World Wide Rally for Freedom movement stands for human freedoms and sovereignty as the corporate-sponsored WHO moves to take charge of every nation’s health policy
CITIES AROUND THE GLOBE MAY 21 / 22 — On the weekend of May 21-22, 2022, people organizing with World Wide Demonstration, a grassroots international freedom movement, hold their eighth weekend of global rallies to support fundamental human rights and sovereignty even as the World Health Organization (WHO) begins their World Health Assembly meeting May 22 in Geneva, Switzerland to amend the International HealthRegulations of 2005 (IHR) and continue negotiations for a new global Pandemic Treaty. The proposed amendments and treaty hearings to-date indicate thecorporate-sponsoredWHOisusing these maneuvers to attempt to gain powers that supersede rightsprotected by national constitutions. By amending existing health regulations, the WHO believes they will be able to bypass the need for direct approval from national government bodies and to avoid public debate or media coverage.
WWD stands for the sovereign right of humans to make their own individual health decisions, free from any corporate or governmental coercion or threats, affirming hard-won human rights accords.
Currently 80% of WHO funding comes from privatecorporations, including pharmaceutical companies, which demonstrates the glaring conflicts of interest the WHO has in devising health recommendations. We recognize their move to amend the IHR and push a new treaty as a straightforward corporate power grab under the guise of “health.” When corporations can use proxy organizations to order everyone in the world to take a product they make, the billions raked in create a powerful incentive to conjure the next crisis. It’s approaching common knowledge that the WHO’s draconian recommendations over the past two years were put in place not to improve human health, but to create windfall Pharma profits, to fuel fears, and to groom the population to accept tyrannical control levers over each person’s individual decisions that can be wielded by a few unelected billionaires.
World Wide Rally for Freedom events will take place in many cities in many countries all over the world. Check the official WWD telegram channel for an updated list.
One Day. Everyone Together. We Will All Be There.
We stand for 5 important Freedoms:
Freedom of Speech.
Freedom of Movement
Freedom of Choice.
Freedom of Assembly.
Freedom of Health.
Many of our 5 important Objectives are being realized one by one. We continue to rally to ensure these damaging infringements of rights are ended foralltime:
End Lockdowns
End Mask Mandates
Prevent Vaccine Mandates and Coercion
Return to Standard International and Domestic Travel
End all State of Emergency Declarations
We have built our Movement upon 5 important Principles:
Decentralization
Collaboration
Community
Stability
Peace
We advocate for 5 Solutions:
Non-Compliance
Empowerment
Freedom Preserving Institutions
Freedom Culture
Shift The Narrative
We will not allow our inalienable Human Rights to be re-packaged as Human Privileges, to be conditioned upon compliance with authoritarianism.
Throughout history, humanity has been tried and tested in difficult times, but in the end, freedom always wins.
We can overcome any fears by building new social relationships and new systems that do function in respect of human rights.
###
World Wide Demonstration: In the spring of 2020, the idea of a world wide demonstration to stand up for our human freedoms in the face of never-ending lockdowns was born. The idea spread virally — the idea resonated around the world — and resulted in millions of everyday people taking to the street in peaceful rallies in hundreds of cities beginning March 2021. We believe that fundamental rights are not privileges, and we stand for peace, freedom, democracy and solidarity. We are mothers and fathers, children and grandchildren, grandmothers and grandfathers, brothers and sisters, young and old. We are the People. We are the Society.
“I would love to be able to bring back our country into a great form of unity,” Trump said. “Without a major event where people pull together, that’s hard to do. But I would like to do it without that major event because usually that major event is not a good thing.” – Donald Trump, Jan 30th 2018
By April of 2020, within two years of Donald Trump’s prophetic message, millions of people had bowed the government’s request to “unite” by “social distancing,” under a “Live Exercise” revealed by Trump’s Secretary of State Mike Pompeo. About half of the world’s population agreed to some form of lockdown. More than 3.9 billion people in more than 90 countries had been asked or ordered to stay at home by their governments. And they did.
In unison, millions donned a ritual mask to protect themselves against an invisible enemy. The effect was dubbed virtue signaling – an attempt to show other people that you are a good person, by expressing opinions that will be acceptable to them, especially on social media. How did so many people fall into lock-step to give up their freedom when they had previously been openly skeptical of government ethics and policies?
Social Engineering
The earliest social experiments had been successful using the tried-and true strategy of The Hegelian Dialectic: Problem • Reaction • Solution. Introduce a Problem and roll out the Solution! Past experiments included “The New Deal” under Franklin Roosevelt in the 1930s, and “Great Society” under Lyndon Johnson in the 1960s. Then came the “financially sound” government programs of Social Security, Medicare, and Medicaid.
Money and politics aside, why trust a government’s blanket medical solution when it comes to health, a personal responsibility?
If we understand the mechanism and motives of the group mind, it is now possible to control and regiment the masses according to our will without them knowing it. – Edward Bernays
After three years of government-induced COVID, there is still no approved government Solution to the COVID Problem because the FDA-approved vaccine is still not officially available to anyone, and may never be. Nonetheless, the Live Exercise of testing, tracking, experimentation, and restrictions, continues unabated.
While vaccine makers, such as Pfizer, insisted they need 75 years of data before releasing results to the public, the “adverse events” of the public subjects are being tracked and published in medical journals, even if not widely reported.
In any true experiment, there are two groups: the cases and the controls. All subjects who consented, received vaccine lots coded by color and number. Did they receive a vaccine with a Red cap or blue cap? Did they receive saline solution or the COVID spike protein? Did they go from a “fully vaccinated” to “double boosted? Did they opt out?
Let The Experiment Continue!
They say a picture is worth a thousand words, even if the subject matter, a spike protein, has never been officially isolated, or seen with the naked eye. As of this writing, there is no proof the cause of COVID exists.
Since no quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted… — CDC 2109 document
Even without proof, millions of people eagerly jumped aboard The Spike Protein Train to protect themselves with a mask, based on an image of a virus they believed in.
Then, by design, came the vaccines. A vaccine has always been the response to a government-declared pandemic. Recall the 1976 Swine Flu and the 1918 Spanish Flu? [See The Making of a Pandemic for more information]. Vaccine deployment is followed by the damage reports.
In any Live Exercise or Experiment, scientists cannot be expected to have any answers now, or possibly ever. Meanwhile, new symptoms to experimental mRNA vaccines create new, “rare” medical diagnoses. A quick search of Pubmed quickly shows that symptoms are the opposite of rare.
With the introduction of vaccines came the subsequent introduction of Vaccine Inflammatory Syndromes. From Autoimmune Inflammatory Syndrome Induced by Adjuvants,(ASIA), to Post Vaccination Inflammatory Syndrome (PVIS), and Multisystem Inflammatory Syndrome (MIS), all related acronyms describe one cause: Vaccine toxicity.
Since the deployment of COVID injections, the new COVID is Long COVID, ranging from back pain to sleep and digestive disorders, that go beyond 6 months. Symptoms also include postural tachycardia syndrome or POTS.
POTS affects the autonomic nervous system, or the parasympathetic nervous system that regulates voluntary and involuntary actions, as well as thinking, communication, and memory. These symptoms have been long studied as conditions of vaccine injury. Therefore, the injected spike proteins that bring on autoimmune-mediated endothelial injuries can also lead to POTS, especially in the lungs, as evidenced by this study in Clin Auton Res.
Simply go to the VAERS database to search and download the data collected from vaccine-induced injuries the government lists on its own website. VAERS data released by the CDC included a total of 7oo,ooo adverse event reports from all age groups following COVID vaccines, including 15,386 deaths between December 14, 2020, and September 17, 2021. Vaccine-injured patients become lifelong customers of pharmaceutical treatments, with doctors and scientists knowing that many will never return to their normal lifestyles.
All patients were treated with non-pharmacologic therapies, and most required pharmacologic therapies. Six to 8 months after COVID-19, 17 (85%) patients had residual autonomic symptoms, with 12 (60%) unable to return to work.
Published mRNA Vaccine Toxicity Studies: Dizziness
Whether by case study, small study, epidemiological study, or case-control study, all studies are ongoing and accumulating. Searching Pubmed by “dizziness or vertigo” and “COVID vaccine” and find dozens of studies. Here are a few:
Among all the symptoms reported, localized pain, generalized weakness, headache, myalgia, chills, fever, nausea, joint pains, sweating, localized swelling at the injection site, dizziness, itching, rash, decreased appetite, muscle spasm, decreased sleep quality, and brain fogging were the most commonly reported symptoms (in descending order of occurrence). Most of the symptoms reported were nonlife threatening.
Vestibular neuritis (VN) is an acute vestibular syndrome that causes acute and spontaneous vertigo due to unilateral vestibular deafferentiation, leading to nausea or vomiting and unsteadiness that can last from days to weeks. Reactivation of latent type 1 herpes simplex virus, autoimmune disorders, and microvascular ischemia are hypothesized to be etiologies.
We reported for the first time a case of neuromyelitis optica spectrum disorder (NMOSD) that developed after the first dose of inactivated virus vaccine for COVID-19. The patient developed mild fever, vomiting, diarrhea, and cough after receiving the first dose of inactivated virus vaccine. Two months later, she experienced dizziness and unsteady walking. MRI scanning of the brain revealed lesions in area postrema and bilateral hypothalamus, typical for NMOSD. Serum antibodies for AQP4, ANA, SSA, SSB, Ro-52, and p-ANCA were positive. The patient was diagnosed as AQP4-positive NMOSD with coexisting systemic autoimmunity.
The most frequently reported adverse events were headache, myalgia, and dizziness. Of the 835 reported deaths after COVID-19 vaccination, 2 vaccine-related deaths were confirmed.
A 67-year-old man who was medicated for hypertension and diabetes was admitted complaining of fever, maculopapular rash, diarrhea, headache, chills, and dizziness 6 days after the first vaccination of ChAdOx1 nCoV-19 in Korea. The COVID-19 test was negative but with low blood pressure, leukocytosis, skin rash, pulmonary edema, and increased inflammation markers. His lab findings and clinical course were consistent with those of MIS after COVID-19 vaccination.
The 9 patients had an evoked nystagmus pathognomonic for benign paroxysmal positional vertigo; in the remaining 17 cases, peripheral vestibular dysfunction could be excluded and central disorder may be suggested. Due to the prevalence of nystagmus of non-peripheral origin, a central nervous system involvement could not be excluded.
38% mild side effects were observed from vaccination. Following were the general side-effects: myalgia (18.2%), the feeling of sickness (16%), fever (15.6%), dizziness (7.8%), joint pain (7.4%), chills (4.8%), and flu (4.8%). Following were the common neurological side-effects reported: headache (18.2%), fatigue (16.5%), muscle pain (16%), numbness/tingling (3%), and migraine (2.6%). Nausea and diarrhoea were reported in only 3.5% of respondents.
The three most frequent AEFI recorded were vagal response (30%), anxiety reaction (24%) and dizziness (21%). AEFI were more frequently observed among women [aOR= 2.24 (95%CI= 2.00 – 2.50)], and those with at least one previous disease [aOR= 1.47 (95%CI= 1.22-1.76)].
The most common AEFI was pain/tenderness at the injection site experienced by 59.3% of those who experienced any AEFI followed by headache/dizziness (35.3%), itching/rashes at the injection site (8.1%), nausea/vomiting (5.8%) and fever/chills (4.7%).
The patient was a health care worker, aged 34-year old. Past medical history was unremarkable and had not used heparin. Over the next couple of days after the vaccination, he reported headache, nausea, and dizziness as well as abdominal pain. His general status and the laboratories studies deteriorate quickly by increasing liver enzymes and severe coagulopathy. Clinically he had presented acute hepatic failure. He had been received blood products, prednisolone pulse along with broad antibiotics without benefit. He died on the sixth day.
Herein, we describe a 48 years old man presenting with rapidly progressive cognitive decline and hyponatremia diagnosed with anti LGI1 AE, occurring shortly after the second dose of mRNA COVID -19 vaccine and possibly representing a severe adverse event related to the vaccination.
Are we living out a medical experiment or social/behavioral experiment?
Has the world been Trumped?
The government forever claims that people must plan for rising healthcare costs. In 2019, U.S. medical health spending increased by 4.6% to $3.8 trillion or $11,582 per person. If the U.S. medical system is the best in the world then shouldn’t the numbers be doing down?
Whether the crisis is called The Opioid Epidemic or The COVID Pandemic, it is a Crisis of Humanity. The conclusion is always the same when the requirement for more dollars and more research takes precedence over individual healing and freedom from government tyranny:
VAERS data released Friday by the Centers for Disease Control and Prevention show 1,261,149 reports of adverse events from all age groups following COVID-19 vaccines, including 27,968 deaths and 228,477 serious injuries between Dec. 14, 2020, and May 6, 2022.
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,261,149 reports of adverse events following COVID-19 vaccines were submitted between Dec. 14, 2020, and May 6, 2022, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 27,968 reports of deaths — an increase of 210 over the previous week — and 228,477 serious injuries, including deaths, during the same time period — up 1,774 compared with the previous week. There were 5,794 additional total adverse events reported to VAERS over the previous week.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 12,899 U.S. deaths reported as of May 6, 16% occurred within 24 hours of vaccination, 20% occurred within 48 hours of vaccination and 59% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 578 million COVID-19 vaccine doses had been administered as of May 6, including 341 million doses of Pfizer, 218 million doses of Moderna and 19 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
20 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department.
The Defender has noticed over previous weeks that reports of myocarditis and pericarditis have been removed by the CDC from the VAERS system in this age group. No explanation was provided.
65 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
650 reports of myocarditis and pericarditis with 638 cases attributed to Pfizer’s vaccine.
166 reports of blood clotting disorders with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to May 6, 2022, for all age groups combined, show:
20% of deaths were related to cardiac disorders.
54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
Pfizer’s COVID efficacy fades rapidly just weeks after second and third doses
Second and third doses of Pfizer’s COVID-19 vaccine provide protection against the Omicron variant for only a few weeks, according to peer-reviewed research published today in JAMA Network Open.
“Our study found a rapid decline in Omicron-specific serum neutralizing antibody titers only a few weeks after the second and third doses of [the Pfizer-BioNTech] BNT162b2,” the authors of the research letter wrote.
The authors said their findings “could support rolling out additional booster shots to vulnerable people as the variant drives an uptick in new cases across the country,” Forbes reported.
Danish researchers studied adults who received two or three doses of BNT162b2 between January 2021 and October 2021, or were previously infected prior to February 2021 and then vaccinated.
They found that after an initial increase in Omicron-specific antibodies after the second Pfizer shot, levels dropped rapidly, from 76.2% at week 4, to 53.3% at weeks 8 to 10, and 18.9% at weeks 12 to 14.
After the third shot, neutralizing antibodies against Omicron fell 5.4-fold between week 3 and week 8.
COVID vaccines for kids under 6 won’t have to meet FDA 50% efficacy standard
The FDA’s top vaccine official told a congressional committee on May 6 that COVID-19 vaccines for kids under 6 will not have to meet the agency’s 50% efficacy threshold for blocking symptomatic infections required to obtain Emergency Use Authorization.
“If these vaccines seem to be mirroring efficacy in adults and just seem to be less effective against Omicron like they are for adults, we will probably still authorize,” Dr. Peter Marks, director of the Center for Biologics Evaluation and Research at the FDA told the House Select Subcommittee on the Coronavirus Crisis.
The FDA is reviewing data from Moderna’s two-shot vaccine for infants and toddlers 6 months to 2 years old, and for children 2 to 6 years old. The company asked the FDA on April 28 to approve its COVID-19 mRNA-1273 vaccine for children, citing different efficacy numbers than it disclosed in March.
The FDA is still awaiting data on Pfizer and BioNTech’s three-dose regimen for children under age 5 after two doses of its pediatric vaccine failed to trigger an immune response in 2-, 3- and 4-year-olds comparable to the response generated in teens and adults.
COVID vaccine injury ends surgeon’s 20-year career
In an interview on CHD.TV’s “The People’s Testaments,” Dr. Joel Wallskog described how he was diagnosed with transverse myelitis after getting the Moderna COVID-19 vaccine, and why he now devotes his time to helping others injured by the vaccine.
In September 2020, Wallskog said, staff members in the clinic he referred patients to began coming down with COVID-19. Although Wallskog did not feel ill, he got an antibody test and it was positive.
When a close friend came down with COVID-19 and had to be intubated, Wallskog decided he should get vaccinated, despite reservations and having already acquired natural immunity.
About a week after receiving his vaccine, Wallskog’s feet became numb and he developed “electrical sensations” down his legs when he bent his head forward. When he began having trouble standing, he ordered emergent MRIs and was found to have a lesion on his spinal cord.
A neurologist diagnosed Wallskog with transverse myelitis, a disorder caused by inflammation of the spinal cord.
Despite various treatments and rest, Wallskog suffers pain and numbness and is unable to stand long enough to perform surgery. His career came to an end in early 2021.
Rheumatologist: 40% of 3,000 vaccinated patients reported vaccine injury
Dr. Robert Jackson, a practicing rheumatologist for 35 years said 40% of the vaccinated patients in his practice reported a vaccine injury, and 5% are still injured. Jackson has more than 5,000 patients, about 3,000 of whom received a COVID-19 vaccine.
Jackson said he’s had 12 patients die following the shot, whereas he normally sees one or two deaths in his patient base a year. About 5% of his patients developed a new condition that makes them susceptible to blood clotting.
Jackson’s observations are consistent with a study published in the BMJ that assessed the safety of vaccines against SARS-CoV-2 in people with inflammatory/autoimmune rheumatic and musculoskeletal disease from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry.
The study showed 37% of 5,121 participants had adverse events and 4.4% of patients had a flare-up of their disease after vaccination.
TORONTO: The Justice Centre has engaged lawyer Phillip Millar to represent serving members of the Canadian Armed Forces (CAF) who have declined the Covid vaccine on the basis of health concerns or conscientious objections. One of client, Warrant Officer James Topp, is a member of the CAF reserve force facing the charge of “Conduct to the Prejudice of Good Order and Discipline,” which has the potential to result in Court Martial. The Justice Centre also represents 15 other CAF members facing discipline and possible job loss over mandatory Covid vaccine policies implemented by the military.
Mr. Topp, who has been a serving member of the CAF for 28 years, has gained national headlines for his 4,293 kilometre “Canada marches” walk across the country, in protest of mandatory vaccine mandates, forced quarantines, mandatory testing, and other conditions of employment or provision of services.
Mr. Topp began his march on February 20, the same day police forces began using physical force against unarmed Freedom Convoy protesters in Ottawa. Facing job loss for refusing a Covid shot, Mr. Topp is averaging 30 km a day along the highway. His goal is to reach the Tomb of the Unknown Soldier in Ottawa by June 22.
Mr. Topp says government overreach has spread into all aspects of the personal lives of Canadians. “I’m not here for profit, and I don’t want to be a celebrity, but I need to do something,” Mr. Topp told about 100 supporters in Vancouver, who came out on a cold winter day to see him off on his march. “We need to do something to repair us because we’ve been deeply fractured by what has happened…” He adds, “We have to “ensure our government upholds the laws that support Canada’s Charter of Rights and Freedoms.”
Mr. Millar will represent Mr. Topp and 15 other military members in Federal Court, seeking an injunction against the release of CAF members until their grievances are heard. The Justice Centre maintains that military members are entitled to have their constitutional freedoms such as freedom of religion and conscience protected, as CAF members have fought and served to protect the freedoms of all Canadians.
Mr. Millar is a former full-time Combat Officer in the CAF Infantry, former Assistant Crown Attorney, and experienced trial lawyer who has already successfully sued the Department of National Defence (DND) in the past.
“The mandatory vaccine is a flawed policy based on a stubborn refusal to acknowledge that the underlying justification for the mandate has changed. The government is using the Canadian Armed Forces as a policy arm to promote its vaccine mandates. The policy hurts the operational effectiveness, morale, and integrity of the system,” says Mr. Millar.
He notes that the “military chain of command is fast-tracking the release of service members who refuse to get vaccinated under administrative processes, trampling their rights and denying them due process by sidestepping the proper procedures.”
“The DND cannot claim that service members are disobeying a lawful order and then refuse to allow the issue to be tried in the military justice system where a judge can make a determination if it is in fact a “lawful order”,” adds Mr. Millar.
The government is using a “5F release,” which was never meant to be applied in this manner.
“We cannot let them get away with ruining the lives and careers of dedicated Canadians who serve their country. Our soldiers, sailors and air force personnel deserve more. They are highly trained, and many have served their country for years,” Mr. Millar concludes.
Good day, South Africa. My name is Ricardo Maarman and I’m from the Show Us the Virus movement.
Today is the 28th of April, 2022. It is the very day that our Leave to Appeal to High Court to challenge the negative judgment we had, with the cost order against me, was due. And so this is why I am giving you this update today.
Now before we proceed I just want to give you a background on the case and what has been happening so far.
You see, for the past two years (or more than two years) the president of South Africa, and many other presidents around the world as well — but in particular president of South Africa — came forward and made a claim.
He claimed that there was a virus called SARS-CoV-2 and this virus is causing a pandemic. And because of this, he has to take away all of the rights, or a lot of the rights, of the people of South Africa. And he has to impose these draconian lockdown, tyrannical regulations on the people.
And for the past two years, while he has been doing this, people have said many things.
You know, people have said this and that and the other in the showing their disapproval of what is going on and they’re opposition of what is going.
We at the Show Us the Virus movement have said one thing — can be summed up in one question that we have asked throughout this whole period. And that question is: Show us the virus. Show us the virus!
You make a claim that there is a virus, so show it to us.
And what we are faced with is controlled opposition who are trying to distract people from this question.
The president decided to fight the legal battle against me — a long protracted legal battle — and seemingly using all of his influence in the judiciary and his power to win this battle against me, to prevent me from ever being able to have this question answered.
But I think his silence has answered it already. And his actions. His dismissal.
He’s maneuvering has shown to us what the answer to the question is. There is no virus here.
The media has chosen to ignore what we’re doing, sort of an unofficial ban on this — never covering this court case. Showing anything else but this.
And the controlled opposition has been trying to distract people’s attention away from this. ‘No, that’s not an important question. THIS is more important than that.’ This is what has been happening.
And we have stayed consistent. We have said the same thing. Because when you speak the truth, and when you are focused on the truth, you do not have to change your tune every now and again. And that’s why you’ve heard the very same thing from us time and again. Show us the virus.
And that won’t change. We won’t be deterred. We will grasp onto the truth and we will pursue it no matter what, hell or highwater.
Now, what has happened as far as the case is concerned as I say that on the 28th of April, which is today, 2022, this is when our would Leave to Appeal is due. And we have successfully launched an application to the judge for Leave to Appeal.
But a strange thing has happening again. One week before this, on the 22nd of April 2022, the Constitutional Court dismissed our Rescission Application. Rescission Application is a sort of appeal to the Constitutional Court. And they have dismissed it.
Now, this is very important because the judge has dismissed our Interdict Application in the High Court because she says there was no case in front of the Constitutional Court, there was no appeal, there was no decision and, therefore, she has dismissed the case. And, therefore, she has ordered that I pay punitive cost of the billionaire president and also the pretty wealthy and rich Minister of CoGTA [Co-Operative Governance and Traditional Affairs]. I must pay their legal cost, based on the fact that there is actually no case in front of the Constitutional Court pending.
The fact that the Constitutional Court — one week before the time — has dismissed my decision application without a hearing, is proof that the judge was wrong in her judgment. There was a case pending. There was an appeal pending in the Constitutional Court.
The fact that the Constitutional Court now has dismissed it a week before, it is supposed to have helped their cause but it doesn’t really. I think that is a little bit of miscommunication or there’s a miscoordination because it doesn’t really help their case. It advances ours. It proves, without a doubt, that when the judge made her decision she was factually mistaken. She was legally mistaken.
And that is why we are — we have launched this Leave to Appeal and we are successful with the merits of our case.
You must remember, at the end of the day, we have gone to the courts and we have said to the courts: The president made a claim. He said there’s a virus. We ask him to show the virus.
And the just and legal thing to do would be that he must prove his claim. He who claims must prove it.
The courts have, thus far, been dismissive of this basic and fundamental legal issue. And, as I’ve said, the media has tried to basically ban this, hide this very important, very fundamental, issue from the people of South Africa.
The controlled opposition. Now, who are the controlled opposition?
Controlled opposition are all those who say they oppose the government in this tyranny that the government is perpetrating against the people of South Africa, based on the SARS CoV-2 virus, but they agree with the claim of the government. They also promote the idea that there is a virus. And they feel that any lawsuit, or any case, that has to do with the Show Us the Virus question is not important. Other cases are important that focus on other things.
And I say to you, quite frankly Show Us the Virus is the fundamental issue here. Nothing is more fundamental than that.
Without the virus claimed there would be no pandemic and no other thing that anybody has a problem with.
And so anyone who is trying to say that they oppose the government but they agree with this basic premise is, quite frankly, controlled opposition. And the purpose of what they are trying to do is to distract you from what is really important. You’ll see this controlled opposition sellouts in politics and everywhere else, trying to distract the South African people, divide the South African people. It’s no different here.
And you see it — these kinds of thing pop up every time we release a message or every time that we are in the middle of a case of, there’s efforts to try and distract. Go look at the background and history and you will see the same.
As I’ve told you already, for this simple question Show Us the Virus, the president has chose to fight a legal battle with me for the past two years. The judiciaries tried to dismiss it. A basic premise of justice, they’ve tried to dismiss it.
Now, the fact that we have lodged our Leave to Appeal should show you — and the fact that we are still asking the same question for two years — should show you that we don’t give up easily and that we will not be easily distracted. And that we will not be easily deterred. And the fight is far, far from over.
Now, unfortunately, this is not the first time that this situation is happening in South Africa. It’s not the first time. Previously it was the HIV virus, that supposedly caused the AIDS pandemic. And the media did the same.
Anyone that opposes this is called an AIDS denialist. Anyone who raises any questions is ridiculed and attacked in the media quite viciously.
There was also protected court cases going on. And I’ll explain to you those court cases that went on. And, unfortunately, the result is very similar to what we are seeing today.
But first, there was also controlled opposition then. There was the Treatment Action Campaign that was pushing for pregnant women to receive toxic drugs (nevirapine). They were pretending to be on the side of the people and demanding that the people be given this toxic drug, sort of as a mandatory drug from the pharmaceutical industry that were the beneficiaries of this poisonous drug.
We have the same. Those people today who are controlled opposition for the government and for these people pushing this tyranny on us, they’re doing the same. They say it’s a bioweapon. They say it’s not so bad, but the virus is there. They are advocating people use ivermectin which is a toxic drug. They saying people should use other toxins, many other toxins.
I’m not a doctor. I will not be able to specify all of them. But many, many, many toxins. You can go check it yourself. All of those who claim to be opposing the government but they believe there is a virus or they advocate there’s a virus without providing any proof, they are also advocating toxic drugs.
The same that was happening during the time of the HIV issue as the Treatment Action Campaign did then. There was a … big court case happening then where the government then was challenging and saying no we shouldn’t be giving people nevirapine, it’s a dangerous, toxic drug. Eventually this matter ended up in the Constitutional Court then. And in the Constitutional Court Dr. Sam Mhlongo, he raised the issue to the court that the HIV virus has never been isolated and purified. Basically, the HIV virus was never shown to exist. So, you know, they were basically in their way asking the same question then: Show us the HIV virus.
And the court decided to dismiss Dr. Sam Mhlongo and say no that will not be entertained. The court will not answer such a question. Again, basic premise of justice. They claim there’s an HIV virus. Dr. Sam Mhlongo is asking them — is saying to the court they’ve never proven it. And therefore they should not be giving people toxic drugs like nevirapine if they haven’t proven the virus to exist. And the Constitutional Court dismissed Dr. Sam Mhlongo, as they are now trying to dismiss me again. It’s a repeat of history.
Sadly, soon after this whole debacle, Dr. Sam Mhlongo lost his life in mysterious circumstances — car accident and he lost his life. And this is how dangerous it can be to just ask a simple question.
To demand justice can be deadly when you are facing with such force of tyranny and injustice. And sadly, this is the case with Dr. Sam Mhlongo.
Now, as I’ve explained to you here — now this is twice in a row — that there has been, every time we go to the High Court, where we are supposed to go to the High Court, we are supposed to appeal, then the Constitutional Court issues orders. issues orders that will seemingly be very convenient for the president’s legal team and for the High Court then to to use together to judge against me.
There seems to be … I can’t say very clear. I was not in meetings where I see them discuss, but what I see is that within a week — every time we are going to the High Court, within a week the Constitutional Court comes back with a decision supposedly against us and supposedly in favor of the president. And that can then be used to help the High Court make its decision.
So this is a determined effort to see that the question of Show Us the Virus is never the answered and that I must be, you know, saddled with this legal cost. Because the financial cost would be quite substantial. They haven’t issued the bill yet and so this is hanging over my head. But what can happen here quite easily, if my Leave to Appeal is dismissed, my appeal is dismissed, and then I’m saddled with this cost. And then this could mean that they could see sequestrate me. It could render me to lose all of my assets and to be impoverished. So this is the threat that is hanging here — all because of asking a question. Show us the virus.
So, they are very dangerous, you know, in terms of their power that they wield and the threats that they have. As I’ve said here, Dr. Sam Mhlongo has lost his life… I have the knowledge that he lost his life for asking that question. And I’m asking that question. I’m asking the question for them to show the proof of these virus claims of theirs, including the one that Dr. Sam Mhlongo asked about HIV. And I’m asking in addition to that.
So I’m sure for me asking his question and redoubling that question with another one, with another virus, then I should be very careful about car accidents as well.
And, of course, in addition to this financial threat that they now directing towards me. But I am not deterred. And as I’m sure Dr. Sam Mhlongo was not deterred. That his death, and that if any such similar thing happens to me or loss of property, then my debt, my loss of property — or my death in the event that they do the same kind or try the same kind of thing against me — will be a witness against them, a witness against the tyranny, a witness against their falsehood. It will be a witness against their injustice. Because why should this man lose property? Why should this man lose his life for asking you to show us the virus when you have made this claim. This is the height of injustice.
They are determined to see that I lose these cases.
They are determined to see that I am silenced.
They are determined to ensure, with the help of their controlled opposition, that people’s attentions are directed elsewhere.
I’m saying to South Africa, we have been fooled once by these people and their tactics, their intimidation, they’re controlled opposition, sellouts, etcetera.
They fooled us in the past. We should not allow them to fool us again.
For them, having fooled us in the past, shame on them. But if we allow them to fool us and divide us again, then shame on us.
It is time for us to redouble our efforts. Here at the Show Us the Virus movement we have no intention to submit ourselves to evil or to falsehood. No intention whatsoever.
We will redouble our efforts as this lodging of this Leave of Appeal application has shown you. There has been many attempts to distract you in the meantime.
From my request, I asked you and I said South Africa please support me, please help me. I am facing these kind of threats, financial threats. And there has come a whirlwind, a whirlwind to try and distract you away from helping me away, from supporting this cause and standing for truth and justice.
I ask you not to allow yourself to be distracted like this I ask you to stand with me as I redouble my efforts to fight against this tyranny and oppression.
I will not surrender. And I want to implore you that, don’t think others will come and save you. Our situation will not change unless we change it ourselves.
We have to redouble our efforts. We have to pray and turn to God to help us to defeat this evil. And we have to stand together. And we must ensure that we focus. We stand as one. And we never relented evil. We stop it. We fight it. Whatever stumbling blocks there are, we jump over it. Whatever walls there are, we go through it if we have to.
So please let’s stand together. Support me as much as you can. Support our cause. We still have an uphill battle to fight.
We will let you know how the Leave of Appeal application goes. And after, that we’ll follow the appeal itself in our efforts to see that justice is done and that an unjust court order be overturned.
“Covid ‘vaccines’ caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.”
This week MEP Christine Anderson (AfD) gave her first speech before the European Union’s new “COVID-19 inquiry committee”. The German MEP condemned the EU’s Covid policies and demanded an investigation into the clear human rights violations under the pretext of combatting a virus.
Anderson railed against the “false claims regarding the safety of the vaccines, their alleged definitive approval, and so-called effectiveness.” The MEP pointed out that the European Medicines Agency (EMA) database shows that in seven months, the Covid “vaccines” caused 20 times as many serious side effects and 23 times as many deaths as all other vaccines in the past 20 years combined.
