereby exosomes would serve as a quality control system to verify the “recyclability” of membrane molecules.”
“At first exosomes were thought to function as “cellular garbage bags”, but now these nano-sized extracellular vesicles are being studied for their role in progression and metastasis.”
This description of tiny particles which were considered garbage bags that also transport information and cargo between cells can be applied to both exosomes and apoptotic bodies. In fairness, these particles both fall under the larger umbrella term of extracellular vesicles. However, there is much more blurring the lines between these particles other than their definitions. It is stated that they both fall into the same size range (along with ectosomes and “viruses”) and that understanding and completely distinguishing these entities based on their differences has been overlooked:
“There are other types of microvesicle, including apoptotic bodies and ectosomes, which are derived from cells undergoing apoptosis and plasma membrane shedding, respectively. Although apoptotic bodies, ectosomes and exosomesare all roughly the same size (typically 40–100 nm) and all also contain ‘gulps’ of cytosol, they are different species of vesicles and understanding differences between them is of paramount importance but has too often been overlooked.”
This blurring of the line does not stop there. In an article from January 2020, it is discussed that exosomes are in fact released by apoptosis thus showing that exosomes and apoptotic bodies are both created from the same cell death process. This is further evidence that they are in fact the same exact particles just at different stages and given different names and functions:
“Apoptosis, a type of programmed cell death that plays a key role in both healthy and pathological conditions, releases extracellular vesicles such as apoptotic bodies and microvesicles, but exosome release due to apoptosis is not yet commonly accepted. Here, the reports demonstrating the presence of apoptotic exosomes and their roles in inflammation and immune responses are summarized, together with a general summary of apoptosis and extracellular vesicles. In conclusion, apoptosis is not just a ‘silent’ type of cell death but an active form of communication from dying cells to live cells through exosomes.”
They want you to believe that the slightly bigger circle is different from the slightly smaller ones.
Why is this connection between apoptotic bodies and exosomes important? As both have been coined garbage bags and considered cellular debris/waste that occur during cell death, it can be seen that these particles, if they represent anything at all, are just waste material from dying cells which serve no purpose whatsoever. This makes much more sense logically rather than assigning functions which can not be observed onto these dead particles which can only be seen after heavy sample altering processes such as fixation, dehydrating, staining, and embedding which are used for electron microscopy preparation. It is important to note that exosomes, like “viruses,” are regularly “isolated” through the process of cell culture. Many of us who challenge the evidence for the existence of “viruses” state that the particles seen in EM are most likely nothing more than cellular debris created through the culturing process. While the cell is kept outside the body in unnatural conditions, it is bombarded with antibiotics, antifungals, foreign DNA/materials, minimal nutrients, and physiologically unsuitable conditions. After being incubated for days, the cell is usually blasted with fresh heapings of many of the previously listed components and incubated further until the cell begins to break apart. While the cellular breakdown observed has been coined the cytopathogenic effect, it is a part of the process of cell death that is blamed on the invisible “virus.” And it is a fact that this very process of cell culturing can lead to the process of cell death known as apoptosis:
“Apoptosis is a genetically regulated process by which cells can be eliminated in vivo in response to a wide range of physiological and toxicological signals. Cells in vitro may be induced to die by apoptosis, e.g., by depletion of nutrients or survival factors from the culture media.”
Hmmm…those particles coming from both healthy and apoptotic cells sure look similar…
Thus, it should be easy to see that these particles which have been called exosomes, apoptotic bodies, extracellular vesicles, “viruses,” etc. are created from the very cell destroying processes that the cell is put through in order to find the particles later in EM imaging. They are not the cause of the cell death but are the effect; a creation resulting from the process. Once the sample is put through purification steps such as ultracentrifugation and ultrafiltration, the bigger cellular debris particles are broken apart and eventually separated into smaller particles through unnaturally high g-forces and various chemical means. These particles are further altered during preparation for EM imaging and are presented as many different entities with varying theoretical functions applied to the same dead waste products.
The Exosome Concept
We already know that “viruses” began first as an idea in the early 1900’s once it was discovered that bacteria were unable to be blamed for every disease and were also found regularly in healthy subjects. It was assumed that there must be something smaller than bacteria in the fluids causing disease. The concept of the “virus” came before there was ever any evidence submitted for the existence of this invisible entity. Over 100 years later, we still have no direct evidence as to the existence of “viruses,” only indirect evidence used to infer their existence. And so it goes with exosomes which also started off as a concept before the entities were ever indirectly inferred into existence:
“The concept of exosomes was first proposed by Trams et al (1) in 1981, while soon after, exosomes were identified in a study of reticulocyte differentiation as a consequence of multivesicular endosome fusion with the plasma membrane.”
As I was intrigued by how the idea of exosomes came about, I decided to break down the 1981 Trams paper in order to see what I could find out. What you will see, upon reading this study, is that just like their “viral” counterparts, the particles claimed to be exosomes were first visually recognized in cell culture fluids. In this study, many cell lines were used to look for the particles eventually picked as the representation for exosomes. They included:
Established cultures
Mouse neuroblastomas, N-18 and NB41A3
Rat glioma, C-6
Mouse melanoma, B-16
Derived from embryonic or neonatal tissue as primary cultures
Rat aorta, RA-B
Mouse astroblast, D-34
Grown from biopsy material
Human melanoma, CL
Human foreskin fibroblasts, KIN
The researchers noticed that in their studies on two enzymes, ecto-ATPases and ecto-5′-nucleotidases, these enzymes were released into the superfusate media of cultured cell lines. Due to their measuring of these two enzymes in the cultured cell media, the researchers decided to go looking for a cause. They proceeded to passage many cell lines and regularly tested the enzyme levels. The researchers eventually filtered the superfusate and subjected it to electron microscopy. After fixation of the pellets in buffered glutaraldehyde, they discovered two populations of vesicles; one which consisted of irregularly shaped vesicles approximately 500 to 1000 nm in diameter and another within the larger vesicles which was a population of smaller, spherical vesicles with an average size of about 40 nm. They then determined that these particles were the cause of their enzymatic effect without ever directly proving this by utilizing the scientific method.
Interestingly, upon finding these various particles, the researchers admitted that the vesicles could be fragments from the dying of lysed cells. Lysis is the breaking down of the membrane of a cell which is said to be caused by “viral,” enzymic, or osmotic mechanisms. In other words, these particles claimed as exosomes were possibly caused by the same process which creates “viral” particles when the cell breaks down as well as that which releases apoptotic bodies as the cell dies from apoptosis. This means that exosomes, “viruses,” apoptotic bodies, etc. are all the same particles released as the cell dies after being subjected to toxic conditions, such as the culturing of the cells for experimentation. They were just given different names and functions by different researchers.
Trams et. al attempted to state, through indirect compositional differences based off of enzymatic readings of unpurified preparations, that these particles were not the product of lysed cells. However, they admitted that their smaller particles resembled vesicles “purified” from pig brain or from calf, rat and rabbit brain, while some of the more densely shadowed small vesicles resembled C-type “virus” particles. In other words, exosomes resembled “viruses” (which come from lysed cells) and the same exact particles were being found everywhere, not just in virology studies. These particles were being found in entirely healthy cell lines and in cultures containing no “viral” material whatsoever. Oddly enough, upon trying to find these same particles in the blood, they concluded that there was no firm evidence that plasma membrane derived microvesicles were present in the circulation. As the results came only from the cell culture process, the researchers wondered if the shedding of microvesicles and their interaction with a target cell or target organ represents a physiologic phenomenon that takes place in vivo (i.e. within a living organism)?
Obviously, this revelation of finding “virus” particles in healthy cultures would destroy the cell culture technique as being valid for “viruses” (even though John Franklin Enders admitted to finding measles “virus” particles in cultures without measles material). This type of study actually shows that “virus-like” particles are found within cell cultures without “viral” material, thus serving as a control of sorts for virology, the likes of which it regularly ignores. This obviously could not stand so these particles had to be something new. While no proof for the functioning of these particles was provided, a hypothesis was established. The researchers concluded that the intercellular transport of some trophic substances or nutrients might involve such vehicles as the microvesicles which they harvested from cell culture superfusates. As this could be a possibility, they decided to refer to these particles as exosomes rather than “viruses.” Thus the exosome concept was born.
The full 1981 Trams paper is presented below:
Exfoliation of membrane ecto-enzymes in the form of micro-vesicles
“Cultures from various normal and neoplastic cell lines exfoliated vesicles with 5′-nucleotidase activity which reflected the ecto-enzyme activity of the parent monolayer culture. The ratio of 5′-nucleotidase to ATPase activity in the microvesicles indicated that cellular ecto-ATPase was conserved in the exfoliative process. Phospholipids of the microvesicles contained significantly increased amounts of sphingomyelin and total polyunsaturated fatty acids. It was concluded that the shedded vesicles constituted a select portion of the plasma membrane. Examination by electron microscopy showed the vesicles had an average diameter of 500 to 1000 nm and often contained asecond population of vesicles about 40 nm in diameter. As much as 70% of the plasma membrane ecto-5′-nueleotidase activity of a culture was released into the medium over a 24-h period. Phosphoesterhydrolases from C-6 glioma or N-18 neuroblastoma microvesicles dephosphorylated cell surface constituents when in contact with monolayer cultures. Exfoliated membrane vesicles may serve a physiologic function; it is proposed that they be referred to as exosomes.
Introduction
Plasma membrane ecto-ATPases and ecto-5′-nucleotidases have been found and characterized in a variety of eukaryotic cells and it is probable that each enzyme subserves more than one function on the cell surface. Both enzymes exhibit a broad specificity for the base moiety of nucleotide substrates [1] but it is not established that ATP or AMP are the predominant endogenous substrates. Ecto-ATPases have the properties of glycolipoproteins and are rather firmly bound to the plasma membrane, while ecto-5′-nucleotidases are composed of glycoprotein which appears to be collocated with sphingomyelin in situ and can be removed from the membrane matrix by fairly mild procedures [2]. During our investigations on the functional roles of these two ecto-enzymes we have observed that ATPase (EC 3.6.1.3) and 5′-nucleotidase (EC 3.1.3.5) were released into the superfusate media of cultured cell lines. We established that this release was not caused by cytolysis of moribund cells. The enzymes were released in the form of vesicles which are probably derived from specific domains of the plasma membrane. Whether or not the exfoliated microvesicles mediate physiologic processes in vivo has not been established.
Methods and Materials
Cell cultures. Cell lines employed in this study were established cultures (e.g. mouse neuroblastomas, N-18 and NB41A3; rat glioma, C-6; mouse melanoma, B-16), or derived from embryonic or neonatal tissue as primary cultures (rat aorta, RA-B; mouse astroblast, D-34) or grown from biopsy material (human melanoma, CL; human foreskin fibroblasts, KIN). Cells were grown in the appropriate medium as monolayers in 75 cm 2 plastic flasks (Falcon Plastics, Oxnard, CA) or on 530 cm 2 NUNC Bioassay dishes (A/S NUNC, Roskilde, Denmark). Passage numbers for a culture refer to the number of times the stock cell line has been subcultured by trypsinization, dilution and explantation into maintenance or experimental culture vessels. In particular, we have used the term ‘low passage’ for the rat glioma cell line C-6 when the parent cell was obtained from the American Type Culture Collection (Rockville, MD) at the earliest available passage (P-38). During repeated passage of this line we have observed over a number ofyears that ecto-5′-nucleotidase activity decreased sharply after about 20 passages and that ecto-ATPase activity increased. The term low passage is used for the C-6 line for P-38 to P-55 and high passage for passages P-65 to P-160.
Enzyme assays. ATPase activity was assayed on intact monolayer cultures or on isolated vesicles by a modified method of Weil-Malherbe and Green [3] by addition of [r 32p] ATP (New England Nuclear Corp., Boston, MA) to a superfusate buffer or to the vesicle suspension. The activity of 5′-nucleotidase was determined in a similar manner with [32p]AMP as substrate (New England Nuclear Corp.). Complete tissue culture growth media usually contain traces of ATPase and 5′-nucleotidase derived from the fetal calf serum component. Therefore, the cultures were washed prior to each experiment several times with a modified medium devoid of serum and routine incubations were performed in serum free media. We have used the term superfusate for modified media which were applied to confluent monolayer cultures in which enzyme accumulation was measured.
Lipid analyses. Phospholipid distribution in intact cells or extruded vesicles was estimated by two-dimensional TLC of a chloroform-methanol extract (2:1, v/v) according to Rouser et al. [4]. After development of the chromatogram, the TLC plates were charred with 50% (NH4)HSO4 and phosphate content of individual spots was determined by the method of Nelson [5]. For fatty acid analysis, aliquots of total lipid extracts were evaporated to dryness and methylated with BFa in methanol according to Morrison and Smith [6]. The fatty acid methyl esters were resolved and quantified on a Hewlett Packard 5840 gas chrom7atograph employing an SP 2330 column operated at 190°C.
Results
We have found that 5′.nucleofidase and ATPase were released into serum-free medium (superfusates) of monolayer cultures of normal and neoplastic cells. When a comparison was made between the ratio of ecto-5′-nucleotidase to ecto-ATPase activity in several cell lines and the activity of the two enzymes released into medium over a 24-h period, it was found that there was a proportionately larger release of 5′-nucleotidase (Table I). As we shall demonstrate below, the released enzymes had been derived from the corresponding plasma membrane ecto-enzymes. The relative preponderance of 5′-nucleotidase over ATPase in the microvesicles, compare ratios (1)/(2) to (3)/(4), indicated that either the ATPases were more labile, or that they had been conserved. When the decay of the catalytic activity of the released enzymes was measured by continued incubation in cell-free medium, it was found that 5′-nucleotidase lost from 3 to 20% of its activity in 24 h while the released ATPase averaged a catalytic loss of about 33% in the same period. Therefore, while the ATPases were somewhat more labile than the 5′-nucleotidases, the 2- to 13-fold enrichment of 5′-nucleotidase in the released microvesicles suggested a conservation of plasma membrane ecto-ATPases.
The release of 5′-nucleotidase activity into 24-h superfusates ranged from 2 to 70% ofmeasured monolayer ecto-5′-nucleotidase activity and it was characteristic for a particular cell line and passage number. With increasing passage number, ecto-5′-nucleotidase/ecto-ATPase activity ratios changed in several cell lines and the amount of enzymes released into superfusates also changed. While duplication was satisfactory when measurements were made within a few days or within a few passages, comparisons made several months apart were not amenable tostatistical treatment.
The results diplayed in Table II on the release of 5′-nucleotidase from a variety of cell lines should be viewed as representative. Release of the enzyme was found to be low from the NB-41A3 mouse neuroblastoma clone and highest in a primary culture derived from neonatal mouse astroblasts (D-34). Only in superfusates from mouse melanoma B-16 was there no measurable enzyme activity released into superfusates, but there was also no detectable ecto-5′-nucleotidase in the monolayer cultures. The rate of enzyme accumulation in the superfusates was linear with time in low density cultures but increased somewhat when cell density was high as shown for two separate duplicate experiments on the rat glioma cell line (Fig. 1). The rate of ATPase accumulation (not shown in Fig. 1) was very similar to that obtained with 5′-nucleotidase. The C-6 glioma culture generally exhibits a high ecto-5′-nucleotidase activity at low passage but the specific activity of the ecto-enzyme does not change substantially over a 30-h period (Fig. 1).
The rate of enzyme liberation was not changed significantly by modification of fetal calf serum concentration in the medium (0 to 20%) or by the addition of 0.5% trypsin to the medium. The release of 5′-nucleotidase activity into superfusates was altered by several compounds; in C-6 glioma cultures the extrusion of enzyme was inhibited by 93 +_ 3% in the presence of 10-6M concanavalin A. With 10 -s M cycloheximide, inhibition was 32 + 24% over a 24-h period. An increase of enzyme extrusion was found in the presence of 10 -6 M colchicine (141 + 35% over control) or when the medium contained 0.5 ug. m1-1 of cytochalasin B (95 -+ 43% over control).
Filtration of superfusates showed that from 97 to 99% of 5′-nucleotidase activity was retained on 0.22 um filters while about 80% passed through an 0.45 um filter. The released enzyme activity was particulate and the particles could also be harvested by centrifugation. In Fig. 2, we show residual medium ATPase and 5′-nucleotidase after subjecting superfusate from glioma cultures (C-6) to increasing centrifugal forces. Cellular debris and unattached cells sedimented at or below 5 • 10^3 • gh (Sorvall SS-34 rotor at 10 a Xg for 0.5 h). The particulate enzymes contained in those supernates could be collected by centrifugation at high speeds. For routine collections of extruded enzyme, the Sorvall supernates were centrifuged for 90 min in a Spinco Ti-70 rotor at 310 000 × g. The small gelatinous pellet could be removed in toto or resuspended in buffer. ATPase activity sedimented at a faster rate than 5′-nucleotidase which indicated that the particle population was not homogeneous. Electronmicroscopy after fixation of the pellets in buffered glutaraldehyde revealed two populations of vesicles, one of which consisted of irregularly shaped vesicles approximately 500 to 1 000 nm in diameter. Contained within those vesicles was another population of smaller, spherical vesicles with an average size of about 40 nm (Fig. 3).
Conceivably, the vesicles were fragments from dying of lysed cells, but the liberation of as much as 70% of its 5′-nucleotidase activity from a healthy monolayer culture in 24 h would result in the accumulation of many other subcellular fragments if that were the case. Analysis of a representative high speed pellet of 6.5 mg protein from rat glioma superfusates yielded 5′-nucleotidase activity of 1.003 panol AMP hydrolyzed • min -1 • mg -1 protein, while marker enzymes for other subcellular particles were virtually absent. Activities of glucose-6-phosphatase (EC 3.1.3.9), cytochrome c oxidase (EC 1.9.3.1) and N-acetylhexosaminiclase (EC 3.2.1.52) were nil and (Na ÷, K+)-ATPase (EC 3.6.1.3) was low (25 nmol • min -1 • mg -1 protein). The 5′-nucleotidase/LDH ratio in C-6 conditioned medium was several fold higher than in cell homogenates and there was no DNA detectable in sedimented vesicles. A comparison of the optimal requirements for divalent cations of the released ATPase showed that stimulating and inhibitory concentrations of Mg 2+, Ca 2+ and Mn 2+ were identical with those required for the respective monolayer ecto-ATPase. Ecto-5′-nucleotidases have a high binding affinity for concanavalin A and about 70% of the nucleotidase activity of C-6 conditioned media was retained by a Sepharose-4G-Con A column, suggesting also a similarity between the ecto-enzyme and the released enzyme. Analysis of vesicle pellets from glioma superfusates disclosed an RNA content of about 5% and lipid content of 30 to 40%. Two-dimensional TLC of vesicle phospholipids [4] gave a pattern which was different from that of lipid extracts of whole cells and from plasma membrane preparations in which 5′-nucleotidase was enriched about 8-fold (Table III). The vesicles contained significantly increased amounts of sphingomyelin and decreased phosphatidylinositol. Comparison of total lipid fatty acid composition of whole cells with vesicles showed that the latter contained increased palmitic acid and total polyunsaturated fatty acids and decreased oleic acid. These compositional differences were further evidence that the exfoliated vesicles had not been derived from lysed cells.
That the vesicles had been derived from the plasma membrane of the respective monolayer cell lines was suggested by the observation that the specific activities of microvesicle and monolayer enzymes were roughly of the same order of magnitude (Table I).Both 5′-nucleotidase and ATPase are classical plasma membrane marker enzymes, but the conservation ofATPase in the exfoliative process strongly suggests that the microvesicles were derived from specific domains of the plasma membrane. Another plasma membrane marker GM 1 (as measured by cholera toxin binding) was not conserved (Salem, N., Lauter, C.J. and Trams, E.G., unpublished results). This may indicate, that ecto-5′-nucleotidase and ecto-ATPase do not serve an interdependent function on the cell surface, as for instance in the catabolism of translocated cytoplasmic ATP [2].
The morphologic similarity of the extruded vesicles to synaptosomal preparations suggested a possible transport function for them. Cells transfer substances to target cells in order to support discrete functions and examples of trophic substances are fibroblast- or nerve growth-factors [7,8].
Our working hypothesis was that one or more of the ecto-phosphoester hydrolases might play a role ina recognition and/or transport process. For instance, the carbohydrate moiety of ecto-5′-nucleotidase might serve as an address which was recognized by a recipient cell and the catalytic moiety of the enzyme would serve to dephosphorylate a receptor constituent and thereby facilitate a transfer mechanism between vesicle and cell. To test this hypothesis, mouse neuroblastoma cells (N-18) were incubated with 32Pi-containing medium with the intent to label cell surface phosphorous-containing compounds. After removal of the isotopic incubation medium, the N-18 cultures were first washed with unlabeled medium and then vesicle suspensions harvested from C-6 glioma conditioned medium were added; normal culture medium served as a control. There was a significant increase in 32p release into the medium (over background 32p diffusion from the cells) when gila-derived vesicles were in contact with the neuroblastoma monolayer cultures (Table IV). In another experiment, 32P-prelabeled C-6 cultures were superfused with either C-6 or with N-18 vesicles. There was a larger release of 32p when glioma cells were incubated with N-18 derived vesicles than when they were incubated with homologous vesicles which suggested that there were either quantitative or qualitative differences between the two experiments. We have no evidence at present to show that the increases of 32p release in the presence of the vesicles was due only to dephosphorylation of cell surface constituents, but the experiments indicate that some interaction between the monolayer cells and the vesicles had taken place.
Because the release of microvesicles occurred in all cell-lines which we have studied so far, we conducted some preliminary tests for their presence in the circulation. Plasma levels of 5′-nucleotidase may be elevated significantly in several diseases [9,10] and the enzyme might normally or pathologically be derived from plasma membranes. We assumed that the presence of such vesicles would be recognizable by their enzyme activity after filtration or centrifugation of blood plasma. We assayed heparinized blood from 16 randomly selected patients and found plasma 5′-nucleotidase activities ranging from 3.4 to 26 nmol AMP hydrolyzed • min -1 • m1-1 plasma. Only a minor fraction of that activity was sedimentable, however, or retained on Millipore filters and there is at present no firm evidence that plasma membrane derived microvesicles are present in the circulation.
Discussion
Our observations suggest that exfoliation of membranous vesicles might occur in many different normal and neoplastic cells. The accumulation of as much as 70% of plasma membrane 5′-nucleotidase in microvesicular form in the medium over a 24-h period suggests a fairly high membrane tumover. This is not extraordinary, because it has been calculated that macrophages and L-cells were capable of interiorizing the equivalent of their cell surface every 33 and 125 min, respectively [11]. Replacement of apical plasma membrane in the lactating mammary gland requires formidable capapcity for membrane synthesis [12] and replacement of exfoliated membrane is a requirement that presumably is easily met by most cells. We have presented evidence that the microvesicles harvested from tissue culture superfusates were not mere fragments from the cytolysis of moribund cells. The preferential release of plasma membrane ecto-5′-nucleotidase over ecto-ATPase furthermore suggests that the exfoliative process was selective and that the microvesicles consisted of specific domains of the plasma membrane. The substantial enrichment of sphingomyelin in the microvesicular fraction supports this contention. A similar fmding of increased sphingomyelin in extracellular membranous vesicles associated with a murine ascitic leukemia was reported by Van Blitterswijk et al. [13]. Microvillous membrane accumulation in media of cultured chick embryo intestines was observed recently by Black et al. [14] and extracellular membrane-invested vesicles have been described by Anderson [15]. The latter particles appear to play a role in mineralization processes and they have been referred to as matrix vesicles. Their size ranged from 300 to 1000 nm and it was postulated that they were derived from the plasma membrane of chondrocytes by budding [15]. Their lipid composition was very similar to that of chondrocyte plasma membrane [16] and similar to the lipid composition of the vesicles which we have collected from rat glioma cultures. The electronmicroscopic images of the particles from our rat glioma culture superfusates suggest that the larger membranes were of plasmalemma origin. The smaller population has some similarities to vesicles purified from pig brain [17] or from calf, rat and rabbit brain [18], while some of the more densely shadowed small vesicles resemble C-type virus particles (Todaro, G., personal communication).
The dephosphorylation, presumably of monolayer cell surface components by microvesicle ecto-phosphoesterhydrolases, suggested an interaction between vesicles and cells. We also have recently found that isotopically labeled constituents of the microvesicles can be transfered to recipient cells (Trams, E.G., Lauter, C.J. and Salem, N., unpublished results) and the question must be asked if the shedding of microvesicles and their interaction with a target cell or target organ represents a physiologic phenomenon that takes place in vivo? Inter-cellular transfer of a quantum of material by means of vesicles has been recognized in neurochemical transmission and there is evidence that metabolic cooperation by packaged transfer of substances may occur elsewhere, such as the transport of macromolecules between glia and neurons [19-21]. It is also conceivable that the vesicle in part or in toto can be incorporated into a recipient cell, thereby producing a modification of the host cell. Such an effect was observed when exfoliated vesicles from a B-16 mouse melanoma subline were fused experimentally with cells from another B-16 subline [22]. Attempts are made currently in several laboratories to design packaged substances for targeted therapeutic use. As an example, liposomes are provided with an organ-specific address [23] and it is hoped that such models will find application, for instance in the treatment of metabolic dystrophies by enzyme replacement. Conceivably, the physiologic distribution of some cellular products between cells or organs is achieved in a similar way, i.e. they are packaged and provided with an address, rather than simply diffused through extracellular fluid compartments. The inter-cellular transport of some trophic substances or nutrients might involve such vehicles as the microvesicles which have been harvested from cell culture superfusates. In a preliminary report we have suggested that such plasma membrane derived vesicles could be referred to generically as exosomes [24].”
doi: 10.1016/0005-2736(81)90512-5.
All the same particles created from the same process.
In Summary:
Exosomes and “viruses” can not be separated from each other(as they are the same particles) which has created a problem for researchers: 1. How can exosome researchers be sure that they are isolating and quantifying extracellular vesicles rather than enveloped “viruses” present in the sample?
2. How can “viral” researchers know that they are not detecting similarly sized “non-viral” vesicles or empty vectors?
It is currently virtually impossible to specifically separate and identify EVs that carry “viral” proteins, host proteins, and “viral” genomic elements from enveloped “viral” particles that carry the same molecules
To date, a reliable method that can actually guarantee a complete separation of these particles does not exist
Exosomes have been disregarded as cellular debris and as garbage carriers and were once thought to be biomarkers of a diseased state
They are now thought to be biologically active
Despite 20 years of research, the very basics of exosome biology are in their infancy and we know little of the part they play in normal cellular physiology(i.e. it is all guesswork)
Other particles said to be garbage bags as well as carriers of cellular information are apoptotic bodies created during apoptosis, a process of cell death:
Cell shrinks
Cell fragments
Cytoskeleton collapses
Nuclear envelope disassembles
Cells release apoptotic bodies
Apoptotic bodies, ectosomes and exosomes are all roughly the same size (typically 40–100 nm) and all also contain cytosol
Understanding differences between them is of paramount importance but has too often been overlooked
Cells in vitro (i.e. cell culture) may be induced to die by apoptosis,e.g.,by depletion of nutrients or survival factors from the culture media
The exosome concept was created by Trams et. al in 1981
Exosomes were first “discovered” in cell cultures and were admitted to potentially be cellular debris
In other words, exosomes=”viruses”=apoptotic bodies=cellular debris
Cultures from various normal and neoplastic cell linesexfoliated vesicles with 5′-nucleotidase activity which reflected the ecto-enzyme activity of the parent monolayer culture
Examination by electron microscopy showed the vesicles had an average diameter of 500 to 1000 nm andoften contained a second population of vesicles about 40 nm in diameter
Exfoliated membrane vesicles may serve a physiologic function; it is proposed that they be referred to as exosomes
In other words, the particles came from cell cultures and ranged anywhere from 40 to 1000 nm, showing that these were not purified preparations of a single substance
During the investigations on the functional roles of two ecto-enzymes, the researchers stated that they “observed” that ATPase and 5′-nucleotidase were released into the superfusate media of cultured cell lines
They claimed to have established that this release was not caused by cytolysis (the dissolution or disruption of cells, especially by an external agent)of moribund cells
The enzymes were released in the form of vesicles which were probably derived from specific domains of the plasma membrane
Whether or not the exfoliated microvesicles mediate physiologic processes in vivo(in the living body)had not been established
In other words, they found particles in the size range of “viruses” which they decided were not a product of cell disintegration by pathological means and assumed they were different and provided functions without direct proof
Cell lines employed in this study were:
Established cultures
Mouse neuroblastomas, N-18 and NB41A3
Rat glioma, C-6
Mouse melanoma, B-16
Derived from embryonic or neonatal tissue as primary cultures
Rat aorta, RA-B
Mouse astroblast, D-34
Grown from biopsy material
Human melanoma, CL
Human foreskin fibroblasts, KIN
Cells were grown in the appropriate medium as monolayers in 75 cm 2 plastic flasks
Passage numbers for a culture refer to the number of times the stock cell line has been subculturedby trypsinization, dilution and explantation into maintenance or experimental culture vessels
During repeated passage of the rat glioma cell line C-6, they observed over a number of years that ecto-5′-nucleotidase activity decreased sharply after about 20 passages and that ecto-ATPase activity increased
Complete tissue culture growth media usually contain traces of ATPase and 5′-nucleotidase derived from the fetal calf serum component
Therefore, the cultures were washed prior to each experiment several times with a modified medium devoid of serum and routine incubations were performed in serum free media
They used the term superfusate for modified media which were applied to confluent monolayer cultures in which enzyme accumulation was measured
They found that 5′.nucleofidase and ATPase were released into serum-free medium (superfusates) of monolayer cultures of normal and neoplastic cells
The release of 5′-nucleotidase activity into 24-h superfusates ranged from 2 to 70% of measured monolayer ecto-5′-nucleotidase activity and it was characteristic for a particular cell line and passage number
With increasing passage number, ecto-5′-nucleotidase/ecto-ATPase activity ratios changed in several cell lines and the amount of enzymes released into superfusates also changed
While duplication was satisfactory when measurements were made within a few days or within a few passages, comparisons made several months apart were not amenable to statistical treatment
In other words, the results related directly to the cell line used and the amount of passages performed and duplication was not satisfactory after a few months
The rate of enzyme liberation was not changed significantly(i.e. there was a change) by modification of fetal calf serum concentration in the medium (0 to 20%) or by the addition of 0.5% trypsin to the medium
The release of 5′-nucleotidase activity into superfusates was altered by several compounds
Thus we can see that adding compounds can alter the results obtained
ATPase activity sedimented at a faster rate than 5′-nucleotidase which indicated that the particle population was not homogeneous(i.e. it was a mixed population of different particles)
Electronmicroscopy after fixation of the pellets in buffered glutaraldehyde revealed two populations of vesicles:
One of which consisted of irregularly shaped vesicles approximately 500 to 1000 nm in diameter
Contained within those vesicles was another population of smaller, spherical vesicles with an average size of about 40 nm
FYI: exosomes are said to be anywhere from 30-150 nm meaning this was not strictly the presumed exosomes in the mixture, i.e. not purification/isolation
Conceivably, the vesicles were fragments from dying of lysed cells, but they excuse this conclusion due to the liberation of as much as 70% of its 5′-nucleotidase activity from a healthy monolayer culture in 24 h as they claim this would result in the accumulation of many other subcellular fragments if that were the case
They looked to compositional differences to provide further evidence that the exfoliated vesicles had not been derived from lysed cells(yet, without purifying and isolating the particles, how would compositional differences be ascertained…?)
That the vesicles had been derived from the plasma membrane of the respective monolayer cell lines was suggested by the observation that the specific activities of microvesicle and monolayer enzymes were roughly of the same order of magnitude
They claim both 5′-nucleotidase and ATPase are said to be classical plasma membrane marker enzymes, but the conservation of ATPase in the exfoliative process strongly suggested that the microvesicles were derived from specific domains of the plasma membrane
The morphologic similarity of the extruded vesicles to synaptosomal preparations suggested a possible transport function for them (i.e. the particles looked the same as those found in cultures from the brain)
The working hypothesis was that one or more of the ecto-phosphoester hydrolases might play a role in a recognition and/or transport process
They carried out two experiments to test this hypothesis and concluded that they had no evidence at present to show that the increases of 32p release in the presence of the vesicles was due only to dephosphorylation of cell surface constituents, but they felt the experiments indicated that some interaction between the monolayer cells and the vesicles had taken place
Because the release of microvesicles occurred in all cell-lines which were studied, they conducted some preliminary tests for their presence in the circulation
They assumed that the presence of such vesicles would be recognizable by their enzyme activity after filtration or centrifugation of blood plasma
After testing, they concluded that there was no firm evidence that plasma membrane derived microvesicles are present in the circulation
The researchers felt that their observations suggest that exfoliation of membranous vesicles might occur in many different normal and neoplastic cells
They claimed to have presented evidence that the microvesicles harvested from tissue culture superfusates were not mere fragments from the cytolysis of moribund cells(which they admitted to be a conceivable possibility)
The preferential release of plasma membrane ecto-5′-nucleotidase over ecto-ATPase furthermore suggested that the exfoliative process was selective and that the microvesicles consisted of specific domains of the plasma membrane
The electronmicroscopic images of the particles from their rat glioma culture superfusates suggested that the larger membranes were of plasmalemma origin
The smaller population had some similarities to vesicles purified from pig brain or from calf, rat and rabbit brain, while some of the more densely shadowed small vesicles resemble C-type “virus” particles
In other words, they found the exact same particles seen in animal brain cultures as well as “viruses” but assigned them a different name and function based on indirect chemical results from mixed unpurified preparations coming from cell cultures
The dephosphorylation, presumably of monolayer cell surface components by microvesicle ecto-phosphoesterhydrolases, suggested an interaction between vesicles and cells
They stated that the question must be asked if the shedding of microvesicles and their interaction with a target cell or target organ represents a physiologic phenomenon that takes place in vivo?
In other words, they did not know whether the process they created in their culture soup actually occurs within a living organism
It is also conceivable(i.e. capable of being imagined) that the vesicle in part or in toto can be incorporated into a recipient cell, thereby producing a modification of the host cell(sounds like a “virus…”)
Conceivably, the physiologic distribution of some cellular products between cells or organs is achieved in a similar way, i.e. they are packaged and provided with an address, rather than simply diffused through extracellular fluid compartments
The inter-cellular transport of some trophic substances or nutrients might involve such vehicles as the microvesicles which have been harvested from cell culture superfusates
In a preliminary report they suggested that such plasma membrane derived vesicles could be referred to generically as exosomes
“Viruses” and EV’s sure seem to blur the lines here.
“Since vesicles resemble viruses, the question of course is whether the first extracellular vesicles were primitive viruses and the viruses learned from extracellular vesicles or vice versa.”
“Viruses can replicate and vesicles cannot. But there are many variants in between. Where do viruses start, and where do extracellular vesicles start?”
We need to be careful replacing one fraudulent theory with another. Sadly, many have fallen into this trap of scraping the “virus” concept and replacing it with the exosome concept. What they do not realize is that these two concepts are built upon the same fraudulent foundation. Both are tied to the cell culture process and come from the same cell death initiated by toxilogical overload. This is why researchers are having a hard time separating not only the particles but also their theoretical functioning from each other. When the lies become overly complicated, they begin to entangle with each other and the illusion begins to fall apart.
Whatever name you want to call them, the broken down cellular debris known as exosomes, “viruses,” apoptotic bodies, extracellular vesicles, etc. are all the same particles consisting of the same size, density, and morphology. They are assigned different names and functions based on the researchers looking at them. While they are claimed to be separate entities, the particles are unable to be purified and isolated from everything else in order to be independently studied and characterized. Their functioning can not be observed within a living organism thus the same particles are given theoretical roles within the body based on the researchers performing the experiments. None of these particles have met the burden of proof of being established through rigorous testing and adherence to the scientific method. As they can never be observed in nature and must be created to be “seen,” they fail the very first criteria. As they can not be separated, they fail at being a valid independent variable. Without a valid independent variable, cause and effect can not be determined. This means that the scientific method can not and is not being applied to these particles. Thus all of the indirect evidence accumulated for this cellular debris assuming multiple identities is nothing but pseudoscientific fairy tales.
‘The End of Germ Theory’ Documentary: An Easy-to-Understand, Step-by-Step Analysis of the History of Germ & Virus Theory, the Erroneous “Science” Behind Vaccination & a Close Look at What Really Makes Us Sick — The Big Pharma Cartel & the Deep Deception of Viral Pandemics
Dr Rosenau / US Public Health Service failed Spanish Flu contagion experiments
Goat Island / US Public Health Service failed Spanish Flu contagion experiments
Johns Hopkins / Dr Sellard failed Measles contagion experiments
Dr. Alfred F Hess failed Chicken Pox varicella contagion experiments
NY State Health Department / US Public health Service failed Polio contagion
experiments
Dr. Eleanor McBean vaccination caused Spanish Flu pandemic research
Dr Frederick Lamont Gates / US Army Antimenigitis vaccination fiasco
Black Death, Spanish Flu outbreak follows 14-25 vaccinations per person
Unvaccinated doctors and families did not catch the Spanish Flu from patients
Masha & Dasha, conjoined twins who never caught flu, colds, measles from eachother
What is Polio really? Lead Arsenate and DDT trends vs outbreaks
False vaccine disease eradication claims and trends
7 common causes of Polio
What is a “virus particle”?
What is Cytopathic Effect “Theory”?
What is Viral Replication “Theory”?
What is a virology cell or tissue “Culture”?
Cytopathic Effect Theory debunked
Autolysis and Apoptosis
Virus particle Isolation and Purification
PCR test fraud and misuse
CDC Covid PCR diagnostic test fraud
“Insilico” imaginary genomes
John Enders’ debunked Measles experiments
Studies admitting virus particles are indistinguishable from cellular debris
Fraudulent Australian failed Covid isolation experiments
Fetal Bovine Calf Serum RNA
Dr Stefan Lanka control experiments debunk virus theory once and for all
1947 fraudulent Polio isolation experiments debunked
Virology fails Koch’s postulates
Antibodies, Antigen test fraud, HIV
Antibody vaccine theory debunked
Big Pharma re-name disease game
Monkeypox fraud
Real causes of Pox diseases
1957 Monkeypox failed contagion experiments and controls debunk virology
Why do some but not all people sometimes but not always seem sick together?
At the end of April, Dr. Jordan Grant gave a remarkable 2-part lecture breaking down the various philosophical issues related to our modern healthcare system. He deconstructed the germ theory of disease and brilliantly showcased why it is based on pseudoscience rather than natural science. Dr. Grant has been at the forefront of calling out virology for its inadherence to the scientific method and he has pinpointed the many logical fallacies surrounding the germ theory fraud.
I have been anxiously awaiting the time that I could share his presentation with you. If you know Dr. Grant, you would understand why. I am fortunate enough to call Jordan a friend. We crossed paths at the beginning of this pandemic through the Infectious Myth Facebook group created by the late David Crowe. From reading Jordan’s conversations with others in our group, I immediately realized that this was a man who carried a wealth of knowledge and he was someone from which I could learn a great deal from. He may not realize it, but Jordan has been a mentor to me in various ways and I am grateful for all of the knowledge I have gained from our conversations. My hope is that you are able to come away with many nuggets of wisdom from this excellent series! At the very least, you will learn one thing you may have never known that can kill a guinea pig.
The Philosophy of Modern Medicine
What Makes Us Ill and How Can We Optimize Health? The modern medical-industrial complex has its focus on drugs and symptom suppression. It is a “sick care” system. We need to understand this philosophy and then empower ourselves with information on true causes of “illness” in order to better understand ways to optimize our health.
