by Jon Rappoport, No More Fake News
February 3, 2022
What proof would I accept? What sort of proof would convince me that SARS-CoV-2 exists?
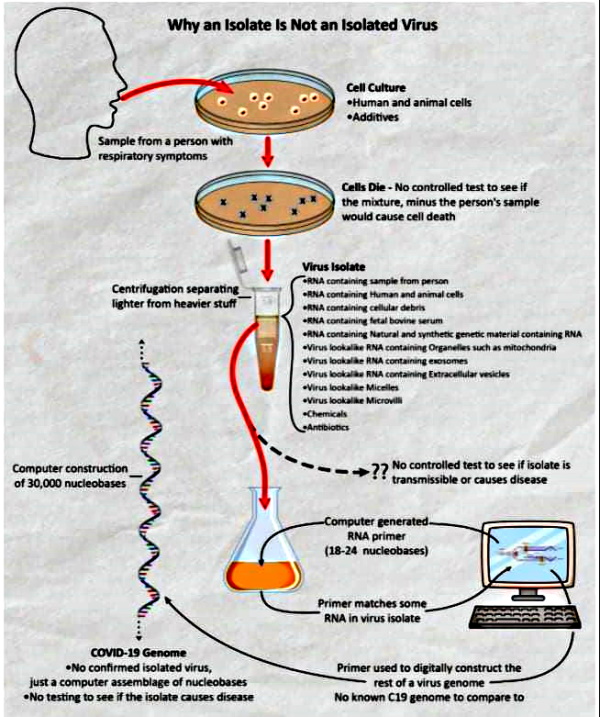
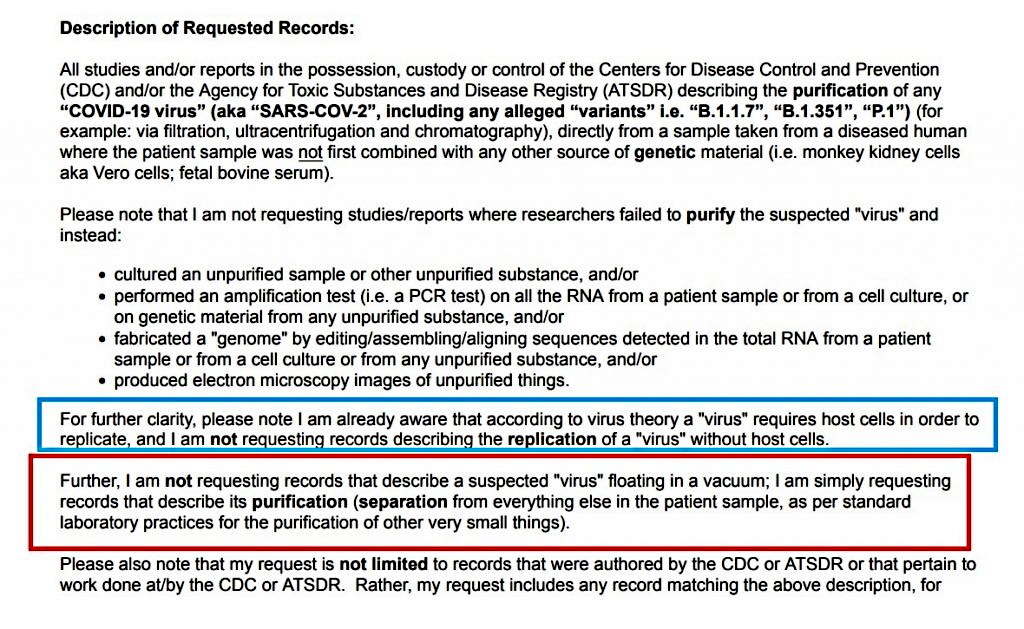
Suppose, for example, a study described how researchers actually DID separate a virus from all the material surrounding it in their cell-soup in the lab?
Would that be enough?
And the answer is no.
Why?
Because I don’t trust studies based on research conducted in elite labs where no independent outsiders are allowed. And that’s the situation, when it comes to purported virus isolation.
These labs are like the famous bunkers where key government officials are taken, in the event of a massive attack against the country.
Try getting in off the street.
And who are these researchers in the super-secret labs? To put it another way, what sort of establishment do they represent?
Is it a clean establishment with a track record of honesty? Or is it a cartel with a criminal history?
If it’s a cartel, why should I accept the “scientific methods” of these researchers or their honesty?
As my long-time readers know, I’ve spent decades exposing lies and crimes of the medical cartel. Chapter and verse. (For example this: Medical weapons of mass destruction)
When it comes to vital issues that mean the difference between life and death—drug/vaccine-fueled destruction of human life; mistreatment and errors in hospitals; faked disease case and death numbers; inaccurate, meaningless, and deceptive diagnostic tests; the fabricated existence of a whole range of phony diseases and disorders and syndromes; the true numbers of medically caused deaths—medical authorities have been lying and sliming their way out of accountability for MANY decades.
And all this doesn’t touch on the history of public health declarations of epidemics that have turned out to be duds.