“Why isn’t that being investigated,” questioned the MEP. She explained that the government’s Covid policies had nothing to do with public health. Instead, it seems it has been “a money-making exercise for the pharmaceutical industry.”
Why were alternative methods to fight Covid not investigated or given to the public, questioned Anderson? Instead, she exclaimed, everything in your whole Covid policy “boiled down solely to: “vaccinate, vaccinate, vaccinate.”
Issues Committee Must Address
Anderson pointed out other issues that the committee must investigate. She first zeroed in on the “implementation of vaccine contracts.” Little information is available on vaccine makers’ contracts due to the committee withholding the information. She questioned how she could “properly do her job as an elected MEP” and educate her constituents without the data.
The massive “restrictions of fundamental rights that are unworthy of a democracy” must also be investigated, exclaimed the MEP. “From job losses, discrimination and marginalization, we have experienced a redefinition of fundamental rights.” According to the new definition, our rights are now privileges to which the government picks and chooses who to grant them.
The MEP demanded answers as to why the committee is not investigating the “marginalization and criminalization of critics” who condemned their “anti-democratic measures.”
She went on to say that it is unacceptable for the World Health Organization (WHO) to sign new contracts with EU member states. As Anderson has previously explained, the WHO is fighting for de facto governing power over EU member states in the event of a pandemic:
Dr. Joseph Yi (StreetMD) with Drs. Tom Cowan, Andrew Kaufman & Mark Bailey: A Response to Claims by Drs. Robert Malone, Peter McCullough & Ryan Cole That SARS-CoV-2 Has Been Isolated & Is a Disease-Causing Virus
Dr Joseph Yi, AKA “StreetMD” asked Drs Bailey, Cowan and Kaufman to respond to Drs Malone, McCullough and Cole’s claims that SARS-CoV-2 has been isolated and shown to exist. Boom!
Dr. Sam Bailey with Eric Coppolino — On the Monumental Task of Documenting & Examining the Covid-19 Chronology: “Knowledge Coming to Light Changes Things”
“Knowledge coming to light changes things.” ~ Eric Coppolino
Recently, I have been fortunate to have connected with the inspiring Eric Coppolino, who is based in New York State.
Eric has an incredible history of exposing scientific fraud and environmental pollution cover-ups. He was one of the first to start investigating the COVID-19 scam and is putting something big together to help all of us who are questioning the narrative.
GREENWICH, CT — Robert F. Kennedy, Jr. has acknowledged the controversy within his own community over whether SARS-CoV-2 physically exists, and whether any viruses exist, or make people sick. He made the comments at a fundraising event here Sunday, April 24, 2022.
Kennedy said that the issue erupts regularly on the email discussion list of Children’s Health Defense (CHD), the vaccine safety and education organization that he founded in 2016.
“On our list, there’s a number of people who make those kinds of arguments” about how viruses allegedly don’t exist, Kennedy said in his remarks. “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
He made the remarks in reply to a question about why no government can produce evidence of having a sample of SARS-CoV-2 taken from a patient, rather than artificially created using a computer model.
Kennedy, the son of Sen. Robert F. Kennedy and the nephew of Pres. John F. Kennedy, is considered one of the leading voices in the international movement against covid-related mandates, lockdowns and safety issues over covid injections. It is the first time he has publicly commented on the virus-existence issue.
Scientists on all sides of the issue agree that viral particles have not been physically
isolated (with purified samples) and then sequenced.
What is Being Used to Prime the Covid Test?
The matter of whether the SARS-CoV-2 virus physically exists has dual significance. The obvious issue is that if there is not a virus, what then is making people sick? And what are they being vaccinated against?
Second, and less obvious: If the government cannot prove that it has a sample of natural SARS-CoV-2, then what is being used to prime the PCR test that is supposed to match and find the genetic code of an actual virus in a patient?
Scientists on all sides of the issue agree that viral particles have not been physically isolated (with purified samples) and then sequenced. Rather, hypothetical viruses are assembled from mixed biological samples, and these “in silico genomes” are then assumed to not only exist in nature but come from inside a pathogenic particle. They have many names: “mimicked human specimens” and “contrived viruses” (in the words of the CDC); or “synthetic nucleotide technology” (in the words words of the authors of the WHO test for covid).
One virologist told me in July 2020 that SARS-C0V- 2 was being assembled “like pages from a book,” necessary because no natural virus particle was available to sequence. The problem is that nobody has demonstrated these pages actually belong to the proposed book.
Covid tests look for sequences attributed to the “virus” merely via computer models —
but these “found” sequences almost always originate from somewhere else (including
the testing process itself).
CDC document pertaining to detection limits in the CDC “covid” test, admitting that
purified isolates of SARS-CoV-2 are not available. Yet this long, technical paragraph
admits something else: how they go about making their contrived virus (mimicked human
specimen), rather than sequencing actual virus. Were viruses available to anyone, it would
be the federal government of the United States. What they are admitting is that the virus
has not been isolated or purified; the writer admits outright that they are using made-up
samples that mimic clinical specimens. The technical notes describe the manufacturing
process for in silico sequences that are used in the “covid” test. The notes make reference
to MN908947, a synthetic, claimed, partial metagenomic transcript (not actual sequencing)
of the “N-gene” — which was later abandoned in its entirety in the Corman-Drosten assay.
Metagenomics: The Creation of Hypothetical Sequences
These hypothetical sequences are developed using technology called metageonomics — without any reference to actual purified suspected viruses. This artificial-intelligence process assembles a hypothetical “virus” from information gathered either from a crude human body fluid sample, or by making a “cell culture” experiment by mixing the fluid with monkey cells, cervical cancer cells, fetal calf serum, antibiotics and other poisons. In all cases where covid is concerned, scientists have used the latter. Because there is no actual virus available as a reference, there is no way to verify if the proposed sequences are valid. They are all theoretical, and no two are alike.
Said another way, in the absence of a real virus specimen, covid tests look for sequences attributed to the “virus” merely via computer models — but these “found” sequences almost always originate from somewhere else. And “positive” results can emerge from nearly anywhere, including the testing process itself). Yet if someone “tests positive” for one of these claimed viral sequences, they are said to be “infected” with SARS-CoV-2.
Previously, the U.S. Centers for Disease Control and Prevention (CDC) has admitted that the polymerase chain reaction has had a 100% false positive rate and has caused several widely-documented “false epidemics.”
The claimed existence, transmissibility and pathogenicity of SARS-CoV-2 were used to declare a global pandemic that by March 31, 2020 had 4.5 billion people around the world living under a stay-at-home order or house arrest.
“On our list, there’s a number of people who make those kinds of arguments. And
other people on the list server, and these are all very brilliant people, ridicule them
and dismiss them, and have them produce a lot of evidence.” — Robert F. Kennedy, Jr.
Seeking Documents from Governments, Agencies and Institutions
At a Q-and-A session at a fundraising event here Sunday, April 24, I asked Kennedy about the work of Christine Massey in the Toronto area, a statistician who is coordinating the worldwide effort to officially query governments, agencies and institutions about whether they have a sample of the claimed virus taken from a human.
“Christine Massey in Toronto has amassed 182 responses under various Freedom of Information Law requests from institutions, provincial state, and federal, national governments, which all say that no one has a sample of SARS CoV-2 taken from a human. Would you please comment on that?”
Kennedy replied: “On our list, there’s a number of people who make those kinds of arguments. And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence. I actually saw an exchange yesterday, where somebody made that exact statement and then 10 people jumped on him on with examples, of where that’s not true.”
The issue over the nature and existence of viruses represents the single biggest split in the covid-truth and anti-mandates movements. I first documented this divide in May of 2020.
“RFK Jr. now relies on popular opinion and ridicule to evaluate science?
When did he declare incompetence with simple logic?” — Christine Massey, statistician and coordinator of the virus FOIA project
‘I Am Amused Reading These Exchanges’
He added: “I am kind of amused reading the exchanges, and my inclination is that the viruses do exist and they do make people sick. I could be wrong. It could all be a big hoax, but to me, it all seems like viruses are real.”
But Kennedy answered a different question than the one I asked. I did not present him with an argument, or ask him whether he thought viruses were real. He admits that he uses a kind of mob rule to make up his mind over critical scientific issues when he says, “And other people on the list server, and these are all very brilliant people, ridicule them and dismiss them, and have them produce a lot of evidence.”
Reading Kennedy’s response, Christine Massey said, “RFK Jr. now relies on popular opinion and ridicule to evaluate science? When did he declare incompetence with simple logic? And why is a man dedicated to protecting children from medical harm uninterested in one of the greatest medical frauds of all time?”
She also demanded the data from the 10 people on Kennedy’s list who claimed to prove that the virus had been isolated.
So far, no governments have produced a scientific paper saying that they or anyone
have such a sample, despite the claim that a contagious virus has killed more than
5 million people worldwide.
Asked About a Legal Issue — Not Scientific
Kennedy said he believed viruses exist, but I did not ask him about that. Rather, I presented him with a legal issue, asking him to comment about how someone well-known and established in covid truth circles over the past two years has collected 182 responses from top-level government agencies and institutions, all saying they do not have a sample of SARS-CoV-2 extracted from a human host.
So far, no governments have produced a scientific paper saying that they or anyone have such a sample, despite the claim that a contagious virus has killed more than 5 million people worldwide.
I followed up and said to him, “The governments have said they don’t have a sample.”
Kennedy, an attorney, responded: “Freedom Information Laws do not require the government agency to do science, or to answer specific questions. What they do is, the Freedom of Information Laws make it obligatory for the government to give you existing documents. So if you are telling the government, ‘I want you to verify these, there are documents’, they say, listen there’s nothing to verify it. It doesn’t mean it’s not true. It means they’ve got nothing.”
So far all have said no such records exist. This includes the U.S. CDC and the FDA, as
well as Health Canada and the National Health Service (NHS) of the UK. None of the
182 agencies and governments queried have replied in the affirmative.
‘Kennedy hasn’t read any of my records requests’
Massey replied to this in an email: “It appears that Kennedy hasn’t read any of my records requests. I didn’t ask governments to ‘do science’ or answer ‘specific questions’. All of my requests have been for studies/reports in the possession, custody or control of an institution.”
I asked Massey how she words her letters seeking documentation of a sample of the claimed virus from a human host.
She provided this example of what she is seeking, and what so far all governments she has queried deny having:
“All studies and/or reports in the possession, custody or control of the Centers for Disease Control and Prevention (CDC) and/or the Agency for Toxic Substances and Disease Registry (ATSDR) describing the purification of any “COVID-19 virus” (aka “SARS-COV-2”, including any alleged “variants” i.e. “B.1.1.7”, “B.1.351”, “P.1”) (for example: via filtration, ultracentrifugation and chromatography), directly from a sample taken from a diseased human where the patient sample was not first combined with any other source of genetic material (i.e. monkey kidney cells aka Vero cells; fetal bovine serum).”
And so far all have said no such records exist. This includes the U.S. CDC and the FDA, as well as Health Canada and the National Health Service (NHS) of the UK. None of the 182 agencies and governments queried have replied in the affirmative.
“It erodes popular faith in democracy when public officials insist that their arbitrary
policies are ‘science based’ and yet cannot produce a single study to support sweeping
mandates.” — Robert F. Kennedy, Jr.
‘No Records Exist’ is an Important Response
Getting a “no records exist” reply is common, and seeking such a reply is a common strategy for establishing that there has not actually been a regulatory process for a policy issue. It is one of the most important uses of open records laws.
In late 2020, the New York State Department of Health (NYS-DOH) responded to an open records request saying it had no studies to prove that masks are safe or effective at preventing the spread of viruses or other diseases. For that same kind of “sorry no documents” FOIL reply, Kennedy was much more outspoken.
At the time, he wrote to his Instagram followers, “It erodes popular faith in democracy when public officials insist that their arbitrary policies are ‘science based’ and yet cannot produce a single study to support sweeping mandates. This letter illustrates the hazard of abandoning due process.”
Previously, he had remained agnostic on the issue of masks and whether masks work. He finally took a position in response
New York State saying it had absolutely no data about whether masks are safe or effective.
“It’s a needlessly divisive issue, with people screaming, on both sides, as if it were
the key to this whole thing — which it isn’t.” — Prof. Mark Crispin Miller
“They did not isolate a virus,” Wallach said. “The reason it’s so confusing for people is that they claim to have done so in the titles of the key scientific papers, but if you read the methodology sections, it’s blatantly clear: they never isolated a virus. They never found anything. The evidence is overwhelming.”
He added: “I respect the importance of political leaders like RFK Jr. keeping an open tent, they have to. But at the same time, this is an issue that should be front and center for the world public, and nobody should be repeating this dogma about the existence of viruses.”
Mark Crispin Miller, professor of communication at New York University, said, “It’s a needlessly divisive issue, with people screaming, on both sides, as if it were the key to this whole thing — which it isn’t. What will make the whole narrative collapse is not the argument that there are no viruses, but the recognition that the authorities we’ve all been listening to — the medical establishment, Big Pharma, Academia, the media et al. — are malign, and intent on killing us.
“That’s it. Everything else is a distraction. Whether the ravages of COVID-19 have been exaggerated, or whether there’s no virus there at all, is ultimately beside the point. And since Bobby’s role is in large part political, as he attempts to keep this movement in one piece, his disinclination to take sides here ought to be respected.”
“Are all based on in-silico modeled synthetic phenomena, which has never been
scientifically proven as coming from an actual virus.” — Dr. Kevin Corbett, expert in diagnostic testing
‘This was what happened with HIV’
Dr. Kevin Corbett did his doctoral work on diagnostic testing associated with HIV and AIDS, including research into the PCR. He said this week that the existence of SARS-CoV-2 and associated tests, “Are all based on in-silico modeled synthetic phenomena, which has never been scientifically proven as coming from an actual virus.
“This was what happened with ‘HIV’, which The Perth Group of scientists [in the 1990s] first proved was never isolated or purified. Those powerful voices like Robert F. Kennedy, Jr., who sadly ignore this issue, are badly misguided, because they fail to address this fundamental caveat in ‘covid science’.”
Corbett cautioned, “Their efforts will only act to further socially embed the popular hysteria of there being a contagion, and therefore will enable further public health mandates forcing masks, social distancing and the latest covid killshot.”
On April 25th, a federal judge stuck down the mask mandate for mass transit.Part of the reasoning was based on fact that the CDC skipped the otherwise-mandatory public notice and comment period as required by the Administrative Procedures Act (APA). However, the main reasoning was to show that government officials do not recognize the limits of their power. Apparently, neither do the masses.
The ruling sent COVID doomsdayers into panic mode. Federal agencies are creatures of statute and are bound by law to operate within the law imposed by Congress. Agencies are not separate entities that may act as they wish.
Their authority is limited to what Congress grants them. So the CDC is governed by Congress – not by any President – and certainly not by career bureaucrats like Fauci. – Phillip Holloway, Esq
Up until COVID, it was illegal to wear a mask to conceal the face in public, with few exceptions. Under COVID, “the science” reversed the mask laws overnight, illegally. Few people questioned the authority of politicians practicing medicine without a license. Perhaps COVID is a lesson to understand that when “science” enters the political picture, its time to question authority. In other words, public health orders do not trump legal orders.
Science and Freedom Do Not Mix
Contrary to popular belief, the law is not based on the latest “science” because science and law are separate spheres of knowledge. Science cannot prove that something is true. Science tests theories, and explains what is observed under a specific set of conditions. Science is a tool. Like any tool, it is neither good or bad, but it can be used according to the will of the “scientist” who wields it. Science does not reveal truth.
Science cannot give you truth. All it can determine is internal self-consistency” based on data within the confines of time and distance. Everything else must be rejected. —William A. Tiller
Science does not usurp the law. Neither do mandates usurp the law. Mandates are public health policies, made by government agencies who use science and fear to manipulate behavior. Yet, federal agencies have NO authority under the law to tell people how to live when it comes to making health decisions.
For those who claim that science “raises awareness,” realize that awareness exercises do nothing to ensure freedom. Real freedom is preserved outside of science, lest people become slaves to a system that is set up to manipulate and engineer consent (as with mandates). Without true consent, there is only implied consent, the illusion of choice, based on the limited options you are provided. An illusion of choice brings an illusion of freedom.
The federal judge made clear that CDC and government officials violated the APA in issuing the mandate.
Despite the protestations by Fauci to the contrary, the CDC was created by a law, is governed by a law, and must act within the confines of that law. – Phil Holloway, Esq. Twitter
Live Exercise
The COVID exercise is a test of people’s ability to know truths from falsehoods. Did anyone investigate the legality of a mandate… or how it may differ from a man date? Did anyone question the blank package insert of the experimental injections? Did anyone know to separate the science from the law?
Early on, the Secretary of State, Mike Pompeo, disclosed, in the media, that COVID is a “live exercise.” Did anyone notice how the media then went back to its regularly scheduled programming; Tel-A-Vision?
Why did it take so long for the courts to intervene, especially when the CDC mask order was set to expire on May 3? Is this court opinion too little, too late? Many would argue the damage has already been done. People’s lives and minds have been altered. Kids breathed their own carbon dioxide to participate in school. Babies did not see the facial expressions of their parents.
What about the Covidians who continue to sport “the mask” in public places? Do they do it “to protect others” as the media tells them to do? Does the media guilt people into “taking responsibility” by wearing a mask? Is health no longer a personal responsibility? Can Fauci run a mile to help you lose weight? Can your doctor wear a life jacket to keep you afloat?
The law is supposed to protect the rights of people to decide for themselves…… but only if people know the laws! Know this: neither Congress, the CDC, nor the media can legislate choice when it comes to your body.
Stay tuned. The Department of Justice has filed a notice of appeal to the 11th Circuit Court of Appeals. This filing is expected to go nowhere, and do nothing, except to save face, since there was no motion for a stay included in the notice of appeal.
While the mask mandate may have ended, the live exercise continues…
On Saturday, Apr. 9, 2022, American Airlines (AA) flight 1067 departed Denver International Airport for its 1-hour and 46-minute flight to Dallas-Fort Worth (DFW). The nearly $100 million Airbus A321 aircraft and its 200 passengers were under the care of AA Captain Bob Snow, who has been with the company for over 31 years. Immediately after pulling into Gate 6 at DFW, Captain Snow—who was forced to get the COVID jab on Nov. 7, 2021, or lose his job—suffered a life-threatening cardiac arrest in the cockpit and almost died. If the tragic event had happened six minutes earlier, there could have been a mass casualty in the skies.
Swiftly, Captain Snow, who passed out and had to be shocked three times, was rushed to Baylor, Scott, and White Health Center ten minutes away. Thankfully, he survived. Snow, who spent time in the hospital’s Intensive Care Unit and is now home, is confident his heart attack directly resulted from the COVID-19 experimental “vaccine” he was mandated to receive. Tellingly, no one from AA or the airline union called Snow while he was in the hospital or stopped by to visit him. While in the hospital, he recorded a video, stating:
“My name is Bob Snow. I am an [American Airlines] Captain and have been a Captain for a number of years. My total service with the company is over 31 years. On Nov. 7, I was mandated to receive a vaccine. Quite literally, I was told if I did not receive the vaccination, I would be fired. This [order] was from our director of flight. So, under duress, I received the vaccine.
Now just a few days ago, after landing in Dallas, six minutes after we landed, I passed out. I coded. I required three shocks. I had to be intubated. I’m now in ICU in Dallas. This is what the vaccine has done for me. I will probably never fly again, based upon the criteria the FAA establishes for pilots. I was hoping to teach my daughter to fly; she wants to be a pilot. [Now] that will probably never happen, all courtesy of the vaccine. This is unacceptable, and I’m one of the victims.
You can see that this is an actual result of the vaccine for some of us. Mandatory, no questions asked, get the shot, or you’re fired. This is not the American way.”
American Airlines Told Captain Robert Snow to Get Vaccinated or Be Fired!
Remarkably, Captain Snow’s COVID-19 vaccine-related cardiac arrest and the myriad of pilot and flight attendant lawsuits currently underway against COVID mask and vaccine mandates are not being reported by mainstream media. Still, it is a subject that many concerned Americans, including Steve Kirsch, Executive Director of the Vaccine Safety Research Foundation, are paying attention to.
Pilots Are Speaking Up About Adverse Events From COVID Jab
Kirsch, who believes that “vaccine injury cover-up is in the interest of all affected parties (except the flying public),” recently interviewed Josh Yoder of US Freedom Flyers about AA Captain Bob Snow. Yoder, a pilot himself, has been a staunch advocate against “vaccine” mandates in the airline industries.
In the interview, Yoder shared with Kirsch that his group has received hundreds of reports about pilots flying planes while suffering from adverse side effects from the COVID jabs. He also noted that cardiologist Dr. Peter McCullough told him that if the airlines were conducting health screenings, 30 percent of the pilots currently flying would most likely be disqualified due to vaccine-induced heart conditions. Yoder told Kirsch:
“He [McCullough] said that if every vaccinated pilot were to be screened, there would be somewhere around a 30 percent loss in manpower.”
Yoder mentioned that the most prominent health issues reported include chest pains, myocarditis, and pericarditis. He noted that “three vaccinated pilots called him yesterday” and said they’re “currently flying with chest pains.” Another said a cardiologist is treating him. Yoder added that the pilots want to remain anonymous because they don’t want to lose their jobs.
Airline pilot Latane Campbell interview: A pilot’s view of COVID policies
On Dec. 15, 2021, McCullough, joined by other experts, including Robert F. Kennedy, Jr., pathologist Dr. Ryan Cole, and Lt. Col. Teresa Long, M.D., signed a 53-page letter to the Federal Aviation Administration (FAA) and major airlines, urging them to flag all vaccinated pilots and administer D-dimer tests, troponin tests, cardiac MRIs, and EKGs to assess their health.
The letter—noting that pilots have died post-vaccination—describes the side effects suffered by numerous pilots, many of whom have been afraid to report them for fear of being grounded. Some have had to seek medical attention and report their injuries due to the significance of the COVID-19 “vaccine” related adverse event. A professional agricultural pilot explained his horrible ordeal, stating in part:
“I am a 33-year-old husband and father of two young boys. I have been healthy my whole life, with no underlying conditions. I received my first dose of the Pfizer COVID Vaccine on February 1. Within thirty minutes, I developed a severe stabbing headache, which later became a burning sensation in the back of my neck. Two days after my vaccination, I got in my airplane to do a job that would only take a few hours.
Immediately after taking off, I knew that something was not right with me. I was starting to develop tunnel vision, and my headache was getting worse. Approximately two hours into flying, I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears.
Instantly, I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God, I was able to land my plane without incident, although I do not remember doing this.”
Cody Flint: 33 Y/O Airline Pilot Develops Brain Swelling, Can No Longer Fly Following Jab
Yoder argued that the overall behavior of the FAA, the airlines, and the pilots’ unions demonstrate a contempt for the safety of the flying public and the well-being of airline employees. Kirsch agrees, adding that we have seen a general tone of “belligerence” from nearly all hospitals towards patients who seek second opinions on vaccine-related injury issues. Yoder told Kirsch that the airline industry seems unwilling to address the potentially catastrophic incident.
Yoder pointed out that “AA is trying to create as much distance between themselves and this incident as possible,” adding, “so are the unions. We can’t even get a response.” Still, according to Yoder, Snow will be speaking out soon. When he does, Yoder warned:
“You’re going to hear some very interesting details that are going to be very damning for American Airlines, the Allied Pilots Association, the FAA, and everyone else involved.”
Steve Kirsch, Full Interview with Josh Yoder re: American Airlines Captain Bob Snow vax injury
The Biden administration’s vaccine mandates purporting to force U.S. military members to take the experimental Covid injections are unconstitutional and, because of the potential for genetic changes, may have implications involving patents and intellectual property, super lawyer Todd Callender tells The New American magazine’s Alex Newman in this episode of Conversations That Matter.
To protect the U.S. military, the rights of troops, and the U.S. Constitution, Callender has joined forces with other attorneys such as Tom Renz to sue the Department of Defense. The case is beyond fascinating, and you won’t want to miss this powerful interview.
AttorneyThomas Renz: “They say, ‘Well, we don’t count anyone as vaccinated until 14 days after their full vaccination,’ so that means until 14 days after your second dose, it’s not counted. Well, they did that because they know most reactions occur within 14 days of either your first or second dose… [As of] November/December [2021], there were 52,000ish [people aged 65 and up] who died within 14 days.” Watch:
Transcript of Dr. Sam Bailey’s introduction, provided by TCTL editor:
Last month, we were fortunate to have microbiologist and colloidal chemistry expert Dr. Robin Wakeling present his analysis of Pfizer Comirnaty under the microscope. Since that time Dr. Wakeling has continued to investigate the injections and is also linked up with other New Zealand teams who have shared their findings with him.
In Part 1 of his analysis, Dr. Wakeling presented the appearances of Comirnaty straight from the vial and has some new information regarding how these complexes form.
But perhaps, more importantly, in this video for the first time he is going to analyze the blood of some Pfizer-injected subjects who have suffered adverse reactions.
He’ll explain what he thinks is happening to the red blood cells and some of the most bizarre images he has ever seen in his long career.
In addition to Comirnaty, the teams have also been investigating recent influenza vaccines under the microscope, with some surprising findings that the officially disclosed ingredient don’t appear to explain.
Dr. Wakeling joins my husband, Dr. Mark Bailey, to present round two of Pfizer Under the Microscope.
OTTAWA: After repeatedly calling on the University of Ottawa (U of O) to end its abusive and discriminatory practices, the Justice Centre is pleased announce that the University has stated it will cancel its mandatory vaccine policy for students as of May 1, 2022.
The Justice Centre represented a pregnant student who was suspended from her university program after deciding against the Covid vaccine. Her doctor advised her that her pregnancy was at high-risk for reasons unrelated to Covid and recommended that she complete her mandatory internship virtually, which was allowed by the curriculum.
However, the University of Ottawa refused to accommodate her, falsely claiming that she was trying to circumvent the vaccination policy and that there were no places available for a virtual internship.
Throughout the process, U of O made little to no effort to find a mutually acceptable solution, the student alleges, and refused to justify its decisions in light of the facts of the case.
“It is clear that the University of Ottawa did not intend to follow the ‘reasonable accommodation’ basic criteria set out by the Supreme Court of Canada more than 15 years ago,” notes Samuel Bachand senior external counsel for the Justice Centre in the province of Québec.
After negotiations and discussions with lawyers from the Justice Centre, the student managed to find a suitable placement for virtual internship on her own, which was finally approved by the University.
“The brazenness and bad faith of the University in this matter are appalling. There are clearly, among the people in authority there, bureaucrats who are willing to sacrifice the mission of their institution to irrational health concerns,” comments Mr. Bachand,
“It is well accepted in the scientific community that the Covid vaccines do not prevent infection or transmission of the virus. There was no basis for the vaccine mandate at the University of Ottawa or any other post-secondary institution given that being vaccinated confers no special status or protection,” concludes Mr. Bachand.
“The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent
“SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and
animal “coronaviruses” created in the very same way. Attempting to claim any connections between the
random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated
into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place.
Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely
related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines,
the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have
a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a
singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial
evidence that is easily debunked.”
“My story has never been to create fear, panic, and anxiety about water.” He said he told Peters that he believes “there’s actually a snake venom connection to all of COVID-19, and I think that’s the weapon.” – Dr. Bryan Ardis
Summarizing his theory, Dr. Ardis said, “They are using Krait venom and Cobra venom, calling it Covid-19, you’re drinking it, it’s getting into your brainstem and it’s paralyzing your diaphragm’s ability to breathe.”
I really didn’t want to write this article. I was hopeful that people would easily see right through the unsubstantiated claims of Dr. Bryan Ardis that snake venom is the cause of “Covid.” I was hopeful that people would take the time to research the information presented in support of the snake venom theory to see if it held any merit at all. I thought his whirlwind alternative media tour on the who’s who of questionable sources (including the likes of Stew Peters, Mike Adams, and Infowars) would have people questioning why this theory was allowed to be so heavily promoted so quickly. I thought that the fact that the man who created the “Covid” snake venom theory was actually selling his own anti-venom line of supplements would be enough grounds to be skeptical of his motive and his claims.
It seems I was wrong. Just like the baseless vaccine shedding and gain of function/bioweapons narratives, this new snake venom theory has sadly spread through the “Truther” community like wildfire, with many who rightfully challenge the existence of “viruses” clinging to the idea of a new invisible enemy to defeat. They believe that it must be a new toxin. It can’t possibly be the same factors we have seen each and every year leading to disease. This toxin must be hiding in the vaccines, the drugs, and/or even the very water we drink. What these “Truthers” do not realize is that this very line of thinking gives credibility to the idea of a new disease which requires new treatments in order to combat it. This is exactly what the pharmaceutical companies want you to believe.
However, there is NO NEW DISEASE. There is no need for any new or even existing pharmaceutical interventions to treat the same symptoms of detoxification people go through each and every year. In fact, the current treatments can easily be shown to have led to numerous unnecessary deaths. There is no new threat known as “Covid-19” which is being caused by any one factor. The factors leading to the symptoms of disease people are experiencing are multi-causal as they are every year.
Now this is not to say that the vaccines, the drugs, or even the water supply are free of toxins. These are all sources of toxicity and should be investigated as to their composition and effects on our health. However, the theory that there is one factor in all of these sources, i.e. snake venom, and this one factor is leading to the symptoms of disease people are experiencing is, at present time, completely baseless. And it all begins at the very foundation of the fraudulent genome.
The Fradulent Genome
You take that snake or that serpent and you figure out how to isolate genes from that serpent and get those genes of that serpent to insert itself into your God-given created DNA. I think this is the plan all along, was to get the serpents’, the evil one’s DNA, into your God-created DNA.”
He also said genetic sequence testing done on sick patients in Wuhan found their genetic sequence matched two snakes, the Chinese Krait and King Cobra, not bats.”
From Dr. Ardis’ interview with Mike Adams, he supplied the article “Snakes could be the source of the Wuhan coronavirus outbreak” from CNN as his starting point for the “Covid”/snake connection. Within the article, you can see that this claim originates from the fraudulent genomes:
“The researchers used an analysis of the protein codes favored by the new coronavirus and compared it to the protein codes from coronaviruses found in different animal hosts, like birds, snakes, marmots, hedgehogs, manis, bats and humans. Surprisingly, they found that the protein codes in the 2019-nCoV are most similar to those used in snakes.” https://www.google.com/amp/s/amp.cnn.com/
To anyone who actually researched the creation of the original “SARS-COV-2” genome, it is readily apparent that it is a fraudulent computer-generated creation stemming from the unpurified lung fluid of a single patient. The sequenced material could have come from multiple sources, including host DNA/RNA, bacteria, and microbes/microorganisms. It could have even come from outside contamination. There is no way to tell what the origin of the RNA is or even if it was a single source as no particles assumed to be “SARS-COV-2” were ever properly purified and isolated directly from the fluids of the sick patient before being sequenced. Thus, any relation this fabricated sequence has to any other sequence is invalid as the source was never identified to exist as a physical entity to begin with. Considering that the bat and snake “coronavirus” sequences for which the “SARS-COV-2” sequence was then compared to also come from unpurified sources, it is easy to see that any claims as to the origins of the sequenced material is a horrible foundation to build upon for an origin theory of a nonexistent “virus” and/or disease.
Even if this snake-venom connection was valid, the enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom. These peptides are “almost identical” to the venoms of animals and yet they are regularly found in healthy humans and other mammals. From his own source:
Like Venom Coursing Through the Body: Researchers Identify Mechanism Driving COVID-19 Mortality
“Researchers from the University of Arizona, in collaboration with Stony Brook University and Wake Forest School of Medicine, analyzed blood samples from two COVID-19 patient cohorts and found that circulation of the enzyme – secreted phospholipase A2 group IIA, or sPLA2-IIA, – may be the most important factor in predicting which patients with severe COVID-19 eventually succumb to the virus.
The sPLA2-IIA enzyme, which has similarities to an active enzyme in rattlesnake venom, is found in low concentrations in healthy individuals and has long been known to play a critical role in defense against bacterial infections, destroying microbial cell membranes.”
Thus, the snake enzymes are in fact normal human enzymes that are regularly found in healthy individuals. There is no mystery as to why these would be present in a sample. We should be able to put this “Covid” snake venom nonsense to bed right here. However, let’s press on a see what else we can uncover.