The Philosophy of Modern Medicine – Dr. Jordan Grant (2022 Conference) – Delivered 04/30/2022 – Dr. Jordan Grant – Berean Bible Church –
Science, Pseudoscience, and The Germ Theory of Disease
For over 150 years, the “germ theory” of disease has dominated mainstream thought regarding many illnesses. Is this theory scientific? Are there holes in the paradigm? We will explore what “science” means, first and foremost, and then apply that to dogmas surrounding contagion and infection.
Science, Pseudoscience, and The Germ Theory of Disease – Dr. Jordan Grant (2022 Conference) – Delivered 04/30/2022 – Dr. Jordan Grant. – Berean Bible Church –
If you are interested in joining the Infectious Myth Facebook group (there are a few due to censorship) to converse with Dr. Grant and many other amazing like-minded people, you can find us here:
In a groundbreaking article for Children of God For Life, titled “Forsaking God For the Sake of Science,” [1] [1b] Debra Vinnedge outlines how the Rockefeller-Harriman eugenics movement gave rise to the practice of medical abortions for research purposes, including live births during which the infant was murdered and its organs harvested:
“…Abortion wasn’t legal yet; this was 1936. But abortion was most certainly legal and acceptable [to eugenicists] if it meant ending the life of a child who would be born to a ‘feeble-minded’ woman, one who might end up less than perfect or who might have to rely on society to pay for their care.”
And therefore, why not perform abortions for medical research? Behind closed doors, out of view, this was happening in several countries, including the US.
Consider this research report: “Human embryos of two and one-half to five months gestation were obtained from the gynaecological department of the Toronto General Hospital…No macerated specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
Here is the citation [2]: Joan C. Thicke, Darline Duncan, William Wood, A. E. Franklin and A. J. Rhodes; Cultivation of Poliomyelitis Virus in Tissue Culture; Growth of the Lansing Strain in Human Embryonic Tissue, Canadian Journal of Medical Science, Vol. 30, pg 231-245. [June 1952]
The authors are certainly describing an infant who was taken from the womb alive, and after cells were harvested, was killed. For research on “growing virus in cell culture.”
Here is another research report that indicates the infant was born alive, its tissues taken, and then killed:
“Embryos of between 12-18 weeks gestation have been utilized. Rarely tissues were obtained from stillborn fetuses, or from premature infants at autopsy…In the experiments 3 sorts of embryonic materials were used: elements of skin, connective tissue, muscle; intestinal tissue; brain tissue…Whenever possible the embryo was removed from the amniotic sac.., transferred to a sterile towel and kept at 5 C until dissected.”
The citation [3]: Thomas H. Weller, John F. Enders, Studies on the Cultivation of Poliomyelitis Viruses in Tissue Culture : I. The Propagation of Poliomyelitis Viruses in Suspended Cell Cultures of Various Human Tissue; Journal of Immunology 1952;69;645-671. [June 1952]
Again, the infant’s tissue was used, in the lab, to “grow virus in cell culture.” The cells were from the infant.
My readers know that, for the past year, I’ve been exposing virologists’ absurd claims that they’re isolating viruses in their labs. [4] [4b] [4c]
In fact, they create soups in dishes, containing toxic drugs and chemicals, monkey cells and human cells, and a mucus sample from a patient. When the cells start dying, they claim this is proof the virus is in the mucus, in the soup, and is deadly.
Of course, this is nonsense, because the toxic drugs and chemicals are perfectly capable of killing the cells; and the cells in the soup are being starved of nutrients, which would also lead to cell-death.
The isolation of viruses is no isolation at all. It’s a fraud.
But it never occurred to me, until now, that some of these human cells in the soup in the lab came from infants, taken from the mother’s womb alive, for harvesting, who were then killed.
This completes a circle of evil.
Of course, out of the virological research fraud and infant murder come THE VACCINES, including the COVID vaccines, which are causing huge numbers of injuries and deaths across the world.
People of faith everywhere must see that declaring a religious exemption from the shots is a DUTY, whether or not the authorities allow the exemption.
The last time I looked, appealing to Pontius Pilate for an exemption didn’t work, and the status of Anthony Fauci is not higher than the Authority to whom, at minimum, four billion people of faith pray.
A growing number of young healthy adults are mysteriously dying. Watch Jefferey Jaxen and Del try to make sense of, what is now being called, “Sudden Adult Death Syndrome” (SADS).
A film by award-winning filmmaker Andy Wakefield, Robert F. Kennedy, Jr. and Children’s Health Defense. Watch the chilling tale of African women whose fertility was tragically stripped away through an experimental tetanus vaccination program. Are women everywhere next?
“When they’re through with Africa, they’re coming for you.” ~ Dr. Stephan Karanja
The chilling, harrowing story of how a World Health Organization (WHO) population control experiment, under the guise of a vaccination program, resulted in the sterilization of millions of women in Africa without their knowledge or consent.
How the ability to carry a pregnancy to term has been tragically stripped away from these women as their government attempts to cover up the evidence.
About a brave, Kenyan doctor — Dr. Stephen Karanja — who warned the world that once they’re done with Africa, they’re coming for the children and everyone else.
Perspectives from leading experts expressing their concerns regarding other vaccines that could cause infertility in women around the world, including the COVID shot.
Andrew Kaufman is a Medical Doctor, Psychiatrist and Molecular Biologist who received his training and degrees from Duke University, MIT and South Carolina Medical University. He says there are no such things as “viruses” and the “Coronavirus Global Pandemic” is a “manufactured event.”
The conversation around whether or not viruses exist, appears to conjure up all kinds of emotions, and is met with resistance. My guess is because virology is a deeply entrenched paradigm, and it is what we were taught as kids.
A cult-like approach would be to dismiss dissenting views and, instead, to perpetuate a previously held belief. David Rasnick refers to this as the Tyranny Of Dogma.
Scientists are doing an awful lot of damage to the world in the name of helping it. I don’t mind attacking my own fraternity because I am ashamed of it.
In late 2019, I joined two other Israeli criminologists and a health risk communications expert in a research project to study the suppression of scientific dissent around the topic of vaccines. At the time, none of us could have ever imagined what was looming right around the corner.
Two of them (Natti Ronel and Ety Elisha) had written a review of a Hebrew-language book called “Turtles All The Way Down,” which was a critical review of vaccine safety science. The thing about the book is that it was published anonymously, as the author(s) feared the potential retribution that might ensue.
Their review was published in the Hebrew-language journal, Medicine (Refuah), which is the journal of the Israeli Medical Association, sort of like the Israeli equivalent of JAMA. I won’t go into how it ever got published in the book review section, but the review simply focused on the absurdity of a scientist who felt the need to publish a scientific book anonymously due to fear of the consequences. Ironically, the publication of the review caused a huge uproar (you can read more about that here where it was covered in Science), and the review itself was retracted, or more precisely it simply disappeared from the on-line version of the journal.
So we started a project to study the phenomena of scientific censorship and suppression of scientific dissent in the field of vaccines by interviewing scientists and doctors who had either had their papers retracted or who had faced attempts to suppress their views. Notably, the only retracted papers in the field of vaccinology that we could identify all raised questions about the safety of vaccines. And this was all BEFORE the COVID pandemic hit. (We’ve got another one that covers the COVID period that should be coming out fairly soon.)
In other words, everything it describes happened before the pandemic. The censorship and suppression we’ve witnessed these last two years already existed — it has only kicked into overdrive. The deliberate dismantling of science didn’t start two years ago.
If it isn’t clear why criminologists would be interested in this topic, consider the following general definition of crime: force or fraud in the pursuit of self-interest.
So without further ado, you can read both papers embedded (hopefully) below:
Symptoms may include a desire to swing from tree to tree, to pick breakfast bugs off your mate, and to screech, yell, and generally monkey around. But seriously….
According to the Centers for Disease Creation (CDC), the agency that created at least eight Genus categories of Pox Diseases, Monkeypox is called a “rare disease.” However, Monkeypox cannot be considered “rare,” if the CDC also claims that Monkeypox is spreading.
After all, where there is a will, there is a vaccine patent!
In February 2021, patent application #20210260182 was filed for RECOMBINANT POXVIRUS BASED VACCINE AGAINST SARS-CoV-2 VIRUS. This is a combination pox/COVID vaccine patent filed over a year ago:
The terms “chimeric” or “engineered” or “modified” (e.g., chimeric poxvirus, engineered polypeptide, modified polypeptide, engineered nucleic acid, modified nucleic acid) or grammatical variations thereof are used interchangeably herein to refer to a non-native sequence that has been manipulated to have one or more changes relative a native sequence.
In some embodiments, the SARS-CoV-2 protein is inserted into the Thymidine Kinase (TK) locus (Gene ID HPXV095; positions 992077-92610; SEQ ID NO: 1) of the horsepox virus or the synthetic horsepox virus.
The official story from the CDC is that “Monkeypox” was discovered in 1958 “when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research” … and injected with Smallpox.
Not too long ago, in 2018, the Horsepox virus had its heyday when researchers told the story of the”infectious virus” synthesized in a lab. Symptoms may include a desire to neigh, snort, and gallop with the herd. But seriously… Horsepox was said to be the cousin of the Smallpox virus, which health authorities claimed had been eradicated from the planet in 1980. Why eradicate one “deadly” virus only to revive its cousin? What is the purpose of Franken-science?
The official answer was “to develop cancer treatments and vaccines,” especially since the current Smallpox vaccine (Variola) has some serious adverse side effects, including death. Note: nothing is ever said about curing cancer, only about “developing treatments and vaccines.” From the 2018 paper, Synthetic viruses—Anything new?:
…it comes as no surprise that it is possible to generate infectious viruses by using synthesized DNA fragments. The first synthetic virus, poliovirus, was produced by Wimmer and colleagues and made us aware of the fact that we entered a new era of reverse genetics that allows for the generation of synthetic viruses without the need for a nucleic acid template.
Chapter 3: “A new era of reverse genetics”
Many scientific papers published since 2018 have questioned the wisdom of engineering viruses from deadly Smallpox, which they admit could lead to the reemergence of Smallpox, as well as to future pandemics. What if the lab-created monkey virus or the horse virus escaped into the wild? What then?
Previously, scientists had blamed monkeys, as well as other species, for the consequences of their genetic experiments: in monkeys (SV40); in pigs (Swine flu (H1N1)); in birds (Avian flu (H5N1) different from Chickenpox; and in insects (Zika mosquito borne virus).
Note: the same molecular signature, protein (PB1-F2), is present in both the 1918 Spanish flu virus and in the highly lethal h5N1 chicken viruses. Coincidence?
These synthesized varieties were not selected to become “epidemics,” only beta tests on behavioral dynamics; except for the Swine Flu Epidemic, which resulted in a mass vaccine campaign, and was subsequently repealed after widespread vaccine injuries and deaths [See my 2018 blog Beware the Horsepox Vaccine!].
With many stories in the media, it is important to know that there is something called The Species Barrier. Even in the Age of Ignorance, the Species Barrier still exists, and The UK Dictionary defines it as:
The natural mechanisms that prevent a virus or disease from spreading from one species to another.
In short, people cannot “catch” diseases from animals, birds, reptiles, insects, vegetables, or minerals. But, as long as people have short attention spans, and continue to be misled by the story, animals will continue to be wrongly blamed and punished for human-engineered, chimeric experiments.
Why create animalpox outbreaks that appear go viral?
The ultimate purpose of any “viral threat” is to roll out the “vaccine solution.” And what exactly is the reason to push an agenda of vaccines? To engineer consent to reengineer humanity for deeper control: Monkey see-Monkey do. Therefore, any true global “viral threat” is not complete without a patented, engineered, controllable, injectable chimeric virus, coming soon to a city near you.
Chapter 4: The Twist: Monkeypox rash
Back to the monkeys!
The media generates associations by first showing computer-generated images of microscopic cells that appear to be bacteria (not viruses). Then, they release images of raised blisters or a rash labelled as “Monkeypox.” Looking closer, any image labelled “Monkeypox” could double as an image labelled Shingles.
Is there a relationship between the pox and the rash, or is it between the COVID vaccine/boosters and the rash?
Because the world complied so quickly to the illegal Coronavirus countermeasures, brought on by governments around the world, there is no need to wait years for the next epidemic! The “flying monkeys” are here to do the bidding of their creators.
What the WHO and CDC have not disclosed is that vaccine ingredients are widely known to cause rashes, often a full body rash. A vaccine-associated rash is a consequence of an influx of toxins to the body that results in a suppressed immune system. Frequent Strep Throat infections are another indication of a suppressed immune system. A.S.I.A is not a continent when it comes to vaccine damage. A.S.I.A is Autoimmune/Inflammatory Syndrome Induced by Adjuvants, (ie, induced by toxins), where adjuvants are vaccine ingredients (eg. aluminum sulphate). Keep this in mind. Do your own research.
Prior to the COVID injections, a rash was not indicated as a symptom of “Coronavirus,” which is a family of cold/flu viruses. According to officials, Coronaviruses can produce runny nose, sore throat, headache, fever, cough, and a general feeling of being unwell. True viruses, those not engineered in a lab, cannot survive outside the cell, they cannot transmit an infection because they are not alive (like bacteria). In this way, viruses are exosomes, produced by the cell in response to a toxic exposure, to help to clean the cell to regain balance and health.
Exosome biogenesis is a mechanism of protein quality control, and once released, exosomes have activities as diverse as remodeling the extracellular matrix and transmitting signals and molecules to other cells. This pathway of intercellular vesicle traffic plays important roles in many aspects of human health and disease, including development, immunity, tissue homeostasis, cancer, and neurodegenerative diseases.
While the virus itself is not a sexually transmitted infection, which are generally spread through semen and vaginal fluids, the most recent surge in cases appears to have been spread among men who have sex with other men, WHO officials said, emphasizing that anyone can contract monkeypox.
Is that science or science fiction? Are we back to HIV-AIDS? Did we ever leave it?
“The HIV/AIDS hypothesis is one hellof a mistake”- Kary Mullis, 1996, p. 14..– Nobel Laureate in Chemistry, 1993, inventor of PCR test.
With so many stories still unfinished, has Monkeypox arrived on the scene as a hoax? A test of humanity? Another virus that divides and discriminates against bi-sexual and gay men? What about the devastation of 500,000 deaths caused by the prescription Opioid Epidemic from 1999 to 2019 that continue? What about more than 150 people who die each year from taking the OTC, FDA-approved drug Tylenol?
Chapter 6: Nature rules
Nature has always ruled and Nature will continue to rule, but only if Nature’s Law is followed. Nature does not discriminate on the basis of race, religion, politics, education, vaccine status, or sex. Only patented lab-created viruses do.
Just because the media stories report on a Monkeypox viral threat, does not mean that humans need fear monkeys or eradicate them, like they did when they agreed to put chickens into lockdown from Pennsylvania to France then exterminated them out of fear.
Fear is False Evidence Appearing Real. Fear freezes people’s ability to be reasonable and rational. Fear separates and isolates. Fear masks identity. Fear disconnects humans from Nature, from each other, and from themselves. Going forward, if choosing fear, refrain from making any decisions or they will be made for you.
Perhaps humans should fear only humans with a god-complex, those who would unleash a lab-created/patented monkeypox/Smallpox/Horsepox/SARS-CoV2 virus into the population via injection for the purpose of reverse genetics.
Forget the Horsepox and Monkeypox stories. Could humanity be looking at a re-deployment of the original Smallpox?
As you know, I’ve spent two years presenting evidence that the discovery of SARS-CoV-2 was a fake.
But I still press on. I examine the reality machine to see why people have such a problem acknowledging the virus—and by extension, all viruses—are nothing more than fairy tales.
I’ve come up with a number of explanations.
For example: DOCTORS.
Rejecting viruses is rejecting doctors. Doctors are security guards around the reality machine.
“Doctors can’t be wrong.”
“I can’t live in a world where doctors are so wrong.”
“I would never be able to stop weeping for the doctors who are so wrong.”
“If I told my doctor I didn’t believe in viruses, he would cut me off, and I couldn’t stand that.”
“I’m a journalist, and my best sources are doctors. The good doctors. And they all say viruses are real. I need my sources.”
“Without information from doctors, the world would spin into chaos.”
“My mind instructs me to believe doctors are only guilty of making mistakes up to a certain threshold. Beyond that, they simply can’t be criticized.”
OK, that takes care of the doctor fixation. But then we have what I call the world-view fixation:
“I don’t want to live in a world where there are no viruses. I would feel lonely and afraid.”
“I need the assurance that this world of ours is filled with tiny invisible killers. When I accept that, I can maintain equilibrium. You know, their threat and our response. It makes sense.”
“I love the idea of tiny killers. It comforts me.”
“I know precisely what to be afraid of in this world. Otherwise, I would start to see ghosts in closets at night again. I remember them from childhood. Those bastards were PERSONAL. They were coming for ME. Viruses are neutral. They don’t know me. To them, I’m just cells. They don’t PREFER me. They’ll take anyone. I like that.”
“Even if viruses are bullshit, they’re sophisticated bullshit. I favor that over some sort of primitive bullshit.”
“Rejecting viruses would equal rejecting my college education. I need that education to assert my superior position against the Lower Ignorant Ones.”
“The ecological chain of life includes viruses. If we remove them from the chain, Nature makes no sense. That’s what I hear.”
“The world is a dangerous place. This is good, because it helps me to explain my problems and lack of determination. Without viruses, the danger factor would be reduced, and I can’t have that.”
“The nature of reality dictates that when you’re right, you should be psychotically nasty about being right. If I’m not right about the existence of viruses, I can’t be as nasty as I want to be. And that would be a tragedy.”
“My father is a doctor, and he is a great man. At least as great as Al Capone.”
During crises, people ask questions, and the Covid crisis is no exception. People are asking, “Is there any real or new illness called Covid-19—apart from vaccinations and the treatments themselves?” We are not alone in proposing that we must take a cold look at the viral theory touted as the cause of this alleged disease.
Journalist Jeremy Hammond has been the most outspoken critic of our contention that the SARS-CoV-2 “virus” does not exist and therefore does not cause Covid. In a video posted in March 2021,1 he outlines the following arguments for the existence of the “virus.” We answer his arguments, point by point.
Definition of Isolation
Hammond states that people in our camp have changed the definition of isolation, but we use the actual definition of the word “isolation” in the English language. It’s the virologists who have changed the meaning of the word from “separated from other things” to meaning “combined with other things in a foreign cell culture.”
Isolation Technology
Hammond claims that scientists do not yet have the technology to purify viral particles. Actually, scientists have been able to purify particles equivalent in size to so-called viruses for decades. The traditional method, in use since at least the 1940s, involves what is called density gradient ultracentrifugation. It uses different densities of a sucrose solution spun into layers at high speeds with an ultracentrifuge, so that the densest layer ends up on the bottom. The sample will separate into bands based on different densities, and one of those bands could contain the so-called viral particles if they existed.
For example, a 2015 article published in Methods in Molecular Biology,2 provides electron microscopy photographs of purified exosomes (see Figure 1). Exosomes are roughly the same size as that of claimed viral particles, around fifty to one hundred nanometers, and they have the same morphology and characteristics of alleged virus particles.
If you can purify exosomes, you can purify viruses using the same techniques. Scientists take exosomes directly from a body fluid; they don’t take the exosomes and put them in a cell culture. One of the challenges the authors discuss is the fact that the exosomes are present in low numbers; also, there are many different types of extracellular particles in the bodily fluid from which to separate the exosomes. These are some of the problems that have been put forth as a reason why it’s difficult to purify virus particles, but the researchers have overcome these problems with exosomes.
Bacteriophages, known as “the viruses of bacteria,” can also be purified, as shown in a 2018 article (again published in Methods in Molecular Biology)33 (see Figure 1). Bacteriophages are particles of similar size to viruses, and they also can be purified by chromatography and other methods. Mr. Hammond alleges that you can’t get a pure sample—a sample where you see only one thing in a vacuum. However, as you can see in the photos of exosomes and bacteriophages, all the objects are the same—they are the only thing in the microscope field because these have been isolated and purified, and there is nothing else in the sample, just exosomes or bacteriophages.
FIGURE 1. Isolated exosomes, isolated bacteriophages and “isolated” viruses
Isolated, purified exosomes
Isolated, purified bacteriophages
Sample taken from human fluids and grown in a tissue culture, said to be “purified” and “isolated” virus.So, biologists clearly have this technology, and it’s been around for quite a long time. It’s just that when they tried to do isolate viral particles, back in the 1940s and 1950s, after they had electron microscopes, they were actually unable to find any particle in the tissues or fluids of anyone who was ill. The problem is that they are unable to find the viral particles, not that they don’t have the technology to isolate and purify.
Cell Culture is the Gold Standard
Hammond admits that you need a cell culture to “isolate” a virus, because the virus needs cells in which to replicate in order to have enough virus to detect. According to the viral theory, the virus causes an infection in the lung, for example, when it invades the lung cells and then reproduces in the lung tissue, right in those cells, and then produces more viral particles. So, all we would need to do is go right to that tissue culture in the sick person, not one that we create in a laboratory with other conditions that are not natural.
In other words, why would we do this kind of indirect experiment when we have a cell culture right in the host—namely, virus-invaded lung tissue—from which we could extract the virus? Why can’t we do a proper isolation, where you go to the host, the natural source of the virus, which is a sick person with an infection, and purify the viral particles right out of that person’s bodily tissues or fluids?
Cytopathic Effects
Virologists claim that the pathogenic nature of viruses is evident in light microscope images of tissue cultures showing cytopathic effects (meaning cell breakdown). But what the images of “viruses” from an electron microscope show is a mixture of cellular material from the cell culture and a variety of different types of particles (see Figure 1, third image). How can we know what any of those particles actually are? And how do we know the particle didn’t come from the foreign cell culture, such as the kidney cells it was cultured in? How do we know it’s not an exosome, a particle produced inside the cell? How do we know it’s not an apoptotic body (from cellular breakdown)? How do we know it’s not another type of extracellular vesicle? How do we know it’s a virus (since it doesn’t have a label and has not been isolated and purified)? While virologists can show images of small particles, they have no way of identifying the nature or identity of any of those particles.
Genetic Sequencing
Hammond claims that scientists can do genetic sequencing of the particles found in tissue cultures. There are actually two ways of doing genetic sequencing. One way is to extract genetic material from only one organism, and then sequence the genome in its entirety. That’s how you can discover the genome sequence of a new organism.
But for viruses, scientists use a different technique, variously termed “genomic” sequencing, “next generation” sequencing or “in silico” sequencing (meaning carried out in a computer). Whatever they call it, this kind of sequencing is just piecemeal.
Hammond describes the method accurately, in that they start with lots of pieces of genetic material, and then a computer does sophisticated calculations and simulations to put them together. The problem—which Hammond does not describe—is that the starting material for these experiments is not a pure organism; it’s not just a virus. What they’re starting with is, in most cases, the lung fluid from a patient diagnosed with Covid by a PCR test. (And we know the PCR test is invalid. See sidebar page 20.)
The fluid they start with has genetic material from many different organisms—from a variety of bacteria species, probably some fungal and yeast species, as well as all of the human genetic material from the host and then anything that happened to be in the air that this person inhaled for the few breaths before they took the sample. In other words, there are many sources of genetic material. When they put those little bits of genetic material into the computer, the computer doesn’t know which organism they’re from—since they are not starting with a pure virus, there’s no way to tell.
When the computer runs the simulation and tries to fit these little strands of sequences together by overlapping ends, they don’t know whether the computer is making a real sequence of an organism, or if it’s putting little bits from different organisms together into some kind of mishmash or chimera. They have no way to check it against a reference standard, because there’s never been any true sequence of these viruses. What we end up with is just a simulation.
To give an idea of the problem, in the first sequence that they did this way with SARS-CoV-2, they actually had over fifty-six million little pieces or sequences, and they had not one but two different software programs independently take those pieces and try to construct them into a longer strand that they said was the size of a typical coronavirus genome. With one of the software programs, they just threw out the data because it didn’t give them what they wanted. So, they’re picking and choosing at each stage: “We think this is good. . . we want to use this.”
The other software program came up with over a million different possible sequences, but they just picked one. And there was no rhyme or reason to how they picked it. It was just an arbitrary selection. With all of the uncertainty about the origin of each individual piece of DNA, they just randomly select one of millions of possible combinations spit out by a computer. How could anyone believe these results represent the real genome of an actual organism? It would be impossible.
Lack of Proper Controls
Hammond states that virologists do a control experiment when they do the tissue cultures. That statement is not quite accurate. In a proper control, you have only one variable different, and as far as we know, virologists have never actually done this. The proper way to do it would be to take lung fluid from someone who is sick, but does not have Covid—sick with influenza or pneumonia, for example—or even lung fluid from someone who is healthy. Then, they would continue the experiment using the exact same methods, the same cell cultures, the same concentrations of antibiotics, the exact same nutrients, and any other additives or environmental conditions such as the same temperature, the same amount of agitation, the same protocols all around—that would be a proper control. No one is doing this type of proper control for virus identification.
Some of the papers about SARS-CoV-2 have mentioned what’s called a “mock infected culture,” but this is not the same as a control. In fact, we don’t know exactly what they do with these mock infected cultures. They’re not reported on in every paper, but in a couple they are. And curiously, they don’t describe these mock infected cultures at all. If you go to the methods sections, you don’t see any explanation of what a mock infected culture is. And they don’t mention the word “control.”
If they’re doing a true control experiment, why wouldn’t they call it a control culture? They have to use different words because they’re not really doing a proper control, but they’re trying to pass it off as one, which is why they change the words. We have read hundreds and hundreds of scientific papers on other subjects, and they always refer to the control group; they don’t say the “mock treatment group.” So, the mock infected culture is some kind of trick. We even tried to communicate with a couple of the corresponding authors on these publications. We asked an open-ended question: “Can you tell us the procedure for the mock infected cells listed in this figure?” In most cases, they didn’t reply at all.
In one case, we were unable to get a clear answer. The reply we received was, “They’re treated the same.” But what does that mean? “Can you tell us the exact conditions?” We even put our queries into a yes or no question like, “Did you use the same antibiotics at the same concentration? Did you use the same nutrition at the same concentration?” But we could not get a clear response, which suggests that they are probably hiding something.
We do have two examples of studies that included a control sample. The first comes from a 1954 article published in Proceedings of the Society for Experimental Biology and Medicine by Enders and Peebles.4 This was the first published paper to use the cell culture technique, which later became known as “virus isolation.”
In this study on measles, the authors put the patient specimen in a foreign culture of monkey kidney cells and then they got cytopathic effects—meaning they were able to show some damage to the cell culture.
An interesting quote in this paper describes the results of the control experiment. “Monkey kidney cultures may therefore be applied for the study of these agents [referring to measles] in the same manner as cultures of human kidney. In doing so, however, it must be borne in mind that cytopathic effects which superficially resemble those resulting from infection by the measles agents may possibly be induced by other viral agents present in a monkey kidney tissue or by unknown factors.”
In other words, they saw a cytopathic effect in the cell culture that was alleged to be a result of damage from the measles virus itself—but it might not necessarily have come from the measles virus; it could have been caused by something in the kidney cells themselves, which they call viruses, or from unknown factors.
Continuing, the two authors said, “A second agent was obtained from an uninoculated culture of monkey kidney cells.” Now, that means they did not put any sample from a measles patient in the culture; they ran the cell culture without a source of virus—just the cell culture with no patient sample in it. According to the authors, “The cytopathic changes induced in the unstained preparations could not be distinguished with confidence from the viruses isolated from measles [emphasis added].” In other words, the sample with nothing added to it produced the same results as the sample containing fluid from the measles patient.
Since the control was positive, that means that the experimental procedure itself, and not the measles virus, caused the cytopathic changes.
An important recent control experiment was carried out by Dr. Stefan Lanka, who is the only virologist we are aware of who has recognized the truth about the nonexistence of a virus—and who left the field. What he did was carry out just the control experiment. There is no possible source of virus anywhere in this experiment. As you can see in Figure 2, the top row of panels is Day One and the second row is Day Five of the experiment.
FIGURE 2. Control experiment by Dr. Stefan LankaDay One is when they changed the cell culture conditions. Previous to Day One, all of these cell cultures were kept healthy with normal cell culture procedures; then, on Day One, they changed the condition. In the first column, they used the full nutrition (GlutaMAX plus 10 percent fetal calf serum) and antibiotics at the normal concentration. In the second column, they reduced the nutrition and kept the same concentration of antibiotics. There was no change on Day Five for either of these two procedures, no cytopathic effects.
The third column simulates what they do in virus cell culture isolation experiments, using reduced nutrition while increasing the antibiotic to three times the normal concentration. (The protocols use either two times or three times the normal concentration.) You can see that on Day Five, there were cytopathic effects—the cells developed vacuoles and started to break down. Normally, virologists would give this as proof of the existence of a virus, except that there’s no virus in this experiment.
In the fourth column, Lanka added yeast RNA, which doesn’t contain any viruses—it’s a pure yeast RNA specimen bought from a laboratory supply company with good quality control. You can see even more cytopathic effects on Day Five in that culture.
So, both these control experiments show that the experimental procedure itself produces the cytopathic effects. If you took the culture materials from the two dishes with cytopathic effects and looked at them under an electron microscope, you would see particles in there that you could call a virus.
Coronavirus Fringe Pattern
According to Hammond, virologists can see the characteristic coronavirus spikes on the particles they are calling viruses. Let’s review a couple of studies to see what is going on. The first was published in 2020 in Kidney360.5 In this study, researchers were looking at biopsies of people with kidney disease, mostly from before the Covid era. In the electron microscope photographs, they saw particles with the characteristic coronavirus spikes (see Figure 3). The researchers said that these were indistinguishable from coronavirus particles, which was a source of confusion for virologists. The authors pointed this out, and they even referenced a previous paper from the CDC that found the same thing.
FIGURE 3. “Viral-like particles in non-COVID19 patients’ biopsies. Electron microscopy images of viral-like particles within podocytes in a case of thrombotic microangiopathy in a (A) native kidney biopsy specimen and (B) acute cellular rejection in an allograft. Note the presence in both cases of single vesicles with an electrondense rim likely representing endocytic coated vesicles, as well as larger multivesicular bodies (arrows), which could be confounded with vesicle packets containing virions. Inset in (A): the individual small coated pits in the exterior of the vesicle bear resemblance to a viral corona. (C) Similar intracytoplasmic vesicles within tubules in an allograft with changes suspicious for acute cellular rejection.”They also said that they identified the protein that made up the spikes, and it was not the spike protein, but a protein called clathrin. So, seeing the characteristic spikes is completely meaningless; it doesn’t identify something as a coronavirus. Remember that these kidney biopsies were from people who had no disease that anyone thought was related to a virus, and it was before even the “discovery” of so-called SARS-CoV-2.
The second example comes from a “virus isolation” paper published in the Medical Journal of Australia in 2020.6 A very interesting quote occurs in this paper: “Electron micrographs. . . showed cytoplasmic membrane-bound vesicles containing coronavirus particles. Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin into the cell culture medium immediately improved virion morphology.” In other words, they didn’t see any spikes so they added the digestive enzyme trypsin, which breaks or cleaves proteins at a certain sequence, and then looked at it again under the microscope—and then saw the spikes! (See Figure 4.)
FIGURE 4: “Following several failures to recover virions with the characteristic fringe of surface spike proteins, it was found that adding trypsin into the cell culture medium immediately improved virion morphology.”Now, isn’t that convenient? In other words, they put a spike suit on the particles so they could look like they’re supposed to look, instead of saying, “Hey, maybe there is no coronavirus in the sample.” If we have to digest a protein to make it look a certain way, then how could we say that’s what it is? It’s like having a cat but really wanting a dog, so you put a little microphone around the cat’s neck that makes a barking sound and then call it a dog. We would call this cheating.
Genome Sequencing
As Hammond and other adherents of viral theory have often stated, genome sequencing has been repeated thousands of times, and the results are published in international databases, so they can’t be a hoax. Actually, the in silico genome-sequencing procedure that we have described has been repeated over two million times—far more than Hammond claims. And of course, each time they get different results, because they can’t repeat results in an invalid experiment, so the different results are all published.
As described earlier, the way they do this is to take a bunch of pieces of unknown origin, which they run through different software simulations, and then pick out the one they like. And then they do some further magic on it by just popping things in or taking things out somewhat arbitrarily to make it look more like what they think a coronavirus genome should look like. Then they claim that this sequence is a “reference sequence” and against all of those couple of million experiments that they have repeated, they can template a reference genome. So, of course, the computer is able to put things together in such a way that it matches the so-called reference sequence somewhat closely, because the sequences that make this up are probably mostly just human sequences of non-coding RNA. (A recent analysis shows this and will soon be published.) Thus, you should be able to have similar enough sequences that you can put something together that’s close, but not exactly identical—which they then call “variants.”
Now Hammond claims that if the procedures were fraudulent, then tens of thousands of scientists all over the world would be participating together in a conspiracy; but that’s not the case at all because almost none of these scientists realizes that what they’re doing is not good science—they never question it. Doctors rarely question the things they’re taught; they just learn them and accept them as true. That’s why I (Andrew Kaufman) was recommending vaccines and using antibiotics earlier in my career, because I also just accepted those things and did them without question. Now I realize that they’re quite lethal, so I don’t do them anymore. There was a kind of individual process that I went through for that.
But the scientists involved in “virus isolation” don’t realize that they’re doing fraudulent science because they’ve never looked at it carefully. And one of the ways that science allows this kind of thing to happen is by a high degree of compartmentalization, where they don’t collaborate or talk with other people in different fields. They don’t learn how other scientists do their experiments and also how they do control experiments. And they don’t seem to talk to exosome scientists, often because they would then see that exosome scientists are able to extract and purify exosomes right from the source. And then they would try to do that and fail, because there aren’t any viruses, and then they would have to have a different conclusion and change their opinion.
But the truth is, it doesn’t matter whether all of the thousands of scientists doing “virus isolation” are in a conspiracy, and it doesn’t matter whether they’re completely ignorant, because the only thing that’s important is to look at the actual science itself—the experiments—and ask the question, can you learn something from this? Can you conclude anything from this experiment? And if the answer is no, it doesn’t matter how many people think you’re wrong, it only matters that the answer is no. It shouldn’t be terribly surprising that the virologists have gotten this wrong, because in medicine this happens frequently. Take the example of beta blockers and heart failure. For many decades, it was an absolute contraindication to prescribe a beta blocker to someone with heart failure, because beta blockers make your heart beat less strongly and less rapidly. So, that was seen to make your heart weaker. But then research showed that actually, adding a beta blocker slows the progression of heart failure and allows people to live longer. It took some time for that scientific finding to be integrated into medicine, but there was no truth to the notion that doctors everywhere were in a conspiracy to hasten the death of heart failure patients. They were just ignorant to the truth of the scientific relationship between that drug in that condition. We could interpret “virus isolation” as a similar phenomenon; virologists who are doing these experiments are not able to actually show the results or provide the conclusive evidence because they are just ignorant of that fact, because they haven’t looked at it. It’s quite as simple as that.
Response to Mercola
Entering the virus debate on January 17, 2022, Dr. Joseph Mercola published a “fact-checked” article entitled, “Yes, SARS-CoV-2 is a Real Virus,”1 in which he insisted that SARS-CoV-2 has been isolated, photographed, genetically sequenced, and exists as a pathogenic entity.
Mercola cites studies from Italy, Germany, India, Columbia, Canada, Australia, Korea and the U.S., which claim to have isolated SARS-CoV-2 and characterized it by genome sequencing. However, none of these studies isolated any virus from the fluids of the patient; all of these studies used culturing techniques that can lead to tissue breakdown and the creation of exosomes (identical in form to “viruses”); none of these studies had a meaningful control; and all used questionable computer techniques to generate a genome in silico. Remember that these tissue cultures would also contain genetic material from the kidney cells of the culture and the bovine serum used as a nutrient medium. Even if the tissue cultures did contain viral particles, how can anyone know that the DNA the computer is analyzing comes from the virus?
As Mercola states, “Another sticking point for some is whether or not SARS-CoV-2 has ever been isolated from a human subject without passing it through animal cells, as such media could be contaminated and therefore the source of the virus.”
Indeed, this is the “sticking point!” All of the studies that Mercola cites as proof passed the sample through animal cells—cultures contaminated with fetal bovine serum and toxic antibiotics, and starved with a minimal nutrient medium.
Furthermore, no paper has proven that an isolated or pure virus obtained from a cell culture has ever made an animal or human sick in any way. Therefore, it is illogical, irrational and anti-scientific to claim that the “virus” is a pathogen.
According to Mercola, “At least part of the confusion appears to be rooted in how the term ‘isolated’ is defined. Some insist a virus is not isolated unless it’s also purified, while others say a virus doesn’t have to be purified in order to be ‘isolated.’” Actually, as we have pointed out, the confusion—deliberate confusion—results from virologists using the word “isolated” to mean “not isolated,” and insisting that “purified” and “isolated” do not mean the same thing.
More Genome Sequencing
One study Mercola highlights is a “genome sequencing” study published in January 2021 in Gut Pathology.7 In this study, the genetic material (RNA) was extracted directly from stool samples of a patient identified as having Covid-19 using the meaningless PCR test.
This paper relies on an in silico genome-sequencing procedure whereby they extract all of the RNA that is present in a body fluid or tissue sample, which would include a number of different sources of genetic material, including the person’s own. The material would include non-coding DNA that has been transcribed, spliced and recombined to make all sorts of novel sequences.
They then throw out the long fragments and just look at the short ones. This is a really important point, because the longer the sequence, the more you can be sure that it came from one source; whereas if you have short sequences, when they put them together in a longer sequence, parts of it could have come from different sources. It’s more reliable to have longer sequences, but then they can’t do the sequencing as fast. So, they put all those short sequences into the computer and let various computer software programs put them together, mapping them to the “reference” standard genome—which has been done in the same way—and then give you a result. The result is a little bit different each time, which is why they have over two million “variants.”
In this 2021 paper, they used fecal material, which they said contained the same genetic material as that extracted from the nose using a nasal swab. And interestingly, in this case, they did use a control group, which is very unusual—they actually used a purchased heat-inactivated SARS-CoV-2 toxic cell culture that served as a negative control.
The other unusual procedure was that they used shorter strands of RNA than normal. Usually, they look at strands of up to one hundred fifty base pairs, but in this study, they limited the length to seventy-six base pairs. This would result in even more error in terms of the source of each particular little strand.
They also skipped an important step, which they call making “contigs” (from the word contiguous). Usually, what they do is take all those little sequences of short strands—there are often over fifty million of them—and put them into software number-crunching programs that try to pair up overlapping sequences on the ends to make longer and longer strands—this is what they call “contig.” Then they pick one of the longest strands and use that as the base genome.
In this case, they didn’t do that. They just took the sequence strands and templated them right away against the reference standard from the database. In other words, they chose the pieces that would fit into the puzzle and entered them into the program, and then the software filled in the gaps and rearranged things as necessary. In this way, they made sure that the genome looked the way they wanted it to look.
All of the studies Mercola lists as proving the existence of the SARS-CoV-2 virus are done in similar fashion to come up with a computer simulation, not a real genome taken intact from a real organism.
When Hammond talks about finding a genome of twenty-eight to twenty-nine thousand base pairs, it’s important to understand that they have never found this genome in any bodily fluid, just like they have never found anything they could call a virus. They have never found a strand of twenty-nine thousand base pairs; instead, they have created it in the computer by matching pieces together based on a template. In other words, they find the sequence only because that’s the sequence they’re telling it to find. This is not science!