Nor does it include the overall history of Rockefeller medicine, which is based on the fatuous notion that there are thousands of separate and distinct diseases, each one of which is caused by a germ that must be treated by a profit-making drug.
Nor does it include the history of vicious suppression of innovative treatments developed by individuals who’ve worked outside the mainstream.
Therefore, suspicion is warranted. Is absolutely necessary. And “suspicion” is a vast understatement.
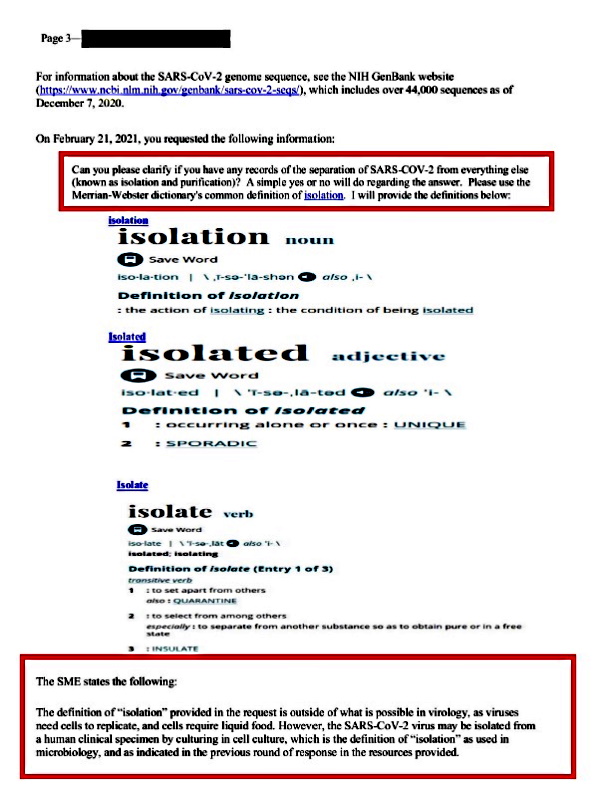
I refuse to trust the researchers who simply claim they’re isolating viruses.
When it comes to the so-called basic building blocks of MANY so-called diseases—which ARE “the viruses”—all the discovery-research HAS BEEN conducted by insiders in their off-limit labs. Without independent witnesses. Without educated witnesses who can watch and question each and every step of “the accepted method” for isolation of new viruses.
Frankly, you would have to be crazy to accept anything coming out of these insider-club labs.
So NO. I don’t accept such findings.
Before I describe how outsiders SHOULD be allowed to witness and participate in secret lab work, let me give you two quotes to consider.
They come from decidedly mainstream and elite editors of elite medical journals. These editors have read and explored and probed and lifted the fake cover from published medical material for decades. Material they themselves have published. Therefore, these are CONFESSIONS.
ONE: “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” (Dr. Marcia Angell, NY Review of Books, January 15, 2009, “Drug Companies & Doctors: A Story of Corruption)
TWO: “The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness…”
“The apparent endemicity of bad research behaviour is alarming. In their quest for telling a compelling story, scientists too often sculpt data to fit their preferred theory of the world. Or they retrofit hypotheses to fit their data. Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours. Our acquiescence to the impact factor fuels an unhealthy competition to win a place in a select few journals. Our love of ‘significance’ pollutes the literature with many a statistical fairy-tale…Journals are not the only miscreants. Universities are in a perpetual struggle for money and talent…” (Dr. Richard Horton, editor-in-chief, The Lancet, in The Lancet, 11 April, 2015, Vol 385, “Offline: What is medicine’s 5 sigma?”)
Suspicion is warranted. It’s absolutely necessary. And again, “suspicion” is a vast understatement.
More than a year ago, I mentioned how virus-isolation research—if the word “research” applies at all—should be done.
And I issue this now, as a challenge, to the entire insider-club of virologists, all of whom claim their established method of finding and sequencing new viruses is scientific and rigorous:
Let’s have a film crew on site. As you work. In your lab. Looking over your shoulders and recording every move you make.
And with the film crew, let’s have several knowledgeable, outside, independent researchers. People whom you would ordinarily refuse to give the time of day. People who are insightful. Possibly, people like Dr. Stefan Lanka, Dr. Andrew Kaufman, Dr. Tom Cowan.
As the film crew works, and as you conduct and describe your step-by-step “isolation” of a new virus, these outsiders can stop you at any moment and question you. In depth.
“Why did you just do that?” “Why didn’t you record that step?” “Explain that answer you just gave me. It makes no sense.” “Exactly what did you just withdraw from the solution in the dish, and how do you know what it was?”
This is not a public relations exercise or an educational documentary for medical students. This is REAL. This is research about your research. No holds barred.
You give a slippery answer to a question; you evade with a vague generality; you try to pull rank; you get nailed to the wall. On film.
THIS is the procedure I want.
All the way from start to finish. Including the so-called sequencing of the “new virus.”
And then we would know a great deal more about what you’re actually doing and not doing in your labs. In the absence of what I’m proposing and demanding, THERE IS NO REASON TO ASSUME THE PROCESS OF VIRUS-ISOLATION IS LEGITIMATE.