Antivenom = Monoclonal Antibodies
One thing I will give Dr. Ardis credit for is spotlighting the connection between the creation of antivenoms with the creation of monoclonal antibodies. The processes for both are very similar and the desired outcome is the exact same: the creation of theoretical antibodies. In the case of snake antivenom, it is normally created by a series of injections of the venom of a snake into an animal and then collecting the blood after a period of time. This is usually done through horses but other animals can be used as the host as well. Thus, the antivenom used for a snakebite victim is typically an injection of horse blood.
Both of these therapies have their basis in animal blood and the creation of the theoretical antibodies. Both are associated with toxic side effects. Sadly, while he was originally right about the fact that monoclonal antibodies are toxic and should not be used to treat the symptoms now collectively known as “Covid,” Dr. Ardis changed his tune when another doctor texted him asking if he would use antivenom for a snake bite:
“Last December, Dr Bryan Ardis received a text message from an Emergency Room physician friend of his that sent him down an unexpected and bizarre rabbit hole that may explain the adverse events from the vaccines that we’ve been reporting. The text read: “Hey Dr Ardis…If you got bit by a rattlesnake, would you go to a hospital and get anti-venom?”
“He says, “I realized, all of a sudden, monoclonal antibodies ARE anti-venom. The Federal Government doesn’t want us using anti-venom. Why are they fighting anti-venom and why are we finding anti-venom works against COVID? Is it not a virus? Is it a venom? This is what I want to know: Is COVID a venom and is this why they don’t want you using monoclonal antibodies?”
Do you see the trick? They want you to equate monoclonal antibodies with antivenom. This is supposed to be an “aha” moment where you realize that there is no way that you would not inject antivenom (i.e. horse blood) into yourself if bitten by a snake. It’s a no-brainer, right? We have all seen the movies where a person is bitten by a venomous snake and quickly dies if not given the antivenom.
If you are willing to accept the injection of horse blood into your body to survive a snake bite, why wouldn’t you also inject the cancer-cell cultured blood of genetically altered mice in order to combat “Covid?”
As Dr. Ardis points out, monoclonal antibodies are essentially antivenom. However, he wrongly states that monoclonal antibodies are an effective therapy. According to a September 2021 Cochrane review of the available studies, they found insufficient evidence to claim that monoclonal antibodies are an effective treatment for “SARS-COV-2:”
Are laboratory-made, COVID-19-specific monoclonal antibodies an effective treatment for COVID-19?
“The evidence for each comparison is based on single studies. None of these measured quality of life. Our certainty in the evidence for all non-hospitalised individuals is low, and for hospitalised individuals is very low to moderate.We consider the current evidence insufficient to draw meaningful conclusions regarding treatment with SARS-CoV-2-neutralising mAbs.”
In other words, the evidence for the usefulness of monoclonal antibodies is non-existent. Unfortunately, the Cochrane Review failed to point out that there are various risks and adverse reactions associated with their use:
Do mAbs have risks?
“Therapeutic mAbs, typically administered by intravenous (IV) infusion, have been a valuable and generally safe treatment option for a variety of conditions for many years. However, they are also known to cause a range of side effects and reactions, which can be immediate or delayed.Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity.”
In January 2022, the FDA restricted the use of some monoclonal therapies (Bamlanivimab and Etesevimab) that are authorized against “Covid-19” as they were shown to be ineffective:
Coronavirus (COVID-19) Update: FDA Limits Use of Certain Monoclonal Antibodies to Treat COVID-19 Due to the Omicron Variant
“In light of the most recent information and data available, today, the FDA revised the authorizations for two monoclonal antibody treatments– bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
Because data show these treatments are highly unlikely to be active against the omicron variant,which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. And like other infectious organisms, SARS-CoV-2 can mutate over time, resulting in certain treatments not working against certain variants such as omicron. This is the case with these two treatments for which we’re making changes today.”
On April 16th, 2022, the FDA revoked the use of Bamlanivimab alone as it’s benefits were shown not to outweigh its risks. Somehow despite this evidence, the FDA still allows for it to be used in combination with Etesevimab, even though they previously revoked their use together in January 2022:
Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab
“Today, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate COVID-19 in adults and certain pediatric patients. Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of SARS-CoV-2 viral variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure,the FDA has determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use. Therefore, the agency determined that the criteria for issuance of an authorization are no longer met and has revoked the EUA.
On Nov. 9, 2020, based on the totality of scientific evidence available at the time, the FDA issued an EUA to Eli Lilly and Co. authorizing the emergency use of bamlanivimab alone for the treatment of mild to moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progressing to severe COVID-19 and/or hospitalization. Importantly, although the FDA is now revoking this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone. The FDA believes that these alternative monoclonal antibody therapies remain appropriate to treat patients with COVID-19 when used in accordance with the authorized labeling based on information available at this time.”
If the FDA’s confusing revoking of the EUA’s of these monoclonal antibodies has you concerned that you will not be able to use them against an imaginary “virus,” don’t worry. The FDA authorized the use of a new “Omicron-specific” monoclonal antibody called Bebtelovimab on February 11th, 2022. Granted, it still carries the same risks, adverse side effects, and uncertainty over clinical worsening listed for the previously ineffective antibody therapies. From the FDA fact sheet:
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
“Possible side effects of bebtelovimab include itching, rash, infusion-related reactions, nausea and vomiting. Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other SARS-CoV2 monoclonal antibodies and could occur with bebtelovimab. In addition, clinical worsening following administration of other SARS-CoV-2 monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19.”
Coronavirus (COVID-19) Update: FDA Authorizes New Monoclonal Antibody for Treatment of COVID-19 that Retains Activity Against Omicron Variant
Hypersensitivity Including Anaphylaxis and Infusion-Related Reactions: Serious hypersensitivity reactions, including anaphylaxis, have been observed with administration of other SARS-CoV-2 monoclonal antibodies and could occur with administration of bebtelovimab. If clinically significant hypersensitivity reactions occur, discontinue and initiate appropriate supportive care. Infusion-related reactions may occur up to 24 hours post injection. These reactions may be severe or life threatening. (5.1)
Clinical Worsening After SARS-CoV-2 Monoclonal Antibody Administration: Clinical worsening of COVID-19 after administration of SARS-CoV-2 monoclonal antibody treatment has been reported and may include signs or symptoms of fever, hypoxia or increased respiratory difficulty, arrhythmia (e.g., atrial fibrillation, sinus tachycardia, bradycardia), fatigue, and altered mental status. Some of these events required hospitalization. It is not known if these events were related to SARS-CoV-2 monoclonal antibody use or were due to progression of COVID-19. (5.2)
Limitations of Benefit and Potential for Risk in Patients with Severe COVID-19: Treatment with bebtelovimab has not been studied in patients hospitalized due to COVID-19. Monoclonal antibodies, such as bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with COVID-19 requiring high flow oxygen or mechanical ventilation. (5.3)
It should be fairly clear that, unlike Dr. Ardis’ claims, monoclonal antibodies are not effective, carry numerous risky side effects, and can actually worsen the disease they are supposed to treat. Interestingly, this same risk of dangerous side effects and worsening disease outcomes is associated with snake antivenom as well. From the fact sheet of a commonly used antivenom for rattlesnake bites, we find these admitted side effects:
Rattlesnake Antivenin Side Effects Center
“Rattlesnake Antivenin (antivenin crotalidae polyvalent) is an antivenin product used only to treat envenomation caused by bites of crotalids (pit vipers) including rattlesnakes, copperhead and cottonmouth moccasins, and others. Common side effects of Rattlesnake Antivenin include allergic reactions such as flushing, itching, hives, swelling of the face/tongue/throat, cough, shortness of breath, blue color to the skin, vomiting, and anaphylaxis (severe allergic reaction).”
“Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered. An immediate reaction (e.g. shock, anaphylaxis) usually occurs within 30 minutes. Symptoms and signs may develop before the needle is withdrawn and may include apprehension, flushing, itching, urticaria; edema of the face, tongue, and throat; cough, dyspnea, cyanosis, vomiting, and collapse. There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use.”
“Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered.30 The incubation period may be less than 5 days, especially in those who have received horse-serum-containing preparations in the past. The usual symptoms and signs are malaise, fever, urticaria, lymphadenopathy, edema, arthralgia, nausea, and vomiting. Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis. Peripheral neuritis usually involves the shoulders and arms. Pain and muscle weakness are frequently present, and permanent atrophy may develop.”
Maybe the use of antivenom to treat a snakebite isn’t the super cure it has been sold to be? Is it possible that, as with many pharmaceutical products and interventions, the antivenom itself is creating the very symptoms it is said to treat? For some further insight, let’s look at a few highlights from an paper from September 2019, right before this “crisis,” which reviewed the use of antivenom and had a few revealing claims about the “anti” toxin. You will see it reiterated that the injection of antivenom created from either horse, sheep, goats, and/or rabbits can cause immediate hypersensitivity and anaphylaxis or a delayed “serum sickness” which can occur weeks after the treatment. It is stated that the antivenom has limited efficacy and can be entirely ineffective based on the geographic location. Improper use of antivenom contributes to increased servere outcomes and the production of antibodies in animals leads to a large number (70%) of immunoglobulins that do not react to snake venom:
Perspective on the Therapeutics of Anti-Snake Venom
3. Current Information in the Design of New Antivenoms
“Currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses [14,15]. Hyperimmunized animals produce antibodies against the venom proteins and serum is extracted from their blood for the treatment of envenomation [6,16]. Conventional serum therapy aims to bind and neutralize the snake venom proteins [17]. It is a fact that the antivenom allows the body to try to reverse the damage caused by the venom. However, it is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia. Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects [18];
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability;
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes;
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both.
“Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom. Around 70% of the immunoglobulins obtained do not act directly against venom toxins [26]. Despite the abovementioned facts, this is the only FDA approved therapy to treat snake venom.”
A few other studies also point out the severe reactions regularly attributed to the use of antivenom. The first is a study from 2016 which points out that not only are adverse reactions common, they occur at a high rate. It is stated that this is due to poor quality control and manufacturing problems:
Adverse reactions to snake antivenom, and their prevention and treatment
“Antivenom is the mainstay of treatment of snakebite envenoming. However, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent. Both acute (anaphylactic or pyrogenic) and delayed (serum sickness type) reactions occur. Acute reactions are usually mild but severe systemic anaphylaxis may develop, often within an hour or so of exposure to antivenom. Serum sickness after antivenom has a delayed onset between 5 and 14 days after its administration. Ultimately, the prevention reactions will depend mainly on improving the quality of antivenom.”
“The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors. This highlights the importance of addressing issues related to poor quality and potentially unsafe antivenom. Ultimately, the prevention of reactions will depend mainly on improving the quality of antivenom. Until these improvements take place, doctors will have to depend on pharmacological prophylaxis as well as careful observation of patients receiving antivenom in preparation for prompt management of acute as well as delayed reactions when they occur.”
This next source is from 2018 and it points out that early antivenoms were unsafe and caused severe life-threatening events. While they now have “acceptable” safety profiles, antivenoms still have varying quality and range from 10% adverse reactions to greater than 50%. This same variation in quality is seen in the production of monoclonal antibodies:
Antivenom therapy: efficacy of premedication for the prevention of adverse reactions
“However, in their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects [8]. The main reason was that first antivenoms were poorly purified preparations or crude sera. Over the years, for many of the original applications, heterologous serums were replaced by other drugs with better safety profiles, such as antibiotics, vaccines and homologous serums. However, in cases of envenomation by snakes, scorpions or arachnids, antivenoms remain the only effective treatment [4]. Currently, after many improvements, antivenoms exhibit acceptable safety profiles [1, 9, 10]. Nevertheless, antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50% [11, 12].”
In is interesting to note that there are many factors that are said to influence the severity of a venomous snakebite including the age, sex, and health of the person bitten as well as the type of snake, the geographical location of the snake, the season the bite occurred in, what the snake ate, and how recently the snake released its venom. Antivenoms themselves have been shown to have varying effects in quality due to the geographical location of the snake which somehow renders the antivenom ineffective and even dangerous in different countries and continents, even against the same type of snake. It is said that this has kept locals from seeking out medical care and sticking to traditional healers:
“Snake venoms are highly complicated. At least 26 separate enzymes have been identified with 10 of these enzymes common to all snake venoms (though in different concentrations). All snake bites are not equal. The quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously.”
“A study led by Dr Fry has found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions.
Researchers tested the effectiveness of two African and two Indian saw-scaled viper antivenoms against saw-scaled vipers from 10 regions.
The results showed that the two African antivenoms were only effective against snakes from restricted ranges.
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers.
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regions. It failed completely against African saw-scaled vipers.
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry says.
“In Kenya, snakebite deaths have increased dramatically after hospitals switched supplies of a very effective African antivenom with a cheaper Indian variety.”
“This creates a knock-on effect in these communities. It’s hard enough to convince people living in these regions not to go to traditional healers to treat snakebite. And if someone does seek proper medical care but dies because of ineffective antivenom, it will be even harder to convince the next victim to seek out antivenom.”
Viper venom’s lethal evolution
It’s the variety of the saw-scaled viper’s prey, from rodents to insects, that researchers say could be the reason why antivenom from one region might not work in another.
“Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes,” UQ PhD candidate in Toxinology Bianca op den Brouw wrote in an article for The Conversation.
“Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet.
“Different saw-scaled viper populations feed on different prey. The physiology of these prey animals differs, and this dictates what makes a toxin effective.
“From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom.”
Maybe the proceeding information on how snakebite antivenoms are created as well as the high rate of adverse events from the antibodies used for antivenom now has you questioning that initial “no-brainer” thought: “Of course I would use antivenom if bit by a snake.” If so, you are on the right track as, based on information from the African Snakebite Institute, in most snake bite cases, antivenom is not used and many snake bites are often unattended and/or unreported. In fact, it is apparently a well-known “myth” (i.e. truth in this case) that the antivenom kills more people than the snake venom itself. Most people (over 80%) never receive antivenom as, like the previous sources stated, it can have disastrous side-effects. Most snake bites do not cause symptoms warranting the use of something so toxic. In fact, snake bite victims are not immediately injected with antivenom and typically are sent home after observation:
“Yet people often have a poor understanding of how it works and there are endless myths about antivenom killing more people than the snake venom itself.”
“Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite) as most victims are not severely envenomated or the bite may be from a snake that is not considered potentially deadly or is not covered by the antivenom (Rhombic Night Adder, Berg Adder and Stiletto Snake). Antivenom is relatively scarce, expensive and can have disastrous side-effects. The biggest danger is an acute allergic reaction (anaphylaxis) or, to a lesser degree, serum sickness that can affect the immune system several days after treatment.”
“Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use. The majority of snakes have control over their venom glands and are quite reluctant to waste their venom on humans. They very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious. Such patients are usually hospitalised for a day, carefully monitored and then sent home.”
“As already mentioned, some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used. Some of those victims go into anaphylactic shock which is a life-threatening medical condition and must be treated with adrenaline. This has to do with the fact that our antivenom is made from horse blood and the allergy is basically an allergy to horse proteins.”
Bill Haast – repeated snake bite victim from the world’s deadliest snakes tragically died at the young age of 100 from natural causes. ?
If snake bites regularly do not cause symptoms and do not require the use of antivenom, are snake bites really as toxic and harmful as we previously thought? Are the dangerous side effects linked to snake bites really just the reactions to having horse blood injected into the body as treatment? Is this another case where the treatment causes the symptoms of disease it was supposed to prevent? If the examples of these next few individuals are taken into consideration, it’s entirely plausible to conclude that we have been misled about the dangers stemming from snakebites in order to cover for the toxic effects of the treatment:
Repeated snake bite for recreation: Mechanisms and implications
“There is a debate in the fatality/immunity due to repeated snake bites in human beings either accidentally or incidentally. Haast and Winer[11] reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus[11] and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier.”
This snake-man got himself bitten over 200 times to become immune to venom
“Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was fatally injured about 20 times.”
“In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times as per the report published in Today I Found Out.“
Man makes deadly snakes bite him 160 times in hunt for human antidote
“An amateur scientist has deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom.
Tim Friede is obsessed by finding a human antidote to poisonous snake bites, which kill an estimated 100,000 people every year.
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra.
He said he experienced a “real throbbing sensation” but he “felt great” after the bites.
“It really hurts and it swells but that’s it,” he said.”
Poison pass: the man who became immune to snake venom
“A lot has been written about Steve Ludwin, widely known as the man who injects snake venom, and lately his life has turned into a non-stop frenzy of international journalists and film crews revelling in the seeming sheer insanity of it.”
“He’s been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years. “Snakes are fucking everywhere. The symbol for medicine is two snakes. They’re ingrained in our brain and DNA,” he tells me, proudly insisting that he hasn’t been ill for decades and has developed “a superhuman immune system”. And it’s tempting to believe him. He does look undeniably fit.”
The Photographer Who Was Bitten by a Black Mamba… and Got the Shot “After several minutes and then hours passed and Laita was still feeling fine — experts recommend heading straight for a hospital, by the way — the crew concluded that Laita didn’t have any venom in his system. The photographer believes that it was either a “dry bite,” when a snake doesn’t release any venom, or that his heavy flow of blood pushed out the venom.”
As can be seen, there are numerous examples of people being deliberately and accidentally bitten by the world’s deadliest snakes who are completely fine and do not require treatment from antivenom whatsoever. Are we to conclude that these people are the lucky few who somehow have amazing super-human “immune” systems that render snake venom ineffective? Or have snake bites and the associated symptoms of venom toxicity been blown out of proportion? Could this be a case where some have had bad reactions to a snake bite just as there are those who have severe allergic reactions to bee stings while the majority of snake bite and bee sting victims come away unscathed? Could this be similar to the supposed rabies cases where the majority of those who were bitten by “rabid” animals actually went on to be just fine without getting the rabies vaccination?
The Treatments Are Worse Than the Disease
It’s very apparent that in the case of monoclonal antibodies and anivenom, the adverse effects of the drugs are actually worse than the supposed diseases they are meant to treat. Could this be due to the fact that, like “viruses,” so-called antibodies have never been properly purified, isolated, and proven to exist? The results of studies using antibodies are regularly unreproducible and irreplicable. It is well-known that antibodies are in fact not as specific as are they are claimed to be and are said to regularly bind to the wrong proteins. Perhaps it is difficult to produce safe and effective products when the entities that are supposed to be produced and supplied in the animal blood are entirely theoretical? Maybe the ridiculous snake venom theory should be viewed in the context that it is a bad idea to be injecting anything, let alone animal blood, into our bodies in an attempt to make ourselves feel better when trusting the body and allowing it to heal is often times the best course of action we can take.
In Summary:
Dr. Bryan Ardis put forth a theory that snake venom is the cause of “Covid-19” primarily based on fraudulent genomic data
The snake connection stems from research linking proteins from the fabricated “SARS-COV-2” genome to bat and snake “coronavirus” proteins
The enzyme phospholipase A2 group IIA or sPLA2-IIA, which Dr. Ardis bases much of his claims on, only has similarities to rattlesnake venom
These peptides are “almost identical” to the venoms of animals and are regularly found in healthy humans and other mammals
Dr. Ardis pointed out that, based on a text, he uncovered the connection between antivenom and monoclonal antibodies and stated that theyare the same thing
He wrongly concluded that monoclonal antibodies are an effective treatment for snake poisons that could be in the vaccines, Remdesivir, and water
According to a Sept 2021 Cochrane Review, their certainty in the evidence for the use of monoclonal antibodies in the treatment of “Covid” for all non-hospitalised individuals was low, and for hospitalised individuals was very low to moderate
They considered the current evidence insufficient to draw meaningful conclusions regarding treatment with “SARS-CoV-2-neutralising” mAbs
Monoclonal antibodies are known to cause a range of side effects and reactions, which can be immediate or delayed
Serious adverse events associated with mAbs include infusion reactions, acute anaphylaxis, and serum sickness, as well as longer-term complications such as infections, cancer, autoimmune disease, and cardiotoxicity
In February 2022, the FDA revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments
The data showed these treatments are highly unlikely to be active against the omicron variant which is circulating at a very high frequency throughout the United States
These treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens
In April 2022, the U.S. Food and Drug Administration revoked the emergency use authorization (EUA) that allowed for the investigational monoclonal antibody therapy bamlanivimab, when administered alone, to be used for the treatment of mild-to-moderate “COVID-19” in adults and certain pediatric patients
Based on its ongoing analysis of emerging scientific data, specifically the sustained increase of “SARS-CoV-2 viral” variants that are resistant to bamlanivimab alone resulting in the increased risk for treatment failure, the FDA determined that the known and potential benefits of bamlanivimab, when administered alone, no longer outweigh the known and potential risks for its authorized use
Importantly, although the FDA revoked this EUA, alternative monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab, administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously authorized for bamlanivimab alone
In other words, the use of Bamlanivimab and Etesevimab was revoked as well as the use of Bamlanivimab but they can still be used together as an alternative to Bamlanivimab alone…
For the Omicron-specific Bebtelovimab authorized by the FDA in February 2022, possible side effects include
Itching
Rash
Infusion-related reactions
Nausea
Vomiting
Serious and unexpected adverse events including hypersensitivity, anaphylaxis and infusion-related reactions have been observed with other “SARS-CoV2” monoclonal antibodies and could occur with bebtelovimab
In addition, clinical worsening following administration of other “SARS-CoV-2” monoclonal antibody treatment has been reported and therefore is possible with bebtelovimab
The FDA claims that it is not known if these events were related to “SARS-CoV-2” monoclonal antibody use or were due to progression of “COVID-19”
Treatment with Bebtelovimab has not been studied in patients hospitalized due to “COVID-19”
Monoclonal antibodies, such as Bebtelovimab, may be associated with worse clinical outcomes when administered to hospitalized patients with “COVID-19” requiring high flow oxygen or mechanical ventilation
Antivenom carries the same risks of severe side effects and worsening condition as monoclonal antibodies
The listing for common side effects of Rattlesnake Antivenin include allergic reactions such as:
Flushing
Iitching
Hives
Swelling of the face/tongue/throat
Cough
Shortness of breath
Blue color to the skin
Vomiting, and anaphylaxis (severe allergic reaction)
Immediate systemic reactions (allergic reactions or anaphylaxis) can occur whenever a horse-serum-containing product is administered
There have been isolated reports of cardiac arrest and death associated with Antivenin (Crotalidae) Polyvalent (equine origin) use
Serum sickness usually occurs 5 to 24 days after administration and its frequency may be related to the number of Antivenin vials administered
The usual symptoms and signs are:
Malaise
Fever
Urticaria
Lymphadenopathy
Edema
Arthralgia
Nausea
Vomiting
Occasionally, neurological manifestations develop, such as meningismus or peripheral neuritis
Peripheral neuritis usually involves the shoulders and arms and pain and muscle weakness are frequently present, and permanent atrophy may develop
A 2019 review on antivenom stated that currently, the only accepted treatment for snakebite envenomation involves intravenous administration of conventional antivenoms comprising antibodies or antibody fragments derived from the plasma of large mammals (generally horses, but also sheep, goats, or rabbits) that have been previously immunized with non-lethal venomous doses
It is known that such therapy can cause problems related to different antivenom characteristics, such as:
Immediate hypersensitivity reaction to the alien immunoglobulins, including anaphylactic and pyrogenic reactions such as chills, rigor, headache, and tachycardia.
Delayed antivenom reactions or serum sickness is observed after 8 to 12 days of treatment; these are characterized by cutaneous eruptions, fever, and allergies, among other effects
Limited efficacy of antivenom therapy to protect the affected organ/s against immediate local tissue damage and low stability
Ineffectiveness of the antivenom due to significant geographic variation in the composition of the venom;
Antigenic reactivity due to the taxonomic diversity of the snakes
Improper use of the antivenom due to incorrect medical management, which contributes to a high incidence of adverse reactions, a low toxin neutralizing potency, or both
Current antibody production faces challenges during the immunization of the animal (equine or ovine), leading to the production of a huge number of antibodies that are not related to the snake venom
Around 70% of the immunoglobulins obtained do not act directly against venom toxins
According to a 2016 study, adverse reactions to snake antivenom that is available are common in many parts of the world where snakebite is prevalent
The high rate of acute adverse reactions to antivenom is an example of how poor manufacturing and quality control by antivenom producers cause problems for patients and their doctors
The prevention of reactions will depend mainly on improving the quality of antivenom
According to their initial applications, antivenoms did not exhibit good safety results and could even cause life-threatening side effects
Currently, after many improvements, antivenoms exhibit “acceptable” safety profiles yet antivenom quality still varies widely depending on the producer, while some antivenoms exhibit adverse reaction rates of less than 10%, others have values of greater than 50%
All snake bites are not equal and the quality of venom depends not only on the type of snake but on the season, the geographical region, the age of the snake, and how recently it has released venom previously
A study led by Dr. Fry found that antivenoms produced using snakes from one region may perform poorly or fail completely against the same species of snakes from other regions
The results showed that the two African antivenoms were only effective against snakes from restricted ranges
One antivenom performed well against West African saw-scaled vipers and the other performed best against the East African saw-scaled vipers
The Indian antivenom only worked against saw-scaled vipers from the region where the antidote was produced and failed against toxins from other Indian regionand it failed completely against African saw-scaled vipers
“These antivenoms are being sold and used interchangeably to treat all saw-scaled viper bites, and in many cases they are not working,” Dr Fry said
If someone does seek proper medical care but dies because of ineffective antivenom,it will be even harder to convince the next victim to seek out antivenom
Antivenom is effective and reliable when venom composition does not vary greatly between individual snakes
Unfortunately, the venom composition from saw-scaled vipers varies between populations and is thought to be partly due to an evolutionary adaptation linked to their diet
From a medical perspective, this means that the antibodies in an antivenom may not be able to adequately recognise and fight all the harmful toxins in the venom
There are endless myths about antivenom killing more people than the snake venom itself
Few snakebite victims are treated with antivenom (less than 20 % of those hospitalised after a snakebite
Antivenom is relatively scarce, expensive and can have disastrous side-effects
Snakebite victims are not automatically injected with antivenom as most of them never experience symptoms severe enough to justify its use
Snakes very often give ‘dry’ bites with no subsequent symptoms of envenomation or the snake might inject a little bit of venom that will cause discomfort or some symptoms but nothing serious
Such patients are usually hospitalised for a day, carefully monitored and then sent home
Some snakebite victims quickly have an allergic reaction to antivenom and this happens in more than 40% of all cases where antivenom is used
This has to do with the fact that antivenom is made from horse blood and the allergy is basically an allergy to horse proteins
Haast and Winer reported complete recovery of a patient without any specific therapy even after bitten by a deadly snake Bangarus Caeruleus and the authors attributed it to cross protection of existing antibody between species of Bangarus and Indian, African and Egyptian cobras, as he had a history of bites from these snakes earlier
Bill Haast, a scientist turned snake-man from America, was bitten at least 173 times by poisonous snakes in his life till mid-2008 of which he was seriously injured about 20 times
In the 1950s, he had few ill-effects and didnt need any anti-venom in spite of the fact that he was bitten by the cobras about 20 times
An amateur scientist named Tim Friede deliberately endured more than 160 self-inflicted snake bites in a bid to become immune to venom
Mr Friede was recently bitten by a taipan and a black mamba, two deadly snakes he keeps at his home in Wisconsin, USA, in addition to his two rattlesnakes and water cobra
He said he experienced a “real throbbing sensation” but he “felt great” after the bites
Steve Ludwin, widely known as the man who injects snake venom, has been shooting, swallowing and scratching venom into his skin from some of the world’s deadliest snakes for 30 years
He hasn’t been ill for decades and has developed “a superhuman immune system”
A photographer was bit by the deadliest snake, a Black Mamba, and after hours passed, he was still feeling fine and needed no treatment
The snake venom theory by Dr. Bryan Ardis is built upon the interpretation of the unpurified fraudulent “SARS-COV-2” genome which is itself built upon references to other fraudulent genomes of human and animal “coronaviruses” created in the very same way. Attempting to claim any connections between the random A,C,T,G’s in a computer database is a useless and pointless exercise as the RNA that was fabricated into the genome of a “virus” was never purified, isolated, and proven to physically exist in the first place. Thus any connections between the protein codes said to belong to a “virus” which are then said to be closely related to supposed snake “coronaviruses” is immediately invalid.
Using this invalid premise to then claim that people have been poisoned by snake venom in the vaccines, the drugs, and the water supply is nothing but unsubstantiated science fiction that seems designed to have a few purposes:
To keep people engaged in the lie that a new disease known as “Covid-19” exists and that there is a singular cause.
To restore faith in monoclonal antibodies and other toxic alternative treatments.
To use the theory to promote and sell anti-venom supplements.
To divide and distract those questioning the official narrative.
To make the “Truther” community look foolish by falling for loosely tied-together circumstantial evidence that is easily debunked.
If we are to take the claims of Dr. Ardis seriously that the symptoms associated with snake venom is the true cause of a disease known as “Covid-19,” how does his theory explain for the fact that the antivenom and monoclonal antibody treatments cause the exact same symptoms of the disease they are supposed to treat? How would it be determined that the worsening clinical outcomes after injection are from the snake bites/venom rather than the antivenom/monoclonal antibodies given as treatment? How does his theory account for the numerous instances where people have been deliberately bitten by snakes, injected with the venom of snakes, and drank of the venom of the snakes with little to no harmful effects whatsoever? How does his theory account for the fact that the vast majority of “Covid” cases are asymptomatic and the vast majority of snake bite cases need no treatment at all? There are many holes in this theory which will easily be picked apart to make those who follow it look foolish for having done so.
There is no “SARS-COV-2.” There is no “Covid-19.” There is no new disease nor any new symptoms of disease requiring treatment from vaccines, monoclonal antibodies, Remdesivir, Hydroxychloroquine, Ivermectin, NAC, nor any other treatment. There is no need for any anti-venom supplements.
Beware those who will sell you the cause of the disease and the solution.
In a stunning move – soon to be filed under the “completely lost touch with America” folder – the Biden administration is reportedly planning to appeal the ruling that lifted the COVID mask mandate on travel, just hours after most major airlines and airports (and ground transportation) has dropped their mask rules.
It was evident this was coming earlier in the day after White House spokesperson Jen Psaki warned and Xavier Becerra, Biden’s health secretary, told reporters in Nevada, that “we are right now in the process of deciding, and we likely will appeal that ruling, but stay tuned.”
Jonathan Turley offered some insight before the actual decision was made to appeal if CDC thinks it necessary:
The Administration is going to have a hard time making this cat walks backwards. The cheering of passengers and pilots seemed as much as a communication to the Administration as it was a celebration. A large number of airlines immediately declared the mandate to be dead and unenforceable. It is like throwing a retirement party for an employee before they have decided to go. It is a tad awkward to express doubts when someone is showing you the door.
That is why those cheering videos could have a greater impact on the White House than any CDC or DOJ recommendation. The Biden Administration could still appeal as it has in past such cases. There will certainly be many DOJ lawyers asserting that they could win on appeal on the basis of agency deference. The question is who would tell the public. They may have to wait for the “ding, dong” parties to end.
But, given all that, they decided it was worth it…
Justice Department Issues Statement on Ruling in Health Freedom Defense Fund Inc, et. al. v. Biden, et. al.
WASHINGTON – The U.S. Department of Justice today released the following statement on Health Freedom Defense Fund Inc., et. al. v. Biden, et. al. from spokesman Anthony Colev:
“The Department of Justice and the Centers for Disease Control and Prevention (CDC) disagree with the district court’s decision and will appeal, subject to CDC’s conclusion that the order remains necessary for public health. The Department continues to believe that the order requiring masking in the transportation corridor is a valid exercise of the authority Congress has given CDC to protect the public health. That is an important authority the Department will continue to work to preserve.
“On April 13,2022, before the district court’s decision, CDC explained that the order w’ould remain in effect while it assessed current public health conditions, and that the Transportation Security Administration would extend its directive implementing the order until May 3 to facilitate CDC’s assessment.
“If CDC concludes that a mandatory order remains necessary for the public’s health after that assessment, the Department of Justice wall appeal the district court’s decision.“
So, if the CDC – against all the actual science – concludes that wearing a mask should remain mandatory, instead of leaving it as a personal decision, the Biden DoJ will appeal the ruling that was celebrated by most.