More Covid-19 Virus Studies
Another paper cited by Mercola comes from Italy, published in the Annals of Internal Medicine in August 2020.8 The researchers took a sputum sample from a sixty-five-year-old woman and diagnosed her with Covid-19 using a PCR test. Then they cultured the sample in kidney cells, followed by genome sequencing as described above. It’s the same in all the studies that Mercola cites. Nobody isolates the virus from the patient directly; nobody takes that virus and determines the genetic material in that virus; nobody takes that virus and exposes somebody else to it and shows that it causes disease.
Mercola cites a study from Colombia that is the same exact experiment—a nose swab cultured in a toxic cell culture, followed by genetic sequencing and electron microscopy.9 According to the researchers, “Electron microscopy images obtained from infected cells showed the presence of structures compatible with SARS-CoV-2”—not structures that are, but that are compatible.
These structures are also “compatible” with kidney failure and probably many other things. The authors state that the genetic composition of their isolates was consistent with the predominant variant—not saying it was the predominant variant. In other words, they are hedging at every turn.
At the end of his article, Mercola mentions “antibody dependent enhancement (ADE),” but there is absolutely no scientific evidence to support something called ADE. Virus theory posits that we make antibodies against viral diseases. In July 2020, the head of the Bulgarian Pathology Association stated that they had found no monoclonal (coming from the same cell) antibodies in any of the people said to have died of Covid.10
This is like saying that no one has died of Covid, because since they haven’t found antibodies, they must conclude that the patients didn’t have Covid.
Does It Matter?
Hammond dismisses those who question the viral theory of disease as his “pet peeve” and “divisive” of the health freedom movement. According to Mercola, “Getting too far into the weeds of theories that refute the existence of viruses altogether will only slow down and hamper the truth movement rather than aid it along, and I would strongly discourage anyone from engaging in this highly unproductive narrative.” In other words, if you question the viral theory, you are the bad guy, hindering the movement for health freedom. One virus advocate has referred to “virus-deniers” as domestic terrorists!
And yet the virus debate has immense importance to the health freedom movement. All the objectionable “public health” measures— masks, social distancing, isolation, testing and above all toxic vaccines—are predicated on the belief that we are threatened by a virulent, contagious virus. If there is no virus—not for Covid-19, not for any disease—then the justification for forcing these measures on the public disappears.
SIDEBARS
Electron Microscopy
Scientists use an electron microscope in order to see the structures inside a cell. To view a sample under the electron microscope, they must prepare it using special procedures. One reason is that the beams of the electron microscope are extremely powerful and can heat the sample up to 150 degrees C. The preparation method requires the following steps:
FIXATION: The sample is placed in some kind of chemical fixative, such as formalin, glutaraldehyde or osmium tetroxide. This preserves the structure of the tissue.
DEHYDRATION: This step requires bathing the tissue many times in alcohol (ethanol or acetone) to remove all water from the tissue.
EMBEDDING: The tissue is put inside a small mold that is filled with paraffin wax or epoxy resin, which is then cooled to harden.
SLICING: The hardened resin is sliced into extremely thin pieces.
STAINING: The tissue is stained with some type of heavy metal, such as uranyl acetate, another name for uranium, or lead acetate, so you can have more contrast when you’re viewing the tissue through the electron microscope.
These methods will obviously have effects on biological samples. For example, formalin in the staining process is formaldehyde, a known human carcinogen and neurotoxin; glutaraldehyde is specifically dangerous for the gastrointestinal tract and the lungs, and osmium tetroxide causes pulmonary edema. Ethanol used in the alcohol baths can cause severe liver damage, and acetone damages the kidneys, the lungs and the brain. Paraffin wax and epoxy resin used for embedding can also affect biological tissues.
Most toxic are the heavy metals uranium and lead used for staining; they are bound to have toxic effects on biological samples. The result is that what you see using the electron microscope has little resemblance to living tissue—it is an artifact and a distortion, from which no conclusions about cell structure can be made.
A Mouse Study
Recently, Dr. Robert Malone stated that the omicron variant is not as dangerous as the others and that we should rethink our vaccines. One of the papers he cited was “Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model,” published in December 2021 in Emerging Microbes and Infections.11
In the abstract of this paper we read, “Older individuals are at higher risk of SARS-CoV-2 infection and severe outcomes, but the underlying mechanisms are incompletely understood. In addition, how age modulates SARS-CoV-2 re-infection and vaccine breakthrough infections remain largely unexplored. Here, we investigated age-associated SARS-CoV-2 pathogenesis, immune responses, and the occurrence of re-infection and vaccine breakthrough infection utilizing a wild-type C57BL/6N mouse model. We demonstrated that interferon and adaptive antibody response upon SARS-CoV-2 challenge are significantly impaired in aged mice compared to young mice, which results in more effective virus replications and severe disease manifestations in the respiratory tract. Aged mice also showed increased susceptibility to re-infection due to insufficient immune protection acquired during the primary infection.”
Now, when well-known spokesmen such as Dr. Robert Malone comment on the importance of a study like this, it works to convince the public that SARS-CoV-2 is real and the omicron variant is real. Maybe omicron is not so bad, maybe it is worse in the elderly, but in any event, the new “variant” is real.
According to Malone, the reason this study is important is that it explains the significant adverse event profile of the vaccines. We would agree that these adverse events combined with a milder disease profile of omicron raise the possibility that boosters may not be good medicine, even for the elderly, but the suggestion that viruses have anything to do with this only perpetuates the kind of misinformation that justifies everything that is wrong with how the health authorities have handled the pandemic—masks, social distancing, isolation, hand sanitizing and vaccinations.
According to the authors, the antibody response was severely impaired in aged mice leading to more severe disease. In the Materials and Methods section, we see that the SARS-CoV-2 variant was “isolated” from a confirmed Covid-19 patient in Hong Kong and that the virus was cultured in Vero (kidney) cells and stored at negative 80 degrees C.
Now, the important part: they expose the mice to a “variant” of the “virus”—to what they think is the omicron variant. One would expect that what scientists would do is take purified virus and expose the mice in the way that humans are exposed, by breathing it in the air. But what did these scientists do? They did a standard viral culture, meaning they inoculated monkey kidney cells (Vero cells) with fetal calf serum and an unpurified sample from a person with alleged “Covid.” (Fetal bovine serum, by the way, is taken from live aborted slaughterhouse calves whose blood is sucked directly from their hearts.) So, they didn’t, in fact, use a virus—that is a flat-out lie. Instead of a virus, they used a culture of kidney cells that contained some of the primers allegedly from a variant strain, a variant that has never been isolated.
Now, you would think that they must have sprayed this culture onto the mice, or gently into their noses, but that’s not what they did. Instead, they anesthetized the mice with toxic drugs—essentially poisoning them—and then squirted a mixture of phosphate-buffered saline and the toxic kidney culture under high pressure down their noses through an intranasal cannula directly into their lungs. No rational person would say that this type of experiment has any relation to what happens in old or young people or to anybody exposed to a “virus.” It’s ridiculous to call this science.
And then they found out whether the young mice did better than the old mice. Upon intranasal inoculation, the young mice transiently lost a maximum of 5 percent body weight for a short period. In contrast, the older mice lost 12 percent of body weight, and they didn’t recover. Moreover, the young mice did not show any sign of disease. The older mice showed hunched postures and labored breathing, which was more severe at higher doses of toxic cell culture injection into their lungs.
If you wanted to be precise in your language, you would say that young mice—injected, anesthetized and subjected to high-pressure squirts of toxins directly into their lungs—seemed to be okay; they just lost a little weight. That’s probably the definition of a bad day for a mouse. But they seemed to recover, whereas the older mice didn’t do as well. That’s what they found.
And then they did all kinds of biochemical histological genetic studies, analyzing the tissue after they ground up the nasal turbinates, the lungs and so forth. They then concluded, “Yep,” these mice have a lot more antibodies than they should—which means they are trying to protect themselves against being poisoned with toxic cell cultures injected right into their lungs.
The authors found that the staining of the nucleocapsid protein was more intense at higher doses of the stuff squirted up the mice’s lungs. Later, they say these findings indicate that SARS-CoV-2 “replicates more effectively in the respiratory tract of aged mice than young mice upon virus exposure.” We would submit that they never actually took out any virus and never saw any replication of any virus in any lung of any mouse.
In other words, the researchers essentially said, “This study does not prove what we thought it was proving, but is just another way to convince us that there is a virus and that the virus is the cause of disease.” When in fact, all this study really tells us is that older, poorly-fed mice do worse when exposed to poisons than younger ones.
Does it matter whether this disease is caused by a virus or not? When the Chief Medical Officer of the World Health Organization predicts that half of the United States is going to get sick in the next six to eight weeks, yes, it does matter. The problem with all this talk about viruses is that it completely obscures the reasons why people are getting sick. We know that a lot of people are getting sick from the injections, but they are not the only people getting sick. Unfortunately, as long as we stick to this nonsense called the viral narrative, we will never ask the right questions, and we will never get any answers as to what otherwise is making people sick.
Rapid Tests for Covid-19 Virus
Recently, the CDC announced—quietly and without explanation—that as of January 1, 2022, they were no longer going to use PCR tests for “diagnosing Covid.” Many people saw this as a kind of capitulation by the CDC, as if to say they had finally seen the light; or perhaps there was enough pressure on CDC that they realized they had to back down quietly from the PCR test. Many people interpreted the CDC’s move as an end to testing, and since this pandemic is really a pandemic of testing, they believed this would go a long way toward ending the pandemic. After all, if they stopped doing the test, nobody would test positive. However, the CDC didn’t say they were going to end testing.
The problem is that these people are playing chess, while the rest of us are playing checkers—if they’re playing chess, we need to play chess, too, and understand the motivations and the rationale behind some of the moves we’re hearing about. And this is particularly true in the case of things that seem to be small victories—sometimes even fairly large victories—because upon closer examination, they don’t all turn out to be the victories that we imagined.
The PCR (Polymerase Chain Reaction) is not a diagnostic test, it’s a manufacturing tool, and it does not test whether or not anybody has any virus. Rather, the PCR is a method to rapidly make millions to billions of copies (complete copies or partial copies) of a specific DNA sample, allowing scientists to take a very small sample of DNA and amplify it (or a part of it) to a large enough amount to study in detail. The inventor, Kary Mullis, was emphatic that his test could not be used to diagnose or determine disease.
The PCR amplifies the DNA sample anywhere from twenty to forty cycles in order to get enough genetic material to detect—the test does this by showing a color change. To use the PCR as a diagnostic test requires two assumptions. The first is that you know that the genetic sequence you are amplifying comes from the virus you are looking for; the second is that there are no other biological organisms in the sample—no microbes, bacteria, fungi or human DNA. To repeat, the premise of using the PCR for diagnosis is that you already know the sequence of the virus, and you know that this primer sequence is one of the pieces of the entire virus genome, and that no other biological organism has that same sequence of DNA. We know that both these premises are not true with PCR Covid tests. Actually, one of the people who came up with the original primer sequences was Christian Drosten, who admitted in a paper that they never had a copy of any virus.12
Now, just think about that for a minute. If you never had a copy of the virus, how can you possibly know that this piece of the genome is a piece of the virus, that it actually came from a virus? If we gave you a sentence and asked you whether this sentence came from a certain book, the obvious common-sense question that any rational human being would ask is, can you show me the book? How can you know whether a sentence comes from a certain book if you don’t have the book?
Furthermore, how can you prove that no other living being has this same sequence? You can determine this by doing what is called a BLAST search, which searches the database of all the genome sequences of all the organisms that have ever been sequenced. Scientists have done this and found out that the same sequence used in the PCR test primers for SARS-CoV-2 is found in at least ninety human sequences and ninety microbial sequences (meaning bacterial or fungal sequences).
Thus, the second premise, that a sequence is unique to a specific virus, is also not true. The sequence is found in humans and in bacteria. If you start with a sample that has sequences that come from humans and that has bacteria and fungus in it, there is no way of knowing whether the positive match—the sticking of the primer to a sequence in the sample that will then be amplified—comes from a virus, the person, bacteria, fungus or maybe from something else.
So, the PCR test is invalid—there are no “false positives,” there are no “false negatives,” there are just false results. So, shouldn’t we applaud when the CDC finally acknowledges that they are not going to do a PCR test anymore?
The question is, what are they going to replace it with? According to government announcements, they are going to use a “higher throughput and multiplexed assay with biotinylated primers.” To explain further: “This developed invention is multiplex and uses the Luminex bead-based liquid assay, which contains one hundred different unique bead oligonucleotide probes with sequences complementary to the target sequences covalently coupled to these unique beads. These capture beads are mixed with viral samples obtained from the patient via cheek swabbing or throat wash and subjected to PCR in a conventional thermocycler. The amplified target sequences then hybridize to complementary capture oligonucleotide probes via forward biotinylated primers; if this bead probe amplicon unit contains the target nucleic acid, it will be bound by the reporter molecule and fluorescence will be detected by flow site cytometer. This multiplex assay would thus be able to detect and identify respiratory pathogens present in hospital and clinical settings.”
English translation: Instead of the old PCR test, they are going to use one hundred different unique beads. These beads contain the primer sequences, and they’re all attached to the other beads. These beads are mixed with viral samples from the patient, and then they are put into PCR amplification cycles.
Now, the only real difference between this and the normal PCR test is that there are more of the primer sequences—like one hundred more—attached to a compound called biotin. These biotinylated primers stick easily to the sequences in the sample, which then get put into the old-fashioned PCR thermocycler, so that they can be amplified. And then you get a result. Now, instead of a PCR test for Covid, one test will test for all the “viruses.”
The upshot of this is that now they will be able to say that you have many different viruses, all at the same time. Since all these viruses can make you sick (so they will argue), you may need a vaccine for each one of them.
This is a checkmate: They now are able to find the code for the original “virus” as well as the delta variant and the lambda variant, right on through the Greek alphabet, because they can make it look like you have multiple different sequences. These sequences amplify more easily because they figured out a way to make the primer sequences stick more readily to whatever is in your sample. And this is not a single-plex test. This is a multiplex assay, which means they can find any number they want, just by increasing the amplifications. And checkmate, they got us.
So, they replaced the old-fashioned PCR with something that will make the whole thing even worse. The lesson is that we should not be fooled by false minor victories, because they are not necessarily good news.
The Seven U.S. Government Payoffs to Kill You in Hospitals
by Dr. Peterson Pierre13
If you have Covid, and you end up in the hospital, you’re put on a rigid protocol. There’s a high mortality rate in the hospital, and your family is kept in the dark about what is happening. So, what’s going on here?
The CARES Act is providing bonus payments to hospitals whenever they have a diagnosis of Covid, while the Center for Medicare and Medicaid Services is waiving patient rights. This is a deadly combination.
The hospital gets the first payment when they offer a free Covid test in the emergency room, and they get another payment if they can come up with a diagnosis of Covid. Number three, they get another bonus payment if they admit a patient with Covid. Number four, they get another bonus payment if the patient is put on remdesivir. Number five, another bonus payment if the patient is put on a mechanical ventilator. Number six, another 20 percent bonus if the diagnosis on your death certificate says Covid, even though you may not have died from Covid. And then number seven, there are bonus payments for the coroners.
Does the public understand the gravity of what’s happening right now? The government is literally paying hospitals to kill you. That’s what’s happening. These are real human lives we’re talking about, priceless human lives. It’s estimated that about one hundred thousand dollars per patient is what the hospital is getting. Think about that.
Rai A, Fang H, Fatmous M, et al. A protocol for isolation, purification, characterization, and functional dissection of exosomes. Methods Mol Biol. 2021;2261:105-149.
Vanderheuvel D, Rombouts S, Adriaenssens EM. Purification of bacteriophages using anion-exchange chromatography. Methods Mol Biol. 2018;1681;59-69.
Enders JF, Peebles TC. Propagation in tissue cultures of cytopathogenic agents from patients with measles. Proc Soc Exp Biol Med. 1954;86(2):277-286.
Cassol CA, Gokden N, Larsen CP, et al. Appearances can be deceiving – Viral-like inclusions in COVID-19 negative renal biopsies by electron microscopy. Kidney360. 2020;1(8):824-828.
Caly L, Druce J, Roberts J, et al. Isolation and rapid sharing of the 2019 novel coronavirus (SARS-CoV-2) from the first patient diagnosed with COVID-19 in Australia. Med J Aust. 2020;212(10):459-462.
Papoutsis A, Borody T, Dolai S, et al. Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing. Gut Pathog. 2021;13(1):7.
Colavita F, Lapa D, Carletti F, et al. SARS-CoV-2 isolation from ocular secretions of a patient with COVID-19 in Italy with prolonged viral RNA detection. Ann Intern Med. 2020;173(3):242-243.
Díaz FJ, Aguilar-Jiménez W, Flórez-Álvarez L, et al. Isolation and characterization of an early SARS-Cov-2 isolate from the 2020 epidemic in Medillin, Colombia. Biomedica. 2020;40(Supl. 2):148-158.
Chen Y, Li C, Liu F, et al. Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model. Emerg Microbes Infect. 2022;11(1):368-383.
Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):2000045.
“A pill with a tiny chip that sends a signal to relevant authorities when [the pill] has been digested…imagine the implications…the compliance…”
Patient compliance is a very big deal in the pharma/medical universe. The patient gets his orders. He follows them.
From a purely $$ perspective, the chip is a major advance. No pills left in bottles. People finish their meds. They go back to the doctor. He authorizes a new script or changes the drug. More pills taken, more money rolls in.
But of course, the larger bonus is control.
“You see, Mr. Jones, we know you didn’t finish taking the meds you were prescribed. So we can’t keep treating you. It’s a waste of time if you won’t follow orders…”
And this is just the first phase of ultimate control. Over time, it gets heavier. Cancelation of health insurance for non-compliance. Mandates.
COVID has been a training ground for citizen obedience. But the medical dictatorship wants more. Always more. And they’ll dream up one occasion after another to secure more.
Bird flu. Monkeypox. Smallpox. Whatever STORYTELLING it takes.
The medical cartel is in the business of making horror movies and promoting them as real.
A pill with a chip is the soft version of nanotech—by which tiny transmitters and receivers are placed in the body and brain. The nanos are also sensors. They report on all sorts of ongoing body processes—which leads to medical diagnoses, toxic drugs, and toxic vaccines in an endless parade.
This is not science fiction. This is not a hundred years in the future. We’re almost there.
Don’t make the mistake of thinking that humans are going to be on the receiving end of all the reports which the nano sensors issue from inside humans. This operation is planned as AI. Eventually, algorithms will interpret those reports and make decisions about treatment.
Many doctors will eventually take on roles as comforting guides, PR flacks, pitchmen, counselors. “Of course this is all for your benefit, Jim. It’s a good diagnosis. The treatment is standard. Think of Carol and the kids and what they need you to do. We caught it in time. You’ll be fine. But for God sakes, stop reading that nonsense online about toxic side effects. What do you think clinical trials are for? We did the prep work. The FDA approved this drug. It’s safe. I looked at your chart myself. The Pfizer antiviral is the preferred choice in your case. This is routine. If you need a human therapist, rather than the AI psychologist, I can recommend a good man. He lives in your town. Your insurance will cover it. But just suck it up and take the medicine. Believe me, you don’t want to progress to the stage where surgery is necessary. Then we would be talking hospitalization and recovery…”
Some of your children will be talking about earning a PhD in Bedside Manner.
Health Freedom and Medical Freedom are the alternative.
Everything coming down the medical pipeline makes this freedom absolutely vital. YOU decide what’s good for your body and mind, and what’s bad.
You assert that right, come hell or high water.
No matter how many court cases are won or lost, FREEDOM to say yes or no to medical treatment is the ultimate back up. This is what I kept writing and saying early on in the COVID hustle.
Meanwhile, the Pfizer CEO, Albert Boura, is a shark. In every sense of the word.
“Monkeypox” – who could have seen it coming? Well, apparently the organisation founded by Ted Turner in 2001 called the ‘Nuclear Threat Initiative’ (NTI) saw it coming when they published a report in November 2021 called, “Strengthening Global Systems to Prevent and Respond to High-Consequence Biological Threats.” The report states that in March 2021, they partnered with the Munich Security Conference to run an exercise scenario involving a, “deadly, global pandemic involving an unusual strain of monkeypox virus that emerged in the fictional nation of Brinia and spread globally over 18 months…the fictional pandemic resulted in more than three billion cases and 270 million fatalities worldwide.”
The Nuclear Threat Initiative introduces Plandemic 2.0? This time it is even bigger and monkeypox takes centre stage.
Amazingly, the scenario had the monkeypox outbreak emerging as a result of an act of bioterrorism in May 2022, right where we are now. We have dealt with gain of function garbage involving non-existent viruses in several other videos, while Dr Stefan Lanka has also dismantled such fallacies. Regardless, the NTI’s report suggests that what is required in a fantasy outbreak is, “aggressive measures to slow virus transmission by shutting down mass gatherings, imposing social-distancing measures, and implementing mask mandates”. The winning countries, in their hallucination implemented, “large-scale testing and contact-tracing operations and scaled-up their health care systems.”
Their charts, which seem to be produced by Neil Ferguson’s calculator, show that countries that don’t comply with their restrictions and medical interventions will be far worse off. The report goes on to state, “both the exercise scenario and the COVID-19 response demonstrate that early actions by national governments have significant, positive impacts in managing the impact of the disease”. When they say “positive impacts” it is not quite clear who is on the receiving end, although they note that “the COVID vaccine market will exceed $150 billion in 2021.” All in all the NTI’s report reads like Event 201 on Ritalin. (Event 201 took place on 18 October, 2019. It was an exercise involving a, “coronavirus pandemic” just months before the COVID-19 “pandemic” was declared.)
Monkeypox attacks right on cue!
As with COVID-19 it appears that other parties have also been eagerly awaiting a market such a “pandemic” would present. Likewise, these fortune-tellers were preparing vaccines to go where no vaccine had gone before. In this case the biotech company Bavarian Nordic gained approval from the FDA in 2019 to market JYNNEOS, a smallpox and monkeypox vaccine. Other health authorities were also primed to react to a previously rare condition that has been of no concern for their nations…until now apparently. For example, on May 20, 2022, the UK Health Security Agency published a document titled, “Recommendations for the use of pre and post exposure vaccination during a monkeypox incident”. Like COVID-19, it’s starting to feel like all roads lead to vaccines again…
Just a matter of time before the “rare” monkeypox vaccine comes to your neighbourhood.
So now that the scene has been set we can get into the “science” of monkeypox starting with an official description of the alleged viral disease. The CDC states that, “Monkeypox was first discovered in 1958 when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research, hence the name ‘monkeypox.’ The first human case of monkeypox was recorded in 1970 in the Democratic Republic of Congo.” They go on to state that, “in humans, the symptoms of monkeypox are similar to but milder than the symptoms of smallpox.” The illness is said to be flu-like with the addition of lymph node swelling and then development of a rash, and then lesions that progress from macules to vesicles to scabs.
In terms of the lethality of monkeypox, the CDC state that, “in Africa, monkeypox has been shown to cause death in as many as 1 in 10 persons who contract the disease.” This 10% fatality rate has already stoked the fear narrative and was also used as the case fatality rate in the NTI’s monkeypox pipe dream. It should be noted that historically monkeypox has been virtually unheard of in first world countries and the rare cases are usually in people that have recently arrived from Africa.
Indeed, one of the only recorded “outbreaks” of monkeypox in the first world was in the United States in April 2003. Cases were declared in 6 states and said to be caused by rodents that were imported to Texas from Ghana. This was the first time monkeypox had been reported outside of Africa and the CDC published a paper in 2006 analysing the incident. The paper states that, “person-to-person spread of the virus is thought to occur principally via infectious oropharyngeal exudates” although it is clear that this has never been scientifically established. They continue to say that, “the virus is thought to have been transmitted from African animals” – in other words, it’s another species-jumping pathogen tale.
Blaming it on minority groups, when have we seen that before?
They reported that, “individuals who had illness onset within 21 days after exposure to MPXV [Monkeypox virus] who experienced fever (defined as a body temperature greater 37.4°C) and vesicular pustular rash or rash (potentially uncharacterized) plus orthopox IgM antibodies were classified as having probable cases of infection.” Now 37.4°C is not a fever in our book, it is a normal body temperature and we would suggest 37.6°C and above qualifies as a fever. We noted in their chart that they were using the classification ≥39.4°C, but this appears to be an error as in another paper, we’ll get to soon, it was once again 37.4°C. The second paper even said the “fever” could be subjective, so they appear to be using this loose criteria and pathologising a normal state. Additionally, the CDC’s weekly report from the 11th of July 2003, stated that from a total of 71 cases, only “two patients, both children, had serious clinical illness; both of these patients have recovered.” The remainder had a variety of respiratory and gastrointestinal symptoms.
The CDC’s cases were confirmed on the basis of specimens that showed: “monkeypox virus isolation, detection of monkeypox-specific nucleic acid signatures, positive electron-microscopy findings, or positive immunohistochemical findings”. We had a look at the electron micrographs presented by the CDC including the image shown below of a skin sample from one of the patients. The caption informs us that the round particles on the right are immature monkeypox virions, while the oval particles on the left are mature viruses. However, all they have is a static image of dead tissue and no conclusions can be made about the biological role of the imaged particles. None of them have been shown to be replication-competent disease-causing intracellular parasites and so should not be called ‘viruses’.
Looking at the CDC’s weekly report from 2003 again, it appears that the 35 “laboratory-confirmed cases” all involved polymerase chain reaction (PCR) “tests”, so we investigated the scientific evidence behind this claim. One of the citations for the development of PCR detection of monkeypox is a 2004 paper titled “Real-Time PCR System for Detection of Orthopoxviruses and Simultaneous Identification of Smallpox Virus”. Now a PCR protocol requires them to know the genetic sequences of the alleged monkeypox virus, which takes us to this 2001 paper titled, “Human monkeypox and smallpox viruses: genomic comparison”. The paper claimed to have “isolated” the monkeypox virus in a rhesus monkey kidney cell culture from a scab of a monkeypox patient. Here the virologists are up to their old tricks again by asserting that: (a) the patient’s scab contains the monkeypox virus, and (b) it is now in their culture brew. They claimed to have sequenced the “viral genome” by referring to a process described for sequencing an alleged variola virus in 1993.
But when we look at this paper there is no virus demonstrated either, simply an assertion that it was “isolated” from, “the material from a patient from India” in 1967. They go on to make the claim that, “the virions were purified by differential centrifugation and viral DNA was isolated” – however, there is no demonstration of what they purified or how they were determined to be virions. In none of these experiments did they perform any controls by seeing what sequences can be detected from other human-derived scabs or similar specimens from unwell individuals. This is where we need to remind the virologists of what a virus is supposed to be – that is a replication-competent intracellular parasite that infects and causes disease in a host. It is not detecting genetic sequences contained within scabs and claiming that it belongs to a virus.
So returning to the CDC’s paper describing the 2003 “outbreak”, it is unclear how they established they could be diagnosing anyone with monkeypox by using the PCR. Their PCR can only have been calibrated to sequences of unproven provenance. Additionally, it doesn’t matter what kind of analytical specificity their PCR protocol had, there was no established diagnostic specificity – in other words it was not a clinically-validated test, an issue that goes beyond whether the “virus” exists or not. (From the MIQE Guidelines: Analytical specificity refers to the qPCR assay detecting the appropriate target sequence rather than other, nonspecific targets also present in a sample. Diagnostic specificity is the percentage of individuals without a given condition whom the assay identifies as negative for that condition.)
The 47 US cases they ended up describing were all in some sort of contact with imported African prairie dogs and the CDC’s paper concludes that, “individuals contracted MPXV infections from infected prairie dogs; no human-to-human transmission was documented, but there were many different potential scenarios of infection involving respiratory and/or muco-cutaneous exposures, percutaneous and/or inoculation exposures”. Now there were some problems with the study design which they admitted to including that, “the analyses were limited by incomplete reporting or recall of information by patients. And, because of the retrospective nature of the study, we were unable to obtain highly detailed data”.
However, even allowing some wriggle room for them here, the inconsistencies go further still. Firstly, no one in the US incident died from the disease which is said to have a 10% fatality rate in Africa. No doubt, the inconsistent lethality rates will be attributed to different “variants”, but there can’t be variants of something that doesn’t exist.
There were few images available of the skin lesions that were reported in the 2003 incident but two of the US cases are depicted below and an image from a monkeypox case in Africa is shown for comparison. The reader can make up their own mind but those skin reactions do not look remotely comparable to us.
Next, the CDC claim that, “the natural reservoir of monkeypox remains unknown. However, African rodents and non-human primates (like monkeys) may harbor the virus and infect people” – in other words it’s all rather vague and remains an unproven hypothesis. Now, obviously some people became unwell in the US in 2003 but with the viral theory we are supposed to believe that it jumped from some prairie dogs to some humans and the latter became infected with the alleged virus…but then no human could pass it on to another human. The theory falls flat – a virus needs to spread, if it can’t spread, it’s dead and thus it’s not a virus. And the historical patterns of alleged monkeypox virus outbreaks make no sense – why did it pass to these people so easily and yet it can go a decade between alleged “outbreaks”?
Unfortunately, the 2003 incident was investigated as though the viral contagion theory had already been established and other explanations were ignored. If people were allegedly getting sick from these African rodents, wouldn’t it be a good idea to check the animals for other toxicities, particularly in their faeces and also for any ticks or parasites? We did note another reference state that with regards to the US cases, “many of the people had initial and satellite lesions on palms, soles, and extremities”. However, according to the CDC, monkeypox usually starts on the face so the clinical picture in the US cases was not consistent with cases that are typically described in Africa.
In any case, a review of the scientific evidence revealed that with regards to monkeypox: (a) there is no evidence of a physical particle that meets the definition of a virus, (b) there is no evidence of anything transmitting between humans, and (c) there is no way to confirm a diagnosis of monkeypox unless you believe in clinically-unvalidated tests such as the PCR kits that have been produced. In other words, if we see a monkeypox “pandemic” that is used as an excuse to role out more globalist terrorism, it will be on the back of another PCR pandemic, not one that has any basis in nature.
For those of you wanting to explore more problems with the various monkeypox claims, Mike Stone of ViroLIEgy has written a couple of interesting commentaries. The first article is, “Was Smallpox Really Eradicated?”, which among other things deals with the convenient emergence of monkeypox while smallpox was apparently being eradicated. The second article is, “Did William Heberden Distinguish Chickenpox From Smallpox in 1767?” This outlines the fact that the pox conditions are not as readily distinguishable from each other as the text books suggest and appear to relate more to the severity of a similar disease process. You can also watch our video, “Chickenpox Parties and Varicella Zoster Virus?” to see why there is no evidence of a virus in that related condition either.
From the perspective of terrain theory it is a fundamental mistake to attribute a person’s illness to a supposed virus, as the subsequent “treatments” don’t address the underlying issues. If someone is unwell, then they are usually deficient in nutrients and need to restore balance, or they have been exposed to environmental toxins and need to help the body detoxify. Wars against alleged pathogens that involve treating everyone the same way with civil rights restrictions and vaccines are certainly not about heath. It is good to see more people waking up to the COVID-19 fraud so there is hope that a monkeypox scamdemic, if attempted, will bring even more light to the situation. As always, your best health is in your own hands, not in the hands of a globalist cult and their cronies.
If you have been outsourcing your health, there has never been a better time to free yourself from the virus fear narrative and begin manifesting your full potential instead.
The doctors, scientists and journalists featured in THE VIRAL DELUSION examine in detail the scientific papers that were used to justify the pandemic, and what they find is shattering. In this shocking, five-part, seven hour documentary series, they explode every single major claim, from the “isolation” of the virus to its so-called genetic sequencing, from the discovery of how to “test” for SARS-CoV2 to the emergence of “variants” that in reality, they explain, exist only on a computer. Their point: that the so-called SARS-CoV2 virus exists only as a mental construct whose existence in the real world has been disproven by the science itself.
They then go back through history to reveal how the birth and growth of virology has led to massive misunderstanding and misdiagnosis of disease: from Smallpox to the Spanish Flu, Polio to AIDS, to COVID itself – putting the pandemic in a whole new context better understood not as settled science, but the tragic culmination of misunderstood biology by the growing cult of virology, built on pseudo-science, to which much of the rest of the medical profession defers without understanding or examination, and the tragic consequences that have been wrought in its name.
In 2019, the virologists took center stage, and for the first time on film, their methods, miscues and tragedy they have wrought are put under the spotlight, revealing the extraordinary leaps of fantasy buried in their methodology, the contradictions quietly acknowledged in their papers, their desperate effort to change language to justify their findings, the obvious incongruence of their conclusions and the extraordinary stakes for our entire society in whether we continue to blindly follow their lead into a full-scale war against nature itself.
Featuring: Andrew Kaufman, MD; Tom Cowan, MD; Stefan Lanka, Virologist; Torsten Engelbrecht, journalist; Claus Kohnlein, MD; Kevin Corbett, PhD RN; David Rasnick, Biochemist PhD; Mark Bailey, MD; Dawn Lester and David Parker, Authors; Stefano Scoglio, Biochemist PhD; Saeed Qureeshi, Chemist PhD; Celia Farber, Journalist; Harold Wallach, PhD; Pam Popper, PhD, ND; Charles Geshekter, PhD; Amandha Vollmer ND, Jim West, Author; Larry Palevsky MD; and more.
The Viral Delusion (2022) Episode 1:The Tragic Pseudoscience of SARS-CoV-2
When doctor Andrew Kaufman began reading the first virology papers out of Wuhan in December 2019, he was shocked to discover that the scientists had come nowhere close to proving that a new virus had emerged… yet saw the media and authorities already claiming a viral pandemic was on it’s way.
In this extraordinarily revealing opening episode, a group of biologists, chemists, doctors and journalists take apart the SARS-COV-2 narrative piece by piece — from the non-isolation of the virus, to the hidden problems with purported photographs of the virus, to the claims that it has been genetically sequenced, to the invalidity of the PCR “covid-test.”
From the treatment protocols for COVID to the assumption of its transmission, Episode One unpacks the science of the claims that changed the world – in which these doctors and scientists make the case that every single claim the authorities made about the so-called SARS-COV2 virus has been based not on evidence, but pseudoscience.
The Viral Delusion (2022) Episode 2: Monkey Business: Polio, Measles And How It All Began
How did it all begin?
How could the scientific establishment have possibly gotten so big a story so wrong?
Everyone knows the story of Polio…or do they?
What from that story is actual history and what is medical marketing?
How did a small branch of the scientific establishment come to convince the world polio was the result of a virus and not from environmental toxins?
Learn what the actual experiments were upon which this theory was based — and how shockingly unconvincing they are.
Discover too how the medical establishment’s efforts to squeeze the symptoms of polio into a virus model formed the very foundation of modern virology, and how that commercially successful model has steered modern science ever since, evidence be damned.
The Viral Delusion (2022) Episode 3: The Mask of Death – The Plague, Smallpox and The Spanish Flu
What about Smallpox?
The Spanish Flu?
The Black Plague?
Go back, back, back in time to examine the claims and counter-claims as to what truly caused these deadly epidemics.
Are the rats of Europe innocent? Turns out they have to be…
And in that discovery we see how the superstitions of our time have clouded the eyes of “science” to avoid the most obvious of insights about disease.
The Viral Delusion (2022) Episode 4: AIDS, The Deadly Deception
AIDS. It was the defining epidemic of a generation.
But it was also the coming of age for many leading scientists and doctors who came to realize that blaming the illnesses known as AIDS on a virus was not only unsupported by science, it was downright nonsensical.
What were the true causes of the many illnesses labelled AIDS around the world?
How many suffered from their misdiagnosis?
How the scientific establishment fell into the deadly AIDS delusion is crucial to understanding the pandemic, and health, today.
The Viral Delusion (2022) Episode 5: Sequencing The Virus, Without The Virus
With the rise of computing and genetic research in the 90’s the virologists go high-tech.
They move away from experiments altogether and into genetic modeling — but do the models have any connection to reality?
The wonders of genetic sequencing have been pointed to as the proof of virology’s explanatory power — but when the claimed sequencing of SARS-COV2 is put under the microscope, has the game changed from the realm of science, to science fiction?
What’s really going on the claim of genetically identifying the SARS-CoV-2 virus is made?
“Here’s another fun fact. The entire medical cartel thrives on the insane proposition—launched
with fervor more than a hundred years ago—that people suffer from thousands of distinct
diseases, each of which is caused by a single germ, which must be treated by a toxic drug and
prevented by a toxic vaccine.
It is this great lie that that has killed millions upon millions upon millions of people.”
The headline of this article has become a battle cry among some “alternative journalists,” activists, lawyers, and doctors.
As my readers know, I’ve devoted considerable space, over the past two years, to presenting evidence that SARS-CoV-2 is a scientific fairy tale, a con, and the virus doesn’t exist.
So when I hear this battle cry, I’m motivated to mention a few significant points.
Let me start by countering the claim that debating the existence of the virus is wasting time.
Here’s a shocker. A person can do more than one thing at the same time. For example, he can expose/oppose the toxic vaccine. He can expose the murderous COVID treatments (ventilators, sedatives, antiviral drugs). He can expose using simple flu-like illness to create fraudulent COVID case numbers.
And he can ALSO expose the fact that the virus has never been isolated (discovered) or sequenced.
So highlighting the non-existence of the virus doesn’t rule out dealing with other vital concerns.
This may come as a surprise, but it’s even possible to go to court to challenge a vaccine mandate, while ALSO arguing elsewhere that the virus doesn’t exist. I know. Amazing, right?
Those alarmed by “the virus doesn’t exist” also say: making that statement leaves us open to being called whackos, and leaves us unable to convince people that all our other criticisms of the pandemic are true.
I would counter that in two ways. Millions of people already believe we’re whackos, even those of us who take a sacred blood oath that the virus is real.
And second, people going against the grain, when their vital issue is still in the budding stage, are always called nuts. Trust me, there was a time when criticizing vaccines made people look like total whackos in the eyes of the general public—and it took decades of fighting the consensus to bring that criticism into the open, where many people saw the truth about jabs.
Here’s another fun fact. The entire medical cartel thrives on the insane proposition—launched with fervor more than a hundred years ago—that people suffer from thousands of distinct diseases, each of which is caused by a single germ, which must be treated by a toxic drug and prevented by a toxic vaccine.
It is this great lie that that has killed millions upon millions upon millions of people.
Therefore, the very real question about the existence of viruses in general is more than a weird preoccupation.
Next, those who claim, “OF COURSE viruses exist,” don’t know what the hell they’re talking about. They’re merely PARROTING what they learned in school or what researchers baldly claim in studies.
“Well, all virologists can’t be wrong.”
Yes, Virginia, they can all be wrong. Just as vaccinologists can all be wrong about “the remarkable safety and efficacy of vaccines.”
Some of the OF COURSE VIRUSES EXIST people are new to the way blogs and videos work. They’ve never encountered commenters in any great numbers before. So when a few dozen committed people suddenly tell them they should examine their premises more carefully and consider what really goes on in virology labs, these OF COURSE people are annoyed and irritated. They don’t like being challenged on basic issues. They don’t like feeling that the floor might suddenly shift under their feet. So they turn on their arrogance machines.
So be it.
The issue isn’t going away. Nor should it.
Despite growing digital censorship, the internet is still the Wild West in certain respects. People are going to say THE VIRUS DOESN’T EXIST, and VIRUSES DON’T EXIST.
And foundations will shake.
Foundations of the medical cartel, and foundations underlying people’s cherished assumptions.
In any area of human life, there are conflicts between “this is strategy” and “this is the truth.” There always will be.
Trying to shortchange the truth or casually say the truth is a lie doesn’t work.
NO ONE who is reading this article has ever been in a virology lab and witnessed the step by step process of “discovering a new virus.” I find that stunning. And yet all sorts of people are quite ready to assert with great finality that they know all about isolating viruses.