Virologists, your work affects every human on Earth. Profoundly. To see this, all a person has to do is look around him these days, at what is called “COVID.” It proceeds from your so-called discovery of SARS-CoV-2.
I view you virologists as I would view the court magicians and soothsayers and high priests who surrounded and advised the leaders of tribes and nations in ancient times.
Those “experts” huddled with the leaders in their very private rooms and spun stories and predictions, and recommended strategies to deal with supposed ongoing and looming crises.
And then the leaders took actions that affected the lives of all the people.
So it is now. With you virologists.
So my demands are entirely within bounds. If you have a shred of honesty, and if you stop and think about it, what I’m demanding is prosaically simple:
You account for every step you take. In real time. Where you work. Right there, you submit yourselves to the detailed scrutiny of independent outsiders.
That’s my bottom line.
And I challenge any scientist, analyst, investigator, doctor, researcher, reporter, alt. reporter who says what I’m demanding is not necessary. You’re wrong. You’re dead wrong.
You either haven’t thought things through, or you’re lying.
Someone is going to tell me what I’m demanding, as proof, is impossible. It would never happen. “They” would never let it happen. They would never let independent outsiders into their holy labs.
You think I don’t know that?
If outsiders can’t get into their labs, what does that tell you?
And someone will say, “We just have to rely on the best evidence we have.”
No we don’t. Because the best available evidence is no evidence.
In a vast sea of death-dealing medical lies, a sea that has existed for more than a hundred years (actually much longer), if experts tell you they’re discovering viruses in labs you can’t enter, and they say you must believe them, and you buy that…
I have condos for sale on the far side of the moon. Full cash only, no payments.
Here it is: Virologists are saying and writing they’ve found a purple man with pink hair and green lips and four arms living a thousand miles under the surface of a planet in the next solar system over. And he causes disease.
Then they’re saying, “Prove us wrong.”
On top of that, they’re saying, “You can’t watch us work while we discover such creatures.”
Conclusion: the purple man doesn’t exist.
Virologists, text me when you’ll let my people into your lab.
Until then, get lost.
Dear reader, the elephant in the room is trust, not data.
When it comes to the “discovery of viruses,” there are no reliable data. We, on the outside, are told that what happens behind locked doors is irrefutable. Period.
We’re told we just can’t understand what the pros are doing. The problem is our lack of knowledge, our lack of training.
We’re the peasants toiling in the valley. Our better, the baron, is up in his castle on top of the mountain. He’s planning our lives, he’s taking care of us.
Sure. Of course. Uh-huh.
Sounds familiar. It’s pretty much the history of the world.
Or it was, until people who came before us finally staked out a territory called freedom, which involved opening locked doors and finding out what lay behind them.
Consider a parochial example: the mafia. They, too, plan behind closed doors. They concoct methods of carrying out crimes. They record their profits. Then, finally, a prosecutor announces, “We were able to get into their books. We saw the details. We made arrests.”
I want my independent accountants to get into the virologists’ books. But not after the fact. I want my people to BE there while the virologists are creating the books, entry by entry, in the lab.
“Why did you just make that entry? Where did your conclusion come from? Who are you trying to kid? You’re just fabricating this stuff? You know, that’s called RICO. That’s a RICO case. Continuing criminal enterprise. They’ll send you away for a long time…”
And all of a sudden, the high and mighty virologist, who’s been able to con the world with his hustle, who knows how to come off sounding superior in every way, feels a dent in his armor. A big dent. He smells his own blood.
And he starts talking.
He wants to make a deal. He’ll roll over on his colleagues. He’ll expose the whole sham.
“…You don’t understand. It’s the money. It’s all about the money. Where it comes from. We have to do this kind of work. Otherwise, we starve. They cut us off. I know the people on the funding committees. I’ll give you their names. They take orders, too. The whole thing is a system. I can draw you a map. I can’t go to jail. I have a family. I’m paying eighty grand a year just to send my kids to college. There’s the mortgage, and the cottage on the Cape…”
The whole bluff POPS and deflates, and we begin to hear words we understand, at last. The words of confession. The down-to-earth sordid truth.
There was never a towering mystery in the castle on the hill.
There was just the passing of the buck. The soiled buck. From hand to hand.
The “science” was the front.
“…You see, it works this way. The pharmaceutical companies have to have new viruses. For every fake virus, they develop a real drug and a real vaccine. It’s marketing. That’s what they’re doing. That’s what they’ve always been doing. This is much bigger than anyone realizes. I’m just a little fish. The big boys run the whole show. They pay the Congress and the FDA. They pay everybody…”
He keeps talking. He can’t stop. He’s way past “isolation, purification and sequencing.” They’re in his rear-view mirror. Now he’s fighting for his freedom from prison. Now he’s telling the truth.
And the ever-present storm clouds over the valley where we peasants toil are blowing away. The air is fresher.
We’re breathing easier.
The big-cheese baron is really a shrunken little man—when he takes his perp walk in chains.
Connect with Jon Rappoport
cover image credit: Tumisu / pixabay





 The Treatments
The Treatments
.jpg){kind=link}