The more we ponder this decision, the more this smells like The DoJ throwing The CDC under the bus. The reason being that The CDC now has to come up with some “science” reason to re-mandate the masks (which we know they can’t) and therefore The DoJ is therefore covered if people try to blame them for not appealing.
And the winner of the most ironic sentence of the day goes to White House spokesperson Jen Psaki, who after relying on court ruling after court ruling to enforce varying levels of health tyranny for the last 15 months, uttered the following in her out-loud voice…
“Public health decisions shouldn’t be made by the courts. They should be made by public health experts.”
Who said the left doesn’t do humor… talking of which…
Babylon Bee has some advice for those still living in fear:
It can be difficult, though, to suddenly see all those triggering human faces after the government coddled you and fed your psychotic delusion and fear for the last two years.
Here are seven ways to cope:
Close your eyes and imagine everyone is wearing a full hazmat suit. – It’s a neat little trick that actually works.
Scream at the sky. – This is a well-known coping mechanism. It works especially well if you record your scream onto your TikTok account.
Play The Sims 4 and manage other people’s lives like you’re an all-powerful god to your heart’s content. – Now you can drown people by surrounding their swimming pools with an impenetrable wall of potted plants. You’re in charge here!
Upgrade to 3 or 4 masks, or just roll around in a giant hamster ball. – Keep upping the number of masks you wear, but if that’s not enough, go the hamster ball route.
Get your pilot’s license and start your own airline. – aIrLiNeS aRe PrIvAtE cOmPaNiEs ThEy CaN dO wHaT tHeY wAnT!
Just remember, we’re all in this together. – It’s just for a little while. It’s a small sacrifice to make. If it saves one toddler from a speech impediment it’s all worth it.
Never go outside again. – Curl up in a ball and live out the rest of your days in the corner of your home, completely safe from COVID.
Bear in mind that nothing is stopping the fearful from ‘masking up’ against the virus…
“you are free to wear masks if you like… if they work, they will protect you, if they don’t why mandate them?”
Presumably there are a number of “political science” reasons for the appeal:
1) “Trump” judge
2) Offering a bone to whatever is left on the ‘Democratic base’ amid the unhinged rantings of the blue-checks on Twitter as the dissonance suddenly strikes that they have been wearing face diapers for 2 years for no reason.
3) Making sure to maintain the role as the “party of science“…
4) …ok we couldn’t think of any more… apart from ‘scream to the sky’
Following a federal judge vacating the federal mask mandate on transportation, the TSA responded, “TSA (Transportation Security Administration) will not enforce its Security Directives and Emergency Amendment requiring mask use on public transportation and transportation hubs at this time.”
Within hours various airlines began notifying customers the mask mandate is gone:
♦ American Airlines – “In accordance with the Transportation Security Administration no longer enforcing the federal face mask mandate, face masks will no longer be required for our customers and team members at U.S. airports and on domestic flights.” (link)
♦ Southwest Airlines – “As a result of this development, effectively immediately, Southwest Employees and Customers will be able to choose whether they would like to wear a mask, and we encourage individuals to make the best decision to support their personal wellbeing.” (link)
♦ Delta Airlines – “Effective immediately, masks are optional for all airport employees, crew members and customers inside U.S. airports and on board all aircraft domestically, as well as on most international flights.” (link)
♦ Alaska Airlines – “Effective immediately, all Alaska Airlines and Horizon Air guests and employees have the option to wear a mask while traveling in the U.S. and at work. Masks are no longer required for travel and will be optional.” (link)
♦ United Airlines – No press release. “Masks are no longer required on domestic flights, select international flights (dependent upon the arrival country’s requirements) or at U.S. airports. More comfortable keeping yours on? Go right ahead… the choice is yours (you look dino-mite either way)!” ~Twitter
Various videos show airline employees in a state of jubilation cheering the announcements.
The professional political left is very sad, apoplectic and filled with anxiety. However, the overwhelming majority are happy. This example again reflects how small that minority of rabid maskers was. Easily a 4:1 ratio. Additionally, with all the major carriers and the TSA making official statements, it would be almost impossible to reinstate the mask mandate now. It’s over.
Plane applauded as the stewardess announced the end of the mandate. She broke into tears as she got to take off her mask for the first time in 2 years pic.twitter.com/WlCpZk30QM
“Ladies and gentlemen, this is your pilot speaking. This is the most important announcement I’ve ever made. The federal mask mandate is over. Take off your mask if you choose!”
A federal judge in Tampa, Florida has vacated the federal transportation mask mandate for planes, trains, buses and public Transportation. [PDF Ruling Available Here]
In essence, U.S. District Judge Kathryn Kimball Mizelle found the CDC exceeded its statutory authority with the mask mandate and violated the rules that guide CDC regulations. After Joe Biden arbitrarily announced the federal transportation mandate, the CDC triggered enforcement of the mask mandate without any required time for public feedback on a new regulation.
Within the ruling, one of the commonsense arguments against the federal mandate was noted. Prior to Joe Biden taking office there was no mask mandate. At the time Joe Biden took office and invoked the mask mandate, there was nothing substantively different in/around the spread of COVID-19 and the mitigation efforts underway.
The federal mask mandate was arbitrary and capricious with no justification from the CDC and no required time for the public to provide feedback. The government’s legal argument was that public feedback, comments on rulemaking, was irrelevant because the mandate was going to be enforced regardless of public opinion. That argument was summarily dispatched by the judge saying, just because the government has a pre-determined outcome in mind does not relinquish them from the obligation to follow the rules.
Sensing they were going to lose the case, remarkably the government lawyers argued that only the original plaintiffs in the lawsuit should be granted relief. Meaning, only the two people who filed the lawsuit should be exempt from the federal mask mandate. That didn’t work.
The federal transportation mask mandate is vacated.
Dr. Tom Cowan on “the Snake Venom Stuff”: Covid Caused by a Specific Snake Venom Is Looking Like Pure Fantasy & Remdesivir Is Definitely Not Snake Venom
Right I can imagine there still may be a lot of questions about the snake venom stuff. And we are still looking into that, so I don’t want to say too much.
For those of you who want something to look at right away, I would say I would check out Amandha Vollmer’s — she did a webinar or talk or something. And if somebody has that they could put that in the chat. So that would be a good place to start.
There’s been a lot of other people who’ve weighed in on that. And all I can say for sure that we found out right now is that remdesivir is definitely not snake venom. And that putting any kind of snake venom in the water and have it orally ingested would probably do nothing. In fact it would do nothing.
And the idea that there’s a covid specific disease caused by a specific poisoning with a specific snake venom is looking like pure fantasy.
But hopefully we’ll have more information about that. In the meantime, there’s some places to check out that really go through this in some detail.
For those interested in the difference between being bitten (or injected) with snake venom and drinking venom (note that this is pure venom, not diluted in a vast water supply), we share this video:
“Darkness has the ability to cover up; light has the ability to uncover! Darkness is the enemy of truth; light is the friend of truth!
~ Mehet Murat ildan
Sometimes acceptance of obvious truth is so stark and thought to be fraught with treachery, that it is literally ignored by the many; making it more comfortable to remain hidden in madness amidst the shadows of deception and lies. While taking responsibility is the only way forward, fear of the truth often wins out, as reliance on collective ignorance gives the false illusion of safety. This behavior is always severely destructive over time, and any psychological relief always temporary, but much more often than not, it is the easy way out for the non-thinking and frightened societal herd. This natural flaw in the makeup of man is well known by the ruling class, and therefore taken advantage of in order to quell dissent and rebellion while gaining further control.
Considering our recent and current history, this was the tactic used for the entirety of the ‘covid’ scam. So long as voluntary acceptance of state propaganda by the masses prevails, this strategy will continually be used going forward in order to perpetuate the advancement of the takeover of humanity in the name of the “Great Reset.” That brings us to the latest threat by the purveyors of evil who have been allowed to rule without resistance. They claim, as voiced by former Trump appointed director of the CDC, Robert Redfield, that the next wave of monumental death worldwide will be due to a non-existent mystery bird flu. This approach by government to manufactured threats, has been around for a very long time, and in the past has been used to frighten the weak, but it is simply a lie.
Threats of avian bird flu, swine flu, including SARS, among many others, have been weapons of the state meant to accelerate panic where none is warranted for very many years. It is imperative to understand that these toxic concoctions are all manmade in labs using gain of function to create bio-weapons. They are not natural, or some lethal strain that just so-happened to affect birds or other animals by accident, and magically jumped to humans. Even the idea of this is ludicrous. If in fact, any such sickness or disease of these types were actually causing mass death, it would only be due to a purposeful release of a bio-weapon by the state, not any innate strain of a normal malady. Knowing this, how could entire populations continue to be so fooled by propaganda?
In 1997, the CDC said that “avian influenza A(H5N1) viruses first spread from poultry to infect humans in Hong Kong resulting in the deaths of 6 of 18 infected persons.” Because of this, the evil WHO and the U.S. sought to increase pandemic preparedness, obviously knowing that this would be useful indoctrination in order to create panic due to future plans to gain power over society. All of this was aligned with the WHO’s “global framework.”
In 2002, SARS was said to be the new disease to fear, and SARS-CoV was to be the “model for future pandemics.” In March of 2003, the ‘novel’ coronavirus, SARS-CoV, was said to be isolated, a lie, and identified and sequenced by nothing other than PCR, an impossibility. There was even the spectre of a future “catastrophic pandemic,” and investigations of live animal markets, as the supposed first case was found in Hong Kong, and said to be able to spread by infected persons traveling by airplane. Does this sound familiar or suspicious to any thinking individual? Is this not the same exact fraud that took place beginning in 2020, two decades later?
In March of 2006, Michael Chertoff, head of Homeland Security, an obvious expert on bird flu, was worried about a bird flu strike any day. “I can’t predict, but I certainly have to say that we should be prepared for the possibility that at some point in the next few months, a wild fowl will come over the migratory pathway and will be infected with H5N1.”
As far back as 1976, the H1N1 Swine Flu hoax took center stage, as the government and its controlled media propaganda campaign went into high gear in order to create a pandemic fraud so as to mass-vaccinate the U.S. population against a non-existent ‘swine flu.’ This conspiracy was also used as a way to get all ‘vaccinations’ available into every person possible. This led directly to 45 million people getting unnecessary injections. At the time, the CDC stated that 80% of the population needed to be ‘vaccinated,’ just as was sought in the ‘covid’ scam.
Again in 2009, the H1N1 fraud was revived, and another government call for mass ‘vaccination’ was issued. As always, the collusion between national and global ‘health organizations, government and government officials, pharmaceutical companies, and corporate insiders was evident. Nothing today has changed, it has only gotten worse, and in fact, the risk now due to the world takeover plot is much more sinister, and globally structured.
In the distant past, while control was a key factor, money from mass ‘vaccination’ was the primary goal. Today, money is a factor, but control of the minds and bodies of the proletariat herds is the result most desired by the ruling ‘elites.’ In addition, depopulation and eugenic transformation of the rest of society, all by way of controlling and lethal injection of a bio-weapon, is what is needed in order to finish the global takeover agenda.
This is a long-term plot to fool the public into believing and expecting that a future pandemic of epoch proportions is imminent. The very idea that ‘natural’ pandemics are inevitable has long been planned and embedded in the minds of the people. This is a multi-decade brainwashing of the common people in order to prepare them for not only mass sickness and death, but also for acceptance of a global governing body with unlimited power.
The most sought-after goal at this time is mass ‘vaccination,’ but this time is different in that the preferred injections are much more dangerous, much more able to physically and psychologically control large numbers of those who have taken the jab, and cause mass death beyond anything seen before. In order to accomplish such a deadly and evil agenda, the people will need to be fooled once again. They will have to believe the lies, and accept that all the impending deaths due to the weaponized ‘covid’ injections, are in fact due to a fraudulent and purposely crafted plot to place blame on a non-existent ‘virus’ that is being called an “avian bird flu.”
The ‘warning’, or more accurately, the foretelling of mass death by the ruling class, as outlined by the ex-CDC commandant Robert Redfield, is that 800 million to 4 billion of us will die due to some mystery bird flu. When the mass deaths occur, it will not be due to any flu or ‘virus,’ it will be due only to the toxic poison that has been previously injected into billions of unsuspecting, order-following slaves to the state.
What type of contamination might be found in a spiked COVID vaccine?
“A foreign body.”
The lot is being recalled due to a foreign body being found in one vial in the lot manufactured at the company’s contract manufacturing site, ROVI – Moderna and ROVI Pharma Industrial Services
Moderna Pharmaceutical, formerly named ModeRNA Therapeutics, became a public company in 2018, specializing in infectious diseases. Prior to the IPO, AstraZeneca was its third-largest investor.
Moderna’s coronavirus shot, known as “SPIKEVAX,” was said to have been approved by the U.S. Food and Drug Administration (FDA) for adults 18 and older on Jan. 31, 2022. But according the the FDA Factsheet, the shot is still only Emergency Use Authorized or EUA. Not approved!
Since November 2020, two of the 4 Biotech companies working to manufacture mRNA “therapies,” — Johnson & Johnson and AstraZenica — had to halt trials over safety concerns. And now the spotlight shines on Moderna’s mRNA vaccine deployment in Europe.
The contaminated lot in question was manufactured at the ROVI site in Spain, and distributed in Norway, Poland, Portugal, Spain, and Sweden from 13-14 January 2022. Reports tie the recalled batches to the Spanish company, ROVI.
Criminal Acts
Will Moderna be investigated for fraud, product safety, death by vaccine?
In February 2021, US officials investigated and acknowledged a “likely association” between Moderna and Pfizer vaccines and myocarditis in adolescents and young people. Of course, the PREP Act and CARES Act both limit liability for death or serious physical injury resulting from these products. See also Moderna’s disclosure in the SPIKEVAX package insert, referencing Myocarditis and Pericarditis, Section 5.2.
All Phase 3 COVID-19 vaccine trails are ongoing and not due to conclude until late 2022/early 2023. The treatments are currently experimental with only 1 year of short-term data and no long term safety data available.
In November 2020 Dr Andreas Noack, a German chemist and one of the EU’s top graphene experts, released a video explaining that he had discovered graphene hydroxide contained in the COVID-19 experimental treatments. He described how the graphene hydroxide nano structures injected into the human body act as ‘razor blades’ inside the veins of recipients and how they would not show up on an autopsy or normal toxicology tests given their atomic size. On 26th November 2021, just hours after publishing his latest video about graphene hydroxide, he died in suspicious circumstances. [See Summary].
Professor Dr Pablo Campra, University of Almeria, Spain also examined Covid-19 experimental treatments in November 2021 using Micro-Raman Spectroscopy, the study of frequencies. He also confirmed the presence of graphene oxide.
Today’s high drug prices show little has changed since 1963, when The Federal Trade Commission ruled that six of the nation’s largest drug companies were conspiring to fix prices on tetracycline, the most widely used antibiotic. The Kefauver drug hearings confirmed the existence of a national crime syndicate and revealed lax enforcement that continues to this day. Note, one of the “big six” criminals, Wyeth Pharmaceuticals, was absorbed by Pfizer.
Gene Therapy or Gene Reset?
Experts contend that the technology in the Pfizer/BioNTech and Moderna shots are not “gene therapy.” But that is not how the experimental products had first been marketed.
According to a November 2021 article at LifeSiteNews, during the 2021 Global Health Summit in Berlin, Bayer executive, Stefan Oelrich, told fellow “experts” that the mRNA COVID “vaccines” are actually “cell and gene therapy” that would have otherwise been rejected by the public if not for a “pandemic” and favorable marketing.
Oelrich also highlighted the term, “Bio Revolution” as:
a confluence of advances in biological science and accelerating development of computing, automation, and artificial intelligence [that] is fueling a new wave of innovation.
As part of his company’s role for “sustainability” Bayer also pledged to push contraception on 100 million women across the world. This rhetoric fits hand-in-glove with Klaus Schwab’s Socialist plan for the “Great Reset.”
Damage from the mRNA injectables are surfacing. According to an October 2021 study in the American Journal of Cardiology:
Sixty percent of the myocarditis related COVID-19 vaccine cases were associated with the Pfizer-BioNTech vaccine, 33% were associated with the Moderna vaccine, and 7% were associated with the Johnson & Johnson vaccine.
According to a November 2021 abstract published in the Journal Circulation titled, “Observational Findings of PULS Cardiac Test Findings for Inflammatory Markers in Patients Receiving mRNA Vaccines:”
…the mRNA vacs numerically increase all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle…
Ignorance Is No Excuse
Ignorance is no excuse in the Age of Information. As more information surfaces, do not expect drug companies to change their criminal ways.
The information is available and viewable for anyone who can do a Google search. Drug companies have subtly disclosed the information if you can read about it here.
If any change will come of these revelations, that change rests with each of us. There are no “good” or “bad” experiences. There is only “experience” from which we all choose to learn more.
Children today are being systematically and deliberately destroyed – both mentally and physically.
We are horrified at the way children were pushed up chimneys in the 19th century. Making children work long, arduous hours was considered normal at the time but the children abused in this way were scarred physically and mentally for life.
Today, we like to think that that sort of cruelty is today confined to those parts of the world where children are employed as slave labour in order to dig out the rare minerals needed to make batteries for electric cars.
And, of course, to the factories where slave labourers make overpriced plimsolls or manufacture mobile phones – all at such a low prices that billionaires can progress up the ladder and become even richer.
We like to think that most countries in the so-called developed world have moved on. We close our eyes to the billionaires growing ever richer on the backs of slave labour children.
Those pulling down statues of 19th century slave traders still buy the electric cars, the mobile phones and the absurd shoes and ignore the uncomfortable truths about how they were made.
In the 19th century, child labour was seen as normal and acceptable. In both physical and psychological terms what we are doing now is even worse.
For no sensible, medical reason our world has been turned upside down and millions of children will never recover. (In Africa, of course, millions of children will die as a result of the lockdowns and deliberately staged global panic.)
There is evidence that as a result of the covid hysteria many children have become withdrawn and frightened of approaching strangers – especially if they are not wearing masks.
A children’s charity has seen a massive rise in the incidence of mental and emotional problems in children under 11 years of age. Children are worried about dying, about their friends and family dying, about their future, about missing school, about loneliness, about future epidemics. The AIDS hysteria of the 20th century has become the covid hysteria of the 21st century.
As a result many are either not eating, or eating too much, and they are not sleeping. Panic attacks are becoming commonplace. A study of 10,000 parents showed that 30% of children were worried about catching the virus and 30% were worried about missing their education. Even more worrying 16% were afraid to leave their homes. More than half of the parents were worried about their children.
And yet deaths among healthy children are so rare that it has been suggested that lightning is a bigger threat to children and that it would make more sense to tell children to wear helmets to protect them against meteors than to recommend that they wore masks or practised social distancing.
Nevertheless, schools introduced masks and social distancing, and many teachers and parents want the restrictions to continue indefinitely – until the very last virus on earth has disappeared.
In Ohio, electronic beams were introduced to track school pupils and to enforce social distancing.
In China, robots have been installed to ensure that children wash their hands properly.
Some schools have installed thermal imaging cameras to see if children have a temperature. (This is entirely pointless).
One educational establishment in the US made a viral tracking app mandatory and students were constantly tracked. Students who turned off the app or tried to leave the campus without permission were expelled.
Under normal circumstances, young children touch and hug one another and derive great comfort from this.
Forcing children to remain isolated has created huge psychological problems. Children from poorer families or where there is an unhappy home life have suffered most. Also, the lack of exercise will result in health problems and obesity.
The problems have been exacerbated by threats that children who do not obey the rules `may kill granny’. (The irony is that their government wants to kill granny with blanket DNR notices in hospitals and care homes and by denying medical treatment to older citizens.) Children have seen adults frightened and as a result child terror has been exacerbated.
Many children have become socio-phobic and are developing OCD.
Figures for suicide are nigh on impossible to obtain but suicide is widely recognised to be a leading cause of death in the 5-19 age group, and one survey showed a 50% increase in suicides in 2020 compared to 2019. I suspect the figure will grow.
In an attempt to escape from reality, children are spending vast amounts of time on the internet. Gaming addiction is becoming an increasing problem with cyberbullying adding to anxiety and depression. Sports and out of school activities have been abandoned or disrupted leading to increased boredom, loneliness and depression.
Equally worrying is the fact that altered behaviour in children will frequently be diagnosed as ADHD and drugs such as Ritalin will be prescribed as a long-term remedy.
All this for an infection which children hardly ever catch and hardly ever transmit.
It’s all madness.
The whole fraud was deliberately designed by billionaires and their evil supporters.
And although politicians, their advisors and the medical establishment are guilty of mass genocide for the part they have played, parents and school teachers must also be held responsible.
If parents and teachers had done a little research, they would have known (and would know) that the covid-19 scare is fraudulent.
Their children’s lives have been sacrificed for nothing.
Last November, 2021, news reports threatened that if people who die of COVID were not vaccinated, their families may not get death benefits they would otherwise have received.
If the only guarantee in life is death, then at least there is life insurance, right?
Wrong! Fast forward to the Post-COVID Era, and the fallout from Emergency Use Authorized (EUA) vaccines. According to Forbes Magazine, if today you choose to receive a COVID-19 injection, it could prevent you from receiving a death benefit from your life insurance.
Say what?
No More Death Benefit
According to an article by Brain Peckford, a recent post-Covid vaccine death in France was ruled to be “a suicide” by a judge, due to the experimental nature of the “vaccine.” The insurance company refused to pay. No death benefit. The article reads:
A wealthy elderly man with a high value Life Insurance policy to the amount of millions of euros… dies from the covid jab. His death as a consequence of being jabbed is not disputed by the doctors, nor his life insurers. The Insurance company refused to pay the policy, citing that the taking of experimental drugs, treatments, etc., is excluded from the policy. The family takes the insurance company to court and they have just lost the case.
The judge stated, “the experimental vaccine side effects are publicised and the deceased could not claim not to have known about them when he voluntarily took the jab. There is no law or mandate in France which forced him to be jabbed. Therefore, his death is essentially suicide”.
Suicide is explicitly excluded from this particular policy and in fact from all life insurance policies in general.
This has been the finding of a major western world court system and there is zero doubt that insurance companies world wide will cite this case as legal fact.
Therefore, if anyone ever challenges you on whether these jabs are experimental or not, and that neither the pharma companies, nor govts, nor anyone else but YOU are responsible for accepting them and if you die, legally you have committed suicide.
No insurance, no payouts, no refunds. You are on your own!
Listen to Dr. Pierre describe the same story and explain the view of the American Council of Life Insurers; that insurance companies may deny payment of death benefit if death results from the experimental COVID injection.
How could this possibly be? One moment the experimental vaccine and the boosters protect you against COVID, but the next moment they do not? One moment you are insured with the injection, but the next moment, you are not? As the French say, “C’est la vie. C’est la guerre!” Meaning? Such is life! That’s war. It can’t be helped!
Changing Narratives
Changing narratives happen by design. Those who own the narrative control the outcome. Moreover, in America, under the Smith-Mundt Modernization Act, the media is free to legally propagandize Americans. The EUA vaccines, once advertised to “save lives by preventing deaths” from COVID-19 coronavirus infections, are now “suicidal.”
In May 2021 it was a different story. According to the American Council of Life Insurers, life insurers could not deny a death benefit because the deceased was vaccinated against COVID-19:
A social media post appears to be behind the spread of entirely false information, suggesting a COVID-19 vaccine could be a factor a life insurer considers in the claims-paying process. The fact is that life insurers do not consider whether or not a policyholder has received a COVID vaccine when deciding whether to pay a claim. Life insurance policy contracts are very clear on how policies work, and what cause, if any, might lead to the denial of a benefit. A vaccine for COVID-19 is not one of them. Policyholders should rest assured that nothing has changed in the claims-paying process as a result of COVID-19 vaccinations.
But good propaganda shifts with the winds. Today’s America is not yesterday’s America. America has been hijacked, morally corrupted, debauched, and sold to the highest bidder.
In fact, if you received the Pfizer/BioNTech, Moderna, or Johnson & Johnson COVID-19 vaccines, you received a vaccine deemed “emergency use authorization” (EUA) from the FDA. No EUA injections are FDA-approved vaccines. Further, the first injections deployed were labelled “experimental.” Thus, participants who consented, without proper Informed Consent, became subjects in an ongoing clinical study. Note: Life insurance companies do not cover experiments.
In other news, if you are unvaccinated and hospitalized, insurance may not pay either. A news release from the University of Michigan states:
“Many insurers claim that it is justified to charge patients for COVID-19 hospitalizations now that COVID-19 vaccines are widely available,” said lead author Kao-Ping Chua, M.D., Ph.D., a health policy researcher and pediatrician at Michigan Medicine and the Susan B. Meister Child Health Evaluation Research Center. “However, some people hospitalized for COVID-19 aren’t eligible for vaccines, such as young children, while others are vaccinated patients who experienced a severe breakthrough infection. Our study suggests these patients could substantial bills.”
To recap: if you are 1) Unvaccinated and hospitalized, or 2) vaccinated pre-death, then life Insurance does not pay what you might expect, if at all.
The Double-edged Sword
Read the article Dissolving a Pandemic of Fear, to understand that this trend first began in distant lands during the summer of 2021 with unusual side effects to the globally-deployed experimental vaccines:
Because of the uncertainties from unauthorized tests and experimental vaccines, insurance companies in India and Korea are limiting what they will cover if someone becomes sick from the COVID injections:
Contrary to popular perception, existing health insurance policies are unlikely to cover the cost of vaccination and adverse reactions, if any. Only policies designed purely for the COVID vaccination process — there is none at the moment — will cover the costs.
If you consented to an EUA injection, your life insurance policy has changed. You can’t win for losing, and you can’t claim your life insurance for dying. Something that cuts both ways is known as a double-edged sword.
Justice Through the Courts?
The federal PREP Act and CARES Act prevent practically all civil litigation, ranging from COVID “vaccines” to “tests,” to doctors/pharmacists/nurses. All have blanket civil (but not criminal) protections. All prosecutions are 100.0% discretionary, meaning that even if one admits to a criminal (COVID) act, no private citizen has the power to prosecute any alleged criminal act. That power rests solely with the district attorney and attorney generals — not citizens.
What does this mean? ALL prosecutions are political. In other words, The ONLY way to legally challenge all the “COVID” treason is confined to CRIMINAL prosecutions. Evidence proving criminal fraud has been submitted to the appropriate authorities, and yet there have been no criminal prosecutions through the Department of Justice. Why not? Good question.
What about life insurance fraud? Can insurers be prosecuted in the courts if the Life Insurance Council COVID policy is against the policy holder?
In response to a FOIA request, a federal district judge recently ordered Pfizer Inc. to release 55,000 pages of documents each month, after Pfizer claimed it would not disclose any data for 75 years. That means all the Pfizer vaccine data should be made public by the end of September 2022, rather than the year 2097.
Yet, who is in charge of sifting through the flood of information? What are the consequences of learning the truth that was meant to be hidden? No one knows. What about the fact that government appears to be practicing medicine without a license? How could this possibly be?
Because the narrative is always written by those who control the pen, you must do your own research and captain your own ship. Call your insurance company directly. Ask an “expert” if getting the vaccine will affect your life insurance coverage in any way. Ask if future EUA jabs will affect your premiums or payouts.
Then ask yourself if paying those high insurance premiums is worth the outcome in The COVIDIAN Age, or if it is better to put your money elsewhere.
Dr. Naomi Wolf at Defeat the Mandates Rally: “You Hurt Our Kids & Watch Out. Because You Have Never Faced the Rage of Thousands of Mothers & Stepmothers”
In an exclusive interview with The Defender, Jeffrey Beauchine said his mother, Carol, knew her Creutzfeldt-Jakob Disease was related to the Moderna shot. Watching her death was like “something you see out of a movie,” he said.
In an exclusive interview with The Defender, Carol’s son, Jeffrey Beauchine, said it was excruciating to watch his 70-year-old mother — who was healthy until she got the vaccine — die from a disease he believes the vaccine caused.
“I’ve seen a lot in my 20 years as a police officer,” Beauchine said. “I’ve seen hundreds of people shot and this affected me more than anything.”
Beauchine said Carol received her first dose of Moderna on Feb. 16, 2021, and didn’t report any complaints. After getting the second dose on March 17, Carol immediately said she “felt different.”
Beauchine said:
“On March 17, she got her second dose and immediately started having reactions to the second dose. She just had this malaise. She just didn’t feel right and said she just felt ‘off.’ She had what she described as pain and burning at the injection site — like someone was tying a hot rope around her arm. Then she explained it as this numbness setting in around the injection site.”
Beauchine said he and his family members didn’t think it was a usual side effect, but they also didn’t think it was unusual.
“We just thought it was a result of the jab working through the system,” Beauchine said. “Then the numbness spread up through her neck and down her left arm.”
The numbness altered Carol’s hearing and spread “down through her hands” until the left hand lost sensation and mobility.
Beauchine said:
“At this point, it was her entire left arm. She started to develop insomnia. She would go a couple of days at a time without sleep and then she was fatigued. This numbness continued to spread. It went down to her hip and moved to her knees, then the entire left side. You could almost bisect her body and the left side was numb and the right side was normal.”
Beauchine said Carol went to the doctors — who initially thought she had suffered a stroke — but her MRI scans were completely normal.
“Nobody could find anything wrong with her so they sent her home,” Beauchine said. “It was almost like reassurance, while at the same time I wondered why they couldn’t.”
Carol then developed tremors in her left arm.
“It was almost like her arm would start jerking involuntarily,” Beauchine said. “Then the tremors moved on to the left leg.”
Beauchine added:
“My mother began to complain that something was wrong with her brain. She said she couldn’t put thoughts together or make sense of things but she could still communicate. Over the phone, you wouldn’t see the altered version of my mom I knew for 44 years.”
Then Carol developed double vision that ultimately led to blindness, and she began to hallucinate.
“She would see herself falling out of the chair and she would physically see herself on the ground,” Beauchine said. “It was weird to understand. She developed a fear of water and would become scared she was near a body of water.”
Doctors believed Carol was suffering from anxiety because of the shot and started treating her for anxiety. Meanwhile, Carol lost the ability to walk.
Beauchine said:
“She was still at home at this time because the hospital couldn’t find anything wrong with her. She was pretty much in a wheelchair. She went from the one who takes care of everybody to my 70-year-old father taking care of her. Then it got too hard for him and during one doctor’s visit they admitted her to see if they could dive into it further.
Beauchine said doctors ran every test “under the sun,” including an MRI, but couldn’t find anything. The only things doctors noticed were the obvious mobility problems on the left side of her body and balance problems.
The doctors also said there was “something off with her cerebellum but they didn’t know what it was,” he added. Carol tried to explain to the doctors that there was something “internally” wrong with her.
“She was then released to a nursing home,” Beauchine said. “It was the first time I saw my mom really sick.”
He said:
“She was in a nursing home where all this COVID was going on and we had to stand outside the window and yell through the air conditioner hole to talk to my mom. She felt defeated and scared, and my father cared for her 18 hours a day — spoon-feeding her — until the end. It just happened so fast.”
Eventually, Carol was able to get into a skilled nursing home, but she deteriorated rapidly.
“She lost the ability to feed herself because she couldn’t get the food on her fork to put it in her mouth,” Beauchine said. “It crushed me because I could see in her eyes without us having any convo, the fear and like she was defeated.”
Beauchine said there were no more good days and his mother lost the ability to communicate.
“By mid-end of July my mom was just a complete rigid person,” he said. “Lips stopped moving. She could only get a couple of syllables out. She would almost be falling out of a wheelchair in a forward position. She couldn’t tell if she was sitting up.”
Beauchine said his mother knew from the very beginning her condition was related to the shot.
“We all knew from the very beginning it was related to the shot, but we didn’t know the future significance of how bad this would get,” Beauchine said. “People have bad reactions all the time but you get over them. She didn’t get over them.”
Beauchine said the doctors didn’t know what to do because “it was just so new.”
“I’m more content with a doctor telling me they don’t know if it’s the shot because there’s no research than the doctors who say it’s definitely not the shot,” he said. “I got more ‘I don’t knows’ than denials.”
By the end of July, Carol’s husband couldn’t wake her up at the nursing home and the family had a meeting and decided their mother needed to go back to the hospital.