If by chance, someone reading this article HAS actually been in a lab and “discovered a virus,” you can bet your bottom dollar he won’t let you or me in there with a full film crew and our outlier experts asking very pointed questions about each “scientific” move he makes, as he “isolates a virus.”
To which somebody might reply: “Well, I’ve never seen a car being made in a factory, but I drive one with full confidence.”
Yes, but when the “virus discovered in a lab” results in you or someone you love being dosed with a drug or vaccine that maims you or kills your family member, you damn well should want to get into “that factory where the car is made.”
But you can’t. They won’t let you…
…Despite the fact that, as I’ve documented many times, the US medical system kills, by a very conservative estimate, 225,000 people a year, or 2.25 million people per decade. [0]
Chew on THAT for a while.
Here is one of my articles on the subject of virus isolation:
The global medical community has been asserting that “a pandemic is being caused by a virus, SARS-Cov-2.”
But what if the virus doesn’t exist?
People have been asking me for a step-by-step analysis of a mainstream claim of virus-isolation. Well, here it is.
“Isolation” should mean the virus has been separated out from all surrounding material, so researchers can say, “Look, we have it. It exists.”
I took a typical passage from a published study, a “methods” section, in which researchers describe how they “isolated the virus.” I sent it to Dr. Andrew Kaufman [1], and he provided his analysis in detail.
I found several studies that used very similar language in explaining how “SARS-CoV-2 was isolated.” For example, “Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States, (Emerging Infectious Diseases, Vol. 26, No. 6 — June 2020)” [2].
First, I want to provide a bit of background that will help the reader understand what is going on in the study.
The researchers are creating a soup in the lab. This soup contains a number of compounds. Human cells, monkey cells, antibiotics, other chemicals, random genetic material.
The researchers assume, without evidence, that “the virus” is in this soup, because they’re dropped a mucus sample from a patient in the soup. At no time do they separate the purported virus from the surrounding material in the soup. Isolation of the virus is not occurring.
They set about showing that the monkey (and/or human cells) they put in the soup are dying. This cell-death, they claim, is being caused by “the virus.” However, as you’ll see, Dr. Kaufman dismantles this claim.
There is no reason to infer that SARS-CoV-2 is in the soup at all, or that it is killing cells.
Finally, the researchers assert, with no proof or rational explanation, that they were able to discover the genetic sequence of “the virus.”
Here are the study’s statements claiming isolation, alternated with Dr. Kaufman’s analysis:
STUDY: “We used Vero CCL-81 cells for isolation and initial passage [in the soup in the lab]…”
KAUFMAN: “Vero cells are foreign cells from the kidneys of monkeys and a source of contamination. Virus particles should be purified directly from clinical samples in order to prove the virus actually exists. Isolation means separation from everything else. So how can you separate/isolate a virus when you add it to something else?”
STUDY: “…We cultured Vero E6, Vero CCL-81, HUH 7.0, 293T, A549, and EFKB3 cells in Dulbecco minimal essential medium (DMEM) supplemented with heat-inactivated fetal bovine serum (5% or 10%)…”
KAUFMAN: “Why use minimal essential media, which provides incomplete nutrition [to the cells]? Fetal bovine serum is a source of foreign genetic material and extracellular vesicles, which are indistinguishable from viruses.”
STUDY: “…We used both NP and OP swab specimens for virus isolation. For isolation, limiting dilution, and passage 1 of the virus, we pipetted 50 μL of serum-free DMEM into columns 2–12 of a 96-well tissue culture plate, then pipetted 100 μL of clinical specimens into column 1 and serially diluted 2-fold across the plate…”
KAUFMAN: “Once again, misuse of the word isolation.”
STUDY: “…We then trypsinized and resuspended Vero cells in DMEM containing 10% fetal bovine serum, 2× penicillin/streptomycin, 2× antibiotics/antimycotics, and 2× amphotericin B at a concentration of 2.5 × 105 cells/mL…”
KAUFMAN: “Trypsin is a pancreatic enzyme that digests proteins. Wouldn’t that cause damage to the cells and particles in the culture which have proteins on their surfaces, including the so called spike protein?”
KAUFMAN: “Why are antibiotics added? Sterile technique is used for the culture. Bacteria may be easily filtered out of the clinical sample by commercially available filters (GIBCO) [3]. Finally, bacteria may be easily seen under the microscope and would be readily identified if they were contaminating the sample. The specific antibiotics used, streptomycin and amphotericin (aka ‘ampho-terrible’), are toxic to the kidneys and we are using kidney cells in this experiment! Also note they are used at ‘2X’ concentration, which appears to be twice the normal amount. These will certainly cause damage to the Vero cells.”
STUDY: “…We added [not isolated] 100 μL of cell suspension directly to the clinical specimen dilutions and mixed gently by pipetting. We then grew the inoculated cultures in a humidified 37°C incubator in an atmosphere of 5% CO2 and observed for cytopathic effects (CPEs) daily. We used standard plaque assays for SARS-CoV-2, which were based on SARS-CoV and Middle East respiratory syndrome coronavirus (MERS-CoV) protocols…”
STUDY: “When CPEs were observed, we scraped cell monolayers with the back of a pipette tip…”
KAUFMAN: “There was no negative control experiment described. Control experiments are required for a valid interpretation of the results. Without that, how can we know if it was the toxic soup of antibiotics, minimal nutrition, and dying tissue from a sick person which caused the cellular damage or a phantom virus? A proper control would consist of the same exact experiment except that the clinical specimen should come from a person with illness unrelated to covid, such as cancer, since that would not contain a virus.”
STUDY: “…We used 50 μL of viral lysate for total nucleic acid extraction for confirmatory testing and sequencing. We also used 50 μL of virus lysate to inoculate a well of a 90% confluent 24-well plate.”
KAUFMAN: “How do you confirm something that was never previously shown to exist? What did you compare the genetic sequences to? How do you know the origin of the genetic material since it came from a cell culture containing material from humans and all their microflora, fetal cows, and monkeys?”
—end of study quotes and Kaufman analysis—
My comments: Dr. Kaufman does several things here. He shows that isolation, in any meaningful sense of the word “isolation,” is not occurring.
Dr. Kaufman also shows that the researchers want to use damage to the cells and cell-death as proof that “the virus” is in the soup they are creating. In other words, the researchers are assuming that if the cells are dying, it must be the virus that is doing the killing. But Dr. Kaufman shows there are obvious other reasons for cell damage and death that have nothing to do with a virus. Therefore, no proof exists that “the virus” is in the soup or exists at all.
And finally, Dr. Kaufman explains that the claim of genetic sequencing of “the virus” is absurd, because there is no proof that the virus is present. How do you sequence something when you haven’t shown it exists, and you don’t have an isolated specimen of it?
Readers who are unfamiliar with my work (over 375 articles on the subject of the “pandemic” during the past year [4]) will ask: Then why are people dying? What about the huge number of cases and deaths? I have answered these and other questions in great detail. The subject of this article is: have researchers proved SARS-CoV-2 exists?
I came across this Facebook post recently by Dr Tom Cowan. He is yet another qualified and intelligent voice of reason steadfastly and dedicatedly censored by the corporate media in an ongoing and increasingly desperate effort to prevent the People getting wise to things they don’t want you to know.
The truth of the matter is these highly qualified a voices of reason are growing in number and ubiquity at an accelerating rate and the enemies of Humanity are having dickens of a job keeping lid on the volcano.
The entire biochemical paradigm of the pharmaceutical-industrial complex that results in the systemic poisoning of Man, which itself is intended to render human beings tired, sick and introverted on their health – and thus neutralised as potential sources of trouble (ie liberty) -is now in jeopardy.
All we have to do is keep going, keep speaking out, keep right on advocating Reason and common sense and keep on bringing to the attention of the People the huge reservoir of wisdom and more workable paradigms that are being kept from them by those with a vested interest in prolonging the Dark Age 0f their barbarism.
In other words, simply REFUSE to shut up.
And the more we can unite and work together, the sooner the Dark Age will be over and the Age of Reason begun.
Dr Tom Cowan is a highly recommended voice of reason.
And here by way of a taster is his post from Facebook
As you can see from this blockbuster article published on Aug. 9, 2016, in the prestigious journal Nature, researchers conclusively demonstrated that whenever fetal calf serum is added to any cell culture (as is done in virtually all modern virology studies, including those used during the past two years), it is simply impossible to use the results of this culture to determine the RNA sequence of any new vîru$. As they demonstrate, fetal calf serum itself is a rich source of many types of RNA sequences. Once this is introduced into the cell culture, from then on, there is no way to determine the origin of the RNA that researchers find.
The significance of this study cannot be overstated and validates what we’ve been saying for many months. Virologists use cell cultures to prove the existence of a new vîru$ and its cytopathic effect. If the culture is contaminated, as this study demonstrates, any claims about a new vîru$ and its genetic makeup are meaningless.
1. Every thirty seconds vivisectors around the world kill another thousand animals. They use cats, dogs, puppies, kittens, horses, sheep, rats, mice, guinea pigs, rabbits, monkeys, baboons and any other creature you can think of.
2 .While waiting to be used in laboratory experiments, animals are kept in solitary confinement in small cages. Alone and frightened they can hear the screams of the other animals being used.
3. Some of the animals used in laboratory experiments are pets which have been kidnapped, taken off the streets and sold to the vivisectors.
4. Animals used in experiments are blinded, burned, shot, injected and dissected. They have their eyes sewn up or their limbs broken. Chemicals are injected into their brains and their screams of anguish are coldly recorded.
5. Three quarters of the experiments performed by vivisectors are done without any anaesthetic.
6. Most vivisectors have no medical or veterinary training.
7. Scientists claim that animals are not sentient creatures and are incapable of suffering mental or physical pain.
8. All animals respond differently to threats of any kind depending on their circumstances (diet, cage size, etc.). None of these factors is allowed for by vivisectors. By locking an animal up in a cage, experimenters have already invalidated their experiment because by altering the animal’s surroundings, the experimenter alters the animal’s susceptibility, its habits, its instincts and its capacity to heal itself. Since these variations are not controlled (cages and surroundings differ) experiments performed on animals kept in cages are of no scientific value.
9 Many of the diseases which kill or cripple human beings do not affect any other members of the animal kingdom. It is, therefore, impossible to use different species to test drug therapies for these illnesses.
10. Doctors wouldn’t test a drug intended for old people on children (or the other way round). So why test drugs intended for pregnant women on rats? No one would test a drug for premenstrual problems on small boys and yet that would make far more sense than testing such a drug on male rats.
11. Drug tests done on animals can produce dangerously unreliable and misleading information. Thalidomide safely passed tests on animals. Penicillin and aspirin both kill cats. When Alexander Fleming discovered penicillin growing on a culture dish in 1928, he tested the drug on rabbits and discarded it when it seemed useless. Later the drug was tested on a cat and a human patient at the same time. The cat died and the human being lived. If doctors had relied upon animal experiments to decide whether or not penicillin was of any value, the drug would have been discarded long ago. Penicillin even kills guinea pigs – the classic test animal for many drugs. Aspirin can be toxic to rats, mice, dogs, monkeys and guinea pigs as well as cats. Morphine sedates human beings but excites cats, goats and horses. Digitalis, one of the best established and most effective drugs for the treatment of heart disease, is so toxic to animals that if we had relied on animal tests it would have never been cleared for use by humans.
12. Vivisectors admit that most animal experiments are unreliable and produce results which are not relevant to human patients. But they don’t know which experiments are unreliable. Logically, that means that all animal experiments are useless. If you don’t know which experiments you can rely on, you can’t rely on any of them.
13. The very unreliability and unpredictably of animal experiments is what makes them commercially valuable. Drug companies test on animals so that they can say that they have tested their drugs before marketing them. If the tests show that the drugs do not cause serious disorders when given to animals the companies say: `There you are! We have tested our drug – and have proved it to be safe!’ If, on the other hand, tests show that a drug does cause serious problems when given to animals the companies say: `The animal experiments are, of course, unreliable and cannot be used to predict what will happen when the drug is given to humans. We have, however, tested our drug.’ Tests which show that a drug causes cancer or some other serious disease when given to animals are ignored on the grounds that animals are different to people. However, tests which show that a new drug doesn’t kill animals are used as evidence that the drug is safe for human consumption. If you try a drug on enough different animals you can usually end up with at least one set of results which suggest that a drug is safe. Scores of drugs which cause cancer or other serious health problems in animals are widely prescribed for human patients. (See www.vernoncoleman.com for the names of 50).
14. Four out of ten patients who take a prescribed drug which has been tested for safety on animals can expect to suffer severe or noticeable side effects.
15. Surveys show that most practising doctors are opposed to vivisection on scientific grounds.
Taken from The Wisdom of Animals by Donna Antoinette Coleman and Vernon Coleman. Available as a paperback and an eBook.
I wrote this article in 2010. It’s truer now than it was then:
DECEMBER 5, 2010. About ten years ago, I decided that the medical cartel could become the most dangerous of all power groups on the planet. I have not changed my mind.
My decision is based on looking up the road 40 or 50 years and inferring what the picture will look like then.
It’s clear to me that drug companies, as they carve up markets and create new markets, are eagerly anticipating the day when every human, from cradle to grave—actually from inside the womb—has the status of Patient.
A person is born a patient and dies a patient. And in between, he receives 40 or 50 key diagnoses of physical and mental diseases/disorders and takes prescribed drug and surgery treatments.
More than that, though, he is stamped with the label, Patient, and he learns that everyone is in the same boat. “We’re all patients, this is a medical world, and it’s normal to be disabled in some way.”
People become proud, yes, proud to be victims. They wear their diagnoses as badges of honor. If you can’t see this trend, you’re not looking.
And universal health care insurance guarantees continuous treatment all the way along the line.
Every medical diagnosis becomes an excuse not to perform, not to excel, not to pursue big goals with large ambition.
Nowhere in the search to gain recognition as a victim do circumstances conspire so well as in the medical arena. It’s perfect. There’s no argument. The doctor told you you have X disease. That’s that. It’s not political. It’s not agenda-driven. It’s science. The proof is laid out on a silver platter. You ARE a victim.
In the coming future, every move a person makes, every step he takes will come under the umbrella of the doctor.
And, again, the main supporter of this system will be the patient himself. That’s how beautiful the marketing is.
In case you’ve been living in a cave for the last 30 years, drug companies and their researchers can invent any vague disease label they want to—and then they can invent five or six sub-categories of the label—and they can set out rules on how to diagnose each sliver of the label—and of course the doctors will make these diagnoses and prescribe drugs. It’s marketing and “healing” at the same time.
Parents who don’t have a clue will submit their children to this system—especially if the government pays for it—and the children will grow up trained to think of themselves as patients/victims…and the only contest will be: who has the most drastic diagnoses and treatments? Who can most proudly wear the badge of honor as Patient?
“Last month, they had to remove my head for five minutes while they fixed my brain.”
“Wow. Well, they put me in a body cast for three months and I couldn’t move, except for my left thumb.”
Cradle to grave.
If you go back and read Huxley’s Brave New World again, you’ll notice the factor of “patient pride.” It isn’t just that the society is controlled, the citizens are idealistic about it.
That’s where the victim industry is heading.
Against it, we have, what?
A little thing called individual freedom. Which includes the right to refuse medical treatment, no matter who prescribes it under what regulations.
People imagine that this right is some arcane matter best debated in medical-ethics journals. It’s an obscure curio.
They couldn’t be more wrong.
As I’ve been writing, the ObamaCare plan contains the seeds of a future in which, by law, the citizen will have less freedom to determine his own medical fate. The walls will gradually close in.
The Founders knew what they were talking about when they warned of the incursion of government and the loss of freedom. At every crossroad, since then, the issue of freedom has resurfaced as the unavoidable key factor.
Dr. Sam Bailey: On Health Freedom Advocates Who Attack Anyone Who Dares to Question Virus & Germ Theory | How RFK, Jr. Was Recently Drawn Into the Viral Existence Debate
Truth Comes to Light editor‘s note: In the video below, Dr. Sam Bailey talks about specific attacks, coming from within the health freedom movement, on the work of those who are questioning the foundations of virus theory.
At this point, most people in the health freedom movement, not to mention the general population, don’t even know that there is a strong debate about the existence of viruses. But awareness is growing.
The so-called, ‘settled science’ of virology must be looked into carefully because, as Dr. Sam Bailey has stated, virus and germ theory “is a system that can and will be used repeatedly to promulgate fear and compliance in the population.”
Dr. Bailey is careful to emphasize that RFK, Jr. is not one of those attacking the work of those who question virology. In this video she shares a segment from a recent public Q&A session wherein Eric Coppolino asks RFK, Jr. some basic questions, pointing to the fact that SARS-C0V-2 has never been shown to exist outside of imagined computer models.
You will find a transcript below the video with links to referenced articles and papers.
RFK, Jr. has been a tireless campaigner in warning the public about the problems of vaccines. However, with regards to the viral existence problem, he has been reluctant to get involved.
Let’s find out what happened when he was drawn into the debate in a recent Q&A session…
Questioning the existence of viruses can be a risky business, as myself and others have found out. However, once you’ve seen the problems with viral theory, it’s not something that can be unseen. It becomes a realization that much of what you were told is factual is not founded in scientific evidence at all. You start to research the material and find that many of the narratives are driven by industry participants and folklore rather than organic science.
While most probably don’t have a dog in the fight, those defending the virus narrative can get pretty hostile.
However, others such as RFK, Jr. simply appear uneasy about mentioning the virus existence issue.
So let’s find out what happened when one of the champions of the health freedom movement was unexpectedly drawn into the debate.
From the start I would like to make it clear that I consider RFK Jr. an ally in promoting health freedom and autonomy. He is a world leader and raising awareness about the risks and ineffectiveness of many vaccines.
I would also say that he has not been ambiguous with regards to his public statements relating to the existence of SARS-CoV-2 or other viruses. As far as I’m aware, he has stated that he believes such viruses exist. Although, in many cases the risks to health and the necessity for a lot of vaccines have been overstated.
I’d also suggest that the virus existence debate does not mean the current health freedom movement will be fractured as some seem to fear.
I don’t mind if other people believe in viruses and germ theory. However, as we point out in ‘Virus Mania’ that is a system that can and will be used repeatedly to promulgate fear and compliance in the population. Once the fatal flaws in the contagion theory are understood, people no longer buy into any of it and don’t get distracted trying to explain different aspects of the scam.
But before we get into RFK Jr.’s recent statements, there have been a few other prominent health freedom fighters who have made forays into the virus existence debate this year.
One was Steve Kirsch. He has been very outspoken about the dangers of the Covid-19 vaccine. Kirsch has realized that many doctors, governments and pharmaceutical companies are playing a game of deception with the public.
But then, on the issue of virus existence he places his faith in the high priests of virology. In early January this year, he decided to announce in his popular blog that SARS-Cov-2 has been isolated and shown to exist.
First, he smeared Drs. Lanka, Kaufman and Cowan with completely inaccurate portrayals of their work and received a huge backlash from his followers in the comment section. Instead of realizing that he might need to conduct his own research into this topic, he then decided to include Christine Massey and myself in the smears.
In a subsequent article 11 days later, curiously Kirsch suggested that we would not front if a live debate was offered.
Well, I can tell you from a series of emails that took place, which Kirsch was part of, that Drs. Bailey times two [Drs. Mark and Samantha Bailey], along with Stefano Scoglio, Drs. Lanka, Cowan and Kaufman, all volunteered to take part in a live debate with any experts that Kirsch was able to produce.
Instead of admitting that he was in over his head, Kirsch posted a third article the following week, embarrassing himself even further with declarations such as: ‘The reason nobody has purified the virus is there is no need to do so in today’s world where gene sequencing is readily available.’ And, ‘if the virus doesn’t exist, then how can 600 labs across the country find the same sequences for the virus in infected samples.’
These kind of statements indicate he’s unaware of the fundamentals of the virus existence debate.
Kirsch doesn’t see that he relies on other “experts” to inform him on the issue. And my husband Mark has written about why this is not a good idea, outlining the nature of the evidence such experts present in his article ‘Warning Signs You’ve Been Tricked by Virologists‘.
As Kirsch has worked out that people selling vaccines may be misleading people, then we would suggest that he peel back another layer to check whether the pharmaceutical and virology establishment, who have billions of dollars of vested interests, may be misleading people with regards to viruses as well.
And some other information I can give you is that I reached out to Steve after he posted his articles offering him a chance to connect, as well as a complimentary copy of ‘Virus Mania’. But he never responded.
In any case, he seems to have gone quiet on the virus existence front, perhaps because he genuinely thinks it’s […] science. Although I would hope that he has some inkling now that there’s more to this than he thought.
Another interesting smear attack against me from a supposed health freedom fighter came from Dr. Roger Watson, writing for The Daily Sceptic in March this year.
This was surprising on a number of fronts. Firstly, because the website developed out of lockdown sceptics and has the motto “question everything”.
However, it seems that questioning the existence of SARS-CoV-2 and the existence of viruses in general is a bridge too far for the so-called ‘Sceptic’.
Secondly, along with my allies including Andy Kaufman and Kevin Corbett, Watson co-signed the viral challenge letter to Boris Johnson demanding that the British prime minister provide proof of the Covid-19 virus. And, if not, then all measures against the nonexistent virus should be dropped.
Obviously, Watson changed his mind at some point and I’m not clear on why that happened. In any case, I had some fun dismantling Watson’s various allegations in my articles ‘The COVID “Sceptics” Who Spread Viral Dogma‘.
Watson’s article was arguably worse […]
Like Kirsch, Watson did not want to enter into a debate about the topic and couldn’t find anyone to front up in his place either. But at least he responded to our emails.
So, now we get to RFK, Jr., which is a slightly different story, as he has not been involved in any smears against me.
In fact, those of you familiar with ‘Virus Mania’ will know that he wrote an important section for our book titled ‘Greed, Negligence and Deception in the Vaccine Industry’.
RFK, Jr. is certainly aware of the controversy surrounding the existence of HIV. As he outlined in his 2022 publication ‘The Real Anthony Fauci’, our friend Tom Cowan even gets a mention in the book when he says: “The first time that someone — Dr. Tom Cowan, a physician from northern California — suggested to me that HIV was not the sole cause of AIDS, I dismissed the comment as ridiculous.”
However, in Chapter 5, ‘The HIV Heresies’, RFK, Jr. goes on to explain how his own research made him realize that there were major problems with the HIV theory.
He is even aware of The Perth Group and the devastating criticisms of the very existence of an infectious HIV particle. Commenting, “In my conversations with Turner and Papadopulos, and in my reading of their paper, I find their arguments clear and convincing. However, I recognize that there are some fifty thousand articles on AIDS in the scientific literature. A casual novitiate like myself has little chance of unraveling this baroque controversy in a vacuum.”
However, most of RFK, Jr.’s focus in the book is on the fact that Anthony Fauci has been instrumental in controlling the HIV/AIDS model and has ruthlessly suppressed dissenting voices.
My hope is that he will read The Perth Group paper ‘HIV – a virus like no other’ one more time and he’ll see there’s no evidence that a pathogenic particle termed HIV exists. And there is no need to read most of the fifty thousand AIDS articles if they fallaciously assert otherwise.
So what happened on April 24 this year — the fundraising event taking place at the Grand Hyatt Hotel in Greenwich, Connecticut?
During the Q&A session, my friend and journalist extraordinaire, Eric Coppolino, was there to put some key questions about the existence of SARS-CoV-2 to RFK Jr.
So let’s take a listen to the exchange that takes place between the two of them on that Sunday afternoon.
Eric Coppolino:
Hi Bobby. Thank you. Christine Massey in Toronto has amassed 182 responses under various Freedom of Information law requests from institutions, provincial, state, and federal, national governments which all say no one has a sample of SARS-C0V-2 taken from a human. Would you please comment on that?
RFK, Jr.:
Yeah, I really am not qualified to comment on it, but … My inclination if there are people who say that viruses don’t exist, that there is no virus… I don’t, you know, my inclination is that that simply is not, you know, that’s not true.
Dr. Sam Bailey:
At least he has admitted that he is relying on inclination, rather than having looked into the evidence himself as he has done with vaccines.
RFK, Jr.:
I can’t argue with you, and I can’t…I actually, on our list there’s a number of people who make those kind of arguments. And other people on the list server…and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.
Dr. Sam Bailey:
It’s hard to know exactly what he’s talking about here. If it’s the same virology papers we’ve been looking at, it is certainly unclear how this constitutes a lot of evidence. In my experience, they are usually reciting the paper’s title without critiquing the methodology, which is where all the problems are.
RFK, Jr.:
I am kind of amused reading the exchanges and my inclination is that viruses do exist and do make people sick. I could be wrong. It could all be a big hoax, but to me, it seems like viruses are real, and … look, I should have just shut up from the beginning and say I’m not gonna answer that question.
Eric Coppolino:
The governments have said they don’t have a sample.
RFK, Jr.:
…You know what? Actually I saw an email exchange yesterday where somebody made exactly that statement and then ten people jumped on him with examples of where that’s not true.
Dr. Sam Bailey:
This was news to me and I know it was news to Christine Massey, coordinator of the SARS-CoV-2 Freedom of Information Project, who demanded the data from the 10 people on Kennedy’s list who claim to prove that the virus had been isolated.
RFK, Jr.:
…The other thing is, I do know this, when you make a freedom of information request, the freedom of information laws do not require the government agency to do science, or to answer questions, specific questions. What they do is, they, the Freedom of Information laws make it obligatory for the government to give you existing documents. So, if you’re telling the government, “I want you to verify this.” They look at their documents and say, “There’s nothing here to verify it.” It doesn’t mean it’s not true. It means they’ve got nothing. But, listen, again, I am not a … scientist. I don’t pretend to be. I find those arguments interesting. And there’s a guy in California, who I deeply respect, Tom Cowan, who makes those arguments and it really… I can’t answer the question.
Dr. Sam Bailey:
This is another interesting statement and perhaps a chance for RFK, Jr. to reflect on the same battle he faces regarding raising awareness about vaccine problems. The mainstream could dismiss RFK Jr.’s arguments as “not being taken seriously by a lot of other people” because the majority of the medical industry still promote all vaccines. However, ‘appeal to popularity’ is a form of faulty reasoning and has no place in a scientific discussion such as this one.
My experience, and I’m sure Tom Cowan and all others in the movement can attest to, is that the majority of people are simply unaware of this debate and don’t even know that questioning the existence of a virus is a thing. And the individuals and corporations that gain from the virus theory often engage in active suppression of the debate.
Prior to widespread internet usage, dissident authors such as The Perth Group were refused publication opportunities in the medical journals. And in the modern era, material such as mine is banned on all the big tech platforms.
The virus theory was put forward in the late 1800s and, for most of us, it is a revelation to go back through the scientific literature and see the key postulants have not been fulfilled .
One of the most amusing, and perhaps tragic, things you’ll see is websites such as AIDSTruth claiming that the science is settled. In 2015 they announced that they were retiring the website because apparently their work was done. The first sentence of their self-congratulatory announcement shows just how disingenuous they are when they use the term ‘AIDS denialism’, knowing very well that what is in dispute is the HIV/AIDS theory or whether an infectious particle, termed HIV, actually exists.
The group also referred to ‘bumps in the early years of treatment’ which is an obscene way to refer to deaths caused by AZT.
In any case, I wonder if the team might consider resurrecting their website or if they are now too busy working on other projects under organizations such as the World Economic Forum and Johns Hopkins.
I think if they do decide to get back into it, they’ll find that the number of individuals and groups opposing their position on the HIV/AIDS theory has gone up dramatically.
Mike Stone of Viroliegy, put together a collection of some of the websites questioning viral theory. And many of them, including Viroliegy itself, have appeared in the last two years.
All the individuals I have personally spoken with, that have or are currently pointing out the flaws in viral theory, they share a number of things in common. Firstly, they all believed in the viral theory at some stage. But when they investigated it for themselves, something changed their minds. Secondly, they have all paid a price whether being publicly censured, smeared or blocked from working in the professions. Thirdly, they are all incredibly generous with their time and share the knowledge with everyone that is interested. And lastly, and perhaps most importantly, they have a passion for exploring the possibilities and following the scientific trail to wherever it takes them by freeing themselves from the shackles of institutional policies, industry capture and public regulatory bodies.
My feeling is that far more people are moving into the questioning the viral theory camp rather than the other way around.
Who knows. Perhaps now that the door has been opened, RFK. Jr. might take more of a look around.
So that we don’t lose touch please find me at drsambailey.com and sign up for my free newsletter.
Dr. Tom Cowan: A Close Look at Dr. Judy Mikovits’ Work Where She Attempts to Explain ‘SARS-CoV-2’
Dr. Tom Cowan has recently created a series of videos where he takes a close look at what some leaders in the anti-covid-vax arena are presenting as science. Dr. Cowan’s videos can be found at his Rumble and BitChute channels.
For those of you who listen to a lot of alternative “anti-vax” presentations about the origins of SARS-CoV-2 and end up feeling that you’ve just listened to a lot of faux-science gobbledygook, you’re not alone.
Below, Truth Comes to Light has clipped two key segments from the longer video where Dr. Cowan looks into Dr. Judy Mikovits’ presentations and papers related to SARS-C0V-2. Dr. Tom Cowan’s full video is also found below.
“Science has become the enterprise of people using words and concepts to make things, that everybody otherwise would understand, basically incomprehensible.”
“There are some basic ways that all of us — men, women, human beings — understand the world. It’s very clear and simple to us. And if we applied that same thinking to subjects in science and biology and medicine I think it would be fairly easy for us to find our way and to see what’s true and what isn’t true.
The problem has become that so-called scientists, especially virologists and medical doctors, have made the whole thing so confusing that most people seem to lose their bearings as far as understanding just the usual, common sense, logical, rational way of thinking and end up believing something that they wouldn’t possibly believe if they really understood the issues.”
“I’m not anti-vaccine. I just want them to be safer and more effective.”
I love that statement. It’s a lullaby. When I can’t go to sleep at night, I just repeat it to myself a few times, and I’m out cold.
It’s typical of half a revolution, which never wins.
For the past 32 years, I’ve presented overwhelming evidence that no vaccine was ever safe or effective. The whole “science” of vaccination is a rank fraud.
But stuffed-shirt journalists, who sort of go against the grain while maintaining a front of respectability, don’t want to venture that far. They know the price they’ll have to pay. They’re hedging their bets.
Occasionally, one of them will take a swipe at me. It cements their position as middle of the road. Which is where they want to be.
Except, liberty and freedom, which is what we’re fighting for, against a global coup by mass medical murders, isn’t something you win in the middle of the road.
You don’t win by trying to come off like a Washington Post reporter who just happens to have different and dissenting ideas. That’s what half-ass looks like.
That sort of person is basically saying, “I have a machine mind like other machine minds. The difference is, I’m inputting different data and therefore drawing different conclusions. If you, too, have a machine mind, read what I write and let’s establish truth and justice…”
The long-term effect of that is like pissing through a fire hose to put out a conflagration taking down a city.
This is simple. If one group of “superior” machine minds wins against another group of machine minds—regardless of which issues come out on top—there is no revolution. LIFE AND FREEDOM have been excised out of the equation.
A considerable amount of money and effort have gone into building a modern culture composed of what looks like science and rationality, but isn’t. It’s a cartoon. A fucking cartoon.
There’s no JUICE in it.
That’s why I use the phrase machine-minds. Minds that calculate and process and collate and compare and then exude “better answers.” This is your educated class. Careful, cautious. Circumspect.
“Delivery, sir. Here are flowers you ordered. I’m sorry they’re dead.”
“I don’t mind dead. But I ordered roses and you brought me tulips. I can prove it. Let me just find the receipt here on my cell phone. And then I can show you these withered blossoms are actually tulips. There are 32 differences between the two types of flowers…”
That’s your educated class.
See, I’ve been at this for 38 years. Reporting. Writing. Actually, I’ve been writing for 66 years. I’ve made the cases I wanted to make. I’ve shoved the evidence in people’s faces. The overall medical cartel is waging a VERY successful war against the people.
You have to turn that evidence with torque, with leverage, into a flamethrower. You’re not just trying to set the record straight and bring in truth, you’re using the truth to crash the gold-plated systems of machine minds.
Those minds are remote. Distant. Distant is where Big Tech domeheads operate from. They profile, they plan, they crunch trillions of pieces of data, and they develop strategies to build a civilization that looks like their minds and their computers.
When one of these high-IQ blown dry characters develops his version of a conscience, and turns whistleblower, he’s a hero to his ilk. He speaks their language. He thinks the way they do. He geeks like they geek.
If I have to guess which guy has more freedom in his belly and his brain, I’m going with the man who lives up in the hills of Tennessee with a shotgun and a dog. If he doesn’t like what I’m writing, I might think about his reasons for a half-hour. Whereas, when an “alt. journalist” claims I’m “going too far,” I know exactly what his game is. He’s spraying his usual brand of sanitizing respectable room-deodorant.
I’ll put this another way. Two men are discussing how to choose a wife. They’re looking at two different lists of characteristics a man should consider and check. But neither man mentions LOVE, so it doesn’t matter which list they decide is superior. They don’t know what love is. What they’re really discussing are machine-thoughts.
If the COVID narrative had never been launched, if we were living now as we did in 2018, we would still have a medical cartel taking away our freedom and killing and maiming an extraordinary number of people. And that will still be the case, even if all COVID mandates and restrictions are defeated.
Plus, the Brave New World on the drawing boards is fronted by medical people. Three of its main features are genetic engineering, nanotechnology, and human-computer interfaces and hybrids. If you think all possible freedom is now under fire, you haven’t seen anything yet.
Way back when, I was briefly trained in two schools. The first was formal logic, taught by a beloved college professor with an extraordinarily sophisticated mind and a huge heart. The second school consisted of two or three encounters with Ida Honorof, activist and author. She was barely five feet tall, and she had the energy, in her 70s, of ten tigers. She explained to me one afternoon, on a street corner, that officials in Los Angeles were spraying a version of deadly Agent Orange in the Angeles National Forest. She handed me a few pounds of corporate and government documents detailing the massive toxicity of a variety of pesticides. She kick-started my life as a reporter.
Neither one of these people engaged in coddling. They didn’t sit around planning their fronts and poses of respectability. They didn’t want half a revolution. They didn’t equivocate.
I’ve never been a big fan of equivocation. I’m over at the I-don’t-give-a-shit end of the spectrum.
Find answers—then shove in all your chips. At the end of the night, don’t leave anything on the table.
Fortunately for all of us, there is a life after this one. But we’re here now, so we’re fighting.
Make it COUNT.
In the wind and the rain and the storm, issue no apologies.
Good day, South Africa. My name is Ricardo Maarman and I’m from the Show Us the Virus movement.
Today is the 28th of April, 2022. It is the very day that our Leave to Appeal to High Court to challenge the negative judgment we had, with the cost order against me, was due. And so this is why I am giving you this update today.
Now before we proceed I just want to give you a background on the case and what has been happening so far.
You see, for the past two years (or more than two years) the president of South Africa, and many other presidents around the world as well — but in particular president of South Africa — came forward and made a claim.
He claimed that there was a virus called SARS-CoV-2 and this virus is causing a pandemic. And because of this, he has to take away all of the rights, or a lot of the rights, of the people of South Africa. And he has to impose these draconian lockdown, tyrannical regulations on the people.
And for the past two years, while he has been doing this, people have said many things.
You know, people have said this and that and the other in the showing their disapproval of what is going on and they’re opposition of what is going.
We at the Show Us the Virus movement have said one thing — can be summed up in one question that we have asked throughout this whole period. And that question is: Show us the virus. Show us the virus!
You make a claim that there is a virus, so show it to us.
And what we are faced with is controlled opposition who are trying to distract people from this question.
The president decided to fight the legal battle against me — a long protracted legal battle — and seemingly using all of his influence in the judiciary and his power to win this battle against me, to prevent me from ever being able to have this question answered.
But I think his silence has answered it already. And his actions. His dismissal.
He’s maneuvering has shown to us what the answer to the question is. There is no virus here.
The media has chosen to ignore what we’re doing, sort of an unofficial ban on this — never covering this court case. Showing anything else but this.
And the controlled opposition has been trying to distract people’s attention away from this. ‘No, that’s not an important question. THIS is more important than that.’ This is what has been happening.
And we have stayed consistent. We have said the same thing. Because when you speak the truth, and when you are focused on the truth, you do not have to change your tune every now and again. And that’s why you’ve heard the very same thing from us time and again. Show us the virus.
And that won’t change. We won’t be deterred. We will grasp onto the truth and we will pursue it no matter what, hell or highwater.
Now, what has happened as far as the case is concerned as I say that on the 28th of April, which is today, 2022, this is when our would Leave to Appeal is due. And we have successfully launched an application to the judge for Leave to Appeal.
But a strange thing has happening again. One week before this, on the 22nd of April 2022, the Constitutional Court dismissed our Rescission Application. Rescission Application is a sort of appeal to the Constitutional Court. And they have dismissed it.
Now, this is very important because the judge has dismissed our Interdict Application in the High Court because she says there was no case in front of the Constitutional Court, there was no appeal, there was no decision and, therefore, she has dismissed the case. And, therefore, she has ordered that I pay punitive cost of the billionaire president and also the pretty wealthy and rich Minister of CoGTA [Co-Operative Governance and Traditional Affairs]. I must pay their legal cost, based on the fact that there is actually no case in front of the Constitutional Court pending.
The fact that the Constitutional Court — one week before the time — has dismissed my decision application without a hearing, is proof that the judge was wrong in her judgment. There was a case pending. There was an appeal pending in the Constitutional Court.
The fact that the Constitutional Court now has dismissed it a week before, it is supposed to have helped their cause but it doesn’t really. I think that is a little bit of miscommunication or there’s a miscoordination because it doesn’t really help their case. It advances ours. It proves, without a doubt, that when the judge made her decision she was factually mistaken. She was legally mistaken.
And that is why we are — we have launched this Leave to Appeal and we are successful with the merits of our case.
You must remember, at the end of the day, we have gone to the courts and we have said to the courts: The president made a claim. He said there’s a virus. We ask him to show the virus.
And the just and legal thing to do would be that he must prove his claim. He who claims must prove it.
The courts have, thus far, been dismissive of this basic and fundamental legal issue. And, as I’ve said, the media has tried to basically ban this, hide this very important, very fundamental, issue from the people of South Africa.
The controlled opposition. Now, who are the controlled opposition?
Controlled opposition are all those who say they oppose the government in this tyranny that the government is perpetrating against the people of South Africa, based on the SARS CoV-2 virus, but they agree with the claim of the government. They also promote the idea that there is a virus. And they feel that any lawsuit, or any case, that has to do with the Show Us the Virus question is not important. Other cases are important that focus on other things.
And I say to you, quite frankly Show Us the Virus is the fundamental issue here. Nothing is more fundamental than that.
Without the virus claimed there would be no pandemic and no other thing that anybody has a problem with.
And so anyone who is trying to say that they oppose the government but they agree with this basic premise is, quite frankly, controlled opposition. And the purpose of what they are trying to do is to distract you from what is really important. You’ll see this controlled opposition sellouts in politics and everywhere else, trying to distract the South African people, divide the South African people. It’s no different here.
And you see it — these kinds of thing pop up every time we release a message or every time that we are in the middle of a case of, there’s efforts to try and distract. Go look at the background and history and you will see the same.
As I’ve told you already, for this simple question Show Us the Virus, the president has chose to fight a legal battle with me for the past two years. The judiciaries tried to dismiss it. A basic premise of justice, they’ve tried to dismiss it.
Now, the fact that we have lodged our Leave to Appeal should show you — and the fact that we are still asking the same question for two years — should show you that we don’t give up easily and that we will not be easily distracted. And that we will not be easily deterred. And the fight is far, far from over.