Beauchine said:
“When I rounded the corner, I saw my mom and it was like she was like yelling or howling. Her eyes were completely fixed in the open position. Her mouth was stuck in the open position and she had violent tremors that wouldn’t stop. She didn’t understand what was going on. The only way I can put it is a bomb went off inside of her head.
“It was excruciating for all of us. My dad was like a deer in the headlights — a blank look I had never seen before. And I’ve seen a lot of stuff in my life with my job but this was like … a bomb went off in my mom’s head and all of her limbs were convulsing and tremoring.
“It’s like something you see out of a movie. They say with this disease you come to the cliff and it’s just a drop-off and once you drop off you’re able to physically see that dropping point — and you could see it that night.”
Doctors sent Carol to Strong Memorial in Rochester, New York, and within weeks they confirmed she had CJD.
“We didn’t know what CJD was, but we were told it was like mad cow disease but like a different variant or different mode of getting it,” Beauchine said. “Same disease but a different way of getting it.”
Carol’s prognosis was fatal and the family was told she had only days left. Beauchine said a panel consisting of doctors and students who were overseeing Carol’s case were open to the fact they did not know what caused her CJD.
“People were learning and they said ‘we don’t know if this is related to the vaccine or not. We don’t know because the vaccine is new and there weren’t a lot of studies on the vaccine. We won’t know until the long-term.’”
Carol passed away on Aug. 2, 202, from CJD — a condition she did not have prior to receiving her second dose of Moderna a few months earlier. Her doctors filed a report with the Centers for Disease Control and Prevention’s Vaccine Adverse Event Reporting System (VAERS I.D. 2180699).
VAERS is the primary government-funded system for reporting vaccine adverse vaccine reactions in the U.S. According to the CDC’s website, “CDC and [U.S. Food and Drug Administration] clinicians review reports of death to VAERS including death certificates, autopsy and medical records.”
Beauchine confirmed the family has never received any contact from the CDC regarding his mother’s death, and to his knowledge, her doctors haven’t either.
Beauchine said Carol was a relatively healthy person with no previous history of COVID. Her only underlying condition was arthritis.
“She was always taking care of other people and when the whole COVID thing broke out in the media, she wanted to stay protected so she could see her kids and grandkids,” Beauchine said. “She didn’t want to be hindered by the virus, so when the opportunity arose for her age group, she got the first dose with no complaints.”
Beauchine said he also received the COVID vaccine because it was required for his job.
“At the time, there was a little smidgeon of excitement because they had you so feared over COVID-19 and finally there was a little light at the end of the tunnel,” he said. “And it was going to be okay.”
He added:
“I got the vax. My wife got the vax. My father got the vax. My children will never get the vax. I’m not against a COVID-19 vaccine but it takes years and years and years of clinical trials and studies to deem something safe to put in the human body, and that wasn’t done. We all turned a blind eye to it at the time in moments of hope.
“I didn’t know any of this stuff that we know now, and then you come to find out that hydroxychloroquine and ivermectin have been used off label for years, but to get the Emergency Use Authorization (EUA), you have to show there’s no treatment available to be able to give that authorization, so they killed the treatments, gave the EUA, but there’s no liability on their end.
“It’s just scary nobody knew that at the time. If somebody wants to make an informed decision, let them know what they’re up against.”
Beauchine said when he talks to people, or his mother comes up in conversation, everyone seems to know someone who had a very serious reaction to a COVID vaccine.
“I am not an anti-vaxxer. I’m not crazy or anything like that,” Beauchine said. “But if I or my family can do anything to help somebody or inform somebody or even be a statistic that could come to some sort of positive resolution in all of this, so be it.”
He added:
“Watching someone slowly walk this path and their health degrading right before your eyes from day to day over a few months is terrible. It’s awful. No one should have to go through this. We all just felt for my mom the whole time. It affected us all.”
The Defender has received numerous reports of people who died from sporadic CJD after receiving a COVID vaccine — all women who were between the ages of 60 and 70. This includes Cheryl Cohen and Jennifer Deason Sprague.
According to the latest data from VAERS, between December 14, 2020, and April 1, 2022, there were 19 reported deaths due to CJD attributed to COVID vaccines. The majority of cases occurred in the 65 to 75 age range and involved a sudden onset of symptoms.
Over the past year-plus, athletes across the world have been dropping like flies as they compete in games. If they aren’t passed out cold, they are seen gripping their chests in agony, unable to breathe due to sudden cardiac events that hit in the heat of the competition.
This wave of heart issues is unprecedented, to say the least. Never before have we seen young, healthy, world-class athletes experiencing heart issues en masse like this. It has never happened, ever. Furthermore, the timing of this sweeping phenomenon could not be more relevant, coinciding perfectly with the rollout of the experimental Covid-19 vaccines.
In December nearly 300 athletes reportedly collapsed or suffered cardiac arrests after taking the COVID vaccines.
But it gets worse. Thanks to a new explosive report by OAN that pegs the number of affected athletes in the hundreds.
In all, their investigation found a jaw-dropping 769 men and women who collapsed with heart issues during competition over the past year (between March 2021 and March 2022).
Most shockingly, the average age of those who experienced full-blown cardiac arrest was just 23.
Considering the timing of this never-before-seen issue in healthy athletes, and the universal push for Covid jabs, all signs point to one culprit: the experimental vaccine.
After detailing two recent high-profile cases, in which two tennis players were forced to recuse themselves from last month’s Miami Open, OAN’s Pearson Sharp reviewed their shocking investigation and asked a few pressing questions that should be answered if you are still questioning what is driving these heart issues in young individuals:
“These are just two o more than 769 athletes who have collapsed during a game on the field over the last year. From March of 2021 to March of this year. The average age of the players suffering cardiac arrest is just 23-years-old.
How many 23-year-old athletes were collapsing and suffering heart attacks before this year? Do you know any 23-year-old people who had heart attacks before now?
And these are just the ones we know about. How many have gone unreported? Nearly 800 athletes – young, fit people in the prime of life falling down on the field. In fact, 500% more soccer players in the EU are dropping dead from heart attacks than just one year ago.”
Just in case there is any lingering inclination to call this a coincidence, Sharp sets the record straight.
“Coincidence? When the Pfizer vaccine is known to cause heart inflamation? No. In fact, many doctors treating these players list their injuries and deaths as being directly caused by the vaccine…
This is not a coincidence – healthy teenagers dying after getting the Pfizer injection. Doctors warned the FDA before they released the experimental vaccine that it would ‘almost certainly cause terrible organ damage.’”
The only question left is: when do we see some accountability?
In a World First on Maria Zeee Uncensored, Australian Senator Malcolm Roberts exposes the Nanotech found in the COVID-19 Vaccines, declaring this is genocide.
We discuss the incoming Digital Identity and the government’s plan to enslave humanity through their plans for a New World Order.
Dr. Naomi Wolf discusses the war on children and on Western values. Forcing children to wear masks is abusive because new studies show that this prevents them from developing normal facial recognition and the practice has a now-measurable effect on their IQ levels.
With all the new information surfacing from the WarRoom/DailyClout volunteers regarding the formerly secret Pfizer documents, and with attorney Stevan Looney’s new essay on the redacted documents in the secret Pfizer tranche now published on DailyClout.io, it is becoming clear that informed consent before receiving the vaccine was never even possible.
Bombshell: in order to process just the paperwork from the “large number of adverse events” — Pfizer’s own words — Pfizer had to hire 2,400 new, full-time employees and the company proudly informed the FDA of these thousands of new hires to grapple with the flood of adverse events they saw as early as February 28, 2021. Yet they did not disclose these adverse events to the public and neither did the FDA.
Hold the line, hold the line
Won’t let them steal our sovereignty with their lies
This is spiritual warfare
Between the light and darkness
It’s an empirical nightmare
What they’re tryna inject inside us
We’re not signing up
For their experiment
Try to coerce and force us
But they’ll never penetrate our temples cause we
Hold the line, hold the line
Won’t let them steal our sovereignty with their lies, so we
Hold the line, hold the line
We stand together and we do not comply, yeah we hold the line
We are the doctors and nurses
Sleepless nights and overtime on the front lines
We are police in the cities
And firefighters, we’re protecting the families
Kicked us to the curb for the shot we refuse
It’s our body and our right to choose
It don’t matter, we will weather this storm
Cause God is with us in this battle, come and join us as we
Hold the line, hold the line
Won’t let them steal our sovereignty with their lies, so we
Hold the line, hold the line
We stand together and we do not comply, yeah we hold the line
We hold the line in love, hold the line
Show ‘em what we’re made of, hold the line
Hold the line, hold the line
Won’t let them steal our sovereignty with their lies, so we
Hold the line
To the parents of the children
We’re sending hope to you
Pull ‘em out of the system
We’ll build a better school
Hold the line
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
‘Defeat the Mandates Coast to Coast’, Next Stop: Los Angeles, CA, April 10, 2022
Thankfully some mandates are dropping across the country, but there are still vaccine mandates that persist in schools, colleges, businesses, hospitals, and corporations. Restrictions on doctors who treat COVID, censorship by Big Tech, the unnecessary COVID-19 vaccination of children, silencing of scientific debate, and the extension of the Emergency Powers Act beyond March 1st for the coronavirus pandemic are a few of the main concerns.
In California, an aggressive slate of COVID-19-related bills—mandating vaccines for children and all employees, and allowing 12 to 17-year-olds to get the vaccine without parental consent—remain under consideration by the California state assembly.
Starting at 12:00 noon we will hold a day-long rally in the heart of Los Angeles at Grand Park where a wide range of featured guests including prominent doctors, recording artists, actors, journalists and premier thought leaders will give a series of inspiring talks and musical performances.
Pfizer hired about 600 additional full-time employees to process adverse event reports during the three months following authorization of its COVID-19 vaccine, with plans to hire 1,800 more by June 2021, newly released documents reveal.
Pfizer hired about 600 additional full-time employees to process adverse event reports during the three months following the Emergency Use Authorization (EUA) of its COVID-19 vaccine, newly released documents reveal.
According to the documents, Pfizer said, “More are joining each month with an expected total of more than 1,800 additional resources by the end of June 2021.”
The information was contained in a 10,000-page document cache released April 1 by the U.S. Food and Drug Administration (FDA) and made public as part of a court-ordered disclosure schedule stemming from an expedited Freedom of Information Act (FOIA) request.
The latest revelations appeared in a document, “Cumulative analysis of post-authorization adverse event reports” of the Pfizer-BioNTech vaccine, highlighting such adverse events identified through Feb. 28, 2021.
The document was previously released in November 2021, but was partially redacted. The redactions included the number of employees Pfizer hired and/or was planning to hire.
According to the unredacted document released April 1:
“Pfizer has also taken a multiple actions [sic] to help alleviate the large increase of adverse event reports. This includes significant technology enhancements, and process and workflow solutions, as well as increasing the number of data entry and case processing colleagues.
“To date, Pfizer has onboarded approximately 600 additional full-time employees (FTEs).
“More are joining each month with an expected total of more than 1,800 additional resources by the end of June 2021.”
The unredacted version also revealed the number of Pfizer-BioNTech vaccine doses shipped worldwide between December 2020 and February 2021:
“It is estimated that approximately 126,212,580 doses of BNT162b2 [the Pfizer EUA vaccine] were shipped worldwide from the receipt of the first temporary authorisation for emergency supply on 01 December 2020 through 28 February 2021.”
The number of shipped doses previously was redacted.
“The rollout of the Pfizer vaccine has led to an unprecedented number of adverse events reported — 158,000 adverse events in the first two-plus months of the rollout means that the rate of reported AE [adverse events] was approximately 1:1000, with many of the AEs graded as serious. This is based on a denominator of 125,000,000 vaccines distributed.
“It is no wonder that an army of 1,800 individuals was needed to process all of the information.”
Hooker noted the total number (1,205,755) of COVID vaccine adverse events reported to the Vaccine Adverse Event Reporting System between Dec. 14, 2020 and March 25, 2022, now eclipses the total number (930,952) of adverse events reported in the 32-year history of the database.
Dr. Madhava Setty, a board-certified anesthesiologist and senior science editor for The Defender, previously reported on the same Pfizer document, before the unredacted version was released.
“In that piece, I alluded to Pfizer’s admission that they needed more staff to process all of the adverse events being reported to them,” Setty said.
“It seems this document has now been updated. 600 FTEs [full-time employees]! … I wonder how many extra people the CDC [U.S. Centers for Disease Control and Protection] has hired? Given how they are operating, I would say zero.”
Pfizer downplayed adverse reactions in request for full FDA license
The April 1 document release also included “request for priority review” — the documentation Pfizer in May 2021 submitted to the FDA for full licensure of its Comirnaty COVID vaccine.
In this document, Pfizer described its vaccine as fulfilling an “unmet medical need,” claiming:
“Mass immunization with a safe and effective vaccine against COVID-19 can dramatically alter the trajectory of the pandemic.
“According to policy briefing by the Institute for Health Metrics and Evaluation published on 31 March 2021, COVID-19 remains a leading cause of death in the US with up to 100,000 additional deaths projected in the US between March and July 2021, many of which can likely be prevented with COVID-19 vaccination.”
Pfizer expressed “concerns” about lifting COVID-related measures, such as lockdowns, on the basis that the lifting of such restrictions would “counteract the impacts of this vaccination effort.”
“Vaccination against COVID-19 began with EUA/conditional approvals in December 2020, in a phased rollout defined by national/regional guidance.
“However, there continue to be concerning trends that may counteract the impacts of this vaccination effort, including:
“[L]imitations in access to obtaining a vaccine due to infrastructure challenges (ie, clinic and appointment capacity and systems)
“[I]ncreasing viral transmission fueled by relaxed compliance with mitigations as the pandemic surpasses the 1-year mark (ie, masks, physical distancing, limiting travel)
“[I]ncreasing circulation of emerging variants of concern (which are currently driving continued spread of viral infection in Europe despite extensive mitigation mandates).”
Pfizer justified its request for full licensure of its COVID vaccine on the following basis:
“A vaccine program must be implemented expediently and rapidly expanded to have a significant impact on the pandemic course.
“Licensure of BNT162b2 is likely to enhance vaccine uptake by facilitating supply of vaccine from Pfizer/BioNTech directly to pharmacies and healthcare providers/facilities.
“The greatest impact of BNT162b2 licensure may be direct supply to healthcare providers who serve vulnerable populations such as elderly patients and those who live in rural and underserved communities (ie, individuals who might be unable to navigate the challenges of securing vaccine access using the systems in place for EUA).
“Expansion of vaccine via licensure would ultimately improve the prospect of achieving population herd immunity to bring the pandemic under control.”
The same document glossed over the adverse effects for which the company previously admitted it hired a significant number of new employees to process, claiming:
“Based on Phase 1 data from the FIH Study BNT162-01, BNT162b1 and BNT162b2 [various vaccines tested during the trial period] were safe and well-tolerated in healthy adults 18 to 55 years of age, with no unanticipated safety findings.
“Phase 2/3 safety data were generally concordant with safety data in Phase 1 of the study, both overall and with regard to younger and older participants.”
This is despite hard figures regarding adverse reactions provided later in the document:
“Through 28 February 2021 (data lock point aligned with Pharmacovigilance Plan), there were a total of 42,086 case reports (25,379 medically confirmed and 16,707 non-medically confirmed) containing 158,893 events. Cases were received from 63 countries.
“Consistent with what was seen in Phase 2/3 of Study C4591001, most reported AEs were in System Organ Classes (SOCs) with reactogenicity events: general disorders and administration site conditions (51,335), nervous system disorders (25,957), musculoskeletal and connective tissue disorders (17,283), and gastrointestinal disorders (14,096).
“Post-authorization data have also informed the addition of adverse drug reactions (ADRs) related to the experience of reactogenicity to the product labeling.”
Release of Pfizer vaccine documents still in progress
Many of the documents released as part of the April 1 tranche appear to include more mundane information and data related to the Pfizer COVID vaccine trials.
These documents include:
Peer-reviewed scientific articles funded by Pfizer-BioNTech, titled “Phase 1/2 Study of COVID-19 RNA Vaccine” (August 2020) and “Safety and Immunogenicity of Two RANA-Based Covid-19 Vaccine Candidates,” published in the New England Journal of Medicine in October 2020.These studies supported “further evaluation of this mRNA vaccine candidate” despite the apparent appearance of serious adverse effects in one of the 12 participants receiving 30 μg and 100 μg doses of the BNT162b1 candidate vaccine during the trial phase. This, however, does not appear to have been the final vaccine formulation that ultimately received an EUA.
A questionnaire that vaccine trial participants were required to complete, along with a study book displaying the information to be collected from those participating.
Documentsoutlining the randomization scheme used for identifying vaccine trial participants and those who received doses of the vaccine or a placebo.
Documentslisting anonymized demographic characteristics of vaccine trial participants.
An anonymized listing of important protocol deviations.
Consent forms that vaccine trial participants were asked to complete, as well as other related documents submitted by Pfizer for Institutional Review Board (IRB) approval, and information regarding institutions participating in the IRB process.
“‘Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“To obtain embryo cells [for research on vaccines and other pharma products], embryos from spontaneous abortions cannot be used, nor can those obtained by means of abortions performed via the vagina: in both cases, the embryo will be contaminated by micro-organisms.”
“The correct way consists in having recourse to Caesarian section or to the removal of the uterus. Only in this way can bacteriological sterility be guaranteed.”
“In either case, then, to obtain embryo cells for culture a programmed abortion must be adopted, choosing the age of the embryo and dissecting it while still alive, in order to remove tissues to be placed in culture media.”
“Given these premises, we face the dilemma of whether the deliberate systematic destruction of a human creature to obtain cell material can be justified, when it is recognized that this is of great interest to fundamental research and for the diagnosis of some human diseases. Are research and diagnosis of such great value that they justify the destruction of human beings?”
“The Geneva Declaration affirms that the doctor has the duty to take the greatest care to safeguard the life of a human being from its conception and will not, even under threat, use his knowledge to infringe humanitarian laws.” (1986-04-26; Herranz, Gonzalo; Il Sabato, no.15…Professor Herranz was, at the time, president of the Committee of Medical Ethics of Spanish Doctors and vice-president of the Permanent Committee of Medical Ethics of the European Community.)”
What exactly happened in 1972 or 1973, in the Netherlands, where an infant girl was aborted, and her kidneys used to make a cell line that would be used, going forward, in the testing of vaccines?
That cell line is called HEK 293, and it has been used to test COVID vaccines.
I have already presented evidence for concluding the abortion involved removing the living infant from her mother’s womb, and taking her kidneys, which of course killed her.
This evidence rests on the realization that, in order to extract viable and useful kidney tissue, the baby had to have a functioning blood supply, which meant she was alive.
But the evidence ALSO comes from knowing many other abortions have been carried out, in order to harvest tissue for medical research, by murdering living babies.
I have found a very informative article (2/9/2021) at the Centre for Bio-Ethical Reform UK, by Christian Hacking, titled, “What the HEK?!” by Christian Hacking. Quoting from the article:
“HEK 293 is a human cell line created using a kidney from a dissected unborn baby in the Netherlands between 1972 and 1973. It is the second most common cell line and is used extensively in ‘pharmaceutical and biomedical research’. It is also used in vaccine creation and cancer research.”
“It was used, along with other human cell lines, to develop a genetically engineered spike protein (that the mRNA vaccine codes for) in the original development stage of the vaccine. The ‘new technology’ Pfizer vaccine and the Moderna Vaccine were tested on HEK 293 before they began human trials. This testing is ongoing for all new batches. Finally the ‘old technology’ Oxford AstraZeneca vaccine grew a weakened viral strain in HEK 293 cell culture…”
“The kidney in question was dissected from a healthy Dutch baby girl of unknown origin by the team at Leiden University in the Netherlands in 1972. Despite the inclusion of the term ‘embryonic’ in the title, the baby in question was probably 12-13 weeks old when she was killed so as to secure functioning kidney cells. The man in charge of the research was named Alex Jan Van der Eb; he is still alive and still based in Holland.”
“When questioned on the matter by the FDA in 2001, Dr Van der Eb confirmed it was an intentional abortion of a ‘fetus’ but gave hazy details of the exact experiments.”
“’So the kidney material, the fetal kidney material was as follows: the kidney of the fetus was, with an unknown family history, obtained in 1972 probably. The precise date is not known anymore. The fetus, as far as I can remember, was completely normal. Nothing was wrong. The reasons for the abortion were unknown to me. I probably knew it at that time, but it got lost, all this information’.”
Author Hacking continues: “…extracting and growing living cells is incredibly difficult. In order to give oneself the best chance of success you need to ensure the child is healthy, fresh, intact and sterile. As one embryologist and Emeritus Professor of Anatomy confirms:”
“’In order to sustain 95% of the cells, the live tissue would need to be preserved within 5 minutes of the abortion. Within an hour the cells would continue to deteriorate, rendering the specimens useless’.”
[That statement was made by “Dr C Ward Kischer, embryologist and Emeritus Professor of Anatomy; specialist in Human Embryology, University of Arizona College of Medicine…”]
[My comment: This suggests the abortion, in the Netherlands, in 1972, was planned and technicians were standing by. I would say that, to ensure the viability of the tissue, the infant had a functioning blood supply and was alive when her kidneys were removed, killing her.]
Hacking:
“In order for the organs to be at ‘optimal viability’, the child needs to be dissected and organs extracted within 5 minutes of delivery. Anaesthetic also cannot be used so as to not change the cellular activity of the organs the researcher wants to obtain.”
“Acclaimed Doctor, Ian Donald, the pioneer of the ultrasound scanner, also claims to have witnessed the WI-38 [another cell-line] dissections [1962], conducted at the Karolinska Institute; he described them such:
“’Experiments were being performed on near-term alive aborted babies who were not even afforded the mercy of anesthetic as they writhed and cried in agony, and when their usefulness had expired, they were executed and discarded as garbage’.”
“In his dense book ‘The Foetus As Transplant Donor the Scientific, Social, and Ethical Perspectives’, immunologist Dr Peter McCullagh relays detailed descriptions of the methods used on dozens of ‘fetal tissue donors’ from the 1970’s onward, including the deaths of babies between 7 and 26 weeks gestation by decapitations, exposure, dissection and drug testing. Gynaecologist and ex-abortionist Dr Bernard Nathanson, relaying his own understanding of abortion, and citing McCullagh’s book claims the Swedish experiments took place thus:
“’…in Sweden they have been puncturing the sac of a pregnant woman at let us say 14 to 16 weeks, and then they put a clamp on the head of the baby, pull the head down into the neck of the womb, drill a hole into the baby’s head, and then put a suction machine into the brain and suck out the brain cells….. Healthy human fetuses from 7 to 21 weeks from legal abortions were used. This is in Sweden. The conception age was estimated from crown rump length and so on. Fetal liver and kidney were rapidly removed and weighed. Now at 21 weeks, what they were doing, or 18 weeks, or 16 weeks, was what is called prostaglandin abortions. They would inject a substance into the womb. The woman would then go into mini-labor and pass this baby. 50% of the time, the baby would be born alive, but that didn’t stop them. They would just simply open up the abdomen of the baby with no anesthesia, and take out the liver and kidneys, etc.’”
“A research paper from the University of Toronto from June 1952 commenting on the method of their experiments suggests that these techniques were universal with researchers working in close proximity to the abortions.”
“’No macerated [softened after death] specimens were used and in many of the embryos the heart was still beating at the time of receipt in the virus laboratory.”
“According to Gonzalo Herranz, former head of the Committee of Medical Ethics of Spanish doctors, the best way to prevent ‘contamination by microorganisms’ is to deliver the child by caesarean section or the removal of the uterus.”
“A 1982 review of a history of tissue donation affirms this, and much of the above evidence:”
“’Fetal tissue for transplantation must be “harvested” within a few minutes of delivery. Ideally this is by hysterectomy, with the fetus delivered in utero. Drugs which reduce fetal physiological activity need to be avoided. The fetus is therefore in as alive and aware a state as possible when being opened’.”
From Hacking’s article, it’s quite clear how the standard procedure of infant-murder is carried out.
It’s entirely reasonable to assume fetal cell line HEK 293—used for COVID vaccine testing—was originally produced, in 1972, by the murder of an infant. Refusal to take a COVID vaccine on the basis of conscience and religion is more than justified.
Given the weight of the circumstantial case, I would say that for all people of faith, refusal is essential.
Lunatic medical murderers and their allies will say anything to avoid blame and the application of true justice to themselves. They will invent “science” at the drop of a hat and couch it in humanitarian terms. They will claim the ends justify the means. They will commit gross forgery to pretend those ends are vital.
But we don’t have to stand by and passively believe them.
Billions of people of faith can stand against them.
The implementation of a digital passport system is a crucial element in this plan, which would go on to enable the creation of a Central Bank Digital Currency (CBDC) that eventually will be able strip you of your assets and turn them into a credit courtesy of governments led by authoritarian technocrats. You can not use money any longer unless someone “higher up” agrees to it. Together with plans to turn dissentic voices into “domestic terrorists” that would be the end of all of the freedoms our forefathers paid with their lives to defend.
One of these systems that could be turned into a didgital concentration camp is the Digital Green Certificate introduced by the European Union in June 2021 under the pretext of “enabling freedom of travel”. It turned out to be quite the opposite.
Consequently, brave parliamentarians such as Mr Roos have started an initiative to block the EU commission’s attempt to extend the “Covid Pass”/Green Certificate until at least 2023.
While CHD is not endorsing political platforms but focuses on advocacy for Children’s Health and Fundamental Human Rights, we kindly ask you to please take 90 seconds and listen to this video which Mr Roos has put out, and also follow the link to object to these plans of the EU Commission’s website:
“The European Commission, wants to extend the covid pass until June 2023. In one and a half minutes, I will explain to you why you should care, and what you can do to stop this.
The covid pass was introduced by the European Union in June 2021. They claimed it would make travel within the European Union easier. But that never worked. Countries still kept introducing their own restrictions. Within just a few months, member states transformed the covid pass into something much bigger. All of a sudden, you needed a QR code to enter a restaurant or even to go to work. But it was never introduced for that.
Now, Omicron is the dominant strain of the virus. To most people, it’s not dangerous anymore. The vaccine doesn’t stop the spread. Science shows that the QR system does not come with any health benefit anymore, while undermining fundamental rights.
This is the moment to abolish the covid pass once and for all.
But the European Commission wants to extend it until at least June 2023, an extremely bad idea.
Together with several colleagues in the Parliament, I will do everything I can to stop this. But we have to do it together.
We need your help, please follow this link to the European Commission website and tell them that you oppose this extension. Please do it as soon as possible, because conditional freedom is NO freedom!”
Senator Malcolm Roberts, Queensland, Australia: To All Who Perpetrated Covid Vaccine Injuries & Death — “We Won’t Let You Get Away With It. We Are Coming for You.”
The evidence continues to mount that these vaccines do not deserve the continuing provisional approval given to them by the TGA.
Concerns about possible adverse side effects are too big to ignore any longer, especially after my COVID Under Question inquiry which you can watch by clicking here.
Transcript
As a servant to the people of Queensland and Australia, tonight I’m speaking on this parliament’s therapeutic response to COVID-19 and the horrific medical harm and loss of life in that response.
Last week, leading Australian parliamentarians came together in an event I organised called COVID Under Question to present documented evidence and victim testimony proving a catastrophic failure of Australia’s regulatory framework.
COVID vaccine injuries are hidden behind anonymous government data, while supposed COVID virus harm is splashed across prime time.
The very least we can do for the victims of COVID vaccines is to say their names—victims like Caitlin Georgia Gotze, a healthy and vibrant 23-year-old studying at Griffith University to become a vet while working as a horse strapper. Caitlin dropped dead at work of a heart attack following a second Pfizer shot. Her death was recorded as asthma, a condition Caitlin had never had.
Reginald Shearer, a formerly healthy fit and active man, quickly went downhill and passed away from effects that began after receiving the AstraZeneca vaccine.
Daniel Perkins, a 36-year-old healthy father from Albion Park, died of a heart attack in his sleep following his second Pfizer injection.
Douglas James Roberts died after taking AstraZeneca. His family are concerned that his GP didn’t warn him of the side-effects of the vaccine. In other words, no informed consent was obtained. Neurosurgeons at the Royal Brisbane and Women’s Hospital attributed his death to a stroke, despite no family history and a clean bill of health. They refused to report his death to the TGA—refused!
The Australian Health Practitioner Regulatory Agency, Ahpra, has been bullying medical practitioners into not reporting or even for talking about the harm they’re seeing.
The TGA erased 98 per cent of the 800 vaccine deaths—98 per cent erased!—that physicians reported. The TGA did so without autopsy or suitable consideration of all the patient medical data.
TGA, ATAGI and Ahpra are the three monkeys of the pharmaceutical industry: hear no evil, see no evil, speak no evil.
Section 22D(2) of the Therapeutic Goods Act 1989 requires the Secretary of the Department of Health to ensure the quality, safety and efficacy of the vaccines were satisfactorily established for each cohort for which the provision of approval is being granted.
Data recently revealed in court papers in the United States clearly shows that vaccine harm was apparent in the clinical trials that Pfizer, BioNTech and others conducted. This information, if ATAGI had bothered to ask for it, should have resulted in a refusal of the application for provisional use.
No data was provided to the secretary regarding individual test subjects—technically, anonymized patient clinical data. No independent analysis of the fundamental issues surrounding novel mRNA vaccines was conducted in Australia—none in Australia!
Instead, the secretary took Pfizer, AstraZeneca and Moderna’s word for it.
I will say that again: the secretary took pharmaceutical companies’ word for the safety of their products.
These are the same pharmaceutical companies that have been fined over and over for criminal behaviour.
AstraZeneca got a US$355 million fine for fraud and, separately, a $550 million fine for making unfounded claims about efficacy.
Pfizer got a $430 million fine for making unfounded claims about efficacy, and a $2.3 billion fine—that’s billion dollars—for making unfounded claims about efficacy and for paying kickbacks.
This is who the Liberal-Nationals, Labor and Greens—our very own pharmaceutical lobby—want to pay more money to. That’s not on the basis of extensive local testing and inquiry, it’s simply on the basis of taking pharmaceutical companies safety assurances. There’s no testing. It’s an assurance made easy by indemnity against any damage that the vaccines cause. What deceit! What criminal incompetence!
The Labor Party and the Liberal-National Party have accepted $1 million each from the pharmaceutical establishment in this election cycle alone. Billions more are being set aside in this week’s budget to pay the pharmaceutical companies to keep the COVID-19 gravy train going. What great value this parliament provides for those electoral donations.
Mention should be made of the TGA’s decision to ban safe, fully approved and widely accepted alternatives to COVID-19 vaccines. This includes hydroxychloroquine and ivermectin; vitamins, minerals and natural antivirals; as well as proven messaging around healthy eating and lifestyles. The decision to ban proven, safe, affordable and accessible alternative treatments that are working around the world was taken to ensure the fastest and widest-possible adoption of the vaccines.
The TGA’s own customers fund the TGA. That means pharmaceutical companies fund their own product’s approval. That fails the pub test. Where are the checks and balances? There are none.
The Australian Bureau of Statistics is culpable in this scandal and cover-up. The Australian Bureau of Statistics’ annual budget is $400 million. The most recent mortality data they provide is from November last year, four months behind. The most recent breakdown of mortality by cause and age is from 2020.
The most recent data on live births is from 2020. Birth data used to be available six weeks after, not 15 months and counting. Are they hiding miscarriages?
At what point do we consider the actions of the TGA, ATAGI and the Australian Bureau of Statistics as interfering with the operation of the Senate? Peer-reviewed and soon-to-be-published data that must require the secretary to cancel the provisional approval of the vaccines has been released from outside of the government.
Let me review those quickly so the Senate fully understands the extent to which we have been misled.
Firstly, freedom of information documents indicate the TGA has failed to assess the reproductive toxicology of the COVID vaccines. Freedom of information documents indicate the TGA has failed to assess the impact of microRNA sequences and related molecular genetic issues on the human body.
Peer-reviewed and published in-vitro research shows gene based vaccine-generated spike proteins can migrate into human cell nuclei to disrupt DNA repair mechanisms. The TGA has dealt with this abysmally—murderously?
Vaccine-derived RNA can be reverse transcribed, leading to possible integration into the human genome, which the TGA denies, based only on pharmaceutical companies telling them to deny it.