Now, unfortunately, this is not the first time that this situation is happening in South Africa. It’s not the first time. Previously it was the HIV virus, that supposedly caused the AIDS pandemic. And the media did the same.
Anyone that opposes this is called an AIDS denialist. Anyone who raises any questions is ridiculed and attacked in the media quite viciously.
There was also protected court cases going on. And I’ll explain to you those court cases that went on. And, unfortunately, the result is very similar to what we are seeing today.
But first, there was also controlled opposition then. There was the Treatment Action Campaign that was pushing for pregnant women to receive toxic drugs (nevirapine). They were pretending to be on the side of the people and demanding that the people be given this toxic drug, sort of as a mandatory drug from the pharmaceutical industry that were the beneficiaries of this poisonous drug.
We have the same. Those people today who are controlled opposition for the government and for these people pushing this tyranny on us, they’re doing the same. They say it’s a bioweapon. They say it’s not so bad, but the virus is there. They are advocating people use ivermectin which is a toxic drug. They saying people should use other toxins, many other toxins.
I’m not a doctor. I will not be able to specify all of them. But many, many, many toxins. You can go check it yourself. All of those who claim to be opposing the government but they believe there is a virus or they advocate there’s a virus without providing any proof, they are also advocating toxic drugs.
The same that was happening during the time of the HIV issue as the Treatment Action Campaign did then. There was a … big court case happening then where the government then was challenging and saying no we shouldn’t be giving people nevirapine, it’s a dangerous, toxic drug. Eventually this matter ended up in the Constitutional Court then. And in the Constitutional Court Dr. Sam Mhlongo, he raised the issue to the court that the HIV virus has never been isolated and purified. Basically, the HIV virus was never shown to exist. So, you know, they were basically in their way asking the same question then: Show us the HIV virus.
And the court decided to dismiss Dr. Sam Mhlongo and say no that will not be entertained. The court will not answer such a question. Again, basic premise of justice. They claim there’s an HIV virus. Dr. Sam Mhlongo is asking them — is saying to the court they’ve never proven it. And therefore they should not be giving people toxic drugs like nevirapine if they haven’t proven the virus to exist. And the Constitutional Court dismissed Dr. Sam Mhlongo, as they are now trying to dismiss me again. It’s a repeat of history.
Sadly, soon after this whole debacle, Dr. Sam Mhlongo lost his life in mysterious circumstances — car accident and he lost his life. And this is how dangerous it can be to just ask a simple question.
To demand justice can be deadly when you are facing with such force of tyranny and injustice. And sadly, this is the case with Dr. Sam Mhlongo.
Now, as I’ve explained to you here — now this is twice in a row — that there has been, every time we go to the High Court, where we are supposed to go to the High Court, we are supposed to appeal, then the Constitutional Court issues orders. issues orders that will seemingly be very convenient for the president’s legal team and for the High Court then to to use together to judge against me.
There seems to be … I can’t say very clear. I was not in meetings where I see them discuss, but what I see is that within a week — every time we are going to the High Court, within a week the Constitutional Court comes back with a decision supposedly against us and supposedly in favor of the president. And that can then be used to help the High Court make its decision.
So this is a determined effort to see that the question of Show Us the Virus is never the answered and that I must be, you know, saddled with this legal cost. Because the financial cost would be quite substantial. They haven’t issued the bill yet and so this is hanging over my head. But what can happen here quite easily, if my Leave to Appeal is dismissed, my appeal is dismissed, and then I’m saddled with this cost. And then this could mean that they could see sequestrate me. It could render me to lose all of my assets and to be impoverished. So this is the threat that is hanging here — all because of asking a question. Show us the virus.
So, they are very dangerous, you know, in terms of their power that they wield and the threats that they have. As I’ve said here, Dr. Sam Mhlongo has lost his life… I have the knowledge that he lost his life for asking that question. And I’m asking that question. I’m asking the question for them to show the proof of these virus claims of theirs, including the one that Dr. Sam Mhlongo asked about HIV. And I’m asking in addition to that.
So I’m sure for me asking his question and redoubling that question with another one, with another virus, then I should be very careful about car accidents as well.
And, of course, in addition to this financial threat that they now directing towards me. But I am not deterred. And as I’m sure Dr. Sam Mhlongo was not deterred. That his death, and that if any such similar thing happens to me or loss of property, then my debt, my loss of property — or my death in the event that they do the same kind or try the same kind of thing against me — will be a witness against them, a witness against the tyranny, a witness against their falsehood. It will be a witness against their injustice. Because why should this man lose property? Why should this man lose his life for asking you to show us the virus when you have made this claim. This is the height of injustice.
They are determined to see that I lose these cases.
They are determined to see that I am silenced.
They are determined to ensure, with the help of their controlled opposition, that people’s attentions are directed elsewhere.
I’m saying to South Africa, we have been fooled once by these people and their tactics, their intimidation, they’re controlled opposition, sellouts, etcetera.
They fooled us in the past. We should not allow them to fool us again.
For them, having fooled us in the past, shame on them. But if we allow them to fool us and divide us again, then shame on us.
It is time for us to redouble our efforts. Here at the Show Us the Virus movement we have no intention to submit ourselves to evil or to falsehood. No intention whatsoever.
We will redouble our efforts as this lodging of this Leave of Appeal application has shown you. There has been many attempts to distract you in the meantime.
From my request, I asked you and I said South Africa please support me, please help me. I am facing these kind of threats, financial threats. And there has come a whirlwind, a whirlwind to try and distract you away from helping me away, from supporting this cause and standing for truth and justice.
I ask you not to allow yourself to be distracted like this I ask you to stand with me as I redouble my efforts to fight against this tyranny and oppression.
I will not surrender. And I want to implore you that, don’t think others will come and save you. Our situation will not change unless we change it ourselves.
We have to redouble our efforts. We have to pray and turn to God to help us to defeat this evil. And we have to stand together. And we must ensure that we focus. We stand as one. And we never relented evil. We stop it. We fight it. Whatever stumbling blocks there are, we jump over it. Whatever walls there are, we go through it if we have to.
So please let’s stand together. Support me as much as you can. Support our cause. We still have an uphill battle to fight.
We will let you know how the Leave of Appeal application goes. And after, that we’ll follow the appeal itself in our efforts to see that justice is done and that an unjust court order be overturned.
cover image based on creative commons work of Alexas_Fotos
Dr. Joseph Yi (StreetMD) with Drs. Tom Cowan, Andrew Kaufman & Mark Bailey: A Response to Claims by Drs. Robert Malone, Peter McCullough & Ryan Cole That SARS-CoV-2 Has Been Isolated & Is a Disease-Causing Virus
Dr Joseph Yi, AKA “StreetMD” asked Drs Bailey, Cowan and Kaufman to respond to Drs Malone, McCullough and Cole’s claims that SARS-CoV-2 has been isolated and shown to exist. Boom!
cover image based on creative commons work of Briam-Cute & geralt
Dr. Sam Bailey with Eric Coppolino — On the Monumental Task of Documenting & Examining the Covid-19 Chronology: “Knowledge Coming to Light Changes Things”
“Knowledge coming to light changes things.” ~ Eric Coppolino
Recently, I have been fortunate to have connected with the inspiring Eric Coppolino, who is based in New York State.
Eric has an incredible history of exposing scientific fraud and environmental pollution cover-ups. He was one of the first to start investigating the COVID-19 scam and is putting something big together to help all of us who are questioning the narrative.
GREENWICH, CT — Robert F. Kennedy, Jr. has acknowledged the controversy within his own community over whether SARS-CoV-2 physically exists, and whether any viruses exist, or make people sick. He made the comments at a fundraising event here Sunday, April 24, 2022.
Kennedy said that the issue erupts regularly on the email discussion list of Children’s Health Defense (CHD), the vaccine safety and education organization that he founded in 2016.
“On our list, there’s a number of people who make those kinds of arguments” about how viruses allegedly don’t exist, Kennedy said in his remarks. “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
He made the remarks in reply to a question about why no government can produce evidence of having a sample of SARS-CoV-2 taken from a patient, rather than artificially created using a computer model.
Kennedy, the son of Sen. Robert F. Kennedy and the nephew of Pres. John F. Kennedy, is considered one of the leading voices in the international movement against covid-related mandates, lockdowns and safety issues over covid injections. It is the first time he has publicly commented on the virus-existence issue.
Scientists on all sides of the issue agree that viral particles have not been physically
isolated (with purified samples) and then sequenced.
What is Being Used to Prime the Covid Test?
The matter of whether the SARS-CoV-2 virus physically exists has dual significance. The obvious issue is that if there is not a virus, what then is making people sick? And what are they being vaccinated against?
Second, and less obvious: If the government cannot prove that it has a sample of natural SARS-CoV-2, then what is being used to prime the PCR test that is supposed to match and find the genetic code of an actual virus in a patient?
Scientists on all sides of the issue agree that viral particles have not been physically isolated (with purified samples) and then sequenced. Rather, hypothetical viruses are assembled from mixed biological samples, and these “in silico genomes” are then assumed to not only exist in nature but come from inside a pathogenic particle. They have many names: “mimicked human specimens” and “contrived viruses” (in the words of the CDC); or “synthetic nucleotide technology” (in the words words of the authors of the WHO test for covid).
One virologist told me in July 2020 that SARS-C0V- 2 was being assembled “like pages from a book,” necessary because no natural virus particle was available to sequence. The problem is that nobody has demonstrated these pages actually belong to the proposed book.
Covid tests look for sequences attributed to the “virus” merely via computer models —
but these “found” sequences almost always originate from somewhere else (including
the testing process itself).
CDC document pertaining to detection limits in the CDC “covid” test, admitting that
purified isolates of SARS-CoV-2 are not available. Yet this long, technical paragraph
admits something else: how they go about making their contrived virus (mimicked human
specimen), rather than sequencing actual virus. Were viruses available to anyone, it would
be the federal government of the United States. What they are admitting is that the virus
has not been isolated or purified; the writer admits outright that they are using made-up
samples that mimic clinical specimens. The technical notes describe the manufacturing
process for in silico sequences that are used in the “covid” test. The notes make reference
to MN908947, a synthetic, claimed, partial metagenomic transcript (not actual sequencing)
of the “N-gene” — which was later abandoned in its entirety in the Corman-Drosten assay.
Metagenomics: The Creation of Hypothetical Sequences
These hypothetical sequences are developed using technology called metageonomics — without any reference to actual purified suspected viruses. This artificial-intelligence process assembles a hypothetical “virus” from information gathered either from a crude human body fluid sample, or by making a “cell culture” experiment by mixing the fluid with monkey cells, cervical cancer cells, fetal calf serum, antibiotics and other poisons. In all cases where covid is concerned, scientists have used the latter. Because there is no actual virus available as a reference, there is no way to verify if the proposed sequences are valid. They are all theoretical, and no two are alike.
Said another way, in the absence of a real virus specimen, covid tests look for sequences attributed to the “virus” merely via computer models — but these “found” sequences almost always originate from somewhere else. And “positive” results can emerge from nearly anywhere, including the testing process itself). Yet if someone “tests positive” for one of these claimed viral sequences, they are said to be “infected” with SARS-CoV-2.
Previously, the U.S. Centers for Disease Control and Prevention (CDC) has admitted that the polymerase chain reaction has had a 100% false positive rate and has caused several widely-documented “false epidemics.”
The claimed existence, transmissibility and pathogenicity of SARS-CoV-2 were used to declare a global pandemic that by March 31, 2020 had 4.5 billion people around the world living under a stay-at-home order or house arrest.
“On our list, there’s a number of people who make those kinds of arguments. And
other people on the list server, and these are all very brilliant people, ridicule them
and dismiss them, and have them produce a lot of evidence.” — Robert F. Kennedy, Jr.
Seeking Documents from Governments, Agencies and Institutions
At a Q-and-A session at a fundraising event here Sunday, April 24, I asked Kennedy about the work of Christine Massey in the Toronto area, a statistician who is coordinating the worldwide effort to officially query governments, agencies and institutions about whether they have a sample of the claimed virus taken from a human.
“Christine Massey in Toronto has amassed 182 responses under various Freedom of Information Law requests from institutions, provincial state, and federal, national governments, which all say that no one has a sample of SARS CoV-2 taken from a human. Would you please comment on that?”
Kennedy replied: “On our list, there’s a number of people who make those kinds of arguments. And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence. I actually saw an exchange yesterday, where somebody made that exact statement and then 10 people jumped on him on with examples, of where that’s not true.”
The issue over the nature and existence of viruses represents the single biggest split in the covid-truth and anti-mandates movements. I first documented this divide in May of 2020.
“RFK Jr. now relies on popular opinion and ridicule to evaluate science?
When did he declare incompetence with simple logic?” — Christine Massey, statistician and coordinator of the virus FOIA project
‘I Am Amused Reading These Exchanges’
He added: “I am kind of amused reading the exchanges, and my inclination is that the viruses do exist and they do make people sick. I could be wrong. It could all be a big hoax, but to me, it all seems like viruses are real.”
But Kennedy answered a different question than the one I asked. I did not present him with an argument, or ask him whether he thought viruses were real. He admits that he uses a kind of mob rule to make up his mind over critical scientific issues when he says, “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
Reading Kennedy’s response, Christine Massey said, “RFK Jr. now relies on popular opinion and ridicule to evaluate science? When did he declare incompetence with simple logic? And why is a man dedicated to protecting children from medical harm uninterested in one of the greatest medical frauds of all time?”
She also demanded the data from the 10 people on Kennedy’s list who claimed to prove that the virus had been isolated.
So far, no governments have produced a scientific paper saying that they or anyone
have such a sample, despite the claim that a contagious virus has killed more than
5 million people worldwide.
Asked About a Legal Issue — Not Scientific
Kennedy said he believed viruses exist, but I did not ask him about that. Rather, I presented him with a legal issue, asking him to comment about how someone well-known and established in covid truth circles over the past two years has collected 182 responses from top-level government agencies and institutions, all saying they do not have a sample of SARS-CoV-2 extracted from a human host.
So far, no governments have produced a scientific paper saying that they or anyone have such a sample, despite the claim that a contagious virus has killed more than 5 million people worldwide.
I followed up and said to him, “The governments have said they don’t have a sample.”
Kennedy, an attorney, responded: “Freedom Information Laws do not require the government agency to do science, or to answer specific questions. What they do is, the Freedom of Information Laws make it obligatory for the government to give you existing documents. So if you are telling the government, ‘I want you to verify these, there are documents’, they say, listen there’s nothing to verify it. It doesn’t mean it’s not true. It means they’ve got nothing.”
So far all have said no such records exist. This includes the U.S. CDC and the FDA, as
well as Health Canada and the National Health Service (NHS) of the UK. None of the
182 agencies and governments queried have replied in the affirmative.
‘Kennedy hasn’t read any of my records requests’
Massey replied to this in an email: “It appears that Kennedy hasn’t read any of my records requests. I didn’t ask governments to ‘do science’ or answer ‘specific questions’. All of my requests have been for studies/reports in the possession, custody or control of an institution.”
I asked Massey how she words her letters seeking documentation of a sample of the claimed virus from a human host.
She provided this example of what she is seeking, and what so far all governments she has queried deny having:
“All studies and/or reports in the possession, custody or control of the Centers for Disease Control and Prevention (CDC) and/or the Agency for Toxic Substances and Disease Registry (ATSDR) describing the purification of any “COVID-19 virus” (aka “SARS-COV-2”, including any alleged “variants” i.e. “B.1.1.7”, “B.1.351”, “P.1”) (for example: via filtration, ultracentrifugation and chromatography), directly from a sample taken from a diseased human where the patient sample was not first combined with any other source of genetic material (i.e. monkey kidney cells aka Vero cells; fetal bovine serum).”
And so far all have said no such records exist. This includes the U.S. CDC and the FDA, as well as Health Canada and the National Health Service (NHS) of the UK. None of the 182 agencies and governments queried have replied in the affirmative.
“It erodes popular faith in democracy when public officials insist that their arbitrary
policies are ‘science based’ and yet cannot produce a single study to support sweeping
mandates.” — Robert F. Kennedy, Jr.
‘No Records Exist’ is an Important Response
Getting a “no records exist” reply is common, and seeking such a reply is a common strategy for establishing that there has not actually been a regulatory process for a policy issue. It is one of the most important uses of open records laws.
In late 2020, the New York State Department of Health (NYS-DOH) responded to an open records request saying it had no studies to prove that masks are safe or effective at preventing the spread of viruses or other diseases. For that same kind of “sorry no documents” FOIL reply, Kennedy was much more outspoken.
At the time, he wrote to his Instagram followers, “It erodes popular faith in democracy when public officials insist that their arbitrary policies are ‘science based’ and yet cannot produce a single study to support sweeping mandates. This letter illustrates the hazard of abandoning due process.”
Previously, he had remained agnostic on the issue of masks and whether masks work. He finally took a position in response
New York State saying it had absolutely no data about whether masks are safe or effective.
“It’s a needlessly divisive issue, with people screaming, on both sides, as if it were
the key to this whole thing — which it isn’t.” — Prof. Mark Crispin Miller
“They did not isolate a virus,” Wallach said. “The reason it’s so confusing for people is that they claim to have done so in the titles of the key scientific papers, but if you read the methodology sections, it’s blatantly clear: they never isolated a virus. They never found anything. The evidence is overwhelming.”
He added: “I respect the importance of political leaders like RFK Jr. keeping an open tent, they have to. But at the same time, this is an issue that should be front and center for the world public, and nobody should be repeating this dogma about the existence of viruses.”
Mark Crispin Miller, professor of communication at New York University, said, “It’s a needlessly divisive issue, with people screaming, on both sides, as if it were the key to this whole thing — which it isn’t. What will make the whole narrative collapse is not the argument that there are no viruses, but the recognition that the authorities we’ve all been listening to — the medical establishment, Big Pharma, Academia, the media et al. — are malign, and intent on killing us.
“That’s it. Everything else is a distraction. Whether the ravages of COVID-19 have been exaggerated, or whether there’s no virus there at all, is ultimately beside the point. And since Bobby’s role is in large part political, as he attempts to keep this movement in one piece, his disinclination to take sides here ought to be respected.”
“Are all based on in-silico modeled synthetic phenomena, which has never been
scientifically proven as coming from an actual virus.” — Dr. Kevin Corbett, expert in diagnostic testing
‘This was what happened with HIV’
Dr. Kevin Corbett did his doctoral work on diagnostic testing associated with HIV and AIDS, including research into the PCR. He said this week that the existence of SARS-CoV-2 and associated tests, “Are all based on in-silico modeled synthetic phenomena, which has never been scientifically proven as coming from an actual virus.
“This was what happened with ‘HIV’, which The Perth Group of scientists [in the 1990s] first proved was never isolated or purified. Those powerful voices like Robert F. Kennedy, Jr., who sadly ignore this issue, are badly misguided, because they fail to address this fundamental caveat in ‘covid science’.”
Corbett cautioned, “Their efforts will only act to further socially embed the popular hysteria of there being a contagion, and therefore will enable further public health mandates forcing masks, social distancing and the latest covid killshot.”
College term paper referenced by Dr. Cowan was actually a published paper by Eleni Papadopulos-Eleopulos, et al. (Dr. Cowan made this correction at the start of a video on the snake venom controversy, streamed on 4/22/2022.)
In this webinar, my friend and colleague Mike Donio analyzed the main points of Dr. Ardis’ recent snake venom warning. Tune in to find out what we think of these claims.
“The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent
“SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and
animal “coronaviruses” created in the very same way. Attempting to claim any connections between the
random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated
into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place.
Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely
related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines,
the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have
a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a
singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial
evidence that is easily debunked.”
“My story has never been to create fear, panic, and anxiety about water.” He said he told Peters that he believes “there’s actually a snake venom connection to all of COVID-19, and I think that’s the weapon.” – Dr. Bryan Ardis
Summarizing his theory, Dr. Ardis said, “They are using Krait venom and Cobra venom, calling it Covid-19, you’re drinking it, it’s getting into your brainstem and it’s paralyzing your diaphragm’s ability to breathe.”
I really didn’t want to write this article. I was hopeful that people would easily see right through the unsubstantiated claims of Dr. Bryan Ardis that snake venom is the cause of “Covid.” I was hopeful that people would take the time to research the information presented in support of the snake venom theory to see if it held any merit at all. I thought his whirlwind alternative media tour on the who’s who of questionable sources (including the likes of Stew Peters, Mike Adams, and Infowars) would have people questioning why this theory was allowed to be so heavily promoted so quickly. I thought that the fact that the man who created the “Covid” snake venom theory was actually selling his own anti-venom line of supplements would be enough grounds to be skeptical of his motive and his claims.
It seems I was wrong. Just like the baseless vaccine shedding and gain of function/bioweapons narratives, this new snake venom theory has sadly spread through the “Truther” community like wildfire, with many who rightfully challenge the existence of “viruses” clinging to the idea of a new invisible enemy to defeat. They believe that it must be a new toxin. It can’t possibly be the same factors we have seen each and every year leading to disease. This toxin must be hiding in the vaccines, the drugs, and/or even the very water we drink. What these “Truthers” do not realize is that this very line of thinking gives credibility to the idea of a new disease which requires new treatments in order to combat it. This is exactly what the pharmaceutical companies want you to believe.
However, there is NO NEW DISEASE. There is no need for any new or even existing pharmaceutical interventions to treat the same symptoms of detoxification people go through each and every year. In fact, the current treatments can easily be shown to have led to numerous unnecessary deaths. There is no new threat known as “Covid-19” which is being caused by any one factor. The factors leading to the symptoms of disease people are experiencing are multi-causal as they are every year.
Now this is not to say that the vaccines, the drugs, or even the water supply are free of toxins. These are all sources of toxicity and should be investigated as to their composition and effects on our health. However, the theory that there is one factor in all of these sources, i.e. snake venom, and this one factor is leading to the symptoms of disease people are experiencing is, at present time, completely baseless. And it all begins at the very foundation of the fraudulent genome.
The Fradulent Genome
You take that snake or that serpent and you figure out how to isolate genes from that serpent and get those genes of that serpent to insert itself into your God-given created DNA. I think this is the plan all along, was to get the serpents’, the evil one’s DNA, into your God-created DNA.”
He also said genetic sequence testing done on sick patients in Wuhan found their genetic sequence matched two snakes, the Chinese Krait and King Cobra, not bats.”
From Dr. Ardis’ interview with Mike Adams, he supplied the article “Snakes could be the source of the Wuhan coronavirus outbreak” from CNN as his starting point for the “Covid”/snake connection. Within the article, you can see that this claim originates from the fraudulent genomes:
“The researchers used an analysis of the protein codes favored by the new coronavirus and compared it to the protein codes from coronaviruses found in different animal hosts, like birds, snakes, marmots, hedgehogs, manis, bats and humans. Surprisingly, they found that the protein codes in the 2019-nCoV are most similar to those used in snakes.” https://www.google.com/amp/s/amp.cnn.com/
To anyone who actually researched the creation of the original “SARS-COV-2” genome, it is readily apparent that it is a fraudulent computer-generated creation stemming from the unpurified lung fluid of a single patient. The sequenced material could have come from multiple sources, including host DNA/RNA, bacteria, and microbes/microorganisms. It could have even come from outside contamination. There is no way to tell what the origin of the RNA is or even if it was a single source as no particles assumed to be “SARS-COV-2” were ever properly purified and isolated directly from the fluids of the sick patient before being sequenced. Thus, any relation this fabricated sequence has to any other sequence is invalid as the source was never identified to exist as a physical entity to begin with. Considering that the bat and snake “coronavirus” sequences for which the “SARS-COV-2” sequence was then compared to also come from unpurified sources, it is easy to see that any claims as to the origins of the sequenced material is a horrible foundation to build upon for an origin theory of a nonexistent “virus” and/or disease.
Even if this snake-venom connection was valid, the enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom. These peptides are “almost identical” to the venoms of animals and yet they are regularly found in healthy humans and other mammals. From his own source:
Like Venom Coursing Through the Body: Researchers Identify Mechanism Driving COVID-19 Mortality
“Researchers from the University of Arizona, in collaboration with Stony Brook University and Wake Forest School of Medicine, analyzed blood samples from two COVID-19 patient cohorts and found that circulation of the enzyme – secreted phospholipase A2 group IIA, or sPLA2-IIA, – may be the most important factor in predicting which patients with severe COVID-19 eventually succumb to the virus.
The sPLA2-IIA enzyme, which has similarities to an active enzyme in rattlesnake venom, is found in low concentrations in healthy individuals and has long been known to play a critical role in defense against bacterial infections, destroying microbial cell membranes.”
Thus, the snake enzymes are in fact normal human enzymes that are regularly found in healthy individuals. There is no mystery as to why these would be present in a sample. We should be able to put this “Covid” snake venom nonsense to bed right here. However, let’s press on a see what else we can uncover.
Antivenom = Monoclonal Antibodies
One thing I will give Dr. Ardis credit for is spotlighting the connection between the creation of antivenoms with the creation of monoclonal antibodies. The processes for both are very similar and the desired outcome is the exact same: the creation of theoretical antibodies. In the case of snake antivenom, it is normally created by a series of injections of the venom of a snake into an animal and then collecting the blood after a period of time. This is usually done through horses but other animals can be used as the host as well. Thus, the antivenom used for a snakebite victim is typically an injection of horse blood.
Both of these therapies have their basis in animal blood and the creation of the theoretical antibodies. Both are associated with toxic side effects. Sadly, while he was originally right about the fact that monoclonal antibodies are toxic and should not be used to treat the symptoms now collectively known as “Covid,” Dr. Ardis changed his tune when another doctor texted him asking if he would use antivenom for a snake bite:
“Last December, Dr Bryan Ardis received a text message from an Emergency Room physician friend of his that sent him down an unexpected and bizarre rabbit hole that may explain the adverse events from the vaccines that we’ve been reporting. The text read: “Hey Dr Ardis…If you got bit by a rattlesnake, would you go to a hospital and get anti-venom?”
“He says, “I realized, all of a sudden, monoclonal antibodies ARE anti-venom. The Federal Government doesn’t want us using anti-venom. Why are they fighting anti-venom and why are we finding anti-venom works against COVID? Is it not a virus? Is it a venom? This is what I want to know: Is COVID a venom and is this why they don’t want you using monoclonal antibodies?”
Do you see the trick? They want you to equate monoclonal antibodies with antivenom. This is supposed to be an “aha” moment where you realize that there is no way that you would not inject antivenom (i.e. horse blood) into yourself if bitten by a snake. It’s a no-brainer, right? We have all seen the movies where a person is bitten by a venomous snake and quickly dies if not given the antivenom.
If you are willing to accept the injection of horse blood into your body to survive a snake bite, why wouldn’t you also inject the cancer-cell cultured blood of genetically altered mice in order to combat “Covid?”
As Dr. Ardis points out, monoclonal antibodies are essentially antivenom. However, he wrongly states that monoclonal antibodies are an effective therapy. According to a September 2021 Cochrane review of the available studies, they found insufficient evidence to claim that monoclonal antibodies are an effective treatment for “SARS-COV-2:”
Are laboratory-made, COVID-19-specific monoclonal antibodies an effective treatment for COVID-19?
“The evidence for each comparison is based on single studies. None of these measured quality of life. Our certainty in the evidence for all non-hospitalised individuals is low, and for hospitalised individuals is very low to moderate.We consider the current evidence insufficient to draw meaningful conclusions regarding treatment with SARS-CoV-2-neutralising mAbs.”
In other words, the evidence for the usefulness of monoclonal antibodies is non-existent. Unfortunately, the Cochrane Review failed to point out that there are various risks and adverse reactions associated with their use:
Do mAbs have risks?
“Therapeutic mAbs, typically administered by intravenous (IV) infusion, have been a valuable and generally safe treatment option for a variety of conditions for many years. However, they are also known to cause a range of side effects and reactions, which can be immediate or delayed.Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity.”
In January 2022, the FDA restricted the use of some monoclonal therapies (Bamlanivimab and Etesevimab) that are authorized against “Covid-19” as they were shown to be ineffective:
Coronavirus (COVID-19) Update: FDA Limits Use of Certain Monoclonal Antibodies to Treat COVID-19 Due to the Omicron Variant
“In light of the most recent information and data available, today, the FDA revised the authorizations for two monoclonal antibody treatments– bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
Because data show these treatments are highly unlikely to be active against the omicron variant,which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. And like other infectious organisms, SARS-CoV-2 can mutate over time, resulting in certain treatments not working against certain variants such as omicron. This is the case with these two treatments for which we’re making changes today.”
On April 16th, 2022, the FDA revoked the use of Bamlanivimab alone as it’s benefits were shown not to outweigh its risks. Somehow despite this evidence, the FDA still allows for it to be used in combination with Etesevimab, even though they previously revoked their use together in January 2022:
Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab
“Today, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate COVID-19 in adults and certain pediatric patients. Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of SARS-CoV-2 viral variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure,the FDA has determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use. Therefore, the agency determined that the criteria for issuance of an authorization are no longer met and has revoked the EUA.
On Nov. 9, 2020, based on the totality of scientific evidence available at the time, the FDA issued an EUA to Eli Lilly and Co. authorizing the emergency use of bamlanivimab alone for the treatment of mild to moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progressing to severe COVID-19 and/or hospitalization. Importantly, although the FDA is now revoking this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone. The FDA believes that these alternative monoclonal antibody therapies remain appropriate to treat patients with COVID-19 when used in accordance with the authorized labeling based on information available at this time.”
If the FDA’s confusing revoking of the EUA’s of these monoclonal antibodies has you concerned that you will not be able to use them against an imaginary “virus,” don’t worry. The FDA authorized the use of a new “Omicron-specific” monoclonal antibody called Bebtelovimab on February 11th, 2022. Granted, it still carries the same risks, adverse side effects, and uncertainty over clinical worsening listed for the previously ineffective antibody therapies. From the FDA fact sheet:
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
“Possible side effects of bebtelovimab include itching, rash, infusion-related reactions, nausea and vomiting. Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other SARS-CoV2 monoclonal antibodies and could occur with bebtelovimab. In addition, clinical worsening following administration of other SARS-CoV-2 monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19.”
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
Hypersensitivity Including Anaphylaxis and Infusion-Related Reactions: Serious hypersensitivity reactions, including anaphylaxis, have been observed with administration of other SARS-CoV-2 monoclonal antibodies and could occur with administration of bebtelovimab. If clinically significant hypersensitivity reactions occur, discontinue and initiate appropriate supportive care. Infusion-related reactions may occur up to 24 hours post injection. These reactions may be severe or life threatening. (5.1)
Clinical Worsening After SARS-CoV-2 Monoclonal Antibody Administration: Clinical worsening of COVID-19 after administration of SARS-CoV-2 monoclonal antibody treatment has been reported and may include signs or symptoms of fever, hypoxia or increased respiratory difficulty, arrhythmia (e.g., atrial fibrillation, sinus tachycardia, bradycardia), fatigue, and altered mental status. Some of these events required hospitalization. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19. (5.2)
Limitations of Benefit and Potential for Risk in Patients with Severe COVID-19: Treatment with bebtelovimab has not been studied in patients hospitalized due to COVID-19. Monoclonal antibodies, such as bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with COVID-19 requiring high flow oxygen or mechanical ventilation. (5.3)
It should be fairly clear that, unlike Dr. Ardis’ claims, monoclonal antibodies are not effective, carry numerous risky side effects, and can actually worsen the disease they are supposed to treat. Interestingly, this same risk of dangerous side effects and worsening disease outcomes is associated with snake antivenom as well. From the fact sheet of a commonly used antivenom for rattlesnake bites, we find these admitted side effects:
Rattlesnake Antivenin Side Effects Center
“Rattlesnake Antivenin (antivenin crotalidae polyvalent) is an antivenin product used only to treat envenomation caused by bites of crotalids (pit vipers) including rattlesnakes, copperhead and cottonmouth moccasins, and others. Common side effects of Rattlesnake Antivenin include allergic reactions such as flushing, itching, hives, swelling of the face/tongue/throat, cough, shortness of breath, blue color to the skin, vomiting, and anaphylaxis (severe allergic reaction).”
“Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered. An immediate reaction (e.g. shock, anaphylaxis) usually occurs within 30 minutes. Symptoms and signs may develop before the needle is withdrawn and may include apprehension, flushing, itching, urticaria; edema of the face, tongue, and throat; cough, dyspnea, cyanosis, vomiting, and collapse. There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use.”
“Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered.30 The incubation period may be less than 5 days, especially in those who have received horse-serum-containing preparations in the past. The usual symptoms and signs are malaise, fever, urticaria, lymphadenopathy, edema, arthralgia, nausea, and vomiting. Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis. Peripheral neuritis usually involves the shoulders and arms. Pain and muscle weakness are frequently present, and permanent atrophy may develop.”
Maybe the use of antivenom to treat a snakebite isn’t the super cure it has been sold to be? Is it possible that, as with many pharmaceutical products and interventions, the antivenom itself is creating the very symptoms it is said to treat? For some further insight, let’s look at a few highlights from an paper from September 2019, right before this “crisis,” which reviewed the use of antivenom and had a few revealing claims about the “anti” toxin. You will see it reiterated that the injection of antivenom created from either horse, sheep, goats, and/or rabbits can cause immediate hypersensitivity and anaphylaxis or a delayed “serum sickness” which can occur weeks after the treatment. It is stated that the antivenom has limited efficacy and can be entirely ineffective based on the geographic location. Improper use of antivenom contributes to increased servere outcomes and the production of antibodies in animals leads to a large number (70%) of immunoglobulins that do not react to snake venom:
Perspective on the Therapeutics of Anti-Snake Venom
3. Current Information in the Design of New Antivenoms
“Currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses [14,15]. Hyperimmunized animals produce antibodies against the venom proteins and serum is extracted from their blood for the treatment of envenomation [6,16]. Conventional serum therapy aims to bind and neutralize the snake venom proteins [17]. It is a fact that the antivenom allows the body to try to reverse the damage caused by the venom. However, it is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia. Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects [18];
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability;
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes;
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both.
“Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom. Around 70% of the immunoglobulins obtained do not act directly against venom toxins [26]. Despite the abovementioned facts, this is the only FDA approved therapy to treat snake venom.”
A few other studies also point out the severe reactions regularly attributed to the use of antivenom. The first is a study from 2016 which points out that not only are adverse reactions common, they occur at a high rate. It is stated that this is due to poor quality control and manufacturing problems:
Adverse reactions to snake antivenom, and their prevention and treatment
“Antivenom is the mainstay of treatment of snakebite envenoming. However, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent. Both acute (anaphylactic or pyrogenic) and delayed (serum sickness type) reactions occur. Acute reactions are usually mild but severe systemic anaphylaxis may develop, often within an hour or so of exposure to antivenom. Serum sickness after antivenom has a delayed onset between 5 and 14 days after its administration. Ultimately, the prevention reactions will depend mainly on improving the quality of antivenom.”
“The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors. This highlights the importance of addressing issues related to poor quality and potentially unsafe antivenom. Ultimately, the prevention of reactions will depend mainly on improving the quality of antivenom. Until these improvements take place, doctors will have to depend on pharmacological prophylaxis as well as careful observation of patients receiving antivenom in preparation for prompt management of acute as well as delayed reactions when they occur.”
This next source is from 2018 and it points out that early antivenoms were unsafe and caused severe life-threatening events. While they now have “acceptable” safety profiles, antivenoms still have varying quality and range from 10% adverse reactions to greater than 50%. This same variation in quality is seen in the production of monoclonal antibodies:
Antivenom therapy: efficacy of premedication for the prevention of adverse reactions
“However, in their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects [8]. The main reason was that first antivenoms were poorly purified preparations or crude sera. Over the years, for many of the original applications, heterologous serums were replaced by other drugs with better safety profiles, such as antibiotics, vaccines and homologous serums. However, in cases of envenomation by snakes, scorpions or arachnids, antivenoms remain the only effective treatment [4]. Currently, after many improvements, antivenoms exhibit acceptable safety profiles [1, 9, 10]. Nevertheless, antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50% [11, 12].”
In is interesting to note that there are many factors that are said to influence the severity of a venomous snakebite including the age, sex, and health of the person bitten as well as the type of snake, the geographical location of the snake, the season the bite occurred in, what the snake ate, and how recently the snake released its venom. Antivenoms themselves have been shown to have varying effects in quality due to the geographical location of the snake which somehow renders the antivenom ineffective and even dangerous in different countries and continents, even against the same type of snake. It is said that this has kept locals from seeking out medical care and sticking to traditional healers:
“Snake venoms are highly complicated. At least 26 separate enzymes have been identified with 10 of these enzymes common to all snake venoms (though in different concentrations). All snake bites are not equal. The quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously.”
“A study led by Dr Fry has found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions.
Researchers tested the effectiveness of two African and two Indian saw-scaled viper antivenoms against saw-scaled vipers from 10 regions.
The results showed that the two African antivenoms were only effective against snakes from restricted ranges.
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers.
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regions. It failed completely against African saw-scaled vipers.
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry says.
“In Kenya, snakebite deaths have increased dramatically after hospitals switched supplies of a very effective African antivenom with a cheaper Indian variety.”
“This creates a knock-on effect in these communities. It’s hard enough to convince people living in these regions not to go to traditional healers to treat snakebite. And if someone does seek proper medical care but dies because of ineffective antivenom, it will be even harder to convince the next victim to seek out antivenom.”
Viper venom’s lethal evolution
It’s the variety of the saw-scaled viper’s prey, from rodents to insects, that researchers say could be the reason why antivenom from one region might not work in another.
“Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes,” UQ PhD candidate in Toxinology Bianca op den Brouw wrote in an article for The Conversation.
“Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet.
“Different saw-scaled viper populations feed on different prey. The physiology of these prey animals differs, and this dictates what makes a toxin effective.
“From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom.”
Maybe the proceeding information on how snakebite antivenoms are created as well as the high rate of adverse events from the antibodies used for antivenom now has you questioning that initial “no-brainer” thought: “Of course I would use antivenom if bit by a snake.” If so, you are on the right track as, based on information from the African Snakebite Institute, in most snake bite cases, antivenom is not used and many snake bites are often unattended and/or unreported. In fact, it is apparently a well-known “myth” (i.e. truth in this case) that the antivenom kills more people than the snake venom itself. Most people (over 80%) never receive antivenom as, like the previous sources stated, it can have disastrous side-effects. Most snake bites do not cause symptoms warranting the use of something so toxic. In fact, snake bite victims are not immediately injected with antivenom and typically are sent home after observation:
“Yet people often have a poor understanding of how it works and there are endless myths about antivenom killing more people than the snake venom itself.”
“Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite) as most victims are not severely envenomated or the bite may be from a snake that is not considered potentially deadly or is not covered by the antivenom (Rhombic Night Adder, Berg Adder and Stiletto Snake). Antivenom is relatively scarce, expensive and can have disastrous side-effects. The biggest danger is an acute allergic reaction (anaphylaxis) or, to a lesser degree, serum sickness that can affect the immune system several days after treatment.”
“Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use. The majority of snakes have control over their venom glands and are quite reluctant to waste their venom on humans. They very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious. Such patients are usually hospitalised for a day, carefully monitored and then sent home.”
“As already mentioned, some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used. Some of those victims go into anaphylactic shock which is a life-threatening medical condition and must be treated with adrenaline. This has to do with the fact that our antivenom is made from horse blood and the allergy is basically an allergy to horse proteins.”
Bill Haast – repeated snake bite victim from the world’s deadliest snakes tragically died at the young age of 100 from natural causes. ?