Internal Pfizer data released in February indicate they accept 1,272 different adverse vaccine events, including paralysis and death.
German and US insurance actuarial data suggests the TGA’s database of adverse event notifications is underreporting side effects ninefold.
Freedom of information documents from 2018 show the TGA keeps two databases of adverse event notifications: one internal, showing all reports of harm; and one public, showing only a part of those.
This means vaccine harm is most likely significantly higher than reported.
Without honest and accurate data, the Senate has no way of deciding how much harm is too much harm.
German pathologists describe pathological aggregates of spike proteins and lymphocyte infiltrations in inflamed organs in autopsies related to death post vaccination.
In response, the TGA is failing to conduct autopsies on the 800 Australians the patients’ own doctors have reported as having died from the vaccines. What the hell is the TGA hiding?
Whistleblowers to the British Medical Journal provided reports of inadequacies, irregularities and possible fraudulent practices in the Pfizer vaccine trial—you know, the same trial for which the TGA took Pfizer’s word.
From a modern immunological perspective, two frequent vaccines for respiratory viruses run the risk of desensitising the immune responses to the virus, and that leads to hypoimmunity and worse illness than without the immunisation. To put that simply: repeated vaccination is doing more harm than good.
These are the matters I sought today to refer to the Senate Select Committee on COVID-19 without success. I thank Senators Hanson, Abetz, Rennick and Antic for their support, integrity and courage.
The truth is the Select Committee on COVID-19 has been running a protection racket for the pharmaceutical industry, and today’s vote proves it.
This unprecedented betrayal of the Australian people must be referred immediately to a royal commission. To the Prime Minister, the health minister, the federal health department and all those in the Senate and the House of Representatives—all of you who have perpetrated this crime—I direct one question: how the hell do you expect to get away with it?
We’re not going to let you get away with it. We won’t let you get away with it. We are coming for you. We have the stamina to hound you down and we damn well will.
COVID UNDER QUESTION is a cross-party inquiry into the Government’s response to COVID held on 23rd March 2022. COVID Under Question was hosted by Senator Malcolm Roberts (One Nation Federal Senator for Queensland) and attended by Stephen Andrew (One Nation Queensland State MP for Mirani), George Christensen (Federal Nationals MP for Dawson), Gerard Rennick (Federal Liberal Senator for Queensland), Alex Antic (Federal Liberal Senator for South Australia) and Craig Kelly (Federal Palmer United Australia MP for Hughes).
Parliamentarians heard from a range of Doctors, experts, economists and everyday people about how the Government’s response to COVID has affected them and at times defied belief. The absurdity of Chief Health Officer dictates and power hungry politicians is all laid bare.
The full day’s proceedings were recorded and available for public viewing.
“To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough
to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out.
This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs.
Instead of being held, rocked, and comforted in the time intervening between their birth and
their death, they have organs cut out of them alive.”
With the release of COVID vaccines, and then the mandates, we’ve seen a new resurgence of people attempting to gain religious exemptions.
Many of these attempts focus on fetal tissue obtained through abortion.
On January 19, 2021, AnnaMaria Cardinalli published an explosive article in Crisis Magazine, headlined, “Catholic Conscience and the COVID-19 Vaccine.”
Cardinalli details the collection of fetal tissue for the cell line named HEK 293.
The tissue was taken from an aborted infant in the Netherlands in 1972-3.
This cell line was used for “testing” the Moderna and Pfizer vaccines.
Cardinalli writes: “We know that the Pfizer and Moderna vaccines do not use any cells derived from abortion in the production process. That is, we know that we are not being directly injected with fetal cells or their engineered descendants (though this fact differs with other manufacturers). We hear that the abortion-derived cell lines were only used in testing, which should somehow comfort us, though it still means that the vaccines from which we seek to benefit depend on the involvement of abortion. We are told that the cell line used in testing came from one abortion, which took place decades ago. These things are all true, but they do not serve to inform us fully.”
“What we may not know follows. The most prominent cell line, called HEK 293, comes from an abortion performed in the 1970’s…”
“HEK stands for human embryonic kidney. To harvest a viable embryonic kidney for this purpose, sufficiently healthy children old enough to have adequately-developed kidneys must be removed from the womb, alive, typically by cesarean section, and have their kidneys cut out. This must take place without anesthesia for the child, which [anesthesia] would lessen the viability of the organs. Instead of being held, rocked, and comforted in the time intervening between their birth and their death, they have organs cut out of them alive.”
“There is no way that a spontaneous abortion could result in the cell line (as the kidneys cannot remain viable past the brief window in which they must be harvested) or that some brilliant researcher found a way for great good to come out of a rare tragedy by making use of a child’s body donated to science after it was aborted. The deliberate killing of an unwanted child (a little girl, in the case of HEK 293) took place in the tortuous manner it did precisely to obtain her organs for research. The harvest of her organs was the direct cause of her death, prior to which, she was a living child, outside the womb.”
“I fear that Pope Francis and Pope Emeritus Benedict may not have had this information when they received the vaccines. If we re-examine the Vatican statement that ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from aborted fetuses in their research and productions process,’ we see that it does not apply here. It does not imagine this scenario. To approve of the currently-available vaccines, it would have to read ‘it is morally acceptable to receive COVID-19 vaccines that have used cell lines from living persons, killed by the harvest of their organs for use in medical research and productions processes,’ but the Church’s moral teachings could never truly bend so far.
Similar to the human rights abuses exposed by international tribunal in today’s China, where unwanted individuals such as religious and political dissidents are executed by the harvest of their organs for profit, the little girl whose cells gave rise to the COVID-19 vaccines was brutally sacrificed for the purpose, as were all the children whose cell lines failed before her.”
After reading Cardinalli’s analysis—not only should the granting of religious exemptions from vaccination be a foregone conclusion; the whole field of fetal tissue research, going back many years and involving many pharmaceutical products, should be put on trial.
The people who have been carrying out the murders, the people who have been using the harvested tissue, the companies—all of them—on trial.
I hope many medical professionals will take Cardinalli’s article as a springboard, and weigh in on what she is very clearly stating.
And not just doctors. All people who are shocked by her conclusions.
So far, I see one counter-claim to Cardinalli’s assertions:
The notion that the kidneys of the aborted baby must be harvested very quickly is false. The kidneys can survive for a longer period.
On that score, I refer you to a devastating video interview conducted by Robert Kennedy Jr. His guest was SOUND CHOICE PHARMACEUTICAL INSTITUTE “President and Founder, Dr. Theresa Deisher Ph.D., [with] over 30 years of pharmaceutical research and leadership experience. She discovered adult cardiac derived stem cells, has worked on their therapeutic uses as an alternative to human fetal DNA, and leads a team of scientists at AVM Biotechnology dedicated to changing what a diagnosis of cancer, autoimmunity, or chronic infectious disease means to patients and their loved ones. As a result of this work, Dr. Deisher is named as an inventor on over 47 patents.”
In the first 15 minutes of the interview, Deisher makes it quite clear that infants in the womb are taken out alive, with their blood supply functioning (essential) and then killed by cutting out their hearts or their brains. This is what is done in order to obtain tissue that will be turned into fetal cell lines.
Since this act of murder is standard practice, it would appear it was committed against the live baby whose kidney cells became cell line HEK 293, used in testing the COVID vaccines.
At the top of the interview, Kennedy said he didn’t want to get into the moral aspect of fetal cell lines. But after listening to Deisher, he was quite shaken. He said so. He said they would have to cover the moral aspect.
The whole world has to.
Here is the basic ramification: THERE IS A RELIGIOUS EXEMPTION FOR THE WHOLE WORLD.
For all people of faith. Every faith.
“According to my religious belief, the murder of an undeniably live infant for any reason is unconscionable and evil, and I refuse the vaccine.”
Here is a Force against which no government, no establishment, no secret society, no wealth can stand.
I fully understand all sorts of professionals will spout language that purports to show “the aborted infant was not alive, the lab followed all the legal guidelines, this is an old argument that has been debunked…”
But this is not just an old argument. This is the equivalent of an opening statement in a murder trial. Nothing less.
If religious leaders will read AnnaMaria Cardinalli’s article, they will see how important her charge is.
The question isn’t “will people of faith wake up and do what they should”; the question is “how can any person of faith NOT do what they should”.
If they will make a stand; if all people of faith will; the entire dire situation we are facing changes in the blink of an eye.
Solomon to God: “You have made Your servant king instead of my father David, but I am a little child; I do not know how to go out or come in…Therefore give to Your servant an understanding heart to judge Your people, that I may discern between good and evil.”
Gautama Buddha: “To cease from evil, to do good, and to purify the mind yourself, this is the teaching of all the Buddhas.”
John 10:10: “The thief comes only to steal and kill and destroy. I came that they may have life and have it abundantly.”
Would any church, any religion in the world say that God wants the killing of live infants for the purpose of medical research?
In the midst of this COVID tyranny, haven’t we all been looking for a truth that will galvanize huge numbers of people?
And not as some kind of stunt. But rather as an inevitable outcome of deep faith.
Faith and justice come from the same everlasting tree.
The People’s Convoy will head back to California on Mar. 31 to protest “10 objectionable COVID-19 bills” being debated in the CA state legislature. They are leaving just a few days short of a month-long stay at the Hagerstown Speedway in Maryland. Prior to its Mar. 4 arrival in Hagerstown, the Convoy embarked on a 10-day cross-country slow roll from Adelanto, CA, beginning Feb. 23. The Convoy plans to return to the D.C. area after the protest in Sacramento.
The follow-up convoy will first stop on Apr. 10 for a Defeat the Mandates Rally with the Convoy’s partner, The Unity Project, in the Los Angeles area. They will then head to Sacramento for their protest against the proposed COVID-19 bills.
California Legislature COVID-19 Bills/The People’s Convoy/The Unity Project
The Unity Project
Contrary to some reporting, the Defeat the Mandates Rallies led by The Unity Project are not anti-vax rallies. Rather, the rallies are meant to reinforce the belief that “mandates are government overreach and that getting a vaccine should be a personal choice.”
The Unity Project/Statement of IntentionSpearheaded by several physicians and scientists, including well-respected, experienced physicians like Dr. Malone, Dr. McCullough, and Dr. Harvey Risch, the Unity Project has spoken forcefully against the vaccine mandates. Quoting Pfizer and Moderna, who state that the shots are “gene therapy” and are experimental, the participating doctors and scientists believe receiving the shots should be left to personal choice. They also think that handling the COVID-19 pandemic has subjected citizens worldwide to egregious measures that were completely unnecessary in many instances. Drs. Paul Alexander and Pierre Kory have often traveled with the Convoy and spoken at several of its rallies. Dr. Malone spoke at a Mar. 26 event in Hagerstown.
The Unity Project is now sponsoring a canvassing campaign powered by volunteers to educate Californians on the dangers of the COVID-19 bills that are currently on the floor. The website also features a series of videos to educate Californians about what is in the bills and why Californians should beware. The flier for the canvassing campaign is available in both English and Spanish. If passed, the bills will, among other things, add COVID-19 shots to the childhood immunization list for public and private schools and will classify “anti-COVID medical opinion as ‘unprofessional conduct.’”
Information on The People’s Convoy website contends that passing the bills is not only dangerous but would “set the stage for other states to introduce similar laws.”
These universally dangerous bills are about to be voted on in the California legislature! If passed, these bills will change everything for people who want to Live, Work or Learn in the State of CA while exercising their right to medical freedom.
If passed, these bills set the stage for other states to introduce similar laws. We know that what starts in CA, spreads to other blue and purple states and potentially at a federal level. This affects everyone!
The Route
A Mar. 28 press release from the Convoy explains that the trip to California represents a continuation of their mission to end emergency orders and mandates—The People’s Convoy “is in this for the long haul,” said one of its organizers, Marcus Sommers.
The truckers’ website has posted a tentative route for the Convoy. Still, specific stops and rally points will be withheld until the day of travel, just as was the protocol for their earlier cross-country trip for the safety and security of its participants. The Convoy will begin its journey on I-81 heading south, picking up I-40 to head West and then to I-20 and I-10 into California. It will then travel I-5 up to Sacramento after a brief stop in the Los Angeles area.
Map/Hagerstown to Sacramento/The People’s ConvoyPublicity for The People’s Convoy has been disappointingly scarce, and their rolls of the beltway have, at times, been met with significant resistance from authorities. However, the truckers and their allies have been undeterred. The Convoy rolled the beltway almost daily, and leadership members managed to secure meetings with Senators Ted Cruz (R-TX), Ron Johnson (R-WI), and other government officials. Senator Ted Cruz also made the trip to the Speedway on Mar. 10 to speak with the Convoy, and he then joined lead organizers Mike Landis and Brian Brase for a roll on the beltway before they delivered him to his press conference in D.C. later in the day. Several truckers were also able to make it into D.C. proper on several occasions, despite the blockades on exits to the Capitol and surrounding areas.
UncoverDC traveled with the Convoy on its initial trip. Conversations with several original truckers indicate that many in that group have had to leave to go back to work. Several truckers who have left the Convoy told UncoverDC that their “savings have been depleted,” and they have to make up for time lost; however, they will continue to work locally to ensure they are better represented in the future. Trucker Bonnie Kelly says she hopes that the convoy “will pick up steam again” along the way, just as it did with the original trip.
A compilation of videos and stills from the February/March trip shows consistent and massive support for the truckers’ mission on overpasses, highways, and cities—big and small—along the way.
In an appearance on “RFK Jr. The Defender Podcast,” Michael Nevradakis, Ph.D., a reporter for The Defender, explained how the two global asset giants pushing for vaccine passports also stand to profit greatly from orchestrating them.
Financial houses BlackRock and The Vanguard Group, two of the world’s “Big Three” asset managers, have profited “enormously” from the COVID-19 pandemic, according to Robert F. Kennedy, Jr.
On the March 23 episode of “RFK Jr. The Defender Podcast,” Kennedy interviewed Michael Nevradakis, Ph.D., a reporter for The Defender, about what Nevradakis uncovered about the far-reaching influence of these two corporations.
In an article he wrote last month for The Defender, Nevradakis exposed BlackRock and Vanguard as two of the top three shareholders in COVID vaccine makers Pfizer, Moderna and Johnson & Johnson.
Kennedy pointed out that BlackRock and Vanguard are the two biggest financial houses in the world. “They control a huge part of the world economy,” Kennedy said.
In 2020, Bloomberg called BlackRock “the fourth branch of government,” said Nevradakis.
He added:
“There’s this very strange cross-ownership where Vanguard is the biggest shareholder in BlackRock and BlackRock is the biggest shareholder in Vanguard … regardless of how some people may try to spin it, it’s obvious that these two companies are closely linked and their fortunes are closely linked.”
The two firms own many major and influential U.S. companies, including American Express, T-Mobile, Twitter and Disney, as well as Big Food and Big Pharma interests.
Nevradakis and Kennedy discussed the connection between BlackRock or Vanguard ownership and vaccine passports.
“[BlackRock and Vanguard] own companies that are at the speartip of pushing for vaccine passports, and also that stand to profit greatly from making and controlling and orchestrating the vaccine passports,” said Kennedy.
In his article, Nevradakis listed major U.S. employers that, as of Feb. 16, mandated COVID vaccines for their employers, and quantified these companies’ relationships with BlackRock and/or Vanguard.
Most of these companies are owned in large part by one or both of the firms. They include pharmaceutical company Abbvie, grocery store Albertsons, health insurer Anthem, Chevron, Delta Airlines and Cigna, among many others.
The “sinister aspect” of these revelations is the idea that competitive capitalism may be an illusion in the U.S., Kennedy pointed out.
Nevradakis agreed. He said:
“The original idea in theory behind [capitalism] is that of competition. And I think that we’re not seeing that in reality. We have very, very large companies, and those large companies are owned by even larger asset management companies. And then … the two largest ones of all also happen to own each other. So I don’t think there’s any way that that could be spun as a competitive situation.”
Watch the podcast here:
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
Below you will find a video presentation by Dr. Tom Cowan. The questions Dr. Cowan raises, the facts he presents, and the clarity he brings to the discussion of “viruses” and the field of virology are essential to our global conversation and quest to understand the truth. Truth Comes to Light has provided a basic transcript and added links to references for added clarity.
Over the past few years, we have shared many articles on this site related to this inquiry into the truth about “viruses” and the whole field of virology, including information on terrain theory vs germ theory. Find links here: Viruses, Vaccines & the History of Modern Medicine. At the end of this post you will find a selected list of related articles.
A few quotes from Dr. Cowan’s video:
“Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?”
“They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
“Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.”
“So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
“So I ask myself how did they do that?”
“What in the heck are these guys doing in these labs? What is gain of function research?”
“Do we really know if mRNA is in these vaccines?
“Where is the paper? Where is the evidence that there actually is mRNA in these injections?”
Okay, so before I get into talking about the question that so many people keep asking me: What about gain of function, lab-created viruses, bio labs now allegedly in the Ukraine?
So what is the science behind that?
So we’ll get into that in a minute. And before that I have a very short, little clip to play.
So that clip pretty much sums it up. That was from our friend Dr. Sam Bailey and our other good friend Stefan Lanka.
So on that note, the reason I wanted to talk about this subject is there was a recent paper that was put out by Dr. Mercola…
So let’s just read the first couple paragraphs there. So this is a summary:
“A study published February 21, 2022, (so very recently) in Frontiers in Virology claims to have discovered that a sequence of the virus’ spike protein is a 100% match to a modified messenger RNA (mRNA) sequence patented by Moderna in 2016.
The genetic sequence patented by Moderna is part of a human DNA repair gene called MSH3. This patented sequence is found in SARS-CoV-2’s furin cleavage site in the spike protein — the part that gives the virus such easy access into human cells.
According to Moderna’s patent application, the gene sequence was modified “for the production of oncology-related proteins and peptides,” ostensibly for use in cancer research.
According to the researchers, the chance that SARS-CoV-2 would have randomly acquired this furin cleavage site through natural evolution is 1 in 3 trillion.”
Okay, so why is this important? So obviously, there’s been a lot of attention in the political sphere and in the anti-vax community. There have been movies written about this.
There are many lectures, many prominent people in the “freedom” or “anti-vax” community who are investigating these patents, and saying that these patents — and as Dr. Mercola said, this study in Frontiers in Virology is literally the smoking gun proving that Moderna patented a sequence, which ended up in SARS-CoV-2, “the virus”, and the only way it could have gotten there is, not through natural evolution (that is a one in three trillion chance) but if it was introduced into the virus by some laboratory technique.
This theory is crucial to our understanding, not only of whether there were crimes committed, but the whole theory of virology and gain-of-function research and all that.
So, obviously, and this should go without saying, that the most important part of this is: Is there actually a SARS-CoV-2 virus? And, if there is, what is the genome? And how was it found?
The rest of the article goes on to talk about what we know about this MSH3 sequence and the protein that it allegedly codes for.
But I want to emphasize again and again and again — the whole point of this is: This sequence which was patented by Moderna in 2016 is identical to the sequence found in SARS-CoV-2.
That is the point.
If we can demonstrate that there is no SARS-CoV-2 and this is not the genome of this alleged virus, then none of the rest of this has any validity or is of any use at all.
It’s all just a sort of smokescreen or a way to throw us off the track about finding out what really is going on.
I cannot emphasize how important this is.
So for the next few minutes we’re going to actually look at how the authors of the article in Frontiers of Virology — what were they claiming was the SARS-CoV-2 genome?
What were they claiming was the evidence that there is a SARS-CoV-2 virus that they could then compare the patent to?
Again, if there’s no virus and there’s no genome then they can’t possibly have put this sequence into a virus or a genome. And it can’t possibly be the thing that’s affecting the world.
So, now let’s be clear about the next step. There is no mention in this story by Dr. Mercola of how the Frontiers in Virology authors found the genome or found the virus.
[…]
In other words, there is no information in here of how Dr. Mercola actually knows there’s a SARS-CoV-2 genome.
But the authors of the Frontiers in Virology paper said that they were comparing the sequence, the mRNA sequence patented by Moderna in 2016, to the genome found in our old friend paper by Chinese virologist Fan Wu.
So it isn’t that we picked this paper by random. It isn’t that I picked this paper to investigate how they found the genome or what their evidence for the virus was. This is the paper that the authors of the Frontiers in Virology use to compare the Moderna patent to.
So we’re using their information and this is their evidence, their proof that the virus exists.
So this is about: Did the paper by Fan Wu prove that the virus existed — the SARS-CoV-2 virus exists — and that this is the genome of the virus?
Again, in order to say that the patented sequence matches 100% to the genome of the virus, obviously, obviously, you have to know that this is actually a virus.
So, this is an old friend, we’ve been through this many times, but let’s see what they say.
So here is the paper, published in the prestigious journal, I believe, Nature — February 3, 2020.
So this is the paper, again, that was cited by the authors of Frontiers in Virology paper that is used as the reference genome.
So how did they do it?
So first we have a summary.
So how did they identify the “virus”? So I’m gonna run down the steps that they used and then we will show the clips, the actual wording from the paper, so that you know that this is actually the facts.
Okay, so we’re looking to find a virus and then find the genome of that virus — a virus that had never been found before.
So first thing they take lung fluid from one person. That’s a huge sample size (that’s a little tongue-in-cheek). That’s obviously just one person. That is a kind of ridiculous experiment to find a new virus.
Then they isolated the RNA, which is a genetic material, from the fluid in that person’s lung. They did not attempt to purify any particles that they could say you were a virus. They did not do any pictures of any virus. They did not do any maceration, filtration, ultracentrifugation to see if they had any such particles. None of that.
They took RNA from the lung fluid, of which we have many possible sources. We have bacterial sources, fungal sources, human sources, possibly viral sources, exosome sources, multivesicular body sources — many sources of RNA. We have no idea the source of that RNA.
Then they create what’s called an mRNA library, which is a catalog of all of the RNA pieces that are in that lung fluid.
This requires that they amplify these pieces of RNA with the process called RT-PCR. And, as we have demonstrated over and over again. and is completely substantiated in the literature, doing PCR amplification of RNA cycles inevitably creates new sequences of RNA which weren’t there in the original sample.
In some cases, if you do enough amplification cycles — up to even 80% of the sequences — after 45 cycles are made de novo, or anew, by the actual PCR process itself.
So now we have yet another source of our RNA. Not only do we have potential viruses, exosomes, multivesicular bodies, apoptotic bodies, human lung tissue, human epithelial lung tissue…, fungal RNA, bacterial RNA — we also have new pieces of RNA generated by the test itself.
Then they performed pair and sequencing that generates 150 base pair reads. That means they matched the sequence by pairing the ends. And you end up with sequences that are basically 150 base pairs long. That’s a fairly small amount. And this results in 56.5 million of these 150 base pair sequences known as reads.
So to be clear, they take this mass, not knowing any idea the origin of these mRNA, they chopped them up into sequences that are 150 base pairs (that’s fairly short) long by pairing the ends. They have 56.5 million of these reads. And then they start doing what’s called de novo assemble.
So there is no sequencing here. There is assembly. And, as it says, you can make a lot of genomes with that many reads.
So they put these 56 million, 150 base pair, reads in aa assembly computer program and… they actually put it in two different computer programs. And one of the computer programs generated 384,000 different sequences. The other one generated over a million sequences.
So now these sequences — all 384,000 of them — are meant to be the possible genomes of this virus. For some reason, they threw away the program that made over a million of these sequences and said the one that made 384,000 — I think that was Megahit — one of those must be the right sequence, the actual sequence of the virus.
Just to be clear, at no point did they ever find a particle. At no point did they purify or isolate a particle.
At no point did they find in any particle… an entire string of RNA, which they then sequenced one by one to find out the sequence of the genetic material of this particle.
None of that was done. All they did was chop up RNA from many different possible sources, put that in a computer program, generate 384,000 and a million in another, and then they went hunting for infectious agents and performed a search of those sequences.
The two longest sequences were a close match to a bat SARS-like coronavirus genome, found 15 years ago or so, that was made in exactly the same way — never having isolated or purified a particle, never having found an intact genome, never having sequenced the genome.
They just did the same sort of assembly, no sequencing of RNA from God knows where. And, this one, the longest one was a 89% match to the previous SARS coronavirus that they did in the same way.
And, as we say: Boom! There is the new novel human coronavirus — even though, as we’ve said over and over again, humans and chimpanzees are about a 96% match. So to say it was an 89% match is essentially like saying there’s no way this could have been anywhere similar to the previous bat SARS-like coronavirus.
In other words, they never found a virus. They never found a genome of this alleged virus. And so there is no possible way they could say that the Moderna patent was found in this virus. Because the virus simply doesn’t exist.
Therefore, any attempt to say that this was a lab-created, engineered virus is simply anti-scientific because there is no genome that was actually found that it could have been made into.
This is a manuscript draft and I don’t know when it will be published.
When I read this, just remember that all these articles that go into The Lancet have to pay homage to the virus god. But I will explain what they mean here.
So this is the interpretation of the entire article. I won’t go through their methods.
“The RNA code counted in PCR tests, previously attributed to SARS-CoV-2, belongs instead to a respiratory-virus-induced immune system response by human cells that liberate exosomes, and that vitiate PCR test results. PCR tests have zero specificity in vivo due to the exosome RNA.”
[…]
And they go on in this article, just as we’re saying — the reality is all of these RNA sequences, all of these reads which were assembled into a viral genome, actually when you do careful analysis, come from human epithelial lung cells.
In other words, just as we’ve been saying all along, these are not viruses. These are breakdown products of our own tissue. And the misconception in calling them a virus needs to stop.
And this idea that they put this patented sequence into a virus can’t possibly be true because, simply, there is no virus.
And all the rest of the article is for not — because nobody put a RNA sequence, patented or otherwise, into a virus.
Now just to show you that we got this from the article — so here is the one patient presenting with cough, etc. So that’s the evidence that we were correct about the one patient.
Here is the evidence that the paired and 150 base pair reads sequencing of the RNA library was performed on this computer platform. So the sequencing yields reads of only 150 base pairs. The whole SARS-CoV-2 genome is supposed to be 30,000.
That means they had to stitch it together using a computer program. This was an assembled genome, out of little bits from God knows where.
And here we see the 56.5 million reads were assembled using Megahit and Trinity. Trinity, they got over a million. They generated a total of 384,000 contigs (that’s sequences).
Trinity generated 1.3 million. They don’t like those because they weren’t long enough. They compared those with the database and compared and found that it was somewhat, although not really similar to a previous bat coronavirus. So, as he says, sequencing results in more than 56 million reads.
How can you possibly differentiate what is from a potential virus from everything else? The answer is you can’t.
And finally… The longest contig is generated by Megahits. The longest one by Trinity is 11,000. How come they didn’t use this one?
Both showed similarity to bat coronavirus. They were found at high abundance. It was only 89 percent similar. That means 11 percent didn’t match. That is a huge amount.
Then they just moved on to develop primers all from this one assay without isolating anything, and from one patient.
And, my friends, that is not science; that is propaganda, as is the entire story of a lab engineered virus.
Now, the real issue here and one of the reasons why this, to me, is so important, is if you go by this unscientific theory that there’s a lab-created virus, you actually miss what I would say are the three most important questions to be asked, and then answered, about this situation.
And so now I’m talking — I would say theory. Where everything else was what I would call simply facts.
So the question that should be asked (and it would be nice to have answers for, and which I don’t have the answers for, but I have some theories) is, to me, the most interesting thing is —
So we have this published genome, fraudulent as it is, by a bunch of Chinese virologists. Right? They come up with this fraudulent, irrational genome. And, lo and behold, it matches a patent taken out by a company called Moderna in 2016.
So I ask myself how did they do that? How did they make — like there’s two theories, there’s two ways of looking at this.
One is: They don’t want that to happen and so it was a mistake.
But, if we think, which I’m inclined to do, that “they” (meaning Moderna and other people) wanted this to happen so that they could throw people off and essentially create a kind of patsy out there, how did they do it?
So I have three possible theories as to how they did it.
Now, let me be clear.
What I’m trying to figure out is these guys Fan Wu and others, Chinese virologists, having, I don’t think, any connection with Moderna, come up with a bogus, anti-scientific genome and for some unbelievable coincidence — let’s say for now — it actually matches exactly one of the patented sequences from the Moderna patent of four years prior. How did that happen?
So possibility number one: It was dumb luck. They just made this sequence and it just so happened to match the Moderna patent. And, frankly, I don’t think that’s actually the right answer.
The second possibility: … Somebody from Moderna or somebody — I don’t know who — calls up Fan Wu and says ‘I want you to make a genome out of nothing and I want it to have this particular sequence in it so some day people will find this out and say “you see, they genetically engineered this sequence”‘. Got it? In other words, there was collusion between the patenters (that’s Moderna) and Fan Wu and his team.
Now I gotta tell you, I actually don’t think that’s true. I would actually love to find out if it is true and if there is a phone call from doctor head of Moderna saying, you know, ‘Hey Wu, would you put this sequence in there so that we can — people find out that it was a genetically engineered sequence?’ But I just don’t think that happens.
And then I came up with a third possibility which is: Once I discovered all these people who are looking into all these patents, that there was at least 70 different patents taken out, of different sequences of RNA, that could end up in a genome. Now, my guess is … I would think it’s a good possibility that one of those sequences may end up in the final genome. And then you would then implant the story that this was a genetically engineered organism and there you go.
So you wouldn’t have to rely on luck, you wouldn’t have to actually have collusion, you could just patent a whole lot of different sequences, for instance, that came in the SARS-1 genome. You could patent all kinds of sequences knowing that, at the end of the day, when somebody makes up this new fraudulent genome it’s bound to have one of them in there. Somebody will find it some day, say it’s the smoking gun and you then implanted the story of the century which does nothing but throws people off.
So those are my three options. I’d be happy to hear about any other possible options. But those were the only three that I could come up with.
Now, the final question then is: What in the heck are these guys doing in these labs? What is gain of function research?
And, I must say, I don’t know what they’re doing in the labs and I don’t think really anybody knows — including in the Chinese labs or Ukrainian labs or North Carolina labs or any other labs.
So again, I have some possibilities.
One is the following …
Screenshot image from BrandNewTube video (specific video source unknown)
They’re doing this.
In other words, what the virologists do is they dress up in hazmat suits and they go on to their computer and start making sequences. And the hazmat suits are crucial, because, as we all know, it’s very possible for the sequences to jump from the computer into their eyes. So it’s very important, as you can see, that they wear goggles and protective head gear to prevent the computer sequences from jumping directly in their eyes.
In other words, they may be just doing nothing and it may be just a whole lot of hooey to get people to worry about things. And to implant in their minds that there is this horrible engineered virus, that we should all be scared of viruses, etc. So that’s one possibility.
Another one is they’re making some sort of proteins or genetic material which can be injected into people. In other words, they’re making toxins. And that is certainly possible.
So those are the two main categories that I came up with. Either they’re just doing nothing and they’re just a front, or a smoke screen, or they’re actually making stuff which isn’t good for people.
And that gets into my final thing that I want to point out.
… This section right here. this is something I’ve been very interested. So this is again from the Mercola article:
“For clarity, this may have nothing to do with Moderna’s patented MSH3 sequence specifically, because the RNA code in the jab is not identical to the RNA code of the actual virus. (I’m not going to get into that.) The RNA in the jab has been genetically altered yet again to resist breakdown and ensure the creation of abundant copies of the spike protein. 11“
Now, I have been asking the question now for months: Where is the paper? Where is the evidence (a) that there actually is mRNA in these injections? They say there is. That’s the whole point. But when people look there either seems to be not there or in variable amounts depending on which injection and which batch.
So it could be that even the whole mRNA in the jab is a actual smokescreen or cover for what’s really in these injections –which is a lot worse stuff like self assembling nanoparticles which we’ve heard about a lot.
So I was very interested to see that this was… stated as fact, because I can’t find a paper, and my friends can’t find a paper, that confirms that abundant copies of this protein are actually made when you inject this sequence.
And this would be like saying — if I wanted to get investors for my new pencil factory, my investors might ask me to see the pencils that we make. And so it would be natural for me to produce copies of the pencils — maybe tens or hundreds or thousands or millions of them — to show that my technology for making pencils actually works.
One would think that if the whole point of these jabs is to make you make spike proteins that, therefore, “confer immunity”, there would be scores, hundreds, thousands of papers showing here’s the amount of spike proteins in an unjabbed person. And then you jab them and then 10 minutes, half an hour, three hours, two weeks, six months, 12 years later, here’s the amount of spike protein. That would prove that the concept is real and that you can actually genetically alter a human being.
Because I have my doubts. So I’m looking for a reference to show this is true. And, lo and behold, here is the reference. Number 11. [see page 3 of Mercola article] So where is the reference from? CBS News.
Now, I could say — I would say if it was from Fox or MSNBC then I would be skeptical. But the fact it’s from CBS, that must mean it’s true. And obviously I’m kidding. Let’s see the reference.
If the whole point of this is to put RNA into injections, make you make a spike protein which is allegedly from the virus, let’s actually see that it works. And here’s a quote saying there’s at least 73 patents.
My guess is one of them was bound to show up in the imaginary sequence. Bingo! We’ve got proof that it’s there, that it was a genetically engineered virus.
And the whole thing, hopefully you now see, comes crashing down like a house of cards if, as we showed, there was no virus genetically engineered or otherwise in the first place.
[At this point in the video, Tom takes questions from the viewers.]
Question: So this one is related, but it has to do with Dr. Bush‘s reference to 10 to the 30th power of viruses within our blood, as well as in the oceans, in the soil. His purpose is to provide constant flow of updated genomic information that we need to in order to adapt and survive. And they’re not pathogens. That we need not fear, etc., etc.
Answer: So he also has said that, of course, viruses are pathogens. The real issue here is how did they find these 10 to the 30th power viruses? And I’ve gone over this, especially in reference to a paper, and I don’t remember the name, but it’s called the ….something to do with the renaming or the re-evaluating of viral…virome…viral world or something like that.
The reason people say this is because they don’t realize that they’re not talking about actual organisms or particles called viruses. They’re talking about liberated pieces of either RNA or DNA — little snippets of RNA or DNA which then get amplified in what’s called metagenomics sequencing and so there are billions and billions and billions of these breakdown products. None of them have anything to do with a virus. They’re simply little bits of genetic garbage that are coming off of our cells and tissues all the time. They have no particular meaning or function that anybody has been able to prove. They’re just little bits of garbage. And the misconception that they’re somehow actual particles and could possibly hurt you or could possibly help you is just a misunderstanding of how they found viruses in the first place.
They don’t find particles. They don’t purify particles. There haven’t been 10 to the 30th purified particles. We’re talking about little pieces of DNA or RNA that get amplified, called viruses, which is a misconception big time.
[Additional questions include speculation about the patent links to the Fan Wu team “discovery” as well as a question about allergies.]
Articles mentioned in this video presentation:
Moderna Patented Key COVID Spike Protein Sequence in 2016 by Dr. Joseph Mercola [originally published March 7, 2022 at this link — https://articles.mercola.com/sites/articles/archive/2022/03/07/moderna-patented-spike-protein.aspx — and was mirrored around the web. It can still be found at Dr. Mercola’s paid archive membership.] Dr. Cowan has provided a pdf file of the article here: https://brandfolder.com/s/fv2q4h7fp84bm5vb3ppn37
We’ve seen the unbelievable microscopy images of the experimental jabs from other investigators around the world, but we wanted to see it for ourselves! There are now 4 teams working on this in New Zealand and Dr Robin Wakeling has agreed to go public with his findings.
He compares the Pfizer jab to other vaccines and discusses the startling findings with Dr Mark Bailey.
For the past two years humanity has been under attack. And entire populations have been put under draconian restrictions under the claim that there is a pandemic.
For those of us that can see there is no evidence of a virus, the war on humanity is even more egregious.
However, within the wider circle of those questioning the covid narrative, a common theme is that something is badly wrong with the offered solution in the form of experimental vaccines.
By early 2020 globalist organizations were indicating the rollout of their touted universal vaccines and an injection in every arm.
In 2021 citizen scientists began examining the injections under the microscope and the revelations was startling.
At the forefront of the research has been the La Quinta Columna team who have produced many light and electron micrograph images, as well as detailed analysis of self-assembling particles, graphene components and potential nanotechnology.
Here in New Zealand we also have several teams who have backed up these findings.
Of course, there have been dismissals that we are just seeing artifacts or, in a sense, crystals.
That’s why we asked Dr. Robin Wakeling, a senior microbiologist and nano-emulsion delivery technology expert, to perform his own analysis of the Pfizer BioNtech product.
He joined my husband, Dr Mike Bailey, to explain the behavior of the product under the microscope. Over time and under the influence of various environmental factors, he compares his findings to known colloidal structures and other vaccines.
And, as the other investigators around the world, reaches some disturbing conclusions.
Dr. Mark Bailey
Welcome everyone. I’m doctor Mark Bailey in Christchurch, New Zealand, and it’s my pleasure to be speaking with Dr Robin Wakeling, coming in from Wellington, New Zealand.
Robin is a microbiologist, PhD and world expert in decay and mold forensics. He’s supervised polymerase chain reaction research and been a vocal critic of the pseudoscience taking place in the alleged covid pandemic.
Robin has thousands of hours of microscopy experience and has previously been involved in the development of patented nano- emulsion delivery technologies. So what better person to take a look at the Pfizer BioNTech products up close?
Now we’ve seen from some of the electromicroscopy images, coming in from other countries such as Spain and Germany, which have demonstrated that the injections contain what appear to be undeclared constituents including graphene oxide, and what could be interpreted as being nanotechnology.
Today we’re gonna take a look at the Pfizer products under the light microscope for ourselves and see how it behaves on a slightly larger scale and how perhaps that coheres to the overseas proceeds findings.
So Robin I’ll hand over to you and perhaps you can stop by telling the audience what kind of microscope you’re using and the grades of magnification we’re looking at.
Dr. Robin Wakeling
Okay, thanks Mark. Yes I use a compound light microscope with a basic magnification of 650 although the software that puts it on the computer screen sort of doubles that approximately.
I use phase contrast most of the time. A couple of the images are using bright field and polarized light.
And then I included a few images of other workers which were dark field. But most of my work was with phase contrast. And the magnification and scale, I’ll remind the audience of as we go through.
Okay, so the overarching theme of this presentation is what …. are the undisclosed ingredients in Comirnaty. We know that there are at least two declared undisclosed ingredients.
In other words they’re just coded. We don’t know what they are on the basis that they are proprietary excipients. So we know that there are some unknowns and possibly some undeclared unknowns also.
So that’s really the overarching question that we’re addressing.
[…]
There are three main findings of the microscopic images that we’re producing or suggesting — the key findings.
So the first one is that the lipid nanoparticles that are contained in Comirnaty — and I’ll explain what LNPs are in a moment — but it appears that they are continuing to self assemble in a way that forms much larger colloidal structures of some highly varied and somewhat rarefied forms.
The second main key finding was that these colloidal structures then seem to change their form in response to collision with interfaces like the glass surfaces of the microscope, preparations, or air bubbles, or other interfaces — whereby they start to take on a much more structured and unnatural formation with a lot of straight lines and right angles — sort of things that don’t usually occur in nature outside of crystallography.
And what we’re going to be showing most of the time has some profound differences to crystal structure. So we’ll cover that too.
And so the third finding, which is where the other two kind of lead to, and it’s where other workers have sort of jumped into the deep end with some of the dark field work that’s been done.
These right-angled sheets and wires seem to form colloidal structures… in some situations, where it appears that some environmental triggers are involved….
They seem to order themselves in a highly-ordered complex way — a way that is quite unusual. Certainly not something that the people who are looking at this have seen before. And these are people who should be familiar with this sort of thing…
Because some human beings care about their children, VAERS was established in 1990 as an early warning system to identify negative reactions and side effects of vaccination, which makes sense.
But there are major problems. It is managed by the FDA and the CDC, which explains why the VAERS database requires a class to learn how to find anything.
Taking the time to actually file a report is voluntary. And out of fear of losing their jobs or being considered an anti-vaxxer, nobody wants to speak ill of the all-holy vaccine, let alone make an official report.
It is estimated that only one percent of vaccine injuries ever get reported to VAERS. So that means when VAERS reports over 44,000 adverse reactions and 90 deaths, one can expect it to be as much as 4.4 million adverse reactions and 9,000 deaths.
And these numbers are only from the age 5 to 17 group.
Conservative numbers put it at 10 percent, which is half a million children that have been wounded and killed from an unneeded, unwanted, experimental gene therapy shot that we were lied to about every step of the way.
Thanks to the OpenVAERS project, which is built upon the VAERS data, the public can easily search these reports and see for themselves.
People are reporting adverse reactions such as chronic pain, loss of hearing and taste, talking gibberish, and acting out aggressively. And these are the mild cases.
There is a tsunami of major brain damage, heart disease and fatalities. Edward Dowd has analyzed the data and has reported an 84 percent increase in deaths among ages 25 through 40, which is the same amount of lives lost to the Vietnam War.
Toby Rogers estimates that Big Pharma kills twice as many people that died in World War II every single year.
The press ignores this because it’s not enough.
They want your newborn babies as well.
Pfizer is pushing to have children as young as 6 months old given a shot that we know is potentially fatal, even though children were never at risk and are still not at risk.
The United States has been force-injecting infants and children with experimental vaccines for years. And now they want to add the infamous ‘clot shot’.
Thanks to virtue-signaling mothers, some children have already been getting it in the womb which is resulting in miscarriages, still births, and deaths from breast feeding on toxic genetically-modified mother’s milk.
Pfizer is planning on submitting another application for emergency use authorization in early April.
That’s about 18 million children under five who could be sacrificed to the altar of Big Pharma and political correctness.
If Pfizer can achieve permanent liability protection from the FDA, who they control, then they can add the mRNA gene therapy shot to the childhood vaccine schedule where it will enjoy permanent liability protection under the 1986 National Childhood Vaccine Injury Act.
These same crooks are putting a judge on the Supreme Court who openly defends leniency towards crimes that involve child rape.
They’re coming for your children and they will not stop.
If you still care about the human race and are looking for something you can do right now, you can go to Toby Rogers at substack and read his urgent call to action for more info.
Dr. David Martin recently filed the first in a series of lawsuits in Federal Court “to get the truth out” about COVID-19 gene therapy injections and “take back America from the COVID pandemic scare.” In what he calls a “multi-step process,” Martin explains the first lawsuit will put into the public record “that the COVID vaccine is not a vaccine.” Instead, Martin explains the Injections are experimental gene therapies “known to kill people, known to actually stay inside of the human body for over 60 days producing pathogens that are scheduled toxins.”
The lawsuit, Griner v. Biden et al., was filed on Mar. 4, 2022, in the U.S. District Court in Utah on behalf of Devan Griner, MD, a double-board certified surgeon and widely published author who has transformed the lives of hundreds of children in Utah and beyond. Besides naming Joe Biden, defendants include Xavier Becerra of the U.S. Department of Health and Human Services (HHS), as well as the Centers for Medicare and Medicaid Services (CMS) and its leaders.
Martin maintains we need to stop forcing and bribing people to get the shot, stating, “Those are illegal acts in the United States and cannot be done.” Martin explains that the first lawsuit is in part litigation for discovery—revealing the criminal conspiracy Martin has talked about for years—as much as it is a litigation for the facts, as both are equally important. Martin is confident the disclosures that will have to be filed by the Federal Government in response to the first case “are, in fact, going to be incriminating for our next case.” Looking forward to obtaining evidence of the felony, Martin explained:
“We wrote this case so that the immunity shield falls away from the manufacturers and all of the injuries and deaths become civil liabilities to the manufacturers.”
Martin, who indicated that Utah is the perfect jurisdiction to begin his campaign, pointed out that when a term like “vaccination” is used, the public believes they are getting something that will keep them from getting sick or transmitting sickness. Instead, Martin asserts that after receiving the COVID-19 injection(s), individuals turn into a biological weapons factory. Explaining further, he declares:
“And [vaccination] is actually defined in the statute exactly that it’s the ability to put something into the body that stimulates the immune system. It turns out that the mRNA that’s being injected into people is not that. In fact, specifically, what it does is take a little computer-simulated strand of mRNA, it sends it into the body, and the body becomes a biological weapons factory. It manufacturers spike proteins. The injection does not stimulate any immunity.
[Instead], it is the instructions to make a scheduled pathogen. And the scheduled pathogen is defined under three different parts of the code, but it specifically includes genetic sequences derived from—are you ready for this—SARS coronavirus. That’s actually a scheduled, known toxin on the scheduled list of biological weapons in the United States code.”
The 32-page lawsuit, with 171 pages of Exhibits, begins by highlighting that the CMS mandate requires almost every employee of any healthcare facility receiving Medicaid or Medicaid funding to “receive one of the three Injections authorized for emergency use by the Food and Drug Administration as COVID-19 vaccines (the “Injections”).”
CMS Mandate Must Be Struck Down
The suit further explains that Plaintiff, Dr. Griner—who has natural immunity and refuses to take one of the injections—is a “highly skilled and well-known plastic surgeon licensed to practice in Utah whose passion is healing children who suffer from cleft palates and other congenital defects.” The doctor has traveled the world on more than twenty medical missions, donating his time to help unfortunate children. However, the lawsuit asserts that the CMS Mandate prevents Dr. Griner from continuing to heal children—unless he takes one of the Injections. Noting that Dr. Griner enjoys robust and durable natural immunity after having recovered from COVID-19, the lawsuit explains:
Dr. Griner is subject to the CMS Mandate because the hospitals in which he has the right to practice receive CMS funding. Thus, Dr. Griner must choose not just between his “job and the jab,” as the Fifth Circuit has phrased it, he must also choose between pursuing his passion for healing children with congenital defects and taking the Injection. This despite the fact that the only justification for forcing Dr. Griner to take the injection is the assertion that doing so will prevent Dr. Griner from transmitting SARS-CoV-2 to his patients and other health care workers with whom he comes in contact, something the CDC readily admits the Injection simply does not do.
The lawsuit insists the CMS Mandate must be “struck down” because overwhelming evidence—along with admission by the CDC Director—shows that the injections do not prevent transmission, infection, or reinfection in those who receive them. And despite the windfall profits being made by the big pharma giants making the Injections, the CDC has admitted that both the “vaccinated” and “unvaccinated” are equally likely to spread COVID-19.
Regardless of CDC Definition Change, Injections Are Treatments, Not Vaccines
Furthermore, the lawsuit states the Injections fail to confer immunity “but are claimed to reduce the severity of symptoms experienced by those infected by SARS-CoV-2.” With this in mind, Plaintiff argues the shots are instead treatments and not vaccines, as that term has already been defined in the law. Displaying the CDC’s changing narrative connected to COVID “vaccines” in the brief, and the fact the CMS Mandate rests squarely on the basis that the Injection prevents transmission, the suit reveals:
In fact, the CDC has actually changed its definitions of “vaccine” and “vaccination” so that the Injections would fit within the new definition. Until recently, the Centers for Disease Control defined a “Vaccine” as: “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.
The CDC also previously defined “Vaccination” as: “The act of introducing a vaccine into the body to produce immunity to a specific disease.”
Both prior definitions fit the common understanding of those terms. To be vaccinated meant that the recipient should have lasting, robust immunity to the disease targeted by the vaccine.
But on Sept. 1, 2021, the CDC quietly rewrote these definitions. It changed the definition of a “Vaccine” to: “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease preparation that is used to stimulate the body’s immune response against diseases.” It changed the definition of “Vaccination” to: “The act of introducing a vaccine into the body to produce immunity to protection from a specific disease.”
Thus, the CDC has eliminated the word “immunity” from its definitions of “Vaccine” and “Vaccination.” Upon information and belief, the CDC did so because it recognizes that the Injections do not produce immunity to the disease known as COVID-19.
This is a critical factual and legal distinction. The Supreme Court has long held that the right to refuse medical treatment is a fundamental human right. Since the Injections do not stop the transmission of SARS-CoV-2, as a matter of fact, they are not “vaccines” as a matter of law. Instead, they are a therapeutic or medical treatment which Dr. Griner has the fundamental human right to refuse.
In great detail, the lawsuit expands on the conviction held by numerous experts that the Injections are treatments, not vaccines. The claim reminds us that the FDA categorizes the shots as “CBER-Regulated Biologics,” otherwise known as “therapeutics,” which falls under the “Coronavirus Treatment Acceleration Program.”
Indeed, among the eight professional examples offered in the suit to corroborate that the Injections do not create an immunity that prevents the transmission of COVID-19 to others, the case quoted NIAID Director Dr. Anthony Fauci’s declaration to NPR on July 27, 2021, when he stated, “We know now as a fact that [vaccinated people with COVID-19] are capable of transmitting the infection to someone else.” Additionally, the head of the Oxford vaccine team Professor Sir Andrew Pollard, is quoted in the case as saying on Oct. 8, 2021:
“We don’t have anything that will stop transmission, so I think we are in a situation where herd immunity is not a possibility, and I suspect the virus will throw up a new variant that is even better at infecting vaccinated individuals.”
Martin Insists Injections are Gene Therapy Medical Devices
Furthermore, Plaintiff declares that with rapidly waning effects, the Injections are not “vaccines,” but are instead “gene therapy medical devices” and should be appropriately classified as such. As illustrated in the screenshot below, Moderna (Pfizer uses the same technology) recognizes that its mRNA platform is not a vaccine. Instead, it is “gene therapy in the form of biological “software” developed to genetically “hack” the machinery of human cells to construct a specific protein.
Elaborating further on the role the mRNA plays in the Injections, the lawsuit summarizes that the specific protein that human cells are “hacked” to create is the spiked protein of the disease. Essentially, the Injections genetically modify human cells to make the same toxic protein that the disease itself creates—the spiked protein. With no known method to reverse the detrimental effects of the Injections, the lawsuit continues, explaining:
These spiked proteins adhere to the endothelial cells of humans, the very cells that line the entire cardiovascular system. The spike proteins adhere to the interior of the cardiovascular system like thorns on a rose bush, causing a variety of detrimental effects, the short- and long-term impact of which are currently unknown and unknowable.
According to a June 01, 2021, bio-distribution study from the Japanese Regulator Agency, the spike protein of the “…coronavirus gets into the blood where it circulates for several days post-vaccination…” and that it concentrates “…in spleen, liver, adrenals, and ovaries in high concentrations…”
Causes of Action As Campaign Gets Underway
The lawsuit lays out three Causes of Action against Defendants, the first being the “Violation of Fifth and Fourteenth Amendment Substantive Due Process.” According to Plaintiff, the CMS Mandates violates the liberty protected by the Fifth and Fourteenth Amendments to the Constitution, including “rights of personal autonomy, self-determination, bodily integrity and the right to reject medical treatment.” With no compelling interest available to Defendants to prove the necessity of mandating the shots, Plaintiff again reminds that the Injections “are simply ineffective against the current variant” and were only somewhat effective against the original SARS-CoV-2 strain.
The Second Cause of Action explains Defendant’s Violation of the Fifth and Fourteenth Amendments related to the Equal Protection Clause, which “prohibits classifications that affect some groups of citizens differently than others.” By creating two classes of healthcare workers—the injected and uninjected—the CMS Mandate dictates the members of one class (the uninjected) get terminated. These unvaccinated employees cannot advance their careers, provide for their families, or pay their mortgages. On the other hand, the injected get to keep their jobs, advance their careers, and pay their bills. Yet, the situations of these two classes are indistinguishable because vaccinated healthcare workers can become infected and reinfected with SARS-CoV-2 and can transmit the disease to fellow workers, patients, and visitors. The lawsuit asserts:
Discriminating against the uninjected controverts the goals of the Equal Protection Clause—i.e., to abolish barriers presenting unreasonable obstacles to advancement on the basis of individual merit.
Pursuant to the Fifth and Fourteenth Amendments, Plaintiff is entitled to temporary, preliminary, and permanent injunctive relief restraining Defendants from enforcing the CMS Mandate.
The Third Cause of Action insists that by issuing the CMS Mandate, Defendants are violating the Constitution of the United States “in that they invade and encroach upon sovereign powers that reside solely in the States and have never been relinquished by the States to the Federal Government.” According to the lawsuit, the CMS Mandate rests upon a general police power asserted by the Federal Government—a power it does not have. Therefore, the CMS Mandate is an ultra vires act taken by the Federal Government because the powers the Federal Government claims to assert belong to and are retained by the States.
With the filing of Griner v. Biden, Dr. Martin’s campaign to expose the illegal corruption behind the pandemic “vaccine” narrative is underway. Emphatically, Martin states that without hesitation, the vaccine needs to be called what it is—a gene therapy injection. Noting a desperate need for “truth in advertising,” he explains:
“If we start calling [the “vaccine”] the “gene therapy injection,” a lot less people will roll up their sleeves—and roll up the sleeves of their children—to actually get the shot. And by the way, if you decide to roll up your own sleeve for an experimental gene therapy, have at it, I don’t care. What I do care about is forcing other people to do it, and coercing other people to do it. And holding their jobs or their livelihoods at gunpoint to get them to do it.”
Del Bigtree: “Less than a third of the total population of the United States of America [has received a booster shot]. [The CDC] boasts that it’s about 44% of the vaccinated… That means, at the very best, there’s a 60% group of people, even that are vaccinated, that don’t listen to the CDC any longer!”
Some people who have received COVID-19 shots experience a range of debilitating symptoms or death
Healthy teenagers, athletes and doctors are among those who have died within hours or days of receiving COVID-19 shots
Others have experienced stroke-like symptoms, paralysis, tics, partial blindness and seizures following the shots
Increasing numbers of people are becoming compelled to speak out and share their stories of how COVID-19 shots altered their lives
Despite assurances of safety from health officials, it’s what the long-term effects of COVID-19 shots will be. Spike proteins from the shots can circulate in your body after injection, causing damage to cells, tissues and organs. “Spike protein is a deadly protein,” Dr. Peter McCullough, an internist, cardiologist and trained epidemiologist, said.1
Experimental and observational evidence show that the human immune response to COVID-19 shots is very different than the response induced by exposure to SARS-CoV-2, and people who’ve received COVID-19 shots may have damage to their innate immune system that’s leading to a form of vaccine acquired immunodeficiency syndrome (VAIDS), due to the impairment in interferon signaling.2
Further, likely due to monocyte activation by the spike protein from the vaccine, some people who have received COVID-19 shots experience a range of debilitating symptoms similar to those found in long haul COVID-19 syndrome, such as headaches, fatigue, cognitive dysfunction, joint pain and chest pain.3
For some, however, the shot’s adverse effects occur quickly, resulting in life-changing debilitation. You can see 10 powerful examples below, ranging from deaths to lives upended due to illogical quarantine rules that illustrate the absurdity of COVID-19 tyranny.
These are real people with real stories to share, and the more people who see them, the more awareness can grow to provide those who survived with the help and medical care they deserve — while warning others of the potentially deadly consequences of COVID-19 injections.
If you find these stories helpful and motivating then I would encourage you to visit our breaking news blog on our site as this is where the stories below were initially posted. The blog posts stay up continuously and are not removed after 48 hours.
10 People Whose Lives Changed After COVID-19 Shots
1. Jim Ashby — Learning to Walk Again
Ashby was forced to get a COVID-19 shot by December 3, 2021, or his employer would consider him “voluntarily resigned.” Eight days after receiving the Pfizer jab, he had a major hemorrhagic stroke.
He’s been in rehab since October 2021, suffering from complete paralysis on the left side of his body. He still has a long way to go in recovery, and still can’t feel or use his left arm or walk without assistance. His rehab is excruciatingly painful, he says, and he spends up to six hours a day learning how to walk again.
What’s worse, his employer isn’t covering the medical bills for the costs of this stroke. “My life has been totally changed, all because of the vaccine mandate … my old life is dead,” he says, “and I have started my new life as a paraplegic.”
2. Athletes Collapsing and Dying
Healthy athletes around the world are dying of heart attacks and strokes. The numbers are exploding, with athletes suffering neurological problems, too. What’s happened in the last six months to a year that’s different? Is there anything in common that’s changed that hooks all these athletes together? They all have had COVID-19 shots. Among them:
Abou Ali, 22-year-old football (soccer) player, who suffered from cardiac arrest in Denmark on September 11, 2021
Caddy Alberto Olguin collapsed and died from a heart attack on the golf course on October 9, 2021
30-year-old Venezuelan marathon champion Alexaida Guedez, 30, died of a heart attack during a 5,000-meter race on August 22, 2021
Andrea Astolfi, 45, sports director of Calcio Orsago in Italy, died of a heart attack on September 11, 2021 after returning from training
Ava Azzopardi, 14, collapsed on a soccer field in the U.S. on October 15, 2021, suffering from cardiac arrest; she had to be put in a medically induced coma to survive
3. Dr. Neil Singh Dhalla, Died From Myocarditis
Dr. Neil Singh Dhalla fell asleep four days after he got a COVID-19 booster shot — and died from a heart attack. The autopsy stated myocarditis — inflammation of the heart muscle that’s a recognized adverse effect of mRNA COVID-19 shots.4 A CEO of a major health clinic, he was only 48 years old and had never had heart problems in his life.
4. Faith Ranson, 16-Year-Old Plagued by Convulsions and Tics
A happy, healthy 16-year-old girl in Australia who got the Pfizer COVID-19 shot is now crippled with convulsions, persistent nausea and visible tics. The problems began three days after her second shot and have been ongoing for months. Health officials actually admitted “there is no question Faith has had a delayed reaction to the second Pfizer vaccination” and is suffering adverse reactions from the shot. Her story even made it to mainstream news.
5. Nurse With COVID Told to Go Back to Work
In this video, a “triple vaxxed” nurse from New York explains how she tested positive for COVID-19, and her employer told her to come back to work even though she hadn’t been in quarantine for five days — against CDC recommendations.Since she was asymptomatic, she was cleared to go to back to work in a health care setting, but told she still had to quarantine in all other aspects of her life. In short, she can go to work to care for patients while actively positive for COVID-19, but she can’t go to a grocery store or a gas station. Not to mention, her kids were quarantined for 10 days, but she was expected to go back to work in less than five.
6. Stroke-Like Symptoms in a Healthy Woman
Complaints of neurological problems and stroke-like reactions continue to pile up. Immediately after receiving the AstraZeneca COVID-19 shot, this previously healthy woman experienced headaches and dizziness and blacked out “a few times.”
Within days, she started experiencing numbness to the point that she couldn’t stand up. Eight days later, she’s in the hospital with loss of feeling in her left arm, left leg and face. She states that 19 women were brought in to her hospital ward with the same symptoms over the span of one weekend.
7. Two Teenage Boys Die From Myocarditis in Their Sleep
Epidemiologists have confirmed that two teenage boys from different U.S. states died in their sleep of myocarditis days after getting the Pfizer shot. Both had received second doses of the shot, and McCullough said that in his view, the shots led to the deaths of the teenagers. In a study that examined the autopsy findings, it’s reported that the “myocarditis” described in the boys’ deaths is “not typical myocarditis pathology”:5
“The myocardial injury seen in these post-vaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.”
8. 59-Year-Old Woman Dies Hours After Shot
A 59-year-old front line health care worker in the U.K. took the COVID-19 shot and died a few hours later. In the video, her acquaintance states, “Now I know it’s a given the vaccine’s going to have some casualties — but people are threatened they are going to lose their jobs if they don’t take it … You have the right to take that risk, but you should have the right to refuse it as well — without jeopardizing your job or your freedom of entry or freedom from discrimination.”
9. Vaccine Advocate Nearly Goes Blind
The man in this video describes himself as a believer in “science” and a “vaccine advocate,” but this didn’t spare him from the shot’s adverse effects. Five days after his first Pfizer COVID-19 shot, he started having blurry vision in his left eye. Within three days, he had lost 60% of his vision in that eye.
After several medical examinations, doctors, optometrists and retina specialists diagnosed him with central serous retinopathy (CSR), in which a small vein ruptured, leading fluid to accumulate under the retina, causing retinal detachment and partial blindness.
Other cases of CSR have also been reported following COVID-19 shots, he says, and in a case report published in the American Journal of Ophthalmology it’s stated, “Acute CSR may be temporally associated with mRNA Covid-19 immunization.”6 The man’s doctor told him that the risk of getting additional COVID-19 shots outweighs the potential benefit for him and tried to help him get an official exemption from further shots, but it was denied. He states:
“I have been deprived of my human rights as a citizen … I try to gather all my strength so many times during the past few months to just go and receive my second dose in order to follow the laws.
But the fact that the science says there is an above-average chance that I may lose more of my sight has driven me to anxiety attacks, night terrors and disabling depression … This is a direct violation of my constitutional rights as a citizen and a human being.”
10. Young Woman Suffers From Seizures, Nearly Dies
Beginning her story by stressing she is NOT anti-vaccine or pro-conspiracy theory, this young woman describes what happened to her after she received a Moderna COVID-19 shot, which she decided to get so she and her husband could join some friends on a cruise.
The day after the shot she started feeling “weird,” delirious and “disassociated from herself,” she says. Soon after, she blacked out in the bathroom, and when her husband tried to revive her, she began seizing. She had three seizures between the time her husband called 911 and when the ambulance got her to the hospital.
She was intubated and suffered other severe effects, she says. She spent days in the hospital and is now taking anti-seizure medication, while living with ongoing anxiety about her near-death experience, which she believes was caused by the shot. “Go out there and do your research so you can make an informed decision,” she says. “Because you don’t want to put something in your body that could potentially harm you.”
Let Your Voice Be Heard
If you or a loved one has been injured by a COVID-19 shot, I will help you share your testimony. Vaccine mandates have led to injuries, devastation and deaths — while the brainwashing “get your vaccine now” campaign is being used to divide and conquer. One spark is all that is required to start a fire. There is a revolution building — a revolution for freedom to live your life without medical mandates or dictators calling the shots.
Please share your story with us, and encourage others you know who have a story to share theirs. It’s never been more important than now, for you and your family, to take control of your health.
The CEOs of the nation’s largest airlines are asking the Biden administration to drop the federal mask mandate on airplanes, along with the pre-departure testing requirement for international travelers. Although COVID-19 cases in the U.S. have fallen sharply in the last two months and restrictions are being lifted across the country, the Centers for Disease Control and Prevention earlier this month extended its mass transit mask mandate by 30 days, until mid-April, and masking guidelines for airlines remain in place.
“Now is the time for the administration to sunset federal transportation travel restrictions – including the international predeparture testing requirement and the federal mask mandate – that are no longer aligned with the realities of the current epidemiological environment,” the CEOs of 10 U.S.-based passenger and cargo airlines, including Delta, American and United, wrote in a letter to President Biden.
The letter states that while the airlines and their employees supported the federal mask mandate when it was first implemented, especially because it did away with the possibility for airline-by-airline rules in the early days of the pandemic, they now feel it is no longer necessary.
After a request from the FDA to suppress vaccine data for the next 75 years, a 55,000-page set of Pfizer documents has recently been released. Vaccine efficiency aside – why has it been so hard to gain access to data about vaccines that we the public paid for?
#Pfizer #Covid #Vaccines
OTTAWA: The Justice Centre announced today that its legal team has eleven affidavits in the Federal Court lawsuit to strike down the federal government’s mandatory Covid-19 vaccine requirements for air travellers (the “Travel Ban”). The Notice of Application was initially filed on February 1, 2022 behalf of several Canadians from across Canada challenging the Travel Ban on the basis that their Charter rights and freedoms have been infringed.
The main applicant in the case is former Newfoundland Premier, The Honourable A. Brian Peckford. Mr. Peckford is the only surviving drafter and signatory to the 1982 Constitution and the Canadian Charter of Rights and Freedoms.
In his sworn affidavit, Mr. Peckford states: “What I find perhaps the most disturbing is that the federal government has mandated a two-tiered society where one group of people has benefits while another group is disadvantaged. As a person who has chosen not to receive the new medical treatment, I am all of a sudden treated as an outcast, labelled a “racist” and “misogynist”, and as an undesirable person not fit to be seated with vaccinated people on an airplane … The Covid-19 vaccinated are allowed to travel by airplane and to see their families and the unvaccinated are not. This is not the Canada I know and love, and this type of segregation causes me utmost sadness.”
In October of 2021, the federal government announced that anyone travelling by air, train, or ship, must have taken the requisite number of mRNA Covid shots (currently two).
The travel vaccination mandate has prevented approximately 6 million vaccine-free Canadians (15% of Canada’s population) from travel within Canada and prevents them from flying out of Canada. The evidence filed with the court shows how the Canadians involved in the lawsuit cannot travel to help sick loved ones, cannot get to work, cannot visit family and friends, cannot access health care outside of Canada, cannot take international vacations, and cannot live ordinary lives.