If snake bites regularly do not cause symptoms and do not require the use of antivenom, are snake bites really as toxic and harmful as we previously thought? Are the dangerous side effects linked to snake bites really just the reactions to having horse blood injected into the body as treatment? Is this another case where the treatment causes the symptoms of disease it was supposed to prevent? If the examples of these next few individuals are taken into consideration, it’s entirely plausible to conclude that we have been misled about the dangers stemming from snakebites in order to cover for the toxic effects of the treatment:
Repeated snake bite for recreation: Mechanisms and implications
“There is a debate in the fatality/immunity due to repeated snake bites in human beings either accidentally or incidentally. Haast and Winer[11] reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus[11] and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier.”
This snake-man got himself bitten over 200 times to become immune to venom
“Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was fatally injured about 20 times.”
“In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times as per the report published in Today I Found Out.“
Man makes deadly snakes bite him 160 times in hunt for human antidote
“An amateur scientist has deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom.
Tim Friede is obsessed by finding a human antidote to poisonous snake bites, which kill an estimated 100,000 people every year.
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra.
He said he experienced a “real throbbing sensation” but he “felt great” after the bites.
“It really hurts and it swells but that’s it,” he said.”
Poison pass: the man who became immune to snake venom
“A lot has been written about Steve Ludwin, widely known as the man who injects snake venom, and lately his life has turned into a non-stop frenzy of international journalists and film crews revelling in the seeming sheer insanity of it.”
“He’s been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years. “Snakes are fucking everywhere. The symbol for medicine is two snakes. They’re ingrained in our brain and DNA,” he tells me, proudly insisting that he hasn’t been ill for decades and has developed “a superhuman immune system”. And it’s tempting to believe him. He does look undeniably fit.”
The Photographer Who Was Bitten by a Black Mamba… and Got the Shot “After several minutes and then hours passed and Laita was still feeling fine — experts recommend heading straight for a hospital, by the way — the crew concluded that Laita didn’t have any venom in his system. The photographer believes that it was either a “dry bite,” when a snake doesn’t release any venom, or that his heavy flow of blood pushed out the venom.”
As can be seen, there are numerous examples of people being deliberately and accidentally bitten by the world’s deadliest snakes who are completely fine and do not require treatment from antivenom whatsoever. Are we to conclude that these people are the lucky few who somehow have amazing super-human “immune” systems that render snake venom ineffective? Or have snake bites and the associated symptoms of venom toxicity been blown out of proportion? Could this be a case where some have had bad reactions to a snake bite just as there are those who have severe allergic reactions to bee stings while the majority of snake bite and bee sting victims come away unscathed? Could this be similar to the supposed rabies cases where the majority of those who were bitten by “rabid” animals actually went on to be just fine without getting the rabies vaccination?
The Treatments Are Worse Than the Disease
It’s very apparent that in the case of monoclonal antibodies and anivenom, the adverse effects of the drugs are actually worse than the supposed diseases they are meant to treat. Could this be due to the fact that, like “viruses,” so-called antibodies have never been properly purified, isolated, and proven to exist? The results of studies using antibodies are regularly unreproducible and irreplicable. It is well-known that antibodies are in fact not as specific as are they are claimed to be and are said to regularly bind to the wrong proteins. Perhaps it is difficult to produce safe and effective products when the entities that are supposed to be produced and supplied in the animal blood are entirely theoretical? Maybe the ridiculous snake venom theory should be viewed in the context that it is a bad idea to be injecting anything, let alone animal blood, into our bodies in an attempt to make ourselves feel better when trusting the body and allowing it to heal is often times the best course of action we can take.
In Summary:
Dr. Bryan Ardis put forth a theory that snake venom is the cause of “Covid-19” primarily based on fraudulent genomic data
The snake connection stems from research linking proteins from the fabricated “SARS-COV-2” genome to bat and snake “coronavirus” proteins
The enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom
These peptides are “almost identical” to the venoms of animals and are regularly found in healthy humans and other mammals
Dr. Ardis pointed out that, based on a text, he uncovered the connection between antivenom and monoclonal antibodies and stated that theyare the same thing
He wrongly concluded that monoclonal antibodies are an effective treatment for snake poisons that could be in the vaccines, Remdesivir, and water
According to a Sept 2021 Cochrane Review, their certainty in the evidence for the use of monoclonal antibodies in the treatment of “Covid” for all non-hospitalised individuals was low, and for hospitalised individuals was very low to moderate
They considered the current evidence insufficient to draw meaningful conclusions regarding treatment with “SARS-CoV-2-neutralising” mAbs
Monoclonal antibodies are known to cause a range of side effects and reactions, which can be immediate or delayed
Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity
In February 2022, the FDA revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments
The data showed these treatments are highly unlikely to be active against the omicron variant which is circulating at a very high frequency throughout the United States
These treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens
In April 2022, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate “COVID-19” in adults and certain pediatric patients
Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of “SARS-CoV-2 viral” variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure, the FDA determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use
Importantly, although the FDA revoked this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone
In other words, the use of Bamlanivimab and Etesevimab was revoked as well as the use of Bamlanivimab but they can still be used together as an alternative to Bamlanivimab alone…
For the Omicron-specific Bebtelovimab authorized by the FDA in February 2022, possible side effects include
Itching
Rash
Infusion-related reactions
Nausea
Vomiting
Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other “SARS-CoV2” monoclonal antibodies and could occur with bebtelovimab
In addition, clinical worsening following administration of other “SARS-CoV-2” monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab
The FDA claims that it is not known if these events were related to “SARS-CoV-2” monoclonal antibody use or were due to progression of “COVID-19”
Treatment with Bebtelovimab has not been studied in patients hospitalized due to “COVID-19”
Monoclonal antibodies, such as Bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with “COVID-19” requiring high flow oxygen or mechanical ventilation
Antivenom carries the same risks of severe side effects and worsening condition as monoclonal antibodies
The listing for common side effects of Rattlesnake Antivenin include allergic reactions such as:
Flushing
Iitching
Hives
Swelling of the face/tongue/throat
Cough
Shortness of breath
Blue color to the skin
Vomiting, and anaphylaxis (severe allergic reaction)
Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered
There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use
Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered
The usual symptoms and signs are:
Malaise
Fever
Urticaria
Lymphadenopathy
Edema
Arthralgia
Nausea
Vomiting
Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis
Peripheral neuritis usually involves the shoulders and arms and pain and muscle weakness are frequently present, and permanent atrophy may develop
A 2019 review on antivenom stated that currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses
It is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia.
Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both
Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom
Around 70% of the immunoglobulins obtained do not act directly against venom toxins
According to a 2016 study, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent
The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors
The prevention of reactions will depend mainly on improving the quality of antivenom
According to their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects
Currently, after many improvements, antivenoms exhibit “acceptable” safety profiles yet antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50%
All snake bites are not equal and the quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously
A study led by Dr. Fry found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions
The results showed that the two African antivenoms were only effective against snakes from restricted ranges
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regionand it failed completely against African saw-scaled vipers
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry said
If someone does seek proper medical care but dies because of ineffective antivenom,it will be even harder to convince the next victim to seek out antivenom
Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes
Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet
From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom
There are endless myths about antivenom killing more people than the snake venom itself
Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite
Antivenom is relatively scarce, expensive and can have disastrous side-effects
Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use
Snakes very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious
Such patients are usually hospitalised for a day, carefully monitored and then sent home
Some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used
This has to do with the fact that antivenom is made from horse blood and the allergy is basically an allergy to horse proteins
Haast and Winer reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier
Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was seriously injured about 20 times
In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times
An amateur scientist named Tim Friede deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra
He said he experienced a “real throbbing sensation” but he “felt great” after the bites
Steve Ludwin, widely known as the man who injects snake venom, has been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years
He hasn’t been ill for decades and has developed “a superhuman immune system”
A photographer was bit by the deadliest snake, a Black Mamba, and after hours passed, he was still feeling fine and needed no treatment
The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent “SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and animal “coronaviruses” created in the very same way. Attempting to claim any connections between the random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place. Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines, the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial evidence that is easily debunked.
If we are to take the claims of Dr. Ardis seriously that the symptoms associated with snake venom is the true cause of a disease known as “Covid-19,” how does his theory explain for the fact that the antivenom and monoclonal antibody treatments cause the exact same symptoms of the disease they are supposed to treat? How would it be determined that the worsening clinical outcomes after injection are from the snake bites/venom rather than the antivenom/monoclonal antibodies given as treatment? How does his theory account for the numerous instances where people have been deliberately bitten by snakes, injected with the venom of snakes, and drank of the venom of the snakes with little to no harmful effects whatsoever? How does his theory account for the fact that the vast majority of “Covid” cases are asymptomatic and the vast majority of snake bite cases need no treatment at all? There are many holes in this theory which will easily be picked apart to make those who follow it look foolish for having done so.
There is no “SARS-COV-2.” There is no “Covid-19.” There is no new disease nor any new symptoms of disease requiring treatment from vaccines, monoclonal antibodies, Remdesivir, Hydroxychloroquine, Ivermectin, NAC, nor any other treatment. There is no need for any anti-venom supplements.
Beware those who will sell you the cause of the disease and the solution.
The Bill and Melinda Gates Foundation have funded the development and distribution of polio vaccines in developing regions like Asia and Africa (Image Source: GRAIN)
Current NHS information describes it as a ‘serious viral infection’ but adds that most people won’t even know they are infected. While some will experience ‘flu-like’ symptoms, others may become temporarily or permanently paralysed.
The term ‘polio’ is a description of spinal pathology: an inflammation of the grey marrow (polio muelos) of the brain stem and spinal cord. Symptoms vary wildly from none to fever, vomiting, bowel irritation, back pain, neck stiffness, problems with swallowing and breathing, paralysis, and death.
Poliovirus is an enterovirus that is activated in the human gut. The corporate science machine maintains that it is a dangerous pathogen spread by infected faecal matter but Dr Suzanne Humphries explains in her book, Dissolving Illusions, that it is a naturally occurring common bowel irritant that existed for millennia before it began crippling people — which poses the question: what changed?
One factor is pesticide usage, which is implicated in other neurological conditions such as Parkinson’s disease. Polio incidence and pesticide usage closely correlate; if you plot them on a graph, they follow the same lines.
What came to be known as polio was once called ‘summer diarrhoea’ because local outbreaks occurred after crop spraying had taken place in the spring. Children played in contaminated soils and ate unwashed fruit; their parents reported finding them paralysed in apple orchards.
High consumption of sugary foods in the summer lowered immunity by suppressing white blood cell activity, creating the perfect environment for toxic pesticides to interact with viruses in the gut and cause illness.
Doctors noted that symptoms of polio resembled food poisoning.
Poor diet increased susceptibility to poliovirus infection – especially a diet full of refined sugar, white flour, and processed foods, which were introduced to the public during the industrial revolution, around the time that polio began to emerge.
British physician Michael Underwood first observed ‘debility of the lower extremities’ in children in 1789. It was the height of the industrial and agricultural revolutions in Europe and pesticide use skyrocketed. Most pesticides contained toxic metals such as lead and arsenic.
Lead and arsenic bind tightly to soil and do not deteriorate; they remain within the first 12-18 inches of topsoil for generations and contaminate waterways. Redevelopment of former rural sites without proper clearance of toxic soil has the potential to poison whole areas of people.
Crops were heavily sprayed with pesticides that were designed to attack the nervous systems of insects — unfortunately they had the same effect on humans. They were inhaled and absorbed through the skin and oral cavity, causing nausea, vomiting, diarrhoea, brain dysfunction, and bone malformation – all of which are common symptoms of heavy metal poisoning and polio.
Heavy metals were present in everyday products in the 18th, 19th, and early 20th centuries. Arsenic was used in synthetic dyes and syphilis treatments; mercury was used in teething powders, dental fillings, and medical preparations.
Lead, arsenic, and mercury are neurotoxic environmental poisons – all are fat-soluble and therefore can affect fatty areas of the body such as the brain and nerves.
Orthopaedist Jacob von Heine observed ‘infantile spinal paralysis’ in 1840 and speculated that it was a contagious disease. It was named ‘acute anterior poliomyelitis’ by Wilhelm Heinrich Erb in 1875, by which time outbreaks had started to occur.
Regional patterns of disease led physicians to believe that polio was a contagious virus, but it was an unproven assumption. Scientists had no idea what a virus was in the nineteenth century — nobody had seen one because the electron microscope, which enabled observation of viruses, was not invented until 1931.
A study of 2,000 case histories carried out by Harvard Infantile Paralysis Commission concluded that tonsillectomies (introduced in 1909 and carried out routinely as a preventative measure) provoked respiratory paralysis due to bulbar polio. This was known at the time as authorities prohibited removal of tonsils and adenoids during epidemics. Bulbar polio was the type that required use of an iron lung and had the highest death rate.
The case fatality rate in the early 1900s was very high. England and Wales made polio a notifiable disease in 1912, and it was endemic from then on. The New York epidemic of 1916 saw patients experimented on with spinal injections of disinfectant and adrenaline. Roughly half of those treated died and were recorded as polio deaths.
A new pesticide, DDT — labeled ‘the killer of killers’ — was introduced just as WW2 began. People were led to believe it was good for them and even sprayed it on their children’s lunches. It is a cumulative poison and can be absorbed through the skin and mucosa. Governments started to ban DDT in the early 1950s, but the damage was done. The UK outlawed it in 1986, and it was banned worldwide in 2001, though it continues to be used in areas with high malaria incidence.
Epidemics peaked in the 1940s and 50s and physicians began to notice a correlation between certain medical interventions and polio paralysis. Children treated for congenital syphilis with arsenic-based Salvarsan often developed paralysis in their injected limbs.
Cases of polio rose in line with the expansion of vaccination programmes for diphtheria, pertussis, and tetanus.
The diphtheria vaccine was introduced in the UK in 1942 and was noted for its adverse effects. The British Medical Association published news on the 10th of April 1950 that the diphtheria vaccine was responsible for childhood paralysis attributed to polio.
A doctor at Guy’s Hospital in London found that 80 children developed paralysis within a month of receiving the shots; a health ministry doctor reported that another 65 children had developed paralysis within a fortnight; the St. Pancras medical officer found 40 more cases. Some children recovered from the paralysis, but others were still paralysed 18 months after onset. Two of the cases followed injection of penicillin.
Anne McLaren, writing for Cambridge University Press in 1957, stated that, “It is now well established that intramuscular inoculation with combined diphtheria-pertussis prophylactics can affect the course of poliomyelitic infection in children. Localisation of paralysis in the limb injected with vaccines was reported by McCloskey, Martin, Geffen, Hill & Knowelden, and Benjamin in 1950.”
In 1951, Dr Ralph Scobey and Dr Mortind Biskind testified in front of the U.S Congress that the paralysis around the country known as ‘polio’ was being caused by industrial poisons, and that a virus theory was purposely fabricated by the chemical industry and the government to deflect litigation away from both parties.
The diagnostic criteria for polio were very loose prior to trials for the vaccine in 1954.Only after the vaccine was introduced was there any effort to distinguish polio from other types of paralytic disease.
The first polio vaccine, created by Jonas Salk in 1955, caused a great deal of controversy. The ‘Cutter Incident’ happened when 120,000 children were injected with a live virus instead of a weakened one: 40,000 developed polio, 200 were paralysed, and ten died. When the immunisation program was eventually rolled out to the public, a different, untested, rapidly approved formula was used.
Salk later admitted that live virus vaccines against influenza or poliomyelitis might produce the diseases they intended to prevent (Science, 4th March 1977).
In 1956, the American Medical Association ordered that doctors could no longer diagnose paralysis as polio – it had to be called ‘acute flaccid paralysis’. This reduced polio statistics dramatically and gave the appearance that the vaccine programme had succeeded, when really the definition of the disease had just changed.
Simple, timely changes to diagnostic criteria meant the number of paralytic cases dropped irrespective of the vaccine programme.
Laboratory testing for polio wasn’t introduced until 1958. Before then, all manner of other diseases could be classed as polio, including other enteroviruses, lead, arsenic, and DDT poisoning, Guillain-Barré syndrome, transverse myelitis, post-polio syndrome, viral or aseptic meningitis, traumatic neuritis, and Reye’s syndrome. How many were misdiagnosed and put on the wrong path of treatment as a result?
It is claimed that the polio vaccine eradicated polio due to overblown, tightly controlled propaganda campaigns, but the truth is that cases plummeted because of changes in pesticide use, elimination of toxic metals in everyday products, improved diets and sanitary behaviour, and redefinition of the disease.
There is no convincing evidence of polio as a contagious viral disease. Naturally occurring polio is all but obsolete in the modern world and the only ‘polio’ we see nowadays is vaccine-induced, courtesy of immunisation programmes run by the World Health Organisation.
There has been a huge rise in vaccine-induced polio paralysis in India. In 2011 there were an extra 47,000 cases, which were directly proportionate to the amount of oral vaccines administered. In 2018 a vaccine tainted with eradicated type-2 polio was given to children in Uttar Pradesh. The country remains vulnerable to polio due to its continued use of DDT, intramuscular injection of antibiotics, and diets high in sugar and low in vitamins.
Research scientist Viera Scheibner says that modern day vaccine advocates have forgotten the ‘polio provocation’ of the past. She believes that vaccines represent a assault on the immune system, which seems to be clearly implicated in the shadowy history of polio.
Vaccines were not needed to combat polio. Dr Fred Klenner published results of a study that used intravenous vitamin C to cure polio and other viral diseases 73 years ago — six years before the vaccine was introduced. With a success rate of 100%, we have to ask why this simple, non-toxic, affordable cure was completely overlooked and ignored by the medical community. Why is it still ignored?
The answer may lie in the criminal deceptions peddled by medical-industrial-pharmaceutical cartels that control the narrative of disease in order to sustain their gravy train of ill-gotten gain. A customer cured is a customer lost and there is no profit to be made from a healthy population.
“The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica…
[….]
“What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice.”
virus, infectious agent of small size and simple composition that can multiply only in living cells of animals, plants, or bacteria. The name is from a Latin word meaning “slimy liquid” or “poison.”
I have purposefully stayed away from the whole “SARS-COV-2” as a gain of function/bioweapon disinformation campaign as it is obvious to anyone who has ever read any “virus” paper, there is absolutely zero credible evidence for the existence of “SARS-COV-2” or any of these other invisible entities. At no point has any virologist ever properly purified and isolated the particles assumed to be “viruses” directly from a sick patient and then proven them pathogenic in a natural way. As this is a fact that is even admitted by virologists themselves, it should also be obvious that if they can not find the particles assumed to be “viruses” in nature, they can not tinker around and modify these fictional entities in a lab in order to create some sort of contagious bioweapon.
Somehow, this logic escapes many. Even though some have woken to the truth and accepted that “SARS-COV-2” does not exist in nature, they still believe that it must have been developed in a lab and unleashed upon the world in order to create a new contagious disease which is wrecking havoc on the elderly and immunocompromised. What they fail to realize is that there simply is no new disease and that none of the symptoms associated with “SARS-COV-2” are new, unique, or specific. There is zero proof of transmission and/or contagion beyond highly flawed epidemiological studies. There is no new “virus,” no new disease, and no contagious bioweapon. It is pure fiction based upon faulty cell culture and genomic experiments.
Before diving into the experimental evidence presented for gain of function studies, I figured it would be a good idea to get some background information on what exactly these kinds of studies entail first. From the October 2021 Nature article highlighted below, we learn that the gain of function concept earned widespread recognition in 2012 due to a pair of studies which both looked to tweak an avian influenza “virus” in order to make it transmissable by air between ferrets. Disregarding the contradictory fact that aerosol transmission is supposedly the way an upper respiratory “virus” is supposed to spread, many became concerned that this kind of work may eventually lead to the release of a super “virus” which could result in the next pandemic. These ferret studies were apparently pivotal with bringing virology into the gain of function field, even though it could be easily argued that virology has been performing these kinds of experiments throughout its existence.
The gain of function term refers to any research that improves a pathogen’s abilities to cause disease or spread from host to host. This is done by fiddling with cell culture material in a lab combined with genomic sequencing. They do this either by inserting genetic material into the cell culture or by way of animal models where the animal is said to be genetically altered in some way to be more susceptible to the “viral” material.
The article provides an example where mice were genetically modified to become susceptible to MERS. However, the mice did not become ill upon being challenged with the “virus.” Thus, the researchers resorted to passaging the “virus” between mice, which involved infecting a couple of mice, giving the “virus” two days to take hold, and then killing the mice and grinding up the lung tissue to inject into other mice. They repeated these steps at least 30 times which eventually made some mice sick. This process of culturing toxic material, injecting animals with the concoction, killing them and grinding up their remains, and then injecting this emulsified goop into other animals in an attenpt to make them sick is what GOF is all about. While this horrific process is getting recognized today, these kinds of experiments have been a staple of virology since the very beginning:
The shifting sands of ‘gain-of-function’ research
“The term first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza virus, using genetic engineering and directed evolution, until it could be transmitted between ferrets2,3. Many people were concerned that publishing the work would be tantamount to providing a recipe for a devastating pandemic, and in the years that followed, research funders, politicians and scientists debated whether such work required stricter oversight, lest someone accidentally or intentionally release a lab-created plague. Researchers around the world voluntarily paused some work, but the issue became particularly politicized in the United States.
US funding agencies, which also support research abroad, later imposed a moratorium on gain-of-function research with pathogens while they worked out new protocols to assess the risks and benefits. But many of the regulatory discussions have taken place out of the public eye.
Now, gain-of-function research is once again centre stage, thanks to SARS-CoV-2 and a divisive debate about where it came from. Most virologists say that the coronavirus probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the virus was first reported. But a group of scientists and politicians argues that a laboratory origin has not been ruled out. They are demanding investigation of the Wuhan Institute of Virology, where related bat coronaviruses have been extensively studied, to determine whether SARS-CoV-2 could have accidentally leaked from the lab or crossed into humans during collection or storage of samples.”
“The term GOF didn’t have much to do with virology until the past decade. Then, the ferret influenza studies came along. In trying to advise the federal government on the nature of such research, the US National Science Advisory Board for Biosecurity (NSABB) borrowed the term — and it stuck, says Gigi Gronvall,a biosecurity specialist at the Bloomberg School of Public Health at Johns Hopkins University in Baltimore, Maryland. From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host.
Virologists do regularly fiddle with viral genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models. “People do all of these experiments all the time,” says Juliet Morrison, a virologist at the University of California, Riverside. For example, her lab has made mouse viruses that are more harmful to mice than the originals. If only mice are at risk, should it be deemed GOF? And would it be worrying?
The answer is generally no. Morrison’s experiments, and many others like them, pose little threat to humans. GOF research starts to ring alarm bells when it involves dangerous human pathogens, such as those on the US government’s ‘select agents’ list, which includes Ebola virus and the bacteria responsible for anthrax and botulism. Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza viruses and coronaviruses. “For the most part, we’re worried about respiratory viruses because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School. GOF studies with those viruses are “a really tiny part” of virology, he adds.”
“Animal research — although fraught with its own set of ethical quandaries — allows scientists to study how pathogens work and to test potential treatments, a necessary precursor to trials in people. That’s what Perlman and his collaborators had in mind when they set out to study the coronavirus responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012. They wanted to use mice, but mice can’t catch MERS.
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells. So, the team altered the mice, giving them a human-like version of the gene for DPP4. The virus could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill. “Having a model of mild disease isn’t particularly helpful to understand why people get so sick,” says collaborator Paul McCray, a paediatric pulmonologist also at the University of Iowa.
So, the group used a classic technique called ‘passaging’ to enhance virulence. The researchers infected a couple of mice, gave the virus two days to take hold, and then transferred some of the infected lung tissue into another pair of mice. They did this repeatedly — 30 times9. By the end of two months, the virus had evolved to replicate better in mouse cells. In so doing, it made the mice more ill; a high dose was deadly, says McCray. That’s GOF of a sort because the virus became better at causing disease. But adapting a pathogen to one animal in this way often limits its ability to infect others, says Andrew Pekosz, a virologist at the Bloomberg School of Public Health.”
“With all the challenges inherent in GOF studies, why do them? Because, some virologists say, the viruses are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match. “We can either wait for something to arise, and then fight it, or we can anticipate that certain things will arise, and instead we can preemptively build our arsenals,” says Morrison. “That’s where gain-of-function research can come in handy.”
This next source is from 2015. The authors admit that virology is heavily reliant on gain or loss of function studies. They offer an alternative definition for GOF research which is any selection process involving an alteration of genotypes and their resulting phenotypes. Obviously, this definition leans far more into the genomics side of the equation. This is due to the claim that these kinds of studies are used by virologists in order to understand a “viruses” genetic make-up. It is stated that researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA. In other words, they mix genetic material from different sources, poison and/or kill lab animals by injecting them with this toxic soup, and then analyze the resulting mixture using computers so that they can claim that the generated model is a new creation. However, it is admitted that these kinds of mutations happen “naturally” with “viruses” every time a person is infected, thus confirming what we already know: virologists can not sequence the same exact “virus” every time:
Gain-of-Function Research: Background and Alternatives
“The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function. In order to understand the role of such studies in virology, Dr. Kanta Subbarao from the Laboratory of Infectious Disease at the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health (NIH) gave an overview of the current scientific and technical approaches to the research on pandemic strains of influenza and Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) coronaviruses (CoV). As discussed in greater detail later in this chapter, many participants argued that the word choice of “gain-of-function” to describe the limited type of experiments covered by the U.S. deliberative process, particularly when coupled with a pause on even a smaller number of research projects, had generated concern that the policy would affect much broader areas of virology research.
TYPES OF GAIN-OF-FUNCTION (GOF) RESEARCH
Subbarao explained that routine virological methods involve experiments that aim to produce a gain of a desired function, such as higher yields for vaccine strains, but often also lead to loss of function, such as loss of the ability for a virus to replicate well, as a consequence. In other words, any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research, even if the U.S. policy is intended to apply to only a small subset of such work.
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of viruses and added that much basic knowledge is still lacking for SARS-CoV and MERS-CoV. Subbarao introduced the key questions that virologists ask at all stages of research on the emergence or re-emergence of a virus and specifically adapted these general questions to the three viruses of interest in the symposium (see Box 3-1). To answer these questions, virologists use gain- and loss-of-function experiments to understand the genetic makeup of viruses and the specifics of virus-host interaction. For instance, researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant viruses from cloned cDNA, and deep sequencing that are critical for studying how viruses escape the host immune system and antiviral controls. Researchers also use targeted host or viral genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool.
During Session 3 of the symposium, Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments. The first category, which he called “gain of function research of concern,” includes the generation of viruses with properties that do not exist in nature. The now famous example he gave is the production of H5N1 influenza A viruses that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type. The second category deals with the generation of viruses that may be more pathogenic and/or transmissible than the wild type viruses but are still comparable to or less problematic than those existing in nature. Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates will improve their replication in mammalian cells. Finally, the third category, which is somewhere in between the two first categories, includes the generation of highly pathogenic and/or transmissible viruses in animal models that nevertheless do not appear to be a major public health concern. An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans. During the discussion, Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature.”
“Imperiale explained that, with respect to the GoF terminology, whenever researchers are working with RNA viruses, GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.” He also commented that the term GoF was understood a certain way by attendees of this symposium, but when the public hears this term “they can’t make that sort of nuanced distinction that we can make here” so the terminology should be revisited.”
Hopefully the above two sources have shown that GOF studies are nothing more than the exact same cell culture experiments utilizing the exact same genomic sequencing technologies and tricks that virologists have always used. The only difference is that they are combining different culture supernatant and genetic materials together into one in order to create a brand new synthetic computer-generated sequence. At no point in time are any purified/isolated particles ever used in these studies. In fact, there are no EM images of the new “virus” of any kind. It should therefore not be surprising that we can see the exact same pattern of unscientific methods and illogical reasoning in GOF studies as found in any of the original “virus” papers.
Seeing as to how the 2012 avian flu studies brought GOF research to the forefront, it seemed ideal to step into this area a bit more to see what actually transpired. The main study presented as evidence of GOF research was led by a man named Ron Fouchier. If that name sounds familiar, that’s because it should. Fouchier was involved in the 2003 “SARS-COV-1” study which proclaimed the satisfaction of Koch’s Postulates for proving a microorganism causes disease yet it failed miserably by not only not being able to satisfy Koch’s four original Postulates, but also Thomas River’s six revised Postulates made strictly for virology. In other words, it was an epic fail.
In Fouchier’s 2012 avian flu GOF study, he attempted to make the H5N1 “virus” infectious through the air. This was done through a process involving cell culturing combined with genetic engineering as well as passaging the material through numerous ferrets. Sounds familiar to the mice example from before, correct? You also see this same process with the early polio and influenza studies as well as in many other virology papers. The main difference is the genomic narrative and the use of modern technology such as reverse genetics to claim the insertion of specific genes.
Highlights from the below paper provide an overview of what was done during this study. It details how the material was collected from a flu strain in Indonesia, genetically altered in a Petri dish, and then transferred to ferrets in a series of experiments using the “wildtype” strain along with different modified strains. Fouchier and Co. were repeatedly unsuccessful in their endeavors of infecting ferrets until they started passaging the “virus” in the animals by injecting them with the cultured soup, grinding up their lung tissues, and injecting other ferrets in the same manner. They repeated this process 6 times and then changed up the experiment by switching to nasal turbinates for the last 4 passage attempts. The only illness said to be achieved via airborne exposure was a loss of appetite, lethargy, and ruffled fur. Upon sequencing the “viruses,” there were only two amino acid switches shared by all six “viruses.” There were several other mutations, but none that occurred in all six airborne “viruses.” In other words, they could not sequence the same “virus” at any point:
Fouchier study reveals changes enabling airborne spread of H5N1
“A study showing that it takes as few as five mutations to turn the H5N1 avian influenza virus into an airborne spreader in mammals—and that launched a historic debate on scientific accountability and transparency—was released today in Science, spilling the full experimental details that many experts had sought to suppress out of concern that publishing them could lead to the unleashing of a dangerous virus.
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 virus that can spread among ferrets without direct contact.
They say their findings show that H5N1 viruses have the potential to evolve in mammals to gain airborne transmissibility, without having to mix with other flu viruses in intermediate hosts such as pigs, and thus pose a risk of launching a pandemic.”
Indonesian H5N1 strain used
Fouchier’s team started with an H5N1 virus collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 viruses more human-like in how they bind to airway cells or in other ways. Avian flu viruses prefer to bind to alpha2,3-linked sialic acid receptors on cells, whereas human flu viruses prefer alpha2,6-linked receptors. In both humans and ferrets, alpha2,6 receptors are predominant in the upper respiratory tract, while alpha 2,6 receptors are found mainly in the lower respiratory tract.
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the virus’s HA protein, the viral surface molecule that attaches to host cells. Q222L and G224S together change the binding preference of H2 and H3 subtype flu viruses, changes that contributed to the 1957 and 1968 flu pandemics, according to the report. And N182K was found in a human H5N1 case.
The scientists created three mutant H5N1 virus strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes, the report explains. They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 virus. Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type virus shed far more virus than those infected with the mutants.
In a second step, the team used a mutation in a different viral gene, PB2, the polymerase complex protein. The mutation E627K in PB2 is linked to the acquisition by avian flu viruses of the ability to grow in the human respiratory tract, which is cooler than the intestinal tract of birds, where the viruses usually reside, according to the report.
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a virus that grew more vigorously in ferrets, and the virus did not spread through the air from infected ferrets to uninfected ones.
The passaging step
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract—the move that Fouchier called “really, really stupid,” according to a report of his initial description of the research at a European meeting last September.
They inoculated one ferret with the three-mutation strain and another with the wild-type virus and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs). Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times. For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest viruses that were secreted from the upper respiratory tract.
The amount of mutant virus found in the nasal turbinate and nose swab samples increased with the number of passages, signaling that the virus was increasing its capacity to grow in the ferret upper airway. In contrast, viral titers in the samples from ferrets infected with the wild-type virus stayed the same.
The next step was to test whether the viruses produced through passaging could achieve airborne transmission. Four ferrets were inoculated with samples of the “passage-10” mutant virus, and two ferrets were inoculated with the passage-10 wild strain. Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact.
The ferrets exposed to those with the wild virus remained uninfected, but three of the four ferrets placed near those harboring the mutant virus did get infected, the researchers found. Further, they took a sample from one of the “recipient” ferrets and used it to inoculate another ferret, which then transmitted the virus to two more ferrets that were placed near it.
Thus, a total of six ferrets became infected with the mutant virus via airborne transmission. However, the level of viral shedding indicated the airborne virus didn’t transmit as efficiently as the 2009 H1N1 virus does.
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur. One of the directly inoculated ferrets died, but all those infected via airborne viruses survived.
When the scientists sequenced the genomes of the viruses that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six viruses: H103Y and T156A. They noted several other mutations, but none that occurred in all six airborne viruses.
“Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of [highly pathogenic avian flu] H5N1 virus,” the researchers wrote.
In further steps, the researchers inoculated six ferrets with high doses of the airborne-transmissible virus; after 3 days, the ferrets were either dead or “moribund.” “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia,” the report notes.”
While the proceeding article did an excellent job of providing the main points from Fouchier’s 2012 GOF study, I wanted to showcase relevant highlights directly from the paper to flesh out the methods used even further. Here you will see that Fouchier’s team claimed that they genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets. They used Influenza “virus” A/Indonesia/5/2005 (A/H5N1) which they said was isolated from a human case of HPAI “virus” infection. This was passaged once in embryonated chicken eggs which was followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000. They then used the QuickChange multisite-directed mutagenesis kit to introduce the desired amino acid substitutions. Site-directed mutagenesis is a synthetic process utilizing PCR to make artificial changes in a DNA sequence. They then took their synthetically-created cultured soup and experimented on ferrets while manipulating the methods until they achieved the results that they desired.
At no point in the paper was a “virus” of any kind ever purified and isolated. At no point were any electron microscope images of the newly mutated “viruses” ever shown. The only “evidence” of an airborne strain is genomic sequencing data from consensus genomes which did not match up. Fouchier and Co. even admitted that airborne transmission could be tested in a second mammalian model system such as guinea pigs, but even this would still not provide conclusive evidence that transmission among humans would occur. They also stated that the mutations they had identified needed further testing to determine their effect on transmission in other A/H5N1 “virus” lineages, and that further experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals. In other words, their study only told them that they could create mutated genomes and not that they created more “virulent viruses” that are transmissable by air:
Airborne Transmission of Influenza A/H5N1 Virus Between Ferrets
“Highly pathogenic avian influenza A/H5N1 virus can cause morbidity and mortality in humans but thus farhas not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”)between humans. To address the concern that the virus could acquire this ability under natural conditions,we genetically modified A/H5N1 virus by site-directed mutagenesis and subsequent serial passage inferrets. The genetically modified A/H5N1 virus acquired mutations during passage in ferrets, ultimatelybecoming airborne transmissible in ferrets. None of the recipient ferrets died after airborne infection withthe mutant A/H5N1 viruses. Four amino acid substitutions in the host receptor-binding protein hemagglutinin, and one in the polymerase complex protein basic polymerase 2, were consistently present in airborne-transmitted viruses. The transmissible viruses were sensitive to the antiviral drug oseltamivir and reacted well with antisera raised against H5 influenza vaccine strains. Thus, avian A/H5N1 influenza viruses can acquire the capacity for airborne transmission between mammals without recombination in an intermediate host and therefore constitute a risk for human pandemic influenza.
Influenza A viruses have been isolated from many host species, including humans, pigs, horses, dogs, marine mammals, and a wide range of domestic birds, yet wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the virus reservoir in nature (1). Influenza A viruses belong to the family Orthomyxoviridae; these viruses have an RNA genome consisting of eight gene segments (2, 3). Segments 1 to 3 encode the polymerase proteins: basic polymerase 2 (PB2), basic polymerase 1 (PB1), and acidic polymerase (PA), respectively. These proteins form the RNA-dependent RNA polymerase complex responsible for transcription and replication of the viral genome.”
Since the late 1990s, HPAI A/H5N1 viruses have devastated the poultry industry of numerous countries in the Eastern Hemisphere. To date, A/H5N1 has spread from Asia to Europe, Africa, and the Middle East, resulting in the death of hundreds of millions of domestic birds. In Hong Kong in 1997, the first human deaths directly attributable to avian A/H5N1 virus were recorded (11). Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 virus infections in humans have been reported from 15 countries (12). Although limited A/H5N1 virus transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 virus has not been detected (13–15). Whether this virus may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness. Although our knowledge of viral traits necessary for host switching and virulence has increased substantially in recent years (16, 17), the factors that determine airborne transmission of influenza viruses among mammals, a trait necessary for a virus to become pandemic, have remained largely unknown (18–21). Therefore, investigations of routes of influenza virus transmission between animals and on the determinants of airborne transmission are high on the influenza research agenda.
The viruses that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza viruses (22). However, given that viruses from only four pandemics are available for analyses, we cannot exclude the possibility that a futurepandemic may be triggered by a wholly avian virus without the requirement of reassortment. Several studies have shown that reassortment events between A/H5N1 and seasonal human influenza viruses do not yield viruses that are readily transmitted between ferrets (18–20, 23). In our work, we investigated whether A/H5N1 virus could change its transmissibility characteristics without any requirement for reassortment.
We chose influenza virus A/Indonesia/5/2005 for our study because the incidence of human A/H5N1 virus infections and fatalities in Indonesia remains fairly high (12), and there are concerns that this virus could acquire molecular characteristics that would allow it to become more readily transmissible between humans and initiate a pandemic. Because no reassortants between A/H5N1 viruses and seasonal or pandemic human influenza viruses have been detected in nature and because our goal was to understand the biological properties needed for an influenza virus to become airborne transmissible in mammals, we decided to use the complete A/Indonesia/5/2005 virus that was isolated from a human case of HPAI A/H5N1 infection.
We chose the ferret (Mustela putorius furo) as the animal model for our studies. Ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza viruses (24). After infection with human influenza A virus, ferrets develop respiratory disease and lung pathology similar to that observed in humans. Ferrets can also transmit human influenza viruses to other ferrets that serve as sentinels with or without direct contact (fig. S1) (25–27).”
Human-to-human transmission of influenza viruses can occur through direct contact, indirect contact via fomites (contaminated environmental surfaces), and/or airborne transmission via small aerosols or large respiratory droplets. The pandemic and epidemic influenza viruses that have circulated in humans throughout the past century were all transmitted via the airborne route, in contrast to many other respiratory viruses that are exclusively transmitted via contact. There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols. However, it is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols. Because we did not measure particle size during our experiments, we will use the term “airborne transmission” throughout this Report.”
“Using a combination of targeted mutagenesis followed by serial virus passage in ferrets, we investigated whether A/H5N1 virus can acquiremutations that would increase the risk of mammalian transmission (34). We have previously shown that several amino acid substitutions in the RBS of the HA surface glycoprotein of A/Indonesia/5/2005 change the binding preference from the avian a-2,3–linked SA receptors to the human a-2,6–linked SA receptors (35). A/Indonesia/5/2005 virus with amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S (numbers refer to amino acid positions in the mature H5 HA protein; N, Asn; Q, Gln; L, Leu; G, Gly; S, Ser) in HA display attachment patterns similar to those of human viruses to cells of the respiratory tract of ferrets and humans (35). Of these changes, we know that together, Q222L and G224S switch the receptor binding specificity of H2 and H3 subtype influenza viruses, as this switch contributed to the emergence of the 1957 and 1968 pandemics (36). N182K has been found in a human case of A/H5N1 virus infection (37).
Our experimental rationale to obtain transmissible A/H5N1 viruses was to select a mutant A/H5N1 virus with receptor specificity for a-2,6–linked SA shed at high titers from the URT of ferrets. Therefore, we used the QuickChange multisite-directed mutagenesis kit (Agilent Technologies, Amstelveen, the Netherlands) to introduce amino acid substitutions N182K, Q222L/G224S, or N182K/Q222L/G224S in the HA of wild-type (WT) A/Indonesia/5/2005, resulting in A/H5N1HA N182K, A/H5N1HA Q222L,G224S, and A/H5N1HA N182K,Q222L,G224S. Experimental details for experiments 1 to 9 are provided in the supplementary materials (25). For experiment 1, we inoculated these mutant viruses andthe A/H5N1wildtype virus intranasally into groups of six ferrets for each virus (fig. S3). Throat and nasal swabs were collected daily, and virus titerswere determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify virus shedding from the ferret URT. Three animals were euthanized after day 3 to enable tissue sample collection. All remaining animals were euthanized by day 7 when the same tissue samples were taken. Virus titers were determined in the nasal turbinates, trachea, and lungs collected post-mortem from the euthanized ferrets. Throughout the duration of experiment 1, ferrets inoculated intranasally with A/H5N1wildtype virus produced high titers in nose and throat swabs—up to 10 times more than A/H5N1HA Q222L,G224S, which yielded the highest virus titers of all three mutants during the 7-day period (Fig. 1). However, no significant difference was observed between the virus shedding of ferrets inoculated with A/H5N1HA Q222L, G224S or A/H5N1HA N182K during the first 3 days when six animals per group were present. Thus, of the viruses with specificity for a-2,6–linked SA, A/H5N1HA Q222L,G224S yielded the highest virus titers in the ferret URT (Fig. 1).
As described above, amino acid substitution E627K in PB2 is one of the most consistent host-range determinants of influenza viruses (29–31). For experiment 2 (fig. S4), we introduced E627K into the PB2 gene of A/Indonesia/5/2005 by site-directed mutagenesis and produced the recombinant virus A/H5N1HA Q222L,G224S PB2 E627K. The introduction of E627K in PB2 did not significantly affect virus shedding in ferrets, because virus titers in the URT were similar to those seen in A/H5N1HA Q222L,G224S-inoculated animals [up to 1 × 104 50% tissue culture infectious doses (TCID50)] (Mann-Whitney U rank-sum test, P = 0.476) (Fig. 1 and fig. S5). When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously (27), A/H5N1HA Q222L,G224S PB2 E627K was not transmitted (fig. S5).
Because the mutant virus harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, we designed an experiment to force the virus to adaptto replication in the mammalian respiratory tract and to select virus variants by repeated passage (10 passages in total) of the constructedA/H5N1HA Q222L,G224S PB2 E627K virus and A/H5N1wildtype virus in the ferret URT (Fig. 2 and fig. S6). In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K. Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs. The nasal turbinates were homogenized in 3 ml of virus-transport medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate thenext ferret intranasally (passage 2). This procedure was repeated until passage 6.
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi. To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise tothe nostrils of the ferrets to induce sneezing. Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml. The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10. We changed the source of inoculum during the course of theexperiment, because passaging nasal washes may facilitate the selection of viruses that were secreted from the URT. Because influenza viruses mutate rapidly, we anticipated that 10 passages would be sufficient for the virus to adapt to efficient replication in mammals.
Virus titers in the nasal turbinates of ferrets inoculated with A/H5N1wildtype ranged from ~1 × 105 to 1 × 107 TCID50/gram tissue throughout 10 serial passages (Fig. 3A and fig. S7). In ferrets inoculated with A/H5N1HA Q222L,G224S PB2 E627K virus, a moderate increase in virus titers in the nasal turbinates was observed as the passage number increased. These titers ranged from 1 × 104 TCID50/gram tissue at the start of the experiment to 3.2 × 105 to 1 × 106 TCID50/gram tissue in the final passages (Fig. 3A and fig. S7). Notably, virus titers in the nose swabs of animals inoculated with A/H5N1HA Q222L,G224S PB2 E627K also increased during the successive passages, with peak virus shedding of 1 × 105 TCID50 at 2 dpi after 10 passages (Fig. 3B).These data indicate that A/H5N1HA Q222L,G224S PB2 E627K was developing greater capacity to replicate in the ferret URT after repeated passage, with evidence for such adaptation becoming apparent by passage number 4. In contrast, virus titers in the nose swabs of the ferrets collected at 1 to 4 dpi throughout 10 serial passages with A/H5N1wildtype revealed no changes in patterns of virus shedding.
Passaging of influenza viruses in ferrets should result in the natural selection of heterogeneous mixtures of viruses in each animal with a variety of mutations: so-called viral quasi-species (38). The genetic composition of the viral quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform (Roche, Woerden, the Netherlands) (tables S1 and S2). The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the virus population after 10 consecutive passages at a frequency >99.5% (Fig. 4 and table S1). Numerous additional nucleotide substitutions were detected in all viral gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kafter passaging, except in segment 7 (tables S1 and S2). Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions.The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627Kwas T156A (T, Thr; A, Ala) in HA. This substitution removes a potential N-linked glycosylation site (Asn-X-Thr/Ser; X, any amino acid) in HA and was detected in 99.6% of the A/H5N1wildtype sequences after 10 passages. T156A was detected in 89% of the A/H5N1HA Q222L,G224S PB2 E627K sequences after 10 passages, and the other 11% of sequences possessed the substitution N154K, which removes the same potential N-linked glycosylation site in HA.
In experiment 4 (see supplementary materials), we investigated whether airborne-transmissible viruses were present in the heterogeneous virus population generated during virus passaging in ferrets (fig. S4). Nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were usedin transmission experiments to test whether airborne-transmissible virus was present in the virus quasi-species. For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally: two for passage 10 A/H5N1wildtype and four for passage 10 A/H5N1HA-Q222L,G224S PB2 E627K virus.
The following day, a naïve recipient ferret was placed in a cage adjacent to each inoculated donor ferret. These cages are designed to prevent direct contact between animals but allow airflow from a donor ferret to a neighboring recipient ferret (fig. S1) (27). Although mutations had accumulated in the viral genome after passaging of A/H5N1wildtype in ferrets, we did not detect replicating virus upon inoculation of MDCKcells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype virus(Fig. 5, A and B). In contrast, we did detect virus in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627Kvirus.Three (F1 to F3) out of four (F1 to F4) naïve recipient ferrets became infected as confirmed by the presence of replicating virus in the collected nasal and throat swabs (Fig. 5, C and D). A throat-swab sample obtained from recipient ferret F2, which contained the highest virus titer among the ferrets in the first transmission experiment, was subsequently used for intranasal inoculation of two additional donor ferrets. Both of these animals, when placed in the transmission cage setup (fig. S1), again transmitted the virus to the recipient ferrets (F5 and F6) (Fig. 6, A and B). Avirus isolate was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi. The virus from F5 was inoculated intranasally into two more donor ferrets. One day later, these animals were paired with two recipient ferrets (F7 and F8) in transmission cages, one of which (F7) subsequently became infected (Fig. 6, C and D).
We used conventional Sanger sequencing to determine the consensus genome sequences ofviruses recovered from the six ferrets (F1 to F3 and F5 to F7) that acquired virus via airborne transmission (Fig. 4 and table S3). All six samples still harbored substitutions Q222L, G224S,and E627K that had been introduced by reverse genetics. Surprisingly, only two additional amino acid substitutions, both in HA, were consistently detected in all six airborne-transmissible viruses: (i) H103Y (H, His; Y, Tyr), which forms part of the HA trimer interface, and (ii) T156A, which is proximal but not immediately adjacent to the RBS (fig. S8). Although we observed severalother mutations, their occurrence was not consistent among the airborne viruses, indicating that of the heterogeneous virus populations generated by passaging in ferrets, viruses with different genotypes were transmissible. In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible viruses because, for example, the consensus sequence of virus isolated from F6 differed from the sequence of parental virus isolated from F2.
Together, these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 virus between mammals. The airborne-transmissible virus isolate with the least number of amino acid substitutions, compared with the A/H5N1wildtype, was recovered from ferret F5. This virus isolate had a total of nine amino acid substitutions; in addition to the three mutations that we introduced (Q222L and G224S in HA and E627K in PB2), this virus harbored H103Y and T156A in HA, H99Y and I368V (I, Ile; V, Val) in PB1, and R99K (R, Arg) and S345N in NP (table S3). Reverse genetics will be needed to identify which of the five to nine amino acid substitutions in this virus are essential to confer airborne transmission.
During the course of the transmission experiments with the airborne-transmissible viruses, ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation. One of eight inoculated animals died upon intranasal inoculation (Table 1). In previously published experiments, ferrets inoculated intranasally with WTA/ Indonesia/5/2005 virus at a dose of 1 × 106 TCID50 showed neurological disease and/or death (39, 40). It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 virus and the subsequent course of disease is not representative of the natural situation in humans.Importantly, although the six ferrets that became infected via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment. Moreover, previous infections of humans with seasonal influenza viruses are likely to induce heterosubtypic immunity that would offer some protection against the development of severe disease (41, 42). It has been shown that mice and ferrets previously infected with an A/H3N2 virus are clinically protected against intranasal challenge infection with an A/H5N1 virus (43, 44).
After intratracheal inoculation (experiment 5; fig. S9), six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible virus F5 in a 3-ml volume of PBS died or were moribund at day 3. Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia (45), as is done for vaccination-challenge studies. At necropsy, the six ferrets revealed macroscopic lesions affecting 80 to 100% of the lung parenchyma with average virus titers of 7.9 × 106 TCID50/gram lung (fig. S10). These data are similar to those described previously for A/H5N1wildtype in ferrets (Table 1). Thus, although the airborne-transmissible virus is lethal to ferrets upon intratracheal inoculation at high doses, the virus was not lethal after airborne transmission.”
“Although our experiments showed that A/H5N1 virus can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear. Previous data have indicated that the 2009 pandemic A/H1N1 virus transmits efficiently among ferrets and that naïve animals shed high amounts of virus as early as 1 or 2 days after exposure (27). When we compare the A/H5N1 transmission data with that of reference (27), keeping in mind that our experimental design for studying transmission is not quantitative, the data shown in Figs. 5 and 6 suggest that A/H5N1 airborne transmission was less robust, with less and delayed virus shedding compared with pandemic A/H1N1 virus.
Airborne transmission could be tested in a second mammalian model system such as guinea pigs (59), but this would still not provide conclusive evidence that transmission among humans would occur. The mutations we identified need to be tested for their effect on transmission in other A/H5N1 virus lineages (60), and experiments are needed to quantify how they affect viral fitness and virulence in birds and mammals. For pandemic preparedness, antiviral drugs and vaccine candidates against airborne-transmissible virus should be evaluated in depth. Mechanistic studies on the phenotypic traits associated with each of the identified amino acid substitutions should provide insights into the key determinants of airborne virus transmission. Our findings indicate that HPAI A/H5N1 viruses have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in humans. Identification of the minimal requirements for virus transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness (34).”
“Influenza virus A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI virus infection and passaged once in embryonated chicken eggs followed by a singlepassage in Madin-Darby Canine Kidney (MDCK) cells. All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000 (63-64). Mutations of interest (N182K, Q222L, G224S in HA and E627K in PB2) were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit (Aligent, Amstelveen, The Netherlands) according to the instructions of the manufacturer. Recombinant viruses were produced upon transfection of 293T cells and virus stocks were propagated and titrated in MDCK cells as described (63).
Cells
MDCK cells were cultured in Eagle’s minimal essential medium (EMEM, Lonza Benelux BV, Breda, the Netherlands) supplemented with 10% fetal calf serum (FCS), 100 IU/ml penicillin, 100 μg/ml streptomycin, 2 mM glutamine, 1.5 mg/ml sodium bicarbonate (Lonza), 10 mM Hepes (Lonza), and non-essential amino acids (MP Biomedicals Europe, Illkirch, France). 293T cells were cultured in Dulbecco modified Eagle’s medium (DMEM, Lonza) supplemented with 10% FCS, 100 IU/ml penicillin, 100 mg/ml streptomycin, 2mM glutamine, 1mM sodium pyruvate, and non-essential amino acids.
Virus titration in MDCK cells
Virus titrations were performed as described previously (27). Briefly, MDCK cells were inoculated with tenfold serial dilutions of virus preparations, homogenized tissues, nose swabs, and throat swabs.Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with 100 U/mlpenicillin, 100 μg/ml streptomycin, 2mM glutamine, 1.5mg/ml sodium bicarbonate, 10mM Hepes, non-essential amino acids, and 20 μg/ml trypsin (Lonza). Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of virus replication in the cells. Infectious virus titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the virus preparations by the method of Spearman-Karber (65).”
The term “Gain of Function” first gained a wide public audience in 2012, after two groups revealed that they had tweaked an avian influenza “virus,” using genetic engineering and directed evolution, until it could be transmitted between ferrets
Most virologists say that the “coronavirus” probably emerged from repeated contact between humans and animals, potentially in connection with wet markets in Wuhan, China, where the “virus” was first reported
However, a group of scientists and politicians argues that a laboratory origin has not been ruled out
The term GOF didn’t have much to do with virology until the past decade when the ferret influenza studies came along
From that usage, it came to mean any research that improves a pathogen’s abilities to cause disease or spread from host to host
Virologists regularly fiddle with “viral” genes to change them, sometimes enhancing virulence or transmissibility, although usually just in animal or cell-culture models
Other major concerns are ‘pathogens of pandemic potential’ (PPP) such as influenza “viruses” and “coronaviruses”
“For the most part, we’re worried about respiratory “viruses” because those are the ones that transmit the best,” says Michael Imperiale, a virologist at the University of Michigan Medical School
He added that GOF studies with those “viruses” are “a really tiny part” of virology
Perlman and his collaborators set out to study the “coronavirus” responsible for Middle East Respiratory Syndrome (MERS-CoV), which emerged as a human pathogen in 2012
They wanted to use mice, but mice can’t catch MERS
The rodents lack the right version of the protein DPP4, which MERS-CoV uses to gain entry to cells and so the team altered the mice, giving them a human-like version of the gene for DPP4
The “virus” could now infect the humanized mice, but there was another problem: even when infected, the mice didn’t get very ill
So, the group used a classic technique called ‘passaging’ to enhance “virulence”
The researchers infected a couple of mice, gave the “virus” two days to take hold, and then transferred some of the infected lung tissue into another pair of mice
They did this repeatedly — 30 times and by the end of two months, the “virus” had evolved to replicate better in mouse cells
In so doing, it made the mice more ill; a high dose was deadly
Some virologists say “viruses” are constantly mutating on their own, effectively doing GOF experiments at a rate that scientists could never match
The field of virology, and to some extent the broader field of microbiology, widely relies on studies that involve gain or loss of function
Any selection process involving an alteration of genotypes and their resulting phenotypes is considered a type of Gain-of-Function (GoF) research
Subbarao emphasized that such experiments in virology are fundamental to understanding the biology, ecology, and pathogenesis of “viruses” and added that much basic knowledge is still lacking for “SARS-CoV” and “MERS-CoV”
Virologists use gain- and loss-of-function experiments to understand the genetic makeup of “viruses” and the specifics of “virus-host” interaction
Researchers now have advanced molecular technologies, such as reverse genetics, which allow them to produce de novo recombinant “viruses” from cloned cDNA (i.e. they are synthetic lab creations)
Researchers also use targeted host or “viral” genome modification using small interfering RNA or the bacterial CRISPR-associated protein-9 nuclease as an editing tool
Dr. Yoshihiro Kawaoka, from the University of Wisconsin-Madison, classified types of GoF research depending on the outcome of the experiments:
The fisrt category is “gain of function research of concern,” includes the generation of “viruses” with properties that do not exist in nature
The now famous example he gave is the production of H5N1 influenza A “viruses” that are airborne-transmissible among ferrets, compared to the non-airborne transmissible wild type
The second category deals with the generation of “viruses” that may be more pathogenic and/or transmissible than the wild type “viruses” but are still comparable to or less problematic than those existing in nature (which is odd considering no “viruses” have been found in nature…)
Kawaoka argued that the majority of strains studied have low pathogenicity, but mutations found in natural isolates (there are no natural isolates) will improve their replication in mammalian cells
The third category, which is somewhere in between the first two categories, includes the generation of highly pathogenic and/or transmissible “viruses” in animal models that nevertheless do not appear to be a major public health concern
An example is the high-growth A/PR/8/34 influenza strain found to have increased pathogenicity in mice but not in humans
Dr. Thomas Briese, Columbia University, further described GoF research done in the laboratory as being a “proactive” approach to understand what will eventually happen in nature
GoF mutations are naturally arising all the time and escape mutants isolated in the laboratory appear “every time someone is infected with influenza.”
In other words, they can never sequence the same “virus” every time so what they do in the lab in GoF studies is no different than how they culture and “isolate viruses” in order to sequence the genomes in the first place
A 2012 study supposedly showed that it takes as few as five mutations to turn the H5N1 avian influenza “virus” into an airborne spreader in mammals—and this launched a historic debate on scientific accountability and transparency
In the lengthy report, Ron Fouchier, PhD, of Erasmus Medical Center in the Netherlands and colleagues describe how they used a combination of genetic engineering and serial infection of ferrets to create a mutant H5N1 “virus” that can spread among ferrets without direct contact
Fouchier’s team started with an H5N1 “virus” collected in Indonesia and used reverse genetics to introduce mutations that have been shown in previous research to make H5N1 “viruses” more human-like in how they bind to airway cells or in other ways
The amino acid changes the team chose included N182K, Q222L, and G224S, the numbers referring to positions in the “virus’s” HA protein, the “viral” surface molecule that attaches to host cells
The scientists created three mutant H5N1 “virus” strains to launch their experiment: one containing N182K, one with Q222L and G2242, and one with all three changes
They then launched their lengthy series of ferret experiments by inoculating groups of six ferrets with one of these three mutants or the wild-type H5N1 “virus”
Analysis of samples during the 7-day experiment showed that ferrets infected with the wild-type “virus” shed far more “virus” than those infected with the mutants
In a second step, the team used a mutation in a different “viral” gene, PB2, the polymerase complex protein
The researchers found that this mutation, when added to two of the HA mutations (Q224L and G224S), did not produce a “virus” that grew more vigorously in ferrets, and the “virus” did not spread through the air from infected ferrets to uninfected ones
Seeing that the this mutant failed to achieve airborne transmission, the researchers decided to “passage” this strain through a series of ferrets in an effort to force it to adapt to the mammalian respiratory tract
This was the move that Fouchier called “really, really stupid” (are we sure he wasn’t referring to the whole study?)
They inoculated one ferret with the three-mutation strain and another with the wild-type “virus” and took daily samples until they euthanized the animals on day 4 and took tissue samples (nasal turbinates and lungs)
Material from the tissue samples was then used to inoculate another pair of ferrets, and this step was carried out six times
For the last four passages, the scientists used nasal-wash samples instead of tissue samples, in an effort to harvest “viruses” that were secreted from the upper respiratory tract
In other words, they completely changed the source material from tissue to nasal secretions more than halfway through the experiment
It was said that the amount of mutant “virus” found in the nasal turbinate and nose swab samples increased with the number of passages while “viral” titers in the samples from ferrets infected with the wild-type “virus” stayed the same
Quick Sidenote From the Supplemtary Materials:
“After inoculation with A/H5N1wildtype, virus titers in the nasal turbinates were variable but high, ranging from 1.6 x 105 to 7.9 x 106 TCID50/gram tissue (panel A), with no further increase observed with repeated passage. After inoculation with A/H5N1HA Q222L,G224S PB2 E627K, virus titers in nasal turbinates averaged 1.6 x 104 in the first three passages, 2.5 x 105 in passage four to seven and 6.3 x 105 TCID50/gram tissue in the last three passages, suggestive of improved replication and virus adaptation. In the lungs, no apparent adaptation was observed for animals inoculated with either virus. Virus titers in lungs were highly variable; presumably it was a matter of chance whether the virus reached the lower airways.”
In other words, the “wildtype virus” titers remained and stayed high while the “mutant virus” started low and elevated throughout passaging yet was still underneath the amount seen in the “wildtype” strain. They also note that finding “virus” in the lungs was a “matter of chance” with either “virus.”
End Quick Sidenote.
The next step was to test whether the “viruses” produced through passaging could achieve airborne transmission so four ferrets were inoculated with samples of the “passage-10” mutant “virus,” and two ferrets were inoculated with the passage-10 wild strain
Uninfected ferrets were placed in cages next to the infected ones but not close enough for direct contact
The ferrets exposed to those with the wild “virus” remained uninfected, but three of the four ferrets placed near those harboring the mutant “virus” did get infected (“infected” meaning they found “viral” RNA)
Thus, a total of six ferrets became “infected” with the mutant “virus” via airborne transmission
However, the level of “viral” shedding indicated the airborne “virus” didn’t transmit as efficiently as the 2009 H1N1 “virus”
In the course of the airborne transmission experiments, the ferrets showed signs of illness, including lethargy, loss of appetite, and ruffled fur (no consideration is given to the fact that the animals were caged, tortured, and experimented on)
One of the directly inoculated ferrets died, but all those infected via airborne “viruses” survived
When the scientists sequenced the genomes of the “viruses” that spread through the air, they found only two amino acid switches, both in HA, that occurred in all six “viruses:” H103Y and T156A
They noted several other mutations, but none that occurred in all six airborne “viruses”
In other words, once again they were unable to sequence the exact same genome in the samples from each ferret
In further steps, the researchers inoculated intratracheallysix ferrets with high doses of the airborne-transmissible “virus;” after 3 days, the ferrets were either dead or “moribund”
They stated: “Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of viruses to cause pneumonia”
Highly “pathogenic” avian influenza A/H5N1 “virus” can cause morbidity and mortality in humans but thus far has not acquired the ability to be transmitted by aerosol or respiratory droplet (“airborne transmission”) between humans
To address the concern that the “virus” could acquire this ability under natural conditions, the researchers genetically modified A/H5N1 “virus” by site-directed mutagenesis and subsequent serial passage in ferrets
In other words, in order to test whether the “virus” could mutate naturally, they mutated it synthetically…
The genetically modified A/H5N1 “virus” acquired mutations during passage in ferrets, ultimately becoming airborne transmissible in ferrets (all “viruses” aquire mutations every time they are sequenced as no “viral” genome is ever the same as the original)
None of the recipient ferrets died after airborne infection with the mutant A/H5N1 “viruses”
Wild birds in the orders Anseriformes (ducks, geese, and swans) and Charadriiformes (gulls, terns, and waders) are thought to form the “virus” reservoir in nature
Since 2003, more than 600 laboratory-confirmed cases of HPAI A/H5N1 “virus” infections in humans have been reported from 15 countries
Although limited A/H5N1 “virus” transmission between persons in close contact has been reported, sustained human-to-human transmission of HPAI A/H5N1 “virus” has not been detected
Whether this “virus” may acquire the ability to be transmitted via aerosols or respiratory droplets among mammals, including humans, to trigger a future pandemic is a key question for pandemic preparedness
The factors that determine airborne transmission of influenza “viruses” among mammals, a trait necessary for a “virus” to become pandemic, have remained largely unknown
The “viruses” that caused the major pandemics of the past century emerged upon reassortment (that is, genetic mixing) of animal and human influenza “viruses”
However, given that “viruses” from only four pandemics are available for analyses, they cannot exclude the possibility that a future pandemic may be triggered by a wholly avian “virus” without the requirement of reassortment
No reassortants between A/H5N1 “viruses” and seasonal or pandemic human influenza “viruses” have been detected in nature and their goal was to understand the biological properties needed for an influenza “virus” to become airborne transmissible in mammals
They chose the ferret (Mustela putorius furo) as the animal model for the studies as ferrets have been used in influenza research since 1933 because they are susceptible to infection with human and avian influenza “viruses”
There is no exact particle size cut-off at which transmission changes from exclusively large droplets to aerosols
It is generally accepted that for infectious particles with a diameter of 5 mm or less, transmission occurs via aerosols
The researchers used the QuickChange multisite-directed mutagenesis kit to introduce amino acid substitutions in the HA of wild-type “virus”
For experiment 1, they inoculated these mutant “viruses” and the A/H5N1wildtype “virus” intranasally into groups of six ferrets for each “virus”
Throat and nasal swabs were collected daily, and “virus” titers were determined by end-point dilution in Madin Darby canine kidney (MDCK) cells to quantify “virus” shedding from the ferret URT
When four naïve ferrets were housed in cages adjacent to those with four inoculated animals to test for airborne transmission as described previously, A/H5N1HA Q222L,G224S PB2 E627K was not transmitted
Because the mutant “virus” harboring the E627K mutation in PB2 and Q222L and G224S in HA did not transmit in experiment 2, they designed an experiment to force the “virus” to adapt to replication in the mammalian respiratory tract and to select “virus” variants by repeated passage (10 passages in total) of the constructed A/H5N1HA Q222L,G224S PB2 E627K “virus” and A/H5N1wildtype “virus” in the ferret URT
In experiment 3, one ferret was inoculated intranasally with A/H5N1wildtype and one ferret with A/H5N1HA Q222L,G224S PB2 E627K
Throat and nose swabs were collected daily from live animals until 4 days postinoculation (dpi), at which time the animals were euthanized to collect samples from nasal turbinates and lungs
The nasal turbinates were homogenized in 3 ml of “virus-transport” medium, tissue debris was pelleted by centrifugation, and 0.5 ml of the supernatant was subsequently used to inoculate the next ferret intranasally (passage 2)
This procedure was repeated until passage 6
From passage 6 onward, in addition to the samples described above, a nasal wash was also collected at 3 dpi
To this end, 1 ml of phosphate-buffered saline (PBS) was delivered dropwise to the nostrils of the ferrets to induce sneezing
Approximately 200 ml of the “sneeze” was collected in a Petri dish, and PBS was added to a final volume of 2 ml
The nasal-wash samples were used for intranasal inoculation of the ferrets for the subsequent passages 7 through 10
They changed the source of inoculum during the course of the experiment, because passaging nasal washes may facilitate the selection of “viruses” that were secreted from the URT
Because influenza “viruses” mutate rapidly, they anticipated (i.e.guessed arbitrarily) that 10 passages would be sufficient for the “virus” to adapt to efficient replication in mammals
The genetic composition of the “viral” quasi-species present in the nasal washe of ferrets after 10 passages of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was determined by sequence analysis using the 454/Roche GS-FLX sequencing platform
The mutations introduced in A/H5N1HA Q222L,G224S PB2 E627K by reverse genetics remained present in the “virus” population after 10 consecutive passages at a frequency >99.5%
Numerous additional nucleotide substitutions were detected in all “viral” gene segments of A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K after passaging, except in segment 7
Of the 30 nucleotide substitutions selected during serial passage, 53% resulted in amino acid substitutions
The only amino acid substitution detected upon repeated passage of both A/H5N1wildtype and A/H5N1HA Q222L,G224S PB2 E627K was T156A
In experiment 4, nasal-wash samples, collected at 3 dpi from ferrets at passage 10, were used in transmission experiments to test whether airborne-transmissible “virus” was present in the “virus” quasi-species
For this purpose, nasal-wash samples were diluted 1:2 in PBS and subsequently used to inoculate six naïve ferrets intranasally
Although mutations had accumulated in the “viral” genome after passaging of A/H5N1wildtype in ferrets, they did not detect replicating “virus” upon inoculation of MDCK cells with swabs collected from naïve recipient ferrets after they were paired with donor ferrets inoculated with passage 10 A/H5N1wildtype “virus”
In contrast, they did detect “virus” in recipient ferrets paired with those inoculated with passage 10 A/H5N1HA Q222L,G224S PB2 E627K “virus”
Three out of four naïve recipient ferrets became “infected” as confirmed by the presence of replicating “virus” in the collected nasal and throat swabs (in other words, they saw CPE in a cell culture and claimed “virus” was present)
A “virus isolate” was obtained after inoculation of MDCK cells with a nose swab collected from ferret F5 at 7 dpi
They used conventional Sanger sequencing to determine the consensus genome sequences of viruses recovered from the six ferrets that acquired “virus” via airborne transmission and all six samples still harbored substitutions Q222L, G224S, and E627K that had been introduced by reverse genetics
In other words, they created consensus sequencing through alignment to reference genomes using computer software and algorithms from unpurified material
They observed several other mutations for which their occurrence was not consistent among the airborne “viruses,” indicating that of the heterogeneous “virus” populations generated by passaging in ferrets, “viruses” with different genotypes were transmissible
In other words, they were unable to sequence the exact same “virus” genome every time…and if that wasn’t clear
In addition, a single transmission experiment is not sufficient to select for clonal airborne-transmissible “viruses” because, for example, the consensus sequence of “virus” isolated from F6 differed from the sequence of parental “virus” isolated from F2
Together, they claim that these results suggest that as few as five amino acid substitutions (four in HA and one in PB2) may be sufficient to confer airborne transmission of HPAI A/H5N1 “virus” between mammals
During the course of the transmission experiments with the airborne-transmissible “viruses,” ferrets displayed lethargy, loss of appetite, and ruffled fur after intranasal inoculation
It should be noted that inoculation of immunologically naïve ferrets with a dose of 1 × 106 TCID50 of A/H5N1 “virus” and the subsequent course of disease is not representative of the natural situation in humans
Importantly, although the six ferrets that became “infected” via respiratory droplets or aerosol also displayed lethargy, loss of appetite, and ruffled fur, none of these animals died within the course of the experiment
After intratracheal (in the throat) inoculation, six ferrets inoculated with 1 × 106 TCID50 of airborne-transmissible “virus” F5 in a 3-ml volume of PBSdied or were moribund at day 3
Intratracheal inoculations at such high doses do not represent the natural route of infection and are generally used only to test the ability of “viruses” to cause pneumonia, as is done for vaccination-challenge studies
Although the airborne-transmissible “virus” is lethal to ferrets upon intratracheal inoculation at high doses, the “virus” was not lethal after airborne transmission
They openly admit that the route of injection and the amount of toxic culture goo injected causes the severity of disease, which does not require the “virus” as an explanation
They state that although experiments showed that A/H5N1 “virus” can acquire a capacity for airborne transmission, the efficiency of this mode remains unclear
They pointed out that their experimental design for studying transmission is not quantitative (i.e. they do not know how much “virus” is required for airborne transmission and assume it occurs via PCR results)
They airborne transmission could be tested in a second mammalian model system such as guinea pigs, but this would still not provide conclusive evidence that transmission among humans would occur
The mutations they identified need to be tested for their effect on transmission in other A/H5N1 “virus” lineages, and experiments are needed to quantify how they affect “viral” fitness and “virulence” in birds and mammals
Their findings indicate that HPAI A/H5N1 “viruses” have the potential to evolve directly to transmit by aerosol or respiratory droplets between mammals, without reassortment in any intermediate host, and thus pose a risk of becoming pandemic in human
Of course, the only place reassortment occurs is in a lab so they never need a host…
Identification of the minimal requirements for “virus” transmission between mammals may have prognostic and diagnostic value for improving pandemic preparedness
Influenza “virus” A/Indonesia/5/2005 (A/H5N1) was isolated from a human case of HPAI “virus” infection and passaged once in embryonated chicken eggs followed by a single passage in Madin-Darby Canine Kidney (MDCK) cells
All eight gene segments were amplified by reverse transcription polymerase chain reaction and cloned in a modified version of the bidirectional reverse genetics plasmid pHW2000
Mutations of interest were introduced in reverse genetics vectors using the QuikChange multi-site-directed mutagenesis kit
Recombinant “viruses” were produced upon transfection of 293T cells and “virus” stocks were propagated and titrated in MDCK cells
MDCK cells (canine) were cultured in Eagle’s minimal essential medium supplemented with:
10% fetal calf serum (FCS)
100 IU/ml penicillin
100 μg/ml streptomycin
2 mM glutamine
1.5 mg/ml sodium bicarbonate
10 mM Hepes
Non-essential amino acids
293T cells (human embryonic kidney) were cultured in Dulbecco modified Eagle’s medium supplemented with:
10% FCS
100 IU/ml penicillin
100 mg/ml streptomycin
2mM glutamine
1mM sodium pyruvate
Non-essential amino acids
For “virus” titrations, MDCK cells were inoculated with tenfold serial dilutions of “virus” preparations, homogenized tissues, nose swabs, and throat swabs
Cells were washed with PBS one hour after inoculation and cultured in 200μl of infection media, consisting of EMEM supplemented with:
100 U/ml penicillin
100 μg/ml streptomycin
2mM glutamine
1.5mg/ml sodium bicarbonate
10mM Hepes
Non-essential amino acids
20 μg/ml trypsin
Three days after inoculation, supernatants of infected cell cultures were tested for agglutinating activity using turkey erythrocytes as an indicator of “virus” replication in the cells
Infectious “virus” titers were calculated from four replicates each of the homogenized tissue samples, nose swabs, and throat swabs and for ten replicates of the “virus” preparations by the method of Spearman-Karber
The only way that the gain of function/bioweapon narrative makes any sense is if the original Latin definition for the word “virus” is used to explain what is happening in this research. In Latin, “virus” means “liquid poision” and what virologists are doing is simply creating a liquid poison in a lab using cell cultures. What they are not doing is creating “infectious agents of a small size and simple composition that can multiply only in living cells of animals, plants, or bacteria” which is the modern definition for the word according to the Britannica. The only way the liquid poison can potentially harm one is through injection. Cell cultured soup is not transmitted through the air nor is it infectious and/or contagious. In other words, GOF studies are not creating “viruses” in the modern sense of the word and can only be considered as such if viewed through the original Latin lens.
What must be realized about the GOF studies and the bioweapon narrative is that these stories are designed to keep people believing in the lies of Germ Theory. This is yet another fear-based tactic utilized by those in power to ensure that the masses are frightened of an invisible enemy that can be unleashed upon the world either accidentally or intentionally at a moments notice. There will be figureheads who appear to be on the side of truth, questioning the natural existence of “SARS-COV-2,” challenging the safety of the vaccines, promoting alternative therapies, etc. who will also continue to push the idea that “viruses” exist and can be manipulated in a lab. These people are the Pied Pipers leading those who are going astray back into the fold. There is no need to create a “virus” bioweapon when all that was needed to control the masses is a PCR test and some well-designed propaganda.
To anyone who may have been taken in by this GOF/Bioweapon narrative, remember that there is no evidence of any purified and isolated “viral” particles ever coming directly from human samples that are then proven pathogenic in a natural way. Virology does not dispute this. If they can not find a “virus” in nature, they can not create one in a lab. That is truly all you need to know.
“‘Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“To obtain embryo cells [for research on vaccines and other pharma products], embryos from spontaneous abortions cannot be used, nor can those obtained by means of abortions performed via the vagina: in both cases, the embryo will be contaminated by micro-organisms.”
“The correct way consists in having recourse to Caesarian section or to the removal of the uterus. Only in this way can bacteriological sterility be guaranteed.”
“In either case, then, to obtain embryo cells for culture a programmed abortion must be adopted, choosing the age of the embryo and dissecting it while still alive, in order to remove tissues to be placed in culture media.”
“Given these premises, we face the dilemma of whether the deliberate systematic destruction of a human creature to obtain cell material can be justified, when it is recognized that this is of great interest to fundamental research and for the diagnosis of some human diseases. Are research and diagnosis of such great value that they justify the destruction of human beings?”
“The Geneva Declaration affirms that the doctor has the duty to take the greatest care to safeguard the life of a human being from its conception and will not, even under threat, use his knowledge to infringe humanitarian laws.” (1986-04-26; Herranz, Gonzalo; Il Sabato, no.15…Professor Herranz was, at the time, president of the Committee of Medical Ethics of Spanish Doctors and vice-president of the Permanent Committee of Medical Ethics of the European Community.)”
What exactly happened in 1972 or 1973, in the Netherlands, where an infant girl was aborted, and her kidneys used to make a cell line that would be used, going forward, in the testing of vaccines?
That cell line is called HEK 293, and it has been used to test COVID vaccines.
I have already presented evidence for concluding the abortion involved removing the living infant from her mother’s womb, and taking her kidneys, which of course killed her.
This evidence rests on the realization that, in order to extract viable and useful kidney tissue, the baby had to have a functioning blood supply, which meant she was alive.
But the evidence ALSO comes from knowing many other abortions have been carried out, in order to harvest tissue for medical research, by murdering living babies.
I have found a very informative article (2/9/2021) at the Centre for Bio-Ethical Reform UK, by Christian Hacking, titled, “What the HEK?!” by Christian Hacking. Quoting from the article:
“HEK 293 is a human cell line created using a kidney from a dissected unborn baby in the Netherlands between 1972 and 1973. It is the second most common cell line and is used extensively in ‘pharmaceutical and biomedical research’. It is also used in vaccine creation and cancer research.”
“It was used, along with other human cell lines, to develop a genetically engineered spike protein (that the mRNA vaccine codes for) in the original development stage of the vaccine. The ‘new technology’ Pfizer vaccine and the Moderna Vaccine were tested on HEK 293 before they began human trials. This testing is ongoing for all new batches. Finally the ‘old technology’ Oxford AstraZeneca vaccine grew a weakened viral strain in HEK 293 cell culture…”
“The kidney in question was dissected from a healthy Dutch baby girl of unknown origin by the team at Leiden University in the Netherlands in 1972. Despite the inclusion of the term ‘embryonic’ in the title, the baby in question was probably 12-13 weeks old when she was killed so as to secure functioning kidney cells. The man in charge of the research was named Alex Jan Van der Eb; he is still alive and still based in Holland.”
“When questioned on the matter by the FDA in 2001, Dr Van der Eb confirmed it was an intentional abortion of a ‘fetus’ but gave hazy details of the exact experiments.”
“’So the kidney material, the fetal kidney material was as follows: the kidney of the fetus was, with an unknown family history, obtained in 1972 probably. The precise date is not known anymore. The fetus, as far as I can remember, was completely normal. Nothing was wrong. The reasons for the abortion were unknown to me. I probably knew it at that time, but it got lost, all this information’.”
Author Hacking continues: “…extracting and growing living cells is incredibly difficult. In order to give oneself the best chance of success you need to ensure the child is healthy, fresh, intact and sterile. As one embryologist and Emeritus Professor of Anatomy confirms:”
“’In order to sustain 95% of the cells, the live tissue would need to be preserved within 5 minutes of the abortion. Within an hour the cells would continue to deteriorate, rendering the specimens useless’.”
[That statement was made by “Dr C Ward Kischer, embryologist and Emeritus Professor of Anatomy; specialist in Human Embryology, University of Arizona College of Medicine…”]
[My comment: This suggests the abortion, in the Netherlands, in 1972, was planned and technicians were standing by. I would say that, to ensure the viability of the tissue, the infant had a functioning blood supply and was alive when her kidneys were removed, killing her.]
Hacking:
“In order for the organs to be at ‘optimal viability’, the child needs to be dissected and organs extracted within 5 minutes of delivery. Anaesthetic also cannot be used so as to not change the cellular activity of the organs the researcher wants to obtain.”