Expert medical evidence now filed with the court ranges from scientific evidence about Covid spread among both vaccinated and unvaccinated; risks associated with taking the new Covid vaccines; vaccine harms such as myocarditis and possible effects on fertility; and the superiority of natural immunity.
The Federal Court has consolidated the Justice Centre action with three other similar cases, brought by other unrelated parties, asking for the travel ban to be ruled unconstitutional. All applicants have asked the Federal Court to hear the case on an expedited basis given the serious infringement on Canadians’ mobility and other rights. The parties have agreed to the following timelines, and hope to have the matter heard in September of this year at the latest:
March 11 – Service of Applicants’ Affidavits and Documentary Exhibits April 25 – Service of Respondent’s Affidavits and Documentary Exhibits May 16 – Completion of cross-examination on Affidavits June 6 – Service and filing of Applicants’ Records June 27 – Service and filing of Respondent’s Record Fall 2022 – Hearing (proposed timeline)
“Canada is the only country in the developed world that bans unvaccinated citizens from air travel,” states Keith Wilson, Q.C., lead counsel on the case for the Justice Centre. Mr. Wilson adds, “Canada’s ban on unvaccinated flying is especially egregious given Canada is the second largest country in the world by landmass and Canadians have a far greater need to use air travel for work, family and health reasons than do the citizens of most other countries.”
“Our experts confirm that both the vaccinated and unvaccinated spread Covid. This means the government’s rationale for the ban on air travel is fatally flawed and there is no justification for the serious infringement on Canadians’ Charter rights,” notes Mr. Wilson.
“Our evidence refutes government claims that infringing the mobility, conscience, security and privacy rights of Canadians is justified,” states Justice Centre lawyer Allison Pejovic.
“Canadians have the right not to be discriminated against, and this Charter challenge seeks to enforce that right,” adds Ms. Pejovic.
The Justice Centre for Constitutional Freedoms is a non-profit national constitutional law organization funded by voluntary donations from concerned Canadians.
David Freiheit, a.k.a Viva Frei, tells us why he hosted marathon livestreams in Ottawa, and gets into the nitty-gritty of the Emergencies Act and the anti-honk legal battles.
During the Freedom Convoy, Viva Frei was on the ground reporting and interviewing people, speaking with truck drivers and on-the-ground supporters. He was present during the three weeks of the main protest, and it was interesting to hear his opinion, legally speaking, about all the tactics and measures used by the government against the demonstration.
In this video, we discuss the seizure of bank accounts, cancellation of licence plates, the state of emergencies called in Ontario and Ottawa, and the use of the federal Emergencies Act.
Did you know a legal case is currently happening against some people involve with the Freedom Convoy, for the modest sum of $306-million? David gives us his thoughts on the legal side of the story, and his own opinion of how he perceived the Freedom Convoy.
VAERS data released Friday by the Centers for Disease Control and Prevention included a total of 1,183,495 reports of adverse events from all age groups following COVID vaccines, including 25,641 deaths and 208,209 serious injuries between Dec. 14, 2020, and March 11, 2022.
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,183,495 reports of adverse events following COVID-19 vaccines were submitted between Dec. 14, 2020, and March 11, 2022, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 11,728 U.S. deaths reported as of March 11, 17% occurred within 24 hours of vaccination, 22% occurred within 48 hours of vaccination and 60% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 556 million COVID vaccine doses had been administered as of March 11, including 328 million doses of Pfizer, 209 million doses of Moderna and 19 million doses of Johnson & Johnson (J&J).
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
The most recent death involves a 7-year-old boy (VAERS I.D. 2152560) from Washington who died 13 days after receiving his first dose of Pfizer’s COVID vaccine when he went into shock and suffered cardiac arrest. He was unable to be resuscitated and died in the emergency department.
17 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department.
The most recent deaths involve a 17-year-old boy (VAERS I.D. 2171083) from Illinois with Duchenne muscular dystrophy who died from cardiac arrest after receiving his second dose of Pfizer’s COVID vaccine, and 14-year-old boy from Guam (VAERS I.D. 2157944) who died one week after his first dose of Pfizer when he suddenly committed suicide.
The boy’s VAERS report states:
“Sudden suicide one week after the vaccine. Patient was a perfectly happy child. After the vaccine, he became much more tired and achy and lost interest in doing his sports. One week later, without any warning, he hung himself.”
68 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
646 reports of myocarditis and pericarditis, with 634 cases attributed to Pfizer’s vaccine.
162 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to March 11, 2022, for all age groups combined, show:
20% of deaths were related to cardiac disorders.
54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
Moderna asks FDA to authorize 4th dose for adults 18 and up
Moderna on Thursday asked the FDA to amend Emergency Use Authorization (EUA) of its COVID vaccine to include a fourth dose for adults 18 and older.
According to The Associated Press, the request is broader than Pfizer’s. Pfizer earlier this week asked the agency to authorize a fourth dose of its COVID vaccine for adults 65 and older.
In a press release, Moderna said the request to include adults over 18 was made “to provide flexibility for the U.S. Centers for Disease Control and Prevention and healthcare providers to determine the appropriate use of an additional booster dose of mRNA-1273, including for those at higher risk of COVID-19 due to age or comorbidities.”
Moderna said its decision to seek FDA approval was based on studies from the U.S. and Israel about the Omicron variant, but didn’t provide further information. Booster doses of Moderna are half the dose of the first and second doses.
Pfizer and BioNTech ask FDA to authorize fourth vaccine dose for older adults Pfizer and BioNTech on Tuesday said they submitted a request to the FDA for EUA of an additional booster dose of their COVID vaccine for adults 65 and older.
The companies’ request was not based on robust, peer-reviewed U.S. data, but on two recent studies from Israel — both published on preprint servers without peer review.
The first study was done in conjunction with Israel’s Ministry of Health and involved a review of 1.1 million health records. The study concluded rates of COVID in those who received a fourth dose of Pfizer’s COVID vaccine were lower compared to those who received only three doses.
According to the preprint published on medRxiv, since Jan. 2 Israel has been administering a fourth dose of the Pfizer vaccine only to people over 60 and at-risk populations.
In the second study of Israeli healthcare workers, results showed a fourth dose of either Pfizer’s or Moderna’s vaccine boosted antibody levels, but neither was effective at preventing infections.
CDC deletes thousands of reported COVID-19 deaths in children
The CDC removed tens of thousands of deaths linked to COVID, including nearly a quarter of deaths it had attributed to those younger than 18, The Epoch Times reported. The change was made on March 15 on its COVID data tracker website.
“Data on deaths were adjusted after resolving a coding logic error. This resulted in decreased death counts across all demographic categories,” the CDC said on the website. The agency also acknowledged COVID death data is not complete.
Before the change, the CDC listed 1,755 deaths in children from COVID, along with 851,000 others, according to Kelley Krohnert, a Georgia resident who tracks the CDC’s updates.
The CDC removed 416 deaths among children and more than 71,000 other reported deaths — arriving at a total of about 780,000.
The CDC’s statistics are frequently cited by physicians and experts when pushing for children to receive COVID vaccines. Dr. Rochelle Walensky, the CDC’s director, referred to the tracker’s death total on November 2021 while pushing for an expert panel to advise her agency to recommend vaccination for all children 5 to 11 years old.
Vaccine researcher develops tinnitus 90 minutes after COVID shot, calls for more research
A vaccinologist at the Mayo Clinic in Minnesota said he developed tinnitus after receiving his second dose of an mRNA COVID vaccine.
Dr. Gregory Poland’s symptoms began 90 minutes after receiving the vaccine. He described the condition as “fairly severe” and “extraordinarily bothersome, interfering with sleep and the ability to concentrate.”
Dr. Gregory Poland, a vaccinologist at the Mayo Clinic in Minnesota, developed tinnitus after his second dose of an mRNA COVID-19 vaccine. He is raising questions about this side effect from the vaccine and suggesting more research is needed.https://t.co/9IXhO9P0cv
— Robert F. Kennedy Jr (@RobertKennedyJr) March 16, 2022
According to the National Institutes of Health, tinnitus is a sign that something is wrong with the auditory system. It is commonly described as a ringing in the ears, but it also can sound like roaring, clicking, hissing, or buzzing that accompanies soft, loud or high pitches.
According to the most recent VAERS data released on March 11, 19,851 people have reported developing tinnitus after a COVID vaccine, with 12,027 cases attributed to Pfizer’s COVID vaccine.
CEO of German health insurer fired after releasing data on underreported COVID vaccine injuries
The CEO of one of Germany’s largest health insurance companies was abruptly fired last month after he released data suggesting German health authorities are significantly underreporting COVID-19 vaccine injuries.
The data, released by Andreas Schofbeck of BKK/ProVita, have since been scrubbed from the company’s website.
Schofbeck, who noticed an unexpected jump in vaccine-related health insurance claims, in February notified the Paul Ehrlich Institute (PEI) — the German equivalent of the CDC — that BKK billing data indicated the PEI was underreporting adverse events to COVID vaccines.
I’m “If these figures are extrapolated to the whole year and to the population in Germany, probably 2.5-3 million people in Germany have received medical treatment for vaccination side effects after Corona vaccination.”
Dr. Dirk Heinrich, chairman of NAV-Virchow Bund, an association of private medical practitioners in Germany, said PEI and BKK would be working closely to examine the billing code data. Heinrich also stated that the conclusions from Schofbeck’s letter are “complete nonsense.”
“The small fringe minority of people who are on their way to Ottawa, who are holding unacceptable views that they’re expressing, do not represent the views of Canadians.”
Words from protestors in Ottawa:
“I’m not a misogynist. I’m not a racist. I have no problem with white people/ I have no problem with other… It is the vocabulary that has been spreading in many countries… This is a consorted effort to use the same vocabulary colloquially so that people get brainwashed, divide themselves and insult their friends, their neighbor. It’s organized for that. And people have to see beyond the trap. It’s really important. We’re a very compliant society. We’re also very polite, and so we will agree. But the problem now is, it is the time to fight…”
“If you come here and see what’s happening, you will feel it…When you come here, you feel in in your heart. You feel what’s happening around here and you can’t do anything but smile. Take our gas. Take our diesel. Take our propane. Take everything you want. But you will not take our freedom. You will not take our love.”
“Freedom over fear.
“Love over hate.”
Vera Sharav, Holocaust survivor
“I think the best thing that’s happened so far are the truckers in Canada. Who hopefully will be a model for other truckers and other working class people who will rise up and say enough. They are our hope. And it’s a fact that we really, really need to recognize.
“People who are not totally brainwashed can see the big lie. And they’re really prompted to get up and take their chances and do what has to be done to stop it. I hope that others follow and that we will be willing to support them. We really need to put the perpetrators on trial. This is terribly important.
“I want to stress that the vital lessons from the Holocaust… what facilitated the Holocaust was the silence and indifference of those who watched and did nothing to prevent it.”
“Silence in the face of evil is itself evil: God will not hold us guiltless.
Not to speak is to speak. Not to act is to act.” ~ Dietrich Bonhoeffer
Dietrich Bonhoeffer was a German Lutheran pastor and theologian. He was also a participant in the German Resistance movement against Nazism, a founding member of the Confessing Church
[As a service to protect truth from censorship and to share widely, mirrored copies of this video are available at Truth Comes to Light Odysee, BitChute and Brighteon channels. All credit, along with our sincere thanks, goes to the original source of this video. Please follow links provided to support their work.]
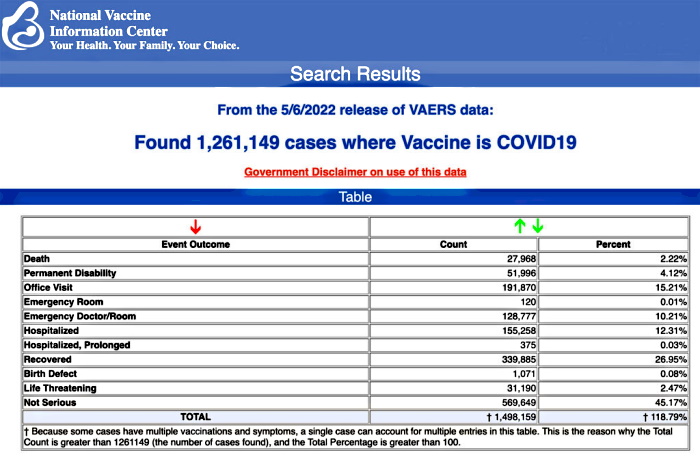
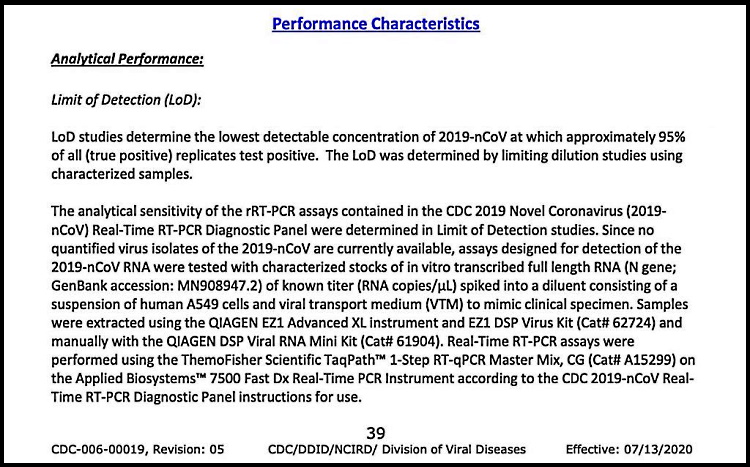
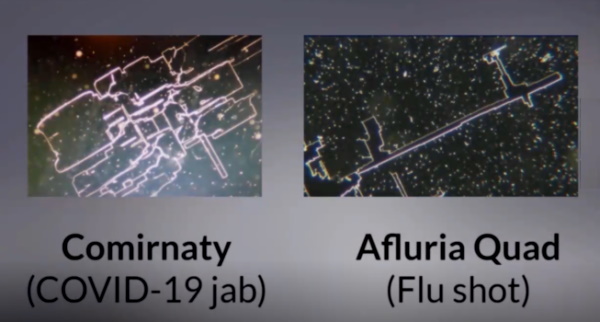
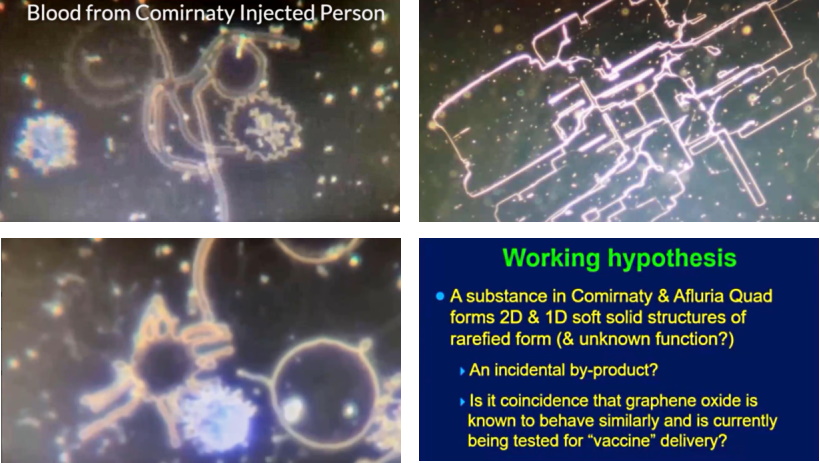
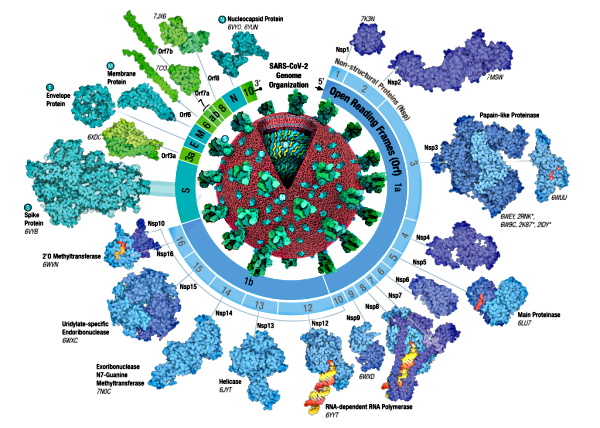
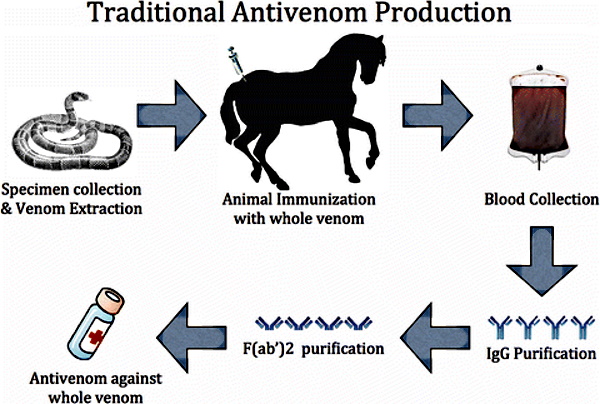
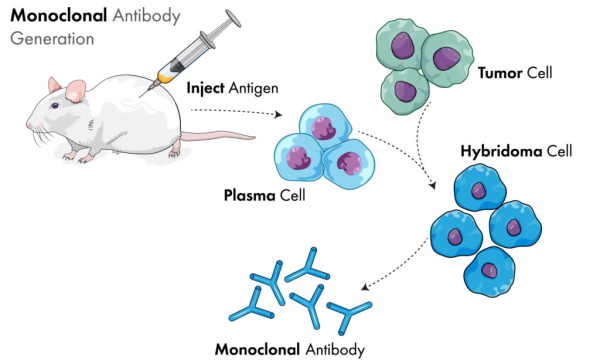
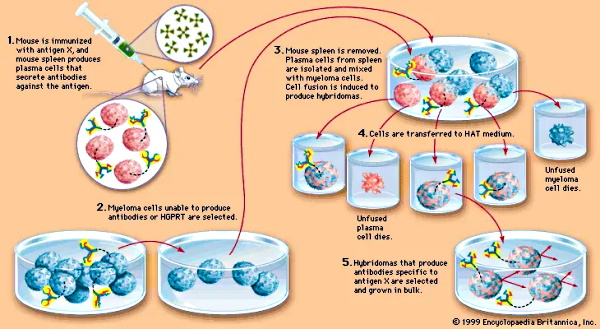


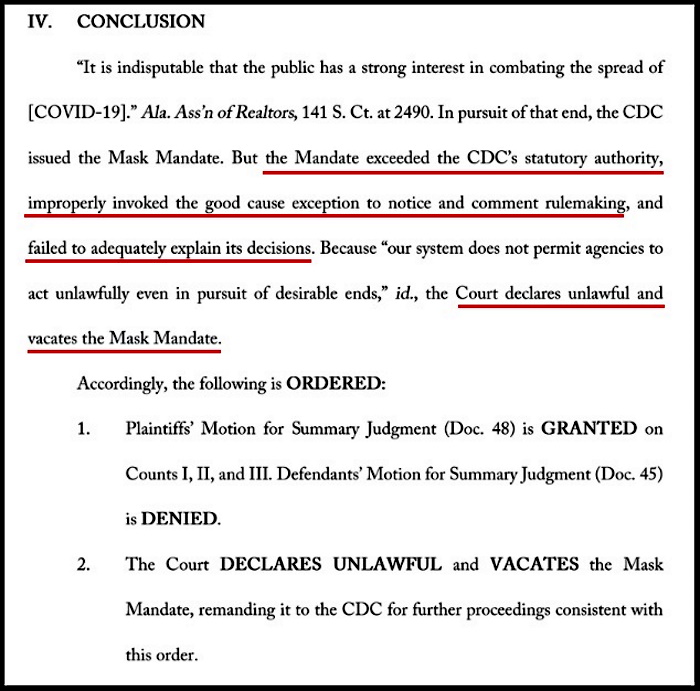

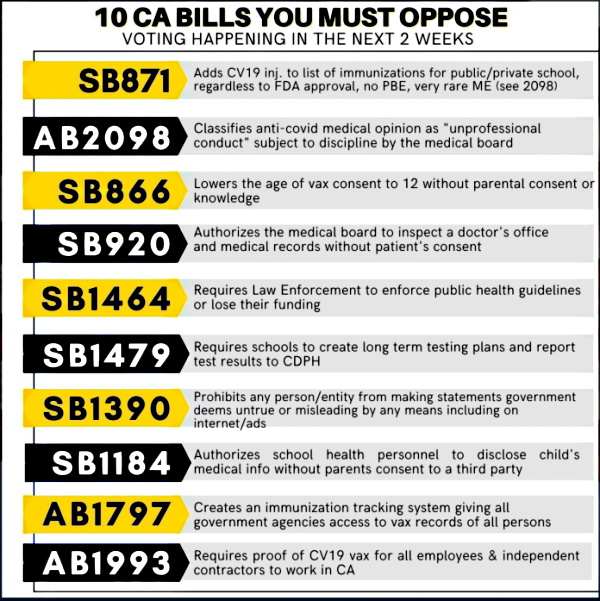
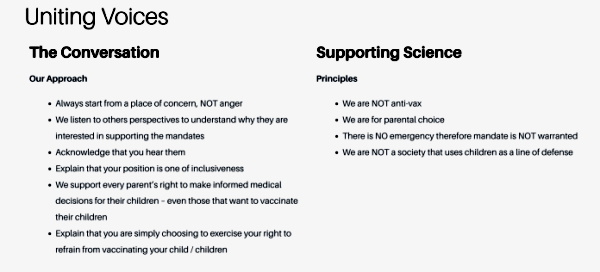


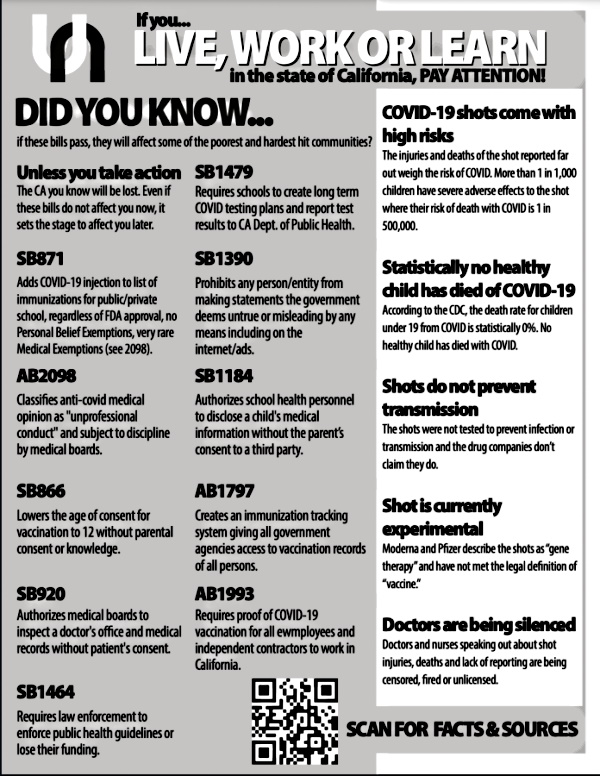
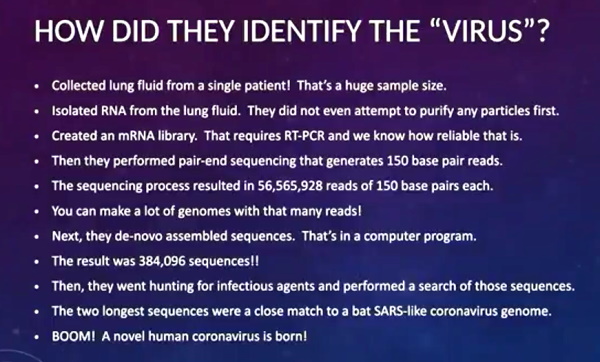
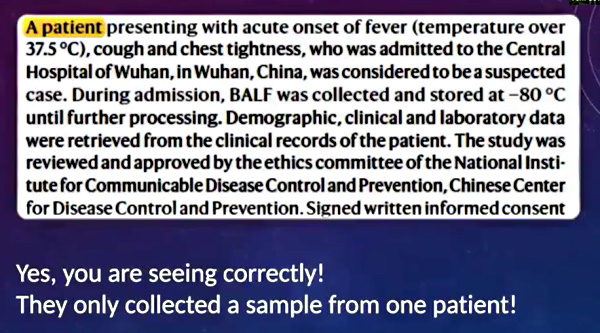
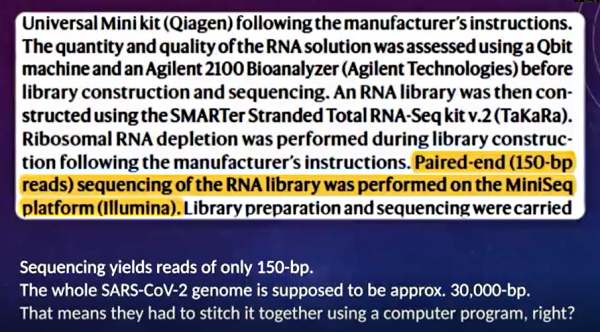
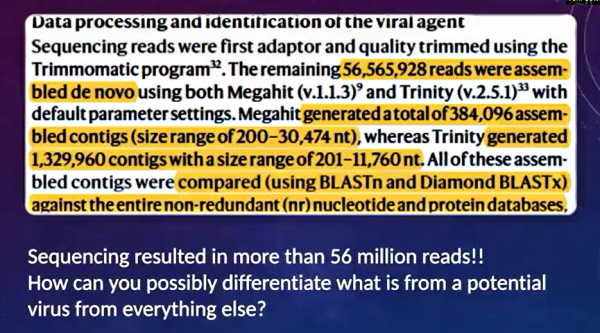
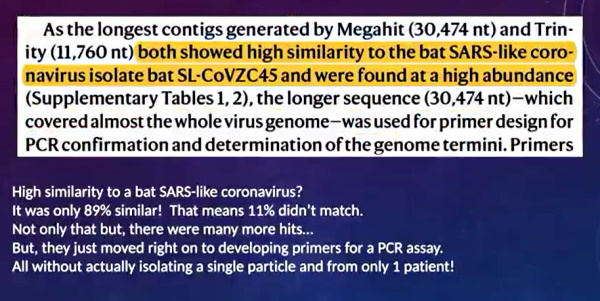

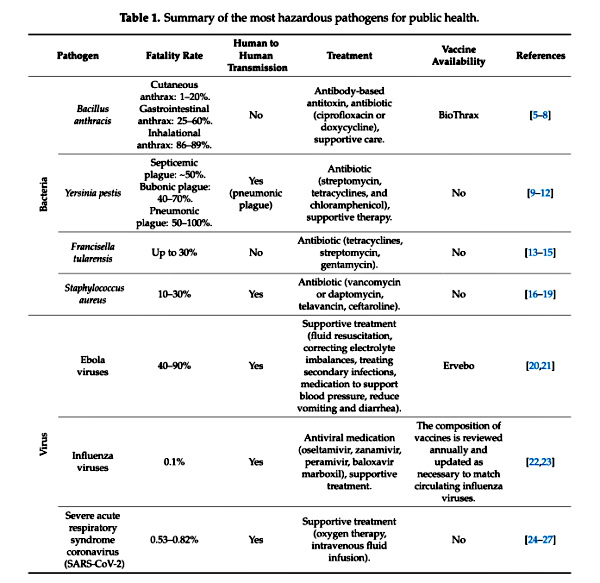
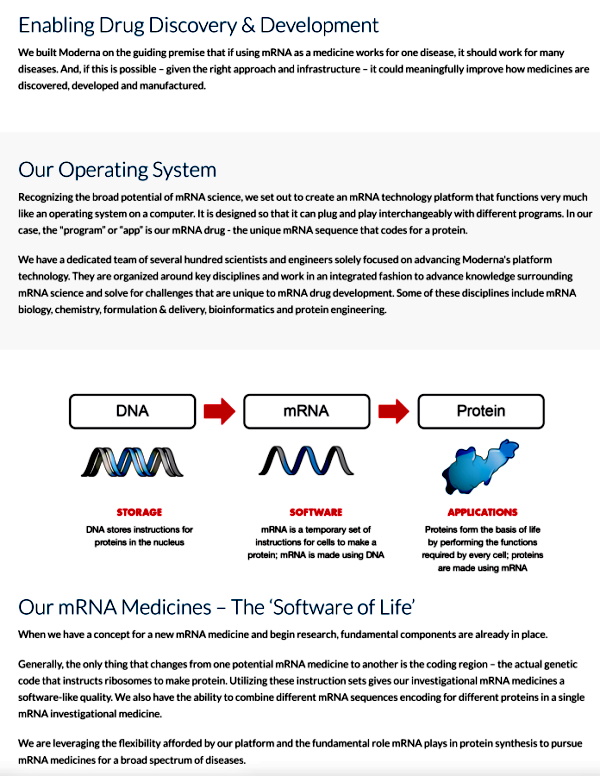 Screenshot /
Screenshot / 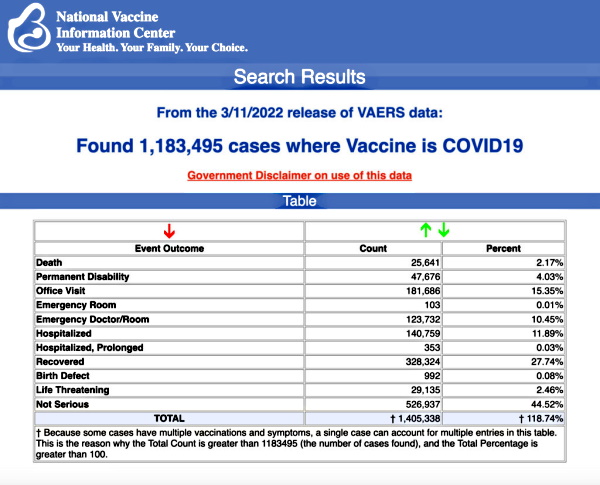

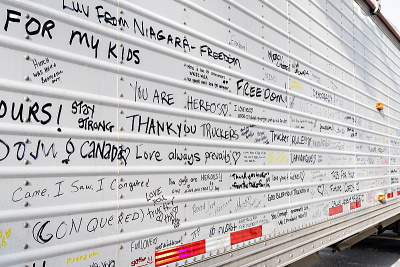











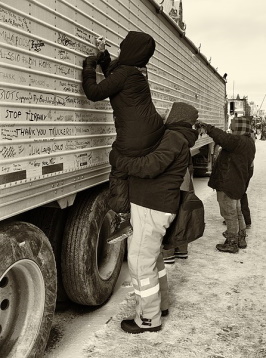







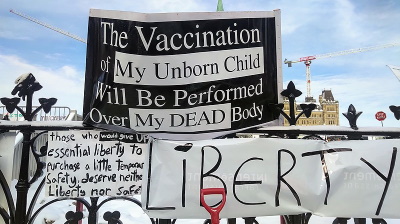





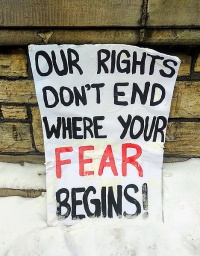













 “I’m not a misogynist. I’m not a racist. I have no problem with white people/ I have no problem with other… It is the vocabulary that has been spreading in many countries… This is a consorted effort to use the same vocabulary colloquially so that people get brainwashed, divide themselves and insult their friends, their neighbor. It’s organized for that. And people have to see beyond the trap. It’s really important. We’re a very compliant society. We’re also very polite, and so we will agree. But the problem now is, it is the time to fight…”
“I’m not a misogynist. I’m not a racist. I have no problem with white people/ I have no problem with other… It is the vocabulary that has been spreading in many countries… This is a consorted effort to use the same vocabulary colloquially so that people get brainwashed, divide themselves and insult their friends, their neighbor. It’s organized for that. And people have to see beyond the trap. It’s really important. We’re a very compliant society. We’re also very polite, and so we will agree. But the problem now is, it is the time to fight…”

{kind=link}
{kind=link}
_J.jpg){kind=link}
.jpg){kind=link}