“Acclaimed Doctor, Ian Donald, the pioneer of the ultrasound scanner, also claims to have witnessed the WI-38 [another cell-line] dissections [1962], conducted at the Karolinska Institute; he described them such:
“’Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“In his dense book ‘The Foetus As Transplant Donor the Scientific, Social, and Ethical Perspectives’, immunologist Dr Peter McCullagh relays detailed descriptions of the methods used on dozens of ‘fetal tissue donors’ from the 1970’s onward, including the deaths of babies between 7 and 26 weeks gestation by decapitations, exposure, dissection and drug testing. Gynaecologist and ex-abortionist Dr Bernard Nathanson, relaying his own understanding of abortion, and citing McCullagh’s book claims the Swedish experiments took place thus:
“’…in Sweden they have been puncturing the sac of a pregnant woman at let us say 14 to 16 weeks, and then they put a clamp on the head of the baby, pull the head down into the neck of the womb, drill a hole into the baby’s head, and then put a suction machine into the brain and suck out the brain cells….. Healthy human fetuses from 7 to 21 weeks from legal abortions were used. This is in Sweden. The conception age was estimated from crown rump length and so on. Fetal liver and kidney were rapidly removed and weighed. Now at 21 weeks, what they were doing, or 18 weeks, or 16 weeks, was what is called prostaglandin abortions. They would inject a substance into the womb. The woman would then go into mini-labor and pass this baby. 50% of the time, the baby would be born alive, but that didn’t stop them. They would just simply open up the abdomen of the baby with no anesthesia, and take out the liver and kidneys, etc.’”
“A research paper from the University of Toronto from June 1952 commenting on the method of their experiments suggests that these techniques were universal with researchers working in close proximity to the abortions.”
“’No macerated [softened after death] specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
“According to Gonzalo Herranz, former head of the Committee of Medical Ethics of Spanish doctors, the best way to prevent ‘contamination by microorganisms’ is to deliver the child by caesarean section or the removal of the uterus.”
“A 1982 review of a history of tissue donation affirms this, and much of the above evidence:”
“’Fetal tissue for transplantation must be “harvested” within a few minutes of delivery. Ideally this is by hysterectomy, with the fetus delivered in utero. Drugs which reduce fetal physiological activity need to be avoided. The fetus is therefore in as alive and aware a state as possible when being opened’.”
From Hacking’s article, it’s quite clear how the standard procedure of infant-murder is carried out.
It’s entirely reasonable to assume fetal cell line HEK 293—used for COVID vaccine testing—was originally produced, in 1972, by the murder of an infant. Refusal to take a COVID vaccine on the basis of conscience and religion is more than justified.
Given the weight of the circumstantial case, I would say that for all people of faith, refusal is essential.
Lunatic medical murderers and their allies will say anything to avoid blame and the application of true justice to themselves. They will invent “science” at the drop of a hat and couch it in humanitarian terms. They will claim the ends justify the means. They will commit gross forgery to pretend those ends are vital.
But we don’t have to stand by and passively believe them.
Billions of people of faith can stand against them.
If you are looking for one of the most masterful takedowns of virology to date, this presentation by Alec Zeck, Dr. Jordan Grant, Mike Donio,Jacob Diaz, and John Blaid is one of the best out there. When I first watched it a month ago, I was blown away and I had intended to share it here but, as often happens, I got sidetracked and sadly forgot to upload it. I hope you can take away a great deal of value from this presentation as the guys delve into the numerous fallacies and assumptions related to this fraudulent field.
In this presentation, you will find:
A break down of the ridiculous cell culture experiments
The lack of adhering to the scientific method
The foundational issues with virology from the very beginning
The inherent problems with and the limitations of electron microscopy imaging
The lack of any purified and isolated physical “viral” particles found directly in human samples
The issues related to the creation of the theoretical genome
The fabrication and lack of validation of the PCR test for “SARS-COV-2”
A thorough explanation of the Stefan Lanka control experiments
The myths of contagion and other possible explanations for dis-ease
The FOI requests and the burden of proof
As I said, a masterful takedown of the pseudoscience called virology!
Virology’s Unproven Assumptions
In this episode, Alec Zeck has a discussion with Mike Donio, Jacob Diaz, Dr. Jordan Grant MD, and John Blaid on the fallacious reasoning, unproven assumptions, and lack of proof for virus theory.


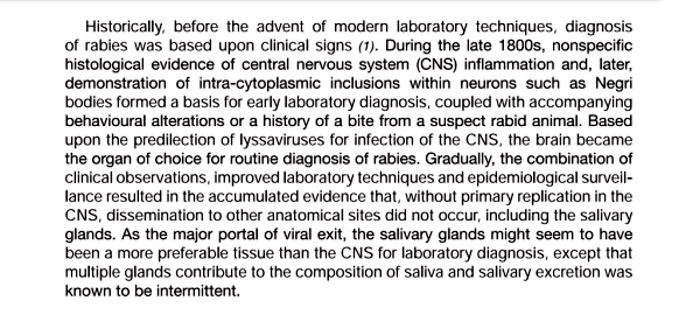
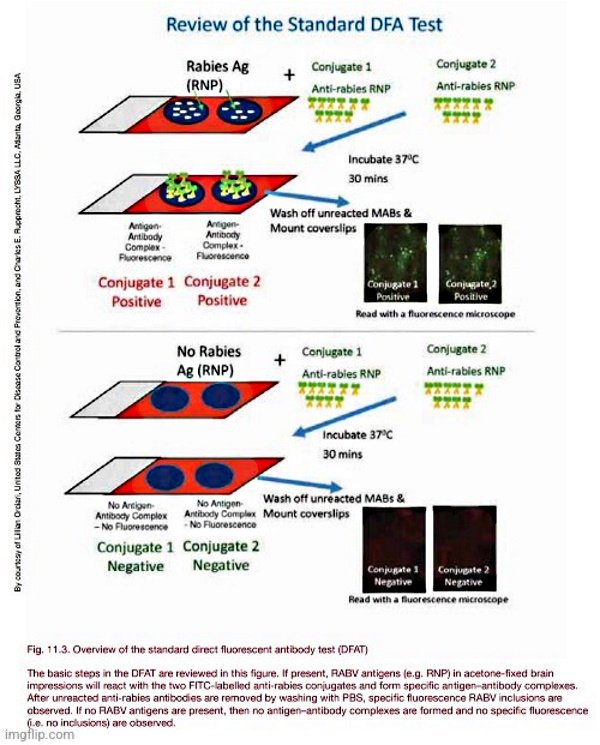
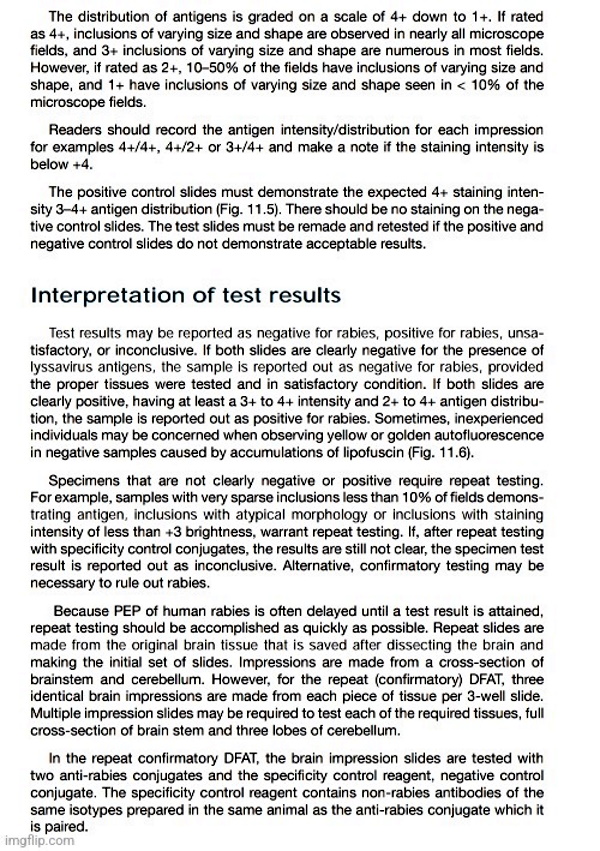
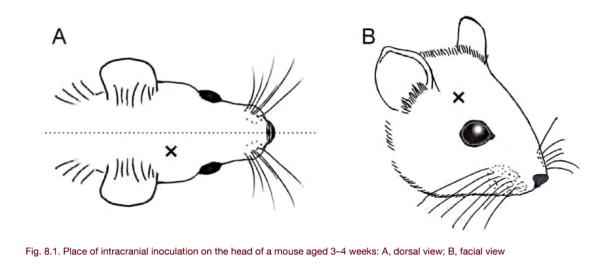
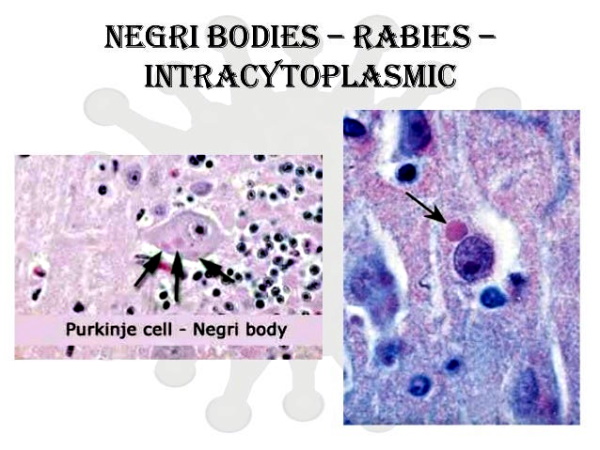
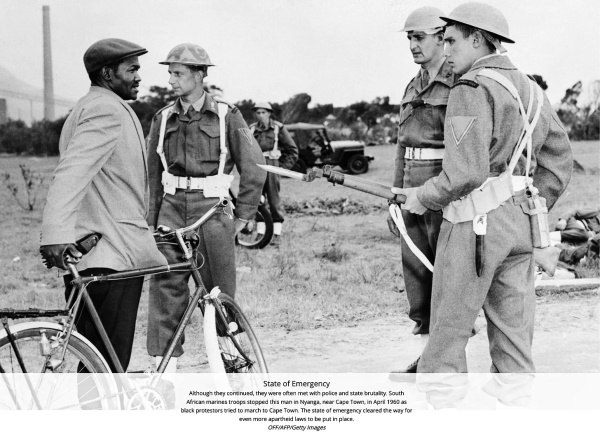
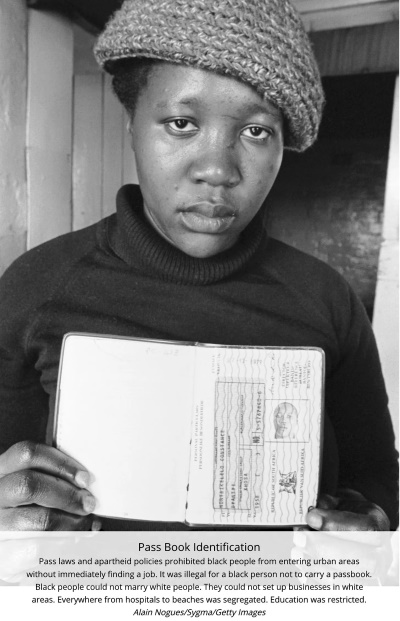
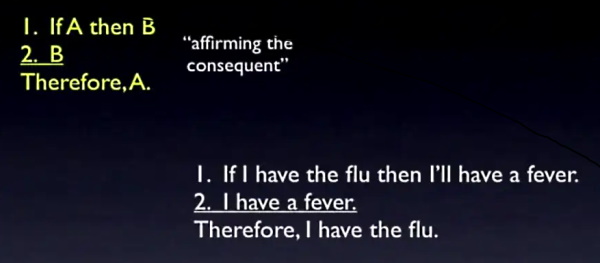
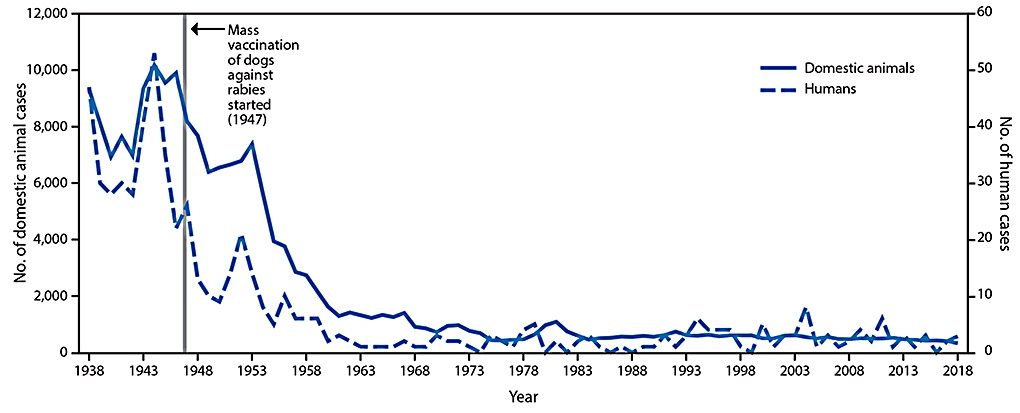
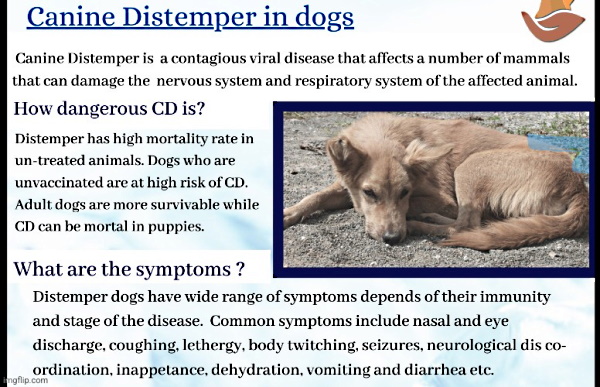

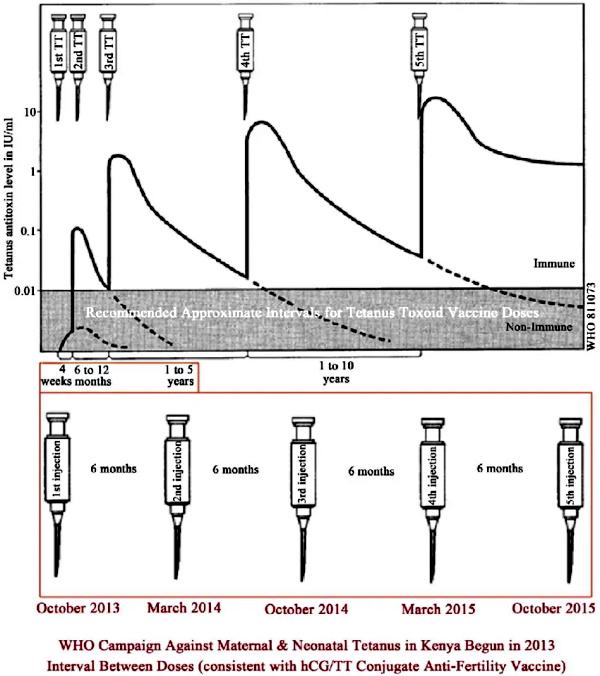
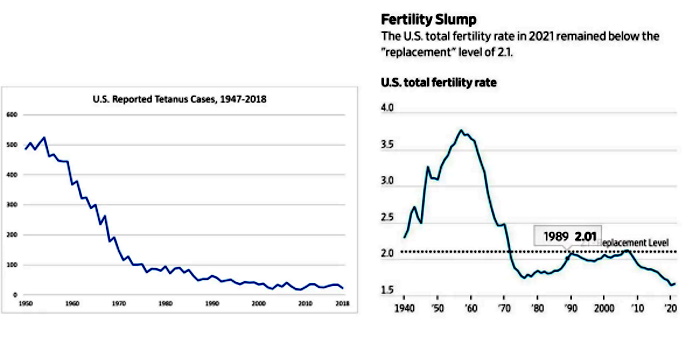

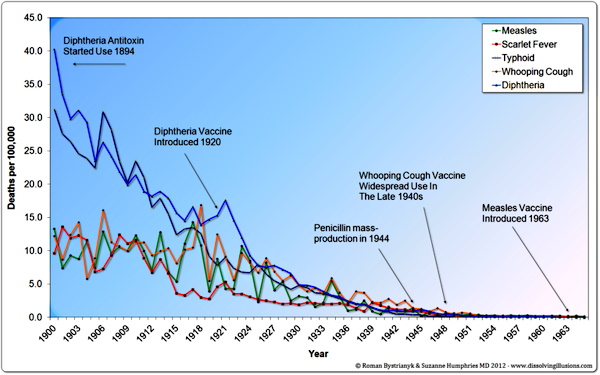
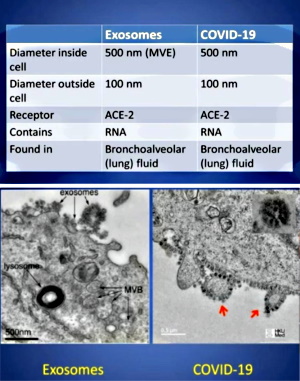
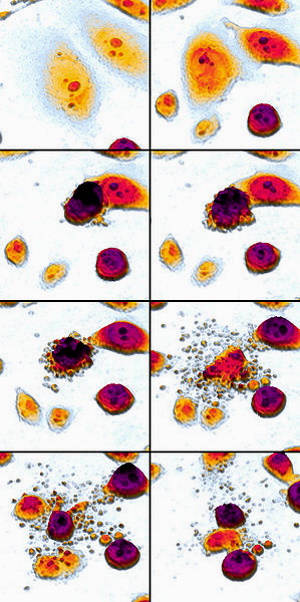
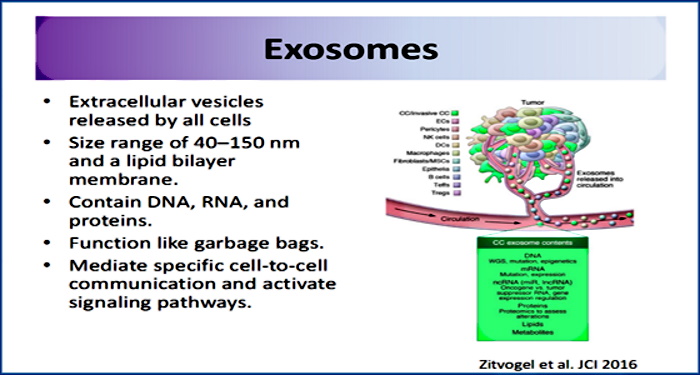
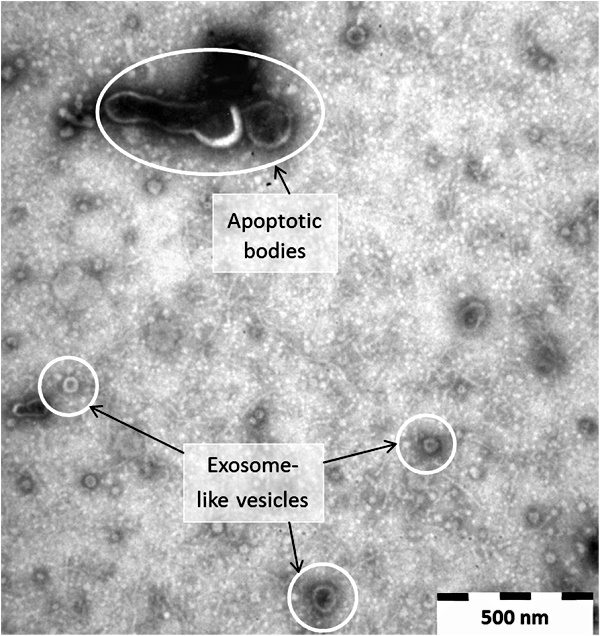
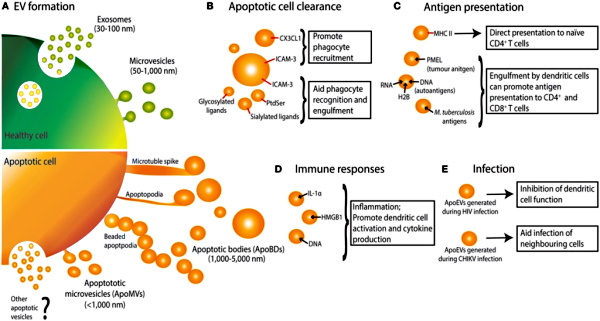
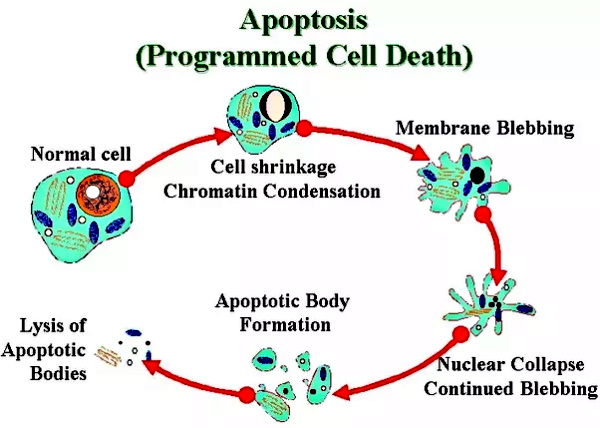
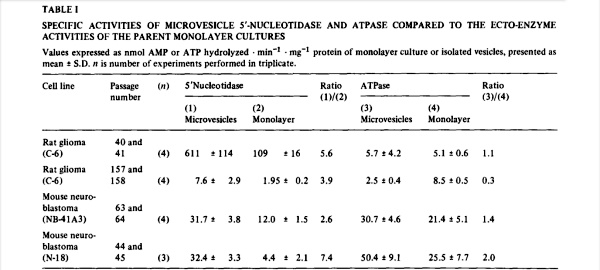
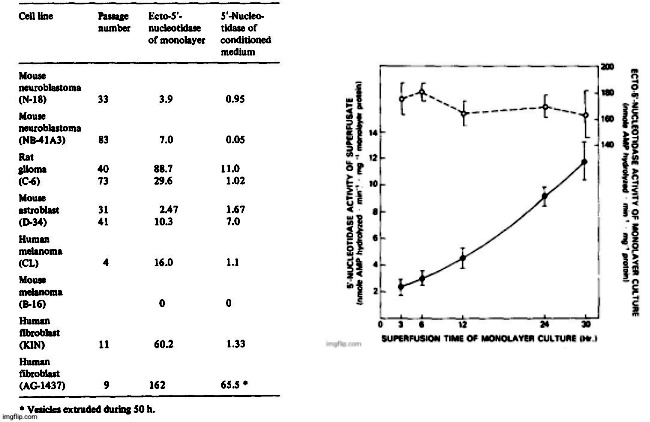
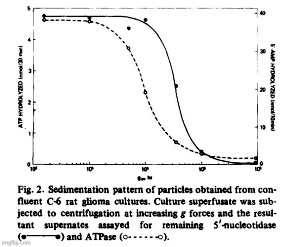
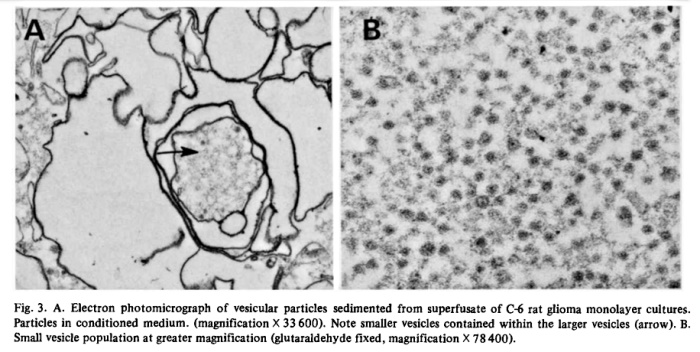
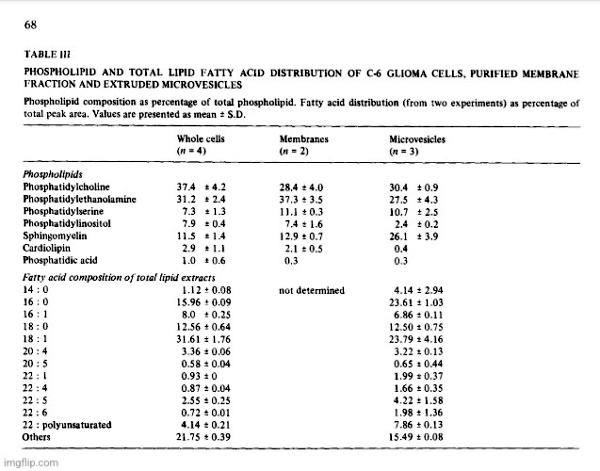
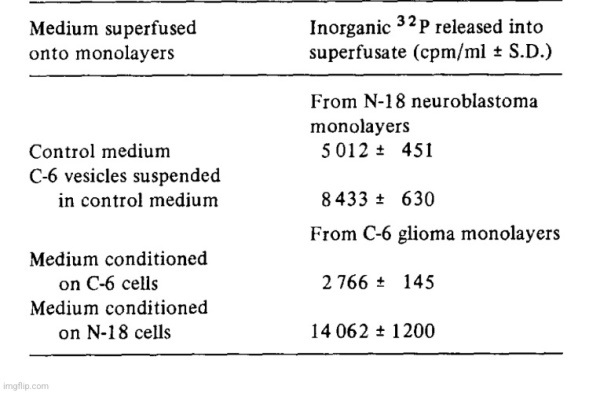

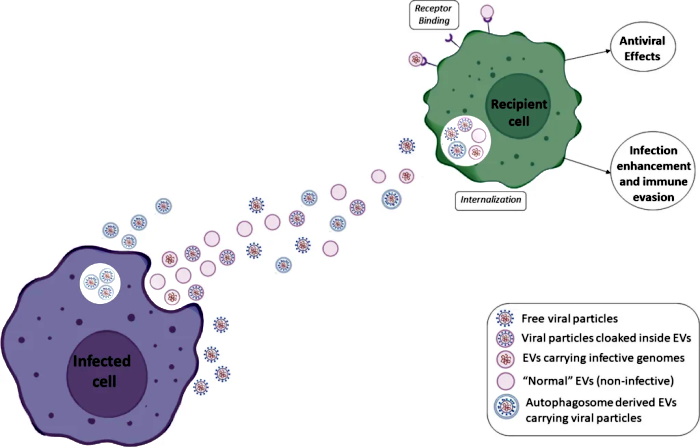
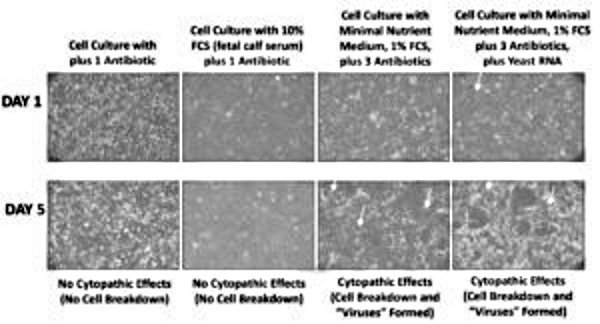
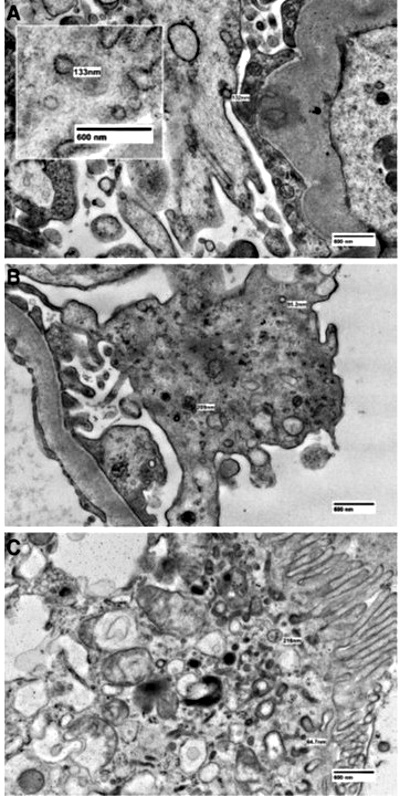
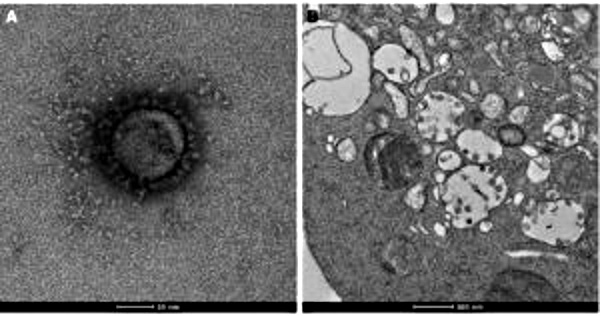

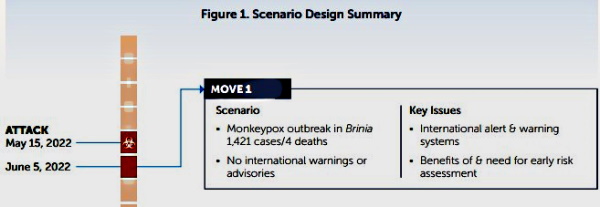

 Next, the
Next, the 
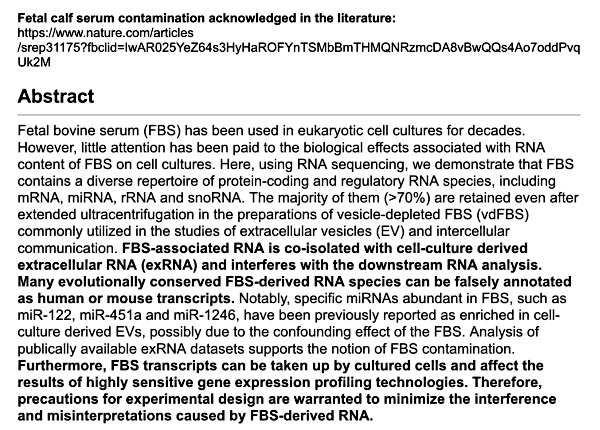
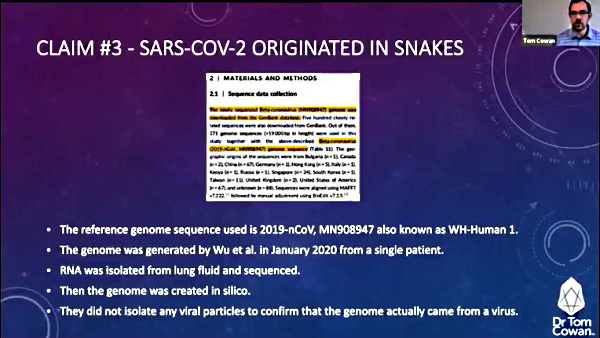
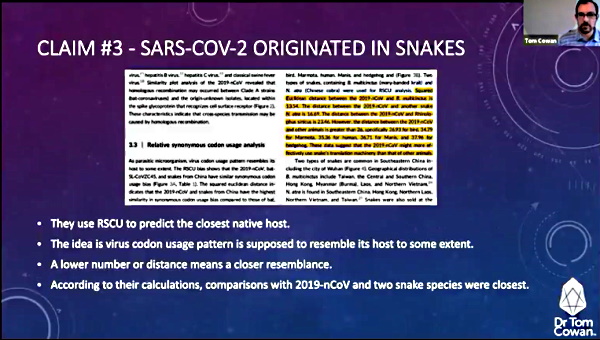
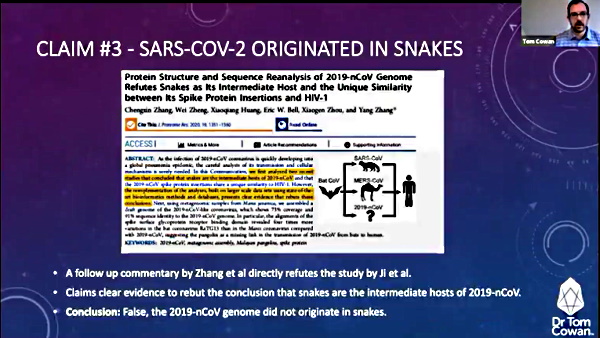
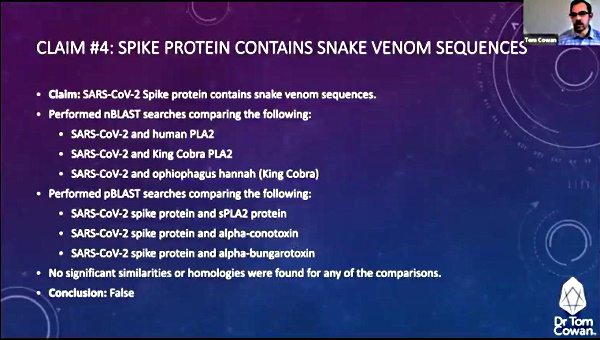
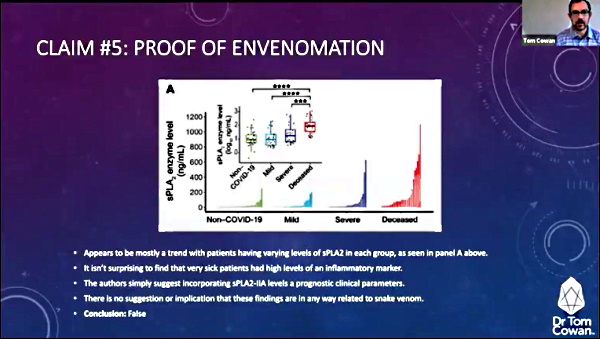
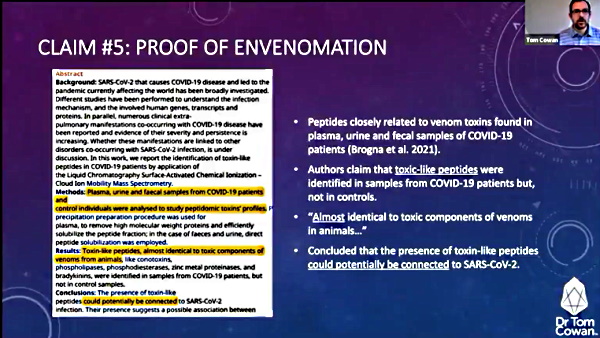
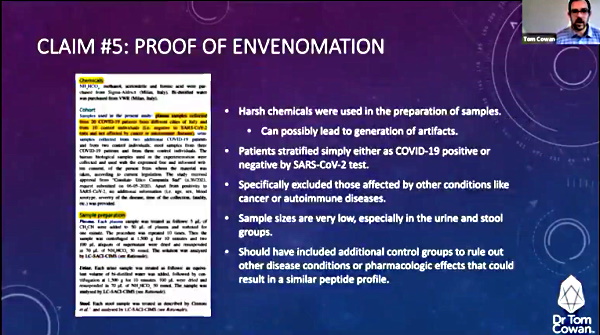
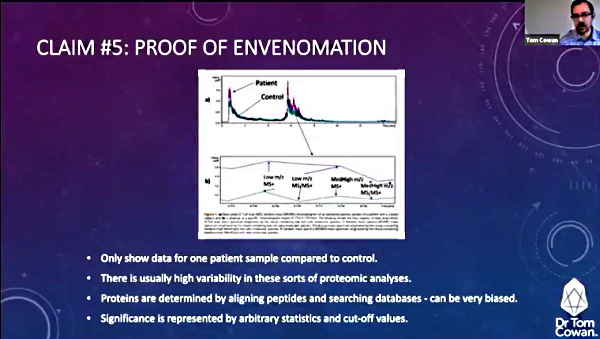
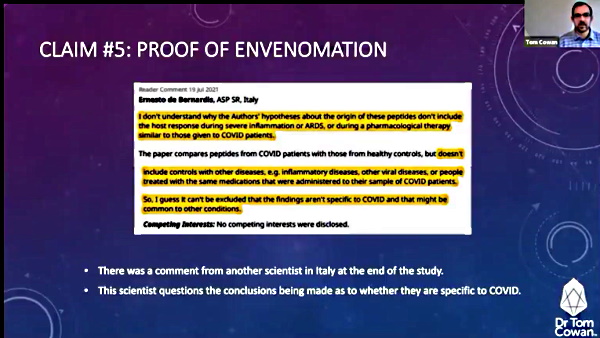
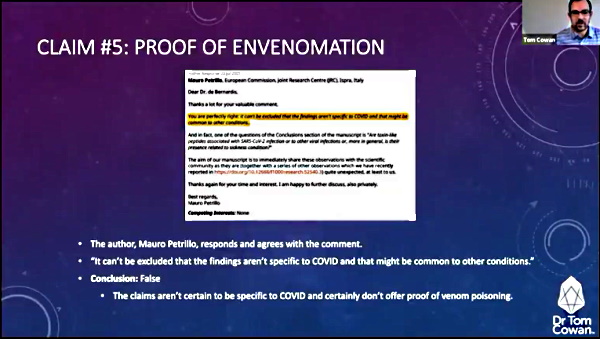
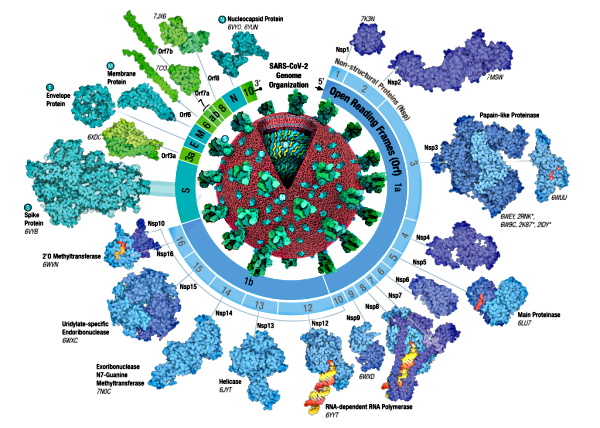
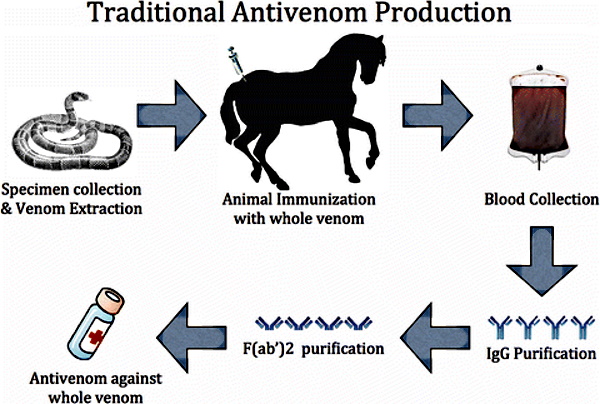


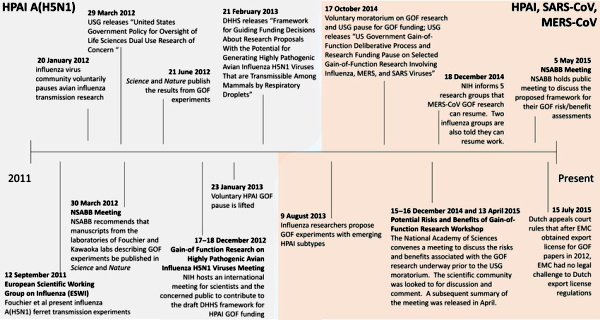
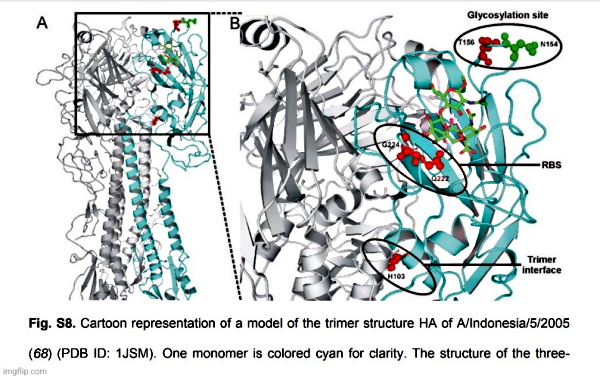


{kind=link}
{kind=link}
{kind=link}